Diagnosa Keperawatan.docx
10
Diagnosa Keperawatan : 1. Resiko Cidera 2. Gangguan Persepsi Sensori 3. Gangguan Citra Tubuh 4. Gangguan Menelan 5. Ketidakefektifan Pola Napas 6. Gangguan Pertukaran Gas 7. Ketidakefektifan Bersihan Jalan Napas 8. Gangguan Komunikasi Verbal 9. Hambatan Mobilitas Fisik 10. Nyeri 11. Mual Prioritas Masalah : 1. Ketidakefektifan Bersihan Jalan Napas 2. Ketidakefektifan Pola Napas NIC NOC Diagnosa Keperawatan 1. Ketidakefektifan Bersihan Jalan Napas NIC : Activities :
-
Upload
neneng-fitriani -
Category
Documents
-
view
114 -
download
2
Transcript of Diagnosa Keperawatan.docx

Diagnosa Keperawatan :
1. Resiko Cidera2. Gangguan Persepsi Sensori 3. Gangguan Citra Tubuh 4. Gangguan Menelan5. Ketidakefektifan Pola Napas6. Gangguan Pertukaran Gas7. Ketidakefektifan Bersihan Jalan Napas8. Gangguan Komunikasi Verbal 9. Hambatan Mobilitas Fisik
10. Nyeri11. Mual
Prioritas Masalah :
1. Ketidakefektifan Bersihan Jalan Napas2. Ketidakefektifan Pola Napas
NIC NOC Diagnosa Keperawatan
1. Ketidakefektifan Bersihan Jalan NapasNIC :
Activities :
1. Determine the need for oral and/or tracheal suctioning2. Auscultate breath sounds before and after suctioning3. Inform the patient and family abaout suctioning

4. Aspirate the nasopharynx, with a bulb syringe or suction device, as appropriate5. Provide sedation, as appropriate6. Use universal precautions gloves, glogges, and mask , as appropriate7. Insert a nasal airway to facilitate nasotracheal suctioning, as appropriate8. Instruct the patient to take several deep breaths before nasotracheal suctioning and the use supplemental oxygen, as appropriate9. Hyperoxygenate with 100% oxygen, using the ventilator or manual resusitation bag
10. Use sterile disposable equipment for each tracheal suction procedure11. Select a suction catheter that is one half the internal diameter of the endotracheal tube, tracheostomy tube or patients airway 12. Instruct patient to take slow , deep breaths during insertion of the suction catheter via the nasotracheal route13. Leave the patient connected to the ventilator during suctioning. If a closed tracheal suction system or an oxygen insufflation
device adaptor is being used.14. Use the lowest amount of wall suction necessary to remove secretions (e.g. 80 to 100 mmHg for adults)15. Monitor patients oxygens status (SaO2 and SvO2 levels) and hemodynamic status (MAP level and cardiac rhytms) immediately
