A Multistate Examination of Partnership Activity Among Local Public Health Systems Using the...
10
A Multistate Examination of Partnership Activity Among Local Public Health Systems Using the National Public Health Performance Standards Priscilla A. Barnes, MPH, PhD, MCHES; Amy B. Curtis, PhD, MPH; Laura Hall-Downey, DrPH, MS; Ramal Moonesinghe, PhD T his study examines whether partnership-related measures in the second version of the National Public Health Performance Standards (NPHPS) are useful in evaluating level of activity as well as identifying latent constructs that exist among local public health systems (LPHSs). In a sample of 110 LPHSs, descriptive analysis was conducted to determine frequency and percentage of 18 partnership-related NPHPS measures. Principal components factor analysis was conducted to identify unobserved characteristics that promote effective partnerships among LPHSs. Results revealed that 13 of the 18 measures were most frequently reported at the minimal-moderate level (conducted 1%-49% of the time). Coordination of personal health and social services to optimize access (74.6%) was the most frequently reported measure at minimal-moderate levels. Optimal levels (conducted >75% of the time) were reported most frequently in 2 activities: participation in emergency preparedness coalitions and local health departments ensuring service provision by working with state health departments (67% and 61% of respondents, respectively) and the least optimally reported activity was review partnership effectiveness (4% of respondents). Factor analysis revealed categories of partnership-related measures in 4 domains: resources and activities contributing to relationship building, evaluating community leadership activities, research, and state and local linkages to support public health activities. System-oriented public health assessments may have questions that serve as proxy measures to examine levels of interorganizational partnerships. Several measures from the NPHPS were useful in establishing a national baseline of minimal J Public Health Management Practice, 2012, 18(5), E14–E23 Copyright C 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins and optimal activity levels as well as identifying factors to enhance the delivery of the 10 essential public health services among organizations and individuals in public health systems. KEY WORDS: evaluation, local public health systems, partnerships, performance standards In the 1988 and 2002, Institute of Medicine’s The Future of the Public’s Health reports, the use of interor- ganizational partnerships was noted as an effective approach in expanding coordination of public health services. 1,2 These partnerships also play an important role in enhancing the organizational capacity of state and local public health departments and improving the overall performance of public health systems. 3-6 Several studies have examined collaborative activities occurring among public health departments and their community partners. 7-11 However, few national studies look at the levels of performance related to interorga- nizational partnerships as reported by representatives Author Affiliations: Department of Applied Health Science, Indiana University School of Public Health-Bloomington (Dr Barnes); Interdisciplinary Health Sciences, College of Health and Human Services, Western Michigan University, Kalamazoo (Dr Curtis); School of Human Sciences, Mississippi State University (Dr Hall-Downey); and Office of Minority Health and Health Disparities, Office of the Director, Centers for Disease Control and Prevention, Atlanta, Georgia (Dr Moonesinghe). Support for this research was provided by University of Kentucky Center for Public Health Systems and Services Research. The findings and conclusions in this article are those of the author(s) and do not necessarily represent the official position of the Centers for Disease Control and Prevention. Disclosure: The authors declare no conflicts of interest. Correspondence: Priscilla A. Barnes, MPH, PhD, MCHES, 1025 E 7th St, HPER 116, Bloomington, IN 47405 ([email protected]). DOI: 10.1097/PHH.0b013e31822ca424 Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. E14
Transcript of A Multistate Examination of Partnership Activity Among Local Public Health Systems Using the...
A Multistate Examination of Partnership ActivityAmong Local Public Health Systems Using theNational Public Health Performance Standards
Priscilla A. Barnes, MPH, PhD, MCHES; Amy B. Curtis, PhD, MPH; Laura Hall-Downey, DrPH, MS;Ramal Moonesinghe, PhD� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �
This study examines whether partnership-related measures
in the second version of the National Public Health
Performance Standards (NPHPS) are useful in evaluating
level of activity as well as identifying latent constructs that exist
among local public health systems (LPHSs). In a sample of 110
LPHSs, descriptive analysis was conducted to determine
frequency and percentage of 18 partnership-related NPHPS
measures. Principal components factor analysis was conducted
to identify unobserved characteristics that promote effective
partnerships among LPHSs. Results revealed that 13 of the 18
measures were most frequently reported at the
minimal-moderate level (conducted 1%-49% of the time).
Coordination of personal health and social services to optimize
access (74.6%) was the most frequently reported measure at
minimal-moderate levels. Optimal levels (conducted >75% of
the time) were reported most frequently in 2 activities:
participation in emergency preparedness coalitions and local
health departments ensuring service provision by working with
state health departments (67% and 61% of respondents,
respectively) and the least optimally reported activity was review
partnership effectiveness (4% of respondents). Factor analysis
revealed categories of partnership-related measures in 4
domains: resources and activities contributing to relationship
building, evaluating community leadership activities, research,
and state and local linkages to support public health activities.
System-oriented public health assessments may have questions
that serve as proxy measures to examine levels of
interorganizational partnerships. Several measures from the
NPHPS were useful in establishing a national baseline of minimal
J Public Health Management Practice, 2012, 18(5), E14–E23Copyright C© 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins
and optimal activity levels as well as identifying factors to
enhance the delivery of the 10 essential public health services
among organizations and individuals in public health systems.
KEY WORDS: evaluation, local public health systems,partnerships, performance standards
In the 1988 and 2002, Institute of Medicine’s TheFuture of the Public’s Health reports, the use of interor-ganizational partnerships was noted as an effectiveapproach in expanding coordination of public healthservices.1,2 These partnerships also play an importantrole in enhancing the organizational capacity of stateand local public health departments and improvingthe overall performance of public health systems.3-6
Several studies have examined collaborative activitiesoccurring among public health departments and theircommunity partners.7-11 However, few national studieslook at the levels of performance related to interorga-nizational partnerships as reported by representatives
Author Affiliations: Department of Applied Health Science, IndianaUniversity School of Public Health-Bloomington (Dr Barnes); InterdisciplinaryHealth Sciences, College of Health and Human Services, Western MichiganUniversity, Kalamazoo (Dr Curtis); School of Human Sciences, Mississippi StateUniversity (Dr Hall-Downey); and Office of Minority Health and Health Disparities,Office of the Director, Centers for Disease Control and Prevention, Atlanta,Georgia (Dr Moonesinghe).
Support for this research was provided by University of Kentucky Center forPublic Health Systems and Services Research.
