Bahan Untuk Referat OA
7
Essentials of Diagnosis Joint pain brought on and exacerbated by activity and relieved with rest. Stiffness that is self-limited upon awakening in the morning or when rising from a seated position after an extended period o f inactivity. Absence of prominent constitutional symptoms. Examination notable for increased bony prominence at the joint margins, crepitance or a grating sensation upon joint manipulation, and little if any associated joint effusion. Diagnosis supported by radiographic features of joint space n arrowing and spur (or osteophyte) formation. General Considerations Osteoarthritis is the leading cause of arthritis in the adult American population and affects an estimated 20 million people in the United States. Joint pain is a frequent symptom that often prompts a patient to seek medical attention, for which osteoarthritis figures prominently in the differential diagnosis. The challenge for clinicians is to correctly identify the cause o f the patient's pain and to initiate appropriate therapy, both medicinal and nonmedicinal. Synonymous with degenerative joint disease, osteoarthritis is characterized by joint pain related to u se, the absence of pain at rest, self-limited morning stiffness, an audible grating sound or crepitus on palpation, reduction in joint range of motion, and minimal to no associated joint swelling or warmth. Characteristic sites of involvement in the peripheral skeleton include the hand (distal interphalangeal joint, proximal interphalangeal [PIP] joint, and first carpometacarpal joint), kn ee, and hip. Common axial sites with a predilection for osteoarthritis are the lumbar and cervical spine. Constitutional symptoms are characteristically absent. Other than pain or discomfort in the involved joint, the patient with osteoarthritis most often feels well and reports good health. The diagnosis of osteoarthritis can usually be made relatively easily and confidently based on the history and examination alone. The b edside diagnosis of osteoarthritis can be supported b y plain radiography. Epidemiology At the population level, osteoarthritis results in substantial morbidity and disability, particularly among the elderly. It is the leading indication for several hundred thousand knee and hip replacement surgeries performed each year in the United States. Therefore, much effort has been invested in improving the understanding of the epidemiology of this disorder, including identifying the factors that predispose persons to osteoarthritis, especially those risk factors that
-
Upload
meilani-ayu-lestari -
Category
Documents
-
view
225 -
download
0
Transcript of Bahan Untuk Referat OA
7/27/2019 Bahan Untuk Referat OA
http://slidepdf.com/reader/full/bahan-untuk-referat-oa 1/7
Essentials of Diagnosis
Joint pain brought on and exacerbated by activity and relieved with rest.
Stiffness that is self-limited upon awakening in the morning or when rising from aseated position after an extended period of inactivity.
Absence of prominent constitutional symptoms.
Examination notable for increased bony prominence at the joint margins, crepitanceor a grating sensation upon joint manipulation, and little if any associated joint effusion.
Diagnosis supported by radiographic features of joint space narrowing and spur (or
osteophyte) formation.
General Considerations
Osteoarthritis is the leading cause of arthritis in the adult American population and affects an
estimated 20 million people in the United States. Joint pain is a frequent symptom that often
prompts a patient to seek medical attention, for which osteoarthritis figures prominently in thedifferential diagnosis. The challenge for clinicians is to correctly identify the cause of the
patient's pain and to initiate appropriate therapy, both medicinal and nonmedicinal. Synonymous
with degenerative joint disease, osteoarthritis is characterized by joint pain related to use, the
absence of pain at rest, self-limited morning stiffness, an audible grating sound or crepitus on palpation, reduction in joint range of motion, and minimal to no associated joint swelling or
warmth.
Characteristic sites of involvement in the peripheral skeleton include the hand (distalinterphalangeal joint, proximal interphalangeal [PIP] joint, and first carpometacarpal joint), knee,
and hip. Common axial sites with a predilection for osteoarthritis are the lumbar and cervicalspine. Constitutional symptoms are characteristically absent. Other than pain or discomfort in the
involved joint, the patient with osteoarthritis most often feels well and reports good health.
The diagnosis of osteoarthritis can usually be made relatively easily and confidently based on the
history and examination alone. The bedside diagnosis of osteoarthritis can be supported by plain
radiography.
