A prospective study of isolation and mortality in a cohort of elderly Navajo Indians
15
STEPHEN J. KUNITZ AND JERROLD E. LEVY A PROSPECTIVE STUDY OF ISOLATION AND MORTALITY IN A COHORT OF ELDERLY NAVAJO INDIANS ABSTRACT. The prospective association between social isolation and mortality in a sample of 271 elderly Navajo Indian men and women living on their reservation in northern Arizona is reported. The follow-up period averaged three years from the time of interview in 1982--3. Self-reported level of physical functioning was predictive of mortality. Of the psycho-social measures, only marital status among men was predictive of increased risk of death, with the unmarried being at higher risk than the married. These results are attributed to the fact that Navajo society is traditionally matrilineal and matrilocal, with the mother-daughter bond being especially significant and with men being relatively more peripheral than their wives to the kin group. Thus unmarried men are far more likely to be isolated from kin than unmarried women and married people of either sex. Key Words: Aged, marriage, mortality, Navajo Indians, social isolation. Though the association between social isolation and mortality has been the subject of empirical investigation for almost a century, it has been only within the past decade that a spate of prospective cohort studies of the phenomenon has been published (House et al. 1982; Reed et al. 1984; Berkman and Syme 1979; Zuckerman et al. 1984; Blazer 1982; Schoen- bach et al. 1986; Welin et al. 1985). The results have been mixed: some showing an association, others showing none. An effort to resolve some of the anomalies suggested that the most important difficulties were those having to do with: (1) differences between the sexes in urban and rural areas, and (2) differences between whites and non-whites (Berkman 1986). With respect to the first issue, an association between isolation and increased risk of death has been observed in each sex in urban areas, but only among men in rural areas. With respect to the second issue, effects are weak or non-existent among Black men and women in Evans County, Georgia and Japanese-American men in Hawaii, and significant among whites. These observations suggest that a problem shared by all the studies has been that they have not adequately described the social organization of the study populations. For instance, while the Japanese are not a kin-based society in the classical sense of the word, since they have no clan system, family solidarity is an overwhelmingly important value (Lebra 1976). A survey of elderly Issei (Japanese-born immigrants to the United States) found that 14 percent lived entirely alone, though many of the solitaries belonged to various formal and informal associations (Montero 1979). This contrasts with 25 percent of a sample of elderly American Indians Journal of Cross-Cultural Gerontology 3 (1988) 71--85. © 1988 by Kluwer Academic Publishers.
Transcript of A prospective study of isolation and mortality in a cohort of elderly Navajo Indians

S T E P H E N J. K U N I T Z A N D J E R R O L D E. L E V Y
A P R O S P E C T I V E S T U D Y OF I S O L A T I O N
A N D M O R T A L I T Y IN A C O H O R T OF E L D E R L Y
N A V A J O I N D I A N S
ABSTRACT. The prospective association between social isolation and mortality in a sample of 271 elderly Navajo Indian men and women living on their reservation in northern Arizona is reported. The follow-up period averaged three years from the time of interview in 1982--3. Self-reported level of physical functioning was predictive of mortality. Of the psycho-social measures, only marital status among men was predictive of increased risk of death, with the unmarried being at higher risk than the married. These results are attributed to the fact that Navajo society is traditionally matrilineal and matrilocal, with the mother-daughter bond being especially significant and with men being relatively more peripheral than their wives to the kin group. Thus unmarried men are far more likely to be isolated from kin than unmarried women and married people of either sex.
Key Words: Aged, marriage, mortality, Navajo Indians, social isolation.
Though the association between social isolation and mortality has been the subject of empirical investigation for almost a century, it has been only within the past decade that a spate of prospective cohort studies of the phenomenon has been published (House et al. 1982; Reed et al. 1984; Berkman and Syme 1979; Zuckerman et al. 1984; Blazer 1982; Schoen- bach et al. 1986; Welin et al. 1985). The results have been mixed: some showing an association, others showing none. An effort to resolve some of the anomalies suggested that the most important difficulties were those having to do with: (1) differences between the sexes in urban and rural areas, and (2) differences between whites and non-whites (Berkman 1986). With respect to the first issue, an association between isolation and increased risk of death has been observed in each sex in urban areas, but only among men in rural areas. With respect to the second issue, effects are weak or non-existent among Black men and women in Evans County, Georgia and Japanese-American men in Hawaii, and significant among whites.
