







Bahasa
Halaman
Hukum


Educational Assessment, Interventions, and Outcomes
480 http://ap.psychiatryonline.org Academic Psychiatry, 30:6, November-December 2006
Visualizing the Future:Technology Competency Development in Clinical Medicine,
and Implications for Medical Education
Malathi Srinivasan, M.D., Craig R. Keenan, M.D., Joel Yager, M.D.
Received February 2, 2006; revised May 1, 2006; accepted May 23,2006. Drs. Srinivasan and Keenan are affiliated with the Departmentof Internal Medicine, University of California, Davis, Sacramento,California. Dr. Yager is affiliated with the Department of Psychiatry,University of New Mexico, Albuquerque, New Mexico. Address cor-respondence to Dr. Srinivasan, 2315 Stockton Boulevard, Sacra-mento, CA 95817; [email protected] (e-mail).
Copyright � 2006 Academic Psychiatry
Objective: In this article, the authors ask three questions. First,what will physicians need to know in order to be effective in thefuture? Second, what role will technology play in achieving thathigh level of effectiveness? Third, what specific skill sets will phy-sicians need to master in order to become effective?
Method: Through three case vignettes describing past, present,and potential future medical practices, the authors identify trendsin major medical, technological and cultural shifts that willshape medical education and practice.
Results: From these cases, the authors generate a series of tech-nology-related competencies and skill sets that physicians willneed to remain leaders in the delivery of medical care. Physicianswill choose how they will be end-users of technology, technologydevelopers, and/or the interface between users and developers.These choices will guide the types of skills each physician willneed to acquire. Finally, the authors explore the implications ofthese trends for medical educators, including the competenciesthat will be required of educators as they develop the medicalcurriculum.
Conclusions: Examining historical and social trends, includinghow users adopt current and emerging technologies, allows us toanticipate changes in the practice of medicine. By consideringmarket pressures, global trends and emerging technologies, medi-cal educators and practicing physicians may prepare themselvesfor the changes likely to occur in the medical curriculum and inthe marketplace.
Academic Psychiatry 2006; 30:480–490
Thinking about competencies related to current andemerging information technologies raises several in-
teresting questions for physicians: What will they need toknow about information technology in order to be effectivein the future? What role will technology play in achievinghigh levels of effectiveness? And what specific skill sets willphysicians require to achieve and maintain these levels ofeffectiveness?
To address these questions, we paint the picture of apotential medical future, briefly outline emerging technol-ogies that will shape that future, and discuss how physi-cians may lead in the use of these technologies and, con-currently, expect to use them on a daily basis. We close byconsidering competencies related to medical technologiesand their implications for clinical educators preparinglearners for a new medical world.
To quickly envision how technology has affected medicalpractice over the years, consider these brief scenarios re-garding the assessment and treatment of a mid-40s malewith fever, chills, and a hacking cough.
The Past, Circa 1890
A physician in a horse-drawn carriage arrives at the pa-tient’s home, summoned earlier in the day by the man’swife, who sent her son on horseback to the physician’s of-fice several miles away. At the age of 40, the man is alreadyapproaching the end of his natural life but has now devel-oped a fever, chills, and a hacking cough. Physical exami-nation leads to the diagnosis of pneumonia, an often fatalcondition. The physician prescribes a morphine tonic withalcohol to relieve the patient’s pain and dyspnea. Hespends time comforting the distraught family who realizesthat the patient may die. The physician will return the nextday to the patient’s home. He creates a written patientrecord in his notebook and returns to his private hospital.Using his microscope, he sees the causative organism in

SRINIVASAN ET AL.
Academic Psychiatry, 30:6, November-December 2006 http://ap.psychiatryonline.org 481
the patient’s sputum sample. Therapeutic options are lim-ited. The physician looks through his few books on medi-cine and surgery and discusses the case with a colleaguedown the street.
The Present, Circa 2006
In his urgent care clinic, a physician sees the patient,whom he has never met, for fever, chills, and a hackingcough. The man is in the prime of his life—mid-40s witha young family. He has traveled about 20 miles by car forthis appointment, driven by his wife. The physician logsonto the hospital’s electronic medical record system andquickly reviews prior appointments and laboratory results.After diagnosing pneumonia on the basis of a quickly ob-tained chest X-ray, the physician prescribes antimicrobialagents to be picked up at the local pharmacy. The patient’swife asks about resistant bacteria and further instructionsfor care. Using the in-room desktop computer, the physi-cian does a quick online search for local bacterial resis-tance patterns and prints out current information from aproprietary medical database. The physician asks the pa-tient to call his nurse the next day. If the patient fails toimprove, he is instructed to return to the office for re-evaluation and possible hospital admission.
The Near Future, Circa 2025
A physician on call in his office in India receives a video-conference call from a patient suffering from fever, chills,and a hacking cough. The patient, located 8,500 miles awayin his local med-terminal, is a member of an internationalhealth network. In his mid-40s, he is a young man withanother 60 to 70 years of life ahead of him. The physicianpulls up the patient’s records from his computer terminal.With the patient in the med-terminal, the physician per-forms a noninvasive MRI-like scan remotely and diagnosespneumonia. Vital signs are taken automatically by meansof pressure gauges. The patient enters a biometric accesscode to allow the physician to obtain his pharmaco-ge-nomic profile from an embedded microchip to begin coun-seling. The patient’s personal digital assistant captures keywords of their conversation via voice recognition softwareand displays pertinent patient-related information for thepatient to view synchronously. The physician prescribes along-acting antibiotic, which the patient receives on-sitefrom an injection terminal. His counseling is complete af-ter the patient receives standardized information from amedical database about self-care. The patient uses a con-tinuous home monitoring device (pulse, blood pressure,
oxygenation), which routes his vital signs to the local phy-sician network to monitor trends and complications. If thepatient’s vital signs fall below acceptable parameters, anambulance network will be automatically notified and hewill be transported to a local hospital for reevaluation andadditional therapy. The Indian physician does a quick lit-erature search on aspects of caring for American patientswith pneumonia and enters his thoughts and lessonslearned into a learning portfolio for his own CME credit.The patient completes his customer satisfaction form onthe insurance company’s Web site in order to receive hisparticipation bonus of a reduced copayment.
This view of the future simply extends already existingmajor medical trends that represent market force pres-sures for cost containment (1, 2), globalization/outsourcing(3–6), and data consolidation (7–11). Another equallyplausible view of the medical future might envision betterpersonal relationships between patients and their physi-cians (12, 13), using local coverage networks and personalcommunications modalities (e.g., next evolution of e-mail,home monitoring) to allow longitudinal and home-basedinteractions. Optimists might even imagine that doctorsmight make home visits (14–16) because their patient poolhas become smaller due to their negotiated rates increas-ing and with risk pools shared across demographic groups.
The major fallacy of trying to predict a medical futurebased on present technologies or current social/economic/political trends is that major shifts are difficult to antici-pate. For instance, while functional nanotechnology andincreased domestic terrorism are recognized as near-fu-ture possibilities, the next major paradigm shift is as yetunknown. These shifts (such as Internet-based shared net-works, massive inexpensive computing power, ease of in-ternational travel, changing unemployment) have a dra-matic impact on the medical horizon in unpredictable,nonlinear ways.
