Young South Asian deaf people and their families: negotiating relationships and identities 1
A guide for people with cancer, their families and friends
Cancer information
www.cancervic.org.au
Understanding Melanoma

Understanding MelanomaA guide for people with cancer, their families and friends
First published January 1996. This edition October 2012.© Cancer Council Victoria 2012ISBN 978 1 921619 72 4
Understanding Melanoma is reviewed approximately every two years. Check the publication date above to ensure this copy of the booklet is up to date. For a more recent copy, phone Cancer Council Helpline 13 11 20.
Acknowledgements This edition has been developed by Cancer Council Victoria on behalf of all other state and territory Cancer Councils as part of a National Publications Working Group initiative.
We thank the reviewers of this booklet: Prof Grant McArthur, Consultant Medical Oncologist, Head of the Translational Research Group and Head of the Molecular Oncology Laboratory, Peter MacCallum Cancer Centre, VIC; Jay Allen, Consumer and Community Coordinator, Melanoma Institute Australia, NSW; Annie Angle, Cancer Council Helpline Nurse, Cancer Council Victoria; Prof Michael P Brown, Director, Cancer Clinical Trials Unit, Senior Medical Oncologist, Royal Adelaide Cancer Centre, SA; Dr Vanessa Estall, Head Radiation Oncologist, Melanoma and Skin Service, Peter MacCallum Cancer Centre, VIC; Clinton Heal, Consumer and CEO and Founder of Melanoma WA; Prof John Thompson, Professor of Melanoma and Surgical Oncology at the University of Sydney and Director, Melanoma Institute Australia, NSW; and members of the SunSmart Victoria team.
Thank you to David Rees and John Paegle for sharing their stories about melanoma. We would also like to thank the health professionals and consumers who have worked on previous editions of this title.
Editor: Jenny MothoneosDesigner: Paula MarchantPrinter: SOS Print + Media Group
Note to readerAlways consult your doctor before beginning any health treatment. This booklet is intended as a general introduction to the topic and should not be seen as a substitute for your doctor’s or other health professional’s advice. However, you may wish to discuss issues raised in this booklet with them. All care is taken to ensure that the information in this booklet is accurate at the time of publication.
Interpreting service: Deaf or hearing or speech impairedIf you use text-based communication, call Cancer Council Helpline 13 11 20 through the National Relay Service (NRS) 13 36 77. If you can hear and still use your voice, but have a speech impairment, call Cancer Council Helpline through NRS 1300 555 727.
Generous Victorians who fundraise to fight cancer make many Cancer Council services, including the publication of this booklet, possible. For information on how you can help, visit www.cancervic.org.au or call 1300 65 65 85.
Cancer Council Victoria1 Rathdowne Street, Carlton VIC 3053Cancer Council Helpline 13 11 20Telephone 03 9635 5000 Facsimile 03 9635 5290Email [email protected] Website www.cancervic.org.au
This booklet has been prepared to help you understand more about melanoma.
Understandably, many people feel shocked and upset when told they have melanoma. It is important to remember that the prognosis for most people diagnosed with melanoma is good.
This booklet aims to help you to understand how melanoma is diagnosed and treated. We also include information about support services you may like to use.
We cannot give you advice about the best treatment for you. You need to discuss this with your doctors. However, we hope this information will answer some of your questions and help you think about other questions you may want to ask your treatment team.
This booklet does not need to be read from cover to cover – just read the parts that are useful to you. Some medical terms that may be unfamiliar are explained in the glossary. You may also like to pass this booklet to your family and friends for their information.
How this booklet was developedThis information was developed with help from medical experts and people who have been diagnosed with melanoma.
Introduction
Cancer Council Helpline 13 11 20 can arrange telephone support in different languages for non-English speakers. You can also call the Translating and Interpreting Service (TIS) direct on 13 14 50.

ContentsWhat is cancer? ................................................................ 4
The skin ............................................................................. 6
Key questions ................................................................... 8What is melanoma? ..............................................................................8
What are the types of melanoma? .......................................................8
How common is melanoma? ..............................................................10
What causes melanoma? ...................................................................10
What are the signs and symptoms? ...................................................13
Diagnosis ......................................................................... 14Physical examination ..........................................................................14
Removing the mole (excision biopsy) .................................................14
Checking the lymph nodes .................................................................16
Staging the melanoma .......................................................................17
Prognosis ...........................................................................................18
Which health professionals will I see? ................................................18
Treatment for early melanoma ...................................... 22Surgery ...............................................................................................22
Removing the lymph nodes (dissection) ............................................24
Adjuvant therapies ..............................................................................26
Treatment for advanced melanoma .............................. 28Surgery ...............................................................................................28
Radiotherapy ......................................................................................28
Targeted therapies ..............................................................................30
Biological therapies ............................................................................30

Chemotherapy ....................................................................................32
Palliative treatment .............................................................................33
Making treatment decisions .......................................... 35Talking with doctors ...........................................................................36
A second opinion ...............................................................................36
Taking part in a clinical trial ................................................................37
Living with melanoma .................................................... 38Healthy eating ....................................................................................38
Staying active .....................................................................................38
Complementary therapies ..................................................................38
Relationships with others ...................................................................39
Sexuality, intimacy and cancer ...........................................................39
Life after treatment .............................................................................40
Coping with advanced melanoma ......................................................40
After treatment: follow up .............................................. 42Will I get another melanoma? .............................................................42
How much sun is enough? .................................................................42
Seeking support ............................................................. 45Practical and financial help ................................................................45
Cosmetic care ....................................................................................45
Useful websites .............................................................. 46Question checklist .......................................................... 47Glossary .......................................................................... 48How you can help ........................................................... 52

What is cancer?
Cancer is a disease of the cells, which are the body’s basic building blocks. Our bodies constantly make new cells to help us grow, to replace worn-out cells and to heal damaged tissue after an injury.
Normally cells grow and multiply in an orderly way, but sometimes something goes wrong with this process and cells grow in an uncontrolled way. This uncontrolled growth may result in a lump called a tumour or may develop into abnormal blood cells.
A tumour can be benign (not cancer) or malignant (cancer). A benign tumour does not spread to other parts of the body. However, a malignant tumour is made up of cancer cells, which are able to spread. The cancer that first develops in a tissue or organ is called the primary cancer.
Malignant or invasive cancer
Abnormal cells
Cancer in-situ Angiogenesis
Abnormal cells multiply
Abnormal cells
How cancer starts
Normal cells
Normal cells
Lymph vessel
Boundary
Blood vessel
4 Cancer Council

