Motherhood and Resilience among Rwandan Genocide-Rape Survivors
29
MOTHERHOOD AND RESILIENCE 411 Motherhood and Resilience among Rwandan Genocide-Rape Survivors Maggie Zraly Sarah E. Rubin Donatilla Mukamana Abstract Anthropological scholarship on motherhood offers frameworks for studying the everyday lives of mothers to reveal a deeper understanding of what mothering means and how motherhood relates to broader sociocultural forms. Theory emerging from psychological anthropology explores the interplay of resilience and suffering in contexts of extreme adversity. Bringing together these bodies of work, this article engages with a lacuna in the scholarship and examines how motherhood shapes women’s resilience among Rwandan genocide- rape survivors. We elucidate how motherhood opened them to new forms of sociality in the context of postgeno- cide Rwanda. Maternal desire gave rise to a motherhood assemblage that fostered diverse modes of resilience, created the potential for new life possibilities, and placed limitations on opportunities. Our findings suggest that emotional experience is crucial to resilience among Rwandan genocide-rape survivors who are mothers and point to future directions for research and health promotion among populations affected by conflict-related sexual violence. [resilience, motherhood, gender, Rwanda] An estimated 42% of state militaries, militias, and rebel groups that engaged in armed conflict in Africa since 2000 are reported to have committed acts of conflict-related sexual violence (Nord˚ as 2011). Among the approximately 350,000 women and girls who were raped during the 1994 genocide against the Tutsi in Rwanda, perhaps 50,000 survived (Bijleveld et al. 2009). In this article, the term genocide-rape (gufata ku ngufu muri jenocide) is considered synonymous with genocidal rape and rape as an act of genocide. It refers to forced sexual penetration that is “committed with intent to destroy, in whole or in part, a national, ethnical, racial or religious group” (OSAPG 2010) by inflicting bodily and mental harm, causing death or group destruction, or preventing future births (Reid-Cunningham 2008). Rwandan survivors of genocide-rape have been publicly recognized on the local and global levels as victims of genocide and crimes against humanity (The Prosecutor v. Jean-Paul Akayesu, ICTR-96-4-T [1998]; Barnes 2005). Collective violence, such as genocide, increases the likelihood of mental health morbidi- ties among affected populations (WHO 2002). However, human resilience, the capacity to function or adapt during or following exposure to adversity, can function to protect men- tal health among violence-affected populations (Panter-Brick 2010; Zraly & Nyirazinyoye 2010). For female survivors of conflict-affected sexual violence, maternal resilience, defined in the psychological literature as “the capacity for mothers to survive the vicissitudes of the ETHOS, Vol. 41, Issue 4, pp. 411–439, ISSN 0091-2131 online ISSN 1548-1352. C 2013 by the American Anthropological Association. All rights reserved. DOI: 10.1111/etho.12031
Transcript of Motherhood and Resilience among Rwandan Genocide-Rape Survivors

MOTHERHOOD AND RESILIENCE 411
Motherhood and Resilience amongRwandan Genocide-Rape Survivors
Maggie ZralySarah E. RubinDonatilla Mukamana
Abstract Anthropological scholarship on motherhood offers frameworks for studying the everyday lives of
mothers to reveal a deeper understanding of what mothering means and how motherhood relates to broader
sociocultural forms. Theory emerging from psychological anthropology explores the interplay of resilience and
suffering in contexts of extreme adversity. Bringing together these bodies of work, this article engages with a
lacuna in the scholarship and examines how motherhood shapes women’s resilience among Rwandan genocide-
rape survivors. We elucidate how motherhood opened them to new forms of sociality in the context of postgeno-
cide Rwanda. Maternal desire gave rise to a motherhood assemblage that fostered diverse modes of resilience,
created the potential for new life possibilities, and placed limitations on opportunities. Our findings suggest
that emotional experience is crucial to resilience among Rwandan genocide-rape survivors who are mothers
and point to future directions for research and health promotion among populations affected by conflict-related
sexual violence. [resilience, motherhood, gender, Rwanda]
An estimated 42% of state militaries, militias, and rebel groups that engaged in armedconflict in Africa since 2000 are reported to have committed acts of conflict-related sexualviolence (Nordas 2011). Among the approximately 350,000 women and girls who wereraped during the 1994 genocide against the Tutsi in Rwanda, perhaps 50,000 survived(Bijleveld et al. 2009). In this article, the term genocide-rape (gufata ku ngufu muri jenocide) isconsidered synonymous with genocidal rape and rape as an act of genocide. It refers to forcedsexual penetration that is “committed with intent to destroy, in whole or in part, a national,ethnical, racial or religious group” (OSAPG 2010) by inflicting bodily and mental harm,causing death or group destruction, or preventing future births (Reid-Cunningham 2008).Rwandan survivors of genocide-rape have been publicly recognized on the local and globallevels as victims of genocide and crimes against humanity (The Prosecutor v. Jean-Paul Akayesu,ICTR-96-4-T [1998]; Barnes 2005).
Collective violence, such as genocide, increases the likelihood of mental health morbidi-ties among affected populations (WHO 2002). However, human resilience, the capacity tofunction or adapt during or following exposure to adversity, can function to protect men-tal health among violence-affected populations (Panter-Brick 2010; Zraly & Nyirazinyoye2010). For female survivors of conflict-affected sexual violence, maternal resilience, definedin the psychological literature as “the capacity for mothers to survive the vicissitudes of the
ETHOS, Vol. 41, Issue 4, pp. 411–439, ISSN 0091-2131 online ISSN 1548-1352. C© 2013 by the American AnthropologicalAssociation. All rights reserved. DOI: 10.1111/etho.12031

412 ETHOS
parenting experience itself,” (Baraitser and Noack 2007:171), may be an additional mentalhealth resource. Previous studies have identified maternal resilience as a defining aspect ofmotherhood among mothers facing adverse conditions or challenging circumstances (Barnesand Murphy 2009; Hartblay 2006).
This article aims to address the question of the role that motherhood plays in processesof resilience among women in conflict-affected settings, particularly among those who sur-vived the 1994 genocide in Rwanda against the Tutsi. The intersection of motherhoodand resilience among women living in African cultural contexts has received little to noattention in the published literature on the aftermath of political violence and warfare,genocide and rape. Therefore, we examine the ways motherhood shapes resilience amongRwandan genocide-rape survivors, describe modes of maternal resilience among Rwandangenocide-rape survivors, and advance understanding of how the intersection of motherhoodand resilience influences the life chances of Rwandan genocide-rape survivors in the culturalcontext of postgenocide Rwanda.
Background
Ethnohistory of Motherhood in RwandaThis cursory historical overview of motherhood in Rwanda focuses specifically on the com-plexity of motherhood as an identity that could endow a woman with a highly regardedsocial status (Amadiume 1997; Vansina 2004). In precolonial Rwandan society, girls becamewomen through marriage and subsequent childbearing. Mothers commanded respect aschild bearers as long as they bore children that extended their husbands’ patrilineal line ofdescent. In contrast, unmarried, pregnant girls were regularly exiled or put to death until the1920s (de Lame 1998; Uwineza et al. 2009). Throughout the 20th century, a glance froman illegitimate child was understood to be potentially powerful enough to destroy a family’sproperty, an entire lineage, or a whole hillside community (May et al. 1990).
In the postcolonial period, beginning in the 1960s, Rwandan cultural ideals of womanhoodincluded being a mother, transmitting life, transmitting cultural knowledge to one’s children,and protecting children from danger (Bagilishya 2000; Jefremovas 1991; May et al. 1990).Up until the genocide, fertility rates in Rwanda ranked among the highest in the world, withtotal fertility rates of 8.5 and 6.2 in 1983 and 1992, respectively (Jayaraman et al. 2009).Having children in the context of marriage bestowed happiness, honor, prestige, and powerto parents and provided security for their old age (May et al. 1990). However, by the 1980s,it was estimated that in some areas of Rwanda up to 22 percent of births occurred amongunmarried mothers (Tallon 1989). This widespread bearing of children outside of marriagewas not culturally valued and was declared a public health problem (ONAPO 1985).
Consistent with centuries of mother valorization, the social identity of motherhood wasintimately bound up with the social harmony of the nation at the historical moment of the1994 genocide against the Tutsi (Baines 2003). During the genocide, pregnant Tutsi womenwere eviscerated (Taylor 1999), Tutsi girls and women were forcibly impregnated with

MOTHERHOOD AND RESILIENCE 413
“Hutu babies,” and pregnant Hutu women married to Tutsi men were killed (The Prosecutor v.Jean-Paul Akayesu, ICTR-96-4-T [1998]). Rwandan women were also forced into “marriage”and sexual slavery either during the genocide and/or when they were abducted by Hutu menwho fled the country when the Rwandan Patriotic Front ousted the genocidal regime frompower (African Rights 2004; Taylor 1999). An estimated 5,000 children were born fromgenocide-rape in Rwanda (Nowrojee et al. 1996).
Resilience in Postgenocide RwandaIn the immediate aftermath of the genocide, the majority of Rwandan genocide-rape sur-vivors were living in conditions characterized by extremely low income, chronic hunger, andinsecure housing (Cohen et al. 2005). They were coping with the risk of social exclusionfrom the stigma of rape, the emotional pain of having children born from genocide-rape,and severe health complications, including disproportionately high rates of HIV/AIDS andpersistent psychiatric suffering (African Rights 2004; Hagengimana et al. 2003; Nowrojeeet al. 1996). In the postgenocide years, grassroots networks of Rwandan women servedas crucial resources for women and girls who had survived genocide and genocide-rape(African Rights 2004). Ethnographic research conducted 12 years postgenocide with mem-bers of such networks characterized three culturally specific Rwandan concepts that relatedto resilience: kwihangana, an intrapsychic creative process of drawing strength from withinthe self in order to withstand suffering; kwongera kubaho, affirmation of the reestablish-ment of the existential conditions for being; and gukomeza ubuzima, the moving forwardin life by accepting ongoing struggles and fighting for survival (Zraly and Nyirazinyoye2010).
Of the three resilience-related concepts, kwihangana, a reflexive verb, is found most ubiqui-tously in everyday Rwandan life, especially in the command form, “Ihangane”: be patient; bestrong; withstand. Though common, it is a potent and compelling command. For example,when someone cuts in front of another who is waiting in a long line for something importantlike medical care, electricity switch-on payment, or banking services, onlookers are likelyto counsel the wronged party, “Ihangane,” meaning, be patient, withstand your emotionaldiscomfort or anger. Ihangane is also used for more somber occasions, such as hearing thatsomeone has died. One then says to the mourning family members, “Ihangane,” meaning,be strong, get through this pain and grief. In both circumstances, the command carries theassumption that eventually, the person’s suffering will come to an end, but patience andstrength are necessary to make it to that moment.
Kwihangana is performed within yourself. One genocide-rape survivor described the processthusly: “‘When I say to make myself strong, there is a time, I mean, as we talk about it, Ifeel palpitations, and then, but I keep quiet and think that everything is possible. You cre-ate in yourself something to be strong and you withstand’” (Zraly 2007:244). Kwihangana,therefore, is a creative process whereby the self imagines the possibility of something otherthan the present mode of suffering, even if that possibility is yet undefined, and by doingso generates the durability to continue living. The capacity for kwihangana is important to