The findings and conclusions in this article are those of the author(s) and donot necessarily represent the official position of the Centers for Disease Controland Prevention.
Disclosure: The authors declare no conflicts of interest.
Correspondence: Priscilla A. Barnes, MPH, PhD, MCHES, 1025 E 7th St,HPER 116, Bloomington, IN 47405 ([email protected]).
DOI: 10.1097/PHH.0b013e31822ca424
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
E14

Multistate Examination of Partnership Among LPHSs Using the NPHPS ❘ E15
from multiple organizations and individual volunteersin public health systems.4,5 Therefore, the purpose ofthis study is to examine observed and latent measuresof interorganizational partnerships as reported by pub-lic health systems in local communities.
Public health systems are intricate networks madeof sundry horizontal and vertical relationships be-tween governmental or nongovernmental organiza-tions at federal, state, and local levels.3,12 These orga-nizations include, but are not limited to public healthdepartments, public safety agencies, health care agen-cies, community-based and faith-based organizations,businesses, media, and economic and philanthropicorganizations.1,2 Individuals, elected officials, grass-roots and community leaders, and volunteers also arepart of this system. In general, public health systemsare responsible for improving the coordination and de-livery of the 10 essential public health services (hereinreferred to as the essential services) in states, counties,cities, regions, and districts.1,2,13 These services act asa guiding framework for public health practitioners“to prevent the spread of diseases, promote healthybehaviors, protect the public against environmentalhazards, and assure quality and accessibility of healthservices.”14
Effective delivery of the essential services requiresupport from numerous organizations and commu-nity leaders, which expands beyond the traditionalparadigm of governmental public health departmentsbeing solely responsible for improving populationhealth.15,16 Therefore, public health systems may use in-terorganizational partnerships to increase performanceof these services.6 National agencies such as Centersfor Disease Control and Prevention (CDC), the Associ-ation of State and Territorial Officials (ASTHO), and theNational Association of County and City Health Offi-cials (NACCHO) recommend that the formation of in-terorganizational partnerships ought to occur to lever-age human, material, and organizational resources.17-19
These partnerships provide a shared space for organi-zations and individual volunteers to engage in a par-ticipatory process to coordinate a collective responseto natural and man-made disasters, provide primaryand secondary prevention services, and develop andenforce public health policies.20-23 Interorganizationalpartnerships exist in informal and formal structures(eg, coalitions, task forces, and alliances), serve differ-ent functions, and are at various stages of developmentand sustainability.6
Because partnerships transpire in different ways, re-searchers are critically assessing factors contributingto the effective operation of public health systems.7,24
Several assessments have been developed to exam-ine various facets of interorganizational partnerships.The Program to Analyze, Record, and Track Networks
to Enhance Relationships (PARTNER) tool evaluatesconnectivity of existing relationships between localhealth departments and their community partners.25
Reciprocity, trust, membership, and organizationalvalue to collaborate are some of the elements thatinfluence the effectiveness of these partnerships inachieving a specific outcome.25 The Partnership Syn-ergy assessment considers the presence of 5 determi-nants (resources, partner characteristics, relationshipsamong partners, partnership characteristics, and exter-nal environment) contributing to the function and op-eration of collaboration.26 Another tool, the NationalPublic Health Performance Standards (NPHPS), con-tains questions that can serve as proxy measures inexamining interorganizational partnerships occurringin public health systems. In general, the NPHPS as-sesses baseline and ongoing improvements made byboth governmental and nongovernmental organiza-tions in building the public health infrastructure.27 De-veloped in 1998, several national public health agenciesconstructed 3 assessments (a state, local, and a localboard of health tool) to identify areas of improvementin the delivery and quality of 10 essential services.28,29
One of the guiding concepts in the NPHPS develop-ment is that performance is not the sole responsibil-ity of governmental public health agencies, but shouldbe based on the collective contributions of both gov-ernmental and nongovernmental organizations.27 EachNPHPS assessment comprises performance standardsthat serve as benchmarks in activities public health sys-tems should strive to obtain. As a result of the assess-ment findings, public health systems should define ar-eas where additional human or financial resources areneeded or improve coordination or distribution of ser-vices. Standards are developed using optimal measures(greater than 75% of the activity is met) and shouldnot be viewed as an “average” or “below average”rating since varying capacities exist across all pub-lic health systems.30 Public health systems completethe NPHPS assessment with representatives from or-ganizations and individual volunteers by discussingand deciding by consensus the appropriate rating re-flecting their performance in delivering the essentialservices.30
In the local NPHPS assessment, questions relatedto interorganizational partnerships span across severalessential services.27 The fourth essential service, mo-bilizing community partnerships, specifically consid-ers processes used to form a constituency of organiza-tions and individuals interested in addressing publichealth issues.27,30 The third, fifth, seventh, eighth, ninth,and tenth essential services include at least one part-nership measure that assesses design, implementation,and coordination and of programs and services basedon the needs of the population within the community,
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

E16 ❘ Journal of Public Health Management and Practice
leadership, building communication capacity, develop-ment and evaluation of strategic plans, and partnershipassessments to improve community outcomes.27,30
Considering that a goal of the local NPHPS is tobuild local public health systems’ (LPHSs) capacityto acquire resources, identifying the current status ofperformance in these partnership measures is impor-tant to further integrate efforts in working as a net-work. Several research studies report LPHSs’ capac-ity in mobilizing community partnerships at moderateto significant levels of performance.4,5,31 These studies,however, do not describe performance levels in specificpartnership measures within the fourth and other es-sential services. In addition, latent constructs may existin the NPHPS that can further determine if there is apattern in building interorganizational partnerships inLPHSs. By examining partnerships in this manner, pub-lic health practitioners and researchers would be able tofurther consider critical elements that are necessary inimproving the manner in which these systems operate.
● Methods
Population and study design
Descriptive analysis was conducted on 18 partnership-related measures (Table 1) from the second version ofthe NPHPS local assessment. The dataset included rawscores reported by LPHSs voluntarily completing theassessment from January 2008 to September 2009 andare filed in an electronic system at the Public HealthFoundation (Washington, District of Columbia). Thedataset includes more than 100 (n = 116) LPHSs from21 states. For the purposes of assessment administra-tion, LPHSs’ jurisdictions were on the basis of the localhealth department area of service (eg, county, city, dis-trict, and regional). Respondents’ self-assessment rat-ings refer to the public health system, not the individuallocal agencies. The CDC granted permission to use theNPHPS dataset and the Western Michigan universityinstitutional review board approved the research pro-cedures.
