
A retrospective non-randomized study on the impact of INTEGUSEAL, a preoperative microbial skin...
6
A retrospective non-randomized study on the impact of INTEGUSEAL, a preoperative microbial skin sealant, on the rate of surgical site infections after cardiac surgery Pascal M. Dohmen a, *, Davide Gabbieri a , Alexander Weymann a , Jo ¨ rg Linneweber a , Torsten Geyer b , Wolfgang Konertz a a Department of Cardiovascular Surgery, Charite ´ Hospital, Medical University Berlin, Chariteplatz 1, D-10117 Berlin, Germany b Department of Anesthesiology, Charite ´ Hospital, Medical University Berlin, Berlin, Germany 1. Introduction The incidence of sternal surgical site infection (SSI) reported in the literature varies from 2% to 20%, with severe deep sternal wound infection occurring in up to 8% of patients in some reported series. 1–6 Such infections remain a substantial cause of morbidity and mortality. A number of preventive measures have been adopted to reduce the risk of SSI, including improvements in patient and skin preparation, hand hygiene, antibiotic prophylaxis, operative room management, asepsis and surgical technique, and postoperative incision care. 7 However, as it is impossible to completely decontaminate the patient’s skin, the risk of wound contamination and subsequent SSI is always present during surgery, even under optimal conditions. Microbial skin sealant INTEGUSEAL is an innovative approach to reducing the risk of contamination of the surgical wound by skin flora throughout the surgical procedure. When applied to the skin as a liquid during preoperative skin preparation, moisture and proteins present in the stratum corneum trigger polymerization of the n-butyl cyanoacrylate. During this process, the compound bonds to the skin to form a barrier that immobilizes the bacteria surviving the application of antimicrobial skin preparations before surgery. The skin sealant wears off gradually as skin exfoliates over the following 3–7 days. Towfigh et al. were able to show the advantages of this microbial skin sealant in a prospective, randomized, multicenter clinical trial of patients undergoing an open inguinal hernia repair. 8 The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were used to improve the quality of this trial. 9 This study was performed to evaluate the impact of a cyanoacrylate microbial skin sealant to extend preventive measures to reduce SSI in cardiac surgery. International Journal of Infectious Diseases 15 (2011) e395–e400 ARTICLE INFO Article history: Received 24 August 2010 Received in revised form 14 January 2011 Accepted 8 February 2011 Corresponding Editor: William Cameron, Ottawa, Canada Keywords: Surgical site infection Cardiac surgery Coronary artery bypass graft Microbial skin sealant Infection prevention SUMMARY Objective: Surgical site infection (SSI) remains a serious potential complication after cardiac surgery. This study evaluated the impact of a cyanoacrylate microbial skin sealant (INTEGUSEAL) on the rate of SSI in cardiac surgery patients. Methods: Between January 2006 and July 2008, 580 patients underwent cardiac surgery by a single surgeon (PMD). Standard preoperative skin preparation was performed in 280 patients (control group), and 300 patients (microbial skin sealant group) received microbial skin sealant in addition to standard preoperative preparation. Patient characteristics and preoperative and combined pre/intraoperative risk scores were evaluated. The primary study endpoint was freedom from SSI within 30 days. Results: Both groups were established in a 15-month period. Carotid artery disease, diabetes mellitus, congestive heart failure, previous cardiac surgery, and bilateral internal mammary artery use were significantly more common in the skin sealant group. Preoperative risk scores for the development of SSI in the two groups were similar. In the skin sealant group, the combined operative risk score for SSI was significantly higher (9.8 Æ 4.0 vs. 8.7 Æ 3.7; p < 0.001) nevertheless the incidence of SSI was significantly lower (2.3% vs. 6.8%; p = 0.011) than in the control group. Conclusion: Changing a surgeon’s standard preoperative practice by including a microbial skin sealant pretreatment significantly reduced the rate of SSI. ß 2011 International Society for Infectious Diseases. Published by Elsevier Ltd. All rights reserved. * Corresponding author. Present address: Oberarzt Herzchirurgie, Herzzentrum Leipzig, Universita ¨ t Leipzig, Struempellstr. 39, D-04289 Leipzig, Germany. Tel.: +49 341 865 251001. E-mail address: [email protected] (P.M. Dohmen). Contents lists available at ScienceDirect International Journal of Infectious Diseases journal homepage: www.elsevier.com/locate/ijid 1201-9712/$36.00 – see front matter ß 2011 International Society for Infectious Diseases. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.ijid.2011.02.004
-
Upload
uni-heidelberg -
Category
Documents
-
view
1 -
download
0
Transcript of A retrospective non-randomized study on the impact of INTEGUSEAL, a preoperative microbial skin...

