lapkas chf
55
CHF FC III/IV ec CAD PEMBIMBING: Dr. PARLINDUNGAN MANIK, Sp.JP PRESENTATOR : ANDITHA NAMIRA REZKY SITOMPUL RAJA HASAYANGAN SIREGAR FAKULTAS KEDOKTERAN UNIVERSITAS SUMATERA UTARA MEDAN 2014
-
Upload
anditha-namira-rs -
Category
Documents
-
view
59 -
download
2
description
laporan kasus chronic heart failure
Transcript of lapkas chf
-
CHF FC III/IV ec CAD
PEMBIMBING:Dr. PARLINDUNGAN MANIK, Sp.JP
PRESENTATOR :ANDITHA NAMIRA REZKY SITOMPULRAJA HASAYANGAN SIREGAR
FAKULTAS KEDOKTERAN UNIVERSITAS SUMATERA UTARAMEDAN 2014
-
HEART FAILURE
-
DEFINISIGagal jantung merupakan sindroma klinis yang kompleks akibat gangguan struktural atau fungsional jantung yang menyebabkan kegagalan pemompaan (sistolik) atau pengisian (diastolik) darah ke dalam ventrikel sehingga jantung gagal untuk memenuhi kebutuhan oksigen dan metabolisme jaringan.
-
ETIOLOGIGAGAL JANTUNG KIRIGangguan kontraktilitasInfark miokardiumTransient myocardial ischemiaBeban volume: regurgitasi katup (mitral atau aorta)Kardiomiopati dilatasi
-
Peningkatan afterload (beban tekanan)Hipertensi sistemikObstruksi aliran: stenosis aortaObstruksi pengisian ventrikel kiriStenosis mitralKonstriksi pericardial atau tamponade Gangguan relaksasi ventrikelHipertrofi ventrikel kiriKardiomiopati hipertrofiKardiomiopati restriktif
-
GAGAL JANTUNG KANAN
Penyebab jantungGagal jantung kiriStenosis katup pulmonalInfark ventrikel kananPenyakit parenkim paruPenyakit paru obstruksi kronisPenyakit paru interstisial
-
Adult respiratory distress syndrome Infeksi paru kronis atau bronkiektasisPenyakit vaskular paruEmboli paruHipertensi pulmonal primer
-
PATOFISIOLOGI
-
Patofisiologi
-
KLASIFIKASI
-
Kriteria Framingham
-
DIAGNOSA
-
Pemeriksaan penunjang
-
Penatalaksanaan
-
PENYAKIT JANTUNG KORONER
-
DEFINISIPenyakit jantung koroner umumnya ditandai dengan episode ketidakseimbangan kebutuhan dan persediaan oksigen otot jantung, terkait dengan iskemia atau hipoksia, yang biasanya diinduksi oleh aktivitas, emosi atau stres lainnya, dan juga dapat terjadi spontan.
-
FAKTOR RISIKOTIDAK DAPAT DIMODIFIKASIDAPAT DIMODIFIKASIJenis kelamin Usia Riwayat keluarga
DislipidemiaTekanan darah tinggi Merokok Diabetes melitusObesitasKurang olahraga Alkohol
-
KLASIFIKASIAngina pektoris ialah sindrom klinis yang ditandai dengan rasa tidak nyaman di dada, rahang, bahu, punggung, atau lengan, biasanya ditimbulkan oleh aktivitas atau stres emosional dan hilang dengan istirahat atau nitrogliserin. Infark miokard adalah perkembangan cepat dari nekrosis otot jantung yang disebabkan oleh ketidakseimbangan antara suplai dan kebutuhan oksigen.
