







Bahasa
Halaman
Hukum


Supporting medication-related decision making with information model-based digital
documents
Thesis submitted in fulfilment of the requirements for the award of the degree of Doctor of Philosophy
Submitted: March 2007
Jean-Pierre Calabretto
B.Pharm. (South Australian Institute of Technology)M.Comput.St. (Deakin University)
School of Computer and Information Science,Division of Information Technology, Engineering and the Environment,
University of South Australia

Table of contents
Table of contents i
List of Figures ix
List of Tables xi
List of Publications xiii
Glossary xiv
Abstract xvi
Declaration xviii
Acknowledgements xix
Chapter 1 The challenges of the health care system: an introduction 1
1.1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1.2. The health of the health care system . . . . . . . . . . . . . . . . . . . . . . . . . . 2
1.3. Medication and chronic illness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51.3.1. Adherence to medication therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51.3.2. Medications and patient safety . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
1.4. The promise of information technology in Health . . . . . . . . . . . . . . . . 81.4.1. Electronic health records . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101.4.2. Decision support systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Page i
1.4.3. Mobile health applications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
1.5. The problems of information technology in Health . . . . . . . . . . . . . . 141.5.1. Information and context of use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141.5.2. knowledge use by health professionals. . . . . . . . . . . . . . . . . . . . . . . . . . . . 151.5.3. Electronic health records . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 151.5.4. Decision support, alerts and reminders . . . . . . . . . . . . . . . . . . . . . . . . . . . . 161.5.5. Mobile computing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171.5.6. privacy & security . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181.5.7. The bottom line with IT in Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
1.6. Medication management and pharmacists. . . . . . . . . . . . . . . . . . . . . 20
1.7. The research problem. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
1.8. Scope of the research. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
1.9. Significance and contributions of the research . . . . . . . . . . . . . . . . . 27
1.10. Outline of the thesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Chapter 2 Addressing the problem of medication-related decision support for pharmacists: investigating the literature 31
2.1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
2.2. Identifying appropriate medication management support for pharmacists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
2.2.1. Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 322.2.2. Finding evidence in the literature. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 322.2.3. Finding other evidence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 362.2.4. Was any evidence missed?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
2.3. Looking for a technology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 412.3.1. Why a document? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 432.3.2. What is a document?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
2.3.2.1. The historical perspective . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .442.3.2.2. What is a digital document? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .442.3.2.3. Managing documents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .452.3.2.4. Genres . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .46
2.3.3. The expression of information in documents. . . . . . . . . . . . . . . . . . . . . . . . 472.3.4. Documents in communication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 502.3.5. Workflow in Health. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
2.3.5.1. The flow of work in Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .522.3.6. Collaboration, Cooperation and Coordination . . . . . . . . . . . . . . . . . . . . . . . 542.3.7. Other advantages of documents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
2.3.7.1. Self awareness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .552.3.7.2. Social roles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .552.3.7.3. The paper-record as a work tool. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .55
2.3.8. Wrapping up the document discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
2.4. Chapter summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
Chapter 3 Methodology 60
Page ii
3.1. Introduction and Research Framework. . . . . . . . . . . . . . . . . . . . . . . . 60
3.2. Research dimensions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 613.2.1. How the research was done . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 623.2.2. The purpose of the project. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 623.2.3. Ensuring relevance and rigour. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 633.2.4. Contribution to knowledge and theory . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643.2.5. Contribution to practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
3.3. Overview of IS research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 653.3.1. Philosophical framework . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 653.3.2. The direction of theory. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 653.3.3. The research paradigm . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 663.3.4. Prevailing paradigms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
3.3.4.1. Positivism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .673.3.4.2. Interpretivism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .683.3.4.3. Critical theory . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .69
3.3.5. Methods of analysis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 693.3.6. Applicability of IS research approaches to the health environment. . . . . . . 71
3.4. Methods in IS research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 713.4.1. A taxonomy of research methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 713.4.2. Comparison of candidate research methods. . . . . . . . . . . . . . . . . . . . . . . . 73
3.4.2.1. Action Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .733.4.2.2. Ethnography . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .743.4.2.3. Grounded theory. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .743.4.2.4. Case study research. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .753.4.2.5. Design Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .75
3.4.3. Selection and justification of the research method . . . . . . . . . . . . . . . . . . . 77
3.5. Research Plan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 783.5.1. The hospital context (Part 1) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 793.5.2. The community context: prototype bench testing (Part 2A). . . . . . . . . . . . . 803.5.3. Medication review field study (Part 2B) . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
3.6. Data collection techniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 833.6.1. Quantitative and qualitative data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 833.6.2. Validity through triangulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 833.6.3. Data collection techniques. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84
3.6.3.1. Literature review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .843.6.3.2. Use of questionnaires . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .843.6.3.3. Use of interviews . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .843.6.3.4. Work practice observation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .853.6.3.5. Use of focus groups . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .853.6.3.6. Documents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .863.6.3.7. Prototyping . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .86
3.7. Data analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 873.7.1. Modelling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 873.7.2. Prototyping . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 883.7.3. Descriptive statistics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 883.7.4. Content analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 883.7.5. Evaluation of research goals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89
3.8. Technology and Standards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 903.8.1. XForms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 903.8.2. The impact of standards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91
3.8.2.1. CDA/HL7. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .913.8.3. User interface design. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92
3.9. Limitations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
Page iii

3.10. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
Chapter 4 Design research in complex environments 95
4.1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
4.2. Design – what’s in a name? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96
4.3. Dealing with complexity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 99
4.4. Design research in education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100
4.5. Design research in information systems . . . . . . . . . . . . . . . . . . . . . 105
4.6. Designing a better health technology intervention . . . . . . . . . . . . . 108
4.7. Design research foundations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1114.7.1. The design research cycle. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1144.7.2. Design research outputs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 116
4.8. Aligning the research plan and design research process . . . . . . . 118
4.9. Chapter summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 121
Chapter 5 Formulating the information model: the hospital scenario 122
5.1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 122
5.2. The Data Gathering Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1235.2.1. Questionnaires and interviews . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1235.2.2. Work practice observations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 125
5.2.2.1. Clinical pharmacy practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1255.2.2.2. The medication review process in the ward . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .125
5.2.3. Documents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 127
5.3. Analysis and discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1285.3.1. Missing information and surrogate value. . . . . . . . . . . . . . . . . . . . . . . . . . 130
5.3.1.1. Missing Information relevant to Medical Officers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1315.3.1.2. Missing Information relevant to Pharmacists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1315.3.1.3. Pharmacist techniques for obtaining missing information. . . . . . . . . . . . . . . . . . . . . . . . . .1325.3.1.4. Medical Officers as a source of information for pharmacists . . . . . . . . . . . . . . . . . . . . . . .1335.3.1.5. Alternative information sources for MOs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1345.3.1.6. Work practice confirmation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1355.3.1.7. The implications of missing information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .136
5.3.2. Information granularity. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1395.3.2.1. Information required by medical officers to initiate a medication order. . . . . . . . . . . . . . . .1395.3.2.2. Information used by pharmacists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1395.3.2.3. Observed information use by pharmacists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .140
5.3.3. Conversation and communication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1425.3.3.1. Pharmacist communication with Medical Officers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1425.3.3.2. Communication with nursing professionals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1425.3.3.3. Other pharmacists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1435.3.3.4. Other health professionals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1435.3.3.5. Pharmacist conversations observed during work practice . . . . . . . . . . . . . . . . . . . . . . . . .143
5.3.4. Time constraints and summary information. . . . . . . . . . . . . . . . . . . . . . . . 1455.3.5. Decision support tools . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 146
5.3.5.1. Decision support tools used by pharmacists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .146
Page iv

5.3.5.2. Pharmacists' understanding of decision support . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1475.3.5.3. Decision support and Medical Officers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1475.3.5.4. Fitting decision support into work practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1475.3.5.5. Is decision support a realistic expectation? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1495.3.5.6. An ideal decision support tool?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1495.3.5.7. The acceptability of alerts and reminders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1515.3.5.8. The acceptance of blocking medication orders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .152
5.3.6. Complementary and Over-the-Counter medication. . . . . . . . . . . . . . . . . . 1535.3.7. Document analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 154
5.4. Formulation of the information model . . . . . . . . . . . . . . . . . . . . . . . 156
5.5. The digital document . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1595.5.1. Some preliminary activities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1595.5.2. Developing the digital document . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 160
5.5.2.1. Patient details page . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1615.5.2.2. Treatment information page . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1645.5.2.3. Medication information page. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1655.5.2.4. Investigations page. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1685.5.2.5. Health Professional contacts page . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .168
5.5.3. Experiences with XForms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 169
5.6. Chapter summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 170
Chapter 6 Modelling for the community context: benchtop testing 172
6.1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172
6.2. The data gathering process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1736.2.1. Questionnaires and interviews . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1736.2.2. Prototype testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 174
6.2.2.1. Accredited pharmacists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1746.2.2.2. The HMR process. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .175
6.2.3. The focus group. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1766.2.4. Document analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 176
6.3. Analysis and discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1766.3.1. Missing information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 178
6.3.1.1. Missing information for HMR pharmacists in GPs’ referrals . . . . . . . . . . . . . . . . . . . . . . . .1786.3.1.2. Pharmacists coping with missing information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1806.3.1.3. The implications of missing information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .181
6.3.2. Information granularity. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1826.3.3. Conversation and communication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1836.3.4. Time constraints and summary information. . . . . . . . . . . . . . . . . . . . . . . . 1836.3.5. Decision support tools . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 184
6.3.5.1. Decision support tools used by pharmacists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1846.3.5.2. Pharmacists’ understanding of decision support . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1846.3.5.3. Fitting decision support into work practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1856.3.5.4. Is decision support a realistic expectation? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1856.3.5.5. An ideal decision support tool. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .185
6.3.6. Systems for experts rather than expert systems . . . . . . . . . . . . . . . . . . . . 1866.3.7. A technology-poor practice paradigm. . . . . . . . . . . . . . . . . . . . . . . . . . . . 1876.3.8. The ‘viewpoints’ of professional practice tools . . . . . . . . . . . . . . . . . . . . . 1886.3.9. Pharmacists’ perceptions of GPs in the HMR process . . . . . . . . . . . . . . . 1896.3.10. Prototype testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 190
6.3.10.1. User reactions to the prototype. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1916.3.10.2. User suggestions for the prototype. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1916.3.10.3. User innovations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1926.3.10.4. Functional prototype issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .193
6.3.11. Document analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1946.3.11.1. Referral documents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1946.3.11.2. Reports . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .195
Page v

6.3.12. Opportunities for the digital document to improve HMR practice . . . . . . 1956.3.12.1. The medication management review process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1956.3.12.2. Opportunities to improve the patient outcomes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .196
6.4. The community aligned information model. . . . . . . . . . . . . . . . . . . 196
6.5. The digital document and the server service . . . . . . . . . . . . . . . . . . 1996.5.1. The VB Browser . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1996.5.2. The digital document . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 201
6.5.2.1. Patient details page . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2046.5.2.2. Treatment details page . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2066.5.2.3. Medication page . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2076.5.2.4. Investigations page. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2106.5.2.5. Health Professional Contacts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .210
6.5.3. The server service . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2116.5.3.1. Security. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2136.5.3.2. Server pages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2146.5.3.3. Summary of the technical changes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .220
6.6. Chapter summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 221
Chapter 7 Evaluating the digital document: field studies 224
7.1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 224
7.2. The data gathering process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2257.2.1. Enrolling the participants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2257.2.2. Data sources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 227
7.2.2.1. Field use of the digital document . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2277.2.2.2. HOMR testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2287.2.2.3. General Practitioner discussions and interviews . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2287.2.2.4. Patient-related data used for the trial . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2287.2.2.5. Accredited pharmacists’ meetings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2297.2.2.6. Other conversations and meetings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2297.2.2.7. Logs of telephone calls and email communication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2297.2.2.8. HMR pharmacists’ focus group. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .230
7.2.3. Issues encountered during data gathering . . . . . . . . . . . . . . . . . . . . . . . . 2307.2.3.1. Field studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2307.2.3.2. HOMR testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2317.2.3.3. Meetings with GPs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2317.2.3.4. Patient-related data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2337.2.3.5. Email. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2357.2.3.6. The focus group . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .235
7.3. Analysis and discussion of findings . . . . . . . . . . . . . . . . . . . . . . . . . 2357.3.1. Missing information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2367.3.2. Information granularity and the language of health professionals . . . . . . . 2437.3.3. Conversation and communication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2457.3.4. Time constraints and summary information. . . . . . . . . . . . . . . . . . . . . . . . 2467.3.5. The use of alerts and reminders. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2477.3.6. Systems for experts rather than expert systems . . . . . . . . . . . . . . . . . . . . 2487.3.7. A technology-poor practice paradigm . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2497.3.8. The ‘viewpoints’ of professional practice tools . . . . . . . . . . . . . . . . . . . . . 2507.3.9. Pharmacists’ perceptions of GPs in the HMR process . . . . . . . . . . . . . . . 2537.3.10. The Practice nurse . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2537.3.11. Complementary medicines and over-the-counter medication . . . . . . . . . 2547.3.12. Field study experiences. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 255
7.3.12.1. HMRs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2557.3.12.2. HOMRs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2567.3.12.3. RMMRs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2577.3.12.4. The technically aware GP. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .257
7.3.13. Evaluation of the intervention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2597.3.13.1. Evaluation of the technology aspects of system use . . . . . . . . . . . . . . . . . . . . . . . . . . . .260
Page vi

7.3.13.2. Evaluation of the human aspects of system use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .262
7.4. The information model . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 269
7.5. The digital document and the server service . . . . . . . . . . . . . . . . . . 2717.5.1. The VB Browser . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2717.5.2. The digital document . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2717.5.3. The XSL report . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2737.5.4. The server service . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 277
7.6. Chapter Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 278
Chapter 8 Summary and conclusions 280
8.1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 280
8.2. Project summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 280
8.3. Themes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2828.3.1. Missing information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2838.3.2. Information granularity. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2848.3.3. Conversation and communication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2858.3.4. Time constraints and summary information. . . . . . . . . . . . . . . . . . . . . . . . 2868.3.5. Alerts and reminders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2878.3.6. Decision support tools . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2888.3.7. Systems for experts rather than expert systems . . . . . . . . . . . . . . . . . . . . 2908.3.8. A technology-poor practice paradigm . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2918.3.9. The ‘viewpoints’ of professional practice tools . . . . . . . . . . . . . . . . . . . . . 2918.3.10. Complementary and Over-the-Counter medication. . . . . . . . . . . . . . . . . 2938.3.11. Pharmacists’ perceptions of GPs in the HMR process . . . . . . . . . . . . . . 2948.3.12. The role of the Practice Nurse. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 294
8.4. The evolution of the information model . . . . . . . . . . . . . . . . . . . . . . 297
8.5. research questions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 299
8.6. Research contributions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3048.6.1. Contributions to theory . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3048.6.2. Contributions to practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 305
8.7. Future work . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3068.7.1. More extensive field trials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3068.7.2. A ‘working document’ for medication management in a hospital. . . . . . . . 3068.7.3. HMR referral generation by Practice Nurses. . . . . . . . . . . . . . . . . . . . . . . 3068.7.4. A digital document approach in an Aged Care Facility . . . . . . . . . . . . . . . 3068.7.5. A digital document approach for information exchange for
discharged hospital cardiac patients. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3078.7.6. A portable medication record. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3078.7.7. A digital document approach for patient groups with
extensive medication use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3078.7.8. A shared record with health consumers . . . . . . . . . . . . . . . . . . . . . . . . . . 3088.7.9. A shared record with other health professionals . . . . . . . . . . . . . . . . . . . . 3088.7.10. GP information behaviour with GP desktop systems . . . . . . . . . . . . . . . 308
References 309
Page vii
Appendices 328
Page viii

List of Figures
Chapter 1 The challenges of the health care system: an introduction 1
1-1 The medication management pathway (Stowasser, Allinson & O'Leary 2004) . . . . . . . . . 211-2 Patient care skills for pharmacists adapted from Gowan & Roller (2004). . . . . . . . . . . . . . 261-3 Relationship of chapters and appendices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Chapter 2 Addressing the problem of medication-related decision support for pharmacists: investigating the literature 31
2-1 Process and results for pharmacy decision support information sources. . . . . . . . . . . . . . 38
Chapter 3 Methodology 60
3-1 Research questions in relation to research phases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 823-2 The HOT fit model (Yusof, Paul & Stergioulas 2006) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
Chapter 4 Design research in complex environments 95
4-1 The Design Research cycle (Vaishnavi & Kuechler 2005) . . . . . . . . . . . . . . . . . . . . . . . 1134-2 Design Research outputs (Purao 2002) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1174-3 Project iterative research cycle and outputs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 119
Chapter 5 Formulating the information model: the hospital scenario 122
5-1 Hospital medication review process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1275-2 The information model from document analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1555-3 Missing information model . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1575-4 The hospital information model. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1585-5 Visual Basic document viewer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1605-6 Patient details page . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1625-7 Edit patient details form . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1635-8 New allergy form. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1645-9 Treatment information page . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1645-10 Medication page . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1655-11 Edit medication form . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1665-12 New medication form . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1665-13 Medication history . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1675-14 Edit social issues form . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1675-15 Investigations page. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1685-16 Health professional contacts page . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 169
Chapter 6 Modelling for the community context: benchtop testing 172
6-1 Home medication review process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1756-2 The community-aligned information model . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1986-3 Visual Basic document viewer (version 2) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1996-4 VB Medication Management Document Printer form . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2006-5 VB HTML output of the digital document . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2016-6 Referral details page. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2026-7 Referral details page – after the review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203
Page ix

6-8 New reason for referral form . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2036-9 Extended reasons for referral form . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2046-10 Patient details page . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2056-11 New reason for referral form – falls. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2066-12 Medication page . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2076-13 Edit immunisations form . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2086-14 Medication history . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2096-15 Edit medications form – after review. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2106-16 Pathways for the HMR digital document. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2126-17 Server service for medication management document. . . . . . . . . . . . . . . . . . . . . . . . . . 2136-18 Server options after log-in. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2146-19 Document viewer with a ‘blank page’ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2156-20 Open patient document. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2166-21 The patient document displayed on the server . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2176-22 Print patient document from the server. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2186-23 HMR report output in new browser window . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2196-24 Save patient file locally . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220
Chapter 7 Evaluating the digital document: field studies 224
7-1 Modified Hot Fit model . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2607-2 The final information model. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2707-3 Digital document referral page prior to review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2727-4 Digital document referral page after review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2737-5 HTML output of document before the HMR review. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2747-6 HTML output of document after review. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2757-7 HTML report output – calculated values . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 276
Chapter 8 Summary and conclusions 280
8-1 Project themes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2828-2 The evolution of the information model. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2988-3 Research questions in relation to research phases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 299
Page x

List of Tables
Chapter 1 The challenges of the health care system: an introduction 1
1-1 Health system challenges. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31-2 Unintended consequences of CPOE (Campbell et al. 2006) . . . . . . . . . . . . . . . . . . . . . . . 16
Chapter 2 Addressing the problem of medication-related decision support for pharmacists: investigating the literature 31
2-1 NEDST criteria for selection of publications of EDSS (National Electronic Decision Support Taskforce 2002) . . . . . . . . . . . . . . . . . . . . . . . . . . 33
2-2 Categorisation of types of EDSS by the NEDST (National Electronic Decision Support Taskforce 2002) . . . . . . . . . . . . . . . . . . . . . . . . . . 33
2-3 Pharmacy-related electronic decision support systems revealed in literature . . . . . . . . . . 352-4 Desirable features for the digital document . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
Chapter 3 Methodology 60
3-1 Research approaches (Neuman 2003, p. 31). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 623-2 Common methods in IS research (Choudrie & Dwivedi 2005) . . . . . . . . . . . . . . . . . . . . . . 723-3 Qualitative measures for the HMR field test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
Chapter 4 Design research in complex environments 95
4-1 Comparisons of natural science and design science enquiry (Lee 2000). . . . . . . . . . . . . . 974-2 Dimensions of DR in education, IS and health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1124-3 Design research criteria (Rossi & Sein 2003) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118
Chapter 5 Formulating the information model: the hospital scenario 122
5-1 Technical appendices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1235-2 The distribution of hospital participants. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1245-3 Data-related appendices. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1285-4 Questions posed to pharmacists and MOs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1295-5 Research themes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1305-6 Missing information experienced by pharmacists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1355-7 Missing information – interviews and observed . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1365-8 Information sources used by pharmacists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1415-9 Conversations between pharmacists and other professionals . . . . . . . . . . . . . . . . . . . . . 144
Chapter 6 Modelling for the community context: benchtop testing 172
6-1 Technical appendices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1736-2 Data-related appendices. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1776-3 Questions posed to HMR pharmacists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1776-4 Research themes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1786-5 Risk factors for adverse outcomes for patients taking medications . . . . . . . . . . . . . . . . . 1796-6 Workflow and technology use in the HMR process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1876-7 Pharmacists’ suggestions for changes to the digital document prototype . . . . . . . . . . . . 1926-8 User innovations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1926-9 Information elements added to the model for the community context . . . . . . . . . . . . . . . 197
Page xi

