MANAGEMEN KEPERAWATAN PADA PASIEN SHOCK · PDF filePASIEN SHOCK Agus K Anam,M.Kep. Definisi...
34
MANAGEMEN KEPERAWATAN PADA PASIEN SHOCK Agus K Anam,M.Kep
Transcript of MANAGEMEN KEPERAWATAN PADA PASIEN SHOCK · PDF filePASIEN SHOCK Agus K Anam,M.Kep. Definisi...
MANAGEMEN KEPERAWATAN PADA
PASIEN SHOCK
Agus K Anam,M.Kep
Definisi
Suatu sindroma dimana Suatu sindroma dimana Suatu sindroma dimana Suatu sindroma dimana PERFUSI JARINGAN TIDAK PERFUSI JARINGAN TIDAK PERFUSI JARINGAN TIDAK PERFUSI JARINGAN TIDAK
ADEKUATADEKUATADEKUATADEKUAT, akibat dari ketidak mampuan sistem , akibat dari ketidak mampuan sistem , akibat dari ketidak mampuan sistem , akibat dari ketidak mampuan sistem
sirkulasi untuk mensuplai oksigensirkulasi untuk mensuplai oksigensirkulasi untuk mensuplai oksigensirkulasi untuk mensuplai oksigensirkulasi untuk mensuplai oksigensirkulasi untuk mensuplai oksigensirkulasi untuk mensuplai oksigensirkulasi untuk mensuplai oksigen
Shock
• Perfusi jaringan tidak adekuat
• Penurunan suplai oksigen • Penurunan suplai oksigen
• Metabolisme anaerobik
• Akumulasi “metabolic waste”
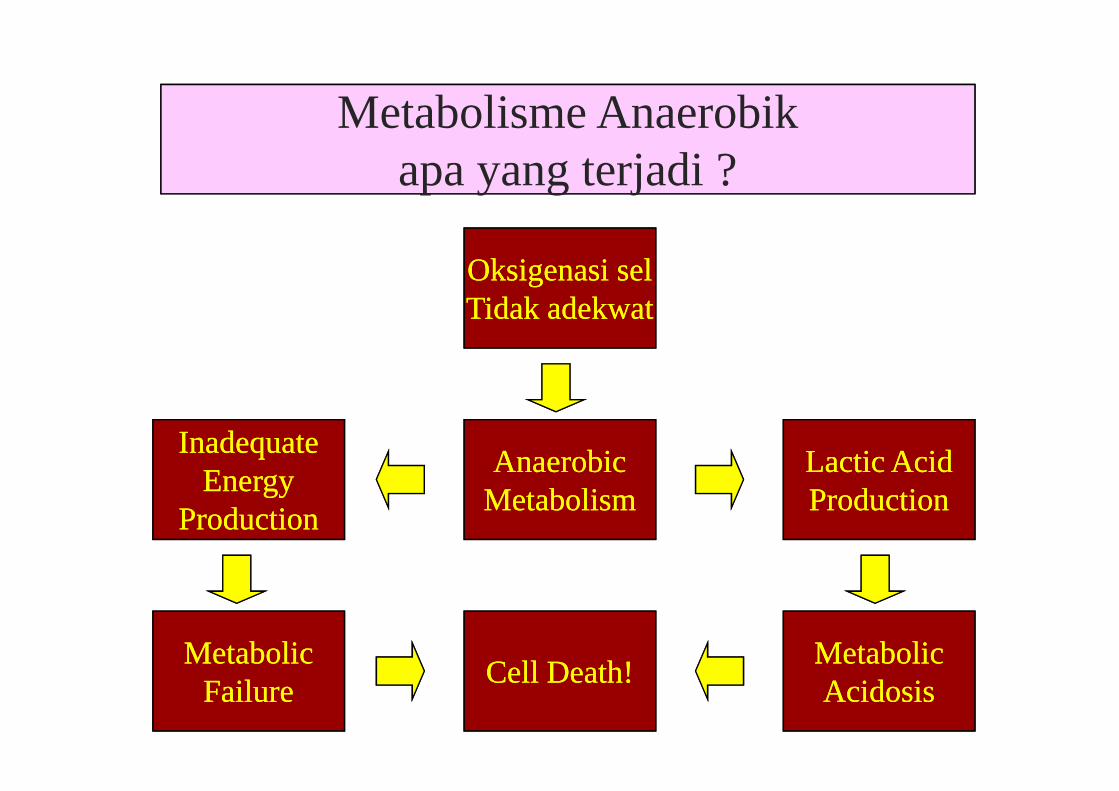
apayang terjadi?Metabolisme Anaerobik
apa yang terjadi ?
