A Simulation Tool for Analyzing and Improving the Maternity Block Management
10
A Simulation Tool for Analyzing and Improving the Maternity Block Management Michelle Chabrol 1 , Denis Gallot 2 , Michel Gourgand 1 , and Sophie Rodier 1,2 1 LIMOS UMR CNRS 6158, University of Blaise Pascal, Campus des C´ ezeaux, 63000 Clermont-Ferrand, France 2 University Hospital of Clermont-Ferrand, Bd L´ eon Malfreyt, 63058 Clermont-Ferrand Cedex 1, France {chabrol,gourgand,rodier} @isima.fr, {dgallot,srodier}@chu-clermontferrand.fr Abstract. The pregnant women enter and leave hospitals 24 hours a day throughout the year. So, the designers of models have to consider the day, the time and the method of arrival, the degrees of emergency, the alternative placement, and the staff availability. The discrete event simulation has been widely used in attempts to improve the delivery of healthcare. In this paper, the method used to develop a simulation tool for a maternity block is described. This paper surveys the application of discrete-event simulation modeling to healthcare systems and presents the decision-making aid tool designed for a maternity block in order to improve their management. Future directions of research and applica- tions are also discussed. abstract environment. Keywords: Modeling, simulation, healthcare, decision-making aid tool, maternity block. 1 Introduction At the end of 2009, the “Hˆ otel Dieu”, a unit of the University Hospital (UH) of Clermont-Ferrand will transfer its activities on a new site: the “Nouvel Hˆ opital Estaing” (NHE). The UH managers have to reconsider the organization of the maternity block which will gather in a single place two obstetrics units now distinct: the “Maternity” and the “Polyclinic”. The maternity and the polyclinic of the “Hˆ otel Dieu” are two separated obstetrics units in two different buildings. We define the maternity block as a hospital unit where the pregnant women undergo a medical treatment before and after child birth. The new obstetrical unit must provide health services for women, which includes the full range of the maternity care and the gynaecology care (only for emergency examinations). The maternity service provides care for pregnant women in the antenatal, intrapartum and postnatal period. The maternity unit has to respond to an uncertain demand from patients. Some demands can be treated within the maternity block, others are admit- ted to the hospital for further treatment as inpatients (complications). In this H.A. Le Thi, P. Bouvry, and T. Pham Dinh (Eds.): MCO 2008, CCIS 14, pp. 59–68, 2008. c Springer-Verlag Berlin Heidelberg 2008
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of A Simulation Tool for Analyzing and Improving the Maternity Block Management

A Simulation Tool for Analyzing and Improvingthe Maternity Block Management
Michelle Chabrol1, Denis Gallot2, Michel Gourgand1, and Sophie Rodier1,2
1LIMOS UMR CNRS 6158, University of Blaise Pascal, Campus des Cezeaux,63000 Clermont-Ferrand, France
2University Hospital of Clermont-Ferrand, Bd Leon Malfreyt,63058 Clermont-Ferrand Cedex 1, France{chabrol,gourgand,rodier}@isima.fr,
{dgallot,srodier}@chu-clermontferrand.fr
Abstract. The pregnant women enter and leave hospitals 24 hours aday throughout the year. So, the designers of models have to considerthe day, the time and the method of arrival, the degrees of emergency,the alternative placement, and the staff availability. The discrete eventsimulation has been widely used in attempts to improve the delivery ofhealthcare. In this paper, the method used to develop a simulation toolfor a maternity block is described. This paper surveys the application ofdiscrete-event simulation modeling to healthcare systems and presentsthe decision-making aid tool designed for a maternity block in order toimprove their management. Future directions of research and applica-tions are also discussed. abstract environment.
Keywords: Modeling, simulation, healthcare, decision-making aid tool,maternity block.
1 Introduction
At the end of 2009, the “Hotel Dieu”, a unit of the University Hospital (UH) ofClermont-Ferrand will transfer its activities on a new site: the “Nouvel HopitalEstaing” (NHE). The UH managers have to reconsider the organization of thematernity block which will gather in a single place two obstetrics units nowdistinct: the “Maternity” and the “Polyclinic”. The maternity and the polyclinicof the “Hotel Dieu” are two separated obstetrics units in two different buildings.We define the maternity block as a hospital unit where the pregnant womenundergo a medical treatment before and after child birth.
The new obstetrical unit must provide health services for women, whichincludes the full range of the maternity care and the gynaecology care (onlyfor emergency examinations). The maternity service provides care for pregnantwomen in the antenatal, intrapartum and postnatal period.
