A Critical Comparison of Davis’ Principles of Plastic Surgery with Gillies’ Plastic Surgery of...
11
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright
Transcript of A Critical Comparison of Davis’ Principles of Plastic Surgery with Gillies’ Plastic Surgery of...
This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
A critical comparison of Davis’ Principles of PlasticSurgery with Gillies’ Plastic Surgery of the face*
M. Felix Freshwater*
University of Miami School of Medicine, Department of Surgery, 9100 S. Dadeland Blvd. Suite 502,Miami FL 33156-7815, USA
Received 17 January 2010; accepted 4 March 2010
KEYWORDSHistory of PlasticSurgery;John Staige Davis;Harold Delf Gillies,Frederick Strange Kolle;Manchot;Tansini
Summary Introduction: The second decade of the 20th century saw the publication of twolandmark books - John Staige Davis’ Plastic Surgery its Principles and Practice published in Phi-ladelphia in 1919 and Major Harold Gillies’ Plastic Surgery of the Face published in the UnitedKingdom early 1920. The aim of this paper is to compare the books critically as scholarlyachievements in their time and note their present day relevance.Material and Methods: Copies of both books are available online having been scanned by Goo-gle and Microsoft. They were analyzed with Acrobat software for key words. A senior plasticsurgeon with over 30 years of clinical experience reviewed both books for current relevance.Key results: Davis’ book was more comprehensive as it encompassed reconstructive plasticsurgery from head to toe while Gillies’ book focused on the face. Davis’ book contained a bibli-ography over 2000 references, while Gillies’ book had one reference. Despite Davis’s title con-taining the word ‘Principles’, Gillies’ book not only mentioned principles almost five times asoften, but almost all of Gillies’ principles remain relevant 90 years later. Furthermore, thequality of Gillies’ post-operative results are far outshines to Davis’.Conclusion: While Davis’ book demonstrates his honesty and scholarship, now it is as inter-esting as a historical curiosity. Gillies’ book remains valuable as it shows his originality andthe continued relevance of his principles.ª 2010 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
In June 2009 Johns Hopkins’ plastic surgery reunion speakerproudly declared that in 1919, John Staige Davis hadwritten ‘a unique textbook in a new field’. I knew that Davisand Sir Harold Gillies were contemporaries and I wonderedhow their books, published within a year of each other,compared. Before comparing the content, it is worthwhileto discuss the authors’ motives for writing their books. Both
* Presented at the 2009 Winter Meeting of the British Associationof Plastic Reconstructive and Aesthetic Surgeons, December 3,2009.
* Tel.: þ1 305 670 9988; fax: þ1 305 670 0770.E-mail address: [email protected]
1748-6815/$-seefrontmatterª2010BritishAssociationofPlastic,ReconstructiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.doi:10.1016/j.bjps.2010.03.009
Journal of Plastic, Reconstructive & Aesthetic Surgery (2011) 64, 17e26
Author's personal copy
Davis and Gillies shared the same motive in writing theirbooksdfrustration. Each was frustrated by the state ofplastic surgery as he experienced it. To better understandthe source of their frustrations, it is important to learnsomething about these authors.
Who was John Staige Davis?
Davis was born in Virginia on January 15, 1872 and was namedafter his grandfather who was surgeon during Civil War. Hisfather was a physician in our Public Health Service. Davis grewup in the Dakota Territory and headed back to the East Coastfor high school and for his bachelor’s degree that he receivedfrom Yale in 1895. Davis moved from New Haven to Baltimorewhere he joined the class of 1899 of a new medical schoolnamed after a Quaker merchant named Johns Hopkins. Davisperformed well enough at Hopkins to be asked to stay at JohnsHopkins Hospital for one year as an intern. He completed4-month rotations in medicine under Sir William Osler,Obstetrics under Howard Kelly and Surgery under WilliamHalsted. Next, he completed three years of surgery training atwhat is now Union Memorial Hospital, whose chief of surgery,John Finney, had been Halsted’s first associate at Hopkins.1
Davis wrote that it was Finney who suggested that hespecialize in plastic surgery.
‘‘He said that every general surgeon was operating onthese cases because they had to be taken care of, butthat no one in this country was doing the work properlyand that the field was undeveloped.’’2
After completing his surgery training, Davis became thefirst American to limit his practice to plastic surgery, and, inaddition, he did research at Hopkins, published a number ofexperimental papers and taught at the now defunct Wom-en’s Medical College in Baltimore.
