
A Prospective Trial of Subxiphoid Pericardiotomy in the Diagnosis and Treatment of Large Pericardial...
6
ANNALS OF SURGERY Vol. 218, No. 6, 777-782 © 1993 J. B. Lippincott Company A Prospective Trial of Subxiphoid Pericardiotomy in the Diagnosis and Treatment of Large Pericardial Effusion A Follow-Up Report Peter Van Trigt, M.D.,* James Douglas, M.D.,* Peter K. Smith, M.D.,* Paul T. Campbell, M.D.,t Thomas C. Wall, M.D.,t Richard T. Kenney, M.D.,t Christopher M. O'Connor, M.D.,t Khalid H. Sheikh, M.D.,t and G. Ralph Corey, M.D.t From the Departments of Surgery* and Medicinet, Duke University Medical Center, Durham, North Carolina Objective This study was designed to determine the cause of large pericardial effusions and evaluate the efficacy of subxiphoid pericardiotomy. Summary Background Data Despite great advances in the techniques used to diagnose pericardial effusions, much controversy remains concerning their cause and the optimal treatment of these effusions. Methods In a prospective consecutive case series, 57 patients underwent a thorough preoperative evaluation followed by a subxiphoid pericardiotomy. All tissue and fluid was exhaustively evaluated. Postoperatively, all patients were followed for a least 1 year. Results Surgery was performed under local anesthesia in 77% of patients, and the complications of surgery were minimal. Pericardial tissue and fluid established or aided in establishing a diagnosis in 81% of patients. Infection and malignancy were the leading causes; the condition in only 4 patients remained undiagnosed. Follow-up revealed recurrent effusion in nine (16%) patients, but only five (9%) required further surgery. The mortality rate at 30 days was 12%, and at 1 year, it was 37%. Fourteen of the 21 deaths occurred in patients with malignancies. Conclusions These data show that the cause of most large pericardial effusions can be determined by a thorough evaluation accompanied by subxiphoid pericardiotomy. In addition, subxiphoid pericardial biopsy and window creation is safe and effective in the treatment of these effusions. 777
Transcript of A Prospective Trial of Subxiphoid Pericardiotomy in the Diagnosis and Treatment of Large Pericardial...
ANNALS OF SURGERYVol. 218, No. 6, 777-782© 1993 J. B. Lippincott Company
A Prospective Trial of SubxiphoidPericardiotomy in the Diagnosisand Treatment of LargePericardial EffusionA Follow-Up ReportPeter Van Trigt, M.D.,* James Douglas, M.D.,* Peter K. Smith, M.D.,* Paul T. Campbell, M.D.,tThomas C. Wall, M.D.,t Richard T. Kenney, M.D.,t Christopher M. O'Connor, M.D.,tKhalid H. Sheikh, M.D.,t and G. Ralph Corey, M.D.t
From the Departments of Surgery* and Medicinet, Duke University Medical Center,Durham, North Carolina
ObjectiveThis study was designed to determine the cause of large pericardial effusions and evaluate theefficacy of subxiphoid pericardiotomy.
Summary Background DataDespite great advances in the techniques used to diagnose pericardial effusions, muchcontroversy remains concerning their cause and the optimal treatment of these effusions.
MethodsIn a prospective consecutive case series, 57 patients underwent a thorough preoperativeevaluation followed by a subxiphoid pericardiotomy. All tissue and fluid was exhaustivelyevaluated. Postoperatively, all patients were followed for a least 1 year.
ResultsSurgery was performed under local anesthesia in 77% of patients, and the complications ofsurgery were minimal. Pericardial tissue and fluid established or aided in establishing a diagnosisin 81% of patients. Infection and malignancy were the leading causes; the condition in only 4patients remained undiagnosed. Follow-up revealed recurrent effusion in nine (16%) patients, butonly five (9%) required further surgery. The mortality rate at 30 days was 12%, and at 1 year, itwas 37%. Fourteen of the 21 deaths occurred in patients with malignancies.