The maternity unit has to respond to an uncertain demand from patients.Some demands can be treated within the maternity block, others are admit-ted to the hospital for further treatment as inpatients (complications). In this
H.A. Le Thi, P. Bouvry, and T. Pham Dinh (Eds.): MCO 2008, CCIS 14, pp. 59–68, 2008.c© Springer-Verlag Berlin Heidelberg 2008

60 M. Chabrol et al.
work, our main goals is to provide to the hospital managers and to the medicalteams, a decision-making aid tool which allows them to improve and optimizethe management of their new structure.
We have built a discrete-event simulation model to show visually and numer-ically the flow of patients through the maternity block on a typical week. Thesimulation shows the impact of variability in demand, and process capability.
We start by briefly describing the main simulation approaches used for thesetypes of model, namely discrete-event simulation. We propose our approach forthe design of decision-making aid tools, and we present the modeling tools used.Next, we present the decision-making aid tool designed for a maternity block.We conclude with a glimpse at the future.
2 Literature Survey
The literature survey on maternity blocks, except medical publications, is poor.This is partly due to the complexity of this system, which meet very different ac-tivities difficult to forecast (the emergency examinations, the delivery, the medi-cal termination of pregnancy, etc.). The maternity block includes different areas,different methods of operation, different asepsis levels and technicality levels (theexamination rooms, the operating rooms,. . . ), which involve somematerial andhu-man resources (doctors, midwives, anesthesiologist, operating room nurses, anaes-thetic nurses). Unlike a conventional surgical unit, the planned or “programmable”operations do not represent the majority of the activity, and emergencies quicklybecome vital for the patient, as for baby, requiring management and priority rulesvery specific. So, it appears necessary to model such systems to develop decision-making aid tools. A choice is to develop a simulation model, that represents all theoperations of an unit in sufficient detail for the experimentation of different sce-narii of organization and the test of several system loads. Computer or simulationmodels provide an insight into the working of a system and can be used to predictthe outcome of a change in strategy. This is particularly useful when the system isvery complex and/or when the experimentation is not possible. Several healthcareadministrators have used discrete-event simulation as an effective tool for allocat-ing scarce resources to improve patient flow, while minimising health care deliverycosts and increasing patient satisfaction
The potential benefit of the simulation of the health care systems is huge. Theliterature shows that with no doubt, the most widely used simulation approachin health is discrete-event simulation (DES). In DES, entities have character-istics which determine their pathway through the system, in exactly the sameway as patients have individual characteristics which determine their pathwaythrough the hospital system [1]. Model designers have to lead the effort to developmodels, by improving their understanding of health care needs and challenges(model designing) and communication of user-friendly models, to help provideanswers to the complex health care issues. In this work, Royston [2] studies thefuture challenges and opportunities in health care modeling and simulation andproposes to compare experiment and modeling (Tab. 1).

A Simulation Tool for Analyzing and Improving 61
Table 1. Experiment vs Modeling
Attribute Experiment Modeling and simulationVeracity Often high, within its do-
mainContingent on logic, ele-ments and data
Timescale Often long Can be quickCost Often high Can be lowRisk Can be high Generally low
Extendablity Limited High
Jun et al. [3] have surveyed an approximately 30 year period, from the early1960s to the late 1990s, applications of simulation in healthcare. They have re-viewed 117 journal articles and have classified them according to theirobjectives. Their main interest is the impact of patient and resource schedulingon patient and work flows, followed by the allocation of resources such as beds,rooms and staff. They also have searched for studies of more complex, integratedand multi-facility systems and have concluded that there seems to be a lack ofsuch work reported in the literature. They suggest that the major reasons for thisshortage are first, the level of complexity and the data needs. Wilson [4] has sur-veyed 200 simulation projects in healthcare but has found only 16 projects whichreported a successful implementation. Common factors in these 16 projects areat least one author who worked at the institution concerned, a problem of highpriority to that institution, an external funding, and/or a detailed description ofdata collection. Twenty years later, a systematic review of healthcare simulationmodels [5] has founded 182 papers published between 1980 and 1999. They haveidentified five broad topic areas: the hospital scheduling and organization, the in-fection and communicable disease, the costs of illness and the economic evaluation,the screening and the miscellaneous. We are interested in hospital scheduling andorganization area. This domain includes 94 (52 per cent) of the 182 papers in thereview. Patient scheduling and admissions policies were popular topics for mod-eling on many sytems : outpatient clinics [6], a walk-in clinic [7], an intensive careunit [8] and operating room scheduling [9] [10] [11]. Fone et al. note that very fewpapers reported that models had been implemented. The authors said “. . . we wereunable to reach any conclusions on the value of modeling in health care because theevidence of implementation was so scant.” ([5], p. 333) As Brailsford said [1], onepossible barrier to implementation is that of generalizability. All healthcare mod-elers stress the importance of working closely with clinical or managerial practi-tioners, in order to gain buy-in and acceptance.
