TUGAS THT Nurul Jadi

of 16
-
Upload
nurul-afifah -
Category
Documents
-
view
218 -
download
0
Transcript of TUGAS THT Nurul Jadi
-
8/13/2019 TUGAS THT Nurul Jadi
1/16
TUGAS THT
Diajukan untuk Memenuhi Tugas dan Melengkapi Syarat dalam Menempuh Program Pendidikan
Profesi Dokter di Bagian Ilmu Kesehatan THT-KL
S!D Tugurejo Semarang
Disusun oleh "
#urul $fifah
%&'(%)'*+,(
$K!LT$S K.D/KT.$#
!#I0.SIT$S ISL$M S!LT$# $1!#1
S.M$$#1
(%&2
-
8/13/2019 TUGAS THT Nurul Jadi
2/16
&' Kriteria diagnosis sinusitis 3erdasarkan task for4e5 saphiro dan ra4helesky
$' Sinusitis akut menurut Task or4e
M$6/ MI#/
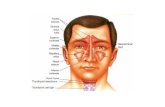
- #yeri pada 7ajah
- /3struksi nasal 8 hidung 3untu
- Post nasal drip
- Hiposmia 8anosmia
- Se4ret nasal purulen
- Demam 9 akut:
- Kongesti nasal
- #yeri gigi 9 terutama gigi
geraham:
- Sakit kepala
- Halotosis
- Batuk
- Demam 9kronis:
- asa lelah- Sakit telinga 8 terasa ada
tekanan di telinga 8 perasaan
penuh di telinga
; Di4urigai 3ila didapatkan ( gejala mayor atau & gejala mayor dan ( gejala minor atau
le3ih dengan gejala < + hari=
B' Sinusitis kronis menurut Saphiro Dan a4helesky
Mayor Minor
1ejala dan tanda - Se4ret hidung yang
purulen
- Se4ret faring yang
purulen
- Batuk
- .dem praor3ita
- #yeri pada 7ajah
- #yeri pada gigi
- Disfagia
- Mengi
- #yeri kepala
- /talgia
- Halitosis
- Demam 9 kronis:Diagnosis - gam3aran radiologi
7ater>s terdapat
- pemeriksaan sitologi
nasal neutrofil atau
-
8/13/2019 TUGAS THT Nurul Jadi
3/16
osifikasi5 air fluid
le?el atau
pene3alan mukosa
*%@ dari antrum
- sintigrafi karena
terdapat pene3alam
8 opafikasi sinus
3akteremia
- pemeriksaan
ultrasonografi
Diagnosis klinis "
- 1ejala dan tanda ( kriteria mayor atau & mayor dan ( minor
- Pemeriksaan diagnosti4 " & mayor " konfirmasi
& minor " menyokong
; diagnosis ditegakkan 3ila gejala terse3ut le3ih dari 2 3ulandengan atau tanpa
mem3utuhkan anti3ioti4 ;
2. Harga normal diffcount
#ilai #ormal La3oratorium Patologi Klinik
PRIA
HematologiAenis Spesimen " darah
Darah Lengkap
.ritrosit " ,'* *'C 9,'* *'*: 9juta8ul:
Haemoglo3in 9H3: " &2'* &+'* 9&2 &: 9g8dl:Hematokrit 9Ht: " ,&'% *2'% 9,% *,: 9@:
http://panji1102.blogspot.com/2008/10/nilai-normal-laboratorium-patologi.htmlhttp://panji1102.blogspot.com/2008/10/nilai-normal-laboratorium-patologi.html -
8/13/2019 TUGAS THT Nurul Jadi
4/16
Trom3osit " &*%'%%% ,,%'%%% 9&*%'%%% ,%%'%%%: 98ul:
Leukosit " ,'%%% &&'%%% 9*'%%% &%'%%%: 98ul:
Laju .ndap Darah 9L.D: " % &% 9mm8jam:
Diff count / Hitung Jenis eu!osit
Basofil " % & 9@:
.osinofil " & 2 9@:
Batang " ( 9@:
Segmen " *% +% 9@:
Limfosit " (% ,% 9@:
Monosit " ( ) 9@:
Urinalisa
Aenis Spesimen " urine midstream 8 porsi tengah
!rine Lengkap
Earna " kuning
Kejernihan " jernih
1lukosa " negatifBiliru3in " negatif
Keton " negatif
Berat jenis " &'%%* &'%2% 9&'%%2 &'%2%:
