00-0Content CNS&ND-DT 19-10
9
CNS & Neurological Disorders - Drug Targets Send Orders for Reprints to [email protected] CNS & Neurological Disorders - Drug Targets, 2020, 19, 741-749 741 REVIEW ARTICLE A Novel Approach to Refractory Epilepsy by Targeting Pgp Peripherally and Centrally: Therapeutic Targets and Future Perspectives Urvashi Langeh 1 , Pooja Chawla 2 , Ghanshyam Das Gupta 3 and Shamsher Singh 4,* 1 Research Scholar, Department of Pharmacology, ISF College of Pharmacy, Moga, Punjab-142001, India; 2 Depart- ment of Pharmaceutical Chemistry, ISF College of Pharmacy, Moga, Punjab-142001, India; 3 Department of Pharma- ceutics, ISF College of Pharmacy, Moga, Punjab-142001, India; 4 Neuroscience Division, Department of Pharmacolo- gy, ISF College of Pharmacy, Moga, Punjab-142001, India ARTICLE HISTORY Received: February 10, 2020 Revised: June 19, 2020 Accepted: June 30, 2020 DOI: 10.2174/1871527319999200819093109 Abstract: Refractory epilepsy is a type of epilepsy involving seizures uncontrolled by first or se- cond-line anticonvulsant drugs at a regular therapeutic dose. Despite considerable growth in epilep- tic pharmacotherapy, one-third of the patients are resistant to current therapies. In this, the mech- anisms responsible for resistant epilepsy are either increased expulsion of antiepileptic drugs (AED- s) by multidrug resistance (MDR) transporters from the epileptogenic tissue or reduced sensitivity of drug in epileptogenic brain tissue. The difficulty to treat refractory epilepsy is because of drug re- sistance due to cellular drug efflux, use of drug monotherapy, and subtherapeutic dose administra- tion. Increased expression of Pgp is also responsible for resistance epilepsy or refractory epilepsy. Increased glutamate expression via inhibition of cyclooxygenase-II (COX-II) enzyme also upregu- late P-glycoprotein (Pgp) expression and augment instance of recurrent seizures. Peripheral and central inhibition of Pgp is a powerful tool to control this drug resistant epilepsy. Drug resistance primarily involves multidrug resistance (MDR1) gene responsible for encoding P-glycoprotein (Pg- P1 or MDR1). Currently, there is no drug under clinical practice which inhibits MDR1. The pre- sent review cites some drugs like Calcium Channel Blockers (CCBs), COX-II inhibitors, and gluta- mate receptors antagonists that inhibit P-gp. The exploitation of these targets may emerge as a bene- ficial approach for patients with drug-resistant epilepsy. The present review further highlights the mechanistic role of Pgp in drug-resistant epilepsy, glutamate role in drug efflux, and management approach. Keywords: Refractory epilepsy, pharmacotherapy, drug resistance, resistance epilepsy, epileptogenic brain, P-glycoprotein. 1. INTRODUCTION Epilepsy is the oldest disorder described firstly by Hip- pocrates in the 5th century BC as an unwalkable disease [1]. Epilepsy is the disorder of the Central Nervous System (CN- S) characterized by recurrent spontaneous seizures due to hy- perexcitability and hypersynchrony of cortical neurons and other subcortical regions of the brain [2]. At present, there are over 70 million people worldwide suffering from active epilepsy with ongoing seizures that require treatment, and 30% of patients are suffering from refractory epilepsy also called Drug-Resistant Epilepsy (DRE) [3]. DRE may be a growing multifaceted condition with risks of brain structural damage and associated with cognitive decline, psychosocial dysfunction, co-morbidities like osteoporosis, fractures and raised incidences of death from suicide, accidents, pneumo- nia, and sudden unexpected death, etc [4, 5]. Over 70 mil- lion people around the world are affected with epilepsy cur- rently, while nearly 70-80% of new-onset epilepsy patients * Address correspondence to this author at the Neuroscience Division, De- partment of Pharmacology, ISF College of Pharmacy, Moga, Punjab, India -142001; Tel: +91-9779980588; E-mail: [email protected] could be partly cured and ultimately reach a comparatively better situation during management [6]. Every year in the de- veloped countries, around 40-70 number of new cases are re- ported per 100,000 persons in the general population acquir- ing epilepsy. Currently, common epilepsy treatment in- cludes drugs like phenytoin and carbamazepine. The re- search and development for effective antiepileptic drugs is still a critical concern [7]. In India, more than 10 million peo- ples are suffering from epilepsy, and out of this 56.3% are having chronic refractory epilepsy [8]. The majority of cases with epilepsy are successfully managed with AEDs, but out of which 20-30% of epileptic patients are pharmacoresistant [9]. The epileptogenesis is a highly dynamic alteration from the normal state to reduced neuronal threshold for seizures or generation of spontaneous seizures [10]. Long term epilep- togenic seizure at the latter phase can develop to frequent spontaneous seizures that affect one hemisphere and treat- ment of refractory epilepsy consists of the epileptogenic zone [11, 12]. Further, epileptogenesis is a chronic process that gradually changes the excitability of neurons, establish- es significant interconnections, and possibly requires com- plex structural alterations before the primary occurrence of 1996-3181/20 $65.00+.00 © 2020 Bentham Science Publishers
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of 00-0Content CNS&ND-DT 19-10

C
NS
& N
euro
logi
cal D
isor
ders
- D
rug
Targ
ets
��� ��:<=:�>6=?���� ��:;;@�?:<:
������������
�� ���������������
Send Orders for Reprints to [email protected]
CNS & Neurological Disorders - Drug Targets, 2020, 19, 741-749
741
REVIEW ARTICLE
A Novel Approach to Refractory Epilepsy by Targeting Pgp Peripherallyand Centrally: Therapeutic Targets and Future Perspectives
Urvashi Langeh1, Pooja Chawla2, Ghanshyam Das Gupta3 and Shamsher Singh4,*
1Research Scholar, Department of Pharmacology, ISF College of Pharmacy, Moga, Punjab-142001, India; 2Depart-ment of Pharmaceutical Chemistry, ISF College of Pharmacy, Moga, Punjab-142001, India; 3Department of Pharma-ceutics, ISF College of Pharmacy, Moga, Punjab-142001, India; 4Neuroscience Division, Department of Pharmacolo-gy, ISF College of Pharmacy, Moga, Punjab-142001, India
A R T I C L E H I S T O R Y
Received: February 10, 2020Revised: June 19, 2020Accepted: June 30, 2020
DOI:10.2174/1871527319999200819093109
Abstract: Refractory epilepsy is a type of epilepsy involving seizures uncontrolled by first or se-cond-line anticonvulsant drugs at a regular therapeutic dose. Despite considerable growth in epilep-tic pharmacotherapy, one-third of the patients are resistant to current therapies. In this, the mech-anisms responsible for resistant epilepsy are either increased expulsion of antiepileptic drugs (AED-s) by multidrug resistance (MDR) transporters from the epileptogenic tissue or reduced sensitivityof drug in epileptogenic brain tissue. The difficulty to treat refractory epilepsy is because of drug re-sistance due to cellular drug efflux, use of drug monotherapy, and subtherapeutic dose administra-tion. Increased expression of Pgp is also responsible for resistance epilepsy or refractory epilepsy.Increased glutamate expression via inhibition of cyclooxygenase-II (COX-II) enzyme also upregu-late P-glycoprotein (Pgp) expression and augment instance of recurrent seizures. Peripheral andcentral inhibition of Pgp is a powerful tool to control this drug resistant epilepsy. Drug resistanceprimarily involves multidrug resistance (MDR1) gene responsible for encoding P-glycoprotein (Pg-P1 or MDR1). Currently, there is no drug under clinical practice which inhibits MDR1. The pre-sent review cites some drugs like Calcium Channel Blockers (CCBs), COX-II inhibitors, and gluta-mate receptors antagonists that inhibit P-gp. The exploitation of these targets may emerge as a bene-ficial approach for patients with drug-resistant epilepsy. The present review further highlights themechanistic role of Pgp in drug-resistant epilepsy, glutamate role in drug efflux, and managementapproach.