International Journal of Infectious Diseases 15 (2011) e395–e400
A retrospective non-randomized study on the impact of INTEGUSEAL, apreoperative microbial skin sealant, on the rate of surgical site infectionsafter cardiac surgery
Pascal M. Dohmen a,*, Davide Gabbieri a, Alexander Weymann a, Jorg Linneweber a,Torsten Geyer b, Wolfgang Konertz a
a Department of Cardiovascular Surgery, Charite Hospital, Medical University Berlin, Chariteplatz 1, D-10117 Berlin, Germanyb Department of Anesthesiology, Charite Hospital, Medical University Berlin, Berlin, Germany
A R T I C L E I N F O
Article history:
Received 24 August 2010
Received in revised form 14 January 2011
Accepted 8 February 2011
Corresponding Editor: William Cameron,
Ottawa, Canada
Keywords:
Surgical site infection
Cardiac surgery
Coronary artery bypass graft
Microbial skin sealant
Infection prevention
S U M M A R Y
Objective: Surgical site infection (SSI) remains a serious potential complication after cardiac surgery. This
study evaluated the impact of a cyanoacrylate microbial skin sealant (INTEGUSEAL) on the rate of SSI in
cardiac surgery patients.
Methods: Between January 2006 and July 2008, 580 patients underwent cardiac surgery by a single
surgeon (PMD). Standard preoperative skin preparation was performed in 280 patients (control group),
and 300 patients (microbial skin sealant group) received microbial skin sealant in addition to standard
preoperative preparation. Patient characteristics and preoperative and combined pre/intraoperative risk
scores were evaluated. The primary study endpoint was freedom from SSI within 30 days.
Results: Both groups were established in a 15-month period. Carotid artery disease, diabetes mellitus,
congestive heart failure, previous cardiac surgery, and bilateral internal mammary artery use were
significantly more common in the skin sealant group. Preoperative risk scores for the development of SSI
in the two groups were similar. In the skin sealant group, the combined operative risk score for SSI was
significantly higher (9.8 � 4.0 vs. 8.7 � 3.7; p < 0.001) nevertheless the incidence of SSI was significantly
lower (2.3% vs. 6.8%; p = 0.011) than in the control group.
Conclusion: Changing a surgeon’s standard preoperative practice by including a microbial skin sealant
pretreatment significantly reduced the rate of SSI.
� 2011 International Society for Infectious Diseases. Published by Elsevier Ltd. All rights reserved.
Contents lists available at ScienceDirect
International Journal of Infectious Diseases
journa l homepage: www.e lsev ier .com/ locate / i j id
1. Introduction
The incidence of sternal surgical site infection (SSI) reported inthe literature varies from 2% to 20%, with severe deep sternalwound infection occurring in up to 8% of patients in some reportedseries.1–6 Such infections remain a substantial cause of morbidityand mortality. A number of preventive measures have beenadopted to reduce the risk of SSI, including improvements inpatient and skin preparation, hand hygiene, antibiotic prophylaxis,operative room management, asepsis and surgical technique, andpostoperative incision care.7 However, as it is impossible tocompletely decontaminate the patient’s skin, the risk of woundcontamination and subsequent SSI is always present duringsurgery, even under optimal conditions.
* Corresponding author. Present address: Oberarzt Herzchirurgie, Herzzentrum
Leipzig, Universitat Leipzig, Struempellstr. 39, D-04289 Leipzig, Germany.
Tel.: +49 341 865 251001.
E-mail address: [email protected] (P.M. Dohmen).
1201-9712/$36.00 – see front matter � 2011 International Society for Infectious Disea
doi:10.1016/j.ijid.2011.02.004
Microbial skin sealant INTEGUSEAL is an innovative approach toreducing the risk of contamination of the surgical wound by skinflora throughout the surgical procedure. When applied to the skinas a liquid during preoperative skin preparation, moisture andproteins present in the stratum corneum trigger polymerization ofthe n-butyl cyanoacrylate. During this process, the compoundbonds to the skin to form a barrier that immobilizes the bacteriasurviving the application of antimicrobial skin preparations beforesurgery. The skin sealant wears off gradually as skin exfoliates overthe following 3–7 days.
Towfigh et al. were able to show the advantages of this microbialskin sealant in a prospective, randomized, multicenter clinical trialof patients undergoing an open inguinal hernia repair.8
The Strengthening the Reporting of Observational Studies inEpidemiology (STROBE) guidelines were used to improve thequality of this trial.9
This study was performed to evaluate the impact of acyanoacrylate microbial skin sealant to extend preventivemeasures to reduce SSI in cardiac surgery.
ses. Published by Elsevier Ltd. All rights reserved.

P.M. Dohmen et al. / International Journal of Infectious Diseases 15 (2011) e395–e400e396
2. Patients and methods
This before/after trial included 580 adult hospitalized patientsundergoing cardiac surgery by a single surgeon (PMD) at theDepartment of Cardiovascular Surgery, Charite Hospital, Berlinbetween January 2006 and July 2008. The study populationincluded all adult patients of this single surgeon undergoingcardiac surgery in which cardiopulmonary bypass (CPB) wasneeded. Patients operated on without using CPB were excluded.Operative techniques with regard to CPB, cardioplegia, reperfusion,and anesthesia (hemodynamics, oxygenation, glucose control andtemperature control), as well as postoperative care, were similar inall patients. All patients received standard institutional preopera-tive care, and 300 patients (skin sealant group) received amicrobial skin sealant (INTEGUSEAL Microbial Sealant, Kim-berly-Clark Corp.; http://www.kchealthcare.com) in addition tothe standard preoperative care. The 280 patients who did notreceive the microbial skin sealant comprised the control group.Each group was established within a period of 15 months toinvestigate the influence of the additional use of a new microbialskin sealant to reduce SSI after cardiac surgery. This period of timewas chosen in order to be able to include an adequate number ofpatients for statistical analysis.
