







Bahasa
Halaman
Hukum


500835-L-os-Dieleman500835-L-os-Dieleman500835-L-os-Dieleman500835-L-os-Dieleman Processed on: 12_10_2015Processed on: 12_10_2015Processed on: 12_10_2015Processed on: 12_10_2015
THE UTERINENICHE IN THE
CAESAREAN SCARImaging, symptoms
and risk factors
Marjolein Dieleman-
Bij de Vaate
THE U
TERINE N
ICHE IN
THE CAESAREAN
SCAR M
arjolein Dielem
an-Bij de Vaate
UITNODIGING
voor het bijwonen van de openbare verdediging van
mijn proefschrift
The uterine niche in the caesarean scar
Imaging, symptoms and risk factors
Op woensdag 27 januari 2016 om 11.45 uur in de aula van de
Vrije Universiteit,De Boelelaan 1105
te Amsterdam
Na afloop bent u van harte welkom op de receptie
ter plaatse
PARANIMFEN
Inge Bij de Vaate&
Marja-Liisa Hendriks
Marjolein Dieleman-Bij de Vaate
Amersfoortseweg 523951 LC Maarn
500835-os-Dieleman.indd 1 19-11-15 08:39


500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
THE UTERINE NICHE IN THE CAESAREAN SCARImaging, symptoms and risk factors
Marjolein Dieleman - Bij de Vaate

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
The uterine niche in the caesarean scarImaging, symptoms and risk factors
Marjolein Dieleman-Bij de Vaate
Thesis VU University Medical Center, Amsterdam – with summary in Dutch.
The studies in this thesis were performed at the Department of Obstetrics and Gynaecology, VU University Medical Center, Amsterdam, and the Department of Obstetrics and Gynaecology, St. Antonius Hospital, Nieuwegein.
Financial support for printing of this thesis was kindly provided by
Biomedic B.V., BMA BV (Mosos), Olympus Nederland B.V., Covidien
Cover design: François DielemanLay-out: Brenda Knoll (persoonlijkproefschrift.nl)Printed by: Ipskamp Drukkers
Copyright © 2015, A.J.M. Dieleman-Bij de Vaate, Amsterdam, The NetherlandsNo part of this thesis may be reproduced in any form or by any means, by print, photocopy, microfilm, or any other means without permission of the author.
ISBN: 978-94-6259-964-2 (printed version)ISBN: 978-94-6259-965-9 (digital version)

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
VRIJE UNIVERSITEIT
THE UTERINE NICHE IN THE CAESAREAN SCARImaging, symptoms and risk factors
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad Doctor aande Vrije Universiteit Amsterdam,
op gezag van de rector magnificusprof.dr. V. Subramaniam,
in het openbaar te verdedigenten overstaan van de promotiecommissie
van de Faculteit der Geneeskundeop woensdag 27 januari 2016 om 11.45 uur
in de aula van de universiteit,De Boelelaan 1105
door
Antoinet Johanna Marjolein Bij de Vaate
geboren te Utrecht

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
promotor: prof.dr. H.A.M. Brölmanncopromotor: dr. J.A.F. Huirne

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Table of contents
Chapter 1
PART I Diagnostics
Chapter 2
Chapter 3
PART II Gynaecological symptoms and risk factors
Chapter 4
Chapter 5
Chapter 6
PART III Niche pregnancy
Chapter 7
Chapter 8
Chapter 9
Appendices
General introduction
Reproducibility of three-dimensional ultrasound for the measurement of a niche in a caesarean scar and assessment of its shape (Eur J Obstet Gynecol Reprod Biol 2015)
Ultrasound evaluation of the Cesarean scar: relation between a niche and postmenstrual spotting (Ultrasound Obstet Gynecol 2011)
Long-term complications of caesarean section. The niche in the scar: a prospective cohort study on niche prevalence and its relation to abnormal uterine bleeding (BJOG 2014)
Prevalence, potential risk factors for development and symptoms related to the presence of uterine niches following Cesarean section: systematic review (Ultrasound Obstet Gynecol 2014)
Therapeutic options of caesarean scar pregnancy: case series and literature review (J Clin Ultrasound 2010)
General discussion and future perspectives
Summary
Nederlandse samenvatting
List of publications
Dankwoord
About the author
Gel instillation sonohysterography (GIS) and saline contrast sonohysterography (SCSH): comparison of two diagnostic techniques (Ultrasound Obstet Gynecol 2010)
7
15
25
39
53
71
105
123
134
138
145
149
155

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
11|General introductionGeneral introduction

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
General introduction
In recent decades, the percentage of caesarean deliveries has increased in most developed countries. There are some well-known complications, such as uterine rupture and pathologically adherent placenta in future pregnancy.1,2
Only recently, the presence of a niche at the site of a caesarean scar in the uterus has been observed.3-6 A niche is mainly a sonographic finding and has been defined as an indentation representing myometrial discontinuity at the site of the caesarean scar that communicates with the uterine or cervical cavity as seen on contrast-enhanced sonohysterography (SHG)7 (Figure 1). Alternative terms for a niche are caesarean scar defect3,8,9, deficient caesarean scar10, diverticulum11, pouch5 and isthmocele12. We believe that the terms ‘deficient’ or ‘defect’ should be avoided, as they imply a relationship between the appearance of a niche and function13, particularly in a future pregnancy, and therefore we prefer the term niche.
8 | Chapter 1
Figure 1: Longitudinal section of a uterus, performed with the use of contrast-enhanced sonohysterography. The black arrow shows the niche at the site of the caesarean scar.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
General introduction | 9
1
ImagingUntil now, there is no gold standard for the detection and measurement of a niche. The niche is mostly evaluated with the use of transvaginal sonography (TVS)4,8-
10,14,15 and SHG4,15-19, and a minority is evaluated with the use of hysteroscopy5,12,16 or hysterosalpingography11. TVS without contrast is a widely used method to identify niches, but SHG may facilitate their detection as it provides a more clear delineation of a niche as the uterine cavity is filled with a contrast medium18. Using saline as a contrast medium is called saline contrast sonohysterography (SCSH) and filling the uterine cavity with gel is called gel instillation sonohysterography (GIS). A problem that occurs during SCSH is unstable filling and inadequate distension of the uterine cavity owing to backflow of saline. As gel has a higher viscosity, GIS may produce a more stable filling of the uterine cavity.20 However, it is unknown if GIS is a better diagnostic method in comparison with the more regularly used SCSH for examination of the uterine cavity. No consensus exists regarding the gold standard for the detection and measurement of a niche. As a result, a wide range in niche prevalence has been reported up to now, and each study uses different methods for niche measurement. In addition, no studies have been performed yet in which the reproducibility of niche measurement was evaluated in non-pregnant women. Risk factorsAs mentioned above, there is a wide range in the reported prevalence of a niche. For TVS, the prevalence varies between 42% and 70% in studies with a random population of women with a history of one or multiple caesarean sections (CSs)3,8,18 and the prevalence for SHG varies between 58% and 84% in studies with a random population.6,15,18 If also studies with a selected population of women with gynaecological symptoms are included, then there is even more variation in prevalence.9,10,16,17,21,22 We do know from these studies that not all women with a history of CS develop a niche. Therefore, it is relevant to study risk factors for the development of niches and risk factors for the development of symptoms in women undergoing a CS.
SymptomsThere is growing interest in possible associations between the presence of a niche and various gynaecological symptoms, and in the mechanisms behind the development of these symptoms. Several studies reported that there is a relation between the presence of a niche and postmenstrual spotting.5,9,19 Different hypotheses have been postulated to explain the aetiology of bleeding disorders in relation to a niche. Postmenstrual spotting may be due to the retention of menstrual blood in the niche, which is intermittently expelled after the majority

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
10 | Chapter 1
of the menstruation has ceased.19,23 This may depend on poor contractility of the uterine muscle around the scar19 and the presence of (fibrotic) tissue below the niche, which may impair the drainage of menstrual flow through the cervix23. At the time of designing our two prospective cohort studies, large prospective cohort studies that consecutively included women with a history of CS and assessed the association between a niche and abnormal uterine bleeding, were lacking. Other reported symptoms in women with a niche are dysmenorrhea, chronic pelvic pain, dyspareunia and urinary symptoms.9 In addition, a pregnancy may develop in a niche, which is a rare form of ectopic pregnancy. The incidence of caesarean scar pregnancies (CSPs) ranges from 1:1800-1:2216 pregnancies and constitutes 6.1% of all ectopic pregnancies in patients with a history of at least 1 caesarean delivery.24,25 Because a CSP can lead to uterine scar rupture and haemorrhage, a life threatening condition for both mother and child may occur if the pregnancy is allowed to continue, even in the first trimester.26 However, there is still no consensus about an optimal treatment modality for a CSP.
Aim of this thesisThe aim of this thesis is to evaluate the diagnostics (part I), clinical consequences of a niche and risk factors (part II), and treatment modalities of a niche pregnancy (part III). The studies aim to answer the following questions:
Part I (diagnostics)- What is the difference between saline contrast sonohysterography (SCSH) and gel instillation sonohysterography (GIS) as diagnostic method for the evaluation of the uterine cavity? Which technique is preferable?- What is the reproducibility of the measurement of the size and volume of a niche, its residual myometrial thickness (RMT) and assessment of its shape, with the use of three-dimensional (3D) ultrasound volumes?- What is the prevalence of a niche in women with a history of CS using both TVS and SHG?
Part II (gynaecological symptoms and risk factors)- What is the relationship between the presence of a niche and abnormal uterine bleeding and urinary symptoms?- Are sonographic features of a niche, such as niche size and volume, related to these symptoms?- What are risk factors for the development of a niche?
Part III (niche pregnancy)- What is the best treatment modality for a CSP?

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
General introduction | 11
1
Outline of the thesisThe first part of this thesis focuses on sonographic evaluation of the uterus, including the niche. In the second part, risk factors for a niche and niche related symptoms are evaluated. In the last part of this thesis, treatment modalities for a niche pregnancy are described.
Chapter 2 compares the effect of two different types of distension fluid, either saline or gel, on diagnostic features in the evaluation of intrauterine abnormalities and patient discomfort during SHG in a prospective cohort study. In chapter 3, the inter- and intraobserver agreement for the measurement and assessment of niches is evaluated using stored 3D TVS volumes.
In Chapters 4 and 5, the prevalence of a niche and related symptoms are evaluated in two different cohort studies with different populations, using both TVS and GIS. In chapter 4, 3D SHG is also used for the assessment of niche volume. Chapter 6 is a systematic review of the medical literature, evaluating the prevalence of a niche using various diagnostic methods, potential risk factors for the development of a niche and niche-related gynaecological symptoms in non-pregnant women.
Chapter 7 reports 4 cases of women with a CSP and their treatment and follow-up. An overview of the literature is provided concerning treatment and follow-up of CSPs. Based on our experience and the literature, treatment recommendations for CSP are given.
In Chapter 8, we discuss the results of our studies and clinical implications, and we will provide suggestions for future research. Finally, a summary of this thesis in English and Dutch is provided in Chapter 9.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
12 | Chapter 1
1. Clark SL, Koonings PP Phelan JP. Placenta previa/accreta and prior cesarean section. Obstet Gynecol 1985; 66: 89-92.
2. Diaz SD, Jones JE, Seryakov M Mann WJ. Uterine rupture and dehiscence: ten-year review and case-control study. South Med J 2002; 95: 431-435.
3. Armstrong V, Hansen WF, Van Voorhis BJ Syrop CH. Detection of cesarean scars by transvaginal ultrasound. Obstet Gynecol 2003; 101: 61-65.
4. Bij de Vaate AJ, Brolmann HA, van der Voet LF, van der Slikke JW, Veersema S Huirne JA. Ultrasound evaluation of the Cesarean scar: relation between a niche and postmenstrual spotting. Ultrasound Obstet Gynecol 2011; 37: 93-99.
5. Fabres C, Aviles G, De La Jara C, Escalona J, Munoz JF, Mackenna A, Fernandez C, Zegers-Hochschild F Fernandez E. The cesarean delivery scar pouch: clinical implications and diagnostic correlation between transvaginal sonography and hysteroscopy. J Ultrasound Med 2003; 22: 695-700; quiz 701-692.
6. Regnard C, Nosbusch M, Fellemans C, Benali N, van Rysselberghe M, Barlow P Rozenberg S. Cesarean section scar evaluation by saline contrast sonohysterography. Ultrasound Obstet Gynecol 2004; 23: 289-292.
7. Bij de Vaate AJ, van der Voet LF, Naji O, Witmer M, Veersema S, Brolmann HA, Bourne T Huirne JA. Prevalence, potential risk factors for development and symptoms related to the presence of uterine niches following Cesarean section: systematic review. Ultrasound Obstet Gynecol 2014; 43: 372-382.
8. Osser OV, Jokubkiene L Valentin L. High prevalence of defects in Cesarean section scars at transvaginal ultrasound examination. Ultrasound Obstet Gynecol 2009; 34: 90-97.
9. Wang CB, Chiu WW, Lee CY, Sun YL, Lin YH Tseng CJ. Cesarean scar defect: correlation between Cesarean section number, defect size, clinical symptoms and uterine position. Ultrasound Obstet Gynecol 2009; 34: 85-89.
10. Ofili-Yebovi D, Ben-Nagi J, Sawyer E, Yazbek J, Lee C, Gonzalez J Jurkovic D. Deficient lower-segment Cesarean section scars: prevalence and risk factors. Ultrasound Obstet Gynecol 2008; 31: 72-77.
11. Surapaneni K Silberzweig JE. Cesarean section scar diverticulum: appearance on hysterosalpingography. AJR Am J Roentgenol 2008; 190: 870-874.
12. Borges LM, Scapinelli A, de Baptista Depes D,
Lippi UG Coelho Lopes RG. Findings in patients with postmenstrual spotting with prior cesarean section. J Minim Invasive Gynecol 2010; 17: 361-364.
13. Naji O, Abdallah Y, Bij De Vaate AJ, Smith A, Pexsters A, Stalder C, McIndoe A, Ghaem-Maghami S, Lees C, Brolmann HA, Huirne JA, Timmerman D Bourne T. Standardized approach for imaging and measuring Cesarean section scars using ultrasonography. Ultrasound Obstet Gynecol 2012; 39: 252-259.
14. Chen HY, Chen SJ Hsieh FJ. Observation of cesarean section scar by transvaginal ultrasonography. Ultrasound Med Biol 1990; 16: 443-447.
15. Menada Valenzano M, Lijoi D, Mistrangelo E, Costantini S Ragni N. Vaginal ultrasonographic and hysterosonographic evaluation of the low transverse incision after caesarean section: correlation with gynaecological symptoms. Gynecol Obstet Invest 2006; 61: 216-222.
16. El-Mazny A, Abou-Salem N, El-Khayat W Farouk A. Diagnostic correlation between sonohysterography and hysteroscopy in the assessment of uterine cavity after cesarean section. Middle East Fertil Soc J 2011; 16: 72-76.
17. Monteagudo A, Carreno C Timor-Tritsch IE. Saline infusion sonohysterography in nonpregnant women with previous cesarean delivery: the “niche” in the scar. J Ultrasound Med 2001; 20: 1105-1115.
18. Osser OV, Jokubkiene L Valentin L. Cesarean section scar defects: agreement between transvaginal sonographic findings with and without saline contrast enhancement. Ultrasound Obstet Gynecol 2010; 35: 75-83.
19. Thurmond AS, Harvey WJ Smith SA. Cesarean section scar as a cause of abnormal vaginal bleeding: diagnosis by sonohysterography. J Ultrasound Med 1999; 18: 13-16; quiz 17-18.
20. Exalto N, Stappers C, van Raamsdonk LA Emanuel MH. Gel instillation sonohysterography: first experience with a new technique. Fertil Steril 2007; 87: 152-155.
21. Chang Y, Tsai EM, Long CY, Lee CL Kay N. Resectoscopic treatment combined with sonohysterographic evaluation of women with postmenstrual bleeding as a result of previous cesarean delivery scar defects. Am J Obstet Gynecol 2009; 200: 370 e371-374.
22. Uppal T, Lanzarone V Mongelli M. Sonographically detected caesarean section scar defects and
References

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
General introduction | 13
1
menstrual irregularity. J Obstet Gynaecol 2011; 31: 413-416.
23. Fabres C, Arriagada P, Fernandez C, Mackenna A, Zegers F Fernandez E. Surgical treatment and follow-up of women with intermenstrual bleeding due to cesarean section scar defect. J Minim Invasive Gynecol 2005; 12: 25-28.
24. Jurkovic D, Hillaby K, Woelfer B, Lawrence A, Salim R Elson CJ. First-trimester diagnosis and management of pregnancies implanted into the lower uterine segment Cesarean section scar. Ultrasound Obstet Gynecol 2003; 21: 220-227.
25. Seow KM, Huang LW, Lin YH, Lin MY, Tsai YL Hwang JL. Cesarean scar pregnancy: issues in management. Ultrasound Obstet Gynecol 2004; 23: 247-253.
26. Fylstra DL. Ectopic pregnancy within a cesarean scar: a review. Obstet Gynecol Surv 2002; 57: 537-543.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
22|Gel instillation sonohysterography (GIS) and Gel instillation sonohysterography (GIS) and
saline contrast sonohysterography (SCSH): saline contrast sonohysterography (SCSH): comparison of two diagnostic techniquescomparison of two diagnostic techniques
A.J.M. Bij de VaateA.J.M. Bij de VaateH.A.M. Brölmann H.A.M. Brölmann
J.W. van der Slikke J.W. van der Slikke M.H. Emanuel M.H. Emanuel
J.A.F. HuirneJ.A.F. Huirne
Ultrasound Obstet Gynecol 2010;35(4):486-9.Ultrasound Obstet Gynecol 2010;35(4):486-9.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Abstract
ObjectiveTo compare gel instillation sonohysterography (GIS) with saline contrast sonohysterography (SCSH) as diagnostic methods for the evaluation of the uterine cavity.
MethodsA prospective cohort study was performed at the Department of Obstetrics and Gynecology of the VU University Medical Center, Amsterdam, between September 2007 and April 2008. We included 65 women suspected of having an intrauterine abnormality with an indication for SCSH/GIS. First SCSH and subsequently GIS were performed in all women. Distension of the uterine cavity, image quality, visualization of intrauterine abnormalities and pain experienced on a visual analog scale (VAS score) were recorded for both procedures.
ResultsThe mean distension with GIS was 9.0 mm and with SCSH it was 8.5 mm (P = 0.15). The mean image quality, on a scale from 0 to 5, for SCSH was 4.0 and for GIS it was 3.6 (P = 0.01). No difference was found for the visualization of intrauterine abnormalities, and the VAS scores for pain experienced on SCSH and GIS were 1.5 and 1.6, respectively (P = 0.62).
ConclusionsThe image quality of SCSH is slightly better than that of GIS. This difference is likely to be attributable to the presence of air bubbles in the gel. The small difference in uterine cavity distension in favor of GIS and comparable stable distension during at least 4 min make GIS a suitable alternative for SCSH if air bubbles can be prevented.
16 | Chapter 2

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Introduction
Abnormal uterine bleeding is highly prevalent and an important factor in female health. Saline contrast sonohysterography (SCSH) is an appropriate technique for the detection of focally growing lesions such as polyps and fibroids1,2. With a sensitivity of 0.95 and a specificity of 0.88 it is an accurate diagnostic tool in the evaluation of the uterine cavity in premenopausal and postmenopausal women3. The uterine cavity is distended with physiological saline, which serves as a contrast medium and enables visualization of the endometrial surface. A problem that occurs during SCSH is unstable filling and inadequate distension of the uterine cavity owing to backflow of saline. In addition, patients experience discomfort owing to fluid leakage. In trying to overcome these disadvantages, the SCSH technique can be modified by instilling gel instead of saline. In one study hydroxyethyl glycerin gel was used, showing good distension and stable filling without backflow problems4. Comparison of both procedures has not been published yet. The purpose of this study was to compare gel instillation sonohysterography (GIS) with SCSH as diagnostic methods for the evaluation of the uterine cavity, with the focus on distension of the cavity.
Methods
This study was performed at our department of obstetrics and gynecology between September 2007 and April 2008. Women attending the department and suspected of having an intrauterine abnormality were asked to participate in the study. The following were used as inclusion criteria: all premenopausal women with abnormal uterine bleeding; postmenopausal women with abnormal uterine bleeding and endometrial thickness > 4 mm; women with infertility in combination with irregular endometrium and/or endometrial thickness > 10 mm; women with a history of premature birth in combination with irregular endometrium and/or endometrial thickness > 10 mm. Because of logistic reasons inclusion was not possible on certain days, while on other days women who met the inclusion criteria were included consecutively. Exclusion criteria were risk of pelvic inflammatory disease, presence of cervical cancer, pregnancy or being premenopausal and in the luteal phase without use of contraception.
Gynecologists and sufficiently trained residents performed first SCSH and subsequently GIS with the Goldstein Sonohysterography Catheter, which is 26 cm in length and 2.4 mm in diameter (Cook Medical, Spencer, USA). Most patients were pretreated with a non-steroidal anti-inflammatory drug (500 mg naprosine 1 day and 1 h before the procedure). Before performing SCSH, sterile saline
Comparison of SCSH with GIS | 17
2
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
18 | Chapter 2
was flushed through the catheter to rid it of small amounts of air and the cervix was cleaned with povidone–iodine solution. The catheter was inserted through the cervical canal and the ‘acorn’ of the catheter was adjusted at the external cervical os to reduce leakage of instilled saline. The transvaginal transducer was introduced and real-time ultrasonographic imaging (Accuvix XQ, Medison, Korea) was performed with the simultaneous, continuous instillation of sterile saline solution (0.9% sodium chloride) into the uterine cavity. Distension was assessed by measuring the greatest distance between the anterior and posterior uterine walls in the midsagittal section. A score between 0 and 5 was given for image quality, with 0 expressing low image quality and 5 expressing high image quality with optimal visualization. The score was based on the following criteria: contrast, sharpness and brightness of the image; air bubbles and other artifacts; distension; visualization in case of an intrauterine abnormality (e.g. contrast around the abnormality, possibility of assessing the intracavitary protrusion). In case of an intrauterine abnormality, the sonographer recorded the nature (e.g. submucous fibroid, polyp, Müllerian duct anomaly or artifact). The women were asked to express the pain experienced during instillation of the fluid using a visual analog scale (VAS), which is a measure of pain intensity, with 0 equivalent to no pain and 10 equivalent to the worst pain imaginable.
Immediately after this procedure GIS was performed with the same catheter and with the use of Endosgel (Farco-Pharma, Köln, Germany) instead of saline solution. Endosgel is a sterile gel preparation, which has long been used by urologists for intraurethral instillation before cystoscopy, and contains chlorhexidine gluconate, sodium lactate, methyl hydroxybenzoate, propyl hydroxybenzoate, hydroxyethylcellulose and purified water. A syringe was connected to the base of the catheter, which was still located in the uterine cavity. A vacuum was created in the curette by withdrawing the plunger and negative pressure was applied until no fluid appeared in the catheter. A syringe was filled with Endosgel, connected to the base of the catheter and realtime ultrasonographic imaging was performed with the simultaneous instillation of gel. The instillation of gel was stopped when the patient felt slight menstrual-like cramps, backflow started or a maximum of 10 mL had been reached. The greatest distance between the anterior and posterior walls was measured, a score for the image quality and pain (VAS) during instillation of gel was given, and the presence of intrauterine abnormalities was recorded.
To evaluate the distension in time with GIS, distension curves were created. The distension in five consecutive women who were suspected of having an intrauterine abnormality was measured at different time points between 0 and 5 min after the instillation of gel and removal of the catheter.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Comparison of SCSH with GIS | 19
2
Statistical analysisThe primary outcome was a difference in distension of the uterine cavity. A difference of 1.5 mm in distension was considered to be clinically relevant. Because of a lack of prior studies and in order to prevent an underpowered study, a standard deviation of 4.0 mm was chosen to perform a power calculation. To achieve 80% power and an alpha of 5%, 56 women would be needed to detect a difference of 1.5 mm in distension. Anticipating technical or procedural failures, we decided to include 65 patients.
The difference in distension between SCSH and GIS was evaluated with the paired samples t-test and the difference in visualization of intrauterine abnormalities was tested with the chi-square test. The Wilcoxon signed-rank test was used to evaluate the difference in quality of the ultrasound images and VAS score. All statistical analysis was performed two-sided using Statistical Packages for the Social Sciences software (SPSS, Inc., Chicago, IL, USA), and P of less than 0.05 was considered statistically significant.
Results
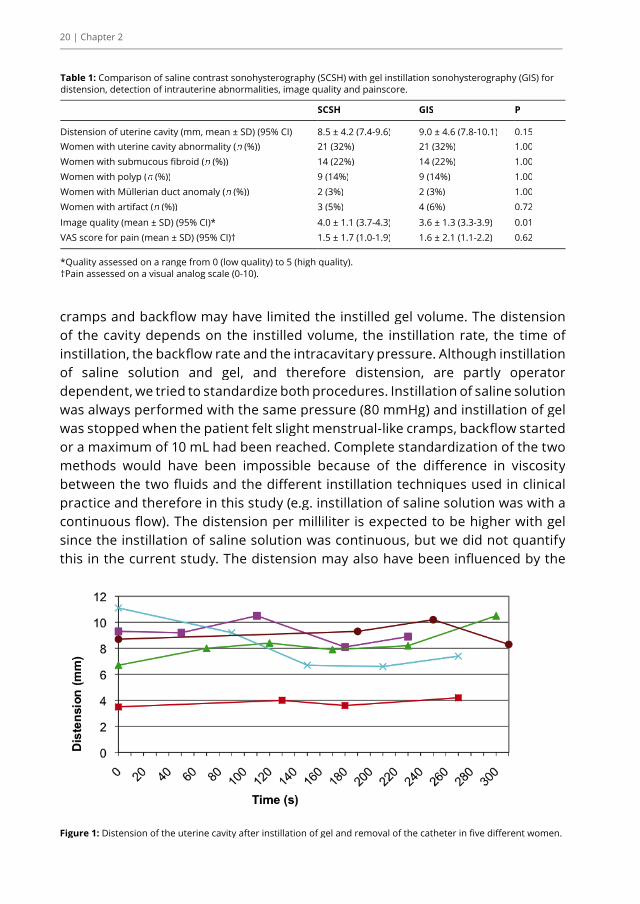
SCSH and GIS were performed in 65 women suspected of having an intrauterine abnormality, after they had given informed consent. Most women undergoing SCSH/GIS had complained of heavy and/or irregular menstrual bleeding (49%) or infertility (20%). The findings for SCSH and GIS are presented in Table 1. Distension after GIS was slightly higher than with SCSH (9.0 mm vs. 8.5 mm), but this difference did not reach statistical significance (P = 0.15). All relevant intrauterine abnormalities detected with SCSH were also identified using GIS (P = 1.00): 14 fibroids (22%), nine polyps (14%) and two Müllerian duct anomalies (3%). Four (6%) artifacts (not air bubbles) were seen with GIS, while three (5%) were seen with SCSH (P = 0.72). The mean image quality for SCSH and GIS was 4.0 and 3.6, respectively, on a scale from 0 to 5 (P = 0.01). The pain experienced was comparable for SCSH and GIS, with mean VAS scores of 1.5 and 1.6, respectively (P = 0.62). Distension curves were created for five women, and show that the distension was stable during at least 4–5 min (Figure 1).
Discussion
Distension of the uterine cavity was 6% greater when using GIS than when using SCSH but this difference did not reach statistical significance. We expected more distension with GIS owing to the higher viscosity of the gel, but menstrual-like
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
20 | Chapter 2
Figure 1: Distension of the uterine cavity after instillation of gel and removal of the catheter in five different women.
Table 1: Comparison of saline contrast sonohysterography (SCSH) with gel instillation sonohysterography (GIS) for distension, detection of intrauterine abnormalities, image quality and painscore.
SCSH GIS P
Distension of uterine cavity (mm, mean ± SD) (95% CI) 8.5 ± 4.2 (7.4-9.6) 9.0 ± 4.6 (7.8-10.1) 0.15Women with uterine cavity abnormality (n (%))n (%))n 21 (32%) 21 (32%) 1.00Women with submucous fibroid (n (%))n (%))n 14 (22%) 14 (22%) 1.00Women with polyp (n (%))n (%))n 9 (14%) 9 (14%) 1.00Women with Müllerian duct anomaly (n (%))n (%))n 2 (3%) 2 (3%) 1.00Women with artifact (n (%))n (%))n 3 (5%) 4 (6%) 0.72
Image quality (mean ± SD) (95% CI)* 4.0 ± 1.1 (3.7-4.3) 3.6 ± 1.3 (3.3-3.9) 0.01VAS score for pain (mean ± SD) (95% CI)† 1.5 ± 1.7 (1.0-1.9) 1.6 ± 2.1 (1.1-2.2) 0.62
*Quality assessed on a range from 0 (low quality) to 5 (high quality). †Pain assessed on a visual analog scale (0-10).
cramps and backflow may have limited the instilled gel volume. The distension of the cavity depends on the instilled volume, the instillation rate, the time of instillation, the backflow rate and the intracavitary pressure. Although instillation of saline solution and gel, and therefore distension, are partly operator dependent, we tried to standardize both procedures. Instillation of saline solution was always performed with the same pressure (80 mmHg) and instillation of gel was stopped when the patient felt slight menstrual-like cramps, backflow started or a maximum of 10 mL had been reached. Complete standardization of the two methods would have been impossible because of the difference in viscosity between the two fluids and the different instillation techniques used in clinical practice and therefore in this study (e.g. instillation of saline solution was with a continuous flow). The distension per milliliter is expected to be higher with gel since the instillation of saline solution was continuous, but we did not quantify this in the current study. The distension may also have been influenced by the

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Comparison of SCSH with GIS | 21
2
study design, since SCSH was always performed first and we did not succeed in all cases in removing the saline solution from the cavity completely. Nevertheless, it seems likely that the remainder of the saline solution was expelled by the gel through the cervix or Fallopian tubes.
It would have been appropriate to report the proportion of cases reaching a certain threshold volume using each technique, but the disadvantage with this approach is that the appropriate threshold volume is different for every woman and this would be difficult to assess. Our previous experience has suggested that greater distension results in better image quality and we therefore decided to compare the maximum uterine distension observed during each of the two procedures.
The image quality for SCSH was better than that for GIS. It must be noted that the score was a subjective impression, and therefore observer bias cannot be excluded. An important reason for the difference in quality is the presence of air bubbles in the gel. The currently used GIS technique may not be optimal in terms of avoiding air bubbles, because the syringe was filled manually with Endosgel. In addition, the catheter was not removed from the uterine cavity between SCSH and GIS in order to reduce inconvenience for the patient, although filling the catheter with gel before entering the uterine cavity may have reduced the occurrence of air bubbles. Another hypothesis is that the presence of air bubbles may have been promoted by rising temperature, negative pressure while filling the syringe, turbulence during gel instillation and dissolved molecules.
For better performance of GIS, commercial products are available containing gel with a smaller amount of dissolved molecules, no need to transfer the gel manually from one syringe to another and with a special cervical applicator preventing cervical backflow or leakage. It may be questioned whether a difference of 10% in image quality (4.0 vs. 3.6 on a scale from 0 to 5) should be considered clinically relevant, since intrauterine abnormalities could be visualized by SCSH as well as GIS in all cases. On the other hand, performing GIS after SCSH in all women may have caused review bias, because visualization of an abnormality with the first procedure makes it easier to recognize the same abnormality using the second procedure. Although it would have been appropriate to use a cross-over design, it appeared that it would be impossible to clear all the gel from the uterus and perform SCSH immediately afterwards. Alternatively, we could have chosen to perform GIS and SCSH at different times by different examiners, blinded to the results of the other test. However, we did not use this design for two reasons: inconvenience to the patient at having to undergo the same procedure twice; and interobserver variation. Future studies may overcome this problem by recording

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
22 | Chapter 2
both SCSH and GIS for retrospective random assessment by independent examiners blinded to the results of the tests.
The mean VAS score for pain during fluid instillation was low and practically the same for both SCSH and GIS, which demonstrates that both procedures are well tolerated. In our experience, the introduction of the speculum and catheter causes more discomfort than the instillation of saline solution or gel. Because SCSH was always performed first, the pain score of SCSH may have been influenced by insertion of the catheter. Therefore, a cross-over design would have been more appropriate.
GIS is an easy diagnostic method to perform and the higher viscosity of the gel causes less fluid leakage. Although backflow could not be prevented completely, Figure 1 demonstrates that GIS gives stable distension during at least 4–5 min, which is sufficient to complete the ultrasound evaluation. Small fluctuations of the distension in time may be caused by contractions of the uterine muscle.
The introduction of three-dimensional (3D) ultrasound enhances visualization of the uterine cavity, and improves diagnostic accuracy of SCSH or GIS5. Gel is considered to be advantageous when performing 3D ultrasound. More stable filling of the uterine cavity without continuous flow of fluid allows extension of the observation time, resulting in better 3D sonohysterographic images with fewer artifacts and moving tissue elements4.
We have noticed that some women experience vasovagal cramps after GIS. To prevent this discomfort, the amount of gel should be as small as possible. With an average of 4 mL, an optimal distension of the uterine cavity can be achieved4.
In conclusion, a small but significant difference in image quality between GIS and SCSH was found in favor of SCSH, which may be caused by the presence of air bubbles while performing GIS. This disadvantage of GIS may be less prominent if another technique is used (e.g. use of commercially available prefilled gel syringes). With a comparable low level of experienced pain, the slightly higher distension with GIS makes it a suitable alternative to SCSH if air bubbles can be prevented. Moreover, a beneficial effect of GIS is expected for 3D ultrasonography and it must be questioned if GIS should replace SCSH when using two-dimensional (2D) imaging. Additional prospective studies should be performed to determine the diagnostic accuracy of 2D and 3D GIS in comparison with SCSH, in which both procedures are assessed independently and preferably blinded.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Comparison of SCSH with GIS | 23
2
References1. Goldstein SR, Zeltser I, Horan CK, Snyder JR,
Schwartz LB. Ultrasonography-based triage for perimenopausal patients with abnormal uterine bleeding. Am J Obstet Gynecol 1997; 177: 102–108.
2. Dijkhuizen FP, De Vries LD, Mol BW, Brölmann HA, Peters HM, Moret E, Heintz AP. Comparison of transvaginal ultrasonography and saline infusion sonography for the detection of intracavitary abnormalities in premenopausal women. Ultrasound Obstet Gynecol 2000; 15: 372–376.
3. de Kroon CD, de Bock GH, Dieben SWM, Jansen FW. Saline contrast hysterosonography in abnormal uterine bleeding: a systematic review and meta-analysis. BJOG 2003; 110: 938–947.
4. Exalto N, Stappers C, van Raamsdonk LAM, Emanuel MH. Gel instillation sonohysterography: first experience with a new technique. Fertil Steril 2007; 87: 152–155.
5. de Kroon CD, Louwe LA, Trimbos JB, Jansen FW. The clinical value of 3-dimensional saline infusion sonography in addition to 2-dimensional saline infusion sonography in women with abnormal uterine bleeding: work in progress. J Ultrasound Med 2004; 23: 1433–1440.
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
33|Reproducibility of three-dimensional Reproducibility of three-dimensional
ultrasound for the measurement of ultrasound for the measurement of a niche in a caesarean scar and a niche in a caesarean scar and
assessment of its shapeassessment of its shape
A.J. Marjolein Bij de VaateA.J. Marjolein Bij de VaateIngeborg H. LinskensIngeborg H. LinskensLucet F. van der VoetLucet F. van der Voet
Jos W.R. TwiskJos W.R. TwiskHans A.M. BrölmannHans A.M. Brölmann
Judith A.F. HuirneJudith A.F. Huirne
Eur J Obstet Gynecol Reprod Biol 2015;188:39-44.Eur J Obstet Gynecol Reprod Biol 2015;188:39-44.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Abstract
ObjectiveTo evaluate the inter- and intraobserver agreement for measurement of the size and volume of a niche and assessment of the shape, with the use of three-dimensional (3D) ultrasound.
Study designIn this reproducibility study, 20 3D ultrasound volumes of uteri with a niche were selected, based on complete visualisation of the uterus and niche in both the longitudinal and transversal plane. Niche measurements were performed off-line twice by one observer and once by another observer. Niche measurements and assessment of shape were performed in the longitudinal and transversal plane, and niche volume in the longitudinal plane.
The mean difference, 95% limits of agreement, the intraclass correlation coefficient (ICC) and Cohen’s kappa were calculated to assess the inter- and intraobserver agreement.
ResultsThe interobserver agreement was excellent for all niche measurements (ICC >0.86), including depth and residual myometrial thickness (RMT), except for width at niche base in the transversal plane (ICC 0.74) and niche volume (ICC 0.79), which were classified as good agreement. Wide limits of agreement and a high mean difference were found for maximal width in the transversal plane.
The intraobserver agreement was excellent for all measurements (ICC >0.80), except for RMT in the longitudinal and transversal plane, which were classified as good agreement (ICC 0.73 and 0.62, respectively). Wide limits of agreement were found for maximal width and width at niche base in the transversal plane.The overall agreement in the transversal plane was lower than in the longitudinal plane, but still all in the range of good agreement. The inter- and intraobserver agreement was good to poor for the assessment of niche shape.
ConclusionUsing 3D ultrasound, various niche parameters, including depth (both perpendicular to niche base and maximal depth), maximal width, width at niche base, RMT and volume, can be measured with a high level of agreement, in particular if measured in the longitudinal plane.
26 | Chapter 3

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Introduction
Since the turn of the century, the interest for the uterine niche has increased. A niche can be observed during sonography at the site of the uterine caesarean scar and has been defined as any indentation representing myometrial discontinuity at the site of a caesarean scar that communicates with the uterine or cervical cavity [1]. The diagnostic method for the detection of a niche is mainly transvaginal sonography (TVS) and contrast-enhanced sonohysterography (SHG). The prevalence of a niche in a random population of women with a history of caesarean section (CS) differs between 24% and 70% for TVS and between 56% and 84% for SHG [1].
Apart from the well-known complications, such as uterine rupture and caesarean scar pregnancy, there are indications that a niche is responsible for symptoms, such as postmenstrual spotting [2], [3], [4] and [5] and subfertility [3]. One study reported a relatively large volume of a niche in women with postmenstrual spotting [2] and another study reported a larger width of the niche in women with postmenstrual spotting, dysmenorrhea and chronic pelvic pain [5]. Interest is growing to learn which niches are responsible for symptoms. Therefore, different classifications for niches have been used, based on size [6] and [7] or shape [2]. However, there is no agreement about a definition for the various subgroups of niches, neither how to measure the niche.
In order to be able to compare studies concerning niche prevalence, classification, size and symptoms, we formulated definitions for the used niche parameters and methods for assessment that may be used for future studies. No studies have been performed up to now, in which the reproducibility of the measurement of a niche was evaluated in non-pregnant women. The objective of the current study is to evaluate the inter- and intraobserver agreement for measurement of the size and volume of a niche, and assessment of the shape, with the use of 3D ultrasound volumes.
Materials and methods
This inter- and intraobserver study was conducted in January 2014 at the Department of Obstetrics and Gynaecology of the VU University Medical Center in Amsterdam. Transvaginal ultrasound images of uteri without using contrast in women with a history of CS were stored for research purposes between 2007 and 2012. The images were performed using an Accuvix ultrasound machine (Medison, Hoofddorp, The Netherlands; currently Samsung Medison) in women
Reproducibility study of niche measurement | 27
3

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
28 | Chapter 3
with their bladder empty. Stored 3D volumes, acquired in the longitudinal plane, of uteri with a niche were selected for this inter- and intraobserver study. Informed consent of all women was obtained at the time of inclusion and the study was approved by the local research ethics committee.
From a data set of 150 anonymized volumes, the first 20 3D volumes with complete visualisation of the uterus and niche in both the longitudinal and transversal plane were selected for both the inter- and intraobserver study. The images were measured twice by one observer (M.B.) in a different random order, with a time interval between the two measurements of four weeks. For the evaluation of the interobserver agreement, another observer (I.L.) performed the same measurements once. The first measurements of the first observer were selected for assessment of interobserver variability and the observers were blinded to each other’s results. The measurements were performed off-line with the use of off-line software (Medison XI Viewer) in the longitudinal and transversal plane.
The most optimal midsagittal section of the uterus was obtained by rotating around the x- and y-axis. The lower uterine segment was examined in the longitudinal plane to identify the area likely to contain the niche. The section with the largest surface area of the niche was identified. In case of multiple previous CSs and multiple niches, measurements of the largest niche were recorded. The uterus was rotated around the z-axis to obtain the base of the niche in the horizontal position in order to simplify the measurements. The image was zoomed if necessary and the measurements were performed with the calliper placed on the inner border of the endometrium.
The following measurements were performed in the longitudinal plane with the Calliper function of the MultiSlice mode (Fig. 1):- Residual myometrial thickness (RMT) (1): measured from the serosal surface of the uterus (without the white lining of the serosa) or if extraperitoneally where the myometrium ended, to the apex of the niche, perpendicular to niche base.- Depth, perpendicular to niche base (2).- Maximal depth (3): distance between apex of the niche and the estimated middle of the niche base.- Maximal width (4): perpendicular to the line between middle of the niche base and apex (3).- Width at niche base (5).
The niche shape was assessed according to a specified classification, which was also used for a previously published study [2]: triangle, semicircle, rectangle, circle, droplet and inclusion cysts (Fig. 2). The volume of the niche was measured