When it first develops, a malignant tumour may not have invaded nearby tissue. This is known as a cancer in-situ, carcinoma in-situ or localised cancer. As the tumour grows, it may spread and become what is known as invasive cancer.
Cancer cells can spread to other parts of the body by travelling through the bloodstream or the lymphatic system. They may continue to grow into another tumour at this new site. This is called a secondary cancer or metastasis.
A metastasis keeps the name of the original cancer. For example, melanoma that has spread to the liver is still called melanoma, even though the person may be experiencing symptoms relating to cancer in the liver.
How cancer spreads
Angiogenesis – tumours grow their own blood vessels
Metastasis – cells invade other parts of the body via blood vessels and lymph vessels
Primary cancer
Local invasion
Lymph vessel
What is cancer? 5
The skin
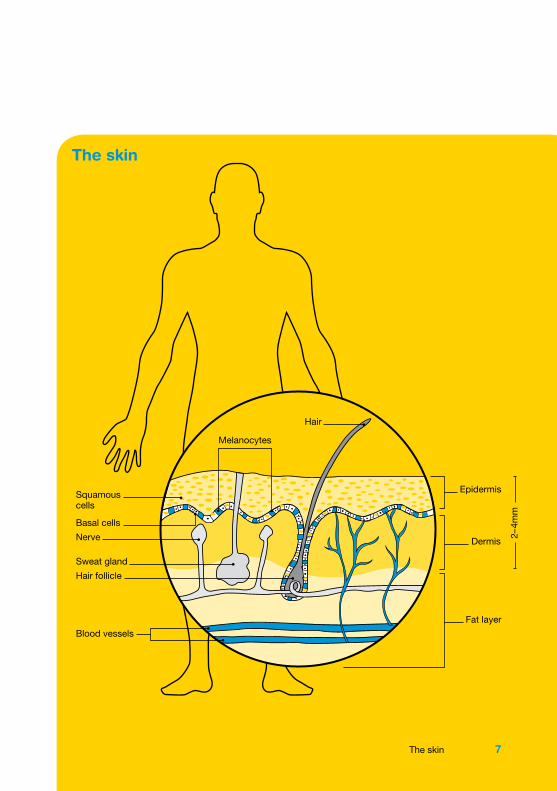
The skin is the largest organ in the body. It covers the body, protecting it from injury, regulating its temperature and preventing it from becoming dehydrated. Skin, like all other body tissues, is made up of cells. It has two main layers called the epidermis and the dermis.
The epidermis is the top, outer layer of the skin. It contains three different kinds of cells: •squamous cells – flat cells that are packed tightly to make up
the top layer •basal cells – tall cells that make up the lower layer •melanocytes – cells that produce a dark pigment called
melanin, the substance that gives skin its colour.
Basal cells multiply constantly and the older cells move upwards in the epidermis. When they flatten out and form a layer they become squamous cells. The top layer of your skin is made up of dead skin cells that eventually fall off.
The dermis is the layer underneath the epidermis. It contains the roots of hairs, sweat glands, blood vessels, lymph vessels and nerves.
Melanocytes
When skin is exposed to the sun, melanocytes make extra melanin to protect the skin from getting burnt. This is what causes skin to tan. Melanocytes are also in non-cancerous (benign) spots on the skin called moles or naevi. Most moles are brown, tan or pink in colour and round in shape.
6 Cancer Council
The skin
Squamouscells
Basal cells
Nerve
Sweat gland
Hair follicle
Blood vessels
Epidermis
Dermis
Fat layer
Hair
Melanocytes
2–4m
m
The skin 7

Key questions
Q: What is melanoma? A: Melanoma is a type of skin cancer. There are three main types
of skin cancer that are named after the cells that are affected: squamous cell carcinoma, basal cell carcinoma and melanoma. Melanoma develops from melanocytes (pigment cells).
It usually occurs on parts of the body that have been overexposed to the sun. However, melanoma can also start in a part of the skin or an other part of the body that has never been exposed to the sun, such as the nervous system, eye and mucous membrane (lining of the mouth and digestive tract).
Melanoma is the least common skin cancer but it is the most serious because it can spread to other parts of the body. If found early, melanoma is often curable. If detected later, it may have grown down deeper into the dermis where it may spread.
Q: What are the types of melanoma? A: Skin melanomas are called cutaneous melanomas. Cutaneous
melanomas are categorised by how thick they are, how far they have spread and the way they look.
Superficial spreading melanoma – This is the most common type of melanoma, making up almost 65% of all cases. It starts as a brown or black spot that spreads across the outer layer of the skin (epidermis). This type of melanoma becomes dangerous when it invades the lower layer of the skin (dermis).
8 Cancer Council
Nodular melanoma – Makes up about 15% of melanomas. It is usually a raised lump on the surface of the skin that is very dark brownish-black or black in colour. However, nodular melanoma can sometimes be pink or red, or have no pigment at all.
Lentigo maligna melanoma (LMM) – This type of melanoma is most common in older people. It makes up about 10% of melanomas.
LMM begins as a large freckle (lentigo maligna) in an area of skin that has had a lot of sun exposure, such as the face, ears, neck and head. It may grow slowly and superficially over many years until it penetrates more deeply into the skin.
Acral lentiginous melanoma – A rare type of melanoma that is most commonly found on the palms of the hands, soles of the feet or under the fingernails or toenails.
Other types of melanoma – There are some other rarer types of melanoma, which start in the eyes, tissues that line the inside of the nose, anus, genital tract (urethra and vagina) and nervous system.
Melanoma in-situ
This is when the abnormal cancer cells are only in the epidermis and have not penetrated into the dermis.
Key questions 9
Q: How common is melanoma? A: Australia and New Zealand have the highest rates of
melanoma in the world. More than 10,000 people are diagnosed with melanoma in Australia every year.
Melanoma of the skin is the fourth most common cancer in both men and women. It accounts for 10% of all cancer diagnoses. One in 19 Australians will be diagnosed with melanoma before age 85.
It is the most common type of cancer in young Australians aged 15–44 (20% of all cases).
Q: What causes melanoma? A: The main cause of all types of skin cancers is exposure to
ultraviolet (UV) radiation from the sun or another source, such as a solarium tanning machine. Each time your unprotected skin is exposed to UV radiation, it changes the structure of cells and affects what they do.
Exposure to UV radiation permanently damages the skin. This damage adds up over time. The most important years for sun protection are during childhood. However, increased protection against sun exposure will prevent skin cancer at whatever age it is used.
Sometimes melanoma happens by chance and isn’t linked to sun exposure. However, this is uncommon.
10 Cancer Council
Family history of melanomaSometimes melanoma runs in families. For most people this is due to factors such as similar skin type or too much sun exposure in childhood. However, in a small number of people (5–10%), melanoma may be caused by an inherited faulty gene. Some of these genes have been identified.
The signs that melanoma could be due to an inherited faulty gene include:
•Two or more close relatives who have, or had, melanoma. These relatives could be on the same side of the family (e.g. mother’s or father’s side). Close relatives include parents, siblings or children.
•Another risk factor may be someone who has had more than one melanoma on different areas of the skin or someone who has been diagnosed with melanoma before the age of 40.
If you are concerned that you have family risk factors, talk to your doctor about having regular skin checks or ask for a referral to a family cancer clinic. To find out more call Cancer Council Helpline.
Research shows that people who first use tanning machines (solariums) before the age of 35 have an 87% higher risk of developing melanoma.
Key questions 11