These observations suggest that a problem shared by all the studies has been that they have not adequately described the social organization of the study populations. For instance, while the Japanese are not a kin-based society in the classical sense of the word, since they have no clan system, family solidarity is an overwhelmingly important value (Lebra 1976). A survey of elderly Issei (Japanese-born immigrants to the United States) found that 14 percent lived entirely alone, though many of the solitaries belonged to various formal and informal associations (Montero 1979). This contrasts with 25 percent of a sample of elderly American Indians
Journal of Cross-Cultural Gerontology 3 (1988) 71--85. © 1988 by Kluwer Academic Publishers.

72 S T EPHEN J. K U N I T Z AND J E R R O L D E. LEVY
and 38 percent of a sample of elderly residents of Cleveland, Ohio (National Indian Council on Aging 1981).
Conversely, so far as can be determined the white subjects are predom- inantly from Northwest Europe or have assimilated the norms of family organization characteristic of Northwest Europe and its overseas exten- sions, most importantly the establishment of a new household at marriage (neolocality). This is an old pattern in Northwest Europe, long antedating industrial development and urban growth. It is not common in Southern Europe or in areas to the East of a line drawn from Leningrad to Trieste (Hajnal 1965, 1982; Laslett 1983); and it is reflected in differences in living arrangements of elderly people in several European countries at present (WHO 1983). This is important for it suggests, first that the patterns of family organization generally thought to be the characteristic consequences of industrialization and urbanization (usually called "Mod- ernization") may not be inevitable; and second, that studies done in white or non-white kin-based societies may show entirely different patterns of association between isolation and mortality than those observed in the populations studied so far. In the Balkans, for example, urbanization may not be associated with isolation and increased risk of death. In addition, social relationships may have entirely different significance in different societies so that mechanically repeating the same measures from one study to another may not lead to illuminating results.
Finally, it is by no means clear what the causal mechanism, if any, is between isolation and mortality: neglect? loneliness? Or are isolation and increased risk of death themselves often the effects of a common cause?
To explore some of these issues, we report here the results of a prospective cohort study of isolation and mortality in a kin-based society, the Navajo Indians living on a 24,000 square mile reservation in northern Arizona, southern Utah, and northwestern New Mexico. The questions in which we are interested are: (1) whether in a society such as this isolation of elderly people is common enough to be associated with increased risk of death, and (2) if so, what characterizes isolated people?
The Navajos are a matrilineal, matrilocal tribe. That is to say, tradition- ally a child was a member of his or her mother's clan (matrilineality), and the typical co-resident domestic group (the camp) was composed of a senior couple, their married daughters and their husbands and children, plus the senior couple's unmarried children (matrilocality).
In such a situation the husband is in a particularly vulnerable position, for he is peripheral to his wife's family and no longer resident in his own natal camp. His wife, on the other hand, is resident in her natal household. Women are thus much more deeply embedded in an extended domestic group than men, who are attached only through their wives. Usually it is only after many years of marriage that the husband, too, may become

I S O L A T I O N A N D M O R T A L I T Y IN E L D E R L Y N A V A J O S 73
central to the kin group. Perhaps as a result, Navajo marriages have tended to be unstable.
This traditional pattern of family organization is not found in the majority of cases at present, and perhaps was never as fixed as the classification "matrilineal-matrilocal" would suggest (Levy and Kunitz 1974). Domestic arrangements have always been fluid and continue so at present. Nonetheless the bond between a mother and her daughters has been and still is of crucial importance.
M A T E R I A L S AND M E T H O D S
The original sample was composed of 279 Navajo men and women who in 1982 were 65 years of age or older. They were a 50 percent random sample from a computer-generated list of all people born in 1917 or earlier who: (1) had been treated at least once in an Indian Health Service clinic or hospital in the previous ten years and (2) had given an address within the Tuba City Service Unit (land management districts 1 and 3), the catchment area of approximately 5,000 square miles forming the universe to which we limited our attention (Kunitz 1983). Eight people (2.9 per cent) refused to be interviewed. The final sample was 271.
