Chronic Venous Insufficiency.dana
41
Pembimbing : dr. Witra Pembimbing : dr. Witra Sp.B(K)V Sp.B(K)V Oleh : Anggi Calapi Oleh : Anggi Calapi FK TRISAKTI 03011028 FK TRISAKTI 03011028 PRESENTASI REFERAT CHRONIC VENOUS INSUFFICIENCY (CVI)
-
Upload
anggi-calapi -
Category
Documents
-
view
299 -
download
27
description
cvi
Transcript of Chronic Venous Insufficiency.dana

Pembimbing : dr. Witra Pembimbing : dr. Witra Sp.B(K)VSp.B(K)V
Oleh : Anggi CalapiOleh : Anggi Calapi
FK TRISAKTI 03011028FK TRISAKTI 03011028
PRESENTASI REFERATCHRONIC VENOUS
INSUFFICIENCY(CVI)

PENDAHULUANPENDAHULUAN Gangguan aliran balik venaGangguan aliran balik vena
CVI terjadi pada vena Ekstremitas bawahCVI terjadi pada vena Ekstremitas bawah
Mempengaruhi hingga 20% dari orang dewasa.Mempengaruhi hingga 20% dari orang dewasa.
Pada usia 50 ~ 40% wanita dan 20% pria Pada usia 50 ~ 40% wanita dan 20% pria memiliki masalah vena yang signifikan.memiliki masalah vena yang signifikan.

Gangguan menetap Gangguan menetap pada aliran darah balik pada aliran darah balik dari perifer ke vena dari perifer ke vena sentral beserta sentral beserta komplikasikomplikasi
Definisi

The Edinburgh Vein Studi disaring 1566 subjek dengan USG dupleks untuk refluks menemukan CVI di 9,4% pria dan 6,6% wanita, setelah penyesuaian usia, yang naik secara signifikan dengan usia (21,2% pada pria berusia> 50 tahun, dan 12,0% pada wanita berusia> 50 tahun). 2
The San Valentino Vascular skrining Proyek ditemukan di antara 30 000 subyek dievaluasi oleh penilaian klinis dan USG dupleks prevalensi 7% untuk varises dan 0,86% untuk "gejala" CVI. 3
prevalensi varises sebesar 7% dan CVI simptomatik 0,86%. prevalensi varises sebesar 7% dan CVI simptomatik 0,86%. Framingham Heart Study diperkirakan bahwa insiden tahunan Framingham Heart Study diperkirakan bahwa insiden tahunan varises pada perempuan 2,6% dan pada pria 1,9%.2varises pada perempuan 2,6% dan pada pria 1,9%.2
Di AS, diperkirakan 2,5 juta orang menderita CVI dan 20%-Di AS, diperkirakan 2,5 juta orang menderita CVI dan 20%-nya berkembang menjadi ulkus vena.nya berkembang menjadi ulkus vena.
Indonesia ?Indonesia ?
Epidemiologi

Vena ekstremitas Vena ekstremitas terbagi dua : terbagi dua : deepdeep dan dan superficialsuperficial
Vena superfisial terletak Vena superfisial terletak di permukaan kulit dan di permukaan kulit dan mengalirkan darah ke mengalirkan darah ke vena dalahvena dalah
Vena dalam terletak di Vena dalam terletak di dekat jaringan otot > dekat jaringan otot > kontraksi dan relaksasi kontraksi dan relaksasi otot mempengaruhi otot mempengaruhi pergerakan aliran darahpergerakan aliran darah
AnatomiAnatomi

Fisiologi venaFisiologi vena
Secara fisiologi vena berfungsi Secara fisiologi vena berfungsi mengembalikan darah dari kapiler ke mengembalikan darah dari kapiler ke jantungjantung
Sebagai reservoir darahSebagai reservoir darah Kapasitas vaskuler sebagai pompa Kapasitas vaskuler sebagai pompa
darahdarah Kapasitas vaskuler sebagai pompa Kapasitas vaskuler sebagai pompa
darahdarah Pengaturan suhu tubuhPengaturan suhu tubuh

