BBS1-FL1-K24.ppt
46
Keseimbangan Cairan, Elektrolit dan Asam-Basa Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera Utara
-
Upload
gheavita-chandra-dewi -
Category
Documents
-
view
4 -
download
2
description
fisiologi
Transcript of BBS1-FL1-K24.ppt
Keseimbangan Cairan, Elektrolit dan Asam-Basa
Departemen Fisiologi
Fakultas Kedokteran
Universitas Sumatera Utara

1. Menjelaskan fungsi cairan tubuh.
2. Menjelaskan input dan output cairan.
3. Menjelaskan kompartemen cairan intrasel dan ekstrasel.
4. Menjelaskan komposisi elektrolit dan zat terlarut lain dalam kompartemen.
5. Menjelaskan osmolaritas & tekanan osmotik cairan tubuh.
6. Menjelaskan peran elektrolit dalam mempertahankan homeostasis pH cairan tubuh.
Specific Learning Objectives:

• Infants have low body fat, low bone mass, and are 73% or more water
• Total water content declines throughout life• Healthy males are about 60% water; healthy females
are around 50%• This difference reflects females’:
– Higher body fat – Smaller amount of skeletal muscle
• In old age, only about 45% of body weight is water
Body Water Content

• Regulating body temperature
• As protective cushion & lubricant
• As reactant
• As solvent
• As transporter
Functions of Body Water

The body maintains a balance of water intake and output by a series of negative feedback loop involving the endocrine system and autonomic nervous system
Water Homeostasis

• To remain properly hydrated, water intake must equal water output
• Water intake sources
– Ingested fluid (60%) and solid food (30%)
– Metabolic water or water of oxidation (10%)
Water Balance and ECF Osmolality
Water output
Urine (60%) and feces (4%)
Insensible losses (28%), sweat (8%)
Increases in plasma osmolality trigger thirst and release of antidiuretic hormone (ADH)
Water Balance and ECF Osmolality

Water Intake and Output

Daily WATER BALANCE
DRINK
1500 ml/Day
DRINK
1500 ml/Day
METABOLISM294 ml/day
METABOLISM294 ml/day
BODY
Vaporization from lungs 400 ml/day
Insensible perspiration 600 ml/day
In feces100 ml/day
URINE1500 ml/day
Adapted from Goldberger, Water, Electrolyte, Acid base balance.
Water intakeWater intake Water excretionWater excretion
( Total 2600 ml )( Total 2600 ml ) approxapprox ( Total 2600 ml )( Total 2600 ml )
In solid food 800 ml/day
In solid food 800 ml/day
We are We are approximatapproximat
elyely two-two-thirds thirds waterwater

• Water occupies two main fluid compartments• Intracellular fluid (ICF) – about two thirds by
volume, contained in cells• Extracellular fluid (ECF) – consists of two major
subdivisions– Plasma – the fluid portion of the blood– Interstitial fluid (IF) – fluid in spaces between cells
Fluid Compartments

Intracellular fluid
Volume = 28 L, 2/3 TBW
Interstitial fluid volume = 11 L
80% of ECF
IV (Plasma Volume )
= 3L
20% of ECF
TBW
ECF (Internal environment)
Volume= 14 L, 1/3 TBW
Kidneys Guts Lungs Skin
Fluid shifts / intakes
Distribution/Compartment of Body FluidsTotal Body Water ( TBW) = 60% wt ( 70 kg -> 42 L 0 …… varies due to ?
40% TBW 20% TBW
• Water is the universal solvent
• Solutes are broadly classified into:
– Electrolytes – inorganic salts, all acids and bases, and some proteins
– Nonelectrolytes – examples include glucose, lipids, creatinine, and urea
Composition of Body Fluids