Keywords: Refractory epilepsy, pharmacotherapy, drug resistance, resistance epilepsy, epileptogenic brain, P-glycoprotein.
1. INTRODUCTIONEpilepsy is the oldest disorder described firstly by Hip-
pocrates in the 5th century BC as an unwalkable disease [1].Epilepsy is the disorder of the Central Nervous System (CN-S) characterized by recurrent spontaneous seizures due to hy-perexcitability and hypersynchrony of cortical neurons andother subcortical regions of the brain [2]. At present, thereare over 70 million people worldwide suffering from activeepilepsy with ongoing seizures that require treatment, and30% of patients are suffering from refractory epilepsy alsocalled Drug-Resistant Epilepsy (DRE) [3]. DRE may be agrowing multifaceted condition with risks of brain structuraldamage and associated with cognitive decline, psychosocialdysfunction, co-morbidities like osteoporosis, fractures andraised incidences of death from suicide, accidents, pneumo-nia, and sudden unexpected death, etc [4, 5]. Over 70 mil-lion people around the world are affected with epilepsy cur-rently, while nearly 70-80% of new-onset epilepsy patients
* Address correspondence to this author at the Neuroscience Division, De-partment of Pharmacology, ISF College of Pharmacy, Moga, Punjab, India-142001; Tel: +91-9779980588; E-mail: [email protected]
could be partly cured and ultimately reach a comparativelybetter situation during management [6]. Every year in the de-veloped countries, around 40-70 number of new cases are re-ported per 100,000 persons in the general population acquir-ing epilepsy. Currently, common epilepsy treatment in-cludes drugs like phenytoin and carbamazepine. The re-search and development for effective antiepileptic drugs isstill a critical concern [7]. In India, more than 10 million peo-ples are suffering from epilepsy, and out of this 56.3% arehaving chronic refractory epilepsy [8]. The majority of caseswith epilepsy are successfully managed with AEDs, but outof which 20-30% of epileptic patients are pharmacoresistant[9].
The epileptogenesis is a highly dynamic alteration fromthe normal state to reduced neuronal threshold for seizuresor generation of spontaneous seizures [10]. Long term epilep-togenic seizure at the latter phase can develop to frequentspontaneous seizures that affect one hemisphere and treat-ment of refractory epilepsy consists of the epileptogeniczone [11, 12]. Further, epileptogenesis is a chronic processthat gradually changes the excitability of neurons, establish-es significant interconnections, and possibly requires com-plex structural alterations before the primary occurrence of
1996-3181/20 $65.00+.00 © 2020 Bentham Science Publishers

742 CNS & Neurological Disorders - Drug Targets, 2020, Vol. 19, No. 10 Langeh et al.
spontaneous seizure [13]. The complex structural changesare neuronal loss, reduced neuronal regeneration, alterationin the plasticity of dendrites, chemotaxis of inflammatorymediators, and extracellular matrix reconstitution. Recently,the desirable therapeutic approach for refractory epilepsy in-cluded immunosuppressant, leucocytes to endothelial cellsbond blocking by using antibodies, expression of neurotroph-ic factors driven by gene therapy, pharmacological neurosti-mulation, or the use of common antiepileptic drugs, but it isstrenuous to manage [14].
However, despite increased development and utilizationof approved antiepileptic drugs over the last 25 years, ap-proximately one-third of the patients are epileptic and unma-nageable [15]. Although there is wide progress in the re-search of epilepsy, still antiepileptic medications show vari-ous limitations [16]. The refractory epilepsy incidence isstill high despite the availability of various AEDs over thelast 10 years. Refractory epileptic patients do not share simi-lar drug treatment resistance mechanisms. To overcome this,targeted drug therapy must be used that might be a better op-tion to improve treatment-related outcomes. In this review,we focused on one targeted pharmacoresistant mechanism ofrefractory epilepsy mediated by efflux transporter P-gp [17].
2. REFRACTORY EPILEPSY: DRUG RESISTANTEPILEPSY
The most common symptoms of epilepsy are seizuresmainly characterized by uncontrolled electrical activity,which leads to minor physiological signs like convulsion,thought conflictions, physiological signs, etc [18]. Around30 to 40% of people with epilepsy have uncontrolledseizures by the first or second line of anticonvulsant treat-ment at the regular therapeutic dose and are thus consideredas refractory epilepsy. Many different terms used for refrac-tory epilepsy are drug-resistant, treatment non-responders,as well as intractable [19]. Refractory epilepsy is related tothe elevated level of morbidness, death, psychosocial disabil-ity, mental problems, including decreased social interactionwith reduced marriage rates and reduced quality of life [20].
International League Against Epilepsy (ILAE), definedepilepsy as brief signs and symptoms that occurred due to ex-cessive abnormal brain neuronal activity and at least two un-provoked seizures happening >24 h distantly [21]. Epilepticpatients are considered as sufferers of refractory epilepsy ifseizures continue to persist, despite the appropriate use oftwo anti-seizure drugs alone or in combination. In this condi-tion, patients will be first referred to multidisciplinary epilep-sy centers where they perform specialized diagnostic tests todetermine whether they are pharmacoresistant and further, ifso, providing alternative treatments [22]. Various treatmentsare available for epilepsy as phenytoin, carbamazepine, sodi-um valproate, etc, which inhibit the neuronal excitability byblocking the GABAergic system (benzodiazepine, barbitu-rates, vigabatrin, and tiagabine) or by blocking sodium chan-nels (phenytoin, lamotrigine, and carbamazepine) [23]. Be-sides the number of unsuccessful AEDs, the reliable refracto-
ry epilepsy predictors have increased frequency of seizuresin the early disease phase, a neurological insufficiency dur-ing the initiation of disease, and structural damage as mani-fested by MRI. Though uncontrollable epilepsy is not at alltimes considered to be drug-resistant and pseudoresistant be-cause of incorrect identification, unsuitable AED or unsuit-able dosage must be lined out before classifying a patient’sseizures as refractory or drug-resistant [4]. A study per-formed in Finland enrolled 144 patients suffering from child-hood epilepsy, followed from the diagnosis time for an aver-age of 37 years. In this, 16% of patients were instantaneous-ly free from seizure and 19% were resistant to treatmentwithout remission and the remaining patients had a non-fre-quent seizure for a short time [24].
3. MECHANISM OF PHARMACORESISTANCE INEPILEPSY
There is growing evidence that drug-resistant epilepsyowes its origin to more than one reason and thus is consid-ered multifactorial, a claim which is also supported by exam-ination of patients who have undergone epilepsy surgery. Re-sistance to drugs might be explained as a failure on the partof AEDs to reach molecular targets [25]. The current hypoth-esis states that the efflux of AEDs plays a significant role inrefractory epilepsy by decreasing therapeutic concentrationat the site of action [26].
