7. 2. lntroduction
8
deBaat C, van Waas MAJ JPP A 2074; 02(01): s1-58 OralAnatomy Related to !mpression Making for Complete Dentures C. de Baatl, M.A.J. van Waas2 7. Department of Oral Function and Prosthetic Dentistry, Radbouduniversity medical center, P.O. Box 9101, 6500 HB Nijmegen, The Netherlands. 2. Department of Oral Function, Academic Centre for Dentistry Amsterdam, Gustav Mahlerlaan 30L4, 1081 LA Amsterdam, The Netherlands. Correspondence,'Professor Dr. Cees de Baat. Email: [email protected] ABSTRACT Making an impression of the edentulous maxillary and mandibular residual alveolar ridge is an important part of fabricating removable complete dentures, because the proper functioning of the dentures is partially dependent on the volume and shape of the resldual alveolar ridges and the surrounding soft tissues, in particular the muscles. Before an impression is made, an insight into the anatomy of the edentulous maxilla and mandible as well as of the soft oral tissues is essential. A S-phase approach for impression making has been introduced, containing guidelines for consecutively making the preliminary impressions, fabricating the'preliminary casts and the individual impression trays, making the individual impressions, and fabricating the master casts. ln each phase, the concern is to achleve the best possible stability of the removable complete dentures. Adequate stability can only be achieved by developing the functional borders of the dentures adequately. How to cite this drticle:de Baat C, van Waas MAJ.Oral anatomy related to impression making for complete dentures. J Pak ProsthodontAssoc 2OL4;02 (01): 51 - 58. lntroduction softenedthermoplastic impression compound is put Making impressions of the edentulous maxillary and on the borders of the individual impression trays and mandibular residual alveolar ridge is one of the most the patient is requested to make functional orofacial difficult components of fabricating removable movements, supported by muscle moulding by the complete dentures, because developing the dentist, until the optimal border position at functional borders of the future dentures in the oral unimpaired function has been obtained. This method cavity needs accurate attention. ln case the flanges of requires accuracy and some experience. lf the the future dentures are too short, the dentures lack thermoplastic impression compound has not been stability and retention on the residual alveolar ridges softened sufficiently, it is not plastic in the oral cavity during functional movements of ihe orofacial and if it has been heated too much, it flows off or muscles. ln case the flanges of the future dentures even damages the oral mucosal tissues. Moreover, a are too long, the dentures will dislodge because the large individual difference exists in the intensity of orofacial muscles will remove them from the residual functional orofacial movements which people can alveolar ridges. ln other words, both the under- make. The only method to reach a good result is to extended and over-extended denture flanges are use the anatomy of the oral cavity as the basis for problematic. ln many text books on removable assessing the correct flange borders of the future complete dentures, developing the functional borders removable complete dentures. To fabricate a is recommended to solve this problem. Developing complete denture which stays stable in position in the the functional borders through border moulding is oral cavity during movements of the mandible, the carried out after shortening the flanges of the lips and the cheeks, the strengths of the orofacial individual impression trays approximately 2 mm from muscles applied to the removable complete denture the expected final length of the flanges of the future have to be considered. This aspect is important in complete dentures. Subsequently, a heat- case a residual alveolar ridge is not atrophic, but it 51
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of 7. 2. lntroduction

- - -- --i01): 47-50
':::-:: S COnfOfmS
-:::-:r s fabrication-- :' catlent, thus
='. -' -ovement of- :':-. iris Position..:'.:= :'csthetic eYe
-. -. :'ocedure (iris
: : - :: difficult and
:' --= :oerator' The
: -:::': :SeS a StOCk
. . :- :VefCOme the- - ,:: n making a
-::i "rih minimal
: - -' -.:Ce Prosthesis
:., .' .3refabricated- , =:=: crosthesis.
: -: :re clinician is
:' . :':'abricated eYe
: =: :', Paft.
: , .'. -' . steps and
. '" ::rkaj Vashisht ,
=- -' :rosthodontics,
.-: :','lsceration. ln:
::: l.ane's clinical
' =- ,.' ar Prosthesis J
. --::(', :: ' ed imPression
' :. -. Am J OPthalmol
i'.' -: .' Positioning the
' . -- ..- ar Prosthesis J
: -- Maxillofacial
:: -: - and surgical
- - : ','C, lsiYaku Euro
- -- r6s-77.1998.
