







Bahasa
Halaman
Hukum


Ezzati, Christopher J.L. Murray and Mohsen NaghaviAndrew E. Moran, Mohammad H. Forouzanfar, Gregory A. Roth, George A. Mensah, Majid
The Global Burden of Disease 2010 StudyTemporal Trends in Ischemic Heart Disease Mortality in 21 World Regions, 1980 to 2010:
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2014 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.113.004042
2014;129:1483-1492; originally published online February 26, 2014;Circulation.
http://circ.ahajournals.org/content/129/14/1483World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2014/02/26/CIRCULATIONAHA.113.004042.DC1.htmlData Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from

1483
Ischemic heart disease (IHD) was the leading cause of death worldwide in 2010.1 Age-standardized IHD mor-
tality has declined in high-income nations since 1980, in large part, because of a combination of improved primary prevention (improvements in risk factors) and improved secondary prevention (improved treatment of acute and chronic IHD).2–5 On average, IHD deaths have been pushed to older ages in the high-income regions. However, in the past, the IHD epidemic has evolved variably in different regions and nations.6 In some low- and middle-income regions, accelerated lifestyle changes, economic stresses, and other factors may be leading to increased IHD inci-dence often occurring in middle-aged adults, and changing the late 20th century paradigm of IHD as a disease of the affluent and the elderly.7
Editorial see p 1459 Clinical Perspective on p 1492
Measuring total IHD deaths and age-standardized IHD mor-tality rates is essential for assessing the burden of IHD and planning prevention programs. Global and regional analysis of IHD mortality trends is complicated by numerous factors, including changes in International Classification of Diseases (ICD) categories over time, sparse or low-quality original vital registration data in some regions, and variations in the degree of incorrect coding of IHD deaths. As part of the Global Burden of Diseases, Injuries, and Risk Factors (GBD) 2010 Study, we used novel estimation methods to assess the numbers of IHD deaths, IHD mortality rates, and years of life lost (YLL) attrib-utable to IHD for 21 world regions over the years 1980 to 2010, and provide uncertainty ranges for these estimates.
Background—Ischemic heart disease (IHD) is the leading cause of death worldwide. The Global Burden of Diseases, Risk Factors and Injuries 2010 Study estimated global and regional IHD mortality from 1980 to 2010.
Methods and Results—Sources for IHD mortality estimates were country-level surveillance, verbal autopsy, and vital registration data. Regional income, metabolic and nutritional risk factors, and other covariates were estimated from surveys and a systematic review. An estimation and validation process led to an ensemble model of IHD mortality for 21 world regions. Globally, age-standardized IHD mortality has declined since the 1980s, and high-income regions (especially Australasia, Western Europe, and North America) experienced the most remarkable declines. Age-standardized IHD mortality increased in former Soviet Union countries and South Asia in the 1990s and attenuated after 2000. In 2010, Eastern Europe and Central Asia had the highest age-standardized IHD mortality rates. More IHD deaths occurred in South Asia in 2010 than in any other region. On average, IHD deaths in South Asia, North Africa and the Middle East, and sub-Saharan Africa occurred at younger ages in comparison with most other regions.
Conclusions—In most world regions, particularly in high-income regions, age-standardized IHD mortality rates have declined significantly since 1980. High age-standardized IHD mortality in Eastern Europe, Central Asia, and South Asia point to the need to prevent and control established risk factors in those regions and to research the unique behavioral and environmental determinants of higher IHD mortality. (Circulation. 2014;129:1483-1492.)
Key Words: epidemiology ◼ mortality ◼ myocardial ischemia ◼ trends ◼ world health
© 2014 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.113.004042
Received May 24, 2013; accepted November 4, 2013.From the Division of General Medicine, Department of Medicine, Columbia University Medical Center, New York, NY (A.E.M.); Institute for Health
Metrics and Evaluation, University of Washington, Seattle, WA (M.H.F., G.A.R., C.J.L.M., M.N.); Division of Cardiology, Department of Medicine, University of Washington, Seattle, WA (G.A.R.); Center for Translation Research and Implementation Science (CTRIS), National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, MD (G.A.M.); and MRC-HPA Centre for Environment and Health and Department of Epidemiology and Biostatistics, Imperial College London, London, UK (M.E.).
The online-only Data Supplement is available with this article at http://circ.ahajournals.org/lookup/suppl/doi:10.1161/CIRCULATIONAHA. 113.004042/-/DC1.
Correspondence to Andrew Moran, MD, MPH, Herbert Irving Assistant Professor of Medicine, Columbia University, Division of General Medicine. Presbyterian Hospital East room 105, 622 West 168th St, New York, NY 10032. E-mail [email protected]
Temporal Trends in Ischemic Heart Disease Mortality in 21 World Regions, 1980 to 2010The Global Burden of Disease 2010 Study
Andrew E. Moran, MD, MPH; Mohammad H. Forouzanfar, PhD; Gregory A. Roth, MD, MPH; George A. Mensah, MD; Majid Ezzati, PhD; Christopher J.L. Murray, MD, DPhil;
Mohsen Naghavi, MD, MPH, PhD
Epidemiology and Prevention
at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from

1484 Circulation April 8, 2014
MethodsDefinition of IHD DeathDetailed IHD mortality definitions and estimation methods are avail-able elsewhere.8,9 In brief, IHD deaths fall into 2 categories: acute myocardial infarction deaths and sudden cardiac deaths. IHD has been consistently defined as an underlying cause of death across ICD revisions (most recently ICD-10 I20–I25 and ICD-9 410–414).8 A proportion of IHD deaths are erroneously assigned on death certifi-cates to either nonfatal ICD conditions (eg, senility) or conditions not defined as an underlying cause of death (eg, heart failure, hyperten-sion, or cardiac conduction disorders). The GBD developed meth-ods for systematically reallocating these undefined or erroneously assigned deaths to IHD based on the total distribution of actual causes of death by the country, sex, age, and year.8,10
IHD Mortality Source DataCause-specific mortality data were gathered from vital registration, verbal autopsy, surveillance systems, surveys/censuses, or police report and aggregated in a central database. Data sources and avail-ability varied substantially among GBD 2010 regions (Tables I and II in the online-only Data Supplement). Causes of death were mapped across revisions and national variations of the ICD over time, incom-plete data were adjusted for reporting bias, erroneously coded deaths were redistributed, deaths were distributed to GBD age categories, and trends were smoothed to eliminate year-to-year fluctuations.1 No gold standard for validating GBD classification and redistribution algorithms exists (such as large-scale autopsy studies), so countries with the most complete vital registration and adherence to recom-mended cause-of-death coding practices were used as the standard. Even in the best of settings, there are problems with erroneous coding of deaths to inappropriate ICD codes, and GBD methods have been demonstrated to improve cause-of-death estimation.11 Overall, num-bers of IHD deaths increased 21.5% after redistribution of undefined- coded deaths to IHD (Table III in the online-only Data Supplement). Globally, 76.9% of deaths incorrectly coded as heart failure, 47.2% incorrectly coded as hypertension, and 89.9% incorrectly coded as all cardiac conduction disorders were redistributed to IHD.9
IHD Mortality ModelsMultilevel IHD mortality regression models were used to improve esti-mation for regions with sparse or outlying mortality data (Online- only Data Supplement Material). Models include fixed effects from covari-ates and nested random effects on super region, region, country, and age. Separate models were developed for males and females. Potential model covariates and their directions of effect were selected based on a comprehensive review by the comparative risk assessment arm of the GBD 2010 study, and included standard IHD risk factors (country mean blood pressure and cholesterol), behavioral variables (physical activity, diet, alcohol consumption), and contextual variables (per capita income, mean education level, and health system access).9 Independent ecologi-cal associations of covariates with IHD mortality were first tested in mixed-effects regressions, adding covariates stepwise, added in order from higher to lower evidence of causal association with IHD in past studies.9 Seventeen covariates produced multivariate coefficients with a plausible direction and were significant at the <0.05 level and were retained for subsequent models. With the use of IHD mortality data and the covariates selected, the Cause of Death Ensemble Model ranked out-of-sample performance of individual IHD mortality statistical models and, with the use of a weighting algorithm, combined the best individ-ual models into ensemble models.12 Out-of-sample predictive validity of the ensemble and individual predictive models were evaluated by ranking each model’s root mean squared error of the natural log of the death rate (the average difference—or error—between model estimates and test set data for each year), the fraction of the time the trend in the prediction matched the temporal trend in the data (trend test), and the proportion of the test data set included in the 95% prediction interval of the model (coverage). All-cardiovascular death and total mortality enve-lopes were estimated independently and used to scale IHD mortality so that the sum of different cardiovascular disease–caused deaths would be equal to the all-cardiovascular disease death envelope, and all-cause deaths would be equal to the total mortality envelope.
Mean body mass index, systolic blood pressure (mm Hg), total cholesterol (mmol/L), and level of tobacco smoking (active smoking prevalence and mean cigarettes per day) were all significant predic-tors of IHD mortality and contributed most frequently to individual IHD models developed for both men and women.9 Alcohol (liters per capita) was the only covariate entered into models without specify-ing the direction of association (ie, not specifying benefit or harm) and contributed to 11% of male models and 42% of female models.
Figure 1. Map of age-standardized ischemic heart disease mortality rate per 100 000 persons in 21 world regions, 2010, the Global Burden of Disease 2010 Study.
at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from

Moran et al Global IHD Mortality Trends, 1980–2010 1485
Contextual covariates such as lower educational status (years per cap-ita), lower income (US dollars per capita), high elevation (percent-age of population dwelling at >1500 m), and high war deaths (rate per 1000 person-years) all contributed more to female than to male ensemble models.9 The prevalence of diabetes mellitus contributed to 30% of male ensemble models, but to zero female models. The root mean squared error of the best male IHD mortality model was 0.58, predicted the correct trend 62% of the time in test data, and included 90% of test data within the 95% confidence intervals around annual estimates. The best female model had a root mean squared error of 0.65, predicted the correct trend 61% of the time in test data sets, and included 91% of the test data within the 95% confidence interval.9
YLL were calculated by multiplying observed IHD deaths for a specific age in the year of interest by the age-specific reference life expectancy estimated by the use of life table methods (eg, 86.0 years at birth).13 Numbers of IHD deaths and YLL attributable to IHD death are reported for all 21 GBD regions for the years 1980 to 2010 (regions listed in Table IV in the online-only Data Supplement). Crude IHD mortality rates were calculated by dividing annual IHD deaths by the total population (all ages) at risk in that year. These rates were also age standardized by the direct method by using the 5-year GBD age categories and the World Health Organization stan-dard population.14 To assist with interpretation, IHD mortality rate trend plots used 7 super regions: Latin America/Caribbean, East Asia/
Figure 2. Total IHD deaths by age group, all world regions (A, males; B, females), 1980 to 2010, the Global Burden of Disease 2010 Study. IHD indicates ischemic heart disease.
at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from

1486 Circulation April 8, 2014
Pacific, South Asia, North Africa/Middle East, sub-Saharan Africa, Eastern Europe/Central Asia, and High Income (Table IV in the online-only Data Supplement).
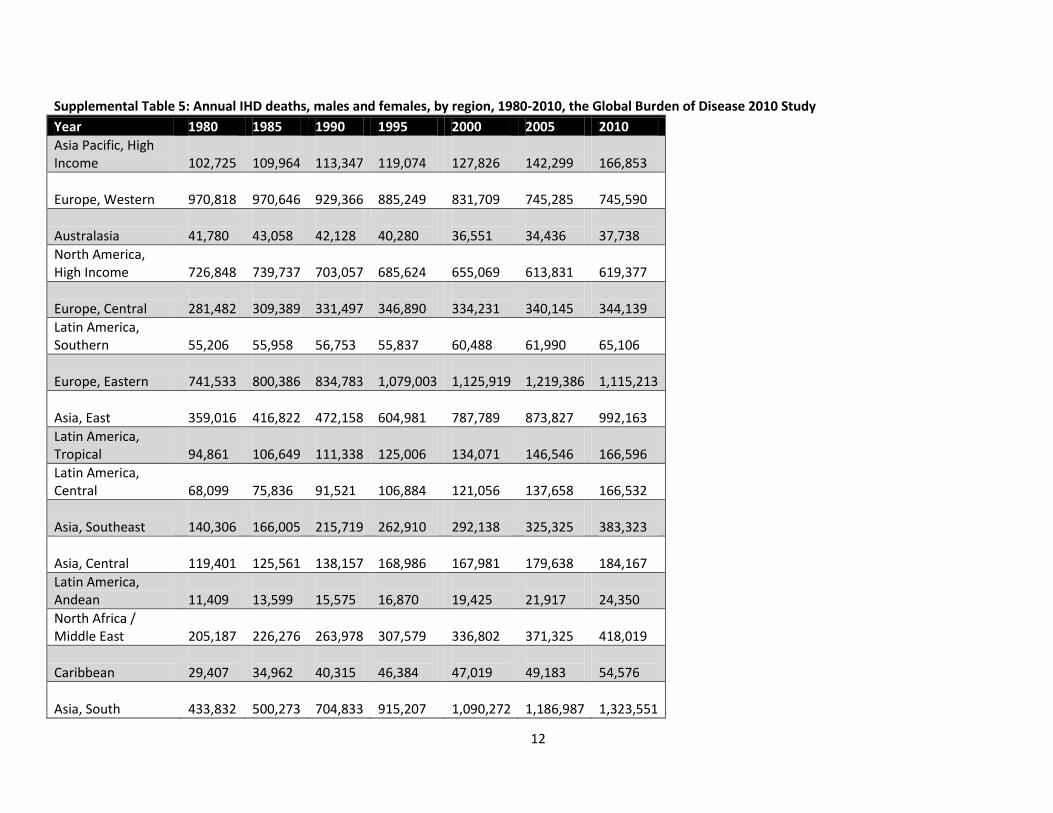
ResultsThere were >7.0 million IHD deaths worldwide in 2010, in comparison with 4.5 million IHD deaths in 1980, 5.2 million in 1990, and 6.3 million in 2000 (Table V in the online-only Data Supplement). In 2010, the highest age-standardized IHD death rates were concentrated in a cluster of regions extend-ing from Eastern Europe and Central Asia to Central Europe, North Africa/Middle East, and South Asia (Figure 1). High age-standardized IHD death rates were also found in the Caribbean region. Of all global IHD deaths in the year 2010, 25.6% occurred in persons <65 years of age (95% confidence interval, 25.9%–27.8%), in comparison with 26.5% in 1980 (95% confidence interval, 23.9%–26.6%).
The number of IHD deaths increased most since 1980 in the ≥80-years age group, the same group in which about half
of all female IHD deaths occurred in 2010 (Figure 2). Rarely, IHD deaths were recorded in infants and children, perhaps because of incorrect cause-of-death reporting. Crude IHD mortality rates in the High Income super regions were among the highest in the world in 1980, but declined substantially by 2005 (Figure I in the online-only Data Supplement). By far the highest crude rates of IHD deaths and the steepest increase since 1980 were observed in the regions of the former Soviet Union (Eastern Europe/Central Asia), especially among males. The South Asia and East Asia/Pacific super regions also saw steady crude IHD death rate increases after 1980.
When mortality rates were age standardized, in comparison with the crude rates, IHD death rates emerged as distinctly higher in North Africa/Middle East and South Asia, 2 regions with younger populations (average age <65 years; Tables 1 and 2, Figure 3). South Asia’s age-standardized death rates increased from ≈1985 to 2000; more recently rates there appear to have leveled off. Age-standardized IHD mortality remained low in sub-Saharan Africa from 1980 to 2010. The largest proportional
Table 1. Age-Standardized IHD Mortality per 100 000 persons, by Region, Males, 1990, 2005, 2010, the Global Burden of Disease 2010 Study
Males
GBD 2010 Super Region 1990 2005 2010
GBD 2010 Region Mean Lower Upper Mean Lower Upper Mean Lower Upper
High income
Asia Pacific, high income 69 60 73 49 45 56 46 42 52
Europe, Western 183 169 192 106 103 122 93 89 108
Australasia 209 190 216 99 94 116 91 83 108
North America, high income 226 209 238 135 129 155 120 112 139
Latin America, Southern 164 154 180 119 113 138 108 102 125
Eastern Europe/Central Asia
Europe, Central 285 263 302 226 215 246 201 192 222
Europe, Eastern 393 380 430 545 497 566 434 396 454
Asia, Central 395 382 427 441 411 459 400 366 430
Latin America/Caribbean
Latin America, Tropical 159 142 170 119 113 139 113 106 132
Latin America, Central 130 121 144 115 101 120 117 103 124
Latin America, Andean 92 85 102 73 66 80 70 63 78
Caribbean 177 163 189 149 144 168 144 137 162
East Asia/Pacific
Asia, Southeast 110 102 124 108 102 132 111 104 133
Asia, East 61 53 86 83 67 91 84 65 92
Oceania 122 106 185 117 101 179 115 98 168
North Africa / Middle East
North Africa / Middle East 228 217 263 197 183 214 189 171 204
South Asia
Asia, South 143 133 165 166 137 178 162 133 186
Sub-Saharan Africa
Sub-Saharan Africa, Southern 122 93 134 76 69 96 77 68 96
Sub-Saharan Africa, East 79 65 87 61 55 76 60 54 77
Sub-Saharan Africa, Central 112 84 134 103 84 124 112 91 135
Sub-Saharan Africa, West 52 47 69 60 54 73 63 56 77
GBD indicates Global Burden of Diseases, Injuries, and Risk Factors; and IHD, ishemic heart disease.
at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from

Moran et al Global IHD Mortality Trends, 1980–2010 1487
increase in age-standardized IHD mortality between 1990 and 2010 occurred in East Asian males (38% increase), although the absolute rate remained comparatively low. On average, IHD deaths occurred at the youngest ages in North Africa/Middle East, South Asia, and sub-Saharan Africa (Figure 4).
Eastern Europe/Central Asia experienced steep increases in the age-standardized IHD death rate after 1990 (around the time of the breakup of the Soviet Union); age-standardized rates there declined starting in the mid-2000s (Figure 3).
Among the high-income regions, age-standardized IHD mortality rates decreased most in Australasia (≈51% decrease from 1990 to 2010), Western Europe (46% decrease), and North America (43% decrease; Tables 1 and 2). The lowest age-standardized IHD mortality rates over the period 1980 to 2010 were observed in the sub-Saharan Africa, Andean Latin America, and Asia/Pacific regions.
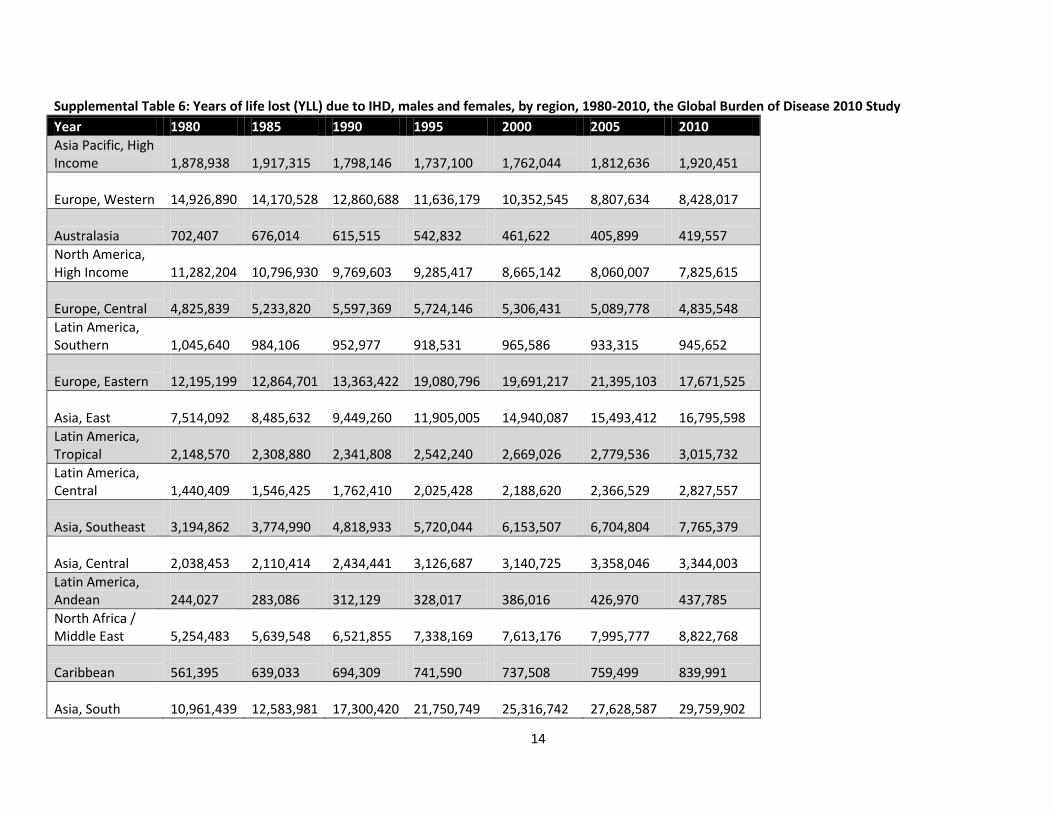
Regional totals of YLL attributable to IHD were highest in regions with larger populations, high IHD mortality rates, and younger average age at IHD death. The highest YLL in all years
was observed in South Asia (a 72% increase since 1990), fol-lowed by Eastern Europe (Table 3, Table VI in the online-only Data Supplement). Despite having among the lowest IHD death rates in the world, East Asia ranked third in IHD YLL in 2010 and has experienced the largest proportional increase in YLL since 1990 (78% higher) because of its large and aging popula-tion. Driven both by lower IHD death rates and older average age at IHD death, the most remarkable decreases in YLL from 1990 to 2010 occurred in the high-income regions of Australasia (34% decrease) and Western Europe (32% decrease).
DiscussionIn the overall GBD study, IHD was the leading cause of death worldwide in 2010.1 Our analysis of IHD mortality trends found that global age-standardized IHD mortality has declined since 1980. At the regional level, another, more complex story emerged: the age-standardized IHD death rate has declined steeply since 1980 in the Western, high-income regions, but has increased in Eastern Europe, Central Asia, South Asia, and
Table 2. Age-Standardized IHD Mortality per 100 000 Persons, by Region, Females, 1990, 2005, 2010, the Global Burden of Disease 2010 Study
Females
GBD 2010 Super Region 1990 2005 2010
GBD 2010 Region Mean Lower Upper Mean Lower Upper Mean Lower Upper
High income
Asia Pacific, high income 44 38 46 28 26 33 27 24 31
Europe, Western 96 85 99 58 56 71 51 49 65
Australasia 113 99 118 58 53 75 55 49 69
North America, high income 126 111 131 83 77 107 76 68 100
Latin America, Southern 84 78 90 62 59 76 58 54 70
Eastern Europe/Central Asia
Europe, Central 161 154 169 131 123 139 117 110 125
Europe, Eastern 224 216 246 272 245 284 235 209 245
Asia, Central 243 238 262 254 241 265 225 213 242
Latin America/Caribbean
Latin America, Tropical 105 95 111 78 73 91 73 68 88
Latin America, Central 86 79 94 77 69 82 74 68 82
Latin America, Andean 72 63 80 60 54 69 55 49 64
Caribbean 133 122 139 116 111 133 112 105 150
East Asia/Pacific
Asia, Southeast 76 69 84 70 65 90 68 63 86
Asia, East 52 46 79 60 45 65 57 40 65
Oceania 79 57 137 86 63 140 87 63 137
North Africa / Middle East
North Africa / Middle East 155 148 173 134 123 143 123 114 131
South Asia
Asia, South 109 98 131 112 89 124 106 86 120
Sub-Saharan Africa
Sub-Saharan Africa, Southern 74 55 83 57 49 76 52 43 72
Sub-Saharan Africa, East 59 45 65 49 42 55 47 41 55
Sub-Saharan Africa, Central 86 67 104 80 65 96 83 68 100
Sub-Saharan Africa, West 62 53 79 59 49 75 59 49 77
GBD indicates Global Burden of Diseases, Injuries, and Risk Factors; and IHD, ishemic heart disease.
at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from

1488 Circulation April 8, 2014
East Asia. Reflecting its large population and relatively young average age at IHD death, the South Asia region had the high-est number of life-years lost to premature IHD deaths.
An IHD epidemic emerged in Eastern Europe and Central Asia after the breakup of the Soviet Union in the early 1990s: this group of regions has had by far the highest crude and age- standardized IHD death rates of any region. Eastern Europe and Central Asia regions experienced a combined 21 million YLL in 2010 because of IHD, second only to South Asia, despite having less than a fifth of South Asia’s population. The
reasons for high IHD death rates in the Eastern Europe region are under debate: peak IHD death-rate years have coincided with economic downturns, and the greatest fluctuations have occurred in the nonmyocardial infarction (ie, cardiac arrest, atherosclerotic heart disease, and other IHD) portion of IHD deaths.15 There is strong evidence that heavy alcohol exposure is the cause of many deaths ascribed to IHD in this region, although the causal pathway needs to be better defined.15,16
Perhaps most concerning are high age-standardized IHD death rates in regions like North Africa/Middle East and
Figure 3. Age-standardized ischemic heart disease mortality rate per 100 000 persons by super region and globally (A, males; B, females), 1980 to 2010, the Global Burden of Disease 2010 Study.
at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from

Moran et al Global IHD Mortality Trends, 1980–2010 1489
South Asia where deaths occurred at younger ages on aver-age, meaning IHD deaths were more likely to occur in pro-ductive, working-age adults. This represents the greatest loss for families and national economies.7,17 In the over-all GBD 2010 study, regions such as South, Central, and East Asia; Central, Andean, and Tropical Latin America; and North Africa/Middle East stood out for having a dou-ble burden of YLL owing to cardiovascular and infectious diseases.
Dietary patterns have shifted worldwide in both high- and low-income regions to more consumption of edible oils, ani-mal fats, and sugar-sweetened beverages.18 Earlier adoption of unhealthy lifestyles and higher risk factor exposures at younger ages may, in part, explain the increasing incidence of IHD at younger ages in regions like South Asia.19,20 East Asia (composed mostly of China) was another region with an IHD mortality increase in our analysis: in an earlier GBD study analysis of cholesterol trends, East Asia was among the few
Figure 4. Average age at the time of IHD death by super region and globally (A, males; B, females), 1980 to 2010, the Global Burden of Disease 2010 Study. IHD indicates ischemic heart disease.
at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from

1490 Circulation April 8, 2014
regions that experienced an increase in mean cholesterol after 1980.21 However, not all IHD epidemics are the same; there are past examples of IHD mortality declines in the face of adverse cholesterol or tobacco trends.22 Our analysis shows that, at a global level, traditional risk factors like tobacco smoke, high cholesterol, and high blood pressure play a cen-tral role in explaining regional differences in IHD mortality rates. Because no causal direction was specified and patterns of alcohol use were not distinguished (ie, binge or heavy compared with moderate alcohol consumption), our analy-sis did not accurately characterize the association of alcohol consumption with IHD. Regional air pollution level was not a significant covariate in the IHD mortality models, but epi-demiological research has established air pollution as a risk factor for IHD,23 and its contribution will be explored in sub-sequent GBD analyses.
The association of lower regional economic and educa-tional status with higher IHD rates suggests that many regions are undergoing an epidemiological transition to higher IHD death rates often associated with economic development.
The populations of many of the transitioning regions (eg, South and East Asia, Latin America/Tropical [Brazil], and North Africa/Middle East) are enormous, and the continued development of these regions depends in part on successfully addressing the threat of cardiovascular disease. To succeed in stemming the tide of IHD mortality in younger adults in the 21st century, as many high-income regions did during the last decades of the 20th century, low- and middle-income regions may need to develop new approaches, emphasizing improved healthcare delivery infrastructure, universal health insurance and affordable essential medicines, and selected population- wide prevention interventions.24,25 Along with the public health community’s emphasis on prevention, the impact of improved access to acute cardiac care should not be forgot-ten. Aspirin and a β-blocker for all acute myocardial infarc-tions and revascularization using low-cost thrombolytic for ST-elevation myocardial infarctions are often life-saving and may be affordable in low-resource settings.26
The strengths of this analysis of global trends in IHD mor-tality were the collection of a comprehensive set of national
Table 3. Years of Life Lost Owing to IHD, Males And Females, by Region, 1990, 2005, and 2010, the Global Burden of Disease 2010 Study
GBD 2010 Super Region 1990 2005 2010
GBD 2010 Region Mean Lower Upper Mean Lower Upper Mean Lower Upper
High income
Asia Pacific, high income 1 798 146 1 620 244 1 900 184 1 812 636 1 692 038 2 018 899 1 920 451 1 752 565 2 116 832
Europe, Western 12 860 688 11 929 341 13 404 064 8 807 634 8 566 677 9 942 095 8 428 017 8 135 515 9 554 209
Australasia 615 515 569 455 632 471 405 899 388 773 462 917 419 557 392 876 482 962
North America, high income 9 769 603 9 109 634 10 256 781 8 060 007 7 735 522 9 068 844 7 825 615 7 351 893 8 948 068
Latin America, Southern 952 977 904 836 1 037 283 933 315 898 505 1 032 393 945 652 905 779 1 055 796
Eastern Europe/Central Asia
Europe, Central 5 597 369 5 242 998 5 831 784 5 089 778 4 920 576 5 468 643 4 835 548 4 650 986 5 210 929
Europe, Eastern 13 363 422 13 020 191 14 332 364 21 395 103 19 746 998 22 075 817 17 671 525 16 219 642 18 315 709
Asia, Central 2 434 441 2 366 917 2 603 885 3 358 046 3 149 985 3 497 223 3 344 003 3 095 362 3 565 863
Latin America/Caribbean
Latin America, Tropical 2 341 808 2 193 945 2 534 789 2 779 536 2 657 763 3 083 571 3 015 732 2 872 578 3 380 191
Latin America, Central 1 762 410 1 637 594 1 905 648 2 366 529 2 129 444 2 484 887 2 827 557 2 550 462 3 012 726
Latin America, Andean 312 129 293 583 351 584 426 970 358 663 456 209 437 785 377 164 474 416
Caribbean 694 309 647 297 739 747 759 499 733 454 832 392 839 991 797 218 1 046 637
East Asia/Pacific
Asia, Southeast 4 818 933 4 360 138 5 246 287 6 704 804 6 383 138 7 672 710 7 765 379 7 361 080 8 864 297
Asia, East 9 449 260 8 689 819 12 168 368 15 493 412 13 436 409 16 405 168 16 795 598 13 989 156 17 913 060
Oceania 71 723 61 923 98 564 107 351 90 631 150 617 122 337 102 152 165 558
North Africa / Middle East
North Africa / Middle East 6 521 855 6 049 947 7 091 033 7 995 777 7 402 525 8 517 971 8 822 768 7 968 594 9 343 464
South Asia
Asia, South 17 300 420 16 157 871 19 323 777 27 628 587 23 082 187 29 334 998 29 759 902 24 854 218 33 295 998
Sub-Saharan Africa
Sub-Saharan Africa, Southern 439 982 351 244 477 998 531 476 491 026 653 461 514 823 468 185 632 563
Sub-Saharan Africa, East 1 414 599 1 148 746 1 545 838 1 628 544 1 446 234 1 803 904 1 781 311 1 600 930 2 000 006
Sub-Saharan Africa, Central 508 418 404 775 597 259 666 283 576 079 770 551 805 163 697 096 940 718
Sub-Saharan Africa, West 1 492 723 1 274 743 1 714 206 1 890 019 1 683 958 2 126 861 2 146 457 1 913 551 2 462 752
GBD indicates Global Burden of Diseases, Injuries, and Risk Factors; and IHD, ishemic heart disease.
at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from

Moran et al Global IHD Mortality Trends, 1980–2010 1491
mortality data from a variety of sources, adjustments for biases introduced by ICD version changes and for death reg-istration coding practices, and methods for accounting for and describing covariate parameter and statistical model selection uncertainty. Limitations of the analysis include incomplete data for many regions, especially sub-Saharan Africa, and the ecological nature of the associations found between covari-ates and IHD mortality. Unexpectedly, diabetes mellitus con-tributed more to male models than to female models, findings that may be explained by the inclusion of nontraditional IHD predictor covariates in the models that absorbed some of these covariates’ effects, or differential competing risk with other causes of death in males in comparison with females.
ImplicationsThe decline in IHD mortality in high-income regions since 1980 is a success story. More troubling are the very high IHD mortality rates in Eastern Europe and Central Asia in 2010, and increased IHD mortality occurring in relatively young adults in South Asia. IHD prevention in the 21st century must extend the control of established risk factors from high- income to low- and middle-income regions while addressing newer social and behavioral determinants of IHD mortality observed in developing regions.
Acknowledgments We sincerely thank the many study participants and investigators of the studies contributing data to this analysis.
Sources of FundingThis research was supported by the Bill and Melinda Gates Foundation, an American Heart Association Postdoctoral Fellowship to Dr Roth, and US National Heart, Lung, and Blood Institute award K08 HL089675-01A1, and a Columbia University Irving Scholarship to Dr Moran.
DisclosuresThe perspectives expressed in this article are those of the authors and do not necessarily represent the views of the National Institutes of Health, Department of Health and Human Services, or any other gov-ernment entity.
References 1. Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V,
Abraham J, Adair T, Aggarwal R, Ahn SY, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Barker-Collo S, Bartels DH, Bell ML, Benjamin EJ, Bennett D, Bhalla K, Bikbov B, Bin Abdulhak A, Birbeck G, Blyth F, Bolliger I, Boufous S, Bucello C, Burch M, Burney P, Carapetis J, Chen H, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahodwala N, De Leo D, Degenhardt L, Delossantos A, Denenberg J, Des Jarlais DC, Dharmaratne SD, Dorsey ER, Driscoll T, Duber H, Ebel B, Erwin PJ, Espindola P, Ezzati M, Feigin V, Flaxman AD, Forouzanfar MH, Fowkes FG, Franklin R, Fransen M, Freeman MK, Gabriel SE, Gakidou E, Gaspari F, Gillum RF, Gonzalez-Medina D, Halasa YA, Haring D, Harrison JE, Havmoeller R, Hay RJ, Hoen B, Hotez PJ, Hoy D, Jacobsen KH, James SL, Jasrasaria R, Jayaraman S, Johns N, Karthikeyan G, Kassebaum N, Keren A, Khoo JP, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Lipnick M, Lipshultz SE, Ohno SL, Mabweijano J, MacIntyre MF, Mallinger L, March L, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGrath J, Mensah GA, Merriman TR, Michaud C, Miller M, Miller TR, Mock C, Mocumbi AO, Mokdad AA, Moran A,
Mulholland K, Nair MN, Naldi L, Narayan KM, Nasseri K, Norman P, O’Donnell M, Omer SB, Ortblad K, Osborne R, Ozgediz D, Pahari B, Pandian JD, Rivero AP, Padilla RP, Perez-Ruiz F, Perico N, Phillips D, Pierce K, Pope CA 3rd, Porrini E, Pourmalek F, Raju M, Ranganathan D, Rehm JT, Rein DB, Remuzzi G, Rivara FP, Roberts T, De León FR, Rosenfeld LC, Rushton L, Sacco RL, Salomon JA, Sampson U, Sanman E, Schwebel DC, Segui-Gomez M, Shepard DS, Singh D, Singleton J, Sliwa K, Smith E, Steer A, Taylor JA, Thomas B, Tleyjeh IM, Towbin JA, Truelsen T, Undurraga EA, Venketasubramanian N, Vijayakumar L, Vos T, Wagner GR, Wang M, Wang W, Watt K, Weinstock MA, Weintraub R, Wilkinson JD, Woolf AD, Wulf S, Yeh PH, Yip P, Zabetian A, Zheng ZJ, Lopez AD, Murray CJ, AlMazroa MA, Memish ZA. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–2128.
2. Tunstall-Pedoe H, Vanuzzo D, Hobbs M, Mähönen M, Cepaitis Z, Kuulasmaa K, Keil U. Estimation of contribution of changes in coronary care to improving survival, event rates, and coronary heart disease mortality across the WHO MONICA Project populations. Lancet. 2000;355:688–700.
3. Kuulasmaa K, Tunstall-Pedoe H, Dobson A, Fortmann S, Sans S, Tolonen H, Evans A, Ferrario M, Tuomilehto J. Estimation of contribution of changes in classic risk factors to trends in coronary-event rates across the WHO MONICA Project populations. Lancet. 2000;355:675–687.
4. Ford ES, Ajani UA, Croft JB, Critchley JA, Labarthe DR, Kottke TE, Giles WH, Capewell S. Explaining the decrease in U.S. deaths from coronary disease, 1980-2000. N Engl J Med. 2007;356:2388–2398.
5. Di Cesare M, Bennett JE, Best N, Stevens GA, Danaei G, Ezzati M. The contributions of risk factor trends to cardiometabolic mortality decline in industrialized countries. Int J Epidemiol. 2013;42:838–848.
6. Mirzaei M, Truswell AS, Taylor R, Leeder SR. Coronary heart disease epidemics: not all the same. Heart. 2009;95:740–746.
7. Leeder S., Raymond S., Greenberg H., Liu H., Esson, K. A Race Against Time: The Challenge of Cardiovascular Disease in Developing Countries. New York, NY: Columbia University Center for Global Health and Economic Development; 2004.
8. Moran AE, Oliver JT, Mirzaie M, Forouzanfar MH, Chilov M, Anderson L, Morrison JL, Khan A, Zhang N, Haynes N, Tran J, Murphy A, Degennaro V, Roth G, Zhao D, Peer N, Pichon-Riviere A, Rubinstein A, Pogosova N, Prabhakaran D, Naghavi M, Ezzati M, Mensah GA. Assessing the Global Burden of Ischemic Heart Disease, Part 1: methods for a system-atic review of the Global Epidemiology of Ischemic Heart Disease in 1990 and 2010. Glob Heart. 2012;7:315–329.
9. Forouzanfar MH, Moran AE, Flaxman AD, Roth G, Mensah GA, Ezzati M, Naghavi M, Murray CJL. Assessing the global burden of ischemic heart failure, Part 2: analytic methods and estimates of the global epidemi-ology of ischemic heart disease in 2010. Global Heart. 2012;7:331–342.
10. Naghavi M, Makela S, Foreman K, O’Brien J, Pourmalek F, Lozano R. Algorithms for enhancing public health utility of national causes-of-death data. Popul Health Metr. 2010;8:9.
11. Murray CJ, Kulkarni SC, Ezzati M. Understanding the coronary heart dis-ease versus total cardiovascular mortality paradox: a method to enhance the comparability of cardiovascular death statistics in the United States. Circulation. 2006;113:2071–2081.
12. Foreman KJ, Lozano R, Lopez AD, Murray CJ. Modeling causes of death: an integrated approach using CODEm. Popul Health Metr. 2012;10:1.
13. Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, Aboyans V, Abraham J, Ackerman I, Aggarwal R, Ahn SY, Ali MK, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Bahalim AN, Barker-Collo S, Barrero LH, Bartels DH, Basáñez MG, Baxter A, Bell ML, Benjamin EJ, Bennett D, Bernabé E, Bhalla K, Bhandari B, Bikbov B, Bin Abdulhak A, Birbeck G, Black JA, Blencowe H, Blore JD, Blyth F, Bolliger I, Bonaventure A, Boufous S, Bourne R, Boussinesq M, Braithwaite T, Brayne C, Bridgett L, Brooker S, Brooks P, Brugha TS, Bryan-Hancock C, Bucello C, Buchbinder R, Buckle G, Budke CM, Burch M, Burney P, Burstein R, Calabria B, Campbell B, Canter CE, Carabin H, Carapetis J, Carmona L, Cella C, Charlson F, Chen H, Cheng AT, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahiya M, Dahodwala N, Damsere-Derry J, Danaei G, Davis A, De Leo D, Degenhardt L, Dellavalle R, Delossantos A, Denenberg J, Derrett S, Des Jarlais DC, Dharmaratne SD, Dherani M, Diaz-Torne C, Dolk H, Dorsey ER, Driscoll T, Duber H, Ebel B, Edmond K, Elbaz A, Ali SE, Erskine H, Erwin PJ, Espindola P, Ewoigbokhan SE, Farzadfar
at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from

1492 Circulation April 8, 2014
F, Feigin V, Felson DT, Ferrari A, Ferri CP, Fèvre EM, Finucane MM, Flaxman S, Flood L, Foreman K, Forouzanfar MH, Fowkes FG, Fransen M, Freeman MK, Gabbe BJ, Gabriel SE, Gakidou E, Ganatra HA, Garcia B, Gaspari F, Gillum RF, Gmel G, Gonzalez-Medina D, Gosselin R, Grainger R, Grant B, Groeger J, Guillemin F, Gunnell D, Gupta R, Haagsma J, Hagan H, Halasa YA, Hall W, Haring D, Haro JM, Harrison JE, Havmoeller R, Hay RJ, Higashi H, Hill C, Hoen B, Hoffman H, Hotez PJ, Hoy D, Huang JJ, Ibeanusi SE, Jacobsen KH, James SL, Jarvis D, Jasrasaria R, Jayaraman S, Johns N, Jonas JB, Karthikeyan G, Kassebaum N, Kawakami N, Keren A, Khoo JP, King CH, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Laden F, Lalloo R, Laslett LL, Lathlean T, Leasher JL, Lee YY, Leigh J, Levinson D, Lim SS, Limb E, Lin JK, Lipnick M, Lipshultz SE, Liu W, Loane M, Ohno SL, Lyons R, Mabweijano J, MacIntyre MF, Malekzadeh R, Mallinger L, Manivannan S, Marcenes W, March L, Margolis DJ, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGill N, McGrath J, Medina-Mora ME, Meltzer M, Mensah GA, Merriman TR, Meyer AC, Miglioli V, Miller M, Miller TR, Mitchell PB, Mock C, Mocumbi AO, Moffitt TE, Mokdad AA, Monasta L, Montico M, Moradi-Lakeh M, Moran A, Morawska L, Mori R, Murdoch ME, Mwaniki MK, Naidoo K, Nair MN, Naldi L, Narayan KM, Nelson PK, Nelson RG, Nevitt MC, Newton CR, Nolte S, Norman P, Norman R, O’Donnell M, O’Hanlon S, Olives C, Omer SB, Ortblad K, Osborne R, Ozgediz D, Page A, Pahari B, Pandian JD, Rivero AP, Patten SB, Pearce N, Padilla RP, Perez-Ruiz F, Perico N, Pesudovs K, Phillips D, Phillips MR, Pierce K, Pion S, Polanczyk GV, Polinder S, Pope CA 3rd, Popova S, Porrini E, Pourmalek F, Prince M, Pullan RL, Ramaiah KD, Ranganathan D, Razavi H, Regan M, Rehm JT, Rein DB, Remuzzi G, Richardson K, Rivara FP, Roberts T, Robinson C, De Leòn FR, Ronfani L, Room R, Rosenfeld LC, Rushton L, Sacco RL, Saha S, Sampson U, Sanchez-Riera L, Sanman E, Schwebel DC, Scott JG, Segui-Gomez M, Shahraz S, Shepard DS, Shin H, Shivakoti R, Singh D, Singh GM, Singh JA, Singleton J, Sleet DA, Sliwa K, Smith E, Smith JL, Stapelberg NJ, Steer A, Steiner T, Stolk WA, Stovner LJ, Sudfeld C, Syed S, Tamburlini G, Tavakkoli M, Taylor HR, Taylor JA, Taylor WJ, Thomas B, Thomson WM, Thurston GD, Tleyjeh IM, Tonelli M, Towbin JA, Truelsen T, Tsilimbaris MK, Ubeda C, Undurraga EA, van der Werf MJ, van Os J, Vavilala MS, Venketasubramanian N, Wang M, Wang W, Watt K, Weatherall DJ, Weinstock MA, Weintraub R, Weisskopf MG, Weissman MM, White RA, Whiteford H, Wiebe N, Wiersma ST, Wilkinson JD, Williams HC, Williams SR, Witt E, Wolfe F, Woolf AD, Wulf S, Yeh PH, Zaidi AK, Zheng ZJ, Zonies D, Lopez AD, AlMazroa MA, Memish ZA. Disability-adjusted life years (DALYs) for 291 dis-eases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2197–2223.
14. Ahmad OB, Boschi-Pinto C, Lopez AD, Murray CJL, Lozano R, Inoue M. Age standardization of rates: a new who standard. GPE discussion paper series: No. 31. Geneva, Switzerland: World Health Organization; 2001.
15. Zaridze D, Maximovitch D, Lazarev A, Igitov V, Boroda A, Boreham J, Boyle P, Peto R, Boffetta P. Alcohol poisoning is a main determinant of
recent mortality trends in Russia: evidence from a detailed analysis of mortality statistics and autopsies. Int J Epidemiol. 2009;38:143–153.
16. Leon DA, Shkolnikov VM, McKee M, Kiryanov N, Andreev E. Alcohol increases circulatory disease mortality in Russia: acute and chronic effects or misattribution of cause? Int J Epidemiol. 2010;39:1279–1290.
17. Huffman MD, Rao KD, Pichon-Riviere A, Zhao D, Harikrishnan S, Ramaiya K, Ajay VS, Goenka S, Calcagno JI, Caporale JE, Niu S, Li Y, Liu J, Thankappan KR, Daivadanam M, van Esch J, Murphy A, Moran AE, Gaziano TA, Suhrcke M, Reddy KS, Leeder S, Prabhakaran D. A cross-sectional study of the microeconomic impact of cardiovascular dis-ease hospitalization in four low- and middle-income countries. PLoS One. 2011;6:e20821.
18. Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pan-demic of obesity in developing countries. Nutr Rev. 2012;70:3–21.
19. Joshi P, Islam S, Pais P, Reddy S, Dorairaj P, Kazmi K, Pandey MR, Haque S, Mendis S, Rangarajan S, Yusuf S. Risk factors for early myocardial infarction in South Asians compared with individuals in other countries. JAMA. 2007;297:286–294.
20. Danaei G, Singh GM, Paciorek CJ, Lin JK, Cowan MJ, Finucane MM, Farzadfar F, Stevens GA, Riley LM, Lu Y, Rao M, Ezzati M; Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group. The global cardiovascular risk transition: associations of four met-abolic risk factors with national income, urbanization, and Western diet in 1980 and 2008. Circulation. 2013;127:1493–502, 1502e1.
21. Farzadfar F, Finucane MM, Danaei G, Pelizzari PM, Cowan MJ, Paciorek CJ, Singh GM, Lin JK, Stevens GA, Riley LM, Ezzati M; Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Cholesterol). National, regional, and global trends in serum total choles-terol since 1980: systematic analysis of health examination surveys and epidemiological studies with 321 country-years and 3.0 million partici-pants. Lancet. 2011;377:578–586.
22. Nicolosi A, Casati S, Taioli E, Polli E. Death from cardiovascular disease in Italy, 1972-1981: decline in mortality rates and possible causes. Int J Epidemiol. 1988;17:766–772.
23. Brook RD, Franklin B, Cascio W, Hong Y, Howard G, Lipsett M, Luepker R, Mittleman M, Samet J, Smith SC Jr, Tager I; Expert Panel on Population and Prevention Science of the American Heart Association. Air pollution and cardiovascular disease: a statement for healthcare professionals from the Expert Panel on Population and Prevention Science of the American Heart Association. Circulation. 2004;109:2655–2671.
24. 2008–2013 action plan for the global strategy for the prevention and con-trol of noncommunicable diseases. Geneva, Switzerland: World Health Organization; 2009.
25. Ebrahim S, Smith GD. Exporting failure? Coronary heart disease and stroke in developing countries. Int J Epidemiol. 2001;30:201–205.
26. Gaziano TA. Cardiovascular disease in the developing world and its cost- effective management. Circulation. 2005;112:3547–3553.
CLINICAL PERSPECTIvEIschemic heart disease (IHD) leads to lost life-years and disability in high-, middle-, and lower-income regions and is the world’s leading cause of death. Monitoring the trends in IHD mortality in diverse world regions requires analyzing a variety of data sources and using statistical modeling that accounts for sparse data in some regions. The Global Burden of Disease 2010 Study estimated IHD mortality in 21 world regions. Since 1980, age-standardized IHD mortality has declined in most world regions, particularly high-income regions. During the same period, age-standardized IHD mortality increased in Eastern Europe, Central Asia, and South Asia. When estimated by using a standard method, age-standardized IHD mortality has trended favorably in most regions since 1980, but unfavorably in a few others. The causes of rising rates in IHD hot-spot regions merit more detailed investigation. Prevention and acute care quality improvements are needed in low- and middle- income regions, where IHD patients die at relatively young ages.
at Columbia University on May 15, 2014http://circ.ahajournals.org/Downloaded from

1
Supplemental Material
Supplemental Methods:
Cause of Death Ensemble Model (CODEm) methods.
Here we summarize ensemble modeling and CODEm methods; interested readers can access more detailed
information about the CODEm method and ensemble modeling elsewhere.1
In brief, ensemble models combine predictions of multiple individual models. Ensemble models estimated
in a variety of fields have demonstrated smaller prediction error than the best individual model. Another
advantage of ensemble models is that they capture not only input parameter uncertainty, but also
uncertainty stemming from model specification. In order to combine predictions from multiple models
(varying in model form, outcome definition, and covariate selection), individual model results are usually
weighted before averaging to produce ensemble estimates.
CODEm worked with two main model forms: linear mixed effects models and spatial-temporal models.
Linear mixed effects models assumed fixed effects of covariates, and hierarchical random effects by super-
region, region, country, and age. Spatial-temporal models begin with the mixed effects models, but
remove the random country effect, instead calculating residuals (predicted – observed estimate) and
performing local regressions on nearby data (in the dimensions of country (“space”) and time (year).
Gaussian Process Regression was used to carry forward sampling and non-sampling variance in the source
data. Two types of dependent cause of death variables were used: mortality rates and “cause fraction”
(e.g., proportion of IHD mortality in all-cardiovascular disease mortality or all-cause mortality). The two
model forms (mixed effects linear models and spatial-temporal models) and two outcome definitions (rate
and cause fraction) led to four model “families” (four combinations of form and outcome) contributing to
ensemble models.
Covariates were added stepwise to models, in order of a prior literature-based assumptions about causal
association and strength of association, and kept in models if the covariate showed estimated direction of
association and if the multivariate covariate coefficient was significant at the <0.05 level.
Biological/physiological covariates (e.g., country mean blood pressure or cholesterol), behavioral covariates
(country mean dietary consumption and physical activity level) and contextual covariates (e.g., mean
education level, per capita income, and health system access) were examined.2 A complete list of
covariates contributing to the IHD mortality models is available elsewhere.3 Multiple models were
developed from combinations of covariate sets in all four model families. We decided to apply more

2
weight to predictions from models that performed better out-of-sample, using monotonically declining
weights based on the model’s performance rank.
Supplemental References
1. Foreman KJ, Lozano R, Lopez AD, Murray CJ. Modeling causes of death: An integrated approach using codem. Population health metrics. 2012;10:1
2. Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Barker-Collo S, Bartels DH, Bell ML, Benjamin EJ, Bennett D, Bhalla K, Bikbov B, Bin Abdulhak A, Birbeck G, Blyth F, Bolliger I, Boufous S, Bucello C, Burch M, Burney P, Carapetis J, Chen H, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahodwala N, De Leo D, Degenhardt L, Delossantos A, Denenberg J, Des Jarlais DC, Dharmaratne SD, Dorsey ER, Driscoll T, Duber H, Ebel B, Erwin PJ, Espindola P, Ezzati M, Feigin V, Flaxman AD, Forouzanfar MH, Fowkes FG, Franklin R, Fransen M, Freeman MK, Gabriel SE, Gakidou E, Gaspari F, Gillum RF, Gonzalez-Medina D, Halasa YA, Haring D, Harrison JE, Havmoeller R, Hay RJ, Hoen B, Hotez PJ, Hoy D, Jacobsen KH, James SL, Jasrasaria R, Jayaraman S, Johns N, Karthikeyan G, Kassebaum N, Keren A, Khoo JP, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Lipnick M, Lipshultz SE, Ohno SL, Mabweijano J, MacIntyre MF, Mallinger L, March L, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGrath J, Mensah GA, Merriman TR, Michaud C, Miller M, Miller TR, Mock C, Mocumbi AO, Mokdad AA, Moran A, Mulholland K, Nair MN, Naldi L, Narayan KM, Nasseri K, Norman P, O'Donnell M, Omer SB, Ortblad K, Osborne R, Ozgediz D, Pahari B, Pandian JD, Rivero AP, Padilla RP, Perez-Ruiz F, Perico N, Phillips D, Pierce K, Pope CA, 3rd, Porrini E, Pourmalek F, Raju M, Ranganathan D, Rehm JT, Rein DB, Remuzzi G, Rivara FP, Roberts T, De Leon FR, Rosenfeld LC, Rushton L, Sacco RL, Salomon JA, Sampson U, Sanman E, Schwebel DC, Segui-Gomez M, Shepard DS, Singh D, Singleton J, Sliwa K, Smith E, Steer A, Taylor JA, Thomas B, Tleyjeh IM, Towbin JA, Truelsen T, Undurraga EA, Venketasubramanian N, Vijayakumar L, Vos T, Wagner GR, Wang M, Wang W, Watt K, Weinstock MA, Weintraub R, Wilkinson JD, Woolf AD, Wulf S, Yeh PH, Yip P, Zabetian A, Zheng ZJ, Lopez AD, Murray CJ, AlMazroa MA, Memish ZA. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the global burden of disease study 2010. Lancet. 2012;380:2095-2128
3. Forouzanfar MH, Moran AE, Flaxman AD, Roth G, Mensah GA, Ezzati M, Naghavi M, Murray CJ. Assessing the global burden of ischemic heart disease, part 2: Analytic methods and estimates of the global epidemiology of ischemic heart disease in 2010. Glob Heart. 2012;7:331-342
Supplemental Table 1: Site-years by decade and source type for the GBD 2010 Study IHD mortality
analysis.
Source Type 1980-1989 1990-1999 2000-2011
Surveillance 0 27 24
Verbal autopsy 14 23 40
Vital Registration 808 966 940

3
Supplemental Table 2: Site-years by GBD 2010 region for the IHD mortality analysis.
GBD Super Region GBD Region Site-years of IHD mortality data
High Income
Asia Pacific, High Income 92
Europe, Western 605
Australasia 56
North America, High Income 60
Latin America, Southern 87
Eastern Europe/Central Asia
Europe, Central 274
Europe, Eastern 194
Asia, Central 186
Latin America/Caribbean
Latin America, Tropical 59
Latin America, Central 218
Latin America, Andean 56
Caribbean 409
East Asia/Pacific
Asia, Southeast
144
Asia, East
71
Oceania
15
North Africa / Middle East 136
South Asia 54
Sub-Saharan Africa
Sub-Saharan Africa, Southern
102
Sub-Saharan Africa, East
18
Sub-Saharan Africa, Central
0
Sub-Saharan Africa, West
8
4
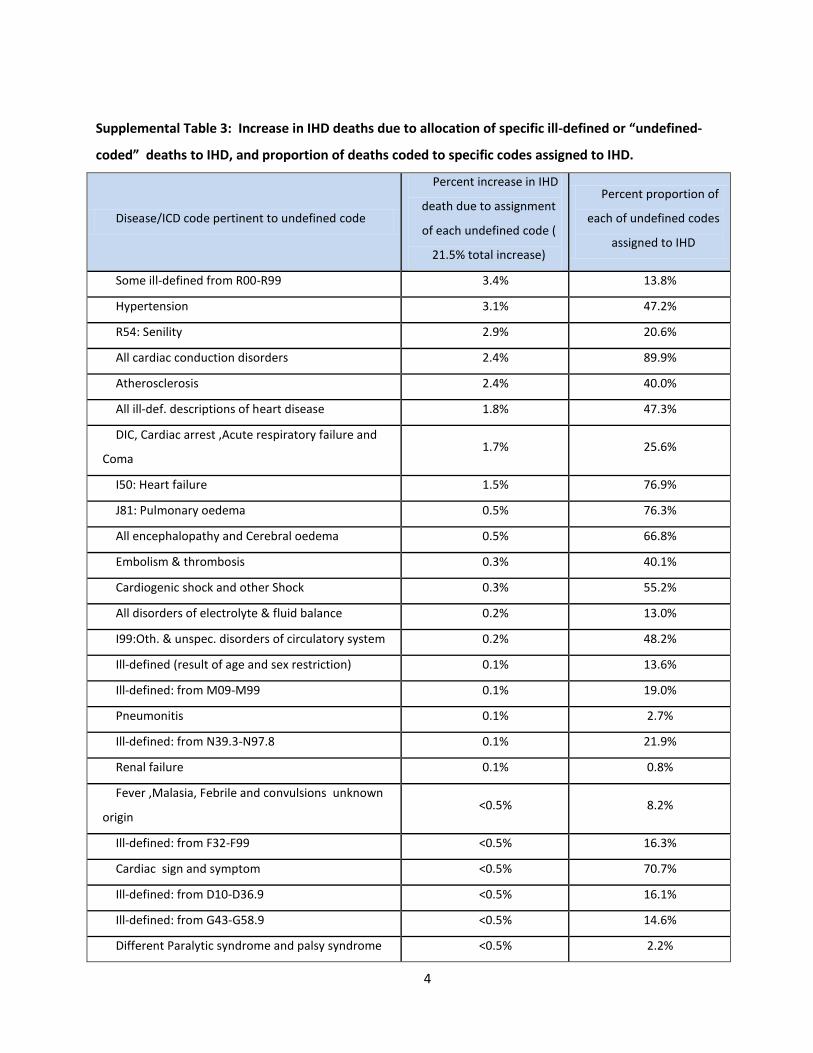
Supplemental Table 3: Increase in IHD deaths due to allocation of specific ill-defined or “undefined-
coded” deaths to IHD, and proportion of deaths coded to specific codes assigned to IHD.
Disease/ICD code pertinent to undefined code
Percent increase in IHD
death due to assignment
of each undefined code (
21.5% total increase)
Percent proportion of
each of undefined codes
assigned to IHD
Some ill-defined from R00-R99 3.4% 13.8%
Hypertension 3.1% 47.2%
R54: Senility 2.9% 20.6%
All cardiac conduction disorders 2.4% 89.9%
Atherosclerosis 2.4% 40.0%
All ill-def. descriptions of heart disease 1.8% 47.3%
DIC, Cardiac arrest ,Acute respiratory failure and
Coma 1.7% 25.6%
I50: Heart failure 1.5% 76.9%
J81: Pulmonary oedema 0.5% 76.3%
All encephalopathy and Cerebral oedema 0.5% 66.8%
Embolism & thrombosis 0.3% 40.1%
Cardiogenic shock and other Shock 0.3% 55.2%
All disorders of electrolyte & fluid balance 0.2% 13.0%
I99:Oth. & unspec. disorders of circulatory system 0.2% 48.2%
Ill-defined (result of age and sex restriction) 0.1% 13.6%
Ill-defined: from M09-M99 0.1% 19.0%
Pneumonitis 0.1% 2.7%
Ill-defined: from N39.3-N97.8 0.1% 21.9%
Renal failure 0.1% 0.8%
Fever ,Malasia, Febrile and convulsions unknown
origin <0.5% 8.2%
Ill-defined: from F32-F99 <0.5% 16.3%
Cardiac sign and symptom <0.5% 70.7%
Ill-defined: from D10-D36.9 <0.5% 16.1%
Ill-defined: from G43-G58.9 <0.5% 14.6%
Different Paralytic syndrome and palsy syndrome <0.5% 2.2%
5
Ill-defined: from L01-L98.9 <0.5% 15.9%
Unspecified liver disease <0.5% 0.9%
Ill-defined: from H00-H99 <0.5% 14.4%
Ill-defined: from K00-k14.9 <0.5% 17.9%
Ill-defined: from A00-B99 <0.5% 14.2%
Ill-defined: from Q10-Q84.9 <0.5% 4.7%
Ill-defined: from J30-J35.9 <0.5% 11.2%
Undefined ICD code <0.5% 31.6%
All unspecified parasitic diseases <0.5% 0.1%
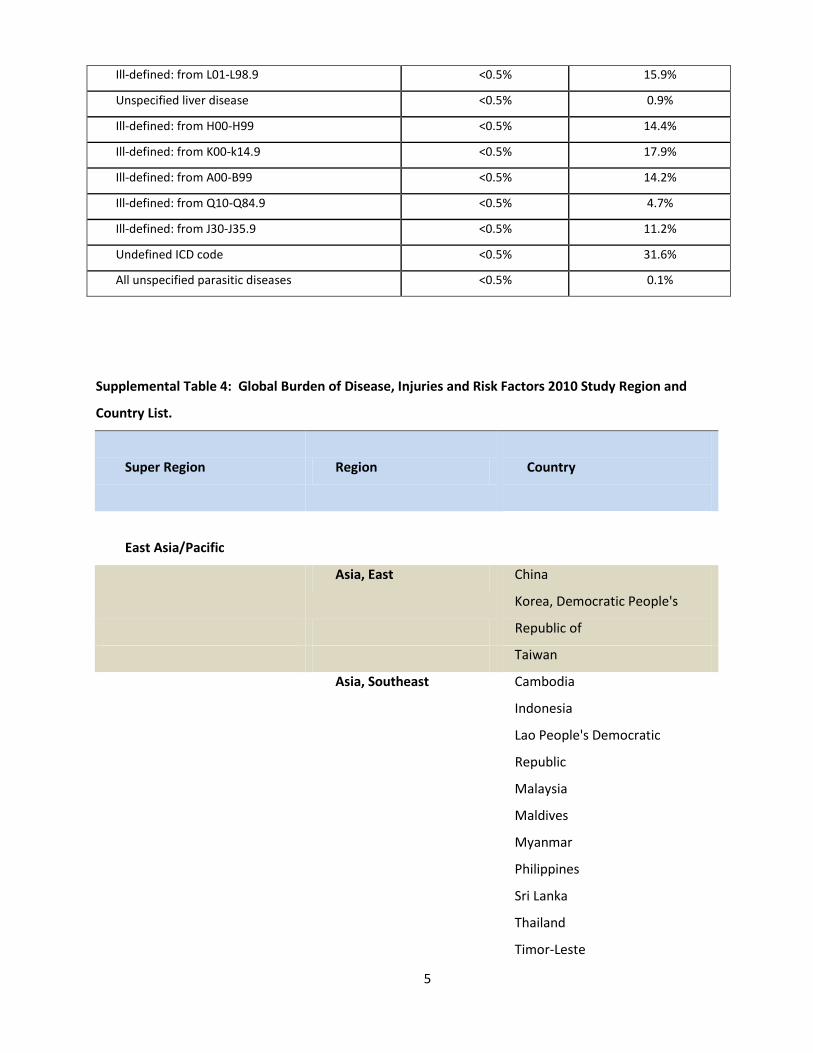
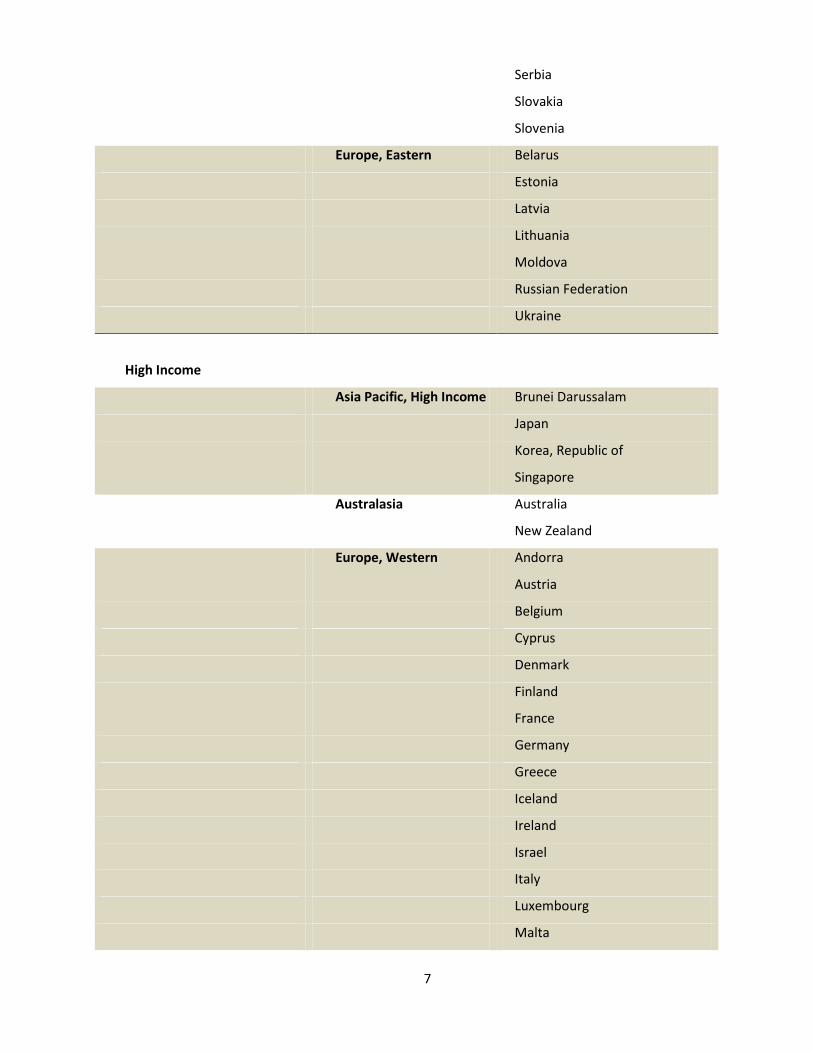
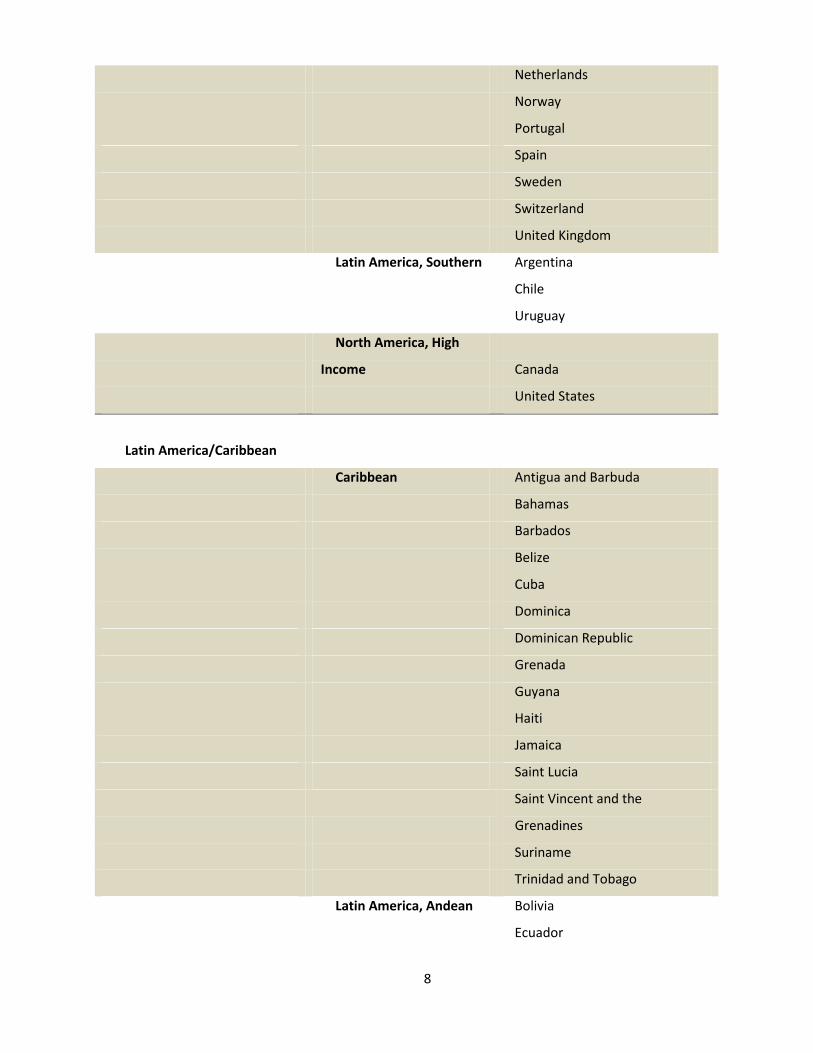
Supplemental Table 4: Global Burden of Disease, Injuries and Risk Factors 2010 Study Region and
Country List.
Super Region Region
Country
East Asia/Pacific
Asia, East China
Korea, Democratic People's
Republic of
Taiwan
Asia, Southeast Cambodia
Indonesia
Lao People's Democratic
Republic
Malaysia
Maldives
Myanmar
Philippines
Sri Lanka
Thailand
Timor-Leste

6
Viet Nam
Oceania Fiji
Kiribati
Marshall Islands
Micronesia, Federated States of
Papua New Guinea
Samoa
Solomon Islands
Tonga
Vanuatu
Eastern Europe/Central Asia
Asia, Central Armenia
Azerbaijan
Georgia
Kazakhstan
Kyrgyzstan
Mongolia
Tajikistan
Turkmenistan
Uzbekistan
Albania
Europe, Central Bosnia and Herzegovina
Bulgaria
Croatia
Czech Republic
Hungary
Macedonia, the Former Yugoslav
Republic of
Montenegro
Poland
Romania
7
Serbia
Slovakia
Slovenia
Europe, Eastern Belarus
Estonia
Latvia
Lithuania
Moldova
Russian Federation
Ukraine
High Income
Asia Pacific, High Income Brunei Darussalam
Japan
Korea, Republic of
Singapore
Australasia Australia
New Zealand
Europe, Western Andorra
Austria
Belgium
Cyprus
Denmark
Finland
France
Germany
Greece
Iceland
Ireland
Israel
Italy
Luxembourg
Malta
8
Netherlands
Norway
Portugal
Spain
Sweden
Switzerland
United Kingdom
Latin America, Southern Argentina
Chile
Uruguay
North America, High
Income Canada
United States
Latin America/Caribbean
Caribbean Antigua and Barbuda
Bahamas
Barbados
Belize
Cuba
Dominica
Dominican Republic
Grenada
Guyana
Haiti
Jamaica
Saint Lucia
Saint Vincent and the
Grenadines
Suriname
Trinidad and Tobago
Latin America, Andean Bolivia
Ecuador

9
Peru
Latin America, Central Colombia
Costa Rica
El Salvador
Guatemala
Honduras
Mexico
Nicaragua
Panama
Venezuela
Latin America, Tropical Brazil
Paraguay
North Africa / Middle East
North Africa / Middle East Algeria
Bahrain
Egypt
Iran, Islamic Republic of
Iraq
Jordan
Kuwait
Lebanon
Libyan Arab Jamahiriya
Morocco
Occupied Palestinian Territory
Oman
Qatar
Saudi Arabia
Syrian Arab Republic
Tunisia
Turkey
United Arab Emirates
Yemen

10
South Asia
Asia, South Afghanistan
Bangladesh
Bhutan
India
Nepal
Pakistan
Sub-Saharan Africa
Sub-Saharan Africa, Central Angola
Central African Republic
Congo
Congo, the Democratic Republic
of the
Equatorial Guinea
Gabon
Sub-Saharan Africa, East Burundi
Comoros
Djibouti
Eritrea
Ethiopia
Kenya
Madagascar
Malawi
Mauritius
Mozambique
Rwanda
Seychelles
Somalia
Sudan
Tanzania, United Republic of
Uganda
Zambia
Sub-Saharan Africa, Southern Botswana
11
Lesotho
Namibia
South Africa
Swaziland
Zimbabwe
Sub-Saharan Africa, West Benin
Burkina Faso
Cameroon
Cape Verde
Chad
Cote d'Ivoire
Gambia
Ghana
Guinea
Guinea-Bissau
Liberia
Mali
Mauritania
Niger
Nigeria
Sao Tome and Principe
Senegal
Sierra Leone
Togo
12
Supplemental Table 5: Annual IHD deaths, males and females, by region, 1980-2010, the Global Burden of Disease 2010 Study
Year 1980 1985 1990 1995 2000 2005 2010
Asia Pacific, High Income
102,725
109,964
113,347
119,074
127,826
142,299
166,853
Europe, Western 970,818
970,646
929,366
885,249
831,709
745,285
745,590
Australasia 41,780
43,058
42,128
40,280
36,551
34,436
37,738
North America, High Income
726,848
739,737
703,057
685,624
655,069
613,831
619,377
Europe, Central 281,482
309,389
331,497
346,890
334,231
340,145
344,139
Latin America, Southern
55,206
55,958
56,753
55,837
60,488
61,990
65,106
Europe, Eastern 741,533
800,386
834,783
1,079,003
1,125,919
1,219,386
1,115,213
Asia, East 359,016
416,822
472,158
604,981
787,789
873,827
992,163
Latin America, Tropical
94,861
106,649
111,338
125,006
134,071
146,546
166,596
Latin America, Central
68,099
75,836
91,521
106,884
121,056
137,658
166,532
Asia, Southeast 140,306
166,005
215,719
262,910
292,138
325,325
383,323
Asia, Central 119,401
125,561
138,157
168,986
167,981
179,638
184,167
Latin America, Andean
11,409
13,599
15,575
16,870
19,425
21,917
24,350
North Africa / Middle East
205,187
226,276
263,978
307,579
336,802
371,325
418,019
Caribbean 29,407
34,962
40,315
46,384
47,019
49,183
54,576
Asia, South 433,832
500,273
704,833
915,207
1,090,272
1,186,987
1,323,551

13
Oceania 1,604
1,980
2,552
3,027
3,377
3,949
4,581
Sub-Saharan Africa, Southern
16,883
18,131
20,094
22,420
22,275
22,721
24,103
Sub-Saharan Africa, East
42,241
47,965
54,706
59,459
60,780
66,701
75,673
Sub-Saharan Africa, Central
15,508
17,923
20,272
22,699
24,269
27,481
33,306
Sub-Saharan Africa, West
37,140
42,668
49,641
56,603
66,515
72,152
84,315
14
Supplemental Table 6: Years of life lost (YLL) due to IHD, males and females, by region, 1980-2010, the Global Burden of Disease 2010 Study
Year 1980 1985 1990 1995 2000 2005 2010
Asia Pacific, High Income
1,878,938
1,917,315
1,798,146
1,737,100
1,762,044
1,812,636
1,920,451
Europe, Western 14,926,890
14,170,528
12,860,688
11,636,179
10,352,545
8,807,634
8,428,017
Australasia 702,407
676,014
615,515
542,832
461,622
405,899
419,557
North America, High Income
11,282,204
10,796,930
9,769,603
9,285,417
8,665,142
8,060,007
7,825,615
Europe, Central 4,825,839
5,233,820
5,597,369
5,724,146
5,306,431
5,089,778
4,835,548
Latin America, Southern
1,045,640
984,106
952,977
918,531
965,586
933,315
945,652
Europe, Eastern 12,195,199
12,864,701
13,363,422
19,080,796
19,691,217
21,395,103
17,671,525
Asia, East 7,514,092
8,485,632
9,449,260
11,905,005
14,940,087
15,493,412
16,795,598
Latin America, Tropical
2,148,570
2,308,880
2,341,808
2,542,240
2,669,026
2,779,536
3,015,732
Latin America, Central
1,440,409
1,546,425
1,762,410
2,025,428
2,188,620
2,366,529
2,827,557
Asia, Southeast 3,194,862
3,774,990
4,818,933
5,720,044
6,153,507
6,704,804
7,765,379
Asia, Central 2,038,453
2,110,414
2,434,441
3,126,687
3,140,725
3,358,046
3,344,003
Latin America, Andean
244,027
283,086
312,129
328,017
386,016
426,970
437,785
North Africa / Middle East
5,254,483
5,639,548
6,521,855
7,338,169
7,613,176
7,995,777
8,822,768
Caribbean 561,395
639,033
694,309
741,590
737,508
759,499
839,991
Asia, South 10,961,439
12,583,981
17,300,420
21,750,749
25,316,742
27,628,587
29,759,902

15
Oceania 45,732
55,796
71,723
85,162
93,788
107,351
122,337
Sub-Saharan Africa, Southern
380,082
402,485
439,982
501,979
525,788
531,476
514,823
Sub-Saharan Africa, East
1,095,487
1,239,823
1,414,599
1,551,138
1,554,534
1,628,544
1,781,311
Sub-Saharan Africa, Central
395,017
450,581
508,418
560,763
597,068
666,283
805,163
Sub-Saharan Africa, West
1,138,204
1,293,544
1,492,723
1,723,077
1,858,139
1,890,019
2,146,457
Totals 83,269,368
87,457,630
94,520,731
108,825,050
114,979,311
118,841,204
121,025,168

16
Supplemental Figure 1a. Males: Crude Ischemic Heart Disease Mortality Rate per 100,000 persons by Super Region and Globally, 1980-2010, the Global Burden of Disease 2010 Study.

17
Supplemental Figure 1b. Females: Crude Ischemic Heart Disease Mortality Rate per 100,000 persons by Super Region and Globally, 1980-2010, the Global Burden of Disease 2010 Study.
Top Related
Copyright © 2022 FDOKUMEN

