A randomised controlled pilot feasibility study of the physical and psychological effects of an...
8
A randomised controlled pilot feasibility study of the physical and psychological effects of an integrated support programme in breast cancer Barbara S. Baker a, * , Julia E. Harrington a , Beak-San Choi b, c , Pascale Kropf b, d , Ingrid Muller b , Caroline J. Hoffman a a The Haven, Effie Road, London SW6 1TB, UK b Department of Immunology, Imperial College, London, St Mary’s Campus, London W2 1NY, UK Keywords: Breast cancer Integrated support programme Complementary therapies Quality of life Immune function abstract A pilot study was conducted to assess recruitment and effectiveness of an integrated support programme in women with breast cancer. Twelve participants were randomised to receive medical care with or without the support programme. Psychosocial questionnaires and immune/hormonal assays were completed at baseline, three and six months. Recruitment was problematic. In the intervention group, mental fatigue was significantly improved (p ¼ 0.016) compared to controls; increased NK cell activity suggested an improvement in immune function. Total stress (p ¼ 0.009), anxiety (p ¼ 0.032) and endocrine-specific(p ¼ 0.032) symptoms were significantly improved in the controls. A large-scale randomisation trial appears warranted, dependent upon effective recruitment. Ó 2012 Elsevier Ltd. All rights reserved. 1. Introduction Patients with cancer are increasingly turning to complementary and alternative medicine (CAM) to use alongside standard cancer treatments. 1e3 Women diagnosed with breast cancer have been reported to use complementary therapies more frequently than individuals diagnosed with other cancers, up to 80% use being reported in a study by Boon et al. 4 The main reasons for this use include the belief that complementary therapies are helpful for recovery, healing and improving health, and that they may boost the immune system, reduce disease symptoms and side effects of cancer treatment, improve emotional health and/or increase the efficacy of standard cancer treatments. A recent systematic review of CAM use showed that the type of CAM most frequently used by women with breast cancer was biologically based (e.g. herbs, vitamins, foods), followed by mind-body medicine (meditation, prayer, emotional healing). 3 Although more rigorous research is needed, there is increasing preliminary evidence to support the beneficial effects of some complementary therapies on the physical and emotional problems experienced by breast cancer patients. A beneficial effect of acupressure on the wrist P6 acupoint was demonstrated for chemotherapy-induced nausea and vomiting in a systematic review of the use of acupoint stimulation for the management of therapy-related side effects in breast cancer patients. 5 Further- more, acupuncture appears to be efficacious in the short-term relief of vasomotor symptoms, a common side effect of the use of hormonal therapies in women with breast cancer. 6e8 In addition, Mindfulness-Based Stress Reduction (MBSR) programmes have been shown in several trials to significantly improve quality of life and mood, and to reduce distress in cancer patients. 9,10 The improvement in quality of life parameters reported in trials of MBSR, cognitive-behavioural therapy, massage and Medical Qigong have also been shown to be associated with altered cortisol and/or immune cell activity, or reduced inflammation. 11e14 The Haven is a charity that offers an integrated programme consisting of information, emotional support, and complementary therapies to help people through the experience of breast cancer, before, during or after their medical treatment. Currently, The Haven has centres in London, Leeds and Hereford, and an outreach programme, The Haven at Home, to extend these support services * Corresponding author. Tel.: þ44 (0) 20 7384 0044; fax: þ44 (0) 20 7384 0001. E-mail addresses: [email protected] (B.S. Baker), julia.harrington@ thehaven.org.uk (J.E. Harrington), [email protected] (B.-S. Choi), Pascale.Kropf@ lshtm.ac.uk (P. Kropf), [email protected] (I. Muller), caroline.hoffman@ thehaven.org.uk (C.J. Hoffman). c Present address: Department of Infectious Diseases, University of Georgia, Athens, Georgia, USA. d Present address: Department of Immunology & Infection, London School of Hygiene and Tropical Medicine, London WC1E 7HT, UK. Contents lists available at SciVerse ScienceDirect Complementary Therapies in Clinical Practice journal homepage: www.elsevier.com/locate/ctcp 1744-3881/$ e see front matter Ó 2012 Elsevier Ltd. All rights reserved. doi:10.1016/j.ctcp.2012.03.002 Complementary Therapies in Clinical Practice xxx (2012) 1e8 Please cite this article in press as: Baker BS, et al., A randomised controlled pilot feasibility study of the physical and psychological effects of an integrated support programme in breast cancer, Complementary Therapies in Clinical Practice (2012), doi:10.1016/j.ctcp.2012.03.002
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of A randomised controlled pilot feasibility study of the physical and psychological effects of an...

at SciVerse ScienceDirect
Complementary Therapies in Clinical Practice xxx (2012) 1e8
Contents lists available
Complementary Therapies in Clinical Practice
journal homepage: www.elsevier .com/locate/ctcp
A randomised controlled pilot feasibility study of the physical and psychologicaleffects of an integrated support programme in breast cancer
Barbara S. Baker a,*, Julia E. Harrington a, Beak-San Choi b,c, Pascale Kropf b,d, Ingrid Muller b,Caroline J. Hoffman a
a The Haven, Effie Road, London SW6 1TB, UKbDepartment of Immunology, Imperial College, London, St Mary’s Campus, London W2 1NY, UK
Keywords:Breast cancerIntegrated support programmeComplementary therapiesQuality of lifeImmune function
* Corresponding author. Tel.: þ44 (0) 20 7384 0044E-mail addresses: [email protected]
thehaven.org.uk (J.E. Harrington), [email protected] (P. Kropf), [email protected] (I.thehaven.org.uk (C.J. Hoffman).
c Present address: Department of Infectious DiseAthens, Georgia, USA.
d Present address: Department of Immunology &Hygiene and Tropical Medicine, London WC1E 7HT, U
1744-3881/$ e see front matter � 2012 Elsevier Ltd.doi:10.1016/j.ctcp.2012.03.002
Please cite this article in press as: Baker BS, eintegrated support programme in breast can
a b s t r a c t
A pilot study was conducted to assess recruitment and effectiveness of an integrated support programmein women with breast cancer.
Twelve participants were randomised to receive medical care with or without the support programme.Psychosocial questionnaires and immune/hormonal assays were completed at baseline, three and sixmonths.
Recruitment was problematic. In the intervention group, mental fatigue was significantly improved(p ¼ 0.016) compared to controls; increased NK cell activity suggested an improvement in immunefunction. Total stress (p ¼ 0.009), anxiety (p ¼ 0.032) and endocrine-specific (p ¼ 0.032) symptoms weresignificantly improved in the controls.
A large-scale randomisation trial appears warranted, dependent upon effective recruitment.� 2012 Elsevier Ltd. All rights reserved.