-
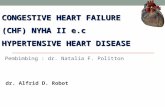
Endothelial DysfunctionFoamCellsFattyStreakIntermediateLesion
AtheromaFibrousPlaqueComplicatedLesion/RuptureEndothelial injurynitric oxideendothelin-1vasodilationLipid accumulationadhesion molecules (ICAM, VCAM)monocyte adhesionmacrophage LDL uptakeInflammationcontinued macrophage/lipid accumulationleukocyte accumulationcytokines (IL-6, TNFa, IFNg )MMP'sCRP (hepatic)oxidized LDLhomocysteinesmokingaginghyperglycemiahypertension35-45 yrs45-55 yrs 55-65 yrs >65 yrsPATOFISIOLOGI
-
DIAGNOSIS
-
PENATALAKSANAAN
-
PENATALAKSANAAN
-
*
-
*Nama: SutrisnoNo. MR: 49.29.18Umur: 45 tahunJ.K.: Laki-lakiPekerjaan: Buruh BangunanAlamat: Jl. Setia Budi Gg Dame No. 14Agama: Islam
-
*KU: Sesak napasT : Hal ini sudah dialami o.s. dalam 2 bulan terakhir, dan dirasakan memberat dalam 1 bulan terakhir. Pada awalnya sesak napas muncul saat beraktivitas berat, namun 1 bulan terakhir sesak juga muncul saat istirahat. PND (+), OT (+). Os merasa lebih baik bila tidur dengan diganjal 2-3 bantal. Sesak napas tidak berhubungan dengan cuaca. Riwayat batuk (-). Riwayat mual-muntah (-). Riwayat demam (-).Riwayat nyeri dada (+) 1 tahun lalu. Nyeri seperti tertusuk-tusuk dan terasa panas di dada sebelah kiri selama > 30 menit, namun saat itu os merasa tidak perlu berobat.
-
Riwayat kaki bengkak (+) sejak 2 minggu terakhir. Riwayat tekanan darah tinggi dan gula darah tinggi disangkal os.
Riwayat merokok (+) selama > 10 tahun sebanyak 4 bungkus / hari. Riwayat minum minuman beralkohol (+) selama > 10 tahun.
Sebelum masuk ke RSHAM, o.s. pernah berobat ke RS Sari Mutiara dan dirawat selama 2 minggu. Namun karena merasa tidak ada perbaikan os pulang.
Faktor risiko PJK: laki-laki, usia . 45 tahun, perokokRPT : tidak jelasRPO : tidak jelas*
-
Status PresensKU: sedang
Kesadaran: CMTD: 120/80 mmHg Pols: 113 x/i, regularRR: 22 x/iSuhu: 37.5C
Sianosis: (-) Ortopnu: (+) Dispnu: (+) Ikterus: (-) Edema: (-) Pucat: (-)*
-
Pemeriksaan Fisik:Kepala : konjungtiva palpebra inferior anemis (-/-), sklera ikterik (-/-)Leher: TVJ: R+3 cmH2ODinding toraks:Inspeksi: simetris fusiformisPalpasi: SF Ka=Ki, kesan normalPerkusi: sonor pada kedua lapangan paru Batas jantung:Atas: ICR III SinistraKanan: ICR IV LSDKiri: ICR V 2 cm lateral LMCS
*
-
AuskultasiJantung:S1 (N) S2 (N) S3 (-) S4 (-) regularMurmur: (-)Tipe: -Grade: -Punctum maximum: -Radiasi: -Paru:Suara pernafasan: vesikulerSuara tambahan: ronki basah basal (+) wheezing (-/-)Abdomen:Palpasi Hepar/Lien: tidak teraba Asites (+)Ekstremitas:Superior: sianosis (-)Clubbing: (-)Inferior: edema (+/+)Pulsasi arteri: (+)Akral: hangat
*
-
Interpretasi EKGST. QRS rate 113x/i. QRS axis (N). P wave (N). PR interval 0,16. QRS duration 0,08. Poor R progression V1-V5. LVH(-). VES (+). ST-T changes (-). T inverted V5-V6, I, aVL.
Kesan: ST + OMI Anteroseptal + Iskemik lateral*
-
Interpretasi Foto ToraksCTR 68%. Ao : normal. Po : normal. Pinggang jantung mendatar. Apex downward. Kongesti (+). Infiltrat (-).