Nosocomial infections were registered and all complicationsduring follow-up were recorded in the German NosocomialInfection Surveillance System (Krankenhaus Infektions Surveil-lance System, KISS).10 Participation in the surveillance system wasapproved by the Institutional Board on the Ethics of ClinicalStudies. Data were de-identified and grouped according todemographics including patient characteristics, operative data,postoperative data, and postoperative complications.
2.1. Risk factors
For each patient, data for the following variables werecollected: age, gender, body mass index (BMI), arterial hyperten-sion, hyperlipidemia, chronic obstructive pulmonary disease(COPD), diabetes mellitus, peripheral vessel disease, carotid arterydisease, cerebral vascular accident, chronic renal failure, ejectionfraction, congestive heart failure, acute myocardial infarct within 1month, previous bypass surgery, and previous valve surgery.
Priority of the surgical procedure was defined as ‘emergency’when surgery was performed immediately, ‘urgent’ when per-formed within 24 h, and ‘elective’ in all other cases. Cardiacprocedures were defined as single coronary artery bypass graft(CABG), single valve surgery, concomitant procedures, and others.The intraoperative variables included number of anastomoses, useof left internal mammary arteries, use of bilateral internalmammary arteries, duration of CPB, and insertion of an intra-aortic balloon pump.
2.2. Preoperative treatment
Preoperative preparation was standardized as previouslyreported.11 In brief, for patients undergoing elective or urgentsurgery, hair removal was performed by depilatory cream (stablepatients) or clippers (unstable patients) in the afternoon of the daybefore surgery. Furthermore stable patients underwent showeringafter shaving, as well as on the morning of surgery. In all of thepatients, soap was used. For patients undergoing emergencysurgery, hair was removed using clippers immediately prior tosurgery. Following hair removal, the skin was disinfected using 1%povidone–iodine in 70% alcohol. Care was taken to allow thedisinfecting solution to dry completely before application ofthe microbial skin sealant. In all patients iodine impregnateddrapes were used, except for those allergic to iodine. Antibiotic
prophylaxis consisted of cefuroxime (before incision and 1.5 gintravenous every 6 h for two subsequent doses).
2.3. Microbial skin sealant
The skin sealant was applied after preoperative skin prepara-tion had been completed and 5–10 min before surgery com-menced. The INTEGUSEAL IS100 applicator was used to apply asingle even layer of skin sealant over an area of approximately50 � 25 cm around the sternal incision mark, which was allowedto dry completely before iodine impregnated drapes werepositioned. In all patients who received this pretreatment, themicrobial skin sealant was used only on the chest incision site andit was not applied at the saphenous or radial donor sites in casesundergoing a CABG procedure.
2.4. Intraoperative management
Intraoperative management was performed as previouslypublished.12 Optimal temperature was maintained in each patientduring and after surgery. Glycemic control was monitored in allpatients and, if needed, insulin was administered intermittently orcontinuously by intravenous infusion if necessary. This interven-tion was performed in diabetic as well as non-diabetic patients.Optimal oxygenation to avoid hypoxia was achieved by performingblood gas analysis during and after surgery.
2.5. SSI risk stratification
Patients were evaluated by the preoperative and combined pre/intraoperative risk scoring system described by Fowler et al.13 Thepredicted risk for development of SSI in the two groups of patientswas calculated and compared.
2.6. Bacteriology
Screening for methicillin-resistant Staphylococcus aureus
(MRSA) was performed in all patients. Nasal, pharyngeal, andinguinal areas were swabbed on the day of admission to hospitaland any strains of S. aureus isolated from swab cultures were testedfor antibiotic susceptibility. For MRSA-positive patients with stableangina, surgery was delayed while patients received intranasalmupirocin therapy, daily chlorhexidine showers and, for thosewith MRSA-positive throat swabs, topical application of chlorhex-idine 0.2% for 3 days.
Generally, in cases with overt SSI, microbiological samples weretaken from the wound and cultured. In cases with a clinicalsuspicion of deep SSI, blood cultures were also taken. Samples werecultured and organisms identified using standard microbiologicaltechniques.
2.7. Clinical endpoint
The study endpoint was freedom from superficial or deep SSI asdefined by the Centers for Disease Control and PreventionNational Nosocomial Infections Surveillance criteria.14 SuperficialSSI was defined as superficial infection of the surgical site treatedwith or without vacuum-assisted closure (VAC) therapy withclosed sternum before discharge and/or readmission within30 days of surgery. Infection was documented by at least one ofthe following: (1) surgical opening of the sternal wound withexcision of tissue (incision and drainage) and application of VACtherapy; (2) positive bacterial culture(s); or (3) treatment withantibiotics. Deep SSI was defined as infection of the surgical sitetreated with VAC therapy before discharge and/or readmissionwithin 30 days of surgery.