414 ETHOS
mental health in that it enables people to maintain emotional integrity. In other words, itaverts an emotional break or breakdown. In the words of another genocide-rape survivor,“‘When one fails to withstand when facing problems, he or she is likely to go mad’” (Zraly2007:244). Importantly, this same ethnographic study of resilience that identified and de-scribed kwihangana among Rwandan genocide-rape survivors also identified “mothering” asa high-stakes context for striving to overcome suffering and adversity in their everyday lives(Rubin and Zraly 2009; Zraly 2007).
Motherhood in Postgenocide RwandaMotherhood continues to be a powerful social marker in contemporary postgenocideRwanda (Mukamana and Brysiewicz 2008), even though remarkable changes in genderrelations, based on principles of human rights, have occurred during the postconflict recon-struction period. Women and girls are gaining access to new cultural avenues for recon-ceiving themselves and their social worlds (Burnet 2008), yet marriage and motherhood arestill seen as the traditional institutions that successfully transform girls into women. Due tothe stigma of rape, young genocide-rape survivors are at risk for being socially labeled un-marriageable, which also perpetuates a notion that the violation of genocide-rape “stripped”them of the opportunity for motherhood (Baines 2003:488). Furthermore, in a marriagemarket with a shortage of available, similarly aged men (Schindler 2011), girls are drivento compete for potential husbands, which increases the perception of young genocide-rapesurvivors’ unmarriageability (Weitsman 2008). Likewise, single mothers, and girls who havelost their virginity through rape, often suffer a problem of social belonging when confrontedwith the loss of identity as being no longer girls, yet not fully transitioned to womanhood(Mukamana and Brysiewicz 2008). In everyday life, the centrality of motherhood is con-stantly acknowledged through the common practice of referring to women as the mothersof their children; i.e., calling them “Mama” followed by the name of their firstborn childor firstborn son. Marrying before becoming a mother helps to ensure that a child fatheredby one’s husband will be socially recognized as legitimate and that a woman will not beostracized from her family (Mukamana and Brysiewicz 2008).
Approaches to the Study of MotherhoodThe feminist critique within anthropology in the 1970s challenged the tendency to representwomen as only mothers and wives in ethnography (Reiter 1975; Rosaldo et al. 1974). Thisshift led to the formation of an “anthropology of women” where motherhood was citedas the root of women’s universal subordination to men (Quinn 1977). However, today,the steadily growing field of the “anthropology of motherhood” champions the importanceof understanding the cultural variation in the conceptions of motherhood and motheringpractices as a linchpin of studies of gender (Barlow and Chapin 2010). This emphasisparallels current directions in the field of “motherhood studies,” which “simultaneouslyinsists on the particularity and specificity of motherhood while at the same time reject[s] anynotion of a fixed or essential aspect of maternal experience, desire, or subjectivity” (Kawash2011, 969; see also Glenn 1994). Across disciplines, studies are advancing knowledge ofmotherhood as a transformational identity and powerful mode of resilience (Barnes and
MOTHERHOOD AND RESILIENCE 415
Murphy 2009; Breen and McLean 2010; Hartblay 2006). This growing attention to culturalvariation, maternal resilience, and the empowering aspects of motherhood is crucial forbridging Western academic theory building with African feminisms. Many African feministsconceive of mothers as powerful in African societies and motherhood as the antidote to(African) women’s oppression (Amadiume 1997; Arnfred 2002). In this way, feminist analysisof motherhood has evolved over time to embrace a more liberating and broad-rangingtheoretical apparatus that includes women worldwide.
The anthropology of motherhood offers frameworks for studying the everyday lives ofmothers to reveal a deeper understanding of what mothering entails and means and howmotherhood relates to broader sociocultural forms (Barlow and Chapin 2010). One frame-work conceives of motherhood, mothering, the mother, and mothers-to-be as lenses throughwhich to understand multilevel social processes (Rubin and Zraly 2009; Walker 1995). While“motherhood” tends to articulate normative and contested cultural models involving ide-ologies, identities, or roles (Walker 1995), “mothering” is positioned as an emergent pro-cess that relates to the practices that women participate in by virtue of “being a mother”that contribute to constructing gender, kinship, and social status and identity (Barlow andChapin 2010). Alternatively, the “mother”—an experience, lived reality, subject, object, ormoral being—draws attention to how mothers make meaning of motherhood and mothering(Arendell 2000). Lastly, studies of “mothers-to-be” generate rich ethnographic data on preg-nancy and birth where motherhood is first shaped and circumscribed (Jordan and Davis-Floyd 1993; Rapp and Ginsburg 1995).
The literature suggests that the transition to motherhood, or the process of becoming amother, often involves a transformation of the self along with the acquisition of a valued,yet possibly contested, identity (Hartrick 1997; Nelson 2003). This transformation may berelated to development of maternal resilience, the capacity to overcome adverse motheringexperiences (Breen and McLean 2010). Becoming and/or being a mother may also affectwomen’s mental health (Becker 1998; Jenkins 1988, 1991; Walters et al. 1999). Becominga mother, especially outside the boundaries of “acceptable” motherhood, appears to engagemothers in maternal resilience practices such as using the symbolic value of motherhoodto overcome stigma (Hartblay 2006) and providing a reason to live (Barnes and Murphy2009).
Motherhood AssemblagesIn order to tease out how and under which conditions motherhood might be oppressive orliberating or both, some feminist theorists have employed Deleuze and Guattari’s (1987)concepts of becoming and machinic assemblage (Shildrick 2010; Trimble 2008). Becoming isthe anticipatory suggestion and transformation of new forms of social relations through “ef-forts to exceed and escape forms of knowledge and power and to express desires that mightbe world altering” (Biehl and Locke 2010:317). A machinic assemblage has been generallydefined as a constellation of various, multiple, interlocking biological and sociological ele-ments, such as bodies, desires, practices, values, and social structures (Biehl and Locke 2010;

416 ETHOS
Deleuze and Guattari 1987). An emergent “anthropology of becoming” suggests that ethno-graphic work can highlight the assemblages through which life chances are constrained, aswell as the ways that desires can break open new possibilities (Biehl and Locke 2010).
In this Deleuze-inspired approach, desire is emphasized for its power and potential both todrive becoming and give rise to assemblages. Maternal desire has been defined as the desireto relate to or “be with” (de Marneffe 2004:xi) one’s child, or in other words, the desire to beengaged in mothering. Built into this definition is the recognition that women often wish fora maternal connection for their own sake, and mothers often view mothering as incrediblyimportant for themselves as well as their children (de Marneffe 2004).
Assemblages produce an ensemble of potential trajectories for the entire system of elementsand interrelations as well as the subjects involved, including the desires and struggles ofactual people to create action and results. Trajectories in the same assemblage may besharply divergent, with some leading to new social forms and others remaking existing forms(Biehl and Locke 2010). From this theoretical ground, Trimble claims that the institutionof Western, patriarchal motherhood is an assemblage that “strives to conserve itself byarresting becoming” (2008:189): it captures women’s efforts through the regulatory notionof the “good mother,” thereby decreasing their energy to create and live other, diversepotentialities. Alternately, Shildrick argues that the “mother machine” assemblage can bereconfigured as “the point of takeoff and production in the generation of new life forms andin mobilising new assemblages” (2010:6): it can spread desire and potentiate new becomings.
We take the concept of motherhood assemblages as a lens through which to better under-stand how resilience can be potentiated among mothers. This approach articulates with acultural and feminist research agenda that calls for investigations into the nature of the humancapacity for resilience “in the face of human horrors” (Jenkins 1991:156; 1998). We use themotherhood assemblage lens to analyze the resilience narratives of Rwandan genocide-rapesurvivors who are also mothers and therefore have survived the experience of the brutal vio-lence of genocide-rape and face the hardships and delights of being a mother. By presentingqualitative data on the subjective experience of resilience as it relates to motherhood amongRwandan genocide-rape survivors, we illuminate multiple maternal-resilience processes.Our analysis explores the interrelations between motherhood and resilience and maps outmaternal desire and divergent postgenocide maternal modes of resilience. Our findings showthat under certain postgenocide conditions, motherhood assemblages can potentiate modesof resilience that empower women and open to expanded opportunities for life chances.Our findings also suggest that a more nuanced understanding of the diversity of possibleresiliences among mothers and other conflict-related sexual-violence survivors is needed toincrease the efficacy of efforts to enhance women’s life chances in postconflict settings.
Methods
This article comes from a larger project investigating resilience as a cultural process—a socially constructed, culturally produced, collective phenomenon with subjective and