Epidemiology
At the population level, osteoarthritis results in substantial morbidity and disability, particularly
among the elderly. It is the leading indication for several hundred thousand knee and hip
replacement surgeries performed each year in the United States. Therefore, much effort has beeninvested in improving the understanding of the epidemiology of this disorder, including
identifying the factors that predispose persons to osteoarthritis, especially those risk factors that
7/27/2019 Bahan Untuk Referat OA
http://slidepdf.com/reader/full/bahan-untuk-referat-oa 2/7
are reversible or modifiable.
Several factors heighten the risk of incident osteoarthritis, including age, gender, and joint injury.While the clinical expression of osteoarthritis begins to manifest during the fourth and fifth
decades of life, the incidence of osteoarthritis continues to increase with each decade of aging.
Moreover, women in their 50s, 60s, and 70s have a greater prevalence of osteoarthritis in thehand, knee, and hip than do men. There is evidence to suggest that racial differences exist in
osteoarthritis prevalence, with greater frequency of knee osteoarthritis in African Americans than
in white Americans. Also, prior trauma to a previously pristine joint, such as a ruptured anterior cruciate ligament or torn medial meniscus, increases the risk of later osteoarthritis at that joint
site.
Pathogenesis
The pathophysiology of this disorder is related to excessive degradation of cartilage within the
involved joint. Elevated production of degradative metalloproteinases, including collagenases,results in tissue breakdown and disruption in assembly of the extracellular matrix. This
disruption to the structural integrity of articular cartilage in turn leads to functional compromise
of the patient
Prevention
At present, there are no definitive data available from randomized controlled trials regarding
what preventive measures can be taken to reduce a patient's risk of developing osteoarthritis.
While certain factors, such as age, gender and race, cannot be altered, others such as body weight
are more amenable to modification. Moreover, findings from observational studies suggest thatweight loss and a change in dietary patterns may reduce a patient's risk of developing
osteoarthritis at the knee or diminish the probability of osteoarthritis progression.
Among women who participated in the Framingham Osteoarthritis Study, those who experienced
a 5-kg or more weight reduction over 10 years had half the risk of developing symptomatic kneeosteoarthritis. Such data support the claim that weight reduction can alter the risk of developing
osteoarthritis. Moreover, higher levels of vitamin D in serum and in the diet and greater intake of
vitamin C were associated with a reduced risk of disease progression. Dietary consumption of
these nutrients was not, however, related to the risk of developing new, or incident,osteoarthritis.
Clinical Findings
Symptoms and Signs
The patient with osteoarthritis affecting a joint in the peripheral skeleton, such as the finger,
knee, or hip, may initially experience relatively minor pain or discomfort with use of the
7/27/2019 Bahan Untuk Referat OA
