
3903A.01 Template SAP - Clinical Trials
49
resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210 This document is confidential. 31 Aug 2020 Page 1 of 49 Statistical Analysis Plan Sponsor Name: resTORbio, Inc. Protocol Number: RTB-101-210 Protocol Title: A Randomized, Double-Blind, Placebo-Controlled Study to Determine if Prophylaxis with RTB101 as Compared to Placebo Reduces the Severity of Laboratory-Confirmed COVID-19 in Adults Age ≥65 Years who Reside in a Nursing Home with One or More Residents or Staff who have Laboratory-Confirmed COVID-19 Protocol Version and Date: Version 4.0 (Amendment 03) 04-June_2020 Author: Patricia Bernardo, ScD, Vice-President Biostatistics and Statistical Programming Notice of Confidential and Proprietary Information: The information contained in this document is confidential belonging to resTORbio, Inc. Acceptance of this document constitutes agreement by the recipient that no information contained herein will be published or disclosed without prior written authorization from an official of resTORbio, Inc. However, this document may be disclosed to appropriate Institutional Review Board and Ethics Committees or duly authorized representatives of a national regulatory authority under the condition that they are requested to keep it confidential. In the event of an actual or suspected breach of this obligation, resTORbio, Inc. should be notified promptly.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of 3903A.01 Template SAP - Clinical Trials

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 1 of 49
Statistical Analysis Plan
Sponsor Name: resTORbio, Inc.
Protocol Number: RTB-101-210
Protocol Title: A Randomized, Double-Blind, Placebo-Controlled Study to Determine if Prophylaxis with RTB101 as Compared to Placebo Reduces the
Severity of Laboratory-Confirmed COVID-19 in Adults Age ≥65 Years who Reside in a Nursing Home with One or More Residents or Staff who have
Laboratory-Confirmed COVID-19
Protocol Version and Date: Version 4.0 (Amendment 03) 04-June_2020
Author: Patricia Bernardo, ScD, Vice-President Biostatistics and Statistical Programming
Notice of Confidential and Proprietary Information:
The information contained in this document is confidential belonging to resTORbio, Inc. Acceptance of this document constitutes agreement by the recipient that no information contained herein will be published or disclosed without prior written authorization from an official of resTORbio, Inc. However, this document may be disclosed to appropriate Institutional Review Board and Ethics Committees or duly authorized representatives of a national regulatory authority under the condition that they are requested to keep it confidential. In the event of an actual or suspected breach of this obligation, resTORbio, Inc. should be notified promptly.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 2 of 49
I confirm that I have reviewed this document and agree with the content.
Approvals
resTORbio, Inc. Approval
M. V. Patricia Bernardo, ScD
Vice President, Biostatistics Signature
Date (DD-Mmm-YYYY)
Joan Mannick
31-AUG-2020
Joan Mannick, MD PhD
Chief Medical Officer
Signature Date (DD-Mmm-YYYY)
31- AUG-2020M. V. Patricia Bernardo

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 3 of 49
Table of Contents Approvals ................................................................................... Error! Bookmark not defined.
Glossary of Abbreviations ................................................................................................... 7
Purpose .............................................................................................................................. 8
Study Objectives ................................................................................................................ 9
Endpoints ......................................................................................................................... 14
Analysis Sets .................................................................................................................... 15

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 4 of 49
Protocol Deviations .......................................................................................................... 16
General Aspects for Statistical Analysis ........................................................................... 17
Demographic, Other Baseline Characteristics and Medication ......................................... 20
Efficacy ............................................................................................................................ 22

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 5 of 49
Safety ............................................................................................................................... 31
Interim Analyses ............................................................................................................... 33
Changes from Analysis Planned in Protocol ..................................................................... 34

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 6 of 49
Programming Considerations ........................................................................................... 35
Quality Control ................................................................................................................. 40
References ....................................................................................................................... 41
Index of Tables ................................................................................................................. 42
Index of Figures................................................................................................................ 45
Index of Listings ............................................................................................................... 46
Appendix 1 ....................................................................................................................... 47

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 7 of 49
Glossary of Abbreviations
Abbreviation Description
AE Adverse Event
ATC Anatomical Therapeutic Chemical
BMI Body Mass index
CI Confidence Interval
COVID-19 Coronavirus Disease-2019
CRF Case Report Form
DMC Data Monitoring Committee
FAS Full Analysis Set
ICH International Conference on Harmonization
IXRS Interactive Voice/Web Response System
MedDRA Medical Dictionary for Regulatory Activities
mITT Modified Intent-to-Treat
PP Per Protocol Set
PT Preferred Term
SAE Serious Adverse Event
SAP Statistical Analysis Plan
SD Standard Deviation
SOC System Organ Class
SOP Standard Operating Procedure
TEAE Treatment Emergent Adverse Event
TFL Table, Figure and Listing

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 8 of 49
Purpose
The purpose of this statistical analysis plan (SAP) is to ensure that the data listings, summary tables, and figures which will be produced, and the statistical methodologies that will be used, are complete and appropriate to allow valid conclusions regarding the study objectives.
Responsibilities
Veristat, LLC will perform the statistical analyses and are responsible for the production and quality control of all tables, figures, and listings.
Timing of Analyses
The study will be unblinded after all subjects have completed dosing for up to 4 weeks and been followed for 4 weeks post-dosing or terminate early from the study and the database is locked.
Analysis of all efficacy and safety endpoints is planned after database lock has occurred.
An independent Data Monitoring Committee (DMC) has been established for the study with the primary goal of performing an ongoing review of safety data. The DMC is an external board comprised of experts with specific knowledge of geriatrics and issues related to conducting clinical studies.
The DMC will be responsible for the following:
• Providing unblinded review of all SAEs throughout the study. • Advising the Sponsor of the need for study stopping or protocol modification/amendments in
order to minimize potential risk for subjects.
Further details are provided in the DMC charter.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 9 of 49
Study Objectives
Primary Objective
The primary objective of this study is to determine if RTB101 decreases the severity of laboratory-confirmed COVID-19 beginning from the first dose of study drug through Week 4 as compared to placebo.
Secondary Objectives
The secondary objectives are:
• To determine if RTB101 decreases the percentage of subjects who develop symptomatic laboratory-confirmed COVID-19 as compared to placebo
• To determine if RTB101 decreases mortality as compared to placebo in patients with laboratory-confirmed COVID-19
• To determine if RTB101 decreases all-cause mortality as compared to placebo
• To determine if RTB101 decreases hospitalizations for COVID-19 as compared to placebo
• To determine if RTB101 decreases, as compared to placebo, the percent of subjects who require mechanicial ventilation, noninvasive ventilation and high flow nasal canula oxygen delivery or ICU admission during hospitalizations for COVID-19
• To assess the safety and tolerability of RTB101 through the end of the study
Exploratory Objectives
• To determine if RTB101 decreases the time to alleviation of moderate and severe symptoms due to laboratory-confirmed COVID-19 as compared to placebo
• To determine if RTB101 decreases the incidence of SARS-CoV-2 infection regardless of symptoms compared to placebo
Brief Description
This is a randomized, double-blind, placebo-controlled, parallel-group Phase 3 study to determine if RTB101 reduces, as compared to placebo, the percentage of subjects who develop laboratory-confirmed COVID-19: with protocol-defined progressive symptoms OR are hospitalized OR die beginning from the first dose of study drug through Week 4 among individuals age ≥65 years who reside in a nursing home with one or more residents or staff who have laboratory-confirmed COVID-19. Eligible subjects will take