MOTHERHOOD AND RESILIENCE 417
intersubjective dimensions. This research aimed to understand the complex phenomenonof resilience among genocide-rape survivors with relation to the experience of survivinggenocide-rape, as well as living in postgenocide Rwanda. Motherhood emerged as a crucialmode of resilience among the survivors, and understanding, parsing, and contextualizingthis emergent mode is the central goal of this article.
This article is based on 14 months of ethnographic fieldwork in Southern Rwanda from2005 to 2006 with genocide survivor-associations’ members who had experienced rapeduring the 1994 genocide. Volunteer study participants were all members of either a pur-posively selected association of genocide-rape survivors and/or a conveniently selected as-sociation of genocide widows. In depth descriptions of multiple methods used to gatherdata in this study have been reported previously (Zraly and Nyirazinyoye 2010; Zraly et al.2011).
The findings reported in this article are based on data gathered through participant-observation in association activities, participant-observation in everyday life, unstructuredinterviews with key informant collaborators who were both genocide-rape survivors andassociation members, and semistructured resilience-narrative interviews with genocide-rapesurvivors who were also association members. The semistructured resilience-narrative inter-view guide was designed in the field, ethnographically grounded, included items to collectdemographic data, and conducted with an English-Kinyarwanda interpreter. Sixty-threesemistructured interviews, averaging two hours in length, were digitally recorded and tran-scribed in English and Kinyarwanda. The Kinyarwanda portions of the transcriptions werethen back-translated into English by a team of four translators.
Quantitative Data AnalysisInterview transcripts and field notes were analyzed to compile data on demographic vari-ables relevant to motherhood for all 63 interviewees: life-course status at the time ofthe genocide (girl or woman), marital status before the genocide, marital status at timeof interview, number of children, and ages of children. Participant-observation had pre-viously revealed that the life-course statuses of “girlhood” and “womanhood” that sur-vivors occupied during the genocide were locally meaningful because of the potentiallydifferent impacts of genocide-rape based on these statuses. Women considered themselvesmarried if they had gone through a traditional, church, or government marriage cere-mony or if they were in a long-term relationship with a partner who lived with them.Genocide-related forced marriage, such as abduction or sexual slavery, was not consid-ered marriage by the community. Women were considered mothers by the community ifthey had ever given birth to a child, and some women considered themselves mothers ifthey were the primary caregiver to adopted or fostered children. Additional salient demo-graphic details were ascertained through analysis to determine whether a participant hadbeen married after the genocide or not, given birth to a child after genocide or not, andgiven birth to a child conceived through genocide-rape/genocide-related forced marriageor not.1

418 ETHOS
Table 1. Initial Motherhood Subcodes
1 children and unmet life expectations2 children take care of mom3 comparing oneself to other mothers*4 desire for motherhood*5 feeding the children6 marriage and HIV7 men and/or marriage not desired8 mothering as a mode of resilience*9 pregnancy from unwanted sex10 social wounds of genocide-rape*11 some women marry12 wanting to raise children as reason to live*13 when motherhood is too much to withstand14 withstanding the challenges of being a mother*15 women’s association as source of childcare16 mothers’ worries for children after their own death
*Bold text indicates codes linked to text describing critical events related to motherhood.
Qualitative Data AnalysisZraly and Rubin investigated mothering in the process of resilience by conducting a fine-grained analysis of its presence in the Rwandan genocide-rape survivors’ resilience-narrativeinterviews. Qualitative data analysis was facilitated by Atlas.ti 5.0 and involved inductive cod-ing, creating cases, narrative analysis, deductive coding, grouping, and recoding (LeCompteand Schensul 1999). Zraly performed the initial inductive coding by constantly conceptualiz-ing and comparing codes (and their linked textual data), categorizing codes, reconceptualiz-ing codes and categories, reclassifying codes into categories, and memoing signs of emergentpatterns regarding the relationships between the codes and categories (Kearney 1998). Oneoutcome of the inductive coding was the naming of a single “mothering” code, identifyingmothering as a broad context that appeared to be pivotal to understanding resilience amongRwandan genocide-rape survivors. That single “mothering” code, which sought to docu-ment the presence of an apparently important connection between mothering and resiliencein the original inductive coding pass, was the analytical starting point for the analyses thatled to the findings presented in this article.
Zraly further analyzed the text that had received the “mothering” code and identified 16motherhood subcodes (Table 1), each of which were linked to at least one quote from thenarrative interviews. The 16 subcodes and their linked quotes were reviewed by both Rubinand Zraly to identify critical events (see LeCompte and Schensul 1999), instances in theinterviews where women shared the events of their lives in ways that provided insight intothe motherhood-resilience nexus in the particular context of postgenocide Rwandan culture.Zraly and Rubin reached consensus that six of the 16 subcodes (indicated in bold text inTable 1) encapsulated such critical events. All six of these subcodes also assembled patternsof similarity across at least two participants, suggesting the possibility that these criticalevents also held shared cultural meaning.
MOTHERHOOD AND RESILIENCE 419
To build on the critical-events analysis and explore the possibility of temporal patterningrelated to these six motherhood subcodes, Zraly selected four participants who depictedone or two of the critical events in their resilience narratives and wrote up four cases,focusing on the temporality and sequencing of the storied nature of resilience experienceas it related to mothering during the genocide, immediately after the genocide, and 12years postgenocide (the time of the interview; see Floersch et al. 2010). This stage of theanalysis revealed two things to us. First, there was a wide conceptual difference between thecritical events that could be categorized as “Motherhood and Gender Wounds,” meaningthe impacts of (and resilience in the face of) the social wounds of stigma, discrimination, andassumptions of unmarriageability for motherhood and mothers, and a second category of allthe other critical events having to do with resilience and motherhood. Second, the events inthis second category of resilience in the context of motherhood appeared to fall into threesubcategories: “Motherhood as a Resilience Resource,” “Living to Mother, Mothering toLive,” and “Mothers Withstanding Motherhood.”
Finally, Zraly returned to the selected interview text that had received the original, single“mothering” code and analyzed it using the four categories above as codes to tag the text. Textthat was not tagged with one of these categorical codes was dropped from further analysis.Resulting data expressing similar experiences, emotions, or desires were then grouped, andeach group was summarized by Rubin and Zraly with a single new theme. This analysisgenerated six themes, each summarizing data that represented a distinct mode of resiliencerelated to motherhood: being a mother, becoming a mother, living for children, cultivatingchildren’s resilience, bearing with children, and enduring distress related to genocide-rapeand children. Quotes that most particularly and clearly exemplified a theme, along withdemographic information or detailed case narrative, were selected for presentation in thesection below. The quotes originate from 14 participants’ semistructured interviews. Allnames have been changed to protect participants’ confidentiality.
Findings
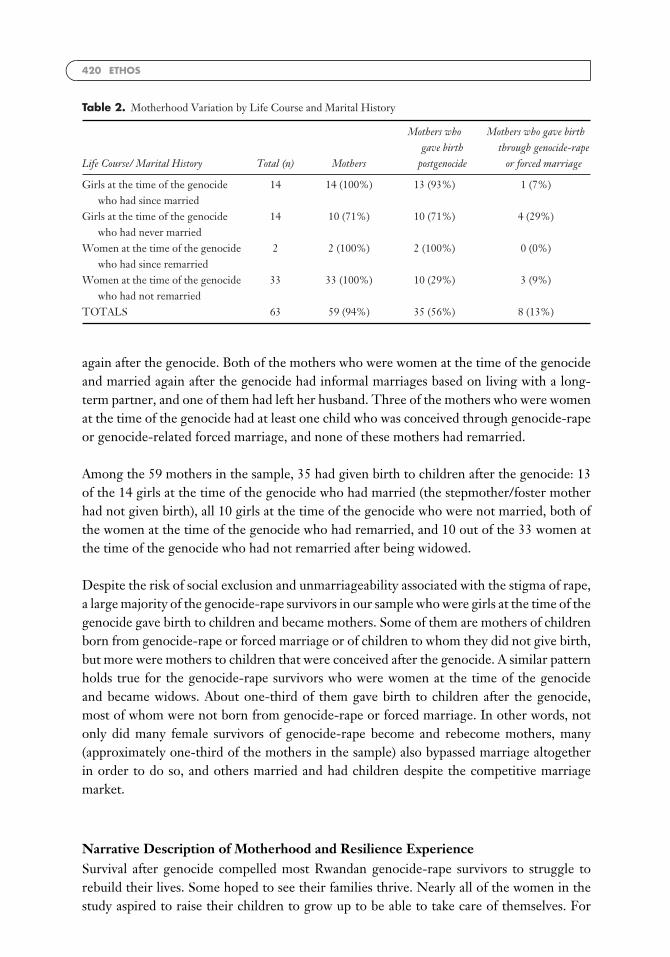
Demographic Description of Motherhood VariationAmong the 63 genocide-rape survivors in this sample of resilience-narrative interviewees,four were not mothers, and only one of the mothers had not given birth (a stepmother whoalso adopted and fostered family members’ children; see Table 2). All four of those whowere not mothers were girls at the time of the genocide. Twenty-four of the girls at the timeof the genocide were mothers at the time of the interview, among whom 14 had married.One of those who had married had subsequently left her husband, and another had beenwidowed after the genocide. Five of the mothers who were girls at the time of the genocidehad at least one child who was conceived through genocide-rape or genocide-related forcedmarriage, and only one of these mothers was married.
All 35 of those who were women at the time of the genocide were mothers. All 35 had alsobeen married before the genocide and widowed during the genocide, and two had married
420 ETHOS
Table 2. Motherhood Variation by Life Course and Marital History
Life Course/ Marital History Total (n) Mothers
Mothers whogave birth
postgenocide
Mothers who gave birththrough genocide-rape
or forced marriage
Girls at the time of the genocidewho had since married
14 14 (100%) 13 (93%) 1 (7%)
Girls at the time of the genocidewho had never married
14 10 (71%) 10 (71%) 4 (29%)
Women at the time of the genocidewho had since remarried
2 2 (100%) 2 (100%) 0 (0%)
Women at the time of the genocidewho had not remarried
33 33 (100%) 10 (29%) 3 (9%)
TOTALS 63 59 (94%) 35 (56%) 8 (13%)
again after the genocide. Both of the mothers who were women at the time of the genocideand married again after the genocide had informal marriages based on living with a long-term partner, and one of them had left her husband. Three of the mothers who were womenat the time of the genocide had at least one child who was conceived through genocide-rapeor genocide-related forced marriage, and none of these mothers had remarried.
Among the 59 mothers in the sample, 35 had given birth to children after the genocide: 13of the 14 girls at the time of the genocide who had married (the stepmother/foster motherhad not given birth), all 10 girls at the time of the genocide who were not married, both ofthe women at the time of the genocide who had remarried, and 10 out of the 33 women atthe time of the genocide who had not remarried after being widowed.
Despite the risk of social exclusion and unmarriageability associated with the stigma of rape,a large majority of the genocide-rape survivors in our sample who were girls at the time of thegenocide gave birth to children and became mothers. Some of them are mothers of childrenborn from genocide-rape or forced marriage or of children to whom they did not give birth,but more were mothers to children that were conceived after the genocide. A similar patternholds true for the genocide-rape survivors who were women at the time of the genocideand became widows. About one-third of them gave birth to children after the genocide,most of whom were not born from genocide-rape or forced marriage. In other words, notonly did many female survivors of genocide-rape become and rebecome mothers, many(approximately one-third of the mothers in the sample) also bypassed marriage altogetherin order to do so, and others married and had children despite the competitive marriagemarket.
Narrative Description of Motherhood and Resilience ExperienceSurvival after genocide compelled most Rwandan genocide-rape survivors to struggle torebuild their lives. Some hoped to see their families thrive. Nearly all of the women in thestudy aspired to raise their children to grow up to be able to take care of themselves. For