John Staige Davis was a prophet without honor in his ownland.3 Neither Halsted nor his successors at Hopkins-DeanLewis and Alfred Blalock supported Davis. The most glaringexample of their failure to support Davis was that they nevergranted him admitting privileges; in other words, he hadneither beds nor operating time. He could only treat patientsin the ‘dispensary’ or outpatient department. Surgery resi-dents could ‘invite’ him to do cases with them and theultimate irony was that he trained at least one Hopkinsresident, Kenneth Pickrell, who without any further trainingbeyond his time with Davis, reigned for over a quarter ofa century as chief of plastic surgery at Duke.4
Pickrell admitted that despite most of the resident casesbeing indigent, it was Davis who operated on all of hispatients while he assisted. In addition, Davis traineda number of preceptees including Edward Hanrahan, whowould become Webster’s brother-in-law, and EdwardKitlowski, the latter of whom Blalock appointed chief ofplastic surgery at Hopkins.
Davis served as a captain in the US Army from 1917 to1919 but never saw service overseas. He wrote PlasticSurgery Its Principles and Practice during this time and itwas published in 1919 when he was 42 years old.
Davis’ frustration was extrinsic. He was frustrated byhow he was treated by Halsted and he was frustrated by thescope of plastic surgery.
Davis wrote in his introduction:
‘‘During the war (1914e1918) plastic surgery was arbi-trarily limited, by regulation, to maxillo-facial recon-struction. This, it is true, is a very important part of thesubject, but it must be remembered - and the factshould be emphasized - that plastic surgery of the trunkand extremities is equally important. The results may beless spectacular, but surely are just as vital to thepatient. The field of plastic surgery extends from the topof the head to the sole of the foot, and no properlytrained plastic surgeon would be willing to limit his workto the face alone.’’5
Davis found frustration with the dearth of plasticteaching when he wrote:
‘‘The teaching of this subject has been absolutelyneglected everywhere, both for medical students andfor post-graduates. There is yet no department forinstruction of this kind in any American University, andno complete textbook has hitherto been written on thesubject.’’
‘‘It has been commonly said that any surgeon who cansuccessfully do an intestinal suture can do plasticsurgery. Careful investigation of this point warrants thestatementewithout qualificationethat few generalsurgeons do plastic surgery as it should be done. Thepossibilities are little understood by the practisingphysician, and hardly more by the general surgeon.There should be a well-trained plastic surgeon on thestaff of every large general hospital, in order that thesepatients may be cared for intelligently.’’6
Davis declared the purpose of his book to be:
‘‘To show the general practitioner the possibilities ofplastic surgery, and start the student or beginner in thissubject on the right track. The more experienced surgeonmay also find methods with which he is unfamiliar, andwhich may be of use to him in dealing with cases.’’6
In 1926 Davis warned Webster that:
‘‘One could not earn a living from the practice of plasticsurgery alone.’’7, a
We may suspect how Davis dealt with this obstacle basedupon this article titled, ’’Baltimore Society Events’’, thatappeared in the January 5, 1902 issue of The New York Times:
‘‘A fitting climax to the day’s entertainments was thebrilliant ball given in the late evening by Mr. and Mrs. W.Graham Bowdoin in honor of their debutante daughterMiss Kathleen Bowdoin. The elegant new residence onNorth Charles Street just completed by Mr. Bowdoinwhich is not only one of the handsomest in Baltimore,but in this section of the country.’’8
Kathleen Bowdoin married Davis in 1907.b Despite havingbeen a debutante, she drew a substantial portion of the
a Pound incorrectly spelled the name Davies and wrote that Daviswas ‘‘a New York pioneer of the specialty.’’
b Op. Cit. reference 1 p. 373.