Who is at risk?
The following factors may increase a person’s risk of developing melanoma:
Skin type – Some people have skin that is more sensitive to UV radiation. This includes people who have pale or fair skin; people who burn easily and don’t tan; and people with light-coloured eyes.
Having lots of moles – Adults with more than 10 moles on their arms and more than 100 on their body should have their skin checked regularly by their GP or a skin specialist (dermatologist).
Childhood tanning/sunburn – Too much sun exposure before the age of 15 greatly increases the chance of getting melanoma in later life because damaged cells have more time to develop into cancer.
Studies show that people who move during adolescence from
low to high UV radiation countries, such as England to Australia, develop melanoma at a lower rate than people born there.
UV exposure – People who occasionally get heavy sun exposure (e.g. on weekends or on holidays) may be more at risk, especially if they get sunburnt. People who are frequently exposed to UV rays through regular sun exposure or solarium use are also at risk.
Age – It is most common in people more than 50 years of age. However, it is the most commonly diagnosed cancer in 15–44 year olds.
Cancer history – A person who has had melanoma or another type of skin cancer (BCC or SCC) is at an increased risk.
12 Cancer Council
Q: What are the signs and symptoms? A: Melanoma can vary greatly in the way it looks. The first
sign of a melanoma is usually a new spot or a change in an existing mole.
Size – The spot may begin to get, or keep getting, larger.
Colour – The mole may appear blotchy with a wide variety of colours, such as brown, black, blue, red, white and/or grey.
Shape or border – An irregular edge (scalloped or notched) or lack of symmetry is a warning sign. That is, if a line was drawn through the middle of the mole, both halves would not match up. The spot may increase in height or become scaly.
Itching or bleeding – A mole that itches from time to time or bleeds may indicate a change to melanoma.
It is normal for new moles to appear and change during childhood and pregnancy. However, all adults who have a new mole should get it examined. Even if you have had a mole checked before and it was assessed as benign, keep an eye on it because it could change in the future. Talk to your doctor immediately about any changes.
Melanoma can occur anywhere on the body. In men, it is more common on the back. Women get more melanomas on their legs.
Key questions 13
Diagnosis
Physical examinationUsually you begin by seeing your general practitioner (GP) who will examine the suspicious spot or mole, and any other moles on your body. Your doctor may use a magnifying instrument, called a dermoscope, to see the spot clearly. The doctor may also feel the lymph nodes near the suspicious spot or mole. The doctor will also ask if you or your family have a history of melanoma.
Removing the mole (excision biopsy)If the doctor suspects that a spot on your skin may be melanoma, you will probably have a biopsy. This is usually a quick and simple procedure. Your family doctor or GP may do it, or you may be referred to a dermatologist or surgeon.
You will have a local anaesthetic injected into the area near the mole. The doctor will use an instrument called a scalpel to remove the spot and a small area of tissue around it. A stitch or stitches will be used to close up the wound. The tissue sample will be sent to a laboratory for examination under a microscope by a tissue specialist (histopathologist).
Results are usually ready in about a week, and a follow-up appointment may be arranged. This waiting period can be an anxious time, and it may help to talk things over with a close friend or relative.
If the mole contained cancerous cells, you will need further surgery, such as a wide local excision (see page 22).
14 Cancer Council

Pathology report
If you have melanoma, the pathologist will prepare a report that provides your treatment team with information to help plan your treatment and determine the prognosis. The following factors may be included:
Breslow thickness – This is a measure of the thickness of the tumour in millimetres. Melanomas are classified into four categories:
•less than 1mm (most people have melanomas in this category)
•1–2mm
•2.1–4mm
•greater than 4mm.
Clark level (level of invasion) – This describes how deeply the cancer has gone through into layers of the skin. It is rated 1–5 with 1 being the most shallow and 5 the deepest. For example, a low Clark level means the cancer is close to the skin’s surface (more superficial); a high level means the cancer has penetrated more deeply into the skin.
Margins – This is the edge of an excision specimen. If there is no tumour touching the margins, the pathologist will describe how close the lesion came to the edge.
Mitotic rate – Mitoses is the process by which one mature cell divides into two identical cells. The pathologist counts the number of actively dividing cells (mitoses) that they see. Averaging this number gives the mitotic count, which is stated as the number of mitoses per square mm.
Ulceration – The breakdown or loss of the epidermis. Ulceration is determined by the pathologist when they review the specimen under the microscope.
Diagnosis 15
Checking the lymph nodesWhen it’s confirmed that you have melanoma, the doctor will check the nearby lymph nodes to see if the cancer has spread. This provides more accurate information about the stage of the melanoma.
Lymph nodes are part of your body’s lymphatic system, which removes excess fluid from tissues; absorbs fatty acids and transports fat; and produces immune cells. Sometimes melanoma can travel through the lymph vessels to other parts of the body.
To check if the melanoma has spread to a lymph node or several lymph nodes, your doctor may recommend that you have a fine needle aspiration biopsy or a sentinel node biopsy.
Fine needle aspiration biopsy – The doctor takes a sample of cells by inserting a needle into a suspicious node and draws tissue into the syringe. This tissue is examined under a microscope to see if it contains cancer cells.
Sentinel node biopsy – This locates the lymph node that drains fluid from the area where the melanoma developed. A small amount of radioactive fluid is injected into the area where the melanoma was removed. This procedure, called lymphoscintigraphy, is done in the nuclear medicine department. The radioactive fluid is not harmful.
After about an hour, the surgeon passes a hand-held machine called a gamma counter over the area to see which node has
16 Cancer Council

absorbed the injected fluid first. This is known as the sentinel node. It is removed in a small operation and checked for cancer cells. If cancer cells are found, the remaining node in the area is removed. This is to try to stop cancer coming back in the same area and to assess the risk of the cancer spreading to other parts of the body.
A sentinel lymph node biopsy can provide information that helps predict the risk of melanoma spread in the future, and can help your doctor plan your treatment.
Staging the melanomaBased on the diagnostic tests, the doctor will be able to tell how far the disease has spread into the skin and whether or not it has moved from the starting point on the skin (the primary site) to the lymph nodes or other parts of the body. This is called staging.
Staging the melanoma helps your health care team decide what treatment is best for you.
Stages 1–2The melanoma has not moved beyond the primary site. This is called localised cancer.
Stage 3The melanoma has spread to lymph nodes near the primary site.
Stage 4 The melanoma has spread to other parts of the body.
Diagnosis 17
PrognosisPrognosis means the expected outcome of a disease. You may wish to discuss your prognosis and treatment options with your doctor, but it is not possible for any doctor to predict the exact course of the disease. The type of melanoma you have, the rate and depth of tumour growth, how well you respond to treatment, and other factors such as age and medical history are also important factors.
Melanoma can be treated most effectively in its early stages when it is still confined to the top layer of the skin (epidermis). The deeper a melanoma penetrates into the skin, the greater the risk that it may spread to draining lymph nodes or other organs.
In Australia, more than 85% of people with melanoma are cured by surgery. With early detection and treatment, the percentage of people cured has grown steadily over the past 20 years.
Which health professionals will I see?You may be cared for by a range of health professionals who specialise in different aspects of your treatment. This is called a multidisciplinary team. Ideally, all your tests and treatment should be available at your hospital, although this may not be possible.
Most people with melanoma will only need to have the melanoma removed surgically. They will not need to see a medical oncologist or a radiation oncologist or have to stay in hospital.
18 Cancer Council

Health professionals for people with early melanoma
dermatologist specialises in the diagnosis and treatment of skin disorders
histopathologist examines tissue to diagnose cancer
surgeon performs operations to remove the melanoma
plastic surgeon specialises in surgery to reconstruct the appearance of the body
specialist nursessupport you throughout your diagnosis and treatment
Health professionals for people with advanced melanoma
medical oncologist prescribes and coordinates the course of chemotherapy
radiation oncologist prescribes and coordinates the course of radiotherapy
specialist nursessupport you throughout your diagnosis and treatment
dietitian recommends an eating plan for you to follow while you are in treatment and recovery
social worker, counsellor,
psychologist, and
physiotherapist
link you to support services and help you with emotional, physical and practical problems
palliative care teamhelp you and your family with any needs you have, including support at home
Diagnosis 19