3 Decision-Making Aid Tool Design: Approach and Tools
A simulation model is able to deal with detail complexity by simulating the lifehistories of individuals and then estimating the population effect from the sumof the individual effects. Each member of the population (entity) included in asimulation model is tracked through a set of options. At each decision point a

62 M. Chabrol et al.
variety of choices is available, and the outcome will depend on, for example, thecharacteristics of the entity and resources, the previous movement through themodel, and the choices that other entities have made.
The main dilemma in a such work is deciding on the appropriate level of detail.An increased detail leads to more realistic representation, which should increasethe confidence of stakeholders. However, an increased detail requires validateddata and it can be expensive and time-consuming to collect all the knowledge ofthe system.
The abstraction level for the simulation model depend of the modeling levelof the formal knowledge. Sinreich and Marmor [12] propose a figure with therange of modeling options and the building blocks used in each case. We adaptand complete it with the classic modeling level for the formalization of the systemknowledge (Fig. 1).
Hight abstraction level
Flexible: models any system and scenario
Difficult to use:Requires knowledge andexperience
Medium abstractionlevel
Flexible: models any system which uses a similar processSimple and intuitive:use friendly after a briefand shortintroduction
Low abstractionlevelDedicated : only models the system it wasdesigned forSimple: easyto use after aquickexplanation
GenericActivities Fixed Process/ ActivityGeneric
Processes
Macroscopic level
Global design, configuration and running
Mesoscopic level
Process design, configuration and running
Microscopic level
Activity design, configuration and running
Knowledge formalization
Simulation modelling
Fig. 1. Abstraction levels for the knowledge formalization and the simulation
The challenge is to develop models at medium abstraction levels, which bothconsider the system complexity and the ease of use. The main goal of our workis to provide for the maternity block teams, a decision-making aid tool:
– To confirm the physical structure size, to specify the staffing requirementsand to plan the resources (functions, allocation. . . ).
– To test and to compare management rules (resources allocation), to studythe system response to random events, to test different scenarii (schedules,load, etc.), to improve the service working.
– To estimate the system performances: indicators evaluation, waiting times,occupancy rates, identification of possible bottleneck.
A second goal is to provide coaching for change to the medical teams. Our workshould allow the maternity teams and the polyclinic teams to work together on theorganisation of the new obstetrical unit. Our approach consists in:
A Simulation Tool for Analyzing and Improving 63
– The data collection on the field (meetings with the executives of health,doctors and midwives).
– The identification of the processes (patient pathways), of the staff tasks ,and of the management rules.
– The modeling of the new maternity block.– The design of a decision-making aid tool based on a simulation model.
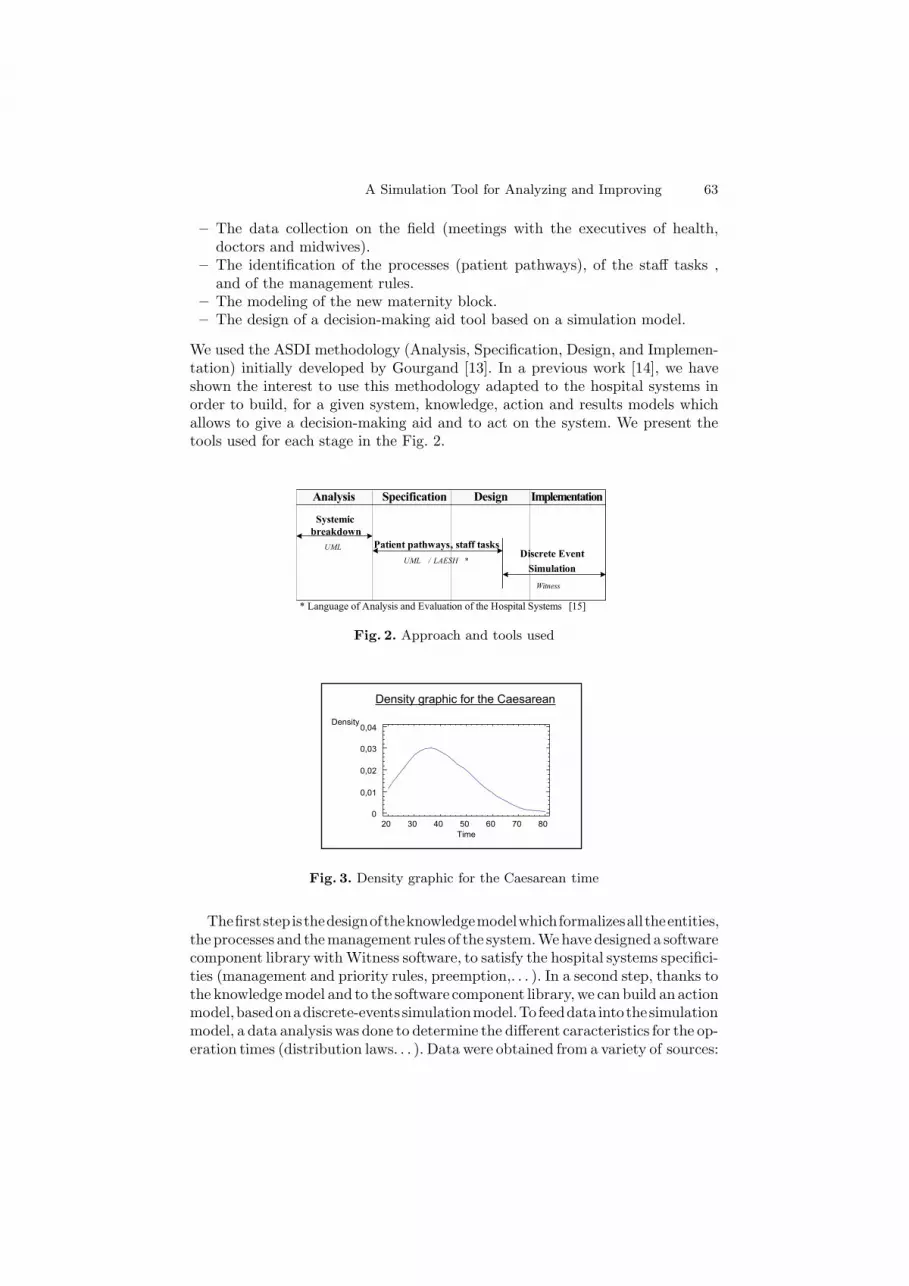
We used the ASDI methodology (Analysis, Specification, Design, and Implemen-tation) initially developed by Gourgand [13]. In a previous work [14], we haveshown the interest to use this methodology adapted to the hospital systems inorder to build, for a given system, knowledge, action and results models whichallows to give a decision-making aid and to act on the system. We present thetools used for each stage in the Fig. 2.
Analysis Specification Design Implementation
Systemic breakdown
UML Patient pathways, staff tasksUML / LAESH * Discrete Event
SimulationWitness
* Language of Analysis and Evaluation of the Hospital Systems [15]
Fig. 2. Approach and tools used
Density graphic for the Caesarean
20 30 40 50 60 70 80
Time
0
0,01
0,02
0,03
0,04Density
Fig. 3. Density graphic for the Caesarean time
Thefirststepisthedesignoftheknowledgemodelwhichformalizesall theentities,the processes and themanagement rules of the system.Wehave designed a softwarecomponent library with Witness software, to satisfy the hospital systems specifici-ties (management and priority rules, preemption,. . . ). In a second step, thanks tothe knowledgemodel and to the software component library,we can build an actionmodel,basedonadiscrete-events simulationmodel.To feeddata intothesimulationmodel, a data analysis was done to determine the different caracteristics for the op-eration times (distribution laws. . . ). Data were obtained from a variety of sources:
64 M. Chabrol et al.
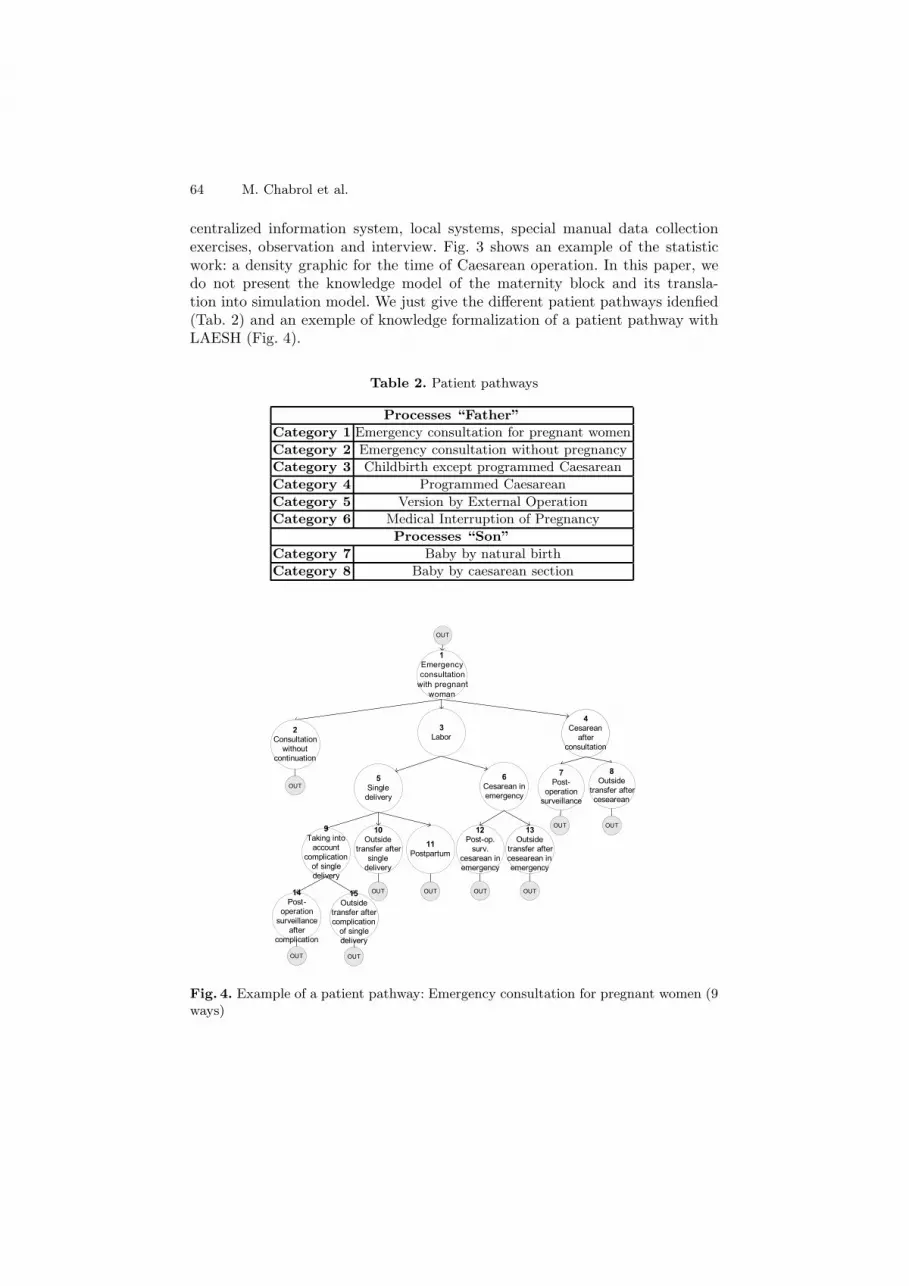
centralized information system, local systems, special manual data collectionexercises, observation and interview. Fig. 3 shows an example of the statisticwork: a density graphic for the time of Caesarean operation. In this paper, wedo not present the knowledge model of the maternity block and its transla-tion into simulation model. We just give the different patient pathways idenfied(Tab. 2) and an exemple of knowledge formalization of a patient pathway withLAESH (Fig. 4).
Table 2. Patient pathways
Processes “Father”Category 1 Emergency consultation for pregnant womenCategory 2 Emergency consultation without pregnancyCategory 3 Childbirth except programmed CaesareanCategory 4 Programmed CaesareanCategory 5 Version by External OperationCategory 6 Medical Interruption of Pregnancy
Processes “Son”Category 7 Baby by natural birthCategory 8 Baby by caesarean section
OUT
4Cesarean
after
consultation
3Labor
1Emergency
consultation
with pregnant
woman
13Outside
transfer after
cesearean in
emergency
14Post-
operation
surveillance
after
complication
15Outside
transfer after
complication
of single
delivery
10Outside
transfer after
single
delivery
9Taking into
account
complication
of single
delivery
12Post-op.
surv.
cesarean in
emergency
11Postpartum
6Cesarean in
emergency
8Outside
transfer after
cesearean
7Post-
operation
surveillance
5Single
delivery
OUT
OUT OUT
OUT OUT
OUT OUT
OUT
2Consultation
without
continuation
OUT
Fig. 4. Example of a patient pathway: Emergency consultation for pregnant women (9ways)

A Simulation Tool for Analyzing and Improving 65
4 Application: A Decision-Making Aid Tool for aMaternity Block
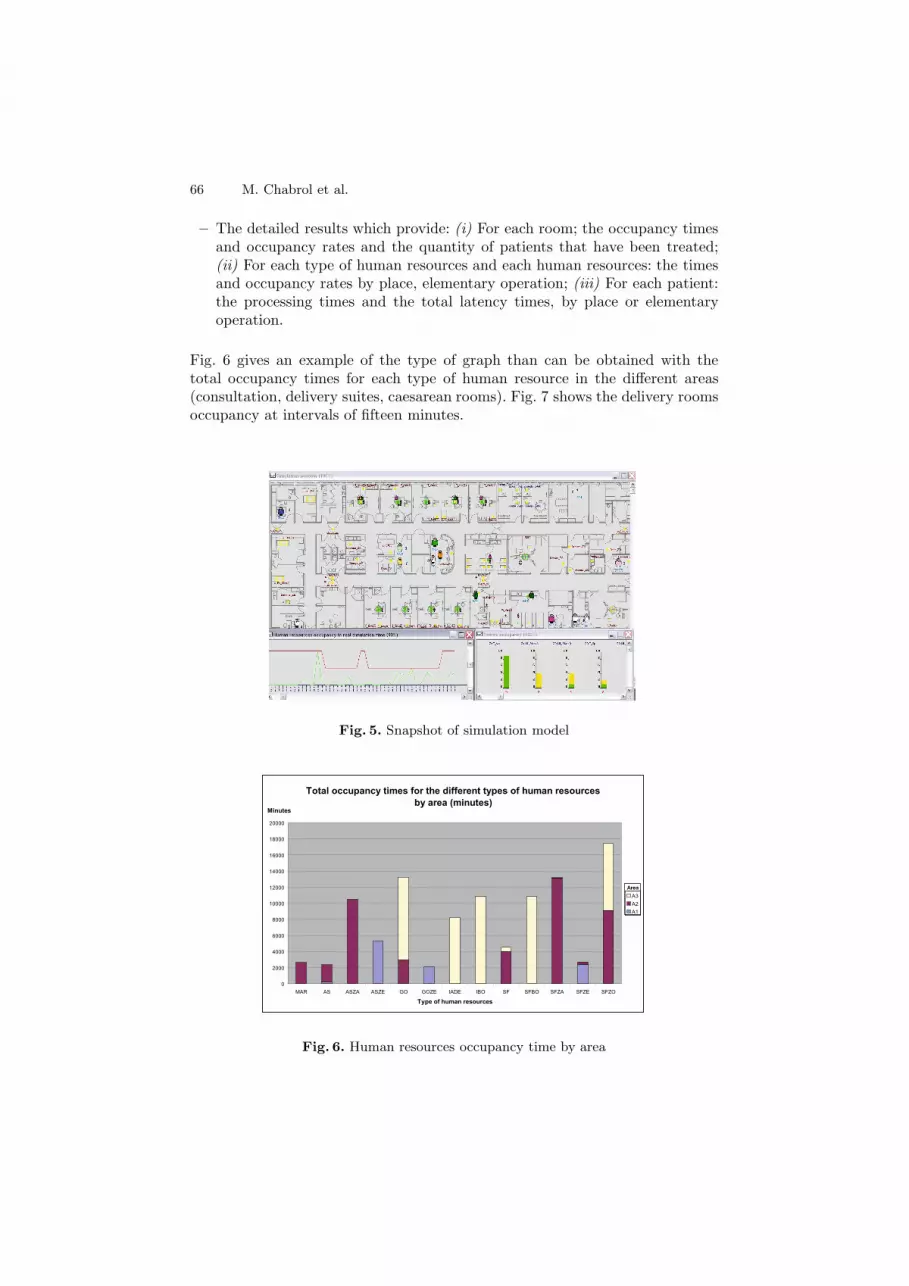
The primary objective in developing the simulation model is to provide a tool fordecision-making in the clinical environment. The simulation tool has to includeseveral modules in order to consider all the requirements described earlier. Thetool has to have a Graphical User Interface that is intuitive and simple to use.Through it, the user can input the system characteristics and the other requireddata and he can get back the different results.