18 M.F. Freshwater
Author's personal copy
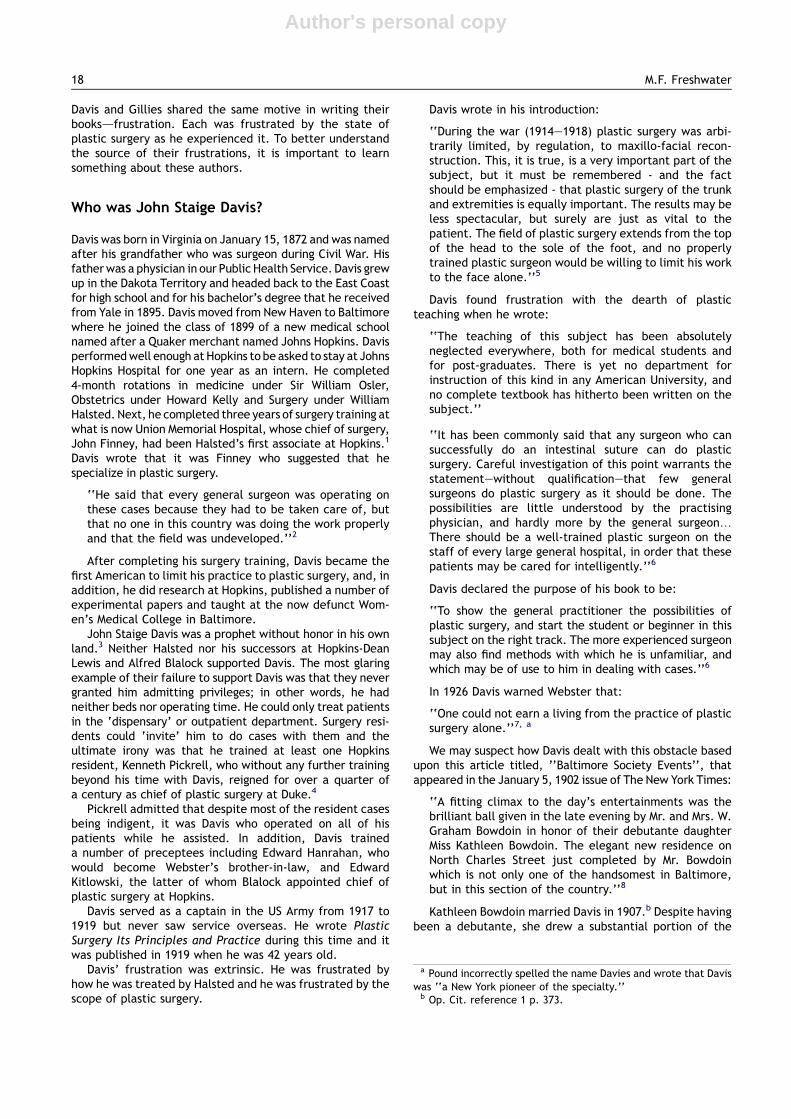
Figure 1 Davis’ depiction of his modification of Tansini’s musculocutaneous flap. In the legend he noted that he did not includemuscles as had Tansini. In the text Davis wrote ‘. plastic operations are not desirable in covering defects left by the radicaloperation for carcinoma of the breast’ (Davis JS. p. 625).
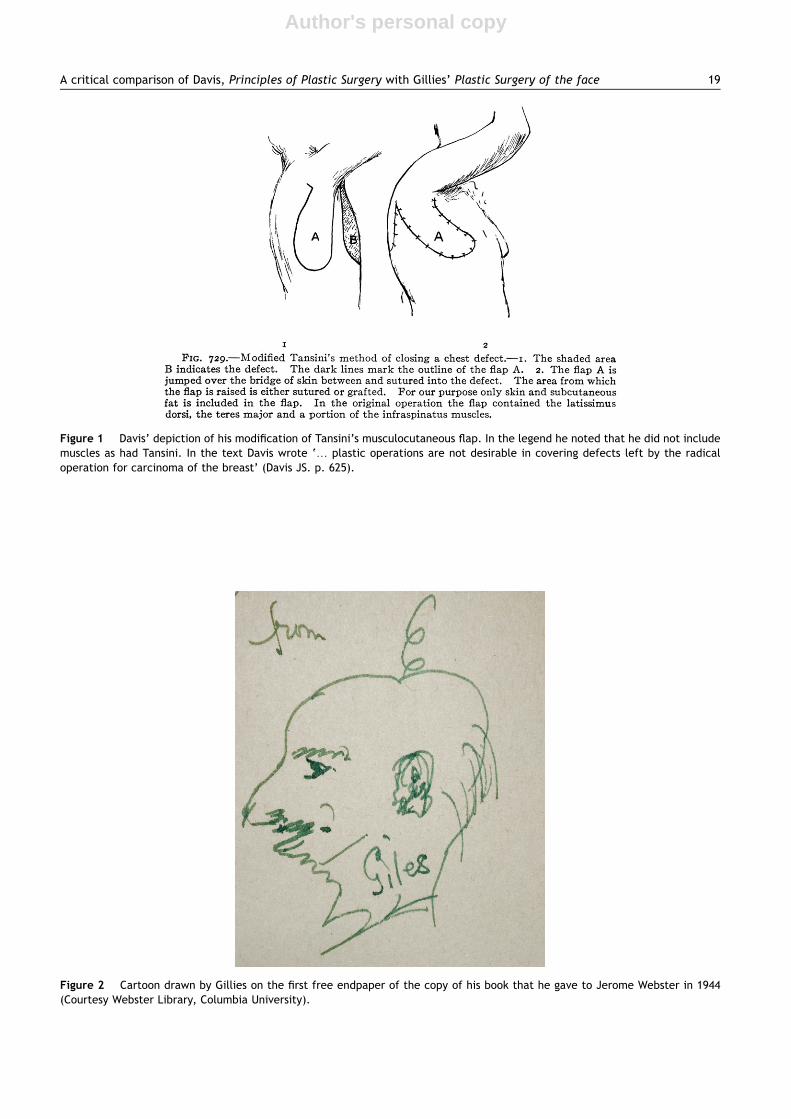
Figure 2 Cartoon drawn by Gillies on the first free endpaper of the copy of his book that he gave to Jerome Webster in 1944(Courtesy Webster Library, Columbia University).