Darah samar " negatif
pH " ,'* )'% 9* ):
Protein " negatif
!ro3ilinogen " %'& &'% 9.!8dl:
#itrit " negatif
.sterase leukosit " negatif
Sedimen
Leukosit " % * 9% 2: 98LPB:
.ritrosit " % & 98LPB:
-
8/13/2019 TUGAS THT Nurul Jadi
5/16
Silinder " negatif 98LPK:
.pitel " F&
Kristal " negatif
Lain-lain " negatif
"imia Dara#
1lukosa # " )% &%% 9mg8dl:
1lukosa PP " &%% - &(% 9mg8dl:
1lukosa S " G &*% 9mg8dl:
Kolesterol total " G (%% 9mg8dl:
Trigliserida " G &*% 9mg8dl:
HDL Kolesterol " < ** 9mg8dl:
LDL kolesterol " G &*% 9mg8dl:
!reum " &* ,% 9mg8dl:
Kreatinin " %'* &'* 9mg8dl:
$sam urat " 2', +'% 9mg8dl:
Biliru3in total " %'( & 9mg @:
Biliru3in direk " % %'( 9mg @:
Biliru3in indirek " %'( %') 9mg @:
S1/T " * ,% 9u8l:
S1PT " * ,& 9u8l:
$lkali osfatase " ,* &C% 9iu8l:
1amma 1T " () 9mu8ml:
Protein total " '& )'( 9gr @:
$l3umin " 2') *'% 9gr @:
1lo3ulin " ('2 2'( 9gr @:
$A%ITA
Hematologi
-
8/13/2019 TUGAS THT Nurul Jadi
6/16
Aenis Spesimen " darah
Darah Lengkap
.ritrosit " , * 9juta8ul:
Haemoglo3in 9H3: " &( &* 9g8dl:
Hematokrit 9Ht: " 2 ,+ 9@:
Trom3o sit " &*%'%%% ,%%'%%%98ul:
Leukosit " *'%%% &%'%%%98ul:
Laju .ndap Darah 9L.D: " G &* 9mm8jam:
Diff count / Hitung Jenis eu!osit
Basofil " % & 9@:
.osinofil " & 2 9@:
Batang " ( 9@:
Segmen " *% +% 9@:
Limfosit " (% ,% 9@:
Monosit " ( ) 9@:
!rinalisa
Aenis Spesimen " urine midstream 8 porsi tengah
!rine Lengkap
Earna " kuning
Kejernihan " jernih
1lukosa " negatif
Biliru3in " negatif
Keton " negatif
Berat jenis " &'%%2 &'%2%
Darah samar " negatif
pH " * )
Protein " negatif
!ro3ilinogen " %'& &'% 9.!8dl:
#itrit " negatif
.sterase leukosit " negatif
-
8/13/2019 TUGAS THT Nurul Jadi
7/16
Sedimen
Leukosit " % 2 98LPB:
.ritrosit " % & 98LPB:
Silinder " negatif 98LPK:
.pitel " F&
Kristal " negatif
Lain-lain " negatif
Kimia Darah
1lukosa # " )% &%% 9mg8dl:
1lukosa PP " &%% - &(% 9mg8dl:
1lukosa S " G &*% 9mg8dl:
Kolesterol total " G (%% 9mg8dl:
Trigliserida " G &*% 9mg8dl:
HDL Kolesterol " < * 9mg8dl:
LDL kolesterol " G &*% 9mg8dl:
!reum " &* ,% 9mg8dl:
Kreatinin " %'* &'* 9mg8dl:
$sam urat " (', *'+ 9mg8dl:
Biliru3in total " %'( & 9mg @:
Biliru3in direk " % %'( 9mg @:
Biliru3in indirek " %'( %') 9mg @:
S1/T " * ,% 9u8l:
S1PT " * ,& 9u8l:
$lkali osfatase " ,* &C% 9iu8l:
1amma 1T " , &) 9mu8ml:
Protein total " '& )'( 9gr @:
$l3umin " 2') *'% 9gr @:
1lo3ulin " ('2 2'( 9gr @:
&. Teori !e'adian (atofisiologi (oli(
-
8/13/2019 TUGAS THT Nurul Jadi
8/16
Pem3entukan polip sering diasosiasikan dengan inflamasi kronik5 disfungsi saraf
otonom serta predisposisi geneti4' Menurut teori Bemstein5 terjadi peru3ahan mukosa
hidung aki3at peradangan atau aliran udara yang 3ertu3ulensi5 terutama di daerah sempit
di kompleks ostiomeatal' Terjadi prolaps su3mukosa yang diikuti oleh reepitelisasi dan
pem3entukan kelanjar 3aru' Auga terjadi peningkatan penyerapan natrium oleh