P.M. Dohmen et al. / International Journal of Infectious Diseases 15 (2011) e395–e400 e397
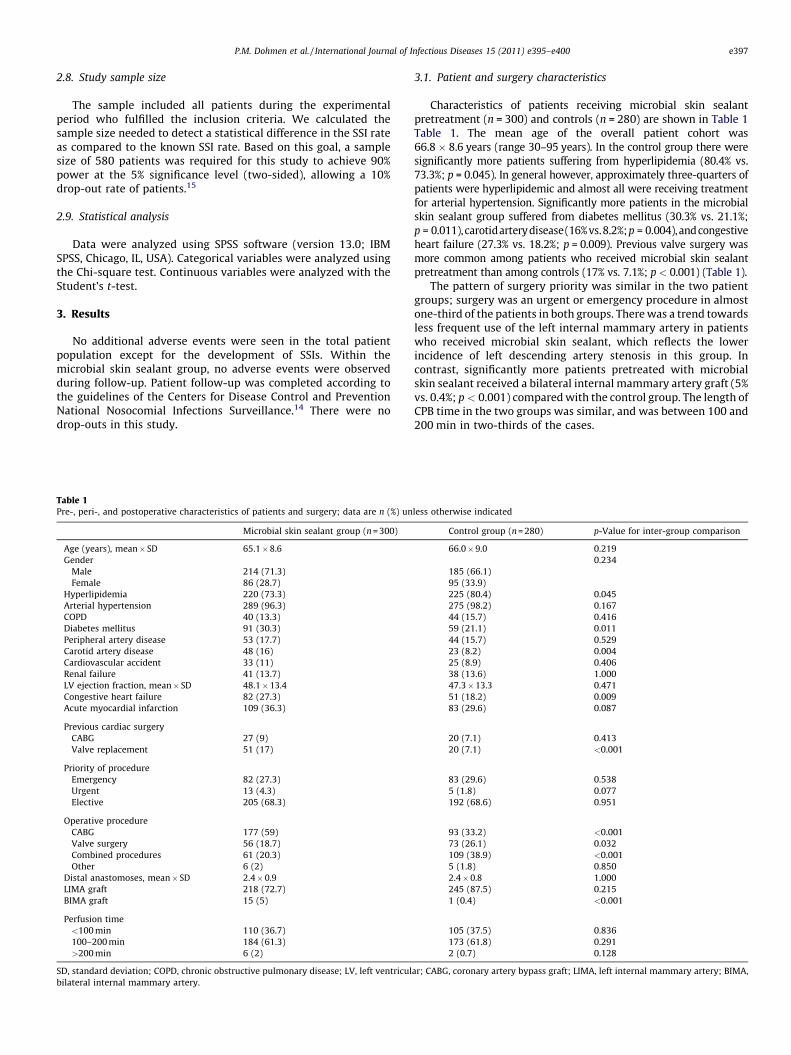
2.8. Study sample size
The sample included all patients during the experimentalperiod who fulfilled the inclusion criteria. We calculated thesample size needed to detect a statistical difference in the SSI rateas compared to the known SSI rate. Based on this goal, a samplesize of 580 patients was required for this study to achieve 90%power at the 5% significance level (two-sided), allowing a 10%drop-out rate of patients.15
2.9. Statistical analysis
Data were analyzed using SPSS software (version 13.0; IBMSPSS, Chicago, IL, USA). Categorical variables were analyzed usingthe Chi-square test. Continuous variables were analyzed with theStudent’s t-test.
3. Results
No additional adverse events were seen in the total patientpopulation except for the development of SSIs. Within themicrobial skin sealant group, no adverse events were observedduring follow-up. Patient follow-up was completed according tothe guidelines of the Centers for Disease Control and PreventionNational Nosocomial Infections Surveillance.14 There were nodrop-outs in this study.
Table 1Pre-, peri-, and postoperative characteristics of patients and surgery; data are n (%) un
Microbial skin sealant group (n = 300)
Age (years), mean� SD 65.1�8.6
Gender
Male 214 (71.3)
Female 86 (28.7)
Hyperlipidemia 220 (73.3)
Arterial hypertension 289 (96.3)
COPD 40 (13.3)
Diabetes mellitus 91 (30.3)
Peripheral artery disease 53 (17.7)
Carotid artery disease 48 (16)
Cardiovascular accident 33 (11)
Renal failure 41 (13.7)
LV ejection fraction, mean� SD 48.1�13.4
Congestive heart failure 82 (27.3)
Acute myocardial infarction 109 (36.3)
Previous cardiac surgery
CABG 27 (9)
Valve replacement 51 (17)
Priority of procedure
Emergency 82 (27.3)
Urgent 13 (4.3)
Elective 205 (68.3)
Operative procedure
CABG 177 (59)
Valve surgery 56 (18.7)
Combined procedures 61 (20.3)
Other 6 (2)
Distal anastomoses, mean� SD 2.4� 0.9
LIMA graft 218 (72.7)
BIMA graft 15 (5)
Perfusion time
<100 min 110 (36.7)
100–200 min 184 (61.3)
>200 min 6 (2)
SD, standard deviation; COPD, chronic obstructive pulmonary disease; LV, left ventricul
bilateral internal mammary artery.