A critical comparison of Davis, Principles of Plastic Surgery with Gillies’ Plastic Surgery of the face 19
Author's personal copy
artwork for her husband’s book that he dedicated to herwith the inscription:
‘‘To K.B.D. whose good counsel and never failingencouragement has meant so much to me in the ups anddowns of life.’’9
Davis’ book was a scholarly achievement and an evenmore amazing accomplishment for a solo author who hadbeen practising, teaching and performing laboratoryresearch. Its 25 chapters covered the field from head totoe. Davis included 2005 references for:
‘‘The reader who wishes to delve more deeply into thatparticular subject.’’10
Two references are particularly notable. The first was thework by Tansini on the use of the latissimus dorsi muscu-locutaneous flap for covering post-mastectomy defects.Sadly, this work was ignored in America for over halfa century. Curiously, Davis said that he specifically excludedany muscle when he used this flap. (Figure 1) 11 The otherreference was the work of Manchot on the arterial supply ofthe skin. Although Davis included many illustrations fromManchot’s work, he did not refer to them in the text.12
GilliesdCoping with frustration
Gillies too had to deal with frustration. Unlike Davis’extrinsic frustration, Gillies’ frustration was intrinsicbecause unlike Davis who was spurned by Halsted, Gillieshad virtually unlimited support and resources throughthe Royal Army Medical Corps (RAMC). His book PlasticSurgery of the Face, published in 1920 by OxfordUniversity Press, delved into the frustrations that hefaced when he had to treat over 2000 facial injuriesbeginning in 1916.
Not only was Gillies better equipped by the RAMC, butalso he was better equipped to deal with frustrations
because he had grown-up overcoming social, physical andpsychological handicaps.
Harold Delf Gillies was born on June 17, 1882, theyoungestamong eight children whose father died when Harold wasthree years old.13 As a child, Gillies fractured his elbow thatresulted in his having permanent limitation of motion.c
Nevertheless, Gillies compensated for his limited mobility,got his Blue on the 1904 championship Cambridge crew andthrough persistent practice served on Cambridge’s golf team.It was through golf that Gillies became well-known to thesporting public winning the St. George’s Challenge Cup forAmateurs in 1913. He had two handicapped and inventeda raised tee that enabled him to drive a ball further than hemight otherwise do particularly in light of his stiff elbow. It islogical to conclude that he invented his ergonomic needleholder to compensate for his limited ability to pronate andsupinate because of his childhood fracture.
Gillies discounted his personal appearance and dealtwith it through humor (Figure 2):
‘‘If I with a bald head and no chin were to wake uptomorrow with curly red hair and a strong chin, imaginehow pleasant my disposition would become?’’14
Plastic Surgery of the Face begins like a Spielberg actionfilm that immediately engages the viewer as in Jaws orJurassic Park, where the shark attacks or velociraptorattacks early in the film. Similarly, on the first page ofchapter one, Gillies sucks you into the maelstrom of hisWorld War I experience. On the first page of chapter one,he tells us that something was rotten in the state of plasticsurgery. He noted:
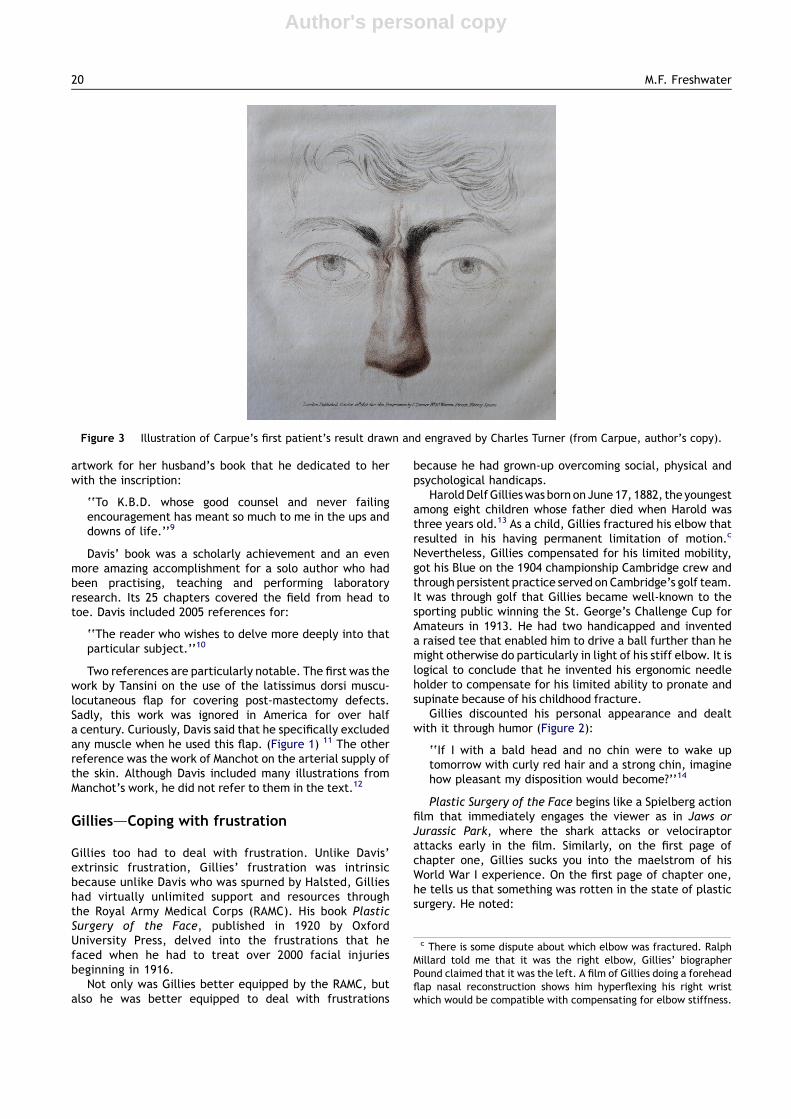
Figure 3 Illustration of Carpue’s first patient’s result drawn and engraved by Charles Turner (from Carpue, author’s copy).
c There is some dispute about which elbow was fractured. RalphMillard told me that it was the right elbow, Gillies’ biographerPound claimed that it was the left. A film of Gillies doing a foreheadflap nasal reconstruction shows him hyperflexing his right wristwhich would be compatible with compensating for elbow stiffness.
20 M.F. Freshwater

Author's personal copy
