A proof of concept study for the integration of robot therapy with physiotherapy in the treatment of...
13
http://cre.sagepub.com Clinical Rehabilitation DOI: 10.1177/0269215508096759 2009; 23; 217 Clin Rehabil Maura Casadio, Psiche Giannoni, Pietro Morasso and Vittorio Sanguineti treatment of stroke patients A proof of concept study for the integration of robot therapy with physiotherapy in the http://cre.sagepub.com/cgi/content/abstract/23/3/217 The online version of this article can be found at: Published by: http://www.sagepublications.com can be found at: Clinical Rehabilitation Additional services and information for http://cre.sagepub.com/cgi/alerts Email Alerts: http://cre.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.co.uk/journalsPermissions.nav Permissions: http://cre.sagepub.com/cgi/content/refs/23/3/217 Citations by Pietro Morasso on April 16, 2009 http://cre.sagepub.com Downloaded from
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of A proof of concept study for the integration of robot therapy with physiotherapy in the treatment of...

http://cre.sagepub.com
Clinical Rehabilitation
DOI: 10.1177/0269215508096759 2009; 23; 217 Clin Rehabil
Maura Casadio, Psiche Giannoni, Pietro Morasso and Vittorio Sanguineti treatment of stroke patients
A proof of concept study for the integration of robot therapy with physiotherapy in the
http://cre.sagepub.com/cgi/content/abstract/23/3/217 The online version of this article can be found at:
Published by:
http://www.sagepublications.com
can be found at:Clinical Rehabilitation Additional services and information for
http://cre.sagepub.com/cgi/alerts Email Alerts:
http://cre.sagepub.com/subscriptions Subscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.co.uk/journalsPermissions.navPermissions:
http://cre.sagepub.com/cgi/content/refs/23/3/217 Citations
by Pietro Morasso on April 16, 2009 http://cre.sagepub.comDownloaded from

Clinical Rehabilitation 2009; 23: 217–228
A proof of concept study for the integrationof robot therapy with physiotherapy in thetreatment of stroke patientsMaura Casadio Neurolab, Department of Informatics, Systems and Telematics (DIST), University of Genova,Psiche Giannoni ART Education and Rehabilitation Center, Genova, Pietro Morasso and Vittorio Sanguineti Neurolab,Department of Informatics, Systems and Telematics (DIST), University of Genova, Italy
Received 14th April 2008; returned for revisions 21st June 2008; revised manuscript accepted 21st July 2008.
Objective: To carry out a proof of concept study for integrating robot therapy with
physiotherapy in the treatment of stroke patients.
Design: A simple and ‘gentle’ paradigm of robot–patient interaction was designed in
order to foster the re-emergence of smooth, active control patterns in coordinated
shoulder/elbow reaching movements. A haptic robot was programmed according to a
strategy of minimal, progressively reduced assistance, with a double representation
of targets: (i) visual (circles on a screen) and (ii) haptic (robot-generated force fields).
The protocol included trials with and without vision, in order to emphasize the role
of proprioceptive feedback. The training paradigm included 10 sessions and more
than 5000 movements.
Subjects: Ten chronic, hemiparetic subjects; four controls provided reference values
for the performance measurements.
Outcome measures: Four performance indicators (derived from the analysis of the
reaching trajectories); clinical/functional measures (Fugl-Meyer and Ashworth scales).
Results: After robot therapy reaching movements became faster and smoother.
The performance in the no-vision trials was at least as good as in the vision trials.
The Fugl-Meyer arm scores also increased significantly and remained approximately
constant at follow-up; the Ashworth scores did not change.
Conclusion: In spite of its simplicity, a limited number of ‘gentle’ robot therapy
sessions appear to be beneficial, even for severely impaired patients, although no
firm conclusion can be drawn at this point. However, the study provides support
material for the careful design of controlled clinical trials and for a better integration
with physiotherapy.
Introduction
In recent years evidence has mounted about thecapacity of the central nervous system to alter itsstructure and function throughout all sorts of lifeexperiences, including following injury, througha complex network of interacting processes.1–4
Address for correspondence: Pietro Morasso, Department ofInformatics, Systems and Telematics (DIST), University ofGenova, Via Opera Pia 13, 16145 Genova, Italy.e-mail: [email protected]
� SAGE Publications 2009Los Angeles, London, New Delhi and Singapore 10.1177/0269215508096759
by Pietro Morasso on April 16, 2009 http://cre.sagepub.comDownloaded from

Animal models of focal brain injuries suggestthat behaviour is probably the most powerful mod-ulator of post-injury recovery.5–7 Beyond the time-dependent spontaneous neurological recovery,8 theprincipal process responsible for functional recov-ery is the use-dependent reorganization of neuralmechanisms made possible by neural plasticity.In view of this, it seems likely that practice is
required to aid recovery from neurologicaldamage, and that guided practice may be themost effective form. Usually such practice isgiven by therapists, but they have limited timeand may not be consistent. In contrast, the useof robots offers a way of giving consistent ongoingopportunities to practise.Conventional physiotherapy and robot therapy
should not be viewed as alternatives but couldcomplement each other in the rehabilitation pro-cess. However, the optimal type of physiotherapyfor patients with stroke is unclear, and only a fewstudies have been carried out to compare in a sys-tematic way the different methods available.A clear consensus on the experimental proceduresis still missing.9–14 Nonetheless, in spite of differ-ences we think that there is a de facto convergence,at least for Bobath15 and MRP16 approaches,towards a system-oriented approach, whichemphasizes problem-solving and skill learning,aiming at the identification for each patient ofspecific milestones that stress the underlyingneural plasticity. This approach to therapy isclearly consistent with ‘gentle’ robot-therapy sys-tems, an example of which is reported in this work.Although the application of robot technologies
to the rehabilitation of neurological patients isabout two decades old, the number of clinicalstudies is still limited, as documented in recentreviews.17,18. A crucial point, in our opinion,is that (robot) rehabilitation techniques can be effi-cient if they can promote increasing levels of motorskill: repetitive use alone, without learning-indu-cing variability, is unlikely to foster the large-scale, long-lasting changes in cortical networksthat are necessary for recovery of function. A rele-vant consequence is that the haptic interactionbetween the patient and the therapist, whetherhuman or robotic, must not be invasive and unidir-ectional but rather should aim at supporting theemergence of functional control patterns bymeans of a minimal degree of assistance when
helping the patient to carry out a movement suchas reaching.19 Therefore, in order to emulate theinherent compliance of human–human interaction,a robot therapist should be highly compliant,allowing a bidirectional interaction with thepatient.20–22 This suggests that certain roboticdevices, such as those frequently derived from thetechnology of industrial robots that enforce passivemovements without requiring any active inter-vention of the patient at the neuromuscular andcognitive levels, should not be used. The robotassistance must match the degree of voluntary con-trol in order to foster its improvement.