CVICVI

SSVena superfisial dan deep vena Vena superfisial dan deep vena
Refluks, obstruksi, otot betis tergangguRefluks, obstruksi, otot betis terganggu
Hipertensi vena menahunHipertensi vena menahun
Edema, ulserasiEdema, ulserasi
Daya elastisitas yang abnormal pada jaringan ikat dinding vena + Katup VarikosesDaya elastisitas yang abnormal pada jaringan ikat dinding vena + Katup VarikosesDilatasi vena tanpa trombosis Varises primerDilatasi vena tanpa trombosis Varises primerRekanalisasi -> menyebabkan vena profunda dan vena perorantes menjadi inkompeten > Rekanalisasi -> menyebabkan vena profunda dan vena perorantes menjadi inkompeten > drainase berkurang dan hipertensi vena > drainase berkurang dan hipertensi vena >
tekanan tekanan
Patogenesis

FAKTOR RESIKO DAN PENYEBAB CVI
UUsia lanjutsia lanjut Riwayat keluarga penyakit venaRiwayat keluarga penyakit vena Kelemahan ligamen (misalnya, hernia, armada datar)Kelemahan ligamen (misalnya, hernia, armada datar) Berdiri lama Peningkatan indeks massa tubuh Merokok Gaya hidup Trauma ekstremitas bawah Trombosis vena sebelumnya (superfisial atau dalam) Arteriovenosa shunt kondisi herediter Tinggi estrogen Kehamilan. [2][2]

Gejala Gejala
Nyeri pada tungkai Nyeri pada tungkai Bengkak pada kakiBengkak pada kaki Betis terasa tertekanBetis terasa tertekan Kaki menjadi cepat lelah saat Kaki menjadi cepat lelah saat
berjalan dan membaik ketika di berjalan dan membaik ketika di istirahatkanistirahatkan

MANIFESTASI CVIMANIFESTASI CVI
ASYMPTOMATICASYMPTOMATIC SUPERFICIAL VENOUS DILATATIONSUPERFICIAL VENOUS DILATATION
Telangiectasias (intradermal) Telangiectasias (intradermal)
Reticular veins (subdermal)Reticular veins (subdermal)

ASYMPTOMATIC VS ASYMPTOMATIC VS SYMPTOMATICSYMPTOMATIC
VARICOSE VEINS (subcutaneous)VARICOSE VEINS (subcutaneous)

CHRONIC VENOUS CHRONIC VENOUS INSUFFICIENCYINSUFFICIENCY
EEdemadema

CHRONIC VENOUS CHRONIC VENOUS INSUFFICIENCYINSUFFICIENCY
Skin changesSkin changes
HyperpigmentationHyperpigmentation

CHRONIC VENOUS CHRONIC VENOUS INSUFFICIENCYINSUFFICIENCY
Skin changesSkin changes
Stasis dermatitisStasis dermatitis

CHRONIC VENOUS CHRONIC VENOUS INSUFFICIENCYINSUFFICIENCY
Skin changesSkin changes Corona phlebectaticaCorona phlebectatica
a. venous cups a. venous cups (veins)(veins)
b. telangiectasiasb. telangiectasias c. reticular veinsc. reticular veins d. stasis spots d. stasis spots
(capillaries)(capillaries)

CHRONIC VENOUS CHRONIC VENOUS INSUFFICIENCYINSUFFICIENCY
LipodermatosclerosisLipodermatosclerosis a form of panniculitis just above the a form of panniculitis just above the
ankles. ankles. 9.9.

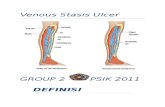
CHRONIC VENOUS INSUFFICIENCYCHRONIC VENOUS INSUFFICIENCYVenous stasis ulceration(s)Venous stasis ulceration(s)