A framework for the development of a generic processes model using thediscrete-event simulation and a visually interactive software (Witness) has beencreated. The framework allows users to input walk-in arrivals hourly, over a24-hour period, over a 7-day week in the Excel spreadsheet interfaces. It alsoallows the user to aim the arrivals through a number of different pathways (emer-gency consultation, programmed Caesarean. . . ) and to set resources within themodeled unit. Input variables of the decision-making aid tool are:
– The human resources with the various time slot of presence (schedules) andthe quantity of persons by time schedule/slot;
– The quantity of patients expected by week;– The patients distribution by “pathway”;– The patients arrival terms by “pathway” (programmed, emergency arrival
laws);– Several probabilities (complications, multiple births, etc.);– The times of elementary operations (constants, variables).
The interface can generate a patients arrival schedule based on the data andparameters captured (the quantity of patients and the distribution’s arrival law).This schedule can be reviewed by the user before running the simulation. Thesimulation’s duration has been set to one week. We have designed a graphicaluser interface. This graphical interface enables the user to visualize the model.As a communication aid with healthcare professionals, this can be invaluable tovalidate the model. During the simulation run, the users can see patients arrivingin real simulation time, observing monitor their travel through the different workareas as defined by their assigned pathways. The simulation also allows usersto see resource use and queue activity throughout the run. A snapshot of thesimulation model is shown in Fig. 5. The generic framework also facilitates thetesting of new scenarios. The resources can be changed and the outputs can becompared after re-running the model. Similarly, process times can be changedand the model re-run to assess impact. Furthermore, the generic framework couldbe used to assign other attributes to patients for modeling. The model was usedto produce detailed predictions of resource requirements for each scenario.
