A new assessment for elders admitted to acute care: reliability of the MDS-AC
15
Aging Clin. Exp. Res. 13: 316-330, 2001 A new assessment for elders admitted to acute care: Reliability of the MDS-AC G.I. Carpenter l , G.F. Teare 2 , K. SteeP, K. Berg 4 , K. Murph y 5, J. Bjornson 6 , P.V. Jonsson 7 , and J.P. Hirdes 8 lCentre for Health Services Studies, George Allen Wing, University of Kent, Canterbury, UK, 2Research Department and Canadian Collaborating Center-interRAI, Providence Center, Scarborough, ON, Canada, 3Department of Geriatric Medicine, New Jersey Medical School, and The Homecare Institute, Hackensack University Medical Center, Hackensack, NJ, USA, 4Brown University, Providence, RI, USA, 5Hebrew Rehabilitation Center for Aged (HRCA), Research and Training Institute, Boston, MA, USA, 6Department of Geriatric Medicine, Diakonhjemmets Hospital, Vinderen, Oslo, Norway, 7Geriatrics University of Iceland, School of Medicine, and Division of Geriatrics, Reykjavik Hospital, Reykjavik, Iceland, 8Department of Health Studies & Gerontology, University of Waterloo, and Canadian Collaborating Center-interRAI, Providence Center, Scarborough, Ontario, Canada ABSTRACT. Assessment of older people rarely includes functional domains critical for ensuring optimum outcome of treatment in acute hospital care. We report the development of a new assessment instrument, and illustrate how differences between pre-hospital and hospital admission status can be systematically evaluated using the Minimum Data Set for Acute Care (MDS-AC). Content was developed by literature review and consultation with professionals working in acute areas. Dual independent assessments were conducted on hospital in-patients in 4 countries. Inter-assessor reliability coefficients were calculated for each item. Kappa was calculated for all binary and multi-level nominal variables. Quadratically weighted Kappa was estimated for all ordinal multi-level variables. Where one level of the variable contained 90% or more of the subjects, total observed agreement is reported. Separate reliability estimates were calculated for pre-hospitalization and inpatient items. Subjects had a mean age of 78. Completion of pre-hospitalization and hospital period assessment (combined) required 20 and 30 minutes. Excluding items for which 90% or more of sub- jects were classified into a single scoring level, average inter-assessor reliability coefficient for the pre-hospital period items was 0.57 and for in hospital 0.58. Overall exact agreement was 83% for prehospitalization assessment items, and 79% for the inhospital items. The reliability achieved in the highly unstable situation of the acute admission phase is suf- ficient for use in clinical care and research. Differences in pre-hospital and admission status necessary for case-mix adjusted comparison of outcomes were illustrated. Development of a means for systematically comparing changes in older people during the course of illness is of increasing importance when addressing questions of the appropriate and inappropriate use of medical technology. (Aging Clin. Exp. Res. 13: 316-330, 2001) ©2001, Editrice Kurtis INTRODUCTION As the number of older people in our societies increase both in absolute numbers and as a percentage of the population, there is increasing pressure on our health and social service systems to provide care, which is both targeted and cost-effective. With ever shorter acute hospital stays outside well established acute geriatric services, comprehensive geriatric assessment is not done at all or is deferred to out-patient settings or post-acute and rehabilitation settings, which may be under threat as in the UK (1) or frequently unavailable, as in the US. Effective assessment is a first pre-requisite of elderly care. This entails not only a thorough systematic enquiry about, and examination of organ systems, but also an evaluation of each individual's cognitive and physical function, including such routine activities as shopping, transportation and managing finances. Key words: Acute care, geriatric assessment, hospitalization, Minimum Data Set for Acute Care (MDS-AC), older people. Correspondence: G.!. Carpenter, M.D., Centre for Health Services Studies, George Allen Wing, University of Kent, Canterbury, Kent CT2 7NF, UK. E-mail: [email protected] Received July 13, 2000; accepted in revised form March 5, 2001. Aging Clin. Exp. Res., Vo!. 13, No. 4 316
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of A new assessment for elders admitted to acute care: reliability of the MDS-AC

Aging Clin. Exp. Res. 13: 316-330, 2001
A new assessment for elders admitted to acute care: Reliability of the MDS-AC G.I. Carpenterl, G.F. Teare2, K. SteeP, K. Berg4, K. Murphy5, J. Bjornson6, P.V. Jonsson7, and J.P. Hirdes8 lCentre for Health Services Studies, George Allen Wing, University of Kent, Canterbury, UK, 2Research Department and Canadian Collaborating Center-interRAI, Providence Center, Scarborough, ON, Canada, 3Department of Geriatric Medicine, New Jersey Medical School, and The Homecare Institute, Hackensack University Medical Center, Hackensack, NJ, USA, 4Brown University, Providence, RI, USA, 5Hebrew Rehabilitation Center for Aged (HRCA), Research and Training Institute, Boston, MA, USA, 6Department of Geriatric Medicine, Diakonhjemmets Hospital, Vinderen, Oslo, Norway, 7Geriatrics University of Iceland, School of Medicine, and Division of Geriatrics, Reykjavik Hospital, Reykjavik, Iceland, 8Department of Health Studies & Gerontology, University of Waterloo, and Canadian Collaborating Center-interRAI, Providence Center, Scarborough, Ontario, Canada
ABSTRACT. Assessment of older people rarely includes functional domains critical for ensuring optimum outcome of treatment in acute hospital care. We report the development of a new assessment instrument, and illustrate how differences between pre-hospital and hospital admission status can be systematically evaluated using the Minimum Data Set for Acute Care (MDS-AC). Content was developed by literature review and consultation with professionals working in acute areas. Dual independent assessments were conducted on hospital in-patients in 4 countries. Inter-assessor reliability coefficients were calculated for each item. Kappa was calculated for all binary and multi-level nominal variables. Quadratically weighted Kappa was estimated for all ordinal multi-level variables. Where one level of the variable contained 90% or more of the subjects, total observed agreement is reported. Separate reliability estimates were calculated for pre-hospitalization and inpatient items. Subjects had a mean age of 78. Completion of pre-hospitalization and hospital period assessment (combined) required 20 and 30 minutes. Excluding items for which 90% or more of sub-jects were classified into a single scoring level, average inter-assessor reliability coefficient for the pre-hospital period items was 0.57 and for in hospital 0.58. Overall exact agreement was 83% for prehospitalization assessment items, and 79% for the inhospital items. The reliability achieved in the highly unstable situation of the acute admission phase is suf-
ficient for use in clinical care and research. Differences in pre-hospital and admission status necessary for case-mix adjusted comparison of outcomes were illustrated. Development of a means for systematically comparing changes in older people during the course of illness is of increasing importance when addressing questions of the appropriate and inappropriate use of medical technology. (Aging Clin. Exp. Res. 13: 316-330, 2001) ©2001, Editrice Kurtis
INTRODUCTION As the number of older people in our societies increase
both in absolute numbers and as a percentage of the population, there is increasing pressure on our health and social service systems to provide care, which is both targeted and cost-effective. With ever shorter acute hospital stays outside well established acute geriatric services, comprehensive geriatric assessment is not done at all or is deferred to out-patient settings or post-acute and rehabilitation settings, which may be under threat as in the UK (1) or frequently unavailable, as in the US.
Effective assessment is a first pre-requisite of elderly care. This entails not only a thorough systematic enquiry about, and examination of organ systems, but also an evaluation of each individual's cognitive and physical function, including such routine activities as shopping, transportation and managing finances.
Key words: Acute care, geriatric assessment, hospitalization, Minimum Data Set for Acute Care (MDS-AC), older people. Correspondence: G.!. Carpenter, M.D., Centre for Health Services Studies, George Allen Wing, University of Kent, Canterbury, Kent CT2 7NF, UK. E-mail: [email protected] Received July 13, 2000; accepted in revised form March 5, 2001.
Aging Clin. Exp. Res., Vo!. 13, No. 4 316

G.I. Carpenter, G.F. Tea re, K. Steel, et af.
During an acute hospital admission, care is routinely focused, with directed use of technically sophisticated diagnostic and therapeutic interventions. Problems other than the "main complaint", if identified at all, are rarely addressed in the acute setting except within specialist geriatric acute services such as exist in the UK.
The importance of systematic evaluation and as-sessment scales in geriatric medicine is well recognized. The Royal College of Physicians and British Geriatrics Society in the United Kingdom (2), and the Danish Medical Bulletin (3) have specifically addressed the contents of an appropriate comprehensive assessment of older people, as have a number of other national and international organizations (4-7). However, it is the experience of almost all health professionals that the assessment of older people in acute care settings frequently remains insufficiently complete. Questions about functional domains, so critical for optimizing treatment outcome within the acute hospital, and then transition to the appropriate care facility or community setting, are frequently omitted.
It is also well established that the pre-morbid state is an important indicator of outcome (8). Additionally, the accurate assessment of both pre-morbid function, and function at the point of admission to acute care will ensure that where problems exist they are identified, so that they might be addressed. Such data, if collected in a standardized manner, can be used for: i) monitoring patient status over time; ii) enhancing communication of patient information across clinical settings; iii) targeting intervention so as to be cost-effective, be it in hospital or after discharge; and iv) case-mix adjustment of performance indicators of specific services and facilities.
To address these needs, a standardized assessment system for old people admitted to hospital with acute illness was developed by a multi-national research collaboration.
