COMMUNITY & PUBLIC HEALTH ADVISORY COMMITTEE ...
51
CPHAC/DiSAC COMMITTEE NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN AGENDA 22 September 2015 1 COMMUNITY & PUBLIC HEALTH ADVISORY COMMITTEE / DISABILITY SUPPORT ADVISORY COMMITTEE NOTICE OF MEETING OPEN MEETING A meeting of the Advisory Committee Members of Nelson Marlborough District Health Board will be held on Tuesday 22 September 2015 at 9.30am St John Meeting Room 93 Seymour Street Blenheim Our VISION is: “leading the way to healthy families” Our MISSION is to: “work with the people of our community to promote, encourage and enable their health, wellbeing and independence.” Our VALUES are: Respect We care about and will be responsive to the needs of our diverse people, communities and staff Innovation We will provide an environment where people can challenge current processes and generate new ways of working and learning Teamwork We create an environment where teams flourish and connect across the organisation for the best possible outcome Integrity We support an environment which expects openness and honesty in all our dealings and maintains the highest integrity at all times
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of COMMUNITY & PUBLIC HEALTH ADVISORY COMMITTEE ...

CPHAC/DiSAC COMMITTEE NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN AGENDA
22 September 2015 1
COMMUNITY & PUBLIC HEALTH ADVISORY COMMITTEE / DISABILITY SUPPORT ADVISORY
COMMITTEE
NOTICE OF MEETING
OPEN MEETING
A meeting of the Advisory Committee Members of Nelson Marlborough District Health Board will be
held on Tuesday 22 September 2015 at 9.30am
St John Meeting Room 93 Seymour Street
Blenheim
Our VISION is: “leading the way to healthy families”
Our MISSION is to: “work with the people of our community to promote, encourage and enable their health, wellbeing and independence.”
Our VALUES are:
RespectWe care about and will be responsive to the needs of our diverse people, communities and staff
InnovationWe will provide an environment where people can challenge current processes and generate new ways of working and learning
TeamworkWe create an environment where teams flourish and connect across the organisation for the best possible outcome
IntegrityWe support an environment which expects openness and honesty in all our dealings and maintains the highest integrity at all times

CPHAC/DiSAC COMMITTEE NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN AGENDA
22 September 2015 2
CPHAC/DiSAC MEETING AGENDA
Section Agenda Item Time Attached Action
PUBLIC FORUM 9.30am
1 Welcome, Karakia, Apologies, Registration of Interests
9.40am Attached Receive
2 Confirmation of previous meeting minutes
9.45am
Attached Resolution 2.1 Action Points
3 General Manager’s Report Attached Resolution
4 Financial Report for August 2015 Attached Resolution
5 PRESENTATIONS: - Hospice Services and Challenges (Frans Dellebeke) - Health of Older People Update (Andrew Lesperance)
11.00am
As Presented
Receive
5.1 Hospice Services and Challenges Attached Note
5.2 Health of Older People – Future State Attached Note
6 Decision: HBSS Contract Renewal Process
12.00pm
Attached Resolution
6.1 PESTEL Analysis Attached Note
7 Decision: Access Criteria for HBSS and ARC
Attached Resolution
7.1 Summary of Entry Criteria Attached Note
8 Glossary Attached Note
There are no items for the Public Excluded section of this meeting.

CPHAC/DiSAC COMMITTEE NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Welcome/Karakia/Apologies 1-1
WELCOME, KARAKIA AND APOLOGIES
Apologies

CPHAC/DiSAC COMMITTEE NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Registrations of Interest 1-2
REGISTRATIONS OF INTEREST – CPHAC/DiSAC MEMBERS
Name Existing – Health Existing – Other Interest Relates To Possible Future Conflicts
Judy Crowe (Chair) Daughter employed at Capital Coast DHB
Human Resources Advisor
Patrick Smith (Deputy Chair)
Member of IHB Managing Director, Patrick Smith HR Ltd
Member on Board of Nelson Tasman Chamber of Commerce
Consultancy services
Contracts held
Focus on primary sector and Maori Working with Maori Health Providers who hold contracts
Jenny Black (Marlborough)
Part Time NMDHB Employee
ACP Practitioner
DN Team Wairau
Pat Heaphy Relative is employee of NMDHB
Spokesperson Knights of Southern Cross
National Spokesperson Opposing Euthanasia
Nurse
Brigid Forrest Contractor to NMDHB
Doctor at Hospice Marlborough (employed by Salvation Army)
Locum GP Marlborough (not a member of PHO)
Base Medical Officer RNZAF Woodbourne (Part time). Employed by Picton Medical Centre
Member SI Alliance Palliative Care Workstream
Community Geriatrician Wairau

CPHAC/DiSAC COMMITTEE NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Registrations of Interest 1-3
Name Existing – Health Existing – Other Interest Relates To Possible Future Conflicts
Jenny Black (ex officio)
Life member of Diabetes NZ
Chair of South Island Alliance Board
Chair of National Chairs
Judith Holmes NMDHB representative on the Mapua, Ruby Bay and Moutere District Health Centre Inc Board
Glenys MacLellan Cancer Society – Bookkeeping Get Sorted (business) – May have contracts with government agencies which may include health and disability agencies
Active at a national level with the Green Party of Aotearoa NZ and spokesperson.
Jenni Gane Employee of Kimi Hauora Wairau
Marlborough Primary Health Organisation
Sonny Alesana Member of IHB Alliance Group PHO
Community Law Service
Luke Katu Employee, Nelson Bays Primary Health
Te Hauora o Ngati Rarua Tane Ora Steering Group
Kaunihera Maori NMIT
Te Hauora o Te Awhina Marae
Member of IHB
Provider Contract Service Provider
Education Provider
Service Provider
As at 16 September 2015

CPHAC / DiSAC
NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Minutes 2-1
MINUTES OF A PUBLIC MEETING OF CPHAC/DISAC COMMITTEES OF NELSON MARLBOROUGH DISTRICT HEALTH BOARD HELD IN SEMINAR CENTRE ROOM 1, BRAEMAR CAMPUS, NELSON HOSPITAL, ON TUESDAY 28 JULY 2015 AT 9.30AM Present: Patrick Smith (Deputy Chair), Judith Holmes, Glenys MacLellan, Jenni Gane, Luke Katu and Sonny Alesana (IHB), Pat Heaphy, Jenny Black (Marlb), Brigid Forrest, Jenny Black (ex officio) Apologies: Judy Crowe, Andrew Lesperance (for lateness) In Attendance: Jessica Bagge, Dawn McConnell, Gerald Hope, Chris Fleming (CE), Eric Sinclair (GM Finance & Performance), Pam Kiesanowski (Director Nursing & Midwifery), Nick Baker (CMO), Ros Gellatly (ACMO – Primary), Vienna Richards (Communications Manager), Gaylene Corlett (Minute Secretary) Karakia: Sonny Alesana
SECTION 1: PUBLIC FORUM There were no attendees in the Public Forum.
SECTION 2: APOLOGIES AND REGISTRATIONS OF INTEREST
Noted.
Moved: Judith Holmes Seconded: Pat Heaphy
RECOMMENDATION:
THAT THE APOLOGIES AND REGISTRATIONS OF INTEREST BE ACCEPTED. AGREED
SECTION 3: MINUTES OF PREVIOUS MEETING 3.1 Minutes of the CPHAC/DISAC Committee Meeting held on 26 May 2015. Noted that the discussion under General Business regarding a seminar for health of older people to be added to the Action List. It was agreed that the CE will raise this suggestion at the next ToSHA meeting.

CPHAC / DiSAC
NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Minutes 2-2
Moved: Judith Holmes Seconded: Luke Katu RECOMMENDATION: THAT THE CPHAC/DISAC MINUTES OF THE MEETING 26 MAY 2015 BE ADOPTED AS A TRUE AND CORRECT RECORD. AGREED
3.2 Matters Arising and Correspondence and Correspondence Noted.
3.3 Action Points Item 1 – Due September 2015 Item 2 – Completed Item 3 – Completed Item 4 – Update from the GM Strategy Planning & Alliance Support to be provided at the next meeting.
SECTION 4: GENERAL MANAGER’S REPORT 4.1 Strategy and Planning National Pharmacy Contract Noted the national Community Pharmacy Service Agreement (CPSA) has been signed by all pharmacists in the Nelson Marlborough district. It is important that the DHB works collaboratively with pharmacists over the next year in order to inform the next contracting round. Discussion was held on how pharmacists can actively manage client medication and provide other services that GPs/Nurses currently provide. Noted Committee members will have an opportunity to provide input into the national agreement through our Community Strategy. ToSHA will also be discussing what services patients can access through their pharmacists. It was noted that education for the community will be required to ensure consumers have a better understanding of what services they can access at pharmacies, eg INR tests for warfarin. There is value for GPs and pharmacists, however team work is needed to get these initiatives in place. Discussion was held on the Community Strategy moving forward. It was noted that it is primary focussed and both local and national initiatives for “doing things smarter” need to be put forward. It was agreed that a focus on pharmacy services be included in the Community Strategy, including education/awareness of the community as to which services they can access at their pharmacy rather than their GP.