Electrolyte Composition of Body Fluids
Figure 26.2

Ionic Composition of Body Fluids
ExtracellularFluid
IntracellularFluid
Cations Anions
Concentration Units are in mEq/L(How many grams of electrolyte (solute) in a liter of plasma
(solution)
Ca2+
Phosphate and Organic Anions
Protein--
More protein And more cations in plasma thanInterstitial fluid
Na+
140
K+
140
Cl
110
HCO3
24
Mg2+
• The tendency for movement of solvent molecules to a region of greater solute concentration can be prevented by applying pressure to the more concentrated solution.
• The pressure necessary to prevent solvent migration is the osmotic pressure of the solution.
OSMOTIC PRESSURE
• The osmolarity is the number of osmoles per liter of solution—eg, plasma—whereas the osmolality is the number of osmoles per kilogram of solvent.
• Therefore, osmolarity is affected by the volume of the various solutes in the solution and the temperature, while the osmolality is not.
• Tonicity: a measure of the ability of a solution to cause a change in cell shape by promoting osmotic flow.
• The term tonicity is used to describe the osmolality of a solution relative to plasma. Solutions that have the same osmolality as plasma are said to be isotonic; those with greater osmolality are hypertonic; and those with lesser osmolality are hypotonic.
TONICITY
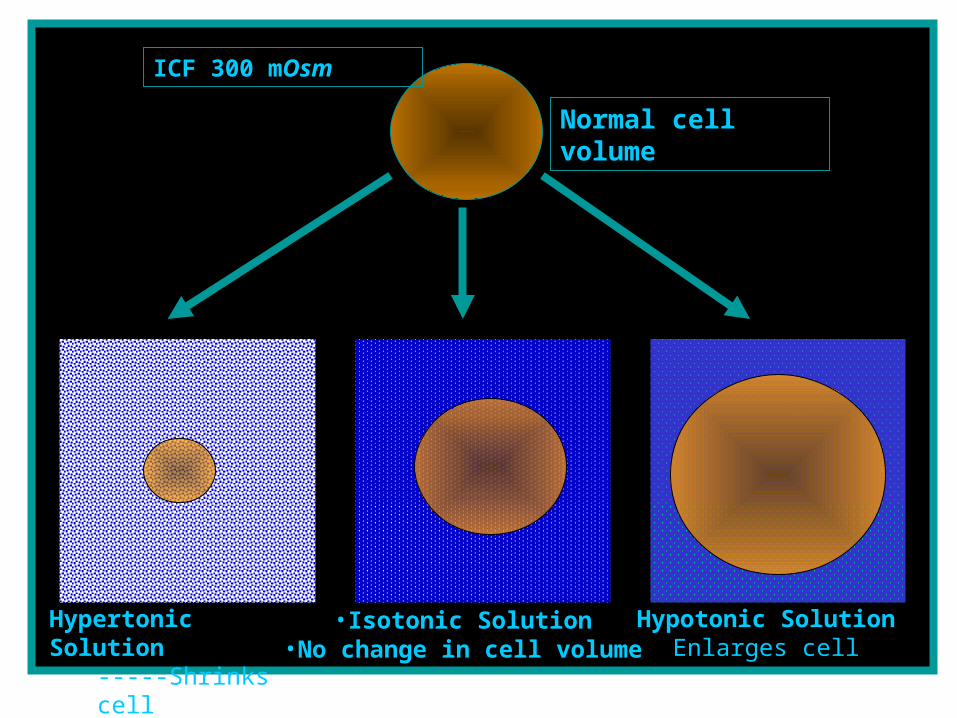
Hypertonic Solution-----Shrinks cell
•Isotonic Solution•No change in cell volume
Hypotonic SolutionEnlarges cell
Normal cell volume
ICF 300 mOsm

• Hypotonic IV solutions if too much water enters the cells eventually it could undergo hemolysis or break open
• Hypertonic IV solutions there is a net flow of water out of the cell and that cause the cell to shrink
Osmosis & IV fluids

• Normal pH of body fluids– Arterial blood is 7.4– Venous blood and interstitial fluid is 7.35– Intracellular fluid is 7.0
• Alkalosis or alkalemia – arterial blood pH rises above 7.45
• Acidosis or acidemia – arterial pH drops below 7.35 (physiological acidosis)
Acid-Base Balance
• Most hydrogen ions originate from cellular metabolism– Breakdown of phosphorus-containing proteins
releases phosphoric acid into the ECF– Anaerobic respiration of glucose produces lactic acid– Fat metabolism yields organic acids and ketone
bodies– Transporting carbon dioxide as bicarbonate releases
hydrogen ions
Sources of Hydrogen Ions

• Concentration of hydrogen ions is regulated sequentially by:– Chemical buffer systems – act within seconds– The respiratory center in the brain stem – acts
within 1-3 minutes– Renal mechanisms – require hours to days to
effect pH changes
Hydrogen Ion Regulation
• One or two molecules that act to resist pH changes when strong acid or base is added
• Three major chemical buffer systems
– Bicarbonate buffer system
– Phosphate buffer system
– Protein buffer system
• Any drifts in pH are resisted by the entire chemical buffering system
Chemical Buffer Systems

