Desired Future Condition Explanatory Report (Final) Carrizo ...
Upload
independentCategory
view
4download
0
Law and Human Behavior, Vol. 22, No. 4, 1998
A Comparison of Forensic and NonforensicMalingerers: A Prototypical Analysis of ExplanatoryModels
Richard Rogers,1 Randall T. Salekin,1 Kenneth W. Sewell,1 Alan Goldstein,2 andKathleen Leonard'
Explanatory models of malingering strive to understand the primary motivationunderlying attempts to feign. Rogers, Sewell, and Goldstein (1994) provided empiricalsupport for the concepiualization of pathogenic, criminological, and adaptationalmodels. In the current study, a prototypical analysis of 221 forensic experts results ina slightly refined formulation: the adaptational model was decomposed into its twobroad dimensions (cost-benefit analysis and adversarial setting). An important findingis that the factor structure for the explanatory models remained stable when applied toboth forensic and nonforensic cases. As a first investigation, significant differences wereobserved in prototypical cases of malingering by the category of referral (forensic ornonforensic) and by type of feigning (mental disorders, cognitive impairment, andmedical syndromes). Surprisingly, the feigning of medical syndromes appeared to playa relatively prominent role in both forensic and nonforensic cases and to be influencedby the apparent adversarial context of the assessment. Finally, important genderdifferences were observed, especially with nonforensic prototypical cases of malingering.
Explanatory models of malingering may have a profound effect on both the con-ceptualization of feigning and clinical methods used for its detection. For example,practitioners who postulate an underlying antisocial motivation for malingering arelikely to be sensitized to the possibility of malingering in psychopathic persons, butless attentive to this consideration in nonpsychopathic persons. Moreover, clinicalmethods are informed by explanatory models; for instance, the assessment of an-tisocial personality disorder (APD) is an essential component for practitioners whoview antisocial motivation as the principal impetus for malingering.
Rogers (1990a, 1990b) described two existing explanatory models of malinger-ing (pathogenic and criminological) and formulated a third (adaptational). Thepathogenic model assumes that the underlying motivation is a mental disorder. As
'University of North Texas, Denton, Texas.2John Jay College. New York, New York.
353
OI47-7307/98/0800-353s15.00/I @ 1998 American Psychology-U* Society/Division 41 of the American Psychological Association

patients grapple for a sense of control over their emerging psychopathology, theyconsciously fabricate symptoms. In many cases, the pathogenic model posits thatthe deteriorative course of the disorder will result in bogus symptoms becomingsupplanted by genuine symptoms. Concerns that criminal defendants and civil liti-gants feign mental disorders to further their own ends foreshadowed the develop-ment of the criminological model (Rogers, 1997b). The criminological model waspromulgated by the publication of the third edition of the Diagnostic and statisticalmanual of mental disorders (DSM-III; American Psychiatric Association [APA],1980) and continues to be espoused by the DSM (APA, 1987, 1994). This modelrests largely on the untested assumption that uncooperative persons with APD back-grounds are likely to malinger when faced with a forensic evaluation. The male fideproduction of symptoms represents primarily a criminal/antisocial motivation.
The formulation of the adaptational model was an effort to free explanatorymodels of malingering from monistic notions of madness (pathogenic) or badness(criminological). The adaptational model suggests that potential malingerers engagein a cost-benefit analysis of their options. When faced with a hostile or indifferentsetting, one option is the fabrication of a mental disorder to achieve a desired ob-jective. Penalties for unsuccessful feigning are often severe, ranging from the ces-sation of mental health services to the curtailment of benefits and negativeoutcomes from litigation. Malingerers are not necessarily accurate in their analyses;data from simulation studies (Kropp, 1992; Linblad, 1991) suggest that malingerersmay overestimate their ability to feign without detection.
Rogers, Sewell, and Goldstein (1994) investigated the three explanatory modelsof malingering via prototypical analysis. Prototype theory was originally developed(Rosch, 1973, 1978) to address fuzzy constructs frequently found in social sciences.According to Livesley (1991, p. 55), prototypes provide "structured representationsof diagnoses with traits organized according to prototypicality." In areas of diag-nostic ambiguity, such as malingering, experts are asked to describe and rate thedistinguishing characteristics of cases most representative of the construct. The pur-pose of prototypical analysis is to evaluate different characteristics for their poten-tial salience in the conceptualization of a disorder or condition. In addressing the"fuzzy" boundaries of clinical constructs, a second purpose is the demarcation ofcharacteristics that are not essential or prototypical. Experts cannot be asked toprovide prototypical ratings exhaustively on all conceivable characteristics; there-fore, past theory and research is typically used to nominate potential characteristics.Unlike other areas of clinical inquiry, random selection of cases is not the objective.Rather, experts are asked to select the most salient or representative cases. Becausesubjectivity cannot be excluded from any judgmental process, substantial numbersof experts are asked to render independent prototypical ratings. With random orquasirandom selection of experts, the direction of such subjectivity is assumed tobe randomly distributed throughout the sample; thus, subjectivity effects are mini-mized by the averaging of ratings across experts.