1. Introduction
Patients with cancer are increasingly turning to complementaryand alternative medicine (CAM) to use alongside standard cancertreatments.1e3 Women diagnosed with breast cancer have beenreported to use complementary therapies more frequently thanindividuals diagnosed with other cancers, up to 80% use beingreported in a study by Boon et al.4 The main reasons for this useinclude the belief that complementary therapies are helpful forrecovery, healing and improving health, and that they may boostthe immune system, reduce disease symptoms and side effects ofcancer treatment, improve emotional health and/or increase theefficacy of standard cancer treatments. A recent systematic reviewof CAM use showed that the type of CAM most frequently used bywomen with breast cancer was biologically based (e.g. herbs,
; fax: þ44 (0) 20 7384 0001.(B.S. Baker), julia.harrington@(B.-S. Choi), Pascale.Kropf@Muller), caroline.hoffman@
ases, University of Georgia,
Infection, London School ofK.
All rights reserved.
t al., A randomised controllecer, Complementary Therap
vitamins, foods), followed by mind-body medicine (meditation,prayer, emotional healing).3
Although more rigorous research is needed, there is increasingpreliminary evidence to support the beneficial effects of somecomplementary therapies on the physical and emotional problemsexperienced by breast cancer patients. A beneficial effect ofacupressure on the wrist P6 acupoint was demonstrated forchemotherapy-induced nausea and vomiting in a systematicreview of the use of acupoint stimulation for the management oftherapy-related side effects in breast cancer patients.5 Further-more, acupuncture appears to be efficacious in the short-term reliefof vasomotor symptoms, a common side effect of the use ofhormonal therapies in women with breast cancer.6e8 In addition,Mindfulness-Based Stress Reduction (MBSR) programmes havebeen shown in several trials to significantly improve quality of lifeand mood, and to reduce distress in cancer patients.9,10 Theimprovement in quality of life parameters reported in trials ofMBSR, cognitive-behavioural therapy, massage and Medical Qigonghave also been shown to be associated with altered cortisol and/orimmune cell activity, or reduced inflammation.11e14
The Haven is a charity that offers an integrated programmeconsisting of information, emotional support, and complementarytherapies to help people through the experience of breast cancer,before, during or after their medical treatment. Currently, TheHaven has centres in London, Leeds and Hereford, and an outreachprogramme, The Haven at Home, to extend these support services
d pilot feasibility study of the physical and psychological effects of anies in Clinical Practice (2012), doi:10.1016/j.ctcp.2012.03.002

B.S. Baker et al. / Complementary Therapies in Clinical Practice xxx (2012) 1e82
to anyone in the UK affected by breast cancer. Analysis of feedbackobtained from visitors to the Haven centres using the MeasureYourself Concerns and Wellbeing (MYCaW) questionnaire showedthat psychological and emotional concerns predominated inwomen diagnosed with breast cancer, and that their two mainconcerns, and well being, significantly improved after receiving theHaven programme.15,16
These preliminary findings showing the benefits of the Havenprogramme suggest that a thorough evaluation of its role as part ofan integrated approach to treatment of women with breast canceris now justified. The first step towards this goal was to carry outa small pilot feasibility study to evaluate the physical and psycho-logical effects of the Haven programme in women with breastcancer compared to controls. This approachwas consistent with therecommendations of a National Cancer Institute Community Clin-ical Oncology Program team that concluded that the most signifi-cant research-design issues in cancer symptom management trialsusing CAM arose as a consequence of the lack of preclinical datafrom pilot studies.17
2. Materials & methods
2.1. Study design
This study was a randomised, controlled pilot feasibility study ofwomen with breast cancer who either received the Haven pro-gramme in conjunction with standard medical care (interventiongroup, n¼ 6), or standard medical care alone (control group, n¼ 6).Patients were randomly allocated, in a 1:1 ratio, in permuted blocksof 4 using a computerised random number generator (Excel).Neither the participants nor the researchers were blinded to thegroup assignment. The participants were given a Study ID numberon enrolment, which was used to code the data, blood and salivasamples collected during the study. The therapists who providedthe programme were unaware of whether the visitors they treatedwere, or were not, part of the research study.
Charing Cross Research Ethics Committee approved the study inJune 2007, and six subsequent changes to the protocol fromNovember 2007 to November 2008. Informed consent wasobtained from participants prior to randomisation, and for thecollection of blood and saliva samples.
2.2. Participants and recruitment
Women with a diagnosis of breast cancer attending the BreastClinics at Charing Cross and St Mary’s Hospitals in London wereenrolled in the study. Inclusion criteria were female patients withstage 0eIII breast cancer, at least 18 yrs old. Exclusion criteria werestage IV metastatic breast cancer (one stage IV breast cancerpatient, whose disease stage was unknown on recruitment, wasincluded in the intervention group), other primary cancer sites,pregnancy or psychosis, autoimmune disease and HIV/AIDS.Patients who were not fluent in English were excluded on prag-matic grounds.
The initial recruitment target was 50 participants, but recruit-ment proved difficult requiring changes to the protocol to allowfurther time for patients to come to terms with their breast cancerdiagnosis. Eligible patients were initially identified by breast carenurses two or three days after diagnosis, then by nurses in the pre-assessment clinic prior to surgery, and finally after surgery andbefore/during further treatments such as chemotherapy, radio-therapy or hormone therapy. The recruitment target was subse-quently reduced to a total of 20 patients on the advice of theCharing Cross Ethics Committee chairman.
Please cite this article in press as: Baker BS, et al., A randomised controlleintegrated support programme in breast cancer, Complementary Therap
2.3. Intervention
The Haven integrated support programme provides psycholog-ical support, information, and a range of complementary therapiesspecifically designed to support the physical and emotional needsof patients with breast cancer before, during and after standardmedical treatment. Individual therapy assessments and reviews,and a personalised programme of care, conducted by experiencedspecialist nurses and therapists, are available to each visitor. A two-day Haven Support Workshop, and a maximum of 12 h of 1:1therapy consultation time was offered, including therapies such asnutrition, counselling, touch therapies, herbal medicine andhomeopathy. Therewere also groups and classes for art therapy, earacupuncture, yoga, meditation and Qigong.
The intervention group was offered the Haven programmeduring the first 1e4 months of the study whilst undergoing stan-dard medical treatment. This is approximate because there wasflexibility within the programme for participants to choose when,and how many, individual therapies they received.
The control group received standard medical treatment alone.To aid recruitment, and for ethical reasons, they were offered theHaven programme at the end of the study.
2.4. Study outcomes
Psychosocial and immune outcomes to be used in a large-scaletrial were measured at baseline, 3 months and 6 months afterrandomisation.
