Kuliah Kesadaran Menurun UNTAR Mei 2012 (Presentasi)
79
KESADARAN MENURUN Hartono Prabowo Bagian Saraf Universitas Tarumanagara Jakarta 10-05-2012
-
Upload
idhar-dewi-pratami-ii -
Category
Documents
-
view
52 -
download
5
Transcript of Kuliah Kesadaran Menurun UNTAR Mei 2012 (Presentasi)

KESADARAN MENURUN
Hartono Prabowo
Bagian Saraf Universitas TarumanagaraJakarta
10-05-2012

Kesadaran Menurun
Seorang pasien pria 65 th diantar ke UGD oleh tetangga rumahnya oleh karena ditemukan dalam keadaan tidak sadarkan diri. Pada pemeriksaan dengan rangsang nyeri didapatkan kelopak mata sedikit terbuka, kedua lengan fleksi disertai kedua tungkai ekstensi dan pasien terdengar “merintih” kesakitan. TD 140/90 mmHg, S 37.20 C, N 88x/menit dan R 24 x/menit

1. Dari data yang ada dapat disimpulkan GCS (Glasgow Coma Scale) pasien tersebut adalah :
A. E2 M2 V2 = 6B. E2 M3 V2 = 7C. E2 M4 V3 = 9D. E3 M3 V2 = 8
Kesadaran Menurun
B

2. Pemeriksaan penunjang yang perlu dipertimbangkan untuk pasien tersebut adalah sebagai berikut, kecuali :
A. Kadar gula darahB. Analisa gas darahC. Fungsi ginjalD. Kadar Potasium darah
Kesadaran Menurun
D

3. Apabila pada pemeriksaan fisik didapatkan adanya kelemahan ekstremitas kiri, maka pemeriksaan yang harus dipertimbangkan adalah sebagai berikut, kecuali :A. Brain CT-Scan / MRI
B. Kadar glukosa darah
C. Kadar potasium darah
D. Analisa gas darah
Kesadaran Menurun
C

4. Tindakan yang harus dikerjakan pada penderita dengan kesadaran menurun adalah sebagai berikut, kecuali :
A. Tindakan Neuroproteksi
B. Segera berikan Piracetam / citicholine
C. Koreksi kelainan sistemik penyebab penurunan kesadaran
D. Jika perlu segera lakukan reperfusi
Kesadaran Menurun C


Kesadaran

Kesadaran
• William James : “consciousness as awareness of one-self and the environment”.
• Phenomenal consciousness : otak dapat mengenali dan memberikan respons yang sesuai terhadap fenomena – fenomena yang terjadi didalam tubuh dan lingkungan

Definisi kesadaran
Kesadaran diartikan sebagai hasil berbagai fungsi yang kompleks dan berdasar pada alertness/ arousal
dan awareness (mengenali dan merespon dengan adekuat terhadap proses dalam diri dan lingkungan).
awareness
AROUSAL
CO
NS
CIO
US
NE
SS
Bedside :•arousal → eye opening. •External awareness → reproducible command following of “non-reflex”/voluntary movements
Thibaut et al, 2012

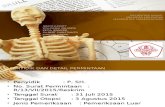
Anatomi Kesadaran
Integritas hubungan antara korteks serebri dengan sistem formasio retikularis pada batang otak.
ARAS menyalurkan impuls dari midpons ke rostral melalui tegmentum menuju nukleus intralaminaris (& nukleus
centromedial) thalamus untuk selanjutnya menuju korteks serebri.

12
Anatomi Kesadaran
Laureys et al, 2002
CO
NS
CIO
US
NE
SS
AROUSAL
AWARENESS
LANGUAGE
MOVEMENTSAppropriateLocalizedAbduction
Brainstem reflexes

13Adopted from Laureys, et al, 2007
TWO AWARENESS NETWORK
• awareness (content of consciousness)• arousal (level of consciousness )

Awareness
@ Sensasi
@ Persepsi
@ Fungsi memori
@ Atensi
@ Kognisi

Neurotransmiter pada alertness / arousal
1. Cholinergic (Ach)
2. Monoaminergic a. noradrenergic
b. dopaminergic
c. serotonergic
3. GABA-nergic.