ConclusionsThese data show that the cause of most large pericardial effusions can be determined by athorough evaluation accompanied by subxiphoid pericardiotomy. In addition, subxiphoidpericardial biopsy and window creation is safe and effective in the treatment of these effusions.
777
778 Van Trigt and Others
Pericardial effusion represents a common sequela to awide variety of insults to the pericardium. The processhas been known since antiquity when Galen recognizedand successfully treated purulent pericarditis with sur-gery.' In recent times, the diagnosis of pericardial effu-sion has been made easier with the advent of echocardi-ography. However, the method ofdetermining the causeand the form of treatment for pericardial effusions havebeen areas of controversy. Some physicians advocatepericardiocentesis;2'3 others, surgery with creation of apericardial window;4'5 and still others, thoracotomy withpericardiectomy.6 7 In addition, thorascopic creation ofa pericardial window, a recently introduced technique todrain large effusions, has gained advocates. Because ofthis lack of consensus and to provide a standard ofcom-parison for newer (thorascopic) techniques, we un-dertook a prospective study to evaluate subxiphoid peri-cardiotomy and drainage in patients with large pericar-dial effusions.8 Fifty-seven ofthe 75 consecutive patientsidentified underwent subxiphoid pericardial biopsy.9 Wepresent here the diagnostic efficacy, mortality rate, com-plications, and 1-year follow-up data.
METHODSAll echocardiograms of patients admitted to Duke
University Medical Center and the Durham Veteran'sAdministration Medical Center during a 20-month pe-riod were screened. Patients with large pericardial effu-sions were selected for entry into the study. Large peri-cardial effusions were defined as those effusions withboth anterior and posterior fluid and 0.5 cm of fluid ei-ther anteriorly or posteriorly during diastole using stan-dard two-dimensional echocardiographic techniques.