‘‘There is hardly an operation hardly a single flap in useto-day that has not been suggested a hundred years ago.The earlier months, then, were spent in a very thoroughtrial of the then known methods. It has been illuminatingto discover the impracticability of many of these, whichwould appear to have been put forward on the study ofone case only, or even on purely theoretical grounds.’’15
The problem that Gillies faced was that the vast body ofplastic surgery literature that had developed in the 19thcentury was for the most part science fiction. Plasticsurgery had begun in London with Joseph Carpue’sanatomic experiments and subsequent clinical cases.16
Carpue was a surgical scientist in the finest tradition ofJohn Hunter and he demanded accurate representations ofhis post-operative results. To achieve this goal, Carpue had
noted artist Charles Turner who creates illustrations.(Figure 3) However, Carpue was unique. All too many textsand papers contained that followed him had results thatwere imaginative at best and dangerous at worst. Here aresome astounding results of mid-19th century Americanplastic surgery for the release of a burn contracture of theneck (Figure 4).17
The nadir of plastic surgery as science fiction was reachedin the United States shortly before World War I. Notwith-standing the statement at the Hopkins reunion, John StaigeDavis did not write the first American textbook of plasticsurgery. He wrote the first honest American textbook ofplastic surgery. A strange character named Frederick StrangeKolle wrote the first 20th century textbook of plastic surgery‘‘Plastic and Cosmetic Surgery’’ published in 1911 by
Figure 4 Series of engravings demonstrating the release of burn contractures using Mutter’s flap (from Pancoast, author’s copy).
A critical comparison of Davis, Principles of Plastic Surgery with Gillies’ Plastic Surgery of the face 21

Author's personal copy
Appleton & Co. in New York and London. Kolle’s topics rangefrom antiseptics, anesthetics, blepharoplasty, otoplasty,cheiloplasty, meloplasty, rhinoplasty and electrolysis. Thelongest chapter containing 130 out of 511 pages was about‘‘Subcutaneous Hydrocarbon Prostheses’’ d paraffin injec-tions. The book is replete with line drawings that demon-strate amazing post-operative results.d
Faced with thousands of patients with injured faces, noreliable anesthesia, no blood transfusions, no antibiotics,the prospect that failure could result in suicide and hardlyany valid techniques to draw upon, Gillies created his ownprinciples that he enumerated in the first chapter. We candivide the principles into pre-operative, operative andpost-operative groups. (Table 1)
Comparing Davis’ and Gillies’ books
In contrast to Davis who exhaustively reviewed the litera-ture upto 1918, Gillies had just one reference. In describingthe permanence of cartilage grafts, Gillies cited anexperimental paper on grafts in dogs from the 1917 volumeof Annals of Surgery by none other than John StaigeDavis!18
One might imagine that a 21st century fillerologist wouldwrite:
Table 1 Gillies’ Principles circa 1920
Pre-Operative1. Mistakes in diagnosis due to inadequate examination are perhaps the commonest cause of indifferent treatment.2. In planning the restoration, function is the first consideration, and it is indeed fortunate that the best
cosmetic results are, as a rule, only to be obtained where function has been restored.3. The restoration is designed from within outwards. The lining membrane must be considered first,
then the supporting structures, and finally the skin covering.4. There is no royal road to the fashioning of the facial scaffold by artificial means: the surgeon must tread
the hard and narrow way of pure surgery.5. It may be laid down as a guiding maxim that the replacement should be as nearly as possible in terms of
the tissues lost, i.e. bone for bone, cartilage for cartilage, fat for fat, etc.