Oksigenasi selOksigenasi selTidak adekwatTidak adekwat
AnaerobicAnaerobicMetabolismMetabolism
MetabolicMetabolicFailureFailure
MetabolicMetabolicAcidosisAcidosis
InadequateInadequateEnergyEnergy
ProductionProduction
Lactic AcidLactic AcidProductionProduction
Cell Death!Cell Death!
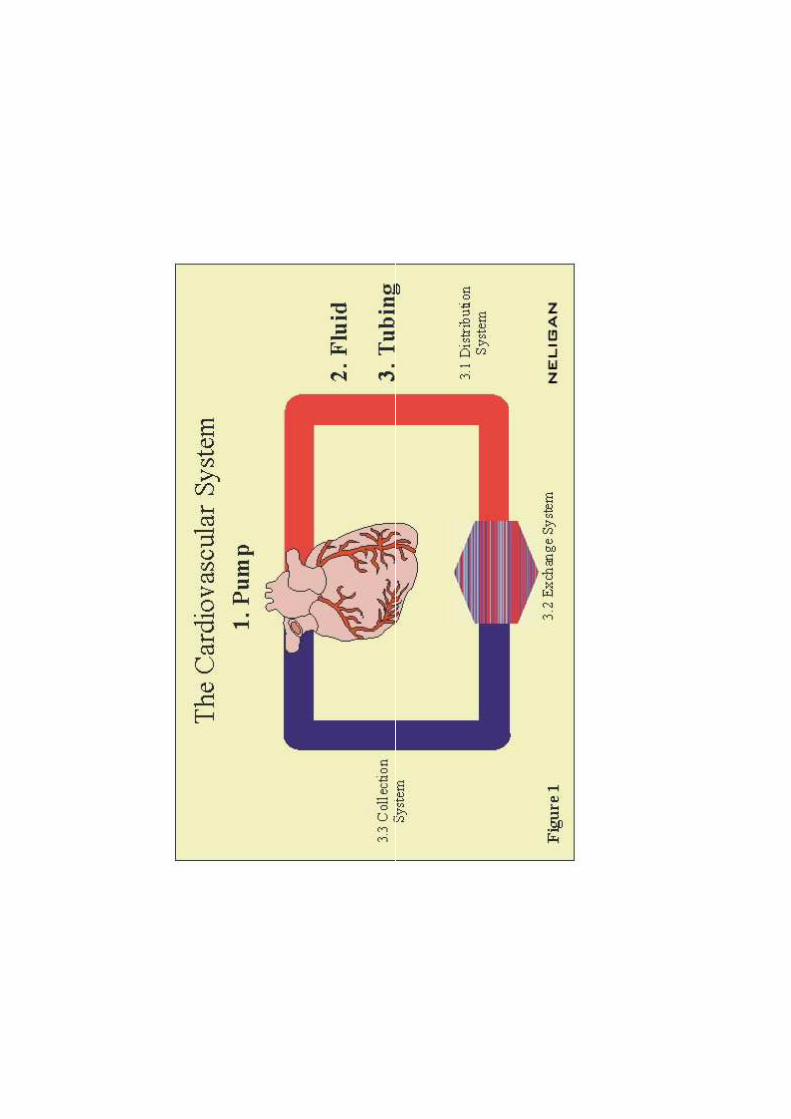
� PUMP tdk bekerja scr optimal
cardiogenic
� FLUID tidak cukup dlm sistem� FLUID tidak cukup dlm sistem
hypovolaemia
� TUBING : gangguan fungsi distribusi
distributive
Kondisi normalKondisi normalKondisi normalKondisi normal
satu komponen mengalami gangguan fungsi
komponen lain berusaha melakukan kompensasi
Pada kondisi Pada kondisi Pada kondisi Pada kondisi shockshockshockshock
satu komponen mengalami gangguan fungsi
elemen lain gagal melakukan kompensasi secara adekuat
Penyebab Shock
• Serangan jantung• Kehilangan darah yg berat atau tiba-tiba• Penurunan cairan tubuh
Core Skills Treat for Shock 8
• Penurunan cairan tubuh• Infeksi• Terpapar lama pada kondisi
panas/dingin yg ekstrem
Klasifikasi Shock
�Syok Kardiogenik
�Syok Hipovolemik�Syok Hipovolemik
�Syok Distributif
�Syok Obstruktif
Cardiogenic shock
• Jantung kehilangan kemampuan u/ memberikan
suplai darah ke seluruh bagian tubuh
• Biasanya akibat kegagalan ventrikel kiri sekunder • Biasanya akibat kegagalan ventrikel kiri sekunder
thd infark miokardial akut infark miokardial akut infark miokardial akut infark miokardial akut & gagal jantunggagal jantunggagal jantunggagal jantung
Hypovolemic Shock
Shock akibat tubuh kehilangan darah, plasma atau cairan tubuh yg lain
Penyebab :� Perdarahan internal atau eksternal � Perdarahan internal atau eksternal
� Trauma
� Dehidrasi
� Kehilangan plasma akibat luka bakar
� Terpapar panas yg berlebihan
� Diuresis osmotik akibat ketoasidosis diabetikum
DISTRIBUTIVE SHOCK
• NEUROGENIC SHOCK
• ANAPHYLAKTIC SHOCK
• SEPTIC SHOCK• SEPTIC SHOCK
Neurogenic Shock
• Results from injury to brain or spinal cord causing an interruption of nerve impulses to the arteries.
• The arteries dilate causing relative hypovolemia.
• Sympathetic impulses to the adrenal glands are lost, preventing the release of catecholamines with theircompensatory effects.
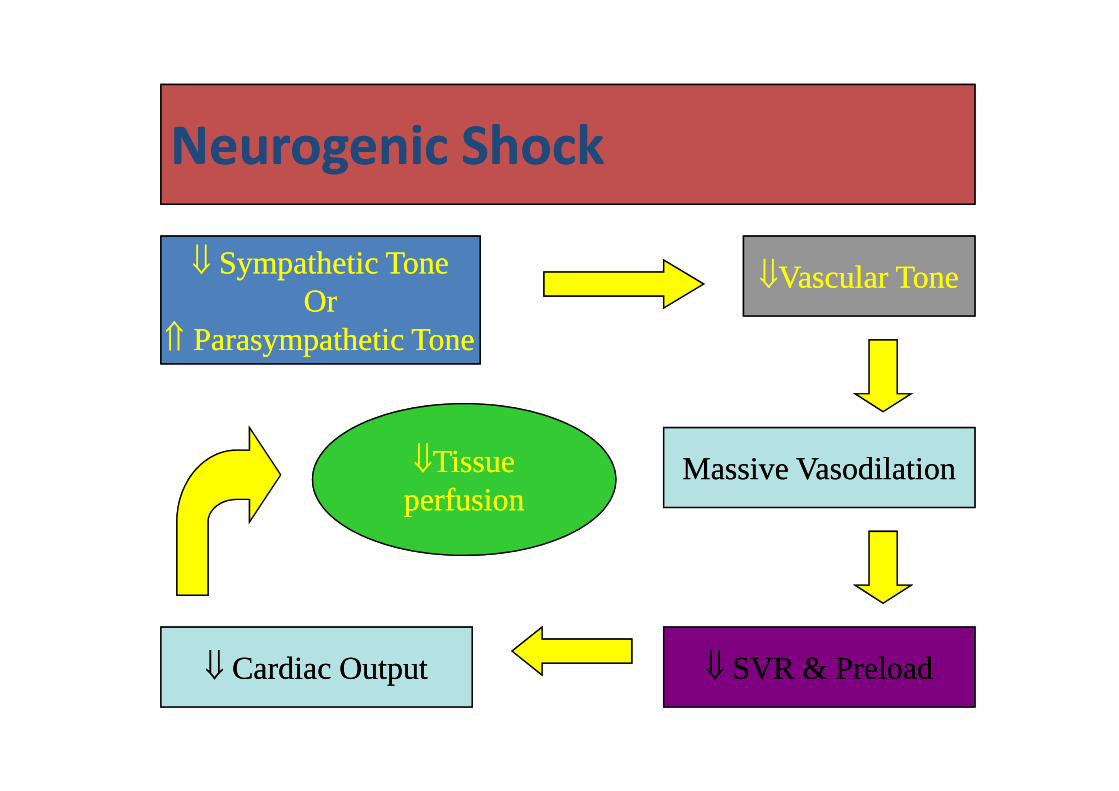
Neurogenic ShockNeurogenic Shock
⇓⇓ Sympathetic ToneSympathetic ToneOrOr
⇑⇑ Parasympathetic ToneParasympathetic Tone
⇓⇓Vascular ToneVascular Tone
Massive VasodilationMassive Vasodilation
⇓⇓ SVR & PreloadSVR & Preload⇓⇓ Cardiac OutputCardiac Output
⇓⇓TissueTissueperfusionperfusion
Anaphylactic Shock
• A severe immune response to a foreign substance.
• Signs and symptoms most often occur within a minute, but can take up to an hour.
• The most rapid reactions are in response to injected substances:– Penicillin injections.– Bees, wasps
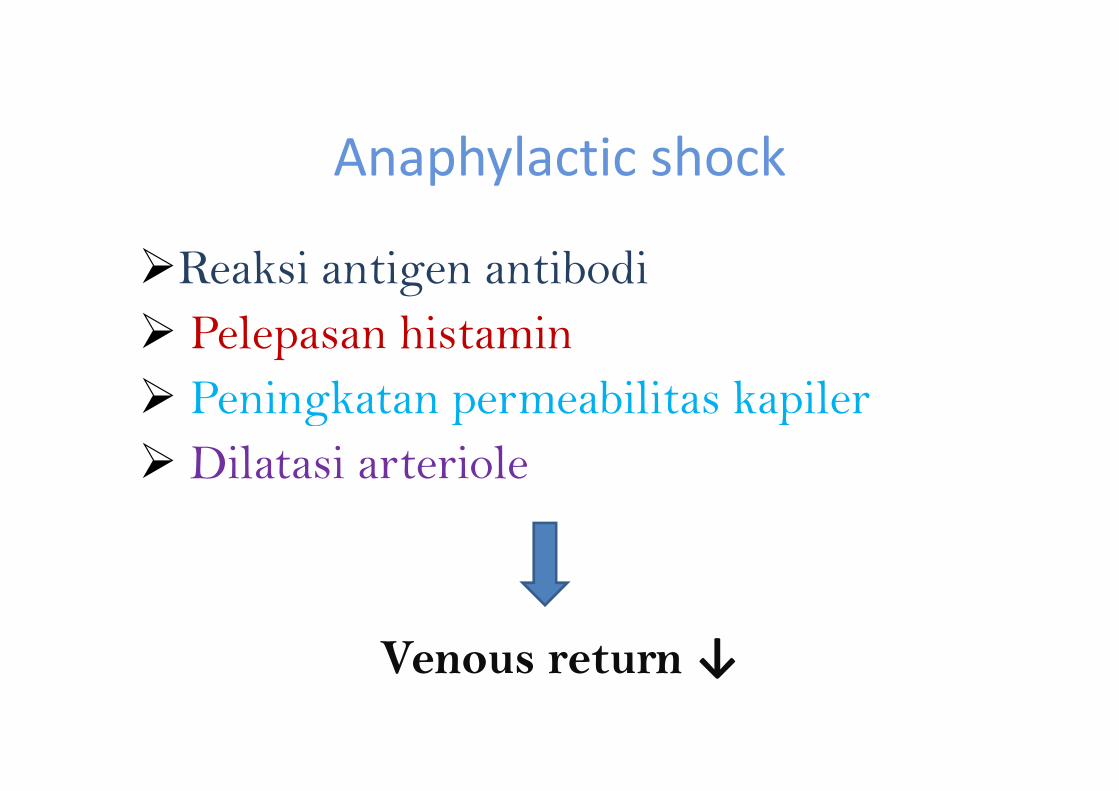
Anaphylactic shock
�Reaksi antigen antibodi
� Pelepasan histamin
� Peningkatan permeabilitas kapiler� Peningkatan permeabilitas kapiler
� Dilatasi arteriole
Venous return ↓
Septic ShockSeptic Shock
�� Shock yg terjadi akibat penyebaranatau invasi kuman
Toksin yg dilepaskan berdampak pada� Toksin yg dilepaskan berdampak padavasodilatasi
• Kompensasi normal :– Vasokonstriksi progresif
– Pe↑ aliran darah ke organ vital
RESPON TUBUH TERHADAP SYOK / KOMPENSASI
– Pe↑ aliran darah ke organ vital
– Pe↑ cardiac output
– Pe↑ kecepatan dan volume pernafasan
– Pe↓ produksi urin
Tanda Shock Akut
• Pe↓ TD sistolik & diastolik secara progresif• Kulit dingin, pucat, dan lembab• Sianosis• Nadi kecil dan cepat• Nadi kecil dan cepat• Pernafasan cepat dan dangkal• Oliguria• Perubahan/Pe↓ tingkat kesadaran
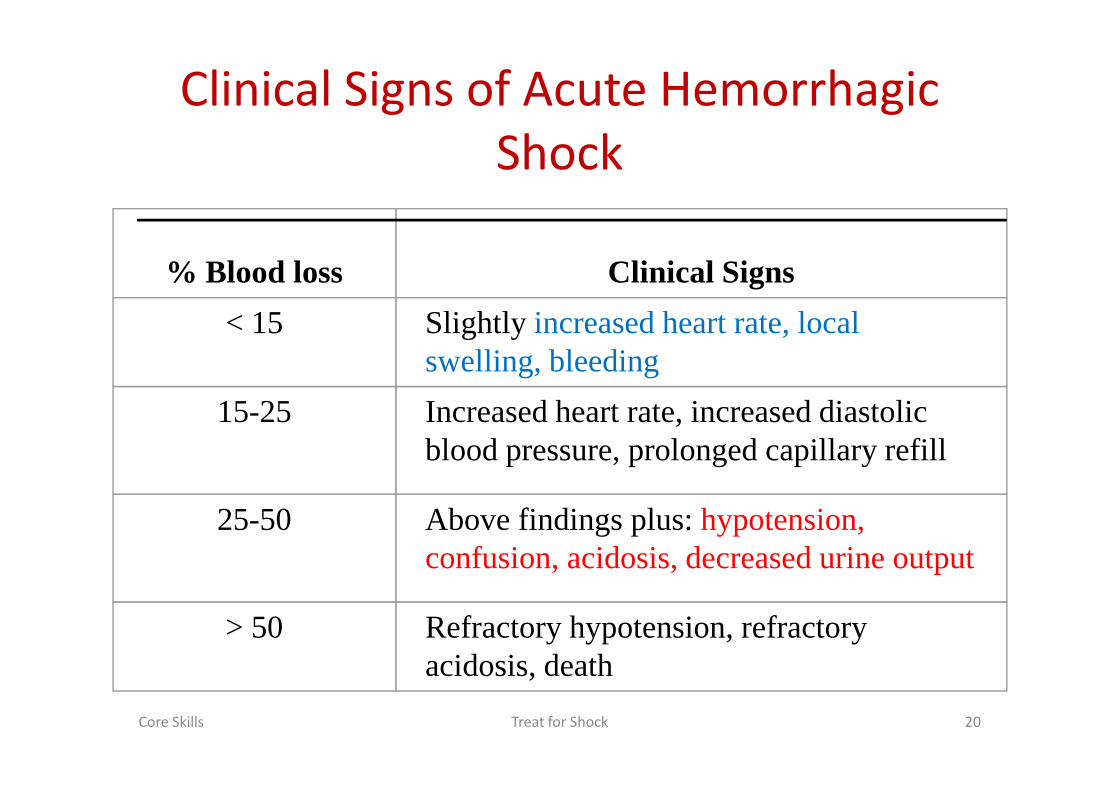
Clinical Signs of Acute Hemorrhagic
Shock
% Blood loss Clinical Signs
< 15 Slightly increased heart rate, local swelling, bleeding
15-25 Increased heart rate, increased diastolic
Core Skills Treat for Shock 20
15-25 Increased heart rate, increased diastolic blood pressure, prolonged capillary refill
25-50 Above findings plus: hypotension, confusion, acidosis, decreased urine output
> 50 Refractory hypotension, refractory acidosis, death
Tingkatan Shock
� Compensatory stage
Respon kompensatorik dpt menstabilkan sirkulasi
� Progressive stage� Progressive stage
Manifestasi dari sistemik hipoperfusi & kemunduran fungsi organ
� Irreversible stage
Kerusakan sel yg hebat tdk dpt dihindari yg akhirnya menujukematian
Compensatory stage assessment
• Restlessness
• oriented
• pupils normal
• heart rate increased
• Diastolic B/P normal or
slight increase
• respirations faster and
deeper
• output = or <• systolic B/P normal or
slight decrease
• output = or <
• pale, cool, may be
thirsty
Role of the RN
• Continuous in-depth assessment of the patient’s hemodynamic status
– Prompt recognition of problems
– Accurate use of emergency orders
Prompt and accurate reports of deviations in – Prompt and accurate reports of deviations in assessment to physician
• Reducing patient anxiety
• Promoting patient safety
Progressive stage assessment
• Listless, agitated,
apathetic, confused
• speech slowed
• pupils dilated
• tachycardia
• Diastolic B/P falling
• respirations rapid and
shallow
• oliguria
• cold, clammy, cyanotic, • tachycardia
• pulses weak
• systolic B/P < 90
• cold, clammy, cyanotic,
marked increase in
thirst
Role of the RN
• Requires expertise in assessing and
understanding shock and the significance of
changes in assessment data
• Managing, implementing and documenting
treatments, medications, fluids along with
continuous assessment and collaboration
Irreversible shock assessment
• Confused, disoriented or unconscious
• reflexes absent
• pupils dilated with minimal response to
• Systolic B/P falling to unobtainable
• Diastolic B/P approaching 0
• Respirations slow and minimal response to light
• HR slow and irregular
• pulses absent (or very weak)
• Respirations slow and shallow, irregular
• output very <or absent
• cold, clammy
• absent bowel sounds
Role of the RN
• Continuing the astute assessment and
interventions begun in previous stages
• Recognizing that the patient is very likely to be
terminalterminal
• Initiating palliative and end-of-life activities
• Support and explanation to family members
Treatment of Shock
Increase tissue perfusion and oxygenation status
• Maintain airway• Control bleeding • Baseline vital signs • Level of consciousness
Treatment of Shock
• Positioning• ABCD approach
• Fluid therapy• Fluid therapy• Drug therapy• Keep patient at normal temperature
– Prevent hypothermia
– Minimize effect of shock
• On-going assessment - every 10-15 minutes
Fluid Replacement
• Crystalloid replacement: NS and LR– Easily available, but can cause rebound overload,
much is lost to tissues
– No oxygen carrying capacity
• Colloids: plasma proteins such as albumin– Large molecules that pull fluids into tissues, but
are harder to obtain, more expensive and run risk of anaphylaxis
– No oxygen carrying capacity
• Blood: if the patient is in hypovolemic
shock, this is the fluid of choice
– Does have oxygen carrying capacity
– Harder and slower to obtain, generally needs
to be cross-matchedto be cross-matched
Vasoactive medications
�Vasopressors: Intropin (dopamine), Dobutrex
(dobutamine)
� Vasodilators: Nipride (nitroprusside), Tridil� Vasodilators: Nipride (nitroprusside), Tridil
(nitroglycerine)
Other medications
• Corticosteroids
• Antibiotics

THANK’S