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Reproducibility study of niche measurement | 29
3
in the longitudinal plane with the use of the eXtended Imaging Virtual Organ Computer-aided Analysis program. The mode “manual 10—planes” was chosen and a diagram of 10 parallel sections of the niche was displayed on the screen. After manual outline of the external niche surface in all selected planes, the software automatically provided the volume of the niche (Fig. 3).
With the niche visible in the longitudinal plane and the blue dot located at the base of the niche, the transversal plane (B plane) was obtained. The section in which the niche had its maximal surface area was identified, and the uterus was rotated around the z-axis to obtain the endometrium (base of the niche) in the horizontal position in order to simplify the measurements. The same measurements as performed in the longitudinal plane were completed in the transversal plane (Fig. 4). In addition, the niche shape according to the same classification (Fig. 2) was recorded.
Figure 1: Niche measurements in the longitudinal plane. 1=residual myometrial thickness; 2=depth perpendicular to niche base; 3=maximal depth; 4=maximal width; 5=width at niche base.
Figure 1: Niche measurements in the longitudinal plane.1=residual myometrial thickness; 2=depth perpendicular to niche base; 3=maximal depth; 4=maximal width; 5=width at niche base.
Figure 2: Classification used to assess the shape of the niche.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
30 | Chapter 3
StatisticsData were analysed using SPSS version 20.0 (SPSS Inc., Chicago, IL, USA). For inter- and intraobserver agreement, the mean difference, 95% limits of agreement and the intraclass correlation coefficient (ICC) were calculated. Bland–Altman plots were used to determine whether the difference was influenced by the magnitude of the measurements [8] and [9]. Cohen’s kappa was calculated for the agreement for categorical variables (i.e. niche shape). For both ICC and kappa, values between 1.0 and 0.81 were considered to show excellent agreement, 0.80–0.61 good, 0.60–0.41 moderate, 0.40–0.21 fair and 0.20–0.00 poor agreement [10].
Figure 4: Niche measurements in the transversal plane.1=residual myometrial thickness; 2=depth perpendicular to niche base; 3=maximal depth; 4=maximal width; 5=width at niche base.
Figure 3: Volume measurement of the niche, demonstrating manual outline of the niche of five of the ten sections, and the calculated volume.
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Reproducibility study of niche measurement | 31
3
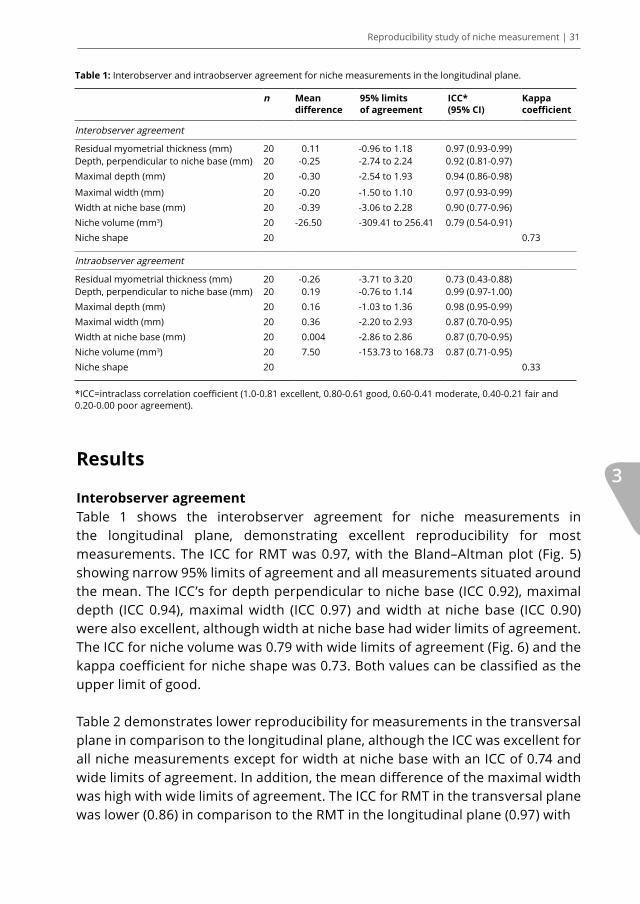
Table 1: Interobserver and intraobserver agreement for niche measurements in the longitudinal plane.
n Mean difference
95% limits of agreement
ICC* (95% CI)
Kappa coefficient
Interobserver agreement
Residual myometrial thickness (mm) 20 0.11 -0.96 to 1.18 0.97 (0.93-0.99)Depth, perpendicular to niche base (mm) 20 -0.25 -2.74 to 2.24 0.92 (0.81-0.97)Maximal depth (mm) 20 -0.30 -2.54 to 1.93 0.94 (0.86-0.98)
Maximal width (mm) 20 -0.20 -1.50 to 1.10 0.97 (0.93-0.99)Width at niche base (mm) 20 -0.39 -3.06 to 2.28 0.90 (0.77-0.96)Niche volume (mm3) 20 -26.50 -309.41 to 256.41 0.79 (0.54-0.91)Niche shape 20 0.73
Intraobserver agreement
Residual myometrial thickness (mm) 20 -0.26 -3.71 to 3.20 0.73 (0.43-0.88)Depth, perpendicular to niche base (mm) 20 0.19 -0.76 to 1.14 0.99 (0.97-1.00)Maximal depth (mm) 20 0.16 -1.03 to 1.36 0.98 (0.95-0.99)Maximal width (mm) 20 0.36 -2.20 to 2.93 0.87 (0.70-0.95)Width at niche base (mm) 20 0.004 -2.86 to 2.86 0.87 (0.70-0.95)Niche volume (mm3) 20 7.50 -153.73 to 168.73 0.87 (0.71-0.95)Niche shape 20 0.33
*ICC=intraclass correlation coefficient (1.0-0.81 excellent, 0.80-0.61 good, 0.60-0.41 moderate, 0.40-0.21 fair and 0.20-0.00 poor agreement).
Results
Interobserver agreementTable 1 shows the interobserver agreement for niche measurements in the longitudinal plane, demonstrating excellent reproducibility for most measurements. The ICC for RMT was 0.97, with the Bland–Altman plot (Fig. 5) showing narrow 95% limits of agreement and all measurements situated around the mean. The ICC’s for depth perpendicular to niche base (ICC 0.92), maximal depth (ICC 0.94), maximal width (ICC 0.97) and width at niche base (ICC 0.90) were also excellent, although width at niche base had wider limits of agreement. The ICC for niche volume was 0.79 with wide limits of agreement (Fig. 6) and the kappa coefficient for niche shape was 0.73. Both values can be classified as the upper limit of good.
Table 2 demonstrates lower reproducibility for measurements in the transversal plane in comparison to the longitudinal plane, although the ICC was excellent for all niche measurements except for width at niche base with an ICC of 0.74 and wide limits of agreement. In addition, the mean difference of the maximal width was high with wide limits of agreement. The ICC for RMT in the transversal plane was lower (0.86) in comparison to the RMT in the longitudinal plane (0.97) with

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
32 | Chapter 3
Figure 5: Bland-Altman plots showing inter- and intraobserver agreement for residual myometrial thickness (RMT) for the longitudinal and transversal plane. Mean (——) and 95% limits of agreement (------) are shown.
Figure 6: Bland-Altman plots showing inter- and intraobserver agreement for niche volume. Mean (——) and 95% limits of agreement (------) are shown.
Diff
eren
ce o
bser
ver
1 - o
bser
ver
2 (m
m)
Diff
eren
ce m
easu
rem
ent 1
- m
easu
rem
ent 2
(mm
)D
iffer
ence
obs
erve
r 1
- obs
erve
r 2
(mm
3)
Diff
eren
ce m
easu
rem
ent 1
- m
easu
rem
ent 2
(mm
3)D
iffer
ence
mea
sure
men
t 1 -
mea
sure
men
t 2 (m
m)
Diff
eren
ce o
bser
ver
1 - o
bser
ver
2 (m
m)
Mean of RMT (mm): interobserver, longitudinal plane Mean of RMT (mm): interobserver, transversal plane
Mean of RMT (mm): intraobserver, longitudinal plane
Mean of niche volume (mm3): interobserver Mean of niche volume (mm3): intraobserver
Mean of RMT (mm): intraobserver, transversal plane

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Reproducibility study of niche measurement | 33
3
Table 2: Interobserver and intraobserver agreement for niche measurements in the transversal plane.
n Mean difference
95% limits of agreement
ICC* (95% CI) Kappa coefficient
Interobserver agreement
Residual myometrial thickness (mm) 20 0.56 -2.56 to 3.67 0.86 (0.68-0.94)Depth, perpendicular to niche base (mm) 20 -0.67 -2.44 to 1.10 0.96 (0.90-0.98)Maximal depth (mm) 20 -0.41 -2.28 to 1.46 0.95 (0.89-0.98)Maximal width (mm) 20 -1.35 -4.82 to 2.12 0.95 (0.87-0.98)Width at niche base (mm) 20 -0.72 -7.14 to 5.69 0.74 (0.46-0.89)Niche shape 20 0.50
Intraobserver agreement
Residual myometrial thickness (mm) 20 -0.71 -5.80 to 4.37 0.62 (0.26-0.83)Depth, perpendicular to niche base (mm) 20 0.20 -2.20 to 2.61 0.91 (0.78-0.96)Maximal depth (mm) 20 0.43 -2.56 to 3.43 0.86 (0.68-0.94)Maximal width (mm) 20 0.18 -4.47 to 4.83 0.88 (0.73-0.95)Width at niche base (mm) 20 0.25 -4.86 to 5.36 0.80 (0.57-0.92)Niche shape 20 0.04
*ICC=intraclass correlation coefficient (1.0-0.81 excellent, 0.80-0.61 good, 0.60-0.41 moderate, 0.40-0.21 fair and 0.20-0.00 poor agreement).
wider limits of agreement (Fig. 5). The kappa coefficient for niche shape in the transversal plane was 0.50.
Intraobserver agreementThe intraobserver agreement in the longitudinal plane was excellent for depth perpendicular to niche base (ICC 0.99), maximal depth (ICC 0.98), maximal width (ICC 0.87), width at niche base (ICC 0.87) and volume (ICC 0.87). Maximal width and width at niche base had both rather wide limits of agreement (Table 1). The intraobserver agreement for RMT was good (ICC 0.73) with wide limits of agreement as shown by the Bland–Altman plot (Fig. 5). The kappa coefficient for niche shape was 0.33.
Also for the intraobserver analyses applies that measurements in the transversal plane were less reproducible than measurements in the longitudinal plane as shown by lower ICC values and wider limits of agreement (Table 2). The ICC for RMT was 0.62 with wide limits of agreement. All other intraobserver measurements in the transveral plane showed excellent agreement, although the limits of agreement were wide for maximal width and width at niche base. The kappa coefficient for niche shape was very low (0.04).

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
34 | Chapter 3
Comment
Main findingsWe demonstrated that both depth perpendicular to niche base and maximal depth can be measured with a high level of agreement. The level of agreement is also high for maximal width and width at niche base if measured in the longitudinal plane, but lower for the same measurements in the transversal plane. Measurement of RMT and volume are reasonably reproducible, as the intraobserver agreement for RMT and interobserver agreement for volume were moderate. Agreement on the assessment of niche shape was poor for both the inter- and intraobserver analyses.
Strengths and limitations of the studyAs far as we know, this is the first study evaluating the reproducibility of niche measurements in non-pregnant women. This study is important for future research, because until now the parameters for niche measurement were different for most studies and therefore difficult to compare. We attempted to make clear definitions for all parameters, which may be used for future research. We did not assess the quotient of the myometrial thickness at the site of the niche and the adjacent normal myometrium, which may nevertheless be a useful parameter.
A limitation of this study is that the results are only applicable to offline analysis of 3D volumes of the niche, not to real-time 2D ultrasound examination. Another limitation is that only ultrasound images performed with TVS were included, and therefore nothing can be said about the reproducibility of SHG images. A number of only 20 included images may also have been a limitation. Finally, two examiners were involved and one of them had also performed the selection of the 20 volumes. Although there was a time gap between the selection of the images and the performance of the reproducibility study, the examiner who selected the 20 volumes might have had a slight advantage.
Interpretation of our findingsConcerning the interobserver study, the mean difference for measurements in the longitudinal plane was mostly negative (Table 1), which means that the measurements of the first observer were in general lower than the second one. After reviewing the measurements, we may explain this finding by the fact that not the largest surface area of the niche was chosen by the first observer for several volumes. However, the mean differences were small (less than 0.50 mm) and therefore acceptable. As it is subjective to estimate the largest surface area of the niche, we suggest measuring the depth and width of the niche three times and to continue measuring in the section with the largest surface area.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Reproducibility study of niche measurement | 35
3
The lower level of intraobserver agreement compared to the interobserver analyses for certain measurements is the opposite from expected, especially for RMT. In order to explain this finding, measurements of the RMT were reviewed and we found that the reproducibility was influenced by the difficulty to recognize the end of the myometrium in some cases, especially if the niche was located extraperitoneally. Although this does not explain the better ICC of the interobserver study in comparison to the ICC of the intraobserver study, this may explain the lower reproducibility in the transversal plane as the serosa and/or end of the myometrium were more difficult to recognize in this plane. Lower reproducibility in the transversal plane in general may be caused by the fact that the resolution of the reconstructed plane (transversal plane) is inferior to that of the acquisition plane (longitudinal plane). In addition, the flection of the uterus in either anteverted or retroverted direction can make it difficult to determine the exact transversal plane perpendicular to the serosa at the site of the niche. A small variation in angle may induce a large effect on the niche depth and RMT.
The ICC values for width at niche base for the transversal plane were lower than the ICC values for the longitudinal plane, which may be explained by the observation that it is difficult to assess the base for the transversal plane in case of intracavitary fluid. The same was observed by O.V. Osser et al. [11], who did not measure the width of the niche in the transversal plane during SHG as they found delineating the niche in the transversal plane difficult.
The intraobserver agreement for niche volume is better in comparison with the interobserver agreement. Measuring a volume requires multiple activities, as the niche surface needs to be manually outlined in 10 different planes, which may introduce slight differences between observers. In addition, we found in retrospect that one observer systematically measured slightly smaller volumes.
The assessment of niche shape is not reproducible, which may be caused by the fact that the classification depends on the section in which the shape is assessed. A lot of niches have branches, which are only present in several sections. In addition, it is difficult to make use of a classification like we did, as a minority of niches meet with a certain predetermined shape. We had not performed any training of the examiners in advance. Training might have improved the reproducibility of the niche shape.
Comparison with other publicationsOnly one reproducibility study [12] on the niche has been published, performed in pregnant women with, similar to our study, niche measurements carried out off-line on stored images. According to the author of this study, RMT does not

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
36 | Chapter 3
vary across the trimesters of pregnancy and is therefore likely to be comparable with our results, although the presence of amniotic fluid in pregnant women acts as a contrast agent and therefore may improve visibility of the margins of the niche. An ICC of 0.71 was found for the interobserver and an ICC of 0.88 for the intraobserver agreement on the measurement of the RMT for all three trimesters combined [12]. Our interobserver agreement for RMT was higher with an ICC of 0.97. Our intraobserver agreement was lower (ICC 0.73), which may be explained by the short delay of only 10 s between the two measurements of Naji et al.
Clinical implicationsOur results indicate that parameters assessing niche size or RMT are highly reproducible in the longitudinal plane using 3D ultrasound. Some of these parameters may have clinical implications. Although still to be proven, they may be associated with the presence of symptoms [2], [5], [13] and [14] and uterine dehiscence or rupture in future pregnancies [15]. In addition, they may be of influence on therapeutical options. Hysteroscopic [16] and [17] or laparoscopic [18] treatment of the niche is performed in some women with gynaecological symptoms, which is dependant on RMT. The RMT must be at least 2–3 mm for hysteroscopic niche resection in order to prevent perforation of the uterus or bladder injury [14]. Based on our results, we suggest measurement of the RMT in both the longitudinal and transversal plane in the section in which the RMT is the smallest instead of taking the maximal surface area of the niche, and to use a volume of sufficient quality in order to be able to recognize the serosa.
Future researchAs we have performed the first study evaluating the inter- and intraobserver agreement for niche measurement, future studies should confirm our results. We believe that the use of a consistent technique for analyzing the 3D volumes and optimization of image quality will improve inter- and intraobserver agreement. Image quality may be improved by adding contrast, and therefore future studies should also evaluate the inter- and intraobserver agreement for SHG images.
Based on the higher reproducibility of niche evaluation in the longitudinal plane, we suggest assessment of the niche in the longitudinal plane in general practice and future studies, except for RMT, which we believe should also be measured in the transversal plane. In addition, given the low reproducibility it may be considered to omit the evaluation of niche shape as performed in our study.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Reproducibility study of niche measurement | 37
3
1. Bij de Vaate AJ, van der Voet LF, Naji O, et al. Prevalence, potential risk factors for development and symptoms related to the presence of uterine niches following cesarean section: systematic review. Ultrasound Obstet Gynecol 2014;43:372–82.
2. Bij de Vaate AJ, Brolmann HA, van der Voet LF, van der Slikke JW, Veersema S, Huirne JA. Ultrasound evaluation of the cesarean scar: relation between a niche and postmenstrual spotting. Ultrasound Obstet Gynecol 2011;37:93–9.
3. Fabres C, Aviles G, De La Jara C, et al. The cesarean delivery scar pouch: clinical implications and diagnostic correlation between transvaginal sonography and hysteroscopy. J Ultrasound Med 2003;22:695–700. quiz 1–2.
4. Thurmond AS, Harvey WJ, Smith SA. Cesarean section scar as a cause of abnormal vaginal bleeding: diagnosis by sonohysterography. J Ultrasound Med 1999;18:13–6. quiz 7-8.
5. Wang CB, Chiu WW, Lee CY, Sun YL, Lin YH, Tseng CJ. Cesarean scar defect: correlation between cesarean section number, defect size, clinical symptoms and uterine position. Ultrasound Obstet Gynecol 2009;34:85–9.
6. Osser OV, Jokubkiene L, Valentin L. High prevalence of defects in cesarean section scars at transvaginal ultrasound examination. Ultrasound Obstet Gynecol 2009;34:90–7.
7. Ofili-Yebovi D, Ben-Nagi J, Sawyer E, et al. Deficient lower-segment cesarean section scars: prevalence and risk factors. Ultrasound Obstet Gynecol 2008;31:72–7.
8. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986;1:307–10.
9. Bland JM, Altman DG. Applying the right statistics: analyses of measurement studies. Ultrasound Obstet Gynecol 2003;22:85–93.
10. Landis JR, Koch GG. The measurement of observer
agreement for categorical data. Biometrics 1977;33:159–74.
11. Osser OV, Jokubkiene L, Valentin L. Cesarean section scar defects: agreement between transvaginal sonographic findings with and without saline contrast enhancement. Ultrasound Obstet Gynecol 2010;35:75–83.
12. Naji O, Daemen A, Smith A, et al. Visibility and measurement of cesarean section scars in pregnancy: a reproducibility study. Ultrasound Obstet Gynecol 2012;40:549–56.
13. Uppal T, Lanzarone V, Mongelli M. Sonographically detected caesarean section scar defects and menstrual irregularity. J Obstet Gynaecol 2011;31:413–6.
14. van der Voet LF, Bij de Vaate AM, Veersema S, Brolmann HA, Huirne JA. Long- term complications of caesarean section. The niche in the scar: a prospective cohort study on niche prevalence and its relation to abnormal uterine bleeding. BJOG 2014;121:236–44.
15. Vikhareva Osser O, Valentin L. Clinical importance of appearance of cesarean hysterotomy scar at transvaginal ultrasonography in nonpregnant women. Obstet Gynecol 2011;117:525–32.
16. Chang Y, Tsai EM, Long CY, Lee CL, Kay N. Resectoscopic treatment combined with sonohysterographic evaluation of women with postmenstrual bleeding as a result of previous cesarean delivery scar defects. Am J Obstet Gynecol 2009;200. 370 e1-370 e4.
17. Feng YL, Li MX, Liang XQ, Li XM. Hysteroscopic treatment of postcesarean scar defect. J Minim Invasive Gynecol 2012;19:498–502.
18. Marotta ML, Donnez J, Squifflet J, Jadoul P, Darii N, Donnez O. Laparoscopic repair of post-cesarean section uterine scar defects diagnosed in nonpregnant women. J Minim Invasive Gynecol 2013;20:386–91.
References

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
44|Ultrasound evaluation of the Cesarean scar: Ultrasound evaluation of the Cesarean scar:
relation between a niche and relation between a niche and postmenstrual spottingpostmenstrual spotting
A.J.M. Bij de VaateA.J.M. Bij de VaateH.A.M. BrölmannH.A.M. BrölmannL.F. van der Voet L.F. van der Voet
J.W. van der Slikke J.W. van der Slikke S. VeersemaS. VeersemaJ.A.F. HuirneJ.A.F. Huirne
Ultrasound Obstet Gynecol 2011;37(1):93-9.Ultrasound Obstet Gynecol 2011;37(1):93-9.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Abstract
ObjectiveTo evaluate the relationship between a niche and abnormal uterine bleeding, and to develop a sonographic classification of niches and evaluate its relationship to abnormal uterine bleeding.
MethodsAn observational prospective cohort study was performed between October 2007 and May 2009. All women who had a Cesarean section performed in our hospital were asked to participate. Two hundred and twenty-five women were included and examined with both transvaginal sonography (TVS) and gel instillation sonohysterography (GIS) 6–12 months after the Cesarean section. In case of a niche, the depth, volume and residual myometrium were measured, and the shape was assessed according to a specified classification. A questionnaire and pictorial blood loss assessment chart were filled in.
ResultsThe prevalence of a niche on evaluation with TVS and GIS was 24.0% and 56.0%, respectively. A niche was considered to be present if the depth was at least 1 mm visualized with GIS. Postmenstrual spotting was reported by 33.6% of women with a niche and 15.2% of women without a niche (P = 0.002). The niche volume was significantly different between women with and without postmenstrual spotting (P = 0.02). Most niches had a semicircular (50.4%) or triangular shape (31.6%). No significant relationship was identified between the shape of the niche and postmenstrual spotting (P = 0.19).
ConclusionsA niche is present in 56.0% of women with a history of Cesarean section when examined by GIS and is associated with postmenstrual spotting. Semicircular and triangular niches are most common, but the shape is not related to postmenstrual spotting.
40 | Chapter 4
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Introduction
In the 1970s the Cesarean section rate began to increase in most Western countries1, as a consequence of which the number of women with a uterine scar is rising. Apart from the well-known complications, such as uterine rupture and pathologically adherent placentas, the long-term effects of this widely used procedure have been poorly studied. Recently, researchers have observed the presence of a niche at the site of the Cesarean scar. A niche is a sonographic finding and is defined as a triangular, anechoic area at the presumed site of incision2. Uterine niches can be identified on transvaginal sonography (TVS), but saline contrast sonohysterography (SCSH) may facilitate their detection2,3, and provides a more clear delineation of scar defects4. An alternative to SCSH is gel instillation sonohysterography (GIS), which has the advantage of creating a more stable filling of the uterine cavity and reducing discomfort for the patient due to the prevention of fluid leakage during the procedure5.
Because of the high Cesarean section rate—15.0% in The Netherlands in 20056 and 31.1% in the USA in 20067—it is important to learn more about the clinical consequences of a niche. Several small studies have demonstrated that a niche may be responsible for abnormal uterine bleeding in women with a previous Cesarean section. However, most studies included women with gynecological complaints2,8-10. No large prospective studies have yet been performed that focus on the relationship between the niche and abnormal uterine bleeding, and in which women with a history of Cesarean section were consecutively asked to participate. The aim of the current study was to evaluate the relationship between the presence of a niche and abnormal uterine bleeding in women with a history of Cesarean section, and to develop a sonographic classification of niches and evaluate its relationship to abnormal uterine bleeding.
Methods
An observational prospective cohort study was performed between October 2007 and May 2009 at the Department of Obstetrics and Gynaecology of the VU University Medical Center, Amsterdam, which is a high-risk pregnancy referral center where about 450 Cesarean sections are carried out every year. The study was approved by the local research ethics committee. All women who had a Cesarean section performed in our hospital were consecutively asked to participate. The women were identified from a database in which all deliveries performed in our hospital are registered. Exclusion criteria were risk of pelvic inflammatory disease, cervical cancer or pregnancy. Women were
Uterine niche and spotting | 41
4

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
42 | Chapter 4
contacted by phone 3–9 months after their Cesarean section and after giving informed consent they visited the hospital 6–12 months after the operation. Medical records, especially details of the pregnancy and Cesarean section, were reviewed and a specific form was filled in, in order to have a complete clinical and obstetric record for each woman. All women underwent both TVS and GIS using an Accuvix ultrasound machine (Medison, Hoofddorp, The Netherlands) to study the presumed site of the uterine scar, performed by one experienced operator (A.B.) in a standardized way.
Except for those not using contraception—who were examined in the follicular phase of their cycle—the women were examined during a random phase of their menstrual cycle and the cycle day was recorded. Patients needed to have their bladder completely empty during the test. TVS was performed first and the following details of the uterus were recorded: position, length, width, endometrial thickness and presence of intracavitary fluid. The uterus was examined for a niche, defined as an anechoic area at the site of the Cesarean scar with a depth of at least 1 mm. If a niche could be detected, the depth of the niche (the vertical distance between the base and apex of the defect) and residual myometrium (from the serosal surface of the uterus to the apex of the niche) were measured (Figure 1), the niche shape was assessed according to a specified classification (Figure 2), and the volume of the niche was measured with the use of three-dimensional ultrasonography and the eXtended Imaging Virtual Organ Computer-aided Analysis program. Subsequently, GIS was performed with the use of an intrauterine insemination catheter (Repromed, IM Services BV, Zwolle, The Netherlands), which was first flushed with sterile gel to rid it of small amounts of air and then introduced into the uterine cavity. Gel was infused through the catheter until the patient felt slight menstrual cramps, backflow started or a maximum of 10 mL was reached5. If a niche with a depth of at least 1 mm could be detected, the same measurements as mentioned above were repeated in the distended uterus. In women without a niche, the thickness of the myometrium at the site of the Cesarean scar (if visible) was measured and recorded as the thickness of the residual myometrium. In patients with multiple niches, only the largest defect was measured. The uterine cavity was examined for the presence of other intrauterine abnormalities, such as submucosal fibroids or polyps.
When the ultrasound examination had been performed, all women were asked to fill in a questionnaire in order to detect abnormal uterine bleeding and especially postmenstrual spotting. Women were asked for the regularity and duration of their menstrual cycle, number of days of blood loss (including the number of days of brownish discharge just before and after the cycle), and the number of days of intermenstrual bleeding. In addition, they were asked to keep

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Uterine niche and spotting | 43
4
a modified pictorial blood loss assessment chart (PBAC)11 to assess the amount of blood loss during their period. Postmenstrual spotting was defined as more than 2 days of brownish discharge at the end of menstruation with a total length of menstruation (including spotting) of more than 7 days, or intermenstrual bleeding which starts within 5 days after the end of menstruation. To prevent any bias patients were not informed about the presence of a niche and the sonographer was not informed about the menstrual pattern.
The primary outcome was the difference in the prevalence of postmenstrual spotting between women with and without a niche. The following secondary outcomes were also evaluated: niche classification based on the shape of the niche and its relationship with abnormal uterine bleeding, and the difference between women with and without a niche concerning other bleeding parameters (i.e. duration of menstruation, intermenstrual bleeding, PBAC score), pain during menstruation and urological symptoms.
In addition we evaluated possible confounders such as amenorrhea, lactation, polyps, smoking, use of oral contraceptives and levonorgestrel-releasing intrauterine system (LNG-IUS).
Statistical analysisTo analyze the relationship between the niche and uterine bleeding parameters and urological symptoms, we used logistic regression analysis, the chi-square test, Student’s t-test or the Mann–Whitney U-test, depending on the type and distribution of the parameter. The relationship between niche classification based on niche shape and postmenstrual spotting was evaluated using Fisher’s exact test. Logistic regression analysis was used to evaluate the influence of possible confounders on postmenstrual spotting in patients with or without a
Figure 1: Schematic diagram demonstrating measurement of depth of the niche (1), thickness of the residual myometrium (2) and total myometrial thickness (3).
Figure 2: Schematic diagram demonstrating classification used to assess niche shape: triangle, semicircle, rectangle, circle, droplet and inclusion cysts.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
44 | Chapter 4
niche. Data were analyzed using Statistical Packages for the Social Sciences (SPSS, Inc., Chicago, IL, USA). Two-sided tests were used and P < 0.05 was considered statistically significant.
Based on a previous study12, a difference of 15% (from 10% to 25%) was expected in the prevalence of abnormal uterine bleeding between women with and without a niche, which was considered clinically relevant. To achieve 80% power with an alpha of 5%, 134 patients with a niche would be needed. Assuming a prevalence of the niche of 59.5% (as ascertained by Menada Valenzano et al.12) in women examined with GIS and with a history of Cesarean section, 225 women had to be included.
632 women underwent acaesarean section during the
research period
132 women not contacted because of:- history of radical vaginal trachelectomy (4)- perinatal death (19)- incorrect phone number (109)
275 women not able to participate:- no possibility to visit the hospital (62)- current pregnancy (22)- refusal to undergo the examinations (191)
500 women contacted by
telephone
225 womenincluded
Figure 3: Flow chart of patients included in the study.
Results
We included 225 women with a history of Cesarean section with a mean age of 34.9 (range, 22–44) years (Figure 3). These women used the following methods of contraception: no contraception, 28.4%; condom, 27.1%; oral contraceptives, 21.8%; LNG-IUS, 10.7%; sterilization, 6.3%; and other methods, 5.7%. Eight women were breast-feeding totally and 10 women partially, of whom three and four, respectively, were amenorrheic. All women underwent TVS. In 16 women the GIS catheter could not be inserted in the uterus or insufficient distension of the uterine cavity was achieved, resulting in 209 patients examined with GIS. A

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Uterine niche and spotting | 45
4
niche could be demonstrated by TVS in 54 out of 225 women (24.0%) and by GIS in 117 out of 209 women (56.0%).
For the following analyses, a niche was considered to be present if visualized with GIS with a depth of at least 1 mm. The baseline characteristics of the study group are demonstrated in Table 1 for women with and without a niche. A significant difference was found for parity (P = 0.01) and for the mean number of previous Cesarean sections (P = 0.001).
Table 1: Baseline characteristics with details of the Cesarean section preceding entry to the study.
Parameter Niche on GIS (n = 117)
No niche on GIS (n = 92)
P
Age (years) 35.2 ± 4.0 34.5 ± 4.4 0.26Parity 1.8 ± 0.9 1.5 ± 0.9 0.01Number of Cesarean sections 1.5 ± 0.7 1.2 ± 0.5 0.001Gestational age at the time of Cesarean section (weeks) 38.2 ± 3.3 37.5 ± 3.9 0.39Indication for last Cesarean section 0.11
Failure of cervical dilation 21 (17.9%) 10 (10.9%)Obstetric history* 21 (17.9%) 9 (9.8%)Fetal distress 20 (17.1%) 30 (32.6%)Breech or transverse presentation 19 (16.2%) 15 (16.3%)Maternal condition (including placental problems) 19 (16.2%) 13 (14.1%)Delayed second stage of labor 15 (12.8%) 11 (12.0%)Patient request 2 (1.7%) 3 (3.3%)Other 0 (0%) 1 (1.1%)
Induction of labour 16 (43.2%) 21 (56.8%) 0.09Labor augmentation 32 (60.4%) 21 (39.6%) 0.46Contractions at the time of Cesarean section† 62 (53.9%) 53 (46.1%) 0.37Dilation at the time of Cesarean section (cm) 3.3 ± 4.0 3.6 ± 4.1 0.68Birth weight (g) 3253 ± 940 3061 ± 986 0.16Time after last Cesarean section at the time of inclusion (weeks) 49.4 ± 4.7 50.1 ± 4.5 0.25
Data are given as mean ± SD or n (%). *Previous failure of labor, cephalopelvic disproportion, multiple Cesarean sections. †Six women excluded because presence of contractions not known. GIS, gel instillation sonohysterography.
Table 2: Sonographic characteristics of uteri of women in the study group.
Characteristic Niche on GIS (n = 117)
No niche on GIS (n = 92)
P
On transvaginal sonographyEndometrial thickness (mm) 5.1 ± 2.9 5.3 ± 3.1 0.73Uterine length (cm) 7.3 ± 1.2 6.9 ± 1.3 0.04Uterine width (cm) 3.8 ± 0.7 3.8 ± 0.9 0.67Intracavitary fluid* 13/98 (13.3%) 5/80 (6.3%) 0.12
On GISMyometrial thickness at site of Cesarean scar (mm) 7.0 ± 2.8 9.6 ± 3.0 <0.001
Data are given as mean ± SD or n (%). *Women between cycle day 1 and 5 of their menstrual cycle were excluded. GIS, gel instillation sonohysterography.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
46 | Chapter 4
Sonographic characteristics of the uterusTable 2 shows the characteristics of the uterus for women with and without a niche. The mean length of the uterus was slightly greater in women with a niche (7.3 cm) than in women without a niche (6.9 cm) (P = 0.04), while the width of the uterus was the same for both groups (3.8 cm). The myometrium at the site of the Cesarean scar during GIS was significantly thinner in women with a niche (7.0 mm) than in women without a niche (9.6 mm) (P < 0.001). After excluding women at days 1–5 of their menstrual cycle (as they may have had menstrual blood in the uterine cavity), TVS demonstrated intracavitary fluid in 13 of 98 patients with a niche (13.3%) and in five of 80 women without a niche (6.3%) (P = 0.12). The mean depth of the niche was 4.9 mm in women with intracavitary fluid and 3.5 mm in women without intracavitary fluid (P = 0.07), and the mean volume of the niche in women with and without intracavitary fluid was 0.14 and 0.04 cm3, respectively (P = 0.01).
Uterine bleeding pattern and urological symptomsThe relationship between the presence of a niche and abnormal uterine bleeding is demonstrated in Table 3. Details of postmenstrual spotting were reported by 208 women; in one woman we were not able to determine the exact cycle pattern. Postmenstrual spotting was present in 39 women with a niche (33.6%) and 14 women without a niche (15.2%). Univariate logistic regression analysis demonstrated a relationship between the presence of a niche and postmenstrual spotting (coefficient = 1.04, odds ratio (OR) = 2.8 (95% CI, 1.4–5.6); P = 0.03). Using univariate analysis, no significant relationship with postmenstrual spotting could be detected for the following potential confounders: amenorrhea (P = 0.10), lactation (P = 0.45), polyps (P = 0.71), smoking (P = 0.44) and use of LNG-IUS (P = 0.73). The only significant relationship was found for the use of oral contraceptives (P = 0.045). Using logistic regression analysis, the coefficient (1.14) changed sufficiently after inclusion of oral contraception as a covariable, confirming oral contraception to be a confounder. After correction for this confounder, the relationship between a niche and postmenstrual spotting became stronger (OR = 3.1 (95% CI, 1.5–6.3); P = 0.002). If women with amenorrhea were excluded from the analyses, postmenstrual spotting was present in 39/110 (35.5%) women with a niche and 14/84 (16.7%) women without a niche (P = 0.004).
As already mentioned, a niche was defined as an anechoic area at the site of the Cesarean scar with a depth of at least 1 mm. Repeating logistic regression analysis with 2 mm as a cut-off value for the depth, the niche was still significantly related to postmenstrual spotting (OR = 2.0 (95% CI, 1.1–3.8); P = 0.03).

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Uterine niche and spotting | 47
4
Information about intermenstrual bleeding was obtained from 197 women, and this symptom was reported by 33 of 110 women with a niche (30.0%) and 9 of 87 women without a niche (10.3%) (P = 0.001). The mean number of days of intermenstrual bleeding was 0.8 for the group with a niche and 0.3 for the group without a niche (P = 0.001). A PBAC was completely filled in by 90 patients, and the total estimated monthly blood loss was similar in both groups (P = 0.97). The pain experienced during menstruation, reported with the use of a visual analog scale (VAS) score, was similar for women with and without a niche (P = 0.95). Urological symptoms were also similar for both groups (Table 3). By using TVS for the detection of a niche, the prevalence of postmenstrual spotting was 29.6% in women with a niche and 22.2% in women without a niche (P = 0.24).
Table 3: Uterine bleeding pattern and urological symptoms of women in the study group.
Characteristic Niche on GIS (n = 117)
No niche on GIS (n = 92)
P
Postmenstrual spotting (n = 208) 39/116 (33.3%) 14/92 (15.2%) 0.002Days of blood loss during menstruation (n = 194) 5.7 ± 2.8 5.8 ± 1.9 0.23Intermenstrual bleeding (n = 197) 33/110 (30.0%) 9/87 (10.3%) 0.001Days of intermenstrual bleeding (n = 197) 0.8 ± 1.7 0.3 ± 1.1 0.001PBAC score (n = 90) 153 ± 161 154 ± 146 0.97VAS score (0-10) (n = 196) 3.5 ± 2.7 3.4 ± 2.3 0.95Incontinence (n = 207) 26/115 (22.6%) 23/92 (25.0%) 0.69Stress incontinence (n = 207) 23/115 (20.0%) 18/92 (19.6%) 0.94Urge incontinence (n = 207) 5/115 (4.3%) 7/92 (7.6%) 0.32
Data are given as n (%) or mean ± SD. GIS, gel instillation sonohysterography; PBAC, pictorial blood loss assessment chart; VAS, visual analog scale for menstrual pain.
Table 4: Niche classification by gel instillation sonohysterography and postmenstrual spotting.
Parameter Prevalence Postmenstrual spotting (n = 28)*
No postmenstrual spotting (n = 66)*
P
Niche classification 0.19Semicircle 59 (50.4%) 14 (50.0%) 32 (48.5%)Triangle 37 (31.6%) 11 (39.3%) 18 (27.3%)Droplet 12 (10.3%) 1 (3.6%) 9 (13.6%)Inclusion cyst(s) 8 (6.8%) 1 (3.6%) 7 (10.6%)Other 1 (0.9%) 1 (3.6%) 0 (0%)
Depth of the niche (mm) 3.7 ± 1.9 3.5 ± 2.1 0.50Volume of niche (cm³)† 0.08 ± 0.13 0.04 ± 0.10 0.02Myometrial thickness at the site of Cesarean scar (mm) 7.5 ± 3.3 8.3 ± 3.2 0.34
Data are given as n (%) or mean ± SD. *As use of oral contraceptives was identified as a confounding factor, women using oral contraceptives (n = 22) were excluded from the analyses. One woman was additionally excluded due to uncertainty with respect to the presence of postmenstrual spotting. †Measured with the use of three-dimensional sonohysterography.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
48 | Chapter 4
Niche classificationThe shape of the niche was assessed with GIS and resulted in the classification presented in Table 4. The most common shapes were semicircular (50.4%), triangular (31.6%), droplet-shaped (10.3%) and inclusion cysts (6.8%) (Figure 4). Women using oral contraceptives were excluded from the following analyses, as the use of oral contraceptives was identified as a confounding factor. No significant relationship was observed between the shape of the niche and postmenstrual spotting (P = 0.19). Both mean depth of the niche and the residual myometrium at the site of the Cesarean scar were not significantly different between the groups with and without postmenstrual spotting (P = 0.50 and 0.34, respectively). However, the niche volume was larger in women with postmenstrual spotting (0.08 cm3) than in women without postmenstrual spotting (0.04 cm3) (P = 0.02).
Figure 4: Ultrasound scans showing the most common niche shapes: the semicircular niche (a), triangular niche (b), droplet-shaped niche (c) and inclusion cysts (d).
Discussion
To the best of our knowledge, this is the first prospective cohort study focusing on the niche and its relationship to abnormal uterine bleeding, in which women were consecutively included 6–12 months after Cesarean section. In order to prevent selection bias, all women who underwent a Cesarean section were

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Uterine niche and spotting | 49
4
included independently of their obstetric history. The prevalence of a niche on TVS was 24.0% in our population, which is comparable with that of 19.4% in a previous study using the same method13. Other authors reported a much lower prevalence of 6.9%10. This difference may have been caused by variation in definitions, level of awareness and methods used. Using GIS, the prevalence in our study increased to 56.0%, which is comparable with other studies3,12. Our findings confirm that the detection rate of niches increases using sonohysterography and that most scar defects appear to be larger with this technique than with TVS.
We have demonstrated a significant relationship between the presence of a niche as seen using GIS and postmenstrual spotting in women with a previous Cesarean section. One in three women with a niche had complaints of postmenstrual spotting, while one in seven women without a niche had these complaints. The relationship between a niche and postmenstrual spotting was independent of amenorrhea, lactation, polyps, smoking, LNG-IUS and oral contraception use. The latter was demonstrated to be a confounder, and after controlling for this factor using logistic regression analysis, the relation between a niche and postmenstrual spotting was even stronger.
Most previous studies included only a selected group of women, who underwent TVS8,10 or SCSH2,9 because of gynecological complaints. This may explain the high prevalence of postmenstrual spotting in these studies, varying between 63.8 and 100%. Only one study has been performed in an unselected population, including 217 women with a history of vaginal delivery or Cesarean section and undergoing both TVS and SCSH. In this study no relationship was found between the presence of a niche and abnormal uterine bleeding, with a prevalence of 24.6% for abnormal uterine bleeding in women with a niche12. We have no clear explanation for why no relationship was found, but three possible explanations may be proposed. First, women were evaluated between 3 months and 10 years after the Cesarean section, and only 17 were examined 3–12 months after the Cesarean section (as were our study population). Secondly, women with multiple parity were excluded, while our study demonstrated that patients with multiple Cesarean sections are at higher risk for the development of a niche. This could be because women with a history of multiple Cesarean sections may have more fibrotic tissue in the myometrium and may be more prone to obstruction of menstrual blood and associated menstrual spotting. Thirdly, although sonohysterography was used in both studies, the method of niche assessment may have been different. The importance of the method used for niche assessment is emphasized by our results of niche evaluation with TVS, as no significant difference for postmenstrual spotting between women with and without a niche was found when TVS was used instead of GIS. Fewer niches