Even with these uncertainties, educators are obliged toprepare their learners for near- and far-future practice sce-narios. They need to consider critical elements embeddedin these known trends, and devise strategies to help learn-ers meet those needs. Similarly, examining critical aspectsof those scenarios (Appendix 1) allows us to describe thespectrum of competencies that physicians may need to de-velop. Foreseeable major trends in medicine include:
• CommunicationEvolution of the doctor-patient relationship into amore client-supplier model (17, 18).Greater emphasis on patient responsibility forhealth (19).

TECHNOLOGY COMPETENCY DEVELOPMENT AND EDUCATION
482 http://ap.psychiatryonline.org Academic Psychiatry, 30:6, November-December 2006
• Information managementAvailability of high quality, transparent medical in-formation for the lay public (20, 21).Internationally available patient medical/pharmacyrecords (22, 23).Stringent new privacy standards, with biometric andother coded data schemas (24–27).User-friendly, decentralized continual education,tailored to individual practices (28).Emphasis on self-directed learning and continuingself-education (29–31).
• DiagnosisDevelopment of pharmocogenomic profiles for in-dividual patients (32–35).Inexpensive high-quality imaging techniques forclinic use (36).Creation of better home monitoring equipment forself/system management (37, 38).
• TherapyInformation management systems for physicianeducation and practice-based updates (39).Compilation of individual patient health statisticsinto searchable databases (40).Testing of complementary, alternative and tradi-tional/local medical practices (41, 42).Increasing emphasis on nonallopathic practice andancillary practitioners (43, 44).
• Quality control and locationDecentralization of medical care via telemedicinetechnologies (45, 46).International standards for medical practice, “in-ternationalizing” medicine (47, 48).Medical outsourcing to other countries for non-emergent treatment (49, 50).
Likelihood of Technology Adoptionby Physicians and Society
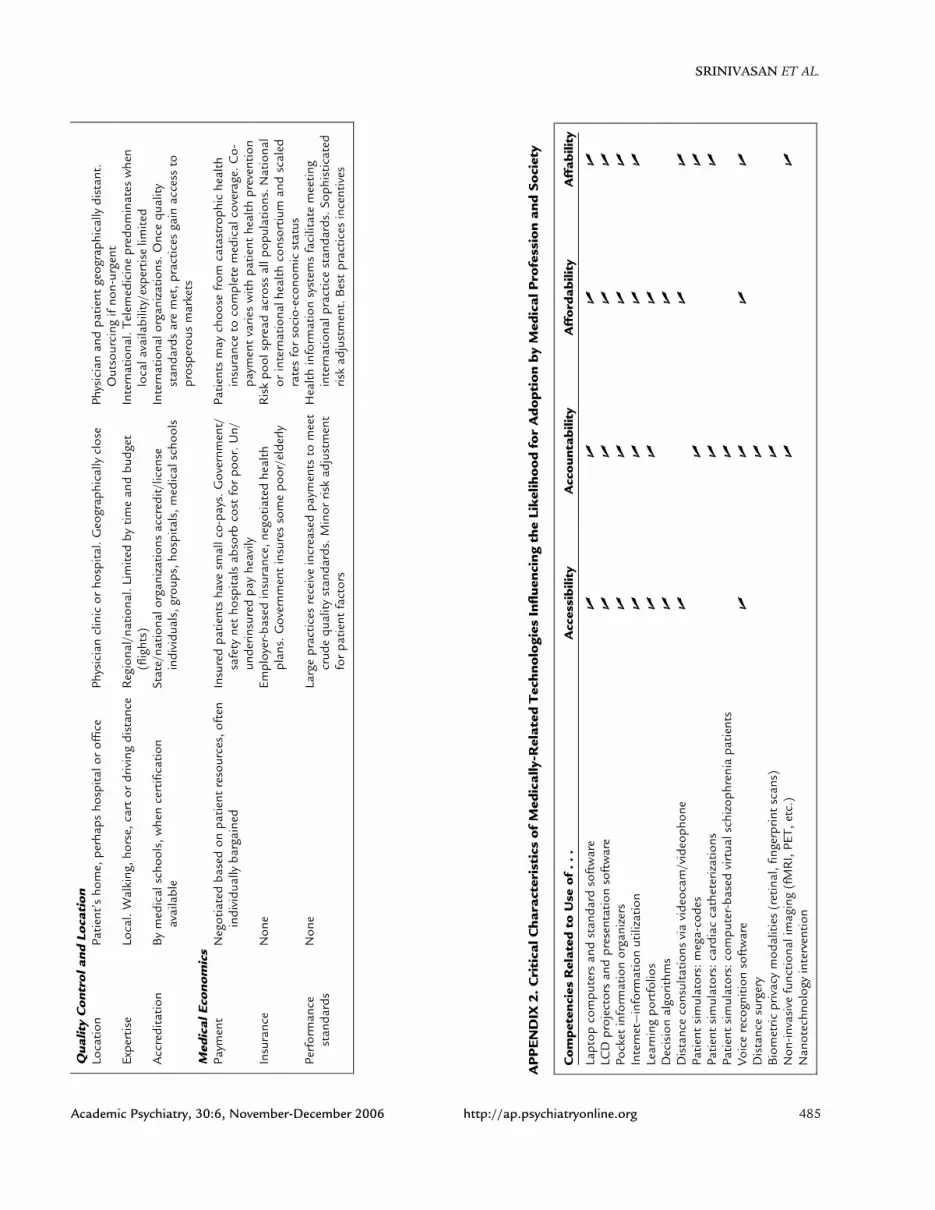
In medicine and the rest of society, the rate of technol-ogy introduction and adoption has been rapid. Enhancedcompetency by physicians may be directly related to tech-nology adoption. The incorporation of new technology inmedical practice is influenced by four strong forces, thefour “As,” which are driving pressures toward greater ef-ficiencies and effectiveness in medical care: accessibility,affordability, accountability, and affability (Appendix 2).These driving pressures are fluid and change over time for
any given technology. For example, as more competitorstry to develop similar products (such as Internet accessproviders [AOL, Comcast, telecom companies]), the tech-nologies will decrease in price (affordability). This de-crease in price and increase in manufacturing/distributionwill increase the consumer’s access to the technology. Witheach iteration, the consumer will find the technology easierto use and more functional (affability). Physicians will berequired to critically assess the cost-benefit-harm-limita-tions for each new technological tool and be accountablefor the use and results of the technologies in practice.
Physician Role Adoption and CompetencyDevelopment
In preparation for this future, physicians will have todecide how involved they will want to be with emergingmedical technologies. Some will elect to remain “end-users” of technology, whereas others will participate in de-veloping and evolving those technologies or will interfacebetween the developers and the end-users (Appendix 3).Physicians who are on the development end of technologywill, of course, need to develop specialized expertise inthose technologies: affecting communication, diagnosticand therapeutic options, data management, self-educationstrategies and other constantly changing areas.