Neuron aminergik pada formasio retikularis
Neurotransmiter Lokasi
Serotonin Nucl. Raphe midbrain, pons, medulla oblongata
Dopamine Tegmentum midbrain.
Norepinephrine Midbrain, pons, medulla oblongata.
Epinephrine Medulla oblongata.

Sistem Cholinergic
Jalur cholinergic berperan pada alertness /arousal sebagai komponen ARAS.
Aktivasi thalamus mengurangi tonus inhibisi nukleus retikularis thalamus
fasilitasi transmisi thalamo-
kortikal. Aktivasi struktur medial diencephalon
emosional erousal.

Noradrenergic
brainstem
dorsal thalamus
o locus ceruleus hipothalamus
hipocampus
neokorteks
Brainstem
o Nukleus tegmental lateralis
Med. Spin.

Terman & Bonica, 2001
Schematic diagram of the noradrenergic systemTo neocortex Anterior thalamic
nucleus
Thalamus
Habenula
PAG
N. Iocuscoeruleus(A6)
Trigeminalspinalnucleus
A1
A5
N. Subcoeruleus (A7)
Hippocampus
Amygdata
DLF
ILC
Modifikasi Meliala, 2003
Locus ceruleus medula oblongata.
Nukleus tegmentum lateralis pons dan medula oblongata.

Serotonergic → inhibisi
• Nukleus raphe tegmentum brainstem → proyeksi ke korteks serebri dan sistem limbik termasuk korteks pyriformis, hypothalamus, hippocampus dan diencephalon.
• Defisiensi serotonin (spt. Withdrawal alkohol) →→→ impulsip, over-reaktip,insomnia
(ggn. Siklus tidur).

Cingulate gyrusFronix
Thalamus
Habenula
PAG
N. Iocuscoeruleus
N. RaphePallidus (B1)
N. Central superior (B6. 8)
Hippocampus
Amygdata
Diagram of the origin and projection of the serotonergic system
N. Raphedorsalis (B7)
N. rapheMagnus(B3)
N. rapheObscurus(B2)
Hippocampus
Septum
DLF
VM
Terman & Bonica, 2001Modifikasi Meliala, 2003

Sistem dopaminergic
• Ventral tegmentum brainstem → neostriatal, mesolimbik dan mesokortikal.
o tu. Fungsi kognitip (lihat efek amphetamine dan obat antipsikotik sbg. Dopamine blocker).
o Peranan dalam arousal kecil tetapi dapat meningkatkan responsiveness.

GABA-nergic
• Neuron GABA-nergic tersebar luas pada SSP dengan fungsi pada kesadaran tidak jelas.
• Inhibisi korteks cerebri, thalamus, ganglion basalis, cerebellum dan med. Spinalis.
• Peningkatan GABA-nergic → alertness dan daya konsentrasi menurun

Glutamat dan aspartat.
• Sintesa pada korteks cerebri.
• Eksitatorik.
• Peranan pada kesadaran kecil.
• Lebih berperan pada komunikasi kortiko – kortikal.