It is conceivable that by choosing the sample in this way we did not include people who had never had any contact with the Public Health Service system of medical care, by far the most significant source of services (free of charge to Indian beneficiaries) on the Reservation. Tiffs is unlikely to have led to significant biases since it seems improbable that a substantial proportion of the population would not have had contact with a health care provider at least once in ten years. Moreover, comparing the size of the population 65 and above as estimated by our method with the number enumerated by the 1980 U.S. Census indicates that the Census missed about 15 per cent of the population 65 and above in this region, and that at the very least we are not likely to have missed many people.
Several sources of data were used: interviews, medical record reviews, and reviews of death certificates in the Arizona state health department. Interviewing was done between Sept. 1, 1982 and August 30, 1983. Interviews generally lasted three or four hours and most often were carried out in Navajo. Data were gathered on family organization and economics; level of physical, social, and intellectual functioning (the Sickness Impact Profile [Department of Health Services 1978]); depres- sion; use of health services; and religious beliefs and practices.
The Sickness Impact Profile is designed to elicit information from the respondent (or a proxy informant) about functional ability in several domains and is thus analogous to other instruments which also measure

74 S T E P H E N J. K U N I T Z A N D J E R R O L D E. L E V Y
activities of daily living. The scales with which we are most concerned in this paper are those devoted to level of physical functioning: ambulation, mobility in and out of bed, independence in dressing and toileting, and so on (PHYSIP).
The measure of depression is based upon a modification of the Diag- nostic Interview Schedule for Depression (DIS-D) recently developed by the National Institute of Mental Health (Robins et al. 1981a, 1981b). It is a fully structured interview designed to enable physicians and non- physicians to make consistent and accurate psychiatric diagnoses in patients and the general population. After encountering several difficulties during pretesting, however, a number of modifications were made that resulted in a shortened format designed to be incorporated in the larger interview without making the entire instrument too unwieldy. In addition the highly structured format was abandoned because respondents felt it too repetitious. More satisfactory results were obtained by allowing respondents to recount their experiences in their own way before the interviewer probed further.
Reviews of medical records were done at the Indian Health Service hospital in Tuba City, Arizona, the source of care mentioned most frequently by our informants. The records included in- and out-patient data as well as summaries of hospitalizations in other facilities. Mortality of the sample was followed by continuing surveillance in the communities, interviews with key informants, and reviews of medical records and death certificates in the state health department. All people were considered to have been under observation from the time of interview to the time of death or until June 30, 1986. Final record reviews in the hospital and state health department were done in June and August, 1986, respectively. Final interviews with key informants were done in June, 1986. The average number of months of observation was 37 per person.
R E S U L T S
Table I displays the age and sex distribution and vital status of the sample as of June 30, 1986. There are two noteworthy results. First, significantly more men than women died below the age of 75. This is consistent with data not presented here, that women below 75 reported the lowest scores on the Sickness Impact Profile, as well as the lowest rates of hospitaliza- tion. Second, there is no significant difference between the sexes at ages 75 and above.
Thirty-seven people died during the period of observation, giving an average annual rate of about 45 per 1,000, close to the top of the range estimated for the entire Navajo population 65 years of age and above. This is lower than the age-specific rate (calculated in five-year age groups)

I S O L A T I O N A N D M O R T A L I T Y IN E L D E R L Y N A V A J O S
TABLE I Mortality by age and sex
75
Status at time of follow-up Age at time of follow-up
< 75 > 75
Male Female Male Female
Dead 8 0 14 15
Alive 40 56 62 75
chi-square 10.111 0.0888 d,f. 1 1 p value < 0.01 > 0.05
observed in the non-Indian population 65 years of age and above. Navajos may thus be one of those populations which experience the so-called mortality "crossover," a phenomenon whose very existence is still a matter of debate (Weatherby et al 1983; Wing et al. 1985; Coale and Kisker 1986).
When the people who died are compared with those who did not, using non-parametric statistical tests such as the Kruskal-Wallis analysis of variance and Mann-Whitney U-test, they had significantly higher scores on all the S.I.P. scales. They also had been hospitalized more often in 1980-3, had spent more days in hospital, and had more diagnostic tests. They did not differ in their responses to questions regarding depression.
Turning to socio-economic variables, there is no difference between the two groups in respect of per capita camp income or income from various sources (e.g., wage work, social security, live stock), number of people per room in the respondent's dwelling, availability of conveniences such as running water and electricity, distance of residence from the nearest hospital, cattle and sheep holdings, and years of education.