2.4.1. Psychosocial outcomesPsychosocial measurements were made using four self-report
questionnaires to determine which ones would be the mostappropriate for use in a larger trial: Functional Assessment of CancerTherapy (FACT-G, 27 items) measures quality of life and is sub-divided into four primary domains e physical, social/family,emotional and functional, plus the Breast (B) and EndocrineSymptom (ES) subscales; Symptoms of Stress Inventory (SOSI, 95items) measures physical, psychological and behavioural responsesto stressful situations; Profile of Mood States (POMS, 65 items) isa measure of affective states comprising a Total Mood DisturbanceScale and six factor-based subscale scores; MultidimensionalFatigue Inventory (MFI, 20 items) measures multi-dimensionalfatigue, including general, physical and mental fatigue, reducedmotivation and reduced activity. Thesemeasures have all been usedin studies of patients with cancer and have shown test-retest reli-ability, concurrent validity to related scales and sensitivity tochange.18e26
2.4.2. Immune/hormonal assaysOn each occasion, a 20 ml heparinised blood sample was
collected from each participant, who provided three serial salivasamples at 8.00 am, 2.00 pm and 8.00 pm using cotton saliva swabs(Sarstedt Ltd., UK) on the following day. The samples were taken orsent in the post, respectively, to the Breakthrough Breast CancerResearch Centre laboratories in London for processing and storage.Plasma and peripheral blood mononuclear cells (PBMCs) wereisolated from the heparinised blood by Ficoll-Hypaque gradientcentrifugation (Lymphoprep, Axis-Shield, UK). The PBMC werewashed, and frozen at �80 �C in 2% DMSO in RPMI 1640 medium(Promocell, UK) plus antibiotics, 2 mM glutamine and 10% heat-inactivated foetal bovine serum (Invitrogen Ltd., UK). The salivasamples were harvested from the cotton swabs by centrifugationand stored at �80 �C.
The following immuneassayswereperformed at the ImmunologyDepartment, Imperial College, StMary’s campus, London: PBMCwere
d pilot feasibility study of the physical and psychological effects of anies in Clinical Practice (2012), doi:10.1016/j.ctcp.2012.03.002

B.S. Baker et al. / Complementary Therapies in Clinical Practice xxx (2012) 1e8 3
thawed, washed and stainedwith conjugatedmonoclonal antibodies(eBioscience) in the following combinations: anti-CD3-FITC/anti-CD4-PB (total CD4þ T cells); anti-CD3-FITC/anti-CD4-PB/anti-CD69-PE-CY7 (early activated CD4þ T cells); anti-CD3-FITC/anti-CD4-PB/anti-CD25-PE (activated CD4þ T cells); anti-CD3-FITC/anti-CD8aPerCP-CY5 (total CD8þ Tcells); anti-CD3-FITC/anti-CD8a-PerCP-CY5/anti-CD69-PE-CY7 (early activatedCD8þ Tcells); anti-CD3-FITC/anti-CD8a-PerCP-CY5/anti-CD25-PE (activated CD8þ T cells) and anti-CD3-APC/anti-CD16-FITC/anti-CD56-PE (natural killer (NK) cells),and analysed by flow cytometry (Becton Dickinson, UK).
NK cell activity was assessed using the CD107 degranulationassay, which measures the expression of CD107a (lysosomal-asso-ciated membrane protein-1) on the surface of activated NK cells,a correlate of NK cell-mediated killing of target cells and cytokinesecretion.27 Briefly, PBMC were thawed, washed and incubatedwith Interleukin (IL)-15 (PeproTech, UK) overnight at 37 �C. Thenext day, PBMC were co-incubated for 1 h at 37 �C with K562 cells(immortalised myelogenous leukaemia cell line which lacks theMHC complex required to inhibit NK cell activity) at an effector:target ratio of 5:1, in the presence of anti-CD107a-APC antibody(eBioscience, UK). After addition of Golgi Stop (BD Bioscience, UK),a protein transport inhibitor, the cells were incubated for a further3 h, washed, stained with anti-CD3-APC/anti-CD16-FITC/anti-CD56-PE and analysed by flow cytometry (Becton Dickinson, UK).
Commercial enzyme-linked immunosorbent assays (ELISAs)were performed according to the manufacturer’s instructions tomeasure levels of Interferon-g (IFN-g) (R & D Systems, UK), TumourNecrosis Factor (TNF)-a (R & D Systems, UK) and solubleinterleukin-6 receptor (sIL-6R) (PeproTech, UK) in plasma, andcortisol (R & D Systems, UK) in saliva.
Arginase, an enzyme that hydrolyses the amino acid L-arginineinto urea and ornithine, was measured in PBMC lysates. Duringimmune responses, depletion of L-arginine by arginase inducesfunctional T cell hyporesponsiveness; this immunomodulatorypathway appears to be important in infection, pregnancy and intumour evasion.28e30 Arginase activity was measured as ureaproduction after incubation of PBMC lysates with L-arginine at 37 �Cfor 15e20min.Oneunit of enzymeactivitywasdefinedas the amountof enzyme that catalysed the formation of 1 mmol of urea per min.31
2.5. Data analysis
Descriptive statistical analysis (mean � SD) was used to detectany preliminary trends in questionnaire score changes and immuneassay levels in the intervention and control groups at 3 and 6months follow-up. The non-parametric ManneWhitney and Wil-coxon tests were used to compare outcomes between and withingroups, respectively. Analyses were performed using PASW v18statistical software.
3. Results
3.1. Patient recruitment
Twenty-nine women with breast cancer were contacted by theHaven research team and assessed for eligibility over a period of 16months from February 2008 to May 2009. Three of these wereineligible due to prior surgery or a poor understanding of English(Fig. 1, Table 1). Recruitment was initially attempted at 2 or 3 daysafter diagnosis, then at pre-assessment prior to surgery and finallypost-surgery, either before or during further treatments such aschemotherapy, radiotherapy and/or hormonal therapies. Noimprovement in the recruitment rate was observed with thesetiming changes, or by additional recruitment at a second hospital(St Mary’s, Paddington, London) within the same NHS Trust.
Please cite this article in press as: Baker BS, et al., A randomised controlleintegrated support programme in breast cancer, Complementary Therap
Of the 26 eligible patients, 14 declined to take part. The reasonsfor declining to take part, obtained from 10 of the 14 women withbreast cancer, were: still coming to terms with their diagnosis andimpending treatment schedule (n ¼ 4), the distance to the Havencentre was considered too far (n ¼ 3), both of these reasons (n ¼ 1),or wanted to receive complementary therapies straight away anddid not want to risk being randomised to the control group (n ¼ 2).Twelve participants took part in the pilot study; six were rando-mised to the intervention group, and six to the control group. Noneof the participants randomised to the control group refused to takepart; they were offered access to the Haven programme at the endof their participation in the study.