A summary diagram of the ascending arousal system
NA : Noradrenaline5-HT : SerotoninDA : DopamineHis : HistamineORX : OrexinMCH : Melanin concentrating hormoneACh : AcetylcholineGABA : Gamma aminobutyric acid
LC : locus coeruleusvPAG : ventral periaqueductal gray matterTMN : Tubero-mammiullary nucleusLH : lateral hypothalamusBF : basal forebrainPPT : pedunculo pontine3
Plum and Posner’s 2007
The cholinergic system, shown in yellow, provides the main input to the relay and reticular nuclei of the thalamus from the upper brainstem. This inhibits the reticular nucleus and activates the thalamic relay nuclei, putting them into transmission mode for relaying sensory information to the cerebral cortex. The cortex is activated simultaneously by a series of direct inputs, shown in red

Kesadaran Menurun
Plum and Posner’s 2007

Kesadaran Menurun
Clouding of consciousness
minimally reduced wakefulness or awareness, hyperexcitability and irritability alternating with drowsiness
Delirium Disoriented (first to time, next to place, and then to persons in their environment ), motor restlessness, hallucination → bilateral impairment of cortical function
Obtundation a mild to moderate reduction in alertness, accompanied by a lesser interest in the environment. Such patients have slower psychologic responses to stimulation - increased number of hours of sleep
Stupor condition of deep sleep or similar behavioral unresponsiveness from which the subject can be aroused only with vigorous and continuous stimulation. Even when maximally aroused, the level of cognitive function may be impaired.
Coma “Deep sleep / Trance” → unresponsiveness in which the patient lies with eyes closed and cannot be aroused to respond appropriately to stimuli even with vigorous stimulation.
• Plum and Posner’s 2007• Huges. Neurological Emergencies. 4th ed. 2003

28
REDUCING CONSCIOUSNESS TO 2 D
Laureys, 2011

PLUM’S DEFINITION
Coma
(unconsciousness)
is an unarousable/ unresponsiveness condition in which , the patient is not
responsive to all stimuli
Coma is caused by disordered arousal rather than impairment of the awareness
J Neurol Neurosurg Psychiatry 2001;71(suppl I):i13–i17

Gangguan fungsi Formatio Retikularis (ARAS) pada tingkat batang otak.
Gangguan fungsi neuron korteks serebri.
Gangguan fungsi interkoneksi Batang Otak (ARAS) dan korteks serebri.
Kesadaran Menurun
• Kelainan bihemisfer serebri
• Bilateral – difus (infeksi, ggn sistemik spt hipoksia, hipoglikemia, uremia hiponatremia, dll)
• Unilateral → dampak pada midbrain
• Kelainan pada batang otak
• Principles and Practice of Emergency Neurology, 2003• Plum and Posner’s 2007• The Merck Manual for Health Care Professionals, 2008

Kesadaran Menurun
Ekstra – kranial Hipoksia / hipercapnea Hipo/hiperglikemia. Uremia. Hepatik ensefalopati. Gangguan elektrolit
(hipo Natremia). Hipoperfusi. Intoksikasi (CO, dll) Asidosis Drugs
Intra – kranial Trauma. CVD stroke Iskemik /
hemoragik. Infeksi (meningitis /
Ensefalitis. Tekanan Intrakranial ↑ Tumor / brain abscess Kejang / status
konvulsivus
• Principles and Practice of Emergency Neurology, 2003• Plum and Posner’s 2007• The Merck Manual for Health Care Professionals, 2008

Peningkatan glikolisis anaerobik
ml/100 g/ menit
ELECTRICAL FAILURE
IONIC FAILURE
Dipertahankan denganautoregulasi
Peningkatan ekstraksi O2 untuk pertahankan CMRO2
Penumbra
Depolarisasi anoksik
Oligemia
Nilai normal
Ringan
Moderat
Berat
ISKEMIA
CBF%
100
80
60
40
20
50
40
30
20
10
Cerebral blood flow (CBF)

Endocrinol Metab Clin N Am 35 (2006) 725–751
Hiperglikemia → kesadaran menurun
Hiperglikemia
Ketosis
Asidosis
DKA
Status Hiperglikemia lain :•DM tidak terkontrol•Stress hyperglycemia•HHS
Status ketosis lain :•Ketotic hypoglycemia•Ketosis alkoholik•Ketosis “starvation”•Isoprophyl alcohol•Hiperemesis
Status asidosis metabolik lain :•Laktat asidosis•Asidosis hiperkloremia•Salicylsm•Asidosis uremikum
• Sekresi insulin ↓• Inefektivitas insulin• Pe ↑ hormon kontra insulin
(glucagon, catecholamine, cortisol dan GH)