The Minimum Data Set for Acute Care (MDS-AC) (see Appendix) is designed to be used by all hospital services, including non-specialists in elderly care. It is a new assessment instrument in the "family" of the MDS assessment instruments which include other tools for use in long-term institutional and homecare settings [the Minimum Data SetlResident Assessment Instrument - MDSIRAI (9), and the MDS for Home Care - MDS-HC (10) respectively], in post-acute care and rehabilitation settings [MDS-Post Acute Care - MDS-PAC], and in psychiatric in-patient settings [MDS for Mental Health - MDS-MH (11)].
The specific objectives were to develop a tool that would provide: - a systematic standardized assessment of pre-mor-
317 Aging Clin. Exp. Res., Vol. 13, No. 4
bid function, and function at the time of admission, so that: 1) problems that might be overlooked by traditional medical and nursing examination are identified; and 2) impairments in, for example, cognition, continence and mobility are recognized as being either new or of long standing,
AND - a systematic pre-discharge assessment linked to pre-
admission and admission assessments so that: 1) problems requiring post-discharge management can be identified; and 2) targeted individualized care packages can be designed.
DESCRIPTION OF THE MDS-AC The MDS-AC covers 14 key domains with 56
standardized assessment items. Assessments are carried out on two occasions. First the individual's prehospital admission status, and the status early in the hospital stay (within 48 hours of admission) are obtained. A second assessment is made later in the hospital stay (within 24-48 hours of discharge), so that problems which require post-hospital follow-up can be identified. A determination of services and treatments needed post hospital stay is then made, and documented.
To develop the content of the assessment tool, the literature covering existing instruments was reviewed. Health care professionals working in acute areas including physicians, nurses, occupational therapists, physiotherapists, social workers, dieticians and respiratory therapists were surveyed. Clinical and social factors important for discharge care planning and making in-hospital referrals, as well as those needed for monitoring outcomes of care were identified. The objective was to develop a standardized assessment tool that addresses major areas of importance in the care of older people, and that facilitates the transfer of information from acute hospital to post-acute nursing homes, and other institution and community care settings. The items for assessment of patient function were identical to those in both the MDS/RAI and the MDS-HC for purposes of continuity and comparability. Additional items (primarily 'administrative') were added that were of particular importance to the hospital stay and discharge planning. Once constructed, the patient assessment items were subjected to a systematic field trial to test interrater reliability, average time for CDmpletion, and clinical utility of the items.
At this time we present findings of the field trials, and illustrate how differences between pre-hospital and hospital admission status can be systematically evaluated using the MDS-AC.

SUBJECTS AND METHODS Reliability Trial The reliability trial involved dual, independent as-
sessments of adults, aged 65 years and older, who were in-patients in acute care hospitals in 4 countries: Canada, Norway, United Kingdom, and the United States. Samples were drawn from hospitals that were willing to participate in the study, and as such do not represent a random sample of older adults receiving acute care services in the participating countries. The sample included dual assessments on 233 acute care patients, 59% from Canada, 24% from Norway, 8% from the United Kingdom and 10% from the United States. A total of 12 acute care sites participated: 5 in Canada, 6 in Norway, 1 in the UK, and 2 in the USA.
At each site, two health care professionals completed independent assessments of elderly patients within a 24-hour period. Patients were recruited into the study after informed consent was obtained from the patient or, when the patient was not competent to decide, from a legal substitute decision-maker. Dual assessments for approximately two-thirds of the subjects (153 of 233) were initiated within 24 hours of their admission to the hospital, and dual assessments of the 80 remaining patients were made between 24 and 48 hours of their anticipated discharge. Assessors were either nurses or doctors, of which 53% had prior experience and/or training in geriatric assessment.
Assessors were prepared for their role by undergoing a standardized face-to-face training program that in-volved detailed instruction in the study procedures and use of the assessment tool. Subsequently, assessors un-dertook two practice assessments at their sites to gain practical familiarity with the detailed data acquisition and coding procedures. Following that experience, they were debriefed to ensure that they were prepared to complete the MDS-AC assessments in accordance with the item specifications. The two assessors at each site did not discuss the patients or their findings with each other until after all information was recorded.
Inter-assessor reliability coefficients of agreement be-yond chance were calculated for each item in the MDS-AC for which no single level of the variable contained 90% or more of the cases. The simple Kappa statistic was calculated for all binary variables and multi-level nominal variables using the Proc Freq procedure of the SAS statistical analysis software (SAS version 6.12). Quadratically weighted Kappa was estimated for all ordinal multi-level variables by calculating an intra-class correlation coefficient (Shrout and Fleiss type 2,1) using a macro (%INTRACC macro) available in SAS (12). Where the distribution of the data was such that one level of the variable contained 90% or more of the subjects, only total ob-
Reliability of the MDS-AC
served agreement is reported. Separate reliability es-timates were calculated for information collected about pre-hospitalization status and in-patient status with respect to each individual MDS-AC item.
Scores on seven Activities of Daily Living (ADL) items (dressing, personal hygiene, toilet use, transfer, locomotion, bed mobility and eating) were summarized using the additive MDS-Long Form summary scale (13). Cognitive impairment was summarized using the Cognitive Performance Scale (14).
RESULTS Sample description The study subjects ranged in age from 60 to 91 years
(mean: 78); 63% were female, 42% were married, and 42% lived alone prior to hospitalization. Table 1 shows the sources of the sample data, and Table 2 the distribution of responses in key pre-hospitalization period and in-hospital assessment items.
Based on the categories of the Cognitive Perfor-mance Scale, in the 30 days prior to hospitalization, 75% were cognitively intact, and 9% had a moderate or more severe cognitive impairment (Table 3). In the pre-hospitalization period, 72% of the sample were in-dependent in ADLs (Table 4), 15% were incontinent at least daily, 25% had some hearing deficit, even with a hearing appliance, and 17% had some visual deficit, even with glasses. Also in that period, 19% had re-ceived one or more special treatments (for example, medication by injection, dialysis, chemotherapy, oxy-gen), and 45% had received one or more health-related services (for example, home care, meals on wheels, physical, occupational or speech therapy). Obstacles to functional mobility inside their home (for example, stairs to the toilet) were reported for 18% of subjects, and informal caregivers were distressed or unable to provide support for 14%.
Reliability trial results Assessors reported that, on average, the assessment
of the pre-hospitalization and the hospital periods (combined) required between 20 and 30 minutes to complete. The most commonly cited reason for a longer assessment time was loquacious patients.
Table 5 shows the inter-assessor reliability results for information gathered with respect to the pre-hospi-talization period (the 30 days prior to the acute event that led to hospitalization), and following admission to the hospital. Excluding items for which 90% or more of subjects were classified into a single scoring level, the average inter-assessor reliability coefficient for items assessed for the pre-hospital period was 0.57, and for the in-hospital period was 0.58. Assessors
Aging Clin. Exp. Res., Vo!. 13, No. 4 318
G.I. Carpenter, G.F. Teare, K. Steel, et af.
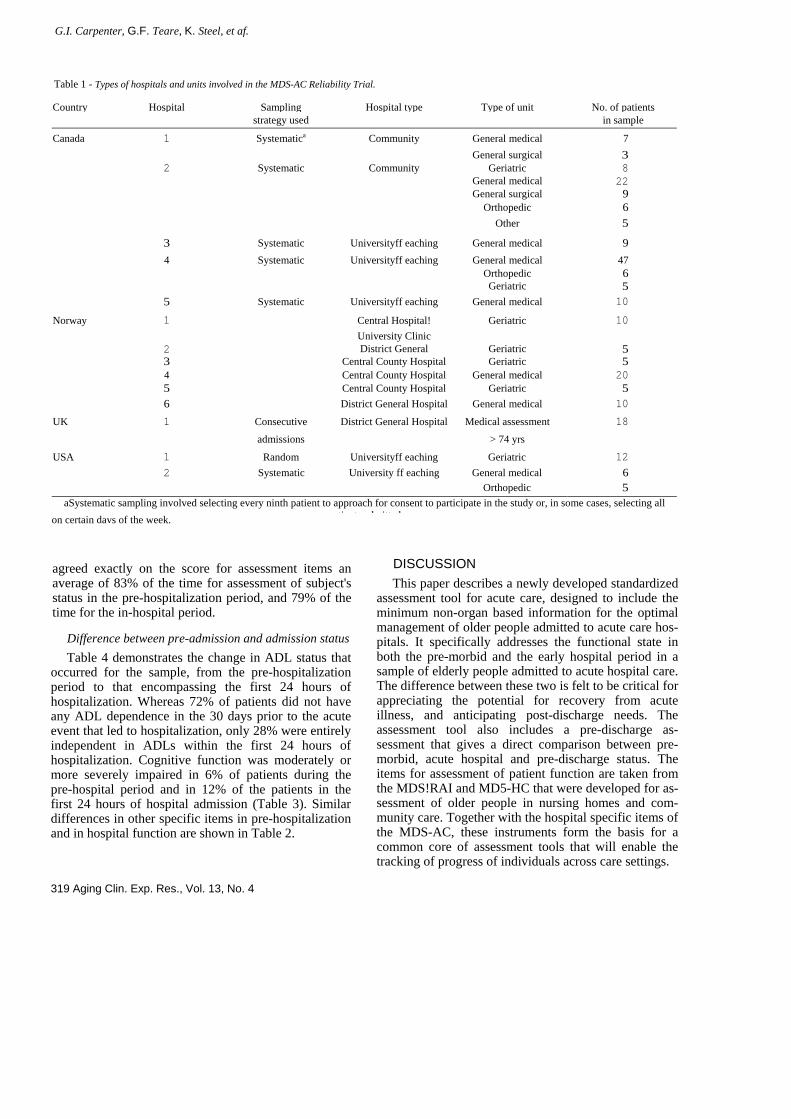
Table 1 - Types of hospitals and units involved in the MDS-AC Reliability Trial. Country Hospital Sampling Hospital type Type of unit No. of patients
strategy used in sample
Canada 1 Systematica Community General medical 7 General surgical 3 2 Systematic Community Geriatric 8 General medical 22 General surgical 9 Orthopedic 6 Other 5
3 Systematic Universityff eaching General medical 9 4 Systematic Universityff eaching General medical 47 Orthopedic 6 Geriatric 5 5 Systematic Universityff eaching General medical 10
Norway 1 Central Hospital! Geriatric 10 University Clinic 2 District General Geriatric 5 3 Central County Hospital Geriatric 5 4 Central County Hospital General medical 20 5 Central County Hospital Geriatric 5 6 District General Hospital General medical 10
UK 1 Consecutive District General Hospital Medical assessment 18
admissions > 74 yrs
USA 1 Random Universityff eaching Geriatric 12 2 Systematic University ff eaching General medical 6 Orthopedic 5
aSystematic sampling involved selecting every ninth patient to approach for consent to participate in the study or, in some cases, selecting all ti t d itt don certain days of the week.