NPHPS partnership measures
In the NPHPS local assessment, 18 questions servedas indicators of interorganizational partnerships.Questions were selected because specific aspects ofpartnerships such as the formation of partnershipsor a description of the process used by organizationsand individuals in “working together” in developingplans or procedures, “coordinating services,” or “build-ing and evaluating relationships” within LPHSs weremeasured. Seven questions related to the mobilization
of community partnerships in identifying and solvingproblems (essential service #4). Eight questions are in 6other essential services: inform, educate, and empowerpeople about health issues (#3); develop policy andplans that support individual and community healthefforts (#5); link people to needed personal health ser-vices and assure the provision of health care (#7); en-sure a competent public health and personal health careworkforce (#8); evaluate effectiveness, accessibility, andquality of personal and population-based health ser-vices (#9); and research new insights and innovativesolutions to health problems (#10) (Table 1). Each mea-sure was rated on a 5-category scale and LPHSs re-ported their level of activity as: no activity (0% of thetime), minimal (1%-24% of the time), moderate (25%-49% of the time), significant (50%-74% of the time),or optimal (≥75% of the time). Minimal and moder-ate activity was combined into one category for someanalyses.
Data analysis
We conducted descriptive analyses using SPSS ver-sion 17. Six of the 116 LPHSs were missing demo-graphic information and were not included in analysis.Following descriptive analysis, exploratory factor anal-ysis was conducted to examine correlation or a linear re-lationship among a set of observed measures to identifyunobserved variables (factors). For this study, underly-ing dimensions of partnership activity were examinedusing the 18 measures of interorganizational partner-ships. Levels of activity—no activity, minimal, moder-ate, significant, and optimal—were assigned scores of0, 1, 2, 3, and 4, respectively. Factor procedures in SAS9.2 (Cary, NC) were used to conduct the principal com-ponent analysis with Varimax rotation. The observedmeasures maximally correlated with each factor (highfactor loadings), but minimally correlated with otherunobserved measures, were grouped together to rep-resent a factor. Measures with factor loadings greaterthan or equal to 0.6 were chosen for interpretation. Thenames of the extracted factors were based on their highloading measures. Medians were calculated to deter-mine which factors were conducted most frequentlyamong LPHSs in the sample.
● Results
Overall, 110 LPHSs, approximately 55% in 2008 and45% in 2009, completed the second version of theNPHPS local assessment. A median of 2 LPHSs (rang-ing from 1 to 23) completed the NPHPS in 21 states.More than 45% of the LPHSs in 2 states (SouthCarolina [n = 5/8, 62.5%] and Virginia [n = 16/35,
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Multistate Examination of Partnership Among LPHSs Using the NPHPS ❘ E17
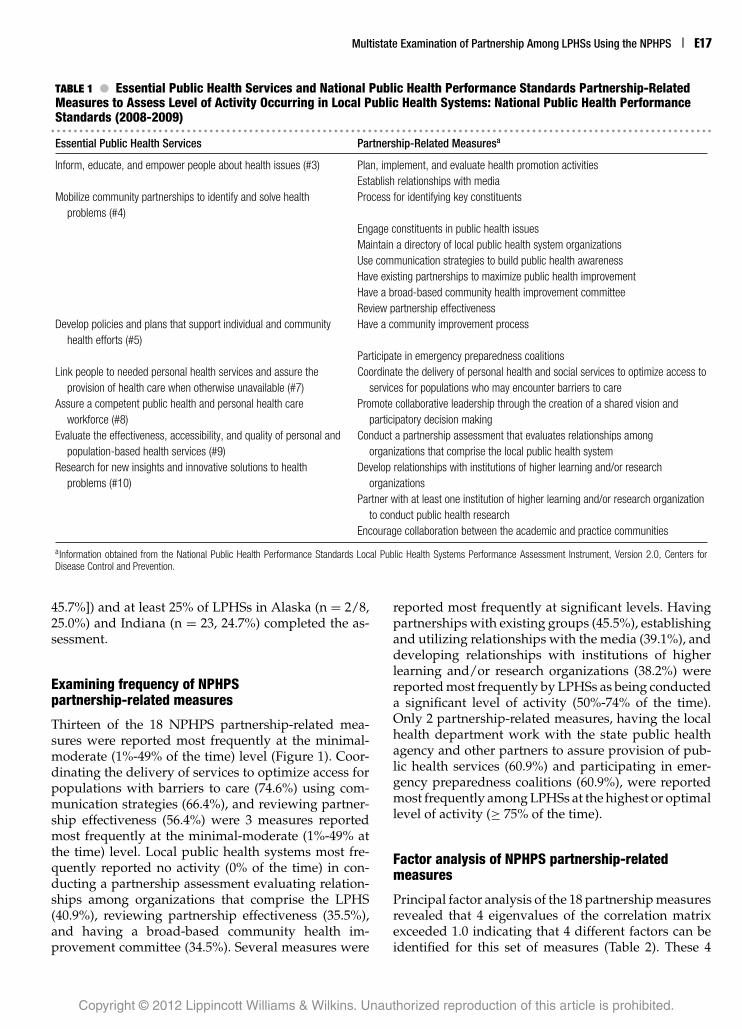
TABLE 1 ● Essential Public Health Services and National Public Health Performance Standards Partnership-RelatedMeasures to Assess Level of Activity Occurring in Local Public Health Systems: National Public Health PerformanceStandards (2008-2009)� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �
Essential Public Health Services Partnership-Related Measuresa
Inform, educate, and empower people about health issues (#3) Plan, implement, and evaluate health promotion activitiesEstablish relationships with media
Mobilize community partnerships to identify and solve healthproblems (#4)
Process for identifying key constituents
Engage constituents in public health issuesMaintain a directory of local public health system organizationsUse communication strategies to build public health awarenessHave existing partnerships to maximize public health improvementHave a broad-based community health improvement committeeReview partnership effectiveness
Develop policies and plans that support individual and communityhealth efforts (#5)
Have a community improvement process
Participate in emergency preparedness coalitionsLink people to needed personal health services and assure the
provision of health care when otherwise unavailable (#7)Coordinate the delivery of personal health and social services to optimize access to
services for populations who may encounter barriers to careAssure a competent public health and personal health care
workforce (#8)Promote collaborative leadership through the creation of a shared vision and
participatory decision makingEvaluate the effectiveness, accessibility, and quality of personal and
population-based health services (#9)Conduct a partnership assessment that evaluates relationships among
organizations that comprise the local public health systemResearch for new insights and innovative solutions to health
problems (#10)Develop relationships with institutions of higher learning and/or research
organizationsPartner with at least one institution of higher learning and/or research organization
to conduct public health researchEncourage collaboration between the academic and practice communities
aInformation obtained from the National Public Health Performance Standards Local Public Health Systems Performance Assessment Instrument, Version 2.0, Centers forDisease Control and Prevention.