Operative1. All normal tissue should be replaced as early as possible, and maintained in its normal position.2. Speaking generally, the use of any foreign body is to be condemned whenever it is possible to substitute
a graft from the patient himself. Any form of a foreign body is a tissue irritant, and tends to givetrouble early or late, in the attempt on the part of the tissues to remove it; whereas grafts,if successful in the early stages, continue satisfactory.
3. The gain of skin below the mouth has to be written off against the loss which occurs when the bed fromwhich it was raised is closed.
4. Apart from those containing a definite artery such as the superficial temporal (the base for which maybe cut quite narrow), the base should be at least as wide as any other part of the flap.
5. The pedicle is returned not earlier than ten days in most cases, and it is of advantage largely toincrease this interval where the blood-supply of the receiving bed is dubious.
Post-Operative1. Disappointment is in store for him who would confine his repair to the surface tissues, heedless of
Nature’s lessons in architecture.2. Satisfactory early results are obtained by very cautious and repeated injections of paraffin wax
in small quantities, but the late results are rarely good and are often appalling.3. For larger hollows, free fat and muscle grafts are used; these are naturally more uncertain
of result. It is not yet established how they will be affected in conditions of wasting, or in old age. The fat-graft,however, owing to fat necrosis, often undergoes a partial absorption.
4. The production of an invisible scar is a question constantly exercising the mind of the plastic surgeon.5. The factors necessary for the production of the optimum scar are:
Asepsis, avoidance of tension on the apposing sutures, perfect apposition of the skin edges, an oftenunknown personal factor in the patient, early removal of sutures.
6. The most frequent cause of failure of a Wolfe graft is lack of pressure firm enough to ensure complete apposition.7. Time is the plastic surgeon’s greatest ally, and at the same time his most trenchant critic.
d Kolle claimed various qualifications including Fellow of NewYork Academy of Medicine, member of the Deutsche MedizinischeGesellschaft and the Kings County Hospital Alumni Society. He hada curious way of citing authorities. He quoted names and had anindex of the names, but, unlike Davis, gave no references. His bookcontained just four clinical cases; a cosmetic otoplasty, a recon-structive otoplasty, a lower lid ectropion, and a nasal rim recon-struction. Kolle’s book had little positive influence on thedevelopment of 20th century plastic surgery and as Gillies saidwhen describing various French and German cheek flaps shouldhave been ‘relegated to the lumber-room’ where it would remainundisturbed for decades.
22 M.F. Freshwater
Author's personal copy
‘‘The technique for the injection . is simple and theinjection can be given, after a little practice, by anyonewho is able to purchase the equipment.’’
However, that was Davis writing about paraffininjections and he listed 22 complications of paraffininjections.19
Occasionally each author let the reader peek behind thecurtain and see what his feelings were. Perhaps with Kollein mind, here is Davis discussing paraffin injections:
‘‘The injection of paraffin is the sheet anchor of the‘quack’ facial specialist.’’20
‘Quack facial specialist’ is a biting phrase. A sheetanchor is an emergency anchor; hence, Davis’s sentencemakes more sense as a scatological pun when sheet ispronounced with a Virginian accent.
Gillies’ puckish sense of humor also is evident in hisbook. For example, in thanking his photographer he wrote:
‘‘Their excellence speaks for itself .[he was] devotedto ensuring that [the photos] shall be an honest and truerecord. He has had to suborn his art to this end, sternlysuppressing the temptation to manipulate the lighting orretouch the negatives.’’21
In discussing nasal reconstruction he wrote:
‘‘No man has ever, previously, had sufficient material toelevate this branch of surgery from its unfavourablestatus, which has been so aptly summed up by theFrench in their saying before he was horrible: now he isridiculous.’’22
By using search technology, one can compare both booksfor key words and references. (Table 2) It assists us inseeing how painfully honest each surgeon was.