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 10 of 49
study drug once a day for 4 weeks and then will continue to be followed for 4 weeks off study drug. Subjects will be monitored per routine standard of care in the nursing home and subjects who develop ≥ 1 COVID-19 symptom will have a nasopharyngeal swab obtained to test for SARS-CoV-2. Data concerning COVID-19 testing results and COVID-19 symptom duration, severity and mortality rates will be obtained from information in the medical records subjectsper standard of care at the nursing homes that will be sites in the study.
Subject Selection
Inclusion Criteria
Subjects eligible for inclusion in this study must fulfill all of the criteria listed in section 4.2 of the protocol.
Exclusion Criteria
Subjects will not be eligible if they meet any of the criteria listed in section 4.3 of the protocol.
Determination of Sample Size
Data on COVID-19 incidence in this patient population is still accumulating. The following table presents the number of subjects needed per arm to achieve 85%-90% power to detect a 30%-50% reduction (compared to the placebo) in the percentage of subjects diagnosed with severe laboratory-confirmed COVID-19 in the RTB101 arm, when the percent of subjects with severe COVID-19 in the control arm is between 40%-50% for a 2-sided significance level of 0.05 . Power calculations were based on a Z-test of the difference of 2 independent proportions.
Proportion of Subjects with Severe COVID-19
Sample Size Per Arm
Placebo
RTB101 (30% Reduction)
85% Power
90% Power
0.4 0.28 276 323
0.45 0.315 229 268
0.5 0.35 191 223
Placebo
RTB101 (40% Reduction)
85% Power
90% Power
0.4 0.24 149 174
0.45 0.27 124 145
resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 11 of 49
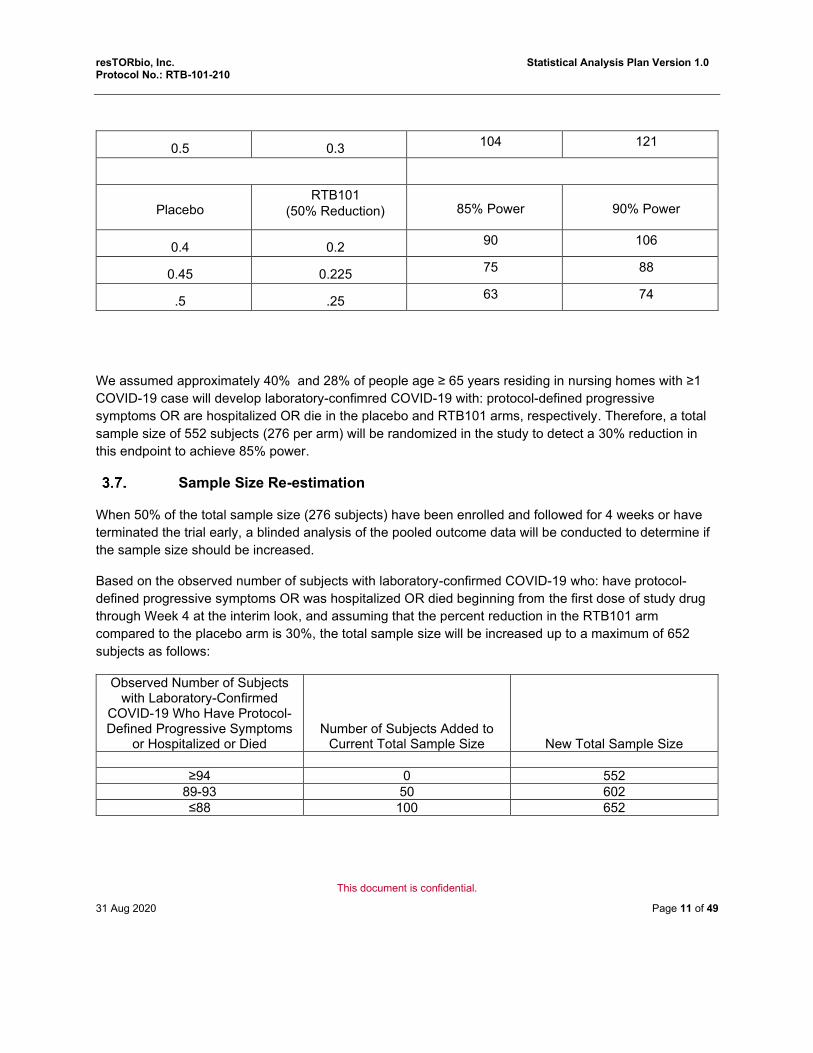
We assumed approximately 40% and 28% of people age ≥ 65 years residing in nursing homes with ≥1 COVID-19 case will develop laboratory-confimred COVID-19 with: protocol-defined progressive symptoms OR are hospitalized OR die in the placebo and RTB101 arms, respectively. Therefore, a total sample size of 552 subjects (276 per arm) will be randomized in the study to detect a 30% reduction in this endpoint to achieve 85% power.
Sample Size Re-estimation
When 50% of the total sample size (276 subjects) have been enrolled and followed for 4 weeks or have terminated the trial early, a blinded analysis of the pooled outcome data will be conducted to determine if the sample size should be increased.
Based on the observed number of subjects with laboratory-confirmed COVID-19 who: have protocol-defined progressive symptoms OR was hospitalized OR died beginning from the first dose of study drug through Week 4 at the interim look, and assuming that the percent reduction in the RTB101 arm compared to the placebo arm is 30%, the total sample size will be increased up to a maximum of 652 subjects as follows:
Observed Number of Subjects with Laboratory-Confirmed
COVID-19 Who Have Protocol-Defined Progressive Symptoms
or Hospitalized or Died
Number of Subjects Added to Current Total Sample Size
New Total Sample Size
≥94 0 552 89-93 50 602 ≤88 100 652
0.5 0.3 104 121
Placebo
RTB101 (50% Reduction)
85% Power
90% Power
0.4 0.2 90 106
0.45 0.225 75 88
.5 .25 63 74

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 12 of 49
This risk of inflating the Type I error rate using this blinded sample size re-estimation technique is generally minimal (Friede and Kieser, 2004, Cong, D, 2016). The information used to re-estimate the sample size does not use any information about the treatment effect and therefore, should not increase the Type I error rate. Results of simulations conducted showed that the Type I error rate is preserved well.
Treatment Assignment & Blinding
After providing informed consent, all eligible subjects will be randomized via the Interactive Voice/Web Response system (IXRS) to one of the treatment arms once ≥ 1 index case of COVID-19 has occurred in the nursing home. The Investigator or his/her delegate will contact the IXRS after confirming that the subject fulfills all the inclusion/exclusion criteria (see Section 3.4 above). The IXRS will prompt the user to randomize the subject. The subject identifier number will be used to link the subject to a treatment arm and a unique medication number for the bottles of study drug to be dispensed to the subject.
Randomization will be stratified by nursing home center to facilitate having a balanced number of subjects randomized to each treatment arm within each nursing home since the incidence and severity of COVID-19 may vary between nursing homes.
The randomization scheme for subjects will be reviewed and approved by a member of the team responsible for Randomization schema.
This is a subject, Investigator and Sponsor-blinded study. Subjects, study staff, and Sponsor will remain blinded until all subjects have completed the 4 week treatment period and the 4 week follow-up period and the database has been hardlocked. The identity of the treatments will be concealed by the use of active study drug that is identical to matched placebo in packaging, labeling, schedule of administration, appearance, and odor. Unblinding a single subject for safety reasons (necessary for subject medical management) will occur via an emergency process in place at the study site.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 13 of 49
Administration of Study Medication
Subjects will be administered one capsule of RTB101 10 mg or matching placebo (depending on their randomization arm) daily with a morning meal for 4 weeks.
Study Procedures and Flowchart
The study will be comprised of up to a 6-week Screening Period, a 4-week Treatment Period and a 4-week follow-up period.
Subjects will have nasopharyngeal swabs obtained for baseline SARS-CoV-2 testing prior to randomization.
Subjects will be administered study drug once daily with breakfast for 4 weeks during the Treatment Period. During that time, the subjects will be monitored for symptoms of COVID-19 listed in Section 6.6.1 of the protocol and Section 7.2.1 below.
Subjects who develop one or more of the symptoms will have a nasopharyngeal swab obtained for SARS-CoV-2 testing as required by standard of care by the nursing home.
The number of subjects in the nursing home who develop laboratory-confirmed COVID-19, the number of subjects who develop laboratory-confirmed COVID-19 with progressive symptoms, hospitalizations and deaths of subjects with laboratory-confirmed COVID-19 beginning from first dose of study drug to end of study treatment (Week 4), and adverse events and serious adverse events from first dose of study drug through Week 5, and deaths due to any cause through Week 8 will be captured in the electronic medical record by the nursing home staff and relevant data from the electronic medical record will be entered into the electronic Case Report Forms.
Details of assessments are provided in Table 6 of the protocol.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 14 of 49
Endpoints
Primary Efficacy Endpoint
The primary endpoint is the percentage of subjects with laboratory-confirmed COVID-19 who: have protocol-defined progressive symptoms OR was hospitalized OR died beginning from first dose of study drug through Week 4.
Secondary Efficacy Endpoints
The secondary endpoints are:
• The percentage of subjects who develop symptomatic laboratory-confirmed COVID-19 beginning from the first dose of study drug through Week 4
• The percentage of subjects who died through Week 8 in subjects with laboratory-confirmed COVID-19 beginning from the first dose of study drug through Week 4
• The percentage of subjects who died through Weeks 2, 4 and 8 for any reason
• The percentage of subjects who are hospitalized due to having one or more predefined COVID-19 symptoms and laboratory-confirmed SARS-CoV-2 from the first dose of study drug through Week 4
• The percentage of subjects who were hospitalized due to having one or more predefined COVID-19 symptoms and laboratory-confirmed SARS-CoV-2 from the first dose of study drug through Week 4 and require mechanical ventilation, noninvasive ventilation and high flow nasal canula oxygen delivery or ICU admission during the hospitalization (to be followed through Week 8)
Exploratory Efficacy Endpoints
• The time to alleviation of moderate and severe symptoms of COVID-19 in subjects with laboratory-confirmed COVID-19 from the first dose of study drug through Week 4 and develop moderate or severe symptoms through Week 8
• The percent of subjects who develop SARS-CoV-2 infection regardless of symptoms beginning from the first dose of study drug through Week 4 among subjects who were SARS-CoV-2 negative at baseline
Safety Endpoints
• Safety and tolerability will be assessed by report of AE/SAEs through Week 5 (4 weeks of study drug treatment and 1 week of follow-up)

