






Bahasa
Halaman
Hukum


Take Charge of Your Health
Utah Foster Care FoundationPreferred ValueCare Network
2015 Member Resources


Get a healthy start to your coverage
step 1 how to find your benefit info Most of what you’ll need you’ll find on our member site, regence.com.
If you’re new to regence.com:
1 Go to regence.com and click Register. 2 Complete the required Plan information fields. Enter your name, member ID and group
numbers as they appear on your member card. 3 Complete the Account Information fields. 4 Create a user name and password. 5 Review your information, accept the User Agreement and click Approve.
Once you’re on regence.com, you will have access to tools that help you track your coverage and make informed decisions about your health care:
Review details of your coverage Manage your claims online and eliminate the paper Explanation of Benefits (EOB) Find a doctor or hospital Access member forms Research treatment options and out-of-pocket cost estimates Learn about medical conditions and medications
.
If you have questions about your benefits or if you need a hard copy of your benefit booklet, give us a call at the number found on the back of your member card.

step 2 finding your providers While your plan is built on a specific provider network, you have a choice of provider (doctors, hospitals, clinics, etc.). All providers set their own fees for their services. We negotiate lower fees (called allowed amounts) with many of them. While most providers accept these allowed amounts, some don’t.
• Find a provider on regence.com by clicking on Find a doctor• Search by name and location or other available search fields.• The search results will give you useful information about network providers, including
specialty, location, education, board certifications, subspecialties and languagesspoken.
Provider Networks Your plan will be based on one of the following provider networks: Preferred Focal Point (PFP), Preferred ValueCare (PVC), Preferred BlueOption (PBO) or Participating (PAR). There are two levels of benefits—in-network and out-of-network. If you visit a provider in your network, your treatments and services will be covered at the highest benefit level, and your out-of-pocket costs will be lowest. If you visit an out-of network (NP) provider, your out-of-pocket costs may be significantly higher.
Reading your member card In the upper right corner of your member card, you will find benefit and network descriptors that will assist you in understanding which providers may be seen for the best benefit.
BlueCard coverage goes with you With the BlueCard Program, you can see providers that are contracted with their local Blue Cross and/or Blue Shield Plan anywhere in the country, as well as contracted providers in 200 countries around the world.
BlueCard Program Advantages
PROVIDER CHOICE You have access to more than 85% of providers and 96% of hospitals nationwide.
BENEFIT CONSISTENCY BlueCard ensures that you receive in-network benefits when choosing participating providers of any Blue Cross and/or Blue Shield Plan.
BILLING PROTECTION Accessing a Blue Cross and/or Blue Shield Plan participating provider ensures that you are not responsible for any balance billed amount.
EASE OF ACCESS It’s quick and easy to locate a participating provider at bcbs.com or by calling 1 (800) 810-BLUE (2583).

step 3 understanding your prescription coverage
Your benefit booklet includes important details about your prescription plan benefits. Any covered prescription medication will fall into one of these categories or “tiers”: Tier 1— Category 1 generic Lowest cost share.
Generic drugs are as effective, safe and high-quality as their brand-name counterparts, yet less expensive.
Tier 2— Category 2 generic and Category 1 brand-name
Because of their value and effectiveness, these are considered to be preferred when there is no Category 1 generic.
Tier 3— Category 2 brand-name These drugs may be more expensive and are less preferred than their alternatives in Tier 1 or Tier 2.
Tier 4— Specialty medications These are used to treat complex medical conditions and are available through our designated specialty pharmacy. They may require more involvement with your doctor and require special storage and handling.
The Essential Formulary is a list of medications your plan covers. If a medication is not on the formulary list (non-formulary medications) the medication is not covered. Your cost share for non-formulary medications would be 100% of the medication cost. You can find the Essential Formulary on regence.com.
You can buy formulary drugs at participating retail, mail-order and specialty pharmacies. We have contracted with RegenceRx for our participating pharmacy network. This network provides with you access to a nationwide network of over 55,000 pharmacies. To receive coverage under your plan’s prescription drug benefit, you need to use a pharmacy in this network and present your member card before purchasing your prescription.
Most pharmacies in your area are likely to be part of the network. There are also network pharmacies throughout the United States. Use Find a doctor on regence.com or call the toll-free 24-hour Pharmacy Locator line at 1 (800) 391-9701 to find a network pharmacy near you.

step 4 how to file a claim Most providers will bill us on your behalf. But if you need to request reimbursement for services you paid for out of your pocket (such as when you see an out-of-network provider), you’ll find the Member Reimbursement Claim Form on the regence.com member site under Resources/Forms & documents/Most used forms & documents.
Send claim forms and original receipts to: Regence BlueCross BlueShield of Utah P.O. Box 30272 Salt Lake City, UT 84130-0272

resources For wellness You have a number of great wellness and health resources available to you. These programs are not insurance but are offered in addition to your medical plan to help you get information and support when you need it.
Integrated Care ManagementThis program provides specialized, targeted attention and support for members whoneed assistance in managing their care. A Personal Care Team of clinical experts isready to assist you and your family with an ongoing medical condition, or seriousillness or injury. Easy access to one-on-one support helps close care gaps andimprove health outcomes. Need help or want to learn more—call 1 (866) 543-5765.
Regence Advice24: Nurse LineIf you’re not sure whether you should take care of a problem at home, call your doctoror go to the ER, registered nurses are there 24 hours a day to help you makeinformed decisions about your health. Call a nurse at 1 (800) 267-6729.
Regence AdvantagesThis members-only discount program offers you savings on health-related productsand services from a number of nationally recognized companies. Discounts includesavings on LASIK surgery, hearing aids, child health and safety products and dentalcare products and more.
have a question? We can help! Call us at the telephone number found on the back of your member card. Monday through Friday, 7 a.m. to 7 p.m. Mountain time.

Regence BlueCross BlueShield of Utah Contact Information and Resources
Customer Service
Hours Services
Toll free number
Monday - Friday, 7:00 a.m. to 7::00 p.m. MT Award-winning team to assist with questions, including finding a doctor, explaining benefits, verifying eligibility, understanding the claims process. Once you receive your member card, you can find the number on the back of the card to make it easy for you to reach us with your questions. 1 (888) 367-2119
Member Website
www.regence.com A complete source of health and wellness information • Review details about your coverage• View claims and personal account information• Compare costs and quality of hospitals, clinics
and providers• Find a doctor and read patient reviews• Member resources—forms, notices, member
discounts• Earn Rewards points for healthy living
RegenceRx www.regenceRx.com
Toll free number
Access to a network of more than 50,000 pharmacies nationwide, including mail-order, tools and information to help you and your doctor discuss medication choices, call center support and more. These tools include: • What’s covered/formulary• Nationwide pharmacy directory• Facts about medications• How your Rx benefits work• About generics
Found on the back of your member card
BlueCard www.bcbs.com
Toll free number
Blue Cross and Blue Shield plans give you access to doctors and hospitals almost everywhere, giving you peace of mind that you’ll always find the care you need. 1 (800) 810-BLUE (2583)
7/23/2014
Reg
ence
Blu
eCro
ss B
lueS
hiel
d of
Uta
h: R
egen
ce In
nova
®C
over
age
Perio
d: 1
2/01
/201
5 –
11/3
0/20
16Su
mm
ary
of B
enef
its a
nd C
over
age:
Wha
t thi
s P
lan
Cov
ers
& W
hat i
t Cos
tsC
over
age
for:
Indi
vidu
al &
Elig
ible
Fam
ily |
Plan
Typ
e: P
PO
Que
stio
ns: C
all 1
(888
) 367
-211
9 or
vis
it us
at w
ww.
Reg
ence
.com
.1
of 9
If y
ou a
ren’
t cle
ar a
bout
any
of t
he u
nder
lined
term
s us
ed in
this
form
, see
the
Glo
ssar
y.Y
ou c
an v
iew
the
Glo
ssar
y at
ww
w.c
ciio
.cm
s.go
v or
cal
l 1 (8
88) 3
67-2
119
to re
ques
t a c
opy.
UT
AH
FO
STE
R C
AR
E F
OU
ND
AT
ION
UU
0115
SIN
NS
This
is o
nly
a su
mm
ary.
If y
ou w
ant m
ore
deta
il ab
out y
our c
over
age
and
cost
s, yo
u ca
n ge
t the
com
plet
e te
rms
in th
e po
licy
or p
lan
docu
men
tat
ww
w.R
egen
ce.c
om o
r by
calli
ng 1
(888
) 367
-211
9.
Impo
rtan
t Que
stio
nsA
nsw
ers
Why
this
Mat
ters
:
Wha
t is
the
over
all
dedu
ctib
le?
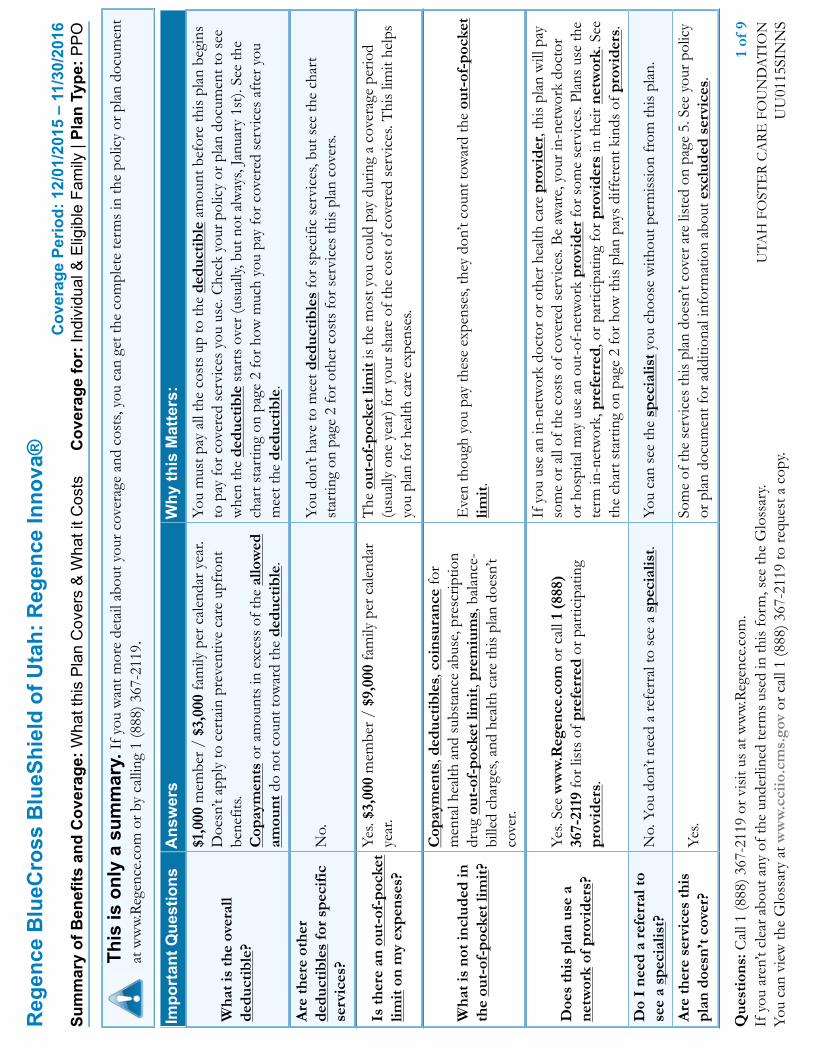
$1,0
00 m
embe
r / $
3,00
0 fa
mily
per
cal
enda
r yea
r.D
oesn
’t ap
ply
to c
erta
in p
reve
ntiv
e ca
re u
pfro
ntbe
nefit
s.C
opay
men
ts o
r am
ount
s in
exc
ess
of th
e al
low
edam
ount
do
not c
ount
tow
ard
the
dedu
ctib
le.
You
mus
t pay
all
the
cost
s up
to th
e de
duct
ible
am
ount
bef
ore
this
pla
n be
gins
to p
ay fo
r cov
ered
ser
vice
s yo
u us
e. C
heck
you
r pol
icy
or p
lan
docu
men
t to
see
whe
n th
e de
duct
ible
sta
rts
over
(usu
ally,
but
not
alw
ays,
Janu
ary
1st).
See
the
char
t sta
rtin
g on
pag
e 2
for h
ow m
uch
you
pay
for c
over
ed s
ervi
ces
afte
r you
mee
t the
ded
ucti
ble.
Are
ther
e ot
her
dedu
ctib
les
for
spec
ific
serv
ices
?N
o.Y
ou d
on’t
have
to m
eet d
educ
tibl
es fo
r spe
cific
ser
vice
s, bu
t see
the
char
tst
artin
g on
pag
e 2
for o
ther
cos
ts fo
r ser
vice
s th
is p
lan
cove
rs.
Is th
ere
an o
ut-o
f-po
cket
limit
on
my
expe
nses
?
Yes.
$3,0
00 m
embe
r / $
9,00
0 fa
mily
per
cal
enda
rye
ar.
The
out
-of-
pock
et li
mit
is th
e m
ost y
ou c
ould
pay
dur
ing
a co
vera
ge p
erio
d(u
sual
ly o
ne y
ear)
for y
our s
hare
of t
he c
ost o
f cov
ered
ser
vice
s. T
his
limit
help
syo
u pl
an fo
r hea
lth c
are
expe
nses
.
Wha
t is
not i
nclu
ded
inth
e ou
t-of
-poc
ket l
imit
?
Cop
aym
ents
, ded
ucti
bles
, coi
nsur
ance
for
men
tal h
ealth
and
sub
stan
ce a
buse
, pre
scrip
tion
drug
out
-of-
pock
et li
mit
, pre
miu
ms,
bal
ance
-bi
lled
char
ges,
and
heal
th c
are
this
pla
n do
esn’
tco
ver.
Eve
n th
ough
you
pay
thes
e ex
pens
es, t
hey
don’
t cou
nt to
war
d th
e ou
t-of
-poc
ket
limit
.
Doe
s th
is p
lan
use
ane
twor
k of
pro
vide
rs?
Yes.
See
ww
w.R
egen
ce.c
om o
r cal
l 1 (
888)
367-
2119
for l
ists
of p
refe
rred
or p
artic
ipat
ing
prov
ider
s.
If y
ou u
se a
n in
-net
wor
k do
ctor
or o
ther
hea
lth c
are
prov
ider
, thi
s pl
an w
ill p
ayso
me
or a
ll of
the
cost
s of
cov
ered
ser
vice
s. B
e aw
are,
you
r in-
netw
ork
doct
oror
hos
pita
l may
use
an
out-
of-n
etw
ork
prov
ider
for s
ome
serv
ices
. Pla
ns u
se th
ete
rm in
-net
wor
k, p
refe
rred
, or p
artic
ipat
ing
for p
rovi
ders
in th
eir n
etw
ork.
See
the
char
t sta
rtin
g on
pag
e 2
for h
ow th
is p
lan
pays
diff
eren
t kin
ds o
f pro
vide
rs.
Do
I ne
ed a
ref
erra
l to
see
a sp
ecia
list?
No.
You
don
’t ne
ed a
refe
rral
to s
ee a
spe
cial
ist.
You
can
see
the
spec
ialis
t you
cho
ose
with
out p
erm
issi
on fr
om th
is p
lan.
Are
ther
e se
rvic
es th
ispl
an d
oesn
’t co
ver?
Yes.
Som
e of
the
serv
ices
this
pla
n do
esn’
t cov
er a
re li
sted
on
page
5. S
ee y
our p
olic
yor
pla
n do
cum
ent f
or a
dditi
onal
info
rmat
ion
abou
t exc
lude
d se
rvic
es.