http://slidepdf.com/reader/full/bahan-untuk-referat-oa 3/7
involved joint (Table 42 – 1). For example, at the outset of osteoarthritis involving the hip joint,
patients may have some difficulty crossing their legs to put on a pair of shoes or pants; however,
once they are dressed and upright, bearing weight and ambulation are still well tolerated. Asosteoarthritis progresses, a patient will gradually experience progressively severe joint
discomfort and increasing difficulty with related activities of daily living.
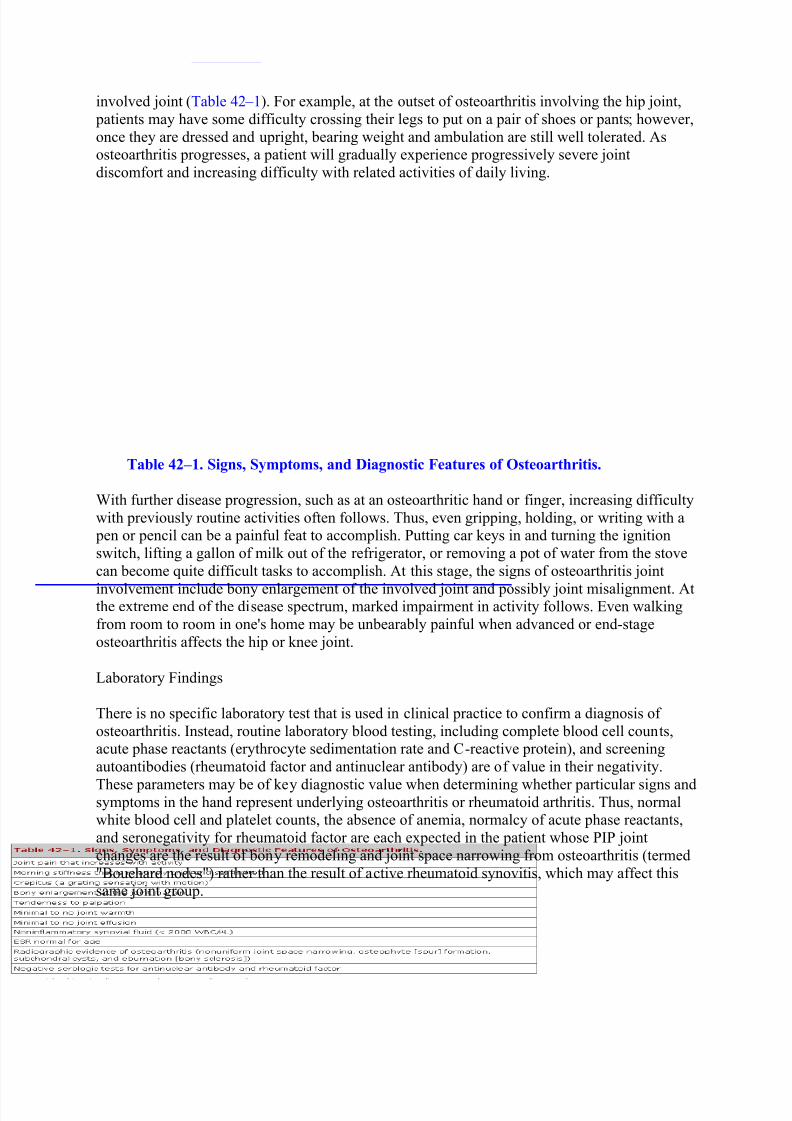
Table 42 – 1. Signs, Symptoms, and Diagnostic Features of Osteoarthritis.
With further disease progression, such as at an osteoarthritic hand or finger, increasing difficulty
with previously routine activities often follows. Thus, even gripping, holding, or writing with a pen or pencil can be a painful feat to accomplish. Putting car keys in and turning the ignition
switch, lifting a gallon of milk out of the refrigerator, or removing a pot of water from the stove
can become quite difficult tasks to accomplish. At this stage, the signs of osteoarthritis joint
involvement include bony enlargement of the involved joint and possibly joint misalignment. Atthe extreme end of the disease spectrum, marked impairment in activity follows. Even walking
from room to room in one's home may be unbearably painful when advanced or end-stage
osteoarthritis affects the hip or knee joint.
Laboratory Findings
There is no specific laboratory test that is used in clinical practice to confirm a diagnosis of
osteoarthritis. Instead, routine laboratory blood testing, including complete blood cell counts,acute phase reactants (erythrocyte sedimentation rate and C-reactive protein), and screening
autoantibodies (rheumatoid factor and antinuclear antibody) are of value in their negativity.
These parameters may be of key diagnostic value when determining whether particular signs andsymptoms in the hand represent underlying osteoarthritis or rheumatoid arthritis. Thus, normalwhite blood cell and platelet counts, the absence of anemia, normalcy of acute phase reactants,
and seronegativity for rheumatoid factor are each expected in the patient whose PIP joint
changes are the result of bony remodeling and joint space narrowing from osteoarthritis (termed
"Bouchard nodes") rather than the result of active rheumatoid synovitis, which may affect thissame joint group.
7/27/2019 Bahan Untuk Referat OA
http://slidepdf.com/reader/full/bahan-untuk-referat-oa 4/7
Imaging Studies
Radiographic imaging can confirm the diagnosis of osteoarthritis. More than 4 decades ago,Kellgren and Lawrence described characteristic radiographic features of osteoarthritis — joint
space narrowing, osteophytes, subchondral cysts, and bony sclerosis (eburnation). To the present,
these parameters remain the radiographic hallmarks of osteoarthritis. While scintigraphy (bonescan) may reveal increased radionuclide uptake at osteoarthritic joints and computed tomography
and magnetic resonance imaging may demonstrate characteristic radiographic features of
osteoarthritis, these imaging modalities are not routinely used to confirm the diagnosis of osteoarthritis.