Melanoma unitsSome people are diagnosed and treated in specialist melanoma units available in major cities around Australia. At these centres, specialists in melanoma work together to assess a patient’s case and recommend the best treatment.
If you are referred to a melanoma unit or a multidisciplinary team meeting, a histopathologist may review your biopsy results, if necessary, to check they are correct and that there is no difference of opinion about your diagnosis. You will be able to talk to a medical specialist who will answer your questions. The specialist will advise you and your doctor about your treatment.
As well as providing treatment advice, melanoma units are involved in research studies and may invite you to participate. They may also seek your permission to collect information, tissue and blood samples from you, for use in melanoma research. People who are at high risk of melanoma are often asked to take part in research studies as well, even if they have not been diagnosed with melanoma. See page 37 for more information on clinical trials.
To find out where a specialist melanoma unit is located, ask your doctor or call Cancer Council Helpline 13 11 20.
20 Cancer Council
Key points
•A melanoma diagnosis starts with an examination of the suspicious spot or mole, and any other moles on your body.
•A GP, dermatologist or surgeon can give you a local anaesthetic and remove a spot on your skin for examination by a histopathologist. This is called an excision biopsy.
•The biopsy will provide information about the thickness of the melanoma (Breslow thickness) and how deeply into the skin the cancer cells have grown (Clark level).
•Your doctor will feel the nearby lymph nodes to work out if the melanoma has spread to other parts of the body. If necessary, you will have a fine needle biopsy or sentinel node biopsy to check the lymph nodes for cancer cells.
•Most people with melanoma will only need to have it
surgically removed. They will not require a hospital stay or further treatment.
•Your doctor may talk to you about your prognosis. This is a general prediction about what may happen to you.
•There are many health professionals who care for people with melanoma. Some health professionals, such as medical oncologists and radiation oncologists, care for people with melanoma that is at risk of spreading or has spread (metastatic melanoma). Most people with melanoma do not need to see these specialists.
•Some people visit specialist melanoma units, which are based in major cities around Australia.
Diagnosis 21
Treatment for early melanomaMelanoma that is found early can be treated successfully. Your medical team will discuss the best treatment for you based on how far the melanoma has spread.
SurgerySurgery is the main treatment for early stage (localised) melanoma. Most of the time this is the only treatment needed.
Wide local excisionThe surgeon will do a wide local excision. This means that the area where the melanoma was and a small amount of normal looking skin will be cut out. This is called a safety margin, and is done to make sure all the cancer cells have been removed. The safety margin is usually between 5mm and 2cm, depending on the thickness of the melanoma. The surgeon will stitch up the wound.
A wide local excision is often performed as a day procedure using local anaesthetic. You will have a general anaesthetic if you have a sentinel node biopsy (see page 16). Many people with melanomas thicker than 1mm also have this procedure at the same time as the wide local excision.
A pathologist will check the tissue around the melanoma for cancer cells. If the sample doesn’t have any cancer cells, it is called a clear margin. If the margins aren’t clear, you may need further treatment. See page 28.
22 Cancer Council
Repairing the woundMost people will be able to have the wound drawn together with stitches. If the surgery wound is too big to close with stitches, the surgeon may cover the wound using some skin from another part of your body. This can be done in two ways:
•Skin flap – Nearby skin and fatty tissue is pulled over the wound and stitched.
•Skin graft – A layer of skin is taken from another part of your body and placed over the area where the melanoma was removed. The skin graft is usually taken from the thigh.
The decision about whether to do a skin graft or flap will depend on many factors, such as where the melanoma is on your body, how much tissue has been removed and your general health.
In either case, the melanoma wound will be covered with a dressing and left for several days. It will then be checked to see if it is healing properly. You will also have dressings on any area from which skin was taken for a graft.
Recovering from the operationYou may be uncomfortable for a few days after a wide local excision. Your doctor will prescribe pain-killers if necessary. If you have a skin graft, the area on which the skin is grafted may look unattractive immediately after the operation. Eventually this area will heal and the redness will fade. Your medical team will tell you how to keep the wound clean to prevent it from becoming infected.
Treatm
ent fo
r early m
ela
nom
a
Treatment for early melanoma 23

In rare cases, the original skin graft fails and a new skin graft is needed.
Your total recovery time varies depending on the thickness of the tumour and the extent of the surgery required. Most people feel better in a week or two. Your doctor can also give you information about any bruising or scarring that you may have after surgery.
Removing the lymph nodes (dissection)If the melanoma has spread to your lymph nodes, they will be removed in an operation called a lymph node dissection or lymphadenectomy. The lymph nodes you have removed will depend on the location of the primary melanoma. There are large groups of lymph nodes in the neck, armpits and groin.
For example, if you have a melanoma in your leg, then the lymph nodes in your groin on the same side will be taken out. If your melanoma is on your head, then the lymph nodes in your neck nearest to the part of your head affected will be removed.
I went to a doctor who specialises in facial and cosmetic surgery. He said it was important to get the melanoma out straightaway. He cut out a larger piece – about the size of a 20-cent coin – and it had clear margins. The cuts from surgery were able to heal into the folds and wrinkles of my face, so the scar is not noticeable. John
24 Cancer Council
Lymphoedema
If the lymph nodes have been surgically removed from the groin or armpit area, swelling of the leg or arm on the same side is the most common problem. This is called lymphoedema and happens due to a build up of lymph fluid in a part of the body.
The likelihood of lymphoedema following treatment depends on the extent of the surgery and whether you’ve had radiotherapy. It can develop a few weeks or even several years after treatment. Though lymphoedema is permanent, it can usually be managed.
How to manage lymphoedema
•Keep the skin healthy and unbroken. This will reduce the risk of infection.
•Wear a well-fitted compression sleeve, stocking or bandaging.
•Always wear gloves for gardening and housework.
•Avoid scratches from pets or insect bites or pricking your finger when sewing.
•Use sunscreen to protect your skin from sunburn.
•Moisturise your skin to prevent dryness and irritation.
•Avoid tight clothing, shoes and jewellery.
•Don’t pick or bite your nails, or push back your cuticles.
•Find activities that help the lymph flow, e.g. swimming, bike riding or light weights.
•Massage the affected area to help move fluid.
•See a lymphoedema specialist – visit the National Lymphoedema Practitioners Register, www.nlpr.asn.au, or talk to your doctor.
•Seek medical help urgently if you suspect infection.
Treatm
ent fo
r early m
ela
nom
a
Treatment for early melanoma 25

Side effectsLike most treatments, having your lymph nodes removed can cause side effects.
Pain – Most people will have some pain after the operation. This usually improves as the wound heals. However, a few people may have pain that continues after the wound has healed. This is most common for people who have lymph nodes removed from the neck.
Shoulder stiffness and pain – These are the most common problems after the lymph nodes in your armpit have been taken out. You may find that you cannot move your arm as freely as you could before the surgery. You may also develop lymphoedema. For information on managing the condition see page 25.
Adjuvant therapiesOccasionally, other treatments are used after surgery if there’s a risk that the melanoma could come back. These are known as adjuvant treatments. They include targeted therapies and biological therapies. See page 30 for more information.
Adjuvant treatments are often given as part of a clinical trial.
26 Cancer Council