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 15 of 49
Analysis Sets
Randomized Set
The Randomized Set (RS) will include all subjects randomized whether treated or not.
Safety Set
The Safety Set (SAF) will include all subjects who were administered at least one dose of any study drug. Subjects will be analyzed per the actual study treatment they received. The follow-up period will include the Week 8 visit which is 4 weeks after the end of the treatment period. The SAF will be used for all analyses and presentation of by-subject listings of all safety endpoints. Subjects will be analyzed according the actual treatment they received.
Full Analysis Set
The Full Analysis Set (FAS) will include all randomized subjects who received at least 1 dose of study drug. Subjects will be analyzed according to randomized treatment. The FAS will be used for all analyses and presentation of by-subject listings of all efficacy endpoints.
Modified Intent-to-Treat
The Modified Intent-to-Treat (mITT) analysis set will exclude all subjects in the FAS who tested positive with SARS-CoV-2 prior to first dose of study drug or whose samples for testing SARS-CoV-2 were taken prior to first dose and the results came back positive after the first dose of study drug date.
Per Protocol Set
The Per Protocol Set (PP) will include all mITT subjects who complete the 4-week treatment period, missed < 20% of doses, and had no major protocol deviations impacting efficacy data. Subjects will be analyzed per the treatment group to which they were randomized.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 16 of 49
Protocol Deviations
A protocol deviations log will be maintained by Insight Therapeutics, LLC, the vendor contracted to perform the study data monitoring. (Protocol deviations will be reviewed by resTORbio on a regular basis.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 17 of 49
General Aspects for Statistical Analysis
General Methods
All analyses and outputs will be produced using SAS® version 9.4 or later. Unless otherwise specified, efficacy and safety summaries will be presented for each treatment. All other summaries will be presented for each treatment and overall. Continuous variables will be summarized using the number of observations (n), mean, standard deviation (SD), median, minimum, and maximum. Categorical variables will be summarized using number of observations (n), frequency, and percentages of subjects.
All relevant subject data will be included in listings. All randomized subjects entered into the database will be included in subject data listings.
Key Definitions
Laboratory-Confirmed COVID-19 with Progressive Symptoms
After randomization, nursing home staff will monitor for the following potential COVID-19 symptoms every 8 hours:
Mild Symptoms:
• New sore throat
• New chest congestion
• New cough
• New headache
• Fever (99.20F or greater)
• New GI symptoms (nausea/vomiting/diarrhea)
• Malaise/Muscle pain
• New loss of taste or smell
Moderate or Severe Symptoms:
• Increased shortness of breath over baseline level
• New onset of tachypnea (respiratory rate of ≥ 22 breaths per minute)
• New onset of tachycardia (more than 100 beats per minute)
• Worsening confusion/change in mental status/decreased responsiveness
• O2 sat decreased by 3% or greater from baseline since last taken, or O2 sat < 93% if baseline O2 sat is unknown
• Imaging indicating a lower respiratory tract infection • Cerebrovascular accident/transient ischemic attack/new neurologic signs
• Functional decline/decline in activities of daily living
Mapping of the data collected on the eCRF into the above mild, moderate and severe symptoms are provided in Section Error! Reference source not found.. Appendix 1.
If a subject has experienced one or more of the symptoms above, the staff will be instructed to contact the physician on call who will order a nasalpharyngeal swab for SARS-CoV-2 testing.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 18 of 49
Subjects who develop ≥ 1 of the moderate or severe symptoms listed above during the 4 weeks of study drug treatment will be defined as having progressive symptoms.
Subjects who have SARS-CoV-2 detected on nasopharyngeal swab during the 4 week treatment period and meet the protocol-defined criteria for progressive symptoms OR are hospitalized OR die will be assessed as having the event defined in the primary endpoint.
A positive SARS-CoV-2 swab that is obtained within 14 days before or after the onset of 1 or more COVID-19 symptoms will be considered laboratory-confirmation of COVID-19.
Only COVID-19 episodes meeting the criteria for the primary endpoint from the first dose of study drug through Week 4 will be included in the primary endpoint analysis.
First Dose Date
For any randomized subject, the first dose date will correspond to the first date subject was administered study drug based on the EMR entry. However, if there are no entries in the EMR indicating the subject took study drug at any time during the study, then the first dose date will be missing and the subject will be considered randomized but not treated.
Study Day
Study Day 1 is defined as the date of the first dose of study drug, regardless of whether this coincides with the date of randomization or not. Subsequent days are numbered consecutively (Day 2, Day 3, etc.). Before the day of the first dose of study drug, study days are numbered sequentially with negative values (i.e., Day -1, Day -2, etc.).
Baseline
Baseline is defined as the last measurement taken before the first dose of study drug, unless otherwise specified.
Missing Data
All data required for this study will be collected by the nursing home staff and entered into the EMR system. Except for the information on study drug received by the subject throughout the treatment period, no additional data will be collected in the EMR for the purpose of this study alone. All data needed to evaluate the endpoints for this trial are collected as part of the standard of care for subjects at this time, when all subjects are being monitored for COVID-19 symptoms. It is expected that there will be very limited missing data in this study.
For the primary efficacy endpoint, subjects who have laboratory-confirmed COVID-19 and discontinue the study prematurely or are lost to follow-up will be imputed to have experienced laboratory-confirmed COVID-19 with: progressive symptoms or hospitalized or died; subjects who discontinue the study prematurely or are lost to follow-up without having laboratory-confirmed COVID-19 will be imputed as not experiencing the event of interest. A sensitivity analysis in which subjects who discontinue the study prematurely or are lost to follow-up will be imputed to have the event of interest, regardless of whether the subjects had laboratory-confirmed COVID-19 or not, will also be conducted.
Partial dates of medications will be imputed solely for the purpose of defining prior/concomitant status for medications. Dates will be defined using the hierarchy of derivations below.
• For missing start day where month and year are present, the start day will be set to the 1st of the

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 19 of 49
month, unless the month and year are the same as the first dose month and year and the 1st of the month is before the first dose date, in which case, the start date will be set to the first dose date.
• For missing start day and month where year is present, the start day and month will be set to January 1st, unless the year is the same as the first dose year and January 1st is before the first dose date, in which case, the start date will be set to the first dose date.
• For missing end day where month and year are present, the end day will be set to the last day of the month, unless the month and year are the same as the trial termination month and year, in which case, the end date will be set to the trial termination date.
• For missing end day and month, where year is present, the end date will be set to the trial termination date if the years are the same. If the trial termination year is greater than the end year, the end day and month will be set to December 31st.
Visit Windows
Visit window will not be used in the summarization or analysis of data.
Pooling of Centres
Data from different nursing home centers will be pooled and not accounted for separately in the logistic regression analyses.
Subgroups
The analyses of the primary and first secondary endpoints (listed below) may be repeated for the following subpopulations of the FAS:
• Age Group (≥85 years old vs. <85 years old) • History of Asthma (Y/N) • Congestive Heart Failure (Y/N)
In each of the subgroup analyses, the independent variable that is used to define the subgroup will be dropped from the model, if applicable.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 20 of 49
Demographic, Other Baseline Characteristics and Medication
Subject Disposition and Withdrawals
Subject disposition will be presented for all screened subjects , the following will be summarized:
• Number of subjects screened
• Number of screen failures
• Reason for screen failure
• Number (%) of subjects randomized
• Number (%) of subjects in the Safety Set
• Number (%) of subjects in the Full Analysis Set
• Number (%) of subjects in the Modified Intent-to-Treat Set
• Number (%) of subjects in the Per-Protocol Set
• Number (%) of subjects who completed the study through Week 4
• Number (%) of subjects who completed the study through Week 8
• Number (%) of subjects who discontinued treatment and their reason
• Number (%) of subjects who discontinued study prematurely and their reason
A separate by-subject listing of subject disposition and withdrawal will also be provided.
Reasons for exclusion from analysis sets will be summarized in the Randomized Set and listed.
Protocol Deviations
All protocol deviations will be listed in the Randomized Set. Major protocol deviations will be summarized in the Randomized Set.
Demographic and Other Baseline Characteristics
Demographics and other baseline characteristics will be summarized for the Full Analysis Set by randomized treatment and overall. Summary statistics and by-subject listings will be provided.
Demographics and baseline characteristics will include age, sex, ethnicity, race, weight, height, body mass index (BMI), age ≥ 85 (Y/N), age ≥ 65 and <85 years, with a medical history of asthma (Y/N), medical history of congestive heart failure (Y/N), medical history of Type 2 Diabetes Mellitus (Y/N) and nursing home residence.
Age at First Dose of Study Drug = (First dose of study drug date - date of birth + 1) / 365.25 and truncated to complete years.
Height (in cm) = height (in inches) * 2.54

