







Bahasa
Halaman
Hukum


Towards a Theory of Sustainable Prevention of Chagas Disease: An Ethnographic
Grounded Theory Study
A dissertation presented to
the faculty of
Ohio University
In partial fulfillment
of the requirements for the degree
Doctor of Philosophy
Claudia Nieto-Sanchez
December 2017
© 2017 Claudia Nieto-Sanchez. All Rights Reserved.

2 This dissertation titled
Towards a Theory of Sustainable Prevention of Chagas Disease: An Ethnographic
Grounded Theory Study
by
CLAUDIA NIETO-SANCHEZ
has been approved for
the School of Communication Studies,
the Scripps College of Communication,
and the Graduate College by
Benjamin Bates
Professor of Communication Studies
Mario J. Grijalva
Professor of Biomedical Sciences
Joseph Shields
Dean, Graduate College

3 Abstract
NIETO-SANCHEZ, CLAUDIA, Ph.D., December 2017, Individual Interdisciplinary
Program, Health Communication and Public Health
Towards a Theory of Sustainable Prevention of Chagas Disease: An Ethnographic
Grounded Theory Study
Directors of Dissertation: Benjamin Bates and Mario J. Grijalva
Chagas disease (CD) is caused by a protozoan parasite called Trypanosoma cruzi
found in the hindgut of triatomine bugs. The most common route of human transmission
of CD occurs in poorly constructed homes where triatomines can remain hidden in cracks
and crevices during the day and become active at night to search for blood sources. As a
neglected tropical disease (NTD), it has been demonstrated that sustainable control of
Chagas disease requires attention to structural conditions of life of populations exposed to
the vector. This research aimed to explore the conditions under which health promotion
interventions based on systemic approaches to disease prevention can lead to sustainable
control of Chagas disease in southern Ecuador. Using Healthy Homes for Healthy Living
(HHHL) as reference, I conducted an ethnographic grounded theory study to answer the
following research questions: RQ1. What are the factors that contribute or limit
sustainable control of Chagas disease in the communities of Chaquizhca, Bellamaria and
Guara under the model proposed by HHHL? RQ2. In what ways, if so, can these factors
be addressed in order to scale up the model to other homes in these communities?
The first three chapters of this document develop the proposal that was approved
for this dissertation. They provide a general overview of the theoretical and
methodological foundations that articulate this research as an interdisciplinary endeavor.
4 The literature review is extended in Chapter 4 through a systematic review that looked
at communication approaches applied to NTD’s eradication, elimination and control. This
systematic review established that behavior change through health education is the most
common goal pursued through communication actions, but no major differences in
media, messages and strategies can be observed for the specific infectious diseases
studied (Guinea worm, lymphatic filariasis, schistosomiasis and Chagas disease). More
complex approaches to communication based on differentiated goals, deep study of local
cultures and deeper understanding of the role of participation in decision-making, are
recommended. Chapter 5 elaborates on fieldwork conducted between 2016 and 2017 to
analyze the experience of local families after implementation of the HHHL model. In
here, I contend that sustainability of CD control under the model proposed by HHHL
largely depends on the systemic capacity of home improvement to activate and sustain
agency in partner families. Agency is explained in this case as the confluence of three
factors: systemic improvement of families’ quality of life, consistent use of protective
measures by partner families, and adaptation to emerging dynamics in communities at
large. Finally, Chapter 6 presents ideas to scale the HHHL model by applying lessons
learnerd in the pilot phase of the project and brosdening its scope to a larger public health
strategy.

5 Dedication
To my parents, for telling me the first story.
A mis padres, por contarme la primera historia.

6 Acknowledgments
My gratitude goes, in first place, to the communities of Chaquizhca, Bellamaria
and Guara. Thanks for receiving all these years of endless questions with an honest smile.
My heart will always admire and be inspired by the courage of those families that
decided to believe in us when we presented the idea of Healthy Homes for Healthy
Living. That act of trust opened multiple avenues for our personal and scientific growth.
Gracias.
Thanks to my colleagues at ITDI and CISeAL for creating spaces of social change
where multiple perspectives and worldviews are welcomed. It has been an honor working
with you all. Special thanks to Darwin Guerrero, Guillermo Gomez, Esteban Baus, Sylvia
Jimenez, Sofia Ocana, Anita Villacis, Cesar Yumiseva and Maria Jose Carrasco for your
lessons of creative and critical thinking. The Healthy Living Initiative is a life changing
experience because you all have invested the best of your energy in making it so.
Thanks to my committee members for their constant support along this process.
Mario, thanks for trusting me with your ideas, for offering me a challenging and inspiring
path through graduate school, and for always setting the highest professional standards as
reference for our group. Thanks for believing in my work and motivations. Thanks for
your economic, scientific and personal support. I am very proud to be called your mentee.
Ben, thanks for your willingness to listen to my ideas and your patient reading of this and
previous versions of this manuscript. Thanks for giving me the ‘yes’ that started my PhD
life and for guiding me in all those critical moments in which I could not see the end of
the road. Tania, thanks for witnessing and shaping my trajectory as a graduate student.
You saw my becoming from a masters student into a doctor and can only join other

7 Commdevers in thanking your presence at Ohio University as faculty and director.
Thanks for always telling me ‘you got this’. To the three of you, thanks for literally
traveling with me to experience that Ecuador that has so deeply impacted my career.
I also want to dedicate some words of gratitude to the voices that constantly guide
and inspire my decisions as scholar. Thanks to Karen Greiner, Adelaida Trujillo, Jair
Vega, Warren Feek, David Mould, Silvio Waisbord, Arving Singhal, Austin Babrow,
Amy Chadwick, Bill Rawlins, and Koen Peeters for modeling the practitioner I am, but
first and foremost, for offering me your friendship in this path of learning. To Rafael
Obregon for believing in me, for insisting every time that fears threaten with holding me
back, and for that perennial hug that reminds me that we are making the road by walking.
My deepest gratitude to the amazing women I have been lucky enough to cross
paths with to understand that there is not solitude in our fights. To Cynthia Hannah,
Karen Greiner, Belen Marco, Diana Marvel, Sofia Ocana, Maria Fernanda Pena, Zulfia
Zaher, Katy Kropf, Piper Kropf, Sharon Casapulla, Adriana Angel, Piedad Mendoza,
Yira Zafra, and so many others sisters I have been reunited with along the way.
Finally, I want to thank my family for embracing my absence with their loving
presence: To my parents, for patiently waiting in the multiple occasions in which work
took over my time and attention; to Camilo and Adriana for showing me the power of
committed love; to my family in the US, for taking that first step that has opened the
doors for many of us and for always offering me a home away from home; and to
Achilles, my Compa, for saying ‘Yes’ to my ‘What if’ question.
My gratitude to all the Gods I have found in the genuine human encounters I have
experienced in these years of travels and learning.

8 Table of Contents
Page
Abstract ............................................................................................................................... 3
Dedication ........................................................................................................................... 5
Acknowledgments............................................................................................................... 6
List of Tables .................................................................................................................... 11
List of Figures ................................................................................................................... 12
Chapter 1: Introduction ..................................................................................................... 13
Neglected Tropical Diseases: The Need for a Paradigm Shift in Disease Prevention 13
Poverty and NTD ........................................................................................................ 18
Chagas Disease ........................................................................................................... 22
Healthy Homes for Healthy Living ............................................................................. 27
Research Purpose ........................................................................................................ 29
Chapter 2: Theoretical Foundations .................................................................................. 31
Living Environments and Health: A Health Systems Perspective .............................. 31
Implementation Research ............................................................................................ 37
Social Construction of Health ..................................................................................... 39
From Persuading Individuals to Dialogic Health Promotion ...................................... 44
Chapter 3: Methods Section .............................................................................................. 49
Methodological Approach and Research Questions ................................................... 49
Research Design: Ethnographic Grounded Theory .................................................... 50
Grounded theory. .................................................................................................. 50
Sustainability as sensitizing concept. .................................................................... 53
Study population. .................................................................................................. 56
Data collection. ..................................................................................................... 57
Data analysis. ........................................................................................................ 62
Final products. ....................................................................................................... 66
Ethics and informed consent procedures. ............................................................. 66
Justification of Methods .............................................................................................. 67
Positionality ................................................................................................................ 69
Chapter 4: Uses of Communication Strategies, Media and Messages in Neglected Tropical Diseases Eradication, Elimination and Control Programs: A Systematic Review........................................................................................................................................... 72

9 Introduction ................................................................................................................. 72
Methods....................................................................................................................... 74
Data sources. ......................................................................................................... 75
Data extraction and synthesis................................................................................ 77
Results ......................................................................................................................... 78
Eradication. ........................................................................................................... 99
Elimination. ......................................................................................................... 102
Control. ............................................................................................................... 106
Discussion ................................................................................................................. 114
References ................................................................................................................. 124
Conclusion ................................................................................................................ 123
Limitations. ......................................................................................................... 124
Chapter 5: Towards a Theory of Sustainable Prevention of Chagas Disease: An Ethnographic Grounded Theory Study ........................................................................... 139
Introduction ............................................................................................................... 139
Home improvement for disease prevention. ....................................................... 141
Systemic approaches to Chagas disease prevention. .......................................... 143
Methods..................................................................................................................... 146
Study area............................................................................................................ 146
Healthy Homes for Healthy Living model (HHHL). .......................................... 147
Data collection and study population. ................................................................. 152
Data analysis. ...................................................................................................... 155
Ethics................................................................................................................... 159
Results ....................................................................................................................... 160
Health impact. ..................................................................................................... 160
Emotional impact. ............................................................................................... 183
Economic impact. ............................................................................................... 187
Social impact. ...................................................................................................... 193
Discussion and Theoretical Development ................................................................ 198
Systemic improvement of families’ quality of life. ............................................ 199
Consistent use of protective measures. ............................................................... 201
Adaptation to emerging dynamics. ..................................................................... 205
Barriers. ............................................................................................................... 206
Conclusion ................................................................................................................ 209

10 Limitations. ......................................................................................................... 211
References ................................................................................................................. 211
Chapter 6: Towards a Theory of Sustainable Prevention of Chagas Disease: Scaling Up Proposal (White Paper) ................................................................................................... 218
Contents .................................................................................................................... 218
Introduction ............................................................................................................... 219
Chagas disease .................................................................................................... 221
CD epidemiology in Loja province. .................................................................... 224
Healthy Homes for Healthy Living Model (HHHL) ................................................ 226
Methods..................................................................................................................... 230
Data collection and study population. ................................................................. 230
Data analysis. ...................................................................................................... 232
Scaling Up Proposal .................................................................................................. 234
Summary of findings ancillary study. ................................................................. 234
Infrastructure improvement. ............................................................................... 237
Dialogic health promotion. ................................................................................. 262
Income generation opportunities. ........................................................................ 267
Conclusion ................................................................................................................ 272
References ................................................................................................................. 273
References ....................................................................................................................... 278
Appendix A: Interview Guide for HHHL Partner Families ........................................... 300
Appendix B: Socio-economic Survey for Communities at Large ................................. 303

11 List of Tables
Page
Table 1. Communication actions advised in articles classified as recommendations. ...... 78
Table 2. Communication strategies implemented in studies classified as interventions. . 82
Table 3. Anti-triatomine measures implemented as part of HHHL infrastructure intervention. .................................................................................................................... 148
Table 4. Health promotion actions developed during the implementation of the HHHL model............................................................................................................................... 148
Table 5. Interviewees in partner families by year and type of intervention (Group 1). .. 154
Table 6. Interviewees in non-partner families (Group 2). .............................................. 155
Table 7. Exemplar of process coding. ............................................................................. 157
Table 8. Exemplar of in-vivo coding. ............................................................................. 158
Table 9. Comparison of 2012 and 2016 decay analysis (summary). .............................. 238
Table 10. Demographic characteristics respondents socio-economic questionnaire. ..... 240
Table 11. Frequency table for quantitative component of socio-economic questionnaire.......................................................................................................................................... 240

12 List of Figures
Page
Figure 1. Flow of search for systematic review. .............................................................. 77
Figure 2. Exemplar of a local home previous intervention. ........................................... 150
Figure 3. Exemplar of a home after HHHL intervention. .............................................. 151

13 Chapter 1: Introduction
Neglected Tropical Diseases: The Need for a Paradigm Shift in Disease Prevention
From terrorism to global warming, current debates about risk are entangled in
complex analyses about the meanings of vulnerability and safety in a context of global
interactions. The last decades have expanded descriptions of risk strictly focused on
personal practices potentially leading to danger (Turner, Skubisz, & Rimal, 2011), to
more sophisticated conceptualizations about multidimensional political, economic, social
and environmental interactions that can threaten modern concepts of health and
wellbeing.
Structural relationships between political and socio-economic conditions and
health are at the core of the conceptualization of neglected tropical diseases (NTD).
Known as ‘the other diseases’ alluded to by the millennium development goal number
six in the Millennium of 2000 (Smith & Taylor, 2013), the NTD group is comprised of
seventeen infectious diseases that mainly affect people living in poverty in tropical
regions of the world (Crompton, 2010). Despite important biological differences
determined by their protozoan (Chagas disease, leishmaniasis, American tripanosimiasis),
bacterial (Buruli ulcer, trachoma, leprocy, yaws), helminthic (trichuriasis, lymphatic
filariasis, onchocerciasis, schistosomiasis), or viral (dengue, and rabies) origin, the World
Health Organization (WHO) decided to group these diseases together in a single category
with the purpose of highlighting poverty as the main risk factor for infectious diseases in
developing countries (Crompton, 2010). Among the political, economic, and social
factors shared by NTD, prevalence in rural or poor urban areas in low-income tropical
countries, high disease burden but low mortality, transmission patterns directly related

14 with habitation settings and productive activities of affected population, and limited
resources invested in their research, prevention, and treatment, are the most salient
(Hotez, Fenwick, Savioli, & Molyneux, 2009).
Since 2003 −year in which WHO coined the acronym NTD− researchers and
organizations have been involved in systematic efforts aimed at obtaining financial and
political support for strategies and programs aimed at preventing, controlling,
eliminating, or eradicating these diseases. The NTD movement has capitalized on the
success claimed by HIV and malaria advocates after the visibility obtained through their
inclusion in the MDG declaration of 2000, up to the point that NTD were included in the
new Sustainable Development Goals launched by the United Nations in 2015 (Engels,
2016).
NTD advocates have focused strategic actions that can facilitate access to
financial and political support for research on these diseases (Kariuki et al., 2011). The
Integrated approach for NTD control has been the main strategy promoted by WHO and
scientists affiliated to institutions in the global North, not only as model for disease
prevention and treatment, but also as a global model for poverty reduction (Allen &
Parker, 2011; Hotez et al., 2007). Since most NTD are endemic of similar geographic
areas, and seven of them show substantial overlap in Sub-Saharan Africa, the integrated
approach basically proposes preventative chemotherapy with antiparasitic drugs
(particularly albendazole, mebendazole, praziquantel, ivermectin, diethylcarbamazine,
and azithromycin) massively distributed to communities at risk in urban and rural settings
of endemic countries (Hotez et al., 2007; Hotez et al., 2006) as main control method.
Four of these drugs are currently donated by pharmaceutical companies (Barry, 2014),
15 which has led WHO and scientists to sustain that around 500 million people in Sub-
Saharan Africa could be treated at an approximate cost of US$ $400 million or less per
year (Hotez et al., 2007). Moreover, there are multiple vaccine trials being conducted for
at least four of these diseases, which has led some authors to think that it is possible to
envision a set of “antipoverty vaccines against all of the neglected tropical diseases”
(Hotez et al., 2007, p. 1025) in the near future.
In addition to preventive chemotherapy, WHO also recommends vector control
and improved surveillance for high-quality care as part of these integrated approaches to
reduce transmission (Daumerie & Kindhauser, 2003). Regional counterparts are
mandated to take these recommendations and adapt them to the specific transmission
dynamics of each disease in different geographical areas.
In Latin America, the Pan American Health Organization (PAHO) has turned
WHO’s general guidelines into a package of seven actions for integrated control of NTD,
including: Integration of preventive chemotherapy; intensive management of cases;
vector control, provision of water and sanitation; management of zoonotic elements of
the disease; community participation; and multisectoral integration (Holveck et al.,
2007).
In spite of minor differences among regions, NTD integrated models share two
main arguments in their conception: a ‘pro-poor’ and ‘rapid impact’ nature. ‘Pro-poor’
approaches have been defined as those in which political actions stimulate economic
growth specifically benefiting the poor (Hotez et al., 2006). A pro-poor approach is one
in which policy-makers work conscientiously to address the needs and priorities of
vulnerable populations such as women, children, small farmers, and informal producers
16 (Molyneux & Nantulya, 2004). Concurrently, the idea of ‘rapid impact’ is defined as a
strategic approach to health systems designed to produce “rapid reductions in disabilities,
improvement in well-being, and, in some cases, interruption of disease transmission”
(Hotez et al., 2007, p. 1022), which in turn can represent gains in productivity, lifespan,
and mortality reduction.
Important critiques against this model have been raised by sectors concerned with
the multiple dimensions of neglect faced by populations exposed to these diseases beyond
the economic limitations alluded by the pro-poor and rapid-impact approaches.
According to WHO’s first report on NTD,
Neglect occurs at three main levels: at the community level, fear and stigma can sometimes lead sufferers and their families to conceal their condition. At the national level, these diseases are often hidden – out of sight, poorly documented, and silent, as those most affected have little political voice (…) Neglected diseases lack visibility at the international level as well. Tied as they are to specific geographical and environmental conditions, they are not perceived as direct threats to industrialized countries (Daumerie, & Kindhauser, 2003, p. 6). This first document published by WHO demanded researchers and policy makers
to shift their implementation paradigm from a disease centered perspective to one focused
on the needs of affected individuals and communities. However, arguments referring to
the intricate relationship between socio-economic conditions and health seem to fade in
the midst of disease oriented narratives reproducing biomedical analytical lenses.
The ‘pro-poor’ and ‘the rapid impact’ approaches correspond with the idea of
economism in health as the determinant logic for resource allocation in health recently
promoted by international health institutions (Sachs, 2005). This approach emphasizes
the economic impacts of disease occurrence by stating that when people are healthy
enough to work, they are boosters of growth instead of burdens for their households; in

17 the long run, individual health is fundamental to the generation of healthy economies
(Leon, 2015). The idea of economism in health emphasizes the market principle of
comparative advantage in allocation of resources for health. Since health is seen as
investment, policy makers are called to prioritize their decisions based on empirical
evidence collected to support decisions about which diseases can generate higher margins
of return (Organisation for Economic Co-operation and Development., 2009). The NTD
strategy embraces this logic and through the London Declaration signed in 2012, gives
definitive support to financial investment in research as the main priority of WHO
advocacy actions until 2020 (Tarleton, Gurtler, Urbina, Ramsey, & Viotti, 2014). Drugs
development, access to medication, and research on new forms of treatment, are at the
core of this agreement between pharmaceuticals, donors, operational partners, and
national NTD control programs.
Critics have pointed out that this strategic approach demonstrates that the NTD
campaign is more effective in rhetorical power than in potential material transformation.
It has been argued that even though working on infectious diseases as causes and
consequences of poverty is an undeniable priority, WHO and its partners have
exaggerated on the real impact of the integrated model for NTD control, especially in
terms of poverty alleviation (Allen & Parker, 2011). From this perspective, institutional
priorities as well as funding issues, force researches to magnify the real impact of the data
collected, and in many cases, disfigure the reality of research sites. Although the
important progress that drug development and effective distribution represent for this
group of diseases is acknowledged (Molyneux & Malecela, 2011), it has also been
recognized that NTD strategy is substantially limited in the goal of effectively addressing

18 the structural issues that determine the specific characteristics of poverty in developing
countries.
Poverty and NTD
Approaching a multi-causal phenomenon such as poverty requires consideration
of diverse and complex human experiences implied in its occurrence. Poverty transcends
income levels to include factors such as education levels, participation opportunities and
living environments in intersection with specific health risks (Adjei & Buor, 2012). The
term NTD has opened a spectrum of research in which the impact of geographical,
demographic, cultural, and social factors can be thoroughly explored by public health
practitioners to arrive to more effective strategies for disease prevention. Deficient water
supply systems and poor sanitary practices, for example, contribute to the spread of
helminth infectious in a different way that urbanization and soil degradation due to
aggressive agriculture contribute to the transmission of vector borne diseases (Gazzinelli,
Correa-Oliveira, Yang, Boatin, & Kloos, 2012). Factors such as land ownership,
geographical conditions that reduce productivity, limitations to satisfy nutrition demands
within the household, and exposure to high temperatures in countries of sub-Saharan
Africa, Asia, Latin America and the Caribbean are also associated with survival
economies that limit people’s capacity to expand their opportunities for living a healthy
life (Franco-Paredes & Santos-Preciado, 2011; Hotez & Aksoy, 2011).
Age, sex and ethnicity have also been studied in relation to NTD transmission
patterns, demonstrating that women and children are particularly vulnerable to experience
the worst consequences of disease in regions such as Sub-Saharan Africa (Armah et al.,
2015). Household composition, social status and, in some cases, educational attainment

19 limit populations’ ability to assess their own health, which in turn affects their capacity
to access preventive treatments delivered through vaccines or antiparasitic drugs (Barry,
2014). Even more problematic could be the fact that once they have fully developed,
infectious diseases can reduce people’s ability to work as a result of the disabilities they
produce, including blindness for onchocerciasis, body deformation and impaired function
for lymphatic filariasis (LF), stunting and cognitive underdevelopment for soil
transmitted helminthiasis (STH), anemia for hookworm disease, and cardiac conditions
for Chagas disease (Gazzinelli et al., 2012).
Due to their reliance on livestock and agricultural production, rural families are in
closer contact with environments that favor transmission of infectious diseases when
compared with their counterparts in the city (Mableson, Okello, Picozzi, & Welburn,
2014). Reductions in agricultural productivity could result from loss of manpower and
rights-based deprivation, mainly experienced by landless tenant farmers, migrant
peasants, and pastoral nomad. Armed conflict can radically increase exposure to NTD
since people can stay under risky environmental conditions while trying to escape, hide
or find survival conditions in spaces that serve as dwellings for vectors as well (Barry,
2014). Migrants are particularly vulnerable to this kind of exposure when they are forced
to leave their lands and bring their belongings with them, which can exacerbate
cohabitation with animals (Bennett et al., 2011). Migrants are more often exposed to the
unsanitary conditions and overcrowding typical of refugee camps and temporary
settlements, increasing their risk of contracting intestinal parasitoses and helminth
infections (Gazzinelli et al., 2012). Moreover, health achievements are threatened during
armed conflict, which in the case of NTD, can result in inability to access chemotherapy

20 and interruption of treatment. This situation is especially troublesome in contexts
where MDA is administered through community health workers that work on voluntary
bases due to lack of opportunities (Hotez & Aksoy, 2011).
Economic, cultural, and social practices intertwine to increase risk-prone —or so
perceived— behaviors leading to disease spreading. The case of shoe wearing in Uganda
illustrates this point (Ayode et al., 2013):
Shoes were thought to confer dignity as well as protection against injury and cold. However, many practical and social barriers prevented the desire to wear shoes from being translated into practice. Limited financial resources meant that people were neither able to purchase more than one pair of shoes to ensure their longevity nor afford shoes of the preferred quality. As a result of this limited access, shoes were typically preserved for special occasions and might not be provided for children until they reached a certain age. While some barriers (for example fit of shoe and fear of labeling through use of a certain type of shoe) may be applicable only to certain diseases, underlying structural level barriers related to poverty (for example price, quality, unsuitability for daily activities and low risk) are likely to be relevant to a range of NTD (p.1). Also at a cultural level, malformations derived from NTD are considered
important sources of stigma and discrimination affecting people’s ability to access
employment and education opportunities.
On top of the isolation and emotional distress derived from these practices, NTD
affected populations face the risk of receiving wrong medical treatment as a result of
health personnel’s lack of training on the specific aspects of these diseases (Gazzinelli et
al., 2012). Dubious quality of existing sources and absence of data create additional
difficulties for accurately estimating population at risk, prevalence, incidence, and
duration of infection, among other critical epidemiologic information necessary to
support decision-making in NTD control strategies (Hotez et al., 2014). This lack of
epidemiological data often coincides with under-diagnosis derived from health providers’

21 poor awareness about NTD’s transmission patterns and treatment, as well as
inaccessibility or unavailability of diagnostic tests (Hotez, 2014). Underreporting, poor
infrastructure for veterinarian and human services, as well as NTD unspecific and
sometimes silent symptomatology also collude to challenge conventional approaches to
disease prevention (Okello et al., 2015).
Particularly, the MDA strategy faces operational challenges associated with
communities’ voluntary involvement, as well as effective monitoring and evaluation
(Prichard et al., 2012). Structural limitations faced by populations living in contexts of
poverty are consistently neglected by researchers’ approach to the underlying social and
economic causes of poverty. Preference for ethnomedicine, people’s tendency to save
drugs for the future, and conspiracy theories about the ‘real’ goals of preventive
chemotherapy distributed through MDA campaigns (Prichard et al., 2012), are some of
the factors previously associated with limited effectiveness of MDA strategies. Critiques
of this approach point out to lack of consultation with afflicted communities leading to
increasing gaps between decision makers and populations at risk, which in turn maintains
or exacerbate social inequalities.
Noteworthy is a consistent reference to issues of implementation in NTD
literature, particularly focused on advocacy for research and development of treatment,
elimination, eradication, and control measures. The so-called ‘vaccine diplomacy’,
consisting in promoting political collaborations between countries for vaccine
development (Hotez, 2010), is a concrete example of how the NTD research agenda has
pushed political interests beyond the specific realm of health. However, policies focused
on social inequalities themselves have been claimed to be more definitive for effectively

22 addressing the needs of health sectors in developing nations than the current influx of
inter-sectorial collaborations and aid resources promoted through the NTD campaign
(Gazzinelli et al., 2012).
The spectrum of risks posed by poverty to the spread and occurrence of NTD
surpasses the specific health challenges produced by infectious diseases themselves.
Epidemiological, economic, technical and environmental arguments are included in this
configuration of risk, sometimes to demonstrate the relevance of NTD for scientific
communities, sometimes to support or complement WHO’s advocacy purposes.
Chagas Disease
The case of Chagas disease (CD) exemplifies the complexities and intertwined
levels of neglect previously described. CD is caused by a protozoan parasite called
Trypanosoma cruzi (T. cruzi) that can be found the hindgut of blood-sucking bugs known
as triatomines. The most common route of human transmission of CD occurs in poorly
constructed domiciliary environments where triatomines can remain hidden in cracks and
crevices during the day and become active at night to search for blood sources.
Triatomines usually feed on people’s blood when they are sleeping; in order to make
room for larger meals, they defecate while feeding and leave the parasite on their feces on
people’s skin. Inadvertently, people bring T. cruzi to their system by rubbing the
punctured wound where triatomines have been feeding from or through the mucus
membranes of mouth and eyes.
Once the parasite enters the human system, it can invade cells and multiply inside
them. In some cases, this first phase of invasion expresses as a swelling of the area of
entry, known as chagoma. After multiplication in the cells, T.cuzi acquires a rounded

23 form called trypomastigote, which can easily circulate through the blood system and
reach vital organs (CDC, 2016). Once organs are invaded, people can experience
symptoms such as fever, headache, edemas, and in some cases, enlargement of heart,
liver and spleen. This period is known as CD’s acute phase. People can also remain
asymptomatic for a very long time, until they develop the next phase of T. cruzi infection
known as chronic. At this stage people can experience arrhythmias, palpitations, chest
pain, and develop severe cardiopathies (Gascon, Vilasanjuan, & Lucas, 2014).
Development of megacolon and mefaesophagus are also possible at this latter stage of the
disease.
No vaccine has been developed for CD. Medicines such as nifurtimox (Bayer)
and benznidazole (Roche) have been used to treat symptoms in the acute phase, but both
drugs have shown side effects that become more serious as a patient’s age increases,
including renal and hepatic complications (Viotti et al., 2014). Even though CD exhibits a
highly inefficient transmission cycle, ongoing contact between humans and vectors over
time increases the possibilities of contracting the infection and developing the disease.
Therefore, WHO has recommended control programs to focus on interrupting the
transmission cycle between vectors and humans. Selective or communitywide indoor
fumigation with deltrametine accompanied by information and education programs
constitute the core of the control measures currently promoted by WHO to control
intradomiciliary transmission (Gilson et al., 2011; Grijalva, Villacis, Ocana-Mayorga,
Yumiseva, & Baus, 2011; Grijalva et al., 2015)
CD has been classified as a neglected tropical disease because it mainly affects
populations in rural regions or impoverished areas in urban settings in the Americas.

24 Different species of triatomines have been identified in Mexico, Central America, the
Andean region (Colombia, Ecuador, Venezuela, and Peru), the Southern Cone
(Argentina, Brazil, Bolivia, Chile, Paraguay, and Uruguay), and the south of the US
(Hotez et al., 2012). The biology of these different species creates specific conditions for
control programs. For example, the South Cone Initiative, recognized for being highly
effective in vector control, directed most of its efforts toward Triatoma infestans, a
species mainly restricted to human created environments (Dias, 2007). Since this species
can only be found in natural environments in some Bolivian regions, vector control
programs in Argentina, Brazil, Paraguay and Chile were highly successful at controlling
triatomines’ domiciliary infestation with sustained indoor fumigation, which lead to
significant decrease in CD transmission in the region (Schofield & Dias, 1999). That is
not the case of Central America where the main vector, Triatoma dimidiate, has been
found in association with palm trees and other sylvatic environments surrounding
traditional homes in countries such as Guatemala and Mexico (C. Barbu, Dumonteil, &
Gourbiere, 2009; Bustamante, Monroy, Rodas, Juarez, & Malone, 2007). Since effective
control methods focused on the palms have not been developed, international guidelines
recommend multiple spraying of the homes, which usually derives in reinfestation after
the residual effect of the insecticide, has receded (Grijalva et al., 2011).
Control efforts in areas where the vectors are endemic require different, and in
most cases, complex approaches to disease prevention at multiple levels. In these cases it
is necessary to understand a series of associations between vectors, reservoirs, hosts and
natural environment, in order to propose alternative approaches that can more effectively
and sustainably interrupt CD transmission cycle. That is the case in Ecuador, where

25 sixteen species of triatomines have been identified (Abad-Franch et al., 2001). Given
Ecuador’s geographical diversity, these different species show particular patterns of
association with natural environments in coastal and mountainous areas. Some of these
associations are determined by geographical characteristics that allow settlement of
particular species, such T. dimidiata, Rhodnius ecuadoriensis, and Panstrongylus howardi
in domestic and peridomestic areas of Manabi (Abad-Franch et al., 2001; Grijalva,
Suarez-Davalos, Villacis, Ocana-Mayorga, & Dangles, 2012), and Triatoma carrioni,
Panstrongylus chinai, and P. rufotuberculatus in the highlands, particularly Loja province
(Grijalva et al., 2015). Other associations are determined by factors such as proximity of
human dwellings to the natural environment. In Manabi, for example, researchers have
identified squirrels’ nests, rodents, opossums, and a particular species of palm acting as
hosts and reservoirs of P. howardi (Grijalva et al., 2011). The interactions of these
elements facilitate an ongoing circulation of vectors from peridomestic areas and to the
natural environment and vice versa, which increases the likelihood of contact with human
beings.
In addition to these ecological factors, control programs recommend to attend to
socio-economic conditions, productive activities and cultural practices that could
constitute risk factors for disease transmission. That is the case of Loja province where
triatomines presence has been associated with traditional elements of rural life such as
pigs and goats breeding, as well as lack of latrines and storage units (Grijalva et al.,
2015). Considerations about home structures are also relevant in this case since
triatomines presence inside domiciliary areas has been particularly found in structures
built with adobe walls, clay tiles, and dirt floors (Grijalva et al., 2012).
26 Additionally, CD faces challenges associated with lack of awareness in affected
populations and government authorities, limited funds assigned for research, low access
to diagnostic tools and treatment, but main and foremost, sustained marginalization
determining the conditions of life of populations at risk (Viotti et al., 2014). All these
characteristics are present in the Ecuadorian context, where the cycle of poverty and
disease is exacerbated by the limited capacity of the national control program. These
structural issues are very likely to remain unaddressed since control programs very rarely
take scientific knowledge into consideration when designing interventions at local,
provincial, and national levels. Some progress has been made, but political issues
affecting resource allocation have to be taken into consideration in order to achieve
sustainable CD control (Dumonteil et al., 2016).
Contributing to the problem of CD is its slow-onset, which makes difficult for
individuals to detect and treat the infection in its early stages. This condition added to the
disease’s disproportionate occurrence in segments of the population that have limited
access to healthcare, limits the possibility of detecting the disease in early stages. Thus,
efforts aimed at disease prevention are pivotal to address the endemic issue of CD in the
rural Americas (Ventura-Garcia et al., 2013).
CD’s epidemiology is alarming due not only to its high prevalence and extended
under-diagnosis, but also for the significant health and economic difficulties that it brings
to affected individuals and families. Statistics suggest that a third of individuals with the
disease will develop gastrointestinal and cardiovascular issues, including heart disease
(Bonney, 2014), which is one of the leading causes on unemployment worldwide.
Considering that health implications associated with CD are cause of disability (e.g.,

27 heart disease), it is not surprising that there are also important economic consequences
associated with this disease. Research estimates that the annual economic cost of CD is 7
billion dollars, surpassing the annual GDP of 192 individual countries –based on GDP
estimates of the United Nations (Lee, Bacon, Bottazzi, & Hotez, 2013).
Prevention programs aimed at sustainable control of CD require serious
consideration of CD transmission cycle, as well as the socio-economic factors associated
to its occurrence. In first place, attempts to contain the spread of the illness through
eradication of bugs have proven successful only in the short term; once the residual effect
of insecticide goes away, triatomines are likely to recolonize fumigated dwellings
(Grijalva, Palomeque-Rodriguez, Costales, Davila, & Arcos-Teran, 2005). Additionally,
the issue of CD is relatively unacknowledged both at large and small scales. Lack of
awareness could be theoretically tied to the aforementioned slow-onset of the illness,
decreasing the temporal connection between infection with the virus and its associated
negative consequences. Due to this weak temporal connection, it should not be a surprise
that CD takes a back seat for affected communities when compared to issues perceived as
more salient or urgent. Therefore, preventative strategies capable to address
epidemiological risks while engaging in sustainable, enduring and effective efforts to
understand the dynamics of the disease in contexts of poverty are needed.
Healthy Homes for Healthy Living
The Healthy Living Initiative (HLI) is a health promotion program designed to
address socio-economic dynamics leading to CD in southern Ecuador. This initiative
emerged from entomological data collected by the Infectious and Tropical Disease
Institute (ITDI) at Ohio University (ITDI) and the Center for Research on Health in Latin

28 America (CISEAL) showing that traditional control strategies at the household level
are effective only for short periods of time but not enough to interrupt transmission in the
long run (Grijalva, Palomeque-Rodriguez, Costales, Davila, & Arcos-Teran, 2005).
HLI’s main goal is to create a sustainable model for CD prevention adapted to the
specific conditions of transmission in Loja province. Three premises support HLI’s
actions: a) poverty is a complex phenomenon underlying the dynamics of transmission;
b) as a complex phenomenon, poverty expresses in multiple forms of exclusion
experienced by local individuals and communities, including inequalities in their access
to health and health-seeking behaviors; c) working closely with local populations in the
definition of a sustainable model for disease prevention can facilitate the design of a
general framework that addresses not only risk factors for CD transmission, but also
social priorities for local populations.
An initial needs assessment conducted in 2010, as well as subsequent
reassessments formulated in 2011 and 2012, suggested three action lines that have
constituted HLI’s general framework: infrastructure improvement, income generation,
and health promotion. The communities focused by HLI, Chaquizhca, Bellamaria, and
Guara, are located in Loja province, an area characterized by high elevation, poor roads
and limited transportation alternatives, all of them factors that increase the isolation and
marginalization faced by local populations in relation to other towns. This situation also
restricts their access to larger markets and, consequently, their economic participation
and competitiveness.
Construction of drinking water systems, formalization of income generation
initiatives, and support of collaborative efforts aimed at strengthening negotiating skills

29 among local leaders in these rural communities have also been part of HLI’s efforts
from its inception. They are considered fundamental for understanding existing dynamics
of collaboration, as well as for generating stable and trustworthy working relationships
between local population and external actors.
HLI’s main project is Healthy Homes for Healthy Living (HHHL), a strategy
focused on designing, building, and promoting living environments conceived to deter
triatomines presence in intra and peridomestic areas of the homes located in these
communities. The project has worked to rebuild four homes and improve two more since
2013, with an equal number of partnerships established with local families. Once this
phase is completed, HLI expects to extend the current HHHL model to as many homes as
possible in this area via full reconstruction or improvement.
Research Purpose
After five years of implementation at small scale, HHHL has accumulated an
important wealth of knowledge derived from direct experiences of implementation that
could be systematically elaborated to advance knowledge on CD control and prevention.
Consequently, this research aimed to explore the conditions under which home
improvement can lead to sustainable control of CD in southern Ecuador. Using HHHL as
reference, I conducted ethnographic grounded theory to understand factors and dynamics
within the home space that could lead to sustainability of control measures in a living
environment such as the ones proposed by this project. I looked at the role that dialogic
approaches to disease prevention can play in accomplishing this idea of sustainability
when working with marginalized populations such as the ones participating in HHHL.
Finally, I provided ideas about how this theoretical construction of sustainability can
30 inform implementation of the HHHL model at medium and large scales in Loja
province. Finally, this study aimed to generate knowledge on how to translate
populations’ experience of poverty and marginalization into population-centered models
of implementation for NTD programs.

31 Chapter 2: Theoretical Foundations
Living Environments and Health: A Health Systems Perspective
In 1909, Brazilian scientist Carlos Chagas described the transmission cycle of
Chagas disease as follows:
[triatomines] inhabit human domiciles, attacking human beings at night after lights are turned off and keeping themselves hidden during the day in walls’ cracks, houses’ roofs, in general, in any place where they can find shelter (…) more abundantly in poorly built constructions, mainly in huts with unfinished walls and grass coverage (p.1).
This description depicted a panorama of complex interactions between human
beings, insects, and living environments potentially leading to disease. It also illustrated
a scenario of systemic dynamics in which changes in one factor could affect the final
result of the entire interaction. Ever since, CD’s preventive interventions have been
focused on interrupting its transmission cycle by preventing home infestation through
different routes.
The measure most strongly recommended by WHO to prevent CD has been
insecticide spraying with delthametrine (Bayer), a highly effective substance that
basically eliminates triatomines presence for periods varying from three to six months
depending on specific environmental conditions (Grijalva et al., 2011). However, once
insecticides’ residual effect disappears, sylvatic triatomines rapidly re-colonize housing
units. In order to improve systematic control, delthametrine has been used in combination
with other preventive measures such as improved sanitation and provision of high quality
and durable plastering materials (Bustamante et al., 2009); amelioration of ventilation
and illumination openings (Rojas de Arias, Ferro, Ferreira, & Simancas, 1999); and
community surveillance (Abad-Franch, Vega, Rolon, Santos, & Rojas de Arias, 2011).

32 The most recent roadmap for NTDs control programs states that the objective
for CD in Latin America is to interrupt transmission via intradomiciliary vectors,
particularly in peri-domiciliary areas. The idea of controlling transmission patterns in
intra and peri-domestic areas immediately takes control measures from organizational
spaces where technical decisions are made, to the very private spaces constituted by
houses of individuals and families in marginalized communities of developing countries.
This approach demands attention to systemic interactions occurring at the
household at multiple levels. WHO has identified four interrelated dimensions of housing
with influence over the physical, social and mental health of occupiers (Braubach, 2011):
the physical structure; the psychosocial, economic and cultural construction of the home;
the neighborhood infrastructure; and the communities constituted around the
neighborhood. Specifically for vector control, inadequate housing has been defined as
houses that do not meet the minimum requirements of low-income families, do not
comply with building regulations, and are pre-disposed to pest infestation and
inhabitants’ illness (Schofield, Briceño-Leon, Kolsprut, Webb & White, 1990). Extreme
weather, household air pollution, and lack of clean water and sanitation are also likely to
attract diseases of vectorial origin in low-income settings (Haines et al., 2013).
Additionally, a recent study conducted by the Schools of Architecture, Design and
Conservation at The Royal Danish Academy of Fine Arts established that housing
designs interested in vectorial control in hot humid tropical areas might consider low
thermal mass, light walls, light roofs, cross ventilation, buildings raised above the
ground, long facades, light or reflective colors, ventilated roof cavities, and vegetation
characteristics in order to maximize their use as facilitators of temperature control. In

33 order to avoid major investments that could probably fail in meeting cultural and
scientific requirements, it has also been recommended to build prototypes and evaluate
their effectives by creating mixed systems combining criteria such as feasibility,
acceptability, performance, thermal comfort, and entomological rates (Knudsen & von
Seidlein, 2014).
However, home improvement directly impacts socio cultural dynamics beyond
the physical elements of the construction. Aspects such as time constraints, lifestyle,
culture, family composition, motivation, social class, reference groups, and perception of
wellness have been suggested to assess housing preferences in resource-limited
environments (Gibler & Nelson, 2003). Similarly, it has been identified that availability
of construction materials, populations’ income levels, relationships with local authorities,
access to alternative models of housing, possibilities of collaboration between designers
and local populations, access to training, and the role of the state to secure tenure of land
for marginalized communities, are crucial elements for planning interventions focused on
creating safer environments for vector control (Hardoy, Cairncross, & Satterthwaite,
1990).
Considering the high impact that safer structures can have on the overall
environment of the house, it is not rare to find associations between infrastructural
interventions such as wall plastering and ceiling elevations and the control of one or more
vector transmitted diseases (Lindsay et al., 2003; Lucero et al., 2013). It has been
documented, for example, that malaria was eradicated in the United States and
substantially reduced during the construction of the Panama Canal through specific
infrastructural measures, including installation of screens in doors and windows (Lindsay,

34 Emerson, & Charlwood, 2002). Similarly, a recent study conducted in Uganda
demonstrated that home design is likely to explain some of the heterogeneity of malaria
transmission even in highly endemic areas (Wanzirah et al., 2015), as well as high
temperatures outside the house have been associated with contracting sleeping sickness
inside homes in Zimbabwe (Vale, Chamisa, Mangwiro, & Torr, 2013)
In spite of these important linkages between living environments and health,
housing improvement is a measure highly contested from a health finances point of view
(Haines et al., 2013). In first place, home improvement is a control measure that involves
multiple factors, some of them directly related with diseases targeted by prevention
strategies, but most of them only partially linked to them. This makes even harder to
isolate factors in order to establish causal relationships between home improvement and
better health (Vale et al., 2013), which has lead health economists to argue that more
specific, cheaper, and faster solutions for disease prevention might exist (Knudsen & von
Seidlein, 2014).
This is, however, an argument contested by systemic perspectives applied to
health interventions: technological solutions —such as mass drug administration—
provide an easy fix that is not necessarily effective and might not be sustainable in the
long run. On the other hand, it has been demonstrated that even small changes in
infrastructure can increase the perceived value of the dwellings and motivate owners to
invest additional resources in maintaining and improving the home space (Lindsay et al.,
2002). Moreover, it has been stated that since homes constitute a particular space where
multiple decisions about disease prevention and control are made, good quality housing
should be considered a structural element of any health system (Lindsay et al., 2002).

35 Systemic perspectives have been considered in NTD prevention when
attempting to include not only the biomedical conditions experienced as a consequence of
infectious diseases, but also the different forms of exclusion that constitute the experience
of marginalization for neglected population. Integrative models such as ecosystems
approaches to health, Ecohealth (Briceno-Leon, 2009; Dumonteil et al., 2013) and One
Health (Webster, Gower, Knowles, Molyneux, & Fenton, 2016) have been applied with
varied results for disease control (Gurtler & Yadon, 2015).
Ecohealth (Forget & Lebel, 2001) has been proposed as a way to improve
people’s health, while strengthening communities and promoting environmental
sustainability. Six principles guide research conducted under eco-health perspectives:
systems thinking, transdisciplinary research, participation, sustainability, gender and
social equity, and knowledge to action (Charron, 2009). Eco-health researchers
acknowledge that the practice of systems thinking generates important challenges for the
actual implementation of control measures, particularly because they require balance
between methodological flexibility and rigor, which in turn generates challenges for
evaluating their effectiveness both in terms of disease control and costs. When applied to
Chagas disease, Ecohealth approaches have been developed in projects interested in
improving infrastructure with specific variations according to the implementation
context. For example, educational workshops, improved insecticide spraying for tiled
roofs and walls, participatory rodent control measures, waste management, productive
household activities and participant based reflective process have been used in Guatemala
(Bustamante, De Urioste-Stone, Juarez, & Pennington, 2014); low-cost housing
improvement techniques, promotion of house cleaning activities, removal of chickens and

36 dogs from human dwellings, and community participation have been combined in
Bolivia (Lardeux, Depickere, Aliaga, Chavez, & Zambrana, 2015); and installation of
window screens and education workshops addressing management and cleaning of
chicken coops has been implemented in Mexico (Waleckx et al., 2015). Although
important improvements in the general health of the population were achieved in all these
cases, additional resources are required to follow up and appraise the sustainability of
these efforts. Comprehensive approaches including community mobilization,
interdisciplinary collaborations, and multi-stakeholder strategies might be necessary to
achieve sustainable vector and disease control (Gurtler & Yadon, 2015).
Similarly, the One-Health approach highlights the need for interdisciplinary and
comprehensive approaches to health promotion when addressing intersections between
health, cohabitation with animals, and ecosystems (Webster et al., 2016). This approach
has made visible synergistic dynamics facilitating infectious disease occurrence in
contexts of poverty by highlighting interactions between living conditions and disease
(Webster et al., 2016). The One Health approach advocates for understanding the
knowledge and values of populations at risk of NTD beyond the operative restrictions
that conceptualizations about their role as beneficiaries might suggest (WHO, 2012). One
Health heavily relies on systems thinking to propose potential routes of action and
evaluating interventions’ effectiveness under premises of sustainability by recognizing
the dynamic nature of all the constitutive elements of human environments: sustainability
not only refers to time, it also refers to space and the finitude of resources. One Health
proposes an ecological interpretation of disease in which both current and future
variations and effects of infectious diseases, including evolutionary factors driving to
37 drug resistance, change of hosts, hybridization and unexpected changes of infectious
agents resultant from particular control measures, are considered (Webster et al., 2016).
Implementation Research
The health systems perspective proposes implementation research as a
fundamental piece for addressing NTD (WHO, 2012). Defined as a scientific endeavor
interested in understanding processes and resources required for disease prevention and
control in real-world settings, implementation research is focused in context-specific and
evidence-informed knowledge (Peters, Adam, Alonge, Agyepong, & Tran, 2013). Given
that NTD occur in contexts determined by complex social, economic and political factors,
implementation research explores interactions between disease and larger social
structures with actual and potential consequences for affected populations (WHO, 2012).
Implementation research has been informed by pragmatic thinking focused not only in
the identification of barriers for the execution of plans, but also on creative ways of
defining effectiveness under real —instead of probabilistic— circumstances (Gilson et
al., 2011).
Implementation research expands narrow perspectives suggested by top down
disease prevention strategies and proposes complex approaches to question traditional
ways of conceptualizing and designing health interventions’. In spite of important
limitations for integration of concepts and methods in interdisciplinary work, as well as
divergent interests driving the values and priorities of funding institutions and local
populations, implementation research has been identified as a key instrument for bridging
gaps and developing more equitable partnerships between stakeholders, researchers and
populations involved in scientific endeavors.
38 Implementation research intends to understand organizational, social, and
political processes constructed through communication and management practices that
could affect the effectiveness of specific interventions (Sheikh et al., 2011). A recent
study conducted by the Center for Mental Health Services Research and the Institute of
Medicine identified ten elements defining allocation of resources for implementation
research based on conceptual and methodological gaps of the field in the US (Proctor,
Powell, Baumann, Hamilton, & Santens, 2012). One of those gaps is theoretical
development. According to the authors, theory has been largely underutilized in
implementation research, which in turn has limited researchers’ ability to identify
contextual factors and suggest specific implementation strategies.
These findings coincide with theoretical perspectives that have already identified
the value of systems thinking in health promotion. However, as complexity of the
proposed solution increases, new challenges associated with its implementation also
emerge. The lack of theoretical references is particularly problematic when trying to scale
up control measures for vectorial transmission in NTD (Colley, 2014; Okorie, Bockarie,
Molyneux, & Kelly-Hope, 2014). Considering that scaling up processes specifically aim
to bring the benefits of pilot or experimental projects for which enough evidence of
positive results exist (WHO, 2012), they are usually challenged by their capacity to
determine the specific breadth and depth of the intervention in which the proposed
solution will work and maintain those results (Mangham & Hanson, 2010). Additionally,
high costs associated with the distribution of solutions, lack of interdisciplinary work and
intersectoral integration, as well as important failures in access to health systems, have
been identified as particularly limiting factors when trying to take systemic models to

39 large sectors of population in Latin America and the Caribbean (Ault & Nicholls,
2010) (Ault & Nicholls, 2010).
All these concerns are of critical importance as they determine future questions in
scientific research, as well as the use of financial resources for disease control. However,
in this case the question for sustainability entails particular relevance because it alludes to
the long-term aspiration of poverty alleviation as main goal of the NTD strategy.
Social Construction of Health
But, how are these system perspectives implemented? How do these theoretical
constructions translate into programs and actions directly affecting populations’ health?
As a concrete form of social interaction, health efforts do no happen in a vacuum. They
are the result of specific conditions that alter the practices and resources framing our
understanding of disease and health as social phenomena. Babrow and Mattson (2003)
argued that health efforts are constructed in a complex interweaving between bodily,
emotional, cognitive and social experiences that allow specific levels of interaction
around the concepts of disease and wellbeing. In this sense, health promotion
interventions should address one or some of these levels of interaction in order to
generate context specific agendas that better interpret individual, interpersonal,
community and political circumstances of the different stakeholders involved in a
particular effort.
As an illustration of this point, the definition of household changes across cultures
by emphasizing specific elements of the system such as kinship, composition, activities,
structures, locations, and trajectories of change that define members’ belonging to a
concrete space (Sajeck, 1996). For example, for the Japanese culture a household is
40 defined by the concept of shotai, referred to individuals sharing a common budget,
while in the Hindu culture home is organized around the idea of zadruga, numerically
prominent social groups conformed by multiple households sharing a common kitchen.
However, Sajeck explains, a general agreement in the anthropological field is to consider
three characteristics to define membership to a household: sleeping, eating, or making
economic contributions. These three characteristics exemplify deeply entangled
behavioral, socio-economic and health related dynamics influencing decision making
within this social structure that can also be relevant when analyzing health issues.
The origins of health communication are located in post-positivistic perspectives
that looked at communication as a tool to facilitate the delivery of health products and
services. The underlying assumption in this perspective was that the evaluation of good
or ill health had to rely on assessments conducted under the lens of specialized/scientific
knowledge. Whether biological, psychological, or medical, scientific expertise concerned
with body functioning, and specifically with disease occurrence, was privileged. Under
this perspective, communication played a “support role” in unidirectional processes
mainly interested in spreading technical information about health. Media theories popular
in the 50’s and 60’s supported this perspective under the assumption that health issues
could be prevented if people were effectively informed and educated about the risks they
faced. Concurrently, psychological theories provided explanations about cognitive
functions underlying individual mental processes that informed the design of persuasive
campaigns and messages for behavior change.
The field of communication expanded in subsequent years through the
development of socio-cultural perspectives that questioned traditional transmission

41 models and proposed communication as the constitutive material of social life. With
this turn, health communicators were faced with profound questions about the factors that
influence and define individual and social conceptualizations of health. Processes and
actions carried out on daily basis to fulfill our expectations of wellbeing and deal with the
implications of illness are broad and complex, deeply entrenched in physical, political,
economic, social and cultural structures. Obtaining information, applying preventive
practices, measuring risk, looking for treatment, dealing with disease, and assuming
death, are all processes that reveal the conceptualization of health hold by individuals and
social groups, but more importantly, give meaning to human experiences in relation to
life beyond the individual body.
In this sense, the meaning of health, as any social issue, is determined by who
participates in its definition, under what role, and through which languages. As sustained
by Deetz (1996a), meaning is constructed based on epistemological orientations derived
from individuals’ relationships with larger structures. Our knowledge of the world is
produced, not simply transmitted, during that relationship. Since personal orientations are
determinant in that process, it is of the highest value to understand that multiple
interpretations can derive from the same event and that all of them can be equally valid
from specific points of view. Craig (1999) supported this thesis with the Constitutive
Model of Communication (CMC). The CMC states that construction of meaning is the
result of endless reflexive processes informed and maintained by everyday practice.
Consequently, communication is the fundamental human mode of explaining and being
in the world. Because of its symbolic character, communication lies at the core of our
definition of physical states in relation to spiritual, emotional, and ethical systems. As a

42 metalanguage, communication processes and resources allow us to name the world
considering embodied experiences, social relationships, and ideological expectations, and
in doing so, we are able to provide our existence with symbolic character.
Symbolic interactionism (Mead, 1934) explains meaning construction as a
fundamental element of human nature by emphasizing that people assign meanings to
their experiences and act in relation to those meanings. Consequently, meanings are not
fixed and are, instead, constantly constructed and reconstructed in social interaction.
Human beings cannot avoid the ongoing practice of meaning-making because it defines
our being in the world (Pearce, 1989); by connecting regular micro-practices with larger
ontological and epistemological structures, individuals are able to build their
interpretations of reality based on the constitutive patterns of their existence.
In this sense, health communication professionals are faced with challenges
derived from the interplay between practices at micro and macro levels fundamental in
the creation and recreation of human experience in relation to health. The simple act of
defining a health problem relies on ideological foundations and rhetorical constructions
that orient us to do so. What kind of discourses inform our definitions of good or ill
health, which factors should be considered to evaluate our susceptibility toward particular
risks, and what types of knowledge should be considered valid when making decisions
regarding healthcare, are expressions of how particular social orders are enacted,
transformed, and sustained through communication resources and practices.
In the reconstruction of reality, some level of coordination between the object as
constructed and the object as perceived is required. That coordination, however, is a
fundamentally challenging process: actions often do not derive in the results initially

43 expected for them, and even if executed as planned, can have counterproductive effects
(Pearce, 1989). As extensively studied in the field of health communication, unintended
consequences result from the fact that health promotion actions come into being in realms
of human experience that do not necessarily coincide with the ones that initially conceive
them (Cho & Salmon, 2007).
The NTD strategy, in particular has been criticized for adopting the idea of
‘bringing health’ to populations in need as its flagship project without consideration of
gender norms, social class, historical relations, language, and organizational systems that
more significantly determine the adoption or rejection of healthcare practices for specific
cultures (Manderson, Aagaard-Hansen, Allotey, Gyapong, & Sommerfeld, 2009). This
criticism coincides with positions put forward by communications specialists aligned
with the field of participatory communication that have pointed out the limited capacity
of information-education-communication (IEC) strategies to promote sustainable
behavior change and agency among marginalized populations (Airhihenbuwa &
Obregon, 2000; Obregon & Waisbord, 2010; Wakefield, Loken, & Hornik, 2010).
The study of culture in health promotion provides important arguments to
understand the contextual nature of communication in health (Airhihenbuwa, Ford, &
Iwelunmor, 2014; Dutta & Basu, 2008). Cultures are dynamic systems that create and re-
create themselves in the enactment of the relationship with the other. This recreation
limits and opens spaces to reformulate alternative ways of structuring health interventions
that could more effectively attend the situation of exclusion faced by populations at risk
of NTD. Health promotions strategies focused on reducing health disparities are called to

44 attend social exclusion not merely as technical concern, but also as lived experience for
neglected populations (Tacket, 2009).
From Persuading Individuals to Dialogic Health Promotion
The need for systematic approaches to disease prevention has been supported by
policy documents and resolutions published by multilateral agencies, as well as academic
actors involved in health research. While describing socio-economic dynamics leading to
disease occurrence, these policy documents also state the need to generate conditions for
participation of multiple actors, particularly affected populations, in health promotion
strategies. The Alma Ata Declaration, for example, claims that people have the right to
participate in planning and implementing strategies to promote their health care.
Subsequently, the Ottawa Charter stated that communities should be involved at all
stages of the health promotion planning processes: from setting priorities, to making
decisions about planning and implementation strategies. More recently, the “One World,
One Health” Declaration gave a step further to establish invite collaboration between
governments, local people, and the private and public (i.e. non-profit) sectors to address
global health challenges and promote biodiversity conservation. Although these
declarations recognize the interdependence of environmental, political and social factors
in the preservation of human health, as well as the need to create conditions to facilitate
individual and community involvement in decisions that directly affect their lives, they
do not suggest ways in which populations’ perspectives should affect programs’ priorities
and definition of future directions. Although significant as general frameworks, they do
not approach structural issues of power and culture that significantly limit programs’
capacity for social transformation.