EVALUASIEVALUASI
KARAKTERISTIKKARAKTERISTIK VENVENAA ARTERIARTERI
INSPEKSIINSPEKSI Irregular, Irregular, hiperhiperpigmentapigmentasisi, , sometimes fibrotsometimes fibrotikik, , granulagranulasisi, usually shallow., usually shallow.
Irregular, smooth edge, Irregular, smooth edge, minimum to no granulation, minimum to no granulation, usually deep with a usually deep with a punched out appearance.punched out appearance.
LOLOKASIKASI Distal lower leg, medial Distal lower leg, medial malleolus.malleolus.
Distal lower leg/feet/toes, Distal lower leg/feet/toes, lateral malleolus, anterior lateral malleolus, anterior tibial area.tibial area.
PEDAL PULSESPEDAL PULSES Usually present.Usually present. May be diminished or May be diminished or absent.absent.
NYERINYERI May be present. Usually May be present. Usually improves with leg elevation.improves with leg elevation.
Usually painful especially Usually painful especially with leg elevation.with leg elevation.
DRAINADRAINASESE sedangsedang sampaisampai banyakbanyak.. sedikitsedikit sampai tidak adasampai tidak ada..
TEMPERATURTEMPERATUR Dapat meningkatDapat meningkat.. menurunmenurun
PERUBAHAN PERUBAHAN KULITKULIT
Flaking, dry, Flaking, dry, hyperpigmented.hyperpigmented.
Thin, shiny, hairless, yellow Thin, shiny, hairless, yellow nails. nails. 3.3.

KLASIFIKASI KLASIFIKASI CEAP – an international consensus conference initiated the Clinical-Etiology-CEAP – an international consensus conference initiated the Clinical-Etiology-
Anatomy-Pathophysiology classification.Anatomy-Pathophysiology classification. C 0 – no evidence of venous disease.C 0 – no evidence of venous disease. C 1 – telangiectasias/reticular veins.C 1 – telangiectasias/reticular veins. C 2 – varicose veins.C 2 – varicose veins. C 3 – edema associated with vein disease.C 3 – edema associated with vein disease. C 4a – pigmentation or eczema.C 4a – pigmentation or eczema. C 4b – lipodermatosclerosis.C 4b – lipodermatosclerosis. C 5 – healed venous ulcer.C 5 – healed venous ulcer. C 6 – active venous ulcer.C 6 – active venous ulcer. E c – congenitalE c – congenital E p – primary venous disease.E p – primary venous disease. E s – secondary venous disorder.E s – secondary venous disorder. E n – not specified.E n – not specified. A s – superficial veins.A s – superficial veins. A d – deep veins.A d – deep veins. A p – perforating veins.A p – perforating veins. A n – not specified.A n – not specified. P r – venous reflux.P r – venous reflux. P o – venous obstruction.P o – venous obstruction. P n – not specified. P n – not specified. 7.7.

PEMERIKSAAN PEMERIKSAAN PENUNJANGPENUNJANG
Tes TrendelenburgTes Trendelenburg• Untuk menentukan derajat insuffisiensi katup pada vena Untuk menentukan derajat insuffisiensi katup pada vena
komunikanskomunikans Ultrasonografi DopplerUltrasonografi Doppler
• Dapat menunjukkan dengan tepat lokasi katup yang Dapat menunjukkan dengan tepat lokasi katup yang abnormalabnormal
Duplex UltrasonographyDuplex Ultrasonography• merupakan modalitas pencitraan standar untuk diagnosis merupakan modalitas pencitraan standar untuk diagnosis
sindrom insuffsiensi vena dan untuk perencanaan sindrom insuffsiensi vena dan untuk perencanaan pengobatan serta pemetaan sebelum operasipengobatan serta pemetaan sebelum operasi
PlebographyPlebography• Plebography Plebography merupakan pemeriksaan invasif yang merupakan pemeriksaan invasif yang
menggunakan medium kontrasmenggunakan medium kontras

PENATALAKSAANPENATALAKSAAN OF OF CVICVI
KONSERVTIFKONSERVTIF• Terapi kompresi stocking komprestion dengan gradient tekanan Terapi kompresi stocking komprestion dengan gradient tekanan
antara 30-40mmhg atau 40-50 mmhg pada pergelangan kakiantara 30-40mmhg atau 40-50 mmhg pada pergelangan kaki• Skleroterapi, menyuntikan bahan kimia ke dalam pembuluh darah Skleroterapi, menyuntikan bahan kimia ke dalam pembuluh darah
yang terkenayang terkena• MedikamentosaMedikamentosa• PentoxifyllinePentoxifylline, yang meningkatkan aliran darah melalui , yang meningkatkan aliran darah melalui
pembuluh, dapat digunakan dalam kombinasi dengan terapi pembuluh, dapat digunakan dalam kombinasi dengan terapi kompresi untuk membantu menyembuhkan borok kaki.kompresi untuk membantu menyembuhkan borok kaki.
• DiuretikDiuretik (obat yang digunakan untuk menarik kelebihan cairan (obat yang digunakan untuk menarik kelebihan cairan dari tubuh melalui ginjal) dapat digunakan untuk mengurangi dari tubuh melalui ginjal) dapat digunakan untuk mengurangi pembengkakan.pembengkakan.
LEG ELEVATION – heart level for 30 minutes 3-4 times daily LEG ELEVATION – heart level for 30 minutes 3-4 times daily improves micro-circulation reduces edema, and promotes healing of improves micro-circulation reduces edema, and promotes healing of venous ulcers.4venous ulcers.4
LATIHANLATIHAN – daily walking and simple ankle flexion exercises – daily walking and simple ankle flexion exercises..