2 of
9U
TA
H F
OST
ER
CA
RE
FO
UN
DA
TIO
NU
U01
15SI
NN
S
●C
opay
men
ts a
re fi
xed
dolla
r am
ount
s (f
or e
xam
ple,
$15
) you
pay
for c
over
ed h
ealth
car
e, u
sual
ly w
hen
you
rece
ive
the
serv
ice.
●C
oins
uran
ce is
your
sha
re o
f the
cos
ts o
f a c
over
ed s
ervi
ce, c
alcu
late
d as
a p
erce
nt o
f the
allo
wed
am
ount
for t
he s
ervi
ce. F
or e
xam
ple,
if th
e pl
an’s
allo
wed
am
ount
for a
n ov
erni
ght h
ospi
tal s
tay
is $
1,00
0, y
our c
oins
uran
ce p
aym
ent o
f 20%
wou
ld b
e $2
00. T
his
may
cha
nge
if yo
u ha
ven’
t met
your
ded
ucti
ble.
●T
he a
mou
nt th
e pl
an p
ays
for c
over
ed s
ervi
ces
is b
ased
on
the
allo
wed
am
ount
. If a
n ou
t-of
-net
wor
k pr
ovid
er c
harg
es m
ore
than
the
allo
wed
amou
nt, y
ou m
ay h
ave
to p
ay th
e di
ffer
ence
. For
exa
mpl
e, if
an
out-
of-n
etw
ork
hosp
ital c
harg
es $
1,50
0 fo
r an
over
nigh
t sta
y an
d th
e al
low
edam
ount
is $
1,00
0, y
ou m
ay h
ave
to p
ay th
e $5
00 d
iffer
ence
. (T
his
is c
alle
d ba
lanc
e bi
lling
.)●
Thi
s pl
an m
ay e
ncou
rage
you
to u
se p
refe
rred
and
par
ticip
atin
g pr
ovid
ers
by c
harg
ing
you
low
er d
educ
tibl
es, c
opay
men
ts a
nd c
oins
uran
ceam
ount
s.
Com
mon
Med
ical
Even
tSe
rvic
es Y
ou M
ayN
eed
Your
cos
t if y
ouus
e a
Pref
erre
dPr
ovid
er
Your
cos
t if
you
use
aPa
rtic
ipat
ing
Prov
ider
Your
cos
t if y
ouus
e a
Non
-pa
rtic
ipat
ing
Prov
ider
Lim
itatio
ns &
Exc
eptio
ns
Prim
ary
care
vis
it to
trea
tan
inju
ry o
r illn
ess
$30
copa
y /
visi
t,ot
her s
ervi
ces
20%
coin
sura
nce
$45
copa
y /
visi
t,ot
her s
ervi
ces
40%
coin
sura
nce
25%
coi
nsur
ance
Spec
ialis
t vis
it$3
0 co
pay
/ vi
sit,
othe
r ser
vice
s 20
%co
insu
ranc
e
$45
copa
y /
visi
t,ot
her s
ervi
ces
40%
coin
sura
nce
25%
coi
nsur
ance
Cop
aym
ent a
pplie
s to
eac
h pr
efer
red
or p
artic
ipat
ing
upfr
ont o
ffic
e vi
sit o
nly,
dedu
ctib
le w
aive
d. A
ll ot
her s
ervi
ces
are
cove
red
at th
e co
insu
ranc
e sp
ecifi
ed, a
fter
dedu
ctib
le.
Oth
er p
ract
ition
er o
ffic
evi
sit
20%
coi
nsur
ance
for
spin
al m
anip
ulat
ions
40%
coi
nsur
ance
for
spin
al m
anip
ulat
ions
40%
coi
nsur
ance
for
spin
al m
anip
ulat
ions
Cov
erag
e is
lim
ited
to 1
0 sp
inal
man
ipul
atio
ns /
yea
r.
If y
ou v
isit
a h
ealth
care
pro
vide
r’s o
ffic
eor
clin
ic
Prev
entiv
e ca
re/
scre
enin
g/im
mun
izat
ion
No
char
geN
o ch
arge
25%
coi
nsur
ance
No
char
ge fo
r chi
ldho
od im
mun
izat
ions
from
non
-par
ticip
atin
g pr
ovid
ers.
Dia
gnos
tic te
st (x
-ray
,bl
ood
wor
k)
No
char
ge fo
rth
e fir
st $
400
/ye
ar, t
hen
20%
coin
sura
nce
No
char
ge fo
rth
e fir
st $
400
/ye
ar, t
hen
40%
coin
sura
nce
No
char
ge fo
rth
e fir
st $
400
/ye
ar, t
hen
40%
coin
sura
nce
If y
ou h
ave
a te
st
Imag
ing
(CT
/PE
T s
cans
,M
RIs
)
No
char
ge fo
rth
e fir
st $
400
/ye
ar, t
hen
20%
coin
sura
nce
No
char
ge fo
rth
e fir
st $
400
/ye
ar, t
hen
40%
coin
sura
nce
No
char
ge fo
rth
e fir
st $
400
/ye
ar, t
hen
40%
coin
sura
nce
No
char
ge fo
r the
firs
t $40
0 pe
r yea
r for
upfr
ont o
utpa
tient
labo
rato
ry a
nd ra
diol
ogy
serv
ices
, ded
ucti
ble
wai
ved.
Onc
e th
e lim
it ha
s be
en m
et a
nd fo
r all
inpa
tient
ser
vice
s, se
rvic
es a
re c
over
ed a
t the
coin
sura
nce
spec
ified
, aft
er d
educ
tibl
e.

3 of
9U
TA
H F
OST
ER
CA
RE
FO
UN
DA
TIO
NU
U01
15SI
NN
S
Com
mon
Med
ical
Even
tSe
rvic
es Y
ou M
ayN
eed
Your
cos
t if y
ouus
e a
Pref
erre
dPr
ovid
er
Your
cos
t if
you
use
aPa
rtic
ipat
ing
Prov
ider
Your
cos
t if y
ouus
e a
Non
-pa
rtic
ipat
ing
Prov
ider
Lim
itatio
ns &
Exc
eptio
ns
Gen
eric
dru
gs$1
0 co
pay
/ re
tail
pres
crip
tion
$30
copa
y /
mai
l ord
er p
resc
riptio
n$1
0 co
pay
/ se
lf-ad
min
istr
able
can
cer c
hem
othe
rapy
dru
gs
Pref
erre
d br
and
drug
s
35%
coi
nsur
ance
/ re
tail
pres
crip
tion
35%
coi
nsur
ance
/ m
ail o
rder
pre
scrip
tion
35%
coi
nsur
ance
up
to $
300
/ se
lf-ad
min
istr
able
can
cer
chem
othe
rapy
dru
gs
Non
-pre
ferr
ed b
rand
drug
s
50%
coi
nsur
ance
/ re
tail
pres
crip
tion
50%
coi
nsur
ance
/ m
ail o
rder
pre
scrip
tion
50%
coi
nsur
ance
up
to $
300
/ se
lf-ad
min
istr
able
can
cer c
hem
othe
rapy
dru
gs
If y
ou n
eed
drug
s to
trea
t you
r ill
ness
or
cond
itio
n
Mor
e in
form
atio
nab
out p
resc
ript
ion
drug
cov
erag
eis
ava
ilabl
e at
ww
w.R
egen
ce.c
om.
Spec
ialty
dru
gsR
efer
to g
ener
ic, p
refe
rred
bra
nd a
nd n
on-p
refe
rred
bra
nd d
rugs
abov
e.
Out
-of-
Poc
ket l
imit
:$50
00 /
mem
ber /
year
.C
over
age
is li
mite
d to
a 3
0-da
y su
pply
reta
ilor
90-
day
supp
ly m
ail o
rder
.M
edic
atio
ns u
sed
as p
art o
f an
outp
atie
ntca
ncer
dru
g tr
eatm
ent r
egim
en th
at is
prov
ided
and
dis
pens
ed in
a p
rofe
ssio
nal
setti
ng w
ill b
e su
bjec
t to
thes
e pr
escr
iptio
nbe
nefit
s.Y
ou a
re re
spon
sibl
e fo
r the
diff
eren
ce in
cost
bet
wee
n a
disp
ense
d br
and-
nam
e dr
ugan
d th
e eq
uiva
lent
gen
eric
dru
g, in
add
ition
to th
e co
paym
ent a
nd/o
r coi
nsur
ance
.
Faci
lity
fee
(e.g
.,am
bula
tory
sur
gery
cent
er)
20%
coi
nsur
ance
40%
coi
nsur
ance
40%
coi
nsur
ance
––––
––––
–––n
one–
––––
––––
––If
you
hav
eou
tpat
ient
sur
gery
Phys
icia
n/su
rgeo
n fe
es20
% c
oins
uran
ce40
% c
oins
uran
ce40
% c
oins
uran
ce––
––––
––––
–non
e–––
––––
––––
Em
erge
ncy
room
serv
ices
20%
coi
nsur
ance
afte
r $10
0 co
pay
20%
coi
nsur
ance
afte
r $10
0 co
pay
20%
coi
nsur
ance
afte
r $10
0 co
pay
––––
––––
–––n
one–
––––
––––
––
Em
erge
ncy
med
ical
tran
spor
tatio
n20
% c
oins
uran
ce20
% c
oins
uran
ce20
% c
oins
uran
ce––
––––
––––
–non
e–––
––––
––––
If y
ou n
eed
imm
edia
te m
edic
alat
tent
ion
Urg
ent c
are
Cov
ered
the
sam
e as
the
If y
ou v
isit
a h
ealth
car
e pr
ovid
er’s
offi
ce o
r cl
inic
or I
f you
hav
e a
test
Com
mon
Med
ical
Eve
nts.
––––
––––
–––n
one–
––––
––––
––
Faci
lity
fee
(e.g
., ho
spita
lro
om)
20%
coi
nsur
ance
40%
coi
nsur
ance
40%
coi
nsur
ance
––––
––––
–––n
one–
––––
––––
––If
you
hav
e ho
spit
alst
ayPh
ysic
ian/
surg
eon
fee
20%
coi
nsur
ance
40%
coi
nsur
ance
40%
coi
nsur
ance
––––
––––
–––n
one–
––––
––––
––
If y
ou h
ave
men
tal
heal
th, b
ehav
iora
lM
enta
l/B
ehav
iora
l hea
lthou
tpat
ient
ser
vice
s50
% c
oins
uran
ce50
% c
oins
uran
ce50
% c
oins
uran
ceC
over
age
is li
mite
d to
12
outp
atie
nt v
isits
/ye
ar.

4 of
9U
TA
H F
OST
ER
CA
RE
FO
UN
DA
TIO
NU
U01
15SI
NN
S
Com
mon
Med
ical
Even
tSe
rvic
es Y
ou M
ayN
eed
Your
cos
t if y
ouus
e a
Pref
erre
dPr
ovid
er
Your
cos
t if
you
use
aPa
rtic
ipat
ing
Prov
ider
Your
cos
t if y
ouus
e a
Non
-pa
rtic
ipat
ing
Prov
ider
Lim
itatio
ns &
Exc
eptio
ns
Men
tal/
Beh
avio
ral h
ealth
inpa
tient
ser
vice
s50
% c
oins
uran
ce50
% c
oins
uran
ce50
% c
oins
uran
ce
Subs
tanc
e us
e di
sord
erou
tpat
ient
ser
vice
s50
% c
oins
uran
ce50
% c
oins
uran
ce50
% c
oins
uran
cehe
alth
, or
subs
tanc
eab
use
need
s
Subs
tanc
e us
e di
sord
erin
patie
nt s
ervi
ces
50%
coi
nsur
ance
50%
coi
nsur
ance
50%
coi
nsur
ance
Cov
erag
e is
lim
ited
to 8
inpa
tient
day
s /
year
Pren
atal
and
pos
tnat
alca
re20
% c
oins
uran
ce40
% c
oins
uran
ce40
% c
oins
uran
ceIf
you
are
pre
gnan
tD
eliv
ery
and
all i
npat
ient
serv
ices
20%
coi
nsur
ance
40%
coi
nsur
ance
40%
coi
nsur
ance
Cov
erag
e fo
r ado
ptio
n ex
pens
es is
lim
ited
to$4
,000
/ p
regn
ancy
.
Hom
e he
alth
car
e20
% c
oins
uran
ce40
% c
oins
uran
ce40
% c
oins
uran
ceC
over
age
is li
mite
d to
130
vis
its /
yea
r.
Reh
abili
tatio
n se
rvic
es20
% c
oins
uran
ce40
% c
oins
uran
ce40
% c
oins
uran
ce
Cov
erag
e is
lim
ited
to 1
5 in
patie
nt d
ays
/ye
ar.
Cov
erag
e is
lim
ited
to 4
0 ou
tpat
ient
vis
its /
year
.
Hab
ilita
tion
serv
ices
20%
coi
nsur
ance
40%
coi
nsur
ance
40%
coi
nsur
ance
Cov
erag
e fo
r neu
rode
velo
pmen
tal t
hera
py is
limite
d to
40
outp
atie
nt v
isits
/ y
ear.
Cov
erag
e fo
r neu
rode
velo
pmen
tal t
hera
py is
limite
d to
ser
vice
s fo
r mem
bers
thro
ugh
age
6.
Skill
ed n
ursi
ng c
are
20%
coi
nsur
ance
40%
coi
nsur
ance
40%
coi
nsur
ance
Cov
erag
e is
lim
ited
to 6
0 in
patie
nt d
ays
/ye
ar.
Dur
able
med
ical
equi
pmen
t20
% c
oins
uran
ce40
% c
oins
uran
ce40
% c
oins
uran
ce––
––––
––––
–non
e–––
––––
––––
If y
ou n
eed
help
reco
veri
ng o
r ha
veot
her
spec
ial h
ealth
need
s
Hos
pice
ser
vice
20%
coi
nsur
ance
40%
coi
nsur
ance
40%
coi
nsur
ance
Cov
erag
e is
lim
ited
to 1
4 re
spite
day
s /
lifet
ime.
Eye
exa
mN
ot c
over
edN
ot c
over
edN
ot c
over
ed––
––––
––––
–non
e–––
––––
––––
If y
our
child
nee
dsde
ntal
or
eye
care
Gla
sses
Not
cov
ered
Not
cov
ered
Not
cov
ered
––––
––––
–––n
one–
––––
––––
––

5 of
9U
TA
H F
OST
ER
CA
RE
FO
UN
DA
TIO
NU
U01
15SI
NN
S
Com
mon
Med
ical
Even
tSe
rvic
es Y
ou M
ayN
eed
Your
cos
t if y
ouus
e a
Pref
erre
dPr
ovid
er
Your
cos
t if
you
use
aPa
rtic
ipat
ing
Prov
ider
Your
cos
t if y
ouus
e a
Non
-pa
rtic
ipat
ing
Prov
ider
Lim
itatio
ns &
Exc
eptio
ns
Den
tal c
heck
-up
Not
cov
ered
Not
cov
ered
Not
cov
ered
––––
––––
–––n
one–
––––
––––
––

6 of
9U
TA
H F
OST
ER
CA
RE
FO
UN
DA
TIO
NU
U01
15SI
NN
S
Exc
lude
d Se
rvic
es &
Oth
er C
over
ed S
ervi
ces:
Serv
ices
You
r P
lan
Doe
s N
OT
Cov
er (
Thi
s is
n’t a
com
plet
e lis
t. C
heck
you
r po
licy
or p
lan
docu
men
t for
oth
er e
xclu
ded
serv
ices
.)●
Acu
punc
ture
●B
aria
tric
sur
gery
●C
osm
etic
sur
gery
, exc
ept c
onge
nita
l ano
mal
ies
●D
enta
l car
e (A
dult)
●H
earin
g ai
ds●
Infe
rtili
ty tr
eatm
ent
●Lo
ng-t
erm
car
e●
Priv
ate-
duty
nur
sing
●R
outin
e ey
e ca
re (A
dult)
●R
outin
e fo
ot c
are
exce
pt fo
r dia
betic
pat
ient
s●
Vis
ion
hard
war
e●
Wei
ght l
oss
prog
ram
s ex
cept
for n
utrit
iona
lco
unse
ling
Oth
er C
over
ed S
ervi
ces
(Thi
s is
n’t a
com
plet
e lis
t. C
heck
you
r po
licy
or p
lan
docu
men
t for
oth
er c
over
ed s
ervi
ces
and
your
cos
ts fo
r th
ese
serv
ices
.)●
Chi
ropr
actic
car
e●
Non
-em
erge
ncy
care
whe
n tr
avel
ing
outs
ide
the
U.S
.