Key points
•Melanoma can be treated successfully if it is caught early. This is called early stage or localised melanoma.
•Treatment is based on how far the melanoma has spread.
•Melanomas are always surgically removed. The surgeon will cut out the melanoma and some skin around it (safety margin). This is called a wide local excision.
•In a wide local excision, small wounds are stitched up. For larger wounds, skin will be pulled over the wound and stitched (skin flap) or a thin layer of skin will be taken from another part of the body, such as the thigh, and placed over the wound (skin graft).
•Depending on the extent of the surgery, recovery time will vary. Most people recover in about two weeks.
•Most people treated for localised melanoma do not have any further trouble with the disease. However, if the melanoma has spread to other parts of your body, you will need further treatment.
•If cancer has spread to nearby lymph nodes, they will be removed in a surgical procedure called lymph node dissection or lymphadenectomy. This procedure may cause side effects, such as lymphoedema.
•Lymphoedema can be managed. This occurs when lymph fluid build ups and causes swelling.
•Treatments that are used after surgery in case the melanoma comes back are called adjuvant therapies.
Treatm
ent fo
r early m
ela
nom
a
Treatment for early melanoma 27
Treatment for advanced melanomaAdvanced melanoma (also called metastatic or secondary melanoma) means the cancer has spread to distant skin sites, lymph nodes or internal organs. Treatment may include surgery, radiotherapy, biological therapies and chemotherapy.
SurgeryIn some cases the surgeon will be able to do a wide local excision to treat metastatic melanoma (see page 22). This is usually possible if the cancer involves other parts of the skin. The surgeon will also remove nearby lymph nodes if they are cancerous. This procedure is called a lymphadenectomy or lymph node dissection.
If the melanoma has spread to internal organs, surgery may still be possible, but this will depend on a number of other factors. The type of operation you have will depend on the part of your body that is affected. Talk to your medical team for more information or call Cancer Council Helpline.
RadiotherapyRadiotherapy treatment uses x-rays to kill cancer cells or injure them so they cannot multiply.
It is sometimes given after surgery to prevent the melanoma coming back. Radiotherapy is mostly used if the cancer has spread to the lymph nodes. If the melanoma has spread to other parts of the body, it may be used to control cancer growth or relieve symptoms.
28 Cancer Council
Before starting treatment you will have a planning appointment where a CT scan is performed. The radiotherapy team will use this to plan your treatment. The technician may make some permanent small tattoos or temporary small marks on your skin so that the same area is targeted during each treatment session.
During treatment, you will lie on a table under a machine that aims radiation at the affected part of your body. The whole process takes about 20–30 minutes, and you don’t feel any pain – similar to having an x-ray. Treatment sessions are usually given over 1–4 weeks. The length of your treatment will depend on the size and location of the tumour, and your general health.
Side effectsRadiotherapy can cause some temporary side effects, such as fatigue. Many people will develop side effects during their treatment, which will depend on the part of the body that receives radiotherapy and how long you are having the treatment. Your treatment team will monitor you closely.
Skin in the treatment area may become red and sore during or immediately after treatment. You will need to take care washing and avoid shaving the area or wearing clothing that can rub. Your treatment team will tell you how to look after your skin.
For a free booklet about radiotherapy and its side effects, call the Helpline on 13 11 20 or visit your local Cancer Council website.
Treatm
ent fo
r adva
nce
d m
ela
nom
a
Treatment for advanced melanoma 29

Targeted therapiesThere have been a number of new developments in the use of targeted therapies for the treatment of advanced melanoma.
Targeted therapies are substances that target the differences between cancer cells and normal cells by selectively targeting proteins in the cancer cell that signal the cancer cell to grow. They have been shown to help specific groups of people with melanoma.
Vemurafenib (Zelboraf®)This drug can reduce the size of melanoma in people with advanced melanoma who have a change in a gene called BRAF. This gene signals cancer cells to multiply. By testing a piece of melanoma tissue removed during diagnostic tests or surgery doctors can identify if you have the BRAF gene mutation. About half the people with melanoma have this gene change. The change in the BRAF gene is only found in the melanoma cells and cannot be passed from parents to children.
Vemurafenib is taken as a tablet twice a day. Common side effects include a rash, increased sun sensitivity, joint pain, hair loss and tiredness. Your treatment team will let you know if this drug is a suitable treatment for you.
Biological therapiesThere have been a number of recent developments in the use of drug treatments known as biological therapies for the treatment of advanced melanoma.
30 Cancer Council
Biological therapies are substances that activate cells in the body to fight the cancer. They can stimulate the body’s immune system to fight the melanoma.
Different types of biological therapies may be used to treat advanced melanoma, including ipilimumab and interferon.
Ipilimumab (Yervoy®)This new drug helps temporarily slow or stop the growth of melanoma in people who have already had other treatments. It works by activating the immune system to attack cancer cells.
The drug is injected into a vein (intravenously) over about 90 minutes. It is usually given once every three weeks for up to four doses. Ask your oncologist how often and for how long you may need ipilimumab injections.
The most common side effects of ipilimumab include skin rashes, itching, and diarrhoea. Less commonly, it can cause severe inflammation in different parts of the body, such as the bowel, liver, skin and hormone glands. This may lead to some serious side effects, including persistent diarrhoea, changes in the way the liver works, skin rashes, severe fatigue and blisters affecting several areas of the body.
It’s important to report these side effects immediately to your medical team. If these side effects occur, you will usually be prescribed high doses of steroids to help reduce the inflammation caused by the ipilimumab.
Treatm
ent fo
r adva
nce
d m
ela
nom
a
Treatment for advanced melanoma 31
InterferonThis drug is sometimes offered as a treatment for advanced melanoma. Interferon is made naturally by the body to fight infection but is also made artificially in laboratories for use as a cancer treatment. It can help stimulate the body’s immune system to attack abnormal cells, such as melanoma cells.
Interferon is usually injected under the skin, although it can also be given into a vein (intravenously). Your medical oncologist will explain how often and for how long you may need interferon.
Interferon can cause side effects similar to flu symptoms, including chills, fevers, headaches, tiredness and muscle and joint pain.
Interferon may also affect your mood and thinking abilities. It can also reduce the number of normal cells in your blood. For example, your red and white blood cells and platelets. It may also affect your liver, which your doctor may pick up on blood tests. These side effects are usually worse in the first month of treatment and will disappear once you finish your treatment. It is important to discuss these side effects with your doctor.
ChemotherapyChemotherapy is the treatment of cancer with anti-cancer (cytotoxic) drugs. The aim of chemotherapy is to kill or slow the growth of cancer cells while doing the least possible damage to healthy cells. Treatment is given to cure or slow the growth of melanoma, or as palliative treatment (see opposite page).
32 Cancer Council

Chemotherapy treatment is usually given over 3–12 months. The number of treatment sessions and their frequency will vary according to the type of melanoma you have and the drugs used.
Side effects Most of the chemotherapy drugs used to treat melanoma do not cause major side effects. However, some drugs do cause nausea, vomiting, fatigue, and thinning or loss of hair. These side effects are temporary and steps can be taken to prevent or reduce them. Cancer Council’s free booklet on chemotherapy has more information about treatment and side effects. Call 13 11 20 for a copy or visit your local Cancer Council website.
Palliative treatmentPalliative treatment helps to improve people’s quality of life by alleviating symptoms of cancer without trying to cure the disease. It is particularly important for people with advanced cancer. However, it is not just for people who are about to die, and it can be used at different stages of cancer.
For some people the focus of treatment is on pain relief and stopping the spread of cancer. However, for many it can also involve the management of other physical and emotional symptoms (e.g. depression, nausea, fatigue and sleeping difficulties) and improving quality of life.
To find out more, call the Helpline for booklets on palliative care and advanced cancer or view them online.
Treatm
ent fo
r adva
nce
d m
ela
nom
a
Treatment for advanced melanoma 33