permukaan sel epitel yang 3eraki3at retensi air sehingga ter3entuk polip' Teori lain
mengatakan karena ketidak seim3angan saraf ?asomotor terjadi peningkatan
permea3ilitas kapiler dan gangguan regulasi ?as4ular yang mengaki3atkan dilepasnya
sitokin-sitokin dari sel mast5 yang akan menye3a3kan edema dan lama-lama menjadi
polip' Bila proses terus 3erlanjut5 mukosa yang sem3a3 makin mem3esar menjadi polip
dan kemudian akan turun ke rongga hidung dengan mem3entuk tangkai'
Pem3entukan polip sering dihu3ungkan dengan proses inflamasi kronik5 disfungsi
sistem saraf otonom dan predisposisigenetik' Be3erapa teori telah dikemukakan5 tetapi
tidak ada satupun yang dapat menjelaskan patofisiologi polip hidungse4ara lengkap'
Menurut teori Bernstein5 inflamasi pertama terjadi di mukosa dinding lateral hidung atau
mukosa sinusse3agai aki3at dari peradangan oleh alergan5 polutan5 atau agen infeksius
9?irus 8 3akteri: atau karena adanya aliran udarayang 3ertur3ulensi' Pada se3agian 3esarkasus5 polip 3erasal dari area sempit di kompleks ostiomeatal 9K/M: di meatusmedia'
Terjadi kerusakan atau prolaps mukosa yang diikuti dengan reepitelisasi dan
pem3entukan kelenjar 3aru' Selamaproses terse3ut polip dapat ter3entuk dari mukosa
karena proses inflamasi dari sel epitel5 sel endotel pem3uluh darah5 danfi3ro3last
3erpengaruh pada integritas 3ioelektik natrium 4hannel pada mukosa hidung' Hal ini
menye3a3kan meningkatnyaa3sorpsi natrium sehingga terjadi retensi air dan
pem3entukan polip'Pada teori kerusakan epitel menjelaskan 3ah7a rusaknya epitel pada
mukosa hidung dise3a3kan karena dalam keadaansakit 9alergi5infeksi: terjadi
peningkatan turgor jaringan' Kerusakan terse3ut menye3a3kan prolaps lamina propia
mukosasehingga terjadi pem3entukan polip yang dapat 3ertam3ah ukurannya karena efek
gra?itasi atau o3struksi ?ena yangdise3a3kan polip'Dari penelitian ditemukan 2+@ pasien
fi3rosis kistik menderita polip hidung' i3rosis kistik adalah penyakit herediter autosomal
-
8/13/2019 TUGAS THT Nurul Jadi
9/16
resesif yang dise3a3kan karena adanya kerusakan pada gen 4ysti4 fi3rosis transmem3rane
regulator 9T: dikromosom +' 1en ini mengatur 4hloride 4hannel pada sel epitel pada
3er3agai organ5 termasuk saluran nafas' Kerusakanpada gen ini menye3a3kan
terganggunya pem3ersihan sekret dan dihasilkannya sekret kental yang dapat
menye3a3kano3struksi dan merupakan predisposisi infeksi pada paru-paru dan sinus
paranasal
Introduction
During the past century several theories have been proposed to
explain the etiopathogenesis of nasal polyposis. The fact that so many
theories have been proposed is the evidence of our poor knowledge of
this topic. Majority of these theories are based on tissue oedema,
increase in the number of tubulo-alveolar glands, presence of cysts of
mucous glands.
