
A qualitative exploration of the cancer experience among long-term survivors: comparisons by cancer...
11
PSYCHO-ONCOLOGY Psycho-Oncology 15: 248–258 (2006) Published online 7 June 2005 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/pon.942 A QUALITATIVE EXPLORATION OF THE CANCER EXPERIENCE AMONG LONG-TERM SURVIVORS: COMPARISONS BY CANCER TYPE, ETHNICITY, GENDER, AND AGE KRISTIE LONG FOLEY a, *, DEBORAH F. FARMER a , VIDA M. PETRONIS b , ROSELYN G. SMITH b , SARAH MCGRAW c , KEVIN SMITH c , CHARLES S. CARVER b and NANCY AVIS a a Department of Public Health Sciences, Wake Forest University School of Medicine, Winston-Salem, NC, USA b University of Miami, Coral Gables, FL, USA c New England Research Institutes, Watertown, MA, USA SUMMARY Background: To elucidate meanings ascribed to the cancer experience by long-term survivors. Methods: Semi-structured interviews were conducted with 58 cancer survivors (415 years post-diagnosis). Respondents described how cancer affected their quality of life (QOL) generally and in 17 domains. Systematic content analyses were conducted to extract themes relating to meanings assigned to the cancer experience. Themes were analyzed by cancer type, gender, and age and confirmed using quantitative assessments of self-rated health and QOL. Results: Four themes were identified: Personal Growth, That’s Life. Relinquishing Control, and Resentment. Women more frequently acknowledged Personal Growth, and men more often indicated minimal impact on their lives (That’s Life). Older survivors were disproportionately classified as That’s Life and younger survivors as Personal Growth. No differences were observed by cancer type or ethnicity. Those who saw cancer as personal growth had the highest QOL, while those who resented cancer had the lowest QOL. Conclusions: Most long-term survivors retrospectively report that cancer either positively influenced their lives or had little long-term impact. Those who express Resentment report that pain, physical deformities, and social isolation significantly reduced their QOL. This qualitative study highlights how cancer survivors incorporate the cancer experience within their overall lives. Copyright # 2005 John Wiley & Sons, Ltd. KEY WORDS: cancer; long-term survivor; quality of life; psychosocial aspects INTRODUCTION Improved early detection and treatment of cancer has resulted in half of all cancer patients surviving 5 or more years, with 9.8 million cancer survivors in the United States in 2001 (Rowland et al., 2004; Parker et al., 1997). Increasing numbers and length of survival have heightened interest in studying the long-term effects of cancer on quality of life (QOL). Quantitative studies have shown that long-term survivors continue to experience residual effects, such as fatigue, pain, low energy levels, and sleep disturbance long after treatment ends (Kornblith et al., 2003; Broeckel et al., 2002; Wenzel et al., 2002; Hammerlid and Taft, 2001; Bower et al., 2000; Gotay and Muraoka, 1998; Dow et al., 1996; Ferrell et al., 1995a,b). Breast cancer survivors often have difficulty with lymphedema and numb- ness (Kornblith et al., 2003) and head and neck cancer survivors experience problems with swal- lowing, localized pain, and dry mouth (Hammerlid and Taft, 2001; Wijers et al., 2002). While these Received 21 August 2004 Copyright # 2005 John Wiley & Sons, Ltd. Accepted 14 April 2005 *Correspondence to: Department of Public Health Sciences, Section on Social Sciences and Health Policy, Wake Forest University, School of Medicine, Piedmont Plaza II-2nd Floor, Winston-Salem, NC 27157-1063, USA. E-mail: kfoley@ wfubmc.edu
Transcript of A qualitative exploration of the cancer experience among long-term survivors: comparisons by cancer...

PSYCHO-ONCOLOGY
Psycho-Oncology 15: 248–258 (2006)Published online 7 June 2005 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/pon.942
A QUALITATIVE EXPLORATION OF THECANCER EXPERIENCE AMONG LONG-TERM
SURVIVORS: COMPARISONS BY CANCER TYPE,ETHNICITY, GENDER, AND AGE
KRISTIE LONG FOLEYa,*, DEBORAH F. FARMERa, VIDA M. PETRONISb, ROSELYN G. SMITHb, SARAH
MCGRAWc, KEVIN SMITHc, CHARLES S. CARVERb and NANCY AVISaaDepartment of Public Health Sciences, Wake Forest University School of Medicine, Winston-Salem, NC, USA
bUniversity of Miami, Coral Gables, FL, USAcNew England Research Institutes, Watertown, MA, USA
SUMMARY
Background: To elucidate meanings ascribed to the cancer experience by long-term survivors.Methods: Semi-structured interviews were conducted with 58 cancer survivors (415 years post-diagnosis).
Respondents described how cancer affected their quality of life (QOL) generally and in 17 domains. Systematiccontent analyses were conducted to extract themes relating to meanings assigned to the cancer experience. Themeswere analyzed by cancer type, gender, and age and confirmed using quantitative assessments of self-rated health andQOL.Results: Four themes were identified: Personal Growth, That’s Life. Relinquishing Control, and Resentment.
Women more frequently acknowledged Personal Growth, and men more often indicated minimal impact on theirlives (That’s Life). Older survivors were disproportionately classified as That’s Life and younger survivors asPersonal Growth. No differences were observed by cancer type or ethnicity. Those who saw cancer as personalgrowth had the highest QOL, while those who resented cancer had the lowest QOL.Conclusions: Most long-term survivors retrospectively report that cancer either positively influenced their lives or
had little long-term impact. Those who express Resentment report that pain, physical deformities, and socialisolation significantly reduced their QOL. This qualitative study highlights how cancer survivors incorporate thecancer experience within their overall lives. Copyright # 2005 John Wiley & Sons, Ltd.
KEY WORDS: cancer; long-term survivor; quality of life; psychosocial aspects
INTRODUCTION
Improved early detection and treatment of cancerhas resulted in half of all cancer patients surviving5 or more years, with 9.8 million cancer survivorsin the United States in 2001 (Rowland et al., 2004;Parker et al., 1997). Increasing numbers and lengthof survival have heightened interest in studying the
long-term effects of cancer on quality of life(QOL).