These major trends will have significant implications forphysician training and competency development (51, 52).As with other professionals, all physicians will be requiredto become “technology literate”—understanding how touse basic software programs, communication/e-mail pro-grams, messaging systems, common organizers, commonpresentation-related hardware. Psychiatrists, for example,might be expected to acquire skills for interacting with re-mote patients via teleconferencing (tele-psychiatry) (53).Most of these technologies currently exist and are alreadybeing used in tele-consultation. Physicians who bridge twoassociated fields of medicine (e.g., electronic medical rec-ord development) and medical practitioners will requirefamiliarity with practice patterns/usage in the associatedfields. As physicians seek additional leadership opportu-nities, those who are dually trained will enjoy competitiveadvantages in the medical marketplace, where obtainingand disseminating medical information will become in-creasingly simple. Medical informatics, the field of man-aging and interfacing with medical information, will com-prise only a subset of the total types of skills that dualcompetency physicians may acquire.

SRINIVASAN ET AL.
Academic Psychiatry, 30:6, November-December 2006 http://ap.psychiatryonline.org 483
Implications for Medical Training
Future medical school selection committees may be in-creasingly inclined to recruit physician leaders who bringsubstantial experiences outside of medicine to their medi-cal education. Because of the increasingly rapid expansionand evolution of the knowledge base, students will need tospend more time learning to assess data critically. Withubiquitous information access, the amount of basic knowl-edge that physicians will need to memorize may decrease.They will also require skills in new ways of communicatingwith their patients via remote means. These shifts may en-courage some physicians to spend more time than in thepast understanding the systems and social implications ofpractice (health economics, health disparities, evidence as-sessment, research training, epidemiology).
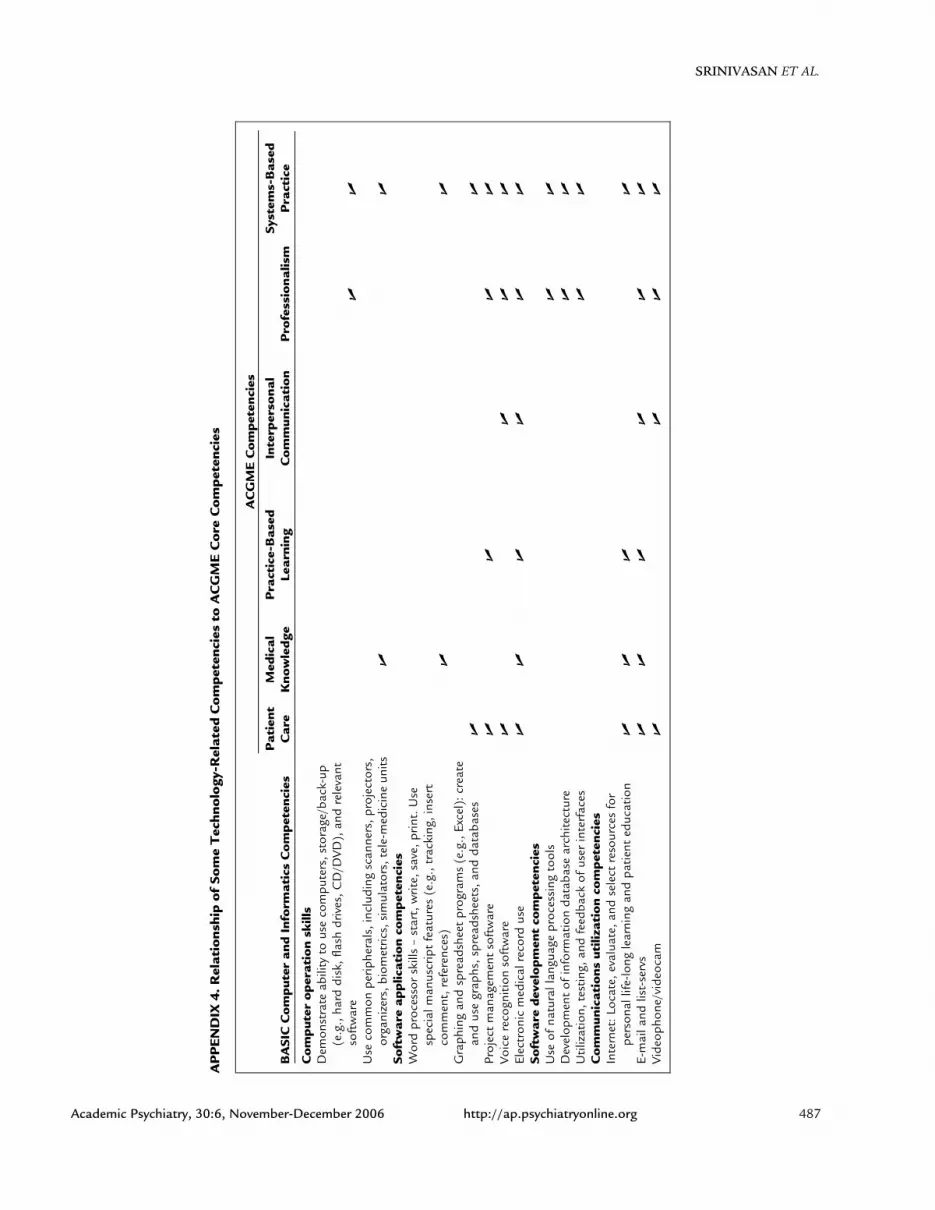
Currently, the competencies outlined by the ACGME(54) are flexible enough to allow incorporation of the tech-nology-related skills into a standard residency training pro-gram. Educators will be faced with an even more compli-cated task: keeping their core curriculum (e.g.,pathophysiology) stable while incorporating new infor-mation at a reasonable pace. In Appendix 4, we havemapped a few very basic technology-related competenciesfor the end-user physician, who may have minimal inputinto technology development. Educators will need to con-sider core skill sets for each user type from a competencyperspective. Since many of the core skills affect the differ-ent areas of medical practice, educators will need to care-fully consider how “stacked” they want their competencygrids to appear.
Medical educators will be faced with the even morecomplicated tasks of retaining their fundamental core cur-riculum requirements (e.g., pathophysiology) while incor-porating new information at a reasonable pace. Traditionalmedical education models are already challenged, as medi-
cal students already acquire and assimilate knowledge viatheir wireless laptops and PDAs during classes, seminars,and at the bedside. Inexpensive, high-quality digital videorecording technologies allow easy demonstration of best/worst communication and clinical skills practices in class-rooms. As high quality core curricula become universallyavailable through the Web, educators will have to deter-mine the best use of classroom time—how much time tospend to deliver core content and/or using a small groupsetting to assess learner understanding and push skills incontent application. Each of the specific competencies thateducators will instruct or encourage will entail knowledge,skills, attitudes, and habits. Some competencies related tothe incorporation of these technologies into a medical ed-ucator’s practice are detailed in Appendix 5.
Conclusions
Cultural and technological shifts often provoke anxietyabout a loss of values or autonomy while simultaneouslyprovoking excitement about new opportunities. The prac-tice of medicine is evolving quickly, and global trends inthe marketplace place pressure to reduce cost while in-creasing quality. The American physician of the future willface international competition, and all competitors will beequipped with powerful new tools for patient care, datamanagement, and communication. Examining these majortrends can help educators understand the new technolog-ical competencies that will be required of physicians.Medical education itself will evolve in learner selection,content, and methods. Physician leaders in education willhelp guide the appropriate implementation of medicaltechnologies in practice, fostering practices that use tech-nology to increase accessible, affordable, accountable, andaffable medical care.

