
A Cognitive-Developmental Model for Marital and Family Therapy Supervision
26
Transcript of A Cognitive-Developmental Model for Marital and Family Therapy Supervision









TABLE 1. Supervisee Cognitive-Developmental Orientations
The following descriptions illustrate how therapists might operatewithin each of the orientations. Competencies represent howtherapists able to access a variety of orientations might utilize aparticular perspective. Constraints reflect what might occur fortherapists over-reliant on one particular orientation.
ORIENTATION COMPETENCIES CONSTRAINTSSensorimotorThese supervisees use their immediate Therapeutic strengths include the Therapists who over-rely on this framesensory experiences to make sense of ability to directly experience and track are susceptible to emotional hyper-their work. Common supervisory client emotions without becoming stimulation in the client and/orrequests include assistance to reactive or overwhelmed, and to themselves. Their intense affectiveorganize fragmented pieces of clinical identify personal feelings during involvements interfere with cognitivedata, to make sense of strong therapy and supervision. This allows conceptualization and behavioralemotional exchanges, and to therapists to work through transference execution. Interventions are based onbehaviorally ground treatment plans. and countertransference issues. what ‘‘feels’’ right at the time, which can
lead to random, haphazard treatmentIllustration: I refused to state that his planning.wife was crazy. Maybe that was amistake. I don’t think she is crazy. Illustration: I get caught with him . . .But, in a sense, there is a part of me in part . . . I have issues with this man.that feels--in this whole system--who I feel bad reactions toward him. He’swouldn’t be crazy, including me, loud and it’s hard for me to get him tobecause it feels crazy when I’m there. stop. I feel I engage more with him
even though I want his wife to beheard. It feels strange in the room,because I’m aware of what I am doing,but can’t stop.
TABLE 1. Supervisee Cognitive-Developmental Orientations
The following descriptions illustrate how therapists might operatewithin each of the orientations. Competencies represent howtherapists able to access a variety of orientations might utilize aparticular perspective. Constraints reflect what might occur fortherapists over-reliant on one particular orientation.
ORIENTATION COMPETENCIES CONSTRAINTSSensorimotorThese supervisees use their immediate Therapeutic strengths include the Therapists who over-rely on this framesensory experiences to make sense of ability to directly experience and track are susceptible to emotional hyper-their work. Common supervisory client emotions without becoming stimulation in the client and/orrequests include assistance to reactive or overwhelmed, and to themselves. Their intense affectiveorganize fragmented pieces of clinical identify personal feelings during involvements interfere with cognitivedata, to make sense of strong therapy and supervision. This allows conceptualization and behavioralemotional exchanges, and to therapists to work through transference execution. Interventions are based onbehaviorally ground treatment plans. and countertransference issues. what ‘‘feels’’ right at the time, which can
lead to random, haphazard treatmentIllustration: I refused to state that his planning.wife was crazy. Maybe that was amistake. I don’t think she is crazy. Illustration: I get caught with him . . .But, in a sense, there is a part of me in part . . . I have issues with this man.that feels--in this whole system--who I feel bad reactions toward him. He’swouldn’t be crazy, including me, loud and it’s hard for me to get him tobecause it feels crazy when I’m there. stop. I feel I engage more with him
even though I want his wife to beheard. It feels strange in the room,because I’m aware of what I am doing,but can’t stop.
101101

TABLE 1 (continued)
ORIENTATION COMPETENCIES CONSTRAINTSFormalThese therapists are capable of Competent therapists can synthesize These therapists often intellectualizeanalyzing situations from multiple ideas and strategies from various and eloquently assess clients andperspectives and demonstrate models and are able to modify discuss treatment objectives inreflective and circular reasoning. treatment plans based on emerging supervision, but are unable to transferCommon supervisory requests include data. They can examine their own this knowledge to effective technicalasking for assistance, deciphering a patterns as these impact on the skills in session. They minimizetypical pattern within or across cases therapeutic and supervisory affective and behavioral data andor in relation to the self, or help in encounters. They can see the bridge prefer to conceptualize abstractly, butexamining theoretical or therapeutic between techniques and the overall cannot challenge the assumptionthemes. treatment plan. underlying their constructions.