Chapter 7 Evaluating the digital document: field studies 224
7-1 Technical appendices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2257-2 Summary of data sources from the field studies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2277-3 The digital document paths in the field studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2317-4 Summary of interaction with GPs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2337-5 Patient data sources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2347-6 Research themes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2367-7 Comparison of missing information in referral documents – referral information . . . . . . . 2377-8 Comparison of missing information in referral documents – personal information . . . . . . 2397-9 Comparison of missing information in referral documents – treatment information . . . . . 2407-10 Comparison of missing information in referral documents – medication information . . . 2417-11 Comparison of missing information in referral documents – laboratory information . . . . 2427-12 GP desktop reports used to provide HMR referral information . . . . . . . . . . . . . . . . . . . . 2517-13 Net benefit comments from GP4 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2597-14 Technology aspects of the intervention – 1a. System quality . . . . . . . . . . . . . . . . . . . . . 2617-15 Technology aspects of the intervention – 1b. Information quality . . . . . . . . . . . . . . . . . . 2627-16 Human aspects of the intervention – 2a System use . . . . . . . . . . . . . . . . . . . . . . . . . . . 2637-17 Human aspects of the intervention – 2b. User satisfaction. . . . . . . . . . . . . . . . . . . . . . . 2647-18 Organisational aspects of the intervention – Structure . . . . . . . . . . . . . . . . . . . . . . . . . . 2657-19 Organisational aspects of the intervention – Environment . . . . . . . . . . . . . . . . . . . . . . . 2667-20 Net benefits of the intervention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 267
Chapter 8 Summary and conclusions 280
8-1 The implications of project themes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 295
Page xii

Page xiii
List of Publications
The following publications emerged from this research.
Submitted to the European Journal of Information Systems – Special Issue on: HIS Research, Revelations and Visions – after acceptance of peer reviewed abstract.Building systems for experts: designing digital documents to support medication management, Jean-Pierre Calabretto, Paula MC Swatman, School of Computer and Information Science, University of South Australia, Adelaide, SA, Australia
In Press
Towards a working document to support medication management, J-P Calabretto, PMC Swatman, British Computer Society Health Informatics Forum (HC2007), 19-21 March 2007, Harrogate, England
Peer Reviewed
Supporting a Medication Management Model with Digital Documents, Jean-Pierre Calabretto, Paula M C Swatman, Jim Warren, Proceedings of the Australasian Confer-ence on Information Sciences (ACIS 2006), December 2006, Adelaide, South Australia
XForms for the Support of Medication Management, Jean-Pierre Calabretto, Debdeep Banerjee, Jim Warren, Linda Bird, Poster Abstract (peer-reviewed), Proceedings of the American Medical Informatics Association Conference 2005, Austin, Texas
Pharmacy decision support – where is it? – a systematic literature review, Jean-Pierre Calabretto, Jim Warren, Linda Bird, International Journal of Pharmacy Practice, Vol. 13, No. 3, pp 1-7, September 2005
Missing Information for Decision Making in Medication Management, Jean-Pierre Calabretto, Jim Warren, Linda Bird, Proceedings of the Thirteenth National Health Informatics Conference, Melbourne, Australia, 31st July – 2nd August, 2005(cited by Bindoff et al. #)
Citations# Bindoff, IK, Tenni, PC, Peterson, GM, Kang, BH & Jackson, SL 2007, 'Development of an intelligent decision support system for medication review', Journal of Clinical Pharmacy and Therapeutics, vol. 32, no. 1, pp. 81-88.

Glossary
AACP . . . . . . . . . . . . . Australian Association of Accredited PharmacistsACF. . . . . . . . . . . . . . . Aged Care FacilityADE. . . . . . . . . . . . . . . Adverse Drug EventADR . . . . . . . . . . . . . . Adverse Drug ReactionADRAC . . . . . . . . . . . . Australian Drug Reactions Advisory Committee AE . . . . . . . . . . . . . . . . Adverse EventAMH . . . . . . . . . . . . . . Australian Medicines HandbookAR . . . . . . . . . . . . . . . . Action ResearchASP. . . . . . . . . . . . . . . Active Server PagesBMI . . . . . . . . . . . . . . . Body Mass IndexBP . . . . . . . . . . . . . . . . Blood pressureCCl . . . . . . . . . . . . . . . Creatinine ClearanceCDA . . . . . . . . . . . . . . Clinical Document ArchitectureCDSS . . . . . . . . . . . . . Clinical Decision Support SystemCIG . . . . . . . . . . . . . . . Computer Interpretable GuidelineCM . . . . . . . . . . . . . . . Complementary MedicineCoP . . . . . . . . . . . . . . . Communities of PracticeCPOE . . . . . . . . . . . . . Computer Physician Order EntryCS . . . . . . . . . . . . . . . . Computer ScienceCSCW . . . . . . . . . . . . . Computer-Supported Collaborative WorkCSS. . . . . . . . . . . . . . . Cascading Style SheetsDMMR. . . . . . . . . . . . . Domiciliary Medication Management ReviewDR. . . . . . . . . . . . . . . . Design ResearchDSS. . . . . . . . . . . . . . . Decision Support SystemDUE . . . . . . . . . . . . . . Drug Utilisation EvaluationE/DMS. . . . . . . . . . . . . Electronic/Document Management SystemEDM . . . . . . . . . . . . . . Electronic Document ManagementEDSS . . . . . . . . . . . . . Electronic Decision Support SystemEHR . . . . . . . . . . . . . . Electronic Health RecordEKP. . . . . . . . . . . . . . . Emergent Knowledge-intensive ProcessEP . . . . . . . . . . . . . . . . Electronic PrescribingGFR . . . . . . . . . . . . . . Glomerular Filtration RateGP. . . . . . . . . . . . . . . . General PractitionerHI . . . . . . . . . . . . . . . . Health Informatics HIC . . . . . . . . . . . . . . . Health Insurance CommissionHIS . . . . . . . . . . . . . . . Health Information SystemHL7 . . . . . . . . . . . . . . . Health Level 7HMR . . . . . . . . . . . . . . Home Medication Review HOMR . . . . . . . . . . . . . Hospital Outreach Medication Review HOT Fit . . . . . . . . . . . . Human-Organisation-Technology FitICU . . . . . . . . . . . . . . . Intensive Care UnitIE. . . . . . . . . . . . . . . . . Internet ExplorerIS. . . . . . . . . . . . . . . . . Information SystemsIT. . . . . . . . . . . . . . . . . Information TechnologyMD . . . . . . . . . . . . . . . Medical DirectorMIMS. . . . . . . . . . . . . . Monthly Index to Medical Specialities (monthly/annual)MM . . . . . . . . . . . . . . . Medication Management MO . . . . . . . . . . . . . . . Medical OfficerNEDST . . . . . . . . . . . . National Electronic Decision Support Task Force
Page xiv

OTC . . . . . . . . . . . . . . Over-the-CounterPBS . . . . . . . . . . . . . . Pharmaceutical Benefits SchemePC . . . . . . . . . . . . . . . . Personal ComputerPDA. . . . . . . . . . . . . . . Personal Digital AssistantQoL . . . . . . . . . . . . . . . Quality of LifeQUM . . . . . . . . . . . . . . Quality Use of MedicinesRCF. . . . . . . . . . . . . . . Residential Care FacilitiesRDNS . . . . . . . . . . . . . Royal District Nursing ServiceRMMR. . . . . . . . . . . . . Residential Medication Management ReviewSHPA . . . . . . . . . . . . . Society of Hospital Pharmacists of AustraliaTAIS . . . . . . . . . . . . . . Therapeutic Advice and Information ServiceUK . . . . . . . . . . . . . . . . United KingdomUML . . . . . . . . . . . . . . Unified Modelling LanguageUniSA . . . . . . . . . . . . . University of South AustraliaUS . . . . . . . . . . . . . . . . United StatesVB . . . . . . . . . . . . . . . . Visual Basic
Page xv

Abstract
Medication is vital in treating chronic disease. Increasing use of medication, however, can lead to (potentially preventable) medication-related adverse events. Medication management offers a means of addressing such adverse events and pharmacists have an important role in this solution, especially in terms of reviews of patient medication.
Improved availability and sharing of patient-related information are critical factors in medication management, so that providing access to this information becomes a major factor in effective medication reviews. Although clinical decision support tools can significantly assist doctors in accessing relevant point-of-care information for greater patient safety, it has proven difficult to ensure the availability and appropriate structure of patient-related information for such support tools. These information access and input problems are further exacerbated by a lack of existing research into suitable decision support solutions for pharmacists.
This research project explored the suitability of an ‘essential’ information model to support an electronic document solution to support clinical documentation and allow effective communication between pharmacists and doctors for medication reviews. The project investigated whether this approach could improve safety, quality and efficiency in the medication review process; as well as more generally identifying factors influencing development and uptake of document-based support tools in the Health sector.
The project used a qualitative Design Research approach and iterated through three scenarios:
• The first, information-rich, hospital scenario developed an information model of essential medication management components, which underpinned the development of a digital document prototype – implemented using XForms technology
• in the second scenario, accredited pharmacists evaluated the digital document to enable refinement of the information model and its associated digital document for the broader ‘community’ context
• The third scenario involved field studies which evaluated the digital document (and thus the underlying information model) within the community, assessing its contribution to quality, safety and efficiency throughout the medication review process.
The investigation identified a number of themes which guided design and development of the prototype; and which appeared likely to have a broader impact on successful uptake of decision support tools.
Missing information proved to be a constant and serious problem for health professionals – although, in this project, it also became a way of determining the value of an information element and thus its inclusion in the information model. Conversation played a significant role in the hospital environment to help supply pharmacists’ information needs. Information granularity, the ‘language’ of health professionals; and their time constraints were major factors influencing design. Health professionals’ extensive use of their personal knowledge also suggested decision support tools in this sector should be ‘systems for experts’ rather than expert systems, i.e. the decision support tool and its user’s personal knowledge should complement one another.
The results of this proof-of-concept project suggest practice improvement in medication management is possible, with perceived improvements in safety, quality and efficiency of the
Page xvi

medication management process. These benefits, however, now need to be affirmed in larger field studies.
The contributions of this research are two-fold: firstly, it is possible to develop a model of essential medication-related information which is succinct, relevant and can be understood and shared by health professionals – in conjunction with the individual’s personal knowledge. Secondly, a document metaphor is a natural fit with health professionals for representing and communicating information. Expressing this metaphor as digital document overcomes the main problems of paper-based documents – sharing and communication; and the dynamic properties of digital documents assist in decision-making.
Page xvii

Page xviii
Declaration
I declare that:
this thesis presents work carried out by myself and does not incorporate without acknowledgment any material previously submitted for a degree or diploma in any university;
to the best of my knowledge it does not contain any materials previously published or written by another person except where due reference is made in the text; and all substantive contributions by others to the work presented, including jointly authored publications, is clearly acknowledged.
Jean-Pierre CalabrettoMarch 2007

Page xix
Acknowledgements
Foremost, I would like to thank my supervisor, Professor Paula Swatman for seeing me to completion of this thesis. Her generosity with time, advice and guidance, is unrivalled; and I am particularly grateful to her for the considerable effort she made to my supervision. In addition, her ability to accept a PhD student mid-way through their research project and keep this going smoothly is remarkable. I have valued her friendship and good humour during this time.
I thank the people who paved the way for my venture. Professor Jim Warren, who moved to Auckland, my first supervisor (now an Associate Supervisor), for his support and friendship in the first half of my project. Kingsley Coulthard, the Director of Pharmacy at the Women’s and Children’s Hospital, my colleague and friend for many years, whose unselfish support and encouragement I will remember.
For a mature-aged student, moving from full-time employment to full-time study can be daunting. As well as an Australian Postgraduate Award, I was very fortunate to receive support from the Distributed Systems Technology Centre (DSTC). For this, I thank Dr. Kerry Raymond, Mark Gibson and Jim Warren. I would also like to thank Dr. Linda Bird who was an Associate Supervisor for the life of the DSTC, and other staff of the DSTC (particularly Dr. Hoylen Sue) for their support and friendship. I also acknowledge the support of Professor Andy Koronios, the Head of the School of Computer and Information Science.
Of special note, is my rewarding association with the Australian Medicines Handbook; and especially thank Simone Rossi, Peter Farrell, Tony Loan, Lawrence Lim and Ceryle Gaehl.
There also many other academic and administrative staff (present and past) within the University that have facilitated my time as a student, offered advice, guidance and friendship. To these people I extend my gratitude. Professor Paul Swatman for his role during my change of supervisors; Associate Professor Carole Alcock, my Associate Supervisor; Roger Tagg; and Professor David Kearney. The administrative and support staff who are essential to smooth sailing within any organisation – Nicole Howard, Vicky Cini, Denise Manocchio, Marela Vuckov, Judy Pollock, Rita Jones, Lisa Brookling, Andrew Beveridge and Kate Pollitt. The IT support staff that allows work to occur – Malcolm Bowes, Steve Allen, Angelo Pace and Harry Sukamar. I acknowledge the help of David Gardiner, the many individuals from the University library and others who ran workshops that were invaluable in my pursuit of resources and necessary skills.
There is also an anonymous group of individuals who deserve some acknowledgement – the journal and conference reviewers who contributed to the betterment of my research writing.
Of course, the life of a research student would not be complete without the value and pleasure of interacting with other research students. These include my previous PhD chums Chunlan Ma, Sistine Barretto and Eric Browne with whom I had many meaningful conversations – and more recent student companions, particularly Nhiem Lu, Kuan Tan, Christian Voigt and David Raisey.
No research occurs without participants. Although they must remain anonymous, it would be remiss of me not to thank my participants. I am grateful for the generosity of the pharmacists, doctors and others who were part of my research. I would also like to thank the many other health professionals, particularly pharmacists, who were not directly part of my studies but supported me and contributed in other ways.
There is no way that I could have embarked on this venture without the love and support of my family – Helen my partner, my son Seb and my daughter Sophie. Despite the fact that Helen endured her own PhD, my family remained remarkably calm and supportive after I expressed my desire to do this. There is no doubt that a family will ‘keep it real’ and enables you to experience and share the things that are the most important in life. It is to Helen, Seb and Sophie; and to my father Lino who died in the month before I began this work, that I dedicate this thesis.

Chapter 1
The challenges of the health care system: anintroduction
1.1 Introduction
Health care should be safe, effective, patient-centred, timely, efficient, and equitable (Institute of Medicine 2001)
Using the Institute of Medicine’s goals for health care as starting points, this chapter introduces
the health system environment and the significant issues and challenges that face it. This
discussion carried out with both International and Australian perspectives, as although health
system structures may vary from country to country, the health care issues in Western
countries are common.
The chapter is structured as follows:
• the health system and the issues faced by it in Western countries are introduced in
Section 1.2
• the role of medication in the treatment of chronic disease and the subsequent concerns
with medication safety are discussed in Section 1.3
• Section 1.4 introduces the role and promise of using Information Technology (IT) in
health care and in particular, decision support
• the challenges to the use of IT and decision support in the health care domain are
discussed in Section 1.5
• the emerging and important role of pharmacists in medication management is discussed
in Section 1.6; and
• the research problem is disclosed Section 1.7
• the scope of the research is discussed in Section 1.8
• Section 1.9 explains the significance and contributions of the research project; and
• the thesis outline is described in Section 1.10
Page 1

1.2 The health of the health care systemGreenes (2001) suggests that it is not difficult to agree on some basic goals for achieving
quality in health care:
• universal health care coverage
• reduction of unnecessary variability and the adoption of best practices
• error reduction and safety
• increased patient-provider interaction and shared decision-making
• accountability of the health care system for cost-effectiveness
• protection of privacy; and
• more emphasis on disease prevention and health maintenance.
Yet, despite the ease with which any reader can see how important these goals are, the health
system is an exceptionally complex environment undergoing rapid change (both
organisationally and technologically); forced to cope with an aging population, the rapid growth
of new therapies and technologies and with the significant costs these new solutions bring with
them – and all of this set against a background of shrinking resources (National Health
Information Management Advisory Council 2001; Ortiz, Meyer & Burstin 2002).
There are some substantial challenges for the long-term sustainability of our health care
system (referred to as Health in this thesis), ranging from system-wide issues to those affecting
institutions and individuals. Table 1-1 presents a summary of some of these challenges,
compiled from: National Health Information Management Advisory Council (2001); European
Commission (2004); Southon (2003) and Greenes (2001).
Page 2

Southon (2003) believes that since no-one seems able to co-ordinate the conflicting
perspectives existing within Health, few of the major problems have effective solutions.
The problem is further complicated by the ‘epidemic’ of chronic disease affecting developed
and developing countries – related to dietary and lifestyle changes – responsible for 60% of
world deaths (World Health Organisation 2002). The shifting dietary patterns relate to the
increased consumption of energy-dense diets high in fat (particularly saturated fat), salt and
sugar (World Health Organisation 2002); together with the increased consumption of foods
that are low in unrefined carbohydrates (World Health Organisation 2003b). Of Australia’s 20.3
million people (as at June 2005), an estimated 2.5 million adults were obese – about 1 in 5
males aged 18 years; and 1 in 6 females. A further 4.9 million adults were estimated to be
overweight but not obese (Australian Institute of Health and Welfare 2006, p.15).
Table 1-1: Health system challenges
Challenge BackgroundAging The increasing proportion of older persons in the population.
Consumerism The increasing demand for; and changing expectations of consumers for health services.
New technologies The rapid increase and availability in the number of new services and products resulting from advances in research.
Financial return Difficulties experienced by public authorities in matching investment in technology with investment in complex organisational changes needed to exploit technology’s potential.
Mobility The increasing mobility of patients and health professionals within the health system.
Equity The continuing inequalities in health care and outcomes among disadvantaged groups.
Occupational issues The need to limit occupational accidents and diseases, to reinforce well-being at work and to address new forms of work-related diseases.
Emerging disease Responding to emerging disease risks (e.g. new communicable diseases such as Severe Acute Respiratory Syndrome).
Information management The management of enormous amounts of health information that need to be available securely, accessibly; and in a timely manner at the point of need.
Budgetary constraints The need to provide the best possible health care under limited budgetary conditions.
Workforce issues The increasing difficulty of maintaining a health workforce in light of many becoming alienated, retiring early, or moving to other careers.
Competition The increasing complexity of the system leading to the perception of competing stakeholders rather than cooperating partners.
Competing demands The difficulty of concurrently aiming for both quality and conservation of resources.
Lack of accountability The inability to measure what practices are effective without an overall system of accountability.
Information relevance The need for increased data collection (in part to achieve accountability) by practitioners that have little time or positive incentive to do so.
Time demands The time that is necessary to ensure quality may have negative effects on productivity – the primary basis for the current reward system.
Health professional-consumer relationships
Monitoring and accountability are among major irritants seen as interfering with physician liberties and the physician-patient relationship.
Page 3
Paradoxically, while one billion adults in the world are overweight and 300 million are clinically
obese in the more advantaged countries, poor countries have 170 million underweight
children, of whom over three million died in 2002 (World Health Organisation 2002).
Together with shifting dietary patterns, people in developed countries are experiencing a
decline in energy expenditure associated with a sedentary lifestyle resulting from motorised
transport, labour-saving devices, the phasing out of physically demanding manual tasks in the
workplace and leisure time largely devoted to physically undemanding pastimes (World Health
Organisation 2003b). In 2004, about half of Australia’s adults did not undertake leisure-time
physical activity at levels recommended for health benefits (Australian Institute of Health and
Welfare 2006, p.15).
As a result of these changes in diet and exercise, chronic non-communicable diseases (such
as obesity, diabetes mellitus, cardiovascular disease, hypertension and stroke; and some
types of cancer), are becoming increasingly significant causes of disability and premature
death, placing additional burdens on already overtaxed national health budgets (World Health
Organisation 2003b). In 2002, cardiovascular disease, cancer, chronic respiratory disease and
diabetes caused 29 million deaths worldwide (Yach et al. 2004). This pattern also exists in
Australia – the chronic diseases which contribute the most to morbidity, disability and mortality
are heart disease, stroke, cancer, diabetes, asthma and osteoarthritis. Some of these chronic
diseases are now considered to be of epidemic proportions (Australian Institute of Health and
Welfare 2006, p.76). For example, in 2004, cardiovascular disease accounted for 47,637
deaths (36% of all deaths) in Australia; and is also one of the leading causes of disability (about
1.4 million people). Cardiovascular disease is also the most expensive disease group in terms
of direct health care expenditure, at $5.5 billion – 11% of Australia’s total allocated health
system expenditure in 2000–01 (Australian Institute of Health and Welfare 2006, p.77). The
1999-2000 Australian Diabetes, Obesity and Lifestyle Study (AusDiab) indicated that 30% (or
3.7 million) of Australians aged 25 years or over had high systolic or diastolic blood pressure,
or were on medication for high blood pressure. The proportion of males and females with high
blood pressure also increases with age (Australian Institute of Health and Welfare 2006,
p.194).
The use of medication has become vital in the treatment of disease and medicines are now
part of most people's lives – especially for the elderly and chronically ill (Ihara, Summer &
Shirey 2002). This topic is examined next in Section 1.3.
Page 4