• The respiratory system regulation of acid-base balance is a physiological buffering system
• There is a reversible equilibrium between:– Dissolved carbon dioxide and water– Carbonic acid and the hydrogen and
bicarbonate ions
CO2 + H2O H2CO3 H+ + HCO3¯
Physiological Buffer Systems
• Chemical buffers can tie up excess acids or bases, but they cannot eliminate them from the body
• The lungs can eliminate carbonic acid by eliminating carbon dioxide
• Only the kidneys can rid the body of metabolic acids (phosphoric, uric, and lactic acids and ketones) and prevent metabolic acidosis
• The ultimate acid-base regulatory organs are the kidneys
Renal Mechanisms of Acid-Base Balance

Imbalances• Illness
• Altered fluid intake
• Prolonged vomiting or diarrhea
• Result From:
Imbalances Affect:
Respiration
Metabolism
Function of Central Nervous System

Dehydration is loss of water and important blood salts like potassium (K+) and sodium (Na+).
Dehydration

CAUSES OF DEHYDRATION GI losses
Vomiting Diarrhea Malabsorption disorders
Increased insensible loss Fever Hyperventilation High environmental
temperatures
Increased sweating Medical conditions High environmental
temperatures
Internal loss - loss of fluids into various body compartments, especially from intravascular into interstitial. Illness - peritonitis, pacreatitis, bowel
obstruction Poor nutritional states
Plasma losses Burns Surgical drains Fistulas (Abnormal tubelike passage
from a normal cavity to another cavity or free standing surface).
Open wounds

Types of dehydration Dehydration is classified as mild, moderate, or severe based on the percentage of body weight lost during the acute illness:Depending on age,
Mild dehydration -- a loss of 3-5% of body weight
Moderate dehydration -- a loss of 6-10% of body weight
Severe dehydration -- a loss of more than 9-15% of body weight. This is a life-threatening emergency ! ! !
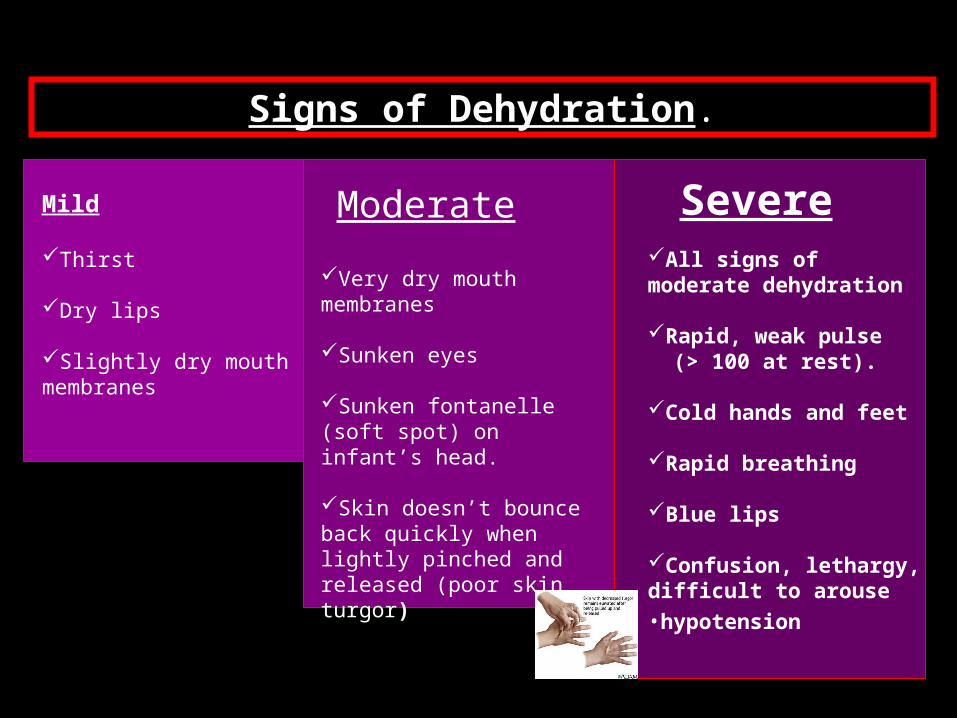
Signs of Dehydration.
Mild
Thirst
Dry lips
Slightly dry mouth membranes
Very dry mouth membranes
Sunken eyes
Sunken fontanelle (soft spot) on infant’s head.
Skin doesn’t bounce back quickly when lightly pinched and released (poor skin turgor)
All signs of moderate dehydration
Rapid, weak pulse (> 100 at rest).
Cold hands and feet
Rapid breathing
Blue lips
Confusion, lethargy, difficult to arouse•hypotension
Moderate Severe

Intravenous fluids and hospitalization may be necessary
Treatment Treat the cause of the dehydration.!!!
Mild dehydration.
Drinking fluids is often sufficient
Moderate to Severe dehydration.