'' :-: : oning Prosthetic
:, . r':sthet Dentt977;
:cular Prostheses-
--:nt 1996; 75:1-3'
deBaat C, van Waas MAJ JPP A 2074; 02(01): s1-58
OralAnatomy Related to !mpression Making for Complete Dentures
C. de Baatl, M.A.J. van Waas27. Department of Oral Function and Prosthetic Dentistry, Radbouduniversity medical center, P.O. Box
9101, 6500 HB Nijmegen, The Netherlands.2. Department of Oral Function, Academic Centre for Dentistry Amsterdam, Gustav Mahlerlaan 30L4,
1081 LA Amsterdam, The Netherlands.
Correspondence,'Professor Dr. Cees de Baat. Email: [email protected]
ABSTRACT
Making an impression of the edentulous maxillary and mandibular residual alveolar ridge is an importantpart of fabricating removable complete dentures, because the proper functioning of the dentures is partially
dependent on the volume and shape of the resldual alveolar ridges and the surrounding soft tissues, in
particular the muscles. Before an impression is made, an insight into the anatomy of the edentulous maxilla
and mandible as well as of the soft oral tissues is essential. A S-phase approach for impression making has
been introduced, containing guidelines for consecutively making the preliminary impressions, fabricatingthe'preliminary casts and the individual impression trays, making the individual impressions, and fabricatingthe master casts. ln each phase, the concern is to achleve the best possible stability of the removablecomplete dentures. Adequate stability can only be achieved by developing the functional borders of thedentures adequately.How to cite this drticle:de Baat C, van Waas MAJ.Oral anatomy related to impression making for complete
dentures. J Pak ProsthodontAssoc 2OL4;02 (01): 51 - 58.
lntroduction softenedthermoplastic impression compound is putMaking impressions of the edentulous maxillary and on the borders of the individual impression trays and
mandibular residual alveolar ridge is one of the most the patient is requested to make functional orofacialdifficult components of fabricating removable movements, supported by muscle moulding by thecomplete dentures, because developing the dentist, until the optimal border position atfunctional borders of the future dentures in the oral unimpaired function has been obtained. This methodcavity needs accurate attention. ln case the flanges of requires accuracy and some experience. lf thethe future dentures are too short, the dentures lack thermoplastic impression compound has not been
stability and retention on the residual alveolar ridges softened sufficiently, it is not plastic in the oral cavityduring functional movements of ihe orofacial and if it has been heated too much, it flows off ormuscles. ln case the flanges of the future dentures even damages the oral mucosal tissues. Moreover, a
are too long, the dentures will dislodge because the large individual difference exists in the intensity oforofacial muscles will remove them from the residual functional orofacial movements which people can
alveolar ridges. ln other words, both the under- make. The only method to reach a good result is toextended and over-extended denture flanges are use the anatomy of the oral cavity as the basis forproblematic. ln many text books on removable assessing the correct flange borders of the futurecomplete dentures, developing the functional borders removable complete dentures. To fabricate a
is recommended to solve this problem. Developing complete denture which stays stable in position in thethe functional borders through border moulding is oral cavity during movements of the mandible, thecarried out after shortening the flanges of the lips and the cheeks, the strengths of the orofacialindividual impression trays approximately 2 mm from muscles applied to the removable complete denturethe expected final length of the flanges of the future have to be considered. This aspect is important incomplete dentures. Subsequently, a heat- case a residual alveolar ridge is not atrophic, but it
51
deBaat C, van Waas MAJ
becomes essential in case of an atrophic residualalveolar ridge.
This article presents a S-phase approach for theprocedure of making an impression of edentulous,whether or not atrophic, residual maxillary andmandlbular alveolar ridges, taking into considerationthe anatomy of the maxilla and the mandible as wellas the functions of the orofacial muscles which willinterfere with the future removable completedentures.
5-Phase approachThe procedure of maklng impressions of edentulousresidual alveolar ridges comprises of 5 phases:preliminary impressions, preliminary casts, individualimpression trays, individual impressions, and mastercasts. A shortcoming somewhere in the 5-phaseapproach has consequences for the next phase(s),leading to removable complete dentures withinsufficient stability and retention.
