2020 - Kementerian Kesihatan Malaysia
114
HTA HEALTH TECHNOLOGY ASSESSMENT REPORT MaHTAS Malaysian Health Technology Assessment Section MEDICAL DEVELOPMENT DIVISION MINISTRY OF HEALTH PRE-DIALYSIS EDUCATION PROGRAMME MOH/P/PAK/ 449.20(TR)-e 2020
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of 2020 - Kementerian Kesihatan Malaysia

HTA
HE
ALT
H T
EC
HN
OLO
GY
AS
SE
SS
ME
NT
RE
PO
RT
MaHTASMalaysian Health Technology Assessment Section
MEDICAL DEVELOPMENT DIVISIONMINISTRY OF HEALTH
PRE-DIALYSIS EDUCATIONPROGRAMME
MOH/P/PAK/ 449.20(TR)-e
2020


HEALTH TECHNOLOGYASSESSMENT REPORT
MALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)MEDICAL DEVELOPMENT DIVISION
MINISTRY OF HEALTH
PRE-DIALYSIS EDUCATION PROGRAMME

PRE-DIALYSIS EDUCATION PROGRAMME
DISCLAIMER
This Health Technology Assessment has been developed from analysis, interpretation and synthesis of scientific research and/or technology assessment conducted by other organizations. It also incorporates, where available, Malaysian data, and information provided by experts to the Ministry of Health Malaysia. While effort has been made to do so, this document may not fully reflect all scientific research available. Additionally, other relevant scientific findings may have been reported since completion of the review.
Please contact: [email protected] if you would like further information.
Published by Malaysian Health Technology Assessment Section, (MaHTAS)Medical Development Division, Ministry of Health MalaysiaLevel 4, Block E1, Complex E, Precinct 1Federal Government Administrative Centre62590, Putrajaya, MalaysiaTel: 603 88831246
CopyrightThe copyright owner of this publication is the Malaysian Health Technology Assessment Section (MaHTAS), Medical Development Division, Ministry of Health Malaysia. Content may be reproduced in any number of copies and in any format or medium provided that a copyright acknowledgement to the Malaysian Health Technology Assessment Section (MaHTAS) is included and the content is not changed, not sold, nor used to promote or endorse any product or service, and not used in an inappropriate or misleading context.
e ISBN : 978-967-2887-12-6
Available on the MOH website: http://www.moh.gov.my/v/hta
This HTA report was endorsed in HTA & CPG Council Meeting Bil. 1/2020 on 13th November 2020.
i

HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
AUTHORS:
DR. NUR FARHANA BINTI MOHAMADSenior Principal Assistant Director Malaysian Health Technology Assessment Section (MaHTAS)Medical Development DivisionMinistry of Health Malaysia
MDM. ROS AZIAH MOHD RASHIDSenior Assistant DirectorMalaysian Health Technology Assessment Section (MaHTAS)Medical Development DivisionMinistry of Health Malaysia
MISS GAN YAN NEEPrincipal Assistant DirectorMalaysian Health Technology Assessment Section (MaHTAS)Medical Development DivisionMinistry of Health Malaysia
MDM. KU NURHASNI KU ABDUL RAHIMSenior Principal Assistant DirectorMalaysian Health Technology Assessment Section (MaHTAS)Medical Development DivisionMinistry of Health Malaysia
DR. HANIN FARHANA KAMARUZAMANSenior Principal Assistant DirectorMalaysian Health Technology Assessment Section (MaHTAS)Medical Development DivisionMinistry of Health Malaysia
INFORMATION SPECIALIST:
MDM. WONG WAI CHEEMatron Malaysian Health Technology Assessment Section (MaHTAS)Medical Development DivisionMinistry of Health Malaysia
MDM. NORHARLINA BT CHE ZAKARIANursing OfficerMalaysian Health Technology Assessment Section (MaHTAS)Medical Development DivisionMinistry of Health Malaysia
ii

PRE-DIALYSIS EDUCATION PROGRAMME
EXPERT COMMITTEE
YBHG. DATO’ DR ONG LOKE MENGSenior Consultant Nephrologist & Head of Nephrology Service, Ministry of Health, MalaysiaHospital Pulau Pinang
DR. RAFIDAH BINTI ABDULLAHConsultant NephrologistHospital Putrajaya
DR. SUNITA BAVANANDANConsultant NephrologistHospital Kuala Lumpur
DR. LEONG CHONG MENNephrologistHospital Kulim
DR. IRENE WONGNephrologistHospital Tengku Ampuan Rahimah, Klang
DR. NORAZINIZAH AHMAD MISWAN NephrologistHospital Ampang
DR. WAN HAZLINA WAN MOHAMAD NephrologistHospital Kuala Lumpur
DR. KHOR SU MEE DietitianHospital Pulau Pinang DR. NOORAINI BINTI DARUSClinical Psychologist and Head of ProfessionHospital Kuala Lumpur
MDM. RUWAIDA NUR BT ZAINUL ABIDINPharmacist UF52Pharmacy Department Hospital Serdang
MDM. CHOONG CHIAU LINGPharmacist UF52Pharmacy DepartmentHospital Selayang
iii

HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
MDM. HJH. NOR FARIDAH BINTI MOHD ZAIDIMedical Social Officer S52Hospital Pulau Pinang
MISS CHAN PEK HARClinical PsychologistHospital Kuala Lumpur
MDM. ARSYURAHMAH BT ABDULL RAHMANDietitian Hospital Sultanah Nur Zahirah, Kuala Terengganu
MDM. MAHANI AHMADHead of NurseCAPD UnitHospital Tuanku Ja’afar, Seremban
DR. JUNAINAH BINTI SABIRIN(Public Health Physician)Former Deputy DirectorMalaysian Health Technology Assessment Section (MaHTAS)Medical Development Division Ministry of Health Malaysia
DR. IZZUNA MUDLA MOHAMED GHAZALI(Public Health Physician)Deputy DirectorMalaysian Health Technology Assessment Section (MaHTAS)Medical Development Division Ministry of Health Malaysia
EXTERNAL REVIEWERS
YBHG. DATUK DR. GHAZALI AHMADConsultant Nephrologist Institut Jantung Negara (IJN) YBHG. PROF MADYA DR. LIM SOO KUNFaculty of MedicineUniversiti Malaya
DR. ANITA MANOCHAConsultant NephrologistHospital Seberang Jaya, Pulau Pinang
iv

PRE-DIALYSIS EDUCATION PROGRAMME
ACKNOWLEDGEMENT
The authors for this Health Technology Assessment Report would like to express their gratitude and appreciation to the following for their contribution and assistance:
• Health Technology Assessment and Clinical Practice Guidelines Council.
• Technical Advisory Committee for Health Technology Assessment.
• Nephrology clinics staff of Hospital Kuala Lumpur (HKL), Hospital Tengku Ampuan Rahimah Klang (HTAR) and Hospital Ampang.
DISCLOSURE
The authors of this report have no competing interest in this subject and the preparation of this report is totally funded by the Ministry of Health, Malaysia.
v

HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
EXECUTIVE SUMMARYBackground
Chronic Kidney Disease (CKD) is a growing public health concern which is responsible for various complications including all-cause and cardiovascular mortality, progression to end-stage renal disease (ESRD), cognitive decline, anaemia, mineral and bone disorders. The Global Burden of Disease 2015 study estimated that, in 2015, about 1.2 million people died from kidney failure, an increase of 32% since 2005. In Malaysia, the prevalence of CKD has increased from 9.1% in the 2011 Malaysian National Health and Morbidity Survey to 15.5% in 2018. The number of patients with CKD is expected to significantly rise in the future largely due to the increasing prevalence of diabetes, hypertension as well as the aging population in Malaysia.
It is known that timely referral to nephrologist is recommended for renal replacement therapy (RRT) in people with progressive CKD. In the Malaysian Clinical Practice Guideline (CPG) for Management of Chronic Kidney Disease (Second Edition) 2018, it is stated in the recommendation that CKD patient with rapidly declining renal function (stage 4 to stage 5) should be referred to a nephrologist/physician. The UK Renal Association recommends that all patients with severe CKD (stage 5 and progressive stage 4), alongside their families and carers, should be offered pre-dialysis education programme (PDEP).
This programme aims at improving knowledge and understanding of the condition, as well as assisting them in making decisions for RRT. However, in most studies, it is reported that about 40% to 60% of patients with CKD start dialysis in an unplanned fashion and/or under urgent circumstances despite regular follow-up by a nephrologist. This is of concern since in unplanned dialysis, patients forego the opportunity to make an informed, shared decision regarding the timing and modality of RRT as options for RRT under urgent conditions are often limited. This highlights the importance of a structured and comprehensive PDEP in preparing advanced-stage CKD patients for RRT.
At present, there is no standard national programme established in Ministry of Health for pre-dialysis education. Pre-dialysis education for advanced CKD patients is often done in different ways across the country. Effectiveness of such methods in delivering pre-dialysis education for advanced CKD patients is largely unknown. Therefore, this health technology assessment (HTA) was requested by Head of Nephrology Services, Ministry of Health, Malaysia to review the available evidence and feasibility of structured PDEP for advanced CKD patients before its adoption into national programme in Malaysia.
Technical featuresPre-dialysis education programme (PDEP) often described as multidisciplinary education programme, which consists of multiple education sessions where patients are educated by three or more health care professionals such as nephrologist, nurse, dietitian, medical social officer, home-dialysis coordinator, pharmacist, technician, or by other dialysis patients. This programme usually caters CKD patients who are in stage 4 and 5. There are variations in practice, however, PDEP usually includes individualised one-to-one sessions with a member or members of the multidisci plinary team and group discussions, peer counselling as well as problem-solving sessions have been described. The aims of this programme are mainly to provide patients with information on ESRD treatment options, help decision-making between treatments, and encourage self-care to improve quality of life.
vi

PRE-DIALYSIS EDUCATION PROGRAMME
Policy QuestionShould a structured PDEP be expanded in all Ministry of Health facilities?
Objectivei. To assess the effectiveness and safety of PDEP for advanced CKD patientsii. To assess the organisational, ethical, legal and societal implications related to PDEP for
advanced CKD patients iii. To assess the cost-effectiveness of PDEP for advanced CKD patients iv. To assess the most suitable PDEP for Malaysian context
Research questionsi. Is PDEP effective and safe for advanced CKD patients?ii. What are the organisational, ethical, legal and societal implications of PDEP for advanced
CKD patients? iii. Is PDEP cost-effective for advanced CKD patients?
MethodsStudies were identified by searching the electronic database for published literatures pertaining to PDEP for advanced CKD patients. The following electronic databases were searched through the Ovid interface: Ovid MEDLINE® In-process and other Non-indexed citations and Ovid MEDLINE® 1946 to present, EBM Reviews - Health Technology Assessment (4th Quarter 2016), EBM Reviews - Cochrane Database of Systematic Review (2005 to Dec 2019), EBM Reviews - Cochrane Central Register of Controlled Trials (Dec 2019), EBM Reviews - Database of Abstracts of Reviews of Effects (1st Quarter 2016), EBM Reviews - NHS Economic Evaluation Database (1st Quarter 2016). Parallel searches were run in PubMed and INAHTA database. No limits were applied to the search. Detailed search strategy is as in Appendix 3. The last search was performed on 2nd December 2019. Additional articles were identified from reviewing the references of retrieved articles.
Results and conclusions:A. SYSTEMATIC REVIEW OF LITERATUREA total of 251 records were found to be potentially relevant and were screened using the inclusion and exclusion criteria. Sixteen out of 75 full text articles comprised of one SR with meta-analysis, one SR, one RCT, three cohort studies, two retrospective cohort studies, two pre- and post- intervention studies, four cross-sectional studies and two qualitative studies were finally included in this review. All studies included were published in English language between 2003 and 2018. Most studies were conducted in Taiwan, United States of America (USA) and Europe. Others were conducted in Brunei, The Netherlands, Turkey, Canada, Philippines and United Kingdom (UK).
EffectivenessThere was limited fair level of retrievable evidence to suggest that participation of advanced CKD patients in PDEP contributed to greater survival probability and higher one-year survival rate compared to those who did not. However, no significant difference reported after two years. Limited fair to good level of retrievable evidence to suggest lower mortality and morbidity rates in patients who had PDEP. Limited evidence demonstrated that patients who had PDEP had longer time to dialysis and better blood profiles compared to those who did not. Significantly lower peritonitis-related mortality rates and lower peritonitis-related morbidity rates were also noted in PD patients.
SafetyThere was no retrievable evidence on the safety issues with regards to PDEP for advanced CKD patients.
vii

HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
OrganisationalHospitalisation / Length of stayThere was fair to good level of retrievable evidence to suggest that PDEP was associated with significantly lower frequency of temporary catheter use, lower rates of hospitalisation at dialysis initiation and post- dialysis, as well as shorter length of hospital stay.
Components of programmeThe evidence showed great variation in the components of the programmes described, from the multidisciplinary team members, to the educational process including timing, delivery styles, formats for content, structure, conduct of the programme and materials. However, most evidence reported involvement of multidisciplinary team members almost always comprised of nephrologists, nurses, dietitians and medical social officers, with few had pharmacist, clinical psychologist and patient volunteers. Most studies mentioned multiple individual sessions with few had mixed of individual sessions and group sessions as well as patients’ involvement. Majority involved patients with CKD stage 4 and 5 in the programme, with content tailored according to the patients’ CKD stage and principally focused on knowledge on nutrition, lifestyle modification, nephrotoxin avoidance, compliance to medications, preparation for RRT and modality choices with few reported hands-on and demonstration. Materials used ranged from video materials, printed materials, and website materials. Frequency of the sessions and follow-up were mostly depended on the CKD stage.
GuidelinesFew guidelines from UK, USA, France, Europe and a position statement following an expert meeting in Switzerland have been issued outlining the recommendations on the conduct of PDEP.
Social / PsychologicalThere was fair to good level of retrievable evidence to suggest significant association between PDEP and patient’s choice as well as receipt of PD and home dialysis for RRT. Limited evidence also showed higher rates of pre-emptive kidney transplantation rates, higher levels of knowledge of ESRD and RRT options as well as higher levels of adherence, lower depression levels and anxiety levels, and better HRQL were noted in patients who had PDEP.
Limited evidence also showed that patient factors including individualisation, educational factors including tailored education, appropriate time/information, and available resources as well as support systems were the influential factors on patients’ decision for RRT. Sub-optimal education, different perspectives between patients and staff, and the influence of patient experience were the three themes identified which related to improving PDEP.
Cost-effectivenessBased on two cost-analyses, significant reduction in medical expenditure after initiation of HD were noted in patients who had PDEP and the cost-saving effect came through the early preparation of vascular access and reduced hospitalisations.
B. LOCAL SURVEY ON PRE-DIALYSIS EDUCATION PROGRAMMEA multi-centre cross-sectional questionnaire survey was conducted in January 2020 to identify the essential components of pre-dialysis education programme based on the preferences of patients, carers and healthcare workers. A total of 39 respondents were recruited via purposive sampling from three public hospitals. Based on the survey findings, patients and carers preferred to have a 30-minute single session with multiple educators every three months delivered by a multidisciplinary team consisting of doctor, dietitian, patient representative, medical social officer, psychologist, pharmacist, nurse and medical assistant with a mix of education materials such as hands-on session or demonstration, audio-visual aids, leaflets or pamphlets and information about websites or online videos in the hospital setting. The pre-dialysis education may be given as an individual (one-to-one) or group session depending on the patient’s preference. The pre-dialysis education should be initiated approximately six months before starting treatment of choice, allowing patients and carers to have sufficient time to understand about available treatment options. Patients and carers agreed
viii

PRE-DIALYSIS EDUCATION PROGRAMME
that being part of a patient support group would be helpful in solving real-life problems and that shared decision-making between doctors and patients is important to them. The healthcare workers expressed different preferences in terms of delivery method, time of initiation, duration, frequency, and venue which may arise from consideration of practical aspects such as daily burden of workload and capacity in delivering the education sessions, which should be taken into consideration when designing the PDEP.
RecommendationBased on the above review, a standardised approach to PDEP should be outlined before its expansion to all Ministry of Health, Malaysia facilities. A multidisciplinary team involving well-trained personnel, and optimally with mixed individual and group sessions as well as using interactive mixed education materials should be established. Comprehensive and more personalised content tailored according to the CKD stage taking account individual needs, emotional support, psychosocial aspects, involvement of family as well as caregivers and additional support from patients’ support group are advocated.
ix

HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
TABLE OF CONTENTSDisclaimer iAuthors iiExpert committee iiiExternal reviewers ivAcknowledgement and Disclosure vExecutive summary viAbbreviations xii
1 CHAPTER 1 : INTRODUCTION1.1 BACKGROUND1.2 TECHNICAL FEATURES1.3 POLICY QUESTIONS
1133
2 CHAPTER 2: SYSTEMATIC REVIEW2.1 OBJECTIVES 2.2 RESEARCH QUESTIONS2.3 METHODS2.3.1 LITERATURE SEARCH STRATEGY2.3.2 STUDY SELECTION2.3.3 QUALITY ASSESSMENT STRATEGY2.3.4 DATA EXTRACTION STRATEGY2.3.5 METHODS OF DATA SYNTHESIS2.4 RESULTS2.4.1 RESULTS OF THE SEARCH2.4.2 DESCRIPTION OF THE INCLUDED STUDIES2.4.3 RISK OF BIAS ASSESSMENT2.4.4 EFFECTIVENESS2.4.4.1 PERITONITIS AND PERITONITIS-RELATED DEATH2.4.4.2 SURVIVAL RATE2.4.4.3 MORBIDITY AND MORTALITY 2.4.5 SAFETY2.4.6 ORGANISATIONAL ISSUES2.4.6.1 HOSPITALISATION AND LENGTH OF STAY2.4.6.2 COMPONENTS OF PROGRAMME2.4.6.3 GUIDELINES2.4.7 SOCIAL IMPLICATION2.4.7.1 MODALITY CHOICE2.4.7.2 PATIENTS’ SATISFACTION2.4.7.3 PATIENTS’ AND STAFF INSIGHTS2.4.7.4 PATIENTS’ KNOWLEDGE2.4.7.5 PSYCHOLOGICAL IMPLICATION2.4.8 COST-EFFECTIVENESS2.5 DISCUSSION
444444667779171919202022222224272929333435363738
x
PRE-DIALYSIS EDUCATION PROGRAMME
3 CHAPTER 3: LOCAL SURVEY ON PRE-DIALYSIS EDUCATION PROGRAMME3.1 AIM3.2 METHODS3.3 RESULTS3.4 DISCUSSION AND CONCLUSION3.5 REFLECTION/CRITICAL PERSPECTIVES
4040414748
4 CHAPTER 4: CONCLUSIONS AND RECOMMENDATIONS4.1 CONCLUSIONS4.1.1 SYSTEMATIC REVIEW4.1.2 PATIENT AND PUBLIC INVOLVEMENT IN PRE-DIALYSIS EDUCATION PROGRAMME4.2 RECOMMENDATIONS
51515152
52
5 REFERENCES 53
6 APPENDICESAppendix 1- Hierarchy of evidence for effectiveness studiesAppendix 2- Health Technology Assessment ProtocolAppendix 3- Search strategyAppendix 4- Evidence Table (Included studies)Appendix 5- List of excluded studiesAppendix 6- Survey questionnairesAppendix 7-Suggestions to improve Pre-dialysis Education Programme
56576364899296
xi

HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
AbbreviationsAIDET Acknowledge, Introduce, Duration, Explanation, Thank youADL Activities of Daily LivingCKD Chronic Kidney DiseaseCASP Critical Appraisal Skills ProgrammeCI Confidence IntervalCPE Comprehensive Pre-dialysis EducationCPG Clinical Practice GuidelineDVD Digital Versatile DiscESRD End-Stage Renal DiseaseeGFR Estimated Glomerular Filtration RateEU European UnionFDA Food Drug AdministrationGFR Glomerular Filtration RateGUIDE Structured Pre-dialysis Education Programme in The NetherlandsGRIPP2-SF Guidance for Reporting Involvement of Patients and the PublicHCW Healthcare WorkersHD HaemodialysisHTA Health Technology AssessmentHR Hazard Ratiohs-CRP High-sensitivity C-reactive ProteinINAHTA International Network of Agencies for Health Technology Assess-
mentiPTH intact Parathyroid HormoneIQR Interquartile rangeKDIGO Kidney Disease Improving Global OutcomesMaHTAS Malaysian Health Technology Assessment SectionMPE Multidisciplinary Pre-dialysis EducationMDM Multidisciplinary MeetingNIH National Institute of HealthNHI National Health InsuranceN/A Not-applicableOT Occupational TherapistOR Odds RatioPD Peritoneal dialysisPDEP Pre-dialysis Education ProgrammePPI Patient and Public InvolvementQoL Quality of liferHuEPO Recombinant Human ErythropoietinRRTOE Renal Replacement Therapy Options Educati nRRT Renal Replacement Therapy
xii

PRE-DIALYSIS EDUCATION PROGRAMME
RCT Randomised controlled trialSR Systematic ReviewUSA United States of AmericaUK United Kingdom
xiii

1
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
CHAPTER 1: INTRODUCTION
1.1 BACKGROUND
Chronic Kidney Disease (CKD) is a growing public health concern which is responsible for various complications including all-cause and cardiovascular mortality, progression to end-stage renal disease (ESRD), cognitive decline, anaemia, mineral and bone disorders.1 The Global Burden of Disease 2015 study estimated that, in 2015, about 1.2 million people died from kidney failure, an increase of 32% since 2005.2 In 2010, it was estimated that around 2.3 to 7.1 million people with ESRD died without access to chronic dialysis.2 However, despite of these growing figures, the awareness remains low among patients and health-care providers.1
In Malaysia, the prevalence of CKD has increased from 9.1% in the 2011 Malaysian National Health and Morbidity Survey3,4 to 15.5% in 20185. Awareness of CKD was hardly improved in seven years from 4% of respondents in 20115 to 5% in 2018.6 In the year of 2011, there were 27,572 patients on renal replacement therapy (RRT) in Malaysia5 and the figures have grown to a total of 37,183 patients on regular dialysis in 2015, with 7,595 new patients entering dialysis.3 The number of patients with CKD is expected to significantly rise in the future largely due to the increasing prevalence of diabetes, hypertension as well as the aging population in Malaysia.3 This will certainly contribute to the major increase in the future needs for RRT and impose a large burden on health care budget.
According to Malaysian Clinical Practice Guideline (CPG) for Management of Chronic Kidney Disease (Second Edition) published in 2018, CKD is defined as an estimated glomerular filtration rate (eGFR) of <60 ml/min/1.73 m2 that is present for more than three months with or without evidence of kidney damage, or evidence of kidney damage that is present for more than three months with or without eGFR <60 ml/min/1.73 m2.3 Markers for kidney damage includes albuminuria (albumin excretion rate ≥30 mg/24 hours or albumin-creatinine ratio ≥3 mg/mmol), urine sediment abnormalities, abnormalities detected by histology, structural abnormalities detected by imaging and history of kidney transplantation.3 Classification of CKD is currently based on cause, glomerular filtration rate (GFR) category, and albuminuria category and follows Kidney Disease Improving Global Outcomes (KDIGO) 2012 guidelines which has health and prognostic implications.3,7 The GFR categories mapping to the previous five-stage classification have been retained but with subdivision of the G3 category of 30 to 59 mL/min per 1.73 m2 into categories G3a (45 to 59 mL/min per 1.73 m2) and G3b (30 to 44 mL/min per 1.73 m2).8 This was driven by data supporting different outcomes and risk profiles in these categories.8 Severity is expressed by level of GFR and albuminuria and is linked to risks for adverse outcomes, including death and kidney outcomes.8

2
PRE-DIALYSIS EDUCATION PROGRAMME
Table 1. Prognosis of CKD by GFR and albuminuria category3,7
It is known that timely referral to nephrologist is recommended for RRT in people with progressive CKD in whom the risk of kidney failure within one year is 10–20% or higher, as determined by validated risk prediction tools.7 In the Malaysian CPG for Management of Chronic Kidney Disease (Second Edition) 2018, it is stated in the recommendation that CKD patient with rapidly declining renal function [loss of eGFR >5 ml/min/1.73 m2 in one year or >10 ml/min/1.73 m2 within five years] or eGFR <30 ml/min/1.73 m2 (eGFR categories G4 to G5) should be referred to a nephrologist/physician3. UK Renal Association recommends that all patients with severe CKD (stage 5 and progressive stage 4), alongside their families and carers, should be offered pre-dialysis education programme (PDEP).9
This programme aims at improving knowledge and understanding of the condition, as well as assisting them in making decisions for RRT.9 However, in most studies, it was reported that about 40% to 60% of patients with CKD start dialysis in an unplanned fashion and/or under urgent circumstances despite regular follow-up by a nephrologist.10 This is of concern since in unplanned dialysis, patients forego the opportunity to make an informed, shared decision regarding the timing and modality of RRT as options for RRT under urgent conditions are often limited.10 Studies reported that advanced age, increased comorbidity burden, late referral to nephrology, and lower GFR at dialysis initiation were the most common independent risk factors for unplanned dialysis.10,11 In addition, patients who had unplanned dialysis were found much less likely to have received formal pre-dialysis education about the different options for RRT.10,11 This highlights the importance of a structured and comprehensive PDEP in preparing advanced-stage CKD patients for RRT as unplanned dialysis is known to be associated with increased patient morbidity, mortality, hospitalisations, needs for temporary catheter insertion which subsequently increase the risk of catheter related sepsis and inevitably contribute further to the economic burden of CKD.
At present, there is no standard national programme established in Ministry of Health for pre-dialysis education. Pre-dialysis education for advanced CKD patients is often done in different ways across the country. Several centres in Peninsular Malaysia have specific programme for pre-dialysis education while numerous other centres lack such a programme. Certain hospitals conduct half-day talk monthly which involves sharing experiences by peritoneal

3
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
dialysis (PD), haemodialysis (HD) and kidney transplant nurses as well as exploring the funding options by the medical social officer and inputs by dietitian for CKD patients and family members. Effectiveness of such method in delivering pre-dialysis education for advanced CKD patients is largely unknown. Therefore, this health technology assessment (HTA) was requested by Head of Nephrology Services, Ministry of Health, Malaysia to review the available evidence and feasibility of structured PDEP for advanced CKD patients before its adoption into national programme in Malaysia.
1.2 TECHNICAL FEATURES
Pre-dialysis education programme (PDEP) often described as multidisciplinary education programme, which consists of multiple education sessions where patients are educated by three or more health care professionals such as nephrologist, nurse, dietitian, medical social officer, home-dialysis coordinator, pharmacist, technician, or by other dialysis patients.11 This programme usually caters CKD patients who are in stage 4 and 5.11 There are variations in practice, however, PDEP usually includes individualised one-to-one sessions with a member or members of the multidisci plinary team and group discussions, peer counselling as well as problem-solving sessions have been described wherein patients discuss treatment modalities, as well as barriers, benefits, and troubleshooting of possible problems with other patients.11 Topics covered in this programme mostly include patients’ renal care, nutrition, lifestyle, nephrotoxin avoidance, medications, preparation for RRT and modality choices depending on the CKD stage. Variety of formats have been described in the delivery style of the programme such as group lectures, interactive workshops, open forum sessions as well as written and audio-visual materials to take home.11,12
The multidisciplinary team should include or have access to dietary counselling, education and counselling about different RRT modalities including HD, PD, home dialysis, and transplant options, vascular access surgery, as well as ethical, psychological and social care.8 The aims of this programme are mainly to provide patients with information on end-stage kidney disease treatment options, help decision-making between treatments, and encourage self-care to improve quality of life.12 A systematic approach with PDEP is thought to assist patients in preparation for RRT and prevent the complications of unplanned dialysis subsequently reduce the complications of ESRD.
1.3 POLICY QUESTION
Should a structured PDEP be expanded in all Ministry of Health facilities?

4
PRE-DIALYSIS EDUCATION PROGRAMME
CHAPTER 2: SYSTEMATIC REVIEW
2.1 OBJECTIVE
2.1.1 To assess the effectiveness and safety of PDEP for advanced CKD patients2.1.2 To assess the organisational, ethical, legal and societal implications related to PDEP
for advanced CKD patients 2.1.3 To assess the cost-effectiveness of PDEP for advanced CKD patients2.1.4 To assess the most suitable PDEP for Malaysian context
2.2 RESEARCH QUESTIONS 2.2.1 Is PDEP effective and safe for advanced CKD patients? 2.2.2 What are the organisational, ethical, legal and societal implications of PDEP for
advanced CKD patients? 2.2.3 Is PDEP cost-effective for advanced CKD patients?
2.3 METHODS
2.3.1 Literature search strategy
Studies were identified by searching the electronic database for published literatures pertaining to PDEP for advanced CKD patients. The following electronic databases were searched through the Ovid interface: Ovid MEDLINE® In-process and other Non-indexed citations and Ovid MEDLINE® 1946 to present, EBM Reviews - Health Technology Assessment (4th Quarter 2016), EBM Reviews - Cochrane Database of Systematic Review (2005 to Dec 2019), EBM Reviews - Cochrane Central Register of Controlled Trials (Dec 2019), EBM Reviews - Database of Abstracts of Reviews of Effects (1st Quarter 2016), EBM Reviews - NHS Economic Evaluation Database (1st Quarter 2016). Parallel searches were run in PubMed and INAHTA database. No limits were applied to the search. Detailed search strategy is as in Appendix 3. The last search was performed on 2 December 2019. Additional articles were identified from reviewing the references of retrieved articles.
2.3.2 Study selection
Based on the policy questions, the following inclusion and exclusion criteria were used: -

5
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Inclusion criteria
a. Population Adults patients with advanced CKD stage 4, 5
b. Intervention
Pre-dialysis education programme (PDEP):i. Multidisciplinary team comprised of nephrologists/
dietitians/ medical social officers/ pharmacists/ nurses/ psychologists/ HD or PD patient volunteers etc.
ii. Multiple sessionsiii. Relatively detailed description of the programme,
such as sessions frequency, content of sessions, and descriptions of educators
c. Comparator i. No PDEP ii. No comparator
d. Outcomesi. Effectiveness of PDEP
- Mortality- Morbidity- Quality of life (QoL)
ii. Safety- Complications- Adverse events
iii. Organisational- Unplanned dialysis- Hospital admission- Length of hospital stay- Components of pre-dialysis education
programme(content, structure, delivery style, timing)
- Training- Guidelines
iv. Ethical, legal implications
v. Psychological/Societal implications:
- Compliance- Acceptance- Patient satisfaction- Patient preference/ dialysis modality choice- Mental health issues
vi. Economic impact- Cost- Cost analysis- Cost-effectiveness- Economic evaluation

6
PRE-DIALYSIS EDUCATION PROGRAMME
e. Study design
HTA reports, systematic review (SR), SR with meta- analysis, randomised controlled trial (RCT), cohort study, case-control study, cross-sectional study and economic evaluation studies
f. Full text articles published in English
Exclusion criteria
a. Study design: animal study, narrative review, case series, case reports and early stage CKD patients.
b. Non-English full text article
Based on the above inclusion and exclusion criteria, study selection was carried out independently by two reviewers. Disagreement was resolved by discussion.
2.3.3 Quality assessment strategy
The methodological quality of all the relevant full text articles retrieved was assessed using the relevant checklist of Cochrane Collaboration Assessment tools, NIH and Critical Appraisal Skills Programme (CASP) depending on the type of the study design. Assessment of the risk of bias was done by two reviewers and achieved by answering a pre-specified question of criteria assessed and assigning a judgement relating to the risk of bias as either:
+ Indicates YES (low risk of bias)
? indicates UNKNOWN risk of bias
- Indicates NO (high risk of bias)
All full text articles were then graded based on guidelines from the U.S./Canadian Preventive Services Task Force (Appendix 1).
2.3.4 Data extraction strategy
Data were extracted from the included studies by a reviewer using a pre-designed data extraction form (evidence table as shown in Appendix 4) and checked by another reviewer. Disagreements were resolved by discussion. Details on: (1) methods including study design, (2) study population (3) type of intervention, (4) comparators, (5) outcome measures including effectiveness of PDEP, safety, cost, cost-effectiveness, economic evaluation, organisational and social issues were extracted. Other information on author, journal and publication year, and study objectives were also extracted. The extracted data were presented and discussed with the expert committee.

7
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
2.3.5 Methods of data synthesis
Data on the effectiveness, safety, cost-effectiveness, organisational and social implication of PDEP for advanced CKD patients were presented in tabulated format with narrative summaries. No meta-analysis was conducted for this review.
2.4 RESULTS
2.4.1 Search resultsAn overview of the search is illustrated in Figure 1. A total of 332 records were identified through the Ovid interface: MEDLINE, EBM Reviews-Cochrane Database of Systematic Reviews (2005 to December 2019), EBM Reviews-Cochrane Central Register of Controlled Trials (December 2019), EBM Reviews-Health Technology Assessment (4th Quarter 2016), EBM Reviews-DARE, EBM Reviews-NHS Economic Evaluation Database (1st Quarter 2016) and Embase. Searches were also conducted in PubMed, Horizon Scanning database, INAHTA database, and FDA database. The last search was run on 02 December 2019.
Thirty-nine additional records were identified from references of retrieved studies. After removal of 120 duplicates, a total of 251 records were found to be potentially relevant and were screened using the inclusion and exclusion criteria. Of these, 75 relevant abstracts were retrieved in full text. After reading, appraising and applying the inclusion and exclusion criteria to the 75 full text articles, 16 full text articles were included. A total of 59 full text articles were excluded due to irrelevant study design (n = 17), irrelevant intervention (n = 28) and irrelevant population (n = 14). The excluded articles are listed in Appendix 5.

8
PRE-DIALYSIS EDUCATION PROGRAMME
Number of records identified through
electronic databases searching (n=332)
Number of additional records identified from other sources (n=39)
Number of records after duplicates removed (n=251)
Number of records screened (n=251)
Number of full-text articles assessed
for eligibility (n=75)
Number of full-text articles included in qualitative
synthesis (n=16)
Number of full-text articles excluded
(n=59) with reasons:
- Irrelevant study design (n=17)-Irrelevant intervention(n=28) -Irrelevant population (n=14)
Number of records excluded (n=176)
Figure 1: Flow chart of retrieval of articles used in the results

9
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
2.4.2 Description of the included studies: Sixteen full text articles included in this review comprised of one SR with meta-analysis,
one SR, one RCT, three cohort studies, two retrospective cohort studies, two pre- and post- intervention studies, four cross-sectional studies and two qualitative studies. All studies included were published in English language between 2003 and 2018. Most studies were conducted in Taiwan, United States of America (USA) and Europe. Others were conducted in Brunei, The Netherlands, Turkey, Canada, Philippines and United Kingdom (UK).
Of the 16 included studies, one SR, two cohort studies and one retrospective cohort study were included in the effectiveness section of this review. One RCT, two cohort studies and two retrospective cohort studies covered organisational issues related to hospitalisation; one SR with meta-analysis, one SR, and three cross-sectional studies covered organisational issues related to modality choice; one SR and meta-analysis, two qualitative studies and one pre- and post- intervention study covered societal implications related to patients’ satisfaction, insights and knowledge; and the other one pre- and post- intervention study covered psychological implications. Studies which covered few different sections were mentioned more than once. Two cost- analysis which were conducted alongside RCT and retrospective cohort study were included in the cost-effectiveness section of this review. No retrievable evidence was found on the safety aspects of pre-dialysis education programme for advanced CKD patients.
Description of 16 full-text articles included in qualitative synthesis are presented in Table 2.

10
PRE-DIALYSIS EDUCATION PROGRAMME
Tabl
e 2.
Des
crip
tion
of th
e in
clud
ed s
tudi
es: s
tudy
des
ign,
num
ber o
f pat
ient
s, in
terv
entio
n, c
ompa
rison
, com
pone
nts
of p
rogr
amm
e an
d su
mm
ary
of re
sults
.
Stud
ySt
udy
desi
gnN
umbe
r of
pat
ient
sIn
terv
entio
n &
Com
paris
onC
ompo
nent
s of
pre
-dia
lysi
s ed
ucat
ion
prog
ram
me
Sum
mar
y of
resu
lts
Hsu
CK
et
al. (
2018
)13
-Tai
wan
Coh
ort s
tudy
-f/up
5 y
ears
398
PD p
atie
nts:
169
PDEP
22
9 N
o PD
EP
befo
re s
tarti
ng
PD.
Mul
tidis
cipl
inar
y pr
e-di
alys
is
educ
atio
n (P
DEP
)vs
. Cus
tom
ary
care
(No-
PDEP
)
•Ed
ucat
ion
by m
ultip
le in
divi
dual
se
ssio
ns w
ith te
am m
embe
rs•
Com
pris
ed a
nur
se o
f cas
e m
x, m
edic
al
soci
al o
ffice
rs, d
ietit
ians
, nep
hrol
ogis
ts,
and
HD
&PD
pat
ient
vol
unte
ers
•Kn
owle
dge
on n
utrit
ion,
life
styl
e m
odifi
catio
n, n
ephr
otox
in a
void
ance
, m
edic
atio
ns a
nd g
iven
acc
. to
CKD
st
age
•Pr
epar
atio
n fo
r RRT
, mod
ality
cho
ices
gi
ven
to la
te s
tage
CKD
-PD
EP g
roup
had
sig
nific
antly
:•
less
per
itoni
tis•
low
er p
erito
nitis
-rela
ted
deat
h ra
tes
•lo
nger
med
ian
time
to fi
rst
perit
oniti
s
-No
sign
ifica
nt d
iffer
ence
in n
o. o
f ho
spita
lisat
ion
and
tech
niqu
e fa
ilure
s
Zukm
in K
et
al.14
(201
7)-B
rune
i
Ret
rope
ctiv
e co
hort
stud
y-f/
up 2
yea
rs
350
new
cas
es
of E
SRD
:18
0 PD
EP16
8 N
o PD
EP-M
edia
n eG
FR
4.0
mL/
min
/ 1.7
3 m
2 ,
PDEP
vs. N
o PD
EP•
Educ
atio
n by
mul
tiple
indi
vidu
al s
essi
ons
with
team
mem
bers
•Te
am in
clud
es n
ephr
olog
ists
, tra
ined
nu
rse,
die
titia
ns, a
nd m
edic
al s
ocia
l of
ficer
s•
Stra
tegi
es to
impr
ove
com
plia
nce,
nu
tritio
nal n
eeds
, nep
hrot
oxin
s av
oida
nce,
fast
trac
k va
scul
ar s
ervi
ces
for fi
stul
a, e
arly
RRT
•C
ultu
ral a
ccep
tanc
e an
d re
ligio
us
coun
sellin
g al
so c
over
ed
-PD
EP g
roup
had
sig
nific
antly
:•
bette
r sur
viva
l pro
babi
lity
•de
crea
sed
risk
of d
ying
•hi
gher
1-y
ear s
urvi
val r
ate

11
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Stud
ySt
udy
desi
gnN
umbe
r of
pat
ient
sIn
terv
entio
n &
Com
paris
onC
ompo
nent
s of
pre
-dia
lysi
s ed
ucat
ion
prog
ram
me
Sum
mar
y of
resu
lts
Van
den
Bosc
h J
et
al. (
2015
)11
SR29
stu
dies
:19
qua
si-
expe
rimen
tal
desi
gn10
nar
rativ
e re
view
s
- 19
stud
ies
wer
e an
alys
ed
for e
ffect
ive
com
pone
nts
of
PDEP
PDEP
Des
crip
tions
of t
he e
duca
tiona
l pro
cess
var
ied
and
incl
uded
indi
vidu
al a
nd g
roup
edu
catio
n,
mul
tidis
cipl
inar
y in
terv
entio
n, a
nd v
aryi
ng
dura
tion
and
frequ
ency
of s
essi
ons.
•7
artic
les
desc
ribed
PD
EP c
onsi
sts
of
mul
tiple
edu
catio
n se
ssio
ns b
y 3
or
mor
e he
alth
car
e pr
ofes
sion
als
such
as
neph
rolo
gist
, nur
se, d
ietit
ian,
med
ical
so
cial
offi
cer,
hom
e-di
alys
is c
oord
inat
or,
phar
mac
ist,
tech
nici
an, o
r by
othe
r di
alys
is p
atie
nts
•Ed
ucat
ion
deliv
ery
styl
e ca
n ei
ther
be
one-
on-o
ne s
essi
ons
or c
lass
room
te
achi
ng s
tyle
, but
a m
ix o
f one
-on-
one
and
grou
p se
ssio
ns is
adv
ocat
ed•
eGFR
< 3
0 m
L/m
in (s
tage
4 C
KD) h
as
been
repo
rted
as id
eal f
or re
ferra
l to
CKD
clin
ic
PDEP
gro
up:
•8
stud
ies
repo
rted
bette
r mor
talit
y an
d m
orbi
dity
rate
s in
PD
EP
grou
p •
6/9
stud
ies
repo
rted
high
er
prop
ortio
n of
pat
ient
s se
lect
ing
hom
e di
alys
is (P
D o
r ano
ther
ho
me
mod
ality
)•
4/19
qua
si-e
xper
imen
tal s
tudi
es
repo
rted
high
er le
vels
of
know
ledg
e of
ESR
F an
d R
RT•
Two
stud
ies
repo
rted
on lo
wer
le
ngth
of h
ospi
tal s
tay
Wu
IW e
t al
. (20
09)15
-Tai
wan
Coh
ort s
tudy
f/up
1 ye
ar57
3 C
KD
patie
nts:
-287
PD
EP-2
86 N
o PD
EPC
KD S
tage
3
(27.
4%)
Stag
e 4
(21.
5%)
Stag
e 5
(51.
1%)
PDEP
vs.
cu
stom
ary
care
(N
o PD
EP)
•Ed
ucat
ion
by m
ultip
le in
divi
dual
ses
sion
s w
ith te
am m
embe
rs•
Com
pris
ed a
nur
se fo
r cas
e m
x, m
edic
al
soci
al o
ffice
rs, d
ietit
ians
, HD
and
PD
pa
tient
vol
unte
ers
and
neph
rolo
gist
s•
Indi
vidu
al le
ctur
es o
n re
nal c
are,
nu
tritio
n, li
fest
yle,
nep
hrot
oxin
av
oida
nce,
and
med
icat
ions
dep
endi
ng
on C
KD s
tage
•Pr
epar
atio
n fo
r RRT
, mod
ality
cho
ices
gi
ven
to la
te s
tage
CKD
PDEP
gro
up h
ad s
igni
fican
tly:
•lo
nger
tim
e to
dia
lysi
s•
bette
r blo
od p
rofil
es•
low
er fr
eque
ncy
of te
mpo
rary
va
scul
ar c
athe
ter u
se•
grea
ter p
ost-d
ialy
sis
body
w
eigh
ts•
high
er P
D in
take
•lo
wer
ove
rall
mor
talit
y •
high
er m
edia
n su
rviv
al ti
me
•lo
wer
1-y
ear h
ospi
talis
atio
n ra
te

12
PRE-DIALYSIS EDUCATION PROGRAMME
Stud
ySt
udy
desi
gnN
umbe
r of
pat
ient
sIn
terv
entio
n &
Com
paris
onC
ompo
nent
s of
pre
-dia
lysi
s ed
ucat
ion
prog
ram
me
Sum
mar
y of
resu
lts
Yu Y
J et
al.
(201
4)16
-Tai
wan
RC
T w
ith
cost
-ana
lysi
s44
5 ad
vanc
ed
CKD
pat
ient
s:-2
32 P
DEP
-213
No
PDEP
Mea
n eG
FR 7
.49
± 3.
1 (M
PE) a
nd
7.87
± 3.
6 in
No
PDEP
gro
up
PDEP
vs.
No
PDEP
•Ed
ucat
ion
by m
ultip
le in
divi
dual
lect
ure
sess
ions
with
team
mem
bers
•C
ompr
ised
a n
urse
for c
ase
mx,
med
ical
so
cial
offi
cers
, die
titia
ns, H
D, P
D p
atie
nt
volu
ntee
rs a
nd n
ephr
olog
ists
•Le
ctur
es fo
cuse
d on
nut
ritio
n, li
fest
yle,
ne
phro
toxi
n av
oida
nce,
die
tary
pr
inci
ples
, and
pha
rmac
olog
ical
re
gim
ens
PDEP
gro
up h
ad s
igni
fican
tly:
•fe
wer
and
sho
rter l
engt
hs o
f ho
spita
lisat
ion
•lo
wer
car
diov
ascu
lar
hosp
italis
atio
n in
firs
t 6 m
onth
s po
st d
ialy
sis
•fe
wer
vas
cula
r acc
ess
rela
ted
surg
erie
s•
low
er to
tal m
edic
al c
ost i
n fir
st
6 m
onth
s af
ter H
D in
itiat
ion
and
low
er m
edic
al c
ost o
f inp
atie
nt
serv
ice
Wei
SY
et
al. (
2010
)17
Taiw
an
Ret
rosp
ectiv
e co
hort
stud
y-f/
up 6
m
onth
s be
fore
di
alys
is a
nd
at d
ialy
sis
initi
atio
n
140
inci
dent
ES
RD
:71
PD
EP69
No
PDEP
CKD
Car
e Pr
ogra
mm
e (P
DEP
) vs.
N
ephr
olog
ist
Car
e G
roup
(N
o PD
EP)
•Ed
ucat
ion
by m
ultip
le in
divi
dual
ses
sion
s w
ith te
am m
embe
rs•
Incl
uded
nep
hrol
ogis
ts, r
enal
nur
ses
and
diet
itian
s as
cor
e m
embe
rs o
f tea
m•
Diff
eren
t goa
ls a
nd e
duca
tion
cont
ents
, acc
ordi
ng C
KD s
tage
s an
d pr
e-se
t clin
ical
pro
toco
ls, d
eliv
ered
ap
prox
imat
ely
30–4
5 m
in a
t eac
h vi
sit.
PDEP
gro
up h
ad:
•hi
gher
cre
atio
n of
vas
cula
r ac
cess
bef
ore
dial
ysis
•Lo
wer
hos
pita
lisat
ion
for d
ialy
sis
initi
atio
n•
Mor
e fre
quen
t out
patie
nt v
isits
du
ring
6 m
onth
s be
fore
dia
lysi
s’ bu
t low
er h
ospi
talis
atio
n an
d sh
orte
r len
gth
of s
tay
‘at d
ialy
sis
initi
atio
n’Ye
oh H
H e
t al
. (20
03)18
-USA
Ret
rosp
ectiv
e co
hort
stud
y-f/
up 1
0 da
ys b
efor
e in
itiat
ion
and
90 d
ays
post
di
alys
is
103
patie
nts
with
C
KD:
-68
PDEP
-35
No
PDEP
PDEP
vs.
No
PDEP
•Ed
ucat
ion
by c
lass
es a
cc. t
o C
KD
stag
es:
Kidn
ey C
lass
- mild
to m
oder
ate
CKD
Cho
ices
Cla
ss-m
oder
ate
to s
ever
e C
KD
or a
bout
3 to
6 m
onth
s be
fore
dia
lysi
s•
Afte
r com
plet
ion
of c
lass
es, p
atie
nts
wer
e fo
llow
ed u
p by
team
mem
bers
in
clud
ed n
urse
s, n
ephr
olog
ists
, di
etiti
ans,
med
ical
soc
ial o
ffice
rs, c
ase
man
ager
s, a
nd p
harm
acis
ts
PDEP
gro
up h
ad s
igni
fican
tly:
•lo
wer
use
of t
empo
rary
cat
hete
rs•
low
er A
V gr
aft p
lace
men
t•
high
er P
D c
athe
ter p
lace
men
t•
low
er e
mer
genc
y ro
om v
isits
and
lo
wer
hos
pita
l sta
y
13
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Stud
ySt
udy
desi
gnN
umbe
r of
pat
ient
sIn
terv
entio
n &
Com
paris
onC
ompo
nent
s of
pre
-dia
lysi
s ed
ucat
ion
prog
ram
me
Sum
mar
y of
resu
lts
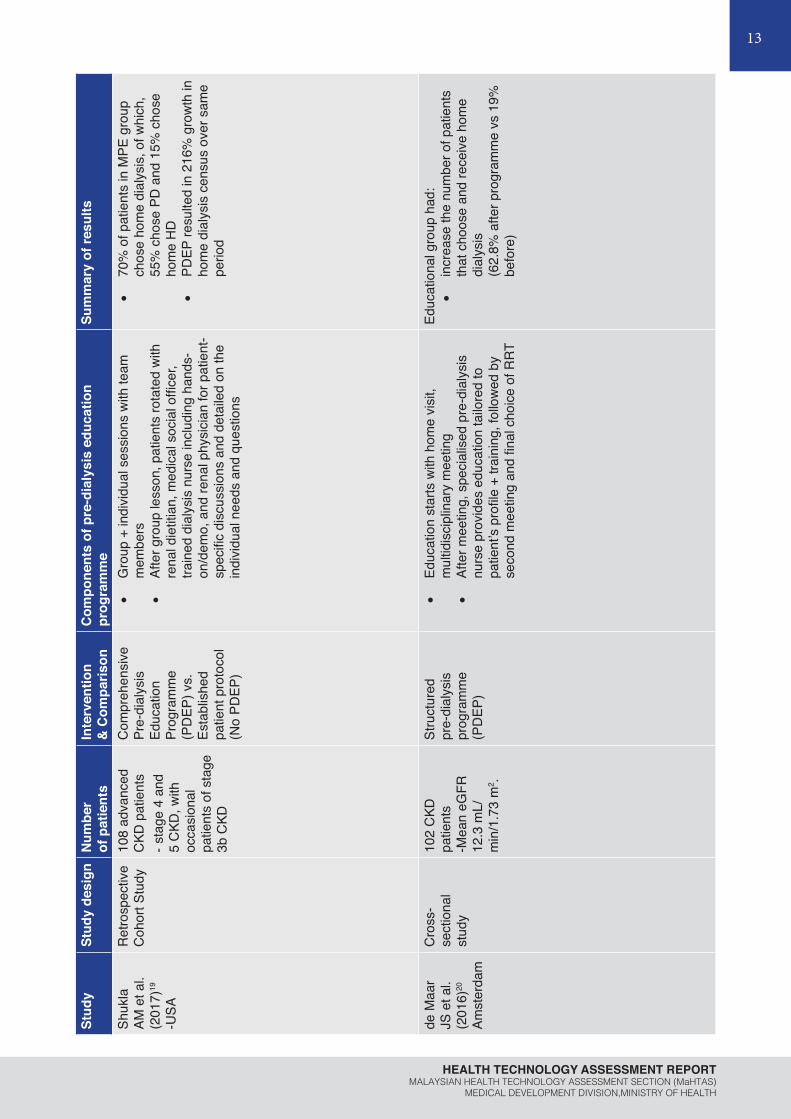
Shuk
la
AM e
t al.
(201
7)19
-USA
Ret
rosp
ectiv
e C
ohor
t Stu
dy10
8 ad
vanc
ed
CKD
pat
ient
s- s
tage
4 a
nd
5 C
KD, w
ith
occa
sion
al
patie
nts
of s
tage
3b
CKD
Com
preh
ensi
ve
Pre-
dial
ysis
Ed
ucat
ion
Prog
ram
me
(PD
EP) v
s.
Esta
blis
hed
patie
nt p
roto
col
(No
PDEP
)
•G
roup
+ in
divi
dual
ses
sion
s w
ith te
am
mem
bers
•Af
ter g
roup
less
on, p
atie
nts
rota
ted
with
re
nal d
ietit
ian,
med
ical
soc
ial o
ffice
r, tra
ined
dia
lysi
s nu
rse
incl
udin
g ha
nds-
on/d
emo,
and
rena
l phy
sici
an fo
r pat
ient
-sp
ecifi
c di
scus
sion
s an
d de
taile
d on
the
indi
vidu
al n
eeds
and
que
stio
ns
•70
% o
f pat
ient
s in
MPE
gro
up
chos
e ho
me
dial
ysis
, of w
hich
, 55
% c
hose
PD
and
15%
cho
se
hom
e H
D
•PD
EP re
sulte
d in
216
% g
row
th in
ho
me
dial
ysis
cen
sus
over
sam
e pe
riod
de M
aar
JS e
t al.
(201
6)20
Amst
erda
m
Cro
ss-
sect
iona
l st
udy
102
CKD
pa
tient
s -M
ean
eGFR
12
.3 m
L/m
in/1
.73
m2 .
Stru
ctur
ed
pre-
dial
ysis
pr
ogra
mm
e (P
DEP
)
•Ed
ucat
ion
star
ts w
ith h
ome
visi
t, m
ultid
isci
plin
ary
mee
ting
•Af
ter m
eetin
g, s
peci
alis
ed p
re-d
ialy
sis
nurs
e pr
ovid
es e
duca
tion
tailo
red
to
patie
nt’s
profi
le +
trai
ning
, fol
low
ed b
y se
cond
mee
ting
and
final
cho
ice
of R
RT
Educ
atio
nal g
roup
had
:•
incr
ease
the
num
ber o
f pat
ient
s th
at c
hoos
e an
d re
ceiv
e ho
me
dial
ysis
(6
2.8%
afte
r pro
gram
me
vs 1
9%
befo
re)

14
PRE-DIALYSIS EDUCATION PROGRAMME
Stud
ySt
udy
desi
gnN
umbe
r of
pat
ient
sIn
terv
entio
n &
Com
paris
onC
ompo
nent
s of
pre
-dia
lysi
s ed
ucat
ion
prog
ram
me
Sum
mar
y of
resu
lts
Cas
sidy
BP
et a
l. (2
018)
21
-Can
ada
Qua
litat
ive
stud
y12
par
ticip
ants
-4
pat
ient
s fro
m
each
dia
lysi
s m
odal
ity
(In-c
entre
HD
, PD
, Hom
e-PD
)
PDEP
•Ed
ucat
ion
by m
ater
ials
and
sm
all g
roup
se
ssio
ns•
Kidn
ey F
ound
atio
n of
Can
ada
bind
er, L
ivin
g w
ith K
idne
y D
isea
se,
4th
editi
on, 4
mul
timod
al s
mal
l gro
up
clas
ses,
pat
ient
par
tner
s, a
nd a
list
of
trust
ed C
KD o
nlin
e re
sour
ces
3 th
emes
influ
ence
d m
odal
ity
deci
sion
-mak
ing
proc
ess:
•
Patie
nt F
acto
rs (i
ndiv
idua
lisat
ion,
au
tono
my,
and
emot
ions
), •
Educ
atio
nal F
acto
rs (t
ailo
red
educ
atio
n, a
ppro
pria
te ti
me/
info
rmat
ion,
and
ava
ilabl
e re
sour
ces)
, •
and
Supp
ort S
yste
ms
(par
tner
ship
with
hea
lth c
are
team
and
fam
ily/fr
iend
s)
Dev
oe
DJ
et a
l. (2
016)
22
- 7 s
tudi
es
from
Nor
th
Amer
ica,
5
from
Eu
rope
, 3
from
Asi
a.
SR +
M
eta-
anal
ysis
15 s
tudi
es
incl
uded
:-7
pre
and
pos
t in
terv
entio
n st
udie
s,
-5 c
ohor
t stu
dies
-2 c
ase-
cont
rol
stud
ies
-1 R
CT
-Mea
n eG
FR
rang
ed fr
om
≤15
to 2
0.4
ml/
min
/1.7
3 m
2
Pre-
dial
ysis
ed
ucat
iona
l in
terv
entio
ns
(PD
EP)
vs. S
tand
ard
care
(No
PDEP
)
Vary
gre
atly
bet
wee
n st
udie
s•
7 st
udie
s in
clud
ed p
hysi
cian
as
an
educ
ator
, 10
incl
uded
a n
urse
, and
4
incl
uded
mul
tidis
cipl
inar
y te
am•
8 st
udie
s ca
rried
out
edu
catio
nal
inte
rven
tions
in g
roup
ses
sion
s, 5
had
1
to 1
ses
sion
onl
y an
d 2
incl
uded
bot
h
Educ
atio
nal g
roup
had
:•
incr
ease
in th
e od
ds o
f cho
osin
g PD
(2-4
x)•
3-fo
ld in
crea
se in
odd
s of
re
ceiv
ing
PD a
s th
e in
itial
tre
atm
ent m
odal
ity