This paper reports a pilot clinical study, in whichthe paretic arm of chronic hemiparetic patients wastreated with a protocol of robot therapy thatassisted the patients in performing reaching move-ments by means of a smooth robot-activated forcefield. An element of novelty is that target represen-tation is both visual (on a computer screen) andhaptic (by the assistive force field), thus allowingalternate trials with force field plus vision, or withonly force field; the latter, in particular, are meantto focus the patient’s attention on the propriocep-tive aspects of movements. The results of the pilotstudy show the emergence of features that are typi-cal of normal reaching movements (approximatelystraight paths with bell-shaped velocity peaks23),suggesting that the patients have recovered atleast part of their ability to generate coherent activepatterns. Moreover, the ability to perform the taskin the absence of vision supports the claim that thesubjects may have improved the perception of theirparetic limb. We believe that this study is relevantfor physiotherapists and rehabilitation teamsbecause it helps them understand what can beexpected of a robot, which features are under con-trol, which measurements can be carried out, andwhich general considerations are appropriate forthe design of optimal rehabilitation protocols thatcombine human and robot intervention. In the end,this is the prerequisite for going from a proof ofconcept study to a controlled clinical trial.
Materials and methods
SubjectsTen hemiparetic subjects (3 men, 7 women, age
53� 13 years) participated in this study (Table 1).
218 M Casadio et al.
by Pietro Morasso on April 16, 2009 http://cre.sagepub.comDownloaded from

Subjects were recruited among those followedas outpatients of the ART Rehabilitation andEducational Center in Genova. When theyentered the robot therapy protocol they had beenattending regular rehabilitation sessions, accord-ing to the Bobath concept (on average onceper week), for at least six months. This routinewas continued throughout the study. The inclu-sion criteria were chronic (at least one year afterstroke) and stable (at least one month beforeentering robot therapy) clinical conditions. Theexclusion criteria were inability to understandinstructions about the exercise protocol andother neurocognitive problems. Preference wasgiven to patients with a high degree of motorimpairment.
In the population of patients disease durationwas 46.2� 41.5 months, with a majority of ischae-mic aetiology (7/10). The level of impairment wasevaluated by means of the Fugl-Meyer score, lim-ited to the arm section (FMA).24 Two therapistswith more than 20 years of experience adminis-tered the clinical evaluations; one of them wasblinded to the type of robot therapy provided toensure the consistency of the testing procedure.Five patients had a severe impairment(FMA510/66); 3 patients had an impairment ofintermediate level (105FMA520); 2 patients hada mild impairment (FMA420). The average FMA
score was 15� 13. The average Ashworth Scalescore of muscle spasticity25 was 2.1� 0.8.
We also carried out a preliminary test of theassistance protocol with four control subjectsaged 29.8� 2.5 years. The purpose of this testwas double: (1) to verify that the experimentalsetup, for the range of force fields used with thepatients, did not alter the general features ofreaching movements reported in the literature23;(2) to provide reference values for the performanceindicators described in the following.
The research conforms to the ethical standardslaid down in the 1964 Declaration of Helsinki,which protect research subjects, and to ethicalbylaws of the International Association ofBobath Instructors (IBITA: art. IV of the statute).Each subject signed a consent form that conformsto these guidelines.
Experimental apparatusThe robot (Braccio di Ferro) is a planar manip-
ulandum with 2 degrees of freedom, which hasbeen fully described elsewhere.22 It has a rigid par-allelogram structure with two direct-drive motorsthat provide a low intrinsic mechanical impedanceat the end-effector and a full backdriveability. Therobot is impedance-controlled in order to transmit
Table 1 Demographic and clinical data of subjects
Subject Age (years) Disease duration(months)a
FMA Ashworth Sex Aetiologyb Paretichand
S1 72 28 6 3 M I LS2 59 39 5 3 F I RS3c 53 154 8 3 M I LS4 69 25 12 1þ F I RS5 57 39 17 3 M I LS6 34 24 13 1þ F I RS7 30 12 6 2 F I LS8 46 26 6 2 F H RS9 53 39 41 1 F H RS10 55 76 36 1 F H L
Mean 52.8 46.2 15.0 2.1SD 13.4 41.5 13.0 0.8
aRefers to the initiation of the robot therapy.bEither ischemic (I) or haemorrhagic (H).cSubject 3 quit after the sixth session.FMA, arm portion of Fugl-Meyer score (0–66); Ashworth, scale of muscle spasticity (0–4), at thebeginning of robot therapy.