Adenoma fibroma theory of Billroth:
illroth in his studies found a large number of tubular glands in the
nasal polypoidal tissue studied. !e concluded that these glands were
not normally seen in such large numbers in the nasal mucosa. !e
hence interpreted nasal polyp to be adenomas that began growing
under the nasal mucosa pushing the epithelium and nasal glands
outwards. !owever !opmann disagreed with this hypothesis saying
that the glandular tissue found in the tissue samples of nasal polypi
studied contained only mucous glands normally found in the nasalmucosa and concluded that nasal polypi could be soft fibromas and
used the term fibroma theory to explain this. These two theories are
not currently accepted at present.
-
8/13/2019 TUGAS THT Nurul Jadi
10/16
"igure showing increase in the number of nasal mucosal glands
"igure showing development of nasal polypi due to increase in the number
of nasal mucosal glands #$denoma theory%
Necrotizing ethmoiditis theory of Woakes:
This theory suggests that ethmoiditis causes periostitis and ostitis of
ethmoid bone causing bone necrosis. The necrotic bone initiates mucosal
reaction leading on to mucosal oedema and polyp formation. This theory
has been flawed from the very begining as no evidence of bone necrosis
could be found in the polypoidal tissue studied so far.
Glandular cyst theory:
&vidently this theory is based on the presence of cystic glands and
mucous filled cysts in the nasal polypoid tissue. The probable cause for
the formation of these glandular cysts could be oedema of submucosa
causing obstruction to the drainage of mucoid glands present in the nasal
-
8/13/2019 TUGAS THT Nurul Jadi
11/16
mucosa. These mucous cysts expands outwards pushing the nasal
mucosa causing the polyp to occur. Taylor in his meticulous study has
proved that mucous glandular cysts usually occur after the polyp has
formed and hence he believed that glandular cysts could be caused by
nasal polyposis and not vice versa.
Mucosal exudate theory of Hayek:
!ayek beleived that nasal polyp formed due to accumulation of exudate
localised deep in the mucosa. This accumulation of exudate causes the
mucosa to bulge leading to polyp formation. 'asal mucosal glands and
tubuloalveolar glands are also
displaced outwards. These glands are hence found in the distal part of the
polyp.
Theory of cystic dilatation due to obstruction of excretory ducts of nasal
glands and blood vessel obstruction(
"igure showing cystic enlargement of nasal mucosal glands
-
8/13/2019 TUGAS THT Nurul Jadi
12/16
"igure showing cyst formation prior to nasal polyposis
)n chronic inflammation involving nasal mucosa blocks the excretory ducts
of nasal tubulo alveolar glands causing the glands to dilate due to pent up
secretions within. The blood vessels #capillaries and veins% surrounding
these distending glands are also stretched. *tretching of these blood
vessels impedes blood circulation and causes tissue oedema due to
transudation of fluid. This theory is not valid due to the fact that dilatation
of mucous glands occur only after formation of nasal polypoidal tissue.
Blockade theory of Jenkins:
This theory is based on the premise that development of nasal polypi is
almost always preceded by certain degree of nasal mucosal inflammation.
The inflammation could be the result of either infection + allergy.
!istologically polyp itself is accumulation of intracellular fluid dammed up
in a localied tissue. )f this blockage persists polyp develop, if the
blockage covers a large area then multiple polypi forms. This theory
doesnt explain why nasal polyp prefers certain areas of nasal cavity.
eri!hlebitis " !erilym!hangitis theory of #ggston and Wolff:
This theory is based on the premise that recurrent infections of nasal
mucosa blocks intercellular fluid transport mechanism in the mucosa. This
is always associated with oedema of lamina propria. This theory is based
on the demonstration of chronic vascular changes in the nasal mucosa in
-
8/13/2019 TUGAS THT Nurul Jadi
13/16
response to inflammation. !istologically these changes are supposed to
be rather diffuse and hence cannot be used to explain the pathogenesis of
nasal polypi which can always be localised to certain areas of nasal cavity.