The transporter hypothesis recommends that overexpres-sion of efflux transporters Pgp at the BBB confines AED’sbrain penetration. These ATP dependent transporters (Pgp)are found at the endothelial cells apical cell membrane andprevent lipophilic drug penetration into brain parenchyma.On the other hand, it is surprising that various AEDs that aremade lipophilic for better brain penetration appear to be tar-geted by BBB multidrug efflux transporters [27]. Moreover,other mechanisms of refractory epilepsy are also reported,such as subicular pyramidal neuronal cells that are engagedin the phenytoin dependent DRE. Selectively activating th-ese cells by chemo or optogenetics leads to resistance ofphenytoin, while inhibiting these cells selectively is helpfulin reversing phenytoin resistance [28]. Additionally, in carba-mazepine drug resistance, use-dependent Na channel block-age loss is the most important development factor. Seizureepisodes itself might lead to altered properties of Na channelthat causes channel protein insensitivity to CBZ. This mech-anism proposes that resistance to CBZ can build up duringthe epileptogenesis course [29].
4. PGP ACTING CENTRALLY AND PERIPHER-ALLY
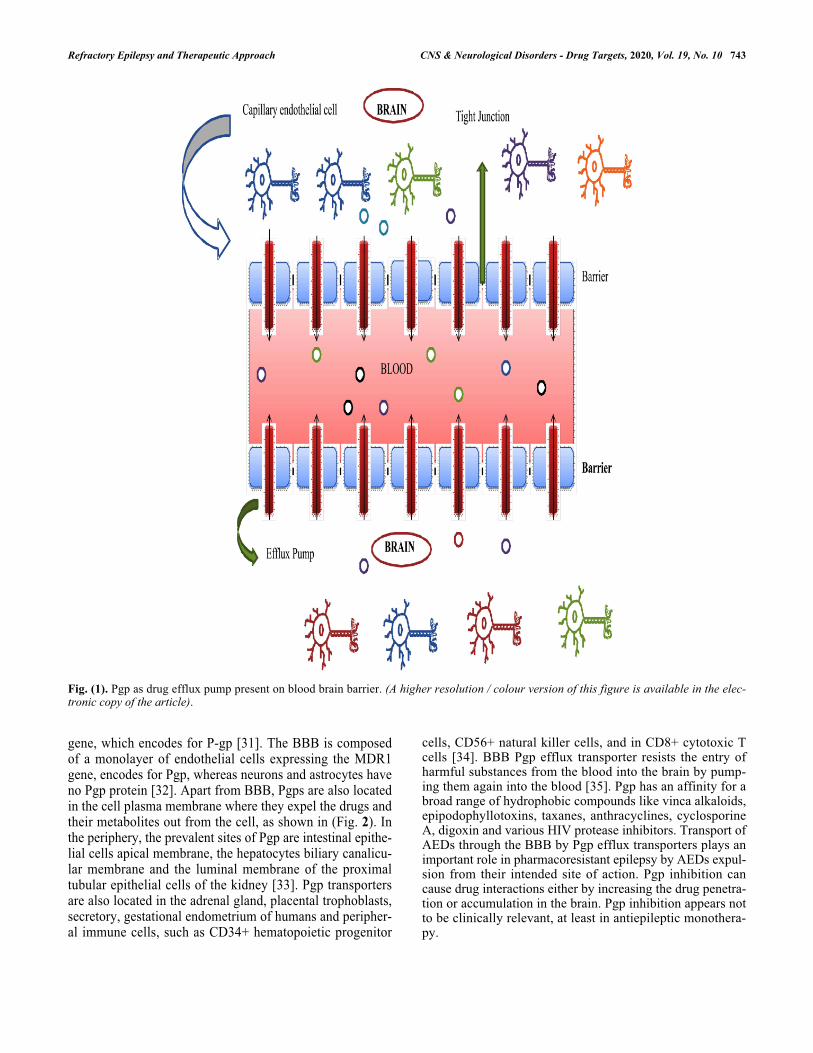
Pgp is the N-glycosylated proteins made up of about1280 amino acids forming an important part of the BBB. Th-ese efflux transporters are greatly found in endothelial cellsof capillary and astrocytes that structure the Blood-BrainBarrier (BBB). They maintain intracellular substrate concen-tration by expelling substrate from the cell via an activeATP dependent mechanism shown in (Fig. 1) [30]. The pri-mary cause behind the AEDs resistance is due to the MDR1
Refractory Epilepsy and Therapeutic Approach CNS & Neurological Disorders - Drug Targets, 2020, Vol. 19, No. 10 743
Fig. (1). Pgp as drug efflux pump present on blood brain barrier. (A higher resolution / colour version of this figure is available in the elec-tronic copy of the article).
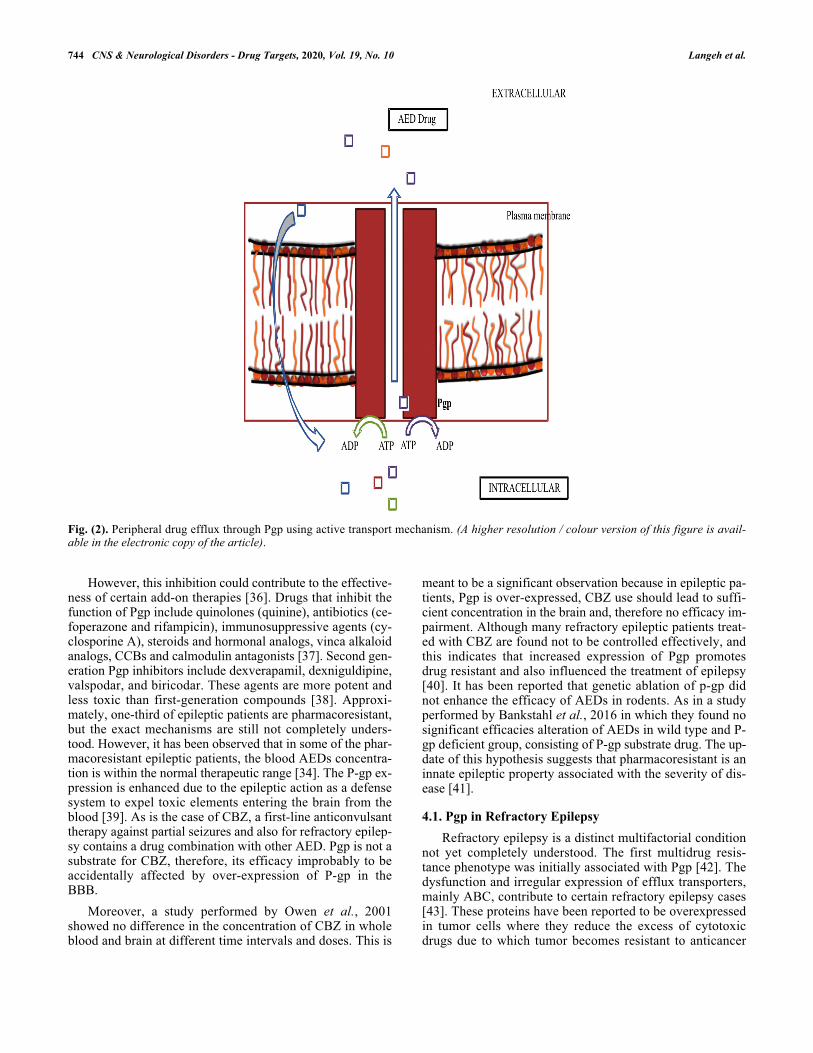
gene, which encodes for P-gp [31]. The BBB is composedof a monolayer of endothelial cells expressing the MDR1gene, encodes for Pgp, whereas neurons and astrocytes haveno Pgp protein [32]. Apart from BBB, Pgps are also locatedin the cell plasma membrane where they expel the drugs andtheir metabolites out from the cell, as shown in (Fig. 2). Inthe periphery, the prevalent sites of Pgp are intestinal epithe-lial cells apical membrane, the hepatocytes biliary canalicu-lar membrane and the luminal membrane of the proximaltubular epithelial cells of the kidney [33]. Pgp transportersare also located in the adrenal gland, placental trophoblasts,secretory, gestational endometrium of humans and peripher-al immune cells, such as CD34+ hematopoietic progenitor
cells, CD56+ natural killer cells, and in CD8+ cytotoxic Tcells [34]. BBB Pgp efflux transporter resists the entry ofharmful substances from the blood into the brain by pump-ing them again into the blood [35]. Pgp has an affinity for abroad range of hydrophobic compounds like vinca alkaloids,epipodophyllotoxins, taxanes, anthracyclines, cyclosporineA, digoxin and various HIV protease inhibitors. Transport ofAEDs through the BBB by Pgp efflux transporters plays animportant role in pharmacoresistant epilepsy by AEDs expul-sion from their intended site of action. Pgp inhibition cancause drug interactions either by increasing the drug penetra-tion or accumulation in the brain. Pgp inhibition appears notto be clinically relevant, at least in antiepileptic monothera-py.