7 of
9U
TA
H F
OST
ER
CA
RE
FO
UN
DA
TIO
NU
U01
15SI
NN
S
Your
Rig
hts
to C
ontin
ue C
over
age:
If y
ou lo
se c
over
age
unde
r the
pla
n, th
en, d
epen
ding
upo
n th
e ci
rcum
stan
ces,
Fede
ral a
nd S
tate
law
s m
ay p
rovi
de p
rote
ctio
ns th
at a
llow
you
to k
eep
heal
thco
vera
ge. A
ny s
uch
right
s m
ay b
e lim
ited
in d
urat
ion
and
will
requ
ire y
ou to
pay
a p
rem
ium
, whi
ch m
ay b
e si
gnifi
cant
ly h
ighe
r tha
n th
e pr
emiu
m y
ou p
ay w
hile
cove
red
unde
r the
pla
n. O
ther
lim
itatio
ns o
n yo
ur ri
ghts
to c
ontin
ue c
over
age
may
als
o ap
ply.
For m
ore
info
rmat
ion
on y
our r
ight
s to
con
tinue
cov
erag
e, c
onta
ct th
e pl
an a
t 1 (8
88) 3
67-2
119.
You
may
als
o co
ntac
t you
r sta
te in
sura
nce
depa
rtm
ent,
the
U.S
.D
epar
tmen
t of L
abor
, Em
ploy
ee B
enef
its S
ecur
ity A
dmin
istr
atio
n at
1 (8
66) 4
44-3
272
or w
ww.
dol.g
ov/e
bsa,
or t
he U
.S. D
epar
tmen
t of H
ealth
and
Hum
anSe
rvic
es a
t 1 (8
77) 2
67-2
323
x615
65 o
r ww
w.cc
iio.c
ms.g
ov.
Your
Grie
vanc
e an
d A
ppea
ls R
ight
s:If
you
hav
e a
com
plai
nt o
r are
dis
satis
fied
with
a d
enia
l of c
over
age
for c
laim
s un
der y
our p
lan,
you
may
be
able
to a
ppea
l or f
ile a
gri
evan
ce. F
or q
uest
ions
abou
t you
r rig
hts,
this
not
ice,
or a
ssis
tanc
e, y
ou c
an c
onta
ct th
e pl
an a
t [C
usto
mer
Serv
iceP
hone
Num
ber]
or v
isit
ww
w.R
egen
ce.c
om. Y
ou m
ay a
lso
cont
act y
our
stat
e in
sura
nce
depa
rtm
ent a
t 1 (8
00) 4
39-3
805
or w
ww.
insu
ranc
e.ut
ah.g
ov o
r the
U.S
. Dep
artm
ent o
f Lab
or, E
mpl
oyee
Ben
efits
Sec
urity
Adm
inis
trat
ion
at 1
(866
)44
4-32
72 o
r ww
w.do
l.gov
/ebs
a/he
alth
refo
rm.
Doe
s th
is C
over
age
Prov
ide
Min
imum
Ess
entia
l Cov
erag
e?T
he A
ffor
dabl
e C
are
Act
requ
ires
mos
t peo
ple
to h
ave
heal
th c
are
cove
rage
that
qua
lifie
s as
“m
inim
um e
ssen
tial c
over
age.”
Thi
s pl
an o
r po
licy
does
pro
vide
min
imum
ess
enti
al c
over
age.
Doe
s th
is C
over
age
Mee
t the
Min
imum
Val
ue S
tand
ard?
In o
rder
for c
erta
in ty
pes
of h
ealth
cov
erag
e (f
or e
xam
ple,
indi
vidu
ally
pur
chas
ed in
sura
nce
or jo
b-ba
sed
cove
rage
) to
qual
ify a
s m
inim
um e
ssen
tial c
over
age,
the
plan
mus
t pay
, on
aver
age,
at l
east
60
perc
ent o
f allo
wed
cha
rges
for c
over
ed s
ervi
ces.
Thi
s is
cal
led
the
“min
imum
val
ue s
tand
ard.
” T
his
heal
th c
over
age
does
mee
t th
e m
inim
um v
alue
sta
ndar
d fo
r th
e be
nefi
ts it
pro
vide
s.
Lang
uage
Acc
ess
Serv
ices
:N
AVA
JO (D
ine)
: Din
ek'e
hgo
shik
a at
'ohw
ol n
inis
ingo
, kw
iijig
o ho
lne'
1 (8
88) 3
67-2
119.
––––
––––
––––
––––
––––
––To
see e
xam
ples
of ho
w th
is pl
an m
ight c
over
costs
for a
sam
ple m
edica
l situ
ation
, see
the n
ext p
age.–
––––
––––
––––
––––
––––
–

8 of
9U
TA
H F
OST
ER
CA
RE
FO
UN
DA
TIO
NU
U01
15SI
NN
S
Abo
ut th
ese
Cov
erag
eEx
ampl
es:
The
se e
xam
ples
sho
w h
ow th
is p
lan
mig
ht c
over
med
ical
car
e in
giv
en s
ituat
ions
. Use
thes
e ex
ampl
esto
see
, in
gene
ral,
how
muc
h fin
anci
al p
rote
ctio
n a
sam
ple
patie
nt m
ight
get
if th
ey a
re c
over
ed u
nder
diff
eren
t pla
ns. Th
is is
not a
cos
tes
timat
or.
Don
’t us
e th
ese
exam
ples
toes
timat
e yo
ur a
ctua
l cos
tsun
der t
his
plan
. The
act
ual
care
you
rece
ive
will
be
diff
eren
t fro
m th
ese
exam
ples
,an
d th
e co
st o
f tha
t car
e w
illal
so b
e di
ffer
ent.
See
the
next
pag
e fo
rim
port
ant i
nfor
mat
ion
abou
tth
ese
exam
ples
.
Hav
ing
a ba
by(n
orm
al d
eliv
ery)
■A
mou
nt o
wed
to p
rovi
ders
: $7,
540
■Pl
an p
ays:
$5,
200
■Pa
tient
pay
s: $
2,34
0
Sam
ple
care
cos
ts:
Hos
pita
l cha
rges
(mot
her)
$2,7
00R
outin
e ob
stet
ric c
are
$2,1
00H
ospi
tal c
harg
es (b
aby)
$900
Ane
sthe
sia
$900
Labo
rato
ry te
sts
$500
Pres
crip
tions
$200
Rad
iolo
gy$2
00V
acci
nes,
othe
r pre
vent
ive
$40
Tot
al$7
,540
Patie
nt p
ays:
Ded
uctib
les
$1,0
00C
opay
s$2
0C
oins
uran
ce$1
,170
Lim
its o
r exc
lusi
ons
$150
Tot
al$2
,340
Man
agin
g ty
pe 2
dia
bete
s(r
outi
ne m
aint
enan
ce o
fa
wel
l-co
ntro
lled
cond
itio
n)
■A
mou
nt o
wed
to p
rovi
ders
: $5,
400
■Pl
an p
ays:
$3,
580
■Pa
tient
pay
s: $
1,82
0
Sam
ple
care
cos
ts:
Pres
crip
tions
$2,9
00M
edic
al E
quip
men
t and
Sup
plie
s$1
,300
Off
ice
Vis
its a
nd P
roce
dure
s$7
00E
duca
tion
$300
Labo
rato
ry te
sts
$100
Vac
cine
s, ot
her p
reve
ntiv
e$1
00T
otal
$5,4
00
Patie
nt p
ays:
Ded
uctib
les
$290
Cop
ays
$440
Coi
nsur
ance
$1,0
50Li
mits
or e
xclu
sion
s$4
0T
otal
$1,8
20

Que
stio
ns a
nd a
nsw
ers
abou
t the
Cov
erag
e Ex
ampl
es:
Que
stio
ns: C
all 1
(888
) 367
-211
9 or
vis
it us
at w
ww.
Reg
ence
.com
.9
of 9
If y
ou a
ren’
t cle
ar a
bout
any
of t
he u
nder
lined
term
s us
ed in
this
form
, see
the
Glo
ssar
y.Y
ou c
an v
iew
the
Glo
ssar
y at
ww
w.c
ciio
.cm
s.go
v or
cal
l 1 (8
88) 3
67-2
119
to re
ques
t a c
opy.
UT
AH
FO
STE
R C
AR
E F
OU
ND
AT
ION
UU
0115
SIN
NS
Wha
t are
som
e of
the
assu
mpt
ions
behi
nd th
e C
over
age
Exam
ples
?●
Cos
ts d
on’t
incl
ude
prem
ium
s.●
Sam
ple
care
cos
ts a
re b
ased
on
natio
nal
aver
ages
sup
plie
d by
the
U.S
. Dep
artm
ent o
fH
ealth
and
Hum
an S
ervi
ces,
and
aren
’t sp
ecifi
cto
a p
artic
ular
geo
grap
hic
area
or h
ealth
pla
n.●
The
pat
ient
’s co
nditi
on w
as n
ot a
n ex
clud
ed o
rpr
eexi
stin
g co
nditi
on.
●A
ll se
rvic
es a
nd tr
eatm
ents
sta
rted
and
end
edin
the
sam
e co
vera
ge p
erio
d.●
The
re a
re n
o ot
her m
edic
al e
xpen
ses
for a
nym
embe
r cov
ered
und
er th
is p
lan.
●O
ut-o
f-po
cket
exp
ense
s ar
e ba
sed
only
on
trea
ting
the
cond
ition
in th
e ex
ampl
e.●
The
pat
ient
rece
ived
all
care
from
in-n
etw
ork
prov
ider
s. I
f the
pat
ient
had
rece
ived
car
efr
om o
ut-o
f-ne
twor
k pr
ovid
ers,
cos
ts w
ould
have
bee
n hi
gher
.
Wha
t doe
s a
Cov
erag
e Ex
ampl
esh
ow?
For e
ach
trea
tmen
t situ
atio
n, th
e C
over
age
Exa
mpl
e he
lps
you
see
how
ded
ucti
bles
,co
paym
ents
, and
coi
nsur
ance
can
add
up.
It a
lso
help
s yo
u se
e w
hat e
xpen
ses
mig
ht b
e le
ft u
p to
you
to p
ay b
ecau
se th
e se
rvic
e or
trea
tmen
t isn
’tco
vere
d or
pay
men
t is
limite
d.
Doe
s th
e C
over
age
Exam
ple
pred
ict
my
own
care
nee
ds?
✖N
o. T
reat
men
ts s
how
n ar
e ju
st e
xam
ples
.T
he c
are
you
wou
ld re
ceiv
e fo
r thi
sco
nditi
on c
ould
be
diff
eren
t bas
ed o
n yo
urdo
ctor
’s ad
vice
, you
r age
, how
ser
ious
you
rco
nditi
on is
, and
man
y ot
her f
acto
rs.
Doe
s th
e C
over
age
Exam
ple
pred
ict
my
futu
re e
xpen
ses?
✖N
o. C
over
age
Exa
mpl
es a
re n
ot c
ost
estim
ator
s. Y
ou c
an’t
use
the
exam
ples
toes
timat
e co
sts
for a
n ac
tual
con
ditio
n. T
hey
are
for c
ompa
rativ
e pu
rpos
es o
nly.
You
row
n co
sts
will
be
diff
eren
t dep
endi
ng o
n th
eca
re y
ou re
ceiv
e, th
e pr
ices
you
r pro
vide
rsch
arge
, and
the
reim
burs
emen
t you
r hea
lthpl
an a
llow
s.
Can
I us
e C
over
age
Exam
ples
toco
mpa
re p
lans
?
✔Ye
s. W
hen
you
look
at t
he S
umm
ary
ofB
enef
its a
nd C
over
age
for o
ther
pla
ns,
you’
ll fin
d th
e sa
me
Cov
erag
e E
xam
ples
.W
hen
you
com
pare
pla
ns, c
heck
the
“Pat
ient
Pays
” bo
x in
eac
h ex
ampl
e. T
he s
mal
ler
that
num
ber,
the
mor
e co
vera
ge th
e pl
anpr
ovid
es.
Are
ther
e ot
her c
osts
I sh
ould
cons
ider
whe
n co
mpa
ring
plan
s?
✔Ye
s. A
n im
port
ant c
ost i
s th
e pr
emiu
m y
oupa
y. G
ener
ally,
the
low
er y
our p
rem
ium
,th
e m
ore
you’
ll pa
y in
out
-of-
pock
etco
sts,
such
as
copa
ymen
ts, d
educ
tibl
es,
and
coin
sura
nce.
You
sho
uld
also
cons
ider
con
trib
utio
ns to
acc
ount
s su
ch a
she
alth
sav
ings
acc
ount
s (H
SAs)
, fle
xibl
esp
endi
ng a
rran
gem
ents
(FSA
s) o
r hea
lthre
imbu
rsem
ent a
ccou
nts
(HR
As)
that
hel
pyo
u pa
y ou
t-of
-poc
ket e
xpen
ses.

