2015 Sharp HealthCare Office Management Education Series
54
2015 Sharp HealthCare Office Management Education Series Final Steps to ICD‐10 Success Paul Belton, Vice President Corporate Compliance, Sharp HealthCare May 6, 2015 – Sharp Coronado Hospital May 7, 2015 – Sharp Chula Vista Medical Center May 29, 2015 – Sharp Metropolitan Medical Campus June 26, 2015 – Sharp Grossmont Hospital
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of 2015 Sharp HealthCare Office Management Education Series

2015Sharp HealthCare
Office Management Education SeriesFinal Steps to ICD‐10 Success
Paul Belton, Vice President Corporate Compliance, Sharp HealthCare
May 6, 2015 – Sharp Coronado HospitalMay 7, 2015 – Sharp Chula Vista Medical Center
May 29, 2015 – Sharp Metropolitan Medical CampusJune 26, 2015 – Sharp Grossmont Hospital

Last Call for ICD‐9‐CMFor October 1 signifies the end of an era; it is the effective date of the final ICD‐9‐CM update before ICD‐10‐CM/PCS codes kick in on October 1, 2015.
In 1979:In 1979:
TOP MOVIES INCLUDED: SUPERMAN THE MOVIE, THE DEER HUNTER, THE MUPPET MOVIE, ROCKY II
TOP MOVIES INCLUDED: SUPERMAN THE MOVIE, THE DEER HUNTER, THE MUPPET MOVIE, ROCKY II
MARGARET THATCHER WS ELECTED PRIME MINISTER IN THE UK
MARGARET THATCHER WS ELECTED PRIME MINISTER IN THE UK
THE BOARD GAM TRIVIIAL PURSUIT WAS LAUNCHEDTHE BOARD GAM TRIVIIAL PURSUIT WAS LAUNCHED
VISICALC BECAME THE FIRST SPREADSHEET PROGRAM
VISICALC BECAME THE FIRST SPREADSHEET PROGRAM POPULAR SONGS
INCLUDED: “MY SHARONA” BY THE KNACK; “HOT STUFF” AND “BAD GIRLS BY GLORIA GAYNOR; PINK FLOYD RELEASED “THE WALL”
POPULAR SONGS INCLUDED: “MY SHARONA” BY THE KNACK; “HOT STUFF” AND “BAD GIRLS BY GLORIA GAYNOR; PINK FLOYD RELEASED “THE WALL”
THE AVERAGE COST OF A NEW HOUSE WAS $58,000
THE AVERAGE COST OF A NEW HOUSE WAS $58,000
THE AVERAGE INCOME WAS $17,500
THE AVERAGE INCOME WAS $17,500
THE SONY WALKMAN DEBUTED, RETAILING FOR $200
THE SONY WALKMAN DEBUTED, RETAILING FOR $200
AVERAGE MONTHLY RENT WAS $280
AVERAGE MONTHLY RENT WAS $280
A GALLON OF GAS WAS 86 CENTS
A GALLON OF GAS WAS 86 CENTS
In 1979:
TOP MOVIES INCLUDED: SUPERMAN THE MOVIE, THE DEER HUNTER, THE MUPPET MOVIE, ROCKY II
MARGARET THATCHER WS ELECTED PRIME MINISTER IN THE UK
THE BOARD GAM TRIVIIAL PURSUIT WAS LAUNCHED
VISICALC BECAME THE FIRST SPREADSHEET PROGRAM POPULAR SONGS
INCLUDED: “MY SHARONA” BY THE KNACK; “HOT STUFF” AND “BAD GIRLS BY GLORIA GAYNOR; PINK FLOYD RELEASED “THE WALL”
THE AVERAGE COST OF A NEW HOUSE WAS $58,000
THE AVERAGE INCOME WAS $17,500
THE SONY WALKMAN DEBUTED, RETAILING FOR $200
AVERAGE MONTHLY RENT WAS $280
A GALLON OF GAS WAS 86 CENTS
“For those of us who have been maintaining or using ICD‐9‐CM since the code set’s implementation in 1979, this is a historic occasion.”“ICD‐9‐CM is down to its last five months. A reflective toast to ICD‐9‐CM.