Special Tests
Pursuit of a histologic diagnosis via synovial or bone biopsy is not a conventional strategy in the
evaluation of a patient with suspected osteoarthritis. However, in the appropriate setting, a jointtap is a valuable test when encountering a patient with presumptive osteoarthritis. When there is
subtle —
if not moderate evidence —
of a mild joint effusion, diagnostic arthrocentesis may be akey aid to confirm the clinical impression. This is because a synovial fluid cell count of 200 –
2000 cells/ L is characteristic of an osteoarthritic effusion; this synovial fluid white bloodcell count is intermediate between the upper bound of normal and the lower bound of an
inflammatory arthritis.
Differential Diagnosis
The challenge when evaluating a patient with joint pain is to effectively use the history,
examination, and available tests to arrive at the correct diagnosis. The presence of pain at thesymptomatic joint, brought on by activity and relieved with rest, is quite suggestive of adegenerative arthropathy. Moreover, the absence of constitutional signs and symptoms and the
presence of bony enlargement at the joint margin, with little if any evidence of joint
inflammation, serve to reinforce this clinical impression. Finally, the pattern of joint involvement
is meaningful because primary osteoarthritis has a predilection for particular joint sites in the peripheral skeleton, predominantly the hands (distal interphalangeal joints, PIP joints, first
carpometacarpal joint), knees, and hips. The cervical and lumbar spine are preferentially
involved sites of involvement in the axial skeleton. These features serve to distinguishosteoarthritis from inflammatory arthropathies (such as rheumatoid arthritis and gout) that have
overlapping sites of involvement.
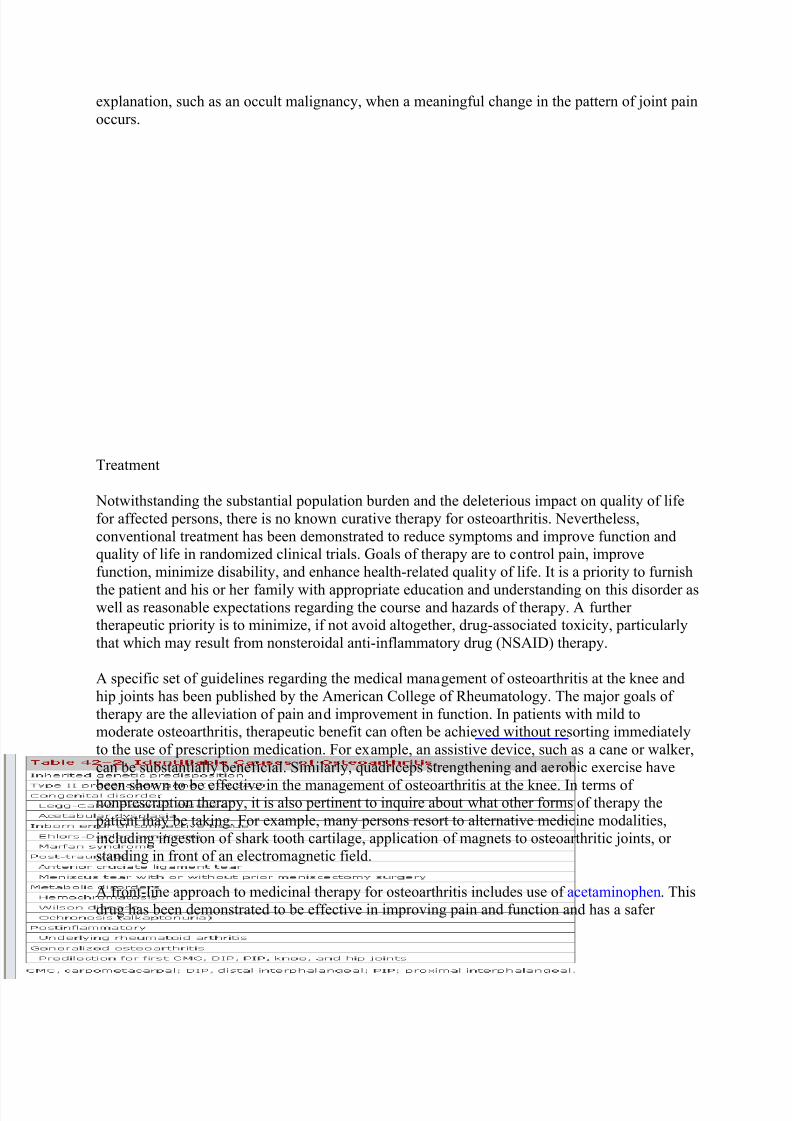
It is also worth noting that a variety of secondary disorders represent identifiable causes of
osteoarthritis. Several such disorders, including those resulting from inborn errors of metabolism
and metabolic derangements, are listed in Table 42 – 2. Recognition of their distinct features, suchas predilection for involvement of the second and third metacarpophalangeal joints in
hemochromatosis-associated arthropathy, may serve to identify the true underlying cause of the
oint pain and may impact upon therapeutic decision making. Finally, one need also bear in mind
that the presence of known osteoarthritis does not negate consideration of an alternate
7/27/2019 Bahan Untuk Referat OA
http://slidepdf.com/reader/full/bahan-untuk-referat-oa 5/7
explanation, such as an occult malignancy, when a meaningful change in the pattern of joint pain
occurs.