Hiperglikemia → kesadaran menurun
Hiperglikemia
Ketosis
Asidosis
Osmolaritas ↑Dehidrasi neuron
serebral
pH serebral ↓
Edema serebri
Metabolisme neuron
serebral ↓
Kesadaran ↓
Endocrinol Metab Clin N Am 35 (2006) 725–751

• Suppression / inhibition of insuline release
• Pancreas : secretion of glucagon & pancreatic polypeptide
• Adrenal medulla : secretion of epinephrine & norepinephrine (NE)
• Adrenal cortex : secretion of cortisol
• Sympathetic postganglionic nerve terminal : secretion of NE
• Pituitary gland : secretion of GH
Hipoglikemia (<70 mg/dl)
• Glucogenolysis ↑ • Gluconeogenesis ↑• Lipolysis ↑• Reduces glucose uptake in peripheral tissue
4 hrs
CLINICAL DIABETES. Volume 24, Number 3, 2006•

• Suppression / inhibition of insuline release• Pancreas : secretion of glucagon & pancreatic polypeptide• Adrenal medulla : secretion of epinephrine & norepinephrine (NE)• Adrenal cortex : secretion of cortisol• Sympathetic postganglionic nerve terminal : secretion of NE• Pituitary gland : secretion of GH
Hipoglikemia (<70 mg/dl)
• Glucogenolysis ↑ • Gluconeogenesis ↑• Lipolysis ↑• Reduces glucose uptake in peripheral tissue
4 hrs
CLINICAL DIABETES. Volume 24, Number 3, 2006•
Autonomic symptoms
Brain neuronal glucose
deprivation symptoms

Neurogenic (ANS) symptoms Neuroglycopenic symptoms
Shakiness (limbung) Abnormal mentation
Trembling (gemetar) Irritability
Anxiety (cemas) Confusion
Nervousness (gelisah) Difficulty in thinking
Palpitasion Dissiculty speaking
Clamminess (tangan basah/lembab)
Ataxia
Sweating (berkeringat dingin) Paresthesia
Dry mouth Headaches
Hunger Stupor
Pallor (pucat) Coma
Pupil dilation Death (if untreated)
Hipoglikemia
CLINICAL DIABETES. Volume 24, Number 3, 2006•

Ensefalopati Hepatikum
Ggn fungsi hati
Ammonia darah ↑
Uptake ammonia otak ↑
Metab Ammonia dalam Astrosit →
glutamin ↑
Permeabilitas BBB ↑ tanpa kerusakan membran basal
Edema serebri
TIK ↑ CBF ↓
Plum and Posner’s 2007
Kesadaran ↓

Hiponatremia Hipernatremia
Plum and Posner’s 2007
Ensefalopati hiper / hipo-Natremia

Obat-obat berpengaruh pada kesadaran
• Sedativa
• Barbiturates
• Tranquilisers
• Alkohol
• Opiates
• Anticholinergics
• Lithium
• Psikotropika
• Paraldehyde
Kesadaran ↓
• Principles and Practice of Emergency Neurology, 2003• Plum and Posner’s 2007• The Merck Manual for Health Care Professionals, 2008

• Diagnosis dan ABC koma harus simultan
• Ukur kadar Glucose darah segera → hipoglikemia?
• Pada kasus trauma dengan kesadaran menurun → imobilisasi leher sampai dapat dibuktikan tidak ada kelainan pada vertebra servikalis
Evaluasi penderita kesadaran menurun
The Merck Manual for Health Care Professionals, 2008The Merck Manual for Health Care Professionals, 2008