Illustration: I can see it from his point Illustration: I have this couple I haveof view, as well as from her’s. It’s hard been seeing for three months, and I’mfor me to reconcile, as both have valid really doing couple therapy, and itviews. I would like to construct a feels like we have moved a lot.reframe that captures both However, I’m getting stuck, whichperspectives and provides a direction often happens to me after threefor treatment. months when I’m doing this kind of
work. Things go along real well, wedo some stuff, and then we get stuck.I’d like to use this case to talkgenerally about what happens to mywork once I have worked with a couplefor a short while. That is, why is it thatI have difficulty doing longer termmore intensive treatment with couples.
TABLE 1 (continued)
ORIENTATION COMPETENCIES CONSTRAINTSFormalThese therapists are capable of Competent therapists can synthesize These therapists often intellectualizeanalyzing situations from multiple ideas and strategies from various and eloquently assess clients andperspectives and demonstrate models and are able to modify discuss treatment objectives inreflective and circular reasoning. treatment plans based on emerging supervision, but are unable to transferCommon supervisory requests include data. They can examine their own this knowledge to effective technicalasking for assistance, deciphering a patterns as these impact on the skills in session. They minimizetypical pattern within or across cases therapeutic and supervisory affective and behavioral data andor in relation to the self, or help in encounters. They can see the bridge prefer to conceptualize abstractly, butexamining theoretical or therapeutic between techniques and the overall cannot challenge the assumptionthemes. treatment plan. underlying their constructions.
Illustration: I can see it from his point Illustration: I have this couple I haveof view, as well as from her’s. It’s hard been seeing for three months, and I’mfor me to reconcile, as both have valid really doing couple therapy, and itviews. I would like to construct a feels like we have moved a lot.reframe that captures both However, I’m getting stuck, whichperspectives and provides a direction often happens to me after threefor treatment. months when I’m doing this kind of
work. Things go along real well, wedo some stuff, and then we get stuck.I’d like to use this case to talkgenerally about what happens to mywork once I have worked with a couplefor a short while. That is, why is it thatI have difficulty doing longer termmore intensive treatment with couples.
102102

ConcreteThese supervisees are adept Competent therapists can apply if/then Rigid therapists hold on to ‘‘thedescribers of action and events. They reasoning and linear hypotheses to method, theory, or technique.’’ Theycan articulate cause and effect anticipate clinet reactions. Their have difficulty viewing the situationrelations which allows them to operate descriptions of basic dynamics are from abstract or affectual perspectiveswith some degree of predictability. often accurate and logical. and cannot apply circular reasoning.Common supervisory requests include They are not able to recognize howasking how to accomplish specific Illustration: I would like feedback specific interventions fit into a largerinterventions and develop treatment regarding my treatment plan, treatment plan.plans, and asking for validation specifically couples work, intermittentregarding observations and behaviors. with individual psychotherapy. I’m Illustration: She’s having a hard time
also interested in what to do about the with her son. She calls the policealcohol. Next session, he might say when he’s violent. The psychiatrist firstthat he will stop drinking on his own said he needed to be hospitalized.terms. How should I react? When he called the advocate he
changed his mind. I don’t know . . . Idon’t have an in. Without permissionfrom the son, I can’t call the advocateto find out what’s up. If I work with themother, I think I’m pulling her out ofthe family again. Do you agree withthat direction? I think it’s my only way. . . to work with the mother . . . but theconsequences may be the same.
ConcreteThese supervisees are adept Competent therapists can apply if/then Rigid therapists hold on to ‘‘thedescribers of action and events. They reasoning and linear hypotheses to method, theory, or technique.’’ Theycan articulate cause and effect anticipate client reactions. Their have difficulty viewing the situationrelations which allows them to operate descriptions of basic dynamics are from abstract or affectual perspectiveswith some degree of predictability. often accurate and logical. and cannot apply circular reasoning.Common supervisory requests include They are not able to recognize howasking how to accomplish specific Illustration: I would like feedback specific interventions fit into a largerinterventions and develop treatment regarding my treatment plan, treatment plan.plans, and asking for validation specifically couples work, intermittentregarding observations and behaviors. with individual psychotherapy. I’m Illustration: She’s having a hard time
also interested in what to do about the with her son. She calls the policealcohol. Next session, he might say when he’s violent. The psychiatrist firstthat he will stop drinking on his own said he needed to be hospitalized.terms. How should I react? When he called the advocate he
changed his mind. I don’t know . . . Idon’t have an in. Without permissionfrom the son, I can’t call the advocateto find out what’s up. If I work with themother, I think I’m pulling her out ofthe family again. Do you agree withthat direction? I think it’s my only way. . . to work with the mother . . . but theconsequences may be the same.