Kesan : kardiomegali + kongesti*
-
Hasil Echocardiography*
-
*
-
Hasil LaboratoriumHematologi Hb 13.40 gr% RBC 4.32 x 106 /mm3 WBC 9.69 x 103/mm3 PLT 245 x 103/mm3 Ht 38.70 %
Metabolisme CHO:KGD adR: 113.9 mg/dL
GinjalUreum 29.50 mg/dL Kreatinin 0.96 mg/dLElektrolitNatrium: 129 mEq/LKalium: 3.5 mEq/LKlorida: 106 m Eq/LEnzim JantungCK-MB: 38 U/LTroponin T: - g/LCK-NAC: 100 U/L*
-
Analisa Gas DarahpH : 7.506pCO2 : 27.7 mmHgpO2 : 159.9 mmHgHCO3 : 21.4 mmol/LTotal CO2 : 22.3 mmol/LBE : -0.8Saturasi O2 : 99.5%*
-
*CHF Fc. III/IV ec. CAD
Fungsional : CHF Fc. III/IVAnatomi : MiokardiumEtiologi : CAD
Diagnosis
-
*- Bed Rest semi fowler- O2 2-4 L/i- IVFD NaCl 0,9% 10 gtt/i (mikro)Inj. Furosemide 20 mg/8 jam- Captopril 3 x 6.25 mgBisoprolol 1 x 1.25 mgAspilet 1 x 80 mg- Simvastatin 1 x 20 mg
Pengobatan
-
*Darah RutinECGLipid profileEchocardiographyAngiography coronerPenjajakan
-
Follow Up 25 Des 2013*
TanggalVital Sign & PFDiagnosaPenatalaksanaan25-12-13S: sesak napasO: Sens: CMTD: 120/80 mmHgHR: 110 x/iRR: 30 x/i Temp: 36.5CKepala: mata: anemia (-), sklera ikterik (-)Leher: TVJ R + 3 cm H2OAuskultasiJantung: S1(N), S2(N), Murmur : (-)Paru: Suara pernafasan : Vesikuler Suara tambahan : ronki basah basal (+)Abdomen:Soepel, H/L/R ttbAsites (+)Ekstremitas:Akral hangat, Oedem pretibial (+/+)CHF Fc. III/IV ec. CAD Bed Rest semi fowlerO2 2 -4 L/iIVFD NaCl 0,9% 10 gtt/i (mikro)Inj. Furosemide 20 mg/8 jamCaptopril 3 x 6.25 mgBisoprolol 1 x 2.5 mgAspilet 1 x 80 mgSimvastatin 1 x 20 mg
-
Follow Up 26 Des 2013*
TanggalVital Sign & PFDiagnosaPenatalaksanaan26-12-13S: sesak napasO: Sens: CMTD: 120/80 mmHgHR: 92 x/iRR: 28 x/i Temp: 36.7CKepala: mata: anemia (-), sklera ikterik (-)Leher: TVJ R + 2 cm H2OAuskultasiJantung: S1(N), S2(N), Murmur : (-)Paru: Suara pernafasan : Vesikuler Suara tambahan : ronki basah basal (+)Abdomen:Soepel, H/L/R ttbAsites (+)Ekstremitas:Akral hangat, Oedem pretibial (+/+)CHF Fc. III/IV ec. CAD (OMI Anteroseptal) Bed Rest semi fowlerO2 2 -4 L/iIVFD NaCl 0,9% 10 gtt/i (mikro)Inj. Furosemide 20 mg/6 jamInj. Dobutamin 5 mg/ kgBB/iCaptopril 2 x 12.5 mgAspilet 1 x 80 mgISDN 5 mgSimvastatin 1 x 20 mgLaxadin 1 x CIAlprazolam 1 x 0.5 mgUSR 2 x 600 mg
-
Follow Up 27 Des 2013*
TanggalVital Sign & PFDiagnosaPenatalaksanaan27-12-13S: sesak napasO: Sens: CMTD: 120/80 mmHgHR: 92 x/iRR: 26 x/i Temp: 36.9CKepala: mata: anemia (-), sklera ikterik (-)Leher: TVJ R + 2 cm H2OAuskultasiJantung: S1(N), S2(N), Murmur : (-)Paru: Suara pernafasan : Vesikuler Suara tambahan : ronki basah basal (+)Abdomen:Soepel, H/L/R ttbAsites (+)Ekstremitas:Akral hangat, Oedem pretibial (+/+)CHF Fc. III/IV ec. CAD (OMI Anteroseptal) Bed Rest semi fowlerO2 2 -4 L/iIVFD NaCl 0,9% 10 gtt/i (mikro)Inj. Furosemide 20 mg/6 jamInj. Dobutamin 5 mg/ kgBB/iCaptopril 2 x 12.5 mgAspilet 1 x 80 mgISDN 5 mgSimvastatin 1 x 20 mgLaxadin 1 x CIAlprazolam 1 x 0.5 mgUSR 2 x 600 mg