agreed exactly on the score for assessment items an average of 83% of the time for assessment of subject's status in the pre-hospitalization period, and 79% of the time for the in-hospital period.
Difference between pre-admission and admission status Table 4 demonstrates the change in ADL status that
occurred for the sample, from the pre-hospitalization period to that encompassing the first 24 hours of hospitalization. Whereas 72% of patients did not have any ADL dependence in the 30 days prior to the acute event that led to hospitalization, only 28% were entirely independent in ADLs within the first 24 hours of hospitalization. Cognitive function was moderately or more severely impaired in 6% of patients during the pre-hospital period and in 12% of the patients in the first 24 hours of hospital admission (Table 3). Similar differences in other specific items in pre-hospitalization and in hospital function are shown in Table 2.
319 Aging Clin. Exp. Res., Vol. 13, No. 4
DISCUSSION This paper describes a newly developed standardized
assessment tool for acute care, designed to include the minimum non-organ based information for the optimal management of older people admitted to acute care hos-pitals. It specifically addresses the functional state in both the pre-morbid and the early hospital period in a sample of elderly people admitted to acute hospital care. The difference between these two is felt to be critical for appreciating the potential for recovery from acute illness, and anticipating post-discharge needs. The assessment tool also includes a pre-discharge as-sessment that gives a direct comparison between pre-morbid, acute hospital and pre-discharge status. The items for assessment of patient function are taken from the MDS!RAI and MD5-HC that were developed for as-sessment of older people in nursing homes and com-munity care. Together with the hospital specific items of the MDS-AC, these instruments form the basis for a common core of assessment tools that will enable the tracking of progress of individuals across care settings.
Overall, the reliability achieved for the MDS-AC items gives a degree of confidence for their use in clin-ical care (kappa >0.4 is sufficient to be of practical use). The results were achieved in what is the highly unstable situation of the acute admission phase where functional status can change rapidly, and when the abilities of acutely ill older people, in particular, may change a great deal during the course of a day. The values of Kappa achieved did not reflect the fact that, on most items, a very high proportion of paired assessments had complete agreement. This apparent "suppression" of Kappa in situations where observations are not evenly distributed among the scoring lev-
Reliability of the MDS-AC
els of an item, as occurred in this study, is a wellknown phenomenon (15-17).
As a result of the reliability study, coding for a number of the assessment items has been simplified, in particular those for assessment of pain, caregiver status, foot problems and oral problems. Also the majority have had minor amendments to the item definitions in line with the on-going developments in the family of MDS assessment instruments. These are taking place in parallel with the development of the MDS for Post Acute Care (MDS-PAC) under a US Federal contract at the Hebrew Rehabilitation Center for the Aged, Boston (Morris J., personal communi-
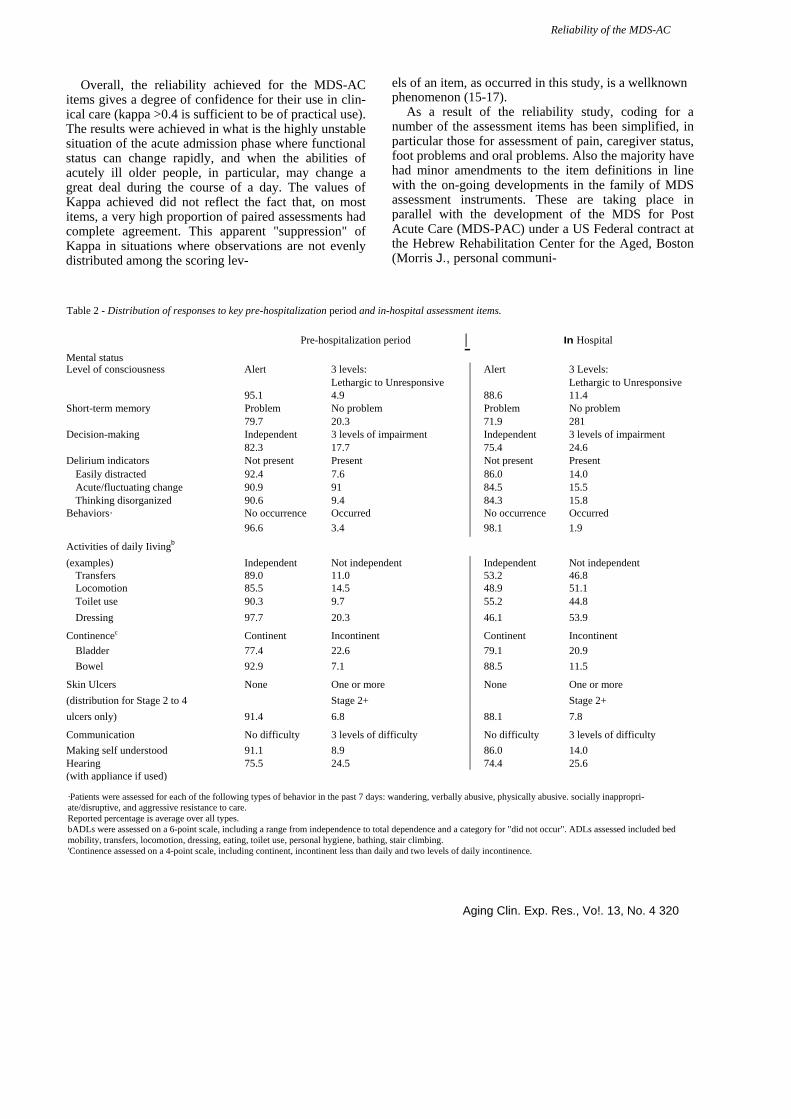
Table 2 - Distribution of responses to key pre-hospitalization period and in-hospital assessment items.
Pre-hospitalization period I In Hospital
Mental status Level of consciousness Alert 3 levels: Alert 3 Levels:
Lethargic to Unresponsive Lethargic to Unresponsive 95.1 4.9 88.6 11.4
Short-term memory Problem No problem Problem No problem 79.7 20.3 71.9 281
Decision-making Independent 3 levels of impairment Independent 3 levels of impairment 82.3 17.7 75.4 24.6
Delirium indicators Not present Present Not present Present Easily distracted 92.4 7.6 86.0 14.0 Acute/fluctuating change 90.9 91 84.5 15.5 Thinking disorganized 90.6 9.4 84.3 15.8
Behaviors· No occurrence Occurred No occurrence Occurred 96.6 3.4 98.1 1.9
Activities of daily Iivingb (examples) Independent Not independent Independent Not independent
Transfers 89.0 11.0 53.2 46.8 Locomotion 85.5 14.5 48.9 51.1 Toilet use 90.3 9.7 55.2 44.8 Dressing 97.7 20.3 46.1 53.9
Continencec Continent Incontinent Continent Incontinent Bladder 77.4 22.6 79.1 20.9 Bowel 92.9 7.1 88.5 11.5
Skin Ulcers None One or more None One or more (distribution for Stage 2 to 4 Stage 2+ Stage 2+ ulcers only) 91.4 6.8 88.1 7.8
Communication No difficulty 3 levels of difficulty No difficulty 3 levels of difficulty Making self understood 91.1 8.9 86.0 14.0 Hearing 75.5 24.5 74.4 25.6 (with appliance if used)
·Patients were assessed for each of the following types of behavior in the past 7 days: wandering, verbally abusive, physically abusive. socially inappropri-ate/disruptive, and aggressive resistance to care. Reported percentage is average over all types. bADLs were assessed on a 6-point scale, including a range from independence to total dependence and a category for "did not occur". ADLs assessed included bed mobility, transfers, locomotion, dressing, eating, toilet use, personal hygiene, bathing, stair climbing. 'Continence assessed on a 4-point scale, including continent, incontinent less than daily and two levels of daily incontinence.
Aging Clin. Exp. Res., Vo!. 13, No. 4 320

G.I. Carpenter, G.F. Tea re, K. Steel, et al.
Table 3 - Distribution of "Cognitive Performance Sca/e" (CPS) scores for the 30-day period prior to hospitalization and in the first 24 hours of hospitalization.