Quantitative studies have shown that long-termsurvivors continue to experience residual effects,such as fatigue, pain, low energy levels, and sleepdisturbance long after treatment ends (Kornblithet al., 2003; Broeckel et al., 2002; Wenzel et al.,2002; Hammerlid and Taft, 2001; Bower et al.,2000; Gotay and Muraoka, 1998; Dow et al., 1996;Ferrell et al., 1995a,b). Breast cancer survivorsoften have difficulty with lymphedema and numb-ness (Kornblith et al., 2003) and head and neckcancer survivors experience problems with swal-lowing, localized pain, and dry mouth (Hammerlidand Taft, 2001; Wijers et al., 2002). While these
Received 21 August 2004Copyright # 2005 John Wiley & Sons, Ltd. Accepted 14 April 2005
*Correspondence to: Department of Public Health Sciences,Section on Social Sciences and Health Policy, Wake ForestUniversity, School of Medicine, Piedmont Plaza II-2nd Floor,Winston-Salem, NC 27157-1063, USA. E-mail: [email protected]

quantitative studies offer insights into sympto-matic complaints among long-term survivors, theyoften fail to represent the full effect of cancer andthe survivor’s interpretation of the overall cancerexperience. For example, some breast cancerpatients report marked benefits from beingcancer survivors (Helgeson et al., 2004; Tomichand Helgeson, 2004; Sears et al., 2003). Qualitativestudies afford researchers an opportunity to fullyevaluate cancer meaning. They can offer a uniqueperspective on survivorship and provide a rich andcoherent picture of individual cancer experiences.In one qualitative study, Wyatt and colleagues(1996) found that some long-term female cancersurvivors emerge from the experience as ‘newwomen’ who put their physical changes intoperspective and focus more on relationships,existential issues, and the pursuit of health. Otherqualitative studies have identified positive aspectsof cancer generally not assessed with traditionalquestionnaires such as increases in spirituality,living in the ‘here and now’ and greater apprecia-tion for life (Osoba et al., 1997; Borghede andSullivan, 1996; Cella et al., 1993; Ringdal andRingdal, 1993; Wyatt et al., 1993, p. 445; Schipperet al., 1984).
Many of these qualitative studies, however,recognize that long-term survivors continue toexperience unresolved issues, such as fear ofrecurrence and concern that health care providersdo not take their concerns seriously. These studiesprovide a perspective on long-term survivorshipthat includes both the positive and negativeaspects of having cancer, as well as a gestalt ofhow individuals define (or redefine) their existenceafter living through and beyond cancer. Previousqualitative studies, however, tend to focus onhomogeneous samples typically representingone cancer type, limiting generalizability andcomparability across cancer types, and tend to begender-specific as a function of including onlyone cancer type (e.g. prostate or breast cancersurvivors).
The current study attempts to fill the gaps in thelong-term survivorship literature by analyzing in-depth qualitative interviews of diverse long-termsurvivors with different types of cancer. Thegoal of this study was to evaluate individualinterpretations of the cancer experience andhow these interpretations affect QOL 5 or moreyears post-diagnosis. Special attention is givento differences by cancer type, ethnicity, gender,and age.
METHODS
Participants
Data for this investigation comes from a largereffort to develop and evaluate a new QOL measuredesigned specifically for long-term cancer survi-vors: the QOL in Adult Cancer Survivors(QLACS) (Avis et al., in press). The first task inthe development of the QLACS was to identifyQOL domains and items that were most relevantto long-term cancer survivors using data from in-depth, in-person semi-structured interviews. Theseinterviews form the basis of the study reportedhere.
Detailed information about recruitment andparticipants is found in Avis et al. (in press).Briefly, participants lived in southeast Florida andhad been diagnosed at least 5 years earlier withcancers of the breast, head/neck, cervix/ovaries,bladder, prostate, or colon/rectum. These cancerswere selected because they have large numbers oflong-term survivors. Participants were recruitedthrough the Florida Cancer Data System (FCDS)which is a database containing the names andaddresses of all persons in two South Floridacounties (Miami-Dade and Broward). Followingconsent to participate, research assistants con-ducted in-depth interviews and brief self-adminis-tered questionnaires were completed in theperson’s home or preferred meeting place.
Data collection and measures
The self-administered questionnaire combinedbasic demographics (gender, age, race, education,employment status), self-rated health, and twoglobal QOL scales. Self-rated health was measuredon a standard 5-point scale from poor to excellent.Taken from the MOS SF-36, this item has beenassociated with various objective health measures(e.g. functional status, mortality) and QOL (Wareand Sherbourne, 1992; Idler and Benyamini,1997). Global QOL was assessed with the Ladderof Life and a Visual Analogue Scale (VAS). TheLadder of Life is a single-item measure developedby Cantril (1965) and modified by Andrews andWithey (1976). Respondents are shown a steplad-der with rungs from 1 to 10 where ‘1’ representsthe worst possible life and ‘10’ represents the bestpossible life and asked to circle the number that
CANCER EXPERIENCE AMONG LONG-TERM SURVIVORS 249
Copyright # 2005 John Wiley & Sons, Ltd. Psycho-Oncology 15: 248–258 (2006)
represents how they felt at the present time. TheLadder has been used with variations by others(Avis et al., 2004; Ganz et al., 2002: Brown et al.,1981; Palmore and Luikart, 1972). The VAS is a100mm bar where respondents are asked to marktheir current QOL on a scale from 0 to 100 where 0represents the lowest possible QOL and 100represents the highest possible quality. Single-itemratings of this sort have been shown to be goodsummary measures of QOL with test–retestreliabilities ranging from 0.70 to 0.87 (deBoeret al., 2004; Gudex et al., 1996; Youngblut andCasper, 1993; Schag et al., 1990).
Following completion of this brief question-naire, a semi-structured interview was conducted.The interview began by asking participants todescribe themselves, the history of their diagnosis,how cancer and its treatment affected their lives atthe time. Respondent were then asked to describeareas in their lives most affected by having hadcancer. The entire transcribed interview was usedfor data analytical purposes.
Although the semi-structured interview specifi-cally targeted aspects of QOL, the respondentsascribed meaning to the cancer experience withinthe context of their prior and current QOL. Forexample, when a person was asked ‘How was yourlife affected at that time by being diagnosed withcancer?’ and later asked ‘Do you have any specialconcerns in life now because you have had cancer?’respondents often discussed how they assignedmeaning to the cancer diagnosis and how suchmeaning affected their overall QOL at the time ofdiagnosis and at the time of the interview.
Data analyses
Transcripts of participant interviews were ana-lyzed using a 5-step framework approach (Popeet al., 2000). The first step involved familiarizationand immersion in the raw data; two investigators(K.F. and D.F.) independently read the tran-scribed interviews and extracted key commentsassociated with how individuals ascribed meaningto the cancer experience. The second step was theidentification of a thematic framework. Theinvestigators met to discuss the abstracted infor-mation related to cancer meaning and identifiedprimary and secondary themes that emerged.Disagreements between researchers in the identifi-cation of themes provided insights that were usedto refine coding (Barbour, 2001). Research has
shown that experienced qualitative researchersanalyzing the same transcript show close agree-ment in identifying themes (Armstrong et al.,1997).