TECHNOLOGY COMPETENCY DEVELOPMENT AND EDUCATION
484 http://ap.psychiatryonline.org Academic Psychiatry, 30:6, November-December 2006
AP
PE
ND
IX1.
Pas
tP
rese
ntN
ear
Futu
re
Cha
ract
eris
tic
Com
mun
icat
ion
Patie
ntro
lePa
ssiv
e,lit
tlem
edic
alkn
owle
dge
Part
icip
ator
yPa
rtic
ipat
ory,
perh
aps
dire
ctiv
ePh
ysic
ian
role
Dire
ctiv
eD
irect
ive
orpa
rtic
ipat
ory
Cus
tom
erse
rvic
eor
ient
atio
npr
edom
inat
es.
Com
petit
ion
incr
ease
sfo
rpa
tient
rost
erPa
tient
-phy
sici
anre
latio
nshi
pK
now
nea
chot
her
intim
atel
yov
ertim
eR
elat
ions
hip
islo
cal,
but
phys
icia
nm
ayno
tkn
owpa
tient
Rel
atio
nshi
pde
cent
raliz
ed,i
nter
natio
nal.
Phys
icia
nm
ayno
tkn
owpa
tient
Fam
ilyro
leC
areg
iver
sfo
ral
lpat
ient
need
sW
hen
patie
ntsi
gnifi
cant
lyill
,mos
tca
rede
liver
edin
the
hosp
ital
Sign
ifica
ntca
regi
ving
,sin
cem
uch
med
ical
care
istr
ansf
erre
dto
the
hom
eD
iagn
osis
Dia
gnos
ticop
tions
Lim
ited
tohi
stor
y,ph
ysic
al,a
ndm
icro
scop
icex
amin
atio
nN
on-in
vasi
vedi
agno
stic
sdo
nein
spec
ific
depa
rtm
ents
,not
inph
ysic
ian’
sdi
rect
offic
eN
on-in
vasi
vedi
agno
stic
sav
aila
ble
atpo
int
ofin
tera
ctio
n(t
erm
inal
s,of
fices
,etc
.).H
ome
mon
itorin
gw
ithhe
alth
-sys
tem
inte
rfac
eT
hera
pyTh
erap
eutic
optio
nsSu
rger
y,an
alge
sics
,her
balt
inct
ures
,co
mpo
unds
,com
fort
Ther
apeu
ticop
tions
base
don
patie
ntde
mog
raph
ics
(age
,sm
okin
g,et
hnic
ity)
Cus
tom
ized
ther
apeu
ticop
tions
base
don
patie
nt’s
indi
vidu
alge
nom
icpr
ofile
Evid
ence
base
Ane
cdot
alm
edic
ine,
case
serie
s,‘‘e
min
ence
-ba
sed
med
icin
e’’
Evid
ence
-bas
ed,f
rom
popu
latio
n-ba
sed
ther
apeu
ticou
tcom
esda
taPo
pula
tion
and
indi
vidu
alpr
obab
ilist
icou
tcom
esfr
omin
tern
atio
nalo
utco
mes
data
base
sIn
form
atio
nM
anag
emen
tPa
tient
reco
rds
Indi
vidu
alcl
inic
note
ske
ptby
phys
icia
nLo
cald
ata
netw
orks
incr
ease
.Mod
erat
epr
ivac
yst
anda
rds
Inte
rnat
iona
llyav
aila
ble
reco
rds,
with
strin
gent
priv
acy
stan
dard
sPa
tient
outc
omes
(pos
itive
,no
chan
ge,a
dver
se)
Not
edby
phys
icia
n,pa
tient
,and
fam
ilyN
oted
byph
ysic
ian,
patie
nt,a
ndfa
mily
.Adv
erse
outc
omes
trac
ked
byhe
alth
syst
emPa
tient
outc
omes
auto
mat
ical
lyen
tere
din
toin
tern
atio
nald
atab
ases
.Mon
itorin
gal
low
sea
rlyad
vers
eou
tcom
esal
erts
Med
ical
info
rmat
ion
Lear
ned
inm
edic
alsc
hool
,few
upda
tes
Lear
ned
inm
edic
alsc
hool
and
resi
denc
ypr
ogra
ms
Perio
dic
upda
tes
Poin
tof
serv
ice
info
rmat
ion
deliv
ery.
Info
rmat
ion
deliv
ery
sim
ulta
neou
sly
topa
tient
and
phys
icia
nC
onti
nuin
gEd
ucat
ion
Phys
icia
n’s
cont
inui
nged
ucat
ion
Not
muc
hch
ange
sinc
em
edic
alsc
hool
.Tex
t-ba
sed
lear
ning
.Opi
nion
lead
erdi
scus
sion
sR
ecer
tifica
tion
ever
y5
to10
year
s,w
ithst
ate-
man
date
ded
ucat
ion
hour
sfo
rlic
ensu
re.
Educ
atio
nis
spor
adic
and
idio
sync
ratic
Con
tinua
lcer
tifica
tion,
each
patie
ntas
ace
rtifi
catio
nca
se.R
eflec
tion-
base
dpo
rtfo
liosy
stem
slin
ked
toC
ME.
Info
rmat
ion
syst
ems
man
age
CM
Ean
dph
ysic
ian
time
Phys
icia
nou
tcom
esM
edic
alkn
owle
dge
Med
ical
know
ledg
e,so
me
proc
edur
al/
com
mun
icat
ion
skill
sM
edic
alkn
owle
dge,
skill
s,at
titud
es,h
abits
,sel
f-re
flect
ion
Prof
essi
onal
inte
ract
ions
Loca
lphy
sici
ans,
limite
dco
nfer
ence
sLo
cala
ndna
tiona
lmee
tings
.Mai
nly
loca
lin
tera
ctio
nsw
ithco
lleag
ues
Virt
ualm
eetin
gsin
tern
atio
nally
,sup
plem
enta
ryin
-pe
rson
mee
tings
SRINIVASAN ET AL.
Academic Psychiatry, 30:6, November-December 2006 http://ap.psychiatryonline.org 485
Qua
lity
Con
trol
and
Loca
tion
Loca
tion
Patie
nt’s
hom
e,pe
rhap
sho
spita
lor
offic
ePh
ysic
ian
clin
icor
hosp
ital.
Geo
grap
hica
llycl
ose
Phys
icia
nan
dpa
tient
geog
raph
ical
lydi
stan
t.O
utso
urci
ngif
non-
urge
ntEx
pert
ise
Loca
l.W
alki
ng,h
orse
,car
tor
driv
ing
dist
ance
Reg
iona
l/na
tiona
l.Li
mite
dby
time
and
budg
et(fl
ight
s)In
tern
atio
nal.