744 CNS & Neurological Disorders - Drug Targets, 2020, Vol. 19, No. 10 Langeh et al.
Fig. (2). Peripheral drug efflux through Pgp using active transport mechanism. (A higher resolution / colour version of this figure is avail-able in the electronic copy of the article).
However, this inhibition could contribute to the effective-ness of certain add-on therapies [36]. Drugs that inhibit thefunction of Pgp include quinolones (quinine), antibiotics (ce-foperazone and rifampicin), immunosuppressive agents (cy-closporine A), steroids and hormonal analogs, vinca alkaloidanalogs, CCBs and calmodulin antagonists [37]. Second gen-eration Pgp inhibitors include dexverapamil, dexniguldipine,valspodar, and biricodar. These agents are more potent andless toxic than first-generation compounds [38]. Approxi-mately, one-third of epileptic patients are pharmacoresistant,but the exact mechanisms are still not completely unders-tood. However, it has been observed that in some of the phar-macoresistant epileptic patients, the blood AEDs concentra-tion is within the normal therapeutic range [34]. The P-gp ex-pression is enhanced due to the epileptic action as a defensesystem to expel toxic elements entering the brain from theblood [39]. As is the case of CBZ, a first-line anticonvulsanttherapy against partial seizures and also for refractory epilep-sy contains a drug combination with other AED. Pgp is not asubstrate for CBZ, therefore, its efficacy improbably to beaccidentally affected by over-expression of P-gp in theBBB.
Moreover, a study performed by Owen et al., 2001showed no difference in the concentration of CBZ in wholeblood and brain at different time intervals and doses. This is
meant to be a significant observation because in epileptic pa-tients, Pgp is over-expressed, CBZ use should lead to suffi-cient concentration in the brain and, therefore no efficacy im-pairment. Although many refractory epileptic patients treat-ed with CBZ are found not to be controlled effectively, andthis indicates that increased expression of Pgp promotesdrug resistant and also influenced the treatment of epilepsy[40]. It has been reported that genetic ablation of p-gp didnot enhance the efficacy of AEDs in rodents. As in a studyperformed by Bankstahl et al., 2016 in which they found nosignificant efficacies alteration of AEDs in wild type and P-gp deficient group, consisting of P-gp substrate drug. The up-date of this hypothesis suggests that pharmacoresistant is aninnate epileptic property associated with the severity of dis-ease [41].
4.1. Pgp in Refractory EpilepsyRefractory epilepsy is a distinct multifactorial condition
not yet completely understood. The first multidrug resis-tance phenotype was initially associated with Pgp [42]. Thedysfunction and irregular expression of efflux transporters,mainly ABC, contribute to certain refractory epilepsy cases[43]. These proteins have been reported to be overexpressedin tumor cells where they reduce the excess of cytotoxicdrugs due to which tumor becomes resistant to anticancer

Refractory Epilepsy and Therapeutic Approach CNS & Neurological Disorders - Drug Targets, 2020, Vol. 19, No. 10 745
drugs [44]. The role of Pgp is to guard susceptible organsagainst harmful xenobiotic compounds by preventing theircytosolic entry and their expulsion through the membrane.Therefore, they increase the metabolic and xenobiotics secre-tion into the urine, bile, and the gastrointestinal tract lumen.Animal model of refractory epilepsy has found upregulatedexpression of Pgp and an add-on therapy of Pgp inhibitorwith standard AED shown to overcome drug-resistant epilep-sy [44-46].
Pgp transporter along with other efflux transporters helpto expel toxic drug substances (metabolites) to prevent or-gan associated toxicity and simultanesously lower the levelof antiepileptic drugs at the target site [26]. There are four--generation inhibitors of Pgp. The first-generation is a non-specific inhibitor of Pgp such as verapamil and cyclosporineA. Second-generation is morepeculiar for Pgp e.g., PSC833(valspodar), a cyclosporine A analog, but their interferenceis shown with metabolizing enzyme CYP3A4. Third-genera-tion is specific to P-gp and shows no metabolizing enzymeinterference. A non-competitive inhibitor of Pgp Tariquidar(XR9576) having a high affinity for Pgp. Fourth-generationinhibitors possess greater potency with lesser toxicity. How-ever, they are still in developing phase and need to be evalu-ated for human use, e.g., the cyclic peptide QZ59SE and thenatural drugs like lamellar and gomisin A [20]. Literature re-ports support the simultaneous therapy of Pgp/MRP inhibi-tors along with AED as an approach to promote AED con-centration in brain, their efficacy, and to conquer pharma-coresistant. CCBs such as verapamil, nifedipine, and dilti-azem co-administered with AED, inhibit P-gp because oftheir intrinsic anticonvulsant activity and inhibitory functionon CYP3A4. Additionally, CCBs also elevates AED concen-tration in CNS, thereby decreasing seizures [45].
5. THERAPEUTIC TARGETS FOR REFRACTORYEPILEPSY
5.1. Voltage Gated Calcium Channel in RefractoryEpilepsy
The calcium channels are the membrane-associated pro-tein that form the plasma membrane pore for the movementof Ca2+ ions driven by the generation of an electrochemicalgradient. The movement of Ca2+ ions helps to initiate cellu-lar signaling, but excessive firing leads to seizure develop-ment [47]. Various CCBs are used to control refractoryepilepsy via inhibiting anti-epileptic drug efflux through Pgppresent on BBB. Kwan et al. have found that the inhibitionof Pgp by verapamil as encouraging molecule for drug-resis-tant epilepsy syndrome [48]. The VGCC are found ubiqui-tously throughout the CNS and are involved in neuronal exci-tation and transmission of synapse, which make them poten-tial targets [49]. The three neurological diseases associatedwith innate defects of voltage-gated calcium channels in-clude epilepsy, ataxia, and migraine, but the role of VGCCin seizure disorder has brought greater interest. In the ner-vous system, calcium channels support various natural pro-cesses such as expression of the gene, potentiation of intra-cellular signaling, membrane potential oscillation, and re-
lease of neurotransmitters [50, 51]. These calcium channelshave their valuable role in the influx of calcium to controlthe excitation of neurons and regulating the intracellular cal-cium-dependent signaling pathways, but the primary reasonbehind the epileptic seizures needs to be understood com-pletely [52].