MOTHERHOOD AND RESILIENCE 421
many women in the study, their resilience narratives speak to the fact that motherhood isone of the most meaningful aspects of their lives. For most of the women in the study,raising children requires financial resources that they cannot always secure. The narrativesalso portray the everyday adversities that Rwandan genocide-rape survivors face, as well astheir resilience processes, in vivid detail.
Being a MotherFor some women, being a mother was a source of resilience. For example, Alicia was marriedwith three children before the genocide. During the genocide, her husband was killed, andshe and her children survived. In 2006, she was in her late forties making her living as alivestock breeder and serving in leadership positions in her community. In her resiliencenarrative, she expressed gratitude for being a mother, especially as a survivor of genocide-rape.
I take [genocide-rape] as something that never existed. I say to myself: “it happened andit ended, this is how things are.” I look back and remember my fellows who experiencedthe same situation and who were killed in the end. So I say to myself: “even this womanwas not fed up with life, or what about this one who experienced it while all her childrenwere killed?” Now I say that God deserves thanks because even though it happened tome, at least I still have my children, and this is enough to me.
Alicia found satisfaction in surviving with her children, particularly when she comparedherself to other women who were raped during the genocide and either died or lost all oftheir children. Her gratefulness for being a mother and still having her children was part ofwhat made it possible for her to accept genocide-rape as a part of her past and to imaginethat it had never occurred at all.
Being a mother also bolstered Delores’s resilience. She considered herself lucky to havesurvived the genocide with five of her children (others had been killed), and she had alsoadopted two orphaned children:
When life gets difficult, some of the things that keep me going are my children, who Ilive with. The reason is that there are survivors who did not get the chance to remainwith even one child, which makes them stay in the house sleeping. That is why I thankGod for this. I am with the children when they come home from school. One may talkwith me when I am sick, whereas another may take care of me. So these things help meto withstand [kwihangana].
Like Alicia, when Delores compared herself to other genocide survivors who no longer hadany children, she was divinely grateful. In her experience, being a mother protected her fromsuccumbing to social isolation and disengagement. She found that her relationships with herchildren conferred within her the capacity to persist through difficult times, such as episodesof illness.
In the Rwandan context, the potential for resilience by virtue of being a mother may dependon mothering one’s own children. For example, Comforte was a single head of household

422 ETHOS
in her early forties living with and taking care of five children between the ages of 5 and16 years old, none of whom were her biological children. During the genocide, her fiancewas killed, and she was raped multiple times by both people she knew and strangers whohid her and forced her to be their wife (bari barangize umugore wabo). A few years afterthe genocide, Comforte married, but her husband died six months later. At the time ofthe interview, Comfort was mothering two of her late husband’s children from a formermarriage, a sister’s child, a brother’s child, and her own sibling. Comforte was also livingwith HIV. She reasoned, “ . . . if they hadn’t come to rape me, I probably would have beenhealthy.” She expressed that being infected with HIV prevented her from giving birth to achild of her own, which was a source of exquisitely profound distress.
Most times, I feel that in my life after the war I have not been able to be happy. Andtherefore, I can see that the problems I experienced are because of the war, and I feelthat not having had a baby is a painful wound.
I’ve never been happy in my life for not living like other mothers, and I’ve lived miserablyinstead.
The fact that Comforte had not given birth to a child was a misery-inducing wound. Shewas unable to find a sense of peace in her postgenocide life. She perceived of herself as amother, but also as different from other mothers. Unlike Alicia and Delores, the sheer natureof being a mother was not an opportunity for Comforte to engage in resilience because ofthe pain, alienation, and injustice she felt from not having had a baby. Instead, her sense of“not living like other mothers” was a reminder of the violence she had endured during thegenocide.
Becoming a MotherThe process of becoming a mother was also a mode of resilience expressed in the narrativesof Rwandan genocide-rape survivors. At the onset of the genocide, Yvonne was married andtwo months pregnant with her first child. In the following months, her husband was killedand Yvonne was raped by three different men, one of whom hid her in his house wherehe repeatedly raped her until the genocide ended. Yvonne remembers being afraid that theviolence of being raped would cause her to lose her baby.
In the immediate aftermath of the genocide, Yvonne became very ill. Seven months intoher pregnancy, she was brought to a hospital where she stayed until she gave birth. Yvonnethen spent the better part of the next 12 years seeking shelter with relatives and others whohad vacant rooms in their houses. It was during these years that Yvonne gave birth to asecond child. When asked about her second child’s father, Yvonne made it clear that shehad neither lived with nor married the man. She described her encounter with him as ameeting of wanderers sharing temporary lodging. She explained that because she was notsatisfied with having only one child, “nahashye umwana,” interpreted literally as “I shoppedfor a baby.”
MOTHERHOOD AND RESILIENCE 423
Look, when you are not married to a man, it’s just that you were staying together inthe same house, you can give birth to a child normally, like that, it’s like you shoppedfor her [wamuhashye], that’s what we call it . . . Only because we were widowed whenwe were young, it’s like you were having one little kid, which meant “don’t refrain frombearing another, don’t miss to have two little kids.”
In the local context, the phrase guhaha umwana (shopping for a baby) referred to gettingpregnant from a man who is not one’s husband in a way that alluded to a sense of practicalitydirected toward realizing conception and motherhood. Yvonne’s outlook on becoming amother outside of marriage ran counter to the discourses of shame and public health nui-sance that shaped single motherhood before the genocide. She seemed to draw upon theexceptional circumstances of the genocide to provide a rationale for a possibly new form ofbecoming a mother—desiring motherhood and making it happen.
Over the course of the fieldwork, Yvonne was the only person who spontaneously used thephrase “shopping for a baby.” However, a number of women expressed similar desires forchildren. For example, in 1993, Linette had a child with her husband. During the genocide,her husband was killed, and she was raped multiple times in the house where she was hiddenwith her child, as well as when she was taken out of the house at night by men patrolling thearea. Like Yvonne, Linette spoke of her unhappiness about having only a single child andher willingness to take action to have a second:
After the war I realized that I have one child and I was wondering what if by accidenthe dies, what will I remain with? So, I got a husband but we did not stay together forlong, it was my way to get a child. So, after producing that child, I just went back to mymum with the other one. . . . I was realizing that I was not happy to stay with only onechild.
Linette wanted a second child, and she got one. She became a mother her way.
The desire to have children and the willingness to act on that desire was not limited towomen who already had children fathered by husbands who had been killed during thegenocide. For example, in Mistique’s case, when the genocide broke out, she was a girl inher early twenties who had not yet married or given birth. She was raped multiple timesduring the genocide and abducted by the people who hid her when they went into exile. Sheexplained that “because of what I went through,” she had rejected approaches from men,telling them “I don’t want a husband.” However, she did have a child with a man who residedin another part of the country with whom she did not maintain a relationship:
I mean, because [genocide-rape] happened, we’re now, look I thought I’d never marrya man, but because they raped us many times, one after the other, we ended up sayingwhy can’t we marry and have kids to console us since we’re now women? . . . what mademe bore this child is because people used to talk about me, and I was thinking abouthow I’ll die unmarried, so what made me do it is because my sister was going to schooland I stayed home alone. But when I’m alone, my little kid keeps me company.

424 ETHOS
Though Mistique did not want to be married, she questioned the idea that being rapedas a girl would prevent her and others in her position from having children. She reasonedthat if she was already a woman, there was nothing to stop her from becoming a mother.In addition, she did not relish the prospect of being childless and alone or becoming thesubject of local gossip. For her, becoming a mother was a solution to the socially isolatingcircumstances she faced as a survivor of genocide-rape.
Notably, both Linette and Mistique were aware of being HIV-positive before they becamepregnant. For them, having a child was a vital component of striving for happiness and socialwell-being, which outweighed the risk of transmitting HIV to their children. Mistique’sdecision to have a child without having ever been married is also significant given theprevailing notion that the experience of genocide-rape would prevent girls from being ableto achieve motherhood (Baines 2003:488). Mistique found a way to mitigate this threat andbreak through and beyond the expectations initially defined for girls who survived genocide-rape. She exercised her agency to improve the conditions of her life. She engaged in resilienceby becoming a mother.
Not all Rwandan genocide-rape survivors who had the desire for children engaged in thebecoming-a-mother mode of resilience. For those who did not opt to shop for children, theexperience of genocide-rape could leave their desires unfulfilled. For example, Heloise hadher first child with her husband in the months immediately preceding the genocide. Herhusband was killed, and she was infected with HIV through genocide-rape.
[Genocide-rape] continues to affect my life, to only think about this disease and feel thatthere is nowhere else I have got it, and again I think that I am going to die while I haveonly one child because I have no idea of looking for other men.
Though Heloise was not satisfied with having “only one child,” she experienced the impactsof genocide-rape as precluding her from getting pregnant and giving birth. Her HIV positivestatus and her reluctance to imagine entering into a sexual relationship with a man left herresigned to the idea that she would never become a mother again. Reflecting on her situationreminded her of the effects of genocide-rape on her life.
Living for ChildrenBeing a mother and mothering gave some genocide-rape survivors a life purpose. Mariellawas a girl in her late teens when the genocide began; she was raped multiple times in avariety of circumstances and abducted for three months. Four years after the genocide, shehad a child with a man who lived nearby. They were not involved in an ongoing relationship,and he did not contribute in any way to the child’s needs. Mariella expressed that her mainreason for living again (kwongera kubaho) was her child:
. . . I feel I have to live on, work, and earn a living for my child, so that if I die, I’ll leavehim with something.
MOTHERHOOD AND RESILIENCE 425
I wish that my child could live well. I don’t want my child to go and ask for help fromsomeone who harmed me. I will do my best to try and earn an independent living.
Mariella’s determination to craft a self-sufficient life stemmed from her desire to ensurethat her child would never need to seek assistance from perpetrators of genocide crimes.Financial independence and providing for her child, even after her death, was a matter ofdignity.
Like Mariella, Comforte’s mothering of the children in her care contributed to her experi-ence of living again (kwongera kubaho) after genocide-rape. Though being a mother was nota mode of resilience for her, living for her children was.
I say that if God helps me to perhaps live a little longer, those children can grow up,that’s all I ask for. I never have problems that make me think that it’s time for me todie, because there are my husband’s children, and if I die, I realize that they might livemiserably.
Though genocide-rape had disrupted her ability to identify as a mother like other mothers,she was able to engage resilience through mothering, especially through mothering her latehusband’s children. Comforte deeply hoped to continue living in order to help her childrengrow up and to protect them from potential suffering.
Both Mariella and Comforte thought about how their deaths might negatively impact theirchildren and found meaning in being alive and living life through mothering. Comfortealso rejected thoughts of her own death because she had an obligation to take care of herchildren. Likewise, Soleil, another genocide-rape survivor and mother, described doing herbest to not consider death as an option due to her sense of duty to raise her children.
I try not to think about death because I have kids. But sure [genocide-rape] is worse thandeath though one can’t choose death when you still have responsibilities to look afterkids.
For Soliel, staying alive after surviving genocide-rape involved overcoming a fate worse thandeath, and she found the strength to do so because of her mothering responsibilities.
Yvonne, who had described shopping for her second child, was also living for her children,which for her included not just staying alive but also protecting her health. The imperativeto take care of her children motivated her to take actions to prevent her acquisition ofadditional burdens of illness and disease.
I have to take care of my own life, no carelessness, no playing around, and I have to takecare of my kids. Because if I don’t take care of my life, look, it may have bad consequencesand I may not be able to look after my kids.
In speaking of avoiding the bad consequences that could result from carelessness and playingaround, Yvonne was directly referring to the possibility of becoming infected with HIV