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 21 of 49
Weight (in kg) = weight (in lbs) * 0.4536
BMI (kg/m2) = Weight(kg)/[Height(m)2]
By-subject listing of all demographic and baseline disease characteristic data will be provided for the Full Analysis Set.
Medical History
A summary table of the number and percentage of subjects by medical history, system organ class (SOC) and preferred term will be produced from the Full Analysis Set. Medical history will be sorted alphabetically by SOC and in descending order of subjects per preferred term within each SOC.
Medical history will be coded using the Medical Dictionary for Regulatory Activities (MedDRA) version 23.0 (Hierarchy) or higher.
A separate by-subject listing of medical history will also be provided.
Medication
All prior and concomitant medications will be summarized in 2 separate tables based on classification using the Anatomical Therapeutic Chemical (ATC) classification and preferred drug name from the World Health Organization Drug Dictionary Global B3 Mar 1, 2020 version, or later in the Safety Set.
A separate by-subject listing of prior and concomitant medications will also be provided for the Safey Set.
Prior Medication
Prior medications are defined as medications entered in the eCRF that either start or end before the first dose of study medication. Prior medications will be summarized by ATC level 2 and preferred drug name for the Safety Population. Only medications received up to 30 days prior to first dose of study drug will be collected.
Prior medications which continue after first dose of study medication will also be classified as a concomitant medication.
Concomitant Medication
Concomitant medications are defined as medication entered in the eCRF that are taken on, after, or are ongoing at the start date of dosing. Concomitant medications will be summarized by ATC level 2 and preferred drug name for the Safety Population.
Surgeries and Procedures
Prior surgeries and procedures are surgeries and procedures that occurred before the first dose of study medication.
Current surgeries and procedures are surgeries and procedures that occurred on or after the first dose of study drug.
By-subject listings of prior and current surgeries and procedures will be provided for the Safey Set.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 22 of 49
Efficacy
Multiple Testing Strategy
A fixed sequence gate-keeping strategy will be used to control the study-wise error rate at a 2-sided α-level of 0.05. The primary and secondary efficacy endpoints will be tested in the sequence specified below:
Order H1 Percentage of subjects with laboratory-confirmed COVID-19 who: have protocol-defined
progressive symptoms OR was hospitalized OR died beginning from the first dose of study drug through Week 4
H2 Percentage of subjects who develop symptomatic laboratory-confirmed COVID-19 beginning from the first dose of study drug through Week 4
H3 Percentage of subjects who are hospitalized due to having one or more predefined COVID-19 symptoms and laboratory-confirmed SARS-CoV-2 from the first dose of study drug through Week 4
H4 Percentage of subjects who were hospitalized due to having one or more predefined COVID-19 symptoms and laboratory-confirmed SARS-CoV-2 from the first dose of study drug through Week 4 and require mechanical ventilation, noninvasive ventilation and high flow nasal canula oxygen delivery or ICU admission during the hospitalization (to be followed through Week 8)
H5 Percentage of subjects who died through Week 8 in subjects with laboratory-confirmed COVID-19 beginning from the first dose of study drug through Week 4
H6 Percentage of subjects who died through Weeks 2, 4 and 8 for any reason
H7 The time to alleviation of moderate and severe symptoms of COVID-19 in subjects with laboratory-confirmed COVID-19 from the first dose of study drug through Week 4 and develop moderate or severe symptoms through Week 8
H8 Percentage of subjects who develop SARS-CoV-2 infection regardless of symptoms beginning from the first dose of study drug through Week 4 among subjects who were SARS-CoV-2 negative at baseline
The primary endpoint, H1, will be tested first at a 2-sided significance level of 0.05. The subsequent endpoints will be tested in the order specified above also at a 2-sided 0.05 alpha-level, if and only if the preceding endpoint was found to be statistically significant. If the preceding endpoint in the sequence fails to meet statistical significance, then testing of subsequent endpoints will be stopped and no further statistical conclusions will be made.
Estimands
This section presents a structured framework that links trial objectives with suitable and precise definitions of how treatment effects are to be estimated. The estimand, which is the target of estimation to address the scientific question of interest posed by the trial objective, with its 4 attributes as specified in the ICH

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 23 of 49
E9(R1) Draft Addendum on Estimands and Sensitivity Analysis in Clinical Trials 2017, are provided below for the primary objective and key secondary objectives.
Primary Objective Estimand
The estimand used to address the primary objective “To determine if RTB101 decreases the severity of laboratory-confirmed COVID-19 beginning from the first dose of study drug through Week 4 as compared to placebo” is defined by the following:
• Population:
• Subjects in the FAS population
• Variable:
• Occurrence of laboratory-confirmed COVID-19 with: protocol-defined progressive symptoms OR hospitalization OR death beginning from the first dose of study drug through Week 4
• Intercurrent events:
• If a subject discontinues study prematurely or is lost to follow-up and has a laboratory-confirmed SARS-CoV-2 infection, impute the subject has the event of interest
• If a subject discontinues study prematurely or is lost to follow-up without a laboratory-confirmed SARS-CoV-2 infection, impute the subject did not have the event of interest
• Population-level summary:
• Odds ratio, i.e. the odds of having laboratory-confirmed COVID-19 with: protocol-defined progressive symptoms OR hospitalization OR death beginning from the first dose of study drug through Week 4 in subjects treated with RTB101 divided by the odds in subjects treated with placebo
Secondary Objective Estimands
1. The estimand for the secondary objective “To determine if RTB101 decreases the percentage of
subjects who develop symptomatic laboratory-confirmed COVID-19 beginning from the first dose of study drug through Week 4 as compared to placebo” is defined by the following:
• Population:
• Subjects in FAS population
• Variable:
• Occurrence of any degree (mild, moderate or severe) of symptomatic laboratory-confirmed COVID-19 beginning from the first dose of study drug through Week 4
• Intercurrent events:

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 24 of 49
• If a subject discontinues study prematurely or is lost to follow-up and has a laboratory-confirmed SARS-CoV-2 infection, impute the subject had the event of interest
• If a subject discontinues study prematurely or is lost to follow-up without a laboratory-confirmed SARS-CoV-2 infection, impute the subject did not have the event of interest
• Population-level summary:
• Odds ratio, i.e. the odds of having any symptomatic laboratory-confirmed COVID-19 in subjects treated with RTB101 beginning from the first dose of study drug through Week 4 divided by the odds in subjects treated with placebo
2. The estimand for the secondary objective “To determine if RTB101 decreases mortality as compared to placebo in patients who develop laboratory-confirmed COVID-19 from the first dose of study drug through Week 4” is defined by the following: • Population:
• Subjects in FAS population
• Variable:
• Occurrence of death through Week 8 in subjects who developed laboratory-confirmed COVID-19 from first dose of study drug through Week 4
• Intercurrent events:
• If a subject discontinues study prematurely or is lost to follow-up and has a laboratory-confirmed SARS-CoV-2 infection, impute the subject had the event of interest
• If a subject discontinues study prematurely or is lost to follow-up without a laboratory-confirmed SARS-CoV-2 infection, impute the subject did not have the event of interest
• Population-level summary:
• Odds ratio, i.e. the odds of death through Week 8 in subjects who develop laboratory-confirmed COVID-19 from the first dose of study drug through Week 4 in subjects treated with RTB101 divided by the odds in subjects treated with placebo
3. The estimand for the secondary objective “To determine if RTB101 decreases all-cause mortality as compared to placebo” is defined by the following: • Population:
• Subjects in FAS population
• Variable:
• Occurrence of death through Weeks 2, 4 and 8 due to any cause
• Intercurrent events:

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 25 of 49
• If a subject discontinues study prematurely or is lost to follow-up, impute the subject did not have the event of interest
• Population-level summary:
• Odds ratio, i.e. the odds of death through Weeks 2, 4 and 8 due to any cause in subjects treated with RTB101 divided by the odds of death in subjects treated with placebo
4. The estimand for the secondary objective “To determine if RTB101 decreases hospitalizations for COVID-19 as compared to placebo” is defined by the following: • Population:
• Subjects in FAS population
• Variable:
• Occurrence of hospitalization through Week 8 due to having one or more predefined COVID-19 symptoms and laboratory-confirmed SARS-CoV-2 from the first dose of study drug through Week 4
• Intercurrent events:
• If a subject discontinues study prematurely or is lost to follow-up and has a laboratory-confirmed SARS-CoV-2 infection, impute the subject had the event of interest
• If a subject discontinues study prematurely or is lost to follow-up and did not have laboratory-confirmed SARS-CoV-2 infection, impute the subject did not have the event of interest
• Population-level summary:
• Odds ratio, i.e. the odds hospitalization due to having one or more predefined COVID-19 symptoms and laboratory-confirmed SARS-CoV-2 from the first dose of study drug through Week 4 in subjects treated with RTB101 divided by the odds in subjects treated with placebo
5. The estimand for the secondary objective “To determine if RTB101 decreases, as compared to placebo, the percent of subjects who require mechanicial ventilation, noninvasive ventilation and high flow nasal canula oxygen delivery or ICU admission during hospitalizations for COVID-19” is defined by the following: • Population:
• Subjects in FAS population
• Variable:
• Hospitalization due to having one or more predefined COVID-19 symptoms and laboratory-confirmed SARS-CoV-2 from the first dose of study drug through Week 4 and requirement of mechanicial ventilation, noninvasive ventilation and high flow nasal canula