3.2. Demographic and clinical characteristics of participants
Baseline demographic and clinical characteristics of the partic-ipants are shown in Table 2. The participants in the interventionand control groups came from almost identical socio-economicgroups, and were of similar marital status, but differed in theireducational level. Differences in the intervention and controlgroups were also noted regarding stage of disease and type ofmedical treatments received. Participants in the intervention grouptended to have milder disease and were less likely to have under-gone amastectomy or to have received chemotherapy than those inthe control group.
3.3. Quality of life questionnaires
The mean (�SD) scores obtained for the intervention andcontrol groups at baseline, three and six months for the POMS,FACT, SOSI and MFI total and subscale scores are shown inTables 3e6.
In the intervention group, the total mood disturbance score(POMS) was non-significantly higher at baseline, indicatinga poorer mood state, compared to the control group (Table 3). Thiswas partly due to a significantly higher confusion/bewildermentsubscale score (p ¼ 0.015). Both intervention and control groupsshowed decreases in the total mood disturbance score at 3 and 6months follow-up suggesting improvement in mood state. For theintervention group, the decrease in the confusion/bewildermentsubscale score at 3 months compared to baseline was statisticallysignificant (p ¼ 0.046) indicating improvement during participa-tion in the support programme.
A small trend in improvement (as shown by amoderate increasein scores) in quality of life (FACT-G) and breast-specific symptoms(FACT-G þ B)/(FACT-G þ B TOI) was also seen in both interventionand control groups at 6 months follow-up (Table 4). The baselineFACT emotional well being subscale score was significantly lower inthe intervention group versus control (p ¼ 0.041), but increasedsignificantly at 6 months in the intervention group (p ¼ 0.043), andat 3 months in the control group (p ¼ 0.042) indicating improve-ment. However, endocrine-related symptoms were significantlybetter in the control versus intervention group at 6 months (FACT-ES, p ¼ 0.032; FACT-G þ ES TOI, p ¼ 0.016).
The total stress score (SOSI) also appeared higher at baseline,indicating worse stress, in the intervention compared to controlgroup, but this difference was not significant (Table 5). The controlgroup showed improvement in stress symptoms (SOSI) at 6months, whilst the intervention group worsened at 3 months andremained at this level at 6 months. However, in the interventiongroup, the SOSI cognitive subscale score was significantly improvedat 3 months compared to baseline (p ¼ 0.046). The control groupshowed significantly lower scores than the intervention group fortotal stress at 3 months (p¼ 0.009) and for the anxiety subscale at 6months (p ¼ 0.032).
d pilot feasibility study of the physical and psychological effects of anies in Clinical Practice (2012), doi:10.1016/j.ctcp.2012.03.002

Fig. 1. CONSORT Diagram.
B.S. Baker et al. / Complementary Therapies in Clinical Practice xxx (2012) 1e84
A trend in improvement in physical fatigue (MFI) was observedin the intervention group at 6 months follow-up, whilst in contrast,the control group showed a worsening of fatigue symptoms by theend of the study as shown by an increase in scores (Table 6). Thescore for the mental fatigue subscale was significantly lower in theintervention vs control group at 6 months (p ¼ 0.016).
3.4. Immune and hormonal assays
Little change in the mean numbers of total and activated CD4þ
and CD8þ T cell subsets and NK cells, or in the levels of IFN-g, TNF-a or sIL-6R were observed in the blood or plasma of participants inboth the intervention and control groups over the 6-month studyperiod (data not shown).
In the intervention group, NK cell activity, as measured by theCD107 degranulation assay, increased at 3 months compared to
Table 1Recruitment levels at different stages of treatment.
Stage of treatment Hospital Time pe
2e3 days post-diagnosis Charing Cross Feb 08ePre-assessment prior to surgery Charing Cross Jun 08ePost-surgery, (before/after start
of further treatments)Charing Cross and St Mary’s Jan 09e
Total
Please cite this article in press as: Baker BS, et al., A randomised controlleintegrated support programme in breast cancer, Complementary Therap
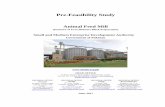
baseline and was maintained at 6-months follow-up (Fig. 2A). Thiscontrasted with the control group whose baseline NK cell activitywas higher than that of the intervention group, and graduallydecreased over the 6-month study period (Fig. 2A).
Similarly, in the intervention group, PBMC arginase levelsincreased at 3 months compared to baseline and remained higherthan baseline at 6-months follow-up. In contrast, the baselinePBMC arginase level in the control group, which was higher thanthat of the intervention group, gradually decreased over the 6-month study period (Fig. 2B). Differences in NK cell activity orPBMC arginase levels between the intervention and control groupsduring the study were not statistically significant.
A moderate (non-significant) decrease in mean daily salivarycortisol levels was noted at 6 months in the intervention groupalone compared to baseline: 878.3 � 564.73 (n ¼ 6) vs1424.1 � 747.3 (n ¼ 4), respectively.
riod Numberrecruited
Numberineligible
Numberdeclined
Totalnumber
May 08 3 2 4 9Dec 08 4 1 6 11May09 5 0 4 9
12 3 14 29
d pilot feasibility study of the physical and psychological effects of anies in Clinical Practice (2012), doi:10.1016/j.ctcp.2012.03.002

Table 2Participant baseline characteristics.
Interventioncount (n ¼ 6)
Controlcount (n ¼ 6)
Age in years at randomisation (mean � SD) 52.3 � 11.3 53.3 � 6.4Socio-economic statusManagerial/Professional 1 1Intermediate 3 3Small employers and own account workers 1 0Lower supervisory/technical 0 1Unclassified 1 1
Marital statusMarried or living as married 2 4Single 1 1Separated 1 0Divorced 1 0Widowed 1 1
Ethnic groupWhite 4 6Asian or Asian British 2 0
Education levelDegree 3 2Teaching or other higher qualification 3 0A level 0 3GCSE or 0 level 0 1
MenopausalPremenopausal 2 3Going through 2 0Postmenopausal 1 1Non-menopausal 0 1Do not know 1 1
Disease stageStage I 3 0Stage II/IIIa 1 4Stage IV 1 0Unknown 1 2
Type of surgeryb
Lumpectomy 3 0Mastectomy 2 4Unknown 1 2
Chemotherapyb
Yes 1 3No 5 3
Radiotherapyb
Yes 3 3No 3 3
Hormone therapyb
Yes 4 2No 0 0Unknown 2 4
a Provisional classification based upon lymph node positivity.b Treatment received before and/or during study.