Writing about surgical correction, Davis states that thecosmetic results for ear reconstruction were fair or poor.Gillies used the word ‘cosmetic’ almost twice as often.When Gillies used the word ‘cosmetic’ the word ‘function’frequently appears nearby. Often Gillies qualified hisresults:
‘‘The result of this implantation was satisfactory froma cosmetic point of view but, surgically speaking, it wasnot gratifying on account of a small leak into the nose,causing later infection of the graft.’’
‘‘In one such case its adoption has resulted in a markedcosmetic improvement, and also a small improvement infunction.’’
‘‘Improvement has been achieved to a greater or lesserextent, and in three, the cosmetic result has beendistinctly indifferent.’’
Remembering that both surgeons were operating beforethe development of antibiotics and blood transfusions,each reported patients dying. Davis reported one patientdying from pneumonia and one cleft palate child almostsuccumbing from undiagnosed hemophilia. Gillies describedhow two of his burn reconstruction patients died from post-operative infection.
Despite Davis’s title containing the word ‘Principles’,Gillies’ book without ‘Principles’ in its title, mentions
principles 102 times compared to Davis’ 28 times. While mostof Davis’ 28 times are adjectives or adverbs Gillies’ principleswere the solid foundation of his work.
Although Davis wrote:
‘‘If this book should prove of use in bringing relief to anyone of our wounded soldiers who’ require the aid of theplastic surgeon, I shall feel fully repaid for the timespent in its preparation.’’23
He had no military cases. In contrast, the overwhelmingmajority of Gillies’ book was a record of military plasticsurgery. Just one chapter with four pages of text called‘Plastic Surgery of Civil Cases’ had civilian work. Interest-ingly, that chapter describes the theoretical use of a tubedpedicle flap for post-mastectomy breast reconstruction.24
(Figure 5)
What were the career consequences of these books?
Despite being under-appreciated by Halsted, the short-term consequences for Davis were most interesting. In1925, Yale awarded him an honorary M.A. degree. Thecitation read:
‘‘He has been a pioneer in plastic surgery. His volumi-nous treatise on the subject published in 1919 is anacknowledged authority. In this field he stands at thehead of his profession, his combined original researchwith practical services to humanity, stimulating theminds of his pupils, colleagues, and healing the bodies ofsufferers.’’e
There were no short-term career consequences forGillies because of his book, he was appointed O.B.E. in1919, was promoted C.B.E. in 1920, and was knighted in1930 for his military service and not for his writing.25
From a surgical perspective, Davis’ and Gillies’ worksbest can be compared as shown in (Table 3).
Davis’ longest lasting technical advance was the smalldeep skin graft. It was an ideal advance for the generalsurgeon who faced a difficult wound coverage problem, asit was easy to perform requiring no complex equipment andhardly any skill. The results, though aesthetically poor,were long lasting. (Figure 6) Gillies’ longest lasting
Table 2 Keyword and reference comparison of Davisand Gillies
Davis Gillies
Principle(s) 28 102Cosmetic 12 23Cure 10 16Death (patient) 2 2Mistake 2 9Safe 3 4Simple (method) 24 22References 2005 1
e Op. cit. reference 1 p. 375.
A critical comparison of Davis, Principles of Plastic Surgery with Gillies’ Plastic Surgery of the face 23

Author's personal copy
Figure 5 These three line drawings are the final stages of Gillies’ theoretical breast reconstruction. He believed that ‘‘The gapleft by removal of the female breast should be remediable in terms of tubed flaps designed to carry large masses of fat, e.g. fromthe buttock.’’ (from Gillies, author’s personal copy).
24 M.F. Freshwater

Author's personal copy
technical advance was the tubed pedicle flap. It wasa demanding and requiring planning, operative skill andjudgment and complex post-operative care. Davis’ deepgraft was designed to be permanent, but Gillies’ tubedpedicle flap was designed to be only a temporary deliverysystem for tissue d a means to an end. If Davis had ‘con-nected the dots’ about the arterial supply of the skin fromhis references to Tansini and Manchot, then Gillies’ tubedpedicle flap may have reached obsolescence after WorldWar I rather than have lasted as a viable technique fordelivering tissue for over 60 years.
One objective means of comparing the value of thebooks is to compare their economic appreciation. Although,both books has a similar list price when first published, theasking price for an original copy of Gillies’ has nowincreased by almost 3½ times as much as the value of Davis’(Table 4).
Despite the dear current costs of hard copies of bothbooks, each can be enjoyed and studied for free as they areboth accessible on the internet and can be downloaded by
anyone. Davis’ book has been digitized by Google.26 Gillies’book is part of the Internet Archive.27
Competing interests
I did my plastic surgery fellowship at Johns Hopkins thatnow proudly claims John Staige Davis as its first plasticsurgeon. I did my plastic surgery residency under RalphMillard, who was Gillies co-author and disciple.