45 Anthropological work conducted around the ideas of ethnomedicine and
medical pluralism have demonstrated that the biomedical model is rooted in Western
ideologies —such as individualism and empiricism— that fundamentally contradict the
realities of multiple social groups around the world. In very diverse contexts, social
groups have conducted what they consider a healthy life within the parameters of their
culture, even in the presence of disease and in absence of technical solutions for health
maintenance (Airhihenbuwa et al., 2014). A consequence of this imposition of Western
values in the design and implementation of health promotion programs has been a
conceptualization of culture as an aggregate of faulty individual behaviors, instead as a
system functioning under its own logics (Escobar, 1995). Socio-cultural perspectives that
questioned the traditional interest of communication models’ for diffusion of information
regardless of contextual factors, have pushed for a reformulation of the health
communication field towards more complex perspectives in which physical, political,
economic, social, and cultural structures could be more effectively considered and
addressed.
Dialogic approaches emerge in this context as a concrete communication stance
interested in questioning power relations traditionally existing in research contexts.
Arthur Frank (2005) describes dialogical research as an encounter in which both the
researcher and participants are subjects of change as a result of an unfolding relationship
that takes place in a unique time and space. In attempting to sustain the dialogical nature
of the encounter, researchers make conscious choices to overcome categorical definitions
assigned by the technicalities of scholarly work to research participants in order to
capture the multiple voices interacting between him/her and research participants. In

46 Frank’s words, “research is, in the simplest terms, one person’s representation of
another” (p. 966). Therefore, researchers assume a responsibility when exploring and
representing the complexities of life as experienced by research participants. Responsible
representation is understood as an ethical imperative to produce more accurate
knowledge about the issues at hand. Instead of assuming the position of a detached
external observer, the dialogical researcher fully recognizes his/her involvement in the
accomplishment of a particular site of knowledge articulated through research, and
commits him/herself to the generation of new dialogues and new learning.
Concurrently, dialogic social change ( Greiner, 2010) takes the ideas of dialogical
research to reclaim the communicative character of interventions’ design and propose
invitational rhetoric as a generative element of social transformation. Greiner (2010)
asserts that dialogic interventions are designed to invite rather than require action,
making possible for interlocutors in dialogue to meaningfully participate in processes of
change. From this perspective, facilitating agency and informed decision making should
be pursued as goals of any social change intervention, regardless of the specific social
issue intended to approach. However, when specifically applied to health, dialogic social
change sustains that communication could be misleading and ineffective when focused
on decontextualized persuasion. Greiner (2010) expands on this idea by sustaining that
individuals “cannot be developed, modernized, nor empowered” (p. 6); therefore,
interventions can render very different results if organized as perspectives being offered
to a community of autonomous individuals with valid criteria for decision-making, rather
than as a set of predefined messages strategically articulated to persuade masses of
people. Porous interventions are more suited to offer the options through structures that

47 require more pulling than pushing, being pushing the classic format of mediated
information campaigns and pulling the voluntary engagement of information seekers. In
Greiner’s words “Intervention designers with a dialogic orientation know that if their
intervention is well designed, interesting and accessible, they do not have to push their
ideas on others, the others will come to them” (p. 12).
Dialogic social change does not vilify persuasion as a rhetorical exercise; neither
does it dismiss its relevance at specific moments in health promotion efforts. What this
perspective actually proposes is that social change is an endeavor that requires profound
understanding of communication as a structuring social process beyond its rhetorical
capacity. Consequently, a common element on dialogic approaches is acknowledging that
behavior change is not the only outcome to be expected from health promotion
interventions, and even when possible, it is not necessarily positive. The specific and
complex contexts in which health decisions are made forces a deeper analysis of a wider
range of explanations for people’s behavior that more effectively could lead to
sustainable good health, as well as multiple routes of action in which behavior change or
maintenance are equally sound alternatives.
Historically, communities and individuals have been subject of characterizations
about their patterns of actions that do not necessarily consider their own understanding of
wellbeing, which can also be seen as another form of social exclusion. Social exclusion is
generally articulated through languages that marginalize, silence, reject, isolate,
segregate, and disenfranchise populations by reinforcing unequal relations (Taket, 2009),
a dynamic particularly true for the field of biomedical research, in which credentials and
formal expertise have been historically privileged over the lived experience and suffering

48 of patients and communities at risk (Kleinman, 2013). Dialogic social change proposes
that interventions communicate from the very first moment in which they are conceived
because that conception reflects ideologies underlying personal theories about the world
functioning, as well as positionalities assumed by program designers in relation to the
other.
HHHL has implemented dialogic approaches to research in an attempt to combine
scientific research and local knowledge to build living environments designed to deter
CD (Nieto-Sanchez, Baus, Guerrero, & Grijalva, 2015). By combining narrative and
assets-based research methods and traditional biomedical research, the initiative has
intended to reduce dynamics of marginalization by facilitating local communities’
empowerment as active agents in the design of solutions for their own health. Even
though it was not initially formulated under this premise, HHHL’s methodological
flexibility has allowed the initiative to grow in understanding the complexity entailed in
social phenomena such as poverty, and the enormous power of dialogue for reframing
knowledge about the impact of poverty over neglected diseases. In this sense, the
potential contribution of HHHL as an experience of dialogic social change relies not only
in their capacity to expand knowledge on NTD occurrence, but even more importantly, to
enhance the effectiveness of control strategies to improve the life of affected populations.
This research intends to understand the actual contributions of dialogical approaches to
NTD interventions’ design and health promotion efforts, as well as the viability of
applying this approach to medium and large-scale interventions.
49 Chapter 3: Methods Section
This research was formulated with the purpose of advancing knowledge on the
possibilities and limitations of implementing Healthy Homes for Healthy Living (HHHL)
as a large scale health promotion strategy for sustainable prevention of Chagas Disease
(CD) in Southern Ecuador. HHHL uses an interdisciplinary approach that includes homes
improvement, health promotion, and associativity as key elements to reduce social
exclusion affecting populations at risk of neglected tropical diseases (NTD). In doing so,
I looked at practices, rhetorical constructions, and relational dynamics (Ager, 2011) that
could support or undermine HHHL’s sustainability model in order to inform
implementation of the project at medium and large scales.
Methodological Approach and Research Questions
HHHL asserts that homes’ structural improvement, long-term health promotion at
the micro-level of the household, and community involvement in locally driven income
generation opportunities, are the basic action lines of a strategy that could potentially lead
to sustainable CD prevention. Actions in these three areas are articulated through
abductive analysis (Tavory & Timmermans, 2014) formulating that HHHL could inform
the design of interventions focused on prevention of CD, NTD, and other diseases that
are structurally connected with poverty. Even more importantly, HHHL designers state
that CD can be controlled in Loja province, and by extension, in areas where triatomines
are endemic and show sylvatic dynamics, using systemic rather than disease-centered
approaches to health promotion.
Consequently, this research aimed to address the following research questions:

50 RQ1: What factors contribute to or limit sustainable control of Chagas disease in the
communities of Chaquizhca, Bellamaria and Guara under the model proposed by Healthy
Homes for Healthy Living?
RQ2: In what ways, if so, can these factors (contributions and limitations) be addressed
in order to scale up the model to other homes in the aforementioned communities?
Research Design: Ethnographic Grounded Theory
Grounded theory.
Grounded theory (GT) is usually defined as a systematic approach to data
collection and analysis interested in generating explanations of social reality based on
emerging information grounded in actual data rather than in theory (Charmaz, 2014;
Glaser & Strauss, 1967; Strauss & Corbin, 1998). GT was initially proposed by Glaser
and Strauss (1967) while arguing that qualitative research has its own logics and capacity
to generate theories. By proposing the constant comparative method (CCM), Glasser and
Strauss developed a systematic approach to qualitative data analysis based on observation
of relationships between codes and categories that could be consistently used to develop
empirical explanations of social phenomena, as well as to assess analytical rigor in
qualitative research. CCM requires ongoing comparison of codes emerged from the data
and memo writing as basic activities leading to what they call developmental theories,
“theories of process, sequence, and change pertaining to organizations, positions, and
social interaction” (p. 114). In spite of later critiques, Glaser and Strauss are
acknowledged for moving forward scientific discussions about the reach and impact of
qualitative data with scientific purposes. Most importantly, both authors pioneered the
idea of developing middle range theories out of systematically analyzed data, and by

51 doing so, they opened the space to question generalization as only criterion to assess
the validity of emerging explanations about social phenomena (Charmaz, 2014).
Subsequent variations of GT departed from this initial formulation by
emphasizing the constructed nature of the relations observed in the data, as well as the
role of researchers and participants in the definition of meanings that could potentially
lead to theory development. Corbin and Strauss (2008), for example, emphasized the role
of the analyst in maintaining methodological rigor and making decisions about what is
relevant in a particular data set. In order to arrive to a theory, Corbin and Strauss
recommended making comparisons not only of incidents, but also of properties,
dimensions, and potential explanations (theories), as well as interrogating the data with
sensitizing, theoretical, practical and guiding questions that allow ongoing reflection
along the analytical process.
Constructivist approaches to grounded theory see both data and analysis as the
product of experiences co-created by participants, researchers, and emerging data
(Atkinson, Delamont, & Housley, 2008). Since constructivism is focused on how and
why participants construct meanings in specific situations (Deetz, 1996b; Pearce, 1989),
its extension to grounded theory looks at how, when, and to what extent the studied
experience is embedded in larger social structures in order to explain and represent
research findings (Charmaz, 2006). Constructivist Grounded Theory (CGT) claims the
main tenants of sociology as proposed by authors affiliated to the Chicago School,
particularly those alluding to the open-ended nature of social processes, the value of
human agency in meaning making, and the fundamental role played by language,
interpretation, action and temporality in research (Charmaz, 2014). Consequently,

52 ongoing reflections about data, linkages in coding structures, and researchers’
positionality, constitute basic inputs in theoretical elaborations emerged from this
perspective. Similarly, simultaneous analysis and data collection; emphasis on actions
and processes rather than dimensions and themes; use of comparative methods;
development of inductive analytic categories through systematic thinking; reliance on
theoretical sampling; and decisive interest in theory construction, are considered
minimum requirements for a grounded theory study to be considered constructivist in
nature (Charmaz, 2014).
It is the process of developing theory, not theoretical construction itself, that
concerns grounded theory. Middle range theories such as the ones proposed by GT value
the systematic effort for explanation considering the interpretive nature of the analytical
processes conducted by individuals (Suddaby, 2006). Theories developed through GT are
not intended at hypothesis testing but at generating alternative explanations to
phenomena by “accounting for what people do in specific situations and linking it to how
they do to it as contingent relationships” (Charmaz, 2014, p. 228). Different from grand
theories’ interest on explanation, middle range theories emphasize understanding of
phenomena and ongoing construction of meaning in social groups.
When coupled with ethnographic methods of data collection, GT receives the
name of ethnographic grounded theory. This method is particularly useful to
contextualize conclusions emerged from sustained involvement with the processes under
study. As such, social action is studied in its own dynamics across multiple sites and
actors. Ethnographic grounded theory is focused on the studied phenomenon or process
rather than in the richness of the context traditionally expected of ethnographic studies

53 (Charmaz, 2014). This means that research issues belonging to the realm of
ethnographic research (such as access to the context intended to study, involvement with
participants over time, direct observation, and ongoing search for diversity within the
data), get translated into the analytical requirements of grounded theory development
(Ager, 2011). Later on, this diversity of inputs facilitate constant comparison of data and
categories during the entire process of collection and analysis, as well as the development
of theory as a result of the emerging relationships between codes and categories
(Charmaz, 2014). While keeping the process open to emerging data, grounded theory
provides tools for systematic analysis and interpretation using ethnographic approaches.
Sustainability as sensitizing concept.
Sensitizing concepts can be defined as interpretive devices used to guide
researchers’ thinking in qualitative inquiry (Tracy, 2013). In GT, these concepts provide
initial ideas about issues to explore throughout the variety of methods included in a
particular researchavor. Rather than limiting factors defining the scope of inquiry and
analysis, sensitizing concepts should be treated as “points of departure for studying the
empirical world while retaining the openness for exploring it” (Charmaz, 2014, p. 30).
Considering HHHL’s interest in sustainability, I will use it as sensitizing concept.
Multiple definitions have been used in health literature to address issues of
sustainability. Some definitions emphasize elements of ownership and appropriation. The
Ecohealth approach, for example, suggests that sustainable initiatives are those capable of
effectively addressing local priorities, switching external perceptions and motivating
wider economic, political, or even environmental changes, while facilitating their
adoption (Charron, 2012). More popular are definitions that talk about sustainability as a

54 time-bounded concept. Terms such as ‘maintained’, ‘continued’, ‘durable’, ‘integrated’
or ‘institutionalized’ are popular in this perspective (Peters, Adam, Alonge, Agyepong, &
Tran, 2013). The health systems approach, for example, proposes that sustainability is
achieved when short, medium and long-term needs of health systems —and the people
they serve— are met in a balanced way (Adam & de Savigny, 2012). Finally, systems’
thinking reframes sustainability as a physical constant and a fundamental element of
resilient systems. From this perspective, a system is sustainable because it can respond to
the movements, changes, and behaviors of its constitutive elements and environment
(Bosschaert, 2012). These four elements (ownership, use of resources, temporality, and
systemic responsiveness) will be used for data collection and observed in the analysis
phase of this research (Hearld, Bleser, Alexander, & Wolf, 2016; Iwelunmor et al., 2016).
I am also interested in identifying ‘power or capacity claims’ for sustainability
(Cartwright, 2011). Cartwright asserts that notions of effectiveness in public health can
be positively impacted by the development of new theoretical perspectives departing
from the widely established notion of evidence under ‘ideal and perfect’ circumstances.
This perspective sustains that social scientists can significantly contribute to scientific
thinking by proposing arguments that can express capacity or potential beyond the
philosophy promoted through randomized control trials. Consequently,
For policy and practice we do not need to know “it works somewhere”. We need evidence for “it-will-work-for-us” claims: the treatment will produce the desired outcome in our situation as implemented there (…) Knowledge like this involves a third kind of causal claim, a power or capacity claim: the treatment reliably promotes the outcome, or reliably contributes across a given range of circumstances (Cartwright, 2011, p. 1401)
55 Similarly, characterizing the spectrum of intended and unintended
consequences derived from NTD control programs could be an important step towards
furthering notions of sustainability structurally connected with the idea of complexity
promoted by systems thinking. The unintended consequences of purposive social action
should not be considered necessarily negative, since their nature as unintended is not
axiological but overly humane in nature (Merton, 1936). Even under extreme
circumstances of rationality, human actions are co-constructed; therefore, they will
always bring unexpected results. Merton sustains that unintended consequences are often
ignored in organized action, as it usually demands an explicit set of goals to be achieved
in order to advance in the purpose of organization itself. However, Merton asserts, there
are important lessons to be learned when attention is posed not only on planned action,
but also on the unplanned actions occurring in wider interactions surrounding the
intervention or treatment. First of all, unplanned effects can inform new routes of action
derived not from the usual result of a known action, but from its unusual response. It can
also define errors in a particular context and generate arguments to question the
immediacy of results as preferred observation parameter in processes of social change.
The relevance of this element lies in the fact that “Public predictions of future social
developments are frequently not sustained precisely because the prediction has become a
new element in the concrete situation, thus tending to change the initial course of
development” (Merton, 1936, p. 904). This idea is relevant for the field of global health,
full of examples of interventions with often harmful unintended consequences (Guttman,
2000; Roberto, Murray-Johnson, & Witte, 2011). However, this continuous occurrence

56 also validates the needs to keep theorizing about pragmatic alternatives that allow
revaluation of existing theoretical models.
Study population.
I conducted purposive sampling for this research. Participants were selected from
inhabitants of the communities of Bellamaria, Chaquizhca, and Guara in southern
Ecuador that have directly or indirectly experienced interventions led by HHHL. The
study population was divided into three groups:
The first group included partner families, ergo, six families that have specifically
agreed to partner with HHHL to build or improve their homes by implementing anti-
triatomine measures. The term partner family refers to a specific conceptualization
developed by HHHL as an alternative to the term beneficiary traditionally used in
development interventions. HHHL adapted the idea of partnership that could be
explained as a means of addressing local needs through collaborative activities and
decision-making sensitive to local concerns and interests (Seddon, Billett, & Clemans,
2004). Interviews and participant observation during health promotion activities were
conducted. Family members older than 14 years old were included. In this case, minors'
assent and parents' informed consent was required.
Considering the principle of maximum variation (Lindlof & Taylor, 2011; Tracy,
2013) , the second group included an equal number of families (6) that have not
implemented an HHHL intervention. They were selected to closely match the decay
category of the homes and socio-economic conditions of HHHL partners. The purpose of
this part of the study was to observe the same criteria previously mentioned in families
that have not applied the HHHL model. Following the same methodology applied for the

57 partner families, members of these families were interviewed at different points in time
to address the questions included in the interview guide. Interviews lasted no more than
one hour and were conducted in participants' homes.
The third group included members of the communities at large. Current records
facilitated by HHHL register the existence of 35 homes in Bellamaria, 42 in Chaquizhca,
and 32 in Guara. Heads of household of all the homes in the communities were
approached to answer questions about the physical structure of their home, as well as the
socio-economic status of their family. These families were approached in their homes and
asked informed consent in case of being interested in taking part of this research. This
group also included community members that have worked directly in any HHHL
construction projects.
These populations guided the initial sampling, but as proposed by grounded
theory, sampling was not complete until reaching theoretical saturation. Theoretical
saturation occurs “when gathering fresh data no longer sparks new theoretical insights”
(Charmaz, 2014, p. 213), consequently, it was reached when the main theoretical
constructs were sufficiently rich and no more data was required.
Finally, considering the different characteristics of the families in this area, the
concept of household was defined based on verbal identification of a particular nucleoid
as ‘home’ and permanent inhabitation of a common house.
Data collection.
This research was conducted in three phases: Phases 1 and 2 were mainly focused
on issues included in RQ1, whereas Phase 3 addressed issues included in RQ2.

58 Phase 1: Construction of ethnographic cases.
Using an ethnographic perspective, I approached families that have partnered with
HHHL since 2011. As mentioned before, the concept of partnership has been defined by
HHHL as the result of multiple dialogic interactions leading to time bounded
commitment between the families and the project to adopt and implement the HHHL
model. In depth interviews, participant observation, documents review and informal
conversations were conducted to develop this ethnographic phase of the study.
a. In-depth interviews: In-depth interviews (Kvale & Brinkmann, 2009) were conducted
with partner families. In this case, I interviewed three members of the partner families
currently inhabiting the home. Interview guides were constructed to capture the factors
leading to decision-making within the family before, during, and after the intervention.
These interviews were conducted to explore appropriation of the space by different
family members, as well as the construction of the household as a physical and symbolic
microsystem. Themes explored in the interview guides at this stage included: Uses of the
space; human interactions with the natural environment; home-health relationship;
perceived value of the home; health seeking behaviors occurring within the home space;
income generation and micro-planning; perceived socio-economic development; pros and
cons of the construction; familial interactions conducted within the home space; and
future plans for the family and the home (see Appendix A).
In addition, I considered WHO’s specific recommendations for integrated control
of NTD transmitted by vectors (Holveck et al., 2007). For Latin America, the Pan
American Health Organization (PAHO) has turned WHO’s general guidelines into a
package of actions aimed at simultaneously addressing the circumstances of transmission
59 of the twelve NTD present in the region (dengue, rabis, buruli ulcer, leprosy, and CD,
among others). These actions include: Vector control; provision of water and sanitation;
management of zoonotic elements of the disease; community participation social capital;
and multisectoral integration. Interview guides were modified as new themes emerged
and new participants were identified.
b. Participant observation: The HHHL model proposes specific health promotion actions
designed to connect the ideas of home and health. These actions include post-
construction visits, follow up to a check-list of healthy practices recommended to avoid
insects presence in local homes, and regular meetings to address potential doubts in
relation to uses of the space. These actions occur in a process that combines families’
adaptation to the new house with practices traditionally conducted in the home space
before the intervention. In order to observe how this interaction evolves over time, I
conducted participant observation (Tracy, 2013) while accompanying health promotion
activities led by the HHHL local facilitator. I took part of this process by assisting the
facilitator in completing the check list designed by HHHL. This checklist was completed
while walking around the house with one of the heads of household to observe uses of
doors and windows, spaces used for storage, use of roofs and ceilings; location of
chicken, guinea pigs, dogs, and pigs, sanitary facilities, and debris and other materials
exposed in peridomestic areas.
I joined the team in their visits during three different periods: one from mid-June
to July 2016, other in January 2017, and the last one from May to June 2017. These
periods were chosen considering the different uses of the space registered during the dry
and rainy season of the year. Similarly, this participant observation complemented the

60 responses obtained through previous interviews in aspects such as uses of the space,
interactions between individuals and the natural environment, health related practices
conducted within the home space, perceived value of the home, maintenance and
cleaning practices, income generation practices carried out at the home level, perceived
economic development, and family dynamics enacted within the home space. Aspects
such as distance from the road, particular smells, and additions or modifications of the
construction were also considered for observation.
c. Documents review: Annual reports produced by HHHL were reviewed in order to
develop a wider understanding of the implementation process during the different phases
of the project. These documents were used as secondary sources to guide the
development of interview schedules (Lindlof & Taylor, 2011), but most importantly,
contributed to the immersion required to develop the ethnographic perspective proposed
in this study. Reviewed documents included research reports submitted in 2013, 2014,
2015 and 2016, as well as weekly reports produced by HLI’s field coordinator between
2013 and 2016.
Phase 2: Validation.
a. Socio-economic surveys for communities at large: I conducted domiciliary visits to
each of the homes currently registered in HHHL records (35 in Bellamaria, 42 in
Chaquizhca, and 32 Guara), in order to apply a socio-economic survey designed to a)
compare the current status of the local families with previous records in order to identify
major changes in the general socio-economic conditions of the communities, and b)
identify factors that influence decision-making in relation to housing and health. Heads of
household of the communities at largewere approached to answer questions about the

61 physical conditions of their home, as well as the socio-economic status of the family.
This questionnaire was administered in individual household visits, separately form the
interviews previously mentioned. Each one of the questions was read to the participants
and their answers registered by the interviewer in paper printed questionnaires. The
questionnaire explored key areas identified in previous HHHL implementation
experiences, including family composition, education level, legal tenure of the land, uses
of the space, income level, productive activities, and access to the road, basic services,
and credit. This questionnaire also explored external sources of financial support, health
status of family, potential sources of income, and concrete interest in home improvement.
Additionally, pictures of the walls, floors, and roofs of the homes were taken in order to
establish the decay status of the construction. These pictures exclusively focused the
external areas of the home and never included its inhabitants. Photographical data was
optional and did not compromise families' participation in this study. I was also interested
in identifying the most salient arguments used by local families to assess the actions
conducted and promoted by HHHL (see Appendix B).
b. Community consultation: Once the aforementioned phases of data collection with
partner families and community at large were completed, an updated new version of the
HHHL model was produced (Chapter 6, white paper). This new version considered
emerging theorizations about sustainability formulated during the initial phases of
analysis the data.
Field notes were collected in all the phases of this research. They were taken as
descriptive memos right after leaving the homes where interviews, surveys, and

62 participant observation were conducted. Later on these notes were turned into extended
analytical memos that were also part of the analysis.
Data analysis.
The development of grounded theory in the context of implementation research is
even more influenced by pragmatic thinking than other applications of this perspective.
The interplay between theory, observation and methodology suggested by abductive
thinking is applied in this case as a way of bringing larger structures of knowledge into
the data collected with the purpose of substantiating theorization emerged from repeated
or accumulated observations (Tavory, 2016). Therefore, analytical processes conducted
within this research were not intended at generating new theories of sustainability but to
extend our understanding of this concept by adding contextualized data emerged from
HHHL implementation.
In order to arrive to that point of theorization about sustainability, I followed the
main tenants of Constructivist Grounded Theory (CGT). This means that I was interested
in interacting with the data collected along this research as ongoing co-constructions
emerged from the specific positionalities of participants and researcher. In order to
maintain the abductive nature of this analysis I was also interested in sustaining iterative
strategies that allow me to interact with emerging data and codes using different forms of
comparative methods.
Observations, interviews, implementation reports, field notes, as well as emerging
materials used in participatory exercises were analyzed in two phases: initial and focused
coding (Saldana, 2016). The initial coding phase involved assigning names to words or
larger segments of data, whereas the second phase aimed to identify the most significant
63 codes initially identified in order to sort, synthesize, integrate, and organize large
amounts of data toward theory construction (Charmaz, 2014). Focused coding moves the
research ahead by elaborating upon the codes we have created and or identifying extant
theories that can support emerging theories. Since this research was conducted in
Ecuador with Spanish-speaking communities, initial coding schemes were constructed in
Spanish using a line-by-line approach. This facilitated interaction with research materials
and provided opportunities to remain close to the data.
I used in-vivo and process coding for the initial coding phase of this project
(Charmaz, 2014; Saldana, 2016). Process coding is an approach to coding particularly
associated to CGT. It uses gerunds “to connote action in the data, both simple observable
activities as well as larger process” (Saldana, 2016, p. 111). The purpose of using process
coding is preserving the fluidity of participants’ experience (Charmaz, 2014). This type
of coding was particularly suitable for this research because of its evolving character:
participants’ experiences were situated in the temporal, physical, and emotional
reconstructions they made of HHHL as a process and the coding system reflected that
evolution.
In vivo coding complemented the actions described through process coding. In-
vivo is “a word or short phrase from the actual language found in the qualitative data
record” (Saldana, 2016, p. 105). While paying attention to the actual language used by
research participants, researchers can amplify their voices and presence in subsequent
phases of data collection and analysis. This method demands rigorous line-by-line coding
in order to have contextualized pieces of language that can be integrated into larger
theoretical development (Charmaz, 2014). Accordingly, I used in-vivo coding to capture

64 essential features of participants’ verbatim reconstruction of their experience with
HHHL model.
I intended to keep this in-vivo and process coding during the analysis phase for as
long as possible; however, I turned into English for the focused coding phase of the
analysis, as well as for memo writing, code book, and final report.
I used several forms of comparative methods for the focused coding phase of this
reserach (Charmaz, 2014); this allowed me to observe complex interactions around the
idea of sustainability from different perspectives. Charmaz suggests that using
comparative methods allows the researcher to identify processes different from the ones
described by participants, as well as assessing comparability and transferability of
theoretical constructions. While comparing the cases of partners and non-partners, for
example, specific attention was placed on the elements proposed by PAHO as conditions
for sustainable control of NTD (vector control, intersection with water sources and
hygiene, management of zoonotic elements of the disease, community participation and
social capital). This analysis provided ideas about the actual impact of HHHL in areas
expected by the project, but also suggested ideas about unintended or overlooked
consequences (Merton, 1936), as well as contribution claims (Cartwright, 2011). Other
kinds of comparisons were made using temporal references, such as appropriation and
use throughout the years, as well as throughout or in different climatological seasons.
Decisions about the specific areas to be compared emerged as data analysis progresses.
In general, I followed the guidelines for CGT as proposed by Bryant and Charmaz
(2007):
a. Data collection, analysis and theoretical development were simultaneously conducted;

65 b. Coding started with the initial instances of data collection;
c. Memo writing started simultaneously with data processing;
d. Theoretical sampling was consistently conducted through pattern searching;
e. Data was collected until theoretical saturation was reached; and
f. I aimed to identify social processes that could lead to theory construction grounded in
the data.
These steps facilitated the subsequent generation of theory that was not only the
product of the research but the analytical framework that guided the analysis of the data.
It is important to emphasize that I intended to pay particular attention to the
contextualized actions and expressions that research participants used in relation to their
environment, their health, and HHHL actions. I followed dialogic ways of representing
emerging elements for theorizing. In this sense,
[emerging] themes are tentative beginnings of the more significant task of representing individual struggles in all their ambivalence and unfinalizability; in particular, how is each voice the site of multiple voices, and what is the contest among these voices. Personal stories are, again, not to be understood as strictly individual. Any person’s story is the site of struggles permeated by multiple voices. (Frank, 2005, p. 972) Additionally, I followed Charmaz (2014) criteria of quality for grounded theory
studies (credibility, originality, resonance, and usefulness) to provide evidence of rigor in
conducting this research. Credibility was pursued by reimaning close to the data
throughout the phases of coding, meaning-making, theorization and dissemination of this
research. I used the ontological tenants of grounded theory to maximize participants’
involvement in the co-construction of potential answers to the research questions
proposed in this study. Resonance and usefulness was pursued by applying a pragmatic

66 orientation towards CGT. As previously explained, the theory of sustainability
produced by this research should partially inform decision-making for implementation of
the HHHL model at medium and large scale. Understanding the actual impact of HHHL
in the lives of local families, as well as identifying the resources and barriers currently
existing in the communities, constitute essential elements to consider in a public health
intervention of this nature. My aim was building complex analyses capable of expanding
the notion of partnership currently promoted by the program in order to approach
marginalized populations with concepts and ideas relevant in their own context.
Final products.
The results of this research will be delivered in the following pages as separate
chapters under the following formats:
a. Chapter 4. Uses of Communication Strategies, Media and Messages in Neglected
Tropical Diseases Eradication, Elimination and Control programs: A systematic review
(journal article)
b. Chapter 5. Towards a theory of sustainable prevention of Chagas disease: An
ethnographic grounded theory study (journal article)
c. Chapter 6. Towards a theory of sustainable prevention of Chagas disease: Scaling up
proposal (White paper)
Ethics and informed consent procedures.
IRB protocols were filed and approved by the Ethical Committee for Research on
Human Subjects at Ohio University (16-X-209) and the Research Ethical Committee at
Pontifical Catholic University from Ecuador (Oficio-CEISH-232-2016). Since I visited
participant's homes for interviews, participant observation and questionnaires’

67 administration, I orally explained the purpose of this study at the beginning of my visit.
After identifying the members of the research team that had access to their testimonies, I
stated potential risks and benefits and emphasized the right of refusing to participate in
this research. Signed informed consent was collected at the beginning of each interview.
In cases when participants could not sign, I read the informed consent and asked an
authorized witness to sign the form. Informed consent included authorization for
recording the interviews and taking pictures of the home during the administration of the
questionnaire. For minors, I collected informed consent of the parents and assent from the
minor.
Justification of Methods
Constructivist grounded theory is a method particularly suited to pursue goals of
social justice (Charmaz, 2005; Denzin, Lincoln, & Smith, 2008). It demands researchers
to stay close to their data, an analytical tool that facilitates identification of new lines of
thinking about data itself, as well as research participants and their context. Charmaz
(2011) explains that in the process of understanding researchers’ rationale for coding, for
example, assumptions about access to resources, hierarchies, policies, and practices,
among other constitutive factors of social justice, are made visible. Similarly, by making
a conscientious effort to represent participants’ voices and views as vividly as possible,
researches are making explicit their commitment with pragmatic and participatory
orientations to research. CGT proposes “a systematic approach to social justice inquiry
that fosters integrating subjective experience with social conditions” (Charmaz, 2014, p.
326); consequently, it can be used to impact policy-making and interventions’ designed

68 to make explicit the actual connections between formulation, implementation and
consequences of specific programs.
In this case, CGT’ pragmatic approach lead me to deconstruct small actions
enacted in the micro system of the home as a reflection of major dynamics of social,
political and economic systems.GT has been used in public health and health systems
research similarly to other data driven methodologies such as realist evaluation (Pawson,
Greenhalgh, Harvey, & Walshe, 2005) and theory of change (De Silva et al., 2014). As a
quintessential qualitative research method, it has been deemed suitable to address the
most important questions for implementation research: what works for whom, under what
circumstances, why, and how (Jagosh et al., 2015). In the field of tropical diseases,
grounded theory has been applied to implementation research on issues as varied as the
study of patterns of Chagas disease in migrants in Peru (Bayer et al., 2009); use of
antimalarial hammocks in Vietnam (Peeters Grietens et al., 2012); impact of multidrug
resistance in tuberculosis on children (Franke et al., 2014); community engagement in a
dengue elimination program in Australia (Kolopack, Parsons, & Lavery, 2015); and
community responses to Ebola (Abramowitz et al., 2015).
Similarly, this research emphasized the idea of sustainability as enacted in the
experience of local families, beyond epidemiological, architectural and social data
previously collected by HLI in relation to CD. Since the question for sustainability often
refers to the capacity of the project to address the structural causes of disease beyond its
physical manifestations, this research aimed to understand how this concept can be
expanded in order to include local families’ voices in subsequent decision-making

69 processes. In summary, I intended to explore how, if so, previous and future partners
see HHHL as a source of health and wellbeing in the long run.
As a socio-constructivist scholar, I am interested in conducting research capable
to inform practice from culture-specific perspectives, research that value the role of social
norms, emotions, and non-strategic evaluations of social processes that better depict the
multiple features of human character. From my point of view, facilitating spaces of
participation to voices emerging from traditionally silent sectors of population —the ill,
the marginalized, the colonized— can lead to more complex, accurate, but mainly, more
ethical understandings of health as a situated concept. From this perspective, I want to
challenge power structures that magnify scientific knowledge in opposition to
idiosyncratic experience. Consequently, the methodological decisions previously outlined
respond to my orientation as a socio-constructivist scholar, as well as my interest in
social justice as fundamental goal of my academic work.
Positionality
The selection of grounded theory, and particularly ethnographic grounded theory,
was ontological and epistemologically linked to the research questions guiding this
project, as well as the nature of my position in the conceptualization of HHHL. Through
my role as Coordinator of the Healthy Living Initiative for the last five years, I have been
able to establish relationships with HHHL partner families and other community
members. Rather than neglecting the impact of power dynamics associated with this
position and the institutions I represent, I expect to use them as a criterion to advance
specific conclusions in the development of this research.

70 From a socio-constructivist point of view, communication is not a subject of
our talk, but the talk itself, the raw material of any human interaction. What we know of
the world, we know it because we are able to assign meaning to it, and we do so, because
we can recognize the resources necessary to understand our realities and incorporate them
in larger referents. Communication becomes the lenses through which we can access
larger forms of organization in knowledge and in life itself.
My understanding of the major role that human agency plays in the construction
of the world is one derived from recognizing human capacity for creating meaningful
explanations of the experiences that define and inform our identity. Emerging definitions
of health reveal particular worldviews and positionalities that, as an interpretive scholar, I
am interested in exploring. Is the construction of the self in relation to the other and
his/her environment what attracted me in first place to the study of health
communication. I support the ontological assumption that individuals’ perceptions of
health are constituted by the meanings they assign to the specific events they have to
experience in their bodies, as well as epistemological conceptions of health
intersubjectively constructed with family members, health providers, and institutions
present in their particular world (Babrow & Mattson, 2011).
In doing so, I can locate myself in what Deetz (1996a) called the “consensus-
pole” of the interpretive/critical tradition: most of my interests in research are oriented
towards gaining understanding of the explanations that people provide of their lived`
experiences, more that evaluating them against some ‘objective’ reality. In my opinion,
making an effort to describe and incorporate populations’ perspectives in health
interventions is one of the main responsibilities of the researcher interested in health

71 promotion. In order to counter the dynamics of manipulation and false-consensus
associated with earliest model of health communication, a particular emphasis on
dialogue has to be made. Concepts such as heteroglossia and unfinalizability (Bakhtin &
Holquist, 1981) are central to the construction of my idea of otherness, and more
concretely, to the possibility of change I embrace. These concepts question the role that
scientific knowledge should play when approaching social realities with a transformative
impetus. By maintaining an open attitude towards the experience of otherness as
recreated in dialogue, I feel better equipped to depict the uniqueness of the context I
intend to approach with this research and formulate ideas of health promotion more
suited to those specific realities.
After five years of work in Ecuador, I have had the opportunity to challenge my
own definitions of wellbeing. My experience as coordinator of the Healthy Living
Initiative has been greatly enriched by the intense learning derived from the possibility of
applying and questioning what I have learned in the classroom while creating meaningful
relations with local populations and colleagues in these communities. Consequently, this
research responds both to my experience with the project and the relationship I have
established with families in this area. I understand that the position I hold in the project
provides a particular perspective informed by processes and sources not exclusively
limited to the experiences of the families. However, as a qualitative scholar, I recognize
myself as my main research instrument and I hope I have used in its best capacity to
address the questions I proposed in previous pages.

72 Chapter 4: Uses of Communication Strategies, Media and Messages in Neglected
Tropical Diseases Eradication, Elimination and Control Programs: A Systematic
Review
Introduction
During the last decade, tropical disease researchers have argued for the need to
include social sciences in the design and implementation of interventions aimed at
addressing neglected tropical diseases, NTD (Allotey, Reidpath, & Pokhrel, 2010; Azoh
Barry, 2014; Bardosh, 2014; Houweling et al., 2016; Manderson et al., 2009; Pokhrel,
Reidpath, & Allotey, 2011; Reidpath, Allotey, & Pokhrel, 2011). Known as ‘the other
diseases’ alluded to by the Millennium Declaration of 2000 (Allen & Parker, 2011; Hotez
et al., 2007; D. H. Molyneux & Malecela, 2011; Smith & Taylor, 2013), the NTD group
includes seventeen infectious diseases that mainly affect people living in poverty
(Crompton, 2010). Snails, mosquitoes, and other insects serve as vectors in areas where
they are naturally present and reach human populations through their living
environments, work settings, and recreational spaces, among other routes. Despite
important differences derived from their protozoan, bacterial, helminthic, and viral origin,
NTD share characteristics of social and political order that make them particularly
relevant for social scientists. First, NTD are endemic in rural or poor urban areas in low-
income tropical countries where continuous interactions with natural environments are
more common (Webster et al., 2016). NTD show high disease burden but low mortality
in affected people, adding an important load of stigma and discrimination to the regular
lives of affected population (Franco-Paredes & Santos-Preciado, 2011). Additionally,
limited resources have been invested in NTD research and treatment, which has led not

73 only to poor alternatives for prevention and treatment, but also to lack of knowledge in
medical communities and general public (Kariuki et al., 2011). Poor documentation,
particularly high impact in marginalized populations, lack of visibility in the media, and
lack of resources to assess and prevent emerging cases, are other factors identified as
leading to neglect around this group of diseases (Ventura-Garcia et al., 2013).
Addressing NTD has been presented as concrete mechanism towards poverty
alleviation and reduction of global inequalities (Hotez et al., 2009). The London
Declaration, promoted and signed by pharmaceutical companies, donors, operational
partners, and national NTD programs in 2012 , committed resources to drugs’
development, access to medication, and research on new forms of treatment for disease
eradication, elimination and control (Molyneux, 2017) . However, it has been argued that
the strategic decisions taken in this context are not nearly enough to achieve the
ambitious social justice goals proposed for this group of diseases (Allen & Parker, 2011).
The use of the term ‘neglect’ has opened a spectrum of research in which the
impact of geographical, demographic, cultural, and social factors can be thoroughly
explored by public health practitioners to arrive to more effective communication
strategies for disease prevention (Azoh Barry, 2014; Bardosh, 2014; Kariuki et al., 2011;
Ventura-Garcia et al., 2013). Even though NTD literature often includes references to
health education, health promotion, and health communication activities, it is important
to understand to what extent those approaches have been conceived to address the
different angles of neglect included in the definition of the NTD category. As stated by
the World Health Organization (WHO),

74 Neglect occurs at three main levels: at the community level, fear and stigma can sometimes lead sufferers and their families to conceal their condition. At the national level, these diseases are often hidden – out of sight, poorly documented, and silent, as those most affected have little political voice (…) Neglected diseases lack visibility at the international level as well. Tied as they are to specific geographical and environmental conditions, they are not perceived as direct threats to industrialized countries (Daumerie, & Kindhauser, 2003, p. 6). This paper is focused on identifying communication strategies involved in the
design and implementation of NTD interventions. Specifically, we aimed to identify
communication strategies implemented in the context of dracunculiasis (Guinea worm)
eradication, lymphatic filariasis elimination, and schistosomiasis and Chagas disease
control programs. Our goal was to understand whether, and if so, the extent to which, the
public health goals established for each one of these diseases, as well as the different
biomedical and environmental factors involved in their occurrence, have affected
decision-making about communication practices recommended and implemented to
effectively approach populations at risk.
Methods
This systematic review identified studies published between January 2012 and
April 2017 that described or recommended implementation of communication strategies
in NTD eradication, elimination or control efforts. This five year period was selected in
consideration to the launch of the London Declaration in January 2012 and the April
2017 NDT Summit that commemorated five years of this event. The selection of these
four diseases responded to two criteria: a) The stage they are facing in terms of
eradication, elimination, and control; and b) the prevention and control methods most
commonly applied in each case. Guinea worm (GW) was included in this review because
it is exemplary of a disease that has reached the eradication stage mainly through

75 community-based prevention and health education programs —unlike smallpox that
was eradicated through vaccination (Visser, 2012). Lymphatic filariasis (LF) and
schistosomiasis (STH), were included due to the significant resources they have received
from mass drug administration programs (MDA) for their elimination and control,
respectively. Lastly, Chagas disease (CD), also in control stage, was included in attention
to the environmental interactions involved in its occurrence. Our rationale for this
selection was to have sufficient scope to obtain a broad panorama that could help us
understand how the diversity of contexts, transmission cycles, and prevention and
treatment methods characteristic of the NTD group has impacted decisions in relation to
communication methods (Table 1), while being narrow enough to carefully examine the
decisions made in each case.
Data sources.
Full searches were conducted using five electronic databases: Medline-Pubmed,
CINAHL, PsycINFO, Lilac and Social Science Citation Index -Science Citation Index. In
order to identify the most common terms associated with communication actions, an
initial search was carried out using the word communication as descriptor. Based on the
results obtained, three more terms were used to refine the search: message, media, and
participation. Expressed in Boolean terms, the search strategy was: “(dracunculiasis OR
guinea worm OR lymphatic filariasis OR schistosomiasis OR Chagas disease) AND
(communication OR message OR media OR participation).” Studies were not excluded
on the basis of design or methods.
Articles were selected in two phases. First, the titles, abstracts and key words of
all the identified studies were examined. A total of 1,040 articles were included at this

76 stage. Once duplicated results were eliminated, 846 abstracts were reviewed. Exclusion
criteria included communication as biological transmission or type of contribution (e.g.
short communication); media as environmental condition in laboratory settings or
publication; and participation as enrolment or interaction in biological processes.
Introductions to special numbers, theses, news reports and congress presentations were
also excluded. Health education was excluded as search term due to the existence of a
journal of the same name; however, pieces mentioning health education in the abstract
were included for second screening. Of these articles, 172 were retained. The first author
used two specific criteria to narrow the selection: focus on the specific diseases being
studied, and concrete use of search terms in programs’ implementation or as
recommended path of action. Fifty-eight articles were excluded due to tangential mention
of issues of interest. Considering that this review is focused on actual communication
uses and practices, policy statements and articles focused on NTD as a general category
were also excluded, unless they included specific sections on the diseases of interest.
Studies were divided into two major groups: articles describing some form of
communication intervention, and articles that referred to communication as a
recommended course of action. Studies were considered interventions when they
described communication actions actually developed in a particular context;
recommendations, on the other hand, were less elaborated statements —usually included
in the final sections of the manuscripts— suggesting communication activities for future
interventions. As showed in Figure 1, a total of 114 articles were finally included in this
review. Only studies conducted in English, French, Spanish, and Portuguese were
examined.
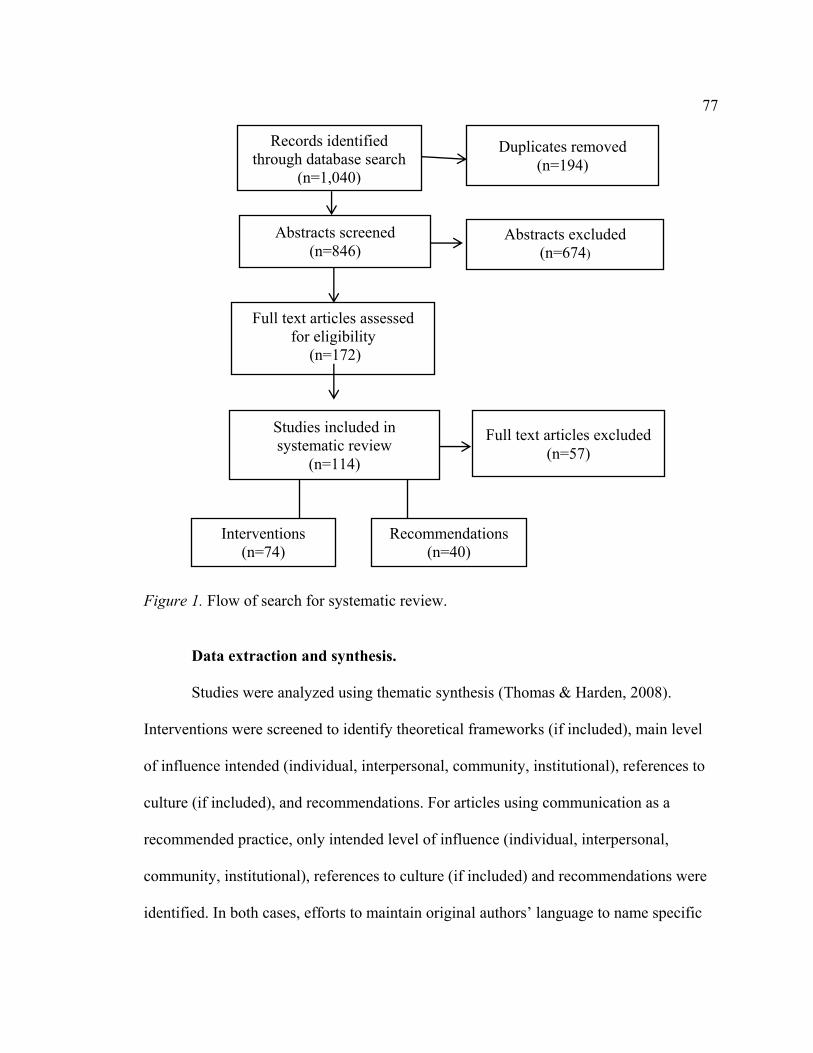
77
Figure 1. Flow of search for systematic review.
Data extraction and synthesis.
Studies were analyzed using thematic synthesis (Thomas & Harden, 2008).
Interventions were screened to identify theoretical frameworks (if included), main level
of influence intended (individual, interpersonal, community, institutional), references to
culture (if included), and recommendations. For articles using communication as a
recommended practice, only intended level of influence (individual, interpersonal,
community, institutional), references to culture (if included) and recommendations were
identified. In both cases, efforts to maintain original authors’ language to name specific
Records identified
through database search
(n=1,040)
Abstracts screened
(n=846)
Duplicates removed
(n=194)
Full text articles assessed for eligibility
(n=172)
Full text articles excluded
(n=57)
Studies included in
systematic review
(n=114)
Interventions (n=74)
Recommendations (n=40)
Abstracts excluded (n=674)

78 actions were made. Findings were stored and coded by category in Excel. Quality of
the selected articles was assessed in relation to their capacity to answer questions
proposed for this study.
Results
A total of 114 articles were identified: 74 of them were included in the
intervention category and 40 in the recommendation group (Tables 2 and 3). Eleven (11)
articles were identified for Guinea worm, 29 articles for lymphatic filariasis, 29 for
schistomiasis, and 45 for Chagas disease.
Table 1. Communication actions advised in articles classified as recommendations. NTD Authors Recommendation Reference
culture Level of influence
GW (Awofeso, 2013) Community education campaigns Health education Booklets Culturally appropriate language
N Individual, interpersonal, community
GW (Jones et al., 2014) Combination of directive and participatory decision-making
N Institutional
GW (Mojoyinola & Blinkhorn, 2013).
Health promotion Advocacy Community mobilization
N Individuals, community, institutional
GW (Whitty, 2015) Advocacy Messaging Anthropological analysis
N Community, institutional

79 Table 1: continued.
LF (Abd Elaziz, El-Setouhy, Bradley, Ramzy, & Weil, 2013)
Educational messages through electronic media
N Institutional
LF (Adhikari, Sherchand, Mishra, Ranabhat, & Wagle, 2015)
Community engagement through government and community structures
Y Individual, interpersonal, community
LF (Gazzinelli et al., 2012) Health education Mass media Community participation
Y Institutional
LF (Krentel, Fischer, & Weil, 2013)
Trust building Face to face interaction Information provision through multiple sources Promotional materials Anthropological studies Management of adverse events Messaging Toolbox for difficult areas
Y
Individual
LF (Martindale et al., 2014)
Community awareness
N Institutional
LF (Mwakitalu, Malecela, Pedersen, Mosha, & Simonsen, 2013)
Community engagement N Community
LF (Mutheneni, Upadhyayula, Kumaraswamy, Kadiri, & Nagalla, 2015)
Community-based health education campaigns Disease awareness programs
N Individual, interpersonal
LF (Rosanti, Mardihusodo, & Artama, 2016)
Community involvement (drug compliance observers)
N Individual
LF (Wijesinghe & Wickremasinghe, 2015)
Hygiene promotion (home-based)
N Individual
LF (Stanton et al., 2016) Community-based support Health education
N Individual, interpersonal
LF (Upadhyayula, Mutheneni, Kadiri, Kumaraswamy, & Nagalla, 2012)
Health education/awareness campaigns
N Communities
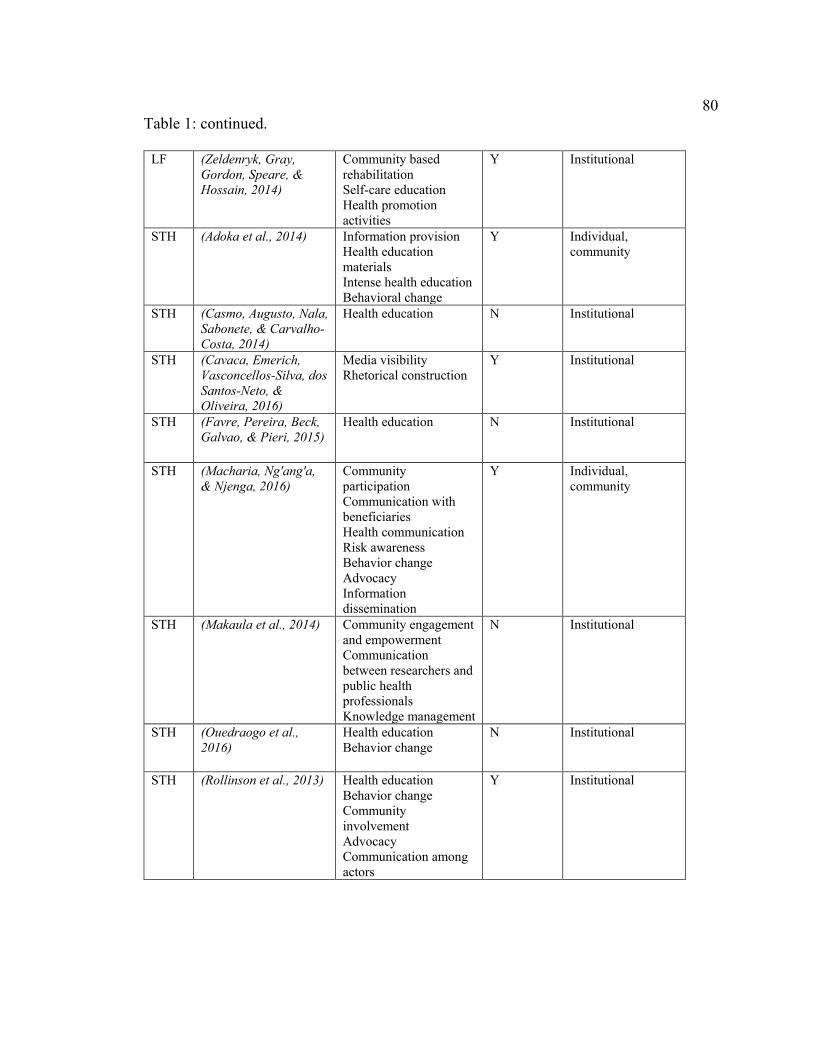
80 Table 1: continued.
LF (Zeldenryk, Gray, Gordon, Speare, & Hossain, 2014)
Community based rehabilitation Self-care education Health promotion activities
Y Institutional
STH (Adoka et al., 2014) Information provision Health education materials Intense health education Behavioral change
Y Individual, community
STH (Casmo, Augusto, Nala, Sabonete, & Carvalho-Costa, 2014)
Health education N Institutional
STH (Cavaca, Emerich, Vasconcellos-Silva, dos Santos-Neto, & Oliveira, 2016)
Media visibility Rhetorical construction
Y Institutional
STH (Favre, Pereira, Beck, Galvao, & Pieri, 2015)
Health education N Institutional
STH (Macharia, Ng'ang'a, & Njenga, 2016)
Community participation Communication with beneficiaries Health communication Risk awareness Behavior change Advocacy Information dissemination
Y Individual, community
STH (Makaula et al., 2014) Community engagement and empowerment Communication between researchers and public health professionals Knowledge management
N Institutional
STH (Ouedraogo et al., 2016)
Health education Behavior change
N Institutional
STH (Rollinson et al., 2013) Health education Behavior change Community involvement Advocacy Communication among actors
Y Institutional

81 Table 1: continued.
STH (Uneke et al., 2015) Capacity enhancement N Institutional
CH (Arenas-Monreal, Pina-Pozas, & Gomez-Dantes, 2015)
Community involvement Gender perspective in health promotion and education campaigns Eco-health
Y Individual, interpersonal
CH (Alviarez & Ferrer, 2014)
Eco-health N Community
CH (Breniere et al., 2013) Inhabitant-based participation Awareness and education campaigns
N Community
CH (Cantillo-Barraza et al., 2015)
Community participation
N Community
CH (de Maio, Llovet, & Dinardi, 2014)
Awareness raising Advocacy
N Institutional
CH (da Silva et al., 2012) Pharmaceutical care (interpersonal communication between pharmacist and patient)
N Individual, community
CH (do Nascimento & Puschel, 2013)
Health education for patients Social support
N Institutional
CH (Donovan, Stevens, Sanogo, Masroor, & Bearman, 2014)
Collaborative education Prevention campaigns
Y Individual
CH (Dumonteil et al., 2013)
Eco-health Y Community
CH (Feliciangeli, 2014) Health education programs Community participation
Y Institutional
CH (Hurtado et al., 2014) Community participation Information provision Sensitization Health education
N Individual, interpersonal, community
CH (Kasten-Monges et al., 2016)
Physician awareness Participative educational models
N Individual, institutional
CH (Provecho, Gaspe, Fernandez, & Gurtler, 2017)
Social participation Y Interpersonal, community
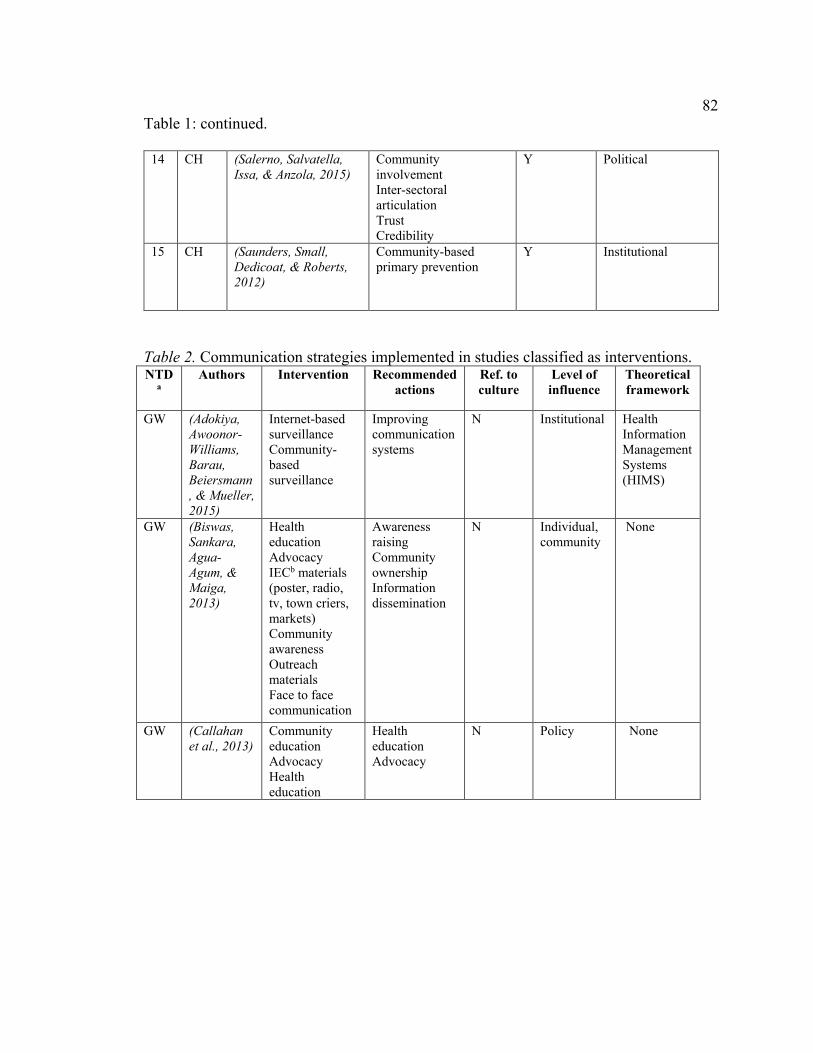
82 Table 1: continued.
14 CH (Salerno, Salvatella, Issa, & Anzola, 2015)
Community involvement Inter-sectoral articulation Trust Credibility
Y Political
15 CH (Saunders, Small, Dedicoat, & Roberts, 2012)
Community-based primary prevention
Y Institutional
Table 2. Communication strategies implemented in studies classified as interventions. NTD
a Authors Intervention Recommended
actions Ref. to culture
Level of influence
Theoretical framework
GW (Adokiya, Awoonor-Williams, Barau, Beiersmann, & Mueller, 2015)
Internet-based surveillance Community-based surveillance
Improving communication systems
N Institutional Health Information Management Systems (HIMS)
GW (Biswas, Sankara, Agua-Agum, & Maiga, 2013)
Health education Advocacy IECb materials (poster, radio, tv, town criers, markets) Community awareness Outreach materials Face to face communication
Awareness raising Community ownership Information dissemination
N Individual, community
None
GW (Callahan et al., 2013)
Community education Advocacy Health education
Health education Advocacy
N Policy None

83 Table 2: continued.
GW (Molyneux & Sankara, 2017)
Advocacy Health education Awareness raising Follow up of rumors Reporting system
N Individual, interpersonal
None
GW (Mbong et al., 2015)
Health education Behavior change Community-based surveillance
Sustained surveillance
N Community None
GW (Ede, Nwaokoro,Iwala,Amadi, & Akpelu, 2014)
Health education Information provision (through media, village health workers, school, and partner organizations).
Advocacy Community mobilization
Y Individual, community
None
GF (Visser, 2012)
Advocacy Community mobilizations Awareness campaigns Health education
Health education Advocacy
N Community None
LF (Aboagye-Antwi et al., 2015)
Community participation
Health education campaigns Community participation
N Individual, community
None

84 Table 2: continued.
LF (Aggithaya et al., 2013)
Community-based self-care integrative treatment Health promotion Community camp workshops IEC Media (booklets and videos) Social mobilization
Community-based LF camps
N Individual None
LF (Byrne & Collins, 2015b)
Health education Hands-on demonstrations Pictures and diagrams.
Treatment plan and follow up care
N Individual.
LF (Ghosh, Samanta, & Kole, 2013)
Community awareness IEC (leaflets, poster, microphone campaigns)
Pre-MDA motivational campaigns Community involvement
N Individual, community
None
LF (Hussain, Sitha, Swain, Kadam, & Pati, 2014)
Intensive behavior change communication (BCC) Community awareness
Awareness Community-based education IEC Sensitization of populations at risk Community mobilization Connecting actors
Y Individual, community, organization
Behavior Change Communication (BCC)
LF (Kisoka et al., 2014)
Social mobilization Media (local radio and television stations)
Dissemination of accurate information Face to face household visits Community and stakeholder involvement
Y Individual, community
None
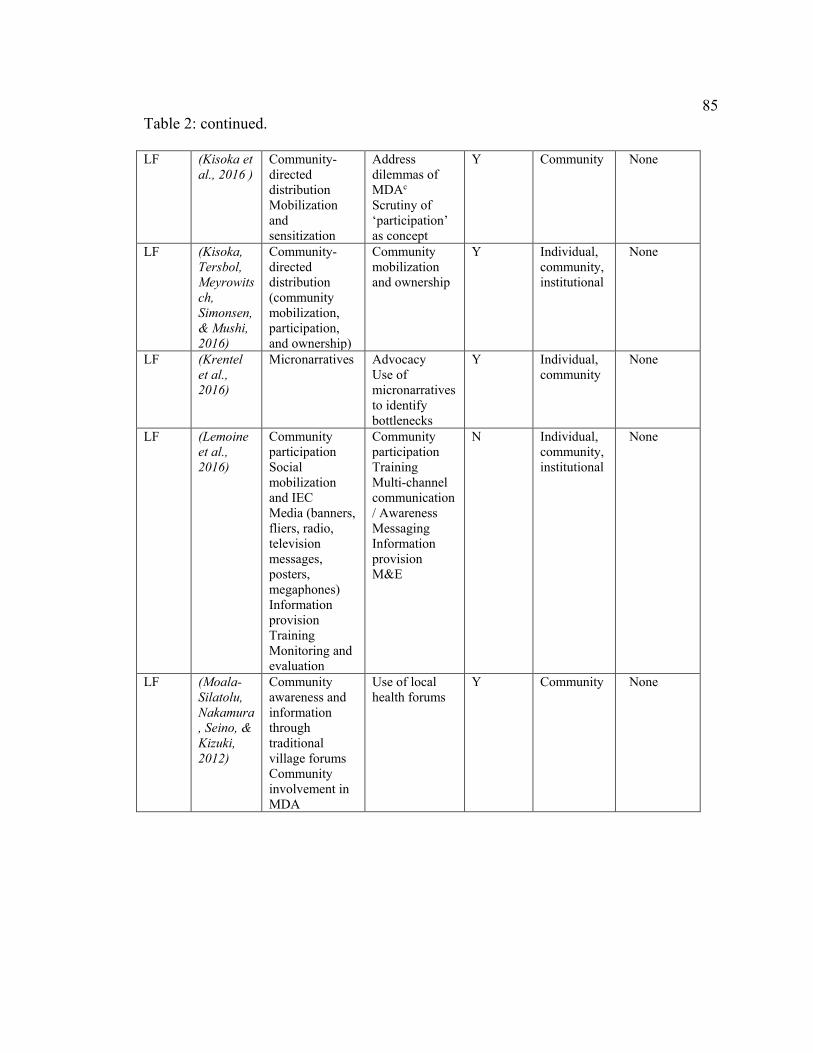
85 Table 2: continued.
LF (Kisoka et al., 2016 )
Community-directed distribution Mobilization and sensitization
Address dilemmas of MDAc Scrutiny of ‘participation’ as concept
Y Community None
LF (Kisoka, Tersbol, Meyrowitsch, Simonsen, & Mushi, 2016)
Community-directed distribution (community mobilization, participation, and ownership)
Community mobilization and ownership
Y Individual, community, institutional
None
LF (Krentel et al., 2016)
Micronarratives Advocacy Use of micronarratives to identify bottlenecks
Y Individual, community
None
LF (Lemoine et al., 2016)
Community participation Social mobilization and IEC Media (banners, fliers, radio, television messages, posters, megaphones) Information provision Training Monitoring and evaluation
Community participation Training Multi-channel communication/ Awareness Messaging Information provision M&E
N Individual, community, institutional
None
LF (Moala-Silatolu, Nakamura, Seino, & Kizuki, 2012)
Community awareness and information through traditional village forums Community involvement in MDA
Use of local health forums
Y Community None

86 Table 2: continued.
LF (Nandha, Krishnamoorthy, & Jambulingam, 2013)
Social mobilization Propaganda (newspapers, posters, radio, announcements, and local health workers) Interpersonal communication
Preparation of community for MDA Social mobilization
N Individual, community
None
LF (Njomo, Amuyunzu-Nyamongo, Magambo, & Njenga, 2012)
Community directed treatment Community participation House by house sensitization Community participation
Community involvement Health education messages Community sensitization Community mobilization
N Individual None
LF (Parker & Allen, 2013)
Social mobilization Advocacy Media (radio, posters, film shows, and mobile megaphones)
MDA campaign - change of focus Acknowledging and understanding local concerns. Social empowerment Knowledge transfer for informed decision-making
Y Community, institutional
None
LF (Sime et al., 2014)
Integrated mapping of NTD Smartphones for data collection Community mobilization
In-country leadership Mobile technology
N Institutional Mobile health (mHealth)
LF (Stanton et al., 2016)
SMS Apps
SMS Apps
N Community Mobile health (mHealth)

87 Table 2: continued.
LF (Ziperstein et al., 2014).
Training Health education Information spread (prefect, village, chief, town crier) Support system Message dissemination (radio, during MDA
Personal home visits Village volunteers Patients’ follow up Community awareness
N Individual, community
None
STH (Amin & Abubaker, 2017)
Health education Community participation
Behavior change supported by health education
Y Community, institutional
None
STH (Barkia et al., 2014)
Door to door visits by mobile teams providing curative and preventive care Health education Information Communication activities Awareness raising Media (Popular songs, audio and video messages)
Involvement of mobile teams for prevention and control activities
Y Community None
STH (Boelee et al., 2013)
Participatory approaches Community awareness and action
Participatory approaches
N Community None

88 Table 2: continued.
STH (Cabello et al., 2016)
Health education Health prevention and promotion Community mobilization
Introducing STH-related activities tailored to local realities Including teachers as health promotion agents Participatory actions
N Individual, community
None
STH (Celone et al., 2016)
Training on participatory research methods Health communication messages and behavior change activities through Madrassas (religious education institutions)
Enhancing credibility and reach of community level and behavior change activities by including religious leaders as change agents
Y Interpersonal, community
Human Centered Design and Adult Learning Theory
STH (Chaula & Tarimo, 2014 )
Advocacy campaigns Information, Education Communication (IEC) and Behavior Change Communication (BCC) Community participation
Effective MDA advocacy campaigns Effective health promotion to induce behavior change Health promotion campaigns
Y Individual, community
None
STH (Hastings, 2016)
Community sensitization Vertical top-down information Unusual communication channels
Explaining rationale for treatment Administering drugs in health centers and not in schools Acknowledging the socio-political context of NTD
Y Individual, community, institutional
None

89 Table 2: continued.
STH (Leonardo et al., 2016)
Health promotion Networking and linkages Health education Multidisciplinary, multisectoral, participatory and consultative methods
Information dissemination Articulation with other poverty alleviation initiatives Community participation Advocacy Health education
Y Institutional None
STH (Liu et al., 2017)
Health education
Sensitive surveillance-response systems
N Policy None
STH (Mewabo et al., 2017)
Sensitization and education Community engagement
Community-based surveillance Contextual behavioral communication changes Leveraging on advances on mhealth and social media
Y Community None
STH (Monde, Syampungani, & van den Brink, 2016)
Health education IEC materials
Information provision
Y Institutional None
STH (Muhumuza, Olsen, Katahoire, Kiragga, & Nuwaha, 2014)
Health education Education messages
Education messages
N Community None
STH (Muhumuza, Olsen, Katahoire, & Nuwaha, 2015)
Education messages
Health education Behavioral change Sensitization
N Community None
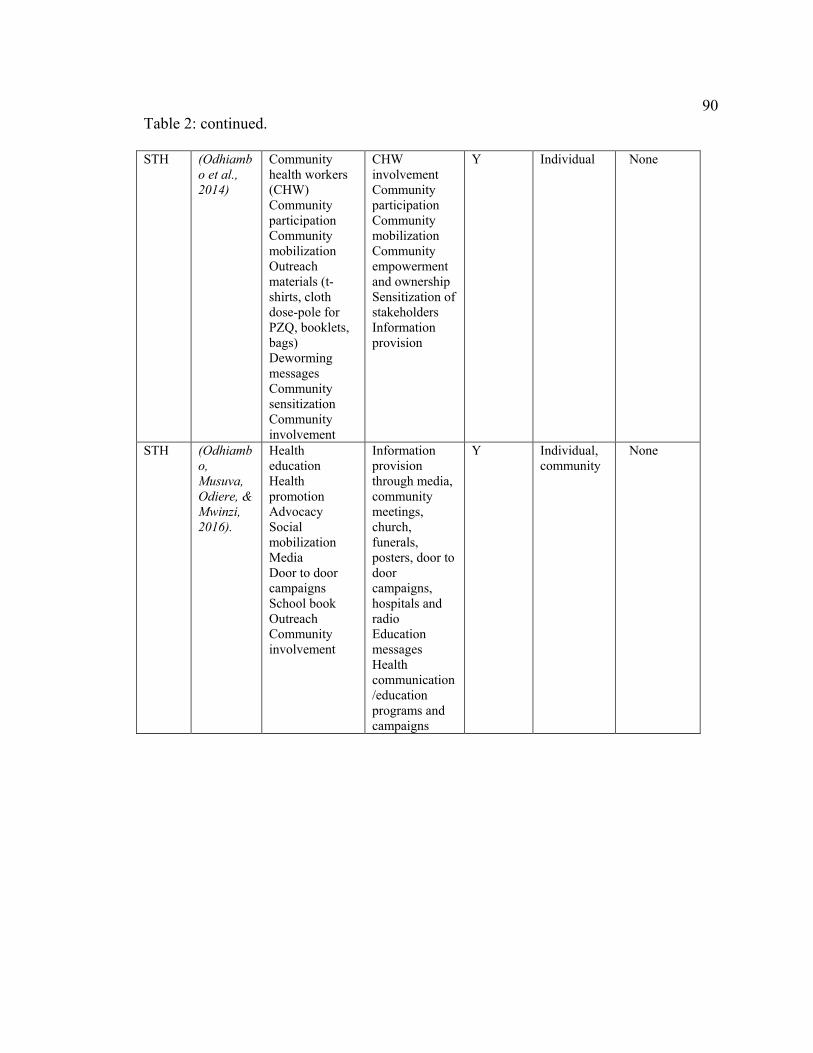
90 Table 2: continued.
STH (Odhiambo et al., 2014)
Community health workers (CHW) Community participation Community mobilization Outreach materials (t-shirts, cloth dose-pole for PZQ, booklets, bags) Deworming messages Community sensitization Community involvement
CHW involvement Community participation Community mobilization Community empowerment and ownership Sensitization of stakeholders Information provision
Y Individual None
STH (Odhiambo, Musuva, Odiere, & Mwinzi, 2016).
Health education Health promotion Advocacy Social mobilization Media Door to door campaigns School book Outreach Community involvement
Information provision through media, community meetings, church, funerals, posters, door to door campaigns, hospitals and radio Education messages Health communication /education programs and campaigns
Y Individual, community
None

91 Table 2: continued.
STH (Omedo et al., 2012)
Community health workers (CHW) Community sensitization
Motivation of CHW with outreach materials (umbrellas, gum boots or bicycles) Health education and mobilization Mass media
Y Individual, community
None
STH (Omedo et al., 2014)
Health communication Community sensitization Health education through community forums Community mobilization Messaging to increase awareness, lead to motivation and then behavior change Media (radio, leaflets, and interpersonal communication) Road shows (loud speakers, distributing brochures and answering questions)
Health communication Improving knowledge and awareness Mass media strategies Integrating communication channels Health messages presented in locally relevant ways Communication campaigns Community-based participatory reserach
Y Individual, community
Community-based participatory research (CBPR)
STH (Phongluxa, van Eeuwijk, Soukhathammavong, Akkhavong, & Odermatt, 2015)
IEC Health education
Health education Direct communication with health professionals Training of opinion leaders
N Community None

92 Table 2: continued.
STH (Rochat et al., 2015).
Preventive messages
Prevention messages
N Individual None
STH (Wang, Carlton, Chen, Liu, & Spear, 2013)
Health education Media (posters, display boards, informal tutoring, video, pamphlets) Outreach materials (towels, school bags)
Combination of various educational formats and multiple media to encourage attention
N Individual, community
Diffusion of innovations
CD (Buttenheim et al., 2014)
Door to door visits (Sensibilizadoras)
Community participation Social norms Health campaigns Outreach materials
Y Individual, community
Health Belief Model
CD (Bustamante et al., 2014)
Door to door visits Household Vector Card
Community KAP
Y Individual, community
None
CD (Charron, 2012)
Health promotion Youth mobilization and education Systems thinking Transdisciplinary research Participation Sustainability Gender and social equity Knowledge to action
Emergent design Iterative cycles of knowledge generation, action, and validation or reassessment Research starts at any phase (participatory research design; knowledge development; intervention strategy development; and systematization of knowledge)
Y Community, institutional
None

93 Table 2: continued.
CD (Barbu et al., 2014)
Community participation
Community participation
N Community None
CD (Cormick et al., 2015)
Follow-up home visits Messaging Text messages Training
SMS communication
Y Individuals Mobile health (mHealth)
CD (Curtis-Robles, Wozniak, Auckland, Hamer, & Hamer, 2015)
Community engagement Educational campaign Information provision and collection of bugs Media (printed pamphlets, phone communication, educational website, email address)
Community engagement in vector surveillance
N Individual Citizen science
CD (De Urioste-Stone et al., 2015)
Community participation Participatory education Community-based participatory processes to develop, implement, and evaluate the intervention. Participatory action research (PAR)
Socio-culturally sensitive education approaches Community-based interventions
Y Community Participatory action research PRECEDE-PROCEED model
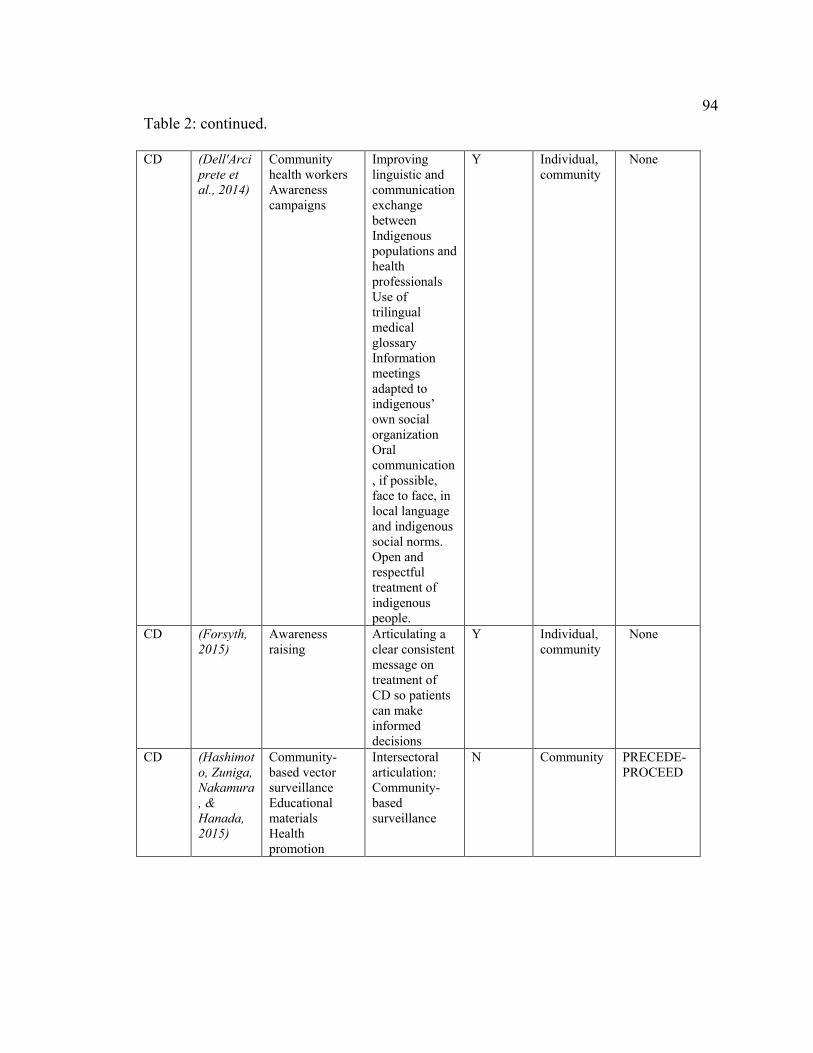
94 Table 2: continued.
CD (Dell'Arciprete et al., 2014)
Community health workers Awareness campaigns
Improving linguistic and communication exchange between Indigenous populations and health professionals Use of trilingual medical glossary Information meetings adapted to indigenous’ own social organization Oral communication, if possible, face to face, in local language and indigenous social norms. Open and respectful treatment of indigenous people.
Y Individual, community
None
CD (Forsyth, 2015)
Awareness raising
Articulating a clear consistent message on treatment of CD so patients can make informed decisions
Y Individual, community
None
CD (Hashimoto, Zuniga, Nakamura, & Hanada, 2015)
Community-based vector surveillance Educational materials Health promotion
Intersectoral articulation: Community-based surveillance
N Community PRECEDE-PROCEED

95 Table 2: continued.
CD (Hashimoto, Zuniga, Romero, Morales, & Maguire, 2015)
Community involvement Comunity-based surveillance Health education Outreach materials ( posters, brochures, T-shirts)
Advocacy Community organization
N Community None
CD (Maeda & Gurgel-Gonçalves, 2012)
Community participation Community surveillance
Health education Education methodologies that favor transformation of knowledge into practice Entomological surveillance based on community participation Informative and educational materials (booklets, manuals, posters and videos) Intensified communication between local population and health personnel.
N Individual, community
None
CD (Dias, Queiroz, Diotaiuti, & Pires, 2016)
Home visits Community participation Health education
Community participation
N Individuals None

96 Table 2: continued.
CD (Lardeux et al., 2015).
Situational analysis Interpersonal communication Community mobilization Lobby with community leaders Supported advertisement House to house visits Community participation
Community participation Behavior change Community participation Basic teaching on cleaning activities Eco-health approaches
Y Individual, interpersonal
None
CD (Lucero et al., 2013)
Community education
Community-based participatory approaches Eco-health interventions
N Community None
CD (Munoz-Vilches et al., 2013)
Information provision to medical personnel
Capacity building
N Individual, institutional
None
CD (Paz-Soldan et al., 2016).
Community participation
Information provision Health education campaigns Awareness raising Strategies for gaining community trust Community participation Peer educators (people affected with CD)
Y Community Theory of Planned Behavior

97 Table 2: continued.
CD (Reyes, Torres, Esteban, Florez, & Araujo, 2017)
Community surveillance Community sensitization
Community participation Health education
N Community None
CD (Rojas-Cortez et al., 2016)
Community-oriented surveillance program Educational folder on how to search triatomines
Public awareness approach using a folder as surveillance method
N Individual, interpersonal
None
CD (Rosecrans, Cruz-Martin, King, & Dumonteil, 2014).
Community participation
Health education
Y Individual Health Belief Model
CD (Sanmartino, Avaria, Gomez Prat, Parada, & Albajar-Viñas, 2015)
Social mobilization with affected people IEC Sensitization and dissemination through short video Dialogic communication
Information world-wide campaign Reinforce communication and education efforts among actors Research to inform communication and education resources Production of mass communication materials
Y Individual, community, institutional
None
CD (Santos, Bedin, Wilhelms, & Villela, 2016)
Community participation Health education
Participatory procedures Education
Y Community, institutional
None

98 Table 2: continued.
CD (Santana Rangel, Monreal, & Ramsey, 2016)
Community participation Community-based surveillance Health education
Community resilience Community participation Strengthening organizational processes
Y Community None
CD (Sartor et al., 2017)
Community participation Social empowerment Multisector cooperation Preparatory meetings with local authors Community workshops Permanent communication channels with local referents Participatory planning Media (radio broadcasts, cell phones and written messages)
Community workshops to raise awareness Two-sided commitment to implement interventions Community involvement
Y Community None
CD (Streiger et al., 2012)
Interdisciplinary approaches with participatory perspective Community organization for fumigation and surveillance
Interdisciplinary approaches Listen to community voices Community participation
Y Individual, community, institutional
None
CD (Triana et al., 2016)
Community participation Knowledge sharing
Community participation
Y Individual, interpersonal, community
None

99 Table 2: continued.
CD (Valdez-Tah, Huicochea-Gomez, Ortega-Canto, Nazar-Beutelspacher, & Ramsey, 2015)
Community participation Participatory approach to promote knowledge sharing, and social and gender equity Eco-health approach
Communication strategies to increase women’s knowledge of CD prevention and control Communication and collaborative networks based on gender roles Participatory activities to promote information exchange and collaborative practices
Y Individual, community
None
CD (Waleckx et al., 2015)
Community participation
Education and awareness programs Eco-health apporaches
Y Individual, interpersonal, community
None
CD (Yevstigneyev, Camara-Mejia, & Dumonteil, 2014)
Health education
Health education and awareness
Y Individual Social Cognitive Learning Theory (SCLT)
CD (Yoshioka, 2013)
Community mobilization Community participation
Community mobilization Training Public awareness Advocacy
N Community None
a NTD: Neglected Tropical Diseases; GW: Guinea worm; LF: lymphatic filariasis; STH: schistosomiasis; and CD: Chagas disease. bIEC: Information, education, communication. c MDA: Mass Drug Administration.
Eradication.
For Dracunculiasis (Guinea worm - GW), four (n=4) of the articles were
recommendations, and the other seven (n=7) were interventions. In GW, all levels of
100 influence were addressed for both recommendations (individual [n=2], interpersonal
[n=1], community [n=3], institutional [n=3]) and interventions (individual [n=2],
interpersonal [n=1], community [n=1], institutional [n=1], political [n=1]). Only one
(n=1) recommendation and none intervention addressed culture. Most interventions (n=6)
did not refer to theory in designing their communication interventions.
GW and yaws are the only NTD currently targeted for eradication. WHO’s GW
eradication strategy includes five specific actions to be implemented at national and
regional levels: surveillance, focused on case management and containment; provision of
safe drinking-water sources; vector control; health education; and, certification of
eradication for regions that have met expected transmission targets (2011). The context of
eradication creates very specific communication demands at institutional levels,
particularly in terms of data collection and case tracking. Standardization of medical
records (Awofeso, 2013), as well as management of rumors about new cases (D.
Molyneux & Sankara, 2017; Visser, 2012) are critical in this case.
Additionally, prevention at local levels remains a pressing need. Health education
messages disseminated in studies included in this review were mainly focused on GW’s
transmission cycle (61.5%), as well as preventive and disease management practices to be
applied at home and community levels (72.7%) (Callahan et al., 2013; Ede, Nwaokoro,
Iwuala, Amadi, & Akpelu, 2014; D. Molyneux & Sankara, 2017; Visser, 2012).
Considering the difficulties of creating a compelling message about risk of transmission
as elimination efforts succeed, authors recommend containing the optimism tone
permeating strategies addressing diseases reaching eliminations stages (Whitty, 2015).
Emphasizing problem solving capacity over prohibitions in populations at risk (Awofeso,

101 2013), empowering families and communities in case identification and management
(Mojoyinola & Blinkhorn, 2013) and including participatory decision making in
interventions of vertical nature (Biswas et al., 2013; Jones et al., 2014), are seen as ways
to bring sustainability and broad commitment around prevention efforts at local levels.
Preferred media to disseminate information at local levels included traditional channels
such as posters, radio, television, town criers, schools, parents, markets and village by
village community mobilization, and films (Biswas et al., 2013; Visser, 2012).
Studies suggested strengthening networks of community surveillance in case of
rumors of reemergence by extending the role of community volunteers and health
workers (Callahan et al., 2013; Mbong et al., 2015), and providing them with tools to
make visible the immediate and long term rewards of a strategy of this nature (Awofeso,
2013; Ede et al., 2014). As hard to reach populations gain prominence because of their
influence in emerging cases, activating population networks willing to share success
stories and generating mechanisms to counter positions of clearly opposing groups, might
be required (Awofeso, 2013; Whitty, 2015). Additionally, authors made a concrete call to
advocate for resources to manage the needs of already affected people, since they can be
overlooked as visibility of cases efforts decreases (Mojoyinola & Blinkhorn, 2013).
Current GW eradication efforts are considered a powerful advocacy tool in
complementary public health and development interventions (Callahan et al., 2013).
Importantly, authors recommend to make visible the unprecedented impact of
coordinated health education actions and face to face communication in programs aimed
at controlling diseases that, like GW, do not count with vaccine or drug based treatments
(Visser, 2012).

102 Elimination.
For lymphatic filariasis (LF), twelve (n=12) of the articles were classified as
recommendations, and seventeen (n=17) as interventions. In LF recommendations, all
levels of influence, except political, were addressed (individual [n=8], interpersonal
[n=2], community [n=3], institutional [n=4]). Interventions did not include the
interpersonal or political levels (individual [n=11], community [n=13], institutional
[n=4]). Most recommendations (n=7) did not address culture, whereas most interventions
(n=11) mentioned issues of culture. Most interventions (n=13) did not refer to theory in
designing their communication intervention.
WHO has targeted four NTD for elimination by 2020: lymphatic filariasis (LF),
leprosy, human African trypanosomiasis (sleeping sickness) and blinding trachoma. LF’s
elimination strategy is aimed at stopping transmission, mainly through community wide
administration of anti-parasitic drugs —albendazole (GlaxoSmithKline), ivermectin
(Merck & Co. Inc.), and diethylcarbamizine, DEC (Eisai)— in endemic areas for a
minimum of five years, as well as reducing burden of the disease in people already
affected through management of lymphedema and hydrocele (Zhou et al., 2016). An
alternative community-wide regimen in endemic regions is the use of common table salt
or cooking salt fortified with DEC (Freeman et al., 2001).
Because of its high reliance on mass drug administration (MDA), it is not
surprising that an important number of publications (69%) included in this review were
focused on issues of compliance. In most cases (58.6%), health education was
recommended as an effective tool to provide information and induce behavior change in
relation to MDA. In the goal of sensitizing and mobilizing local leaders, health workers,
103 and general population to join MDA campaigns, these strategies have relied on
administering information about LF transmission patterns (Njomo et al., 2012), treatment
options (Ziperstein et al., 2014), as well as benefits of the strategy (Aboagye-Antwi et al.,
2015; Hussain et al., 2014). Higher levels of compliance have been associated with trust
in drug distributors, timely provision of information regarding access to treatment, and
visibility of positive results (Krentel et al., 2016).
In terms of messaging, some studies have identified the need to address concerns
about side effects and safety of MDA, as well as presenting LF elimination as a ‘shared
responsibility’ (Rosanti et al., 2016). Segmenting publics by educational and socio-
economic status (Kisoka et al., 2014), as well as disseminating information through
frequently visited social settings and authorities already respected by local communities
(Moala-Silatolu et al., 2012), are practices recommended for effective message
dissemination . Radio, television, posters, newspaper, and town criers have been some of
the communication channels involved in these strategies (Kisoka et al., 2014; Parker &
Allen, 2013). Short message services (SMS) and apps to support community health
workers’ in their roles of data collection and report (Stanton, Molineux, Mackenzie, &
Kelly-Hope, 2016), as well as text messages to reach younger populations and involving
them in local MDA activities (Krentel et al., 2016), have also been tested. Innovative
approaches such as packaging research data and making it readily available for decision-
makers (Uneke et al., 2015), as well as designing toolkits with information specifically
directed to contexts of post-conflict or natural-disaster (Krentel et al., 2013) have been
proposed.
104 Since community participation is mostly equated with compliance (Kisoka et
al., 2014), particular interest has been posed in identifying community perceptions that
act as barriers in the achievement of programmatic goals (Aboagye-Antwi et al., 2015;
Hussain et al., 2014). Those barriers include lack of trust in drugs’ quantities, safety, and
packing (Krentel et al., 2013), as well as worries about the need of treating these diseases
instead of others that are perceived as more prevalent and urgent in local contexts
(Kisoka et al., 2017; Parker & Allen, 2013).
This utilitarian definition of participation has been problematized, as it dismisses
the political and cultural relevance of communities’ opinions, beliefs and perceptions as
simple ‘barriers to elimination’ (Parker & Allen, 2013). Arguments about increasing
communities’ engagement in interventions designs (Parker & Allen, 2013), facilitating
communities’ involvement in health workers’ selection (Njomo et al., 2012), and going
beyond persuasion goals (Moala-Silatolu et al., 2012), have been presented. In these
cases the authors have favored provision of relevant information that responds to rational
and legitimate local concerns, over production of sophisticated communication strategies
and materials aimed at reducing populations’ resistance. These studies have demonstrated
that current strategies are based on ideas about populations living in poverty as apolitical
and homogenous (Kisoka et al., 2017; Mutheneni et al., 2015), which in turn increases
the distance between policy makers and populations at risk.
Nevertheless, more comprehensive approaches have also been attempted in LF
elimination campaigns. Aggithaya et al. (2013) describe an approach to health promotion
in which allopathic and ayurvedic medicine are combined in self-treatment of
lymphedemas. Information about LF and its effect is provided in workshops supported by
105 booklets and videos supported facilitators’ interaction during these workshops.
Similarly, Zeldenryk, Gray, Speare, Gordon and Melrose (2011), propose to go beyond
the shortcomings of strategies founded on the idea of lack of knowledge, to propose
community-driven rehabilitation programs designed to address issues of stigma and
psychological burden faced by LF patients. Considering that these issues go beyond the
individual realm, this approach suggests health education integrated into self-care
management, re-engagement in social activities and health promotion.
At a larger scale, the Haitian program for NTD management combined rigorous
selection of community health workers —under criteria of being known and respected
inhabitants in their districts—with a highly visible social mobilization strategy. The
program used a cascade model of information designed to secure that all actors involved
were capable of addressing critical messages. Flyers, banners, sound tracks, radio
programs, television spots, and community meetings held in schools, churches, and
markets were used as main vehicles. A knowledge attitudes and practices (KAP) study
conducted previous implementation served as formative research for selection of
channels and message design. The authors attributed part of the success of this program
to the high levels of community awareness derived from evidence-based, multi-channel,
and highly visible communication and education campaigns, as well as a well-trained
network of drug distributors highly trusted by community members.
In the same vein, other programs have also given special attention to the
characteristics of community health workers in charge of drug distribution and
community education. Turning knowledge about their communities into public support,
involving family members during their home visits, as well as establishing differentiated

106 approaches according to the priorities of treatment (Aggithaya et al., 2013; Byrne &
Collins, 2015a; Kisoka et al., 2014; Sime et al., 2014; Ziperstein et al., 2014), are
methods that have rendered positive results for community health workers in terms of
adherence to treatment. Krentel, Fischer and Weil (2013) described in detail the
conditions required to build trust in drug distributors, all of them associated with effective
communication processes at individual and institutional levels. Those conditions include
acknowledged reputation and credentials of information providers, training on
communicating knowledge related to MDA, willingness to answer questions, and belief
on the relevance of the program.
Increasing awareness about the physical and psychological consequences of LF in
all actors involved in elimination efforts and not only exclusively on recipient
communities, and facilitating wide distribution of knowledge on best practices
(Martindale et al., 2014; Uneke et al., 2015), have been other communication oriented
recommendations identified for LF elimination.
Control.
Schistosomiasis.
For schistosomiasis (STH) control, nine (n=9) of the articles were
recommendations, whereas twenty (n=20) were interventions. All levels of influence
were addressed either in recommendations (individual [n=2], community [n=2],
institutional [n=7]) or interventions (individual [n=9], interpersonal [n=1], community
[n=14], institutional [n=3], policy [n=1]). Most recommendations (n=6) and interventions
(n=12) mentioned issues of culture. Most interventions (n=12) did not refer to theory in
designing their communication interventions.

107 Similar to LF, schistosomiasis (STH) is another NTD treated through MDA.
Current SC control programs are focused in providing praziquantil to target populations
under different frequencies and distribution methods, being annual MDA of all
community members in targeted areas the most intensive one (Secor, 2015).
Consequently, 14 out of the 29 articles about STH identified in this review dealt with
issues of compliance. Most of these studies described routes towards compliance with
MDA regimes framed on a general framework of health education based on information
provision as an affective route towards behavior change (Leonardo, 2016; Monde et al.,
2016; Ouedraogo et al., 2016; Phongluxa et al., 2015).
Advocacy, health education, and IEC campaigns have been deigned to
disseminate messages about MDA potential benefits ( Odhiambo et al., 2016; Chaula &
Tarimo, 2014; Odhiambo et al., 2014; Omedo et al., 2014), as well as disease focused
information such as dangers of SC infection, risk of contact with contaminated water, and
recommendations to avoid secondary effects (Muhumuza et al., 2014; Rochat et al.,
2015). Debates about the actual need of convening very detailed information about
STH’s transmission cycle in populations’ at risk emerged as an interesting concern in
message design. While some authors emphasized that this knowledge is necessary to
foster the distribution and acceptance of preventive treatment (Odhiambo et al., 2014;
Phongluxa et al., 2015), others argued that knowledge about risk factors is not the most
important variable in behavior change and should be replaced by concrete cues to action
that can more directly lead to health protection (Rochat et al., 2015). In this context,
studies recommended segmenting publics and crafting information for specific groups,
such as less advantaged members of the community (Adokiya et al., 2015) and travelers

108 (Rochat et al., 2015). Similarly, increasing policy makers’ understanding about how
context, religious practices and socio-economic status affect risk-prone behaviors (Amin
& Abubaker, 2017; Celone et al., 2016; Macharia et al., 2016; Monde et al., 2016;
Muhumuza et al., 2015) was recommended. Preferred media in STH strategies included
radio road shows, school booklets, posters, display boards, and pamphlets (Dumonteil et
al., 2013; Feliciangeli, 2014; Ouedraogo et al., 2016). Mhealth and social media
(Provecho et al., 2017) was considered an important tools to explore by future
interventions.
This high reliance on health education was questioned by some authors that see
this approach as insufficient to deal with very serious and valid concerns about MDA
expressed by populations at risk (Rochat et al., 2015; Wang et al., 2013). Hastings (2016)
problematized the scope of schistosomiasis’ MDA campaigns in terms of reaching
populations at risk through current communication efforts. As rumors that reinforced
negative reactions against an MDA campaign being conducted in Tanzania increased, the
author identified a series of mistakes that made of communication efforts more
undermining than enhancing factors: provision of information through unauthorized
voices (school teachers instead of health authorities), lack of time for parents to
understand why the medicine was provided to their kids, insufficient health education to
school teachers as the drug distributors of choice, and wrong messages emphasized
during the campaign, were some of them. Other studies also emphasized the spread of
rumors associated with religious objection and the “real” purpose of treatment, as
definitive factors for derailing campaigns’ activities and purposes (Omedo et al., 2012).
109 Including target populations during the planning cycle of these interventions
was recommended as a mechanism to reduce this resistance (Omedo et al., 2012).
Although conceptualizations about participation as enrolment are also common in this
case (Chaula & Tarimo, 2014), efforts to include community members in the selection of
community health workers, as well as community health workers’ perspectives in
decisions about distribution strategies (Boelee et al., 2013; Omedo et al., 2014; Omedo et
al., 2012; Wang et al., 2013), were made. These actions were identified as effective
mechanisms to gain insights into community perceptions and include during the planning
phase of programs and interventions.
Some studies applied a wider approach to analyze the impact of socio-economic
aspects of disease in prevention (Celone et al., 2016; Liu et al., 2017; Muhumuza et al.,
2014). Celone et al., (2016), for example, demonstrated the impact of infrastructure in
populations’ capacity to implement recommended behaviors. Construction of male and
female urinals, safe play areas, and laundry spaces were treated as necessary mechanisms
to address pressing needs of local communities, as well as strategies to create natural
spaces for message dissemination. Following the Human Centered Design approach,
researchers worked with local communities to make decisions about how to address local
priorities in association with externally defined programmatic goals. Other studies also
recommended attention to socio-economic conditions to enhance behavior change, such
as provision of snacks to reduce the side effects of medicine intake (Favre et al., 2015;
Muhumuza et al., 2015) and improvement of water supply systems (Amin & Abubaker,
2017).

110 Several studies described positive impacts of social mobilization as a
mechanism to enhance community health workers’ position, reduce resistance to
treatment and increase programs’ capacity to cover existing demands (Odhiambo et al.,
2016; Omedo et al., 2012; Omedo et al., 2014). Social mobilization activities identified in
this review included door to door campaigns (Barkia et al., 2014), sensitization through
community gatherings (Celone et al., 2016), use of public spaces such as funeral
ceremonies and congregations (Odhiambo et al., 2016), and replication of messages used
in mass media in forums organized by community leaders (Omedo et al., 2014).
Articulating actions with religious organizations was identified as an effective way to
convene community members’ attention through already trusted spaces (Celone et al.,
2016). Training of religious authorities and local teachers on STH prevention can be
strategic in the goal of securing provision of information on regular basis at local levels.
Chagas disease.
For Chagas disease (CD) control, fifteen (n=15) of the articles were
recommendations, whereas thirty (n=30) were interventions. All levels of influence were
addressed either in recommendations (individual [n=5], interpersonal [n=3] community
[n=7], institutional [n=4], political [n=1]) or interventions (individual [n=18],
interpersonal [n=4], community [n=22], institutional [n=5]). Most recommendations
(n=12) and interventions (n=16) did not address culture as a particular subject. Most
interventions (n=22) did not refer to the use of theory when designing their
communication actions.
Control methods for CD differ substantially from the ones proposed for GW, LF
and STH. No vaccine has been developed for CD; medicines such as nifurtimox (Bayer)

111 and benznidazole (Roche) have been used to treat patients in the acute phase of the
disease, but both drugs have shown side effects that become more serious as a patient’s
age increases, including severe kidney damage (Viotti et al., 2014). Consequently, control
strategies recommended by WHO are mostly focused in interrupting CD’s transmission
cycle between vectors and humans thorough selective or community wide indoor
fumigation with deltrametine, accompanied by information and education activities
(Gilson et al., 2011; Grijalva et al., 2011; Grijalva et al., 2015). Similarly, multiple
interventions have attempted environmental modifications through home reconstruction
or modification (Nieto-Sanchez, Baus, Guerrero, & Grijalva, 2015; Rojas de Arias et al.,
1999).
Due to the intricate web of economic, social and environmental dynamics leading
to CD transmission, strategies considered participatory in nature -such as community
surveillance and home improvement- have been widely applied in this case (71%).
However, uses made of the idea of participation vary through a wide range of actions and
conceptualizations, including convincing community members of accepting interventions
at their household —particularly spraying campaigns (Bustamante et al., 2014;
Buttenheim et al., 2014) and infrastructure interventions (Waleckx et al., 2015)—,
triatomines’ report and collection (Curtis-Robles et al., 2015; Dias, Queiroz, Diotaiuti, &
Pires, 2016; Maeda & Gurgel-Gonçalves, 2012), and involvement of community
members in health promotion activities (Lardeux et al., 2015; Sanmartino et al., 2015;
Yevstigneyeva et al., 2014). Approaching local populations to collect traditional
knowledge (Lucero et al., 2013), as well as getting insights into the experience of patients
and affected communities (Sanmartino et al., 2015; Streiger et al., 2012), have been more

112 complex attempts at bringing the political implication of participatory practices. In
some cases, this complexity expresses as involvement of local communities under gender
sensitive lens (Triana et al., 2016; Valdez-Tah et al., 2015), as well as identification of
local dynamics through which local responsiveness can be motivated (Dell'Arciprete et
al., 2014; Rangel et al., 2016).
Consistently, multiple projects (29%) applied or recommended an Eco-health
perspective when designing CD prevention interventions (Arenas-Monreal et al., 2015;
Charron, 2012; Dumonteil et al., 2013; Hurtado et al., 2014a; Lardeux et al., 2015;
Lucero et al., 2013; Santos et al., 2016; Triana et al., 2016; Waleckx et al., 2015).
Consideration of environmental and behavioral factors in these cases has opened avenues
to think of different communication strategies to activate interactions at individual,
interpersonal, communitarian and institutional levels. Interventions at the household
level, for example have emphasized collaboration among family members to reconstruct
areas that can facilitate triatomines’ entrance and hiding (Triana et al., 2016), whereas
strategies focused on community levels have worked to engage community members in
epidemiological and entomological surveillance (Rangel et al., 2016), as well as
participatory planning and implementation (Waleckx et al., 2015). These interventions
have generated important information about behavior change associated with
modification of living environments under systemic perspectives (Dumonteil et al., 2016;
Lardeux et al., 2015). They have also emphasized the need of long term health promotion
integrated into local health systems in order to extend application of protective practices
over time (Lardeux et al., 2015; Lucero et al., 2013).

113 Besides traditional health education activities, health promoters in CD control
strategies play an active role in facilitating community surveillance for vector control.
This surveillance includes providing information about triatomines’ detection in domestic
and peridomestic areas, safe collection, reporting to health centers, as well as feedback
and follow up (Hashimoto et al., 2012; Hashimoto, Zuniga, Romero, et al., 2015; Rojas-
Cortez et al., 2016). Some authors have explored the advantages of this long term
involvement to generate trust in local communities (Paz-Soldan et al., 2016), as well as
acquiring insights into communities symbolic and meaning-making processes
(Dell'Arciprete et al., 2014). Awareness raising (Yoshioka, 2013) and critical thinking
about existing conditions for environmental modifications (De Urioste-Stone et al.,
2015), have also been pursued through CD health education strategies.
From the studies included in this review, CD articles were the ones that more
often included references to theoretical frameworks commonly used in health
communication: 27% compared to 16% in GW, 18.7% in LF, and 15% in SC.
Specifically, the Health Belief Model, HBM (Becker & Maiman, 1975) and Social
Networks Analysis (Valente & Fosados, 2006) were applied to identify patterns and
interactions that could be influential in diffusion process and behavior modification
(Buttenheim et al., 2014; Triana et al., 2016); HBM was also used to measure threat
perception as a result of perceived severity and susceptibility to CD (Rosecrans et al.,
2014). The PRECEDE-PROCEED model (Green & Kreuter, 2005) was used as
analytical framework in an intervention aimed at providing tools to reduce rodents as
reservoir for triatomines (De Urioste-Stone et al., 2015) and as planning methodology to
integrate data from six different sites in a pilot study about community surveillance in
114 Central America (Hashimoto, Zuniga, Nakamura, et al., 2015). Recent approaches
such as mhealth have been applied to design interventions exploring text message
capacity to improve appointment attendance in pregnant women diagnosed with CD
(Cormick et al., 2015), as well as identification and report of household triatomines
through a web based platform (Curtis-Robles et al., 2015). Given the participatory
emphasis mentioned by several programs, it is interesting that only one concrete
reference about participation theory was identified in this research (De Urioste-Stone et
al., 2015).
Discussion
Even though it could be assumed that different public health goals demand
specific communication interventions, this review showed a general use of
communication as a set of support tools or supplemental activities aimed at reinforcing
the achievement of biomedical goals in the four studied conditions, regardless of their
stages of eradication, elimination, or control. Attention to cultural, and social practices is
given mainly in the context of media selection and message dissemination.
Behavior change was identified as the most prominent outcome of interest in this
review (38.5%). Communication strategies varied in channels and approaches mostly as a
response to the behaviors identified as risk-prone according to the transmission cycle of
the disease. Health communication, health education, and awareness raising campaigns
were the strategies most commonly referred in this expectation of behavior change. Using
rationales, language, and tones associated with risk framing —mostly for awareness,
instruction and persuasion— behavior change is pursued in alignment with protective
practices and acceptance of treatment. As an example, while interventions focused on LF

115 and STH were mainly focused in health education to secure compliance with MDA
goals at individual and community levels, CD programs included a variety of cleaning
and reconstruction practices promoted at the household levels and expected to be
followed by exposed families. Inclusion of stories about social incentives, rewards, and
best practices are promising in terms of expanding social and scientific narratives about
populations exposed to neglected diseases.
Noteworthy is the effort to include formative research (generally KAP and
perception studies) for the development of communication materials and subsequent
phases of implementation (Lemoine et al., 2016; Macharia et al., 2016; Omedo et al.,
2014). Several studies showed the need of testing materials and methods such as
micronarratives (Krentel et al., 2016), focus groups (Zeldenryk et al., 2014) and mhealth
tools (M. Stanton et al., 2016) to validate language, acceptability, and effectiveness. This
finding is consistent with previous literature emphasizing the need of going through more
in depth processes of research for interventions design (Muela Ribera, Hausmann-Muela,
Gryseels, & Peeters Grietens, 2016).
These results present avenues attempted by NTD interventions in order to
approach social dynamics in the context of infectious diseases’ eradication, elimination
and control. Even though there is an ongoing interest in finding avenues to increase
effectiveness of suggested treatments, a more complex understanding of the processes
and capacities offered by the health communication field is required in order to make a
sound use of them and approach the social justice goals proposed for this group of
diseases.

116 Health communication efforts do no happen in a vacuum. They are the result
of specific conditions that alter the practices and resources framing populations’
understanding of health as a social phenomenon. Babrow and Mattson (2011) argued that
health efforts are constructed in a complex interweaving between bodily, emotional,
cognitive and social experiences that allow specific levels of interaction around the
concepts of disease and wellbeing. In this sense, health promotion interventions are
meant to address these levels of interaction in order to generate context specific agendas
that better interpret individual, interpersonal, community and political circumstances of
the different stakeholders involved in a particular effort.
Accordingly, I present three areas in which the field of health communication can
substantially contribute to the effectiveness of NTD efforts: differentiated approaches for
different agendas; configuration of culture-centered over culture-sensitive frameworks;
and complex analyses of the political aspects involved in communities’ participation.
Different agendas, different communication approaches.
The complex network of factors involved in NTD occurrence demand a more
specialized approach to the issues intended to address through communication actions.
Understanding the level of individual knowledge about a particular condition is as
important as contextualizing the system of values, norms and resources operating when
individuals and communities decide to apply (or not) that knowledge in the direction
expected by interventions’ designers. For example, deficient water supply systems and
poor sanitary practices contribute to the spread of LF in a radically different way from
how urbanization and soil degradation contribute to the transmission of CD (Gazzinelli et
117 al., 2012); therefore, both contexts cannot be addressed under the sole parameter of
health promotion.
Guttman (2000) suggests that program designers should identify the locus of
problem, solution, benefit, and evaluation in order to generate coherent strategies toward
public health goals. This coherence allows communication researchers and implementers
to understand the level(s) of the intended change (individual, family, organizational,
community, marketplace, societal, and cultural-normative), as well as the extent to which
specific types of change (environmental, power-based, behavioral, educational,
collaboration-based or policy-oriented) can be promoted.
Understanding that persuasion towards behavior change is one, but not the only
outcome to be expected from communication strategies is particularly important in the
case of MDA campaigns. As explained by multiple authors in this review (Boelee et al.,
2013; Bustamante et al., 2009; Cavaca et al., 2016; Donovan et al., 2014; Mewabo et al.,
2017), epidemiological, economic, technical and environmental arguments are included
in the configuration of risk made by local communities. If populations’ acceptance of
arguments posed by MDA promoters programs is considered a valid response under
biomedical parameters, rejecting them on the bases of fear and mistrust are equally valid
reactions under historical, spiritual and culture-specific lenses. The MDA strategy has
been conceptualized under a series of challenging premises and difficult messages that
demand even more attention from a communication point of view (Ziperstein et al.,
2014). Dismissing local arguments as irrational and opting for persuasion as the fastest
route to invalidate populations’ positions will only limit interventions’ response capacity
in the long run.

118 Similarly, the MDA strategy faces operational challenges associated with
communities’ voluntary involvement, as well as effective monitoring and evaluation
(Prichard et al., 2012). Structural limitations faced by populations living in contexts of
poverty are consistently neglected by researchers’ approach to the underlying social and
economic causes of poverty. Critics point out that lack of consultation with afflicted
communities leads to increasing gaps between decision makers and populations at risk,
which in turn maintains or exacerbates social inequalities (Bardosh, 2014). Generating
spaces and languages that facilitate encounters between community members,
researchers, funders and program designers to define expected changes and potential
routes of action can be a concrete way of reducing tensions identified in this area. Areas
such as interpersonal communication and organizational communication count with
thoroughly studied theoretical and methodological frameworks designed to generate
productive dialogues in this direction.
Framing communication interventions under specific theoretical perspectives can
substantially enhance achievement of programmatic expectations. Studies included in this
review (Celone et al., 2016; M. O. Omedo et al., 2012) illustrated specific uses of
theoretical perspectives that even if not exclusive of the health communication field, can
substantially enhance communication goals. In this context, it is important to note that the
field has experienced a conceptual and practical movement from theories oriented to
individual behavior change toward approaches more interested in identifying processes
through which people make sense of their health priorities under specific social contexts,
posing particular attention to the way in which these priorities are communicated and
negotiated (Obregon et al., 2009; Obregon & Waisbord, 2010). Strategies that show

119 flexibility to adapt communication activities to local resources and provide autonomy
to local providers for decision-making in communication issues are better equipped to
respond to local concerns from different angles (Tufte & Mefalopulos, 2009). This
approach does not dismiss the relevance of individual behavior change, but prioritizes
community strengthening as the most important expected outcome in public health
interventions (Greiner, 2012; Greiner, 2010).
Culture-sensitive vs. culture-centered approaches.
The study of culture in health promotion provides important arguments to
understand the contextual nature of communication (Airhihenbuwa et al., 2014; Dutta &
Basu, 2008). Two parallel approaches have focused their attention in the interactions
between community members and health personnel in multidisciplinary health promotion
efforts: the culture-sensitive and culture-centered approaches to health communication
(Airhihenbuwa et al., 2014; Airhihenbuwa & Obregon, 2000; Dutta & Basu, 2008; Dutta
& de Souza, 2008). Although these two approaches acknowledge the relevant role of
culture when setting specific health objectives, they hold distinct assumptions about the
role it plays in the consolidation of a healthy life. From a culture-sensitive perspective,
culture is often viewed as a barrier to achieving “desired” health-outcomes; consequently,
studies are focused in identifying these barriers in order to frame health behaviors in a
way that is acceptable for the local cultural landscape (i.e., system of beliefs, social and
material relationships). Said differently, the end-goal of culture-sensitive approaches is to
bring into action preconceived health behaviors (and outcomes) by turning existing
cultural features from barriers into allies (Dutta & de Souza, 2008). Culture-centered
approaches, on the other hand, see culture and local capabilities as the contextual factors

120 that should define the logics of health interventions. Instead of barriers, they
constitute a space to confront the dynamics of marginalization within which these
communities are situated (Dutta & Basu, 2008; Dutta et al., 2017). In this sense, the end-
goal of culture-centered approaches is to challenge power inequalities that affect the
material conditions of these communities with the aim of facilitating the improvement of
health outcomes as part of a more decisive process of social change (Jamil & Dutta,
2012).
Although an important number of publications (53%, n=60) included in this
review did not even refer to cultural factors, the ones that did it operated between these
two approaches. For those interventions supporting culture sensitive approaches (47.2%),
a tone of sensitization and persuasion was commonly used. The appreciation of culture as
a barrier is constituted and reinforced through a series of actions aimed at reducing
resistance in local populations. Studies conducted under more culture-centered
perspectives (52.8%) (Dell'Arciprete et al., 2014; W. Kisoka et al., 2017; Parker & Allen,
2013) included local contexts and community reactions in order to inform
implementation with a more complex set of arguments, as well as critical perspectives
about issues of power in current NDT strategies. As stated by Hastings (2016), changing
the tone of messages or using more sophisticated communication channels might not be
enough to addressed the concerns of local population when it comes to drug intake or
interaction with external actors; these interactions should be taken as expressions of
realities that more often than not, occur in very distant political and geographical spaces.
This space usually expresses as distance between the locus from where strategies are
framed and the realities of populations in the receiving end of the equation.

121 Consequently, designing complex approaches to work not only within the
cultural boundaries of populations at risk, but also to question dynamics that define
structural marginalization, emerge as an important priority of NTD programs.
Recommendations for making efforts to inform interventions design with contextualized
information should be taken seriously, as rumors, non-compliance, fear, and mistrust will
continue emerging under the current logics of control, eradication and elimination
strategies.
Political aspects of participation.
Even though the concept of participation is a common place in public health
literature nowadays, its implementation is still challenging. This review showed uses of
the term that range from active engagement in interventions’ design (De Urioste-Stone et
al., 2015; Lemoine et al., 2016) to mere compliance and enrolment. Important actions
were identified in this review to extend the reach and scope of community participation,
including engaging community members in the planning phase of interventions, relying
on community knowledge for interventions design, and using locally relevant scenarios to
enhance decision-making at community levels. We also identified conceptualizations that
considered community participation merely as mechanism to reduce resistance towards
implementation, a perspective that can be problematized because it prioritizes
programmatic objectives over the essential goal of acknowledging the needs of neglected
populations in decision-making about issues that affect their health (International
Conference on Primary Health, 1978; Turner et al., 2011). Context-specific particularities
at the individual, household, community and social levels are determinant to describe the
specific shape that community involvement can take in each case. This review

122 highlighted actions such as selecting local volunteer workers, involving peer
educators, providing community training, and using local resources as ways to promote
community participation in communicable diseases’ control programs.
Similarly, moving from instrumental perspectives that see participation as a goal
in itself, rather than a necessary process to stimulate social change, can open the door to
design more comprehensive involvement of local priorities beyond persuasion (Omedo et
al., 2012; Stanton et al., 2016). In this review, interventions that deployed multiple
channels and diverse entry points also reported higher levels of engagement. In this
sense, Eco-health interventions provide important references for health promotion
initiatives under systemic lenses open to consider local knowledge, as well as issues of
gender and power in interventions design (Celone et al., 2016; Lucero et al., 2013).
Similarly, acknowledging the evolving character of establishing relationships with
community members is a fundamental element in the generation of ownership and
sustainability for health promotion efforts of this nature. As stated by Macharia et al.
(2016), “Anticipating community participation in a programme is not an intelligent guess,
as this is a learning process for beneficiaries and the stakeholders which can be earned
through the sharing of experiences by all the concerned actors” (p. 2). In this sense, focus
on processes more than outputs, according local realities and beyond programmatic
demands, can be considered an important step towards developing a kind of involvement
that acknowledges and addresses NTD social-economic impacts, and goes beyond
populations’ buy in.

123 Conclusion
Because of its nature as fundamental human mode of explaining and being in the
world (Pearce, 1989), communication lies at the core of the human experience of physical
spiritual, emotional, and ethical states. Communication operates through a wide range of
practices at micro and macro levels fundamental in the creation and recreation of
individual, interpersonal, communal and institutional ideas about health, illness and
wellbeing.
In this context, it is important to acknowledge that multiple forms of silence have
determined the dynamics of NTD: unawareness, stigma, and political inaction, among
others. These dynamics articulate issues of power, representation, framing, deployment
and construction of realities around health issues expressed in strategies’ orientations and
purposes. This review kept a broad focus in order to include implementation of
communication strategies in specific contexts, as well as recommendations generated by
studies interested in using communication knowledge and resources. Contemporary
debates about the social construction of health (Babrow & Mattson, 2011; Deetz, 1996b),
the role of local communities in determining their health priorities (Obregon et al., 2012)
and the implications of cultural perspectives in health promotion (Dutta & Basu, 2008;
Dutta & de Souza, 2008), can effectively inform decision-making in interventions
focused in NTD eradication, elimination and control. As stated in previous studies, the
choice of the world ‘neglect’ entails a concrete call to acknowledge responsibility in the
realization of social justice objectives (Allotey et al., 2010). In this context, reducing the
distance between neglecters and neglected through effective communication actions

124 becomes not only a strategic priority but also an ethical imperative for scientists,
program designers, and researchers involved in NTD research.
Limitations.
Search terms might not reflect the full spectrum of communication strategies in
NTD literature; however, we consider that the terms applied for this review are
overarching and depict the dynamics of the field. Similarly, it is possible that implicit
definitions of culture and cultural approaches to disease prevention are included in the
reviewed articles; however, we decided to focus on explicit references in order to
maintain authors’ perspectives in our analyses. This review was limited to academic
literature published in indexed journals. However, communication issues previously
identified are better addressed in grey literature and implementation reports available
through different channels. Considering that most of the articles included in this selection
were not specifically focused on communication but in biomedical aspects of the selected
conditions, issues of space could have affected the extent to which communication
information was presented. This review included papers in English, French, Portuguese
and Spanish, but relevant information in other languages might also been excluded.
References
Abd Elaziz, K. M., El-Setouhy, M., Bradley, M. H., Ramzy, R. M., & Weil, G. J. (2013). Knowledge and practice related to compliance with mass drug administration during the Egyptian national filariasis elimination program. Am J Trop Med Hyg, 89(2), 260-264. doi: 10.4269/ajtmh.12-0491
Aboagye-Antwi, F., Kwansa-Bentum, B., Dadzie, S. K., Ahorlu, C. K., Appawu, M. A., Gyapong, J., . . . Boakye, D. A. (2015). Transmission indices and microfilariae prevalence in human population prior to mass drug administration with ivermectin and albendazole in the Gomoa District of Ghana. Parasit Vectors, 8, 562. doi: 10.1186/s13071-015-1105-x
Adhikari, R. K., Sherchand, J. B., Mishra, S. R., Ranabhat, K., & Wagle, R. R. (2015). Awareness and Coverage of Mass Drug Administration for Elimination of

125 Lymphatic Filariasis: A Community Based Cross Sectional Study in Nepal. Journal of Community Health, 40(1), 34-40. doi: 10.1007/s10900-014-9891-1
Adoka, S. O., Anyona, D. N., Abuom, P. O., Dida, G. O., Karanja, D., Vulule, J. M., . . . Ofulla, A. V. (2014). Community Perceptions of Schistosomiasis Transmission, Prevalence and Control in Relation to Aquatic Habitats in the Lake Victoria Basin of Kenya. East Afr Med J, 91(7), 232-244.
Adokiya, M. N., Awoonor-Williams, J. K., Barau, I. Y., Beiersmann, C., & Mueller, O. (2015). Evaluation of the integrated disease surveillance and response system for infectious diseases control in northern Ghana. BMC Public Health, 15, 75. doi: 10.1186/s12889-015-1397-y
Aggithaya, M. G., Narahari, S. R., Vayalil, S., Shefuvan, M., Jacob, N. K., & Sushma, K. V. (2013). Self care integrative treatment demonstrated in rural community setting improves health related quality of life of lymphatic filariasis patients in endemic villages. Acta Tropica, 126(3), 198-204. doi: 10.1016/j.actatropica.2013.02.022
Airhihenbuwa, C. O., Ford, C. L., & Iwelunmor, J. I. (2014). Why culture matters in health interventions: lessons from HIV/AIDS stigma and NCDs. Health Educ Behav, 41(1), 78-84. doi: 10.1177/1090198113487199
Airhihenbuwa, C. O., & Obregon, R. (2000). A critical assessment of theories/models used in health communication for HIV/AIDS. J Health Commun, 5 Suppl, 5-15. doi: 10.1080/10810730050019528
Allen, T., & Parker, M. (2011). The "other diseases" of the Millennium Development Goals: rhetoric and reality of free drug distribution to cure the poor's parasites. Third World Q, 32(1), 91-117.
Allotey, Pascale, Reidpath, Daniel D., & Pokhrel, Subhash. (2010). Social sciences research in neglected tropical diseases 1: the ongoing neglect in the neglected tropical diseases. Health research policy and systems, 8, 32.
Alviarez, Y., & Ferrer, E. (2014). Aproximación a la problemática de la coendemicidad enfermedad de Chagas-Leishmaniasis desde un enfoque de Ecosalud. Comunidad Salud, 12(2), 55-61.
Amin, M., & Abubaker, H. (2017). Control of Schistosomiasis in the Gezira Irrigation Scheme, Sudan. J Biosoc Sci, 49(1), 83-98. doi: 10.1017/S0021932016000079
Arenas-Monreal, L., Pina-Pozas, M., & Gomez-Dantes, H. (2015). [Challenges and inputs of the gender perspective to the study of vector borne diseases]. Salud Publica Mex, 57(1), 66-75.
Awofeso, N. (2013). Towards global Guinea worm eradication in 2015: the experience of South Sudan. Int J Infect Dis, 17(8), e577-582. doi: 10.1016/j.ijid.2013.03.003
Azoh Barry, Jose. (2014). Social sciences research on infectious diseases of poverty: too little and too late? Plos Neglected Tropical Diseases, 8(6), e2803.
Babrow, A., & Mattson, M. . (2011). Building health communciation theories in the 21st Century. In R. Parrot, T. L. Thompson & J. Nussbaum (Eds.), The Routlege Handbook of Health Communication (pp. xii, 753 pages).
Barbu, C. M., Buttenheim, A. M., Pumahuanca, M. L. H., Calderon, J. E. Q., Salazar, R., Carrion, M., . . . Levy, M. Z. (2014). Residual Infestation and Recolonization during Urban Triatoma infestans Bug Control Campaign, Peru. Emerging Infectious Diseases, 20(12), 2055-2063. doi: 10.3201/eid2012.131820

126 Bardosh, K. (2014). Global aspirations, local realities: the role of social science
research in controlling neglected tropical diseases. Infect Dis Poverty, 3(1), 35. doi: 10.1186/2049-9957-3-35
Barkia, H., Barkia, A., Yacoubi, R., Alemad, A., El Kharim, K., & Belghyti, D. (2014). Contribution of Mobile Teams to Efforts to Eliminate Schistosomiasis at Schistosoma haematobium in Morocco- Narrative Review Article. Iran J Public Health, 43(9), 1167-1175.
Becker, M. H., & Maiman, L. A. (1975). Sociobehavioral determinants of compliance with health and medical care recommendations. Med Care, 13(1), 10-24.
Biswas, G., Sankara, D. P., Agua-Agum, J., & Maiga, A. (2013). Dracunculiasis (guinea worm disease): eradication without a drug or a vaccine. Philos Trans R Soc Lond B Biol Sci, 368(1623), 20120146. doi: 10.1098/rstb.2012.0146
Boelee, E., Yohannes, M., Poda, J. N., McCartney, M., Cecchi, P., Kibret, S., . . . Laamrani, H. (2013). Options for water storage and rainwater harvesting to improve health and resilience against climate change in Africa. Regional Environmental Change, 13(3), 509-519. doi: 10.1007/s10113-012-0287-4
Breniere, S. F., Salas, R., Buitrago, R., Bremond, P., Sosa, V., Bosseno, M. F., . . . Barnabe, C. (2013). Wild populations of Triatoma infestans are highly connected to intra-peridomestic conspecific populations in the Bolivian Andes. PLoS One, 8(11), e80786. doi: 10.1371/journal.pone.0080786
Bustamante, D. M., De Urioste-Stone, S. M., Juarez, J. G., & Pennington, P. M. (2014). Ecological, social and biological risk factors for continued Trypanosoma cruzi transmission by Triatoma dimidiata in Guatemala. PLoS One, 9(8), e104599. doi: 10.1371/journal.pone.0104599
Bustamante, D. M., Monroy, C., Pineda, S., Rodas, A., Castro, X., Ayala, V., . . . Trampe, R. (2009). Risk factors for intradomiciliary infestation by the Chagas disease vector Triatoma dimidiatain Jutiapa, Guatemala. Cad Saude Publica, 25 Suppl 1, S83-92.
Buttenheim, A. M., Paz-Soldan, V., Barbu, C., Skovira, C., Quintanilla Calderon, J., Mollesaca Riveros, L. M., . . . Levy, M. Z. (2014). Is participation contagious? Evidence from a household vector control campaign in urban Peru. J Epidemiol Community Health, 68(2), 103-109. doi: 10.1136/jech-2013-202661
Byrne, S. K., & Collins, S. D. (2015a). Lymphatic Filariasis in Children in Haiti. MCN Am J Matern Child Nurs, 40(4), 227-233. doi: 10.1097/NMC.0000000000000144
Byrne, S. K., & Collins, S. D. (2015b). Lymphatic Filariasis in Children in Haiti. Mcn-the American Journal of Maternal-Child Nursing, 40(4), 227-233.
Cabello, R., Beck, L., Massara, C. , Murta, F., Guimaraes, R., Pieri, O., . . . Favre, T. . (2016). Schistosoma mansoni infection and related knowledge among schoolchildren in an endemic area of Minas Gerais, Brazil, prior to educational actions. Acta Tropica, 164, 208-215. doi: 10.1016/j.actatropica.2016.09.015
Callahan, K., Bolton, B., Hopkins, D. R., Ruiz-Tiben, E., Withers, P. C., & Meagley, K. (2013). Contributions of the Guinea worm disease eradication campaign toward achievement of the Millennium Development Goals. PLoS Negl Trop Dis, 7(5), e2160. doi: 10.1371/journal.pntd.0002160

127 Cantillo-Barraza, O., Garces, E., Gomez-Palacio, A., Cortes, L. A., Pereira, A.,
Marcet, P. L., . . . Triana-Chavez, O. (2015). Eco-epidemiological study of an endemic Chagas disease region in northern Colombia reveals the importance of Triatoma maculata (Hemiptera: Reduviidae), dogs and Didelphis marsupialis in Trypanosoma cruzi maintenance. Parasit Vectors, 8, 482. doi: 10.1186/s13071-015-1100-2
Casmo, V., Augusto, G., Nala, R., Sabonete, A., & Carvalho-Costa, F. A. (2014). The effect of hookworm infection and urinary schistosomiasis on blood hemoglobin concentration of schoolchildren living in northern Mozambique. Rev Inst Med Trop Sao Paulo, 56(3), 219-224.
Cavaca, A. G., Emerich, T. B., Vasconcellos-Silva, P. R., dos Santos-Neto, E. T., & Oliveira, A. E. (2016). Diseases Neglected by the Media in Espirito Santo, Brazil in 2011-2012. Plos Neglected Tropical Diseases, 10(4). doi: ARTN e0004662 10.1371/journal.pntd.0004662
Celone, M., Person, B., Ali, S. M., Lyimo, J. H., Mohammed, U. A., Khamis, A. N., . . . Knopp, S. (2016). Increasing the reach: Involving local Muslim religious teachers in a behavioral intervention to eliminate urogenital schistosomiasis in Zanzibar. Acta Tropica, 163, 142-148. doi: 10.1016/j.actatropica.2016.08.004
Charron, D. F. (2012). Ecosystem approaches to health for a global sustainability agenda. Ecohealth, 9(3), 256-266. doi: 10.1007/s10393-012-0791-5
Chaula, S. A., & Tarimo, D. S. (2014). Impact of praziquantel mass drug administration campaign on prevalence and intensity of Schistosoma haemamtobium among school children in Bahi district, Tanzania. Tanzan J Health Res, 16(1), 1-8.
Cormick, G., Ciganda, A., Cafferata, M. L., Ripple, M. J., Sosa-Estani, S., Buekens, P., . . . Althabe, F. (2015). Text message interventions for follow up of infants born to mothers positive for Chagas disease in Tucuman, Argentina: a feasibility study. BMC Res Notes, 8, 508. doi: 10.1186/s13104-015-1498-9
Crompton, D. (2010). Working to overcome the global impact of neglected tropical diseases first WHO report on neglected tropical diseases (pp. ix, 172 p.). Retrieved from http://site.ebrary.com/lib/yale/Doc?id=10430901
Curtis-Robles, R., Wozniak, E. J., Auckland, L. D., Hamer, G. L., & Hamer, S. A. (2015). Combining Public Health Education and Disease Ecology Research: Using Citizen Science to Assess Chagas Disease Entomological Risk in Texas. PLoS Negl Trop Dis, 9(12), e0004235. doi: 10.1371/journal.pntd.0004235
da Silva, G. M. S., Chambela, M. C., Sousa, A. S., Sangenis, L. H. C., Xavier, S. S., Costa, A. R., . . . Saraiva, R. M. (2012). Impact of pharmaceutical care on the quality of life of patients with Chagas disease and heart failure: randomized clinical trial. Trials, 13. doi: Artn 244 10.1186/1745-6215-13-244
De Maio, F. G., Llovet, I., & Dinardi, G. (2014). Chagas disease in non-endemic countries: 'sick immigrant' phobia or a public health concern? Critical Public Health, 24(3), 372-380. doi: 10.1080/09581596.2013.836589
De Urioste-Stone, S. M., Pennington, P. M., Pellecer, E., Aguilar, T. M., Samayoa, G., Perdomo, H. D., . . . Juarez, J. G. (2015). Development of a community-based intervention for the control of Chagas disease based on peridomestic animal

128 management: an eco-bio-social perspective. Trans R Soc Trop Med Hyg, 109(2), 159-167. doi: 10.1093/trstmh/tru202
Deetz, S. (1996). The positioning of the researcher in studies of organizations: De-hatching literacy theory - Commentary. Journal of Management Inquiry, 5(4), 387-391. doi: Doi 10.1177/105649269654014
Dell'Arciprete, A., Braunstein, J., Touris, C., Dinardi, G., Llovet, I., & Sosa-Estani, S. (2014). Cultural barriers to effective communication between Indigenous communities and health care providers in Northern Argentina: an anthropological contribution to Chagas disease prevention and control. Int J Equity Health, 13, 6. doi: 10.1186/1475-9276-13-6
Dias, J. V., Queiroz, D. R., Diotaiuti, L., & Pires, H. H. (2016). Knowledge of triatomine insects and of the Chagas disease among people from localities which have different levels of vector infestations. Cien Saude Colet, 21(7), 2293-2304. doi: 10.1590/1413-81232015217.07792015
Dias, J.V.L., Queiroz, D.R.M., Diotaiuti, L, & Pires, H. H. R. (2016). Knowledge of triatomine insects and of the Chagas disease among people from localities which have different levels of vector infestations. . Ciência & Saúde Coletiva, 21(7), 2293-2304. doi: https://dx.doi.org/10.1590/1413-81232015217.07792015
do Nascimento, H. R., & Puschel, V. A. D. (2013). Self-care actions in patients with heart failure. Acta Paulista De Enfermagem, 26(6), 601-607.
Donovan, S. D., Stevens, M., Sanogo, K., Masroor, N., & Bearman, G. (2014). Knowledge and perceptions of Chagas disease in a rural Honduran community. Rural Remote Health, 14(3), 2845.
Dumonteil, E., Herrera, C., Martini, L., Grijalva, M. J., Guevara, A. G., Costales, J. A., . . . Waleckx, E. (2016). Chagas Disease Has Not Been Controlled in Ecuador. PLoS One, 11(6), e0158145. doi: 10.1371/journal.pone.0158145
Dumonteil, E., Nouvellet, P., Rosecrans, K., Ramirez-Sierra, M. J., Gamboa-Leon, R., Cruz-Chan, V., . . . Gourbiere, S. (2013). Eco-bio-social determinants for house infestation by non-domiciliated Triatoma dimidiata in the Yucatan Peninsula, Mexico. PLoS Negl Trop Dis, 7(9), e2466. doi: 10.1371/journal.pntd.0002466
Dutta, M. J., & Basu, A. (2008). Meanings of health: interrogating structure and culture. Health Commun, 23(6), 560-572. doi: 10.1080/10410230802465266
Dutta, M. J., Comer, S., Teo, D., Luk, P., Lee, M., Zapata, D., . . . Kaur, S. (2017). Health Meanings among Foreign Domestic Workers in Singapore: A Culture-Centered Approach. Health Commun, 1-10. doi: 10.1080/10410236.2017.1292576
Dutta, M. J., & de Souza, R. (2008). The past, present, and future of health development campaigns: reflexivity and the critical-cultural approach. Health Commun, 23(4), 326-339. doi: 10.1080/10410230802229704
Ede, A. O., Nwaokoro, J. C., Iwuala, C. C., Amadi, A. N., & Akpelu, U. A. (2014). The provision of potable water in eradication of Guinea worm infection in Ezza North, Southeastern, Nigeria. J Community Health, 39(5), 980-986. doi: 10.1007/s10900-014-9842-x
Favre, T. C., Pereira, A. P., Beck, L. C., Galvao, A. F., & Pieri, O. S. (2015). School-based and community-based actions for scaling-up diagnosis and treatment of

129 schistosomiasis toward its elimination in an endemic area of Brazil. Acta Tropica, 149, 155-162. doi: 10.1016/j.actatropica.2015.04.024
Feliciangeli, M. D. (2014). Leishmaniasis in Venezuela: Current status, actions and prospects for vector control in the context of a multi-sectorial control program. Boletin De Malariologia Y Salud Ambiental, 54(1), 1-7.
Forsyth, C. (2015). Controlled but not cured: Structural processes and explanatory models of Chagas disease in tropical Bolivia. Soc Sci Med, 145, 7-16. doi: 10.1016/j.socscimed.2015.09.022
Franco-Paredes, C., & Santos-Preciado, J. I. (2011). Freedom, justice, and neglected tropical diseases. PLoS Negl Trop Dis, 5(8), e1235. doi: 10.1371/journal.pntd.0001235
Freeman, A. R., Lammie, P. J., Houston, R., LaPointe, M. D., Streit, T. G., Jooste, P. L., . . . Addiss, D. G. (2001). A community-based trial for the control of lymphatic filariasis and iodine deficiency using salt fortified with diethylcarbamazine and iodine. Am J Trop Med Hyg, 65(6), 865-871.
Gazzinelli, A., Correa-Oliveira, R., Yang, G. J., Boatin, B. A., & Kloos, H. (2012). A research agenda for helminth diseases of humans: social ecology, environmental determinants, and health systems. PLoS Negl Trop Dis, 6(4), e1603. doi: 10.1371/journal.pntd.0001603
Ghosh, S., Samanta, A., & Kole, S. (2013). Mass drug administration for elimination of lymphatic filariasis: Recent experiences from a district of West Bengal, India. Trop Parasitol, 3(1), 67-71. doi: 10.4103/2229-5070.113917
Gilson, L., Hanson, K., Sheikh, K., Agyepong, I. A., Ssengooba, F., & Bennett, S. (2011). Building the field of health policy and systems research: social science matters. PLoS Med, 8(8), e1001079. doi: 10.1371/journal.pmed.1001079
Global programme to eliminate lymphatic filariasis: progress report, 2015. (2016). Wkly Epidemiol Rec, 91(39), 441-455.
Green, L.W., & Kreuter, M.W. (2005). Health Program Planning: An Educational and Ecological Approach (M.-H. H. Education Ed. 4th edition ed.). NY.
Greiner, K. (2012). Participatory Health Communication Research In R. Obregon & S. Waisbord (Eds.), The handbook of global health communication (pp. 348-373). Chichester, England: Wiley-Blackwell.
Greiner, Karen P. (2010). Exploring dialogic social change (pp. 1 electronic text). Retrieved from http://rave.ohiolink.edu/etdc/view?acc_num=ohiou1273197688
Grijalva, M. J., Villacis, A. G., Ocana-Mayorga, S., Yumiseva, C. A., & Baus, E. G. (2011). Limitations of selective deltamethrin application for triatomine control in central coastal Ecuador. Parasit Vectors, 4, 20. doi: 10.1186/1756-3305-4-20
Grijalva, M. J., Villacis, A. G., Ocana-Mayorga, S., Yumiseva, C. A., Moncayo, A. L., & Baus, E. G. (2015). Comprehensive Survey of Domiciliary Triatomine Species Capable of Transmitting Chagas Disease in Southern Ecuador. PLoS Negl Trop Dis, 9(10), e0004142. doi: 10.1371/journal.pntd.0004142
Guttman, N. (2000). Public health communication interventions values and ethical dilemmas (pp. 1 online resource (xviii, 286 p).
Hashimoto, K., Alvarez, H., Nakagawa, J., Juarez, J., Monroy, C., Cordon-Rosales, C., & Gil, E. (2012). Vector control intervention towards interruption of transmission of

130 Chagas disease by Rhodnius prolixus, main vector in Guatemala. Mem Inst Oswaldo Cruz, 107(7), 877-887.
Hashimoto, K., Zuniga, C., Nakamura, J., & Hanada, K. (2015). Integrating an infectious disease programme into the primary health care service: a retrospective analysis of Chagas disease community-based surveillance in Honduras. BMC Health Serv Res, 15, 116. doi: 10.1186/s12913-015-0785-4
Hashimoto, K., Zuniga, C., Romero, E., Morales, Z., & Maguire, J. H. (2015). Determinants of Health Service Responsiveness in Community-Based Vector Surveillance for Chagas Disease in Guatemala, El Salvador, and Honduras. PLoS Negl Trop Dis, 9(8), e0003974. doi: 10.1371/journal.pntd.0003974
Hastings, J. (2016). Rumours, Riots and the Rejection of Mass Drug Administration for the Treatment of Schistosomiasis in Morogoro, Tanzania. J Biosoc Sci, 48 Suppl 1, S16-39. doi: 10.1017/S0021932016000018
Hotez, P. J., Fenwick, A., Savioli, L., & Molyneux, D. H. (2009). Rescuing the bottom billion through control of neglected tropical diseases. Lancet, 373(9674), 1570-1575. doi: 10.1016/S0140-6736(09)60233-6
Hotez, P. J., Molyneux, D. H., Fenwick, A., Kumaresan, J., Sachs, S. E., Sachs, J. D., & Savioli, L. (2007). Control of neglected tropical diseases. N Engl J Med, 357(10), 1018-1027. doi: 10.1056/NEJMra064142
Houweling, T. A., Karim-Kos, H. E., Kulik, M. C., Stolk, W. A., Haagsma, J. A., Lenk, E. J., . . . de Vlas, S. J. (2016). Socioeconomic Inequalities in Neglected Tropical Diseases: A Systematic Review. PLoS Negl Trop Dis, 10(5), e0004546. doi: 10.1371/journal.pntd.0004546
Hurtado, L. A., Calzada, J. E., Pineda, V., Gonzalez, K., Santamaria, A. M., Caceres, L., . . . Saldana, A. (2014). Knowledge and risk factors related to Chagas' disease in two Panamanian communities where Rhodnius pallescens is the main vector. Biomedica, 34(2), 260-270. doi: 10.7705/biomedica.v34i2.2133
Hussain, M. A., Sitha, A. K., Swain, S., Kadam, S., & Pati, S. (2014). Mass drug administration for lymphatic filariasis elimination in a coastal state of India: a study on barriers to coverage and compliance. Infect Dis Poverty, 3, 31. doi: 10.1186/2049-9957-3-31
International Conference on Primary Health, Care. (1978). Declaration of Alma-Ata. WHO Chron, 32(11), 428-430.
Jamil, R., & Dutta, M. J. (2012). A culture-centered exploration of health: constructions from rural Bangladesh. Health Commun, 27(4), 369-379. doi: 10.1080/10410236.2011.586989
Jones, A. H., Becknell, S., Withers, P. C., Ruiz-Tiben, E., Hopkins, D. R., Stobbelaar, D., & Makoy, S. Y. (2014). Logistics of Guinea worm disease eradication in South Sudan. Am J Trop Med Hyg, 90(3), 393-401. doi: 10.4269/ajtmh.13-0110
Kariuki, T., Phillips, R., Njenga, S., Olesen, O. F., Klatser, P. R., Porro, R., . . . Hanne, D. (2011). Research and capacity building for control of neglected tropical diseases: the need for a different approach. PLoS Negl Trop Dis, 5(5), e1020. doi: 10.1371/journal.pntd.0001020
Kasten-Monges, M. D., Cabrera-Pivaral, C. E., Lozano-Kasten, F., Aguilar-Velasco, H. M., Hidalgo-Ottolenghi, R., & Zavala-Gonzalez, M. A. (2016). Evaluation of the

131 clinical competence in mexican resident physicians for the diagnosis and treatment of Chagas disease. Gaceta Medica De Mexico, 152(4), 516-520.
Kisoka, W. J., Simonsen, P. E., Malecela, M. N., Tersbol, B. P., Mushi, D. L., & Meyrowitsch, D. W. (2014). Factors influencing drug uptake during mass drug administration for control of lymphatic filariasis in rural and urban Tanzania. PLoS One, 9(10), e109316. doi: 10.1371/journal.pone.0109316
Kisoka, W. J., Tersbol, B. P., Meyrowitsch, D. W., Simonsen, P. E., & Mushi, D. L. (2016). Community Members' Perceptions of Mass Drug Administration for Control of Lymphatic Filariasis in Rural and Urban Tanzania. J Biosoc Sci, 48(1), 94-112. doi: 10.1017/S0021932015000024
Kisoka, W., Mushi, D., Meyrowitsch, D. W., Malecela, M., Simonsen, P. E., & Tersbol, B. P. (2016). Dilemmas of Community-Directed Mass Drug Administration for Lymphatic Filariasis Control: A Qualitative Study from Urban and Rural Tanzania. J Biosoc Sci, 49(4), 447-462. doi: 10.1017/S0021932016000365
Krentel, A., Damayanti, R., Titaley, C. R., Suharno, N., Bradley, M., & Lynam, T. (2016). Improving Coverage and Compliance in Mass Drug Administration for the Elimination of LF in Two 'Endgame' Districts in Indonesia Using Micronarrative Surveys. PLoS Negl Trop Dis, 10(11), e0005027. doi: 10.1371/journal.pntd.0005027
Krentel, A., Fischer, P. U., & Weil, G. J. (2013). A review of factors that influence individual compliance with mass drug administration for elimination of lymphatic filariasis. PLoS Negl Trop Dis, 7(11), e2447. doi: 10.1371/journal.pntd.0002447
Lardeux, F., Depickere, S., Aliaga, C., Chavez, T., & Zambrana, L. (2015). Experimental control of Triatoma infestans in poor rural villages of Bolivia through community participation. Trans R Soc Trop Med Hyg, 109(2), 150-158. doi: 10.1093/trstmh/tru205
Lemoine, J. F., Desormeaux, A. M., Monestime, F., Fayette, C. R., Desir, L., Direny, A. N., . . . Baker, M. (2016). Controlling Neglected Tropical Diseases (NTDs) in Haiti: Implementation Strategies and Evidence of Their Success. PLoS Negl Trop Dis, 10(10), e0004954. doi: 10.1371/journal.pntd.0004954
Leonardo, L., Chigusa, Y., Kikuchi, M., Kato-Hayashi, N., Kawazu, S., Angeles, J. M., . . . Chua, J. C. (2016). Schistosomiasis in the Philippines: Challenges and Some Successes in Control. Southeast Asian Journal of Tropical Medicine and Public Health, 47(4), 651-666.
Liu, Y., Zhong, B., Wu, Z. S., Liang, S., Qiu, D. C., & Ma, X. (2017). Interruption of schistosomiasis transmission in mountainous and hilly regions with an integrated strategy: a longitudinal case study in Sichuan, China. Infect Dis Poverty, 6(1), 79. doi: 10.1186/s40249-017-0290-6
Lucero, D. E., Morrissey, L. A., Rizzo, D. M., Rodas, A., Garnica, R., Stevens, L., . . . Monroy, M. C. (2013). Ecohealth interventions limit triatomine reinfestation following insecticide spraying in La Brea, Guatemala. Am J Trop Med Hyg, 88(4), 630-637. doi: 10.4269/ajtmh.12-0448
Macharia, J. W., Ng'ang'a, Z. W., & Njenga, S. M. (2016). Factors influencing community participation in control and related operational research for urogenital

132 schistosomiasis and soil-transmitted helminths in rural villages of Kwale County, coastal Kenya. Pan Afr Med J, 24, 136. doi: 10.11604/pamj.2016.24.136.7878
Maeda, M.H., & Gurgel-Gonçalves, R. (2012). Conhecimentos e práticas de moradores do Distrito Federal, Brasil, em relação à Doença de chagas e seus vetores. Rev. patol. trop, 41(1), 15-26.
Makaula, P., Sadalaki, J. R., Muula, A. S., Kayuni, S., Jemu, S., & Bloch, P. (2014). Schistosomiasis in Malawi: a systematic review. Parasit Vectors, 7, 570. doi: 10.1186/s13071-014-0570-y
Manderson, L., Aagaard-Hansen, J., Allotey, P., Gyapong, M., & Sommerfeld, J. (2009). Social research on neglected diseases of poverty: continuing and emerging themes. PLoS Negl Trop Dis, 3(2), e332. doi: 10.1371/journal.pntd.0000332
Martindale, S., Mkwanda, S. Z., Smith, E., Molyneux, D., Stanton, M. C., & Kelly-Hope, L. A. (2014). Quantifying the physical and socio-economic burden of filarial lymphoedema in Chikwawa District, Malawi. Trans R Soc Trop Med Hyg, 108(12), 759-767. doi: 10.1093/trstmh/tru154
Mbong, E. N., Sume, G. E., Danbe, F., Kum, W. K., Mbi, V. O., Fouda, A. A., & Atem, P. (2015). Not every worm wrapped around a stick is a guinea worm: a case of Onchocerca volvulus mimicking Dracunculus medinensis. Parasit Vectors, 8, 374. doi: 10.1186/s13071-015-1004-1
McLeroy, K. R., Bibeau, D., Steckler, A., & Glanz, K. (1988). An ecological perspective on health promotion programs. Health Educ Q, 15(4), 351-377.
Mewabo, A. P., Moyou, R. S., Kouemeni, L. E., Ngogang, J. Y., Kaptue, L., & Tambo, E. (2017). Assessing the prevalence of urogenital schistosomaisis and transmission risk factors amongst school-aged children around Mape dam ecological suburbs in Malantouen district, Cameroon. Infect Dis Poverty, 6(1), 40. doi: 10.1186/s40249-017-0257-7
Moala-Silatolu, A., Nakamura, K., Seino, K., & Kizuki, M. (2012). Greater Adherence to Mass Drug Administration Against Lymphatic Filariasis through Traditional Village Forums in Fiji. J Rural Med, 7(2), 65-72. doi: 10.2185/jrm.7.65
Mojoyinola, J.K. , & Blinkhorn, F.A. . (2013). Impact of Guinea Worm Disease on the socio-economic well-being of a rural community in Oke-Gun areas of Oyo State, Nigeria. International Journal of Health Promotion and Education, 51(4), 180-184.
Molyneux, D. H., & Malecela, M. N. (2011). Neglected tropical diseases and the millennium development goals: why the "other diseases" matter: reality versus rhetoric Parasit Vectors (Vol. 4, pp. 234).
Molyneux, D., & Sankara, D. P. (2017). Guinea worm eradication: Progress and challenges- should we beware of the dog? PLoS Negl Trop Dis, 11(4), e0005495. doi: 10.1371/journal.pntd.0005495
Molyneux, David H. (2017). The London Declaration on Neglected Tropical Diseases: 5 years on. Transactions of the Royal Society of Tropical Medicine and Hygiene.
Monde, C., Syampungani, S., & van den Brink, P. J. (2016). Natural and human induced factors influencing the abundance of Schistosoma host snails in Zambia. Environ Monit Assess, 188(6), 370. doi: 10.1007/s10661-016-5351-y

133 Muela Ribera, J., Hausmann-Muela, S., Gryseels, C., & Peeters Grietens, K. (2016).
Re-imagining adherence to treatment from the "other side": local interpretations of adverse anti-malarial drug reactions in the Peruvian Amazon. Malar J, 15, 136. doi: 10.1186/s12936-016-1193-x
Muhumuza, S., Olsen, A., Katahoire, A., Kiragga, A. N., & Nuwaha, F. (2014). Effectiveness of a pre-treatment snack on the uptake of mass treatment for schistosomiasis in Uganda: a cluster randomized trial. PLoS Med, 11(5), e1001640. doi: 10.1371/journal.pmed.1001640
Muhumuza, S., Olsen, A., Katahoire, A., & Nuwaha, F. (2015). Reduced uptake of mass treatment for schistosomiasis control in absence of food: beyond a randomized trial. BMC Infect Dis, 15, 423. doi: 10.1186/s12879-015-1158-7
Munoz-Vilches, M. J., Salas-Coronas, J., Gutierrez-Izquierdo, M. I., Metz, D., Salvador-Sanchez, J., & Gimenez-Sanchez, F. (2013). [Health professionals' knowledge on Chagas disease in the province of Almeria, Spain]. Rev Esp Salud Publica, 87(3), 267-275. doi: 10.4321/S1135-57272013000300006
Mutheneni, S. R., Upadhyayula, S. M., Kumaraswamy, S., Kadiri, M. R., & Nagalla, B. (2015). Impact of socioeconomic factors on the prevalence of lymphatic filariasis in Andhra Pradesh, India. Journal of Public Health-Heidelberg, 23(4), 231-240. doi: 10.1007/s10389-015-0673-8
Mwakitalu, M. E., Malecela, M. N., Pedersen, E. M., Mosha, F. W., & Simonsen, P. E. (2013). Urban lymphatic filariasis in the city of Tanga, Tanzania, after seven rounds of mass drug administration. Acta Tropica, 128(3), 692-700. doi: 10.1016/j.actatropica.2013.10.004
Nandha, B., Krishnamoorthy, K., & Jambulingam, P. (2013). Towards elimination of lymphatic filariasis: social mobilization issues and challenges in mass drug administration with anti-filarial drugs in Tamil Nadu, South India. Health Educ Res, 28(4), 591-598. doi: 10.1093/her/cyt042
Nieto-Sanchez, C., Baus, E. G., Guerrero, D., & Grijalva, M. J. (2015). Positive deviance study to inform a Chagas disease control program in southern Ecuador. Memorias Do Instituto Oswaldo Cruz, 110(3), 299-309. doi: 10.1590/0074-02760140472
Njomo, D. W., Amuyunzu-Nyamongo, M., Magambo, J. K., & Njenga, S. M. (2012). The role of personal opinions and experiences in compliance with mass drug administration for lymphatic filariasis elimination in Kenya. PLoS One, 7(11), e48395. doi: 10.1371/journal.pone.0048395
Obregon, R., Chitnis, K., Morry, C., Feek, W., Bates, J., Galway, M., & Ogden, E. (2009). Achieving polio eradication: a review of health communication evidence and lessons learned in India and Pakistan. Bull World Health Organ, 87(8), 624-630.
Obregon, R., & Waisbord, S. (2010). The complexity of social mobilization in health communication: top-down and bottom-up experiences in polio eradication. J Health Commun, 15 Suppl 1, 25-47. doi: 10.1080/10810731003695367
Obregon, Rafael, Waisbord, Silvio R., Wiley InterScience (Online service), & Alumni and Friends Memorial Book Fund. (2012). The handbook of global health communication Handbooks in communication and media (pp. 1 online resource (xx, 658 p). doi:99953324588

134 Odhiambo, G. O., Musuva, R. M., Atuncha, V. O., Mutete, E. T., Odiere, M. R.,
Onyango, R. O., . . . Mwinzi, P. N. (2014). Low levels of awareness despite high prevalence of schistosomiasis among communities in Nyalenda informal settlement, Kisumu city, western Kenya. PLoS Negl Trop Dis, 8(4), e2784. doi: 10.1371/journal.pntd.0002784
Odhiambo, G. O., Musuva, R. M., Odiere, M. R., & Mwinzi, P. N. (2016). Experiences and perspectives of community health workers from implementing treatment for schistosomiasis using the community directed intervention strategy in an informal settlement in Kisumu City, western Kenya. BMC Public Health, 16, 986. doi: 10.1186/s12889-016-3662-0
Okorie, P. N., Bockarie, M. J., Molyneux, D. H., & Kelly-Hope, L. A. (2014). Neglected tropical diseases: a systematic evaluation of research capacity in Nigeria. PLoS Negl Trop Dis, 8(8), e3078. doi: 10.1371/journal.pntd.0003078
Omedo, M. O., Matey, E. J., Awiti, A., Ogutu, M., Alaii, J., Karanja, D. M., . . . Mwinzi, P. N. (2012). Community health workers' experiences and perspectives on mass drug administration for schistosomiasis control in western Kenya: the SCORE Project. Am J Trop Med Hyg, 87(6), 1065-1072. doi: 10.4269/ajtmh.2012.12-0435
Omedo, M., Ogutu, M., Awiti, A., Musuva, R., Muchiri, G., Montgomery, S. P., . . . Mwinzi, P. (2014). The effect of a health communication campaign on compliance with mass drug administration for schistosomiasis control in western Kenya--the SCORE project. Am J Trop Med Hyg, 91(5), 982-988. doi: 10.4269/ajtmh.14-0136
Ouedraogo, H., Drabo, F., Zongo, D., Bagayan, M., Bamba, I., Pima, T., . . . Zhang, Y. (2016). Schistosomiasis in school-age children in Burkina Faso after a decade of preventive chemotherapy. Bull World Health Organ, 94(1), 37-45. doi: 10.2471/BLT.15.161885
Parker, M., & Allen, T. (2013). Will mass drug administration eliminate lymphatic filariasis? Evidence from northern coastal Tanzania. Journal of biosocial science, 45(4), 517-545.
Paz-Soldan, V. A., Bauer, K. M., Hunter, G. C., Castillo-Neyra, R., Arriola, V. D., Rivera-Lanas, D., . . . Buttenheim, A. M. (2016). To spray or not to spray? Understanding participation in an indoor residual spray campaign in Arequipa, Peru. Glob Public Health, 1-18. doi: 10.1080/17441692.2016.1178317
Pearce, W. Barnett. (1989). Communication and the human condition. Carbondale: Southern Illinois University Press.
Phongluxa, K., van Eeuwijk, P., Soukhathammavong, P. A., Akkhavong, K., & Odermatt, P. (2015). Perceived illness drives participation in mass deworming campaigns in Laos. Acta Tropica, 141(Pt B), 281-288. doi: 10.1016/j.actatropica.2014.03.022
Pokhrel, S., Reidpath, D., & Allotey, P. (2011). Social sciences research in neglected tropical diseases 3: Investment in social science research in neglected diseases of poverty: a case study of Bill and Melinda Gates Foundation. Health Res Policy Syst, 9, 2. doi: 10.1186/1478-4505-9-2
Prichard, R. K., Basanez, M. G., Boatin, B. A., McCarthy, J. S., Garcia, H. H., Yang, G. J., . . . Lustigman, S. (2012). A research agenda for helminth diseases of humans:

135 intervention for control and elimination. PLoS Negl Trop Dis, 6(4), e1549. doi: 10.1371/journal.pntd.0001549
Provecho, Y. M., Gaspe, M. S., Fernandez, M. D. P., & Gurtler, R. E. (2017). House Reinfestation With Triatoma infestans (Hemiptera: Reduviidae) After Community-Wide Spraying With Insecticides in the Argentine Chaco: A Multifactorial Process. J Med Entomol, 54(3), 646-657. doi: 10.1093/jme/tjw224
Rangel, J.A.S., Monreal, L.A., & Ramsey, J.M. . (2016). Resiliencia comunitaria y enfermedad de Chagas en una región rural de México. Revista de Saúde Pública, 50(46).
Reidpath, D. D., Allotey, P., & Pokhrel, S. (2011). Social sciences research in neglected tropical diseases 2: A bibliographic analysis. Health Res Policy Syst, 9, 1. doi: 10.1186/1478-4505-9-1
Reyes, M., Torres, A., Esteban, L., Florez, M., & Angulo, V. (2017). Riesgo de transmisión de la enfermedad de Chagas por intrusión de triatominos y mamíferos silvestres en Bucaramanga, Santander, Colombia. Biomédica: Revista Del Instituto Nacional De Salud, 37(1), 68-78. doi:10.7705/biomedica.v37i1.3051
Rochat, L., Bizzini, A., Senn, N., Bochud, P. Y., Genton, B., & de Valliere, S. (2015). Acute schistosomiasis: a risk underestimated by travelers and a diagnosis frequently missed by general practitioners-a cluster analysis of 42 travelers. J Travel Med, 22(3), 168-173. doi: 10.1111/jtm.12187
Rojas de Arias, A., Ferro, E. A., Ferreira, M. E., & Simancas, L. C. (1999). Chagas disease vector control through different intervention modalities in endemic localities of Paraguay. Bull World Health Organ, 77(4), 331-339.
Rojas-Cortez, M., Pinazo, M. J., Garcia, L., Arteaga, M., Uriona, L., Gamboa, S., . . . Monteiro, F. A. (2016). Trypanosoma cruzi-infected Panstrongylus geniculatus and Rhodnius robustus adults invade households in the Tropics of Cochabamba region of Bolivia. Parasit Vectors, 9, 158. doi: 10.1186/s13071-016-1445-1
Rollinson, D., Knopp, S., Levitz, S., Stothard, J. R., Tchuem Tchuente, L. A., Garba, A., . . . Utzinger, J. (2013). Time to set the agenda for schistosomiasis elimination. Acta Tropica, 128(2), 423-440. doi: 10.1016/j.actatropica.2012.04.013
Rosanti, T. I., Mardihusodo, S. J., & Artama, W. T. (2016). Directly observed treatment increases drug compliance in lymphatic filariasis mass drug administration. Universa Medicina, 35(2), 119-127. doi: 10.1805/UnivMed.2016.v35.119-127
Rosecrans, K., Cruz-Martin, G., King, A., & Dumonteil, E. (2014). Opportunities for improved chagas disease vector control based on knowledge, attitudes and practices of communities in the yucatan peninsula, Mexico. PLoS Negl Trop Dis, 8(3), e2763. doi: 10.1371/journal.pntd.0002763
Salerno, R., Salvatella, R., Issa, J., & Anzola, M. C. (2015). A regional fight against Chagas disease: lessons learned from a successful collaborative partnership. Rev Panam Salud Publica, 37(1), 38-43.
Sanmartino, M., Avaria, A. , Gopmez Prat, J., Parada, M., & Albajar-Viñas, P. (2015). Que no tengan miedo de nosotros: El Chagas según los propios protagonistas. Interface - Comunicação, Saúde, Educação, 19(55), 1063-1075. doi: https://dx.doi.org/10.1590/1807-57622014.1170
136 Santos, C. V., Bedin, C., Wilhelms, T. S., & Villela, M. M. (2016). Assessment of the
Housing Improvement Program for Chagas Disease Control in the Northwestern municipalities of Rio Grande do Sul, Brazil. Rev Soc Bras Med Trop, 49(5), 572-578. doi: 10.1590/0037-8682-0386-2016
Sartor, P., Colaianni, I., Cardinal, M. V., Bua, J., Freilij, H., & Gurtler, R. E. (2017). Improving access to Chagas disease diagnosis and etiologic treatment in remote rural communities of the Argentine Chaco through strengthened primary health care and broad social participation. PLoS Negl Trop Dis, 11(2), e0005336. doi: 10.1371/journal.pntd.0005336
Saunders, M., Small, A., Dedicoat, M., & Roberts, L. (2012). The development and validation of a risk score for household infestation by Triatoma infestans, a Bolivian vector of Chagas disease. Trans R Soc Trop Med Hyg, 106(11), 677-682. doi: 10.1016/j.trstmh.2012.07.006
Secor, W. E. (2015). Early lessons from schistosomiasis mass drug administration programs. F1000Res, 4. doi: 10.12688/f1000research.6826.1
Sime, H., Deribe, K., Assefa, A., Newport, M. J., Enquselassie, F., Gebretsadik, A., . . . Davey, G. (2014). Integrated mapping of lymphatic filariasis and podoconiosis: lessons learnt from Ethiopia. Parasit Vectors, 7, 397. doi: 10.1186/1756-3305-7-397
Smith, J., & Taylor, E. M. (2013). MDGs and NTDs: reshaping the global health agenda. PLoS Negl Trop Dis, 7(12), e2529. doi: 10.1371/journal.pntd.0002529
Stanton, M. C., Best, A., Cliffe, M., Kelly-Hope, L., Biritwum, N. K., Batsa, L., & Debrah, A. (2016). Situational analysis of lymphatic filariasis morbidity in Ahanta West District of Ghana. Trop Med Int Health, 21(2), 236-244. doi: 10.1111/tmi.12643
Stanton, M., Molineux, A., Mackenzie, C., & Kelly-Hope, L. (2016). Mobile Technology for Empowering Health Workers in Underserved Communities: New Approaches to Facilitate the Elimination of Neglected Tropical Diseases. JMIR Public Health Surveill, 2(1), e2. doi: 10.2196/publichealth.5064
Streiger, M, Mainero, M.C., Bizai, M.L., Fabbro, D., Mendicino, D., Barco, M., . . . Arias, E. (2012). Perspectiva interdisciplinaria para el abordaje de una enfermedad infecciosa: chagas o tripanosomiasis americana. Rev. salud pública (Córdoba), 16(1).
Thomas, J., & Harden, A. (2008). Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol, 8, 45. doi: 10.1186/1471-2288-8-45
Triana, D. R., Mertens, F., Zuniga, C. V., Mendoza, Y., Nakano, E. Y., & Monroy, M. C. (2016). The Role of Gender in Chagas Disease Prevention and Control in Honduras: An Analysis of Communication and Collaboration Networks. Ecohealth, 13(3), 535-548. doi: 10.1007/s10393-016-1141-9
Tufte, Thomas, & Mefalopulos, Paolo. (2009). Participatory communication : a practical guide. Washington, D.C.: World Bank.
Turner, M.M., Skubisz, C., & Rimal, R.N. (2011). Theory and practice in risk communication: A review of the literature and visions of the future. In T. L.

137 Thompson, R. Parrott & J. F. Nussbaum (Eds.), The Routledge Handbook of health communication (Second ed.). New York: Routledge.
Uneke, C. J., Ezeoha, A. E., Uro-Chukwu, H., Ezeonu, C. T., Ogbu, O., Onwe, F., & Edoga, C. (2015). Enhancing the Capacity of Policy-Makers to Develop Evidence-Informed Policy Brief on Infectious Diseases of Poverty in Nigeria. Int J Health Policy Manag, 4(9), 599-610. doi: 10.15171/ijhpm.2015.100
Upadhyayula, S. M., Mutheneni, S. R., Kadiri, M. R., Kumaraswamy, S., & Nagalla, B. (2012). A cohort study of lymphatic filariasis on socio economic conditions in Andhra Pradesh, India. PLoS One, 7(3), e33779. doi: 10.1371/journal.pone.0033779
Valdez-Tah, A., Huicochea-Gomez, L., Ortega-Canto, J., Nazar-Beutelspacher, A., & Ramsey, J. M. (2015). Social Representations and Practices Towards Triatomines and Chagas Disease in Calakmul, Mexico. PLoS One, 10(7), e0132830. doi: 10.1371/journal.pone.0132830
Valente, T. W., & Fosados, R. (2006). Diffusion of innovations and network segmentation: the part played by people in promoting health. Sex Transm Dis, 33(7 Suppl), S23-31. doi: 10.1097/01.olq.0000221018.32533.6d
Ventura-Garcia, L., Roura, M., Pell, C., Posada, E., Gascon, J., Aldasoro, E., . . . Pool, R. (2013). Socio-cultural aspects of Chagas disease: a systematic review of qualitative research. PLoS Negl Trop Dis, 7(9), e2410. doi: 10.1371/journal.pntd.0002410
Viotti, R., Alarcon de Noya, B., Araujo-Jorge, T., Grijalva, M. J., Guhl, F., Lopez, M. C., . . . Latin American Network for Chagas Disease, Nhepacha. (2014). Towards a paradigm shift in the treatment of chronic Chagas disease. Antimicrob Agents Chemother, 58(2), 635-639. doi: 10.1128/AAC.01662-13
Visser, B. J. (2012). Dracunculiasis eradication--finishing the job before surprises arise. Asian Pac J Trop Med, 5(7), 505-510. doi: 10.1016/S1995-7645(12)60088-1
Waleckx, E., Camara-Mejia, J., Ramirez-Sierra, M. J., Cruz-Chan, V., Rosado-Vallado, M., Vazquez-Narvaez, S., . . . Dumonteil, E. (2015). An innovative ecohealth intervention for Chagas disease vector control in Yucatan, Mexico. Trans R Soc Trop Med Hyg, 109(2), 143-149. doi: 10.1093/trstmh/tru200
Wang, S., Carlton, E. J., Chen, L., Liu, Y., & Spear, R. C. (2013). Evaluation of an educational intervention on villagers' knowledge, attitude and behaviour regarding transmission of Schistosoma japonicum in Sichuan province, China. Acta Tropica, 127(3), 226-235. doi: 10.1016/j.actatropica.2013.05.009
Webster, J. P., Gower, C. M., Knowles, S. C., Molyneux, D. H., & Fenton, A. (2016). One health - an ecological and evolutionary framework for tackling Neglected Zoonotic Diseases. Evol Appl, 9(2), 313-333. doi: 10.1111/eva.12341
Whitty, C. J. (2015). Political, social and technical risks in the last stages of disease eradication campaigns. Int Health, 7(5), 302-303. doi: 10.1093/inthealth/ihv049
Wijesinghe, R. S., & Wickremasinghe, A. R. (2015). Physical, psychological, and social aspects of quality of life in filarial lymphedema patients in Colombo, Sri Lanka. Asia Pac J Public Health, 27(2), NP2690-2701. doi: 10.1177/1010539511434140
Yevstigneyeva, V., Camara-Mejia, J., & Dumonteil, E. (2014). Analysis of children's perception of triatomine vectors of chagas disease through drawings:

138 opportunities for targeted health education. PLoS Negl Trop Dis, 8(10), e3217. doi: 10.1371/journal.pntd.0003217
Yoshioka, K. (2013). Impact of a community-based bug-hunting campaign on Chagas disease control: a case study in the department of Jalapa, Guatemala. Mem Inst Oswaldo Cruz, 108(2), 205-211.
Zeldenryk, L., Gray, M., Gordon, S., Speare, R., & Hossain, M. (2014). The use of focus groups to develop a culturally relevant quality of life tool for lymphatic filariasis in Bangladesh. Qual Life Res, 23(1), 299-309. doi: 10.1007/s11136-013-0455-0
Ziperstein, J., Dorkenoo, M., Datagni, M., Drexler, N., Murphy, M., Sodahlon, Y., & Mathieu, E. (2014). Final program evaluation methods and results of a National Lymphedema Management Program in Togo, West Africa. J Epidemiol Glob Health, 4(2), 125-133. doi: 10.1016/j.jegh.2013.11.001
Zhou, X., Yap, P., Tanner, M., Bergquist, R., Utzinger, J., & Zhou, X. (2016). Surveillance and response systems for elimination of tropical diseases: summary of a thematic series in Infectious Diseases of Poverty. Infectious Diseases of Poverty, 5(1), 49. doi:10.1186/s40249-016-0144-7

139 Chapter 5: Towards a Theory of Sustainable Prevention of Chagas Disease:
An Ethnographic Grounded Theory Study
Introduction
Chagas disease is caused by Trypanosoma cruzi (T. cruzi), a protozoan parasite
that can be found the hindgut of blood-sucking bugs known as triatomines. The most
common route of human transmission of CD occurs in domiciliary environments where
triatomines can remain hidden in cracks and crevices during the day and become active at
night to search for blood sources. Triatomines feed on people’s blood while they are
sleeping; in order to make room for larger meals, triatomines defecate and leave the
parasite on people’s skin. Inadvertently, bitten individuals bring T. cruzi to their system
by rubbing the punctured wound where triatomines have been feeding from or through
the mucus membranes in mouth and eyes. Once the parasite enters the human system, it
invades cells around the entry site and multiplies inside them. At this point, the parasite
turns into trypomastigotes that are released into de blood system, starting the acute phase
of the infection. People can show mild symptoms or remain asymptomatic for long
periods of time, until they develop the next phase of T. cruzi infection known as chronic.
At this stage people can experience arrhythmias, palpitations, and chest pain (Gascon et
al., 2014). About 30% to 40% of the affected population develops cardiopathies,
alterations of the gastrointestinal system such as megacolon and mefaesophagus,
neurological or a mix of these clinical manifestations in latter stages of the disease
(Soriano-Arandes et al., 2014).
CD has been classified as a neglected tropical disease because it is commonly
found among people living in poverty in tropical and subtropical regions of Central and

140 South America, as well as the south of the United States (Hotez, 2014). No vaccine
has been developed, and medicines used to treat its symptoms in the acute phase —
nifurtimox (Bayer) and benznidazole (Roche)— have shown side effects that become
more serious as a patient’s age increases, including renal and hepatic complications
(Viotti et al., 2014). Other forms of transmission include intake of contaminated food,
vertical transmission from mothers to infants, and blood transfusion (World Health
Organization, 2012b).
Recent estimates from the World Health Organization (WHO) showed that around
5,742,167 people are infected with T. cruzi in Latin America, approximately 199,872 of
them in Ecuador (World Health Organization, 2015). Ecuador shows the highest
percentage of population at risk due to domiciliary infestation in the continent (28.99%),
an estimated incidence of 14 people per 100,000 inhabitants —the highest after Bolivia,
Argentina and Paraguay—, and mortality rates around 2.5% per 100,000 inhabitants per
year (Dumonteil et al., 2016). In spite of successful control efforts developed by the
National Chagas Disease Control Program since 2003 (Dumonteil et al., 2016; Quinde-
Calderon, Rios-Quituizaca, Solorzano, & Dumonteil, 2016), CD is still present in the
country, particularly in areas where environmental factors and living conditions create
favorable spaces for triatomine infestation. In 2003, Loja province in southern Ecuador,
was identified as one of those areas. It has been established that around 35% of
households in some areas of this province have shown infestation with triatomines, with
seroprevalences between 3.6% and 3.9% (Grijalva et al., 2005; Thomson, Thomas,
Sellstrom, & Petticrew, 2008). Domiciliary infestation in the province has been
associated with presence of pigs and goats in perdomestic areas, lack of latrine/toilet,
141 storage of agricultural products inside the house and presence of fruit trees (Grijalva
et al., 2015).
Even though CD exhibits a very complex transmission cycle (Noireau, Diosque,
& Jansen, 2009), ongoing contact between humans and vectors increases the possibilities
of contracting the infection and developing the disease (Bustamante et al., 2009).
Consequently, multiple control programs focused on interrupting CD transmission cycle
by improving living environments of populations at risk have been developed in the last
few years. Following the World Health Organization (WHO) recommendations (World
Health Organization, 2012b), such programs have implemented measures such direct
spraying with delthametrine and community surveillance in combination with different
types of infrastructural interventions, including improved sanitation and provision of high
quality and durable plastering materials (Bustamante et al., 2009); amelioration of
ventilation and illumination openings (Rojas de Arias et al., 1999); cracks fixing
(Lardeux et al., 2015); and, complete replacement of dwellings (Santos et al., 2016).
Home improvement for disease prevention.
Considering the high impact that housing structures can have on the overall health
of their inhabitants (Haines et al., 2013; Thomson & Petticrew, 2007; Thomson,
Sellstrom, & Thomas, 2007; Thomson et al., 2008), it is not rare to find associations
between infrastructural interventions and control of one or more vector transmitted
diseases (Lindsay et al., 2003; Lucero et al., 2013). It has been documented, for example,
that malaria was eradicated in the United States and substantially reduced in Panama
during the construction of the Panama Canal through specific infrastructural measures,
including installation of screens in doors and windows (Lindsay et al., 2002).

142 However, home improvement measures are considered difficult to justify from
scientific and financial points of view. Confounding factors make difficult to establish a
causal relationships between home improvement and better health (Thomson et al., 2008;
Vale et al., 2013), and cost-effectiveness arguments indicate that cheaper, faster, and
more specific solutions for disease prevention might exist (Knudsen & von Seidlein,
2014; Thomson, 2005). Even if relevant from implementation points of view, these
arguments do not reflect potential impacts of home improvement over comprehensive
public health agendas (Haines et al., 2013).
In the specific case of Chagas disease, previous studies have shown promising
results, including significant reductions of infestation by Triatoma infestants in dwellings
of indigenous communities in Bolivia (Lardeux et al., 2015); sustained reduction of
Triatoma dimidiata homestead presence for over five years in rural communities of
Guatemala (Lucero et al., 2013), and, elimination of domestic transmission with T.
infestants in highly endemic areas of Bolivia, Paraguay, North Argentina and in the
Brazilian states of Minas Gerais, Bahia, and Rio Grande do Sul (Dias, 2007).
Additionally, increased knowledge about vectors and awareness on Chagas disease
transmission cycles has been associated with participatory approaches to housing
improvement (Waleckx et al., 2015). However, more information is needed to understand
the impact of home improvement over other socio-economic factors associated with
Chagas disease transmission, as well as the sustainability of these efforts (Gurtler &
Yadon, 2015).

143 Systemic approaches to Chagas disease prevention.
Different from disease-centered approaches, systemic approaches to disease
prevention identify and anticipate synergies, reactions and interactions between actors
and contexts that should be considered by policy designers when addressing issues of
social justice such as the ones claimed by the NTD category (Gilson et al., 2011).
Systemic perspectives have been considered in NTD prevention when attempting to
include not only the biomedical conditions experienced as a consequence of infectious
diseases, but also the different forms of exclusion that constitute the experience of
marginalization for neglected populations.
Good quality housing can be considered a constitutive element of functional
health systems (Lindsay et al., 2002). Home improvement directly impacts socio cultural
dynamics beyond the physical elements of the construction. Aspects such as lifestyle,
culture, family composition, motivation, social class, time constraints, and perception of
wellness influence decision-making about materials and structure of dwellings (Gibler &
Nelson, 2003). In resource-constrained settings, additional elements, such as availability
of construction materials, populations’ income levels, relationships with local authorities,
and access to alternative models of housing, should also be considered (Hardoy,
Cairncross, & Satterthwaite, 1990).
Integrative models such as Ecohealth (Briceno-Leon, 2009; Dumonteil et al.,
2013) and One Health (Webster et al., 2016) have worked under a systemic perspective
with varied results for Chagas disease prevention. Eco-health (Forget & Lebel, 2001) has
been proposed as a way to improve people’s health, while strengthening communities and
promoting environmental sustainability. Six principles guide research conducted under

144 eco-health perspectives: systems thinking, transdisciplinary research, participation,
sustainability, gender and social equity, and knowledge to action (Charron, 2012). Eco-
health researchers acknowledge that the practice of systems thinking generates important
challenges for the actual implementation of control measures, particularly because they
require balance between methodological flexibility and rigor, which in turn generates
challenges for evaluating their effectiveness both in terms of disease control and costs
(Gurtler & Yadon, 2015).
When applied to Chagas disease, Eco-health approaches have been applied in
projects interested in improving infrastructure with some variations according to specific
implementation contexts. In Guatemala, for example, educational workshops, improved
insecticide spraying for tiled roofs and walls, participatory rodent control measures,
waste management, productive household activities and participant based reflective
process were developed (Bustamante et al., 2014). Similarly, low-cost housing
improvement techniques, promotion of house cleaning activities, removal of chickens and
dogs from human dwellings, and community participation have been combined in Bolivia
(Lardeux et al., 2015), whereas installation of window screens and education workshops
addressing management and cleaning of chicken coops have been implemented in
Mexico (Waleckx et al., 2015). Although important improvements in the general health
of the population were achieved in all these cases, additional resources are required to
follow up and appraise the sustainability of these efforts.
Similarly, the One-Health approach highlights the need for interdisciplinary and
comprehensive approaches to health promotion when addressing intersections between
health and ecosystems (Webster et al., 2016). By highlighting interactions between living

145 conditions and disease, this approach has made visible synergistic dynamics
facilitating infectious disease occurrence in contexts of poverty (Mackey & Liang, 2012).
One Health heavily relies on systems thinking to propose potential routes of action and
evaluating interventions’ effectiveness under premises of sustainability. Considering the
dynamic nature of all the constitutive elements of human environments, sustainability not
only refers to time, but also to space and the finitude of resources (World Health
Organization, 2012a). One Health proposes an ecological interpretation of disease in
which both current and future variations and effects of infectious diseases, including
evolutionary factors driving to drug resistance, change of hosts, and hybridization and
unexpected changes of infectious agents resultant from particular control measures, are
considered (Webster et al., 2016). The One Health approach advocates for a better
understanding of the knowledge and values of populations at risk of NTD beyond the
operative restrictions that those conceptualizations about their role as beneficiaries might
suggest (WHO, 2012).
Healthy Homes for Healthy Living (HHHL), a Chagas disease control program
currently developed in Loja province (Ecuador), follows the logics proposed by systemic
approaches to disease prevention. By studying HHHL, we intend to advance knowledge
on sustainability of Chagas disease control programs based on home improvement.
Consequently, I aimed to answer the following research question: What factors contribute
to or limit sustainable control of Chagas disease in the communities of Chaquizhca,
Bellamaria and Guara under the model proposed by Healthy Homes for Healthy Living?

146 Methods
Study area.
This study was conducted in Calvas county in Loja province, southern Ecuador.
Loja province shows a series of environmental conditions that favor presence of several
species of triatomines. The species Triatoma carrioni has been found in the northern and
southern areas of the province (altitudes ranging from 831 to 2,242 masl), while
Pastrongelous chinai has been found in in a wide range of altitude (175 to 2,003 masl)
and four ecological zones (Grijalva et al., 2015). Rhodnius ecuadoriensis —the most
common species in Calvas county—has been found in areas with altitudes ranging from
275 to 1,948 masl in the central and western portions of the province (Grijalva et al.,
2012). These areas are usually abundant in fruit trees that can host rodents and bird nests,
both factors previously associated with triatomines’ presence in sylvatic environments
(Grijalva et al., 2012; Suarez-Davalos, Dangles, Villacis, & Grijalva, 2010).
Climatological conditions associated with dry low mountain forest and dry tropical forest
common in this region have ben also identified as favorable for triatomines’ infestation
(Abad-Franch et al., 2001)
Socio-economic conditions have also been referred as risk factors in CD
transmission. Being an agricultural region, most families in Loja province rely on
economic activities that require ongoing association with their living environments. This
association is closely linked with practices previously identified as risk factors for CD
transmission, including accumulation of produce in the surrounding areas of the home,
interaction with pigs, as well as presence of dogs and guinea pigs (Grijalva et al., 2015).
Deficient housing has also been referred as a fundamental element of CD transmission in

147 Loja province, particularly when dwellings are built with adobe walls and earthen
floors (Grijalva et al., 2005) or do not have sanitary facilities available (Grijalva, Villacis,
Ocana-Mayorga, Yumiseva, & Baus, 2011).
This research was conducted in Bellamaria (36 homes), Chaquizhca (42 homes),
and Guara (48 homes), three communities of Loja province where HHHL’s intervention
has taken place. Socio-economic conditions are adversely affected by limited job
opportunities, as well as deficient access to basic services such as water, health and
education (Nieto-Sanchez, Baus, Guerrero, & Grijalva, 2015). Poor roads and limited
transportation alternatives increase isolation and marginalization faced by local families,
and restricts their access, participation and competitiveness in larger markets. These
communities were chosen as focus of HHHL’s intervention due to particularly high rates
of triatomine’s infestation registered during entomological searches conducted by the
Malaria National Service in Loja province between 2005 and 2009 (Grijalva et al., 2015).
Healthy Homes for Healthy Living model (HHHL).
The Healthy Living Initiative (HLI) is a health promotion program designed to
address socio-economic dynamics leading to CD occurrence in Loja province (Nieto-
Sanchez et al., 2015). Led by the Infectious and Tropical Disease Institute (ITDI) at Ohio
University (OU) and the Center for Research in Health in Latin America (CISeAL) at
Pontifical Catholic University of Ecuador (PUCE), the project is interested in exploring
strategies for long-term Chagas disease control as a way to address questions raised by
previous research showing that traditional control strategies suggested by WHO are
effective only for short periods immediately after fumigation (Grijalva et al., 2005).

148 HLI’s main project is Healthy Homes for Healthy Living (HHHL), a strategy
focused on designing, building, and promoting living environments conceived to deter
triatomines’ presence in intra and peridomestic areas of the homes located in these
communities. HHHL proposes a prevention model based on homes’ structural
improvement (Table 4), long-term health promotion at the micro-level of the household
(Table 5), and community involvement in locally driven income generation opportunities.
Actions in these three areas are articulated through ongoing communication between
actors with the purpose of informing decision-making at individual, interpersonal, and
institutional levels (McLeroy et al., 1988). However, due to its direct intervention in local
households, most of the work conducted by HHHL emphasizes impacts at the family
level.
Table 3. Anti-triatomine measures implemented as part of HHHL infrastructure intervention.
Intervention in domiciliary areas For full reconstruction Rationale Demolition of existing home. Avoiding reoccupation of endangered areas. Construction of a new home that includes kitchen, two or three rooms (depending on the size of the family), and social area (porch).
Reducing overcrowding.
Walls made out of small adobe blocks secured by mesh and plastered with compressed earth block (CEB) and stucco.
Securing resistance of the construction and adherence of plastering to avoid cracks and crevices that could host triatomines for extended periods of time.
Floors made out of compressed earth block (CEB).
Reducing holes in the floor where triatomines could hide.
Roofs structured with wood beams and covered by clay tiles and sheets of waterproofed asphalt.
Improving safety, reducing storage areas in ceilings that can host triatomines and improving ventilation.
Triple protection in windows (mesh, glass and wood) .
Facilitating cross-ventilation and reducing insects’ entrance.
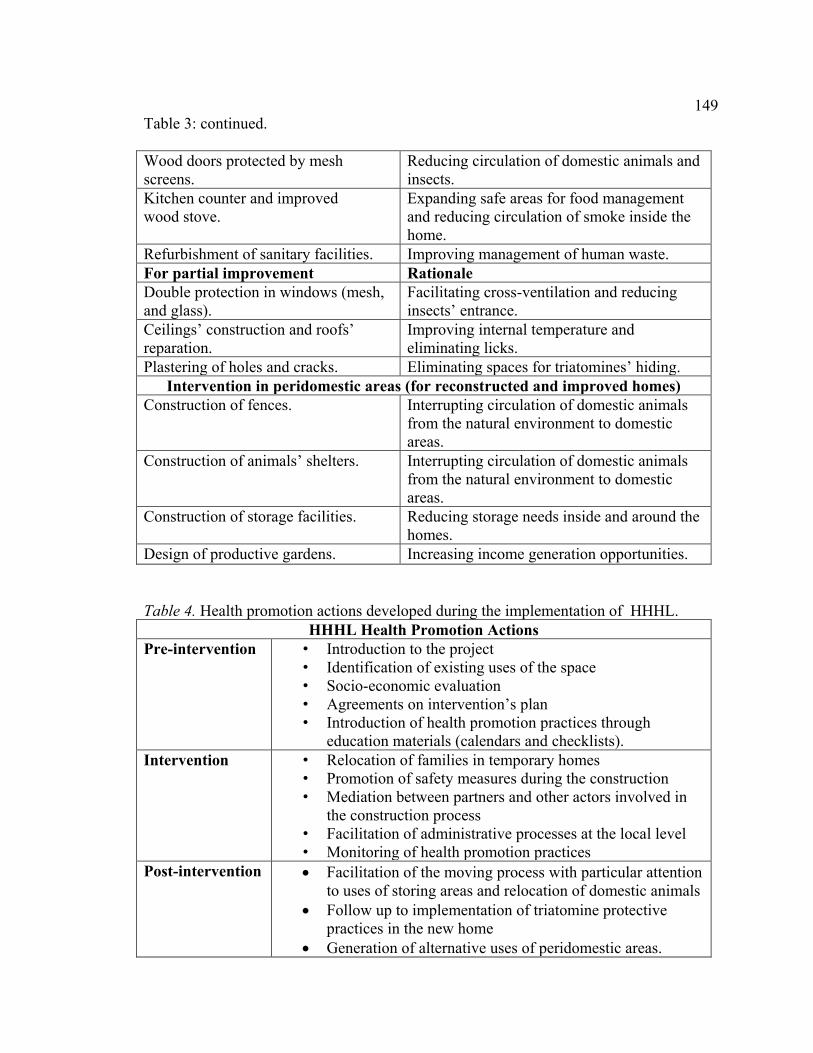
149 Table 3: continued.
Wood doors protected by mesh screens.
Reducing circulation of domestic animals and insects.
Kitchen counter and improved wood stove.
Expanding safe areas for food management and reducing circulation of smoke inside the home.
Refurbishment of sanitary facilities. Improving management of human waste. For partial improvement Rationale Double protection in windows (mesh, and glass).
Facilitating cross-ventilation and reducing insects’ entrance.
Ceilings’ construction and roofs’ reparation.
Improving internal temperature and eliminating licks.
Plastering of holes and cracks. Eliminating spaces for triatomines’ hiding. Intervention in peridomestic areas (for reconstructed and improved homes)
Construction of fences. Interrupting circulation of domestic animals from the natural environment to domestic areas.
Construction of animals’ shelters. Interrupting circulation of domestic animals from the natural environment to domestic areas.
Construction of storage facilities. Reducing storage needs inside and around the homes.
Design of productive gardens. Increasing income generation opportunities.
Table 4. Health promotion actions developed during the implementation of HHHL. HHHL Health Promotion Actions
Pre-intervention • Introduction to the project • Identification of existing uses of the space • Socio-economic evaluation • Agreements on intervention’s plan • Introduction of health promotion practices through
education materials (calendars and checklists). Intervention • Relocation of families in temporary homes
• Promotion of safety measures during the construction • Mediation between partners and other actors involved in
the construction process • Facilitation of administrative processes at the local level • Monitoring of health promotion practices
Post-intervention
Facilitation of the moving process with particular attention to uses of storing areas and relocation of domestic animals
Follow up to implementation of triatomine protective practices in the new home
Generation of alternative uses of peridomestic areas.

150 Between 2013 and 2016, HHHL worked in the reconstruction and
refurbishment of six homes in the communities of Bellamaria (n=2), Chaquizhca (n=2),
and Guara (n=2). During this period (Pilot phase), HHHL collected information about
technical and social implications of implementing infrastructure interventions in this area
according to different purposes. The 2013’s intervention was carried out with only one
family and was focused on prototyping an anti-triatomine home, as well as designing
health promotion processes to facilitate appropriation and implementation of protective
measures in an entirely reconstructed home. The 2014’s intervention aimed to understand
how to introduce anti-triatomine measures in dwellings that did not require full
reconstruction; two homes were intervened in this period, including one previously built
by the National Ministry of Housing (MIDUVI, by its acronym in Spanish). Finally,
HHHL simultaneously built three homes (one in each community) between 2015 and
2016 in order to identify logistical demands, as well as behavioral and socio-economic
impacts of conducting differentiated interventions around home improvement for CD
prevention.
Figure 2. Exemplar of a local home previous intervention.

151
Figure 3. Exemplar of a home after HHHL intervention.
In order to conduct the physical intervention of the space, HHHL has worked
under a model of partnership that examines the contributions that different stakeholders
can make to the definition and realization of healthy environments as conceived in this
particular context. Family members, neighbors, local facilitators, academic communities,
and representatives of the local government are expected to maximize existing resources
by contributing in different capacities to the execution of plans individually conceived
according to partner families’ specific socio-economic conditions. Partner families in
each stage of intervention were selected according to a number of criteria, including
interest in reconstructing their homes, capacity to commit resources to the project, and
decay status of their dwellings.
The level of decay of local construction was established after a study conducted in
2012 by PUCE’s Architecture School (unpublished data). This study identified seven
criteria to determine urgency of infrastructure intervention in the homes of these three
communities, including constructive pathologies, thermal performance, use of culturally
acceptable materials, access to water and sanitation, access to natural sunlight,
ventilation, potential risks, and cost of the required intervention. Five categories were

152 established under these criteria. Category 1 includes homes that are safe enough to
implement anti-triatomine measures without a major intervention, at an approximate cost
of USD $49.23 per m2. Categories 2 and 3 indicate some form of refurbishment required
before implementing those measures, at an approximate cost of USD $70.30 per m2 in the
former and USD $120.63 in the later category. Finally, categories 4 and 5 are specific for
homes that demand full reconstruction in order to solve structural issues that endanger the
safety of inhabitant families beyond CD transmission. Intervention costs in this case can
go from USD $158.74 for category 4 and USD $218.89 for category 5.
HHHL uses the term ‘partner family’ to refer to families that have agreed to build
or improve their homes according to the model proposed by HHHL. This rhetorical
decision was made as an alternative to the term “beneficiary” traditionally used in
development interventions. Calling local families “partners” makes visible a relationship
in which involved actors make specific contributions during the intervention, including
economic resources, labor, knowledge, and social capital. HHHL has adopted the idea of
partnership as a means of addressing local needs through collaborative activities and
decision-making sensitive to local concerns and interests as proposed by Seddon, Billett,
and Clemans (2004).
Data collection and study population.
Ethnographic grounded theory was used as main methodological framework for
this research. Grounded theory (GT) is a systematic approach to data collection and
analysis interested in generating explanations of social realities based on emerging
information grounded in actual data rather than in theory (Glaser & Strauss, 1967; Strauss
& Corbin, 1998). Constructivist approaches to grounded theory see both data and analysis

153 as the product of experiences co-created by participants, researchers, and emerging
data (Atkinson et al., 2008). Since constructivism is focused on how and why participants
construct meanings in specific situations (Deetz, 1996b; Pearce, 1989), its extension to
grounded theory looks at how, when, and to what extent the studied experience is
embedded in larger social structures in order to explain and represent research findings
(Charmaz, 2006). Constructivist Grounded Theory (CGT) alludes to the open-ended
nature of social processes, the value of human agency in meaning making, and the
fundamental role played by language, interpretation, action and temporality in research
(Strauss & Corbin, 1998). When coupled with ethnographic methods of data collection,
GT receives the name of ethnographic grounded theory.
CGT was considered an appropriate method to depict local populations’ practices,
discursive constructions, and relational dynamics that could support or limit sustainability
of the HHHL model. Consequently, participants were selected from inhabitants of the
communities of Bellamaria, Chaquizhca, and Guara in southern Ecuador that have
directly or indirectly experienced interventions led by HHHL. The study population was
divided into three groups: partner families; non-partner families, and heads of household
across the community.
The first group (Group 1) included the six families that have specifically agreed to
partner with HHHL to build or improve their homes according to the above-described
model (Table 6). At least three members of each family were interviewed in three
different moments of field visits: the first one between June and July 2016; the second in
January of 2017; and the last between May and June 2017. Participant observation during
health promotion activities was also conducted. Members of the family older than 14

154 years old were also included. In this case, minors' assent and parents' informed
consent was requested.
Table 5. Interviewees in partner families by year and type of intervention (Group 1). Year Fam.
size Community Decay
level Phase and type of
intervention Interviewees
2013 9 Guara 5 Prototype – full reconstruction
Male (55), Female (56), Male (15)
2014 7 Chaquizhca 3 Refurbishment - Partial improvement
Female (98), Female (38), Female (16)
2014 4 Bellamaria 1 Refurbishment Partial improvement
Female (81), Male (48), Female (50)
2015 6 Bellamaria 5 Simultaneous construction - Full reconstruction
Male (55), Female (56), Male (17).
2015-2016
5 Guara 5 Simultaneous construction - Full reconstruction
Male (54), Female (42), Female (77)
2015-2016
5 Chaquizhca 5 Simultaneous construction - Full reconstruction
Male (44), Female (37), Female (17).
Considering the principle of maximum variation (Lindlof & Taylor, 2011; Tracy,
2013) , the second group included an equal number of families (6) that have not
implemented HHHL intervention. They were selected to closely match the decay
category and socio-economic conditions of HHHL partners. The purpose of this part of
the study was to observe families that have not applied the HHHL model in order to
depict their understanding of health in relation to home and compare it with the
information obtained from the previous group. Following the same methodology applied
with the partner families, members of these families were interv iewed at different points

155 in time to address the questions included in the interview guide. Interviews lasted no
more than one hour and were conducted in participants' homes. Considering that the
relationships established between the researcher and families included in this group was
not as extensive as with families included in group 1, only two members of these families
were interviewed during the same periods of data collection.
Table 6. Interviewees in non-partner families (Group 2). Case Total
Inhabitants Community Decay
level Interviewees
1 11 Bellamaria 5 Male (46), Female (42) 2 6 Bellamaria 3 Male (30), Female (28)
3 5 Chaquizhca 1 Male (48), Female (49) 4 7 Bellamaria 5 Male (33), Female (29) 5 4 Guara 5 Male (71), Female (60) 6 8 Chaquizhca 5 Male (40), Female (42)
The third group (Group 3) included heads of household of the communities at
large (n=102). Participants completed a facilitated paper-based forty-one (41) item
questionnaire that included questions about physical conditions of the dwelling, socio-
economic status of the family, and interest in home improvement in the near future (see
Appendix 2). This information was collected in order to create a larger picture of the
communities at large that could serve as reference for theory development in later stages
of analysis. Group 3 is cross-sectional and not exclusive of groups 1 and 2. Information
collected with this group will be further analyzed in a separate paper.
Data analysis.
The analytical processes conducted within this research were aimed at expanding
understanding of sustainability of CD control programs based on home improvement by

156 including contextualized data emerged from HHHL implementation. Therefore,
‘sustainability’ was used as sensitizing concept. Sensitizing concepts are interpretive
devices used as “points of departure for studying the empirical world while retaining the
openness for exploring it” (Charmaz, 2014, p. 30). In order to operationalize
sustainability as concept, I used the Pan American Health Organization (PAHO)
parameters for sustainable management of NTD in the region (Holveck et al., 2007): (i)
vector control; (ii) provision of water and sanitation; (iii) management of zoonotic
elements of the disease; and (iv) community participation. Interview protocols and
questionnaires were structured around these parameters.
More than 40 hours of interviews with partner and non-partner families, 150
pages of implementation reports, 102 questionnaires, as well as field notes taken during
informal conversations and participant observation, were analyzed in two phases of
coding (Saldana, 2016). The initial coding phase involved assigning codes to words or
larger segments of transcribed materials, whereas the second phase aimed to identify the
most significant codes in order to sort, synthesize, integrate, and organize them toward
theory construction (Charmaz, 2014). Since this research was conducted in Ecuador with
Spanish-speaking communities, initial coding schemes were constructed in Spanish using
a line-by-line approach.
For the phase of initial coding, I used process and in-vivo coding. Process coding
is an approach particularly associated to CGT, as it uses gerunds “to connote action in the
data, both simple observable activities as well as larger process” (Saldana, 2016, p. 111).
Process coding was particularly suitable for this research because it preserves the fluidity

157 of participants’ experience (Charmaz, 2014), which can lead to situated
reconstructions of HHHL as a process. Examples of process coding are provided in Table
7.
Table 7. Exemplar of process coding.
Original quote Translation Codes (Initial coding - Spanish)
Category (Focused coding – English)
“Ecuatorianos habíamos muchísimos en España y ahora pues tengo intenciones de devolverme. Pero por supuesto si me consiguen un contrato de trabajo. Sin contrato pues no me voy porque ya sé lo que es el sufrimiento.”
“There were many Ecuadorians in Spain and now I still have the intention of going back. But of course, only if they [his family] get me a job contract. I will not go without a contract because I already know how much you have to suffer.”
Migrando
Social dynamics
In vivo coding completed the actions described through process coding. In-vivo is
“a word or short phrase from the actual language found in the qualitative data record”
(Saldana, 2016, p. 105). While paying attention to the actual language used by research
participants, I intended to amplify their voices and presence in subsequent phases of data
collection and analysis. Examples of In-vivo coding are provided in Table 8.

158 Table 8. Exemplar of in-vivo coding.
Original quote Translation Codes Category
“Así cómo quedan estas [casas] son lindas, bien aseaditas. Pero cuando queda el adobe visto es guardadero de chinches y de cucarachas. Pero en estas terminadas así no se mete nada.”
“These homes end up being pretty, very clean. But when the adobe is exposed it stores chinches and cockroaches. In these homes, when finished up this way, nothing comes in.”
Aseadito
References – Intervened home
Guardadero de chinches
References – Non-intervened home
For the phase of focused coding, I used several forms of comparative methods
(Charmaz, 2014), including comparison between partner and non-partner families, as
well as temporality and types of interventions conducted by HHHL. The 382 codes
identified and organized in Nvivo 11.4 software (QSR International, 2016) during the
initial phase of coding, were synthesized into six main categories after memo writing:
infrastructure in intervened homes, infrastructure in non-intervened homes, social
structures, community relations, relationships with HHHL staff, and future perspectives.
These categories were then sorted during the phase of theoretical sampling and integrated
into four theoretical concepts (Charmaz, 2014; Timmermans & Tavory, 2007): health
impact, emotional impact, economic impact, and social impact.
In addition to this extensive process, analytical rigor was pursued through several
avenues. In first place, I used Charmaz (2014) criteria of quality for grounded theory
studies as permanent reference along this study: credibility, originality, resonance, and
usefulness. In doing so, I remained close to the data throughout the phases of coding,
meaning-making, and theorization. My intention has been to use the ontological tenants

159 of grounded theory to maximize participants’ involvement in the co-construction of
potential answers to the research questions proposed in this study.
This goal has also been pursued by applying a pragmatic orientation towards
CGT. Considering that the theoretical elaborations emerged from this research will
partially inform decision-making for implementation of the HHHL model at medium and
large scales, understanding the actual impact of HHHL in the lives of local families, as
well as identifying the resources and barriers currently existing in the studied
communities, constitute essential information.
Finally, I acknowledge that the design of this research has been undoubtedly
influenced by my involvement in HHHL’s conceptualization and implementation. The
main rationale driving the conception of this research has been to approach the
experience of partner and non-partner families with concepts and ideas relevant in their
own context in order to depict the complexity of their viewpoints in interaction with
external actors. Rather than a limitation, I consider that my previous involvement with
this project has equipped me with background knowledge useful to make methodological
decisions and contextualize collected data. Since I had interacted with most research
participants at some point during my work on this area, this involvement also facilitated
their decision to take part of this process under informed references. As a result, their
answers showed not only willingness to participate, but also openness to discuss sensitive
issues that can significantly contribute to the quality of the results hereafter presented.
Ethics.
IRB protocols approved by the Ethical Committee for Research on Human
Subjects at Ohio University (16-X-209) and the Research Ethical Committee at Pontifical

160 Catholic University from Ecuador (Oficio-CEISH-232-2016). Minors' assent and
parents' informed consent were requested when appropriate.
Results
This study aimed to approach the experiences of partner families in relation to the
construction and use of the homes promoted as anti-triatomine solution. I also intended to
identify factors that contribute to or limit sustainable control of Chagas disease under the
model proposed by HHHL. Consequently, the following section will expand on four
theoretical concepts emerged once the categories identified during the phase of focused
coding (infrastructure in intervened homes, infrastructure in non-intervened homes, social
structures, community relations, relationships with HHHL staff, and future perspectives).
were sorted and integrated into analytical memos during the phase of theoretical sampling
(Charmaz, 2014). These theoretical categories are: health impact, emotional impact,
economic impact, and social impact.
Health impact.
According to local families, HHHL’s model promotes conditions for better health
expressed in five areas: safety; vector control; water, hygiene, and sanitation; separation
from animals; and storage options.
Safety.
When people ask about my house, I always tell them that this model has three benefits: these homes are elegant, clean, and healthy. They are elegant because they are modern; clean because no animal comes in, not even bugs or cats; and healthy because they are natural (…) Clay tiles, wood, and adobe are natural materials, and with these larger windows, air circulates in and out all the time. Male, 54, Guara.
161 Community members referred to HHHL model as the “Golden House” (Casa
de Oro), in reference to difference between the structures proposed by HHHL and
traditional housing models existing in this area. They called them ‘luxurious’, ‘elegant’,
and ‘similar to a city house.’ The idea of luxury comes from elements of the new
construction that are not considered necessary in traditional homes. Even though most
homes in these communities are also made out of adobe (over 73% according to HLI
unpublished data), they follow a basic construction pattern in which adobe walls are
raised on top of stone foundations assembled above the ground, followed by dirt floors,
wooden beams, bamboo ceilings, and clay tile’ roofs. Under this model, walls and
foundations remain visible and exposed to environmental conditions throughout the
years. HHHL homes are also built with adobe blocks, but under most recent construction
techniques that reduce their size and bring more stability to the construction. In order to
slow down its natural decay and avoid cracks, adobe walls are covered with mesh and
plastered with cement. Underground foundations made out of concrete, cement columns,
and steel rods are fundamental for the general structure as they make it more solid and
seismic resistant.
Formative research conducted to formulate the HHHL model showed perceived
advantages of adobe constructions over other materials in this area (Nieto-Sanchez et al.,
2015). In general, adobe is considered fresher and more affordable than bricks because
local families can make it with materials freely available in the natural environment such
as manure, grass and water. Moreover, since most families have built their homes with
this material, there is a base of available and affordable expertise when needed. Built
around 40 years ago, the first constructions fully made out of this material were the local

162 schools. However, only for half of that time people have been using adobe for their
own homes. When compared with plastered bamboo (the most common construction
technique previously used by local families), adobe required the additional effort of
bringing water and dirt to the construction site, sometimes located so far away from the
sources that multiple trips by donkey or horse were needed. Slowly, knowledge spread
and adobe homes started to be perceived as safer and warmer, especially because of their
capacity to sustain tile roofs.
Even if safer than previous models, traditional adobe homes face important
structural problems. A decay analysis conducted to determine HHHL’s intervention
priorities established that around 52.4% of the homes in the communities require
investments of more than US$100 per square meter in order to solve structural issues
such as lack of foundations, broken walls, and unstable roofing structures. Many of these
problems do not come from the adobe itself, but from the quality of the dirt used to make
it. According to the interviewees, ‘good dirt’ can make durable adobe homes that can
resist more than 20 years of use without major issues. Bad dirt, instead, can easily molder
and substantially diminish the thickness and resistance of the walls over time. This
condition is also associated with the presence of cracks that host triatomines and other
insects. One of the interviewees expressed that even though traditional homes tend to
have a useful life of 10 to 12 years, he had to reconstruct his after only 8 years of
occupation because it had been built with muddy dirt. He was contacted by HHHL in
2013 when the prototype house was built, but he rejected the offer arguing that his house
would not resist all the time required to complete the project:

163 My house couldn't resist more. I was very concerned thinking that it would collapse during the next rainy season because the walls had profound cracks. I had no option but immediately building a new house. Male, 48, Chaquizhca. Similar sense of urgency moved partner families to accept the idea of
reconstructing their homes using the HHHL model. None of them mentioned particular
concerns regarding triatomines or disease presence; instead, safety of their families was
mentioned as a determinant factor to make this decision:
Our previous house was about to kill us. Everything was poorly done, poorly built… it was moldering. Female, 56, Bellamaria. Safety was mentioned by all family members when asked about contributions of
the new model to their health. Arguments about safety referred to resistance to tremors
derived from walls sustained with steel rods, foundations that can take all the weight of
the structure, and efficiency of the roof to prevent leaks. HHHL’s homes are also
perceived as of better quality because the adobes used to build them are mechanically
compressed and contain less residual materials, which makes them stronger and more
compact. Cement plastering is perceived as an efficient way of protecting the home from
decay.
Local families perceive damages in the roof as more serious than other structural
problems, particularly during the rainy season. Winter comes with constant rain, strong
winds, and mudslides that make more visible the structural problems of the homes. Since
most families place tiles on the roof without a system that secures them, they tend to
move easily with the wind or animals’ activity. Families wait until the first rains to locate
leaks produced by broken tiles. It is common having to deal with water, garbage and
guano falling from the roofs to their beds during this time of the year. This problem can

164 be so serious that families cannot stay or need to reorganize themselves inside the
house to find protection. Collecting water coming from the roof with black plastic bags
internally attached to the tiles, as well as moving beds to avoid the leaks, are other
common practices. If major issues emerge or worsen during this period, families have no
other alternative than living with them for as long as the rainy season lasts because adobe
constructions cannot be repaired with wet dirt. Rain can create additional problems when
adobe surfaces’ are washed off as a result of ongoing friction with water. As explained in
the following quote, partner families expressed satisfaction because the last rainy season
was particularly intense (because of El Niño phenomenon occurring at that time in Latin
America) and they did not experience any problem with leaks:
What I like the most about this new house is that we don't have to deal with rain during the night. The previous house had so many leaks that we had to squeeze one against the other in our beds in order to avoid them. Also, there is no dirt falling to our beds because water cannot bring it in anymore. Male,17, Bellamaria. Of the intervened homes, only the repaired ones present issues with leaks.
Structural problems were not fully corrected by HHHL’s intervention in these cases
because it was only intended at installing anti-triatomine measures and improving
internal comfort. As a result, leaks were not sealed and are creating additional problems
in wooden ceilings installed by the program.
Another important difference between reconstructed and improved homes is that
while the former are considered fresh, the later keep registering elevated temperatures in
the interior of the homes. Partner families of fully reconstructed homes coincided in that
tile roofs and adobe walls contribute to the amelioration of interior temperatures. Even
when compared with options that can speed up the construction process (such as bricks or

165 cement blocks), lower temperatures are considered an important advantage of adobe
construction:
I feel so confortable and happy with my house because it is really fresh. I can even sleep with the windows wide open: the mesh protects us and nothing else is necessary. Male, 55, Guara. This is not the situation for improved homes. In the case of the family whose
home was initially constructed by MIDUVI, the house is rarely used during daytime due
to the heat accumulated through the fiber-cement roof. Cooking and social activities are
conducted in an old abobe home remaining next to the improved construction, while the
renovated one is only used at night and mainly to sleep. The other refurbished home also
reports high temperatures, particularly during nighttime. In this case, the family only
closes the door screens at night and sleeps with doors and windows wide open.
Partner families reported only opening their window covers when they are at
home, even during the dry season. Glass protection is closed most of the time to prevent
dust from coming into the house. Having natural light is also reported as an advantage of
maintaining windows open at all times and only strong winds that threat with breaking
the glass protection would force them to close wood shutters.. HHHL models have been
designed considering cross ventilation between doors and windows in all rooms in order
to reduce the temperature of the house. However, families do not seem to be aware of this
measure and often stay in the house with one of the two windows or the door closed.
Non-partner families, on the other hand, reported keeping doors and windows
closed at all times to reduce presence of animals and dust:
We close everything because it gets cold inside. Sometimes mosquitoes and chinchorros [local name for triatomines] want to come in, so we prefer to close them around six or seven. Female, 41, Chaquizhca.

166 Vector control.
Both partner and non-partner families identified presence of triatomines in their
communities. Participants mentioned that it is usual to see them flying around light bulbs:
I don't think they live in my house, but I’ve seen them climbing the wall. I pick and kill them, but they don’t have any blood inside. Female, 22, Guara Only one of the partner families has reported presence of a triatomines after the
intervention. The first time they collected them and reported to the HHHL staff; the next
time they just crushed it:
My kids found a chinchorro in one of the rooms but they crushed it right away. It did not have any blood inside, so it hadn’t eaten yet. Male, 55, Guara.
Statements like this demonstrate certain level of knowledge about Chagas disease
and its transmission cycle. This knowledge can be associated with previous campaigns
conducted by HLI with adults and kids. As explained by one of the partners:
Our homes were built because of that disease called Chagas, the chinchorro’s disease. Before the program [HHHL] came, we didn’t know anything about it. We knew that there were a lot of ‘chinches’ in the countryside and that they used to come to the houses when the lights were on. In the old times, we used to cook only with firewood and sometimes chinches came to the homes in the shell of a tree called faique. Male, 55, Guara. In spite of this familiarity, people identify insects as sources of disease. Partner
families mentioned absence of insects in relation to health improvement through the
HHHL homes. As described by one participant,
We still have some bugs coming from time to time, but you cannot compare with the previous house. We can rest assured at home because there are not even mosquitoes around. In the old house, they didn't let us sleep during the rainy season. If there were no bugs, we had rats peeing on the beds or falling from the roof. We don't have any of that anymore. Male, 54, Guara. When asked about the health of the family in traditional homes, non-partner
families expressed several concerns. The head of household of one of them mentioned

167 that her home could only partially protect his health because of the multiple problems
derived from the structure of the home:
I can protect my family from the cold and the wind with cloth rags or bed sheets. But I cannot do anything about diseases that come from flies, mosquitoes or chinchorros. They come inside because there are many cracks and we cannot cover them all. Even if I cover the cracks in the walls, they will come through the roof because we have only tiles, not a ceiling. So, I cannot protect my family from them, bugs will always find a way to come in. Male, 46, Bellamaria. Members of the partner families described similar issues in regard to their
previous homes:
There were bugs at all times: cundiles (cattle flees), centipedes, fleas... Male, 17, Bellamaria At some point in time we had to sleep under a mosquito net because bugs used to bite the kids very badly. Our ceiling was made out of bad bamboo, so bugs could easily live in there. Female, 56, Bellamaria When I had to stay late to do my homework, there were little moths flying and falling around me. They bothered me because they stained my notebooks. It is not like that anymore here. Female, 17, Chaquizhca. Some plagues are more difficult to control. Seasonal plagues such as churumbos
(locust) invariably come to the homes during the rainy season. These insects are noisy
and smell bad after dying. Since light bulbs attract them, family members remain in
darkness for longer periods of time while eating or using the social areas of the house.
Later in the night, they turn on the lights of the porch to ensure that churumbos remain
outside and do not try to access the rooms. Additionally, one of the partner families
decided to block minor spaces under the door with rags and toilet paper to avoid them
from coming to the house. Partner families also pointed out that cockroaches are
frequent; their capacity to infest the house via pipes, sacks and cardboard boxes make
them even more difficult to control.

168 The use of mesh is one of the measures promoted by HHHL to prevent
triatomines’ entry to the homes. This element is not common in this region, not even in
more affluent areas of the province. HHHL has tested different materials and models,
most of them showing quality problems. Participants identified strong winds, quality of
construction materials, kids introducing objects or pushing the door from the mesh,
installation issues, and faulty design as the main causes for the openings found in the
mesh in all homes. Spaces that have more circulation of people, particularly kitchens,
showed even more problems.
Besides these quality issues, partner families showed acceptance of screens in
windows and doors. Keeping and repairing them when broken (although not
immediately), are some of the practices that illustrate this acceptance. Similarly, multiple
bugs were found outside the mesh in windows of kitchens and rooms during the visits
conducted for this research. Families reported sleeping only with the mesh protection
most of the year.
With the purpose of reducing openings for bugs’ circulation, HHHL installed
small weights to keep doors’ screens closed. This solution has served this purpose in
bedrooms that are not used very often during the day, but not in areas of more circulation
like the kitchen, especially when all members of the family or guests are present. In those
cases, families install objects to lock the doors open in order to facilitate circulation of
people.
Besides bugs, non-partner families reported presence of reptiles and scorpions in
accumulations of debris, as well as sacks with corn and cardboard boxes with clothes.
Two of the non-partner families also reported permanent use of mosquito nets as

169 protective measures regardless of the season. Concerns about insects are explained in
the following quote:
We are exposed to rats, chinchorros, leaks, humidity, dirtiness coming from the roof… there are many risks here in the countryside. There are also mosquitoes that bite us often, and some people get sick with paludism [Malaria]. If we see insects around, we just turn the light on and kill them. Male, 71, Guara. Consequently, fumigation remains the most common control measure for plagues’
control in the area. We observed that partner families continue relying on this traditional
control method in combination with the measures proposed by the model. Products
commonly used in this practice include Nuvan (DDVP), Malation (malaoxon), Bala
(chlorpyrifos and cipermetrina), Pix (cipermetrina), and Puñete (chlorpyrifos), and
sometimes plants that are considered natural insecticides such as porotillo (Fallopia
convolvulus), moshquera (Croton sp.), florblanca (Buddleja utilis, also known as mon-
teramirez) and chamana (Dodonaea viscosa). The most common times for fumigation are
the beginning of the rainy season (January or February), and October, the preferred time
for hens’ incubation. Interviewees reported fumigating in the morning, leaving the house,
and coming back when they calculate that smell has evaporated, after four or six hous.
Interviewees mentioned that they fumigate to control fleas, chinchorros, moths, ants,
cockroaches, cattle fleas, and yuyes (Paederus irritans). People also referred often to the
fumigation conducted by HLI during entomological visits in 2011 and 2012 with
delthametrine (Bayer) as particularly effective. According to them, it was highly effective
and perceived as non-toxic:
The remedy used by the Universities doesn't smell. It is not stinky, like the ones we use. And it kills all sorts of bugs. That winter [after fumigation] we didn't have anything, not even mosquitoes. Male, 30, Bellamaria.

170 Flies and mosquitos are so common that they are usually ignored. Their
presence is also associated with accumulations of fresh produce and food kept in the
kitchen. Since freezers are rare in this area, families use traditional methods to keep meat
fresh and useful for consumption, including drying it under the sun and conserving it in
covered pots in the fresh areas of the house. Flies are usually around reserved meat, even
in spaces protected by mesh. None of the interviewees considered them dangerous or
annoying.
Water, hygiene, and sanitation.
In this region, water is treasured as the most valuable resource for agriculture and
animals rising. All the interviewees declared having regular access to water at their
homes obtained through recently constructed water systems. HLI has had an active
involvement in securing access to drinking water systems for the intervened
communities. The project concluded the distribution phase of a water system in Guara in
partnership with Fundación Uriel; built a new system for Chaquizhca in partnership with
the Spanish NGO Ayuda en Accion; and improved the water collection and distribution
system in Bellamaria in partnership with Rotary Club International. Both partner and
non-partner families expressed appreciation for having this resource at hand to cover their
cooking, hygiene, and animals’ feeding needs at home. These three systems cover now
approximately 70 families in these three communities.
The experience of lacking water at home and the need to secure access to it during
the dry season has reinforced the practice of storing rainwater and water coming from the
local system in buckets and laundry tanks. This situation is especially visible in
Bellamaria, where intermittent access to water has been a historical problem with

171 devastating effects on productive activities. Community members have fresh
memories of transporting water using donkeys to their homes, as well as having to
depend exclusively on water coming from the Catamayo River up to 2016. Even though
this community is the closest to the river, they have had to experience how the increased
current of the river during the rainy season has sedimented its bed to the extent that plots
are now located at a higher altitude. For this reason, if families want to make use of water
from the river for irrigation purposes, they have to use motor pumps capable to bring
water from the river to their plots. Since this very expensive, local families prefer to
collect as much water as possible during the rainy season and keep it in their homes or
plots.
Community members that do not have access to the general water systems argued
lack of money or manpower to secure their access (as community projects, water systems
demand regular work during the construction phase or payment for usage rights from all
the beneficiaries). In these cases, community members cover their needs for water by
bringing it through hoses or carrying it in buckets from untreated sources near their
homes.
Sanitary facilities in this region are generally composed by a toilet that is filled
with water coming from a tank in the house. Disposals are conducted to a septic tank
located in the peridomestic area. The availability of water in families’ plots has facilitated
the use of latrines; therefore, most of HHHL interventions in this aspect have been
focused on bringing water to latrines and showers through hoses or pipes. All partner
families reported regular use of these facilities even before HHHL’s intervention in their
homes.
172 Partner families stated that cleaning practices have not radically changed with
the new home structure. The main difference they can perceive is that their work in this
area is more visible. Activities such as sweeping and mopping are conducted on regular
basis, usually by the mother or younger members of the family. Most families use
conventional brooms to sweep the home on daily basis, and brooms made out of bushes
to sweep the peridomestic area one or two times a week. Local bushes (mushquera,
florblanca, chamana) are known for having acidic properties that make of them effective
natural insecticides and particularly useful to control flees. Although partner families are
hesitant to use them against the cement floor due to the green stain they produce, they are
widely used in the communities. Throwing buckets of water in the floor every couple of
weeks, as well as sweeping walls and intersections in the roof to eliminate spider nets, are
complementary cleaning practices in the new homes.
Even when it takes more time than it used to, partner families think that HHHL
homes are easier to clean. Some of them acknowledge that they feel more motivated to
clean now than they were in the previous house:
I remember that my previous house was quite messy because we used to keep animals inside. I remember that my chickens were everywhere and since my kitchen was made out of bahareque [intertwined canes put together with mud], it did not look so clean (…) Cleaning and organizing takes more of my time now, but I feel more comfortable. Unlike myself, I want my kids to grow in a clean place. Female, 38, Chaquizhca. The whole purpose [of HHHL] is leaving healthier, living far away from rats, bugs, chinches… in the homes we used to have there were a lot of rats, cats… If you were not paying attention, you could get cat’s pee coming from the roof. It was terribly dirty. Male, 54, Guara. Non-partner families can also appreciate cleanliness as an advantage: Those homes have the advantage of looking clean and organized. When you have something like that, you feel like having flowers, keeping it pretty, clean it. I think

173 they are easier to clean because of the cement floor and the ceramic. In houses like mine (traditional) you can sweep and sweep, but there is no way that you can make them look clean. Female, 60, Guara, Families report that a more thorough cleaning of the house is part of the
agreement reached with the program. In some cases, I observed that partner families
apologized with HHHL local facilitator because they had no time to clean and organize
their homes before his visit. Regular cleaning, as well as keeping animals and insects
away from the house, was referred by partner families as effective ways of keeping the
house in good conditions. However, this activity demands ongoing work from local
families. Due to the dry nature of the terrain, there is ongoing circulation of dust that
covers belongings and food inside the home. Even sweeping the dirt floors produces
additional dust that families have to contain by throwing water on them. Other activities
characteristic of rural life, such as threshing corn or peanuts, produce additional detritus
that remain in the surroundings of the homes to be reused as food for domestic animals or
fertilizers.
Cleaning becomes more essential as more productive activities are conducted at
home. For example, according to traditional knowledge, guinea pigs grow better in places
where they can stay warm in contact with firewood stoves. They are treated with special
care because they are considered important nutrition sources, as well as a delicacy for
special occasions. Families usually throw grass and leftovers to the kitchen floor where
guinea pigs can feed themselves. Although practical because they do not demand a
separate structure, this practice requires ongoing removal of feces from the kitchen to
avoid bad smells and food contamination.

174 This practice has slightly changed for partner families. Only two of them have
kept guinea pigs after the intervention, but in both cases, they have created alternative
structures outside the homes where they can replicate traditional practices. Made out of
rags and mesh, these structures provide an intermediate solution between the demands of
the program and families’ priorities. Challenges associated with cleaning of these areas
remain. Similarly, families that work on pig’s raising need to keep important amounts of
leftovers to feed them. Collecting and keeping this food in the kitchen creates additional
challenge such as dealing with flies, cockroaches and domestic animals.
Generational conflicts emerge around some of the practices recommended by
HHHL. For example, the program insists on de-cluttering the house by making a
conscious selection of materials that the family wants to keep before moving in.
However, some family members, especially elders, are more prone to keep artifacts they
perceive as valuable or potentially useful in the future, including plastic bottles, bags,
wrapping paper, old posters and calendars. This conflict is illustrated in the following
quote:
I tell her [grandmother] not to stack sacks here. If she finds a pretty piece of cardboard, she will take it to her room. Then, when I come to clean, I try to throw it away, but she says, ‘This is my room, I can keep it here.’ Then I tell her that even if this is her room, she has to keep it clean. ‘We are not going to live as we used to. We will live better.’ Sometimes I get mad at her and we argue because my kids also sleep in her room. Female, 38, Chaquizhca. This practice could be associated with the unavailability of resources at hand to
solve practical problems in this area. Both the isolation of the communities, as well as the
lack of resources at hand, have created some sense of anticipation to unforeseen needs
that often calls for storing apparently unnecessary materials. I observed, for example, the

175 wool of an old mattress being washed, dried and stored in bags for families to make
another mattress when needed, water that comes from the shower being reused to irrigate
gardens at home, organic residuals being used to feed domestic animals, and animal feces
collected in sacks to be used as fertilizers.
Following this rationale, unlike the prototype home that was demolished using
machinery, the most recent homes intervened by HHHL were manually disassembled.
Families expressed their appreciation for this practice, not only because it reduced the
emotional impact of that moment, but also because it allowed them to reserve an
important number of pieces from the previous house that they could reuse in the future.
Wood and tiles were used in pigs, guinea pigs and goats shelters; old doors were given
away to other neighbors; and some wood beams were used in the construction of fences.
Finally, it is important to mention that these three communities show important
issues in relation to residuals’ management. Most community members throw residuals to
the open environment. As most families in this area, partner families burn plastic, paper
and hygiene products within the confines of the peridomestic zone with a frequency
varying from two times a week to once every two weeks. Even more serious is the use of
septic tanks even after surpassing their capacity. When they reach that point, community
members keep using them until another sort of problem occurs (filtration to another
family’s land, for example). This is problematic, as these tanks are located within the
confines of the home and can potentially become sources of infections and disease.

176 Separation from animals.
The practice of separating animal shelters from the family’s space is constantly
reinforced through HHHL’s health promotion activities. As explained by one of the
partners:
One thing the program wanted us to do was living separated from chickens, preventing them from nesting in our rooms. We decided to send animals to sleep far away from the homes and now they are in their own place. Male, 44, Chaquizcha. Creating a physical separation between animals and families is a significant
change in families’ routines. Only one of them had a proper fence before the intervention.
In some cases, cohabitation was so close that pigs were sleeping in bedrooms and internal
areas of the house. However, this change has been gradual and not free of conflict.
Different perspectives about the best way to raise animals have emerged among family
members, especially with elders who are used to traditional ways of animals’ raising.
These practices include keeping chickens and guinea pigs in areas of the house where
they can stay warm and ‘grow better,’ such as the kitchen and under the beds. Insistence
of the project about this practice has generated clashes than in some cases have derived
into establishing specific practices for animals’ keeping according to who owns them.
One of the female partners explained:
We have struggled a lot trying to convince my grandmother of sending animals away. She wants chicken to keep nesting in her bed. I have to be strong with her and always end up arguing because if I don't want her to keep animals inside, even less so will I let them nest here. I gave up at the end and let her feed her chickens in the porch. She is old, almost 99, you know? She cannot walk much, so I agreed. I feed my chicken outside the fence and she feeds hers here, in front of the house. Female, 38, Chaquizhca.

177 HHHL’s interventions have secured the construction of a fence that could
function as permanent separation between animals and families. However, this separation
is highly dynamic, as animals and produce circulate from and to the families’ plots on
regular basis. For example, domestic animals look for a covered shelter more often
during the rainy season; therefore, it is more common to see them around the porch and
other roofed areas of the house during this period. It also takes more effort from family
members to feed their chickens far away from the home when it is raining. I observed
more frequent presence of chicken in peridomestic areas inside the fence during the rainy
season than during the summer months. As explained by one of the heads of household,
Since we are by ourselves here, sometimes we get lazy to walk to the chicken coops to feed our chicken. We might feed them here [close to the house] but always send them back to their place afterwards. Male, 55, Guara. None of the partner families reported presence of animals inside the house.
However, we observed a hen nesting on the top of a wall in one of the intervened homes.
When we asked for the reasons to keep it there, the head of household argued that the hen
had been brought in by her husband because it can produce good fighting cocks.
Regardless of his wife’s complains, the hen was considered valuable and he was not
willing the expose it to other animals and thieves. According to the interviewee, her
husband was responsible for setting a cusha for the hen in the room and placing an egg
on it to motivate the chicken to incubate in that place. Chickens came after the first one
and they were also found on top of undone beds.
Similarly, cats and dogs are kept in the porch because they are used for safety
purposes. Nearly every house, including partner families, owns at least one cat that is
used to control mice and rats. Rats usually come from the natural environment to the

178 homes, especially during the rainy season. Two interviewees in the partner homes
reported recent presence of mice, in both cases controlled through cats and plastic bottles
installed in electricity cables that make rats fall when trying to reach the homes.
According to the interviewees, cats sleep on the porch but never in the rooms or kitchen.
A similar situation occurs with dogs, used as protection against strangers. They usually
bark when somebody is approaching the house, and can also run after foxes (locally
known as chucurillos) when they approach to attack the chickens.
Even though there is more tolerance about keeping animals such as dogs, cats and
chickens in peridomestic areas, community members value the benefits of having a fence
as an efficient mechanism to separate animals —particularly pigs and goats— from
activities conducted in the house. Families have identified practical advantages derived
from this practice as explained in the following quotes:
I’m better now because animals are not around and I can keep the water tank that they [HHHL] built for us. It has been really helpful (…) We didn't try to have a garden before because the patio was open and there were animals eating the seeds and the sprouting plants every time I tried. Female, 37, Chaquizhca Partners also mentioned that it is easier to clean the patio now that animals are not
around because they do not have to deal with their feces and leftovers. Besides the
construction of fences, families have adopted the practice of keeping animals away by
feeding them and locating their food far from the main structure of the house:
Animals used to come to the house because I had a bucket full of leftovers for the pigs and they had learned to come here for food. It is not like that anymore because now we bring the leftovers up to the place where we keep the pigs. They do not come to the house at all. That is better because they used to defecate here, next to us. It is much better now because they eat, stay and defecate in their own place. Male, 55, Guara.

179 Despite these benefits, the economic situation of the families impacts their
decisions about the best way to keep their animals, as explained in the following quote:
Our pigs stay free most of the time because they can feed themselves with the grass they find around. They grow better this way because we do not have the money to buy enough food or to build a proper pigsty, so our pigs only eat leftovers from what we grow and whatever they find around. If they depend on the food we can provide for them when they are locked in their corrals, they will be thin and we won’t be able to sell them. Female, 56, Guara. Protecting their animals also influences families’ rationales for bringing them into
the house. Goats, for example, are usually kept in basic structures outside the
peridomestic area (most frequently, a zinc roof sustained on wood planks that provides
them with some shade). Families collect goats at the end of the day to keep them in a
corral and leave them free during the say so they can feed with grass. However, when a
goat has just given birth, mother and calf are kept for some time inside the fence in order
to protect the newborns from other animals.
Fences have also faced quality issues. Some of them were built with fresh wood,
which impeded the wire to stick properly. In other cases, animals have eaten part of it.
Keeping fences in good shape implies an important expense for the families, since they
need generous amounts of wire to create multiple rows around the property that can
effectively prevent animals from coming inside. Even though openings in most fences
observed for this research are still minor, they can become more serious if families do not
repair them promptly.
Storage.
The presence of elements from the natural environment is also stimulated by
accumulation of materials inside the dwellings. Local homes have to fulfill multiple

180 storage needs, including crops, daily food, tools, firewood, construction materials
(that are usually collected to be reutilized), clothes, and kitchen utensils. However, it is
not common to have storage units separated from the home; instead, families adapt free
spaces inside and outside to store what is needed in different times of the year.
Using the space under beds, as well as the corners between roof and walls in
rooms and kitchens to store valuables indistinctively of their use, is a well-established
practice. Considering that the regular size of local homes is about 65 m2 and have to host
families of four to ten members in average, available space is very limited. Some families
have built small rooms made out of wood boards attached to the house or basic covered
huts in their plots to store agriculture tools. These spaces are also used to store fertilizers
and crops when the space in the house is not sufficient.
One of the interviewees in the non-partner families explained that he usually
builds a troje (elevated box closed with mesh and wood) in his bedroom to store his
produce and keep it protected from domestic animals during the harvest season. When the
troje is full, he throws the crops on the floor on top of plastic bags secured with wood
sticks that have been previously treated with insecticide. These plastic bags remain in the
floor for as long as there are crops to be sold or consumed by the family. Other storage
alternatives include leaving produce with family or neighbors, as well as locating cane
and firewood in shaded areas near the home (usually attached to walls and windows).
HHHL has included different forms of storage units in the model. The size and
specific devise used in each case depends on the specific needs and resources available in
each family. For example, an external troje and internal shelves were built for a family of
a single mom with no regular agricultural production, whereas an external storage room
181 with more capacity was built for families expecting larger production during the
harvest season. Plastic boxes and deep cans have also been provided to facilitate
organization of food and clothes.
Even though some storage units built by the project present structural problems,
all of them are consistently used. In general, these storage solutions seem to be
insufficient for the needs of local families.
This problem becomes even more serious during the rainy season when crops are
collected and stored temporally at home. During this time of the year partner families use
their porch or the back wall of their home to place valuables, specially crops, tools,
insecticides, and fertilizers. During the observation periods conducted for this research, I
saw one of the families using available space in the rooms and kitchen to store corn; the
other five families had maintained the recommendation of avoiding this practice, even if
it means pilling up their belongings in corners around the house. In this sense, trusses
have demonstrated to be an efficient measure to address the problem of storing spaces in
between ceilings and roofs that can host triatomines and other insects. They remain free
and secure in all the homes, with the only exception of the first communion dress of a girl
in a partner family whose mom wanted to keep it safe and separated from other clothes.
An additional need in terms of storage space is firewood. As in most rural areas,
kitchens constitute one of the most important spaces in the house. Its use is determined
both by the diet and resources available for the household. Local families combine
cooking with gas and firewood on daily basis. Firewood is preferred for the taste it gives
to food, but also because certain products (such as beans and corn) require more cooking
time, which is makes use of gas inefficient. In general, gas is perceived as a more
182 expensive resource, not only because they have to pay for it, but also because they
need to make important efforts to bring gas tanks from Cariamanga, the closest city (7 to
25 km. away from the communities), to their homes. These costs include transportation to
and from the city, paying for the tank and bringing it by donkey or other mediums to their
homes. Regardless, it is usually available to cook food that can be ready very quickly,
particularly at breakfast time.
Considering these two factors, HHHL decided to incorporate an improved
firewood kitchen to the model. This is considered a healthier cooking alternative because
the stove counts with a chimney that takes the smoke out of the house in less time than
regular ones, as well as small burners specifically adjusted to the size of the pots used by
the families. This reduces the amount of firewood and time required to cover families’
cooking needs. Even though this type of kitchen has been considered highly efficient for
some families, it has also shown important flaws. Most of the families faced problems
during the first experiences of use, including height (initial models were too tall for the
average stature of people in this area), overheating of the chimney, and even more
production of smoke when the burners are not exactly the same size of the pots used for
cooking. As a result, most partner families have been using firewood stoves as tables or
storage areas in the kitchen.
Four out of the six partner families have built a traditional firewood burner in the
peridomicile; two of them have chosen it as their permanent cooking area. Reasons
argued for this decision include fear of a fire derived from high temperatures of the
chimney pipe in contact with the wood ceiling, as well as smoke accumulation derived
from cluttering of the chimney after some years of consistent use. Partner families also

183 showed concerns for the aesthetics of the house after soot is accumulated in the walls
of the kitchen and surrounding areas. It is important to point out that other homes
reconstructed without HHHL’s support have adopted similar solutions (attaching a
traditional kitchen to the reconstructed home); this way, families can secure a space to
cook with firewood without altering the appearance of the new construction. However,
we did not observe accumulation of firewood in any of the reconstructed homes; instead,
small amounts were kept in all of them for daily purposes.
In general, the ‘health’ category showed concrete configurations of risk
constructed around ongoing interactions with the natural environment. Families described
practices carried out to counter potential risks in relation to safety, vector control, water
and hygiene, separation from animals, and storing both in previous and new homes.
Perceptions of risk portrayed in this category showed areas that are conferred the status of
life protective, and therefore, associated with health status.
Emotional impact.
Additionally to this perceived impact over health issues, families expressed
emotional impacts experienced along the processes of decision-making, construction and
occupation of HHHL homes. Ongoing comparison between previous or traditional homes
and the ones built through their partnership with HHHL were commonly established in
quotes included in this theoretical category.
The adjective most commonly used to describe the intervened homes, both by
partner and non-partner families, was ‘beautiful.’ According to research participants,
what makes HHHL homes beautiful is that ‘adobe is not exposed’; ‘they look clean’;
‘they are much better than previous homes’; ‘they are well done’; ‘it is a pleasure coming
184 to visit’; ‘they have more space and everything looks more organized’; and ‘it is easy
to keep them clean’, among others.
References to traditional homes in partner families established comparisons
between past and present conditions. When asked about memories of their previous
homes, partner families mentioned the general condition of decay experienced before the
construction:
What I recall about the previous house is that I don't want that to happen to me again. I have always had family members that came to visit us and I used to feel ashamed for the house I was living in. I didn’t feel comfortable. Male, 55, Bellamaria. Similarly, they referred to the space available for their daily chores and the
substantial improvement it represents for the family:
I do not miss anything from my previous house. I think of it, but not in the sense that I would like to go back because my house was really destroyed. I love my house, the one that the project built for me. Female, 56, Guara. Sometimes I think of our house with some sadness because we lived there for many years. So many years living there and suddenly the entire house is on the floor! Female, 37, Chaquizhca. When asked about the most significant changes experienced in the new homes,
families’ narratives included practical factors such as more capacity to receive visitors
and ease to conduct activities at home, to more comprehensive ideas about the impact of
the home on families’ lives. The following quotes explain this wide range of factors:
What has changed the most is that we don't have to live surrounded by dirt and dust now. Of course, we still get some, but you cannot even compare it with the past. We don't have to spend the night dealing with water anymore, we don't have to sleep all together to avoid the leaks and the there is no dust falling from the walls all the time. We sleep without worries now (…) Additionally, when our extended family comes to visit, we have space for them. The house is cleaner, more organized… my old house was not nice. Male, 17, Bellamaria.

185 In my opinion, what have changed the most are the bedrooms. We have more space now and I feel very happy because I can sleep only with my female daughters now. The house is more organized. And I feel more comfortable because I have the bathroom right here… we don't have to go in the open air anymore. Female, 38, Chaquizhca. For me, this is a new way of living. Our previous house was full of cracks, and bugs and animals could come very easily, but they don't come here anymore, they are always outside (…) I like living this way because animals can transmit diseases to us, but since they are far away, we have a better way of living now. Female, 17, Chaquizhca. As illustrated in the following quote, partners’ comments connect factors such as
hygiene, absence of animals, and access to water and sanitation as promoted in the health
promotion aspect of the program, with immediate changes emerged from modifications in
the structure of the house itself:
Everything has changed in our own health because there is a little bit of control, more cleanliness. We have water directly in the kitchen, we don't have to go to the river to bring it in tanks. We can just open the faucet and there it is (…) Considering the extreme conditions we have faced, this is progress. It is pure happiness when I come from my plot and I can just sit anywhere without the concern of animals coming to bother me (…) My new granddaughter will not have to grow up with animals’ feces everywhere, unlike my kids that had to step on that dirtiness (…) I think I am good, things have improved, thanks God. Male, 55, Bellamaria. Elders living with three of the partner families were more skeptical about the
project and expressed resistance to change their living environments. In their opinion, the
new constructions can affect their comfort and health in different ways: a skylight
installed in one of the refurbished homes as a solution for the lack of windows was
regarded as uncomfortable to sleep at night, whereas cement floors were considered
slippery and prone to falls. The mother of one of the partners used to live with his son
when the construction project started; once finished, she decided to go back to an old

186 adobe home that had been abandoned for some years. When asked about her decision,
she replied:
This is firm-land and my cane does not slip when I walk. Here I have all what I need: my mat, my little teddy bear and a portrait of Jesus’ Sacred Heart. I do not like mattresses because they make you warm at night, so I prefer this way. I do not want to go anywhere and I prefer to finish my days here. If you can help me plastering my room with cement, fine, but I’m not doing anything to the floor. I already know the holes of this dirt floor and do not want anything else. Female, 77, Guara. An important element when families evaluate the construction process is their
understanding of the homes as a joint project. Partner families acknowledge having
received contributions from HHHL and also from the national government through
MIDUVI to accomplish the kind of improvements obtained with this construction. At the
same time, families refer to the construction as a result of their own efforts. Words such
as ‘endurar’ (be strong), sacrificar (sacrifice), luchar (struggle) and sufrir (suffering) are
common in partner statements:
I never thought I could have a house like this, but I got it through my own efforts. Of course, I had to work very hard, put my hands at work, but I cannot compare the kind of house I have now with what I had before. This was built with all the strength I put into it. Male, 55, Bellamaria. When the engineer [local facilitator] came for the second time to talk with us, I saw that my house was in very bad shape and I said: we need to be strong, make an effort and try to do it, even if we need to suffer for it. Female, 37, Chaquizhca. I made as many sacrifices as I was capable of. Even if I was sick, I kept on working. Female, 56, Guara. This notion of effort is interpreted as an element directly related with ownership
over the final product:
When people ask to me what I had to contribute for the project, I always tell them that I have to give all my work for the entire summer. Some people really dislike that idea. But I tell them that for anything you want, you need to work. If there is

187 someone who is offering to help you, that is even better and you have to put even more effort into it. Nobody will give you everything for free; at the bare minimum, you need to work hard so you can appreciate what you have done. You have to make an effort, know that you have sweat for what you have, so you can also take care of it. Male, 55, Guara. The emotional impacts previously described showed an experience of wellbeing
beyond the material aspects of the intervention. Systemic perspectives are operated when
families link infrastructure-related changes with more overarching concepts such as ‘life
style’, ‘progress’, and ‘happiness’. This sense of wellbeing is also stated as positive
evaluations of the future associated with a significant change in life conditions for
younger members of the family if compared with the old times. A renovated sense of
ownership and self-esteem can also be observed in this category.
Economic impact.
Families used different forms of funding to sustain their involvement with the
project. These forms included acquiring loans, getting support from family and friends,
selling animals and produce, and investing their labor exclusively in their work with the
project for as long as needed. Given the constrained economic situation experienced by
local families, finding the necessary resources to conduct a project of this nature
generates important economic demands for partner families.
Even though most of the partner families had had experience with credits —
either with financial institutions (banks or cooperatives), government offices, and/or
family and friends— only two of them acquired a formal loan to cover their part of the
agreement. In some cases, the existence of previous loans deterred families from
acquiring new financial commitments:

188 The first time you approached us with the project we were still paying the debt we acquired to buy our house 13 years ago. On top of that, we had to take another loan to pay the expenses of our kids when they started high school. We have been living like that for years: asking for more loans to pay previous debts. We need to work very hard to be able to do this. If we have animals, we can sell them to be able to pay both loans when the installments coincide and we don't have the money. We keep doing that to be on time with the installments because otherwise the bank will not help us again. Female, 37, Chaquizchca. In other cases, older children of the family —normally migrants established in
larger Ecuadorian cities or abroad—provided the resources to cover these installments.
Involvement of older members of the family also expressed as actual work in the
construction and remittances focused on covering payments for the construction crew or
food for the family. Decision-making processes about assuming the costs of the
intervention are illustrated in the following quote:
When the project first came with the offer of building the house I said to myself ‘I do not have that money.’ But I kept thinking and then I said ‘I need to find a way, what can I do?’ Immediately after I decided to ask for a loan to a cooperative in town and then called my sons in Quito. They said, ‘Yes Dad, we can help you to pay’, and they are the ones who have helped me so far. My wife and I have put the rest of the work and that way it was not so difficult. Male, 55, Guara. Loans requested to cover expenses associated with the project have ranged from
US$500 to US$2,000, and in all cases, have been covered within 18 months after the
construction. Illustrating the relationship between financial institutions and economic
performance in their context, one partner stated:
We had to work a lot to get this house complete, but you have to work a lot or get loans for anything you want in life, right? Do you want to have something? You need to ask for a loan, get a debt; otherwise, things will not just come to you. Male, 54, Guara

189 Families’ dependence on agriculture is reinforced by the lack of paid jobs in
the region. This issue emerged constantly in the answers regarding family’s economy for
all interviewees. As explained by one of the partners,
Here we don't have a factory or a boss that can hire us for a monthly salary. It is impossible to think that we will get a job for one or two months here. Male, 55, Bellamaria. Under these circumstances, community members are forced to migrate constantly
to places with more job opportunities, usually gold mines and shrimp production
companies located in provinces nearby. Some of the participants also complained about
how hard it was for them to find people that could work with them over the entire
construction process. Other community members are the most readily available resource
at hand but they can only work when they are not attending their own plots. This is
particularly true during the rainy season, when they need to count on the labor of
neighbors to be able to collect products as fast as possible before they get rotten.
Finally, the use that people make of animals for economic purposes is very similar
in partner and non-partner families. While chickens and goats are used as regular meals
in the household or as meals to be provided to community members as payment for their
labor, cattle and pigs are raised and reserved to cover important expenses (such as school
enrollment or paid labor). Pigs are rarely used for internal consumption of the household,
except for their fat. In words of one of the interviewees, having pigs is like having a
‘money box’ because they can be sold for a good amount of money (around US$25) at
any moment:
You have a warranty with pigs: you can buy them when they are little, feed them with cane from your plot, keep them without disease, and when they are ready, sell them for much more than you initially bought them. Female, 42, Chaquizhca.

190 Because of the perceived difference between the investment made by partner
families and the final result, some community members, visitors and external contractors
have referred to the new homes as a ‘gift’. Families acknowledge that in economic terms,
the contribution of HHHL was important. Even considering that some of them were
saving resources for minor repairs or full reconstruction, the scale of these interventions
was much larger than what they had in mind:
I always say that we have this house because the Universities helped us; we didn’t have the money to build anything like this. Female, 49, Guara. HHHL homes are also seen as investment towards the future as they reduce the
need to attend problems associated with the natural decay and structural damages of old
homes, as explained in the following quote:
I don't have to worry now about how to fix my house, how to buy more materials, or how to get the money to pay for more loans. That pain is gone and my only concern now is how to get through life. Female, 56, Bellamaria Similarly, the word ‘stretching’ (estirar), common in sayings from the popular
culture, was often used by interviewees to illustrate the absence of resources and the
ongoing struggle for making means meet needs:
Once we got the loan to buy the house, we had to ‘stretch the blanket’, as we say here. The house was not in good condition, but we had to wait until being done with the payments of the previous loan to consider the possibility of improving it. Female, 37, Chaquizhca Families rarely used the word ‘poverty’; however, it came more often in answers
describing the struggles of rural life:
Life in the countryside is harsh and requires sacrifice, but it is also peaceful. Even if there is no money, or if there is poverty, you can live in peace. Male, 33, Bellamaria.
191 Dependency on their individual capacity is what defines the situation of
poverty for local families according to one of the partners:
Like most people around here, we are poor. We depend on our work, on what we can produce week by week, to sustain our family. We do not have capital or a regular salary. If we do not sweat on daily basis, who is going to give us a coin? Therefore, when we had to work for the house, we had to assume that nobody would get any income during the entire construction time. It was an entire summer thinking, ‘what am I going to live from?’ Male, 54, Guara. Although these constrains still exist for partner families, new economic activities
have also emerged with the new living environments. Having a productive garden
associated to the HHHL model, for example, has been promoted with two purposes:
generating additional sources of income for the families, and creating an additional
barrier for animals’ presence in the peridomestic areas. Four out of the six partner
families have tried to organize a productive garden in the surrounding areas of the house.
Two of them have implemented basic systems of drip irrigation in an attempt to sustain
their production during the dry season. Even if used for internal consumption of the
household, these gardens represent savings in products that families would have to buy
otherwise. For the family that has a small store in their home administrated by the female
head of household, this garden provides new alternatives of products to sell in her
community:
I want to grow a bit of everything, because if I plant just one thing, I will have to pile and waste a lot. But if I have a bit of everything, you will get little amounts and nothing would be wasted. We use cilantro for everything, parsley for stew, radish for sauces, sprouts for salad… we use everything. Female, 37, Chaquizhca. Other products grown by partner families in their gardens include achiote,
oranges, grapefruit, avocado, papaya, passion fruit, tomato, onion, cassava, and beans,
among others.

192 I also observed that after the intervention, partner families invested additional
resources in other productive activities, such as tilapia production and poultry. One of the
families decided to invest additional resources to buy certified corn seeds that will
increase their level of production: if a bag with 100 pounds of regular seeds costs around
US$20, a quintal of certified seeds can be worth US$220. Even though this could seem
expensive at first look, income for this family is likely to substantially increase over time:
with regular seeds, families can get up to 20 hundredweights per hectare, whereas with
the improved ones, they can get up to 120. Interestingly, these new assets can also
become an additional element to consider in the adaptation of the HHHL in terms of
organization of the space: in this case, increased corn production creates new storing
demands.
Finally, five out of the six families decided to acquire at least one new mattress,
blankets and beds before moving to the new space. As explained by one of the
interviewees,
Yes, things are better now because we did not have all this. We used to have things everywhere. Our beds used to have mats made out of bamboo and bugs used to live there. Things are different now because my uncle helped us to buy new beds when he saw the new house, thanks God. Female, 38, Chaquizhca. We also observed acquisition of services and assets of more economic value such
as refrigerators (n=2), motorcycles (n=1), sound speakers (n=2), and satellite television
(2). Similarly, two of the partner families, have considered more technical ways of
chicken rising and have already developed specific corrals closed with mesh and wood.
Even though it is not possible to state that these decisions demonstrate an improvement in

193 the economic situation of the families as a result of implementing the HHHL model,
they illustrate signs of increasing purchase power.
Economic dynamics characteristic of rural life in this area of Ecuador became
visible under this category. Participants talked about their dependence on daily labor, as
well as restrictions to get access to funding sources due to the unpredictability of their
work as farmers. The economic cost of implementing a project that demands ongoing
contributions in labor and cash over an extended period of time is a factor that cannot be
minimized in a project of this nature. However, this section also showed resources used
by local families to address these restrictions and commit to the project until completion.
Social impact.
The last theoretical category emerged in this phase of analysis was social impacts.
Unlike the health, emotional and economic impacts previously described, this category
expands the limits of the household level and connects HHHL implementation with larger
social structures already existing in the communities. Social impacts also include
interactions occurring at the household level that have been affected by the modification
of the space.
Following existing dynamics of community organization, family members have
worked closely in the construction of the model. Women and younger members of the
family have been in charge of cooking for the construction crews and organizing
peridomestic areas in all cases. Additionally, they have been involved in the production
of adobe: unlike the traditional blocks, the size of the improved blocks facilitates this
possibility. Considering that almost all community members know and have participated

194 in the production of adobe for their own homes, it was easy for the families to speed
up the construction process with their own resources:
We all, each and every member of my family, worked for this house and worked very hard. Some of my children used to come at the end of the day, when the rest of the construction crew had left, to help me with the adobe. Male, 55, Guara. I did a lot of things: I helped making the adobe, passing cement, stones, and bricks, smoothing the floor, passing threads through the tiles, and sticking mesh to the wall. Male, 15, Guara. Family members also participated in the preparation of tiles and painting. One of
the families even got a door for the peridomestic area produced by one of their sons
currently enrolled in high-school:
We reached a point when we needed to complete the peridomicile and there was no money for the door. Since I am taking a class in metallurgy at school, I asked my older brothers to buy the materials for me and I made it. I cut, took measures and welded, and at the end I thought it was better because I put in practice what I already knew and learned more. At the beginning, it didn't come up well… but it was my first real job in metallurgy. Male, 17, Bellamaria. Similarly, the construction of HHHL homes has generated additional sources of
jobs in the communities. In first place, the project has hired people previously certified in
construction techniques by the National Professional Training Service (Servicio Nacional
del Capacitación Profesional de Ecuador, SECAP). This training, organized by HLI in
2012, provided a base of knowledge in constructions with clay that is now replicated.
People who took this training have been prioritized for adobe production, trusses
assembly, and home construction. The cycle of learning is explained by one of the
trainees:
I have learned a lot from this project. Unlike other [community members] that didn’t even go to the [SECAB] classes, I’ve been practicing what we learned. It was not knowledge to keep on paper. I think that it was not interesting for some people, but it was interesting to me. I just missed one class and then I talked to the professor, caught up and passed the test (…) The only thing I cannot do in these

195 homes is the floor because it needs precise measures. Other than that, I can do everything: I have produced adobe, raised walls, installed doors and windows, built roofs, and fixed kitchens. I can even read blueprints. Male, 30, Bellamaria. In this context, an ongoing interplay between existing and specialized knowledge
hold by local families, external contractors, and architects took place along the
construction process. The following quote described how local families valued their
knowledge and questioned the information provided by external actors:
One day all the partners talked among us. We said that people from the construction crew were organizing the process but they didn't have as much experience with adobe production as we had. We have built all the homes in this region with adobe! One day, after getting a number of adobes that were turning into dust in our hands, we decided to organize ourselves and do things differently. We knew that we were adding to much sand into the mix, so we modified the formula. Then we showed the quality of those adobes to the construction crew and they agreed that our method was better. Male, 54, Guara. We decided to put in practice what we knew. At the beginning the bricks were weak and twisted. Then we decided how much of sand, water, and grass we had to add. Once we found the right mix, we progressed a lot. Male, 55, Bellamaria. Traditional knowledge has also been applied in the new homes as a resource to
improve the mix that was applied in the improved kitchens by one of the partner families
with the purpose of making it more resistant to constant use:
Once the improved stove was finished, I decided to give it some cohesion in the way that we traditionally use here. I made some plastering with dry donkey and horse’s manure. It has to be so dry that you can turn it into dust. Then you throw it in a hole and leave it there until is rotten. Finally, you put it on top of the adobe and it doesn't let any garbage coming from the adobe to fall or collapse. The walls of my previous bedroom were sealed like that. Male, 54, Guara. Similarly, partner families with more experience in construction provided
opinions and advice regarding different phases of the process, such as the lay out of
foundations and of roofs. Their existing knowledge helped them to supervise construction

196 and also to consult with more experienced neighbors that had been involved in other
constructions. That knowledge remains with the families as part of the process:
I can tell you that if someone comes today to ask for help in the construction of this type of house, I would gladly provide it. If they want to make adobe, I can explain to them because I already know how to make it (…) I remember everything about the construction because I was there from beginning to end. I never abandoned it. That’s why when they [construction workers] did something wrong, I could call them out (…) I have everything in my mind now. Male, 55, Guara. Partner families have hired community members as construction workers to reach
the number of non-qualified labor required to conclude the process within the agreed
timeframe (two to four months). During the negotiation, partner families agreed to have
at least two people working at all times in the construction (one of them was generally
one member of the family). The possibility of supporting community members with
emerging jobs was explained by one of the community members hired by HHHL:
I was working in the construction of the homes when the construction of the water system in Bellamaria began. Since it was not possible for me to be in both places, I hired my brother in law to cover my part in the water system. That way I was making some money and paying him a little bit less, but we both had a job. Male, 30, Bellamaria The participation of women in productive activities also opens spaces for them to
get involved in decision-making at the household level. Even when most of the
negotiations between HHHL and partner families occurred through the male head of
household, women played a definitive role in the decision of joining the project:
I remember the first time that the engineer talked to me about my house: he brought a design, a little house made of cardboard to explain how it would look like so I could say if I liked it or not. And I say that I liked it, but with the front towards the valley, not like my previous house. Female, 49, Guara.

197 While both men and women are in charge of planting and harvesting, women
are the ones usually in charge of taking produce to the market. This role gives them a
prominent role as administrators of resources at home in addition to their regular
activities:
I paid for most of the construction with my work. My husband helped in the adobe production and then in the construction; but most of the money we used to pay the people that helped here came from my work at the market, what we got from selling animals, and money that my older sons sent to us. I had built my old home by myself after my previous husband abandoned us, so this was not the first time. Female, 56, Bellamaria. Similarly, women in non-partner families have expressed interest in start creating
the conditions for a potential intervention in their homes in the near future:
As you know, everything is a matter of reaching an agreement. We have seen the [HHHL] houses and now we know how they are. I would like to have one of those, especially because of my kids. They are still young and I would like a house that looks pretty and organized for them. What you do is help for us and we can also help with a part. If the project can help me later on, I can start saving during the vacation time of my kids. We can start saving and saving and see what happens. Female, 42, Chaquizhca. Finally, it is noteworthy that two of the heads of household in the partner families
became Presidents of the water committees in their communities —probably the strongest
form of local organization in this area— right after the intervention in their homes was
concluded.
Family and community members were able to directly participate in the
construction of HHHL homes, not only with their physical, but also with their intellectual
capacities. Knowledge exchange between actors helped them to strengthen existing skills
and gain ownership over the project. Power dynamics were visible in this section, as
partner families assumed an active role as counterparts of the project, following but also

198 questioning external knowledge on the basis of their own experience. Importantly,
women demonstrated influence over decisions taken in immediate and future investments
at the household level.
Discussion and Theoretical Development
The implementation of HHHL has provided important criteria to consider the
relevance of living environments in CD prevention. Conceiving home environments as
entry point for disease prevention, facilitates inclusion of factors such as long-lasting
impact (Peters et al., 2013), ownership (Charron, 2012), use of existing resources (Adam
& de Savigny, 2012), and flexibility (Bosschaert, 2012) in the design of sustainable
public health strategies. In this context, we aimed to identify potential contributions of
the systemic approach proposed by HHHL to the construction of sustainable control
measures for CD prevention.
Based on the four theoretical categories outlined in the previous section, I theorize
that sustainability of CD control under the model proposed by HHHL largely depends on
the systemic capacity of home improvement to activate and sustain agency in partner
families. That agency is expressed in the different levels of impact previously outlined
and evolves as an integrated set of capacities toward health promotion and disease
prevention.
So far, the program has been able to create scenarios of social inclusion for
populations at risk of CD in interaction with program designers and health institutions.
Those scenarios are spaces where individual and group agency in relation to health is
invited and maintained. Besides the direct intervention on the homes, HLI has facilitated
construction of drinking water systems, formalization of income generation initiatives,

199 and collaborative efforts aimed at strengthening negotiating skills of local leaders,
among other actions. In this way, the program has attended to the dynamics of the various
elements that constitute the local context and has responded with opportunities for local
families to improve their health according to resources available to them. Instead of
limiting control measures to individuals’ capacity to react to risk factors, the program has
invested important resources in addressing local priorities, while at the same time has
generated stable working relationships with local populations and collected relevant
information to inform implementation processes. This study suggests that by doing so,
HHHL has been able to extend active sense-making in local families’ expressed as
agency in the construction of healthier living environments resilient to their specific
conditions.
From this perspective, agency around the model, and therefore, sustainability of
the intervention can be seen as the confluence of three factors: systemic improvement of
families’ quality of life, consistent use of protective measures, and adaptation to
emerging dynamics.
Systemic improvement of families’ quality of life.
Different from disease-centered approaches, systems thinking emphasizes that
social structures are not just aggregates of parts: they are systems acting under concrete
logics that produce and reproduce social orders through practices and relationships
among actors (Giddens, 1984). This means that human beings are not only pieces of these
structures, but agents in their capacity to reconfigure their environment and the larger
social groups they belong to through reflexive thinking articulated in discursive and
practical action (Suddaby, 2006). This study has shown that systemic interventions

200 around living environments have the potential to generate positive impacts in areas
such as vector control and water and sanitation, but also in aspects such as emotional
wellbeing and social relations at the household level, all of them constitutive of an
integrative idea of health (Haines et al., 2013). As illustrated in the theoretical categories
of Health and Emotional impact —and in the following quote— partner families
acknowledge the systemic nature of the intervention:
The benefits of this process are obvious; everybody in the house feels them. Fencing our land, for example, reduces the entrance of garbage and animals; because of that, we don't have to deal with their excrements and as a result, we are protected from diseases. Male, 55, Bellamaria.
By integrating a broader analysis of the determinants of health (Bardosh, 2014;
Hashimoto, Zuniga, Romero, et al., 2015), HHHL and partner families have been able to
implement a model that conceives healthy living environments within the home space,
while protecting and potentiating local livelihoods. HHHL homes integrate ongoing
interactions between local families and their natural environment in the construction of an
idea of health that acknowledges the dynamics of rural life in the context of CD
transmission in southern Ecuador. However, instead of focusing exclusively on CD’
transmission dynamics, the project has addressed areas perceived as more pressing by
local families, including the urgency of living in a safe space. During this study, partner
families evaluated HHHL’s infrastructure intervention according to criteria that are
relevant within their own context, including its capacity to avoid leaks, keeping pleasant
temperatures, allowing circulation of air without increasing insects’ presence, and
reducing animals’ circulation within the home space, among other factors.

201 Ecohealth interventions have previously shown that comprehensive control
programs encompassing complementary control measures can efficiently prevent
triatomines’ reinfestation in exposed dwellings (Gurtler & Yadon, 2015; Lucero et al.,
2013). However, when these interventions aim to control more than one health threat,
such as plagues of rodents or multiple insects, their perceived protective capacity
increases (De Urioste-Stone et al., 2015; Rosecrans et al., 2014; Santos et al., 2016;
Waleckx et al., 2015). As illustrated in the health impacts’ section, a strategy such as
HHHL is positively impacted by identifying intersections with other sources of disease
that can be potentiated through similar preventive behaviors, such as reduction of
mosquitoes in water based breathing sites or cohabitation with animals. Since local
families showed shared concerns about insects’ presence, they can be empowered in the
application of preventive practice resilient to emerging conditions. Recent
recommendations have been made in this direction for emergent vector-borne diseases
such as zika virus, dengue and chikunguna (Heydari et al., 2017).
Consistent use of protective measures.
As expressed across all themes, HHHL homes are perceived as beautiful,
aesthetically and technically superior to other homes in the area. This factor allows
families to take pride on an asset they have actively achieved with their effort and
commitment. Narratives of parents and children include a renovated sense of self-esteem
expressed not only in their statements of ownership over the construction (‘my house’),
but also in complains about failures of the process and intentions of maintaining the home
in the best possible conditions (social impact category). This finding is consistent with
previous literature indicating that even small changes in infrastructure can increase the

202 perceived value of the dwellings and motivate owners to invest additional resources
in maintaining and improving the home space (Lindsay et al., 2002).
Similar to previous interventions focused on infrastructural improvement
(Hashimoto, Zuniga, Romero, et al., 2015; Lucero et al., 2013; Pellecer, Dorn,
Bustamante, Rodas, & Monroy, 2013), the use of local materials, reutilization of recycled
ones and deployment of passive construction and demolition techniques, has increased
acceptability of protective measures. In spite of its association with Chagas disease
transmission (Grijalva et al., 2015; Meymandi et al., 2017; Montenegro, Vera, Zuleta,
Llanos, & Junqueira, 2016; Saunders et al., 2012), HHHL adobe constructions have
shown efficiency in insect control, as well as substantial contributions to the duration and
comfort of the construction. This efficiency cannot be isolated from other protective
measures applied within the home space, particularly those operating in peridomiciliary
areas; however they show an important contribution of the technology implemented in
this case.
Moreover, all families reported a substantial reduction of insects inside the home
space. As it has occurred in other cases of partial or full reconstruction, it cannot be
claimed that this reduction is caused exclusively by the HHHL intervention (Donovan et
al., 2014; Hurtado et al., 2014b; Santos et al., 2016); however, they show an element of
protection that is acknowledged by local families as beneficial. In this case, families
showed active engagement with bug control measures, such as consistent use of screens
in doors and windows, as well as reduction of accumulated materials and separation from
domestic animals. Internal and external walls have been also kept clear and cleaning
practices recommended by the program reported to be regularly applied. Special attention

203 should be given to substances used for fumigation, as well as the patterns followed in
this practice (Charron, 2012).
HHHL has contributed with knowledge that can be used by local families as a
resource to react to social dynamics affecting their lives. It includes specific productive
skills, as well as concrete knowledge on how CD and living environments can affect their
health. However, further research is needed in order to understand the extent to which
this knowledge will alter families’ behavior around CD prevention in the long run. As
showed in previous studies, the fact that local populations can identify specific stages of
the transmission cycle, cannot be equated with accurate evaluations of risk and
subsequent behavior change (Dell'Arciprete et al., 2014; Parker & Allen, 2013; Rochat et
al., 2015; Sanmartino & Crocco, 2000). However, previous interventions (Bustamante et
al., 2014; Lardeux et al., 2015; Lucero et al., 2013; Monroy et al., 2009; Waleckx et al.,
2015) have shown that participatory approaches that facilitate interactions between
existing knowledge an external expertise can increase communities’ awareness and
agency towards sustainable disease prevention. In this case, community involvement has
expanded the level of influence of a partnership designed for a concrete reconstruction
effort, to a wider idea about health promotion in which partner families themselves
become promoters of control measures. As explained by one of the partners,
Being ‘partners’ means that we help each other: you have helped me and I can help you. Being partners is also a matter of having the house as clean as possible to prevent chinchorros from coming inside (…) I’m thankful because this is the result of everybody’s work. Male, 55, Guara Interactions between acquired knowledge and emerging needs also determine
application of protective measures in the long run. The family that built the prototype

204 home in 2013, for example, continues applying a good number of practices such
preventing animals from coming into the home, usage of the storage room as main space
for storing crops and tools, and repairing windows and doors’ screens when they break.
At the same time, they have added new spaces and activities to their home space,
including tilapia and doves’ production, as well as improved husbandry. Even though
most of these activities are not conducted within the immediate space of the home, they
create ongoing influx of supplies and animals to and from areas surrounding the home.
Further research is required to understand how dynamics inspired and facilitated by the
model suggest new needs in terms of health promotion.
Emphasis of the project in the interpersonal sphere of the socio-ecological model
(McLeroy et al., 1988) has also facilitated ownership of this solution from different
members of the household. As expressed by a young member of a partner family,
My parents made a good decision because this house benefits the entire family. It is good not only for us, but for our extended family as well. Female, 17, Chaquizhca
Unlike programs emphasizing individual responses, programs focused on
promoting responses from multiple actors increase their capacity to suggest specific
actions adjusted to the context of the intervention (Norman, 2009). Since NTD programs
have already received recommendations for involving women, youngsters, extended
families and communities at large in order to measure the social impact of control
interventions (Arenas-Monreal et al., 2015; Monroy et al., 2009; Triana et al., 2016),
emphasis on health promotion at the family level can be important contribution of the
HHHL model to NTD literature.

205 Finally, regular health promotion once the construction phase of the
intervention has been concluded is highly recommended. Reinforcing protective
behaviors can be more important as vector and disease become even less visible (Whitty,
2015). The fact that community members consider safety a definite priority in their
decision making about maintaining and repairing their homes is important in terms of the
general framing of the strategy for future interventions. A comprehensive idea of health
and safety can constitute a more relevant argument for potential partners than CD
prevention itself, and definitely a more accurate argument if the experience of partner
families is considered as main reference.
Adaptation to emerging dynamics.
Similarly, the systemic nature of the HHHL’s intervention, operated under a
dialogic approach to health promotion (Frank, 2005; Greiner, 2010), has facilitated
modification of the conditions of the program according to the resources and priorities
available in each phase. Complex interactions between scientists, program staff, and local
communities around the home space were especially visible under the categories of
economic and social impacts. These interactions created opportunities to pose questions,
discuss potential courses of action, and arrive to joint solutions. This is not to say that
these interactions were free of conflict; on the contrary, conflict emerged often as
individual interest, disciplinary perspectives and administrative priorities demanded
attention. However, withdrawing from the process was a costly decision that compelled
involved actors to find solutions once disagreement aroused, especially under the
perspective of a given word. In words of one of the interviews,

206 I have said this before: to do this [building the house], you have to be tough and strong. You will have to suffer a little bit, but by the same token, you get a beautiful house. Male, 55, Guara. In this sense, the multiple levels of impact involved in the proposed solution
comprise a number of responses to be considered before making a decision for ‘no
compliance’. The perceived value of the intervention motivates reactions from involved
actors that can derive into increasing ownership.
As previously explained in systems’ literature, this emergent response is an
important attribute of systemic interventions: rather than providing a set of fixed answers,
systems put resources in place to be able to identify disarrangement and modify
interventions as they evolve (Charron, 2012). Different from interventions exclusively
evaluated under the lens of compliance —that even out populations’ political and social
circumstances (Bardosh, 2014), a systemic intervention of this nature facilitates the
design of intermediate forms of implementation, flexible enough to incorporate elements
that are relevant for local populations—not only for implementers— and enhance
decision-making power. Consequently, and as shown across categories, families have
responded with agency, creativity, resilience, and problem-solving capacity to conclude
all the interventions proposed by the program.
Barriers.
Sustaining that level of flexibility will be fundamental to enhance participation of
community members in order to bring the HHHL model up to scale. When asked about
interest on replicating the HHHL model in their homes, 60 out of the 102 heads of
household interviewed for this study (Group 3) expressed interest in this possibility. It is
possible to think that this interest is not only sparked by the end product, but also by

207 respondents involvement in the intervention: 57.1% of the heads of household who
expressed interest in implementing HHHL’s model have participated in HHHL’s
construction activities, and 72.7% have participated in at least one of the HLI’s projects.
These findings echo previous studies on local influence in health promotion efforts
(Buttenheim et al., 2014; Lardeux et al., 2015), as well as the position of one of the
partners who mentioned that the intervention would act as a ‘mirror’ for other community
members interested in improving their living environments.
However, covering their involvement with the program is a high cost for local
families, even under this model of partnership. The general cost of HHHL homes has
varied between US$2,000 and US$4,000 for refurbished homes, and US$15,000 to
US$20,000 in fully reconstructed homes. According to partner families, their cover
around USD $2,000 to USD $3,000 of this cost, mainly expressed as the cost of their own
and hired labor. Additionally, working for three months exclusively in this project can
generate a negative impact on families’ economy during the implementation period.
Expansion of the HHHL model should consider important levels of stress emerged from
the need to meet agreements made with the program and lack of economic resources
available to supply daily needs. As explained by one of the partners,
When I saw my house turned down after the demolition, I thought I had lost all what I had in my life. I only had the hope for something better coming soon for my family to move forward. Male, 55, Guara. Some of these costs can be reduced if processes such as adobe making and
construction strategy are revised in order to make them more efficient. Important delays
in the construction were caused by miscalculations of the actual time that certain
activities would take, while in other cases responded to lack of materials, environmental

208 conditions, physical capacity of the construction crew, and partner families’ need to
attend other activities. All of them could be corrected under more realistic planning
processes adjusted to the actual capacities of partner families.
Efficiency should also be considered in reference to the materials being used in
the construction. Extreme temperatures and profuse rains in this area create
environmental conditions that demand increased resistance from construction materials.
However, elements of the construction such as stoves, mesh, and wood have shown
quality issues that required additional resources form partner families to repair them.
Since the need for additional resources can act as an important barrier toward behavior
change, addressing this quality issues is fundamental to enhance a long lasting usage of
protective measures.
A more detailed analysis of sustainability in refurbished homes is recommended.
A fully reconstructed home can potentiate preventive behaviors under the perspective of
ownership generated through the construction process, which is not necessarily the case
for those families that do not experience a drastic change. It was observed that partial
interventions are challenged with structural issues that can render HHHL intervention
irrelevant in the long run. Specific health promotion strategies should be designed to
reinforce sense of ownership and usefulness in these cases.
Finally, the flexibility and adaptability showed by the HHHL to facilitate
participation of local families under differentiated funding models could be strengthened
and replicated by this and other programs applying systemic approaches to disease
prevention. During this pilot phase of the project, local facilitators and staff had
institutional support to emphasize negotiation processes over blunt indicators of cost-

209 effectiveness (Bardosh, 2014; Odhiambo et al., 2016; Parker & Allen, 2013), which
rendered important results in terms of trust building and appropriateness of the applied
solution. Building on the knowledge accumulated during this process, HHHL can
continue working to establish strategic partnerships with governmental or private
institutions with the experience and infrastructure necessary to conduct this kind of
endeavor at larger scales. An important precedent in this direction was the partnership
established with MIDUVI for the phase of simultaneous reconstruction in 2015. Since
intersectoral collaboration is a baseline condition for sustainability of systemic
interventions (Charron, 2012; Dias, 2007; Santos et al., 2016), extending this type of
association with national, international, and multilateral institutions is recommended.
Conclusion
To conclude, I contend that systemic approaches to disease prevention should be
considered a route to avoid fixed, hopeless, and finished ideas about neglected
populations that limit researchers’ capacity to come up with solutions that can effectively
address populations’ priorities. The term NTD has opened a spectrum of research in
which the impact of geographical, demographic, cultural, and social factors can be
thoroughly explored by public health practitioners to arrive to more effective strategies
for disease prevention. However, addressing a multi-causal phenomenon such as poverty
requires consideration of diverse and complex human experiences implied in its
occurrence. Poverty transcends income levels to include factors such as access to
education, participation opportunities and living environments, all of them articulated in
one way or another with specific health risks (Adjei & Buor, 2012). Exclusion
experienced by neglected populations go beyond their access to immediate sources of

210 income, and include limited support from financial institutions, discrimination in
legal procedures, limited access to job and education opportunities, and early adulthood,
among many others. They also express as an ongoing need to work in association with
their living environment, not only in their plots and farms, but also in the space where
domiciliary activities are conducted. Bugs and other animals find in the home an
extension of their natural environment and cohabitation with one another is deeply
engrained in cultural dynamics that do not see them as a risk.
The four theoretical categories outlined in previous sections show a set of impacts
at different levels capable to activate agency, hence, promote sustainability of HHHL
around three factors: systemic improvement of families’ quality of life, consistent use of
protective measures, and adaptation to emerging dynamics. These three factors also
showed limitations, including need for ongoing health promotion as vector and risk
factors become less visible, low quality of some construction materials, families’
financial capacity to sustain and replace protective measures, and capacity to react to the
dynamic nature of living environments.
In this context, sustainability of the systemic health promotion model proposed by
HHHL relies on is its capacity to enhance the effectiveness of control strategies while
directly improving the quality of life of individuals and communities at risk. A systemic
perspective like this can be a useful resource to help researchers to create complex forms
of engagement that could lead to more effective health promotion efforts, as well as help
populations at risk to better understand the purpose and relevance of research in their own
context.
211 Limitations.
The first author of this paper has participated in HLI activities for an extended
period of time. It is possible that respondents were influenced by their identification of
this author as member of HHHL and expectations about potential benefits to be obtained
through her advocacy capacity. Member checking of the full results was not possible due
to financial and geographical limitations; however, some preliminary ideas about
theoretical categories were tested with a limited number of community members during
the third field visit. Lastly and in spite of the authors’ efforts to stay close the data,
richness of local language and intentionality of the original words used by research
participants might have gotten lost in translation.
References
Abad-Franch, F. (2007). Control de la enfermedad de Chagas en el Ecuador. OPS/OMS - Ministerio de Salud Publica del Ecuador. Quito, Ecuador.
.Abad-Franch, F., Paucar, A., Carpio, C., Cuba, C. A., Aguilar, H. M., & Miles, M. A. (2001). Biogeography of Triatominae (Hemiptera: Reduviidae) in Ecuador: implications for the design of control strategies. Mem Inst Oswaldo Cruz, 96(5), 611-620.
Adam, T., & de Savigny, D. (2012). Systems thinking for strengthening health systems in LMICs: need for a paradigm shift. Health Policy Plan, 27 Suppl 4, iv1-3. doi:10.1093/heapol/czs084
Adjei, P. O. W., & Buor, D. (2012). From poverty to poor health: Analysis of socio-economic pathways influencing health status in rural households of Ghana. Health Sociology Review, 21(2), 232-241.
Arenas-Monreal, L., Pina-Pozas, M., & Gomez-Dantes, H. (2015). [Challenges and inputs of the gender perspective to the study of vector borne diseases]. Salud Publica Mex, 57(1), 66-75.
Atkinson, P., Delamont, S., & Housley, W. (2008). Contours of culture : complex ethnography and the ethnography of complexity. Walnut Creek, CA: AltaMira Press.
Bardosh, K. (2014). Global aspirations, local realities: the role of social science research in controlling neglected tropical diseases. Infect Dis Poverty, 3(1), 35. doi:10.1186/2049-9957-3-35
Bosschaert, T. (2012). The SiD definition of Sustainability. Retrieved from http://www.except.nl/en/#.en.articles.204-the-sid-definition-of-sustainability

212 Briceno-Leon, R. (2009). [Chagas disease in the Americas: an ecohealth perspective].
Cad Saude Publica, 25 Suppl 1, S71-82. Bustamante, D. M., De Urioste-Stone, S. M., Juarez, J. G., & Pennington, P. M. (2014).
Ecological, social and biological risk factors for continued Trypanosoma cruzi transmission by Triatoma dimidiata in Guatemala. PLoS One, 9(8), e104599. doi:10.1371/journal.pone.0104599
Bustamante, D. M., Monroy, C., Pineda, S., Rodas, A., Castro, X., Ayala, V., . . . Trampe, R. (2009). Risk factors for intradomiciliary infestation by the Chagas disease vector Triatoma dimidiatain Jutiapa, Guatemala. Cad Saude Publica, 25 Suppl 1, S83-92.
Buttenheim, A. M., Paz-Soldan, V., Barbu, C., Skovira, C., Quintanilla Calderon, J., Mollesaca Riveros, L. M., . . . Levy, M. Z. (2014). Is participation contagious? Evidence from a household vector control campaign in urban Peru. J Epidemiol Community Health, 68(2), 103-109. doi:10.1136/jech-2013-202661
Charmaz, K. (2006). Constructing grounded theory. London ; Thousand Oaks, Calif.: Sage Publications.
Charmaz, K. (2014). Constructing grounded theory (2nd edition ed.). London ; Thousand Oaks, Calif.: Sage.
Charron, D. F. (2012). Ecosystem approaches to health for a global sustainability agenda. Ecohealth, 9(3), 256-266. doi:10.1007/s10393-012-0791-5
De Urioste-Stone, S. M., Pennington, P. M., Pellecer, E., Aguilar, T. M., Samayoa, G., Perdomo, H. D., . . . Juarez, J. G. (2015). Development of a community-based intervention for the control of Chagas disease based on peridomestic animal management: an eco-bio-social perspective. Trans R Soc Trop Med Hyg, 109(2), 159-167. doi:10.1093/trstmh/tru202
Deetz, S. (1996). The positioning of the researcher in studies of organizations: De-hatching literacy theory - Commentary. Journal of Management Inquiry, 5(4), 387-391. doi:Doi 10.1177/105649269654014
Dell'Arciprete, A., Braunstein, J., Touris, C., Dinardi, G., Llovet, I., & Sosa-Estani, S. (2014). Cultural barriers to effective communication between Indigenous communities and health care providers in Northern Argentina: an anthropological contribution to Chagas disease prevention and control. Int J Equity Health, 13, 6. doi:10.1186/1475-9276-13-6
Dias, J. C. (2007). Southern Cone Initiative for the elimination of domestic populations of Triatoma infestans and the interruption of transfusional Chagas disease. Historical aspects, present situation, and perspectives. Mem Inst Oswaldo Cruz, 102 Suppl 1, 11-18.
Donovan, S. D., Stevens, M., Sanogo, K., Masroor, N., & Bearman, G. (2014). Knowledge and perceptions of Chagas disease in a rural Honduran community. Rural Remote Health, 14(3), 2845.
Dumonteil, E., Herrera, C., Martini, L., Grijalva, M. J., Guevara, A. G., Costales, J. A., . . . Waleckx, E. (2016). Chagas Disease Has Not Been Controlled in Ecuador. PLoS One, 11(6), e0158145. doi:10.1371/journal.pone.0158145
213 Dumonteil, E., Nouvellet, P., Rosecrans, K., Ramirez-Sierra, M. J., Gamboa-Leon, R.,
Cruz-Chan, V., . . . Gourbiere, S. (2013). Eco-bio-social determinants for house infestation by non-domiciliated Triatoma dimidiata in the Yucatan Peninsula, Mexico. PLoS Negl Trop Dis, 7(9), e2466. doi:10.1371/journal.pntd.0002466
Forget, G., & Lebel, J. (2001). An ecosystem approach to human health. Int J Occup Environ Health, 7(2 Suppl), S3-38.
Frank, A. W. (2005). What is dialogical research, and why should we do it? Qualitative Health Research, 15(7), 964-974. doi:10.1177/1049732305279078
Gascon, J., Vilasanjuan, R., & Lucas, A. (2014). The need for global collaboration to tackle hidden public health crisis of Chagas disease. Expert Rev Anti Infect Ther, 12(4), 393-395. doi:10.1586/14787210.2014.896194
Gilson, L., Hanson, K., Sheikh, K., Agyepong, I. A., Ssengooba, F., & Bennett, S. (2011). Building the field of health policy and systems research: social science matters. PLoS Med, 8(8), e1001079. doi:10.1371/journal.pmed.1001079
Glaser, B. G., & Strauss, A. L. (1967). The discovery of grounded theory; strategies for qualitative research. Chicago,: Aldine Pub. Co.
Greiner, K. P., Ohio University., & OhioLINK Electronic Theses and Dissertations Center. (2010). Exploring dialogic social change (pp. 1 electronic text). Retrieved from http://rave.ohiolink.edu/etdc/view?acc_num=ohiou1273197688
Grijalva, M. J., Palomeque-Rodriguez, F. S., Costales, J. A., Davila, S., & Arcos-Teran, L. (2005). High household infestation rates by synanthropic vectors of Chagas disease in southern Ecuador. J Med Entomol, 42(1), 68-74.
Grijalva, M. J., Suarez-Davalos, V., Villacis, A. G., Ocana-Mayorga, S., & Dangles, O. (2012). Ecological factors related to the widespread distribution of sylvatic Rhodnius ecuadoriensis populations in southern Ecuador. Parasit Vectors, 5, 17. doi:10.1186/1756-3305-5-17
Grijalva, M. J., Villacis, A. G., Ocana-Mayorga, S., Yumiseva, C. A., Moncayo, A. L., & Baus, E. G. (2015). Comprehensive Survey of Domiciliary Triatomine Species Capable of Transmitting Chagas Disease in Southern Ecuador. PLoS Negl Trop Dis, 9(10), e0004142. doi:10.1371/journal.pntd.0004142
Gurtler, R. E., & Yadon, Z. E. (2015). Eco-bio-social research on community-based approaches for Chagas disease vector control in Latin America. Trans R Soc Trop Med Hyg, 109(2), 91-98. doi:10.1093/trstmh/tru203
Haines, A., Bruce, N., Cairncross, S., Davies, M., Greenland, K., Hiscox, A., . . . Wilkinson, P. (2013). Promoting health and advancing development through improved housing in low-income settings. J Urban Health, 90(5), 810-831. doi:10.1007/s11524-012-9773-8
Hashimoto, K., Zuniga, C., Romero, E., Morales, Z., & Maguire, J. H. (2015). Determinants of Health Service Responsiveness in Community-Based Vector Surveillance for Chagas Disease in Guatemala, El Salvador, and Honduras. PLoS Negl Trop Dis, 9(8), e0003974. doi:10.1371/journal.pntd.0003974
Heydari, N., Larsen, D. A., Neira, M., Beltran Ayala, E., Fernandez, P., Adrian, J., . . . Stewart-Ibarra, A. M. (2017). Household Dengue Prevention Interventions,

214
Expenditures, and Barriers to Aedes aegypti Control in Machala, Ecuador. Int J Environ Res Public Health, 14(2). doi:10.3390/ijerph14020196
Holveck, J. C., Ehrenberg, J. P., Ault, S. K., Rojas, R., Vasquez, J., Cerqueira, M. T., . . . Periago, M. R. (2007). Prevention, control, and elimination of neglected diseases in the Americas: pathways to integrated, inter-programmatic, inter-sectoral action for health and development. BMC Public Health, 7, 6. doi:10.1186/1471-2458-7-6
Hotez, P. J. (2014). Neglected parasitic infections and poverty in the United States. PLoS Negl Trop Dis, 8(9), e3012. doi:10.1371/journal.pntd.0003012
Hurtado, L. A., Calzada, J. E., Pineda, V., Gonzalez, K., Santamaria, A. M., Caceres, L., . . . Saldana, A. (2014). [Knowledge and risk factors related to Chagas' disease in two Panamanian communities where Rhodnius pallescens is the main vector]. Biomedica, 34(2), 260-270. doi:10.1590/S0120-41572014000200012
Lardeux, F., Depickere, S., Aliaga, C., Chavez, T., & Zambrana, L. (2015). Experimental control of Triatoma infestans in poor rural villages of Bolivia through community participation. Trans R Soc Trop Med Hyg, 109(2), 150-158. doi:10.1093/trstmh/tru205
Lindlof, T. R., & Taylor, B. C. (2011). Qualitative communication research methods (3rd ed.). Thousand Oaks, Calif.: SAGE.
Lindsay, S. W., Emerson, P. M., & Charlwood, J. D. (2002). Reducing malaria by mosquito-proofing houses. Trends Parasitol, 18(11), 510-514.
Lindsay, S. W., Jawara, M., Paine, K., Pinder, M., Walraven, G. E., & Emerson, P. M. (2003). Changes in house design reduce exposure to malaria mosquitoes. Trop Med Int Health, 8(6), 512-517.
Lucero, D. E., Morrissey, L. A., Rizzo, D. M., Rodas, A., Garnica, R., Stevens, L., . . . Monroy, M. C. (2013). Ecohealth interventions limit triatomine reinfestation following insecticide spraying in La Brea, Guatemala. Am J Trop Med Hyg, 88(4), 630-637. doi:10.4269/ajtmh.12-0448
Mackey, T. K., & Liang, B. A. (2012). Threats from emerging and re-emerging neglected tropical diseases (NTDs). Infect Ecol Epidemiol, 2. doi:10.3402/iee.v2i0.18667
McLeroy, K. R., Bibeau, D., Steckler, A., & Glanz, K. (1988). An ecological perspective on health promotion programs. Health Educ Q, 15(4), 351-377.
Meymandi, S. K., Forsyth, C. J., Soverow, J., Hernandez, S., Sanchez, D., Montgomery, S. P., & Traina, M. (2017). Prevalence of Chagas Disease in the Latin American-born Population of Los Angeles. Clin Infect Dis, 64(9), 1182-1188. doi:10.1093/cid/cix064
Monroy, C., Bustamante, D. M., Pineda, S., Rodas, A., Castro, X., Ayala, V., . . . Moguel, B. (2009). House improvements and community participation in the control of Triatoma dimidiata re-infestation in Jutiapa, Guatemala. Cad Saude Publica, 25 Suppl 1, S168-178.
Montenegro, D., Vera, M., Zuleta, L., Llanos, V., & Junqueira, A. (2016). [Strategy for determining a baseline in areas of vector interruption for Chagas disease]. Rev Panam Salud Publica, 39(6), 341-351.

215 Nieto-Sanchez, C., Baus, E. G., Guerrero, D., & Grijalva, M. J. (2015). Positive deviance
study to inform a Chagas disease control program in southern Ecuador. Memorias Do Instituto Oswaldo Cruz, 110(3), 299-309. doi:10.1590/0074-02760140472
Noireau, F., Diosque, P., & Jansen, A. M. (2009). Trypanosoma cruzi: adaptation to its vectors and its hosts. Vet Res, 40(2), 26. doi:10.1051/vetres/2009009
Norman, C. D. (2009). Health promotion as a systems science and practice. J Eval Clin Pract, 15(5), 868-872. doi:10.1111/j.1365-2753.2009.01273.x
Odhiambo, G. O., Musuva, R. M., Odiere, M. R., & Mwinzi, P. N. (2016). Experiences and perspectives of community health workers from implementing treatment for schistosomiasis using the community directed intervention strategy in an informal settlement in Kisumu City, western Kenya. BMC Public Health, 16, 986. doi:10.1186/s12889-016-3662-0
Parker, M., & Allen, T. (2013). Will mass drug administration eliminate lymphatic filariasis? Evidence from northern coastal Tanzania. Journal of biosocial science, 45(4), 517-545.
Pearce, W. B. (1989). Communication and the human condition. Carbondale: Southern Illinois University Press.
Pellecer, M. J., Dorn, P. L., Bustamante, D. M., Rodas, A., & Monroy, M. C. (2013). Vector blood meals are an early indicator of the effectiveness of the Ecohealth approach in halting Chagas transmission in Guatemala. Am J Trop Med Hyg, 88(4), 638-644. doi:10.4269/ajtmh.12-0458
Peters, D. H., Adam, T., Alonge, O., Agyepong, I. A., & Tran, N. (2013). Implementation research: what it is and how to do it. BMJ, 347, f6753. doi:10.1136/bmj.f6753
Quinde-Calderon, L., Rios-Quituizaca, P., Solorzano, L., & Dumonteil, E. (2016). Ten years (2004-2014) of Chagas disease surveillance and vector control in Ecuador: successes and challenges. Trop Med Int Health, 21(1), 84-92. doi:10.1111/tmi.12620
Rochat, L., Bizzini, A., Senn, N., Bochud, P. Y., Genton, B., & de Valliere, S. (2015). Acute schistosomiasis: a risk underestimated by travelers and a diagnosis frequently missed by general practitioners-a cluster analysis of 42 travelers. J Travel Med, 22(3), 168-173. doi:10.1111/jtm.12187
Rojas de Arias, A., Ferro, E. A., Ferreira, M. E., & Simancas, L. C. (1999). Chagas disease vector control through different intervention modalities in endemic localities of Paraguay. Bull World Health Organ, 77(4), 331-339.
Rosecrans, K., Cruz-Martin, G., King, A., & Dumonteil, E. (2014). Opportunities for improved chagas disease vector control based on knowledge, attitudes and practices of communities in the yucatan peninsula, Mexico. PLoS Negl Trop Dis, 8(3), e2763. doi:10.1371/journal.pntd.0002763
Saldana, J. (2016). The coding manual for qualitative researchers (Third ed.). Los Angeles, Calif. ; London: SAGE.
Sanmartino, M., & Crocco, L. (2000). [Knowledge about Chagas' disease and risk factors in Argentina communities with different epidemiological trends]. Rev Panam Salud Publica, 7(3), 173-178.
216 Santos, C. V., Bedin, C., Wilhelms, T. S., & Villela, M. M. (2016). Assessment of the
Housing Improvement Program for Chagas Disease Control in the Northwestern municipalities of Rio Grande do Sul, Brazil. Rev Soc Bras Med Trop, 49(5), 572-578. doi:10.1590/0037-8682-0386-2016
Saunders, M., Small, A., Dedicoat, M., & Roberts, L. (2012). The development and validation of a risk score for household infestation by Triatoma infestans, a Bolivian vector of Chagas disease. Trans R Soc Trop Med Hyg, 106(11), 677-682. doi:10.1016/j.trstmh.2012.07.006
Seddon, T., Billett, S., & Clemans, A. (2004). Politics of social partnerships: a framework for theorizing. Journal of Education Policy, 19(2), 123-142. doi:10.1080/0144341042000186309
Soriano-Arandes, A., Basile, L., Ouaarab, H., Claveria, I., Gomez i Prat, J., Cabezos, J., . . . Jane, M. (2014). Controlling congenital and paediatric chagas disease through a community health approach with active surveillance and promotion of paediatric awareness. BMC Public Health, 14, 1201. doi:10.1186/1471-2458-14-1201
Strauss, A. L., & Corbin, J. M. (1998). Basics of qualitative research : techniques and procedures for developing grounded theory (2nd ed.). Thousand Oaks: Sage Publications.
Suarez-Davalos, V., Dangles, O., Villacis, A. G., & Grijalva, M. J. (2010). Microdistribution of sylvatic triatomine populations in central-coastal Ecuador. J Med Entomol, 47(1), 80-88.
Suddaby, R. (2006). From the editors: What grounded theory is not. Academy of Management Journal, 49(4), 633-642.
Thomson, H., & Petticrew, M. (2007). Housing and health - Heating improvements may hold most promise for developing healthy housing policy. British Medical Journal, 334(7591), 434-435. doi:10.1136/bmj.39133.558380.BE
Thomson, H., Sellstrom, E., & Thomas, S. (2007). Housing improvement as a strategy to improve health and reduce health inequalities: a systematic review of best available evidence. European Journal of Public Health, 17, 127-127.
Thomson, H., Thomas, S., Sellstrom, E., & Petticrew, M. (2008). Best available evidence on housing improvement and health: A systematic review. Journal of Epidemiology and Community Health, 62, A4-A5.
Timmermans, S., & Tavory, I. (2007). Advancing Ethnographic Research through Grounded Theory Practice. In A. Bryant & K. Charmaz (Eds.), The Sage Handbook of Grounded Theory (pp. 493-512). USA: Sage Publications.
Tracy, S. J. (2013). Qualitative research methods : collecting evidence, crafting analysis, communicating impact. Chichester, West Sussex, UK: Wiley-Blackwell.
Triana, D. R., Mertens, F., Zuniga, C. V., Mendoza, Y., Nakano, E. Y., & Monroy, M. C. (2016). The Role of Gender in Chagas Disease Prevention and Control in Honduras: An Analysis of Communication and Collaboration Networks. Ecohealth, 13(3), 535-548. doi:10.1007/s10393-016-1141-9
Vale, G. A., Chamisa, A., Mangwiro, C., & Torr, S. J. (2013). A neglected aspect of the epidemiology of sleeping sickness: the propensity of the tsetse fly vector to enter houses. PLoS Negl Trop Dis, 7(2), e2086. doi:10.1371/journal.pntd.0002086

217 Viotti, R., Alarcon de Noya, B., Araujo-Jorge, T., Grijalva, M. J., Guhl, F., Lopez, M. C.,
. . . Latin American Network for Chagas Disease, N. (2014). Towards a paradigm shift in the treatment of chronic Chagas disease. Antimicrob Agents Chemother, 58(2), 635-639. doi:10.1128/AAC.01662-13
Waleckx, E., Camara-Mejia, J., Ramirez-Sierra, M. J., Cruz-Chan, V., Rosado-Vallado, M., Vazquez-Narvaez, S., . . . Dumonteil, E. (2015). An innovative ecohealth intervention for Chagas disease vector control in Yucatan, Mexico. Trans R Soc Trop Med Hyg, 109(2), 143-149. doi:10.1093/trstmh/tru200
Webster, J. P., Gower, C. M., Knowles, S. C., Molyneux, D. H., & Fenton, A. (2016). One health - an ecological and evolutionary framework for tackling Neglected Zoonotic Diseases. Evol Appl, 9(2), 313-333. doi:10.1111/eva.12341
Whitty, C. J. (2015). Political, social and technical risks in the last stages of disease eradication campaigns. Int Health, 7(5), 302-303. doi:10.1093/inthealth/ihv049
World Health Organization. (2012a). Global Report for Research on Infectious Diseases of Poverty. Retrieved from Geneva: WHO/TDR on behalf of Special Programme for Research and Training in Tropical Diseases (TDR): http://www.who.int/tdr/publications/global_report/en/
World Health Organization. (2012b). Research priorities for Chagas disease, human African trypanosomiasis and leishmaniasis. World Health Organ Tech Rep Ser(975), v-xii, 1-100.
World Health Organization. (2015). Chagas disease in Latin America: an epidemiological update based on 2010 estimates. Wkly Epidemiol Rec, 90(6), 33-43.

218
Chapter 6: Towards a Theory of Sustainable Prevention of Chagas Disease:
Scaling Up Proposal (White Paper)
Contents
1. Introduction 2. Background
2.1. Chagas disease 2.2. Chagas disease epidemiology in Loja Province (Ecuador)
3. Healthy Homes for Healthy Living 4. Methodology
4.1. Data collection and study population 4.2. Data Analysis
5. Scaling up proposal 5.1. Infrastructure improvement
5.1.1. Summary of findings Grounded Theory study 5.1.2. General interest 5.1.3. Infrastructure improvement
5.1.3.1. Local interest in scaling up 5.1.3.2. Implementation considerations 5.1.3.3. Economic considerations 5.1.3.4. Strategic considerations
5.1.4. Dialogic health promotion 5.1.5. Income generation
6. Conclusion

219 Introduction
Probably one of the most important challenges currently faced by researchers
working on public health is how to translate scientific research into practice, and even
more importantly, into practice relevant for populations affected by specific health risks.
Translational, operational, formative, and implementation research have been the subject
of advocacy efforts interested in promoting science as a socially relevant endeavor
capable to mobilize resources for social change (Pokhrel et al., 2011; Sommerfeld et al.,
2015).
The health systems perspective proposes implementation research as a
fundamental piece to address social inequalities lying at the core of neglected tropical
diseases (NTD) occurrence (World Health Organization, 2012a). Defined as a scientific
endeavor interested in understanding processes and resources required for disease
prevention and control in real-world settings, implementation research is focused in
context-specific and evidence-informed knowledge (Peters, Adam, Alonge, Agyepong, &
Tran, 2013). Given that NTD occur in contexts determined by complex social, economic
and political factors, implementation research explores interactions between disease and
larger social structures with actual and potential consequences for affected populations
(WHO, 2012). Informed by pragmatic thinking, it is not only focused on the
identification of barriers for the execution of plans, but also on creative ways of defining
effectiveness under real —instead of hypothetical— circumstances (Gilson et al., 2011).
Implementation research expands narrow perspectives suggested by top down
disease prevention strategies and proposes complex approaches to health promotion that

220 question traditional ways of conceptualizing and designing health interventions. As a
result, it has been identified as a key instrument for bridging gaps and developing more
equitable partnerships between stakeholders, researchers and populations involved in
scientific endeavors, as well as a vehicle to understand organizational, social, and
political processes constructed through communication practices that could affect
effectiveness of health interventions (Sheikh et al., 2011).
After five years of implementation of its pilot phase, Healthy Homes for Healthy
Living (HHHL) has accumulated an important wealth of knowledge about systemic
approaches to Chagas Disease (CD) prevention (Briceno-Leon, 2009; Bustamante et al.,
2014; Lucero et al., 2013; Santos et al., 2016). This white paper aims to explore the
conditions under which HHHL could be scaled up in the focal communities of
Chaquizhca, Bellamaria and Guara in Loja province (Ecuador). Information included in
this report was collected as part of a larger study aimed at identifying factors that
contribute to or limit sustainable control of CD under the model proposed by HHHL.
Since those results have been reported elsewhere (see Chapter 5), this document will
specifically include information about strategies to potentially expand HHHL model
considering previously identified factors. Consequently, this white paper will specifically
address the question: In what ways can the contributions and limitations in the HHHL
model be addressed in order to scale it up to other homes in the focal communities of
Loja province?

221
Chagas disease.
Chagas disease (CD) is caused by Trypanosoma cruzi (T. cruzi), a protozoan
parasite that can be found the hindgut of blood-sucking insects known as triatomines. CD
is commonly found among people living in poverty in rural areas of tropical and
subtropical regions of the Americas. Different species of triatomines have been
identified in Mexico, Central America, the Andean region (Colombia, Ecuador,
Venezuela, and Peru), the Southern Cone (Argentina, Brazil, Bolivia, Chile, Paraguay,
and Uruguay), and the south of the US (Hotez, 2014; Hotez et al., 2012). Ongoing
migratory flows have created new epidemiological contexts in urban centers (De Maio et
al., 2014; Dias et al., 2016).
The most common route of human transmission of CD occurs in poorly
constructed domiciliary environments where triatomines can remain hidden in cracks and
crevices during the day and become active at night to search for blood sources.
Triatomines feed on people’s blood while they are sleeping; in order to make room for
larger meals, they defecate and leave the parasite on people’s skin. Inadvertently, bitten
individuals bring T. cruzi to their system by rubbing the punctured wound where
triatomines have been feeding from or through the mucus membranes in mouth and eyes
(CDC, 2017). Once the parasite enters the human system, it invades cells around the
entry site and multiplies inside them. At this point, the parasite turns into trypomastigotes
that are released into de blood system, starting the acute phase of the infection. People
can show mild symptoms or remain asymptomatic for long periods of time, until they
develop the next phase of T. cruzi infection known as chronic. At this stage people can
222 experience arrhythmias, palpitations, and chest pain (Gascon et al., 2014). About 30% to
40% of the affected population develops cardiopathies, alterations of the gastrointestinal
system such as megacolon and mefaesophagus, neurological or a mix of these clinical
manifestations latter stages of the disease (Soriano-Arandes et al., 2014).
No vaccine has been developed for CD, and medicines used to treat its symptoms
in the acute phase —nifurtimox (Bayer) and benznidazole (Roche)— have shown side
effects that become more serious as a patient’s age increases, including renal and hepatic
complications (Viotti et al., 2014). Other forms of transmission include intake of
contaminated food, vertical transmission from mothers to infants, and blood transfusion
(World Health Organization, 2012b).
The biology of the different species of triatomines involved in CD transmission
creates specific conditions for control programs. For example, the Southern Cone
Initiative, known for a significant impact in reduction of infestation rates in highly
endemic areas of Bolivia, Paraguay, North of Argentina and the Brazilian states of Minas
Gerais, Bahia, and Rio Grande do Sul, directed most of its efforts toward Triatoma
infestans, a species mainly restricted to human created environments (Dias, 2007). This
condition determined that control programs could focus almost exclusively in domiciliary
infestation with sustained indoor fumigation, which lead to significant decrease in CD
transmission in the region (Schofield & Dias, 1999).
Control efforts in areas where vectors are found in association with sylvatic
habitats require different, and in most cases, complex approaches to disease prevention at
multiple levels. In these cases it is necessary to understand a series of associations
223 between vectors, reservoirs, hosts and natural environment in order to determine routes of
contact between triatomines and blood sources (C. Barbu et al., 2009). That is the case of
Central America, where the main vector, Triatoma dimidiate, has been found in
association with palm trees, around rock piles, and in traditional homes surrounded by
dogs and chicken (Dumonteil et al., 2013). International guidelines recommend multiple
spraying of those homes, which usually derives into reinfestation after the residual effect
of the insecticide has receded (Bustamante et al., 2009).
In Ecuador, sixteen species of triatomines have been identified (Abad-Franch et
al., 2001). Given Ecuador’s geographical diversity, these different species show
particular patterns of association with natural environments in coastal and mountainous
areas of the country. Some of these associations are determined by geographical
characteristics that allow settlement of particular species, such T. dimidiata, Rhodnius
ecuadoriensis, and Panstrongylus howardi in domestic and peridomestic areas of Manabi
(Abad-Franch et al., 2001; Grijalva et al., 2012), and Triatoma carrioni, Panstrongylus
chinai, and Panstrongylus rufotuberculatus in the highlands, particularly Loja province
(Grijalva et al., 2015). Other associations are determined by factors such as proximity of
human dwellings to the natural environment. That is the case of Manabi, where
researchers have identified squirrels’ nests, rodents, opossums, and a particular species of
palm acting as hosts and reservoirs of P. howardi (Grijalva et al., 2011). The interactions
of these elements facilitate an ongoing circulation of vectors from peridomestic areas to
the natural environment and vice versa, which increases the likelihood of contact with
human beings.

224
In addition to these ecological factors, it has been recommended that CD control
programs attend to socio-economic conditions, productive activities, and cultural
practices that could constitute risk factors for disease transmission (Sommerfeld &
Kroeger, 2015; Ventura-Garcia et al., 2013). That is the case of Loja province where
triatomines presence has been associated with traditional elements of rural life such as
pigs and goats breeding, as well as lack of latrines and storage units (Grijalva et al.,
2015). Since triatomines’ presence inside domiciliary areas has been predominantly
found in structures built with adobe walls, clay tiles, and dirt floors (Grijalva et al., 2012;
Grijalva et al., 2015), considering home structures is fundamental in this case.
Additionally, CD faces challenges associated with lack of awareness in affected
populations and medical personnel, limited funds assigned for research, low access to
diagnostic tools and treatment, but main, and foremost, sustained socio-economic
marginalization determining the conditions of life of populations at risk (Viotti et al.,
2014). These conditions play a fundamental role in the classification of CD as a neglected
tropical disease (NTD).
CD epidemiology in Loja province.
Loja province is considered at high risk for CD transmission given registered
domiciliary presence of triatomines and evidence of transmission through primary vectors
(Abad-Franch, 2003; Grijalva & Villacis, 2009). Environmental and socio-economic
factors have been identified in this transmission dynamics. Located bellow 2,200 meters
above sea level (masl), Loja is abundant with trees that host rodents and birds’ nests,
factors associated with presence of R. ecuadoriensis in sylvatic environments (Grijalva et

225 al., 2012) . Dogs, guinea pigs and pigs are common in local households (Grijalva et al.,
2005). As a predominantly rural region, communities rely on economic activities that
require ongoing association with their natural environment, mainly agriculture and cattle
rising. Accumulation of produce –harvested and used for cattle feed– in the surrounding
areas of the home, collection of firewood for cooking purposes and presence of fruit
trees, are common (Grijalva et al., 2015). Finally, conditions of living environments
associated with triatomine infestation such as inhabitation of dwellings built with adobe
walls and earthen floors (Grijalva et al., 2005; Grijalva et al., 2012), as well as lack of
access to sanitary facilities (Grijalva, Villacis, Ocana-Mayorga, Yumiseva, & Baus,
2011), are also part of this context.
This research was focused in the communities of Bellamaria (39 homes),
Chaquizhca (50 homes), and Guara (46 homes), a region that showed particularly high
rates of triatomines’ infestation during entomological searches conducted by the Malaria
National Service between 2005 and 2009 in Loja province (Grijalva et al., 2015). Houses
in this area are located within the dry mountain subtropical forest ecological zone and
range in altitude from 1.100 to 2.200 m above sea level. The terrain is characteristic of
the western slopes of the southern Ecuadorian Andes mountain range. The region has a
yearly annual rainfall between 1600 and 3200 mm, with an average relative humidity of
78% and a rainy season that goes from December to April (Campozano, Celleri, Trachte,
Bendix, & Samaniego, 2016). The main economic activity of local population is
subsistence agriculture and day labor. Socio-economic conditions of most families in
these communities are adversely affected by limited job opportunities, poor access to

226 sanitary facilities, as well as deficient health and education services (Nieto-Sanchez,
Baus, Guerrero, & Grijalva, 2015). Poor roads and limited transportation alternatives
increase isolation and marginalization faced by local populations, and restricts their
access, participation and competitiveness in larger markets.
The cycle of poverty and disease in relation to CD is exacerbated in this region by
the limited capacity of the national control program (Quinde-Calderon, Rios-Quituizaca,
Solorzano, & Dumonteil, 2016). Some progress has been made in terms of disease
surveillance and prevention campaigns, but political issues have limited the resource
allocation necessary to achieve sustainable CD control (Dumonteil et al., 2016).
Given this combination of factors, previous studies have indicated the need for
systematic vector control interventions focused on housing improvement and community
participation as potentially effective mechanism for sustainable control of CD disease in
this region (Grijalva et al., 2012; Grijalva et al., 2015). Healthy Homes for Healthy
Living (HHHL) was designed to respond to this need.
Healthy Homes for Healthy Living Model (HHHL)
The Healthy Living Initiative (HLI) is a health promotion effort designed to
address socio-economic dynamics leading to Chagas Disease (CD) occurrence in Loja
province (Nieto-Sanchez et al., 2015). Led by the Infectious and Tropical Disease
Institute (ITDI) at Ohio University (OU) and the Center for Research in Health in Latin
America (CISeAL) at Pontifical Catholic University of Ecuador (PUCE), this initiative is
interested in exploring strategies for long term CD control.

227
Three premises support HLI’s actions: a) poverty is a complex phenomenon
underlying the dynamics of CD transmission (Houweling et al., 2016; Manderson et al.,
2009; Pokhrel et al., 2011) ; b) as a complex phenomenon, poverty expresses in multiple
forms of exclusion experienced by local individuals and communities, including
inequalities in their access to health and health-seeking behaviors (De Maio et al., 2014;
Dell'Arciprete et al., 2014; Sanmartino et al., 2015); c) working closely with local
populations in the definition of a sustainable model for disease prevention can facilitate
the design of a general framework that addresses not only risk factors for CD
transmission, but also socioeconomic priorities of local populations (Abad-Franch et al.,
2011; Gurtler & Yadon, 2015).
HLI’s main project is Healthy Homes for Healthy Living (HHHL), a Chagas
disease prevention effort focused in designing, building, and promoting living
environments conceived to deter triatomines’ presence in intra and peridomestic areas of
the homes in Loja province. Previous research has shown that traditional control
strategies –mainly fumigation with deltrametrine (Bayer) – are effective to prevent
triatomines’ infestation for short periods of time, but not to sustainably prevent CD in the
long run (Grijalva et al., 2005). That is, triatomines come back to spread dwellings
between 6 to 12 months after fumigation (Grijalva et al., 2011).
Consequently, HHHL proposes a prevention model that aims to address the
structural causes of disease transmission in this region. This model is based on homes’
structural improvement (Table. 4), long-term health promotion at the micro-level of the
household (Table. 5), and community involvement in locally driven income generation

228 opportunities. Actions in these three areas are articulated through ongoing
communication among involved actors aimed at informing decision-making at individual,
communitarian, and institutional levels. However, most of the activities promoted by
HHHL’s occur at the family -interpersonal- level.
Between 2013 and 2016, HHHL worked in the reconstruction and refurbishment
of six homes in the communities of Bellamaria (n=2), Chaquizhca (n=2), and Guara
(n=2). During this period (Pilot phase), HHHL collected information about technical and
social implications of implementing infrastructure interventions in this area according to
different purposes. The 2013’s intervention was carried out with only one family and was
focused on prototyping the process of fully reconstructing a home to make it anti-
triatomine, as well as designing health promotion processes to facilitate appropriation and
implementation of this new space. The goals of the 2014’s intervention was
understanding how to introduce anti-triatomine measures in dwellings that did not require
full reconstruction. Two homes were intervened during that year, including one home
built by the National Ministry of Housing (MIDUVI, by its acronym in Spanish). Finally,
HHHL simultaneously rebuilt three homes (one in each community) between 2015 and
2016, in order to identify logistical demands, as well as behavioral and socio-economic
impacts of conducting differentiated interventions around home improvement for CD
prevention. These interventions were funded through research schemes available at Ohio
University (OU) and Pontifical Catholic University of Ecuador (PUCE), as well as local
families and institutional partners, including the National Ministry of Housing (MIDUVI)
and the local government.

229
HHHL has worked under a model of partnership that examines the contributions
that different stakeholders can make to the definition and realization of healthy
environments as conceived in this particular context. Family members, neighbors, local
facilitators, academic communities, and representatives of the local government are
expected to maximize existing resources by contributing in different capacities to the
execution of plans individually conceived considering families’ socio-economic
conditions. Partner families in each stage of intervention were selected according to a
number of criteria, including interest in reconstructing their homes, capacity to commit
resources to the project, and decay status of their dwellings.
The level of decay of local construction was established after a study conducted in
2012 by PUCE’s Architecture School (unpublished data). This study identified seven
criteria to determine urgency of infrastructure intervention in the homes of these three
communities, including constructive pathologies, thermal performance, use of culturally
acceptable materials, access to water and sanitation, access to natural sunlight,
ventilation, potential risks, and cost of the required intervention. Five categories were
established under these criteria. Category 1 includes homes that are safe enough to
implement anti-triatomine measures without a major intervention, at an approximate cost
of USD $49.23 per m2. Categories 2 and 3 indicate some form of refurbishment required
before implementing those measures, with an approximate cost of USD $70.30 per m2 in
the former and USD $120.63 in the later. Finally, categories 4 and 5 are specific for
homes that demand full reconstruction in order to solve structural issues that endanger the

230 safety of inhabitant families at a cost USD $158.74 for category 4 and USD $218.89 for
category 5. A new study aimed at updating this data was conducted in 2016.
HHHL uses the term ‘partner family’ to refer to families that have agreed to build
or improve their homes according to the model proposed by HHHL. This rhetorical
decision was made as an alternative to the term “beneficiary” traditionally used in
development interventions. Calling local families “partners” makes visible a relationship
in which involved actors make specific contributions during the intervention, including
economic resources, labor, and social capital. HHHL has adapted the idea of partnership
as a means of addressing local needs through collaborative activities and decision-making
sensitive to local concerns and interests proposed by Seddon, Billett, and Clemans
(2004).
Methods
Data collection and study population.
Ethnographic grounded theory was used as main methodological framework for
this research. Grounded theory (GT) is a systematic approach to data collection and
analysis interested in generating explanations of social realities based on emerging
information grounded in actual data rather than in theory (Charmaz, 2014; Glaser &
Strauss, 1967; Strauss & Corbin, 1998). Constructivist approaches to grounded theory see
both data and analysis as the product of experiences co-created by participants,
researchers, and emerging data (Atkinson et al., 2008). Since constructivism is focused
on how and why participants construct meanings in specific situations (Deetz, 1996b;
Pearce, 1989), its extension to grounded theory looks at how, when, and to what extent

231 the studied experience is embedded in larger social structures in order to explain and
represent research findings (Charmaz, 2006). Constructivist Grounded Theory (CGT)
alludes to the open-ended nature of social processes, the value of human agency in
meaning making, and the fundamental role played by language, interpretation, action and
temporaryity in research (Strauss & Corbin, 1998). When coupled with ethnographic
methods of data collection, GT receives the name of ethnographic grounded theory.
Participants for this reserach were selected from inhabitants of the communities of
Bellamaria, Chaquizhca, and Guara in southern Ecuador that have directly or indirectly
experienced interventions led by HHHL. The study population was divided into three
groups: partner families; non-partner families, selected as matched pairs; and a third
group of heads of household selected across the community.
The first group (Group 1) included the six families that have specifically agreed to
partner with HHHL to build or improve their homes according to the above-described
model (Table 3). At least three members of each family were interviewed in three
different moments of field visits: the first one between June and July 2016; the second in
January of 2017; and the last between May and June 2017.
Considering the principle of maximum variation (Lindlof & Taylor, 2011; Tracy,
2013), an equal number of families (6) that have not implemented the HHHL model also
participated in in-depth interviews for this research (Group 2). They were purposely
selected with the purpose of mirroring partner’s situation previous intervention,
particularly in terms of family composition and decay status of the home. Two members
of these families were interviewed during the same periods of data collection.

232
The third group (Group 3) included members of the communities at large
(n=102). Heads of household that accepted to participate completed a facilitated paper-
based forty-one (41) item questionnaire including questions about physical conditions of
the dwelling, socio-economic status of the family, and interest in home improvement in
the near future. This information was collected in order to create a larger picture of the
communities that could serve as reference for theory development in later stages of
analysis. Group 3 is cross-sectional and not exclusive of groups 1 and 2.
Data analysis.
The analytical processes conducted within this research were not intended at
generating new theories of sustainability; instead, they aimed to extend understanding of
this concept by adding contextualized data emerged from HHHL implementation.
Therefore, I used ‘sustainability’ as sensitizing concept. Sensitizing concepts are
interpretive devices used as “points of departure for studying the empirical world while
retaining the openness for exploring it” (Charmaz, 2014, p. 30). In order to operationalize
sustainability as concept, I used the Pan American Health Organization (PAHO)
parameters for sustainable management of NTD in the region (Holveck et al., 2007): (i)
vector control; (ii) provision of water and sanitation; (iii) management of zoonotic
elements of the disease; and (iv) community participation social capital. Interview
protocols and questionnaires were structured around these parameters.
A total of 102 questionnaires from community members, more than 40 hours of
interviews with partner and non-partner families, as well as more than 150 pages of
implementation reports, and field notes about informal conversations and participant

233 observation were analyzed in two phases of coding (Saldana, 2016). The initial coding
phase involved assigning codes to words or larger segments of transcribed materials,
whereas the second phase aimed to identify the most significant codes initially identified
in order to sort, synthesize, integrate, and organize them toward theory construction
(Charmaz, 2014). Since this research was conducted in Ecuador with Spanish-speaking
communities, initial coding schemes were constructed in Spanish using a line-by-line
approach.
Questionnaires were analyzed in two separate ways. First, quantitative data were
analyzed using frequency tables. Subsequently, a univariate logistic regression model was
fitted for the “interest in reconstructing home under the HHHL model” variable in each of
the outcomes. All quantitative data were analyzed using R (version 3.4.1). Descriptive
coding was applied to the qualitative portion of each question. Descriptive coding is a
method intended at identifying and summarizing the most salient elements of a portion of
qualitative data (Saldaña, 2016). This process was intended at expanding the information
provided by partner and non-partner families included in the interviews by adding a more
general perspective from the communities at large.
These descriptive codes were integrated in the Focused coding phase described in
a separate manuscript (see Chapter 5). The questionnaire included 41 questions, 38 of
them with a potential qualitative follow up question. In order to process this information,
a workbook in Excel with different tabs (sheets) for each one of the questions was used.
The first part of the process consisted on entering the answers for each one of the
respondents (102) in the corresponding tab. Subsequent coding was conducted in each

234 one of the existing Excel sheets using the Comment function available in the Review
menu of the program.
Scaling Up Proposal
Summary of findings ancillary study.
The ideas for scaling up the HHHL’s model proposed here build upon a larger
study aimed at identifying contributions and limitations to sustainable control of CD
under the model proposed by HHHL. Since those results have been discussed at length in
a separate paper, I will only provide a summary for readers’ reference.
The study “Towards a theory of sustainable prevention of Chagas disease: An
ethnographic grounded theory study” aimed to identify factors that contribute to or limit
sustainable control of Chagas disease under the model proposed by HHHL in three
communities of Loja province. It approached the experiences of local families in relation
to the construction and use of the homes promoted as anti-triatomine solution by HHHL.
Four theoretical concepts emerged once the categories identified during the phase
of focused coding (infrastructure in intervened homes, infrastructure in non-intervened
homes, social structures, community relations, relationships with HHHL staff, and future
perspectives) were sorted and integrated into analytical memos during the phase of
theoretical sampling (Charmaz, 2014). These theoretical categories were health impact,
emotional impact, economic impact and social impact.
Applying these lenses, I theorized that sustainability of CD control under the
model proposed by HHHL largely depends on the systemic capacity of home
improvement to activate and sustain agency in partner families. That agency is expressed

235 in the different levels of impact previously outlined and evolves as an integrated set of
capacities toward health promotion and disease prevention.
So far, the program has been able to create scenarios of social inclusion for
populations at risk of CD in interaction with program designers and health institutions.
Those scenarios are spaces where individual and group agency in relation to health is
invited and maintained. Besides the direct intervention on the homes, HHHL has
facilitated construction of drinking water systems, formalization of income generation
initiatives, and collaborative efforts aimed at strengthening negotiating skills of local
leaders, among other actions. This way, the program has attended to the dynamics of
various elements constitutive the local context and has responded with opportunities for
local families to improve their health according to resources available to them. Instead of
limiting control measures to individuals’ capacity to react to risk factors, the program has
invested important resources in addressing local priorities, generating stable working
relationships with local populations and collecting relevant information to inform
implementation processes. This study suggests that by doing so, HHHL has been able to
extend active sense-making in local families’ expressed as agency in the construction of
healthier living environments resilient to their specific conditions.
From this perspective, agency around the model, and therefore, sustainability of
the intervention can be seen as the confluence of three factors: systemic improvement of
families’ quality of life, consistent use of protective measures, and adaptation to
emerging dynamics. These three factors also showed limitations, including need for
ongoing health promotion as vector and risk factors become less visible, low quality of

236 some construction materials, families’ financial capacity to sustain and replace protective
measures, and capacity to react to the dynamic nature of living environments.
Moreover, I argued that the flexibility and adaptability showed by the HHHL to
facilitate participation of local families under differentiated funding models could be
strengthened and replicated by this and other programs applying systemic approaches to
disease prevention. During this pilot phase of the project, local facilitators and staff had
institutional support to emphasize negotiation processes over blunt indicators of cost-
effectiveness (Bardosh, 2014; Odhiambo et al., 2016; Parker & Allen, 2013), which
rendered important results in terms of trust building and appropriateness of the applied
solution.
Building on the knowledge obatined during this process, it was recommended that
HHHL keeps working on establishing strategic partnerships with governmental and
private institutions with the experience and infrastructure necessary to implement home
improvement projects at larger scales, but sustain its involvement in the health promotion
efforts conducted along the process. Since intersectoral collaboration is a baseline
condition for sustainability of systemic interventions (Charron, 2012; Dias, 2007; Santos,
Bedin, Wilhelms, & Villela, 2016), this model of partnership can provide the necessary
tools for the intervention to continue as a systemic approach to disease prevention. In this
sense, it is important to sustain mechanisms generated with government institutions,
NGOs, and private partners interested in promoting the idea of healthy housing. An
important precedent of this kind of collaboration is the partnership established with the
Ecuadorian Ministry of Housing in 2015. Possibilities of extending this type of

237 association with national, international, and multilateral institutions should be further
explored.
Accordingly, scaling up the HHHL model will be understood in this paper as the
process of bringing up to scale the model’s capacity to engage and activate agency
around disease prevention in other families in this area. Although some operational issues
in relation to infrastructure will be presented, I will elaborate on ideas to sustain the
systemic nature of intervention while extending it to the other families in these
communities.
Infrastructure improvement.
Existing interest in the HHHL model.
Updated data resulted from the decay analysis conducted in 2012 (n=126) in
Chaquizhca, Bellamaria, and Guara showed significative progression towards decay in
local homes (Table 8). While 23.5% (n=31) of the homes were classified under category
3, 19.7% (n=26) under category 4, and 15.15% (n=20) under category 5 of decay in 2012
(n=132) in 2012, the most recent analysis included 8.73% (n=11) of the homes in
category 3, 11.11% (n=14) in category 4, and 41.27% (n=42) in category 5. The increase
in category 5 can be explained by the natural progression of adobe constructions when
they are built with traditional techniques. According to local families, a traditional adobe
construction that does not include additional protection measures —such as cement
plastering— is expected to last 10 to 12 years without major repairs. After that period,
walls become thinner and start showing major cracks.
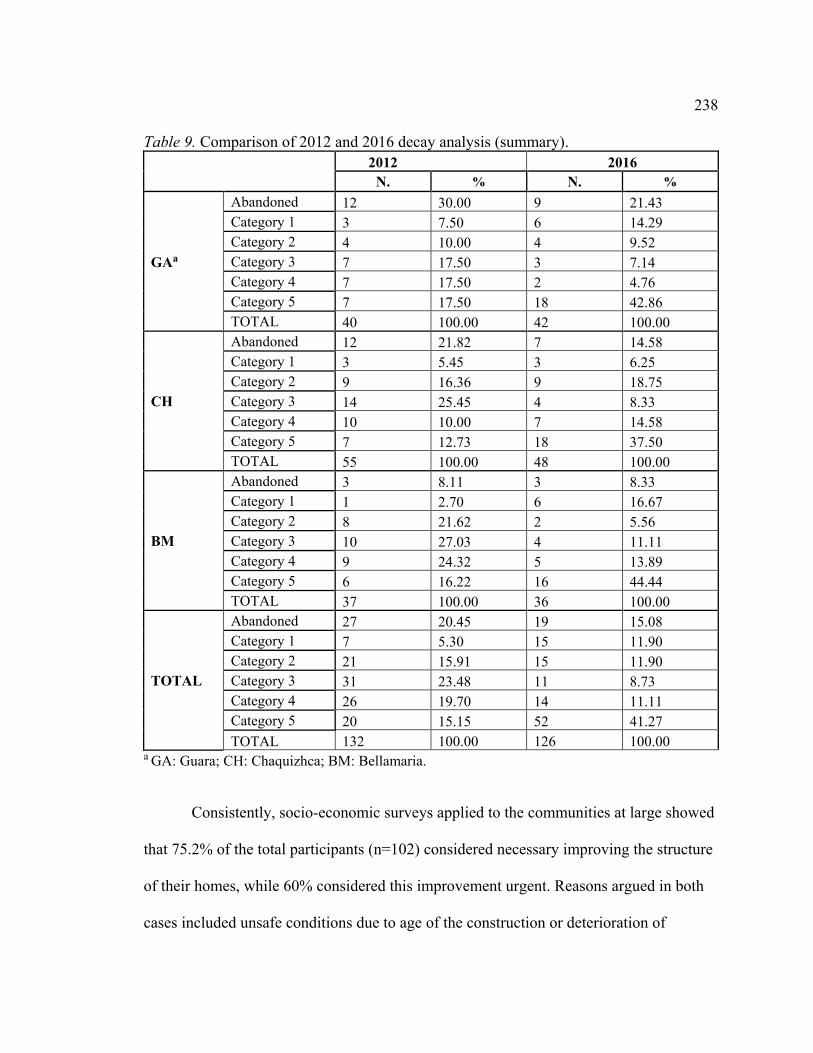
238 Table 9. Comparison of 2012 and 2016 decay analysis (summary).
2012
2016
N. % N. %
GAa
Abandoned 12 30.00 9 21.43 Category 1 3 7.50 6 14.29 Category 2 4 10.00 4 9.52 Category 3 7 17.50 3 7.14 Category 4 7 17.50 2 4.76 Category 5 7 17.50 18 42.86 TOTAL 40 100.00 42 100.00
CH
Abandoned 12 21.82 7 14.58 Category 1 3 5.45 3 6.25 Category 2 9 16.36 9 18.75 Category 3 14 25.45 4 8.33 Category 4 10 10.00 7 14.58 Category 5 7 12.73 18 37.50 TOTAL 55 100.00 48 100.00
BM
Abandoned 3 8.11 3 8.33 Category 1 1 2.70 6 16.67 Category 2 8 21.62 2 5.56 Category 3 10 27.03 4 11.11 Category 4 9 24.32 5 13.89 Category 5 6 16.22 16 44.44 TOTAL 37 100.00 36 100.00
TOTAL
Abandoned 27 20.45 19 15.08 Category 1 7 5.30 15 11.90 Category 2 21 15.91 15 11.90 Category 3 31 23.48 11 8.73 Category 4 26 19.70 14 11.11 Category 5 20 15.15 52 41.27 TOTAL 132 100.00 126 100.00
a GA: Guara; CH: Chaquizhca; BM: Bellamaria.
Consistently, socio-economic surveys applied to the communities at large showed
that 75.2% of the total participants (n=102) considered necessary improving the structure
of their homes, while 60% considered this improvement urgent. Reasons argued in both
cases included unsafe conditions due to age of the construction or deterioration of

239 original adobe, lack of comfort (high temperatures and darkness), presence of leaks, and
interest in improving the health of family members. Additionally, 56.6% of the
respondents mentioned that they would consider full reconstructions of their homes,
while 67.4% expressed interest in their homes being intervened under the HHHL model
(Table 9). Arguments stated to support this interest include aesthetics and infrastructure
considerations (the homes are ‘more organized and clean’, ‘pretty’, ‘allow individual
rooms for members of the family’, ‘more comfortable to receive visitors’, ‘good for
earthquakes and tremors’), appreciations about the lifestyle promoted by HHHL homes
(‘they help us to live better’, ‘healthy’, ‘reduce bugs and dust’, ‘good to live far away
from animals’), and evaluations of HHHL contribution (‘it is good help’, ‘built by people
that know [about technical construction]’, ‘families do not spend a lot of money’, ‘we
like what you guys do’), among others.
Families that were not interested in implementing the HHHL model expressed
concerns about costs (‘it is too expensive and we are poor’), workload (‘it is too much
work’, ‘I am a single a mom and do not have anybody that could work for me’), and size
(‘those homes seem small for larger families’). Participants also mentioned preference for
other materials (‘I would like to build my next home with bricks’) and lack of interest for
altering their current lifestyles (‘we have lived this way all our life and we are too old
now’).

240 Table 10. Demographic characteristics respondents socio-economic questionnaire N % Respondent gender Female 58 56.9% Male 44 43.1% Respondent age 18-30 13 12.7% 31-40 17 16.7% 41-50 16 15.7% 51-60 21 20.6% 61-70 14 13.7% 71-80 11 10.8% 81-90 10 9.8% Inhabitants 1 to 3 49 48.0% 4 to 6 33 32.3% >6 20 19.6% House age <14 41 40.2% 15-29 45 44.1% >30 16 15.7%
Table 11. Frequency table for quantitative component of socio-economic questionnaire. Question Answers N. % General socio-economic factors
Members of the family living in another city Yes 81 79.4 No 21 20.6 DN/DA 0 0
Breadwinner in the house
Mom 14 13.7 Dad 32 31.4 Both 3 36.3 Children 16 15.6 Other? 3 2.9
Transportation method more often used
Car 14 13.7 Ranchera 78 76.5 Animal 5 4.9 Walking 2 2 Other? 2 2

241 Table 11: continued.
DN/DA 1 1
Distance to the closest road
Less than 1 hour 99 97.1 Between 1 and 2 hours 3 2.9
Over two hours 0 0 DN/DA 0 0
Regular fumigation of the household
Yes 63 62.4 No 38 37.6 DN/DA 0 0
Currently receiving subsidy from the government Yes 68 66.7 No 34 33.3 DN/DA 0 0
Have received subsidy from the Ministry of Housing
Yes 4 4 No 98 96 DN/DA 0 0
Currently receiving disability subsidy Yes 11 10.8 No 91 89.2 DN/DA 0 0
Access to community water system Yes 66 64 No 36 36 DN/DA 0 0
Sanitary facility
Toilet 36 35.6 Latrine 37 36.6 Bushes 29 27.7 DN/DA 0 0
Source of water used for cooking
Open source water 30 29.4
Bore hole/well 3 2.9 Tap 64 62.7 Other 4 3.9
Space for cooking
Kitchen 83 81.3 Patio 13 12.7 Bedroom 5 4.9 Other? 1 0.9
Affiliated to Farmers Social Insurance Yes 61 59.8 No 41 40.2 DN/DA 0 0

242 Table 11: continued.
Monthly income
Under 100 41 40.2 Between 100 and 300 43 42.1
Between 300 and 500 9 8.8
More than 500 2 2 DN/DA 7 6.9
Staying in their homes for the next five years Yes 90 88.2 No 7 6.9 NS/NR 5 4.9
Legal titles over the land where the house was built
Yes 44 43.1 No 56 55 DN/DA 2 1.9
Legal titles over productive plot Yes 72 71.3 No 28 27.7 DN/DA 2 1.9
Interest in home improvement and HHHL
Infrastructural changes recently implemented in the house
Yes 47 46 No 53 52 DN/DA 2 1.9
Need to improve infrastructure of the home
Not necessary 15 14.7 Small need 9 8.8 Somehow needed 20 19.6 Needed 36 35.2 Really needed 16 15.6 DN/DA 6 5.8
Urgency to improve infrastructure of the home
Not urgent 23 22.5 Not very urgent 15 14.7 Somehow urgent 19 18.6 Urgent 28 27.4 Very urgent 13 12.7 DN/DA 3 2.9
Interest in full reconstruction
Yes 46 45 No 42 41.1 Maybe 10 9.8 DA/DA 3 2.9
Preferred materials for full reconstruction Adobe 28 27.4 Bricks 40 39.2

243 Table 11: continued.
Cement 7 6.9 Block 2 7.4 Other 5 1.9 DN/DA 22 21.5
Have heard of HHHL homes Yes 89 87.2 No 12 11.8 DN/DA 1 0.9
Have participated in HHHL construction activities Yes 53 52 No 46 45 DN/DA 3 2.9
Interest in implementing HHHL model
Yes 60 58.8 No 23 22.5 Maybe 4 3.9 DN/DA 15 14.7
Have participated in HLI activities Yes 72 70.5 No 25 24.5 DN/DA 5 4.9
From the households that expressed interest in implementing the HHHL model,
32% are located in Bellamaria (n=21), 37.5% are in Chaquizhca (n=24), and 29.7%
(n=19) are in Guara. Approximately 41.3% of the families currently hold titles over their
land, 71.4% own a plot to cultivate their products, and 65.6% receive the government
subsidy. Even though 85.7% reported monthly incomes under US$300, all families
(100%) mentioned willingness to contribute some resource to complete a project of this
nature, including produce and cattle sales, family loans, remittances, labor, and credits
with banks, cooperatives, or official institutions. Around 48.4% of them have conducted
some form of infrastructure repair in their homes during the last year and 46.5% would be
willing to fully reconstruct their dwellings.

244
These results show favorable conditions to scale up the HHHL model under most
of the criteria previously established to select partner families. Most importantly, they
indicate accuracy of the factors observed by the project during the phase of simultaneous
reconstruction to establish differentiated models of funding for partner families, including
property over their land, access to the Human Development Subsidy (government
subsidy), regular income (obtained through produce sold at the local market, animals’
commerce or weekly salary), as well as access to additional sources of funding of income
(remittances or credits, among others). However, I recommend to consider economic,
infrastructure, and strategic factors to design an scaling up process at community levels.
Economic considerations.
The general cost of HHHL homes varied between US$2,000 and US$4,000 for
refurbished homes, and US$15,000 to US$20,000 in fully reconstructed homes.
Differences were brought by the size of the home, as well as the type of intervention
carried out in each case. Additionally, the project was forced to deal with unexpected
budget increments derived from overprice in basic materials, lack of providers,
transportation to and from the construction sites, and lack of experience in this type of
interventions.
Considering that the construction of a traditional house in this region could be
completed at a total cost of US$1,000, the US$2,000 to US$3,000 invested by partner
families is significant. Moreover, it is more than the US$1,000 recommended by previous
studies conducted to determine the value of affordable, comfortable, and sustainable
housing for resource constrained settings (Haines et al., 2013).

245
However, HHHL’s partner families were not required to contribute the same
amount of financial resources to complete the project. Even though they brought assets
such as social capital and knowledge, all of them identified labor as the most important
resource they contributed with to the intervention: partner families were required to work
full time in the construction for periods of time ranging from eight to 15 weeks. Since
most families in the region depend exclusively on their work for daily subsistence,
working for three months in this project represents a high cost for them. Individuals that
work in one of the local haciendas, for example, can make US$10 a day for five days a
week during the corn production season (January to September). Considering that
constructions took place during that time of the year due to more favorable climatological
conditions, the approximate cost of a partner’s full involvement in the project could have
been around US$750 (this cost excludes the value of food and produce that some workers
can get as part of their payment).
Additionally, partners had to partially cover the cost of hired labor: if a regular
home can be built by two or three people within a month, HHHL homes required crews
of minimum four people to complete it within two or three months. In this case, partner
families had to identify resources to cover one or two construction workers (if a member
of the family was not capable of willing to contribute with his/her own labor) at a cost of
US$10 per day if breakfast and dinner were provided by the hiring family, or U$13 a day
if that was not the case.
Since community members have access to different forms of income, specific
analyses of the socio-economic conditions of each family were conducted in order to

246 understand the viability of their participation in the construction process. For example,
while one of the partner families had five kids under the age of 17, all of them attending
school, the other three families involved in full reconstruction processes had adult
children willing to support their family either with their work or money. While the first
family had important debts to cover, the other three families did not have any or had
small ones. Similarly, the first family did not own a plot to work and the head of
household depended on being hired by landlords from the area for daily subsistence,
whereas the other three families owned their plots and had spaces to sell their crops in the
local market. Considering that these elements could compromise not only the family’s
capacity to engage in the project, but also their economic performance during the
construction months, HHHL decided to partially accept the offer of the head of household
of the first family when he suggested that his labor could be paid by the project instead of
taken it as an in-kind contribution (he was paid at the local rate during two days for each
week of the construction). Additionally, the mother made arrangements to cook for the
construction crew in order to complete the cash necessary to cover weekly expenses.
Under this model, the family was able to participate and conclude the process within the
stipulated timeframes.
This example illustrates a model in which each actor has been able to contribute
with resources derived from their agency and advocacy capacity under specific
circumstances suggested by their economic situations. In order to implement this
differentiated approach, some factors demand special attention.

247
Children’s school attendance is considered one of the most difficult expenses to
cover for families in this region. Even though education in Ecuador is stated by the
government to be free because parents do not need to cover tuition fees, they still need to
acquire textbooks, transportation, and materials for all their kids. Besides these regular
expenses, families in these communities have to pay for relocation of their children when
they start secondary school. Even though Cariamanga −the urban center where most
schools are located− is only 15 km. away from the communities, the conditions of the
road can make the ride to the closest of them (Guara) about 1 hour and 20 minutes long.
Since classes start at 7 AM, school kids have to leave their homes before 5 AM and are
not be back until 3:30 PM. The inconvenience of this long day, added to transportation
costs (US$1.50 each way on daily basis), has forced most families to rent a room in
Cariamanga where children can stay during the week. The cost of these rooms can range
from US$35 to US$50 per month. Many families cover these costs with the monthly
subsidy provided by the national government to families living under the poverty line, as
well as sales of animals and produce. Additionally, families reserve a portion of their
products to leave with their kids in the city. In these cases, costs increase as more kids in
the family join secondary schools.
Availability of resources is a determinant factor for families to embark in
construction endeavors. It is rare for local families to have all the resources necessary to
bring a construction project from beginning to end in an anticipated fashion. Instead, they
tend to repair or start reconstructing what is needed when they have a job that gives them
extra resources to get materials and continue with the construction as new sources of

248 income emerge. As a result, constructions can extend over long periods of time and it is
not unusual to find constructions that mix different types of materials, including bricks,
wood boards, bahareque and block, depending on the income available at the moment of
the construction. This is particularly problematic in terms of safety: different types of
materials also demand different types of foundations and structural conditions, but
families can easily dismiss technical demands due to the lack of available resources.
Another aspect that deserves particular attention is the level of indebtedness that
families are assuming at the moment of the intervention. Acquiring debts with one or
multiple parties constitutes an option at hand that many families have attempted to
address lack of resources in different periods of the year. Loans with family and friends
are preferred over financial institutions, first, because most of the time these loans come
with no interest, and second, because the payment periods are more flexible. These loans
can also be paid with labor if they are acquired with people from the same area (usually
landlords). Additionally, it is not unusual for local families to acquire new loans to cover
previous ones. Applying for loans guaranteed by the national government subsidy or to
the local water system committee have been other resources used by partner families in
HHHL’s pilot phase.
However, financial institutions also generate mistrust in community members.
Partner and non-partner families mentioned unwillingness to work with banks and
cooperatives because of the uncertainty of being able to pay within the expected monthly
deadlines. This concern is associated with the unpredictable nature of agricultural
production, as explained in the following quote by a member of a non-partner family:

249
I asked for a loan but it turned out really bad for me… I broke. A year ago, I asked for US$3,000 to plant corn, but the person in the store sold me very bad seeds. The corn that came after them was white and small; it became dust in my hands. It was not even useful to feed the pigs. Nobody wanted to buy it and the money we had used to pay people for planting, supplies, and all the harvest, was wasted. I’m still paying US$485 every three months for money I never saw. Male, 33, Bellamaria. In spite of these unfortunate experiences that warn about challenges of working
with the official financial system, approximately a third (24) of the families that
expressed interest in implementing HHHL’s model showed willingness to apply for
credits with banks or cooperatives.
The analysis of the specific conditions of partner families has facilitated decision-
making in relation to families that require additional support from the project. It has also
created an interaction of reciprocity between families and HHHL in which the interests of
both actors are acknowledged and deemed relevant.
Community members considered that the contributions made by HHHL are
essential to carry out an infrastructure improvement as substantial as the one achieved
through this process. Partner families argued that they would be able to produce the
adobe themselves, but they would still need the cement, beams, rods and additional
materials required to work with adobe under the proposed structure. As explained by one
of the interviewees:
People have received almost all the materials they need and all what they’ve had to contribute with is their labor. That’s good (…) What they [HHHL] do is good and on top of that they give jobs to other community members. Male, 30, Bellamaria

250
For these reasons, it is recommended that this differentiated approach is sustained
in subsequent phases of the project. During this pilot phase of the project, two types of
partner were identified:
Full partners, in reference to partners that assumed all the costs of the intervention
without additional support.
Hired partners, families that assumed all the cost of the intervention, but required
to be hired by the program in order to cover those costs.
As explained before, elements to consider in order to make a decision in relation
to this classification include:
Property of the terrain where the family lives
Access to the Human Development Subsidy
Potential sources of income
Major species sold in the last month or being raised at the moment (including
pigs, goats, and cattle)
Minor species being raised for sale (mainly chicken)
Tenancy of regular space to sale cattle, agricultural or other products (such as
handcrafts) in the local market
Additional sources of income (panela production, fishing, tilapia production,
construction jobs, etc.)
Recent migration to urban centers for income generation purposes (gold mines or
shrimp companies, for example)

251
Number of family members bringing resources to the household (explore
contributions made by older children).
Weekly food related expenses
Health conditions being attended on regular basis
Transportation demands
Utilities
School expenses (number of children currently enrolled in school and currently
living in other cities)
Projection of agriculture related expenses throughout the year (fertilizers,
harvesting, and irrigation, among others)
It is highly possible that this information cannot be obtained in a single visit or
through a single instrument. Relevance of regular face-to-face interactions cannot be
overemphasized. These regular interactions may lead to greater trust by families and
greater willingness to disclose their economic opportunities and constrains, information
that becomes critical to inform decision-making at this stage. Families do not tend to give
away information about their economic situation easily, in some case because they
identify potential benefits to be obtained if they report lower levels of income, but also
because their lack of resources is a sensitive issue for them. Evaluating the socio-
economic conditions of the family should be considered a process that includes not only
data collection, but also observation of household dynamics and construction of
relationships with potential partner families.
252
This deep level of analysis might not be necessary for homes included in category
1, that will experience minor levels of economic impact; its relevance increases as homes
considered for potential interventions approach category 5 of decay. Since these cases
demand larger economic investments, as well as long term involvement with the project,
establishing a trustworthy relationship from the beginning is crucial.
Implementation considerations.
Processes such as adobe production, quality of construction materials and
sequence of the interventions should be revised in order to make a more efficient use of
available resources. Important delays in the construction were caused by miscalculations
in the actual time that certain activities would take, while in other cases were produced by
lack of materials, environmental conditions, physical capacity of the construction crew,
and partner families’ production needs. These issues could be addressed under more
detailed planning processes based on realistic implementation conditions learned
throughout the pilot phase of the project(Gilson et al., 2011). Consequently, this section
will describe some implementation issues identified during this research, as well as
suggested routes of action.
Adobe production.
Adobe production has evolved during the different stages of implementation of
the pilot phase. Knowledge about specific characteristics of the mix (four volumes of dirt,
two of grass or cane bagasse and two of water), location of dirt mines with the required
acidic concentrations, social organization for mass production and costs associated to
transportation, have been identified throughout the process. Partner families involved in
253 adobe production during the simultaneous construction phase mentioned that use of
machinery to compact the block makes the process less tiring, reduced back pain (if
compared with traditional methods), speeds up drying for use (5 days instead of 20),
reduced the amounts of raw material required (especially water), and produced less waste
during the construction. Moreover, families acknowledged comfort derived from the
characteristics of compact blocks in reconstructed homes.
In order to facilitate involvement of community members and speed up the
process, it is recommended that adobe production can be conducted in each community.
Transportation constitutes an important burden for community members as there are not
many options and the existing ones can be expensive. Adjusting to rancheras’ times (only
public transportation system available) affects availability of people, as they only
circulate at 6 AM and 3 PM.
Other recommendations made by partner families to add efficiency to adobe
production include:
a. Increasing the size of the molds currently used in the block press machine to produce
more blocks in one operation
b. Securing presence of groups of 4 people during the operation hours: 2 people are in
charge of making the mix and 2 more in charge of compressing the blocks.
c. Adding a sanding machine to the production process
d. Install the adobe factory in each community (moving machinery as production moves
from one community to another)

254 e. Facilitating association for production and mobilization of adobe blocks to the homes
—even through hiring of some community members
Importantly, information about advantages of technical production of adobe has
not been shared with community members. That could partially explain why around
42.1% of questionnaire respondents preferred bricks when considering reconstruction
projects, while only 29.5% is considering adobe. Respondents mainly referred to
production advantages such faster and less demanding construction processes to explain
this preference; however, they also mentioned problems of adobe constructions that have
been addressed with the new technology, such as cleanliness and decay. Given the
availability of resources (including existence of machinery readily available for
community members), information about the advantages of this method should be made
public and accessible.
Quality of construction materials.
Efficiency should also be considered in reference to the quality of materials being
used in the construction and some elements of the design that have not worked as
expected. Extreme temperatures and profuse rains in this area create environmental
conditions that demand particular resistance from construction materials. Stoves, mesh,
and wood have shown quality issues that will need to be addressed by the program in
order to secure a long lasting usage of these measures. Additionally, partner families
recommended:
a. Screens: Plastic mesh installed in small panels has been the screen’s design that more
resistance to use and environmental conditions has shown. This resistance is also

255 dependent of the presence of animals in the peridomestic area; major damages were
found in homes that keep cats and dogs in the porch.
b. Kitchen: Improved stoves require more consistent follow up to secure their use. Two
out of five kitchens repaired to this day are only used to store utensils and food. In these
cases, families have built an external kitchen where they cook, store crops, raise guinea
pigs and store firewood, which could suggest that the actual model does not meet the
requirements of local families. Partner families recommended lowering the height of
stove, making more than one pot for each burner, using local manure mix to adapt
burners to the exact size of the pot and securing that chimney pipes are circular and have
a 15 cms. Diameter to avoide ash blockages, as potential ways of stimulating stoves’
usage.
c. Storage units: Defining a concrete structure for the storage unit that can efficiently
serve production demands of local families is important. One of the storage units built in
the most recent phase of the project was built with adobe under the same conditions of
the house. It required another month of work to be completed, but since the peak of
agricultural production had not been reached, the family did not see an immediate need to
complete it. In the meanwhile, produce was stored in the surrounding areas of the house.
Once finished, the storage unit did not seem to meet actual demands from the family
because more production was obtained as a result of their apparent improved economic
situation. Another family decided to reuse some of the adobe resultant from the old house
in their storage unit. Even though the adobe production equipment was offered to them,
the family opted for traditional adobe arguing problems to mobilize the new ones from
256 and to the construction site. Additionally, the family deemed unnecessary investing
money in the construction materials required by the new type of adobe for a storage unit.
Since the number of adobes kept from the previous home was insufficient for the size of
the desired construction, those adobes remain in the peridomestic areas as potential focus
of triatomines. Finally, one more unit was built with bricks, but without the necessary
safety measures to sustain it. Since family members think it can be easily open by
robbers, it is only used to half of its capacity.
d. Water and sanitation: Most of the latrines existing in these communities were built
seven years ago by an NGO called Foundation Uriel, in partnership with the local
government of Cariamanga and Loja Province Assembly. Observation conducted for this
research found structural problems such as falling doors, filtering roofs, and broken
toilets in most of the sanitary facilities built as part of that initiative. Depending on the
extent of the damages, families tend to leave them without reparation for long periods of
time and use provisional solutions in the meanwhile. For example, pipes conducting
residuals to the septic tanks can become exposed in the ground due to the continuous
activity of animals in the preridomestic area. Bringing more dirt can easily repair this
kind of damage and families usually act promptly to solve it. On the other hand, specific
damages that require additional resources, such as a broken hose or an unattached base
demanding reparations with cement, remain broken until some money is available. Most
families keep making use of the latrines until the decay forces them to find other
alternatives, usually the open fields. When asked about the health risks of this practice, a
community member expressed:

257
The latrine that the government gave to us is useless now; therefore, we have to defecate in the open air. That creates contamination because that is what dogs, chicken, pigs are going to eat later on. And of course that is a risk because those are also the animals we eat at home. Male, 33, Bellamaria.
Three out of the six non-partner families interviewed for this research—the three
of them located in Bellamaria— did not have sanitary facilities at all. The heads of
household of these families are younger members of the community, two of them sons of
the original families, who grew up making use of sanitary facilities at home. When the
need to build their own home came, they did not have enough money to build adobe
homes; therefore, they replicated traditional construction techniques in which sanitary
facilities were not included (mainly wood boards mixed with bahareque). They argued
that having a latrine is of interest for the family, but subjected to availability of resources.
In contrast, some of the homes recently constructed (with family resources, not HHHL
homes) included latrines located in the interior of the homes, an important variation from
traditional homes. Reasons argued for this decision include the presence of elders that
could be at risk while walking at night to the reach the bathroom, as well as reducing
exposure to environmental conditions leading to disease, especially during the rainy
season. Due to the high levels of specificity that construction of disposal systems
demands, studying partnerships with institutions specialized in the construction and
donation of these facilities is recommended.
Strategic considerations.
Under the assumption that subsequent phases of HHHL are going to be
implemented by institutions with more resources and expertise in construction projects,
the following strategy is suggested.
258 a. Intervention by community: A sequential intervention community by community is
suggested. Both community members and civil engineers involved in the Pilot phase of
HHHL mentioned increased costs derived from centralized production of adobe in one of
the communities. Therefore, intervening one community at a time while preparing the
other two to continue is recommended. This sequential intervention of infrastructure
improvement would start by mobilizing machinery for adobe production and conclude
with the construction of storage units. Health promotion efforts would continue for an
extended period of time.
Of the intervened communities, Bellamaria is the one that counts with better
conditions to be intervened with a full reconstruction project in the near future. In first
place, 32 of the families are included in a common title that gives them legal access to the
land they inhabit and work. This model of shared ownership was popular in the 60’s after
a land reform that facilitated occupation of haciendas by workers established within their
limits. Even though most of the signatories of the original tittles are dead or in late stages
of life, the initial agreement gave them the possibility of passing two occupations rights
to family members that have been taken by younger families currently established in
Bellamaria. This process has not been legalized in most cases; however, it depends more
of internal arrangements among inhabitant families than from external actors. It would
require additional support for HHHL to promote these dialogues among community
members.
Other conditions facilitating a prompt intervention at the community level in
Bellamaria are availability of resources derived from its closeness to the river —which

259 guarantees access to water sources throughout the year for agriculture purposes, as well
as extensive areas of shared property that provide appropriate conditions for cattle rising.
Additionally, 44% of the homes in this community were classified under category
5 by 2016’s decay analysis and 13.89% were classified under category 4, creating the
highest proportion of risk in the three communities. This data indicate a substantial
potential impact of the HHHL model in this community, first and foremost in terms of
health and safety.
These conditions also suggest that impact of the HHHL would be highest in
Bellamaria, which could generate important impacts for replication in other communities.
While the intervention in Bellamaria is occurring, it is suggested that HHHL facilitators
work in two specific factors in Chaquizhca and Guara (in that order): legalization of titles
and land tenure, as well as preparation of roads in partnership with the local government.
Even though Chaquizhca and Guara also present high proportions of risk (52.1% in the
former and 47.6% in the latter), accessibility and land tenure are major limitations faced
by community members that could substantially affect the intervention. Also, presence of
more homes in Category 1 of decay in Guara suggests that priority of the intervention is
lower.
b. Peridomiciles first: It is also recommended to start the intervention with reorganization
of peridomestic areas. A proper fence should be built first by partner families because it
facilitates relocation of animals and installation of separation practices for a longer period
of time. It is important to consider, however, that some homeowners have chosen
locations distant from community centers precisely with the purpose of keeping an

260 important number of animals around their home without bother other neighbors.
Addressing animals’ relocation as a priority previous to the intervention is particularly
important in Bellamaria, where ownership of domestic animals is substantially higher.
c. Temporary home: One of the conditions more difficult to follow for partner families is
the need to find a temporary house during the construction time. Even though it has been
solved in different ways (using an abandoned house, an empty room in a neighbor’s
home, a tent, or a provisional shelter), families had to experience multiple inconveniences
during this period. Moreover, it is possible to argue that in some cases they were even
more exposed to environmental conditions than in their original home. Family’s
transition to the temporary house requires planning and facilitation. It can constitute a
teachable moment as it provides opportunities to identify risk factors and special needs of
the family. This part of the process should only be done when the need of demolishing
the house is imminent due to the beginning of the construction. However, it is also
important to proceed in a sensitive manner, as families have expressed reticence to leave
their dwellings and expose their belongings. At this stage of the process it is useful to
count with outreach materials that can also supply storage needs for the family,
particularly plastic boxes and cans that can help to organize crops, produce and clothes.
d. Demolition: One of the main changes applied between the first home built by HHHL
and the simultaneous construction phase was that in the second case, homes were not
turned down through machinery but manually disassembled. Partner families expressed
their appreciation for this practice, not only because it reduced the emotional impact of
that moment in the process, but also because it allowed them to reserve an important

261 number of pieces from the previous house that they could reuse in the future. Wood and
tiles were used in pigs, guinea pigs and goat shelters, old doors were given away to other
neighbors, and some adobes were kept to be reused in basic shelters built to protect crops
in productive plots. This process can be done in two days with two people saving and
organizing materials, and two more tearing the house down. Selection of reusable
materials should also be planned with the partner family. It is important for the project to
count with strong arguments at this stage to advise partner families about materials that
can constitute a risk for triatomines’ reinfestation. Natural conflict can emerge because of
the different motivations of the involved actors: while HHHL frames risk in terms of
exposure to CD transmission dynamics, partner families understand these dynamics from
the point of view of their financial situation.
e. Construction times: Construction periods should be restricted to the dry season of the
year (mid-May through November). In first place, it is not possible to make adobe once
the rainy season has started because it slows down the drying period. Local families do
not have covered spaces that can protect all the adobes required for the construction for
such a long period of time. Additionally, humid dirt is not useful for adobe production
and it would not be possible for local families to collect the raw material for the
construction. Most importantly, people are especially busy working in their plots during
the rainy season (preparing the land for their own production) and can rarely work for
somebody else.
f. Animals’ shelters and storage units post-construction: These two points should be the
final phase of the infrastructure intervention. They cannot be underestimated, as

262 availability of animals’ shelters and storage unit facilitates implementation of health
promotion practices to be conducted within the home space. Particular attention should
be given to chicken, as families are quite used to feed them while conducting social
activities in peridomestic areas. Families have usually built chicken coops in trees
surrounding the house for them to nest and sleep, but it is important to reemphasize the
need to feed them as well in order to secure their relocation. Similarly, corn storage has
specific demands, as it has to be available throughout the year to feed chickens, pigs and
other domestic animals. During the harvesting time, it can be collected in important
amounts and families might need to use the space at home if no other alternative is
available. This last period has also been used to install productive gardens within the
home space.
Dialogic health promotion.
Trust is fundamental element in this systemic approach to disease prevention. By
accepting an intervention in their homes, families have allowed us to dismantle their
more valuable asset under the idea that they will be able to obtain a safer home. In this
context, it was important that representatives of the program were present at key
moments of the project not only to address questions and collect feedback, but also to
demonstrate knowledge and control over the intervention. As explained by one of the
interviewees, supervision of the process is critical:
The architect was always here (…) She supervised the construction crew and that is good. Many times she saw mistakes in the process and demanded construction workers to turn everything down to start from scratch. We could trust that things were correctly done because she was there to control them. Female, 37, Chaquizhca.
263
In this sense, different worldviews emerging during the intervention illustrated the
need to consider research as an ongoing learning experience that is constantly reframed
on the bases of what communities and staff learn about each other over time. An
interesting case occurred with one of the partners who asked to the local facilitator if the
intervention was being conducted in his home because he or any member of his family
had been diagnosed with CD. Since medical information of the family was never
requested or collected, his concern shows potential forms of stigma that could be
emerging as unintended consequence of the intervention. Research in this aspect is
recommended.
Similar to this case, community members have their own interpretation of the
actions conducted by HHHL. Many of the respondents in the socio-economic
questionnaire referred to HHHL contributions as ‘help’, which reaffirms existing
perceptions of HHHL as an aid —not necessarily health oriented—project. Participants in
the questionnaire posed questions about the temporarily of HHHL presence in the area
(‘How long are you guys going to be here?’) and directly requested support for
productive initiatives, as well as construction of irrigation systems and fences. These
requests could be an expression of how the health goals of the intervention are
overshadowed by the visibility of dynamics associated with the construction.However,
the health promotion model applied by HHHL purposely opens spaces for this kind of
requests, under the premise that knowing the priorities of the communities is critical to
inform decision making that enhances programmatic goals.

264
In any case, clearly informing and reinforcing the goals of the intervention to all
the actors involved at different stages of the process is a basic element of transparency
with the communities that should be systematically included in HHHL activities.
The role of local facilitation in this context cannot be overemphasized. In HHHL’s case,
local facilitators have led projects related with legalization of homes and plots,
construction of water systems, and multiple mediation processes on behalf of the
community with the local government, including legalization of electric systems. Their
understanding of the systemic nature of CD as a neglected condition, as well as the
systemic nature of home improvement as a life change opportunity, has been critical to
complete the proposed interventions.
The fact that the local facilitator that is permanently working in the communities
has experience in community organization, as well as many of the topics that are of
interest for community members, has increased trust in his work. From that perspective,
he has been able to provide important advice on construction issues and relationships
with local providers, as well as valuable ideas for the design of productive initiatives.
Similarly, local facilitators’ capacity to mingle and work along community
members has increased their capacity to conduct horizontal dialogues, particularly when
delicate or private issues are discussed. That was the case of initial dialogues about
families’ financial situation. The level of trust of local families in the role of the local
facilitation team is illustrated in the following quotes:
The facilitator walks, works and understands people down here. Male, 48, Bellamaria.

265
When all the work was completed at the end of the day, we used to sit with them in the porch to laugh for a little bit. I actually missed them when the construction was over. Female, 17, Chaquizhca. Many times I tell the engineer to stay with us for dinner. When we had good food, we share, but if we didn’t, we also felt comfortable offering whatever we had to him. Male, 55, Guara. Considering the relevance of the role played by local facilitators in the
implementation of the HHHL model, having one per community during the scaling up
phase of the project is recommended. This can facilitate interactions when more actors
are involved and secure consistency of health promotion processes when brought to scale.
Communication spaces.
The most important communication space created by HHHL is called “Visitas de
Porche” (Porch visits). This is a basic space of encounter created with partner families to
present the conditions of the intervention, follow up on potential doubts, design a plan
once the proposal has been accepted, and carry out data collection for research purposes.
Since it is conducted at the front porch of the home, it provides a transparent mechanism
to involve all family members from the very beginning of the process. It also creates
spaces of contact with community members and offers the opportunity to observe social
dynamics at the household level.
During the pre-intervention phase, Porch Visits were mainly focused in
explaining contributions expected from partner families along the process, including
labor, supervision and knowledge. However, the most recent intervention conducted in
partnership with Ecuador’s Ministry of Housing, also required contributions in cash.
Families came back to a folder containing the characteristic of the intervention when

266 rumors about the use of this money emerged. Providing that information in a printed
format was also important for the families to be able to review and pose questions later
on. A minimum of three visits followed this first encounter in order to collect doubts,
solve them when possible or transmit them to the team when needed. This moment in the
process requires paying close attention to all the questions suggested by the family and
providing answers as soon as possible.
The project also generated spaces for knowledge sharing between former and new
partners during the pre-intervention phase of the process. These scenarios have served as
an organic way of peer support that can complement the perspective provided by the
program with the critical reviews of families that have already gone through this
experience. These spaces have facilitated informed decision-making by expanding
information sources beyond the HHHL’s narratives. This level of community
involvement also made visible the extent of the impact of the intervention, which could
be associated with community members interest in subsequent phases of the program:
57.1% of the heads of household who expressed interest in implementing HHHL’s model
have participated in HHHL’s construction activities (developed with partner families),
72.7% have participated in any of the HLI’s projects, and 93.8% have heard about HHHL
homes.
During the construction process, empowering heads of household to assume a
supervision role and oversight has shown positive results because it facilitates
appropriation from early stages of the process. This appropriation can be illustrated in the
following quote:

267
I explained to the contractor that it was important to keep a level of understanding between the two of us. ‘If anything happens, you just need to tell me. My role, as owner of this house, is to tell you what I think works best for me.’ He gave me a lot of ideas and also asked me if I liked what he was doing. Because of that we could work well together. Male, 44, Chaquizhca. Similarly, the follow up process that comes after the intervention has been
perceived as a moment of knowledge exchange:
The facilitator only comes for a short time in each visit. It is good that he comes to visit to learn how the home was built, to ask questions. Sometimes he can see that something was not done well and correct to do things better the next time. Female, 43, Guara. Due to the private nature of some of the practices proposed in the follow up
phase, it is important to have an instance of reflection to provide an explanation about the
rationale for them. Mentioning that these practices have already been implemented by
other community members with positive results (Nieto-Sanchez et al., 2015), could
facilitate their adoption.
In terms of the health outcomes of the intervention, it is fundamental to bring the
purpose of creating healthy environments to the forefront of the process. Considering the
invasive nature of homes’ intervention, it is important to clearly state the protective
aspect of it. Making visible partners’ opinions about the impacts they have experienced,
could serve this purpose. Generating outreach materials for construction workers,
architects, local facilitators, and all members of the team in regular contact with partner
families can also be useful to maximize spaces of health promotion along the process.
Income generation opportunities.
While conceiving the home space as a system in itself, HHHL model has also
looked for opportunities to connect the intervention with larger communitarian dynamics.

268 Community members, for example, often refer to water systems construction as a project
of high impact at the community level:
What was done with the water system was excellent help, very good, no doubts. Male, 30, Bellamaria However, income opportunities associated to home’s construction have been
approached by the project in a systematic way. As mentioned before, local families are
used to participate in the construction of their own homes, but also to hire neighbors or
construction workers to complete difficult or physically demanding tasks such as
installing roofs or making the adobe for their homes. A community member who has
worked in HHHL construction processes compares traditional home construction
techniques with the ones proposed by HHHL:
The problem of this [traditional] adobe is that it has to be mixed with your feet. You need to make a hole in the ground that will be turned into a pool to fit around 30 wheelbarrows of dirt, two or three sacks of grass and lots of water (I don’t know the exact amount because you need to refill when water filters). With that amount you can get up to 20 adobes. For the other adobe, you need more people because three will be mixing in the machine and one more will be refilling the molds. The other problem with the old adobe is the weight: it is extremely heavy when you have to complete in the final parts of the wall, whereas the new adobe never weights more than 12 pounds. It is really easy to lift it or even throwing to somebody else if that person is at the top of the wall. Male, 30 year, Bellamaria. Because of the efficiency of the new techniques, community members think that
adobe production could be an interesting income generation alternative:
It is a very good idea to have groups of people making adobe. If a person cannot make his own adobe and can afford paying for it, you are generating job opportunities for those who don't have one. Male, 44, Bellamaria. The possibility of selling adobes can be explored, as there is an established
practice of paying community members for making the blocks under traditional models.

269 There has also been interest from people external to the communities in the technique
applied in HHHL homes. Using the acquired knowledge as an expertise now existing in
the communities is an interesting option to be explored in following stages of the process.
It is also important to consider that home construction, as well as other productive
activities can expect collaboration of community members under specific circumstances.
Even though the minga model (community work) has been part of the organizational
structure of these areas, it has been losing relevance in the last decades. Some of the
interviewees showed nostalgia of previous times when community work used to happen
in a more spontaneous and organic way:
There was a time when people used to help one another in harvesting times. Back then people were not focused on their plot but there were organized in groups of nine people to work every day in a different plot. That was beautiful. Female, 29, Bellamaria. However, larger interventions should not be planned under the assumption of
community work being provided for free. Since labor is the main resource for every
family, unpaid collaborations can only last for short periods of time, as people have to
return to their work as soon as possible. In these cases, families that request this kind of
collaboration from their neighbors have to pay back with work when requested and
provide food for all the crew. Partner families have used this structure for construction of
fences, excavation of canals, and adobe production.
The construction of HHHL homes has generated additional sources of jobs in the
communities. In first place, the project has hired people previously certified in
construction techniques by the National Professional Training Service (Servicio Nacional
del Capacitación Profesional de Ecuador, SECAP). This training, organized by HLI in

270 2012, provided a base of knowledge in constructions with mud that is now replicated.
People who took this training have been prioritized for adobe production, trusses
assemble, and home construction. The cycle of learning is explained by one of the
trainees:
I have learned a lot from this project. Unlike others that didn’t even go to the [SECAB] classes, I’ve been practicing what we learned. It was not knowledge to keep on paper. I think that it was not interesting for some people, but it was interesting to me. I just missed one class and then I talked to the professor, caught up and passed the test (…) The only thing I cannot do in these homes is the floor because it needs precise measures. Other than that, I can do everything: I have made adobe, raised walls, installed doors and windows, built roofs, and fixed kitchens. I can even read blueprints. Male, 30, Bellamaria. Similarly, partner families have hired community members as construction
workers to reach the number of non-qualified labor required to conclude the process
within the agreed timeframe (two to four months). During the negotiation, partner
families agreed to have at least two people working at all times in the construction (one
of them was generally one member of the family). The possibility of supporting
community members with emerging jobs was explained by one of the community
members hired by HHHL:
I was working in the construction of the homes when the construction of the water system in Bellamaria began. Since it was not possible to be in both places, I hired my brother in law to cover my part in the water system. That way I was making some money and paying to him a little bit less, but we both had a job. Male, 30, Bellamaria.
Exploring home construction techniques under a more systematic model of
community work is recommended. Partner families and community members who have
taken part of previous construction processes should be consulted to generate an
organization model that could be adjusted to the dynamics of agriculture production.

271
Finally, the lack of jobs in the region creates other challenge that should be
carefully observed by the program: ongoing migration. Interviewees explained the impact
of this situation in their decision about staying or leaving the communities:
Here we don't have a factory or a boss that can hire us for a monthly salary. It is impossible to think that we will get a job for one or two months here. Male, 55, Bellamaria. Recently my wife and my daughter have been sick, so poverty is striking us. We don't have a lot of sources to get money from. Here you can pass the day with cassava and salt because the weather is good. However, there is no money, nor jobs. If we want a job, we need to go somewhere else. Male, 46, Bellamaria. Under these circumstances, community members are forced to migrate constantly
to places with more job opportunities, usually gold mines, or shrimp production
companies located in provinces nearby. Internal common destinations are Quito,
Guayaquil, and Santo Domingo in Ecuador, whereas USA and Spain are usually the route
of international migrants. This factor is brought both by lack of paid jobs and education
opportunities, as well as ongoing trend of urbanization in the country. The words of a
community member expressed this concern:
Our situation in these communities has worsened throughout the years because young people do not want to work here anymore. Only old people like me. Young people here do not like the countryside anymore, they only want to go to the city. When I was young, most children wanted to stay with their parents and help them working the land. We used to help our parents, our neighbors. But that has changed a lot (…) Sometimes I wonder about our future: what is going to happen with us if our children do not want to stay here? Male, 49, Chaquizhca. Cultural values dictate ongoing responsibility and reciprocity from children to
parents, expressed as economic and social supervision over time. In this sense, the
presence of adult children that work in other cities has facilitated families’ decision-
making about assuming financial responsibilities associated with home improvement.

272 However, current trends create an important question for HHHL model: what is the
expected time of usage of an improved home in terms of family occupation? Most of the
questionnaire respondents (86%) stated that they are planning to stay in the communities
for the next five years; however, this answer should be carefully analyzed under the
scope that most heads of household interviewed for this research were in the 51 to 60 age
group, which represents people that are already established in the communities, and do
not include younger members of the family with other perspectives for their own lives.
Studying migration routes to determine foci of CD transmission in migrant population is
also recommended (Ventura-Garcia et al., 2013).
Conclusion
Several authors have called for a reassessment of the idea of cost-effectiveness as
most important criteria to establish viability of eradication, elimination, and control
interventions in NTD (Bardosh, 2014; Hastings, 2016; Parker & Allen, 2013). Instead,
they have proposed deeper understanding of the realities of families exposed to these
diseases that could lead to solutions designed to address structural inequities that are at
the roots of individual and communities’ most pressing needs. In this document I have
outlined a plan for scaling up Healthy Homes for Healthy Living’s model that addresses
strengths and limitations for sustainability identified by partner families as explained in
ancillary grounded theory study. Together, these documents provide criteria to look at
sustainability as a factor of families’ agency over the proposed solution. HHHL has
created opportunities to expand knowledge derived from systemic approaches to disease
prevention in which direct encounters between scientists, architects, health promoters and

273 communities come together to address the complexity of Chagas disease problematic. I
am convinced that HHHL is not only a sound approach to disease prevention, but first
and foremost, an opportunity for social transformation that can truly impact the lives of
marginalized populations.
References
Abad-Franch, F. (2003). Control de la Enfermedad de Chagas en Ecuador. Retrieved from Quto, Ecuador:
Abad-Franch, F., Paucar, A., Carpio, C., Cuba, C. A., Aguilar, H. M., & Miles, M. A. (2001). Biogeography of Triatominae (Hemiptera: Reduviidae) in Ecuador: implications for the design of control strategies. Mem Inst Oswaldo Cruz, 96(5), 611-620.
Abad-Franch, F., Vega, M. C., Rolon, M. S., Santos, W. S., & Rojas de Arias, A. (2011). Community participation in Chagas disease vector surveillance: systematic review. PLoS Negl Trop Dis, 5(6), e1207. doi:10.1371/journal.pntd.0001207
Atkinson, P., Delamont, S., & Housley, W. (2008). Contours of culture : complex ethnography and the ethnography of complexity. Walnut Creek, CA: AltaMira Press.
Barbu, C., Dumonteil, E., & Gourbiere, S. (2009). Optimization of control strategies for non-domiciliated Triatoma dimidiata, Chagas disease vector in the Yucatan Peninsula, Mexico. PLoS Negl Trop Dis, 3(4), e416. doi:10.1371/journal.pntd.0000416
Bardosh, K. (2014). Global aspirations, local realities: the role of social science research in controlling neglected tropical diseases. Infect Dis Poverty, 3(1), 35. doi:10.1186/2049-9957-3-35
Briceno-Leon, R. (2009). [Chagas disease in the Americas: an ecohealth perspective]. Cad Saude Publica, 25 Suppl 1, S71-82.
Bustamante, D. M., De Urioste-Stone, S. M., Juarez, J. G., & Pennington, P. M. (2014). Ecological, social and biological risk factors for continued Trypanosoma cruzi transmission by Triatoma dimidiata in Guatemala. PLoS One, 9(8), e104599. doi:10.1371/journal.pone.0104599
Bustamante, D. M., Monroy, C., Pineda, S., Rodas, A., Castro, X., Ayala, V., . . . Trampe, R. (2009). Risk factors for intradomiciliary infestation by the Chagas disease vector Triatoma dimidiatain Jutiapa, Guatemala. Cad Saude Publica, 25 Suppl 1, S83-92.
Campozano, L., Celleri, R., Trachte, K., Bendix, J., & Samaniego, E. (2016). Rainfall and Cloud Dynamics in the Andes: A Southern Ecuador Case Study. Advances in Meteorology. doi:Artn 3192765 10.1155/2016/3192765
274 Charmaz, K. (2006). Constructing grounded theory. London ; Thousand Oaks, Calif.:
Sage Publications. Charmaz, K. (2014). Constructing grounded theory (2nd edition ed.). London ; Thousand
Oaks, Calif.: Sage. De Maio, F. G., Llovet, I., & Dinardi, G. (2014). Chagas disease in non-endemic
countries: 'sick immigrant' phobia or a public health concern? Critical Public Health, 24(3), 372-380. doi:10.1080/09581596.2013.836589
Deetz, S. (1996). The positioning of the researcher in studies of organizations: De-hatching literacy theory - Commentary. Journal of Management Inquiry, 5(4), 387-391. doi:Doi 10.1177/105649269654014
Dell'Arciprete, A., Braunstein, J., Touris, C., Dinardi, G., Llovet, I., & Sosa-Estani, S. (2014). Cultural barriers to effective communication between Indigenous communities and health care providers in Northern Argentina: an anthropological contribution to Chagas disease prevention and control. Int J Equity Health, 13, 6. doi:10.1186/1475-9276-13-6
Dias, J. C. (2007). Southern Cone Initiative for the elimination of domestic populations of Triatoma infestans and the interruption of transfusional Chagas disease. Historical aspects, present situation, and perspectives. Mem Inst Oswaldo Cruz, 102 Suppl 1, 11-18.
Dias, J. C. P., Ramos, A. N., Gontijo, E. D., Luquetti, A., Shikanai-Yasuda, M. A., Coura, J. R., . . . Alves, R. V. (2016). 2nd Brazilian Consensus on Chagas Disease, 2015. Revista Da Sociedade Brasileira De Medicina Tropical, 49, 3-59. doi:10.1590/0037-8682-0505-2016
Dumonteil, E., Nouvellet, P., Rosecrans, K., Ramirez-Sierra, M. J., Gamboa-Leon, R., Cruz-Chan, V., . . . Gourbiere, S. (2013). Eco-bio-social determinants for house infestation by non-domiciliated Triatoma dimidiata in the Yucatan Peninsula, Mexico. PLoS Negl Trop Dis, 7(9), e2466. doi:10.1371/journal.pntd.0002466
Gascon, J., Vilasanjuan, R., & Lucas, A. (2014). The need for global collaboration to tackle hidden public health crisis of Chagas disease. Expert Rev Anti Infect Ther, 12(4), 393-395. doi:10.1586/14787210.2014.896194
Gilson, L., Hanson, K., Sheikh, K., Agyepong, I. A., Ssengooba, F., & Bennett, S. (2011). Building the field of health policy and systems research: social science matters. PLoS Med, 8(8), e1001079. doi:10.1371/journal.pmed.1001079
Glaser, B. G., & Strauss, A. L. (1967). The discovery of grounded theory; strategies for qualitative research. Chicago,: Aldine Pub. Co.
Grijalva, M. J., Palomeque-Rodriguez, F. S., Costales, J. A., Davila, S., & Arcos-Teran, L. (2005). High household infestation rates by synanthropic vectors of Chagas disease in southern Ecuador. J Med Entomol, 42(1), 68-74.
Grijalva, M. J., Suarez-Davalos, V., Villacis, A. G., Ocana-Mayorga, S., & Dangles, O. (2012). Ecological factors related to the widespread distribution of sylvatic Rhodnius ecuadoriensis populations in southern Ecuador. Parasit Vectors, 5, 17. doi:10.1186/1756-3305-5-17

275 Grijalva, M. J., & Villacis, A. G. (2009). Presence of Rhodnius ecuadoriensis in sylvatic
habitats in the southern highlands (Loja Province) of Ecuador. J Med Entomol, 46(3), 708-711.
Grijalva, M. J., Villacis, A. G., Ocana-Mayorga, S., Yumiseva, C. A., & Baus, E. G. (2011). Limitations of selective deltamethrin application for triatomine control in central coastal Ecuador. Parasit Vectors, 4, 20. doi:10.1186/1756-3305-4-20
Grijalva, M. J., Villacis, A. G., Ocana-Mayorga, S., Yumiseva, C. A., Moncayo, A. L., & Baus, E. G. (2015). Comprehensive Survey of Domiciliary Triatomine Species Capable of Transmitting Chagas Disease in Southern Ecuador. PLoS Negl Trop Dis, 9(10), e0004142. doi:10.1371/journal.pntd.0004142
Gurtler, R. E., & Yadon, Z. E. (2015). Eco-bio-social research on community-based approaches for Chagas disease vector control in Latin America. Trans R Soc Trop Med Hyg, 109(2), 91-98. doi:10.1093/trstmh/tru203
Haines, A., Bruce, N., Cairncross, S., Davies, M., Greenland, K., Hiscox, A., . . . Wilkinson, P. (2013). Promoting health and advancing development through improved housing in low-income settings. J Urban Health, 90(5), 810-831. doi:10.1007/s11524-012-9773-8
Hastings, J. (2016). Rumours, Riots and the Rejection of Mass Drug Administration for the Treatment of Schistosomiasis in Morogoro, Tanzania. J Biosoc Sci, 48 Suppl 1, S16-39. doi:10.1017/S0021932016000018
Holveck, J. C., Ehrenberg, J. P., Ault, S. K., Rojas, R., Vasquez, J., Cerqueira, M. T., . . . Periago, M. R. (2007). Prevention, control, and elimination of neglected diseases in the Americas: pathways to integrated, inter-programmatic, inter-sectoral action for health and development. BMC Public Health, 7, 6. doi:10.1186/1471-2458-7-6
Hotez, P. J. (2014). Neglected parasitic infections and poverty in the United States. PLoS Negl Trop Dis, 8(9), e3012. doi:10.1371/journal.pntd.0003012
Hotez, P. J., Dumonteil, E., Woc-Colburn, L., Serpa, J. A., Bezek, S., Edwards, M. S., . . . Bottazzi, M. E. (2012). Chagas disease: "the new HIV/AIDS of the Americas". PLoS Negl Trop Dis, 6(5), e1498. doi:10.1371/journal.pntd.0001498
Houweling, T. A., Karim-Kos, H. E., Kulik, M. C., Stolk, W. A., Haagsma, J. A., Lenk, E. J., . . . de Vlas, S. J. (2016). Socioeconomic Inequalities in Neglected Tropical Diseases: A Systematic Review. PLoS Negl Trop Dis, 10(5), e0004546. doi:10.1371/journal.pntd.0004546
Lindlof, T. R., & Taylor, B. C. (2011). Qualitative communication research methods (3rd ed.). Thousand Oaks, Calif.: SAGE.
Lucero, D. E., Morrissey, L. A., Rizzo, D. M., Rodas, A., Garnica, R., Stevens, L., . . . Monroy, M. C. (2013). Ecohealth interventions limit triatomine reinfestation following insecticide spraying in La Brea, Guatemala. Am J Trop Med Hyg, 88(4), 630-637. doi:10.4269/ajtmh.12-0448
Manderson, L., Aagaard-Hansen, J., Allotey, P., Gyapong, M., & Sommerfeld, J. (2009). Social research on neglected diseases of poverty: continuing and emerging themes. PLoS Negl Trop Dis, 3(2), e332. doi:10.1371/journal.pntd.0000332

276 Nieto-Sanchez, C., Baus, E. G., Guerrero, D., & Grijalva, M. J. (2015). Positive deviance
study to inform a Chagas disease control program in southern Ecuador. Memorias Do Instituto Oswaldo Cruz, 110(3), 299-309. doi:10.1590/0074-02760140472
Odhiambo, G. O., Musuva, R. M., Odiere, M. R., & Mwinzi, P. N. (2016). Experiences and perspectives of community health workers from implementing treatment for schistosomiasis using the community directed intervention strategy in an informal settlement in Kisumu City, western Kenya. BMC Public Health, 16, 986. doi:10.1186/s12889-016-3662-0
Parker, M., & Allen, T. (2013). Will mass drug administration eliminate lymphatic filariasis? Evidence from northern coastal Tanzania. Journal of biosocial science, 45(4), 517-545.
Pearce, W. B. (1989). Communication and the human condition. Carbondale: Southern Illinois University Press.
Pokhrel, S., Reidpath, D., & Allotey, P. (2011). Social sciences research in neglected tropical diseases 3: Investment in social science research in neglected diseases of poverty: a case study of Bill and Melinda Gates Foundation. Health Res Policy Syst, 9, 2. doi:10.1186/1478-4505-9-2
R Core Team. (2017). R: A language and environment for statistical computing. Retrieved from Vienna, Austria: https://www.R-project.org/.
Saldana, J. (2016). The coding manual for qualitative researchers (Third ed.). Los Angeles, Calif. ; London: SAGE.
Sanmartino, M., Avaria, A., Gopmez Prat, J., Parada, M., & Albajar-Viñas, P. (2015). Que no tengan miedo de nosotros: El Chagas según los propios protagonistas. Interface - Comunicação, Saúde, Educação, 19(55), 1063-1075. doi:https://dx.doi.org/10.1590/1807-57622014.1170
Santos, C. V., Bedin, C., Wilhelms, T. S., & Villela, M. M. (2016). Assessment of the Housing Improvement Program for Chagas Disease Control in the Northwestern municipalities of Rio Grande do Sul, Brazil. Rev Soc Bras Med Trop, 49(5), 572-578. doi:10.1590/0037-8682-0386-2016
Schofield, C. J., & Dias, J. C. (1999). The Southern Cone Initiative against Chagas disease. Adv Parasitol, 42, 1-27.
Seddon, T., Billett, S., & Clemans, A. (2004). Politics of social partnerships: a framework for theorizing. Journal of Education Policy, 19(2), 123-142. doi:10.1080/0144341042000186309
Sheikh, K., Gilson, L., Agyepong, I. A., Hanson, K., Ssengooba, F., & Bennett, S. (2011). Building the field of health policy and systems research: framing the questions. PLoS Med, 8(8), e1001073. doi:10.1371/journal.pmed.1001073
Sommerfeld, J., & Kroeger, A. (2015). Innovative community-based vector control interventions for improved dengue and Chagas disease prevention in Latin America: introduction to the special issue. Trans R Soc Trop Med Hyg, 109(2), 85-88. doi:10.1093/trstmh/tru176
Sommerfeld, J., Ramsay, A., Pagnoni, F., Terry, R. F., Guth, J. A., & Reeder, J. C. (2015). Applied research for better disease prevention and control. PLoS Negl Trop Dis, 9(1), e3378. doi:10.1371/journal.pntd.0003378

277 Soriano-Arandes, A., Basile, L., Ouaarab, H., Claveria, I., Gomez i Prat, J., Cabezos, J., .
. . Jane, M. (2014). Controlling congenital and paediatric chagas disease through a community health approach with active surveillance and promotion of paediatric awareness. BMC Public Health, 14, 1201. doi:10.1186/1471-2458-14-1201
Strauss, A. L., & Corbin, J. M. (1998). Basics of qualitative research : techniques and procedures for developing grounded theory (2nd ed.). Thousand Oaks: Sage Publications.
Tracy, S. J. (2013). Qualitative research methods : collecting evidence, crafting analysis, communicating impact. Chichester, West Sussex, UK: Wiley-Blackwell.
Ventura-Garcia, L., Roura, M., Pell, C., Posada, E., Gascon, J., Aldasoro, E., . . . Pool, R. (2013). Socio-cultural aspects of Chagas disease: a systematic review of qualitative research. PLoS Negl Trop Dis, 7(9), e2410. doi:10.1371/journal.pntd.0002410
Viotti, R., Alarcon de Noya, B., Araujo-Jorge, T., Grijalva, M. J., Guhl, F., Lopez, M. C., . . . Latin American Network for Chagas Disease, N. (2014). Towards a paradigm shift in the treatment of chronic Chagas disease. Antimicrob Agents Chemother, 58(2), 635-639. doi:10.1128/AAC.01662-13
World Health Organization. (2012). Global Report for Research on Infectious Diseases of Poverty. Retrieved from Geneva: WHO/TDR on behalf of Special Programme for Research and Training in Tropical Diseases (TDR): http://www.who.int/tdr/publications/global_report/en/

278
References
Abad-Franch, F. (2003). Control de la Enfermedad de Chagas en Ecuador. Quto, Ecuador: OPS/OMS – Ministerio de Salud Pública del Ecuador.
Abad-Franch, F., Paucar, A., Carpio, C., Cuba, C. A., Aguilar, H. M., & Miles, M. A. (2001). Biogeography of Triatominae (Hemiptera: Reduviidae) in Ecuador: implications for the design of control strategies. Mem Inst Oswaldo Cruz, 96(5), 611-620.
Abad-Franch, F., Vega, M. C., Rolon, M. S., Santos, W. S., & Rojas de Arias, A. (2011). Community participation in Chagas disease vector surveillance: systematic review. PLoS Negl Trop Dis, 5(6), e1207. doi: 10.1371/journal.pntd.0001207
Abd Elaziz, K. M., El-Setouhy, M., Bradley, M. H., Ramzy, R. M., & Weil, G. J. (2013). Knowledge and practice related to compliance with mass drug administration during the Egyptian national filariasis elimination program. Am J Trop Med Hyg, 89(2), 260-264. doi: 10.4269/ajtmh.12-0491
Aboagye-Antwi, F., Kwansa-Bentum, B., Dadzie, S. K., Ahorlu, C. K., Appawu, M. A., Gyapong, J., . . . Boakye, D. A. (2015). Transmission indices and microfilariae prevalence in human population prior to mass drug administration with ivermectin and albendazole in the Gomoa District of Ghana. Parasit Vectors, 8, 562. doi: 10.1186/s13071-015-1105-x
Abramowitz, S. A., McLean, K. E., McKune, S. L., Bardosh, K. L., Fallah, M., Monger, J., . . . Omidian, P. A. (2015). Community-centered responses to Ebola in urban Liberia: the view from below. PLoS Negl Trop Dis, 9(4), e0003706. doi: 10.1371/journal.pntd.0003706
Adam, T., & de Savigny, D. (2012). Systems thinking for strengthening health systems in LMICs: need for a paradigm shift. Health Policy Plan, 27 Suppl 4, iv1-3. doi: 10.1093/heapol/czs084
Adhikari, R. K., Sherchand, J. B., Mishra, S. R., Ranabhat, K., & Wagle, R. R. (2015). Awareness and Coverage of Mass Drug Administration for Elimination of Lymphatic Filariasis: A Community Based Cross Sectional Study in Nepal. Journal of Community Health, 40(1), 34-40. doi: 10.1007/s10900-014-9891-1
Adjei, P. O. W., & Buor, D. (2012). From poverty to poor health: Analysis of socio-economic pathways influencing health status in rural households of Ghana. Health Sociology Review, 21(2), 232-241.
Adoka, S. O., Anyona, D. N., Abuom, P. O., Dida, G. O., Karanja, D., Vulule, J. M., . . . Ofulla, A. V. (2014). Community Perceptions of Schistosomiasis Transmission, Prevalence and Control in Relation to Aquatic Habitats in the Lake Victoria Basin of Kenya. East Afr Med J, 91(7), 232-244.
Adokiya, M. N., Awoonor-Williams, J. K., Barau, I. Y., Beiersmann, C., & Mueller, O. (2015). Evaluation of the integrated disease surveillance and response system for infectious diseases control in northern Ghana. BMC Public Health, 15, 75. doi: 10.1186/s12889-015-1397-y

279 Ager, D. L. (2011). The emotional impact and behavioral consequences of post-M&A
integration: An ethnographic case study in the software industry. Journal of Contemporary Ethnography, 40(2), 199-230. doi: 10.1177/0891241610387134
Aggithaya, M. G., Narahari, S. R., Vayalil, S., Shefuvan, M., Jacob, N. K., & Sushma, K. V. (2013). Self care integrative treatment demonstrated in rural community setting improves health related quality of life of lymphatic filariasis patients in endemic villages. Acta Tropica, 126(3), 198-204. doi: 10.1016/j.actatropica.2013.02.022
Airhihenbuwa, C. O., Ford, C. L., & Iwelunmor, J. I. (2014). Why culture matters in health interventions: lessons from HIV/AIDS stigma and NCDs. Health Educ Behav, 41(1), 78-84. doi: 10.1177/1090198113487199
Airhihenbuwa, C. O., & Obregon, R. (2000). A critical assessment of theories/models used in health communication for HIV/AIDS. J Health Commun, 5 Suppl, 5-15. doi: 10.1080/10810730050019528
Allen, T., & Parker, M. (2011). The "other diseases" of the Millennium Development Goals: rhetoric and reality of free drug distribution to cure the poor's parasites. Third World Q, 32(1), 91-117.
Allotey, Pascale, Reidpath, Daniel D., & Pokhrel, Subhash. (2010). Social sciences research in neglected tropical diseases 1: the ongoing neglect in the neglected tropical diseases. Health research policy and systems, 8, 32.
Alviarez, Y., & Ferrer, E. (2014). Aproximación a la problemática de la coendemicidad enfermedad de Chagas-Leishmaniasis desde un enfoque de Ecosalud. Comunidad Salud, 12(2), 55-61.
Amin, M., & Abubaker, H. (2017). Control of Schistosomiasis in the Gezira Irrigation Scheme, Sudan. J Biosoc Sci, 49(1), 83-98. doi: 10.1017/S0021932016000079
Andrus, J., Bottazzi, M. E., Chow, J., Goraleski, K. A., Fisher-Hoch, S. P., Lambuth, J. K., . . . Hotez, P. J. (2013). Ears of the Armadillo: Global Health Research and Neglected Diseases in Texas. PLoS Negl Trop Dis, 7(6), e2021. doi: 10.1371/journal.pntd.0002021
Arenas-Monreal, L., Pina-Pozas, M., & Gomez-Dantes, H. (2015). [Challenges and inputs of the gender perspective to the study of vector borne diseases]. Salud Publica Mex, 57(1), 66-75.
Armah, F. A., Quansah, R., Luginaah, I., Chuenpagdee, R., Hambati, H., & Campbell, G. (2015). Historical Perspective and Risk of Multiple Neglected Tropical Diseases in Coastal Tanzania: Compositional and Contextual Determinants of Disease Risk. PLoS Negl Trop Dis, 9(8), e0003939. doi: 10.1371/journal.pntd.0003939
Atkinson, Paul, Delamont, Sara, & Housley, William. (2008). Contours of culture : complex ethnography and the ethnography of complexity. Walnut Creek, CA: AltaMira Press.
Ault, S. K., & Nicholls, R. S. (2010). [Integrated approach to neglected tropical diseases in Latin America and the Caribbean: an ethical imperative to reach justice and social equity]. Biomedica, 30(2), 159-163.
Awofeso, N. (2013). Towards global Guinea worm eradication in 2015: the experience of South Sudan. Int J Infect Dis, 17(8), e577-582. doi: 10.1016/j.ijid.2013.03.003

280 Ayode, D., McBride, C. M., de Heer, H. D., Watanabe, E., Gebreyesus, T., Tora, A., . . .
Davey, G. (2013). A qualitative study exploring barriers related to use of footwear in rural highland ethiopia: implications for neglected tropical disease control. PLoS Negl Trop Dis, 7(4), e2199. doi: 10.1371/journal.pntd.0002199
Azoh Barry, Jose. (2014). Social sciences research on infectious diseases of poverty: too little and too late? Plos Neglected Tropical Diseases, 8(6), e2803.
Babrow, Austin S., & Mattson, M. . (2011). Building health communciation theories in the 21st Century. In R. Parrot, T. L. Thompson & J. Nussbaum (Eds.), The Routlege Handbook of Health Communication (pp. xii, 753 pages).
Bakhtin, M. M., & Holquist, Michael. (1981). The dialogic imagination : four essays. Austin: University of Texas Press.
Barbu, C., Dumonteil, E., & Gourbiere, S. (2009). Optimization of control strategies for non-domiciliated Triatoma dimidiata, Chagas disease vector in the Yucatan Peninsula, Mexico. PLoS Negl Trop Dis, 3(4), e416. doi: 10.1371/journal.pntd.0000416
Barbu, C. M., Buttenheim, A. M., Pumahuanca, M. L. H., Calderon, J. E. Q., Salazar, R., Carrion, M., . . . Levy, M. Z. (2014). Residual Infestation and Recolonization during Urban Triatoma infestans Bug Control Campaign, Peru. Emerging Infectious Diseases, 20(12), 2055-2063. doi: 10.3201/eid2012.131820
Bardosh, K. (2014). Global aspirations, local realities: the role of social science research in controlling neglected tropical diseases. Infect Dis Poverty, 3(1), 35. doi: 10.1186/2049-9957-3-35
Barkia, H., Barkia, A., Yacoubi, R., Alemad, A., El Kharim, K., & Belghyti, D. (2014). Contribution of Mobile Teams to Efforts to Eliminate Schistosomiasis at Schistosoma haematobium in Morocco- Narrative Review Article. Iran J Public Health, 43(9), 1167-1175.
Barry, J. A. (2014). Social Sciences Research on Infectious Diseases of Poverty: Too Little and Too Late? Plos Neglected Tropical Diseases, 8(6). doi: ARTN e2803 10.1371/journal.pntd.0002803
Bayer, A. M., Hunter, G. C., Gilman, R. H., Cornejo Del Carpio, J. G., Naquira, C., Bern, C., & Levy, M. Z. (2009). Chagas disease, migration and community settlement patterns in Arequipa, Peru. PLoS Negl Trop Dis, 3(12), e567. doi: 10.1371/journal.pntd.0000567
Becker, M. H., & Maiman, L. A. (1975). Sociobehavioral determinants of compliance with health and medical care recommendations. Med Care, 13(1), 10-24.
Bennett, S., Agyepong, I. A., Sheikh, K., Hanson, K., Ssengooba, F., & Gilson, L. (2011). Building the field of health policy and systems research: an agenda for action. PLoS Med, 8(8), e1001081. doi: 10.1371/journal.pmed.1001081
Biswas, G., Sankara, D. P., Agua-Agum, J., & Maiga, A. (2013). Dracunculiasis (guinea worm disease): eradication without a drug or a vaccine. Philos Trans R Soc Lond B Biol Sci, 368(1623), 20120146. doi: 10.1098/rstb.2012.0146
Boelee, E., Yohannes, M., Poda, J. N., McCartney, M., Cecchi, P., Kibret, S., . . . Laamrani, H. (2013). Options for water storage and rainwater harvesting to

281
improve health and resilience against climate change in Africa. Regional Environmental Change, 13(3), 509-519. doi: 10.1007/s10113-012-0287-4
Bonney, K. M. (2014). Chagas disease in the 21st century: a public health success or an emerging threat? Parasite, 21, 11. doi: 10.1051/parasite/2014012
Bosschaert, T. (2012). The SiD definition of Sustainability. November 25, 2016, from http://www.except.nl/en/ - .en.articles.204-the-sid-definition-of-sustainability
Braubach, M. (2011). Key challenges of housing and health from WHO perspective. Int J Public Health, 56(6), 579-580. doi: 10.1007/s00038-011-0296-y
Breniere, S. F., Salas, R., Buitrago, R., Bremond, P., Sosa, V., Bosseno, M. F., . . . Barnabe, C. (2013). Wild populations of Triatoma infestans are highly connected to intra-peridomestic conspecific populations in the Bolivian Andes. PLoS One, 8(11), e80786. doi: 10.1371/journal.pone.0080786
Briceno-Leon, R. (2009). [Chagas disease in the Americas: an ecohealth perspective]. Cad Saude Publica, 25 Suppl 1, S71-82.
Bryant, A., & Charmaz, K. (2007). The SAGE handbook of grounded theory (pp. 1 online resource (xxx, 623 p).
Bustamante, D. M., De Urioste-Stone, S. M., Juarez, J. G., & Pennington, P. M. (2014). Ecological, social and biological risk factors for continued Trypanosoma cruzi transmission by Triatoma dimidiata in Guatemala. PLoS One, 9(8), e104599. doi: 10.1371/journal.pone.0104599
Bustamante, D. M., Monroy, C., Pineda, S., Rodas, A., Castro, X., Ayala, V., . . . Trampe, R. (2009). Risk factors for intradomiciliary infestation by the Chagas disease vector Triatoma dimidiatain Jutiapa, Guatemala. Cad Saude Publica, 25 Suppl 1, S83-92.
Bustamante, D. M., Monroy, M. C., Rodas, A. G., Juarez, J. A., & Malone, J. B. (2007). Environmental determinants of the distribution of Chagas disease vectors in south-eastern Guatemala. Geospat Health, 1(2), 199-211. doi: 10.4081/gh.2007.268
Buttenheim, A. M., Paz-Soldan, V., Barbu, C., Skovira, C., Quintanilla Calderon, J., Mollesaca Riveros, L. M., . . . Levy, M. Z. (2014). Is participation contagious? Evidence from a household vector control campaign in urban Peru. J Epidemiol Community Health, 68(2), 103-109. doi: 10.1136/jech-2013-202661
Byrne, S. K., & Collins, S. D. (2015a). Lymphatic Filariasis in Children in Haiti. MCN Am J Matern Child Nurs, 40(4), 227-233. doi: 10.1097/NMC.0000000000000144
Byrne, S. K., & Collins, S. D. (2015b). Lymphatic Filariasis in Children in Haiti. Mcn-the American Journal of Maternal-Child Nursing, 40(4), 227-233.
Cabello, R., Beck, L., Massara, C. , Murta, F., Guimaraes, R., Pieri, O., . . . Favre, T. . (2016). Schistosoma mansoni infection and related knowledge among schoolchildren in an endemic area of Minas Gerais, Brazil, prior to educational actions. Acta Tropica, 164, 208-215. doi: 10.1016/j.actatropica.2016.09.015
Callahan, K., Bolton, B., Hopkins, D. R., Ruiz-Tiben, E., Withers, P. C., & Meagley, K. (2013). Contributions of the Guinea worm disease eradication campaign toward achievement of the Millennium Development Goals. PLoS Negl Trop Dis, 7(5), e2160. doi: 10.1371/journal.pntd.0002160

282 Campbell, S. J., Savage, G. B., Gray, D. J., Atkinson, J. A., Soares Magalhaes, R. J.,
Nery, S. V., . . . Clements, A. C. (2014). Water, Sanitation, and Hygiene (WASH): a critical component for sustainable soil-transmitted helminth and schistosomiasis control. PLoS Negl Trop Dis, 8(4), e2651. doi: 10.1371/journal.pntd.0002651
Campozano, L., Celleri, R., Trachte, K., Bendix, J., & Samaniego, E. (2016). Rainfall and Cloud Dynamics in the Andes: A Southern Ecuador Case Study. Advances in Meteorology. doi: Artn 3192765 10.1155/2016/3192765
Cantillo-Barraza, O., Garces, E., Gomez-Palacio, A., Cortes, L. A., Pereira, A., Marcet, P. L., . . . Triana-Chavez, O. (2015). Eco-epidemiological study of an endemic Chagas disease region in northern Colombia reveals the importance of Triatoma maculata (Hemiptera: Reduviidae), dogs and Didelphis marsupialis in Trypanosoma cruzi maintenance. Parasit Vectors, 8, 482. doi: 10.1186/s13071-015-1100-2
Cartwright, N. (2011). A philosopher's view of the long road from RCTs to effectiveness. Lancet, 377(9775), 1400-1401.
Casmo, V., Augusto, G., Nala, R., Sabonete, A., & Carvalho-Costa, F. A. (2014). The effect of hookworm infection and urinary schistosomiasis on blood hemoglobin concentration of schoolchildren living in northern Mozambique. Rev Inst Med Trop Sao Paulo, 56(3), 219-224.
Cavaca, A. G., Emerich, T. B., Vasconcellos-Silva, P. R., dos Santos-Neto, E. T., & Oliveira, A. E. (2016). Diseases Neglected by the Media in Espirito Santo, Brazil in 2011-2012. Plos Neglected Tropical Diseases, 10(4). doi: ARTN e0004662
10.1371/journal.pntd.0004662 Celone, M., Person, B., Ali, S. M., Lyimo, J. H., Mohammed, U. A., Khamis, A. N., . . .
Knopp, S. (2016). Increasing the reach: Involving local Muslim religious teachers in a behavioral intervention to eliminate urogenital schistosomiasis in Zanzibar. Acta Tropica, 163, 142-148. doi: 10.1016/j.actatropica.2016.08.004
Charmaz, K. (2014). Constructing grounded theory (2nd edition ed.). London ; Thousand Oaks, Calif.: Sage.
Charmaz, K. (2005). Grounded Theory in the 21st Century: Applications for Advancing Social Justice Studies. In N. K. Denzin & Y. S. Lincoln (Eds.), The SAGE handbook of qualitative research (3rd ed ed., pp. 507-535). Thousand Oaks: Sage Publications.
Charmaz, K. (2006). Constructing grounded theory. London ; Thousand Oaks, Calif.: Sage Publications.
Charmaz, K. (2011). A Constructivist Grounded Theory Analysis of Losing and Regaining a Valued Self. In Frederick J. Wertz (Ed.), Five ways of doing qualitative analysis : phenomenological psychology, grounded theory, discourse analysis, narrative research, and intuitive inquiry (pp. 165-204). New York: Guilford Press.
Charron, D. F. (2012). Ecosystem approaches to health for a global sustainability agenda. Ecohealth, 9(3), 256-266. doi: 10.1007/s10393-012-0791-5

283 Chaula, S. A., & Tarimo, D. S. (2014). Impact of praziquantel mass drug administration
campaign on prevalence and intensity of Schistosoma haemamtobium among school children in Bahi district, Tanzania. Tanzan J Health Res, 16(1), 1-8.
Cho, H. Y., & Salmon, C. T. (2007). Unintended effects of health communication campaigns. Journal of Communication, 57(2), 293-317.
Corbin, J., & Strauss, A. (2008). Strategies for qualitative data analysis. Basics of qualitative research (pp. 65-86). Los Angeles, CA: Sage.
Cormick, G., Ciganda, A., Cafferata, M. L., Ripple, M. J., Sosa-Estani, S., Buekens, P., . . . Althabe, F. (2015). Text message interventions for follow up of infants born to mothers positive for Chagas disease in Tucuman, Argentina: a feasibility study. BMC Res Notes, 8, 508. doi: 10.1186/s13104-015-1498-9
Craig, R. T. (1999). Communication theory as a Field. Communication Theory, 9(2), 119-161.
Crompton, D. (2010). Working to overcome the global impact of neglected tropical diseases first WHO report on neglected tropical diseases (pp. ix, 172 p.). Retrieved from http://site.ebrary.com/lib/yale/Doc?id=10430901
Curtis-Robles, R., Wozniak, E. J., Auckland, L. D., Hamer, G. L., & Hamer, S. A. (2015). Combining Public Health Education and Disease Ecology Research: Using Citizen Science to Assess Chagas Disease Entomological Risk in Texas. PLoS Negl Trop Dis, 9(12), e0004235. doi: 10.1371/journal.pntd.0004235
da Silva, G. M. S., Chambela, M. C., Sousa, A. S., Sangenis, L. H. C., Xavier, S. S., Costa, A. R., . . . Saraiva, R. M. (2012). Impact of pharmaceutical care on the quality of life of patients with Chagas disease and heart failure: randomized clinical trial. Trials, 13. doi: Artn 244 10.1186/1745-6215-13-244
De Maio, F. G., Llovet, I., & Dinardi, G. (2014). Chagas disease in non-endemic countries: 'sick immigrant' phobia or a public health concern? Critical Public Health, 24(3), 372-380. doi: 10.1080/09581596.2013.836589
De Silva, M. J., Breuer, E., Lee, L., Asher, L., Chowdhary, N., Lund, C., & Patel, V. (2014). Theory of Change: a theory-driven approach to enhance the Medical Research Council's framework for complex interventions. Trials, 15, 267. doi: 10.1186/1745-6215-15-267
De Urioste-Stone, S. M., Pennington, P. M., Pellecer, E., Aguilar, T. M., Samayoa, G., Perdomo, H. D., . . . Juarez, J. G. (2015). Development of a community-based intervention for the control of Chagas disease based on peridomestic animal management: an eco-bio-social perspective. Trans R Soc Trop Med Hyg, 109(2), 159-167. doi: 10.1093/trstmh/tru202
Deetz, S. (1996a). Describing differences in approaches to organization science: Rethinking Burrell and Morgan and their legacy. Organization Science, 7(2), 191-207. doi: DOI 10.1287/orsc.7.2.191
Deetz, S. (1996b). The positioning of the researcher in studies of organizations: De-hatching literacy theory - Commentary. Journal of Management Inquiry, 5(4), 387-391. doi: Doi 10.1177/105649269654014

284 Dell'Arciprete, A., Braunstein, J., Touris, C., Dinardi, G., Llovet, I., & Sosa-Estani, S.
(2014). Cultural barriers to effective communication between Indigenous communities and health care providers in Northern Argentina: an anthropological contribution to Chagas disease prevention and control. Int J Equity Health, 13, 6. doi: 10.1186/1475-9276-13-6
Denzin, N., Lincoln, Y., & Smith, L. (2008). Handbook of critical and indigenous methodologies. Los Angeles: Sage.
Dias, J. C. (2007). Southern Cone Initiative for the elimination of domestic populations of Triatoma infestans and the interruption of transfusional Chagas disease. Historical aspects, present situation, and perspectives. Mem Inst Oswaldo Cruz, 102 Suppl 1, 11-18.
Dias, J. C. P., Ramos, A. N., Gontijo, E. D., Luquetti, A., Shikanai-Yasuda, M. A., Coura, J. R., . . . Alves, R. V. (2016). 2nd Brazilian Consensus on Chagas Disease, 2015. Revista Da Sociedade Brasileira De Medicina Tropical, 49, 3-59. doi: 10.1590/0037-8682-0505-2016
Dias, J. V., Queiroz, D. R., Diotaiuti, L., & Pires, H. H. (2016). Knowledge of triatomine insects and of the Chagas disease among people from localities which have different levels of vector infestations. Cien Saude Colet, 21(7), 2293-2304. doi: 10.1590/1413-81232015217.07792015
Dias, J.V.L., Queiroz, D.R.M., Diotaiuti, L, & Pires, H. H. R. (2016). Knowledge of triatomine insects and of the Chagas disease among people from localities which have different levels of vector infestations. . Ciência & Saúde Coletiva, 21(7), 2293-2304. doi: https://dx.doi.org/10.1590/1413-81232015217.07792015
do Nascimento, H. R., & Puschel, V. A. D. (2013). Self-care actions in patients with heart failure. Acta Paulista De Enfermagem, 26(6), 601-607.
Donovan, S. D., Stevens, M., Sanogo, K., Masroor, N., & Bearman, G. (2014). Knowledge and perceptions of Chagas disease in a rural Honduran community. Rural Remote Health, 14(3), 2845.
Dumonteil, E., Herrera, C., Martini, L., Grijalva, M. J., Guevara, A. G., Costales, J. A., . . . Waleckx, E. (2016). Chagas Disease Has Not Been Controlled in Ecuador. PLoS One, 11(6), e0158145. doi: 10.1371/journal.pone.0158145
Dumonteil, E., Nouvellet, P., Rosecrans, K., Ramirez-Sierra, M. J., Gamboa-Leon, R., Cruz-Chan, V., . . . Gourbiere, S. (2013). Eco-bio-social determinants for house infestation by non-domiciliated Triatoma dimidiata in the Yucatan Peninsula, Mexico. PLoS Negl Trop Dis, 7(9), e2466. doi: 10.1371/journal.pntd.0002466
Dutta, M. J., & Basu, A. (2008). Meanings of health: interrogating structure and culture. Health Commun, 23(6), 560-572. doi: 10.1080/10410230802465266
Dutta, M. J., Comer, S., Teo, D., Luk, P., Lee, M., Zapata, D., . . . Kaur, S. (2017). Health Meanings among Foreign Domestic Workers in Singapore: A Culture-Centered Approach. Health Commun, 1-10. doi: 10.1080/10410236.2017.1292576
Dutta, M. J., & de Souza, R. (2008). The past, present, and future of health development campaigns: reflexivity and the critical-cultural approach. Health Commun, 23(4), 326-339. doi: 10.1080/10410230802229704

285 Ede, A. O., Nwaokoro, J. C., Iwuala, C. C., Amadi, A. N., & Akpelu, U. A. (2014). The
provision of potable water in eradication of Guinea worm infection in Ezza North, Southeastern, Nigeria. J Community Health, 39(5), 980-986. doi: 10.1007/s10900-014-9842-x
Engels, D. (2016). Neglected tropical diseases in the Sustainable Development Goals. Lancet, 387(10015), 223-224. doi: 10.1016/S0140-6736(16)00043-X
Favre, T. C., Pereira, A. P., Beck, L. C., Galvao, A. F., & Pieri, O. S. (2015). School-based and community-based actions for scaling-up diagnosis and treatment of schistosomiasis toward its elimination in an endemic area of Brazil. Acta Tropica, 149, 155-162. doi: 10.1016/j.actatropica.2015.04.024
Feliciangeli, M. D. (2014). Leishmaniasis in Venezuela: Current status, actions and prospects for vector control in the context of a multi-sectorial control program. Boletin De Malariologia Y Salud Ambiental, 54(1), 1-7.
Forget, G., & Lebel, J. (2001). An ecosystem approach to human health. Int J Occup Environ Health, 7(2 Suppl), S3-38.
Forsyth, C. (2015). Controlled but not cured: Structural processes and explanatory models of Chagas disease in tropical Bolivia. Soc Sci Med, 145, 7-16. doi: 10.1016/j.socscimed.2015.09.022
Franco-Paredes, C., & Santos-Preciado, J. I. (2011). Freedom, justice, and neglected tropical diseases. PLoS Negl Trop Dis, 5(8), e1235. doi: 10.1371/journal.pntd.0001235
Frank, A. W. (2005). What is dialogical research, and why should we do it? Qualitative Health Research, 15(7), 964-974. doi: 10.1177/1049732305279078
Franke, M. F., Del Castillo, H., Pereda, Y., Lecca, L., Fuertes, J., Cardenas, L., . . . Murray, M. (2014). Parasite infection and tuberculosis disease among children: a case-control study. Am J Trop Med Hyg, 90(2), 279-282. doi: 10.4269/ajtmh.13-0425
Freeman, A. R., Lammie, P. J., Houston, R., LaPointe, M. D., Streit, T. G., Jooste, P. L., . . . Addiss, D. G. (2001). A community-based trial for the control of lymphatic filariasis and iodine deficiency using salt fortified with diethylcarbamazine and iodine. Am J Trop Med Hyg, 65(6), 865-871.
Gascon, J., Vilasanjuan, R., & Lucas, A. (2014). The need for global collaboration to tackle hidden public health crisis of Chagas disease. Expert Rev Anti Infect Ther, 12(4), 393-395. doi: 10.1586/14787210.2014.896194
Gazzinelli, A., Correa-Oliveira, R., Yang, G. J., Boatin, B. A., & Kloos, H. (2012). A research agenda for helminth diseases of humans: social ecology, environmental determinants, and health systems. PLoS Negl Trop Dis, 6(4), e1603. doi: 10.1371/journal.pntd.0001603
Ghosh, S., Samanta, A., & Kole, S. (2013). Mass drug administration for elimination of lymphatic filariasis: Recent experiences from a district of West Bengal, India. Trop Parasitol, 3(1), 67-71. doi: 10.4103/2229-5070.113917
Gilson, L., Hanson, K., Sheikh, K., Agyepong, I. A., Ssengooba, F., & Bennett, S. (2011). Building the field of health policy and systems research: social science matters. PLoS Med, 8(8), e1001079. doi: 10.1371/journal.pmed.1001079

286 Glaser, B. G., & Strauss, A. L. (1967). The discovery of grounded theory; strategies for
qualitative research. Chicago,: Aldine Pub. Co. Global programme to eliminate lymphatic filariasis: progress report, 2015. (2016). Wkly
Epidemiol Rec, 91(39), 441-455. Green, L.W., & Kreuter, M.W. (2005). Health Program Planning: An Educational and
Ecological Approach (M.-H. H. Education Ed. 4th edition ed.). NY. Greiner, K. (2012). Participatory Health Communication Research In R. Obregon & S.
Waisbord (Eds.), The handbook of global health communication (pp. 348-373). Chichester, England: Wiley-Blackwell.
Greiner, Karen P. (2010). Exploring dialogic social change (pp. 1 electronic text). Retrieved from http://rave.ohiolink.edu/etdc/view?acc_num=ohiou1273197688
Grijalva, M. J., Palomeque-Rodriguez, F. S., Costales, J. A., Davila, S., & Arcos-Teran, L. (2005). High household infestation rates by synanthropic vectors of Chagas disease in southern Ecuador. J Med Entomol, 42(1), 68-74.
Grijalva, M. J., Suarez-Davalos, V., Villacis, A. G., Ocana-Mayorga, S., & Dangles, O. (2012). Ecological factors related to the widespread distribution of sylvatic Rhodnius ecuadoriensis populations in southern Ecuador. Parasit Vectors, 5, 17. doi: 10.1186/1756-3305-5-17
Grijalva, M. J., & Villacis, A. G. (2009). Presence of Rhodnius ecuadoriensis in sylvatic habitats in the southern highlands (Loja Province) of Ecuador. J Med Entomol, 46(3), 708-711.
Grijalva, M. J., Villacis, A. G., Ocana-Mayorga, S., Yumiseva, C. A., & Baus, E. G. (2011). Limitations of selective deltamethrin application for triatomine control in central coastal Ecuador. Parasit Vectors, 4, 20. doi: 10.1186/1756-3305-4-20
Grijalva, M. J., Villacis, A. G., Ocana-Mayorga, S., Yumiseva, C. A., Moncayo, A. L., & Baus, E. G. (2015). Comprehensive Survey of Domiciliary Triatomine Species Capable of Transmitting Chagas Disease in Southern Ecuador. PLoS Negl Trop Dis, 9(10), e0004142. doi: 10.1371/journal.pntd.0004142
Gurtler, R. E., & Yadon, Z. E. (2015). Eco-bio-social research on community-based approaches for Chagas disease vector control in Latin America. Trans R Soc Trop Med Hyg, 109(2), 91-98. doi: 10.1093/trstmh/tru203
Guttman, N. (2000). Public health communication interventions values and ethical dilemmas (pp. 1 online resource (xviii, 286 p).
Haines, A., Bruce, N., Cairncross, S., Davies, M., Greenland, K., Hiscox, A., . . . Wilkinson, P. (2013). Promoting health and advancing development through improved housing in low-income settings. J Urban Health, 90(5), 810-831. doi: 10.1007/s11524-012-9773-8
Hashimoto, K., Alvarez, H., Nakagawa, J., Juarez, J., Monroy, C., Cordon-Rosales, C., & Gil, E. (2012). Vector control intervention towards interruption of transmission of Chagas disease by Rhodnius prolixus, main vector in Guatemala. Mem Inst Oswaldo Cruz, 107(7), 877-887.
Hashimoto, K., Zuniga, C., Nakamura, J., & Hanada, K. (2015). Integrating an infectious disease programme into the primary health care service: a retrospective analysis

287
of Chagas disease community-based surveillance in Honduras. BMC Health Serv Res, 15, 116. doi: 10.1186/s12913-015-0785-4
Hashimoto, K., Zuniga, C., Romero, E., Morales, Z., & Maguire, J. H. (2015). Determinants of Health Service Responsiveness in Community-Based Vector Surveillance for Chagas Disease in Guatemala, El Salvador, and Honduras. PLoS Negl Trop Dis, 9(8), e0003974. doi: 10.1371/journal.pntd.0003974
Hastings, J. (2016). Rumours, Riots and the Rejection of Mass Drug Administration for the Treatment of Schistosomiasis in Morogoro, Tanzania. J Biosoc Sci, 48 Suppl 1, S16-39. doi: 10.1017/S0021932016000018
Hearld, L. R., Bleser, W. K., Alexander, J. A., & Wolf, L. J. (2016). A systematic review of the literature on the sustainability of Community Health Collaboratives. Med Care Res Rev, 73(2), 127-181. doi: 10.1177/1077558715607162
Heydari, N., Larsen, D. A., Neira, M., Beltran Ayala, E., Fernandez, P., Adrian, J., . . . Stewart-Ibarra, A. M. (2017). Household Dengue Prevention Interventions, Expenditures, and Barriers to Aedes aegypti Control in Machala, Ecuador. Int J Environ Res Public Health, 14(2). doi: 10.3390/ijerph14020196
Holveck, J. C., Ehrenberg, J. P., Ault, S. K., Rojas, R., Vasquez, J., Cerqueira, M. T., . . . Periago, M. R. (2007). Prevention, control, and elimination of neglected diseases in the Americas: pathways to integrated, inter-programmatic, inter-sectoral action for health and development. BMC Public Health, 7, 6. doi: 10.1186/1471-2458-7-6
Hotez, P. J. (2010). Peace through vaccine diplomacy. Science, 327(5971), 1301. doi: 10.1126/science.1189028
Hotez, P. J. (2014). Neglected parasitic infections and poverty in the United States. PLoS Negl Trop Dis, 8(9), e3012. doi: 10.1371/journal.pntd.0003012
Hotez, P. J., & Aksoy, S. (2011). An interfaith dialogue on the neglected tropical diseases. PLoS Negl Trop Dis, 5(12), e1240. doi: 10.1371/journal.pntd.0001240
Hotez, P. J., Alvarado, M., Basanez, M. G., Bolliger, I., Bourne, R., Boussinesq, M., . . . Naghavi, M. (2014). The global burden of disease study 2010: interpretation and implications for the neglected tropical diseases. PLoS Negl Trop Dis, 8(7), e2865. doi: 10.1371/journal.pntd.0002865
Hotez, P. J., Dumonteil, E., Woc-Colburn, L., Serpa, J. A., Bezek, S., Edwards, M. S., . . . Bottazzi, M. E. (2012). Chagas disease: "the new HIV/AIDS of the Americas". PLoS Negl Trop Dis, 6(5), e1498. doi: 10.1371/journal.pntd.0001498
Hotez, P. J., Fenwick, A., Savioli, L., & Molyneux, D. H. (2009). Rescuing the bottom billion through control of neglected tropical diseases. Lancet, 373(9674), 1570-1575. doi: 10.1016/S0140-6736(09)60233-6
Hotez, P. J., Molyneux, D. H., Fenwick, A., Kumaresan, J., Sachs, S. E., Sachs, J. D., & Savioli, L. (2007). Control of neglected tropical diseases. N Engl J Med, 357(10), 1018-1027. doi: 10.1056/NEJMra064142
Hotez, P. J., Molyneux, D. H., Fenwick, A., Ottesen, E., Ehrlich Sachs, S., & Sachs, J. D. (2006). Incorporating a rapid-impact package for neglected tropical diseases with programs for HIV/AIDS, tuberculosis, and malaria. PLoS Med, 3(5), e102. doi: 10.1371/journal.pmed.0030102

288 Houweling, T. A., Karim-Kos, H. E., Kulik, M. C., Stolk, W. A., Haagsma, J. A., Lenk,
E. J., . . . de Vlas, S. J. (2016). Socioeconomic Inequalities in Neglected Tropical Diseases: A Systematic Review. PLoS Negl Trop Dis, 10(5), e0004546. doi: 10.1371/journal.pntd.0004546
Hurtado, L. A., Calzada, J. E., Pineda, V., Gonzalez, K., Santamaria, A. M., Caceres, L., . . . Saldana, A. (2014a). Knowledge and risk factors related to Chagas' disease in two Panamanian communities where Rhodnius pallescens is the main vector. Biomedica, 34(2), 260-270. doi: 10.7705/biomedica.v34i2.2133
Hurtado, L. A., Calzada, J. E., Pineda, V., Gonzalez, K., Santamaria, A. M., Caceres, L., . . . Saldana, A. (2014b). [Knowledge and risk factors related to Chagas' disease in two Panamanian communities where Rhodnius pallescens is the main vector]. Biomedica, 34(2), 260-270. doi: 10.1590/S0120-41572014000200012
Hussain, M. A., Sitha, A. K., Swain, S., Kadam, S., & Pati, S. (2014). Mass drug administration for lymphatic filariasis elimination in a coastal state of India: a study on barriers to coverage and compliance. Infect Dis Poverty, 3, 31. doi: 10.1186/2049-9957-3-31
International Conference on Primary Health, Care. (1978). Declaration of Alma-Ata. WHO Chron, 32(11), 428-430.
Iwelunmor, J., Blackstone, S., Veira, D., Nwaozuru, U., Airhihenbuwa, C., Munodawafa, D., . . . Ogedegebe, G. (2016). Toward the sustainability of health interventions implemented in sub-Saharan Africa: a systematic review and conceptual framework. Implement Sci, 11, 43. doi: 10.1186/s13012-016-0392-8
Jagosh, J., Bush, P. L., Salsberg, J., Macaulay, A. C., Greenhalgh, T., Wong, G., . . . Pluye, P. (2015). A realist evaluation of community-based participatory research: partnership synergy, trust building and related ripple effects. BMC Public Health, 15, 725. doi: 10.1186/s12889-015-1949-1
Jamil, R., & Dutta, M. J. (2012). A culture-centered exploration of health: constructions from rural Bangladesh. Health Commun, 27(4), 369-379. doi: 10.1080/10410236.2011.586989
Jones, A. H., Becknell, S., Withers, P. C., Ruiz-Tiben, E., Hopkins, D. R., Stobbelaar, D., & Makoy, S. Y. (2014). Logistics of Guinea worm disease eradication in South Sudan. Am J Trop Med Hyg, 90(3), 393-401. doi: 10.4269/ajtmh.13-0110
Kariuki, T., Phillips, R., Njenga, S., Olesen, O. F., Klatser, P. R., Porro, R., . . . Hanne, D. (2011). Research and capacity building for control of neglected tropical diseases: the need for a different approach. PLoS Negl Trop Dis, 5(5), e1020. doi: 10.1371/journal.pntd.0001020
Kasten-Monges, M. D., Cabrera-Pivaral, C. E., Lozano-Kasten, F., Aguilar-Velasco, H. M., Hidalgo-Ottolenghi, R., & Zavala-Gonzalez, M. A. (2016). Evaluation of the clinical competence in mexican resident physicians for the diagnosis and treatment of Chagas disease. Gaceta Medica De Mexico, 152(4), 516-520.
Kisoka, W. J., Simonsen, P. E., Malecela, M. N., Tersbol, B. P., Mushi, D. L., & Meyrowitsch, D. W. (2014). Factors influencing drug uptake during mass drug administration for control of lymphatic filariasis in rural and urban Tanzania. PLoS One, 9(10), e109316. doi: 10.1371/journal.pone.0109316

289 Kisoka, W. J., Tersbol, B. P., Meyrowitsch, D. W., Simonsen, P. E., & Mushi, D. L.
(2016). Community Members' Perceptions of Mass Drug Administration for Control of Lymphatic Filariasis in Rural and Urban Tanzania. J Biosoc Sci, 48(1), 94-112. doi: 10.1017/S0021932015000024
Kisoka, W., Mushi, D., Meyrowitsch, D. W., Malecela, M., Simonsen, P. E., & Tersbol, B. P. (2017). Dilemmas of Community-Directed Mass Drug Administration for Lymphatic Filariasis Control: A Qualitative Study from Urban and Rural Tanzania. J Biosoc Sci, 49(4), 447-462. doi: 10.1017/S0021932016000365
Kleinman, A. (2013). From illness as culture to caregiving as moral experience. N Engl J Med, 368(15), 1376-1377. doi: 10.1056/NEJMp1300678
Kolopack, P. A., Parsons, J. A., & Lavery, J. V. (2015). What makes community engagement effective?: Lessons from the Eliminate Dengue Program in Queensland Australia. PLoS Negl Trop Dis, 9(4), e0003713. doi: 10.1371/journal.pntd.0003713
Krentel, A., Damayanti, R., Titaley, C. R., Suharno, N., Bradley, M., & Lynam, T. (2016). Improving Coverage and Compliance in Mass Drug Administration for the Elimination of LF in Two 'Endgame' Districts in Indonesia Using Micronarrative Surveys. PLoS Negl Trop Dis, 10(11), e0005027. doi: 10.1371/journal.pntd.0005027
Krentel, A., Fischer, P. U., & Weil, G. J. (2013). A review of factors that influence individual compliance with mass drug administration for elimination of lymphatic filariasis. PLoS Negl Trop Dis, 7(11), e2447. doi: 10.1371/journal.pntd.0002447
Kvale, Steinar, & Brinkmann, Svend. (2009). InterViews : learning the craft of qualitative research interviewing (Second edition ed.).
Lardeux, F., Depickere, S., Aliaga, C., Chavez, T., & Zambrana, L. (2015). Experimental control of Triatoma infestans in poor rural villages of Bolivia through community participation. Trans R Soc Trop Med Hyg, 109(2), 150-158. doi: 10.1093/trstmh/tru205
Lee, B. Y., Bacon, K. M., Bottazzi, M. E., & Hotez, P. J. (2013). Global economic burden of Chagas disease: a computational simulation model. Lancet Infect Dis, 13(4), 342-348. doi: 10.1016/S1473-3099(13)70002-1
Lemoine, J. F., Desormeaux, A. M., Monestime, F., Fayette, C. R., Desir, L., Direny, A. N., . . . Baker, M. (2016). Controlling Neglected Tropical Diseases (NTDs) in Haiti: Implementation Strategies and Evidence of Their Success. PLoS Negl Trop Dis, 10(10), e0004954. doi: 10.1371/journal.pntd.0004954
Leon, Joshua K. (2015). The rise of global health : the evolution of effective collective action.
Leonardo, L., Chigusa, Y., Kikuchi, M., Kato-Hayashi, N., Kawazu, S., Angeles, J. M., . . . Chua, J. C. (2016). Schistosomiasis in the Philippines: Challenges and Some Successes in Control. Southeast Asian Journal of Tropical Medicine and Public Health, 47(4), 651-666.
Lindlof, Thomas R., & Taylor, Bryan C. (2011). Qualitative communication research methods (3rd ed.). Thousand Oaks, Calif.: SAGE.

290 Lindsay, S. W., Emerson, P. M., & Charlwood, J. D. (2002). Reducing malaria by
mosquito-proofing houses. Trends Parasitol, 18(11), 510-514. Lindsay, S. W., Jawara, M., Paine, K., Pinder, M., Walraven, G. E., & Emerson, P. M.
(2003). Changes in house design reduce exposure to malaria mosquitoes. Trop Med Int Health, 8(6), 512-517.
Liu, Y., Zhong, B., Wu, Z. S., Liang, S., Qiu, D. C., & Ma, X. (2017). Interruption of schistosomiasis transmission in mountainous and hilly regions with an integrated strategy: a longitudinal case study in Sichuan, China. Infect Dis Poverty, 6(1), 79. doi: 10.1186/s40249-017-0290-6
Lucero, D. E., Morrissey, L. A., Rizzo, D. M., Rodas, A., Garnica, R., Stevens, L., . . . Monroy, M. C. (2013). Ecohealth interventions limit triatomine reinfestation following insecticide spraying in La Brea, Guatemala. Am J Trop Med Hyg, 88(4), 630-637. doi: 10.4269/ajtmh.12-0448
Mableson, H. E., Okello, A., Picozzi, K., & Welburn, S. C. (2014). Neglected zoonotic diseases-the long and winding road to advocacy. PLoS Negl Trop Dis, 8(6), e2800. doi: 10.1371/journal.pntd.0002800
Macharia, J. W., Ng'ang'a, Z. W., & Njenga, S. M. (2016). Factors influencing community participation in control and related operational research for urogenital schistosomiasis and soil-transmitted helminths in rural villages of Kwale County, coastal Kenya. Pan Afr Med J, 24, 136. doi: 10.11604/pamj.2016.24.136.7878
Mackey, T. K., & Liang, B. A. (2012). Threats from emerging and re-emerging neglected tropical diseases (NTDs). Infect Ecol Epidemiol, 2. doi: 10.3402/iee.v2i0.18667
Maeda, M.H., & Gurgel-Gonçalves, R. (2012). Conhecimentos e práticas de moradores do Distrito Federal, Brasil, em relação à Doença de chagas e seus vetores. Rev. patol. trop, 41(1), 15-26.
Makaula, P., Sadalaki, J. R., Muula, A. S., Kayuni, S., Jemu, S., & Bloch, P. (2014). Schistosomiasis in Malawi: a systematic review. Parasit Vectors, 7, 570. doi: 10.1186/s13071-014-0570-y
Manderson, L., Aagaard-Hansen, J., Allotey, P., Gyapong, M., & Sommerfeld, J. (2009). Social research on neglected diseases of poverty: continuing and emerging themes. PLoS Negl Trop Dis, 3(2), e332. doi: 10.1371/journal.pntd.0000332
Martindale, S., Mkwanda, S. Z., Smith, E., Molyneux, D., Stanton, M. C., & Kelly-Hope, L. A. (2014). Quantifying the physical and socio-economic burden of filarial lymphoedema in Chikwawa District, Malawi. Trans R Soc Trop Med Hyg, 108(12), 759-767. doi: 10.1093/trstmh/tru154
Mbong, E. N., Sume, G. E., Danbe, F., Kum, W. K., Mbi, V. O., Fouda, A. A., & Atem, P. (2015). Not every worm wrapped around a stick is a guinea worm: a case of Onchocerca volvulus mimicking Dracunculus medinensis. Parasit Vectors, 8, 374. doi: 10.1186/s13071-015-1004-1
McLeroy, K. R., Bibeau, D., Steckler, A., & Glanz, K. (1988). An ecological perspective on health promotion programs. Health Educ Q, 15(4), 351-377.
Merton, Robert King. (1936). The unanticipated consequences of purposive social action. Indianapolis, Indiana: Bobbs-Merrill, College Division.

291 Mewabo, A. P., Moyou, R. S., Kouemeni, L. E., Ngogang, J. Y., Kaptue, L., & Tambo,
E. (2017). Assessing the prevalence of urogenital schistosomaisis and transmission risk factors amongst school-aged children around Mape dam ecological suburbs in Malantouen district, Cameroon. Infect Dis Poverty, 6(1), 40. doi: 10.1186/s40249-017-0257-7
Meymandi, S. K., Forsyth, C. J., Soverow, J., Hernandez, S., Sanchez, D., Montgomery, S. P., & Traina, M. (2017). Prevalence of Chagas Disease in the Latin American-born Population of Los Angeles. Clin Infect Dis, 64(9), 1182-1188. doi: 10.1093/cid/cix064
Moala-Silatolu, A., Nakamura, K., Seino, K., & Kizuki, M. (2012). Greater Adherence to Mass Drug Administration Against Lymphatic Filariasis through Traditional Village Forums in Fiji. J Rural Med, 7(2), 65-72. doi: 10.2185/jrm.7.65
Mojoyinola, J.K. , & Blinkhorn, F.A. . (2013). Impact of Guinea Worm Disease on the socio-economic well-being of a rural community in Oke-Gun areas of Oyo State, Nigeria. International Journal of Health Promotion and Education, 51(4), 180-184.
Molyneux, D. H., & Malecela, M. N. (2011). Neglected tropical diseases and the millennium development goals: why the "other diseases" matter: reality versus rhetoric Parasit Vectors (Vol. 4, pp. 234).
Molyneux, D., & Nantulya, V. (2004). Linking disease control programmes in rural Africa: a pro-poor strategy to reach Abuja targets and millennium development goals. BMJ, 328(7448), 1129-1132. doi: 10.1136/bmj.328.7448.1129
Molyneux, D., & Sankara, D. P. (2017). Guinea worm eradication: Progress and challenges- should we beware of the dog? PLoS Negl Trop Dis, 11(4), e0005495. doi: 10.1371/journal.pntd.0005495
Molyneux, David H. (2017). The London Declaration on Neglected Tropical Diseases: 5 years on. Transactions of the Royal Society of Tropical Medicine and Hygiene.
Monde, C., Syampungani, S., & van den Brink, P. J. (2016). Natural and human induced factors influencing the abundance of Schistosoma host snails in Zambia. Environ Monit Assess, 188(6), 370. doi: 10.1007/s10661-016-5351-y
Monroy, C., Bustamante, D. M., Pineda, S., Rodas, A., Castro, X., Ayala, V., . . . Moguel, B. (2009). House improvements and community participation in the control of Triatoma dimidiata re-infestation in Jutiapa, Guatemala. Cad Saude Publica, 25 Suppl 1, S168-178.
Montenegro, D., Vera, M., Zuleta, L., Llanos, V., & Junqueira, A. (2016). [Strategy for determining a baseline in areas of vector interruption for Chagas disease]. Rev Panam Salud Publica, 39(6), 341-351.
Muela Ribera, J., Hausmann-Muela, S., Gryseels, C., & Peeters Grietens, K. (2016). Re-imagining adherence to treatment from the "other side": local interpretations of adverse anti-malarial drug reactions in the Peruvian Amazon. Malar J, 15, 136. doi: 10.1186/s12936-016-1193-x
Muhumuza, S., Olsen, A., Katahoire, A., Kiragga, A. N., & Nuwaha, F. (2014). Effectiveness of a pre-treatment snack on the uptake of mass treatment for

292
schistosomiasis in Uganda: a cluster randomized trial. PLoS Med, 11(5), e1001640. doi: 10.1371/journal.pmed.1001640
Muhumuza, S., Olsen, A., Katahoire, A., & Nuwaha, F. (2015). Reduced uptake of mass treatment for schistosomiasis control in absence of food: beyond a randomized trial. BMC Infect Dis, 15, 423. doi: 10.1186/s12879-015-1158-7
Munoz-Vilches, M. J., Salas-Coronas, J., Gutierrez-Izquierdo, M. I., Metz, D., Salvador-Sanchez, J., & Gimenez-Sanchez, F. (2013). [Health professionals' knowledge on Chagas disease in the province of Almeria, Spain]. Rev Esp Salud Publica, 87(3), 267-275. doi: 10.4321/S1135-57272013000300006
Mutheneni, S. R., Upadhyayula, S. M., Kumaraswamy, S., Kadiri, M. R., & Nagalla, B. (2015). Impact of socioeconomic factors on the prevalence of lymphatic filariasis in Andhra Pradesh, India. Journal of Public Health-Heidelberg, 23(4), 231-240. doi: 10.1007/s10389-015-0673-8
Mwakitalu, M. E., Malecela, M. N., Pedersen, E. M., Mosha, F. W., & Simonsen, P. E. (2013). Urban lymphatic filariasis in the city of Tanga, Tanzania, after seven rounds of mass drug administration. Acta Tropica, 128(3), 692-700. doi: 10.1016/j.actatropica.2013.10.004
Nandha, B., Krishnamoorthy, K., & Jambulingam, P. (2013). Towards elimination of lymphatic filariasis: social mobilization issues and challenges in mass drug administration with anti-filarial drugs in Tamil Nadu, South India. Health Educ Res, 28(4), 591-598. doi: 10.1093/her/cyt042
Nieto-Sanchez, C., Baus, E. G., Guerrero, D., & Grijalva, M. J. (2015). Positive deviance study to inform a Chagas disease control program in southern Ecuador. Memorias Do Instituto Oswaldo Cruz, 110(3), 299-309. doi: 10.1590/0074-02760140472
Njomo, D. W., Amuyunzu-Nyamongo, M., Magambo, J. K., & Njenga, S. M. (2012). The role of personal opinions and experiences in compliance with mass drug administration for lymphatic filariasis elimination in Kenya. PLoS One, 7(11), e48395. doi: 10.1371/journal.pone.0048395
Noireau, F., Diosque, P., & Jansen, A. M. (2009). Trypanosoma cruzi: adaptation to its vectors and its hosts. Vet Res, 40(2), 26. doi: 10.1051/vetres/2009009
Norman, C. D. (2009). Health promotion as a systems science and practice. J Eval Clin Pract, 15(5), 868-872. doi: 10.1111/j.1365-2753.2009.01273.x
Nwaka, S., Besson, D., Ramirez, B., Maes, L., Matheeussen, A., Bickle, Q., . . . Geary, T. (2011). Integrated dataset of screening hits against multiple neglected disease pathogens. PLoS Negl Trop Dis, 5(12), e1412. doi: 10.1371/journal.pntd.0001412
Obregon, R., Chitnis, K., Morry, C., Feek, W., Bates, J., Galway, M., & Ogden, E. (2009). Achieving polio eradication: a review of health communication evidence and lessons learned in India and Pakistan. Bull World Health Organ, 87(8), 624-630.
Obregon, R., & Waisbord, S. (2010). The complexity of social mobilization in health communication: top-down and bottom-up experiences in polio eradication. J Health Commun, 15 Suppl 1, 25-47. doi: 10.1080/10810731003695367
Obregon, Rafael, Waisbord, Silvio R., Wiley InterScience (Online service), & Alumni and Friends Memorial Book Fund. (2012). The handbook of global health
293
communication Handbooks in communication and media (pp. 1 online resource (xx, 658 p). doi:99953324588
Odhiambo, G. O., Musuva, R. M., Atuncha, V. O., Mutete, E. T., Odiere, M. R., Onyango, R. O., . . . Mwinzi, P. N. (2014). Low levels of awareness despite high prevalence of schistosomiasis among communities in Nyalenda informal settlement, Kisumu city, western Kenya. PLoS Negl Trop Dis, 8(4), e2784. doi: 10.1371/journal.pntd.0002784
Odhiambo, G. O., Musuva, R. M., Odiere, M. R., & Mwinzi, P. N. (2016). Experiences and perspectives of community health workers from implementing treatment for schistosomiasis using the community directed intervention strategy in an informal settlement in Kisumu City, western Kenya. BMC Public Health, 16, 986. doi: 10.1186/s12889-016-3662-0
Okello, A. L., Beange, I., Shaw, A., Moriyon, I., Gabriel, S., Bardosh, K., . . . Welburn, S. C. (2015). Raising the political profile of the neglected zoonotic diseases: three complementary European commission-funded projects to streamline research, build capacity and advocate for control. PLoS Negl Trop Dis, 9(3), e0003505. doi: 10.1371/journal.pntd.0003505
Okorie, P. N., Bockarie, M. J., Molyneux, D. H., & Kelly-Hope, L. A. (2014). Neglected tropical diseases: a systematic evaluation of research capacity in Nigeria. PLoS Negl Trop Dis, 8(8), e3078. doi: 10.1371/journal.pntd.0003078
Omedo, M. O., Matey, E. J., Awiti, A., Ogutu, M., Alaii, J., Karanja, D. M., . . . Mwinzi, P. N. (2012). Community health workers' experiences and perspectives on mass drug administration for schistosomiasis control in western Kenya: the SCORE Project. Am J Trop Med Hyg, 87(6), 1065-1072. doi: 10.4269/ajtmh.2012.12-0435
Omedo, M., Ogutu, M., Awiti, A., Musuva, R., Muchiri, G., Montgomery, S. P., . . . Mwinzi, P. (2014). The effect of a health communication campaign on compliance with mass drug administration for schistosomiasis control in western Kenya--the SCORE project. Am J Trop Med Hyg, 91(5), 982-988. doi: 10.4269/ajtmh.14-0136
Organisation for Economic Co-operation and Development. (2009). Aid effectiveness : a progress report on implementing the Paris Declaration. Paris: OECD.
Ouedraogo, H., Drabo, F., Zongo, D., Bagayan, M., Bamba, I., Pima, T., . . . Zhang, Y. (2016). Schistosomiasis in school-age children in Burkina Faso after a decade of preventive chemotherapy. Bull World Health Organ, 94(1), 37-45. doi: 10.2471/BLT.15.161885
Parker, M., & Allen, T. (2013). Will mass drug administration eliminate lymphatic filariasis? Evidence from northern coastal Tanzania. Journal of biosocial science, 45(4), 517-545.
Pawson, R., Greenhalgh, T., Harvey, G., & Walshe, K. (2005). Realist review--a new method of systematic review designed for complex policy interventions. J Health Serv Res Policy, 10 Suppl 1, 21-34. doi: 10.1258/1355819054308530
Paz-Soldan, V. A., Bauer, K. M., Hunter, G. C., Castillo-Neyra, R., Arriola, V. D., Rivera-Lanas, D., . . . Buttenheim, A. M. (2016). To spray or not to spray?

294
Understanding participation in an indoor residual spray campaign in Arequipa, Peru. Glob Public Health, 1-18. doi: 10.1080/17441692.2016.1178317
Pearce, W. Barnett. (1989). Communication and the human condition. Carbondale: Southern Illinois University Press.
Peeters Grietens, K. , Xuan, X. N., Muela Ribera, J., Duc, T. N., Bortel, Wv, Ba, N. T., . . . Erhart, A. (2012). Social determinants of long lasting insecticidal hammock use among the Ra-glai ethnic minority in Vietnam: implications for forest malaria control. PLoS One, 7(1), e29991. doi: 10.1371/journal.pone.0029991
Pellecer, M. J., Dorn, P. L., Bustamante, D. M., Rodas, A., & Monroy, M. C. (2013). Vector blood meals are an early indicator of the effectiveness of the Ecohealth approach in halting Chagas transmission in Guatemala. Am J Trop Med Hyg, 88(4), 638-644. doi: 10.4269/ajtmh.12-0458
Peters, D. H., Adam, T., Alonge, O., Agyepong, I. A., & Tran, N. (2013). Implementation research: what it is and how to do it. BMJ, 347, f6753. doi: 10.1136/bmj.f6753
Phongluxa, K., van Eeuwijk, P., Soukhathammavong, P. A., Akkhavong, K., & Odermatt, P. (2015). Perceived illness drives participation in mass deworming campaigns in Laos. Acta Tropica, 141(Pt B), 281-288. doi: 10.1016/j.actatropica.2014.03.022
Pokhrel, S., Reidpath, D., & Allotey, P. (2011). Social sciences research in neglected tropical diseases 3: Investment in social science research in neglected diseases of poverty: a case study of Bill and Melinda Gates Foundation. Health Res Policy Syst, 9, 2. doi: 10.1186/1478-4505-9-2
Prichard, R. K., Basanez, M. G., Boatin, B. A., McCarthy, J. S., Garcia, H. H., Yang, G. J., . . . Lustigman, S. (2012). A research agenda for helminth diseases of humans: intervention for control and elimination. PLoS Negl Trop Dis, 6(4), e1549. doi: 10.1371/journal.pntd.0001549
Provecho, Y. M., Gaspe, M. S., Fernandez, M. D. P., & Gurtler, R. E. (2017). House Reinfestation With Triatoma infestans (Hemiptera: Reduviidae) After Community-Wide Spraying With Insecticides in the Argentine Chaco: A Multifactorial Process. J Med Entomol, 54(3), 646-657. doi: 10.1093/jme/tjw224
Quinde-Calderon, L., Rios-Quituizaca, P., Solorzano, L., & Dumonteil, E. (2016). Ten years (2004-2014) of Chagas disease surveillance and vector control in Ecuador: successes and challenges. Trop Med Int Health, 21(1), 84-92. doi: 10.1111/tmi.12620
R Core Team. (2017). R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing.
Rangel, J.A.S., Monreal, L.A., & Ramsey, J.M. . (2016). Resiliencia comunitaria y enfermedad de Chagas en una región rural de México. Revista de Saúde Pública, 50(46).
Reidpath, D. D., Allotey, P., & Pokhrel, S. (2011). Social sciences research in neglected tropical diseases 2: A bibliographic analysis. Health Res Policy Syst, 9, 1. doi: 10.1186/1478-4505-9-1
Roberto, A. J., Murray-Johnson, L., & Witte, K. (2011). International health communication campaigns in developing countries. In T. L. Thompson, R. Parrott

295
& J. F. Nussbaum (Eds.), The Routledge handbook of health communication (2nd ed. ed., pp. 220-234). New York, NY: Routledge.
Rochat, L., Bizzini, A., Senn, N., Bochud, P. Y., Genton, B., & de Valliere, S. (2015). Acute schistosomiasis: a risk underestimated by travelers and a diagnosis frequently missed by general practitioners-a cluster analysis of 42 travelers. J Travel Med, 22(3), 168-173. doi: 10.1111/jtm.12187
Rojas de Arias, A., Ferro, E. A., Ferreira, M. E., & Simancas, L. C. (1999). Chagas disease vector control through different intervention modalities in endemic localities of Paraguay. Bull World Health Organ, 77(4), 331-339.
Rojas-Cortez, M., Pinazo, M. J., Garcia, L., Arteaga, M., Uriona, L., Gamboa, S., . . . Monteiro, F. A. (2016). Trypanosoma cruzi-infected Panstrongylus geniculatus and Rhodnius robustus adults invade households in the Tropics of Cochabamba region of Bolivia. Parasit Vectors, 9, 158. doi: 10.1186/s13071-016-1445-1
Rollinson, D., Knopp, S., Levitz, S., Stothard, J. R., Tchuem Tchuente, L. A., Garba, A., . . . Utzinger, J. (2013). Time to set the agenda for schistosomiasis elimination. Acta Tropica, 128(2), 423-440. doi: 10.1016/j.actatropica.2012.04.013
Rosanti, T. I., Mardihusodo, S. J., & Artama, W. T. (2016). Directly observed treatment increases drug compliance in lymphatic filariasis mass drug administration. Universa Medicina, 35(2), 119-127. doi: 10.1805/UnivMed.2016.v35.119-127
Rosecrans, K., Cruz-Martin, G., King, A., & Dumonteil, E. (2014). Opportunities for improved chagas disease vector control based on knowledge, attitudes and practices of communities in the yucatan peninsula, Mexico. PLoS Negl Trop Dis, 8(3), e2763. doi: 10.1371/journal.pntd.0002763
Sachs, Jeffrey. (2005). The end of poverty : economic possibilities for our time. New York: Penguin Press.
Saldana, Johnny. (2016). The coding manual for qualitative researchers (Third ed.). Los Angeles, Calif. ; London: SAGE.
Salerno, R., Salvatella, R., Issa, J., & Anzola, M. C. (2015). A regional fight against Chagas disease: lessons learned from a successful collaborative partnership. Rev Panam Salud Publica, 37(1), 38-43.
Sanmartino, M., Avaria, A. , Gopmez Prat, J., Parada, M., & Albajar-Viñas, P. (2015). Que no tengan miedo de nosotros: El Chagas según los propios protagonistas. Interface - Comunicação, Saúde, Educação, 19(55), 1063-1075. doi: https://dx.doi.org/10.1590/1807-57622014.1170
Sanmartino, M., & Crocco, L. (2000). [Knowledge about Chagas' disease and risk factors in Argentina communities with different epidemiological trends]. Rev Panam Salud Publica, 7(3), 173-178.
Santos, C. V., Bedin, C., Wilhelms, T. S., & Villela, M. M. (2016). Assessment of the Housing Improvement Program for Chagas Disease Control in the Northwestern municipalities of Rio Grande do Sul, Brazil. Rev Soc Bras Med Trop, 49(5), 572-578. doi: 10.1590/0037-8682-0386-2016
Sartor, P., Colaianni, I., Cardinal, M. V., Bua, J., Freilij, H., & Gurtler, R. E. (2017). Improving access to Chagas disease diagnosis and etiologic treatment in remote rural communities of the Argentine Chaco through strengthened primary health
296
care and broad social participation. PLoS Negl Trop Dis, 11(2), e0005336. doi: 10.1371/journal.pntd.0005336
Saunders, M., Small, A., Dedicoat, M., & Roberts, L. (2012). The development and validation of a risk score for household infestation by Triatoma infestans, a Bolivian vector of Chagas disease. Trans R Soc Trop Med Hyg, 106(11), 677-682. doi: 10.1016/j.trstmh.2012.07.006
Schiavo, Renata. (2014). Health communication : from theory to practice (Second edition. ed.).
Schneider, M. C., Aguilera, X. P., Barbosa da Silva Junior, J., Ault, S. K., Najera, P., Martinez, J., . . . Periago, M. R. (2011). Elimination of neglected diseases in Latin America and the Caribbean: A mapping of selected diseases. PLoS Negl Trop Dis, 5(2), e964. doi: 10.1371/journal.pntd.0000964
Schofield, C. J., & Dias, J. C. (1999). The Southern Cone Initiative against Chagas disease. Adv Parasitol, 42, 1-27.
Secor, W. E. (2015). Early lessons from schistosomiasis mass drug administration programs. F1000Res, 4. doi: 10.12688/f1000research.6826.1
Seddon, T., Billett, S., & Clemans, A. (2004). Politics of social partnerships: a framework for theorizing. Journal of Education Policy, 19(2), 123-142. doi: 10.1080/0144341042000186309
Sheikh, K., Gilson, L., Agyepong, I. A., Hanson, K., Ssengooba, F., & Bennett, S. (2011). Building the field of health policy and systems research: framing the questions. PLoS Med, 8(8), e1001073. doi: 10.1371/journal.pmed.1001073
Sime, H., Deribe, K., Assefa, A., Newport, M. J., Enquselassie, F., Gebretsadik, A., . . . Davey, G. (2014). Integrated mapping of lymphatic filariasis and podoconiosis: lessons learnt from Ethiopia. Parasit Vectors, 7, 397. doi: 10.1186/1756-3305-7-397
Smith, J., & Taylor, E. M. (2013). MDGs and NTDs: reshaping the global health agenda. PLoS Negl Trop Dis, 7(12), e2529. doi: 10.1371/journal.pntd.0002529
Sommerfeld, J., & Kroeger, A. (2015). Innovative community-based vector control interventions for improved dengue and Chagas disease prevention in Latin America: introduction to the special issue. Trans R Soc Trop Med Hyg, 109(2), 85-88. doi: 10.1093/trstmh/tru176
Sommerfeld, J., Ramsay, A., Pagnoni, F., Terry, R. F., Guth, J. A., & Reeder, J. C. (2015). Applied research for better disease prevention and control. PLoS Negl Trop Dis, 9(1), e3378. doi: 10.1371/journal.pntd.0003378
Soriano-Arandes, A., Basile, L., Ouaarab, H., Claveria, I., Gomez i Prat, J., Cabezos, J., . . . Jane, M. (2014). Controlling congenital and paediatric chagas disease through a community health approach with active surveillance and promotion of paediatric awareness. BMC Public Health, 14, 1201. doi: 10.1186/1471-2458-14-1201
Stanton, M. C., Best, A., Cliffe, M., Kelly-Hope, L., Biritwum, N. K., Batsa, L., & Debrah, A. (2016). Situational analysis of lymphatic filariasis morbidity in Ahanta West District of Ghana. Trop Med Int Health, 21(2), 236-244. doi: 10.1111/tmi.12643
297 Stanton, M., Molineux, A., Mackenzie, C., & Kelly-Hope, L. (2016). Mobile Technology
for Empowering Health Workers in Underserved Communities: New Approaches to Facilitate the Elimination of Neglected Tropical Diseases. JMIR Public Health Surveill, 2(1), e2. doi: 10.2196/publichealth.5064
Strauss, Anselm L., & Corbin, Juliet M. (1998). Basics of qualitative research : techniques and procedures for developing grounded theory (2nd ed.). Thousand Oaks: Sage Publications.
Streiger, M, Mainero, M.C., Bizai, M.L., Fabbro, D., Mendicino, D., Barco, M., . . . Arias, E. (2012). Perspectiva interdisciplinaria para el abordaje de una enfermedad infecciosa: chagas o tripanosomiasis americana. Rev. salud pública (Córdoba), 16(1).
Suarez-Davalos, V., Dangles, O., Villacis, A. G., & Grijalva, M. J. (2010). Microdistribution of sylvatic triatomine populations in central-coastal Ecuador. J Med Entomol, 47(1), 80-88.
Suddaby, R. (2006). From the editors: What grounded theory is not. Academy of Management Journal, 49(4), 633-642.
Taket, A. R. (2009). Theorising social exclusion. London ; New York: Routledge. Tarleton, R. L., Gurtler, R. E., Urbina, J. A., Ramsey, J., & Viotti, R. (2014). Chagas
disease and the london declaration on neglected tropical diseases. PLoS Negl Trop Dis, 8(10), e3219. doi: 10.1371/journal.pntd.0003219
Tavory, I. (2016). The pragmatist wave of theory construction. Br J Sociol, 67(1), 50-56. doi: 10.1111/1468-4446.12187
Tavory, I., & Timmermans, S. (2014). Abductive analysis : theorizing qualitative research. Chicago: The University of Chicago Press.
Thomas, J., & Harden, A. (2008). Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol, 8, 45. doi: 10.1186/1471-2288-8-45
Thomson, H., & Petticrew, M. (2007). Housing and health - Heating improvements may hold most promise for developing healthy housing policy. British Medical Journal, 334(7591), 434-435. doi: 10.1136/bmj.39133.558380.BE
Thomson, H., Sellstrom, E., & Thomas, S. (2007). Housing improvement as a strategy to improve health and reduce health inequalities: a systematic review of best available evidence. European Journal of Public Health, 17, 127-127.
Thomson, H., Thomas, S., Sellstrom, E., & Petticrew, M. (2008). Best available evidence on housing improvement and health: A systematic review. Journal of Epidemiology and Community Health, 62, A4-A5.
Timmermans, S., & Tavory, I. (2007). Advancing Ethnographic Research through Grounded Theory Practice. In A. Bryant & K. Charmaz (Eds.), The Sage Handbook of Grounded Theory (pp. 493-512). USA: Sage Publications.
Timmermans, S., & Tavory, I. (2012). Theory construction in qualitative research: From grounded theory to abductive analysis. Sociological Theory, 30(3), 167-186. doi: 10.1177/0735275112457914
Tracy, Sarah J. (2013). Qualitative research methods : collecting evidence, crafting analysis, communicating impact. Chichester, West Sussex, UK: Wiley-Blackwell.

298 Triana, D. R., Mertens, F., Zuniga, C. V., Mendoza, Y., Nakano, E. Y., & Monroy, M. C.
(2016). The Role of Gender in Chagas Disease Prevention and Control in Honduras: An Analysis of Communication and Collaboration Networks. Ecohealth, 13(3), 535-548. doi: 10.1007/s10393-016-1141-9
Tufte, Thomas, & Mefalopulos, Paolo. (2009). Participatory communication : a practical guide. Washington, D.C.: World Bank.
Turner, M.M., Skubisz, C., & Rimal, R.N. (2011). Theory and practice in risk communication: A review of the literature and visions of the future. In T. L. Thompson, R. Parrott & J. F. Nussbaum (Eds.), The Routledge Handbook of health communication (Second ed.). New York: Routledge.
Uneke, C. J., Ezeoha, A. E., Uro-Chukwu, H., Ezeonu, C. T., Ogbu, O., Onwe, F., & Edoga, C. (2015). Enhancing the Capacity of Policy-Makers to Develop Evidence-Informed Policy Brief on Infectious Diseases of Poverty in Nigeria. Int J Health Policy Manag, 4(9), 599-610. doi: 10.15171/ijhpm.2015.100
Upadhyayula, S. M., Mutheneni, S. R., Kadiri, M. R., Kumaraswamy, S., & Nagalla, B. (2012). A cohort study of lymphatic filariasis on socio economic conditions in Andhra Pradesh, India. PLoS One, 7(3), e33779. doi: 10.1371/journal.pone.0033779
Valdez-Tah, A., Huicochea-Gomez, L., Ortega-Canto, J., Nazar-Beutelspacher, A., & Ramsey, J. M. (2015). Social Representations and Practices Towards Triatomines and Chagas Disease in Calakmul, Mexico. PLoS One, 10(7), e0132830. doi: 10.1371/journal.pone.0132830
Vale, G. A., Chamisa, A., Mangwiro, C., & Torr, S. J. (2013). A neglected aspect of the epidemiology of sleeping sickness: the propensity of the tsetse fly vector to enter houses. PLoS Negl Trop Dis, 7(2), e2086. doi: 10.1371/journal.pntd.0002086
Valente, T. W., & Fosados, R. (2006). Diffusion of innovations and network segmentation: the part played by people in promoting health. Sex Transm Dis, 33(7 Suppl), S23-31. doi: 10.1097/01.olq.0000221018.32533.6d
Ventura-Garcia, L., Roura, M., Pell, C., Posada, E., Gascon, J., Aldasoro, E., . . . Pool, R. (2013). Socio-cultural aspects of Chagas disease: a systematic review of qualitative research. PLoS Negl Trop Dis, 7(9), e2410. doi: 10.1371/journal.pntd.0002410
Viotti, R., Alarcon de Noya, B., Araujo-Jorge, T., Grijalva, M. J., Guhl, F., Lopez, M. C., . . . Latin American Network for Chagas Disease, Nhepacha. (2014). Towards a paradigm shift in the treatment of chronic Chagas disease. Antimicrob Agents Chemother, 58(2), 635-639. doi: 10.1128/AAC.01662-13
Visser, B. J. (2012). Dracunculiasis eradication--finishing the job before surprises arise. Asian Pac J Trop Med, 5(7), 505-510. doi: 10.1016/S1995-7645(12)60088-1
Wakefield, M. A., Loken, B., & Hornik, R. C. (2010). Use of mass media campaigns to change health behaviour. Lancet, 376(9748), 1261-1271. doi: 10.1016/S0140-6736(10)60809-4
Waleckx, E., Camara-Mejia, J., Ramirez-Sierra, M. J., Cruz-Chan, V., Rosado-Vallado, M., Vazquez-Narvaez, S., . . . Dumonteil, E. (2015). An innovative ecohealth

299
intervention for Chagas disease vector control in Yucatan, Mexico. Trans R Soc Trop Med Hyg, 109(2), 143-149. doi: 10.1093/trstmh/tru200
Wang, S., Carlton, E. J., Chen, L., Liu, Y., & Spear, R. C. (2013). Evaluation of an educational intervention on villagers' knowledge, attitude and behaviour regarding transmission of Schistosoma japonicum in Sichuan province, China. Acta Tropica, 127(3), 226-235. doi: 10.1016/j.actatropica.2013.05.009
Wanzirah, H., Tusting, L. S., Arinaitwe, E., Katureebe, A., Maxwell, K., Rek, J., . . . Lindsay, S. W. (2015). Mind the gap: house structure and the risk of malaria in Uganda. PLoS One, 10(1), e0117396. doi: 10.1371/journal.pone.0117396
Webster, J. P., Gower, C. M., Knowles, S. C., Molyneux, D. H., & Fenton, A. (2016). One health - an ecological and evolutionary framework for tackling Neglected Zoonotic Diseases. Evol Appl, 9(2), 313-333. doi: 10.1111/eva.12341
Whitty, C. J. (2015). Political, social and technical risks in the last stages of disease eradication campaigns. Int Health, 7(5), 302-303. doi: 10.1093/inthealth/ihv049
Wijesinghe, R. S., & Wickremasinghe, A. R. (2015). Physical, psychological, and social aspects of quality of life in filarial lymphedema patients in Colombo, Sri Lanka. Asia Pac J Public Health, 27(2), NP2690-2701. doi: 10.1177/1010539511434140
World Health Organization. (2012a). Global Report for Research on Infectious Diseases of Poverty. Geneva: WHO/TDR on behalf of Special Programme for Research and Training in Tropical Diseases (TDR).
World Health Organization. (2012b). Research priorities for Chagas disease, human African trypanosomiasis and leishmaniasis. World Health Organ Tech Rep Ser(975), v-xii, 1-100.
World Health Organization. (2015). Chagas disease in Latin America: an epidemiological update based on 2010 estimates. Wkly Epidemiol Rec, 90(6), 33-43.
Yevstigneyeva, V., Camara-Mejia, J., & Dumonteil, E. (2014). Analysis of children's perception of triatomine vectors of chagas disease through drawings: opportunities for targeted health education. PLoS Negl Trop Dis, 8(10), e3217. doi: 10.1371/journal.pntd.0003217
Yoshioka, K. (2013). Impact of a community-based bug-hunting campaign on Chagas disease control: a case study in the department of Jalapa, Guatemala. Mem Inst Oswaldo Cruz, 108(2), 205-211.
Zeldenryk, L., Gray, M., Gordon, S., Speare, R., & Hossain, M. (2014). The use of focus groups to develop a culturally relevant quality of life tool for lymphatic filariasis in Bangladesh. Qual Life Res, 23(1), 299-309. doi: 10.1007/s11136-013-0455-0
Ziperstein, J., Dorkenoo, M., Datagni, M., Drexler, N., Murphy, M., Sodahlon, Y., & Mathieu, E. (2014). Final program evaluation methods and results of a National Lymphedema Management Program in Togo, West Africa. J Epidemiol Glob Health, 4(2), 125-133. doi: 10.1016/j.jegh.2013.11.001

300
Appendix A: Interview Guide for HHHL Partner Families
Title of Research: Towards a theory and scaling up strategy of a model for sustainable prevention of Chagas disease: An ethnographic grounded theory study
Date: Interviewee (position in the family): Age: Introduction Thank you so much for welcoming me into your house and accepting talking to me. I would like to talk to you today about the use you give to your home. The questions I am going to ask to you are about activities you conduct inside and outside the house, as well as your cleaning and maintenance practices. I also would like to know about the changes you have experienced after occupying this new space. In case that you want to participate in this study, I’ll check with you a document in which I explain that all the information you share with me during this interview will be confidential, that I will protect your privacy, and that you can refuse to answer any question or stop this interview at any given time. Once you have signed that document, we can start with the interview. Administration: The following set of questions will be considered generative and will be asked to all the participants. Follow up questions will be introduced as a result of their answers. Considering the length of this questionnaire, this interview can be administered by specific segments. Informed consent will be obtained in each administration. Before and after implementing the Healthy Homes for Healthy Living Model
How do you remember the previous house? What do you remember of the design process? Why did you decide to accept the proposal suggested by HHHL? What is your most important memory of the construction process? In your opinion, what is the most significant change that has occurred after the
construction of the new house? Have you identified any negative impact? What do you think is the most significant change experienced by the family in
general? Have you noticed any change at the community level? How have your neighbors
reacted to the new construction? What do you think of the house? What do you think of the new peridomicile? Are there any new activities that you do in this house that you did not use to do in
the old house? Are there activities that you use to do in the previous house that you do not do in
the new house? Are there new people living in your house now?

301
Is there any particular place of the old house that you miss/want back? Why? Is there any particular spot of the house that you particularly like? Would you like
to take a picture of it? Why do you like it?
Vector transmission control
• Have you seen chinchorros inside the new house? Can you remember where and which time of the year? Have you seen them lately?
• Have you seen chinchorros in the patio of your house? Where and in which time of the year? Have you seen them once the construction was completed?
• Have you seen any other bug inside he house lately? Did you use to see them more often in your previous house?
• What use do you give to doors and windows? Have you had any problem using them?
Intersection with sanitation and water sources
Where does your family usually take showers? Has this changed after the construction was complete?
Where does you family Do you have any sanitary facility? Does you family use it? Where do disposal go
to? Has this changed since the construction was completed? Where does the water you use at home come from? Where does trash go?
Management of zoonotic aspects of Chagas disease
• Where were domestic animals placed before the construction? Where are they placed now?
• Have you noticed important changes in these animals as a result of this change? • What is the main use you give to the animals present in your patio? • What are the main activities you conduct in domestic and peridomestic areas of
your home? • What are the main uses you give to the plants around the home? • Have you seen squirrels and raposas around your home? • What do you use the piles of materials stored around the home? • Where do you store crops and tools?
Community participation
In which moments during the construction process did you count with the help of other members of the community?
What do you think of their help?

302
Would have you liked to count with more support form other members of the community in this process?
How did the adobe factory work? What do you think of the idea of producing abobe as an income generation
alternative for members of the community? Why? If that is the case, how should it work? What do you thin of working with other community members in productive
activities? Which comments have you received of other community members about the new
house? How have your neighbors reacted to the new house?
Integration with the health sector
Did any institution help you out during the constriction process? Which ones? Do you think this house protects the health of your family? If so, how? Has any member of you family felt sick in the last weeks? If that was the case,
which type of treatment did they receive? Has any member of your family visited any doctor in the last few weeks? What
was the reason? Do you have medicinal plants around your house? Would you like to have some?
Family economy
How did you fund the construction process? Did you get any financial commitment to complete the payment for the house? How was the economic situation of the family before the construction? How was the economic situation of the family during the construction? How is the economic situation of the family after the construction? Are you spending more money now? If so, how?
Future plans
What would you like to do with your house in the future? What would you like to change of this house if you could? What do you think is
necessary to accomplish this change? How do you picture this house in five years? How do you picture it in 20 years
from now? How do you imagine your community in ten years from now?
303
Appendix B: Socio-economic Survey for Communities at Large
Title of Research: Towards a theory and scaling up strategy of a model for sustainable prevention of Chagas disease: An ethnographic grounded theory study
Community: Home code: Date: Interviewer: Interviewee (position in the family): Age: N. Question Answers Codes Follow up question
1 Who lives in your house?
Relationship, ages, sex, permanent or temporal
2 Is any member of your
immediate family living in another city?
Yes 1 Where? No 2
DN/DA 99
3 Who is the breadwinner in the house?
Mom 1 Why? Dad 2
Both 3 Children 4 Other? 99
4 Do you have legal titles
over the land where your house is bult?
Yes 1 Why? No 2
DN/DA 99
5 Do you have legal titles over the land you work?
Yes 1 Why? No 2
DN/DA 99
6 How long have you lived in this house?
7 How long ago was this
house built?
8 Have you modified this house recently?
Yes 1 How? No 2

304
DN/DA 99
9 How far is the closest road?
More than 1 hour 1 How ofthen do you go to that road?
Between 1 and 2 hours 2
More than two hours 3 DN/DA 99
10 Which form of transport do you use more often?
Car 1
What do you use this form transport for? How frequently?
Ranchera 2 Animal 3 Walking 4 Other? 5 DN/DA 99
11 How necessary do tou
think it is to improve the structure of your home?
Not necessary 1 Why? Small need 2 Somehow needed 3 Needed 4 Really needed 5 DN/DA 99
12 How urgent do tou think
it is to improve the structure of your home?
Not urgent 1 Why? Not very urgent 2 Somehow urgent 3 Urgent 4 Very urgent 5 DN/DA 99
13 if you could, which part of the house would you
like to modify first?
Roof 1
Which kind of improvement would you like to carry out?
windows 2 Floors 3 Walls 4 Doors 5 DN/DA 99
14 if you could, which part
of the peridomicile would you like to modify first?
Fence Why? Door Garen Animal shelters

305
Storage Other
15 Would you like to rebuild your house entirely?
Yes 1 Why? No 2 Maybe 3 DA/NA 99
16 If that is the case, which materila would you use?
Adobe 1 Why? Bricks 2 Cement 3 Block 4 Other 5 DN/DA 99
17
Have you heard of the houses built by Catholic
University (Healthy Homes for Healthy
Living)?
Yes 1 What is your opinion about these homes?
No 2
DN/DA 99
18
Have you or any other member of your family
participated in any of the construction activities
associated with HHHL?
Yes 1 Which ones? No 2
DN/DA 99
19 Would you like your
house to participate of a similar process?
Yes 1 Why? No 2 DN/DA 99
20
Nothing 11
Which resources would you be willing to invest to fund this improvement?
Savings 1 How much?
Products' commerce 2 What kind of products?
Animal's commerce 3 What kind of animals?
Loans with family and
friends 4 Remittances 5

306
Credits with the national
government 6 Credits with banks 7 ¿Cuáles bancos?
Labor 8 Loans with small
funding agencies 9 Other? 10 ¿Cuál?
DN/DA 99
21 Which of the following activities do you work
on?
Farmer in your own plot 1 Which one of these is your main activity?
Farmer in somebody else's plot 2
Do other members of your family work in any of the previous activities?
Construction worker 3
How frequently does the head of household travel to other regiosn to find jobs?
Driver 4 To which regions? Animals raising 5
Day laborer 6 Other 7
22 Do you receive any
subsidy from the government?
Yes 1 Who was it assigned to? When did you get it? How muh did you get?
NO 2
DN/DA 99 23 Have you received any Yes 1 Who was it assigned

307
subsidy from MIDUVI? NO 2 to? When did you get it? How muh did you get? DN/DA 99
24 Does anybody in the
house receive the disability subsidy?
Yes 1 Who was it assigned to? When did you get it? How muh did you get?
NO 2
DN/DA 99
25 Do you have access to the community water system
in your community?
Yes 1 Why? Did you participate in that process? For how long?
NO 2
DN/DA 99
26
Which of the following options do you use more often for your sanitary
needs?
Toilet 1 Latrine 2 Bushes 3 DN/DA 99
Open water source (River/lake/stream/pond)
1 Why?
27 Where does the water you
use for cooking come from? Bore hole/well
2
Tap 3 Other 4 Kitchen 1 Why? Outside the house 2
28 Where do you cook? Bedroom 3 Other? 4
29 What is the most common source of energy for cooking in the house?
Gas 1 Why?
Firewood 2 Other? 3
30
What did you invest your money in durimg the last month?
Food 1 What was the most importat expense you had to assume? Health 2
Home refurbishment 3 Education 4 Animals' care 5
Agricultural production 6 Transportation 7 Other 8
31 Are you insured to the Yes 1 Why? Which services

308
Farmers' insurance? No 2 do you receive?
DN/DA 99
32 Are you member of any local organization?
Farmers organization 1 Which one? What do you think of it?
Savings cooperative 2 Artisans 3 Union 4 Other? DN/DA 99
33 Do you know if this organization funds housing projects?
Yes 1 NO 2 DN/DA 99
34 In dolars, how much is the monthly income of
your family?
Under 100 1 Where does this income come from?
Between 100 and 300 2
Between 300 and 500 3 More than 500 4 DN/DA 99
35 Are there times of the
year in which your income increases?
January-March 1 Which ones? April-June 2 July- September 3 October-December 4 DN/DA 99
36 In those times of the year,
how much does your income increase?
Up to 100 1 Why?
Bteween 100 and 300 2 More than 300 3 DN/DA 4
37 Are there times of the
year in which your income decreases?
January-March 1 Which ones?
April-June 2 July- September 3 October-December 4 DN/DA 99
38 In those times of the year,
how much does your income decrease?
Up to 100 1 Why?
Bteween 100 and 300 2 More than 300 3

309
DN/DA 99
39 Would you like to stay in this community for the
next five years?
Yes 1 Why?
NO 2 DN/DA 99
40
Have you participated in any of the activities
conducted by the Healthy Living Initiative?
Yes 1 Which ones? Why?
NO 2
DN/DA 99
41 Do you have any question for us?

!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
!!
Thesis and Dissertation Services
Top Related
Copyright © 2022 FDOKUMEN