Third, the thematic framework, including allthemes, was applied to all data (Pope et al., 2000).Fourth, charts were made of primary and second-ary themes for all participants. These charts weresorted to further elucidate the relevance of themesby cancer type, age, gender, and race/ethnicity.Finally, the charts were interpreted to capture therichness of the data.
The process employed to collect, analyze andreanalyze the data was useful in elucidating QOLthemes of long-term survivors of a variety ofcancer types. The themes centered on individualinterpretations of the cancer experience and howthese interpretations related to long-term QOL.Special attention was given to commonalities anddifferences across cancer type, gender, and age.These themes were then validated using structuredsurvey items on self-rated health and two globalQOL indices.
RESULTS
Description of the sample
A total of 58 cancer survivors were interviewed.The sample was distributed among cancer types asfollows: bladder (n ¼ 6), breast (n ¼ 12), colo-rectal (n ¼ 11), gynecologic (n ¼ 10), head andneck (n ¼ 9), and prostate (n ¼ 10). The samplewas predominately Caucasion and female andranged in age at diagnosis from 25 to 86. SeeTable 1 for sample characteristics.
Meaning of the cancer experience
The majority of survivors described cancer asanother of life’s hurdles to be managed and movedbeyond. For some, however, cancer dramaticallychanged their lives for better or worse many yearspost-diagnosis. Ultimately, four primary themeswere identified: That’s Life, Personal Growth,Relinquishing Control and Resentment. Althoughspirituality did not emerge as a primary theme, itwas nonetheless a common thread throughoutmany interviews and was classified as an importantsecondary theme.
K. L. FOLEY ET AL.250
Copyright # 2005 John Wiley & Sons, Ltd. Psycho-Oncology 15: 248–258 (2006)

That’s Life (n ¼ 38). Many individuals re-ported that they approached the diagnosis andtreatment in a very matter-of-fact manner. Theyaccepted the diagnosis, pursued the appropriatecourse of treatment, and went on with life withlittle incident. They indicated that their currentQOL had little to do with cancer or its treatment.
An elderly prostate cancer survivor reportedthat his life did not change, other than theinconvenience of going for radiation treatmentsevery day for 2 months. ‘I just took it as I would atoothache or whatever it was, except there was nopain involved.’ One breast cancer survivor saidthat cancer did not have any effect on her life otherthan the inconvenience of chemotherapy; ‘I don’tblame the cancer for anything. I certainly didn’thave to change my lifestyle for it. I made itaccommodate to me.’ In a similar fashion, a
different breast cancer survivor reported thatcancer made a minimal difference in her life; ‘Lifegoes on. That wasn’t my time.’
A male colorectal cancer survivor, a ministerwho had to wait 6 weeks to get back into the pulpitreported, ‘I just accept it as part of life.’ Anotherfemale colorectal cancer survivor stated, ‘Youknow, you feel like that’s the past, over and donewith. Get a move on.’ A 6-year bladder cancersurvivor who suffered a recurrence of cancer 2years prior to the interview states that cancer hasnot changed his life; ‘Like I told you before, I havebeen very, very fortunate and I don’t think that theBig C has changed me one iota, nothingwhatsoever.’
Personal Growth (n ¼ 12). Many cancer survi-vors reported that their immediate interpretationand sustaining force throughout treatment waspositive. They report they always expected tosurvive and the cancer had relatively little short- orlong-term negative impact on their lives. In fact,cancer had a positive impact on long-term QOL. Itfostered a greater appreciation for life and adetermination to enjoy life without letting littlethings upset them. In general, the cancer experi-ence amplified the person’s pre-existing innerstrengths. For a head and neck cancer survivorwho was 28 years old at the time of diagnosis,separated and raising two young children, thecancer experience with the disfiguring aftermath ofsurgery and radiation was viewed as a positivegrowth experience.
I really couldn’t ask for a better life. Even with myphysical appearance and everything that I’ve beenthrough, if I had to do it again, I would. . . .I couldn’t ask for a better thing to happen to mebecause I have matured and I have developed aspecial relationship with God, and my parents, andmy life in general is better.
An older prostate cancer survivor whose dreamsof a comfortable retirement evaporated when heused his retirement nest egg to pay for cancertreatment and whose subsequent incontinencemakes it impossible for him to get a job, none-theless regards his cancer experience as positive. ‘Ithink that the cancer has made me a morecomplete human being. . . . I feel like I am hereon earth to do something else.’ A man who wasconsidering divorce at the time of his diagnosis,who ultimately sold his business, rearranged hispriorities in life, and who now 26 years later has
Table 1. Description of the study sample (N ¼ 58)
Characteristic n (%)
Cancer type
Bladder 6 (10.3)
Breast 12 (20.7)
Colorectal 11 (19.0)
Gynecological 10 (17.2)
Head and Neck 9 (15.5)
Prostate 10 (17.2)
Gender
Female 32 (55.2)
Male 26 (44.8)
Age at diagnosis (years)
550 10 (17.2)
50–64 16 (27.6)
65+ 32 (55.2)
Race
Black 9 (15.5)
Hispanic 8 (13.9)
White 41 (70.7)
Years since diagnosis (mean) 7.7
5 18 (31.0)
6–9 29 (50.0)
10+ 11 (19.0)
Educational level
Less than high school 6 (10.3)
High school grad/some college 33 (27.6)
College grad 19 (55.2)
CANCER EXPERIENCE AMONG LONG-TERM SURVIVORS 251
Copyright # 2005 John Wiley & Sons, Ltd. Psycho-Oncology 15: 248–258 (2006)

been married 46 years, states ‘Cancer for me atleast was the best thing that ever happened.’
A woman who had a mastectomy, lymphect-omy, and chemotherapy found that cancer en-riched her life. When asked if having had cancerhad any positive impact on her life she replied: ‘AsI said, to be more appreciative of living today andtaking advantage of it. It was a philosophy before,now it is almost a crusade to me.’ Some survivorsare very vocal in stating that cancer improved theirlives. A cervical cancer survivor found that cancerand its treatment made her stronger and moreconfident. ‘It has just given me a better outlook. . .Actually I can honestly say I am glad for theexperience because it has affected me in a positivemanner.’
Resentment (n ¼ 6). Survivors rarely definedtheir cancer experience with complete negativity.Individuals were able to identify some positiveaspect of cancer, in spite of residual pain, fears ofrecurrence, etc. However, some experienced con-siderable depression and/or anger related to thecancer diagnosis and treatment and its long-termeffects. Physical deformities, health problemsresulting from cancer and its treatment, residualpain and social isolation in particular, led to asignificantly reduced QOL and a clear resentmentfor having had cancer. A 17-year head and neckcancer survivor who had increasing difficulty withpain from scar tissue forming in his mouth, littleenergy, and concern about his appearance was nolonger able to work and had removed himselfalmost completely from public life. He stated:
I’m a mean person. I have a lot of anger in me,because I can’t do the things that I want to do. And Iattribute it to the aftermath of what has happened tome. . . I mean, the cancer and the surgery and all thethings that are gone and done with it. . .