Distribution of patientso.b CPS score
o 1 2 3 4 5 6
Cognitive status
Intact Borderline intact
Mild impairment Moderate impairment Moderately severe impairment Severe impairment
Very severe impairment
No. (%)in pre-hospitalization period
101 (75) 22 (16)
4 (3) 3 (2) o 4 (3) 1 (1)
No. (%) in early hospitalization period
90 (67) 21 (16) 6 (4) 7 (5) o
7 (5) 3 (2)
aDue to missing values for one or more items in the CPS, the scale was calculated for the pre-hospital period for 135 patients and the early hospital period for 134 patients of the 153 patients assessed within 24 hours of admission. bColumns do not total to exactly 100% due to rounding.
cation), and the development of the MDS for Palliative Care (MDS-PC).
Although very many admission assessment protocols exist, particularly in geriatric services in the UK, we are unaware of any attempts to address the questions of reliability of assessment in acute settings for such a comprehensive range of assessment items. The demon-stration of a high degree of reliability of the items on pre-morbid function in particular shows that pre-morbid function can be reliably recorded, and used for comparison with data about function at hospital admission. Others have recently shown that valid retrospective assessment of pre-hospitalization function is feasible (18).
Our results have illustrated differences between pre-morbid ADL and cognitive function and function at admission. Although the number of people with a sig-nificant difference in cognitive function was small, these are the people who may have reversible cognitive im-pairment (i.e., delirium). For pre-morbid status, there was
an 83% agreement for short-term memory, 85% for de-CiSion-making and 94% for eating. These items, together with "comatose" comprise the variables of the MDS Cognitive Performance Scale. Other widely used standard assessments of cognitive function such as the Abbreviated Mental Test and Mini-Mental State Examination (MMSE) cannot be completed retrospectively.
While demonstrating reliability of the MDS-AC as-sessment in these and other domains does not imply that it will improve outcome of care, there is ample evidence that comprehensive geriatric assessment improves outcome of care (19). A recent trial of the MDSHC has demonstrated its role in a study that showed a significant reduction in hospital admissions (20). It is probable that using a structured assessment such as the MDS-AC, at least in some countries and specialties, may show benefits in improving rates of successful discharge home and reducing admissions to long-term care.
The MDS-AC has been designed for completion by
Table 4 - Activities of Daily Living (ADL) self-performance for the 30-day period prior to hospitalization and in the first 24 hours of hospitalization.
Distribution of patientso,b Modified MDS ADL-Long Form additive summary scale score (13)
o 1 to 7 8 to 14 15 to 21 22 to 28
No. (%) in pre-hospitalization period
71 (74) 20 (21) 4 (4) 1 (1) o
No. (%) in early hospitalization period
42 (44) 40 (41) 11 (10)
3 (3) o
'Case deleted if any of 7 ADL items in the ADL-Long Form scale was scored "did not occur", leaving 96 of 153 subjects assessed within 24 hours of admission for the analysis. bColumns do not total to exactly 100% due to rounding.
321 Aging Clin. Exp. Res., Vol. 13, No. 4

Reliability of the MDS-AC
Table 5 - Inter-assessor agreement for assessment items on the MDS-AC.
Assessment area Number of Inter-assessor Kappa Proportion of items on reliability assessments with MDS-AC (the average where more complete agreement than one item) Pre-hospital In hospital Pre-hospital In hospital
Pain Acute pain present 1 0.57 0.53 0.62 0.61 Pain controlled by medication 1 0.44 0.39 0.65 0.60 Chronic pain present 1 0.54 n/aa 0.77 n/a
Mental Status Level of consciousness 1 #b 0.65 0.89 0.90 Memory 1 0.49 0.54 0.83 0.74 Decision-making 1 0.70 0.74 0.85 0.82 Indicators of delirium 3 # 0.58 0.90 0.89 Indicator of depression/sad mood 1 0.39 0.44 0.68 0.69 Change in mental status 1 0.43 n/a 0.84 n/a
Behavior problems 5 # # 0.92 0.98 Physical functioning
ADL self-performance 9 0.50 0.58 0.82 0.65 IADL self-performance 7 0.53 n/a 0.73 n/a
Incontinence Bladder 2 0.67 0.69 0.85 0.83 Bowel 2 # # 0.97 0.94
Skin condition Pressure/Stasis ulcers 2C 062 0.65 0.92 0.89 History of pressure ulcers 1 # n/a 0.91 n/a Foot status 1 0.61 0.57 0.79 0.79 Surgical wounds 4 0.62 n/a 0.92 n/a
Sensory function (vision, hearing) 2 0.62 0.67 0.79 0.78 Communication 1 # 0.67 0.88 0.86 Oral status 1 0.36 0.50 0.83 0.82 Informal caregiver issues 1 0.53 0.56 0.68 0.59 Medication compliance 1 0.58 0.75 Drug allergy 1 0.74 0.90 Advance directive 1 0.68 0.84 Falls (last 180 days) 1 0.71 0.87 Tobacco / Alcohol use 2 0.64 0.95 Potential indicators of neglect 1 # 0.94
aNot assessed. These items assessed only for the pre-hospitalization period. b90% or more of subjects were in only one level of the coding range. 'One of the pressure ulcer items was missing data too frequently for reliability to be estimated.
physicians (interns, house officers depending on coun-try), or nurses. The assessment time of 20-30 minutes should be within the acceptable limits for assessment of these factors in the acute setting. The routine use of the instrument would in addition enable case-mix adjusted comparison of outcomes of care of older people, especially for those circumstances where premorbid functional ability and functional recovery is important.
As a research tool, its use could contribute to un-derstanding the causes for change in function that may occur in the acute phase of illness in older people. De-
velopment of a systematic way of observing changes occurring during illness in older people is of increasing importance when addressing questions of the ap-propriate and inappropriate use of medical technology.
At the hospital of one of the authors (K.S.), elders now account for 51% of patient days, yet they represent only 13% of the catchment population. With a budget now in excess of $500,000,000, even a small reduction in length of stay or widely used but inappropriate interventions would result in very substantial savings. Should use of the MDS-AC in practice be shown to increase the time taken for admission as-
Aging Clin. Exp. Res., Vo!. 13, No. 4 322

2. G.I. Carpenter, G.F. Tea re, K. Steel, et af. 3.
sessment, this cost must be weighed against the demonstrated benefits. These matters will be the subject of studies that go beyond the remit of this paper.
The MDS-AC is currently being further evaluated in studies in Canada, Norway, Iceland, Italy, the United Kingdom, and the United States.
APPENDIX
MINIMUM DATA SET - ACUTE CARE (MDS-AC) Draft 1.12
SECTION A. PATIENT IDENTIFICATION (Complete any information not found in Ihe addressograph)
1 NAME OF PATIENT
a_ LAST/FAMIL Y NAME
b. FIRST NAME t. MIDDLE INITIAL
2 BIRTHDATE
DODO-DO-DD YEAR MON
THDAY
3 GENDER 1. Male 2. Fem I
4 DATE OF Date this hospital stay began. ADMISSION
DODO-DO-DD YEAR MON
THDAY
5 HOSPITAL
CHART No. 0000000000 6 HEALTH
CARE No. 0000000000000
PRECIPITAT-ITime of onset of the precipitating event/problem or ING EVENT! destabllization that directly led to this DESTABllIZ· hospitalization (time prior to date of admission A4)
AllON (Le., how long ago was patient's health/function relatively stable)
O. Within last week 3. 31-60 days prior 1.8-14 days prior 4. More than 60 days prior
2. 15-30 da s rior 4 IMOST Most recent acute hospital admission(s) during the RECENT 3 months prior to current admission HOSPITAL- O. None IZA TION 1. 1-30 days prior to current admission
2. 31-90 da s rior to current admission ADVANCE Does the patient have an advance directive? DIRECTIVE (e.g. Do not resuscitate; No "heroic measures") O. No 1. Yes 9. Unknown
SECTION B. SOCIODEMOGRAPHICS
LANGUAGE la. Primary Language: O. English 2. Other 1. French Specify
b. Interpreter needed O. No 1. Yes
SECTION D. ASSESSMENT INFORMATION
SIGNATURES OF PERSONS COMPLETING THE ASSESSMENTS
a. Signature of Assessment Coordinator: I b. Title:
CHECK <v) to confirm completion of the following:
Pre-morbid and early and late in-hospital columns completed c.
Discharge Date, Resources. Diagnoses etc (page 7 ) completed d.
List Of Medications taken/ordered while in hospital is attached e.
I. Date Assessment Coordinator signed that assessments are DODO-DO-DD complete YEAR MONTH DAY
g. Other signatures Title Sections/Items Date
h.
,. J.
k.
I.
O. Married/Partner 3. Separated/Divorced 1.Never married 4. Other 2. Widowed 1. No schooling 2. 8~ grade/less 3. 9-11 grades 4. High school 5. Technical or trade school 6. Diploma/Bachelor's degree 7. Graduate deqree
MARITAL STATUS
EDUCATION (highest level completed)
SECTION C. ADMISSION DETAIL ADMITTED
FROM (At dale of entry-M)
1.Private home, apt or 5. Acute care hospital- room, no home care not rehabilitation 2. Private home/apUroom 6. Rehabilitation unit with home care or hospital 3.Board and care or 7. Psychiatric assisted living or group hospital/unit home 8. Emergency Dept. 4. Long term care facility 9. Other (nursing home or Specify ________ _
chronic hospital) a. 1. Primarily a medical problem
2.Primarily a surgical problem 3. Both
b. 1. New problem 2. Exacerbation of existing problem 3. 80th 1 and 2
REASON FOR CURRENT HOSPITAL-IZATION
I Addressograph
SECTION E. ASSESSMENT DATES
1 ASSESS- MENT a. Assessment for first in-hospital period (i.e. first 24
h i DODO-DO-DDREFERENC hospital) DATES (date YEAR MONTH DAY
assessment b. Assessment for second in-hospital period (Le. first of: Daypelformed) 7 or within 24 hrs of discharge) DODO-DO-DD
YEAR MONTH DAY C. Assessment for third in·hospital period (Le. latter of: Day
or upon ALC designation) DODO-DO-DD YEAR MONTH DAY
323 Aging Clin. Exp. Res., Vo!. 13, No. 4

4.