1.3 Medication and chronic illness An Australian report suggests that in any two-week period, about 7 in 10 Australians (and 9 in
10 older Australians) will have taken at least one medicine (Roughead & Semple 2002).
Medication alone was also the most common treatment given to patients by General
Practitioners (GPs), occurring on 37% of visits (at a rate of 101.5 prescriptions per 100
encounters or 69.8 prescriptions per 100 problems) – compared to clinical treatment alone
(e.g. counselling) on 11% of occasions (Australian Institute of Health and Welfare 2006,
p.365). The most commonly used drugs in Australia in 2004-05 were atorvastatin (used for
lowering blood cholesterol) followed by simvastatin (also for lowering blood cholesterol) and
ramipril (for treating chest pain and high blood pressure) (Australian Institute of Health and
Welfare 2006, p.365).
These figures relate only to prescription medications – but there is another group of
medications which contributes to this increasing trend of use. The Australian Institute of Health
and Welfare (2006) estimated that, in 2004, along with the 233 million prescriptions dispensed
in community pharmacies, Australians also spent $1.7 billion on Over-the-Counter (OTC)
medications such as analgesics, cough medicines and vitamins; and $0.8 billion on natural and
other Complementary Medications (CMs). The use of OTC and CM medications accounted for
over 14% of the recurrent Health expenditure in 2003-04 – taking medication to resolve
feelings of unwellness is a frequent health-related action taken by Australians.
1. 3.1 Adherence to medication therapyThe widespread use of medication has led to an increasing concern within the health
community about adherence to (prescription) medication regimens in the elderly and
chronically ill groups – adherence to long-term therapy for chronic illnesses in developed
countries averages about 50% (World Health Organisation 2003a).
The consequences of poor adherence to medication regimens for the chronically ill include:
poor health outcomes; poorer quality of life; and increased health care costs through such
factors as increased hospital emergency room visits, hospital admissions or visits to
community doctors (Ihara, Summer & Shirey 2002; World Health Organisation 2003a).
Conversely, good adherence to beneficial drug therapy has been associated with a decreased
risk of mortality (Simpson et al. 2006). Good adherence per se however, does not necessarily
constitute a good outcome, as good adherence to proved harmful drug therapy has been
shown to increase the risk of mortality (Simpson et al. 2006).
Osterberg and Blaschke (2005) have suggested some general approaches for improving
adherence to medication therapy, including: patient education, improved medication dosing
Page 5

schedules for patients, increased patient accessibility to doctors (i.e. shorter waiting times) and
better communication between doctors and patients. The study by Bajramovic, Emmerton and
Tett (2004) confirmed that information sharing between health professionals and consumers
was an important issue – not helped by the perceived lack of time in doctor-consumer
interactions; and the lack of systems to support good information-sharing. The authors of this
study went on to suggest that improvements in information sharing between doctors,
pharmacists and consumers were crucial to the future of health care (Bajramovic, Emmerton
& Tett 2004).
A further important issue is that much of the care needed in chronic illness involves a degree
of patient self-management which if not supported by the health system may leave patients at
risk (World Health Organisation 2003a). Increasing the ability of patients to self-manage (and
shifting the cost of medications more directly to the consumer) is also a motivation of many
governments. This motivation is reflected in the trend of making prescription medication
(including some for the prevention of serious illness) available Over-the-Counter (Cohen,
Paquette & Cairns 2005). This trend has implications for both the health care team and
patients themselves in terms of improving the safety of self-medication – the implications are
the need for better information for patients and more collaborative care involving better
communication between doctors, nurses and pharmacists (Bradley & Blenkinsopp 1996).
With the increasing involvement of patients in their own care, interventions by health
professionals (to improve patient adherence to medication therapy) are seen as positive
returns on investment – through the primary prevention of risk factors for medication therapy
and the secondary prevention of adverse health outcomes (World Health Organisation 2003a).
The increasing recognition of this fact is stated by the World Health Organisation:
Increasing the effectiveness of adherence interventions may have a far greater impact on the health of the population than any improvement in specific medical treatments (World Health Organisation 2003a)
The importance of adherence to medication therapy also raises the issue of medication safety.
The use of medicines is not without risks and this issue has been raised as an international
concern. The issue of medication-related adverse effects is discussed next in Subs-section
1.3.2.
1. 3.2 Medications and patient safetyThe landmark and widely quoted report To Err Is Human: Building a Safer Health System
(Kohn, Corrigan & Donaldson 1999) identified the extent and cost of preventable iatrogenic
injuries in the United States (US) hospital system – estimated to affect 3%-4% of US hospital
patients and account for over 7,000 deaths annually. The cost of dealing with preventable
Page 6
adverse drug events (ADEs) for US hospital inpatients was estimated to be about US $2 billion.
Similarly, findings from the United Kingdom (UK) suggested that inpatient medication errors
cost about £500 million a year (UK Audit Commission 2001).
Australian figures place medication-related hospital admissions at 2.5%, rising to 30% for
those patients aged over 75 – with up to three-quarters of these medication-related admissions
being potentially preventable. People aged over 65 years are considered to have higher rates
of medication incidents compared to younger people, as the elderly are taking more
medications (Roughead & Semple 2002). A review of high-risk individuals in the community
found 2.8 medication-related problems per person (Runciman et al. 2003). Other Australian
data suggest that of the 100 million or more annual general practice encounters in Australia,
about 400,000 are thought to involve medication-related adverse drug events (Roughead &
Semple 2002)
Roughead E.E. and Lexchin (2006) in an editorial in the Medical Journal of Australia,
commented that in light of more than 30 Australian studies estimating the number of ADEs in
a variety of settings: ’it is clear that counting is not enough — it is time for action’. Roughead
and Lexchin (2006) suggested that a way forward was through developing a ‘no blame’ culture
with better doctor-patient communication, better inter-health professional communication and
the use of technology. Some technology-based strategies which have been shown to reduce
medication incidents include: computerised prescribing with clinical decision-support,
information about medicines for health care providers on-line, or in prescribing or dispensing
software; and computerised adverse drug alerts (Roughead & Lexchin 2006).
Further, as the distinction between primary (community-based) and secondary (hospital-
based) care blurs, an urgent need exists to review medication management across the health
continuum (UK Audit Commission 2001).
The recognition of these-health related problems on a wide-spread scale has led to
government or national strategies to address these problems, many underpinned by IT. This
is discussed next in Section 1.4.
Page 7

1.4 The promise of information technology in HealthThe National Health Information Management Advisory Council (2001) suggested that
emerging priorities for governments included:
• maximising the health of individuals and the community
• achieving a balance in the investment of health resources in individual and community
health
• responding flexibly to community and consumer needs
• providing services that are integrated and coordinated
• relying on an evidence basis for health care to achieve best practice in health services;
and
• concentrating on proven services and on agreed priority areas
Alongside these priorities, there is an increasing recognition by governments of the importance
of increased and better use of health information. This includes: access to up-to-date health
information for both consumers and health providers; new and improved methods of
communicating information among and between consumers and health providers; the sharing
of information between consumers and health providers; and collecting, collating and
analysing information/data across health settings and populations (National Health Information
Management Advisory Council 2001).
However, the amount and complexity of health-related information and knowledge has
increased to such a degree that information processing in itself has become a major activity
for any health organisation (European Commission 2004). This overwhelming amount of
information makes it virtually impossible for individual health clinicians to provide high-quality,
error-free care on a consistent basis, since they are ‘inherently fallible information processors’;
and clinicians are supported by poor systems that allow errors to occur (Ortiz, Meyer & Burstin
2002). The problems of managing this 'explicit', increasingly evidence-based knowledge are
compounded by consideration of individuals’ 'tacit' knowledge which deals mainly with
experience; and the increasingly informed patient (Sowerby Centre for Health Informatics
2000).
To address the problems of this information-intensive health environment, governments
increasingly see IT as a valuable tool. IT promises substantial productivity gains, the ability to
cope with increasing demand on health care services, the ability to reshape the health care
delivery to make it more citizen-centred (European Commission 2004); and the ability to
address issues of quality and safety (Bates & Gawande 2003; Electronic Prescribing Initiative
2004). Safe care is now considered to require a degree of individualisation which would be
unimaginable without computerised decision support (Bates & Gawande 2003).
Page 8

The ubiquity of IT in health has given rise to the term e-Health: ‘the application of information
and communications technologies across the whole range of functions that affect the health
sector’ (European Commission 2004). This term is used to describe a wide range of
technology-based tools in Health such as: Internet-based applications; health information
networks; electronic health records; telemedicine services; personal wearable and portable
communicable systems; and health portals (European Commission 2004). The notion of e-
Health is that the ubiquity, flexibility and potential reach of the Internet will allow for the delivery
of high-quality, low-cost services (Sowerby Centre for Health Informatics 2000).
The main roles for IT in Health are seen to lie in: the management of information and
knowledge (Sowerby Centre for Health Informatics 2000); electronic prescribing (Electronic
Prescribing Initiative 2004); and clinical decision support (Bates & Gawande 2003). Decision
support tools – particularly, clinical practice guidelines, prescribing alerts and those providing
current patient information at the point of care – offer opportunities to reduce the numbers of
adverse events, unnecessary hospitalisations, reduce the duplication of diagnostic tests and
enhance decision-making for providers and consumers (thus increasing the quality of care and
health outcomes) (National Health Information Management Advisory Council 2001). Bates
and Gawande (2003) suggest that the types of tools able to prevent errors and adverse events
are those which can improve communication, make knowledge more readily accessible, assist
with calculations, perform checks in real time; and assist with monitoring. Although, many
areas of decision support activity have considerable overlap, the researcher will now provide
a brief introduction to some of the main areas of activity.
Page 9
1. 4.1 Electronic health recordsThe Australian National Electronic Health Records Taskforce (2000) defined an electronic
health record (EHR) as:
An electronic longitudinal collection of personal health information usually based on the individual, entered or accepted by health care providers, which can be distributed over a number of sites or aggregated at a particular source. The information is organised primarily to support continuing, efficient, and quality health care. The record is under the control of the consumer and is stored and transmitted securely (National Electronic Health Records Taskforce 2000, p. xv).
The advantages of EHRs seem very clear from this definition – again based on the report of
the same taskforce, they include:
• better consumer access to their own health information, thus allowing consumers to
make more informed decisions about their health care
• better provider access to information (with consumer consent) at the point of care
• fewer diagnostic tests (including the elimination of redundant tests)
• improved warnings and alerts to counter avoidable error (e.g. adverse drug interactions);
and
• better planned and co-ordinated care (including the capacity to develop comprehensive
care plans that providers and consumers alike would use)
EHRs are seen as fundamental to the ability of some electronic decision support tools to
function as the EHR will provide the source of patient data upon which many of these tools will
function (National Electronic Decision Support Taskforce 2002).
Substantial efforts to develop national shared EHR networks have been made by some
countries, including Brazil, Canada, England and Australia – the latter with a national project
named HealthConnect (Schloeffel 2004a). A major advance in the area of EHR design was the
Good European Health Record (GEHR) project – a large European Union-funded project
undertaken within eight European countries between 1992 and 1994 – which later evolved (in
2002) into the openEHR model (Schloeffel 2004b), which is based on archetypes1.
Other efforts in area of EHRs have ranged from those supporting specific patients groups such
as diabetics (Austin et al. 2003), community-based practices (Baron et al. 2005) and across
primary care and specialty practices in community networks (Poon et al. 2006).
1. 4.2 Decision support systemsAs previously mentioned, there is a great deal of overlap in what constitutes a decision support
system (DSS) so for this discussion the researcher will also include Computerised Physician
1. Archetypes define domain-specific concepts which can range from simple concepts such as ‘blood pressure’ or more complex concepts such as ‘family history’; and are important components for seman-tic interoperability.
Page 10

Order Entry (CPOE) or electronic prescribing (EP), as many alerting and reminder functions
(considered to be decision support) are part of CPOE systems.
There are also very many definitions for decision support systems. Clinical decision support
systems (CDSS) have been described as active knowledge systems which use two or more
items of patient data to generate case-specific advice, and are typically designed to integrate
a medical knowledge base, patient data and an inference engine to generate case specific
advice (OpenClinical 2004).
Although decision support is a key interest for this research project, it is well beyond the scope
of this thesis to discuss DSS in detail – rather, a synopsis of DSS follows. The properties of
decision support systems already described include:
• providing clinicians with access to relevant, evidence-based information at the point of
care (Delaney et al. 1999)
• comparisons of patient characteristics (with a credible knowledge base) that guide a
clinician by offering patient-specific and situation-specific advice (General Practice
Computing Group 1999; Eccles et al. 2002)
• providing access to laboratory test interpretations, calculation of drug dosages,
automated warnings and alerts, practice guidelines; and decision analysis (Remmlinger
2002)
• complex systems that can model the likelihood of future events and the effectiveness of
proposed interventions, based on individual patient data, the 'knowledge' of risks and the
effectiveness of interventions (Delaney et al. 1999)
• reminders, advice or interpretation specific to a given patient at a particular time (Wyatt
2000)
• use of active knowledge systems which use two or more items of patient data to
generate case-specific advice (Wyatt & Spiegelhalter 1991)
• access to electronically stored knowledge to aid patients, carers, and service providers in
making decisions on health care (National Electronic Decision Support Taskforce 2002).
Bates et al. (2003) summarised the features of DSS as supports which include passive and
active referential information as well as reminders, alerts, and guidelines. More generically,
decision support can describe any computer application which enhances a human's ability to
make decisions (Coiera 2003a).
Page 11

Examples of DSS from the literature are many and varied. Some include:
• guideline-based tools for emergency department clinicians (‘the asthma kiosk’, a patient-
driven decision-support tool which provides ED clinicians with tailored recommendations
for guideline-based treatment (Porter et al. 2006)
• a computer-assisted patient screening support for health care workers in India (Peters et
al. 2006)
• a hospital-based management of antimicrobial utilisation (McGregor et al. 2006); and
• the provision of on-line clinical decision-support information for health professionals
(Walther et al. 2002)
The importance given to electronic decision support in Australia was evidenced by the
establishment of the Australian National Electronic Decision Support Taskforce (NEDST). The
task of NEDST was to consider the benefits and difficulties electronic decision support and
recommend a way forward to ensure a consistent national approach to the development of
electronic decision support in Australia (National Electronic Decision Support Taskforce 2002).
A DSS can thus embody many definitions and exhibit a range of features – the considerable
overlap which results makes it very difficult to describe what a DSS ‘is’. Nevertheless, the
potential benefits that DSS offer to health care practice suggests an enduring quest to discover
what elements will afford effective decision support for health care professionals.
A significant feature of health care workers is their mobility which has in turn led to investigation
of the use of technology to support this mobile (nomadic) work. Mobile computing is discussed
in the next sub-section.
1. 4.3 Mobile health applicationsMobile computing is broadly described as computing technology – software, hardware and
communications – associated with mobility i.e. technology that is not fixed and is capable of
being portable (Hameed 2003). Examples of this technology include Personal Digital
Assistants (PDAs), laptop computers and mobile telephones. These mobile devices can also
include technology enabling users to communicate over a network, or directly with one other
using both wired and wireless technology (Hameed 2003).
The use of mobile technologies such as PDAs within hospital environments is not new
(Sargent et al. 2005) – applications based upon PDAs have included commercial medical or
drug references, medical calculators and personal organisation software, such as calendars
and address books (Barretta, Strayera & Schubarta 2004; Carroll & Christakis 2004). PDAs
are used less commonly for writing prescriptions or medical billing (Carroll & Christakis 2004).
Page 12

A study by Rothschild et al. (2006) demonstrated that PDA-based software (which included a
pharmacopoeia, an infectious disease reference, a medical diagnostic and therapeutic
reference; and transmitted medical alerts and other notifications during PDA-computer
synchronisations) was used frequently and improved patient care. Providing clinicians with up-
to-date drug-information alerts and warnings was considered especially valuable.
A promising area of use for mobile devices is remote access to information for primary health
care workers – as mobile portals for information access; and for the transmission of data from
remote locations to a central system (Hameed 2003). A challenge, however, for community
health services, is that many rely on legacy and paper-based systems (Sargent et al. 2005).
For the benefits of mobile devices to be fully realised requires the mapping of clinical pathways
to these devices so that they progress beyond the confines of traditional 'bricks and mortar'
hospital infrastructures – this non-trivial challenge should not be underestimated (Sargent et
al. 2005). An example of such an approach is the e-Therapeutics tools planned by the
Canadian Pharmacists Association (CPhA). These tools will combine evidence-based content
from CPhA, information from Health Canada (and others) and other applications (e.g. e-
prescribing, EHR) – this content will be delivered through multiple channels including a web
portal and be downloadable to a PDA (Canadian Pharmacists Association 2004a).
User acceptance of mobile devices is equally important. One way of achieving user
acceptance while simultaneously enhancing deliverability of the system – providing a ‘best fit’
with end user needs – is to address user concerns as they arise during development (Cooper,
Alcock & Burgess 2003). Cooper, Alcock and Burgess (2003) demonstrated this approach with
a proposed electronic point-of-care (ePOC) information system for ambulatory care services.
This system allowed the collection, delivery and exchange of timely information at point of care
to match complex health care workflow requirements, as well as allowing immediate updating
of health care records. The project enabled more timely and effective information access and
management – particularly, freeing up nurses from paper work and allowing more time for
consultation with patients (Cooper, Alcock & Burgess 2003).
Wireless technology has been used within a hospital environment with hand-held devices to
extend a clinical information system allowing improved information access and communication
at the point of care by providing: access to information resources, event monitoring and a
virtual whiteboard (Mendonca et al. 2004). Wireless technology can also be used to make
better use of clinicians’ time by allowing them to access the latest patient-related data when
they are located outside of a hospital campus (Holleran et al. 2003).
Page 13

1.5 The problems of information technology in HealthAlthough the benefits of IT in health care have been widely promoted, the health industry has
been a slow adopter of IT: estimates place IT expenditure in public health care at about 1.5%
of total revenue, which is significantly lower than that spent by other industries (e.g. banking
or the resources sector) (England 2001). The development of clinical DSS (CDSS) in health
care has, however, mirrored the general trend of IT adoption (Garg et al. 2005). The particular
problem of DSS uptake in Health is that tasks are often fuzzy, complicated and involves a great
number of people and technologies, whose activities are intricately linked – organisations
facing such tasks need high levels of information processing and exchange (Winthereik &
Vikkelsø 2005). A predicament is that existing patient care information systems often appear
to be based on formal, stepwise notions of health care work – these systems cannot handle all
potential exceptions and become impossible to maintain and to use (Ash, Berg & Coiera 2004),
so that failures of health information systems are common (Heeks 2006).
Some specific problem areas for IT in health care are now discussed in the following
subsections.
1. 5.1 Information and context of useThe health care environment is a paradox – characterised by an enormous amount of rapidly
changing information but at the same time hampered by the unavailability of critical information
at the point of clinical decision-making (National Electronic Decision Support Taskforce 2002).
For clinicians, the enormous amount of information they encounter in their job is a day-to-day
problem:
a wealth of information creates a poverty of attention, and a need to allocate that attention efficiently among the overabundance of information sources that might consume it (Varian 1995).
Consequently, information needs to be located, filtered and summarised – otherwise, the
technology which produces and distributes information is effectively useless (Varian 1995).
There is also a belief that, because of the overwhelming amount of information available to
clinicians, clinicians will intuitively understand the importance of problem-solving and learning
skills (such as how to find relevant answers quickly); and will see that clinical practice is not
simply about learning facts (Wyatt & Sullivan 2005). Unfortunately, however, this intuitive
understanding does not always take place.
Missing information in doctor-patient encounters is common and can affect both doctor-patient
interaction as well as clinical decision-making (Elder & Hickner 2005). The problem is further
complicated by the fact that information inaccuracies are common, for example:
Page 14