B.S. Baker et al. / Complementary Therapies in Clinical Practice xxx (2012) 1e8 5
3.5. Study dropouts, missing data/samples and patient compliance
None of the participants from either group dropped out of thestudy. Three patients failed to attend and complete the question-naire at 6 months. This was due to bereavement and/or ill health
Table 3Profile of Mood States: total and subscale scores.
Subscale scores Time 1 Time 2
Intervention(n ¼ 6)
Control(n ¼ 6)
p value Intervent(n ¼ 6)
Tension/anxiety 15.67 � 8.29 9.2 � 5.19 0.180 8.33 � 6Depression/dejection 17.50 � 14.25 9.2 � 9.66 0.394 12.83 � 1Anger/hostility 11.83 � 11.07 8.33 � 7.12 0.589 10.67 � 8Vigour/activity 17.83 � 7.31 14.95 � 9.43 0.699 18.00 � 4Fatigue/inertia 10.33 � 7.03 5.94 � 4.87 0.310 9.17 � 7Confusion/bewilderment 12.67 � 4.37 5.83 � 3.19 0.015 8.17 � 3Total Mood Disturbance 85.83 � 45.00 53.40 � 31.27 0.240 67.17 � 2
Statistically significant differences between the intervention and control group are show
Please cite this article in press as: Baker BS, et al., A randomised controlleintegrated support programme in breast cancer, Complementary Therap
(n¼ 2), or other commitments (n¼ 1). A questionnaire was sent outto them to complete; however, none of these questionnaires werereturned.
Six of 36 blood samples were not obtained for analysis due topoor veins, phlebotomist unavailable or participant non-attendance; seven of the 36 sets of saliva (each taken at threetime points over the day) were not collected by participants.
In the intervention group, one of the six participants did notaccess the Haven programme during the study, and two did notbook an initial consultation appointment until they had been in thestudy for 3 months. Furthermore, these two participants receivedonly 1 h of massage or 3 h acupuncture, respectively, in addition totheir initial 1-h appointment. The non-use of therapies was eitherdue to a lack of need of support or, in one case, a misunderstandingon the part of the participant as to the procedure for obtainingtherapy appointments. The remaining three participants in theintervention group received 12, 14 or 14.5 h of one-to-one treat-ment, which encompassed a range of different complementarytherapies. In addition, the two participants who received the mosthours of therapy, also attended 13 or 16.5 h of groups, classes,workshops and/or seminars. Participants reported no adverseevents during this study.
In the control group, one of the six participants received occa-sional massage treatment at home and attended Pilates classes,whilst another visited another support charity to obtain cosmetic/wig and financial advice.
4. Discussion
This small pilot study has provided preliminary trends relatingto the physical and psychological effects of the support pro-gramme offered at The Haven to women diagnosed with breastcancer.
In the intervention group, mental fatigue was significantlyimproved compared to controls. A moderate improvement inphysical fatigue was also observed, which contrasted with a wors-ening of fatigue symptoms in the control group. However, thisimprovement in fatigue was not associated with changes innumbers of early activated CD69þ T cells or in levels of sIL-6R inplasma (data not shown), both previously reported biologicalmarkers of fatigue in breast cancer survivors.32 The increasedfatigue experienced by the control group participants may beexplained by the more frequent use of chemotherapy compared tothat of the intervention group.
In addition, an improvement in immune function in the inter-vention group was suggested by an increase in NK cell activity,accompanied by a moderate decrease in salivary cortisol levels. Incontrast in the control group, NK cell activity decreased over thestudy period. Increased NK cell activity compared to controls,accompanied by reduced cortisol levels and improved quality of
Time 3
ion Control(n ¼ 6)
p value Intervention(n ¼ 5)
Control(n ¼ 4)
p value
.50 8.17 � 2.32 0.699 8.00 � 3.16 2.50 � 3.11 0.0631.03 5.33 � 7.42 0.310 3.40 � 3.51 1.75 � 2.22 0.556.57 5.83 � 4.71 0.485 9.40 � 10.31 2.00 � 2.31 0.190.05 17.17 � 8.95 0.937 14.60 � 3.21 10.25 � 6.60 0.413.22 8.00 � 6.36 0.937 3.60 � 2.51 2.00 � 2.16 0.286.37 5.83 � 2.86 0.310 5.00 � 2.24 3.25 � 2.63 0.2869.42 50.33 � 24.81 0.394 44.00 � 14.75 21.75 � 13.67 0.063
n in bold.
d pilot feasibility study of the physical and psychological effects of anies in Clinical Practice (2012), doi:10.1016/j.ctcp.2012.03.002

Table 4Functional Assessment of Cancer Therapy (FACT-G), Breast (B) and Endocrine Symptom (ES): total and subscale scores.
Subscale Scores Time 1 Time 2 Time 3
Intervention(n ¼ 6)
Control(n ¼ 6)
p value Intervention(n ¼ 6)
Control(n ¼ 6)
p value Intervention(n ¼ 5)
Control(n ¼ 4)
p value
FACT-G: Physical wellbeing (PWB)
22.33 � 3.56 23.17 � 4.53 0.589 20.67 � 3.98 23.17 � 5.00 0.394 23.80 � 3.03 25.25 � 1.71 0.556
FACT-G: Social wellbeing (SWB)
21.08 � 7.12 22.14 � 5.92 0.589 17.17 � 6.34 19.83 � 5.04 0.589 18.20 � 9.00 23.50 � 5.80 0.286
FACT-G: Emotional wellbeing (EWB)
12.17 � 4.49 18.67 � 2.50 0.041 17.33 � 4.59 21.00 � 1.79 0.180 20.20 � 2.39 21.75 � 2.63 0.556
FACT-G: Functional wellbeing (FWB)
19.33 � 5.92 19.17 � 6.43 0.937 17.50 � 2.74 18.17 � 4.26 0.699 21.40 � 1.52 23.63 � 4.27 0.286
Breast-specific (B) 22.83 � 4.75 24.17 � 5.49 0.699 23.83 � 8.18 23.33 � 5.65 0.937 26.00 � 3.00 27.50 � 5.26 0.413Endocrine-specific (ES) 59.78 � 6.50 63.05 � 3.22 0.485 60.67 � 7.61 59.67 � 5.16 0.818 56.80 � 2.77 65.50 � 6.03 0.032Total ScoresFACT-G 74.92 � 16.30 83.14 � 16.37 0.310 72.67 � 12.36 82.17 � 12.94 0.240 83.60 � 9.71 94.13 � 12.69 0.111FACT-G þ B 97.75 � 16.41 107.31 � 17.73 0.394 96.50 � 19.74 105.50 � 14.61 0.589 109.60 � 11.63 121.63 � 11.15 0.111FACT-G þ ES 134.79 � 17.65 146.19 � 18.13 0.240 133.33 � 18.52 141.83 � 14.12 0.394 140.40 � 8.73 159.63 � 11.10 0.063FACT-B TOI (PWB þ FWB þ B) 64.50 � 8.73 66.50 � 13.55 0.589 62.00 � 12.25 64.67 � 10.01 0.937 71.20 � 5.40 76.38 � 3.86 0.111FACT-ES TOI (PWB þ FWB þ ES) 101.45 � 11.85 105.38 � 12.40 0.310 98.83 � 11.51 101.00 � 10.37 0.589 102.00 � 3.87 114.38 � 4.46 0.016
Statistically significant differences between the intervention and control group are shown in bold.