426 ETHOS
through sexual activity. By taking care of herself, she sought to avoid the risk of disease.She valued her life based, at least in part, on its importance to her children. She engaged inresilience in order to ensure that she would have the capacity to take care of her kids. (Thispart of Yvonne’s narrative also highlights that she distinguished shopping for a baby fromcareless sexual play.)
Cultivating Children’s ResilienceBeyond living for children, Helene engaged in a mode of resilience that she hoped bolsteredher children’s resilience. She had two teenage children from her marriage to a man whowas killed during the genocide, as well as an infant whose father was not part of their lives.Helene went to great lengths to try to ensure that her children would never doubt her abilityto provide them with basic necessities even though she struggled to acquire these resources.By doing this, she was striving to affirm that they really knew she was, in her words, their“true mother”:
The way I try to stand for myself, for example if there is nothing in the house, whenthere isn’t any food for [the children], in such a case the 15-year-old son asks you:“Mom, why haven’t you cooked anything so far?” And I tell him: “please wait a bit, letme do this, let me collect firewood first, let me do this.” This is when I must withstand[kwihangana] to avoid showing him that there isn’t anything in the house. But when youhave really failed, you call him and tell him to withstand and sleep, and you promise himthat tomorrow you will go and buy something because now the night is coming. Youpromise to go tomorrow, and that you will be back by eight o’clock [in the morning].This gives him some courage.
Helene strove to be a model of resilience for her children, which was one way she continuedto fight to keep herself going.
To continue living [gukomeza ubuzima] is not an imperative to me only because I evenwant the children to look at me and see that I don’t have any problem, that I am notangry. So even when you have a problem, you should keep it inside of you, otherwiseyour children could discover that you are distraught. You should avoid speaking to themangrily, being angry. If I am in need of anything, they should not realize it. By doingthis, I am trying to continue living [gukomeza ubuzima].
She aimed to instill in her children a sense of security in life by protecting them fromdetecting any emotional distress that she herself might be feeling. She reasoned that byattempting to shield her children from her own worries and distress, she was promotingtheir emotional well-being, especially with respect to her teenage daughter, Juliette, whohad also been raped during the genocide.
. . . it is a kind of courage I want to create in her so that she keeps feeling happy as shebelieves that she will never want.
As a genocide-rape survivor and mother, Helene was driven to do everything possible topromote positive emotion and remove any sense of lack among her children.
MOTHERHOOD AND RESILIENCE 427
Bearing with ChildrenHowever, in some circumstances where Rwandan genocide-rape survivors who were moth-ers were not able to meet their children’s material needs, maternal resilience consisted ofwithstanding (kwihangana) suffering. In Renee’s case, she was a genocide widow with foursurviving children, one of whom she gave birth to during the genocide, as well as twochildren that she had adopted from her in-law’s family, which had been decimated in thegenocide. During the genocide, Renee was raped by two men and infected with HIV. Afterthe genocide, she entered into a sexual relationship with a man who was financially betteroff than herself and had offered to help her take care of her children. She gave birth to twomore children with this man (both of whom were not infected with HIV), who ended up notcontributing anything to support her family’s survival. Reflecting back, Renee realized thathe had taken advantage of her precarious situation to coerce her into having sex with him,and in her resilience narrative, she described what transpired as “a kind of rape.”
Renee was faced with the responsibility to care for eight children while enduring the painfulknowledge that this man, who was morally obliged to help her, had abused and abandonedher instead.
You may also be richer than I may be yet you do not solve a problem for me while you areaware of it. In this time, I withstand and spend the night on an empty stomach togetherwith my children. Moreover, I tell my children that this is how problems are. This iswhat I mean by withstanding [kwihangana]. Indeed, the person got me pregnant andcame back to get me pregnant again while he had not helped me. Yet I have withstoodand not gone mad. This is withstanding [kwihangana].
Renee engaged in kwihangana to prevent herself from having a debilitating mental breakdownfrom the stress of experiencing sexual coercion (after genocide-rape) and not being able toprovide food for herself and her children. When they were hungry and without enoughto eat, Renee explained to her children the reality of the problems she was facing. UnlikeHelene, who when facing similar circumstances entered a mode of resilience to transmitcourage and hope to her children, Renee’s resilience was more focused on keeping herselffrom losing her mind while witnessing her children suffer.
When you are sick without having some food, and the children are crying because theydo not have food and things like that, you feel more pain and hence grow weaker.
Lack of food interfered with Renee’s ability to adhere to her HIV medication regimen, andhearing her children’s cries while feeling helpless to attend to their needs drained her. Heronly recourse at these times was engaging in withstanding to maintain her sanity.
Like Renee, Madeline was also a genocide-rape survivor and genocide widow living withHIV and had developed a relationship with a man in hopes that he would take care of herand her two surviving children. Wanting another child, Madeline moved in with the manand became pregnant. Unfortunately, he left her and provided no support for their child.Unable to find the means to keep her children in school, Madeline used kwihangana not only
428 ETHOS
to manage the situation of her life in general, but also to tolerate the responsibility of beinga mother.
Regarding withstanding [kwihangana]? I am referring to withstanding problems relatedto the fact that I have school children for whom I am not able to find school equipmentin addition to being infected. Therefore, the children are a load to me because they aredismissed from school due to the lack of notebooks and shoes, or finding food. That isall I withstand.
Not able to meet the needs of her children, they became a burden for Madeline to withstand.In the contexts of poverty and living with HIV, Madeline and Renee both had tried to arrangefor material security for themselves and their children through establishing relationships withmen to whom they were not married. When this tactic failed, being a mother in postgenocideRwanda meant having to persevere through trying times when they could not find a way toprovide for their children.
Enduring Distress Related to Genocide-Rape and ChildrenFor some women, pressing on through tribulations related to motherhood required peri-odically facing emotional distress directly related to both children and genocide-rape. Forexample, Helene, who earnestly endeavored to consistently foster courage in her children,was sometimes disturbed by memories of genocide-rape, especially by those that involvedher daughter Juliette. At one point during the genocide, Helene and Juliette had beensimultaneously gang raped.
When I think back and remember how I was raped, of course I realize that it is verydiscouraging to me. When I remember how I was raped—sometimes you could beraped by one man, and this was not very problematic, but when you imagine a numberof people, you really feel . . . it is the way I was raped which disturbs me.
It is over . . . I am no longer thinking about it too much, I only think about it when aproblem arises, for example problems related to children, especially with Juliette.
In her resilience narrative, Helene repeatedly said “it’s over,” referring to putting her experi-ences of genocide-rape in the past. However, she tended to temporarily dwell on dispiritingmemories of perverse, multiple rapes when she encountered difficulties raising Juliette. ForHelene, mothering a child who had also survived genocide-rape meant necessarily revisitingher own genocide-rape memories from time to time, enduring her own pain, and living withthe knowledge of the sexual violence that her child had experienced. Through it all, sheprioritized shielding her children as best she could from any distress in the present.
For other women, genocide-rape had resulted in pregnancy and childbirth. The relationshipsbetween mothers and children born from genocide-rape were particularly fraught withagonizing emotion. Annabelle was in her late teens when she was raped repeatedly by a manwho forcibly took her as his “wife” during the genocide, then abducted her to live with himfor a few years in a neighboring country. She bore two children from the years of rape. Upon
MOTHERHOOD AND RESILIENCE 429
returning to Rwanda, she placed both children in an orphanage. Her decision to separatefrom her children was partly influenced by her own family’s rejection of them and partlyinfluenced by her choice to marry and start a family with a man who would not accept themin his household. After getting married, Annabelle gave birth to two more children with herhusband. However, Annabelle remained distraught about not living with or being able tohelp her first two children:
. . . . what happened happened, I was raped like others, but nothing else grieves me morethan my children.
Annabelle had accepted genocide-rape as something that had happened in her past andnormalized her experiences by comparing herself to other survivors. She had reintegratedinto postgenocide society as a married woman and mother, and her resilience to do soinvolved managing the persistently devastating grief of being separated from her childrenconceived through rape.
In her resilience narrative, Chloe also spoke about her experience being mother to childthat was conceived through genocide-rape. She had experienced multiple rapes during thegenocide, by neighbors and soldiers, and her husband and previous children had been killed.Chloe was HIV-positive, and so was her child. They lived together and Chloe struggledwith having ambivalent feelings for her child.
I have begun to love that child of mine now since I have known God, normally I didn’tlove her because I knew that, I felt she is a Hutu indeed, thus a killer, I felt . . . I feelthat God gave her to me and my children are not, now I finally love her. Then in thisloving her when I think that she will not live, I’m grieved more. This is what makes mylife decrease.
Chloe had always been Catholic, but after the genocide, she had not felt a connectionto divinity until she became part of a religious group practicing a charismatic form ofCatholicism. She attributed finally feeling love for her child to her newfound spiritualstrength, which allowed her to see her child as sacred rather than inherently evil. Being ableto love her child was an emotional achievement for her. Yet, in making herself vulnerable tothat love, she encountered the dread of losing her child to HIV. Chloe’s emotional journeyillustrates a maternal mode of resilience among genocide-rape survivors who develop thecapacity to have affection for a child whose very existence can be a perpetual signifier of thebrutality they’ve experienced. This requires tremendous fortitude in everyday life. Chloehad the mettle to be willing to love her child even though she felt that to do so was makingthe chances of her own survival more precarious.
Discussion
Rwandan genocide-rape survivors challenged analysts’ expectations that they would not beable to become mothers in the postgenocide social context. Perhaps the most unexpectedfinding from this study was that more than half of the Rwandan genocide-rape survivors inthis sample had become first-time mothers or given birth to additional children postgenocide,