A cervical cancer survivor who became sociallyisolated as a result of cancer and the aftermath ofits treatment says: ‘(Life) It’s not full at all. It’sreally not even a life. It’s just an existence. . . It’sdone everything to me. It’s the big C.’ A middle-aged prostate cancer survivor who constantlyworries about recurrence and stays home due toincontinence problems says:
Sometimes I think I’m going to go nuts. I startthinking of the cancer, and my situation. Sometimes,for no reason at all. . . . I am unhappy. . . . I feel sorryfor myself. I feel forgotten. . . . Sometimes I feel angrywith God and I feel so desperate, you know? So
desperate. I say, ‘Why me? Why should I be goingthrough all of this. . .’?
Relinquishing Control (n ¼ 2). A few survivorsreported that they dealt with the cancer experienceby learning to let go and relinquish control of theirlives. As a middle-aged female, head and neckcancer survivor stated:
My outlook is that whatever will be will be, and Ireally have no control over it. . . . There’s a reason foreverything, but I don’t question it anymore; I acceptit. Because it’s fate, it’s what it’s supposed to be.
A breast cancer survivor noted:
And I had to really be punched in the face before Ilearned that we really have no control, that we aregiven so many days, so many minutes, and it’s whatyou make of those minutes that makes life what it is.
Secondary themes. For the majority of cancersurvivors, assessment of their cancer experienceevoked varied responses. Many classified as That’sLife also acknowledged the positive benefits ofhaving had cancer. Spirituality was a commonsecondary theme. Most individuals who expressedPersonal Growth indicated they had grownspiritually and developed a deeper appreciationor commitment to their faith. Surviving canceroffered them the opportunity to begin life again ina more dedicated, spiritual way. One breast cancersurvivor whose cancer forced her to declarebankruptcy and who cried ‘for about two years,’reported that cancer also spurred her to turn herlife around.
And so, the day that I was diagnosed with cancer, Isaid, ‘Well,’ I said, ‘God, is this your way of talkingto me? Well, if it is, I lay everything aside and start tolive my life, you know, to please you.’
A female cervical cancer survivor who curtailedmany of her activities due to the effects ofradiation and other health problems, says:
I think my religious beliefs are stronger. Having hadcancer. I have always attended church and I knewthere was a Supreme Being, but I think after gettingthis far with the cancer I know that the Lord isworking through my doctors.
A few survivors who viewed cancer as anopportunity for Personal Growth also adopted aThat’s Life focus and one expressed Resentment.
K. L. FOLEY ET AL.252
Copyright # 2005 John Wiley & Sons, Ltd. Psycho-Oncology 15: 248–258 (2006)
Two survivors whose main theme was Resentmentand two whose main theme was RelinquishingControl also noted that they had experiencedPersonal Growth in dealing with cancer. Only twowhose main theme was Resentment were con-sumed by this feeling and could not find anythingpositive in the cancer experience.
Other secondary themes were mentioned lessfrequently than spirituality. Awareness of one’sown mortality and fear of recurrence were notedby several survivors. A few talked about lifestylechanges they had made. Some stopped taking theirhealth for granted, changed their eating habits,quit smoking, and began taking better care ofthemselves. For example, one breast cancersurvivor became a vegetarian and a nudist, begana spiritual journey, changed jobs, began volunteer-ing, and engaged in a number of self-helpactivities. A cervical cancer survivor who was 38years old at diagnosis began eating healthier,exercising more, spending more time with herchildren, and took steps to reduce her stress.
Some survivors found that the cancer experiencedrew them closer to family and friends and madethem more appreciative of their time together,while others found that relationships with family
or friends deteriorated. Concerns such as weightgain, fatigue and lack of energy, incontinence andbowel problems, impotence and sexual dysfunc-tion, gas, difficulties with concentration andmemory, problems with eating and talking, aswell as financial and insurance hardships werenoted. Some accepted these changes philosophi-cally as part of life; others were resentful, curtailedactivities and became more socially isolated.
A number of emotions were expressed: anger,frustration, mood swings and depression as well asincreased optimism and hopefulness. Some survi-vors felt that the cancer experience had made themstronger, and many stated they had changed theirpriorities and adopted a new attitude toward life.
Cancer meaning by type, ethnicity, gender, and ageat diagnosis