Phase 1: Preliminary impressionsThe quality of a preliminary impression is highlydependent on the correct size of the confection(stock) impression tray used. A set of anatomically-shaped confection impression trays is needed toselect the optimal tray from the set. When using a
tray of such set, one should realise that the design
JPP A 201,4; 02(01): 51-58
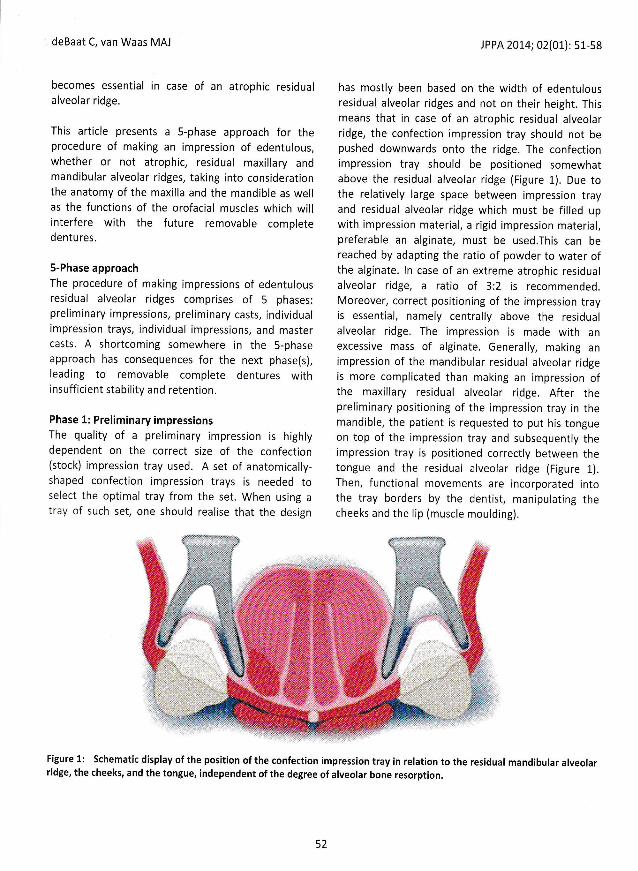
has mostly been based on the width of edentulousresidual alveolar ridges and not on their height. Thismeans that in case of an atrophic residual alveolarridge, the confection impression tray should not bepushed downwards onto the ridge. The confectionimpression tray should be positiqned somewhatabove the residual alveolar ridge (Figure 1). Due tothe relatively large space between impression trayand residual alveolar ridge which must be filled upwith impression material, a rigid impression material,preferable an alginate, must be used.This can bereached by adapting the ratio of powder to water ofthe alginate. ln case of an extreme atrophic residualalveolar ridge, a ratio of 3:2 is recommended.Moreover, correct positioning of the impresslon trayis essential, namely centrally above the residualalveolar ridge. The impression is made with anexcessive mass of alginate. Generally, making animpression of the mandibular residual alveolar ridgeis more complicated than making an impression ofthe maxillary residual alveolar ridge. After thepreliminary positioning of the impression tray in themandible, the patient is requested to put his tongueon top of the impression tray and subsequently theimpression tray is positioned correctly between thetongue and the residual alveolar ridge (Figure 1).Then, functional movements are incorporated intothe tray borders by the dentist, manipulating thecheeks and the lip (muscle moulding).
deBaat C van Hda:
IFigure 2: Schernati tattachment for the hpteryto-mandibuk ilmylohyoid musde frmandible and frorn disl
Phase 2: prelimimrycTo be able to rfurbimpression trala, ttstudied in relation tc tthe mandible. Surslborders of the firEu,re r
are recorded on lhe ppencil.
Preliminory mariilxyaDorsally to th€pte rygo m axil la ry fissr-r.rby the pterygornaxiiliPterygomandibular +oldto the retromolar @ o
Figure 1: Schematic display of the position of the confection impression tray in relation to the residual mandibular alveolarridge, the cheeks, and the tongue, independent of the degree of alveolar bone resorption.
52

t2014;02(01): 51-58
ritth of edentulousqr their height. This
lrk residual alveolar
tr traY should not be
lEe. The confection
ritinned somewhat
;e (Figure 1). Due to
reen imPression tray
ilr must be filled uP
I impression material,
be used.This can be
lf powder to water of
Erne atrophic residual
b2 is recommended'
irf the imPression traY
J above the residual
rr is made with an
Generally, making an
residual alveolar ridge
ling an imPression of
ular ridge. After the
rimpression traY in the
r*ed to Put his tongue
y and subsequenilY the
correctlY between the
rolar ridge (Figure 1)'
i are incorPorated into
ntist, maniPulating the
lr.ilding).
':: :-a rrandibular alveolar
deBaat C, van Waas MAJ )PP A 20L4; 02(01): 51-58
Ptfl1'eol,tEcrnatG i. .ILUEUOrrlsr!***ctr H#k
kp*r:* Phrnrg*iCm*r:*sri{uxir
K*r*pola:Tr:gonr*x
r
;F
Phase 2: Preliminary casts
To be able to fabricate adequate individualizedimpression trays, the preliminary casts must bestudied in relation to the anatomy of the maxilla andthe mandible. Subsequently, the intended flangeborders of the future removable complete denturesare recorded on the preliminary casts, using a sharppencil.