• ± 30 ml / kg B.W. Daily of
water
and
electroly
te
requiremen
ts
70 kg adult 2000ml/day
• Fever water needs ± 15% for each 1°C rise in the patient's temperature
Adapted
from
Goldberger,
Wate
r,
Electro
lyte, A
cid
base bala
nce.

Daily of
water
and
electrolyt
e
requirements
Fever or sweating water needed ± 500 to 2000 ml (if
the patient's temperature is > 38.3°C or room temperature is > 32°C( 101°F)
• More 4 mEq K , will be needed
• Na, 100 mEq( 5,9 g NaCl)
• K, 60 mEq daily ( 4,5 g KCl)
Adapted from Goldberger, Water, Electrolyte, Acid base balance.
VolumVolume e of of
Fluid Fluid NeedeNeede
dd
a water loss of 4000 ml is
present.How much the patient needs ?
There are several
methods of calculating the
volume of water needed to treat water
loss.
The patient needs not only the 4000 ml but an additional 1500 ml or more water daily to cover the daily water losses due to insensible perspiration, urinary output, and other causes.
Adapted from Goldberger, Water, Electrolyte, Acid base balance.
Volume of
Fluid Needed
Method 1. A simple way to
calculate the water deficit is the following :
If thirst is present, but other clinical signs are minimal, assume that the water deficit is about 2% of the body weight. In a 70 kg patient, the water deficit ± 1400 ml.
If the patient has gone 3 to 4 days without water, and if there is marked thirst, a dry mouth and oliguria, ……… the water deficit is approximately 6% of the b. w.
In a 70 kg patient, the water deficit ± 4200 ml. The above signs are present. In addition, if
there are marked physical weakness and severe mental changes, such as confusion or delirium, ………the water deficit is 7 to 14% of the body weight.
In a 70 kg patient, the water deficit ± 5 to 10 liters.Adapted from Goldberger, Water, Electrolyte, Acid base balance.
Method 2.
If the patient has been weighed daily, and it is known, for example, that he has lost 4 kg weight during an acute period of desiccation, the water deficit is …………………….
Adapted from Goldberger, Water, Electrolyte, Acid base balance.
approximately 4000 ml, or 4 liters.

Method 3.based on the fact that the plasma sodium concentration varies inversely with the volume of extracellular water. It assumes, however, that only water has been lost and the sodium content of the body has remained unchanged.
Adapted from Goldberger, Water, Electrolyte, Acid base balance.
•The formula is :Na2 X BW2 = Na1 X BW1
• Na2 presents the present serum sodium concentration. • BW2 represents the present body water volume.• Na1 represents the original, or normal, serum sodium concentration
of 142 mEq/L. • BW1 represents the original volume of body water. This is 60% of the
body weight of a man (50 % in a woman).• The loss of body water therefore equals BW1 – BW2.

Method 3.based on the fact that the plasma sodium concentration varies inversely with the volume of extracellular water. It assumes, however, that only water has been lost and the sodium content of the body has remained unchanged.
Example :Man, weighing approximately 70 kg. Present
serum sodium concentration, 162 mEq/LNa2 X BW2 = Na1 X BW1162 x X = 142 X 42 X = 142 X 42 = 37 liters.
162
The water loss is therefore 42 – 37 = 5 liters.
Adapted from Goldberger, Water, Electrolyte, Acid base balance.


How Does a Clinician Determine How Does a Clinician Determine ECF and ICF Volumes in a ECF and ICF Volumes in a
Patient?Patient?• ECF volume : CLINICAL EXAMECF volume : CLINICAL EXAM
– Plasma volume: Plasma volume: • jugular venous pressurejugular venous pressure• central venous pressure (with a catheter)central venous pressure (with a catheter)• examine chest for pulmonary edema (or examine chest for pulmonary edema (or
Xray)Xray)• postural hypotension - not specificpostural hypotension - not specific
– Interstitial volumeInterstitial volume• edemaedema

How Does a Clinician How Does a Clinician Determine ECF and ICF Determine ECF and ICF Volumes in a Patient?Volumes in a Patient?
Intracellular Volume
• Serum sodium concentration and serum osmolality– Hyponatremia and hyposmolality = ICFV– Hypernatremia = ICFV

What are the expected losses ?
• Measurable:– urine ( measure hourly if necessary )– GI ( stool, stoma, drains, tubes )
• Insensible:– sweat– exhaled

Hypertonic Solution-----Shrinks cell
•Isotonic Solution•No change in cell volume
Hypotonic SolutionEnlarges cell
Normal cell volume
ICF 300 mOsm