After identification, the patient's physician was con-tacted for permission to proceed. The patient was evalu-ated by one of the authors and a physical examinationand laboratory and radiologic work-up were performed.This included a complete blood count; coagulation stud-ies; levels of serum electrolytes, serum creatinine, bloodurea nitrogen, calcium, albumin, and protein; liver func-tion studies; lactate dehydrogenase (LDH) levels; thyroidstudies; antinuclear antibody determination; rheuma-toid factor analysis; skin tests; appropriate cultures; chestx-ray; and electrocardiogram. Acute and convalescentviral serologic tests for herpes simplex (HSV), lympho-cytic choriomeningitis virus, cytomegalovirus (CMV),influenza, and Coxsackie B1-4"10"'1 were drawn. Other se-rologic titers included Toxoplasma, Legionella, Myco-
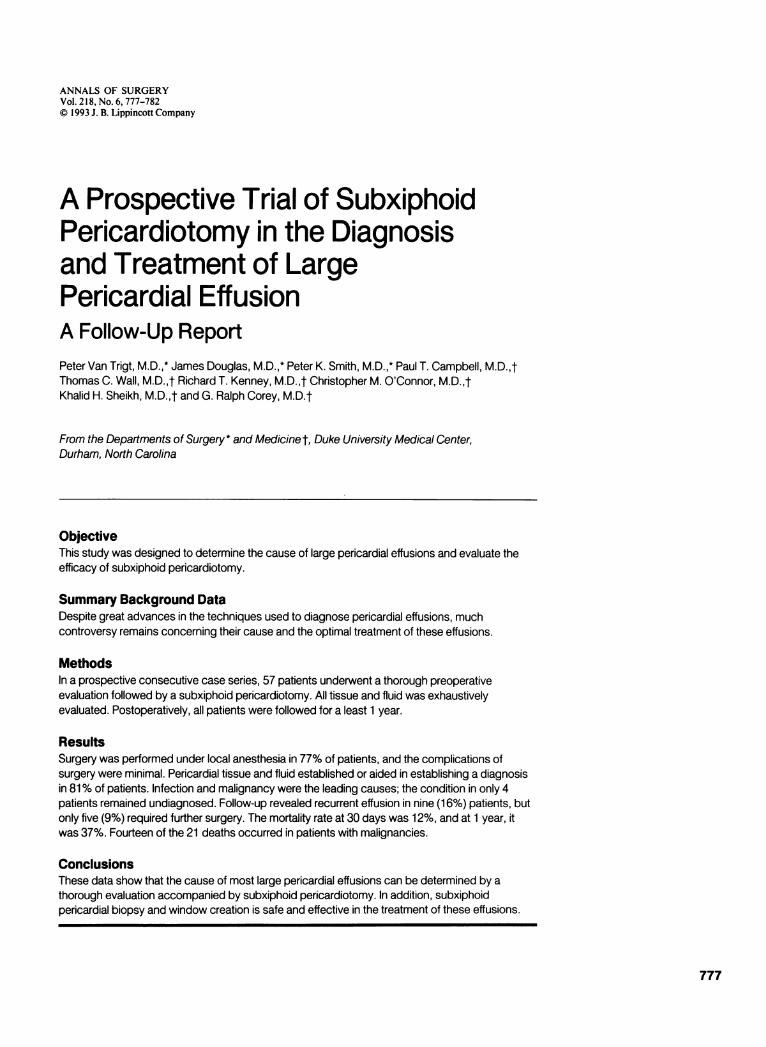
Figure 1. Transverse computed tomographic image shows a large sym-metric pericardial effusion (arrow). Uremic effusion was diagnosed after allother studies gave negative results.
plasma, Venereal Disease Research Laboratories, andLeptospira. Computed tomography, magnetic resonanceimaging, and right heart catheterization were done onselected patients (Figs. 1 to 3).
Ifthought to be clinically indicated, a subxiphoid peri-cardial biopsy and drainage was performed according toa published method.4 The procedure was performed un-der local anesthesia with a supplemental intravenoussedative-hypnotic being given as needed. A 5- to 6-cmincision centered over the xiphoid was made and carriedthrough the rectus fascia. The xiphoid process was ex-cised, and the lower aspect of the sternum was gently el-evated with a retractor. The fibroareolar tissue anteriorto the pericardium was removed with sharp and blunt
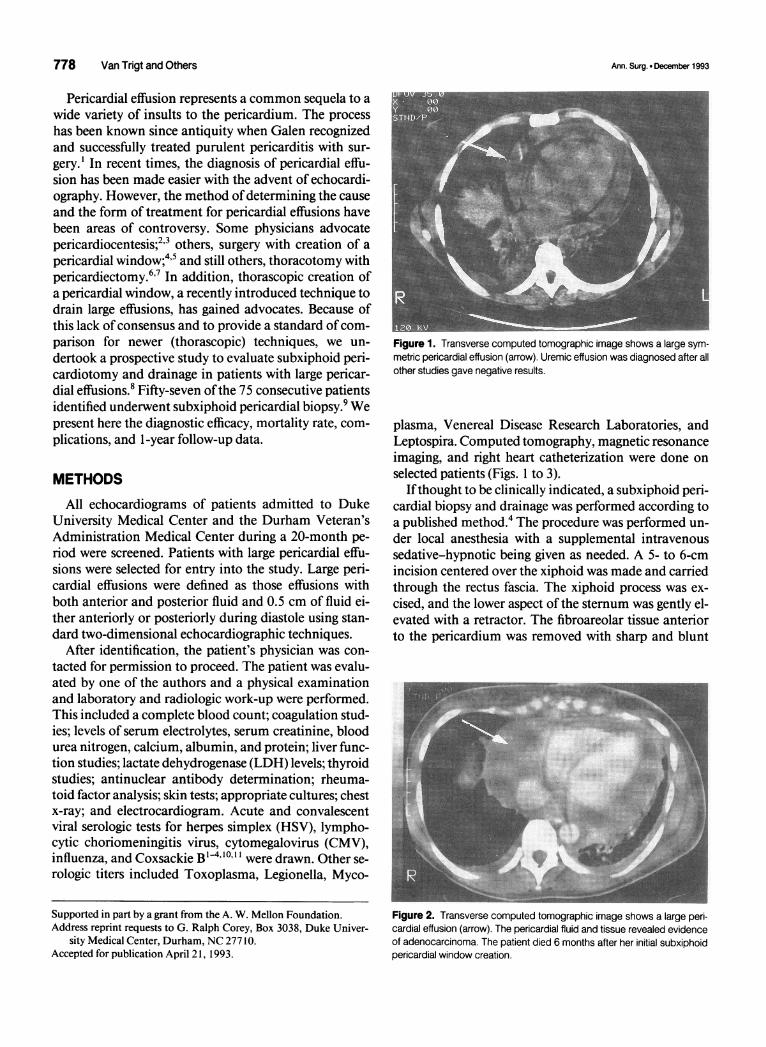
Figure 2. Transverse computed tomographic image shows a large peri-cardial effusion (arrow). The pericardial fluid and tissue revealed evidenceof adenocarcinoma. The patient died 6 months after her initial subxiphoidpericardial window creation.