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 26 of 49
oxygen delivery or ICU admission during the hospitalization (to be followed through Week 8)
• Intercurrent events:
• If a subject discontinues study prematurely or is lost to follow-up and has a laboratory-confirmed SARS-CoV-2 infection, impute the subject had the event of interest
• If a subject discontinues study prematurely or is lost to follow-up and did not have laboratory-confirmed SARS-CoV-2 infection, impute the subject did not have the event of interest
• Population-level summary:
• Odds ratio, i.e. the odds of hospitalization due to having one or more predefined COVID-19 symptoms and laboratory-confirmed SARS-CoV-2 from the first dose of study drug through Week 4 and requirement of mechanicial ventilation, noninvasive ventilation and high flow nasal canula oxygen delivery or ICU admission in subjects treated with RTB101 divided by the odds in subjects treated with placebo
Exploratory Objective Estimands
1. The estimand for the exploratory objective “To determine if RTB101 decreases the time to alleviation of moderate and severe symptoms as compared to placebo in subjects who develop moderate or severe laboratory-confirmed COVID-19 beginning from the first dose of study drug through Week 4” is defined by the following:
• Population:
• Subjects in FAS population with laboratory-confirmed COVID-19 from the first dose of study drug through Week 4 who develop moderate or severe symptoms through Week 8
• Variable: Time to alleviation of moderate and severe symptoms due to laboratory-confirmed COVID-19
• Intercurrent events:
• If a subject discontinues study prematurely or is lost to follow-up and time to alleviation of moderate and severe COVID-19 symptoms has not been reached, subject is censored on the date of last contact
• Population-level summary:
• Difference in the median time to alleviation between RTB101 and placebo
2.The estimand for the exploratory objective “To determine if RTB101 decreases the incidence of SARS-CoV-2 infection regardless of symptoms compared to placebo” is defined by the following:
• Population:

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 27 of 49
• Subjects in FAS population
• Variable:
• Occurrence of laboratory-confirmed SARS-CoV-2 infection regardless of symptoms beginning from the first dose of study drug through Week 4
• Intercurrent event:
• If a subject discontinues study prematurely or is lost to follow-up without a laboratory-confirmed SARS-CoV-2 infection, impute the subject did not have the event of interest
• Population-level summary:
• Odds ratio, i.e. the odds of having a laboratory-confirmed SARS-CoV-2 infection regardless of symptoms in subjects treated with RTB101 beginning from the first dose of study drug through Week 4 divided by the odds in subjects treated with placebo
Primary Efficacy Endpoint Analysis
Primary Analysis of the Primary Endpoint
The primary efficacy endpoint is the percentage of subjects with laboratory-confirmed COVID-19 with: protocol-defined progressive symptoms OR hospitalization OR death beginning from the first dose of study drug through Week 4 (H1). Week 4 is defined as Study Day 28. The protocol-defined progressisve symptoms is defined in Section 7.2.1 above.
The primary efficacy endpoint will be analyzed through a logistic regression model to obtain an estimate of the population odds ratio, i.e. the odds of having laboratory-confirmed COVID-19 with protocol-defined progressive symptoms OR hospitalization OR death in subjects treated with RTB101 compared to the odds of having laboratory-confirmed COVID-19 with protocol-defined progressive symptoms OR hospitalization OR death in subjects treated with placebo and its associated confidence interval. The logistic regression model will be adjusted for factors that are known to be prognostic of outcome, specifically age (continuous covariate), nursing home facility, medical history of diabetes mellitus type 2 (T2DM, Y/N), medical history of congestive heart failure (CHF, Y/N) and asthma (Y/N).
Analysis of the primary efficacy endpoint will be based on the estimand for the primary objective described above.
Summary statistics will be presented along with a full data listing.
Sensitivity and Supplemental Analyses for the Primary Endpoint
The following sensitivity and supplemental analyses are planned to provide evidence in support of the strength of treatment of RTB101 10 mg as compared to placebo.
9.3.2.1. Sensitivity Analysis
As a sensitivity analysis, the primary efficacy endpoint will be analyzed based on the estimand for the primary objective described above; however, all subjects who discontinue study prematurely or are lost to follow-up will be imputed with the subjects having the event of interest, whether or not a laboratory-confirmed SARS-CoV-2 infection was observed.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 28 of 49
9.3.2.2. Supplemental Analyses
1. The primary analysis described in 9.3.1 above will be conducted in the Per Protocol (PP) population.
2. The primary analysis described in 9.3.1 above will be conducted in the mITT population.
Analyses of Secondary Efficacy Endpoints
The percentage of subjects who develop symptomatic laboratory-confirmed COVID-19 beginning from the first dose of study drug through Week 4
The percentage of subjects who develop symptomatic (any degree) laboratory-confirmed COVID-19 beginning from the first dose of study drug through Week 4 (H2), as assessed by the criteria specified in Section 7.2.1, will be analyzed in the same manner as the primary efficacy analysis as described in 9.3.1
based on the estimand for the secondary objective corresponding to this endpoint described in 9.2.2 above. Analyses will be conducted in the FAS, mITT and PP populations.
Summary statistics will be presented along with a full data listing by treatment group.
Percentage of subjects who died through Week 8 in subjects with laboratory-confirmed COVID-9 infection beginning from the first dose of study drug through Week 4
The percentage of subjects who died through Week 8 due to laboratory-confirmed COVID-19 beginning from randomizaiton through Week 4 (H5) will be analyzed in the same manner as the primary efficacy endpoint, as described in 9.3.1 above based on the estimand for the secondary objective corresponding to this secondary endpoint as described in 9.2.2 above. Analyses will be conducted in the FAS population.
Summary statistics will be presented along with a full data listing by treatment group.
Percentage of subjects who died through Weeks 2, 4 and 8 for any reason
The percentage of subjects who died through Weeks 2, 4 and 8 due to any cause (H6) will be analyzed in the same manner as the primary efficacy endpoint, as described in 9.3.1 above based on the estimand for the secondary objective corresponding to this secondary endpoint as described in 9.2.2 above. Week 2 is defined as Study Day 14, Week 4 as Study Day 28 and Week 8 as Study Day 56. Analyses will be conducted in the FAS population.
Percentage of subjects who are hospitalized due to having one or more predefined COVID-19 symptoms and laboratory-confirmed SARS-CoV-2 from first dose of study drug through Week 4
The percentage of subjects who were hospitalized due to laboratory-confirmed COVID-19 (H3) will be analyzed in the same manner as the primary efficacy endpoint, as described in 9.3.1 above based on the estimand for the secondary objective corresponding to this secondary endpoint as described in 9.2.2 above. Analyses will be conducted in the FAS population.
Percentage of subjects who require mechanical ventilation, noninvasive ventilation and high flow nasal canula oxygen delivery or ICU admission during the hospitalization