103103
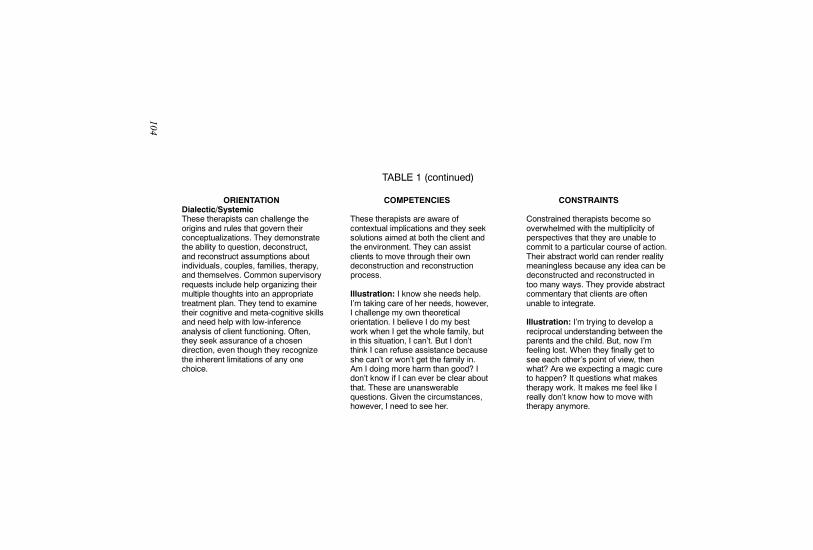
TABLE 1 (continued)
ORIENTATION COMPETENCIES CONSTRAINTSDialectic/SystemicThese therapists can challenge the These therapists are aware of Constrained therapists become soorigins and rules that govern their contextual implications and they seek overwhelmed with the multiplicity ofconceptualizations. They demonstrate solutions aimed at both the client and perspectives that they are unable tothe ability to question, deconstruct, the environment. They can assist commit to a particular course of action.and reconstruct assumptions about clients to move through their own Their abstract world can render realityindividuals, couples, families, therapy, deconstruction and reconstruction meaningless because any idea can beand themselves. Common supervisory process. deconstructed and reconstructed inrequests include help organizing their too many ways. They provide abstractmultiple thoughts into an appropriate Illustration: I know she needs help. commentary that clients are oftentreatment plan. They tend to examine I’m taking care of her needs, however, unable to integrate.their cognitive and meta-cognitive skills I challenge my own theoreticaland need help with low-inference orientation. I believe I do my best Illustration: I’m trying to develop aanalysis of client functioning. Often, work when I get the whole family, but reciprocal understanding between thethey seek assurance of a chosen in this situation, I can’t. But I don’t parents and the child. But, now I’mdirection, even though they recognize think I can refuse assistance because feeling lost. When they finally get tothe inherent limitations of any one she can’t or won’t get the family in. see each other’s point of view, thenchoice. Am I doing more harm than good? I what? Are we expecting a magic cure
don’t know if I can ever be clear about to happen? It questions what makesthat. These are unanswerable therapy work. It makes me feel like Iquestions. Given the circumstances, really don’t know how to move withhowever, I need to see her. therapy anymore.
TABLE 1 (continued)
ORIENTATION COMPETENCIES CONSTRAINTSDialectic/SystemicThese therapists can challenge the These therapists are aware of Constrained therapists become soorigins and rules that govern their contextual implications and they seek overwhelmed with the multiplicity ofconceptualizations. They demonstrate solutions aimed at both the client and perspectives that they are unable tothe ability to question, deconstruct, the environment. They can assist commit to a particular course of action.and reconstruct assumptions about clients to move through their own Their abstract world can render realityindividuals, couples, families, therapy, deconstruction and reconstruction meaningless because any idea can beand themselves. Common supervisory process. deconstructed and reconstructed inrequests include help organizing their too many ways. They provide abstractmultiple thoughts into an appropriate Illustration: I know she needs help. commentary that clients are oftentreatment plan. They tend to examine I’m taking care of her needs, however, unable to integrate.their cognitive and meta-cognitive skills I challenge my own theoreticaland need help with low-inference orientation. I believe I do my best Illustration: I’m trying to develop aanalysis of client functioning. Often, work when I get the whole family, but reciprocal understanding between thethey seek assurance of a chosen in this situation, I can’t. But I don’t parents and the child. But, now I’mdirection, even though they recognize think I can refuse assistance because feeling lost. When they finally get tothe inherent limitations of any one she can’t or won’t get the family in. see each other’s point of view, thenchoice. Am I doing more harm than good? I what? Are we expecting a magic cure
don’t know if I can ever be clear about to happen? It questions what makesthat. These are unanswerable therapy work. It makes me feel like Iquestions. Given the circumstances, really don’t know how to move withhowever, I need to see her. therapy anymore.