3.1. Patient and surgery characteristics
Characteristics of patients receiving microbial skin sealantpretreatment (n = 300) and controls (n = 280) are shown in Table 1Table 1. The mean age of the overall patient cohort was66.8� 8.6 years (range 30–95 years). In the control group there weresignificantly more patients suffering from hyperlipidemia (80.4% vs.73.3%; p = 0.045). In general however, approximately three-quarters ofpatients were hyperlipidemic and almost all were receiving treatmentfor arterial hypertension. Significantly more patients in the microbialskin sealant group suffered from diabetes mellitus (30.3% vs. 21.1%;p = 0.011),carotidarterydisease(16%vs.8.2%;p = 0.004), and congestiveheart failure (27.3% vs. 18.2%; p = 0.009). Previous valve surgery wasmore common among patients who received microbial skin sealantpretreatment than among controls (17% vs. 7.1%; p < 0.001) (Table 1).
The pattern of surgery priority was similar in the two patientgroups; surgery was an urgent or emergency procedure in almostone-third of the patients in both groups. There was a trend towardsless frequent use of the left internal mammary artery in patientswho received microbial skin sealant, which reflects the lowerincidence of left descending artery stenosis in this group. Incontrast, significantly more patients pretreated with microbialskin sealant received a bilateral internal mammary artery graft (5%vs. 0.4%; p < 0.001) compared with the control group. The length ofCPB time in the two groups was similar, and was between 100 and200 min in two-thirds of the cases.
less otherwise indicated
Control group (n = 280) p-Value for inter-group comparison
66.0�9.0 0.219
0.234
185 (66.1)
95 (33.9)
225 (80.4) 0.045
275 (98.2) 0.167
44 (15.7) 0.416
59 (21.1) 0.011
44 (15.7) 0.529
23 (8.2) 0.004
25 (8.9) 0.406
38 (13.6) 1.000
47.3�13.3 0.471
51 (18.2) 0.009
83 (29.6) 0.087
20 (7.1) 0.413
20 (7.1) <0.001
83 (29.6) 0.538
5 (1.8) 0.077
192 (68.6) 0.951
93 (33.2) <0.001
73 (26.1) 0.032
109 (38.9) <0.001
5 (1.8) 0.850
2.4�0.8 1.000
245 (87.5) 0.215
1 (0.4) <0.001
105 (37.5) 0.836
173 (61.8) 0.291
2 (0.7) 0.128
ar; CABG, coronary artery bypass graft; LIMA, left internal mammary artery; BIMA,

[(Figure_1)TD$FIG]
Figure 1. Incidence of surgical site infection (SSI) in patients undergoing cardiac
surgery who were treated with microbial skin sealant as part of preoperative skin
preparation and patients who received only standard preoperative preparation
(controls). The incidence of SSI was significantly lower in the microbial skin sealant
group than in the control group (2.3% vs. 6.8%, p = 0.011).
P.M. Dohmen et al. / International Journal of Infectious Diseases 15 (2011) e395–e400e398
3.2. SSI risk stratification
The preoperative risk score for SSI was 11.0 � 4.5 for themicrobial skin sealant group and 10.6 � 4.7 for the control group(p = 0.293). The risk scores for SSI according to combined preopera-tive–intraoperative factors were 9.8 � 4.0 and 8.6 � 3.7, respectively(p < 0.001). The associated predicted risks for SSI were 3.5%(preoperative) and 3.2% (combined) for the microbial skin sealantgroup and 3.0% (preoperative) and 2.6% (combined) for the controlgroup.
3.3. Incidence of SSI
At the end of the study, SSI was recorded for 26 patients. Thosewith SSI included seven patients in the microbial skin sealantgroup (2.3%; one with superficial SSI and six with deep SSIs) and 19patients in the control group (6.8%; 15 superficial SSIs and fourdeep SSIs). The inclusion of skin sealant in preoperative prepara-tions resulted in a statistically significant reduction in SSI(p = 0.011) (Figure 1 Figure 1). Moreover, there was a 34% relativerisk reduction in SSIs observed in the microbial skin sealant groupcompared with the SSI rate predicted by preoperative risk factors(2.3% vs. 3.5%).