LEG ELEVATION – heart level for 30 LEG ELEVATION – heart level for 30 minutes 3-4 times daily improves micro-minutes 3-4 times daily improves micro-circulation reduces edema, and promotes circulation reduces edema, and promotes healing of venous ulcers.4healing of venous ulcers.4
EXERCISEEXERCISE– daily walking and simple – daily walking and simple ankle flexion exercises.ankle flexion exercises.

MANAGEMENT OF CVI – MANAGEMENT OF CVI – COMPRESSION THERAPYCOMPRESSION THERAPY
Compression bandages – elastic or Compression bandages – elastic or non-elastic with single or multi-non-elastic with single or multi-layers.layers.

COMPRESSION STOCKINGCOMPRESSION STOCKING

MANAGEMENT OF CVI –MANAGEMENT OF CVI –COMPRESSION COMPRESSION
STOCKINGSSTOCKINGS4.4.
CLASSCLASS PRESSUREPRESSURE LEVEL OF LEVEL OF SUPPORTSUPPORT
INDICATIOINDICATIONN
CEAPCEAP
OTCOTC <15 mmHg<15 mmHg MinimalMinimal Asymptomatic,Asymptomatic,
comfort only.comfort only.0, 10, 1
II 15-20 mmHg15-20 mmHg MildMild Minor varicosities, Minor varicosities, tired aching legs, tired aching legs, minor swelling.minor swelling.
1, 2, 31, 2, 3
IIII 20-30 mmHg20-30 mmHg ModerateModerate Moderate to Moderate to severe severe varicosities, varicosities, moderate moderate swelling,phlebitis, swelling,phlebitis, following ablation.following ablation.
3, 4 3, 4
IIIIII 30-40 mmHg30-40 mmHg FirmFirm Severe Severe varicosities, varicosities, swelling, swelling, management of management of ulcerations, ulcerations, following DVT, following DVT, post surgery.post surgery.
4, 5, 64, 5, 6
IVIV >40 mmHg>40 mmHg Extra firmExtra firm Lymphedema.Lymphedema. NANA

MANAGEMENT OF CVIMANAGEMENT OF CVI
PNEUMATIC COMPRESSION PNEUMATIC COMPRESSION THERAPYTHERAPY

CHRONIC VENOUS CHRONIC VENOUS INSUFFICIENCY VERSUS INSUFFICIENCY VERSUS
LYMPHEDEMALYMPHEDEMA

MANAGEMENT OF CVI - MANAGEMENT OF CVI - MEDICATIONSMEDICATIONS
Diuretics – one of the most inappropriate treatments.Diuretics – one of the most inappropriate treatments. Aspirin – may accelerate the healing of chronic ulcers.Aspirin – may accelerate the healing of chronic ulcers. Pentoxifylline – more effective for complete or partial Pentoxifylline – more effective for complete or partial
ulcer healing then placebo.ulcer healing then placebo. Stanozolol – an anabolic steroid that stimulates Stanozolol – an anabolic steroid that stimulates
fibrinolysis and improves lipodermatosclerosis and fibrinolysis and improves lipodermatosclerosis and possibly ulcer healing.possibly ulcer healing.
Escin (horseshoe chestnut) – 50mg twice daily Escin (horseshoe chestnut) – 50mg twice daily reduces leg volume and edema. It stimulates the reduces leg volume and edema. It stimulates the release of F series prostaglandins which induce release of F series prostaglandins which induce venoconstriction, decreasing the permeability of venoconstriction, decreasing the permeability of vessel walls to low molecular proteins, water, and vessel walls to low molecular proteins, water, and electrolytes. electrolytes.
Hydroxyethylrutoside, Sulodexide, Prostacyclin Hydroxyethylrutoside, Sulodexide, Prostacyclin Analogues – not available in the United States. Analogues – not available in the United States. 4.4.