Two levels of results are obtained. Overall results:
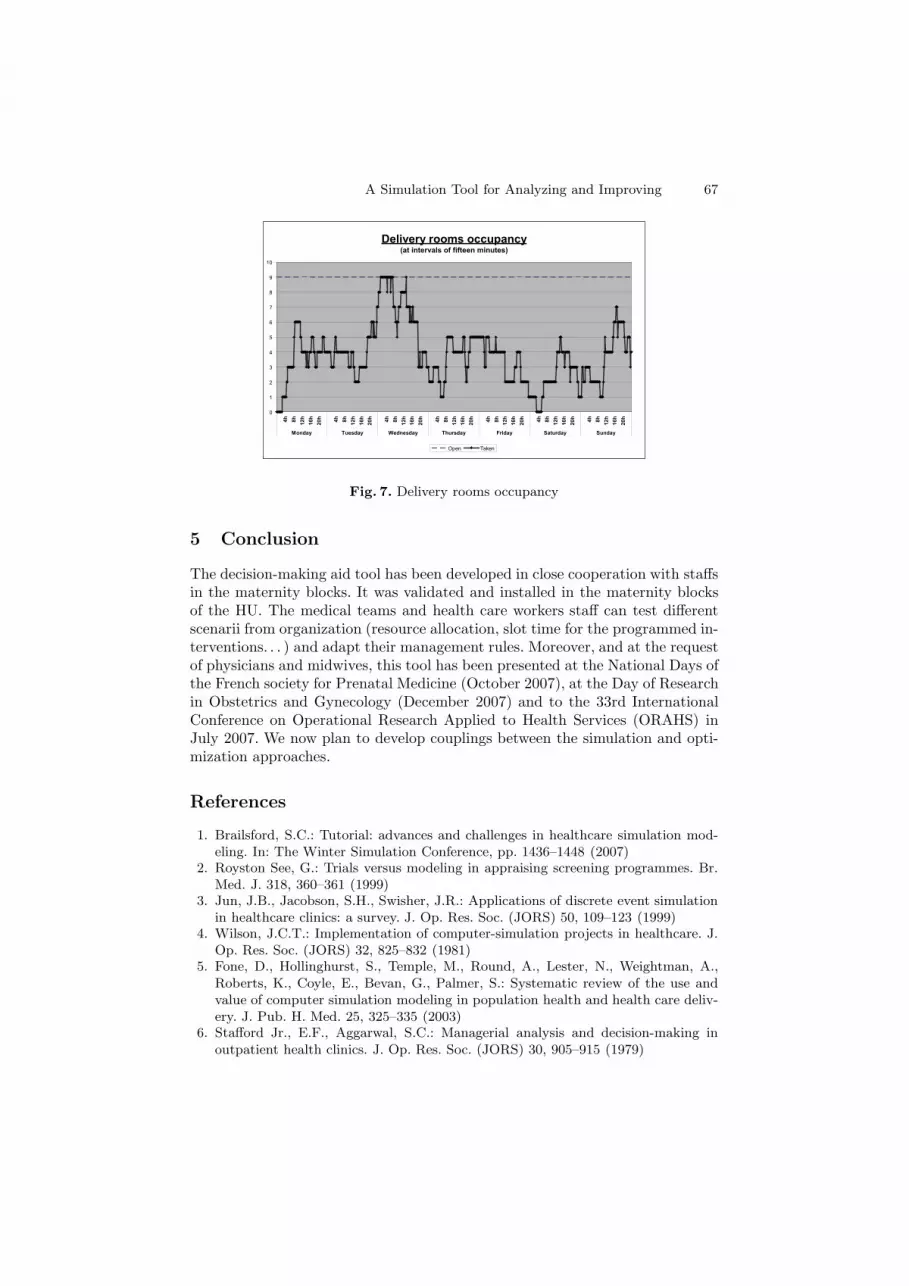
– The overall results: the passive resources (rooms) and active resourcesoccupancy (recorded every fifteen minutes), the total time spent in thesystem by each patient and the quantity of births of each type (naturalchildbirth and cesarean section).
66 M. Chabrol et al.
– The detailed results which provide: (i) For each room; the occupancy timesand occupancy rates and the quantity of patients that have been treated;(ii) For each type of human resources and each human resources: the timesand occupancy rates by place, elementary operation; (iii) For each patient:the processing times and the total latency times, by place or elementaryoperation.
Fig. 6 gives an example of the type of graph than can be obtained with thetotal occupancy times for each type of human resource in the different areas(consultation, delivery suites, caesarean rooms). Fig. 7 shows the delivery roomsoccupancy at intervals of fifteen minutes.