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
50 | Chapter 4
were identified on TVS and therefore GIS should be used to exclude a niche in cases of postmenstrual spotting. Some selection may have occurred in our study since women with complaints are generally more willing to participate in a study. However, women were not informed whether or not a niche was observed to prevent possible bias in reporting their bleeding pattern.
The ideal moment for sonographic evaluation is probably the early follicular phase, assuming that a thin endometrium may improve the identification of a niche and measurement of its depth and size. Although standardized measurement during the early follicular phase was not possible for our participants due to their private schedules, no difference in mean endometrial thickness and cycle day between the groups with and without a niche was found. Women will be followed for a period of 5 years, which should allow identification of patients with later onset of postmenstrual spotting, but these follow-up data are not yet available. It has been suggested that the frequency of abnormal uterine bleeding—defined as spotting after the end of menstruation and/or noncyclic bleeding not related to menstruation—is higher in women who were evaluated after a longer period12.
Several hypotheses have been postulated to explain the etiology of bleeding disorders in relation to the niche. It has been assumed that abnormal uterine bleeding may be due to the retention of menstrual blood in the niche, which is intermittently expelled after the majority of the menstruation has ceased, causing postmenstrual spotting9,14. Thurmond et al.9 reported that this condition may depend on poor contractility of the uterine muscle around the scar. In addition, the presence of fibrotic tissue below the niche may impair the drainage of menstrual flow through the cervix14. It cannot be ruled out that the accumulated blood is produced in situ, as suggested by Morris15 based on the presence of free blood cells in the endometrial stroma, suggesting recent hemorrhage.
The positive relationship between niche volume and postmenstrual spotting indicates an increased capacity to collect blood and underlies the theories mentioned above. Our hypotheses that the depth and shape of the niche may be related to abnormal uterine bleeding could not be confirmed, which may be explained by the group size being insufficient to test these secondary outcome parameters. The presence of intracavitary fluid seemed to be more frequent in women with a niche than in women without a niche, but a larger study group will be needed to assess this. In addition, the volume of the niche was higher in women with intracavitary fluid. We propose that the presence of a niche, especially one with a large volume, may be associated with intracavitary fluid, which affects postmenstrual spotting. It has been suggested that subfertility after a Cesarean section might be caused by the presence of a niche14. More
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Uterine niche and spotting | 51
4
research should be undertaken to study the relationship between the niche, intracavitary fluid and infertility.
In conclusion, we have performed the first prospective study in which the prevalence of the niche and its relationship to abnormal uterine bleeding were evaluated. Our results demonstrate that 56.0% of women with a history of Cesarean section have a niche when examined by GIS and that a niche is associated with postmenstrual spotting. Therefore, we encourage gynecologists to include the niche as a differential diagnosis in patients with postmenstrual spotting and a previous Cesarean section. Future research should increase our knowledge about the etiology of a niche.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
52 | Chapter 4
1. Notzon FC, Placek PJ, Taffel SM. Comparisons of national cesarean-section rates. N Engl J Med 1987; 316: 386–389.
2. Monteagudo A, Carreno C, Timor-Tritsch IE. Saline infusion sonohysterography in nonpregnant women with previous cesarean delivery: the “niche” in the scar. J Ultrasound Med 2001; 20: 1105–1115.
3. Regnard C, Nosbusch M, Fellemans C, Benali N, van Rysselberghe M, Barlow P, Rozenberg S. Cesarean section scar evaluation by saline contrast sonohysterography. Ultrasound Obstet Gynecol 2004; 23: 289–292.
4. Vikhareva Osser O, Jokubkiene L, Valentin L. Cesarean section scar defects: agreement between transvaginal sonographic findings with and without saline contrast enhancement. Ultrasound Obstet Gynecol 2010; 35: 75–83.
5. Bij de Vaate AJM, Brölmann HAM, Van der Slikke JW, Emanuel MH, Huirne JAF. Gel instillation sonohysterography (GIS) and saline contrast sonohysterography (SCSH): comparison of two diagnostic techniques. Ultrasound Obstet Gynecol 2010; 35: 486–489.
6. Kramer HM, Kwee A, Bremer HA. Once a C-section, always a C-section? Ned Tijdschr Geneeskd 2009; 153: 136–140.
7. MacDorman MF, Menacker F, Declercq E. Cesarean birth in the United States: epidemiology, trends, and outcomes. Clin Perinatol 2008; 35: 293–307, v.
8. Fabres C, Aviles G, De La Jara C, Escalona J, Muñoz JF, Mackenna A, Fernández C, Zegers-Hochschild F, Fernández E. The cesarean delivery scar pouch: clinical implications and diagnostic correlation between transvaginal sonography and
hysteroscopy. J Ultrasound Med 2003; 22: 695–700.9. Thurmond AS, Harvey WJ, Smith SA. Cesarean
section scar as a cause of abnormal vaginal bleeding: diagnosis by sonohysterography. J Ultrasound Med 1999; 18: 13–16.
10. Wang CB, Chiu WW, Lee CY, Sun YL, Lin YH, Tseng CJ. Cesarean scar defect: correlation between Cesarean section number, defect size, clinical symptoms and uterine position. Ultrasound Obstet Gynecol 2009; 34: 85–89.
11. Higham JM, O’Brien PM, Shaw RW. Assessment of menstrual blood loss using a pictorial chart. Br J Obstet Gynaecol 1990; 97: 734–739.
12. Menada Valenzano M, Lijoi D, Mistrangelo E, Costantini S, Ragni N. Vaginal ultrasonographic and hysterosonographic evaluation of the low transverse incision after caesarean section: correlation with gynaecological symptoms. Gynecol Obstet Invest 2006; 61: 216–222.
13. Ofili-Yebovi D, Ben-Nagi J, Sawyer E, Yazbek J, Lee C, Gonzalez J, Jurkovic D. Deficient lower-segment Cesarean section scars: prevalence and risk factors. Ultrasound Obstet Gynecol 2008; 31: 72–77.
14. Fabres C, Arriagada P, Fernández C, Mackenna A, Zegers F, Fernández E. Surgical treatment and follow-up of women with intermenstrual bleeding due to cesarean section scar defect. J Minim Invasive Gynecol 2005; 12: 25–28.
15. Morris H. Surgical pathology of the lower uterine segment caesarean section scar: is the scar a source of clinical symptoms? Int J Gynecol Pathol 1995; 14: 16–20.
References

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
55|Long-term complications of Long-term complications of
caesarean section. The niche in the scar: caesarean section. The niche in the scar: a prospective cohort study on niche a prospective cohort study on niche
prevalence and its relation to abnormal prevalence and its relation to abnormal uterine bleedinguterine bleeding
L.F. van der Voet L.F. van der Voet A.J.M. Bij de VaateA.J.M. Bij de Vaate
S. Veersema S. Veersema H.A.M. BrölmannH.A.M. Brölmann
J.A.F. HuirneJ.A.F. Huirne
BJOG 2014;121(2):236-44.BJOG 2014;121(2):236-44.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Abstract
ObjectiveTo study the prevalence of niches in the caesarean scar in a random population, and the relationship with postmenstrual spotting and urinary incontinence.
DesignA prospective cohort study.
SettingA teaching hospital in the Netherlands.
PopulationNon-pregnant women delivered by caesarean section.
MethodsTransvaginal ultrasound (TVU) and gel instillation sonohysterography (GIS) were performed 6–12 weeks after caesarean section. Women were followed by questionnaire and menstruation score chart at 6–12 weeks, 6 months, and 12 months after caesarean section.
Main outcome measuresPrevalence of a niche 6–12 weeks after caesarean section, using TVU and GIS. Secondary outcomes: relation to postmenstrual spotting and urinary incontinence 6 and 12 months after caesarean section; and niche characteristics, evaluated by TVU and GIS.
ResultsTwo hundred and sixty-three women were included. Niche prevalence was 49.6% on evaluation with TVU and 64.5% with GIS. Women with a niche measured by GIS reported more postmenstrual spotting than women without a niche (OR 5.48, 95% CI 1.14–26.48). Women with residual myometrium at the site of the uterine scar measuring <50% of the adjacent myometrial thickness had postmenstrual spotting more often than women with a residual myometrial thickness of >50% of the adjacent myometrial thickness (OR 6.13, 95% CI 1.74–21.63). Urinary incontinence was not related to the presence of a niche.
ConclusionsA niche is present in 64.5% of women 6–12 weeks after caesarean section, when examined by GIS. Postmenstrual spotting is more prevalent in women with a niche and in women with a residual myometrial thickness of <50% of the adjacent myometrium.
54 | Chapter 5

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Introduction
Concern regarding the association between delivery by caesarean section and long-term maternal morbidity is growing, as the rate of caesarean section continues to increase. In the Netherlands the caesarean section rate increased from 7.4 to 15.8% during the period 1990–2008,1 and in the USA it increased from 21.2 to 32.8% from 1990 to 2011.2 The long-term complications of caesarean section in relation to future reproduction have been comprehensively examined.3,4 In the past decade several articles have described a defect that can be seen on ultrasound at the site of the caesarean section scar, known as a ‘niche’.5,6 A niche is defined as a triangular anechoic structure at the site of the scar or a gap in the myometrium of the anterior lower uterine segment at the site of a previous caesarean section.7,8 Niche prevalence depends on the method used for evaluation and the population investigated.9-16 In non-pregnant women the scar is visible with transvaginal ultrasonography (TVU) and contrast sonohysterography using either saline (saline infusion sonohysterography, SIS) or gel (gel instillation sonohysterography, GIS).5,6 There have been several reports of an association between abnormal bleeding and a niche.8,10-12,15 In particular, postmenstrual spotting seems to be a predominant symptom in women with a niche10,11; however, most of these studies included symptomatic patients, resulting in a possible selection bias. Given the proximity of the niche to the bladder, it has been postulated that the local accumulation of fluid and scarring might disturb bladder function11; however, prospective studies assessing both bleeding symptoms and urinary symptoms in relation to the presence of a niche in a random population of women with a history of caesarean section are scarce. As far as we are aware, none of the reported studies asked women to participate at the time of caesarean section. The aim of our study was to determine the prevalence of niches in the caesarean section scar in a random population of women enrolled immediately after caesarean section, using both TVU and GIS 6–12 weeks after caesarean section, and to examine the relationship between the niche and postmenstrual spotting and urinary incontinence.
Methods
Study design and populationWe conducted a prospective observational cohort study. The trial was registered in the Dutch trial register (trial number NTR-2887). The study was performed in St Antonius Hospital, Nieuwegein: a teaching hospital in the Netherlands. The protocol was approved by the local medical ethics committee (VCMO NL18722.100.07 R-07.14A/SCAR.). Participants were recruited between November 2007 and
Niche prevalence and abnormal uterine bleeding | 55
5

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
56 | Chapter 5
September 2010. Specially trained midwives asked all women over 18 years of age who underwent a caesarean section at St Antonius Hospital during the inclusion period to participate, within 3 days of the caesarean section. Exclusion criteria were twin pregnancies, known uterine anomalies, or the suspicion of a uterine infection, defined as a positive culture or fever and abdominal pain with discharge. After providing written informed consent, all participants were evaluated by TVU followed by GIS 6–12 weeks after the caesarean section. A GIS was not performed when there were suspected placental remnants, intrauterine haematomas, intrauterine fluid accumulation, or a possible pregnancy (i.e. a visit during the midluteal phase in women not using adequate contraception). Women were followed by questionnaires and menstruation score charts at 6–12 weeks, 6 months, and 12 months after the caesarean section.
Transvaginal ultrasoundAll TVU and GIS procedures were performed at St Antonius Hospital by three experienced examiners (L.V., S.V., and M.S.). TVU was performed using a 7.5–MHz transducer (Philips Sonicare HD 11.XE, Philips Medical Systems, Eindhoven, the Netherlands). Women were examined after emptying their bladder. The uterus, uterine scar, and niche, if present, were examined in a standardised way. The position, length, and width of the uterus and double thickness of the endometrium were registered in the midsagittal plane. A niche was defined as an anechoic space (with or without fluid) at least 2 mm deep at the presumed site of the caesarean section scar. The uterus was screened for the presence of caesarean section scar(s) using parallel sagittal planes going from left to right, until the plane with the largest niche depth was defined. The uterus was also scanned in the transverse plane. When a niche was identified, it was measured in the sagittal plane in which the niche had the greatest depth; the depths of the niche and of the residual myometrium at the site of the scar and of the adjacent normal myometrium were measured in real time (see Figure 1). In cases when more than one caesarean section scar was present the largest niche was measured.
Figure 1. Schematic presentation of niche measurement. The following measurements were performed: (1) niche depth (in the sagittal plane); (2) residual myometrium (RM), from the serosal surface of the uterus (without the white lining of the serosa) to the apex of the niche, perpendicular to the endometrium (in sagittal plane); (3) adjacent myometrial thickness (AMT). Adapted from Bij de Vaate et al.11!
!!
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Niche prevalence and abnormal uterine bleeding | 57
5
Gel instillation sonographyA speculum was inserted and a catheter (SIS Rudigoz Catheter, CCD International, Paris, France) was placed inside the uterus. Gel (Endosgel, Farco-Pharma GmbH, Köln, Germany) was flushed inside the uterine cavity and cervix while retracting the catheter. A maximum volume of 10 cm3 was instilled, or less if uterine cramps occurred or reflux was observed from the cervix. The speculum was removed, the vaginal probe was reinserted, and the presence of a niche was recorded in the sagittal plane where the niche had the greatest depth. Niche characteristics were measured and recorded as described above (Figure 1). The shape was classified according to the previous classifications published by Bij de Vaate et al.11 The presence of uterine polyps, fibroids, or other intrauterine abnormalities was noted.
Data collectionThe characteristics of participants, including contraceptive use, breastfeeding, bleeding characteristics before pregnancy, and detailed obstetric history (dates ofprevious caesarean section, indication, and characteristics of the last pregnancy and caesarean section) were noted immediately after informed consent was given. Current contraceptive use and bleeding pattern were recorded at 6–12 weeks after the caesarean section. Women completed and returned a questionnaire at 6 and 12 months after the caesarean section. The questionnaire included questions on current medication or contraceptive use, breastfeeding, bleeding pattern (including duration of menstruation, postmenstrual spotting, vaginal discharge, and urinary incontinence). They were also asked to complete a validated menstrual score chart: the Pictorial Blood Assessment Chart (PBAC).17 All data were recorded in a web-based database by two research nurses. The results of the ultrasound scans were not recorded in the case notes, and women and their doctors were not informed of the ultrasound findings. All women who underwent TVU were included in the analyses. Only women who underwent both TVU and GIS were included in the comparison of TVU and GIS measurement outcomes.
The primary outcome was the prevalence of a niche as measured by TVU and GIS 6–12 weeks after caesarean section. Secondary outcome measures included details of the bleeding pattern, including postmenstrual spotting (defined as more than 2 days of brownish discharge after the end of the menstrual period), number of days of menstrual bleeding, urinary incontinence at 6 and 12 months after caesarean section, and the relationship of these with a niche, and niche characteristics (i.e. depth, residual myometrium, and the ratio of the residual myometrium divided by the total thickness of the adjacent anterior myometrium), identified by TVU and GIS.
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
58 | Chapter 5
Statistical analysesData were analysed using the spss 20 (SPSS Inc., Chicago, IL, USA). Differences in baseline characteristics were compared using the chi-square test, Fisher’s exact test, Student’s t–test, or the Mann–Whitney U–test, depending on the type and distribution of the variables. Logistic regression analysis was planned to analyse the relationship between the presence of a niche and postmenstrual spotting. Potential confounding factors were predefined, and included age, breastfeeding, body mass index (BMI), BMI above 25 kg/m2, oral contraceptive use, and use of the levonorgestrel intrauterine system (LNG-IUS). These potential confounding factors were tested using univariate analysis. All tests were two-sided. A two-tailed P < 0.05 was considered to be statistically significant.
Results
Between November 2007 and September 2010, 350 women gave informed consent to participate in the study within 3 days of their caesarean section at St Antonius Hospital. Of these, 276 were willing to receive a TVU at 6–12 weeks, and 263 women could be included. TVU was used to examine 263 women, and 197 underwent both TVU and GIS (see Figure 2). Two women underwent a second caesarean section during the study period, but only the results of the first caesarean section and the related TVU and GIS were included in the study. TVU and GIS were performed at a mean of 7.6 ± 1.7 (SD) weeks after caesarean section. In total, 72% (191/263) of all women who underwent a TVU completed the questionnaire at 6 months, and 69% (172/249) of the women who received a questionnaire at 12 months after the caesarean section completed it. Of all the women who completed the questionnaire at 12 months, 45 were pregnant again. Of the women who underwent both a TVU and GIS the response rate was 73% at 12 months. Baseline characteristics and sonography results at 6–12 weeks after caesarean section are shown in Table 1. The majority of the women (71%) analysed had had only one previous caesarean section. Sixty-four (24%) had had two and eleven (4%) had had three previous caesarean sections. One caesarean section was carried out by a J–shaped or ‘hockey stick’ incision. All other women had a transverse lower segment incision. The uterus was closed in two layers in four women and in one layer in all others. Most caesarean sections (55%) were performed because of an emergency. During the sonographic evaluation at 6–12 weeks after caesarean section, 55% of the women were breastfeeding and 77% were amenorrhoeic. At 6–12 weeks, the women reported using the following methods of contraception: no contraception, 36%; oral contraceptives, 10%; progesterone only pill, 3%; sterilisation, 4%; condoms, 42%; and other, 5%. The difference in contraceptive use was not statistically significant between patients with or without a niche.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Niche prevalence and abnormal uterine bleeding | 59
5
Figure 2. Flow diagram of study participants.
Excluded (n = 87): • Women not willing to undergo TVU at 6–12 weeks after CS (74)
• Twin pregnancy (6) • Uterus anomaly (1) • New pregnancy (2) • > 12 weeks after CS (1) • Pelvic inflammatory disease (1) • Woman’s 2nd CS during study-‐period (2)
Transvaginal ultrasound (TVU) (n = 263)
Excluded from GIS (n = 66): • Placental remnant/haematoma (8) • Pelvic inflammatory disease (6) • Woman's request (6) • Unprotected intercourse (3) • Failed GIS (no distension) (11) • Failed GIS (pain) (12): • Intrauterine fluid (13) • 0ther (7)
Gel instillation sonography (GIS) (n =197)
Questionnaire completed 12 months after CS (n =172)
Nonresponders (77) Lost to follow-‐up (14) • Incorrect address/moved (12) • Refusal to continue the study (2)
Women willing to participate (n = 350)
There were no differences regarding the rate of primary or emergency caesarean section, age, or parity between women who were included in our analyses and those who refused to participate, those who did not undergo a GIS, or those who did not complete the questionnaire at 12 months.
Niche prevalence and characteristicsNiche prevalence was 49.6% when evaluated by TVU and 64.5% when evaluated by GIS. In three women it was not possible to identify the scar in the uterus with TVU. With GIS all scars were visible. In women with one caesarean section, 62% who underwent GIS had a niche, compared with 68.2% of women with two caesarean sections and 77.8% of women with three caesarean sections. Sonographic characteristics of the uterus are shown in Tables 1 and 2. The length and width of the uterus were no different between women who had or did not have a niche. The niche was deeper when examined by GIS than by TVU (2.32 ± 3.35 and 3.03 ± 3.1 mm, respectively; P < 0.001). The thickness of the residual myometrium at the site of the uterine scar was approximately 2 mm less in women with a niche compared with those without a niche, as measured by TVU and GIS (P < 0.001 and P = 0.005, respectively; see Table 1). The mean

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
60 | Chapter 5
Tabl
e 1.
Cha
ract
eris
tics
of th
e st
udy
part
icip
ants
.
A
ll w
omen
( n
= 2
63)
Nic
he (T
VU)
(n =
129
)N
o ni
che
(TVU
) (n
= 1
31)
P*N
iche
(GIS
) (n
= 1
27)
No
nich
e (G
IS)
(n =
70)
P**
Base
line
char
acte
ristic
s
Age
(yea
rs),
mea
n (±
SD)
32.4
6 (±
4.15
)32
.66
(±4.
16)
32.2
6 (±
4.15
)0.
4432
.51
(±4.
11)
32.7
3 (±
3.85
)0.
72Pa
rity
, mea
n (±
SD)
1.54
(±0.
70)
1.55
(±0.
73)
1.54
(±0.
68)
0.96
1.57
(±0.
78)
1.50
(±0.
68)
0.52
BMI (
kg/m
2 ), m
ean
(±SD
)25
.70
(±5.
58)
26.1
5 (±
5.48
)25
.28
(±5.
66)
0.28
25.9
8 (±
5.83
)24
.98
(±5.
19)
0.29
Num
ber
of c
aesa
rean
sec
tions
, mea
n (±
SD)
1.33
(±0.
56)
1.35
(±0.
57)
1.31
(±0.
54)
0.55
1.35
(±0.
59)
1.26
(±0
.50)
0.26
Visi
t at 6
–12
wee
ks a
fter
cae
sare
an s
ectio
n
Wee
ks a
fter
cae
sare
an s
ectio
n, m
ean
(±SD
)7.
58 (±
1.74
)7.
40 (±
1.40
)7.
74 (±
2.01
)0.
127.
66 (±
1.77
)7.
72 (±
1.92
)0.
82Br
east
feed
ing,
num
ber
(per
cent
age)
***
142
(55%
)67
(52%
)75
(±59
%)
0.38
64 (5
3%)
41 (6
1%)
0.29
Ultr
ason
ogra
phic
resu
lts a
t 6–1
2 w
eeks
aft
er c
aesa
rean
sec
tion
Dou
ble
endo
met
rial
thic
knes
s TV
U (m
m),
mea
n (±
SD)
5.49
(±3.
80)
5.61
(±3.
85)
5.36
(±5.
77)
0.61
5.36
(±3.
57)
4.86
(±3.
33)
0.34
Ute
rus
leng
th T
VU (c
m),
mea
n (±
SD)
7.18
(±1.
43)
7.29
(±1.
52)
7.07
(±1.
32)
0.23
7.09
(±1.
38)
7.11
(±1.
47)
0.92
Ute
rus
wid
th T
VU (c
m),
mea
n (±
SD)
4.23
(±0.
94)
4.26
(±0.
81)
4.19
(±1.
07)
0.59
4.27
(±0.
84)
4.17
(±1.
20)
0.49
Thic
knes
s of
myo
met
rium
at s
ite o
f CS
scar
(mm
), m
ean
(±SD
)9.
59 (±
4.18
)8.
51 (±
3.90
)10
.73
(±4.
18)
<0.0
018.
59 (±
3.81
)10
.20
(±3.
59)
0.00
5
BMI,
body
mas
s in
dex;
TVU
, tra
nsva
gina
l ultr
asou
nd; G
IS, g
el in
still
atio
n so
nohy
ster
ogra
phy.
*P v
alue
bet
wee
n ni
che
and
no n
iche
dur
ing
TVU
.**
P va
lue
betw
een
nich
e an
d no
nic
he d
urin
g G
IS.
***N
o in
form
atio
n on
bre
astf
eedi
ng fo
r 13
pat
ient
s at
6–1
2 w
eeks
aft
er C
S.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Niche prevalence and abnormal uterine bleeding | 61
5
ratio between the thickness of the residual myometrium at the site of the niche and the thickness of the adjacent myometrium was 0.74 ± 0.58 in all women who underwent GIS. The ratio was <0.5 in 22% of these women. Most niches detected by GIS had a semicircular shape (55%); 24% had a triangular shape, 10% had a droplet shape, 6% were inclusion cysts, and 7% had another shape.
Table 2. Comparison of transvaginal ultrasound (TVU) and gel instillation sonohysterography (GIS) results (n = 197)*.
TVU GIS P (95%CI)
Niche depth of all women, mean (±SD)** 2.32 (±3.35) 3.03 (±3.1) <0.001 (0.38–1.02)Niche depth of women with niche on GIS, mean (±SD)** 3.43 (±3.67) 4.77 (±2.64) <0.001 (0.92–1.79)Residual myometrial thickness of all women, mean (±SD) 9.58 (±4.39) 9.11 (±3.8) 0.06 (–0.24–0.96)Residual myometrial thickness of women with niche on GIS, mean (±SD)
9.30 (±4.67) 8.59 (±3.75) 0.03 (0.09–1.38)
*Of the 263 women in total, only the 197 women who underwent both TVU and GIS were included in this table.**Niche depth was recorded as 0 when no niche was observed.
Bleeding pattern and urological symptomsThe questionnaire at 6 months was completed by 191 women. Information on the menstrual cycle was available for only 59 women. Given the large proportion of women who were still breastfeeding or who did not yet have a regular menstrual cycle we decided not to analyse the outcomes at 6 months. The questionnaire at 12 months was completed by 172 women. The menstrual pattern could not be analysed in 45 of these women because of a subsequent pregnancy. Ten of these women completed the information on the basis of their menstruation pattern before pregnancy. Information on the menstrual cycle and contraceptive use was available for 137 women, of whom 17 were amenorrhoeic because of LNG-IUD or another hormonal contraceptive. Postmenstrual spotting was reported by 13 out of 45 (28.9%) women with a niche detected by GIS, compared with two women out of 29 (6.9%) without a niche detected by GIS (OR 5.48, 95% CI 1.14–26.48; Table 3). Including only primiparae, again postmenstrual spotting was reported more frequently in women with a niche detected by both TVU or GIS compared with those without a niche (31 versus 4% for TVU and 32 versus 0% for GIS; OR 9.7, 95% CI 1.1–85.6). Women with a ratio of residual myometrium of less than half of the adjacent myometrium (ratio <0.5) measured by TVU or GIS reported postmenstrual spotting more often than women with a ratio of >0.5 (OR 7.2, 95% CI 1.74–21.62, and OR 6.1, 95% CI 1.94–26.70, respectively; Table 4).Using univariate analyses none of the predefined confounding factors or baseline characteristics were related to postmenstrual spotting: all had P > 0.1 (LNG-IUD use, P = 0.11; oral contraceptive use, P = 0.24; breastfeeding, P = 1.0; age, P = 1.0; BMI, P = 1.0; BMI > 25 kg/m2, P = 0.40), and therefore the planned

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
62 | Chapter 5
Tabl
e 3.
Ute
rine
ble
edin
g pa
tter
n an
d ur
olog
ical
sym
ptom
s at
12
mon
ths
afte
r ca
esar
ean
sect
ion.
Nic
he (T
VU)
No
nich
e (T
VU)
P*N
iche
(GIS
)
No
nich
e (G
IS)
P**
OR
(95%
CI)
No.
of w
omen
with
pos
tmen
stru
al s
pott
ing
( n =
91/
74)*
**13
(26)
5 (1
2)0.
1013
(28.
9)2
(6.9
)0.
025.
48 (1
.14–
26.4
8)D
ays
of b
lood
loss
dur
ing
men
stru
atio
n, m
ean
(±SD
) (n
= 91
/83)
***
5.9
(±2.
57)
6.1
(±2.
84)
0.75
5.5
(±2.
1)5.
5 (±
1.4)
0.98
No.
of w
omen
with
vag
inal
dis
char
ge (n
= 1
37/9
8)**
*11
(14)
11 (1
8)0.
847
(11)
8 (2
3)0.
15
No.
of w
omen
taki
ng o
ral c
ontr
acep
tives
(n =
137
/109
)***
19 (2
5)13
(21)
0.61
19 (2
8)10
(24)
0.82
No.
of w
omen
with
LN
G-IU
D (n
= 1
37/1
09)*
**9
(12)
8 (1
3)0.
8210
(15)
2 (5
)0.
21N
o. o
f wom
en w
ith a
men
orrh
oea
(n =
137
/109
)***
12 (1
6)5
(8)
0.18
9 (1
3)3
(7)
0.53
No.
of w
omen
with
inco
ntin
ence
(n =
115
/90)
***
20 (3
1)17
(34)
0.71
19 (3
3)10
(29)
0.82
No.
of w
omen
with
str
ess
inco
ntin
ence
(n =
115
/90)
***
15 (2
3)11
(22)
0.89
14 (2
5)6
(17)
0.45
No.
of w
omen
with
urg
e in
cont
inen
ce (n
= 1
15/9
0)**
*4
(6)
3 (6
)0.
972
(4)
2 (6
)0.
63
No.
of p
regn
ant w
omen
(n =
260
/197
)***
17 (1
3)28
(21)
0.08
21 (1
6.5)
15 (2
1)0.
40N
o. lo
st to
follo
w-u
p/no
n-re
spon
ders
(n =
263
/197
)42
(33)
49 (3
7)0.
4145
(35)
18 (2
6)0.
16To
tal (
n =
260/
197)
***
129
(49.
6)13
1 (5
0.4)
127
(64.
5)70
(35.
5)
Dat
a ar
e pr
esen
ted
as n
umbe
r (%
) unl
ess
indi
cate
d w
ith m
ean
(±SD
).G
IS, g
el in
still
atio
n so
nohy
ster
ogra
phy;
TVU
, tra
nsva
gina
l ultr
asou
nd; L
NG
-IUD
, lev
onor
gest
rel i
ntra
uter
ine
devi
ce.
Thre
e w
omen
for
who
m th
e pr
esen
ce o
f a n
iche
cou
ld n
ot b
e de
term
ined
wer
e ex
clud
ed.
* P v
alue
bet
wee
n ni
che
and
no n
iche
dur
ing
TVU
.**
P va
lue
betw
een
nich
e an
d no
nic
he d
urin
g G
IS.
***N
umbe
r of
wom
en w
ho c
ompl
eted
the
ques
tionn
aire
for
a sp
ecifi
c pa
ram
eter
and
who
und
erw
ent T
VU/G
IS, r
espe
ctiv
ely.
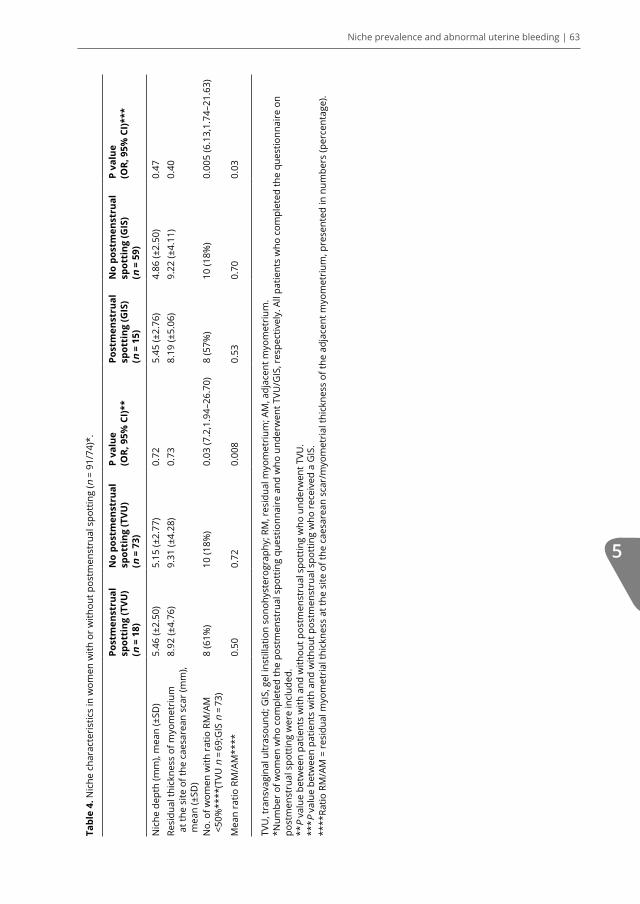
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Niche prevalence and abnormal uterine bleeding | 63
5
Tabl
e 4.
Nic
he c
hara
cter
istic
s in
wom
en w
ith o
r w
ithou
t pos
tmen
stru
al s
pott
ing
(n =
91/
74)*
.
Po
stm
enst
rual
sp
otti
ng (T
VU)
( n =
18)
No
post
men
stru
al
spot
ting
(TVU
) (n
= 7
3)
P va
lue
(OR,
95%
CI)*
*Po
stm
enst
rual
sp
otti
ng (G
IS)
(n =
15)
No
post
men
stru
al
spot
ting
(GIS
) (n
= 5
9)
P va
lue
(OR,
95%
CI)*
**
Nic
he d
epth
(mm
), m
ean
(±SD
)5.
46 (±
2.50
)5.
15 (±
2.77
)0.
72
5.45
(±2.
76)
4.86
(±2.
50)
0.47
Re
sidu
al th
ickn
ess
of m
yom
etri
um
at th
e si
te o
f the
cae
sare
an s
car
(mm
), m
ean
(±SD
)
8.92
(±4.
76)
9.31
(±4.
28)
0.73
8.
19 (±
5.06
)9.
22 (±
4.11
)0.
40
No.
of w
omen
with
rat
io R
M/A
M<5
0%**
**(T
VU n
= 6
9;G
IS n
= 7
3)8
(61%
)10
(18%
)0.
03 (7
.2,1
.94–
26.7
0)8
(57%
)10
(18%
)0.
005
(6.1
3,1.
74–2
1.63
)
Mea
n ra
tio R
M/A
M**
**0.
500.
720.
008
0.53
0.70
0.03
TVU
, tra
nsva
gina
l ultr
asou
nd; G
IS, g
el in
still
atio
n so
nohy
ster
ogra
phy;
RM
, res
idua
l myo
met
rium
; AM
, adj
acen
t myo
met
rium
.*N
umbe
r of
wom
en w
ho c
ompl
eted
the
post
men
stru
al s
pott
ing
ques
tionn
aire
and
who
und
erw
ent T
VU/G
IS, r
espe
ctiv
ely.
All
patie
nts
who
com
plet
ed th
e qu
estio
nnai
re o
n po
stm
enst
rual
spo
ttin
g w
ere
incl
uded
.**
P va
lue
betw
een
patie
nts
with
and
with
out p
ostm
enst
rual
spo
ttin
g w
ho u
nder
wen
t TVU
.**
* P v
alue
bet
wee
n pa
tient
s w
ith a
nd w
ithou
t pos
tmen
stru
al s
pott
ing
who
rec
eive
d a
GIS
. **
**Ra
tio R
M/A
M =
res
idua
l myo
met
rial
thic
knes
s at
the
site
of t
he c
aesa
rean
sca
r/m
yom
etri
al th
ickn
ess
of th
e ad
jace
nt m
yom
etri
um, p
rese
nted
in n
umbe
rs (p
erce
ntag
e).

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
64 | Chapter 5
logistic regression was not performed. We did not find any significant differences between women with or without a niche concerning the existence of (combined) urinary incontinence, urge incontinence, or stress incontinence (see Table 3).
Discussion
Main findingsAll caesarean section scars could be identified using GIS. Using this technique the prevalence of niches at the site of these caesarean section scars was high (64.5%) in a random population. Comparing the results of GIS with TVU, niche prevalence was higher, measured niche depth was greater, and residual myometrium was thinner when detected by GIS. Postmenstrual spotting 1 year after caesarean section was strongly related to the presence of a niche detected by both TVU and GIS. One out of three women with a niche detected by GIS reported postmenstrual spotting, compared with one out of ten women without a niche. Postmenstrual spotting was related to a residual : adjacent myometrium ratio of <50%, which might indicate that this is a relevant parameter for niche size. The prevalence of urinary incontinence was not related to the presence or absence of a niche.
Strengths and limitations of the studyTo the best of our knowledge this is the first study that has recruited participants at a very early stage after their caesarean section (within 3 days), followed by early examination (within 3 months) by both TVS and GIS, and with the sequential completion of menstrual questionnaires up to 1 year after the caesarean section. Only two prospective studies have evaluated niches in an unselected population.11,18 Both these studies recruited patients at 6–12 months after caesarean section. The Bij de Vaate et al.11 study was carried out by our study group, but in a different population and with the examinations performed by a different examiner. In the present study, early scanning (3 months after the caesarean section) meant that the vast majority of the women were still amenorrhoeic, so the influence of abnormal uterine bleeding on the willingness of women to participate (selection bias) is expected to be limited. An additional advantage of early sonographic evaluation is that, because of amenorrhoea in most patients, the potential confounding effect of variations in timing of the measurements during the menstrual cycle and related endometrial thickness is limited. In addition, women were consecutively asked to participate by research midwives, and the registration of the results was independent of clinical considerations. Women and their doctors were not informed whether or not a niche was observed to prevent possible bias in reporting their bleeding pattern. Although complete post-caesarean section scar healing may take up

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Niche prevalence and abnormal uterine bleeding | 65
5
to 6 months6, we do not know the exact time needed to develop a niche. We defined a niche as an anechoic space (with or without fluid) with a depth of at least 2 mm at the presumed site of the caesarean section scar. This should not be confused with the caesarean section scar itself. As demonstrated in this study, a scar is almost always visible and is reflected as a hypoechoic indentation of the myometrium at the location of the caesarean section. We expect the uterine scar to continue to heal beyond 6–12 weeks, and this might differ in performance with time. However, we consider it very unlikely that niches (i.e. discontinuations and fluid-stained spaces in the myometrium) will heal after this period. However, changes in a niche over time are not unlikely. Sustained accumulation of fluid may, in theory, increase niche size over time, but no data are currently available to confirm this theory.
A possible limitation of our study is that not all women who were delivered by caesarean section during the study period were asked to participate. Women were asked consecutively by trained midwives during their day and night shifts, but these midwives were not always present. Because the absence of the midwives was randomly distributed over the week, we consider this potential effect on selection bias to be minor. This is underlined by the lack of differences in baseline characteristics between women who were asked to participate and those who were not, with regards to elective or emergency caesarean section, age, and parity. In addition, we did not observe any differences in these parameters between included and excluded women, or those who were not willing to undergo a GIS or who did not complete the questionnaire.
Patients with a previous twin pregnancy or a known uterine anomaly were excluded in order to assemble a homogeneous group and to prevent undesired effects of unknown confounding factors; however, whether these factors would in fact introduce significant confounding effects is a topic for further discussion. We also decided not to perform a GIS in patients with a placental remnant, haematoma, or fluid in the uterine cavity detected by TVU. Consequently, a relatively small proportion of all patients who provided informed consent were analysed. Whether it is correct to exclude women with intrauterine fluid collection from examination by GIS should be further discussed. This was decided before the start of the study, and was included in the study protocol; however, it can be postulated that this group might have been particularly symptomatic and prone to postmenstrual spotting. We could not observe any relationship between niches and urinary incontinence, but we did not report other urinary symptoms, such as urgency. An additional shortcoming of the study is that we did not measure the niche width in the sagittal plane or the niche length in the transverse plane, as recently proposed by Naji et al.5 (our study had already begun before