Robot therapy with physiotherapy 219
by Pietro Morasso on April 16, 2009 http://cre.sagepub.comDownloaded from

smoothly modulated force fields to the hand of thepatient.The subject sits in a chair, with chest and wrist
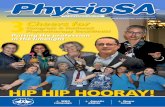
restrained by means of suitable holders, andgrasps the Braccio di Ferro handle. A light, softsupport is connected to the forearm in order toallow low-friction sliding on the horizontal surfaceof a table. Only the shoulder and elbow can moveand motion is restricted to the horizontal plane,with no influence of gravity. The height of the seatis adjusted so that the arm can be kept approxi-mately horizontal. A 19-inch LCD screen is posi-tioned in front of the patients at a distance ofabout 1m in order to display the positions ofhand and target in the form of 2-cm-diameter cir-cles of different colours (Figure 1).
Experimental design and training protocolThe experimental design was specifically
focused on facilitating active execution of large,outward-reaching movements and thus thechosen task consisted of reaching a set of targets,
arranged in the horizontal plane (Figure 1)according to three shell layers: inner (A, 3 targets),middle (B, 3 targets) and outer (C, 7 targets),which required an almost full arm extension.
Target sequences were generated according tothe following scheme: A!C!B!A. When atarget was selected, it was presented to the subjectin two modalities: visual (as a circle on the com-puter screen, with a 2-cm diameter) and haptic (asa robot-generated force field, directed toward thetarget whichever the position of the hand). Thiscontrol scheme does not impose any constrainton either the timing of the reaching movement orthe trajectory that subjects have to follow in orderto reach the target.
Two types of trials were alternated in thetreatment protocol: (1) open-eyes trials and (2)closed-eyes trials. In the latter case the subjectcould perceive the direction of the target fromthe direction of the force vector applied to thehand. In this way, the robot-generated force fieldcarried out two complementary functions: (1) itprovided motor assistance and (2) it induced thepatient to focus his or her attention on the pro-prioceptive feedback. For this reason, the forcefield was activated immediately at the targetonset, but not in a step-like manner, in order toavoid a jerky pull: we used instead a smooth acti-vation profile, with a rise-time of 1 second. Thisduration was chosen to minimize the influence ofthe robot as reaching patterns approached thetypical performance of normal subjects: approx.0.25 s of reaction time þ approx. 0.75 s of reachingtime. The value of the field intensity achieved atthe end of activation profile was chosen accordingto the protocol explained below. The force wasswitched off as soon as the subject hit the target.The next target was presented after a pause of 1 s.This pause was introduced because whereas anormal subject is likely to stay on target afterthe force field is turned off, we may expect patientsto perform a ‘rebound movement’, with a velocitypeak that is higher, the higher their hypertonus.This gives us an opportunity to detect if the hyper-tonus of the patients goes up or down as a side-effect of the treatment, by looking at the velocitypeak of the rebound movement.
In addition to the assistive force field describedabove, the haptic environment implemented by therobot included two additional components: a mild
Figure 1 A view from above of a subject holding the
manipulandum of the Braccio di Ferro haptic robot.
The subject’s shoulders are strapped to a chair; the forearm
slides on the table surface; the wrist is stabilized by means
of a skateboard wrist brace and the hand grasp by means of
a Velcro holder. The targets (circles with a 2 cm diameter)
are arranged on three shell layers: A, B, C. The distance
between adjacent shells is 10 cm; the distance between
targets on the same shell is 6.26 cm (shell A), 8.77 cm (shell
B), 5.65 cm (shell C). The C shell is in front of a virtual wall.
The basic sequence of target activation is A!C!B!A
and it is repeated 3� 7� 3¼63 times in a random order.
220 M Casadio et al.
by Pietro Morasso on April 16, 2009 http://cre.sagepub.comDownloaded from

viscous field, which was intended to damp occa-sional hand oscillations, and a stiff virtual wall, inorder to prevent going beyond the C shell of tar-gets and, at the same time, provide a propriocep-tive feedback about the successful achievement ofthe movement to the outward target. The param-eters of this haptic control scheme were chosenduring preliminary experiments with normal sub-jects: rise time of the assistive field¼ 1 s; viscouscoefficient¼ 12Ns/m, and elastic coefficient of thewall¼ 1000N/m.
Each treatment session consisted of severalblocks of trials that included repetitions of theA!C!B!A sequence with different targetsin random order, for a total of 3� 3� 7¼ 63movements. The protocol started with a testphase, in which the patient was familiarized withthe apparatus and with the range of assistiveforces. This phase was supervised by a physicaltherapist, who observed the response to the differ-ent force levels and selected the minimum levelcapable of inducing at least a partial movementin the direction of the target. In this manner,the patients could indeed reach the targets butusually after a sequence of several submovements.Open-eyes and closed-eyes blocks of trials werealternated in the same session.
The first training session used the same level offorce determined in the test session for a total of126 movements (63 with open eyes and 63 withclosed eyes). After a little rest, the therapist con-sidered the level of performance and asked thesubject about fatigue. The decision could be (1)to terminate the session, (2) to continue with thesame force level, (3) to continue with a reducedforce that was 10–20% smaller than the previouslyused force. The procedure was iterated, with pos-sibly reduced assistive force levels until the deci-sion to stop was agreed by the patient and thetherapist and in any case no later than 75 minutesafter the initiation of the session.