Reliability of the MDS-AC
Throughout the MDS-AC assessment: Assessment for Premorbid Period (Column 'A') to reflect typical activity/function during the 30 days prior to the destabilization or acute event that resulted in this hospital admission (see item C3), unless otherwise indicated.
Assessment for In-Hospital Periods ('B' Columns) to reflect activity/functioning during the past 24 hours, unless otherwise indicated.
SECTION F: PHYSICAL FUNCTION 1 ACTIVITIES OF (A) For pre-morbid performance: Code for typical dailv self-performance in the 30 days prior to the destabilization
DAILY LIVING or acute event that led to this admission (see item C3).
B) For immediate pre-admission and in-hospltal performance: Code for self-performance in most dependent episode during the past 24 hours.
CODE: O. INDEPENDENT - no help setup, or supervision provided nor needed 1. SETUP HELP ONLY - article or device given to or placed within reach of patient on one or more occasions 2. SUPERVISION - oversight, encouragement or cueing provided on one or more occasions 3. PHYSICAL ASSISTANCE - patient involved in activity BUT
received physical assistance (non-weight bearing or weight bearing) to complete the task on one or more occasions
4. TOTAL DEPENDENCE-full performance of activity by other(s)
8. ACTIVITY DID NOT OCCUR Including moving to and from lying position, turning side to side, and positioning body while in bed Including moving to and between surfaces to/from bed, chair,
heelchair, standing position (Note: Excludes to/from bath/toilew t) How patient moves between locations within a room and on same floor. If in wheelchair, self-sufficiency once in wheelchair How patient eats and drinks (regardless of skill). Includes intake of nourishment by other means (e.g .• tube feeding, total parenteral nutrition) Including using the toilet room or commode, bedpan, urinal, transferring on/off toilet, cieaning self after toilet use or incontinent episode, changing pad, managing any special devices required (ostomy or catheter), and adjusting clothes How patient maintains personal hygiene. Includes combing hair, brushing teeth, shaving, applying makeup, controlling body odour, washing/drying face, hands, and perineum (EXCLUDE baths and showers)
(B1) The 24 hrs
prior to admission
(B2) First of:
-C-H-E-C-K-("~) all that apply:
(A)
Day 7 or 24 hrs pre-discharge
(B3) Latter of: Pre-morbid
periOd Day 14 or upon ALe designation
a. MOBILITY IN BED
b. TRANSFER
c.ILOCOMOTION
d.IEATING
e.ITOILET USE
f.IPERSONAL HYGIENE
2 I LOCOMOTION DEVICES
Cane/crutch
Walker
Wheeled
3 INSTRUMENTAL (A) Typical pre-morbld FUNCTlON/NG in routine activities at home or in the community prior to destabilization or ACTIVITIES OF acute event that led to this hospital admission (see item C3)
DAILY LIVING
(B) CAPACITY to perform the activities as independently as possible. Speculate and code what you think the patient's ability would have been during the past 24 hrs.
CODE: IADL SELF-PERFORMANCE CODE O. INDEPENDENT-<Jid on own 1 . SOME HELP- performed with help some of the time 2.FULL HELP- performed with help all of the time 3. BY OTHERS- performed by others
(A) Pre-morbid
period
(B3) Latter of:
Day 14 or upon ALC deslanation
3. Column A: ACTIVITY DID NOT OCCUR Columns B2-3 : NOT APPLICABLE
a. b.
c. d.
e.
g.
Aging Clin. Exp. Res., Vo!. 13, No. 4 324
G.I. Ca':penter, G.F. Teare, K. Steel, et al.
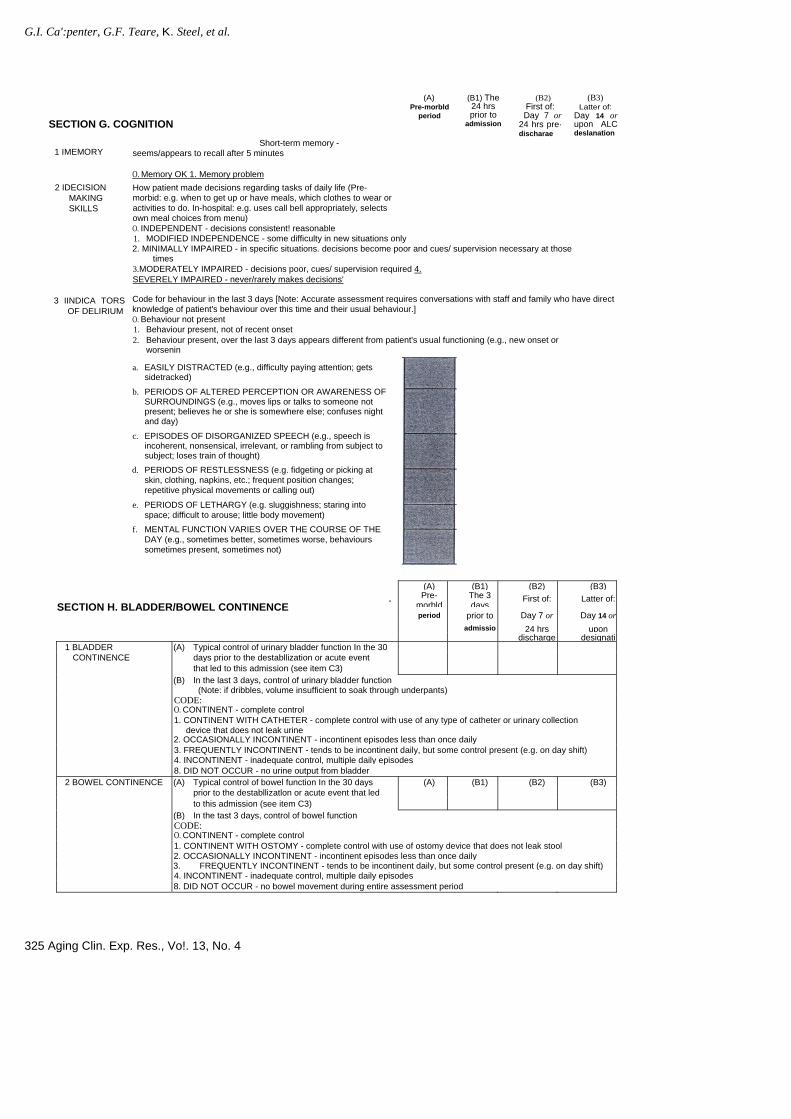
1 IMEMORY
Short-term memory - seems/appears to recall after 5 minutes
(A) Pre-morbld
period
(B1) The 24 hrs prior to
admission
(B2) First of: Day 7 or
24 hrs pre· discharae
(B3) Latter of:
Day 14 or upon ALC deslanation
2 IDECISION
MAKING SKILLS
3 IINDICA TORS OF DELIRIUM
O. Memory OK 1. Memory problem How patient made decisions regarding tasks of daily life (Pre-morbid: e.g. when to get up or have meals, which clothes to wear or activities to do. In-hospital: e.g. uses call bell appropriately, selects own meal choices from menu) O. INDEPENDENT - decisions consistent! reasonable 1. MODIFIED INDEPENDENCE - some difficulty in new situations only 2. MINIMALLY IMPAIRED - in specific situations. decisions become poor and cues/ supervision necessary at those
times 3. MODERATELY IMPAIRED - decisions poor, cues/ supervision required 4. SEVERELY IMPAIRED - never/rarely makes decisions'
Code for behaviour in the last 3 days [Note: Accurate assessment requires conversations with staff and family who have direct knowledge of patient's behaviour over this time and their usual behaviour.] O. Behaviour not present 1. Behaviour present, not of recent onset 2. Behaviour present, over the last 3 days appears different from patient's usual functioning (e.g., new onset or
worsenin a. EASILY DISTRACTED (e.g., difficulty paying attention; gets
sidetracked)
b. PERIODS OF ALTERED PERCEPTION OR AWARENESS OF SURROUNDINGS (e.g., moves lips or talks to someone not present; believes he or she is somewhere else; confuses night and day)
c. EPISODES OF DISORGANIZED SPEECH (e.g., speech is incoherent, nonsensical, irrelevant, or rambling from subject to subject; loses train of thought)
d. PERIODS OF RESTLESSNESS (e.g. fidgeting or picking at skin, clothing, napkins, etc.; frequent position changes; repetitive physical movements or calling out)
e. PERIODS OF LETHARGY (e.g. sluggishness; staring into space; difficult to arouse; little body movement)
f. MENTAL FUNCTION VARIES OVER THE COURSE OF THE DAY (e.g., sometimes better, sometimes worse, behaviours sometimes present, sometimes not)
(A) (B1) (B2) (B3)
. Pre-morbld
The 3 days
First of: Latter of: SECTION H. BLADDER/BOWEL CONTINENCE
period prior to Day 7 or Day 14 or admissio 24 hrs upon
discharge designati1 BLADDER (A) Typical control of urinary bladder function In the 30
CONTINENCE days prior to the destabllization or acute event that led to this admission (see item C3)
(B) In the last 3 days, control of urinary bladder function (Note: if dribbles, volume insufficient to soak through underpants)
CODE: O. CONTINENT - complete control 1. CONTINENT WITH CATHETER - complete control with use of any type of catheter or urinary collection
device that does not leak urine 2. OCCASIONALLY INCONTINENT - incontinent episodes less than once daily 3. FREQUENTLY INCONTINENT - tends to be incontinent daily, but some control present (e.g. on day shift) 4. INCONTINENT - inadequate control, multiple daily episodes 8. DID NOT OCCUR - no urine output from bladder
2 BOWEL CONTINENCE (A) Typical control of bowel function In the 30 days (A) (B1) (B2) (B3) prior to the destabllizatlon or acute event that led to this admission (see item C3)
(B) In the tast 3 days, control of bowel function CODE: O. CONTINENT - complete control 1. CONTINENT WITH OSTOMY - complete control with use of ostomy device that does not leak stool 2. OCCASIONALLY INCONTINENT - incontinent episodes less than once daily 3. FREQUENTLY INCONTINENT - tends to be incontinent daily, but some control present (e.g. on day shift) 4. INCONTINENT - inadequate control, multiple daily episodes 8. DID NOT OCCUR - no bowel movement during entire assessment period
325 Aging Clin. Exp. Res., Vo!. 13, No. 4
SECTION G. COGNITION
Reliability of the MDS-AC
(A) (B1)
5.