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
66 | Chapter 5
that publication). Therefore, we could not analyse the relationship between these parameters and niche symptomatology. We also did not determine the reproducibility of our measurements.
Clinical implications of the findings and relation to published dataWe were able to identify the caesarean section scar with GIS in 100% of the women. This is in line with another study examining women within 3 months of a caesarean section.19 The observed niche prevalence rate of 49.6% using TVU is comparable with the reported prevalence (42%) in a prospective cohort study of an unselected population.9 Different prevalence rates (28 and 61%) were reported in prospective studies in populations evaluated at 6 months and at 6–12 months after a caesarean section.11,13 Different definitions of a niche and different timing after the caesarean section may both affect the niche detection rate. Vikhareva Osser et al.13 used the definition ‘any visible defect’, and Bij de Vaate et al.11 used ‘any indentation of at least 1 mm’. We used a cut-off level of 2 mm; however, consensus on the exact cut-off levels is lacking. Early scanning may facilitate the recognition of the location of the caesarean section scar in the uterine wall as a result of incomplete scar healing, and this may increase the detection of small niches. In addition, the related thin endometrium resulting from breastfeeding in the majority of the women may also improve niche recognition and measurement.
We used the same terminology as that suggested by Naji et al.5, and measured the depth and residual myometrial thickness in the sagittal plane as described. Niche prevalence using GIS was 64.5% in our study, which is comparable with the reported prevalence using GIS or SIS in random, unselected populations (56, 59.5, 59, and 78%).10,11,14,18 Niche prevalence was higher using GIS than with TVU only. These findings are in line with the reported findings of three studies comparing GIS or SIS with TVU.10,11,18 These studies showed a higher niche prevalence with sonohysterography than with TVU without contrast, and thus GIS may be more accurate at detecting niches. Although the niches that were detected using GIS but were missed using TVU were smaller than those detected by both TVU and GIS, they can be clinically relevant. This is underlined by the strong relationship we found between postmenstrual spotting and niches on GIS.11 An additional argument for using GIS rather than TVU is that the residual myometrium measured using GIS was significantly thinner. The residual myometrium is considered to be the main limiting factor for eventual hysteroscopic niche resections to treat related bleeding symptoms. Most publications report a required residual myometrium of 2–3 mm for hysteroscopic niche resection, given the risk of perforation and/or bladder injury.20 In order to prevent undesired complications during hysteroscopic niche resections we propose that a GIS or SIS be used rather than TVU for the preoperative evaluation of the residual myometrium. Several previous studies
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Niche prevalence and abnormal uterine bleeding | 67
5
indicated a relationship between large niches and postmenstrual spotting. Bij de Vaate et al.11 reported the niche volume to be related to postmenstrual spotting. We were not able to calculate niche volume because of the lack of stored three-dimensional volumes. In order to assess the relationship between large niches and postmenstrual spotting, we decided not to take an absolute measurement of residual myometrium, but to relate it to the adjacent myometrium. We defined large niches as those with a residual myometrium with thickness of <50% of that of the adjacent myometrium. This parameter was significantly related to postmenstrual spotting. This parameter and cut-off level were also used by Ofilli-Yebovi et al.15, who reported a high prevalence of women with a ratio of less of than 50% in a population with gynaecological symptoms. A potential relationship between niche size and postmenstrual spotting is in line with the hypothesis that spotting is induced by the accumulation of blood inside the niche.6,7 A depth of more than half the myometrial thickness makes the anterior part of the niche possibly large enough to obstruct the direct outflow of menstrual blood. This, in combination with lower contractility as a result of fibrosis, may induce the accumulation of blood in a niche.
One out of three women with a niche observed by GIS reported postmenstrual spotting. This is in line with the previous reported prevalence of postmenstrual spotting in patients with a niche.10,11 Given the high prevalence of postmenstrual spotting after caesarean section, this should be part of routine counselling before elective caesarean section.
Future perspectivesFuture research should focus on the relationship of niches to subsequent fertility, obstetric complications such as uterine rupture, and on the impact of a niche on a woman’s well-being. There is a lack of information on the impact of niche-related bleeding disorders on women’s quality of life, their sexual function, and their willingness to undergo treatment for related symptoms.
Conclusion
In conclusion, the caesarean section scar was visible in all women at 6–12 weeks after caesarean section using GIS. The prevalence of niches detected by GIS is high after caesarean section (64.5%), and more niches are detected using GIS than using TVU, with a larger observed niche size and reduced residual myometrial thickness. The presence of a niche is related to postmenstrual spotting. Postmenstrual spotting is more frequent in patients with large niches (defined as a residual myometrium of thickness <50% of that of the adjacent myometrium) than in patients with smaller niches.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
68 | Chapter 5
Acknowledgements
We thank K.W. Van den Berg-Swart and C. van Dam-Bourens, research nurses, for recording all the collected data in the database. We thank M. Stigter-de Vries MD for performing the ultrasounds.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Niche prevalence and abnormal uterine bleeding | 69
5
1. Stichting Perinatale Registratie Nederland. Perinatale zorg in Nederland 2008. Utrecht: Stichting Perinatale Registratie Nederland. 2011 [www.perinatreg.nl]. Accessed 25 April 2013.
2. [http://www.cdc.gov/nchs/data/nvsr/nvsr61/nvsr61_05.pdf] Accessed 29 April 2013.
3. Silver RM. Implications of the first cesarean: perinatal and future reproductive health and subsequent cesareans, placentation issues, uterine rupture risk, morbidity, and mortality. Semin Perinatol 2012;36:315–23.
4. Miller ES, Hahn K, Grobman A. Consequences of a primary elective Cesarean Delivery Across the Reproductive Life. Obstet Gynecol 2013;121:789–97.
5. Naji O, Abdallah Y, Bij de Vaate AJ, Smith A, Pexsters A, Stalder C, et al. Standardised approach for imaging and measuring Cesarean section scars using ultrasonography. Ultrasound Obstet Gynecol 2012;39:252–9.
6. Roberghe S, Boutin A, Chaillet N, Moore L, Jastrow N, Demers S, et al. Systematic review of cesarean scar assessment in the nonpregnant state: imaging techniques and uterine scar defect. Am J Perinatol 2012;29:465–72.
7. Monteagudo A, Carreno C, Timor-Tritsch IJ. Saline infusion sonohysterography in nonpregnant women with previous caesarean delivery: the “niche” in the scar. J Ultrasound Med 2001;20:1105–15.
8. Thurmond AS, Harvey WJ, Smith SA. Cesarean section scar as a cause of abnormal vaginal bleeding: diagnosis by sonohysterography. J Ultrasound Med 1999;18:13–6.
9. Armstrong V, Hansen WF, Van Voorhis BJ, Syrop CH. Detection of cesarean scars by transvaginal ultrasound. Obstet Gynecol 2003;101:61–5.
10. Valenzano M, Lijoi D, Mistrangelo E, Constantini S, Ragni N. Vaginal ultrasound and hysterosonographic evaluation after caesarean section: correlation with gynaecological symptoms. Gynecol Obstet Invest 2006;61:216–22.
11. Bij de Vaate AJM, Brolmann HAM, van der Voet LF, van der Slikke JW, Veersema S, Huirne JAF. Ultrasound evaluation of the caeserean scar:
relation between a niche and postmenstrual spotting. Ultrasound Obstet Gynecol 2011;37:93–9.
12. Uppal T, Lanzarone V, Mongelli M. Sonographically detected caesarean section scar defects and menstrual irregularity. J Obstet Gynaecol 2011;31:413–6.
13. Vikhareva Osser O, Jokubkiene L, Valentin L. High prevalence of defects in Cesarean section scars at transvaginal ultrasound examination. Ultrasound Obstet Gynecol 2009;34:90 – 7.
14. Regnard C, Nobusch M, Fellemans C, Benali N, Van Rijsselberghe M, Rozenberg S. Caesarean section scar evaluation by saline contrast sonohysterography. Ultrasound Obstet Gynecol 2004;3:289–92.
15. Ofilli-Yebovi D, Ben-Nagi J, Swayer E, Lee C, Gonzalez J, Jurkovic D. Deficient lower-segment Cesarean section scars: prevalence and risk factors. Ultrasound Obstet Gynecol 2008;31:72–7.
16. Wang CB, Chiu WW, Lee CY, Sun YL, Lin YH, Tseng CJ. Cesarean scar defect: correlation between Cesarean section number, defect size, clinical symptoms and uterine position. Ultrasound Obstet Gynecol 2009;34:85–9.
17. Janssen CA, Scholten PC, Heintz AP. A simple visual assessment technique to discriminate between menorrhagia and normal menstrual blood loss. Obstet Gynecol 1995;8 5:977–82.
18. Vikhareva Osser O, Jakubkiene L, Valentin l. Cesarean section scar defects: agreement between transvaginal sosnographic findings with and without saline contrast enhancement. Ultrasound Obstet Gynecol 2010;35:75–83.
19. Chen HY, Chen SJ, Hsieh FJ. Observation of caesarean section scar by transvaginal ultrasonography. Ultrasound Med Biol 1990;16:443–7.
20. Chang Y, Tsai EM, Long CY, Lee CL, Kay N. Resectoscopic treatment combined with sonohysterographic evaluation of women with postmenstrualbleeding as a result of previous cesarean delivery scar defects. Am J Obstet Gynecol 2009;200:370.e1–4.
References

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
66|Prevalence, potential risk factors for Prevalence, potential risk factors for
development and symptoms related to development and symptoms related to the presence of uterine niches following the presence of uterine niches following
Cesarean section: systematic reviewCesarean section: systematic review
A.J.M. Bij de VaateA.J.M. Bij de VaateL.F. van der Voet L.F. van der Voet
O. Naji M. Witmer M. Witmer
S. Veersema S. Veersema H.A.M. BrölmannH.A.M. Brölmann
T. BourneT. BourneJ.A.F. HuirneJ.A.F. Huirne
Ultrasound Obstet Gynecol 2014;43(4):372-82.Ultrasound Obstet Gynecol 2014;43(4):372-82.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
72 | Chapter 6
Abstract
ObjectiveTo review systematically the medical literature reporting on the prevalence of a niche at the site of a Cesarean section (CS) scar using various diagnostic methods, on potential risk factors for the development of a niche and on niche-related gynecological symptoms in non-pregnant women.
MethodsThe PubMed and EMBASE databases were searched. All types of clinical study reporting on the prevalence, risk factors and/or symptoms of a niche in non-pregnant women with a history of CS were included, apart from case reports and case series.
ResultsTwenty-one papers were selected for inclusion in the review. A wide range in the prevalence of a niche was found. Using contrast-enhanced sonohysterography in a random population of women with a history of CS, the prevalence was found to vary between 56% and 84%. Nine studies reported on risk factors and each study evaluated different factors, which made it difficult to compare studies. Risk factors could be classified into four categories: those related to closure technique, to development of the lower uterine segment or location of the incision or to wound healing, and miscellaneous factors. Probable risk factors are single-layer myometrium closure, multiple CSs and uterine retroflexion. Six out of eight studies that evaluated niche-related symptoms described an association between the presence of a niche and postmenstrual spotting.
ConclusionsThe reported prevalence of a niche in non-pregnant women varies depending on the method of detection, the criteria used to define a niche and the study population. Potential risk factors can be categorized into four main categories, which may be useful for future research and meta-analyses. The predominant symptom associated with a niche is postmenstrual spotting.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 73
6
Introduction
In recent decades, the percentage of Cesarean section (CS) deliveries has dramatically increased in most developed countries. An average rate of 21.1% for developed countries has been reported, with a range between 6.2% and 36%1. There are some well-known complications, such as uterine rupture and pathologically adherent placenta in future pregnancy2,3, but there is now an increasing interest in the long-term effects of this procedure. Recently, the presence of a niche at the site of a CS scar has been observed4-7. A niche is mainly a sonographic finding and has been defined as a triangular anechoic area at the presumed site of incision8. However, a generally accepted definition of a niche is still under debate. Alternative terms for a niche are Cesarean scar defect4,9,10, deficient Cesarean scar11, diverticulum12, pouch6 and isthmocele13. Interest in the potential clinical relevance of a niche has increased in the last few years and a growing number of studies on the subject have been published. Various methods to detect and measure a niche have been described. The majority of papers have evaluated the niche with the use of transvaginal sonography (TVS)5,9-11,14,15 and contrast-enhanced sonohysterography (SHG)5,8,15-18, but a minority have used hysteroscopy6,13,16 or hysterosalpingography12. At present there is no consensus regarding the gold standard for the detection and measurement of a niche. As not all women with a history of CS develop a niche, it is of interest to identify the risk factors that may predict their development. In addition, there is growing interest in possible associations between the presence of a niche and various gynecological symptoms, and in the mechanisms behind the development of these symptoms. A common symptom reported to be associated with the presence of a niche is postmenstrual spotting5,6,10,18.
The objective of the current review was to give a systematic overview of the available literature on the prevalence of a niche using various diagnostic methods, on potential risk factors for the development of a niche and on niche-related gynecological symptoms in non-pregnant women.
Methods
Search strategyIn February 2013, we searched the PubMed and EMBASE databases for words in the title or abstract and MeSH terms. All possible combinations of known terms for niche (cicatrix, scar, isthmocele, anechoic, pouch, wound dehiscence, diverticulum), uterus (uterine diseases, myometrium, endometrium, myoendometrium) and CS (Cesarean, caesarean, c section, abdominal delivery,

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
74 | Chapter 6
postCesarean, postcaesarean) were used. The complete electronic search strategy is provided in Appendix S1. Reference lists of the studies were cross-checked to identify cited articles not captured by the electronic search.
Study selection criteriaWe included all types of clinical study reporting on the prevalence, risk factors and/or symptoms of a niche in non-pregnant women, using TVS, SHG or hysteroscopy. Studies in the English language published as full papers in peer-reviewed journals were included. Case reports or small case series were excluded. Given the limited number of cohort studies or randomized controlled trials, we did not apply additional methodological filters for paper selection. The types of study we expected to find were randomized controlled trials, prospective cohort studies (following a group of similar individuals over time), retrospective cohort studies (comparison of patients’ medical records for a particular outcome), cross-sectional studies (observation of a population at one specific point in time) and case–control studies (comparing subjects who have a certain condition with patients who do not, in order to identify a factor that may contribute to this condition).
Studies were selected in a two-stage process by two researchers ( J.H. and A.B.). First, eligibility was assessed based on the titles and abstracts. Full manuscripts were obtained for all selected studies. In the second step, the decision for final inclusion was made after examination of the full papers. The outcomes of this review are the prevalence of a niche in women with a history of CS, risk factors for the development of a niche and symptoms related to the presence of a niche.
Presentation of dataThe PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) statement was used for reporting the methods, results and discussion sections of the current review and the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement was used to obtain an impression of the quality of the included studies19,20. Included papers were ordered in the tables according to the outcome of the most relevant items of the STROBE checklist, such as clear definition of the study population and clear description of the method of evaluation. The extended STROBE checklist, including all STROBE items, is provided in Appendix S2. The QUADAS (Quality Assessment of Diagnostic Accuracy) checklist was used for assessing the methodological quality of the studies reporting on the accuracy of diagnostic tests21.
The included studies were divided into papers reporting on niche prevalence, risk factors and symptoms. The tables were subdivided into two sections: a section

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 75
6
with studies performed in a random population of women with a history of CS, and a section with studies performed in a population of women with gynecological symptoms. All studies were assessed for potential risk of bias. Papers were ranked based on methodological criteria, which means that randomized controlled trials and studies with a clear definition of study population and method of evaluation were placed at the top of the tables. In the table reporting on risk factors, studies including women with one previous CS and in which multivariate analysis was used were placed in the first few columns.
Results
Literature identificationThe electronic search in PubMed and EMBASE generated 2953 records. Four additional records were identified through cross-checking. After screening 2957 abstracts, 27 papers were thought to meet the inclusion criteria and were selected for full assessment. Six papers were excluded for the following reasons: study design (two case reports), three publications did not meet the outcome measures and in one study women were examined at 14–16 weeks’ gestation. We included two studies that were subgroups of a study by Vikhareva Osser et al.9 as new outcome parameters were tested17,22. The final study included 21 papers (Figure 1).
1370 records identified through searching
Pubmed
4 additional records identified through
cross-checking
2957 records screened2930
records excluded
21 studies included
6 publications excluded:-2 case reports-3 publications did not meet the outcome measures -In 1 publication women were examined at 14-16 weeks’ gestation
1583 records identified through searching
Embase (Pubmed results were
excluded)
27 full-text articles assessed for
eligibility
Figure 1: Flow diagram of literature search for articles on uterine niches following Cesarean section.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
76 | Chapter 6
Table 1: Methodological characteristics, based on the STROBE-statement, of included studies performed either in a random population of women with a history of Cesarean section (CS) or in women with a history of CS and gynecological symptoms (i.e. subject to selection bias).
Study Design Clear definition of study population
Clear description of niche assessment
Clear description of assessment of all outcomes
Description of missing data
Correction for confounders
Random population
Yazicioglu, 200626
RCT Yes Yes No Yes Yes
Vikhareva Osser, 201022
Prosp. cohort Yes Yes Yes NA Yes
Bij de Vaate, 20115
Prosp. cohort Yes Yes Yes Yes Yes
Hayakawa, 200625
Prosp. cohort Yes Yes Yes NA Yes
Valenzano, 200615
Case-control Yes Yes Yes NA No
Vikhareva Osser, 201017
Prosp. cohort Yes Yes Yes NA No
Vikhareva Osser, 20099
Case-control Yes Yes Yes NA No
Ceci, 201223
Prosp. cohort Yes Yes Yes Yes No
Armstrong, 20034
Case-control Yes Yes Yes NA No
Regnard, 20047
Prosp. cohort No Yes Yes NA No
Chen, 199014
Prosp. cohort No No No NA No
Glavind, 201224
Retro. cohort Yes Yes Yes NA No
Women with gynecological symptoms
Ofili-Yebovi, 200811
Prosp. cohort Yes Yes Yes Yes Yes
El-Mazny, 201116
Cross-sectional Yes Yes Yes NA No
Monteagudo, 20018
Prosp. cohort Yes Yes Yes NA No
Wang, 200910
Cross-sectional No Yes Yes NA Yes
Chang, 200927
Prosp. cohort No Yes No NA No
Uppal, 201128
Prosp. cohort No No Yes No Yes
Borges, 201013
Prosp. cohort No No No NA No
Thurmond, 199918
Prosp. cohort No No No NA No
Fabres, 20036
Retro. cohort No Yes No NA No
Only first author is listed for each study. Prosp., prospective; RCT, randomized controlled trial; Retro., retrospective.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 77
6
The niche was evaluated in a random population of women with a history of CS in 12 studies4,5,7,9,14,15,17,22-26. In these studies, women with a history of CS were included regardless of the presence of symptoms. The other nine studies evaluated women who were referred for a variety of gynecological symptoms, such as abnormal uterine bleeding or infertility6,8,10,11,13,16,18,27,28. The included studies with a random population and those with a population of women with symptoms are reported in Table 1. The diagnostic methods used for evaluation of the uterine cavity were TVS in 16 studies4-6,9-11,14,15,17,22-28, SHG in eight studies5,7,8,15-18,22 and hysteroscopy in four studies6,13,16,23.
PrevalenceThe prevalence of a niche was reported in 15 papers. Seven studies were performed in a random population of women with a history of CS (Table 2) and eight in a population of women with gynecological symptoms (Table 3).
Using TVS, the reported prevalence of a niche varied between 24% and 70% in four studies with a random population of women with a history of one or multiple CSs4,5,9,17. All four studies met the STROBE criteria in terms of a clear description of study population and method of evaluation. Using SHG, the prevalence of a niche varied between 56% and 84% in three studies with a random population that met the STROBE criteria5,15,17. The prevalence of a niche as ascertained by hysteroscopy was only evaluated in populations of women with gynecological symptoms13,16 (Table 3).
Two studies meeting the STROBE criteria and conducted in a random population of women with a history of CS reported the prevalence of a niche using both TVS and SHG5,17. Vikhareva Osser et al.17 reported a niche prevalence of 84% with SHG and 70% with TVS, with a niche defined as any indentation or other defect in the scar. The same authors found that the length and height of Cesarean scar defects were greater when evaluated using SHG than when evaluated using TVS, and that more scars were seen and classified subjectively as large by SHG without a change being noted in the shape. Bij de Vaate et al.5 found a niche prevalence of 56% with SHG and 24% with TVS, and defined a niche as an anechoic area at the site of the CS scar with a depth of at least 1 mm.
Another study performed in women with gynecological symptoms compared the accuracy of SHG with hysteroscopy as the reference technique and demonstrated that SHG is comparable to hysteroscopy for the diagnosis of a niche as shown by the sensitivity (87%), specificity (100%), positive predictive value (100%), negative predictive value (95%) and overall accuracy (96%)16. This study did not meet

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
78 | Chapter 6
Tabl
e 2:
Pre
vale
nce
of a
nic
he in
rel
atio
n to
dia
gnos
tic m
etho
d in
a r
ando
m p
opul
atio
n of
wom
en w
ith a
his
tory
of C
esar
ean
sect
ion
(CS)
.
Stud
yD
esig
nn
Popu
lati
onD
efini
tion
of a
ni
che
Out
com
eN
iche
pr
eval
ence
on
TVS
(%)
Nic
he
prev
alen
ce
on S
HG
(%)
Resu
lts
Popu
latio
n w
ith h
isto
ry o
f onl
y on
e CS
Vale
nzan
o,
2006
15Ca
se-
cont
rol
116
with
pr
evio
us
CS
(n =
217
)
Rand
om s
elec
tion
of
wom
en w
ith fi
rst
deliv
ery
betw
een
1995
an
d 20
04: v
agin
al b
irth
(n
= 1
01) o
r CS
(n =
116
)
Tria
ngul
ar, a
nech
oic
ar
ea a
t pre
sum
ed s
ite
of in
cisi
on
Prev
alen
ce o
f m
orph
olog
ical
ch
ange
s
of L
US,
on
TVS
or S
HG
60%
Nic
he p
reva
lenc
e si
mila
r in
w
omen
who
had
und
ergo
ne C
S at
3-1
2 m
onth
s, 1
-5 y
ears
and
5-
10 y
ears
aft
er C
S
Popu
latio
n w
ith h
isto
ry o
f one
or m
ultip
le C
Ss
Bij d
e Va
ate,
20
115
Pros
p.
coho
rt22
5Co
nsec
utiv
e
incl
usio
n
6-12
mon
ths
af
ter
CS
Anec
hoic
are
a at
site
of
CS
scar
with
dep
th
of a
t lea
st 1
mm
Prev
alen
ce, d
epth
an
d vo
lum
e of
nic
he
on T
VS a
nd S
HG
, an
d so
nogr
aphi
c cl
assi
ficat
ion
(SH
G)
base
d on
sha
pe
24%
56%
Mos
t com
mon
sha
pes
sem
icir
cula
r (5
0.4%
), tr
iang
ular
(3
1.6%
), dr
ople
t-sh
aped
(1
0.3%
) and
incl
usio
n cy
sts
(6.8
%)
Vikh
arev
a O
sser
, 20
1017
*
Pros
p.
coho
rt
108
His
tory
of C
S in
pr
eced
ing
6-9
mon
ths,
w
ho h
ad u
nder
gone
TV
S an
d SH
G
Any
visi
ble
defe
ct o
r in
dent
atio
n in
sca
r, ho
wev
er s
mal
l
Agre
emen
t bet
wee
n TV
S an
d SH
G w
ith
rega
rd to
pre
vale
nce,
le
ngth
, hei
ght
and
shap
e of
nic
he
70%
†84
%†
Mos
t sca
r de
fect
s tr
iang
ular
in
shap
e. S
hape
did
not
cha
nge
at S
HG
, but
was
eas
ier
to
delin
eate
bor
ders
of s
car
defe
ct; p
reva
lenc
e of
(lar
ge)
nich
es h
ighe
r on
SH
G.
Vikh
arev
a O
sser
, 20
099
Case
- co
ntro
l 16
2 w
ith
prev
ious
CS
(n =
287
)
Del
iver
ed 6
-9 m
onth
s
befo
re e
xam
inat
ion:
pr
imip
arae
with
un
com
plic
ated
vag
inal
de
liver
y (n
= 1
25) o
r w
omen
del
iver
ed b
y CS
at
leas
t onc
e (n
= 1
62).
Any
visi
ble
defe
ct o
r in
dent
atio
n in
sca
r, ho
wev
er s
mal
l
Prev
alen
ce, s
ize,
sh
ape
and
loca
tion
of C
S sc
ar d
efec
ts
on T
VS
69%
Mos
t sca
r de
fect
s tr
iang
ular
in
shap
e (8
3%),
som
e ro
und
(2%
) or
ova
l (4%
), an
d 10
% to
tal
defe
cts;
sca
rs w
ith d
efec
ts
loca
ted
low
er in
ute
rus
than
in
tact
sca
rs
Arm
stro
ng,
2003
4Ca
se-
cont
rol
32 w
ith
prev
ious
CS
(n
= 7
0)
Volu
ntee
rs a
ged
18-4
0 w
ith h
isto
ry o
f vag
inal
(n
= 3
8) o
r ce
sare
an
(n =
32)
del
iver
y w
ithin
pr
eced
ing
5 ye
ars
Sono
grap
hic
dem
onst
ratio
n of
flui
d w
ithin
CS
scar
Prev
alen
ce o
f CS
scar
de
fect
s on
TVS
42%

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 79
6
Tabl
e 2:
Con
tinue
d.
Stud
yD
esig
nn
Popu
lati
onD
efini
tion
of a
ni
che
Out
com
eN
iche
pr
eval
ence
on
TVS
(%)
Nic
he
prev
alen
ce
on S
HG
(%)
Resu
lts
Regn
ard,
20
047
Pros
p.
coho
rt
33H
isto
ry o
f CS
plan
ning
a
furt
her
preg
nanc
yTr
iang
ular
, ane
choi
c
area
at p
resu
med
site
of
inci
sion
Prev
alen
ce o
f nic
he
and
freq
uenc
y of
de
hisc
ence
at s
ite o
f ut
erin
e sc
ar o
n SH
G
58%
6% p
reva
lenc
e of
sca
r de
hisc
ence
(dep
th o
f nic
he
at le
ast 8
0% o
f ant
erio
r m
yom
etri
um)
Chen
, 19
9014
‡
Pros
p.
coho
rt
47H
isto
ry o
f CS,
pe
rfor
med
bet
wee
n
7 da
ys a
nd 8
yea
rs
prev
ious
ly
Vari
ous
patt
erns
of C
S sc
ar d
efine
d Ev
alua
tion
of L
US
on
TVS
49%
sho
wed
nor
mal
pat
tern
s,
21%
wed
ge d
efec
t, 15
%
outw
ard
prot
rusi
on, 6
% in
war
d pr
otru
sion
, 4%
hem
atom
a an
d 4%
inw
ard
retr
actio
n
Onl
y fir
st a
utho
r is
list
ed fo
r ea
ch s
tudy
. *Su
bgro
up a
naly
sis
of V
ikha
reva
Oss
er9 .
†Wom
en w
ho h
ad u
nder
gone
one
or
two
CSs.
‡Pr
egna
nt w
omen
in th
e st
udy
popu
latio
n w
ere
excl
uded
from
this
rev
iew
. LU
S, lo
wer
ute
rine
seg
men
t; Pr
osp.
, pro
spec
tive;
SH
G, c
ontr
ast-
enha
nced
son
ohys
tero
grap
hy; T
VS=t
rans
vagi
nal s
onog
raph
y.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
80 | Chapter 6Ta
ble
3: P
reva
lenc
e of
a n
iche
in r
elat
ion
to d
iagn
ostic
met
hod
in a
pop
ulat
ion
of w
omen
with
a h
isto
ry o
f Ces
area
n se
ctio
n (C
S) a
nd g
ynec
olog
ical
sym
ptom
s (i.
e. s
ubje
ct to
se
lect
ion
bias
).
Stud
yD
esig
nn
Popu
lati
onD
efini
tion
of a
ni
che
Out
com
eN
iche
pr
eval
ence
on
TVS
(%)
Nic
he
prev
alen
ce
on S
HG
(%)
Nic
he
prev
alen
ce
on H
S (%
)
Resu
lts
Popu
latio
n un
derg
oing
gyn
ecol
ogic
al u
ltras
ound
for a
var
iety
of i
ndic
atio
ns, w
ith h
isto
ry o
f one
or m
ultip
le C
Ss
Ofil
i-Yeb
ovi,
2008
11Pr
osp.
co
hort
32
4H
isto
ry o
f tra
nsve
rse
low
er-s
egm
ent C
S,
refe
rred
for
vari
ety
of
gyne
colo
gica
l ind
icat
ions
Any
dete
ctab
le
thin
ning
of
myo
met
rium
at s
ite
of C
S sc
ar
Prev
alen
ce o
f CS
scar
def
ects
and
de
scri
ptio
n of
m
orph
olog
ical
fe
atur
es o
n TV
S
19%
Scar
def
ect s
ever
e (≥
50%
of d
epth
of
myo
met
rium
) in
10%
El-M
azny
, 20
1116
Cros
s-se
ctio
nal
75H
isto
ry o
f CS
in p
rece
ding
1-
5 ye
ars,
exa
min
ed fo
r in
fert
ility
, men
stru
al
diso
rder
s or
rec
urre
nt
preg
nanc
y lo
ss
Filli
ng d
efec
t in
CS
scar
, defi
ned
as
tria
ngul
ar, a
nech
oic
area
at p
resu
med
si
te o
f inc
isio
n
Accu
racy
of
SHG
ver
sus
gold
st
anda
rd H
S fo
r de
tect
ion
of n
iche
an
d th
ickn
ess
of
scar
27%
31%
SHG
com
para
ble
to
HS
as s
how
n by
sen
s.
(87%
), sp
ec. (
100%
), PP
V (1
00%
), N
PV (9
5%) a
nd
over
all a
ccur
acy
(96%
) in
diag
nosi
s of
nic
he; s
car
thic
knes
s lo
wer
at S
HG
th
an a
t HS
(P =
0.0
16)
Mon
teag
udo,
20
018
Pros
p.
coho
rt
44H
isto
ry o
f CS,
und
erw
ent
SHG
for
vari
ety
of
gyne
colo
gic
indi
catio
ns
Tria
ngul
ar a
nech
oic
stru
ctur
e at
pr
esum
ed s
ite o
f CS
sca
r
Prev
alen
ce a
nd
char
acte
rist
ics
of
nich
e on
SH
G
100%
Wan
g,
2009
10Cr
oss-
sect
iona
l 20
7*
His
tory
of C
S, e
xam
ined
on
TVS
for
vari
ous
gyne
colo
gica
l ind
icat
ions
, di
agno
sed
with
a
CS s
car
defe
ct
Hyp
oech
ogen
ic a
rea
with
in m
yom
etri
um
of L
US
at s
ite o
f pr
evio
us C
S in
cisi
on
Prev
alen
ce o
f CS
scar
def
ect o
n TV
S7%
Upp
al,
2011
28
Pr
osp.
co
hort
71
† Re
ferr
ed fo
r gy
neco
logi
cal u
ltras
ound
; 71
wom
en h
ad h
isto
ry
of C
S
Flui
d-fil
led
defe
ct in
hy
ster
otom
y in
cisi
onFr
eque
ncy
and
appe
aran
ce o
f CS
scar
def
ects
on
TVS
in w
omen
with
hi
stor
y of
CS
40%
Dia
met
er o
f sca
r de
fect
(a
vera
ge in
long
itudi
nal
and
tran
sver
sal p
lane
s)
rang
ed fr
om 3
to 1
2 m
m
with
mea
n of
6.5
mm

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 81
6
Tabl
e 3:
Con
tinue
d.
Stud
yD
esig
nn
Popu
lati
onD
efini
tion
of a
ni
che
Out
com
eN
iche
pr
eval
ence
on
TVS
(%)
Nic
he
prev
alen
ce
on S
HG
(%)
Nic
he
prev
alen
ce
on H
S (%
)
Resu
lts
Popu
latio
n w
ith p
ostm
enst
rual
spo
ttin
g an
d hi
stor
y of
one
or m
ultip
le C
Ss
Chan
g,
2009
27Pr
osp.
co
hort
57
Post
men
stru
al s
pott
ing
afte
r CS
Tria
ngul
ar a
nech
oic
imag
e in
ant
erio
r lo
wer
ute
rus
mus
cle,
at
trib
utab
le to
pri
or
CS d
eliv
ery
Prev
alen
ce o
f CS
scar
def
ect o
n TV
S;
com
pari
son
with
SH
G c
once
rnin
g th
ickn
ess
of r
esid
ual
myo
met
rium
and
de
pth
of s
car
defe
ct
(n =
22)
88%
‡SH
G s
how
ed s
imila
r th
ickn
ess
of r
esid
ual
myo
met
rium
and
larg
er
dept
h of
the
CS s
car
defe
ct in
com
pari
son
with
TVS
(p<0
.05)
Borg
es,
2010
13Pr
osp.
co
hort
43
Post
men
stru
al s
pott
ing
and
hist
ory
of C
S in
pr
eced
ing
2-25
yea
rs
On
HS:
cav
ity a
t sc
ar s
ite, s
uper
ior
fibro
tic r
ing,
infe
rior
fib
rotic
rin
g, b
lood
in
inva
gina
tion
site
an
d ce
rvic
al c
anal
di
amet
er a
t hei
ght
of u
pper
fibr
osis
Prev
alen
ce o
f is
thm
ocel
e w
ith H
S
88%
Popu
latio
n w
ith n
iche
dem
onst
rate
d on
TVS
and
his
tory
of o
ne o
r mul
tiple
CSs
Fabr
es,
2003
6Re
tro.
co
hort
92
His
tory
of C
S an
d po
uch
at s
ite o
f CS
scar
on
TVS;
H
S pe
rfor
med
in 4
4% o
f pa
tient
s w
ith a
bnor
mal
ut
erin
e bl
eedi
ng
Filli
ng d
efec
t of
uter
ine
cavi
ty
loca
ted
in r
elat
ion
to
ante
rior
isth
mus
Des
crip
tion
of
sono
grap
hic
char
acte
rist
ics
of p
ouch
and
as
sess
men
t of
ass
ocia
tion
betw
een
TVS
and
hyst
eros
copy
In a
ll w
omen
def
ect w
as
visu
aliz
ed a
s tr
iang
ular
an
echo
ic a
rea
with
ba
se o
n po
ster
ior
wal
l of
cer
vica
l cha
nnel
an
d ve
rtex
opp
osite
ba
se p
oint
ing
tow
ard
ante
rior
wal
l of i
sthm
us;
HS
show
ed 1
00%
co
rrel
atio
n w
ith T
VS in
de
tect
ion
of p
ouch
Onl
y fir
st a
utho
r is
list
ed fo
r ea
ch s
tudy
. *42
50 w
omen
with
his
tory
of C
S ex
amin
ed. †
Tota
l n =
318
(71
with
pre
viou
s CS
). ‡I
f nic
he w
as n
ot n
oted
at fi
rst v
isit,
TVS
was
pe
rfor
med
dur
ing
post
men
stru
al s
pott
ing
(n =
18)
. Sev
en w
omen
wer
e lo
st to
follo
w-u
p an
d ex
clud
ed. H
S, h
yste
rosc
opy;
LU
S, lo
wer
ute
rine
seg
men
t; N
PV, n
egat
ive
pred
ictiv
e va
lue;
PPV
, pos
itive
pre
dict
ive
valu
e; P
rosp
., pr
ospe
ctiv
e; R
etro
., re
tros
pect
ive;
sen
s., s
ensi
tivity
; SH
G, c
ontr
ast-
enha
nced
son
ohys
tero
grap
hy; s
pec.
, spe
cific
ity;
TVS=
tran
svag
inal
son
ogra
phy.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
82 | Chapter 6
two criteria of the QUADAS checklist21. First, the study population consisted of women with gynecological symptoms. Second, the hysteroscopy findings were interpreted with prior knowledge of the SHG results. Another study reported that hysteroscopy as the reference technique showed 100% correlation with TVS in the detection of a niche6. However, this study did not meet the QUADAS criteria either, as it was a retrospective study in women with a niche assessed using TVS, and hysteroscopy was performed in a subgroup of women who wanted to become pregnant (verification bias).
Niche shapeFive studies reporting on niche shape evaluated the shape in the sagittal plane with TVS or SHG5,6,9,14,17. Most authors described the niche as being triangular in shape with TVS6,9,14. Vikhareva Osser et al.9 reported that 83% of niches were triangular, 2% were round, 4% were oval and 10% showed no remaining myometrium over the defect. The same group demonstrated that the shape did not change when evaluated by SHG17. Another study demonstrated that the niche was visualized as a triangular anechoic area in all women6. In addition, it was reported that a wedge defect was present in 21% of women with a history of CS, inward protrusion (internal surface of the scar bulging toward the uterine cavity) in 6%, outward protrusion (external surface bulging toward the bladder or abdominal cavity) in 15%, hematoma (echogenic mass adjacent to the wound site of the anterior wall of the lower uterine segment) in 4% and inward retraction (external surface of the scar dimpled toward the myometrial layer) in 4%14. Bij de Vaate et al.5, using SHG, found that 50% of niches were semicircular, 32% were triangular and 10% were droplet-shape; inclusion cysts accounted for 7%.
If we consider only the methodologically well-performed studies according to the STROBE criteria with a random population of women with a history of CS, triangular and semicircular are found to be the most commonly described shapes 5,9.
Niche sizeEight studies evaluated niche size, but the studies describing large niches used different definitions for this5,7,9,11,16,17,27,28. Vikhareva Osser et al.9 classified a niche as large or as a total defect based on subjective evaluation in a random population of women with a history of CS examined by TVS. At least one defect was classified as large in 14%, 23% and 45% of the women with one, two and at least three CSs, respectively. At least one total defect (with no remaining myometrium over the defect) was observed in 6%, 7% and 18% of the women with one, two and at least three CSs, respectively. In another study by the same authors, a niche was defined as large if the remaining myometrium

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 83
6
measured ≤ 2.2 mm in thickness using TVS and ≤ 2.5 mm using SHG in women with one previous CS17. According to the authors, these cut-off values were the measurements that best discriminated between defects estimated subjectively as being large or not in women with a history of one CS. Regnard et al.7 reported that two out of 19 niches (11%) had a depth of at least 80% of the anterior myometrium, which was demonstrated with SHG in a random population of women with a history of CS. Ofili-Yebovi et al.11 demonstrated that, when using TVS in a group of women with gynecological symptoms, half of them had a large niche, i.e. one involving more than 50% of the myometrial thickness.
The abovementioned studies demonstrate that there is currently no uniform definition of a large niche. The definitions used for a large niche were a niche penetrating to a depth of at least 50% or 80% of the anterior myometrium, or the remaining myometrial thickness ≤ 2.2 mm when evaluated by TVS and ≤ 2.5 mm when evaluated by SHG. A total defect was defined as no remaining myometrium over the defect.
Risk factorsRisk factors that are associated with the presence or size of a niche were evaluated in nine studies (Table S1). Various risk factors were investigated, but none of the papers studied exactly the same ones. In addition, some factors are known to be mutually related. For example, several indications for CS (duration of labor, oxytocin augmentation) affect cervical dilatation or the development of the lower uterine segment22. For this reason, we classified all risk factors into four main categories: factors related to closure technique, development of the lower uterine segment or location of the incision, wound healing and miscellaneous factors (Table 4). In addition, studies were classified according to their design, with studies including only one previous CS and/or those using multivariate analysis presented first. Three studies were performed in a population of women with a history of only one CS and analyzed with the use of multivariate analysis, and will be discussed below22,25,26.
Closure techniqueTwo studies evaluated the relationship between closure technique and the presence of a niche25,26. A randomized controlled trial reported a lower frequency of a niche in women treated by full thickness suturing (including the endometrial layer) in comparison with split thickness suturing (excluding the endometrial layer)26, while a prospective cohort study reported a reduced risk of niche development after double-layer myometrium closure or single-layer myometrium closure with endometrial suture in comparison with single-layer myometrium closure without endometrial suture25. Another prospective cohort
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
84 | Chapter 6
study reported large niches more frequently in women with one-layer uterine closure (90.9%) in comparison with two-layer closure (9.1%), but this was not a statistically significant difference22. A niche was classified as large in the latter study if the remaining myometrium measured ≤ 2.2 mm in thickness using TVS and ≤ 2.5 mm in thickness using SHG.
Development of lower uterine segment or scar locationThree studies reported a relationship between the presence or size of a niche and the factors potentially affecting the development of the lower uterine segment or scar location (Table 4)22,25,26. In one of these studies, the risk of a large niche increased if the station of the presenting part of the fetus at CS was below the pelvic inlet, cervical dilatation was ≥ 5 cm or duration of labor was ≥ 5 h22. Another study, on the other hand, reported that an increased risk for the presence of a niche was related to less cervical dilatation26. Hayakawa et al.25 reported that an increased risk was associated with premature rupture of membranes and increased gestational age at delivery, while Yazicioglu et al.26 found that there was no relationship with gestational age. Emergency CS and the presence of labor were reported not to be risk factors for the presence of a niche25,26.
Wound healingOne study reported a relationship between uterine retroflexion and a large niche, and another reported a relationship between pre-eclampsia and the presence of a niche22,25. We classified these risk factors as ones with a potential negative effect on wound healing. Other factors that were classified in this category (infection or maternal body mass index) were not related to the presence of a niche25. In a study performed in women with a history of one or multiple CSs, multivariate analysis demonstrated a relationship between the presence of a niche and multiple CSs or uterine retroflexion11.
SymptomsThe identification of niche-related symptoms was evaluated in eight studies, using TVS, SHG or hysteroscopy for niche assessment (Table S2). Two studies were performed in a random population of women with a history of CS5,15; both studies fulfilled the STROBE criteria, except for the correction for confounders in one study15. Bij de Vaate et al.5 reported postmenstrual spotting in 34% of women with a niche using SHG, which was significantly higher than in women without a niche. Menada Valenzano et al.15 did not find an association between the presence of a niche identified with SHG and abnormal uterine bleeding, defined as spotting after the end of menstruation and/or non-cyclic bleeding not related to menstruation. However, the same authors found that abnormal uterine bleeding was more frequent in women with diverticula (anechoic round

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 85
6
structures) and deformation of the cervical canal at the scar site, identified on TVS. In addition, abnormal bleeding was more frequent in women with a history of CS than in women with a previous vaginal birth in this study, indicating some relationship between the presence of a CS scar and postmenstrual spotting.
Six studies were performed in a population of women with gynecological symptoms (Table S2), and a high prevalence of postmenstrual spotting in women with a niche compared with women without a niche was reported in three studies6,10,18. In one cross-sectional study the prevalence of postmenstrual spotting in women with a niche examined by TVS for various gynecological reasons was 64%10. In a very small prospective cohort study all women with a niche demonstrated by SHG had postmenstrual spotting18. A retrospective study of all TVS examinations conducted for a variety of gynecological reasons reported abnormal bleeding in 83% and postmenstrual spotting in 76% of premenopausal women with a niche6.
Three studies reported an association between the size of a niche and postmenstrual spotting5,10,28. In one study, performed in a random population of women with a history of CS, the depth and shape of the niche were not significant factors, while a larger niche volume was described in women with postmenstrual spotting5. The other two studies, performed in a population of women with gynecological symptoms, demonstrated that niches were significantly wider in women with postmenstrual spotting, dysmenorrhea or chronic pelvic pain, and that the prevalence of postmenstrual spotting or prolonged menstrual bleeding was higher with a larger diameter of the niche10,28. Other reported symptoms in women with a niche were dysmenorrhea (53.1%), chronic pelvic pain (36.9%) and dyspareunia (18.3%)10.
Discussion
In a random population of women with a history of CS, the prevalence of a niche ranged from 24% to 70% and 56% to 84% when assessed by TVS and SHG, respectively. Probable risk factors are single-layer myometrium closure, multiple CSs and retroflexed uterus. The predominant symptom related to a niche is postmenstrual spotting.
The ideal study reporting on symptoms would be performed in a random sample of women with a history of CS in order to prevent selection bias, but also including a group of patients who had only experienced vaginal birth in order to distinguish the effects of CS and niche. Only one study performed in a random