MANAGEMENT OF CVI – MANAGEMENT OF CVI – SKIN CARESKIN CARE
Skin cleansing – wash with a mild non-Skin cleansing – wash with a mild non-soap cleanser (e.g. Dove, Olay, Caress).soap cleanser (e.g. Dove, Olay, Caress).
Emollients – provides a film of oil to Emollients – provides a film of oil to lubricate the skin (e.g. Vaseline, lubricate the skin (e.g. Vaseline, Lubriderm, Aveeno).Lubriderm, Aveeno).
Barrier preparations – physically block Barrier preparations – physically block chemical irritants and moisture.(e.g. Zinc chemical irritants and moisture.(e.g. Zinc oxide, Vaselineoxide, Vaseline). ).
Topical corticosteroids – often used to Topical corticosteroids – often used to treat stasis dermatitis.treat stasis dermatitis. 4.4.

MANAGEMENT OF CVI – MANAGEMENT OF CVI – VENOUS STASIS ULCERSVENOUS STASIS ULCERS
Surgical debridement – used to remove Surgical debridement – used to remove devitalized tissue.devitalized tissue.
Enzymatic agents – used to break down Enzymatic agents – used to break down necrotic tissue (e.g. Santyl).necrotic tissue (e.g. Santyl).
Growth factors – synthesized by many cell Growth factors – synthesized by many cell types such as platelets, neutrophils, and types such as platelets, neutrophils, and epithelial cells (e.g. Regranex).epithelial cells (e.g. Regranex).
Bioengineered tissue – used for a variety of Bioengineered tissue – used for a variety of non-healing ulcers (e.g. Apligraf, non-healing ulcers (e.g. Apligraf, Dermagraft).Dermagraft).
Skin grafting – an option for non-healing Skin grafting – an option for non-healing ulcers. ulcers. 4.4.

MANAGEMENT OF CVI – MANAGEMENT OF CVI – VENOUS STASIS ULCERSVENOUS STASIS ULCERS
Dressings – depend upon the ulcer characteristics, Dressings – depend upon the ulcer characteristics, frequency of dressing changes, and cost.frequency of dressing changes, and cost.
-Occlusive dressings may be fully occlusive -Occlusive dressings may be fully occlusive (impermeable to gases and liquids) or semi-(impermeable to gases and liquids) or semi-impermeable (impermeable to liquids and partially impermeable (impermeable to liquids and partially permeable to gases and water vapor). permeable to gases and water vapor).
It stimulates collagen synthesis, angiogenesis, and It stimulates collagen synthesis, angiogenesis, and speeds reepithelialization.speeds reepithelialization.
-Low adherent gauze dressings – frequent changes -Low adherent gauze dressings – frequent changes but inexpensive.but inexpensive.
-Hydrogels and alginate dressings are highly -Hydrogels and alginate dressings are highly absorbent to handle heavily exudative ulcers, while absorbent to handle heavily exudative ulcers, while hydrocolloids can help with wound debridement and hydrocolloids can help with wound debridement and skin protection.skin protection.
-Silver can be incorporated if the ulcer is infected. -Silver can be incorporated if the ulcer is infected. 4.4.

MANAGEMENT OF CVI – MANAGEMENT OF CVI – ABLATION THERAPYABLATION THERAPY
Indications – patients with persistent Indications – patients with persistent signs/symptoms of venous disease signs/symptoms of venous disease after a minimum of 3 months of after a minimum of 3 months of medical therapy (e.g. compression) medical therapy (e.g. compression) and documented reflux (e.g. >0.5 and documented reflux (e.g. >0.5 seconds of reflux GSV).seconds of reflux GSV).
Absolute contraindications – acute Absolute contraindications – acute DVT or phlebitis and pregnancy. DVT or phlebitis and pregnancy. 5,6.5,6.
Radiofrequency versus laser Radiofrequency versus laser endovenous ablation therapy.endovenous ablation therapy.