-
Follow Up 28 Des 2013*
TanggalVital Sign & PFDiagnosaPenatalaksanaan28-12-13S: sesak napasO: Sens: CMTD: 100/70 mmHgHR: 98 x/iRR: 26 x/i Temp: 36.6CKepala: mata: anemia (-), sklera ikterik (-)Leher: TVJ R + 2 cm H2OAuskultasiJantung: S1(N), S2(N), Murmur : (+) PSM grade 3/6 di apeksParu: Suara pernafasan : Vesikuler Suara tambahan : ronki basah basal (+)Abdomen:Soepel, H/L/R ttbAsites (+)Ekstremitas:Akral hangat, Oedem pretibial (+/+)CHF Fc. III/IV ec. CAD (OMI Anteroseptal) Bed Rest semi fowlerO2 2 -4 L/iIVFD NaCl 0,9% 10 gtt/i (mikro)Inj. Furosemide 20 mg/6 jamInj. Dobutamin 5 mg/ kgBB/iCaptopril 2 x 12.5 mgAspilet 1 x 80 mgISDN 5 mgSimvastatin 1 x 20 mgBisoprolol 1 x 1.25 mgLaxadin 1 x CIAlprazolam 1 x 0.5 mgUSR 2 x 600 mg
-
Follow Up 29 Des 2013*
TanggalVital Sign & PFDiagnosaPenatalaksanaan29-12-13S: sesak napasO: Sens: CMTD: 100/70 mmHgHR: 98 x/iRR: 26 x/i Temp: 36.6CKepala: mata: anemia (-), sklera ikterik (-)Leher: TVJ R + 2 cm H2OAuskultasiJantung: S1(N), S2(N), Murmur : (+) PSM grade 3/6 di apeksParu: Suara pernafasan : Vesikuler Suara tambahan : ronki basah basal (+)Abdomen:Soepel, H/L/R ttbAsites (+)Ekstremitas:Akral hangat, Oedem pretibial (+/+)CHF Fc. III/IV ec. CAD (OMI Anteroseptal) Bed Rest semi fowlerO2 2 -4 L/IDiet jantung IIIIVFD NaCl 0,9% 10 gtt/i (mikro)Inj. Furosemide 20 mg/6 jamInj. Dobutamin 5 mg/ kgBB/iCaptopril 2 x 12.5 mgAspilet 1 x 80 mgISDN 5 mgSimvastatin 1 x 20 mgBisoprolol 1 x 1.25 mgLaxadin 1 x CIAlprazolam 1 x 0.5 mgUSR 2 x 600 mgSpironolacton 1 x 25 mg
-
*
TanggalVital Sign & PFDiagnosaPenatalaksanaan30-12-13S: sesak napasO: Sens: CMTD: 100/70 mmHgHR: 68 x/iRR: 28 x/i Temp: 36.6CKepala: mata: anemia (-), sklera ikterik (-)Leher: TVJ R + 2 cm H2OAuskultasiJantung: S1(N), S2(N), Murmur : (+) PSM grade 3/6 di apeksParu: Suara pernafasan : Vesikuler Suara tambahan : ronki basah basal (+)Abdomen:Soepel, H/L/R ttbAsites (+)Ekstremitas:Akral hangat, Oedem pretibial (+/+)CHF Fc. III/IV ec. CAD (OMI Anteroseptal) Bed Rest semi fowlerO2 2 -4 L/IDiet jantung IIIIVFD NaCl 0,9% 10 gtt/i (mikro)Inj. Furosemide 20 mg/6 jamInj. Dobutamin 5 mg/ kgBB/iCaptopril 2 x 12.5 mgAspilet 1 x 80 mgISDN 5 mgSimvastatin 1 x 20 mgBisoprolol 1 x 1.25 mgLaxadin 1 x CIAlprazolam 1 x 0.5 mgUSR 2 x 600 mgSpironolacton 1 x 25 mg
-
*