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
86 | Chapter 6
Tabl
e 4:
Cla
ssifi
catio
n of
ris
k fa
ctor
s fo
r pr
esen
ce o
r si
ze o
f a C
esar
ean
sect
ion
(CS)
sca
r ni
che.
Vik
h.,
2010
22H
aya.
, 20
0625
Yazi
.,
2005
26O
fil.,
20
0811
Ceci
,
20
1223
Gla
v.,
2012
24A
rms.
, 20
034
Wan
g,
20
0910
Mon
t.,
2001
8
Stud
y ch
arac
teri
stic
s
Incl
uded
pat
ient
s (n
)10
813
770
324
6014
932
207
44Pr
evio
us C
Ss (n
)1
11
≥11
1≥1
≥1≥1
Risk
fact
ors:
In m
ultiv
aria
te a
naly
sis
(n)
814
72
00
00
0In
uni
vari
ate
anal
ysis
(n)
200
08
11
22
1Fo
r pr
esen
ce o
f nic
he/la
rge
nich
eLa
rge
Pres
.Pr
es.
Pres
.La
rge
Larg
e Pr
es.
Larg
e La
rge
Repo
rted
pot
enti
al r
isk
fact
ors
for
nich
e
Fact
ors
affec
ting
clos
ure
tech
niqu
e
Sutu
ring
tech
niqu
eN
oYe
s*Ye
s*N
AYe
sYe
sN
AN
AN
AYe
ars
of s
urgi
cal e
xper
ienc
eN
AN
o*N
AN
AN
AN
AN
AN
AN
AAn
y cl
osur
e fa
ctor
rel
ated
?N
oYe
s*Ye
s*N
AYe
sYe
sN
AN
AN
A
Fact
ors
affec
ting
deve
lopm
ent o
f LU
S or
low
er lo
catio
n of
inci
sion
Adva
nced
sta
ge p
rese
ntin
g pa
rt a
t CS
Yes*
NA
NA
NA
NA
NA
NA
NA
NA
Scar
at l
evel
of i
nter
nal c
ervi
cal o
sYe
sN
AN
AN
oN
AN
AN
AN
AN
ACe
rvic
al d
ilata
tion
Yes*
§N
AYe
s*¶
NA
NA
NA
NA
NA
NA
Pres
ence
/dur
atio
n of
labo
r at
CS
Yes*
NA
No*
NA
NA
NA
Yes
NA
NA
Oxy
toci
n du
ring
labo
rYe
sN
AN
AN
AN
AN
AN
AN
AN
APr
emat
ure
rupt
ure
of m
embr
anes
NA
Yes*
NA
NA
NA
NA
NA
NA
NA
Emer
genc
y CS
No
No*
NA
No
NA
NA
NA
NA
NA
Ges
tatio
nal a
ge a
t del
iver
yYe
s‡Ye
s*†
No*
No
NA
NA
NA
NA
NA
Any
LUS
fact
or r
elat
ed?
Yes*
Yes*
Yes*
No
NA
NA
Yes
NA
NA
Fact
ors
with
pot
entia
l neg
ativ
e in
fluen
ce o
n w
ound
hea
ling
Mul
tiple
CSs
NA
NA
NA
Yes*
NA
NA
Yes
Yes
No
Ute
rine
ret
rofle
xion
Yes*
NA
NA
Yes*
NA
NA
NA
Yes
NA
Dia
bete
s**
NA
NA
NA
NA
NA
NA
NA
NA
Ster
oids
dur
ing
preg
nanc
y**
NA
NA
NA
NA
NA
NA
NA
NA

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 87
6
Tabl
e 4:
Con
tinue
d.
Vik
h.,
2010
22H
aya.
, 20
0625
Yazi
.,
2005
26O
fil.,
20
0811
Ceci
,
20
1223
Gla
v.,
2012
24A
rms.
, 20
034
Wan
g,
20
0910
Mon
t.,
2001
8
Pre-
ecla
mps
ia**
Yes*
NA
NA
NA
NA
NA
NA
NA
Peri
- or
post
part
um in
fect
ion
No
No*
NA
NA
NA
NA
NA
NA
NA
Intr
aope
rativ
e co
mpl
icat
ions
No
NA
NA
NA
NA
NA
NA
NA
NA
Mat
erna
l BM
IN
oN
o*N
AN
AN
AN
AN
AN
AN
AAn
y he
alin
g fa
ctor
rel
ated
?Ye
s*Ye
s*N
AYe
s*N
AN
AYe
sYe
sN
o
Oth
er
Mat
erna
l age
Yes
No*
NA
No
NA
NA
NA
NA
NA
Mul
tiple
pre
gnan
cies
NA
Yes*
NA
No
NA
NA
NA
NA
NA
Num
ber
of v
agin
al b
irth
sN
oN
AN
AN
oN
AN
AN
AN
AN
APl
acen
ta p
revi
aN
AN
o*N
AN
AN
AN
AN
AN
AN
APf
anne
nstie
l or
vert
ical
inci
sion
NA
No*
NA
NA
NA
NA
NA
NA
NA
Intr
aope
rativ
e bl
ood
loss
No
No*
NA
NA
NA
NA
NA
NA
NA
Plat
elet
s/he
mat
ocri
t/he
mog
lobi
nN
oN
AN
o*N
AN
AN
AN
AN
AN
AFe
tal w
eigh
tN
AN
AN
o*N
AN
AN
AN
AN
AN
ARe
gion
al o
r ge
nera
l ane
sthe
sia
NA
No*
NA
NA
NA
NA
NA
NA
NA
Ope
ratin
g tim
eN
AN
AN
o*N
AN
AN
AN
AN
AN
A
Onl
y na
mes
of fi
rst a
utho
rs a
re g
iven
, abb
revi
ated
to fo
ur le
tter
s. *
Resu
lts o
btai
ned
with
use
of m
ultiv
aria
te a
naly
sis
(par
amet
ers
that
wer
e no
t ris
k fa
ctor
s w
ere
not i
nclu
ded
in
this
tabl
e). §
Mor
e ce
rvic
al d
ilata
tion.
¶Le
ss c
ervi
cal d
ilata
tion.
‡D
ecre
ased
ges
tatio
nal a
ge a
t del
iver
y. †
Incr
ease
d ge
stat
iona
l age
at d
eliv
ery.
**N
umbe
r of
wom
en to
o sm
all f
or
stat
istic
al c
alcu
latio
ns. B
MI,
body
mas
s in
dex;
LU
S, lo
wer
ute
rine
seg
men
t; N
A, n
ot a
sses
sed;
Pre
s, p
rese
nce.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
88 | Chapter 6
population described a positive relationship between a niche and postmenstrual spotting5. This association was not found by Menada Valenzano et al.15, who did report a relationship between postmenstrual spotting and a previous CS. The discrepancy in the findings of these two studies can be explained by variations in methodology, such as definition of a niche, timing of the ultrasound scans and exclusion of multiple CSs in the population of Menada Valenzano et al. In the majority of the studies evaluating niches in women with gynecological symptoms, selection bias is likely to play a role, which is underlined by the higher prevalence of postmenstrual spotting in these women than in a random population of women with a history of CS6,10,13,18,28. Several hypotheses have been put forward to explain the etiology of abnormal uterine bleeding in women with a niche, such as poor contractility of the uterine muscle around the niche, which may result in retention of menstrual blood within it18.
Two studies report that closure technique during CS affects niche development. It seems to be more appropriate to use double-layer or full thickness suturing, a finding that should be confirmed in future studies25,26. Although the results of the current review are inconclusive, we hypothesize that potential factors affecting the development of the lower uterine segment (such as duration of labor, dilatation, stage of the presenting part) may influence development of a niche. It has been postulated that the characteristics of the myometrium alter during labor and that, for example, a thinner myometrium may be less well vascularized, which may lead to insufficient wound healing and niche development29. In addition, a lower position of the CS incision, in particular in the cervical part of the uterus, may be more prone to the development of a niche9.
The current review is the first systematic review to give an overview of the available literature relating to the prevalence of a niche, potential risk factors and symptoms associated with a niche. Given the inconsistency in methodology between the studies, we were not able to perform meta-analyses. However, we ranked the included papers based on criteria for quality assessment in order to improve the interpretation of the current reported evidence.
The lack of consistency in methodology is based on three aspects. The principal issue was the method of niche detection. Although TVS has been considered an accurate method for detecting a niche, SHG may facilitate their detection and measurement, an idea that is supported by the higher prevalence and identification of larger niches with SHG than with TVS in two comparative studies5,17. Application of saline or gel contrast enables differentiation between niches that communicate with cervical wall defects and cervical (mucous) cysts. In addition, small indentations or defects at the site of the scar can be identified

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 89
6
more precisely if contrast is used. Therefore, we propose SHG in non-pregnant patients as the gold standard in future studies on niche prevalence.
The second major issue is the lack of agreement about the definition of a niche. First of all, it is important to distinguish a niche from the CS scar itself. Naji et al.30 described a standardized measurement technique and registration method for the evaluation of CS scars using TVS in pregnant and non-pregnant women. However, there is no agreement about how to define the margins of a niche, whether cervical diverticula should be included or if there is a minimal size to the anechoic area for it to qualify as a niche. We propose the following definition: any indentation representing myometrial discontinuity at the site of the Cesarean scar that communicates with the uterine or cervical cavity as seen on SHG. The problem with reporting on risk factors for a large niche is the lack of predefined definitions for them. In one study, the cut-off value for a large niche was based on study outcome, and therefore has a risk of data-driven definition22. We propose the use of predefined cut-off values for a large niche based on interquartile ranges or standard deviations, or on the ratio of niche depth and total thickness of adjacent myometrium, e.g. a ratio of more than 50%11.
Finally, there is significant heterogeneity in the patient populations reported, consisting of women with a history of CS who were assessed for a variety of gynecological symptoms or women with a history of CS (and vaginal birth), independent of their symptoms.
As the CS rate increases, the potential morbidity associated with CS scars is likely to become increasingly important. If we are to understand the relevance of the presence of a niche, it is essential that agreed criteria and definitions are used in future studies as well as standardized outcomes. In addition, identification of potential risk factors provides insight into etiology, but more importantly it would be useful for the prevention of future niche development and related symptoms.
At present we do not know the importance of a niche in future pregnancies and it must be questioned whether it is appropriate to report on the morphology of CS scars using ultrasound in view of the fact that we do not know how to act on this information. It seems increasingly likely that niches may be a cause of abnormal uterine bleeding, and we await good interventional trials to see if correction in these circumstances is effective. The possible impact of a niche on fertility is an important subject, but we have little information on this topic to guide us.
In conclusion, niches are frequently identified after CS and are related to postmenstrual spotting. A uniform definition of a niche and a method for

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
90 | Chapter 6
assessment should be formulated in order to enable future meta-analyses. We propose to use SHG and define a niche as any indentation representing myometrial discontinuity at the site of the Cesarean scar that communicates with the uterine or cervical cavity. More well-designed research on risk factors is needed in order to obtain tools to prevent future niche development.
Acknowledgements
We thank J.C.F. Ket for his assistance with the literature search.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 91
6
1. Betrán AP, Merialdi M, Lauer JA, Bing-Shun W, Thomas J, Van Look P, Wagner M. Rates of caesarean section: analysis of global, regional and national estimates. Paediatr Perinat Epidemiol 2007; 21: 98–113.
2. Diaz SD, Jones JE, Seryakov M, Mann WJ. Uterine rupture and dehiscence: ten-year review and case–control study. South Med J 2002; 95: 431–435.
3. Clark SL, Koonings PP, Phelan JP. Placenta previa/accreta and prior Cesarean section. Obstet Gynecol 1985; 66: 89 – 92.
4. Armstrong V, Hansen WF, Van Voorhis BJ, Syrop CH. Detection of Cesarean scars by transvaginal ultrasound. Obstet Gynecol 2003; 101: 61–65.
5. Bij de Vaate AJ, Brolmann HA, van der Voet LF, van der Slikke JW, Veersema S, Huirne JA. Ultrasound evaluation of the Cesarean scar: relation between a niche and postmenstrual spotting. Ultrasound Obstet Gynecol 2011; 37: 93 – 99.
6. Fabres C, Aviles G, De La Jara C, Escalona J, Muñoz JF, Mackenna A, Ferna ́ndez C, Zegers-Hochschild F, Fernández E. The cesarean delivery scar pouch: clinical implications and diagnostic correlation between transvaginal sonography and hysteroscopy. J Ultrasound Med 2003; 22: 695–700.
7. Regnard C, Nosbusch M, Fellemans C, Benali N, van Rysselberghe M, Barlow P, Rozenberg S. Cesarean section scar evaluation by saline contrast sonohysterography. Ultrasound Obstet Gynecol 2004; 23: 289–292.
8. Monteagudo A, Carreno C, Timor-Tritsch IE. Saline infusion sonohysterography in nonpregnant women with previous cesarean delivery: the ‘‘niche’’ in the scar. J Ultrasound Med 2001; 20: 1105–1115.
9. Osser OV, Jokubkiene L, Valentin L. High prevalence of defects in Cesarean section scars at transvaginal ultrasound examination. Ultrasound Obstet Gynecol 2009; 34: 90–97.
10. Wang CB, Chiu WW, Lee CY, Sun YL, Lin YH, Tseng CJ. Cesarean scar defect: correlation between Cesarean section number, defect size, clinical symptoms and uterine position. Ultrasound Obstet Gynecol 2009; 34: 85–89.
11. Ofili-Yebovi D, Ben-Nagi J, Sawyer E, Yazbek J, Lee C, Gonzalez J, Jurkovic D. Deficient lower-segment Cesarean section scars: prevalence and risk factors. Ultrasound Obstet Gynecol 2008; 31: 72 – 77.
12. Surapaneni K, Silberzweig JE. Cesarean section scar diverticulum: appearance on hysterosalpingography. AJR Am J Roentgenol 2008;
190: 870–874.13. Borges LM, Scapinelli A, de Baptista Depes D,
Lippi UG, Coelho Lopes RG. Findings in patients with postmenstrual spotting with prior cesarean Section. J Minim Invasive Gynecol 2010; 17: 361–364.
14. Chen HY, Chen SJ, Hsieh FJ. Observation of cesarean section scar by transvaginal ultrasonography. Ultrasound Med Biol 1990; 16: 443–447.
15. Menada Valenzano M, Lijoi D, Mistrangelo E, Costantini S, Ragni N. Vaginal ultrasonographic and hysterosonographic evaluation of the low transverse incision after caesarean section: correlation with gynaecological symptoms. Gynecol Obstet Invest 2006; 61: 216–222.
16. El-Mazny A, Abou-Salem N, El-Khayat W, Farouk A. Diagnostic correlation between sonohysterography and hysteroscopy in the assessment of uterine cavity after cesarean section. Middle East Fertil Soc J 2011; 16: 72 – 76.
17. Osser OV, Jokubkiene L, Valentin L. Cesarean section scar defects: agreement between transvaginal sonographic findings with and without saline contrast enhancement. Ultrasound Obstet Gynecol 2010; 35: 75–83.
18. Thurmond AS, Harvey WJ, Smith SA. Cesarean section scar as a cause of abnormal vaginal bleeding: diagnosis by sonohysterography. J Ultrasound Med 1999; 18: 13–16.
19. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health-care interventions: explanation and elaboration. BMJ 2009; 339: b2700.
20. Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, Poole C, Schlesselman JJ, Egger M; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. PLoS Med 2007; 4: e297.
21. Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J. The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol 2003; 3: 25.
22. Vikhareva Osser O, Valentin L. Risk factors for incomplete healing of the uterine incision after caesarean section. BJOG 2010; 117: 1119 – 1126.
23. Ceci O, Cantatore C, Scioscia M, Nardelli C, Ravi
References

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
92 | Chapter 6
M, Vimercati A, Bettocchi S. Ultrasonographic and hysteroscopic outcomes of uterine scar healing after cesarean section: comparison of two types of single-layer suture. J Obstet Gynaecol Res 2012; 38: 1302 – 1307.
24. Glavind J, Madsen L, Uldbjerg N, Dueholm M. Ultrasound evaluation of Cesarean scar after single- and double-layer uterotomy closure: a cohort study. Ultrasound Obstet Gynecol 2013; 42: 207 – 212.
25. Hayakawa H, Itakura A, Mitsui T, Okada M, Suzuki M, Tamakoshi K, Kikkawa F. Methods for myometrium closure and other factors impacting effects on cesarean section scars of the uterine segment detected by the ultrasonography. Acta Obstet Gynecol Scand 2006; 85: 429 – 434.
26. Yazicioglu F, Gökdogan A, Kelekci S, Aygün M, Savan K. Incomplete healing of the uterine incision after caesarean section: Is it preventable? Eur J Obstet Gynecol Reprod Biol 2006;124: 32 – 36.
27. Chang Y, Tsai EM, Long CY, Lee CL, Kay N. Resectoscopic treatment combined with
sonohysterographic evaluation of women with postmenstrual bleeding as a result of previous cesarean delivery scar defects. Am J Obstet Gynecol 2009; 200: 370.e1 – 4.
28. Uppal T, Lanzarone V, Mongelli M. Sonographically detected caesarean section scar defects and menstrual irregularity. J Obstet Gynaecol 2011; 31: 413 – 416.
29. Buhimschi CS, Buhimschi IA, Yu C, Wang H, Sharer DJ, Diamond MP, Petkova AP, Garfield RE, Saade GR, Weiner CP. The effect of dystocia and previous cesarean uterine scar on the tensile properties of the lower uterine segment. Am J Obstet Gynecol 2006; 194: 873 – 883.
30. Naji O, Abdallah Y, Bij De Vaate AJ, Smith A, Pexsters A, Stalder C, McIndoe A, Ghaem-Maghami S, Lees C, Brolmann HA, Huirne JA, Timmerman D, Bourne T. Standardized approach for imaging and measuring Cesarean section scars using ultrasonography. Ultrasound Obstet Gynecol 2012; 39: 252 – 259.
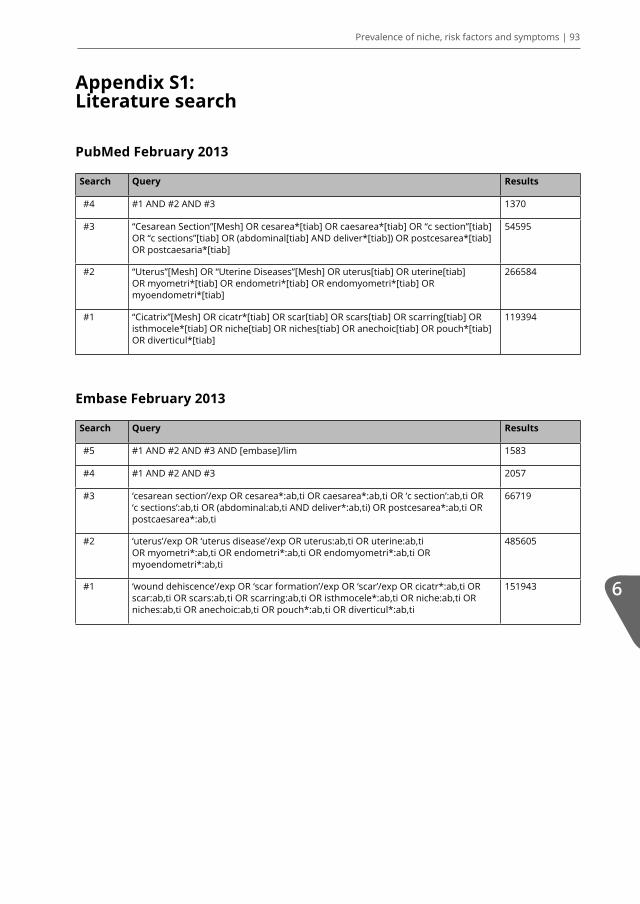
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 93
6
Appendix S1: Literature search
PubMed February 2013
Search Query Results
#4 #1 AND #2 AND #3 1370
#3 “Cesarean Section”[Mesh] OR cesarea*[tiab] OR caesarea*[tiab] OR “c section”[tiab] OR “c sections”[tiab] OR (abdominal[tiab] AND deliver*[tiab]) OR postcesarea*[tiab] OR postcaesaria*[tiab]
54595
#2 “Uterus”[Mesh] OR “Uterine Diseases”[Mesh] OR uterus[tiab] OR uterine[tiab] OR myometri*[tiab] OR endometri*[tiab] OR endomyometri*[tiab] OR myoendometri*[tiab]
266584
#1 “Cicatrix”[Mesh] OR cicatr*[tiab] OR scar[tiab] OR scars[tiab] OR scarring[tiab] OR isthmocele*[tiab] OR niche[tiab] OR niches[tiab] OR anechoic[tiab] OR pouch*[tiab] OR diverticul*[tiab]
119394
Embase February 2013
Search Query Results
#5 #1 AND #2 AND #3 AND [embase]/lim 1583
#4 #1 AND #2 AND #3 2057
#3 ‘cesarean section’/exp OR cesarea*:ab,ti OR caesarea*:ab,ti OR ‘c section’:ab,ti OR ‘c sections’:ab,ti OR (abdominal:ab,ti AND deliver*:ab,ti) OR postcesarea*:ab,ti OR postcaesarea*:ab,ti
66719
#2 ‘uterus’/exp OR ‘uterus disease’/exp OR uterus:ab,ti OR uterine:ab,ti OR myometri*:ab,ti OR endometri*:ab,ti OR endomyometri*:ab,ti OR myoendometri*:ab,ti
485605
#1 ‘wound dehiscence’/exp OR ‘scar formation’/exp OR ‘scar’/exp OR cicatr*:ab,ti OR scar:ab,ti OR scars:ab,ti OR scarring:ab,ti OR isthmocele*:ab,ti OR niche:ab,ti OR niches:ab,ti OR anechoic:ab,ti OR pouch*:ab,ti OR diverticul*:ab,ti
151943

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
94 | Chapter 6A
ppen
dix
S2: S
TRO
BE c
heck
list
Des
crip
tion
of i
tem
sVi
khar
eva
O
sser
and
Va
lent
in
(201
0)
Bij d
e Va
ate
et
al.
(201
1)
Gla
vind
et
al.
(2
012)
Hay
akaw
a et
al.
(200
6)
Vale
nzan
oet
al.
(200
6)
Yazi
ciog
lu
(200
6)Vi
khar
eva
Oss
er
et a
l. (2
010)
Viha
reva
O
sser
et
al.
(200
9)
Ofili-
Yebo
vi
et a
l. (2
008)
El-M
azny
et
al.
(201
1)
Wan
g
et a
l. (2
009)
1 a St
udy
desi
gn is
cle
ar in
title
or
abst
ract
11
11
11
00
01
1
b Ab
stra
ct p
rovi
des
an in
form
ativ
e an
d ba
lanc
ed s
umm
ary
11
11
11
11
11
1
2 Ex
plai
n th
e sc
ient
ific
back
grou
nd a
nd
ratio
nale
for
the
inve
stig
atio
n be
ing
repo
rted
11
11
11
11
11
1
3 St
ate
spec
ific
obje
ctiv
es, i
nclu
ding
any
pr
espe
cifie
d hy
poth
eses
11
11
11
11
11
1
4 Pr
esen
t key
ele
men
ts o
f stu
dy d
esig
n ea
rly
in th
e pa
per
11
11
11
00
01
1
5 D
escr
ibe
the
sett
ing,
loca
tions
, and
re
leva
nt d
ates
, inc
ludi
ngpe
riod
s of
rec
ruitm
ent,
expo
sure
, fol
low
-up
, and
dat
a co
llect
ion
11
11
11
00
00
0
6 a G
ive
the
elig
ibili
ty c
rite
ria
and
the
sour
ces
and
met
hods
of s
elec
tion
of
part
icip
ants
; des
crib
e m
etho
ds o
f fol
low
-up
11
11
11
11
11
0
b Fo
r m
atch
ed s
tudi
es, g
ive
mat
chin
g cr
iteri
a an
d nu
mbe
r of
exp
osed
and
un
expo
sed
NA
NA
NA
NA
1N
AN
AN
AN
AN
AN
A
7 Cl
earl
y de
fine
all o
utco
mes
, exp
osur
es,
pred
icto
rs, p
oten
tial c
onfo
unde
rs, a
nd
effec
t mod
ifier
s; g
ive
diag
nost
ic c
rite
ria,
if
appl
icab
le
11
11
10
11
11
1
8 Fo
r ea
ch v
aria
ble
of in
tere
st, g
ive
data
sou
rces
and
det
ails
of m
etho
ds o
f as
sess
men
t1
11
11
11
11
11
9 D
escr
ibe
any
effor
ts to
add
ress
pot
entia
l so
urce
s of
bia
s1
10
01
11
10
00

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 95
6
App
endi
x S2
: STR
OBE
che
cklis
t: C
ontin
ued.
Des
crip
tion
of i
tem
sVi
khar
eva
O
sser
and
Va
lent
in
(201
0)
Bij d
e Va
ate
et
al.
(201
1)
Gla
vind
et
al.
(2
012)
Hay
akaw
a et
al.
(200
6)
Vale
nzan
oet
al.
(200
6)
Yazi
ciog
lu
(200
6)Vi
khar
eva
Oss
er
et a
l. (2
010)
Viha
reva
O
sser
et
al.
(200
9)
Ofili-
Yebo
vi
et a
l. (2
008)
El-M
azny
et
al.
(201
1)
Wan
g
et a
l. (2
009)
10 E
xpla
in h
ow th
e st
udy
size
was
arr
ived
at
11
11
11
11
00
0
11 E
xpla
in h
ow q
uant
itativ
e va
riab
les
wer
e ha
ndle
d in
the
anal
yses
; if
appl
icab
le, d
escr
ibe
whi
ch g
roup
ings
wer
e ch
osen
and
why
00
00
00
00
10
0
12
a D
escr
ibe
all s
tatis
tical
met
hods
11
11
11
11
11
1
b D
escr
ibe
any
met
hods
use
d to
exa
min
e su
bgro
ups
and
inte
ract
ions
NA
NA
NA
NA
0N
AN
AN
AN
AN
AN
A
c Ex
plai
n ho
w m
issi
ng d
ata
wer
e ad
dres
sed
00
00
00
00
00
0
d Ex
plai
n ho
w lo
ss to
follo
w-u
p w
as
addr
esse
dN
AN
AN
AN
AN
A0
NA
NA
NA
NA
NA
e D
escr
ibe
any
sens
itivi
ty a
naly
ses
NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
13
a Re
port
num
bers
of i
ndiv
idua
ls a
t eac
h st
age
of s
tudy
11
11
11
11
11
1
b G
ive
reas
ons
for
non-
part
icip
atio
n at
ea
ch s
tage
11
11
11
11
11
1
c Co
nsid
er u
se o
f a fl
ow d
iagr
am0
11
00
00
00
00
14
a G
ive
char
acte
rist
ics
of s
tudy
par
ticip
ants
an
d in
form
atio
n on
exp
osur
es a
nd
pote
ntia
l con
foun
ders
11
11
11
11
11
0
b In
dica
te n
umbe
r of
par
ticip
ants
with
m
issi
ng d
ata
for
each
var
iabl
e of
inte
rest
NA
1N
AN
AN
A1
NA
NA
1N
AN
A

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
96 | Chapter 6
c Su
mm
ariz
e fo
llow
-up
time
NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
15. R
epor
t num
bers
of o
utco
me
even
ts o
r su
mm
ary
mea
sure
s ov
er ti
me
11
11
11
11
11
1
16
a G
ive
unad
just
ed e
stim
ates
and
, if
appl
icab
le, c
onfo
unde
r-ad
just
ed e
stim
ates
an
d th
eir
prec
isio
n
11
01
01
00
10
1
b Re
port
cat
egor
y bo
unda
ries
whe
n co
ntin
uous
var
iabl
es w
ere
cate
gori
zed
1N
AN
AN
AN
AN
A0
0N
AN
AN
A
c If
rele
vant
, con
side
r tr
ansl
atin
g es
timat
es o
f rel
ativ
e ri
sk in
to a
bsol
ute
risk
fo
r a
mea
ning
ful t
ime
peri
od0
00
00
00
00
00
17 R
epor
t oth
er a
naly
ses
done
NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
18 S
umm
ariz
e ke
y re
sults
with
ref
eren
ce
to s
tudy
obj
ectiv
es1
11
10
01
11
11
19 D
iscu
ss li
mita
tions
of t
he s
tudy
, tak
ing
into
acc
ount
sou
rces
of p
oten
tial b
ias
or
impr
ecis
ion.
10
11
00
11
00
1
20. G
ive
a ca
utio
us o
vera
ll in
terp
reta
tion
of r
esul
ts1
11
11
11
11
11
21. D
iscu
ss th
e ge
nera
lisab
ility
of t
he
stud
y re
sults
00
00
00
00
00
0
22. G
ive
fund
ing
sour
ces
10
10
00
11
00
0
Sum
mar
y22
/27
(81.
5%)
21/2
7 (7
7.8%
)20
/26
(76.
9%)
19/2
6 (7
3.1%
)18
/28
(64.
3%)
18/2
8 (6
4.3%
)17
/27
(63.
0%)
17/2
7(6
3.0%
)16
/27
(59.
3%)
15/2
6(5
7.7%
)15
/26
(57.
7%)
App
endi
x S2
: STR
OBE
che
cklis
t: C
ontin
ued.
Des
crip
tion
of i
tem
sVi
khar
eva
O
sser
and
Va
lent
in
(201
0)
Bij d
e Va
ate
et
al.
(201
1)
Gla
vind
et
al.
(2
012)
Hay
akaw
a et
al.
(200
6)
Vale
nzan
oet
al.
(200
6)
Yazi
ciog
lu
(200
6)Vi
khar
eva
Oss
er
et a
l. (2
010)
Viha
reva
O
sser
et
al.
(200
9)
Ofili-
Yebo
vi
et a
l. (2
008)
El-M
azny
et
al.
(201
1)
Wan
g
et a
l. (2
009)
App
endi
x S2
: STR
OBE
che
cklis
t: C
ontin
ued.
Des
crip
tion
of i
tem
sU
ppal
et a
l. (2
011)
Ceci
et
al.
(201
2)A
rmst
rong
et
al.
(2
003)
Borg
es e
t al
. (2
010)
Mon
teag
udo
et a
l.
(200
1)
Regn
ard
et
al. (
2004
)Fa
bres
et
al.
(200
3)
Chan
g et
al
. (2
009)
Thur
mon
d (1
999)
Chen
et a
l. (1
990)
1 a St
udy
desi
gn is
cle
ar in
title
or
abst
ract
01
00
00
10
00
b Ab
stra
ct p
rovi
des
an in
form
ativ
e an
d ba
lanc
ed s
umm
ary
11
11
11
01
01
2 Ex
plai
n th
e sc
ient
ific
back
grou
nd a
nd
ratio
nale
for
the
inve
stig
atio
n be
ing
repo
rted
11
11
10
11
01
3 St
ate
spec
ific
obje
ctiv
es, i
nclu
ding
any
pr
espe
cifie
d hy
poth
eses
11
11
01
10
00
4 Pr
esen
t key
ele
men
ts o
f stu
dy d
esig
n ea
rly
in th
e pa
per
11
01
00
11
00
5 D
escr
ibe
the
sett
ing,
loca
tions
, and
re
leva
nt d
ates
, inc
ludi
ng
pe
riod
s of
rec
ruitm
ent,
expo
sure
, fol
low
-up
, and
dat
a co
llect
ion
11
01
00
01
00
6 a G
ive
the
elig
ibili
ty c
rite
ria
and
the
sour
ces
and
met
hods
of s
elec
tion
of
part
icip
ants
; des
crib
e m
etho
ds o
f fol
low
-up
01
10
10
00
00
b Fo
r m
atch
ed s
tudi
es, g
ive
mat
chin
g cr
iteri
a an
d nu
mbe
r of
exp
osed
and
un
expo
sed
NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
7 Cl
earl
y de
fine
all o
utco
mes
, exp
osur
es,
pred
icto
rs, p
oten
tial c
onfo
unde
rs, a
nd
effec
t mod
ifier
s; g
ive
diag
nost
ic c
rite
ria,
if
appl
icab
le
11
10
11
10
00
8 Fo
r ea
ch v
aria
ble
of in
tere
st, g
ive
data
sou
rces
and
det
ails
of m
etho
ds o
f as
sess
men
t0
11
01
10
00
0

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 97
6
App
endi
x S2
: STR
OBE
che
cklis
t: C
ontin
ued.
Des
crip
tion
of i
tem
sU
ppal
et a
l. (2
011)
Ceci
et
al.
(201
2)A
rmst
rong
et
al.
(2
003)
Borg
es e
t al
. (2
010)
Mon
teag
udo
et a
l.
(200
1)
Regn
ard
et
al. (
2004
)Fa
bres
et
al.
(200
3)
Chan
g et
al
. (2
009)
Thur
mon
d (1
999)
Chen
et a
l. (1
990)
1 a St
udy
desi
gn is
cle
ar in
title
or
abst
ract
01
00
00
10
00
b Ab
stra
ct p
rovi
des
an in
form
ativ
e an
d ba
lanc
ed s
umm
ary
11
11
11
01
01
2 Ex
plai
n th
e sc
ient
ific
back
grou
nd a
nd
ratio
nale
for
the
inve
stig
atio
n be
ing
repo
rted
11
11
10
11
01
3 St
ate
spec
ific
obje
ctiv
es, i
nclu
ding
any
pr
espe
cifie
d hy
poth
eses
11
11
01
10
00
4 Pr
esen
t key
ele
men
ts o
f stu
dy d
esig
n ea
rly
in th
e pa
per
11
01
00
11
00
5 D
escr
ibe
the
sett
ing,
loca
tions
, and
re
leva
nt d
ates
, inc
ludi
ng
pe
riod
s of
rec
ruitm
ent,
expo
sure
, fol
low
-up
, and
dat
a co
llect
ion
11
01
00
01
00
6 a G
ive
the
elig
ibili
ty c
rite
ria
and
the
sour
ces
and
met
hods
of s
elec
tion
of
part
icip
ants
; des
crib
e m
etho
ds o
f fol
low
-up
01
10
10
00
00
b Fo
r m
atch
ed s
tudi
es, g
ive
mat
chin
g cr
iteri
a an
d nu
mbe
r of
exp
osed
and
un
expo
sed
NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
7 Cl
earl
y de
fine
all o
utco
mes
, exp
osur
es,
pred
icto
rs, p
oten
tial c
onfo
unde
rs, a
nd
effec
t mod
ifier
s; g
ive
diag
nost
ic c
rite
ria,
if
appl
icab
le
11
10
11
10
00
8 Fo
r ea
ch v
aria
ble
of in
tere
st, g
ive
data
sou
rces
and
det
ails
of m
etho
ds o
f as
sess
men
t0
11
01
10
00
0

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
98 | Chapter 6
App
endi
x S2
: STR
OBE
che
cklis
t: C
ontin
ued.
9 D
escr
ibe
any
effor
ts to
add
ress
pot
entia
l so
urce
s of
bia
s0
01
00
00
00
0
10 E
xpla
in h
ow th
e st
udy
size
was
arr
ived
at
00
01
10
10
10
11 E
xpla
in h
ow q
uant
itativ
e va
riab
les
wer
e ha
ndle
d in
the
anal
yses
; if a
pplic
able
, de
scri
be w
hich
gro
upin
gs w
ere
chos
en
and
why
00
00
00
00
00
12
a D
escr
ibe
all s
tatis
tical
met
hods
11
10
00
00
00
b D
escr
ibe
any
met
hods
use
d to
exa
min
e su
bgro
ups
and
inte
ract
ions
NA
NA
NA
NA
NA
NA
NA
NA
NA
0
c Ex
plai
n ho
w m
issi
ng d
ata
wer
e ad
dres
sed
00
00
00
00
00
d Ex
plai
n ho
w lo
ss to
follo
w-u
p w
as
addr
esse
dN
A0
NA
NA
NA
NA
NA
NA
NA
NA
e D
escr
ibe
any
sens
itivi
ty a
naly
ses
NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
13 a Re
port
num
bers
of i
ndiv
idua
ls a
t eac
h st
age
of s
tudy
1
11
10
10
11
0
b G
ive
reas
ons
for
non-
part
icip
atio
n at
ea
ch s
tage
11
11
11
01
11
c Co
nsid
er u
se o
f a fl
ow d
iagr
am0
00
00
00
00
0
14
a G
ive
char
acte
rist
ics
of s
tudy
par
ticip
ants
an
d in
form
atio
n on
exp
osur
es a
nd
pote
ntia
l con
foun
ders
00
11
00
10
00
b In
dica
te n
umbe
r of
par
ticip
ants
with
m
issi
ng d
ata
for
each
var
iabl
e of
inte
rest
0N
AN
AN
AN
AN
AN
AN
AN
AN
A
c Su
mm
ariz
e fo
llow
-up
time
NA
1N
AN
AN
AN
AN
AN
AN
AN
A

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 99
6
App
endi
x S2
: STR
OBE
che
cklis
t: C
ontin
ued.
15 R
epor
t num
bers
of o
utco
me
even
ts o
r su
mm
ary
mea
sure
s ov
er ti
me
11
11
11
11
11
16
a G
ive
unad
just
ed e
stim
ates
and
, if
appl
icab
le, c
onfo
unde
r-ad
just
ed e
stim
ates
an
d th
eir
prec
isio
n
10
00
00
00
00
b Re
port
cat
egor
y bo
unda
ries
whe
n co
ntin
uous
var
iabl
es w
ere
cate
gori
zed
NA
NA
NA
NA
NA
1N
A0
NA
NA
c If
rele
vant
, con
side
r tr
ansl
atin
g es
timat
es
of r
elat
ive
risk
into
abs
olut
e ri
sk fo
r a
mea
ning
ful t
ime
peri
od0
00
00
00
00
0
17 R
epor
t oth
er a
naly
ses
done
N
AN
AN
AN
AN
AN
AN
AN
AN
AN
A
18 S
umm
ariz
e ke
y re
sults
with
ref
eren
ce
to s
tudy
obj
ectiv
es0
00
01
11
00
0
19 D
iscu
ss li
mita
tions
of t
he s
tudy
, tak
ing
into
acc
ount
sou
rces
of p
oten
tial b
ias
or
impr
ecis
ion.
1
01
01
10
00
0
20 G
ive
a ca
utio
us o
vera
ll in
terp
reta
tion
of r
esul
ts
11
11
11
11
11
21 D
iscu
ss th
e ge
nera
lisab
ility
of t
he s
tudy
re
sults
10
00
00
00
00
22 G
ive
fund
ing
sour
ces
10
00
00
00
00
Sum
mar
y15
/27
(55.
6%)
15/2
8(5
3.6%
)14
/26
(53.
8%)
11/2
6(4
2.3%
)11
/26
(42.
3%)
11/2
7(4
0.7%
)10
/26
(38.
5%)
8/27
(29.
6%)
5/26
(19.
2%)
5/27
(18.
5%)
STRO
BE: S
tren
gthe
ning
the
Repo
rtin
g of
Obs
erva
tiona
l Stu
dies
in E
pide
mio
logy
, NA:
not
app
licab
le.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
100 | Chapter 6
Tabl
e S1
: Ris
k fa
ctor
s fo
r th
e pr
esen
ce o
f a n
iche
and
fact
ors
asso
ciat
ed w
ith n
iche
siz
e.
Lead
ing
auth
orD
esig
n n
Popu
lati
onO
utco
me
Defi
niti
on o
f nic
he a
nd
met
hod
of e
valu
atio
nRe
sult
s
Rand
om s
ampl
e of
wom
en w
ith a
his
tory
of C
S,re
port
ing
abou
t fac
tors
ass
ocia
ted
with
the
pres
ence
of a
nic
he:
Yazi
ciog
lu
et a
l.
2005
26
Rand
omiz
ed
cont
rolle
d tr
ial
70N
ullip
ar p
regn
ant
patie
nts
with
an
indi
catio
n fo
r CS
, w
ith o
r w
ithou
t la
bour
.
The
effec
t of s
utur
ing
tech
niqu
e (fu
ll th
ickn
ess
incl
udin
g th
e en
dom
etri
al
laye
r ve
rsus
spl
it th
ickn
ess
excl
udin
g th
e en
dom
etri
al la
yer)
on
the
inci
denc
e of
ces
area
n sc
ar d
efec
t.
Defi
nitio
n: A
ny d
evia
tion
from
the
full
appo
sitio
n of
the
cran
ial a
nd c
auda
l ed
ges
of th
e ut
erin
e in
cisi
on c
ausi
ng
a ba
lloon
ing
out t
owar
ds th
e an
teri
or
abdo
min
al w
all.
Met
hod:
TVS
The
freq
uenc
y of
inco
mpl
ete
heal
ing
was
si
gnifi
cant
ly lo
wer
in th
e gr
oup
trea
ted
by fu
ll th
ickn
ess
sutu
ring
(OR
0.2
[95%
CI 0
.06-
0.99
]; p=
0.04
8). P
atie
nts
with
inco
mpl
ete
heal
ing
had
less
cer
vica
l dila
tatio
n pr
ior
to s
urge
ry
(OR
0.5
[95%
CI 0
.3-0
.8];
p=0.
007)
.
Hay
akaw
a
et a
l.
2006
25
Pros
pect
ive
coho
rt s
tudy
137
Wom
en w
ho
unde
rwen
t firs
t CS
bet
wee
n 26
an
d 41
wee
ks o
f ge
stat
ion
with
a
tran
sver
se lo
wer
ut
erin
e se
gmen
t in
cisi
on, w
ith o
r w
ithou
t lab
our.
Asso
ciat
ion
betw
een
wed
ge d
efec
t one
m
onth
aft
er C
S an
d m
etho
d fo
r m
yom
etri
um
clos
ure
as w
ell a
s ot
her
peri
oper
ativ
e pa
ram
eter
s.
Defi
nitio
n: C
onca
vity
at t
he
pres
umed
site
of i
ncis
ion
with
a
dept
h of
mor
e th
an 5
mm
.
Met
hod:
TVS
Fact
ors
asso
ciat
ed w
ith w
edge
def
ect w
ere
myo
met
rium
clo
sure
tech
niqu
e (d
oubl
e-la
yer:
OR
0.3
[95%
CI 0
.09-
0.9]
; p=0
.04)
, si
ngle
-laye
r w
ith d
ecid
ual s
utur
e: O
R 0.
08
[95%
CI 0
.01-
0.5]
; p=0
.007
), ge
stat
iona
l wee
k (O
R 1.
4 [9
5% C
I 1.1
-1.8
]; p=
0.02
), m
ultip
le
preg
nanc
ies
(OR
8.9
[95%
CI 2
.0-4
0.6]
; p=
0.00
5), p
rem
atur
e ru
ptur
e of
mem
bran
es
(OR
8.7
[95%
CI 1
.3-5
9.7]
; p=0
.03)
and
pr
e-ec
lam
psia
(OR
8.7
[95%
CI 1
.7-4
4.5]
; p=
0.00
9).
Arm
stro
ng
et a
l.
2003
4
Pros
pect
ive
coho
rt s
tudy
32 w
ith
prev
ious
CS
(n
= 7
0)
Volu
ntee
rs
betw
een
ages
18
and
40
with
a
hist
ory
of o
ne o
r m
ultip
le v
agin
al
(n =
38)
or
cesa
rean
de
liver
ies
(n =
32)
with
in th
e pr
eced
ing
5 ye
ars.
Asso
ciat
ion
betw
een
cesa
rean
sca
r de
fect
s an
d th
e ob
stet
ric
hist
ory.
Defi
nitio
n: F
luid
with
in th
e sc
ar a
nd in
cont
inui
ty w
ith
the
endo
cerv
ical
can
al.
M
etho
d: T
VS
Prol
onge
d la
bour
pri
or to
ces
area
n de
liver
y (p
=0.0
1) a
nd m
ultip
le C
Ss (p
<0.0
4) w
ere
asso
ciat
ed w
ith th
e pr
esen
ce o
f ces
area
n sc
ar d
efec
ts.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 101
6
Tabl
e S1
: Con
tinue
d.
Lead
ing
auth
orD
esig
nn
Popu
lati
onO
utco
me
Defi
niti
on o
f nic
he a
nd
met
hod
of e
valu
atio
nRe
sult
s
repo
rtin
g ab
out f
acto
rs a
ssoc
iate
d w
ith n
iche
siz
e:
Vikh
arev
a O
sser
and
Va
lent
in
20
1022
(s
ubgr
oup
of V
ikha
reva
O
sser
et
al.
20
099 )
Pros
pect
ive
coho
rt s
tudy
108
Wom
en w
ith a
hi
stor
y of
one
CS
in th
e pr
eced
ing
6-9
mon
ths.
Fact
ors
incr
easi
ng th
e ri
sk o
f lar
ge c
esar
ean
scar
def
ects
in w
omen
w
ith a
his
tory
of o
nly
one
CS.
Defi
nitio
n: A
ny in
dent
atio
n in
the
scar
, how
ever
sm
all.
Met
hod:
TVS
and
SH
G.
Incr
ease
d ce
rvic
al d
ilata
tion
at C
S (0
cm
, 1-4
cm
, 5-7
cm
, ≥8
cm; O
R 4.
4 [9
5% C
I 0.7
-28.
5],
26.5
[4.3
-161
.8],
32.4
[6.1
-171
.0];
p<0.
001)
an
d st
atio
n of
the
pres
entin
g pa
rt a
t CS
belo
w p
elvi
c in
let (
OR
14.1
[95%
CI 4
.6-4
3.1]
; p<
0.00
1) w
ere
inde
pend
ent v
aria
bles
as
soci
ated
with
a la
rge
nich
e. R
etro
flexe
d ut
erus
(OR
2.9
[95%
CI 1
.0-8
.3];
p=0.
047)
and
du
ratio
n of
act
ive
labo
ur (0
, 1-4
, 5-9
, ≥10
ho
urs;
OR
2.0
[95%
CI 0
.2-2
3.8]
, 13.
0 [2
.2-
76.6
], 33
.1 [6
.6-1
66.9
]; p<
0.00
1) w
ere
also
as
soci
ated
with
a la
rge
nich
e.
Ceci
et
al.
20
1223
Pros
pect
ive
coho
rt s
tudy
60Si
ngle
ton
prim
ipar
ae
who
wer
e no
t in
labo
ur a
nd
unde
rwen
t the
ir
first
CS.
The
outc
ome
of
the
cesa
rean
sca
r, co
mpa
ring
2 ty
pes
of
sing
le-la
yer
sutu
res
(lock
ed c
ontin
uous
vs.
in
terr
upte
d su
ture
s).
Defi
nitio
n: B
ell-s
hape
d po
uch
area
.
M
etho
d: T
VS a
nd h
yste
rosc
opy.
The
prev
alen
ce o
f a u
teri
ne w
all d
efec
t was
85
.7%
, and
the
area
und
er th
e po
uch
was
la
rger
in w
omen
with
con
tinuo
us s
utur
es a
s co
mpa
red
to in
terr
upte
d su
ture
s (p
=0.0
3).
Hys
tero
scop
y co
nfirm
ed th
e pr
esen
ce o
f th
e po
uche
s, b
ut d
iffer
ent h
yste
rosc
opic
ou
tcom
es w
ere
obse
rved
.
Gla
vind
et
al.
2012
24
Retr
ospe
ctiv
e co
hort
stu
dy14
9W
omen
who
un
derw
ent
thei
r fir
st C
S in
sin
glet
on
preg
nanc
y at
leas
t 6
mon
ths
ago
and
who
wer
e no
t in
labo
ur.
A di
ffer
ence
in r
esid
ual
myo
met
rial
thic
knes
s an
d si
ze o
f the
ces
area
n sc
ar d
efec
t bet
wee
n si
ngle
- and
dou
ble-
laye
r ut
erot
omy
clos
ure.
Defi
nitio
n: A
ny in
dent
ed
wed
ge-s
hape
d ar
ea s
tret
chin
g be
yond
the
sugg
este
d an
teri
or
linin
g of
the
endo
met
rium
.
Met
hod:
TVS
The
med
ian
resi
dual
myo
met
rial
thic
knes
s w
as 5
.8 m
m in
dou
ble-
laye
r vs
. 4.6
mm
in
sing
le-la
yer
clos
ures
(p=0
.04)
. The
sca
r de
fect
le
ngth
dec
reas
ed fr
om 6
.8 m
m in
sin
gle-
laye
r to
5.6
mm
in d
oubl
e-la
yer
clos
ures
(p
=0.0
1). H
eigh
t and
wid
th w
ere
sim
ilar
in
both
gro
ups.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
102 | Chapter 6
Tabl
e S1
: Con
tinue
d.
Lead
ing
auth
orD
esig
nn
Popu
lati
onO
utco
me
Defi
niti
on o
f nic
he a
nd
met
hod
of e
valu
atio
nRe
sult
s
Sele
cted
pop
ulat
ion
cons
istin
g of
wom
en w
ith g
ynae
colo
gica
l sym
ptom
s,re
port
ing
abou
t fac
tors
ass
ocia
ted
with
the
pres
ence
of a
nic
he:
Ofil
i-Yeb
ovi
et a
l.
20
0811
Pros
pect
ive
coho
rt s
tudy
324
Wom
en w
ith a
hi
stor
y of
one
or
mul
tiple
tr
ansv
erse
lo
wer
-seg
men
t CS
s, r
efer
red
for
a va
riet
y of
gy
naec
olog
ical
in
dica
tions
.
The
iden
tifica
tion
of
fact
ors
asso
ciat
ed w
ith
the
pres
ence
of c
esar
ean
scar
def
ects
.
Defi
nitio
n: D
etec
tabl
e m
yom
etri
al
thin
ning
at t
he s
car
site
.
Met
hod:
TVS
A hi
stor
y of
mul
tiple
CSs
(OR
1.9
[95%
CI
1.3-
2.9]
; p=0
.001
), ut
erin
e re
trofl
exio
n (O
R 2.
4 [9
5% C
I 1.3
-4.8
]; p=
0.01
) and
the
inab
ility
to
vis
ualiz
e al
l ces
area
n sc
ars
in w
omen
with
a
hist
ory
of m
ultip
le C
Ss (O
R 0.
31 [9
5% C
I 0.
13-0
.75]
; p=0
.01)
wer
e as
soci
ated
with
the
pres
ence
of c
esar
ean
scar
def
ects
.
repo
rtin
g ab
out f
acto
rs a
ssoc
iate
d w
ith n
iche
siz
e:
Wan
g
et a
l.
2009
10
Cros
s-se
ctio
nal
stud
y20
7W
omen
with
a
hist
ory
of o
ne
or m
ultip
le C
Ss,
exam
ined
with
TV
S fo
r va
riou
s gy
naec
olog
ical
in
dica
tions
, di
agno
sed
with
a
cesa
rean
sca
r de
fect
.
Asso
ciat
ion
betw
een
the
size
of c
esar
ean
scar
de
fect
s, u
teri
ne p
ositi
on
and
the
num
ber
of C
Ss.
Defi
nitio
n: H
ypoe
chog
enic
are
a w
ithin
the
myo
met
rium
of t
he
low
er u
teri
ne s
egm
ent,
at th
e si
te
of a
pre
viou
s ce
sare
an in
cisi
on.
M
etho
d: T
VS
The
mea
n w
idth
and
dep
th o
f the
sca
r de
fect
w
ere
larg
er in
wom
en w
ho h
ad u
nder
gone
m
ultip
le C
Ss (p
=0.0
01 a
nd p
=0.0
02) a
nd th
e m
ean
wid
th w
as la
rger
in w
omen
with
a
retr
oflex
ed u
teru
s (p
<0.0
01).
Mon
teag
udo
et a
l. 2
0018
Pros
pect
ive
coho
rt s
tudy
44W
omen
with
a
hist
ory
of o
ne
or m
ultip
le C
Ss,
who
und
erw
ent
SHG
for
a va
riet
y of
gyn
aeco
logi
c in
dica
tions
.
Asso
ciat
ion
betw
een
the
num
ber
of C
Ss a
nd
the
size
of t
he n
iche
and
th
ickn
ess
of th
e re
sidu
al
myo
met
rium
.
Defi
nitio
n: T
rian
gula
r an
echo
ic s
truc
ture
at t
he s
ite
of a
pre
viou
s ce
sare
an s
car.
Met
hod:
SH
G
Ther
e w
as n
o as
soci
atio
n be
twee
n th
e nu
mbe
r of
CSs
and
the
dept
h of
the
nich
e or
th
e th
ickn
ess
of th
e re
sidu
al m
yom
etri
um.
CS=c
esar
ean
sect
ion;
TVS
=tra
nsva
gina
l son
ogra
phy;
SH
G=s
onoh
yste
rogr
aphy
.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 103
6
Tabl
e S2
: Sym
ptom
s as
soci
ated
with
the
pres
ence
of a
nic
he.
Lead
ing
auth
orD
esig
nn
Popu
lati
onO
utco
me
Defi
niti
on o
f nic
he a
nd
met
hod
of e
valu
atio
nSp
ecifi
cati
on o
f ble
edin
g di
sord
er a
nd m
etho
d of
ev
alua
tion
Resu
lts
No
sele
ctio
n bi
as, r
ando
m s
ampl
e of
wom
en w
ith a
his
tory
of C
S:
Bij d
e Va
ate
et a
l.
2011
5
Pros
pect
ive
coho
rt s
tudy
225
Cons
ecut
ive
incl
usio
n of
wom
en
6-12
mon
ths
afte
r a
CS.
Rela
tions
hip
betw
een
nich
e an
d ab
norm
al
uter
ine
blee
ding
.
Defi
nitio
n: A
nech
oic
area
at t
he s
ite o
f the
ce
sare
an s
car
with
a
dept
h of
at l
east
1 m
m.
Met
hod:
SH
G
Post
men
stru
al s
pott
ing:
M
ore
than
2 d
ays
of
brow
nish
dis
char
ge
at th
e en
d of
the
men
stru
atio
n w
ith a
tota
l le
ngth
of m
enst
ruat
ion
of m
ore
than
7 d
ays,
or
inte
rmen
stru
al b
leed
ing
whi
ch s
tart
s w
ithin
5
days
aft
er th
e en
d th
e en
d of
the
men
stru
atio
n.
M
etho
d: Q
uest
ionn
aire
an
d PB
AC.
Post
men
stru
al s
pott
ing
was
re
port
ed b
y 34
% o
f wom
en
with
a n
iche
and
15%
with
out
a ni
che
(p=0
.002
). La
rger
nic
he
volu
me
was
see
n in
wom
en
with
pos
tmen
stru
al s
pott
ing
than
with
out p
ostm
enst
rual
sp
ottin
g (p
=0.0
2,) a
nd
no r
elat
ion
was
foun
d be
twee
n ni
che
shap
e an
d po
stm
enst
rual
spo
ttin
g.
Vale
nzan
o et
al.
2006
15
Case
-con
trol
st
udy
116
with
pr
evio
us
CS
(n =
217
)
Rand
om s
elec
tion
of w
omen
who
gav
e bi
rth
for
the
first
tim
e be
twee
n 19
95
and
2004
: vag
inal
bi
rth
(n =
101
) or
CS
(n =
116
).
Asso
ciat
ion
betw
een
mor
phol
ogic
al
chan
ges
of th
e lo
wer
ut
erin
e se
gmen
t aft
er
CS a
nd th
e fr
eque
ncy
of a
bnor
mal
ute
rine
bl
eedi
ng.
Defi
nitio
n: T
rian
gula
r, an
echo
ic a
rea
at th
e pr
esum
ed s
ite o
f inc
isio
n.
Met
hod:
TVS
, and
onl
y ni
ches
with
SH
G
Abno
rmal
ute
rine
bl
eedi
ng: S
pott
ing
blee
ding
af
ter
the
end
of th
e m
enst
ruat
ion
and/
or n
on-
cycl
ic b
leed
ing
not r
elat
ed
to th
e m
enst
ruat
ion.
M
etho
d: Q
uest
ions
wer
e as
ked.
Abno
rmal
ble
edin
g w
as
mor
e fr
eque
nt in
the
CS
grou
p as
com
pare
d w
ith th
e va
gina
l bir
th g
roup
(p=0
.041
). N
o as
soci
atio
n w
as fo
und
betw
een
abno
rmal
ble
edin
g an
d th
e pr
esen
ce o
f a n
iche
(p
=0,8
18),
but a
n as
soci
atio
n w
as fo
und
with
div
ertic
ula
(p=0
.012
) and
def
orm
atio
n of
th
e ce
rvic
al c
anal
(p=0
.031
), w
hich
was
mor
e si
gnifi
cant
in
wom
en w
ho h
ad a
CS
5-10
ye
ars
ago.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
104 | Chapter 6
Tabl
e S2
: Con
tinue
d.
Lead
ing
auth
orD
esig
nn
Popu
lati
onO
utco
me
Defi
niti
on o
f nic
he a
nd
met
hod
of e
valu
atio
nSp
ecifi
cati
on o
f ble
edin
g di
sord
er a
nd m
etho
d of
ev
alua
tion
Resu
lts
Sele
cted
pop
ulat
ion
cons
istin
g of
wom
en w
ith g
ynae
colo
gica
l sym
ptom
s:
Upp
al
et a
l.
20
1128
Pros
pect
ive
coho
rt s
tudy
71 w
ith
prev
ious
CS
(n
= 3
18)
Wom
en r
efer
red
for
gyna
ecol
ogic
al
ultr
asou
nd. 7
1 w
omen
had
a
hist
ory
of C
S.
Asso
ciat
ion
betw
een
cesa
rean
sca
r de
fect
s an
d ab
norm
al
vagi
nal b
leed
ing.
Defi
nitio
n: F
luid
fil
led
defe
ct in
the
hyst
erot
omy
inci
sion
.
M
etho
d: T
VS
Abno
rmal
ble
edin
g pa
tter
n: p
erio
ds lo
nger
th
an 7
day
s an
d/or
sp
ottin
g af
ter
the
peri
od.
M
etho
d: Q
uest
ionn
aire
an
d re
cord
s of
the
wom
en
wer
e re
view
ed.
The
pres
ence
of a
ces
area
n sc
ar d
efec
t was
sig
nific
antly
as
soci
ated
abn
orm
al b
leed
ing
(OR
1.96
[95%
CI 1
.16-
3.32
]; p<
0.05
). Th
e la
rger
the
defe
ct,
the
high
er w
as th
e in
cide
nce
of a
bnor
mal
vag
inal
ble
edin
g.
Thur
mon
d et
al.
1999
18
Pros
pect
ive
coho
rt s
tudy
310
Wom
en r
efer
red
for
abno
rmal
ute
rine
bl
eedi
ng, w
ho w
ere
eval
uate
d w
ith S
HG
, in
depe
nden
t of t
heir
ob
stet
ric
hist
ory.
Des
crip
tion
of a
ca
use
of a
bnor
mal
va
gina
l ble
edin
g re
late
d to
a h
isto
ry
of C
S.
Defi
nitio
n: A
gap
in th
e an
teri
or lo
wer
ute
rine
se
gmen
t myo
met
rium
at
the
expe
cted
site
of
the
scar
from
pri
or
cesa
rean
del
iver
ies.
M
etho
d: S
HG
Post
men
stru
al
spot
ting:
2 to
12
days
of
pos
tmen
stru
al
disc
harg
e of
dar
k re
d or
bro
wn
mat
eria
l.
M
etho
d: N
ot s
peci
fied.
9 w
omen
with
a h
isto
ry o
f CS
dem
onst
rate
d a
nich
e an
d al
l th
ese
wom
en h
ad a
his
tory
of
2 to
12
days
of p
ostm
enst
rual
sp
ottin
g.
Wan
g et
al.
2009
10
Cros
s-se
ctio
nal
stud
y20
7W
omen
with
a
hist
ory
of C
S,
exam
ined
with
TV
S fo
r va
riou
s gy
naec
olog
ical
in
dica
tions
, di
agno
sed
with
a
cesa
rean
sca
r de
fect
.
The
prev
alen
ce
of v
ario
us c
linic
al
sym
ptom
s in
pat
ient
s w
ith c
esar
ean
scar
de
fect
s an
d th
e as
sess
men
t of t
he
asso
ciat
ion
betw
een
the
size
of t
he
cesa
rean
sca
r de
fect
an
d sy
mpt
oms.
Defi
nitio
n: H
ypoe
chog
enic
ar
ea w
ithin
the
myo
met
rium
of t
he
low
er u
teri
ne s
egm
ent,
at th
e si
te o
f a p
revi
ous
cesa
rean
inci
sion
.
M
etho
d: T
VS
Blee
ding
dis
orde
r no
t defi
ned.
Met
hod:
Med
ical
hi
stor
ies
wer
e re
view
ed.
Que
stio
nnai
res
and
mis
sing
dat
a w
ere
obta
ined
by
dire
ct p
hone
co
ntac
t.
Prol
onge
d po
stm
enst
rual
sp
ottin
g w
as th
e m
ost
com
mon
sym
ptom
(64%
), fo
llow
ed b
y dy
smen
orrh
ea
(53%
), ch
roni
c pe
lvic
pai
n (4
0%) a
nd d
yspa
reun
ia (1
8%).
The
mea
n de
fect
wid
th w
as
sign
ifica
ntly
larg
er in
wom
en
with
pos
tmen
stru
al s
pott
ing
(p<0
.001
), dy
smen
orrh
ea
(p=0
.001
) and
chr
onic
pel
vic
pain
(p<0
.001
). N
o as
soci
atio
n be
twee
n de
pth
or th
ickn
ess
of
the
resi
dual
myo
met
rium
and
sy
mpt
oms
was
foun
d.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Prevalence of niche, risk factors and symptoms | 105
6
Tabl
e S2
: Con
tinue
d.
Lead
ing
auth
orD
esig
nn
Popu
lati
onO
utco
me
Defi
niti
on o
f nic
he a
nd
met
hod
of e
valu
atio
nSp
ecifi
cati
on o
f ble
edin
g di
sord
er a
nd m
etho
d of
ev
alua
tion
Resu
lts
Fabr
es
et a
l.20
036
Retr
ospe
ctiv
e co
hort
stu
dy92
Prem
enop
ausa
l w
omen
with
a
hist
ory
of C
S an
d a
pouc
h at
the
site
of
the
cesa
rean
sc
ar d
emon
stra
ted
with
TVS
, who
wer
e as
sess
ed fo
r ot
her
gyna
ecol
ogic
al
reas
ons.
Asso
ciat
ion
betw
een
the
pres
ence
of t
he
pouc
h an
d bl
eedi
ng
dist
urba
nces
.
Defi
nitio
n: A
filli
ng d
efec
t of
the
uter
ine
cavi
ty
loca
ted
in r
elat
ion
to
the
ante
rior
isth
mus
.
Met
hod:
TVS
Blee
ding
dis
orde
r an
d m
etho
d no
t defi
ned.
83
% o
f the
wom
en w
ith
a po
uch
had
abno
rmal
ut
erin
e bl
eedi
ng. A
mon
g th
ese
wom
en, 7
6% h
ad
post
men
stru
al s
pott
ing,
16%
m
idcy
cle
met
rorr
hagi
a an
d 6%
bot
h sy
mpt
oms.
Mon
teag
udo
et a
l.20
018
Pros
pect
ive
coho
rt s
tudy
44W
omen
with
a
hist
ory
of C
S,
who
und
erw
ent
SHG
for
a va
riet
y of
gyn
aeco
logi
c in
dica
tions
.
The
prev
alen
ce o
f ab
norm
al u
teri
ne
blee
ding
in w
omen
w
ith a
nic
he.
Defi
nitio
n: T
rian
gula
r an
echo
ic s
truc
ture
at
the
pres
umed
si
te o
f a C
S sc
ar.
M
etho
d: S
HG
Blee
ding
dis
orde
r an
d m
etho
d no
t defi
ned.
75%
of w
omen
with
a n
iche
ha
d ab
norm
al u
teri
ne
blee
ding
, 36%
had
fibr
oids
an
d 18
% h
ad e
ndom
etri
al
poly
ps.
Borg
es e
t al.
2010
13Pr
ospe
ctiv
e co
hort
stu
dy43
Wom
en w
ith
post
men
stru
al
spot
ting
and
a hi
stor
y of
CS
in
the
prec
edin
g 2-
25
year
s.
Asse
ssm
ent o
f th
e hy
ster
osco
py
findi
ngs
in w
omen
w
ith a
his
tory
of C
S an
d po
stm
enst
rual
sp
ottin
g, s
tres
sing
th
e di
agno
sis
of
isth
moc
ele.
Defi
nitio
n no
t spe
cifie
d.
Met
hod:
Hys
tero
scop
yBl
eedi
ng d
isor
der
and
met
hod
not d
efine
d.Th
e hy
ster
osco
pic
diag
nosi
s of
isth
moc
ele
was
con
clus
ive
in 3
8 pa
tient
s (8
8.4%
). Th
e av
erag
e tim
e of
po
stm
enst
rual
spo
ttin
g w
as 6
ye
ars
and
the
mea
n du
ratio
n of
eac
h ep
isod
e w
as 6
day
s.
CS=c
esar
ean
sect
ion;
TVS
=tra
nsva
gina
l son
ogra
phy;
SH
G=s
onoh
yste
rogr
aphy
; PBA
C=pi
ctor
ial b
lood
loss
ass
essm
ent c
hart
.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
77|Therapeutic options of Therapeutic options of
caesarean scar pregnancy: case series caesarean scar pregnancy: case series and literature reviewand literature review
A.J.M. Bij de Vaate A.J.M. Bij de Vaate H.A.M. Brölmann H.A.M. Brölmann
J.W. van der Slikke J.W. van der Slikke M.G.A.J. Wouters M.G.A.J. Wouters
R. Schats R. Schats J.A.F. Huirne J.A.F. Huirne
J Clin Ultrasound 2010;38(2):75-84.J Clin Ultrasound 2010;38(2):75-84.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Abstract
We describe our experience with the treatment of 4 caesarean scar pregnancies and provide an overview of current literature. Four women diagnosed with a caesarean scar pregnancy in our hospital between 1996 and 2007 were treated with local or systemic methotrexate and had a steady decline of the serum ß-hCG level. The uterus was preserved in all women and 3 of them had an uneventful subsequent pregnancy and delivery. We suggest that transcervical needle aspiration of amniotic fluid followed by intra-amniotic injection of methotrexate should be the treatment of choice, followed by surgical treatment only if methotrexate fails.
108 | Chapter 7

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Introduction
Pregnancy developing in a scar from a caesarean section (CS) is the rarest form of ectopic pregnancy. In that case, the pregnancy is located outside the uterine cavity and is completely surrounded by myometrium and the fibrous tissue of the scar. Invasion of the conceptus into the myometrium is believed to occur through a defect in the caesarean scar. This defect may be due to fibrosis and poor vascularity, resulting in impaired postoperative healing.1 Because a caesarean scar pregnancy (CSP) can lead to uterine scar rupture and hemorrhage, a life-threatening condition for both mother and child may occur if the pregnancy is allowed to continue, even in the 1st trimester.2
Since the 1970s the CS rate has dramatically increased in most Western countries.3 The consequence is an increase in the incidence of CSPs. Currently, the incidence ranges from 1:1,800–1:2,216 pregnancies and constitutes 6.1% of all ectopic pregnancies in patients with a history of at least 1 caesarean delivery.1,4 Because of the low frequency of CSPs, no clinical trials are available that can help determine the optimal clinical management. Therefore, there is no consensus on the most preferred treatment modality. The purpose of this report is to describe our experience with the treatment and follow-up of 4 CSPs, summarized in Table 1, and to provide an overview of current literature. Therefore, the Medline database was searched with all known terms for CSP in combination with all known terms for methotrexate treatment, and reference lists were cross-checked. Based on our experience and the literature search, we suggest treatment recommendations for CSP.
Case descriptions
Case 1A 36-year-old woman, gravida 5 para 3, presented with lower abdominal pain and a positive pregnancy test at a gestational age of 6 weeks and 6 days (GA 6+6) according to her last menstrual period. The obstetric history included 2 uneventful caesarean deliveries, 1 spontaneous abortion, and 1 induced delivery because of intra-uterine fetal death. Sonography (US) revealed an empty uterine cavity and the serum ß-human chorionic gonadotrophin (ß-hCG) level was 2,018 mIU/ml. Expectant management with regular measurements of the serum ß-hCG level and US examinations was proposed. After 8 days (GA 8+0), she presented with lower abdominal pain and slight vaginal bleeding. US examination using an Aloka SSD 3500 scanner with a 2–6-MHz curved-array transducer (Aloka, Wallingford, CT) demonstrated a gestational sac (GS) in the anterior
Caesarean scar pregnancy | 109
7

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
110 | Chapter 7
isthmic wall of the uterus, containing an embryo with fetal cardiac activity and a crown-rump length corresponding to 6 weeks and 2 days gestation (Figure 1) with a serum ß-hCG level of 40,000 mIU/ml. US-guided transcervical aspiration of the GS, followed by intra-amniotic injection of 50 mg methotrexate (1 mg/kg body weight), was performed successfully. Intermittent bleeding and abdominal pain improved after a few weeks followed by normal menstrual periods, and serum
ß-hCG levels dropped below 2 mIU/ml after 5 months (Figure 2).
Figure 1: Transvaginal ultrasound image of a longitudinal section of retroverted uterus showing a ceasarean scar pregnancy (arrow).
Figure 2: Graphic representation of the serum ß-hCG levels after treatment in the 4 cases of caesarean scar pregnancy.*Local injection of methotrexate **Systemic injection of methotrexate
010000
20000300004000050000
6000070000
0 10 20 30 40 50 60 70
Days after methotrexate injection
Ser
um b
eta-
hCG
leve
l (m
IU/m
l)
Patiënt 1*Patiënt 2*Patiënt 3*Patiënt 4**

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Caesarean scar pregnancy | 111
7
Case 2A 38-year-old woman, gravida 6 para 1, presented with vaginal spotting after a positive pregnancy test at 4 weeks and 1 day gestation (GA 4+1). The obstetrical history included 2 induced abortions, 1 primary CS because of a breech presentation, an evacuation of a missed abortion, and 1 tubal pregnancy followed by right salpingectomy. In vitro fertilization was performed because of tubal factor infertility and she became pregnant after the 1st attempt. The 1st transvaginal US examination at 5 weeks and 1 day gestation (GA 5+1) revealed an empty uterine cavity and suspicion of a pregnancy in the caesarean scar. Three days later (GA 5+4), she presented with profuse vaginal bleeding and the serum ß-hCG level was 14,000 mIU/ml. US-guided transcervical aspiration of the GS and intra-amniotic injection of 75 mg methotrexate (1 mg/kg body weight) were performed. Vaginal bleeding stopped 1 day after the procedure and the patient was discharged in good condition. Regular measurements of serum ß-hCG showed a steady decline, and the ß-hCG level was undetectable (<2 mIU/ml) 3 months after methotrexate injection (Figure 2). Two months later, transvaginal US showed almost complete regression of the GS. She started again with in vitro fertilization therapy 5 months after the procedure, resulting in a pregnancy after the 6th attempt and a primary CS after 37 weeks and 4 days gestation.
Case 3A 31-year-old woman, gravida 3 para 1, presented with minimal vaginal blood loss at 6 weeks and 6 days gestation (GA 6+6) according to her last menstrual period. Her obstetrical history included 1 secondary CS because of failure to progress during labor and a curettage after incomplete abortion. US examination revealed an empty uterine cavity and a hypoechoic structure (11 mm in diameter) located in the right side of the uterus. The serum ß-hCG level was 21,100 mIU/ml. The patient was admitted with a suspicion of ectopic pregnancy. However, diagnostic laparoscopy showed a normal abdomen and uterus without signs of a tubal, adnexal, or intra-abdominal pregnancy. The US was repeated after 4 days (GA 7+3) and revealed a GS (22 x 23 x 19 mm) containing an embryo with fetal cardiac activity implanted in the anterior wall of the uterus, protruding into the vesico-uterine space. MRI confirmed the CSP. Transcervical aspiration of the amniotic fluid and intra-amniotic injection of 50 mg methotrexate (1 mg/kg body weight ) under US guidance was performed successfully. The serum ß-hCG levels decreased steadily, and the ß-hCG level was below the detection limit (<2 mIU/ml) 4 months after the procedure (Figure 2). Nine weeks after methotrexate treatment, US still showed a hypoechoic structure with a hyper-echoic wall (24 x 23 x 14 mm) between the uterus and bladder. Diagnostic hysteroscopy was performed and an extracavitary space with trophoblastic tissue was seen in the anterior wall of the uterus, close to the internal os. Laparotomy was performed

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
112 | Chapter 7
Patië
nt
no.
Pres
entin
g sy
mpt
oms
Ges
tatio
nal
age
(wee
ks)a
Prim
ary
diag
nost
ic
tool
Feta
l he
art
activ
ity
Pre-
trea
tmen
t ß-
hCG
le
vels
(m
IU/m
l)
Trea
tmen
tTi
me
afte
r tr
eatm
ent
for
ß-hC
G
to r
each
no
rmal
leve
ls
(day
s)
Subs
eque
nt
preg
nanc
y re
port
edPr
imar
ySe
cond
ary
1Ab
dom
inal
pai
n,
vagi
nal b
leed
ing
7+1
Sono
grap
hic
Yes
40.0
00Tr
ansc
ervi
cal a
spir
atio
n an
d in
tra-
amni
otic
inje
ctio
n of
50
mg
met
hotr
exat
e
Non
e16
7N
/A
2Va
gina
l ble
edin
g5+
1So
nogr
aphi
cN
o14
.000
Tran
scer
vica
l asp
irat
ion
and
intr
a-am
niot
ic in
ject
ion
of 7
5 m
g m
etho
trex
ate
Non
e92
Yes
3Va
gina
l ble
edin
g7+
3So
nogr
aphi
c,
lapa
rosc
opy,
M
RI
Yes
26.4
00Tr
ansc
ervi
cal a
spir
atio
n an
d in
tra-
amni
otic
inje
ctio
n of
50
mg
met
hotr
exat
e
Lapa
roto
my
131
Yes
4N
one
8+3
Sono
grap
hic
No
63.0
00Ex
pect
ant m
anag
emen
tSy
stem
ic in
ject
ion
of
50 m
g m
etho
trex
ate,
la
paro
tom
y
103
Yes
a Ges
tatio
nal a
ge a
t dia
gnos
is a
ccor
ding
to th
e la
st m
enst
rual
per
iod.
Tabl
e 1:
Cha
ract
eris
tics
of th
e 4
patie
nts
with
a c
aesa
rean
sca
r pr
egna
ncy.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Caesarean scar pregnancy | 113
7
Patië
nt
no.
Pres
entin
g sy
mpt
oms
Ges
tatio
nal
age
(wee
ks)a
Prim
ary
diag
nost
ic
tool
Feta
l he
art
activ
ity
Pre-
trea
tmen
t ß-
hCG
le
vels
(m
IU/m
l)
Trea
tmen
tTi
me
afte
r tr
eatm
ent
for
ß-hC
G
to r
each
no
rmal
leve
ls
(day
s)
Subs
eque
nt
preg
nanc
y re
port
edPr
imar
ySe
cond
ary
1Ab
dom
inal
pai
n,
vagi
nal b
leed
ing
7+1
Sono
grap
hic
Yes
40.0
00Tr
ansc
ervi
cal a
spir
atio
n an
d in
tra-
amni
otic
inje
ctio
n of
50
mg
met
hotr
exat
e
Non
e16
7N
/A
2Va
gina
l ble
edin
g5+
1So
nogr
aphi
cN
o14
.000
Tran
scer
vica
l asp
irat
ion
and
intr
a-am
niot
ic in
ject
ion
of 7
5 m
g m
etho
trex
ate
Non
e92
Yes
3Va
gina
l ble
edin
g7+
3So
nogr
aphi
c,
lapa
rosc
opy,
M
RI
Yes
26.4
00Tr
ansc
ervi
cal a
spir
atio
n an
d in
tra-
amni
otic
inje
ctio
n of
50
mg
met
hotr
exat
e
Lapa
roto
my
131
Yes
4N
one
8+3
Sono
grap
hic
No
63.0
00Ex
pect
ant m
anag
emen
tSy
stem
ic in
ject
ion
of
50 m
g m
etho
trex
ate,
la
paro
tom
y
103
Yes
a Ges
tatio
nal a
ge a
t dia
gnos
is a
ccor
ding
to th
e la
st m
enst
rual
per
iod.
Tabl
e 1:
Cha
ract
eris
tics
of th
e 4
patie
nts
with
a c
aesa
rean
sca
r pr
egna
ncy.
8 months after methotrexate treatment to remove pregnancy debris and repair the anterior uterine wall. There were no intra- or postoperative complications and the patient became pregnant 3 months after laparotomy. An elective CS was performed at a gestational age of 37 weeks and 4 days.
Case 4A 38-year-old woman, gravida 3 para 1, had her 1st US examination at 8 weeks and 3 days gestation (GA 8+3) according to her last menstrual period. Her obstetrical history included 1 CS because of pre-eclampsia and suspicion for placental abruption and 1 vacuum evacuation because of a missed abortion. US evaluation showed a fetus with a crown-rump length of 8 mm without fetal cardiac activity located in the scar from the CS. Management options and risks were explained, and the patient decided to wait for a spontaneous abortion. After 16 days without a sign of spontaneous abortion, a single injection of 50 mg methotrexate (1 mg/kg body weight) was administered intramuscularly. The serum ß-hCG levels declined from 75,000 mIU/ml 7 days before methotrexate treatment to 12,000 mIU/ml 7 days after injection. Although serum ß-hCG levels declined steadily (Figure 2), the GS was still visible by US 3 weeks after methotrexate treatment. Laparotomy was performed 2 months after the procedure to resect the gestational tissue from the anterior uterine wall and the caesarean scar defect was repaired. The patient had an uneventful postoperative recovery and serum ß-hCG levels were below the detection limit 3 months after methotrexate treatment (Figure 2). She became pregnant 6 months after laparotomy, resulting in an uneventful CS at 38 weeks and 2 days gestation.
DiscussionNo general treatment guidelines for a CSP have been established to date and evidence-based data are lacking. A treatment policy should preferentially not be based on anecdotal reports only, but given the infrequent event of CSP, much is to be learned from each report. Current data indicate that expectant management is rarely successful and particularly unsuitable for women with vital scar pregnancies.1,5 In a hemodynamically stable patient, 2 options may be considered , medical or surgical, both aimed to eliminate the GS and retain the patient’s fertility.5
Medical TreatmentThe administration of local or systemic methotrexate for this indication has shown high success rates. All reported cases of CSP treated with methotrexate, including our patients (no. 1–4), are summarized in Table 2. Systemic methotrexate in general is described as safe and effective, and virtually without

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
114 | Chapter 7
side effects.6 A single intramuscular dose of 50 mg/m2 followed by expectant
management can be used for CSPs with a gestational age of less than 6–8 weeks without fetal cardiac activity.7 Some authors reported systemic methotrexate to be more effective in women with serum ß-hCG levels below 5,000 mIU/ml.4,8 Systemic treatment with methotrexate was reported in 25 cases and successful in 9 cases (Table 2). In 13 cases7,9–17 complementary medical or surgical
treatment was indicated because of rising ß-hCG levels, persistence of cardiac motion, increase of the GS, or prolonged vaginal bleeding. In 1 case18 dilation and curettage was performed because of vaginal bleeding, which resulted in copious hemorrhaging. Laparatomy was performed in 2 cases because of increasing size of the viable fetus and profuse vaginal bleeding, and 1 of these cases resulted in a hysterectomy.19 One of our patients with a CSP without fetal cardiac activity was treated with systemically injected methotrexate. Despite a rapid decline of serum ß-hCG levels, US did not show regression of the GS. It can be debated whether systemic methotrexate is the treatment of choice, since fibrous tissue may be involved in placentation. Due to impaired vascularization of this tissue, the penetration of methotrexate to the fetal sac may be insufficient.16 For this reason, others advocate local injection of methotrexate,20 which can be injected into the GS by a transabdominal or transvaginal route. The transvaginal approach may be preferable because of the shorter distance to the GS.4 Local treatment with methotrexate was reported in 22 cases and successful in 18 cases (Table 2). In 8 cases with detectable embryonic cardiac activity, embryocide was performed 1st by the intracardiac injection of potassium chloride (KCl). Jurkovic et al1 reported 18 CSPs diagnosed in a period of 4 years, and 6 of these cases were treated with local injection of 25 mg methotrexate and intra-cardiac injection of 0.1–0.2 nmol potassium chloride (KCl) in case of detectable embryonic cardiac activity. Four women were treated successfully with a serum ß-hCG resolution time between 6 and 10 weeks. Two women with vital pregnancies corresponding to 6 and 8 weeks’ gestation required additional surgical intervention and blood transfusion due to heavy vaginal bleeding. The women who did not receive medical treatment were managed either surgically, which was successful in all cases, or expectantly, which was successful in 1 of 3 cases. Lai et al21 reported an emergency laparotomy after local treatment because of active vaginal bleeding and pelvic pain. Complementary medical treatment was indicated in 1 case22 because of increase of the GS and rising ß-hCG level. The uterus was preserved in all women treated with local methotrexate. Combined local and systemic methotrexate treatment was performed in 8 women and was successful in 7 cases (Table 2). Smorgick et al23 evaluated combined local and systemic methotrexate treatment in 31 patients with a viable ectopic pregnancy, which was successful in all CSP cases (n = 5). Although a 2nd dose was required in 4 of 5 cases of CSP, surgical intervention could be avoided.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Caesarean scar pregnancy | 115
7
Figure 2 shows that in our 4 cases the serum ß-hCG level initially increased after local treatment with methotrexate, which was followed by a steady decline. In contrast, systemic methotrexate caused an immediate decline of the serum ß-hCG level.
On rare occasions, rupture of the scar and heavy bleeding may occur after medical treatment. This may even happen 15 days following methotrexate treatment.21 Therefore, some authors propose a combination of the medical approach with bilateral uterine artery embolization to minimize the risk of such complications.24
Surgical TreatmentBecause of the persistence of pregnancy tissue after medic al treatment, 2 of our patients underwent laparotomy with good results. Several authors consider laparotomy to be the preferred option as primary treatment,2,25–27 allowing the simultaneous removal of the pregnancy and repair of the defect. Resection of the old scar and new closure may reduce the risk of recurrence of a CSP.26 Others advocate laparotomy only if conservative medical or laparoscopic treatment fails, if the patient presents late, or if facilities and expertise for operative endoscopy are not available. Laparotomy is mandatory when uterine rupture is suspected. Removal of pregnancy tissue during laparotomy results in a rapid decline of serum ß-hCG levels within 1 or 2 weeks28 but has the drawbacks of a larger surgical wound, longer hospitalization, and longer recovery time in comparison to medical treatment.29

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
116 | Chapter 7
Tabl
e 2:
Clin
ical
dat
a of
rep
orte
d ca
ses
of c
aesa
rean
sca
r pr
egna
ncy
trea
ted
with
met
hotr
exat
e, in
clud
ing
our
patie
nts
(no.
1-4
).
Ges
tati
onal
ag
e (w
eeks
)a
Feta
l he
art
acti
vity
Pre-
trea
tmen
t ß
-hCG
leve
ls
(mIU
/ml)
Prim
ary
trea
tmen
tSu
cces
sSe
cond
ary
trea
tmen
t an
d/or
mat
erna
l out
com
e
Loca
l MTX
Patie
nt n
o. 1
7+1
Yes
40.0
00Tr
ansc
ervi
cal a
spir
atio
n an
d lo
cal M
TX
(1 m
g/kg
)Ye
sN
one
Patie
nt n
o. 2
5+1
No
14.0
00Tr
ansc
ervi
cal a
spir
atio
n an
d lo
cal M
TX
(1 m
g/kg
)Ye
sN
one
Patie
nt n
o. 3
7+3
Yes
26.4
00Tr
ansc
ervi
cal a
spir
atio
n an
d lo
cal M
TX
(1 m
g/kg
) Ye
sLa
paro
tom
y af
ter
8 m
onth
s to
rem
ove
preg
nanc
y de
bris
and
rep
air
uter
ine
scar
c Has
egaw
a et
al.,
200
534
12+0
No
Unk
now
nLo
cal M
TX
Yes
Repe
at c
aesa
rean
sca
r pr
egna
ncy
succ
essf
ully
trea
ted
with
loca
l MTX
Hw
u et
al.,
200
511
ca
se 2
6+0
Yes
29.3
77Tr
ansc
ervi
cal a
spir
atio
n an
d lo
cal M
TX (5
0 m
g)Ye
sN
one
Lai e
t al.,
199
521
7+
0Ye
s5.
789
Tran
sabd
omin
al a
spir
atio
n an
d lo
cal M
TX
(50
mg)
No
Lapa
roto
my
Pasc
ual e
t al.,
200
735U
nkno
wn
No
11.8
38As
pira
tion
and
loca
l MTX
(5
0 m
g)Ye
s N
one
b Seo
w e
t al.,
200
036
7+0
Yes
23.3
28Lo
cal M
TX
(50
mg)
Yes
Non
e
Seow
et a
l., 2
0044
case
46+
0Ye
s16
.628
Tran
sabd
omin
al a
spir
atio
n an
d lo
cal M
TX
(1m
g/kg
)Ye
sN
one
case
56+
4Ye
s19
.086
Tran
sabd
omin
al a
spir
atio
n an
d lo
cal M
TX
(1m
g/kg
)Ye
sN
one
case
68+
4Ye
s47
.752
Tran
scer
vica
l asp
irat
ion
and
loca
l MTX
(1
mg/
kg)
Yes
Non
e
case
76+
1Ye
s24
.195
Tran
scer
vica
l asp
irat
ion
and
loca
l MTX
(1
mg/
kg)
Yes
Non
e
case
96+
2N
o20
.122
Tran
scer
vica
l asp
irat
ion
and
loca
l MTX
(1
mg/
kg)
Yes
Non
e
Tan
et a
l., 2
00522
case
18+
5N
o58
7Tr
ansc
ervi
cal a
spir
atio
n an
d lo
cal M
TX
(50
mg)
No
Syst
emic
MTX
(70
mg)

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Caesarean scar pregnancy | 117
7
Tabl
e 2:
Con
tinue
d.
Ges
tati
onal
ag
e (w
eeks
)a
Feta
l he
art
acti
vity
Pre-
trea
tmen
t ß
-hCG
leve
ls
(mIU
/ml)
Prim
ary
trea
tmen
tSu
cces
sSe
cond
ary
trea
tmen
t an
d/or
mat
erna
l out
com
e
Loca
l MTX
with
KCl
God
in e
t al.,
199
7379+
0Ye
s62
.000
Loca
l MTX
(6
0 m
g) w
ith 8
MEq
KCl
Ye
sN
one
Jurk
ovic
et a
l., 2
0031
case
16+
0Ye
s23
.700
Tran
scer
vica
l loc
al M
TX
(25
mg)
with
0,1
-0,2
nm
ol K
ClYe
sN
one
case
28+
0Ye
s18
.090
Tran
scer
vica
l loc
al M
TX
(25
mg)
with
0,1
-0,2
nm
ol K
ClN
oD
ilatio
n an
d cu
rett
age
case
36+
0Ye
s15
.540
Tran
scer
vica
l loc
al M
TX
(25
mg)
with
0,1
-0,2
nm
ol K
ClYe
sN
one
case
45+
0Ye
s3.
823
Tran
scer
vica
l loc
al M
TX
(25
mg)
with
0,1
-0,2
nm
ol K
ClYe
sN
one
case
56+
0Ye
s64
.299
Tran
scer
vica
l loc
al M
TX
(25
mg)
with
0,1
-0,2
nm
ol K
ClN
oEm
boliz
atio
n, d
ilatio
n an
d cu
rett
age
b cas
e 6
9+0
Yes
92.8
80Tr
ansc
ervi
cal l
ocal
MTX
(2
5 m
g) w
ith 0
,1-0
,2 n
mol
KCl
Yes
Non
e
Tan
et a
l., 2
00522
case
28+
0Ye
s18
6.64
3Tr
ansc
ervi
cal a
spir
atio
n an
d lo
cal M
TX
(50
mg)
with
7.4
5% K
Cl (5
ml)
Yes
Syst
emic
MTX
aft
er 4
8 da
ys b
ecau
se
of a
larg
e ve
nous
sin
us a
roun
d th
e ge
stat
iona
l sac
Syst
emic
MTX
Patie
nt n
o. 4
8+3
No
63.0
00Sy
stem
ic M
TX
(1 m
g/kg
)Ye
sLa
paro
tom
y af
ter
2 m
onth
s to
rem
ove
preg
nanc
y de
bris
and
rep
air
uter
ine
scar
Ayas
et a
l., 2
00638
6+4
Yes
18.9
14Sy
stem
ic M
TX
(50
mg/
m2)
on
days
0 a
nd 8
Yes
Non
e
b Deb
et a
l., 2
0079
6+0
No
39.2
41Sy
stem
ic M
TX
(50
mg/
m2 )
No
Hys
tero
scop
y af
ter
15 w
eeks
Gra
essl
in e
t al.,
200
5106+
0Ye
s9.
585
Thre
e do
ses
of s
yste
mic
MTX
(1
mg/
kg) o
n da
ys 0
, 3 a
nd 7
No
Dila
tion
and
cure
ttag
e af
ter
34 d
ays

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
118 | Chapter 7
Tabl
e 2:
Con
tinue
d.
Ges
tati
onal
ag
e (w
eeks
)a
Feta
l he
art
acti
vity
Pre-
trea
tmen
t ß
-hCG
leve
ls
(mIU
/ml)
Prim
ary
trea
tmen
tSu
cces
sSe
cond
ary
trea
tmen
t an
d/or
mat
erna
l out
com
e
Hai
mov
-Koc
hman
et a
l.,
2002
7 - c
ase
113
+0N
o3.
559
Syst
emic
MTX
(5
0 m
g/m
2 )Ye
sN
one
case
26+
0N
o6.
684
Syst
emic
MTX
(5
0 m
g/m
2 )N
oSy
stem
ic M
TX (5
0 m
g/m
2 ) w
ith a
ltern
ate
day
folin
ic a
cid
c Hol
land
and
Bie
nsto
ck,
2008
396+
0N
o7.
619
Syst
emic
MTX
(5
0 m
g/m
2 )Ye
sN
one
Hw
u et
al.,
200
511
case
16+
0Ye
s12
.755
Four
dos
es o
f sys
tem
ic M
TX
(1 m
g/kg
) with
alte
rnat
e da
y fo
linic
aci
dN
oTr
ansc
ervi
cal a
spir
atio
n an
d lo
cal M
TX
(50
mg)
Iyib
ozku
rt e
t al.,
200
8405+
4N
o10
.440
Four
dos
es o
f sys
tem
ic M
TX
(1 m
g/kg
) with
alte
rnat
e da
y fo
linic
aci
dYe
s N
one
Lam
and
Lo,
200
212
7+0
Yes
6.16
0M
ultip
le-d
ose
syst
emic
MTX
(1
mg/
kg) w
ith a
ltern
ate
day
folin
ic a
cid
No
Seco
nd c
ours
e of
MTX
and
folin
ic a
cid
Lam
et a
l., 2
00419
case
17+
0Ye
s12
0.00
0M
ultip
le-d
ose
syst
emic
MTX
(1
mg/
kg) w
ith a
ltern
ate
day
folin
ic a
cid
No
Lapa
roto
my
case
28+
0N
o12
.300
Mul
tiple
-dos
e sy
stem
ic M
TX
(1m
g/kg
) with
alte
rnat
e da
y fo
linic
aci
dN
oLa
paro
tom
y an
d hy
ster
ecto
my
Mar
chio
lé e
t al.,
200
41811
+0N
o6.
380
Syst
emic
MTX
(1
00 m
g)N
oD
ilatio
n an
d cu
rett
age,
Fol
ey c
athe
ter
beca
use
of h
emor
rhag
e, a
nd
embo
lizat
ion
May
mon
et a
l., 2
00441
ca
se 4
7+0
No
1.40
0Sy
stem
ic M
TX
(50
mg/
m2 )
Yes
Non
e
McK
enna
et a
l., 2
00813
case
26+
5Ye
s29
.652
Two
dose
s of
sys
tem
ic M
TX
(50
mg)
No
Tran
scer
vial
loca
l MTX
(50
mg/
m2 )
and
syst
emic
MTX
(50
mg)
the
follo
win
g da
y

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Caesarean scar pregnancy | 119
7
Tabl
e 2:
Con
tinue
d.
Ges
tati
onal
ag
e (w
eeks
)a
Feta
l he
art
acti
vity
Pre-
trea
tmen
t ß
-hCG
leve
ls
(mIU
/ml)
Prim
ary
trea
tmen
tSu
cces
sSe
cond
ary
trea
tmen
t an
d/or
mat
erna
l out
com
e
Mur
aji e
t al.,
200
914
case
1La
te 5
wee
ksN
o21
.675
Syst
emic
MTX
(5
0 m
g/m
2 )N
oTr
ansc
ervi
cal a
spir
atio
n an
d lo
cal M
TX
(50
mg)
, com
bine
d sy
stem
ic (5
0 m
g/m
2 ) an
d lo
cal M
TX (5
0 m
g)
case
2Ea
rly
5 w
eeks
No
3.91
3Sy
stem
ic M
TX
(50
mg/
m2 )
No
Syst
emic
MTX
(50
mg/
m2 )
case
3Ea
rly
5 w
eeks
No
8.19
8Sy
stem
ic M
TX
(50
mg/
m2 )
No
Syst
emic
MTX
(50
mg/
m2 )
Pers
adie
et a
l., 2
00515
7+0
Yes
37.4
64Fo
ur d
oses
of s
yste
mic
MTX
(1
mg/
kg) w
ith a
ltern
ate
day
folin
ic a
cid
No
Loca
l MTX
(25
mg)
Ravh
on e
t al.,
199
7168+
0Ye
s12
.000
Syst
emic
MTX
(5
0 m
g/m
2 )N
oTr
ansc
ervi
cal a
spir
atio
n of
per
sist
ent
sac
afte
r 9
wee
ks
Seow
et a
l., 2
0044
case
25+
0N
o3.
217
Syst
emic
MTX
Ye
sN
one
case
85+
2N
o4.
280
Syst
emic
MTX
Yes
Non
e
Shuf
aro
and
Nad
jari
, 20
0142
7+0
Yes
11.3
06Fo
ur d
oses
of s
yste
mic
MTX
(1
mg/
kg) w
ith a
ltern
ate
day
folin
ic a
cid
Yes
Non
e
Yan,
200
717
case
16+
3N
o6.
117
Syst
emic
MTX
(4
5 m
g) w
ith fo
linic
aci
d,
repe
ated
aft
er 2
day
s
No
Ute
rine
art
ery
embo
lizat
ion
afte
r 16
da
ys
case
27+
0Ye
s15
7.69
0Sy
stem
ic M
TX
(75.
5 m
g)N
oSe
cond
dos
e of
MTX
(75.
5 m
g),
twic
e ut
erin
e ar
tery
em
boliz
atio
n,
lapa
rosc
opy

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
120 | Chapter 7
Tabl
e 2:
Con
tinue
d.
Ges
tati
onal
ag
e (w
eeks
)a
Feta
l he
art
acti
vity
Pre-
trea
tmen
t ß
-hCG
leve
ls
(mIU
/ml)
Prim
ary
trea
tmen
tSu
cces
sSe
cond
ary
trea
tmen
t an
d/or
mat
erna
l out
com
e
Com
bine
d lo
cal a
nd s
yste
mic
MTX
c Mab
uchi
et a
l., 2
00943
5+0
Unk
now
nU
nkno
wn
Loca
l (50
mg)
and
sys
tem
ic M
TX
(50
mg/
m2 )
No
Lapa
roto
my
May
mon
et a
l., 2
00441
case
18+
0Ye
s16
.620
Tran
scer
vica
l asp
irat
ion
and
loca
l (2
5 m
g) +
sys
tem
ic M
TX (5
0 m
g/m
2 )Ye
sN
one
case
26+
0Ye
s7.
700
Tran
scer
vica
l asp
irat
ion
and
loca
l (2
5 m
g) +
sys
tem
ic M
TX (5
0 m
g/m
2 )Ye
sN
one
case
36+
0Ye
s12
.000
Tran
scer
vica
l asp
irat
ion
and
loca
l (2
5 m
g) +
sys
tem
ic M
TX (5
0 m
g/m
2 )Ye
sN
one
McK
enna
et a
l., 2
00813
case
17+
2Ye
s35
.535
Tran
scer
vica
l loc
al
(50
mg/
m2 )
and
syst
emic
(80
mg)
MTX
Ye
sN
one
Naw
roth
et a
l., 2
00132
8+3
Yes
45.7
74Tr
ansa
bdom
inal
loca
l and
sys
tem
ic M
TX
(1 m
g/kg
), re
peat
ed o
n da
y 4
Yes
Non
e
Seow
et a
l., 2
0044
case
17+
3N
o36
.023
Tran
sabd
omin
al a
spir
atio
n an
d lo
cal
(1m
g/kg
) + s
yste
mic
MTX
Yes
Non
e
b cas
e 3
6+1
No
23.3
28Tr
ansa
bdom
inal
asp
irat
ion
and
loca
l (1
mg/
kg) +
sys
tem
ic M
TX
Yes
Non
e
MTX
=met
hotr
exat
e; K
Cl=p
otas
sium
chl
orid
e; ß
-hCG
=ß–h
uman
cho
rion
ic g
onad
otro
phin
. a G
esta
tiona
l age
at t
he ti
me
of tr
eatm
ent a
ccor
ding
to th
e la
st m
enst
rual
per
iod.
b Pre
gnan
cy in
duce
d by
in-v
itro
fert
iliza
tion
and
embr
yo tr
ansf
er.
c Rec
urre
nt c
aesa
rean
sca
r pr
egna
ncy.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Caesarean scar pregnancy | 121
7
A minimally invasive alternative is endoscopic surgery. An operative hysteroscopic approach should be chosen for a CSP that grows toward the uterine cavity, whereas laparoscopy is more appropriate for a deeply implanted pregnancy growing toward the abdominal cavity and the bladder.28,30 Hysteroscopy enables the identification of the embryonic sac and the distribution of vessels at the implantation site. The embryonic sac can be separated from the uterine wall and the vessels can be electrocoagulated to achieve hemostasis. The success rate of hysteroscopy is encouraging, but the number of cases are too small to draw solid conclusions.28
Laparoscopy is suitable if the woman is hemodynamically stable and appropriate facilities are available with a trained surgeon. The pregnancy mass in the caesarean scar is incised and the pregnancy tissue is removed in an endobag.28 For the prevention of massive operative blood loss, blocking uterine perfusion with bilateral occlusion of the uterine arteries can be performed at the beginning of the procedure.29
In the study of Wang et al,29 laparoscopic treatment was performed in 4 women and hysteroscopic treatment in 6 women, and 1 woman underwent combined treatment with laparoscopy and hysteroscopy. No complications occurred and serum ß-hCG levels declined to a normal limit within 4 weeks after surgery.
Curettage should not be considered as the 1st choice of therapy, because the trophoblastic tissue will not always be reached due to its location and because of the risk of scar rupture and severe hemorrhage.2
Follow-upThe proposed follow-up protocol for CSP is a weekly outpatient clinical assessment and measurement of serum ß-hCG levels until they are below the detection limit. US examination is performed on a monthly basis to evaluate the size of the retained products of conception until no further pregnancy tissue can be detected.1 Follow-up in our patients consisted of 1 or 2 weekly out-patient clinical assessments and measurements of serum ß-hCG. Even though serum ß-hCG levels had declined under the detection limit, the trophoblastic tissue in 2 patients persisted for many weeks and was resected by laparotomy. One possible explanation for the persistence of pregnancy tissue is that the scanty venous flow within the fibrous scar tissue makes the absorption of residual gestational tissue difficult. A 2nd explanation might be related to the proliferation of fibrous tissue in the isthmic portion of the uterus in response to myometrial injury induced by placental villi invasion.4

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
122 | Chapter 7
It can be questioned if it was necessary to remove the persisting pregnancy tissue in 2 of our patients, because the women had no complaints and the tissue might have disappeared spontaneously in the following months. It was also found by several authors4,16,28 that it is hard to predict when the gestational mass completely resolves, and that aspiration of the gestational tissue may be required because of the slow absorption. Wang et al31 performed a prospective cohort study with 71 cases of CSP and reported that methotrexate treatment followed by dilation and curettage results in a shorter time to resolution of the CSP and serum ß-hCG. Dilation and curettage was offered when serum ß-hCG levels decreased to <50 mIU/ml, no subtrophoblastic blood flow could be detected, and a connection between the GS and the uterine cavity was demonstrated on transvaginal US.
Although there are little data to suggest any danger in conceiving soon after a CSP, an interval of 3–6 months up to 2 years has been advised.4,32 The low prevalence of recurrent CSPs indicates that implantation into the scar is more likely to be a chance event, rather than the result of a particular affinity of a pregnancy for implanting into the scar.33 To date only 3 cases of recurrent CSP have been reported.28 Ben Nagi et al33 reported a case with 3 recurrences and suggested that the risk of scar implantation might be directly related to the size of the anterior uterine wall defect. In our case series, 3 of 4 patients had a successful pregnancy after the CSP; the 4th patient has no desire for a pregnancy yet.
In conclusion, based on literature and our own experience, we believe that transcervical needle aspiration of the GS and intra-amniotic injection of methotrexate, which may be combined with systemic methotrexate, should be the preferred treatment option. This treatment can avoid unnecessary surgery and preserve the woman’s fertility but requires time and patience for the serum ß-hCG levels to drop to normal and the pregnancy tissue to resolve completely. If medical treatment fails, additional surgical treatment can be chosen. Depending on the localization of the pregnancy tissue and the available experience, this may be by laparoscopy, laparotomy, or hysteroscopy.
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Caesarean scar pregnancy | 123
7
1. Jurkovic D, Hillaby K, Woelfer B, et al. First-trimester diagnosis and management of pregnancies implanted into the lower uterine segment Cesarean section scar. Ultrasound Obstet Gynecol 2003;21:220.
2. Fylstra DL. Ectopic pregnancy within a cesarean scar: a review. Obstet Gynecol Surv 2002;57:537.
3. Notzon FC, Placek PJ, Taffel SM. Comparisons of national cesarean-section rates. N Engl J Med 1987;316:386.
4. Seow KM, Huang LW, Lin YH, et al. Cesarean scar pregnancy: issues in management. Ultrasound Obstet Gynecol 2004;23:247.
5. Maymon R, Halperin R, Mendlovic S, et al. Ectopic pregnancies in a Caesarean scar: review of the medical approach to an iatrogenic complication. Hum Reprod Update 2004;10:515.
6. Stovall TG, Ling FW, Gray LA. Single-dose methotrexate for treatment of ectopic pregnancy. Obstet Gynecol 1991;77:754.
7. Haimov-Kochman R, Sciaky-Tamir Y, Yanai N, et al. Conservative management of two ectopic pregnancies implanted in previous uterine scars. Ultrasound Obstet Gynecol 2002;19:616.
8. Rotas MA, Haberman S, Levgur M. Cesarean scar ectopic pregnancies: etiology, diagnosis, and management. Obstet Gynecol 2006;107:1373.
9. Deb S, Clewes J, Hewer C, et al. The management of Cesarean scar ectopic pregnancy following treatment with methotrexate—a clinical challenge. Ultrasound Obstet Gynecol 2007;30:889.
10. Graesslin O, Dedecker FJ, Quereux C, et al. Conservative treatment of ectopic pregnancy in a cesarean scar. Obstet Gynecol 2005;105:869.
11. Hwu YM, Hsu CY, Yang HY. Conservative treatment of caesarean scar pregnancy with transvaginal needle aspiration of the embryo. BJOG 2005;112:841.
12. Lam PM, Lo KW. Multiple-dose methotrexate for pregnancy in a cesarean section scar. A case report. J Reprod Med 2002;47:332.
13. McKenna DA, Poder L, Goldman M, et al. Role of sonography in the recognition, assessment, and treatment of cesarean scar ectopic pregnancies. J Ultrasound Med 2008;27:779.
14. Muraji M, Mabuchi S, Hisamoto K, et al. Cesarean scar pregnancies successfully treated with methotrexate. Acta Obstet Gynecol Scand 2009;88:720.
15. Persadie RJ, Fortier A, Stopps RG. Ectopic pregnancy in a caesarean scar: a case report. J
Obstet Gynaecol Can 2005;27:1102.16. Ravhon A, Ben-Chetrit A, Rabinowitz R, et al.
Successful methotrexate treatment of a viable pregnancy within a thin uterine scar. Br J Obstet Gynaecol 1997;104:628.
17. Yan CM. A report of four cases of caesarean scar pregnancy in a period of 12 months. Hong Kong Med J 2007;13:141.
18. Marchiole P, Gorlero F, de Caro G, et al. Intramural pregnancy embedded in a previous Cesarean section scar treated conservatively. Ultrasound Obstet Gynecol 2004;23:307.
19. Lam PM, Lo KW, Lau TK. Unsuccessful medical treatment of cesarean scar ectopic pregnancy with systemic methotrexate: a report of two cases. Acta Obstet Gynecol Scand 2004;83:108.
20. Donnez J, Godin PA, Bassil S. Successful methotrexate treatment of a viable pregnancy within a thin uterine scar. Br J Obstet Gynaecol 1997;104:1216.
21. Lai YM, Lee JD, Lee CL, et al. An ectopic pregnancy embedded in the myometrium of a previous cesarean section scar. Acta Obstet Gynecol Scand 1995;74:573.
22. Tan G, Chong YS, Biswas A. Caesarean scar pregnancy: a diagnosis to consider carefully in patients with risk factors. Ann Acad Med Singapore 2005;34:216.
23. Smorgick N, Vaknin Z, Pansky M, et al. Combined local and systemic methotrexate treatment of viable ectopic pregnancy: outcomes of 31 cases. J Clin Ultrasound 2008;36:545.
24. Ghezzi F, Lagana D, Franchi M, et al. Conservative treatment by chemotherapy and uterine arteries embolization of a cesarean scar pregnancy. Eur J Obstet Gynecol Reprod Biol 2002;103:88.
25. Shih JC. Cesarean scar pregnancy: diagnosis with three-dimensional (3D) ultrasound and 3D power Doppler. Ultrasound Obstet Gynecol 2004;23:306.
26. Vial Y, Petignat P, Hohlfeld P. Pregnancy in a cesarean scar. Ultrasound Obstet Gynecol 2000;16:592.
27. Fylstra DL, Pound-Chang T, Miller MG, et al. Ectopic pregnancy within a cesarean delivery scar: a case report. Am J Obstet Gynecol 2002;187:302.
28. Ash A, Smith A, Maxwell D. Caesarean scar pregnancy. BJOG 2007;114:253.
29. Wang CJ, Chao AS, Yuen LT, et al. Endoscopic management of cesarean scar pregnancy. Fertil Steril 2006;85:494.
30. Wang CJ, Yuen LT, Chao AS, et al. Caesarean scar pregnancy successfully treated by operative
References

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
124 | Chapter 7
hysteroscopy and suction curettage. BJOG 2005;112:839.
31. Wang JH, Xu KH, Lin J, et al. Methotrexate therapy for cesarean section scar pregnancy with and without suction curettage. Fertil Steril 2009;92:1208.
32. Nawroth F, Foth D, Wilhelm L, et al. Conservative treatment of ectopic pregnancy in a cesarean section scar with methotrexate: a case report. Eur J Obstet Gynecol Reprod Biol 2001;99:135.
33. Ben Nagi J, Ofili-Yebovi D, Sawyer E, et al. Successful treatment of a recurrent Cesarean scar ectopic pregnancy by surgical repair of the uterine defect. Ultrasound Obstet Gynecol 2006;28:855.
34. Hasegawa J, Ichizuka K, Matsuoka R, et al. Limitations of conservative treatment for repeat Cesarean scar pregnancy. Ultrasound Obstet Gynecol 2005;25:310.
35. Pascual MA, Hereter L, Graupera B, et al. Three-dimensional power Doppler ultrasound diagnosis and conservative treatment of ectopic pregnancy in a cesarean section scar. Fertil Steril 2007;88:706.
36. Seow KM, Cheng WC, Chuang J, et al. Methotrexate for cesarean scar pregnancy after in vitro fertilization and embryo transfer. A case report. J
Reprod Med 2000;45:754.37. Godin PA, Bassil S, Donnez J. An ectopic pregnancy
developing in a previous caesarian section scar. Fertil Steril 1997;67:398.
38. Ayas S, Akoz I, Karateke A, et al. Successful medical treatment of cesarean scar pregnancy: a case report. Clin Exp Obstet Gynecol 2007;34:195.
39. Holland MG, Bienstock JL. Recurrent ectopic pregnancy in a cesarean scar. Obstet Gynecol 2008;111:541.
40. Iyibozkurt AC, Topuz S, Gungor F, et al. Conservative treatment of an early ectopic pregnancy in a cesarean scar with systemic methotrexate—case report. Clin Exp Obstet Gynecol 2008;35:73.
41. Maymon R, Halperin R, Mendlovic S, et al. Ectopic pregnancies in Caesarean section scars: the 8 year experience of one medical centre. Hum Reprod 2004;19:278.
42. Shufaro Y, Nadjari M. Implantation of a gestational sac in a cesarean section scar. Fertil Steril 2001;75:1217.
43. Mabuchi S, Kawase C, Muraji M, et al. A case of recurrent cesarean scar pregnancy. Acta Obstet Gynecol Scand 2009;88:1059.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
88|General discussion and General discussion and
future perspectivesfuture perspectives

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Main findings
ImagingVarious methods for the detection and measurement of a niche have been described, but most often transvaginal sonography (TVS) or sonohysterography (SHG) are used. In Chapter 6, we propose SHG in non-pregnant women as the gold standard for the detection of a niche and assessment of the prevalence for future studies. In case SHG is used, we demonstrated in Chapter 2 that gel instillation sonohysterography (GIS) is a suitable alternative for saline contrast sonohysterography (SCSH). Although the image quality of SCSH was slightly better than that of GIS, which was likely to be attributable to the presence of air bubbles in the gel, the small difference in uterine cavity distension in favour of GIS and stable distension during at least 4 minutes make GIS a suitable alternative for SCSH if air bubbles can be prevented. More stable filling of the uterine cavity with gel is especially an advantage when performing 3D ultrasound. For our reproducibility study in Chapter 3, we used 3D TVS. The results of this study demonstrated that a niche could be measured with a high level of agreement with the use of 3D ultrasound, in particular if measured in the longitudinal plane.
Naji et al.1 suggested a standardized approach to describe niches by measuring the width, depth and residual myometrial thickness (RMT) in the longitudinal plane and length in the transverse plane. We propose the same measurements, but we defined our measurements in more detail and performed some additional measurements in both the longitudinal and transversal plane in the section with the greatest surface area of the niche: depth (perpendicular to niche base), maximal depth (distance between apex of the niche and the estimated middle of the niche base), maximal width (perpendicular to the line between middle of the niche base and apex) and width at niche base (Chapter 3). In addition, we suggest measuring niche volume in the longitudinal plane, and the RMT in both the longitudinal and transversal plane in the section in which the RMT is the smallest.
PrevalenceIn Chapter 4, a niche was defined as an anechoic area with a depth of at least 1 mm, which resulted in a niche prevalence of 24% for TVS and 56% for GIS. In Chapter 5, a niche depth of at least 2 mm was used, resulting in a prevalence of 50% for TVS and 65% for GIS. Chapter 6 shows that each study found a different niche prevalence, varying between 56% and 84% for a random population of women with a history of caesarean section (CS) examined with the use of SHG.
126 | Chapter 8

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Risk factorsIn our systematic review (Chapter 6), we describe that possible risk factors for the presence or size of a niche are single-layer myometrium closure, multiple CSs and retroflected uterus. The problem with reporting on risk factors for a large niche is the lack of predefined definitions, resulting in different cut-off values for a large niche for each study. As each study evaluated different risk factors and some risk factors are interdependent, we propose to categorize risk factors into four main categories: factors related to closure technique, development of the lower uterine segment or location of the incision, wound healing and miscellaneous factors. This may be helpful for future research, including meta-analyses.
SymptomsThis thesis contains two prospective cohort studies reporting on symptoms associated with a niche (Chapter 4 and 5). We demonstrated that women with a niche more often report postmenstrual spotting in comparison to women without a niche after a CS and that niche size is related to postmenstrual spotting as well. In Chapter 4 was demonstrated that women with postmenstrual spotting have a larger niche volume. In Chapter 5, we demonstrated that women with a RMT measuring <50% of the adjacent myometrial thickness have more often complaints of postmenstrual spotting than women with a RMT >50% of the adjacent myometrial thickness (Chapter 5). A systematic review of the literature showed that our results are in line with the findings of other studies (Chapter 6). Six out of eight studies that evaluated niche-related symptoms demonstrated an association between the presence of a niche and postmenstrual spotting.
A rare but serious complication of a subsequent pregnancy after a CS is a caesarean scar pregnancy (CSP). Chapter 7 describes four cases of CSP and a literature review reporting on the options for treatment.
Strengths and limitations
The strength of this thesis is that it contains two prospective cohort studies reporting on niche prevalence and related symptoms (Chapter 4 and 5). In addition, the literature was reviewed in Chapter 6 on the same subject, and we evaluated the reproducibility of niche measurements and tried to define clear definitions for various niche parameters (Chapter 3).
However, the studies of this thesis have some limitations as well. The niche prevalence using TVS in the study reported in Chapter 4 was rather low compared with the study in Chapter 5 (24% versus 50%), which was not expected as a niche
General discussion and future perspectives | 127
8

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
128 | Chapter 8
was defined as an anechoic space of at least 1 mm in Chapter 4 and at least 2 mm in Chapter 5. The prevalence of 50% reported in Chapter 5 is comparable with the reported prevalence in other studies (Chapter 6). One explanation for the higher prevalence in Chapter 5 may be a difference in timing of scanning, as the women of Chapter 5 were scanned only 6-12 weeks after their CS and the women of Chapter 4 6-12 months after their CS. Shortly after a CS, the scar in the myometrium has a more transonic aspect, improving the visualization of the niche. In addition, the endometrium is thinner shortly after a CS as most women are still breast-feeding, which may also improve the visibility of a niche. Another explanation is that the sonographer of Chapter 5 was more experienced in comparison with the sonographer of Chapter 4, resulting in a higher detection rate in Chapter 5. However, the latter is not underlined by the comparable niche detection rates in both studies using GIS. These prevalences (56% for Chapter 4 and 65% for Chapter 5) were also comparable with other studies, and showed no outliers (Chapter 6). In both Chapters 4 and 5 was reported that postmenstrual spotting is the main symptom related to a niche, which was confirmed by the systematic review in Chapter 6.
Another limitation of this thesis is that only TVS was evaluated in our reproducibility study of Chapter 3, even though we postulated in Chapters 4, 5 and 7 that the performance of SHG is preferable to TVS. In our prospective cohort studies (Chapters 4 and 5), the niche was only evaluated in the longitudinal plane. We also wanted to include measurements in the transversal plane for our reproducibility study. However, we learned that it was difficult to delineate the niche in the transversal plane using SHG in several cases, and therefore we decided to start using only TVS for evaluating the inter- and intraobserver agreement.
A third limitation is that for the comparison of GIS versus SCSH in Chapter 2, niche detection and measurement were not included. However, one may expect that more stable distension with GIS is also an advantage for niche detection and measurement, and therefore also preferable for the evaluation of a niche, in particular if 3D ultrasound is used. We did not repeat this study in patients with a niche before we designed our prospective studies in Chapter 4 and 5.
Comparison to literature
NicheIn a recently published review2, it was postulated that the ‘disorder’ caused by a niche is a syndrome that should be defined by the associated symptoms. The authors propose that a previous caesarean scar defect is the formation of

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
General discussion and future perspectives | 129
8
a pouch at the site of an old caesarean incision at the anterior lower uterine segment, uterine isthmus or in the upper segment of the cervical canal with (among other symptoms) prolonged menstruation, dysmenorrhoea, intermenstrual spotting, the presence of a fluid-filled pouch and infertility. We do not agree with this definition, as we believe that a niche can exist without the presence of symptoms, and therefore we also prefer to avoid the term ‘defect’. In the same review was suggested that niches with ‘valves’ are the ones that lead to symptoms, as the ‘valve’-like lower edge impedes menstrual flow and allows for the accumulation of fluid in the niche. Although we found that a larger niche volume (Chapter 4) and RMT <50% of the adjacent myometrium (Chapter 5) are related to postmenstrual spotting, we believe that the exact mechanism that leads to symptoms is still under debate and an issue for future research. For example, one may hypothesize that postmenstrual bleeding is induced by abnormal vessel formation in the niche, including fragile vessels that are prone to bleeding.
Another recently published review article3 reported that a number of factors contribute to the varying niche prevalence between studies. These factors include heterogeneity of the studied populations, no accepted guidelines for the diagnostic criteria of a niche, and niches even with symptoms being unrecognized because of lack of knowledge of the condition. Like mentioned in our Letter to the Editor4, several of the populations reported in this review3 were selected based on gynaecological symptoms, which may bias the prevalence. In addition, no distinction was made between TVS and SHG while reporting the prevalence. The authors of this review proposed a staging system for the niche based on RMT, ratio RMT to the adjacent total myometrial thickness, number of scars, number of previous CSs and menstrual pattern.3 We agree with a standard approach for describing the niche, according to Naji et al.1. In addition, we support the suggestion to classify the morphological appearance of a niche as mild, moderate and severe based on the mean values3. We propose to add volume to the variables of this classification, as we found that it was associated with postmenstrual spotting (Chapter 4). However, instructions and training are necessary in order to obtain reproducible 3D volume measurements (Chapter 3). In addition, we suggest to consider the addition of some extra dimensions described in our reproducibility study (Chapter 3), measured in the longitudinal plane, in order to map the niche more accurately. RMT should be measured in both the longitudinal and transversal plane, as women with gynaecological complaints are treated with either hysteroscopy or laparoscopy based on the RMT. A value between 2 and 3 mm should be chosen as cut-off value in the classification3, as this is the lower limit for hysteroscopic resection of the niche in order to prevent perforation of the uterus or bladder injury5.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
130 | Chapter 8
Caesarean scar pregnancyMany case reports, case series and reviews on a CSP and its treatment were published, but there are still no universal treatment guidelines for the management of CSPs. A difference should be made between CSPs protruding towards the uterine cavity (type 1) and CSPs protruding towards the bladder (type 2). In addition, it is relevant to measure the RMT, ß-human chorionic gonadotrophin (ß-hCG) level and vascularity since this may affect the success rate of different therapies and the complication rates. Several recent studies will be discussed below.
We report in Chapter 7 that we believe that transcervical needle aspiration of the gestational sac and intra-amniotic injection of methotrexate may be the treatment of choice. However, there is still no evidence for the optimal treatment modality. In one review6, the authors advocated medical treatment with methotrexate alone (local, systemic or combined) or in conjunction with aspiration, in women who are hemodynamically stable with an unruptured CSP of less than 8 weeks’ gestation and a myometrial thickness of less than 2 mm between the gestational sac and the bladder. In a recent retrospective case series7, 19 patients with a CSP were successfully treated with 25 mg of methotrexate into the area of the embryo, 25 mg into the placental area and an additional 25 mg was administered intramuscularly. The authors found after the treatment an initial increase in the serum ß-hCG level followed by a steady decline, just as we observed in our three patients treated with local methotrexate (Chapter 7). In another recent review8, it was reported that the lowest complication rates were achieved with intra-amniotic injection of methotrexate or potassium chloride as well as hysteroscopic resection. Based on these results, hysteroscopic removal may be considered in certain cases, but only if a CSP grows toward the uterine cavity with a sufficient thick residual myometrium. Hysteroscopic removal was reported to be associated with less bleeding and complications if it was performed after a decrease in ß-hCG after pretreatment with local methotrexate or uterine artery embolization.9 Despite the higher ß-hCG levels and thinner residual myometrium in the pretreated groups, the outcomes were equal or better in comparison with immediate hysteroscopic removal of the CSP. Although it is not always needed to perform surgical removal of a CSP after medical treatment, some publications reported that ß-hCG levels resolve quicker.10-12 Therefore we suggest to consider hysteroscopy in patients with a sufficient thick myometrium after pretreatment with local methotrexate if medical treatment fails, i.e. in case of persistent symptoms, ß-hCG and/or pregnancy tissue. However, one should take into account that it may take 30 to 140 days before ß-hCG levels and the vascularity of a CSP are non-detectable after local methotrexate treatment, and disappearance of the CSP tissue may even take longer.7 In case the CSP grows towards the

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
General discussion and future perspectives | 131
8
bladder and medical treatment fails, laparoscopic13-15 or vaginal16 removal of the pregnancy may be considered, which has the advantage of closing the niche in the same session. These therapies may be combined with temporary occlusion of the uterine arteries to reduce bleeding or after local methotrexate therapy.
Clinical implications
Until now, the awareness for the presence of a niche is low. However, we demonstrated that a niche is present in a majority of women with a history of CS (Chapters 4 and 5) and that a niche may have serious long-term consequences. First of all, about a third of the women with a niche have complaints of postmenstrual spotting (Chapters 4 and 5). Dysmenorrhea, chronic pelvic pain and dyspareunia were also reported to be associated with a niche (Chapter 6). Secondly, a pregnancy may develop in a niche, which can lead to a life-threatening condition if the pregnancy is allowed to continue (Chapter 7). Thirdly, there are indications that a niche may lead to subfertility. In a recent review and meta-analysis was reported that women with a history of CS had approximately 10% lower pregnancy rates compared to women with a previous vaginal delivery. However, it must be noted that studies controlling for maternal age or those that were least prone to bias found smaller effects.17 The relation between a niche and subfertility has not been studied yet. Two proposed mechanisms that may contribute to subfertility are the persistence of menstrual blood or fluid in the niche and uterus, impairing sperm penetration through cervical mucus and embryo implantation, and a chronic inflammatory state.3 In one prospective cohort study, 41 women with a niche, secondary infertility and postmenstrual spotting were included. Hysteroscopic niche resection and coagulation of niche vessels resulted in a spontaneous pregnancy and resolution of postmenstrual spotting in all patients.18 Finally, one may hypothesize that the presence of a (large) niche is a risk factor for uterine scar dehiscence or rupture in a future pregnancy, but only one small study has evaluated this association. The authors of this prospective cohort study with 156 women with a history of CS suggested that an association is likely between large niches detected by TVS and uterine rupture or dehiscence.19

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
132 | Chapter 8
Future research
It is important for future research that a uniform definition and standard method for niche assessment is used. In our review (Chapter 6), we propose the following definition for a niche: any indentation representing myometrial discontinuity at the site of the caesarean scar that communicates with the uterine or cervical cavity seen on SHG. However, for standardization reasons we suggest to define a niche as an indentation of at least 1 mm. A cut off value of 1 mm was also used in Chapter 4, and this study demonstrated that even niches with a depth between 1 and 2 mm were associated with postmenstrual spotting. However, additional research is needed to set the exact threshold for a niche, which should be based on related symptoms and its impact on patients. As mentioned in the proposed definition, SHG should be used for detection and measurement of a niche. In addition, we suggest to use the measurements described in Chapter 3, both in the longitudinal and transversal plane, to describe the niche accurately. A standard classification should be used, which includes at least niche volume and RMT. We believe that more uniformity will result in a smaller range in the prevalence of a niche.
The focus for future research should be on the aetiology of the development of a niche and related symptoms. If more is known about the aetiology of the development of a niche, the prevalence of niches may be reduced. Possible risk factors contributing to niche development, such as location of the incision and suturing method of the uterine scar, need to be studied. We know that full thickness suturing (including the endometrium) partly prevents the development of a niche (Chapter 6). However, randomized controlled trials (RCTs) need to be performed to determine whether single- or double-layer closure, using unlocked sutures, is superior in preventing niches and related symptoms. There are also indications that a niche is related to factors affecting development of lower uterine segment (LUS) during labour. One study reported that the risk of a large niche increased if the station of the presenting part of a foetus at CS was below pelvic inlet, cervical dilatation was ≥5 cm or duration of labour was ≥5 hours (Chapter 6). If these findings can be confirmed in future studies, it is relevant to learn if this relation is caused by a thin LUS during CS, by the low uterine incision or both. Also factors with potential negative influence on wound healing should be evaluated in future studies, as there are indications that a retroflected uterus, pre-eclampsia and multiple CSs are related to a niche (Chapter 6).
We should learn more about the aetiology of symptoms, in order to be able to treat the niche effectively. In Chapter 4, we report that several hypotheses have been postulated to explain the aetiology of postmenstrual spotting. It may be
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
General discussion and future perspectives | 133
8
due to the retention of menstrual blood in the niche, which may depend on poor contractility of the uterine muscle around the scar and/or fibrotic tissue below the niche impairing the drainage of menstrual flow. Another hypothesis is that accumulated blood is produced in situ as was demonstrated by Morris20, which may be further elucidated by microscopic research on caesarean scar tissue. Research on scar tissue should also demonstrate if there is a condition of chronic inflammation at the site of a niche.
More research is needed to confirm if there is a relation between a niche and subfertility, to learn more about the mechanism behind this and to find out if a niche affects future pregnancies. No studies were published that evaluated the relation between a niche and subfertility. One prospective cohort study found no increase in spontaneous abortion rates in the CS group compared to the non-CS group. However, in eight pregnancies in which the implantation site crossed the scar, seven of them resulted in a spontaneous abortion.21 A small study did indicate that there may be a relation between a large niche and uterine dehiscence or rupture19. As a growing number of women with large niches are treated to prevent uterine rupture or dehiscence, a large prospective study should be performed to confirm this result.
Minimally invasive therapies are used to treat the symptoms related to the niche. One review22 included twelve studies, reporting on hysteroscopic niche resection, laparoscopic repair, (laparoscopic assisted) vaginal repair and oral contraceptives. Abnormal uterine bleeding improved in the vast majority of the patients after these interventions. However, the methodological quality of the papers was considered to be moderate to poor and therefore well-designed RCTs, which should include expectant management, are needed. In addition, studies with a long-term follow-up are needed, as not much is known about the chance for recurrence of a niche on the long term after treatment.
It is important that the awareness for the presence of a niche in women with a history of CS increases among doctors and patients, as a niche can cause complaints that can be treated successfully. Both small and large niches can cause symptoms. Women need to be informed about the risk to develop a niche and the related symptoms during the counselling for a primary CS. We need to learn more about the risk factors for a niche to enable surgeons to prevent the development of a niche during a CS. Therapies must be improved in order to treat women with a niche and symptoms successfully, and more research should be performed to get to know the optimal treatment modality and to tailor treatment to individual needs.
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
134 | Chapter 8
1. Naji O, Abdallah Y, Bij De Vaate AJ, Smith A, Pexsters A, Stalder C, et al. Standardized approach for imaging and measuring Cesarean section scars using ultrasonography. Ultrasound Obstet Gynecol 2012;39(3):252-9.
2. Allornuvor GF, Xue M, Zhu X, Xu D. The definition, aetiology, presentation, diagnosis and management of previous caesarean scar defects. J Obstet Gynaecol 2013;33(8):759-63.
3. Tower AM, Frishman GN. Cesarean scar defects: an underrecognized cause of abnormal uterine bleeding and other gynecologic complications. J Minim Invasive Gynecol 2013;20(5):562-72.
4. Brolmann HA, BijdeVaate M, van der Voet L, Naji O, Hehenkamp W, Bourne T, et al. Letter to the Editor JMIG on the Article “Cesarean scar defects: an underrecognized cause of abnormal uterine bleeding and other gynecologic complications” (2013;20; 562-572). J Minim Invasive Gynecol 2014;21(3):498-9.
5. van der Voet LF, Bij de Vaate AM, Veersema S, Brolmann HA, Huirne JA. Long-term complications of caesarean section. The niche in the scar: a prospective cohort study on niche prevalence and its relation to abnormal uterine bleeding. BJOG 2014;121(2):236-44.
6. Osborn DA, Williams TR, Craig BM. Cesarean scar pregnancy: sonographic and magnetic resonance imaging findings, complications, and treatment. J Ultrasound Med 2012;31(9):1449-56.
7. Timor-Tritsch IE, Monteagudo A, Santos R, Tsymbal T, Pineda G, Arslan AA. The diagnosis, treatment, and follow-up of cesarean scar pregnancy. Am J Obstet Gynecol 2012;207(1):44 e1-13.
8. Litwicka K, Greco E. Caesarean scar pregnancy: a review of management options. Curr Opin Obstet Gynecol 2013;25(6):456-61.
9. Li YR, Xiao SS, Wan YJ, Xue M. Analysis of the efficacy of three treatment options for cesarean scar pregnancy management. J Obstet Gynaecol Res 2014;40(11):2146-51.
10. Ash A, Smith A, Maxwell D. Caesarean scar pregnancy. BJOG 2007;114(3):253-63.
11. Deans R, Abbott J. Hysteroscopic management of cesarean scar ectopic pregnancy. Fertil Steril 2010;93(6):1735-40.
12. Wang CJ, Chao AS, Yuen LT, Wang CW, Soong YK, Lee CL. Endoscopic management of cesarean scar
pregnancy. Fertil Steril 2006;85(2):494 e1-4.13. Fuchs N, Manoucheri E, Verbaan M, Einarsson
J. Laparoscopic management of extrauterine pregnancy in caesarean section scar: description of a surgical technique and review of the literature. BJOG 2015;122(1):137-40.
14. Lee CL, Wang CJ, Chao A, Yen CF, Soong YK. Laparoscopic management of an ectopic pregnancy in a previous Caesarean section scar. Hum Reprod 1999;14(5):1234-6.
15. Wang G, Liu X, Bi F, Yin L, Sa R, Wang D, et al. Evaluation of the efficacy of laparoscopic resection for the management of exogenous cesarean scar pregnancy. Fertil Steril 2014;101(5):1501-7.
16. He M, Chen MH, Xie HZ, Yao SZ, Zhu B, Feng LP, et al. Transvaginal removal of ectopic pregnancy tissue and repair of uterine defect for caesarean scar pregnancy. BJOG 2011;118(9):1136-9.
17. Gurol-Urganci I, Bou-Antoun S, Lim CP, Cromwell DA, Mahmood TA, Templeton A, et al. Impact of Caesarean section on subsequent fertility: a systematic review and meta-analysis. Hum Reprod 2013;28(7):1943-52.
18. Gubbini G, Centini G, Nascetti D, Marra E, Moncini I, Bruni L, et al. Surgical hysteroscopic treatment of cesarean-induced isthmocele in restoring fertility: prospective study. J Minim Invasive Gynecol 2011;18(2):234-7.
19. Vikhareva Osser O, Valentin L. Clinical importance of appearance of cesarean hysterotomy scar at transvaginal ultrasonography in nonpregnant women. Obstet Gynecol 2011;117(3):525-32.
20. Morris H. Surgical pathology of the lower uterine segment caesarean section scar: is the scar a source of clinical symptoms? Int J Gynecol Pathol 1995;14(1):16-20.
21. Naji O, Wynants L, Smith A, Abdallah Y, Saso S, Stalder C, et al. Does the presence of a Caesarean section scar affect implantation site and early pregnancy outcome in women attending an early pregnancy assessment unit? Hum Reprod 2013;28(6):1489-96.
22. van der Voet LF, Vervoort AJ, Veersema S, BijdeVaate AJ, Brolmann HA, Huirne JA. Minimally invasive therapy for gynaecological symptoms related to a niche in the caesarean scar: a systematic review. BJOG 2014;121(2):145-56.
References

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
99|SummarySummary
SamenvattingSamenvatting

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Summary
This thesis is about the niche, defined as an indentation of at least 1 mm representing myometrial discontinuity at the site of the caesarean scar that communicates with the uterine or cervical cavity, and mainly diagnosed using sonography and in particular with contrast-enhanced sonohysterography (SHG). Part I reports on diagnostics of the niche, part II on gynaecological symptoms and risk factors associated with a niche, and part III on niche pregnancy.
Chapter 1 is a general introduction and describes the outline of this thesis. The caesarean section (CS) rate is rising, and with that also the niche prevalence and interest for the niche. The niche is mostly evaluated with the use of transvaginal sonography (TVS) and SHG, but up to now there is no gold standard for the detection and measurement of a niche. As a result, a wide range in niche prevalence has been reported. In the first part of this thesis, we tried to learn more about the diagnostics and prevalence of a niche.
We do know that not all women with a history of CS develop a niche, and therefore it is relevant to study the risk factors for the development of a niche. In addition, there are indications that a niche is associated with symptoms, especially with postmenstrual spotting. In the second part we tried to identify symptoms and risk factors associated with a niche.
Furthermore, caesarean scar pregnancies (CSPs) have been described in the literature. In the third part, we aimed to report favourable treatment modalities for CSPs.
Part ISHG is a widely used method for the assessment of the uterine cavity and for the detection and measurement of a niche. In Chapter 2, we compared gel instillation sonohysterography (GIS) with saline contrast sonohysterography (SCSH) for the evaluation of the uterine cavity. First SCSH and subsequently GIS were performed in 65 women suspected of having an intrauterine abnormality. Distension of the uterine cavity, image quality, visualization of intrauterine abnormalities and pain were recorded for both procedures. We found that the image quality of SCSH was slightly better than that of GIS, which was likely to be attributable to the presence of air bubbles in the gel. We concluded that the small difference in uterine cavity distension in favour of GIS and stable distension during at least 4 minutes make GIS a suitable alternative for SCSH if air bubbles can be prevented. More stable filling of the uterine cavity with gel is especially an advantage when performing 3D ultrasound.
136 | Chapter 9

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
9
In Chapter 3 we studied the reproducibility of niche measurement with 3D sonography. We evaluated the inter- and intraobserver agreement for measurement of niche size and volume, and assessment of shape with the use of three-dimensional (3D) ultrasound. Twenty 3D ultrasound volumes of uteri with a niche were selected and niche measurements were performed off-line twice by one observer and once by another observer in the longitudinal and transversal plane. The following measurements were performed: residual myometrial thickness (RMT), depth perpendicular to niche base, maximal depth, maximal width, width at niche base and the volume of the niche. In addition, we assessed the shape of the niche. We have shown that these niche parameters can be measured with a high level of agreement, in particular in the longitudinal plane. Our results demonstrated low reproducibility for niche shape.
Part IIChapter 4 and 5 describe two prospective cohort studies, evaluating the niche prevalence and its relation with symptoms. In Chapter 4, 225 women were examined with the use of sonography six to twelve months after CS. The included women completed a questionnaire and pictorial blood loss assessment chart (PBAC). A niche (defined as an anechoic area with a depth of at least 1 mm) was present in 24% of women with TVS and 56% with GIS, and was found to be associated with postmenstrual spotting. The volume of the niche was significantly larger in women with postmenstrual bleeding. We made a classification based on the sonographic shape of the niche. Niche shape was not associated with abnormal uterine bleeding. In Chapter 5, 263 women were included and sonography was performed six to twelve weeks after their CS. Women were followed by questionnaire and PBAC at six to twelve weeks, six months and twelve months after CS. The prevalence of a niche (defined as an anechoic area with a depth of at least 2 mm) was 50% with TVS and 65% with GIS, and women with niche had more often complaints of postmenstrual spotting twelve months after CS. In addition, the prevalence of postmenstrual spotting was higher in women with a RMT <50% of the adjacent myometrium than in women with a RMT >50%. Urinary incontinence was not related to the presence of a niche.
Chapter 6 contains a systematic review of the medical literature on the prevalence of a niche using various diagnostic methods, on potential risk factors for the development of a niche and on niche-related gynaecological symptoms in non-pregnant women. Reported niche prevalence varies depending on the method of detection, the criteria used to define a niche and the study population. As each study evaluated different risk factors, we classified the risk factors into four categories: those related to closure technique, to development of the lower uterine segment or location of the incision, to wound healing, and
Summary| 137

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
138 | Chapter 9
miscellaneous factors. Probable risk factors for the development of a niche are single-layer myometrium closure, multiple CSs and uterine retroflexion. Finally, we demonstrated with our review that the predominant symptom associated with a niche is postmenstrual spotting.
Part IIIWe describe our experience with the treatment of four caesarean scar pregnancies (CSPs) and provide an overview of the available literature in Chapter 7. Based on these cases and the literature, we postulate that transcervical needle aspiration of amniotic fluid followed by intra-amniotic injection of methotrexate is a good option for the treatment of a CSP, which may prevent surgical treatment in a lot of cases. Surgical treatment can still be performed if methotrexate fails. A disadvantage of medical treatment in comparison with surgical treatment is that it requires more time for the serum ß-HCG levels to drop to normal and the pregnancy tissue to resolve completely.
Chapter 8 provides the main findings of this thesis, a general discussion of the results and suggests future research strategies.
There is a high variance in niche prevalence between studies, which may be explained by the heterogeneity of the studied populations and the lack of consensus on diagnostic criteria for a niche. The exact mechanism that leads to symptoms in women with a niche is still under debate. As a niche does not preclude a normal function of the lower uterine segment, with or without pregnancy, we prefer to avoid the term ‘defect’.
There are still no universal treatment guidelines for the management of CSP’s. We believe that transcervical needle aspiration of the gestational sac and intra-amniotic injection of methotrexate is a preferable treatment option as surgical intervention and the related risk for complications can be prevented in the majority of cases. If medical treatment fails, we suggest hysteroscopy in patients with a sufficient thick myometrium, and laparoscopic or vaginal removal of the pregnancy in case the CSP grows toward the bladder.
Future research on the niche needs a uniform definition and standard method for niche assessment. In the absence of evidence for the correct cut-off value for niche depth, we propose the following definition for a niche: an indentation of at least 1 mm representing myometrial discontinuity at the site of the caesarean scar that communicates with the uterine or cervical cavity seen on SHG. Future research should demonstrate if this is the correct cut off value. In addition, we propose to use the parameters described in our reproducibility study

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Summary| 139
9
(Chapter 3). At least volume and RMT should be included, as we demonstrated that these parameters are related to postmenstrual spotting. In addition, RMT is an important factor in the decision to treat with either hysteroscopy or laparoscopy in women with gynaecological complaints. The focus for future research should be on the aetiology of niche development and related symptoms, and its impact on patients functioning, including sexuality. More research is needed to confirm if a niche is related to subfertility and/or to uterine dehiscence and rupture in a subsequent pregnancy. In addition, well-designed RCT’s are needed to get to know the optimal treatment modality of a niche, tailored to niche characteristics and symptoms of individual patients.
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Nederlandse samenvatting
Dit proefschrift gaat over de niche. De niche is een inkeping in de baarmoederwand van tenminste 1 mm ter plaatse van het keizersnedelitteken en staat in verbinding met de baarmoederholte. De niche kan zichtbaar worden gemaakt door middel van echoscopie, en dan vooral met behulp van contrastechoscopie. Deel I van dit proefschrift gaat over de diagnostiek van de niche, deel II over gynaecologische symptomen als gevolg van de niche en risicofactoren voor een niche, en deel III over zwangerschappen in de niche.
Hoofdstuk 1 is de introductie en beschrijft de achtergronden en doelstellingen van dit proefschrift. Het aantal keizersnedes neemt wereldwijd toe en daarmee ook de prevalentie van de niche en de interesse hiervoor. Hoewel de niche meestal wordt gediagnosticeerd met behulp van echoscopie, bestaat er nog geen gouden standaard voor de diagnostiek van een niche. Om die reden is de variatie in de gerapporteerde prevalentie van de niche groot. In het eerste deel van dit proefschrift wordt ingegaan op de diagnostiek en prevalentie van de niche.
Niet alle vrouwen ontwikkelen een niche na een keizersnede. Het is van belang om te weten te komen welke vrouwen nu een niche ontwikkelen en wat risicofactoren zijn voor het ontstaan van een niche. Daarnaast hebben sommige vrouwen klachten als gevolg van een niche, zoals spotting na afloop van de menstruatie. In het tweede deel van dit proefschrift onderzoeken we welke risicofactoren geassocieerd zijn met een niche en de symptomen die bij een niche kunnen horen.
In zeldzame gevallen nestelt een zwangerschap zich in een niche, wat een bedreiging vormt voor moeder en kind bij het vorderen van de zwangerschap. In het derde deel gaan we in op de behandeling van een zwangerschap in de niche.
Deel IContrastechoscopie is een veel gebruikte onderzoeksmethode voor het in beeld brengen van de baarmoederholte, en ook voor het in beeld brengen van de niche. De baarmoeder wordt hierbij gevuld met een vloeistof, wat zorgt voor contrast, waarna een echo wordt gemaakt. Bij de uitvoering van dit onderzoek kan de baarmoederholte worden gevuld met gel (GIS, gel instillation sonohysterography) of met een fysiologische zoutoplossing (SCSH, saline contrast sonohysterography). In Hoofdstuk 2 hebben we beide methodes vergeleken door bij 65 vrouwen die verdacht werden van een afwijking in de baarmoederholte, zoals bijvoorbeeld een myoom of een poliep, eerst een contrastecho met fysiologische zoutoplossing en vervolgens met gel uit te voeren. Beide methodes werden vergeleken op de
140 | Chapter 9

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Samenvatting | 141
9
volgende punten: distensie van de baarmoederholte, kwaliteit van de echo, het in beeld kunnen brengen van een afwijking in de baarmoederholte en pijn. We vonden dat de beeldkwaliteit met fysiologische zoutoplossing iets beter was dan met gel, wat meest waarschijnlijk werd veroorzaakt door de aanwezigheid van luchtbellen in de gel. Aangezien de distensie van de baarmoeder beter was met gel en de distensie stabiel bleef gedurende 4 minuten, concludeerden we dat gel een goed alternatief is voor fysiologische zoutoplossing als luchtbellen in de gel kunnen worden voorkomen. De stabielere vulling met gel is met name een belangrijk voordeel bij het maken van 3D-echo’s.
In Hoofdstuk 3 werd de reproduceerbaarheid van het opmeten van de niche met behulp van 3D-echografie onderzocht. We hebben de overeenkomst tussen de bevindingen van twee onderzoekers onderzocht en tussen de herhaalde bevindingen van dezelfde onderzoeker. Twintig 3D-echobeelden werden geselecteerd en de metingen werden offline verricht in het longitudinale en in het transversale vlak. De volgende metingen werden verricht: resterende dikte van de baarmoederwand ter plaatse van de niche, de diepte van de niche loodrecht op de basis, de maximale diepte van de niche, de maximale breedte van de niche, de breedte ter plaatse van de basis van de niche en het volume van de niche. Ook hebben we de vorm van de niche bepaald. Onze studie heeft aangetoond dat de reproduceerbaarheid van het opmeten van de niche met behulp van 3D-echografie goed is, met name in het longitudinale vlak. De reproduceerbaarheid van de bepaling van de vorm van de niche bleek slecht te zijn.
Deel IIHoofdstuk 4 en 5 beschrijven 2 prospectieve cohortstudies. Beide studies hebben de prevalentie van de niche onderzocht en gekeken welke symptomen veroorzaakt kunnen worden door een niche. Hoofdstuk 4 beschrijft de studie waarbij 225 vrouwen zes tot twaalf maanden na hun keizersnede werden onderzocht met behulp van een echo. Alle vrouwen vulden een vragenlijst en een menstruatiescorekaart (PBAC; pictorial blood loss assessment chart) in. Een niche (gedefinieerd als een inkeping met een diepte van tenminste 1 mm) was aanwezig bij 24% van de vrouwen met een normale vaginale echo en bij 56% van de vrouwen met GIS (contrastecho met gel). We vonden ook dat vrouwen met een niche vaker last hadden van spotting na de menstruatie, en dat het volume van de niche groter was bij vrouwen met deze klachten. We hebben een classificatie gemaakt gebaseerd op de vorm van de niche die we zagen met de echo, maar vonden geen relatie tussen de vorm en menstruatieklachten. In het onderzoek van Hoofdstuk 5 werden 263 vrouwen geïncludeerd en werd zes tot twaalf weken na de keizersnede een echo gemaakt. Ook deze vrouwen

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
142 | Chapter 9
kregen een vragenlijst en menstruatiescorekaart (PBAC; pictorial blood loss assessment chart) die op 3 tijdstippen werden ingevuld: zes tot twaalf weken na de keizersnede, zes maanden na de keizersnede en twaalf maanden na de keizersnede. De prevalentie van de niche (gedefinieerd als een inkeping van minstens 2 mm) was in dit onderzoek 50% met een normale vaginale echo en 65% met GIS (contrastecho met gel). Twaalf maanden na de keizersnede hadden vrouwen met een niche vaker klachten van spotting na de menstruatie. Spotting na de menstruatie kwam vaker voor bij vrouwen bij wie de resterende dikte van de baarmoederwand ter plaatse van de niche minder was dan 50% van de volledige dikte van de baarmoederwand (RMT <50%) in vergelijking met vrouwen bij wie de resterende dikte meer was dan 50% (RMT >50%). Urine-incontinentie bleek niet geassocieerd te zijn met de aanwezigheid van een niche.
Hoofdstuk 6 is een systematisch review van de medische literatuur, waarbij de diagnostiek en bijbehorende prevalentie van de niche werden onderzocht, de mogelijke risicofactoren voor de ontwikkeling van een niche en de symptomen die geassocieerd zijn met een niche bij niet-zwangere vrouwen. Er bleek grote variatie te zijn in de gerapporteerde prevalentie van een niche, afhankelijk van de gebruikte diagnostische methode, de gebruikte definitie voor een niche en de studiepopulatie. Omdat iedere geïncludeerde studie andere risicofactoren had onderzocht, werden alle risicofactoren geclassificeerd in 4 categorieën: risicofactoren die te maken hebben met hechttechniek, risicofactoren die te maken hebben met de ontwikkeling van het onderste uterussegment tijdens de bevalling of de locatie van de incisie tijdens de keizersnede, risicofactoren die te maken hebben met wondgenezing en overige risicofactoren. Uit ons review bleek dat enkellaags hechten van de baarmoederwand tijdens een keizersnede, een voorgeschiedenis met meerdere keizersnedes en een baarmoeder in retroflexie risicofactoren zijn voor de ontwikkeling van een niche. Ook hebben we aangetoond dat spotting na de menstruatie het belangrijkste symptoom is dat is geassocieerd met de aanwezigheid van een niche.
Deel IIIIn Hoofdstuk 7 beschrijven we onze ervaring met de behandeling van 4 zwangerschappen in een niche en geven we een overzicht van de literatuur die gaat over de behandeling van deze zeldzame zwangerschappen. Gebaseerd op onze ervaring en de literatuur concludeerden we in dit hoofdstuk dat opzuigen van het zwangerschapsweefsel met een naald via de cervix, gevolgd door het achterlaten van Methotrexaat een goede primaire behandeling is van een zwangerschap in een niche, waardoor een operatie in veel gevallen kan worden voorkomen. In het geval dat Methotrexaat onvoldoende effect heeft, kan dan altijd nog tot een operatie worden overgegaan. Een nadeel van deze medicamenteuze behandeling

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Samenvatting | 143
9
ten opzichte van een operatie is dat het langer duurt totdat het ß-HCG in het bloed is gedaald tot normale waarden en het zwangerschapsweefsel volledig is verdwenen.
Hoofdstuk 8 beschrijft de belangrijkste conclusies van dit proefschrift, en de sterke en minder sterke methodologische aspecten van alle hoofdstukken. Ook bespreken we onze bevindingen in het licht van andere literatuur en doen we aanbevelingen voor toekomstig onderzoek. Er is een grote variatie in de gerapporteerde prevalentie van de niche, wat zou kunnen worden verklaard door heterogene studiepopulaties en het gebrek aan eenduidige diagnostische criteria voor de niche. Het exacte mechanisme waardoor vrouwen met een niche klachten krijgen, is nog steeds niet opgehelderd. Wij zijn voorstander van het vermijden van de term ‘defect’ als we praten over een keizersnedelitteken met een niche, aangezien deze term impliceert dat sprake is van een pathologische functie van het onderste uterussegment. Voor dit laatste is geen bewijs.
Er zijn nog steeds geen richtlijnen voor de behandeling van een zwangerschap in een niche. Onze voorkeur gaat uit naar het opzuigen van het zwangerschapsweefsel met een naald via de cervix, gevolgd door het achterlaten van Methotrexaat, zodat een operatie en de bijbehorende mogelijke complicaties kunnen worden vermeden in een meerderheid van de gevallen. Als deze medicamenteuze behandeling niet slaagt, adviseren wij een hysteroscopische behandeling bij patiënten bij wie de baarmoederwand ter plaatse van de zwangerschap voldoende dik is, en laparoscopische behandeling of een operatie via de vagina bij vrouwen met een dunne baarmoederwand bij wie de zwangerschap richting de blaas groeit.
Voor toekomstig onderzoek is het belangrijk dat een uniforme definitie bestaat voor de niche en een gestandaardiseerde methode voor de detectie en het in kaart brengen van een niche. Hoewel er nog geen bewijs is voor een bepaalde afkapwaarde van de diepte van de niche stellen wij de volgende definitie van de niche voor: een inkeping in de baarmoederwand van tenminste 1 mm ter plaatse van het keizersnedelitteken, waarbij verbinding is met de baarmoederholte, vastgesteld met een contrastecho. Toekomstig onderzoek moet aantonen of dit de juiste afkapwaarde is. Ook stellen wij voor om de parameters uit ons reproduceerbaarheidsonderzoek (Hoofdstuk 3) te gebruiken. In elk geval moeten het volume van de niche en de resterende dikte van de baarmoederwand ter plaatse van de niche worden opgemeten, aangezien we hebben aangetoond dat deze parameters geassocieerd zijn met spotting na de menstruatie. Daarnaast

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
144 | Chapter 9
is de resterende dikte van de baarmoederwand een belangrijke factor voor de beslissing ofwel een hysteroscopische ofwel een laparoscopische behandeling uit te voeren bij vrouwen die behandeld willen worden voor de klachten als gevolg van een niche. De focus van toekomstig onderzoek moet ons inziens liggen op de etiologie van de ontwikkeling van een niche en gerelateerde symptomen, en de impact hiervan op het functioneren van patiënten (onder andere de impact op de sexualiteit). Meer onderzoek is nodig om aan te tonen dat er een relatie is tussen een niche en subfertiliteit, en dehiscentie of ruptuur tijdens een volgende zwangerschap. RCT’s zijn nodig om te weten te komen wat de beste behandeling is van een niche, afgestemd op de individuele karakteristieken van een niche en individuele klachten van een patiënt.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
6|List of publicationsList of publications

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
List of publications
Hornberg JJ, Bruggeman FJ, Binder B, Geest CR, de Vaate AJ, Lankelma J, Heinrich R, Westerhoff HV. Principles behind the multifarious control of signal transduction. ERK phosphorylation and kinase/phosphatase control. FEBS J 2005;272(1):244-58.
Bij de Vaate AJ, van Doorninck CE, Visser M, van der Slikke JW, Brölmann HA. Endometrial aspiration before or after saline infusion sonography and the effect on specimen quality: a randomized study. J Minim Invasive Gynecol 2008;15(5):580-83.
Bij de Vaate AJ, Huirne JA, van der Slikke JH, Schats R, Brölmann HA. Medical treatment of cesarean scar pregnancy. J Minim Invasive Gynecol 2010;17(1):133.
de Vaate AJ, Brölmann HA, van der Slikke JW, Wouters MG, Schats R, Huirne JA. Therapeutic options of caesarean scar pregnancy: case series and literature review. J Clin Ultrasound 2010;38(2):75-84.
Bij de Vaate AJ, Brölmann HA, van der Slikke JW, Emanuel MH, Huirne JA. Gel instillation sonohysterography (GIS) and saline contrast sonohysterography (SCSH): comparison of two diagnostic techniques. Ultrasound Obstet Gynecol 2010;35(4):486-89.
Brölmann HAM, Bij de Vaate AJM, Vonk Noordegraaf A, Janssen PF, Huirne JAF. Hysterectomy or a minimal invasive alternative? A systematic review on quality of life and satisfaction. Gynecol Surg 2010;7(3):205-10.
Bij de Vaate AJ, Brölmann HA, van der Voet LF, van der Slikke JW, Veersema S, Huirne JA. Ultrasound evaluation of the Cesarean scar: relation between a niche and postmenstrual spotting. Ultrasound Obstet Gynecol 2011;37(1):93-99.
Naji O, Abdallah Y, Bij De Vaate AJ, Smith A, Pexsters A, Stalder C, McIndoe A, Ghaem-Maghami S, Lees C, Brölmann HA, Huirne JA, Timmerman D, Bourne T. Standardized approach for imaging and measuring Cesarean section scars using ultrasonography. Ultrasound Obstet Gynecol 2012;39(3):252-59.
van der Voet LF, Bij de Vaate AM, Veersema S, Brölmann HA, Huirne JA. Long-term complications of caesarean section. The niche in the scar: a prospective cohort study on niche prevalence and its relation to abnormal uterine bleeding. BJOG 2014;121(2):236-44.
146 | Appendices

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Brölmann HA, BijdeVaate M, van der Voet L, Naji O, Hehenkamp W, Bourne T, Huirne JA. Letter to the Editor JMIG on the Article “Cesarean scar defects: an underrecognized cause of abnormal uterine bleeding and other gynecologic complications”. J Minim Invasive Gynecol 2014;21(3):498-9.
van der Voet LF, Vervoort AJ, Veersema S, BijdeVaate AJ, Brölmann HA, Huirne JA. Minimally invasive therapy for gynaecological symptoms related to a niche in the caesarean scar: a systematic review. BJOG 2014;121(2):145-56.
Bij de Vaate AJ, van der Voet LF, Naji O, Witmer M, Veersema S, Brölmann HA, Bourne T, Huirne JA. Prevalence, potential risk factors for development and symptoms related to the presence of uterine niches following Cesarean section: systematic review. Ultrasound Obstet Gynecol 2014;43(4):372-82.
Nieuwenhuis LL, de Vaate MA, Hehenkamp WJ, Heymans MW, van Baal MW, Brölmann HA, Huirne JA. Diagnostic and clinical value of 3D gel installation sonohysterography in addition to 2D gel installation sonohysterography in the assessment of intrauterine abnormalities. Eur J Obstet Gynecol Reprod Biol 2014;175:67-74.
Nieuwenhuis LL, Bij de Vaate MA, Hehenkamp WJ, Heymans MW, van Baal MW, Brölmann HA, Huirne JA. Reproducibility of three-dimensional gel installation sonohysterography in the assessment and classification of intrauterine abnormalities. Eur J Obstet Gynecol Reprod Biol 2014;179:141-46. mei
Bij de Vaate AJ, van der Voet LF, Naji O, Witmer M, Veersema S, Brölmann HA, Bourne T, Huirne JA. Reply: Niche risk factor for uterine rupture? Ultrasound Obstet Gynecol 2014;44(3):371-72.
Marjolein Bij de Vaate AJ, Linskens IH, van der Voet LF, Twisk JW, Brölmann HA, Huirne JA. Reproducibility of three-dimensional ultrasound for the measurement of a niche in a caesarean scar and assessment of its shape. Eur J Obstet Gynecol Reprod Biol 2015;188:39-44.
List of publications | 147

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
6|DankwoordDankwoord

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
150 | Appendices
Dankwoord
Het is eindelijk zover! De afgelopen jaren heb ik steeds met plezier gewerkt aan het onderzoek en het opschrijven van de resultaten. Aan dit proefschrift en de weg ernaar toe hebben vele mensen bijgedragen, die ik hier wil bedanken.
Allereerst wil ik alle vrouwen bedanken die hebben deelgenomen aan de SECURE-studie. Dankzij hen hebben we veel kunnen leren over de niche. Ik was verrast door de bereidheid waarmee zij meededen aan het onderzoek. Velen van hen waren zelfs bereid deel te nemen aan de vervolgonderzoeken.
Ik wil mijn promotoren bedanken voor hun hulp bij het tot stand komen van dit proefschrift. Prof. dr. H.A.M. Brölmann, beste Hans, ik kan me nog goed herinneren dat je me vroeg om naast mijn coschappen een onderzoekje te komen doen. Ik deed mijn examen voor het coschap gynaecologie bij ‘de professor’ en wilde graag verder in de gynaecologie. Ik nam me voorafgaand aan het examen voor dat ik van deze gelegenheid gebruik moest maken om dit kenbaar te maken, maar werd tot mijn verrassing door jou gevraagd onderzoek te komen doen. Van het een kwam het ander en uiteindelijk begon ik met de opleiding Verloskunde en Gynaecologie. Hoewel dat uiteindelijk voor mij niet het juiste vak bleek te zijn, heb ik absoluut geen spijt van alle jaren die ik op jouw afdeling heb doorgebracht. Ik wil je bedanken voor alle kansen die je mij hebt gegeven. Ik begon als een leek in het doen van onderzoek (“Wat is een CRF?”) en ben je erkentelijk voor het vele dat ik heb geleerd tijdens mijn onderzoeksjaren. Dank voor het zelfvertrouwen dat je mij hebt gegeven in mijn eerste jaren als arts!
Dr. J.A.F. Huirne, beste Judith, dank dat jij er later bij kwam als copromotor. Ik heb het enorm gewaardeerd dat jij er altijd was als klankbord en dat ik mijn stukken telkens weer per ommegaande terugkreeg met waardevol commentaar. Ik moet bekennen dat ik er wel eens van heb gebaald als een stuk erg snel over ‘de schutting’ terugkwam voorzien van jouw grondige commentaar; de blijdschap ervan af te zijn was dan slechts van korte duur. Het troostte me dat ik wist dat het artikel er altijd beter van zou worden! Ik bewonder je om de grote berg werk die je verzet en om jouw multitask-kwaliteiten. Ooit belden we op een zaterdag toen je aan het werk was en tegelijkertijd koekjes bakte met de kinderen. Dank ook voor je persoonlijke interesse en steun!
Dr. J.W. van der Slikke, beste Hans, bedankt voor de begeleiding tijdens de eerste jaren van mijn promotie-onderzoek en niet te vergeten tijdens het Madonnaproject. Het was een plezier om samen met jou mijn vuurdoop van het spreken op een internationaal congres (in Sint Petersburg) te beleven.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Dankwoord | 151
Geachte leden van de promotiecommissie, prof. dr. M.Y. Bongers, prof. dr. T. Bourne, prof. dr. O. Donnez, dr. W.J.K. Hehenkamp, prof. dr. F.W. Jansen, prof. dr. C.B. Lambalk, prof. dr. H. de Vries, hartelijk dank voor uw deelname en voor het kritisch beoordelen van het manuscript.
Alle co-auteurs wil ik bedanken voor hun bijdragen en nuttig commentaar op alle conceptversies van de artikelen.
Beste Lucet, beiden hebben we vele jaren gewerkt aan onderzoek naar de niche. Ik hoop dat jouw proefschrift gauw zal volgen.
Beste echoscopisten, beste Annemieke, Annelieke, Marijke, Monique, Sara en Charlotte, van jullie heb ik het maken van echo’s geleerd. Fijn dat jullie altijd bereid waren mee te denken en me attendeerden op ‘mooie niches’.
Alle mede-onderzoekers van het VUmc - Annemarie, Chantal, Dorien, Els, Esther, Ingeborg, Iris, Lisette, Lucas, Maaike, Marieke, Mariëlle, Marja-Liisa, Petra, Sylvia, Tamar, Ton en Yolanda - wil ik bedanken voor de mooie onderzoeksjaren. Kamergenoten, Jacqueline, Afra en Mariëlle, wat hebben we goede tijden beleefd; vooral de koffiepauzes om 10.30 uur waren hoogtepuntjes van de soms lange onderzoeksdagen. Annemarie en Yolanda, ook al zijn onze wegen gesplitst en is er veel gebeurd in de afgelopen tijd, onze ‘gesprekken van de koffiepauze’ gaan nog steeds door en ik hoop dat ze nog heel lang door zullen gaan. Yolanda en Petra, we hebben mooie tijden beleefd op congressen; bedankt voor jullie gezelligheid! Ingeborg, bedankt dat je tijd vrij hebt willen maken om naar echobeelden te kijken voor mijn laatste artikel.
Beste Anne-To Boddeus, Leo van Velzen, Rikste Hinloopen en Willy Lemmen, wat een voorrecht dat jullie mijn opleiders in het eerste en derde jaar van de huisartsopleiding zijn (geweest). Jullie hebben mij begeleid tijdens de eerste stappen in het huisartsenvak - de kennis moest in het begin van ver komen -, mij de liefde voor het vak bijgebracht en ervoor gezorgd dat ik straks met een rugzak vol kennis en zelfvertrouwen zelf als huisarts aan de slag ga. Ik hoop jullie nog regelmatig tegen te komen in huisartsenland!
Lieve Marieke, Linda en Marja-Liisa, studievriendinnen (letterlijk) van de eerste dag. Super dat we elkaar nog steeds met enige regelmaat zien. Dank voor jullie vriendschap!
Lieve Femke, Alexandra en Janet, dank voor jullie vriendschap die nu al zeker 20 jaar (!) bestaat. Door de drukte van het leven zien we elkaar soms wat minder,

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
152 | Appendices
maar dat doet niet af aan onze vriendschap. Ongetwijfeld volgen er nog veel gezellige weekendjes als er even niet wordt gebaard of verhuisd.
Lieve paranimfen, Inge en Marja-Liisa, dank dat jullie aan mijn zijde willen staan tijdens de verdediging van mijn proefschrift. Geen seconde heb ik na hoeven denken over mijn keuze voor jullie. Lieve zus, we werken dan wel op totaal verschillende terreinen, onze carrières vertonen vele overeenkomsten. Tegelijk genoten we van het student zijn, gingen we aan het werk en maakten we mooie reizen samen. Hoewel allebei in een andere stad vonden we altijd wel de tijd om bij te kletsen. Een tijdje was het vaste prik om even te bellen na middernacht als we allebei weer richting huis gingen of dronken we een snelle kop koffie op plaatsen waar onze wegen kruisten. Beiden hebben we ons hart gevolgd en een carrièreswitch gemaakt, waar we tot op de dag van vandaag nog steeds gelukkig mee zijn. Ik hoop dat onze levens nooit te druk zullen zijn voor het bijkletsen onder het genot van een kop koffie, en dat Peter en Anne-Sophie veel kunnen genieten van hun tante. Lieve Marja-Liisa, we hebben elkaar, met Linda en Marieke, ontmoet op dag 1 van onze studententijd. We kwamen naast elkaar te wonen en haalden de schotten tussen onze balkonnetjes weg, wat het grote Amsterdam net iets kleiner maakte. Daarna nam ik jouw studentenkamer over en begonnen we allebei bij de Verloskunde en Gynaecologie. Een aantal jaar later kondigden we op dezelfde avond allebei aan te switchen naar de huisartsopIeiding; in de beide opleidingen en de promotie ging jij mij net een stap voor. Je stond en staat altijd klaar met een goed advies. Bedankt daarvoor en ook voor onze fijne vriendschap!
Lieve Jan-Bart, wat leuk om te zien dat jij nu écht je plekje hebt gevonden. Hoewel jij in mijn hart mijn kleine broer zult blijven, ging je me voor in het trouwen, kopen van een eigen huis en krijgen van kinderen. Ik respecteer je om de manier waarop je in het leven staat en je gulle levenshouding!
Lieve Jacqueline, Hélène, Rien, Edith, Willem, Ruth, Ben en Marianne, dank voor jullie meeleven tijdens het schrijven van dit proefschrift. Belangrijker nog, bedankt voor alle goede tijden die we als familie met elkaar hebben!
Lieve pa en ma Dieleman, bedankt dat ik er zulke fijne schoonouders bij ‘kado’ heb gekregen. Wat leuk dat ik in uw voetsporen ga treden als huisarts! Bedankt dat u altijd voor ons klaar staat!
Lieve pa en ma, dank voor alle kansen die jullie mij hebben geboden en voor jullie onvoorwaardelijke steun! Ik realiseer me steeds meer dat het een groot goed is dat ik altijd het gevoel had dat jullie achter me stonden, zelfs als jullie

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
Dankwoord | 153
niet onverdeeld blij waren met een voornemen. Wat heerlijk om een stabiele thuisbasis te hebben, waar we altijd op terug kunnen vallen!
Lieve François, Peter en Anne-Sophie, wat ben ik dankbaar voor jullie aanwezigheid in mijn leven! François, dankzij jou heeft dit proefschrift enige vertraging opgelopen. Ik had me voorgenomen om mijn dankwoord nooit te hoeven eindigen met “het proefschrift is nu af, vanaf nu ga ik genieten”. Nee liefste, wat hebben wij genoten van de afgelopen jaren samen en ik hoop dat er nog velen zullen volgen. Ik hou van je! Peter en Anne-Sophie, wat genieten we elke dag van jullie schaterlachen, prachtige opmerkingen en dikke knuffels. Lieve Peter, bedankt dat je ’s middags af en toe nog een (kort of lang) tukkie deed, dankzij jou is dit proefschrift dan toch nog afgekomen. En lieve Anne-Sophie, jij vond het alleen maar gezellig om naast mij in je wipstoel te zitten als ik achter mijn computer zat te typen. Geen peuter vrolijker dan jij! Jullie zijn onze grootste schatten!

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
6|About the authorAbout the author

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
156 | Appendices

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman
About the author | 157
About the author
Marjolein Dieleman-Bij de Vaate werd op 5 juli 1979 geboren te Utrecht. Zij is de oudste dochter van J. Bij de Vaate en W. Bij de Vaate-Sterk en groeide samen met haar zus en broer op in Zoetermeer. In 1997 behaalde zij haar Gymnasiumdiploma aan het Christelijk Gymnasium Sorghvliet te Den Haag.
Daarop startte zij met de studie Medische Biologie aan de VU in Amsterdam. Na drie jaar werd zij ingeloot voor de studie Geneeskunde, die zij volgde aan dezelfde universiteit. In 2005 behaalde zij haar doctoraal Medische Biologie en in 2006 haar artsexamen. Aansluitend begon zij onder begeleiding van prof. dr. H.A.M. Brölmann, en later ook onder begeleiding van dr. J. Huirne, aan het promotieonderzoek dat tot dit proefschrift heeft geleid.
In 2010 begon Marjolein met de opleiding Verloskunde en Gynaecologie in het Spaarne Ziekenhuis in Hoofddorp. Na ruim een jaar besloot zij de gynaecologie te verruilen voor de huisartsgeneeskunde. In het voorjaar van 2016 hoopt zij de huisartsopleiding te Utrecht af te ronden.
Marjolein is woonachtig in Maarn en gelukkig getrouwd met François Dieleman. Samen zijn zij de trotse ouders van Peter en Anne-Sophie.

500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman500835-L-bw-Dieleman


500835-L-os-Dieleman500835-L-os-Dieleman500835-L-os-Dieleman500835-L-os-Dieleman Processed on: 12_10_2015Processed on: 12_10_2015Processed on: 12_10_2015Processed on: 12_10_2015
THE UTERINENICHE IN THE
CAESAREAN SCARImaging, symptoms
and risk factors
Marjolein Dieleman-
Bij de Vaate
THE U
TERINE N
ICHE IN
THE CAESAREAN
SCAR M
arjolein Dielem
an-Bij de Vaate
UITNODIGING
voor het bijwonen van de openbare verdediging van
mijn proefschrift
The uterine niche in the caesarean scar
Imaging, symptoms and risk factors
Op woensdag 27 januari 2016 om 11.45 uur in de aula van de
Vrije Universiteit,De Boelelaan 1105
te Amsterdam
Na afloop bent u van harte welkom op de receptie
ter plaatse
PARANIMFEN
Inge Bij de Vaate&
Marja-Liisa Hendriks
Marjolein Dieleman-Bij de Vaate
Amersfoortseweg 523951 LC Maarn
500835-os-Dieleman.indd 1 19-11-15 08:39
Top Related
Copyright © 2022 FDOKUMEN