3
Learning Objectives• Introduction to ICD-10
• Key Components & Challenges
• Importance & Benefits
• Impacts, Suggested Learning & Documentation Examples
• Implementation
• ICD-10 and CPT & Resources

4
Challenges of Physician/Clinician ICD-10 Education
• Specialties have different educational needs• All physician/clinicians need ICD-10 general awareness• Need to address diagnoses and inpatient procedures• Multiple coding concepts and principles: specificity, laterality,
contemporary language• Need to reach audience via multiple delivery options and multiple
viewings• Facilities need to educate on specific documentation review and
EHR template changes• Time constraints of physician/clinician audience

5
Training Solution
• Specialty programs separately address diagnoses and inpatient procedure changes
• Programs prepare physicians for facility documentation education and EHR modifications
• Focus on the impact of documentation• Programs are 15-30 minutes in length• 24/7 access via desktops, laptops, and mobile devices• Module programs can be assigned at staff level• Custom module options to support client specific content requirements

6
Key Components of General Training Module
• ICD-9 to ICD-10 Comparisons• New Concepts• Specificity• Laterality• Combination Codes• Seven Character Layout• Contemporary Language• Impact of Documentation

7
Reimbursement: Impact of Documentation Details
Adm for COPD exacerbation w/acute bronchitis. Stools occult + EGD confirms gastritis.• PDx: COPD exacerbation, Secondary Dx:
Gastritis w/+ occult– DRG 192 COPD w/o CC/MCC– LOS 2.9 r.w. 0.72220 = $3,690
• PDx: COPD exacerbation, Secondary Dx: GI Bleed
– DRG 191 COPD w/CC– LOS 3.6 r.w. 0.9735 = $4, 967
• PDx: COPD exacerbation, Secondary Dx: Gastritis w/GI bleed
– DRG 190 COPD w/MCC– LOS 4.3 r.w. 1.1924 = $6,188

8
Physician Profiling
• Some types are performance, economic, and disease management. Ideally, each Doctor would have an average cost per case of 1.0. The expected cost is the average cost per case for plan, age, sex, and severity-adjusted.
Z Score < 1.0 1.1 to 1.5 1.6 to 2.0 2.1 to 2.5Premium or Co-Pay
$100/Month$10
$150/Month$20
$200/Month$20
$250/Month$25

9
Contemporary Language: AsthmaICD-10-CM
Mild intermittent asthma• Uncomplicated• With exacerbation• With status asthmaticus
Mild persistent asthma• Uncomplicated• With exacerbation• With status asthmaticus
Moderate persistent asthma• Uncomplicated• With exacerbation• With status asthmaticus
Severe persistent asthma• Uncomplicated• With exacerbation• With status asthmaticus
ICD-9-CMExtrinsic with• Status Asthmatics• Exacerbation• Unspecified
Intrinsic with• Status Asthmatics• Exacerbation• Unspecified

10
Details for Injuries
ICD-10-CMS82.101C Initial encounter for open fracture type IIIA, upper end of right tibia
S82.101F Subsequent encounter with routine healingS82.101J Subsequent encounter with delayed healingS82.101N Subsequent encounter with nonunionS82.101R Subsequent encounter with malunionS82.101S Sequela
ICD-9-CM823.10 Open fracture, tibia, upper end
ICD-10 use Gustilo classification for open fractures.