P reli mi n o ry m axi lla ry co st :Dorsally to the maxillary tuberosity, thepterygomaxillary fissure is situated, dorsally Iimitedby the pterygomaxillary or hamular notch. Thepterygomandibular fold connects the hamular notchto the retromolar pad of the mandible and functions
as attachment for the buccinators as well as thepharyngeal constrictor muscle (Figure 2)
For the posterior flange border of the future maxlllarydenture, the pterygo-mandibular fold is importantbecause it indicates the position of the pterygo-maxillary fissure. Dorsally at both sides, the denture isextended until the deepest point of the pterygo-maxillary fissure and forms the posterior border ofthe denture directly dorsally to the maxillarytuberosities. When the posterior border of thedenture extends beyond the pterygo-maxillaryfissure, the denture will dislodge while opening themouth extremely through tightening the buccinatormuscle at the attachment to the pterygo-mandibularfold.
#tylotuyo*d Ri*ge
Figure 2: Schematic display of the lingual side of the right mandible. The pterygo-mandibular fold functions ventrally asattachment for the buccinator muscle and dorsally as attachment for the pharyngeal constrictor muscle. The border of thepterygo-mandibular fold reaches caudally until the retromolar pad or somewhat lingually of the retromolar pad. Themylohyoid muscle attaches to the mylohyoid line, in the anterior region somewhat cranially of the caudal border of themandible and from this point in cranial direction until the retromolar pad.
53
deBaat C, van Waas MAJ
It is more difficult to assess the posterior border ofthe future maxillary denture between the twomaxillary tuberosities. Two key anatomical structures
are available. The first one is at the junction between
the hard to the soft palate, the vibrating line. The
hard palate is a part of the maxilla, usually the bone is
ending dorsally with an angle perpendicular to thecaudal surface, but the angle may also be oblique
with the cranial border of the palatal bone somewhat
more dorsally than the caudal border. When
available,'this minor dorsal 'lengthening' of the hardpalate can be used as additional base for the futureremovable maxillary denture. The not bone-
supported soft palate is part of the posterior
boundary 'of the oral cavity. lt is mobile and itsmovements are essential when swallowing and
speaking. The junction between the hard to the softpalate becomes slightly visible when a patient says
"ah" when the oral cavity is open. When saying "ah",
the soft palate is moving cranially. lt is possible tolocate the junction somewhat more clearly when a
patient is requested to exhale or to blow his nose
strongly while the oral cavity is open and the nose is
pinched. ln those cases, the soft palate is bulged outinto the caudal direction. A second key anatomical
structures..... to assess the posterior border of the
future complete maxillary denture are the palatine
foveas, small depressions on the hard palate near thejunction between the hard and soft palates, left and
right of the median palatine suture. These structures
are rudimentary ducts of salivary glands. They are
frequently directly visible in the oral cavity and mostly
also in the preliminary impression and on thepreliminary cast.
The next boundary which should be assessed for a
good function of the future removable maxillary
denture is the dorso-buccal flange. Between themaxillary tuberosity and the mandibular ramus, a
transversal niche is located which provides space toenable the mandible to make movements. The futureremovable maxillary denture can be extended intothis space to cover the maxilla until its vestibular
sulcus, because no muscle attachments, which could
dislodge the removable denture, are present in this
space. However, lt is a pertinent prerequisite that the
JPP A 2Ot4; 02(0L): 51-58
dorso-buccal flange of the denture is thin to prevent
contact with the mandibular ramus when themandible is moving. ln case the mandibular ramus
touches the removable maxillary denture whilemoving, the denture will dislodge.