CPHAC / DiSAC
NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Minutes 2-3
Under 13s Free Service Noted all GPs in Nelson and Tasman have signed up for the Under 13s free services, however there are challenges in Marlborough around providing the service after hours. All Marlborough practices, except one, have signed up to the under 13s service during day hours, however at the moment none have agreed to provide free after hours service. Noted there is a degree of risk around the Commerce Commission legislation and legal advice has been obtained and passed to the PHO. We are not pursuing that pathway yet, as the PHO has indicated there is progressive movement. We will, however, revisit this situation at a later date. It was agreed that the GM Strategy Planning & Alliance Support check on whether the PHO is in breach of their contract by not having this service in place by 1 July 2015. Discussion was held on education for the community around this service whereby parents could be encouraged to have their year 8 daughters visit their GP for a general check including the vaccine for cervical screening. It was agreed that we would allow the new service to settle before looking at how we can promote visits. Primary Care Strategy A Primary Care Strategy day has been scheduled for Saturday 19 September to allow an opportunity for local primary providers to gain a collective understanding of primary care in 2030. 4.2 Disability Support Services The CE gave a brief background update on DSS and the proposal being presented to the Board to separate DSS into a business unit which will operate under the restrictions of the DHB. As part of the business unit it is proposed to set up a business unit advisory group. A request will be made to the Board to appoint the Chair of the advisory group to the CPHAC/DiSAC Committee as either a member or ex officio. 4.3 ARRC, HBSS and Palliative Care Discussion was held on the increase in aged care noting there was a large increase in October that has trended on. It was agreed that the CE, on behalf of the GM Strategy Planning & Alliance Support, investigate the cause of the blip in October. Discussion held on supporting Kaumatua into aged care. It was agreed that the GM Strategy Planning & Alliance Support report on the number of Maori residents in aged care facilities and the number of Maori receiving home support in his report at the next meeting. Discussion held on the need to continually focus on supporting the home based support needs of the aged person. It was agreed that whilst we are prescriptive of what home based support is, we need to relook at what home support provides, eg not all clients require housework when some would prefer a walk to the corner etc. It was noted that the GM report was very informative and of value.
Moved: Luke Katu Seconded: Jenny Black (Marlb) RECOMMENDATION:

CPHAC / DiSAC
NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Minutes 2-4
THAT THE GENERAL MANAGER’S REPORT BE RECEIVED. AGREED
SECTION 5: UPDATES 5.1 Suicide Facts and Prevention John Allen, Manager of the Mental Health Mobile Community Crisis Team (and other branches of community teams) attended for this item. The MOH recently released the publication Suicide Facts: Deaths and Intentional Self Harm Hospitalisations 2012. This is an annual publication for the purpose of reporting numbers, trends and demographic profiles of people who die by suicide or seriously self harm themselves. The report noted that in 2012 there were markedly higher rates of suicide in males, particularly youth (15-24 years) and those aged 40-44, and Maori (compared with non Maori). Maori males and Maori youth showed high suicide rates. NMDHB district suicide rate for the five years between 2007 and 2011 was not statistically different to the national suicide rates. It was noted that long term unemployment for young men has a high rate of suicide. Noted youth tend to move away from Nelson but often come home when ill. Identifying as early as possible the reason for the return and ensuring support is in place is important. It is also around how much resilience skills our youth receive whilst in secondary school. NZ has one of the highest suicide rates in the OCED. At NMDHB the mental health team utilise the strength and skills of the mental health directorate which traverses primary and secondary care to work cohesively. They work collaboratively with others that may help clients, not just the medicine end, but also around resilience building, coping skills etc. Noted more resources are going into men’s mental and social health, eg the Men’s Shed, farming community etc. Discussion held on the background of those who have committed suicide, eg reasons, that may assist us in helping clients. Noted that the coronial autopsy looks back at the death to see if there are any commonalities. The first signs are low mood and depression, but what is that? It is a large number of things like response to life circumstances, eg genes, relationships, loss of spouse or separation, job loss, substance use etc. Linking these you see that they affect men differently to women. Middle aged men have a statistic blip with more deaths which is worrying. How to fix this is a global problem. Need to start looking at how we help our men. There is a new process where the Chief Medical Officer receives coronial notification of suicides. They are usually in a number of groups, eg older people who are often

CPHAC / DiSAC
NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Minutes 2-5
terminally ill and make the decision to commit suicide, older people that have no medical illness but have had “enough”, middle aged people, youth, etc so we do have a rough idea of trends. The youth suicides are studied in great detail. Noted it is difficult to get men to engage in their health responsibility. We do not have good services for men to go to if they do have mental illness. Discussion held on failed suicides and whether there is follow up if they present to ED, either through primary or secondary care. Noted that Mental Health Services try to pick up people before it gets to that point. It is about staying healthy, keeping in touch with family, friends and neighbours – it is about the fabric of community. If parts are missing by failure to provide by either community or personal issues, then problems occur. If isolated then depression sets in, especially for men. Need whole of system approach. The Mental Health Service are seeing a change with the single referral system – better triage of every referral. Noted that many of the larger organisations have good EAP systems which assist in supporting staff, however the challenge is often getting staff to use it. Need to ensure managers are aware of their staff and their circumstances. Noted one provider has a package that clips onto their first aid training that gives managers etc approval to ask staff how they really are which is proving beneficial.
Moved: Patrick Smith Seconded: Brigid Forrest RECOMMENDATIONS: 1 NOTE THE RECENT SUICIDE FACTS PUBLICATIONS AND THE
RELEVANT NELSON MARLBOROUGH STATISTICS 2 NOTE SOME OF THE PROPOSED ACTIONS FOR THE SUICIDE
PREVENTION PLANS WHICH ONCE FINALISED WILL BE SUBMITTED TO THE MINISTRY OF HEALTH.
AGREED
SECTION 6: FINANCE REPORT 6.1 Financial Report for June 2015 Revenue is favourable to plan by $337k for the month, and $1,021k for the year. Discussion held on patient portals and the cost of registration to the patient, noting that it is up to the GP practice on how much to charge. The initiative is still in the early stages with some practices not having many patients registered. The PHOs are promoting the initiative. Practices can decide what patients have access to, eg making appointments, results, etc. It was agreed that the CE/Ros Gellatly present to ToSHA on the challenges of business models around patient portals and the implications.

CPHAC / DiSAC
NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Minutes 2-6
Moved: Brigid Forrest Seconded: Judith Holmes RECOMMENDATION: THAT THE COMMITTEE RECEIVES THE FINANCIAL REPORT. AGREED
SECTION 7: DECISIONS 7.1 DHB Fluoridation Position Statement Peter Burton (SM Public Health) and Ed Kiddle (Medical Officer of Health) attended for this item. Noted the fluoridation campaign needs to be community led with the DHB providing support. Need to get organisations like Grey Power and parenting groups behind it. Need to consider how to engage the community. Noted in 2011 62% of the NMDHB population were keen for fluoridation. The position statement on fluoridation was endorsed by the Committee.
Moved: Judith Holmes Seconded: Brigid Forrest
RECOMMENDATION:
THAT CPHAC/DiSAC CONSIDER AND ENDORSE THE POSITION STATEMENT ON WATER FLUORIDATION FOR THE NELSON MARLBOROUGH DISTRICT HEALTH BOARD.
SECTION 8: PRESENTATION 8.1 Oral Health Including Fluoridation Rob Beaglehole presented to the Committee on water fluoridation. Tooth decay is the number one non communicable disease in the world. If you have poor oral health as a child, it is predicted you will have poor oral health as an adult. Tooth decay is the most common reason for child admissions to hospital. Last year NMDHB had 242 children under general anaesthetic for removal of one or more teeth, and most of those children were still in nappies. Water fluoridation would reduce tooth decay by 40% at a cost of only 50cents per person per annum.

CPHAC / DiSAC
NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Minutes 2-7
Sugary drinks are the number one cause of tooth decay, obesity, and diabetes. NMDHB is leading the way with excluding sugary drinks from the hospital cafe. NCC and MDC have come onboard by excluding sugary drinks at their events.

CPHAC / DiSAC
NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Minutes 2-8
NMDHB Strategic Plan 2005 - 2015 Water fluoridation is known to reduce dental decay by up to 40% and has been shown to be particularly effective in reducing socio-economic and ethnic differences in oral health. Strategies to improve oral health include “stimulating an informed discussion within the community on the merits of water fluoridation.” Draft NMDHB Position Statement on Community Water Fluoridation • Considers dental decay to be an important public health issue with significant
ethnic and socioeconomic health • Endorses community water fluoridation as an important public health measure • Supports the Ministry of Health’s position recommending the fluoridation of
drinking water supplies • Acknowledges that community water fluoridation is a safe, effective and
affordable population-based strategy for the prevention of dental decay. • Is committed to promoting health messages endorsing fluoridation of water
supplies as a cornerstone of oral health in conjunction with eating healthy food, reducing sugar intake, twice daily brushing with fluoride toothpaste and regularly visiting a dental provider
• Is committed to working with local government, central government and other public health organisations to actively promote the fluoridation of community water supplies.
Noted WINZ provide dental assistance of $300.00 per year (not changed since 1985) which is not enough for low income users to get dental treatment.

CPHAC / DiSAC
NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Minutes 2-9
Discussion: Noted there are currently 75 Councils with 34 currently providing fluoride in their drinking water. In terms of population, 52% have fluoridated water. Discussion held on the amount of sugar in fruit juice. WHO recommend that children have 3 teaspoons of sugar per day and adults 6 teaspoons per day. Noted the dental hubs were initially set up by the Ministry to treat low income people with CSC after hours, however this has not been put into use. Noted it is also about education and changing behaviours of people that do drink sugary drinks and smoke. Discussion held on whether the DHB can escalate fluoridation through the NZ Health Strategy. It was agreed that a deliberate strategy and action submission be put to the Health Strategy when submissions are called. Noted fluoride tablets are not recommended as too much fluoride is not good for you and you have to remember to take the tablet. Fluoride in the water attacks the plaque as well as decay. Need to promote the drinking of water! NCC has a water tanker attending events promoting water drinking rather than sugary drinks.
SECTION 9: GENERAL BUSINESS Patient Story Rob Beaglehole told a patient story where an older woman turned up to a private dentist in pain. As she could not afford the treatment, the dentist sent her off to the hospital. Current government policy is that we need to see people within 4 months. However she could not wait 4 months. She ended up in ED in pain demanding her teeth be taken out, however they could only provide her with antibiotics, pain relief and advice to visit a private dentist. The criteria has been modified, as previously those with CSC could access one complete treatment which would involve tooth extractions, cleaning, fillings etc. The new criteria means we cannot provide routine dental care, but see them for pain relief and that means taking out their teeth. The woman met with Rob and an x-ray showed a huge abscess. She is addicted to coca cola – drinking two 1.5 litre bottles per day. She is also a heavy smoker. The only treatment we could provide was to take out the two problem teeth. If this woman was not drinking a lot of coca cola and smoking so much, her teeth would not have needed treatment. Because she is in the poverty cycle she cannot afford teeth treatment in private, cannot be treated at ED unless it is a life threatening situation, cannot see dental department as we only take out teeth and no longer provide dental care. Five years ago we saw 580 cases of acute swelling and infection in ED; this year we saw 890, mostly Maori males aged 22-35? If we were able to see these people earlier we would be able to prevent extractions by general anaesthetic. Dental infections were a huge cause of death before antibiotics were introduced.

CPHAC / DiSAC
NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Minutes 2-10
Rob has recently seen three people (21, 28 and 32 years old) having full extractions of all teeth! Noted there is no criteria for making dentures if all teeth are extracted. Noted people can come with broken bones or other injuries and we fix them but not for teeth. Karakia: Luke Katu Meeting closed at 12.23pm.

NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Action Points – CPHAC / DiSAC Open 2.1-1
ACTION POINTS – NMDHB – CPHAC / DiSAC Open Meeting
Held on 28 July 2015
Action Item #
Action Discussed
Action Requested Person Responsible
Meeting Raised In
Due Date Status
1 GM Report: Palliative Care / Dementia Beds
Advanced Care Planning be discussed as part of the CPHAC/DiSAC workplan at the September meeting.
Further discussion be held on respite care, training family members who care for the elderly etc at the meeting in September
Andrew Lesperance
24 March 2015
26 May 2015
22 September 2015
In report and examples to be provided 22 Sept
2 GM Report: Dementia Beds
Discussion on planning/older persons strategy to be added to the Committee’s workplan for next year
Andrew Lesperance/ Judy Crowe
26 May 2015
24 November 2015?
3 GM Report: Healthier Homes
Follow up on whether the Kaumatua flats beside the Marae are insulated
Andrew Lesperance
26 May 2015 22 September 2015
Verbal update to be provided

CPHAC / DiSAC Nelson Marlborough District Health Board OPEN MEETING
General Manager’s Report 3-1
Status This report contains: For decision Update Regular report
For information
MEMO To: CPHAC/DiSAC Members
From: Andrew Lesperance, GM Strategy Planning & Alliance Support
Date: 16 September 2015
Subject: General Manager’s Report
(I) STRATEGY & PLANNING With the Health Needs Assessment and Health Services Plans largely completed and presented to the Hospital Advisory Committee in August, there is now an opportunity to look forward and consider how this information will shape, guide and direct the planning of our services in the 16/17 and out years planning round. In addition to the above, the information collected has been used to inform and forecast the DHBs future bed requirements. Service managers have been provided with historical volumes and bed numbers, and asked a series of questions to help inform bed capacity for the next 20 or more years. Assumptions around models of care and where services should best be delivered for our community will then be reviewed via a moderating panel (composed of clinicians, the executive and expertise from Health Partners group (now Ernst & Young)). Once reviewed and agreed, the report will be made available for the October Board to consider and review. Annual Planning Process We have begun considering how best to approach the annual planning cycle, with the need to ensure we ideally sequence capital planning, board input to new initiatives and direction, budget planning (high level and detail) and Ministry requirements. A brief timeline for these activities has been provided to the Executive and will be included in the board pack for their general awareness. Advanced Care Planning CPHAC have previously asked for information about the Advanced Care Planning Process. Advanced Care Planning (ACP) is a way to help think, talk and share a person’s wishes about future health care. There are two programmes that support the discussions about a person’s wishes. Conversations that Count is designed to equip volunteers to speak to their community in a consistent manner, presenting the ACP concept to people. The Conversations that Count trained communicator encourages people to start a conversation and make a plan. They do not help a person write a plan. ACP is the course that takes trainees to the next level (L1, L2, L3) with a programme facilitated by SIAPO (South Island Alliance Programme Office). There have been a number of community members and staff who have expressed an interest in being part of the Training for ACP. The next course has just closed for expressions of interest and

CPHAC / DiSAC Nelson Marlborough District Health Board OPEN MEETING
General Manager’s Report 3-2
will be held in Nelson at the beginning of December. For people who have applied to attend this course it will take attendees to L2 ACP with the ability to assist others to write a plan and discuss their wishes with family. (II) DISABILITY SUPPORT SERVICES (DSS) Update on issues relating to the aging population within DSS Within DSS the Intellectual Disability Service Stream (IDSS) the average age of the people we are supporting is 55. Many of the individuals are getting frail and requiring different levels of support. The service works hard to ensure that the people being supported are able to remain in their home right through to end of life. DSS currently provides residential support services to 60 people who are between the ages of 61 to 90 yrs of age. It is predicted that over the next 5 years that there will be up to 60 deaths. As previously predicted the natural attrition rate for the people supported by DSS in the Intellectual Disability Service Stream is slowly increasing with three deaths over the last month and two people receiving terminal care. Over the last five years there has been a reduction of service users from 210 people in IDSS residential supported living to 183. During this time there have been 32 deaths, 18 discharges and 29 new referrals into the service. The Physical Disability Support Services (PDSS) to date has grown from 6 beds to 25, and over the next 6 to 12 months the number of beds will grow to 40 to meet the current demand. 15 beds (9 in Nelson and 7 in Blenheim) are currently in the early stages of development. This growth in PDSS has kept DSS overall average occupancy in the 90% range, which has helped the overall service to remain viable as a business unit. DSS is also working with a number of individuals/ families who are looking for suitable flatting opportunities. This group is being far more specific in regards to what they require, to meet these needs we will need to be able to adapt our current service models. The DSS strategic plan for the next 10 years will focus on the natural attrition rate and its implications along with the required changes to DSS methods of providing support services to people who have a disability. Future developments will be in line with Government strategies and enabling good lives document. The proposed business unit advisory group will be able to assist with the development of the strategic plan.

CPHAC / DiSAC Nelson Marlborough District Health Board OPEN MEETING
General Manager’s Report 3-3
Utilisation/Activity

CPHAC / DiSAC Nelson Marlborough District Health Board OPEN MEETING
General Manager’s Report 3-4
Key Performance Indicator Report: August 2015
CUSTOMER EXPERIENCE: To deliver person-centred care every time.
Performance Areas Target Previous
Month Actual Comment
ILPs current within 12 month time frame
100% 82% 80%
Key workers identified for all Service Users
100% 100% 100%
Service User Board in place. Service Users involved at all levels
10 mtgs/
financial year 1 2
Customer Survey results indicate overall satisfaction with the quality of care received.
100% na na Surveying started end of August
Number of complaints and resolution completed within 20 days.
100% 100% 100%
FINANCES: To ensure stewardship and financial strength.
Performance Areas Target Previous
Month YTD
Actual Comment
To achieve financial viability, income contribution to overheads
7% of revenue 16.0% 7.71%
August comments - YTD actual contribution $227k as a % of total income $2.946k = 7.71%
Growth of business
1% 1.01% .995%
June 15 = 211 August 15 = 210 people
Redn 3 people in Aug, offset with increase of 2 in July. Net change reduction 1
Occupancy of houses 95% 98% 98% Current month ID 97% PD 109% (7rms)
Homes covering costs and contributing to overheads 100% 85.5% 78.6%
Based on YTD actual – bottom line contribution

CPHAC / DiSAC Nelson Marlborough District Health Board OPEN MEETING
General Manager’s Report 3-5
STAFF LEARNING AND GROWTH: To enable our people.
Performance Areas Target Previous
Month Actual Comment
Staff who have attained NZQA qualification completion rate. No target.
Report periods are Jan-June & July-Dec.
2 staff over January – June 2015
National Certificate in Health, Disability & Aged Support: Foundation Skills (Lev 2): 6 staff
National Certificate in Brain Injury (Lev 4): 0 staff
Staff turnover rate YTD (Financial year) < 12% 0.94% 1.24%
Staff performance reviewed within 12 months
100% 93.6% 96%
Staff current with mandatory skills 100% 90.5% 83.25%
Annual leave balances managed within DHB policy
100% Policy >2 years accumulated leave.
Sick leave rate - % of staff taking sick leave
<=2.7% 3.1% 2.85% YTD = 2.85% Current Month 2.61%
Strengthen the cultural competencies of DSS staff through the development and delivery of Maori cultural training.
US 23380 achieved
- -
9 staff attended the meeting 21.7.2015
Next Whanau Group meeting 15.8.2015
PROCESSES: To deliver excellent services in the most efficient way.
Performance Areas Target Previous
Month Actual Comment
External Audit requirements met within timeframes
100%
SILC Trust Cultural Audit – 28 recommendations in Workplan May 2015
DSS policies current 100% 100% 100%
Health & Disability Service Standards achieved
100% na na Certification due early 2016
% Right Medication New measure January 2015. Safety 1
st and new
target March 2015 100% 90% 82%
No. errors: Jun=15 Jul=21 Aug = 37
No. SU: Jun=211 Jul=213 Aug = 210
Monitor and evaluate whether Maori needs are being met He Taura
Tieke audit Actions
1. ToW principles in person centred planning. - DSS Workplan.
2. Collect SU & staff ethnicity data. – With Corporate 3. Establish a network of Maori SU. - Whanau Group 4. Celebrate Te Reo week. - Whanau Group
(III) ARRC, HBSS AND PALLIATIVE CARE ARRC – Expenditure
Results for the month ending August 2015 detail an overspend of $156k in the Health of Older People portfolio. The highest overspend is seen in Residential or Hospital level care, with lowest seen in rest home care. A small overspend has also been incurred in

CPHAC / DiSAC Nelson Marlborough District Health Board OPEN MEETING
General Manager’s Report 3-6
the community support services ($22k). Some of the overspend results from accruals that have flowed through June and July. The volumes forecast for this financial year is accurate for all but hospital level care where there has been a much higher than anticipated entry and access. The level of acuity upon entry into aged residential care has increased, with patients entering from the community directly into hospital level care rather than the historical pattern of rest home entry into hospital level care. This direct entry is a sign that we have supported individuals to live well in the community for longer, however does impact our hospital level care bed numbers and budget. ARRC Volumes Since the last reporting period Psycho-geriatric care increased to 18 residents in the month of August. Marlborough Dementia care bed occupancy rate continues to operate near capacity. We are aware of additional capacity being considered and planned. There were three beds available at the end of June 2015, one bed at the end of July and zero beds at the end of August in Blenheim. There remain vacant dementia beds in Nelson and Tasman. Of note is that since June 2014 Support Works has been responsible for authorisation of entry into Rest Home and Hospital level care in Nelson, along with the Geriatricians. Since March 2015 Support Works in Blenheim has been responsible for patient sign off at Hospital level care (historically completed for Rest Home level care). Previously this signing off of care has been solely held by the Wairau Geriatricians or Psychogeriatrician. The intention is to have Support Works and clinicians work as a team to ensure consistent application of criteria for access to residential care across our entire district. A separate short paper outlines the proposed criteria for each care category, and will be reviewed with CPHAC via a presentation on the day.
1,140
1,160
1,180
1,200
1,220
1,240
1,260
0
100
200
300
400
500
600
700
800
T
o
t
a
l
C
o
u
n
t
S
e
r
v
i
c
e
L
e
v
e
l
C
o
u
n
t
No of ARC residents at end of month
Rest home Dementia Hospital level care Psychogeriatric Total Residents