Evaluasi penderita kesadaran menurun
• Riwayat penyakit • Pemeriksaan fisik umum• Pemeriksaan neurologis termasuk (pemeriksaan
mata) • Pemeriksaan Laboratorium (darah, urin dan jika
perlu AGD ) • Neuroimaging (Brain CTScan / MRI, Ro-Thorax)• Ukur tekanan intrakranial (jika perlu dan mungkin) • Bila diagnosa tidak jelas → LP / EEG

Pemeriksaan fisik
• Keadaan umum• Tanda vital• Pola pernafasan dan “odor” spesifik• Jantung / paru / abdomen• Pupils• RBO (Refleks batang otak)• Reaksi terhadap rangsang nyeri• Fungsi traktus piramidalis• Tanda rangsang meningeal • Tanda TIK ↑

Observasi umum
• Gerakan menelan “brain function is still intact”• Asterixis dan “multifocal myoclonus” → ggn
metabolik (uremia, ensefalopati hepatikum, encephalopati hipoksik, intoksikasi obat) →ggn fungsi otak difus
• Psychogenic ? → tonus otot / refleks fisiologis / refleks batang otak normal (lateralisasi / refleks patologis negatip)
• Principles and Practice of Emergency Neurology, 2003• Plum and Posner’s 2007• The Merck Manual for Health Care Professionals, 2008

Penilaian kesadaran
Kwalitatip
CMSomnolen
SoporSoporokoma
Koma
KwantitatipGCS
(Glasgow Coma Scale)
Skala lain penilaian kesadaran•Innsbruck Coma Scale•Edinburgh-2 Coma Scale•Reaction Level Scale•Coma Recovery Scale Revised•FOUR Score (Full Outline of Unresponsiveness)•AVPU•ACDU

Metoda rangsang nyeri pada kesadaran menurun
Plum and Posner’s 2007

Verbal response Oriented to person, place, and date = 5 Converses but is disoriented = 4 Says inappropriate words = 3 Says incomprehensible sounds = 2 No response = 1
Glasgow Coma ScaleEye opening Spontaneous = 4 To speech = 3 To painful stimulation = 2 No response = 1
Motor response Follows commands = 6 Makes localizing movements to pain = 5 Makes withdrawal movements to pain = 4 Flexor (decorticate) posturing to pain = 3 Extensor (decerebrate) posturing to pain = 2 No response = 1
• Principles and Practice of Emergency Neurology, 2003• Plum and Posner’s 2007• The Merck Manual for Health Care Professionals, 2008

STEREOTYPED MOTOR RESPONSE
Flaccidity without movement → the lower brain stem is not affecting movement
Flaccidity without movement → the lower brain stem is not affecting movement
Decorticate → hemispheric damage with preservation of motor centers in the upper portion of the brain stem (eg, rubrospinal tract).
Decerebrate → the upper brain stem motor centers damage → only the lower brain stem centers (eg, vestibulospinal tract, reticulospinal tract), which facilitate extension, are responding to sensory stimuli.
• Principles and Practice of Emergency Neurology, 2003• Plum and Posner’s 2007• The Merck Manual for Health Care Professionals, 2008

Pola pernafasan dikaitkan lokasi lesi
Cheyne Stokes lesi pada hemisfer serebri / batang otak bagian atas
Central neurogenic hyperventilaion
= 40-70/m (Kussmaul/ Biot ) lesi pada tegmentum serebri / bagian atas pons
• Principles and Practice of Emergency Neurology, 2003• Plum and Posner’s 2007• The Merck Manual for Health Care Professionals, 2008

Apneustic lesi pada Pons (bilateral)
Ataksik lesi pada bagian dorsomedial formatio reticularis dan medula oblongata
Apnea lesi pada bagian Ventrolateral Medulla (bilateral)