On the other hand, as Table II indicates, there was a significant difference in marital status between the two groups when men and women were considered separately. More men than women were married, and among the unmarried men who were 75 and above at time of death or end of the period of observation, a higher proportion (about 41 per cent) died than among the married men (about 11 per cent). There were no differ- ences between married and unmarried women or men below the age of 75. There were no comparable differences when number of children living in the camp, number of households in the camp, generational depth of the camp, or camp composition (neolocal vs. extended) were considered.
Among Navajos women now outnumber men at all ages, as they do in

76 S T E P H E N J. K U N I T Z A N D J E R R O L D E. L E V Y
T A B L E II Mortality and marital status
M e n
Vital Status Unde r 75 75 and above
Marr ied Unmar r ied Married Unmar r ied
Dead 6 2 7 7
Alive 3 9 52 10
Chi-square 3.03 7.545 d.f. 1 1 p value > 0.05 < 0.01
W o m e n
Vital Status U n d e r 75 75 and above
Married Unmar r ied Marr ied Unmar r i ed
Dead 0 0 3 12
Alive 23 33 20 55
Chi-square - - 0.292 d.f. - - 1 p value - - > 0.05
the United States in general (Kunitz and Slocumb 1976). For that reason we thought that the unmarried men in our sample might be more likely than the married men to have some physical or psychological problems that would keep them from marrying, even when sufficient numbers of women were available from which to choose a wife. On the other hand, unmarried women would not be as likely to differ from married women. Thus it seemed reasonable to hypothesize that marital status was simply a reflection of other variables more directly associated with increased mortality among men.
To examine this possibility Sickness Impact Profile and Depression scores of married with unmarried men, and married with unmarried women were compared. There were no differences between the two groups of men. Unmarried women, however, had significantly higher scores than married women on the Sickness Impact Profile scales, a finding accounted for by the fact that unmarried women were older than married women, having outlived their spouses, a subject to which we shall return below. There is no evidence that marital status is associated with a

ISOLATION AND MORTALITY IN ELDERLY NAVAJOS 77
reduced level of physical or psychological functioning that might also influence the risk of death.
To explore the issue further we have done the following analyses. Figure 1 is a display of four Kaplan-Meier curves. The apparent difference between married and unmarried men is statistically significant at p -- 0.016 (using a one-tailed test because of the expectation that unmarried people are at greater risk of death than married people). For approximate tests of hypotheses we have used Cox proportional hazards regression. Under the regression model, single males have approximately 2.5 times
r r
> >
o'3
O ' r -
O"1 C)
C O
O
O
(.O O
t.lb o 1-
- - T F " ............. : L I~__ {
i
J I _ _ '
I ~ j ~ " t
i [ . . . . .
Fig. 1.
- I-- ~ Married F I I I Low PHYSIP
' 1 II
I [ . . . . . . . . . . . . . . . . . . . . . . . . . . . r - - - - ]
] , i . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Married High PHYSIP
I
I ] Unmarried ] Low PHYSIP
I
I i.___
Unmarried High PHYSIP
I I I I
10 2 0 3 0 4 0
T i m e in M o n t h s
Survival curves for males by marital status and PHYSIP score.
50
78 STEPHEN J. KUNITZ AND JERROLD E. LEVY
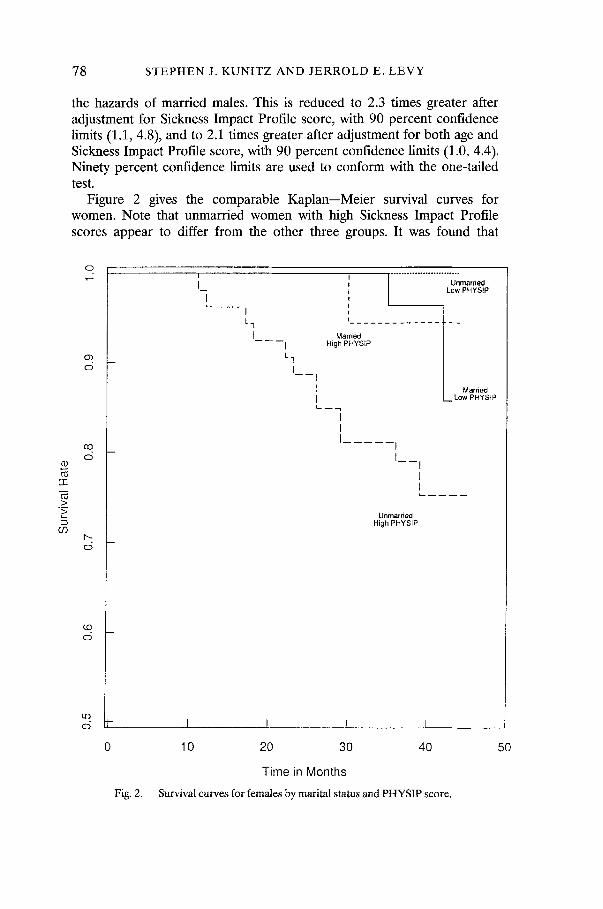
the hazards of married males. This is reduced to 2.3 times greater after adjustment for Sickness Impact Profile score, with 90 percent confidence limits (1.1, 4.8), and to 2.1 times greater after adjustment for both age and Sickness Impact Profile score, with 90 percent confidence limits (1.0, 4.4). Ninety percent confidence limits are used to conform with the one-tailed test.