Reg
ence
Blu
eCro
ss B
lueS
hiel
d of
Uta
h: R
egen
ce H
SA 3
.0SM
Cov
erag
e Pe
riod:
12/
01/2
015
– 11
/30/
2016
Sum
mar
y of
Ben
efits
and
Cov
erag
e: W
hat t
his
Pla
n C
over
s &
Wha
t it C
osts
Cov
erag
e fo
r: In
divi
dual
& E
ligib
le F
amily
| Pl
an T
ype:
PPO
Que
stio
ns: C
all 1
(87
7) 5
08-7
360
or v
isit
us a
t ww
w.R
egen
ce.c
om.
1 of
8If
you
are
n’t c
lear
abo
ut a
ny o
f the
und
erlin
ed te
rms
used
in th
is fo
rm, s
ee th
e G
loss
ary.
You
can
vie
w th
e G
loss
ary
at w
ww
.cci
io.c
ms.
gov
or c
all 1
(87
7) 5
08-7
360
to re
ques
t a c
opy.
UT
AH
FO
STE
R C
AR
E F
OU
ND
AT
ION
UU
0115
SH
H3S
This
is o
nly
a su
mm
ary.
If y
ou w
ant m
ore
deta
il ab
out y
our c
over
age
and
cost
s, yo
u ca
n ge
t the
com
plet
e te
rms
in th
e po
licy
or p
lan
docu
men
tat
ww
w.R
egen
ce.c
om o
r by
calli
ng 1
(87
7) 5
08-7
360.
Impo
rtan
t Que
stio
nsA
nsw
ers
Why
this
Mat
ters
:
Wha
t is
the
over
all
dedu
ctib
le?
$1,5
00 s
ingl
e /
$3,0
00 fa
mily
per
cal
enda
r yea
r.D
oesn
’t ap
ply
to c
erta
in p
reve
ntiv
e ca
re.
Am
ount
s in
exc
ess
of th
e al
low
ed a
mou
nt d
o no
tco
unt t
owar
d th
e de
duct
ible
.
Sing
le: Y
ou m
ust p
ay a
ll th
e co
sts
up to
the
sing
le d
educ
tibl
e am
ount
bef
ore
this
plan
beg
ins
to p
ay fo
r cov
ered
ser
vice
s yo
u us
e.Fa
mily
: Mem
bers
col
lect
ivel
y m
ust p
ay a
ll th
e co
sts
up to
the
fam
ily d
educ
tibl
eam
ount
bef
ore
this
pla
n be
gins
to p
ay fo
r any
mem
ber’s
cov
ered
ser
vice
s.C
heck
you
r pol
icy
or p
lan
docu
men
t to
see
whe
n th
e de
duct
ible
sta
rts
over
(usu
ally,
but
not
alw
ays,
Janu
ary
1st).
See
the
char
t sta
rtin
g on
pag
e 2
for h
owm
uch
you
pay
for c
over
ed s
ervi
ces
afte
r you
mee
t the
ded
ucti
ble.
Are
ther
e ot
her
dedu
ctib
les
for
spec
ific
serv
ices
?N
o.Y
ou d
on’t
have
to m
eet d
educ
tibl
es fo
r spe
cific
ser
vice
s, bu
t see
the
char
tst
artin
g on
pag
e 2
for o
ther
cos
ts fo
r ser
vice
s th
is p
lan
cove
rs.
Is th
ere
an o
ut-o
f-po
cket
limit
on
my
expe
nses
?Ye
s. $5
,000
sin
gle
/$1
0,00
0 fa
mily
per
cal
enda
r yea
r.
The
out
-of-
pock
et li
mit
is th
e m
ost y
ou c
ould
pay
dur
ing
a co
vera
ge p
erio
d(u
sual
ly o
ne y
ear)
for y
our s
hare
of t
he c
ost o
f cov
ered
ser
vice
s. T
his
limit
help
syo
u pl
an fo
r hea
lth c
are
expe
nses
.
Wha
t is
not i
nclu
ded
inth
e ou
t-of
-poc
ket l
imit
?P
rem
ium
s, b
alan
ce-b
illed
cha
rges
, and
hea
lth c
are
this
pla
n do
esn’
t cov
er.
Eve
n th
ough
you
pay
thes
e ex
pens
es, t
hey
don’
t cou
nt to
war
d th
e ou
t-of
-poc
ket
limit
.
Doe
s th
is p
lan
use
ane
twor
k of
pro
vide
rs?
Yes.
See
ww
w.R
egen
ce.c
om o
r cal
l 1 (
877)
508-
7360
for l
ists
of i
n-ne
twor
k or
out
-of-
netw
ork
prov
ider
s.
If y
ou u
se a
n in
-net
wor
k do
ctor
or o
ther
hea
lth c
are
prov
ider
, thi
s pl
an w
ill p
ayso
me
or a
ll of
the
cost
s of
cov
ered
ser
vice
s. B
e aw
are,
you
r in-
netw
ork
doct
oror
hos
pita
l may
use
an
out-
of-n
etw
ork
prov
ider
for s
ome
serv
ices
. Pla
ns u
se th
ete
rm in
-net
wor
k, p
refe
rred
, or p
artic
ipat
ing
for p
rovi
ders
in th
eir n
etw
ork.
See
the
char
t sta
rtin
g on
pag
e 2
for h
ow th
is p
lan
pays
diff
eren
t kin
ds o
f pro
vide
rs.
Do
I ne
ed a
ref
erra
l to
see
a sp
ecia
list?
No.
You
don
’t ne
ed a
refe
rral
to s
ee a
spe
cial
ist.
You
can
see
the
spec
ialis
t you
cho
ose
with
out p
erm
issi
on fr
om th
is p
lan.
Are
ther
e se
rvic
es th
ispl
an d
oesn
’t co
ver?
Yes.
Som
e of
the
serv
ices
this
pla
n do
esn’
t cov
er a
re li
sted
on
page
5. S
ee y
our p
olic
yor
pla
n do
cum
ent f
or a
dditi
onal
info
rmat
ion
abou
t exc
lude
d se
rvic
es.

2 of
8U
TA
H F
OST
ER
CA
RE
FO
UN
DA
TIO
NU
U01
15SH
H3S
●C
opay
men
ts a
re fi
xed
dolla
r am
ount
s (f
or e
xam
ple,
$15
) you
pay
for c
over
ed h
ealth
car
e, u
sual
ly w
hen
you
rece
ive
the
serv
ice.
●C
oins
uran
ce is
your
sha
re o
f the
cos
ts o
f a c
over
ed s
ervi
ce, c
alcu
late
d as
a p
erce
nt o
f the
allo
wed
am
ount
for t
he s
ervi
ce. F
or e
xam
ple,
if th
e pl
an’s
allo
wed
am
ount
for a
n ov
erni
ght h
ospi
tal s
tay
is $
1,00
0, y
our c
oins
uran
ce p
aym
ent o
f 20%
wou
ld b
e $2
00. T
his
may
cha
nge
if yo
u ha
ven’
t met
your
ded
ucti
ble.
●T
he a
mou
nt th
e pl
an p
ays
for c
over
ed s
ervi
ces
is b
ased
on
the
allo
wed
am
ount
. If a
n ou
t-of
-net
wor
k pr
ovid
er c
harg
es m
ore
than
the
allo
wed
amou
nt, y
ou m
ay h
ave
to p
ay th
e di
ffer
ence
. For
exa
mpl
e, if
an
out-
of-n
etw
ork
hosp
ital c
harg
es $
1,50
0 fo
r an
over
nigh
t sta
y an
d th
e al
low
edam
ount
is $
1,00
0, y
ou m
ay h
ave
to p
ay th
e $5
00 d
iffer
ence
. (T
his
is c
alle
d ba
lanc
e bi
lling
.)●
Thi
s pl
an m
ay e
ncou
rage
you
to u
se in
-net
wor
k an
d ou
t-of
-net
wor
k pr
ovid
ers
by c
harg
ing
you
low
er d
educ
tibl
es, c
opay
men
ts a
nd c
oins
uran
ceam
ount
s.
Com
mon
Med
ical
Eve
ntSe
rvic
es Y
ou M
ayN
eed
Your
Cos
t If Y
ouU
se a
n In
-net
wor
kPr
ovid
er
Your
Cos
t If Y
ou U
sean
Out
-of-n
etw
ork
Prov
ider
Lim
itatio
ns &
Exc
eptio
ns
Prim
ary
care
vis
it to
trea
tan
inju
ry o
r illn
ess
20%
coi
nsur
ance
40%
coi
nsur
ance
Spec
ialis
t vis
it20
% c
oins
uran
ce40
% c
oins
uran
ce––
––––
––––
–non
e–––
––––
––––
Oth
er p
ract
ition
er o
ffic
evi
sit
20%
coi
nsur
ance
for
spin
al m
anip
ulat
ions
40%
coi
nsur
ance
for
spin
al m
anip
ulat
ions
Cov
erag
e is
lim
ited
to 1
0 sp
inal
man
ipul
atio
ns /
yea
r.
If y
ou v
isit
a h
ealth
care
pro
vide
r’s o
ffic
eor
clin
ic
Prev
entiv
e ca
re/
scre
enin
g/im
mun
izat
ion
No
char
ge25
% c
oins
uran
ceD
educ
tibl
e w
aive
d.
Dia
gnos
tic te
st (x
-ray
,bl
ood
wor
k)20
% c
oins
uran
ce40
% c
oins
uran
ceIf
you
hav
e a
test
Imag
ing
(CT
/PE
T s
cans
,M
RIs
)20
% c
oins
uran
ce40
% c
oins
uran
ce––
––––
––––
–non
e–––
––––
––––
Gen
eric
dru
gs20
% c
oins
uran
ce /
reta
il an
d m
ail o
rder
pre
scrip
tion
Pref
erre
d br
and
drug
s20
% c
oins
uran
ce /
reta
il an
d m
ail o
rder
pre
scrip
tion
If y
ou n
eed
drug
s to
trea
t you
r ill
ness
or
cond
itio
n
Mor
e in
form
atio
nab
out p
resc
ript
ion
drug
cov
erag
eis
ava
ilabl
e at
ww
w.R
egen
ce.c
om.
Non
-pre
ferr
ed b
rand
drug
s20
% c
oins
uran
ce /
reta
il an
d m
ail o
rder
pre
scrip
tion
Cov
erag
e is
lim
ited
to a
90-
day
supp
ly fr
om a
reta
il or
mai
l ord
er s
uppl
ier.
Cov
erag
e is
lim
ited
to a
30-
day
supp
ly fo
r sel
f-in
ject
able
med
icat
ions
from
eith
er re
tail
or m
ail o
rder
sup
plie
r.D
educ
tibl
e do
es n
ot a
pply
to c
erta
in p
reve
ntiv
edr
ugs,
wom
en’s
cont
race
ptiv
es o
r im
mun
izat
ions
at a
part
icip
atin
g ph
arm
acy.
Med
icat
ions
use
d as
par
t of a
n ou
tpat
ient
can
cer d
rug
trea
tmen
t reg
imen
that
is p
rovi
ded
and
disp
ense
d in
a

3 of
8U
TA
H F
OST
ER
CA
RE
FO
UN
DA
TIO
NU
U01
15SH
H3S
Com
mon
Med
ical
Eve
ntSe
rvic
es Y
ou M
ayN
eed
Your
Cos
t If Y
ouU
se a
n In
-net
wor
kPr
ovid
er
Your
Cos
t If Y
ou U
sean
Out
-of-n
etw
ork
Prov
ider
Lim
itatio
ns &
Exc
eptio
ns
Spec
ialty
dru
gsR
efer
to g
ener
ic, p
refe
rred
bra
nd a
ndno
n–pr
efer
red
bran
d dr
ugs
abov
e.pr
ofes
sion
al s
ettin
g w
ill b
e su
bjec
t to
thes
e pr
escr
iptio
nbe
nefit
s.
Faci
lity
fee
(e.g
.,am
bula
tory
sur
gery
cent
er)
20%
coi
nsur
ance
40%
coi
nsur
ance
––––
––––
–––n
one–
––––
––––
––If
you
hav
eou
tpat
ient
sur
gery
Phys
icia
n/su
rgeo
n fe
es20
% c
oins
uran
ce40
% c
oins
uran
ce––
––––
––––
–non
e–––
––––
––––
Em
erge
ncy
room
serv
ices
20%
coi
nsur
ance
20%
coi
nsur
ance
––––
––––
–––n
one–
––––
––––
––
Em
erge
ncy
med
ical
tran
spor
tatio
n20
% c
oins
uran
ce20
% c
oins
uran
ce––
––––
––––
–non
e–––
––––
––––
If y
ou n
eed
imm
edia
te m
edic
alat
tent
ion
Urg
ent c
are
Cov
ered
the
sam
e as
the
If y
ou v
isit
ahe
alth
car
e pr
ovid
er’s
off
ice
or c
linic
or I
fyo
u ha
ve a
test
Com
mon
Med
ical
Eve
nts.
––––
––––
–––n
one–
––––
––––
––
Faci
lity
fee
(e.g
., ho
spita
lro
om)
20%
coi
nsur
ance
40%
coi
nsur
ance
––––
––––
–––n
one–
––––
––––
––If
you
hav
e a
hosp
ital
stay
Phys
icia
n/su
rgeo
n fe
e20
% c
oins
uran
ce40
% c
oins
uran
ce––
––––
––––
–non
e–––
––––
––––
Men
tal/
Beh
avio
ral h
ealth
outp
atie
nt s
ervi
ces
50%
coi
nsur
ance
50%
coi
nsur
ance
Men
tal/
Beh
avio
ral h
ealth
inpa
tient
ser
vice
s50
% c
oins
uran
ce50
% c
oins
uran
ce
Subs
tanc
e us
e di
sord
erou
tpat
ient
ser
vice
s50
% c
oins
uran
ce50
% c
oins
uran
ce
If y
ou h
ave
men
tal
heal
th, b
ehav
iora
lhe
alth
, or
subs
tanc
eab
use
need
s
Subs
tanc
e us
e di
sord
erin
patie
nt s
ervi
ces
50%
coi
nsur
ance
50%
coi
nsur
ance
Cov
erag
e is
lim
ited
to 1
2 ou
tpat
ient
vis
its /
yea
r.C
over
age
is li
mite
d to
8 in
patie
nt d
ays
/ ye
ar.
Pren
atal
and
pos
tnat
alca
re20
% c
oins
uran
ce40
% c
oins
uran
ceIf
you
are
pre
gnan
tD
eliv
ery
and
all i
npat
ient
serv
ices
20%
coi
nsur
ance
40%
coi
nsur
ance
Cov
erag
e fo
r ado
ptio
n ex
pens
es is
lim
ited
to $
4,00
0 /
preg
nanc
y.