Treatment
Notwithstanding the substantial population burden and the deleterious impact on quality of life
for affected persons, there is no known curative therapy for osteoarthritis. Nevertheless,
conventional treatment has been demonstrated to reduce symptoms and improve function andquality of life in randomized clinical trials. Goals of therapy are to control pain, improve
function, minimize disability, and enhance health-related quality of life. It is a priority to furnish
the patient and his or her family with appropriate education and understanding on this disorder aswell as reasonable expectations regarding the course and hazards of therapy. A further therapeutic priority is to minimize, if not avoid altogether, drug-associated toxicity, particularly
that which may result from nonsteroidal anti-inflammatory drug (NSAID) therapy.
A specific set of guidelines regarding the medical management of osteoarthritis at the knee and
hip joints has been published by the American College of Rheumatology. The major goals of
therapy are the alleviation of pain and improvement in function. In patients with mild tomoderate osteoarthritis, therapeutic benefit can often be achieved without resorting immediately
to the use of prescription medication. For example, an assistive device, such as a cane or walker,
can be substantially beneficial. Similarly, quadriceps strengthening and aerobic exercise have
been shown to be effective in the management of osteoarthritis at the knee. In terms of nonprescription therapy, it is also pertinent to inquire about what other forms of therapy the
patient may be taking. For example, many persons resort to alternative medicine modalities,
including ingestion of shark tooth cartilage, application of magnets to osteoarthritic joints, or standing in front of an electromagnetic field.
A front-line approach to medicinal therapy for osteoarthritis includes use of acetaminophen. Thisdrug has been demonstrated to be effective in improving pain and function and has a safer
7/27/2019 Bahan Untuk Referat OA
http://slidepdf.com/reader/full/bahan-untuk-referat-oa 6/7
toxicity profile, particularly with regard to the gastrointestinal tract, than other NSAIDs. For
many years, the NSAIDs have been widely used in the management of osteoarthritis. Via their
inhibition of cyclooxygenase (COX), particularly the inducible isoform at sites of joint damage,symptomatic benefit is achieved.
However, the toxicity profile of NSAID therapy remains a major concern, at both the individualand population aggregate level. An estimated 10,000 Americans die each year of gastrointestinal
complications resulting from NSAID therapy. The following factors increase the risk of such
toxicity:
Persons with prior peptic ulcer disease.
Persons older than 65 years.
Concomitant tobacco and alcohol use.
Coadministration of glucocorticoids or anticoagulation therapy.
Comorbid Helicobacter pylori infection.
In 1999, a new category of NSAID agents, the selective COX-2 antagonists, that selectively and
preferentially inhibit the inducible isoform at the site of joint injury (but not the constitutive form
of the enzyme that has gastroprotective properties) was introduced into the marketplace. Their
use has exploded in just the last 4 years, on the strength of furnishing a safer gastrointestinal profile. However, this improved safety profile has been questioned, including concern of an
enhanced cardiovascular toxicity profile that may offset the improved gastrointestinal benefits.
Increasing evidence now exists to support use of glucosamine sulfate, a component of humanarticular cartilage, in the medical management of osteoarthritis. In particular, two recent
European reports have furnished evidence from randomized, placebo-controlled trials thatdemonstrated improvement in joint pain and functionality in patients with knee osteoarthritis
managed with oral glucosamine at a dose of 1500 mg/d compared with placebo. Moreover, in
both trials glucosamine was also shown to halt radiographic progression of joint spacenarrowing. The concept that a therapeutic intervention may actually arrest or reverse structural
compromise to an osteoarthritic joint is a novel and highly noteworthy development in the
management of osteoarthritis. Whether similar benefit may be accrued with use of chondroitin
sulfate (also commercially available) — or whether additive benefit can be obtained fromconcomitant administration of both glucosamine and chondroitin — remains to be determined.