before, during and after suctioning16. Base the duration of each tracheal suction pass on the incressity to remove secretions and patients respone to suctioning17. Hyperinflate and hyperoxygenate beetwen each tracheal suction pass and after the final suction pass 18. Suction the oropharynx after completion of tracheal suctioning 19. Clean area around tracheal stoma after completion of tracheal suctioning, as appropriate20. Stop tracheal suctioning and provide supplemental oxygen if patient experiences brachycardia in increase in ventricular octops
and/or desaturation21. Vary suctioning techniques, based on the clinical response of the patient22. Note type and amount of secretion obtained23. Send secretion for culture and sensitivity test, as appropriate24. Instruct the patient and/or family how to suction the airway, as appropriate
NOCRespiratory status : Airway Patency (0410)Domain – Physiologic Health ( II)Class – Cardiopulmonary (E)Scale – Extremely compromised to Not compromised (a)Definition : extent to which the tracheo brochial passages remain open
Respiratory status : Airway patency
Extremely compromised
1
Substantially compromised
2
ModeratelyCompromised
3
MildlyCompromised
4
Not compromised
5Indicators
111
1
1
1
1
1
222
2
2
2
2
2
333
3
3
3
3
3
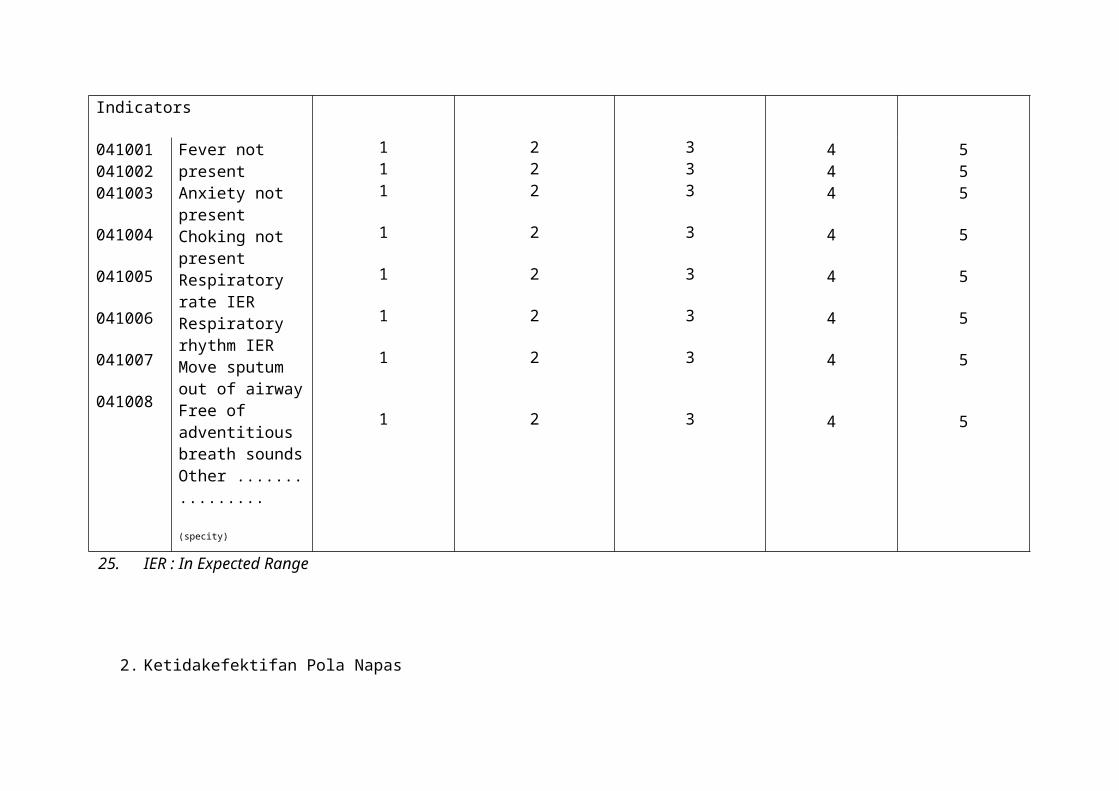
041001041002041003
041004
041005
041006
041007
041008
Fever not presentAnxiety not presentChoking not presentRespiratory rate IERRespiratory rhythm IERMove sputum out of airwayFree of adventitious breath soundsOther ................ (specity)
444
4
4
4
4
4
555
5
5
5
5
5
25. IER : In Expected Range
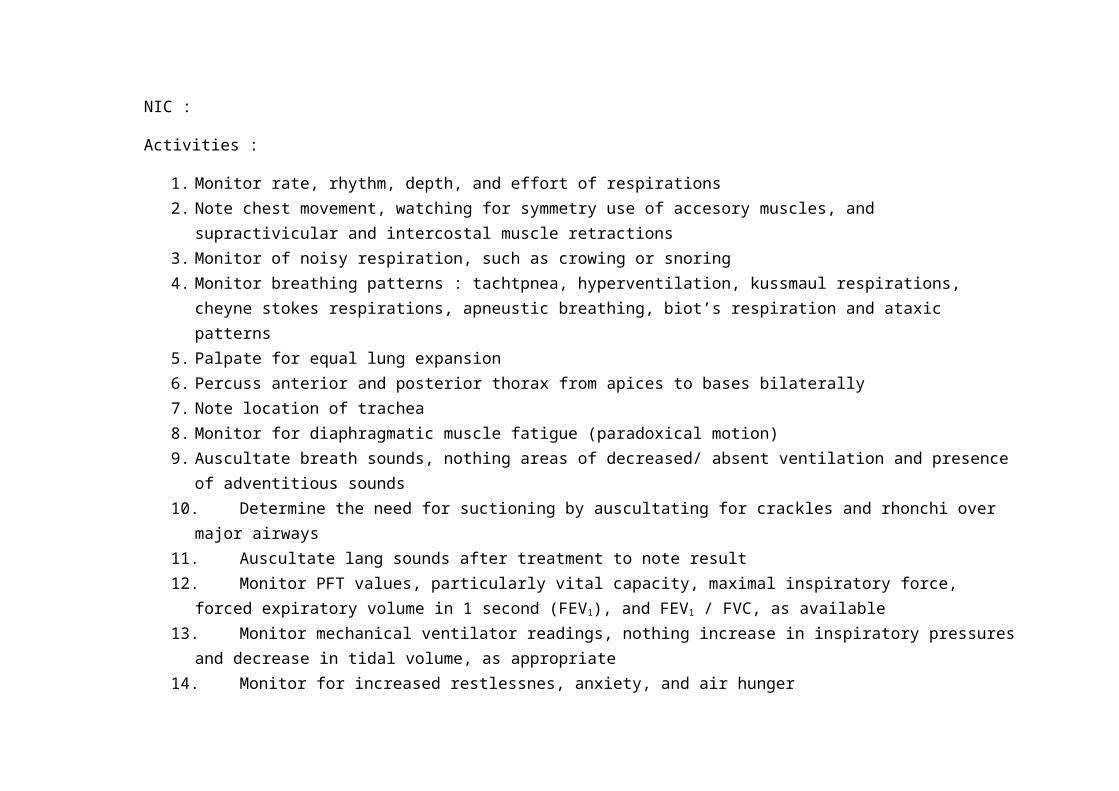
2. Ketidakefektifan Pola NapasNIC :
Activities :
1. Monitor rate, rhythm, depth, and effort of respirations2. Note chest movement, watching for symmetry use of accesory muscles, and supractivicular and intercostal muscle retractions3. Monitor of noisy respiration, such as crowing or snoring4. Monitor breathing patterns : tachtpnea, hyperventilation, kussmaul respirations, cheyne stokes respirations, apneustic breathing,
biot’s respiration and ataxic patterns5. Palpate for equal lung expansion6. Percuss anterior and posterior thorax from apices to bases bilaterally7. Note location of trachea8. Monitor for diaphragmatic muscle fatigue (paradoxical motion)9. Auscultate breath sounds, nothing areas of decreased/ absent ventilation and presence of adventitious sounds10. Determine the need for suctioning by auscultating for crackles and rhonchi over major airways11. Auscultate lang sounds after treatment to note result12. Monitor PFT values, particularly vital capacity, maximal inspiratory force, forced expiratory volume in 1 second (FEV1), and