3.4. Bacteriology
All patients included in this study were free of MRSA duringscreening. Among the 26 patients suffering from SSIs, wound
Table 2Isolated pathogens; data are n unless otherwise indicated
Microbial skin
sealant group
(n = 300)
Control group
(n = 280)
Methicillin-susceptible
Staphylococcus aureus
1 1
Methicillin-resistant
Staphylococcus aureus
2 1
Coagulase-negative Staphylococcus 1 5
Pseudomonas aeruginosa 2
Enterococcus faecalis 2
Klebsiella pneumoniae 1 1
Enterobacter cloacae 1
cultures were positive in 18 cases (69.2%; Table 2). The mostcommonly isolated pathogen was S. aureus, which caused five(27.8%) of the microbiologically confirmed SSIs, including threecases of MRSA. Other organisms obtained from sternal site samplesincluded Staphylococcus epidermidis (n = 6), Klebsiella pneumoniae
(n = 2), Enterococcus faecalis (n = 2), Pseudomonas aeruginosa
(n = 2), and Enterobacter cloacae (n = 1). The majority of patients(61.1%) had a polymicrobial infection, and a monomicrobialinfection was seen in only seven of the 18 patients (38.9%) withpositive wound cultures. Blood cultures were positive in 13 of the26 patients (50%) with SSI. All except one of those patients in themicrobial skin sealant group with SSI had positive blood culturesand in three of these six patients (50%) positive blood cultures werefound prior to microbiological confirmation of sternal siteinfection. In the control group, blood cultures were positive forseven of the 12 patients (58.3%) with positive sternal site samples.
4. Discussion
Median sternotomy has become established as the standardapproach for most open cardiac surgery procedures since thetechnique was introduced by Julian et al. in 1957.16 SSI is still aserious potential complication of sternotomy that, with highassociated morbidity and mortality, leads to prolonged hospitali-zation, repeated surgical procedures, and increased healthcarecosts.17–19 The development of a sternal SSI is a multifactorialprocess. Numerous studies have identified a multitude of clinicaland perioperative variables as being contributory. A comparison ofrates of infection at the sternal site after cardiac surgery reported inthe literature is therefore difficult, as different studies haveincluded patients with different characteristics undergoing sur-gery involving different specific procedures. However, largestudies are helpful to analyze risk factors. For example, in amultivariate logistic regression analysis of more than 9000consecutive adult patients undergoing full sternotomy, Gummertet al.20 showed that the presence of diabetes, use of single orbilateral internal mammary artery graft(s), intensive care unit stayof more than 5 days, re-exploration, and BMI >30 kg/m2,significantly increased the risk of a deep SSI. Old age and thepresence of COPD and renal failure are also established risk factorsfor SSI.21–24
In this study, patients in the two treatment groups were ofsimilar mean age, and similar proportions of patients in each groupwere suffering from COPD and renal failure. In contrast, asignificantly higher proportion of patients in the skin sealantgroup than in the control group had diabetes mellitus (30.3% vs.21.1%; p < 0.011), and both internal mammary arteries were usedin significantly more patients in the skin sealant group comparedwith the control group (5% vs. 0.4%; p < 0.001). Such inter-groupdifferences in important risk factors for SSI suggest that one groupmight be at higher risk than the other. We therefore evaluated riskfactors and calculated the predicted rate of SSI of both groups usingthe risk stratification system of Fowler et al.13 According to pre-operative risk scores, both patient groups were at similar risk ofdeveloping SSI. The combined risk score based on pre- andintraoperative variables showed a higher risk for SSI in the skinsealant group compared with the control group. This appears toreflect longer CPB times and more frequent intraoperativeapplication of an intra-aortic balloon pump in the skin sealantgroup. Although each of these factors alone did not differsignificantly between groups, their combined effect had a greaterimpact on the risk score in this risk evaluation system. Notably,despite the similar (preoperative) or increased (combined) risk inthe microbial skin sealant group, use of this adjunct to preopera-tive skin preparation significantly reduced the observed incidenceof SSI to a rate corresponding to a third lower than that predicted

P.M. Dohmen et al. / International Journal of Infectious Diseases 15 (2011) e395–e400 e399
for superficial and deep SSI by preoperative factors. In addition, thefrequency of SSI observed in the control group, which was morethan two-fold higher than predicted, suggests that the risk scoringsystem may have underestimated SSI risk in this series of patients.
The risk of developing SSI after surgery depends in part on the‘dose’ of bacterial contamination, i.e., the number of bacteria thatcolonize the surgical wound.14 While the operative woundfollowing cardiac surgery is considered to be ‘clean’,14 the surgicalsite may be contaminated by airborne bacteria-carrying particlesin the operating room and intensive care unit, by bacteria fromendogenous sources such as the patient’s mucous membranes thatare spread on the hands of theatre personnel, or by directcontamination by the patient’s normal skin microflora. Patientsincluded in this study were operated on at the same clinical centreby the same surgeon, thereby minimizing differences in medicalenvironment, preoperative preparation, surgical technique, andpostoperative care that are likely to occur in a multicenter study.On the other hand, ‘standard’ techniques and the clinical practiceof individual clinical staff may have changed during the 31-monthperiod in which the data were collected, which is a limitation ofthis study. The number of patients and the duration of the studyshould, however, have limited any effect of seasonal differences onthe SSI risk of the two treatment groups. Additional studies havebeen initiated to collect data during equivalent periods. Althoughthis was not a randomized comparison, which represents a furtherlimitation, the data were collected from patients undergoingroutine operations carried out in a cardiovascular surgery unit andare thus more representative of clinical reality.