In the plasma membrane, the VGCC form selectivepores for calcium influx into the cell. The higher concentra-tion of calcium outside the cell to an inner low calcium con-centration generates an electrochemical gradient that medi-ates calcium flow in cells. Neuronal cell membrane depo-larization occurs due to increased calcium influx, which in-duces firing of action potential and membrane oscillations.The intracellular signaling pathways and biochemicalmachinery are regulated by calcium influx [50]. The rise ofintracellular calcium plays a crucial role to elicit seizure andits propagation. The entry of calcium ion through Volt-age-Dependent Calcium Channels (VDCCs) transmit an elec-trical signal to cascade intracellular transduction in variouscells such as muscle, neuronal and endocrine cells. VDCCsare the key element of electric excitement and convertingcell surface action potential signals to transient intracellularcalcium. The alteration in the function of VDCC can lead toabnormal cellular events following disease conditions. VD-CC causes synaptic transmission in neurons and epilepsy pa-tients. Increased currents from VDCC with changed proper-ties occur in epileptic patient's neurons [53].
It has also been suggested that recurrent seizures may re-sult in the production of stress signals locally together withglutamate evoked responses that could induce Pgp expres-sion in neurons and cells of the BBB [54]. High Voltage Ac-tivated (HVA) channels expressed postsynaptically lead tolong-term depolarization and changes in expression can pro-duce a significant effect on the neuronal firing property.Moreover, these channels play a major role in low thresholdburst-firing where more amounts of Ca2+ throughout burst-ing are accomplished [55]. These HVA channels are also pre-sent presynaptically and involved in neurotransmitter re-lease. The neuronal function dependence on synaptic trans-mission reveals that a small variation in the presynaptic calci-um channels, shows a considerable effect on neuronal firingleading to epileptic seizures [49]. Iannetti et al. reported acase study of a child suffering from refractory status epilepti-cus, not responsive to conventional AEDs. The intravenousverapamil administration to the patient produced a dramaticresponse by the direct anticonvulsant action of the drug andalso verapamil is a known Pgp inhibitor that facilitates thebrain penetration of AEDs [56].
A Voltage-Gated Calcium Channel (VGCC) blocker, Ve-rapamil used in drug-resistant epileptic patients produced ex-pectable results. Verapamil might be responsible for increas-ing the AEDs brain influx by inhibiting Pgp and also modu-lates the neuronal abnormal influx of calcium for maintain-ing resting membrane potentials that is responsible for hyper-excitation of the membrane and augument seizures [57].

746 CNS & Neurological Disorders - Drug Targets, 2020, Vol. 19, No. 10 Langeh et al.
5.2. Selective COX II Inhibition in Refractory EpilepsyBauer et al. 2007 demonstrated that overexpression of
Pgp can be locally induced by glutamate microinjection,which increases the COX-2 level [58]. A further report byBauer confirmed that nanomolar injection of glutamatethrough intracerebral route increases Pgp expression locallywith no seizure. The Pgp level was found to be elevated inexisting capillary endothelium. The glutamate locally up-reg-ulates Pgp via COX-2, and can be prevented with COX-2 in-hibitors. Targeting these pathway may be an innovative ap-proach to overcome Pgp expression in the epileptic brainand improve the brain delivery of antiepileptic drugs.
Another in vivo experiment, reported the low level ofPgp and decrease status epilepticus attacks inpilocarpine-in-duced seizure treated with non-selective COX inhibitors in-domethacin and celecoxib, a selective COX-2 inhibitor [58].
Van Vliet et al. determined selective COX-2 inhibitioneffect on the expression of Pgp. The study confirmed thatCOX-2 inhibition efficiently controls the expression ofepileptic brain Pgp and promotes the delivery of AED pheny-toin into the brain. Various studies have indicated thatseizure-induced BBB Pgp is a characteristic in acute seizureand chronic models of epilepsy [59]. Zibell et al., in the firstexperiment established that NS-398 and indomethacinheptyl ester, COX-2 inhibitors, block glutamate-mediated el-evated expression of Pgp. Similarly, one more epileptic ani-mal model of rat experiment, confirmed that celecoxib medi-ated selective inhibition prevents the upregulation of en-dothelial Pgp in the brain. Thus, the data strongly hypothe-sized that seizure-induced increased expression of BBB ef-flux transporter can be prevented by using selective COX-2inhibitor [60]. Hartz et al. revealed that glutamate causedPgp elevation locally through COX-2 that can be preventedby using COX-2 inhibitors [61].
Moreover, Prostaglandin (PG) E2, a major product of cy-clooxygenase (COX)-2 acts as a proconvulsant by increas-ing hyperexcitability of neurons, death of neurons, and func-tional impairment of BBB. PGE2 has been associated withup-regulated BBB Pgp due to seizure [62, 63]. Underseizure pathological conditions, in non-neuronal cells, de-layed COX-II produced hippocampal PGE2 that facilitatethe death of neurons. The repetitive and subacute cure willprobably be obtained by selective inhibitors of COX-2matching the elevation period of PGE2 following seizuresonset for the treatment to avoid the death of neurons [64].
6. GLUTAMATE RECEPTOR ANTAGONISTIn a study, diazepam was administered past 90 min of sta-
tus epilepsy with simultaneous administration of vehicle orMK-801 (dizocilpine), an inhibitor glutamate receptor. Inthe vehicle-treated group, Pgp expression was elevated inthe endothelial cells of the brain hippocampus up to twofolds, fully inhibited by MK-801. Moreover, the hippocam-pus and parahippocampus region neurodegeneration was pre-vented by the glutamate blocking agents. Whereas, tariqui-dar, a known Pgp inhibitor, showed no effect in the status of
epilepticus induced Pgp elevation and neurodegeneration.The study indicates that MK-801 prevents the epileptic gluta-mate release responsible for Pgp expression. Furthermore, itwas found that dizocilpine prevents the upregulation of Pgpas well as neurodegeneration if given after SE. It provides aclinically beneficial treatment useful in refractory SE pa-tients [65]. Moreover, there are some natural molecules ofplant origin like moringin, Ginko-Biloba, quercetin, naringinbeing used in animal models, but no useful clinical out-comes are observed because of their bioavailability hin-drance or low BBB penetrability. So, for medically resistant,patient’s surgery as well as vagal stimulation techniques, pro-vide significant relief [66].
6.1. AcetazolamideAcetazolamide is a carbonic anhydrase inhibitor and an
unsubstituted sulfonamide. The drug was since used actuallyfor focal and generalized refractory and catamenial epilepsytreatment [67]. Acetazolamide, an adjuvant valuable agentin the epileptic pharmacotherapy and an agent to be ob-served in refractory epilepsy. Even though, it is also usefulin the absence, partial, myoclonic, primarily generalized ton-ic-clonic seizures that are not controlled by other agents[68]. Acetazolamide injection into the rat's MTLE model sig-nificantly inhibits MDR protein (MRP1). The inhibition ofMRP1 increases the AED's efficacy via increasing drug avai-lability locally [69]. The finding suggests that acetazolamiderepresses expression of P-gp significantly in the rat model ofMTLE [70]. Chen et al. 2013 also reported that MRP1 up--regulation is essential in the brain cells AEDs drug resis-tance in amygdale kindling rats [71]. There are severalforms of carbonic anhydrase present in the brain which, man-ages the amount of CNS activity. So, any modifications intheir activity might precipitate seizures due to alteringGABAergic excitation, pH, and ionic imbalance [72]. In thebrain, acetazolamide reported to inhibit carbonic anhydraseisozymes like II, IV, V, VII, XII, and XIV but its clinical uti-lization is still limited that is why this is preferred as an adju-vant to the treatment of refractory epilepsy [73].