TanggalVital Sign & PFDiagnosaPenatalaksanaan31-12-13S: sesak napasO: Sens: CMTD: 100/70 mmHgHR: 78 x/iRR: 28 x/i Temp: 36.6CKepala: mata: anemia (-), sklera ikterik (-)Leher: TVJ R + 2 cm H2OAuskultasiJantung: S1(N), S2(N), Murmur : (+) PSM grade 3/6 di apeksParu: Suara pernafasan : Vesikuler Suara tambahan : ronki basah basal (+)Abdomen:Soepel, H/L/R ttbAsites (+)Ekstremitas:Akral hangat, Oedem pretibial (+/+)CHF Fc. III/IV ec. CAD (OMI Anteroseptal) Bed Rest semi fowlerO2 2 -4 L/IDiet jantung III + ekstra putih telurIVFD NaCl 0,9% 10 gtt/i (mikro)Inj. Furosemide 20 mg/6 jamInj. Dobutamin 5 mg/ kgBB/iCaptopril 2 x 12.5 mgAspilet 1 x 80 mgISDN 5 mgSimvastatin 1 x 20 mgBisoprolol 1 x 1.25 mgLaxadin 1 x CIAlprazolam 1 x 0.5 mgUSR 2 x 600 mgSpironolacton 1 x 25 mg
-
*
TanggalVital Sign & PFDiagnosaPenatalaksanaan1-1-14S: sesak napasO: Sens: CMTD: 100/70 mmHgHR: 78 x/iRR: 28 x/i Temp: 36.6CKepala: mata: anemia (-), sklera ikterik (-)Leher: TVJ R + 2 cm H2OAuskultasiJantung: S1(N), S2(N), Murmur : (+) PSM grade 3/6 di apeksParu: Suara pernafasan : Vesikuler Suara tambahan : ronki basah basal (+)Abdomen:Soepel, H/L/R ttbAsites (+)Ekstremitas:Akral hangat, Oedem pretibial (+/+)CHF Fc. III/IV ec. CAD (OMI Anteroseptal) Bed Rest semi fowlerO2 2 -4 L/IDiet jantung III + ekstra putih telurIVFD NaCl 0,9% 10 gtt/i (mikro)Inj. Furosemide 20 mg/6 jamInj. Dobutamin 5 mg/ kgBB/iCaptopril 2 x 12.5 mgAspilet 1 x 80 mgISDN 5 mgSimvastatin 1 x 20 mgBisoprolol 1 x 1.25 mgLaxadin 1 x CIAlprazolam 1 x 0.5 mgUSR 2 x 600 mgSpironolacton 1 x 25 mg
-
*
TanggalVital Sign & PFDiagnosaPenatalaksanaan2-1-14S: sesak napasO: Sens: CMTD: 100/70 mmHgHR: 78 x/iRR: 28 x/i Temp: 36.6CKepala: mata: anemia (-), sklera ikterik (-)Leher: TVJ R + 2 cm H2OAuskultasiJantung: S1(N), S2(N), Murmur : (+) PSM grade 3/6 di apeksParu: Suara pernafasan : Vesikuler Suara tambahan : ronki basah basal (+)Abdomen:Soepel, H/L/R ttbAsites (+)Ekstremitas:Akral hangat, Oedem pretibial (+/+)CHF Fc. III/IV ec. CAD (OMI Anteroseptal) Bed Rest semi fowlerO2 2 -4 L/IDiet jantung III + ekstra putih telurIVFD NaCl 0,9% 10 gtt/i (mikro)Inj. Furosemide 20 mg/6 jamInj. Dobutamin 5 mg/ kgBB/iCaptopril 2 x 12.5 mgAspilet 1 x 80 mgISDN 5 mgSimvastatin 1 x 20 mgBisoprolol 1 x 1.25 mgLaxadin 1 x CIAlprazolam 1 x 0.5 mgUSR 2 x 600 mgSpironolacton 1 x 25 mg
-
terimakasihI LOVE MY HEART, LET IT BEAT
*****Pathophysiology of AtherosclerosisAtherosclerosis is the main pathology underlying cardiovascular diseases, in the coronaries leading eventually leading to myocardial ischemia or infarction when it occurs in the coronary arteries, and to transient ischemic attacks and stroke when it occurs in the carotid or cerebral arteries. Atherosclerosis is a chronic, progressive process.
One of the earliest manifestations of atherosclerosis is thought to be dysfunction of the vascular endothelium, caused by one or more insults to the endothelium shown in the green box: LDL (especially the oxidized form) and other atherogenic lipoproteins, homocysteine, components in cigarette smoke, aging, hyperglycemia, and hypertension are examples. Endothelium dysfunction leads to a decrease in release of the vasodilator, nitric oxide, and an increase in production of the vasoconstrictor, endothelin-1, and can be detected non-invasively via ultrasound determination of vasodilation in the brachial artery. Although endothelial dysfunction occurs early in the atherosclerotic process, it continues throughout the progression of the disease.