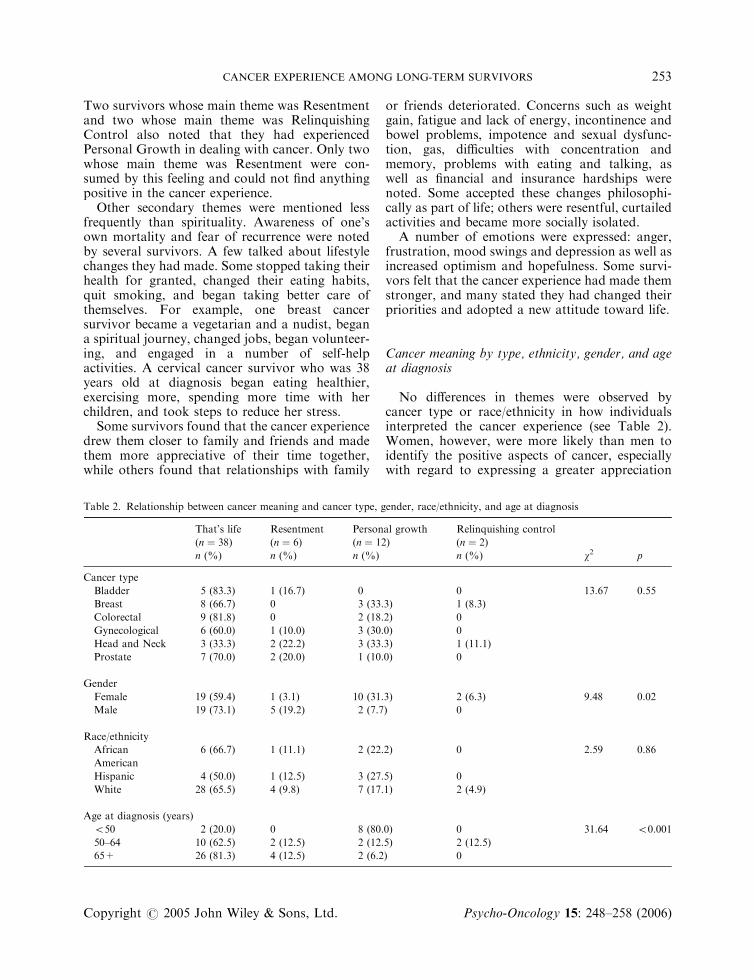
No differences in themes were observed bycancer type or race/ethnicity in how individualsinterpreted the cancer experience (see Table 2).Women, however, were more likely than men toidentify the positive aspects of cancer, especiallywith regard to expressing a greater appreciation
Table 2. Relationship between cancer meaning and cancer type, gender, race/ethnicity, and age at diagnosis
That’s life Resentment Personal growth Relinquishing control
(n ¼ 38) (n ¼ 6) (n ¼ 12) (n ¼ 2)
n (%) n (%) n (%) n (%) w2 p
Cancer type
Bladder 5 (83.3) 1 (16.7) 0 0 13.67 0.55
Breast 8 (66.7) 0 3 (33.3) 1 (8.3)
Colorectal 9 (81.8) 0 2 (18.2) 0
Gynecological 6 (60.0) 1 (10.0) 3 (30.0) 0
Head and Neck 3 (33.3) 2 (22.2) 3 (33.3) 1 (11.1)
Prostate 7 (70.0) 2 (20.0) 1 (10.0) 0
Gender
Female 19 (59.4) 1 (3.1) 10 (31.3) 2 (6.3) 9.48 0.02
Male 19 (73.1) 5 (19.2) 2 (7.7) 0
Race/ethnicity
African 6 (66.7) 1 (11.1) 2 (22.2) 0 2.59 0.86
American
Hispanic 4 (50.0) 1 (12.5) 3 (27.5) 0
White 28 (65.5) 4 (9.8) 7 (17.1) 2 (4.9)
Age at diagnosis (years)
550 2 (20.0) 0 8 (80.0) 0 31.64 50.001
50–64 10 (62.5) 2 (12.5) 2 (12.5) 2 (12.5)
65+ 26 (81.3) 4 (12.5) 2 (6.2) 0
CANCER EXPERIENCE AMONG LONG-TERM SURVIVORS 253
Copyright # 2005 John Wiley & Sons, Ltd. Psycho-Oncology 15: 248–258 (2006)

for life, moving them towards a more fulfillingexistence, and a commitment to the greater goodthrough volunteerism. Men reflected upon thecancer experience in a very matter-of-fact manner.They acknowledge and respect that it is a part oftheir lives, but indicate that cancer had neitherpositive nor negative long-term implications onQOL.
Age at diagnosis (but not age at interview ortime since diagnosis) was related to how indivi-duals view the cancer experience. For the oldercancer patient, a diagnosis is perceived to be a partof ‘aging’ and, for many, is compared to othermorbidities that are more greatly influencing theircurrent QOL. These survivors have difficultydifferentiating between the late effects of cancerand its treatment and ‘old age.’ As an 82 year oldretired salesman and prostate cancer survivor putit, ‘I don’t know if it’s the cancer or it’s the old age.Like I would like. . . to be able to play ball, and Ihave the time. . . But I just can’t do it.’ Or as a 91year old retired schoolteacher and 5-year color-ectal cancer survivor states, ‘It [my life] is moreaffected by my eyes and my incontinence, not thecancer.’ As an 82 year old ovarian cancer survivorstates, ‘My physical, the things that I am botheredby now have nothing to do with having hadcancer.’ A 71 year old head and neck cancersurvivor says, ‘Ever hear of Old-timer’s? I lay itmostly to being 71 years old, as far as memorygoes.’
The older patient diagnosed with cancer is alsomore likely to compare the cancer experience toother immediate concerns, such as care giving for afrail spouse and/or the death of a loved one.Difficulties with concentration, for example, sud-denly seem rather insignificant when confrontedwith the death of a lifelong partner. A 78 year oldretired mechanical engineer, widowed 2 yearsearlier, says that he has had to adjust his lifestyledue to cancer but that it was not as difficult asadjusting to widowhood: ‘Yes. No question aboutit. But the worse thing was [going from] beingmarried to not being married.’ An 80 year oldretired Air Force Lieutenant Colonel and formersecurity business owner whose cancer of the vocalcords has left him with a diminished speakingvoice reports he is more concerned about hisdaughter than about himself: ‘What bothered memore is for my daughter to have had cancer.’
Survivors diagnosed at young ages often re-ferred to cancer as a life-changing event, some-thing that reshaped their outlook on life and, in
many cases, led to changes in work or personalrelationships. One 47 year old breast cancersurvivor said ‘This (life) isn’t a dress rehearsal,this is it, you know.’ She goes on to describe howshe lives moment-by-moment and each day to itsfullest solely as a result of having had cancer.Another young breast cancer survivor (35 at thetime of diagnosis) ended a difficult marriage afterdiagnosis with cancer and continues to commitconsiderable time volunteering for cancer-relatedorganizations and support groups. She says thebenefits of cancer ‘. . .were finding that I have moreinner strength than I knew I had, finding that Icould make changes in my life that were bene-ficial.’ When describing the 5-years after diagnosiswith breast cancer, ‘. . .it’s been a wonderful fiveyears, just action-packed.’ Life-changing experi-ences were not solely among young breast cancerpatients. A 51 year old head and neck cancersurvivor quit a stressful job after diagnosis,married, and became more committed to herspiritual well-being.