In this study, the bacterial species isolated most commonlyfrom sternal wound SSI were S. aureus and S. epidermidis. Sternalinfection with S. aureus in particular is associated with seriousmorbidity, high mortality, and a poor prognosis.25,26 Coagulase-negative staphylococci are also major pathogens in sternalinfections, particularly when implanted material is intro-duced.24,27,28 Importantly, the endogenous route of SSI aftercardiac surgery has been demonstrated for both S. aureus andcoagulase-negative staphylococci.27,28 In some patients, the strainof S. aureus isolated from surgical wound infections followingcardiac surgery has been shown to be identical to that colonizingthe nose,29,30 but the majority of such infections are likely to becaused by staphylococci and other species of the patient’s skinmicroflora.14,28,31 Microbiological screening showed the absence ofMRSA in this patient population, and decolonization of carriersprior to surgery was not required. Although colonization atadmission may have been undetected and thus cannot beexcluded, the finding of MRSA isolated from the sternal SSI inthree patients is consistent with nosocomial rather than endoge-nous transmission, as reported elsewhere.30 Given the predomi-nant role of the skin microbial flora in SSI, inhibiting the migrationof endogenous potential pathogens appears to be a rationalapproach to reducing surgical wound contamination. Importantadvantages of this approach to immobilizing all skin-bornemicroorganisms in situ is that it targets all types of pathogenand does not promote the common mechanisms of bacterialresistance to antibiotics.
Pretreatment with the skin sealant is convenient and its use hasbeen easily integrated with existing routine preoperative pre-parations used at this surgical centre. No cases of skin sensitivity orother reaction following application of the skin sealant were notedand it can be used safely after a variety of skin preparationsolutions and without the need for a specific wound closuretechnique.
In conclusion, this comparison of outcomes from a singlesurgeon’s patients shows that including a microbial skin sealantprior to cardiac surgery significantly reduced the rate of SSI. Theskin sealant may thus be a useful addition to the multimodal
prevention approach needed to minimize bacterial contaminationof surgical incisions.
4.1. Study limitations
This study is limited by the fact that it was a single center, non-randomized, retrospective study. Furthermore the patient char-acteristics were not identical for both groups and thereforepatients were at different risk of developing an SSI. However, inthis study we were able to see a significant reduction in SSI eventhough the microbial skin sealant group was at higher risk ofdeveloping an SSI. To date there are no other data available for thereader on this microbial skin sealant to determine the value of thisadditional tool except for a prospective, randomized, multicenterclinical trial in patients undergoing an open inguinal herniarepair.8
Acknowledgements
Neil McKendrick PhD provided assistance in preparing andediting the manuscript with the financial support of Kimberly-Clark Europe.
Conflict of interest: PMD has been a member of a speaker facultyfor, and has received lecture fees from, Kimberly-Clark Healthcare.He has also received a research grant from Kimberly-ClarkHealthcare for a separate study. DG, TG, WK, JL and AW have noconflicts of interest.
References
1. Brown IW, Moor GF, Hummel BW, Marshall WG, Collins JP. Toward furtherreducing wound infections in cardiac operations. Ann Thorac Surg 1996;62:1783–9.
2. Fry DE. The surgical infection prevention project: processes, outcomes, andfuture impact. Surg Infect (Larchmt) 2006;7(Suppl 3):S17–26.
3. Borger MA, Rao V, Weisel RD, Ivanov J, Cohen G, Scully HE, et al. Deep sternalwound infection: risk factors and outcomes. Ann Thorac Surg 1998;65:1050–6.
4. Milano CA, Kesler K, Archibald N, Sexton DJ, Jones RH. Mediastinitis aftercoronary artery bypass graft surgery: risk factors and long-term survival.Circulation 1995;92:2245–51.
5. Mekontso-Dessap A, Kirsch M, Brun-Buisson C, Loisance D. Poststernotomymediastinitis due to Staphylococcus aureus: comparison of methicillin-resistantand methicillin-susceptible cases. Clin Infect Dis 2001;32:877–83.
6. Munoz P, Menasalvas A, Bernaldo DQ, Desco M, Vallejo JL, Bouza E. Postsurgicalmediastinitis: a case–control study. Clin Infect Dis 1997;25:1060–4.
7. Gardlund B. Postoperative surgical site infections in cardiac surgery—an over-view of preventive measures. APMIS 2007;115:989–95.
8. Towfigh S, Cheadle WG, Lowry SF, Malangomi MA, Wilson SE. Significantreduction in incidence of wound contamination by skin flora through use ofmicrobial sealant. Arch Surg 2008;143:885–91.
9. Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. TheStrengthening the Reporting of Observational Studies in Epidemiology(STROBE) statement: guidelines for reporting observational studies. J ClinEpidemiol 2008;61:344–9.