Supported in part by a grant from the A. W. Mellon Foundation.Address reprint requests to G. Ralph Corey, Box 3038, Duke Univer-
sity Medical Center, Durham, NC 27710.Accepted for publication April 21, 1993.
Ann. Surg. * December 1993

Subxiphoid Pericardiotomy for Large Pericardial Effusions 779
Table 1. SYMPTOMS (N = 57)
No.Symptom (%)
SOB/DOEChest painOrthopneaEdemaCoughFeverPNDAbdominal swellingNight sweatsChillsAsymptomaticSyncope
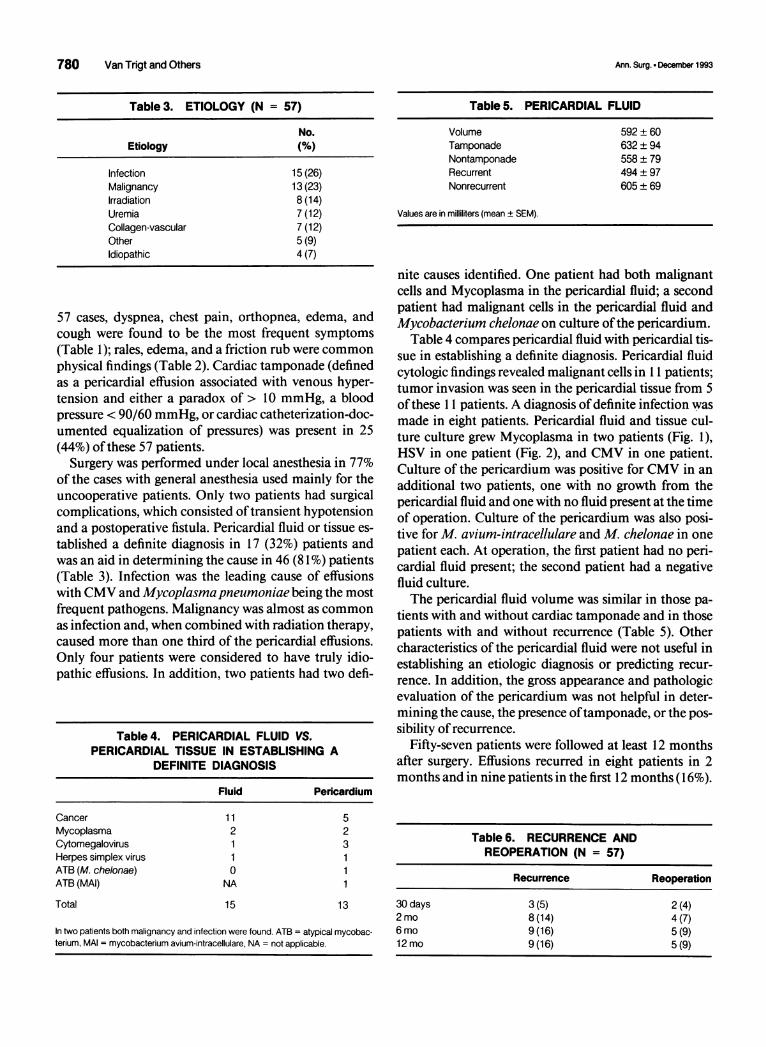
Figure 3. Magnetic resonance image shows a large inhomogeneouspericardial effusion (arrow) in a patient with acquired immune deficiencysyndrome and systemic lupus erythematosus. Pericardial fluid and tissuetests were unrevealing, and the patient died during the following month.