Key points
•If melanoma has spread to other parts of your body (distant skin sites, lymph nodes or internal organs), it is called advanced or metastatic melanoma.
•Treatment for metastatic melanoma may include surgery, radiotherapy, targeted therapies, biological therapies and chemotherapy.
•The surgeon will usually be able to cut out the melanoma metastasis and skin around it (wide local excision). Nearby lymph nodes may also be removed in a procedure called lymph node dissection.
•Radiotherapy uses x-rays to kill cancer cells or injure them so they cannot multiply. Side effects may include skin redness and soreness, and fatigue.
•New developments in the treatment of advanced
melanoma include targeted therapies and biological therapies.
•Targeted therapies block proteins that signal the cancer cell to grow.
•Biological therapies activate cells in the body to fight cancer. The different types that may be used include vemurafenib, ipilimumab and interferon.
•Chemotherapy is drug treatment that kills cancer cells or slows their growth. Most of the chemotherapy drugs used to treat melanoma do not cause major side effects, but you may have temporary side effects such as fatigue and nausea.
•Palliative treatment helps improve quality of life without trying to cure the cancer.
34 Cancer Council
Making treatment decisions
Sometimes it is difficult to decide on the right treatment. You may feel that everything is happening so fast you don’t have time to think things through. If you are feeling unsure about your options, check with your doctor how soon your treatment should start, and take as much time as you can before making a decision. Understanding details about the disease, the available treatments and their possible side effects will help you make a well-informed decision. This decision will also take into account your personal values and the things that are important to you and your family. It is common to feel overwhelmed by information so it may help if you read and talk about the melanoma gradually.
•Weigh up the advantages and disadvantages of different treatments, including the impact of any side effects.
•If only one type of treatment is recommended, ask your doctor why other choices have not been offered.
•If you have a partner, you may want to discuss the treatment options together. You can also talk to friends and family.
You have the right to accept or refuse any treatment offered by your doctors and other health care professionals. Some people with advanced cancer choose treatment even if it only offers a small benefit for a short period of time. Others want to make sure the benefits of treatment outweigh the side effects so they have the best possible quality of life. Some people choose options that focus on reducing symptoms and make them feel as well as possible.
Making treatment decisions 35

Talking with doctorsWhen your doctor first tells you that you have melanoma you may not remember all the details about what you are told. You may want to see the doctor again before deciding on treatment. Ask for the time and support to make your decision.
If you have questions, it may help to write them down before you see the doctor. You can also check the list of suggested questions on page 47. Taking notes or recording the discussion can help too. Many people like to have a family member or friend go with them to take part in the discussion, take notes or simply listen.
If your doctor uses medical terms you don’t understand, ask for an explanation in everyday language. You can also check a word’s meaning in the glossary (see page 48).
A second opinionGetting a second opinion from another specialist may be a valuable part of your decision-making process. It can confirm or clarify your doctor’s recommendations and reassure you that you have explored all of your options.
Some people feel uncomfortable asking their doctor for a second opinion, but specialists are used to people doing this.
If you have several questions for your doctor, ask if it is possible to book a longer appointment.
36 Cancer Council

Your doctor can refer you to another specialist and send your initial results to that person. You can get a second opinion even if you have started treatment or still want to be treated by your first doctor. Alternatively, you may decide you would prefer to be treated by the doctor who provided the second opinion.
Taking part in a clinical trialYour doctor may suggest you consider taking part in a clinical trial. Doctors run clinical trials to test new or modified treatments and ways of diagnosing disease to see if they are better than current treatments. Over the years, trials have improved treatments and led to better outcomes for people diagnosed with melanoma.
If you join what is called a randomised trial for a new treatment, you will be chosen at random to receive either the best existing treatment or a promising new treatment.
To help you decide whether or not to participate, you can talk to your specialist or the clinical trials nurse. If you’re still unsure, you can ask for a second opinion from an independent specialist. If you do decide to take part, you have the right to withdraw from the trial at any time; doing so will not jeopardise your ongoing treatment for cancer.
For more information about clinical trials and other research, including questions to ask your doctor and how to find a suitable study, call Cancer Council Helpline 13 11 20. You can also find trials on the website www.australiancancertrials.gov.au.
Making treatment decisions 37
Living with melanoma
Cancer can affect many areas of your life, causing physical and emotional strain. While most people diagnosed with early melanoma have the cancer removed and need no further treatment, it can still be a worrying time for some people. Eating well, exercising and relaxing may help reduce stress and anxiety, and improve wellbeing. Dealing with changes in your emotions and relationships early on is also very important.
Healthy eatingEating nutritious food will help you keep as well as possible and cope with cancer and treatment side effects. Cancer Council Helpline can send you free information about nutrition and cancer.
Staying activeYou will probably find it helpful to be active and exercise regularly if you can. Physical activity, even if gentle or for a short duration, helps to improve circulation, reduce tiredness and elevate mood. The amount and type of exercise you do will depend on what you are used to, how well you feel and what your doctor advises.
Complementary therapiesComplementary therapies may help you cope better with side effects such as pain. They may also increase your sense of control over the diagnosis, decrease your stress and anxiety, and improve your mood. Examples of complementary therapies include herbal medicine, acupuncture, massage, relaxation and meditation.
38 Cancer Council

Some cancer treatment centres offer these therapies as part of their services, but you may have to see a private practitioner. Self-help CDs or DVDs can also guide you through different techniques.
Relationships with othersGive yourself time to adjust to your cancer diagnosis, and do the same for friends and family. People often react in different ways, for example, being overly positive, playing down fears, or keeping a distance. They are also dealing with the diagnosis and the changes.
Sharing your thoughts and feelings with family, friends and colleagues may help strengthen your relationships with them. If you feel uncomfortable talking about your feelings, take your time and approach others when you are ready.
Sexuality, intimacy and cancerHaving cancer can affect your sexuality in physical and emotional ways. The impact of these changes depends on many factors, such as treatment and side effects, the way you and your partner communicate, the way you see your changed body, and your self-confidence. Talking to your partner about changes can help.
Call the Helpline for booklets about complementary and alternative therapies, and sexuality and cancer, or view online at your local Cancer Council website.
Living with melanoma 39
Life after treatmentLife after cancer treatment can present its own challenges. You may need to take some time to adjust to any physical and emotional changes. You may have mixed emotions. Beforehand, you may have been busy with appointments and focused on treatment, but afterwards you may feel anxious or vulnerable. You might worry about every ache and pain and wonder if the cancer is coming back.
Some people say that after cancer they have changed priorities and see life in a new way. For example, you may decide to travel, spend more time with family, or do volunteer work. Although you might feel pressure to return to normal life, you may find that you don’t want your life to return to how it was before cancer.
You might find it helpful to: •re-establish a new daily routine at your own pace •spend time on a leisure activity you enjoy•schedule regular check-ups with your doctor •share your concerns with family and friends and tell them how
they can support you •call Cancer Council Helpline 13 11 20 to request a free booklet
about life after cancer.
Coping with advanced melanomaWhen you are first told that you have advanced melanoma, you will probably feel a range of emotions, such as shock, anxiety or disbelief. These reactions are normal. You may feel some or all
40 Cancer Council
of these emotions at different times. Talking about your feelings with others may help you deal with them; not talking is likely to be more distressing.
If you have continued feelings of sadness, have trouble getting up in the morning or have lost motivation to do things that previously gave you pleasure, you may be depressed. Depression is quite common among people who have cancer. Counselling or medication may help you – talk to your doctor or call the Helpline for more information.
Talk to someone who’s been thereComing into contact with other people who have had similarexperiences to you can be beneficial. You may feel supportedand relieved to know that others understand what you are goingthrough and that you are not alone.
Types of support services*
Face-to-face support groups – often held in community centres or hospitals
Online discussion forums – where people can connect with each other at any time (see www.cancerconnections.com.au)
Telephone support groups – for certain situations or types of cancer, which trained counsellors facilitate
Peer support programs – match you with a trained volunteer who has had a similar cancer experience, e.g. Cancer Connect * Not available in all areas
Living with melanoma 41