In following sessions, the training always startedwith two blocks of the initially selected force leveland continued with decreasing levels of force assis-tance until one of the previously defined termina-tion conditions occurred. In other words, thestrategy of adaptive reduction of the assistancelevel is non-monotonic in the sense that is charac-terized by a saw-tooth pattern: it decreases withina session but it regains the original level at the
beginning of the next session. If a patient reacheda level of assistance with a force below 4N, theclosed-eye block was eliminated because that levelof force is very close to the perceptual threshold26
and thus is insufficient to allow the patient to per-ceive the direction of the target without vision.
Summing up, the training procedure is tailoredto the individual patients in two respects: (1) theinitial level of the assistance force is tuned accord-ing to the therapist judgement; (2) the number ofblocks of trials depends on the performance of thepatient and the speed of learning from session tosession. Overall, the protocol included 10 sessions(one session per week, with a duration rangingbetween 60 and 75 minutes), plus the initial testsession. During that time, all subjects continuedtheir physiotherapy programme with the sameschedule and the same routine.
The FMA and Ashworth scores were evaluatedat the beginning of the robot therapy protocol andimmediately after its completion. A follow-upevaluation was carried out three months later.The robot training sessions were carried out atNeurolab-DIST, University of Genova, underthe supervision of a physical therapist (PG). Thephysiotherapy sessions were carried out at theART premises.
Data analysis and performance evaluationHand trajectories and the forces generated by
the robot were sampled at 1000Hz and stored at100Hz. Hand speed was estimated by using afourth-order Savitzky–Golay smoothing filter.The analysis focused on the outward movements(A!C) and, in particular, we defined thefollowing performance indicators, which werechosen because it is easy to identify the normalreference values:
� Mean speed (I1): average hand speed, computedfrom the time of target presentation to thetime at which the subject reaches the target.This indicator is expected to increase as trainingproceeds, approaching a normal value of about20 cm/s, which is the average value of controlsubjects.
� Number of submovements (I2), identified by thenumber of peaks in the speed profile, after we
Robot therapy with physiotherapy 221
by Pietro Morasso on April 16, 2009 http://cre.sagepub.comDownloaded from

eliminated ‘spurious’ peaks according to asimple threshold mechanism. (Note: ‘Spurious’velocity peaks were eliminated by means of twocriteria: (1) a threshold on the speed (0.01m/s),(2) a threshold on the time interval between onepeak and the next one (0.3 s).) The reachingmovements of the control subjects were charac-terized by a single-peaked, bell-shaped speedprofile23 and thus this indicator shouldapproach 1, as training proceeds.
� Endpoint error after the first submovement (I3),defined as the distance between hand positionand the position of the target at the end of thefirst submovement. As training proceeds, thisindicator should go down to 0.
� T-ratio (I4), defined as the ratio between theduration of the first submovement and thetotal time required for reaching the target. Astraining proceeds, this indicator should increase,up to the value of 1 (or 100%) that characterizesthe performance of control subjects.
Statistical analysisThe performance improvements of each indica-
tor, which could be attributed to the robot therapysessions, were evaluated in two different manners:
Performance improvements at the beginning of eachsessionRecalling that each session started with the
assistance level selected in the test session, the per-formance improvements were evaluated by meansof a two-way, repeated measures ANOVA, withtwo factors: session (1–10) and vision (yes/no).To assess whether the session effects actually cor-responded to an increase of performance over ses-sions, for each indicator we ran a contrast analysis(linear contrast) of the session effect and of thesession� vision interaction.
Overall performanceThe analysis above evaluates session and condi-
tion effects for a fixed level of robot assistance.However, all indicators (in particular, the meanspeed) are clearly dependent on the assistiveforce value. Therefore, a more complete pictureof training performance can be obtained by
considering all the different levels of assistiveforce experienced by each subject. For this pur-pose, we used a mixed-effect model, with threefixed factors (session, vision and force) and twoadditional random factors (subject and target) toproperly account for the correlations amongrepeated measures from the same subject:
0Indicator0¼ b0 þ b1 � ð0session0 � 1Þ
þ b2 �0 force0 þ b3 �
0vision0 ð1Þ
where ‘indicator’ is one of the four parametersdefined above, ‘session’ is an integer (from 1 to10), ‘force’ is the field intensity (in N), and‘vision’ is a binary variable that designateswhether the exercise was carried out with openor close eyes. Model coefficients can be interpretedas follows:
b0¼ ‘baseline performance level’;b1¼ ‘rate of improvement session by session’;b2¼ ‘rate of improvement dependent on the assis-
tance level’;b3¼ ‘performance bias introduced by presence of
vision’.
Results
Test with control subjectsThe control subjects were exposed to the train-
ing protocol with the full range of forces requiredby the population of patients, from 0N to 25N.In all cases, the subjects could reach the targetswith a single movement, characterized by a velo-city peak, which in most cases occurred before theend of the rise-time of the force field. This meansthat robot assistance automatically becomes lessand less relevant as the performance level of apatient approaches the level of the control subjects.
Improvement of performance indicators for theassistance force selected in the test session
Figure 2 shows the evolution of I1 during thetraining sessions. The level of assistance is differ-ent for the different patients, according to theinitial test session (e.g. F¼ 25N for S1, F¼ 20Nfor S2, etc.). The graphs clearly exhibit a positive
222 M Casadio et al.
by Pietro Morasso on April 16, 2009 http://cre.sagepub.comDownloaded from

trend for all the subjects. Similar curves wereobtained for the other indicators.