7. FUTURE PERSPECTIVESThe failure of two or more AEDs treatments should
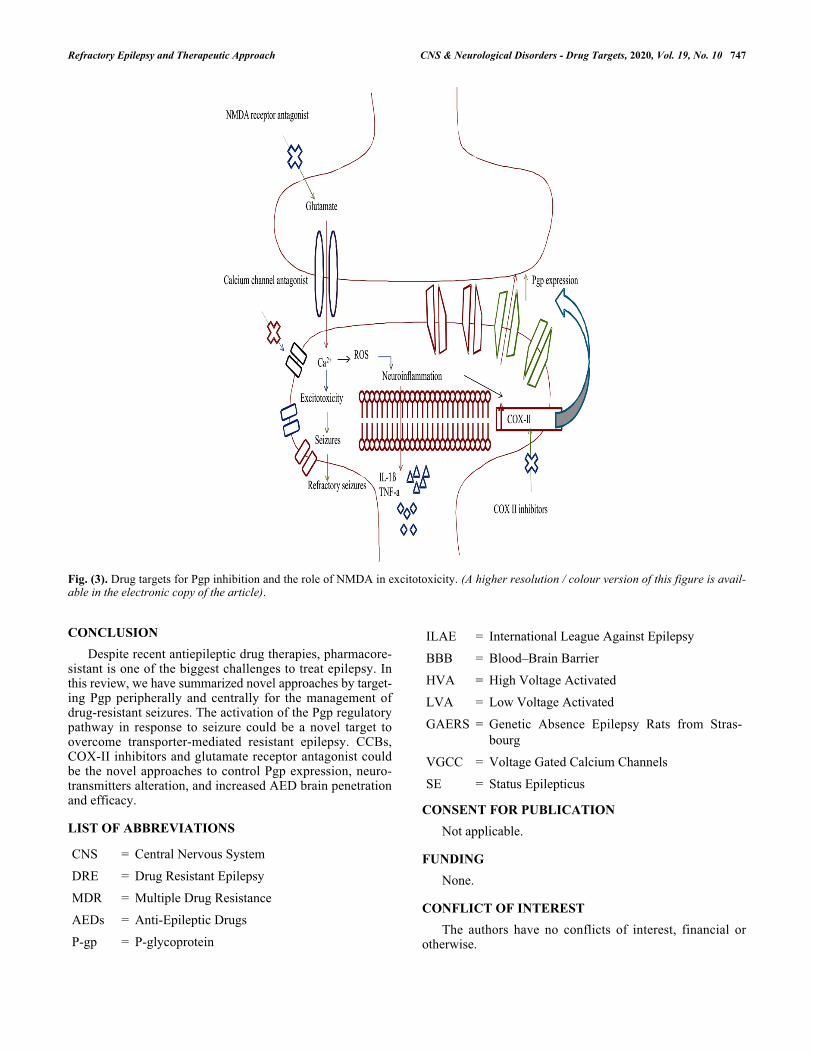
prompt early evaluation of the risk factors for pharmacoresis-tant. Pgp is the major targets responsible for refractoryepilepsy by expelling AED from the target site that eventual-ly leads to a decreased level of AEDs. Novel approaches bytargeting Pgp peripherally and centrally could be considereda novelty in the management of drug-resistant seizures. Pgpinhibitors prevent drug efflux and increase the AED concen-tration at the target site. Pgp inhibitors, in combination withherbal drugs, enhance the bioavailability of herbal medica-tions and promote their antiepileptic action. Elevated COX-II levels potentiate Pgp concentration. Glutamate mediatedcalcium influx and inflammation lead to seizures, whichcould be overcome by CCBs, selective COX-II inhibitor, glu-tamate receptor antagonist as an add-on treatment that mightbe considered in drug-resistant epilepsy as shown in (Fig. 3).
Refractory Epilepsy and Therapeutic Approach CNS & Neurological Disorders - Drug Targets, 2020, Vol. 19, No. 10 747
Fig. (3). Drug targets for Pgp inhibition and the role of NMDA in excitotoxicity. (A higher resolution / colour version of this figure is avail-able in the electronic copy of the article).
CONCLUSIONDespite recent antiepileptic drug therapies, pharmacore-
sistant is one of the biggest challenges to treat epilepsy. Inthis review, we have summarized novel approaches by target-ing Pgp peripherally and centrally for the management ofdrug-resistant seizures. The activation of the Pgp regulatorypathway in response to seizure could be a novel target toovercome transporter-mediated resistant epilepsy. CCBs,COX-II inhibitors and glutamate receptor antagonist couldbe the novel approaches to control Pgp expression, neuro-transmitters alteration, and increased AED brain penetrationand efficacy.
LIST OF ABBREVIATIONS
CNS = Central Nervous System
DRE = Drug Resistant Epilepsy
MDR = Multiple Drug Resistance
AEDs = Anti-Epileptic Drugs
P-gp = P-glycoprotein
ILAE = International League Against Epilepsy
BBB = Blood–Brain Barrier
HVA = High Voltage Activated
LVA = Low Voltage Activated
GAERS = Genetic Absence Epilepsy Rats from Stras-bourg
VGCC = Voltage Gated Calcium Channels
SE = Status Epilepticus
CONSENT FOR PUBLICATIONNot applicable.
FUNDINGNone.
CONFLICT OF INTERESTThe authors have no conflicts of interest, financial or
otherwise.
748 CNS & Neurological Disorders - Drug Targets, 2020, Vol. 19, No. 10 Langeh et al.
ACKNOWLEDGEMENTSThe authors are highly thankful to Mr. Parveen Garg,
Chairman, ISFCP for providing excellent research plat-forms.