104104

TABLE 2. Sample Questions Associated with Each Cognitive-Developmental OrientationASSESSMENT QUESTIONS
1. How do you make sense of/conceptualize this family?2. What do you want to focus on in supervision?
EXPLORATORY QUESTIONS FOR HORIZONTAL AND VERTICAL DEVELOPMENT
Client
1. How does this familyexpress emotion?
2. What elements ofverbal and non-verbal behaviorseem most helpful inunderstanding thisfamily?
1. What are theysaying/doing? Howdid they react?
2. Can you tell mewhat interactionsoccurred that leadyou to thatconclusion?
Self as Therapist
1. What were youfeeling in thissession?
2. What did you decideto focus on in orderto make sense ofthings?
1. How would youdescribe what youare doing?
2. How could youbetter execute thatinterventionstrategy?
TherapeuticProcess
1. How are yourfeelings about thisfamily affecting howyou react?
2. How is this familyfeeling toward you?
1. What verbal andnon-verbal behaviorsprompted thatintervention? Whatdid you think wouldhappen? How didthey actually react?What did you donext?
SupervisoryProcess
1. How are yourfeelings about thesupervisory processaffecting you now?
2. What are you feelingbefore you come/after you leavesupervision?
1. What are we doinghere that makes thiseffective/ineffectivefor you?
2. How would youdescribe what wehave been doinghere?
SENSORIMOTOR
CONCRETE
VERTICALDEVELOPMENT
HORIZONTAL DEVELOPMENT
TABLE 2. Sample Questions Associated with Each Cognitive-Developmental OrientationASSESSMENT QUESTIONS
1. How do you make sense of/conceptualize this family?2. What do you want to focus on in supervision?
EXPLORATORY QUESTIONS FOR HORIZONTAL AND VERTICAL DEVELOPMENT
Client
1. How does this familyexpress emotion?
2. What elements ofverbal and non-verbal behaviorseem most helpful inunderstanding thisfamily?
1. What are theysaying/doing? Howdid they react?
2. Can you tell mewhat interactionsoccurred that leadyou to thatconclusion?
Self as Therapist
1. What were youfeeling in thissession?
2. What did you decideto focus on in orderto make sense ofthings?
1. How would youdescribe what youare doing?
2. How could youbetter execute thatinterventionstrategy?
TherapeuticProcess
1. How are yourfeelings about thisfamily affecting howyou react?
2. How is this familyfeeling toward you?
1. What verbal andnon-verbal behaviorsprompted thatintervention? Whatdid you think wouldhappen? How didthey actually react?What did you donext?
SupervisoryProcess
1. How are yourfeelings about thesupervisory processaffecting you now?
2. What are you feelingbefore you come/after you leavesupervision?
1. What are we doinghere that makes thiseffective/ineffectivefor you?
2. How would youdescribe what wehave been doinghere?
SENSORIMOTOR
CONCRETE
VERTICALDEVELOPMENT
HORIZONTAL DEVELOPMENT
105105