Cheyne Stokes lesi pada hemisfer serebri / batang otak bagian atas
Central neurogenic hyperventilaion lesi pada tegmentum serebri / bagian atas pons
Apneustic lesi pada Pons (bilateral)Ataksik lesi pada bagian dorsomedial formatio reticularis dan medula oblongata Apnea lesi pada bagian Ventrolateral Medulla (bilateral)
Pola pernafasan dikaitkan lokasi lesi
• Principles and Practice of Emergency Neurology, 2003• Plum and Posner’s 2007• The Merck Manual for Health Care Professionals, 2008

Lesion Location
Eyes PositionLight
ReflexesPUPIL SIZE
EYES PICTURE
Hemisphere
Conjugate deviation to destructive lesion side
Normal Normal
Thalamus See to the nose Negative Small
Pons Medial eyes (Doll’s eyes)
Negative Small
Cerebellum Medial eyes Normal Big
The PupilsThe Pupils
• Principles and Practice of Emergency Neurology, 2003• Plum and Posner’s 2007• The Merck Manual for Health Care Professionals, 2008

Kelainan pupil dikaitkan lokasi lesiKelainan pupil dikaitkan lokasi lesi
Plum and Posner’s 2007

Refleks Batang Otak (RBO)
Pupil reflexesDoll’s eye
phenomenon
Corneal reflexes
Vomiting reflexes
Oculovestibular reflexes/
cold-water calories testing• Principles and Practice of Emergency Neurology, 2003• Plum and Posner’s 2007• The Merck Manual for Health Care Professionals, 2008

PYRAMIDAL -TRACT LESIONS
Motoric UMN paresis /paralysis
• Physiol Reflexes increase
• Pathol Reflexes (+)
• Muscle Tonus increase

Right Hemiparesis(lesion of left internal capsule)
Crossed Paresis(left midbrain lesion causing left oculomotor nerve palsy
and right hemiparesis
Crossed Paresis(lesion at the level of the
pyramidal decussation causing paresis of right arm
and left leg
Right Left

Intrakranial Herniasi
Plum and Posner’s 2007

Tanda-Tanda awal herniasi unkus
Plum and Posner’s 2007

Tanda-Tanda lanjut herniasi unkus
Plum and Posner’s 2007

Tanda-Tanda awal herniasi sentral / trantentorial
Plum and Posner’s 2007

Tanda-Tanda lanjut herniasi sentral / trantentorial
Plum and Posner’s 2007

Tanda-Tanda herniasi sentral / trantentorial (midbrain-upper pons)
Plum and Posner’s 2007

Tanda-Tanda herniasi sentral / trantentorial (lower pons – med. oblongata)
Plum and Posner’s 2007

DIAGNOSTIC TOOLS
Adopted from Laureys, 2011

Adopted from Laureys, 2011

Bruno et al, 2011

Bruno et al, 2011

Vegetative State / Coma Vigil / Apallic State
• Responsiveness and awareness negatip → fungsi kognitip (-)
• Akibat disfungsi hemisfer serebri dengan batang otak dan diensefalon normal
• Refleks Otonom, refleks motorik dan siklus tidur normal
• > 1 bulan• Principles and Practice of Emergency Neurology, 2003• Plum and Posner’s 2007• The Merck Manual for Health Care Professionals, 2008

• Etiologi : tu pasca hipoksia (ensefalopati) / trauma • Prognosis : dubia • Terapi : Suportip• Harapan hidup : 2 – 5 tahun• C.o.d : infeksi (paru / ISK)
Multi organ failure
Vegetative State / Coma Vigil / Apallic State
• Principles and Practice of Emergency Neurology, 2003• Plum and Posner’s 2007• The Merck Manual for Health Care Professionals, 2008

The locked-in syndrome describes a state in which the patient is de-efferented, resulting in paralysis of all four
limbs and the lower cranial nerves.
LOCK-IN SYNDROME
• Plum and Posner’s 2007• Demerti, 2010