Prototypical ratings not only can provide the cardinal or distinguishing char-acteristics of an ambiguous clinical construct, but also further our understandingof the interrelations of these characteristics to the construct in question (Broughton,1990). In the Rogers et al. (1994) study, 320 experts were asked to rate the pro-
3S4 Rogers, Salekin, Sewell, Goldstein, and Leonard

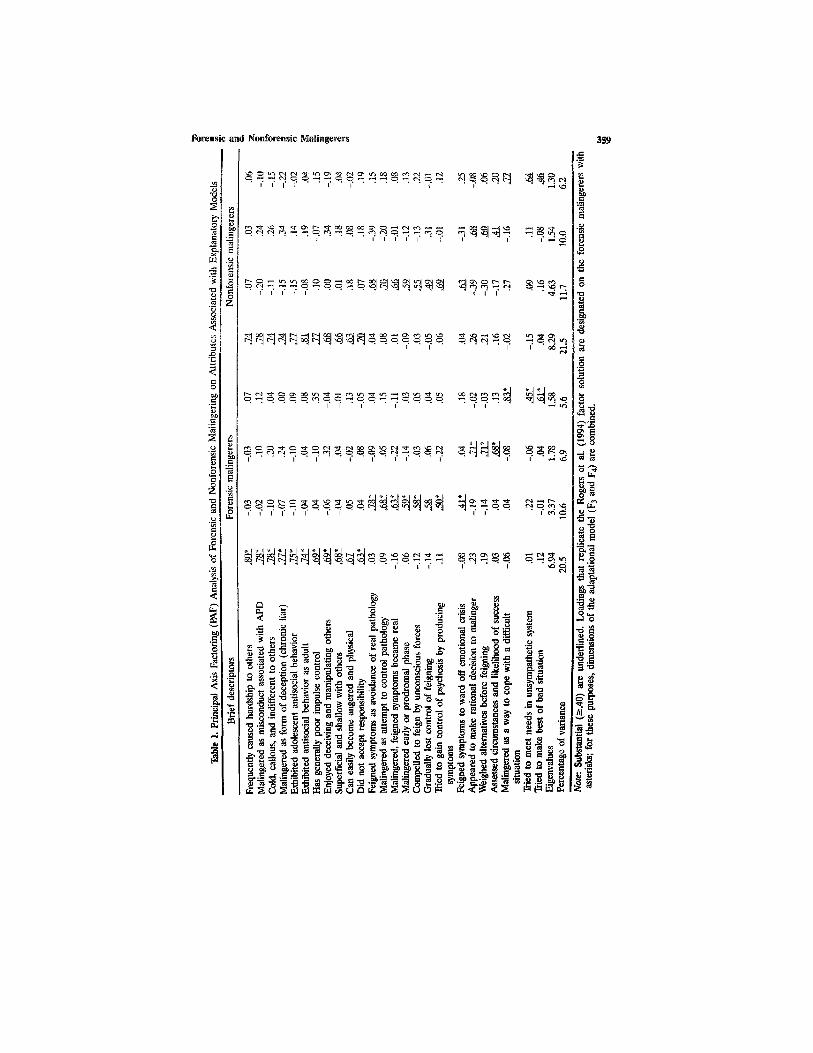
totypicality of attributes associated with each of the three explanatory models. Aprincipal components analysis (PCA) revealed three well-defined factors, account-ing for 41.2% of the variance; these dimensions corresponded closely to the patho-genic, criminological, and adaptational models. Based on a 7-point scale, theadaptational model (M = 4.63) was more prototypical than the criminological (M= 3.95) and pathogenic (M = 2.80) models.
The stability of these dimensions as well as their alignment with the explanatorymodels warrants further investigation. The current study sought to replicate andextend the findings of Rogers et al. (1994) by addressing four research issues. First,we investigated the applicability of explanatory models across forensic and non-forensic settings. One untested hypothesis is that the criminological model may as-sume greater importance in forensic than nonforensic cases. Second, we examinedthe prototypical ratings associated with each explanatory model in light of Rogerset al. (1994). Third, we addressed whether different types of malingering wouldresult in differences across factor scores. In this regard, malingering is grouped bythree nonexclusive categories: (a) fabrication of psychopathology/mental disorders,(b) feigned cognitive impairment (i.e., intellectual and neuropsychological deficits),and (c) simulation of spurious medical symptoms and syndromes (Cunnien, 1997).Potential differences in the prototypicality of explanatory models based on the typeof malingering remain uninvestigated. Fourth, we explored for the first time genderdifferences in prototypical cases on types of malingering.
An important assumption of prototypical analysis is that participants have ex-pertise regarding the construct under investigation. In this regard, forensic psycholo-gists must often grapple with issues of malingering and related response styles.Therefore, we selected clinicians likely to have training and background in malin-gering. Participants for the study were recruited from two sources. Workshop par-ticipants were recruited from the American Academy of Forensic Psychology(AAFP), which is a training component for the American Board of ProfessionalPsychology (ABPP). These participants were recruited from a series of 28 postdoc-toral workshops offered in five cities across the United States during 1994 and 1995.Only one workshop addressed the clinical assessment of malingering and deception.To eliminate the possibility of any subtle influences on respondents, the principalauthor of the explanatory models did not present any workshops during this timeor participate in any manner during these workshops.
Participants were recruited by brief announcements made typically at the be-ginning of workshops. Participants interested in malingering were invited to pickup and complete protocols at a central location during workshop breaks. No per-centages are available regarding the proportion of participants with training/back-ground in malingering that responded to these invitations to participate.
Sample
METHOD
Forensic and Nonforensic Malingerers 355

The second source of participants was diplomates in forensic psychology fromthe ABPP. Unlike the workshop participants, diplomates were contacted via mail.Otherwise, directions and presentation of material were identical to those com-pleted by the postdoctoral workshop participants. Of 149 diplomates, 44 (29.5%)agreed to participate and completed the prototypical ratings in the allotted period(4 weeks).