Figure 2 gives the comparable Kaplan--Meier survival curves for women. Note that unmarried women with high Sickness Impact Profile scores appear to differ from the other three groups. It was found that
03
cc
>
69
O
Ob O
CO O
O
e.D O
O t-
O
Fig. 2.
I I
I ~ - - - - - - j [ "1
I I Lq
I - - - - I
I I
I 1 I
l Unmarried Low PHYSIP
Ma,2 . . . . . . . . . . . } - - High PHYSIP /
| Married [_. Low PHYSlP
/
I I 1
Unmarried High PHYSIP
I ! r
10 20 30 40
Time in Months
Survival curves for females by marital status and PHYSIP score.
50

I S O L A T I O N A N D M O R T A L I T Y IN E L D E R L Y N A V A J O S 7 9
women in the former group have an eight-fold greater hazard of dying than the latter three groups combined. We attempted an approximate age adjustment, and the relative hazards for those 75 and above is approxi- mately six-fold that of women below the age of 75, but even with an age variable in the model the effect of Sickness Impact Profile score remained strong. This result for women seems to be a consequence of the fact that the younger women have the lowest S.I.P. scores, experienced no deaths, and were also most likely to be married, as we have already observed.
The question we must now ask is, why is marital status the only psycho-social variable that is significantly associated with increased risk of death? and why only among men 75 and above?
One possibility is that the low mortality of elderly Navajos is the result of selection at younger ages such that only the healthiest survive. And if they are particularly healthy, perhaps social interaction is simply irrelevant to enhanced survival. If this is the case, it must be sex related since as we have shown, marital status is associated with survival among men but not women.
There seem to be two somewhat different processes at work. In respect of mortality among men, several observations are noteworthy. The only people in our sample who died below age 75 were men. Men are more likely than women to be married at ages above and below 75. When Sickness Impact Profile scores of deceased men and age-matched controls are compared, the men below 75 who died had significantly higher scores, but there was no difference between cases and controls 75 years of age and above. And when number of hospital days is compared, the men under 75 who died had spent significantly more days in hospital in 1980--3 than controls whereas among older men there was again no difference. Thus there is evidence that among the younger men who died were some with serious disabling illnesses requiring lengthy hospital stays. Older men who died did not differ from matched controls who did not die on these measures of severity of pre-existing disease. This would seem to support the possibility that among men there is some sort of selection at work such that those below 75 who die are in discernibly worse health than those who did not die, whereas no such distinction can be made among the older men.
Among women the situation was very different. No women died below age 75, and this group had the lowest Sickness Impact Profile scores and the lowest proport ion that had been hospitalized in 1980--3. Among women 75 and above, only a very few were married. When women who died are compared with age- and sex-matched controls, the former have significantly higher Sickness Impact Profile scores but not significantly more days in hospital.
It appears, then, that one reason marital status makes a difference among men is because mortality is high enough and marital status

80 S TEPHEN J. K U N I T Z AND J E R R O L D E. LEVY
sufficiently varied that its effect is discernible. Marital status may have a discernible effect only among men 75 and above because the men who died below that age were sufficiently sick that psycho-social factors were relatively less important. Among women just the opposite pertains: in the age group where death is common, marital status does not vary. Clearly, the two situations are related, for it is high mortality among younger men that results in the high frequency of unmarried women at older ages. This does not explain why mortality is higher among men than women; it simply contributes to part of an explanation of why no effect of marriage is observed among the women.