430 ETHOS
despite the fact that none of them either had or remained with a husband from before thegenocide. Most of the women who were girls when they were raped during the genocide hadbecome mothers after the genocide, and the majority of their children were not conceivedthrough genocide-rape. In one case in which a woman had two children from genocide-rapeand forced marriage, she opted (painfully) to place them in an orphanage and begin a newfamily. More than half of the mothers who gave birth postgenocide did so without marrying.In fact, some women even actively shopped for their babies, clearly prioritizing becoming amother and doing so without becoming a wife. This practice was observed among womenacross diverse life situations, such as already having a child, not having any children, andliving with HIV.
Rwandan genocide-rape survivors’ motherhood was often bound up with new patterns ofsociality. Some mothers were married, living futures beyond those that were initially thoughtpossible for them due to the cultural norm of unmarriageability associated with the stigmaof rape. Others had become mothers without marrying, in some cases revealing a willingnessto disregard traditionally valued rites of passage for women in order to achieve their goalof having a child. They navigated around previously existing forms of Rwandan culturalknowledge and power regarding womanhood and motherhood and carved out new socialpathways to motherhood. These new forms of sociality highlight what can be interpreted asRwandan genocide-rape survivors’ becoming—a becoming driven by their maternal desire.
Rwandan genocide-rape survivors’ becoming gave rise to a motherhood assemblage withthe potential to foster diverse modes of resilience. The Rwandan genocide-rape survivor-motherhood assemblage that coalesced was essentially comprised of mother, child(ren),mother-child(ren) relationship, emotion, traditional Rwandan cultural expectations of moth-ers, genocide-rape experience, genocide survivor status, postgenocide Rwanda, local socio-economic inequalities, and maternal desire itself. This motherhood assemblage operatedneither as a fundamentally liberating experience necessarily leading to transformation andempowerment, nor as an entrenched, oppressive institution that subordinated all women,nor as a generator and perpetuator of desire (Shildrick 2010; Trimble 2008). Instead, thegenocide-rape survivors’ maternal desire and their mothering practices interacted with otherelements in the assemblage to create the potential both for new, genocide-defying life pos-sibilities to open for some mothers and for limited life opportunities for other mothers toescape genocide-related suffering. In other words, motherhood situated Rwandan genocide-rape survivors, along with their children, hopes, prayers, and desires, at an intersectionof different potential futures that were not overdetermined by their personal biographiesinvolving brutal violence, excruciating pain, myriad illnesses, and disease.
The tendencies for certain modes of resilience appeared to us to be influenced by the meaningof maternal desire across different mother-child(ren) relationships and the meaning of theemotional content of these relationships in the postgenocide Rwandan context. Some modesof resilience resonated with the idea that surviving genocide-rape meant that anything waspossible, particularly for one’s life with one’s children, and that mother and child(ren)’s mereexistence defied the genocide. The “being a mother” mode of resilience hinged on a mother’smiraculously satisfied desire to “be with” one’s own child(ren) despite the catastrophe of

MOTHERHOOD AND RESILIENCE 431
the genocide and was augmented by a state of divine gratitude for having a child and amother-child relationship that survived the genocide. The “becoming a mother” mode ofresilience depended on a mother’s wanting a child and exerting a degree of control overthe process of becoming “with child,” which was empowering in that a mother could bringherself the happiness and comfort of living with that child and also “prove” that genocideperpetrators had failed to destroy her reproductive capacity. The “living for children” modeof resilience required a mother to believe that a happy, dignified future for her child(ren)was possible and that she could acquire the material resources to improve her child(ren)’schances of such a future, thereby creating the possibility that through her determination herfamily would not ultimately be extinguished by the impacts of the genocide. The “living forchildren” mode-of-resilience finding also supports Barnes and Murphy’s (2009) argumentthat maternal resilience can provide some mothers, outside the boundaries of “acceptable”motherhood, with a reason to live. All three of these modes of resilience resonate with theidea that surviving genocide-rape means that anything is possible, particularly for one’s lifewith one’s children, and that mother and child(ren)’s mere existence defies the genocide.
On the other hand, some modes of resilience did not defy the genocide as much as theyunderscored the relentless effect that experiences of genocide-rape had in survivors’ lives;specifically, that mothers’ relationships with their children are inextricably embedded withsuffering borne of the genocide; in other words, their commitment to their children ensnaresthem in a life of suffering. The “bearing with children” mode of resilience occurred whenmother wished to provide for her child(ren) but instead had no other option but to garnerstrength to “be with” them in their suffering with unmet needs and to stay sane, despite herongoing sense of victimization as a genocide-rape survivor. The “enduring distress relatedto children and genocide-rape” mode of resilience required mother to heroically undergorepeated experiences of agonizing emotions related to genocide-rape in order to have arelationship with or mother one’s child(ren), meaning that the violence of the genocide hadnot yet ended for some women. One mode of resilience seems to be at the threshold betweenaccentuating that experiences of genocide-rape continue to affect survivors’ lives and theidea of surviving genocide-rape means that anything is possible. The “cultivating children’sresilience” mode involved a mother extending the courage she had needed to survive thegenocide in order to protect her child(ren) from suffering in the postgenocide environment.The mother’s courage was intensified by her intimate knowledge of the suffering herchild(ren) experienced during the genocide and the courage they needed to live on.
Motherhood, Positive Emotion, and ResilienceIn some instances, motherhood was a resource for overcoming the impacts of genocide-rape, coping with the challenges of everyday life, and imagining and shaping possibilitiesfor postgenocide living. Experiences of being grateful for children, living with children,providing for children, and fostering children’s courage were associated with positive affect,such as appreciation, contentment, empowerment, comfort, and dignity. Previous researchhas shown positive affect to have adaptive value, suggesting that it may be a key compo-nent of resilience and flourishing mental health (Fredrickson and Losada 2005). This sug-gests that the positive emotions and positive moods that Rwandan genocide-rape survivors