More ventr:ally, in the buccal premolar region, thebuccal frenum is situated. lt is a vertical ligament oforal mucosa connecting the residual alveolar ridge tothe modiolus in the cheek. The modiolus is a point
distal to the corner of the mouth where several
muscles converge. Among others, the buccinator
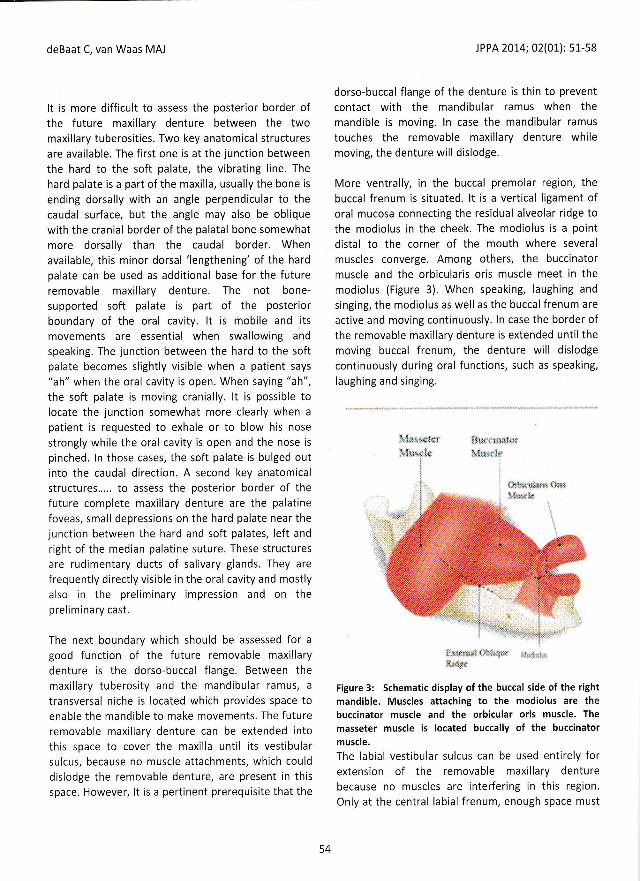
muscle and the orbicularis oris muscle meet in themodiolus (Figure 3). When speaking, laughing and
singing, the modiolus as well as the buccal frenum are
active and moving continuously. ln case the border ofthe removable maxillary denture is extended until themoving buccal frenum, the denture will dislodge
continuously during oral functions, such as speaking,
laughing and singing.
, i -; il !i:t. :i-.N' I11.,. i.. 1r., :.
l
i :'* :.: t ' ,r:'
Figure 3: Schematic display of the buccal side of the rightmandible. Muscles attaching to the modiolus are thebuccinator muscle and the orbicular oris muscle. The
masseter muscle is located buccally of the buccinatormuscle,
The labial vestibular sulcus can be used entirely forextension of the removable maxillary denture
because no muscles are interfering in this region.
Only at the central labial frenum, enough space must
deBaat C, van Waas
be created for nrrthickness of the devestibular sulcus is, i
by the degree of ahrthe degree of atrrelthick the denture flaan aesthetically and iupper lip.
Preliminory mandihThe study of the premandible starts atobserved from veotretromolar pad is srmobile mucosal part r
caudal border of t'rrposterior border of amust be located eusupported part of tile I
Buccally of ihE -.the thin bucc -.:_located. The mabuccal side of thethe zygomaticmandibular cornpspace for theadequately. lf noarise during n-a.: -
retromolar pac -
buccinator n-_., =
horizontally frc *modiolus(Figur: -.pushes the re*: . :downwards tc :-=the stability o. :-exploited by e:r::- :to or somewhat bethe external oblic.muscle attaches theresidual alveoia.external oblrql:visible on the prelirninal
Any further ventralh, tfuSimilar to the maxilla, aconnecting the buccd I
54

- - -- :ii01): 51-58
-: ! :- i to Prevent':*-s when the
': - .': bular ramus
.-"::'ture while
'.'.*. =' region, the
: 2-. r? llgament of
: -. . .eclar ridge to
--t. tls is a Point' - --.' ."1ere several-:-: :-e buccinator
- -,:: meet in the
...-: aughing and
-.- . -- -a-a f renum are
- :::::he border of
: . :,::'ded until the
:=" -'. ',vill dislodge
- -, : -:^ as sPeaking,
Fl}I
[**I rr..t
:-: :-:cal side of the right
:::-: rodiolus are the
'::-:' oris muscle. The
:-::: ' of the buccinator
-,- :. -.ed entirelY for
.. :- --:iillarY denture''--=''. n this region'- - -' . -: -gh space must
deBaat C, van Waas MAJ
be created for movements of the upper lip. The
thickness of the denture flange border in the labial
vestibular sulcus is, among other factors, determinedby the degree of alveolar bone resorption. The higherthe degree of alveolar bone resorption, the morethick the denture flange border has to be to providean aesthetically and functionally good support for theupper lip.
Prelimi na ry ma ndi buld rcdstThe study of the preliminary cast of the edentulousmandible starts at the retromolar pad. Whenobserved from ventral to dorsal aspect, first theretromolar pad is supported by bone and then a
mobile mucosal part can be detected, finishing at thecaudal border of the pterygo-mandibular fold. Theposterior border of a removable mandibular denturemust be located exactly at the end of the bone-supported part of the retromolar pad.