REFERENCES
Adams F. On the sacred disease.The genuine works of Hip-[1]pocrates. London: Sydenham Society 1849; Vol. II: pp. 831-58.Devinsky O, Vezzani A, Najjar S, De Lanerolle NC, Rogawski[2]MA. Glia and epilepsy: excitability and inflammation. Trends Neu-rosci 2013; 36(3): 174-84.PMID: 23298414Thijs RD, Surges R, O’Brien TJ, Sander JW. Epilepsy in adults.[3]Lancet 2019; 393(10172): 689-701.PMID: 30686584Laxer KD, Trinka E, Hirsch LJ, et al. The consequences of refrac-[4]tory epilepsy and its treatment. Epilepsy Behav 2014; 37: 59-70.PMID: 24980390Hamberger MJ, Schevon CA, Seidel WT, McKhann GM II, Morri-[5]son C. Cortical naming sites and increasing age in adults with re-fractory epilepsy: More might be less. Epilepsia 2019; 60(8):1619-26.PMID: 31251399Zang K, Zhang Y, Hu J, Wang Y. The large conductance calci-[6]um-and voltage-activated potassium channel (bk) and epilepsy.(CNS & Neurol Disord Drug Targets) 2018; 17(4): 248-54.Zhu Y, Zhang S, Feng Y, Xiao Q, Cheng J, Tao J. The Yin and[7]Yang of BK channels in epilepsy. (CNS & Neurol Disord DrugTargets) 2018; 17(4): 272-9.Santhosh NS, Sinha S, Satishchandra P. Epilepsy: Indian perspec-[8]tive. Ann Indian Acad Neurol 2014; 17 (Suppl. 1): S3-S11.PMID: 24791085Dalic L, Cook MJ. Managing drug-resistant epilepsy: challenges[9]and solutions. Neuropsychiatr Dis Treat 2016; 12: 2605-16.PMID: 27789949Löscher W. The holy grail of epilepsy prevention: Preclinical ap-[10]proaches to antiepileptogenic treatments. Neuropharmacology2020; 167: 107605-19.PMID: 30980836Binder DK, Schramm J. Multilobar resections and hemispherecto-[11]my.Epilepsy: A Comprehensive Textbook. (2nd ed.). Philadel-phia: Lippincott-Raven 2008; pp. 1879-89.Alba-Ferrara L, Kochen S, Hausmann M. Emotional Prosody Pro-[12]cessing in Epilepsy: Some Insights on Brain Reorganization. FrontHum Neurosci 2018; 12: 92.PMID: 29593517Castaneda-Arellano R, Beas-Zarate C, Feria-Velasco AI, Bi-[13]tar-Alatorre EW, Rivera-Cervantes MC. From neurogenesis to neu-roprotection in the epilepsy: signalling by erythropoietin. FrontBiosci 2014; 19: 1445-55.PMID: 24896364Pitkänen A, Lukasiuk K. Mechanisms of epileptogenesis and po-[14]tential treatment targets. Lancet Neurol 2011; 10(2): 173-86.PMID: 21256455Golyala A, Kwan P. Drug development for refractory epilepsy:[15]The past 25 years and beyond. Seizure 2017; 44: 147-56.PMID: 28017578Dong S, Liu Y, Xu J, Hu Y, Huang L, Wang Z. Synthesis and[16]Evaluation of N-substituted (Z)-5-(benzo [d][1, 3] dioxol-5-yl-methylene)-2-thioxothiazolidin-4-one Derivatives and 5-substitut-edthioxothiazolidindione Derivatives as Potent AnticonvulsantAgents CNS & Neuroll Disord Drug Targets 2019; 18(10):798-807.French JA. Refractory epilepsy: clinical overview. Epilepsia 2007;[17]48 (Suppl. 1): 3-7.PMID: 17316406Sharma AK, Rani E, Waheed A, Rajput SK. Pharmacoresistant[18]epilepsy: a current update on non-conventional pharmacologicaland non-pharmacological interventions. J Epilepsy Res 2015;5(1): 1-8.PMID: 26157666
French JA. Refractory epilepsy: one size does not fit all. Epilepsy[19]Curr 2006; 6(6): 177-80.PMID: 17260051Sirven JI. Epilepsy: a spectrum disorder. Cold Spring Harb Per-[20]spect Med 2015; 5(9): a022848.PMID: 26328931Fisher RS, Acevedo C, Arzimanoglou A, et al. ILAE official re-[21]port: a practical clinical definition of epilepsy. Epilepsia 2014;55(4): 475-82.PMID: 24730690Engel J Jr. Approaches to refractory epilepsy. Ann Indian Acad[22]Neurol 2014; 17 (Suppl. 1): S12-7.PMID: 24791078Islam F, Ahmed S, Yasmeen BN, et al. Recent advances in the ma-[23]nagement of epilepsy. North Int Med Coll J 2014; 5(2): 353-6.Sillanpää M, Schmidt D. Natural history of treated child-[24]hood-onset epilepsy: prospective, long-term population-basedstudy. Brain 2006; 129(Pt 3): 617-24.PMID: 16401617Gidal BE. P-glycoprotein expression and pharmacoresistant epilep-[25]sy: cause or consequence? Epilepsy Curr 2014; 14(3): 136-8.PMID: 24940157Catchpool M, Dalziel K, Mahardya RTK, Harvey AS. Cost-effec-[26]tiveness of epileptic surgery compared with medical treatment inchildren with drug-resistant epilepsy. Epilepsy Behav 2019; 97:253-9.PMID: 31254845Schmidt D, Löscher W. Drug resistance in epilepsy: putative neu-[27]robiologic and clinical mechanisms. Epilepsia 2005; 46(6):858-77.PMID: 15946327Xu C, Wang Y, Zhang S, et al. Subicular pyramidal neurons gate[28]drug resistance in temporal lobe epilepsy. Ann Neurol 2019;86(4): 626-40.PMID: 31340057Remy S, Gabriel S, Urban BW, et al. A novel mechanism underly-[29]ing drug resistance in chronic epilepsy. Ann Neurol 2003; 53(4):469-79.PMID: 12666114Schinkel AH. P-Glycoprotein, a gatekeeper in the blood-brain bar-[30]rier. Adv Drug Deliv Rev 1999; 36(2-3): 179-94.PMID: 10837715Nanayakkara AK, Follit CA, Chen G, Williams NS, Vogel PD,[31]Wise JG. Targeted inhibitors of P-glycoprotein increase che-motherapeutic-induced mortality of multidrug resistant tumorcells. Sci Rep 2018; 8(1): 967.PMID: 29343829Dombrowski SM, Desai SY, Marroni M, et al. Overexpression of[32]multiple drug resistance genes in endothelial cells from patientswith refractory epilepsy. Epilepsia 2001; 42(12): 1501-6.PMID: 11879359Leschziner GD, Andrew T, Pirmohamed M, Johnson MR.[33]ABCB1 genotype and PGP expression, function and therapeuticdrug response: a critical review and recommendations for future re-search. Pharmacogenomics J 2007; 7(3): 154-79.PMID: 16969364Feldmann M, Koepp M. P-glycoprotein imaging in temporal lobe[34]epilepsy: in vivo PET experiments with the Pgp substrate [11C]-verapamil. Epilepsia 2012; 53 (Suppl. 6): 60-3.PMID: 23134497Sukhai M, Yong A, Kalitsky J, Piquette-Miller M. Inflammation[35]and interleukin-6 mediate reductions in the hepatic expression andtranscription of the mdr1a and mdr1b genes. Mol Cell Biol ResCommun 2000; 4(4): 248-56.PMID: 11409920Calatozzolo C, Pollo B, Botturi A, et al. Multidrug resistance pro-[36]teins expression in glioma patients with epilepsy. J Neurooncol2012; 110(1): 129-35.PMID: 22832898Marchetti S. Effect of selected ABC-drug transporters and anti-[37]cancer drug disposition in vitro and in vivo Doctoral dissertation,Utrecht UniversityKrishna R, Mayer LD. Modulation of P-glycoprotein (PGP) medi-[38]
Refractory Epilepsy and Therapeutic Approach CNS & Neurological Disorders - Drug Targets, 2020, Vol. 19, No. 10 749
ated multidrug resistance (MDR) using chemosensitizers: recentadvances in the design of selective MDR modulators. Curr MedChem Anticancer Agents 2001; 1(2): 163-74.PMID: 12678765Rizzi M, Caccia S, Guiso G, et al. Limbic seizures induce P-glyco-[39]protein in rodent brain: functional implications for pharmacoresis-tance. J Neurosci 2002; 22(14): 5833-9.PMID: 12122045Owen A, Pirmohamed M, Tettey JN, Morgan P, Chadwick D,[40]Park BK. Carbamazepine is not a substrate for P-glycoprotein. BrJ Clin Pharmacol 2001; 51(4): 345-9.PMID: 11318771Bankstahl M, Klein S, Römermann K, Löscher W. Knockout of P-[41]glycoprotein does not alter antiepileptic drug efficacy in the in-trahippocampal kainate model of mesial temporal lobe epilepsy inmice. Neuropharmacology 2016; 109: 183-95.PMID: 27288003Amin ML. P-glycoprotein inhibition for optimal drug delivery.[42]Drug target insights 2013; 7: DTI-S12519.Deng X, Xie Y, Chen Y. Effect of neuroinflammation on ABC[43]transporters: possible contribution to refractory epilepsy. (CNS &Neurol Disord Drug Targets) 2018; 17(10): 728-35.Finch A, Pillans P. P-glycoprotein and its role in drug-drug interac-[44]tions. Aust Prescr 2014; 37(4): 137-9.Robey RW, Lazarowski A, Bates SE. P-glycoprotein--a clinical[45]target in drug-refractory epilepsy? Mol Pharmacol 2008; 73(5):1343-6.PMID: 18314494Tang F, Hartz AMS, Bauer B. Drug-resistant epilepsy: multiple[46]hypotheses, few answers. Front Neurol 2017; 8: 301.PMID: 28729850Kambli L, Bhatt LK, Oza M, Prabhavalkar K. Novel therapeutic[47]targets for epilepsy intervention. Seizure 2017; 51: 27-34.PMID: 28772199Kwan P, Brodie MJ. Early identification of refractory epilepsy. N[48]Engl J Med 2000; 342(5): 314-9.PMID: 10660394Zamponi GW, Lory P, Perez-Reyes E. Role of voltage-gated calci-[49]um channels in epilepsy. Pflugers Arch 2010; 460(2): 395-403.PMID: 20091047Cain SM, Snutch TP. Voltage-gated calcium channels in epilepsy.[50]Epilepsia 2010; 51: 11.Simms BA, Zamponi GW. Neuronal voltage-gated calcium chan-[51]nels: structure, function, and dysfunction. Neuron 2014; 82(1):24-45.PMID: 24698266Rajakulendran S, Hanna MG. The role of calcium channels in[52]epilepsy. Cold Spring Harb Perspect Med 2016; 6(1): a022723.PMID: 26729757Xu JH, Tang FR. Voltage-dependent calcium channels, calcium[53]binding proteins, and their interaction in the pathological processof epilepsy. Int J Mol Sci 2018; 19(9): 2735.PMID: 30213136Volk HA, Potschka H, Löscher W. Increased expression of the[54]multidrug transporter P-glycoprotein in limbic brain regions afteramygdala-kindled seizures in rats. Epilepsy Res 2004; 58(1):67-79.PMID: 15066676Brumberg JC, Nowak LG, McCormick DA. Ionic mechanisms un-[55]derlying repetitive high-frequency burst firing in supragranularcortical neurons. J Neurosci 2000; 20(13): 4829-43.PMID: 10864940Iannetti P, Spalice A, Parisi P. Calcium-channel blocker verapamil[56]administration in prolonged and refractory status epilepticus.Epilepsia 2005; 46(6): 967-9.PMID: 15946342Nicita F, Spalice A, Papetti L, Nikanorova M, Iannetti P, Parisi P.[57]Efficacy of verapamil as an adjunctive treatment in children with
drug-resistant epilepsy: a pilot study. Seizure 2014; 23(1): 36-40.PMID: 24113539Bauer B, Hartz AM, Pekcec A, Toellner K, Miller DS, Potschka[58]H. Seizure-induced up-regulation of P-glycoprotein at the blood--brain barrier through glutamate and cyclooxygenase-2 signaling.Mol Pharmacol 2008; 73(5): 1444-53.PMID: 18094072van Vliet EA, Zibell G, Pekcec A, et al. COX-2 inhibition con-[59]trols P-glycoprotein expression and promotes brain delivery ofphenytoin in chronic epileptic rats. Neuropharmacology 2010;58(2): 404-12.PMID: 19786037Zibell G, Unkrüer B, Pekcec A, et al. Prevention of seizure-in-[60]duced up-regulation of endothelial P-glycoprotein by COX-2 inhi-bition. Neuropharmacology 2009; 56(5): 849-55.PMID: 19371577Hartz AM, Bauer B. Regulation of ABC transporters at the blood-[61]-brain barrier: new targets for CNS therapy. Mol Interv 2010;10(5): 293-304.PMID: 21045243Soldner ELB, Hartz AMS, Akanuma SI, et al. Inhibition of human[62]microsomal PGE2 synthase-1 reduces seizure-induced increasesof P-glycoprotein expression and activity at the blood-brain barri-er. FASEB J 2019; 33(12): 13966-81.PMID: 31638830Pekcec A, Unkrüer B, Schlichtiger J, et al. Targeting prostag-[63]landin E2 EP1 receptors prevents seizure-associated P-glycopro-tein up-regulation. J Pharmacol Exp Ther 2009; 330(3): 939-47.PMID: 19494186Takemiya T, Maehara M, Matsumura K, Yasuda S, Sugiura H, Ya-[64]magata K. Prostaglandin E2 produced by late induced COX-2 sti-mulates hippocampal neuron loss after seizure in the CA3 region.Neurosci Res 2006; 56(1): 103-10.PMID: 16837093Bankstahl JP, Hoffmann K, Bethmann K, Löscher W. Glutamate[65]is critically involved in seizure-induced overexpression of P-glyco-protein in the brain. Neuropharmacology 2008; 54(6): 1006-16.PMID: 18394657Kumar GP, Khanum F. Neuroprotective potential of phytochemi-[66]cals. Pharmacogn Rev 2012; 6(12): 81-90.PMID: 23055633Lim LL, Foldvary N, Mascha E, Lee J. Acetazolamide in women[67]with catamenial epilepsy. Epilepsia 2001; 42(6): 746-9.PMID: 11422329Reiss WG, Oles KS. Acetazolamide in the treatment of seizures.[68]Ann Pharmacother 1996; 30(5): 514-9.PMID: 8740334Sun Y, Luo X, Yang K, et al. Neural overexpression of multidrug[69]resistance-associated protein 1 and refractory epilepsy: a meta-a-nalysis of nine studies. Int J Neurosci 2016; 126(4): 308-17.PMID: 26000815Duan L, Di Q. Acetazolamide suppresses multi-drug resistance-re-[70]lated protein 1 and P-Glycoprotein expression by inhibiting aqua-porins expression in a mesial temporal epilepsy rat model. MedSci Monit 2017; 23: 5818-25.PMID: 29217817Chen YH, Wang CC, Xiao X, Wei L, Xu G. Multidrug resis-[71]tance-associated protein 1 decreases the concentrations of an-tiepileptic drugs in cortical extracellular fluid in amygdale kin-dling rats. Acta Pharmacol Sin 2013; 34(4): 473-9.PMID: 23474709Supuran CT. Carbonic anhydrases as drug targets--an overview.[72]Curr Top Med Chem 2007; 7(9): 825-33.PMID: 17504127Thiry A, Dogné JM, Supuran CT, Masereel B. Carbonic anhy-[73]drase inhibitors as anticonvulsant agents. Curr Top Med Chem2007; 7(9): 855-64.PMID: 17504130