The list of attributes3 generated by Rogers et al. (1994) for the three explana-tory models was reproduced for the current study. Rogers constructed the attributesbased on his earlier theoretical work (Rogers, 1990a, 1990b) to address pathogenic,criminological, and adaptational models. The eight pathogenic items posit under-lying psychopathology, deterioration in clinical status, and ineffectual attempts atits control as the impetus for feigning. The 16 criminological items were derivedfrom two sources: the DSM indices of malingering (APA, 1987, 1994) and coretraits of psychopathy as exemplified by the Psychopathy Checklist—Screening Ver-sion (PCL-SV; Hare, Cox, & Hart, 1989; Hart, Cox, & Hare, 1995), which assumeantisocial and psychopathic motives for feigning. The eight adaptational itemsstressed from the malingerer's perspective the adversarial nature of the evaluation,the consideration of malingering among other alternatives, and choice of feigningas a method of achieving an important objective. As a preliminary investigation ofthis attribute list by Rogers et al. (1994), one of us (K.WS.) categorized the attrib-utes independently. He achieved a 100% concordance with Rogers's original clas-sification.
Experts were asked to select from their own professional practices two proto-typical examples of malingering: a forensic case and a clinical (i.e., nonforensic)case. No limitations were placed on the type of malingering or its context. For eachcase, the expert was asked to concentrate throughout the ratings on a specific pro-totypical malingerer. Experts were asked to choose the "clearest and most repre-sentative examples of malingerers" from their own professional practices. Expertsaddressed the extent to which these attributes were evident in the specific prototypicmalingerers from their own clinical and forensic assessments. To further concretizethe process, experts were asked to supply the malingerer's first name, age, race,and gender. The order of cases was counterbalanced. Half of the sample was askedto provide prototypical ratings first for the forensic case, followed by the clinicalcase. The other half completed the prototypical ratings in the reverse order.
Consistent with Rogers et al. (1994), ratings were rendered on a 7-point scalewith higher numbers representing increased importance/relevance to malingering.The scale was anchored by 1: "unimportant to malingering," 4: "moderately impor-tant to malingering" and 7: "Very important to malingering." Experts were alsoasked to supply the sources of clinical data used in the determination of malinger-ing. As a refinement of the Rogers et al. (1994) study, experts provided specific
3S6 Rogers, Salekin, Sewell, Goldstein, and Leonard
3A complete list of the attributes is included in Table 1.
Materials

information about the type of malingering with reference to three nonexclusive cate-gories: (a) psychopathology/mental disorder, (b) intellectual/neuropsychological im-pairment (subsequently described as "cognitive impairment"), and (c) medicalsyndrome or disorder.
Experts were also asked to supply information about their own training andbackground. Experts were asked to estimate the prevalence of malingering in theirpractice (forensic and nonforensic) if they had performed a minimum of 100 evalu-ations.
Results
The sample (N = 221) was composed of mostly doctoral-level psychologists(99.1%) with an average of 17.24 years (SD = 8.53) of postdoctoral experience.Their primary professional settings varied from clinical (137 or 62.0%) to forensic(91 or 41.2%), correctional (29 or 13.1%), and medical (28 or 12.7%).4 Irrespectiveof their professional settings, approximately two thirds (67.9%) of the experts de-voted at least 25% of their professional time to forensic practice.
The prevalence of malingering varied by the type of evaluation. For forensicevaluations, the M percentage is 17.44 (SD = 14.44). Removing two extreme outliers(>4 SD), the prevalence for nonforensic cases is 7.16% (SD = 7.09).
The 200 forensic and 182 nonforensic malingerers used in prototypic cases weregenerally comparable with respect to their sociodemographic backgrounds. The ma-jor exception occurred with gender; females accounted for approximately half(49.9%) of the nonforensic cases, but only 18.5% of the forensic cases, x2(l, N =381) = 39.84, p < .0001. Racial differences were nonsignificant, x2 (7, N = 381)= 5.93, p = .55: (a) for forensic, 70.7% Anglo American, 23.7% African American,3.0% Hispanic American, and 2.6% other; and (b) for nonforensic, 77.0% AngloAmerican, 16.4% African American, 2.7% Hispanic American, and 3.9% other. Theages between the groups were comparable, F(l, N = 381) = 2.54, p = .11, forforensic (M = 35.52, SD = 10.38) and nonforensic (M = 33.67, SD = 12.40) pro-totypical cases.
Applicability of Explanatory Models to Forensic and Nonforensic Cases
Two principal axis factoring (PAF) analyses, rotated to varimax solutions, werecomputed separately for forensic and nonforensic cases. We employed the over-and under-factoring procedures of Pedhazur (1982) to examine three-, four-, andfive-factor solutions. We selected the four-factor solution based on scree test, eigen-values, and interpretability of the solution. In comparison to the four-factor solu-tions, the three-factor solutions resulted in two cross-loadings, accounted forappreciably smaller percentage of the variance (37.5%) for forensic prototypes, and
4Experts were allowed to designate more than one professional setting; therefore, these percentagesexceed 100%.
Forensic end Nonforensic Malingerers 357

evidenced less consistency between forensic and nonforensic PAF analyses. In con-trast, the five-factor solutions yielded a weak fifth factor (only two strong loadings,of which one is cross-loaded for clinical prototypes) and limited interpretability.Results of the PAF analyses are presented in Table 1.