CPHAC / DiSAC Nelson Marlborough District Health Board OPEN MEETING
General Manager’s Report 3-7
Home Based Support Over the past three months the volume of clients receiving home based support has increased slightly (4). However the value of the support provided has decreased. This indicates that the number of hours assigned is reducing as a result of the increasing consistency of Needs Assessments being undertaken by Support Works.
Home Based Support Client Numbers (excludes chronic conditions)
Jun-15 Jul-15 Aug-15
Nelson Tasman 1592 1587 1605
Marlborough 855 858 846
Total 2447 2445 2451
Total Cost Home Based Support Actual Costs May-15 Jun-15 Jul-15
Preventative Maintenance $ 77,229 $ 57,855 $ 55,765
Supporting Independence $ 38,128 $ 31,050 $ 23,668
Enhanced $ - $ - $ 172
Complex Low $ 77,363 $ 65,021 $ 55,385
Complex Medium $ 272,696 $ 214,221 $ 182,297
Complex High $ 355,996 $ 275,443 $ 216,639
Complex Very High $ 29,428 $ 22,912 $ 16,127
Total $ 850,840 $ 666,502 $ 550,053
(excludes chronic conditions)
As the contracts are coming up for renewal, a short paper outlining the Home Based Support Services contractual arrangements is also being provided to CPHAC/DiSAC this month.
Day Programmes – C urrent Spend (August 15)
The actual spend for August 2015 Day programmes was $63,558. At the end of August there were 265 clients attending Day programmes across the district. There is potential for the expansion of day programmes as the population ages. These programmes are of significant assistance for families who continue to support individuals at home.
August-15
Day Programmes
No of days used in month
Cost No of clients at end of month
Geriatric 1016 $ 48,272 178
Dementia 283 $ 15,286 81

CPHAC / DiSAC Nelson Marlborough District Health Board OPEN MEETING
General Manager’s Report 3-8
Palliative Care
The Nelson Tasman Regional Hospice and Hospice Marlborough provide in-patient and community based palliative care services across the District. Hospice services are intended for patients whose needs cannot be managed by Primary Care and require the more specialist services provided by the Hospice multidisciplinary teams
The Ministry of Health has allocated new money to Hospice for services that improve the quality of palliative care in aged residential care, primary care and community settings. Hospices are working with the DHB, PHO and other providers (ARC) to establish the priorities for local outcomes for the funding, and building their individual business cases. Proposals must be submitted to the Ministry by the end of 2015 for implementation in early 2016. This will be a very busy period for our two Hospices in NMDHB as there are also required to work towards the new service specifications that are to be implemented in July 2016. The Hospice sustainability funding was not included in the budget – revenue or expenditure. The unfavourable variance is due to the increased contracted amounts to pass on the funding to the Hospice Providers. This is offset by the favourable MOH revenue variance allocated to the budget Internal Revenue. Hospice services will be discussed during our CPHAC/DiSAC meeting this month by way of a short presentation and discussion.
$000 July 2015
Actual Budget
Budget Variance
625600 - Palliative Care 369,910 341,331 (28,579)
(IV) MENTAL HEALTH & ADDICTIONS Service Development
Mental health services hosted an independent review panel to engage with the DHBs mental health services to consider three areas; the model of care (is it contemporary and fit for the future), the financials of our service delivery (is funding used efficiently and effectively), and organisational culture. Dr. David Codyre, a Psychiatrist from Auckland led a panel of three who spent three days engaging with all aspects of the mental health services. We anticipate a draft report from them toward the end of September.
The review of the Directorate’s Stepped Model of Care has been completed with consult sessions across Nelson and Wairau and the draft document is due end of Sept for comment. The objectives of the review include ensuring the Stepped Model of Care is contemporary and aligned to current government strategic direction, interfaces across the wider health system, organizational culture within the services, and cost structure including the quality of the spend and opportunities for efficiencies.

CPHAC / DiSAC Nelson Marlborough District Health Board OPEN MEETING
General Manager’s Report 3-9
In addition to the above, the major focus for the Directorate for August has been continuing to progress service Integration. The intended direction has been presented to ELT and the Directorate forum (Health Promotion – Primary – Specialist – NGO), and a draft document is currently being prepared for consultation Directorate-wide. The NGO Residential Review for Nelson is out for consultation until the end of September. The results of this combined with the Wairau one will contribute to Service Integration.
The Directorate met with St Mark’s Board to discuss their review and future possible models of care. Next step: Reviewer to meet St Mark’s with Directorate to go through review; then in the afternoon combined with DHB and other Providers to co-design future model of care, linking to Regional plans for South Island Addiction Services (via Alliance).
Alex Hospital refurbishment (MHOP) is progressing well with a slight decrease in reportable events from 2 clients in particular. With closer proximity and noise of men working on the site staff continue to do well managing the environment. Consumer Collective discussion topics: Model of Care for future, Service Review, family advisory input to Specialist Service.
Directorate Reference Group discussion topics:
Workforce Calendar
Service Integration Update (Tipahi status)
Review date notification
Contract Status – Variations at Sector Services
Ongoing discussion on Client Records. Consumers and Families reiterate their concerns on open access
Single Care Plan – agreed across all Providers
Real Time Feedback initiative now implemented throughout NZ. Concerns remain on cost
Family Advisor FTE saving/family input to Specialist queried - resolution could be fee for service from SF.

CPHAC / DiSAC Nelson Marlborough District Health Board OPEN MEETING
General Manager’s Report 3-10
Monthly Quality and Safety KPI Report
Reportable Events 2015/16 YTD

CPHAC / DiSAC Nelson Marlborough District Health Board OPEN MEETING
General Manager’s Report 3-11
Reportable Events for August were 35, which is the highest for some months and primarily due to the employee assaults by client at Tipahi St. Seven of the 11 community reportable events related to the same client. There were four SAC2 events recorded, three in relation to assaults on staff and one to do with the set up of the workstations at the new CAMHS premises in Wairau. MHOP reportable events are 16 for the month which is down from the high of last month and the lowest since April 2015. These are primarily assaults between clients, with one client being involved in six incidents. Activity – Specialist
NB: Seclusion hours were up again in August with 15 seclusion events involving seven people. A challenging young client who MH are in the process of working with an NGO to organise more appropriate accommodation had a difficult month featuring in both the seclusion (30% of seclusion hours related to this client) and also in reportable events (seven). A second client had five seclusion events, so between the two accounted for 60% of the month’s seclusion. Community caseload numbers were unavailable at the time of reporting due to issues with remote access to the database.
Activity – NGO
Year to Date Year End 14/15
Jun-15 Jul-15 Aug-15 Monthly Average Monthly Average
Inpatient Acute Admissions 24 17 26 22 25
Inpatient Acute LOS (days) 12.4 11.03 14.34 12.7 12.4
Inpatient Seclusion Use (hours)* 524.8 92.3 284.0 188.2 234.5
Community Crisis Contacts* 66 139 54 129 129
Community After Hours Call 33 41 51 46 53.9
Community Caseload Numbers 2684 2691 0 2691 2865
Psychogeriatric IP Admissions* 2 5 5 5.0 5.0
Psychogeriatric IP Occupancy (%)* 100.4% 99.2% 99.2% 99.2% 86.7%
*Provisional @ 4 September 2015
Last Three Months

CPHAC / DiSAC Nelson Marlborough District Health Board OPEN MEETING
General Manager’s Report 3-12
Richmond NZ has now merged with another NGO in the sector and has become Emerge. This is continuing to cause delays in reporting of the current year figures. SF Blenheim has been recording all activity from several non DHB funded streams. This has been discussed and in future it is hoped to separate the funding streams/stats. Te Whare Mahana Residential contract finished in February 2015 with the DBT program being nationally funded by MOH as a one year pilot with a fee for service basis paid by any DHB for utilisation. There is currently no one from NMDHB utilising the Te Whare Mahana DBT program.
Andrew Lesperance GENERAL MANAGER STRATEGY PLANNING & ALLIANCE SUPPORT
RECOMMENDATION: THAT THE GENERAL MANAGER’S REPORT BE RECEIVED.

CPHAC/DiSAC COMMITTEE NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Financial Report 4-1
Status This report contains: For decision Update Regular report
For information
MEMO
To: CPHAC/DiSAC Members
From: Andrew Lesperance, General Manager Strategy Planning & Alliance Support
Date: 16 September 2015
Subject: Financial Report for August 2015
Fund Statement of Financial Performance The following report represents a funder only view of the DHB finances to 31 August 2015.
Revenue Revenue is favourable to plan by $169k for the month and $288k year to date (YTD). The significant variances are shown below. Favourable
PBF Adjustment has been made for free U13 GP visits ($55k per month)
Additional funding for sustainable Hospice services ($37k per month) has been devolved from Central Government
Additional elective funding of $60k has been recognized for additional joint procedures provided by Clinical services in July and August 2015.
Expenditure Total expenditure on payments to providers is $42k unfavourable to budget for the month and $290k unfavourable YTD. The major variances in each service category are shown below.
$000 August 2015 $000
Actual Budget
Last
Year
Actual
Budget
Variance
F/ (U)
Actual Budget
Last
Year
Actual
Budget
Variance
F/ (U)
Budget Last Year
Revenue
Ministry of Health 33,724 33,555 33,357 169 67,398 67,111 66,727 288 416,720 400,275
Other Revenue 12 12 32 (0) 24 25 24 (0) 147 152
Total Revenue 33,736 33,568 33,389 168 67,423 67,135 66,752 288 416,867 400,427
Expenditure
Personal Health Expenditure 25,238 25,283 24,319 45 50,534 50,562 48,402 28 302,629 288,684
Mental Health Expenditure 3,279 3,354 3,243 75 6,633 6,709 6,508 76 40,254 39,806
Public Health Expenditure 91 97 90 6 182 193 187 11 1,160 1,050
Disability Support Expenditure 5,575 5,396 5,171 (179) 11,194 10,789 10,266 (405) 64,687 61,256
Hauora Maori Services Expenditure 224 234 261 11 469 469 483 (0) 2,812 2,801
Other Expenses 427 427 569 0 853 853 1,138 0 5,120 6,830
Total Expenditure 34,834 34,791 33,653 (42) 69,865 69,575 66,985 (290) 416,661 400,427
Net Surplus/(Deficit) (1,098) (1,224) (264) 126 (2,442) (2,440) (233) (2) 205 (0)
Year to Date $000 Full Year $000