Excess male mortality is not unique to the Navajos (Verbrugge 1985). In the course of the epidemiologic transition from high to low mortality regimes, female mortality generally declines more rapidly and to lower levels than male mortality (Omran 1971). In low mortality regimes such as exist in developed and some developing nations, female life expectancy is greater than male, and females outnumber males at all ages. There is no universally agreed upon explanation of the phenomenon, but it is usually attributed to differences in behavioral patterns, as the changing incidence of smoking and lung cancer among men and women in the United States, and deaths from accidents among Navajos (Kunitz 1983), suggest. How much of the difference is simply a matter of behavioral patterns such as these and how much is associated with biological differences between the sexes is by no means clear, however.
With respect to the protective effect of marriage among men but not women, there is much evidence from experimental studies among animals, as well as human observational studies, that contact with others reduces the risk of death (Cassel 1976). Recall the point we made about matrilineality at the outset: that the mother-daughter bond seems to be especially significant and that men tend to be peripheral to their wives' families. We may examine this issue more closely by considering whether unmarried men and women differ from married men and women in the degree to which they have contact with other kin. We would expect that unmarried men would be the most isolated and that unmarried women would be at least as closely connected with kin as married men and women, if not more so. Table III displays the pertinent data, which indicate that unmarried men were significantly more likely than others to live in camps without their children. On the other hand, unmarried women were more likely than others to live with their children (Unmarried women were also most likely to live in multi-generation camps; data not shown.)
In addition, of the 27 unmarried men, six lived in single person camps. Of 99 unmarried women, four lived in single person camps (p < 0.01). Which is to say, men are more likely than women to be married. But when men are not married, they are more likely than unmarried women to live in isolation, not only from their children but from other people as well.

I S O L A T I O N A N D M O R T A L I T Y I N E L D E R L Y N A V A J O S
TABLE III Marital status, sex, and number of co-resident children
81
No. of Married Married Unmarried Unmarried Total children men women men women
0 34 16 14 22 86
1 20 14 7 47 88
2 or more 42 15 6 30 93
Total 96 45 27 99 267
chi-square = 21.86 d.f.v. = 6 p < 0.01
Table IV shows that only among men living with no or one child (combined to increase Ns) is being unmarried associated with a signifi- cantly increased risk of death. Among men living with two or more children, as well as among married and unmarried women regardless of the number of children with whom they live, there is no association between marital status and risk of death.
It is puzzling that being unmarried should be associated with increased
TABLE IV Vital status vs. marital status, gender and number of co-resident children
Gender Marital status No. co-resident children
0--1 Children /> 2 Children
Men
dead alive dead alive
Married 6 48 7 35
Unmarried 7 14 1 5
;~2 = 6.8 X2=0
Women Married 2 28 1 14
Unmarried 9 60 3 27
X 2 = 1.62 X2 = 0.08
d.f. = 1 )~2 = 3.84 p = 0.05

82 S T E P H E N J. K U N I T Z A N D J E R R O L D E. L E V Y
risk of death only among men living with 0--1 children and not among women in the same situation. We have reported previously that there was no evidence from the scaled instruments we used to measure depression and level of functioning that there was a difference between married and unmarried men and women that would suggest that less healthy people were unmarried and thus at greater risk of dying. On the other hand, it was observed in the course of interviewing that men often denied depres- sive symptoms or used alcohol to mask them. This was not found to be the case among women. In reviewing our field notes and interviews in search of a possible explanation of the results reported in Table 4, we looked particularly for mention of alcohol abuse. And indeed, of the seven men who died and had been both unmarried and living with 0--1 children, five had recent histories of excessive use. Such histories were not found as commonly for other men.
Unfortunately, because alcohol use was not a central focus of the research to begin with, equally detailed histories were not taken from all respondents. Furthermore, this is a result discovered after the fact rather than a hypothesis with which we began originally. For both reasons, therefore, formal tests of significance would be inappropriate. We believe the finding to be a real one, however.
We have suggested elsewhere that heavy drinking among Navajo men generally ceases by the time they reach their late 30s or early 40s (Levy and Kunitz 1974). Not all men stop or reduce their consumption, however, and some resume drinking as a consequence of a traumatic event such as the death of a wife or a favorite son, both of which happened to men in our sample. Whatever the sequence -- whether heavy drinking among elderly men maintains, exacerbates, or causes isolation -- it seems likely that it contributes to both physical deterioration and increased risk of death.