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 29 of 49
(to be followed through Week 8) in subjects who are hospitalized due to laboratory-confirmed COVID-19 from the first dose of study drug through Week 4
The percentage of subjects who require mechanical ventilation, noninvasive ventilation and high flow nasal canula oxygen delivery or ICU admission among subjects who were hospitalized due to laboratory-confirmed COVID-19 (H4) will be analyzed in the same manner as the primary efficacy endpoint, as described in 9.3.1 above based on the estimand for the secondary objective corresponding to this secondary endpoint as described in 9.2.2 above. Analyses will be conducted in the FAS population.
Analysis of the Exploratory Efficacy Endpoints
The time to alleviation of moderate and severe symptoms of COVID-19 in subjects with laboratory-confirmed COVID-19 from the first dose of study drug through Week 4 who develop moderate or severe symptoms through Week 8
The time to alleviation of moderate and severe symptoms in subjects with laboratory-confirmed COVID-19 beginning from the first dose of study drug through Week 4 who develop moderate or severe symptoms through Week 8 (H7) will be analyzed as an exploratory endpoint.
Time to alleviation of moderate and severe symptoms (days) is defined as:
(the last date moderate or severe symptoms are reported – earliest start date of moderate and severe symptoms) +1
in subjects who develop laboratory-confirmed COVID-19 with moderate or severe symptoms.
Note that only the following moderate and severe symptoms will be followed for alleviation in the analysis:
o Increased shortness of breath over baseline level
o New onset of tachypnea (respiratory rate ≥ 22 breaths per minute)
o New onset of tachycardia (more than 100 beats per minute)
o Worsening confusion/change in mental status/decreased responsiveness
o O2 sat decreased by 3% or greater from baseline or <93%
o Functional decline/decline in activities of daily living
Risk set: Subjects who have laboratory-confirmed COVID-19 with laboratory-confirmed COVID-19 beginning from the first dose of study drug through Week 4 who develop moderate or severe symptoms through Week 8.
Time origin: Earliest start date of any moderate or severe symptom associated with laboratory-confirmed COVID-19 beginning from the first dose of study drug through Week 8.
For subjects with >1 laboratory-confirmed COVID-19 with moderate and severe symptoms through Week 8, the longest time to alleviation of moderate and severe symptoms among the COVID-19 episodes will be used for the analysis.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 30 of 49
For subjects who completed the study but were not observed to have an alleviation of their moderate and severe symptoms, time to alleviation of moderate and severe symptoms will be censored on the date of study completion by the subject .
For subjects who discontinued study prematurely or were lost to follow-up, time to alleviation of moderate and severe symptoms will be censored on the date of last contact.
The distribution of events (alleviation of moderate and severe symptoms) in the RTB101 and placebo arms will be compared using a stratified logrank test with nursing home facility as the stratification factor. Analyses will be conducted in the FAS, mITT and PP populations. Summary statistics and associated survival curves (Kaplan-Meier estimates) will be presented along with a full data listing by treatment group.
9.5.2 Percentage of subjects who develop SARS-CoV-2 infection regardless of symptoms beginning from the first dose of study drug through Week 4 among subjects who were SARS-CoV-2 negative at baseline
The percentage of subjects who develop SARS-CoV-2 infection regardless of symptoms beginning from the first dose of study drug through Week 4 (H8) will be analyzed in the same manner as the primary efficacy endpoint, as described in 9.3.1 above based on the estimand for the exploratory objective corresponding to this exploratory endpoint as described in 9.2.2 above. Analyses will be conducted in the mITT population.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 31 of 49
Safety
Safety analyses will be conducted on the Safety Set (SAF) and will be assessed on the basis of adverse events (AE) reported.
Extent of Exposure
Duration of exposure is defined as the number of days the subject was administered study drug during the 4 week treatment period. Duration of exposure will be summarized using descriptive statistics by treatment group. The duration of exposure (in days) will also be categorized as follows: ≤7, 8-14, 15-21, 22-28 and >28, and tabulated by treatment group..
A listing including study drug administration information from the EMR will be presented.
Treatment Compliance
Treatment compliance will be calculated as follows:
(Number of capsules taken/28) x 100
Subjects are expected to take 1 capsule of study medication once per day through Week 4 (28 days).
Adverse Events
An adverse event is any untoward medical occurrence associated with the use of a drug in humans, whether or not considered drug-related. All adverse events (AEs) will be coded using the MedDRA version 23.0 (Hierarchy) or higher. Only treatment-emergent adverse events, defined as any adverse events that start or increase in intensity on or after the first dose of study drug(Study Day 1) will be included in the safety summaries for this study. The following listings of AEs will be provided by subjects:
• All AEs,
• Serious adverse events (SAEs)
• Severe (Grade 3 or higher) adverse events
• AEs leading to death
• AEs leading to study withdrawal
• AEs leading to study drug discontinuation
• Study drug related AEs
Adverse Events will be included in summary tables by treatment received. An overall summary table of AEs through Week 5 will be produced for the following categories:
• Any AE
• Grade 1 (Mild) AEs, Grade 2 (Moderate) AEs, Grade 3 (Severe) AEs, Grade 4 (Severe and Life Threatening), and Grade 5 (Fatal) AEs

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 32 of 49
• Study drug-related AEs
• Serious AEs
• Study drug-related Serious AEs
• AEs leading to permanent study drug discontinuation
• AEs leading to study discontinuation
• AEs leading to death
All AEs will be classified by SOC and PT. Frequency count of AEs, the number of unique subjects experiencing an AE, percentage of unique subjects experiencing an AE and total number of events will be tabulated by treatment. For the number of unique subjects reporting, if a subject reported more than one AE that was coded to the same SOC or PT, the subject will be counted only once for that specific SOC or PT.
The following summaries of AEs will also be provided:
• AEs by SOC and PT
• AEs by SOC, PT and maximum severity
• AEs by SOC, PT and causality relationship
• Serious AEs by SOC and PT
• AEs leading to study withdrawal by SOC and PT
• TEAEs leading to study drug discontimuation by SOC and PT
• AEs leading to death by SOC and PT
For AEs presented by relationship to study treatment, the strongest relationship to study treatment(s) during the clinical trial will be presented for each subject if coded to the same SOC or PT. For AEs presented by severity, the worst severity during the clinical trial will be presented for each subject if coded to the same SOC or PT. If either relationship or severity is missing, then the strongest relationship (related) or worst severity (severe) will be assigned.
Laboratory Evaluations
No laboratory evaluations will be performed in this study.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 33 of 49
Interim Analyses
Aside from the blinded sample size re-estimation described in Section 3.7 above, there is no other planned interim analysis.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 34 of 49
Changes from Analysis Planned in Protocol
There are no changes from the analyses planned in the protocol.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 35 of 49
Programming Considerations
All tables, figures, listings (TFLs), and statistical analyses will be generated using SAS for Windows, Release 9.4 (SAS Institute Inc., Cary, NC, USA). Computer-generated table, listing and figure output will adhere to the following specifications.
General Considerations
• One SAS program can create several outputs, or a separate SAS program will be created for each output.
• One output file can contain several outputs or each output will be stored in a separate file.
• Output files will be delivered in Word format or portable document format pdf.
• Numbering of TFLs will follow ICH E3 guidance
Table, Listing, and Figure Format
General
• All TFLs will be produced in landscape format on American letter size, unless otherwise specified.
• All TFLs will be produced using the Courier New font, size 8 which is the smallest acceptable point size for the Regulatory Authorities.
• The data displays for all TFLs will have a minimum blank 1-inch margin on all 4 sides.
• Headers and footers for figures will be in Courier New font, size 8 which is the smallest acceptable point size for the Regulatory Authorities.
• Legends will be used for all figures with more than 1 variable, group, or item displayed.
• TFLs will be in black and white (no color), unless otherwise specified
• Specialized text styles, such as bolding, italics, borders, shading, and superscripted and subscripted text, will not be used in the TFLs, unless otherwise specified. On some occasions, superscripts 1, 2, or 3 may be used (see below).
• Only standard keyboard characters will be used in the TFLs. Special characters, such as non-printable control characters, printer-specific, or font-specific characters, will not be used. Hexadecimal-derived characters will be used, where possible, if they are appropriate to help display math symbols (e.g., μ). Certain subscripts and superscripts (e.g., cm2, Cmax) will be employed on a case-by-case basis.
• Mixed case will be used for all titles, footnotes, column headers, and programmer-supplied formats, as appropriate.
Headers
• All output should have the following header at the top left of each page:

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 36 of 49
• resTORbio, Inc. Protocol RTB-101-204 (Syneos Health study number 7001371)
• Draft/Final Run <date>
• All output should have Page n of N at the top or bottom right corner of each page. TFLs are internally paginated in relation to the total length (i.e., the page number should appear sequentially as page n of N, where N is the total number of pages in the table).
• The date output was generated should appear along with the program name as a footer on each page.
Display Titles
• Each TFL are identified by the designation and a numeral. (i.e., Table 14.1.1). ICH E3 numbering is strongly recommended, but sponsor preferences are obtained before final determination. A decimal system (x.y and x.y.z) are used to identify TFLs with related contents. The title is centered. The analysis set are identified on the line immediately following the title. The title and table designation are single spaced. A solid line spanning the margins will separate the display titles from the
• Column headers. There will be 1 blank line between the last title and the solid line.
Table x.y.z First Line of Title
Second Line of Title if Needed (ITT Analysis Set)
Column Headers
• Column headings are displayed immediately below the solid line described above in initial upper-case characters.
• In the case of efficacy tables, the variable (or characteristic) column will be on the far left followed by the treatment group columns and total column (if applicable). P-values may be presented under the total column or in separate p-value column (if applicable). Within-treatment comparisons may have p-values presented in a row beneath the summary statistics for that treatment.
• For numeric variables, include “unit” in column or row heading when appropriate.
• Analysis set sizes will be presented for each treatment group in the column heading as (N=xx) (or in the row headings, if applicable). This is distinct from the ‘n’ used for the descriptive statistics representing the number of subjects in the analysis set.
• The order of treatments in the tables and listings will be Placebo first in the case of placebo controlled studies and Active comparators first in the case of active comparator trials, followed by a total column (if applicable).
Body of the Data Display
13.2.5.1. General Conventions
Data in columns of a table or listing are formatted as follows:

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 37 of 49
• Alphanumeric values are left-justified;
• Whole numbers (e.g., counts) are right-justified; and
• Numbers containing fractional portions are decimal aligned.
13.2.5.2. Table Conventions
• Units will be included where available
• If the categories of a parameter are ordered, then all categories between the maximum and minimum category are presented in the table, even if n=0 for all treatment groups in a given category that is between the minimum and maximum level for that parameter. For example, the frequency distribution for symptom severity would appear as:
Severity Rating
N
severe 0 moderate 8 mild 3
Where percentages are presented in these tables, zero percentages will not be presented and so counts of 0 will be presented as 0 and not as 0 (0%).
• If the categories are not ordered (e.g., Medical History, Reasons for Discontinuation from the Study, etc.), then only those categories for which there is at least 1 subject represented in 1 or more groups are included.
• An Unknown or Missing category are added to each parameter for which information is not available for 1 or more subjects.
• Unless otherwise specified, the estimated mean and median for a set of values are printed out to 1 more significant digit than the original values, and standard deviations are printed out to 2 more significant digits than the original values. The minimum and maximum should report the same significant digits as the original values. For example, for systolic blood pressure:
N XX Mean XXX.X Std Dev X.XX Median XXX.X Minimum XXX Maximum XXX
• P-values are output in the format: “0.xxx”, where xxx is the value rounded to 3 decimal places.
Every p-value less than 0.001 will be presented as <0.001. If the p-value are less than 0.0001, then present as <0.0001. If the p-value is returned as >0.999, then present as >0.999
• Percentage values are printed to one decimal place, in parentheses with no spaces, one space after the count (e.g., 7 (12.8%), 13 (5.4%)). Pre-determine how to display values that round down to 0.0. A common convention is to display as '<0.1', or as appropriate with additional decimal

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 38 of 49
places. Unless otherwise noted, for all percentages, the number of subjects in the analysis set for the treatment group who have an observation will be the denominator. Percentages after zero counts should not be displayed and percentages equating to 100% are presented as 100%, without decimal places.
• Tabular display of data for medical history, prior/concomitant medications, and all tabular displays of adverse event data are presented by the body system, treatment class, or SOC with the highest occurrence in the active treatment group in decreasing order, assuming all terms are coded. Within the body system, drug class and SOC, medical history (by preferred term), drugs (by ATC1 code), and adverse events (by preferred term) are displayed in decreasing order. If incidence for more than 1 term is identical, they should then be sorted alphabetically. Missing descriptive statistics or p-values which cannot be estimated are reported as “-”.
• The percentage of subjects is normally calculated as a proportion of the number of subjects assessed in the relevant treatment group (or overall) for the analysis set presented. However, careful consideration is required in many instances due to the complicated nature of selecting the denominator, usually the appropriate number of subjects exposed. Describe details of this in footnotes or programming notes.
• For categorical summaries (number and percentage of subjects) where a subject can be included in more than one category, describe in a footnote or programming note if the subject are included in the summary statistics for all relevant categories or just 1 category and the criteria for selecting the criteria.
• Where a category with a subheading (such as system organ class) has to be split over more than one page, output the subheading followed by “(cont.)” at the top of each subsequent page. The overall summary statistics for the subheading should only be output on the first relevant page.
13.2.5.3. Listing Conventions
• Listings will be sorted for presentation in order of treatment groups as above, subject number, visit/collection day, and visit/collection time.
• Missing data are represented on subject listings as either a hyphen (“-”) with a corresponding footnote (“- = unknown or not evaluated”), or as “N/A”, with the footnote “N/A = not applicable”, whichever is appropriate.
• Dates are printed in SAS DATE9.format (“ddMMMyyyy”: 01JUL2000). Missing portions of dates are represented on subject listings as dashes (--JUL2000). Dates that are missing because they are not applicable for the subject are output as “N/A”, unless otherwise specified.
• All observed time values are to be presented using a 24-hour clock HH:MM or HH:MM:SS format (e.g., 11:26:45, or 11:26). Time will only be reported if it was measured as part of the study.
• Units will be included where available
13.2.5.4. Figure Conventions
• Unless otherwise specified, for all figures, clinical visits will be displayed on the X-axis and endpoint (e.g., treatment mean change from Baseline) values will be displayed on the Y-axis.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 39 of 49
Footnotes
• A solid line spanning the margins will separate the body of the data display from the footnotes.
• All footnotes will be left justified with single-line spacing immediately below the solid line underneath the data display.
• Footnotes should always begin with “Note:” if an informational footnote, or 1, 2, 3, etc. if a reference footnote. Each new footnote should start on a new line, where possible.
• Subject specific footnotes are avoided, where possible.
• Footnotes will be used sparingly and add value to the table, figure, or listing. If more than six lines of footnotes are planned, then a cover page is strongly recommended to be used to display footnotes, and only those essential to comprehension of the data will be repeated on each page.
• The last line of the footnote section will be a standard source line that indicates the name of the program used to produce the data display, date the program was run, and the listing source (i.e., ‘Program : myprogram.sas Listing source: 16.x.y.z’).

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 40 of 49
Quality Control
SAS programs are developed to produce output such as analysis data sets, summary tables, data listings, figures, or statistical analyses. SOPs of the CRO (Veristat, LLC) contracted to generate the TLFs for this study will be followed.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 41 of 49
References
Friede, T., & Kieser, M. (2004). Sample size recalculation for binary data in internal pilot study designs. Pharmaceutical Statistics: The Journal of Applied Statistics in the Pharmaceutical Industry, 3(4), 269-279.
Cong, D (2016). The effect of sample size re-estimation on Tpe I error rates when comparing two binomial proportions. Master’s Thesis, Department of Statistics, College of Arts and Sciences, Kansas State University.

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 42 of 49
Index of Tables
Table Number Name Analysis Set 14.1.1.1 Subject Disposition All Screened
Subjects 14.1.2.1 Reasons for Exclusion from Analysis Sets Randomized Set 14.1.2.2 Major Protcol Deviations Randomized Set 14.1.3.1 Demographic and Baseline Characteristics Full Analysis Set 14.1.3.2 Medical History Full Analysis Set 14.1.4.1 Prior Medications Safety Set 14.1.4.2 Concomitant Medications Safety Set 14.1.5.1 Treatment Compliance Safety Set 14.2.1.1 Primary Analysis: Percentage of Subjects With
Laboratory-Confirmed COVID-19 Who: Have Protocol-Defined Progressive Symptoms or Were Hospitalized or Died from the First Dose of Study Drug through Week 4
Full Analysis Set
14.2.1.2 Sensitivity Analysis Percentage of Subjects With Laboratory-Confirmed COVID-19 Who: Have Protocol-Defined Progressive Symptoms or Were Hospitalized or Died from the First Dose of Study Drug through Week 4
Full Analysis Set
14.2.1.3 Supplemental Analysis: Percentage of Subjects With Laboratory-Confirmed COVID-19 Who: Have Protocol-Defined Progressive Symptoms or Were Hospitalized or Died from the First Dose of Study Drug through Week 4
Modified Intent-to-Treat Set
14.2.1.4 Supplemental Analysis: Percentage of Subjects With Laboratory-Confirmed COVID-19 Who: Have Protocol-Defined Progressive Symptoms or Were Hospitalized or Died from the First Dose of Study Drug through Week 4
Per Protocol Set
14.2.1.5 Subgroup Analysis: Percentage of Subjects With Laboratory-Confirmed COVID-19 Who: Have Protocol-Defined Progressive Symptoms or Were Hospitalized or Died from the First Dose of Study Drug through Week 4 by Age Group
Full Analysis Set
14.2.1.6 Subgroup Analysis: Percentage of Subjects With Laboratory-Confirmed COVID-19 Who: Have Protocol-Defined Progressive Symptoms or Were Hospitalized or Died from the First Dose of Study Drug through Week 4 by Medical History of Asthma
Full Analysis Set
14.2.1.7 Subgroup Analysis: Percentage of Subjects With Laboratory-Confirmed COVID-19 Who: Have Protocol-Defined Progressive Symptoms or Were Hospitalized or Died from the First Dose of Study Drug through Week 4 by Medical History of Congestive Heart Failure
Full Analysis Set
14.2.2.1 Percentage of Subjects who Develop Symptomatic Laboratory-Confirmed COVID-19 from the First Dose of Study Drug through Week 4
Full Analysis Set
14.2.2.2 Percentage of Subjects who Develop Symptomatic Laboratory-Confirmed COVID-19 from the First Dose of Study Drug through Week 4
Modified Intent-to-Treat Set
14.2.2.3 Percentage of Subjects who Develop Symptomatic Laboratory-Confirmed COVID-19 from the First Dose of Study Drug through Week 4
Per Protocol Set