Financial disclosure
None.
References
1. Davis WB. The life of John Staige Davis. Plast Reconstr Surg1978;62:368e78.
2. Davis JS. Plastic Surgery Its Principles and Practice. Phila-delphia: P. Blackiston’s Sons; 1919. vii.
3. Webster JP. In memoriam-John Staige Davis. Plast ReconstrSurg 1947;2:171e3.
4. Pickrell KL. Recollections of John Staige Davis. Ann Plast Surg1979;2:346e9.
5. Davis JS. Plastic Surgery Its Principles and Practice. Philadelphia:P. Blackiston’s Sons; 1919. viieviii.
6. Davis JS. Plastic Surgery Its Principles and Practice. Philadelphia:P. Blackiston’s Sons; 1919. vii.
7. Pound R. Gillies Surgeon Extraordinary. London: MichaelJoseph; 1964. 78.
8. Baltimore Society Events NY Times. Available from: http://query.nytimes.com/mem/archive-free/pdf?resZ9E03E6DA103DEE32A25756C0A9679C946397D6CF; January 5, 1902 [accessed15.11.09].
9. Davis JS. Plastic Surgery Its Principles and Practice. Philadelphia:P. Blackiston’s Sons; 1919. v.
10. Davis JS. Plastic Surgery Its Principles and Practice. Philadelphia:P. Blackiston’s Sons; 1919. viii.
11. Davis JS. Plastic Surgery Its Principles and Practice. Phila-delphia: P. Blackiston’s Sons; 1919. 627.
12. Davis JS. Plastic Surgery Its Principles and Practice. Phila-delphia: P. Blackiston’s Sons; 1919. 114e115, 607e609, 689e
692.13. Available from: http://www.dnzb.govt.nz/dnzb/default.asp?
Find_Quick.asp?PersonEssayZ3G9 [accessed 15.11.09].14. Pound R. Gillies Surgeon Extraordinary. London: Michael
Joseph; 1964. 72.15. Gillies HD. Plastic Surgery of the Face. London: Henry Frowde;
1920. 3e4.16. Freshwater MF. Priorities in Plastic Surgery. Plast Reconstr Surg
1984;73:987e90.17. Pancoast J. A Treatise on Operative Surgery. Phila-
delphia: Cary and Hart for G.N. Lewis; 1846. 366 plate76.
18. Davis JS. A comparison of the permanence of freetransplants of bone and cartilage. Ann Surg 1917;65:170e4.
19. Davis JS. Plastic Surgery Its Principles and Practice. Phila-delphia: P. Blackiston’s Sons; 1919. 45e46.
20. Davis JS. Plastic Surgery Its Principles and Practice. Philadelphia:P. Blackiston’s Sons; 1919. 47.
21. Gillies HD. Plastic Surgery of the Face. London: Henry Frowde;1920. 3e4.
22. Gillies HD. Plastic Surgery of the Face. London: Henry Frowde;1920. 211.
Table 4 Objective Economic Comparison
Davis Gillies
Publisher’s list price $10 £3.15Amazon price $963 £1338Increase in price 9530% 42376%
Table 3 Subjective Comparison
Davis Gillies
Results Journeyman MasterGoal for target
audienceCookbook Theoretical/
aspirationalMajor technical
advanceSmall deepskin graft
Tubed pedicle flap
Utility of thetechnical advance
Little skill,less judgment
More skill,more judgment,artistry
Figure 6 50-year post-poperative result of a patient who hadsmall deep pinch grafts by John Staige Davis after a street caraccident. Note the hypopigmented donor sites and cobblestoneappearance of the grafts on the foot (photographed by authorJuly 4, 1976).
A critical comparison of Davis, Principles of Plastic Surgery with Gillies’ Plastic Surgery of the face 25
Author's personal copy
23. Davis JS.Plastic Surgery Its Principles and Practice. Philadelphia:P. Blackiston’s Sons; 1919. ix.
24. Gillies HD. Plastic Surgery of the Face. London: Henry Frowde;1920. 393e395.
25. Obituary: Sir Harold Gillies. Br Med J Sep 1960;2:866e7. doi:10.1136/bmj.2.5202.866-c [accessed 11.11.09].
26. Available from: http://books.google.com/books?idZC2AoAAAAYAAJ&printsecZfrontcover&dqZeditions:0Uguck6yTBPURd#vZonepage&qZ&fZfalse [accessed 11.11.09].
27. Available from: http://www.archive.org/details/plasticsur-geryof00gilluoft [accessed 11.11.09].
26 M.F. Freshwater