(B2) (B3) Pre-
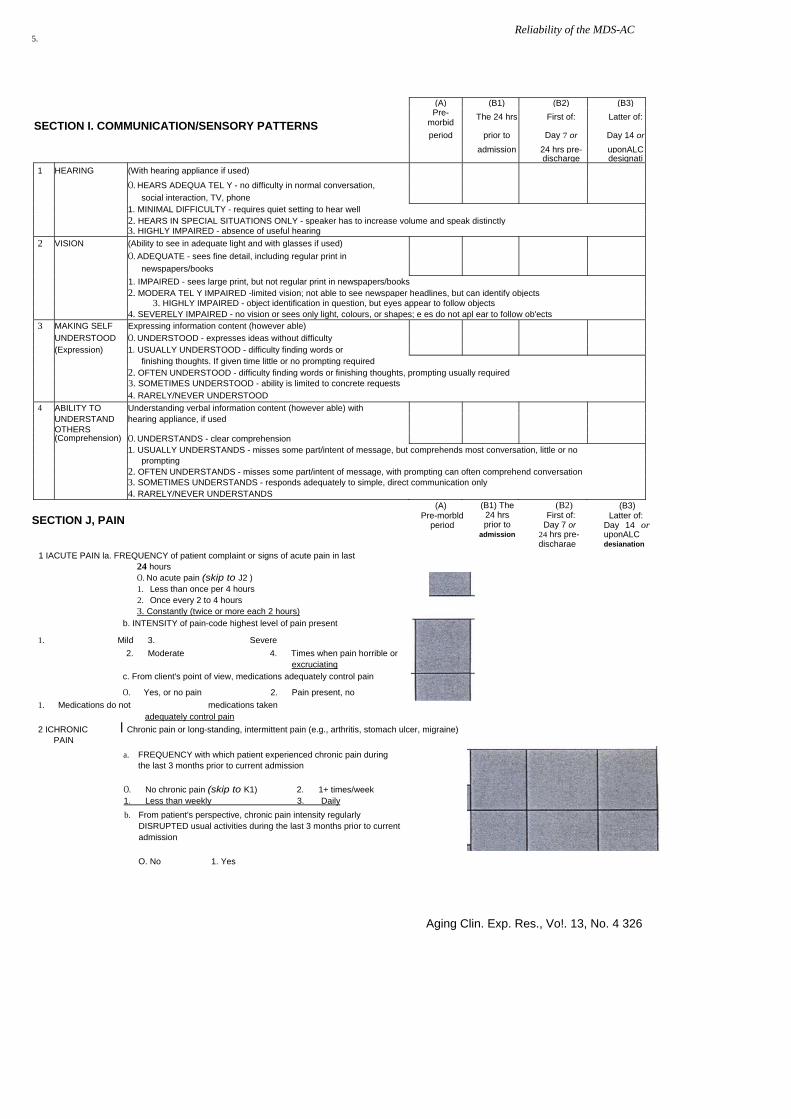
morbid The 24 hrs First of: Latter of: SECTION I. COMMUNICATION/SENSORY PATTERNS
period prior to Day 7 or Day 14 or
admission 24 hrs pre- uponALC discharge designati
1 HEARING (With hearing appliance if used)
O. HEARS ADEQUA TEL Y - no difficulty in normal conversation,
social interaction, TV, phone 1. MINIMAL DIFFICULTY - requires quiet setting to hear well 2. HEARS IN SPECIAL SITUATIONS ONLY - speaker has to increase volume and speak distinctly 3. HIGHLY IMPAIRED - absence of useful hearing
2 VISION (Ability to see in adequate light and with glasses if used) O. ADEQUATE - sees fine detail, including regular print in newspapers/books
1. IMPAIRED - sees large print, but not regular print in newspapers/books 2. MODERA TEL Y IMPAIRED -limited vision; not able to see newspaper headlines, but can identify objects 3. HIGHLY IMPAIRED - object identification in question, but eyes appear to follow objects 4. SEVERELY IMPAIRED - no vision or sees only light, colours, or shapes; e es do not apl ear to follow ob'ects
3 MAKING SELF Expressing information content (however able) UNDERSTOOD O. UNDERSTOOD - expresses ideas without difficulty (Expression) 1. USUALLY UNDERSTOOD - difficulty finding words or finishing thoughts. If given time little or no prompting required 2. OFTEN UNDERSTOOD - difficulty finding words or finishing thoughts, prompting usually required 3. SOMETIMES UNDERSTOOD - ability is limited to concrete requests 4. RARELY/NEVER UNDERSTOOD
4 ABILITY TO Understanding verbal information content (however able) with UNDERSTAND hearing appliance, if used
OTHERS (Comprehension) O. UNDERSTANDS - clear comprehension 1. USUALLY UNDERSTANDS - misses some part/intent of message, but comprehends most conversation, little or no
prompting 2. OFTEN UNDERSTANDS - misses some part/intent of message, with prompting can often comprehend conversation 3. SOMETIMES UNDERSTANDS - responds adequately to simple, direct communication only 4. RARELY/NEVER UNDERSTANDS
SECTION J, PAIN (B2)
First of: Day 7 or
24 hrs pre-discharae
(B3) (A) Pre-morbld
period
(B1) The 24 hrs prior to
admission
Latter of: Day 14 or uponALC desianation
1 IACUTE PAIN la. FREQUENCY of patient complaint or signs of acute pain in last 24 hours O. No acute pain (skip to J2 ) 1. Less than once per 4 hours 2. Once every 2 to 4 hours 3. Constantly (twice or more each 2 hours)
b. INTENSITY of pain-code highest level of pain present
1. Mild 3. Severe 2. Moderate 4. Times when pain horrible or
excruciating c. From client's point of view, medications adequately control pain
O. Yes, or no pain 2. Pain present, no 1. Medications do not medications taken
adequately control pain 2 ICHRONIC I Chronic pain or long-standing, intermittent pain (e.g., arthritis, stomach ulcer, migraine)
PAIN
O. No chronic pain (skip to K1) 2. 1+ times/week
a. FREQUENCY with which patient experienced chronic pain during the last 3 months prior to current admission