After treatment: follow up
Follow up will vary depending on the type of melanoma you have. Your doctor will recommend regular skin checks. Some melanomas require closer monitoring than others. Check with your doctor if you are unsure of your follow-up plan.
Will I get another melanoma?Most people treated for early (localised) melanoma do not have any further trouble with the disease. However, people who have had one melanoma have more than five times the risk of developing another melanoma as an average person of their age.
During your regular follow-up, your doctor will check your melanoma site and lymph nodes to see if the cancer has come back or spread.
It is important to be familiar with your skin, check it for changes (self-examination) and visit your doctor for regular check-ups.
How much sun is enough?After treatment for melanoma it is important to limit exposure to the sun’s UV radiation. Your family members are also at increased risk of developing melanoma and other skin cancers but can reduce their risk by spending less time in the sun and using a combination of sun protection measures.
UV levels vary across Australia, throughout the year, and throughout the day. This means the amount of time you need
42 Cancer Council
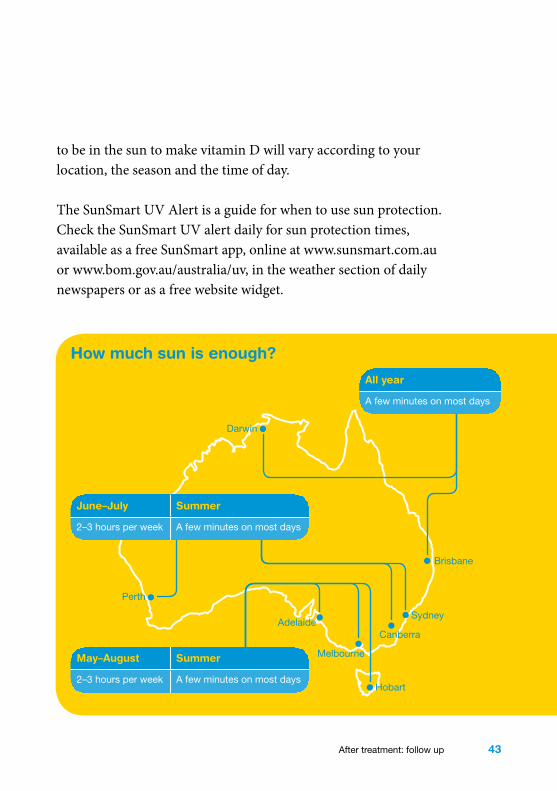
to be in the sun to make vitamin D will vary according to your location, the season and the time of day.
The SunSmart UV Alert is a guide for when to use sun protection. Check the SunSmart UV alert daily for sun protection times, available as a free SunSmart app, online at www.sunsmart.com.au or www.bom.gov.au/australia/uv, in the weather section of daily newspapers or as a free website widget.
How much sun is enough?
May–August Summer
2–3 hours per week A few minutes on most days
Perth
Adelaide
Melbourne
Hobart
Canberra
Sydney
Brisbane
Darwin
All year
A few minutes on most days
June–July Summer
2–3 hours per week A few minutes on most days
After treatment: follow up 43
Protecting your skin from the sun
Use a combination of protective measures to protect your skin from the sun:
•Wear clothing that covers your shoulders, neck, arms, legs and body. Choose closely woven fabric.
•Use a SPF 30+ broad spectrum and water resistant sunscreen. Apply sunscreen 20 minutes before going out and reapply every two hours, or after swimming or any activity that causes you to sweat or rub it off.
•Wear a broad-brimmed hat that shades your face, neck and ears. Adult hats should have at least a 7.5cm brim.
•Use shade from trees, umbrellas, buildings or any type of canopy. UV radiation is reflective and bounces off surfaces, such as concrete, snow, water and sand. If you can see the sky, even if the direct sun is blocked, the shade will not completely protect you from UV.
•Protect your eyes with sunglasses that meet the Australian Standard AS 1067. Wrap-around styles are best.
•Always protect your skin during the sun protection times indicated by the daily SunSmart UV Alert (see previous page for more information).
•Do not use solariums, tanning beds or sun lamps, which give off UV radiation.
•Babies and children should be protected from direct exposure to sunlight. Use shade, umbrellas, clothing and hats to protect them whenever the UV Index is 3 or above. Apply SPF 30+ sunscreen to the areas of a baby’s or child’s skin that cannot be covered with clothing, such as the face and the back of the hands.
44 Cancer Council

Seeking support
Practical and financial helpMelanoma may cause practical and financial difficulties, particularly for people living in rural or remote areas who have to travel for treatment.
Financial assistance – through benefits, pensions and programs – may help pay for the cost of prescription medicines and for travel to medical appointments.
Some people diagnosed with localised melanoma may not feel they need practical, financial or emotional support. People diagnosed with metastatic melanoma may want to ask the hospital social worker or Cancer Council Helpline 13 11 20 which services are available in their area and if they are eligible to receive them.
Cosmetic careSkin cancer treatments such as surgery, skin flaps or grafts often leave noticeable scars. In most cases your doctor will do everything possible to make the scar less noticeable. Scars will fade with time.
You may feel concerned with the appearance of the scar, especially if it’s on your face. Various cosmetics are available to help conceal the scar. Your hairstyle or clothing might also cover scarring. Give yourself time to adapt to any changes. Try to see yourself as a whole person (body, mind and personality) instead of focusing on the parts that have changed. Many people find it helps to talk things through with a counsellor, friend or family member.
Seeking support 45

Useful websites
The internet has many useful resources, although not all websites are reliable. The websites listed below are good sources of information.
AustralianCancer Council Australia ........................................www.cancer.org.au
Adelaide Melanoma Unit.........................................www.rah.sa.gov.au/cancer/melanoma.php
Australian and New ZealandMelanoma Trials Group ..............................................www.anzmtg.org
Melanoma Institute Australia ............................www.melanoma.org.au
Melanoma Patients Australia ..............www.melanomapatients.org.au
Melanoma WA .............................................www.melanomawa.org.au
Peter MacCallum Cancer Centre................ www.petermac.org/skincancerandmelanomainformation
Sunsmart ..........................................................www.sunsmart.com.au
New South Wales GovernmentDark Side of Tanning .........................www.darksideoftanning.com.au
HealthInsite .................................................... www.healthinsite.gov.au
Australian GovernmentDepartment of Health and Ageing ..........................www.health.gov.au
InternationalAmerican Cancer Society ............................................ www.cancer.org
Macmillan Cancer Support ...............................www.macmillan.org.uk
US National Cancer Institute .......................................www.cancer.gov
Melanoma Patients Information Page (US) .................... www.mpip.org
46 Cancer Council
Question checklist
Early-stage melanoma•How thick is the melanoma? •Has the melanoma spread? •What treatment do you recommend and why? •Will a doctor who specialises in melanoma treat me? •Are there other treatment choices for me? If not, why not? •What are the risks and possible side effects of each treatment? •What are the chances I will get lymphoedema as a result of
surgery?•How long will treatment take? Will I have to stay in hospital?
Advanced melanoma•Will the treatment affect me sexually or physically? Will I be able
to do normal things?•Is there anything that can be done to help control the side effects? •How will I know if the treatment is working?•What are my chances of cure?•How much will treatment cost? •Will I have a lot of pain with the treatment? If I do, what will be
done about this? •Are the latest tests and treatments for this type of cancer available
in this hospital? •Are there any clinical trials of new treatments? Will I be eligible to
participate in any of these trials? •How frequently will I have check-ups? •Are there any complementary therapies that might help me? •Is my melanoma hereditary (one that runs in families)? •Is there anyone else with melanoma I can speak to?
Question checklist 47
You may come across new terms when reading this booklet or talking to health professionals. You can check the meaning of other health-related words at www.cancercouncil.com.au/words or www.cancervic.org.au/glossary.
Glossary
acral lentiginous melanoma
A rare type of cutaneous
melanoma that occurs on the
palms of the hands, soles of the
feet or under the nails.
adjuvant treatment
A treatment given with or shortly
after another treatment to
enhance its effectiveness.
advanced cancer
Cancer that has spread deeply
into the surrounding tissues
or away from the original site
(metastasised) and is less likely
to be cured.
anaesthetic
A drug that stops a person
feeling pain during a medical
procedure. A local anaesthetic
numbs part of the body; a general
anaesthetic causes a person to
lose consciousness for a period
of time.
basal cell
One of the three types of cells
that make up the skin’s top layer
(epidermis).
basal cell carcinoma (BCC)
A type of skin cancer that
develops in the basal cells of the
top layer (epidermis) of the skin.
benign
Not cancerous or malignant.
biological therapy
Treatment that activates cells in
the body to fight cancer.
biopsy
The removal of a small sample
of tissue from the body, for
examination under a microscope,
to help diagnose a disease.
Breslow thickness
A description of a melanoma’s
thickness in millimetres, which
is classified into four categories:
less than 1mm, 1–2mm, 2.1–4mm
or greater than 4mm.
48 Cancer Council