Meaning of cancer and QOL
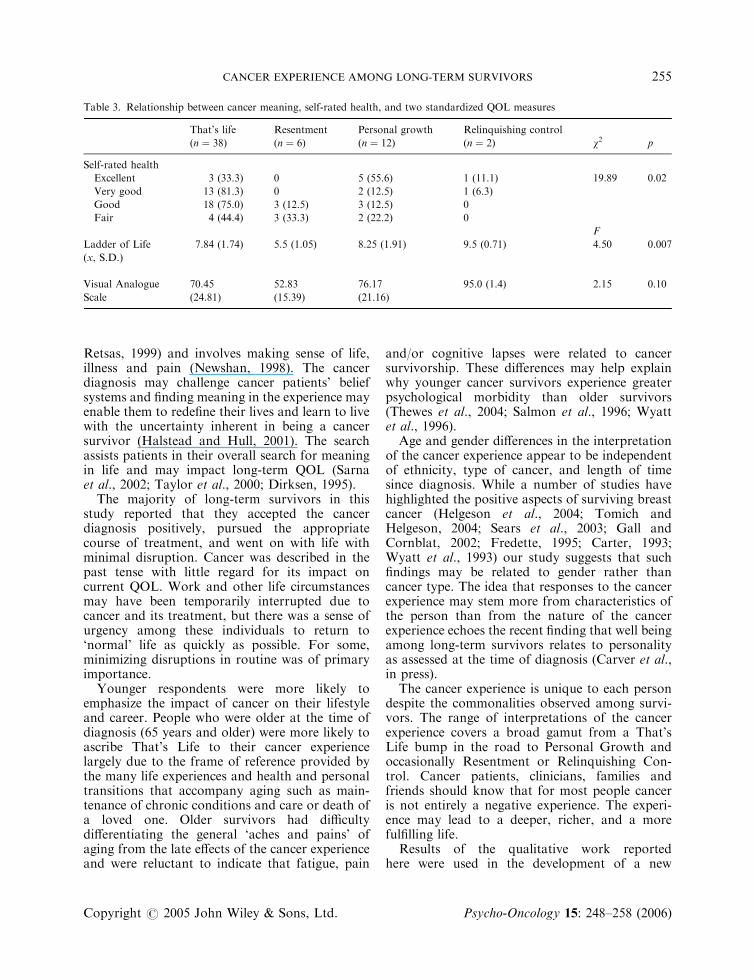
We next examined how these themes related toquantitative measures of self-rated health and ourglobal measures of QOL (see Table 3). Personswho assigned Personal Growth or RelinquishingControl to the cancer were more likely than thosewith That’s Life or Resentment themes to reporttheir health as excellent or very good. Half of thoseclassified as Resentment indicated their health wasfair.
Additionally, global QOL reported on theLadder scale was considerably lower for those inthe Resentment category compared to those inThat’s Life, Personal Growth, or RelinquishingControl (5.5 vs 7.8, 8.3, and 9.5, respectively,p ¼ 0:007). Lastly, QOL on the VAS was alsomuch lower among those in Resentment (52.8);persons assigned Relinquishing Control (95.0) hadthe highest QOL scores.
DISCUSSION
Deriving meaning from the cancer experience is animportant part of adjusting to diagnosis, treatmentand survivorship. The search for meaning comesfrom the need for self-preservation (Thomas and
K. L. FOLEY ET AL.254
Copyright # 2005 John Wiley & Sons, Ltd. Psycho-Oncology 15: 248–258 (2006)
Retsas, 1999) and involves making sense of life,illness and pain (Newshan, 1998). The cancerdiagnosis may challenge cancer patients’ beliefsystems and finding meaning in the experience mayenable them to redefine their lives and learn to livewith the uncertainty inherent in being a cancersurvivor (Halstead and Hull, 2001). The searchassists patients in their overall search for meaningin life and may impact long-term QOL (Sarnaet al., 2002; Taylor et al., 2000; Dirksen, 1995).
The majority of long-term survivors in thisstudy reported that they accepted the cancerdiagnosis positively, pursued the appropriatecourse of treatment, and went on with life withminimal disruption. Cancer was described in thepast tense with little regard for its impact oncurrent QOL. Work and other life circumstancesmay have been temporarily interrupted due tocancer and its treatment, but there was a sense ofurgency among these individuals to return to‘normal’ life as quickly as possible. For some,minimizing disruptions in routine was of primaryimportance.
Younger respondents were more likely toemphasize the impact of cancer on their lifestyleand career. People who were older at the time ofdiagnosis (65 years and older) were more likely toascribe That’s Life to their cancer experiencelargely due to the frame of reference provided bythe many life experiences and health and personaltransitions that accompany aging such as main-tenance of chronic conditions and care or death ofa loved one. Older survivors had difficultydifferentiating the general ‘aches and pains’ ofaging from the late effects of the cancer experienceand were reluctant to indicate that fatigue, pain
and/or cognitive lapses were related to cancersurvivorship. These differences may help explainwhy younger cancer survivors experience greaterpsychological morbidity than older survivors(Thewes et al., 2004; Salmon et al., 1996; Wyattet al., 1996).
Age and gender differences in the interpretationof the cancer experience appear to be independentof ethnicity, type of cancer, and length of timesince diagnosis. While a number of studies havehighlighted the positive aspects of surviving breastcancer (Helgeson et al., 2004; Tomich andHelgeson, 2004; Sears et al., 2003; Gall andCornblat, 2002; Fredette, 1995; Carter, 1993;Wyatt et al., 1993) our study suggests that suchfindings may be related to gender rather thancancer type. The idea that responses to the cancerexperience may stem more from characteristics ofthe person than from the nature of the cancerexperience echoes the recent finding that well beingamong long-term survivors relates to personalityas assessed at the time of diagnosis (Carver et al.,in press).
The cancer experience is unique to each persondespite the commonalities observed among survi-vors. The range of interpretations of the cancerexperience covers a broad gamut from a That’sLife bump in the road to Personal Growth andoccasionally Resentment or Relinquishing Con-trol. Cancer patients, clinicians, families andfriends should know that for most people canceris not entirely a negative experience. The experi-ence may lead to a deeper, richer, and a morefulfilling life.
Results of the qualitative work reportedhere were used in the development of a new
Table 3. Relationship between cancer meaning, self-rated health, and two standardized QOL measures
That’s life Resentment Personal growth Relinquishing control
(n ¼ 38) (n ¼ 6) (n ¼ 12) (n ¼ 2) w2 p
Self-rated health
Excellent 3 (33.3) 0 5 (55.6) 1 (11.1) 19.89 0.02
Very good 13 (81.3) 0 2 (12.5) 1 (6.3)
Good 18 (75.0) 3 (12.5) 3 (12.5) 0
Fair 4 (44.4) 3 (33.3) 2 (22.2) 0
F
Ladder of Life 7.84 (1.74) 5.5 (1.05) 8.25 (1.91) 9.5 (0.71) 4.50 0.007
(x, S.D.)
Visual Analogue 70.45 52.83 76.17 95.0 (1.4) 2.15 0.10
Scale (24.81) (15.39) (21.16)
CANCER EXPERIENCE AMONG LONG-TERM SURVIVORS 255
Copyright # 2005 John Wiley & Sons, Ltd. Psycho-Oncology 15: 248–258 (2006)
instrument}the QOL among Adult Cancer Sur-vivors (QLACS, Avis et al., in press) scale. As aresult of this qualitative work, the QLACSincluded a domain assessing personal growth orbenefits. The QLACS also taps into the That’s Lifetheme with questions about contentment andpositive outlook on life and the Resentment themewith items on distress in relationships, pain,discomfort, and cancer recurrence and itemsreflecting social distancing or isolation. Theinstrument also addresses a number of secondarythemes: fatigue and lack of energy, sexual dysfunc-tion, concentration and memory, financial andinsurance problems, mood swings, and depression.