Locked-in syndrome can be caused by stroke at the level of the basilar artery suppling denying blood to the Pons,
among other causes..
Unlike persistent vegetative state, in which the upper portions of the brain are damaged and the lower portions are spared, locked-in syndrome is caused by damage to specific portions of the lower brain and brainstem with no damage to the upper brain.
Agranoff, 2007
LOCK-IN SYNDROME
• Plum and Posner’s 2007• Demerti, 2010

Brain death
• Kebutuhan penggunaan ventilator jangka panjang.
• Kemungkinan terjadinya pemberian harapan yang tidak tepat kepada keluarga penderita.
Diagnosa Brain death perlu ditegakkan
•1959 (Mollaret & Goulon) → Irreversible coma
•1971 (Mohandas & Chou) → a critical component of severe brain damage
•1979 (Model Brain Death Act / US)→ Irreversible cessation of
• circulatory and respiratory function
• All function of brain
• Principles and Practice of Emergency Neurology, 2003• Plum and Posner’s 2007• The Merck Manual for Health Care Professionals, 2008

• Death :– Irreversible end of
life.
– Irreversible cessation of heartbeat and respiration.
• Brain Death :– Death of the brain
without cessation of the heart beat.
• Principles and Practice of Emergency Neurology, 2003• Plum and Posner’s 2007• The Merck Manual for Health Care Professionals, 2008
Brain death

• Harvard Committee (1968).
• The Minnesota Criteria (1971).
• President’s Commission for the study of Ethical Problem in Medicine and Biomedical and Behavioral Research, USA (1981).
• UK criteria (1995).
• AAN 1995.
Brain Death is defined as the irreversible loss of the capacity for consciousness combined with the
irreversible loss of all brainstem functions including the capacity to breathe.
• Principles and Practice of Emergency Neurology, 2003• Plum and Posner’s 2007• The Merck Manual for Health Care Professionals, 2008
Kriteria MBO (Brain death)

Brain Death Eelco F.M. Wijdicks, M.D.
N Engl J Med, Vol. 344, No. 16 April 19, 2001
• Koma (GCS 3).• Pupil dilatasi
maksimal.
Ventilator
Refleks Batang Otak
• Refleks okulosefalik.• Refleks pupil /
cahaya.• Refleks kornea.• Test irigasi• Refleks batuk /
muntah.• Test Sulfas Atropin. • Test apneu
Singkirkan :– Gangguan
keseimbangan asam-basa dan elektrolit.
– Hipothermia berat ( < 32o C).
– Hipotensi.– Intoksikasi ……
neuromuscular inhibitor.
NEGATIP
Should never be diagnosed hurriedly in the emergency room.

Brain Death (Eelco, 2001)
Evaluasi : 2 x
< 2 mo 48 hrs
2 mo – 1 y 24 hrs
1 – 18 y Facultative.
> 18 y Facultative
Should never be diagnosed hurriedly in the emergency room
Guidelines for determination of death JAMA 246:333,393. 1978

Pemeriksaan tambahan Dx – Brain deathEelco, 2001
Pemeriksaan Keterangan
Cerebral angiography Absence of intra-cerebral filling of the intracranial arteries at the entry into the skull.
EEG electro-cerebral silence
Transcranial Doppler (TCD).
Small systolic peaks in early systole with retrograde (reverberating, oscillation) or absent flow during diastole
Cerebral Scintigraphy
Atropine test Vagal component of 10th nerve
Jugular bulb oxygen saturation
SSEP / BAEP

• Kesadaran menurun merupakan keadaan emergensi • Kesadaran menurun dapat disebabkan oleh berbagai
kelainan baik intra maupun ekstrakranial. • Diagnosis yang cepat dan tepat merupakan tantangan
utama guna penatalaksanaan yang edekuat. • Diagnosis dapat ditegakkan dengan pemeriksaan
fisik, neurologis dan dengan bantuan pemeriksaan penunjang yang sesuai.
Kesimpulan