Tele
med
icin
epr
edom
inat
esw
hen
loca
lava
ilabi
lity/
expe
rtis
elim
ited
Acc
redi
tatio
nB
ym
edic
alsc
hool
s,w
hen
cert
ifica
tion
avai
labl
eSt
ate/
natio
nalo
rgan
izat
ions
accr
edit/
licen
sein
divi
dual
s,gr
oups
,hos
pita
ls,m
edic
alsc
hool
sIn
tern
atio
nalo
rgan
izat
ions
.Onc
equ
ality
stan
dard
sar
em
et,p
ract
ices
gain
acce
ssto
pros
pero
usm
arke
tsM
edic
alEc
onom
ics
Paym
ent
Neg
otia
ted
base
don
patie
ntre
sour
ces,
ofte
nin
divi
dual
lyba
rgai
ned
Insu
red
patie
nts
have
smal
lco-
pays
.Gov
ernm
ent/
safe
tyne
tho
spita
lsab
sorb
cost
for
poor
.Un/
unde
rinsu
red
pay
heav
ily
Patie
nts
may
choo
sefr
omca
tast
roph
iche
alth
insu
ranc
eto
com
plet
em
edic
alco
vera
ge.C
o-pa
ymen
tva
ries
with
patie
nthe
alth
prev
entio
nIn
sura
nce
Non
eEm
ploy
er-b
ased
insu
ranc
e,ne
gotia
ted
heal
thpl
ans.
Gov
ernm
ent
insu
res
som
epo
or/e
lder
lyR
isk
pool
spre
adac
ross
allp
opul
atio
ns.N
atio
nal
orin
tern
atio
nalh
ealth
cons
ortiu
man
dsc
aled
rate
sfo
rso
cio-
econ
omic
stat
usPe
rfor
man
cest
anda
rds
Non
eLa
rge
prac
tices
rece
ive
incr
ease
dpa
ymen
tsto
mee
tcr
ude
qual
ityst
anda
rds.
Min
orris
kad
just
men
tfo
rpa
tient
fact
ors
Hea
lthin
form
atio
nsy
stem
sfa
cilit
ate
mee
ting
inte
rnat
iona
lpra
ctic
est
anda
rds.
Soph
istic
ated
risk
adju
stm
ent.
Bes
tpr
actic
esin
cent
ives
AP
PE
ND
IX2.
Cri
tica
lCha
ract
eris
tics
of
Med
ical
ly-R
elat
edT
echn
olo
gies
Infl
uenc
ing
the
Like
liho
od
for
Ado
ptio
nb
yM
edic
alP
rofe
ssio
nan
dSo
ciet
y
Co
mpe
tenc
ies
Rel
ated
toU
seo
f..
.A
cces
sib
ility
Acc
oun
tab
ility
Aff
ord
abili
tyA
ffab
ility
Lapt
opco
mpu
ters
and
stan
dard
soft
war
e�
��
�LC
Dpr
ojec
tors
and
pres
enta
tion
soft
war
e�
��
�Po
cket
info
rmat
ion
orga
nize
rs�
��
�In
tern
et—
info
rmat
ion
utili
zatio
n�
��
�Le
arni
ngpo
rtfo
lios
��
�D
ecis
ion
algo
rithm
s�
�D
ista
nce
cons
ulta
tions
via
vide
ocam
/vid
eoph
one
��
�Pa
tient
sim
ulat
ors:
meg
a-co
des
��
Patie
ntsi
mul
ator
s:ca
rdia
cca
thet
eriz
atio
ns�
�Pa
tient
sim
ulat
ors:
com
pute
r-ba
sed
virt
uals
chiz
ophr
enia
patie
nts
�Vo
ice
reco
gniti
onso
ftw
are
��
��
Dis
tanc
esu
rger
y�
Bio
met
ricpr
ivac
ym
odal
ities
(ret
inal
,fing
erpr
int
scan
s)�
Non
-inva
sive
func
tiona
lim
agin
g(f
MR
I,PE
T,et
c.)
��
Nan
otec
hnol
ogy
inte
rven
tion

TECHNOLOGY COMPETENCY DEVELOPMENT AND EDUCATION
486 http://ap.psychiatryonline.org Academic Psychiatry, 30:6, November-December 2006
AP
PE
ND
IX3.
Fiel
dso
fE
volv
ing
Kno
wle
dge,
Wit
hSo
me
Exa
mpl
es
Do
mai
nE
volv
ing
Fiel
dSk
ills
for
Phy
sici
anD
evel
opi
ngT
echn
olo
gy
Indi
vidu
alpa
tien
tG
enom
icpr
ofilin
gB
asic
scie
nce
trai
ning
inge
netic
chip
desi
gnan
dge
netic
sequ
enci
ng.U
nder
stan
ding
ofge
netic
patt
ern
varia
tion
Indi
vidu
alda
tase
arch
inte
rpre
tatio
nH
ealth
serv
ices
rese
arch
trai
ning
for
data
base
man
ipul
atio
nan
dco
nstr
uctio
nfo
rus
eful
quer
ies.
Prog
ram
min
gsk
ills
and
data
base
cons
truc
tion
skill
sus
eful
,via
med
ical
info
rmat
ics
trai
ning
Und
erst
andi
ngcu
ltura
lnor
ms
for
deci
sion
-mak
ing
Cul
tura
lant
hrop
olog
yan
dfie
ldex
perie
nce
with
nativ
e/se
lf/ot
her
cultu
res
Und
erst
andi
ngin
divi
dual
care
pref
eren
ces
and
expe
ctat
ions
Com
mun
icat
ion
and
liste
ning
skill
str
aini
ng,i
ndiv
idua
land
syst
ems
chan
gest
rate
gies
Dia
gno
stic
opt
ions
New
noni
nvas
ive
imag
ing
and
test
ing
tech
nolo
gyA
lgor
ithm
and
mat
hem
atic
str
aini
ng.T
rain
ing
innu
clea
rph
ysic
s.Pr
ogra
mm
ing
skill
sU
nder
stan
ding
cultu
ralv
aria
tions
indi
seas
epr
esen
tatio
nC
ultu
rala
nthr
opol
ogy
and
field
expe
rienc
ew
ithna
tive/
self/
othe
rcu
lture
s.Et
hics
trai
ning
toun
ders
tand
soci
etal
confl
ict
The
rape
utic
opt
ions
Nan
otec
hnol
ogy
Trai
ning
inna
note
chno
logy
desi
gnan
dde
velo
pmen
t.C
hip
desi
gnan
dha
rdw
are
desi
gntr
aini
ngG
enet
icm
anip
ulat
ion
Che
mis
try/
gene
tictr
aini
ng.P
rote
omic
san
dce
llula
rbi
olog
ytr
aini
ng.S
oftw
are
prog
ram
min
gsk
ills
Cus
tom
ized
phar
mac
eutic
als
Che
mis
try
and
cellu
lar
biol
ogy
trai
ning
.Res
earc
htr
ials
trai
ning
.Man
agem
ent
and
mar
ketin
gtr
aini
ngU
nder
stan
ding
neur
ocog
nitiv
e-be
havi
oral
links
Neu
roco
gniti
vebi
olog
ytr
aini
ng.M
anip
ulat
ion
and
use
ofne
ural
imag
ing
tech
niqu
esN
on-p
harm
aceu
tical
inte
rven
tions
Test
ing
alte
rnat
ive,
com
plem
enta
rym
edic
ine
via
heal
thse
rvic
esre
sear
chan
dcl
inic
altr
ialt
rain
ing.