SOB/DOE = shortness of breath/dyspnea on exertion, PND = paroxysmal nocturnaldyspnea.
dissection. Keeping the dissection in the midline avoidsentering the pleural space, which rarely occurs. To facil-itate adequate exposure of the pericardium, the fibrousridge oftissue at thejunction between the diaphragm andthe inferior pericardium was grasped with an Allis clampand pulled inferiorly. A longitudinal incision was madein the pericardium in the midline under direct vision andfluid was removed. A 3- to 4-cm piece of anterior peri-cardium was excised. Pericardial fluid and tissue was sentfor appropriate pathologic and microbiologic studies.The pericardial space was gently explored with theoperator's finger, and loculated collections were openedcarefully. The epicardium ofthe left ventricular apex wasvisualized, and the character of the epicardium (e.g.,inflammation or tumor nodules) was noted. An angled28-French soft chest tube was placed in the posteriorpericardial space along the diaphragmatic surface andbrought out through a separate incision. The rectus fas-cia was then reapproximated, followed by a subcutane-ous and subcuticular closure. The chest tube was left un-til the drainage was less than 100 mL/day, and then, itwas removed.
Eighteen patients were excluded from the protocol forthe following reasons: seven patients refused the proce-dure; six physicians refused to perform the procedure;three patients had chronic effusion; and two patientsdied before the procedure could be performed.
Pericardial fluid was sent to determine the levels ofglucose, protein, LDH, leukocytes and differential,erythrocytes, pH, triglycerides, and cholesterol; for cyto-logic examination; and for anaerobic and aerobic bacte-rial, viral, Mycoplasma, fungal, and mycobacterial cul-tures. Pericardial tissue was studied pathologically and
cultured in a manner similar to pericardial fluid. In ad-dition, chlamydial cultures were performed on pericar-dial tissue. Careful follow-up of these patients includedclinic visits with one ofthe authors and echocardiogramsat 1, 3, 6, and 12 months after surgery.
RESULTS
Fifty-seven of 75 consecutive patients with large peri-cardial effusions underwent surgery. In evaluating these
Table 2. SIGNS (N = 57)
Mean
Temperature (OC)Pulse (beats/min)Systolic blood pressure (mmHg)Diastolic blood pressure (mmHg)JVP height (cm H20)Paradoxical pulse (mmHg)
RalesEdemaFriction rubKussmaul'sSoft S2MurmurEwart'sHepatomegalyAscitesNormal
3729813079910
No. of Patients (%)
28 (49)25 (44)15 (26)12(21)11 (19)10 (18)10 (18)10 (18)8(14)4 (7)
JVP = jugular venous pulse.
46(81)31 (54)26 (46)25 (44)24 (42)19 (33)13 (23)12(21)9(16)8(14)3 (5)2 (4)
Vol. 218 - No. 6
780 Van Trigt and Others
Table 3. ETIOLOGY (N = 57)
No.Etiology (%)
Infection 15 (26)Malignancy 13 (23)Irradiation 8 (14)Uremia 7 (12)Collagen-vascular 7 (12)Other 5 (9)Idiopathic 4 (7)
57 cases, dyspnea, chest pain, orthopnea, edema, andcough were found to be the most frequent symptoms(Table 1); rales, edema, and a friction rub were common
physical findings (Table 2). Cardiac tamponade (definedas a pericardial effusion associated with venous hyper-tension and either a paradox of > 10 mmHg, a bloodpressure < 90/60 mmHg, or cardiac catheterization-doc-umented equalization of pressures) was present in 25(44%) of these 57 patients.