Client
1. How do youconceptualize theway this familyunderstands andresponds to thesetypes of issues?
2. Do you notice anycommonalitiesacross situations?
3. Do you see anyrepeating patterns?
1. What rules are thisfamily operatingfrom?
2. When/how/why/werethese rulesestablished?
3. Can they challengethese rules?
Self as Therapist
1. Does your reactionin this situationseem familiar toyou?
2. Have you donesimilar things/feltsimilar ways in yourrelationships withother people?
1. What rules are youoperating from?
2. Can you notice theflaws in these rules?
3. What could you doto change theserules and do thingsdifferently?
TherapeuticProcess
1. What types ofinterventions seemmost congruent withthis family?
2. Can you identify therepeating patterns ofinteraction that areoccurring betweenyou and this family?
1. What assumptionsare you makingabout this family?How are theseassumptions limited?
2. When you recognizethis type of patternbetween you and thefamily what couldyou do to see thingsdifferently?
SupervisoryProcess
1. How is ourrelationship similarto others in yourlife?
2. Can we discuss thispattern that seemsto be occurring inour relationship?
1. What do you see asthe implicit expec-tations we have setfor one another?How would you liketo change these?
2. How do our cultural/gender/religious/value similarities anddifferences come tobear on thisrelationship?
FORMAL
DIALECTIC/SYSTEMIC
VERTICALDEVELOPMENT
HORIZONTAL DEVELOPMENT
TABLE 2 (continued)
Client
1. How do youconceptualize theway this familyunderstands andresponds to thesetypes of issues?
2. Do you notice anycommonalitiesacross situations?
3. Do you see anyrepeating patterns?
1. What rules are thisfamily operatingfrom?
2. When/how/why/werethese rulesestablished?
3. Can they challengethese rules?
Self as Therapist
1. Does your reactionin this situationseem familiar toyou?
2. Have you donesimilar things/feltsimilar ways in yourrelationships withother people?
1. What rules are youoperating from?
2. Can you notice theflaws in these rules?
3. What could you doto change theserules and do thingsdifferently?
TherapeuticProcess
1. What types ofinterventions seemmost congruent withthis family?
2. Can you identify therepeating patterns ofinteraction that areoccurring betweenyou and this family?
1. What assumptionsare you makingabout this family?How are theseassumptions limited?
2. When you recognizethis type of patternbetween you and thefamily what couldyou do to see thingsdifferently?
SupervisoryProcess
1. How is ourrelationship similarto others in yourlife?
2. Can we discuss thispattern that seemsto be occurring inour relationship?
1. What do you see asthe implicit expec-tations we have setfor one another?How would you liketo change these?
2. How do our cultural/gender/religious/value similarities anddifferences come tobear on thisrelationship?
FORMAL
DIALECTIC/SYSTEMIC
VERTICALDEVELOPMENT
HORIZONTAL DEVELOPMENT
TABLE 2 (continued)
106106


TABLE 3. Supervisory Environments Associated with Each Cognitive-Developmental Orientation
Cognitive-developmental supervision is designed to assist supervisees to access skills within each of the various orientations. This holisticframework involves the creation of environments that facilitate both horizontal (skill mastery) and vertical (skill extension) development.
SUPERVISION MODALITIESAND TECHNIQUES
1. Directive, live supervision with bug-in-ear or phone-in.
2. Supervisor/therapist therapy team.3. Team and/or video observationfocused on case conceptualization.
4. Didactic and readings.5. Group supervision.6. Role plays; sculpting.7. Experiential exercises.
1. Live supervision with pre-sessionplanning, mid-session coaching, andpost-session debriefing.
2. Audio/video and case presentationfocused on assessment and skillmastery.
3. Exercises concerning observationand intervention skills.
SUPERVISION OBJECTIVES
SENSORIMOTOR ORIENTATION1. To develop methods of caseconceptualization.
2. To clarify and understand feelings aspresented by self and family.
3. To reduce anxiety.4. To identify countertransferenceissues.
CONCRETE ORIENTATION1. To enact therapeutic strategies andtechniques.
2. To identify and articulate if/thenconceptualizations.
3. To enhance tracking skills.4. To understand decision-makingprocesses of self, family, andtherapeutic encounter.
SUPERVISORY STYLE
Directive: Used to provide a structurethat permits supervisees to safely exploresensory experience and to integratesalient aspects of this experience into acoherent organization.
Coaching: Used to assist supervisees tounderstand thoughts, feelings, andbehaviors of self and family from a linearperspective. Provides demonstrations andmodels of effective therapy.
TABLE 3. Supervisory Environments Associated with Each Cognitive-Developmental Orientation
Cognitive-developmental supervision is designed to assist supervisees to access skills within each of the various orientations. This holisticframework involves the creation of environments that facilitate both horizontal (skill mastery) and vertical (skill extension) development.
