Dm,Rasional

of 56
-
Upload
ghina-ninditasari -
Category
Documents
-
view
216 -
download
0
description
Dm,Rasional
Transcript of Dm,Rasional
-
CURRICULUM VITAENama : DR.Dr. Aris Wibudi, SpPDTgl. Lahir : Walikukun, 27 April 1954Pendidikan .1980 : Lulus FK UI 1991 : Lulus Spesialis Peny. Dalam (FKUI) 1996 : Modul DM 1 (Endokrin FKUI) 1998: Modul DM 2 (Endokrin FKUI) 1992: Edukator DM (PERKENI) 2006: S-3, IPB Bogor Pekerjaan 2005 -: Staf Ahli RSPAD
-
Pengelolaan Rasional Diabetes Tipe-2Aris Wibudi
-
Distribution of oral glucose to tissues of the bodyCherrington, A.D. Diabetes 1999; 48:1198-1214
-
Gangguan Metabolik Utama pada DM-2Resistensi Insulin *
Defek sekresi insulin*
Peningkatan Produksi Glukosa*Diabetes Care, 1999; 22:562
-
backResistensi Insulin
-
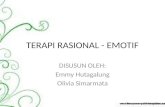
Insulin secretion profiles in Type 2diabetic patients and healthy people8006amInsulin secretion (pmol/min)Time10am2pm6pm10pm2am6am700600500400300200100Healthy peopleType 2 diabetic patientsPolonsky KS. Et al., 1988
-
Patterns of Insulin Response to IV Glucose: Non-Diabetic and Diabetic IndividualsInsulinSecretion1STPhase2NDPhaseNon-DiabeticType 2 DiabetesTime (minutes)InsulinSecretion
-
IGT
Postprandial Hyperglycemia
Type 2DiabetesPhase 1
Type 2DiabetesPhase 2
Type 2DiabetesPhase 3
- 12
- 10
- 6
- 2
0
2
6
10
14
Years from diagnosis
Beta cell function (%)
Stages of type 2 Diabetes in relationship to -cell function
25
0
50
75
100
hypoX-jsk-7-99
-
backInsulin eksogen
-
INSULINGLIKOGEN SINTASEProduksi Glukosa Hati
-
DMdefek
-
HIPER GLIKEMIA
-
prandial hiperglikemia
-
fasting hiperglikemiaSU-SR
-
combinationinsulininsulinOADOAD
-
insulinOADOADinsulin
-
Site of action of OADPencernaanGlukosa ekstraselSekresi insulin selbeta pankreasAGIProduksiglukosahepatikAmbilanglukosaototInsulin sensitizernutrisiAcarboseInsulin sensitizerMetforminInsulin Metforminglinid SU Sekretagog insulininsulinIslet Enhancer
-
Oral Anti DiabeticInsulinobat*
-
OADBiguanid MetforminInsulin sekretagoka. Sulfonilurea: glibenclamide gliclazide glipizid - glikuidon glimepirideb. glinide-glukosidase inhibitor (PGA)Insulin sensitizerIslet Enhancer
-
Kir 6.2SUR 1ATP Binding SiteSulphonylurea Binding SiteBenzoic Acid Binding SiteK+ATPDepolarizationCa++Ca++Mode of Action ofInsulin SecretagoguesThe KATP channel consists of subunits that comprise the inwardrectifying channel (Kir 6.2) and regulatory components (SUR 1). The SUR 1 regulates whether the inward rectifying K channel is open or closed. The SUR 1 subunit contains unique binding sites for ATP, Sulphonylurea, and Benzoic Acid Derivative
-
Percobaan in vitro menunjukkan bahwa glimepiride berikatan pada subunit reseptor sulfonilurea yang berbeda 1Ref.1. Kramer W et al. Diab Res Clin Pract 1995; 28 (Suppl): S67-S80.
-
Pada kondisi resistensi insulin, insulin tidak mampu menggerakkan jumlah GLUT 4 yang cukup ke permukaan sel
-
Terima Kasih
-
SHORT ACTING INTERMEDIATE ACTING
-
Diagnosis
-
DMNormoglikemiKomplikasiTerapi
-
makromikro
-
regulasi glukosa
-
FARMAKO TERAPI Dokter Pasien
-
Aspek pasienGemuk / kurusUsiaGangguan fungsi hati / ginjalLamanya DMHasil pemantauan glukosa darah
-
ASPEK DOKTERPengetahuan tentang obat
-
Pedoman PenatalaksanaanAlgoritmeKerja obatPatofisiologi
-
Pedoman PenatalaksanaanAlgoritmeKerja obatPatofisiologi
-
Algoritme Penatalaksanaan DM Tipe 2
-
INSULIN
-
SU + B / PG INSULINSU + B + PG
-
Pedoman PenatalaksanaanAlgoritmeKerja obatPatofisiologi
-
Natural History of Type 2 DiabetesNormal glucose metabolismImpaired glucose metabolismType 2 diabetesInsulin sensitivityInsulin secretion30%70%100%50%150%100%Diabetes Obes Metab 1999; 1(1): S1IGT50%70-100%
-
IGT
Postprandial Hyperglycemia
Type 2DiabetesPhase 1
Type 2DiabetesPhase 2
Type 2DiabetesPhase 3
- 12
- 10
- 6
- 2
0
2
6
10
14
Years from diagnosis
Beta cell function (%)
Stages of type 2 Diabetes in relationship to -cell function
25
0
50
75
100
hypoX-jsk-7-99
-
Development of Type 2 DiabetesINSULIN RESISTANCEInsulin Resistance and Hyperinsulinemia with Normal Glucose ToleranceInsulin Resistance and Declining Insulin Levels With Impaired Glucose ToleranceType 2 DiabetesImpaired Beta-Cell FunctionAdapted from Diabetes 1996;45:1661
-