4 of
8U
TA
H F
OST
ER
CA
RE
FO
UN
DA
TIO
NU
U01
15SH
H3S
Com
mon
Med
ical
Eve
ntSe
rvic
es Y
ou M
ayN
eed
Your
Cos
t If Y
ouU
se a
n In
-net
wor
kPr
ovid
er
Your
Cos
t If Y
ou U
sean
Out
-of-n
etw
ork
Prov
ider
Lim
itatio
ns &
Exc
eptio
ns
Hom
e he
alth
car
e20
% c
oins
uran
ce40
% c
oins
uran
ceC
over
age
is li
mite
d to
130
vis
its /
yea
r.
Reh
abili
tatio
n se
rvic
es20
% c
oins
uran
ce40
% c
oins
uran
ceC
over
age
is li
mite
d to
15
inpa
tient
day
s /
year
.C
over
age
is li
mite
d to
40
outp
atie
nt v
isits
/ y
ear.
Hab
ilita
tion
serv
ices
20%
coi
nsur
ance
40%
coi
nsur
ance
Cov
erag
e fo
r neu
rode
velo
pmen
tal t
hera
py is
lim
ited
to40
out
patie
nt v
isits
/ y
ear.
Cov
erag
e fo
r neu
rode
velo
pmen
tal t
hera
py is
lim
ited
tose
rvic
es fo
r mem
bers
thro
ugh
age
6.
Skill
ed n
ursi
ng c
are
20%
coi
nsur
ance
40%
coi
nsur
ance
Cov
erag
e is
lim
ited
to 6
0 in
patie
nt d
ays
/ ye
ar.
Dur
able
med
ical
equi
pmen
t20
% c
oins
uran
ce40
% c
oins
uran
ce––
––––
––––
–non
e–––
––––
––––
If y
ou n
eed
help
reco
veri
ng o
r ha
veot
her
spec
ial h
ealth
need
s
Hos
pice
ser
vice
20%
coi
nsur
ance
40%
coi
nsur
ance
Cov
erag
e is
lim
ited
to 1
4 re
spite
day
s /
lifet
ime.
Eye
exa
mN
ot c
over
edN
ot c
over
ed––
––––
––––
–non
e–––
––––
––––
Gla
sses
Not
cov
ered
Not
cov
ered
––––
––––
–––n
one–
––––
––––
––If
you
r ch
ild n
eeds
dent
al o
r ey
e ca
reD
enta
l che
ck-u
pN
ot c
over
edN
ot c
over
ed––
––––
––––
–non
e–––
––––
––––

5 of
8U
TA
H F
OST
ER
CA
RE
FO
UN
DA
TIO
NU
U01
15SH
H3S
Excl
uded
Ser
vice
s &
Oth
er C
over
ed S
ervi
ces:
Serv
ices
You
r P
lan
Doe
s N
OT
Cov
er (
Thi
s is
n’t a
com
plet
e lis
t. C
heck
you
r po
licy
or p
lan
docu
men
t for
oth
er e
xclu
ded
serv
ices
.)●
Acu
punc
ture
●B
aria
tric
sur
gery
●C
osm
etic
sur
gery
, exc
ept c
onge
nita
l ano
mal
ies
●D
enta
l car
e (A
dult)
●H
earin
g ai
ds●
Infe
rtili
ty tr
eatm
ent
●Lo
ng-t
erm
car
e●
Priv
ate-
duty
nur
sing
●R
outin
e ey
e ca
re (A
dult)
●R
outin
e fo
ot c
are
exce
pt fo
r dia
betic
pat
ient
s●
Vis
ion
hard
war
e●
Wei
ght l
oss
prog
ram
s ex
cept
for n
utrit
iona
lco
unse
ling
Oth
er C
over
ed S
ervi
ces
(Thi
s is
n’t a
com
plet
e lis
t. C
heck
you
r po
licy
or p
lan
docu
men
t for
oth
er c
over
ed s
ervi
ces
and
your
cos
ts fo
r th
ese
serv
ices
.)●
Chi
ropr
actic
car
e●
Non
-em
erge
ncy
care
whe
n tr
avel
ing
outs
ide
the
U.S
.
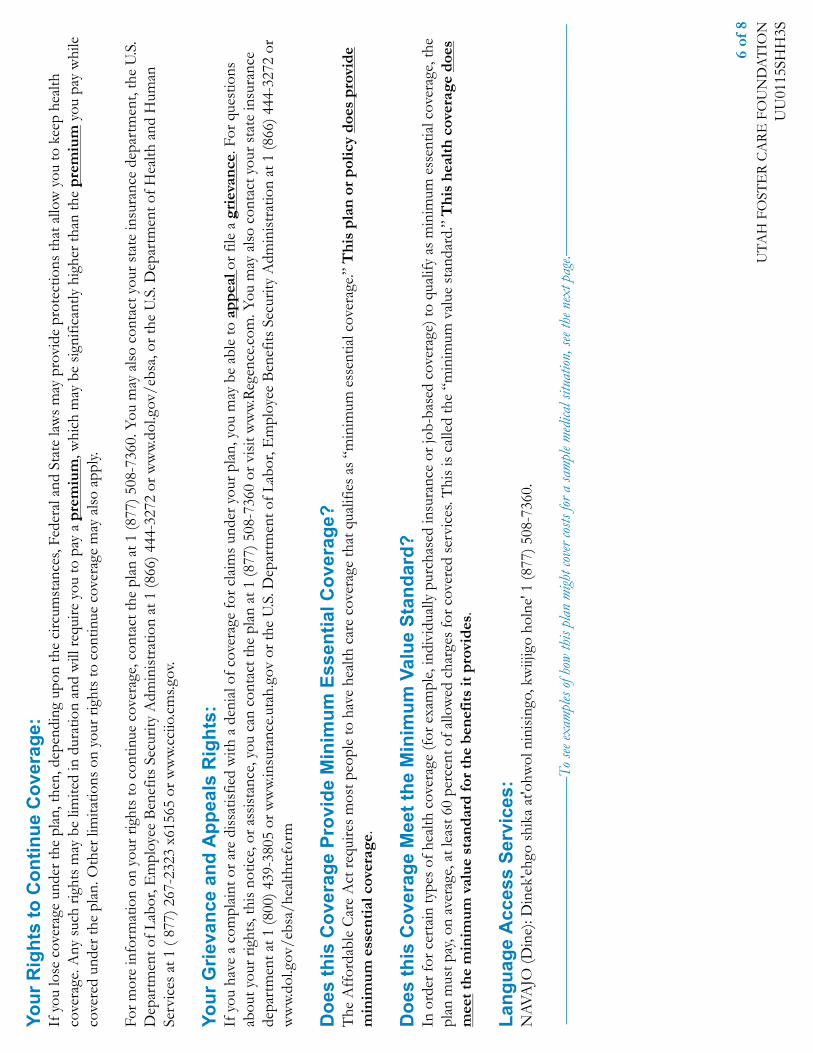
6 of
8U
TA
H F
OST
ER
CA
RE
FO
UN
DA
TIO
NU
U01
15SH
H3S
Your
Rig
hts
to C
ontin
ue C
over
age:
If y
ou lo
se c
over
age
unde
r the
pla
n, th
en, d
epen
ding
upo
n th
e ci
rcum
stan
ces,
Fede
ral a
nd S
tate
law
s m
ay p
rovi
de p
rote
ctio
ns th
at a
llow
you
to k
eep
heal
thco
vera
ge. A
ny s
uch
right
s m
ay b
e lim
ited
in d
urat
ion
and
will
requ
ire y
ou to
pay
a p
rem
ium
, whi
ch m
ay b
e si
gnifi
cant
ly h
ighe
r tha
n th
e pr
emiu
m y
ou p
ay w
hile
cove
red
unde
r the
pla
n. O
ther
lim
itatio
ns o
n yo
ur ri
ghts
to c
ontin
ue c
over
age
may
als
o ap
ply.
For m
ore
info
rmat
ion
on y
our r
ight
s to
con
tinue
cov
erag
e, c
onta
ct th
e pl
an a
t 1 (8
77) 5
08-7
360.
You
may
als
o co
ntac
t you
r sta
te in
sura
nce
depa
rtm
ent,
the
U.S
.D
epar
tmen
t of L
abor
, Em
ploy
ee B
enef
its S
ecur
ity A
dmin
istr
atio
n at
1 (8
66) 4
44-3
272
or w
ww.
dol.g
ov/e
bsa,
or t
he U
.S. D
epar
tmen
t of H
ealth
and
Hum
anSe
rvic
es a
t 1 (
877)
267
-232
3 x6
1565
or w
ww.
cciio
.cm
s.gov
.
Your
Grie
vanc
e an
d A
ppea
ls R
ight
s:If
you
hav
e a
com
plai
nt o
r are
dis
satis
fied
with
a d
enia
l of c
over
age
for c
laim
s un
der y
our p
lan,
you
may
be
able
to a
ppea
l or f
ile a
gri
evan
ce. F
or q
uest
ions
abou
t you
r rig
hts,
this
not
ice,
or a
ssis
tanc
e, y
ou c
an c
onta
ct th
e pl
an a
t 1 (8
77) 5
08-7
360
or v
isit
ww
w.R
egen
ce.c
om. Y
ou m
ay a
lso
cont
act y
our s
tate
insu
ranc
ede
part
men
t at 1
(800
) 439
-380
5 or
ww
w.in
sura
nce.
utah
.gov
or t
he U
.S. D
epar
tmen
t of L
abor
, Em
ploy
ee B
enef
its S
ecur
ity A
dmin
istr
atio
n at
1 (8
66) 4
44-3
272
orw
ww.
dol.g
ov/e
bsa/
heal
thre
form
Doe
s th
is C
over
age
Prov
ide
Min
imum
Ess
entia
l Cov
erag
e?T
he A
ffor
dabl
e C
are
Act
requ
ires
mos
t peo
ple
to h
ave
heal
th c
are
cove
rage
that
qua
lifie
s as
“m
inim
um e
ssen
tial c
over
age.”
Thi
s pl
an o
r po
licy
does
pro
vide
min
imum
ess
enti
al c
over
age.
Doe
s th
is C
over
age
Mee
t the
Min
imum
Val
ue S
tand
ard?
In o
rder
for c
erta
in ty
pes
of h
ealth
cov
erag
e (f
or e
xam
ple,
indi
vidu
ally
pur
chas
ed in
sura
nce
or jo
b-ba
sed
cove
rage
) to
qual
ify a
s m
inim
um e
ssen
tial c
over
age,
the
plan
mus
t pay
, on
aver
age,
at l
east
60
perc
ent o
f allo
wed
cha
rges
for c
over
ed s
ervi
ces.
Thi
s is
cal
led
the
“min
imum
val
ue s
tand
ard.
” T
his
heal
th c
over
age
does
mee
t the
min
imum
val
ue s
tand
ard
for
the
bene
fits
it p
rovi
des.
Lang
uage
Acc
ess
Serv
ices
:N
AVA
JO (D
ine)
: Din
ek'e
hgo
shik
a at
'ohw
ol n
inis
ingo
, kw
iijig
o ho
lne'
1 (8
77) 5
08-7
360.
––––
––––
––––
––––
––––
––––
––––
–––T
o see
exam
ples
of ho
w th
is pl
an m
ight c
over
costs
for a
sam
ple m
edica
l situ
ation
, see
the n
ext p
age.–
––––
––––
––––
––––
––––
––––
––––