D I S C U S S I O N
Several processes seem to be causing the patterns we have observed. First, there does seem to be some sort of selection at work among men such that they develop more serious illness earlier and die at younger ages than women. Second, the most significant relationship for men appears to be with a wife. Women seem to have a larger number of significant relation- ships than men. Combined with their generally better health, women are at lower risk of death than men. Thus when their health does begin to fail, so many of them are unmarried that marital status is not likely to be predictive of death, and they are more likely to be embedded in social relationships than men that being unmarried is less of a risk factor in any event.

I S O L A T I O N A N D M O R T A L I T Y IN E L D E R L Y N A V A J O S 83
This explanation is not too different from the one suggested for the patterns observed in other populations (Verbrugge 1985). It has been said, for example, that American women have larger numbers of intimate friends than men and are thus protected from the impact of loss of a spouse. Of course this does not explain those cases in which there is no association among men, or where there is a significant association among women (see Table V).
TABLE V The association between marital status and mortality in seven prospective cohort studies
Place of Study and Significance of Reference Composition of Population Association
Tecumseh, Michigan White Adults of all ages House et al. 1982 Male Significant Female Not significant
Hawaii [Japanese-American Reed et al. 1984 Adult Men] Not significant
Alameda Co., California Berkman and Syme 1979 Adults of all ages Men Significant Women Not significant
Connecticut [Men and Not available Zuckerman et al. 1984 Women (Elderly)]
North Carolina [Men and Blazer 1982 Women (Elderly)] Not significant
Evans Co., Georgia Schoenbach et al. 1986 White Men Significant White Women Significant Black Men Marginally significant < 60 Black Women Not significant
Gothenburg, Sweden Welin et al. 1985 Middle-aged men "Borderline"
significant (p = 0.052)
But there is more to the issue than that. The observation that the most isolated Navajo men also seem to be the ones most likely to have histories of alcohol abuse leads us to ask whether alcohol abuse is a cause of both isolation and physical deterioration, a reaction to isolation and a cause of physical deterioration, or for some people a cause and for others an effect of isolation. What data we have suggests it is both a cause and effect of isolation. This is an important question to explore further because it raises the very real possibility that in those populations among whom "isolation"

84 STEPHEN J. KUNITZ AND J E R R O L D E. LEVY
(however measured) is found to be associated with an increased risk of death, it may not be isolation per se that is important but some character- istic of the individual that causes him or her to be both isolated and at increased risk of premature death. If our work is an example, some of the most important determinants -- alcohol abuse, for instance -- may not have been searched for carefully enough and thus may lead one to conclude, perhaps wrongly, that social isolation is an important cause of increased risk of death whereas it may turn out in some instances to be simply an epiphenomenon.
Our results thus suggest that: (1) future work might profitably explore characteristics of individuals that may be causally associated with both social isolation and increased risk of death, and (2) the inconsistent results among studies are likely to be resolved by more careful consideration than has generally been the case of the attributes of social relationships characteristic of each population.
A C K N O W L E D G E M E N T S
This study was supported by grant No. 1 R01 AG03403 from the National Institute on Aging. The authors are grateful to Tracy Andrews, Donald Callaway, Chena Dupuy, Eric Henderson, Dennis Parker, and Scott Russell for fieldwork; Diana Strickland and William Martens for data processing; Shirley Eberley, David Oakes, and Charles L. Odoroff for statistical advice and services; and Nancy Hildreth and William H. Barker for useful comments on an early draft.
R E F E R E N C E S
Berkman, L. F. 1986 Social Networks, Support, and Health: Taking the Next Step Forward. American Journal of Epidemiology 123:559--562.
Berkman, L. F. and S. L. Syme 1979 Social Networks, Host Resistance, and Mortality: A Nine-Year Follow-Up Study of Alameda Country Residents. American Journal of Epidemiology 109:186--204.
Blazer, D. G. 1982 Social Support and Mortality in an Elderly Community Population. American Journal of Epidemiology 115: 684--694.
Cassel, J. 1976 The Contribution of the Social Environment to Host Resistance. American Journal of Epidemiology 104:107-- 123.
CoMe, A. J. and E. E. Kisker 1986 Mortality Crossovers: Reality or Bad Data? Population Studies 40: 389--401.
