







Bahasa
Halaman
Hukum


SURGICAL POTPOURRI Huntsville 2018
Erika Allard-Ihala
PGY2 General Surgery

Conflict of Interest Declaration: Nothing to Disclose
I have no financial or personal relationships to disclose.

Bariatric Surgery Indications Acute and long term complications
Benign anorectal disease Anal fissure Hemorrhoids Perianal abscess Fistula
Choosing Wisely preoperative reminders The Hernia
Objectives

BARIATRIC SURGERY

INDICATIONS: BMI >40 with no comorbidities BMI >35 with comorbidities Age < 65
In 18 months, the cost of the surgery will be equivalent to
the patients health care costs from medical issues. In 1-2 months the patients may no longer need oral
hypoglycemics or antihypertensive medications. Less chronic disease overall.
BARIATRIC SURGERY

CONTRAINDICATIONS:
Age <18y or >65 (controversial)
Untreated depression or psychosis
Uncontrolled eating disorders
Substance use
Severe cardiac disease that prohibits them from an anesthetic
Severe coagulopathy
Inability to comply with nutritional requirements
BARIATRIC SURGERY

Pre-op the patient must have thiamine, vitamin B12, folate, iron, vitamin ADEK, calcium, and copper levels.
Post-op the above nutrient levels should be monitored q3-6m
Blood work

ACUTE COMPLICATIONS
Anastomotic leak 0.8-6%
Pulmonary embolism 0.3-1.2%
Hemorrhage 0.4-4% *
Internal hernia 0-5%
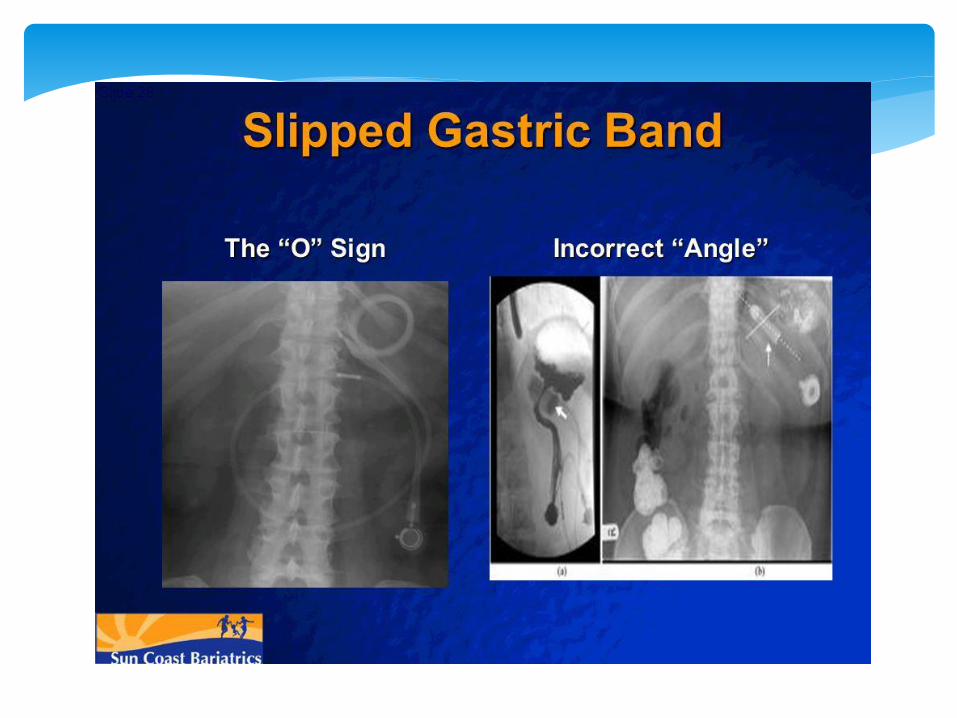
Gastric band slippage 0-20%
Dumping syndrome
Myocardial infarction
Small bowel obstruction
BARIATRIC SURGERY

Abdominal exam is unreliable
May not have vomiting with SBO or internal hernia
NG decompression**
Bariatric patient presenting with tachycardia should be investigated.


ANASTOMOTIC LEAK


CHRONIC COMPLICATIONS
Vitamin and mineral deficiencies
Marginal ulcer 0.6-16%
Internal hernia
Small bowel obstruction (adhesive or stenotic)
Cholelithiasis requiring cholecystectomy
Erosion or slippage of lap band
Dumping syndrome
GERD
BARIATRIC SURGERY

No NSAIDS
No smoking
If patients are on prednisone or ASA they must be on PPI to prevent marginal ulcers
These commonly occur with Roux en Y bypass.
MARGINAL ULCER
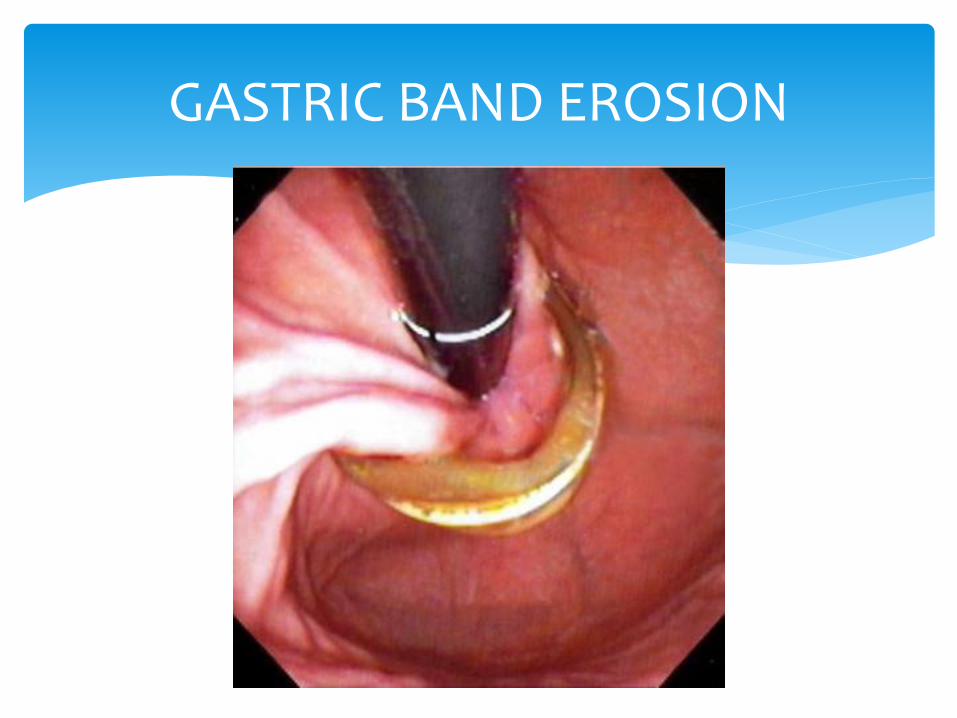
GASTRIC BAND EROSION


Recommended supplements:
Vitamin C 500mg daily
Vitamin B12 500mcg daily
Calcium carbonate 500mg daily
Ferrous fumarate 325mg daily
Vitamin D 2000 units daily
**for sleeve gastrectomy** extra Vitamin B12 and iron
Supplements

BENIGN ANORECTAL DISEASE
Tear in the anoderm that is distal to the dentate line
More common in children and middle aged adults
Acute <6 weeks
Chronic >6 weeks and fails conservative management
Causes: Primary: local trauma from hard stool or prolonged
diarrhea
Secondary: medical/surgical condition, IBD or malignancy
ANAL FISSURES
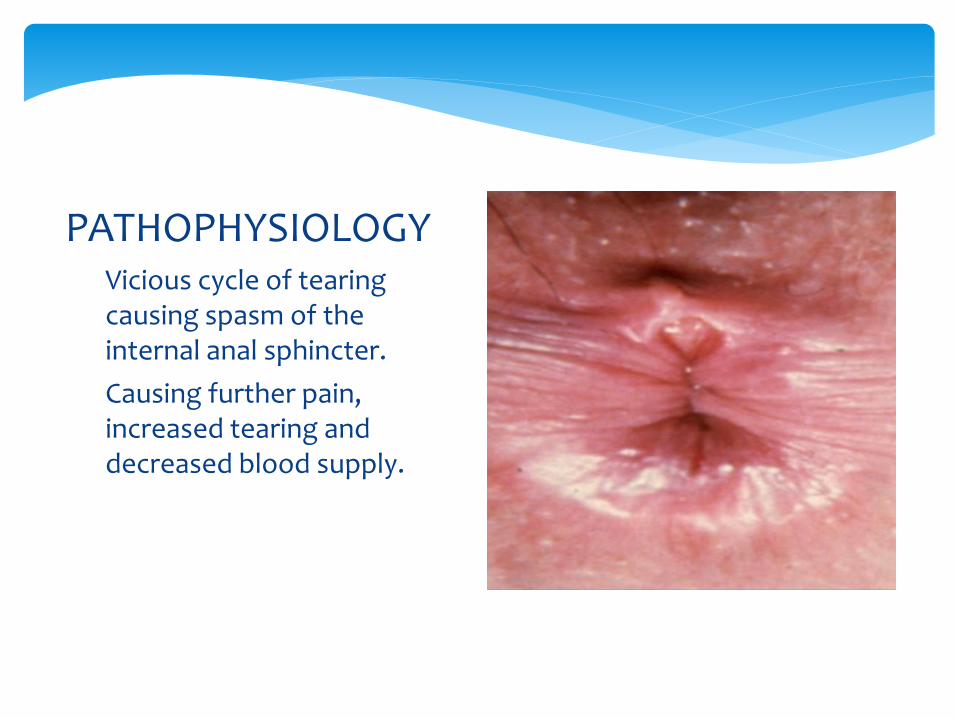
Vicious cycle of tearing causing spasm of the internal anal sphincter.
Causing further pain, increased tearing and decreased blood supply.
PATHOPHYSIOLOGY
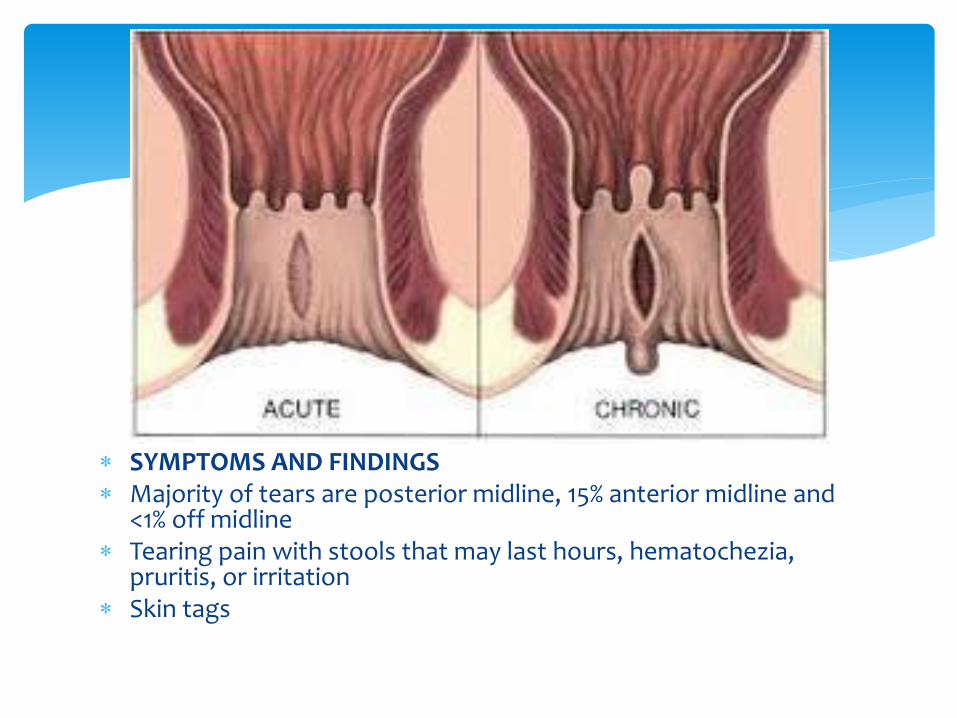
SYMPTOMS AND FINDINGS Majority of tears are posterior midline, 15% anterior midline and
<1% off midline Tearing pain with stools that may last hours, hematochezia,
pruritis, or irritation Skin tags

INITIAL
Stool softeners and high fiber diet
Avoid straining and trauma to the anus
Sitz baths
MEDICATIONS
Nitro ointment 0.2-0.4% QID
Diltiazem 2% gel TID x 8 wks
Nifedipine 0.2% TID x 8 wks
TREATMENT

If there is bleeding, then consider endoscopy.
If the fissure persists > 6 weeks then lateral internal sphincterotomy by dividing a portion of the muscle.
Healing is achieved with >95% of the patients.
TREATMENT

HEMORRHOIDS

Cushions of submucosal tissue containing venules, arterioles and smooth muscle fibers.
Function to be part of the continence mechanism
External: distal to the dentate line
Internal: proximal to the dentate line
HEMORRHOIDS

CLINICAL SYMPTOMS
Hard stools
Bleeding
Anal pruritis
Pain due to thrombosis
Stool leakage



Fiber Metamucil 30g/day
Warm sitz baths and mild soap
Oral and topical analgesicslidocaine gel or cream
Stool softeners
Antispasmodics?
Thrombosed hemorrhoids evacuate clot
CONSERVATIVE TREATMENT




External hemorrhoids do not usually require minimally invasive or surgical treatment BUT if bleeding or thrombosed they may require surgical excision.
Endoscopic assessment
INTERNAL HEMORRHOIDS
PRINCIPLE: Remove or to cause sloughing of excess hemorrhoidal tissue. Healing and scarring fixes the residual tissue to underlying anorectal ring Rubber band ligation, bipolar diathermy, laser photocoagulation,
sclerotherapy, cryosurgery Hemorrhoidectomy usually reserved for grade 4, combined
internal/external or significant prolpase.
ADVANCED TREATMENT


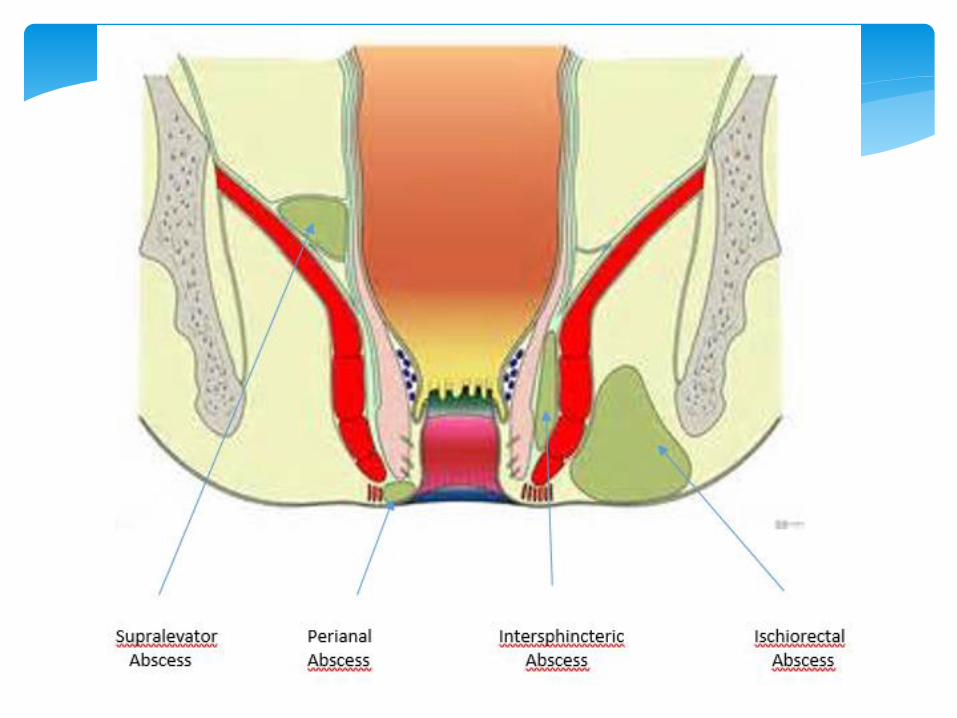
Acute collection of purulent material.
M : F-- 2:1
8-10 anal cryptoglands are arranged circumferentially around the internal sphincter. If the gland becomes obstructed with debris, bacterial growth occurs and abscess forms.
ANORECTAL ABSCESS

CLINICAL SIGNS & SYMPTOMS
Anal pain not associated with BM
Palpable mass in perianal area
Purulent drainage
Area of fluctuance
Patch of erythematous and indurated skin
Fevers and malaise

Often no imaging is needed.
CT or MRI can be useful in supralevator or horseshoe abscess
EUS
Necrotizing infections do occur and the patient present with necrotic skin, bullae or crepitus. They will appear septic and will need early debridement.
DIAGNOSIS

Incise and drain
Sitz baths
When do you give antibiotics?
Valvular heart disease
Immunosuppression
Extensive cellulitis
Necrotizing infection
Diabetes
TREATMENT

Clavulin 10d was found to increase fistula rate.
Ciprofloxacin and Flagyl 10 d decreases fistula rate from 30% to 15%
There has been some research to demonstrating that antibiotics along with drainage reduces the rate of fistula formation.
ANTIBIOTICS

TREATMENT
Outpatient drainage
Local anesthetics: lidocaine with bicarbonate
Cruciate incision
Epithelialized track connecting the abscess to perirectal skin
Drainage of anorectal abscess results in cure for 50% of patients, the rest develop a fistula in ano.
M:F, 2:1
Causes: abscess is most common.
Crohn’s disease, chlamydia, radiation proctitis, foreign bodies and actinomycosis are less common and we should consider them if the fistulas are complex, recurrent or nonhealing.
ANORECTAL FISTULA
Non healing abscess
Chronic purulent drainage
Pustule like lesion in perianal area
Rectal pain
Intermittent drainage
Pruritis
CLINICAL SYMPTOMS

CLINICAL SIGNS
Perianal excoriation
External opening with purulent fluid
DRE for abscess
Do not probe fistula!

5%
23% 70%
2%

Referral to surgeon.
Goals of treatment are to eradicate sepsis without sacrificing continence.
MRI or CT to help further delineate the anatomy.
Majority of cases undergo EUA and seton placement.
TREATMENT
Avoid colorectal cancer screening tests on asymptomatic patients with a life expectancy less than 10 years AND no family or personal history of CRC.

Avoid preoperative CXR for patients with an unremarkable history and physical exam.

THE HERNIA


Groin ultrasounds, who orders these before sending to see the surgeon?
For the surgeons in the room, does this change your management?
THE HERNIA WORKUP

In a recent study from Calgary, they assessed 400 patients (90% male) who underwent assessment for possible groin hernia.
75% had groin ultrasound prior to surgical consultation.
Of the ultrasounds performed 1.7% affected surgical management.
In Alberta, the cost of US for groins that did not affect surgical management was $1.6 million.
THE HERNIA WORKUP

In 2011, Denmark assessed 10 000 inguinal hernias.
They found clinical examination to be the best diagnostic tool.
In 2018, the five continental hernia societies, have agreed that ultrasound is rarely needed.
THE HERNIA WORKUP
When the diagnosis is not apparent or there may be an occult hernia, ultrasound is recommended.
THE HERNIA WORKUP


THANK YOU!
QUESTIONS?

Up to date
Bariatric Complications and Emergencies
Sabistons Surgical Textbook
Schwartz’s Principles of Surgery
International guidelines for groin hernia management Retrieved from https://link.springer.com/article/10.1007/s10029-017-1668-x
The role of groin ultrasound imaging in the management of
inguinal hernias. R. Tong, E. Debru, R. Gill, P. Mitchell, N. Church, A. Reso. From the University of Calgary, Calgary, Alta.
REFERENCES:
Copyright © 2022 FDOKUMEN