MANAGEMENT OF CVI – MANAGEMENT OF CVI – RADIOFREQUENCY RADIOFREQUENCY
ENDOVENOUS ABLATION ENDOVENOUS ABLATION THERAPYTHERAPY
Radiofrequency devices – generate Radiofrequency devices – generate a high frequency alternating a high frequency alternating current for which the energy heats current for which the energy heats the adjacent vein walls to the probe the adjacent vein walls to the probe which alters the protein structure which alters the protein structure of the vein effecting its closure. of the vein effecting its closure. 5.5.
Superficial veins include – Great Superficial veins include – Great Saphenous Vein, Small Saphenous, Saphenous Vein, Small Saphenous, and incompetent perforator veins.and incompetent perforator veins.

MANAGEMENT OF CVI – MANAGEMENT OF CVI – RADIOFREQUENCY RADIOFREQUENCY
ENDOVENOUS ABLATION ENDOVENOUS ABLATION THERAPYTHERAPY

MANAGEMENT OF CVI – MANAGEMENT OF CVI – RADIOFREQUENCY RADIOFREQUENCY
ENDOVENOUS ABLATION ENDOVENOUS ABLATION THERAPYTHERAPY

MANAGEMENT OF CVI – MANAGEMENT OF CVI – RADIOFREQUENCY RADIOFREQUENCY
ENDOVENOUS ABLATION ENDOVENOUS ABLATION THERAPYTHERAPY
BEFORE BEFORE AFTERAFTER

MANAGEMENT OF CVI – MANAGEMENT OF CVI – MECHANICAL ABLATIONMECHANICAL ABLATION
Physical destruction of a vein with Physical destruction of a vein with its partial or complete removal.its partial or complete removal.
- Vein ligation/stripping- Vein ligation/stripping
- Stab phlebectomy- Stab phlebectomy
- Powered phlebectomy- Powered phlebectomy
- Open or endoscopic perforator - Open or endoscopic perforator ligation.ligation.

REFERENCESREFERENCES1.1. 2012 Vascular Disease Foundation. 8206 Leesburg Pike, suite 301, Vienna 2012 Vascular Disease Foundation. 8206 Leesburg Pike, suite 301, Vienna
Virginia 22187.Virginia 22187.
2.2. Alguire PC, Scovell S. Overview and medical management of lower Alguire PC, Scovell S. Overview and medical management of lower extremity chronic venous disease. 2012 UpToDate.extremity chronic venous disease. 2012 UpToDate.
3.3. Venous stasis and arterial ulcer comparison. February 1, 2009. Venous stasis and arterial ulcer comparison. February 1, 2009. http://www.lhsc.on.ca/Health_Professionals/Wound_Care/venous.htm.http://www.lhsc.on.ca/Health_Professionals/Wound_Care/venous.htm.
4.4. Alguire PC, Mathes BM. Medical management of lower extremity chronic Alguire PC, Mathes BM. Medical management of lower extremity chronic venous disease. 2012 UpToDate.venous disease. 2012 UpToDate.
5.5. Scovell S. Radiofrequency ablation for the treatment of lower extremity Scovell S. Radiofrequency ablation for the treatment of lower extremity chronic venous disease. 2012 UpToDate.chronic venous disease. 2012 UpToDate.
6.6. Ihnat DM. Endovenous laser ablation for the treatment of lower extremity Ihnat DM. Endovenous laser ablation for the treatment of lower extremity chronic venous disease. 2012 UpToDate.chronic venous disease. 2012 UpToDate.
7.7. Collins KA. Classification of lower extremity chronic venous disorders. Collins KA. Classification of lower extremity chronic venous disorders. 2012 UpToDate.2012 UpToDate.
8.8. Greenberg DL, Scovell S. Liquid and foam sclerotherapy techniques for Greenberg DL, Scovell S. Liquid and foam sclerotherapy techniques for the treatment of lower extremity veins. 2012 UpToDate.the treatment of lower extremity veins. 2012 UpToDate.
9.9. Alguire PC, Mathes BM. Pathophysiology of chronic venous disease. 2012 Alguire PC, Mathes BM. Pathophysiology of chronic venous disease. 2012 UpToDate.UpToDate.

TERIMATERIMA KASIHKASIH

ANATOMY OF THE LOWER ANATOMY OF THE LOWER EXTREMITY VENOUS EXTREMITY VENOUS
SYSTEMSYSTEM