Statistical analysis showed that the sessioneffect is strongly significant for all indicators.In particular, it provided the following estimatesof the indicator changes from the initial to thefinal session: I1 (mean speed) almost doubles from5.61� 0.94 cm/s at session 1, to 10.00� 0.78 cm/s atsession 10 (F(1,8)¼ 15.47,P¼ 0.004); I2 (number ofpeaks) is reduced from 5.71� 1.04 to 1.69� 0.21(F(1,8)¼ 16.01, P¼ 0.004); I3 (endpoint errorafter the first submovement) is reduced from5.05� 1.22 cm to 3.06� 0.33 cm (F(1,8)¼ 16.98,P¼ 0.003); I4 (the T-ratio) is increased from47.1� 8.9% to 83.8� 5.4% (F(1,8)¼ 29.28,P¼ 0.0006).
All together, the analysis of the performanceindicators shows a linear improvement trend,
thus supporting the choice of a non-monotonicreduction of the assistance profile: the lineartrend means that the patients remain equallyresponsive throughout the training protocol tothe patterns of robotic assistance. With regard tovision, different subjects exhibit different beha-viours, as exemplified in Figure 2 for I1: (a) inthe majority of subjects there is no clear differencebetween the vision and no-vision situations; (b) insome subjects there is a tendency for the no-visionparadigm to prevail; (c) in other subjects the visioncase is clearly better. Therefore, it is not surprisingthat, at the population level, no vision effect orvision� session interaction appears to be statisti-cally significant. However, what is significant fromthe point of view of motor recovery is that in mostsubjects (8 out of 10) the deprivation of an impor-tance sensory channel such as vision does not
18
16
14
12
10
8
6
4
2
18
16
14
12
10
8
6
4
2
18
16
14
12
10
8
6
4
2
18
16
14
12
10
8
6
4
2
18
16
14
12
10
8
6
4
2
18
16
14
12
10
8
6
4
2
18
16
14
12
10
8
6
4
2
18
16
14
12
10
8
6
4
2
18
16
14
12
10
8
6
4
2
18
16
14
12
10
8
6
4
2
2 4 6 8 10 2 4 6 8 10 2 4 6 8 10 2 4 6 8 10
2 4 6 8 102 4 6 8 102 4 6 8 102 4 6 8 102 4 6 8 10
2 4 6
S1F = 25N
S6F = 9N
S7F = 6N
S8F = 5N
S9F = 5N
S10F = 4N
S2F = 20N
S3F = 18N
S4F = 12N
S5F = 9N
Vision No vision
Mean speed (cm/s) vs. session
Figure 2 Each panel shows the evolution of the I1 indicator (mean speed of the outward reaching movements) over the 10
training sessions for the different subjects at a level of assistance selected in the initial session. Bold lines refer to average
values and dashed lines to standard errors. Subjects 8 and 9 initiate no-vision blocks in the second session with the same
force level of the vision ones; subject 3 quit after the sixth session. The reference value (average speed of the normal
population) is Vref¼ 19.3� 4.9 cm/s.
Robot therapy with physiotherapy 223
by Pietro Morasso on April 16, 2009 http://cre.sagepub.comDownloaded from

necessarily imply a deterioration of the reachingperformance; this further supports the workinghypothesis that an experimental design thatemphasizes the role of the proprioceptive channelhas a relevant rehabilitation value.
Evolution of the assistance levelTable 2 shows the progressive reduction of the
assistance level after the initial test session for eachpatient. In the overall population of subjects, theinitial level of assistance ranged between 5N and25N and it was generally higher for patients withlower initial levels of the FMA score. Table 3 shows
complementary information: the number of blocksof trials to which each patient was exposed in thesequence of training sessions.
For example, subject 1 started with three blocks(for a total of 756 movements) and at the end hecould go through 12 blocks (for a total of 3024movements). On average, each subject performedmore than 5000 reaching movements all together.The profile of progressive reduction of the assis-tance level was not always monotonically decreas-ing. In two cases (subject 7, session 6 and subject 8,session 3) the minimum level of assistance wasslightly greater than in the previous session. Thisis due to the fact that according to the protocolduring each session the patient went through the
Table 3 Total number of training blocks used in each therapy sessions
Subjects Sessions
SS1 SS2 SS3 SS4 SS5 SS6 SS7 SS8 SS9 SS10
S1 3 7 8 10 10 10 10 10 11 12S2 6 7 7 9 9 11 11 13 11 13S3a 4 7 8 9 11 11S4 5 9 9 10 11 11 12 14 15 16S5 4 4 5 6 6 6 8 8 8 8S6 4 4 4 5 6 4 7 7 8 8S7 6 6 6 6 7 7 8 8 9 9S8 8 8 10 10 10 11 10 11 11 12S9 7 8 9 10 11 12 11 12 12 12
S10 8 8 10 10 10 12 13 12 12 11
In each session, each subject was exposed to all the previously experienced force levels, indecreasing order, before attempting a further reduction of the force.aSubject 3 quit after the sixth session.