Historical Algorithm ofTherapy for Type 2 DiabetesAdapted from Mudaliar S et al. In: Ellenberg and Rifkins Diabetes Mellitus, 6th ed. New York, NY: Appleton and Lange; 2003:531-557.Inadequate nonpharmacologic therapy
-
Proposed Algorithm ofTherapy for Type 2 DiabetesSevere symptomsSevere hyperglycaemiaKetosisPregnancyInadequate non-pharmacologic therapy
-
DOSISmulai dosis keciltingkatkan bertahap ataukombinasi
-
Monitor PemantauanGlukosa darahPuasa Prandial
-
Kemungkinan yang didapat Glukosa darahINormal Normal Puasa Post Prandial
-
- Insulin basal- Insulin prandial
-
IIIGDN / PP
-
IIGDN / PP
Insulin prandial
-
Ringkasan ( 1 )Penatalaksanaan DMTailored to the patientTeam Work NetworkPenurunan Glukosa segeraPenyerta
-
Ringkasan (2)Pilar PenatalaksanaanEdukasiTerapi NutrisiAktifitas FisikObat (bila perlu)
-
Ringkasan (3)Pedoman Farmakologik ALGORITMA PATOFISIOLOGI KERJA OBAT
-
Ringkasan (4)Tersedia pilihan OAD INSULIN
-
Ringkasan (5)INSULIN Short acting Intermediate Mixed
-
Ringkasan (6) OAD Sulfonilurea : Generasi I Generasi II Generasi III RepaglinidBiguanidPG Insulin Sensitiser
-
Ringkasan (7)Terapi Kombinasi Kapan saja Jangan golongan sama
-
Nature. 2003 Mar 13;422(6928):173-6. Epub 2003 Feb 23. Free fatty acids regulate insulin secretion from pancreatic beta cells through GPR40. Itoh Y et al. Takeda Chemical Industries, Ltd,
Related Articles, Links
-
Fig. Increase cellular levels of malonyl-CoA and FACoAs as a common mechanism causing glucolipotoxicity in various tissues in obesity associated type 2 diabetesPrentki et al. Diabetes 51 (Suppl. 53): S405-S413, 200
-
Increasedmass
Diabetescomplications
AlteredBlood flow andcontractility
ExcessiveGlucoseproduction
AlteredSecretionCell death
Insulinresistance
Hyperglycemia
Malonyl-CoA
FACoA
Hyperlipidemia
Adipose tissue
Muscle
b-cell
Neural
Vascular
Liver
-
(+) FA/glucose storage (+) FA oxidationAdipose tissue(+) glucose oxidation (-) FA oxidationMuscle(-) gluconeogenesis PEPCK liverPPAR FFAFFAEndocrinology(142);3,2001
-
GlucoseGlucoseG-6-PGlucokinaseMetabolismSignal (S)ATPADPK+ATPDepolarizationCa++Ca++SecretoryGranulesGLUT-2Insulin SecretionMechanism of Glucose-MediatedInsulin Secretion
-
Shepherd and Kahn. NEJM 1999; 341:248-257Insulin regulation of GLUT-4 translocation
-
Metabolic Effects of Insulin on Muscle and Fat Cells123
-
Signaling Molecule 1Signaling Molecule 2Plasma MembraneGPI-PLCGlut 4Insulin ReceptorPGlut 4TranslocationGlucoseTransport???GPI-PLCInsulin Saving Mechanism of Glimipiride(Muller et al 1996)abLipid Synthesis GlycogenSynthesisSUR-GLIMGLIM = Glimepiride15
-
10%20%70%dokterpasienedukator
-
Glukosa Darah Sel InsulinResistensi
The endocrine characteristics of type 2 diabetes include peripheral insulin resistance in muscle and fat tissue, decreased pancreatic insulin secretion, and increased hepatic glucose output.35. Insulin secretion profiles in Type 2 diabetic patients and healthy peopleUnder fasting conditions the insulin secretion rate is similar between healthy people and Type 2 diabetic patients. In normal people, insulin secretion increases rapidly after food intake and is followed by a return to basal levels before the next meal. In Type 2 diabetic patients, meal-related increases in insulin secretion are delayed and reduced, and secretion does not return to basal levels between meals.
It has been common practice to reserve insulin therapy until relatively late in the treatment plan for patients with type 2 diabetes. Typically, it is introduced after patients have failed to achieve glycaemic control with diet and with combination therapy using 2 or 3 oral hypoglycaemic agents of escalating dosages1,2Based on the time associated with various oral agent alterations (eg, titration and combination therapy), patients are often out of control for lengthy periods and thus increase the risk of complications related to chronic hyperglycaemia11.Mudaliar S, Henry R. The oral antidiabetic agents. In: Porte D, Jr, Sherwin RS, Baron A. Ellenberg and Rifkins Diabetes Mellitus, 6th ed. New York, NY: Appleton and Lange; 2003:531-557. 2.Riddle MC. Tactics for type II diabetes. Endocrinol Metab Clin North Am. 1997;26:659-677.Clinicians may consider this proposed algorithm for the treatment of patients with type 2 diabetes. In this algorithm, insulin can be integrated into a patients regimen at various stages of the disease