15
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Stud
ySt
udy
desi
gnN
umbe
r of
pat
ient
sIn
terv
entio
n &
Com
paris
onC
ompo
nent
s of
pre
-dia
lysi
s ed
ucat
ion
prog
ram
me
Sum
mar
y of
resu
lts
Prie
to-
Vela
sco
M e
t al.
(201
4)23
-9 re
nal
units
; 6 E
U
coun
tries
-2 u
nits
ea
ch in
UK,
Sw
eden
, Sp
ain
-3 u
nits
in
Fran
ce,
Belg
ium
, Ita
ly
Cro
ss-
sect
iona
l st
udy
4 nu
rses
, 5
neph
rolo
gist
s an
d 1
clin
ical
ps
ycho
logi
st
com
plet
ed
ques
tionn
aire
s ab
out t
heir
rena
l un
it
Ren
al
repl
acem
ent
ther
apy
optio
n ed
ucat
ion
(PD
EP)
•Fe
w h
ave
grou
p ed
ucat
ion
sess
ions
, m
ostly
indi
vidu
al s
essi
ons
•N
urse
s al
way
s in
volv
ed, w
ith
neph
rolo
gist
, die
titia
ns, p
sych
olog
ists
, m
edic
al s
ocia
l offi
cers
, onl
y 1
has
occu
patio
nal t
hera
py, p
hysi
o, p
harm
acis
t•
All h
ad b
ackg
roun
d in
gen
eral
or
neph
rolo
gy n
ursi
ng•
All i
nclu
des
patie
nts
with
CKD
sta
ge 4
or
5, a
nd fa
mily
mem
bers
•Ke
y to
pics
suc
h as
the
‘impa
ct o
f the
di
seas
e’ w
ere
cove
red
by e
very
uni
t, bu
t on
ly a
few
uni
ts d
escr
ibed
all
dial
ysis
m
odal
ities
•M
ost h
ave
visi
ts to
HD
, hom
e di
alys
is
Sam
e as
in c
ompo
nent
s of
pro
gram
me
Dan
guila
n R
A e
t al.
(201
3)24
Philip
pine
s
Pre-
and
pos
t-in
terv
entio
n st
udy
-f/up
6
mon
ths
299
CKD
pa
tient
s:60
% C
KD S
tage
5
and
19%
Sta
ge
4
PDEP
•Ed
ucat
ion
by m
ultip
le in
divi
dual
ses
sion
s w
ith te
am m
embe
rs•
Trai
ned
CKD
edu
cato
rs, a
nur
se a
nd
a ps
ycho
logi
st, c
ondu
cted
stru
ctur
ed
educ
atio
nal m
odul
es a
ccor
ding
to C
KD
stag
e•
Take
-hom
e m
ater
ials
afte
r eac
h vi
sit
Afte
r PD
EP:
•Si
gnifi
cant
incr
ease
in m
ean
over
all p
re-te
st s
core
s of
CKD
kn
owle
dge
(onl
y 28
% p
atie
nts
com
plet
ed th
e m
odul
es)

16
PRE-DIALYSIS EDUCATION PROGRAMME
Stud
ySt
udy
desi
gnN
umbe
r of
pat
ient
sIn
terv
entio
n &
Com
paris
onC
ompo
nent
s of
pre
-dia
lysi
s ed
ucat
ion
prog
ram
me
Sum
mar
y of
resu
lts
Gar
cía-
Llan
a H
et
al. (
2014
)25
Spai
n
Pre-
and
pos
t- in
terv
entio
n st
udy
-f/up
6
mon
ths
42 C
KD p
atie
nts
Mea
n eG
FR
<20m
L/m
in/1
.73
m2
PDEP
•Ed
ucat
ion
by m
ultip
le in
divi
dual
ses
sion
s•
Patie
nt a
ttend
ed re
gula
r app
t with
ne
phro
logi
st, n
urse
and
nut
ritio
nist
•
Each
pat
ient
rece
ived
6 in
divi
dual
m
onth
ly fa
ce-to
-face
ses
sion
s w
ith
heal
th p
sych
olog
ist
Afte
r PD
EP:
•si
gnifi
cant
ly h
ighe
r lev
els
of
adhe
renc
e, lo
wer
dep
ress
ion
and
anxi
ety
leve
ls, a
nd b
ette
r H
RQ
L (i.
e., g
ener
al h
ealth
and
em
otio
nal r
ole
dom
ains
).
Can
kaya
E
et a
l. (2
013)
26
Turk
ey
Cro
ss-
sect
iona
l st
udy
88 li
ve d
onor
ki
dney
tran
spla
nt
reci
pien
ts:
-61
PDEP
-2
7 no
PD
EP
Pre-
dial
ysis
ed
ucat
ion
prog
ram
me
(PD
EP)
vs. N
o PD
EP
•Ed
ucat
ion
usin
g tra
inin
g ki
t•
Spec
ially
pre
pare
d ki
t usi
ng v
isua
ls
and
writ
ten
card
s w
ith 6
mod
ules
giv
en
acco
rdin
g to
CKD
sta
ges
PDEP
gro
up h
ad s
igni
fican
tly:
•H
ighe
r pre
-em
ptiv
e ki
dney
tra
nspl
anta
tion
rate
s co
mpa
red
to
no-P
DEP
gro
up(4
2.6%
vs
18.5
%, P
<0.0
01)
•H
ighe
r don
or tr
ansp
lant
atio
n ra
tes
from
spo
use,
sib
lings
and
ot
her r
elat
ives
C
ombe
s G
et a
l. (2
017)
12
UK
Qua
litat
ive
stud
ySe
mi-s
truct
ured
in
terv
iew
s in
4
hosp
itals
with
96
sta
ff an
d 93
di
alys
is p
atie
nts
PDEP
•Ed
ucat
ion
by o
ne to
one
ses
sion
s +
grou
p se
ssio
ns in
clud
ing
talk
s fro
m
patie
nts
on R
RT
+ w
ritte
n m
ater
ials
/DVD
s to
take
hom
e•
Hom
e vi
sits
by
nurs
e in
sev
eral
site
s
•M
ost p
atie
nts
repo
rted
PDEP
ov
eral
l hel
pful
•3
them
es re
late
d to
impr
ovin
g PD
E id
entifi
ed:
-sub
-opt
imal
edu
catio
n;
-diff
eren
t per
spec
tives
bet
wee
n pa
tient
s an
d st
aff;
-influ
ence
of p
atie
nt e
xper
ienc
e
Foot
note
: AV=
Art
erio
veno
us, C
KD
= C
hron
ic K
idne
y D
isea
se, E
SRD
=End
Sta
ge R
enal
Dis
ease
, eG
FR=
estim
ated
Glo
mer
ular
Filt
ratio
n R
ate,
H
D=H
aem
odia
lysi
s, P
D=P
erito
neal
Dia
lysi
s, P
DEP
=Pre
-dia
lysi
s Ed
ucat
ion
Prog
ram
me,
RR
T=R
enal
Rep
lace
men
t The
rapy
, SR
= Sy
stem
atic
R
evie
w, R
CT=
Ran
dom
ised
Con
trol
led
Tria
l, H
RQ
L=H
ealth
Rel
ated
Qua
lity
of L
ife

17
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
2.4.3 Risk of bias assessment:
Assessment for Systematic Review Studies Using Critical Appraisal Skills Programme (CASP) Checklist Figure 2 shows the summary of the risk of bias of the two included studies based on the Critical Appraisal Skill Programme (CASP) checklist. Both studies were overall at low risk of bias at all domain assessed. For Devoe DJ et al. (2016), meta-analysis was done on four observational studies on association of pre-dialysis educational interventions with the odds of choosing PD and the odds of receiving PD and reported heterogeneity of I2=76.7% and I2=24.9%, respectively.22
Criteria assessed
Aut
hors
look
for t
he ri
ght t
ype
of
pap
ers?
Sele
ctio
n of
stu
dies
(all
rele
vant
stu
dies
in
clud
ed?)
Asse
ssm
ent o
f qua
lity
of in
clud
ed
stud
ies?
If th
e re
sults
of t
he re
view
hav
e be
en
com
bine
d, is
it re
ason
able
to d
o so
(h
eter
ogen
eity
)?
Van den Bosch J et al. (2015)11 + + + ?Devoe DJ et al. (2016)22 + + + +
+ Indicates low risk of bias
? indicates unclear risk of bias
- Indicates high risk of bias
Figure 2: Assessment of risk of bias of SR
Randomised controlled trialsCochrane Risk of Bias Assessment tool was used to assess the risk of bias of the RCT includedin this review. The summary risk of bias assessment of the RCTs is shown in Figure 3.
Criteria assessed
Adeq
uate
seq
uenc
e ge
nera
tion
(sel
ectio
n bi
as)
Allo
catio
n co
ncea
lmen
t (s
elec
tion
bias
)
Blin
ding
of p
artic
ipan
ts a
nd
pers
onne
l (pe
rform
ance
bia
s)
Inco
mpl
ete
outc
ome
data
ad
dres
sed
(attr
ition
bia
s)
Sele
ctiv
e re
porti
ng (r
epor
ting
bias
)
Free
of o
ther
bia
s
Yu YJ et al. (2014)16 + ? ? + + +

18
PRE-DIALYSIS EDUCATION PROGRAMME
+ Indicates low risk of bias
? indicates unclear risk of bias
- Indicates high risk of bias
Figure 3: Assessment of risk of bias of RCT
Yu Y et al. (2014) did not mention the detail of blinding as well as allocation concealment method and thus was classified as unclear risk of bias.16
Assessment Using NIH Quality Assessment Tool For Before-After (Pre-Post) Studies With No Control Group The risk of bias for Pre-Post studies with no control group was assessed using NIH Quality Assessment Tool. Two studies were included in this assessment. Figure 4. shows the summary of the risk of bias for the studies. Both studies have high risk of bias. Danguilan R A et al. (2013) had two high risk criteria which were loss to follow up more than 20% and the study did not use interrupted time series design.24 García-Llana H et al. (2014) had three high risk criteria which included small sample size, the study did not use interrupted time series design and did not take individual level data to determine effects at group level.25
CRITERIA ASSESSED Dan
guila
n R
A
et a
l. (2
013)
24
Gar
cía-
Llan
a H
et
al.
(201
4)25
Question or objective clearly stated? + +Eligibility/selection criteria for study population clearly described? + +Were participants representative for those who would be eligible for the test/ service/intervention in the population of interest?
+ +Were all eligible participants that met the pre-specified entry criteria enrolled? + +Sample size sufficiently large to provide confidence in findings? + -Test/service/intervention clearly described and delivered consistently? + +Outcome measures pre-specified, valid, reliable, and assessed consistently? + +People assessing the outcome measures blinded to participants exposure/ interventions?
NA NA
Loss to follow-up after baseline 20% or less? Loss to follow-up accounted for in the analysis?
- +Statistical methods examine changes in outcome measures from before to after intervention? P value?
+ +Outcome measures taken multiple times before and after intervention? Use interrupted time-series design?
- -

19
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
If intervention conducted at group Level, did statistical analysis take into account of individual Level data to determine effects at group Level?
+ -
+ Indicates low risk of bias
? indicates unclear risk of bias
- Indicates high risk of bias
Figure 4: Assessment of risk of bias of (Pre-Post) Studies with No Control Group
2.4.4 EFFECTIVENESS Four studies reported on effectiveness of PDEP for advanced CKD patients, of which one
was SR, two cohort studies and one retrospective cohort study.
2.4.4.1 Peritonitis and peritonitis-related death Hsu CK et al. (2018) conducted a cohort study in PD patients in Taiwan to investigate the
impact of PDEP on the occurrence of peritonitis, time to first episode of peritonitis and patient outcomes. The study involved 398 patients starting PD at Chang Gung Memorial Hospital, Keelung, Taiwan. Patients were divided into PDEP group (n = 169) and no- PDEP group (n = 229) according to whether the subjects had ever received PDEP before starting RRT. Pre-dialysis education programme (PDEP) recipients were older (63.1±16.2 vs. 58.5±16.4 years old, P = 0.006), were less likely to be man (39.1% vs. 52%, P = 0.01) but had higher prevalence of diabetes (60.4% vs. 43.7%, P< 0.001) compared to the no-PDEP recipients. The PDEP group also had lower baseline educational levels (P < 0.001) and were more likely to use automated PD than patients of no-PDEP group (49.7% vs. 39.7%, P = 0.05). Pre-dialysis education programme (PDEP) was described in the study as education given by a team which comprised of a nurse of case management, medical social officers, dietitians, 10 nephrologists, and HD and PD patient volunteers. The programme included multiple individual sessions on nutrition supplement, lifestyle modification, nephrotoxin avoidance, dietary principles and pharmacological regimens by case-management nurse, according to their CKD stage by National Kidney Foundation Dialysis Outcomes Quality Initiative (NKF/DOQI) guidelines. Monitoring of CKD complications, preparation for timely initiation of RRT, care of vascular or peritoneal access, and registration for inclusion in the renal transplant waiting list were also instructed for late stage CKD patients. Different modality of RRT as well as their benefit, disadvantage and self-care knowledge were explained. Shared decision making was performed for these patients for their choice of renal replacement modality selection. All patients also received dietary counseling biannually from a dietitian. The programme was discontinued once the patients initiate dialysis therapy. Meanwhile, patients in the no-PDEP group received customary care from the same group of nephrologists, who instructed patients regarding the renal function, evaluation of laboratory data and the clinical indicators of renal failure as well as treatment strategies. Writing materials or booklets were given to patients if needed. All patients were subsequently followed up for five years. Incidences of peritonitis and peritonitis-related mortality were compared between the two groups.13 Level II-2
The results showed that after five years of follow-up, the PDEP patients had significantly less peritonitis [0.29±0.72 vs. 0.64±1.5 episodes/person-year or median (Interquartile range, IQR): 0 (0.29) vs. 0.11 (0.69) episodes/person-year, P < 0.001] than no-PDEP patients. The PDEP group had lower peritonitis-related death rates compared to no-PDEP group (3.6% vs. 8.7%, P = 0.04). Patients in the PDEP group had longer median time to first episode of

20
PRE-DIALYSIS EDUCATION PROGRAMME
peritonitis compared the no-PDEP group (46.7 months vs. 33.9 months, P = 0.003). Cox regression analysis revealed that the educational level below elementary [hazard ratio (HR): 1.925; 95% (CI): 1.257, 2.874, P = 0.003] and the use of PDEP (HR: 0.594; 95% CI: 0.434, 0.813, P < 0.001) were significant independent predictors for peritonitis-free survival, after adjusting the baseline characteristics of age, gender, diabetes, hypertension and peritoneal modalities. The authors concluded that an efficient standardised PDEP adhered to the NKF/DOQI guidelines may prolong the time to the first episode of peritonitis and reduce peritonitis rate, independent of age, gender, diabetes, hypertension, educational status and PD modality. Subsequently, decreased peritonitis-related death. The findings provided basis for strategic implementation of PDEP as an efficient method to improve dismal outcome of PD patients.13
Level II-2
2.4.4.2 Survival rate Zukmin K et al. (2017) conducted a retrospective cohort study in Brunei to compare survival probability, sociodemographic, and clinical characteristics of multidisciplinary pre-dialysis educated (PDEP) and no-PDEP/crashlander patients. A total of 350 new cases of ESRD from Raja Isteri Pengiran Anak Saleha Hospital and all dialysis centers in Brunei Darussalam were included in the study. Data were extracted from the computerised clinical registry and patients’ dialysis records. Data extracted included sociodemographic information, clinical information, survival status, pre-dialysis clinic referral, choice of RRT, and types of vascular access (for HD patients). Patients were divided into PDEP group (n = 180) and no-PDEP group (n = 168) according to whether the subjects had ever received PDEP before starting RRT. The PDEP groups were more likely to be older (P = 0.001), diabetics (P = 0.013), and hypertensive (P = 0.016), have ischemic heart disease (P = 0.014), and to be using arteriovenous fistula (P < 0.001). Pre-dialysis education programme (PDEP) was provided in the settings by a multidisciplinary team of professionals which included nephrologists, nurse practitioners, dieticians, and medical social officers. Nurse practitioners comprise specific nurses that specialize in vascular access, HD, PD and transplantation. Geriatricians and palliative care team occasionally involved if patients have pre-emptively decided not to undergo RRT. Clinics were focused on strategies to maintain target blood pressure, improve compliance with medications, nutritional needs, nephrotoxins avoidance, and fast track vascular services for fistula formations and early commencement of RRT. Cultural acceptance and religious counselling were also covered in the clinic to overcome social stigmatisation and improve psychological acceptance. Survival probability, sociodemographic, and clinical characteristics of PDEP and no-PDEP/crashlander patients were compared. The results showed that despite being older and having more comorbidities, PDEP patients have better survival probability (P = 0.028) and a 34% decreased risk of dying. The one-year survival rate was higher in the PDEP group compared to no-PDEP group (79.8% vs. 66.2%, respectively). No significant difference reported for survival rates after two years (57.7% and 60.1%, respectively). The authors concluded that PDEP before the initiation of RRT contributed to greater survival probability in near ESRD patients. The survival benefits were evident despite the presence of inherent risks (older age and presence of comorbidities) in the PDEP population in comparison with the no-PDEP group.14 Level II-2
2.4.4.3 Morbidity and mortality A systematic review was conducted by Van den Bosch J et al. (2015) to review evidence on effective components of PDEP as related to modality choice and selected clinical outcomes. Systematic search was performed on PubMed MEDLINE, Cochrane Library, and Ovid (from January 1, 1995 to December 31, 2013) for studies done on pre-dialysis education programme. Literature also reviewed for any information on processes, pathways, and organisation of the pre-dialysis education programme. The review included 29 relevant studies which consisted of 19 quasi-experimental design and 10 narrative reviews. Nineteen studies were analysed for effective components of PDEP. Descriptions of the educational process varied and included individual and group education, multidisciplinary intervention, and varying duration and frequency of sessions. The review found that there were eight

21
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
studies reported on mortality and morbidity including biochemical indicators, cardiovascular incidents, infection rates, emotional status (Table 3). All studies reported better rates for the group that received pre-dialysis education.11 Level I
Table 3: Studies which reported on mortality and morbidity
Studies Results
Cho et al. (2012)Less unplanned urgent dialysis (8.7% vs 24.2%),
Less cardiac events (2.7% vs 9.4%), less infections (4.0% vs 12.1%)
Klang et al. (1998) Significant better mood, less mobility problems, less functional disabilities and lower anxiety
Lacson et al. (2011) Significant better survival rate (adj. HR 0.61)
Levin et al. (1997) Better biochemical markers: blood pressure, calcium, phosphate, and anemia
Rioux et al. (2011) 35% of all acute starters adopted home dialysis vs 13% before program
Hall G et al (2004) Less infection rates 18.5 vs. 31.8; (p = 0.00349)
Souqiyyeh M Z et al. (2008) Significantly less dropouts for PD (p < 0.02)
Wu IW et al. (2009) conducted a cohort study in Taiwan to evaluate the impact of PDEP on the incidence of dialysis and outcomes of CKD patients in accordance with the guidelines of the National Kidney Foundation Dialysis Outcomes Quality Initiative (NKF/DOQI). The study involved 573 pre-dialysis CKD patients who visited the nephrology outpatient clinics of the Department of Nephrology at Chang Gung Memorial Hospital in Taipei and Keelung from May 2006 to May 2007. Patients were classified into stages 3, 4 or 5 in accordance with the NKF/DOQI classification system. All patients were divided into two cohorts according to the sites; PDEP group at the Keelung centre (n = 287) and no-PDEP group at Taipei centre (n = 286). Pre-dialysis education programme (PDEP) were described given in multiple individual sessions with team members which comprised of a nurse for case mx, medical social officers, dietitians, HD and PD patient volunteers and 10 nephrologists. Programme consisted of integrated course involving individual lectures on renal health, delivered by case-management nurse that focused on nutrition, lifestyle, nephrotoxin avoidance, dietary principles and pharmacological regimens. Standardised interactive educational sessions were conducted intermittently where all patients were interviewed depending on the CKD stage. For stage 3 CKD patients, programme consisted of lectures on healthy renal function, clinical presentation of uraemia, risk factors and complications associated with renal progression and an introduction to the various RRTs. For stage 4 CKD patients, programme included discussions on the management of complications associated with CKD, indications of RRT and evaluation of vascular or peritoneal access. For stage 5 CKD patients, programme included monitoring for timely initiation of RRT, care of vascular or peritoneal access, dialysis-associated complications and registration for inclusion in the renal transplant waiting list. Patients in Stage 3 or 4 CKD were followed-up three-monthly while patients in stage 5 CKD were followed-up monthly. In contrast, patients in customary care group (no-PDEP) were attended by same group of nephrologists who instructed patients regarding renal function, evaluation of laboratory data and clinical indicators of chronic renal failure as well as strategies for its management and treatment. General principles of HD and PD explained when patients enter stage 4 CKD and patients were provided with written instructions. Patients from both

22
PRE-DIALYSIS EDUCATION PROGRAMME
groups were followed up for 12 months for dialysis initiation or mortality from any cause.15 Level
II-2
The study showed that dialysis was initiated in 13.9% of patients in the PDEP group and 43% of the patients in the no-PDEP group, (P < 0.001). Time to dialysis was significantly longer for PDEP group (11.3 months) compared to no-PDEP group (9.2 months) (P < 0.001). Patients in the PDEP group showed better blood profiles [higher serum albumin level (3.8 ± 0.5 vs. 3.4 ± 0.5 g/dL), P = 0.050; lower serum high-sensitive C-reactive protein (hs-CRP) level (3.3±2.8 vs. 5.5±5.6 mg/L), P = 0.032; lower serum ferritin concentration (284 ± 31 vs. 532 ± 59 ng/mL), P = 0.049], higher PD uptake (35% vs. 20.5%, P = 0.023), lower frequency of temporary vascular catheter use (25% vs. 50.4%; P < 0.05) and greater post-dialysis body weights (65±10 vs. 58±11 kg, P = 0.034) than the no-PDEP patients. Overall mortality was reported lower for the PDEP group than the no-PDEP group (1.7% vs.10.1%, P < 0.001). Patients in the PDEP group had higher median survival time compared to the no-PDEP group (11.9 months vs. 11.2 months, P < 0.001). Adjusted hazard ratio (HR) of mortality for PDEP recipients was 0.103 [95% confidential interval (CI) 0.040, 0.265, P < 0.001], after adjustment for age, gender, diabetes, hypertension, eGFR, Hb, serum albumin and hs-CRP. Cox regression analysis revealed that diabetes, eGFR, hs-CRP level and PDEP assignment were significant independent predictors for progression to ESRD. Independent prognostic factors for mortality included age, diabetes, eGFR, hs-CRP and PDEP assignment. The authors concluded that efficient standardised PDEP complying with the NKF/DOQI guidelines may decrease the incidence of dialysis and reduce the all-cause mortality and the overall hospitalisation rate in CKD patients. This valuable information confirms the role of PDEP in the care of CKD patients.15 Level II-2
2.4.5 SAFETY There was no retrievable evidence in the scientific databases on the safety of PDEP for
advanced CKD patients.
2.4.6 ORGANISATIONAL 2.4.6.1 Hospitalisation and length of stay There were one SR, one RCT, two cohort studies, and two retrospective cohort studies which
reported on hospitalisation and length of stay.
In the cohort study which was conducted by Hsu CK et al. (2018), investigating the impact of PDEP on PD patients in Taiwan, reported that after five years of follow-up, there was no significant difference between patients in PDEP group and no-PDEP group in frequency of hospitalisation [median (IQR), episodes/person-year : 1.36 (2.43) in PDEP group vs. 1.15 (2.04) in no-PDEP group, P = 0.66] and the percentage of technique failures requiring shifting of modality to HD [due to either peritonitis; 9.5% in PDEP group vs. 11.8% in no-PDEP group, or poor fluid management; 1.8% in PDEP group vs. 2.2% in no-PDEP group].13 Level II-2
The SR by Van den Bosch J et al. (2015) which examined the evidence on the effective components of PDEP, reported that there were two quasi-experimental studies mentioned on length of hospital stay, which was lower for the education groups (6.5 vs. 13.5 total hospital days; 2.2 vs. 5.1 hospital days/patient per year).11 Level I
Yu YJ et al. (2014) conducted an RCT in Taiwan involving 445 advanced CKD patients who were randomly assigned to PDEP group (n = 232) and no-PDEP group (n = 213). Pre-dialysis education programme (PDEP) in this setting consisted of an integrated course involving individual lectures on renal health, delivered by the case-management nurse. The individual lectures focused on nutrition, lifestyle, nephrotoxin avoidance, dietary principles, and pharmacological regimens. The programme team involved a nurse for case management, medical social officers, dietitians, HD and PD patient volunteers and 10 nephrologists.

23
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Standardised interactive educational sessions were periodically conducted wherein all patients were interviewed depending on their CKD stage, determined earlier by using the NKF/DOQI guideline. Stage 3 or 4 CKD patients were followed up every three months, and stage 5 CKD patients were followed up on a monthly basis. For stage 4 CKD patients, the programme included discussions on the management of complications associated with CKD, indications of RRT, and the evaluation of vascular or peritoneal access. For stage 5 CKD, patients were monitored for timely initiation of RRT, the care of vascular or peritoneal access, dialysis-associated complications, and registration for inclusion in the renal transplantation waiting list. All patients received dietary counselling biannually from a dietitian. In addition, case-management nurse often contacted the participants by telephone to encourage them to inform their nephrologists of their symptoms and to reinforce the importance of medical visits. The programme was discontinued once RRTs were initiated. On the other hand, patients in the no-PDEP group were attended by same group of nephrologists who instructed patients regarding renal function, evaluation of laboratory data and clinical indicators of chronic renal failure as well as strategies for its management and treatment. General principles of HD and PD explained when patients enter stage 4 CKD and patients were provided with written instructions.16 Level II-1
The study reported that PDEP patients had significantly fewer and shorter lengths of hospitalisation than the no-PDEP patients (median (IQR) 0 (15) vs. 8 (27) days, P<0.001). Eighty-eight (37.9%) patients in the PDEP group had at least one hospitalisation, compared with 127 patients (59.6%) in the no-PDEP group (P<0.001). Cardiovascular disease (including uncontrolled hypertension, coronary artery disease, stroke, heart failure, and peripheral artery occlusive disease) was the main cause of first hospitalisation in all patients. The PDEP patients had lower cardiovascular hospitalisation in the first six months post dialysis (18.53% vs. 29.58%, P=0.007) and fewer vascular access related surgeries during the first admission (15.09% vs. 25.82%, P=0.005) compared to the no-PDEP patients.16 Level II-1
Wei SY et al. (2010) conducted a retrospective cohort study involving 140 incident ESRD patients who started HD from August 2004 to July 2005 from the two study hospitals in Taiwan to evaluate the effectiveness of CKD care programme (PDEP) on pre-ESRD care. Patients were divided into two groups; CKD group who received PDEP for at least six months before initiation of HD (n=71) and ‘Nephrologist Care Group’ (no-PDEP) who were cared for by nephrologists alone for at least six months before initiation of dialysis (n=69). The PDEP included nephrologists, renal nurses and dietitians as the core members of a multidisciplinary team responsible in caring for patients at different CKD stages. Patients were invited to join the care program by the nephrologist and were referred to well-trained renal nurses and dieticians. Different goals and education contents were planned according to stages of CKD and pre-set clinical protocols, and were delivered systematically approximately 30 to 45 minutes at each visit. Every patient received follow-up visits with clinical evaluation, laboratory examinations, nursing and dietary education, which was taken every three months for CKD stages 3 and 4, and every one to two months for stage 5 CKD patients. Main goals of the programme included delaying the deterioration of renal function, early preparations for dialysis, reducing of risk of complications, and ensuring smooth and safe transition to RRT. In contrast, “Nephrologist Care Group” were all treated by nephrologists from the same department, but they did not receive nursing education and dietary counselling by CKD nurses and dieticians. Principle of CKD care, including medications and early preparation of vascular access were routinely delivered to patients by the nephrologists. Patients were followed-up six months before dialysis and at dialysis initiation. Dialysis initiation was the end-point of observation. Quality indicators for evaluation included status of recombinant human erythropoietin (rHuEPO) treatment, vascular access preparation and hospitalisation for initiation of dialysis, were compared between two groups.17 Level II-2

24
PRE-DIALYSIS EDUCATION PROGRAMME
The study found that PDEP group had higher creation of vascular access before dialysis. Vascular access had been created before HD in 57.7% of patients in the PDEP Group vs. only 37.7% of the no-PDEP group (P=0.017). Percentage of patients who started HD with created vascular access without the insertion of double lumen catheter was 50.7% PDEP, vs. 29.0% in the no-PDEP group (P=0.009). Percentage of patients who were not hospitalised for initiation of HD was 40.8% in PDEP group, vs. 18.8% in the no-PDEP group (P<0.005). Most patients in no-PDEP group (81.2%) had their first HD through inpatient HD. In terms of frequency of services utilisation, the PDEP group had more frequent outpatient visits during six months before dialysis ((9.9 ± 5.5 vs 5.5 ± 5.5 times/patient, P<0.001), but lower percentage of hospitalisation at dialysis initiation (59.2% vs 81.2%, P= 0.005), and shorter length of stay (6.6days ± 16.2 vs. 16.2days ± 16.2, P <0.001) compared to the no-PDEP group.17 Level II-2
In another cohort study which was conducted by Wu IW et al. (2009) in Taiwan, reported that the one-year hospitalisation rate was lower in the PDEP patients than in the no-PDEP patients (2.8% vs. 16.4%, P=0.034). However, the reason for hospitalisation did not differ significantly between them.15 Level II-2
Yeoh HH et al, (2003) conducted a retrospective cohort study in the United States of America (USA), to compare patients who had PDEP with those who did not due to late referral or refusal to participate, in terms of hospitalisations, emergency room visits and dialysis access placement. The charts of 103 CKD patients who were seen in clinic from 1997 to 2000 were retrospectively reviewed. Data on 68 patients who elected to participate in the pre-dialysis classes and 35 patients who decided not to participate in the classes in spite of encouragement to do so or were referred late and required immediate dialysis were reviewed. The PDEP team who were involved in the delivery of education and care of patients consisted of nurses, nephrologists, dietitians, medical social officers, case managers, and pharmacists. The programme comprised of two separate classes given according to the CKD stages; Kidney Class for patients mild to moderate renal impairment and Choices Class for patients with moderate to severe renal disease or about three to six months before dialysis will be needed. The Kidney Class covered general information about kidney disease, causes of renal failure, and its manifestation. The Choices Class covered options in RRT including HD, PD and renal transplantation. Once the patients attended the classes, they were followed-up by all the members of the team regularly. Data from period beginning 10 days before the initiation of dialysis to 90 days after the first dialysis, for a total period of 100 days was obtained. This period captures hospitalisation for initiation of dialysis. Data for each variable were compared for patients who attended the pre-dialysis class and those who did not. The results showed that compared to the group without PDEP, PDEP group had lower percentage of use of temporary catheters (4.4% vs. 37%, P < 0.001), lower incidence of AV graft placement (18% vs. 51%, P < 0.001) and higher incidence of PD catheter placement (31% vs. 11.4%, P = 0.03). Patients in the PDEP group had lower emergency room visits (0.57 vs. 1.1 per patient, P = 0.035) and lower average length of hospital stay per patient (1.4 days vs. 9.9 days per patient, P < 0.001) than those in no-PDEP group.18 Level II-2
2.4.6.2 Components of programme There was substantial variation noted in various PDEP described in the included studies.
Summary of the components of PDEP in each study which was included in this review were tabulated in Table 2.
Multidisciplinary team
Most studies [Hsu CK et al. (2018), Zukmin K et al. (2017), Wu IW et al. (2009), Yeoh HH et al. (2003), Yu YJ et al. (2014), Shukla AM et al. (2017), de Maar JS et al. (2016), Cassidy BP et al. (2018)] mentioned the involvement of multidisciplinary team in their PDEP. The team

25
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
almost always comprised of nephrologists, nurses, dietitians, and medical social officers. Few had clinical psychologist, pharmacist, and patient volunteers.13 Level II-2, 14 Level II-2, 15 Level II-2, 16
Level II-1, 17 Level II-2, 19 Level II-2, 20 Level II-3, 21
A systematic review and meta-analysis was conducted by Devoe DJ et al. (2016) to examine the relationship between patient-targeted educational interventions and choosing and receiving PD. Fifteen studies of educational interventions designed to increase PD selection were included in the review which consisted of: seven pre- and post- intervention studies, five cohort studies, two case-control studies and one RCT. Of 15 studies, two were excluded from meta-analysis due to missing information. Seven studies from North America, five from Europe and three from Asia. Number of participants ranged from 63 to 21,302 for a total of 31,653. Mean eGFR ranged from ≤15 to 20.4 ml/min/1.73 m2. There was great variation of the educational interventions between the studies. Seven studies included physician as an educator, 10 included a nurse, and four included multidisciplinary team. Four studies included family members in educational interventions.22 Level I
In the systematic review done by Van den Bosch J et al. (2015), the studies included addressed components of PDEP established. Seven articles retrieved from the scientific literature review described PDEP which consisted of multiple education sessions where patients were educated by three or more health care professionals such as nephrologist, nurse, dietitian, medical social officer, home-dialysis coordinator, pharmacist, technician, or by other dialysis patients.11 Level I
Prieto-Velasco M et al. (2014) conducted a cross-sectional study to assess on how is RRT option education being run in European Union (EU) countries. Experts comprised of four nurses, five nephrologists and one clinical psychologist from nine renal units; two units each in UK, Sweden, Spain and three units in France, Belgium, Italy, completed a questionnaire on RRT option education in their unit. The study showed that nurses were almost always responsible for organising the education programme. Seven units also involved nephrologists, five units involved dietitians, four units involved psychologists and three units involved medical social officers. All staff involved had background in general or nephrology nursing.23 Level II-3
Delivery style
Most studies included in this review described PDEP in their settings, which were delivered in multiple individual sessions with mostly multidisciplinary team members as reported in Hsu CK et al. (2018), Zukmin K et al. (2017), Yu YJ et al. (2014), Wu IW et al. (2009), Danguilan R A et al. (2013), García-Llana H et al. (2014), de Maar JS et al. (2016), Cankaya E et al. (2013) and Wei SY et al (2010).13 Level II-2, 14 Level II-2, 15 Level II-2, 17 Level II-2, 15 Level II-2, 20 Level II-3, 24, 25 Level II-3, 26 Level II-3,
Mixed of individual sessions and group sessions has been described in Yeoh HH et al. (2003), Shukla AM et al. (2017), Cassidy BP et al. (2018) and Combes G et al. (2017).18 Level II-2, 19 Level
II-2, 21, 27 Few studies including Hsu CK et al. (2018), Wu IW et al. (2009), Yu YJ et al. (2014), Cassidy BP et al. (2018) and Combes G et al. (2017) described patients involvement in their PDEPs such as giving talks and sharing sessions.12,13 Level II-2, 15 Level II-2, 16 Level II-1, 21
A systematic review and meta-analysis which was conducted by Devoe DJ et al. (2016), reported that of 15 studies included in their review, eight studies carried out educational interventions in group sessions, five had one to one session only and two included both.22 Level I
Van den Bosch J et al. (2015) reported in their systematic review that education delivery style can either be one-on-one sessions or class room teaching style, but a mix of one-on-one and group sessions were advocated. Educational programmes should contain individualised one-on-one counselling sessions with a member or members of multidisciplinary team. In addition to small group discussions, peer counselling and problem-solving or “brainstorming” sessions

26
PRE-DIALYSIS EDUCATION PROGRAMME
have been described wherein patients discuss treatment modalities, barriers and benefits, and troubleshooting of possible problems with other patients or facilitators. Various formats have been described for group sessions such as group lectures, interactive workshops, or open forum sessions.11 level I
Prieto-Velasco M et al. (2014) reported that most renal units included patients visit to in-centre HD unit (8/9 units) and home-dialysis nurse visit to assess suitability (7/9 units). Half of the renal units have formal meeting with ‘expert patient’ as part of the education programme. Group education sessions were used in 3/9 units.23 Level II-3
Frequency, follow-up and duration
Most studies included described the frequency of the sessions and follow-up depended on the stages of CKD. Some studies mentioned stage 3 or 4 CKD patients were followed up every three months while stage 5 CKD patients were followed-up on a monthly basis.15 Level II-2,
16 Level II-1, 17 Level II-2 Devoe DJ et al. (2016), reported that of 15 studies included in their systematic review, eight studies carried out educational interventions two or more days.22 Level I Van den Bosch J et al. (2015) reported that number of sessions and duration per session varies by educational program. There were reports of six individual sessions of one hour, four sessions, one night a week for two hours; or at least four to five interviews.11 Level I
Timing
Van den Bosch J et al. (2015) reported that an estimated glomerular filtration rate of less than 30 mL/min (stage 4 CKD) has been reported as ideal for referral to CKD clinic.11 Level I Others recommended that patients should be referred as early as possible to renal education (less than six months).11 Level I Prieto-Velasco M et al. (2014) reported that education programme for the patient and family began several months before dialysis or according to disease progression and all nine renal units evaluated in their studies have included patients with CKD stage 4 or 5 in the programme.23 Level II-3
Content and structure
There was variation in the content and structure of each pre-dialysis education programme described in the included studies. Most studies reported that the content of the education programme was largely focused on knowledge on nutrition, lifestyle modification, nephrotoxin avoidance, and compliance to medications and tailored according to the patients’ CKD stage.13 Level II-2, 14 Level II-2, 15 Level II-2, 16 Level II-1, 17 Level II-2, 18 Level II-2 Knowledge on preparation for RRT and modality choices as well as fast track vascular services for fistula and early commencement of RRT were given to the patients in advanced CKD stage. 13 Level II-2, 14 Level II-2, 15 Level II-2, 16 Level II-1,
17 Level II-2, 18 Level II-2 Zukmin K et al. (2017) reported that in their PDEP, cultural acceptance and religious counselling were also been covered.14 Level II-2 Shukla AM et al. (2017) mentioned hands-on or demonstration session by trained dialysis nurse.19 Level II-2 A systematic review and meta-analysis which was conducted by Devoe DJ et al. (2016), reported that of 15 studies included in their review, five studies included information on diet, six studies used video material, seven used printed materials, and one used website materials.22 Level I Cankaya E et al. (2013) used specially prepared training kit using visuals and written cards according to CKD stages for patients in their education programme.26 Prieto-Velasco M et al. (2014) reported key topics such as the ‘impact of the disease’ were covered by every unit, but only a few units described all dialysis modalities.23 Level II-3 Materials used in the nine renal units assessed came in a wide variety of forms and from a wide range of sources.23 Level II-3 Booklets were used in all units, online materials and DVDs were used in half of units.23 Level II-3 Cassidy BP et al. (2018) gave a list of trusted CKD online resources21 while Combes G et al. (2017) and Danguilan R A et al. (2013) mentioned take-home materials for patients after each visit.12,

27
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Training
Most studies did not specify details on training for their multidisciplinary team members in PDEP. Only Prieto-Velasco M et al. (2014) reported that all staff administering the programme had a background in general or nephrology nursing.23 Level II-3 Other studies included Shukla AM et al. (2017), Danguilan R A et al. (2013), Wei SY et al (2010) and García-Llana H et al. (2014) only mentioned involvement of trained staff but there was no description of the kind of trainings received by them.19 Level II-2, 24, 17 Level II-2, 25 Level II-3
2.4.6.3 Guidelines
A position statement was compiled by Bagnis C I et al. (2015) following an expert meeting in Zurich, Switzerland in March 2013, involving six nephrologists, eight nurses and one clinical psychologist from a spread of 12 European renal units with established RRT option education programmes. This position statement outlined clear recommendations on important aspects of the programme based on current evidence and in the context of pre-existing guidelines including guidelines from National Collaborating Centre for Chronic Conditions, Royal College of Physicians, UK, The Renal Association, UK, Haute Autorité de santé, France, and Dialysis Advisory Group of the American Society of Nephrology, USA. Overview of the recommendations are as follows27:
vWho should be in the team?The team consists of a nephrologist and a CKD nurse, at a minimum. Optimally, additional members of the team include a dietitian, a psychologist, a medical social officer, a physical therapist and an expert patient.
vWhat knowledge, training and experience should the team have?Knowledge of CKD and hands-on experience of all treatment modalities are minimum requirements for the team members. Optimally, the team also has training in the principles of adult education, motivational interviewing / communication skills and how to avoid bias when giving information.
vWhen should the programme begins?Starting the programme at least 12 months before the predicted start of dialysis allows time to establish dialysis access, for the patient to accept their situation, and take part in the decision-making. If this is not possible, then the programme begins upon referral for dialysis. Optimally, commencement of the programme is based on the level of disease (CKD Stage 4, progressive) and the rate of disease progression.
vWho should receive?The programme is made available to patients in CKD Stage 4 and Stage 5 (planned and unplanned starts), patients expressing an interest in changing modality and all patients upon request. Optimally, family, friends or caregivers of patients also attend the programme.
vShould the programme be individualized? If so, how?The programme ends when the patient has sufficient knowledge to make an informed decision regarding treatment modality. A more individualised approach to the programme is warranted if the patient does not have sufficient knowledge. Optimally, the following are available: (i) A key contact person is present to help the patient work through the material in
the order and speed of the patient’s choosing and help deal with psychological aspects of the disease.
(ii) There are regular updates on the patient’s condition between the education team and the patient’s general practitioner (GP).

28
PRE-DIALYSIS EDUCATION PROGRAMME
(iii) There is regular contact between the patient and the nephrologist/nurse. (iv) There is an option for the programme to be delivered in the patients’ preferred
place (i.e. home or hospital), within time and budget constraints.
vHow many sessions are required?At least one session is required. Optimally, as many sessions as required to independently reach an informed and balanced decision on modality are held.
vWhen should finish?Programme finishes when the predefined objectives have been met. Optimally, the programme finishes when the patient has chosen a form of RRT, with regular follow-ups being conducted into the treatment phase.
vWhat topics should be included?The minimal topics covered in all programmes are: (i) Topics requested by the patient. (ii) Unbiased information on CKD and the four treatment options [HD, PD,
transplantation and conservative care], and how well they match the patient’s beliefs and values.
(iii) An explanation that it is possible for the patient to change modality if there are no contraindications.
(iv) Clarification of the patient’s right to stop dialysis. (v) Ways to delay disease progression.
Optimally, the following topics are also covered: (i) Interviews to understand the patient’s history, lifestyle, pain levels,
comorbidities, physical activity levels, diet, culture, beliefs, wishes and expectations, what the patient knows and wants to know about the disease, patient’s social network, how much the patient wants to be involved in the treatment.
(ii) Implications of CKD upon finances (reduced capacity to work, insurance, treatment costs).
(iii) Impact of CKD upon QoL. (iv) Dealing with emotional stress. (v) Practical topics (e.g. transportation to/from treatments, contacting a patient
association, and making an advanced healthcare directive). (vi) Understanding kidney function test results and blood test results. (vii) Timing of placement of dialysis access. (viii) Medication required.
vWhat materials/resources should be used?Following materials / resources are used in the programme: (i) One-to-one meetings with staff at the unit. (ii) Written booklets appropriate to disease stage, level of education and cultural/
religious background. (iii) Multimedia showing the dialysis modalities in action.
Optimally, the following materials/resources are also used: (i) Patient decision aids(ii) Tours of dialysis facilities(iii) Online material (carefully chosen websites)(iv) Meetings with expert patients. (v) Videos including interviews with dialysis patients. (vi) Group education sessions may be considered.

29
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
vHow should the programme takes account of language and cultural differences?Medical interpreters are necessary and translations of the written material available for key culturally and linguistically diverse populations. Optimally, picture sets are available for sessions with these patients. Religious and cultural perspectives are important with regards to all treatment options. Cultural differences impact the perceived roles of doctor/patient and understanding of health/disease.
vHow should the quality of the programme be evaluated?A quality evaluation uses one or more of the following indicators:(i) The percentage of patients starting treatment with the modality they chose at
the end of the programme(ii) Proportion of planned initiations with established access/pre-emptive
transplantation. (iii) Patient satisfaction with modality choice (iv) Proportion of patients who have undergone a formal education programme
prior to initiation of RRT. (v) Patient satisfaction with the level of information they have received. (vi) Register of patients with End of Life Care needs. (vii) Proportion of those patients identified as having End of Life Care needs who
have a workable Advance Care Plan.
Optimally, one or more of the following indicators can be used: (i) QoL measurements (ii) Measurement of patient involvement(iii) Clearly defined: target population; objectives; curriculum; pedagogical tools;
criteria for evaluating effectiveness (including clinical, QoL); and sources of finance
This position statement endorses current guidelines, and offers further guidance to ensure patients receive high-quality education aimed at helping them make an informed choice of modality.27
The National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative (KDOQI) has provided evidence-based guidelines for all stages of CKD and related complications since 1997. The 2015 update of the KDOQI Clinical Practice Guideline for Haemodialysis Adequacy is intended to assist practitioners caring for patients in preparation for and during haemodialysis. In this updated guideline, it is stated that patients who reach CKD stage 4 (GFR <30 mL/min/1.73 m2), including those who have imminent need for maintenance dialysis at the time of initial assessment, should receive education about kidney failure and options for its treatment, including kidney transplantation, PD, HD in the home or in-centre, and conservative treatment. Patients’ family members and caregivers also should be educated about treatment choices for kidney failure.28
2.4.7 SOCIAL IMPLICATION
There were one SR, one SR with meta-analysis, one retrospective cohort study and two cross-sectional studies retrieved on social implications of PDEP with regards to modality choice. Two qualitative studies found which assessed patients’ satisfaction as well as patients’ and staff insights on PDEP. One SR and one pre- and post- intervention study retrieved examining patients’ knowledge related to PDEP.