7 of
8U
TA
H F
OST
ER
CA
RE
FO
UN
DA
TIO
NU
U01
15SH
H3S
Abo
ut th
ese
Cov
erag
eEx
ampl
es:
The
se e
xam
ples
sho
w h
ow th
is p
lan
mig
ht c
over
med
ical
car
e in
giv
en s
ituat
ions
. Use
thes
e ex
ampl
esto
see
, in
gene
ral,
how
muc
h fin
anci
al p
rote
ctio
n a
sam
ple
patie
nt m
ight
get
if th
ey a
re c
over
ed u
nder
diff
eren
t pla
ns. Th
is is
not a
cos
tes
timat
or.
Don
’t us
e th
ese
exam
ples
toes
timat
e yo
ur a
ctua
l cos
tsun
der t
his
plan
. The
act
ual
care
you
rece
ive
will
be
diff
eren
t fro
m th
ese
exam
ples
,an
d th
e co
st o
f tha
t car
e w
illal
so b
e di
ffer
ent.
See
the
next
pag
e fo
rim
port
ant i
nfor
mat
ion
abou
tth
ese
exam
ples
.
Hav
ing
a ba
by(n
orm
al d
eliv
ery)
■A
mou
nt o
wed
to p
rovi
ders
: $7,
540
■Pl
an p
ays:
$4,
730
■Pa
tient
pay
s: $
2,81
0
Sam
ple
care
cos
ts:
Hos
pita
l cha
rges
(mot
her)
$2,7
00R
outin
e ob
stet
ric c
are
$2,1
00H
ospi
tal c
harg
es (b
aby)
$900
Ane
sthe
sia
$900
Labo
rato
ry te
sts
$500
Pres
crip
tions
$200
Rad
iolo
gy$2
00V
acci
nes,
othe
r pre
vent
ive
$40
Tot
al$7
,540
Patie
nt p
ays:
Ded
uctib
les
$1,5
00C
opay
s$0
Coi
nsur
ance
$1,1
60Li
mits
or e
xclu
sion
s$1
50T
otal
$2,8
10
Man
agin
g ty
pe 2
dia
bete
s(r
outi
ne m
aint
enan
ce o
fa
wel
l-co
ntro
lled
cond
itio
n)
■A
mou
nt o
wed
to p
rovi
ders
: $5,
400
■Pl
an p
ays:
$3,
100
■Pa
tient
pay
s: $
2,30
0
Sam
ple
care
cos
ts:
Pres
crip
tions
$2,9
00M
edic
al E
quip
men
t and
Sup
plie
s$1
,300
Off
ice
Vis
its a
nd P
roce
dure
s$7
00E
duca
tion
$300
Labo
rato
ry te
sts
$100
Vac
cine
s, ot
her p
reve
ntiv
e$1
00T
otal
$5,4
00
Patie
nt p
ays:
Ded
uctib
les
$1,5
00C
opay
s$0
Coi
nsur
ance
$760
Lim
its o
r exc
lusi
ons
$40
Tot
al$2
,300
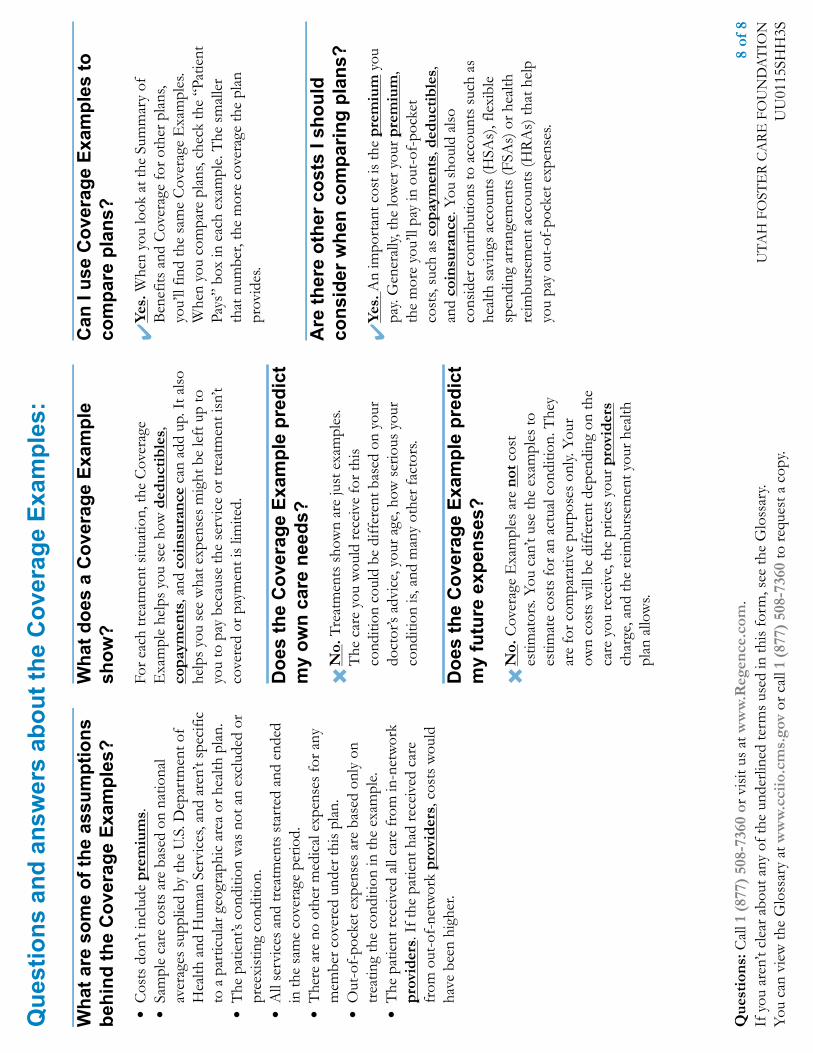
Que
stio
ns a
nd a
nsw
ers
abou
t the
Cov
erag
e Ex
ampl
es:
Que
stio
ns: C
all 1
(87
7) 5
08-7
360
or v
isit
us a
t ww
w.R
egen
ce.c
om.
8 of
8If
you
are
n’t c
lear
abo
ut a
ny o
f the
und
erlin
ed te
rms
used
in th
is fo
rm, s
ee th
e G
loss
ary.
You
can
vie
w th
e G
loss
ary
at w
ww
.cci
io.c
ms.
gov
or c
all 1
(87
7) 5
08-7
360
to re
ques
t a c
opy.
UT
AH
FO
STE
R C
AR
E F
OU
ND
AT
ION
UU
0115
SHH
3S
Wha
t are
som
e of
the
assu
mpt
ions
behi
nd th
e C
over
age
Exam
ples
?●
Cos
ts d
on’t
incl
ude
prem
ium
s.●
Sam
ple
care
cos
ts a
re b
ased
on
natio
nal
aver
ages
sup
plie
d by
the
U.S
. Dep
artm
ent o
fH
ealth
and
Hum
an S
ervi
ces,
and
aren
’t sp
ecifi
cto
a p
artic
ular
geo
grap
hic
area
or h
ealth
pla
n.●
The
pat
ient
’s co
nditi
on w
as n
ot a
n ex
clud
ed o
rpr
eexi
stin
g co
nditi
on.
●A
ll se
rvic
es a
nd tr
eatm
ents
sta
rted
and
end
edin
the
sam
e co
vera
ge p
erio
d.●
The
re a
re n
o ot
her m
edic
al e
xpen
ses
for a
nym
embe
r cov
ered
und
er th
is p
lan.
●O
ut-o
f-po
cket
exp
ense
s ar
e ba
sed
only
on
trea
ting
the
cond
ition
in th
e ex
ampl
e.●
The
pat
ient
rece
ived
all
care
from
in-n
etw
ork
prov
ider
s. I
f the
pat
ient
had
rece
ived
car
efr
om o
ut-o
f-ne
twor
k pr
ovid
ers,
cos
ts w
ould
have
bee
n hi
gher
.
Wha
t doe
s a
Cov
erag
e Ex
ampl
esh
ow?
For e
ach
trea
tmen
t situ
atio
n, th
e C
over
age
Exa
mpl
e he
lps
you
see
how
ded
ucti
bles
,co
paym
ents
, and
coi
nsur
ance
can
add
up.
It a
lso
help
s yo
u se
e w
hat e
xpen
ses
mig
ht b
e le
ft u
p to
you
to p
ay b
ecau
se th
e se
rvic
e or
trea
tmen
t isn
’tco
vere
d or
pay
men
t is
limite
d.
Doe
s th
e C
over
age
Exam
ple
pred
ict
my
own
care
nee
ds?
✖N
o. T
reat
men
ts s
how
n ar
e ju
st e
xam
ples
.T
he c
are
you
wou
ld re
ceiv
e fo
r thi
sco
nditi
on c
ould
be
diff
eren
t bas
ed o
n yo
urdo
ctor
’s ad
vice
, you
r age
, how
ser
ious
you
rco
nditi
on is
, and
man
y ot
her f
acto
rs.
Doe
s th
e C
over
age
Exam
ple
pred
ict
my
futu
re e
xpen
ses?
✖N
o. C
over
age
Exa
mpl
es a
re n
ot c
ost
estim
ator
s. Y
ou c
an’t
use
the
exam
ples
toes
timat
e co
sts
for a
n ac
tual
con
ditio
n. T
hey
are
for c
ompa
rativ
e pu
rpos
es o
nly.
You
row
n co
sts
will
be
diff
eren
t dep
endi
ng o
n th
eca
re y
ou re
ceiv
e, th
e pr
ices
you
r pro
vide
rsch
arge
, and
the
reim
burs
emen
t you
r hea
lthpl
an a
llow
s.
Can
I us
e C
over
age
Exam
ples
toco
mpa
re p
lans
?
✔Ye
s. W
hen
you
look
at t
he S
umm
ary
ofB
enef
its a
nd C
over
age
for o
ther
pla
ns,
you’
ll fin
d th
e sa
me
Cov
erag
e E
xam
ples
.W
hen
you
com
pare
pla
ns, c
heck
the
“Pat
ient
Pays
” bo
x in
eac
h ex
ampl
e. T
he s
mal
ler
that
num
ber,
the
mor
e co
vera
ge th
e pl
anpr
ovid
es.
Are
ther
e ot
her c
osts
I sh
ould
cons
ider
whe
n co
mpa
ring
plan
s?
✔Ye
s. A
n im
port
ant c
ost i
s th
e pr
emiu
m y
oupa
y. G
ener
ally,
the
low
er y
our p
rem
ium
,th
e m
ore
you’
ll pa
y in
out
-of-
pock
etco
sts,
such
as
copa
ymen
ts, d
educ
tibl
es,
and
coin
sura
nce.
You
sho
uld
also
cons
ider
con
trib
utio
ns to
acc
ount
s su
ch a
she
alth
sav
ings
acc
ount
s (H
SAs)
, fle
xibl
esp
endi
ng a
rran
gem
ents
(FSA
s) o
r hea
lthre
imbu
rsem
ent a
ccou
nts
(HR
As)
that
hel
pyo
u pa
y ou
t-of
-poc
ket e
xpen
ses.

URGENT CARE CENTERSSorted by alpha Name
2January 1, 2015
AFTER HOURS MEDICAL LLCDBA MEDALLUS MEDICAL3451 S 5600 W #FSALT LAKE CITY, UT(801) 957-0900
BASIN MEDICAL CLINIC LLC379 N 500 W #1AVERNAL, UT(435) 789-1165
COPPERVIEW MEDICAL CENTER3556 W 9800 S #101SOUTH JORDAN, UT(801) 567-9780
FIRSTMED EAST URGENT CARE1950 E 7000 SSALT LAKE CITY, UT(801) 943-3300
FIRSTMED MURRAY URGENT CARE5911 FASHION PLACE BLVDMURRAY, UT(801) 266-6483
FIRSTMED NORTH URGENT CARE1512 RENAISSANCE TOWNE DR #100BOUNTIFUL, UT(801) 295-6483
FIRSTMED WEST URGENT CARE8822 S REDWOOD RD #E122WEST JORDAN, UT(801) 256-0009
IHC AMERICAN FORK INSTACARE98 N 1100 E #101AMERICAN FORK, UT(801) 492-2550
IHC DRAPER INSTACARE12473 S MINUTEMAN DRDRAPER, UT(801) 495-7970
IHC INSTACARE BOUNTIFUL390 N MAIN STBOUNTIFUL, UT(801) 292-6100
IHC INSTACARE CEDAR CITY962 SAGE DRCEDAR CITY, UT(435) 865-3440
IHC INSTACARE HEREFORDSHIRE1915 W 5950 SROY, UT(801) 387-8100
IHC INSTACARE HOLLADAY6272 S HIGHLAND DRSALT LAKE CITY, UT(801) 871-6400
IHC INSTACARE HURRICANE75 N 2260 WHURRICANE, UT(435) 635-6550
IHC INSTACARE KAYSVILLE CREEKSIDE435 N MAIN STKAYSVILLE, UT(801) 498-6000
IHC INSTACARE LAYTON2075 UNIVERSITY PARK BLVDLAYTON, UT(801) 779-6200
IHC INSTACARE LOGAN412 N 200 ELOGAN, UT(435) 713-2710
IHC INSTACARE MEMORIAL2000 S 900 ESALT LAKE CITY, UT(801) 464-7777
IHC INSTACARE MURRAY196 E WINCHESTER STSALT LAKE CITY, UT(801) 639-5500
IHC INSTACARE NORTH OGDEN2400 N WASHINGTON BLVDNORTH OGDEN, UT(801) 786-7500
IHC INSTACARE NORTH OREM1975 N STATE STOREM, UT(801) 714-5000
IHC INSTACARE PAYSON845 TURF FARM RD #1PAYSON, UT(801) 465-6250
IHC INSTACARE PROVO1134 N 500 W #102PROVO, UT(801) 357-1770
IHC INSTACARE RIVER ROAD577 S RIVER RDSAINT GEORGE, UT(435) 688-6000
IHC INSTACARE SALT LAKE389 S 900 ESALT LAKE CITY, UT(385) 282-2400
IHC INSTACARE SANDY9493 S 700 ESANDY, UT(801) 523-2483
IHC INSTACARE SARATOGA SPRINGS354 W STATE ROAD 73SARATOGA SPRINGS, UT(801) 766-4567
IHC INSTACARE SOUTH OGDEN975 CHAMBERS STSOUTH OGDEN, UT(801) 387-6200
IHC INSTACARE SOUTHRIDGE3723 W 12600 S #150RIVERTON, UT(801) 285-4560
IHC INSTACARE SPRINGVILLE762 W 400 SSPRINGVILLE, UT(801) 489-3244
IHC INSTACARE SUNSET1739 W SUNSET BLVDSAINT GEORGE, UT(435) 634-6000
IHC INSTACARE SYRACUSE745 S 2000 WSYRACUSE, UT(801) 525-2400
IHC INSTACARE TAYLORSVILLE3845 W 4700 STAYLORSVILLE, UT(801) 840-2020
IHC INSTACARE TOOELE777 N MAIN STTOOELE, UT(435) 228-1200
IHC INSTACARE WEST JORDAN2655 W 9000 SWEST JORDAN, UT(801) 256-6399
IHC NORTH CACHE VALLEY INSTACARE4088 N HIGHWAY 91HYDE PARK, UT(435) 563-4888
IHC NORTH TEMPLE CLINIC54 N 800 WSALT LAKE CITY, UT(801) 408-8654
IHC NORTHERN UTAH KIDSCARE2000 S 900 ESALT LAKE CITY, UT(801) 464-77882075 UNIVERSITY PARK BLVDLAYTON, UT(801) 779-62002655 W 9000 SWEST JORDAN, UT(801) 568-99333723 W 12600 S #150RIVERTON, UT(801) 285-45613845 W 4700 S #105TAYLORSVILLE, UT(801) 840-2101390 N MAIN STBOUNTIFUL, UT(801) 294-99334403 HARRISON BLVD #4875OGDEN, UT(801) 387-4500DBA MOUNTAIN VIEW KIDSCARE9720 S 1300 E #100SANDY, UT(801) 501-9933
IHC PARK CITY BONANZA INSTACARE1665 BONANZA DRPARK CITY, UT(435) 649-7640
IHC PARK CITY-CANYONS4000 CANYONS RESORT DRPARK CITY, UT(435) 615-2235
IHC SNOWBIRD CLINICHIGHWAY 210SNOWBIRD, UT(801) 359-3948
OGDEN CLINIC1159 12TH STOGDEN, UT(801) 475-37004650 HARRISON BLVDOGDEN, UT(801) 475-3100
RIVERSIDE MEDICAL CENTER LLCDBA BLUE ROCK MEDICAL CENTER3152 N UNIVERSITY AVE #120PROVO, UT(801) 375-2177
RIVERWOODS URGENT CARE LLC280 RIVER PARK DR #120PROVO, UT(801) 229-2011
TRI CITY MEDICAL CLINIC275 W 200 N #100LINDON, UT(801) 796-1333830 N 2000 WPLEASANT GROVE, UT(801) 756-3511
UUHC URGENT CARE1525 W 2100 SSALT LAKE CITY, UT(801) 213-8841
AFTER HOURS MEDICAL LLC UUHC URGENT CAREValueCare Network

URGENT CARE CENTERSSorted by alpha Name
3January 1, 2015
WEE CARE PEDIATRICS2084 N 1700 W #ALAYTON, UT(801) 773-8644
WEE CARE PEDIATRICS WEE CARE PEDIATRICS

HOSPITAL Preferred ValueCare (PVC)ALTA VIEW HOSPITALAMERICAN FORK HOSPITALASHLEY REGIONAL MEDICAL CENTER XBEAR RIVER VALLEY HOSPITAL XBEAVER VALLEY HOSPITAL XBLUE MOUNTAIN HOSPITAL XBRIGHAM CITY HOSPITAL XCACHE VALLEY HOSPITAL XCASTLEVIEW HOSPITAL XCENTRAL VALLEY MEDICAL CENTER XDAVIS HOSPITAL AND MEDICAL CENTER XDELTA COMMUNITY MEDICAL CENTER XDIXIE REGIONAL MEDICAL CENTER XFILLMORE HOSPITAL XGARFIELD MEMORIAL HOSPITAL XGUNNISON VALLEY HOSPITAL XHEBER VALLEY MEDICAL CENTER XHUNTSMAN CANCER HOSPITAL XINTERMOUNTAIN MEDICAL CENTERJORDAN VALLEY MEDICAL CENTER XKANE COUNTY HOSPITAL XLAKEVIEW HOSPITAL XLDS HOSPITALLOGAN REGIONAL HOSPITAL XLONE PEAK HOSPITAL INC XMCKAY DEE HOSPITALMILFORD MEMORIAL HOSPITAL XMOAB REGIONAL HOSPITAL XMOUNTAIN POINT MEDICAL CENTER XMOUNTAIN VIEW HOSPITAL XMOUNTAIN WEST MEDICAL CENTER XOGDEN REGIONAL MEDICAL CENTER XOREM COMMUNITY HOSPITALPARK CITY MEDICAL CENTER XPRIMARY CHILDRENS HOSPITAL XRIVERTON HOSPITALRIVERTON CHILDREN'S UNIT XSALT LAKE REGIONAL MEDICAL CENTER XSAN JUAN COUNTY HOSPITAL XSANPETE VALLEY HOSPITAL XSEVIER VALLEY MEDICAL CENTER XST MARKS HOSPITAL XTHE ORTHOPEDIC SPECIALTY HOSPITAL (TOSH)TIMPANOGOS REGIONAL HOSPITAL XUINTAH BASIN MEDICAL CENTER XUNIVERSITY HOSPITAL XUNIVERSITY OF UTAH ORTHO CENTER XUTAH VALLEY REGIONAL MEDICAL CENTERVALLEY VIEW MEDICAL CENTER X
6/1/2015
Regence BlueCross BlueShield of Utah
Preferred ValueCare Network Hospitals