B.S. Baker et al. / Complementary Therapies in Clinical Practice xxx (2012) 1e86
life, has previously been reported in breast cancer patientsreceiving mindfulness-based stress reduction.33
Arginase, which is constitutively expressed by poly-morphonuclear cells in peripheral blood,30 is implicated as one ofthe factors involved in the ability of tumour cells to survive despiteimmune surveillance (causes T cell hyporesponsiveness via deple-tion of L-arginine), and high levels of arginase activity have beendemonstrated in the carcinomas of prostate, gallbladder and lung.35
PBMC arginase levels have not to the best of our knowledge beenpreviously investigated in breast cancer patients, although serumlevels of the enzyme have been reported to be elevated in suchpatients, compared to healthy individuals, in a disease stage-dependent manner.34 PBMC arginase levels tended to decrease inthe control group; this may be explained by theirmore frequent useof chemotherapy, which may have caused a decrease in circulatingpolymorphonuclear cells. In contrast, in the intervention group,PBMC arginase levels tended to increase, possibly suggesting animprovement in immune function via increased poly-morphonuclear cell levels. These tentative findings will requirefurther investigationwith a larger number of breast cancer patients.
Improvement in total mood disturbance, quality of life andbreast-specific symptoms were found in both intervention andcontrol groups. However, total stress at 3 months, and anxiety andendocrine-specific symptoms at 6 months were significantly betterin the control compared to the intervention group. The intervention
Table 5Symptoms of stress inventory: mean total and subscale scores.
Subscale meanscores
Time 1 Time 2
Intervention(n ¼ 6)
Control(n ¼ 6)
pvalue
Interventio(n ¼ 6)
Peripheral 0.86 � 0.74 0.40 � 0.55 0.310 1.05 � 0.94Cardio arousal 0.11 � 0.14 0.25 � 0.39 0.818 0.25 � 0.35Cardio respiratory 0.74 � 0.57 0.31 � 0.39 0.132 0.81 � 0.76Cardio Total 0.49 � 0.39 0.29 � 0.23 0.394 0.59 � 0.54Neurological 0.40 � 0.38 0.03 � 0.08 0.093 0.24 � 0.23Gastrointestinal 0.43 � 0.32 0.74 � 0.87 0.937 0.46 � 0.45Muscle 1.07 � 0.93 0.80 � 0.38 1.000 0.83 � 0.93Habitual 0.76 � 0.53 0.60 � 0.39 0.699 0.61 � 0.23Depression 0.98 � 0.63 0.77 � 0.60 0.699 0.52 � 0.52Anxiety 0.45 � 0.18 0.35 � 0.28 0.699 0.42 � 0.32Emotional 0.69 � 0.47 0.58 � 0.71 0.589 0.60 � 0.50Cognitive 1.24 � 0.75 0.79 � 0.66 0.485 0.64 � 0.43Total mean score 0.71 � 0.32 0.53 � 0.28 0.310 1.47 � 1.06
Statistically significant differences between the intervention and control group are show
Please cite this article in press as: Baker BS, et al., A randomised controlleintegrated support programme in breast cancer, Complementary Therap
group tended to have a poorer mood state and higher stress scorecompared to the control group at baseline, which may be of rele-vance to these findings. In addition, not all the participants in theintervention group received a sufficient number of therapy sessionsto help with their emotional and physical issues.
These preliminary findings should be interpreted with cautionas the number of participants was very small. Further, whether thetrends observed here would be reproduced in a larger study is notknown, as stratification of patients according to age, disease stage,menopausal status etc, may dilute out the effects seen with thissmall mixed group of patients. Difficulties in recruitment ofpatients were a major problem and delaying the approach topatients to later in the treatment schedule did not improve therecruitment rate. It is possible that recruitment of womenwho hadjust finished their primary cancer treatment may have been moresuccessful.36The main reason for the recruitment problems wasconsidered to be due to a reliance on busy breast care nurses at thetwo hospitals to recruit patients. It will be necessary in any futureadequately powered large-scale trial to employ a dedicatedresearch nurse or research assistant to ensure that the requirednumbers of participants are obtained. Difficulties in recruitingbreast cancer patients to complementary therapy trials have beenpreviously reported by several authors.36e39 Interestingly, none ofthe participants randomised to the control group refused to takepart as a result, and none subsequently dropped out of the study.
Time 3
n Control(n ¼ 6)
pvalue
Intervention(n ¼ 5)
Control(n ¼ 4)
pvalue
0.79 � 0.62 0.699 1.48 � 0.21 0.50 � 0.82 0.2860.17 � 0.28 0.699 0.30 � 0.49 0.00 � 0.00 0.1900.87 � 1.06 0.937 0.67 � 0.52 0.28 � 0.56 0.2860.59 � 0.59 0.937 0.52 � 0.37 0.17 � 0.33 0.1900.30 � 0.45 0.699 0.12 � 0.18 0.05 � 0.10 0.7300.80 � 0.55 0.310 0.56 � 0.54 0.31 � 0.28 0.5560.43 � 0.48 0.589 0.99 � 0.91 0.11 � 0.22 0.1110.70 � 0.27 0.589 0.82 � 0.33 0.48 � 0.22 0.1900.48 � 0.58 0.937 0.45 � 0.37 0.06 � 0.07 0.1900.18 � 0.15 0.065 0.35 � 0.25 0.07 � 0.05 0.0320.56 � 0.65 0.818 0.73 � 0.50 0.13 � 0.18 0.0630.60 � 0.46 0.937 0.83 � 0.43 0.29 � 0.31 0.0630.55 � 0.23 0.009 1.51 � 1.05 0.23 � 0.09 0.111
n in bold.
d pilot feasibility study of the physical and psychological effects of anies in Clinical Practice (2012), doi:10.1016/j.ctcp.2012.03.002

Table 6Multidimensional fatigue inventory subscale scores.
Subscalea Time 1 Time 2 Time 3
Intervention(n ¼ 6)
Control(n ¼ 6)
p value Intervention(n ¼ 6)
Control(n ¼ 6)
p value Intervention(n ¼ 5)
Control(n ¼ 4)
p value
General 8.33 � 4.08 9.33 � 2.80 0.937 9.33 � 2.16 7.33 � 4.59 0.240 8.40 � 2.30 12.00 � 3.16 0.111Physical 10.33 � 5.13 9.50 � 4.28 0.699 9.83 � 2.23 8.17 � 5.34 0.589 8.00 � 1.87 11.25 � 2.50 0.063Reduced activity 10.17 � 3.97 10.50 � 4.23 0.937 11.33 � 1.75 9.00 � 4.20 0.093 10.80 � 1.30 11.25 � 4.92 0.286Reduced
motivation10.67 � 2.34 11.83 � 4.26 0.485 11.33 � 2.34 9.67 � 2.50 0.310 11.80 � 2.68 13.75 � 2.06 0.413
Mental fatigue 8.67 � 3.14 12.67 � 3.93 0.132 9.33 � 1.86 9.83 � 3.19 0.699 9.00 � 2.35 13.25 � 2.22 0.016
a Total scores are not used for this questionnaire.
B.S. Baker et al. / Complementary Therapies in Clinical Practice xxx (2012) 1e8 7
A further limitation of the study was the differences betweenthe characteristics of the participants in the two groups. Althoughthey were of similar socio-economic and marital status, the inter-vention group participants were more highly educated, more oftendiagnosed with a milder disease and less likely to have undergonea mastectomy or to have received chemotherapy than those in thecontrol group. Stratification of participants would be necessary inany future large trial to ensure that participants in the two groupshave similar demographic and disease characteristics.
CD107+NK cells in intervention and control groups
0
5
10
15
20
T1 T2 T3
Mea
n fo
ld in
crea
se in
CD
107+
NK
cel
ls
CD107+ NK cells - Intervention CD107+ NK cells- Control
PBMC Arginase in intervention and control groups
0
5
10
15
20
T1 T2 T3
PB
MC
Arg
inas
e, m
U/m
g pr
otei
n
PBMC Arginase-Intervention PBMC Arginase-Control
A
B
Fig. 2. Immune function of intervention and control groups over 6-month studyperiod; T1 ¼ baseline, T2 ¼ 3 months, T3 ¼ 6 months. (A) CD107þ cytolytic NK assay.PBMCs were incubated with K562 target cells for 4 h at a 5:1 E:T ratio. Data presentedas mean fold increase of % CD3� CD56þCD16þCD107þ NK cells. (B) PBMC arginaselevels. Data presented as mean PBMC arginase, mU/mg protein.
Please cite this article in press as: Baker BS, et al., A randomised controlleintegrated support programme in breast cancer, Complementary Therap
Despite the small numbers of participants, the dropout rate waslow in both groups, and the amount of missing questionnaire datawas small. In addition, the majority of blood and saliva sampleswere obtained and were suitable for analysis. Data obtained fromthe four self-report questionnaires showed some differences withinand/or between groups for specific emotional and physical symp-toms, which did not appear to overlap, suggesting that all thequestionnaires would be appropriate to use in a larger trial.
The uptake of the Haven programme by the intervention groupwas, however, variable with only half participating in the Havenprogramme from the start of the study. This appeared to bedependent onwhether the individual felt that they needed support,which may have been influenced by the type of treatment theywere receiving at the time. Careful monitoring will be necessary inany future trial to ensure patient compliance.
5. Conclusions
The preliminary findings of this small pilot study suggest thatthe Haven programmemay have beneficial effects on fatigue, mooddisturbance, quality of life, breast-specific symptoms and immunefunction in women with breast cancer that warrant further inves-tigation in a large multi-centre randomised trial. This will requirean effective recruitment strategy to ensure its success.
Conflict of interest statement
None declared.
Acknowledgements
The authors kindly thank GlaxoSmithKline for funding thisstudy, all the Haven staff and Visitors who took part, Professor AlanAshworth who provided laboratory facilities at the BreakthroughBreast Cancer Research Centre, London and Cristina Naceur-Lombardi who processed the blood and saliva samples.
References
1. Molassiotis A, Fernandez-Ortega P, Pud D, Ozden G, Scott JA, Panteli V, et al. Useof complementary and alternative medicine in cancer patients: a Europeansurvey. Ann Oncol 2005;16:655e63.
2. Corner J, Harewood J, Maslin-Prothero S, Lewith G, Maher EJ, Young T, et al.A study of the use of complementary and alternative therapies among peopleundergoing cancer treatment: a quantitative and qualitative study. Final Report.NHS R&D Programme. Department of Health. University of Southampton;January 2006.
3. Wanchai A, Armer JM, Stewart BR. Complementary and alternative medicineuse among women with breast cancer: a systematic review. Clin J Oncol Nurs2011;14(4):E45e55.
4. Boon H, Olatunde F, Zick SM. Trends in complementary/alternative medicineuse by breast cancer survivors: comparing survey data from 1998 and 2005.BMC Women’s Health 2007;7:4.
5. Chao L-F, Zhang AL, Liu H-E, Cheng M-H, Lam H-B, Lao SK. The efficacy ofacupoint stimulation for the management of therapy-related adverse events in
d pilot feasibility study of the physical and psychological effects of anies in Clinical Practice (2012), doi:10.1016/j.ctcp.2012.03.002

B.S. Baker et al. / Complementary Therapies in Clinical Practice xxx (2012) 1e88
patients with breast cancer: a systematic review. Breast Cancer Res Treat2009;118:255e67.
6. Borud EK, Alraek T, White A, Fonnebo V, Eggen AE, Hammar M, et al. Theacupuncture on hot flashes among menopausal women study (ACUFLASH)study, a randomised controlled trial. Menopause 2009;16(3):484e93.
7. Borud EK, Alraek T, White A, Grimsgaard S. The acupuncture on hot flashesamong menopausal women study: observational follow-up results at 6 and 12months. Menopause 2010;17(2):262e8.
8. Kim KH, Kang KW, Kim DI, Kim HJ, Yoon HM, Lee JM, et al. Effects ofacupuncture on hot flashes in perimenopausal and postmenopausal women:a multicentre randomised clinical trial. Menopause 2010;17(2):269e80.
9. Musial F, Bussing A, Heusser P, Choi K-E, Ostermann T. Mindfulness-basedstress reduction for integrative cancer care e a summary of evidence. ForschKomplementmed 2011;18(4):192e202.
10. Hoffman CJ, Ersser SJ, Hopkinson JB, Nicholls PG, Harrington JE, Thomas PW.Effectiveness of mindfulness-based stress reduction in mood, breast- andendocrine-related quality-of-life and wellbeing in stages 0 to III breast cancer:a randomized, controlled trial. J Clin Oncol 2012 Mar 19 [epub ahead of print].