30
PRE-DIALYSIS EDUCATION PROGRAMME
2.4.7.1 Modality choice
Shukla AM et al. (2017) conducted a retrospective cohort study in the USA to report the findings of the initial 22 months of a newly formed comprehensive pre-dialysis education programme (PDEP) clinic for advanced CKD patients and its impact on the rates of home dialysis. The study involved 108 advanced CKD patients with stage 4 and 5 CKD, with occasional patients of stage 3b CKD with rapid renal progression under the care of nephrologists were offered and encouraged transition to the care of PDEP clinic for their routine nephrology care. The PDEP clinic included a renal physician, an advanced nurse practitioner educator, a renal dietitian, and a renal social officer. A pharmacist was added in the PDEP clinic for the latter half of the study period. The PDEP clinic new protocol required patients to attend half-day comprehensive education session. Patients were encouraged to attend with family members, spouse, or caregivers. On arrival, patients were provided with printed material for kidney disease followed by group lesson in classroom format by renal advanced nurse practitioner educator which lasted for a minimum of one hour. After group lesson, patients rotated with renal dietician, social officer, trained dialysis nurse well versed in all dialysis techniques, and renal physician for patient-specific discussions and detailed on the individual needs and questions. Sessions with dialysis nurse included a ‘hands-on’ demonstration of home PD, home HD, and in-centre machine as per the needs and requests from patients. Following that, detailed session with the renal physician which started with an interview of the individual’s family, social, medical, and occupational needs. All previously provided information was reviewed and specific questions addressed. Patients and their caregivers were encouraged to make ‘active choice’ for their RRT. Any remaining misconceptions or fears were addressed during this final discussion and final modality choice was recorded in a passive manner. In contrast, patients who were in established patient protocol group had greater freedom to focus on the areas of their choice for counselling and were routinely seen by the renal physician for nephrology care. Patient preferences for RRT were noted at each clinic visit.19 Level II-2
The study found that over 22 months of PDEP clinic commenced, 70% of patients in PDEP group chose home dialysis, of which, 55% chose PD and 15% chose home HD. Similar rates of home dialysis choice were noted across spectrum of socio-economic variables. Multivariate analysis showed that the choice of RRT modality was unaffected by the patients’ age, gender, race, availability and type of insurance, diabetes status, albumin, or the stage of renal disease. The commencement of PDEP clinic has resulted in a 216% growth in home dialysis census over the same period and resulted in near doubling of home dialysis prevalence to 38% of all dialysis patients within 22 months of initiation.19 Level II-2
Devoe DJ et al. (2016) reported in their systematic review and meta-analysis that six studies reported primary outcome of choosing PD, and five provided sufficient data for meta-analysis. In the RCT (N = 70), educational intervention group was associated with more than 4-fold increase in the odds of choosing PD (OR, 4.60; 95% CI, 1.19,17.74). Meta-analysis results from four observational studies (N = 7,653) showed that patient-targeted educational interventions were associated with a 2-fold increase in the odds of choosing PD (pooled OR, 2.15; 95% CI, 1.07,4.32; I2 = 76.7%). For secondary outcome of receiving PD, 10 studies reported secondary outcome, nine had sufficient data for meta-analysis. Meta-analysis results from nine observational studies (N = 8,229) showed that patient-targeted educational intervention was associated with a three-fold increase in the odds of receiving PD as the initial treatment modality (OR, 3.50; 95% CI, 2.82, 4.35; I2 = 24.9%). The authors concluded that this review demonstrated a strong association between patient-targeted education interventions and the subsequent choice and receipt of PD. The variability in the design of the educational strategies identified and the strength of association across studies highlight the uncertainty about when and how educational interventions should be delivered, as well as likelihood of impact according to baseline PD penetration.22 Level I

31
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
de Maar JS et al. (2016) conducted a cross-sectional study in Amsterdam, The Netherlands to assess the impact of implementation of a structured PDEP named GUIDE with a home-focused approach on the number of pre-dialysis patients that choose home dialysis, and the number of patients that eventually receive home dialysis. Records of all 102 patients that received a treatment recommendation in the GUIDE programme between September 2013 and December 2014 at Meander Medical Centre were retrospectively reviewed. The structured PDEP process starts when a patient has an eGFR of 15 mL/min/1.73 m2. The programme began with home visit from a case manager (social worker) during which first education is given and suitability for home dialysis was assessed. Following that, set of questionnaires were completed by patient, case manager and nephrologist. Patient questionnaire had questions about the patient’s social support system, daily activities, level of independence in activities of daily living (ADL), aspects of life that patient values most and preferences and expectations with regards to RRT. Meanwhile, medical questionnaire comprised the categories transplantation, PD and HD, which contained questions about relative and absolute contraindications for each therapy and nephrologist’s treatment preference. Case manager’s questionnaire covered the suitability of the home, the social environment and the balance between burden and capacity and ended with case manager’s judgment of whether or not home dialysis would be suitable. Subsequently, a multidisciplinary meeting (MDM) was held to determine a specific patient profile and treatment recommendation. In MDM, the most suitable treatment for particular patient was chosen. This was then followed by patient education, a second MDM and finally the selection of the treatment by the patient and the nephrologist. After MDM, specialised pre-dialysis nurse provides education tailored to patient’s profile. General information related to RRT was given to all patients. Training for patient and family members before the start of home dialysis was discussed. Education was provided in a single session, which was repeated upon request. Written brochures and educational videos were also provided. Meetings with other patients were also offered and arranged if requested by the patient or their family. Patient’s response to this educational session was discussed in a second MDM. Following this, patient and nephrologist choose a treatment modality during the next visit to the outpatient clinic.20 Level II-3
The results showed that home dialysis was recommended for 62.8% of the patients who were advised to have dialysis treatment. Of patients that opted for dialysis, 34.2% chose PD and 8.2% chose home HD. About 22.9% started home dialysis as their first therapy, compared with 17.6% in the months before implementation of the programme. The study reported that 32.1% of the patients that received dialysis therapy received home dialysis. In the months before PDEP, an average of just 19.5% of patients that received dialysis received home dialysis. The authors concluded that compared with historical data, the standardised and home-focused PDEP, with its home visit, seems to successfully increase the number of patients that choose and receive home dialysis.20 Level II-3
Van den Bosch J et al. (2015) reported in their systematic review that six out of nine studies reporting on dialysis modality selection showed a higher proportion of patients selecting home dialysis (PD or another home modality) (Table 4) while three studies found no significant difference in modality choice.11 Level I
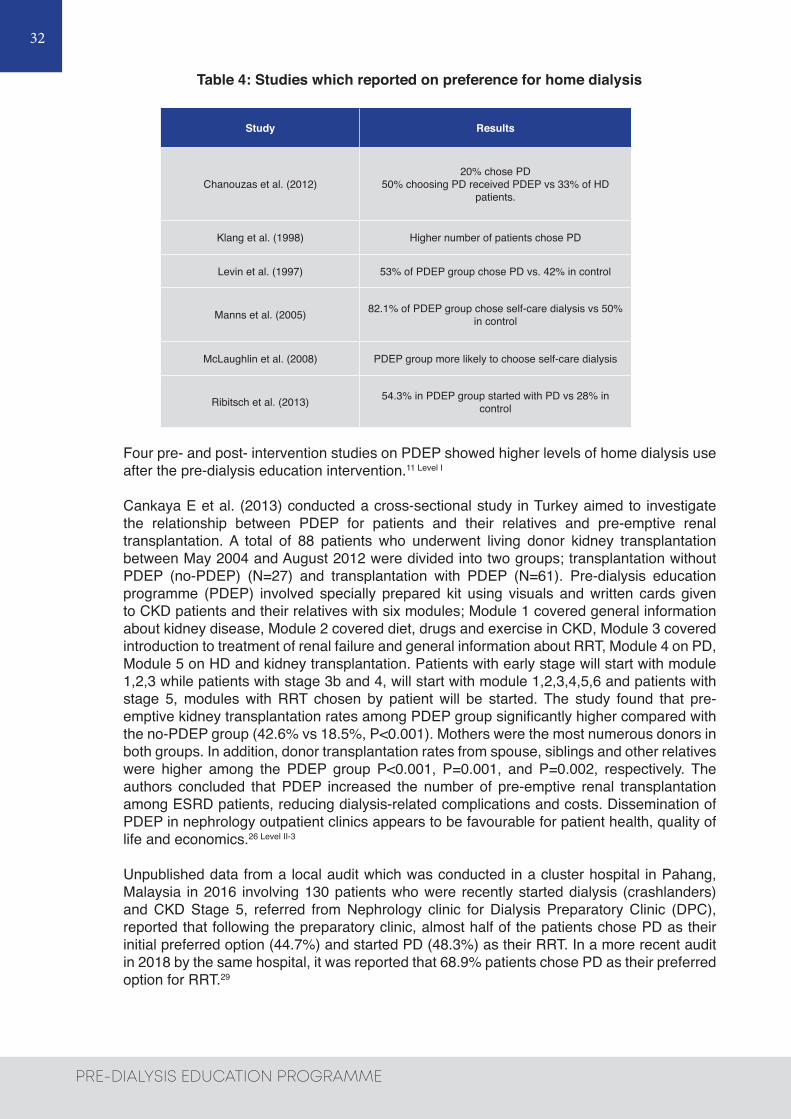
32
PRE-DIALYSIS EDUCATION PROGRAMME
Table 4: Studies which reported on preference for home dialysis
Study Results
Chanouzas et al. (2012)20% chose PD
50% choosing PD received PDEP vs 33% of HD patients.
Klang et al. (1998) Higher number of patients chose PD
Levin et al. (1997) 53% of PDEP group chose PD vs. 42% in control
Manns et al. (2005) 82.1% of PDEP group chose self-care dialysis vs 50% in control
McLaughlin et al. (2008) PDEP group more likely to choose self-care dialysis
Ribitsch et al. (2013) 54.3% in PDEP group started with PD vs 28% in control
Four pre- and post- intervention studies on PDEP showed higher levels of home dialysis use after the pre-dialysis education intervention.11 Level I
Cankaya E et al. (2013) conducted a cross-sectional study in Turkey aimed to investigate the relationship between PDEP for patients and their relatives and pre-emptive renal transplantation. A total of 88 patients who underwent living donor kidney transplantation between May 2004 and August 2012 were divided into two groups; transplantation without PDEP (no-PDEP) (N=27) and transplantation with PDEP (N=61). Pre-dialysis education programme (PDEP) involved specially prepared kit using visuals and written cards given to CKD patients and their relatives with six modules; Module 1 covered general information about kidney disease, Module 2 covered diet, drugs and exercise in CKD, Module 3 covered introduction to treatment of renal failure and general information about RRT, Module 4 on PD, Module 5 on HD and kidney transplantation. Patients with early stage will start with module 1,2,3 while patients with stage 3b and 4, will start with module 1,2,3,4,5,6 and patients with stage 5, modules with RRT chosen by patient will be started. The study found that pre-emptive kidney transplantation rates among PDEP group significantly higher compared with the no-PDEP group (42.6% vs 18.5%, P<0.001). Mothers were the most numerous donors in both groups. In addition, donor transplantation rates from spouse, siblings and other relatives were higher among the PDEP group P<0.001, P=0.001, and P=0.002, respectively. The authors concluded that PDEP increased the number of pre-emptive renal transplantation among ESRD patients, reducing dialysis-related complications and costs. Dissemination of PDEP in nephrology outpatient clinics appears to be favourable for patient health, quality of life and economics.26 Level II-3
Unpublished data from a local audit which was conducted in a cluster hospital in Pahang, Malaysia in 2016 involving 130 patients who were recently started dialysis (crashlanders) and CKD Stage 5, referred from Nephrology clinic for Dialysis Preparatory Clinic (DPC), reported that following the preparatory clinic, almost half of the patients chose PD as their initial preferred option (44.7%) and started PD (48.3%) as their RRT. In a more recent audit in 2018 by the same hospital, it was reported that 68.9% patients chose PD as their preferred option for RRT.29

33
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
2.4.7.2 Patients’ satisfaction
Cassidy B P et al. (2018) conducted a qualitative study in Canada to explore participants’ satisfaction with the education they received, while identifying educational needs, and the influence of the educational process in their dialysis modality decision making. The study included a sample of 12 participants between August and September 2016 with four patients from each dialysis modality (in-centre HD, PD, home PD). Patients’ age ranged from 23 to 77 years old with median age of 62 years old. Highest levels of education attained were high school (33%), college (50%), and postgraduate degree (17%). Pre-dialysis education was provided by multidisciplinary team. Educational supports given included: Kidney Foundation of Canada binder, Living With Kidney Disease, 4th edition, four multimodal small group classes, patient partners, and a list of trusted CKD online resources. The four classes covered self-management, living with CKD, stages of change, videos and demonstrations of each dialysis modality, a patient panel, vascular access, and a tour of the dialysis unit. A 30- to 60-minute semi structured interview using the AIDET (Acknowledge, Introduce, Duration, Explanation, Thank You) protocol was conducted with patients along with any family members present to explore on how patients receive information, its influence on their decisions and how the current educational supports could be improved. Demographic survey on patients were also completed. Keywords, phrases, and descriptions were analysed and categorized into themes. Quotes were extracted to best represent the patient voice and were matched to themes through team consensus.21
The study found that there were three overarching themes which influenced the modality decision-making process; Patient Factors (individualisation, autonomy, and emotions), Educational Factors (tailored education, appropriate time/information, and available resources), and Support Systems (partnership with health care team and family/friends). For patient factors, individual circumstances including transportation, level of activity, living situation, and support systems were the core of many modality decisions (individualisation). In addition, patients had varying levels of independence, ability and willingness to engage, and preferred different quantities of information (autonomy), and without adequate understanding of their current health state, patients experienced fear, denial, regret, anger, and shock (emotions). For educational factors, the study reported that content and format of education delivered to patients influenced decision making, with individual patient factors had impacts on the effectiveness of the educational support. Patients tended to receive information more effectively, with active engagement and motivation to learn when provided in accordance with their preferred learning styles (tailored education). Demographic and generational variance was apparent factors which influenced certain participants wished to receive information. Patients’ requests to improve the current educational support included more face-to-face education from clinicians and patients, videos on dialysis, online educational classes, and written information via pamphlets. It is also reported in the study that providing time and repeated exposure to information enhanced patient-informed decision making (appropriate time/information).21
Different patients needed different appropriate amount of time. Patients felt rushed, barraged with information, and overwhelmed when not given enough time. Patients also reported feeling they did not receive balanced information in terms of both the benefits and drawbacks of each modality and desired a more realistic approach. Educational supports had major impact on patients’ perception for each modality (available resource). However, not all the resources offered were accessed by the patients. Patients benefited from group learning and the shared patient experiences and perceptions. The HD unit tour helped set expectations, ease fears, and increase comfort levels. The written materials and CKD websites appeared to play a larger role in improving patients’ understanding of CKD, the modality options available, and prompting questions to ask the healthcare team. In addition, patients reported consistently referring the healthcare team, family, and friends as an educational resource (support systems).21

34
PRE-DIALYSIS EDUCATION PROGRAMME
As for support systems, nephrologists play a significant role in modality education and decision making. When a trusting partnership was established, patients had an enhanced sense of importance, control, and respect. However, the opposite was found when there was not a sense of partnership with healthcare team. Patients were less likely to identify other healthcare team members as crucial to decision making. However, when able, feedback was generally positive. Patients stated the case manager was an important educator, the social worker helped them cope and ease fears, and nurses provided emotional support. Patients also relied on family and friends, and lack of support often influenced the decision for in-centre HD over a home-based therapy. The authors concluded that patient’s health literacy, willingness to accept information, pre-dialysis lifestyle, support systems, and values were the influential factors in modality decision making. Patient education requires the flexibility to individualise the delivery of a standardised CKD curriculum in partnership with a patient-health care team, to fulfill the goal of informed and shared decision making.21
2.4.7.3 Patients’ and staff insights
Combes G et al. (2017) conducted a qualitative study in Canada to provide insights into what staff and patients think needs to improve related to pre-dialysis education. Mixed methods were used to look at quantitative changes in home dialysis uptake rates and qualitative case studies to explore barriers and success factors for home dialysis. Four hospital renal units were selected from seven West Midlands units. Formal pre-dialysis education in all four sites included one or more one-to-one sessions with a specialist nurse, a group information session, including talks from patients on RRT and written materials as well as DVDs which patients took home. In several sites, specialist nurses undertook home visits where they discussed treatment options with patients. Doctors also discussed treatment options with patients during out-patient appointments. Semi-structured interviews were conducted with 96 clinical and managerial staff and 93 dialysis patients starting their current treatment within 12 months. For patients, the topic guide in the interview covered were how patients came to be on dialysis, experiences of pre-dialysis and dialysis pathways and suggestions for improvement. For staff, the topic guide covered were current practice, how well the pre-dialysis and dialysis pathways work and how the team had been working to increase uptake of home dialysis. Patients and staff were prompted with an open-ended question about how treatment decisions were made if they did not spontaneously talk about the pre-dialysis period. The semi-structured qualitative telephone interviews were undertaken with 20 to 25 patients and semi-structured qualitative face-to-face interviews were undertaken 20 to 30 staff per site until saturation was achieved. All interviews were audio recorded and were transcribed by a specialist transcription team. The written and audio-visual pre-dialysis education materials used in each site were also reviewed. Data was analysed using thematic framework analysis.12
They reported that most staff made favourable comments about pre-dialysis education and valued the role of specialist nursing staff in educating and supporting patients’ treatment decisions. Most patients reported finding it was overall helpful. There were three themes identified which related to improving pre-dialysis education; sub-optimal education (restricted range of teaching materials and methods, and bias in the presentation of information and treatment options), different perspectives between patients and staff (importance of informal education, approaches to treatment decision-making), and influence of patient experience (influence from other patients, impact of distress). Patients desired improvements made to the teaching methods and biases eliminated. Patients indicated that restricted range of teaching materials and methods have made them felt that they were unable to use information given because the high volume and complexity of information. Another perspective on teaching materials came from patients who thought that they were not ‘real’ enough, and struggled to apply the information to their own lives. Seeing different treatments being undertaken by real patients were all suggested as ways of improving the education. On the other hand, from staff perspective, written materials were designed so that patients had information to take

35
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
home and consider over time. However, some patients were unable to take advantage of this positive intention. This suggested that patients would benefit from wider range of teaching methods, including interactive methods. Some patients thought that all treatment options were presented fairly and with equal emphasis, others felt not all options had been presented to them and that they had only found out about viable alternatives once they were on dialysis.
Some of these patients thought that opportunities to talk to patients already on treatment might have helped to give them a more balanced view of what life on dialysis might be like. Staff were also aware of the potential for bias in the presentation of information and treatment options, however, all staff groups thought that the first conversation with doctors about treatment options is crucial in influencing patients’ treatment choice. Staff were less aware than patients of how informal staff-patient conversations can influence patients’ treatment decision-making. Many staff felt ill equipped to talk about all treatment options in a balanced and unbiased way due to lack of training or lacked experience of the full range of treatment options. It was seemed that some patients continued to consider treatment options well after they had started dialysis, and continued gathering information and views about treatment options, some with intention to switch treatment. This highlighted the importance of all staff, irrespective of their role, being able to present all options neutrally and answer basic questions about all types of treatment.12
As for approaches to treatment decision-making, patient decision-making was found to be complex and patients’ abilities to make treatment decisions were adversely affected in the pre-dialysis period by emotional distress. Nearly all staff described a rational fact-based approach to treatment decision-making while most patients talked about a more personalised approach of thinking about their own lives and how different treatment options might work for them. With regards to the influence of other patients on decision-making, some patients valued having opportunities to talk to other patients, particularly those who were already on dialysis, because they were able to portray what treatment is really like and some patients thought this helped to balance any biases from staff. Some staff also recognised that pre-dialysis patients can find it beneficial to converse with patients on RRT however, other staff were more cautious and actively discouraged patient contact, because some patients may have atypical experiences or be biased against certain treatments. The impact of distress on decision-making emerged as a strong theme across all patient groups and sites. Patients described at length, the traumatic and frightening nature of the transition to end-stage renal failure. It seemed likely that distress was a major factor contributed to the difficulties of making treatment decision including for patients who had known for years they would need RRT and who might therefore be expected to be well prepared for treatment decision-making. However, very few staff appeared to appreciate the potential adverse impact of psychological distress on patients’ ability to make treatment decisions.12
2.4.7.4 Patients’ knowledge
One SR and one pre- and post- intervention study were found reporting on patients’ knowledge.
Van den Bosch J et al. (2015) reported in their SR that four of 19 quasi-experimental studies found higher levels of knowledge of end-stage renal disease and of different treatment options for patients receiving pre-dialysis education compared to those who did not receive.11 Level I
Danguillan R A et al. (2013) conducted a pre- and post- intervention study in Philippines to review the efficacy of PDEP and counselling programme in improving CKD knowledge. The study involved 299 CKD patients not yet on RRT from June 2009 to February 2010 and consisted of; 60% CKD Stage 5, 19% Stage 4, 10% Stage 3, 1% Stage 2 and 2% Stage 1. An evaluation tool was administered before and after the education modules to determine its efficacy in improving CKD knowledge. Pre-dialysis education programme (PDEP) involved a team comprised of trained CKD educators, a nurse and a psychologist, who conducted

36
PRE-DIALYSIS EDUCATION PROGRAMME
structured educational modules according to CKD stage. After each module, patients were instructed to return after every out-patient follow-up for completion of the education modules and further counselling. Patients were given take-home materials after each visit and were instructed about the recommended completion times for the modules: within three to four months for CKD stages 1 to 3, within one to two months for CKD stage 4 and within one month for CKD stage 5. Evaluation tools consisted of four self-administered questionnaires; a 30-item tool (22 items on general CKD knowledge and eight items on RRT), three 10-item tools covering lessons learned from each of the three CKD Clinic visits, an eight-item tool on patients’ health-care seeking behaviour prior to consultation at hospital, and a four-item questionnaire on perceived CKD knowledge. The 30-item tool evaluated patients’ baseline or actual knowledge (overall pre-test) and again after the patient completed all the education modules (overall post-test). The 10-item tools were administered after each visit to reinforce the lessons learned. Patients were followed-up for six months and overall pre- and post-test scores were compared to determine if there was improvement in the patient’s CKD knowledge.24
The study found that only 28% patients completed the modules within six-month follow-up period. Most patients who did not complete the programme (83%), no longer presented for follow-up after three months due to various reasons; poor compliance due to financial, came only for diagnosis, too ill to return for follow-up, lack of understanding, and low priority given. For perceived CKD knowledge, majority (34%) had no knowledge about CKD, 30% had little, 28% some, and 8% claimed a great deal of knowledge. Most were unaware of RRT options; 70%, 64.2%, and 54.2% had no knowledge of PD, HD, and transplantation, respectively. No significant association between CKD stage and knowledge of RRT. About 90% scored < 60% on general knowledge of CKD and 90% scored < 50% on the actual knowledge of ESRD treatment options. Among patients who claimed that they had extensive CKD knowledge, all scored < 60% in the actual knowledge questionnaire. For efficacy of education modules, there was significant increase in mean overall pre-test scores of CKD knowledge from 7.0 ± 5.11 (maximum score 30) to 23.0 ± 4.5 (maximum score 30) points in the overall post-test, with 69% scoring ≥75% (P<0.00001). There was an increase in number of patients (58%) who gained knowledge on the different aspects of CKD after completing the educational modules except for the topic on signs and symptoms of CKD. Patients aged < 50 years had significantly higher pre- and post- test results compared to older age groups (P=0.007). The authors concluded that the CKD education and counselling programmes were effective in improving patients’ knowledge of their disease. Elderly and non-high-school graduates of a financially disadvantaged population may need specially designed education modules to improve their comprehension.24
2.4.7.5 Psychological Implication
García-Llana H et al. (2014) conducted pre- and post- intervention study to determine the effectiveness of an individual, pre-dialysis intervention programme in terms of adherence, emotional state and health related quality of life (HRQL) in pre-dialysis patients with advanced CKD. All 52 adult patients with advanced CKD under pre-dialysis treatment with eGFR of ≤ 20ml/min or less were included in the study. The programme involved a six-month individual programme with every patient entering the study attended their regular appointments with nephrologist, the nurse and nutritionist and each patient received six individual monthly face-to-face sessions about 90-minutes duration each time with health psychologist. Every session had two distinct aims; first 45 minutes of sessions provided training in skills that facilitated the patient’s adaptation to the advanced CKD and its treatments, and last 45 minutes helped improve adherence to medication through motivational interviewing. Assessments were administered prior to the intervention and after the intervention. Patients were followed-up for six months and evaluated for adherence, depression, anxiety and HRQL with standardised self-report questionnaires. Biochemical markers were also registered.25 Level II-3

37
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
The study found that after the intervention, patients reported significantly higher levels of adherence [Mean score (SD) range; pre-test 27.12 (2.74), 22–33 vs. post-test 31.45 (2.05), 26–33 (P<0.001)], lower depression levels [(M = 10.92) pre- vs. post- (M = 8.86) intervention] and anxiety levels [(M = 18.22) pre- vs. post- (M = 14.41)]. Health-related quality of life (HRQL) scores on the General Health subscale increased significantly (from M = 37.19 to M = 45.97), as did scores on the Emotional Role subscale (from M = 71.82 to M = 77.57). No effects were found in other domains of HRQL (physical function, physical role, bodily pain, vitality, social function, mental health). Biochemical parameters were found significantly better controlled after the intervention, except for iPTH. The authors concluded that the findings highlighted the potential benefit of applying individual psycho-educational intervention programmes based on motivational interviewing and using the stages of change model to promote adherence and wellbeing in advanced CKD patients.25 Level II-3
2.4.8 COST / COST - EFFECTIVENESS
Yu YJ et al. (2014) conducted RCT with cost-analysis in Taiwan to analyse the medical expenditure and utilisation incurred during the first six months of dialysis initiation in 445 incident HD patients who were randomised into PDEP and no-PDEP groups before reaching ESRD. Medical expenditure and utilisation in the first six months of initiation of haemodialysis in these patients were accurately recorded and compared between PDEP and no-PDEP patients. Medical service utilisation was calculated as the frequency of outpatient visits and the frequency and length of hospitalisation. Medical service expenditures included outpatient expenditures (all costs including physicians’ and nursing fees, examinations, surgery, and medication) and inpatient expenditures (all costs including laboratory testing, imaging testing, medications, surgery and consulting, ward and administrative, nasogastric tube feeding, and haemodialysis fees). The expenditures for each participant were totalled to compute the sum of ambulatory and inpatient medical service utilization costs and expenditures. Analysis of costs only included those medical costs for which our hospitals made reimbursement claims to the NHI. The salaries, overheads, and administrative costs of the care team were not included in the analysis. The results showed that PDEP patients had lower total medical cost in the first six months after HD initiation (9147.6 ± 0.1 USD/patient vs. 11190.6 ± 0.1 USD/patient, p=0.003) compared to the no-PDEP patients. Medical cost of inpatient service was significantly lower in MPE patients (mean 2261.8 ± 5635.8 USD/patient in PDEP patients vs. mean 3698.8 ± 5540.9 USD/patient in no-PDEP patients, p<0.001), principally due to reduced cardiovascular hospitalisation and vascular access-related surgeries. The decreased inpatient and total medical cost associated with PDEP were independent of patients’ demographic characteristics, concomitant disease, baseline biochemistry and use of double-lumen catheter at initiation of haemodialysis. The authors concluded that participation of multidisciplinary education in pre-dialysis period was independently associated with reduction in the inpatient and total medical expenditures of the first six months after dialysis owing to decreased inpatient service utilisation secondary to cardiovascular causes and vascular access–related surgeries.16 Level II-2
Wei SY et al. (2010) conducted a retrospective cohort study with cost-analysis in Taiwan involving 140 incident ESRD patients who started dialysis and divided into two groups; PDEP group who received care and education from multidisciplinary team and Nephrologist Care Group (no-PDEP) who received standard care from nephrologist only. Medical services utilisation and costs were analysed from six months before initiation of dialysis to the time of the first HD, and the time periods were divided into ‘six months before dialysis’, ‘at dialysis initiation’, and the sum of the two periods as the ‘total period of observation’. Outcome measures for service utilisation included average outpatient visits before dialysis, frequency of hospitalisation before dialysis, percentage of patient hospitalisation at dialysis initiation, and average length of stay. Measurement of costs only included direct medical costs for which the study hospitals made claims for reimbursement. Salaries, overheads and indirect costs of the care team were not included in the analysis. The results showed

38
PRE-DIALYSIS EDUCATION PROGRAMME
that PDEP group had higher costs during the six months before dialysis (US$1428 +/- 2049 vs US$675 +/- 962/patient, P < 0.001), but was significantly associated with lower medical costs at dialysis initiation (US$942 +/- 1941 vs US$2410 +/- 2481/patient, P < 0.001) and for the total period of observation (US$2674 +/- 2780 vs US$3872 +/- 3270/patient, P = 0.009). The cost-saving effect resulted from the early preparation of vascular access and the lack of hospitalisation at dialysis initiation. The authors concluded that PDEP had successfully helped pre-ESRD patients to proceed into dialysis initiation with better preparedness, which reduced the probability of emergency dialysis through hospitalisation and saves money.17 Level
II-2
2.5 DISCUSSION
Our systematic review included 16 studies comprised of one SR with meta-analysis, one SR, one RCT, three cohort studies, two retrospective cohort studies, two pre- and post- intervention studies, four cross-sectional studies and two qualitative studies on pre-dialysis education programme for advanced CKD patients. There was no HTA report retrieved. The evidence was gathered according to the outcomes for effectiveness, safety, organisational, social implications and cost-effectiveness. The findings showed that with regards to effectiveness, participation of CKD patients in structured PDEP was associated with significantly better survival probability, mortality and morbidity rates. The one-year survival rate for HD patients who received structured PDEP were found to be higher despite of them being older and having more comorbidities. Peritoneal dialysis (PD) patients who had structured PDEP beforehand also found to have significantly lower peritonitis-related mortality rates and lower peritonitis-related morbidity rates compared to those who did not. These findings highlight that structured PDEP contributed to improved outcomes in advanced CKD patients. Meanwhile, PDEP in MOH facilities in Malaysia vary greatly across the country and have yet to be standardised. Future works are seriously needed to further strengthen PDEP in MOH, Malaysia facilities through standardisation to ensure effective outcomes for advanced CKD patients.
We did not find any retrievable evidence on the safety issues related to the programme. Frequency of temporary catheter use, rates of hospitalisation at dialysis initiation and post- dialysis, as well as length of hospital stay were also found to be significantly lowered in CKD patients who had PDEP. Significantly more patients who participated in the programme had their vascular access created before the initiation of HD. Cost-analyses included in this review, highlighted that medical expenditure after HD initiation significantly reduced in patients who had PDEP and achieved cost-savings principally due to reduced cardiovascular hospitalisation and vascular access–related surgeries.
In terms of modality choice, our findings demonstrated substantial association between PDEP and the subsequent choice and receipt of PD. An increase in rates of home dialysis and pre-emptive kidney transplantation rates were likewise noted. Similarly, the results from the local audits in Malaysia on advanced CKD patients who attended PDEP clinics also showed a higher preference for PD as their option for RRT and these findings are in line with findings from this SR. Higher PD uptake has been shown to have significant impacts on ESRD patients notably in superior social and patient experience compared to HD. In particular, patients treated with PD reported better quality of life,30-34 greater independence34, more flexible lifestyle34 and improved job opportunities.34 Better cognitive functions and lower dementia risk have also been reported in patients treated with PD.35 In addition, most studies suggest that PD is less costly with comparable or better health outcomes than HD.36
In terms of patient’s knowledge and psychological implications, higher levels of ESRD knowledge and of different treatment options, as well as higher levels of adherence, lower depression and anxiety levels, and better HRQL were reported for patients in PDEP. Two qualitative studies in this review explored patients’ satisfaction and insights towards the programme and reported that modality selection is a complex process requiring an

39
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
individualised approach for each patient. Patients’ decisions on RRT were influenced by their own preferences and values, the education delivered to them, and the support systems available to them. Emotional distress was a strong theme described by patients in the transition to end-stage renal failure which then affected their abilities to make treatment decisions. However, the impact of psychological distress on patients was found mostly underappreciated by the healthcare staff.
In general, our results indicated that PDEP had favourable outcomes on advanced CKD patients. However, there was wide variation between the components of programmes outlined in all the included studies in this review. These findings are in line with previous systematic reviews done by Devoe DJ et al. (2016) and Van den Bosch J et al. (2015) which highlighted such a great variation between different components of the programmes.11 Level I, 22 Level I Both SRs reported that the nature of educational interventions varied greatly between studies.11 Level
I, 22 Level I Our review detailed similar findings that most studies described varying educational components and processes. Multidisciplinary team members were almost always comprised of nephrologist, nurses, dietitians, and medical social workers with few programmes had clinical psychologist, pharmacist, and patient volunteers. Delivery style ranged from multiple individual sessions with multidisciplinary team members to mixed of individual sessions and group sessions as well as patients’ involvement particularly in peer sharing sessions. Variety of formats for content, structure, frequency of sessions, follow-up and duration of sessions have been described. Materials used came in a wide variety of forms and sources included printed materials, video and website materials. Timing for PDEP were mentioned at stage 4 and 5 CKD or few months before dialysis commencement. Training for the staff administering the programme was not specified in most included studies.
These findings emphasised on the lack of standardisation in the conduct of PDEP which
could hinder advanced CKD patients from getting optimal quality educational interventions to ensure effective outcomes for RRT and the subsequent improvement in quality of life. A more standardised approach to PDEP is needed to further establish its effectiveness for advanced CKD patients. Since most of the studies included in our review had follow-up duration of between three months to two years with exception of one study on PD patients that had follow-up duration of five years, more studies with longer follow-up period are needed in the future to demonstrate the long-term effects of PDEP for advanced CKD patients.
Limitations
This systematic review has several limitations and these should be considered when interpreting the results. Although there was no restriction in language during the search, only the full text articles in English published in peer-reviewed journals were included in the review, which may have excluded some relevant articles and further limited the study numbers. Firstly, one of the important limitations was the methodological quality of the included reviews and the limitations of the primary studies themselves. The SRs in this review have included mostly quasi-experimental studies and often without control groups or pre- and post- intervention measures. Some studies presented data in comparison to other reports or to previous findings instead of in comparison to control groups. We did not conduct a rigorous assessment of the concordance of the data reported in the SR with those stated in the primary studies. It is presumed that each review generally included the full available and eligible evidence that data extraction was accurate, and that analyses were scientifically sound. Secondly, the huge variation between the PDEP conducted in the included studies would be an important aspect that should be considered when interpreting the results. Most of the included studies in this review were conducted in Taiwan, USA and other parts of Europe which could potentially raise some questions on the applicability of the results to Malaysian population.

40
PRE-DIALYSIS EDUCATION PROGRAMME
CHAPTER 3: PATIENT AND PUBLIC INVOLVEMENT IN
PRE-DIALYSIS EDUCATION PROGRAMOver the years, Malaysian Health Technology Assessment Section (MaHTAS) has continuously ensured patient involvement in the development of HTA and CPG. Patients or their representatives are often involved as committee members for HTA and CPG. This is the first patient and public involvement (PPI) initiative by the authors to obtain perspectives from patients, carers and HCWs via a questionnaire survey as part of the HTA on PDEP. The short form of Guidance for Reporting Involvement of Patients and the Public (GRIPP2-SF) checklist is used for the reporting of this survey which includes five sections: aim, methods, study results, discussion and conclusion, and reflection/critical perspective.37
3.1 AIM
Pre-dialysis education has been offered to CKD patients in several major and minor specialist centres in Malaysia. However, a structured and user-centric PDEP is yet to be established in public health facilities. As each treatment option has its own advantages and disadvantages, sufficient information should be provided for better informed decision-making by the patients and carers. The aim of this survey is to identify the essential components of PDEP based on the preferences of patients, carers and HCWs to inform the development of a structured PDEP in Malaysia.
3.2 METHODS
The survey instrument was developed in English language based on findings from previous studies37-40, informal interview with a 30-year-old Malaysian female CKD patient with 12 months’ dialysis experience, and questions of feasibility and acceptability that the survey was designed to answer. The survey items were revised via professional judgement on relevance to pre-dialysis education in Malaysian public health facilities and appropriateness in terms of simplicity, ambiguity, validity, and sentence structure.
The survey consisted of 20 partial close-ended questions divided in three sections (Appendix 6): (i) socio-demographics (age, sex and level of education); (ii) background/treatment experience (type of respondents, place of treatment/workplace, and experience of dialysis and pre-dialysis education); and (iii) preferences of PDEP (preferred patient educators, types of information needed, delivery method, education materials, time of initiation, duration, frequency, preferred venue, and importance of patient support group and shared decision-making). Respondents were allowed to choose more than one answer for some of the questions.
The multicentre cross-sectional survey was conducted in January 2020 by a team of four researchers at the nephrology clinic or dialysis centre of three selected public hospitals under the Ministry of Health Malaysia (MOH):1) Hospital Kuala Lumpur (HKL)2) Hospital Tengku Ampuan Rahimah Klang (HTAR)3) Hospital Ampang
Inclusion criteria were age ≥18 years old, Malaysian citizens and CKD patients, carers of CKD patients or HCWs involved in the care of CKD patients. Those who were experiencing medical conditions deemed unfit to participate were excluded from the survey. Target sample size was a minimum 30 respondents (10 participants from each study site). Respondents were recruited via purposive sampling by nephrologists or HCWs in charge of the nephrology

41
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
clinic at selected public hospitals. The survey was answered by respondents themselves (self-administered) or administered by researchers if respondents were unable to read the English language. Informed consent was obtained prior to administration of the survey. An additional short interview session was carried out following the survey for participating HCWs to obtain in-depth information on the existing pre-dialysis education being offered to CKD patients at selected public hospitals. Data tabulation and descriptive analysis were performed using Microsoft Excel® version 2016 (Microsoft Corporation, Redmond, WA, USA) software.
3.3 RESULTSA total of 39 respondents consisting of patients, carers and HCWs were recruited from selected public hospitals. About two-third of the respondents were younger than 50 years of age (64.1%) (Table 5). Approximately half of the respondents were female (53.8%) and had completed education up to secondary school (56.4%). Time to complete the survey ranged from 10 to 30 minutes.
Majority of respondents were CKD patients (69.2%) and from HKL (43.6%) (Table 6). Most of the patients and carers of CKD patients (N=31) had received pre-dialysis education prior to initiation of dialysis (67.7%); about 18 of them (58.1%) had been initiated on dialysis with duration of dialysis ranging from less than six months to more than 18 months.
Table 5: Socio-demographics of respondents.
Characteristics (N=39) Frequency, n (%)
Age18-3031-4041-5051-6061-70
4 (10.3)8 (20.5)13 (33.3)9 (23.1)5 (12.8)
GenderMaleFemale
18 (46.2)21 (53.8)
Level of educationPrimarySecondaryTertiary
3 (7.7)22 (56.4)14 (35.9)
Table 6: Respondents’ background/treatment experience.
Background/treatment information Frequency, n (%)
Type of respondent (N=39) Patient Carer HCW
27 (69.2)4 (10.3)8 (20.5)

42
PRE-DIALYSIS EDUCATION PROGRAMME
Hospital/workplace (N=39)HKLHTARHospital Ampang
17 (43.6)12 (30.8)10 (25.6)
Received pre-dialysis education (patients/carers, N=31)Yes No
21 (67.7)10 (32.3)
Initiation of dialysis (patients/carers, N=31)YesNo
18 (58.1)13 (41.9)
Duration of dialysis for those on dialysis (N=18)<6 months6-12 months12-18 months >18 months
4 (22.2)0
2 (11.1)12 (66.7)
In terms of preferred educators, the preference of patients and carers (N=31) in decreasing order was doctor (94%), dietitian (90%), patient representative (84%), medical social officer (81%), psychologist (74%), pharmacist (74%), nurse (68%) and medical assistant (52%) as shown in Figure 5.
Figure 5: Preferred patient educators.
For the type of information needed prior to initiation of dialysis as illustrated in Figure 6, majority of patients/carers (N=31) agreed that it is important to be given the information on dietary advice (100%), advantages and disadvantages of treatment options (97%), medications and supplements associated with each treatment (97%), side effects of dialysis (97%), how dialysis was performed (97%), costs associated with treatment options (87%) and the effects of dialysis to daily lives (87%). However, information on how to dress for dialysis was less required by the patients/carers (39%).

43
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
As for the delivery method, patients and carers (N=31) had a slightly higher preference for individual (one-to-one) sessions (39%), followed by group sessions of 2-5 people (29%) and group sessions of 5-10 people (29%); one respondent voted for group sessions of 15-20 people. The majority of HCWs (N=8) also showed preference for individual (one-to-one) sessions (63%) instead of group sessions of 2-5 people (25%) and group sessions of 5-10 people (12%). A slightly higher proportion of patients and carers (N=31) preferred one single session with multiple educators (32%) compared to multiple sessions by appointment (26%), multiple sessions upon request only (26%) and one single session with a single educator (16%). Meanwhile, half of the HCWs (N=8) voted for multiple education sessions by appointment (50%), followed by one single session with multiple educators (25%) and one single session with a single educator (25%).
Figure 6: Types of information needed by patients/carers prior to initiation of dialysis.
Figure 7: Education materials.

44
PRE-DIALYSIS EDUCATION PROGRAMME
.In terms of education materials, preference of patients and carers (N=31) in decreasing order was hand-on session/demonstration (74%), audio-visual aids (71%), leaflet/pamphlet (64%) and information about websites or online videos (61%), suggesting that a mix of different education materials may be suitable for PDEP.
With regards to the time of initiation, patients and carers (N=31) had the highest preference for pre-dialysis education to be given six months before initiation of dialysis (39%). However, half of HCWs (N=8) voted for pre-dialysis education to be given one month before initiation of dialysis (50%).
For the duration of each session, patients and carers (N=31) preferred a shorter session of 15-30 minutes per session (52%) followed by 30-45 minutes (32%), 45-60 minutes (10%) and >60 minutes (6%). Majority of HCWs (N=8) voted for a longer session of 30-45 minutes for each session (63%).
In terms of frequency, patients and carers (N=31) had the highest preference for pre-dialysis education to be held once every three months (36%), followed by once every two months (29%), once every month (26%) and once a year (7%); one respondent preferred for on an as-needed basis. Similarly, HCWs showed the highest preference for once every three months (50%), followed by once every six months (37%) and once every month (13%).
Majority of patients and carers (N=31) voted for hospitals (65%) as the preferred venue for PDEP, followed by dialysis centres (39%). However, 75% of HCW voted for community clinics. Some of the HCWs commented that PDEP should be expanded to primary care or community level; however, issues on commitment, sustainability and continuity of the programme need to be considered.
Almost all patients and carers (N=31) agreed that being part of a patient support group would be helpful to discuss solving problems faced in real life (96.8%) and that doctor-patient shared decision-making on initiation of dialysis is important (96.8%).
Some of the respondents provided suggestions to improve PDEP (Appendix 7) which were grouped into four themes: individualised, support system, training and comprehensiveness (Table 7).
Based on the information provided by the participating HCWs, the three selected public hospitals had provided pre-dialysis education to their patients with some differences in programme content, structure and component (Table 8). All three programmes involved a multidisciplinary team of HCWs such as doctors, nurses, pharmacists and dietitians.

45
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Table 7: Summary of suggestions to improve PDEPNo. Themes
Individualised Support system Training Comprehensiveness
1. Programme must be well-organised as scheduled and should accommodate the patient’s personal schedule.
Family members/ partners/ friends should be included throughout the patient’s CKD journey.
Educators must be well-qualified, knowledgeable, and experienced to be able to advise and answer patients’ questions correctly.
Contents of the module should be comprehensive and hands-on demonstration should be included.
2. Educators must provide more human touch and be sensitive towards patients’ needs and emotions as they may be very fragile during the pre-dialysis stage.
Consistent attendance from the same family member/ partner/ friend should be encouraged.
Educators must be well-trained in providing adequate emotional support to patients.
Patients and carers should be educated on CKD and its progression, signs and symptoms of ESRD and preventive measures to delay ESRD.
3. Weekend sessions are preferred to minimise interference with daily work.
Carers should be well-educated about CKD, end-stage renal disease (ESRD) and dialysis to provide sufficient support and help patients make informed decisions.
HCWs should know how to communicate effectively with patients to ensure accuracy of information before starting each dialysis such as body weight, dry weight and dietary intake.
Counselling by a psychologist can be given by appointment for patients who need it.
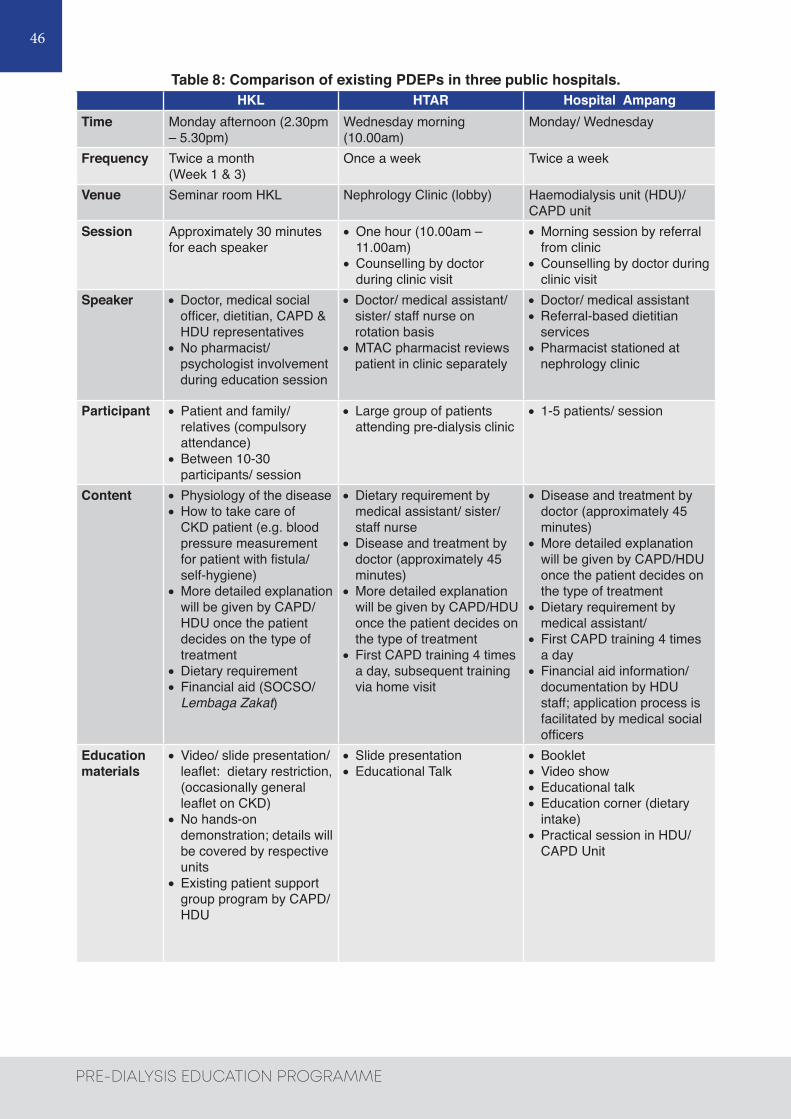
46
PRE-DIALYSIS EDUCATION PROGRAMME
Table 8: Comparison of existing PDEPs in three public hospitals.HKL HTAR Hospital Ampang
Time Monday afternoon (2.30pm – 5.30pm)
Wednesday morning (10.00am)
Monday/ Wednesday
Frequency Twice a month (Week 1 & 3)
Once a week Twice a week
Venue Seminar room HKL Nephrology Clinic (lobby) Haemodialysis unit (HDU)/ CAPD unit
Session Approximately 30 minutes for each speaker
•One hour (10.00am – 11.00am)
•Counselling by doctor during clinic visit
•Morning session by referral from clinic
•Counselling by doctor during clinic visit
Speaker •Doctor, medical social officer, dietitian, CAPD & HDU representatives
•No pharmacist/ psychologist involvement during education session
•Doctor/ medical assistant/ sister/ staff nurse on rotation basis
•MTAC pharmacist reviews patient in clinic separately
•Doctor/ medical assistant •Referral-based dietitian
services•Pharmacist stationed at
nephrology clinic
Participant •Patient and family/ relatives (compulsory attendance)
•Between 10-30 participants/ session
• Large group of patients attending pre-dialysis clinic
• 1-5 patients/ session
Content •Physiology of the disease•How to take care of
CKD patient (e.g. blood pressure measurement for patient with fistula/ self-hygiene)
•More detailed explanation will be given by CAPD/HDU once the patient decides on the type of treatment
•Dietary requirement• Financial aid (SOCSO/
Lembaga Zakat)
•Dietary requirement by medical assistant/ sister/ staff nurse
•Disease and treatment by doctor (approximately 45 minutes)
•More detailed explanation will be given by CAPD/HDU once the patient decides on the type of treatment
• First CAPD training 4 times a day, subsequent training via home visit
•Disease and treatment by doctor (approximately 45 minutes)
•More detailed explanation will be given by CAPD/HDU once the patient decides on the type of treatment
•Dietary requirement by medical assistant/
• First CAPD training 4 times a day
• Financial aid information/ documentation by HDU staff; application process is facilitated by medical social officers
Education materials
•Video/ slide presentation/ leaflet: dietary restriction, (occasionally general leaflet on CKD)
•No hands-on demonstration; details will be covered by respective units
•Existing patient support group program by CAPD/ HDU
•Slide presentation•Educational Talk
•Booklet•Video show•Educational talk•Education corner (dietary
intake)•Practical session in HDU/
CAPD Unit

47
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
3.4 DISCUSSION
The PPI initiative has revealed essential preferences of patients, carers and HCWs for pre-dialysis education which are valuable information for the development of a national, structured and patient-centred PDEP in Malaysia. Engagement of patients and stakeholders not only increases its relevance to users by answering questions of importance to patients and carers, but also empowers them to play a more active role; supports democracy and accountability; improves acceptability of research findings; and accelerates adoption into practice.41 A number of suggestions for improvement has also emerged, highlighting the importance of an individualised approach, strong support system, adequate staff training, and comprehensiveness of the programme. Our findings resonate with results from previous qualitative study where a much more individualised approach is required, taking into account the wide variation of patients’ motivation and interest in making treatment choices, which would demand a higher level of skill and training for staff involved in PDEP.38
Emotional distress in CKD may impede patients’ and carers’ understanding of information. In addition to effective communication skills, HCWs need to be well-informed about all treatment options as well as complexities and difficulties patients and carers face when considering treatment options so that they are able to provide adequate assistance and emotional support. Combes et al. (2017) observed that staff and patients may not conceptualise pre-dialysis education in the same way; patients appeared to place additional value on more informal education, arising from conversations with staff and other patients whilst staff tended to focus on formal pre-dialysis education sessions and discussions during outpatient appointments.38 Hence, HCWs need to be aware of how informal staff-patient conversations can influence patients’ treatment decision-making and be sufficiently trained in providing informal education in an unbiased way.
It is noteworthy that in this survey, patients and carers expressed different preferences in terms of delivery method, time of initiation, duration, frequency and venue compared with HCWs’ preferences. Such differences may arise from varying past experiences of patients and carers. Individual sessions may provide more comfort to those who are emotionally overwhelmed and assistance to those with low health literacy who find it difficult to process and apply health information to their own lives. Some may prefer group sessions which encourage interaction among participants, improving education efficiency, knowledge perception and self-management behaviours.42 Therefore, method of delivery in terms of individual or group sessions should consider patients’ needs and suitability prior to enrolment in PDEP.
Different preferences may also arise from HCWs’ consideration of practical aspects in implementing the programme. For example, in this survey, HCWs voted for pre-dialysis education to be given one month before initiation of dialysis in contrast to patients’ and carers’ preference of six months before initiation of dialysis. This coincides with findings by Morton et al. (2010) where patients and families conveyed the need for more time to absorb information and to adjust to the approaching treatment regardless of the treatment options they were contemplating; however, nephrologists tend to provide information in increasing detail closer to the initiation of renal replacement therapy which would reduce the time available for patients to make decisions, possibly coinciding with patients being symptomatic or cognitively impaired.39 Therefore, the timing of pre-dialysis education should allow sufficient time for patients and carers to understand about treatment options before making treatment decisions. Nevertheless, HCWs may have different perspectives due to the daily burden of workload and capacity in delivering the education sessions, which should be taken into consideration when designing the PDEP.

48
PRE-DIALYSIS EDUCATION PROGRAMME
Another important aspect to be considered is that different healthcare facilities may have varying capacities and needs influencing the delivery of PDEP, which was evident from the comparison of existing PDEPs at the three selected public hospitals in this survey. The lack of standardization of education programmes is acknowledged by professionals in the field of pre-dialysis education.40 The delivery of current PDEP in Malaysia is highly dependent on the availability of human resources, staff competencies, appropriateness of facilities, number of patients and content of the programme. Different structure, components and methods of delivery in these facilities suggests the need for standardisation in the design and implementation of PDEP among the MOH hospitals to ensure effective and standardised educational methods.
The strength of this survey was the experiential knowledge obtained from different categories of respondents (patients, carers and HCWs) which provided unique perspectives to promote more useful evidence that is relevant and responsive to patients’ and stakeholders’ needs. There was variation in the duration of dialysis, ranging from less than six months to more than 18 months which gave a broad perception of PDEP based on the patients’ experience with dialysis. The limitation of this survey is that some respondents required researchers’ help in administering the questionnaire where translation of English language to other languages such as Malay and Mandarin was required, during which translated items may not retain the same meaning as original items. The survey is also limited by a small number of respondents due to a short study period which may not fully represent each category (patients, carers and HCWs). The inclusion of all three study sites in Klang Valley implied limited respondent demography and results may not be generalizable to suburban or rural populations due to limited respondent demography. Nevertheless, this survey provided valuable insights of CKD patients’ and carers’ experiences and preferences which helped stakeholders identify the key areas for the development of a national structured patient-centred PDEP.
Based on the survey findings, the preferences of patients and carers for the PDEP could be concluded as below:
1) Educators: A multidisciplinary team consisting of:a) Doctorb) Dietitianc) Patient representatived) Medical Social officere) Psychologistf) Pharmacistg) Nurseh) Medical assistant
2) Delivery style: According to the patient’s preference; single individual (one-to-one) session or group session with multiple educators every three months
3) Education materials: A mix of materials such as:a) Hands-on session/demonstrationb) Audio-visual aidsc) Leaflet/pamphletd) Information about website/online video
4) Time of initiation: Sufficient time to understand about treatment options; approximately six months before initiation of treatment
5) Duration: Approximately 30 minutes for each session6) Preferred venue: Hospital
3.5 REFLECTION / CRITICAL PERSPECTIVES
The comparison of existing PDEPs in three public hospitals showed different interdisciplinary approaches in which the extent of involving healthcare professionals from different disciplines differed among the hospitals. Based on the survey findings, respondents preferred pre-

49
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
dialysis education to be delivered by a multidisciplinary team consisting of doctor, dietitian, patient representative, medical social officer, psychologist, pharmacist, nurse and medical assistant. Respondents expressed that they had different needs throughout their CKD journey which ought to be addressed by healthcare professionals from different disciplines. A retrospective cohort study reported that recipients of a multidisciplinary PDEP, including nephrologists, dialysis nurses, pharmacists, dietitians, and medical social officers experienced reduced unplanned urgent dialysis, hospital stays, cardiovascular events, and infections as well as improved metabolic status on dialysis initiation compared with non-recipients.43 Interdisciplinary care models that emphasise shared responsibility for CKD education among multiple professionals should be promoted as it may improve patient outcomes and create efficiencies in education delivery.42
In this survey, respondents had emphasised on the inclusion of family members or other carers during pre-dialysis education sessions as they too need to be well informed in order to provide the support and advice that patients need. In addition, carers reported feeling unprepared, having insufficient knowledge and receiving inadequate support from healthcare professionals. For patients with CKD, family members and other carers not only provide important support to them, but also have the potential to help overcome socio-cultural barriers and institutional/medical mistrust which is prevalent among hard-to-reach groups who carry the highest burden of CKD. Support from family and other social groups has also been shown to be a key factor in changing diet patterns (e.g. sodium reduction) and increasing physical activity. Therefore, including family and other carers in pre-dialysis education may better equip them to support the patients who they care for and ultimately yield improved patient outcomes.42
Majority of respondents agreed that being a part of a patient support group would be helpful for CKD patients. Some respondents expressed that they were more comfortable to hear from those with experiential knowledge and were more open to discuss their concerns with them. Indirect involvement of motivated dialysis patients in the PDEP can offer support to other patients through experience-sharing. In a research by Salter et al. (2015), participants acknowledged that other fellow dialysis patients provided emotional support beyond what they were receiving from their friends and family. Many participants described how dialysis patients encouraged one another to keep a positive attitude and formed close bonds, which they considered as social support from their “dialysis family”.44 Having the opportunity to talk to those already on renal replacement therapy could help patients envisage what life on dialysis is really like.38 Hence, sharing sessions by experienced dialysis patients, either by volunteering or through incentive methods, may be incorporated in the PDEP for a more comprehensive programme. However, this may need to be implemented with care as patients’ stories may have more influence than clinical advice on other patients’ treatment choice.38,39
The respondents also agreed that shared decision-making between doctors and patients is important. Shared decision-making, a collaborative process that allows patients and their providers to make healthcare decisions together, taking into account the best scientific evidence available, as well as the patient’s values and preferences, is recognized as a central component of patient-centred care and self-management support.35 Decision-making in ESRD is complex and dynamic, evolving over time and toward death. Patients, families and healthcare professionals should make joint decisions about starting or stopping dialysis treatment to ensure that decisions are informed and consistent with the patient’s preferences. However, factors that affect patients and healthcare professionals in making such decisions must be understood. A systematic review found that for the initiation of dialysis, patients based their choice on “gut instinct”, as well as weighing over the effect of treatment on quality of life and survival. Healthcare professionals, on the other hand, focused on biomedical factors and were led by an instinct to prolong life. Both patients and healthcare professionals described feeling powerless from different aspects of disease management.45 Hence, patients’ input in decision-making is valuable for the healthcare professionals to design an acceptable and

50
PRE-DIALYSIS EDUCATION PROGRAMME
feasible PDEP. By taking into account the differences in values perceived, the feeling of powerlessness for both the patients and healthcare providers can be addressed mutually.
How patients coped with emotions was also an important aspect to be considered. In handling ESRD, two coping mechanisms were highlighted by the patients, which are problem controlling and emotion controlling. The effect of emotions on choice is well described, and it is suggested that an emotional reaction to a stimulus is the most important factor to guide decisions.45 During the survey, some respondents expressed that they were having problems in accepting the fact that they need dialysis and this may not be well-addressed in the current PDEP. As a result, patients faced difficulties in making decisions for dialysis options and hence, kept on delaying in initiating treatments. In the qualitative study by Combes et al. (2017), patients described in detail, the traumatic and frightening nature of the transition to end-stage renal failure; however very few staff appeared to appreciate the potential adverse impact of psychological distress on patients’ ability to make treatment decisions.38 Therefore, the presence of a counsellor or psychologist in the PDEP team to offer counselling sessions regularly or by request would be crucial to specifically address the patient’s emotional needs. Questionnaire survey was the preferred method used to gather information from patients and stakeholders in this PPI initiative given the short timeframe. Moving forward, other complementary methods such as focus group discussion may be conducted to consolidate the survey findings. Qualitative data from focus group discussion may provide new insights on factors influencing patients’ decision-making on treatment choice. In a focus group study by Salter et al. (2015) among patients with ESRD undergoing haemodialysis, participants disclosed their perceptions of being treated poorly by medical professionals, lacking information about renal disease and treatment options, as well as desiring more knowledge about treatment options.37 Focus group discussion may also reveal potential explanations on findings from other quantitative studies, for example, the reasons behind why certain groups of patients were less interested in suggested interventions by the treating doctors. Recommendations for best practice in focus group discussion include clear rationale for the choice of this method, skills and techniques of the moderator or facilitator, methods and results should be reported explicitly, cautious towards biases affecting group discussion, and ensure a clear pathway between the data obtained, coding and subsequent analysis of data.46
During the survey, some patients and HCWs appeared to be facing language barrier in receiving and providing pre-dialysis education, respectively, which was expected as Malaysia is a multicultural and multilingual country. Education materials and sessions may need to be provided in Malay the national language as well as English the second language, both widely spoken in Malaysia. For non-Malay and non-English speaking patients, language barrier may impede their ability to understand with sufficient depth about CKD and treatment options, resulting in their needs being inadequately addressed. In a qualitative study exploring the experience of healthcare decision-making among culturally and linguistically diverse adults receiving in-centre haemodialysis for advanced CKD, patients expressed that while different cultural backgrounds did not influence their communication with healthcare providers, it was much easier understanding their providers and expressing their concerns and questions in language-concordant consultations.47 In the circumstances of language discordance between patient and provider, family member/partner/friend of diverse linguistic background or interpreter may be required to accompany the patient for pre-dialysis education session. The linguistically diverse population in Malaysia further emphasises the importance of an individualised approach in providing pre-dialysis education.