Buccally of the retromolar pad, directly laterally ofthe thin buccinator muscle, the masseter muscle is
located. The masseter muscle is attached to thebuccal side of the body of the mandible as well as tothe zygomatic arch (Figure 3).A removablemandibular complete denture must leave sufficientspace for the masseter muscle to functionadequately. lf not, pain and a traumatic ulcer willarise during mastication. Somewhat ventrally of theretromolar pad, in the vestibule of the oral cavity, thebuccinator muscle can be found, which extendshorizontally from the pterygo-mandibular fold to themodiolus(Figure 2-3). When this muscle tightens, itpushes the removable mandibular complete denturedownwards to the residual alveolar ridge, enhancingthe stability of this denture. This property can beexploited by extending the flange of the denture tightto or somewhat below the buccinator muscle untilthe external oblique line, where the buccinatormuscle attaches the mandible. ln case of an atrophicresidual alveolar ridge, it is rather easy to palpate theexternal oblique line and in some cases this line is
visible on the preliminary cast.
Any further ventrally, the buccal frenum can be seen.Similar to the maxilla, a ligament of oral mucosa is
connecting the buccal frenum with the modiolus.
JPP A 20L4; 02(01): 51-58
Sometimes, the buccal frenum is dominantly present,sometimes it is hardly visible, particularly in olderpeople. A removable complete mandibular dentureshould offer sufficient space for the functionalmovements of the buccal frenum.
The mental foramen is situated buccally at the bodyof the mandible, but in case of an extreme atrophicresidual alveolar ridge it is situated at the cranial side.
Through this foramen, the merital artery, the mentalvein as well as the mental nerve pass from themandibular canal to the lower lip region. The mentalnerve is a branch of the inferior alveolar nerve. Whena removable mandibular complete denture touchesthe cranially of the mandible exposed mental orinferior alveolar nerve during function, a short stab ofpain will occur. To prevent this unpleasantexperience, the mandibular complete denture needs
maximal stability and correct occlusion andarticulation. ln most cases, providing some space in thedenture around the mental foramen is not an
adequate solution because this solution reduces theretention of the denture.
Figure 4: Schematic display of the midline of themandible. ln a dentate mandible, the mental muscle is
situated at the labial part of the mandible (a). In an
edentulous mandible with an atrophic residual alveolarridge, the position of the mental muscle has moved to thecranial side of the mandible (b).
a
55
@
ff,;,h .MSr **:&r tr@,

deBaat C, van Waas MAJ
*Ba&*x:fid*ffi.I(
Figure 5: Schematic display of the lingual side of the leftmandible showing the position of the genial tubercle, thegenioglossus muscle, and the mylohyoid muscle whichattaches at the mylohyoidridga and the hyoid bone.
Lingually, the flange of a removable cempletedenture can be extended until the genial tubercle, theattachment of the genioglossus muscle (Figure 5). Thegenioglossus muscle can move the tongue ventrallyand caudally. ln case of atrophy of the residualalveolar ridge, the genial tubercle is very pronounced(Figure 6).
j. lri,r,-ri,li::,I ]: tr
IPP A 2014; 02(01): s1-58
More dorsally et the lingual side of the mandible, themylohyoid muscle is shaping the floor of the oralcavity, which is extending horizontally in the anteriorregion and almost vertically in the posterior region(Figure 5). This anatomical structure is similar to thecourse of the mylohyoid line, in the anterior regionsomewhat cranially of the caudal border of themandible, directly below the genial tubercle, andfrom this point in cranial direction until theretromolar pad, almost until the forrner plane efocclusion. At the other side, the mylohyoid muscleattaches to the hyoid bone, which is located centrally,posteriorly and caudally of the mandible. As a
consequence, the tightened mylohyoid muscle has a
somewhat vertical position posteriorly, approximately60 degrees to the horizontal plane. ln the anteriorregion, the. lingual flange of a removable completedenture should be extended just cranially of themylohyoid line and in the posterior region it can be
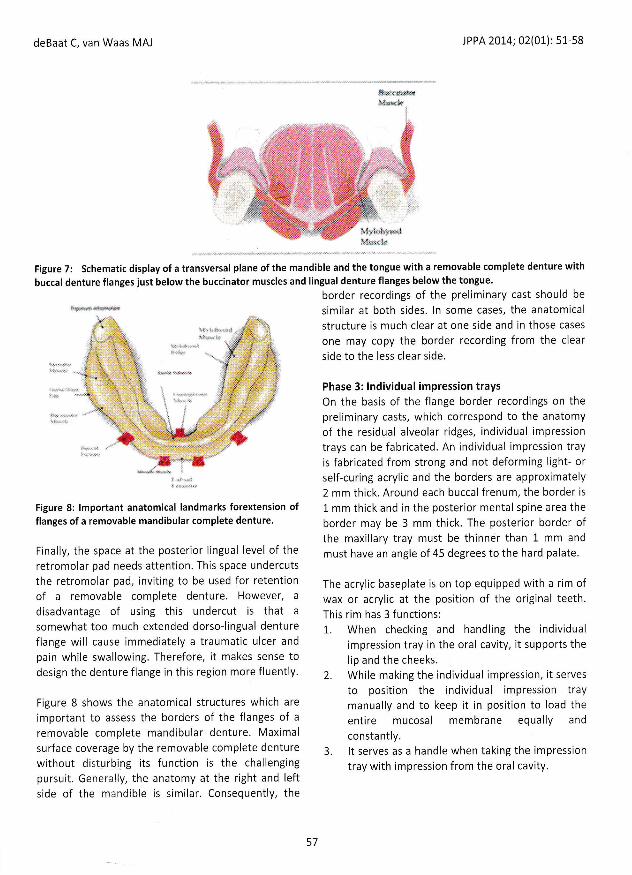
extended just caudally of the mylohyoid line. Thecombination of denture f langes just below thebuccinator muscles bucally and denture flanges belowthe tongue lingually improves the sta bility of a
removable mandibular complete denture (Figure 7).