Wondering what preventive care your plan covers?
Preventive Care CoverageOur plans cover the kind of services that:• Screen for serious conditions• Prevent infectious diseases• Help you stay well
STAYING WELL
Reg
ence
Blu
eCro
ss B
lueS
hiel
d of
Uta
h
is a
n In
de
pe
nde
nt L
ice
nse
e o
f the
Blu
e C
ross
and
Blu
e S
hie
ld A
sso
ciat
ion


1. Evidence-based preventive guidelines are developed and validated by the following government entities: United States Preventive Services Task Force (USPSTF), Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention (CDC), and Health Resources and Services Administration (HRSA).
WHAT YOU NEED TO KNOW ABOUT PREVENTIVE CAREThe federal health care reform law passed in 2010 requires insurers to cover specific preventive care services. We support that initiative. In fact, our plans already covered many preventive care services, as we have long believed that preventive care and early detection are key to the long-term health and well-being of our members.
This brochure explains who’s eligible for preventive care and shows which services are
available to you and the family members covered by your plan.
Who’s eligible for these preventive services? To be eligible for these preventive services, you must first be covered by an active
Regence policy.
Benefits for federally required preventive services may not be available to members
covered by “grandfathered” policies or retiree-only plans. Contact Customer Service by
calling the phone number located on the back of your member card or use the Live Help
chat feature on regence.com for more information.
Do preventive services require pre-authorization?Yes. Some services require pre-authorization and must meet medical necessity criteria.
What preventive services are covered?Regence follows government guidelines to determine which preventive services we cover.1
These guidelines are updated periodically to reflect new scientific and medical advances.
Also, current services could be revised and may have limitations. Benefits are subject to
change. New recommendations must be implemented no later than the first plan or policy
year that is at least one year after the recommendation’s publication.
You can learn more details about these services at healthcare.gov, including recommended
child and adolescent immunization schedules.
Your provider may order preventive services that are outside of the recommended
government guidelines that Regence follows and may result in out-of-pocket costs for you.
What is the coinsurance/copay for these preventive services?The services listed in this brochure will be paid at 100% (no deductible, coinsurance or
copays) when you see preferred (Category 1), participating (Category 2) or in-network
providers. Deductibles and/or coinsurance may apply when you see non-participating
(Category 3) or out-of-network providers.

Men
Wom
en
Preg
nant
Wom
en
Chi
ldre
n (0
-17)
Health screenings, counseling and services for:
Suggested guidelines
Adult abdominal aortic aneurysm Screening is covered once per lifetime for men age 65 and over if they have ever smoked.
ü
Alcohol misuse Screening and behavioral counseling intervention covered for adults age 18 and older.
ü ü
Anemia (iron deficiency) Screening covered up to age 21, and pregnant women. ü ü ü ü
Bacteriuria (urinary tract infection) Screening for asymptomatic pregnant women. ü
Blood pressure Screening covered for adults age 18 and older. ü ü
Breast cancer Screening for women age 40 and older and those at increased risk. Mammograms only.
ü
Breast cancer chemoprevention Counseling for women at increased risk. ü
Breastfeeding equipment Manual and electric breastfeeding pumps are covered when purchased or rented from a licensed provider. Hospital-grade pumps are not covered.
ü ü
Breastfeeding - lactation support and counseling
Lactation support and counseling are covered when provided by a licensed provider.
ü ü
Breastfeeding supplies Initial breastfeeding supplies provided with a breastfeeding pump. ü ü
Cardiovascular disease and prevention Intensive behavioral counseling interventions to promote a healthful diet and physical activity for cardiovascular disease prevention for adults age 18 and older who are overweight or obese with cardiovascular disease risk factors.
ü ü
Cervical cancer Screening for sexually active women. ü
Chlamydia infection Screening for infection. ü
Cholesterol Screening for men age 35 and older and men ages 20-35 who are at increased risk for coronary heart disease. Screening for women age 45 and older and those 20-45 who are at increased risk for coronary heart disease.
ü ü ü
Colorectal cancer Screening for those age 50 and older, once every 5 years for a sigmoidoscopy and every 10 years for a colonoscopy, fecal occult blood testing annually.
ü ü
Congenital hypothyroidism Screening for newborns. ü
Contraceptive education and training Education and training on contraceptive methods. See Note 1. ü ü
Contraceptive devices - implants, cervical caps, intrauterine devices (IUDs), dia-phragms
Generic contraceptive devices are covered. When no generic exists, a brand is covered. If a generic becomes available, the brand will no longer be covered under Preventive Care. See Note 1.
ü ü
Depression screening Screening during wellness exams. ü ü ü
Diabetes (Type 2) Screening for adults with sustained high blood pressure. ü ü
Diabetes (Gestational) Screening for pregnant women after 24 weeks of gestation and the first pre-natal visit for pregnant women at high risk for diabetes.
ü
Diet behavioral counseling Counseling for adults with hyperlipidemia and other risk factors. ü ü
Fluoride treatment Application of fluoride varnish to the primary teeth by a primary care clinician for all infants and children starting at the age of primary tooth eruption up to age 5 years.
ü
Genetic risk assessment and BRCA (breast cancer susceptibility) mutation counseling and testing
For women with family risk of breast, ovarian, tubal and peritoneal cancer. BRCA testing requires pre-authorization and must meet medical necessity criteria. ü
Gonorrhea medication Preventive medication for the eyes of newborns. ü
Gonorrhea screening Screening for males up to age 21 and all females. ü ü ü
Hearing One screening in the first year of life for newborns. ü
Hepatitis B Screening for those at increased risk for infection and pregnant women. ü ü ü ü
COVERED PREVENTIVE SERVICES

Men
Wom
en
Preg
nant
Wom
en
Chi
ldre
n (0
-17)
Hepatitis C Screening for those at increased risk, and a one-time screening for adults born between 1945 and 1965.
ü ü ü
HIV Screening for adolescents and adults ages 15 to 65 years, and younger adolescents and older adults who are at increased risk. Also includes all pregnant women, including those who present in labor who are untested and whose HIV status is unknown.
ü ü ü ü
HPV Screening for women from age 30, every 3 years. ü
Interpersonal and domestic violence Screening and counseling during wellness exams. ü
Lead screening Screening up to age 21. ü ü ü
Lung cancer screening Annual screening for lung cancer with low-dose computed tomography (LDCT) in adults aged 55 to 80 years who have a 30 pack-year smoking history and currently smoke or have quit within the past 15 years. LDCT screening requires pre-authorization and must meet medical necessity criteria.
ü ü
Metabolic screening Screening up to age 2 months. ü
Obesity Screening and (if obese) counseling age 6 and older. ü ü ü
Oral health Risk assessment for preschool children. ü
Osteoporosis Screening for women age 65 and older and all women at increased risk. ü
Phenylketonuria (PKU) Newborn screening for genetic disorders. ü
Prevention of falls Physical therapy for adults age 65 or older residing independently in the community who are at increased risk for falls.
ü ü
RH(D) incompatibility Screening for pregnant women. ü
Sexually transmitted infection (STI) Counseling during wellness exams. ü ü ü
Sickle cell Screening for children up to 12 months old. ü
Skin cancer Counseling for children, adolescents and young adults ages 10 to 24. ü ü ü
Sterilization Sterilization is covered. See Note 1. ü
Syphilis Screening for those at increased risk and those up to age 21; also includes pregnant women.
ü ü ü ü
Tobacco use Counseling and interventions. Does not include programs or classes.See also “Tobacco use” below.
ü ü ü ü
Tuberculosis Skin test for children. ü
Vision Screening for children age 3 up to age 5. ü
Immunization vaccines - please consult your physician for frequency
Diphtheria, pertussis, tetanus (DPT) ü ü ü
Haemophilus influenzae type b (Hib) ü
Hepatitis A ü ü ü
Hepatitis B ü ü ü
Herpes zoster (shingles) Age 60 and older. ü ü
Human papillomavirus (HPV) Up to age 27. ü ü ü
Inactivated poliovirus ü
Influenza ü ü ü
Measles, mumps, rubella (MMR) ü ü ü
Meningococcal ü ü ü
Pneumococcal ü ü ü
Rotavirus ü
Varicella ü ü ü
COVERED PREVENTIVE SERVICES

Men
Wom
en
Preg
nant
Wom
en
Chi
ldre
n (0
-17)
Prescription medications
Only the types of prescription medications listed below are covered under Preventive Care. Medications require a prescription. Get the most value for your health care dollar with preferred medications. Learn more at OmedaRx.com/Member.
Aspirin use for the prevention of cardiovascular disease
For men age 45-79 and women age 55-79.ü ü
Aspirin use (low-dose) for the prevention of preeclampsia
For women after 12 weeks of gestation who are at high risk for preeclampsia.ü
Breast cancer medications Risk-reducing breast cancer medications for asymptomatic women aged 35 years or older.
ü
Contraceptive injectables Generic contraceptive injectables. See Note 1. ü ü
Contraceptive pills Generic contraceptive pills. See Note 1. ü ü
Contraceptive products-topical Diaphragms and patches. See Notes 1 and 2. ü ü
Emergency contraceptive products Generic contraceptive pills. See Notes 1 and 2. ü ü
Fluoride supplements For children 6 months through age 6 without sufficient fluoride ü
Folic acid supplements For all women planning or capable of pregnancy. ü ü
Iron supplements For children age 6-12 months at increased risk - drops only. ü
Tobacco use Refer to OmedaRx.com/Member for a list of covered over-the-counter medications. ü ü
Vitamin D supplement For adults age 65 or older residing independently in the community who are at increased risk for falls.
ü ü
Wellness exams Suggested guidelines
Well-child exams For children through 17 years of age. ü
Annual physical exams Ages 18 and over. ü ü
Notes:1. This benefit may not be available to members of groups who have applied for a religious exemption from contraceptive coverage.2. When no generic exists in the medication category, a formulary brand is covered.
COVERED PREVENTIVE SERVICES


Have questions? Call the Customer Service number on the back of your member card or go to the “Contact Us” link at regence.com.
QUESTIONS?
09499rep08000-ut/05-15 © 2015 Regence BlueCross BlueShield of Utah

Looking for a claim or a doctor?
Want to compare treatment costs?
Visit regence.com for all that and more.
Your complete source of health and wellness informationYou can find everything you need to know about your health plan and
ways to take care of yourself all in one place: regence.com.
Consider health care decisions and explore treatment options to help
you plan your budget:
• Compare cost and quality of hospitals, clinics and providers.
• Research treatment options and out-of-pocket cost estimates.
• Learn about medical conditions and medications.
• Explore health articles and videos.
Discover tools that help you track your coverage and make informed
decisions about your health care:
• Review details about your coverage.
• Manage your claims online and eliminate paper Explanation of Benefits.
• Find a doctor or specialist and read patient reviews.
Healthy living has its own rewards, but Regence Rewards points
can help:
• Earn points for completing a General Health Assessment.
• Receive points for healthy everyday activities—such as eating fruits and veggies and walking the dog, or joining an online wellness program.
• Redeem points for a $25 gift card.
REGENCE.COMGet everything you need to know about your plan
ONLINE RESOURCES
Rege
nce
Blu
eCro
ss B
lueS
hiel
d of
Uta
h is
an
Inde
pend
ent L
icen
see
of th
e B
lue
Cro
ss a
nd B
lue
Shi
eld
Ass
ocia
tion

To get started, just follow these steps:
1. Go to regence.com and click Register.
2. Complete the required Plan Information fields. The name, member ID and group numbers you enter must match your member card.
3. Complete the Account Information fields.
4. Create a user name and secure password.
5. Review your information, accept the User Agreement and
click Approve.
You’re automatically enrolled for Rewards after you register. You get
Rewards points for the following:
• Taking a confidential General Health Assessment. Learn how you’ve been managing your health to date, and get practical tips on how to improve your health and well-being.
• Managing stress and getting into shape. Reach for a healthy lifestyle with wellness programs on weight loss, nutrition, stress relief, smoking cessation and more.
What are you waiting for? Register now at regence.com!
Anyone in your family age 13 and older can register for an account and qualify for the Rewards program.
WELL TIP
08269rep07122-ut/06-14
© 2014 Regence BlueCross BlueShield of Utah

ONLINE PROVIDER DIRECTORYWondering if your doctor is in your network?
Looking for a new one?
Our online directory is quick and easy.
Already a Regence member?Try our enhanced Provider Search by signing in at regence.com to:
• Use cost indicators, which let you know which health care providers,
clinics and hospitals are in your network and provide you with the
lowest cost.
• Find out who’s accepting new patients.
• Check out a provider’s philosophy of care, specialties, credentials
and languages.
• Read online reviews from real patients.
Don’t have time to sign in? Not a member yet?1. Go to regence.com.
2. Click Find a doctor.
3. Review the information about provider networks and continue
to Find a doctor.
4. Choose your network.
5. Search by doctor, hospital or clinic name, specialty or medical condition.
6. Specify your location and hit Search.
Tip: When possible, use the drop-down list that appears when you enter
your search criteria to find the most accurate results.
7. Refine your search results further using filters like Accepting New
Patients or Specialties.
Need to print your results? Simply export results as a PDF.
Prefer to call us directly?Our friendly member services specialists can help. Just call the Member
Services number located on the back of your member ID card.
ONLINE RESOURCES
Rege
nce
Blu
eCro
ss B
lueS
hiel
d of
Uta
h is
an
Inde
pend
ent L
icen
see
of th
e B
lue
Cro
ss a
nd B
lue
Shi
eld
Ass
ocia
tion
09959rep08945-ut/07-15© 2015 Regence BlueCross BlueShield of Utah