Table 2 Assistance force (in N) selected in the ‘test’ session and then the progressive reductionof the minimum force adopted in the therapy sessions (SS1–SS10)
Subjects Tests Sessions
SS1 SS2 SS3 SS4 SS5 SS6 SS7 SS8 SS9 SS10
S1 25 25 18 18 15 15 15 15 13 13 10S2 22 20 18 16 16 14 12 12 12 12 8S3a 18 18 14 14 12 10 10S4 15 13 12 12 10 9 9 6 6 6 6S5 13 10 10 9 8 8 8 7 6 5 4S6 13 8 8 8 7 7 9 6 5 4 4S7 9 6 6 6 5 5 7 5 4 2 2S8 9 5 4 5 3 3 3 3 3 3 2S9 5 3 2 1 0 0 0 0 0 0 0
S10 5 2 1 0 0 0 0 0 0 0 0
aSubject 3 quit after the sixth session.
224 M Casadio et al.
by Pietro Morasso on April 16, 2009 http://cre.sagepub.comDownloaded from

sequence of assistance levels of the previous ses-sion until he or she was willing to perform: in thetwo cases above the patient stopped before the endof the sequence.
Performance indicators: interaction between sessionand force
The dependence of the performance indicatorsupon assistance level and session is shown inFigure 3 for subject 4: the subject initiates thetherapy with a level of assistance of 15N; this isreduced to 9N at session 5, and is further reducedto 5N at session 8. The figure shows that all indi-cators improve as a function of both the sessionand the level of assistance.
This is confirmed by the regression analysis of allthe indicators. More specifically, we found highlysignificant effects of session for I1, I2 and I4, butnot for I3. As regards the level of assistance,
all indicators display a significant effect(I1: P50.0001; I2: P¼ 0.0006; I3: P¼ 0.0009; I4:P50.0001). The b1 coefficients are positive forthe two indicators (I1, I4) for which the improve-ment is indicated by an increase of the indicator(I1: b1¼ 0.36� 0.097 cm/s per session; I4:b1¼ 2.98� 0.77% per session), and negative forthe two indicators (I2, I3) for which improvementis indicated by a decrement (I2: b1¼�0.3� 0.09peaks per session; I3: b1¼�0.29� 0.08 cm per ses-sion). We also used the model of Equation (1) inorder to assess the overall effect of therapy for eachsubject. For each indicator we computed the quan-tity �Ik¼ b1� (‘session’–1), where ‘session’¼ 10and k¼ 1,2,3,4, which estimates the magnitude ofthe session effect at the end of training, extrapo-lated for the case of no assistance (‘force’¼ 0):this is a measure of the portion of the observedvariation of the indicators that can be attributedto training. The results are reported in Table 4.
12
10
8
6
4
2
12
10
8
6
4
2
14
1 2 3 4 6 7 8 9 10
1 2 3 4 6 7 8 9 10 1 2 3 4 6 7 8 9 10
1 2 3 4 6 7 8 9 10
90
70
50
30
10
Robot therapy session Robot therapy session
(%) (cm)
(cm/s)
Mean speed
F = 15N F = 9NF = 5N
Number of sub-movements
F = 15N
F = 9NF = 5N
6
5
4
3
2
1
0
Endpoint errorafter the 1st sub-movement
F = 9NF =5N
F =15N
F = 5N
F = 9NF = 15N
T-Ratio
Figure 3 Interaction of session and assistance level for subject 4. A force of 15 N is used throughout all the sessions; a
force of 9 N is introduced at the fifth session; a force of 5 N is introduced at the eighth session. Other intermediate assistive
force levels were used with this subject (13 N, 12 N, 6 N, 4 N, respectively) but are not plotted for simplicity.
Robot therapy with physiotherapy 225
by Pietro Morasso on April 16, 2009 http://cre.sagepub.comDownloaded from

Fugl-Meyer scoreTable 5 reports the FMA scores evaluated at
three phases of the protocol: (1) before beginningthe robot therapy protocol, (2) just after its termi-nation, and (3) three months later. We found astatistically significant change (P¼ 0.004) fromFMAPRE¼ 15� 13 to FMAPOST¼ 20� 14, corre-sponding to an average �FMA¼ 4.5� 2.6improvement. This is in line with previous stu-dies,17 which report an average improvement of3.7� 0.5. Evaluation of the FMA at follow-up
resulted in a substantial preservation of theimprovement:
FMAfollowup ¼ 20� 13
Modifications of the hypertonusHypertonus of the flexor muscles of the upper
limb is a typical feature of most hemipareticpeople. To assess indirectly whether the trainingprotocol induced an increase of the activation ofthe flexors and, in general, the coactivation level ofshoulder and elbow muscles, we looked at thebouncing movements that occur immediatelyafter a C-target is reached. At that time the forcefield is switched off in a step-like fashion and thepatient remains without robot assistance for1 second before the next target is selected.A normal subject would stay on target, whereasthe hypertonus of hemiparetic patients results in arebound movement, the velocity peak of which is agood indicator of the level of the hypertonus.Statistical analysis showed that the peak speed ofthe rebound movements did not significantlychange over sessions. This result suggests thatthere is no hint, even in severely impaired subjects,that the training protocols induces any kindof spasticity or increase of the muscle tonus.We attribute this important result to the factthat the protocol was designed to be as gentle aspossible. This was also confirmed by the Ashworthscore, which did not increase for any subject overthe robot training period.
Discussion
The first conclusion of this proof of concept studyis that a gentle approach to robot therapy is welltolerated and is also effective for severely impairedsubjects. When patients are put in front of amachine or robot it is important to avoidmaking them feel that they are forced toperform an endless repetition of uninterestingactions. This was avoided in our case by givingthe subjects freedom with regard to time andpath, introducing enough variability in the exer-cise to make it interesting. The Braccio di Ferrowas indeed perceived by our subjects as a benignand gentle agent that did not press them overly.