By checking whether a removable mandibulardenture dislodges when the patient is moving his
tongue along the upper lip, the correct length of thelingual flanges can be assessed. When the denturestays at its position, the lengths of the lingual flang:sare correct. ln case of severe atrephy of the residualalveolar ridge, the floor of the oral cavity may be so
much pronounced that it is not possible to extend a
part of the lingual flanges beyond the mylohyoidlines.
deBaat C, van \tlaas
Figure 7: Schematt-buccal denture flangsi
Eq**-
Figure 6:Schematic display of the lingual side of the leftmandible with a pronounced mentalspine.
Figure g: ,rO.** -lflanges of a remotzble r
Finally, the space at drretromolar pad neecb ethe retromolar pad, inUof a removable contdisadvantage of us-r6somewhat too muah dflange will cause inlrreapain while swallowirg- .n
design the denture flangl
Figure 8 shows the anilimportant to assess Eheremovable complete n-lsurface coverage by trre nwithout disturbing is ipursuit. Generally, til-re aside of the mandibte 6
56
2l)14;02(01): 51-58
f the mandible, the
n floor cf the oral
Flty in the anterior
he Posterior region
Lre is similar to the
r the anterior region
trdal border of the
penial tubercle, and
lrestion until the
lre former Plane ef
ie mYlohyoid muscle
ilr is located centrallY,
[r mandible. As a
lrtryoid muscle has a
Eriorty, aPProximatelY
fne. ln the anterior
t removable comPlete
i.rst craniallY of the
Erior region it can be
r rnylohYoid line' The
6es just below the
I dcnture flanges below
Es the stalilitY of a
lte denture (Figure 7)'
ernovable mandibula,r
patient is moving his
E correst length of the
nd. When the denture
b of the lingual flanges
tatrsphY of the residual
n oral cavitY maY be so
S Possible to extend a
berpnd the mYlohYoid
deBaat C, van Waas MAJ JPP A 201.4; 02(01): 51-58
Es,ew*S{M$r
llS"*ts}s*ht*xS*
Figure 7: Schematic display of a transversal plane of the mandible and the tongue with a removable complete denture with
buccal denture flanges just below the buccinator muscles and lingual denture flanges below the tongue.
border recordings of the preliminary cast should be
similar at both sides. ln some cases, the anatomical
structure is much clear at one side and in those cases
one may copy the border recording from the clear
side to the less clear side.
Phase 3: lndividual impression traysOn the basis of the flange border recordings on the
preliminary casts, which correspond to the anatomy
of the residual alveolar ridges, individual impression
trays can be fabricated. An individual impression trayis fabricated from strong and not deforming light- orself-curing acrylic and the borders are approximately
2 mm ihick. Around each buccal frenum, the border is
1 mm thick and in the posterior mental spine area the
border may be 3 mm thick. The posterior border ofthe maxillary tray must be thinner than 1 mm and
must have an angle of 45 degrees to the hard palate.
The acrylic baseplate is on top equipped with a rim ofwax or acrylic at the position of the original teeth.This rim has 3 functions:1". When cheoking and handling the individual
impression tray in the oral cavity, it supports the
lip and the cheeks.
2. While making the individual impression, it serves
to position the individual impression traymanually and to keep it in position to load the
entire mucosal membrane equally and
constantly.3. lt serves as a handle when taking the impression
tray with impression from the oral cavity.
Figure 8: tmportant r"","r,.",'l]"rmarks forextension offlanges of a removable mandibular complete denture.
Finally, the space at the posterior lingual level of the
retromolar pad needs attention. This space undercuts
the retromolar pad, inviting to be used for retentionof a removable complete denture. However, a
disadvantage of using this undercut is that a
somewhat too much extended dorso-lingual denture
flange will cause immediately a traumatic ulcer and
pain while swallowing. Therefore, it makes sense todesign the denture flange in this region more fluently.