432 ETHOS
experienced in the modes of resilience, “being mother,” “becoming mother,” and “livingfor children” may have contributed to their resilience. Likewise, the experience of positiveemotions may be more important for resilience and flourishing mental health, regardlessof the intensity of negative emotions (Cohn et al. 2009). Therefore, the positive emotionthat Rwandan genocide-rape survivors experienced in the mode of resilience, “cultivatingchildren’s resilience,” may also have contributed to women’s resilience.
Brison has argued that after sexual assault, reestablishing feelings of happiness and trustthrough becoming and being a mother can provide survivors with a reason to live again andhelp them find “meaning in a life caring for and being sustained by others” (2002:158). Shesuggests that, in this way, motherhood can be central to the work of recovery, the work ofremaking the self after violence. This draws attention to the embodied way that motherhoodamong Rwandan genocide-rape survivors, particularly in the “becoming mother” mode ofresilience, can generate new contexts for everyday living and in doing so participate inremaking the world (see Das and Kleinman 2001).
Motherhood, Distress, and ResilienceMotherhood could also be a source of distress and limitation for mothers who were genocide-rape survivors. Unfulfilled desires to have children, feeling like an abnormal mother, sufferingalong with children, and being reminded of genocide-rape by children were associatedwith negative affect, such as loneliness, lack, disempowerment, overwhelm, discouragement,and grief. Research has also shown that the capacity to tolerate negative emotion (distresstolerance) also has adaptive value (Simons and Gaher 2005), which suggests that it too mightbe a key component of resilience (Bernstein et al. 2011). This suggests that the pain andsuffering that Rwandan genocide-rape survivors were withstanding in the “bearing children”and “enduring distress related to genocide-rape and children” modes of resilience mayhave contributed to their resilience. Yet, modes of resilience associated with negative affectin the Rwandan genocide-rape-survivor motherhood assemblage are more complicated tointerpret, because resilience does not wholly justify pain and suffering and because divergentoutcomes arise from the common experience of mothers’ entrapment in suffering due togenocide-rape being embedded in their relationships with their child(ren).
In the “bearing children” mode of resilience, the Rwandan genocide-rape survivors were ableto tolerate distress to differing degrees. The women engaged in kwihangana to withstandsuffering in overwhelming situations that did not seem to be improving for either of them.Renee suffered with her children while teaching them about kwihangana. She expressedrighteous outrage regarding the fact that the man who sexually coerced her did not financiallytake care of her children. Renee’s form of “bearing with children” was significantly moremeaning laden and childcare centered than Madeline’s, who seemed resigned to accept herfate and somewhat disconnected from her children, objectifying them as burdens. Madelinewas clear about the fact that she was tolerating that she was HIV-positive and that she did nothave the financial capacity to pay for her children to go to school. Because Renee’s distresstolerance engaged her children, motherhood was still possibly bolstering to resilience, even
MOTHERHOOD AND RESILIENCE 433
though she reported a general feeling of weakening. For Madeline, motherhood was notlikely contributing anything to her resilience. Therefore, we can posit that this specific formof kwihangana-centered distress tolerance contributes to maternal resilience when it includesmaternal desire. However, if in withstanding the burdens of motherhood one loses the desireto mother, motherhood is not likely to be a resilience resource for women in the “bearingwith children” mode of resilience.
The “enduring distress related to genocide-rape and children” mode is where it is mostchallenging to understand the relationships between suffering, motherhood, and resilience.Because the extraordinary violence of genocide-rape can subtly, yet deeply, affect the ordi-nary, everyday world where mothering and resilience processes unfold, Das’s (2000) conceptof poisonous knowledge is useful for teasing out these relationships. Parson (2010) has arguedthat the swallowing and digesting of poisonous knowledge—an understanding that the rootsof the violence one has suffered oneself and the social world one is rooted in are all part ofthe same social organism—can empower women affected by multiple violences.
Helene—who had been gang raped alongside her daughter Juliette—had confronted thepoisonous knowledge of genocide-rape in heroic steps, like joining the women’s organizationwith Juliette, where everything about genocide-rape had to be spoken out loud in front ofother genocide-rape survivors. Helene felt that sharing their stories in this way helpedstrengthen their relationship. Although Helene chose this method of revisiting her genocideexperiences, she also reluctantly revisited her own internal genocide landscapes when sheworried about Juliette. Revisiting the world of genocide-rape in this unmediated way wasnot a desired journey for Helene, but she felt that if she entirely avoided it, or even tried to, itwould mean that she would be less equipped to handle her own and Juliette’s genocide-rapeissues. Purposefully swallowing poisonous knowledge for the sake of Juliette’s well-beingcontributed to Helene’s resilience as well as her capacity to mother.
Chloe had resisted swallowing the poisonous knowledge of genocide-rape for many years,considering her child born of genocide-rape a killer in her own right; however, throughparticipating in charismatic healing, she was able to come to terms with the fact that she hada child born through genocide-rape and establish new affective ties with her daughter. Byingesting the poisonous knowledge, Chloe became a mother to her daughter, with feelings oflove for her child. Although this new relationship did not immediately contribute to Chloe’sresilience—because it also triggered overwhelming feelings of impending loss and grief dueto the child’s HIV-positive status—it is possible that this newfound motherhood could turnout to be a future pathway toward a new mode of resilience for Chloe.
The painful suffering of “enduring distress related to genocide-rape and children” appearsto be potentially adaptive for some mothers in some circumstances. If mothers engage inprocessing the poisonous knowledge of genocide-rape as it relates to their children, theyseem to be able to develop connection to and compassion for the children who remind themof genocide-rape. Such relationships offer mothers the opportunity to experience positiveemotion (e.g., love, courage) and, in some cases, to find a reason to live.
434 ETHOS
RecommendationsThe findings of this study suggest specific ways of promoting health among populationsof conflict-affected sexual violence survivors. First, given the finding that many survivorsof genocide-rape in Rwanda escaped the expectation that they were doomed to exist onthe social margins of productive and reproductive activity, postconflict mental health andemotional-health-promotion efforts must recognize that motherhood can be an importantsite for conflict-affected sexual-violence survivors to engage in a variety of modes of re-silience. This suggests that postconflict mental-health-promotion activities be designed toreach out deliberately to mothers and that efforts to support mothers’ existing strengths helpfoster the dynamics of diverse forms of resilience.
Second, in African contexts of extreme global/local economic inequality, where populationsface the chronic threat of material deprivation, resilience promotion with conflict-affectedsexual-violence survivors must begin with ensuring that mothers and their children havefood to eat every day. Funding to implement child-support policies and execute child-support frameworks, including those targeting parents not living with children, is warrantedto protect children’s health and security.
Third, because living with the unsatisfied desire for children can be so devastating, especiallywhen it is personally understood as a result of conflict-affected sexual violence, reproductivetechnologies and state-of-the-art HIV/AIDS prevention education must be distributedthroughout Africa in ways that women can access. For example, knowledge about howto prevent mother-to-child transmission of HIV/AIDS and equitable opportunities touse fertility treatments would enable more women who have been biologically, bodily,or psychologically hurt by conflict-affected sexual violence to become pregnant and havechildren if they so desire.
Fourth, specialized interventions to support the mental health of women who have givenbirth to children as a result of genocide- or war-rape must be further developed, translated,and disseminated in order to actualize principles of human rights, gender equity, and socialjustice in individual and social recovery from armed conflict and genocide.
Lastly, more research is needed on the processes and relationships involved in motherhoodand the implications of motherhood for women’s health. Future directions for this workcall for engaging in research in conflict-affected communities and societies with mothersand mothers-to-be to make visible emergent forms of motherhood and their significance formothers’ health and well-being.
Conclusion
This article contributes to the ethnographic scholarship on motherhood, gender, and health.It is well contextualized within the existing anthropological research on mothering andRwanda and offers an analysis that suggests motherhood bolsters Rwandan genocide-rapesurvivor’s resilience through (1) diminishing the stigma of genocide-rape through its sym-bolic value, (2) fostering the experience of positive emotion, (3) providing a reason to live,

MOTHERHOOD AND RESILIENCE 435
(4) practicing maternal desire-mediated distress tolerance, and (5) making meaning of child-related genocide-rape suffering. The voices of the women interviewed stand out and providean effective grounding for a compelling account of the ways in which motherhood is a re-source for daily-life resilience among Rwandan women affected by genocide-rape. Thesedata inform the final recommendation for strategies to increase health and equality forwomen in conflict zones and provide an opportunity to further cultural critique of practicesand institutions surrounding motherhood in Europe and the United States.
As this article illustrates, we need to know far more about the relationship between moth-erhood and mental health in a way that disrupts a universalizing American narrative aboutthe “burdens of motherhood.” According to the women in this study, motherhood can bea transformative process that is potentially powerful and even liberating. This empiricalfinding supports African feminisms’ claims to motherhood as the root of women’s empow-erment (see Amadiume 1997; Arnfred 2002) and creates more space in anthropology forfurther investigations into the relationships between motherhood, women’s mental healthstatus (see Jenkins 1988, 1991), and resilience. In this space, more research attention mustbe dedicated to the yet unshared experiences of positive emotion, distress tolerance, andmeaning making among women who have witnessed and suffered war- or genocide-rape.
The Rwandan women in the study were stunningly resilient and creative in the wake ofunfathomable violence. Alicia took genocide-rape like something that never existed, Yvonneshopped for a baby, Helene created courage in Juliette, and Chloe began to love her daughter.Their creative power to generate new contexts for living, new meaning, new socialities, andnew lives worth living, for their children and themselves, is the hallmark of their becoming.
MAGGIE ZRALY is Assistant Professor of Anthropology at Utah State University.
SARAH E. RUBIN is a Ph.D. Candidate at Case Western Reserve University.
DONATILLA MUKAMANA is Lecturer in Mental Health at the Kigali Health Institute.
Notes
Acknowledgements. This research was approved by Case Western Reserve University IRB and research
clearance was obtained from the National University of Rwanda School of Public Health. It was supported by the
National Science Foundation (Grant No. 0514519), Fulbright IIE, and the Baker-Nord Center for the
Humanities at Case Western Reserve University. We thank the study participants for their generosity in sharing
their experiences, the National University of Rwanda School of Public Health, the Center for Conflict
Management at the National University of Rwanda, the National University of Rwanda Research House,
AVEGA-Agahozo, and Abasa for facilitating this work. We wish to thank the readers at Miami University of Ohio
and Utah State University who contributed productive feedback on earlier drafts of this manuscript. We are also
extremely grateful to Janis Jenkins and the anonymous reviewer for their generous comments on an earlier version
of this article.
1. The interview included demographic questions about current marital status, whether one had ever been married,
and number and ages of children. Asking these questions often led to discussions of which children had been born

436 ETHOS
before, during, or after genocide and the participants’ relationships to children’s fathers. Participant-observation
data were also drawn to determine marital status and motherhood.
References Cited
African Rights2004 Rwanda: Broken Bodies, Torn Spirits: Living with Genocide, Rape, and HIV/AIDS.
Amadiume, Ifi1997 Reinventing Africa: Matriarchy, Religion and Culture. New York: Zed Books.
Arendell, Terry2000 Conceiving and Investigating Motherhood: The Decade’s Scholarship. Journal of Marriage and Family
62(4):1192–1207.Arnfred, Signe
2002 Simone De Beauvoir in Africa: “Woman = the Second Sex?” Issues of African Feminist Thought.JENdA: A Journal of Culture and African Women Studies 2(1). http://www.africaknowledgeproject.org/index.php/jenda/article/view/69
Bagilishya, Deogratias2000 Mourning and Recovery from Trauma: In Rwanda, Tears Flow Within. Transcultural Psychiatry
37(3):337–353.Baines, Erin K.
2003 Body Politics and the Rwandan Crisis. Third World Quarterly 24(3):479–493.Baraitser, Lisa, and Amelie Noack
2007 Mother Courage: Reflections on Maternal Resilience. British Journal of Psychotherapy 23(2):171–188.Barlow, Kathleen, and Bambi L. Chapin
2010 The Practice of Mothering: An Introduction. Ethos 38(4):324–338.Barnes, Catherine
2005 The Functional Utility of Genocide: Towards a Framework for Understanding the Connection Be-tween Genocide and Regime Consolidation, Expansion and Maintenance. Journal of Genocide Research7(3):309–330.
Barnes, Donna B., and Sheigla Murphy2009 Reproductive Decisions for Women with HIV: Motherhood’s Role in Envisioning a Future. Qualitative
Health Research 19(4):481–491.Becker, Anne E.
1998 Postpartum Illness in Fiji: A Socioeconomic Perspective. Psychosomatic Medicine 60(4):431–438.Bernstein, Amit, Anka A. Vujanovic, Teresa M. Leyro, and Michael J. Zvolensky
2011 Research Synthesis and the Future. In Distress Tolerance, Zvolensky Michael J., Amit Bernstein, and AnkaA. Vujanovic, eds. Pp. 263–280. New York: Guilford.
Biehl, Joao, and Peter Locke2010 Deleuze and the Anthropology of Becoming. Current Anthropology 51(3):317–351.
Bijleveld, Catrien, Aafke Morssinkhof, and Alette Smeulers2009 Counting the Countless Rape Victimization during the Rwandan Genocide. International Criminal Justice
Review 19(2):208–224.Breen, Andrea V., and Kate C. McLean
2010 Constructing Resilience: Adolescent Motherhood and the Process of Self-Transformation. In NarrativeDevelopment in Adolescence: Creating the Storied Self. Kate C. McLean and Monisha Pasupathi, eds.Pp. 151–168. New York: Springer.
Brison, Susan J.2002 Outliving Oneself: Trauma, Memory, and Personal Identity. In Gender Struggles: Practical Approaches
to Contemporary Feminism. Constance L. Mui and Julien S. Murphy, eds. Pp. 137–165. Lanham, MD:Rowman & Littlefield.
Burnet, Jennie E.2008 Gender Balance and the Meanings of Women in Governance in Post-Genocide Rwanda. African Affairs
107(428):361–386.Cohen, Mardge H., Anne-Christine d’ Adesky, and Kathryn Anastos
2005 Women in Rwanda: Another World Is Possible. Journal of the American Medical Association 294(5):613–615.
Cohn, Michael A., Barbara L. Fredrickson, Stephanie L. Brown, Joseph A. Mikels, and Anne M. Conway2009 Happiness Unpacked: Positive Emotions Increase Life Satisfaction by Building Resilience. Emotion
9(3):361–368.