Shopping for goods and services?
Looking for healthy savings?
Learn what we can do for you.
Feeling good doesn’t have to cost a lotAs a Regence member, you can enjoy savings on the following health-related products and services. This discount program is offered to all Regence members at no additional cost (although some discounted programs offered by vendors may carry separate fees). Regence Advantages is not insurance but is offered in addition to your medical and/or dental plan(s) to help you stay healthy and live better.
REGENCE ADVANTAGESSave money and feel great!
STAYING WELL
Rege
nce
Blu
eCro
ss B
lueS
hiel
d of
Uta
h is
an
Inde
pend
ent L
icen
see
of th
e B
lue
Cro
ss a
nd B
lue
Shi
eld
Ass
ocia
tion
• EyeMed Vision Care®: Save 35% on a complete pair of glasses (frames and lenses). Save 15% on non-disposable contacts and $10 on contact lens fittings. These discounts are available at leading retailers and many private practice locations.
• QualSight®: QualSight makes LASIK easy for members. You can save 40-50% off the national average price of Traditional LASIK or receive significant savings on procedures such as Custom Bladeless (all laser) LASIK. Find out if you are a potential candidate for this life-changing procedure today.
• Zenni Optical: Zenni Optical offers high quality, affordable and stylish prescription eyeglasses direct from the factory to its customers. Members receive 5% off Zenni’s already low prices, with complete prescription eyewear starting at only $6.95. Zenni’s online store offers over 3,000 frame styles to choose from. You can turn any pair of Zenni eyeglasses into sunglasses, with a wide selection of tinted lenses to choose from.
• TruVision™: Significant discounts are offered on laser vision correction procedures such as LASIK and PRK and 10% to 15% savings on mail-order contact lenses. TruVision uses TLC Laser Eye Centers as their preferred LASIK provider. TLC has performed over 2 million LASIK procedures and offers a Lifetime Savings Commitment®.
• TruHearing®**: Save an average of $890 per hearing aid on a selection of over 90 models and 400 styles from five leading manufacturers. Each purchase includes a 45-day money-back guarantee and extended three-year manufacturers’ warranties, which include one-time loss and damage coverage, along with 48 batteries per hearing aid. All appointments must be scheduled through TruHearing to ensure preferred pricing. Members can purchase an additional 120 batteries for $39.
• Beltone Hearing Care™**: Receive a free screening, a 25% discount on Beltone hearing aids, a one-year supply of hearing-aid batteries and free follow-up visits and testing.
Regence is completely independent from the companies that provide these products and services.Regence does not endorse or guarantee the products and services offered or their effectiveness.Regence reserves the right to change the program at any time without prior notice.
Want to learn more? Access member discounts at regence.com/advantages

08740rep07576-ut/10-14
© 2014 Regence BlueCross BlueShield of Utah
• HearPO®**: Receive a 40% discount on diagnostic services, including hearing exams, and significant savings on hearing aids. You’ll enjoy a 60-day no-risk trial period; one-year follow-up care; a three-year warranty, including coverage for loss and damage; and free batteries (160 cells per hearing aid)—all with a lowest-price guarantee.
• Epic® Dental: Purchase smile-protecting supplies at 25% off, including mouthwash, gums, mints and toothpaste. All items contain xylitol, a natural ingredient that fights cavities.
• Dental Optimizer Lollipops: Now you can put a halt to cavities and tooth decay with cavity-fighting lollipops from the Dental Optimizer. These all-natural lollipops eliminate cavity-causing bacteria, while leaving healthy bacteria intact. Members receive a 15% discount on lollipops and other tooth-friendly products.
• National Allergy Supply: Save 15% on products for non-drug allergy relief, including pillow and mattress encasings, air filtration products, asthma management tools, green cleaning products and personal care products. National Allergy Supply provides discount prices, outstanding service and a 60-day unconditional return policy with no restocking fees.
• CHP CAMaffinity Program: As a Regence member, you’re eligible for the CHP CAMaffinity Program, which provides a 20% discount on complementary and alternative medicine (CAM) services offered through The CHP Group’s growing network of chiropractors, acupuncturists, naturopathic physicians and massage therapists.
• CHP Active and Healthy: CHP Active and Healthy is the discount program that gets you up, moving, and saving money! With discounts offered by thousands of participating vendors (e.g. health clubs, ski resorts, sporting events, museums, etc.) for a small annual fee, it’s your source for great deals on healthy and fun activities.
• Nautilus, Inc.: Enjoy 10% off and free shipping on a number of home gym products from Nautilus, Inc., including its #1 selling home cardio machine: The Bowflex® TreadClimber® TC20. Regardless of your fitness goal or level, these products can help you achieve a healthy and fit lifestyle.
• Take Shape for Life® Independent Certified Health Coach, Tonja Noretto: Save $25 or more on your first month’s order! This safe weight management and health program uses clinically proven Medifast® products and a personal health coach to provide one-on-one guidance and encouragement. The program helps you lose weight and manage disease and health through nutritional intervention, free access to health care professionals, educational materials, and the “Habits of Health” system. There are no hidden costs or start-up fees.
• Jenny®: Jenny Fits Your Life! Pick a program that works with you, not against you! MyDays™ is a flexible, new weight loss choice that gives you the structure you need to stay on track and the freedom to live your life. Each week you can eat five days with Jenny; the other two days you enjoy your own healthy choices. Your consultant will help you find the program that fits your real life.
Members can choose one of these discounted offers from Jenny Craig:
– FREE 30-day Program* – 30% off of the Jenny All Access Membership*
• Safe Beginnings®: Save 15% on Safe Beginnings products, including safety gates, cabinet locks, outlet covers, window guards, and many other baby-proofing products.
• CorCell® Saving Baby’s Cord Blood®: Cord blood stem cells are now being used to treat more than 70 diseases, and research is ongoing to find treatments for even more. Regence has partnered with CorCell to offer a $650 discount when you bank your baby’s umbilical cord blood. Protect your child or give the gift of cord blood preservation to your grandchild, niece, nephew, friend or other loved one.
• Lively: Receive a 10% discount on Lively’s activity-sharing product that enables older adults to live independently longer with a rich connection to family. It has been called the “next big thing” for elder loved ones by respectfully measuring healthy living patterns and giving family members a way to know when help or their care may be needed.
• Everest Funeral Planning and Concierge Service: Save $50 off the enrollment fee for Everest’s suite of funeral-planning services. With advisors available 24 hours a day, you’ll get the information you need to make informed decisions about all funeral-related issues, within your budget, and with a funeral home of your choice.
• Banfield Pet Hospital®: As a Regence member, you receive a waived enrollment fee for Banfield Pet Hospital’s Optimum Wellness Plans®, packages of preventive care that include annual blood work, vaccinations, de-worming, unlimited office visits, plus much more. Banfield is the largest veterinary hospital in the world with 850 locations nationwide.
*Plus the cost of food. Plus the cost of shipping, if applicable. Valid at participating centres. No cash value. One offer per person. Not valid with any other program offers or discounts. Restrictions apply.
** Discounts through HearPO (also includes extended family), TruHearing and Beltone are available to members and their parents and grandparents.

Regence has coveredA c r o s s t h e c o u n t r y A n d
a r o u n d t h e w o r l d.
With coverage from Regence, you take your health care benefits with you–across the country and around the world. The BlueCard Program gives you access to doctors and hospitals nearly everywhere, so you’ll have peace of mind knowing that you can always find the health care provider you need.
ChoicesYour Regence membership gives you a world of choices. Through the BlueCard Worldwide® Program, you’re free to choose doctors and hospitals that best suit you and your family in more than 200 countries and territories around the world.
designed to save moneyIn most cases, when you travel or live outside the Regence service area, you can take advantage of savings the local Blue Plan has negotiated with providers in the area where you are. For covered services, you should not have to pay any amount above these negotiated rates. You should also not have to pay amounts above any applicable out-of-pocket expenses.
Rege
nce
Blue
Cros
s Bl
ueSh
ield
of U
tah
is an
Inde
pend
ent L
icen
see
of th
e Bl
ue C
ross
and
Blu
e Sh
ield
Ass
ocia
tion
the BlueCard® Program
BlueCard Program advantages
PRovIdeR ChoICeYou have access to more than 85% of providers and 96% of hospitals nationwide.
BeneFIT ConsIsTenCYBlueCard ensures that you receive in-network benefits when choosing participating providers of any Blue Cross and/or Blue shield Plan.
BIllIng PRoTeCTIonAccessing a Blue Cross and/or Blue shield Plan participating provider ensures that you are not responsible for any balance billed amount.
eAse oF ACCessIt’s quick and easy to locate a participating provider at regence.com or by calling (1-800-810-BlUe).

03781-ut / 07-10© 2010. The Regence group, all rights reserved.
to learn more about the BlueCard program, call your local Blue Plan or visit regence.com.
BlueCard and BlueCard Worldwide are registered service marks of the Blue Cross and Blue Shield Association.
You see a provider outside the Regence service area
Participating provider provides care for you
local Blue Plan prices the claim and submits it to Regence
Processes the claim andauthorizes payment
sends an explanation ofbenefits to you
local Blue Plan pays provider
how it works

Check out these helpful tips and programs Have a prescription to fill? Wondering if you should switch to a generic or use a mail order pharmacy? Here are some quick tips and programs you need to know about.
Prescription in hand— now what?Head for a participating pharmacy! Most pharmacies in your area are probably in our network. We have participating pharmacies across the United States.
Be sure to show your member card.The pharmacist will use it to send us your claim online and tell you right then and there how much you owe. You’ll be on your way in no time.
Save time and money Formulary Understanding your options when it comes to choosing a medication can help save you money. We've created a preferred medication list/formulary to help you and your doctor make the best decisions on medications that are right for you. Before a medication is added to our preferred list, it's carefully evaluated by a team of doctors and pharmacists. How effective is it? Is it safe? Will it improve health? Our thorough and successful review process has been nationally recognized.
PHARMACY BENEFITS
HERE'S HOW TO
STRETCH YOUR
PHARMACY
DOLLARS.
Science. Insights. Solutions.™
Generics Generics and brand-names have the same strength, quality and purity. But, generics generally cost 20% to 60% less. So, ask your doctor if there is a generic drug that will work for you.
Mail-order You can get some medications—like the ones you take for extended periods of time—through mail order. It cuts out trips to the pharmacy and can even save you a copay or lower your out-of-pocket costs if you have coinsurance.
Specialty Pharmacy If you take a specialty medication (usually injectable drugs and those medications that need special handling), you’ll likely have lower out-of-pocket costs when you use our Specialty Pharmacy partner. In some cases your plan may require that you use our Specialty Pharmacy. The Specialty Pharmacy will help you coordinate refills, monitor side effects, and give you 24-hour access to clinical specialists. You’ll even get injectable supplies for free—and everything can be delivered to your home or location of your choice.
Get the Most Out of Your Pharmacy Benefits.

PHARMACY BENEFITS
| 08130-orx/04-08-152015 OmedaRx
Half-Tablet Program Medications on our Half-Tablet list can save you money! If your medication is in our program, instead of getting 30 pills in your dose, have your doctor give you a prescription for a double-strength dose, then split each one in half to last you two months. That can save you pharmacy visits and up to six copays a year. We’ll even give you a pill splitter.
Blood Glucose Meter Program Our unique program allows all members with diabetes the opportunity to receive a new LifeScan OneTouch glucose meter at no cost. LifeScan meters and test strips are on our formulary. You may order your meter directly from LifeScan by calling 1-855-306-2278.
Understanding prior authorization We review prescriptions for some brand-name medications before we’ll cover them. We do this to make sure that you’re getting the best drug and value. Drugs on the prior-authorization list include many for which equal or more effective and lower cost options exist.
If your drug needs prior authorization, you’ll want to do one of two things:
1. Try a generic first! Most generics don’t need prior authorization, so if your brand-name medication prescription requires prior authorization and has a generic, switching will save you time and money. It’s that easy.
OR
2. Have your doctor or pharmacist request prior authorization for your brand-name medication. You may need to get that authorization before you can get your prescription filled.
Have questions or want to learn more about your prescription benefits? Call the Customer Service number on your member ID card.
WE HAVE MORE THAN 65,000PHARMACIES IN OUR NETWORK.

OmedaRx™ Generic Incentive Program
Brand Medications Generic Alternatives*
Antidepressants (for depression, anxiety, or other conditions)
Celexa, Cymbalta®, Effexor XR, Lexapro, Paxil CR, Pristiq, Prozac Weekly,
Wellbutrin SR, Zoloft
bupropion SA (Wellbutrin SR), fluoxetine (Prozac®)
Antidiabetic Agents (to lower blood sugar)
Actos, Glucophage, Glucotrol, Glucotrol XL
glipizide (Glucotrol®), glipizide XL (Glucotrol XL®), glyburide (Diabeta®), metformin (Glucophage®), metformin ER (Glucophage XR®)
Antihypertensives (to lower blood pressure)
Bystolic®, Lopressor® metoprolol (Lopressor®)
Aceon, Atacand, Avapro, Benicar, Cozaar, Diovan, Lotensin, Micardis, Prinivil, Teveten,
Vasotec, Zestril
benazepril (Lotensin®), lisinopril (Zestril®, Prinivil®), losartan (Cozaar®)
Avalide, Atacand HCT, Benicar HCT, Diovan HCT, Hyzaar, Prinzide, Zestoretic
lisinopril-HCTZ (Zestoretic), losartan-HCTZ (Hyzaar)
Norvasc amlodipine (Norvasc®), felodipine ER
Anti-inflammatories (to treat pain and inflammation)
Arthrotec, Celebrex etodolac (Lodine®), ibuprofen, nabumetone,
naproxen
Antiviral (to treat or suppress herpes simplex virus)
Valtrex acyclovir (Zovirax®)
Bone & Joint (to treat osteoporosis)
Actonel, Atelvia, Boniva, Fosamax alendronate sodium (Fosamax®)
Endocrine/Thyroid (to treat low thyroid)
Levoxyl®, Synthroid, Unithroid levothyroxine
Gastric Acid Agents (to reduce heartburn or stomach acid)
Aciphex, Dexilant™, Nexium, Prevacid, Prilosec, Protonix
omeprazole (Prilosec®), pantoprazole (Protonix®)
Brand Medications Generic Alternatives*
©2015 OmedaRx. All Rights Reserved. 04-2015
*Generic alternatives may not be the exact equivalent of a listed medication; however they can be used to treat similar health conditions.

OmedaRx™ Generic Incentive Program
*Generic alternatives may not be the exact equivalent of a listed medication; however they can be used to treat similar health conditions.
Brand Medications Generic Alternatives*
Hormone Replacement Therapy
Cenestin, Enjuvia, Estrace, Premarin, Vivelle-Dot estradiol (Estrace®)
Hyperlipidemics (to lower cholesterol)
Lopid, Tricor, Trilipix gemfibrozil (Lopid®),
fenofibrate (Lofibra) Men’s Health (for enlarged prostate)
Cardura, Cardura XL, Flomax, Uroxatral doxazosin (Cardura)
Proscar, Avodart finasteride (Proscar)
Migraines
Amerge, Axert, Frova, Imitrex, Maxalt/MLT, Relpax, Treximet, Zomig/ZMT
sumatriptan succinate tablet (Imitrex®)
Neurology (various conditions)
Depakote, Dilantin, Lamictal, Lyrica, Neurontin, Topamax
gabapentin (Neurontin®)
Ophthalmic (to treat glaucoma, eye conditions)
Lumigan®, Travatan Z®, Xalatan®, Zioptan® latanoprost (Xalatan®)
Respiratory (for asthma, seasonal allergies)
Beconase AQ®, Dymista®, Flonase®, Nasacort AQ®, Nasonex®, Omnaris®, Patanase®, Rhinocort Aqua®, Veramyst®, Qnasl®,
Zetonna® fluticasone propionate (Flonase®)
Accolate®, Singulair®, Zyflo/CR® montelukast (Singulair®)
Urinary Agents (for urinary incontinence)
Detrol, Detrol LA, Ditropan XL, Sanctura, Toviaz, Vesicare
oxybutynin
©2015 OmedaRx. All Rights Reserved. 04-2015




Top Related
Copyright © 2022 FDOKUMEN