45.7%]) and at least 25% of LPHSs in Alaska (n = 2/8,25.0%) and Indiana (n = 23, 24.7%) completed the as-sessment.
Examining frequency of NPHPSpartnership-related measures
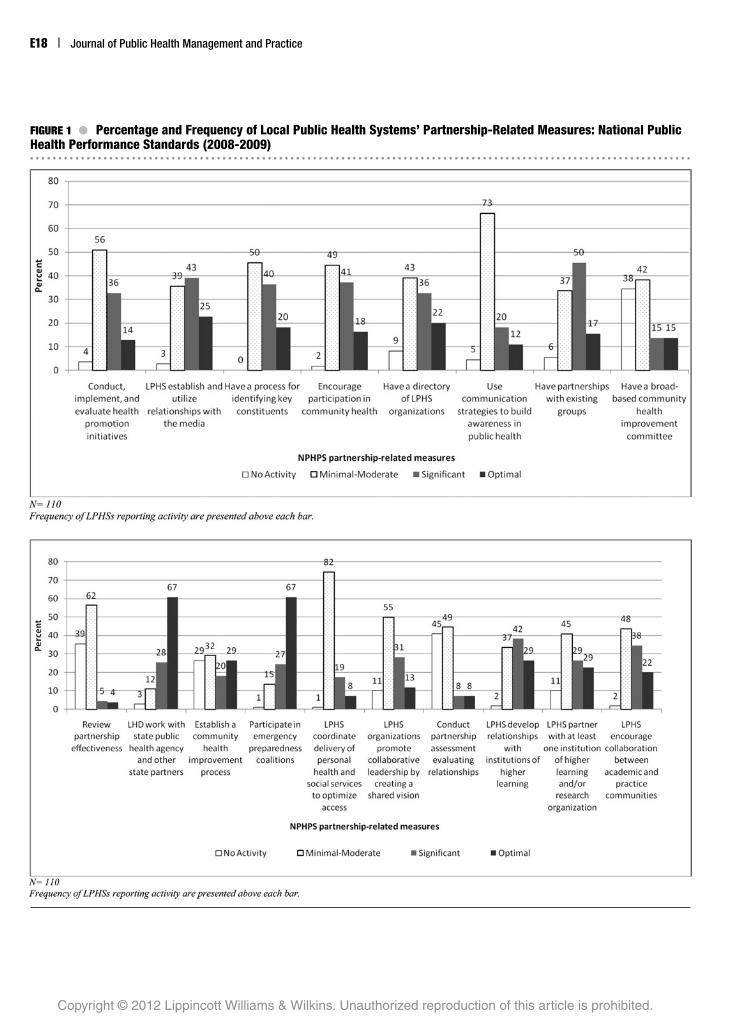
Thirteen of the 18 NPHPS partnership-related mea-sures were reported most frequently at the minimal-moderate (1%-49% of the time) level (Figure 1). Coor-dinating the delivery of services to optimize access forpopulations with barriers to care (74.6%) using com-munication strategies (66.4%), and reviewing partner-ship effectiveness (56.4%) were 3 measures reportedmost frequently at the minimal-moderate (1%-49% atthe time) level. Local public health systems most fre-quently reported no activity (0% of the time) in con-ducting a partnership assessment evaluating relation-ships among organizations that comprise the LPHS(40.9%), reviewing partnership effectiveness (35.5%),and having a broad-based community health im-provement committee (34.5%). Several measures were
reported most frequently at significant levels. Havingpartnerships with existing groups (45.5%), establishingand utilizing relationships with the media (39.1%), anddeveloping relationships with institutions of higherlearning and/or research organizations (38.2%) werereported most frequently by LPHSs as being conducteda significant level of activity (50%-74% of the time).Only 2 partnership-related measures, having the localhealth department work with the state public healthagency and other partners to assure provision of pub-lic health services (60.9%) and participating in emer-gency preparedness coalitions (60.9%), were reportedmost frequently among LPHSs at the highest or optimallevel of activity (≥ 75% of the time).
Factor analysis of NPHPS partnership-relatedmeasures
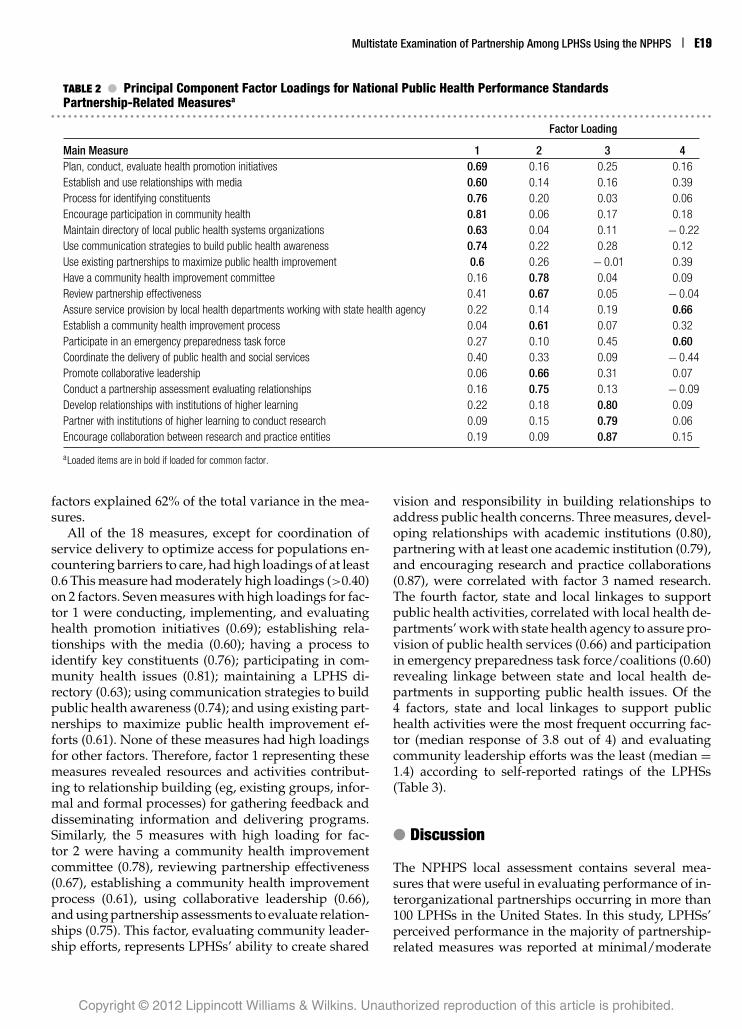
Principal factor analysis of the 18 partnership measuresrevealed that 4 eigenvalues of the correlation matrixexceeded 1.0 indicating that 4 different factors can beidentified for this set of measures (Table 2). These 4
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
E18 ❘ Journal of Public Health Management and Practice
FIGURE 1 ● Percentage and Frequency of Local Public Health Systems’ Partnership-Related Measures: National PublicHealth Performance Standards (2008-2009)� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Multistate Examination of Partnership Among LPHSs Using the NPHPS ❘ E19
TABLE 2 ● Principal Component Factor Loadings for National Public Health Performance StandardsPartnership-Related Measuresa
� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �
Factor Loading
Main Measure 1 2 3 4Plan, conduct, evaluate health promotion initiatives 0.69 0.16 0.25 0.16Establish and use relationships with media 0.60 0.14 0.16 0.39Process for identifying constituents 0.76 0.20 0.03 0.06Encourage participation in community health 0.81 0.06 0.17 0.18Maintain directory of local public health systems organizations 0.63 0.04 0.11 − 0.22Use communication strategies to build public health awareness 0.74 0.22 0.28 0.12Use existing partnerships to maximize public health improvement 0.6 0.26 − 0.01 0.39Have a community health improvement committee 0.16 0.78 0.04 0.09Review partnership effectiveness 0.41 0.67 0.05 − 0.04Assure service provision by local health departments working with state health agency 0.22 0.14 0.19 0.66Establish a community health improvement process 0.04 0.61 0.07 0.32Participate in an emergency preparedness task force 0.27 0.10 0.45 0.60Coordinate the delivery of public health and social services 0.40 0.33 0.09 − 0.44Promote collaborative leadership 0.06 0.66 0.31 0.07Conduct a partnership assessment evaluating relationships 0.16 0.75 0.13 − 0.09Develop relationships with institutions of higher learning 0.22 0.18 0.80 0.09Partner with institutions of higher learning to conduct research 0.09 0.15 0.79 0.06Encourage collaboration between research and practice entities 0.19 0.09 0.87 0.15
aLoaded items are in bold if loaded for common factor.
factors explained 62% of the total variance in the mea-sures.
All of the 18 measures, except for coordination ofservice delivery to optimize access for populations en-countering barriers to care, had high loadings of at least0.6 This measure had moderately high loadings (>0.40)on 2 factors. Seven measures with high loadings for fac-tor 1 were conducting, implementing, and evaluatinghealth promotion initiatives (0.69); establishing rela-tionships with the media (0.60); having a process toidentify key constituents (0.76); participating in com-munity health issues (0.81); maintaining a LPHS di-rectory (0.63); using communication strategies to buildpublic health awareness (0.74); and using existing part-nerships to maximize public health improvement ef-forts (0.61). None of these measures had high loadingsfor other factors. Therefore, factor 1 representing thesemeasures revealed resources and activities contribut-ing to relationship building (eg, existing groups, infor-mal and formal processes) for gathering feedback anddisseminating information and delivering programs.Similarly, the 5 measures with high loading for fac-tor 2 were having a community health improvementcommittee (0.78), reviewing partnership effectiveness(0.67), establishing a community health improvementprocess (0.61), using collaborative leadership (0.66),and using partnership assessments to evaluate relation-ships (0.75). This factor, evaluating community leader-ship efforts, represents LPHSs’ ability to create shared
vision and responsibility in building relationships toaddress public health concerns. Three measures, devel-oping relationships with academic institutions (0.80),partnering with at least one academic institution (0.79),and encouraging research and practice collaborations(0.87), were correlated with factor 3 named research.The fourth factor, state and local linkages to supportpublic health activities, correlated with local health de-partments’ work with state health agency to assure pro-vision of public health services (0.66) and participationin emergency preparedness task force/coalitions (0.60)revealing linkage between state and local health de-partments in supporting public health issues. Of the4 factors, state and local linkages to support publichealth activities were the most frequent occurring fac-tor (median response of 3.8 out of 4) and evaluatingcommunity leadership efforts was the least (median =1.4) according to self-reported ratings of the LPHSs(Table 3).
● Discussion
The NPHPS local assessment contains several mea-sures that were useful in evaluating performance of in-terorganizational partnerships occurring in more than100 LPHSs in the United States. In this study, LPHSs’perceived performance in the majority of partnership-related measures was reported at minimal/moderate
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

E20 ❘ Journal of Public Health Management and Practice
TABLE 3 ● Total Score, Range, and Median of UnderlyingCharacteristics Revealed from Principal ComponentsFactor Loadings for National Public Health PerformanceStandards Partnership-Related Measures� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �
Factors Median
Resources and activities contributing to relationship building 2.5Evaluating community leadership efforts 1.4Research 2.6State and local linkages to support public health activities 3.8
activity. Participation in emergency preparedness coali-tions/task forces and local health departments work-ing with state health agencies to assure public healthservices were rated at optimal levels. Coordination ofpublic health and social services to optimize access,however, was rated at nonoptimal levels. Furthermore,factor analysis presented a different perspective in de-termining areas of partnership activity conducted bythese systems that were indirectly measured in theNPHPS.
One of the intended purposes of the NPHPS is to as-sess the strengths of organizations and individuals todeliver the 10 essential services. This study reveals theoverlapping function of assessing overall system per-formance and actually reviewing the effectiveness ofspecific partnerships as they occur in the system. Whenexamining partnerships outside the essential servicesframework, LPHSs’ perceived higher performance inthe formation, coordination, and implementation ofthese activities as opposed to the evaluation of theirown partnerships. This result suggests that there aredifferent approaches to and perspectives on evaluation(eg, process impact, outcome). The NPHPS is a usefulfirst step in assessing overall capacity of the system’sability to leverage resources,32,33 but other partnershipassessments are needed to evaluate process and out-come measures contributing to effectiveness related tospecific public health priorities. Also, improving effec-tiveness of system partnerships may profit by beingtied to national quality improvement efforts. Althoughthe motivations of this sample to complete the assess-ment are not known; increased use of the NPHPS isexpected because of the launch of national voluntaryaccreditation of public health departments.34
The NPHPS is one of the suggested assessmentsthat LPHSs may use to assess whether they are meet-ing accreditation standards. Several partnership stan-dards require local health departments to support orcatalyze broad-based participation among a diversegroup of organizations and individuals in the system.35
In the accreditation process, strong emphasis is alsoplaced on using community health planning tools, suchas the Mobilizing for Action through Planning and
Partnerships.35 Mobilizing for Action through Planningand Partnerships (NPHPS is one of the 4 assessmentsin the planning tool) can help LPHSs effectively formpartnerships to identify and prioritize public health is-sues in a strategic manner.36 Thus, agency-focused ac-creditation standards recognize the value and impor-tance of partnerships in strengthening the public healthinfrastructure.
This study revealed that LPHSs are performing atself-reported minimal-moderate levels in a majorityof partnership measures. The reasons for this level ofperformance are unknown. Previous studies indicatethat nonoptimal performance may be associated withfragmentation of services existing within the publichealth system.3,37,38 Results from this study suggest thatLPHSs may invest most of their time in respondingto public health issues and providing services ratherthan building system and community capacity to en-sure connectivity between organizations. Specifically,LPHSs reported the highest percentage of minimal-moderate levels in coordinating the delivery of per-sonal health and social services to optimize access tocare. Determining the mechanisms used by LPHSs tocoordinate health services is complex. Coordination isconsidered a form of partnership that involves organi-zations and individuals working together and sharingresources to achieve a goal.39 Being the unit of gov-ernment and mandated to ensure the public’s health,local health departments are viewed as the key coor-dinating entity of population-based services in localcommunities.15,40 One factor that influences coordina-tion is public health mandates.41,42 For example, manylocal health departments are responsible for inspectionof restaurants, daycares, and other facilities to ensureadequate operating procedures as mandated in theirstate or local regulations or Public Health Code.41,42
However, secondary prevention services may be coor-dinated through hospitals, community health centers,and community-based organizations. In certain locales,the local health departments may not be the primaryfacilitating entity.43,44 Therefore, identifying a central co-ordinating entity or “hub” for initiating and carryingout public health priorities may further improve theintegration of services.
Using the NPHPS proved helpful in establishing abaseline measure and identifying areas, which LPHSsare performing at optimal levels, as indicated in thisstudy in the development and administration of emer-gency preparedness coalitions. Increased attention toemergency preparedness is attributed to financial sup-port from federal and national organizations, whichhas been a major focus of national public health effortsto increase security following the events of Septem-ber 11, 2001.45-47 Funding has enabled local health de-partments to work with organizations to create and
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Multistate Examination of Partnership Among LPHSs Using the NPHPS ❘ E21
maintain emergency response plans, to develop profes-sional public health staff, and to enhance informationtechnology. Through federal cooperative agreements,more than 5 billion dollars has been allocated to publichealth departments in the United States to build thepublic health infrastructure from 2002 to 2007.48 Thisincreased attention to emergency preparedness has ex-panded the public’s perception of LPHSs’ role and hasbrought together organizations to improve system co-ordination in program-specific partnerships.
The factor analysis proved to be useful in reveal-ing additional characteristics that are not directlymeasured in the NPHPS. Partnerships between stateand local health departments are critical in establish-ing stronger communication and administration ofpopulation-based services. Local health departmentstypically serve as an intermediary for state health de-partments to provide financial support and techni-cal assistance for certain public health priorities.49,50
Several studies suggest that governing structure (in-dependently operated or decentralized as opposed tostate-operated or centralized) is an important factorthat influences relationships with state health depart-ments. In centralized public health systems, a less dis-tinct relationship may exist among governmental localagencies because they may operate as a subunit of thestate agency. Decentralized systems may have a moredistant relationship between state and local agenciesespecially in the event of state funding to the local com-munities are limited or not available.40 Further exam-ination of the different types of relationships betweenlocal and state health agencies related to interorganiza-tional partnerships is needed to fully understand effec-tive delivery of the essential services.
Use of factor analysis also revealed that evaluatingcommunity leadership is an area that may influence thedevelopment and sustainability of interorganizationalpartnerships. In this study, less than 10% of LPHSs re-ported activity in measuring partnership effectivenessat least 50% of the time. Given the economic challengesthat local health departments encounter, public healthofficials may not have sufficient financial resources tosupport additional analysis of system effectiveness.7
Local public health systems can form interdisciplinarynetworks that utilize formative and participatory ac-tion research methods to assess the impact of policy andprevention and intervention strategies. For example,the Public Health Practiced-Based Research Networks,funded by Robert Wood Johnson Foundation, arenetworks comprise public health agencies, academicinstitutions, and community-based organizations thatexecute research studies to build and inform evidence-based practice.51 These networks provide evidence forstrengthening the capacity of the public health infras-tructure and quality of service delivery.
This study suggests several implications for pub-lic health practice. For LPHSs interested in improv-ing coordination of the essential services, the NPHPSshould be considered as a potential tool to measure mo-bilization and ongoing activity of partnerships withinpublic health systems. A second implication is that na-tional and LPHS leaders need to increase attention incross-cutting partnerships such as community healthimprovement committees, especially given emergencypreparedness coalitions did not lead to optimal lev-els across all partnerships. Emergency preparednessis a programmatic area and does not necessarily in-clude all aspects of LPHSs. It is entirely possible thatwhile emergency preparedness coalitions are strong be-cause of the influx of federal dollars, surveillance, en-forcement, maternal and child health, social services,or other partnerships that LPHSs should establish arelacking. Therefore, participation in emergency pre-paredness coalitions should not serve as the primarymeasure for whether or not “standards”—in general—are being met. Future studies should explore character-istics needed to develop stronger interorganizationalpartnerships outside of emergency preparedness. Last,accreditation of local health departments is one wayof measuring organizations’ capacity and readiness tochange, particularly if these “units of government”serve as the liaison between state and national orga-nizations as well as community partners in their ju-risdiction. Organizations such as the CDC, NACCHO,ASTHO, and other public health organizations work-ing may provide technical assistance to LPHSs to im-prove levels of activity in partnerships.
This is one of the first studies to examine partnershipactivities using the NPHPS and provides public healthpractitioners with a baseline assessment of strengthsand improvements as they continue to work towardbuilding effective systemic partnerships. The NPHPSpartnership questions serve as proxy measures provid-ing summative group ratings from governmental andnongovernmental organizations and individual volun-teers. Questions presented in the local assessment ed-ucate many organizations and individuals about theessential services as well as the areas of strengths andweaknesses within the system. This study adds to thepublic health systems and services research literatureby reemphasizing the importance of building elements,such as established linkages between state and localgovernmental entities and community leadership, informing and sustaining systemic partnerships.
Several limitations are noted in this study. First, be-cause local health systems self-select to participate inthe NPHPS, the sample may not be representative ofthe population. Next, because data were self-reportedand on the basis of the subjective rating of participantsinvolved in completing the NPHPS, researchers do not
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

E22 ❘ Journal of Public Health Management and Practice
know how LPHSs considered the varying opinions oforganizations and individual volunteers in examiningperformance scores as reported in the dataset. Further-more, data are perceived ratings rather than objectivemeasures of performance. Therefore, subjectivity mayhave affected the final rating of partnership activity.Another limitation to the study is that informationwas not available regarding the administration of theNPHPS in local jurisdictions. Strategies for administer-ing the NPHPS local assessment have been describedin a user guide that is available online to organiza-tions and at national technical assistance workshops.Although LPHSs were encouraged to recruit govern-mental and nongovernmental entities and individualvolunteers to participate in the assessment to get a com-prehensive perspective on the overall function of thelocal public health system, the extent of participationis unclear. Last, this study does not take into accountLPHSs completing the first version of the NPHPS.Future studies should identify common measures inboth versions and examine levels of partnerships witha larger sample.
System-oriented public health assessments mayhave proxy measures that can be used to examine levelof partnership activity existing in LPHSs as well as helpidentify latent characteristics that promote coordina-tion and collaboration. This study provides an initialassessment of performance in interorganizational part-nerships from a systemic perspective and reinforcesthe need for coordination of interorganizational part-nerships to occur at multiple levels. Accountabilitymeasures (ie, accreditation) are forthcoming to builda stronger presence of interorganizational partnershipsin the public health infrastructure. As the public healthsystems and services research field continues to grow,increased attention should focus on integrating effortsto ensure ultimate connectivity between organizationsand individual volunteers and 10 essential services aredelivered in a coordinated approach.
REFERENCES
1. Institute of Medicine. The Future of the Public’s Health.Washington, DC: Institute of Medicine; 1988.
2. Institute of Medicine. The Future of the Public’s Health.Washington, DC: Institute of Medicine; 2002.
3. Handler A, Issel M, Turnock B. A conceptual framework tomeasure performance of the public health system. Am J PublicHealth. 2001;91(8):1235-1239.
4. Scutchfield FD, Knight EA, Kelly AV, Bhandari MW,Vasilescu IP. Local public health agency capacity and itsrelationship to public health system performance. J PublicHealth Manag Pract. 2004;10(3):204-215.
5. Mays GP, McHugh MC, Shim K, et al. Identifying dimensionsof performance in local public health systems: results from
the National Public Health Performance Standards Program.J Public Health Manag Pract. 2004;10(3):193-203.
6. Mays GP, Scutchfield FD. Improving public health sys-tem performance through multi-organizational partner-ships. Prev Chronic Dis. 2010;7(6). http:www.cdc.gov/pcd/issues/2010/nov/10_0088.htm. Accessed November 3, 2010.
7. Zahner S. Local public health system partnerships. PublicHealth Rep. 2005;120(1):76-83.
8. Zahner SJ, Kaiser B, Kapelke-Dale J. Local partnerships forcommunity assessment and planning. J Public Health ManagPract. 2005;11(5):460-464.
9. Barnes PA, Curtis AB. A national examination of partnershipsamong local health departments and faith communities in theU.S. J Public Health Manag Pract. 2009;15(3):253-263.
10. Lovelace K. External collaboration and performance: NorthCarolina local public health departments, 1996. Public HealthRep. 2000;115(4):350-357.
11. Cheadle A, Hsu C, Schwartz PM, et al. Involving local healthdepartments in community health partnerships: evaluationresults from the Partnership for the Public’s Health Initiative.J Urban Health. 2008;85(2):162-177.
12. Baker EL, Potter MA, Jones DL, Mercer SL, Cioffi JP, GreenLW, et al. The public health infrastructure and our nation’shealth. Ann Rev Public Health. 2005;26:303-318.
13. Corso LC, Wiesner P, Halverson P, Brown C. Using the essen-tial services as a foundation for performance measurementand assessment of local public health systems. 2000;6(5):1-18.
14. Public Health Functions Steering Committee. Public Healthin America. 1995. http://www.health.gov/phfunctions/public.htm. Accessed August 20, 2009.
15. Turnock BJ. Public Health: What it is and Jow it Works. 2nd ed.Sudbury, MA: Jones & Bartlett Publishing; 2004.
16. National Institutes of Health, U.S. National Library ofMedicine. Public Health Systems and Services ResearchOverview. 2008. Prepared by University of Kentucky Cen-ter for Public Health Systems and Services Research. http://www.nlm.nih.gov/nichsr/phssr/phssrintro.html. Accessedon June 6, 2011.
17. Baker EL, Melton RJ, Stange PV, et al. Health reform and thehealth of the public: forging community health partnerships.JAMA. 1994;272(16):1276-1282.
18. National Association of County and City Health Of-ficials (NACCHO). 2008 National Profile Study of lo-cal health departments. http://www.naccho.org/topics/infrastructure/profile/index.cfm. Accessed November 13,2010.
19. Association of State and Territorial Health Officials (ASTHO).Developing partnerships with community health centersfor emergency preparedness planning. 2007. http://www.astho.org/t/pb/pub.aspx?pageid=5264&terms=%22partnerships%22. Accessed November 13, 2010.
20. Hann NE. Transforming public health through com-munity partnerships. Prev Chronic Dis. http://www.cdc.gov/pcd/issues/2005/nov/05_0072.htm. Accessed June 13,2009.
21. Roussos St, Fawcett SB. A review of collaborative partner-ships as a strategy for improving community health. AnnuRev Public Health. 2000;21:369-402.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Multistate Examination of Partnership Among LPHSs Using the NPHPS ❘ E23
22. Woulfe J, Oliver TR, Zahner SJ, Siemering KQ. Mul-tisector partnerships in population health improvement.Prev Chronic Dis. 2010;7(6). http://www.cdc.gov/pcd/issues/nov/10_0104.htm. Accessed June 6, 2011.
23. Veazie MA, Teufel-Shone N, Silverman GS, Connolly AM,Warne S, King BF. Building community capacity in publichealth: the role of action-oriented partnerships. J Public HealthManag Pract. 2001;7(2):21-32.
24. Provan KG, Milward HB. A preliminary theory of interor-ganizational network effectiveness: a comparative studyof four community mental health systems. Adm Sci Qtrly.1995;40(1):1-33.
25. Varda DM, Chandra A, Stern SA, Lurie N. Core dimensionsof connectivity in public health connectivity. J Public HealthManag Pract. 2008;14(5):E1-E7.
26. Lasker RD, Weiss ES, Miller R. Partnership synergy: a prac-tical framework for studying and strengthening the collabo-rative advantage. Milbank Q. 2001;79(2):179-2005.
27. Centers for Disease Control and Prevention National Pub-lic Health Performance Standards Program. http://www.cdc.gov/nphpsp/index.html. Accessed November 2, 2009.
28. Bakes-Martin R, Corso L, Landrum LB, Fisher VS, Halver-son PK. Developing National Performance Standards forlocal public health systems. J Public Health Manag Pract.2005;11(5):418-421.
29. Corso LC, Lenaway D, Beitsch L, Landrum LB, Deutsch H.The national public health performance standards: drivingquality improvement in public health systems. J Public HealthManag Pract. 2010;16(1):19-23.
30. Centers for Disease Control and Prevention National PublicHealth Performance Standards Program: User Guide.Atlanta, GA: Centers for Disease Control and Pre-vention; 2008. http://www.cdc.gov.gov/od/ocphp/nphpsp/PDF/UserGuide.pdf. Accessed September 13, 2009.
31. Bhandari MW, Scutchfield FD, Charnigo R, Riddell MC,Mays GP. New data, same story? Revisiting studies on therelationship of local public health systems characteristicsto public health performance. J Public Health Manag Pract.2010;16(2):110-117.
32. Barron G., Glad J, Vokotich C. The use of national pub-lic health performance standards to evaluate change incapacity to carry out the 10 Essential Services. J EnvironHealth. 2007;29-31. http://www.cdc.gov/nceh/ehs/capacitybuilding/Docs/Use_of_Natl_PH_Performance_Standards_to_Eval_Change_in_Capacity.pdf. Accessed June 6, 2011.
33. Ellison JH. National public health performance stan-dards: are they a means of evaluating the local publichealth system? J Public Health Manag Pract. 2005;11(5):433-434.
34. Baker SL, Beitsch L, Landrum L, Head R. The role of perfor-mance management and quality improvement in a nationalvoluntary public health accreditation system. J Public HealthManag Pract. 2007;13(4):427-429.
35. Public Health Accreditation Board (PHAB). PHAB standardsand measures version 1.0. http://phaboard.org/index.php/accreditation/standards. Accessed September 5, 2011.
36. Salem E, Hooberman J, Ramirez D. MAPP in Chicago: amodel for public health systems development and com-munity building. J Public Health Manag Pract. 2005;11(5):393-400.
37. Baker EL, Melton RJ, Stange PV, et al. Health reform and thehealth of the public: forging community health partnerships.JAMA. 1994;272(16):1276-1282.
38. Baker EL, Koplan JP. Strengthening the nation’s public healthinfrastructure: historic challenge, unprecedented opportu-nity. Health Aff. 2002;21(6):15-25.
39. Himmelman A. Collaboration for a Change: Definitions,Decision-Making Models, Roles, and Collaboration Process Guide.Minneapolis, MN: Himmelman Consulting; 2002. http://depts.washington.edu/ccph/pdf_files/4achange.pdf.
40. Wholey D, Gregg W, Moscovice I. Public health systems: asocial networks perspective. Health Serv Res. 44(5):1842–1862.
41. Miller CA, Gilbert B, Warren DG, et al. Statutory authoriza-tions for the work of local health departments. Am J PublicHealth. 1977;67(10):940-945.
42. Jones T, Pavlin B, LaFleur BJ, Ingram A, Schaffner W. Restau-rant inspection scores and foodborne disease. Emer Infect Dis.2004;10(4):688-692.
43. Reid WM, Page DP, Cookro DV, Mandel IG, Hostetler RM,Mason KP. Gaining strategic advantages through partner-ships with public health departments. J Health Hum Serv Adm.2000;23(1):24-36.
44. Halverson P, Mays GP, Kaluzny AD, Richards TB. Not-so-strange bedfellows: models of interaction betweenmanaged care plans and public health agencies. Milbank Q.1997;75(1):113-138.
45. Lurie N, Wasserman J, Nelson CD. Public health prepared-ness: evolution or revolution. Health Aff. 2006;25(4):935-945.
46. Nelson C, Lurie N, Wasserman J. Assessing public healthemergency preparedness: concepts, tools, and challenges.Ann Rev Public Health. 2007;28:1-18.
47. Wasserman J, Jacobson P, Lurie N, Nelson C, RicciKA, Shea M. Organizing State and Local Health Depart-ment for Public Health Preparedness. Santa Monica, CA:RAND Corporation. 2006. http://www.rand.org/pubs/technical_reports/TR318. Accessed January 3, 2010.
48. Centers for Disease Control and Prevention. Fundingguidance and technical assistance to states: emergencypreparedness and response. Atlanta, Georgia: Centersfor Disease Control and Prevention. http://emergency.cdc.gov/cdcpreparedness/coopagreement/index.asp. Ac-cessed January 10, 2010.
49. Beitsch LM, Grigg M, Menachemi N, Brooks RG. Roles oflocal public health agencies within the state public healthsystem. J Public Health Manag Pract. 2006;12(3):232-241.
50. Berkowitz B, Nicola RM. Public health infrastructure systemchange: outcomes from the turning point initiative. J PublicHealth Manag Pract. 2003;9(3):224-227.
51. Robert Wood Johnson Foundation. Public health practice-based research networks. Call for proposals. 2009. http://www.publichealthsystems.org/media/file/PBRNPPCFP090409.pdf. Accessed June 6, 2011.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.