
PENATALAKSANAAN PREEKLAMSIA MASA KEHAMILAN,...
54
PENATALAKSANAAN PREEKLAMSIA MASA KEHAMILAN, PERSALINAN DAN NIFAS DALIMAN RS MARGONO SOEKARJO/ FK UNSOED PURWOKERTO Jumat, 08 Maret 2019 1 PENATALAKSANAAN PREEKLAMSIA, SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Transcript of PENATALAKSANAAN PREEKLAMSIA MASA KEHAMILAN,...

PENATALAKSANAAN
PREEKLAMSIA
MASA KEHAMILAN,
PERSALINAN DAN NIFAS
DALIMAN RS MARGONO SOEKARJO/
FK UNSOED
PURWOKERTO
Jumat, 08 Maret 2019 1 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19

INSIDENSI
KELAINAN
HIPERTENSI DALAM
KEHAMILAN (HDK) MERUPAKAN
KOMPLIKASI 5 – 10% DARI SELURUH
KEHAMILAN.
PREEKLAMSIA
TERIDENTIFIKASI 3,9%
DARI SELURUH
KEHAMILAN.
DI NEGARA MAJU 10–16 % KEMATIAN IBU DISEBABKAN OLEH
KELAINAN HIPERTENSI.
PROPORSI 3 PENYEBAB
KEMATIAN LAIN PERDARAHAN
13% , ABORSI 8 %, DAN SEPSIS
2%.
YANG PENTING, BAHWA LEBIH
DARI SETENGAH
HIPERTENSI YANG
DIHUBUNGKAN DENGAN
PENYEBAB KEMATIAN DAPAT
DICEGAH
Jumat, 08 Maret 2019 2 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
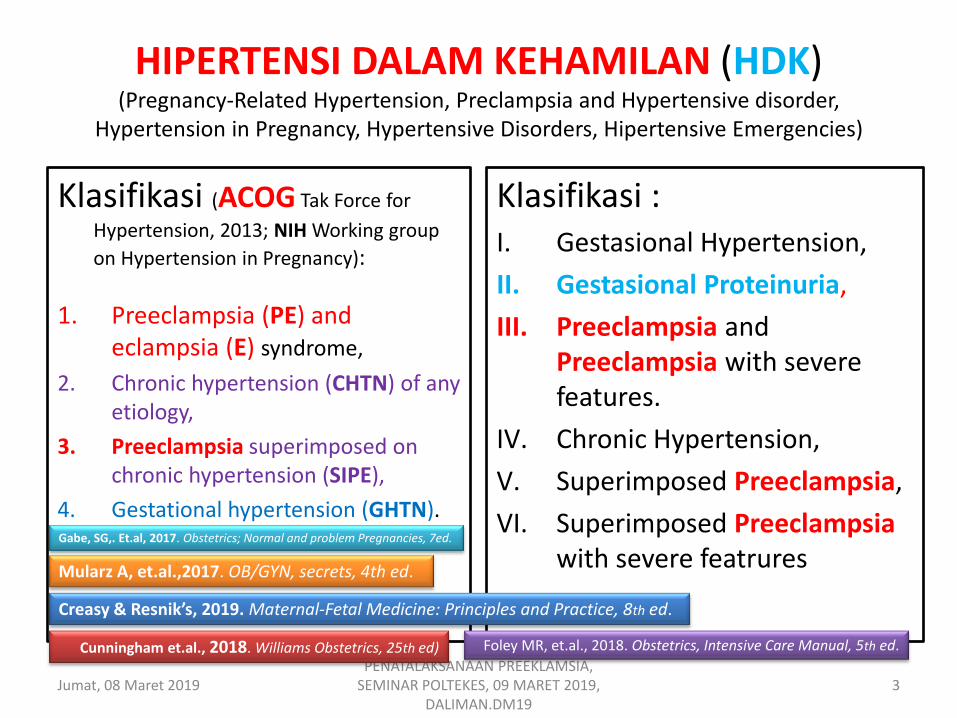
HIPERTENSI DALAM KEHAMILAN (HDK) (Pregnancy-Related Hypertension, Preclampsia and Hypertensive disorder,
Hypertension in Pregnancy, Hypertensive Disorders, Hipertensive Emergencies)
Klasifikasi (ACOG Tak Force for
Hypertension, 2013; NIH Working group
on Hypertension in Pregnancy):
1. Preeclampsia (PE) and eclampsia (E) syndrome,
2. Chronic hypertension (CHTN) of any etiology,
3. Preeclampsia superimposed on chronic hypertension (SIPE),
4. Gestational hypertension (GHTN).
Klasifikasi : I. Gestasional Hypertension,
II. Gestasional Proteinuria,
III. Preeclampsia and Preeclampsia with severe features.
IV. Chronic Hypertension,
V. Superimposed Preeclampsia,
VI. Superimposed Preeclampsia with severe featrures
Jumat, 08 Maret 2019 3 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Creasy & Resnik’s, 2019. Maternal-Fetal Medicine: Principles and Practice, 8th ed.
Cunningham et.al., 2018. Williams Obstetrics, 25th ed) Foley MR, et.al., 2018. Obstetrics, Intensive Care Manual, 5th ed.
Mularz A, et.al.,2017. OB/GYN, secrets, 4th ed.
Gabe, SG,. Et.al, 2017. Obstetrics; Normal and problem Pregnancies, 7ed.
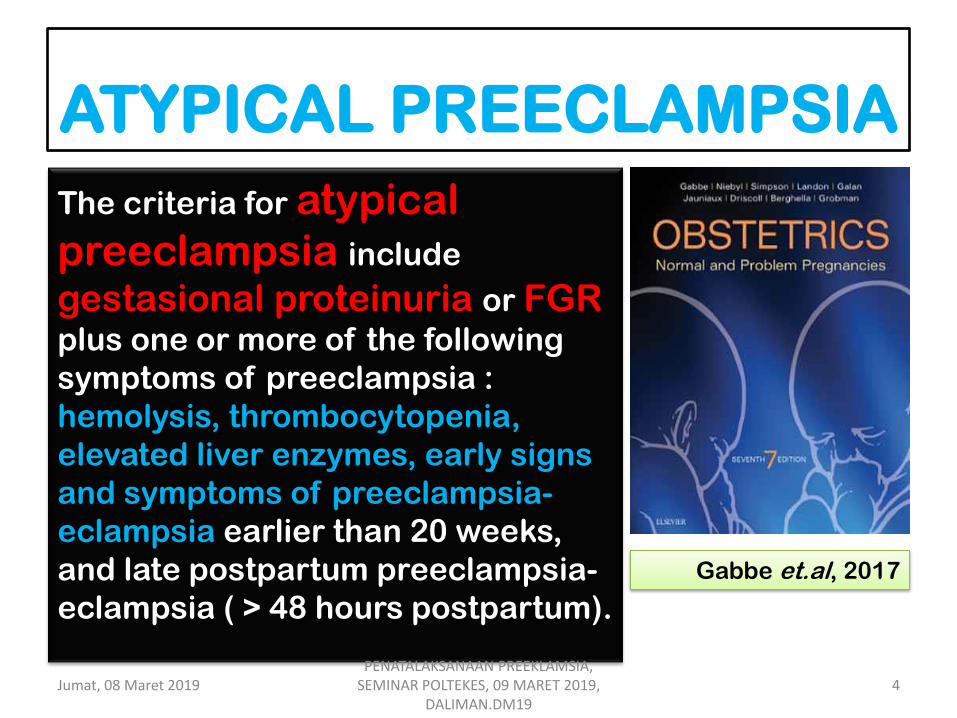
ATYPICAL PREECLAMPSIA
The criteria for atypical
preeclampsia include
gestasional proteinuria or FGR
plus one or more of the following
symptoms of preeclampsia :
hemolysis, thrombocytopenia,
elevated liver enzymes, early signs
and symptoms of preeclampsia-
eclampsia earlier than 20 weeks,
and late postpartum preeclampsia-
eclampsia ( > 48 hours postpartum).
Gabbe et.al, 2017
Jumat, 08 Maret 2019 4 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
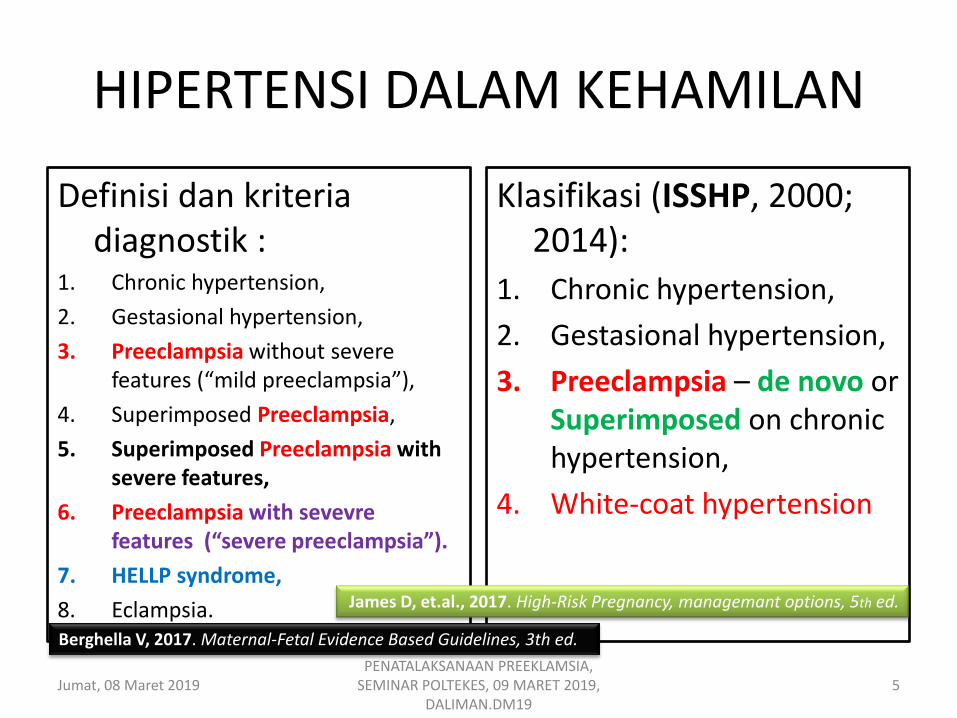
HIPERTENSI DALAM KEHAMILAN
Definisi dan kriteria diagnostik :
1. Chronic hypertension,
2. Gestasional hypertension,
3. Preeclampsia without severe features (“mild preeclampsia”),
4. Superimposed Preeclampsia,
5. Superimposed Preeclampsia with severe features,
6. Preeclampsia with sevevre features (“severe preeclampsia”).
7. HELLP syndrome,
8. Eclampsia.
Klasifikasi (ISSHP, 2000; 2014):
1. Chronic hypertension,
2. Gestasional hypertension,
3. Preeclampsia – de novo or Superimposed on chronic hypertension,
4. White-coat hypertension
Jumat, 08 Maret 2019 5 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Berghella V, 2017. Maternal-Fetal Evidence Based Guidelines, 3th ed.
James D, et.al., 2017. High-Risk Pregnancy, managemant options, 5th ed.