• incorrect recording of primary diagnosis for outpatient visits (57%) (Peabody et al. 2004)
• missing or uncoded medication data stored in electronic records (1.38 medications per
patient) (Wagner & Hogan 1996); and
• missing clinical information in primary care visits (13.6% of visits) (Smith et al. 2005)
In the last of these three studies, the authors noted that this missing clinical information had
the potential to adversely affect patients (44%), potentially resulting in delayed care or
additional services (59.5%); and added that significant time was spent unsuccessfully
searching for missing information (Smith et al. 2005). A recent study has shown that 51% of
hospital clinicians' information needs went unmet during their clinical practice; and that human
interaction was used to meet background information needs more frequently than was a
computer resource (Currie et al. 2003).
A critical feature of information is that it is contextual – its generation, use and value will depend
on the context of use (Shepherd et al. 2006) – specifically, the patient. Berg and Goorman
(1999) consider that information should be conceptualised as being always intertwined with the
context of its production – it is not simply a matter of using technology to transport information.
In addition, the further information has to circulate (i.e. the more diverse contexts in which it
must be usable), the more work is required to disentangle the information from its original
context (Berg & Goorman 1999).
1. 5.2 knowledge use by health professionalsAn important feature of Health is that health professionals need to access information from a
variety of sources. This access is not only to written material, but also involves other health
professionals – experts, specialists and consultants (Swatman et al. 1996). Thus, knowledge
in health care exists in a variety of modalities – tacit, explicit, experiential and social – which
interrelate with one another during a health care process (Shepherd et al. 2006). This provides
a major challenge to the use of knowledge in decision support systems; and for knowledge
management in general. Currently, knowledge management systems do not have the
capability to dynamically map tacit knowledge to the corresponding explicit knowledge
required for problem solving (Shepherd et al. 2006). Quite apart from the lack of a coherent
approach to knowledge management, some health reforms have actually adopted techniques
which have been found to be destructive to knowledge management (Southon & Cook 2001).
1. 5.3 Electronic health recordsDespite the widespread work on EHR, no widespread uptake of EHR standards has taken
place. To date, most successful information EHR systems have been implemented as
proprietary systems, or as unique systems developed by academic medical centres (Greenes
2001). Limited successes of this nature have made it difficult to use the knowledge gained from
Page 15

any of these EHR innovations for more widespread adoptions (Greenes 2001).
1. 5.4 Decision support, alerts and remindersThe Australian experience identified by The National Institute of Clinical Studies (2002) was
that, although substantial development in EDSS had taken place in Australia, much of the
development was fragmented and uncoordinated because of problems of accessibility,
scalability, duplication and lack of integration with existing systems.
The main issue for decision support systems is that their actual level of is limited by the
available medical data (Kuilboer et al. 1997) – in particular, by the paucity of structured data
(Greenes 2001). A clinical decision support system is only as effective as its underlying
knowledge base (Purcell 2005). Bates et al. (2003) suggest that some key issues for EDSS
are the timing of triggers, the ease of use of the system, the helpfulness of the content,
matching the workflow of users; and the need for messages to be highly directive.
The long experience with DSS has now allowed this group of systems to be viewed more
realistically. In particular, recent attention has turned to the unintended consequences of DSS.
A review of CPOEs by Campbell et al. (2006) identified a number of unintended consequences
of such systems, which are summarised in Table 1-2.
A survey of a CPOE system at a tertiary-care teaching hospital found that the CPOE system
facilitated 22 types of medication error risks (Koppel et al. 2005). A recent review by Coiera,
Westbrook and Wyatt (2006) which summarised the safety and quality of DSS concluded that
the usability and performance of DSS was the result of a complex set of cognitive and socio-
technical interactions – and that a deeper understanding of all these issues would result in
intrinsically ‘safer’ systems and better outcomes for the clinicians who use the systems.
The perceived poor specificity of alerts and reminders within DSS systems (e.g. for drug alerts)
Table 1-2: Unintended consequences of CPOE (Campbell et al. 2006)
ConsequenceMore or new work for clinicians.
Unfavourable workflow issues.
Never ending demands by the system.
Problems relating to the persistence of paper.
Untoward changes in communication patterns and practices.
Negative emotions.
The generation of new kinds of errors.
Unexpected changes in the power structure.
An overdependence on the technology.
Page 16
is an important issue which may impede the ability of such alerts to improve patient safety
(Glassman et al. 2002). A study by Weingart et al. (2003) found that physicians overrode
91.2% of drug allergy and 89.4% of high-severity drug interaction alerts – few physicians
changed their prescription in response to a drug allergy or interaction alert. In most of these
cases, alert overrides by physicians were justifiable on the basis of the physicians' personal
knowledge of the patient's situation. Further, while a standard exists for alerts and reminders
– Arden Syntax – collections of exchangeable alerts and reminders are not widely available
(Greenes 2001). This appears to suggest that the alerts and reminders currently available
within existing DSS systems are not sufficiently reliable to promote confidence on the part of
the using clinicians.
To sum up, despite the perception that DSS can improve efficiency and reduce costs, the
current supporting evidence is limited – and the cost effectiveness of these systems remains
unknown. Many studies have suggested that CDSS were inefficient, requiring more time and
effort from users than the paper-based methods they were designed to replace (Garg et al.
2005). Other concerns still outstanding include: workflow integration, compatibility with legacy
applications, system maturity, upgrade availability and the eroded capacity for users’
independent decision-making (Garg et al. 2005). Finally, Garg et al. (2005) believe that in
some cases cheaper, non-computerised alternatives may be equally or more effective in
improving health care and reducing medical errors.
1. 5.5 Mobile computingThe issues affecting the development of applications for mobile devices are similar to those
affecting the development of other computer applications – the most important issue for both
mobile and other technology applications is user acceptance. However, mobile devices also
present particular problems for developers, because of device size and portability.
Arshad, Mascolo and Mellor (2003) consider mobile devices (such as PDAs) to be extremely
resource-constrained in terms of memory, processing power, battery lifetime and screen size
– these issues have been reported as problems in studies on PDA use (Carroll & Christakis
2004). Users often find information difficult to read on PDAs because of the small form factor
and font size (Holleran et al. 2003). These problems require application developers to
consider: how PDA resources are used during runtime; what concessions must be made about
executing processes; and where to store information (i.e. on the PDA or remotely on a more
powerful device (Arshad, Mascolo & Mellor 2003). Addressing these problems of screen size
and computational power has occasionally involved novel approaches e.g. the use of PDAs for
information representation alongside mobile telephones for communication (Schwabe &
Frohberg 2006).
Page 17

An important concern for clinicians is the physical size of the PDA (i.e. how convenient it is to
carry) and the potential for data loss (Barretta, Strayera & Schubarta 2004). The latter is of
particular concern for clinicians if mobile devices are used to store confidential or sensitive
patient-related data.
Although many organisations have considered the use of wireless hand-held computers, such
devices are not yet in widespread use (Kuperman & Gibson 2003). The main obstacle to the
use of wireless networks appears to be speed – users report that transfer of data to their
devices is too slow (Holleran et al. 2003).
1. 5.6 privacy & securityThe public has general concerns about the privacy of their electronically stored information.
There has been recent vindication of these concerns in a study which showed major
deficiencies in compliance with the new Australian Privacy Legislation by Australian
companies – suggesting that concerns about privacy about personal information in health are
justified (Watt et al. 2002).
Health professionals' concerns about the security and privacy of personal (patient) information
are another major barrier to the implementation of DSS (National Electronic Decision Support
Taskforce 2002). Since EHR systems available over networks are vulnerable to attacks and
misuse, EHR systems require a range of security measures such as encryption, public key
infrastructure, firewalls; and network service management, software management, rights
management tools and system vulnerability management tools (Win & Cooper 2004).
Because of some of these concerns, the health community has a seen a move towards using
Intranets to share information – using the same technologies as the Internet but offering more
security (Swatman et al. 1996).
There is evidence that public opinion concerning information privacy may be changing,
however – a recent survey revealed that most of the British public considered the confidential
use of personal, identifiable patient information by the National Cancer Registry for public
health research and surveillance was not an invasion of privacy (Barrett et al. 2006). Whether
this finding will hold true across a range of national opinions, however, remains to be seen.
1. 5.7 The bottom line with IT in HealthIn summary, there are many problems to overcome in realising the full potential of IT within the
health domain. The degree to which IT systems actually support work practices found in
health, particularly clinical work, is a major issue which leads to poor acceptance of IT by
Page 18

clinicians (England 2001). Consequently, this lack of adoption of IT systems by health care
workers around the world means that health care retains the problems associated with paper-
based exchanges: hand-writing, lack of integrated information and limited availability and
capture of information at the point-of-care (Cooper, Alcock & Burgess 2003).
Some DSS strategies (including guideline implementations, alerts and reminders) have been
associated with reduced medication prescribing errors, improved preventive and chronic
disease care; and improved physician and patient satisfaction in controlled trials. But these
DSS cases have occurred predominantly in academic settings or inpatient environments – it is
therefore difficult to generalise these cases to community-based care, where most prescribing
occurs (Smith et al. 2006). Adding to this difficulty is the fact that computer-based clinical
decision support systems (CDSSs) vary greatly in design and function (Sim & Berlin 2003). In
fact, research has been undertaken to ascertain which clinical decisions might benefit from
automation, based on analyses of task complexity (Sintchenko & Coiera 2003). The bottom
line is that, while many CDSSs improve practitioner performance, the effects on patient
outcomes still remain understudied and, when studied, have produced inconsistent findings
(Garg et al. 2005).
The area of DSS is thus a rapidly advancing and unregulated field, with potential for harm as
well as benefit where systems are poorly designed and inadequately evaluated (National
Electronic Decision Support Taskforce 2002). This issue has prompted the question of whether
clinical software should be regulated (Coiera & Westbrook 2006).
Coiera and Westbrook (2006) suggest that clinical software is not subject to any procedure to
prove its safety and efficacy – compared to the complicated and highly controlled process
which occurs during the development of new drugs. They further add that, although stand-
alone software in routine clinical use may undergo rigorous evaluation by its developers,
commercial vendors can still produce (hospital) prescribing systems with significant gaps in
functionality – some even being devoid of decision rules designed to check for errors or to
guide prescribing! Unless a hospital has the expertise to develop and maintain its own
computational knowledge bases – 'an arcane and highly specialised skill set if there ever was
one' (Coiera & Westbrook 2006) – such an outcome is fraught with danger. It is, in fact, the
very strengths of DSS systems – the complex knowledge base and reasoning features and
their ability to influence physician decisions – which give rise to the ethical and legal concerns
about such systems (Berner 2002).
As these systems have the ability to harm patients, the clinician must be able to make informed
decisions on when to follow or to ignore the CDSS’s advice. In addition, knowledge bases must
Page 19

be properly maintained, and users of these systems should know how the systems were
developed and tested, the source of the rules in the system, the expectations of the user when
using the system and what user training is required (Davis et al. 2002). These authors note
that despite the technological sophistication of the American health care system, a
Commonwealth Fund 2001 Health Care Quality Survey revealed that medical care in the
American system fell short of the ideal. They suggested that having the best technology is not
enough; and that perhaps it is more difficult to explain why simple measures which are well-
known to be effective in preventing disease and managing chronic conditions are not
systematically employed (Davis et al. 2002).
So, although IT has a very powerful contribution to make to Health, IT must also be
implemented within a clearly understood framework of the knowledge processes which will
impact on its use (Southon 2003). Kaplan (2001) suggests that although controlled clinical
trials are the 'gold standard' for evaluation of DSS, a social science approach is also needed
to understand whether systems will be used or how they will be used – it is not simply an issue
of IT performance. Importantly, more qualitative studies will help to reveal the unintended
effects of IT in Health and to help understand the observed effects (Ammenwerth 2006).
Information technology has the potential to greatly improve patient safety and quality of care,
but considerably more work is required to evaluate the technologies used and their impact on
outcomes (Ortiz, Meyer & Burstin 2002).
Perhaps the redundancy built into the system of people and technologies is one explanation
why more errors do not occur – e.g. despite the many prescription mistakes made, only a
fraction end in medication administration mistakes (Ash, Berg & Coiera 2004). So, although
'we created external devices that exponentially increased our ability to calculate, analyse, and
learn' – we have some way to go before we can fully realise the potential of these devices in
Health (Jadad & Enkin 2007).
1.6 Medication management and pharmacistsEfforts towards addressing medication-related adverse events have seen the term medication
management (MM) come into common use. This term broadly describes a set of relationships
and decisions through which primary health care practitioners and patients work together to
produce specific drug therapy outcomes (Canadian Pharmacists Association 2004b).
'Medicines Management'1encompasses a range of activities intended to improve the way in
which medicines are used by patients and by government; and describes processes based on
patient need used to design, implement, deliver and monitor patient-focused care (Department
1. Medicines and medication will be used synonymously in this thesis.
Page 20

of Health Social Services and Public Safety 2004).
Stowasser, Allinson and O'Leary (2004) have described a medication management pathway
– shown in Figure 1-1 – which includes nine steps (cognitive and physical) described inside
the loop – and three background processes, shown on the outer part of the pathway loop.
This pathway is intended to apply to medication management independent of the health
setting, health professionals or the funding source (i.e. public or private).
Figure 1-1: The medication management pathway (Stowasser, Allinson & O'Leary 2004)
Page 21

The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) has produced
standards which detail the elements of a medication review process; and the necessary
patient-related and medication-related information required to ensure the review process can
be carried out effectively (Rich 2004):
• appropriateness of the drug, dose, frequency, and route of administration
• therapeutic duplication
• real or potential allergies or sensitivities
• real or potential interactions between the ordered medication and other medications,
food, and laboratory test values
• other contraindications
• variation from organisational criteria for use; and
• other relevant medication-related issues or concerns.
The required patient information elements included:
• age and sex
• current medications
• diagnosis, comorbidities, concurrent conditions
• relevant laboratory test values
• allergies and past sensitivities
• weight and height
• pregnancy and lactation status; and
• any other information required by the organization for safe medication management.
A further term is used in Australia for the use of medication – the Quality of Medicines (QUM)
– which describes an overarching strategy for improving medication management rather than
a list of goals. It includes such aspects as ensuring the right patient receives the right drug in
the right dosage with the appropriate monitoring etc. According to the Australian Department
of Health and Ageing, QUM is: ‘selecting management options wisely; choosing suitable
medicines if a medicine is considered necessary; and using medicines safely and effectively’.
In a broader sense, this can apply equally to individuals and decisions that affect population
health (http://www.health.gov.au/internet/wcms/publishing.nsf/Content/nmp-quality.htm,
viewed 2006-07-11). QUM is a term used commonly used in the Australian health setting (by
pharmacists).
Pharmacists are considered to be drug therapy experts and, because of their knowledge, skills
and accessibility, pharmacists are well-placed to ensure that patients, other health care
professionals (and the health care system) can safely accomplish optimal drug therapy
outcomes (Canadian Pharmacists Association 2004b).
Page 22

The value of medication-related interventions by clinical pharmacists in the hospital setting is
well established and has been shown to be beneficial to patient management, affecting length
of stay, re-admission probability, medical procedures or laboratory monitoring – and leading to
significant savings (Dooley et al. 2003). Some further examples of effective pharmacist
interventions include:
• pharmacist-monitored anticoagulation programmes which have been associated with
reduced thromboembolic events in patients (Poon et al. 2007)
• a medical centre-based pharmacy care program which has led to increases in patients’
medication adherence leading to clinically meaningful reductions in blood pressure (BP)
– a discontinuation of the program was associated with decreased medication
adherence and persistence in patients’ high blood pressure (Lee, Grace & Taylor 2006)
• a pharmacist-based telephone patient counselling service which has been shown to
improve patient adherence and reduced mortality for patients receiving polypharmacy1
(Wu et al. 2006).
It is clear that hospital pharmacists remain important to patient health, even in the presence of
CPOE systems – the CPOE system may effectively intercept inpatient prescribing errors, but
cannot intercept medication administration errors (i.e. the errors which are possible outside the
influence of the CPOE can do that pose the highest risk of patient injury) (Wang et al. 2007).
This supports the view that maximising medication safety requires pharmacist involvement in
addition to a CPOE system (Bobb et al. 2004).
The term 'clinical' when applied to pharmacists is usually used in the context of hospital
pharmacists, although there is an evolving clinical role for community pharmacists similar to
that of the clinical pharmacist in the acute care setting (Gowan & Roller 2004). A 'general
practice pharmacist' role has also been described, in which a pharmacist is employed on-site
in a general medical practice with the aim of helping to rationalise prescribing, provide
consumer counselling on medication-related issues, run consumer-focused2 clinics, offer
prescription review and monitor drug therapy (Whitehead, Sunderland & Benrimoj 2003).
This consumer-focused model for pharmacists implies that medication reviews involve a
broader perspective of the consumer him/herself, in addition to an understanding of the
consumer's medication (Gowan & Roller 2004). These authors suggest this model should also
1. Polypharmacy refers to multiple medication use by a patient, but is mainly used in the context of unnec-essary medications
2. Consumer-focused, patient-focused and patient-centred are terms that can be differentiated on the basis of patient involvement, although there is an overlap in the way these terms are used in the litera-ture. Thus the use of these terms in this thesis will be as employed in the supporting literature, but can be considered synonymous
Page 23

include every aspect of a pharmacist's interaction with that consumer, from hospital discharge
to regular refills of prescriptions and non-prescription product requests in the community.
Consequently, within the (community) primary care setting, pharmacists provide direct patient
care; face-to-face counselling and education for their patients; prescribing advice for other
providers; advice on cost-effective drug therapy and options for treatments; and chronic
disease therapy management. In the combination of these roles, pharmacists are considered
to be essential to optimal primary health care (Canadian Pharmacists Association 2004b).
This evolving role may also lead to the development of different practice levels as hospital,
community and consultant medication management pharmacists merge more closely with
general practice and primary care initiatives (Gowan & Roller 2004). Further activities for
community pharmacists could also include: contributing to developing care programmes and
services for 'at risk' consumer groups; developing protocols for consumer counselling and self-
medication; health promotion; multidisciplinary research; and audit and drug utilisation review
(Department of Health Social Services and Public Safety 2004). Demand for this pharmacist
role is likely to be further increased because of aging populations, reductions in the availability
of GPs, shortfalls in residential care beds for patients and reductions of the informal carer
network in communities (Gowan & Roller 2004).
An important aspect of patient-focused pharmacists is that they work closely with general
practitioners and other health care professionals as a team to provide optimal patient care.
Such collaborative service delivery models involving community doctors and pharmacists have
been shown to be successful in helping resolve medication-related problems of patients
(Gilbert et al. 2002).
There is also an increasing realisation in the health domain of the importance of consumer and
health professional partnerships (National Health Information Management Advisory Council
2001; Commonwealth of Australia 2002). Consumer-centred doctor consultation has been
shown to increase consumer satisfaction, lower patient symptom burden and spare health
service resources (Little et al. 2001). Other literature concerned with physician-patient
relationships confirms the importance of participatory and patient-centred relationships in
improving patient satisfaction, medication adherence and disease and illness outcomes
(Worley-Louis, Schommer & Finnegan 2003). In the same way that good patient-physician
relationships are important for good patient outcomes, these relationships are also likely to be
important for effective patient-pharmacist interactions. However, although the patient-centred
model is widely advocated for doctors, its use in medical practice is probably rather limited –
an important reason for this the pressure on consultation time (Little et al. 2001). Such time
limitations are less likely for pharmacists who have an explicit focus on reviewing a patient’s
Page 24

medication.
MM studies have found that pharmacist interventions for community patients improve the
medication use and clinical outcomes for those patients (Frey 2003). A systematic review of
published studies (1990 to 2003) on the effectiveness of pharmaceutical care services
undertaken by Roughead, Semple and Vitry (2005) concluded that pharmaceutical care
services in the community and outpatient settings were effective. Pharmaceutical care
services demonstrated improved medication use, improved signs and symptoms in people
with asthma and improved surrogate endpoints (blood pressure, cholesterol levels,
glycosylated haemoglobin levels and medication use) – although the services reported did not
provide evidence of improved health-related quality of life for patients. Roughead, Semple and
Vitry (2005) suggested that consideration should be given to the use of adverse drug events
and resolution of medication-related problems as an outcome measure in future studies.
Gowan and Roller (2004) have suggested that in the patient-focused care role described for
pharmacists, an integration of particular knowledge and skills is required – these have been
described in and adapted within Figure 1-2. These additional information and knowledge
requirements for the pharmacist – disease states, evidence-based medicine, non-drug
therapy, interpretation of laboratory results, identification of consumer needs, consumer
monitoring skills and history-taking skills – suggests that the information and knowledge
requirements (and perhaps also the decision support requirements) of the pharmacist may be
similar to those of doctors. The ability of pharmacists to access information appropriate to their
needs has been shown to improve their ability to review the appropriateness of prescribed
drugs and identify drug-related problems (Millonig, Jackson & Ellis 2002).
However, the lack of relevant information is a major cause of medication-related sentinel
events and errors, leading the Joint Commission on Accreditation of Healthcare Organizations
to specify that ready accessibility to patient-specific information should be a principal aim for
those health professionals involved in medication management (Rich 2004).
As poor or missing information affects medical decision-making, the question of whether
missing information presents the same problem for pharmacists involved in medication
management naturally arises. Since pharmacists use the same information components as
doctors, this may very well prove to be the case.
Although IT and DSS have not had widespread success in supporting medical decision-
makers, there still appears to be a significant potential for these systems to be of benefit. This,
in turn, suggests a role for a DSS to support pharmacists involved in medication management.
Page 25