51
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
CHAPTER 4: CONCLUSIONS AND RECOMMENDATIONS
4.1 CONCLUSION4.1.1 SYSTEMATIC REVIEW
EffectivenessThere was limited fair level of retrievable evidence to suggest that participation of advanced CKD patients in PDEP contributed to greater survival probability and higher one-year survival rate compared to those who did not. However, no significant difference reported after two years. Limited fair to good level of retrievable evidence to suggest lower mortality and morbidity rates in patients who had PDEP. Limited evidence demonstrated that patients who had PDEP had longer time to dialysis and better blood profiles compared to those who did not. Significantly lower peritonitis-related mortality rates and lower peritonitis-related morbidity rates were also noted in PD patients.
SafetyThere was no retrievable evidence on the safety issues with regards to PDEP for advanced CKD patients.
OrganisationalHospitalisation / Length of stayThere was fair to good level of retrievable evidence to suggest that PDEP was associated with significantly lower frequency of temporary catheter use, lower rates of hospitalisation at dialysis initiation and post- dialysis, as well as shorter length of hospital stay.
Components of programmeThe evidence showed great variation in the components of the programmes described, from the multidisciplinary team members, to the educational process including timing, delivery styles, formats for content, structure, conduct of the programme and materials. However, most evidence reported involvement of multidisciplinary team members almost always comprised of nephrologists, nurses, dietitians and medical social officers, with few had pharmacist, clinical psychologist and patient volunteers. Most studies mentioned multiple individual sessions with few had mixed of individual sessions and group sessions as well as patients’ involvement. Majority involved patients with CKD stage 4 and 5 in the programme, with content tailored according to the patients’ CKD stage and principally focused on knowledge on nutrition, lifestyle modification, nephrotoxin avoidance, compliance to medications, preparation for RRT and modality choices with few reported hands-on and demonstration. Materials used ranged from video materials, printed materials, and website materials. Frequency of the sessions and follow-up were mostly depended on the CKD stage.
GuidelinesFew guidelines from UK, USA, France, Europe and a position statement following an expert meeting in Switzerland have been issued outlining the recommendations on the conduct of PDEP.
Social/PsychologicalThere was fair to good level of retrievable evidence to suggest significant association between PDEP and patient’s choice as well as receipt of PD and home dialysis for RRT. Limited evidence also showed higher rates of pre-emptive kidney transplantation rates, higher levels of knowledge of end-stage renal disease and RRT options as well as higher levels of adherence, lower depression levels and anxiety levels, and better HRQL were noted in patients who had PDEP.

52
PRE-DIALYSIS EDUCATION PROGRAMME
Limited evidence also showed that patient factors including individualisation, educational factors including tailored education, appropriate time/information, and available resources as well as support systems were the influential factors on patients’ decision for RRT. Sub-optimal education, different perspectives between patients and staff, and the influence of patient experience were the three themes identified which related to improving PDEP.
Cost-effectivenessBased on two cost-analyses, significant reduction in medical expenditure after initiation of HD were noted in patients who had PDEP and the cost-saving effect came through the early preparation of vascular access and reduced hospitalisations.
4.1.2 PATIENT AND PUBLIC INVOLVEMENT IN PRE-DIALYSIS EDUCATION PROGRAMME
Based on the survey findings, patients and carers preferred to have a 30-minute single session with multiple educators every three months delivered by a multidisciplinary team consisting of doctor, dietitian, patient representative, medical social officer, psychologist, pharmacist, nurse and medical assistant with a mix of education materials such as hands-on session or demonstration, audio-visual aids, leaflets or pamphlets and information about websites or online videos in the hospital setting. The pre-dialysis education may be given as an individual (one-to-one) or group session depending on the patient’s preference. The pre-dialysis education should be initiated approximately six months before starting treatment of choice, allowing patients and carers to have sufficient time to understand about available treatment options. Patients and carers agreed that being part of a patient support group would be helpful in solving real-life problems and that shared decision-making between doctors and patients is important to them. The healthcare workers expressed different preferences in terms of delivery method, time of initiation, duration, frequency, and venue which may arise from consideration of practical aspects such as daily burden of workload and capacity in delivering the education sessions, which should be taken into consideration when designing the PDEP.
4.2 RECOMMENDATIONS
Based on the above review, a standardised approach to PDEP should be outlined before its expansion to all Ministry of Health, Malaysia facilities. A multidisciplinary team involving well-trained personnel, and optimally with mixed individual and group sessions as well as using interactive mixed education materials should be established. Comprehensive and more personalised content tailored according to the CKD stage taking account individual needs, emotional support, psychosocial aspects, involvement of family as well as caregivers and additional support from patients’ support group are advocated.

53
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
5.0 REFERENCES1. Jha V, Garcia-Garcia G, Iseki K et al. Chronic kidney disease: global dimension and
perspectives. Lancet.2013;382(9888):260-272.2. Luyckx VA, Tonelli M, Stanifer JW. The global burden of kidney disease and the sustainable
development goals. Bull World Health Organ. 2018;96(6):414-422D.3. Ministry of Health, Malaysia. Clinical Practice Guidelines: Management of Chronic Kidney
Disease (Second Edition). Available at www.moh.gov.my Accessed on 15th October 2019.4. Hooi LS, Ong LM, Ahmad G et al. A population-based study measuring the prevalence of
chronic kidney disease among adults in West Malaysia. Kidney Int. 2013;84(5):1034-1040.5. Ministry of Health, Malaysia. National Action Plan For Healthy Kidneys (ACT-KID 2018-2025).
Available at http://www.moh.gov.my/moh/resources/Penerbitan/Rujukan/NCD/National%20Strategic%20Plan/act_kid-1-min.pdf Accessed on 15th October 2019.
6. Bavanandan S, Saminathan T A, Hooi L S et al. Is Chronic Kidney Disease on the Rise in Malaysia? Findings from a nationwide study. Poster presented at The International Society of Nephrology (ISN) World Congress of Nephrology; 2019 April 12-15; Melbourne, Australia.
7. Kidney Disease:Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney inter., Suppl. 2013; 3:1-150.
8. Stevens PE, Levin A; Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med. 2013 Jun 4;158(11):825-830.
9. UK Renal Association. Clinical Practice Guidelines: Planning, Initiating and Withdrawal of Renal Replacement Therapy (6th Edition). Available at https://renal.org/wp-content/uploads/2017/06/planning-initiation-finalf506a031181561659443ff000014d4d8.pdf Accessed on 15th October 2019.
10. Hassan R, Akbari A, Brown PA et al. Risk Factors for Unplanned Dialysis Initiation: A Systematic Review of the Literature. Can J Kidney Health Dis. 2019;6:2054358119831684.
11. Van den Bosch J, Warren DS, Rutherford PA. Review of predialysis education programmes: a need for standardization. Patient Prefer Adherence. 2015;9:1279-1291.
12. Combes G, Sein K, Allen K. How does pre-dialysis education need to change? Findings from a qualitative study with staff and patients. BMC Nephrol. 2017;18(1):334.
13. Hsu CK, Lee CC, Chen YT et al. Multidisciplinary pre-dialysis education (MPE) reduces incidence of peritonitis and subsequent death in peritoneal dialysis patients: 5-year cohort study. PLoS One. 2018;13(8):e0202781.
14. Zukmin K, Ahmad I, Wynn AK et al. A comparative study to evaluate factors that influence survival in multidisciplinary predialysis educated patients and “Crashlanders”. Saudi J Kidney Dis Transpl. 2017;28(4):743-750.
15. Wu IW, Wang SY, Hsu KH et al. Multidisciplinary predialysis education decreases the incidence of dialysis and reduces mortality--a controlled cohort study based on the NKF/DOQI guidelines. Nephrol Dial Transplant. 2009;24(11):3426-3433.
16. Yu YJ, Wu IW, Huang CY et al. Multidisciplinary predialysis education reduced the inpatient and total medical costs of the first 6 months of dialysis in incident hemodialysis patients. PLoS One. 2014;9(11):e112820.
17. Wei SY, Chang YY, Mau LW et al. Chronic kidney disease care program improves quality of pre-end-stage renal disease care and reduces medical costs. Nephrology (Carlton). 2010;15(1):108-115.
18. Yeoh HH, Tiquia HS, Abcar AC et al. Impact of predialysis care on clinical outcomes. Hemodial Int. 2003;7(4):338-341.
19. Shukla AM, Easom A, Singh M et al. Effects of a Comprehensive Predialysis Education (CPE) Program on the Home Dialysis Therapies: A Retrospective Cohort Study. Perit Dial Int. 2017;37(5):542-547.
20. de Maar JS, de Groot MA, Luik PT et al. GUIDE, a structured pre-dialysis programme that

54
PRE-DIALYSIS EDUCATION PROGRAMME
increases the use of home dialysis. Clin Kidney J. 2016;9(6):826-832.21. Brendan P. Cassidy, Lori Harwood, Leah E et al. Educational Support Around Dialysis
Modality Decision Making in Patients With Chronic Kidney Disease: Qualitative Study. Can J Kidney Health Dis. 2018; 5: 2054358118803323.
22. Devoe DJ, Wong B, James MT et al. Patient Education and Peritoneal Dialysis Modality Selection: A Systematic Review and Meta-analysis. Am J Kidney Dis. 2016;68(3):422-433.
23. Prieto-Velasco M, Isnard Bagnis C, Dean J et al. Predialysis education in practice: a questionnaire survey of centres with established programmes. BMC Res Notes. 2014;7:730.
24. Danguilan R A, Cabanayan-Casasola C B, Evangelista N N et al. An education and counseling program for chronic kidney disease: strategies to improve patient knowledge. Kidney International Supplements.2013;3(2):215-218.
25. García-Llana H, Remor E, del Peso G et al. Motivational interviewing promotes adherence and improves wellbeing in pre-dialysis patients with advanced chronic kidney disease. J Clin Psychol Med Settings. 2014;21(1):103-115.
26. Cankaya E, Cetinkaya R, Keles M et al. Does a predialysis education program increase the number of pre-emptive renal transplantations? Transplant Proc. 2013;45(3):887-889.
27. C I Bagnis, C Crepaldi, J Dean et al. Quality standards for predialysis education: results from a consensus conference. Nephrol Dial Transplant. 2015;30(7):1058–1066.
28. The National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative (KDOQI). KDOQI Clinical Practice Guideline for Haemodialysis Adequacy: 2015 Update. Available at: https://www.kidney.org/sites/default/files/KDOQI-Clinical-Practice-Guideline-Hemodialysis-Update_Public-Review-Draft-FINAL_20150204.pdf. Accessed on 2nd December 2019.
29. Mat Sabri et al. Impact of Dialysis Preparatory Clinic on dialysis modality as first Renal Replacement Therapy. Oral presentation at Congress of Malaysian Society of Nephrology 2016.
30. Alhusaini OA, Wayyani LA, Dafterdar HE et al. Comparison of quality of life in children undergoing peritoneal dialysis versus hemodialysis. Saudi Med J. 2019;40(8):840-843.
31. Hsu CC, Huang CC, Chang YC et al. A comparison of quality of life between patients treated with different dialysis modalities in Taiwan. PLoS One. 2020;15(1):e0227297.
32. Chuasuwan A, Pooripussarakul S, Thakkinstian A, Ingsathit A, Pattanaprateep O. Comparisons of quality of life between patients underwent peritoneal dialysis and hemodialysis: a systematic review and meta-analysis. Health Qual Life Outcomes. 2020;18(1):191.
33. Chuasuwan A, Pooripussarakul S, Thakkinstian A et al. Comparisons of quality of life between patients underwent peritoneal dialysis and hemodialysis: a systematic review and meta-analysis. Health Qual Life Outcomes. 2020;18(1):191.
34. Walker RC, Marshall MR. Increasing the uptake of peritoneal dialysis in New Zealand: a national survey. J Ren Care. 2014;40(1):40-48.
35. Tian X, Guo X, Xia X et al. The comparison of cognitive function and risk of dementia in CKD patients under peritoneal dialysis and hemodialysis: A PRISMA-compliant systematic review and meta-analysis. Medicine (Baltimore). 2019;98(6):e14390.
36. Yang, F., Liao, M., Wang, P. et al. The Cost-Effectiveness of Kidney Replacement Therapy Modalities: A Systematic Review of Full Economic Evaluations. Appl Health Econ Health Policy (2020).
37. Staniszewska S, J Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. BMJ. 2017;358:j3453.
38. Combes G, Sein K, Allen K. How does pre-dialysis education need to change? Findings from a qualitative study with staff and patients. BMC Nephrol. 2017;18(1):334.
39. Morton RL, Tong A, Howard K, et al. The views of patients and carers in treatment decision making for chronic kidney disease: systematic review and thematic synthesis of qualitative studies. BMJ. 2010;340:c112.
40. Van den Bosch J, Warren DS, Rutherford PA. Review of predialysis education programs: a

55
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
need for standardization. Patient Prefer Adherence. 2015;9:1279-1291.41. Esmail L, Moore E, Rein A. Evaluating patient and stakeholder engagement in research:
moving from theory to practice. Journal of comparative effectiveness research. 2015 Mar;4(2):133-145.
42. Narva AS, Norton JM, Boulware LE. Educating patients about CKD: the path to self-management and patient-centered care. Clin J Am Soc Nephrol. 2016;11(4):694-703.
43. Cho EJ, Park HC, Yoon HB, Ju KD, Kim H, Oh YK, Yang J, HWANG YH, Ahn C, OH KH. Effect of multidisciplinary pre‐dialysis education in advanced chronic kidney disease: Propensity score matched cohort analysis. Nephrology. 2012;17(5):472-479.
44. Salter ML, Kumar K, Law AH, et al. Perceptions about hemodialysis and transplantation among African American adults with end-stage renal disease: inferences from focus groups. BMC Nephrol. 2015;16:49.
45. Hussain JA, Flemming K, Murtagh FE, et al. Patient and health care professional decision-making to commence and withdraw from renal dialysis: a systematic review of qualitative research. Clin J Am Soc Nephrol. 2015;10(7):1201-1215.
46. O. Nyumba T, Wilson K, Derrick CJ, et al. The use of focus group discussion methodology: Insights from two decades of application in conservation. Methods Ecol Evol. 2018;9(1):20-32.
47. Muscat DM, Kanagaratnam R, Shepherd HL, et al. Beyond dialysis decisions: a qualitative exploration of decision-making among culturally and linguistically diverse adults with chronic kidney disease on haemodialysis. BMC Nephrol. 2018;19(1):339.

56
PRE-DIALYSIS EDUCATION PROGRAMME
6.0 APPENDICES Appendix 1
HIERARCHY OF EVIDENCE FOR EFFECTIVENESS STUDIES
DESIGNATION OF LEVELS OF EVIDENCE
I Evidence obtained from at least one properly designed randomized controlled trial.
II-I Evidence obtained from well-designed controlled trials without randomization.
II-2 Evidence obtained from well-designed cohort or case-control analytic studies, preferably from more than one centre or research group.
II-3 Evidence obtained from multiple time series with or without the intervention. Dramatic results in uncontrolled experiments (such as the results of the introduction of penicillin treatment in the 1940s) could also be regarded as this type of evidence.
III Opinions or respected authorities, based on clinical experience; descriptive studies and case reports; or reports of expert committees.
SOURCE: US/CANADIAN PREVENTIVE SERVICES TASK FORCE (Harris 2001)

57
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Appendix 2
PTK-Bor-11
HEALTH TECHNOLOGY ASSESSMENT (HTA) PROTOCOLPRE-DIALYSIS EDUCATION PROGRAMME
1.0 BACKGROUND INFORMATIONChronic Kidney Disease (CKD) is a growing public health concern which is responsible for various complications including all-cause and cardiovascular mortality, kidney-disease progression to end-stage kidney disease, cognitive decline, anaemia, mineral and bone disorders.1 The Global Burden of Disease (GBD) 2015 study estimated that, in 2015, about 1.2 million people died from kidney failure, an increase of 32% since 2005.2 In 2010, it is estimated that around 2.3 to 7.1 million people with end-stage kidney disease died without access to chronic dialysis.2 However, despite of these growing figures, the awareness remains low among patients and health-care providers.1 In Malaysia, the prevalence of CKD has increased from 9.1% in the 2011 Malaysian National Health and Morbidity Survey3 to 15.5% in 20185. Awareness of CKD was hardly improved in seven years from 4% of respondents in 20115 to 5% in 2018.6 In the year of 2011, there were 27,572 patients on renal replacement therapy (RRT) in Malaysia5 and the figures have grown to a total of 37,183 patients on regular dialysis in 2015, with 7,595 new patients entering dialysis.3 The number of patients with CKD is expected to significantly rise in the future largely due to the increasing prevalence of diabetes, hypertension as well as the aging population in Malaysia.3 This will certainly contribute to the major increase in the future needs for RRT and impose a large burden on health care budget.
According to Malaysian Clinical Practice Guideline for Management of Chronic Kidney Disease (Second Edition) published in 2018, CKD is defined as an estimated glomerular filtration rate (eGFR) of <60 ml/min/1.73 m2 that is present for more than three months with or without evidence of kidney damage, or evidence of kidney damage that is present for more than three months with or without eGFR <60 ml/min/1.73 m2.3 Markers for kidney damage includes albuminuria (albumin excretion rate ≥30 mg/24 hours or albumin-creatinine ratio ≥3 mg/mmol), urine sediment abnormalities, abnormalities detected by histology, structural abnormalities detected by imaging and history of kidney transplantation.3 Classification of CKD is currently based on cause, GFR category, and albuminuria category (CGA) and follows Kidney Disease Improving Global Outcomes (KDIGO) 2012 guidelines which has health and prognostic implications.3,7 The GFR categories mapping to the previous five-stage classification have been retained but with subdivision of the G3 category of 30 to 59 mL/min per 1.73 m2 into categories G3a (45 to 59 mL/min per 1.73 m2) and G3b (30 to 44 mL/min per 1.73 m2).8 This was driven by data supporting different outcomes and risk profiles in these categories.8 Severity is expressed by level of GFR and albuminuria and is linked to risks for adverse outcomes, including death and kidney outcomes.8

58
PRE-DIALYSIS EDUCATION PROGRAMME
Table 1. Prognosis of CKD by GFR and albuminuria category3,7
It is known that timely referral to nephrologist is recommended for RRT in people with progressive CKD in whom the risk of kidney failure within one year is 10–20% or higher, as determined by validated risk prediction tools.7 In the Malaysian Clinical Practice Guideline for Management of Chronic Kidney Disease (Second Edition) 2018, it is stated in the recommendation that CKD patient with rapidly declining renal function [loss of eGFR >5 ml/min/1.73 m2 in one year or >10 ml/min/1.73 m2 within five years] or eGFR <30 ml/min/1.73 m2 (eGFR categories G4 to G5) should be referred to a nephrologist/physician3. UK Renal Association recommends that all patients with severe CKD (stage 5 and progressive stage 4), alongside their families and carers, should be offered pre-dialysis education programme.9 This programme aims at improving knowledge and understanding of the condition, as well as assisting them in making decisions for RRT.9 However, in most studies, it is reported that about 40% to 60% of patients with CKD start dialysis in an unplanned fashion and/or under urgent circumstances despite regular follow-up by a nephrologist.10 This is of concern since in unplanned dialysis, patients forego the opportunity to make an informed, shared decision regarding the timing and modality of RRT as options for RRT under urgent conditions are often limited.10 Studies reported that advanced age, increased comorbidity burden, late referral to nephrology, and lower GFR at dialysis initiation were the most common independent risk factors for unplanned dialysis.10,11 In addition, patients who had unplanned dialysis were found much less likely to have received formal pre-dialysis education about the different options for RRT.10,11 This highlights the importance of a structured and comprehensive pre-dialysis education programme in preparing advanced-stage CKD patients for RRT as unplanned dialysis is known to be associated with increased patient morbidity, mortality, hospitalisations, needs for catheter insertion for haemodialysis which subsequently increase the risk of catheter related sepsis as well as central vein stenosis, and further, inevitably contribute to the economic burden of CKD.
Pre-dialysis education programme often described as multidisciplinary education programme, which consists of multiple education sessions where patients are educated by three or more health care professionals such as nephrologist, nurse, dietitian, medical social officer, home-dialysis coordinator, pharmacist, technician, or by other dialysis patients.11 There are variations in practice, however, pre-dialysis education programme usually includes individualised one-to-one sessions with a member or members of the multidisci plinary team and group discussions, peer counselling as well as problem-solving sessions have been described wherein patients discuss treatment modalities, as well as barriers, benefits, and troubleshooting of possible problems with other patients.11 Variety of formats have been described in the delivery style of the programme such as group lectures, interactive workshops, open forum sessions as well as written and audio-visual materials to take home.11,12 In its Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease, KDIGO

59
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
recommended that patients with progressive CKD should be managed in a multidisciplinary care setting.8 The multidisciplinary team should include or have access to dietary counselling, education and counselling about different RRT modalities, transplant options, vascular access surgery, and ethical, psychological, and social care.8 The aims for this programme are mainly to provide patients with information on end-stage kidney disease treatment options, helps decision-making between treatments, and encourages self-care to improve quality of life.12 A systematic approach with a pre-dialysis education programme is thought to assist patients in preparation for RRT and prevent the complications of unplanned dialysis subsequently reduce the complications of end-stage renal disease.
At present, there is no standard national programme established in Ministry of Health for pre-dialysis education. Pre-dialysis education for advanced CKD patients is often done in different ways across the country. Several centres in Peninsular Malaysia have specific programme for pre-dialysis education while numerous other centres lack such a programme. Certain hospitals conduct half-day talk monthly which involves sharing experiences by peritoneal dialysis, haemodialysis and kidney transplant nurses as well as exploring the funding options by the medical social officer and inputs by dietitian for CKD patients and family members. Effectiveness of such method in delivering pre-dialysis education for advanced CKD patients is largely unknown. Therefore, this health technology assessment was requested by Head of Nephrology Services, Ministry of Health, Malaysia to review the available evidence and feasibility of structured pre-dialysis education programme for advanced CKD patients before its adoption into national programme in Malaysia.
2.0 POLICY QUESTION
Should a structured pre-dialysis education programme be expanded in all Ministry of Health facilities?
3.0 OBJECTIVES
3.1 To assess the effectiveness and safety of pre-dialysis education programme for advanced CKD patients3.2 To assess the organisational, ethical, legal and societal implications related to pre- dialysis education programme for advanced CKD patients3.3 To assess the cost-effectiveness of pre-dialysis education programme for advanced CKD patients3.4 To assess the most suitable pre-dialysis education programme for Malaysian context
Research Questionsi) Is pre-dialysis education programme effective and safe for advanced CKD patients?ii) What are the organisational, ethical, legal and societal implications of pre-dialysis
education programme for advanced CKD patients?iii) Is pre-dialysis education programme cost-effective for advanced CKD patients?
4.0 METHODS4.1. Search Strategy4.1.1 Electronic databases will be searched for published literatures pertaining to pre-dialysis education programme for advanced CKD patients. The databases are MEDLINE, PubMed, and EBM Reviews-Cochrane Database of Systematic Review, EBM-Reviews-Cochrane Central Register of Controlled Trials, EBM Reviews-Health Technology Assessment,EBM Reviews-Cochrane Methodology Register, EBM Reviews-NHS Economic Evaluation Database, Database of Abstracts of Reviews of Effects (DARE), Horizon Scanning, INAHTA database, and HTA database. 4.1.2 Additional literatures will be identified from the references of the related articles.4.1.3 General search engine will also be used to get additional web-based information. 4.1.4 There will be no limitation applied in the search such as year and language.4.1.5 The search strategy will be included in the appendix.

60
PRE-DIALYSIS EDUCATION PROGRAMME
4.2 Inclusion and Exclusion Criteria
4.2.1 Inclusion Criteria
a. Population :Adults patients with advanced CKD stage 4,5b. Intervention:Pre-dialysis education programme;
i. Multidisciplinary team comprised of nephrologists/ dieticians/ social workers/ pharmacists/ nurses/ psychologists/ HD or PD patient volunteers etc.
ii. Multiple sessionsiii. Relatively detailed description of the programme, such as sessions frequency, content of
sessions, and descriptions of educatorsc.Comparators :
i. No pre-dialysis education programme ii. No comparator
d.Outcome :i. Effectiveness
- Mortality- Morbidity- Quality of life
ii. Safety - adverse events - complications
iii. Organisational issues- Unplanned dialysis - Hospital admission- Length of hospital stay- Components of pre-dialysis education programme
(content, structure, delivery style, timing)- Training- Guidelines
iv. Ethical, legal implications v. Psychological/Societal implications
- Compliance- Acceptance- Patient satisfaction- Patient preference/ dialysis modality choice- Mental health issues
vi. Cost-effectiveness, economic evaluation, cost-analysis
e. Study design :Health technology assessment (HTA) reports, systematic reviews (SRs), randomised controlled trials (RCTs), non-randomised controlled trials (NRCTs), cohort study, case-control study, pre- and post- intervention, cross-sectional study and economic evaluation studies.
f. English full text articles
4.2.2 Exclusion Criteria a. Study design : Animal study, laboratory study, narrative review, case-series, case study, early stage CKD patients
b. Non English full text articles
Based on the above inclusion and exclusion criteria, study selection will be carried out independently by two reviewers. Disagreement will be resolved by discussion.

61
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
4.3 Critical Appraisal of Literature
The risk of bias (methodology quality) of all retrieved literatures will be assessed using the relevant checklist of Cochrane Collaboration Assessment tools, Critical Appraisal Skill Programme (CASP) by two reviewers depending on the type of the study design.
4.4 Analysis and Synthesis of Evidence
4.4.1 Data extraction strategy
The following data will be extracted:i. Details of methods and study population characteristicsii. Detail of intervention and comparatorsiii. Details on outcomes for effectiveness, safety and cost associated with pre-dialysis
education programme for advanced CKDiv. Details on organisational, ethical, legal and societal issues related to the practice
Data will be extracted from selected studies by a reviewer using a pre-designed data extraction form and checked by another reviewer. Disagreements will be resolved by discussion.
4.4.2 Methods of data synthesisData on the efficacy/effectiveness, safety and cost-effectiveness of pre-dialysis education programme will be presented in tabulated format with narrative summaries. Meta-analysis maybe conducted for this Health Technology Assessment.
4.5 Local economic evaluationPublished scientific evidence related to economic evaluation on pre-dialysis education programme will be examined first and if appropriate local data is available, local economic evaluation will be conducted for this HTA.
4.6 Patient involvementAs the target population for pre-dialysis education programme are advanced CKD patients, patients’ acceptance is deemed vital. Thus, patient engagement has been proposed to be included in this HTA. The mechanism of patient engagement will be scrutinised and conducted together in collaboration with nephrologists from Hospital Kuala Lumpur, Hospital Ampang and Hospital Tengku Ampuan Rahimah, Klang.
5.0 Report writing
6.0 References
1. Jha V, Garcia-Garcia G, Iseki K et al. Chronic kidney disease: global dimension and perspectives. Lancet.2013;382(9888):260-272.
2. Luyckx VA, Tonelli M, Stanifer JW. The global burden of kidney disease and the sustainable development goals. Bull World Health Organ. 2018;96(6):414-422D.
3. Ministry of Health, Malaysia. Clinical Practice Guidelines: Management of Chronic Kidney Disease (Second Edition). Available at www.moh.gov.my Accessed on 15th October 2019.
4. Hooi LS, Ong LM, Ahmad G et al. A population-based study measuring the prevalence of chronic kidney disease among adults in West Malaysia. Kidney Int. 2013;84(5):1034-1040.
5. Ministry of Health, Malaysia. National Action Plan For Healthy Kidneys (ACT-KID 2018-2025). Available at http://www.moh.gov.my/moh/resources/Penerbitan/Rujukan/NCD/National%20Strategic%20Plan/act_kid-1-min.pdf Accessed on 15th October 2019.
6. Bavanandan S, Saminathan T A, Hooi L S et al. Is Chronic Kidney Disease on the Rise in Malaysia? Findings from a nationwide study. Poster presented at The International Society of Nephrology (ISN) World Congress of Nephrology; 2019 April 12-15; Melbourne, Australia.

62
PRE-DIALYSIS EDUCATION PROGRAMME
7. Kidney Disease:Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney inter., Suppl. 2013; 3:1-150.
8. Stevens PE, Levin A; Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med. 2013 Jun 4;158(11):825-830.
9. UK Renal Association. Clinical Practice Guidelines: Planning, Initiating and Withdrawal of Renal Replacement Therapy (6th Edition). Available at https://renal.org/wp-content/uploads/2017/06/planning-initiation-finalf506a031181561659443ff000014d4d8.pdf Accessed on 15th October 2019.
10. Hassan R, Akbari A, Brown PA et al. Risk Factors for Unplanned Dialysis Initiation: A Systematic Review of the Literature. Can J Kidney Health Dis. 2019;6:2054358119831684.
11. Van den Bosch J, Warren DS, Rutherford PA. Review of predialysis education programmes: a need for standardization. Patient Prefer Adherence. 2015;9:1279-1291.
12. Combes G, Sein K, Allen K. How does pre-dialysis education need to change? Findings from a qualitative study with staff and patients. BMC Nephrol. 2017;18(1):334.

63
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Appendix 3Search strategy:
Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations and Ovid MEDLINE(R) <1946 to Present>
1 Kidney Failure, Chronic/ 2 (chronic adj2 (kidney failure or renal failure)).tw. 3 esrd.tw. 4 (end stage adj2 (kidney disease or renal disease)).tw. 5 (end-stage adj2 (kidney disease or renal disease or renal failure)).tw. 6 Renal Insufficiency, Chronic/ 7 (chronic adj2 (kidney disease* or renal disease*)).tw. 8 (chronic adj2 (renal insufficienc* or kidney insufficienc*)).tw. 9 esrf.tw.10 Advanced ckd.tw11 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 1012 HEALTH EDUCATION/ 13 community health education.tw.14 health education.tw.15 Pre-dialysis.tw.16 Predialysis.tw.17 Pre-dialysis education.tw.18 Predialysis education.tw.19 Pre-dialysis education program*.tw.20 Predialysis education program*.tw.21 Multidisciplinary pre-dialysis education.tw.22 Multidisciplinary predialysis education.tw.23 12 or 13 or 14 or 17 or 18 or 19 or 20 or 21 or 2224 11 and 23
PubMedSearch (((((((((((Kidney Failure, Chronic/[MeSH Terms]) OR ((chronic adj2 (kidney failure[Title/Abstract] OR renal failure))[Title/Abstract])) OR esrd[Title/Abstract]) OR ((end stage adj2 (kidney disease[Title/Abstract] OR renal disease)).[Title/Abstract])) OR ((end-stage adj2 (kidney disease[Title/Abstract] OR renal disease[Title/Abstract] OR renal failure))[Title/Abstract])) OR Renal Insufficiency, Chronic/[MeSH Terms]) OR ((chronic adj2 (kidney disease*[Title/Abstract] OR renal disease*))[Title/Abstract])) OR ((chronic adj2 (renal insufficienc*[Title/Abstract] OR kidney insufficienc*))[Title/Abstract])) OR esrf[Title/Abstract]) OR Advanced ckd[Title/Abstract])) AND (((((((((((HEALTH EDUCATION/[MeSH Terms]) OR community health education[Title/Abstract]) OR health education[Title/Abstract]) OR Pre-dialysis[Title/Abstract]) OR Predialysis[Title/Abstract]) OR Pre-dialysis education[Title/Abstract]) OR Predialysis education[Title/Abstract]) OR Pre-dialysis education program*[Title/Abstract]) OR Predialysis education program*[Title/Abstract]) OR Multidisciplinary pre-dialysis education[Title/Abstract]) OR Multidisciplinary predialysis education[Title/Abstract])

64
PRE-DIALYSIS EDUCATION PROGRAMME
Evid
ence
Tab
le :
Effe
ctiv
enes
s Q
uest
ion
: How
effe
ctiv
e is
Pre
-dia
lysi
s Ed
ucat
ion
Prog
ram
me
for a
dvan
ced
CKD
pat
ient
s?
Bibl
iogr
aphi
c C
itatio
nSt
udy
Type
/Met
hods
LEN
umbe
r of
Patie
nts
& Pa
tient
C
hara
cter
istic
Inte
rven
tion
Com
paris
onLe
ngth
of
Fol
low
U
p
Out
com
e M
easu
res/
Effe
ct S
ize
Gen
eral
C
omm
ents
1.H
su C
K, L
ee
CC
, Che
n YT
et a
l. M
ultid
isci
plin
ary
pre-
dial
ysis
edu
catio
n (M
PE) r
educ
es
inci
denc
e of
per
itoni
tis
and
subs
eque
nt d
eath
in
per
itone
al d
ialy
sis
patie
nts:
5-y
ear c
ohor
t st
udy.
PLoS
One
. 20
18;1
3(8)
:e02
0278
1.
Taiw
an
Coh
ort s
tudy
Obj
ectiv
eTo
in
vest
igat
e im
pact
of
M
PE
on
the
occu
rrenc
e of
pe
riton
itis,
tim
e to
fir
st
epis
ode
of p
erito
nitis
and
pat
ient
out
com
es
of P
D p
atie
nts
who
rece
ive
this
edu
catio
nal
prog
ram
Met
hod
-All
patie
nts
star
ting
PD a
t D
epar
tmen
t of
N
ephr
olog
y, C
hang
G
ung
Mem
oria
l H
ospi
tal,
Keel
ung,
fro
m J
uly
1, 2
007
to
Dec
embe
r 31
, 20
16 w
ere
enro
lled
and
follo
w-u
p fo
r 5 y
ears
from
PD
initi
atio
n.-P
atie
nts
wer
e di
vide
d in
to M
PE g
roup
and
no
n-M
PE g
roup
acc
ordi
ng to
whe
ther
the
subj
ects
had
eve
r re
ceiv
ed M
PE b
efor
e st
artin
g re
nal r
epla
cem
ent t
hera
py.
-Inci
denc
es o
f pe
riton
itis
and
perit
oniti
s-re
late
d m
orta
lity
wer
e co
mpa
red
betw
een
MPE
reci
pien
ts a
nd n
on-re
cipi
ents
. -C
onte
nt o
f the
MPE
was
sta
ndar
dize
d in
ac
cord
ance
with
the
NKF
/DO
QI g
uide
lines
.-K
apla
n-M
eier
an
alys
is
and
Cox
pr
opor
tiona
l haz
ards
mod
el w
ere
appl
ied
to id
entif
y the
pro
gnos
tic fa
ctor
s ass
ocia
ted
with
per
itoni
tis-fr
ee s
urvi
val.
-Stu
dy e
ndpo
ints
:v
Epis
odes
of p
erito
nitis
v
Out
com
es
afte
r pe
riton
itis
(incl
udin
g ho
spita
lisat
ion,
te
chni
que
failu
re,
switc
hing
of
mod
ality
int
o he
mod
ialy
sis
or
deat
h)
II-2
398
PD p
atie
nts:
169
M
PE
229
No
MPE
be
fore
sta
rting
PD
.
-MPE
reci
pien
ts
olde
r (6
3.1±
16.2
vs.
58
.5±1
6.4
year
s ol
d, P
=0.0
06),
had
high
er p
reva
lenc
e of
dia
bete
s (6
0.4%
vs
43.
7%,
P< 0
.001
) -M
PE g
roup
had
lo
wer
bas
elin
e ed
ucat
iona
l lev
els
(P<
0.00
1)
-No
diffe
renc
es in
in
itial
labo
rato
ry
findi
ngs,
bas
elin
e pe
riton
eal
equi
libra
tion
test
(P
ET) a
nd P
D
adeq
uacy
bet
wee
n tw
o gr
oups
-P
atie
nts
drop
ped
out:
MPE
gro
up (s
witc
h to
HD
27,
dea
th
20) 2
0% v
s N
on-
MPE
gro
up (s
witc
h to
HD
16,
dea
th 6
) 13
%.
Mul
tidis
cipl
inar
y pr
e-di
alys
is
educ
atio
n (M
PE)
-Com
pris
ed a
nu
rse
of c
ase
mx,
so
cial
wor
kers
, di
etiti
ans,
10
neph
rolo
gist
s, a
nd
HD
&PD
pat
ient
vo
lunt
eers
. -D
eliv
ery
of
know
ledg
e on
nut
ritio
n su
pp, l
ifest
yle
mod
ifica
tion,
ne
phro
toxi
n av
oida
nce,
die
tary
pr
inci
ples
and
ph
arm
acol
ogic
al
regi
men
s by
nur
se
acc.
to C
KD s
tage
-M
onito
ring
of C
KD
com
plic
atio
ns,
prep
arat
ion
for
timel
y in
itiat
ion
of R
RT, c
are
of v
ascu
lar o
r pe
riton
eal a
cces
s,
and
regi
stra
tion
for i
nclu
sion
in th
e re
nal t
rans
plan
t w
aitin
g lis
t wer
e C
KP p
atie
nts.
Cus
tom
ary
care
(Non
-MPE
)
-Sam
e gr
oup
of n
ephr
olog
ist
who
inst
ruct
ed
pts
reg.
rena
l fu
nctio
n,
eval
uatio
n of
la
bora
tory
dat
a an
d th
e cl
inic
al
indi
cato
rs o
f re
nal f
ailu
re
as w
ell a
s tre
atm
ent
stra
tegi
es.
-Writ
ing
mat
eria
ls o
r bo
okle
ts g
iven
to
pat
ient
s if
verb
al
inst
ruct
ions
ar
e di
fficu
lt an
d w
ithou
t he
lp o
f cas
e-m
x nu
rse
5 ye
ars
afte
r PD
st
arts
Res
ults
:Af
ter
a 5-
year
s of
follo
w-u
p (m
ean
follo
w-
up d
urat
ion:
29.
4 m
onth
s; 3
0.1
mon
ths
in
MPE
gro
up v
s. 2
8.5
mon
ths;
Perit
oniti
s -M
PE
patie
nts
had
sign
ifica
ntly
le
ss
perit
oniti
s [0
.29±
0.72
vs
. 0.
64±1
.5
epis
odes
/per
son-
year
or
m
edia
n (IQ
R):
0 (0
.29)
vs.
0.1
1 (0
.69)
epi
sode
s/pe
rson
-ye
ar, P
< 0.
001]
than
non
-MPE
pat
ient
s.
Perit
oniti
s-re
late
d de
ath
rate
s-M
PE g
roup
had
low
er p
erito
nitis
-rel
ated
de
ath
rate
s co
mpa
red
to n
on-M
PE g
roup
(3
.6%
ver
sus
8.7%
, P=
0.04
).
Tim
e to
firs
t epi
sode
of p
erito
nitis
-Med
ian
time
to
the
first
ep
isod
e of
pe
riton
itis
in
the
non-
MPE
an
d M
PE
grou
ps w
as 3
3.9
mon
ths
and
46.7
mon
ths,
re
spec
tivel
y (C
ox-M
ante
l log
rank
test
, P =
0.
003)
. -C
ox re
gres
sion
ana
lysi
s re
veal
ed th
at th
e ed
ucat
iona
l lev
el b
elow
ele
men
tary
[h
azar
d ra
tio (H
R):
1.92
5; 9
5% (C
I): 1
.257
, 2.
874,
P=
0.00
3] a
nd th
e us
e of
MPE
(HR
: 0.
594;
95%
CI:
0.43
4, 0
.813
, P<
0.0
01)
wer
e si
gnifi
cant
in
depe
nden
t pr
edic
tors
fo
r pe
riton
itis-
free
surv
ival
, afte
r ad
just
ing
the
base
line
char
acte
ristic
s of
age
, gen
der,
diab
etes
, hy
perte
nsio
n an
d pe
riton
eal
mod
aliti
es
Aut
hors
con
clus
ion
In c
oncl
usio
n, a
n ef
ficie
nt s
tand
ardi
zed
MPE
pro
gram
adh
ered
to th
e N
FK/D
OQ
I
-Sin
gle
cent
re s
tudy
-edu
catio
n by
te
am, m
ultip
le
indi
vidu
al s
essi
ons
App
endi
x 4

65
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Evid
ence
Tab
le :
Effe
ctiv
enes
s Q
uest
ion
: How
effe
ctiv
e is
Pre
-dia
lysi
s Ed
ucat
ion
Prog
ram
me
for a
dvan
ced
CKD
pat
ient
s?Bi
blio
grap
hic
Cita
tion
Stud
yTy
pe/M
etho
dsLE
Num
ber o
f Pat
ient
s &
Patie
nt C
hara
cter
istic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
2. Z
ukm
in K
, Ahm
ad
I, W
ynn
AK e
t al.
A co
mpa
rativ
e st
udy
to e
valu
ate
fact
ors
that
in
fluen
ce s
urvi
val
in m
ultid
isci
plin
ary
pred
ialy
sis
educ
ated
pa
tient
s an
d “C
rash
land
ers”
. Sa
udi J
Kid
ney
Dis
Tra
nspl
. 20
17;2
8(4)
:743
-75
0.
Brun
ei
Ret
rope
ctiv
e co
hort
st
udy
Obj
ectiv
e:To
com
pare
su
rviv
al p
roba
bilit
y, so
ciod
emog
raph
ic, a
nd
clin
ical
cha
ract
eris
tics
of m
ultid
isci
plin
ary
pre-
dial
ysis
edu
cate
d (M
PE)
and
non-
MPE
/cra
shla
nder
pa
tient
s
Met
hods
:- A
ll ne
w E
SRD
pa
tient
s w
ho s
tarte
d fir
st h
emod
ialy
sis
(HD
) fro
m J
anua
ry 2
013
to
Dec
embe
r 201
4 fro
m
Raj
a Is
teri
Peng
iran
Anak
Sa
leha
Hos
pita
l and
all
dial
ysis
cen
ters
in B
rune
i D
arus
sala
m w
ere
enro
lled
-Dat
a ex
tract
ed fr
om
clin
ical
regi
stry
and
dia
lysi
s re
cord
s.
-Dat
a in
clud
ed
soci
odem
ogra
phic
in
form
atio
n, c
linic
al
info
rmat
ion,
com
orbi
ditie
s,
surv
ival
sta
tus,
pre
-dia
lysi
s cl
inic
refe
rral,
choi
ce o
f R
RT, a
nd ty
pes
of v
ascu
lar
acce
ss (f
or H
D p
atie
nts)
.-S
urvi
val p
roba
bilit
y, so
ciod
emog
raph
ic, a
nd
clin
ical
cha
ract
eris
tics
of m
ultid
isci
plin
ary
pre-
dial
ysis
edu
cate
d (M
PE)
and
non-
MPE
/cra
shla
nder
pa
tient
s w
ere
com
pare
d.
II-2
Tota
l 350
new
cas
es
of E
SRD
-Med
ian
age
56.0
ye
ars.
-S
light
ly m
ore
mal
es
-Mal
ays
(86.
6%) n
on-
Mal
ays
(13.
4%)
-Med
ian
estim
ated
G
FR 4
.0 m
L/m
in/
1.73
m2 ,
-119
pat
ient
s (3
4.6%
) w
ere
dece
ased
at t
he
end
of s
tudy
per
iod.
-MPE
gro
ups
olde
r (P
=0.0
01),
diab
etic
s (P
=0.0
13),
and
HTN
(P
=0.0
16),
IHD
(P
=0.0
14),
and
usin
g ar
terio
veno
us fi
stul
a (P
<0.
001)
.
Mul
tidis
cipl
inar
y pr
e-di
alys
is e
duca
tion
(MPE
)(n
=180
)
-Mul
tidis
cipl
inar
y te
am
incl
udes
nep
hrol
ogis
ts,
nurs
e pr
actit
ione
rs,
diet
icia
ns, a
nd m
edic
al
soci
al w
orke
rs-N
urse
com
pris
e sp
ecifi
c nu
rses
that
spe
cial
ize
in
vasc
ular
acc
ess,
HD
, PD
, an
d tra
nspl
anta
tion
-Ger
iatri
cian
s an
d pa
lliativ
e ca
re te
am
occa
sion
ally
invo
lved
if
patie
nts
have
pre
-em
ptiv
ely
deci
ded
not t
o un
derg
o R
RT-C
linic
focu
ses
on
stra
tegi
es to
mai
ntai
n ta
rget
BP,
impr
ove
com
plia
nce
with
m
edic
atio
ns, n
utrit
iona
l ne
eds,
nep
hrot
oxin
s av
oida
nce,
and
fast
trac
k va
scul
ar s
ervi
ces
for
fistu
la fo
rmat
ions
and
ea
rly c
omm
ence
men
t of
RRT
-C
ultu
ral a
ccep
tanc
e an
d re
ligio
us c
ouns
ellin
g al
so c
over
ed in
this
cl
inic
to o
verc
ome
soci
al
stig
mat
izat
ion
and
impr
ove
psyc
holo
gica
l acc
epta
nce
No
MPE
(n=1
68)
2 ye
ars
Res
ults
:Su
rviv
al
Surv
ival
sta
tus
All p
atie
nts
MPE
(%)
Non
MPE
(%)
Aliv
e/ce
nsor
ed22
5 (6
5.4%
)12
7 (5
6.7%
)97
(43.
3%)
Dec
ease
d11
9 (3
4.6%
)52
(44.
1%)
66 (5
5.9%
)
-Des
pite
bei
ng o
lder
and
hav
ing
mor
e co
mor
bidi
ties,
MPE
pa
tient
s ha
ve b
ette
r sur
viva
l pro
babi
lity
(P =
0.0
28) a
nd a
34
% d
ecre
ased
risk
of d
ying
1 ye
ar (%
)2
year
s (%
)
MPE
79.8
%57
.7%
Non
-MPE
66.2
%60
.1%
- Th
e 1-
year
sur
viva
l rat
e w
as h
ighe
r in
MPE
gro
up
com
pare
d to
non
-MPE
(79.
8% v
ersu
s 66
.2%
). -
No
sign
ifica
nt d
iffer
ence
afte
r tw
o ye
ars
(57.
7% a
nd
60.1
%)
- O
lder
age
(P =
0.0
01),
high
ser
um c
reat
inin
e le
vel (
P <0
.001
), lo
wer
est
imat
ed G
FR (P
<0.
001)
, and
low
er
hem
oglo
bin
leve
l (P
= 0.
017)
wer
e as
soci
ated
with
the
redu
ctio
n in
the
surv
ival
pro
babi
lity.
Aut
hors
con
clus
ion:
Mul
tidis
cipl
inar
y pr
e-di
alys
is e
duca
tion
(MPE
) bef
ore
the
initi
atio
n of
RRT
con
tribu
ted
to g
reat
er s
urvi
val p
roba
bilit
y in
nea
r ESR
D p
atie
nts.
The
sur
viva
l ben
efits
wer
e ev
iden
t de
spite
the
pres
ence
of i
nher
ent r
isks
(old
er a
ge a
nd
pres
ence
of c
omor
bidi
ties)
in th
e M
PE p
opul
atio
n in
co
mpa
rison
with
the
non-
MPE
coh
ort.
Mul
ti-ce
ntre
st
udy
Educ
atio
n by
te
am, m
ultip
le
indi
vidu
al
sess
ions

66
PRE-DIALYSIS EDUCATION PROGRAMME
Evid
ence
Tab
le :
Effe
ctiv
enes
s Q
uest
ion
: How
effe
ctiv
e is
Pre
-dia
lysi
s Ed
ucat
ion
Prog
ram
me
for a
dvan
ced
CKD
pat
ient
s?Bi
blio
grap
hic
Cita
tion
Stud
yTy
pe/M
etho
dsLE
Num
ber o
f Pa
tient
s &
Patie
nt
Cha
ract
eris
tic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
3. V
an d
en
Bosc
h J,
War
ren
DS,
Rut
herfo
rd
PA. R
evie
w
of p
redi
alys
is
educ
atio
npr
ogra
ms:
a n
eed
for s
tand
ardi
zatio
n.
Patie
ntPr
efer
Ad
here
nce.
20
15;9
:127
9-12
91.
Syst
emat
ic re
view
Obj
ectiv
e:
To re
view
evi
denc
e on
effe
ctiv
e co
mpo
nent
s of
pre
-dia
lysi
s ed
ucat
ion
prog
ram
mes
as
rela
ted
to m
odal
ity c
hoic
e an
d se
lect
ed
clin
ical
out
com
es.
Met
hod:
-Sys
tem
atic
sea
rch
was
per
form
ed o
n Pu
bMed
MED
LIN
E, C
ochr
ane
Libr
ary,
and
Ovi
d (fr
om J
anua
ry 1
, 199
5 to
Dec
embe
r 31
, 201
3)
-Incl
usio
n cr
iteria
app
lied:
v
Adul
ts o
nly
v
Pre-
dial
ysis
edu
catio
n fo
r CKD
st
age
III, I
V, a
nd V
v
Plan
ned
star
t pat
ient
s, u
npla
nned
st
art p
atie
nts,
and
pat
ient
s on
di
alys
is, i
e, in
cide
nt a
nd p
reva
lent
pa
tient
s.v
Det
aile
d de
scrip
tion
of
prog
ram
me
v
Mul
tiple
ses
sion
sv
Mul
tidis
cipl
inar
y pr
ogra
mm
e in
volv
ing
phys
icia
ns, n
urse
s,
diet
icia
ns, e
tc.
-Out
com
es in
clud
ed:
v
Dia
lysi
s m
odal
ity c
hoic
e an
d th
e nu
mbe
rs o
f pat
ient
s ch
oosi
ng
each
mod
ality
v
Any
clin
ical
out
com
e as
soci
ated
w
ith p
re-d
ialy
sis
educ
atio
n v
Hea
lth-re
late
d qu
ality
of l
ife
v
Mea
sure
s as
soci
ated
with
pat
ient
ch
oice
v
Fina
ncia
l im
pact
of p
atie
nts
choo
sing
mor
e ho
me
ther
apie
s v
Patie
nt s
atis
fact
ion
-Lite
ratu
re a
lso
revi
ewed
for a
ny in
form
atio
n on
pro
cess
es, p
athw
ays,
and
org
aniz
atio
n of
th
e pr
e-di
alys
is e
duca
tion
prog
ram
me
I29
rele
vant
stu
dies
:19
qua
si-e
xper
imen
tal
desi
gn10
nar
rativ
e re
view
s
-19
stud
ies
wer
e an
alys
ed fo
r effe
ctiv
e co
mpo
nent
s of
pre
-di
alys
is e
duca
tion
prog
ram
me
-Des
crip
tions
of
the
educ
atio
nal
proc
ess
varie
d an
d in
clud
ed in
divi
dual
an
d gr
oup
educ
atio
n,
mul
tidis
cipl
inar
y in
terv
entio
n, a
nd
vary
ing
dura
tion
and
frequ
ency
of s
essi
ons.
Pre-
dial
ysis
ed
ucat
ion
prog
ram
mes
Res
ults
:M
orta
lity
and
mor
bidi
ty-8
stu
dies
repo
rted
on m
orta
lity
and
mor
bidi
ty
(incl
udin
g bi
oche
mic
al in
dica
tors
, car
diov
ascu
lar
inci
dent
s, in
fect
ion
rate
s, e
mot
iona
l sta
tus)
. -A
ll st
udie
s re
porte
d be
tter r
ates
for t
he tr
eatm
ent
grou
p.
Cho
et a
l. (2
012)
Less
unp
lann
ed u
rgen
t dia
lysi
s (8
.7%
vs
24.2
%),
less
car
diac
eve
nts
(2.7
% v
s 9.
4%),
less
infe
ctio
ns
(4.0
% v
s 12
.1%
)
Klan
g et
al.
(199
8)Si
gnifi
cant
bet
ter m
ood,
less
mob
ility
prob
lem
s,
less
func
tiona
l dis
abilit
ies
and
low
er a
nxie
ty
Lacs
on e
t al.
(201
1)Si
gnifi
cant
bet
ter s
urvi
val r
ate
(adj
. HR
0.6
1)
Levi
n et
al.
(199
7)Be
tter b
ioch
emic
al m
arke
rs: b
lood
pre
ssur
e,
calc
ium
, pho
spha
te, a
nd a
nem
ia
Rio
ux e
t al.
(201
1)35
% o
f all
acut
e st
arte
rs a
dopt
ed h
ome
dial
ysis
vs
13%
bef
ore
prog
ram
Hal
l G e
t al (
2004
)Le
ss in
fect
ion
rate
s 18
.5 v
s. 3
1.8;
p =
0.0
0349
Souq
iyye
h M
Z e
t al.
(200
8)si
gnifi
cant
ly le
ss d
ropo
uts
for P
D (p
<0.0
2)
Aut
hors
con
clus
ion:
Ther
e is
a n
eed
for a
sta
ndar
dise
d ap
proa
ch
built
on
best
evi
denc
e fro
m C
KD a
nd a
lso
from
ot
her c
linic
al c
ondi
tions
and
exi
stin
g kn
owle
dge
on th
e ev
alua
tion
of c
ompl
ex in
terv
entio
ns to
en
sure
form
al e
valu
atio
n of
pre
dial
ysis
edu
catio
n pr
ogra
mm
es, a
nd th
eir e
ffect
s on
clin
ical
ou
tcom
es a
nd m
odal
ity c
hoic
e.
Mos
t with
out
cont
rol
grou
ps

67
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Evid
ence
Tab
le :
Effe
ctiv
enes
s Q
uest
ion
: How
effe
ctiv
e is
Pre
-dia
lysi
s Ed
ucat
ion
Prog
ram
me
for a
dvan
ced
CKD
pat
ient
s?Bi
blio
grap
hic
Cita
tion
Stud
yTy
pe/M
etho
dsLE
Num
ber o
f Pa
tient
s &
Patie
nt
Cha
ract
eris
tic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
pO
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
4. W
u IW
, Wan
g SY
, Hsu
KH
et a
l. M
ultid
isci
plin
ary
pred
ialy
sis
educ
atio
n de
crea
ses
the
inci
denc
e of
di
alys
is a
nd
redu
ces
mor
talit
y--a
co
ntro
lled
coho
rt st
udy
base
d on
th
e N
KF/D
OQ
I gu
idel
ines
. Nep
hrol
Dia
l Tra
nspl
ant.
2009
;24(
11):3
426-
3433
.
Taiw
an
Coh
ort s
tudy
Obj
ectiv
e:To
eva
luat
e th
e im
pact
of
mul
tidis
cipl
inar
y pr
e-di
alys
is
educ
atio
n (M
PE) o
n th
e in
cide
nce
of d
ialy
sis
and
outc
omes
of C
KD p
atie
nts
in a
ccor
danc
e w
ith th
e gu
idel
ines
of t
he N
atio
nal
Kidn
ey F
ound
atio
n D
ialy
sis
Out
com
es Q
ualit
y In
itiat
ive
(NKF
/DO
QI).
Met
hods
:-A
ll st
udy
parti
cipa
nts
wer
e pr
e-di
alys
is C
KD p
atie
nts
who
vis
ited
the
neph
rolo
gy
outp
atie
nt c
linic
s of
the
Dep
artm
ent o
f Nep
hrol
ogy
at C
hang
Gun
g M
emor
ial
Hos
pita
l in
Taip
ei a
nd
Keel
ung
from
May
200
6 to
M
ay 2
007.
-Pat
ient
s w
ere
clas
sifie
d in
to s
tage
s III
, IV
or V
in
acco
rdan
ce w
ith th
e N
KF/
DO
QI c
lass
ifica
tion
syst
em-In
form
atio
n w
as c
olle
cted
fo
r fur
ther
ana
lyse
s,
incl
udin
g de
mog
raph
ic
varia
bles
, cau
ses
of p
rimar
y re
nal d
isea
se, i
nitia
l sta
tus
of re
nal f
unct
ion,
obv
ious
ur
aem
ic
-All
parti
cipa
nts
wer
e di
vide
d in
to tw
o co
horts
acc
ordi
ng to
th
e si
tes:
v
MPE
gro
up a
t th
e Ke
elun
g ce
ntre
v
Non
-MPE
gro
up
at T
aipe
i cen
tre.
-Pat
ient
s w
ere
atte
nded
by
sam
e gr
oup
of n
ephr
olog
ists
un
der s
ame
follo
w-u
p sc
hem
a, a
nd w
ere
follo
wed
up
for 1
2 m
onth
s fo
r dia
lysi
s in
itiat
ion
or m
orta
lity
from
an
y ca
use.
II-2
Stud
y in
volv
ed 5
73
CKD
pat
ient
s:v
287
rece
ived
M
PE
v
286
Non
M
PE
-317
(55.
3%) w
ere
mal
es a
nd 2
56
(44.
7%) f
emal
es;
-Ave
rage
age
was
63
.4±1
4.8
year
s.-M
ean
eGFR
: 2
3.8
±20.
1 m
L/m
in/1
.73
-Sta
ge II
I 157
(2
7.4%
) S
tage
IV 1
23
(21.
5%)
Sta
ge V
293
(5
1.1%
)- M
PE re
cipi
ents
ol
der
(65.
5±13
.9 v
s 61
.2±1
4.8
year
s ol
d,
P=0.
048)
with
muc
h lo
wer
pre
vale
nce
of
hype
rtens
ion
(5.2
% v
s 22
%,
P <
0.00
1).
Mul
tidis
cipl
inar
y pr
e-di
alys
is
educ
atio
n (M
PE)
-Com
pris
ed a
nur
se fo
r ca
se m
x, s
ocia
l wor
kers
, di
etiti
ans,
HD
and
PD
pa
tient
vol
unte
ers
and
10
neph
rolo
gist
s-P
rogr
amm
e co
nsis
ted
of
inte
grat
ed c
ours
e in
volv
ing
indi
vidu
al le
ctur
es o
n re
nal
heal
th, d
eliv
ered
by
case
-mx
nurs
e-L
ectu
res
focu
sed
on n
utrit
ion,
life
styl
e,
neph
roto
xin
avoi
danc
e,
diet
ary
prin
cipl
es a
nd
phar
mac
olog
ical
regi
men
s-S
tand
ardi
zed
inte
ract
ive
educ
atio
nal s
essi
ons
wer
e pe
riodi
cally
con
duct
ed w
here
al
l pat
ient
s w
ere
inte
rvie
wed
de
pend
ing
on C
KD s
tage
-Sta
ge II
I or I
V C
KD p
atie
nts:
f/u
p 3m
onth
ly, s
tage
V: f
/up
mon
thly
-Sta
ge II
I pat
ient
s:
prog
ram
me
cons
iste
d of
le
ctur
es o
n he
alth
y re
nal
func
tion,
clin
ical
pre
sent
atio
n of
ura
emia
, ris
k fa
ctor
s an
d co
mpl
icat
ions
ass
ocia
ted
with
rena
l pro
gres
sion
and
an
intro
duct
ion
to th
e va
rious
R
RTs
-Sta
ge IV
pat
ient
s:
prog
ram
me
incl
uded
di
scus
sion
s on
the
mx
of
com
plic
atio
ns a
ssoc
iate
d w
ith C
KD, i
ndic
atio
ns o
f RRT
an
d ev
alua
tion
of v
ascu
lar o
r pe
riton
eal a
cces
s.
-Sta
ge V
pat
ient
s:
mon
itore
d fo
r tim
ely
initi
atio
n of
RRT
, car
e of
vas
cula
r or
perit
onea
l acc
ess,
dia
lysi
s-as
soci
ated
com
plic
atio
ns
and
regi
stra
tion
for i
nclu
sion
in
the
rena
l tra
nspl
ant
wai
ting
list
Cus
tom
ary
care
-Sam
e gr
oup
of n
ephr
olog
ist
inst
ruct
ed
parti
cipa
nts
rega
rdin
g re
nal f
unct
ion,
ev
alua
tion
of la
b da
ta
and
clin
ical
in
dica
tors
of
chro
nic
rena
l fa
ilure
as
wel
l as
stra
tegi
es
for m
x &
tx-G
ener
al
prin
cipl
es o
f H
D a
nd P
D
expl
aine
d w
hen
patie
nts
ente
r sta
ge IV
-All
patie
nts
prov
ided
w
ith w
ritte
n in
stru
ctio
ns.
-Com
orbi
dity
fa
ctor
s ev
alua
ted
befo
re re
ferra
l to
nur
se
spec
ializ
ing
in
HD
or P
D.
-Nur
sing
sta
ff pr
ovid
ed
inst
ruct
ions
fo
r dai
ly li
ving
an
d ex
plai
ned
crite
ria fo
r H
D a
nd P
D
sele
ctio
n an
d th
e di
ffere
nce
betw
een
mod
aliti
es.
12 Mon
ths
-Mea
n fo
llow
-up
perio
d w
as
11.7
±0.9
m
onth
s.
Res
ults
:In
cide
nce
of d
ialy
sis
-Dia
lysi
s w
as in
itiat
ed in
13.
9% a
nd 4
3% o
f the
pat
ient
s in
the
MPE
an
d no
n-M
PE g
roup
s, re
spec
tivel
y (P
< 0
.001
)-T
ime
to d
ialy
sis
was
sig
nific
antly
long
er fo
r MPE
gro
up (1
1.3
mon
ths)
vs
Non
-MPE
gro
up (9
.2 m
onth
s) (P
<0.0
01)
-MPE
reci
pien
ts s
how
ed:
v
a hi
gher
ser
um a
lbum
in le
vel (
3.8
± 0.
5 ve
rsus
3.4
±
0.5
g/dL
, P =
0.0
50),
v
low
er s
erum
hs-
CR
P le
vel (
3.3±
2.8
vers
us 5
.5±5
.6
mg/
L, P
=0.0
32),
v
low
er s
erum
ferri
tin c
once
ntra
tion
(284
± 3
1 ve
rsus
532
±
59 n
g/m
L, P
= 0
.049
),
v
high
er P
D u
ptak
e (3
5% v
ersu
s 20
.5%
, P =
0.0
23),
v
low
er fr
eque
ncy
of te
mpo
rary
vas
cula
r cat
hete
r use
(2
5% v
ersu
s 50
.4%
; P <
0.0
5)
v
and
grea
ter p
ost-d
ialy
sis
body
wei
ghts
(65±
10 v
ersu
s 58
±11
kg, P
=0.0
34) t
han
the
non-
MPE
pat
ient
s.
Mor
talit
y-O
vera
ll m
orta
lity
was
1.7
% a
nd 1
0.1%
in th
e M
PE a
nd n
on-M
PE
grou
ps, r
espe
ctiv
ely
(P <
0.0
01).
-Med
ian
surv
ival
tim
e in
the
non-
MPE
and
MPE
gro
ups
was
11.
2 an
d 11
.9 m
onth
s, re
spec
tivel
y (C
ox–M
ante
l log
rank
test
, P<0
.001
)-A
djus
ted
haza
rd ra
tio o
f mor
talit
y fo
r MPE
reci
pien
ts w
as 0
.103
[9
5% c
onfid
entia
l int
erva
l (C
I) 0.
040,
0.2
65, P
< 0
.001
], af
ter
adju
stm
ent f
or a
ge, g
ende
r, di
abet
es, h
yper
tens
ion,
eG
FR, H
b,
seru
m a
lbum
in, h
s-C
RP
-Cox
regr
essi
on a
naly
sis
reve
aled
that
dia
bete
s, e
stim
ated
gl
omer
ular
filtr
atio
n ra
te (e
GFR
), hi
gh-s
ensi
tive
C-re
activ
e pr
otei
n (h
s-C
RP)
and
MPE
ass
ignm
ent w
ere
sign
ifica
nt in
depe
nden
t pr
edic
tors
for p
rogr
essi
on to
ESR
D.
-Inde
pend
ent p
rogn
ostic
fact
ors
for m
orta
lity
incl
uded
age
, di
abet
es, e
GFR
, hs-
CR
P an
d M
PE a
ssig
nmen
t
Aut
hors
con
clus
ion:
An e
ffici
ent s
tand
ardi
zed
MPE
pro
gram
me
com
plyi
ng w
ith th
e N
KF/D
OQ
I gui
delin
es m
ay d
ecre
ase
the
inci
denc
e of
dia
lysi
s an
d re
duce
the
all-c
ause
mor
talit
y an
d th
e ov
eral
l hos
pita
lisat
ion
rate
in
CKD
pat
ient
s. T
his
valu
able
info
rmat
ion
confi
rms
the
role
of M
PE in
th
e ca
re o
f CKD
pat
ient
s
Mul
tiple
in
divi
dual
se
ssio
ns
with
team
m
embe
rs
+ pa
tient
s vo
lunt
eers

68
PRE-DIALYSIS EDUCATION PROGRAMME
Evid
ence
Tab
le :
Org
anis
atio
nal (
HO
SPIT
ALIS
ATIO
N)
Que
stio
n : W
hat a
re th
e or
gani
satio
nal i
ssue
s w
ith re
gard
s to
Pre
-dia
lysi
s Ed
ucat
ion
Prog
ram
me
for a
dvan
ced
CKD
pat
ient
s?Bi
blio
grap
hic
Cita
tion
Stud
yTy
pe/M
etho
dsLE
Num
ber o
f Pat
ient
s &
Patie
nt C
hara
cter
istic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
1.H
su C
K, L
ee C
C, C
hen
YT e
t al.
Mul
tidis
cipl
inar
y pr
e-di
alys
is e
duca
tion
(MPE
) red
uces
inci
denc
e of
per
itoni
tis a
ndsu
bseq
uent
dea
th
in p
erito
neal
dia
lysi
s pa
tient
s: 5
-yea
r coh
ort
stud
y. PL
oS O
ne.
2018
;13(
8):e
0202
781.
Taiw
an
Coh
ort s
tudy
Obj
ectiv
eTo
inve
stig
ate
impa
ct o
f MPE
on
the
occu
rrenc
e of
per
itoni
tis, t
ime
to fi
rst e
piso
de o
f pe
riton
itis
and
patie
nt o
utco
mes
of P
D p
atie
nts
who
rece
ive
this
edu
catio
nal p
rogr
am
Met
hod
-All
patie
nts
star
ting
PD a
t Dep
artm
ent o
f N
ephr
olog
y, C
hang
Gun
g M
emor
ial H
ospi
tal,
Keel
ung,
from
Jul
y 1,
200
7 to
Dec
embe
r 31,
20
16 w
ere
enro
lled
and
pros
pect
ivel
y fo
llow
-up
for 5
yea
rs fr
om P
D in
itiat
ion.
-Pat
ient
s w
ere
divi
ded
into
MPE
gro
up a
nd
non-
MPE
gro
up a
ccor
ding
to w
heth
er th
e su
bjec
ts h
ad e
ver r
ecei
ved
MPE
bef
ore
star
ting
rena
l rep
lace
men
t the
rapy
.-In
cide
nces
of p
erito
nitis
and
per
itoni
tis-re
late
d m
orta
lity
wer
e co
mpa
red
betw
een
MPE
re
cipi
ents
and
non
-reci
pien
ts.
-Con
tent
of t
he M
PE w
as s
tand
ardi
zed
in
acco
rdan
ce w
ith th
e N
KF/D
OQ
I gui
delin
es.
-Kap
lan-
Mei
er a
naly
sis
and
Cox
pro
porti
onal
ha
zard
s m
odel
wer
e ap
plie
d to
iden
tify
the
prog
nost
ic fa
ctor
s as
soci
ated
with
per
itoni
tis-
free
surv
ival
.-S
tudy
end
poin
ts:
v
Epis
odes
of p
erito
nitis
v
Out
com
es a
fter p
erito
nitis
(in
clud
ing
hosp
italis
atio
n, te
chni
que
failu
re, s
witc
hing
of m
odal
ity in
to
hem
odia
lysi
s or
dea
th)
-Pat
ient
s w
ho d
rop-
out f
rom
PD
(dea
th, r
enal
tra
nspl
ant,
switc
h to
hem
odia
lysi
s) b
efor
e de
velo
pmen
t of fi
rst p
erito
nitis
wer
e ce
nsor
ed.
II-2
398
PD p
atie
nts:
169
M
PE
229
No
MPE
bef
ore
star
ting
PD.
-MPE
reci
pien
ts
olde
r (6
3.1±
16.2
vs.
58
.5±1
6.4
year
s ol
d, P
=0.0
06),
had
high
er p
reva
lenc
e of
dia
bete
s (6
0.4%
vs
43.
7%,
P< 0
.001
) -M
PE g
roup
had
lo
wer
bas
elin
e ed
ucat
iona
l lev
els
(P<
0.00
1)
-No
diffe
renc
es in
in
itial
labo
rato
ry
findi
ngs,
bas
elin
e pe
riton
eal
equi
libra
tion
test
(P
ET) a
nd P
D
adeq
uacy
bet
wee
n tw
o gr
oups
-P
atie
nts
drop
ped
out:
MPE
gro
up (s
witc
h to
HD
27,
dea
th 2
0)
20%
vs
Non
-MPE
gr
oup
(sw
itch
to
HD
16,
dea
th 6
) 13
%.
Mul
tidis
cipl
inar
y pr
e-di
alys
is e
duca
tion
(MPE
)
-Com
pris
ed a
nur
se o
f ca
se m
x, s
ocia
l wor
kers
, di
etiti
ans,
10
neph
rolo
gist
s,
and
HD
&PD
pat
ient
vo
lunt
eers
. -D
eliv
ery
of k
now
ledg
e on
nut
ritio
n su
pp,
lifes
tyle
mod
ifica
tion,
ne
phro
toxi
n av
oida
nce,
di
etar
y pr
inci
ples
and
ph
arm
acol
ogic
al re
gim
ens
by n
urse
acc
. to
CKD
sta
ge
-Mon
itorin
g of
CKD
co
mpl
icat
ions
, pre
para
tion
for t
imel
y in
itiat
ion
of
RRT
, car
e of
vas
cula
r or
perit
onea
l acc
ess,
and
re
gist
ratio
n fo
r inc
lusi
on in
th
e re
nal t
rans
plan
t wai
ting
list w
ere
also
inst
ruct
ed fo
r la
te s
tage
CKD
pat
ient
s.
-Sha
red
deci
sion
mak
ing
was
don
e fo
r the
se p
atie
nts
for t
heir
choi
ce o
f RRT
. -B
enefi
t, di
sadv
anta
ge
and
self-
care
for d
iffer
ent
mod
ality
was
exp
lain
ed.
-All
patie
nts
also
rece
ived
di
etar
y co
unse
lling
bian
nual
ly fr
om a
die
titia
n.-M
PE p
rogr
am
disc
ontin
ued
once
the
patie
nts
initi
ate
dial
ysis
th
erap
y
Cus
tom
ary
care
(Non
-MPE
)
-Sam
e gr
oup
of
neph
rolo
gist
w
ho
inst
ruct
ed
pts
reg.
rena
l fu
nctio
n,
eval
uatio
n of
labo
rato
ry
data
and
th
e cl
inic
al
indi
cato
rs o
f re
nal f
ailu
re
as w
ell a
s tre
atm
ent
stra
tegi
es.
-Writ
ing
mat
eria
ls
or b
ookl
ets
give
n to
pa
tient
s if
verb
al
inst
ruct
ions
is
diffi
cult
and
with
out h
elp
of c
ase-
mx
nurs
e
5 ye
ars
afte
r PD
st
arts
Res
ults
:Af
ter a
5-y
ears
of
follo
w-u
p (m
ean
follo
w-u
p du
ratio
n:
29.4
mon
ths;
30.
1 m
onth
s in
MPE
gr
oup
vs. 2
8.5
mon
ths;
Hos
pita
lisat
ion
and
tech
niqu
e fa
ilure
s-N
o si
gnifi
cant
di
ffere
nce
betw
een
two
grou
ps in
fre
quen
cy o
f ho
spita
lizat
ion
(med
ian
(IQR
), ep
isod
es/p
erso
n-ye
ar :
1.36
(2.4
3) in
M
PE g
roup
vs
1.15
(2
.04)
in n
on-M
PE
grou
p, P
=0.6
6 an
d th
e pe
rcen
tage
of
tech
niqu
e fa
ilure
s re
quiri
ng s
hifti
ng o
f m
odal
ity to
HD
(due
to
eith
er p
erito
nitis
; 9.
5% in
MPE
vs.
11
.8%
in n
on-
MPE
, or p
oor fl
uid
man
agem
ent;
1.8%
in
MPE
vs.
2.2
% in
no
n-M
PE)
Sing
lece
ntre
st
udy
-edu
catio
n by
team
, m
ultip
le
indi
vidu
al
sess
ions

69
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Evid
ence
Tab
le :
Org
anis
atio
nal (
HO
SPIT
ALIS
ATIO
N)
Que
stio
n : W
hat a
re th
e or
gani
satio
nal i
ssue
s w
ith re
gard
s to
Pre
-dia
lysi
s Ed
ucat
ion
Prog
ram
me
for a
dvan
ced
CKD
pat
ient
s?Bi
blio
grap
hic
Cita
tion
Stud
yTy
pe/M
etho
dsLE
Num
ber o
f Pa
tient
s &
Patie
nt
Cha
ract
eris
tic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
2. V
an d
en
Bosc
h J,
W
arre
n D
S,
Rut
herfo
rd
PA. R
evie
w
of p
redi
alys
is
educ
atio
npr
ogra
ms:
a
need
for
stan
dard
izat
ion.
Pa
tient
Pre
fer
Adhe
renc
e.
2015
;9:1
279-
1291
.
Syst
emat
ic re
view
Obj
ectiv
e:
To re
view
evi
denc
e on
effe
ctiv
e co
mpo
nent
s of
pre
-dia
lysi
s ed
ucat
ion
prog
ram
mes
as
rela
ted
to m
odal
ity c
hoic
e an
d se
lect
ed
clin
ical
out
com
es.
Met
hod:
-Sys
tem
atic
sea
rch
was
per
form
ed o
n Pu
bMed
MED
LIN
E,
Coc
hran
e Li
brar
y, an
d O
vid
(from
Jan
uary
1, 1
995
to D
ecem
ber 3
1,
2013
) -In
clus
ion
crite
ria a
pplie
d:
v
Adul
ts o
nly
v
Pre-
dial
ysis
edu
catio
n fo
r CKD
pat
ient
s st
age
III, I
V, a
nd
V
v
Plan
ned
star
t pat
ient
s, u
npla
nned
sta
rt pa
tient
s, a
nd
patie
nts
on d
ialy
sis,
ie, i
ncid
ent a
nd p
reva
lent
pat
ient
s.
v
Det
aile
d de
scrip
tion
of p
rogr
amm
e
v
Mul
tiple
ses
sion
s
v
Mul
tidis
cipl
inar
y pr
ogra
mm
e in
volv
ing
phys
icia
ns, n
urse
s,
diet
icia
ns, e
tc.
-Out
com
es in
clud
ed:
v
Dia
lysi
s m
odal
ity c
hoic
e an
d th
e nu
mbe
rs o
f pat
ient
s ch
oosi
ng e
ach
mod
ality
v
Any
clin
ical
out
com
e as
soci
ated
with
pre
-dia
lysi
s ed
ucat
ion
v
Hea
lth-re
late
d qu
ality
of l
ife
v
Mea
sure
s as
soci
ated
with
pat
ient
cho
ice
v
Fina
ncia
l im
pact
of p
atie
nts
choo
sing
mor
e ho
me
ther
apie
s
v
Patie
nt s
atis
fact
ion
-Lite
ratu
re a
lso
revi
ewed
for a
ny in
form
atio
n on
pro
cess
es,
path
way
s, a
nd o
rgan
izat
ion
of th
e pr
e-di
alys
is e
duca
tion
prog
ram
mes
I29
rele
vant
stu
dies
:19
qua
si-
expe
rimen
tal
desi
gn10
nar
rativ
e re
view
s
-19
stud
ies
wer
e an
alys
ed
for e
ffect
ive
com
pone
nts
of p
re-
dial
ysis
edu
catio
n pr
ogra
mm
e
-Des
crip
tions
of
the
educ
atio
nal
proc
ess
varie
d an
d in
clud
ed
indi
vidu
al a
nd
grou
p ed
ucat
ion,
m
ultid
isci
plin
ary
inte
rven
tion,
and
va
ryin
g du
ratio
n an
d fre
quen
cy o
f se
ssio
ns.
Pre-
dial
ysis
ed
ucat
ion
prog
ram
mes
Res
ults
Hos
pita
lisat
ion
Two
stud
ies
repo
rted
on
leng
th o
f hos
pita
l sta
y, w
hich
was
low
er fo
r the
ed
ucat
ion
grou
ps
(6.5
ver
sus
13.5
tota
l ho
spita
l day
s; 2
.2
vers
us 5
.1 h
ospi
tal
days
/pat
ient
per
yea
r).
Mos
tly
with
out
cont
rol
grou
p
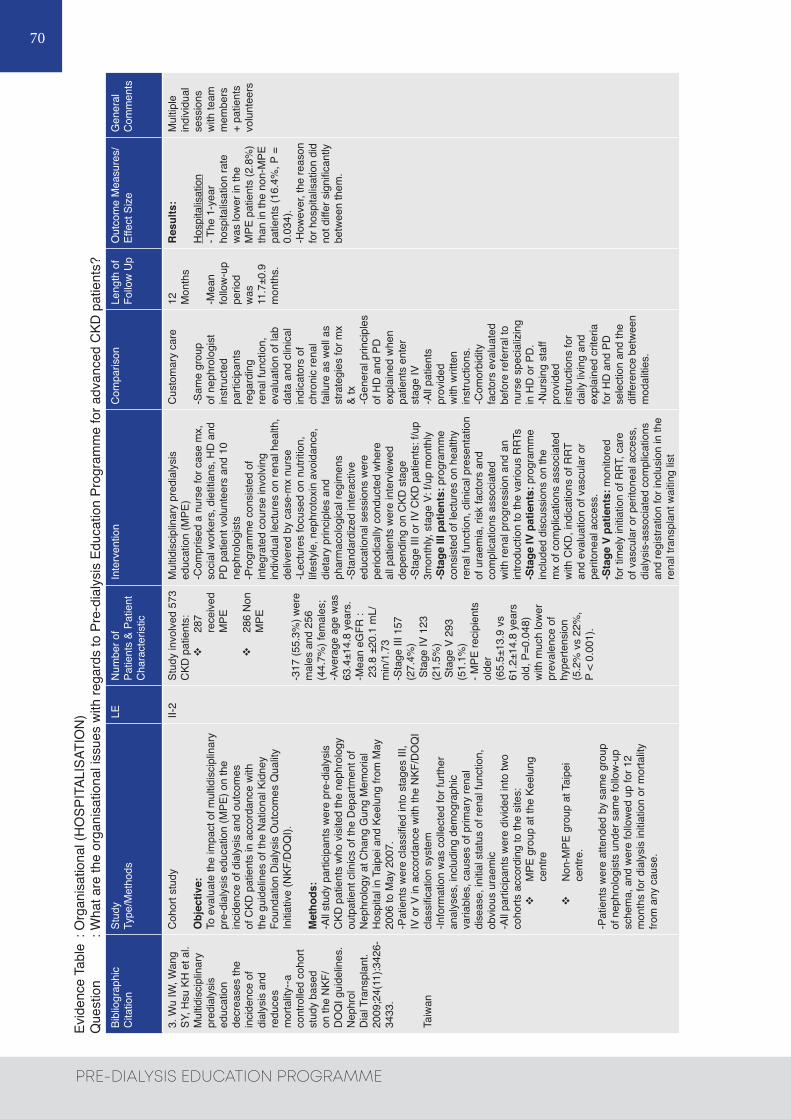
70
PRE-DIALYSIS EDUCATION PROGRAMME
Evid
ence
Tab
le :
Org
anis
atio
nal (
HO
SPIT
ALIS
ATIO
N)
Que
stio
n : W
hat a
re th
e or
gani
satio
nal i
ssue
s w
ith re
gard
s to
Pre
-dia
lysi
s Ed
ucat
ion
Prog
ram
me
for a
dvan
ced
CKD
pat
ient
s?Bi
blio
grap
hic
Cita
tion
Stud
yTy
pe/M
etho
dsLE
Num
ber o
f Pa
tient
s &
Patie
nt
Cha
ract
eris
tic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
3. W
u IW
, Wan
g SY
, Hsu
KH
et a
l. M
ultid
isci
plin
ary
pred
ialy
sis
educ
atio
n de
crea
ses
the
inci
denc
e of
di
alys
is a
nd
redu
ces
mor
talit
y--a
co
ntro
lled
coho
rt st
udy
base
d on
the
NKF
/D
OQ
I gui
delin
es.
Nep
hrol
Dia
l Tra
nspl
ant.
2009
;24(
11):3
426-
3433
.
Taiw
an
Coh
ort s
tudy
Obj
ectiv
e:To
eva
luat
e th
e im
pact
of m
ultid
isci
plin
ary
pre-
dial
ysis
edu
catio
n (M
PE) o
n th
e in
cide
nce
of d
ialy
sis
and
outc
omes
of
CKD
pat
ient
s in
acc
orda
nce
with
th
e gu
idel
ines
of t
he N
atio
nal K
idne
y Fo
unda
tion
Dia
lysi
s O
utco
mes
Qua
lity
Initi
ativ
e (N
KF/D
OQ
I).
Met
hods
:-A
ll st
udy
parti
cipa
nts
wer
e pr
e-di
alys
is
CKD
pat
ient
s w
ho v
isite
d th
e ne
phro
logy
ou
tpat
ient
clin
ics
of th
e D
epar
tmen
t of
Nep
hrol
ogy
at C
hang
Gun
g M
emor
ial
Hos
pita
l in
Taip
ei a
nd K
eelu
ng fr
om M
ay
2006
to M
ay 2
007.
-Pat
ient
s w
ere
clas
sifie
d in
to s
tage
s III
, IV
or V
in a
ccor
danc
e w
ith th
e N
KF/D
OQ
I cl
assi
ficat
ion
syst
em-In
form
atio
n w
as c
olle
cted
for f
urth
er
anal
yses
, inc
ludi
ng d
emog
raph
ic
varia
bles
, cau
ses
of p
rimar
y re
nal
dise
ase,
initi
al s
tatu
s of
rena
l fun
ctio
n,
obvi
ous
urae
mic
-A
ll pa
rtici
pant
s w
ere
divi
ded
into
two
coho
rts a
ccor
ding
to th
e si
tes:
v
MPE
gro
up a
t the
Kee
lung
ce
ntre
v
Non
-MPE
gro
up a
t Tai
pei
cent
re.
-Pat
ient
s w
ere
atte
nded
by
sam
e gr
oup
of n
ephr
olog
ists
und
er s
ame
follo
w-u
p sc
hem
a, a
nd w
ere
follo
wed
up
for 1
2 m
onth
s fo
r dia
lysi
s in
itiat
ion
or m
orta
lity
from
any
cau
se.
II-2
Stud
y in
volv
ed 5
73
CKD
pat
ient
s:v
287
rece
ived
M
PE
v
286
Non
M
PE
-317
(55.
3%) w
ere
mal
es a
nd 2
56
(44.
7%) f
emal
es;
-Ave
rage
age
was
63
.4±1
4.8
year
s.-M
ean
eGFR
: 2
3.8
±20.
1 m
L/m
in/1
.73
-Sta
ge II
I 157
(2
7.4%
) S
tage
IV 1
23
(21.
5%)
Sta
ge V
293
(5
1.1%
)- M
PE re
cipi
ents
ol
der
(65.
5±13
.9 v
s 61
.2±1
4.8
year
s ol
d, P
=0.0
48)
with
muc
h lo
wer
pr
eval
ence
of
hype
rtens
ion
(5.2
% v
s 22
%,
P <
0.00
1).
Mul
tidis
cipl
inar
y pr
edia
lysi
s ed
ucat
ion
(MPE
)-C
ompr
ised
a n
urse
for c
ase
mx,
so
cial
wor
kers
, die
titia
ns, H
D a
nd
PD p
atie
nt v
olun
teer
s an
d 10
ne
phro
logi
sts
-Pro
gram
me
cons
iste
d of
in
tegr
ated
cou
rse
invo
lvin
g in
divi
dual
lect
ures
on
rena
l hea
lth,
deliv
ered
by
case
-mx
nurs
e-L
ectu
res
focu
sed
on n
utrit
ion,
lif
esty
le, n
ephr
otox
in a
void
ance
, di
etar
y pr
inci
ples
and
ph
arm
acol
ogic
al re
gim
ens
-Sta
ndar
dize
d in
tera
ctiv
e ed
ucat
iona
l ses
sion
s w
ere
perio
dica
lly c
ondu
cted
whe
re
all p
atie
nts
wer
e in
terv
iew
ed
depe
ndin
g on
CKD
sta
ge-S
tage
III o
r IV
CKD
pat
ient
s: f/
up
3mon
thly,
sta
ge V
: f/u
p m
onth
ly-S
tage
III p
atie
nts:
pro
gram
me
cons
iste
d of
lect
ures
on
heal
thy
rena
l fun
ctio
n, c
linic
al p
rese
ntat
ion
of u
raem
ia, r
isk
fact
ors
and
com
plic
atio
ns a
ssoc
iate
d w
ith re
nal p
rogr
essi
on a
nd a
n in
trodu
ctio
n to
the
vario
us R
RTs
-Sta
ge IV
pat
ient
s: p
rogr
amm
e in
clud
ed d
iscu
ssio
ns o
n th
e m
x of
com
plic
atio
ns a
ssoc
iate
d w
ith C
KD, i
ndic
atio
ns o
f RRT
an
d ev
alua
tion
of v
ascu
lar o
r pe
riton
eal a
cces
s.
-Sta
ge V
pat
ient
s: m
onito
red
for t
imel
y in
itiat
ion
of R
RT, c
are
of v
ascu
lar o
r per
itone
al a
cces
s,
dial
ysis
-ass
ocia
ted
com
plic
atio
ns
and
regi
stra
tion
for i
nclu
sion
in th
e re
nal t
rans
plan
t wai
ting
list
Cus
tom
ary
care
-Sam
e gr
oup
of n
ephr
olog
ist
inst
ruct
ed
parti
cipa
nts
rega
rdin
g re
nal f
unct
ion,
ev
alua
tion
of la
b da
ta a
nd c
linic
al
indi
cato
rs o
f ch
roni
c re
nal
failu
re a
s w
ell a
s st
rate
gies
for m
x &
tx-G
ener
al p
rinci
ples
of
HD
and
PD
ex
plai
ned
whe
n pa
tient
s en
ter
stag
e IV
-All
patie
nts
prov
ided
w
ith w
ritte
n in
stru
ctio
ns.
-Com
orbi
dity
fa
ctor
s ev
alua
ted
befo
re re
ferra
l to
nurs
e sp
ecia
lizin
g in
HD
or P
D.
-Nur
sing
sta
ff pr
ovid
ed
inst
ruct
ions
for
daily
livi
ng a
nd
expl
aine
d cr
iteria
fo
r HD
and
PD
se
lect
ion
and
the
diffe
renc
e be
twee
n m
odal
ities
.
12 Mon
ths
-Mea
n fo
llow
-up
perio
d w
as
11.7
±0.9
m
onth
s.
Res
ults
:
Hos
pita
lisat
ion
- The
1-y
ear
hosp
italis
atio
n ra
te
was
low
er in
the
MPE
pat
ient
s (2
.8%
) th
an in
the
non-
MPE
pa
tient
s (1
6.4%
, P =
0.
034)
. -H
owev
er, t
he re
ason
fo
r hos
pita
lisat
ion
did
not d
iffer
sig
nific
antly
be
twee
n th
em.
Mul
tiple
in
divi
dual
se
ssio
ns
with
team
m
embe
rs
+ pa
tient
s vo
lunt
eers
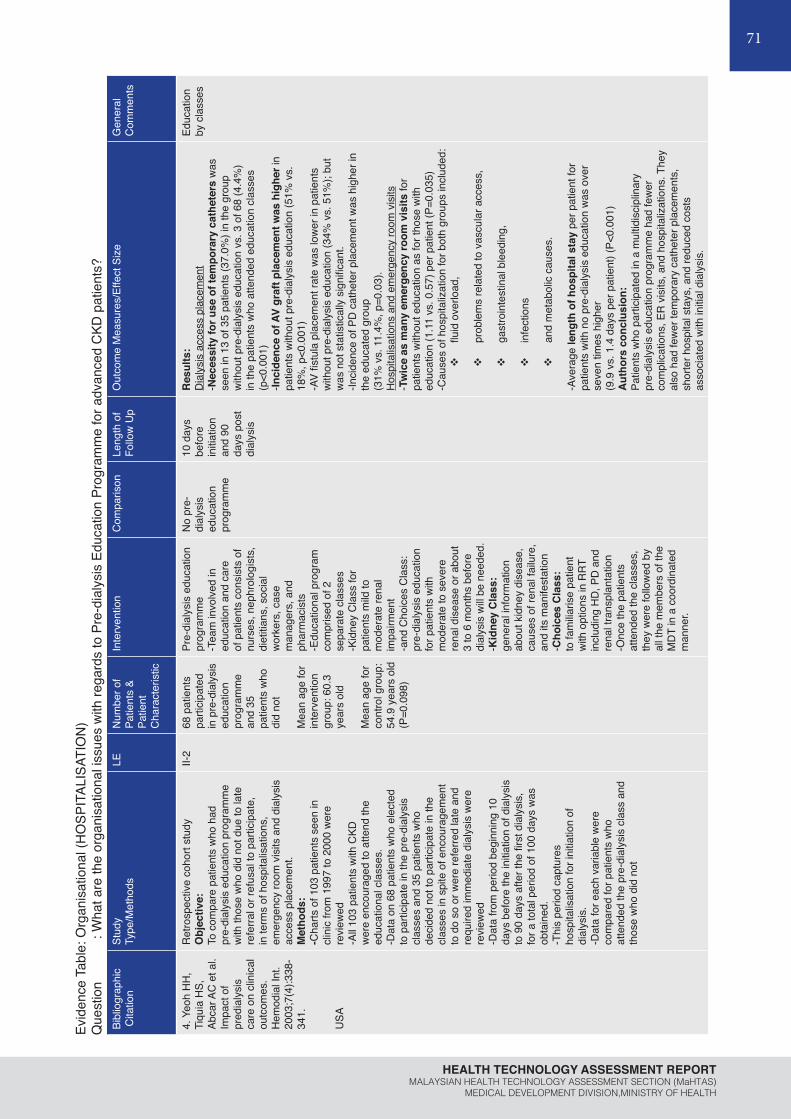
71
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Evid
ence
Tab
le: O
rgan
isat
iona
l (H
OSP
ITAL
ISAT
ION
)Q
uest
ion
: Wha
t are
the
orga
nisa
tiona
l iss
ues
with
rega
rds
to P
re-d
ialy
sis
Educ
atio
n Pr
ogra
mm
e fo
r adv
ance
d C
KD p
atie
nts?
Bibl
iogr
aphi
c C
itatio
nSt
udy
Type
/Met
hods
LEN
umbe
r of
Patie
nts
& Pa
tient
C
hara
cter
istic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
4. Y
eoh
HH
, Ti
quia
HS,
Ab
car A
C e
t al.
Impa
ct o
fpr
edia
lysi
s ca
re o
n cl
inic
al
outc
omes
. H
emod
ial I
nt.
2003
;7(4
):338
-34
1.
USA
Ret
rosp
ectiv
e co
hort
stud
yO
bjec
tive:
To c
ompa
re p
atie
nts
who
had
pr
e-di
alys
is e
duca
tion
prog
ram
me
with
thos
e w
ho d
id n
ot d
ue to
late
re
ferra
l or r
efus
al to
par
ticip
ate,
in
term
s of
hos
pita
lisat
ions
, em
erge
ncy
room
vis
its a
nd d
ialy
sis
acce
ss p
lace
men
t. M
etho
ds:
-Cha
rts o
f 103
pat
ient
s se
en in
cl
inic
from
199
7 to
200
0 w
ere
revi
ewed
-All
103
patie
nts
with
CKD
w
ere
enco
urag
ed to
atte
nd th
e ed
ucat
iona
l cla
sses
. -D
ata
on 6
8 pa
tient
s w
ho e
lect
ed
to p
artic
ipat
e in
the
pre-
dial
ysis
cl
asse
s an
d 35
pat
ient
s w
ho
deci
ded
not t
o pa
rtici
pate
in th
e cl
asse
s in
spi
te o
f enc
oura
gem
ent
to d
o so
or w
ere
refe
rred
late
and
re
quire
d im
med
iate
dia
lysi
s w
ere
revi
ewed
-Dat
a fro
m p
erio
d be
ginn
ing
10
days
bef
ore
the
initi
atio
n of
dia
lysi
s to
90
days
afte
r the
firs
t dia
lysi
s,
for a
tota
l per
iod
of 1
00 d
ays
was
ob
tain
ed.
-Thi
s pe
riod
capt
ures
ho
spita
lisat
ion
for i
nitia
tion
of
dial
ysis
. -D
ata
for e
ach
varia
ble
wer
e co
mpa
red
for p
atie
nts
who
at
tend
ed th
e pr
e-di
alys
is c
lass
and
th
ose
who
did
not
II-2
68 p
atie
nts
parti
cipa
ted
in p
re-d
ialy
sis
educ
atio
n pr
ogra
mm
e an
d 35
pa
tient
s w
ho
did
not
Mea
n ag
e fo
r in
terv
entio
n gr
oup:
60.
3 ye
ars
old
Mea
n ag
e fo
r co
ntro
l gro
up:
54.9
yea
rs o
ld(P
=0.0
98)
Pre-
dial
ysis
edu
catio
n pr
ogra
mm
e-T
eam
invo
lved
in
educ
atio
n an
d ca
re
of p
atie
nts
cons
ists
of
nurs
es, n
ephr
olog
ists
, di
etiti
ans,
soc
ial
wor
kers
, cas
e m
anag
ers,
and
ph
arm
acis
ts-E
duca
tiona
l pro
gram
co
mpr
ised
of 2
se
para
te c
lass
es-K
idne
y C
lass
for
patie
nts
mild
to
mod
erat
e re
nal
impa
irmen
t -a
nd C
hoic
es C
lass
: pr
e-di
alys
is e
duca
tion
for p
atie
nts
with
m
oder
ate
to s
ever
e re
nal d
isea
se o
r abo
ut
3 to
6 m
onth
s be
fore
di
alys
is w
ill be
nee
ded.
-K
idne
y C
lass
: ge
nera
l inf
orm
atio
n ab
out k
idne
y di
seas
e,
caus
es o
f ren
al fa
ilure
, an
d its
man
ifest
atio
n-C
hoic
es C
lass
: to
fam
iliaris
e pa
tient
w
ith o
ptio
ns in
RRT
in
clud
ing
HD
, PD
and
re
nal t
rans
plan
tatio
n-O
nce
the
patie
nts
atte
nded
the
clas
ses,
th
ey w
ere
follo
wed
by
all t
he m
embe
rs o
f the
M
DT
in a
coo
rdin
ated
m
anne
r.
No
pre-
dial
ysis
ed
ucat
ion
prog
ram
me
10 d
ays
befo
re
initi
atio
n an
d 90
da
ys p
ost
dial
ysis
Res
ults
:D
ialy
sis
acce
ss p
lace
men
t-N
eces
sity
for u
se o
f tem
pora
ry c
athe
ters
was
se
en in
13
of 3
5 pa
tient
s (3
7.0%
) in
the
grou
p w
ithou
t pre
-dia
lysi
s ed
ucat
ion
vs. 3
of 6
8 (4
.4%
) in
the
patie
nts
who
atte
nded
edu
catio
n cl
asse
s (p
<0.0
01)
-Inci
denc
e of
AV
graf
t pla
cem
ent w
as h
ighe
r in
patie
nts
with
out p
re-d
ialy
sis
educ
atio
n (5
1% v
s.
18%
, p<0
.001
)-A
V fis
tula
pla
cem
ent r
ate
was
low
er in
pat
ient
s w
ithou
t pre
-dia
lysi
s ed
ucat
ion
(34%
vs.
51%
); bu
t w
as n
ot s
tatis
tical
ly s
igni
fican
t.-In
cide
nce
of P
D c
athe
ter p
lace
men
t was
hig
her i
n th
e ed
ucat
ed g
roup
(3
1% v
s. 1
1.4%
, p=0
.03)
. H
ospi
talis
atio
ns a
nd e
mer
genc
y ro
om v
isits
-Tw
ice
as m
any
emer
genc
y ro
om v
isits
for
patie
nts
with
out e
duca
tion
as fo
r tho
se w
ith
educ
atio
n (1
.11
vs. 0
.57)
per
pat
ient
(P=0
.035
)-C
ause
s of
hos
pita
lizat
ion
for b
oth
grou
ps in
clud
ed:
v
fluid
ove
rload
,
v
prob
lem
s re
late
d to
vas
cula
r acc
ess,
v
gast
roin
test
inal
ble
edin
g,
v
infe
ctio
ns
v
and
met
abol
ic c
ause
s.
-Ave
rage
leng
th o
f hos
pita
l sta
y pe
r pat
ient
for
patie
nts
with
no
pre-
dial
ysis
edu
catio
n w
as o
ver
seve
n tim
es h
ighe
r (9
.9 v
s. 1
.4 d
ays
per p
atie
nt) (
P<0.
001)
Aut
hors
con
clus
ion:
Patie
nts
who
par
ticip
ated
in a
mul
tidis
cipl
inar
y pr
e-di
alys
is e
duca
tion
prog
ram
me
had
few
er
com
plic
atio
ns, E
R v
isits
, and
hos
pita
lizat
ions
. The
y al
so h
ad fe
wer
tem
pora
ry c
athe
ter p
lace
men
ts,
shor
ter h
ospi
tal s
tays
, and
redu
ced
cost
s as
soci
ated
with
initi
al d
ialy
sis.
Educ
atio
n by
cla
sses

72
PRE-DIALYSIS EDUCATION PROGRAMME
Bibl
iogr
aphi
c C
itatio
nSt
udy
Type
/Met
hods
LEN
umbe
r of
Patie
nts
& Pa
tient
C
hara
cter
istic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
5. Y
u YJ
, Wu
IW,
Hua
ng C
Y et
al.
Mul
tidis
cipl
inar
y pr
edia
lysi
s ed
ucat
ion
redu
ced
the
inpa
tient
an
d to
tal m
edic
alco
sts
of th
e fir
st 6
m
onth
s of
dia
lysi
s in
in
cide
nt h
emod
ialy
sis
patie
nts.
PLo
SO
ne.
2014
;9(1
1):e
1128
20.
Taiw
an
Ran
dom
ised
con
trolle
d tri
al w
ith c
ost-a
naly
sis
Obj
ectiv
e:To
ana
lyse
the
med
ical
exp
endi
ture
an
d ut
ilisat
ion
incu
rred
durin
g th
e fir
st 6
m
onth
s of
dia
lysi
s in
itiat
ion
in 4
25 in
cide
nt
haem
odia
lysi
s pa
tient
s w
ho w
ere
rand
omis
ed
into
mul
tidis
cipl
inar
y pr
e-di
alys
is e
duca
tion
(MPE
) and
non
-MPE
gro
ups
befo
re re
achi
ng
ESR
D.
Met
hods
:-A
tota
l of 2
280
patie
nts
wer
e en
rolle
d in
the
stud
y an
d w
ere
rand
omly
div
ided
into
the
MPE
gro
up a
nd th
e no
n-M
PE g
roup
by
usin
g a
rand
om ta
ble
at s
tudy
ent
ry.
-445
pat
ient
s re
ache
d ES
RD
nee
ding
ha
emod
ialy
sis
afte
r a m
ean
follo
w-u
p of
33
±2.6
mon
ths:
232
patie
nts
in th
e M
PE g
roup
21
3 pa
tient
s in
the
non-
MPE
gro
up-P
rogr
am c
onsi
sted
of a
n in
tegr
ated
cou
rse
invo
lvin
g in
divi
dual
lect
ures
on
rena
l hea
lth,
deliv
ered
by
the
case
-man
agem
ent n
urse
-Lec
ture
s fo
cuse
d on
nut
ritio
n, li
fest
yle,
ne
phro
toxi
n av
oida
nce,
die
tary
prin
cipl
es, a
nd
phar
mac
olog
ical
regi
men
s.
-Cas
e-m
anag
emen
t nur
se c
onta
cted
the
patie
nts
to e
nsur
e tim
ely
follo
w-u
p-F
or s
tage
IV C
KD p
atie
nts,
the
prog
ram
in
clud
ed d
iscu
ssio
ns o
n th
e m
anag
emen
t of
com
plic
atio
ns a
ssoc
iate
d w
ith C
KD,
indi
catio
ns o
f ren
al re
plac
emen
t the
rapy
, an
d th
e ev
alua
tion
of v
ascu
lar o
r per
itone
al
acce
ss.
-For
sta
ge V
CKD
wer
e m
onito
red
for t
imel
y in
itiat
ion
of re
nal r
epla
cem
ent t
hera
pies
, the
ca
re o
f vas
cula
r or p
erito
neal
acc
ess,
dia
lysi
s-as
soci
ated
com
plic
atio
ns, a
nd re
gist
ratio
n fo
r in
clus
ion
in th
e re
nal t
rans
plan
tatio
n w
aitin
g lis
t. -A
ll pa
tient
s re
ceiv
ed d
ieta
ry c
ouns
ellin
g bi
annu
ally
from
a d
ietit
ian.
-In
add
ition
, cas
e-m
anag
emen
t nur
se o
ften
cont
acte
d th
e pa
rtici
pant
s by
tele
phon
e to
en
cour
age
them
to in
form
thei
r nep
hrol
ogis
ts
of th
eir s
ympt
oms
and
to re
info
rce
the
impo
rtanc
e of
med
ical
vis
its.
-The
MPE
pro
gram
was
dis
cont
inue
d on
ce
rena
l rep
lace
men
t the
rapi
es w
ere
initi
ate
II-1
445
adva
nced
CKD
pa
tient
s: v
232
patie
nts
in M
PE
grou
p
v
213
patie
nts
in n
on-
MPE
gr
oup
-Mea
n ag
e of
pa
tient
s w
as
63.8
±13.
2 ye
ars,
and
22
1 (4
9.7%
) of t
hem
w
ere
men
-Mea
n eG
FR 7
.49
± 3.
1 M
PE g
roup
and
m
ean
eGFR
7.8
7±
3.6
in th
e no
n-M
PE
grou
p
Mul
tidis
cipl
inar
y pr
e-di
alys
is
educ
atio
n (M
PE)
-MPE
pro
gram
co
mpr
ised
a
nurs
e fo
r cas
e m
anag
emen
t, so
cial
wor
kers
, di
etiti
ans,
ha
emod
ialy
sis,
pe
riton
eal
dial
ysis
pat
ient
vo
lunt
eers
and
10
neph
rolo
gist
s
Non
-MPE
-S
ame
grou
p of
ne
phro
logi
sts
inst
ruct
ed
patie
nts
abou
t re
nal f
unct
ion,
ev
alua
tion
of
labo
rato
ry d
ata,
an
d cl
inic
al
indi
cato
rs o
f ch
roni
c re
nal
failu
re, a
nd
stra
tegi
es fo
r its
mx
and
tx-G
ener
al
prin
cipl
es o
f H
D a
nd P
D
expl
aine
d w
hen
patie
nts
at
Stag
e 4
CKD
6 m
onth
s of
dia
lysi
s in
itiat
ion
Res
ults
:H
ospi
talis
atio
n an
d va
scul
ar a
cces
s re
late
d su
rger
ies
-MPE
pat
ient
s ha
d si
gnifi
cant
ly fe
wer
and
sho
rter
le
ngth
s of
hos
pita
lisat
ion
(med
ian
(IQR
) 0 (1
5) v
s. 8
(27)
day
s, p
<0.0
01]
than
non
-MPE
pat
ient
s).
-Car
diov
ascu
lar d
isea
se (i
nclu
ding
unc
ontro
lled
hype
rtens
ion,
cor
onar
y ar
tery
dis
ease
, st
roke
, hea
rt fa
ilure
, and
per
iphe
ral a
rtery
oc
clus
ive
dise
ase)
was
the
mai
n ca
use
of fi
rst
hosp
italiz
atio
n in
all
patie
nts.
-Eig
hty-
eigh
t (37
.9%
) pat
ient
s in
the
MPE
gro
up
had
at le
ast o
ne h
ospi
talis
atio
n, c
ompa
red
with
12
7 pa
tient
s (5
9.6%
) in
the
non-
MPE
gro
up
(p<0
.001
).-P
artic
ipat
ion
in M
PE p
rogr
am re
duce
d ca
rdio
vasc
ular
hos
pita
lisat
ion
in fi
rst 6
m
onth
s po
st d
ialy
sis
(18.
53%
vs.
29.
58%
, p=
0.00
7).
-MPE
gro
up w
ere
mor
e lik
ely
to h
ave
few
er
vasc
ular
acc
ess
rela
ted
surg
erie
s du
ring
the
first
adm
issi
on [3
5 pa
tient
s (1
5.09
%) v
s. 5
5 (2
5.82
%),
p=0.
005]
.A
utho
rs c
oncl
usio
n:Pa
rtici
patio
n of
mul
tidis
cipl
inar
y ed
ucat
ion
in
pre-
dial
ysis
per
iod
was
inde
pend
ently
ass
ocia
ted
with
redu
ctio
n in
the
inpa
tient
and
tota
l med
ical
ex
pend
iture
s of
the
first
6 m
onth
s po
st-d
ialy
sis
owin
g to
dec
reas
ed in
patie
nt s
ervi
ce u
tiliz
atio
n se
cond
ary
to c
ardi
ovas
cula
r cau
ses
and
vasc
ular
ac
cess
–rel
ated
sur
gerie
s.
Sing
le-
cent
re s
tudy
Educ
atio
n by
indi
vidu
al
sess
ions
with
te
am
Evid
ence
Tab
le :
Org
anis
atio
nal (
HO
SPIT
ALIS
ATIO
N)
Que
stio
n : W
hat a
re th
e or
gani
satio
nal i
ssue
s w
ith re
gard
s to
Pre
-dia
lysi
s Ed
ucat
ion
Prog
ram
me
for a
dvan
ced
CKD
pat
ient
s?
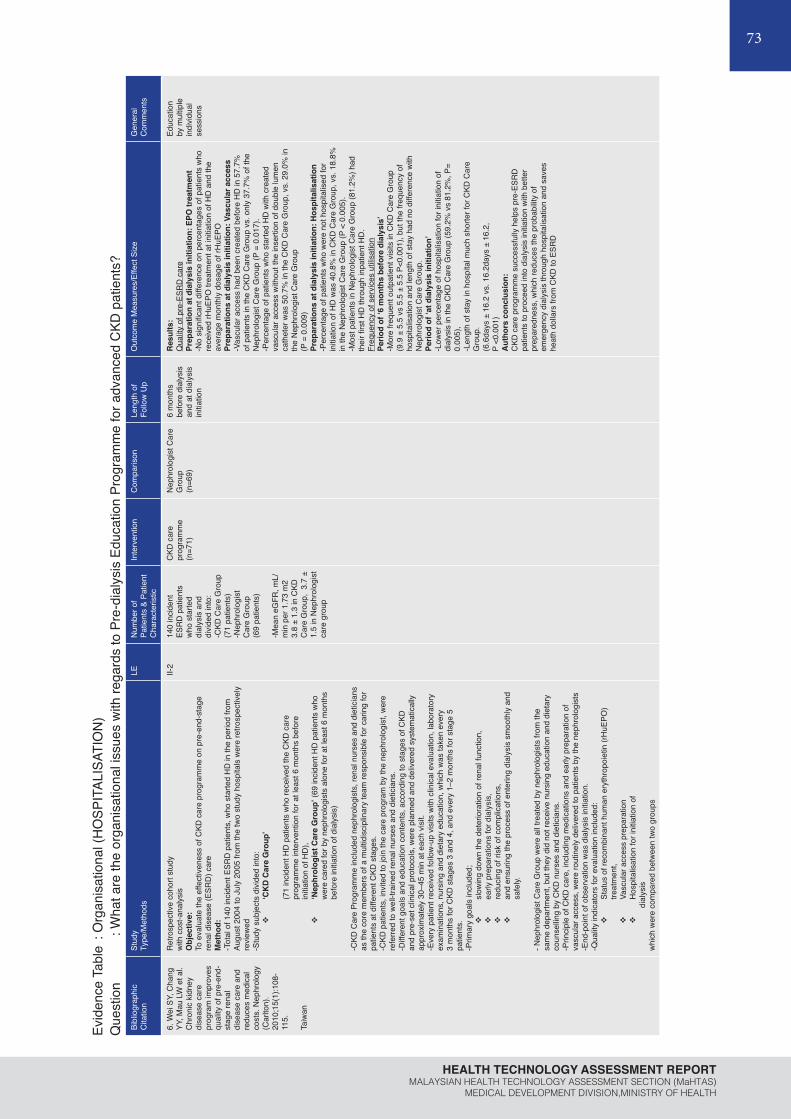
73
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Evid
ence
Tab
le :
Org
anis
atio
nal (
HO
SPIT
ALIS
ATIO
N)
Que
stio
n :
Wha
t are
the
orga
nisa
tiona
l iss
ues
with
rega
rds
to P
re-d
ialy
sis
Educ
atio
n Pr
ogra
mm
e fo
r adv
ance
d C
KD p
atie
nts?
Bibl
iogr
aphi
cC
itatio
nSt
udy
Type
/Met
hods
LEN
umbe
r of
Patie
nts
& Pa
tient
C
hara
cter
istic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
6. W
ei S
Y, C
hang
YY
, Mau
LW
et a
l.C
hron
ic k
idne
y di
seas
e ca
re
prog
ram
impr
oves
qu
ality
of p
re-e
nd-
stag
e re
nal
dise
ase
care
and
re
duce
s m
edic
al
cost
s. N
ephr
olog
y (C
arlto
n).
2010
;15(
1):1
08-
115.
Taiw
an
Ret
rosp
ectiv
e co
hort
stud
yw
ith c
ost-a
naly
sis
Obj
ectiv
e:
To e
valu
ate
the
effe
ctiv
enes
s of
CKD
car
e pr
ogra
mm
e on
pre
-end
-sta
ge
rena
l dis
ease
(ESR
D) c
are
Met
hod:
-Tot
al o
f 140
inci
dent
ESR
D p
atie
nts,
who
sta
rted
HD
in th
e pe
riod
from
Au
gust
200
4 to
Jul
y 20
05 fr
om th
e tw
o st
udy
hosp
itals
wer
e re
trosp
ectiv
ely
revi
ewed
-Stu
dy s
ubje
cts
divi
ded
into
:v
‘CK
D C
are
Gro
up’
(71
inci
dent
HD
pat
ient
s w
ho re
ceiv
ed th
e C
KD c
are
prog
ram
me
inte
rven
tion
for a
t lea
st 6
mon
ths
befo
re
initi
atio
n of
HD
), v
‘Nep
hrol
ogis
t Car
e G
roup
’ (69
inci
dent
HD
pat
ient
s w
ho
wer
e ca
red
for b
y ne
phro
logi
sts
alon
e fo
r at l
east
6 m
onth
s be
fore
initi
atio
n of
dia
lysi
s)
-CKD
Car
e Pr
ogra
mm
e in
clud
ed n
ephr
olog
ists
, ren
al n
urse
s an
d di
etic
ians
as
the
core
mem
bers
of a
mul
tidis
cipl
inar
y te
am re
spon
sibl
e fo
r car
ing
for
patie
nts
at d
iffer
ent C
KD s
tage
s.
-CKD
pat
ient
s, in
vite
d to
join
the
care
pro
gram
by
the
neph
rolo
gist
, wer
e re
ferre
d to
wel
l-tra
ined
rena
l nur
ses
and
diet
icia
ns.
-Diff
eren
t goa
ls a
nd e
duca
tion
cont
ents
, acc
ordi
ng to
sta
ges
of C
KD
and
pre-
set c
linic
al p
roto
cols
, wer
e pl
anne
d an
d de
liver
ed s
yste
mat
ical
ly
appr
oxim
atel
y 30
–45
min
at e
ach
visi
t. -E
very
pat
ient
rece
ived
follo
w-u
p vi
sits
with
clin
ical
eva
luat
ion,
labo
rato
ry
exam
inat
ions
, nur
sing
and
die
tary
edu
catio
n, w
hich
was
take
n ev
ery
3 m
onth
s fo
r CKD
sta
ges
3 an
d 4,
and
eve
ry 1
–2 m
onth
s fo
r sta
ge 5
pa
tient
s.-P
rimar
y go
als
incl
uded
;v
slow
ing
dow
n th
e de
terio
ratio
n of
rena
l fun
ctio
n,
v
early
pre
para
tions
for d
ialy
sis,
v
redu
cing
of r
isk
of c
ompl
icat
ions
,v
and
ensu
ring
the
proc
ess
of e
nter
ing
dial
ysis
sm
ooth
ly a
nd
safe
ly.
- Nep
hrol
ogis
t Car
e G
roup
wer
e al
l tre
ated
by
neph
rolo
gist
s fro
m th
e sa
me
depa
rtmen
t, bu
t the
y di
d no
t rec
eive
nur
sing
edu
catio
n an
d di
etar
y co
unse
lling
by C
KD n
urse
s an
d di
etic
ians
. -P
rinci
ple
of C
KD c
are,
incl
udin
g m
edic
atio
ns a
nd e
arly
pre
para
tion
of
vasc
ular
acc
ess,
wer
e ro
utin
ely
deliv
ered
to p
atie
nts
by th
e ne
phro
logi
sts
-End
-poi
nt o
f obs
erva
tion
was
dia
lysi
s in
itiat
ion.
-Q
ualit
y in
dica
tors
for e
valu
atio
n in
clud
ed:
v
Stat
us o
f rec
ombi
nant
hum
an e
ryth
ropo
ietin
(rH
uEPO
) tre
atm
ent,
v
Vasc
ular
acc
ess
prep
arat
ion
v
Hos
pita
lisat
ion
for i
nitia
tion
of
d
ialy
sis
whi
ch w
ere
com
pare
d be
twee
n tw
o gr
oups
II-2
140
inci
dent
ES
RD
pat
ient
s w
ho s
tarte
d di
alys
is a
nd
divi
ded
into
:-C
KD C
are
Gro
up
(71
patie
nts)
-Nep
hrol
ogis
t C
are
Gro
up
(69
patie
nts)
-Mea
n eG
FR, m
L/m
in p
er 1
.73
m2
3.8
± 1.
3 in
CKD
C
are
Gro
up,
3.7
± 1.
5 in
Nep
hrol
ogis
t ca
re g
roup
CKD
car
e pr
ogra
mm
e(n
=71)
Nep
hrol
ogis
t Car
e G
roup
(n=6
9)
6 m
onth
s be
fore
dia
lysi
s an
d at
dia
lysi
s in
itiat
ion
Res
ults
:Q
ualit
y of
pre
-ESR
D c
are
Prep
arat
ion
at d
ialy
sis
initi
atio
n: E
PO tr
eatm
ent
-No
sign
ifica
nt d
iffer
ence
on
perc
enta
ges
of p
atie
nts
who
re
ceiv
ed rH
uEPO
trea
tmen
t at i
nitia
tion
of H
D a
nd th
e av
erag
e m
onth
ly d
osag
e of
rHuE
POPr
epar
atio
ns a
t dia
lysi
s in
itiat
ion:
Vas
cula
r acc
ess
-Vas
cula
r acc
ess
had
been
cre
ated
bef
ore
HD
in 5
7.7%
of
pat
ient
s in
the
CKD
Car
e G
roup
vs.
onl
y 37
.7%
of t
he
Nep
hrol
ogis
t Car
e G
roup
(P =
0.0
17).
-Per
cent
age
of p
atie
nts
who
sta
rted
HD
with
cre
ated
va
scul
ar a
cces
s w
ithou
t the
inse
rtion
of d
oubl
e lu
men
ca
thet
er w
as 5
0.7%
in th
e C
KD C
are
Gro
up, v
s. 2
9.0%
in
the
Nep
hrol
ogis
t Car
e G
roup
(P
= 0
.009
)Pr
epar
atio
ns a
t dia
lysi
s in
itiat
ion:
Hos
pita
lisat
ion
-Per
cent
age
of p
atie
nts
who
wer
e no
t hos
pita
lised
for
initi
atio
n of
HD
was
40.
8% in
CKD
Car
e G
roup
, vs.
18.
8%
in th
e N
ephr
olog
ist C
are
Gro
up (P
< 0
.005
). -M
ost p
atie
nts
in N
ephr
olog
ist C
are
Gro
up (8
1.2%
) had
th
eir fi
rst H
D th
roug
h in
patie
nt H
D.
Freq
uenc
y of
ser
vice
s ut
ilisat
ion
Perio
d of
‘6 m
onth
s be
fore
dia
lysi
s’-M
ore
frequ
ent o
utpa
tient
vis
its in
CKD
Car
e G
roup
(9
.9 ±
5.5
vs
5.5
± 5.
5 P<
0.00
1), b
ut th
e fre
quen
cy o
f ho
spita
lisat
ion
and
leng
th o
f sta
y ha
d no
diff
eren
ce w
ith
Nep
hrol
ogis
t Car
e G
roup
.Pe
riod
of ‘a
t dia
lysi
s in
itiat
ion’
-Low
er p
erce
ntag
e of
hos
pita
lisat
ion
for i
nitia
tion
of
dial
ysis
in th
e C
KD C
are
Gro
up (5
9.2%
vs
81.2
%, P
= 0.
005)
, -L
engt
h of
sta
y in
hos
pita
l muc
h sh
orte
r for
CKD
Car
e G
roup
.(6
.6da
ys ±
16.
2 vs
. 16.
2day
s ±
16.2
, P
<0.0
01)
Aut
hors
con
clus
ion:
CKD
car
e pr
ogra
mm
e su
cces
sful
ly h
elps
pre
-ESR
D
patie
nts
to p
roce
ed in
to d
ialy
sis
initi
atio
n w
ith b
ette
r pr
epar
edne
ss, w
hich
redu
ces
the
prob
abilit
y of
em
erge
ncy
dial
ysis
thro
ugh
hosp
italis
atio
n an
d sa
ves
heat
h do
llars
from
CKD
to E
SRD
Educ
atio
n by
mul
tiple
in
divi
dual
se
ssio
ns

74
PRE-DIALYSIS EDUCATION PROGRAMME
Evid
ence
Tab
le :
Org
anis
atio
nal (
CO
MPO
NEN
TS O
F PR
OG
RAM
ME)
Que
stio
n : W
hat a
re th
e co
mpo
nent
s of
Pre
-dia
lysi
s Ed
ucat
ion
Prog
ram
me
for a
dvan
ced
CKD
pat
ient
s?Bi
blio
grap
hic
Cita
tion
Stud
yTy
pe/M
etho
dsLE
Num
ber o
f Pat
ient
s &
Patie
nt C
hara
cter
istic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
1. V
an d
en
Bosc
h J,
War
ren
DS,
Rut
herfo
rd
PA. R
evie
w
of p
redi
alys
is
educ
atio
npr
ogra
ms:
a n
eed
for s
tand
ardi
zatio
n.
Patie
nt P
refe
r Ad
here
nce.
20
15;9
:127
9-12
91.
Syst
emat
ic re
view
Obj
ectiv
e:
To re
view
evi
denc
e on
effe
ctiv
e co
mpo
nent
s of
pre
-dia
lysi
s ed
ucat
ion
prog
ram
mes
as
rela
ted
to m
odal
ity
choi
ce a
nd s
elec
ted
clin
ical
out
com
es.
Met
hod:
-Sys
tem
atic
sea
rch
was
per
form
ed o
n Pu
bMed
MED
LIN
E, C
ochr
ane
Libr
ary,
and
Ovi
d (fr
om J
anua
ry 1
, 199
5 to
D
ecem
ber 3
1, 2
013)
-In
clus
ion
crite
ria a
pplie
d:
v
Adul
ts o
nly
v
Pre-
dial
ysis
edu
catio
n fo
r C
KD p
atie
nts
stag
e III
, IV
, and
Vv
Plan
ned
star
t pat
ient
s,
unpl
anne
d st
art p
atie
nts,
an
d pa
tient
s on
dia
lysi
s,
ie, i
ncid
ent a
nd p
reva
lent
pa
tient
s.v
Det
aile
d de
scrip
tion
of
prog
ram
me
v
Mul
tiple
ses
sion
sv
Mul
tidis
cipl
inar
y pr
ogra
mm
e in
volv
ing
phys
icia
ns, n
urse
s,
diet
icia
ns, e
tc.
-Out
com
es in
clud
ed:
v
Dia
lysi
s m
odal
ity c
hoic
e an
d th
e nu
mbe
rs o
f pa
tient
s ch
oosi
ng e
ach
mod
ality
v
Any
clin
ical
out
com
e as
soci
ated
with
pre
-di
alys
is e
duca
tion
v
Hea
lth-re
late
d qu
ality
of
life
v
Mea
sure
s as
soci
ated
with
pa
tient
cho
ice
v
Fina
ncia
l im
pact
of
patie
nts
choo
sing
mor
e ho
me
ther
apie
s v
Patie
nt s
atis
fact
ion
-Lite
ratu
re a
lso
revi
ewed
for a
ny
info
rmat
ion
on p
roce
sses
, pat
hway
s,
and
orga
niza
tion
of th
e pr
e-di
alys
is
educ
atio
n pr
ogra
mm
es
I29
rele
vant
stu
dies
:19
qua
si-e
xper
imen
tal
desi
gn10
nar
rativ
e re
view
s
-19
stud
ies
wer
e an
alys
ed
for e
ffect
ive
com
pone
nts
of p
re-d
ialy
sis
educ
atio
n pr
ogra
mm
e
-Des
crip
tions
of
the
educ
atio
nal
proc
ess
varie
d an
d in
clud
ed in
divi
dual
an
d gr
oup
educ
atio
n,
mul
tidis
cipl
inar
y in
terv
entio
n, a
nd v
aryi
ng
dura
tion
and
frequ
ency
of
sess
ions
.
Pre-
dial
ysis
edu
catio
n pr
ogra
mm
esR
esul
ts:
Com
pone
nts
of p
re-d
ialy
sis
educ
atio
n pr
ogra
mm
es
Mul
tidis
cipl
inar
y ed
ucat
ion
-Pre
-dia
lysi
s ca
re is
del
iver
ed b
y a
mul
tidis
cipl
inar
y te
am in
clud
ing
a ne
phro
logi
st, a
nur
se, a
die
ticia
n, a
nd a
soc
ial w
orke
r.- T
he te
am c
an a
lso
incl
ude:
v
a ph
arm
acis
t who
exp
lain
s in
form
atio
n on
med
icin
es n
eeds
v
a ps
ycho
logi
st e
xper
t, w
hich
cou
ld b
e a
spec
ialis
ed n
urse
for
emot
iona
l sup
port
whe
n ne
eded
;
v
a ca
se m
anag
er;
v
repr
esen
tativ
es fr
om th
e lo
cal p
atie
nt k
idne
y su
ppor
t gro
up;
v
and
othe
r pat
ient
s es
tabl
ishe
d on
mai
nten
ance
dia
lysi
s
-7 a
rticl
es re
triev
ed fr
om th
e sc
ient
ific
liter
atur
e re
view
des
crib
ed
mul
tidis
cipl
inar
y ed
ucat
ion
prog
ram
whi
ch c
onsi
sts
of m
ultip
le e
duca
tion
sess
ions
whe
re p
atie
nts
wer
e ed
ucat
ed b
y th
ree
or m
ore
heal
th c
are
prof
essi
onal
s su
ch a
s ne
phro
logi
st, n
urse
, die
titia
n, s
ocia
l wor
ker,
hom
e-di
alys
is c
oord
inat
or, p
harm
acis
t, te
chni
cian
, or b
y ot
her d
ialy
sis
patie
nts
Del
iver
y st
yle
-Edu
catio
n de
liver
y st
yle
can
eith
er b
e on
e-on
-one
ses
sion
s or
cla
ss ro
om
teac
hing
sty
le, b
ut a
mix
of o
ne-o
n-on
e an
d gr
oup
sess
ions
wer
e ad
voca
ted
-Edu
catio
nal p
rogr
ams
shou
ld c
onta
in in
divi
dual
ised
one
-on-
one
coun
sellin
g se
ssio
ns w
ith a
mem
ber/m
embe
rs o
f mul
tidis
cipl
inar
y te
am.
-Thi
s ca
n be
a p
hysi
cian
, nep
hrol
ogis
t, nu
rse,
die
ticia
n, s
ocia
l wor
ker,
etc.
-In a
dditi
on to
sm
all g
roup
dis
cuss
ions
, pee
r cou
nsel
ling
and
prob
lem
-sol
ving
or
“bra
inst
orm
ing”
ses
sion
s ha
ve b
een
desc
ribed
whe
rein
pat
ient
s di
scus
s tre
atm
ent m
odal
ities
, bar
riers
and
ben
efits
, and
trou
bles
hoot
ing
of p
ossi
ble
prob
lem
s w
ith o
ther
pat
ient
s (o
r fac
ilitat
ors)
.-G
roup
ses
sion
s ca
n ha
ve a
var
iety
of f
orm
ats
such
as
grou
p le
ctur
es,
inte
ract
ive
wor
ksho
ps, o
r ope
n fo
rum
ses
sion
s.
Freq
uenc
y an
d du
ratio
n -N
umbe
r of s
essi
ons
and
dura
tion
per s
essi
on v
arie
s by
edu
catio
nal p
rogr
am.
-The
re w
ere
repo
rts o
f 6 in
divi
dual
ses
sion
s of
1 h
our,
4 se
ssio
ns, 1
nig
ht a
w
eek
for 2
hou
rs; o
r at l
east
4 to
5 in
terv
iew
s
Tim
ing
-An
estim
ated
glo
mer
ular
filtr
atio
n ra
te o
f les
s th
an 3
0 m
L/m
in (s
tage
IV C
KD)
has
been
repo
rted
as id
eal f
or re
ferra
l to
CKD
clin
ic.
-Oth
ers
reco
mm
end
that
pat
ient
s sh
ould
be
refe
rred
as e
arly
as
poss
ible
to
rena
l edu
catio
n (>
6 m
onth
s).
Aut
hors
con
clus
ion:
Ther
e is
a n
eed
for a
sta
ndar
dize
d ap
proa
ch b
uilt
on b
est e
vide
nce
from
C
KD a
nd a
lso
from
oth
er c
linic
al c
ondi
tions
and
exi
stin
g kn
owle
dge
on th
e ev
alua
tion
of c
ompl
ex in
terv
entio
ns to
ens
ure
form
al e
valu
atio
n of
pre
-di
alys
is e
duca
tion
prog
ram
s, a
nd th
eir e
ffect
s on
clin
ical
out
com
es a
nd
mod
ality
cho
ice.
Mos
t stu
dies
w
ithou
t con
trol
grou
p

75
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Evid
ence
Tab
le :
Org
anis
atio
nal (
CO
MPO
NEN
TS O
F PR
OG
RAM
ME)
Que
stio
n : W
hat a
re th
e or
gani
satio
nal i
ssue
s w
ith re
gard
s to
Pre
-dia
lysi
s Ed
ucat
ion
Prog
ram
me
for a
dvan
ced
CKD
pat
ient
s?Bi
blio
grap
hic
Cita
tion
Stud
yTy
pe/M
etho
dsLE
Num
ber o
f Pat
ient
s &
Patie
nt C
hara
cter
istic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al C
omm
ents
2. P
rieto
-Vel
asco
M
, Isn
ard
Bagn
is C
, D
ean
J et
al.
Pred
ialy
sis
educ
atio
nin
pra
ctic
e: a
qu
estio
nnai
re
surv
ey o
f cen
tres
with
est
ablis
hed
prog
ram
mes
. BM
CR
es N
otes
. 20
14;7
:730
.
EU c
ount
ries
Cro
ss-s
ectio
nal s
tudy
Obj
ectiv
e:To
hel
p ad
dres
s kn
owle
dge
gap:
a) h
ow is
rena
l re
plac
emen
t the
rapy
op
tion
educ
atio
n (R
RTO
E) b
eing
run?
Met
hods
:-A
n ex
pert
mee
ting
was
hel
d in
Mar
ch
2013
to fo
rmul
ate
a po
sitio
n st
atem
ent o
n op
timal
way
s to
run
RRT
OE.
-E
xper
ts w
ere
sele
cted
fro
m u
nits
that
had
ex
tens
ive
expe
rienc
e in
RRT
OE
or w
ere
perfo
rmin
g re
sear
ch in
th
is fi
eld.
-Bef
ore
the
mee
ting,
ex
perts
com
plet
ed a
pi
lot q
uest
ionn
aire
on
RRT
OE
in th
eir o
wn
units
.
II-3
Four
nur
ses,
5
neph
rolo
gist
s an
d 1
clin
ical
psy
chol
ogis
t
(9 re
nal u
nits
; 6 E
U
coun
tries
) par
ticip
ated
.
-2 u
nits
eac
h in
UK,
Sw
eden
, Spa
in-3
uni
ts in
Fra
nce,
Be
lgiu
m, I
taly
Ren
al re
plac
emen
t th
erap
y op
tion
educ
atio
n (R
RTO
E)
Res
ults
:St
aff i
nvol
ved
-Nur
ses
wer
e al
mos
t alw
ays
resp
onsi
ble
for o
rgan
isin
g R
RTO
E. (8
/9 u
nits
)-N
ephr
olog
ists
spe
nt 7
.5%
(med
ian)
of t
heir
time
on R
RTO
Ev
Nep
hrol
ogis
ts a
lso
invo
lved
in R
RTO
E pr
ogra
mm
e (7
units
),v
diet
icia
ns (5
uni
ts)
v
psyc
holo
gist
s (4
uni
ts),
v
soci
al w
orke
rs (3
uni
ts),
v
phys
ioth
erap
ist (
1uni
t),v
occu
patio
nal t
hera
pist
(1un
it)v
phar
mac
ist (
1uni
t)
-All
staf
f adm
inis
terin
g th
e pr
ogra
mm
e ha
d ba
ckgr
ound
in g
ener
al o
r nep
hrol
ogy
nurs
ing
Star
ting
RRT
OE
-Edu
catio
n fo
r the
pat
ient
and
fam
ily b
egan
sev
eral
mon
ths
befo
re d
ialy
sis
or a
ccor
ding
to
dise
ase
prog
ress
ion
-RRT
OE
parti
cipa
nts
incl
uded
:v
patie
nts
with
CKD
sta
ge IV
or V
(9
uni
ts),
v
patie
nts
requ
iring
a c
hang
e in
RRT
trea
tmen
t (8
units
),v
fam
ily m
embe
rs o
f pat
ient
s (9
uni
ts)
Con
tent
and
stru
ctur
e-K
ey to
pics
suc
h as
the
‘impa
ct o
f the
dis
ease
’ wer
e co
vere
d by
eve
ry u
nit,
but o
nly
a fe
w
units
des
crib
ed a
ll di
alys
is m
odal
ities
. -M
ost R
RT p
atie
nts
visi
t in
cent
re H
D u
nit (
8/9
units
), pa
tient
s vi
sit h
ome
dial
ysis
nur
se to
as
sess
sui
tabi
lity
(7/9
uni
ts)
-Hal
f of u
nits
hav
e fo
rmal
mee
ting
with
‘exp
ert p
atie
nt’ a
s pa
rt of
RRT
OE
prog
ram
me
-Gro
up e
duca
tion
sess
ions
wer
e us
ed in
3/9
uni
ts.
Dec
isio
n-m
akin
g-M
ost h
ave
form
al d
ecis
ion-
mak
ing
proc
ess
with
writ
ten
supp
ort m
ater
ials
in p
lace
(7/9
uni
ts)
with
bot
h nu
rses
and
nep
hrol
ogis
ts
Mat
eria
ls-M
ater
ials
cam
e in
a w
ide
varie
ty o
f for
ms
and
from
a w
ide
rang
e of
sou
rces
-Boo
klet
s w
ere
used
in a
ll un
its, o
nlin
e m
ater
ials
and
DVD
s w
ere
used
in h
alf o
f uni
ts
Qua
lity
assu
ranc
e m
easu
res
-Mos
t wid
ely
used
(6/9
uni
ts);
v
patie
nt s
atis
fact
ion,
v
num
ber o
f pat
ient
s co
mpl
etin
g th
e pr
ogra
mm
e,
v
linki
ng a
ttend
ance
/com
plet
ion
of p
rogr
amm
e to
clin
ical
follo
w u
p,
v
and
regu
larly
upd
atin
g m
ater
ials
-Mos
t wid
ely
agre
ed u
pon
fact
ors
perc
eive
d to
be
impo
rtant
wer
e na
tiona
l/loc
al g
uide
lines
m
anda
ting
RRT
OE
prog
ram
me
and
the
clin
ical
lead
ersh
ip in
the
rena
l uni
t (ea
ch 6
uni
ts)
Aut
hors
con
clus
ion:
Th
ere
wer
e su
bsta
ntia
l var
iatio
ns in
how
RRT
OE
is ru
n be
twee
n th
e un
its.

76
PRE-DIALYSIS EDUCATION PROGRAMME
Evid
ence
Tab
le :
Soci
etal
impl
icat
ions
(MO
DAL
ITY
CH
OIC
E)Q
uest
ion
: Wha
t are
the
soci
etal
impl
icat
ions
of P
re-d
ialy
sis
Educ
atio
n Pr
ogra
mm
e fo
r adv
ance
d C
KD p
atie
nts?
Bibl
iogr
aphi
cC
itatio
nSt
udy
Type
/Met
hods
LEN
umbe
r of
Patie
nts
& Pa
tient
C
hara
cter
istic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
1. S
hukl
a AM
, Eas
om
A, S
ingh
M e
t al.
Effe
cts
of a
C
ompr
ehen
sive
Pr
edia
lysi
s Ed
ucat
ion
(CPE
) Pro
gram
on
the
Hom
e D
ialy
sis
Ther
apie
s: A
Ret
rosp
ectiv
e C
ohor
t St
udy.
Perit
Dia
l Int
. 20
17;3
7(5)
:542
-547
.
USA
Ret
rosp
ectiv
e C
ohor
t Stu
dy
Obj
ectiv
e:To
repo
rt th
e fin
ding
s of
a
retro
spec
tive
anal
ysis
of
the
initi
al 2
2 m
onth
s of
ne
wly
form
ed C
PE c
linic
for
adva
nced
CKD
sub
ject
s,
and
its im
pact
on
the
rate
s of
hom
e di
alys
is (H
oD)
Met
hods
:-A
ll pa
tient
s w
ith s
tage
4
and
5 C
KD, w
ith o
ccas
iona
l pa
tient
s of
sta
ge 3
b C
KD
with
rapi
d re
nal p
rogr
essi
on
unde
r the
car
e of
ne
phro
logi
sts
wer
e of
fere
d an
d en
cour
aged
tran
sitio
n to
the
care
of C
PE c
linic
un
der a
sin
gle
neph
rolo
gist
fo
r the
ir ro
utin
e ne
phro
logy
ca
re.
-CPE
clin
ic in
clud
ed:
v
a re
nal
phys
icia
n,
v
an a
dvan
ced
nurs
e pr
actit
ione
r (A
NP)
edu
cato
r, v
a re
nal
diet
icia
n,
v
and
a re
nal
soci
al w
orke
r.
-A p
harm
acis
t was
indu
cted
in
the
CPE
clin
ic fo
r the
la
tter h
alf o
f the
stu
dy
perio
d.-A
ll pa
tient
s ad
mitt
ed to
cl
inic
for fi
rst t
ime
wer
e se
en
on n
ew p
atie
nt p
roto
col,
and
retu
rnin
g pa
tient
s w
ere
seen
on
esta
blis
hed
patie
nt
prot
ocol
-Ana
lysi
s 22
mon
ths
of C
PE
clin
ic w
ere
done
II-2
108
adva
nced
C
KD p
atie
nts
-with
ave
rage
eG
FR o
f 18.
34
± 6.
5 m
L/m
in
wer
e se
en in
the
first
22
mon
ths
of th
e C
PE c
linic
-Maj
ority
of
patie
nts
wer
e re
ferre
d to
the
CPE
clin
ic la
te
with
late
sta
ge
4 (e
GFR
16
– 22
mL/
min
) an
d st
age
5 co
mpr
isin
g 74
%
of th
e to
tal C
PE
popu
latio
n.
Com
preh
ensi
ve P
re-d
ialy
sis
Educ
atio
n Pr
ogra
mm
e (C
PE):
-New
pro
toco
l req
uire
d pa
tient
s to
atte
nd
half-
day
com
preh
ensi
ve e
duca
tion
sess
ion.
-Pts
enc
oura
ged
to a
ttend
with
fam
ily
mem
bers
, spo
use,
or c
areg
iver
s.
-On
arriv
al, p
atie
nts
prov
ided
with
prin
ted
mat
eria
l for
kid
ney
dise
ase
fol
low
ed b
y gr
oup
less
on in
cla
ssro
om fo
rmat
by
rena
l AN
P ed
ucat
or, w
hich
last
ed fo
r a m
in. o
f 1
hour
.-A
fter g
roup
less
on, p
atie
nts
rota
ted
with
re
nal d
ietic
ian,
soc
ial w
orke
r, tra
ined
dia
lysi
s nu
rse
wel
l ver
sed
in a
ll di
alys
is te
chni
ques
, an
d re
nal p
hysi
cian
for p
atie
nt-s
peci
fic
disc
ussi
ons
and
deta
iled
on th
e in
divi
dual
ne
eds
and
ques
tions
. -S
essi
ons
with
dia
lysi
s nu
rse
incl
uded
a
‘han
ds-o
n’ d
emon
stra
tion
of h
ome
perit
onea
l di
alys
is (P
D),
hom
e he
mod
ialy
sis
(HD
), an
d in
-cen
ter m
achi
ne a
s pe
r the
nee
ds a
nd
desi
res
of p
ts.
-Vis
it en
ded
with
det
aile
d se
ssio
n w
ith th
e re
nal p
hysi
cian
. -P
rovi
der s
essi
ons
star
ted
with
an
inte
rvie
w
of th
e in
divi
dual
’s fa
mily
, soc
ial,
med
ical
, and
oc
cupa
tiona
l nee
ds.
-All
prev
ious
ly p
rovi
ded
info
rmat
ion
was
re
view
ed a
nd s
peci
fic q
uest
ions
add
ress
ed.
-Pat
ient
s an
d th
eir c
areg
iver
s en
cour
aged
to
mak
e ‘a
ctiv
e ch
oice
’ for
thei
r RRT
. -A
ny re
mai
ning
mis
conc
eptio
ns o
r fea
rs w
ere
addr
esse
d du
ring
this
fina
l dis
cuss
ion.
-T
he la
st m
embe
r of t
he c
linic
team
reco
rded
fin
al m
odal
ity c
hoic
e in
a p
assi
ve m
anne
r.
Esta
blis
hed
patie
nt p
roto
col
-Gre
ater
fre
edom
for
patie
nts
to
focu
s on
the
area
s of
thei
r ch
oice
with
all
clin
ic m
embe
rs
avai
labl
e fo
r co
unse
lling.
-S
een
by th
e re
nal p
hysi
cian
fo
r the
ir ro
utin
e ne
phro
logy
ca
re.
-Pat
ient
pr
efer
ence
s fo
r RRT
wer
e no
ted
at e
ach
clin
ic v
isit
22 m
onth
sR
esul
ts:
Ove
r 22
mon
ths
CPE
clin
ic:
Rat
es o
f hom
e di
alys
is (H
oD)
v
70%
of p
atie
nts
in C
PE g
roup
ch
ose
HoD
, v
Of w
hich
, 55%
cho
se p
erito
neal
di
alys
is (P
D)
v
and
15%
cho
se h
ome
hem
odia
lysi
s (H
HD
).
-Rat
es o
f HoD
cho
ice
wer
e si
mila
r acr
oss
spec
trum
of s
ocio
-eco
nom
ic v
aria
bles
. -5
4.6%
of t
hose
cho
osin
g to
retu
rn fo
r mor
e th
an 1
ses
sion
, 25.
3%, c
hang
ed th
eir m
odal
ity
pref
eren
ce a
fter t
he fi
rst e
duca
tion
sess
ion,
an
d ne
arly
all
reac
hed
a fin
al m
odal
ity
sele
ctio
n by
the
end
of th
ird v
isit.
-M
ultiv
aria
te a
naly
sis
show
ed th
at th
e ch
oice
of
RRT
mod
ality
was
una
ffect
ed b
y th
e pa
tient
s’ ag
e, g
ende
r, ra
ce, a
vaila
bilit
y an
d ty
pe o
f ins
uran
ce, d
iabe
tes
stat
us, a
lbum
in, o
r th
e st
age
of re
nal d
isea
se (p
> 0
.05)
.-In
itiat
ion
of th
e C
PE p
rogr
am re
sulte
d in
a
216%
gro
wth
in H
oD c
ensu
s ov
er th
e sa
me
perio
d an
d re
sulte
d in
nea
r dou
blin
g of
HoD
pr
eval
ence
to 3
8% o
f all
dial
ysis
pat
ient
s w
ithin
22
mon
ths
of in
itiat
ion.
Aut
hors
con
clus
ion
Com
preh
ensi
ve p
atie
nt e
duca
tion
impr
oves
the
choi
ce a
nd p
reva
lenc
e of
HoD
ther
apie
s. W
e fu
rther
find
that
3 s
essi
ons
of C
PE m
ay p
rovi
de
need
ed re
sour
ces
for t
he la
rge
maj
ority
of
subj
ects
for a
dequ
ate
deci
sion
-mak
ing
Gro
up+
indi
vidu
al
sess
ions
w
ith te
am
mem
bers

77
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Evid
ence
Tab
le :
Soci
etal
impl
icat
ions
(MO
DAL
ITY
CH
OIC
E)Q
uest
ion
: Wha
t are
the
soci
etal
impl
icat
ions
of P
re-d
ialy
sis
Educ
atio
n Pr
ogra
mm
e fo
r adv
ance
d C
KD p
atie
nts?
Bibl
iogr
aphi
c C
itatio
nSt
udy
Type
/Met
hods
LEN
umbe
r of P
atie
nts
& Pa
tient
Cha
ract
eris
ticIn
terv
entio
nC
ompa
rison
Leng
th o
f Fo
llow
Up
Out
com
e M
easu
res/
Effe
ct S
ize
Gen
eral
C
omm
ents
2. D
evoe
DJ,
Won
g B,
Ja
mes
MT
et a
l.Pa
tient
Edu
catio
n an
d Pe
riton
eal D
ialy
sis
Mod
ality
Sel
ectio
n:
A Sy
stem
atic
Rev
iew
an
d M
eta-
anal
ysis
. Am
J K
idne
y D
is.
2016
;68(
3):4
22-4
33.
Syst
emat
ic re
view
and
met
a-an
alys
is
Obj
ectiv
e:To
cha
ract
eris
e th
e re
latio
nshi
p be
twee
n pa
tient
-targ
eted
edu
catio
nal i
nter
vent
ions
and
ch
oosi
ng a
nd re
ceiv
ing
PD.
Met
hods
: -S
yste
mat
ic s
earc
h w
ere
done
in M
EDLI
NE,
EM
BASE
, CIN
AHL
and
EBM
R &
incl
uded
co
ntro
lled
obse
rvat
iona
l stu
dies
and
ra
ndom
ized
tria
ls o
f edu
catio
nal i
nter
vent
ions
de
sign
ed to
incr
ease
PD
sel
ectio
n in
the
revi
ew-A
bstra
cts
from
ann
ual m
eetin
g of
the
Amer
ican
Soc
iety
of N
ephr
olog
y fo
r 200
9-20
14 w
ere
revi
ewed
-R
elev
ant a
rticl
es a
lso
hand
sea
rche
d fro
m
refe
renc
e lis
t-T
wo
revi
ewer
s re
view
ed th
e tit
les
and
full
text
for i
nclu
sion
acc
ordi
ng to
crit
eria
:v
adul
ts w
ith C
KDv
repo
rted
patie
nt-ta
rget
ed
educ
atio
n st
rate
gies
abo
ut
avai
labl
e di
alys
is m
odal
ities
v
repo
rted
rele
vant
out
com
es
(cho
osin
g PD
or r
ecei
ving
PD
on
ly o
r cho
osin
g PD
or r
ecei
ving
PD
with
hom
e H
D)
v
and
inco
rpor
ated
sta
ndar
d ca
re
as c
ontro
l gro
up
-Ris
k of
bia
s as
sess
men
t was
don
e-P
rimar
y ou
tcom
e w
as c
hoos
ing
PD, d
efine
d as
inte
ntio
n to
use
PD
rega
rdle
ss o
f whe
ther
PD
was
eve
r use
d.-S
econ
dary
out
com
e, re
ceiv
ing
PD, w
as
defin
ed a
s an
indi
vidu
al re
ceiv
ing
PD a
s hi
s or
her
trea
tmen
t.-M
eta-
anal
ysis
wer
e do
ne, s
tudi
es e
stim
ates
w
ere
pool
ed
IO
f 3,5
40 c
itatio
ns, 1
5 st
udie
s w
ere
incl
uded
:-7
pre
and
pos
t in
terv
entio
n st
udie
s,
-5 c
ohor
t stu
dies
-2 c
ase-
cont
rol
stud
ies
-1 ra
ndom
ised
co
ntro
lled
trial
(RC
T)
-Of 1
5 st
udie
s, 2
w
ere
excl
uded
from
m
eta-
anal
ysis
due
to
mis
sing
info
rmat
ion
-7 s
tudi
es fr
om N
orth
Am
eric
a, 5
from
Eu
rope
, 3 fr
om A
sia.
-Num
ber o
f pa
rtici
pant
s ra
nged
fro
m 6
3 to
21,
302
for
tota
l of 3
1,65
3.-M
ean
age
rang
ed
from
58
to 7
0.8
year
s ol
d-P
erce
ntag
e of
men
ra
nged
from
45%
to
64.3
%-M
ean
eGFR
rang
ed
from
≤15
to 2
0.4
ml/
min
/1.7
3 m
2
-Tw
o st
udie
s in
clud
ed
only
sta
ge 5
or E
SRD
Pre-
dial
ysis
ed
ucat
iona
l in
terv
entio
ns.
-Edu
catio
nal
inte
rven
tions
var
y gr
eatly
bet
wee
n st
udie
s-7
stu
dies
incl
uded
ph
ysic
ian
as a
n ed
ucat
or, 1
0 in
clud
ed a
nur
se,
and
4 in
clud
ed
mul
tidis
cipl
inar
y te
am-8
stu
dies
car
ried
out e
duca
tiona
l in
terv
entio
ns 2
or
mor
e da
ys a
nd 5
st
udie
s in
clud
ed
info
rmat
ion
on d
iet
-8 s
tudi
es c
arrie
d ou
t edu
catio
nal
inte
rven
tions
in g
roup
se
ssio
ns, 5
had
1 to
1
sess
ion
only
and
2
incl
uded
bot
h-6
stu
dies
use
d vi
deo
mat
eria
l, 7
used
pr
inte
d m
ater
ials
, an
d 1
used
web
site
m
ater
ials
-4 s
tudi
es in
clud
ed
fam
ily m
embe
rs
in e
duca
tiona
l in
terv
entio
ns
Stan
dard
car
e
-6 o
ut o
f 15
stud
ies
repo
rted
cont
rol
inte
rven
tion
-of t
he 6
stu
dies
, 2
incl
uded
sta
ndar
d ed
ucat
ion
from
ne
phro
logi
st a
nd
2 ha
d st
anda
rd
educ
atio
n gi
ven
by
mul
tidis
cipl
inar
y te
am
-Dur
atio
n of
follo
w u
p ra
nged
from
12
to 1
44
mon
ths
Res
ults
:Pr
imar
y ou
tcom
e- c
hoos
ing
PD6
stud
ies
repo
rted
prim
ary
outc
ome,
and
5
prov
ided
suf
ficie
nt d
ata
for m
eta-
anal
ysis
:
-In th
e R
CT
(N=7
0), e
duca
tiona
l in
terv
entio
n gr
oup
was
ass
ocia
ted
with
a
mor
e th
an 4
-fold
incr
ease
in th
e od
ds o
f ch
oosi
ng P
D
(OR
, 4.6
0; 9
5% C
I, 1.
19,1
7.74
). -B
ased
on
resu
lts fr
om 4
obs
erva
tiona
l st
udie
s (N
=7,6
53),
patie
nt-ta
rget
ed
educ
atio
nal i
nter
vent
ions
wer
e as
soci
ated
w
ith a
2-fo
ld in
crea
se in
the
odds
of
choo
sing
PD
(poo
led
OR
, 2.1
5; 9
5% C
I, 1.
07,4
.32;
I2 =
76.7
%).
Seco
ndar
y ou
tcom
e-re
ceiv
ing
PD10
stu
dies
repo
rted
seco
ndar
y ou
tcom
e,
only
9 h
ad s
uffic
ient
dat
a fo
r met
a-an
alys
is:
-Bas
ed o
n re
sults
from
9 o
bser
vatio
nal
stud
ies
(N=8
,229
), pa
tient
-targ
eted
ed
ucat
iona
l int
erve
ntio
n w
as a
ssoc
iate
d w
ith a
3-fo
ld in
crea
se in
the
odds
of
rece
ivin
g PD
as
the
initi
al tr
eatm
ent
mod
ality
(O
R, 3
.50;
95%
CI,
2.82
, 4.3
5; I2 =
24.9
%).
Aut
hors
con
clus
ion:
This
sys
tem
atic
revi
ew d
emon
stra
tes
a st
rong
ass
ocia
tion
betw
een
patie
nt-
targ
eted
edu
catio
n in
terv
entio
ns a
nd
the
subs
eque
nt c
hoic
e an
d re
ceip
t of
PD. T
he v
aria
bilit
y in
the
desi
gn o
f the
ed
ucat
iona
l stra
tegi
es id
entifi
ed a
nd th
e st
reng
th o
f ass
ocia
tion
acro
ss s
tudi
es
high
light
the
unce
rtain
ty a
bout
whe
n an
d ho
w e
duca
tiona
l int
erve
ntio
ns s
houl
d be
de
liver
ed, a
s w
ell a
s lik
elih
ood
of im
pact
ac
cord
ing
to b
asel
ine
PD p
enet
ratio
n.

78
PRE-DIALYSIS EDUCATION PROGRAMME
Bibl
iogr
aphi
cC
itatio
nSt
udy
Type
/Met
hods
LEN
umbe
r of
Patie
nts
&Pa
tient
C
hara
cter
istic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
3. d
e M
aar
JS, d
e G
root
M
A, L
uik
PT e
t al
. GU
IDE,
a
stru
ctur
edpr
e-di
alys
is
prog
ram
me
that
incr
ease
s th
e us
e of
ho
me
dial
ysis
. C
lin K
idne
y J.
2016
;9(6
):826
-83
2.
Amst
erda
m,
The
Net
herla
nds
Cro
ss-s
ectio
nal s
tudy
Obj
ectiv
e:To
ans
wer
the
follo
win
g qu
estio
n:
Doe
s th
e im
plem
enta
tion
of a
stru
ctur
ed p
re-d
ialy
sis
prog
ram
me
with
a h
ome-
focu
sed
appr
oach
incr
ease
the
num
ber o
f pre
-dia
lysi
s pa
tient
s th
at c
hoos
e ho
me
dial
ysis
, and
the
num
ber o
f pat
ient
s th
at
even
tual
ly re
ceiv
e ho
me
dial
ysis
?M
etho
ds-R
ecor
ds o
f all
102
patie
nts
that
rece
ived
a tr
eatm
ent
reco
mm
enda
tion
in th
e G
UID
E pr
ogra
mm
e be
twee
n 12
Sep
tem
ber
2013
and
18
Dec
embe
r 201
4 at
Mea
nder
Med
ical
Cen
tre w
ere
retro
spec
tivel
y re
view
ed.
-The
stru
ctur
ed p
re-d
ialy
sis
prog
ram
me
(GU
IDE)
pro
cess
sta
rts
whe
n a
patie
nt h
as a
n eG
FR o
f 15
mL/
min
/1.7
3 m
2 . -B
egin
s w
ith h
ome
visi
t fro
m a
cas
e m
anag
er (s
ocia
l wor
ker)
durin
g w
hich
firs
t edu
catio
n is
giv
en a
nd s
uita
bilit
y fo
r hom
e di
alys
is is
as
sess
ed.
-Nex
t, qu
estio
nnai
res
wer
e co
mpl
eted
by
patie
nt, c
ase
man
ager
an
d ne
phro
logi
st.
-Pat
ient
que
stio
nnai
re c
onta
ins:
v
ques
tions
abo
ut th
e pa
tient
’s so
cial
sup
port
syst
em,
v
daily
act
iviti
es,
v
leve
l of i
ndep
ende
nce
in a
ctiv
ities
of d
aily
livi
ng (A
DL)
, v
aspe
cts
of li
fe th
at p
atie
nt v
alue
s m
ost
v
and
pref
eren
ces
and
expe
ctat
ions
with
rega
rd to
RRT
.
-Med
ical
que
stio
nnai
re c
ompr
ises
the
cate
gorie
s Tr
ansp
lant
atio
n,
PD a
nd H
D, w
hich
con
tain
que
stio
ns a
bout
rela
tive
and
abso
lute
co
ntra
indi
catio
ns fo
r eac
h th
erap
y an
d ne
phro
logi
st’s
treat
men
t pr
efer
ence
. -C
ase
man
ager
’s qu
estio
nnai
re c
over
s th
e su
itabi
lity
of th
e ho
me,
th
e so
cial
env
ironm
ent a
nd th
e ba
lanc
e be
twee
n bu
rden
and
ca
paci
ty a
nd e
nds
with
cas
e m
anag
er’s
judg
men
t of w
heth
er o
r not
ho
me
dial
ysis
wou
ld b
e su
itabl
e.-A
mul
tidis
cipl
inar
y m
eetin
g (M
DM
) is
held
to d
eter
min
e a
spec
ific
patie
nt p
rofil
e (tr
eatm
ent r
ecom
men
datio
n).
-In M
DM
, mos
t sui
tabl
e tre
atm
ent f
or p
artic
ular
pat
ient
is c
hose
n,
whi
le ta
king
into
acc
ount
the
sequ
ence
of p
rogr
amm
e’s
treat
men
t pr
efer
ence
.-T
his
sequ
ence
impl
ies
trans
plan
tatio
n is
reco
mm
ende
d w
hen
poss
ible
ove
r dia
lysi
s an
d ho
me
dial
ysis
ove
r in-
cent
re d
ialy
sis.
-A
n au
tom
ated
GU
IDE
dash
boar
d, w
hich
gen
erat
es a
pro
file
usin
g an
alg
orith
m b
ased
on
answ
ers
to th
e qu
estio
nnai
res
-Thi
s is
follo
wed
by
patie
nt e
duca
tion,
a s
econ
d M
DM
and
fina
lly
the
sele
ctio
n of
the
treat
men
t by
the
patie
nt a
nd th
e ne
phro
logi
st.
II-3
102
patie
nts
wer
e in
clud
ed
who
sta
rted
the
proc
ess
at
a m
ean
eGFR
of
12.
3 m
L/m
in/1
.73
m2 .
-Mea
n ag
e w
as 6
8.6
year
s an
d 44
.1%
w
ere
fem
ale
GU
IDE
(stru
ctur
ed p
re-
dial
ysis
pro
gram
me)
-Afte
r MD
M, s
peci
alis
ed
pre-
dial
ysis
nur
se
prov
ides
edu
catio
n ta
ilore
d to
pat
ient
’s pr
ofile
.-A
ll pa
tient
s re
ceiv
e ge
nera
l RRT
in
form
atio
n-T
rain
ing
that
pat
ient
an
d fa
mily
mem
bers
re
ceiv
es b
efor
e th
e st
art o
f hom
e di
alys
is is
di
scus
sed.
-If
ther
e ar
e no
fam
ily
mem
bers
who
are
w
illing
or a
ble
to
cont
ribut
e, p
assi
ve
HH
D (o
r pas
sive
PD
) w
ith th
e he
lp o
f hom
e ca
re is
dis
cuss
ed.
-If th
e pr
ofile
onl
y in
clud
es C
HD
, no
info
rmat
ion
is p
rovi
ded
on o
ther
mod
aliti
es-E
duca
tion
is p
rovi
ded
in a
sin
gle
sess
ion,
w
hich
is re
peat
ed if
the
patie
nt w
ishe
s.
-Writ
ten
broc
hure
s an
d ed
ucat
iona
l vid
eos
are
also
pro
vide
d.-M
eetin
gs w
ith o
ther
pa
tient
s ar
e of
fere
d an
d ar
rang
ed if
requ
este
d by
the
patie
nt o
r the
ir fa
mily
. -P
atie
nt’s
resp
onse
to
this
edu
catio
nal
sess
ion
is d
iscu
ssed
in
a se
cond
MD
M.
-Fol
low
ing
this
, pat
ient
an
d ne
phro
logi
st
choo
se a
trea
tmen
t m
odal
ity d
urin
g th
e ne
xt
visi
t to
the
outp
atie
nt
clin
ic.
Res
ults
:
v
Hom
e di
alys
is w
as
reco
mm
ende
d fo
r 62.
8% o
f the
pa
tient
s w
ho w
ere
advi
sed
to
have
dia
lysi
s tre
atm
ent.
v
Of p
atie
nts
that
opt
ed
for d
ialy
sis,
34.
2% c
hose
PD
an
d 8.
2% c
hose
HH
D;
v
22.9
% s
tarte
d ho
me
dial
ysis
as
thei
r firs
t the
rapy
, com
pare
d w
ith 1
7.6%
in th
e m
onth
s be
fore
im
plem
enta
tion
of G
UID
E.
v
32.1
% o
f the
pat
ient
s th
at
rece
ived
dia
lysi
s th
erap
y re
ceiv
ed h
ome
dial
ysis
. v
In th
e m
onth
s be
fore
GU
IDE,
an
aver
age
of ju
st 1
9.5%
of p
atie
nts
rece
ived
dia
lysi
s re
ceiv
ed h
ome
dial
ysis
.
Aut
hors
con
clus
ion:
Com
pare
d w
ith h
isto
rical
dat
a, th
e st
anda
rdis
ed a
nd h
ome-
focu
sed
pre
dial
ysis
pro
gram
me
GU
IDE,
with
its
hom
e vi
sit,
seem
s to
suc
cess
fully
incr
ease
the
num
ber o
f pat
ient
s th
at c
hoos
e an
d re
ceiv
e ho
me
dial
ysis
Educ
atio
n st
arts
with
ho
me
visi
t, M
DM
m
eetin
g, a
nd
educ
atio
n+
train
ing,
se
cond
MD
M
and
final
ch
oice
of
RRT
Evid
ence
Tab
le :
Soci
etal
impl
icat
ions
(MO
DAL
ITY
CH
OIC
E)Q
uest
ion
: Wha
t are
the
soci
etal
impl
icat
ions
of P
re-d
ialy
sis
Educ
atio
n Pr
ogra
mm
e fo
r adv
ance
d C
KD p
atie
nts?

79
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Evid
ence
Tab
le :
Soci
etal
impl
icat
ions
(MO
DAL
ITY
CH
OIC
E)Q
uest
ion
: Wha
t are
the
soci
etal
impl
icat
ions
of P
re-d
ialy
sis
Educ
atio
n Pr
ogra
mm
e fo
r adv
ance
d C
KD p
atie
nts?
Bibl
iogr
aphi
c C
itatio
nSt
udy
Type
/Met
hods
LEN
umbe
r of P
atie
nts
& Pa
tient
Cha
ract
eris
ticIn
terv
entio
nC
ompa
rison
Leng
th o
f Fo
llow
Up
Out
com
e M
easu
res/
Effe
ct S
ize
Gen
eral
C
omm
ents
4. V
an d
en B
osch
J,
War
ren
DS,
Rut
herfo
rd
PA. R
evie
w o
f pr
edia
lysi
s ed
ucat
ion
prog
ram
s: a
nee
d fo
r st
anda
rdiz
atio
n. P
atie
nt
Pref
er A
dher
ence
. 20
15;9
:127
9-12
91.
Syst
emat
ic re
view
Obj
ectiv
e:
To re
view
evi
denc
e on
effe
ctiv
e co
mpo
nent
s of
pre
-dia
lysi
s ed
ucat
ion
prog
ram
mes
as
rela
ted
to m
odal
ity c
hoic
e an
d se
lect
ed c
linic
al o
utco
mes
.
Met
hod:
-Sys
tem
atic
sea
rch
was
per
form
ed o
n Pu
bMed
MED
LIN
E, C
ochr
ane
Libr
ary,
and
Ovi
d (fr
om J
anua
ry 1
, 199
5 to
Dec
embe
r 31
, 201
3)
-Incl
usio
n cr
iteria
app
lied:
v
Adul
ts o
nly
v
Pre-
dial
ysis
edu
catio
n fo
r CKD
pa
tient
s st
age
III, I
V, a
nd V
v
Plan
ned
star
t pat
ient
s,
unpl
anne
d st
art p
atie
nts,
and
pa
tient
s on
dia
lysi
s, ie
, inc
iden
t an
d pr
eval
ent p
atie
nts.
v
Det
aile
d de
scrip
tion
of
prog
ram
me
v
Mul
tiple
ses
sion
sv
Mul
tidis
cipl
inar
y pr
ogra
mm
e in
volv
ing
phys
icia
ns, n
urse
s,
diet
icia
ns, e
tc.
-Out
com
es in
clud
ed:
v
Dia
lysi
s m
odal
ity c
hoic
e an
d th
e nu
mbe
rs o
f pat
ient
s ch
oosi
ng e
ach
mod
ality
v
Any
clin
ical
out
com
e as
soci
ated
with
pre
-dia
lysi
s ed
ucat
ion
v
Hea
lth-re
late
d qu
ality
of l
ife
v
Mea
sure
s as
soci
ated
with
pa
tient
cho
ice
v
Fina
ncia
l im
pact
of p
atie
nts
choo
sing
mor
e ho
me
ther
apie
s v
Patie
nt s
atis
fact
ion
-Lite
ratu
re a
lso
revi
ewed
for a
ny
info
rmat
ion
on p
roce
sses
, pat
hway
s, a
nd
orga
niza
tion
of th
e pr
e-di
alys
is e
duca
tion
prog
ram
mes
I29
rele
vant
stu
dies
:19
qua
si-e
xper
imen
tal
desi
gn10
nar
rativ
e re
view
s
-19
stud
ies
wer
e an
alys
ed fo
r effe
ctiv
e co
mpo
nent
s of
pre
-di
alys
is e
duca
tion
prog
ram
me
-Des
crip
tions
of
the
educ
atio
nal
proc
ess
varie
d an
d in
clud
ed in
divi
dual
an
d gr
oup
educ
atio
n,
mul
tidis
cipl
inar
y in
terv
entio
n, a
nd
vary
ing
dura
tion
and
frequ
ency
of s
essi
ons.
Pre-
dial
ysis
ed
ucat
ion
prog
ram
mes
Res
ults
Mod
ality
sel
ectio
n-6
out
of 9
stu
dies
repo
rting
on
dial
ysis
mod
ality
se
lect
ion
note
d a
high
er p
ropo
rtion
of p
atie
nts
sele
ctin
g ho
me
dial
ysis
(PD
or a
noth
er h
ome
mod
ality
)
Cha
nouz
as e
t al.
(201
2)20
% c
hose
PD
. 50
% c
hoos
ing
PD re
ceiv
ed P
DEP
vs
33%
of H
D
patie
nts.
Klan
g et
al.
(199
8)H
ighe
r pat
ient
s ch
ose
PD
Levi
n et
al.
(199
7)53
% o
f PD
EP g
roup
cho
se P
D v
s. 4
2% in
con
trol
Man
ns e
t al.
(200
5)82
.1%
of P
DEP
gro
up c
hose
sel
f-car
e di
alys
is v
s 50
%
in c
ontro
l
McL
augh
lin e
t al.
(200
8)PD
EP g
roup
mor
e lik
ely
to c
hoos
e se
lf-ca
re d
ialy
sis
Rib
itsch
et a
l. (2
013)
54.3
% in
PD
EP g
roup
sta
rted
with
PD
vs
28%
in
cont
rol
-3 s
tudi
es fo
und
no s
igni
fican
t diff
eren
ce in
mod
ality
ch
oice
-4 s
tudi
es w
ith p
re- a
nd p
ost-
inte
rven
tion
(pre
-dia
lysi
s ed
ucat
ion)
mea
sure
men
ts s
how
ed h
ighe
r lev
els
of
hom
e di
alys
is u
se a
fter t
he p
re-d
ialy
sis
educ
atio
n in
terv
entio
n
Mos
tly w
ithou
t co
ntro
l gro
up

80
PRE-DIALYSIS EDUCATION PROGRAMME
Bibl
iogr
aphi
c C
itatio
nSt
udy
Type
/Met
hods
LEN
umbe
r of
Patie
nts
& Pa
tient
C
hara
cter
istic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
If p
atie
nts/
sta
ff di
d no
t spo
ntan
eous
ly ta
lk a
bout
th
e pr
e-di
alys
is p
erio
d, th
ey w
ere
prom
pted
with
an
open
-end
ed q
uest
ion
abou
t how
trea
tmen
t dec
isio
ns
wer
e m
ade
-Sem
i-stru
ctur
ed q
ualit
ativ
e te
leph
one
inte
rvie
ws
wer
e un
derta
ken
with
20–
25 p
atie
nts
per s
ite u
ntil
satu
ratio
n w
as a
chie
ved.
-S
taff
popu
latio
n w
as c
linic
al s
taff
wor
king
with
CKD
st
age
5 pa
tient
s an
d m
anag
eria
l sta
ff.
-Sem
i-stru
ctur
ed q
ualit
ativ
e fa
ce-to
-face
inte
rvie
ws
wer
e un
derta
ken
on-s
ite w
ith 2
0–30
sta
ff pe
r site
unt
il sa
tura
tion
was
ach
ieve
d.
-Inte
rvie
ws
last
ed fo
r 30–
60 m
in a
nd w
ere
unde
rtake
n in
priv
ate
with
onl
y th
e in
terv
iew
er a
nd in
terv
iew
ee
pres
ent
-All
inte
rvie
ws
wer
e au
dio
reco
rded
and
wer
e tra
nscr
ibed
ver
batim
by
a sp
ecia
list t
rans
crip
tion
team
. -T
rans
crip
ts w
ere
chec
ked
by re
sear
cher
s bu
t not
pa
rtici
pant
s-T
he w
ritte
n an
d au
dio-
visu
al P
DE
mat
eria
ls u
sed
in
each
site
wer
e al
so re
view
ed-D
ata
was
ana
lyse
d us
ing
them
atic
fram
ewor
k an
alys
is.
The
impa
ct o
f dis
tres
sv
a st
rong
them
e ac
ross
all
patie
nt g
roup
s an
d si
tes
v
Patie
nts
desc
ribed
at l
engt
h, th
e tra
umat
ic a
nd fr
ight
enin
g na
ture
of t
he tr
ansi
tion
to e
nd-
stag
e re
nal f
ailu
rev
Patie
nts’
abilit
ies
to m
ake
treat
men
t dec
isio
ns w
ere
adve
rsel
y af
fect
ed in
the
pre-
dial
ysis
pe
riod
by e
mot
iona
l dis
tress
v
Very
few
sta
ff ap
pear
ed to
app
reci
ate
the
pote
ntia
l adv
erse
impa
ct o
f psy
chol
ogic
al
dist
ress
on
patie
nts’
abilit
y to
mak
e tre
atm
ent d
ecis
ions
.
v
Auth
ors
conc
lusi
on:
-Sug
gest
ed im
prov
emen
ts to
teac
hing
met
hods
and
edu
catio
nal m
ater
ials
are
in li
ne w
ith p
revi
ous
stud
ies
and
curre
nt c
linic
al g
uide
lines
. -A
ll st
aff,
irres
pect
ive
of th
eir r
ole,
nee
d to
be
train
ed a
bout
all
treat
men
t opt
ions
so
that
info
rmal
co
nver
satio
ns w
ith p
atie
nts
are
not b
iase
d.
-The
stu
dy a
rgue
s fo
r a m
ore
indi
vidu
alis
ed a
ppro
ach
to P
DE
whi
ch is
mor
e lik
e co
unse
lling
than
ed
ucat
ion
and
wou
ld d
eman
d a
high
er le
vel o
f ski
ll an
d tra
inin
g fo
r spe
cial
ist P
DE
staf
f. -T
he s
tudy
con
clud
es th
at e
ven
if th
ese
impr
ovem
ents
are
mad
e to
PD
E, n
ot a
ll pa
tient
s w
ill be
nefit
, be
caus
e so
me
find
deci
sion
-mak
ing
in th
e pr
e-di
alys
is p
erio
d to
o co
mpl
ex o
r are
una
ble
to e
ngag
e w
ith
educ
atio
n du
e to
illn
ess
or e
mot
iona
l dis
tress
. -It
is th
eref
ore
reco
mm
ende
d th
at p
re-d
ialy
sis
treat
men
t de
cisi
ons
are
tem
pora
ry, a
nd th
at P
DE
is re
plac
ed w
ith o
n-go
ing
RRT
edu
catio
n w
hich
pro
vide
s op
portu
nitie
s fo
r per
sona
lised
edu
catio
n an
d on
-goi
ng re
view
of p
atie
nts’
treat
men
t cho
ices
. -E
mot
iona
l sup
port
to h
elp
over
com
e th
e di
stre
ss o
f the
tran
sitio
n to
end
-sta
ge re
nal d
isea
se w
ill al
so b
e es
sent
ial t
o en
sure
all
patie
nts
can
bene
fit fr
om R
RT e
duca
tion.
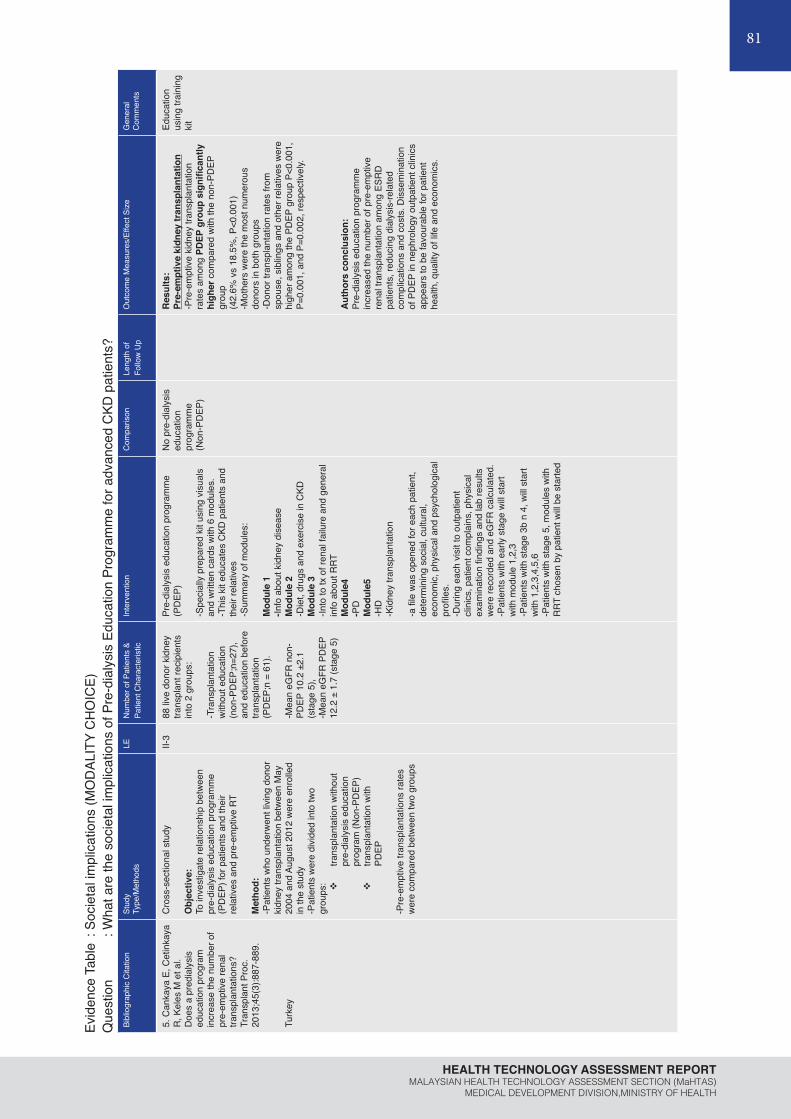
81
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Evid
ence
Tab
le :
Soci
etal
impl
icat
ions
(MO
DAL
ITY
CH
OIC
E)Q
uest
ion
: Wha
t are
the
soci
etal
impl
icat
ions
of P
re-d
ialy
sis
Educ
atio
n Pr
ogra
mm
e fo
r adv
ance
d C
KD p
atie
nts?
Bibl
iogr
aphi
c C
itatio
nSt
udy
Type
/Met
hods
LEN
umbe
r of P
atie
nts
& Pa
tient
Cha
ract
eris
ticIn
terv
entio
nC
ompa
rison
Leng
th o
f Fo
llow
Up
Out
com
e M
easu
res/
Effe
ct S
ize
Gen
eral
C
omm
ents
5. C
anka
ya E
, Cet
inka
ya
R, K
eles
M e
t al.
Doe
s a
pred
ialy
sis
educ
atio
n pr
ogra
m
incr
ease
the
num
ber o
f pr
e-em
ptiv
e re
nal
trans
plan
tatio
ns?
Tran
spla
nt P
roc.
20
13;4
5(3)
:887
-889
.
Turk
ey
Cro
ss-s
ectio
nal s
tudy
Obj
ectiv
e:To
inve
stig
ate
rela
tions
hip
betw
een
pre-
dial
ysis
edu
catio
n pr
ogra
mm
e (P
DEP
) for
pat
ient
s an
d th
eir
rela
tives
and
pre
-em
ptiv
e RT
Met
hod:
-Pat
ient
s w
ho u
nder
wen
t liv
ing
dono
r ki
dney
tran
spla
ntat
ion
betw
een
May
20
04 a
nd A
ugus
t 201
2 w
ere
enro
lled
in th
e st
udy
-Pat
ient
s w
ere
divi
ded
into
two
grou
ps: v
trans
plan
tatio
n w
ithou
t pr
e-di
alys
is e
duca
tion
prog
ram
(Non
-PD
EP)
v
trans
plan
tatio
n w
ith
PDEP
-Pre
-em
ptiv
e tra
nspl
anta
tions
rate
s w
ere
com
pare
d be
twee
n tw
o gr
oups
II-3
88 li
ve d
onor
kid
ney
trans
plan
t rec
ipie
nts
into
2 g
roup
s:
-Tra
nspl
anta
tion
with
out e
duca
tion
(non
-PD
EP;n
=27)
, an
d ed
ucat
ion
befo
re
trans
plan
tatio
n(P
DEP
;n =
61)
.
-Mea
n eG
FR n
on-
PDEP
10.
2 ±2
.1
(sta
ge 5
),-M
ean
eGFR
PD
EP
12.2
± 1
.7 (s
tage
5)
Pre-
dial
ysis
edu
catio
n pr
ogra
mm
e(P
DEP
)
-Spe
cial
ly p
repa
red
kit u
sing
vis
uals
an
d w
ritte
n ca
rds
with
6 m
odul
es.
-Thi
s ki
t edu
cate
s C
KD p
atie
nts
and
thei
r rel
ativ
es-S
umm
ary
of m
odul
es:
Mod
ule
1-In
fo a
bout
kid
ney
dise
ase
Mod
ule
2-D
iet,
drug
s an
d ex
erci
se in
CKD
Mod
ule
3-In
to to
tx o
f ren
al fa
ilure
and
gen
eral
in
fo a
bout
RRT
Mod
ule4
-PD
Mod
ule5
-HD
-K
idne
y tra
nspl
anta
tion
-a fi
le w
as o
pene
d fo
r eac
h pa
tient
, de
term
inin
g so
cial
, cul
tura
l, ec
onom
ic, p
hysi
cal a
nd p
sych
olog
ical
pr
ofile
s.-D
urin
g ea
ch v
isit
to o
utpa
tient
cl
inic
s, p
atie
nt c
ompl
ains
, phy
sica
l ex
amin
atio
n fin
ding
s an
d la
b re
sults
w
ere
reco
rded
and
eG
FR c
alcu
late
d.-P
atie
nts
with
ear
ly s
tage
will
star
t w
ith m
odul
e 1,
2,3
-Pat
ient
s w
ith s
tage
3b
n 4,
will
star
t w
ith 1
,2,3
,4,5
,6-P
atie
nts
with
sta
ge 5
, mod
ules
with
R
RT c
hose
n by
pat
ient
will
be s
tarte
d
No
pre-
dial
ysis
ed
ucat
ion
prog
ram
me
(Non
-PD
EP)
Res
ults
:Pr
e-em
ptiv
e ki
dney
tran
spla
ntat
ion
-Pre
-em
ptiv
e ki
dney
tran
spla
ntat
ion
rate
s am
ong
PDEP
gro
up s
igni
fican
tly
high
er c
ompa
red
with
the
non-
PDEP
gr
oup
(42.
6% v
s 18
.5%
, P<0
.001
)-M
othe
rs w
ere
the
mos
t num
erou
s do
nors
in b
oth
grou
ps-D
onor
tran
spla
ntat
ion
rate
s fro
m
spou
se, s
iblin
gs a
nd o
ther
rela
tives
wer
e hi
gher
am
ong
the
PDEP
gro
up P
<0.0
01,
P=0.
001,
and
P=0
.002
, res
pect
ivel
y.
Aut
hors
con
clus
ion:
Pre-
dial
ysis
edu
catio
n pr
ogra
mm
e in
crea
sed
the
num
ber o
f pre
-em
ptiv
e re
nal t
rans
plan
tatio
n am
ong
ESR
D
patie
nts,
redu
cing
dia
lysi
s-re
late
d co
mpl
icat
ions
and
cos
ts. D
isse
min
atio
n of
PD
EP in
nep
hrol
ogy
outp
atie
nt c
linic
s ap
pear
s to
be
favo
urab
le fo
r pat
ient
he
alth
, qua
lity
of li
fe a
nd e
cono
mic
s.
Educ
atio
n us
ing
train
ing
kit
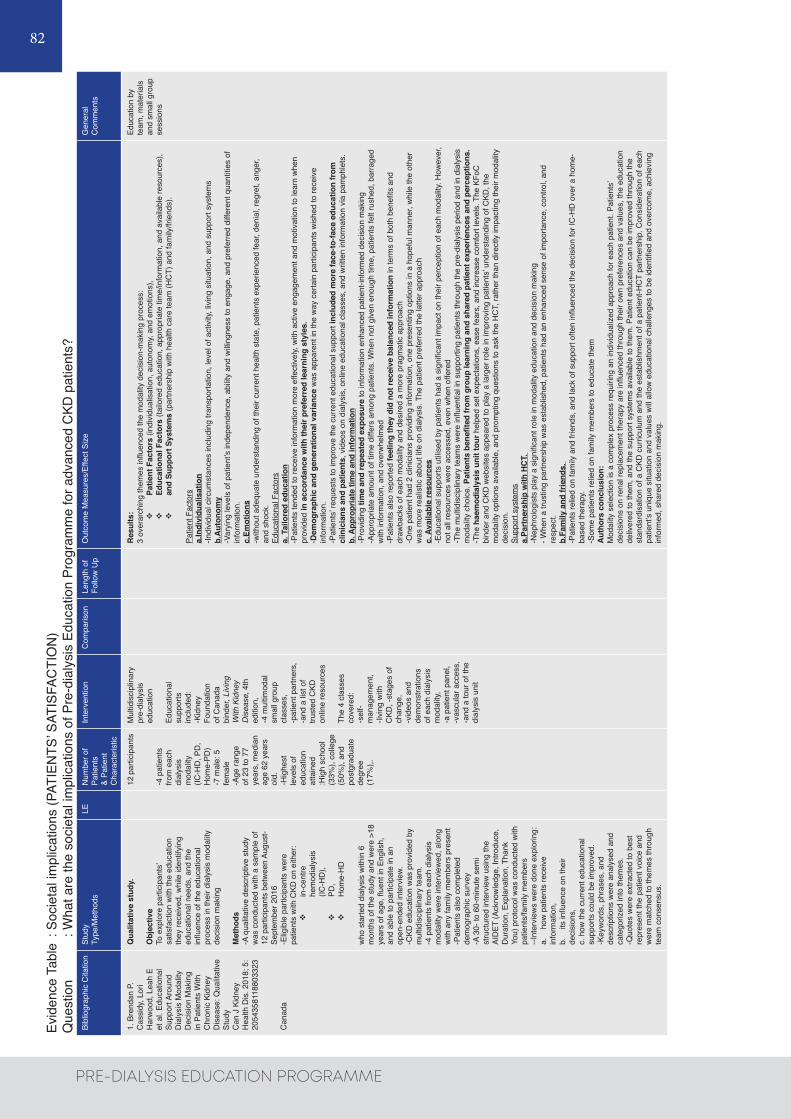
82
PRE-DIALYSIS EDUCATION PROGRAMME
Bibl
iogr
aphi
c C
itatio
nSt
udy
Type
/Met
hods
LEN
umbe
r of
Patie
nts
& Pa
tient
C
hara
cter
istic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
1. B
rend
an P
. C
assi
dy, L
ori
Har
woo
d, L
eah
E et
al.
Educ
atio
nal
Supp
ort A
roun
d D
ialy
sis
Mod
ality
D
ecis
ion
Mak
ing
in P
atie
nts
With
C
hron
ic K
idne
y D
isea
se: Q
ualit
ativ
e St
udy
Can
J K
idne
y H
ealth
Dis
. 201
8; 5
: 20
5435
8118
8033
23
Can
ada
Qua
litat
ive
stud
y.
Obj
ectiv
eTo
exp
lore
par
ticip
ants
’ sa
tisfa
ctio
n w
ith th
e ed
ucat
ion
they
rece
ived
, whi
le id
entif
ying
ed
ucat
iona
l nee
ds, a
nd th
e in
fluen
ce o
f the
edu
catio
nal
proc
ess
in th
eir d
ialy
sis
mod
ality
de
cisi
on m
akin
g
Met
hods
-A q
ualit
ativ
e de
scrip
tive
stud
y w
as c
ondu
cted
with
a s
ampl
e of
12
par
ticip
ants
bet
wee
n Au
gust
-Se
ptem
ber 2
016
-Elig
ible
par
ticip
ants
wer
e pa
tient
s w
ith C
KD o
n ei
ther
: v
in-c
entre
he
mod
ialy
sis
(IC-H
D),
v
PD,
v
Hom
e-H
D
who
sta
rted
dial
ysis
with
in 6
m
onth
s of
the
stud
y an
d w
ere
>18
year
s of
age
, flue
nt in
Eng
lish,
an
d ab
le to
par
ticip
ate
in a
n op
en-e
nded
inte
rvie
w.-C
KD e
duca
tion
was
pro
vide
d by
m
ultid
isci
plin
ary
team
. -4
pat
ient
s fro
m e
ach
dial
ysis
m
odal
ity w
ere
inte
rvie
wed
, alo
ng
with
any
fam
ily m
embe
rs p
rese
nt-P
atie
nts
also
com
plet
ed
dem
ogra
phic
sur
vey
-A 3
0- to
60-
min
ute
sem
i st
ruct
ured
inte
rvie
w u
sing
the
AID
ET (A
ckno
wle
dge,
Intro
duce
, D
urat
ion,
Exp
lana
tion,
Tha
nk
You)
pro
toco
l was
con
duct
ed w
ith
patie
nts/
fam
ily m
embe
rs--I
nter
view
s w
ere
done
exp
lorin
g:a.
h
ow p
atie
nts
rece
ive
info
rmat
ion,
b.
it
s in
fluen
ce o
n th
eir
deci
sion
s,
c. h
ow th
e cu
rrent
edu
catio
nal
supp
orts
cou
ld b
e im
prov
ed.
-Key
wor
ds, p
hras
es, a
nd
desc
riptio
ns w
ere
anal
ysed
and
ca
tego
rized
into
them
es.
-Quo
tes
wer
e ex
tract
ed to
bes
t re
pres
ent t
he p
atie
nt v
oice
and
w
ere
mat
ched
to th
emes
thro
ugh
team
con
sens
us.
12 p
artic
ipan
ts
-4 p
atie
nts
from
eac
h di
alys
is
mod
ality
(IC
-HD
, PD
, H
ome-
PD)
-7 m
ale:
5
fem
ale
-Age
rang
e of
23
to 7
7 ye
ars,
med
ian
age
62 y
ears
ol
d.-H
ighe
st
leve
ls o
f ed
ucat
ion
atta
ined
:H
igh
scho
ol
(33%
), co
llege
(5
0%),
and
post
grad
uate
de
gree
(1
7%),.
Mul
tidis
cipl
inar
y pr
e-di
alys
is
educ
atio
n
Educ
atio
nal
supp
orts
in
clud
ed:
-Kid
ney
Foun
datio
n of
Can
ada
bind
er, L
ivin
g W
ith K
idne
y D
isea
se, 4
th
editi
on,
-4 m
ultim
odal
sm
all g
roup
cl
asse
s,
-pat
ient
par
tner
s,
-and
a li
st o
f tru
sted
CKD
on
line
reso
urce
s
The
4 cl
asse
s co
vere
d:-s
elf-
man
agem
ent,
-livi
ng w
ith
CKD
, -st
ages
of
chan
ge,
-vid
eos
and
dem
onst
ratio
ns
of e
ach
dial
ysis
m
odal
ity,
-a p
atie
nt p
anel
, -v
ascu
lar a
cces
s,
-and
a to
ur o
f the
di
alys
is u
nit
Res
ults
:3
over
arch
ing
them
es in
fluen
ced
the
mod
ality
dec
isio
n-m
akin
g pr
oces
s:
v
Patie
nt F
acto
rs (i
ndiv
idua
lisat
ion,
aut
onom
y, an
d em
otio
ns),
v
Educ
atio
nal F
acto
rs (t
ailo
red
educ
atio
n, a
ppro
pria
te ti
me/
info
rmat
ion,
and
ava
ilabl
e re
sour
ces)
, v
and
Supp
ort S
yste
ms
(par
tner
ship
with
hea
lth c
are
team
(HC
T) a
nd fa
mily
/frie
nds)
.
Patie
nt F
acto
rsa.
Indi
vidu
alis
atio
n-In
divi
dual
circ
umst
ance
s in
clud
ing
trans
porta
tion,
leve
l of a
ctiv
ity, l
ivin
g si
tuat
ion,
and
sup
port
syst
ems
b.A
uton
omy
-Var
ying
leve
ls o
f pat
ient
’s in
depe
nden
ce, a
bilit
y an
d w
illing
ness
to e
ngag
e, a
nd p
refe
rred
diffe
rent
qua
ntiti
es o
f in
form
atio
n.c.
Emot
ions
-with
out a
dequ
ate
unde
rsta
ndin
g of
thei
r cur
rent
hea
lth s
tate
, pat
ient
s ex
perie
nced
fear
, den
ial,
regr
et, a
nger
, an
d sh
ock.
Educ
atio
nal F
acto
rsa.
Tai
lore
d ed
ucat
ion
-Pat
ient
s te
nded
to re
ceiv
e in
form
atio
n m
ore
effe
ctiv
ely,
with
act
ive
enga
gem
ent a
nd m
otiv
atio
n to
lear
n w
hen
prov
ided
in a
ccor
danc
e w
ith th
eir p
refe
rred
lear
ning
sty
les.
-Dem
ogra
phic
and
gen
erat
iona
l var
ianc
e w
as a
ppar
ent i
n th
e w
ay c
erta
in p
artic
ipan
ts w
ishe
d to
rece
ive
info
rmat
ion.
-Pat
ient
s’ re
ques
ts to
impr
ove
the
curre
nt e
duca
tiona
l sup
port
incl
uded
mor
e fa
ce-to
-face
edu
catio
n fr
om
clin
icia
ns a
nd p
atie
nts,
vid
eos
on d
ialy
sis,
onl
ine
educ
atio
nal c
lass
es, a
nd w
ritte
n in
form
atio
n vi
a pa
mph
lets
. b.
App
ropr
iate
tim
e an
d in
form
atio
n-P
rovi
ding
tim
e an
d re
peat
ed e
xpos
ure
to in
form
atio
n en
hanc
ed p
atie
nt-in
form
ed d
ecis
ion
mak
ing
-App
ropr
iate
am
ount
of t
ime
diffe
rs a
mon
g pa
tient
s. W
hen
not g
iven
eno
ugh
time,
pat
ient
s fe
lt ru
shed
, bar
rage
d w
ith in
form
atio
n, a
nd o
verw
helm
ed-P
atie
nts
also
repo
rted
feel
ing
they
did
not
rece
ive
bala
nced
info
rmat
ion
in te
rms
of b
oth
bene
fits
and
draw
back
s of
eac
h m
odal
ity a
nd d
esire
d a
mor
e pr
agm
atic
app
roac
h-O
ne p
atie
nt h
ad 2
clin
icia
ns p
rovi
ding
info
rmat
ion,
one
pre
sent
ing
optio
ns in
a h
opef
ul m
anne
r, w
hile
the
othe
r w
as m
ore
real
istic
abo
ut li
fe o
n di
alys
is. T
he p
atie
nt p
refe
rred
the
latte
r app
roac
hc.
Ava
ilabl
e re
sour
ces
-Edu
catio
nal s
uppo
rts u
tilis
ed b
y pa
tient
s ha
d a
sign
ifica
nt im
pact
on
thei
r per
cept
ion
of e
ach
mod
ality
. How
ever
, no
t all
reso
urce
s w
ere
acce
ssed
, eve
n w
hen
offe
red
-The
mul
tidis
cipl
inar
y te
ams
wer
e in
fluen
tial i
n su
ppor
ting
patie
nts
thro
ugh
the
pre-
dial
ysis
per
iod
and
in d
ialy
sis
mod
ality
cho
ice.
Pat
ient
s be
nefit
ed fr
om g
roup
lear
ning
and
sha
red
patie
nt e
xper
ienc
es a
nd p
erce
ptio
ns.
-The
hae
mod
ialy
sis
unit
tour
hel
ped
set e
xpec
tatio
ns, e
ase
fear
s, a
nd in
crea
se c
omfo
rt le
vels
. The
KFo
C
bind
er a
nd C
KD w
ebsi
tes
appe
ared
to p
lay
a la
rger
role
in im
prov
ing
patie
nts’
unde
rsta
ndin
g of
CKD
, the
m
odal
ity o
ptio
ns a
vaila
ble,
and
pro
mpt
ing
ques
tions
to a
sk th
e H
CT,
rath
er th
an d
irect
ly im
pact
ing
thei
r mod
ality
de
cisi
on.
Supp
ort s
yste
ms
a.Pa
rtne
rshi
p w
ith H
CT.
-N
ephr
olog
ists
pla
y a
sign
ifica
nt ro
le in
mod
ality
edu
catio
n an
d de
cisi
on m
akin
g- W
hen
a tru
stin
g pa
rtner
ship
was
est
ablis
hed,
pat
ient
s ha
d an
enh
ance
d se
nse
of im
porta
nce,
con
trol,
and
resp
ect.
b.Fa
mily
and
frie
nds.
-P
atie
nts
relie
d on
fam
ily a
nd fr
iend
s, a
nd la
ck o
f sup
port
ofte
n in
fluen
ced
the
deci
sion
for I
C-H
D o
ver a
hom
e-ba
sed
ther
apy.
-Som
e pa
tient
s re
lied
on fa
mily
mem
bers
to e
duca
te th
emA
utho
rs c
oncl
usio
n:M
odal
ity s
elec
tion
is a
com
plex
pro
cess
requ
iring
an
indi
vidu
aliz
ed a
ppro
ach
for e
ach
patie
nt. P
atie
nts’
deci
sion
s on
rena
l rep
lace
men
t the
rapy
are
influ
ence
d th
roug
h th
eir o
wn
pref
eren
ces
and
valu
es, t
he e
duca
tion
deliv
ered
to th
em, a
nd th
e su
ppor
t sys
tem
s av
aila
ble
to th
em. P
atie
nt e
duca
tion
can
be im
prov
ed th
roug
h th
e st
anda
rdis
atio
n of
a C
KD c
urric
ulum
and
the
esta
blis
hmen
t of a
pat
ient
-HC
T pa
rtner
ship
. Con
side
ratio
n of
eac
h pa
tient
’s un
ique
situ
atio
n an
d va
lues
will
allo
w e
duca
tiona
l cha
lleng
es to
be
iden
tified
and
ove
rcom
e, a
chie
ving
in
form
ed, s
hare
d de
cisi
on m
akin
g.
Educ
atio
n by
te
am, m
ater
ials
an
d sm
all g
roup
se
ssio
ns
Evid
ence
Tab
le :
Soci
etal
impl
icat
ions
(PAT
IEN
TS’ S
ATIS
FAC
TIO
N)
Que
stio
n : W
hat a
re th
e so
ciet
al im
plic
atio
ns o
f Pre
-dia
lysi
s Ed
ucat
ion
Prog
ram
me
for a
dvan
ced
CKD
pat
ient
s?

83
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Evid
ence
Tab
le :
Soci
etal
impl
icat
ions
(PAT
IEN
TS A
ND
STA
FF IN
SIG
HTS
)Q
uest
ion
: Wha
t are
the
soci
etal
impl
icat
ions
of P
re-d
ialy
sis
Educ
atio
n Pr
ogra
mm
e fo
r adv
ance
d C
KD p
atie
nts?
Bibl
iogr
aphi
c C
itatio
nSt
udy
Type
/Met
hods
LEN
umbe
r of
Patie
nts
& Pa
tient
C
hara
cter
istic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
1. C
ombe
s G
, Se
in K
, Alle
n K.
How
doe
s pr
e-di
alys
is
educ
atio
n ne
ed
to c
hang
e?
Find
ings
from
a
qual
itativ
e st
udy
with
sta
ff an
d pa
tient
s. B
MC
N
ephr
ol.
2017
;18(
1):3
34.
UK
Qua
litat
ive
stud
y
Obj
ectiv
eTo
repo
rt fin
ding
s re
leva
nt to
PD
E fro
m a
larg
er m
ixed
m
etho
ds s
tudy
, pro
vidi
ng in
sigh
ts in
to w
hat s
taff
and
patie
nts
thin
k ne
eds
to im
prov
e.
Met
hods
-Mix
ed m
etho
ds w
as u
sed
to lo
ok a
t qua
ntita
tive
chan
ges
in h
ome
dial
ysis
upt
ake
rate
s an
d qu
alita
tive
case
stu
dies
to e
xplo
re b
arrie
rs a
nd s
ucce
ss fa
ctor
s fo
r hom
e di
alys
is-F
our h
ospi
tal r
enal
uni
ts, s
elec
ted
from
sev
en W
est
Mid
land
s un
its-P
atie
nt p
opul
atio
n w
as d
ialy
sis
patie
nts
aged
18+
st
artin
g th
eir c
urre
nt tr
eatm
ent w
ithin
12
mon
ths,
-Sem
i stru
ctur
ed o
ne-to
-one
inte
rvie
ws
wer
e un
derta
ken
with
dia
lysi
s pa
tient
s an
d cl
inic
al a
nd
man
ager
ial s
taff
-For
pat
ient
s, th
e to
pic
guid
e co
vere
d:
v
how
pat
ient
s ca
me
to b
e on
dia
lysi
s;
v
expe
rienc
es o
f pre
-dia
lysi
s an
d di
alys
is
path
way
s;
v
sugg
estio
ns fo
r im
prov
emen
t.
-For
sta
ff, th
e to
pic
guid
e co
vere
d:
v
curre
nt p
ract
ice,
v
how
wel
l the
pre
-dia
lysi
s an
d di
alys
is
path
way
s w
ork;
v
how
the
team
had
bee
n w
orki
ng to
in
crea
se u
ptak
e of
hom
e di
alys
is;
v
sugg
estio
ns fo
r im
prov
emen
t
- If p
atie
nts/
sta
ff di
d no
t spo
ntan
eous
ly ta
lk a
bout
th
e pr
e-di
alys
is p
erio
d, th
ey w
ere
prom
pted
with
an
open
-end
ed q
uest
ion
abou
t how
trea
tmen
t dec
isio
ns
wer
e m
ade
-Sem
i-stru
ctur
ed q
ualit
ativ
e te
leph
one
inte
rvie
ws
wer
e un
derta
ken
with
20–
25 p
atie
nts
per s
ite u
ntil
satu
ratio
n w
as a
chie
ved.
-S
taff
popu
latio
n w
as c
linic
al s
taff
wor
king
with
CKD
st
age
5 pa
tient
s an
d m
anag
eria
l sta
ff.
-Sem
i-stru
ctur
ed q
ualit
ativ
e fa
ce-to
-face
inte
rvie
ws
wer
e un
derta
ken
on-s
ite w
ith 2
0–30
sta
ff pe
r site
unt
il sa
tura
tion
was
ach
ieve
d.
-Inte
rvie
ws
last
ed fo
r 30–
60 m
in a
nd w
ere
unde
rtake
n in
priv
ate
with
onl
y th
e in
terv
iew
er a
nd in
terv
iew
ee
pres
ent
-All
inte
rvie
ws
wer
e au
dio
reco
rded
and
wer
e tra
nscr
ibed
ver
batim
by
a sp
ecia
list t
rans
crip
tion
team
. -T
rans
crip
ts w
ere
chec
ked
by re
sear
cher
s bu
t not
pa
rtici
pant
s-T
he w
ritte
n an
d au
dio-
visu
al P
DE
mat
eria
ls u
sed
in
each
site
wer
e al
so re
view
ed-D
ata
was
ana
lyse
d us
ing
them
atic
fram
ewor
k an
alys
is.
Sem
i-st
ruct
ured
in
terv
iew
s in
fo
ur h
ospi
tals
w
ith 9
6 cl
inic
al a
nd
man
ager
ial
staf
f and
93
dia
lysi
s pa
tient
s
Pre-
dial
ysis
ed
ucat
ion
(PD
E)
Form
al P
DE
in a
ll fo
ur s
ites
incl
uded
:
-one
or m
ore
one-
to-o
ne
sess
ions
with
a
spec
ialis
t nu
rse;
-a g
roup
in
form
atio
n se
ssio
n,
incl
udin
g ta
lks
from
pat
ient
s on
RRT
; -a
nd w
ritte
n m
ater
ials
/D
VDs
whi
ch
patie
nts
took
ho
me.
-In s
ever
al
site
s,
spec
ialis
t nu
rses
un
derto
ok
hom
e vi
sits
w
here
they
di
scus
sed
treat
men
t op
tions
with
pa
tient
s.
-Doc
tors
als
o di
scus
sed
treat
men
t op
tions
with
pa
tient
s du
ring
out-p
atie
nt
appo
intm
ents
.
Res
ults
:-M
ost s
taff
mad
e fa
vour
able
com
men
ts a
bout
PD
E an
d va
lued
the
role
of s
peci
alis
t nur
sing
sta
ff in
ed
ucat
ing
and
supp
ortin
g pa
tient
s’ tre
atm
ent d
ecis
ions
. -M
ost p
atie
nts
reca
lled
taki
ng u
p pa
rt or
all
of th
e fo
rmal
PD
E on
offe
r and
repo
rted
findi
ng it
hel
pful
ov
eral
l. -3
them
es re
late
d to
impr
ovin
g PD
E id
entifi
ed:
v
sub-
optim
al e
duca
tion;
v
diffe
rent
per
spec
tives
bet
wee
n pa
tient
s an
d st
aff;
v
influ
ence
of p
atie
nt e
xper
ienc
e
a. S
ub-o
ptim
al e
duca
tion
Res
tric
ted
rang
e of
teac
hing
mat
eria
ls a
nd m
etho
dsv
In m
akin
g tre
atm
ent d
ecis
ions
, som
e pa
tient
s fe
lt th
ey u
nabl
e to
use
info
rmat
ion
give
n be
caus
e th
e hi
gh v
olum
e an
d co
mpl
exity
of i
nfor
mat
ion
mea
nt
v
From
sta
ff pe
rspe
ctiv
e, w
ritte
n m
ater
ials
wer
e de
sign
ed s
o th
at p
atie
nts
had
info
rmat
ion
to
take
hom
e an
d co
nsid
er o
ver t
ime.
v
How
ever
, it s
eem
ed th
at s
ome
patie
nts
wer
e un
able
to ta
ke a
dvan
tage
of t
his
posi
tive
inte
ntio
nv
Anot
her p
ersp
ectiv
e on
teac
hing
mat
eria
ls c
ame
from
pat
ient
s w
ho th
ough
t tha
t the
y w
ere
not ‘
real
’ eno
ugh,
and
stru
ggle
d to
app
ly th
e in
form
atio
n to
thei
r ow
n liv
es.
v
Seei
ng d
iffer
ent t
reat
men
ts b
eing
und
erta
ken
by re
al p
atie
nts
wer
e al
l sug
gest
ed a
s w
ays
of im
prov
ing
the
educ
atio
n
-Thi
s su
gges
ts th
at p
atie
nts
wou
ld b
enefi
t fro
m th
e us
e of
a w
ider
rang
e of
teac
hing
met
hods
, inc
ludi
ng
inte
ract
ive
met
hods
.B
ias
in th
e pr
esen
tatio
n of
info
rmat
ion
and
trea
tmen
t opt
ions
v
Som
e pa
tient
s th
ough
t tha
t all
treat
men
t opt
ions
wer
e pr
esen
ted
fairl
y an
d w
ith e
qual
em
phas
is, o
ther
s fe
lt no
t all
optio
ns h
ad b
een
pres
ente
d to
them
and
that
they
had
onl
y fo
und
out a
bout
via
ble
alte
rnat
ives
onc
e th
ey w
ere
on d
ialy
sis.
v
Som
e of
thes
e pa
tient
s th
ough
t tha
t opp
ortu
nitie
s to
talk
to p
atie
nts
alre
ady
on
trea
tmen
t mig
ht h
ave
help
ed to
giv
e th
em a
mor
e ba
lanc
ed v
iew
of w
hat l
ife o
n di
alys
is
mig
ht b
e lik
e.
v
Staf
f wer
e al
so a
war
e of
the
pote
ntia
l for
bia
sv
How
ever
, all
staf
f gro
ups
thou
ght t
hat t
he fi
rst c
onve
rsat
ion
that
doc
tors
hav
e w
ith p
atie
nts
abou
t tre
atm
ent o
ptio
ns is
cru
cial
in in
fluen
cing
trea
tmen
t cho
ice
b. D
iffer
ent p
ersp
ectiv
es b
etw
een
patie
nts
and
staf
f Th
e im
port
ance
of i
nfor
mal
edu
catio
nv
Staf
f wer
e le
ss a
war
e th
an p
atie
nts
of h
ow in
form
al s
taff-
patie
nt c
onve
rsat
ions
can
in
fluen
ce p
atie
nts’
treat
men
t dec
isio
n-m
akin
g.
v
Som
e pa
tient
s m
ay h
ave
atyp
ical
exp
erie
nces
or b
e bi
ased
aga
inst
cer
tain
trea
tmen
ts
Educ
atio
n on
e to
one
se
ssio
ns
+ gr
oup
sess
ions
+
writ
ten
mat
eria
ls

84
PRE-DIALYSIS EDUCATION PROGRAMME
Bibl
iogr
aphi
c C
itatio
nSt
udy
Type
/Met
hods
LEN
umbe
r of P
atie
nts
& Pa
tient
Cha
ract
eris
ticIn
terv
entio
nC
ompa
rison
Leng
th o
f Fo
llow
Up
Out
com
e M
easu
res/
Effe
ct S
ize
Gen
eral
C
omm
ents
1. V
an d
en B
osch
J,
War
ren
DS,
Rut
herfo
rd
PA. R
evie
w o
f pr
edia
lysi
s ed
ucat
ion
prog
ram
s: a
nee
d fo
r st
anda
rdiz
atio
n. P
atie
nt
Pref
er A
dher
ence
. 20
15;9
:127
9-12
91.
Syst
emat
ic re
view
Obj
ectiv
e:
To re
view
evi
denc
e on
effe
ctiv
e co
mpo
nent
s of
pre
-dia
lysi
s ed
ucat
ion
prog
ram
mes
as
rela
ted
to m
odal
ity c
hoic
e an
d se
lect
ed c
linic
al
outc
omes
.
Met
hod:
-Sys
tem
atic
sea
rch
was
per
form
ed o
n Pu
bMed
M
EDLI
NE,
Coc
hran
e Li
brar
y, an
d O
vid
(from
Ja
nuar
y 1,
199
5 to
Dec
embe
r 31,
201
3)
-Incl
usio
n cr
iteria
app
lied:
v
Adul
ts o
nly
v
Pre-
dial
ysis
edu
catio
n fo
r CKD
pa
tient
s st
age
III, I
V, a
nd V
v
Plan
ned
star
t pat
ient
s, u
npla
nned
st
art p
atie
nts,
and
pat
ient
s on
di
alys
is, i
e, in
cide
nt a
nd p
reva
lent
pa
tient
s.v
Det
aile
d de
scrip
tion
of p
rogr
amm
ev
Mul
tiple
ses
sion
sv
Mul
tidis
cipl
inar
y pr
ogra
mm
e in
volv
ing
phys
icia
ns, n
urse
s,
diet
icia
ns, e
tc.
-Out
com
es in
clud
ed:
v
Dia
lysi
s m
odal
ity c
hoic
e an
d th
e nu
mbe
rs o
f pat
ient
s ch
oosi
ng e
ach
mod
ality
v
Any
clin
ical
out
com
e as
soci
ated
w
ith p
re-d
ialy
sis
educ
atio
n v
Hea
lth-re
late
d qu
ality
of l
ife
v
Mea
sure
s as
soci
ated
with
pat
ient
ch
oice
v
Fina
ncia
l im
pact
of p
atie
nts
choo
sing
mor
e ho
me
ther
apie
s v
Patie
nt s
atis
fact
ion
-Lite
ratu
re a
lso
revi
ewed
for a
ny in
form
atio
n on
pr
oces
ses,
pat
hway
s, a
nd o
rgan
izat
ion
of th
e pr
e-di
alys
is e
duca
tion
prog
ram
mes
I29
rele
vant
stu
dies
:19
qua
si-e
xper
imen
tal
desi
gn10
nar
rativ
e re
view
s
-19
stud
ies
wer
e an
alys
ed fo
r effe
ctiv
e co
mpo
nent
s of
pre
-di
alys
is e
duca
tion
prog
ram
me
-Des
crip
tions
of
the
educ
atio
nal
proc
ess
varie
d an
d in
clud
ed in
divi
dual
an
d gr
oup
educ
atio
n,
mul
tidis
cipl
inar
y in
terv
entio
n, a
nd v
aryi
ng
dura
tion
and
frequ
ency
of
ses
sion
s.
Pre-
dial
ysis
ed
ucat
ion
prog
ram
sR
esul
ts
Patie
nt k
now
ledg
e-4
of 1
9 qu
asi-e
xper
imen
tal s
tudi
es
repo
rted
on m
easu
res
of p
atie
nt
know
ledg
e.
v
Gom
ez e
t al.
(199
9)v
King
et a
l. (2
008)
v
Klan
g et
al.
(199
9)v
Man
ns e
t al.
(200
5)
-All
repo
rted
high
er le
vels
of k
now
ledg
e of
end
-sta
ge re
nal d
isea
se a
nd o
f di
ffere
nt tr
eatm
ent o
ptio
ns fo
r pat
ient
s re
ceiv
ing
pre-
dial
ysis
edu
catio
n co
mpa
red
to u
nedu
cate
d pa
tient
s.
Mos
tly w
ithou
t co
ntro
l gro
up
Evid
ence
Tab
le :
Effe
ctiv
enes
s Q
uest
ion
: How
effe
ctiv
e is
Pre
-dia
lysi
s Ed
ucat
ion
Prog
ram
me
for a
dvan
ced
CKD
pat
ient
s?
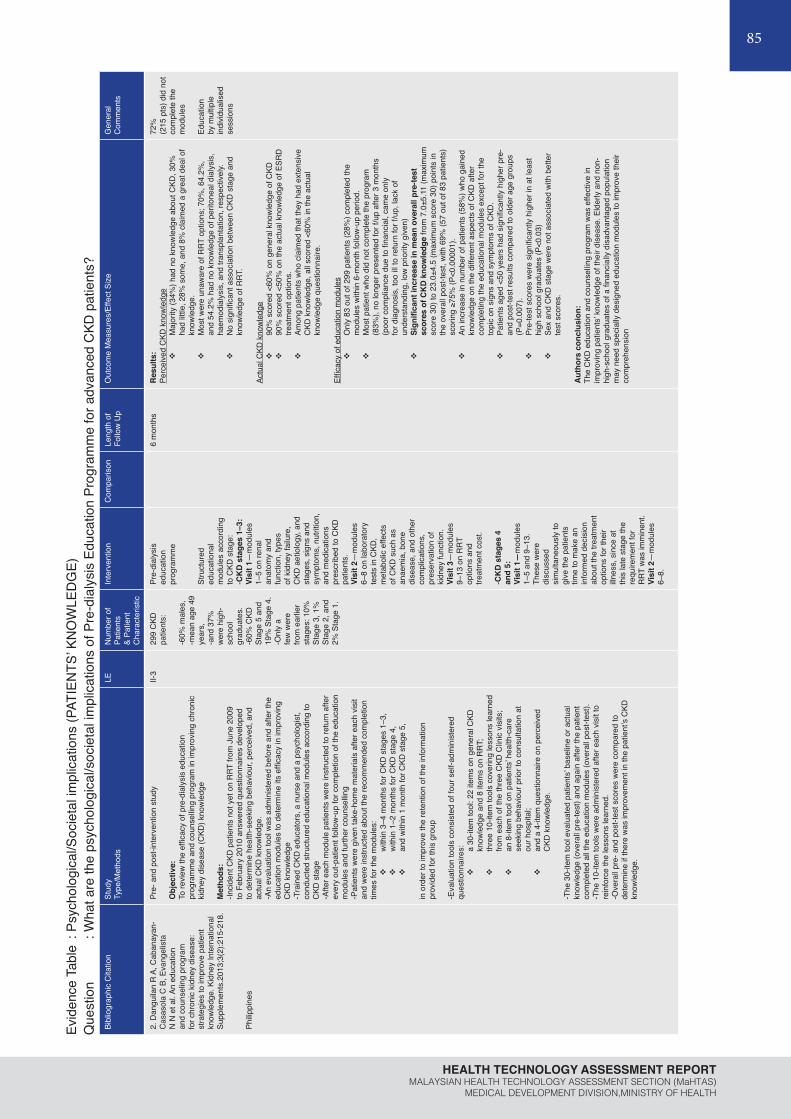
85
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Evid
ence
Tab
le :
Psyc
holo
gica
l/Soc
ieta
l im
plic
atio
ns (P
ATIE
NTS
’ KN
OW
LED
GE)
Que
stio
n : W
hat a
re th
e ps
ycho
logi
cal/s
ocie
tal i
mpl
icat
ions
of P
re-d
ialy
sis
Educ
atio
n Pr
ogra
mm
e fo
r adv
ance
d C
KD p
atie
nts?
Bibl
iogr
aphi
c C
itatio
nSt
udy
Type
/Met
hods
LEN
umbe
r of
Patie
nts
& Pa
tient
C
hara
cter
istic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
2. D
angu
ilan
R A
, Cab
anay
an-
Cas
asol
a C
B, E
vang
elis
ta
N N
et a
l. An
edu
catio
n an
d co
unse
ling
prog
ram
fo
r chr
onic
kid
ney
dise
ase:
st
rate
gies
to im
prov
e pa
tient
kn
owle
dge.
Kid
ney
Inte
rnat
iona
l Su
pple
men
ts.2
013;
3(2)
:215
-218
.
Philip
pine
s
Pre-
and
pos
t-int
erve
ntio
n st
udy
Obj
ectiv
e:To
revi
ew th
e ef
ficac
y of
pre
-dia
lysi
s ed
ucat
ion
prog
ram
me
and
coun
sellin
g pr
ogra
m in
impr
ovin
g ch
roni
c ki
dney
dis
ease
(CKD
) kno
wle
dge
Met
hods
:-In
cide
nt C
KD p
atie
nts
not y
et o
n R
RT fr
om J
une
2009
to
Feb
ruar
y 20
10 a
nsw
ered
que
stio
nnai
res
deve
lope
d to
det
erm
ine
heal
th-s
eeki
ng b
ehav
iour
, per
ceiv
ed, a
nd
actu
al C
KD k
now
ledg
e.-A
n ev
alua
tion
tool
was
adm
inis
tere
d be
fore
and
afte
r the
ed
ucat
ion
mod
ules
to d
eter
min
e its
effi
cacy
in im
prov
ing
CKD
kno
wle
dge
-Tra
ined
CKD
edu
cato
rs, a
nur
se a
nd a
psy
chol
ogis
t, co
nduc
ted
stru
ctur
ed e
duca
tiona
l mod
ules
acc
ordi
ng to
C
KD s
tage
-Afte
r eac
h m
odul
e pa
tient
s w
ere
inst
ruct
ed to
retu
rn a
fter
ever
y ou
t-pat
ient
follo
w-u
p fo
r com
plet
ion
of th
e ed
ucat
ion
mod
ules
and
furth
er c
ouns
ellin
g-P
atie
nts
wer
e gi
ven
take
-hom
e m
ater
ials
afte
r eac
h vi
sit
and
wer
e in
stru
cted
abo
ut th
e re
com
men
ded
com
plet
ion
times
for t
he m
odul
es:
v
with
in 3
–4 m
onth
s fo
r CKD
sta
ges
1–3,
v
with
in 1
–2 m
onth
s fo
r CKD
sta
ge 4
, v
and
with
in 1
mon
th fo
r CKD
sta
ge 5
,
in o
rder
to im
prov
e th
e re
tent
ion
of th
e in
form
atio
n pr
ovid
ed fo
r thi
s gr
oup
-Eva
luat
ion
tool
s co
nsis
ted
of fo
ur s
elf-a
dmin
iste
red
ques
tionn
aire
s:
v
a 30
-item
tool
: 22
item
s on
gen
eral
CKD
kn
owle
dge
and
8 ite
ms
on R
RT;
v
thre
e 10
-item
tool
s co
verin
g le
sson
s le
arne
d fro
m e
ach
of th
e th
ree
CKD
Clin
ic v
isits
; v
an 8
-item
tool
on
patie
nts’
heal
th-c
are
seek
ing
beha
viou
r prio
r to
cons
ulta
tion
at
our h
ospi
tal;
v
and
a 4-
item
que
stio
nnai
re o
n pe
rcei
ved
CKD
kno
wle
dge.
-The
30-
item
tool
eva
luat
ed p
atie
nts’
base
line
or a
ctua
l kn
owle
dge
(ove
rall
pre-
test
) and
aga
in a
fter t
he p
atie
nt
com
plet
ed a
ll th
e ed
ucat
ion
mod
ules
(ove
rall
post
-test
). -T
he 1
0-ite
m to
ols
wer
e ad
min
iste
red
afte
r eac
h vi
sit t
o re
info
rce
the
less
ons
lear
ned.
-Ove
rall
pre-
and
pos
t-tes
t sco
res
wer
e co
mpa
red
to
dete
rmin
e if
ther
e w
as im
prov
emen
t in
the
patie
nt’s
CKD
kn
owle
dge.
II-3
299
CKD
pa
tient
s:
-60%
mal
es,
-mea
n ag
e 49
ye
ars,
-a
nd 3
7%
wer
e hi
gh-
scho
ol
grad
uate
s.
-60%
CKD
St
age
5 an
d 19
% S
tage
4.
-Onl
y a
few
wer
e fro
m e
arlie
r st
ages
: 10%
St
age
3, 1
%
Stag
e 2,
and
2%
Sta
ge 1
.
Pre-
dial
ysis
ed
ucat
ion
prog
ram
me
Stru
ctur
ed
educ
atio
nal
mod
ules
acc
ordi
ng
to C
KD s
tage
:-C
KD
sta
ges
1–3:
Vi
sit 1
—m
odul
es
1–5
on re
nal
anat
omy
and
func
tion,
type
s of
kid
ney
failu
re,
CKD
aet
iolo
gy, a
nd
stag
es, s
igns
and
sy
mpt
oms,
nut
ritio
n,
and
med
icat
ions
pr
escr
ibed
to C
KD
patie
nts.
Vi
sit 2
—m
odul
es
6–8
on la
bora
tory
te
sts
in C
KD,
met
abol
ic e
ffect
s of
CKD
suc
h as
an
aem
ia, b
one
dise
ase,
and
oth
er
com
plic
atio
ns,
pres
erva
tion
of
kidn
ey fu
nctio
n.
Visi
t 3—
mod
ules
9–
13 o
n R
RT
optio
ns a
nd
treat
men
t cos
t.
-CK
D s
tage
s 4
and
5:
Visi
t 1—
mod
ules
1–
5 an
d 9–
13.
Thes
e w
ere
disc
usse
d si
mul
tane
ousl
y to
gi
ve th
e pa
tient
s tim
e to
mak
e an
in
form
ed d
ecis
ion
abou
t the
trea
tmen
t op
tions
for t
heir
illnes
s, s
ince
at
this
late
sta
ge th
e re
quire
men
t for
R
RT w
as im
min
ent.
Visi
t 2—
mod
ules
6–
8.
6 m
onth
sR
esul
ts:
Perc
eive
d C
KD k
now
ledg
ev
Maj
ority
(34%
) had
no
know
ledg
e ab
out C
KD, 3
0%
had
little
, 28%
som
e, a
nd 8
% c
laim
ed a
gre
at d
eal o
f kn
owle
dge.
v
Mos
t wer
e un
awar
e of
RRT
opt
ions
; 70%
, 64.
2%,
and
54.2
% h
ad n
o kn
owle
dge
of p
erito
neal
dia
lysi
s,
haem
odia
lysi
s, a
nd tr
ansp
lant
atio
n, re
spec
tivel
y. v
No
sign
ifica
nt a
ssoc
iatio
n be
twee
n C
KD s
tage
and
kn
owle
dge
of R
RT.
Actu
al C
KD k
now
ledg
ev
90%
sco
red
<60%
on
gene
ral k
now
ledg
e of
CKD
v
90%
sco
red
<50%
on
the
actu
al k
now
ledg
e of
ESR
D
treat
men
t opt
ions
. v
Amon
g pa
tient
s w
ho c
laim
ed th
at th
ey h
ad e
xten
sive
C
KD k
now
ledg
e, a
ll sc
ored
<60
% in
the
actu
al
know
ledg
e qu
estio
nnai
re.
Effic
acy
of e
duca
tion
mod
ules
v
Onl
y 83
out
of 2
99 p
atie
nts
(28%
) com
plet
ed th
e m
odul
es w
ithin
6-m
onth
follo
w-u
p pe
riod.
v
Mos
t pat
ient
who
did
not
com
plet
e th
e pr
ogra
m
(83%
), no
long
er p
rese
nted
for f
/up
afte
r 3 m
onth
s (p
oor c
ompl
ianc
e du
e to
fina
ncia
l, ca
me
only
fo
r dia
gnos
is, t
oo il
l to
retu
rn fo
r f/u
p, la
ck o
f un
ders
tand
ing,
low
prio
rity
give
n)v
Sign
ifica
nt in
crea
se in
mea
n ov
eral
l pre
-test
sc
ores
of C
KD
kno
wle
dge
from
7.0
±5.1
1 (m
axim
um
scor
e 30
) to
23.0
±4.5
(max
imum
sco
re 3
0) p
oint
s in
th
e ov
eral
l pos
t-tes
t, w
ith 6
9% (5
7 ou
t of 8
3 pa
tient
s)
scor
ing
≥75%
(P<0
.000
01).
v
An in
crea
se in
num
ber o
f pat
ient
s (5
8%) w
ho g
aine
d kn
owle
dge
on th
e di
ffere
nt a
spec
ts o
f CKD
afte
r co
mpl
etin
g th
e ed
ucat
iona
l mod
ules
exc
ept f
or th
e to
pic
on s
igns
and
sym
ptom
s of
CKD
. v
Patie
nts
aged
<50
yea
rs h
ad s
igni
fican
tly h
ighe
r pre
- an
d po
st-te
st re
sults
com
pare
d to
old
er a
ge g
roup
s (P
=0.0
07).
v
Pre-
test
sco
res
wer
e si
gnifi
cant
ly h
ighe
r in
at le
ast
high
sch
ool g
radu
ates
(P<0
.03)
v
Sex
and
CKD
sta
ge w
ere
not a
ssoc
iate
d w
ith b
ette
r te
st s
core
s.
Aut
hors
con
clus
ion:
The
CKD
edu
catio
n an
d co
unse
lling
prog
ram
was
effe
ctiv
e in
im
prov
ing
patie
nts’
know
ledg
e of
thei
r dis
ease
. Eld
erly
and
non
-hi
gh-s
choo
l gra
duat
es o
f a fi
nanc
ially
dis
adva
ntag
ed p
opul
atio
n m
ay n
eed
spec
ially
des
igne
d ed
ucat
ion
mod
ules
to im
prov
e th
eir
com
preh
ensi
on
72%
(2
15 p
ts) d
id n
ot
com
plet
e th
e m
odul
es
Educ
atio
n by
mul
tiple
in
divi
dual
ised
se
ssio
ns

86
PRE-DIALYSIS EDUCATION PROGRAMME
Evid
ence
Tab
le :
Psyc
holo
gica
l im
plic
atio
ns (A
DH
EREN
CE,
DEP
RES
SIO
N A
ND
AN
XIET
Y LE
VEL)
Que
stio
n : W
hat a
re th
e ps
ycho
logi
cal i
mpl
icat
ions
of P
re-d
ialy
sis
Educ
atio
n Pr
ogra
mm
e fo
r adv
ance
d C
KD p
atie
nts?
Bibl
iogr
aphi
c C
itatio
nSt
udy
Type
/Met
hods
LEN
umbe
r of P
atie
nts
& Pa
tient
Cha
ract
eris
ticIn
terv
entio
nC
ompa
rison
Leng
th o
f Fo
llow
Up
Out
com
e M
easu
res/
Effe
ct S
ize
Gen
eral
C
omm
ents
1. G
arcí
a-Ll
ana
H,
Rem
or E
, del
Pes
o G
et
al.
Mot
ivat
iona
lin
terv
iew
ing
prom
otes
adh
eren
ce
and
impr
oves
w
ellb
eing
in p
re-
dial
ysis
pat
ient
sw
ith a
dvan
ced
chro
nic
kidn
ey
dise
ase.
J
Clin
Psy
chol
M
ed S
ettin
gs.
2014
;21(
1):1
03-1
5.
Spai
n
Pre-
and
pos
t- in
terv
entio
n st
udy
Obj
ectiv
e:To
det
erm
ine
the
effe
ctiv
enes
s of
an
indi
vidu
al, p
re-d
ialy
sis
inte
rven
tion
prog
ram
in
term
s of
adh
eren
ce, e
mot
iona
l sta
te
and
heal
th re
late
d qu
ality
of l
ife (H
RQ
L) in
pr
e-di
alys
is p
atie
nts
with
adv
ance
d ch
roni
c ki
dney
dis
ease
Met
hod:
-All
52 p
atie
nts
in th
e st
udy
sam
ple
met
the
follo
win
g el
igib
ility
crite
ria:
v
olde
r tha
n 18
yea
rs;
v
diag
nosi
s of
adv
ance
d C
KD
unde
r pre
-dia
lysi
s tre
atm
ent;
v
GFR
of 2
0 m
l/min
or l
ess;
v
no D
SM IV
psy
chia
tric
diag
nose
s;
v
able
to re
ad a
nd s
peak
Sp
anis
h;
v
and
had
acce
pted
and
sig
ned
an in
form
ed c
onse
nt fo
rm to
pa
rtici
pate
in th
e pr
ogra
m
-10
patie
nts
drop
ped
out o
f the
pro
gram
for
the
follo
win
g re
ason
s:v
1 pa
tient
cha
nged
hos
pita
l,v
5 pa
tient
s in
itiat
ed H
D,
v
3 pa
tient
s in
itiat
ed P
D,
v
1 pa
tient
die
d
-42
patie
nts
com
plet
ed th
e pr
ogra
m a
nd
wer
e in
clud
ed in
the
anal
ysis
-Ass
essm
ents
wer
e ad
min
iste
red
prio
r to
the
inte
rven
tion
and
afte
r the
inte
rven
tion.
-Pat
ient
s w
ere
eval
uate
d fo
r adh
eren
ce,
depr
essi
on, a
nxie
ty a
nd H
RQ
L w
ith
stan
dard
ised
sel
f-rep
ort q
uest
ionn
aire
s.
-Bio
chem
ical
mar
kers
wer
e al
so re
gist
ered
.
II-3
42 p
atie
nts
adva
nced
ch
roni
c ki
dney
dis
ease
in
clud
ed
-Ave
rage
age
68y
ears
old
-Mos
t wer
e m
en
(60%
), m
arrie
d (5
9%),
unem
ploy
ed (6
9%)
Pre-
dial
ysis
in
terv
entio
n pr
ogra
m
-6-m
onth
indi
vidu
al
prog
ram
was
m
anag
ed b
y a
train
ed h
ealth
ps
ycho
logi
st.
-Eve
ry p
atie
nt
ente
ring
the
stud
y at
tend
ed
thei
r reg
ular
ap
poin
tmen
ts
with
nep
hrol
ogis
t, th
e nu
rse
and
nutri
tioni
st
-Eac
h pa
tient
re
ceiv
ed 6
in
divi
dual
mon
thly
fa
ce-to
-face
se
ssio
ns (9
0-m
in
dura
tion)
with
hea
lth
psyc
holo
gist
-Eve
ry s
essi
on h
ad
two
dist
inct
aim
s:a.
firs
t 45
min
of
sess
ions
pro
vide
d tra
inin
g in
ski
lls
that
faci
litat
ed th
e pa
tient
’s ad
apta
tion
to th
e AC
KD a
nd it
s tre
atm
ents
, b.
last
45
min
he
lped
impr
ove
adhe
renc
e to
m
edic
atio
n th
roug
h m
otiv
atio
nal
inte
rvie
win
g
6 m
onth
sR
esul
ts:
Afte
r the
inte
rven
tion,
pat
ient
s re
porte
d si
gnifi
cant
ly h
ighe
r lev
els
of
adhe
renc
e, lo
wer
dep
ress
ion
and
anxi
ety
leve
ls, a
nd b
ette
r HR
QL
(i.e.
, ge
nera
l hea
lth a
nd e
mot
iona
l rol
e do
mai
ns).
Adhe
renc
e le
vel
v
Patie
nts
repo
rted
bette
r adh
eren
ce to
trea
tmen
ts a
fter t
he
indi
vidu
al s
essi
on p
rogr
am a
s m
easu
red
by th
e ad
here
nce
to tr
eatm
ent s
urve
y (H
ighe
r sco
re in
dica
tes
grea
ter d
egre
e of
trea
tmen
t adh
eren
ce)
Mea
n sc
ore
(SD
) ran
ge;
Pre-
test
27.
12 (2
.74)
, 22–
33 v
s Po
st-te
st 3
1.45
(2.0
5),
26–3
3 (P
<0.0
01) a
nd b
y th
e M
oris
ky–G
reen
–Lev
ine
Test
(p
<0.0
01).
v
Rat
es o
f non
-adh
eren
ce to
ora
l med
icat
ion,
as
mea
sure
d by
the
Mor
isky
–Gre
en–L
evin
e Te
st, d
ecre
ased
sig
nific
antly
fro
m b
efor
e th
e in
terv
entio
n (2
9 %
) to
afte
r the
inte
rven
tion
(16%
).
Dep
ress
ion
and
anxi
ety
leve
lv
Dep
ress
ion
leve
ls s
igni
fican
tly d
ecre
ased
from
bef
ore
(M
= 10
.92)
to a
fter (
M =
8.8
6) th
e in
terv
entio
n,
v
as d
id a
nxie
ty le
vels
(fr
om M
= 1
8.22
to M
= 1
4.41
)
Hea
lth-re
late
d qu
ality
of l
ife (H
RQ
L)
v
Hea
lth-re
late
d qu
ality
of l
ife (H
RQ
L) s
core
s on
the
Gen
eral
H
ealth
sub
scal
e in
crea
sed
sign
ifica
ntly
(fro
m M
= 3
7.19
to
M =
45.
97),
as d
id s
core
s on
the
Emot
iona
l Rol
e su
bsca
le
(from
M =
71.
82 to
M =
77.
57).
v
No
effe
cts
wer
e fo
und
in o
ther
dom
ains
of H
RQ
L (p
hysi
cal
func
tion,
phy
sica
l rol
e, b
odily
pai
n, v
italit
y, so
cial
func
tion,
m
enta
l hea
lth)
Clin
ical
mar
kers
of a
dvan
ced
CKD
pat
ient
s in
pre
-dia
lysi
s be
fore
and
afte
r th
e pr
ogra
mv
Bioc
hem
ical
par
amet
ers
wer
e co
ntro
lled
sign
ifica
ntly
bet
ter
afte
r the
inte
rven
tion,
exc
ept f
or iP
TH.
Aut
hors
con
clus
ion:
Thes
e fin
ding
s hi
ghlig
ht th
e po
tent
ial b
enefi
t of a
pply
ing
indi
vidu
al
psyc
ho-e
duca
tiona
l int
erve
ntio
n pr
ogra
ms
base
d on
mot
ivat
iona
l in
terv
iew
ing
and
usin
g th
e st
ages
of c
hang
e m
odel
to p
rom
ote
adhe
renc
e an
d w
ellb
eing
in a
dvan
ced
CKD
pat
ient
s.
Smal
l sam
ple
size
,
Educ
atio
n by
mul
tiple
in
divi
dual
se
ssio
ns
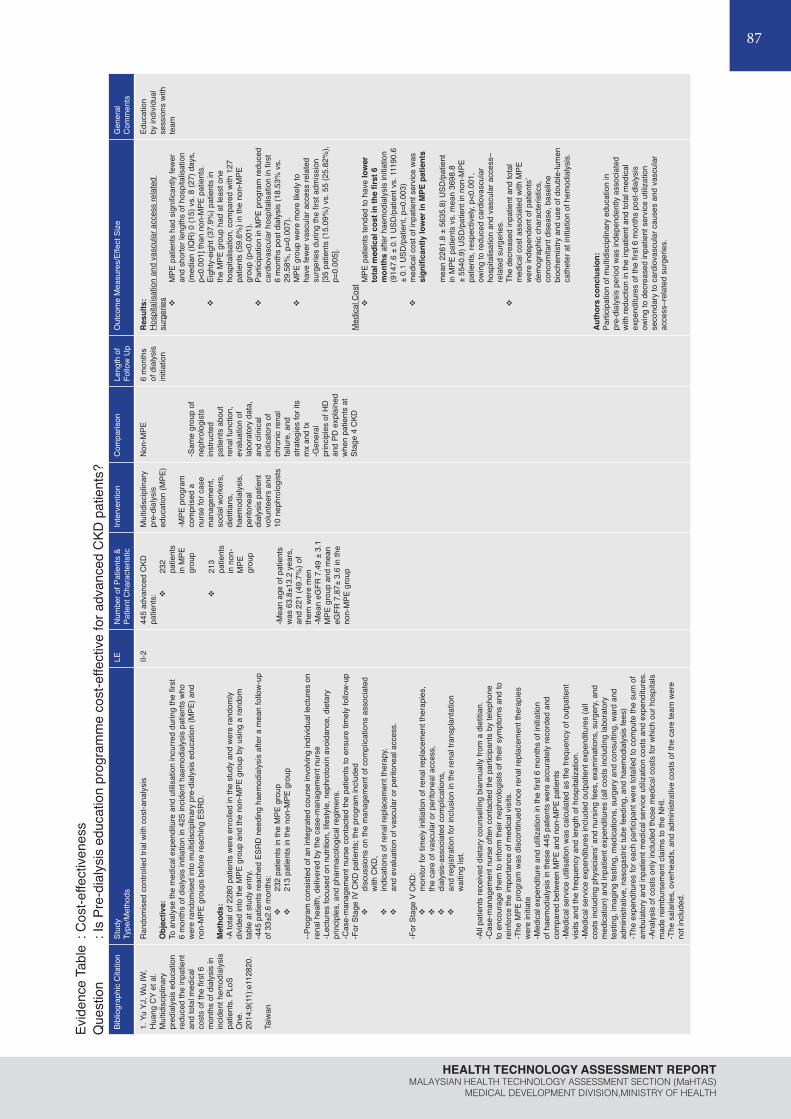
87
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Evid
ence
Tab
le :
Cos
t-effe
ctiv
enes
sQ
uest
ion
: Is
Pre-
dial
ysis
edu
catio
n pr
ogra
mm
e co
st-e
ffect
ive
for a
dvan
ced
CKD
pat
ient
s?Bi
blio
grap
hic
Cita
tion
Stud
yTy
pe/M
etho
dsLE
Num
ber o
f Pat
ient
s &
Patie
nt C
hara
cter
istic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
1. Y
u YJ
, Wu
IW,
Hua
ng C
Y et
al.
Mul
tidis
cipl
inar
y pr
edia
lysi
s ed
ucat
ion
redu
ced
the
inpa
tient
an
d to
tal m
edic
alco
sts
of th
e fir
st 6
m
onth
s of
dia
lysi
s in
in
cide
nt h
emod
ialy
sis
patie
nts.
PLo
SO
ne.
2014
;9(1
1):e
1128
20.
Taiw
an
Ran
dom
ised
con
trolle
d tri
al w
ith c
ost-a
naly
sis
Obj
ectiv
e:To
ana
lyse
the
med
ical
exp
endi
ture
and
util
isat
ion
incu
rred
durin
g th
e fir
st
6 m
onth
s of
dia
lysi
s in
itiat
ion
in 4
25 in
cide
nt h
aem
odia
lysi
s pa
tient
s w
ho
wer
e ra
ndom
ised
into
mul
tidis
cipl
inar
y pr
e-di
alys
is e
duca
tion
(MPE
) and
no
n-M
PE g
roup
s be
fore
reac
hing
ESR
D.
Met
hods
:-A
tota
l of 2
280
patie
nts
wer
e en
rolle
d in
the
stud
y an
d w
ere
rand
omly
di
vide
d in
to th
e M
PE g
roup
and
the
non-
MPE
gro
up b
y us
ing
a ra
ndom
ta
ble
at s
tudy
ent
ry.
-445
pat
ient
s re
ache
d ES
RD
nee
ding
hae
mod
ialy
sis
afte
r a m
ean
follo
w-u
p of
33±
2.6
mon
ths:
v
232
patie
nts
in th
e M
PE g
roup
v
213
patie
nts
in th
e no
n-M
PE g
roup
--Pro
gram
con
sist
ed o
f an
inte
grat
ed c
ours
e in
volv
ing
indi
vidu
al le
ctur
es o
n re
nal h
ealth
, del
iver
ed b
y th
e ca
se-m
anag
emen
t nur
se-L
ectu
res
focu
sed
on n
utrit
ion,
life
styl
e, n
ephr
otox
in a
void
ance
, die
tary
pr
inci
ples
, and
pha
rmac
olog
ical
regi
men
s.
-Cas
e-m
anag
emen
t nur
se c
onta
cted
the
patie
nts
to e
nsur
e tim
ely
follo
w-u
p-F
or S
tage
IV C
KD p
atie
nts;
the
prog
ram
incl
uded
v
disc
ussi
ons
on th
e m
anag
emen
t of c
ompl
icat
ions
ass
ocia
ted
with
CKD
, v
indi
catio
ns o
f ren
al re
plac
emen
t the
rapy
, v
and
eval
uatio
n of
vas
cula
r or p
erito
neal
acc
ess.
-For
Sta
ge V
CKD
: v
mon
itor f
or ti
mel
y in
itiat
ion
of re
nal r
epla
cem
ent t
hera
pies
, v
the
care
of v
ascu
lar o
r per
itone
al a
cces
s,
v
dial
ysis
-ass
ocia
ted
com
plic
atio
ns,
v
and
regi
stra
tion
for i
nclu
sion
in th
e re
nal t
rans
plan
tatio
n w
aitin
g lis
t.
-All
patie
nts
rece
ived
die
tary
cou
nsel
ling
bian
nual
ly fr
om a
die
titia
n.
-Cas
e-m
anag
emen
t nur
se o
ften
cont
acte
d th
e pa
rtici
pant
s by
tele
phon
e to
enc
oura
ge th
em to
info
rm th
eir n
ephr
olog
ists
of t
heir
sym
ptom
s an
d to
re
info
rce
the
impo
rtanc
e of
med
ical
vis
its.
-The
MPE
pro
gram
was
dis
cont
inue
d on
ce re
nal r
epla
cem
ent t
hera
pies
w
ere
initi
ate
-Med
ical
exp
endi
ture
and
util
izat
ion
in th
e fir
st 6
mon
ths
of in
itiat
ion
of h
aem
odia
lysi
s in
thes
e 44
5 pa
tient
s w
ere
accu
rate
ly re
cord
ed a
nd
com
pare
d be
twee
n M
PE a
nd n
on-M
PE p
atie
nts
-Med
ical
ser
vice
util
isat
ion
was
cal
cula
ted
as th
e fre
quen
cy o
f out
patie
nt
visi
ts a
nd th
e fre
quen
cy a
nd le
ngth
of h
ospi
taliz
atio
n.-M
edic
al s
ervi
ce e
xpen
ditu
res
incl
uded
out
patie
nt e
xpen
ditu
res
(all
cost
s in
clud
ing
phys
icia
ns’ a
nd n
ursi
ng fe
es, e
xam
inat
ions
, sur
gery
, and
m
edic
atio
n) a
nd in
patie
nt e
xpen
ditu
res
(all
cost
s in
clud
ing
labo
rato
ry
test
ing,
imag
ing
test
ing,
med
icat
ions
, sur
gery
and
con
sulti
ng, w
ard
and
adm
inis
trativ
e, n
asog
astri
c tu
be fe
edin
g, a
nd h
aem
odia
lysi
s fe
es)
-The
exp
endi
ture
s fo
r eac
h pa
rtici
pant
wer
e to
talle
d to
com
pute
the
sum
of
ambu
lato
ry a
nd in
patie
nt m
edic
al s
ervi
ce u
tiliz
atio
n co
sts
and
expe
nditu
res.
-A
naly
sis
of c
osts
onl
y in
clud
ed th
ose
med
ical
cos
ts fo
r whi
ch o
ur h
ospi
tals
m
ade
reim
burs
emen
t cla
ims
to th
e N
HI.
-The
sal
arie
s, o
verh
eads
, and
adm
inis
trativ
e co
sts
of th
e ca
re te
am w
ere
not i
nclu
ded.
II-2
445
adva
nced
CKD
pa
tient
s: v
232
patie
nts
in M
PE
grou
p
v
213
patie
nts
in n
on-
MPE
gr
oup
-Mea
n ag
e of
pat
ient
s w
as 6
3.8±
13.2
yea
rs,
and
221
(49.
7%) o
f th
em w
ere
men
-Mea
n eG
FR 7
.49
± 3.
1 M
PE g
roup
and
mea
n eG
FR 7
.87±
3.6
in th
e no
n-M
PE g
roup
Mul
tidis
cipl
inar
y pr
e-di
alys
is
educ
atio
n (M
PE)
-MPE
pro
gram
co
mpr
ised
a
nurs
e fo
r cas
e m
anag
emen
t, so
cial
wor
kers
, di
etiti
ans,
ha
emod
ialy
sis,
pe
riton
eal
dial
ysis
pat
ient
vo
lunt
eers
and
10
nep
hrol
ogis
ts
Non
-MPE
-Sam
e gr
oup
of
neph
rolo
gist
s in
stru
cted
pa
tient
s ab
out
rena
l fun
ctio
n,
eval
uatio
n of
la
bora
tory
dat
a,
and
clin
ical
in
dica
tors
of
chro
nic
rena
l fa
ilure
, and
st
rate
gies
for i
ts
mx
and
tx-G
ener
al
prin
cipl
es o
f HD
an
d PD
exp
lain
ed
whe
n pa
tient
s at
St
age
4 C
KD
6 m
onth
s of
dia
lysi
s in
itiat
ion
Res
ults
:H
ospi
talis
atio
n an
d va
scul
ar a
cces
s re
late
d su
rger
iesv
MPE
pat
ient
s ha
d si
gnifi
cant
ly fe
wer
an
d sh
orte
r len
gths
of h
ospi
talis
atio
n (m
edia
n (IQ
R) 0
(15)
vs.
8 (2
7) d
ays,
p<
0.00
1] th
an n
on-M
PE p
atie
nts.
v
Eigh
ty-e
ight
(37.
9%) p
atie
nts
in
the
MPE
gro
up h
ad a
t lea
st o
ne
hosp
italis
atio
n, c
ompa
red
with
127
pa
tient
s (5
9.6%
) in
the
non-
MPE
gr
oup
(p<0
.001
).v
Parti
cipa
tion
in M
PE p
rogr
am re
duce
d ca
rdio
vasc
ular
hos
pita
lisat
ion
in fi
rst
6 m
onth
s po
st d
ialy
sis
(18.
53%
vs.
29
.58%
, p=0
.007
). v
MPE
gro
up w
ere
mor
e lik
ely
to
have
few
er v
ascu
lar a
cces
s re
late
d su
rger
ies
durin
g th
e fir
st a
dmis
sion
[3
5 pa
tient
s (1
5.09
%) v
s. 5
5 (2
5.82
%),
p=0.
005]
.
Med
ical
Cos
tv
MPE
pat
ient
s te
nded
to h
ave
low
er
tota
l med
ical
cos
t in
the
first
6
mon
ths
afte
r hae
mod
ialy
sis
initi
atio
n (9
147.
6 ±
0.1
USD
/pat
ient
vs.
111
90.6
±
0.1
USD
/pat
ient
, p=0
.003
)v
med
ical
cos
t of i
npat
ient
ser
vice
was
si
gnifi
cant
ly lo
wer
in M
PE p
atie
nts
mea
n 22
61.8
± 5
635.
8) U
SD/p
atie
nt
in M
PE p
atie
nts
vs. m
ean
3698
.8
± 55
40.9
) USD
/pat
ient
in n
on-M
PE
patie
nts,
resp
ectiv
ely,
p<0.
001,
ow
ing
to re
duce
d ca
rdio
vasc
ular
ho
spita
lisat
ion
and
vasc
ular
acc
ess–
rela
ted
surg
erie
s.
v
The
decr
ease
d in
patie
nt a
nd to
tal
med
ical
cos
t ass
ocia
ted
with
MPE
w
ere
inde
pend
ent o
f pat
ient
s’ de
mog
raph
ic c
hara
cter
istic
s,
conc
omita
nt d
isea
se, b
asel
ine
bioc
hem
istry
and
use
of d
oubl
e-lu
men
ca
thet
er a
t ini
tiatio
n of
hem
odia
lysi
s.
Aut
hors
con
clus
ion:
Parti
cipa
tion
of m
ultid
isci
plin
ary
educ
atio
n in
pr
e-di
alys
is p
erio
d w
as in
depe
nden
tly a
ssoc
iate
d w
ith re
duct
ion
in th
e in
patie
nt a
nd to
tal m
edic
al
expe
nditu
res
of th
e fir
st 6
mon
ths
post
-dia
lysi
s ow
ing
to d
ecre
ased
inpa
tient
ser
vice
util
izat
ion
seco
ndar
y to
car
diov
ascu
lar c
ause
s an
d va
scul
ar
acce
ss–r
elat
ed s
urge
ries.
Educ
atio
n by
indi
vidu
al
sess
ions
with
te
am

88
PRE-DIALYSIS EDUCATION PROGRAMME
Evid
ence
Tab
le :
Cos
t-effe
ctiv
enes
sQ
uest
ion
: Is
Pre-
dial
ysis
edu
catio
n pr
ogra
mm
e co
st-e
ffect
ive
for a
dvan
ced
CKD
pat
ient
s?Bi
blio
grap
hic
Cita
tion
Stud
yTy
pe/M
etho
dsLE
Num
ber o
f Pa
tient
s &
Patie
nt
Cha
ract
eris
tic
Inte
rven
tion
Com
paris
onLe
ngth
of
Follo
w U
p O
utco
me
Mea
sure
s/Ef
fect
Siz
eG
ener
al
Com
men
ts
2. W
ei S
Y,
Cha
ng Y
Y, M
au
LW e
t al.
Chr
onic
kid
ney
dise
ase
care
pr
ogra
m
impr
oves
qua
lity
of p
re-e
nd-
stag
e re
nal
dise
ase
care
an
d re
duce
s m
edic
al c
osts
. N
ephr
olog
y (C
arlto
n).
2010
;15(
1):1
08-
115.
Taiw
an
Ret
rosp
ectiv
e co
hort
stud
yw
ith c
ost-a
naly
sis
Obj
ectiv
e:
To e
valu
ate
the
effe
ctiv
enes
s of
CKD
car
e pr
ogra
m o
n pr
e-en
d-st
age
rena
l dis
ease
(E
SRD
) car
e
Met
hod:
-Tot
al o
f 140
inci
dent
ESR
D p
atie
nts,
who
sta
rted
HD
in th
e pe
riod
from
Aug
ust
2004
to J
uly
2005
from
the
two
stud
y ho
spita
ls w
ere
retro
spec
tivel
y re
view
ed-S
tudy
sub
ject
s di
vide
d in
to:
v
‘CK
D C
are
Gro
up’
(71
inci
dent
HD
pat
ient
s w
ho re
ceiv
ed th
e C
KD c
are
prog
ram
in
terv
entio
n fo
r at l
east
6 m
onth
s be
fore
initi
atio
n of
HD
), v
‘Nep
hrol
ogis
t Car
e G
roup
’ (69
inci
dent
HD
pat
ient
s w
ho w
ere
care
d fo
r by
neph
rolo
gist
s al
one
for a
t lea
st 6
mon
ths
befo
re in
itiat
ion
of
dial
ysis
)
-CKD
Car
e Pr
ogra
m in
clud
ed n
ephr
olog
ists
, ren
al n
urse
s an
d di
etic
ians
as
the
core
m
embe
rs o
f a m
ultid
isci
plin
ary
team
resp
onsi
ble
for c
arin
g fo
r pat
ient
s at
diff
eren
t C
KD s
tage
s.
-CKD
pat
ient
s, in
vite
d to
join
the
care
pro
gram
by
the
neph
rolo
gist
, wer
e re
ferre
d to
w
ell-t
rain
ed re
nal n
urse
s an
d di
etic
ians
. -D
iffer
ent g
oals
and
edu
catio
n co
nten
ts, a
ccor
ding
to s
tage
s of
CKD
and
pre
-set
cl
inic
al p
roto
cols
, wer
e pl
anne
d an
d de
liver
ed s
yste
mat
ical
ly a
ppro
xim
atel
y 30
–45
min
at e
ach
visi
t. -E
very
pat
ient
rece
ived
follo
w-u
p vi
sits
with
clin
ical
eva
luat
ion,
labo
rato
ry
exam
inat
ions
, nur
sing
and
die
tary
edu
catio
n, w
hich
was
take
n ev
ery
3 m
onth
s fo
r C
KD s
tage
s 3
and
4, a
nd e
very
1–2
mon
ths
for s
tage
5 p
atie
nts.
-Prim
ary
goal
s in
clud
ed:
v
slow
ing
dow
n th
e de
terio
ratio
n of
rena
l fun
ctio
n,
v
early
pre
para
tions
for d
ialy
sis,
v
redu
cing
of r
isk
of c
ompl
icat
ions
,v
and
ensu
ring
the
proc
ess
of e
nter
ing
dial
ysis
sm
ooth
ly a
nd s
afel
y.
-Nep
hrol
ogis
t Car
e G
roup
wer
e al
l tre
ated
by
neph
rolo
gist
s fro
m th
e sa
me
depa
rtmen
t, bu
t the
y di
d no
t rec
eive
nur
sing
edu
catio
n an
d di
etar
y co
unse
lling
by
CKD
nur
ses
and
diet
icia
ns.
-Prin
cipl
e of
CKD
car
e, in
clud
ing
med
icat
ions
and
ear
ly p
repa
ratio
n of
vas
cula
r ac
cess
, wer
e ro
utin
ely
deliv
ered
to p
atie
nts
by th
e ne
phro
logi
sts
-End
-poi
nt o
f obs
erva
tion
was
dia
lysi
s in
itiat
ion.
-Q
ualit
y in
dica
tors
for e
valu
atio
n in
clud
ed:
v
Stat
us o
f rec
ombi
nant
hum
an e
ryth
ropo
ietin
(rH
uEPO
) tre
atm
ent,
v
Vasc
ular
acc
ess
prep
arat
ion
v
Hos
pita
lisat
ion
for i
nitia
tion
of d
ialy
sis
whi
ch w
ere
com
pare
d be
twee
n tw
o gr
oups
-Med
ical
ser
vice
s ut
ilisat
ion
and
cost
s w
ere
anal
ysed
from
6 m
onth
s be
fore
initi
atio
n of
dia
lysi
s to
the
time
of th
e fir
st H
D, a
nd th
e tim
e pe
riods
wer
e di
vide
d in
to ‘6
m
onth
s be
fore
dia
lysi
s’, ‘
at d
ialy
sis
initi
atio
n’, a
nd th
e su
m o
f the
two
perio
ds a
s th
e ‘to
tal p
erio
d of
obs
erva
tion’
. -In
dica
tors
of s
ervi
ce u
tilis
atio
n in
clud
ed:
v
Aver
age
outp
atie
nt v
isits
bef
ore
dial
ysis
, v
Freq
uenc
y of
hos
pita
lisat
ion
befo
re d
ialy
sis,
v
Perc
enta
ge o
f pat
ient
hos
pita
lisat
ion
at d
ialy
sis
initi
atio
n,
v
Aver
age
leng
th o
f sta
y (L
OS)
- Mea
sure
men
t of c
osts
in th
is s
tudy
onl
y in
clud
ed d
irect
med
ical
cos
ts fo
r whi
ch th
e st
udy
hosp
itals
mad
e cl
aim
s to
the
NH
I for
reim
burs
emen
t-S
alar
ies,
ove
rhea
ds a
nd in
dire
ct c
osts
of t
he c
are
team
wer
e no
t inc
lude
d
II-2
140
inci
dent
ES
RD
pa
tient
s w
ho s
tarte
d di
alys
is a
nd
divi
ded
into
:
-CKD
Car
e G
roup
(71
patie
nts)
-Nep
hrol
ogis
t C
are
Gro
up
(69
patie
nts)
-Mea
n eG
FR,
mL/
min
per
1.
73 m
2 3.
8 ±
1.3
in C
KD
Car
e G
roup
, 3.
7 ±
1.5
in
Nep
hrol
ogis
t ca
re g
roup
CKD
car
e pr
ogra
m
Nep
hrol
ogis
t C
are
Gro
up6
mon
ths
befo
re d
ialy
sis
Res
ults
:
Qua
lity
of p
re-E
SRD
car
ePr
epar
atio
n at
dia
lysi
s in
itiat
ion:
EPO
trea
tmen
t-N
o si
gnifi
cant
diff
eren
ce o
n pe
rcen
tage
s of
pat
ient
s w
ho
rece
ived
rHuE
PO tr
eatm
ent a
t ini
tiatio
n of
HD
and
the
aver
age
mon
thly
dos
age
of rH
uEPO
Prep
arat
ions
at d
ialy
sis
initi
atio
n: v
ascu
lar a
cces
s-V
ascu
lar a
cces
s ha
d be
en c
reat
ed b
efor
e H
D in
57.
7%
of p
atie
nts
in th
e C
KD C
are
Gro
up v
s. o
nly
37.7
% o
f the
N
ephr
olog
ist C
are
Gro
up (P
= 0
.017
). -P
erce
ntag
e of
pat
ient
s w
ho s
tarte
d H
D w
ith c
reat
ed v
ascu
lar
acce
ss w
ithou
t the
inse
rtion
of d
oubl
e lu
men
cat
hete
r was
50
.7%
in th
e C
KD C
are
Gro
up, v
s. 2
9.0%
in th
e N
ephr
olog
ist
Car
e G
roup
(P
= 0
.009
)
Prep
arat
ions
at d
ialy
sis
initi
atio
n: h
ospi
talis
atio
n-P
erce
ntag
e of
pat
ient
s w
ho w
ere
not h
ospi
talis
ed fo
r ini
tiatio
n of
HD
was
40.
8% in
CKD
Car
e G
roup
, vs.
18.
8% in
the
Nep
hrol
ogis
t Car
e G
roup
(P <
0.0
05).
-Mos
t pat
ient
s in
Nep
hrol
ogis
t Car
e G
roup
(81.
2%) h
ad th
eir
first
HD
thro
ugh
inpa
tient
HD
.
Freq
uenc
y of
ser
vice
s ut
ilisat
ion
Perio
d of
‘6 m
onth
s be
fore
dia
lysi
s’-M
ore
frequ
ent o
utpa
tient
vis
its in
CKD
Car
e G
roup
(9.9
± 5
.5
vs 5
.5 ±
5.5
P<0
.001
), bu
t the
freq
uenc
y of
hos
pita
lisat
ion
and
leng
th o
f sta
y ha
d no
diff
eren
ce w
ith N
ephr
olog
ist C
are
Gro
up.
Perio
d of
‘at d
ialy
sis
initi
atio
n’-L
ower
per
cent
age
of h
ospi
talis
atio
n fo
r ini
tiatio
n of
dia
lysi
s in
th
e C
KD C
are
Gro
up (5
9.2%
vs
81.2
%, P
= 0.
005)
, -L
engt
h of
sta
y in
hos
pita
l muc
h sh
orte
r for
CKD
Car
e G
roup
.(6
.6da
ys ±
16.
2 vs
. 16.
2day
s ±
16.2
, P
<0.0
01)
Med
ical
cos
tsv
Parti
cipa
tion
in C
KD c
are
prog
ram
, tho
ugh
with
hi
gher
cos
ts d
urin
g th
e 6
mon
ths
befo
re d
ialy
sis
($U
S142
8 +/
- 204
9 vs
US$
675
+/- 9
62/p
atie
nt,
P <
0.00
1),
v
was
sig
nific
antly
ass
ocia
ted
with
low
er m
edic
al
cost
s at
dia
lysi
s in
itiat
ion
($U
S942
+/-
1941
vs
$US2
410
+/- 2
481/
patie
nt, P
< 0
.001
) v
and
for t
he to
tal p
erio
d of
obs
erva
tion
($U
S267
4 +/
- 278
0 vs
$U
S387
2 +/
- 327
0/pa
tient
, P =
0.0
09)
-The
cos
t-sav
ing
effe
ct c
ame
thro
ugh
the
early
pre
para
tion
of v
ascu
lar a
cces
s an
d th
e la
ck o
f hos
pita
lizat
ion
at d
ialy
sis
initi
atio
n.
Aut
hors
con
clus
ion:
CKD
car
e pr
ogra
m s
ucce
ssfu
lly h
elps
pre
-ESR
D p
atie
nts
to p
roce
ed in
to d
ialy
sis
initi
atio
n w
ith b
ette
r pre
pare
dnes
s,
whi
ch re
duce
s th
e pr
obab
ility
of e
mer
genc
y di
alys
is th
roug
h ho
spita
lizat
ion
and
save
s he
ath
dolla
rs fr
om C
KD to
ESR
D
Educ
atio
n by
mul
tiple
in
divi
dual
se
ssio
ns

89
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Appendix 5LIST OF EXCLUDED STUDIES
1. Hassan R, Akbari A, Brown PA et al. Risk Factors for Unplanned Dialysis Initiation: A Systematic Review of the Literature. Can J Kidney Health Dis. 2019;6:2054358119831684.
2. de Oliveira JGR, Askari M, Fahd MGN et al. Chronic Kidney Disease and the Use of Social Media as Strategy for Health Education in Brazil. Studies in health technology and informatics. 2019;264:1945-1946.
3. Cassidy BP, Getchell LE, Harwood L et al. Barriers to Education and Shared Decision Making in the Chronic Kidney Disease Population: A Narrative Review. Canadian Journal of Kidney Health & Disease.5:2054358118803322.
4. Chen NH, Lin YP, Liang SY et al. Conflict when making decisions about dialysis modality. Journal of Clinical Nursing.27(1-2):e138-e146.
5. Noorkhairina SS, Norhasyimah G, ‘Ain IN et al. Educational Needs Assessment and the Management of Chronic Kidney Disease in a Malaysian Setting: A Review. Int J Care Scholars. 2018;1(1):34-38.
6. Ng CY, Lee ZS, Goh KS. Cross-sectional study on knowledge of chronic kidney disease among medical outpatient clinic patients. The Medical journal of Malaysia. 2016;71(3):99-104.
7. Javaid MM, Khan BA et al. Sustained Increase in Peritoneal Dialysis Prevalence through a Structured PD Initiation Service. Peritoneal Dialysis International.38(5):374-376.
8. Li WY, Wang YC, Hwang SJ et al. Comparison of outcomes between emergent-start and planned-start peritoneal dialysis in incident ESRD patients: a prospective observational study. BMC Nephrology.18(1):359.
9. Berkhout-Byrne N, Gaasbeek A, Mallat MJK et al. Regret about the decision to start dialysis: a cross-sectional Dutch national survey. Netherlands Journal of Medicine.75(6):225-234.
10. Lovell S, Walker RJ, Schollum JB et al. To dialyse or delay: a qualitative study of older New Zealanders’ perceptions and experiences of decision-making, with stage 5 chronic kidney disease. BMJ Open.7(3):e014781.
11. Winterbottom A, Bekker H, Mooney A. Dialysis modality selection: physician guided or patient led? Clin Kidney J. 2016;9(6):823-825.
12. Pugh J, Aggett J, Annwen G et al. Frailty and comorbidity are independent predictors of outcome in patients referred for pre-dialysis education. Clinical Kidney Journal. 2016;9:324-329.
13. Molnar AO, Hiremath S, Brown PA, Akbari A. Risk factors for unplanned and crash dialysis starts: a protocol for a systematic review and meta-analysis. Syst Rev. 2016;5(1):117.
14. Begum R, Khan TM, Ming LC. Burden of chronic kidney disease and its risk factors in Malaysia. Journal of epidemiology and global health. 2016;6(4):325-326.
15. Chiang PC, Hou JJ, Jong IC et al. Factors Associated with the Choice of Peritoneal Dialysis in Patients with End-Stage Renal Disease. BioMed Research International.2016:5314719.
16. Phuphaibul R, Teamprathom W, Puckpinyo A et al. Can a community-based multidisciplinary intervention effectively restore renal function? A non-randomized clinical trial. Nursing & Health Sciences.18(4):533-538.
17. Bavanandan S, Ahmad G, Teo AH, Chen L, Liu FX. Budget Impact Analysis of Peritoneal Dialysis versus Conventional In-Center Hemodialysis in Malaysia. Value in health regional issues. 2016;9:8-14.
18. Jha V, Wang AY, Wang H. The impact of CKD identification in large countries: the burden of illness. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2012;27 Suppl 3:iii32-38.
19. Salman M, Khan AH, Adnan AS et al. Attributable causes of chronic kidney disease in adults: a five-year retrospective study in a tertiary-care hospital in the northeast of the Malaysian Peninsula. Sao Paulo medical journal = Revista paulista de medicina. 2015;133(6):502-509.
20. Brown PA, Akbari A, Molnar AO et al. Factors Associated with Unplanned Dialysis Starts in Patients followed by Nephrologists: A Retropective Cohort Study. PloS one.
90
PRE-DIALYSIS EDUCATION PROGRAMME
2015;10(6):e0130080.21. Karkar A, Hegbrant J, Strippoli GF. Benefits and implementation of home hemodialysis: A
narrative review. Saudi Journal of Kidney Diseases & Transplantation.26(6):1095-1107.22. Hussain JA, Flemming K, Murtagh FE et al. Patient and health care professional decision-
making to commence and withdraw from renal dialysis: a systematic review of qualitative research. Clinical Journal of The American Society of Nephrology: CJASN.10(7):1201-1215.
23. Pajek J. Overcoming the Underutilisation of Peritoneal Dialysis. BioMed Research International.2015:431092.
24. Winterbottom AE, Gavaruzzi T, Mooney A et al. Patient Acceptability of the Yorkshire Dialysis Decision Aid (YoDDA) Booklet: A Prospective Non-Randomized Comparison Study Across 6 Predialysis Services. Peritoneal Dialysis International.36(4):374-381.
25. Fortnum D, Ludlow M, Morton RL. Renal unit characteristics and patient education practices that predict a high prevalence of home-based dialysis in Australia. Nephrology (Carlton, Vic). 2014;19(9):587-593.
26. Smart NA, Dieberg G, Ladhani M et al. Early referral to specialist nephrology services for preventing the progression to end-stage kidney disease. The Cochrane database of systematic reviews. 2014(6):Cd007333.
27. Walker RC, Marshall MR. Increasing the uptake of peritoneal dialysis in New Zealand: a national survey. Journal of Renal Care.40(1):40-48.
28. Davis JS, Zuber K. Implementing patient education in the CKD clinic. Adv Chronic Kidney Dis. 2013;20(4):320-325.
29. Hooi LS, Ong LM, Ahmad G et al. A population-based study measuring the prevalence of chronic kidney disease among adults in West Malaysia. Kidney Int. 2013;84(5):1034-1040.
30. Kurella Tamura M, Li S, Chen SC et al. Educational programs improve the preparation for dialysis and survival of patients with chronic kidney disease. Kidney Int. 2014;85(3):686-692.
31. Fabian J, Van Jaarsveld K, Maher HA et al. Early survival on maintenance dialysis therapy in South Africa: evaluation of a pre-dialysis education programme. Clinical & Experimental Nephrology.20(1):118-125.
32. Griva K HLZ, Yuanhong Lai A et al. Perspectives of patients, families, and health care professionals on decision-making about dialysis modality-the good, the bad, and the misunderstandings! Perit Dial Int. 2013;33(3): 280–289.
33. Strand H, Parker D. Effects of multidisciplinary models of care for adult pre-dialysis patients with chronic kidney disease: a systematic review. International journal of evidence-based healthcare. 2012;10(1):53-59.
34. Harwood L, Clark AM. Understanding pre-dialysis modality decision-making: A meta-synthesis of qualitative studies. International journal of nursing studies. 2013;50(1):109-120.
35. Chan YM, Zalilah MS, Hii SZ. Determinants of compliance behaviours among patients undergoing hemodialysis in Malaysia. PloS one. 2012;7(8):e41362.
36. Chanouzas D, Ng KP, Fallouh B et al. What influences patient choice of treatment modality at the pre-dialysis stage? Nephrology Dialysis Transplantation.27(4):1542-1547.
37. Maffei S, Savoldi S, Triolo G. When should commence dialysis: focusing on the predialysis condition. Nephrourology Monthly.5(2):723-727.
38. Castledine C, Gilg J, Rogers C et al. UK Renal Registry 13th Annual Report (December 2010): Chapter 15: UK renal centre survey results 2010: RRT incidence and use of home dialysis modalities. Nephron.119 Suppl 2:c255-267.
39. Bastos MG, Kirsztajn GM. Chronic kidney disease: importance of early diagnosis, immediate referral and structured interdisciplinary approach to improve outcomes in patients not yet on dialysis. Jornal Brasileiro de Nefrologia.33(1):93-108.
40. Demoulin N, Beguin C, Labriola L, Jadoul M. Preparing renal replacement therapy in stage 4 CKD patients referred to nephrologists: a difficult balance between futility and insufficiency. A cohort study of 386 patients followed in Brussels. Nephrology Dialysis Transplantation.26(1):220-226.
41. Chiou CP, Chung YC. Effectiveness of multimedia interactive patient education on knowledge, uncertainty and decision-making in patients with end-stage renal disease. Journal of Clinical Nursing.21(9-10):1223-1231.

91
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
42. Fadem SZ, Walker DR, Abbott G et al. Satisfaction with renal replacement therapy and education: the American Association of Kidney Patients survey. Clinical journal of the American Society of Nephrology : CJASN. 2011;6(3):605-612.
43. Covic A, Bammens B, Lobbedez T et al. Educating end-stage renal disease patients on dialysis modality selection: clinical advice from the European Renal Best Practice (ERBP) Advisory Board. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2010;25(6):1757-1759.
44. Morton RL, Howard K, Webster AC et al. Patient information about options for treatment: Methods of a national audit of information provision in chronic kidney disease. Nephrology.15(6):649-652.
45. Jennette C, Derebail V, Baldwin J et al. Renal replacement Therapy and Barriers to choice: using a Mixed Methods approach to explore the Patient’s Perspective. The Journal of Nephrology Social Work.32:15-26.
46. Yen M, Huang JJ, Teng HL. Education for patients with chronic kidney disease in Taiwan: a prospective repeated measures study. Journal of Clinical Nursing.17(21):2927-2934.
47. Chen YR, Yang Y, Wang SC et al. Effectiveness of multidisciplinary care for chronic kidney disease in Taiwan: a 3-year prospective cohort study. Nephrology Dialysis Transplantation.28(3):671-682.
48. Van Biesen W, Verbeke F, Vanholder R. We don’t need no education ... . (Pink Floyd, The Wall ) Multidisciplinary predialysis education programmes: pass or fail? Nephrology Dialysis Transplantation.24(11):3277-3279.
49. Mason J, Khunti K, Stone M et al. Educational interventions in kidney disease care: a systematic review of randomized trials. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2008;51(6):933-951.
50. Thomas M. Pre-dialysis education for patients with chronic kidney disease. Nephrology. 2007;12:S46-S48.
51. Elizabeth JL, Hanna L, Walker D, Milo E, Koupatsiaris T, De Vos JY, et al. Pre-dialysis education and patient choice. J Ren Care. 2006;32(4):214-220.
52. Owen JE, Walker RJ, Edgell L et al. Implementation of a pre-dialysis clinical pathway for patients with chronic kidney disease. International Journal for Quality in Health Care.18(2):145-151.
53. Devins GM, Mendelssohn DC, Barre PE et al. Predialysis psychoeducational intervention extends survival in CKD: a 20-year follow-up. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2005;46(6):1088-1098.
54. Goldstein M, Yassa T, Dacouris N et al. Multidisciplinary predialysis care and morbidity and mortality of patients on dialysis. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2004;44(4):706-714.
55. Hostetter T, Gladstone EH, Sica DA. National Kidney Disease Education Program in 2004: a program in evolution. Journal of Clinical Hypertension.6(6):299-302.
56. Devins GM, Mendelssohn DC, Barre PE et al. Predialysis psychoeducational intervention and coping styles influence time to dialysis in chronic kidney disease. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2003;42(4):693-703.
57. Golper T. Patient education: can it maximize the success of therapy? Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2001;16 Suppl 7:20-24.
58. Devins GM, Hollomby DJ, Barre PE, Mandin H, Taub K, Paul LC, et al. Long-term knowledge retention following predialysis psychoeducational intervention. Nephron. 2000;86(2):129-134.
59. Harris LE, Luft FC, Rudy DW, Kesterson JG, Tierney WM. Effects of multidisciplinary case management in patients with chronic renal insufficiency. The American journal of medicine. 1998;105(6):464-471.

92
PRE-DIALYSIS EDUCATION PROGRAMME
Appendix 6 SURVEY QUESTIONNAIRE Title of Survey: Pre-dialysis Education Programme for Chronic Kidney Disease (CKD) Patients: How would you like it to be?
Available at: https://tinyurl.com/predialysissurvey
Purpose of survey
The purpose of this survey is to understand the preferences of patients, carers and healthcare staff for pre-dialysis education so that we can develop a programme that better meet their needs. This survey would take no more than 10 minutes.
Informed consent
Your participation in this survey is voluntary. You may choose not to participate. If you decide to participate in this survey, you may withdraw at any time. If you decide not to participate in this survey or if you withdraw from participating at any time, you will not be penalized. Your responses in this survey will be anonymous and confidential.
I have read the above information and I voluntarily agree to be part of this survey and to provide necessary information to the doctor, nurse, or other staff members, as requested.
Yes No
Kindly fill in your name.………………………...
Section 1 of 3: Socio-demographics
1. How old are you?………………………...
2. What is your gender?MaleFemaleOther: ………………………...
3. What is your level of education?Primary schoolSecondary schoolTertiary education (college, university)None

93
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
Section 2 of 3: Patients’ or carers’ treatment experience
4. Are you currently a patient diagnosed with chronic kidney disease (CKD); a carer of family member/ partner/ child diagnosed with CKD or a part of healthcare team for CKD patients?
PatientCarerHealthcare staff (skip question 6 and 7)
5. (If patient or carer) Which hospital are you (or the patient you are caring for) currently under follow-up?
(If healthcare staff) Where do you work?Hospital Kuala LumpurHospital AmpangHospital Tengku Ampuan Rahimah, Klang
6. Did you (or the patient you are caring for) receive pre-dialysis education prior to initiation of dialysis?
Yes No
7. How long have you (or the patient you are caring for) been on dialysis?< 6 months6-12 months12-18 months> 18 monthsNot on dialysis
Section 3 of 3: Patients’ or carers’ preferences
8. Who do you think should be the one to provide pre-dialysis education to CKD patients? (You may select one or more)
Doctor NurseMedical assistantOther: ………………………...
9. Do you think CKD patients would also benefit from receiving counselling or advice from the following healthcare professionals? (You may select one or more)
DieticianPsychologistPharmacistSocial workerPatient representativeOther: ………………………...

94
PRE-DIALYSIS EDUCATION PROGRAMME
10. What type of information do you think is important for CKD patients to know prior to starting dialysis? (You may select one or more) How dialysis is performed Advantages and disadvantages of each treatment option (dialysis, kidney transplantation, conservative care without dialysis) Side effects of dialysis Costs associated with each treatment option (dialysis, kidney transplantation, conservative care without dialysis) Dietary advice (e.g. what to eat before, during and after dialysis) How to dress for dialysis access How dialysis may affect daily life (family, work, school, or leisure activities) Medications & supplements associated with each treatment option (dialysis, kidney transplantation, conservative care without dialysis) Other: ………………………...
11. How do you think pre-dialysis education should be conducted? Individually (one-to-one) GroupSD session (2-5 people) Group session (5-10 people) Other: ………………………...
12. Should it be conducted in a single session or multiple sessions? One single session with one single educator (for example: doctor or nurse) One single session with multiple educators (for example: doctor, nurse, pharmacist, dietician and psychologist) Multiple sessions with each educator by appointment (for example: doctor, nurse, pharmacist, dietician and psychologist) Multiple sessions with each educator upon request only (for example: doctor, nurse, pharmacist, dietician and psychologist) Other: ………………………...
13. What education material(s) should be included in the pre-dialysis education? (You may select one or more) Leaflet / Pamphlet Audio-visual tools such as videos or slide presentations Information about useful online websites or videos to refer at your own free time Hands-on session to show how each dialysis option works Other: ………………………...
14. How soon do you think CKD patients should start receiving pre-dialysis education prior to dialysis? 1 month before 2 months before 3 months before 5 months before 6 months before Not sure

95
HEALTH TECHNOLOGY ASSESSMENT REPORTMALAYSIAN HEALTH TECHNOLOGY ASSESSMENT SECTION (MaHTAS)
MEDICAL DEVELOPMENT DIVISION,MINISTRY OF HEALTH
15. How long should each pre-dialysis education session be?< 15 minutes15-30 minutes30-45 minutes45-60 minutes> 60 minutes
16. How frequent do you think pre-dialysis education should be given?Once a monthOnce every 2 monthsOnce every 3 monthsOnce every 6 monthsOnce a yearOther: ………………………...
17. Which of the venue below would be suitable for pre-dialysis education? (You may select one or more)
HospitalCommunity clinicOne-stop centreDialysis centreOther: ………………………...
18. Do you think it would be helpful to be part of a patient support group to discuss about solving problems faced in real life?
YesNoMaybe
19. Do you have any other comments/suggestions to improve pre-dialysis education?……………………….........................................................................................................................……………………………………………………………………………………....................……………………………………………………………………………………..
20. Following pre-dialysis education, do you think it is important that the doctor shares the decision-making about starting dialysis with the patient?
YesNoMaybe
That’s the end of our survey. Thank you for taking the time to complete this survey.
Your contribution is much appreciated!

96
PRE-DIALYSIS EDUCATION PROGRAMME
Appendix 7
SUGGESTIONS TO IMPROVE PRE-DIALYSIS EDUCATION PROGRAMME
1. Programme must be well-organised according to planned schedule and shouldac commodate the patient’s schedule so that the patient’s own time is not affected.
2. Emotional and spiritual information or support should be provided.3. Educators must be sensitive and provide more human touch to address patients’
needs and emotions as CKD patients may be fragile and depressed during the pre- dialysis stage.
4. Weekend sessions are preferred to minimise interference with daily work.5. Family members should attend pre-dialysis education session with patients toimprove
understanding of the disease and treatment. Family members are very important for patients throughout the CKD journey.
6. There should be consistent attendance from the same family member/partner or friend.7. Carers need to know how to help the patient make decisions.8. Education should be extended to carers as they should know about symptoms of kidney
failure.9. Education to carers should be provided.10. Educators must be qualified and knowledgeable to teach and answer questions correctly.11. Nurses must have sufficient experience before educating patients.12. Good communication between healthcare staff and patients especially before starting
each dialysis is important to ensure accuracy of information such as body weight, dry weight and dietary intake.
13. Prevention of CKD should be included in the module.14. There should be early education on disease progression and preventive measures to
avoid ESRD.15. Counselling by a psychologist can be given by appointment for patients who need it.16. Contents of the module should be comprehensive and include demonstration.17. Pre-dialysis education is very important as it can help patients feel more comfortable to
start dialysis.18. PDEP can be organised with any campaign in other clinics.


KEMENTERIAN KESIHATAN MALAYSIA
Malaysian Health Technology Assessment Section (MaHTAS)Medical Development Division, Ministry og Health Malaysia,
Level 4, Block E1, Complex E, Precint 1,Federal Goverment Administrative Centre
62590, Putrajaya, Malaysia.
Tel: 03-88831229
e ISBN 978-967-2887-12-6
9 7 8 9 6 7 2 8 8 7 1 2 6