11
Major Changes
Major changes for cardiology diagnosis documentation needed for ICD-10-CM:• Hypertension
– Document as underlying cause of cardiac disease– Document the type of angina
• Acute Myocardial Infarction– Documentation of timeframe needed– Documentation of the coronary artery involved needed

12
Major Changes
Major changes for cardiology diagnosis documentation needed for ICD-10-CM:• Congestive Heart Failure
– Documentation of type of congestive heart failure needed
• Cardiac Complications– More specificity needed to capture details of complications

13
Estimated Targeting eLearning
Specialty Number of Diagnosis/Estimated Minutes
Internal Medicine 30/150
Family Practice 60/300
Pediatrics 35/175
Cardiology 19/95
Dermatology 17/85
Emergency 52/260
Gastroenterology 18/90
Hematology/Oncology 35/175
Hospice 31/155
Infectious Disease 18/90
Nephrology 15/75
Specialty Number of Diagnosis/Estimated Minutes
Neurology 17/85
Psychiatry 15/75
Pulmonary 19/95
ENT 13/65
Gen Surgery 19/95
Urology 17/85
Ortho: Spine 15/75
Ortho: Sports 16/80
Ortho: Hand 12/60
Ortho: Foot/Ankle 10/50
OB 13/75
GYN 19/95

14
Suggested Learning Process Rollout
PHASE 1 PHASE 2
• All skills available on web-enabled devices!
* Rollout additional Relevant skills* Utilize Mobile App Library*Keep Primary/Secondary Skills Available
• Top 10 Primary Diagnoses• Top 5 Secondary Diagnoses• By Specialty, By Provider

15
Acute Bronchitis and Bronchiolitis
Acute Bronchitis and Bronchiolitis
J20.1 Acute bronchitis due to hemophilus influenza J20.5 Acute bronchitis due to respiratory syncytial virus J21.0 Acute bronchiolitis due to respirator syncytial virus J21.1 Acute bronchiolitis due to human metapneumovirus
Below are a few example ICD-10 codes selected to help display how the clinical features of this condition align with the documentation requirements of ICD-10.
Example of ICD-10 Codes
Introduction Documentation Codes Relevant Data Example Quiz, Codes, Results

16
ICD-10-CM Impacts
• ICD-10-CM is not just a new code set that will affect how we bill for our services. It is a new patient and disease classification system that will be used throughout our practices.
• ICD-10-cm ushers in significant opportunities for us to improve how we provide and track the care we give to our patients each day.
• Lets take a close look at each of these impacted areas and discuss opportunities to mitigate risks in each situation.
1. Internal Systems2. Internal Process3. Policies4. Reimbursement5. Documentation6. Staff Education

17
Internal Systems
• Translate paper-based charting to ICD-10-CM codes (e.g., encounter forms/superbills).
• Review contracts with all software vendors.
• Ask about system updates, timelines, and associated costs.
• Ask venders about ICD-10-CM testing plans (e.g., when will it start and how long will it take).
• Inquire about backup plans if the vendor is not ready to accommodate ICD-10-CM codes.
Consider these important implementation tips to assist in the ICD-10-CM transition:

18
Internal Processes
Internal processes, such as insurance verification, preauthorization, ordering of labs/pathology, and report generation, will require familiarity with ICD-10-CM.
These systems currently rely on ICD-9-CM codes and will need to be updated for ICD-10-CM.
ExampleA patient needs to be scheduled for surgery occurring after the ICD-10-CM effective date. During the preauthorization process, the insurance company asks for the medical diagnosis code and description necessitating the procedure.
Translation of commonly used ICD-9-CM codes to ICD-10-CM codes will enable office staff to communicate effectively with insurance companies.

19
Internal Processes
Consider these important implementation tips to assist in the ICD-10-CM transition:
• Recruit physicians within the practice to review ICD-9-CM to ICD-10-CM translations to ensure they are clinically correct
• Familiarize staff performing insurance verification and preauthorization with commonly used ICD-10-CM codes and their descriptions.
• Update lab and pathology order forms/systems with ICD-10-CM codes
• Evaluate all internal reports generated with ICD-9-CM codes and update these with ICD-10-CM codes