10. Gastmeier P, Sohr D, Schwab F, Behnke M, Zuschneid I, Brandt C, et al. Tenyears of KISS: the most important requirements for success. J Hosp Infect2008;70(Suppl 1):S11–6.
11. Dohmen PM. Influence of skin flora and preventive measures on surgical siteinfection during cardiac Surgery. Surg Infect 2006;7:S13–7.
12. Dohmen PM, Konertz W. A review of current strategies to reduce intraoperativebacterial contamination of surgical wounds. GMS Krankenhhyg Interdiszip2007;2:Doc38.
13. Fowler VG, O’Brien SM, Muhlbaier LH, Corey GR, Ferguson TB, Peterson ED.Clinical predictors of major infections after cardiac surgery. Circulation2005;112(9 Suppl):I358–65.
14. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for preven-tion of surgical site infection, 1999. Centers for Disease Control and Prevention(CDC) Hospital Infection Control Practices Advisory Committee. Am J InfectControl 1999;27:97–132. quiz 133–4; discussion 96.
15. Vierron E, Giraudeau B. Sample size calculation for multicenter randomizedtrial: taking the center effect into account. Comtemp Clin Trials 2007;28:451–8.
16. Julian OC, Lopez-Belio M, Dye WS, Javid H, Grove WJ. The median sternalincision in intracardiac surgery with extracorporeal circulation; a generalevaluation of its use in heart surgery. Surgery 1957;42:753–61.
17. Salehi Omran A, Karimi A, Ahmadi SH, Davoodi S, Marzban M, Movahedi N, et al.Superficial and deep sternal wound infection after more than 9000 coronary

P.M. Dohmen et al. / International Journal of Infectious Diseases 15 (2011) e395–e400e400
artery bypass graft (CABG): incidence, risk factors and mortality. BMC Infect Dis2007;7:112.
18. Dohmen PM. Antibiotic resistance in common pathogens reinforces the need tominimise surgical site infections. J Hosp Infect 2008;70(Suppl 2):15–20.
19. Fry DE. The economic costs of surgical site infection. Surg Infect (Larchmt)2002;3(Suppl 1):S37–43.
20. Gummert JF, Barten MJ, Hans C, Kluge M, Doll N, Walther T, et al. Mediastinitisand cardiac surgery—an update risk factor analysis in 10,373 consecutive adultpatients. Thorac Cardiovasc Surg 2002;50:87–91.
21. Diez C, Koch D, Kuss O, Silber RE, Friedrich I, Boergermann J. Risk factors formediastinitis after cardiac surgery—a retrospective analysis of 1700 patients. JCardiothorac Surg 2007;2:23.
22. Baskett RJ, MacDougall CE, Ross DB. Is mediastinitis a preventable complica-tion? Ann Thorac Surg 1999;67:462–5.
23. Stahle E, Tammelin A, Bergstrom R, Hambreus A, Nystrom SO, Hansson HE.Sternal wound complications—incidence, microbiology and risk factors. Eur JCardiothorac Surg 1997;11:1146–53.
24. Gardlund B, Bitkover CY, Vaage J. Postoperative mediastinitis in cardiacsurgery—microbiology and pathogenesis. Eur J Cardiothorac Surg 2002;21:825–30.
25. Reddy SL, Grayson AD, Smith G, Warwick R, Chalmers JA. Methicillin-resistantStaphylococcus aureus infections following cardiac surgery: incidence, impactand identifying adverse outcome traits. Eur J Cardiothorac Surg 2007;32:113–7.
26. Haas JP, Evans AM, Preston KE, Larson EL. Risk factors for surgical site infectionsafter cardiac surgery: the role of endogenous flora. Heart Lung 2005;34:108–14.
27. Kuhme T, Isaksson B, Dahlin LG. Wound contamination in cardiac surgery. Asystematic quantitative and qualitative study of the bacterial growth in sternalwounds in cardiac surgery patients. APMIS 2007;115:1001–7.
28. Jakob HG, Borneff-Lipp M, Bach A, von Puckler S, Windeler J, Sonntag H, et al.The endogenous pathway is a major route for deep sternal wound infection. EurJ Cardiothorac Surg 2000;17:154–60.
29. Kluytmans JA, Mouton JW, Ijzerman EP, Vandenbroucke-Grauls CM, Maat AW,Wagenvoort JH, et al. Nasal carriage of Staphylococcus aureus as a major riskfactor for wound infections after cardiac surgery. J Infect Dis 1995;171:216–9.
30. Owens CD, Stoessel K. Surgical site infections: epidemiology, microbiology andprevention. J Hosp Infect 2008;70(Suppl 2):3–10.
31. San Juan R, Chaves F, Lopez Gude MJ, Dıaz-Pedroche C, Otero J, Cortina RomeroJM, et al. Staphylococcus aureus poststernotomy mediastinitis: description oftwo distinct acquisition pathways with different potential preventiveapproaches. J Thorac Cardiovasc Surg 2007;134:670–6.




