1. Less than weekly 3. Daily b. From patient's perspective, chronic pain intensity regularly
DISRUPTED usual activities during the last 3 months prior to current admission
O. No 1. Yes
Aging Clin. Exp. Res., Vo!. 13, No. 4 326
6. G.I. Carpenter, G.F. Tea re, K. Steel, et al.
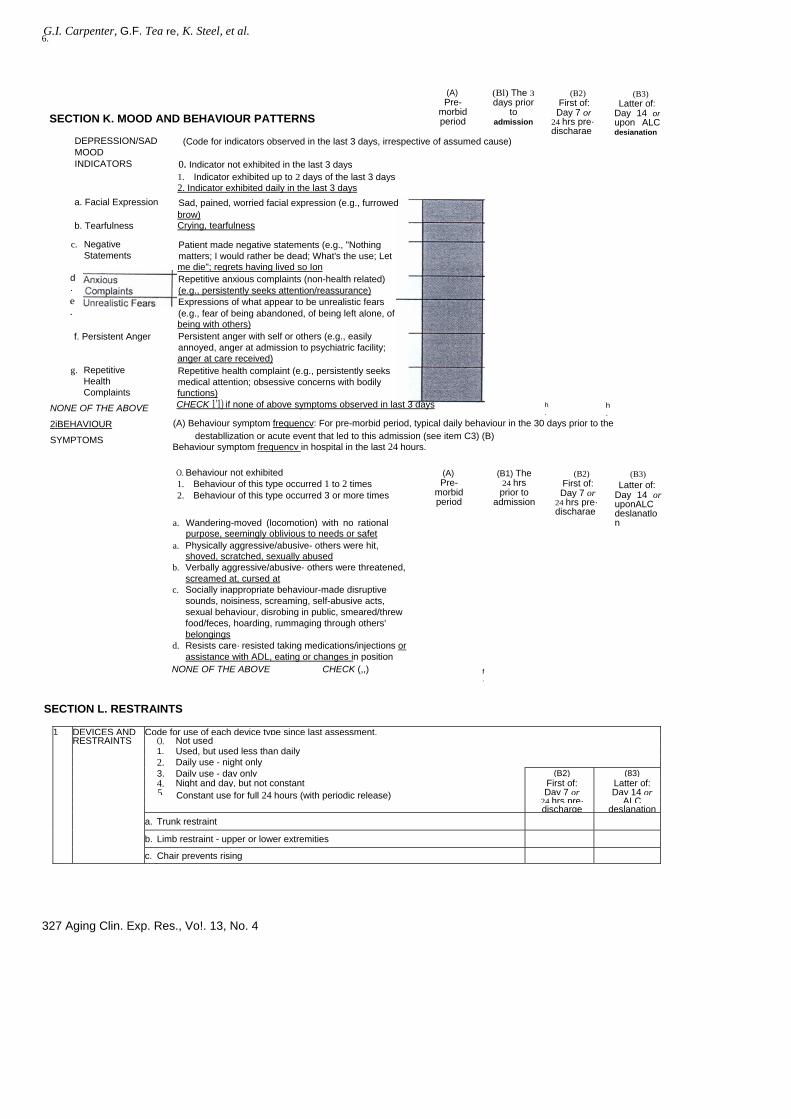
SECTION K. MOOD AND BEHAVIOUR PATTERNS
(A) Pre-
morbid period
(Bl) The 3 days prior
to admission
(B2) First of: Day 7 or
24 hrs pre· discharae
(B3) Latter of:
Day 14 or upon ALC desianation
DEPRESSION/SAD MOOD INDICATORS
(Code for indicators observed in the last 3 days, irrespective of assumed cause)
d.
o. Indicator not exhibited in the last 3 days 1. Indicator exhibited up to 2 days of the last 3 days 2. Indicator exhibited daily in the last 3 days Sad, pained, worried facial expression (e.g., furrowed brow) Crying, tearfulness Patient made negative statements (e.g., "Nothing matters; I would rather be dead; What's the use; Let me die"; regrets having lived so Ion Repetitive anxious complaints (non-health related) (e.g., persistently seeks attention/reassurance) Expressions of what appear to be unrealistic fears (e.g., fear of being abandoned, of being left alone, of being with others) Persistent anger with self or others (e.g., easily annoyed, anger at admission to psychiatric facility; anger at care received) Repetitive health complaint (e.g., persistently seeks medical attention; obsessive concerns with bodily functions)
a. Facial Expression
b. Tearfulness
c. Negative Statements
e.
f. Persistent Anger
g. Repetitive Health Complaints
NONE OF THE ABOVE
2iBEHAVIOUR
SYMPTOMS
CHECK 1'1) if none of above symptoms observed in last 3 days
(A) Behaviour symptom frequencv: For pre-morbid period, typical daily behaviour in the 30 days prior to the
h.
h.
destabllization or acute event that led to this admission (see item C3) (B) Behaviour symptom frequencv in hospital in the last 24 hours.
O. Behaviour not exhibited 1. Behaviour of this type occurred 1 to 2 times 2. Behaviour of this type occurred 3 or more times
(A) Pre-
morbid period
(B1) The 24 hrs prior to
admission
(B2) First of: Day 7 or
24 hrs pre· discharae
(B3) Latter of:
Day 14 or uponALC deslanatlon a. Wandering-moved (locomotion) with no rational
urpose, seemingly oblivious to needs or safet p a. Physically aggressive/abusive- others were hit,
shoved, scratched, sexually abused b. Verbally aggressive/abusive- others were threatened,
screamed at, cursed at c. Socially inappropriate behaviour-made disruptive
sounds, noisiness, screaming, self-abusive acts, sexual behaviour, disrobing in public, smeared/threw food/feces, hoarding, rummaging through others' belongings
d. Resists care· resisted taking medications/injections or assistance with ADL, eating or changes in position
NONE OF THE ABOVE CHECK (,,) f.
SECTION L. RESTRAINTS
1 DEVICES AND Code for use of each device type since last assessment.RESTRAINTS O. Not used
1. Used, but used less than daily 2. Daily use - night only
3. Daily use - day only (B2) (83) 4. Night and day, but not constant First of: Latter of: 5. Day 7 or Day 14 or Constant use for full 24 hours (with periodic release)
24 hrs pre· ALCdischarge deslanation
a. Trunk restraint
b. Limb restraint - upper or lower extremities
c. Chair prevents rising
327 Aging Clin. Exp. Res., Vo!. 13, No. 4
Reliability of the MDS-AC 7.8.
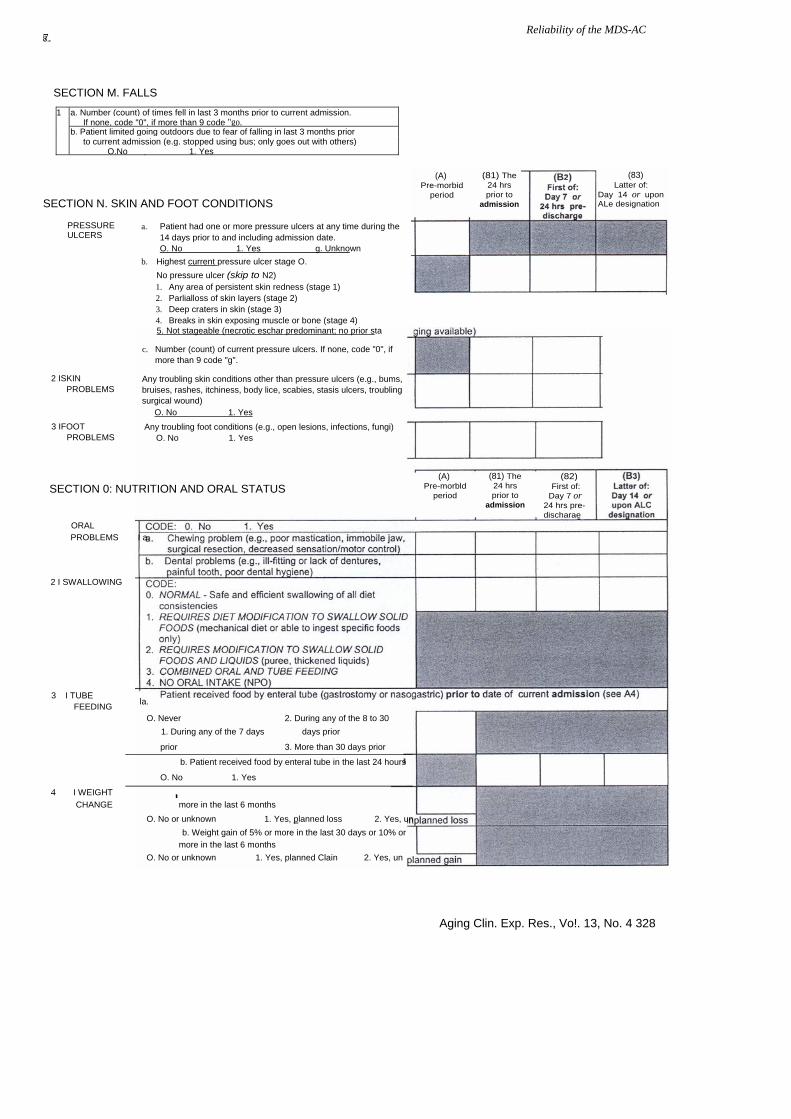
SECTION M. FALLS
1 a. Number (count) of times fell in last 3 months prior to current admission. If none, code "0", if more than 9 code "go.
b. Patient limited going outdoors due to fear of falling in last 3 months prior to current admission (e.g. stopped using bus; only goes out with others)
O.No 1. Yes
(83) Latter of:
(A) Pre-morbid
period Day 14 or upon ALe designation
PRESSURE ULCERS
SECTION N. SKIN AND FOOT CONDITIONS
(81) The 24 hrs prior to
admission
2 ISKIN PROBLEMS
3 IFOOT PROBLEMS
a. Patient had one or more pressure ulcers at any time during the 14 days prior to and including admission date.
O. No 1. Yes g. Unknown b. Highest current pressure ulcer stage O.
No pressure ulcer (skip to N2) 1. Any area of persistent skin redness (stage 1) 2. Parlialloss of skin layers (stage 2) 3. Deep craters in skin (stage 3) 4. Breaks in skin exposing muscle or bone (stage 4) 5. Not stageable (necrotic eschar predominant; no prior sta
c. Number (count) of current pressure ulcers. If none, code "0", if more than 9 code "g".
Any troubling skin conditions other than pressure ulcers (e.g., bums, bruises, rashes, itchiness, body lice, scabies, stasis ulcers, troubling surgical wound) O. No 1. Yes Any troubling foot conditions (e.g., open lesions, infections, fungi)
O. No 1. Yes
(A) Pre-morbld
period
(82) First of:
Day 7 or 24 hrs pre-discharae
SECTION 0: NUTRITION AND ORAL STATUS (81) The 24 hrs prior to
admission
ORAL PROBLEMS I a.
2 I SWALLOWING
3 I TUBE FEEDING la. O. Never 2. During any of the 8 to 30 1. During any of the 7 days days prior
prior 3. More than 30 days prior
b. Patient received food by enteral tube in the last 24 hours
O. No 1. Yes
4 I WEIGHT I CHANGE more in the last 6 months O. No or unknown 1. Yes, planned loss 2. Yes, un b. Weight gain of 5% or more in the last 30 days or 10% or more in the last 6 months O. No or unknown 1. Yes, planned Clain 2. Yes, un
Aging Clin. Exp. Res., Vo!. 13, No. 4 328

G.I. Ca~penter, G.F. Teare, K. Steel, et af.