Table 4 Variation of movement indicators between thebeginning and the end of the robot training
Subject �I1 Meanspeed(cm/s)
�I2 Numberof
submovements
�I3 Endpointerror (cm)
�I4T-ratio
(%)
S1 þ6.7 �3.1 �2.6 þ50.2S2 �0.1 �0.1 �0.1 �1.0S3a þ7.0 �7.7 �1.8 þ50.0S4 þ5.8 �3.3 �2.3 þ41.9S5 þ4.0 �6.5 �6.8 þ32.9S6 þ1.2 �2.4 �5.1 þ23.4S7 þ6.4 �4.4 �3.6 þ50.7S8 þ1.2 �1.2 �0.5 þ10.5S9 þ2.4 �1.4 �1.2 þ13.9S10 þ0.9 �2.9 �1.0 þ6.4
Mean þ3.55 �3.30 �2.50 þ27.9SD 2.36 2.36 2.13 19.84
Computed according to the following equation:�Ik¼ b1� (‘session’–1).aSubject 3 quit after the sixth session.
Table 5 Arm portion of Fugl-Meyer score (FMA, max 66)before initiation of the therapy, at the end and three monthsafterwards
Subject FMApre
FMApost
�FMA �FMA% FMAfollow-up
S1 6 8 2 33 7S2 5 8 3 60 7S3 8 9 1 13 9S4 12 18 6 50 22S5 17 21 4 24 18S6 13 23 10 77 24S7 6 9 3 50 11S8 6 13 7 117 16S9 41 45 4 10 42S10 36 41 5 14 41
Mean 15.0 19.5 4.5 45 19.7SD 13.0 13.6 2.6 34 12.9
aSubject 3 quit after the sixth session.
226 M Casadio et al.
by Pietro Morasso on April 16, 2009 http://cre.sagepub.comDownloaded from

The protocol also included elements of challenge,for example facing reduced levels of assistance,that motivated the repetitions in order to improveperformance.
A negative side-effect of robot–human inter-action could be to induce spasticity, which isvelocity- and acceleration-dependent. This wasavoided by using minimal assistance, which keptthe movement velocity at relatively low levels,without any sharp acceleration peaks, and by thefact that each session started with a ‘warm-up’,using the assistance levels mastered in the previoussessions, before attempting a more challengingtask. A related risk is fatigue, both muscular andcognitive. This study suggests that the challenge ofthe task was well tolerated, even by the mostseverely impaired patients, and the endurance ofthe patients increased with practice. In general,we believe it is important to monitor the willing-ness of the patients to continue the session withoutforcing them to a predetermined sequence.
The results show significant improvements insmoothness and motor coordination for the reach-ing task: we observed a remarkable reduction inthe degree of segmentation and the emergence ofquasi-normal reaching patterns, with bell-shapedvelocity profiles. It may be asked to what extentsuch improvements are also indicative of func-tional recovery. Studies on recovery from neuralinjury have suggested that smoothness is a resultof a learned, coordinative process rather than aconsequence of the structure of the neuromuscularsystem,27 and there is also evidence that the seg-mented structure of arm movements in strokepatients can be attributed to a deficit of interjointcoordination.28 Thus smooth movements resultfrom improved coordination and this is a conditiosine qua non for functional recovery. In any case,our results show that higher smoothness is asso-ciated with better FMA score and this suggeststhat training general motion control abilities canbe as effective as focusing primarily on specificfunctional movements.
A peculiar feature of the proposed approach isthat assistance is kept at a minimum level, thusavoiding as much as possible the risk that move-ments are performed in a passive way: movementsmust be assisted, not enforced by the robot thera-pist. Motor improvement is indeed only part of thestory: all patients reported a better awareness of
their affected limb. This was confirmed by thetherapist when delivering the FMA test, in parti-cular with regard to the test items related to coor-dination (speed, tremor and dysmetria). Trainingin the closed-eyes condition is likely to be crucialin enhancing such awareness: with eyes closedpatients must focus their attention on the purelyhaptic component of the task and this may help toreinforce the internal representation of the armthat is essential for delivering coordinated activecommands.
Having discussed the positive elements of theproposed approach to robot therapy it is alsofair to draw attention to its intrinsic weaknessesand/or limitations. An obvious limitation of theBraccio di Ferro robot is that it only allowsplanar movements that involve the shoulder andelbow. Moreover, these movements are not ‘func-tional’ in a strict sense and one may ask to whatextent the improved smoothness of reachingmovements is useful for functional movementssuch as drinking a glass of water. This is indeedthe main challenge faced in the design of optimal,integrated protocols of robot–human therapy,aimed at the ‘carryover’ of the observed gains inmotor abilities to the activities of daily life.
Our experience with this limited studyemphasizes the need for multidisciplinary rehabi-litation teams that include physiotherapists, reha-bilitation medical doctors and rehabilitationengineers for the rational exploitation of robotsin the rehabilitation of neurological patients.The tasks of the team are multifaceted and includethe following items: (1) quantitative evaluationof the specific deficits/requirements of a patient(for example by using the same robotic systemused for treatment), (2) identification of clearfunctional goals, (3) translation of the goals intorobotic interaction paradigms, tailored for thepatient and endowed with suitable coordination/performance evaluation procedures. Defining,choosing and adapting protocols of robot therapyto the individual needs of different patients, inshort personalizing robot therapy, is an openfield that requires attention and research effortin the future. The purpose of this study was toprovide support material and suggestions for thedesign of controlled clinical trials of integratedhuman–robot therapy.