Glandular hy!er!lasia theory of $ra%ina:
$ccording to rajina chronic inflammation of nasal mucosa cause local
hyperplasia of nasal mucosal glands. These hyperplastic glands will cause
bulging of nasal mucosa. )n addition to glandular hyperplasia changes that
occur in the blood vessels will cause oedema in the region of the middle
meatus. This in turn increases nasal mucosal oedema. *tudies have
shown that the number of nasal mucosal glands are the same in
polypoidal as in the normal tissue.
#!ithelial ru!ture theory:
This is the currently proposed theory. )n this theory the initial stage of
nasal polyp formation starts of as epithelial rupture possibly due to
inflammation and tissue oedema. This is followed by prolapse of lamina
propria through the defect. The adjacent epithelium attempts to cover up
the defect there by forming a lining for the polypoidal tissue. )f the defectin the epithelium is not covered up real fast the prolapsed lamina propria
continues to grow and the polyp complete with its stalk develops. $fter
epitheliation of the polyp the characteristic new long tubular glands are
formed.
-
8/13/2019 TUGAS THT Nurul Jadi
14/16
"igure showing &xudate forming under the nasal mucosa #&xudative
theory%
"igure showing nasal polyp forming after accumulation of exudate
-
8/13/2019 TUGAS THT Nurul Jadi
15/16
"igure showing rupture of epithelium
"igure showing development of nasal polyp following epithelial rupture
&ole !layed by mucous glands:
The glandular elements seen in the nasal polypoidal tissue are nasal
glands. ommonly seen glands are degenerated long glands. The entire
long duct along with their lateral branches are distended due to filled upsecretions. Due to the pent up secretion and distention the secretory
epithelium of the nasal gland become cuboidal and flat losing their
secretory ability. This is followed by degeneration of the gland.
&ole !layed by cellular infilatrates:
-
8/13/2019 TUGAS THT Nurul Jadi
16/16
&osinophilic infiltration is an important feature in the pathogenesis of
chronic rhinosinusitis and nasal polypi. $ccumulation of eosinophils in the
polyp stroma is basically caused by increased transendothelial migration,
increased survival, and increased concentration of interleukin /.
). Per*edaan r#initis alergi+ r#initis ,asomotor+ r#initis medicamentosa dan r#initis
infe!si
hinitis
akut
hinitis kronik hinitis spesifik
hinitisSimplek
hnitishipertrofi
hnitissika
hinitisalergi
musiman
hinitisalergi
tahunan
hinitis?asomotor
hinitismedikamento
sa&tiologi
-hino?irus-Myo?irus-0irus4oasa4kle
-0irus.H/
Infeksi
3erulang
dalam
hidungdan sinus
-/rangtua
yang
3ekerja
di luarruangan
-Penderita
anemia
-Peminum
al4ohol
-1iJi
3uruk
$lergi $lergi
inhalan
9asap
rokok5peru3ahan
4ua4a5
kelem3ap
an yang
tinggi:
Bertam3ah
nya
akti?itas
parasimpatis
-pemakaian
?asokontriksi
topi4al
-drug a3use
*ecret
-sekreten4er9prodr
omal:
-kental
9sekunder:
Se4retmukopuru
len
Mukosayang
kering
9 depan
septumda
n ujung
depan
konka
inferior :
Se4ret4air
Se4ret4air
hinoreyang
mu4us 8
serous
Se4retmukoid
0ejala Demamdan panas
dalam
hidung
#yeri
kepala
hinoko
njungti?i
tis
$lergi
shiner
Hidung
tersum3at
3ergantian
tergantungposisi
.osinofil
pada se4ret
hidung
husus
Sem3uh
sesudah *-
&% hari
Mukosa
hipertrofi
Tim3uln
ya
periodik
Tim3ul
intermitte
n
Tes kulit 9-: