







Bahasa
Halaman
Hukum


Trajectories of Adherence to Airway Clearance Therapy forPatients with Cystic Fibrosis
Avani C. Modi,1 PHD, Amy E. Cassedy,2 PHD, Alexandra L. Quittner,3 PHD, Frank Accurso,4 MD,
Marci Sontag,5 PHD, Joni M. Koenig,6 MSPH, and Richard F. Ittenbach,7 PHD1Cincinnati Children’s Hospital Medical Center, University of Cincinnati College of Medicine, 2Cincinnati
Children’s Hospital Medical Center, 3University of Miami, 4University of Colorado Denver, 5Colorado School
of Public Health, University of Colorado Denver, 6The Children’s Hospital of Denver, and 7Cincinnati
Children’s Hospital Medical Center, University of Cincinnati College of Medicine
All correspondence concerning this article should be addressed to Avani C. Modi, PhD, Division of
Behavioral Medicine and Clinical Psychology, Center for the Promotion of Adherence and Self Management,
Cincinnati Children’s Hospital Medical Center, 3333 Burnet Avenue – MLC 7039, Cincinnati, OH 45229,
USA. E-mail: [email protected]
Received November 25, 2009; revisions received January 19, 2010; accepted February 15, 2010
Objective Although cross-sectional studies have demonstrated poor adherence to airway clearance therapy
(ACT) for patients with cystic fibrosis (CF), no studies have identified longitudinal patterns of adherence.
The objective was to characterize and identify predictors of ACT adherence trajectories for individuals
with CF. Methods Secondary data analyses were conducted for a randomized clinical trial examining
differences in three ACTs. Participants (n¼ 153; M¼ 14.3 years, 55% male, 86% Caucasian, baseline FEV1%
predicted: M¼ 86.7)/primary caregivers completed Daily Phone Diaries, an empirically supported adherence
measure, every 4 months. Results Group-based trajectory modeling revealed the best-fitting solution was
a three-group model: low-adherence (14%), medium-adherence (49%), and high-adherence (37%) groups.
ACT type was the only significant predictor of adherence trajectories. Discussion Three trajectories of
adherence to ACT for patients with CF were found. With the identification of trajectories, adherence inter-
ventions can be targeted for the subgroup at highest risk in order to prevent poor health outcomes.
Key words chest wall oscillation; compliance; developmental; Flutter; group-based models; high frequency;longitudinal; manual chest physiotherapy.
Cystic fibrosis (CF) is a progressive, multi-system pulmon-
ary disease, affecting approximately 30,000 individuals in
the United States (Cystic Fibrosis Foundation, 2009).
Significant advances in medicine have resulted in increased
lifespan for individuals with CF, shifting from 25 years of
age in 1985 to 37.4 years in 2008 (Cystic Fibrosis
Foundation, 2009). Treatment for CF has become increas-
ing complex in the past two decades, often taking patients
several hours to complete each day. Treatment often in-
volves taking several types of pills, including oral antibiot-
ics, pancreatic enzymes, digestive medications, and
vitamins. Because lung disease is the primary cause of
morbidity and mortality in patients with CF, much of the
treatment regimen is devoted to thinning and reducing
mucus, as well as keeping the airways open. This is accom-
plished by prescribing nebulized medications (e.g., bron-
chodilators, dornase alpha for mucus thinning, and
inhaled antibiotics) and airway clearance therapy (ACT).
Evidence from several clinical trials and a recent review
examining the benefits of ACT have identified improved
mucus transport as one of the most prominent benefits
of this treatment (see Bradley, Moran, & Elborn, 2006
for evidence-based review). Several forms of ACT are cur-
rently prescribed, including postural drainage and percus-
sion (PD&P), Flutter, and high-frequency chest wall
oscillation (HFCWO), also known as Vest therapy.
Journal of Pediatric Psychology 35(9) pp. 1028–1037, 2010
doi:10.1093/jpepsy/jsq015
Advance Access publication March 18, 2010
Journal of Pediatric Psychology vol. 35 no. 9 � The Author 2010. Published by Oxford University Press on behalf of the Society of Pediatric Psychology.All rights reserved. For permissions, please e-mail: [email protected]
at University of M
iami - O
tto G. R
ichter Library on February 13, 2014
http://jpepsy.oxfordjournals.org/D
ownloaded from

Although ACT remains a mainstay of CF treatment at
this time, it is time-consuming and can be one of the most
difficult to incorporate into daily routines, often taking as
much as an hour a day (Abbott, Dodd, & Webb, 1996; Modi
& Quittner, 2006a). Not surprisingly, several cross-
sectional studies have suggested poor adherence to ACT
across childhood (Modi et al., 2006; Passero, Remor, &
Salomon, 1981; White, Miller, Smith, & McMahon,
2009), adolescence (Quittner et al., 2000; White et al.,
2009), and adulthood (Abbott et al., 1996; Conway,
Pond, Hamnett, & Watson, 1996; White, Stiller, &
Haensel, 2007). For example, school-aged children demon-
strated ACT adherence rates of 51–74% (Modi et al., 2006).
ACT adherence has also been shown to be poor during ado-
lescence (50%; Quittner et al., 2000) and adulthood
(30–32%; Abbott et al., 1996; Myers & Horn, 2006), with
increasing age associated with worse adherence
(Arias Llorente, Bousono Garcia, & Diaz Martin, 2008). In
addition to age, pulmonary functioning has also been asso-
ciated with adherence in CF (Zindani, Streetman,
Streetman, & Nasr, 2006). In contrast, studies are lacking
or there are inconclusive results regarding the association
between adherence and sex (Myers, 2009; Patterson, Wall,
Berge, & Milla, 2008) and socioeconomic status in CF.
However, it is possible that similar to other pediatric condi-
tions (Berquist et al., 2006; Modi, Morita, & Glauser, 2008),
these may be critical factors affecting ACT adherence.
Although these studies provide important snapshots
of adherence at various developmental stages, no studies
have examined adherence to ACT over time for patients at
different points in their lifespan. Identifying the long-term
patterns of adherence in patients with chronic disease is
important because it allows us to understand their variabil-
ity and potentially identify critical periods for intervention.
Furthermore, it may be the first step in identifying thresh-
olds for efficacy related to treatment. For example, what
level of adherence is necessary to obtain optimal health
outcomes, 75, 80, or 100%? This is especially true for
patients with CF, whose treatment regimen only becomes
more complex over time as a result of worsening symptoms
and deterioration of health. While longitudinal ACT adher-
ence data are unavailable, recent adherence data for neb-
ulized medications using an adaptive aerosol delivery
device indicated significant intra- and inter-patient variabil-
ity in adherence (Latchford, Duff, Quinn, Conway, &
Conner, 2009; McNamara, McCormack, McDonald,
Heaf, & Southern, 2009), which was then used to person-
alize and subsequently improve adherence to this treat-
ment (e.g., reduce treatment from twice to once daily;
(McNamara et al., 2009). Overall, these studies highlight
the need to examine longitudinal patterns of adherence for
individuals with CF, allowing us to target individuals at
highest risk during critical developmental periods.
Empirically supported treatments for adherence are
behaviorally and family based, often requiring eight to 12
sessions (Kahana, Drotar, & Frazier, 2008). However,
these interventions are not readily available (e.g., limited)
to the populations that need them most. By identifying
which patients are at highest risk, the limited resources
needed to improve adherence through intervention can
be better targeted across child and adult chronic disease
populations. Targeting patients at highest risk may also
improve health outcomes, such as pulmonary functioning,
reduction in hospitalizations for pulmonary exacerbations,
the likelihood of becoming infected with drug-resistant
bacteria, and health-related quality of life. In addition,
determining the patient-specific (e.g., age, sex) and
treatment-specific (e.g., ACT type) factors that impact
adherence over time will build upon prior cross-sectional,
correlational studies by delineating what contributes to
adherence trajectories over time. For example, if one par-
ticular ACT type is associated with the poorest adherence,
clinicians may wish to prescribe other forms of ACT that
patients prefer and are thus more likely to adhere to. This
is clinically feasible because to date, there are no data to
suggest differences in health outcomes based on which
ACT is used for patients with CF (Main, Prasad, &
Schans, 2005).
New statistical methods, including group-based trajec-
tory models (GBTM), provide the ability to identify adher-
ence sub-groups, including those with the poorest
adherence (e.g., highest risk). These methods have been
successfully applied to other areas and populations,
including criminology (Jennings & Piquero, 2008),
dental caries (Broadbent, Thomson, & Poulton, 2008),
American Indian youth (Stiffman, Alexander-Eitzman,
Silmere, Osborne, & Brown, 2007), and most recently
dyspnea symptoms in marine transportation workers
(Arrandale, Koehoorn, Macnab, & Kennedy, 2009); how-
ever, it has not been used in pediatric psychology research,
which was the central goal of the current study.
The purpose of this study was 3-fold: (1) to describe
rates of adherence to ACT over time for a sample of chil-
dren, adolescents and adults with CF using the Daily
Phone Diary (DPD), an empirically supported assessment
of adherence (Quittner, Modi, Lemanek, Ievers-Landis, &
Rapoff, 2008), (2) to identify and characterize adherence
trajectories for individuals with CF, and (3) to identify
Adherence Trajectories in Cystic Fibrosis 1029
at University of M
iami - O
tto G. R
ichter Library on February 13, 2014
http://jpepsy.oxfordjournals.org/D
ownloaded from

predictors of adherence trajectories. It was hypothesized
that a minimum of two distinct adherence trajectory sub-
groups (e.g., high and low) would be identified and that
these trajectories would be predicted from patient-specific
factors such as age, sex, airway clearance treatment, base-
line pulmonary functioning, and family income.
MethodsParticipants
This was a secondary analysis of data collected for a ran-
domized, prospective clinical trial examining differences in
efficacy of three types of ACT (e.g., PD&P, flutter device, or
Vest) on pulmonary functioning over a 3-year period.
Participants for the clinical trial included individuals with
CF who were 7 years of age or older across 20 CF centers.
All patients had a confirmed diagnosis of CF based on
either a sweat chloride or two documented CFTR muta-
tions and forced expiratory volume in 1 s predicted
(FEV1% predicted) of at least 45%. Exclusion criterion
included the following: hospitalization for a pulmonary
exacerbation, episode of gross hemoptysis (>249 ml)
within 60 days prior to screening, pneumothorax in the
6 months prior to screening, or unwillingness to be rando-
mized to one of three ACTs. Although a sample size of 180
patients was expected, difficulties with recruitment re-
sulted in a final sample of 166 participants for the larger
clinical trial. Fifteen participants withdrew within the first
60 days after randomization, 11 of whom withdrew on the
day of randomization. The clinical trial ended early because
withdrawal rates were significantly higher in PD&P than in
Flutter or HFCWO groups and in older age groups (Sontag
et al., 2010).
Adherence data were available for at least one time
point for 153 participants; however, there were missing
data (16%) for participants across the five assessment
points (pre-randomization: n¼ 130; 4-month: n¼ 131;
8-month: n¼ 121; 12-month: n¼ 115; and 16-month:
n¼ 100). Forty-three percent of participants had five com-
plete data assessment points. Participants in the study
ranged from 7 to 44 years of age at the time of enrollment
(M¼ 14.3 years, SD¼ 7.9 years), and 55% were male. A
majority of participants were Caucasian (86%), while 7%
were Hispanic, 3% were African–American, and 2% were
other. Baseline FEV1% predicted was 86.7% (SD¼ 19.1),
while the mean FEV1% predicted was 85.1 (SD¼ 18.8) for
participants at Time 5, suggesting mild disease severity at
both time points. A majority of participants were either
children or adolescents (80%) and the type of ACT was
equally distributed across participants (PD&P¼ 33%,
Flutter ¼ 30%, and Vest ¼ 37%).
Procedure
Detailed procedures and results regarding the larger rando-
mized trial are reported elsewhere (Sontag et al., 2010);
however, it is important to note that study consent was
obtained from caregivers of children 7–17 years of age and
adults 18 years and older while assent was obtained from
adolescents. Participants were given instructions and train-
ing on their assigned ACT, which was prescribed twice
daily for 20 min/session. For purposes of this secondary
data analysis, adherence was the primary variable of
interest. Adherence was measured at baseline and every
4 months thereafter. Because adherence data were sparse
after the fifth assessment and the study was discontinued
for most participants by the sixth assessment due to high
drop-out rate in the adult age group (Sontag et al., 2010),
data analyses were performed on the first five assessments.
Institutional Review Board Approval was received from all
20 sites participating in the clinical trial.
Measures
Daily Phone Diary
The DPD, a well-established empirically supported assess-
ment measure of adherence (Quittner et al., 2008), uses a
cued recall procedure to track parents, adolescents, and
adults through their activities over the past 24 hours and
provides a detailed analysis of activity patterns, compan-
ions, and mood (Quittner & Opipari, 1994; Quittner,
Opipari, Regoli, Jacobsen, & Eigen, 1992). For all activities
lasting 5 min or longer, participants (e.g., caregivers of chil-
dren 7–13 years of age, adolescents 14–18 years of age, and
adults 18 years and older) reported the type of activity,
duration, and who was present. The interviewer assisted
participants in reconstructing their day as accurately as pos-
sible by providing prompts, such as the time of day or in-
formation about the previous activity (after you finished
dinner, what did you do next?). As the phone diary was
conducted, each activity was recorded by the interviewer on
a computer screen with clock hands which rotated through
a 24-hour clock, a set of activities, companions, and a rating
of mood ranging from 1 (extremely negative) to 5 (extreme-
ly positive). A set of two DPDs (one weekday and one week-
end day) was conducted by phone at each assessment
point. The DPD has yielded reliable stability coefficients
over a 3-week period (r¼ 0.61–0.71, p < .01) and high
levels of inter-rater reliability (>90%) in a CF population
(Quittner et al., 1992). Strong convergent validity was
1030 Modi et al.
at University of M
iami - O
tto G. R
ichter Library on February 13, 2014
http://jpepsy.oxfordjournals.org/D
ownloaded from

found between adherence calculated through the DPD and
objective measures of adherence (Modi et al., 2006; Modi &
Quittner, 2006b). For the current study, time spent in ACT
was extracted from the DPD to measure the duration (in
minutes) each patient spent in ACT each day.
Demographic Questionnaire
A basic demographic questionnaire, which provided infor-
mation about child age, sex, and family income, was ob-
tained via a case-report form.
Health Status
Respiratory functioning was measured by pulmonary func-
tion tests (PFTs). Specifically, FEV1% predicted using
equations for age, sex, and weight were performed by a
trained technician at all sites.
Statistical Analyses
Data analysis proceeded in two discrete stages: a two-part
descriptive phase in which we first sought to understand
and describe the characteristics of the data in general,
and then identified and described trajectories for specific
subgroups within the broader sample of individuals with
CF; and an inferential phase in which we sought to identify
clinically significant predictors (e.g., age, baseline pulmon-
ary functioning) of these adherence trajectory subgroups.
All data were analyzed using SAS v9.1� (SAS Institute,
Cary, NC, USA) and the PROC TRAJ Macro, a closed
source module developed specifically for use with SAS soft-
ware (http://www.andrew.cmu.edu/user/bjones).
Descriptive Phase (Aim 1)
Univariate statistics, including frequency counts as well as
measures of central tendency, variability, and association,
were used to describe sample characteristics, medical his-
tory, and patterns of adherence for this sample. Adherence
rates were calculated using the number of minutes each
participant engaged in airway clearance over the 2-day
DPD period divided by the number of minutes prescribed
for each individual (e.g., 40 min daily was prescribed for all
participants). For example, if a patient conducted airway
clearance for 30 min on day 1 and 20 min on day 2,
the adherence rate would be as follows: [(30þ 20)/
80]� 100¼ 62.5%. Adherence rates were computed for
each assessment point and for the entire study period.
Group-based Trajectories (Aim 2)
A semi-parametric, group-based approach to model estima-
tion was used to identify and characterize ACT adherence
rates over time. This technique, known as GBTM, draws
from a broader class of mixture models in which a finite
number of subgroups within a broader population are
allowed to have different patterns (or trajectories) of
change over time (Nagin, 2005). GBTM is particularly
useful when the number of subgroups and shapes of the
respective trajectories are unknown. To this extent, a
two-step approach for model estimation was used. First,
two-, three-, and four-group solutions were compared to
identify the optimal number of trajectories based on model
Bayesian Information Criterion (BIC) values, where the
value closest to zero value indicates the best fit. Second,
parameter estimates and Wald-statistics for intercept-only,
linear, quadratic, and cubic polynomials were compared to
determine the preferred model. In this case, the preferred
model included three separate trajectories, which were
then plotted for visual inspection. Assignment of indi-
viduals to the three trajectory subgroups was based
on the highest posterior probability estimate for the
final, best-fitting model. A censored normal probability
distribution served as the reference distribution for
all three curves analyzed here. For linear trajectories, a
mixed model was tested to examine the slope of adherence
over time.
Inferential Phase (Aim 3)
In addition, five cumulative logistic regression models
(i.e., ordinal logistic regression) were specified and tested
to identify patient-specific factors capable of distinguishing
the three adherence trajectory subgroups. Cumulative lo-
gistic regression was chosen due to the ordinal nature of
the adherence groups. Although the specific number of
adherence groups was initially unknown, it was reasonable
to assume that the groups would be ordinal in nature (e.g.,
low, medium, high adherence). The proportional odds
model of cumulative logistic regression has the added
advantage of offering summary odds ratios for each of
the predictors rather than multiple odds ratios for each
pair of outcomes (Gameroff, 2005). The outcome of inter-
est was trajectory group membership. Testable covariates
included patient sex, age, randomized ACT type, baseline
FEV1% predicted, and household income.
ResultsDescriptive Phase (Aims 1 and 2)
Descriptive data, including means and standard deviations
for adherence rates across the five time points, are as
follows: pre-randomization: M¼ 36.1 (SD¼ 30.4);
Adherence Trajectories in Cystic Fibrosis 1031
at University of M
iami - O
tto G. R
ichter Library on February 13, 2014
http://jpepsy.oxfordjournals.org/D
ownloaded from
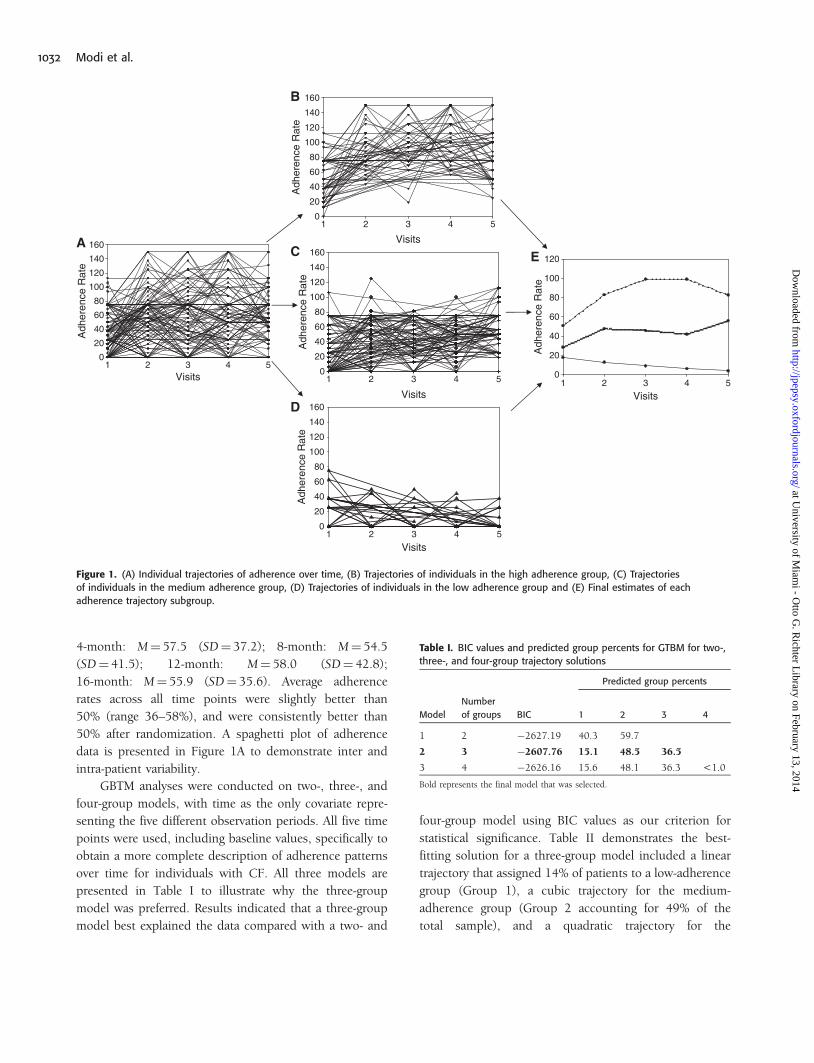
4-month: M¼ 57.5 (SD¼ 37.2); 8-month: M¼ 54.5
(SD¼ 41.5); 12-month: M¼ 58.0 (SD¼ 42.8);
16-month: M¼ 55.9 (SD¼ 35.6). Average adherence
rates across all time points were slightly better than
50% (range 36–58%), and were consistently better than
50% after randomization. A spaghetti plot of adherence
data is presented in Figure 1A to demonstrate inter and
intra-patient variability.
GBTM analyses were conducted on two-, three-, and
four-group models, with time as the only covariate repre-
senting the five different observation periods. All five time
points were used, including baseline values, specifically to
obtain a more complete description of adherence patterns
over time for individuals with CF. All three models are
presented in Table I to illustrate why the three-group
model was preferred. Results indicated that a three-group
model best explained the data compared with a two- and
four-group model using BIC values as our criterion for
statistical significance. Table II demonstrates the best-
fitting solution for a three-group model included a linear
trajectory that assigned 14% of patients to a low-adherence
group (Group 1), a cubic trajectory for the medium-
adherence group (Group 2 accounting for 49% of the
total sample), and a quadratic trajectory for the
Visits
Adh
eren
ce R
ate
0
20
40
60
80
100
120
140
160
Visits
Adh
eren
ce R
ate
0
20
40
60
80
100
120
Visits
Adh
eren
ce R
ate
0
20
40
60
80
100
120
140
160
Visits
Adh
eren
ce R
ate
0
20
40
60
80
100
120
140
160
Visits
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
Adh
eren
ce R
ate
0
20
40
60
80
100
120
140
160
A
B
C
D
E
Figure 1. (A) Individual trajectories of adherence over time, (B) Trajectories of individuals in the high adherence group, (C) Trajectories
of individuals in the medium adherence group, (D) Trajectories of individuals in the low adherence group and (E) Final estimates of each
adherence trajectory subgroup.
Table I. BIC values and predicted group percents for GTBM for two-,
three-, and four-group trajectory solutions
Predicted group percents
Model
Number
of groups BIC 1 2 3 4
1 2 �2627.19 40.3 59.7
2 3 �2607.76 15.1 48.5 36.5
3 4 �2626.16 15.6 48.1 36.3 <1.0
Bold represents the final model that was selected.
1032 Modi et al.
at University of M
iami - O
tto G. R
ichter Library on February 13, 2014
http://jpepsy.oxfordjournals.org/D
ownloaded from

high-adherence group (Group 3 accounting for 37% of the
total sample). Group membership for each trajectory can
be found in Figures 1B through D. Individual trajectories
for the high-adherence Figure 1B, medium-adherence
Figure 1C, and low-adherence Figure 1D groups are
plotted. Final estimates of the trajectories are presented
in Figure 1E. Results indicated a significant negative
slope for the low-adherence group [F(4, 94)¼ 3.22;
p < .05].
Predictors of Adherence Trajectories (Aim 3)
Using the newly created adherence trajectories (low,
medium, and high), patient-specific factors that predicted
group membership were examined. Of the five cumulative
single covariate logistic regression models specified, only
ACT type emerged as a statistically significant predictor of
adherence group membership (Table III). Specifically, we
found significantly more participants using the Flutter
device in the medium-adherence group (see Table IV).
A trend was also noted for family income, in which
patients with a family income greater than $50,000 were
1.87 times more likely to be in the high-adherence trajec-
tory group. Similarly, a positive trend was noted for pul-
monary functioning, in which patients with better FEV1%
predicted were slightly more likely to be in the high adher-
ence group.
Discussion
Results from the current study build upon prior
cross-sectional research examining adherence to ACT for
patients with CF and suggest significant inter-patient vari-
ability. Prior to randomization for the ACT clinical trial,
adherence to this treatment was quite low at �36% for
the entire sample. This translates into patients performing
14 min of ACT each day compared to the recommended
40 min per day. However, as expected, adherence to ACTs
increased with enrollment in a clinical trial to 58%.
Although this rate is still low, it is consistent with prior
studies (Abbott et al., 1996; Modi et al., 2006; Myers &
Horn, 2006; Quittner et al., 2000) and suggests that pa-
tients with CF have poor adherence to this critical aspect of
their treatment regimen. Longitudinal results also indi-
cated that rates of adherence remained relatively stable
over the 16-month study period, indicating that patients
with CF who enroll and remain in a randomized, clinical
trial are able to consistently engage in ACT �50% of the
recommended time.
One novel aspect of this study was its examination of
trajectories of adherence over time in a large cohort of
patients with CF. Data indicated three distinct groups,
including a low, medium, and high adherence group.
Specifically, it appears that patients whose initial adher-
ence was lowest (e.g., 17%) remained low over time.
In contrast, patients who exhibited the highest rate of
adherence initially maintained higher levels of adherence
over time. The medium adherence group, which encom-
passed the largest proportion of individuals with CF
(49%), displayed the most variability in adherence. As sug-
gested by prior studies, this is likely due to ACT barriers,
such as competing activities and forgetting (Abbott et al.,
1996; Modi & Quittner, 2006a), which interfere at various
Table III. Logistic regression: patient predictors of adherence
trajectories
Variable OR CI0.95 p-value
Sex (male as reference category) 1.26 0.69, 2.31 0.46
Age 0.99 0.96, 1.03 0.72
ACT type 0.04
PD&P (reference group)
Flutter 2.46 1.13, 5.36 0.02
Vest 1.08 0.52, 2.23 0.84
Baseline FEV% predicted 1.05 0.99, 1.03 0.06
*Household income
(<$50,000 as
reference category)
1.87 0.92, 3.80 0.08
Note. All models tested met the score test for the proportional odds assumption.
*Multiple iterations were used to examine household income differences,
including a four- and a seven-category income variable with results indicating
no statistically significant relationship.
Table II. Final three-group model for adherence trajectories
Group Parameter Estimate (SE) T p
Low Intercept 17.73 (11.22) 1.58 0.11
Linear model �8.58 (4.13) �2.08 0.03
Medium Intercept �43.82 (25.06) �1.75 0.08
Cubic model 3.61 (1.28) 2.82 <0.01
High Intercept 0.73 (11.42) 0.06 0.94
Quadratic model �8.22 (1.49) �5.53 <0.01
Table IV. ACT type by adherence trajectory subgroup
Group PD&P Flutter Vest
Low adherence (n¼ 22) 7 (14%) 7 (15%) 8 (14%)
Medium adherence (n¼ 75) 20 (40%) 31 (67%) 24 (42%)
High adherence (n¼ 56) 23 (46%) 8 (17%) 25 (44%)
Adherence Trajectories in Cystic Fibrosis 1033
at University of M
iami - O
tto G. R
ichter Library on February 13, 2014
http://jpepsy.oxfordjournals.org/D
ownloaded from

times and occur inconsistently. It is possible that individ-
uals in the high adherence group are better able to problem
solve their barriers to ACT adherence and incorporate
these strategies into daily routines compared to individuals
in the medium adherence group. Overall, these adherence
trajectories allowed for identification of patients who are
highest risk for poor adherence by demonstrating that
patients who exhibit adherence rates below 25% are
likely to maintain these levels over time, placing them at
risk for increased morbidity (e.g., pulmonary exacerba-
tions, acquisition of drug-resistant microorganisms). It is
this subgroup that would benefit from the most intensive
intervention to improve adherence. However, even the high
and medium groups are below 50% and thus would bene-
fit from adherence interventions. Specifically, adherence
interventions that focus on providing education to fill
gaps in knowledge, teaching and ensuring that patients
have the skills to conduct the therapy, identifying and
problem solving around barriers to adherence, and match-
ing the type of therapy that best suits the needs of the
patient and their family are likely the most beneficial
(Homnick, 2007; Kahana et al., 2008).
Interestingly, ACT was the only significant patient-
specific predictor of adherence trajectories. Patients pre-
scribed Flutter were more likely to be in the medium
adherence group compared to PD&P and Vest. The
Flutter can be completed independently once the tech-
nique has been mastered, which is likely desirable for ado-
lescents and adults. However, because the Flutter requires
active participation (versus passive with Vest), patients may
become bored or disinterested in the therapy for the full
prescribed duration. These findings suggest that patients
prescribed the Flutter device are not likely to have high
rates of adherence over time. If, in contrast, patients pre-
scribed PD&P or Vest are more likely to be in the
high-adherence trajectory, it is important to incorporate
patient preference when making decisions about ACTs,
especially given lack of evidence regarding efficacy differ-
ences between the three ACT methods (Main et al., 2005).
Homnick (2007) has suggested the need to adapt ACTs
based on disease severity and patient preference to encour-
age optimal adherence, with frequent monitoring to ensure
health status does not decline.
While age and sex were not associated with adherence
trajectories, a trend was noted for both family income and
baseline pulmonary functioning. Specifically, patients with
CF were almost twice as likely to be in the high adherence
group if their family income was greater than $50,000.
These results are similar to studies in pediatric epilepsy
(Modi et al., 2008) and liver transplant (Berquist et al.,
2006) suggesting a positive association between adherence
and socioeconomic status. In addition, patients with CF
with higher pulmonary functioning trended toward being
in the high adherence group compared to the low adher-
ence group. Future studies with more variability in pul-
monary functioning (e.g., patients with more severe
disease) would better elucidate these findings.
While this study is the first to examine longitudinal
adherence to ACT for children, adolescents, and adults
with CF, several limitations exist that provide directions
for future research. The identification of adherence trajec-
tories and predictors of these trajectories represented the
first step in understanding adherence behaviors over time.
An important next step is to examine the relations between
adherence trajectories and health outcomes, including
pulmonary functioning, nutritional status, and health-
related quality of life. With this information, clinical
researchers may be able to identify optimal levels of adher-
ence, which promote the best outcomes. Future studies
should also include a larger cohort of adults with CF
to elucidate developmental differences in adherence.
Although the use of GBTM techniques was a major
strength of this study, research from other fields has sug-
gested that large sample sizes are necessary to identify
trajectories. While our sample size fell below the suggested
200 cases, studies have successfully used sample sizes con-
sistent with ours (Conklin et al., 2005; Mulvaney,
Lambert, Garber, & Walker, 2006). An important area
for future research is a confirmatory analysis of the low,
medium, and high adherence trajectories we identified.
Finally, these data are a secondary analysis of a randomized
clinical trial examining differences between three ACT
types and thus must be considered within this context.
Sontag et al. (2010) have reported lessons learned from
this trial, including early termination due to differential
drop-out in the adult PD&P study arm, which contributed
to inadequate power to detect group differences. While the
early termination of the trial has important implications for
adherence, because adherence was the primary outcome
variable, we had sufficient longitudinal data to compute
our results.
Overall, this is the first study to use GBTM to examine
adherence behaviors in individuals with a chronic illness
that requires a time-consuming and complex treatment
regimen. Adherence trajectories, such as the ones identi-
fied in this study, are likely to generalize to other chronic
illness populations with complex treatment regimens,
including diabetes, sickle cell disease, and asthma and
1034 Modi et al.
at University of M
iami - O
tto G. R
ichter Library on February 13, 2014
http://jpepsy.oxfordjournals.org/D
ownloaded from

should be evaluated in these populations. Examining ad-
herence trajectories holds promise for identifying the level
of adherence necessary to obtain the best health outcomes
and quality of life.
Acknowledgements
The authors thank all of the children, adolescents, adults,
and their families who participated in this study. In addi-
tion, we would like to thank all the research assistants who
conducted the DPDs. We would also like to acknowledge
the following institutions, Investigators and Coordinators
of the Airway Secretion Clearance Trial: Baylor College of
Medicine (Texas Children’s Hospital), Oermann, Chris,
Morris, Lisa; Tulane University School of Medicine,
Davis, Scott, Broussard, Annette; Baystate Medical
Center, Gerstle, Robert, Pellett, Amira; Schneider
Children’s Hospital/Long Island Medical Center, DeCelie-
Germana, Joan, Hurley, Jody; University of Florida,
Wagner, Mary, Capen, Cindy; Children’s Healthcare of
Atlanta at Scottish Rite, Scott, Peter, Crews, Barbara;
New England Medical Center, Yee, William, Ulles,
Monica; University of California, San Diego, Pian, Mark,
Boone, Debbie; Children’s Hospital of Buffalo, McMahon,
Colin, Prentice, Sandy; Programa Pediatrico Pulmonar de
San Juan, Rodriguez-Santana, Jose, Medina, Vivian;
Connecticut Children’s Medical Center, Lapin, Craig,
Drapeau, Ginny; The University of Texas Southwestern
Medical Center at Dallas, Gelfand, Andy, Urbanczyk,
Brenda; St. Vincent’s Hospital and Medical Center of
New York, Berdella, Maria, Grece, Caroll Anne;
University of Rochester, Voter, Karen, Sierzega, Renata;
Indiana University, Eigen, Howard, Blagburn, Mary;
University of Wisconsin, Rock, Michael, Yngsdal-Krenz,
Rhonda; Wake Forest University, Schechter, Michael,
Hunt, Meagan; Kaiser Permanente Medical Care Program,
Shay, Greg, Farmer, Gail; University of Nebraska Medical
Center, Colombo, John, Acquizzino, Dee; St. Louis
University, Albers, Gary, Lewis, Pat.
Funding
Hill-Rom Inc. (formerly American Biosystems, Inc.) and
the United States Cystic Fibrosis Foundation.
Conflict of interest: American Biosystems provided one of
the three ACT methods used in the larger randomized
clinical trial. Dr. Accurso has served on the advisory
board for American Biosystems.
References
Abbott, J., Dodd, M., & Webb, A.K. (1996). Health
perceptions and treatment adherence in adults with
cystic fibrosis. Thorax, 51, 1233–1238.
Arias Llorente, R.P., Bousono Garcia, C., & Diaz
Martin, J.J. (2008). Treatment compliance in children
and adults with cystic fibrosis. Journal of Cystic
Fibrosis, 7, 359–367.
Arrandale, V.H., Koehoorn, M., Macnab, Y.,
& Kennedy, S.M. (2009). Longitudinal analysis of
respiratory symptoms in population studies with a
focus on dyspnea in marine transportation workers.
International Archives of Occupational and
Environmental Health, 82, 1097–1105.
Berquist, R.K., Berquist, W.E., Esquivel, C.O., Cox, K.L.,
Wayman, K.I., & Litt, I.F. (2006). Adolescent
non-adherence: prevalence and consequences in
liver transplant recipients. Pediatric Transplant, 10,
304–310.
Bradley, J.M., Moran, F.M., & Elborn, J.S. (2006).
Evidence for physical therapies (airway clearance and
physical training) in cystic fibrosis: an overview of
five Cochrane systematic reviews. Respiratory
Medicine, 100, 191–201.
Broadbent, J.M., Thomson, W.M., & Poulton, R. (2008).
Trajectory patterns of dental caries experience in the
permanent dentition to the fourth decade of life.
Journal of Dental Research, 87, 69–72.
Conklin, C.A., Perkins, K.A., Sheidow, A.J., Jones, B.L.,
Levine, M.D., & Marcus, M.D. (2005). The return
to smoking: 1-year relapse trajectories among
female smokers. Nicotine and Tobacco Research, 7,
533–540.
Conway, S.P., Pond, M.N., Hamnett, T., & Watson, A.
(1996). Compliance with treatment in adult patients
with cystic fibrosis. Thorax, 51, 29–33.
Cystic Fibrosis Foundation (2009). About Cystic Fibrosis,
Retrieved from http://www.cff.org/AboutCF/
Gameroff, M.J. (2005). Using the proportional odds
model for health-related outcomes: Why, when, and
how with various SAS� procedures. In: Proceedings
of the 30th annual SAS User’s Group International
Conference. Retrieved from http://www2.sas.com/
proceedings/sugi30/205-30.pdf
Homnick, D.N. (2007). Making airway clearance success-
ful. Paediatric Respiratory Reviews, 8, 40–45.
Jennings, W.G., & Piquero, A.R. (2008). Trajectories of
non-intimate partner and intimate partner homicides,
Adherence Trajectories in Cystic Fibrosis 1035
at University of M
iami - O
tto G. R
ichter Library on February 13, 2014
http://jpepsy.oxfordjournals.org/D
ownloaded from
1980-1999: The importance of rurality. Journal of
Criminal Justice, 36, 435–443.
Kahana, S., Drotar, D., & Frazier, T. (2008). Meta-
analysis of psychological interventions to promote
adherence to treatment in pediatric chronic health
conditions. Journal of Pediatric Psychology, 33,
590–611.
Latchford, G., Duff, A., Quinn, J., Conway, S.,
& Conner, M. (2009). Adherence to nebulised
antibiotics in cystic fibrosis. Patient Education and
Counseling, 75, 141–144.
Main, E., Prasad, A., & Schans, C. (2005). Conventional
chest physiotherapy compared to other airway
clearance techniques for cystic fibrosis. Cochrane
Database System Review, CD002011.
McNamara, P.S., McCormack, P., McDonald, A.J.,
Heaf, L., & Southern, K.W. (2009). Open adherence
monitoring using routine data download from an
adaptive aerosol delivery nebuliser in children with
cystic fibrosis. Journal of Cystic Fibrosis, 8, 258–63.
Modi, A.C., Lim, C.S., Yu, N., Geller, D., Wagner, M.H.,
& Quittner, A.L. (2006). A multi-method assessment
of treatment adherence for children with cystic
fibrosis. Journal of Cystic Fibrosis, 5, 177–185.
Modi, A.C., Morita, D.A., & Glauser, T.A. (2008).
One-month adherence in children with new-onset
epilepsy: white-coat compliance does not occur.
Pediatrics, 121, e961–966.
Modi, A.C., & Quittner, A.L. (2006a). Barriers to
Treatment Adherence for Children with Cystic
Fibrosis and Asthma: What Gets in the Way?
Journal of Pediatric Psychology, 31, 846–858.
Modi, A.C., & Quittner, A.L. (2006b). Utilizing com-
puterized phone diary procedures to assess health
behaviors in family and social contexts. Children’s
Health Care, 35, 29–45.
Mulvaney, S., Lambert, E.W., Garber, J., & Walker, L.S.
(2006). Trajectories of symptoms and impairment for
pediatric patients with functional abdominal pain: a
5-year longitudinal study. Journal of the American
Academy of Child and Adolesccent Psychiatry, 45,
737–744.
Myers, L.B. (2009). An exploratory study investigating
factors associated with adherence to chest phy-
siotherapy and exercise in adults with cystic fibrosis.
Journal of Cystic Fibrosis, 8, 425–427.
Myers, L.B., & Horn, S.A. (2006). Adherence to chest
physiotherapy in adults with cystic fibrosis. Journal
of Health Psychology, 11, 915–926.
Nagin, D. (2005). Group-based modeling of development.
Cambridge: Harvard University Press.
Passero, M.A., Remor, B., & Salomon, J. (1981). Patient-
reported compliance with cystic fibrosis therapy.
Clinical Pediatrics (Phila), 20, 264–268.
Patterson, J.M., Wall, M., Berge, J., & Milla, C. (2008).
Gender differences in treatment adherence
among youth with cystic fibrosis: development of a
new questionnaire. Journal of Cystic Fibrosis, 7,
154–164.
Quittner, A.L., & Opipari, L.C. (1994). Differential
treatment of siblings: interview and diary analyses
comparing two family contexts. Child Development,
65, 800–814.
Quittner, A.L., Opipari, L.C., Regoli, M.J., Jacobsen, J.,
& Eigen, H. (1992). The impact of caregiving and
role strain on family life: Comparisons between
mothers of children with cystic fibrosis and
matched controls. Rehabilitation Psychology, 37,
289–304.
Quittner, A.L., Drotar, D., Ievers-Landis, C.E.,
Seidner, D., Slocum, N., & Jacobsen, J. (2000).
Adherence to medical treatments in adolescents with
cystic fibrosis: The development and evaluation of
family-based interventions. In D. Drotar (Ed.),
Promoting Adherence to Medical Treatment in
Childhood Chronic Illness: Interventions and Methods
(pp. 383–407). Hillsdale, NJ: Erlbaum Associates, Inc.
Quittner, A.L., Modi, A.C., Lemanek, K.L.,
Ievers-Landis, C.E., & Rapoff, M.A. (2008).
Evidence-based assessment of adherence to medical
treatments in pediatric psychology. Journal of
Pediatric Psychology, 33, 916–936.
SAS Institute (Version 9.1). Cary, NC, USA.
Sontag, M.K., Quittner, A.L., Modi, A.C., Giles, D.,
Koenig, J.M., Oermann, C., et al. (2010). Lessons
learned from a randomized trial of airway secretion
clearance techniques in cystic fibrosis. Pediatric
Pulmonology, 45(3), 291–300.
Stiffman, A.R., Alexander-Eitzman, B., Silmere, H.,
Osborne, V., & Brown, E. (2007). From early to late
adolescence: American Indian youths’ behavioral
trajectories and their major influences. Journal of the
American Academy of Child and Adolescent Psychiatry,
46, 849–858.
White, D., Stiller, K., & Haensel, N. (2007). Adherence
of adult cystic fibrosis patients with airway clearance
and exercise regimens. Journal of Cystic Fibrosis, 6,
163–170.
1036 Modi et al.
at University of M
iami - O
tto G. R
ichter Library on February 13, 2014
http://jpepsy.oxfordjournals.org/D
ownloaded from

White, T., Miller, J., Smith, G.L., & McMahon, W.M.
(2009). Adherence and psychopathology in children
and adolescents with cystic fibrosis. European Child
and Adolescent Psychiatry, 18, 96–104.
Zindani, G.N., Streetman, D.D., Streetman, D.S.,
& Nasr, S.Z. (2006). Adherence to treatment in
children and adolescent patients with cystic fibrosis.
Journal of Adolescent Health, 38, 13–17.
Adherence Trajectories in Cystic Fibrosis 1037
at University of M
iami - O
tto G. R
ichter Library on February 13, 2014
http://jpepsy.oxfordjournals.org/D
ownloaded from
Top Related
Copyright © 2022 FDOKUMEN