Complications
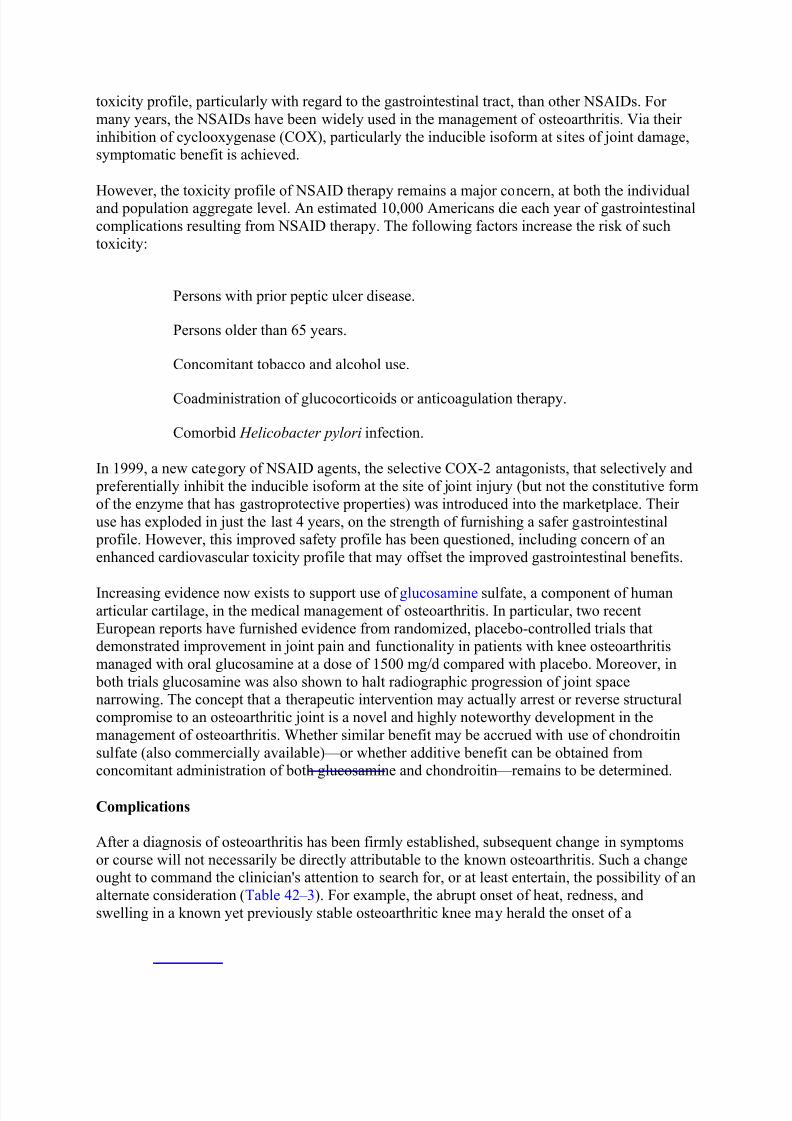
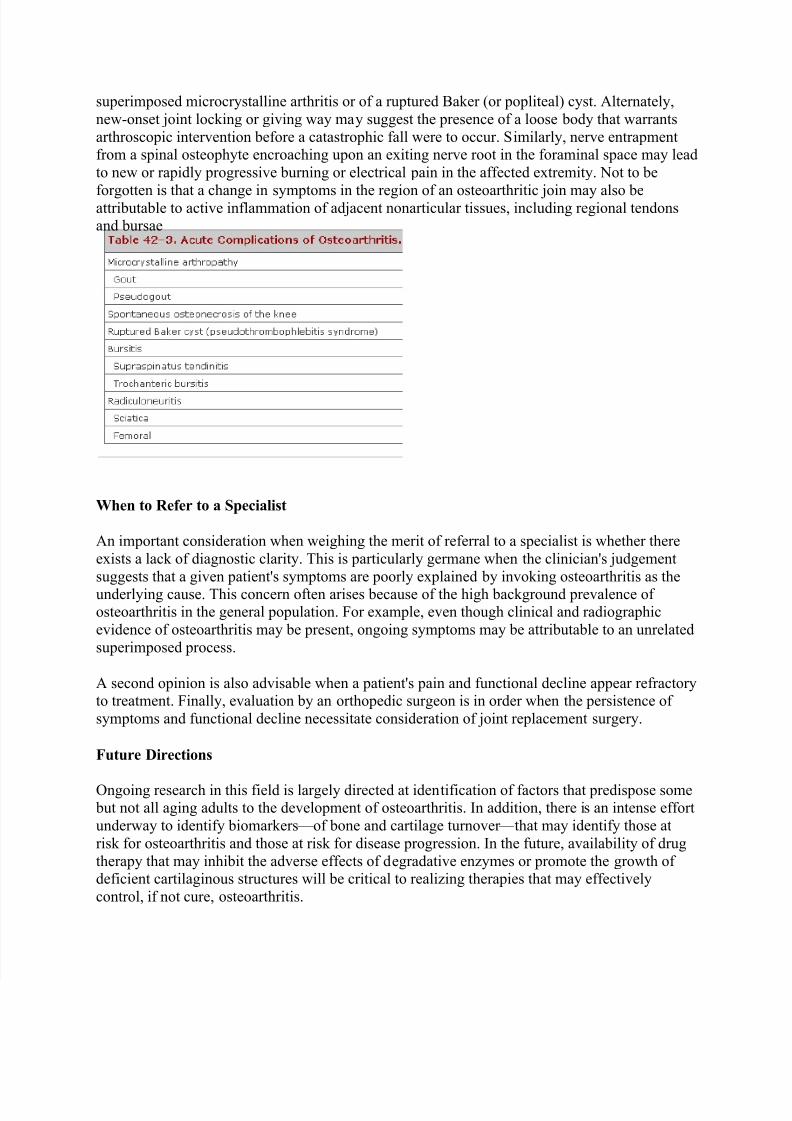
After a diagnosis of osteoarthritis has been firmly established, subsequent change in symptoms
or course will not necessarily be directly attributable to the known osteoarthritis. Such a changeought to command the clinician's attention to search for, or at least entertain, the possibility of an
alternate consideration (Table 42 – 3). For example, the abrupt onset of heat, redness, and
swelling in a known yet previously stable osteoarthritic knee may herald the onset of a
7/27/2019 Bahan Untuk Referat OA
http://slidepdf.com/reader/full/bahan-untuk-referat-oa 7/7
superimposed microcrystalline arthritis or of a ruptured Baker (or popliteal) cyst. Alternately,
new-onset joint locking or giving way may suggest the presence of a loose body that warrants
arthroscopic intervention before a catastrophic fall were to occur. Similarly, nerve entrapmentfrom a spinal osteophyte encroaching upon an exiting nerve root in the foraminal space may lead
to new or rapidly progressive burning or electrical pain in the affected extremity. Not to be
forgotten is that a change in symptoms in the region of an osteoarthritic join may also beattributable to active inflammation of adjacent nonarticular tissues, including regional tendonsand bursae
When to Refer to a Specialist
An important consideration when weighing the merit of referral to a specialist is whether there
exists a lack of diagnostic clarity. This is particularly germane when the clinician's judgement
suggests that a given patient's symptoms are poorly explained by invoking osteoarthritis as the
underlying cause. This concern often arises because of the high background prevalence of osteoarthritis in the general population. For example, even though clinical and radiographic
evidence of osteoarthritis may be present, ongoing symptoms may be attributable to an unrelated
superimposed process.
A second opinion is also advisable when a patient's pain and functional decline appear refractoryto treatment. Finally, evaluation by an orthopedic surgeon is in order when the persistence of
symptoms and functional decline necessitate consideration of joint replacement surgery.
Future Directions
Ongoing research in this field is largely directed at identification of factors that predispose some but not all aging adults to the development of osteoarthritis. In addition, there is an intense effort
underway to identify biomarkers — of bone and cartilage turnover — that may identify those at
risk for osteoarthritis and those at risk for disease progression. In the future, availability of drug
therapy that may inhibit the adverse effects of degradative enzymes or promote the growth of deficient cartilaginous structures will be critical to realizing therapies that may effectively
control, if not cure, osteoarthritis.