Figure 8 shows the anatomical structures which are
important to assess the borders of the flanges of a
removable complete mandibular denture. Maximal
surface coverage by the removable complete denture
without disturbing its function is the challengingpursuit. Generally, the anatomy at the right and leftside of the mandible is similar. Consequently, the
57

deBaat C, van Waas MAJ
A plastic or metal handle instead of a wax or acrylicrim is not practical, because it disturbs the posltion ofthe lip and hampers loading the mucosal membraneequally while making the impression.
Phase 4: lndividual impressionsThe flange borders of the individual impression traysare assessed in the oral cavity by requesting thepatient to make functional oral movements. Special
attention is paid to the posterior border of themaxillary individual impression tray throughrequesting the patient to say "ah" with openedmouth and by checking the position of the border in
relation to the palatine foveas. Finally, the fit and theflange borders are checked, using an easy to removesilicone based soft lining material (Fit Checker@, GC,
Co, Japan).
When the flanges of the individual impression trayare correct initially, the final borders can be assessed,
using a low-fusing thermoplastic impressioncompound. A small quantity of heated softthermoplastic impression compound is introduced tothe flanges of the individual impression trayconcerning an area of less than 3 cm length each
time. Subsequently, the individual impression tray is
put into the oral cavity and the patient is requestedto make functional orofacial movements with the lip,
the tongue and the cheeks, supported by muscle
trimming by the dentist. After assessing the finalflange borders, the individual impression can be
made using a thin silicone impression material andpushing the individual impression tray firmly into thecorrect position.
Phase 5: lndividual casts
With respect to the individual casts, it is essential thatthe carefully assessed flange borders of the individualimpression trays are reflected correctly with a raisedperipheral border wall laterally. When this wall is
lacking, all efforts of border assessment will have
been in vain.
EpilogueWithout thorough knowledge of the oral anatomy, itis impossible to assess the correct flange borders ofremovable complete dentures.
JPP A 201.4; 02(01): 51-58
The term stability has been used frequently in thisarticle, in contrast to the term retention. That is notoccasional because the stability of a removablecomplete denture is more important than its
retentlon. Without adequate stability, (optimal)
retention ls not possible. A prerequisite for stability is
molding the flange borders correctly.
Suggested reading list / References
Massad JJ, Gagna DR. Vinyl polysiloxa.ne impressionmaterial in removable prosthodontics. Part 1:
edentulous impressions. CompendContinEduc Dent2007; 28: 452-459.
McCord JF, Grant AA. A clinical guide to completedental prosthetics. London: BDA Bookshop, BritishDe nta lAssociotio n 2000.
Preston AJ. Removable prostheses revisited:challenges for primary dental care. l. Completedentures. Prim Dent Care 2007; L4: 67-72.
Rahn AO, lvanhoe JR, Plummer KD. Textbook ofcomplete dentures.Shelfon; People's MedicolPubli sh i ng Hou se, 2009.
Shor A, Shor K, Goto ! Rehabilitation of failingdentition with immediate denture prostheses:
technique for a predictable esthetic and functionaloutcome. CompendContinEduc Dent 2006; 27: 168-176.
Zarb GA, Hobkirk J, Eckert S, Jacob R. Prosthodontictreatment for edentulous patients: completedentures and implant-supported prostheses. St. Louis:
Elsevier Mosby, 2013.
Rajasekar.V, Tilak -(
Full Mouth Rr
Report
V.Rajaseka/ iilt. Assistant prof-2. professor & Fle3. Post Graduate
Chennai - 6flI1
Correspondence: h)
Abstract:These days dental trinterested in keep*qanterior teeth resr.rttrduring excursive mqreduction of the ueniWe report descripruthe reduction in r,ertithe permanent recqrdimension with an inroriented treatment Iprincipally to retain ilrKeywords:Worn clouOcclusion,
How to cite this arfrteeth: A case report J I
lntroductionThe gradual wear of dris a normal processindividual. Hower,er,,result in pulpal 3drimpaireddisfigureme.: -_--.patients wrtr ::_ - _ .
a. Excessii,e :-- :dimensic - -the veri :. -. . - .
b. Excessi,,,e _-_ _,,dimensic-:_ _:.
c. Excessrv: ,.,..dimenslc-:_-
The severe oc: _. , . :
58













![[7] PROTA TEMATIK 2](https://static.fdokumen.com/doc/165x107/63233bca078ed8e56c0ac38d/7-prota-tematik-2.jpg)