Surgery was performed under local anesthesia in 77%of the cases with general anesthesia used mainly for theuncooperative patients. Only two patients had surgicalcomplications, which consisted oftransient hypotensionand a postoperative fistula. Pericardial fluid or tissue es-
tablished a definite diagnosis in 17 (32%) patients andwas an aid in determining the cause in 46 (81 %) patients(Table 3). Infection was the leading cause of effusionswith CMV and Mycoplasma pneumoniae being the mostfrequent pathogens. Malignancy was almost as common
as infection and, when combined with radiation therapy,caused more than one third of the pericardial effusions.Only four patients were considered to have truly idio-pathic effusions. In addition, two patients had two defi-
Table 4. PERICARDIAL FLUID VS.PERICARDIAL TISSUE IN ESTABLISHING A
DEFINITE DIAGNOSIS
Fluid Pericardium
CancerMycoplasmaCytomegalovirusHerpes simplex virusATB (M. chelonae)ATB (MAI)
Total
11
2
10
NA
15
523
11
13
In two patients both malignancy and infection were found. ATB = atypical mycobac-terium, MAI = mycobacterium avium-intracellulare, NA = not applicable.
Table 5. PERICARDIAL FLUID
Volume 592 ± 60Tamponade 632 ± 94Nontamponade 558 ± 79Recurrent 494 ± 97Nonrecurrent 605 ± 69
Values are in milliliters (mean ± SEM).
nite causes identified. One patient had both malignantcells and Mycoplasma in the pericardial fluid; a secondpatient had malignant cells in the pericardial fluid andMycobacterium chelonae on culture ofthe pericardium.
Table 4 compares pericardial fluid with pericardial tis-sue in establishing a definite diagnosis. Pericardial fluidcytologic findings revealed malignant cells in 11 patients;tumor invasion was seen in the pericardial tissue from 5of these 11 patients. A diagnosis ofdefinite infection wasmade in eight patients. Pencardial fluid and tissue cul-ture culture grew Mycoplasma in two patients (Fig. 1),HSV in one patient (Fig. 2), and CMV in one patient.Culture of the pericardium was positive for CMV in an
additional two patients, one with no growth from thepericardial fluid and one with no fluid present at the timeof operation. Culture of the pericardium was also posi-tive for M. avium-intracellulare and M. chelonae in onepatient each. At operation, the first patient had no peri-cardial fluid present; the second patient had a negativefluid culture.The pericardial fluid volume was similar in those pa-
tients with and without cardiac tamponade and in thosepatients with and without recurrence (Table 5). Othercharacteristics of the pericardial fluid were not useful inestablishing an etiologic diagnosis or predicting recur-
rence. In addition, the gross appearance and pathologicevaluation of the pericardium was not helpful in deter-mining the cause, the presence oftamponade, or the pos-
sibility of recurrence.Fifty-seven patients were followed at least 12 months
after surgery. Effusions recurred in eight patients in 2months and in nine patients in the first 12 months (16%).
Table 6. RECURRENCE ANDREOPERATION (N = 57)
Recurrence Reoperation
30 days 3(5) 2(4)2 mo 8(14) 4 (7)6 mo 9(16) 5 (9)12 mo 9(16) 5(9)
Ann. Surg. - December 1993

Subxiphoid Pencardiotomy for Large Pericardial Effusions
Table 7. MORTALITY
Etiology Immediate 30 Days 2 Months 6 Months 12 Months
Infection 0/14(0) 0/14 (0) 1/14(7) 1/14 (7) 1/14 (7)Malignancy 0/13(0) 5/13 (38) 7/13 (54) 12/13(92) 12/13 (92)Irradiation 0/8 (0) 0/8 (0) 0/8 (0) 2/8 (25) 2/8 (25)Uremia 0/7 (0) 0/7 (0) 0/7 (0) 3/7 (43) 3/7 (43)Collagen-vascular 0/7 (0) 1/7 (14) 1/7 (14) 1/7 (14) 1/7 (14)Idiopathic 0/4 (0) 1/4 (25) 1/4 (25) 1/4 (25) 1/4 (25)Other 0/5 (0) 0/5 (0) 1/5 (20) 1/5 (20) 1/5 (20)Overall 0/57 (0) 7/57 (12) 11/57 (19) 21/57 (37) 21/57 (37)
Values in parentheses are percentages.