A second major consequence of damage to the endothelium is an up-regulation of expression of various cellular adhesion molecules on the surface, including selectins, ICAM-1 and VCAM-1. These molecules mediate the binding of circulating monocytes to the vascular wall, which then migrate through the vascular wall and take up residence in the vascular wall, where they begin to oxidize and accumulate LDL. Continued accumulation of lipid-laden macrophages, known as foam cells, forms the first visible manifestation of the atherosclerotic lesion known as a fatty streak.
From the fatty streak lesion, the atherosclerotic process continues to progress with continued accumulation of macrophages, and later leukocytes. Pro-inflammatory cytokines (including IL-6, TNFa, and interferons) released by macrophages within the lesion exert local effects that continue to support progression of the lesion. Systemically, these inflammatory cytokines may also stimulate C-reactive protein sythesis from the liver an effect that has been hypothesized to account for the higher levels of circulating CRP observed in patients with CHD compared to those without. Recognition of this process of lipid and macrophage accumulation leading to inflammatory reaction at the vessel wall, which in turn feeds back to support further lipid accumulation, is the basis for the notion that atherosclerosis is an inflammatory disease.
The morphology of the lesion also evolves, from a simple fatty streak lesion to a more complex fibrous plaque, characterized by a core of lipid surrounded by a fibrous cap. These advanced atherosclerotic lesions have been categorized into 2 broad groups: lesions with a thick fibrous cap with a small lipid core and low macrophage content, and lesions with a thin fibrous cap with a large lipid core and high macrophage content. The former is generally considered a stable plaque less prone to rupture, and thus cause an acute event; whereas the latter is considered an unstable, or vulnerable, plaque more prone to rupture and thus cause an acute event. The factors determining the vulnerability of a plaque to rupture is currently an important area of research one of these factors is thought to be the activity of matrix metalloproteinases (MMPs) within the lesion. MMP activity degrades the collogen matrix of the fibrous cap, causing it to thin, weaken, and become for prone to rupture.
*****************