CPHAC/DiSAC COMMITTEE NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Financial Report 4-2
Personal Health – Favourable $45k for the month and $28k YTD. Favourable
Expenditure on Pharmaceutical Cancer Treatments is $86k favourable to budget for the month and $46k favourable YTD. The estimate for the rebate was increased by $30k per month in August based on Pharmac’s June forecast
Community Pharmaceutical expenditure is tracking below budget by $42k for the month and $74k YTD. This is based on the latest DHB forecast drug costs and rebate receivable from Pharmac and is likely to change
Expenditure on Adolescent and School Dental services is $26k below budget for the month. This is likely to be a timing issue due to delayed claims
Delayed implementation of the emergency contraception program (ECP) contributes $19k to the YTD favourable variance
$36k has been credited for the provision made in June for the under 6 after hours visits which did not eventuate contributing to the YTD variance.
Unfavourable
Expenditure on PHO services to Under 13s was not included in the budget. Unfavourable variance of $41k for the month and $88k year to date is offset by additional revenue
Palliative Care is unfavourable $23k for the month and $52k YTD due to the sustainability payment offset by increased revenue
Patient travel and assistance expenditure is over budget by $78k for the month and $87k YTD. This is consistent with the higher volume than planned outflow of patients treated by other DHBs.
Mental Health – $75k favourable for the month and $76k YTD. Favourable
Te Whare Mahana is $29k under spent due to housing & recovery services budget not committed to date
There is $57k unspent funding pending the outcome of the services review. Public Health – Expenditure is favourable to budget by $6k for the month and $11k YTD due to delayed implementation of the maternity smoke free incentives program has resulted in the favourable variance.
Disability Support – $179k unfavourable for the month and $405k YTD.
Aged Residential Care – Expenditure on aged residential care shows an unfavourable variance to budget – $148k for the month and $367k YTD
The August result includes $0.28m of costs associated with residential care for the health of older people that date back to September 2014 which were late claiming by providers. These were not known at the time accruals were completed for the last financial year and therefore were not accrued into the FY 2014/15 financial results
Hospital level care volumes are higher than budget. Rest Home level care volumes are tracking to budget but the number of clients at the higher cost Dementia level is higher than predicted
Home Based Support Services – There has been higher than planned growth in the number of clients receiving personal care packages resulting in an overspend in total Home Based Support expenditure of $23k for the month and $35k YTD.

CPHAC/DiSAC COMMITTEE NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Financial Report 4-3
Hauora Maori – Tracking close to budget.
Andrew Lesperance General Manager Strategy, Planning & Alliance Support
RECOMMENDATION: THAT THE COMMITTEE RECEIVES THE FINANCIAL REPORT

Presentation: Hospice Services and Challenges 5.1-1
22 September 2015
Outline of Nelson Tasman Hospice presentation to CPHAC Members
The Nelson Tasman Region Hospice Trust (NTRHT) is a specialist palliative care service that provides care to patients who have less than 12 months to live. This service is provided by a specialist multi disciplinary team that provides care, support and education to patients, families, carers and other health providers.
The NTRHT has on average 140 patients and has a 10 bed in-patient facility, however most of those patients are cared for in the community. We deliver a 24/7 service by means of our multi-disciplinary team that includes doctors, nurses, physiotherapist, social worker, chaplain, bereavement counsellor and who are supported by health care assistants, admin and maintenance/equipment staff and approximately 260 fantastic volunteers.
The way we deliver our service has remained relatively unchanged for many years, however we are now faced by a number of exciting challenges that include:
1. New Ministry of Health service specifications. These specification require us to have a specialist, registrar or a nurse practitioner. We have none of these and there is a national and international shortage of people with these skills.
2. New Zealand has a rapidly aging population that is going to require a different specialist palliative care service than what is currently provided.
3. Patients in our rural communities are predominantly cared for by their GPs and we believe that they should receive a more comprehensive package of care from our multi disciplinary team.
4. The Nelson Hospital is one of a few hospitals in New Zealand who does not have a specialist palliative care service for patients who are terminally ill. We believe that these patients will benefit from input from our specialist multi-disciplinary team.
5. Information Technology will be a key factor to providing the best care for patients and needs to be embraced.
6. With an aging population and increased co-morbidities we need to ensure that we attract, train/develop and retain our staff.
7. The NTRHT has been asked to look for a new location/building and this provides us with an opportunity to build a purpose built facility that will enable the Hospice to be the specialist palliative care service hub for the Nelson/Tasman region.
8. The Nelson Tasman Hospice is contracted by Nelson Marlborough District Health Board (NMDHB) to provide this service and currently funds 68% of the operational costs. The remaining funds come from the Nelson Tasman Region Funding Trust, grants and regional fundraising events. Funding will always be a challenge and with more and more charities seeking financial support this source of income is likely to be a more challenging task.
Therefore, to enable the NTRHT to proceed on this exciting and challenging path we thought it would be beneficial to ensure that our journey is aligned with the regions strategic health direction. As a result we appreciate the opportunity to present these challenges to CPHAC members and to hear your thoughts.
Frans Dellebeke
CEO – Nelson Tasman Region Hospice Trust

CPHAC/DiSAC COMMITTEE NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Presentation: Health of Older People – Future State 5.2-1
Status This report contains: For decision Update Regular report
For information
MEMO
To: CPHAC/DiSAC Members
From: Andrew Lesperance, General Manager Strategy Planning & Alliance Support
Date: 16 September 2015
Subject: Health of Older People – Future State
Background Defining the Group Currently those born between 1946 and 1964 in the 18 years post war are characterised by the date definition and labelled ‘baby boomers’. In 2011 the first of the early Baby Boomers reached the New Zealand retirement age of 65 years. Statistics further show, that a male has an average life expectancy of 78 years, with 67.4 of those years in full health. This means there are 10.6 years in decline. For a female the average life expectancy is 82 years, with 69.2 of those years in full health, and 12.8 years in decline. It is easy to conclude that within these age groups, the standard of 11.7 years in decline is where the impact will be most felt in health and community services. Aging in place Aging in place is defined as the ability to live in one's own home and community safely, independently, and comfortably, regardless of age, income, or ability level. However, studies have found that whilst people desire to stay in their own homes, there is resistance to making changes which would match the desire to age in place to the reality. Future Vision: Health of Older People People will remain healthy for longer, and older people will be ‘active, valued and celebrated’ members of the community.
People in our community will choose where they grow old, regardless of the changes that may occur with age
The majority of people will choose to remain in their own home, which will be modified to meet their changing needs as they age
Home modifications will involve more than installing grab bars in the bathroom, with new technology developments assisting with everyday activities, from robot vacuums with cameras to detect dirt and can find their way back to a charger, to centralised and automated control of all appliances, and the use of voice commands to operate devices
People will use technology to refill prescriptions, monitor their own vital signs, and connect with their care team – nurses, doctors and specialists
Residential care homes will still be available for older people who can no longer manage the activities of daily living in their own home
When required, access to rehabilitation and convalescent care that supports older people to remain healthy and independent is available

CPHAC/DiSAC COMMITTEE NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Presentation: Health of Older People – Future State 5.2-2
Advanced Care Plans will be commonplace, and everyone in the care team will be aware of what you want for end of life care.
Now that we have verbalised the future state for older people, the work begins to create the reality. How do we support this group to remain in their own environment/homes? By taking a whole of system approach with linkages and key support workers providing access to services across a variety of disciplines and coordinating care across a variety of services. Including but not limited to:
Home Based Support Services
Allied Health in an MDT environment
Transitional rehabilitation in patients home Considerable progress has been made in the Nelson Marlborough region around caring in a “structured way’ for our ageing residents. Our presentation this month will review the system enhancements to date, discuss the desired direction of travel, and include some of the innovations being examined and investigated. Andrew Lesperance General Manager Strategy, Planning & Alliance Support

CPHAC/DiSAC COMMITTEE NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Decision: HBSS Contract Renewal Process 6-1
Status This report contains: For decision Update Regular report For information
MEMO
To: CPHAC/DiSAC Members
From: Kaye Hannagan, Simone Newsham and Andrew Lesperance
Date: 16 September 2015
Subject: DECISION: Health of Older People – Home Based Services Contract Renewal
Aging in Place Aging in place can be defined as the ability to live in one's own home and community safely, independently, and comfortably, regardless of age, income, or ability level. Home Based (HB) Support Services are a cornerstone to achieving the objectives of supporting people to live in their own home for as long as possible. This support comes at a cost. With budget constraints requiring a fine balance between assisting people to live at home and entering Rest Home level care. NMDHB contracts Home Based Support Providers (five in total) to provide services, based on needs assessments, to approximately 2,451 people (excluding chronic conditions) each month. These Home Based Services are demand driven and represent an increasing element of financial risk as the population of those over 65 year olds increases. The cost of providing the HB care amounted to $11m in the 2014/15 financial year, of this, in excess of $1m was Household Maintenance. Home Based Services Environment The Home Based Support Providers have been operating under the same contract since 2010 with yearly renewals. There are significant changes in the environment, both locally and nationally, which will change the way in which services are delivered over the next few years throughout New Zealand. The distribution of the Deloitte Home and Community Financial Review and Risk Analysis has compelled discussion in the sector, with three key impacts defined:
HB providers are signalling that DHB funding increases have not kept pace with minimum wage and inflationary pressures and are limiting HB organisational sustainability
Providers are finding it difficult to retain staff with a level of skill mix, experience and commitment
DHBs are requesting an increased compliance and skill mix for more complex patients remaining in their own home, which increases HB provider internal pressures to match skills and costs.
Nationally there are a number of factors which are driving change, not specifically health related, but these changes will impact on how services are provided in the future:
In between travel; the implementation of which has begun and is being driven by the Ministry of Health, this is likely to impact on how we pay for the provision of care