SUPERVISION MODALITIESAND TECHNIQUES
1. Directive, live supervision with bug-in-ear or phone-in.
2. Supervisor/therapist therapy team.3. Team and/or video observationfocused on case conceptualization.
4. Didactic and readings.5. Group supervision.6. Role plays; sculpting.7. Experiential exercises.
1. Live supervision with pre-sessionplanning, mid-session coaching, andpost-session debriefing.
2. Audio/video and case presentationfocused on assessment and skillmastery.
3. Exercises concerning observationand intervention skills.
SUPERVISION OBJECTIVES
SENSORIMOTOR ORIENTATION1. To develop methods of caseconceptualization.
2. To clarify and understand feelings aspresented by self and family.
3. To reduce anxiety.4. To identify countertransferenceissues.
CONCRETE ORIENTATION1. To enact therapeutic strategies andtechniques.
2. To identify and articulate if/thenconceptualizations.
3. To enhance tracking skills.4. To understand decision-makingprocesses of self, family, andtherapeutic encounter.
SUPERVISORY STYLE
Directive: Used to provide a structurethat permits supervisees to safely exploresensory experience and to integratesalient aspects of this experience into acoherent organization.
Coaching: Used to assist supervisees tounderstand thoughts, feelings, andbehaviors of self and family from a linearperspective. Provides demonstrations andmodels of effective therapy.
109109

SUPERVISION MODALITIESAND TECHNIQUES
1. Audio/video supervision or casepresentation focused on patterns ofdifficulty across cases or therapeuticencounters.
2. Self-analysis inventories.3. Critique of major and personal
models.
1. Audio/video and case presentationfocused on epistemological andontological issues.
2. Co-therapy stressing the dialecticprocesses between supervisor,supervisee, and family.
3. Peer consultation.4. Sharing of supervisor thoughts andanalyses.
5. Analyze self and theories for crosssituational constancy andunrecognized bias.
SENSORIMOTOR ORIENTATION
FORMAL ORIENTATION1. To reflect on self and clinical data.2. Assessment and interventiongeneralization and flexibility.
3. To identify repetitive patterns acrossfamilies and therapeutic encounters,and within self.
4. To construct metaphors and otheranalogs to help families find meaningin therapy.
DIALECTIC/SYSTEMIC ORIENTATION1. To recognize and challengeassumptions underlying major andpersonal models, treatment plans,and supervision.
2. To discern significant contextualissues.
3. To realize how one’s history isreflected in the nature and methodsof construction.
4. To evaluate the limits of their ownconstructions.
SUPERVISORY STYLE
Consultation: Stresses the facilitation ofreflective skills. Used to assistsupervisees to understand the constancyof patterns within self, family, therapeuticencounters, therapy models, andsupervision.
Collaboration: Focuses on thesupervisee’s core cognitive and meta-cognitive processes such as person-environment issues and personalconstructs.
TABLE 3 (continued)
SUPERVISION MODALITIESAND TECHNIQUES
1. Audio/video supervision or casepresentation focused on patterns ofdifficulty across cases or therapeuticencounters.
2. Self-analysis inventories.3. Critique of major and personal
models.
1. Audio/video and case presentationfocused on epistemological andontological issues.
2. Co-therapy stressing the dialecticprocesses between supervisor,supervisee, and family.
3. Peer consultation.4. Sharing of supervisor thoughts andanalyses.
5. Analyze self and theories for crosssituational constancy andunrecognized bias.
SENSORIMOTOR ORIENTATION
FORMAL ORIENTATION1. To reflect on self and clinical data.2. Assessment and interventiongeneralization and flexibility.
3. To identify repetitive patterns acrossfamilies and therapeutic encounters,and within self.
4. To construct metaphors and otheranalogs to help families find meaningin therapy.
DIALECTIC/SYSTEMIC ORIENTATION1. To recognize and challengeassumptions underlying major andpersonal models, treatment plans,and supervision.
2. To discern significant contextualissues.
3. To realize how one’s history isreflected in the nature and methodsof construction.
4. To evaluate the limits of their ownconstructions.
SUPERVISORY STYLE
Consultation: Stresses the facilitation ofreflective skills. Used to assistsupervisees to understand the constancyof patterns within self, family, therapeuticencounters, therapy models, andsupervision.
Collaboration: Focuses on thesupervisee’s core cognitive and meta-cognitive processes such as person-environment issues and personalconstructs.
TABLE 3 (continued)
110110




