Stat
istic
alan
alys
ispa
ckag
eus
eC
om
mun
icat
ion
Dis
tanc
e/re
mot
eco
mm
unic
atio
nst
rate
gies
Com
mun
icat
ion
and
liste
ning
skill
str
aini
ng,w
ithou
tfa
ce-t
o-fa
cevi
sual
cues
.D
ista
nce
phys
ical
exam
inat
ion
and
inte
rven
tions
Com
mun
icat
ing
with
mul
ti-lin
gual
popu
latio
nsEx
pert
ise
and
med
ical
fluen
cyin
mul
tiple
lang
uage
s.Tr
aini
ngin
cultu
ralv
alue
san
dex
pect
atio
nsfo
rth
ose
popu
latio
nsC
usto
mer
-cen
tere
dca
reC
usto
mer
serv
ice
and
reta
iltr
aini
ng.B
usin
ess
man
agem
ent
trai
ning
.Per
sonn
elm
anag
emen
ttr
aini
ngPo
licy
deve
lopm
ent
Com
mun
icat
ion,
med
iare
latio
ns,a
ndad
voca
cytr
aini
ngVa
lues
confl
ict
Ethi
cala
ndco
mm
unic
atio
nstr
aini
ngto
antic
ipat
e,re
cogn
ize,
addr
ess
emer
ging
valu
esco
nflic
ts(e
.g.r
epro
duct
ion
and
life-
prol
ongi
ngca
re)
Dat
am
anag
emen
tTo
ols
tocr
itica
llysy
nthe
size
info
rmat
ion
Trai
ning
inep
idem
iolo
gy,e
duca
tiona
lcon
tent
deliv
ery,
algo
rithm
icde
cisi
onai
ds,
and
info
rmat
ion
deliv
ery
syst
emD
ata
inte
rfac
eto
ols
Trai
ning
inna
tura
llan
guag
epr
oces
sing
,voi
cere
cogn
ition
prog
ram
min
g,da
taar
chite
ctur
e,an
dso
ftw
are
prog
ram
min
gE
duca
tio
nD
ecen
tral
ized
educ
atio
nst
rate
gies
Trai
ning
ined
ucat
iona
lcon
tent
deliv
ery,
soft
war
epr
ogra
mm
ing
(JA
VA,Z
ope,
Flas
h,et
c.),
vide
opr
oduc
tion,
and
Web
-bas
edto
ols
Cre
atio
nof
high
-qua
lity
curr
ent
patie
nt/p
hysi
cian
info
rmat
ion
Trai
ning
ined
ucat
iona
lres
earc
hm
etho
dolo
gy,e
duca
tiona
ldel
iver
ytim
ing/
rein
forc
emen
t,an
dcu
rric
ulum
deve
lopm
ent
Self-
educ
atio
nan
dse
lf-re
flect
ion
stra
tegi
esTr
aini
ngin
refle
ctiv
ele
arni
ngan
dre
info
rcem
ent
stra
tegi
es,e
duca
tiona
ldel
iver
ym
echa
nism
sSi
mul
atio
nte
chno
logy
for
skill
spr
actic
eTr
aini
ngin
educ
atio
nalc
onte
ntde
liver
y,pl
astic
sm
anuf
actu
ring,
hard
war
ede
velo
pmen
t,al
gorit
hmic
&ev
ent-
driv
ende
cisi
on-m
akin
gLi
cens
ure
Inte
rnat
iona
lsta
ndar
dsde
velo
pmen
tfo
rm
edic
alpr
actic
eH
ealth
serv
ices
rese
arch
trai
ning
for
asse
ssm
ent
ofef
ficac
y,co
nten
tex
pert
ise.
Hea
lthad
voca
cytr
aini
ngM
onito
ring
and
enfo
rcem
ent
ofpr
actic
evi
olat
ions
Educ
atio
nala
sses
smen
tex
pert
ise
and
heal
thad
voca
cytr
aini
ng.G
over
nmen
tala
ndpo
licy
trai
ning
Rem
edia
tion
stra
tegi
esfo
rsu
bsta
ndar
dph
ysic
ians
Educ
atio
nalc
urric
ulum
deve
lopm
ent,
facu
ltyde
velo
pmen
t,co
mm
unic
atio
nsk
ills
trai
ning
,and
deci
sion
-mak
ing
anal
ysis
Pri
vacy
Evol
ving
priv
acy
stan
dard
sTr
aini
ngin
med
ical
ethi
cs,m
edic
alec
onom
ics,
med
iare
latio
ns,a
ndhe
alth
advo
cacy
New
met
hods
ofen
surin
gun
ique
info
rmat
ion
acce
ssTr
aini
ngin
biom
etric
s,ge
nom
ics,
and
com
pute
rpr
ogra
mm
ing
SRINIVASAN ET AL.
Academic Psychiatry, 30:6, November-December 2006 http://ap.psychiatryonline.org 487
AP
PE
ND
IX4.
Rel
atio
nshi
po
fSo
me
Tec
hno
logy
-Rel
ated
Co
mpe
tenc
ies
toA
CG
ME
Co
reC
om
pete
ncie
s
AC
GM
EC
om
pete
ncie
s
BA
SIC
Co
mpu
ter
and
Info
rmat
ics
Co
mpe
tenc
ies
Pat
ient
Car
eM
edic
alK
now
ledg
eP
ract
ice-
Bas
edLe
arni
ngIn
terp
erso
nal
Co
mm
unic
atio
nP
rofe
ssio
nalis
mSy
stem
s-B
ased
Pra
ctic
e
Co
mpu
ter
ope
rati
on
skill
sD
emon
stra
teab
ility
tous
eco
mpu
ters
,sto
rage
/bac
k-up
(e.g
.,ha
rddi
sk,fl
ash
driv
es,C
D/D
VD),
and
rele
vant
soft
war
e�
�U
seco
mm
onpe
riphe
rals
,inc
ludi
ngsc
anne
rs,p
roje
ctor
s,or
gani
zers
,bio
met
rics,
sim
ulat
ors,
tele
-med
icin
eun
its�
�So
ftw
are
appl
icat
ion
com
pete
ncie
sW
ord
proc
esso
rsk
ills
–st
art,
writ
e,sa
ve,p
rint.
Use
spec
ialm
anus
crip
tfe
atur
es(e
.g.,
trac
king
,ins
ert
com
men
t,re
fere
nces
)�
�G
raph
ing
and
spre
adsh
eet
prog
ram
s(e
.g.,
Exce
l):c
reat
ean
dus
egr
aphs
,spr
eads
heet
s,an
dda
taba
ses
��
Proj
ect
man
agem
ent
soft
war
e�
��
�Vo
ice
reco
gniti
onso
ftw
are
��
��
Elec
tron
icm
edic
alre
cord
use
��
��
��
Soft
war
ede
velo
pmen
tco
mpe
tenc
ies
Use
ofna
tura
llan
guag
epr
oces
sing
tool
s�
�D
evel
opm
ent
ofin
form
atio
nda
taba
sear
chite
ctur
e�
�U
tiliz
atio
n,te
stin
g,an
dfe
edba
ckof
user
inte
rfac
es�
�C
om
mun
icat
ions
utili
zati
on
com
pete
ncie
sIn
tern
et:L
ocat
e,ev
alua
te,a
ndse
lect
reso
urce
sfo
rpe
rson
allif
e-lo
ngle
arni
ngan
dpa
tient
educ
atio
n�
��
�E-
mai
land
list-
serv
s�
��
��
�Vi
deop
hone
/vid
eoca
m�
��
�

TECHNOLOGY COMPETENCY DEVELOPMENT AND EDUCATION
488 http://ap.psychiatryonline.org Academic Psychiatry, 30:6, November-December 2006
AP
PE
ND
IX5.