CPHAC/DiSAC COMMITTEE NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Decision: HBSS Contract Renewal Process 6-2
Raising the minimum wage; specifically the Bartlett case, has ramifications for this female dominated workforce
Zero hours employment contracts; a move to make these contracts legislatively untenable, especially in the HB environment. HB providers are competing for staff in the arena with public sector employees who pay higher rates and guaranteed hours.
Current Contract NMDHB has a number of service providers (five) in the region. The Home and Community Health Association has raised concerns nationally about the viability of the HBSS sector (Deloitte Report). Requests for price increases are made by local providers on a regular basis; the most increase in the 2015/16 contract which ends this month will be 0.37% across all contract lines. The 2010 contract under which providers currently operate has a strong focus on the restorative care model, however the practical application of the model is not supported by the structure of the contract. The contract separates services into seven sub groups, which are difficult to monitor and measure. HB providers have a desire for a less complex model and have requested changes frequently. Paradoxically, if a provider worked to a fully restorative model their income would potentially reduce (as would the carer who provides the direct service). Carers have no guaranteed income from other clients so it would be counter intuitive to reduce units of care as restoration of full health came about. There have also been enquiries from other providers nationally regarding entry into the local HBSS market. The same providers have delivered the service for 6 years with no opportunity for a free market model or tendering process for new entrants. Since the introduction of the HBSS contracts in 2010 many additional contracts have been introduced. The devolution of the Long Term Chronic Conditions to DHBs in 2012 meant the introduction of new and separate contracts to the same providers for the same services. In addition to this there are contracts for paediatric personal health and palliative HBSS service offered to the same providers as separate contracts. As the contract comes to an end this month, we will look to comply with all of government procurement rules and regulations as we progress the renewal. Attached as item 6.1 is a PESTEL analysis for your general background. RECOMMENDATION: THAT THE CPHAC/DISAC COMMITTEE:
ENDORSE THE CONTRACT RENEWAL FOR ONE YEAR, WHILST NMDHB
WORKS TOWARDS A TENDER PROCESS FOR HOME BASED SERVICES TO
BEGIN IN OCTOBER 2016.
NOTE THAT THE LONG TERM CONDITIONS CONTRACT LINES PREVIOUSLY
DEVOLVED FROM CENTRAL GOVERNMENT WILL BE INCLUDED IN THIS
CONTRACT PROCESS.

CPHAC/DiSAC COMMITTEE NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Decision: HBSS Contract Renewal Process 6-3
NOTE THE DHBS DRIVE TO ENSURE QUALITY AND SUSTAINABILITY OF
SERVICE DELIVERY WILL MEAN THAT CONTRACTS HAVE THREE DISTINCT
THEMES OF SERVICE PROVISION WITH APPROPRIATE PRICING MODELS
THAT REFLECT THE SKILLS AND EXPERTISE REQUIRED TO DELIVER
EACH:
o CLINICALLY STABLE – MINIMAL REVIEW
o VARIABLE – MONITOR TO PREVENT DECLINE
o REHABILITATION – FACILITATING PATIENT IMPROVEMENT AND
WORKING TO A PLAN THAT REDUCES CARE PROVISION IN THE SHORT
TO MEDIUM TERM.
NOTE THAT THE CONTRACT WILL HAVE DISTINCT OUTCOME MEASURES
AND REPORTING TO ENSURE CONSISTENCY OF APPROACH AND
DELIVERY OF SERVICES BY APPROPRIATELY TRAINED STAFF.

PESTEL Analysis 6.1-1
PESTEL Analysis
In considering the process of renewing the current contract, a PESTEL analysis was applied to the current environment, to provide structure to the thinking and approach. It is provided for your general background information.
Political
Market model, public-private partnership approach to age care, including HBSS is favoured by the current government
As the older population grows and the younger population diminishes and shows increasing levels of political disengagement; the over 65 age group present a very large proportion of the voting population.
Economic
Industry drive for increased funding as viability of the providers is being questioned
Increasing level of spending on HBSS with no sign of reducing based on population data
HBSS national review – potential national contract with no local negotiating power on price or model
Social
Aging population, requiring increased level of support to remain in their own home
Technological
Medication compliance technologies now more readily available
Monitoring of support workers entry and exit times increasing being used by providers but not a requirement of the DHB
Increased allied health technical skills to maximise independence in the home
Increased utilisation on InterRAI data to predict and intervene those people who are at risk of requiring residential care, or demonstrate the potential to develop greater independence
Environmental
Nelson’s temperate climate facilitates good health in the elderly. Investment into activity programmes accessing our environmental advantage to delay entry into residential facilities
Need to ensure equity of access to services across our diverse region
Legal
Zero hours contract – potential legislation change
Gender Equality pay – Kristine Bartlett case
MBIE procurement guidelines

CPHAC/DiSAC COMMITTEE NELSON MARLBOROUGH DISTRICT HEALTH BOARD OPEN MEETING
Decision: Access Criteria for HBSS and ARC 7-1
Status This report contains: For decision Update Regular report For information
MEMO
To: CPHAC/DiSAC Members
From: Simone Newsham, Kaye Hannagan and Andrew Lesperance, General Manager Strategy Planning & Alliance Support
Date: 16 September 2015
Subject: DECISION: Access Criteria for Home Based Support Services and Aged Residential Care
The DHB is required to provide Home Based Support Services as well as Aged Related Residential Care (ARRC) services for the district. In order to ensure continuity and consistency of care across the district, a range of access criteria have been developed across the district over time. This criteria has been significantly supplemented by the introduction of the InterRAI tool across New Zealand. InterRAI is an internationally validated tool that has been demonstrated to improve the quality and consistency of assessment for people with disabilities. The InterRAI assessment provides details on a person’s physical, medical, psychological and social situation. A series of algorithms are then automatically generated to provide guidance to the clinician on the areas of concern that require intervention. The InterRAI tool is not a replacement of clinical assessment but complements and supports clinical reasoning to ensure a comprehensive picture of the persons needs is gained. As of July 1st every person must have an InterRAI assessment to enter or move levels in ARRC. It is therefore recommended that the InterRAI assessment and scores is used to ensure consistency of approach to entry into Aged Related Residential Care. Enclosed are the proposed criteria for entry into ARRC at the three different levels. NASC also have a range of criteria for access to Home Based Support Services. Because of the heterogeneous nature of this group 6 main categories of support have been developed in order to monitor and match a person’s support package to their identified need. Attached as item 7.1 is a summary of the entry criteria to each of the six categories. Andrew Lesperance General Manager Strategy, Planning & Alliance Support
RECOMMENDATION: THAT THE CPHAC/DiSAC COMMITTEE RECEIVES THE REPORT AND ENDORSE THE ACCESS CRITERIA.

Summary of Entry Criteria 7.1-1
REST HOME SIGN OFF CHECKLIST – HC COMMUNITY ASSESSMENTS
NAME:
NHI: DATE:
Current code and allocation of support:
Has functional decline only occurred as a result of a medical event in the last 2-4 weeks? If so reversibility must be considered.
QUESTION TICK
ADL Hierarchy 0-3
CPS 0-3
IADL capacity score is 20 or higher
CHESS 2 or more
MAPLe 3 or more
Institutional Risk triggered
Informal Support or Abusive Relationship triggered
Total of above /7
Plus both of the following:
Overnight supervision/care is needed
Unsafe at home with maximal care provided
Total (should be at least 7) /9
Comments:
Summary of Entry Criteria 7.1-2
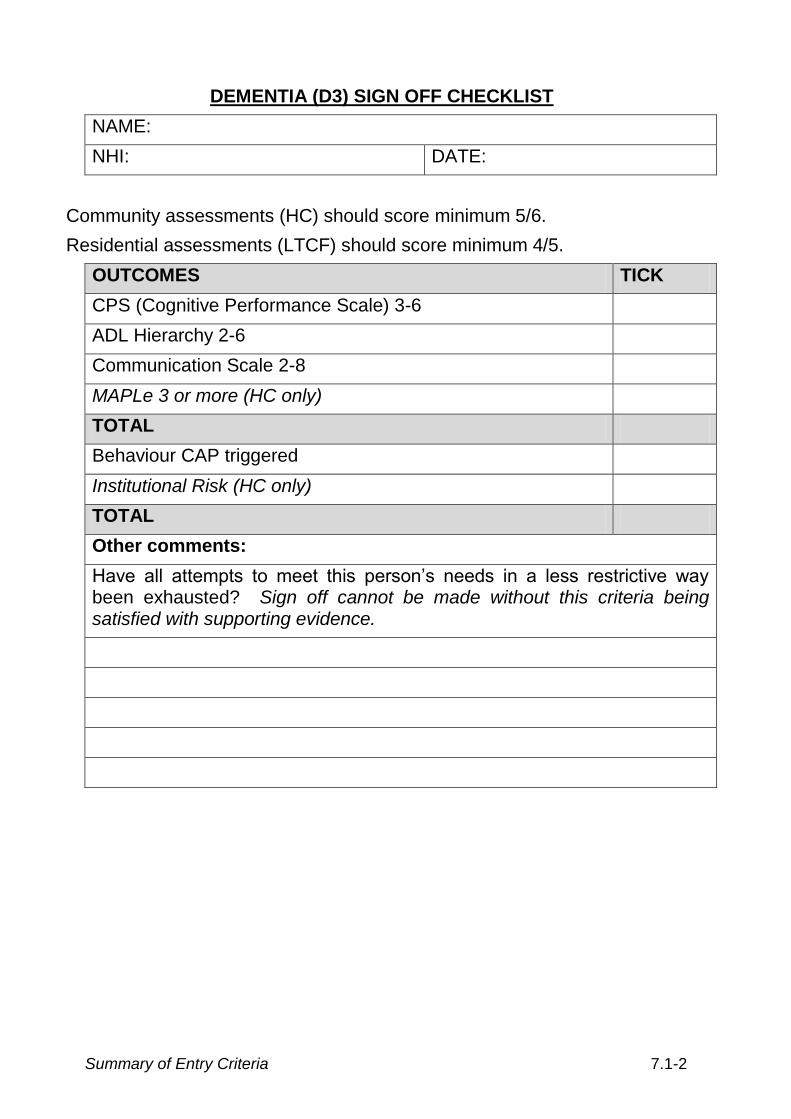
DEMENTIA (D3) SIGN OFF CHECKLIST
NAME:
NHI: DATE:
Community assessments (HC) should score minimum 5/6.
Residential assessments (LTCF) should score minimum 4/5.
OUTCOMES TICK
CPS (Cognitive Performance Scale) 3-6
ADL Hierarchy 2-6
Communication Scale 2-8
MAPLe 3 or more (HC only)
TOTAL
Behaviour CAP triggered
Institutional Risk (HC only)
TOTAL
Other comments:
Have all attempts to meet this person’s needs in a less restrictive way been exhausted? Sign off cannot be made without this criteria being satisfied with supporting evidence.