FEV1 / FVC, as available13. Monitor mechanical ventilator readings, nothing increase in inspiratory pressures and decrease in tidal volume, as appropriate14. Monitor for increased restlessnes, anxiety, and air hunger15. Note changes in SaO2, SvO2, end-tidal CO2, and ABG values, as appropriate16. Monitor patients ability to cough effectively17. Note onset, charcteristics, and duration of cough18. Monitor patients respiratory secretions19. Monitor for dypsnea and events that decrease and worsen it20. Monitor for hoarseness and voice changes every hour in patient with facial burns21. Monitor for crepitus, as appropriate22. Monitor chest x-ray reports
23. Open the airway, using the chin lift or jaw thurst technique, as appropriate24. Place the patient on sude, as indicated, to prevent aspiration; log roll if cervical aspiration is suspected25. Institute resuscitation efforts, ass needed26. Institute respiratory therapy treatmrnts (e.g. nebulizer), as needed.
NOC
Respiratory Status : Ventilation (0403)
Domain – Physiologic Health ( II)
Class – Cardiopulmonary (E)
Scale – Extremely compromised to Not compromised (a)
Definition : movement of air in and out of the lungs
Respiratory status : Airway patency
Extremely compromised
1
Substantially compromised
2
ModeratelyCompromised
3
MildlyCompromised
4
Not compromised
5Indicators
1
1
1
1
1
222
2
2
2
333
3
3
3
040301
040302
040303
040304
040305
Respiratory rate IERRespiratory rhythm IERDepth of inspiration Chest expansion symmetricalEase of breathing
444
4
4
4
555
5
5
5
040306
040307
040308
040309
040310
040311
040312
040313
040314
040315
040316040317
040318
040319
040320
040321
Move sputum out of airwayVocalizes adequatelyExpulsion of air
Accessory muscle use not presentAdventitious breath sound not presentChest retraction not presentPursed lips breathing not presentDypsnea at rest not present Dypsnea with exertion not presentOrthopnea not presentSOB not presentTactile fremitus not presentPercussed sounds IERAusculated breath sounds IERAusculated vocalization IERBronchophony IER
1
1
1
1
1
1
1
1
1
1
11
1
1
1
1
2
2
2
2
2
2
2
2
2
22
2
2
2
2
3
3
333
3
3
3
3
3
33
3
3
3
3
4
4
444
4
4
4
4
4
44
4
4
4
4
5
5
555
5
5
5
5
5
55
5
5
5
5

040322040323
040324040325
040326
040327
040328
Egophony IERWhispered pectoriloquy IERTidal volume IERVital capacity IER
Chest X-ray findings IERPulmonary function test IER
Other ................ (specity)
11
11
1
1
1
22
22
2
2
2
33
33
3
3
3
44
44
4
4
4
55
55
5
5
5
IER : In Expected Range; SOB : Shortness Of Breath
Daftar pustaka
Johnson, Marion., Maas, Meridean dan Moorhead, Sue. 2000. Nursing Outcomes Classification (NOC). Edition : 2nd. USA : Mosby, Inc
Dochterman, JM. Bulechek, GM. 2004. Nursing Interventions Classification (NIC). Edition : 4th.USA : Mosby. Inc




