The four-factor solution with forensic prototypes accounted for 42.7% of thevariance with no cross-loadings. The first factor, criminological, accounted for 20.5%of the variance and was composed of 11 variables with very high loadings. Thesevariables emphasized the antisocial behavior and background, general deception,and impaired interpersonal relationships. The second factor, pathogenic, accountedfor 10.6% of the variance; its variables addressed underlying psychopathology andineffectual attempts to gain control over emerging symptomatology via feigning.The third factor, cost-benefit analysis (6.9% of the variance), addressed malingeringas the weighing of alternatives and likelihood of success. The fourth factor, adver-sarial context (5.6% of the variance), considered malingering as a method of copingwith unsympathetic and difficult circumstances.
The four-factor solution with nonforensic prototypes accounted for 49.3% ofthe variance with no cross-loadings. Its factors and substantial loadings completelymirrored the results of forensic PAF analysis. Small differences were observed inthe percentage of variance accounted for by each factor. For the nonforensic PAFanalysis, the percentages of variance were the following: F1 (21.5%), F2 (11.7%),F3 (10.0%), and F4 (6.2%).
Comparison of Forensic and Nonforensic Solutions
Close correspondence in factor solutions was found between forensic and non-forensic prototypical malingerers. On a descriptive level, these solutions were nearlyidentical across forensic and nonforensic samples. All variables (i.e., 25 of 25) withsubstantial (>.40) loadings on one PAF manifested unique and parallel loadings onthe second PAR For a formal comparison, congruence coefficients were utilized toaddress the degree of correspondence for each factor between the forensic andnonforensic prototypes (Kroonenberg & ten Berge, 1987); the congruence was veryhigh for the first two factors (F1 = .99; F2 = .95) and moderate for the latter twofactors (F3 = .80; F4 = .85). Overall, the congruence coefficients (M = .91) cor-roborated the obvious similarity in factor structures.
Prototypicality of Explanatory Models
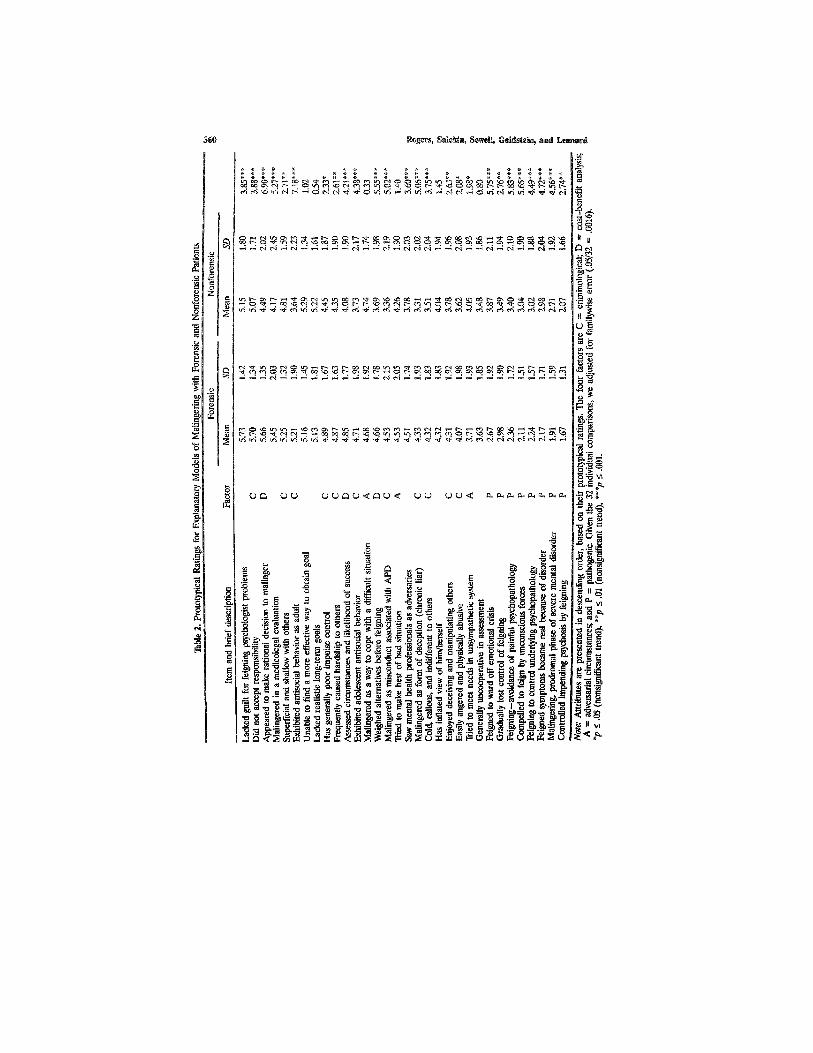
The Rogers et al. (1994) study examined overall differences in magnitude forprototypical ratings associated with each explanatory model. In the current study,we were interested in exploring these differences separately for forensic and non-forensic settings. As primarily descriptive data, the Ms, SDs, and t tests (controlledfor familywise error with an alpha = .05) are presented in Table 2.To test overalldifferences for explanatory models, the two MANOVAs yielded highly significant
358 Rogers, Salekin, Sewell, Goldstein, and Leonard
Forensic and Nonforensic Malingerers 359
360 Rogers, Salekin, Sewell, Goldstein, and Leonard

results: (a) forensic, Wilks lambda = .250, F(3, 198) = 196.67, p < .001, and (b)nonforensic, Wilks lambda = .576, F(3, 179) = 43.89, p < .001.
The prototypical ratings (see Table 2) generally confirmed results of Rogers etal. (1994) regarding the relative unimportance of the pathogenic model. Rogers etal. (1994) found an M rating of 2.49 as compared to the current results of 2.26(forensic) and 3.07 (nonforensic). In each analysis, the pathogenic model had ratingsthat consistently averaged below moderate prototypicality (i.e., <4.00).
Past and current results for the criminological model are rated generally inthe midrange of prototypicality. In the Rogers et al. (1994) study, the M rating forthe criminological model was 3.95. In the current study, the hypothesized difference,t(l, 170) = 4.88; p < .001, was found for the criminological mode! with higherratings for forensic (M = 4.77, SD - 1.37) than nonforensic (M - 4.05, SD =1.55) cases. Inspection of individual ratings in Table 2 reveals that the three highcriminological ratings (>5.00) were derived from the PCL-SV conceptualization ofpsychopathy.
The adaptational model was decomposed into two dimensions: cost-benefitanalysis and adversarial circumstances. Intuitively, the greatest differences be-tween forensic and nonforensic cases would be expected for adversarial circum-stances. However, the averages of these scores were virtually identical (4.31 and4.35) and reflected moderate prototypicality. In contrast, cost-benefit analysis ap-peared to be more salient in forensic M = 5.06, SD = 1.36) than nonforensiccases (M = 4.09, SD = 1.61), t(l, 169) = 6.73; p < .001. For purposes of com-parison, we averaged Rogers et al. (1994) ratings for these dimensions; theyyielded M ratings of 4.40 for adversarial circumstances and 4.50 for cost-benefitanalysis.
Types of Malingering and Explanatory Models
As noted in the Method section, prototypical cases are composed of three ma-jor types of malingering: mental disorder, cognitive impairment, and medical syn-dromes. As a supplementary analysis, we examined differences by the type ofmalingering for each of the four underlying dimensions. For this purpose, we cre-ated four new scales (one for each dimension); attributes with substantial loadings(>.40) were composed into a scale. As displayed in Table 3, we computed ANOVAsfor each scale by the three major types of malingering. Because the types of ma-lingering constitute nonexclusive categories, we only included those prototypicalcases that represented a single type.
Among prototypical forensic cases, only one difference was observed. Feignedcognitive impairment was rated lower than feigned medical syndromes on adver-sarial context. In prototypical nonforensic cases, the pathogenic model appeared tobe the least applicable to feigned cognitive impairment. In addition, the adversarialcontext appeared to be much more salient to the feigned mental disorders in com-parison to the other types.
Forensic and Nonforensic Malingerers 361
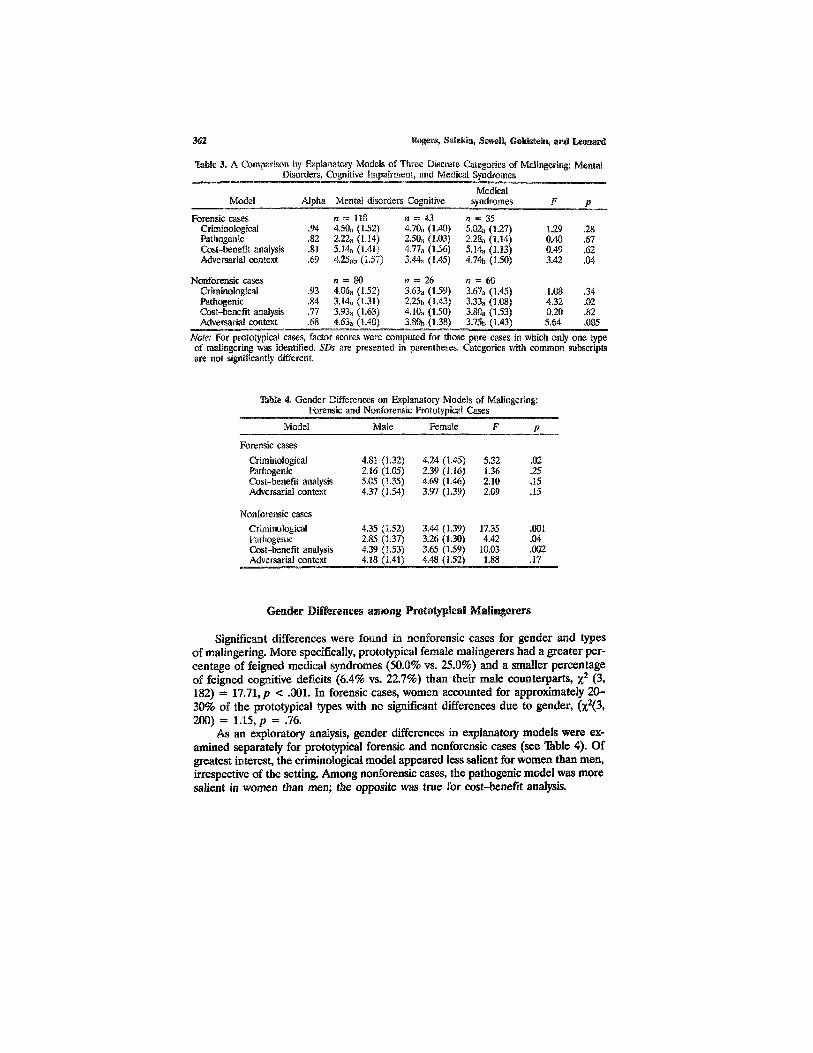
Table 3. A Comparison by Explanatory Models of Three Discrete Categories of Malingering: MentalDisorders, Cognitive Impairment, and Medical Syndromes
Model
Forensic casesCriminologicalPathogenicCost-benefit analysisAdversaria! context
Nonforensic casesCriminologicalPathogenicCost-benefit analysisAdversarial context
Alpha
.94
.82
.81
.69
.93
.84
.77
.68
Mental disorders
n = 1184.50a (1.52)2.22a (1.14)5.14a (1.41)4.25ab (1.57)
n = 804.06a (1.52)3.14a (1.31)3.93a (1.63)4.63a (1.40)
Cognitive
n = 434.70a (1.40)2.50a (1.03)4.77a (1.56)3.44a (1.45)
n = 263.63a (1.59)2.25b (1.43)4.10a (1.50)3.80b (1.38)
Medicalsyndromes
n = 355.02a (1.27)2.28a (1.14)5.14a (1.13)4.74b (1.50)
n = 603.67a (1.45)3.33a (1.08)3.80a (1.53)3.75b (1.43)
F
1.290.400.493.42
1.084.320.205.64
P
.28
.67
.62
.04
.34
.02
.82
.085
Note: For prototypical cases, factor scores were computed for those pure cases in which only one typeof malingering was identified. SDs are presented in parentheses. Categories with common subscriptsare not significantly different.
Table 4. Gender Differences on Explanatory Models of Malingering:Forensic and Nonforensic Prototypical Cases
Model
Forensic cases
CriminologicalPathogenicCost-benefit analysisAdversarial context
Male
4.81 (1.32)2.16 (1.05)5.05 (1.35)4.37 (1.54)
Female
4.24 (1.45)2.39 (1.16)4.69 (1.46)3.97 (1.39)
F
5,321.362.102.09
P
.02
.25
.15
.15
Nonforensic cases
CriminologicalPathogenicCost-benefit analysisAdversarial context
4.35 (1.52)2.85 (1.37)4.39 (1.53)4.18 (1.41)
3.44 (1.39)3.26 (1.30)3.65 (1.59)4.48 (1.52)
17.354.42
10.031.88
.001
.04
.002
.17
Gender Differences among Prototypical Malingerers
Significant differences were found in nonforensic cases for gender and typesof malingering. More specifically, prototypical female malingerers had a greater per-centage of feigned medical syndromes (50.0% vs. 25.0%) and a smaller percentageof feigned cognitive deficits (6.4% vs. 22.7%) than their male counterparts, x2 (3,182) = 17.71, p < .001. In forensic cases, women accounted for approximately 20-30% of the prototypical types with no significant differences due to gender, (x2(3,200) = 1.15, p = .76.
As an exploratory analysis, gender differences in explanatory models were ex-amined separately for prototypical forensic and nonforensic cases (see Table 4). Ofgreatest interest, the xCriminological model appeared less salient for women than men,irrespective of the setting. Among nonforensic cases, the pathogenic model was moresalient in women than men; the opposite was true for cost-benefit analysis.
Rogers, Salekin, Sewell, Goldstein, and Leonard362

The impetus and motivation for malingering are crucial to our conceptualiza-tion of feigning and consequent use of assessment methods. Research by Rogerset al. (1994) provided a general understanding of the three explanatory models andsuggested that the adaptational model had the greatest prototypicality, while thepathogenic model had the least. The current data serve to refine these explanatorymodels, especially with respect to the adaptational model. In addition, we examinetheir application by (a) type of case (forensic vs. nonforensic) and (b) type of ma-lingering (mental disorders, cognitive impairment, and medical syndromes). As aninitial investigation, we explore gender differences in prototypical malingerers. Wealso discuss the prototypical ratings of malingering in the context of professionalpractice and psychological assessment. Finally, we address methodological consid-erations for this and future studies.
Review and Refinement of Explanatory Models
Rogers et al. (1994) concluded that the adaptational model had the highestprototypical ratings and therefore most relevance in understanding the motivationsto malinger. The present study produced less positive results. For forensic malin-gerers, the cost-benefit analysis component of the adaptational model was the onlydimension to produce high M ratings (i.e., > 5.00). However, ratings on this com-ponent were much lower in nonforensic cases. In addition, the adversarial-circum-stances component produced only midrange values. Overall differences between theadaptational (i.e., both components combined) and the criminological models arenegligible.5
The current data suggest an enhancement of the adaptational model with thedelineation of two components: cost-benefit analysis and adversarial context. Asdescribed later, these dimensions may play important roles, based on both the set-ting and type of malingering. One possibility is that the adaptational model shouldbe decomposed into these two dimensions. We do not believe this is necessary forseveral reasons. First, these dimensions were articulated a priori as key elementsof the adaptational model. Second, as noted in Table 1, these dimensions are clearlyaligned with the adaptational model.
The current study confirmed the Rogers et al. (1994) finding that the patho-genic model is not central to our understanding of malingering. It appears to havea modest role with nonforensic malingerers (M = 3.07), but very little relevanceto forensic malingerers. Of course, infrequent cases can occur for which the patho-genic model has salience. By computing M scores for individual cases, we found15 (7.5%) forensic and 54 (29.5%) nonforensic cases in which the pathogenic modelwas at least moderately important (M ratings in a prototypical case >4.00) to ma-lingering. Our point is that the pathogenic model is generally low in prototypicality,although notable exceptions do occur in individual cases.
5Cohen's d is .06 for forensic and .11 for nonforensic cases.
DISCUSSION
Forensic and Nonforensic Malingerers 363

Malingering: Forensic versus Nonforensic Cases
Differences between forensic and nonforensic malingerers were explored forthe first time. Cost-benefit analysis appeared to be the most representative dimen-sion of forensic cases followed by the criminological model and adversarial circum-stances. In contrast, nonforensic cases were most prototypical for the adversarialcircumstances followed by cost-benefit analysis and the criminological model. Al-though predicted differences were found for the criminological model (i.e., moreprototypical in forensic cases), the greatest difference occurred for cost-benefitanalysis. The weighing of alternatives and likely outcomes was viewed as very pro-totypical of forensic malingerers (M = 5.06), but only moderately so for nonforensicmalingerers (M = 4.09).
Types of Malingering
We examined for the first time how the differences among the types of ma-lingering might be reflected in the explanatory models. The adversarial context ap-peared to play a significant but different role, depending on the setting. In a forensicsetting, cases of feigned medical syndromes were more prototypical (M = 4.74)than feigned cognitive impairment (M = 3.44). In nonforensic settings, the adver-sarial context was more salient to feigned mental disorders than either the simu-lation of cognitive impairment or medical syndromes. In both settings, theadversarial context did not appear central to those malingering cognitive impair-ment.
The pathogenic model does not appear to be affected by the type of malin-gering in forensic settings. However, an important difference was found in non-forensic cases: malingerers of cognitive impairment appear to be less influencedthan others by the pathogenic model. This finding is intuitively appealing becausethe antecedents (e.g., motor vehicle accident) to purported impairment are notlikely to be psychopathological.
Gender Differences
In nonforensic cases, the explanatory models do not appear to be importantto our understanding of female malingerers' motivations to feign. With the notableexception of the adversarial context, prototypical female offenders receive ratingsof less than moderate prototypicality (i.e., < 4.00). Although modest in magnitude,the pathogenic model appears somewhat more germane to female than male of-fenders in nonforensic settings.
Gender differences also occurred in nonforensic cases in the type of malinger-ing observed. Essentially unnoticed in the clinical literature, one half of nonforensicfemale malingerers focused on feigned medical syndromes. Gender differences intypes of malingering clearly require further investigation.
364 Rogers, Safekin, Sewell, Goldstein, and Leonard

Implications for Professional Practice
The presence of prototypical features can assist in the accurate classificationof clinical populations (Cantor, Smith, French, & Mezzich, 1980). For example,Horowitz, Post, French, Wallis, and Siegelman (1981) found that the presence ofprototypical characteristics facilitates the diagnosis of depression and that theircomparative absence led to diagnostic disagreements. Applied to malingering, thequestion is raised whether direct methods of assessing prototypical items would in-crease the classificatory accuracy (Broughton, 1990). In this light, three items withhigh prototypicality (i.e., > 5.00; lack of guilt, responsibility, and long-term goals)across both forensic and nonforensic settings were adapted from the PsychopathyChecklist—Screening Version (Hare et al., 1989, 1995). Would the use of theseitems in the context of a PCL-SV interview improve the assessment of malingering?Because the PCL-SV posits a trait model of personality (Rogers, 1995), the inclu-sion of other, more situational characteristics (e.g., setting and referral question)also may facilitate the classification of malingering.
Gender differences must be taken into account in the assessment of malinger-ing. The current data, based only on prototypical cases, would suggest that maleand female malingerers are substantially different in types of feigning, especially innonforensic cases. The issue remains whether clinicians have gender biases in theirviews of feigned medical syndromes, possibly engendered by early formulations ofhysteria, somatoform disorders, and secondary gain from physical disorders (Rogers& Reinhardt, in press). Nevertheless, psychologists need to address more system-atically the possibility of feigned medical syndromes. Strikingly, feigned medical syn-dromes made up 36.1% of prototypical nonforensic cases. We also were surprisedthat 22.7% of prototypical forensic cases were composed solely of feigned medicalsyndromes. Their clinical assessment, generally neglected in the malingering litera-ture, deserves our attention.
Rogers, Bagby, and Dickens (1992, Table 20) recommended the use of specificquestions to address the varying objectives associated with malingering and facti-tious disorders. Perhaps, similar inquiries could be developed to measure persons'perceptions regarding (a) the adversarial context of the evaluation and (b) theirobjectives and their perceived alternatives for reaching these objectives. The sali-ence of cost-benefit analysis especially in forensic cases might augment our assess-ment methods by focusing on the putative motivation in addition to the clinicalpresentation. Obviously, such investigations would need to take into account thepossibility of malingering and dissimulation on these inquiries. Otherwise, cliniciansare in the untenable position of assuming honesty on some responses to prove ma-lingering on others.
Assessment methods (see, e.g., Cercy, Schretlen, & Brandt, 1997; Pankratz &Binder, 1997; Rogers, Harrell, & Liff, 1993) have highlighted the differences in thedetection of feigned mental disorders versus cognitive impairment. Albeit prelimi-nary, the current data hint that this need may extend beyond the detection strategiesthemselves and apply to explanatory models. Based on the setting, gender, and typeof purported impairment, different motivations may assume greater prototypicality.Across forensic and nonforensic settings, better understanding is urgently needed
Forensic and Nonforensic Malingerers 365

On how these explanatory models influence the presentations by malingerers andaffect our detection methods.
Methodological Considerations
The current study offers refinements to the Rogers et al. (1994) study in furtherspecifying the type of malingering (mental disorders, cognitive impairment, andmedical syndromes) and the general setting (forensic and nonforensic). In addition,further specification was achieved by asking experts to rate prototypical cases fromtheir own practices rather than their general experiences of malingerers. Ideally,the next step would be to study contemporaneous (i.e., at the same time the ma-lingerer is evaluated) rather than retrospective prototypical ratings. Although salientcases of malingering are often very memorable, decrements in memory recall areinevitable over time. However, the practicalities of such an undertaking (e.g., severalhundred experts rendering systematic ratings over multiple years) are likely tothwart this methodological refinement. In the absence of such contemporaneousstudies, our understanding of malingering can still be enhanced via prototypicaiitystudies targeted at both specific cases and general attributes.
REFERENCES
American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders (3rd ed.).Washington, DC: Author.
American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disorders (3rd re-vised). Washington, DC: Author.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.).Washington, DC: Author.
Broughton, R. (1990). The prototype concept in personality assessment. Canadian Psychology, 31, 26-37.Cantor, N., Smith, E., French, R. de S., & Mezzich, J. (1980). Psychiatric diagnosis as prototype cate-
gorization. Journal of Abnormal Psychology, 89, 181-193.Cercy, S. P., Schretlen, D. J., & Brandt, J. (1997). Malingered amnesia and false memories. In R. Rogers
(Ed.), Clinical assessment of malingering and deception (2nd ed.; pp. 85-107). New York: Guilford.Cunnien, A. J. (1997). Psychiatric and medical syndromes associated with deception. In R. Rogers (Ed.),
Clinical assessment of malingering and deception (2nd ed.; pp. 23-46). New York: Guilford.Hare, R. D., Cox, D. N., & Hart, S. D. (1989). Preliminary manual far the Psychopathy Checklist: Clinical
Version (PCL-CV). Unpublished manuscript, University of British Columbia, vancouver, British Co-lumbia, Canada.
Hare, R. D., Cox, D. N., & Hart, S. D. (1995). Manual for the Screening Version of Psychopathy ChecklistRevised (PCL-SV). Toronto: Multi-Health Systems.
Hart, S. D., Cox, D. N., & Hare, R. D. (1996). Manual for the Screening Version of Psychopathy ChecklistRevised (PCL-SV). Toronto: Multi-Health Systems.
Horowitz, L. M., Post, D. L., French, R. de S., Wallis, K. D., & Siegelman, E. Y. (1981). The prototypeas a construct in abnormal psychology: Clarifying disagreement in psychiatric judgments, journal ofAbnormal Psychology, 90, 575-585.
Kroonenberg, P. M., & ten Berge, J. M. F. (1987). Cross-validation of the WISC-R factorial structureusing three-mode principal components analysis and perfect congruence analysis. Applied Psycho-logical Assessment, 11, 195-210.
Kropp, P. R. (1992). Antisocial personality disorder and malingering. Unpublished doctoral dissertation,Simon Fraser University, Burnaby, British Columbia, Canada.
Linblad, A. D. (1991). Detection of malingered mental illness with a forensic population: An analoguestudy. Unpublished dissertation, University of Manitoba, Winnipeg, Manitoba, Canada.
366 Rogers, Salekin, Sewell, Goldstein, and Leonard

Livesley, W. J. (1991). Classifying personality disorders: Ideal types, Prototypes, or dimensions? Journalof Personality Disorders, 5, 52-59.
Pankratz, L., & Binder, L. M. (1997). Malingering on intellectual and neuropsychological measures. InR. Rogers (Ed.), Clinical assessment of malingering and deception (2nd ed.; pp. 223-236). New York:Guilford.
Pedhazur, E. J. (1982). Multiple regression in behavioral research: Explanation and prediction (2nd ed.).New York: Holt, Reinhart, and Winston.
Rogers, R. (1990a). Development of a new classificatory model of malingering. Bulletin of the AmericanAcademy of Psychiatry and Law, IS, 323-333.
Rogers, R. (1990b). Models of feigned mental illness. Professional Psychology: Research and Practice, 21,182-188.
Rogers, R. (1995), Diagnostic and structured interviewing: A handbook for psychologists. Odessa, FL: Psy-chological Assessment Resources.
Rogers, R. (Ed.) (1997a). Clinical assessment of malingering and deception (2nd ed.). New York: Guilford.Rogers, R. (1997b). Introduction. In R. Rogers (Ed.), Clinical assessment of malingering and deception
(2nd ed.; pp. 1-19). New York: Guilford.Rogers, R., Bagby, R. M., & Dickens, S. E. (1992). Structured Interview of Reported Symptoms (SIRS)
and professional manual. Odessa, FL: Psychological Assessment Resources.Rogers, R., Harrell, E. H., & Liff, C. D. (1993). Feigning neuropsychological impairment: A critical
review of methodological and clinical considerations. Clinical Psychology Review, 13, 255-274.Rogers, R., & Reinhardt, V R. (in press). Secondary gain: A clinical construct in search of consensus.
In G. P. Koocher, J. C, Norcross, & S. S. Hill III (Eds.), Psychologist's desk reference. Oxford:Oxford University Press.
Rogers, R., Sewell, K. W., & Goldstein, A. (1994). Explanatory models of malingering: A prototypicalanalysis. Law and Human Behavior, 18, 543-552.
Rosen, E. (1973). On the internal structure of perceptual and semantic categories. In T. E. Moore (Ed.),Cognitive development and the acquisition of language (pp. 111-144). New York: Academic Press.
Rosch, E. (1978). Principles of categorization. In E. Rosch & B. B. Lloyd (Eds.), Cognition and catego-rization (pp. 27-48). Hillsdale, NJ: Erlbaum.
Forensic and Nonforensic Malingerers 367
Copyright © 2022 FDOKUMEN