Department of Health Services 1978 The Sickness Impact Profile: A Brief Summary of Its Purpose, Uses, and Administration. Seattle, WA.: University of Washington.
Hajnal, J. 1965 European Marriage Patterns in Perspective. In Population in History. D. V. Glass and D. E. C. Eversley, eds. London: E. Arnold.
Hajnal, J. 1982 Two Kinds of Preindustrial Household Formation System. Population and Development Review 8: 449--494.

ISOLATION AND MORTALITY IN ELDERLY NAVAJOS 85
House, J. S., C. Robbins and H. L. Metzner 1982 The Association of Social Relationships and Activities with Mortality: Prospective Evidence from the Tecumseh Community Health Study. American Journal of Epidemiology 116:123 - - 1 4 0 .
Kunitz, S. J. 1983 Disease Change and the Role of Medicine: The Navajo Experience. Los Angeles and Berkeley: The University of California Press.
Kunitz, S. J. and J. C. Slocumb 1976 The Changing Sex Ratio of the Navajo Tribe. Social Biology 23: 33--44.
Laslett, P. 1983 Family and Household as Work Group and Kin Group: Areas of Traditional Europe Compared. In Family Forms in Historic Europe. R. Wall, J. Robin and P. Laslett, eds. Pp. 513--563. Cambridge: Cambridge University Press.
Lebra T. 1976 Japanese Patterns of Behavior. Honolulu: University of Hawaii Press. Levy, J. E. and S. J. Kunitz 1974 Indian Drinking: Navajo Practices and Anglo-American
Theories. New York: Wiley. Montero, D. 1979 Disengagement and Aging among the Issei. In Ethnicity and Aging. D.
E. Gelfand and A. J. Kutzik, eds. Pp. 193--205. New York: Springer Publishing Company.
National Indian Council on Aging 1981 American Indian Elderly: A National Profile. Albuquerque, N. M.: National Indian Council on Aging, Inc.
Omran, A. 1971 The Epidemiological Transition: A Theory of the Epidemiology of Population Change. Milbank Memorial Fund Quarterly 41: 509--538.
Reed, D., D. McGee and K. Yano 1984 Psychosocial Processes and General Susceptibility to Chronic Disease. American Journal of Epidemiology 119: 356--370.
Robins, L. M., J. E. Helzer, J. Croughan, J. B. W. Williams and R. L. Spitzer 1981a NIMH Diagnostic Interview Schedule: Version IIIm unpublished copy for circulation. Bethesda: National Institute of Mental Health.
Robins, L. N., J. E. Helzer, J. Croughan and K. Ratcliff 1981b The National Institute of Mental Health Diagnostic Interview Schedule: Its History, Characteristics, and Validity. Archives of General Psychiatry 31:759--764.
Schoenbach, V. J., B. H. Kaplan, L. Fredman and D. G. Kleinbaum 1986 Social Ties and Mortality in Evans Country, Georgia. American Journal of Epidemiology 123: 577--591.
Verbrugge, L. M. 1985 Gender and Health: An Update on Hypotheses and Evidence. Journal of Health and Social Behavior 26:156--182.
Weatherby, N. L., C. B. Nam and L. W. Isaac 1983 Development, Inequality, Health Care, and Mortality at the Older Ages: A Cross-National Analysis. Demography 20: 27--43.
Welin, L., K. Svarsudd, S. Ander-Peciva, G. Tibblin, B. Tibblin, B. Larsson and L. Wilhelmsen 1985 Prospective Study of Social Influences on Mortality. Lancet 1: 915--918.
Wing, S., K. G. Manton, E. Stallard, C. G. Hames and H. A. Tyroler 1985 The Black/ White Mortality Crossover: Investigation in a Community-Based Study. Journal of Gerontology 40: 78--84.
World Health Organization 1983 The Elderly in Eleven Countries: A Sociomedical Survey. Public Health in Europe 21. Copenhagen: World Health Organization, Regional Office for Europe.
Zuckerman, D. M., S. V. Kasl and A. M. Ostfeld 1984 Psychosocial Predictors of Mortality among the Elderly Poor. American Journal of Epidemiology 119: 410--423.
Dept. of Preventive Medicine and Community Health, Box 644, University of Rochester School of Medicine, 601 Elmwood A venue, Rochester, N. Y. 14642