9. 10.
NB: COMPLETE INFORMA nON ON THIS PAGE BY EARLIEST OF: DAY 7 or LAST 24 hrs PRIOR TO DISCHARGE. If DISCHARGE is LATER THAN DAY 7, update this page with any new information obtained between Day 7 assessment and discharge date.
SECTION P. DATE OF DISCHARGE 1 I DATE OF DISCHARGE
DODO-DO-DD YEAR MONTH DAY SECTION Q. RESOURCES FOR DISCHARGE 1 LIVING A. CODE for permanent living arrangement prior to ARRANGE- admission MENT B. CODE for permanent arrangement expected at
discharge C. CODE for initial arrangement expected at discharge if
different than Q1 B - otherwise leave blank C A B a. Type of residence p~~:. ~:~~. JI~~~.
1. Private home/apartment 2. Rented Room 1. Board and care/assisted
living/group home 2. Homeless (with or without
shelter) 3. Continuing/Long Term Care
facility 4. Hospice 5. Other
Specify 8. Unknown 9. Deceased
2 AVAILABLE SOCIAL SUPPORTS (Family or close friends)
3
INFORMAL CARE-GIVER STATUS
4 COMPLI-ANCE/ ADHER-ENCE with MEDI-CATIONS
b. Live(d) with
1. Alone 2. Spouse only 3. Spouse and other(s) 4. Child (not spouse) 5. Other relative{s) (not spouse
or children) 6. Friends 7. Group setting 8.Other Specify. 9. Unknown CODE: 0. No 1. Possibly yes 2.
Definitely yes Presence of one or more family members (or close friends) who are willing and able to provide support after discharge
a. Emotional support
b. Intemnittent physical support with ADLs or IADLs-less than daily
c. Intemnittent physical support with DLs or IADLs-<laily A
b. Full time physical support (as ded) with ADLs or IADLs nee
b. All or most of necessary transportation
CODE: . No 1. Yes 0 a. Family (or close friend) overwhelmed by
patient's illness b. Family relationship{s) require unusual
amounts of staff time Compliance with medications prescribed by a physician during the 30 days prior to the destabilization or acute event that led to this admission 0. Always compliant 1 . Compliant 80% of time or more 2. Compliant less than 80 % of time (including did not
purchase prescribed medicines) 3. NO MEDICINES PRESCRIBED for that Deriod
329 Aging Clin. Exp. Res., Vol. 13, No. 4
SECTION R. DIAGNOSES AT DISCHARGE
1. List diagnoses established during or ICD 9 code (if available) responsible for this hospitalization
a. 0000.00 b. 0000.00
0000.00 c
0000.00 d
0000.00 e.
0000.00 f.
SECTION S: REFERRALS AND SERVICES
1 REFERRALS (A) Therapy referrals and services received during & SERVICES the current hospital stay. CHECK (-J) all that
RECEIVED apply.
(B) Patient will receive assessment or service after discharge (i.e. therapy assessment or service
has been ordered). CHECK {-J)all that aoolv.
lA,} IA2} lA,} (Bl Referral Assesse
dTherapy Post
to by Inrovider nrovider rvovided
Discharge
Speech-language a. a. a. a. pathology and audiology
Occupational therapy b. b. b. b.
Physical therapy c c. c c.
Respiratory therapy d. d. d. d.
Psychological therapy e. e. e. e. (any licensed mental health professional) Geriatric service f. f. f. f.
SECTION T. PREVENTIVE HEALTH ISSUES 1 IADDICTIONS I 0. No 1. Yes
a. In the last 3 months prior to current admission, patient felt the need or was told by others to cut down on drinking, or others were concerned with patient's drinking
b. In the last 3 months prior to current admission, patient had to have a drink first thing in the morning to steady nerves (i.e., an "eye opener") or has been in trouble because of drinking
b. Smoked or chewed tobacco daily in month prior to admission
CHECK (-J) all that apply
No pneumovax in last 5 years
2 IOTHER ISSUES NEEDING FOLLOW-UP
a.
If female, no mammogram in past 2 years b.
ACKNOWLEDGEMENTS K. Steel is supported in part by grants from the John A Hartford
Foundation, the Elizabeth and Stephen Bechtel Jr. Foundation, the Grotta Foundation, the Jeanne and Julian Silverberg Endowment Fund, and by the Hunterdon Health Fund as the UMDNJ Endowed Professor of Geriatrics at the New Jersey Medical School.
J.P. Hirdes and G.F. Teare were supported in this work by grants from the Providence Centre Foundation, and the Population Health Fund, Health Canada.
The work was completed with the support of the medical and nursing staff of the following hospitals: Canada: Centenary Health Centre, Scarborough, St. Joseph's Health
Centre, London Ontario; Sunnybrook and Women's College Health Sciences Centre, North York Ontario; the Toronto Hospital, Toronto; Walter Mackenzie Health Sciences Centre, Edmonton, Alberta.
Norway: Ulleval, Aker, Lovisenberg and Diakonhjemmet Hospitals, Oslo; Vest Agder and Ostfold Sentral Regional Hospitals. The Kent and Canterbury Hospital, Canterbury, Kent. Rhode Island Hospital, Providence, Rhode Island; Hackensack University Medical Center and UMDNJ, the New
Jersey Medical School.
REFERENCES 1. Young J., Robinson J., Dickinson E.: Rehabilitation for
older people: At risk in the new NHS. BMJ 316: 1108-1109, 1998.
2. Royal College of Physicians, British Geriatrics Society: Stan-dardised assessment scales for elderly people. Royal College of Physicians of London and the British Geriatrics Society, London, 1992.
3. Sletvold 0., Tilvis R., Jonsson A, Schroll M., Snoedal J., En-gedal K., Schultz-Larsen K., Gustafson Y: Geriatric Work-up in Nordic Countries: The Nordic approach to comprehensive geriatric assessment. Dan. Med. Bull. 43: 350-359, 1996.
4. National Institutes of Health Consensus Development Con-ference Statement: geriatric assessment methods for clinical de-cision-making. J. Am. Geriatr. Soc. 36: 342-347,1988.
5. US VA-NIA-RWJ: Conse.nsus Panel. JAm. Geriatr. Soc. 39: 1S-59S, 1991.
6. Rubenstein L.Z., Wieland D., Bernabei R. (Guest Eds.): Special Issue on Geriatric Assessment. Aging Clin. Exp. Res. 7: 157-260, 1995.
Reliability of the MDS-AC
7. Kellog International Taskforce. Dan. Med. Bull. Special Suppl. 7, 1989.
8. Wieland D., Rubenstein L.: What do we know about patient targeting in geriatric evaluation and management programmes. Aging Clin. Exp. Res. 8: 297-310, 1996.
9. Morris J.N., Hawes C, Fries B.E., Phillips e.D., Mor V., Katz S., Murphy K., Drugovich M.L., Friedlob AS.: Designing the National Resident Assessment Instrument. Gerontologist 30: 293-307,1990.
10. Morris J.N., Fries BE., Steel K., Ikegami N., Bernabei R., Car-penter G.!., Gilgen R., Hirdes J.P., Topinkova E.: Compre-hensive clinical assessment in community setting - Applicability of the MDS-He. J. Am. Geriatr. Soc. 45: 1017-1024, 1997.
11. Hirdes J., Perez E., Curtin-Telegdi N., Prendergast P., Morris J.N., Ikegami N., Fries B.E., Phillips e.: The RAI-MH: Training Manual and Resource Guide Version 1.0. Queen's Printer for Ontario, Toronto, 1999.
12. Shrout P., Fleiss J.: Intraclass correlations: uses in assessing rater reliability. Psych. Bull. 86: 420-428, 1979.
13. Morris J.N., Fries B.E., Morris SA: Scaling ADL's within the MDS. J. Gerontol. 54: M546-M553, 1999.
14. Morris J.N., Fries BE, Mehr DR, Hawes e., Phillips e., Mor V., Lipsitz L.A: The MDS Cognitive Performance Scale. J. Gerontol. 49: 174-182, 1994.
15. Guggenmoos-Holzmann l.: How reliable are chance-corrected measures of agreement? Stat. Med. 12: 2191-2205,1993.
16. Feinstein A, Cicchetti D.: High agreement but low kappa: !. The problems of two paradoxes. J Clin. Epidemiol. 43: 543-549, 1990.
17. Thompson W., WaIter S.: A reappraisal of the kappa coefficient. J. Clin. Epidemiol. 41: 949-958,1988.
UK~ USA:
18. Covinsky K.E., Palm er R.M., Pine Z.M., WaIter L.e., Chren M-M.: Functional status before hospitalization in acutely ill older adults: validity and clinical importance of retrospective reports. J. Am. Geriatr. Soc. 48: 164-169,2000.
19. Stuck AE., Siu AL., Wieland G.D., Adams J., Rubenstein L.Z.: Comprehensive geriatric assessment: a meta-analysis of controlled trials. Lancet 342: 1032-1036, 1993.
20. Landi F., Gambassi G., Pola R., Tabaccanti S., Cavinato T., Carbon in P.U., Bernabei R.: Impact of integrated home care services on hospital use. JAm. Geriatr. Soc. 47: 1430-1434, 1999.
Aging Clin. Exp. Res., Vo!. 13, No. 4 330