11. Carlson LE, Speca M, Faris P, Patel KD. One year pre-post intervention follow-upof psychological, immune, endocrine and blood pressure outcomes ofmindfulness-based stress reduction (MBSR) in breast and prostate canceroutpatients. Brain Behav Immun 2007;21:1038e49.
12. Savard J, Simard S, Ivers H, Morin CM. Randomized study on the efficacy ofcognitive-behavioural therapy for insomnia secondary to breast cancer, part II:immunologic effects. J Clin Oncol 2005;23:6097e106.
13. Hernandez-Reif M, Field T, Ironson G, Beutler J, Vera Y, Hurley J, et al. Naturalkiller cells and lymphocytes increase in women with breast cancer followingmassage therapy. Intern J Neurosci 2005;115:495e510.
14. Oh B, Butow P, Mullan B, Clarke S, Beale P, Pavlakis N, et al. Impact of medicalqigong on quality of life, fatigue, mood and inflammation in cancer patients:a randomised controlled trial. Ann Oncol 2010;21:606e14.
15. Seers HE, Gale N, Paterson C, Cooke HJ, Tuffrey V, Polley MJ. Individualised andcomplex experiences of integrative cancer support care: combining qualitativeand quantitative data. Support Care Cancer 2009;17:1159e67.
16. Harrington JE, Baker BS, Hoffman CJ. Effect of an integrated support pro-gramme on the concerns and wellbeing of women with breast cancer:a national service evaluation. Complement Ther Clin Pract 2012;18:10e5.
17. Buchanan DR, White JD, O’Mara M, Kelaghan JW, Smith WB, Minasian LM.Research-design issues in cancer-symptom-management trials using comple-mentary and alternative medicine: lessons from the National Cancer Institutecommunity clinical oncology program experience. J Clin Oncol 2005;23:6682e9.
18. Brady MJ, Cella DF, Mo F, Bonomi AE, Tulsky DS, Lloyd SR, et al. Reliability andvalidity of the functional assessment of cancer therapy-breast (FACT-B) qualityof life instrument. J Clin Oncol 1997;15:974e86.
19. Fallowfield LJ, Leaity SM, Howell A, Benson S, Cella D. Assessment of qualityof life in women undergoing hormonal therapy for breast cancer: validationof the endocrine system subscale for the FACT-B. Breast Cancer Res Treat1999;55:189e99.
20. Leckie MS, Thompson E. Symptoms of stress inventory. Seattle: University ofWashington; 1979.
21. Carlson LE, Ursuliak Z, Goodey E, Angen M, Speca M. The effects of a mindful-ness meditation-based stress reduction program on mood and symptoms of
Please cite this article in press as: Baker BS, et al., A randomised controlleintegrated support programme in breast cancer, Complementary Therap
stress in cancer outpatients: 6-month follow-up. Support Care Cancer2001;9:112e23.
22. Smets EMA, Garssen B, Bonke B, de Haes JCJM. The multidimensional fatigueinventory (MFI) psychometric qualities of an instrument to assess fatigue.J Psychosom Res 1995;39:315e25.
23. Smets EM, Garssen B, Cull A, de Haes JC. Application of the multidimensionalfatigue inventory (MFI-20) in cancer patients receiving radiotherapy. Brit JCancer 1996;73:241e5.
24. Gotay CC, Stern JD. Assessment of psychological functioning in cancer patients.J Psychosoc Oncol 1995;13:123e60.
25. Cassileth BR, Lusk EJ, Brown LL, Cross PA. Psychosocial status of cancer patientsand next of kin: normative data from profile of mood states. J Psychosoc Oncol1985;3:99e105.
26. McNair DM, Lorr M, Droppleman LF. EITS manual for the profile of mood states.San Diego: Educational and Industrial Testing Service; 1971.
27. Alter G, Malenfant JM, Altfeld M. CD107a as a functional marker for theidentification of natural killer cell activity. J Immunol Methods 2004;294:15e22.
28. Bronte V, Zanovello P. Regulation of immune responses by L-arginine metab-olism. Nat Rev Immunol 2005;5:641e54.
29. Rodriguez PC, Ochoa AC. Arginine regulation by myeloid derived suppressorcells and tolerance in cancer: mechanisms and therapeutic perspectives.Immunol Rev 2008;222:180e91.
30. Munder M. Arginase: an emerging key player in the mammalian immunesystem. Brit J Pharmacol 2009;158:638e51.
31. Kropf P, Baud D, Marshall SE, Munder M, Mosley A, Fuentes JM, et al. Arginaseactivity mediates reversible T cell hyporesponsiveness in human pregnancy.Eur J Immunol 2007;37:935e45.
32. Collado-Hidalgo A, Bower JE, Ganz PA, Cole SW, Irwin MR. Inflammatorybiomarkers for persistent fatigue in breast cancer survivors. Clin Cancer Res2006;12(9):2759e66.
33. Witek-Janusek L, Albuquerque K, Rambo Chroniak K, Chroniak C, Durazo-Arvizu R, Mathews HL. Effect of mindfulness based stress reduction on immunefunction, quality of life and coping in women newly diagnosed with early stagebreast cancer. Brain Behav Immun 2008;22:969e81.
34. Polat MF, TaysI S, Polat S, Boyuk A, Bakan E. Elevated serum arginase activitylevels in patients with breast cancer. Surg Today 2003;33:655e61.
35. Du C, Wang Y. The immunoregulatory mechanisms of carcinoma for its survivaland development. J Exp Clin Cancer Res 2011;30:12e21.
36. Johnston MF, Hays RD, Subramanian SK, Elashoff RM, Axe EK, Li JJ, et al. Patienteducation integrated with acupuncture for relief of cancer-related fatiguerandomized controlled feasibility study. BMC Complement Alternat Med2011;11:49e57.
37. Richardson MA, Post-White J, Singletary SE, Justice B. Recruitment forcomplementary/alternative medicine trials: who participates after breastcancer. Ann Behav Med 1998;20(3):190e8.
38. Ziegler R. Mistletoe preparation iscador: are there methodological concernswith respect to controlled clinical trials? Evid Based Complement Alternat Med2009;6(1):19e30.
39. Sikorskii A, Wyatt GK, Siddiqi A-e-A, Tamkus D. Recruitment and early reten-tion of women with advanced breast cancer in a complementary and alter-native medicine trial. Evid Based Complement Alternat Med 2011:7. doi:10.1093/ecam/nep051. Article ID 734517.
d pilot feasibility study of the physical and psychological effects of anies in Clinical Practice (2012), doi:10.1016/j.ctcp.2012.03.002