cells
The basic building blocks of
the body. A human is made
of billions of cells that are
adapted for different functions.
chemotherapy
The use of cytotoxic drugs to
treat cancer by killing cancer cells
or slowing their growth.
Clark level
A number (1–5) that describes
how far a melanoma has
penetrated into the skin.
cutaneous melanoma
Melanoma that starts in the skin.
dermatologist
A doctor who specialises in
the prevention, diagnosis and
treatment of skin conditions,
including melanoma.
dermis
The lower layer of the two main
layers that make up the skin.
epidermis
The top, outer layer of the two
main layers that make up the
skin.
lentigo maligna melanoma
A type of cutaneous melanoma
that develops in a lentigo maligna
(Hutchinson’s melanotic freckle).
localised melanoma
A melanoma that has not spread
from its starting point to lymph
nodes or other organs.
lymph nodes
Small, bean-shaped structures
forming part of the lymphatic
system. Also called lymph glands.
lymph vessels
Thin tubes that drain the body’s
tissue fluid (lymph) from all over
the body to lymph nodes.
lymphatic system
A network of tissues, capillaries,
vessels and nodes that removes
excess fluid from tissues, absorbs
fatty acids and transports fat, and
produces immune cells.
lymphoscintigraphy
A procedure in which a radioactive
substance is injected into the skin
to identify sentinel lymph nodes.
malignant
Cancer. Malignant cells can
Glossary 49

spread (metastasise) and can
eventually cause death if they
cannot be treated.
melanin
Brown pigment that gives the
skin its colour.
melanocyte
One of the three types of
cells that make up the skin’s
epidermis. Melanocytes produce
melanin.
melanoma
Cancer of the melanocytes.
melanoma in-situ
An early melanoma that has not
penetrated into deeper tissue (the
dermis).
metastasis
A cancer that has spread from
a primary cancer to another
part of the body. Also known as
secondary cancer.
mole
See naevus.
naevus (plural: naevi)
A small dark spot on the skin
that arises from skin cells called
melanocytes. Also called a mole.
nodular melanoma
A type of cutaneous melanoma.
Makes up about 15% of
melanomas, and is often more
aggressive.
primary cancer
The original cancer. Cells from the
primary cancer may break away
and be carried to other parts
of the body, where secondary
cancers may form.
primary site
The part of the body where the
cancer first developed.
prognosis
The expected outcome of a
person’s disease.
radiotherapy
The use of radiation, usually
x-rays or gamma rays, to kill
cancer cells or injure them so
they cannot grow and multiply.
risk factor
A substance or condition that
increases an individual’s chance
of developing a particular type of
cancer.
50 Cancer Council

sentinel node
The first lymph node to receive
lymph fluid directly from a tumour.
skin flap
Moving nearby skin to close a
wound.
skin graft
A shaving of skin moved from
one part of the body to another,
to cover a wound.
squamous cell
One of the three types of cells
that make up the skin’s top layer
(epidermis).
squamous cell carcinoma
(SCC)
A type of skin cancer that begins
in the epidermis.
stage
The extent of a cancer and
whether the disease has spread
from an original site to other parts
of the body.
superficial spreading
melanoma
The most common type of
cutaneous melanoma, making up
almost 65% of all cases.
targeted therapies
Substances that target proteins
in the cancer cells that signal the
cancer cell to grow.
tumour
A new or abnormal growth of
tissue on or in the body. A tumour
may be benign or malignant.
ultraviolet (UV) radiation
The part of sunlight that causes
tanning, sunburn and skin
damage. It is also produced by
solariums, tanning lamps and
sunbeds. UV radiation cannot be
seen or felt.
wide local excision
A surgical procedure to remove
a melanoma with some of the
healthy tissue around it.
Glossary 51

How you can help
At Cancer Council we’re dedicated to improving cancer control. As well as funding millions of dollars in cancer research every year, we advocate for the highest quality care for cancer patients and their families. We create cancer-smart communities by educating people about cancer, its prevention and early detection. We offer a range of practical and support services for people and families affected by cancer. All these programs would not be possible without community support, great and small.
Join a Cancer Council event: Join one of our community fundraising events such as Daffodil Day, Australia’s Biggest Morning Tea, Relay For Life, Girls Night In and Pink Ribbon Day, or hold your own fundraiser or become a volunteer.
Make a donation: Any gift, large or small, makes a meaningful contribution to our work in supporting people with cancer and their families now and in the future.
Buy Cancer Council sun protection products: Every purchase helps you prevent cancer and contribute financially to our goals.
Help us speak out for a cancer-smart community: We are a leading advocate for cancer prevention and improved patient services. You can help us speak out on important cancer issues and help us improve cancer awareness by living and promoting a cancer-smart lifestyle.
Join a research study: Cancer Council funds and carries out research investigating the causes, management, outcomes and impacts of different cancers. You may be able to join a study.
To find out more about how you, your family and friends can help, please call your local Cancer Council.
52 Cancer Council

Cancer Council Helpline 13 11 20
Cancer Council Helpline is a telephone information service provided by Cancer Council Victoria for people affected by cancer.
For the cost of a local call (except from mobiles), you, your family, or friends can talk about your concerns and needs confidentially with experienced cancer nurses. Helpline nurses can send you information and put you in touch with support services in your area.
If you need information in a language other than English, you can call the Multilingual Cancer Information Line (see the back cover).
The Helpline is open Monday to Friday, 9am to 5pm. If calling outside business hours, you can leave a message and your call will be returned the next business day.
Cancer Council Publications
If you found this booklet helpful, you might want to request another free resource from Cancer Council. Call the Helpline if you would like a copy of any of the following resources:
Treatment and side effects
•Understandingchemotherapy•Understandingradiotherapy
•Complementaryand alternative cancer therapies
Coping with cancer and recovery
•Nutritionandexercise•Lifewithcancer•Commonquestionsabout cancer pain
•Copingwithcancerfatigue•Sexualityandcancer•Whencancerwon’tgoaway
For further information and details pleasevisit our website: www.cancervic.org.au
Cancer information in your languageFor the cost of a local call (except from mobiles), you can talk confidentially to a Cancer Council nurse with the help of an interpreter.Simply follow these steps:
1. Call 13 14 50, Monday to Friday, 9am to 5pm.
2. Say the language you need.
3. Wait on the line for an interpreter (may take up to 3 minutes).
4. Ask the interpreter to contact Cancer Council Victoria Helpline 13 11 20.
5. You will be connected to the interpreter and a cancer nurse.
OC
T 2012U
ND
ER
STA
ND
ING
ME
LAN
OM
A
Copyright © 2022 FDOKUMEN