Co
mpe
tenc
ies
Rel
ated
toU
seo
fT
echn
olo
gyin
Med
ical
Edu
cati
on
and
Pat
ient
Edu
cati
on
Dev
elo
ping
Edu
cati
ona
lMat
eria
lB
asic
Kno
wle
dge:
The
educ
ator
shou
ldbe
able
tode
scrib
ean
ddi
scus
s:C
hara
cter
istic
s,st
reng
ths,
and
wea
knes
ses
ofdi
ffer
ent
med
ia,i
nclu
ding
avai
labl
em
edia
com
mun
icat
ion
reso
urce
sSo
cial
,leg
alan
det
hica
liss
ues
rela
ted
tote
chno
logy
use
(fai
rus
e,co
pyrig
hts,
acce
ssib
ility
,HIP
AA
,etc
.)R
ole
ofte
chno
logy
/med
iain
appl
icat
ion
ofco
reed
ucat
iona
lprin
cipl
es(e
.g.,
adul
tle
arni
ng)
Skill
s:Th
eed
ucat
orsh
ould
beab
leto
:D
evel
op,m
aint
ain,
and
mod
ifya
Web
page
Prod
uce
elec
tron
icsl
ides
/ove
rhea
dsus
ing
Pow
erPo
int
orsi
mila
rpr
ogra
ms
tocr
eate
still
s,in
sert
vide
oclip
sO
pera
teba
sic
med
ia-r
elat
edte
chno
logy
:vid
eore
cord
er/p
laye
r,di
gita
lcam
eras
,mon
itor/
TV,L
CD
proj
ecto
rs,c
ompu
ter,
etc.
Edit
voic
e/vi
deo
files
,pro
vide
high
qual
ityvi
deos
and
grap
hics
Use
thes
esk
ills
topr
oduc
ein
tegr
ated
mul
timed
iapr
esen
tatio
ns,i
nclu
ding
non-
linea
rhy
perm
edia
pres
enta
tions
Prod
uce
prin
t-ba
sed
prod
ucts
usin
gde
skto
ppu
blis
hing
Cur
ricu
lum
Dev
elo
pmen
tTh
eed
ucat
orsh
ould
beab
leto
:Id
entif
yta
rget
audi
ence
,lea
rner
need
s,ap
prop
riate
curr
icul
argo
als,
reso
urce
sfo
rcu
rric
ular
deve
lopm
ent/
impl
emen
tatio
nD
evel
opcr
eativ
ean
dus
eful
lear
ning
expe
rienc
es,u
sing
med
iato
pres
ent
mat
eria
lin
aco
mpr
ehen
sibl
em
anne
rLo
cate
,eva
luat
e,an
dse
lect
reso
urce
s/m
ater
ial(
digi
tali
nfor
mat
ion,
loca
lexp
erts
,prim
ary
docu
men
ts/a
rtifa
cts,
text
,etc
.)U
sete
chno
logy
inth
edi
scip
line/
subj
ectf
orle
arni
ngan
dex
tern
alco
mm
unic
atio
nU
sete
chno
logy
tofa
cilit
ate
teac
hing
stra
tegi
essp
ecifi
cto
the
disc
iplin
eD
evel
opph
ysic
alse
ttin
gsan
dor
gani
zatio
nala
ndm
anag
emen
tst
rate
gies
that
supp
ort
activ
est
uden
tin
quiry
and
colla
bora
tion
Inco
rpor
ate
med
iaan
dte
chno
logy
for
teac
hing
whe
reap
prop
riate
,and
supp
ort
lear
ner
expr
essi
onin
ava
riety
ofm
edia
Edu
cati
ona
lAss
essm
ent
The
educ
ator
shou
ldbe
able
to:
Cre
ate
stud
yde
sign
sth
atal
low
deve
lopm
ent
and
test
ing
ofed
ucat
iona
lhyp
othe
sis
Rig
orou
sly
anal
yze
data
from
stud
ies
for
effe
ctiv
enes
sof
inte
rven
tions
Dem
onst
rate
effe
ctiv
enes
sof
lear
ning
mod
ality
Dev
elop
perf
orm
ance
task
sfo
rst
uden
tsto
loca
te/a
naly
zein
form
atio
n,sy
nthe
size
,and
appl
yin
form
atio
nin
new
cont
exts
Dev
elop
need
sas
sess
men
tsus
ing
tool
s,su
chas
Surv
eyM
onke
yU
seap
prop
riate
tech
nolo
gies
effe
ctiv
ely
toco
llect
info
rmat
ion
onst
uden
tle
arni
ng,u
sing
ava
riety
ofm
etho
dsD
isse
min
atio
no
fE
duca
tio
nM
ater
ials
Cre
ate
sust
aina
ble
syst
ems
ofch
ange
with
inin
stitu
tions
and
natio
nsD
evel
opon
-line
e-le
arni
ngco
urse
sus
ing
form
ats
such
asW
ebC
T,A
ngel
,etc
.Es
tabl
ish
on-li
neco
nfer
ence
svi
aW
ebD
evel
opin
tera
ctiv
eW
eb-b
ased
curr
icul
umD
evel
opan
dpr
ovid
efe
edba
ckon
lear
ning
port
folio
sPr
esen
tm
ater
iala
tna
tiona
ledu
cato
ran
dpa
tient
care
conf
eren
ces
Use
med
iato
diss
emin
ate
appr
opria
teed
ucat
iona
lmat
eria
lto
polic
ym
aker
s
Som
eda
taad
apte
dfr
omst
anda
rds
deve
lope
dfo
red
ucat
ors
inN
orth
Car
olin
a(t
ps.d
pi.s
tate
.nc.
us/s
tand
ards
.htm
l)
SRINIVASAN ET AL.
Academic Psychiatry, 30:6, November-December 2006 http://ap.psychiatryonline.org 489
References
1. Scanlon WJ: The future of Medicare hospital payment.Health Affairs 2006; 25:70–80
2. Cromwell J, Drozd EM, Gage B, et al: Variation in patientroutine costliness in U.S. psychiatric facilities. J Ment HealthPolicy Econ 2005; 8:15–28
3. Capko J: Outsourcing: friend or foe? J Med Pract Manage2005; 21:67–71
4. Ghods AJ, Nasrollahzadeh D: Transplant tourism and the Ira-nian model of renal transplantation program: ethical consid-erations. Exp Clin Transplant 2005; 3:351–354
5. Available at http://www.medical-tourism-india.com. AccessedJan 20, 2006
6. Available at http://www.outsourceoperation.com. AccessedJan 20, 2006
7. Kleinke JD: Release 0.0: clinical information technology inthe real world. Health Aff 1998; 17:23–38
8. Kaushal R, Bates DW, Poon EG, et al: Functional gaps inattaining a national health information network: what will ittake to get there in five years? Health Aff 2005; 24:1281–1289
9. Coile RC Jr: The digital transformation of health care. Phy-sician Exec 2000; 26:8–15
10. Forkner-Dunn J: Internet-based patient self-care: the nextgeneration of health care delivery. J Med Internet Res 2003;5:e8
11. Murray E, Lo B, Pollack L, et al: The impact of health infor-mation on the Internet on health care and the physician-pa-tient relationship: national U.S. survey among 1,050 U.S. phy-sicians. J Med Internet Res 2003; 5:e17.