Fig. 5. Snapshot of simulation model
Total occupancy times for the different types of human resourcesby area (minutes)
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
20000
MAR AS ASZA ASZE GO GOZE IADE IBO SF SFBO SFZA SFZE SFZO
Type of human resources
A3
A2
A1
Area
Minutes
Fig. 6. Human resources occupancy time by area
A Simulation Tool for Analyzing and Improving 67
Delivery rooms occupancy(at intervals of fifteen minutes)
0
1
2
3
4
5
6
7
8
9
10
4h 8h 12h
16h
20h 4h 8h 12h
16h
20h 4h 8h 12h
16h
20h 4h 8h 12h
16h
20h 4h 8h 12h
16h
20h 4h 8h 12h
16h
20h 4h 8h 12h
16h
20h
Monday Tuesday Wednesday Thursday Friday Saturday Sunday
Open Taken
Fig. 7. Delivery rooms occupancy
5 Conclusion
The decision-making aid tool has been developed in close cooperation with staffsin the maternity blocks. It was validated and installed in the maternity blocksof the HU. The medical teams and health care workers staff can test differentscenarii from organization (resource allocation, slot time for the programmed in-terventions. . . ) and adapt their management rules. Moreover, and at the requestof physicians and midwives, this tool has been presented at the National Days ofthe French society for Prenatal Medicine (October 2007), at the Day of Researchin Obstetrics and Gynecology (December 2007) and to the 33rd InternationalConference on Operational Research Applied to Health Services (ORAHS) inJuly 2007. We now plan to develop couplings between the simulation and opti-mization approaches.
References
1. Brailsford, S.C.: Tutorial: advances and challenges in healthcare simulation mod-eling. In: The Winter Simulation Conference, pp. 1436–1448 (2007)
2. Royston See, G.: Trials versus modeling in appraising screening programmes. Br.Med. J. 318, 360–361 (1999)
3. Jun, J.B., Jacobson, S.H., Swisher, J.R.: Applications of discrete event simulationin healthcare clinics: a survey. J. Op. Res. Soc. (JORS) 50, 109–123 (1999)
4. Wilson, J.C.T.: Implementation of computer-simulation projects in healthcare. J.Op. Res. Soc. (JORS) 32, 825–832 (1981)
5. Fone, D., Hollinghurst, S., Temple, M., Round, A., Lester, N., Weightman, A.,Roberts, K., Coyle, E., Bevan, G., Palmer, S.: Systematic review of the use andvalue of computer simulation modeling in population health and health care deliv-ery. J. Pub. H. Med. 25, 325–335 (2003)
6. Stafford Jr., E.F., Aggarwal, S.C.: Managerial analysis and decision-making inoutpatient health clinics. J. Op. Res. Soc. (JORS) 30, 905–915 (1979)

68 M. Chabrol et al.
7. Reilly, T.A., Marathe, V.P., Fries, B.E.: A delay-scheduling model for patientsusing a walk-in clinic. J. Med. Syst. 2, 303–313 (1978)
8. Kim, S.-C., Horowitz, I., Young, K.K., Buckley, T.A.: Analysis of capacity man-agement of the intensive care unit in a hospital. Eur. J. Op. Res. (EJOR) 115,36–46 (1999)
9. Dexter, F., Macario, A., Traub, R.D., Hopwood, M., Lubarsky, D.A.: An operat-ing room scheduling strategy to maximize the use of operating room block time:computer simulation of patient scheduling and survey of patients’ preferences forsurgical waiting time. Anesthesia and analgesia 89, 7–20 (1999)
10. Fitzpatrick, K.E., Baker, J.R., Dave, D.S.: An application of computer simulationto improve scheduling of hospital operating room facilities in the United States.Int. J. Comp. App. Teh. 6, 214–224 (1993)
11. Ballard, S.M., Kuhl, M.E.: The use of simulation to determine maximum capacityin the surgical suite operating room. In: The Winter Simulation Conference, pp.433–438 (2006)
12. Sinreich, Marmor: A simple and intuitive simulation tool for analyzing emergencydepartment operations. In: The Winter Simulation Conference, pp. 1994–2002(2004)
13. Gourgand, M.: Outils logiciels pour l’evaluation des performances des systemesinformatiques. Doctorat d’Etat, University of Blaise Pascal, Clermont-Ferrand,France (1984)
14. Chabrol, M., Fenies, P., Gourgand, M., Tchernev, N.: Un environnement demodelisation pour la Supply Chain Hospitaliere: application sur le. Nouvel Hopitald’Estaing. Ingenierie des Systemes d’Information 11, 137–162 (2006)
15. Chabrol, M., Gourgand, M., Rodier, S.: A modeling methodology and its applica-tion to the design of decision-making aid tools for the hospital systems. In: IEEEInternational Conference on Research Challenges in Information Science (2008)