Prior to this work, two instruments assessedQOL in long-term cancer survivors: the QOL-Cancer Survivors scale (QOL-CS; Ferrell et al.,1995a) and the Long-term QOL (LTQL;Wyatt et al., 1996; Wyatt and Donze, 2003).These two measures contain the same items, butorganize them into different domains. They haveone item related to positive change, but neitherhas a benefits scale. The items do not addressthe domains of That’s Life, Resentment orRelinquishing Control or difficulties withmemory and concentration, financial or insurancesequelae, or possible emotional aftermaths ofcancer such as depression, increased hopefulness,or anger. These issues have been incorporated intothe QLACS.
This study of cancer survivors has severalstrengths that differentiate it from other studieson long-term survivorship. First, the participantswere a diversified group in terms of cancer type,race/ethnicity, gender, and age. To the best of ourknowledge, no other study has explored long-termQOL across this broad spectrum of cancersurvivors. Secondly, the one-on-one nature of theinterviews provided breadth and depth of informa-tion. Finally, all participants were at least 5 yearspost-diagnosis, so as not to confound issues oflong-term survivorship with those related to newdiagnoses.
The findings of this study, however, should beinterpreted with some caution. The diversity ofthis study, while a strength, limits in-depthexploration of issues specifically relevant to anyone cancer type. The small number of Hispanicand African American participants limits racial/ethnic comparisons of long-term QOL. While ourstudy was intentionally designed to explore cancermeaning and QOL across a broad spectrumof cancer patients, the small sample size and
qualitative analyses limit the confidence withwhich cancer meaning themes and differencesby cancer type, gender, and age were fullyuncovered. The participants’ impressions of thecancer experience were inherently colored by timeand based on hindsight about the experience.Further, volunteers who participated in this studymay be more optimistic than others who chose notto participate. Thus, the study may underestimatethe prevalence of Resenters in the survivorpopulation. Lastly, the cross-sectional natureof this study does not allow determination ofthe direction of the relationship between themesand QOL.
CONCLUSIONS
The majority of cancer survivors make positiveadjustments following diagnosis and treatmentand incorporate the experience into their dailylives (That’s Life) or use it to make their livesbetter (Personal Growth). However, a minorityview the cancer experience with Resentment,which appears to have a detrimental relationshipwith their overall QOL. Equally plausible is thatpoor QOL leads to considerable resentmentamong long-term survivors.
Future research should extend the findings ofthis study to newly diagnosed patients to see ifsimilar themes are identified and whether suchthemes are related to long-term QOL. Researchtools should be developed to identify patients whointerpret the experience with Resentment andinterventions created to assist in improving theirQOL. Further, the gender and age differences inascribed cancer meaning deserve more attention;these differences may impact patterns of doctor–patient communication, and the manner in whichsurvivors’ needs are addressed. Lastly, this studydemonstrates that symptomatic complaints andpsychological concerns are not necessarily con-comitant with long-term cancer survivorship. Formost survivors, cancer provides perspective oftheir daily lives, but has little impact on their day-to-day functioning.
ACKNOWLEDGEMENTS
This work was supported by grant no. NIH R01CA78995 from the National Institutes of Health.
K. L. FOLEY ET AL.256
Copyright # 2005 John Wiley & Sons, Ltd. Psycho-Oncology 15: 248–258 (2006)
REFERENCES
Andrews FM, Withey SB. 1976. Social indicators ofwell-being. Americans’ Perceptions of Life Quality.Plenum: New York.
Armstrong D, Gosling A, Weinman J, Marteau T. 1997.The place of inter-rater reliability in qualitativeresearch: An empirical study. Sociology 31: 597–606.
Avis NE, Assmann SF, Kravitz HM, Ganz PA, Ory M.2004. Quality of life in diverse groups of midlifewomen: Assessing the influence of menopause, healthstatus and psychosocial and demographic factors.Qual Life Res 13: 933–946.
Avis NE, Smith KW,McGraw S, Smith RG, Petronis VM,Carver CS. 2005. Assessing quality of life in adult cancersurvivors (QLACS). Qual Life Res 14: 1007–1023.
Barbour RS. 2001. Checklists for improving rigour inqualitative research: A case of the tail wagging thedog? Br Med J 322: 1115–1117.
Borghede G, Sullivan M. 1996. Measurement of qualityof life in localized prostatic cancer patients treatedwith radiotherapy. Development of a prostate cancer-specific module supplementing the EORTC QLQ-C30. Qual Life Res 5: 212–221.
Bower JE, Ganz PA, Desmond KA, Rowland JH,Meyerowitz BE, Belin TR. 2000. Fatigue in breastcancer survivors: Occurrence, correlates, and impacton quality of life. J Clin Oncol 18: 743–753.
Broeckel JA, Thors CL, Jocobsen PB, Small M, CoxCE. 2002. Sexual functioning in long-term breastcancer survivors treated with adjuvant chemotherapy.Breast Cancer Res Treatment 75: 241–248.
Brown JS, Rawlinson ME, Hilles NC. 1981. Lifesatisfaction and chronic disease: Exploration of atheoretical model. Med Care 19: 1136–1146.
Cantril H. 1965. The Pattern of Human Concerns.Rutgers University Press: New Brunswick, NJ.
Carter BJ. 1993. Long-term survivors of breast cancer.Cancer Nurs 16: 354–361.
Carver CS, Smith RG, Antoni MH, Petronis VM, WeissS, Derhagopian RP. Optimistic personality andpsychosocial well-being during treatment predictpsychosocial well-being among long-term survivorsof breast cancer. Health Psychol, in press.
Cella DF, Tulsky DS, Gray G et al. 1993. The functionalassessment of cancer therapy (FACT) scale: Develop-ment and validation of the general measure. J ClinOncol 11: 570–579.
deBoer AGEM, van Lanschot JJB, Stalmeir PFM et al.2004. Is a single-item visual analogue scale as valid,reliable and responsive as multi-item scales inmeasuring quality of life? Qual Life Res 13: 311–320.
Dirksen SR. 1995. Search for meaning in long-termcancer survivors. J Adv Nurs 21: 628–633.
Dow KH, Ferrell BR, Leigh S, Ly J, Gulasekaram P.1996. An evaluation of the quality of life among long-term survivors of breast cancer. Breast Cancer ResTreatment 39: 261–273.
Ferrell BR, Dow KH, Grant M. 1995a. Measurement ofthe quality of life in cancer survivors. Qual Life Res 4:523–531.
Ferrell BR, Dow KH, Leigh S, Ly J, Gulasekaram P.1995b. Quality of life in long-term cancer survivors.Oncol Nurs Forum 22: 915–922.
Ferrell BR, Smith SL, Juarez G, Melancon C. 2003.Meaning of illness and spirituality in ovarian cancersurvivors. Oncol Nurs Forum 2: 249–257.
Fredette SL. 1995. Breast cancer survivors: Concernsand coping. Cancer Nurs 18: 35–46.
Gall TL, Cornblat MW. 2002. Breast cancer survivorsgive voice: A qualitative analysis of spiritual factors inlong-term adjustment. Psycho-Oncology 11: 524–535.
Ganz PA, Desmond KA, Leedham B et al. 2002. Qualityof life in long-term, disease-free survivors of breastcancer: A follow-up study. J Natl Cancer Inst 94:39–49.
Gotay CC, Muraoka MY. 1998. Quality of life in long-term survivors of adult-onset cancers. J Natl CancerInst 90: 656–667.
Gudex C, Dolan P, Kind P, Williams A. 1996. Healthstate valuations from the general public using thevisual analogue scale. Qual Life Res 5: 521–531.
Halstead MT, Hull M. 2001. Struggling with paradoxes:The process of spiritual development in women withcancer. Oncol Nurs Forum 28: 1534–1544.
Hammerlid E, Taft C. 2001. Health-related quality oflife in long-term head and neck cancer survivors: Acomparison with general population norms. Br JCancer 84: 149–156.
Helgeson VS, Snyder P, Seltman H. 2004. Psychologicaland physical adjustment to breast cancer over 4 years:Identifying distinct trajectories of change. HealthPsychol 23: 3–15.
Idler EL, Benyamini Y. 1997. Self-rated health andmortality: A review of twenty-seven communitystudies. J Health Soc Behav 38: 21–37.
Kornblith AB, Herdon II JE, Weiss RB et al. 2003.Long-term adjustment of survivors of early-stagebreast carcinoma, 20 years after adjuvant chemother-apy. Cancer 98: 679–689.
Newshan G. 1998. Transcending the physical: Spiritualaspects of pain in patients with HIV and/or cancer.J Adv Nurs 28: 1236–1241.
Osoba D, Aaronson N, Zee B, Sprangers M, te Velde A.1997. Modification of the EORTC QLQ-C30 (version2.0) based on content validity and reliability testing inlarge samples of patients with cancer. Qual Life Res 6:103–108.
Palmore E, Luikart C. 1972. Health and social factorsrelated to life satisfaction. J Health Soc Behav 13:68–80.
Parker SL, Tong T, Bolden S, Wingo PA. 1997. Cancerstatistics. CA Cancer J Clin 47: 5–27.
Pope C, Ziebland S, Mays N. 2000. Qualitative researchin health care. Analysing qualitative data. Br Med J320: 114–116.
CANCER EXPERIENCE AMONG LONG-TERM SURVIVORS 257
Copyright # 2005 John Wiley & Sons, Ltd. Psycho-Oncology 15: 248–258 (2006)
Ringdal GI, Ringdal K. 1993. Testing the EORTCquality of life questionnaire on cancer patients withheterogeneous diagnoses. Qual Life Res 2: 129–140.
Rowland J, Mariotto A, Aziz N et al. 2004. Cancersurvivorship}United States, 1971–2001. MorbidityMortality Weekly Rep 53: 526–529.
Salmon P, Manzi F, Valori RM. 1996. Measuring themeaning of life for patients with incurable cancer: Thelife evaluation questionnaire (LEQ). Eur J Cancer32A: 755–760.
Sarna L, Padilla G, Holmes C, Tashkin D, Brecht ML,Evangelista L. 2002. Quality of life of long-termsurvivors of non-small-cell lung cancer. J Clin Oncol20: 2920–2929.
Schag CA, Heinrich RL, Aadland RL, Ganz PA. 1990.Assessing problems of cancer patients: Psychometricproperties of the cancer inventory of problem situa-tions. Health Psychol 9: 83–102.
Schipper H, Clinch J, McMurray A, Levitt M. 1984.Measuring the quality of life of cancer patients: Thefunctional living index-cancer: Development andvalidation. J Clin Oncol 2: 472–783.
Sears SR, Stanton AL, Danoff-Burg S. 2003. The yellowbrick road and the emerald city: Benefit finding,positive reappraisal coping and posttraumatic growthin women with early-stage breast cancer. HealthPsychol 22: 487–497.
Taylor SE, Kemeny ME, Reed GM, Bower JE,Bruenewald TL. 2000. Psychological resources, posi-tive illusions, and health. Am Psychol 55: 99–109.
Thewes B, Butow P, Girgis A, Pendlebury S. 2004. Thepsychosocial needs of breast versus older survivors.Psycho-Oncology 13: 177–189.
Thomas J, Retsas A. 1999. Transacting self-preserva-tion: A grounded theory of the spiritual dimensions
of people with terminal cancer. Int J Nurs Stud 36:191–201.
Tomich PL, Helgeson V. 2004. Is finding somethinggood in the bad always good? Benefit findingamong women with breast cancer. Health Psychol23: 16–23.
Ware Jr JE, Sherbourne CD. 1992. The MOS36-item short-form health survey (SF-36). I.Conceptual framework and item selection. Med Care30: 473–483.
Wenzel LB, Donnelly JP, Fowler JM et al. 2002.Resilience, reflection, and residual stress in ovariancancer survivorship: A gynecologic oncology groupstudy. Psycho-Oncology 11: 142–153.
Wijers OB, Levendag PC, Braaksma MMJ, BoonzaaijerM, Visch LL, Schmitz PIM. 2002. Patients with headand neck cancer cured by radiation therapy: A surveyof the dry mouth syndrome in long-term survivors.Head Neck 24: 737–747.
Wyatt G, Donze LF. 2003. The long-term quality of lifeinstrument for female cancer survivors. In Measure-ment of Nursing Outcomes (2nd edn), Strickland O(ed.). Springer: New York; 216–225.
Wyatt G, Friedman LL. 1996. Long-term female cancersurvivors: Quality of life issues and clinical implica-tions. Cancer Nurs 19: 1–7.
Wyatt G, Kurtz ME, Friedman LL, Given B, GivenCW. 1996. Preliminary testing of the long-termquality of life (LTQL) instrument for female cancersurvivors. J Nurs Meas 4: 153–170.
Wyatt G, Kurtz ME, Liken M. 1993. Breast cancersurvivors: An exploration of quality of life issues.Cancer Nurs 16: 440–448.
Youngblut JM, Casper GR. 1993. Single-item indicatorsin nursing research. Res Nurs Health 16: 459–465.
K. L. FOLEY ET AL.258
Copyright # 2005 John Wiley & Sons, Ltd. Psycho-Oncology 15: 248–258 (2006)




