12. Maisels MJ, Kring EA: A simple approach to improving pa-tient satisfaction. Clin Pediatr 2005; 44:797–800
13. Bezold C: The future of patient-centered care: scenarios, vi-sions, and audacious goals. J Altern Complement Med 2005;11:S77–84
14. Alexander GC, Kurlander J, Wynia MK: Physicians in retainer(“concierge”) practice: a national survey of physician, patient,and practice characteristics. J Gen Intern Med 2005; 20:1079–1083
15. Marsh AG: A curious 21st century phenomenon: physiciansreviving the house call. Caring 2005; 24:12–16, 18–22, 24
16. Meyer GS, Gibbons RV: House calls to the elderly—a vanish-ing practice among physicians. N Engl J Med 1997; 337:1815–1820
17. Will consumerism lead to better health? Lancet 2005; 366:34318. Robinson JC: Managed consumerism in health care. Health
Aff 2005; 24:1478–148919. Kubiak T, Hermanns N, Schreckling HJ, et al: Evaluation of
a self-management-based patient education program for thetreatment and prevention of hypoglycemia-related problemsin type 1 diabetes. Patient Educ Couns 2006; 60:228–234
20. Murray E, Lo B, Pollack L, et al: The impact of health in-formation on the internet on the physician-patient relation-ship: patient perceptions. Arch Intern Med 2003; 163:1727–1734
21. Baker L, Wagner TH, Singer S, et al: Use of the Internet and
e-mail for health care information: results from a nationalsurvey. JAMA 2003; 289:2400–2406
22. Shortliffe EH: The evolution of electronic medical records.Acad Med 1999; 74:414–419
23. Katehakis DG, Sfakianakis S, Tsiknakis M, et al: An infra-structure for Integrated Electronic Health Record services:the role of XML (Extensible Markup Language). J Med In-ternet Res 2001; 3:e7
24. Hashiyada M: Development of biometric DNA ink for au-thentication security. Tohoku J Exp Med 2004; 204:109–117
25. Pothen DJ, Parmanto B: Biometric authentication: privacyprotection or invasion? J AHIMA 2001; 72:24, 26
26. Woodward JD: Biometric scanning, law & policy: identifyingthe concerns–drafting the biometric blueprint. Univ PittsbgLaw Rev 1997; 59:97–155
27. Garner JC: Final HIPAA security regulations: a review.Manag Care Q 2003; 11:15–27
28. Allison JJ, Kiefe CI, Wall T, et al: Multicomponent Internetcontinuing medical education to promote chlamydia screen-ing. Am J Prev Med 2005; 28:285–290
29. Mandel LS, Goff BA, Lentz GM: Self-assessment of residentsurgical skills: is it feasible? Am J Obstet Gynecol 2005;193:1817–1822
30. Hiramanek N: Self-directed learning and continuing medicaleducation. Aust Fam Physician 2005; 34:879–880
31. Mamary E, Charles P: Promoting self-directed learning forcontinuing medical education. Med Teach 2003; 25:188–190
32. Ginsburg GS, Donahue MP, Newby LK: Prospects for per-sonalized cardiovascular medicine: the impact of genomics. JAm Coll Cardiol 2005; 46:1615–1627
33. Cacabelos R, Fernandez-Novoa L, Corzo L, et al: Genomicsand phenotypic profiles in dementia: implications for phar-macological treatment. Methods Find Exp Clin Pharmacol2004; 26:421–444
34. Ross JS, Schenkein DP, Kashala O, et al: Pharmacogenomics.Adv Anat Pathol 2004;11:211–220
35. Mancama D, Arranz MJ, Kerwin RW: Pharmacogenomics ofpsychiatric drug treatment. Curr Opin Mol Ther 2003; 5:642–649
36. Kobal SL, Atar S, Siegel RJ: Hand-carried ultrasound im-proves the bedside cardiovascular examination. Chest 2004;126:693–701
37. Schlaeper C, Diaz-Buxo JA: Home hemodialysis and remotemonitoring: current technology, requirements and capabili-ties. Blood Purif 2005; 23:18–22
38. Celis H, Den Hond E, Staessen JA: Self-measurement ofblood pressure at home in the management of hypertension.Clin Med Res 2005; 3:19–26
39. Duque G, Finkelstein A, Roberts A, et al: Learning whileevaluating: the use of an electronic evaluation portfolio in ageriatric medicine clerkship. BMC Med Educ 2006; 6:4
40. Joosse P, Goslings JC, Luitse JS, et al: M-study: arguments forregional trauma databases. J Trauma 2005; 58:1272–1276; dis-cussion 1277
41. Kennedy J: Herb and supplement use in the US adult popu-lation. Clin Ther 2005; 27:1847–1858

TECHNOLOGY COMPETENCY DEVELOPMENT AND EDUCATION
490 http://ap.psychiatryonline.org Academic Psychiatry, 30:6, November-December 2006
42. Harle L, Brown T, Laheru D, et al: Omega-3: fatty acids forthe treatment of cancer cachexia: issues in designing clinicaltrials of dietary supplements. J Altern Complement Med2005; 11:1039–1046
43. Ruggie M: Mainstreaming complementary therapies: new di-rections in health care. Health Aff (Millwood) 2005; 24:980–990
44. Sierpina VS, Frenkel MA: Acupuncture: a clinical review.South Med J 2005; 98:330–337
45. Harnett B: Telemedicine systems and telecommunications. JTelemed Telecare 2006; 12:4–15
46. Senapati S, Advincula AP: Telemedicine and robotics: pavingthe way to the globalization of surgery. Int J Gynaecol Obstet2005; 91:210–216.
47. Fernandez RD, Hebert GJ: Global licensure: new modalitiesof treatment and care require the development of new struc-tures and systems to access care. Nurs Adm Q 2004; 28:129–132
48. Paine L, Deshpande R, Margolis JD, et al: Up to code: does
your company’s conduct meet world-class standards? HarvBus Rev 2005; 83:122–133, 154
49. Segouin C, Hodges B, Brechat PH: Globalization in healthcare: is international standardization of quality a step towardoutsourcing? Int J Qual Health Care 2005; 17:277–279
50. Spiegel JM, Labonte R, Ostry AS: Understanding “globali-zation” as a determinant of health determinants: a critical per-spective. J Occup Environ Health 2004; 10:360–367
51. Yager J: The future of psychiatry, in Encyclopedia of the Fu-ture. Edited by Kurian GT, Molitor GTT. Mcmillan, 1995
52. Robinowitz CB, Yager J: The future of psychiatric education,in Annual Review of Psychiatry, volume 15. Edited by Dick-stein LJ, Riba MB, Oldham JM. Arlington, Va, American Psy-chiatric Publishing, 1996, pp 581–604
53. Hilty DM, Marks SL, Urness D, et al: Clinical and educationalapplications of telepsychiatry: a review. Can J Psychiatry 2004;49:12–23
54. Available at http://www.acgme.org/Outcome. Accessed Janu-ary 15, 2006.
Top Related
Copyright © 2022 FDOKUMEN