Robot therapy with physiotherapy 227
by Pietro Morasso on April 16, 2009 http://cre.sagepub.comDownloaded from

References
1 Nudo RJ. Mechanisms for recovery of motorfunction following cortical damage. Curr OpinNeurobiol 2006; 16: 638–44.
2 Lee RG, van Donkelaar P. Mechanisms underlyingfunctional recovery following stroke. Can J NeurolSci 1995; 22: 257–63.
3 Carmichael ST. Plasticity of cortical projectionsafter Stroke. Neuroscientist 2003; 9: 64–75.
4 Dancause N, Barbay S, Frost SB et al. Extensivecortical rewiring after brain injury. J Neurosci 2005;25: 10167–79.
5 Jones TA, Chu CJ, Grande LA, Gregory AD.Motor skills training enhances lesion-inducedstructural plasticity in the motor cortex of adultrats. J Neurosci 1999; 19: 10153–63.
6 Biernaskie J, Corbett D. Enriched rehabilitativetraining promotes improved forelimb motor func-tion and enhanced dendritic growth after focalischemic injury. J Neurosci 2001; 21: 5272–80.
7 Kopp B, Kunkel A, Muhlnickel W, Villringer K,Taub E, Flor H. Plasticity in the motor systemrelated to therapy–induced improvement of move-ments after stroke. Neuroreport 1999; 4: 807–10.
8 Kwakkel G, Kollen B, Twisk J. Impact of time onimprovement of outcome after stroke. Stroke 2006;37: 2348–53.
9 Dickstein R, Hocherman S, Pillar T, Shaham R.Stroke rehabilitation: three exercise therapyapproaches. Phys Ther 1986; 66: 1233–38.
10 Lord JP, Hall K. Neuromuscular reeducationversus traditional programs for stroke rehabilita-tion. Arch Phys Med Rehabil 1986; 67: 88–91.
11 Ernst E. A review of stroke rehabilitation andphysiotherapy. Stroke 1990; 21: 1081–85.
12 Wagenaar RC, Meijer OG et al. The functionalrecovery of stroke: a comparison between neuro-developmental treatment and the Brunstrommethod. Scand J Rehabil Med 1990; 22: 1–8.
13 Langhammer B, Sunnaas S. Bobath or MotorRelearning Programme? A comparison of two dif-ferent approaches of physiotherapy in stroke
rehabilitation: a randomized controlled study.Clin Rehabil 2000; 14: 361–69.
14 van Vliet PM, Lincoln NB, Foxall A. Comparisonof Bobath based and movement science basedtreatment for stroke: a randomised controlled trial.J Neurol Neurosurg Psychiatry 2005; 76: 503–508.
15 Bobath B. Adult hemiplegia: evaluation and treatment,3rd edition. Butterworth-Heinemann, 1990.
16 Carr JH, Shepherd RB. A motor relearning pro-gramme for stroke, Butterworth-Heinemann, 1987.
17 Prange GB, Jannink MJ et al. Systematic review ofthe effect of robot-aided therapy on recovery of thehemiparetic arm after stroke. J Rehabil Res Dev2006; 43: 171–84.
18 Kwakkel G, Kollen BJ, Krebs HI. Effects of robot-assisted therapy on upper limb recovery afterstroke: a systematic review. Neurorehabil NeuralRepair 2008; 22: 111–21.
19 Casadio M, Morasso P, Sanguineti V, Giannoni P.Impedance-controlled, minimally-assistive robotictraining of severely impaired hemiparetic patients.BioRob 2006 (the First IEEE/RAS-EMBS Int Confon Biomedical Robotics and Biomechatronics),Pisa, Italy, 20–22 February 2006.
20 Krebs HI, Hogan N, Volpe BT, Aisen ML,Edelstein L, Diels C. Overview of clinical trials withMIT-MANUS: a robot-aided neuro-rehabilitationfacility. Technol Health Care 1999; 7: 419–23.
21 Harwin WS. Robots with a gentle touch: advancesin assistive robotics and prosthetics. Technol HealthCare 1999; 7: 411–17.
22 Casadio M, Morasso P, Sanguineti V,Arrichiello V. Braccio di Ferro: a new hapticworkstation for neuromotor rehabilitation. TechnolHealth Care 2006; 13: 1–20.
23 Morasso P. Spatial control of arm movements.Exp Brain Res 1981; 42: 223–27.
24 Platz T, Pinkowski C et al. Reliability and validityof arm function assessment with standardizedguidelines for the Fugl-Meyer Test. Clin Rehabil2005; 19: 404–11.
25 Bohannon RW, Smith MB. Interrater reliabilityof a modified Ashworth scale of muscle spasticity.Phys Ther 1987; 67: 206–207.
26 Boff KR, Kaufman I, eds. Cutaneous sensitivity(chapter 12), Kinesthesia (chapter 13), Tactileperception (chapter 31). In Handbook of humanperception and human performance, volume 1.J. Wiley and Sons, 1986.
27 Rohrer B, Fasoli S, Krebs HI et al. Movementsmoothness changes during stroke recovery.J Neurosci 2002; 22: 8297–304.
28 Levin MF. Interjoint coordination during pointingmovements is disrupted in spastic hemiparesis.Brain 1996; 119: 281–93.
Clinical messages
� Design rehabilitation protocols in a patient-oriented way, integrating robot therapy andphysiotherapy.
� Learn to exploit and understand the quanti-tative measurements coming out of patient-robot interaction during treatment.
228 M Casadio et al.
by Pietro Morasso on April 16, 2009 http://cre.sagepub.comDownloaded from