MOTHERHOOD AND RESILIENCE 437
Das, Veena2000 The Act of Witnessing: Violence, Poisonous Knowledge, and Subjectivity. In Violence and Subjectivity. V.
Das, A. Kleinman, M. Ramphele, and P. Reynolds, eds. Pp. 205–225. Berkeley: University of CaliforniaPress.
Das, Veena and Arthur Kleinman2001 Introduction. In Remaking a World: Violence, Social Suffering, and Recovery. Das Veena, Arthur Klein-
man, Margaret Lock, Mamphela Ramphele and Pamela Reynolds, eds. Pp. 1–30. Berkeley: University ofCalifornia Press.
de Lame, Danielle1998 Changing Rwandan Vision of Women and Land, in the Heart of the House, at the Outskirts of the World.
Afrika Focus 15(1–2):3–12.de Marneffe, Daphne
2009 Maternal Desire: On Children, Love, and the Inner Life. New York: Little, Brown. http://books.google.com/books/about/Maternal_Desire.html?id=Z5iuTJGt1ZcC, accessed September 16, 2013.
Deleuze, Gilles and Felix Guattari1987 A Thousand Plateaus: Capitalism and Schizophrenia. Minneapolis: University of Minnesota.
Floersch, Jerry, Jeffrey L. Longhofer, Derrick Kranke, and Lisa Townsend2010 Integrating Thematic, Grounded Theory and Narrative Analysis A Case Study of Adolescent Psychotropic
Treatment. Qualitative Social Work 9(3):407–425.Fredrickson, Barbara L., and Marcial F. Losada
2005 Positive Affect and the Complex Dynamics of Human Flourishing. American Psychologist 60(7):678–686.Glenn, Evelyn Nakano
1994 Social Constructions of Mothering: A Thematic Overview. In Mothering: Ideology, Experience, andAgency. Glenn Evelyn Nakano, Grace Chang, and Linda Rennie Forcey, eds. Pps. 1–32. New York:Routledge.
Hagengimana, Athanase, Devon Hinton, Bruce Bird, Mark Pollack, and Roger K. Pitman2003 Somatic Panic-Attack Equivalents in a Community Sample of Rwandan Widows Who Survived the 1994
Genocide. Psychiatry Research 117(1):1–9.Hartblay, Cassandra
2006 An Absolutely Different Life: Locating Disability, Motherhood, and Local Power in Rural Siberia. HonorsProjects. Macalester College.
Hartrick, Gweneth A.1997 Women Who Are Mothers: The Experience of Defining Self. Health Care for Women International
18(3):263–277.Jayaraman, Anuja, Tesfayi Gebreselassie, and S. Chandrasekhar
2009 Effect of Conflict on Age at Marriage and Age at First Birth in Rwanda. Population Research and PolicyReview 28(5):551–567.
Jefremovas, Villia1991 Loose Women, Virtuous Wives, and Timid Virgins: Gender and the Control of Resources in Rwanda.
Canadian Journal of African Studies 25(3):378–395.Jenkins, Janis H.
1988 Ethnopsychiatric Interpretations of Schizophrenic Illness: The Problem of Nervios among Mexican-American Families. Culture, Medicine and Psychiatry 12(3):301–329.
1991 The State Construction of Affect: Political Ethos and Mental Health among Salvadoran Refugees. Culture,Medicine and Psychiatry 15(2):139–165.
1998 The Medical Anthropology of Political Violence: A Cultural and Feminist Agenda. Medical AnthropologyQuarterly 12(1):122–131.
Jordan, Brigitte, and Robbie Davis-Floyd1993 Birth in Four Cultures: A Crosscultural Investigation of Childbirth in Yucatan, Holland, Sweden, and the
United States. Prospect Heights, IL: Waveland Press.Kawash, Samira
2011 New Directions in Motherhood Studies. Signs 36(4):969–1003.Kearney, Margaret H.
1998 Ready-to-wear: Discovering Grounded Formal Theory. Research in Nursing & Health 21(2):179–186.LeCompte, Margaret Diane, and Jean J. Schensul
1999 Ethnographer’s Toolkit. 5. Analyzing & Interpreting Ethnographic Data. Walnut Creek, CA: Altamira.May, John F., Monique Mukamanzi, and Marcel Vekemans
1990 Family Planning in Rwanda: Status and Prospects. Studies in Family Planning 21(1):20–32.Mukamana, Donatilla, and Petra Brysiewicz
2008 The Lived Experience of Genocide Rape Survivors in Rwanda. Journal of Nursing Scholarship 40(4):379–384.

438 ETHOS
Nelson, Antonia M.2003 Transition to Motherhood. Journal of Obstetric, Gynecologic, & Neonatal Nursing 32(4):465–
477.Nordas, R.
2011 Sexual Violence in Armed Conflicts. Center for the Study of Civil War, Oslo.Nowrojee, Binaifer, Dorothy Q. Thomas, and Janet Fleischman
1996 Rwanda – Sexual Violence during the Rwandan Genocide and Its Aftermath: Shattered Lives. HumanRights Watch.
Office National de la Population, Republique Rwandaise (ONAPO)1985 Rapport Du Seminaire National Sur La Sante Familiale.
Office of the Special Advisor on the Prevention of Genocide (OSAPG)2010 Prevention of Genocide. United Nations.
Panter-Brick, Catherine2010 Conflict, Violence, and Health: Setting a New Interdisciplinary Agenda. Social Science & Medicine
70(1):1–6.Parson, Nia
2010 Transformative Ties: Gendered Violence, Forms of Recovery, and Shifting Subjectivities in Chile. MedicalAnthropology Quarterly 24(1):64–84.
Quinn, Naomi1977 Anthropological Studies on Women’s Status. Annual Review of Anthropology 6(1):181–225.
Rapp, Rayna, and Faye Ginsburg.1995 Conceiving the New World Order: The Global Politics of Reproduction. Berkeley: University of California
Press.Reid-Cunningham, and Allison Ruby
2008 Rape as a Weapon of Genocide. Genocide Studies and Prevention 3(3):279–296.Reiter, Rayna
1975 Toward an Anthropology of Women. New York: Monthly Review.Rosaldo, Michele Zimbalist, Louis Lamphere, and Joan Bamberger
1974 Woman, Culture, and Society. Stanford, CA: Stanford University Press.Rubin, Sarah, and Maggie Zraly
2009 “Shopping for a Baby”: Motherhood as a Mode of Resilience among Rwandan Survivors of Genocide-Rape.American Anthropological Association, Philadelphia, December 5.
Schindler, Kati2011 Do New Opportunities Arise for Women in Post-War Countries? The Case of Rwanda. Weekly Report
(3):13–16.Shildrick, Margrit
2010 Becoming-Maternal: Things to Do with Deleuze. Studies in the Maternal 2(1). www.mamsie.bbk.ac.uk,accessed September 16, 2013.
Simons, Jeffrey S., and Raluca M. Gaher2005 The Distress Tolerance Scale: Development and Validation of a Self-Report Measure. Motivation and
Emotion 29(2): 83–102.Tallon, F.
1989 [Rwandan Experience in Population Policy]. Imbonezamuryango = Famille, Sante, Developpement /Republique Rwandaise, Office National De La Population (ONAPO) 15:21–23.
Taylor, Christopher C.1999 A Gendered Genocide: Tutsi Women and Hutu Extremists in the 1994 Rwanda Genocide. PoLAR:
Political and Legal Anthropology Review 22(1):42–54.Trimble, Sarah S.
2008 (Un)usual Suspects: Mothers, Masculinities, Monstrosities. In Feminist Mothering. O’Reilly Andrea, ed.Pp. 177–190. Albany: State University of New York Press.
Uwineza, Peace, Elizabeth Pearson, and Elizabeth Powley2009 Sustaining Women’s Gains in Rwanda: The Influence of Indigenous Culture and Post-genocide Politics.
Hunt Alternatives Fund.Vansina, Jan
2004 Antecedents to Modern Rwanda: The Nyiginya Kingdom. Madison: University of Wisconsin Press.Walker, Cherryl
1995 Conceptualising Motherhood in Twentieth Century South Africa. Journal of Southern African Studies21(3):417–437.
Walters, Vivienne, Joyce Yaa Avorti, and Nicki Charles.1999 ‘Your Heart Is Never Free’: Women in Wales and Ghana Talking About Distress. Canadian Psychology
40(2):129–142.

MOTHERHOOD AND RESILIENCE 439
Weitsman, Patricia A.2008 The Politics of Identity and Sexual Violence: A Review of Bosnia and Rwanda. Human Rights Quarterly
30(3):561–578.World Health Organization
2002 World Report on Violence and Health. Etienne G. Krug, ed. Geneva, Switzerland: World HealthOrganization.
Zraly, Maggie2007 Bearing: Resilience among Genocide-Rape Survivors in Rwanda. Ph.D. dissertation, Department of An-
thropology, Case Western Reserve University.Zraly, Maggie, and Laetitia Nyirazinyoye
2010 Don’t Let the Suffering Make You Fade Away: An Ethnographic Study of Resilience Among Survivors ofGenocide-rape in Southern Rwanda. Social Science & Medicine 70(10):1656–1664.
Zraly, Maggie, Julia Rubin-Smith, and Theresa Betancourt2011 Primary Mental Health Care for Survivors of Collective Sexual Violence in Rwanda. Global Public Health
6(3):257–270.