Hipertensi Dalam Kehamilan (HDK)
1. Hipertensi (HTN) +,
2. Hipertensi (HTN) -,
3. Proteinuria (PU) +,
4. Proteinuria (PU) -,
5. Hasil laboratorium (Lab) PEB,
6. Gejala atau tanda (G&T) PEB.
HAMIL
HTN +
HTN -
PU +
PU-
LAB PEB
G&T PEB
Jumat, 08 Maret 2019 6 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
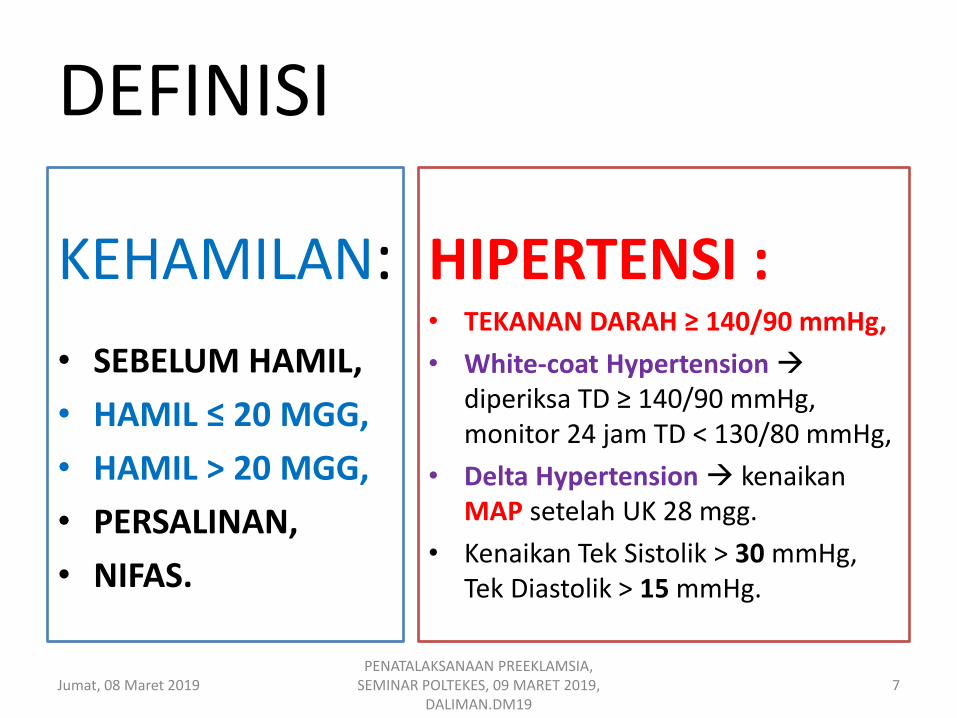
DEFINISI
KEHAMILAN:
• SEBELUM HAMIL,
• HAMIL ≤ 20 MGG,
• HAMIL > 20 MGG,
• PERSALINAN,
• NIFAS.
HIPERTENSI : • TEKANAN DARAH ≥ 140/90 mmHg,
• White-coat Hypertension diperiksa TD ≥ 140/90 mmHg, monitor 24 jam TD < 130/80 mmHg,
• Delta Hypertension kenaikan MAP setelah UK 28 mgg.
• Kenaikan Tek Sistolik > 30 mmHg, Tek Diastolik > 15 mmHg.
Jumat, 08 Maret 2019 7 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
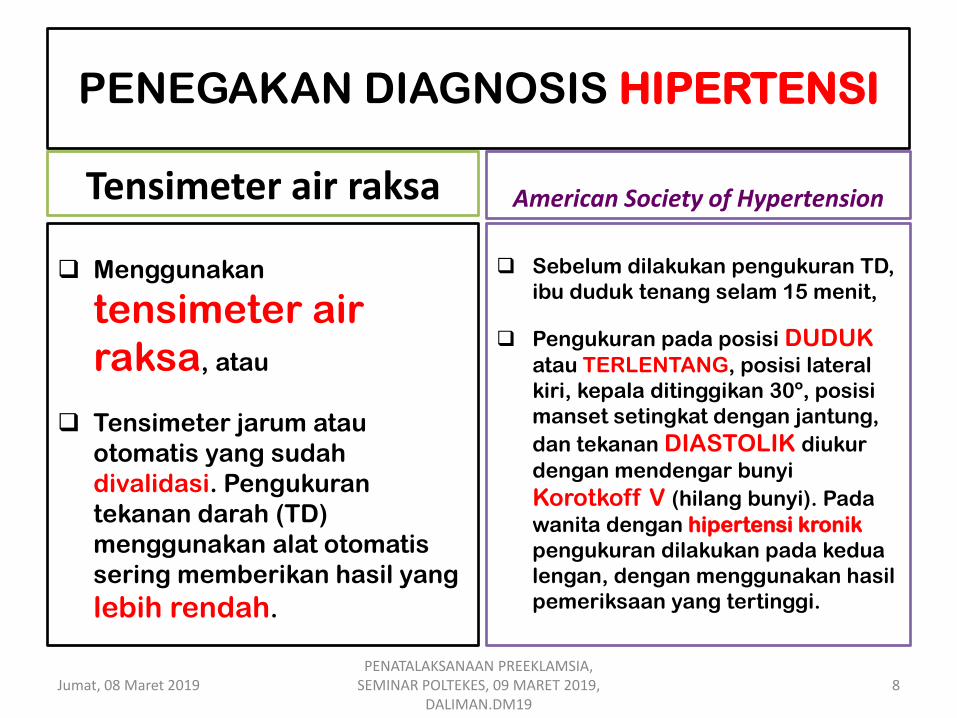
PENEGAKAN DIAGNOSIS HIPERTENSI
Tensimeter air raksa
Menggunakan
tensimeter air
raksa, atau
Tensimeter jarum atau
otomatis yang sudah
divalidasi. Pengukuran
tekanan darah (TD)
menggunakan alat otomatis
sering memberikan hasil yang
lebih rendah.
American Society of Hypertension
Sebelum dilakukan pengukuran TD,
ibu duduk tenang selam 15 menit,
Pengukuran pada posisi DUDUK
atau TERLENTANG, posisi lateral
kiri, kepala ditinggikan 30º, posisi
manset setingkat dengan jantung,
dan tekanan DIASTOLIK diukur
dengan mendengar bunyi
Korotkoff V (hilang bunyi). Pada
wanita dengan hipertensi kronik
pengukuran dilakukan pada kedua
lengan, dengan menggunakan hasil
pemeriksaan yang tertinggi.
Jumat, 08 Maret 2019 8 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19

DELTA HIPERTENSI
Jumat, 08 Maret 2019 9 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Cunningham et.al, 2018. Williams Obstetrics, 25 ed

DEFINISI
Proteinuria + (posistif):
≥ 300 mg/ 24 jam urine tampung,
Rasio creatinin/ protein urine, 1 x pemeriksaan, > 0,3 mg/ dL,
Kualitatif dipstik 1+ (30 mg/ dL)
Lab Preklamsia Berat (PEB):
• Trombositopenia ( < 100.000/ µL),
• Konsentrasi Creatinin serum > 1,1 mg/ dL (2 x nilai NORMAL, tanpa penyakit ginjal lain),
• SGOT/ PT > 2 x NILAI ATAS NORMAL.
Jumat, 08 Maret 2019 10 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19

DEFINISI
Gejala dan tanda PEB:
1. Muncul gangguan baru cerebral atau visual,
2. Edema paru atau SIANOSIS
3. Nyeri menetap epigastrik atau kuadran kanan atas yang tidak respon terapi dan tidak ada alternatif diagnosis.
Jumat, 08 Maret 2019 11 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Creasy & Resnik’s, 2019. Maternal-Fetal Medicine: Principles and Practice, 8th ed.

DIAGNOSIS HDK
HIPERTENSI
≥ 140/90
1
PROTEINURIA
POSITIF 2
PROTEINURIA NEGATIF
2
LAB & GEJALA-TANDA
PEB
1. HTN + PU (-)(LAB PEB -, G&T PEB -) +
UK ≥ 20 HIPERTENSI GESTASIONAL
2. HTN + PU (-) (LAB PEB -, G&T PEB -) +
UK < 20 HIPERTENSI KRONIK
3. HTN + PU (+)/(-) (LAB PEB +, G&T PEB
+) + UK ≥ 20 SINDROMA
PREEKLAMSIA (PE)
4. HTN + PU (-) PU (+)/ (-) (Kenaikan
HTN) pada UK ≥ 20 PREEKLAMSIA
SUPERIMPOSSED (SIPE).
MedScape, Kee-Hak Lim, MD; Ronald M Ramus, MD Preeclampsia Updated: Feb 16, 2018
Cunningham et.al, 2018. Williams Obstetrics, 25 ed and ACOG, 2013
Jumat, 08 Maret 2019 12 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Creasy & Resnik’s, 2019. Maternal-Fetal Medicine: Principles and Practice, 8th ed.
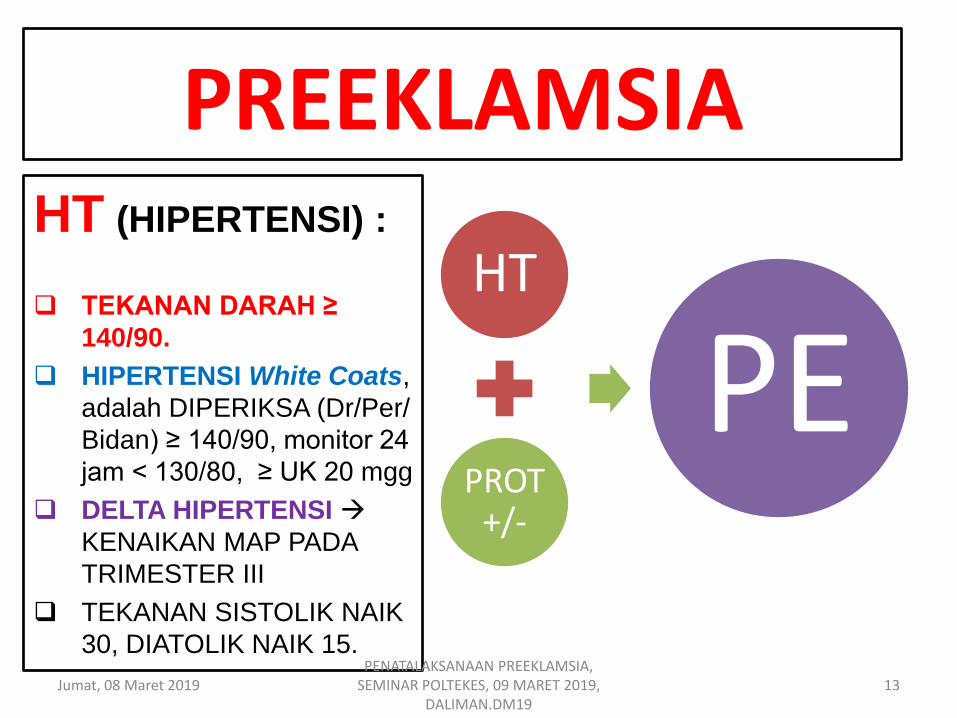
PREEKLAMSIA
HT
PROT +/-
PE
HT (HIPERTENSI) :
TEKANAN DARAH ≥
140/90.
HIPERTENSI White Coats,
adalah DIPERIKSA (Dr/Per/
Bidan) ≥ 140/90, monitor 24
jam < 130/80, ≥ UK 20 mgg
DELTA HIPERTENSI
KENAIKAN MAP PADA
TRIMESTER III
TEKANAN SISTOLIK NAIK
30, DIATOLIK NAIK 15.
Jumat, 08 Maret 2019 13 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19

Sindroma PREEKLAMSIA
Diskripsi yang paling baik, adalah sindroma spesifik
kehamilan yang pada hakekatnya dapat mempengaruhi setiap
sistem organ.
Dasar diagnosis- paling sederhana- adalah TEKANAN DARAH
≥ 140/90 mmHg + POSITIF PROTEINURIA ( gambaran
kerusakan endothelial-karakteristik sindroma Preeklamsia)
Abnormal ekskresi PROTEIN, adalah 300 mg/ 24 jam, atau
rasio protein : kreatinin urine ≥ 0,3, atau persisten 30
mg/dL (1+ dipstik).
Jumat, 08 Maret 2019 14
PENATALAKSANAAN PREEKLAMSIA, SEMINAR POLTEKES, 09 MARET 2019,
DALIMAN.DM19
Sindroma Preeklamsia
Menurut Sibai (2009) dan ACOG
(2013b): diagnosis sindroma
Preeklamsia dapat ditegakkan TIDAK
HARUS PROTEINURIA POSITIF.
HIPERTENSI + DISFUNGSI
MULTIORGAN, seperti trombositopenia
(< 100.000), disfungsi renal (kreatinin >
1,1 mg/dL), nekrosis hepatoseluler
(disfungsi liver)( AST dan ALT > 2 X
NORMAL), pertubasi sistema syaraf
pusat/ SSP (nyeri kepala, gangguan
penglihatan, dan KEJANG), EDEMA
PULMONUM
Jumat, 08 Maret 2019 15 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
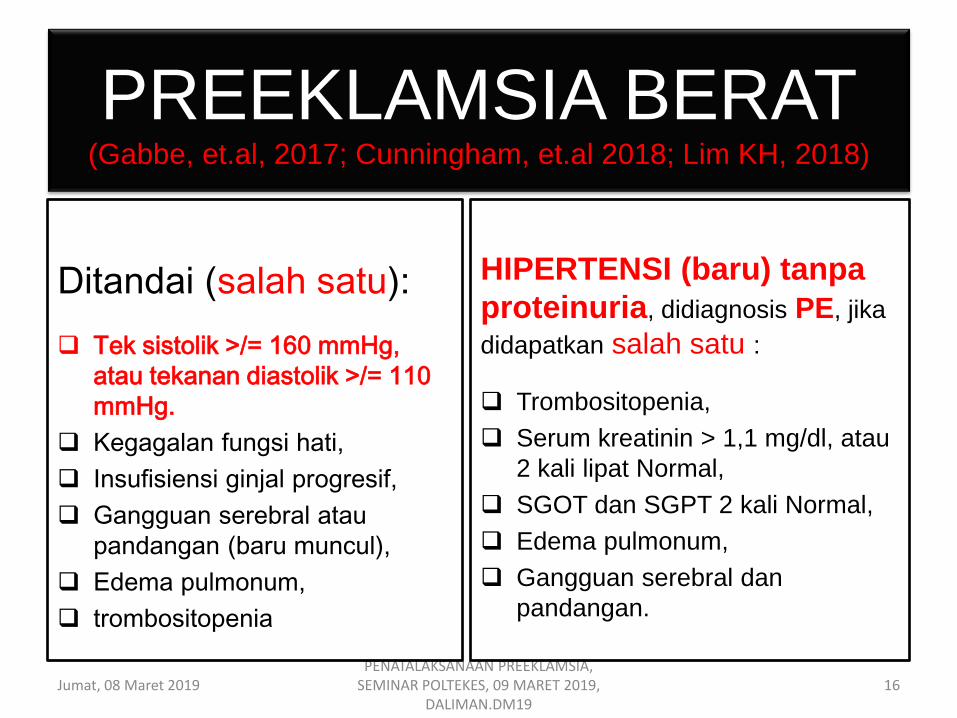
PREEKLAMSIA BERAT (Gabbe, et.al, 2017; Cunningham, et.al 2018; Lim KH, 2018)
Jumat, 08 Maret 2019 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
16
Ditandai (salah satu):
Tek sistolik >/= 160 mmHg,
atau tekanan diastolik >/= 110
mmHg.
Kegagalan fungsi hati,
Insufisiensi ginjal progresif,
Gangguan serebral atau
pandangan (baru muncul),
Edema pulmonum,
trombositopenia
HIPERTENSI (baru) tanpa
proteinuria, didiagnosis PE, jika
didapatkan salah satu :
Trombositopenia,
Serum kreatinin > 1,1 mg/dl, atau
2 kali lipat Normal,
SGOT dan SGPT 2 kali Normal,
Edema pulmonum,
Gangguan serebral dan
pandangan.
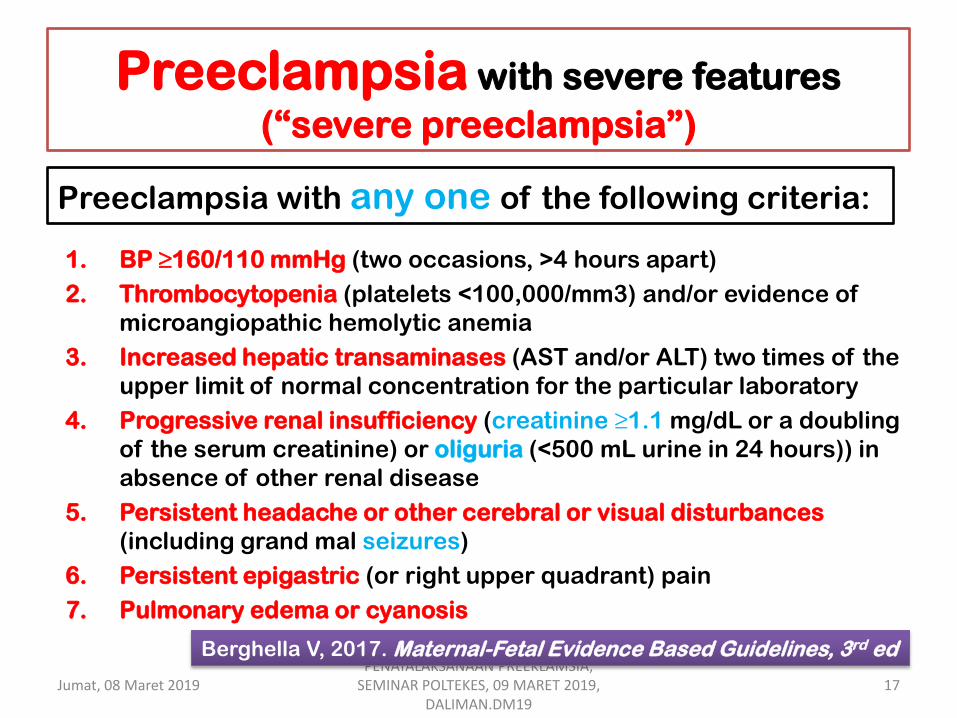
Preeclampsia with severe features
(“severe preeclampsia”)
1. BP ≥160/110 mmHg (two occasions, >4 hours apart)
2. Thrombocytopenia (platelets <100,000/mm3) and/or evidence of
microangiopathic hemolytic anemia
3. Increased hepatic transaminases (AST and/or ALT) two times of the
upper limit of normal concentration for the particular laboratory
4. Progressive renal insufficiency (creatinine ≥1.1 mg/dL or a doubling
of the serum creatinine) or oliguria (<500 mL urine in 24 hours)) in
absence of other renal disease
5. Persistent headache or other cerebral or visual disturbances
(including grand mal seizures)
6. Persistent epigastric (or right upper quadrant) pain
7. Pulmonary edema or cyanosis
Preeclampsia with any one of the following criteria:
Jumat, 08 Maret 2019 17 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Berghella V, 2017. Maternal-Fetal Evidence Based Guidelines, 3rd ed

Superimposed preeclampsia One or more of the following criteria:
1. New onset of proteinuria (≥300 mg in 24 hours without prior proteinuria) after 20 weeks in a woman with chronic HTN or sudden increase in proteinuria in a woman with known proteinuria before or early in pregnancy
2. A sudden increase in hypertension previously well
controlled or escalation of antihypertensive medication to control BP
Jumat, 08 Maret 2019 18 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Berghella V, 2017. Maternal-Fetal Evidence Based Guidelines, 3rd ed
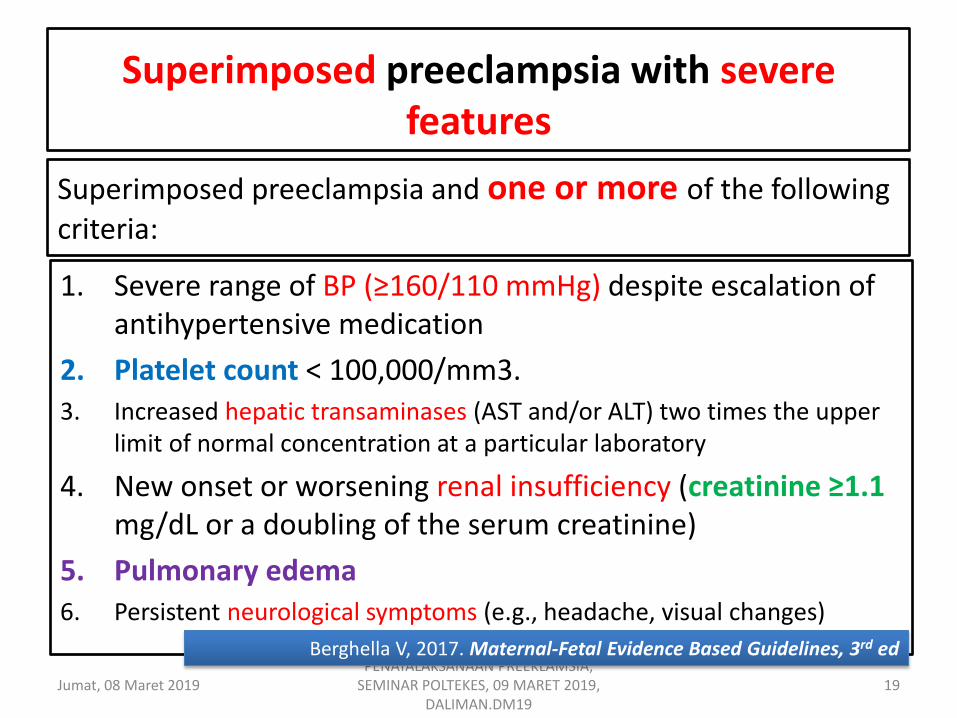
Superimposed preeclampsia with severe features
1. Severe range of BP (≥160/110 mmHg) despite escalation of antihypertensive medication
2. Platelet count < 100,000/mm3. 3. Increased hepatic transaminases (AST and/or ALT) two times the upper
limit of normal concentration at a particular laboratory
4. New onset or worsening renal insufficiency (creatinine ≥1.1 mg/dL or a doubling of the serum creatinine)
5. Pulmonary edema 6. Persistent neurological symptoms (e.g., headache, visual changes)
Superimposed preeclampsia and one or more of the following criteria:
Jumat, 08 Maret 2019 19 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Berghella V, 2017. Maternal-Fetal Evidence Based Guidelines, 3rd ed
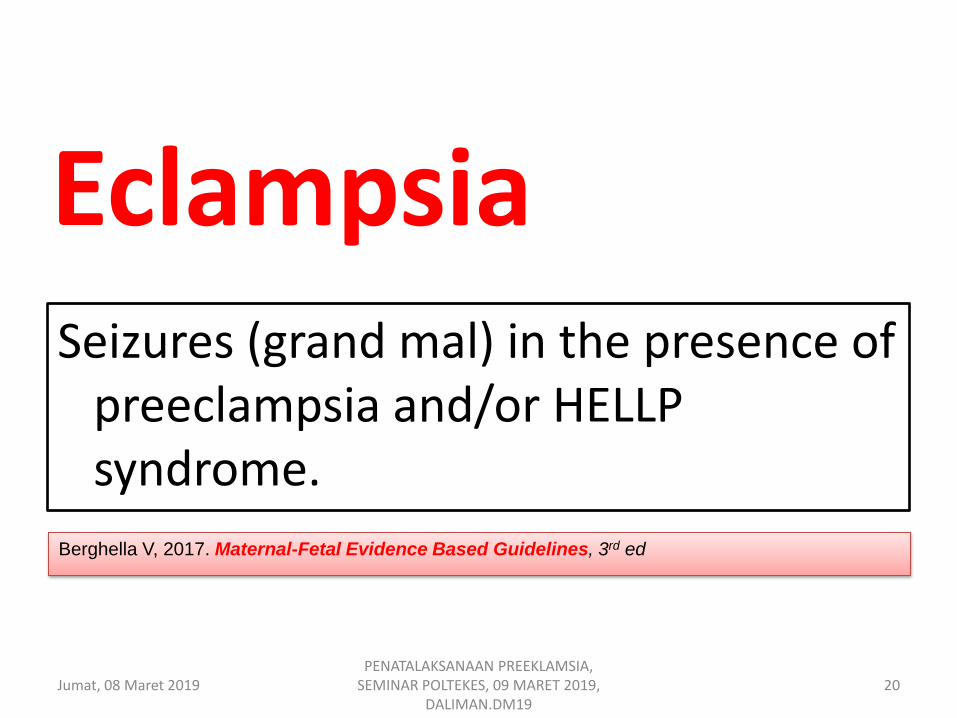
Eclampsia Seizures (grand mal) in the presence of
preeclampsia and/or HELLP syndrome.
Berghella V, 2017. Maternal-Fetal Evidence Based Guidelines, 3rd ed
Jumat, 08 Maret 2019 20 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19

Eklamsia SEKITAR 15% KASUS,
TANPA HIPERTENSI
DAN PROTEINURIA
SEBELUM EKLAMSIA,
LEBIH DARI 50% KASUS TERJADI PADA
KASUS YANG TIDAK
DIDIAGNOSIS PRE-
EKLAMSIA, TETAPI
HANYA PENYAKIT
RINGAN, PRETERM,
DAN TANPA DAPAT
DICEGAH.
Jumat, 08 Maret 2019 21 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
HT PE PEB Ekl
85%
15% (-) HT dan (-) PU
15% ?
?
?

EKLAMSIA
1. Hanya 42%-43% Eklamsia didahului dengan PE 57%-58% tidak didahului PE
2. 30%-50% Eklamsia tidak didahului dengan PEB 50%-70% didahului PEB.
Jumat, 08 Maret 2019 22 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
PE PEB EKL
Creasy and Resnik’s, et.al., 2019. Maternal-Fetal Medicine, Principle and Practice, 8th ed.
42%-43%
50%-70%
≠30%-50%
≠ 57%-58%
25%
MedScape, Kee-Hak Lim, MD; Ronald M Ramus, MD Preeclampsia Updated: Nov 29, 2018
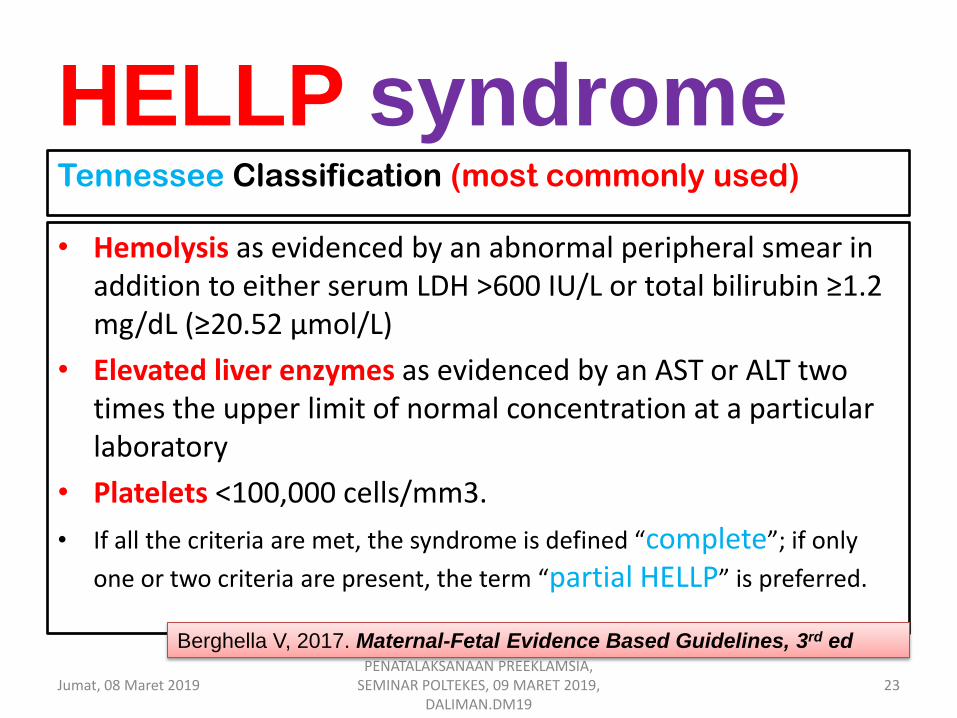
HELLP syndrome
• Hemolysis as evidenced by an abnormal peripheral smear in addition to either serum LDH >600 IU/L or total bilirubin ≥1.2 mg/dL (≥20.52 μmol/L)
• Elevated liver enzymes as evidenced by an AST or ALT two times the upper limit of normal concentration at a particular laboratory
• Platelets <100,000 cells/mm3.
• If all the criteria are met, the syndrome is defined “complete”; if only
one or two criteria are present, the term “partial HELLP” is preferred.
Tennessee Classification (most commonly used)
Jumat, 08 Maret 2019 23 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Berghella V, 2017. Maternal-Fetal Evidence Based Guidelines, 3rd ed
03/08/2019 PEMBELAJARAN TERFOKUS AMP, 150517,
DALIMAN.DM17 24
The basic management objectives
for any pregnancy complicated by
Preeclampsia are (Cunningham, 2018):
1. Termination of pregnancy with the least possible trauma
to mother and fetus
2. Birth of an infant who subsequently thrives
3. Complete restoration of health to the mother.
PENATALAKSANAAN
PREEKLAMSIA
PENCEGAHAN PE Terminologi umum
PENCEGAHAN,
dibagi 3:
1. Pencegahan
PRIMER,
2. Pencegahan
SEKUNDER,
3. Pencegahan
TERSIER.
PRIMER, artinya menghindari
terjadinya PENYAKIT,
SEKUNDER, artinya
memutus proses terjadinya
PENYAKIT yang sedang
berlangsung sebelum timbul
GEJALA atau KEDARURATAN
KLINIS,
TERSIER, berarti
pencegahan dari KOMPLIKASI
yang disesbabkan oleh proses
PENYAKIT TATALAKSANA
Jumat, 08 Maret 2019 25 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
PNPK PREEKLMASIA, HKFM POGI
PENCEGAHAN PRIMER o Pencegahan
yang terbaik,
namun hanya
dapat dilakukan
apabila
penyebab PE
telah diketahui
dengan jelas.
o Dilakukan
dengan prediksi
dan mengontrol
FAKTOR RISIKO
PE 17
1. Umur > 40 th,
2. Nulipara,
3. Multipara dengan riwayat PE,
4. Multipara dengan kehamilan oleh pasangan BARU
(primipaternitas),
5. Multipara yang jarak kehamilan sebelumnya ≥ 7-10 th,
6. Riwayat PE sebelumnya,
7. Riwayat keluarga PE (IBU atau saudara perempuan),
8. Kehamilan multipel,
9. IDDM,
10. Penyakit GINJAL,
11. Penyakit GIGI,
12. APS,
13. Kehamilan dengan inseminasi dodor sperma, oosit atau embryo,
14. OBESITAS sebelum hamil,
15. BMI ≥ 35,
16. Takanan darah DIASTOLIK ≥ 80 mmHg
17. Proteinuria (dipstick ≥+1 pada 2 kali pemeriksaan berjarak 6 jam atau
secara kuantitatif 300 mg/ 24 jam)
Jumat, 08 Maret 2019 26 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
PNPK HKFM POGI. PREEKLAMSIA
Risk factors- Preeclampsia Risk factors for preeclampsia and their odds
ratios are as follows [2] : 1. Nulliparity (3:1)
2. Age older than 40 years (3:1) >35 th (1,2 :1 / 1,1-1,3)
3. Black race (1.5:1)
4. Family history (5:1)
5. Chronic renal disease (20:1)
6. Chronic hypertension (10:1)
7. Antiphospholipid syndrome (10:1)
8. Diabetes mellitus (2:1)
9. Twin gestation (but unaffected by zygosity) (4:1)
10. High body mass index (BMI > 30) (3:1)
11. Homozygosity for angiotensinogen gene T235 (20:1)
12. Heterozygosity for angiotensinogen gene T235 (4:1)
13. TEK SIS > 130, TEK DIASTOLIK > 80 mmHg UK < 20.
14. Interval KEHAMILAN > 7 TH,
15. RIWAYAT PE kehamilan sebelumnya (8,4:1 / 7,1-9,9),
16. Kehamilan dengan ASISSTED REPRODUCTIONS TECHNOLOGY (1,8:1).
17. Riwayat SOLUSIO PLASENTA (2,0:1/ 1,4-2,7), LAHIR MATI (2,4:1)
MedScape, Kee-Hak Lim, MD; Ronald M Ramus, MD Preeclampsia Updated: Nov 29, 2018
Jumat, 08 Maret 2019 27 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
James D., et.al., 2017. High-Risk Pregnancy, Management Options. 5th ed
Gabbe et.al., 2017. Obstetrics, Normal adnd Problem Pregnancies, 7th ed.
Creasy and Resnik’s, et.al., 2019. Maternal-Fetal Medicine, Principle and Practice, 8th ed.
Cunningham, 2018. Williams Obstetrics, 25th ed.)
PENCEGAHAN SEKUNDER
1. Istirahat,
2. Restriksi
garam,
3. ASPIRIN dosis
rendah,
4. Suplemenatsi
KALSIUM,
5. Suplementasi
ANTIOKSIDAN.
KESIMPULAN (ASPIRIN DOSIS RENDAH)
1. Penggunaan Aspirin dosis rendah untuk
PENCEGAHAN PRIMER berhubungan dengan
penurunan risiko PE, persalinan PRETERM,
kematian janin atau neonatus dan BAYI KMK,
sedangkan untuk PENCEGAHAN SEKUNDER
berhubungan dengan penurunan risiko PE,
persalinan PRETEM < 37 mgg, dan BBL < 2500
gram.
2. Efek Asprin lebih nyata didapatkan pada
KELOMPOK RISIKO TINGGI,
3. Pemberian Aspirin dosis > 75 mg lebih baik untuk
menurunkan risiko PE, namun risiko yang
diakibatnya lebih tinggi.
REKOMENDASI
Aspirin dosis 75 mg atau kurang cukup aman
diberikan pada KELOMPOK RISIKO TINGGI
untuk menurunkan risiko PE baik sebagai
pencegahan PRIMER atau SEKUNDER.
03/08/2019 28 PEMBELAJARAN TERFOKUS AMP, 150517,
DALIMAN.DM17
Level evidence Ia, Rekomendasi A

PENCEGAHAN SEKUNDER
1. Istirahat,
2. Restriksi
garam,
3. ASPIRIN dosis
rendah,
4. Suplemenatsi
KALSIUM,
5. Suplementasi
ANTIOKSIDAN.
KESIMPULAN (KALSIUM)
1. Pemberian KALSIUM (1,5-2 gram) berhubungan dengan penurunan HDK
dan PE pada wanita dengan ASUPAN
RENDAH KALSIUM dan risiko tinggi PE,
2. Pemberian Kalsium juga berhubungan
dengan penurunan risiko MORBIDITAS
BERAT dan MORTALITAS MATERNAL,
persalinan PRETERM, dan tekanan
darah diastolik > persentil 95 pada
masa kanak.
REKOMENDASI
Pemberian KALSIUM dapat dilakukan pada
WANITA yang MEMILIKI RISKO TINGGI
PE dan RENDAH ASUPAN KALSIUM
untuk mencegah terjadinya PE.
Jumat, 08 Maret 2019 29 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Level evidence Ia, Rekomendasi A
TOG release: Low dose aspirin and calcium supplementation for prevention of pre-eclampsia
• Low dose aspirin started before 16 weeks
gestation and calcium supplementation after 20 weeks gestation in low-intake populations can prevent the onset of pre-eclampsia in pregnancies at risk of the condition, states a new review published today in The Obstetrician & Gynaecologist (TOG). It is also possible to assess a woman’s risk of developing pre-eclampsia from as early as 11 weeks of pregnancy, say the authors.
18 July 2014
03/08/2019 30 PEMBELAJARAN TERFOKUS AMP, 150517,
DALIMAN.DM17

PENCEGAHAN SEKUNDER
Rekomendasi :
• Istirahat di rumah ( 4jm/ hr atau 2 x 15 menit + suplemen) direkomendasikan untuk pencegahan primer PE,
• Tirah baring TIDAK direkomendasikan untuk memperbaiki luaran pada wanita dengan hipertensi (dengan atau tanpa proteinuria)
Level evidence Ia, Rekomendasi A
Rekomendasi :
• Pembatasan garam untuk mencegah PE dan komplikasinya selama kehamilan TIDAK direkomendasikan.
Level evidence Ia, Rekomendasi A
Jumat, 08 Maret 2019 31 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19

Clinical Risk Assessment for Preeclampsia
Risk Level Risk Factors Recommendation
High History of preeclampsia, especially when accompanied by an adverse outcome, Multifetal gestation, Chronic hypertension, Type 1 or 2 diabetes, Renal disease, Autoimmune disease (systemic lupus erythematous, antiphospholipid syndrome)
Recommend low-dose aspirin if the patient
has ≥1 of these
high-risk factors
Moderate Nulliparity, Obesity (body mass index >30 kg/m2), Family history of preeclampsia (mother or sister), Sociodemographic characteristics (African American race, low socioeconomic status), Age ≥35 years Personal history factors (e.g., low birthweight or small for gestational age, previous adverse pregnancy outcome, >10-year pregnancy interval)
Consider low-dose aspirin if the patient
has several of
these moderate-risk factors.
Low Previous uncomplicated full-term delivery Do not recommend low-dose aspirin
Timing Use of low-dose aspirin was initiated between 12 and 28 weeks of gestation. Evidence did not suggest additional benefit when use of aspirin was started earlier (12 to 16 weeks) rather than later (≥16 weeks) in pregnancy in women at increased risk for preeclampsia 1.
Jumat, 08 Maret 2019 32 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Penanganan Hanya persalinan obat
preeklamsia. Pasien dengan PE tidak berat
perlu induksi setelah umur kehamilan 37 mgg.
Sebelumnya pasien biasanya diawasi dengan ketat atau dirawat untuk perkembangan, perburukan atau komplikasi PE, dan imaturitas janin ditangani ekspektatif dengan pemberian kortikosteroid guna memacu pematangan paru janin untuk persiapan persalinan prematur.
Pasien dengan PEB induksi persalinan seharusnya dilakukan setelah umur kehamilan 34 mgg.
Dalam kasus ini, memberatnya penyakit dipertimbangkan dengan risiko prematuritas janin.
Dalam kondisi darurat kontrol TD dan kejang harus diprioritaskan.
Jumat, 08 Maret 2019 33 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
MedScape, Kee-Hak Lim, MD; Ronald M Ramus, MD Preeclampsia Updated:
Nov 29, 2018

MgSO4 MgSO4 ADALAH OBAT
PILIHAN UNTUK PENCEGAHAN
EKLAMSIA, MENURUNKAN 59%
RISIKO EKLAMSIA, 36%
SOLUSIO PLASENTA, 46% (STATISTIK TIDAK SIGNIFIKAN)
KEMATIAN MATERNAL.
SYARAT PEMBERIAN MgSO4 ADALAH
REFLEKS PATELLA +, URINE OUTPUT >30
CC/JAM, DAN REPIRASI > 16 KALI/MENIT,
SERTA TERSEDIA ANTIDOTUMNYA YAITU
Ca Gluconas.
TOKSISITAS MgSO4 BERUPA
HILANGNYA REFLEKS PATELLA,
DEPRESI RESPIRASI, PERUBAHAN
KONDISI JANTUNG, CARDIAC
ARREST.
DOSIS AWAL 4- 6 gram iv BOLUS, DILANJUTKAN
DENGAN DRIPS 1-2
gram/ JAM.
PEMBERIAN ULANG iv 2
gr (BB≤ 70 kg), ATAU 4
gr (BB> 70 kg), MINIMAL
3-5/ 5-10 MENIT
KEMUDIAN (JARANG),
JIKA PERLU DAPAT DIBERIKAN
Na-AMOBARBITAL 250 mg IV
MINIMAL 3-5 MENIT
Jumat, 08 Maret 2019 34 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
REKOMENDASI PNPK-Preeklamsia
1. Pemberian MgSO4 pada PEB berguna untuk mencegah terjadinya kejang eklamsia atau kejang berulang.
2. Rute administrasi MgSO4 yang dianjurkan adalah IV untuk mengurangi nyeri pada lokasi sutikan.
3. MgSO4 merupakan pilihan utama pada pasien PEB dibandingkan diazepam atau fenitoin, untuk mencegah terjadinya kejang/ eklamsia atau kejang berulang.
Level evidence Ia, Rekomendasi A
Jumat, 08 Maret 2019 35 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19

OBAT ANTIHIPERTENSI
ALTERNATIF OBAT ANTIHIPERTENSI, ADALAH :
1. Labetalol 20 mg iv bolus, dilanjutkan 40 mg, 80 mg, 80 mg jika diperlukan, setiap 10 menit dengan dosis maksimal total 220 mg.
2.Nifedipin 10-20 mg po, diulang
tiap 30 menit (bisa sampai 8 x per 24 jam) (NHBPEP-WG,2000; RCOG,2006: dalam Cunningham 2014).
3. Hydralazine 5-10 mg iv/ im, tiap 20 menit, dosis maksimal 30 mg.
4. Sodium nitroprusside dimulai 0,25 ug/kg/min sampai dosis maksimal 5 ug/kg/min (second line).
DIBERIKAN APABILA
TEKANAN SISTOLIK ≥160 DAN ATAU TEKANAN
DIASTOLIK ≥110
Jumat, 08 Maret 2019 36 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Cunningham, 2018. Williams Obstetrics, 25th ed.)
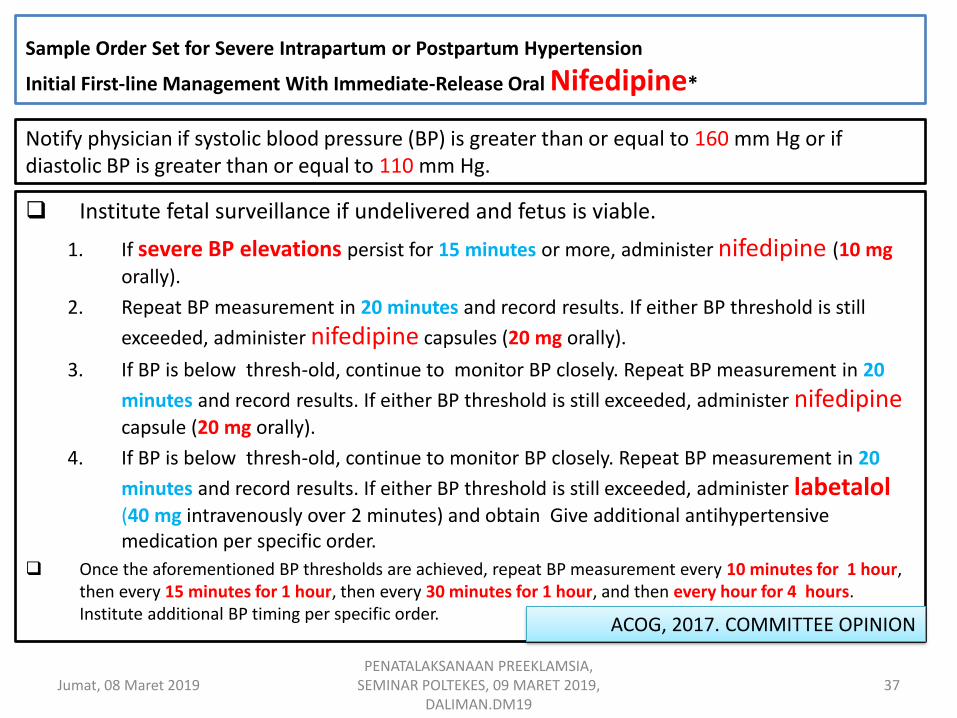
Sample Order Set for Severe Intrapartum or Postpartum Hypertension
Initial First-line Management With Immediate-Release Oral Nifedipine*
Institute fetal surveillance if undelivered and fetus is viable.
1. If severe BP elevations persist for 15 minutes or more, administer nifedipine (10 mg
orally).
2. Repeat BP measurement in 20 minutes and record results. If either BP threshold is still
exceeded, administer nifedipine capsules (20 mg orally).
3. If BP is below thresh-old, continue to monitor BP closely. Repeat BP measurement in 20
minutes and record results. If either BP threshold is still exceeded, administer nifedipine capsule (20 mg orally).
4. If BP is below thresh-old, continue to monitor BP closely. Repeat BP measurement in 20
minutes and record results. If either BP threshold is still exceeded, administer labetalol (40 mg intravenously over 2 minutes) and obtain Give additional antihypertensive medication per specific order.
Once the aforementioned BP thresholds are achieved, repeat BP measurement every 10 minutes for 1 hour, then every 15 minutes for 1 hour, then every 30 minutes for 1 hour, and then every hour for 4 hours. Institute additional BP timing per specific order.
Notify physician if systolic blood pressure (BP) is greater than or equal to 160 mm Hg or if diastolic BP is greater than or equal to 110 mm Hg.
Jumat, 08 Maret 2019 37 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
ACOG, 2017. COMMITTEE OPINION

Jumat, 08 Maret 2019 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
38
TERAPI HIPERTENSI KRONIK
1. PERUBAHAN GAYA HIDUP BERUPA DIET KAYA BUAH, SAYUR, RENDAH LEMAK, MENGURANGI SATURASI DAN TOTAL LEMAK, (MENGURANGI MASUKAN GARAM SAMPAI < 2,4 gram/
HARI TIDAK DIANJURLKAN LAGI).
2. BEDREST DI RS DIHUBUNGKAN PENGURANGAN 42% HIPERTENSI BERAT, 47% PERSALINAN PRETERM.
3. OBAT ANTIHIPERTENSI – METHYLDOPA, LABETALOL,
BETABLOKER, NIFEDIPIN, DIURETIK.
4. ACE-INHIBITOR KONTRAINDIKASI DIBERIKAN PADA TRIMESTER PERTAMA,
DIHUBUNGKAN DENGAN PENINGKATAN 2 KALI TERJADINYA MALFORMASI, DAN JANGKA PANJANG IUGR, OLIGOHIDRAMNION, GAGAL GINJAL DAN KEMATIAN NEONATUS.

MANAJEMEN CAIRAN pada
PEB • Hindari pemberian
diuretik.
• Resusitasi volume cairan yang agresif penyebab utama untuk EDEMA PULMONUM.
• Sedapat mungkin pasien harus RESTRIKSI CAIRAN, minimal sampai periode DIURESIS POSTPARTUM.
TOTAL CAIRAN secara umum seharusnya dibatasi TIDAK LEBIH dari
1. 80 mL/jam, atau
2. 1 mL/kg/jam, atau
3. (60-125 ml/jam)
Jumat, 08 Maret 2019 39 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
MedScape, Kee-Hak Lim, MD; Ronald M Ramus, MD Preeclampsia Updated: Nov 29, 2018
Cunningham, 2018. Williams Obstetrics, 25th ed.)
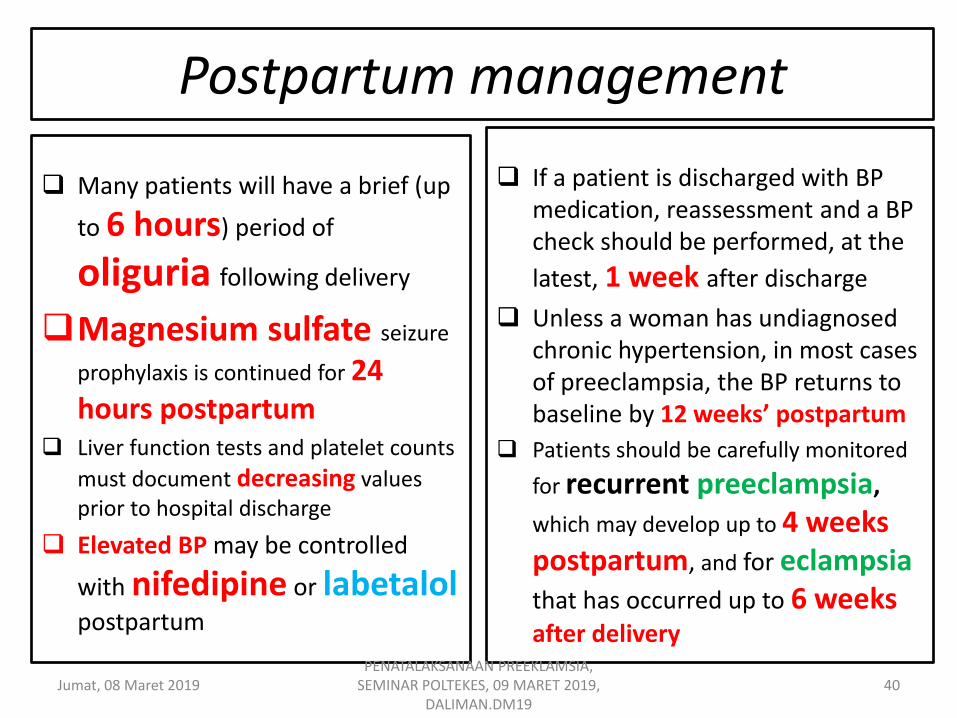
Postpartum management
Many patients will have a brief (up
to 6 hours) period of
oliguria following delivery
Magnesium sulfate seizure
prophylaxis is continued for 24 hours postpartum
Liver function tests and platelet counts
must document decreasing values prior to hospital discharge
Elevated BP may be controlled
with nifedipine or labetalol postpartum
If a patient is discharged with BP medication, reassessment and a BP check should be performed, at the
latest, 1 week after discharge
Unless a woman has undiagnosed chronic hypertension, in most cases of preeclampsia, the BP returns to baseline by 12 weeks’ postpartum
Patients should be carefully monitored
for recurrent preeclampsia,
which may develop up to 4 weeks postpartum, and for eclampsia
that has occurred up to 6 weeks after delivery
Jumat, 08 Maret 2019 40 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Jumat, 08 Maret 2019 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
41
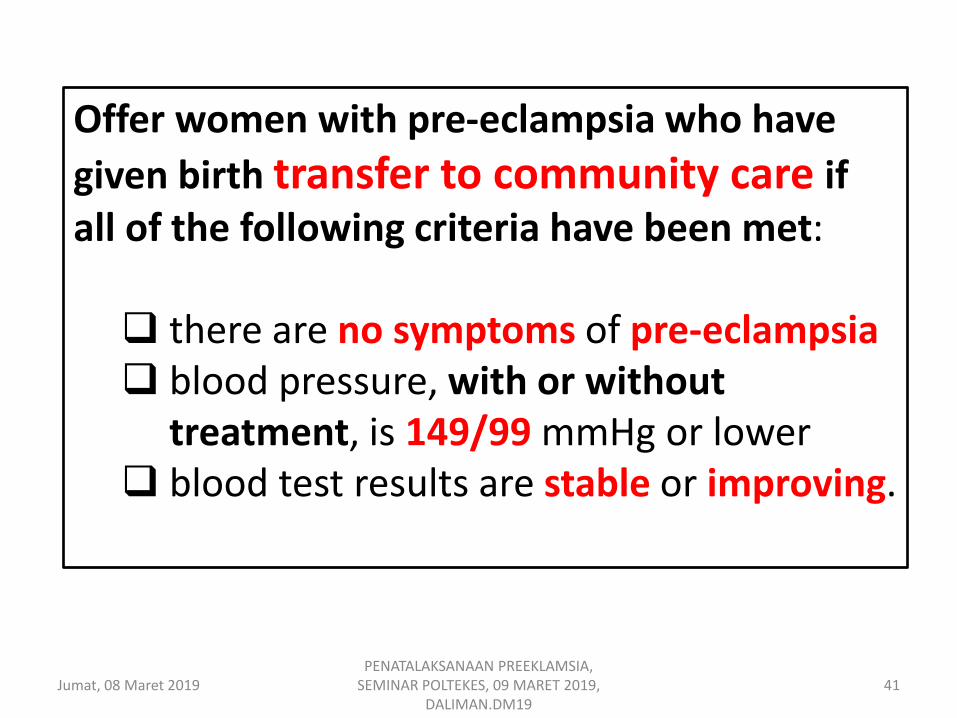
Offer women with pre-eclampsia who have
given birth transfer to community care if all of the following criteria have been met: there are no symptoms of pre-eclampsia blood pressure, with or without
treatment, is 149/99 mmHg or lower blood test results are stable or improving.
Jumat, 08 Maret 2019 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
42
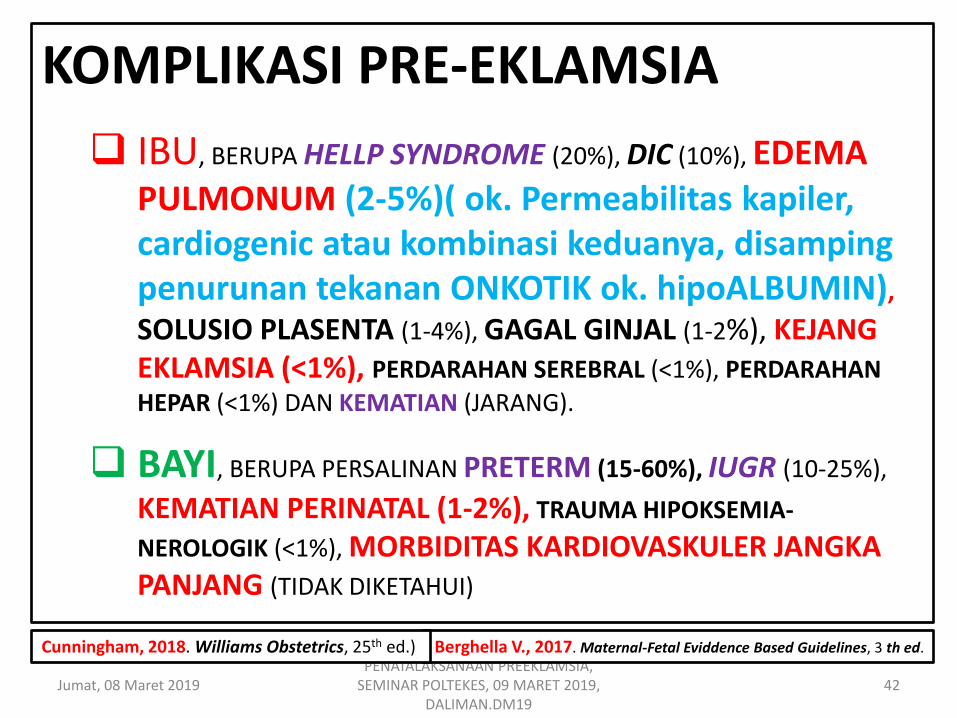
KOMPLIKASI PRE-EKLAMSIA
IBU, BERUPA HELLP SYNDROME (20%), DIC (10%), EDEMA PULMONUM (2-5%)( ok. Permeabilitas kapiler, cardiogenic atau kombinasi keduanya, disamping penurunan tekanan ONKOTIK ok. hipoALBUMIN),
SOLUSIO PLASENTA (1-4%), GAGAL GINJAL (1-2%), KEJANG EKLAMSIA (<1%), PERDARAHAN SEREBRAL (<1%), PERDARAHAN
HEPAR (<1%) DAN KEMATIAN (JARANG).
BAYI, BERUPA PERSALINAN PRETERM (15-60%), IUGR (10-25%),
KEMATIAN PERINATAL (1-2%), TRAUMA HIPOKSEMIA-
NEROLOGIK (<1%), MORBIDITAS KARDIOVASKULER JANGKA PANJANG (TIDAK DIKETAHUI)
Berghella V., 2017. Maternal-Fetal Eviddence Based Guidelines, 3 th ed. Cunningham, 2018. Williams Obstetrics, 25th ed.)