20
• Familiarize physicians and other clinical staff with increased granularity required documentation for the most commonly used diagnoses in the practice.
• Audit current and post go-live documentation for gaps in the required ICD-10-CM specificity
• Implement newly identified documentation requirements prior to the transition to help decrease time spent requesting additional information
• Plan for decreased office productivity in the first year following ICD-10-CM implementation as all staff becomes accustomed to using this new code set.
ICD-10-CM and Documentation
Consider these important implementation tips to assist in the ICD-10-CM transition:

21
Although the current diagnostic coding system (ICD-9-CM) is changing with ICD-10-CM, the procedural coding system in the outpatient and ambulatory settings is not. CPT remains the system we will use for coding and our procedures, tests, and other medical services.
However, CPT is affected in that our diagnostic documentation and coding in ICD-10-CM must prove medical necessity for our CPT codes and show the severity of our patient’s illnesses.
In this way, ICD-10-CM and CPT have a critical symbiotic relationship.
ICD-10-CM and CPT

22
When submitting a claim to a payer, each CPT code must have a corresponding diagnosis code; it provides the reason for the procedure. If a diagnosis code does not effectively illustrate a patient’s medical condition, it can be difficult to justify the medical necessity for the services we provide. ICD-10-CM, with its greater number of granular codes, provides us the ability to do this more effectively, but also creates more scrutiny if we do not use the codes.
Let’s consider the following patient scenario. Although this scenario is not typical for all specialties, it is used to illustrate how ICD-10-CM will enhance our CPT Coding.
ICD-10-CM and CPT

23
A 56 year old with a history of H. pylori and peptic ulcer five years ago presents with complaints of burning in her stomach and lack of appetite due to nausea. She take famotidine daily as prescribed by her physician five years ago. This is the first time she is seeking evaluation and treatment for this problem with your practice.
She indicates the pain occurs between meals and resolves after eating, but she is finding it hard to eat due to nausea. She states the famotidine no longer helps with her symptoms. She has been taking non-steroidal and anti-inflammatory drugs (NSAIDs) twice daily for the past month as prescribed by her family physician for osteoarthritic joint pain in her left knee.
Your plan is to perform an upper GI endoscopy since patient’s last endoscopy was five years ago, she appears to have an adverse reaction to NSAIDs, and she is a new patient with your practice.
Example of CPT and ICD-10
GI report: acute peptic ulcer, no hemorrhage noted.
ICD-10-CM and CPT

24
Here is a comparison of inappropriate and appropriate coding in ICD-10-CM, utilizing the granularity and additional codes available to us.
ICD-10-CM and CPT
Inappropriate Coding Assignment Appropriate Coding Assignment
ICD-10 ICD-10R11.0 Nausea K27.3 Acute peptic ulcer; site unspecified,
without hemorrhage or perforation
CPT R110 Nausea
43235 Upper gastrointestinal endoscopy including esophagus, stomach, and either the duodenum and/or jejunum as appropriate; diagnostic, with or without collection of specimen(s) by brushing or washing (separate procedure)
T39.395A Adverse effect of other NSAID, initial encounter
CPT 43235 Upper gastrointestinal endoscopy
including esophagus, stomach, and either the duodenum and/or jejunum as appropriate; diagnostic, with or without collection of specimen(s) by brushing or washing (separate procedure)
BILL FOR SERVICESBILL FOR SERVICES

25
ICD-10 will impact every service we provide: from the reception desk to the exam or procedure room through the billing process. Educating ourselves and our staff ensures we are prepared to capitalize on all ICD-10 has to offer.
Underestimating the impact of ICD-10 could result in decreased productivity for both clinicians and office staff, an increased number of claims denials, requests for additional documentation, and significant financial risk.
ICD-10-CM and CPT

26
In this course, we will learn how ICD-10-CM can help us better describe diseases and injuries and more
accurately identify trends for tracking and research.
We will also examine the granularity of ICD-10-CM code descriptions and how they will enable us to
illustrate effectively the complete clinical pictures of our patients and offer consistent standards for billing
and payments.
Introduction to ICD-10

27
The coding system we use today, ICD-9-CM was developed over 30 years ago and does not reflect the advances in medical care since that time.
• ICD-9-CM codes are imprecise; this makes it difficult to capture the data needed for quality reporting, medical research, and reporting of public health issues.
• ICD-9-CM is not specific enough to justify the medical necessity of the services we provide; this negatively affects our ability to receive optimal reimbursement.
Why change to ICD-10 Now?

28
The Benefits of ICD-10-CMQuality
MeasurementPublicHealth
Research Reimbursement Severity of Illness
Analysis of the quality of the care we provide will be more complete due to the up-to-date clinical descriptions in ICD-10-CM.
Granularity in ICD-10-CM allows for better capture of emerging and reportable diseases, and the tracking of these diseases throughout the U.S. and internationally.
Improvement in the classification of diseases in ICD-10-CM and correlation with causes, treatments, and outcomes results in better data capture for research and collaboration with our colleagues.
ICD-10-CMprovides better descriptions of our patients’ conditions, making it easier to justify the medical necessity of the services we provide.
Detailed disease descriptions in ICD-10-CM enable us to illustrate effectively the complete clinical pictures of our patients.

29
CPT codes require a corresponding diagnosis code, which provides the reason for the visit or procedure. Granularity in ICD-10-CM allows us to communicate the reason for the patient’s visit and the services provided more effectively with payers.
Justifying the medical necessity of our procedure coding with specific documentation to support ICD-10-CM coding will assist in ensuring we receive appropriate reimbursement for our services.
ICD-10-CM and CPT
ICD-10-CM CPT

30
Documentation and ICD-10-CMICD-10-CM was designed with the idea that healthcare delivery is not static, but constantly changing. To reflect the advances in disease identification and care delivery. ICD-10 has far greater specificity in its code descriptions. Look at these examples below where current documentation will lack the ability to accurately reflect our patient’s severity of illness in the world of ICD-10.
Today The World of ICD-10Diabetes E11.621
(Type II diabetes mellitus with foot ulcer)
COPD J44.1 (Chronic obstructive pulmonary disease with (acute) exacerbation)
Anemia D52.1 (Drug-induced folate deficiency anemia)

31
Documentation and ICD-10-CM
It is critical that we understand the greater level of specificity require in our documentation in order to be successful in ICD-10-CM.
Proper documentation will assist in ensuring appropriate payment, decreasing requests for additional records, and supporting quality record reporting
Here are some impacts on documentation for ICD-10-CM
Key documentation Impacts for ICD-10-CM
• Anatomical Site• Laterality• Acuity• Gender• Encounter Type• Trimester• Severity• Fetus Identification in Multiple Gestations• Fracture Type• Healing Status• Wound Type• Alcohol/Drug/Tobacco Use and Exposure
32
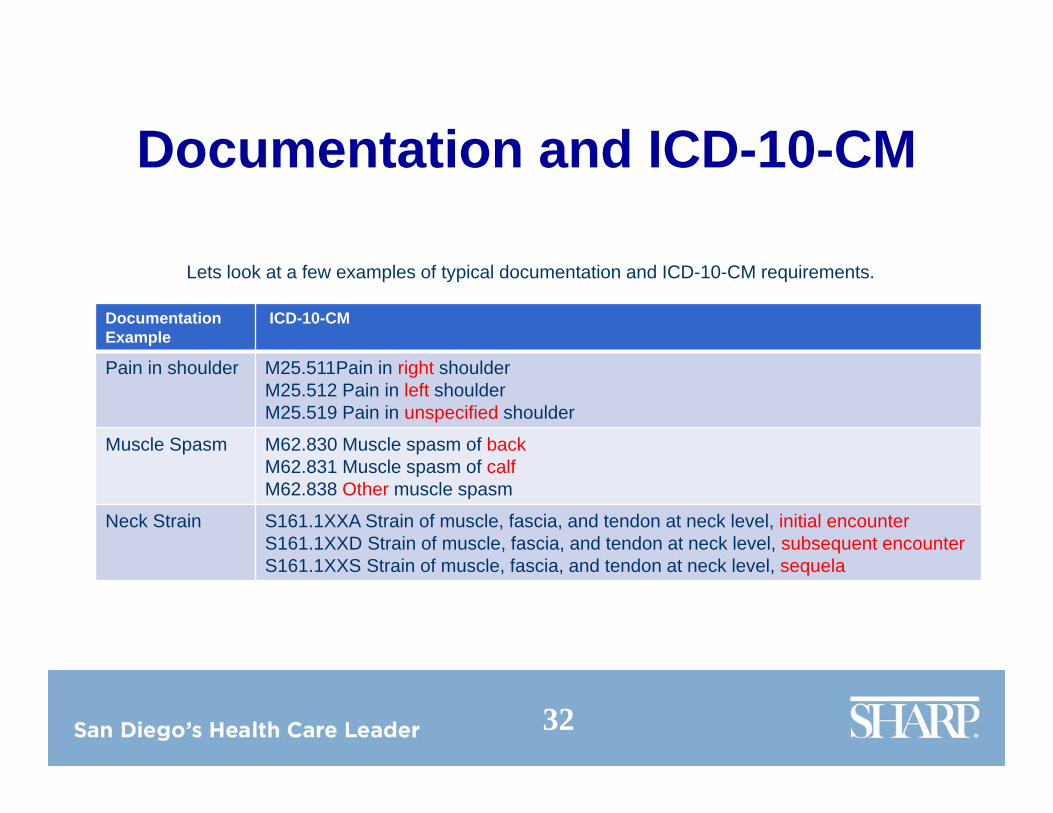
Documentation and ICD-10-CM
Lets look at a few examples of typical documentation and ICD-10-CM requirements.
DocumentationExample
ICD-10-CM
Pain in shoulder M25.511Pain in right shoulderM25.512 Pain in left shoulderM25.519 Pain in unspecified shoulder
Muscle Spasm M62.830 Muscle spasm of backM62.831 Muscle spasm of calfM62.838 Other muscle spasm
Neck Strain S161.1XXA Strain of muscle, fascia, and tendon at neck level, initial encounterS161.1XXD Strain of muscle, fascia, and tendon at neck level, subsequent encounterS161.1XXS Strain of muscle, fascia, and tendon at neck level, sequela

33
E/M CODES AND ICD-10
ICD-10-CM diagnosis codes gives us more opportunities to justify appropriate E/M code levels based on the complexity of our patients. We will be able to more accurately communicate acuity, severity, and duration of illness to payers through our diagnosis coding.
Coding Impacts in ICD-10
ICD-10 diagnosis codes are much more accurate when describing the clinical presentations of our patients. Using this new code set effectively has
the potential to decrease queries from auditors.

34
A 40 year old patient is referred to your practice due to persistent aggravating respiratory symptoms following repeated treatments with prednisone and antibiotics. A comprehensive history indicates she has rheumatoid arthritis (RA) in her hands, hips and knees. She is currently managing her RA with Enbrel. She also has type 1 diabetes mellitus (DM), well managed with insulin.
A comprehensive physical exam exhibits dry, crackling breath sounds bilaterally. A chest x-ray confirms interstitial lung disease associated with RA.
Example of E/M Codes
Diagnosis entered into chart: Interstitial lung disease.
E/M Codes

35
Correct ICD-10 code identification is very important in E/M coding as it helps validate the level of medical decision making.
E/M CodesInappropriate Coding Assignment Appropriate Coding Assignment
ICD-10 ICD-10J84.9 Interstitial pulmonary disease,
unspecifiedK27.3 Interstitial pulmonary disease,
unspecified
CPT M05.19 Rheumatoid lung disease with rheumatoid arthritis of multiple sites
99203 Office visit for E/M of a new patient. Requires a detailed exam, and medical decision making of low complexity.
E10.9 Type 1 diabetes mellitus without complications
Z79.4 Long term (current) use of insulin
CPT 99204 Office visit for E/M of a new patient.
Requires a comprehensive history, a comprehensive exam, and medical decision making of moderate complexity
BILL FOR SERVICESBILL FOR SERVICES

36
Asthma
ICD-9 ICD-1014 Number of codes: 18
Codes are indexed by type of asthma (extrinsic vs. intrinsic)
Disease Indexing
Codes are indexed by severity of asthma and status of Indexing exacerbations.
493.00
493.01
493.02
Extrinsic asthma, unspecified
Extrinsic asthma, with status asthmaticus
Extrinsic asthma, with (acute) exacerbation
ExampleCodeChoices
J45.20 Mild intermittent, asthma uncomplicated
J45.21 Mild intermittent asthma with (acute) exacerbation
J45.22 Mild intermittent asthma with status asthmaticus
In ICD-10, we will code asthma by severity. This will better represent the condition based on standard classifications.
ICD-9 vs. ICD-10 Coding

37
Primary Malignancy of Bronchus and Lung
ICD-9 ICD-106 Number of codes: 5
Codes are indexed by anatomical site. Disease Indexing
Codes are indexed by anatomical site and laterality.
162.2
162.5
162.8
Malignant neoplasm of main bronchus
Malignant neoplasm of lower lobe, bronchus of lung
Malignant neoplasm of other parts of bronchus or lung
ExampleCodeChoices
C34.02 Malignant neoplasm of left main bronchus
C34.31 Malignant neoplasm of lower lobe, right bronchus, or lung
J45.22 Malignant neoplasm of overlapping sites of right bronchus and lung
In ICD-10, the addition of laterality when coding lung cancer will help to support disease tracking and monitoring of treatment interventions.
ICD-9 vs. ICD-10 Coding

38
Acute and Chronic Bronchitis
ICD-9 ICD-103 Number of codes: 15
Acute bronchitis is indexed by acuity. Chronic Bronchitis is indexed by type.
Disease Indexing
Acute bronchitis is indexed by acuity and causal organism. Chronic bronchitis is indexed by type.
466.0
491.0
491.1
Acute bronchitis
Simple chronic bronchitis
Mucopurulent Chronic bronchitis
ExampleCodeChoices
J20.1 Acute bronchitis due to Hemophilus influenzae
J41.1 Mucopurulent chronic bronchitis
J41.8 Mixed simple and mucopurulent chronic bronchitis
In ICD-10, gives us the ability to communicate severity of illness more effectively. This will help expedite pre-authorization for the treatments we provide.
ICD-9 vs. ICD-10 Coding

39
What Physicians need to Know
• ICD-10 will have a direct impact on physicians through:– Physician quality profiles – mortality and morbidity– Physician utilization profiles – efficiency of treating
patients– Physicians’ current and future evaluation and
management levels, including pay for performance– Daily workflow – (if ICD-10 is not properly implemented)
Documentation must be specific, detailed, complete!

40
ICD-10 Benefits for Physicians
• What is the return on investment (ROI) for the physicians?– Accurate payment for new procedures
– physicians are projected to save $100M - $1.2 Billion with a decade of ICD-10 implementation
– Fewer rejected claims – ICD-10 is more detailed and organized than ICD-9
– Better claims adjudication and faster approvals – a reduced claims cycle will lower administrative costs for physicians

41
ICD-10 Benefits for Physicians
• ICD-10 offers a more decisive system to determine payments by offering:– Greater detail on the quality of care provided
• Government payers, insurers, hospitals, health systems, medical groups and others will use ICD-10’s granular data to determine:– Accurate and fair physician compensation– Reimbursement for goods and services
• Under government’s Value-Based Purchasing Program, physicians do not provide precise documentation such as:– Laterality– Specificity– Anatomic sitewill experience reduced payments

42
ICD-10 Benefits for Physicians
• Improved physician documentation will lead to:– Physician profiling/National Registries –
profiling is occurring more frequently with a concentrated move towards transparency
– Quality reporting – CMS has implemented the physician compare website (provides public quality of care information 1/1/14) and PQRS mandated through federal legislation incentivizes MD’s to report quality information

43
Implementation Plan by Specialty
– Provide physician ICD-10 training for Medicare Part A and Part B and include physician office staff
– Customize physician education by specialty and include specific coding guidelines and clinical examples
– Recommend training modalities(instructor led, on-line, blended)
Customize Physician Training Materials

44
Implementation Plan
Prepare Physician Champions to present ICD-10 training materials
Determine styles of learning Provide Train-the-Trainer materials
Leader
Role Model
Advisor
Mentor
Coach
Conduct Train-the-Trainer Sessions

45
Implementation Plan
Roll Out ICD-10 Training
Schedule sessions between now and go-live date
Begin with small doses of information Provide quick reference materials

46
Physician Education
• Conduct Physician education on new documentation requirement for ICD-10 to support:– Coding and DRG Assignment– Medical Necessity– Reduced Future Denials

47
Claims Denials
• Physician and hospitals are at risk for significant increase in denials
• These denials may occur due to:– Changes in remediation of medical policies– Refinements in processing rules based on increased granularity
of the ICD-10 codes– Misinterpretation of the intent of the policies or rules– Errors of translation of ICD-9 to ICD-10 codes– Misinterpretation of the intent of the policies or rules– Errors of translation of ICD-9 to ICD-10 Codes

48
Potential Reimbursement Impacts
• Reimbursement is dependent upon conditions and procedures documented by physicians and what is coded on the claim
• Complex ICD-10 Mappings reinforce the need for ICD-10 Clinical Specialists to customize mapping and maximize payment accuracy

49
Career Step’s Training Solution
• Specialty programs separately address diagnoses and inpatient procedure changes
• Programs prepare physicians for facility documentation education and EHR modifications
• Focus on the impact of documentation• Programs are 15-30 minutes in length• 24/7 access via desktops, laptops, and mobile devices• Module programs can be assigned at staff level• Custom module options to support client specific content requirements

50
Key Components of General Training Module
• ICD-9 to ICD-10 COMPARISONS• NEW CONCEPTS• SPECIFICITY• LATERALITY• COMBINATIONS CODES• SEVEN CHARACTER LAYOUT• CONTEMPORARY LANGUAGE• IMPACT OF DOCUMENTATION

51
Reimbursement: Impact of Documentation Details• Adm for COPD exacerbation w/acute bronchitis. Stools occult +, EGD
confirms gastritis.• PDx: COPD exacerbation, Secondary Dx: Gastritis w/+ occult
• DRG 192 COPD w/o CC/MCC• LOS 2.9 r.w. 0.72220 = $3,690
• PDx: COPD exacerbation, Secondary Dx: GI Bleed• DRG 191 COPD w/CC• LOS 3.6 r.w. 0.9735 = $4,967
• PDx: COPD exacerbation, Secondary Dx: Gastritis w/GI bleed• DRG 190 COPD w/MCC• LOS 4.3. r.w. 1.1924 = $6,188

52
ICD-10 Resources
52

53
Available resources and use them appropriately:
AHIMA Preparation Checklistwww.ahima.org/downloads/pdfs/resources/checklist.pdf
AHIMA Top Tenhttp://library.ahima.org/xpedio/groups/public/documents/ahima/bok1048748.pdf
AHIMA (American Health Information Management Association) ICD-10 Implementation Sitehttp://www.ahima.org/icd10/
American Academy of Professional Coders (AAPC) ICD-10 Implementation Sitehttp://www.aapc.com/icd-10/index.aspx
ICD-10 CM Resources

54
Center for Medicare and Medicaid Services (CMS)
CMS ICD-10 https://www.cms.gov/ICD10/CMS Medicare Fee-for-Service Provider Resources
https://www.cms.gov/ICD10/06_MedicareFeeforServiceProviderResources.asp#TopOfPage
2013 ICD-10-CM Official Coding Guidelines
http://www.cdc.gov/nchs/data/icd10/10cmguidelines2013final.pdf