Five (9%) of these required reoperation (Table 6). Thecauses ofthe recurrent effusions were diverse-two viral,two uremic, two idiopathic, one collagen-vascular, onemalignant, and one radiation. Reoperation, consisting ofa left anterior thoracotomy with an extensive anteriorpericardiectomy, was performed in two patients with vi-ral-induced pericardial effusion and one patient eachwith uremia, collagen-vascular disease, and malignancyas the causes oftheir effusions.The deaths are outlined in Table 7. Although the im-
mediate mortality rate was 0%, the 30-day mortality ratewas 12% (7 of 57). Five of these seven patients had a ma-lignancy. The mortality rate in the malignancy subgroupremained high throughout the study-38% at 1 monthand 92% (12 of 13) at 1 year.
DISCUSSIONSubxiphoid pericardiotomy was used in this study be-
cause it provides a definitive and safe method ofevaluat-ing and treating pericardial effusions without the neces-sity of general anesthesia.4'5' '013 Using this approach,pericardial fluid and pericardial tissue can be examinedand cultured, thus offering a potentially improved diag-nostic yield over pericardiocentesis alone.12 In addition,the subxiphoid pericardiotomy is an effective method ofdrainage even in hemodynamically unstable patientswith cardiac tamponade.9" 3
Pericardiocentesis alone was not used in this study as adiagnostic and therapeutic modality for several reasons.First was the consideration of safety. Despite several re-ports of mortality rates as low as 0% to 4% for this proce-dure, these figures are probably valid for only the mostexperienced cardiologists.2"14"15 Furthermore, pericardio-centesis has an incomplete diagnostic effectiveness with50% positive cultures in tuberculous pericarditis'6 and a50% to 100% yield of malignant cells in neoplastic peri-carditis. 17-21 Finally, pericardiocentesis relieves cardiactamponade in only 61% of patients.2
In this prospective study, careful presurgical evalua-tion of the patients and thorough pathologic and micro-biologic processing of the surgical specimens resulted ina diagnosis in 53 of 57 patients. The condition in onlyfour (7%) patients remained undiagnosed. This is a sig-nificantly lower percentage than that in previous se-ries.2'6"'4'22-24 Nineteen diagnoses in 17 patients resultedfrom fluid and tissue evaluation (Table 4). Althoughpericardial tissue was of particular value in infectiouscauses ofpericarditis, malignancy was diagnosed by fluidcytologic examinations in all 11 patients.Our results also demonstrated that the use of the sub-
xiphoid pericardiotomy with drainage is safe. Seventy-seven per cent of procedures were done under local an-esthesia with only two minor operative complications.Therapeutic efficacy was also demonstrated for this pro-cedure. At the 1-year follow-up, low recurrence (16%)and reoperation rates (9%) were found.
In looking at the 1-year mortality rates, there was littleindication that pericardial effusion per se had any effecton this. Most deaths (67%) occurred in patients with ma-lignancy. No in-hospital deaths were caused by an oper-ative complication or a recurrence of effusion with he-modynamic compromise.On the basis of our experience, we believe that subxi-
phoid pericardiotomy is not only safe and effective diag-nostically, but in contrast to previous literature, we thinkit is extremely effective in treating large pericardial effu-sions of various causes and severities.
References
1. Spodick DH. Medical history of the pericardium. Am J Cardiol1970; 26:447-454.
2. Krikorian JG, Hancock EW. Pericardiocentesis. Am J Med 1978;65:808-814.
3. Hancock EW. Subacute effusive constrictive pericarditis. Circula-tion 1971; 43:183-192.
4. Fontenelle LJ, Cuello L, Dooley BN. Subxiphoid pericardial win-dow. J Thorac Cardiovasc Surg 1971; 62:95-97.
781Vol.218 -No.6

782 Van Trigt and Others
5. Daugirdas JT, Leehey DJ, Popli S, et al. Subxiphoid pericardios-tomy for hemodialysis-associated pericardial effusion. Arch InternMed 1986; 146:1113-1115.