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 43 of 49
Table Number Name Analysis Set 14.2.2.4 Subgroup Analysis: Percentage of Subjects who Develop
Symptomatic Laboratory-Confirmed COVID-19 from the First Dose of Study Drug through Week 4 by Age Group
Full Analysis Set
14.2.2.5 Subgroup Analysis: Percentage of Subjects who Develop Symptomatic Laboratory-Confirmed COVID-19 from the First Dose of Study Drug through Week 4 by Medical History of Asthma
Full Analysis Set
14.2.2.6 Subgroup Analysis: Percentage of Subjects who Develop Symptomatic Laboratory-Confirmed COVID-19 from the First Dose of Study Drug through Week 4 by Medical History of Congestive Heart Failure
Full Analysis Set
14.2.3.1 Percentage of Subjects who Died through Week 8 in Subjects with Laboratory-Confirmed COVID-19 from the First Dose of Study Drug through Week 4
Full Analysis Set
14.2.4.1 Percentage of Subjects who Died through Weeks 2, 4 an 8 for Any Reason
Full Analysis Set
14.2.5.1 Percentage of Subjects who are Hospitalized Due to Having Symptomatic Laboratory-Confirmed COVID-19 from the First Dose of Study Drug through Week 4
Full Analysis Set
14.2.6.1 Percentage of Subjects were Hospitalized Due to Having One or More Predefined COVID-19 Symptoms and Laboratory-Confirmed SARS-CoV-2 from the First Dose of Study Drug through Week 4 and who Require Mechanical Ventilation, Noninvasive Ventilation, High Flow Nasal Canula Oxygen Delivery or ICU Admission During the Hospitalization
Full Analysis Set
14.2.7.1 Time to Alleviation of Moderate and Severe Symptoms of COVID-19 in Subjects with Laboratory-Confirmed COVID-19 from the First Dose of Study Drug through Week 4 who Develop Moderate or Severe Symptoms through Week 8
Full Analysis Set
14.2.7.2 Time to Alleviation of Moderate and Severe Symptoms of COVID-19 in Subjects with Laboratory-Confirmed COVID-19 from the First Dose of Study Drug through Week 4 who Develop Moderate or Severe Symptoms through Week 8
Modified Intent-to-Treat Set
14.2.7.3 Time to Alleviation of Moderate and Severe Symptoms of COVID-19 in Subjects with Laboratory-Confirmed COVID-19 from the First Dose of Study Drug through Week 4 who Develop Moderate or Severe Symptoms through Week 8
Per Protocol Set
14.2.8.1 Percentage of Subjects who Develop SARS-CoV-2 Infection Regardless of Symptoms from the First Dose of Study Drug through Week 4 Among Subjects who were SARS-CoV-2 Negative at Baseline
Modified Intent-to-Treat Set
14.3.1.1 Adverse Events – Overall Summary Safety Set 14.3.1.2 Adverse Events by System Organ Class and Preferred
Term Safety Set
14.3.1.3 Adverse Events by System Organ Class, Preferred Term, and Maximum Severity
Safety Set

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 44 of 49
Table Number Name Analysis Set 14.3.1.4 Adverse Events by System Organ Class, Preferred Term,
and Causality Relationship Safety Set
14.3.1.5 Serious Adverse Events by System Organ Class and Preferred Term
Safety Set
14.3.1.6 Adverse Events Leading to Withdrawal from Study by System Organ Class and Preferred Term
Safety Set
14.3.1.7 Adverse Events Leading to Study Drug Discontinuation by System Organ Class and Preferred Term
Safety Set
14.3.1.8 Adverse Events Leading to Death by System Organ Class and Preferred Term
Safety Set
14.3.2.1 Serious Adverse Events, Listing Safety Set 14.3.2.2 Adverse Events Leading to Death, Listing Safety Set 14.3.2.3 Adverse Events Leading to Withdrawal from Study,
Listing Safety Set
14.3.2.4 Adverse Events Leading to Study Drug Discontinuation, Listing
Safety Set
14.3.2.5 Severe Adverse Events, Listing Safety Set 14.3.3.1 Extent of Exposure Safety Set

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 45 of 49
Index of Figures
Figure Number Name Analysis Set 14.2.1 Kaplan-Meier Curves of Time to Alleviation of Moderate and
Severe Symptoms of COVID-19 in Subjects with Laboratory-Confirmed COVID-19 from the First Dose of Study Drug through Week 4 who Develop Moderate or Severe Symptoms through Week 8
Full Analysis Set

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 46 of 49
Index of Listings
Listing Number Name Analysis Set 16.2.1.1 Subject Disposition All Screened
Subjects 16.2.2.1 Protocol Deviations Randomized Set 16.2.3.1 Inclusion and Exclusion Criteria Violations All Screened
Subjects 16.2.3.2 Reasons for Screen Failure Randomized Set 16.2.4.1 Demographic and Baseline Characteristics Full Analysis Set 16.2.4.2 Medical and Surgical History Full Analysis Set 16.2.4.3 Prior Medications Safety Set 16.2.4.4 Concomitant Medications Safety Set 16.2.5.1 Study Drug Administration Safety Set 16.2.6.1 COVID-19 Signs and Symptoms Full Analysis Set 16.2.6.2 Chest X-Ray Full Analysis Set 16.2.6.3a Change in Condition Evaluation (from eINTERACT form) Full Analysis Set 16.2.6.3b Change in Condition Evaluation (from eINTERACT form) –
Additional Information Full Analysis Set
16.2.6.4 SARS-CoV-2 Diagnostic Test Results at Baseline Full Analysis Set 16.2.6.5 SARS-CoV-2 Diagnostic Test Results After Randomization Full Analysis Set 16.2.6.6 Hospitalization Full Analysis Set 16.2.7.1 Adverse Events Safety Set 16.2.7.2 Deaths Safety Set

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 47 of 49
Appendix 1
Mapping of eCRF data from Presence of COVID-19 Symptoms and eINTERACT forms to the COVID-19 Symptoms
The COVID-19 symptoms are derived from the eCRF as follows:
eCRF Page
COVID-19 Symptoms Presence of COVID-19
Symptoms
eINTERACT Mild New sore throat “Sore throat” is checked New chest congestion “Chest congestion” is checked New cough “Cough” is checked New headache “Headache” is checked Fever (99.2oF or greater) Most Recent Temperature is
≥99.2oF. (If temperature is recorded in oC, convert to oF first)
Chills “Chills and/or shaking chills” is
checked
New GI symptoms (nausea/vomiting/diarrhea)
“Nausea” is checked and/or “Vomiting” is checked and/or “Diarrhea” is checked
In “Change/s in condition, symptoms or signs” section, one or more of the following are checked:
• Diarrhea • Food and/or fluid intake
(decreased or unable to eat and/or drink adequate amounts)
• Nausea/Vomiting
and/or In the “GI symptoms present (check all that apply)” section, one or more of the symptoms listed is checked
Malaise/muscle pain “Malaise and/or muscle pain” is
checked
New loss of taste or smell “New loss of taste or smell” is
checked

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 48 of 49
Moderate or Severe Symptoms
Increased shortness of breath over baseline level
“Increase shortness of breath” is checked
New onset of tachypnea (respiratory rate of ≥ 22 breaths per minute)
Most Recent Respiration is ≥22
New onset of tachycardia (more than 100 beats per minute)
Most Recent Pulse is >100 is checked
Worsening confusion/change in mental status/decreased responsiveness
Worsening confusion is checked
In “Change/s in condition, symptoms or signs” section, one or more of the following are checked:
• Altered mental status • Behavioral symptoms (e.g.
agitation; psychosis) • Pain (uncontrolled) • Unresponsiveness
and/or In the “Mental Status Evaluation” section, one or more of the symptoms listed is checked and/or In the “Behavioral changes (check all that apply)” section, one or more of the symptoms listed is checked and/or In the “Behavioral changes (check all that apply)” section, “Recent onset of significant mood decline, with anorexia, crying, and sleeplessness” is answered “Yes”
O2 sat decreased by 3% or greater from baseline or <93% if no baseline O2 saturation available
O2 Sat decreased by 3% or greater since last taken, and/or Most Recent O2 sats <93%, if no baseline 02 saturation is available

resTORbio, Inc. Statistical Analysis Plan Version 1.0 Protocol No.: RTB-101-210
This document is confidential.
31 Aug 2020 Page 49 of 49
Cerebrovascular accident/transient ischemic attack/new neurologic signs
In “Change/s in condition, symptoms or signs” section, the following is checked:
• Stroke/C VA/TIA/new neurological signs
and/or In the “Neurological symptoms” section, one or more of the symptoms listed is checked
Functional decline/decline in activities of daily living
In “Change/s in condition, symptoms or signs” section, the following is checked:
• Functional decline (worsening function and/or mobility)
and/or In the “Describe functional status changes” section, one or more of the symptoms listed is checked and/or In the “Has there been a decline in the resident's ability to perform the following ADLs?” section, one or more of the symptoms listed is checked
Imaging indicating a lower respiratory tract infection
For this symptom, data will be coming from the Chest X-ray form. The symptom is present if the question “Are the results consistent with Covid-19?” is answered “Yes”.




