Summary of Entry Criteria 7.1-3
CONTINUING CARE SIGN OFF CHECKLIST – HC COMMUNITY ASSESSMENTS
NAME:
NHI: DATE:
Has functional decline only occurred as a result of a medical event in the last 2-4 weeks? If so reversibility must be considered.
Yes should be ticked for at least 5 items.
QUESTION YES NO
ADL hierarchy Scale 3-6
CHESS 2-5
MAPLe 3-5 (HC only)
PUR (Pressure Ulcer Risk) score 2-8
TOTAL /4
If ADL less than 3, consider whether this person could
be managed at rest home level.
Activities of Daily Living CAP
Institutional Risk (HC only)
Any one of the following:
Mood CAP
Falls CAP
Pain
Under-nutrition
COMMENTS: (if less than 6 are there other outcomes to consider?)

Summary of Entry Criteria 7.1-4
CRITERIA FOR ACCESS TO HOME BASED SUPORT SERVICES BASED
Category Entry Criteria Package Parameters
Essential Housework (HSHM)
- No personal care requirements
- Must have a community services card
- Must live alone or with a ‘non-able bodied’ person who would be physically or cognitively unable to complete household tasks
- Must have an age or health related condition that prevents independence e.g. Dyspnoea, identified falls risk, requires walking aid, unable to crouch or bend
- Max 1 hour of household maintenance per fortnight.
- Provide advice on breaking down household task into manageable subtasks.
- Consider referral to allied health for support to regain independence
Strengthening Independence (CHSI)
- Disability impacts on both basic and extended IADL’s, preventing independence with these and, leisure/ social activities.
- They may have experienced a recent acute health episode, from which they are expecting to recover but rehabilitation is slow stream.
- Max package size $110 per week (approx 3 units)
- Consider referrals allied health, fitness programmes.
Low Complex Need (CHSL)
- Disability impacts on basic ADL’s, household management and completing social activities.
- Person requires supervision and/or minimal assistance with ADL’s.
- May have some mild cognitive impairment.
- Max package $140 per week (approx 4 units)
Moderately Complex (CHSM)
- Disability impacts in ADLs, household management and
Max package $300 per week (approx 10 units, but may also include some day
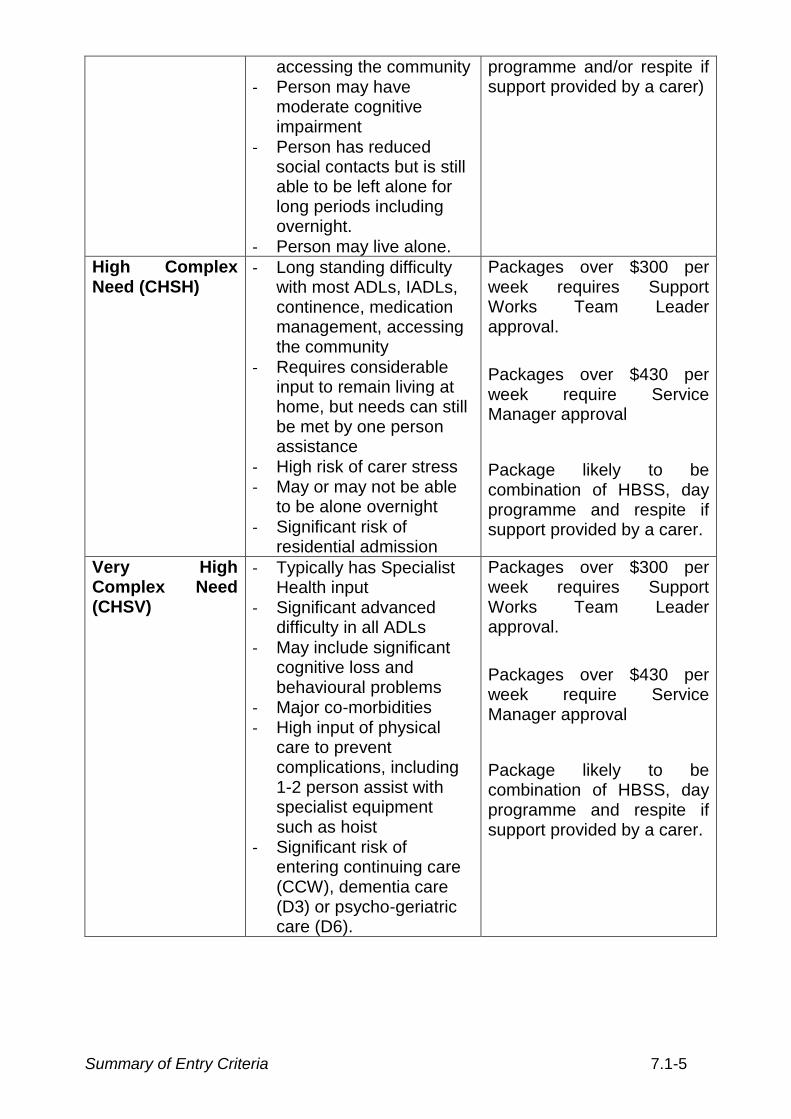
Summary of Entry Criteria 7.1-5
accessing the community - Person may have
moderate cognitive impairment
- Person has reduced social contacts but is still able to be left alone for long periods including overnight.
- Person may live alone.
programme and/or respite if support provided by a carer)
High Complex Need (CHSH)
- Long standing difficulty with most ADLs, IADLs, continence, medication management, accessing the community
- Requires considerable input to remain living at home, but needs can still be met by one person assistance
- High risk of carer stress - May or may not be able
to be alone overnight
- Significant risk of residential admission
Packages over $300 per week requires Support Works Team Leader approval.
Packages over $430 per week require Service Manager approval
Package likely to be combination of HBSS, day programme and respite if support provided by a carer.
Very High Complex Need (CHSV)
- Typically has Specialist Health input
- Significant advanced difficulty in all ADLs
- May include significant cognitive loss and behavioural problems
- Major co-morbidities - High input of physical
care to prevent complications, including 1-2 person assist with specialist equipment such as hoist
- Significant risk of entering continuing care (CCW), dementia care (D3) or psycho-geriatric care (D6).
Packages over $300 per week requires Support Works Team Leader approval.
Packages over $430 per week require Service Manager approval
Package likely to be combination of HBSS, day programme and respite if support provided by a carer.

Nelson Marlborough District Health Board Open Meeting
Glossary 8-1
GLOSSARY OF COMMONLY USED ACRONYMS, ABBREVIATIONS AND MAORI TRANSLATION
ABC Ask about their smoking status; brief advice to quit; cessation A4HC Action for Healthy Children A&D / AOD Alcohol and Drug / Alcohol and Other Drugs A&R Audit & Risk Committee ACC Accident Compensation Corporation ACMO Associate Chief Medical Officer ACNM - Associate Charge Nurse Manager ACU Ambulatory Care Unit ACP Advanced Care Plan ADM Acute Demand Management ADON Associate Director of Nursing AE Alternative Education AEP Accredited Employer Programme AIR Agreed Information Repository ALOS Average Length of Stay ALT Alliance Leadership Team (short version of (TOSHALT) AOD Alcohol and Drug AOHS Adolescent Oral Health Services AP Annual Plan with Statement of Intent ARC Aged Residential Care ARF Audit Risk and Finance ARCC Aged Residential Care Contract ARRC Aged Related Residential Care ASD Autism Spectrum Disorder ASMS Association of Salaried Medical Specialists AT&R Assessment, Treatment & Rehabilitation BSCQ Balanced Score Card Quadrant BA Business Analyst BCTI Buyer Created Tax Invoice BFCI Breast Feeding Community Initiative BFCI Baby Friendly Community Initiative BHE Blenheim BOT Board of Trustees BS Business Support BSI Blood Stream Infection BSMC Better, Sooner, More Convenient CaaG Capacity at a Glance CAMHS Child and Adolescent Mental Health Services CARES Coordinated Access Response Electronic Service CBAC Community Based Assessment Centres CBF Capitation Based Funding CBSD Community Based Service Directorate CE (CEO) Chief Executive (Chief Executive Officer) CEA Collective Employee Agreement CDHB Canterbury District Health Board CCDHB Capital & Coast District Health Board (also called C & C) CCDM Care Capacity Demand Management CCDP Care Capacity Demand Planning CCF Chronic Conditions Framework CCT Continuing Care Team CCU Coronary Care Unit CDEM Civil Defence Emergency Management CDHB Canterbury District Health Board CDM Chronic Disease Management

Nelson Marlborough District Health Board Open Meeting
Glossary 8-2
CEG Coordinating Executive Group (for emergency management) CeTas Central Technical Advisory Support CFA Crown Funding Agreement or Crown Funding Agency CFO Chief Financial Officer CGC Clinical Governance Committee CHFA Crown Health Financing Agency CHS Community Health Services CIMS Coordinated Incident Management System CIO Chief Information Officer CLAB Central Line Associated Bacteraemia CLAG Clinical Laboratory Advisory Group CME Continuing Medical Education CMI Chronic Medical Illness CMO Chief Medical Officer CMS Contract Management System CNM Charge Nurse Manager Concerto IT system which provides clinician’s interface to systems COHS Community Oral Health Service COO Chief Operating Officer COPD Chronic Obstructive Pulmonary Disease COPMI Children of Parents with Mental Illness CPHAC Community and Public Health Advisory Committee CPIP Community Pharmacy Intervention Project CPNE Continuing Practice Nurse Education CP Chief Pharmacist CPO Controlled Purchase Operations
CPSOG Community Pharmacy Services Operational Group
CPU Critical Purchase Units CRG Christchurch Radiology Group CRISP Central Region Information Systems Plan CSR Contract Status Report CSSD Central Sterile Supply Department CSSD Clinical Services Support Directorate CT Computerised Tomography CTA Clinical Training Agency CTC Contributions to Cost CTANAG Clinical Training Agency Nursing Advisory Group CTU Combined Trade Unions CVD Cardiovascular Disease CVDRA Cardiovascular/Diabetes Risk Assessment CWD Case Weighted Discharge CYF Child, Youth and Family CYFS Child, Youth and Family Service DA Dental Assistant DAH Director of Allied Health DAP District Annual Plan DAR Diabetes Annual Review DBI Diagnostic Breast Imaging DBT Dialectical Behaviour Training DHB District Health Board DHBNZ District Health Boards New Zealand DHBRF District Health Boards Research Fund DIFS District Immunisation Facilitation Services DiSAC Disability Support Advisory Committee DGH Director General of Health DMH Director of Maori Health DNA Did Not Attend DONM Director of Nursing and Midwifery