6. Piehler JM, Pluth JR, Schaff HV, et al. Surgical management ofeffusive pericardial disease. J Thorac Cardiovasc Surg 1985; 90:506-516.
7. Pradham DJ, Ikins PM. The role of pericardiotomy in treatmentof pericarditis with effusion. Am Surg 1976; 42:257.
8. Corey RC, Campbell PT, Van Trigt P, et al. Etiology of large peri-cardial effusions. Am J Med 1993; 95:209-213.
9. Wall TC, Campbell PT, O'Connor CM, et al. Diagnosis and man-agement (by subxiphoid pericardiotomy) of large pericardial effu-sions causing cardiac tamponade. Am J Cardiol 1992; 69:1075-1078.
10. Ribot S, Frankel JH, Gielchinsky I, Gilbert L. Treatment ofuremicpericarditis. Clin Nephrol 1974; 2:127-130.
11. Santos GH, Frater RWM. The subxiphoid approach in the treat-ment of pericardial effusion. Ann Thorac Surg 1977; 23:467-470.
12. Ibarra-Perez C, Gonzalez-Radillo L. Diagnosis and treatment ofpericarditis by the subxiphoid approach. Am Surg 1978; 44:602-604.
13. Alcan KE, Zabetakis PM, Marino ND, et al. Management ofacutecardiac tamponade by subxiphoid pericardiotomy. JAMA 1982;247:1143-1148.
14. Permanyer-Miralda G, Sagrista-Sauleda J, Soler-Soler J. Primary
acute pericardial disease: a prospective study of 231 consecutivepatients. Am J Cardiol 1985; 56:623-630.
15. Callahan JA, Seward JB, Hishimura RA, et al. Two-dimensionalecho-cardiographically guided pericardiocentesis: experience in117 consecutive patients. Am J Cardiol 1985; 55:476-479.
16. Rooney JJ, Crocco JA, Lyons HA. Tuberculous pericarditis. AnnIntern Med 1970; 72:73-78.
17. Campbell PT, Van Trigt P, Wall TC, et al. Subxiphoid pericardi-otomy in the diagnosis and management of large pericardial effu-sions associated with malignancy. Chest 1992; 101:938-943.
18. Zipf RE, Johnston WW. The role of cytology in the evaluation ofpericardial effusions. Chest 1972; 62:593-596.
19. Posner MR, Cohen GI, Skarin AT. Pericardial disease in patientswith cancer. Am J Med 1981; 71:407-413.
20. Reyes CV, Strinden C, Banerji M. The role ofcytology in neoplas-tic tamponade. Acta Cytol 1982; 26:299-302.
21. Sulkes A, Weshler Z, Kopolovic Y. Pericardial effusion as the firstevidence of malignancy in bronchogenic carcinoma. J Surg Oncol1982; 20:71-74.
22. Colombo A, Olson HG, Egan J, Gardin JM. Etiology and prognos-tic implications of large pericardial effusion in men. Clin Cardiol1988; 11:389-394.
23. Markiewicz W, Borovic R, Ecker S. Cardiac tamponade in medicalpatients: treatment and prognosis in the echocardiographic era.AmHeartJ 1986; 111:1138-1142.
24. Guberman BA, Fowler NO, Engel PJ, et al. Cardiac tamponade inmedical patients. Circulation 1981; 64:633-640.
Ann. Surg. * December 1993

















![[Clinical and laboratory features of patients with pericardial effusion]](https://static.fdokumen.com/doc/165x107/6325f6805547884b71068814/clinical-and-laboratory-features-of-patients-with-pericardial-effusion.jpg)