Jumat, 08 Maret 2019 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
43
KOMPLIKASI EKLAMSIA
KEMATIAN MATERNAL (1-2%) DI NEGARA
MAJU, LEBIH DARI (10%) DI NEGARA BERKEMBANG.
KEMATIAN PERINATAL (6-12%) DI NEGARA
MAJU, LEBIH DARI (25%) DI NEGARA BERKEMBANG.
SOLUSIO PLASENTA (7-10%), DIC (7-11%), HELLP
(10-15%), EDEMA PULMONUM (3-5%), GAGAL GINJAL (5-9%), PNEUMONIA ASPIRASI (2-3%), CARDIOPULMONARY ARREST (2-5%), PERSALINAN PRETERM (50%).

Jumat, 08 Maret 2019 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
44
MORBIDITAS DAN MORTALITAS
JANGKA PANJANG PENDERITA
PREEKLAMSIA, TERNYATA
MENINGKAT SECARA
BERMAKNA DIBANDINGKAN
BUKAN PENDERITA
PREEKLAMSIA, TERHADAP
KEJADIAN HIPERTENSI,
IHD, STROKE, DAN
PENYEBAB LAIN
KEMATIAN.
Long-term cardiovascular consequences of
preeclampsia. All differences p ≤.001 except p =
0.03 for all-cause mortality. (Data from Bellamy and colleagues, 2007.)

Acute Treatment of Severe Hypertension in Pregnancy
In the setting of severe
hypertension (SBP >160 mm Hg 93% STROKE H;
DBP >110 mm Hg 20% STROKE H), antihypertensive treatment is
recommended.
The goal of hypertension treatment is to lower BP to prevent cerebrovascular and cardiac complications while maintaining uteroplacental blood flow (ie, maintain BP
around 140/90 mm Hg).
Jumat, 08 Maret 2019 45 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Cunningham, 2018. Williams Obstetrics, 25th ed.)

ANTIHYPERTENSIVE and PE
CONTROL of MILDLY increasing BP does not appear to improve PERINATAL MORBIDITY or MORTALITY, and it may, in fact, REDUCE BIRTH WEIGHT.
Jumat, 08 Maret 2019 46 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Antihypertensive treatment decreases the incidence of cerebrovascular problems, is dose not alter the progression of PREECLAMPSIA.
MedScape, Kee-Hak Lim, MD; Ronald M Ramus, MD Preeclampsia Updated: Nov 29, 2018
Prophylactic treatment with
magnesium sulfate Prophylactic treatment with magnesium sulfate is indicated for
all patients with severe preeclampsia. However,
no consensus exists as to whether patients with mild preeclampsia need magnesium seizure prophylaxis.
Although ACOG recommends magnesium sulfate in severe preeclampsia, it has not recommended this
therapy in all cases of mild preeclampsia.
Jumat, 08 Maret 2019 47 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
MedScape, Kee-Hak Lim, MD; Ronald M Ramus, MD Preeclampsia Updated: Nov 29, 2018
Jumat, 08 Maret 2019 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
48
Some Indications for Delivery with Early-Onset Severe Preeclampsia (Cunningham, 2018):
Maternal
1. Persistent severe headache or visual changes; eclampsia 2. Shortness of breath; chest tightness with rales and/or SaO2 < 94
percent breathing room air; pulmonary edema 3. Uncontrolled severe hypertension despite treatment
4. Oliguria < 500 mL/24 hr or serum creatinine 1.5 mg/dL 5. Persistent platelet counts < 100,000/L, 6. AST or ALT > 2 x upper limit of normal with RUQ or epigastric pain,
7. Suspected abruption, progressive labor, and/or ruptured
membranes,
AFI = amnionic fluid index; EGA = estimated gestational age; SaO2 = oxygen saturation.
From Sibai and Barton (2007).
≤ 72 JAM
Foley MR, et., 2018. Obstetric Intensive Care Manual. 5th ed.
ONE OR MORE
MedScape, Kee-Hak Lim, MD; Ronald M Ramus, MD Preeclampsia Updated: Nov 29, 2018

Jumat, 08 Maret 2019 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
49
Fetal
1. Severe growth restriction—< 5th percentile for EGA
2. Persistent severe oligohydramnios —AFI < 5 cm/ DVP < 2 cm.
3. Biophysical profile 4 done 4-6 hr apart 4. Reversed end-diastolic umbilical artery flow 5. Repetitive late or severe variable heart rate
deceleration, 6. Fetal death
Foley MR, et., 2018. Obstetric Intensive Care Manual. 5th ed
≤ 72 JAM ONE OR MORE
MedScape, Kee-Hak Lim, MD; Ronald M Ramus,
MD Preeclampsia Updated: Nov 29, 2018

Jumat, 08 Maret 2019 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
50
Foley MR, et., 2018. Obstetric Intensive Care Manual. 5th ed
Penyebab EDEMA PULMONUM
1.CARDIAC (HIGH PRESSURES) Cardiac dysfunction,
Pulmonary venous dysfunction, Pulmonary Embolism, Airway
Obstruction, Preeclampsia, Miscelaneous, (decreased Left
Ventricular contractility, Mitral stenosis, Mitral regurgitation, INTRAVASCULAR VOLUME OVERLOAD, dysrithmias), (Venous occlusive disease, Neurogenic pulmonary vasoconstriction), (Amniotic fluid, thrombus, fat, air), (edema, astma,
foreign body), (Pulmonary hypertension), (Pneumothorax, tumor, one lung anesthesia (down lung syndrome)).
2.NONCARDIOGENIC (PERMEABILITY) Adult
Respiratory Disterss Syndrome (ARDS), Aspiration Syndrome, Pulmonary Embolism, Abruptio Placentae, Dead Fetus Syndrome, Sepsis.
EDEMA PULMONUM
Jumat, 08 Maret 2019 51 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
DIAGNOSIS PROGRESIF nafas pendek, desaturasi, takhipnea, kadang HIPERTENSI, bilateral RBBH, S3 Gallops (tidak selalu).
FAKTOR PREDISPOSIS KELEBIHAN CAIRAN (fluid overload), PE, terapi TOKOLITIK, HT tak terkontrol.
MANAJEMEN posisi semi-Fowler, kepala dan dada ditinggikan, O2 10 L/m sungkup (facemask) atau CPAP, puls oxymetri kontinyu dan monitor cardiac, PEMBATASAN CAIRAN (30-50 ml/jam), kontrol faktor predisposisi.
Terapi farmakologi MORFIN sulfat : 3-5 mg IV, FUROSEMID : 20-40 mg iv dapat diulang – maksimal dosis 120 mg/jam-pelan untuk menghindari INTOKSIKASI, NITROGLYCERIN 2 in of paste to chest atau 1 pill (1/150) IV, HYDRALAZINE : 5-10 mg IV HT BERAT.
DIAGNOSIS, FAKTOR PREDISPOSISI, MANAJEMEN, TERAPI FARMAKOLOGI, MONITOR.
Foley MR, et., 2018. Obstetric Intensive Care Manual. 5TH ed.
Preparing for Clinical Emergencies in Obstetrics and Gynecology
Examples of Tools for Managing Clinical Emergencies
1. Availability of appropriate emergency supplies in a resuscitation cart (crash cart) or kit
2. Development of a rapid response team
3. Development of protocols that include
clinical triggers 4. Use of standardized communication tools for
huddles and briefs (eg, SBAR)
5. Implementation of emergency drills and simulations
Abbreviation: SBAR, Situation–Background–Assessment–Recommendation.
ABSTRACT: Patient care emergencies may occur at any time in any setting, particularly the inpatient setting. It is important that obstetrician–gynecologists prepare themselves
by assessing potential emergencies, establishing early warning systems, designating specialized first responders, conducting emergency drills, and debriefing staff after actual events to identify strengths and opportunities for improvement. Having such systems in place may reduce or prevent the severity of medical emergencies.
ACOG COMMITTEE OPINION Number 590, March 2014 (Replaces Committee Opinion
Number 487, April 2011) (Reaffirmed 2018)
Jumat, 08 Maret 2019 52 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
Wassalamu’alaikum warahmatullahi wabarakaatuh
Jumat, 08 Maret 2019 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
53
CURICULUM VITAE (CV) • Nama : DALIMAN, dr.Sp.OG(K)FM.
• T/ TL : Klaten, 3 Februari 1956.
• Alamat : Jl. Dr. Angka, 28. PURWOKERTO.
• Email : [email protected]
• Pendidikan :
SD – SMA ,tamat 1974, Wonosobo.
Dokter, FK UGM Angkatan 1975, tamat 1981.
Spesialis Obgin, Sp.OG, FK UGM 1989, tamat 1993.
Konsultan Fetomaternal, (K)FM, FK UGM 2009, tamat 2011.
• Pekerjaan :
Kepala Puskesmas Nanga Sepauk, Sintang, Kalbar (1982-1987)
Direktur RSUD Sintang, Kalbar (1987-1989).
Tenaga Medis Fungsional, Sp.OG, RSUD Sintang, Kalbar (1994-1998).
Wakil Direktur RSUD Margono Soekarjo (2000-2008).
Wakil Dekan FK Unsoed (2001-2004)
Dokter Pendidik Klinis RSUD Margogono Soekarjo/ FKIK Unsoed (2009- SEKARAG).
Jumat, 08 Maret 2019 PENATALAKSANAAN PREEKLAMSIA,
SEMINAR POLTEKES, 09 MARET 2019, DALIMAN.DM19
54




