Nelson Marlborough District Health Board Open Meeting
Glossary 8-3
DR Disaster Recovery DRG Diagnostic Related Group DSP District Strategic Plan DSS Disability Support Services DT Dental Therapist DWCSP District Wide Clinical Services Plan EAP Employee Assistance Programme EBID Earnings Before Interest & Depreciation ECP Emergency Contraceptive Pill ECWD Equivalent Case Weighted Discharge ED Emergency Department EDA Economic Development Agency EDaaG ED at a Glance EFI Energy For Industry ELT Executive Leadership Team EMPG Emergency Management Planning Group ENS Ear Nurse Specialist ENT Ears, Nose and Throat EOI Expression of Interest EPA Enduring Power of Attorney EQP Earthquake Prone Building Policy ERMS ereferral Management System ESA Electronic Special Authority ESOL English Speakers of Other Languages ESPI Elective Services Patient Flow Indicators ESR Environmental Science & Research ESU Enrolled Service Unit EVIDEM Evidence and Value: Impact on Decision Making FCT Faster Cancer Treatment FF&E Furniture, Fixtures and Equipment FFT Future Funding Track FMIS Financial Management Information System FOMHT Friends of Motueka Hospital Trust FOUND Found Directory is an up-to-date listing of community groups and
organisations in Nelson/Tasman FPSC Finance Procurement and Supply Chain FRC Fee Review Committee FSA First Specialist Assessment FST Financially Sustainable Threshold FTE Full Time Equivalent FVIP Family Violence Intervention Programme GM General Manager GMS General Medical Subsidy GP General Practitioner GRx Green Prescription hA healthAlliance HAC Hospital Advisory Committee HBI Hospital Benchmarking Information HBSS Home Based Support Services HBT Home Based Treatment H&DC / HDC Health and Disability Commissioner HDSP Health & Disability Services Plan Programme HDU High Dependency Unit HEA Health Education Assessments He Kawenata Covenant, agreement, treaty, testament (PM Ryan Maori Dictionary pg 104) HEeADSSS Psychosocial tool – Home, Education, eating, Activities, Drugs and Alcohol,
Sexuality, Suicidality (mood), Safety HEHA Healthy Eating Healthy Action

Nelson Marlborough District Health Board Open Meeting
Glossary 8-4
HEP Hospital Emergency Plan HESDJ Ministries of Health, Education, Social Development, Justice HFA Health Funding Authority HHS Hospital and Health Services HIA Health Impact Assessment HM Household Management HMS Health Management System HNA Health Needs Assessment HODs Heads of Department HOP Health of Older People HP Health Promotion HPI Health Practitioner Index HPV Human Papilloma Virus HR Human Resources HR & OD Human Resources and Organisational Development HSP Health Services Plan HQSC Health Quality & Safety Commission IANZ International Accreditation New Zealand IBA Information Builders of Australia IDF Inter District Flow IDSS Intellectual Disability Support Services IFRS International Financial Reporting Standards IHB Iwi Health Board
ILM Investment Logic Mapping
IM Information Management InterRAI Inter Residential Assessment Instrument IoD Institute of Directors New Zealand IPAC Independent Practitioner Association Council IPC Intensive Patient Care IPC Units Intensive Psychiatric Care Units IPG Immunisation Partnership Group IPSAS International Public Sector Accounting Standards IPU In-Patient Unit IS Information Systems ISSP Information Services Strategic Plan IT Information Technology JAMHWSAP Joint Action Maori Health & Wellness Strategic Action Plan JOG Joint Oversight Group KIM Knowledge and Information Management Kotahitanga Unity, accord, coalition, solidarity (PM Ryan Maori Dictionary pg 127) KPI Key Performance Indicator KHW Kimi Hauora Wairau (Marlborough PHO) LA Local Authority LCN Local Cancer Network LIS Laboratory Information Systems LOS Length of Stay LSCS Lower Segment Caesarean Section LTC Long Term Care LTCCP Long Term Council Community Plan LTO Licence to Occupy LTS-CHC Long Term Supports – Chronic Health Condition LTSFSG Long Term Service Framework Steering Group Manaakitanga Goodwill, show respect, or kindness to ((PM Ryan Maori Dictionary pg 172) Manawhenua Power, prestige, authority over land (HW Williams Maori Dictionary pg 172) Manawhenua O Te Tau Ihu O Te Waka A Maui – Referring to the eight iwi who hold tribal
authority over the top of the South Island (no reference) MA Medical Advisor MAC(H) Medicines Advisory Group (Hospital)

Nelson Marlborough District Health Board Open Meeting
Glossary 8-5
MCT Mobile Community Team MDC Marlborough District Council
MDM Multidisciplinary Meetings
MDO Maori Development Organisation MDS Maori Development Service MDT Multi Disciplinary Team MECA Multi Employer Collective Agreement MHAU Mental Health Admission Unit MHC Mental Health Commissioner MHD Maori Health Directorate MHDSF Maori Health and Disability Strategy Framework MHFS Maori Health Foundation Strategy MHINC Mental Health Information Network Collection MHSD Mental Health Service Directorate MHWSF Maori Health and Wellness Strategic Framework MMG Medicines Management Group MOH Ministry of Health MOH Medical Officer of Health MOA Memorandum of Agreement MOSS Medical Officer Special Scale MOU Memorandum of Understanding MOW Meals on Wheels MPDS Maori Provider Development Scheme MQ&S Maternity Quality & Safety Programme MRI Magnetic Resonance Imaging MRT Medical Radiation Technologist (or Technician) MSD Ministry of Social Development MSD Marlborough Services Directorate MSSD Medical Surgical Services Directorate NPA Nutrition and Physical Activity NRAHDD Nelson Region After Hours & Duty Doctor Limited NRL Nelson Radiology Ltd NRT Nicotine Replacement Therapy MRSA Methicillin Resistant Staphylococcus Aureus NHBIT National Health Board IT NASC Needs Assessment Service Coordination NBPH Nelson Bays Primary Health NCC National Capital Committee NCC Nelson City Council NCSP National Cervical Screening Programme NETP Nursing Entry to Practice NGO Non Government Organisation NHCC National Health Coordination Centre NHI National Health Index NIR National Immunisation Register NMDHB Nelson Marlborough District Health Board NMDS National Minimum Dataset NMIT Nelson Marlborough Institute of Technology NN Nelson NPA Nutrition and Physical Activity (Programme) NPV Net Present Value NRAHDD Nelson Regional After Hours and Duty Doctor Ltd NRSII National Radiology Service Improvement Initiative NSU National Screening Unit NTOS National Terms of Settlement NZHIS NZ Health Information Services NZMA New Zealand Medical Association NZNO NZ Nurses Organisation

Nelson Marlborough District Health Board Open Meeting
Glossary 8-6
NZPH&D Act NZ Public Health and Disability Act 2000 OAG Office of the Auditor General OECD Organisation for Economic Co-operation and Development OIA Official Information Act OIS Outreach Immunisation Services OPD Outpatient Department OPF Operational Policy Framework OPJ Optimising the Patient Journey ORL Otorhinolaryngology (previously Ear, Nose and Throat) OSH Occupational Health and Safety OT Occupational Therapy PACS Picture Archiving Computer System PAS Patient Administration System P&F Planning and Funding PANT Physical Activity and Nutrition Team PBF(F) Population Based Funding (Formula) PC Personal Cares P&C Primary & Community PCBU Person Conducting Business Unit PCI Percutaneous Coronary Intervention PCO Primary Care Organisation PCT Pharmaceutical Cancer Treatments PDO Principal Dental Officer PDR Performance Development Review PDRP Professional Development and Recognition Programme PDSA Plan, Do, Study, Act PFG Performance Framework Group (formerly known as Services Framework
Group) PHS Public Health Service PHCS Primary Health Care Strategy PHI Public Health Intelligence PHO Primary Health Organisation PHOA PHO Alliance PHONZ PHO New Zealand PHS Public Health Service PHU Public Health Unit PIA Performance Improvement Actions PICS Patient Information Care System PN Practice Nurse PPE Property, Plant & Equipment assets PPP PHO Performance Programme PSAAP PHO Service Agreement Amendment Protocol PT Patient PTAC Pharmacology and Therapeutics Committee PRIMHD Project for the Integration of Mental Health Data PVS Price Volume Schedule Q&SGC Quality & Safety Governance Committee QA Quality Assurance QHNZ Quality Health NZ QIC Quality Improvement Council QIPPS Quality Improvement Programme Planning System RA Radiology Assistant Rangatiratanga Autonomy, evidence of greatness (HW Williams Maori Dictionary pg 323) RDA Resident Doctors Association RDA Riding for Disabled RIF Rural Innovation Fund RIS Radiology Information System RFI Request for Information

Nelson Marlborough District Health Board Open Meeting
Glossary 8-7
RFP Request for Proposal RICF Reducing Inequalities Contingency Funding RIS Radiology Information System RM Registered Midwife RMO Resident Medical Officer RN Registered Nurse ROI Registration of Interest RSE Recognised Seasonal Employer RSL Research and Sabbatical Leave SAC1 Severity Assessment Code SAC2 Severity Assessment Code SAN Storage Area Network SCBU Special Care Baby Unit SCN Southern Cancer Network SDB Special Dental Benefit Services SHSOP Specialist Health Services for Older People SI South Island SIA Services to Improve Access SIAPO South Island Alliance Programme Office SICF South Island Chairs Forum SICSP South Island Clinical Services Plan SI HSP South Island Health Services Plan SIRCC South Island Regional Capital Committee SISSAL South Island Shared Service Agency SLA Service Level Agreement SLATs Service Level Alliance Teams SLH SouthLink Health SM Service Manager SMO Senior Medical Officer SNA Special Needs Assessment SOI Statement of Intent SOPD Surgical Outpatients Department SOPH School of Population Health
SPaIT Strategy Planning and Integration Team SPAS Strategy Planning & Alliance Support SSBs Sugar Sweetened Beverages SSE Sentinel and Serious Events
TDC Tasman District Council TLA Territorial Local Authority TOW Treaty of Waitangi TOR Terms of Reference ToSHA Top of the South Health Alliance
TPOT The Productive Operating Theatre
TRTT Te Roopu Tupu Tahi UG User Group VLCA Very Low Cost Access VRA Vascular Risk Assessment WAM Wairau Accident & Medical Trust WAVE (Project) Working to Add Value through E-Information WEll Whanau Engagement, Innovation and Integration WIP Work in Progress WR Wairau YOTS Youth Offending Teams YTD Year to Date YTS Youth Transition Service As at 16 September 2015