In the researcher's domain experience (and that of other domain colleagues), there did not
appear to be any existing DSS to support pharmacists, other than the traditional prescribing
and drug information systems which were part of conventional pharmacy practice – creating
an obvious lacuna which needed to be addressed.
1.7 The research problemThis chapter has introduced the health domain – an environment of rapid change, significant
cost increases and shrinking resources. The inherent complexity and problems of the health
domain challenge the ability of health professionals and the health system to deliver quality
health care safely and efficiently.
A focus of the discussion in this chapter has been medication, a treatment modality
increasingly used in the treatment of chronic disease, which now forms the basis for has been
major concerns because of the increasing prevalence of medication-related adverse effects.
Medication management was introduced as a patient-focused process which aims to improve
the way in which medicines are used by patients – to improve patient outcomes – and,
particularly, to improve the safety of medication use. The important and evolving consumer-
focused role of the pharmacist in medication management suggested that the information and
knowledge needs of pharmacists might well be similar to those of doctors involved in patient
care.
Figure 1-2: Patient care skills for pharmacists adapted from Gowan & Roller (2004)
Knowledge of disease statesKnowledge of disease states
Knowledge of evidence-based medicines
Knowledge of evidence-based medicines
Knowledge of non-drug therapyKnowledge of non-drug therapy
Knowledge of self-help servicesKnowledge of self-help services
Knowledge of laboratory monitoring
Knowledge of laboratory monitoring
Ability to provide education Ability to provide education
Ability to identify needsAbility to identify needs
History-taking &interviewing skills History-taking &
interviewing skills
Patient monitoring skills Patient monitoring skills
Communication skillsCommunication skills
Drug information skillsDrug information skills
Medication management
care plans
Medication management
care plans
Patient Care
Page 26

The promise of technology in the broader context has been questioned, because of the
complexity and nature of health-related information and communication – and perhaps partly
because of information technology failures. However, as IT (and clinical decision support
systems in particular) still hold promise in supporting medical decision-making, the question of
whether any existing and relevant technology support for medication management exists
naturally arises, particularly for pharmacists working in the increasingly important area of
medication reviews. The researcher's domain experience (and that of other domain
practitioners) suggested this may not be the case – which formed the basic focus of this
investigation. Consideration of all these issues led to the postulation of the main research
question:
Can we advance medication management for health consumers by supporting decision-making with a patient-focused information model and technology-based intervention?
Clearly, such a question is too complex to be answered as it stands. The sub-questions
emerging from this principal question are discussed in the remaining chapters of this thesis.
1.8 Scope of the researchMedication management is a concept which includes the patient and all health professionals
involved in medication-related treatment of the patient, including hospital and community
settings. However, including all possible health professionals and the patient was too complex
an investigation for a research project of this nature and time-frame. The scope of the research
was thus limited to the two major health professional groups involved in medication
management – the pharmacist and the doctor. As the pharmacist arguably takes the principal
role in medication management, the research project aimed primarily to provide support the
pharmacist's function. By improving the process for the pharmacist, the researcher believed
that the outcomes for the other partners in the medication management process would also
improve. The term 'patient-focused' in this thesis therefore describes a focus on the patient,
rather than direct patient involvement.
1.9 Significance and contributions of the researchThis thesis describes an exploration of an important and topical area of interest – the ability of
information technology to contribute to improved outcomes in health care and, in particular, the
ability of information technology to improve medication-related outcomes for patients. The
research is significant not only because it is carried out in this important area, but also because
it uses a novel empirical approach to do so.
Page 27

It is expected that this thesis will make a contribution to both theory and practice.
In theoretical terms, the research project:
• adds to knowledge and contributes to the literature of an emerging area of interest – the
application of technology to health care and, in particular, decision support tools
• will identify issues which affect the approach to development, implementation and
success of decision support tools
• adds to the empirical evidence for the need for decision support tools by pharmacists
involved in medication management
• investigates issues which underpin the development of an information model for
medication management
• adds to the understanding of decision-making and knowledge use by pharmacists and
doctors involved in medication management
• investigates the relationship between the support offered by medication-related
information models and knowledge use by pharmacists
• examines a document-centric user-interaction approach to support the medication
management process for doctors and pharmacists – in particular, the role played by a
digital document to share and communicate medication-related information
• investigates the importance of dynamic properties to the support offered by a digital
document to medication-related decision-making
• provides a substantial analysis of design research theory, significantly extending existing
studies into this approach.
In practical terms, the research project:
• aims to provide a framework upon which pharmacists and doctors can improve the
practice of medication management – in particular, safety, quality and efficiency of the
process – enabling better outcomes for patients
• identifies technology-related issues which may impact on the ability of researchers or
developers of decision support tools to undertake a technology-based intervention in the
community
• contributes to knowledge within and beyond the project by publishing research findings
• develops technology artefacts that can be used in future research to support and
improve the medication management process.
Page 28

1.10 Outline of the thesisThis thesis is structured into eight chapters which describe the background, methodology,
empirical research and conclusions related to this exploration of technology use in Health.
• Chapter 2 describes two literature reviews. The first review looked for evidence of
existing decision support tools for pharmacists in the area of medication management;
and provided the justification for this project. The second literature review investigated
and justified the technology approach – the digital document – used for this project
• Chapter 3 introduces methodological concepts and describes the selection of the
research approach based on comparisons of candidate research methods
• Chapter 4 elaborates on the chosen research method (Design Research) and discusses
its suitability for complex and dynamic environments – the health care domain – justifying
the novel use of this method in this project
• Chapter 5 is the first of three empirical research chapters, and provides a description of
an investigation of the information-rich hospital environment. Within this environment
there was an exploration of the use of information and knowledge of hospital
pharmacists and doctors involved in medication management. The results from this
scenario formed the basis for the development of the information model and XForms-
based digital document prototype
• Chapter 6 describes the testing of the hospital-centric digital document prototype by
pharmacists accredited to undertake medication reviews on patients in the community
setting. This testing refined and prepared the digital document (and consequently the
underlying information model) for the community context
• Chapter 7 describes the field studies that evaluated the digital prototype intervention –
looking for improvement in the safety, quality and efficiency of the medication
management process. The participants in the field studies were accredited pharmacists
and community doctors who were involved in medication reviews
• Chapter 8 summarises the findings from this research, draws conclusions and suggests
future research directions.
The empirical research resulted in the collection of a large amount of rich data, too substantial
to report in detail in this thesis. Consequently, the detailed analyses of data are contained in
appendices, with summaries of the analyses being included in the thesis chapters. Appendices
were also used to report source code, extensive documentation (such as approvals from
Ethics Committees) and the bibliography. All appendices, formatted as PDF files, are
contained in the CD-ROM which accompanies this thesis. The relationship of chapters and
appendices is shown in Figure 1-3. It should be noted that some appendices (e.g.
development records contained on spreadsheets) may require magnification for comfortable
viewing.
Page 29

Figure 1-3: Relationship of chapters and appendices
Chapter 1: IntroductionChapter 1: Introduction
Chapter 2: Literature reviewsChapter 2: Literature reviews
Chapter 3: MethodologyChapter 3: Methodology
Chapter 4: Design researchChapter 4: Design research
Chapter 5: Hospital scenarioChapter 5: Hospital scenario
Chapter 6: Benchtop testingChapter 6: Benchtop testing
Chapter 7: Field studiesChapter 7: Field studies
Chapter 8: Discussion & conclusionsChapter 8: Discussion & conclusions
Chapters
A: Analysis of pharmacy decision support literature
B: An Investigation of Methodology
E: Hospital Ethics Approval & relevant correspondence
H: Pharmacist Questionnaire
I: Medical Officer Questionnaire
J: Hospital – Full Analysis
K: Hospital – Technical & Development
L: Hospital – VB Viewer Code
M: Hospital – XForms Code
N: Hospital – Patient XML File
O: Benchtop – Full Analysis
R: Benchtop – VB Viewer Code
F: Benchtop Testing Ethics Approval
G: Field Studies Ethics Approval
P: Benchtop – Technical & Development
Q: Development Record (Excel spreadsheet)
T: Benchtop – XForms Code
S: Benchtop – ASP Code
U: Benchtop – Patient XML File
X: Field studies – Full Analysis
Z: Field studies – Technical & Development
AA: Field studies – XForms Code
Y: Field studies – Additional Information &Consent Forms
AD: Bibliography
V: Benchtop – XSL Code
W: Benchtop – Comparison of Model Elements (Excel)
D: HOT Fit Model Items
C: HMR Quality Assurance form
AB: Field studies – Patient XML File
AC: Field studies – XSL Code
Appendices (contained on CD-ROM)
Page 30

Chapter 2
Addressing the problem of medication-relateddecision support for pharmacists: investigating the
literature
2.1 IntroductionChapter 1 set the scenario for this research, by discussing the health domain in relation to the
complexity and problems inherent in the modern day challenges of improving quality, efficiency
and safety in an environment of rapid change, significant cost increases and shrinking
resources.
A particular focus of this discussion was the area of medication, a treatment modality
increasingly used in modern medicine. The promise of technology in the broader context has
been questioned, because of the complexity and nature of health-related information and
communication – and also, perhaps, partly because there have been some widely-publicised
technology failures.
The question for this chapter now relates to whether there is any existing and relevant
technology support for medication management, particularly for pharmacists working in the
increasingly important area of medication reviews. Informal responses from domain
practitioners suggested there was little such technology, other than traditional use of
technology for dispensing and provision of electronic drug information. This, in turn, led to a
further potential question – if no such support was currently extant, what might be a suitable
technology for this purpose?
In summary, the questions addressed by the review of the literature are, firstly:
What support is there for pharmacists for medication-related decision-making?
and, subsequently, if none existed:
What technology might provide this support?
Page 31

This chapter is structured as follows:
• Section 2.2 describes the major literature review undertaken to answer the first
question; and evaluates and summarises the findings
• Section 2.3 describes the minor literature review which provided an answer to the
second question and supported the technology approach of this project
• the chapter summary that brings together the literature findings and identifies the full set
of research questions is found within Section 2.4.
2.2 Identifying appropriate medication management support for pharmacists
2. 2.1 BackgroundAs described in Chapter 1, 2002 saw the establishment of the National Electronic Decision
Support Taskforce (NEDST) to consider the benefits and difficulties of adopting a national
approach to electronic decision support in Australia (The National Institute of Clinical Studies
2002). This taskforce undertook a fairly substantial review of the literature as a preliminary to
identifying possible solutions (National Electronic Decision Support Taskforce 2002), but found
only two pharmacy-related Electronic Decision Support Systems (EDSS), both relatively
simple systems.
Given the significant amount of activity and research in EDSS more broadly, it was
disappointing to see how little evidence there was concerning the use of EDSS in the
pharmacy sector – particularly in light of the evolving role of the pharmacist in medication
management. The major literature review, which follows in this chapter, was born from the
need to investigate any published evidence of research and/or implementation of EDSS to
support pharmacists since the NEDST report. The findings of this literature review formed the
basis for the present research project.
2. 2.2 Finding evidence in the literatureThe aim of the literature review was to identify EDSS which directly supported pharmacists or
pharmacy practice in either a hospital or community setting. This had the potential to: produce
an inventory of systems in use or under development; ascertain what type of research was
(not) being done; identify any observable deficits or gaps for EDS in pharmacy; and identify
opportunities for EDSS in pharmacy. The NEDST report provided a solid starting point but that
review was limited to randomised controlled trials. Because of the paucity of randomised
controlled trials in this area, a wider net was cast to find any implemented system for which
there was an evaluation or evidence of use. In addition, the 'clinicians' mentioned by NEDST
included physicians, nurses and allied health practitioners, while the present project focused
Page 32

on activities directly related to pharmacists and/or pharmacy practice. The NEDST criteria are
shown in Table 2-1.
A brief overview of the literature approach to the question of pharmacy decision support
follows, although a more detailed search strategy and results are shown in Appendix A.
A systematic search strategy was used to identify relevant literature. Although Pubmed was
expected to provide the vast majority of literature, additional sources were also investigated to
minimise the risk of missing any relevant literature. These included journals with known
publication of decision support articles (e.g. the Journal of the American Medical Informatics
Association) and relevant databases (e.g. Science Direct and the Cochrane Reviews
Database).
The search strategy used Medical Subject Headings (MeSH) from the US National Library of
Medicine (determined by use of the text words ‘pharmacy’, ‘pharmaceutical’, ‘decision’,
‘support’ and ’evidence’); together with combinations of selected text words ('pharmacy’,
’decision’, ‘support’, ‘evidence', 'pharmaceutical’, ‘evaluation’). The term 'decision support' has
already been discussed in the context of this research project in Chapter 1 – the project does
not attempt to develop a decision support 'system' in the traditional sense of the word, but the
Table 2-1: NEDST criteria for selection of publications of EDSS (National Electronic Decision Support Taskforce 2002)
CriteriaImplemented and in routine use by clinicians.
Used within the last 5 years (at the time of survey).
Provided clinical, rather than management, support.
Were not embedded into medical instruments.
Table 2-2: Categorisation of types of EDSS by the NEDST (National Electronic Decision Support Taskforce 2002)
Type CategorisationOne Provides categorised information that requires further processing and analysis by
users before a decision can be made.
Two Presents the clinician with trends of patients’ changing clinical status and alerts clinicians to out-of-range assessment results and intervention strategies. Clinicians are prompted to review information related to the alerts before arriving at a clinical decision.
Three Uses deductive inference engines to operate on a specific knowledge base and automatically generates diagnostic or intervention recommendations based on changing patient clinical condition, with the knowledge and inference engines stored in the knowledge base.
Four Uses more complex knowledge management and inference models such as case management reasoning, neural networks, or statistical discrimination analysis to perform outcome or prognostic predictions. Such systems possess self-learning capabilities and use fuzzy set formalism and similarity measures or confidence level computation as mechanisms to deal intelligently and accurately with uncertainty.
Page 33

literature review needed to use this term to ensure pertinent material was found.
This combined search of databases and journals identified 389 unique references. The
abstracts from these references were obtained and evaluated. Of the 389, 104 (27%) were
related to pharmacy; and 23 made reference to ‘decision support’ where this was used in a
very broad sense. One particularly interesting finding was that four papers cited in the NEDST
study were actually missed by this search. So despite what was considered a broad search, it
was still possible for some relevant information to slip through the net – highlighting a problem
when attempting ‘complete’ reviews.
Where possible, full electronic or hard copies were obtained of the 23 decision support papers;
and these were evaluated against the NEDST criteria with only four being successful. The
remaining 19 papers described professional practice or professional issues, drug safety,
pharmaco-economics, information technology, or decision making in general. The EDSS
described in these papers were also classified according to their ‘type’ described in the NEDST
report to give an indication of their level of sophistication (see Table 2-2). And even these four
papers (summarised in Table 2-3), while meeting criteria, did not describe systems of
relevance to this project, i.e. supporting pharmacists with medication management. Rather,
they described relatively simple EDSS according to the NEDST categorisation, three being
concerned with the generation of alerts and one relating to changes in pharmacist work
practices.
Amsden (2003) describes a system perhaps closest to the notion of supporting pharmacists
with medication management. This hospital-based system combined information from a
number of hospital systems and; through a rules-based system, alerts pharmacists to whether
a specific patient required review (monitoring). Although useful in itself, however, this is a good
example of a sophisticated problem-alerting system rather than relating to supporting decision-
making.
The alerting system described by Armstrong & Denemark (1998) informed pharmacists about
possible therapeutic duplication, drug interactions, high or low doses, drug overuse or
underuse; and drug-pregnancy conflicts. This on-line ‘electronic’ alert to the pharmacist was
generated by a Medicaid1 claims processor based on drug utilisation review (DUR) criteria.
This alert provided the possibility for a community pharmacist intervention (usually with the
doctor or patient) prior to dispensing further supplies of medication.
1. Medicaid is the United States’ health insurance program for individuals and families with low incomes.
Page 34

Monane et al. (1998) describe a system based on prescription claims, similar to that developed
by Armstrong & Denemark (1998), although relating to elderly patients within a Managed
Care1 system. When medications were entered into the on-line computerised DUR system
(containing previous medication claims), they could trigger an actionable alert that was sent to
the pharmacist. The alert was intended to trigger communication between the pharmacist and
doctor; and included rationales for the alert, therapeutic alternatives; and possible withdrawal
protocols – this presented an opportunity to change potentially inappropriate medication
before it was dispensed to the patient.
Murray et al. (1998) offered a particularly interesting perspective on the effect of a decision
support system on pharmacists, describing the effects of computer-based prescribing on
pharmacist work patterns following the implementation of Computer Physician Order Entry
1. Managed Care in the United States very generally describes a funded (insurance) plan that controls all aspects of the health care of the insured individuals.
Table 2-3: Pharmacy-related electronic decision support systems revealed in literature
Author(s) Title Description Outcomes Type of EDSS
Amsden, 2003 Push technology in the pharmacy. Clinical decision support helps the pharmacy department of a South Carolina medical center automate monitoring of medication effectiveness.
550 rules-based alerting system for pharmacists that combined information from the pharmacy system, laboratory system, and patient location system for patient monitoring.
38% savings in pharmacist time, 24% increase in interventions. Cost savings of US$50, 000 per annum.
2
Armstrong and Denemark, 1998
How pharmacists respond to on-line, real-time DUR alerts.
Real-time, on-line alerting system for pharmacists for prescription criteria.
20.9% of prescriptions not dispensed (medication over-utilisation, high dose, therapeutic duplication, low dose, drug–pregnancy and drug–drug interaction).
2
Monane et al., 1998
Improving prescribing patterns for the elderly through an on-line drug utilization review intervention: a system linking the physician, pharmacist, and computer.
Pharmacists alerted based on predetermined criteria for elderly patients. The pharmacist then initiated telephone-based therapeutic interventions to physicians.
Rate of change of therapeutic agent was 24% (compared to 2% expected baseline).
2
Murray et al., 1998
Effects of computer-based prescribing on pharmacist work patterns.
Work sampling of pharmacists at a hospital-based outpatient pharmacy before and after the implementation of computer-based prescribing.
Pharmacists spent 12.9% more time correcting prescription problems, 34.0% less time filling prescriptions, 45.8% more time in problem solving and 3.4% less time providing advice.
2
Page 35

(CPOE), rather than describing decision support for pharmacists per se.
Another notable observation was that three of these papers described projects in the mid-
1990’s. Recent activity in medically-based decision support activity did not appear to be
mirrored by similar current (published) activity for pharmacy.
However, a further paper relevant to the literature review was found late in the project –
‘Development of an intelligent decision support system for medication review’. This paper, by
Bindoff et al. (2007), described a knowledge-based system using a multiple classification
ripple-down rules approach, which allowed a user to identify medication-related problems
using the patient’s demographic, medical information and drug-related information. Although
the subject of this paper was highly relevant, it was based on a single test of a prototype
system using one clinical pharmacist. Thus, it still did not fulfil the inclusion criteria as it was
not an implemented system in routine clinical use.
In brief, this systematic literature review concurred with the findings of the NEDST that there
was little published evidence of pharmacy-related decision support outside systems which
traditionally support pharmacists – predominantly dispensing systems.
2. 2.3 Finding other evidenceIt is widely accepted that much information is published on-line and may not even appear in
journals or databases; and this was acknowledged by the inclusion of web sites as sources in
the NEDST review. These web sites were explored with a similar intent as for the literature
review. The web sites (viewed 2004-05-12) included: http://www.coiera.com/ailist/list.html;
http://openclinical.org/aidss.html; and http://medexpert.imc.akh-wien.ac.at/; and revealed 80
unique EDSS systems. Of these, 8 had definitely been decommissioned, but it was difficult to
ascertain whether some of the other systems were still in use. Two systems which involved or
directly supported pharmacy practice were simple alerting systems:
• DoseChecker generated pharmacist alerts for inappropriate drug dosing where it fell
outside guidelines for patients with renal impairment; and
• Microbiology/Pharmacy Expert System is a PC rules-based system producing dBase®
output and used by pharmacists to monitor aminoglycoside antibiotic dosing.
The lack of published evidence of pharmacist-specific decision support was counter to the
researcher’s personal knowledge and domain experience that such activities were occurring,
at least in Australia. And since Canada and the United Kingdom (UK) have similar health care
systems to Australia’s, there should also have been more evidence of these activities in those
locations. The researcher's familiarity with the Australian pharmacy sector prompted and
Page 36

enabled investigation of other, less obvious sources of information including Information
Technology (IT)-related papers presented at the biennial conferences of the Society of
Hospital Pharmacists of Australia (SHPA) and the Australian Quality Use of Medicines Project
Mapping website.
A review of SHPA conference proceedings (1999, 2001 and 2003) revealed that of 39 IT-
related presentations, 14 described clinical decision support (one presentation actually
reported on 4 projects). The vast majority of these were Type 1, and five systems could be
considered of Type 2. The majority of the remaining presentations dealt with use of IT for
management support, administrative or supply functions, discussions of electronic prescribing
or system implementations. About 50% of the presentations for each year concerned the use
of simple local databases for reporting activities. An interesting trend, however, was the
increase in the sophistication of topic areas over time.
The Quality Use of Medicines Project Mapping web site (http://www.qummap.health.gov.au/,
viewed 2004-05-19) provided evidence of other Australian-related activity. This site revealed
four projects of Type 1: one described the conversion of existing drug prescribing guidelines
into portable electronic format; two involved the integration of existing electronic information
products into single products; and one project aimed to provide wireless access to clinical
information for clinical pharmacists. The first three projects were not exclusively directed at
pharmacists.
Examination of the Australian scene, therefore, despite its initially promising appearance,
added little to the evidence sought for presence of pharmacy-related decision support. The
researcher’s impression of decision support activities was that they uniformly related to
information retrieval or alerting systems. The overall picture is represented in Figure 2-1.
Page 37

Without any clues from the literature about what was happening in the UK and Canada, the
path chosen for investigation of pharmacy practice perspectives was through websites of
pharmacy profession organisations in those locations. However, this proved to be a particularly
fruitless avenue.
Although there was clear evidence of IT-related activities in the UK, no status report could be
found. Of note, a conference organised by the Royal Pharmaceutical Society (’2000 and
counting – the application of IT to modern pharmacy practice’) addressed developments in the
IT area, and the introduction of new technologies into pharmacy practice (‘Forum 2000’ 2000).
The importance of IT was signified as the central conference theme, but it was interesting to
note that the developments which took precedence were primarily concerned with information
retrieval – that is, Type 1 systems. National strategies were evident in the general health
environment to support health care professionals with IT-enabled communication, patient
records and information for better patient outcomes (Department of Health 2002) and for
pharmacy IT priorities (Giles-Burness & Roberts 2002).
Personal communication suggested there was a significant amount of pharmacy decision
support activity in Canada, but this was occurring in the commercial environment and thus was
Figure 2-1: Process and results for pharmacy decision support information sources
Literature
Selected NEDST web sites
389Unique references
780Total
46Cochrane reviews
110Databases & selected journals
88PubMed text terms
536PubMed Mesh terms
References
23About ‘decision support’
104Pharmacy-related
8Decommissioned
80Unique EDSS
Australian hospital pharmacy conferences
39IT-related presentations
524Type 2 EDSS
49Type 1 EDSS
Quality Use of Medicines Project mapping site
Information sources meeting criteria
4 2 14 4
Page 38

not reported in the peer reviewed literature:
... there is certainly a lot of activity in pharmacy decision support but not a ton of reports in the peer-reviewed literature because these systems are proprietary in nature. This software area is very competitive in the pharmacy world (personal email communication, (Neil MacKinnon, May 19, 2005).
The Canadian Pharmacist’s Association’s website (http://www.pharmacists.ca/content/hcp/
Resource_Centre/Pharmacy_Practice_Research/cppr_list.cfm, viewed 2004-05-12) provided
a brief description of one information technology related project. This project, Enhancing
Pharmacist-Physician Communication Using Information Technology, was designed to
determine the feasibility of, and the proof of concept for, establishing an electronic network
between pairs of community pharmacists and family physicians to exchange information on
their patients.
Although not Canadian, the ComputerTalk website (http://www.computertalk.com/
index.html?=FromMainFrame=AboutUs.html, viewed 2004-01-19), a North American website
which publishes information about retail and community systems (Computer Talk for
Pharmacists) and hospital information systems (Computer Talk for Health-System
Pharmacies), was also assessed. Any critical evaluation was difficult as features of described
systems were at high functional levels and listed under company profiles. However, the overall
impression of the researcher was that more electronic decision support related to hospital
systems than to retail systems where there is greater emphasis on Point-of-Sale (POS)
integration, inventory, claims management, billing and (dispensing) workflow management.
Electronic information sources and decision support tended to be listed under names of other
third party providers.
2. 2.4 Was any evidence missed?Although an attempt was made to cast a wide net for recent literature, it is possible that some
references were missed. It was mentioned earlier that four of the references evaluated in the
NEDST citation list did not surface in the PubMed literature search. The focus on Australia, the
UK and Canada as areas of interest, although pertinent for comparison, may also have
imposed some limitations. This was ironically verified during the submission of this literature
review for publication in The International Journal of Pharmacy Practice (Calabretto, Warren
& Bird 2005). A European reviewer (personal communication, 31/1/2005) suggested that the
researcher had missed evidence about pharmacy-related decision support tools in Europe.
This may be true, but strengthened the message delivered in that publication that this type of
work is not published (or perhaps was not robust enough to be published?).
Although very general search terms were used, an issue could also be the use of different
keywords allocated to publications by the authors. Additionally, the restriction to the English
Page 39
language may have narrowed the results. The reporting of activities in the literature may also
be underestimated by the increasing trend to publish such information on the world-wide web;
and the fact that much information of this type may be ‘hidden’ in commercial contexts or in
conference proceedings. This adds to the general difficulty of retrieval and is exceedingly
problematic. Despite these limitations, the researcher’s domain knowledge and the use of
adapted criteria should have ensured that the magnitude of the findings was nevertheless
representative of the situation.
Despite the difficulties of identifying publications relating to decision support systems for
pharmacy, the profession is well represented in the literature in more general discussions
about decision support and, in particular, electronic prescribing and medication safety. From
the perspective of other EDS activities, pharmacy dispensing systems (both in the community
and in the hospital settings) do provide levels of electronic decision support. Most commonly,
these are alerts for drug-drug interactions, drug-allergy interactions, drug-food interactions and
drug-dose checking (e.g. maximum and minimum dose and/or frequency). Systems that are
more sophisticated may also provide alerts for drug-disease interactions, drug-laboratory
result interactions, therapeutic duplication, dose alerts in paediatrics, pregnancy or geriatrics
(although the latter are more typically provided in hospital-based systems). While it may be
possible to obtain broad system feature comparisons, there are no publications which critically
evaluate these systems, or evaluate impacts/outcomes of these features. As these systems
are commercial in nature, this is perhaps not surprising.
Therefore in answering the question:
What support is there for pharmacists for medication-related decision-making?
There is little to suggest that decision support exists for pharmacists other than for information
retrieval or some cases of alert systems. While this lack does not detract from the value of
those systems, these are not suitable tools to support the process or related decision-making
in the evolving role of the pharmacist described in Chapter 1. The need to develop such tools
was thus conveyed by the (lack of) literature.
This need for ‘specialist’ support for pharmacists is no different to examples of support for
knowledge management or decision-making in the wider IT community, such as supporting
knowledge management and organisational memory in city councils (Schwabe 1999;
Schwabe & Krcmar 2000a), or integrated knowledge management to meet the challenges of
anti-terrorism initiatives for law enforcement agencies (Chen et al. 2003).
Page 40

Having identified the need to develop such tools, the next step in the research project was to
consider a suitable technology, revealed by a subsequent literature review in Section 2.3.
2.3 Looking for a technologyThe literature from this review and that supporting the introduction (Chapter 1) also provided
some guidance as to the general characteristics for a supporting technology. A sound
decision-related information and workflow model was needed to support or acknowledge:
• the increasing emphasis on continuity of care at the hospital-community interface and
coordinated care (Gowan & Roller 2004)
• the evolving and increasingly clinical role of the pharmacist in the community
(Whitehead, Sunderland & Benrimoj 2003; Department of Health Social Services and
Public Safety 2004; Gowan & Roller 2004)
• a more patient-focused approach (Little et al. 2001; Gowan & Roller 2004)
• increased knowledge and information requirements of the pharmacist (Gowan & Roller
2004) similar to medical professionals
• customisation to fit into local practice patterns, and attention to standards of care and
workflow issues to achieve acceptance by users (National Electronic Health Records
Taskforce 2000)
• the local health care contributions by pharmacists into the broader health system (Giles-
Burness & Roberts 2002).
With the confirmation of the lack of appropriate tools for pharmacists, attention turned to what
might be suitable steps to begin to address this lacuna. As the aim was to develop tools to
support contextual decision-making, an investigation of the context was required. And before
one can be informed about something, this ‘something’ must first be modelled (Berg &
Toussaint 2003). Ely et al. (2000) have suggested that a taxonomy of doctors’ questions about
patient care may enhance the understanding of doctors’ information needs and improve the
ability to meet those needs. Such a taxonomy would be equally useful in assessing the
information needs of pharmacists from the perspective of medication management (MM). The
best way to do this seemed to be to investigate pharmacists directly, as the design of
information and communication systems must include the people who will use them – since
interpretation is dependent upon the user’s specific context, culture, knowledge and resources
(Coiera 2003b). The abstraction of requirements from the ‘messiness and the concrete forms
of the work practices’ as well as being a necessary step in requirements elicitation also
facilitates user interaction in the process (Berg & Toussaint 2003).
As the MM process involves doctors and pharmacists, there was also a need to investigate the
doctors’ involvement in; and perception of the MM process. Bates and Gawande (2003) note
Page 41

that it remains difficult to change clinical practice, adding that it is important to understand the
impact of decision support when identifying the common elements of success in this area.
Therefore, in the first stages of this project it was important to identify a taxonomy that allowed
the categorisation of information needs, sound understanding of the ‘information space’
(Coiera 2003b); and the communication contexts that affected good decision making.
As no tool for this purpose was evident in the literature, there was similarly no expectation that
a taxonomy or model for the concept of medication management would exist – and none was
found. The ‘medication models’ cited most commonly describe processes or guidelines, rather
than the issues relevant to this project.
A commentary by Cameron (2005) on medication management models and other pharmacist
interventions described two models:
• The first Medication Management Model was well described in the literature, although it
actually referred to a medication review process involving a home care nurse, consultant
pharmacist and primary physician using a set of guidelines to address four high risk
medication problems in the high-risk elderly population (Frey & Rahman 2003). These
problems included: prevention of unnecessary therapeutic duplication; issues related to
cardiovascular medication; use of psychotropic drugs in patients with recent falls; or
confusion and psychotropic drugs in patients with assessment of recent confusion.
These guidelines had grown out of earlier published criteria for determining potentially
inappropriate medication use in the elderly (Beers 1997) and have been subsequently
been updated (Fick et al. 2003).
• A second model was the pharmacist intervention program, PHARMAssist which consists
of six monthly meetings between participants and pharmacists to discuss correct and
safe medication use, supported by a medication record that participants are encouraged
to maintain and share with other health care providers (Cameron 2005).
Other (medication management) models mentioned in the literature described broader
applications of the term, including collaborative service delivery (Gilbert et al. 2002), disease-
based pharmaceutical care such as asthma (Saini, Krass & Armour 2004), primary care
pharmacy (Carmichael et al. 2004) and substance use disorders in patients with severe mental
illness (Mueser, Drake & Wallach 1998). Lacking an existing model on which to base this
project, it was clear that one would have to be developed from first principles.
Page 42

However, even if a suitable taxonomy could be described, the next research question
remained:
What technology might provide this support?
Chapter 1 attested to the difficulty of designing ‘decision support systems’ in general and
suggested that important elements were flexible information representation and
communication. Early consideration of a supporting technology by the researcher indicated
that a document metaphor might have the appropriate expressiveness and flexibility to support
the aim of the project. The background to this view is revealed in the next sub-section.
2. 3.1 Why a document?The document remains the pervasive way of representing information regardless of the
progress and similar intent of the Internet; and paper is still an important aspect of information
representation (McNurlin & Sprague 2005, p. 280).
Further, despite various technologies available for content storage and manipulation, much
content for human use is still understood and processed in the form of documents (Honkaranta
2001). Primarily as paper forms, documents are still the most common vehicle for carrying out
processes, carrying information and accumulating input from a chain of people as they
(documents) move through organisations (McNurlin & Sprague 2005, p. 285). In a typical
organisation, 80%-90% of the recorded information is represented as documents rather than
as highly structured data for manipulation (Honkaranta 2001). In addition, as individuals may
have no, or only infrequent access to the Internet, a case could be made for maintaining both
means of representation (McNurlin & Sprague 2005, p. 282).
A document-oriented user-interaction paradigm is an intuitive way of supporting clinical
documentation, as well as an effective mechanism of allowing information communication
between individuals involved in the health care process (Lenz et al. 2002). Berg and Toussaint
(2003) state that what makes paper (documents) particularly well-suited in supporting Western
medical work is their ability to accumulate data during a patient trajectory; and coordinating
activities and events at various locations or times. The researcher’s domain experience
confirms that most health-related information is contained in a broad range of general purpose
and specifically designed documents used to share or communicate information, or as
personal repositories. The document-oriented view of a data structure (supported by XML),
also matches the organisation of health care data very well (Schweiger et al. 2005). In addition
to content and communication, documents (in a broad sense) can also have other benefits for
users, such as allowing adaptability, flexibility, portability and visibility (Fitzpatrick 2000a),
providing virtual meeting places (Toomey, Adams & Churchill 1998); and also taking on social
Page 43

roles (Brown & Duguid 1995) – benefits which are discussed later. The nature of what a
document ‘is’, forms the basis of much debate in the literature. As it is important to understand
what role a document was going to play in the framework of this project, some relevant
discussion is offered.
2. 3.2 What is a document?
2. 3.2.1 The historical perspectiveHistorically a document is associated with paper, e.g. defined by the Macquarie Dictionary as
‘a written or printed paper furnishing information or evidence’ (Delbridge 1982). Other
definitions move away from the object and instead concentrate on the content, e.g. a unit of
'recorded information structured for human consumption' (McNurlin & Sprague 2005, p. 280).
Van der Meer (1994, p. 13) in Uijlenbroek (1997, p. 17) takes this idea further and defines a
document as 'an object which has the purpose, or to which the purpose is given, to serve the
perusal of the information it contains', without mention of the technology required to examine
the document. Therefore, any data-containing item could be regarded as a document, e.g. a
letter, book, computer disk, computer chipset or even a traffic sign (Uijlenbroek 1997, p. 17).
The notion of a document has further changed over time to include reference to the fact that
IT is now a common medium for viewing documents and has progressed from simply the
notion of display, although a definitive characterisation is difficult because of the arbitrary way
in which the ‘frontier’ between documents and non-documents is discussed (Buckland 1998).
A more technology-oriented and broader definition of a document is:
... a snapshot of some set of information that can: incorporate many complex informational types, exist in multiple places across a network, depend on other documents for information, change on the fly (as subordinate documents are updated), have an intricate structure or complex data types such as full-motion video and voice annotations and be viewed and modified by many people simultaneously (if they have permission to do so) (Michalsky 1991)
Documents previously created and stored on paper are now digitally created, stored,
transferred and displayed; and the application of technology to process traditional documents
can change organisational outcomes (McNurlin & Sprague 2005, p. 280). This leads to
consideration of a ‘digital document’ in the next sub-section.
2. 3.2.2 What is a digital document?As organisational information is increasingly created and maintained as formal and informal
digital documents (Murphy 1998), the media or technology used to embody a document can
confuse the understanding of what a document actually is (Honkaranta 2001). Digital
technology consequently rekindles discussions about medium, message and meaning as
technological definitions of a document become more obscure when ‘everything is in bits’
(Buckland 1998). Buckland (1998) adds that the definition of documents needs to move away
from encompassing traditional physical forms to a definition in terms of function. For example,
Page 44

a digital document could be defined as ‘electronically recorded information flexibly structured
for human consumption’ (Murphy 2001).
There are however, some fundamental differences in how traditional and digital documents are
differentiated. Furuta (1995) lists these as:
• permanence – a digital document may never occur in a concrete, discrete form
• the reflection of importance in form – traditional documents usually contain an indication
of the their importance
• size – digital documents can vary enormously in size, ranging from words to megabytes.
Traditional documents may also be large, but unlikely to be so without requiring
computer assistance in preparation.
On the other hand, digital documents must also be differentiated from unstructured computer
files or computer databases. Again, Furuta (1995) provides guidance. A digital document is:
• a self-contained unit or intellectual contribution
• formed from component parts and relationships among those components
• intentionally authored, reflecting the author's intention with semantic relationships among
components.
These characteristics of course, equally apply to the authoring of ‘traditional’ documents.
Given the ubiquitous and blossoming nature of digital documents, no discussion of them in a
business context would be incomplete without giving some attention to the growing problem of
how to manage them – and this usually involves Electronic/Document Management Systems
(E/DMS), discussed next.
2. 3.2.3 Managing documentsDocument management and E/DMS will not be discussed in depth as while this project uses
digital documents, it is not focused on creating a ’system’ to manage digital documents. Should
the life of this digital document exceed the life of the project, however, this may need to be a
future consideration.
The consideration of documents as the knowledge assets of an organisation (in a general
sense), creates a need for mechanisms for collaboration and coordination between authors
and users; and a means to manage and evaluate increasing amounts of knowledge – this is
the intent of a well-designed E/DMS (Ginsburg 2000). Good E/DMS can also be the basis for
quality improvement and process redesign (McNurlin & Sprague 2005, p. 281). The adoption
of XML, which changes (Web) content from a human-readable, static representation (as
HTML) to a form that is ‘computer-readable’, allows more dynamic document content
(McNurlin & Sprague 2005, p. 287). Of course, this assumes that the computer has been ‘told
Page 45
what it means’ and ‘what to do with it’.
McNurlin & Sprague (2005) propose that good content management can be achieved by
understanding the goals of three phases of the content life-cycle – quality, efficiency and
effectiveness – and designing the phase with the particular goal in mind.
Tyrväinen & Päivärinta (1999) also investigate organisational E/DMS using document
classification through their document life cycle perspective (production, storage, processing
and use) and conclude that universal definitions for a ‘document’ are not suitable to conceive
organisational EDMS. They comment that this is affected by purpose of use (to observe facts,
meaning intended by the author, interpretation of data, reuse or co-ordination); and the time of
observations (when the event is recorded or the structure, knowledge or data). Within this
project, purpose of use and reuse are major considerations.
Of course, the intent of sharing document information may be from other perspectives. The
Information Continuum Model, developed by researchers at Monash University in Australia
had as its fundamental concerns, empowerment and social justice (Schauder, Stillman &
Johanson 2005).
Although general E/DMS are not relevant for this project, one particular approach to document
management based on classification did have some relevance. ‘Genres’ are used for
classification of documents for Electronic Document Management (EDM) (Karjalainen et al.
2000) or for the generation of taxonomies used in large unstructured document collections
(Müller et al. 1999). Relevance within this project was based on the potential of the genre
approach to assist with the development of taxonomies.
2. 3.2.4 GenresThe concept of genre has its roots in art and literature, where it examines how the semantic
content of text is shaped and determined by its generic nature and traditions, thus laying down
the structure, format and use of language (Toms & Campbell 1999). Genres represent one of
the many research perspectives within digital documents, which also include: hard vs. soft
documents (the latter containing inconsistencies and duplication); social interactions; support
tools; and searching (Murphy 1998).
Genre analysis involves the classification of documents based on persistent and socially
recognised combinations of form (observable physical and linguistic features) and content
(social motives, themes and topics of communication) – this is valid regardless of the media
used, and so can relate to digital or traditional documents (Honkaranta 2001; Murphy 2001).
Page 46

However, the intent is usually in relation to digital documents and newer genres can emerge
as a result of the diffusion of digital media (Tyrväinen & Päivärinta 1999). Shepherd and
Watters (1998) have described a new class of genre – the cybergenre – resulting from the
combination of the computer and the Internet. They suggest that the cybergenre can be
characterised by the triple, <content, form, functionality>, compared to genres in other media
characterised by the tuple, <content, form>. The functionality afforded by cybergenres allows
the generation of new genres, either not based on previously existing genres or substantially
different from existing genres. One application of cybergenres has been for the automatic
identification of web pages, to distinguish organisational, corporate and personal home pages
(Shepherd, Watters & Kennedy 2004).
Honkaranta (2001) has described the use of a ‘genre lens’ for requirements analysis and for
designing content workflows; and Karjalainen et al. (2000) have described a practice-oriented
method using genre-based metadata for EDM.
Instances of a genre may vary significantly not only in content, but also in ordering and other
structural elements (Murphy 2001). Yoshioka et al. (2001) use this for the formulation of
taxonomies. Genre taxonomy expresses the form of communication (purpose, content,
participants, timing, location, and form); and distinguishes between contexts of use (e.g. a
widely used report vs. a specific technical report). Progression of a genre also allows
understanding of use, change and coordination aspects thus generating ideas for improving
work processes.
As the nature of genre approach is to classify groups of documents, it became clear that this
approach was less relevant to the project. Although discussion of the different document
elements are pertinent to the project, the medication management document can be
considered a particular specialisation of a genre, as the form and communicative actions of the
document are for the specific purpose of supporting medication review.
This discussion now turns to two of the main interests for a document in this project:
information representation; and communication.
2. 3.3 The expression of information in documentsIn discussions about information, definitions of a document often focus on a single aspect and
are often metaphorical, for example ‘captured knowledge’, ’data in context’; and ’an organised
view of information’ (Buckland 1998). Otlet (1934) in Buckland (1998) defined documents as
graphic and written records representing ideas or of objects; and believed that the objects
Page 47

themselves could be regarded as documents if the user was informed by observation of those
objects. Cited examples of such documents include: natural objects, artefacts, objects bearing
traces of human activity (such as archaeological finds), explanatory models, educational
games; and works of art (Buckland 1998).
Furuta (1995) provides a useful description of a document as a meaningful, moderately-sized
unit of information, which serves as a useful abstraction in defining many types of operations.
In addition, this author believes that document components are interrelated, where
relationships are assumed to be intentionally created (by an author) (Furuta 1995). From the
perspective of a digital document, there is no suggestion that the form must be textual or
sequential (Furuta 1995), but it is the variation of content, ordering and other structural
elements (particularly the amount of structure) which provides the greatest value compared to
the invariant structures of databases (Murphy 2001).
Not surprisingly, the digital ‘document metaphor’ (certainly as expressed using XML), is
influenced by documents that individuals commonly use (e.g. faxes, product descriptions,
purchase orders, bank statements, various forms) (Erwig 2003). What makes this metaphor
usable by many is that it reflects common knowledge about the concept of a pattern and
variables that are implicit in a document (Erwig 2003). For the purposes of this project, the MM
document can become an abstraction of meaningful information with a structure reflecting
common use; and this will implicitly support knowledge used by pharmacists during medication
review.
Notwithstanding document representation being tied to intended use, it is important to prevent
structures found in traditional documents (or their computer implementations) from restricting
the interpretation of relationships within digital documents (Furuta 1995).
Murphy (2001) believes that digital documents are often ‘dichotomised’ – at one end as
passive, informal, isolated individual objects (e.g. a word processing file); and at the other as
complex, cooperative, collective, multimedia creations waiting for the right application of
advanced tools and efforts to organise them – there is little discussion about the ‘middle’ of
what is really a continuum.
This interpretive flexibility of documents therefore allows supportable adaptations of ‘messy
reality’, as they can structure practice when required; and also de-structure practice when they
don't match the expected reality (Murphy 2001). A document metaphor can therefore become
an appropriate artefact to support decision-making in ‘wicked problem’ environments such as
Health, as well as more generally in Computer Supported Cooperative Work (CSCW)
Page 48

(Fitzpatrick 1998). Fitzpatrick (1998) states that better solutions (in the CSCW environment)
can only occur through an ongoing exchange between the activities of understanding and
designing. Such knowledge-intensive work areas have also been a problem for the inflexibility
of other models such as: workflow, enterprise resource planning and software process support
(Jørgensen 2002). Therefore, ‘more powerful algorithms’ may not be the answer – new ways
need to be found to allow the human and computers parts of the ‘system’ to cooperate better
(Jørgensen 2002).
A distinct advantage of documents is that they provide visual cues – the layout of a document
contains distinctive features indicating to users the type of content likely to be contained; and
with socially familiar forms, it is even possible to identify function without labels (Toms &
Campbell 1999). The ability to use a digital document should be the same as for a traditional
document providing there is an ability to recognise these formal cues (Toms & Campbell
1999). However, the translation of these built-in clues to the digital environment does not occur
implicitly, as they may not be transferred – or even be transferable – to the digital medium,
requiring additional effort by users to make sense of the document, adding to users’ cognitive
load and potentially leading to misunderstanding and misinterpretation (Toms & Campbell
1999).
Toms & Campbell (1999) suggest that a document can be represented through a set of distinct
layers:
• document function (semantic content represented by text)
• document form (visual appearance and structure such as formatting and layout)
• document interface (how the document is accessed, used and examined).
In the paper world, these layers are represented by a variety of tactile and physical
characteristics such as the size of an item, the texture of the paper etc., and in the digital world
by a common user interface or ‘interface metaphor’. In keeping with the view earlier, these
interface metaphors need to be aligned with users’ mental models of the system, rather than
focusing too closely on system models which may lead to the risk of failure (Toms & Campbell
1999). As Jones & Dumais in Toms & Campbell (1999) note: ‘the intuitions of systems
designers are not always in accord with the needs or abilities of the user'.
It is important that digital documents carry their meaning with them as well as being able to be
read and manipulated with a variety of tools (LaMarca et al. 1999). Investigation of semantic
content in shared documents has shown that concise, unconstrained, free-text communication
is more effective in reducing cognitive overload in coordinated work around complex tasks,
compared to structured and ‘complete’ information entry or retrieval (Ash, Berg & Coiera
Page 49

2004). This is an interesting finding, particularly in light of the current desire to formulate
complete taxonomies and ontologies to support the delivery of health care. In the case of
information sharing, the flexible nature of documents, which allows weak structure for common
use and strong structure use for individual use, also allows them to act as ‘boundary objects’
between groups (Murphy 2001). This role in supporting communication and workflow is
discussed in the next sub-section.
2. 3.4 Documents in communicationAs well as being considered repositories of information, digital documents can be also be
defined as ‘adaptable artefacts, that enable communication and support workflow’
(Honkaranta 2001). This definition is often used in relation to Communities of Practice (CoP)
(Murphy 2001). It is difficult to separate workflow, coordination and communication in
discussions about shareable artefacts, but consideration here needs to turn to ‘workflow’, as
the meaning of this term used for the present project will not reflect that used in the traditional
Information Systems (IS) literature.
Traditionally, IS are designed around an idealised model of tasks (Coiera 2003b); and
Workflow Management Systems (WMS) attempt to support processes by integrating domain
and organisational knowledge (Quaglini et al. 2001). Workflow systems are also often seen as
technologies designed for organisational ordering and accountability (Fitzpatrick 1998). The
Workflow Management Coalition (WMC) defines workflow as:
The automation of a business process, in whole or part, during which documents, information or tasks are passed from one participant to another for action, according to a set of procedural rules (Workflow Management Coalition 1999)
The fundamental property of a traditional workflow process is that it is case-based (e.g. an
insurance claim, tax declaration, customer complaint); and the goal of workflow management
is to handle a large number of similar cases as efficiently and effectively as possible, based on
a process definition that specifies the order in which tasks must be executed (van der Aalst &
Kumar 2001). However, although support for routine, predictable, product-based processes is
desirable, there is the question of how much work is actually routine – probably very little
(Fitzpatrick 1998).
Commercial workflow products also assume a functional relationship between work items and
workers (i.e. each work item is executed by a single entity – either a worker or a team) where
tasks are selected and completed (van der Aalst & Kumar 2001). A problem is that individuals
within teams typically perform different roles (van der Aalst & Kumar 2001). For this reason,
business models are usually represented using data-oriented techniques (e.g. relational
models) or process models (e.g. Petri-nets) as most workflow models lack the semantics to
Page 50
concisely represent specific tasks, roles, processes, goals and organisation structures found
in business (Weigand & van den Heuvel 2002). Formal representations of workflow which exist
are idealisations that hide what is significant about ‘routine’ work, i.e. the problem-solving and
interpretation required to put procedures into action (Fitzpatrick 1998). Business models also
lack mechanisms to adequately represent the informal communication that is used to
coordinate workflows (Weigand & van den Heuvel 2002). In addition, business or health care
demands can be interrupted because of the requirements of the information flow – this can
compromise safety as well as efficiency (Mack 1998). Idealised workflow plans therefore can
become little more than a resource for situated action (Fitzpatrick 1998). LaMarca et al. (1999)
also suggest that the need to deal with content as well as coordination is a fundamental
question in the development of CSCW.
In brief, supporting workflow in a general sense is already a difficult endeavour. The health
environment poses some additional confounders that are discussed next.
2. 3.5 Workflow in HealthRestating the nature of the health domain, this is an area of knowledge intensive work typified
by non-routine work, information processing, dependence on knowledge and motivation of
workers; requiring inter- and cross-disciplinary cooperation; and networked rather than
bureaucratic organisational structures (Jørgensen 2002).
Health care organisations are different from industrial or commercial companies as their main
goals as improving the health of the public rather than achieving profit. Consequently,
outcomes are difficult to measure and processes cannot be well-defined or controlled (Quaglini
et al. 2001). The health care process is typified by many exceptions as: physicians are
independent decision-makers who may not comply with guidelines (Panzarasa et al. 2004);
and patients may be involved in decision-making about their own treatment (Mack 1998; Little
et al. 2001); and be treated by different institutions or health care professionals (Quaglini et al.
2001; Canadian Pharmacists Association 2004b; Panzarasa et al. 2004). The management of
older, chronic patients is a particularly complex process, as several disease processes are
likely to co-exist, requiring a so-called holistic approach to managing information flows
between the different individuals involved (Panzarasa et al. 2004). In addition, workflows in the
health care domain are based on intent rather than results (Klischewski & Wetzel 2003).
The domain-specific hurdles posed by this complexity must be solved before workflow systems
can become useful (Browne 2001). Beyer et al. (2004) investigated the core requirements of
health care professionals and suggested key issues were flexibility, adaptability, robustness,
integration of existing systems and standards, semantic compatibility, security and process
Page 51

orientation. These are a daunting and complex list of demands matching a complex, dynamic
socio-technical system.
Understanding workflow is particularly important when designing applications for clinicians
(Bates et al. 2003). For example, the acceptability of a prescribing DSS is dependant on its
ability to avoid interference with patient-doctor interaction or the consultation workflow (Ahearn
& Kerr 2003). Mack (1998) states that considering workflow in health care actually needs
careful attention to the ‘patient's footsteps’ (Mack 1998).
There have been attempts to create Computer Interpretable Guideline (CIG) representations
for patient-specific decision support that will not interrupt clinical workflow (Elkin et al. 2001).
An example of such a system – although not a particularly successful one – is the 'disease-
state' flow model, used in the PRODIGY Project to represent therapeutic approaches (e.g.
drug monotherapy followed by combination therapy for hypertension) (Barretto et al. 2003).
However, it is import to note that for health professionals, working on a computer is rarely an
isolated task as they are always communicating with others (Ash, Berg & Coiera 2004).
Against this complex picture of health, there is the need to support informal aspects of the work
process (Fitzpatrick 1998), to integrate workflow with aspects of information integration
(Barretto et al. 2003); and support communication (Panzarasa et al. 2004) – this proposes the
use of relatively unstructured workflows (Barretto et al. 2003). This initially suggested that
document-centred collaboration could provide a coordination infrastructure similar to a
workflow process while allowing conventional use of digital documents. Examples of such
approaches to workflow in Health are introduced in the next section.
2. 3.5.1 The flow of work in HealthGiven the flexibility required in the health care domain, it might be better to talk about the ‘flow
of work’, because the nature of the work undertaken can vary for each individual (as opposed
to repeating tasks) and also because the flow is highly dependant on intent or outcomes of the
work task. Some different approaches to workflow in health as a better reflection of needs –
service flow, document flow and ‘care flow’ – are briefly overviewed.
Klischewski & Wetzel (2003) have suggested a service flow modelling approach where: each
workplace is a service point; flowing data represent customer relations (not the products to
work on); process models are resources for personalisation; and process control is
decentralised (there is no central flow engine). In this scenario, information flow accompanies
the patient's move through the service provider network. However, these authors also note that
there are two particular aspects opposing the development of suitable infrastructures in the
Page 52

health domain. Service work might last longer than the patient's presence at a service point
(i.e. treatment issues continue after a visit to a General Practitioner or medical specialist); and
the existing IT infrastructure needs to be considered, as it can range from scenarios of ‘poorly’
IT equipped physicians to large hospitals using sophisticated IT (Klischewski & Wetzel 2003).
Bernauer, Kappel & Michlmayr (2003) suggest traceable document flows (TDF) as an
alternative, light-weight infrastructure for workflow management in environments where a
workflow management system is not available and/or impossible to deploy. This is based on a
peer-to-peer (P2P) model that allows for the collaborative editing of documents. Metadata is
used to describe document flows across a network – in this way, workflow analysis can be
carried out by investigating document flows (Bernauer, Kappel & Michlmayr 2003).
Panzarasa et al. (2004) describe the concept of a Careflow Management System (CfMS)
which handles the information and (internal and external) communication needs that underlie
chronic disease management. A CfMS involves procedures (e.g. documents, shared
information and task assignment) being passed from one participant to another according to a
process definition. Careflows are case-based, a case being the process execution for a
particular patient. When a new instance of a Careflow takes place, a generic task will be
defined as a work item for the care of an individual patient alongside the required resources
(either human or non-human). This application also provides forms for data entry, data retrieval
and visualisation. Of particular importance is that the CfMS deals with possible exceptions
arising during the instance execution and generation of worklists. The CfMS represents the
best practice knowledge suitable for the management of those patients; and optimises the use
of end-user application components, such as electronic patient records, management
systems, and interaction between agents involved in the care process (e.g. patients, nurses,
clinicians, etc.) (Panzarasa et al. 2004).
These examples illustrate attention to a range of factors which require consideration in health
and although this project does not attempt anything as ambitious as these systems, the overall
philosophy is similar.
In summary, even within discussions of 'conventional' workflow models, problems exist
because of the difficulty of exact task definitions, exception handling; and the need to consider
organisational structures and information flows. Health defies the application of conventional
workflow concepts because it is a complex and dynamic environment. In particular, the
interaction between a patient and many health professionals, the large number of exceptions,
and the constant requirement for information sharing and communication points to an
unstructured and flexible workflow process. A natural solution appears to be to fit the ‘workflow’
Page 53

to the patient, where this reflects the flow of care. Although the present project looked at a
smaller component of patient care, namely medication management, the same issues are
relevant. The notion of a document metaphor, implemented as a digital document that was
'self-aware' and supported information sharing and communication by being itself the artefact
of workflow appeared to be a promising approach.
A further important dimension of health care is that information is not simply moved on to the
next user. As the patient moves through the system, there is a requirement for collaboration,
cooperation and coordination to ensure that decision-making considers all appropriate
information and receives the attention of all appropriate health professionals. This dimension
is discussed in the next sub-section.
2. 3.6 Collaboration, Cooperation and CoordinationHealth can be considered to have communities of practice (CoP). In a general sense these are
‘groups of people informally bound together by shared expertise and passion for a joint
enterprise’, who share experiences and knowledge in novel ways, develop new approaches to
problems, promote best practice, develop professional skills, can exist within (business) units
or across divisional boundaries, are self organising and fundamentally informal (Wenger &
Snyder 2000). Not all of these features are found for all health professionals or practice
scenarios, but this does describe many aspects of professional practice well. Aspects of
collaboration, cooperation and coordination are becoming ever more important as the
provision of health care increasingly changes from isolated treatment episodes to a continuous
process involving multiple health care professionals and institutions, with the consequent need
for an ‘information system’ to support processes across the whole of health care (Beyer et al.
2004).
CoPs require tools to carry out practice and to interact with outside entities – digital documents
are possible candidates for this (Murphy 2001). Murphy (2001) sees documents as having
three roles: objects of practice (conveying practice-related information); making practice
visible; and as mechanisms to bridge between CoPs. LaMarca et al. (1999) see collaboration
as a function of a document artefact (rather than the application) and the digital document as
the central means of content exchange. Sometimes, however, electronic communication can
change the nature of boundaries and work-practices in unexpected ways and there is a
challenge to also focus on the social boundaries as artefacts are enacted (Fitzpatrick 2000b).
Fitzpatrick (2000b) cites the advantages of implementing a digital radiography system – this
enabled new forms of communication among individuals with the common goal of shared
patient care. The new forms of communication (electronic orders, digital x-rays and on-line
Page 54
reports) changed the nature of the work practice boundaries, shortened the phases of
interaction, diminished the constraints of physical boundaries; and allowed more direct
interactions between the specialists and the doctors requesting the order. These artefacts had
created transparent communication pathways to support relationships previously unsupported
by the previous pathways (Fitzpatrick 2000b).
As well as supporting information sharing and communication, documents provide other
benefits in and of themselves. Sub-section 2.3.5 mentions some of those benefits which were
of particular interest to this project.
2. 3.7 Other advantages of documents
2. 3.7.1 Self awarenessLaMarca et al. (1991) argued for the need for ’situationally aware’ documents, responsive to
changes in their use and users. They saw the ability to associate computation with content to
give the ability to bind application semantics with content, making the documents in effect
situationally aware. A desirable feature of the artefact in this project was the notion of context
– did the document know ‘where’ it was, for example with a doctor or pharmacist? TDFs
(described earlier) also used versions of documents at different locations to form the basis for
modelling the distribution aspect and allowing a modified relationship to a person (Bernauer,
Kappel & Michlmayr 2003), but such a notion was outside the scope of this project.
2. 3.7.2 Social rolesAnother important aspect of documents is their social role. Society often focuses on the
‘commercial life’ of documents, but Brown & Duguid (1995) believe we should also remember
the social uses of documents. It is this social life or social world (cyberspace) created by digital
documents that has led to the enormous success of the Internet (Brown & Duguid 1995). As
anticipated in this project, the document metaphor can enable authors, in this case the authors
of the medication management document, to connect through ‘virtual communities’ that had
been part of ‘discourses’ of the world of paper technologies (Brown & Duguid 1995). Therefore,
this project not only had the potential to improve the communication and sharing of information,
but also to assist with the social interaction of participants – a valuable ‘side-effect’.
2. 3.7.3 The paper-record as a work toolThe weaknesses of paper-based records are well documented and include illegible
handwriting, incomplete and ambiguous data, data fragmentation, poor availability; and the
danger of becoming voluminous over time, making overview problematic (Roukema et al.
2006). These factors contribute to poor continuity and quality of patient care (Roukema et al.
2006).
Page 55

However, the physical nature of the (paper) working record is embedded into the way that
patient care is practised in the social context of communication and coordination (Fitzpatrick
2000a); and the coded or written information conveyed by paper can be interpreted in different
social contexts, e.g. nursing, medicine, surgery, or the patient (Southon & Cook 2001). For
example, paper is flexible and adaptable (supporting local practice, individual preferences and
different functional views), combines functionality and communication (through location at the
point of care or specific places), embeds conversations/communications (e.g. annotations),
can make the status of work more visible (though location and access); and can be easily
moved to the point of work (Fitzpatrick 2000a). It therefore seems logical that a ‘good’ digital
document should model itself, or at least be conceived with similar notions.
Additionally, Berg & Toussaint (2003) actually suggest the reverse engineering of (some
elements of) the paper-based medical record in the development of an Electronic Patient
Record (EPR), believing that the way in which its role makes primary care processes possible
can help in understanding the models which underlie its functioning; and how they developed.
2. 3.8 Wrapping up the document discussionWith the range and breadth of definitions of documents; and the ways in which they are
implicated in information sharing and communication, it was important for the researcher to
constrain the meaning of a document to something relevant to this project – well as to some
idealised behaviour. A simple yet elegant definition previously synthesised by Uijlenbroek
(1997) was adopted as being broad enough to be inclusive of technology and simple enough
to be understandable:
A set of recorded information, regardless of its carrier, which has or had the possibilities for modification and exchange, and is manageable (Uijlenbroek 1997, p. 17-21)
The ’document’ in this project was to be an embodiment of content and presentation, context
of use, and business rules which guided its use. The purpose of the document was to inform
and to guide decision-making, acknowledging that ‘hard-to-express tacit knowledge’ was less
central than the explicit knowledge with which documents are usually identified (Murphy 2001).
The document was not to be a representation of a workflow process, decision support system
or other clinical system. The document metaphor sought an ideal representation using a digital
document which combined aspects presented in the discussion. These features are
summarised in Table 2-4.
Section 2.4 summarises this chapter’s review of the literature.
Page 56

2.4 Chapter summaryThis chapter reported and discussed the literature that was used to address two questions.
These are addressed consecutively below.
What support is there for pharmacists for medication-related decision-making?
There was very little evidence of suitable technology to support the pharmacy profession other
than a few examples of relatively simple support tools, apart from the traditional practice tools
for dispensing and information retrieval. This suggested a clear need to develop an appropriate
tool to support pharmacists with decision-making or their additional information and knowledge
needs to support their expanding, patient-centred medication management roles – and provide
a means to ensure safe professional practice and optimal medication-related outcomes for
health consumers. The need for this project was consequently justified.
Table 2-4: Desirable features for the digital document
Feature CommentWill ‘look like an appropriate work document’ to the health professional using it.
Different professionals will want to view the order of information differently, for example a medical officer (MO) will likely want to observe the diagnosis or symptoms first and then be concerned about appropriate therapy – a pharmacist may be more likely to view the medication list first and then look at the rationale for use.Formatting/highlighting of information components may be different depending on how important the information is considered by the user. For example in a paediatric context, the weight may be bolded to be more apparent. Similarly, a change in value or a change to a value outside a recommended range may be highlighted.
Will contain relevant information for the decision context.
The document should be able to embody relevant information available for the medication management decision context. For example, current medication history, patient diagnosis, concurrent disease etc.
Will know about, and elicit missing information.
If there is some important information missing in the medication management context, the document should be aware of this and prompt the user to enter the information, with appropriate justification/evidence. Justification may be on the basis of clinical grounds or workflow expectations.
Will change shape as it moves to different users.
The document will be aware of where it is and therefore adapt itself to the user context. This will involve dynamic IT components to change the document for particular user contexts.
Will change shape as it accommodates individual user needs.
The document will allow flexible entry of information based on the need of the user. For example, the ability to add new medications, diagnoses or other observations.
Will be informed by relevant guidelines to support decision-making.
The document should ‘know’ about guidelines to support the requests for information, or provide anticipatory assistance. This is will not be a trivial exercise.
Will support communication between health professionals.
The document will know not only where it is, but also where it came from and where it will go, so that the user can know the information source, and if necessary go back to the source, and will know the next intended audience.
Page 57

What technology might provide this support?
The concept of a ‘document metaphor’, implemented as a digital document suggested itself as
a fitting approach to address this gap. This promised to support information sharing and
communication by means of a metaphor that was familiar to health professionals, as well as
providing the flexibility required for a dynamic and complex health environment. Documents by
their nature also offered other potential advantages, such as supporting some of the social
aspects of work.
The first steps towards developing such a tool were the creation of the underlying model or
taxonomy to provide a guiding foundation and a suitable technology for implementation.
Although the tool was intended for community use, the researcher decided to develop the
preliminary model through an investigation of the hospital context. The reasons for this were,
firstly, that hospital-based and community-based medication reviews have the same aim,
albeit within different contexts. Secondly, the hospital scenario would be a physically easier
environment within which to engage pharmacists and doctors – and that environment is more
‘information-rich’ for those professionals, allowing a more detailed and productive
investigation. The information model and document prototype developed for the hospital
scenario could be subjected to prototype testing to refine the model for community use. The
final model could then be evaluated in community-based medication review field studies for
impact.
These steps can be represented by means of the following research questions:
Investigation of the hospital scenario.
A. Can medication management-related issues in the hospital environment be addressed by the use of technology?
B. What technology approach might be appropriate to do this?
Model and prototype evaluation by community pharmacists
C. What are the differences in the community environment that affect the approach?
Page 58

Field studies
D. Can our intervention improve safety, quality and efficiency?
E. What is the contribution of the information model?
F. What is the contribution of the technology artefact (digital document)?
The approach taken to answer these questions is described next in Chapter 3 - Methodology.
Page 59

Chapter 3
Methodology
3.1 Introduction and Research FrameworkChapter 1 stated the main research question:
Can we advance medication management for health consumers by supporting decision-making with a patient-focused information model and technology-based intervention?
The literature reviews in the previous chapter demonstrated the need and set the ground for
this research project. As evidenced by the literature, the pharmacy profession is poorly
supported by tools to help with decision-making – expanding patient-centred roles and
additional information and knowledge needs clearly require the development of appropriate
tools, to ensure safe professional practice and optimal medication-related outcomes for health
consumers. The literature also suggested a way forward using an information model as the
basis for a digital document to support information sharing and communication.
The document model incorporating support for decision-making and workflow was developed
by the investigation of three different scenarios. The scenarios originally planned were
Australian hospital clinical pharmacy practice, home medication reviews (HMR) and the
primary care community pharmacy in Canada. However, the Canadian context was not
pursued for financial and practical considerations. Further, it was felt that it was better to
investigate the Australian HMR scenario to a greater depth to provide more richness.
Each scenario revealed further sub-goals for research that were expressed as the following
questions:
A. Can medication management-related issues in the hospital environment be addressed by the use of technology?
B. What technology approach might be appropriate to do this?
C. What are the differences in the community environment that affect the approach?
Page 60

D. Can our intervention improve safety, quality and efficiency?
E. What is the contribution of the information model?
F. What is the contribution of the technology artefact (digital document)?
This chapter discusses the methodology and strategy used to answer these research
questions. A more expansive discussion of research methodology can be found in Appendix
B.
This chapter is structured as follows:
• a brief introduction to relevant dimensions of research is done in Section 3.2
• an overview of IS research is given in Section 3.3
• IS methods and the selection of an appropriate method, Design Research, for this
research is discussed in Section 3.4 – a more thorough discussion of this approach and
its novel application to Health in this project is done in Chapter 4
• Section 3.5 introduces research design, however, in an attempt to avoid confusion with
the selected research method, this will be referred to as the Research Plan
• data collection techniques are discussed in Section 3.6
• the techniques used for data analysis are discussed in Section 3.7
• technology and standards applicable to digital documents are overviewed in Section 3.8
• Section 3.9 provides a project summary
• limitations of the research project are discussed in Section 3.10; and
• the chapter is summarised in Section 3.11.
3.2 Research dimensionsResearch – the ‘methodical search for knowledge’ (Friedman 2003) which contributes to the
understanding of a phenomenon (Vaishnavi & Kuechler 2005) – typically begins with real life
issues or problems (Crotty 1998, p.13). The main issues in developing a research proposal are
discussed in this section, including what methods were employed (and how they were justified,
revealing ‘assumptions about reality’) (Crotty 1998, p. 2); and how these assumptions led to
research design and data collection (Myers 2005).
Some of Neuman’s (2002, p. 20) dimensions of research – how it is done (applied or basic),
its purpose (exploratory, descriptive or explanatory) and the data collection techniques used
(quantitative or qualitative), provide a basis for describing the approach of this research. Later
sections focus on relevance and rigour; and on the contributions of the project.
Page 61

3. 2.1 How the research was doneThis project is considered applied research, as it addressed specific concerns and could offer
a solution to a problem (Neuman 2003, p. 22-23), rather than basic or ‘pure research', as the
intent was not to advance fundamental knowledge about the world, refute theory (Neuman
2003, p. 21-22), or contribute to abstract, theoretical understanding (Clarke 2000). The project
approach was also similar to variations of applied research such as instrumentalist research,
where interventions with artefacts/techniques underlie an alternative motivation to better
understand or more effectively 'design interventions' (Clarke 2000), or clinical research which
involves specific forms of professional engagement (Friedman 2003). These are areas where
a sense of research issues, background and experience are needed to distinguish among
kinds of problems and likely alternative solutions (Friedman 2003).
3. 2.2 The purpose of the projectResearch purposes or approaches adapted from Neuman (2003, p. 31) are summarised in
Table 3.1.
The nature of the research questions initially evoked an exploratory research approach, in
keeping with the objectives of becoming more familiar with a topic (Malhotra & Grover 1998),
that is, to look for ‘what’ (Neuman 2003, p. 29-30). However, the project is also descriptive
(Neuman 2003, p. 20) as an intent is the description of ‘how’ supporting the medication
management process with technology can help health professionals (‘who’) achieve better
outcomes. This suggested qualitative techniques for data gathering as they are more open to
using a range of evidence (Neuman 2003, p. 29-30); and data can be refined to identify new
possibilities and areas of interest (Malhotra & Grover 1998). Although this approach rarely
provides definitive answers, serendipity and creative questions are important as everything is
potentially significant (Neuman 2003, p. 29-30).
Explanatory research is devoted to finding causal relationships among variables (Malhotra &
Grover 1998) that is, to know ‘why’ for issues that are already known and described (Neuman
Table 3-1: Research approaches (Neuman 2003, p. 31)
Exploratory Descriptive ExplanatoryBecome familiar with basic facts, setting and concerns.
Provide a detailed, highly accurate picture.
Test a theory's predictions or principle.
Create a general mental picture of conditions.
Locate new data that contradict past data.
Elaborate and enrich a theory's explanation.
Formulate and focus questions for future research.
Create a set of categories or classify types.
Extend a theory to new issues or topics.
Generate new ideas, conjectures or hypotheses.
Clarify a sequence of steps of phases.
Support or refute an explanation or prediction.
Determine the feasibility of conducting research.
Document a causal process or mechanism.
Link issues or topics with a general principle.
Develop techniques for measuring and locating future data.
Report on the background or context of a situation.
Determine which of several explanations is best.
Page 62

2003, p. 31); and involves theory-based expectations on how and why variables should be
related on the basis of testing a relationship using a hypothesis (Malhotra & Grover 1998). This
research project does not begin with a hypothesis, nor does it aim to identify causes and
reasons – it is inductive rather than deductive.
3. 2.3 Ensuring relevance and rigourRelevance and rigour are important elements in any research, as they promise usability and
trustworthiness respectively; and are therefore worthy of some discussion here. Discussions
of relevance and rigour in the IS literature leaves an impression that relevance and rigour were
seen to be in conflict (Fällman & Grönlund 2002) This debate essentially saw academics
seeking rigour in research of interesting problems (e.g. 'unsolvable problems', such as
decision support systems); and practitioners seeking relevance in areas with lower complexity
that would have more immediate pay-offs (Westfall 1999). This section will not report that
debate, but concentrate on general aspects of relevance and rigour.
This project addressed issues or problems that practitioners actually face (Ball 2001; Fällman
& Grönlund 2002) allowing the findings to have validity-in-practice (Davison, Martinsons &
Kock 2004). In particular, the project is grounded on its application to a practical problem faced
by health practitioners, based on literature and the domain experience of the researcher. Truex
(2001) suggests that relevance might also be assured by employing research methods that
require relevance. They noted that Action Research is such a method (Truex III 2001). Design
Research, used in this research project and described later, has many aspects of Action
Research and thus relevance was further assured.
Rigour was sought through a combination of techniques described later in this chapter; and
through the researcher's own domain knowledge. In general terms, rigour can be increased by
reflecting the nature of the domain, producing data which reflect the phenomena under study;
and combining research techniques, so that the weaknesses of some are complemented by
the strengths of others (Clarke 2000), e.g. combining action research with experiments
(Mathiassen 2002).
Another major aspect of any research is its ‘contribution’. While giving general direction about
PhD research projects, Phillips and Pugh (2000, p. 63) suggest a PhD is awarded for ‘an
original contribution to knowledge’, and list ways this could be achieved. The ways that are
pertinent for this project are setting down new information for the first time, carrying out new
empirical work, applying a particular technique in a new area; and looking at areas within a
discipline not looked at before (Phillips & Pugh 2000, p. 63-64). The contributions of this project
in a general sense are discussed next in Section 3.2.4.
Page 63
3. 2.4 Contribution to knowledge and theoryThe contribution by research to knowledge is implicit in its definition as a ‘methodical search
for knowledge’ (Friedman 2003). A definition of research in the Merriam-Webster On-line
Dictionary (viewed 2005-11-13) is:
studious inquiry or examination; especially: investigation or experimentation aimed at the discovery and interpretation of facts, revision of accepted theories or laws in the light of new facts, or practical application of such new or revised theories or laws... and... the collecting of information about a particular subject
Research knowledge is not intrinsically valuable of course; and only becomes so if it is used
in, and improves practice – this is well recognised in the medical field where it is not the
research results that are important per se, but appropriate application of that information in a
clinical context (Moody 2000). Theory is also required to make an important contribution to
knowledge (Mumford 2001) – and central to the conception of theory is causality (Gregor
2002). Theory can be simple (models of elements), dynamic (describing process or action), or
describe relationships (Friedman 2003). The contribution to theory by this project was through
the development of an information model to support medication management; and through the
process of describing the support role offered by the digital document. These models could
then be used by other researchers (Neuman 2003, p. 65) to develop generalisable answers
(Friedman 2003).
Friedman (2003) also states that data and theory are interwoven; and sound theory requires
engagement with empirical reality. Theory frames research by providing concepts and basic
assumptions (Neuman 2003, p. 65); and interaction with further research findings then
becomes the basis for more theory (Gregor 2002; Neuman 2003, p. 65). The inductive
approach in this project developed theory ‘from the ground up’ as data were gathered and
analysed over time to reveal relationships (Neuman 2003, p. 65-66) (rather than being an
exercise in building, testing or extending theory) (Clarke 2000). The dissemination of results is
also a part of the outcomes of this project, ensuring that new knowledge can be applied into
practice – ensuring practical and academic relevance is particularly important in applied
disciplines (Moody 2000) – such as IS and Health.
3. 2.5 Contribution to practiceThe contribution of research to practice is also associated with the concept of relevance and
depends on the intention of the researcher and the research method (Baskerville & Myers
2004). This project had the dual intention (Davison, Martinsons & Kock 2004) of improving
practice; and contributing to theory and knowledge – within and beyond the immediate
confines of the project. In addition, participants in the project were motivated to take part by
the desire to change professional practice (Simpson et al. 2001). This research was seen very
much as a collaborative practice study (practice and research driven) with the desire to
Page 64

improve practice and add to the body of knowledge at the same time (Mathiassen 2002). Dual
intentions can also be evident in research methods. Action Research (and consequently
Design Research) seek simultaneously to create change (i.e. contribute to practice) and study
process (Baskerville & Myers 2004). Where possible, the researcher obtained pre-change
measures of appropriate variables to allow assessment of any practical improvements
(Mumford 2001) – allowing some measure of contribution by the project.
3.3 Overview of IS researchThe previous sections introduced some dimensions of research. This section now discusses
the theoretical aspects of research as a background to the approach of this project. This begins
by an introduction of the philosophical framework of research, the nature of theory and major
research paradigms and methods of analysis that influence the research approach. This
section ends with a more detailed comparison of the IS and health domains suggesting a
similar research approach in both.
3. 3.1 Philosophical frameworkResearch is described by the direction of theory and a paradigm which is the basic position
describing a set of basic assumptions shared by theories (Neuman 2003, p. 51). These two
areas are covered below. The primary focus for theory in this research is substantive (as for
specific areas of social concern) rather than formal (for broad conceptual areas) (Neuman
2003, p. 53-54). The focus also exists at the micro level as it relates to a small number of
people and small slices of time (Neuman 2003, p. 52-53).
3. 3.2 The direction of theoryTheory can be approached from two directions – beginning with abstract theory (deduction) or
observation of empirical evidence (induction). Induction is the direction of this research, first
beginning with observations of empirical evidence and then moving to more abstract
generalisations and ideas (Neuman 2003, p. 51; Crotty 1998, p. 78).
A definition of empirical is:
(an) ‘adjective based on observation or experience rather than theory or pure logic’ (Compact Oxford English Dictionary http://www.askoxford.com/concise_oed/empirical?view=uk, viewed 2006-06-07);
and empirical data:
‘originating in or based on observation or experience’ (Merriam-Webster On-line Dictionary http://www.m-w.com/dictionary/empirical, viewed 2006-06-07).
According to Gregor (2002), some of the primary purposes of the inductive approach in IS are
to build knowledge for analysing and describing (‘what is’), understanding (‘how’ and ‘why’);
and design and action (‘how to do’ something). The descriptive approach taken was in keeping
Page 65

with this dominant approach in empirical research, although it is accepted that most models
resulting from this approach will have limited explanatory power and predictive value (Clarke
2000). The deductive approach was not suitable for this project as there were no initial theories
suggesting what evidence should be gathered to support them (Malhotra & Grover 1998;
Neuman 2003, p. 51).
Having discussed some basic aspects of research, the research paradigm is considered in the
next sub-section. The research paradigm is the fundamental foundation to any research, as it
determines ‘how the researcher engages and comes to know about the world’ (Neuman 2003,
p. 90).
3. 3.3 The research paradigmMiller and Crabtree (1999, p. 8) describe the research paradigm as the patterned set of
assumptions that concern reality (ontology), knowledge of that reality (epistemology); and the
particular ways of knowing about that reality (methodology). There is no individual, correct
approach to research in social science (Neuman 2003, p. 90) and researchers must determine
what approach they will take – and then use methods consistent with that approach (Miller &
Crabtree 1999, p. 8; Neuman 2003, p. 90).
Ontology is the study of 'being', and is concerned with ‘what is’ (Crotty 1998), i.e. reality (Miller
& Crabtree 1999). Epistemology refers to the knowledge about reality (Miller & Crabtree 1999)
and incorporates assumptions of how it can be obtained (Myers 2005). Ontology and
epistemology are intertwined as the theoretical perspective that involves a certain way of
understanding what is (ontology), will also influence the way of understanding what it means
to know (epistemology) (Crotty 1998). The three main paradigms in social research are
discussed in Sub-section 3.3.4.
3. 3.4 Prevailing paradigmsThere are three ideal-type approaches to social research based on different philosophical
assumptions about the purpose of science and the nature of social reality – these approaches
seek to answer basic questions about research differently (Neuman 2003, p. 90; Myers 2005).
Although they are philosophically distinct, this is not always clear cut in the practice of
research, where there is considerable disagreement as to whether these research ‘paradigms’
(or underlying epistemologies) conflict, or can be accommodated within a single study (Myers
2005). However, they have common features as they are empirical, systematic, theoretical,
public, self-reflective and open-ended (Neuman 2003, p. 92). However, no particular paradigm
has a ‘final grasp on truth’ – the choice is most often based on the research aim and personal
preference (Miller & Crabtree 1999, p. 11). For this project, the aims and personal preferences
of the researcher suggest that the ‘truth’ is best realised through an interpretive stance. These
Page 66
three paradigms are now overviewed.
3. 3.4.1 Positivism Positivism (logical empiricism), arising from August Comte (1798-1857), seeks rigorous and
exact measure in 'objective' research where hypotheses are tested by analysing numbers from
measures (Neuman 2003) – the central concept is deduction (Straub, Gefen & Boudreau
2004).
The aim of positivism is to see the world as an:
organized method for combining deductive logic with precise empirical observations of individual behaviour in order to discover and confirm a set of probabilistic causal laws that can be used to predict general patterns of human activity (Neuman 2003)
In essence, the truth is ‘out there’, is ordered and is waiting to be discovered (Neuman 2003,
p. 72).
The ontological view assumes that this reality exists and can be measured independently of
our knowledge of it (Plummer 2001; Dubé & Paré 2003) remaining ‘value free’ (Neuman 2003,
p. 75). Parts of this reality can also be studied independently and later combined to get a
picture of the whole (Neuman 2003, p. 72).
Positivist theory generally begins from a possible causal law, logically linked to quantitative
measurements that can be subjected to statistical analysis (Neuman 2003, p. 75) and be used
for prediction (Plummer 2001; Myers 2005). Positivism also assumes that we all experience
the world in the same way (Neuman 2003, p. 77), that results can be replicated independently
(Neuman 2003, p. 73), meaning is stable and additive (Neuman 2003, p. 72); and can be
communicated to others (Neuman 1997, p. 66). Scientific theory, a cornerstone of positivism,
defines theory as one which can be falsified (Straub, Gefen & Boudreau 2004) through
hypothesis testing (Clarke 2000). Interestingly, Crotty (1998, p. 29) suggests a contradiction in
the objective or ‘scientific’ paradigm as many theories are created as heuristic and explanatory
inventions rather than being direct conclusions from data – i.e. scientists are actively
constructing scientific knowledge rather than passively observing the laws found in nature.
In keeping with the general philosophy, IS research is considered to be positivist if there is
evidence of formal propositions, quantifiable measures of variables, hypothesis testing, and
the drawing of inferences about a phenomenon from a representative sample to a stated
population (Klein & Myers 1999). The models employed are most often causal and are
validated through data (Straub, Gefen & Boudreau 2004). These factors point to a positivist
stance not being appropriate for this project, although positivist methods include field
experiments, laboratory experiments, free simulation experiments, experimental simulations,
Page 67

case studies, adaptive experiments, field studies, opinion research and archival research
(Straub, Gefen & Boudreau 2004).
3. 3.4.2 InterpretivismAs indicated by the researcher in the introduction to this section, this project was true to the
interpretive stance as it used an inductive approach, there was close engagement with
participants; and the research questions were selected and moulded based on domain
experience and intent of the researcher.
Interpretivism can be traced to the German sociologist Max Weber (1864-1920) asserting that
'facts' and 'truth' are a fantasy, that 'objective' observation is impossible and that the act of
observation-and-interpretation is dependent on the observer’s perspective (Clarke 2000).
Varieties of interpretive social science include: hermeneutics, constructionism,
ethnomethodology, and cognitive, idealist, phenomenological, subjectivist and qualitative
sociology. (Neuman 2003, p. 76). The interpretive ontological perspective is that society
constructs a social reality that is perceived differently by different individuals and meaning
comes through shared understanding – this reality can only be interpreted, not discovered
(Plummer 2001)
Neuman (2003, p. 76) describes this practically oriented approach as:
(a) systematic analysis of socially meaningful action through the direct detailed observation of people in natural settings in order to arrive at understandings and interpretations of how people create and maintain their social words.
This approach not only takes into account the researcher’s reasons and social context of
action (Neuman 2003, p. 76), but also difficulties presented by the nature of the research
domain, particularly intangible factors and relationships such as the dependence of outcomes
on the selection and definition of the research question, design of the research framework, and
definition and measurement of variables (Clarke 2000). Interpretive social science theory
essentially tells a story, representing a concept or idea, arrived at through an inductive process
(Neuman 2003, p. 77-78). Such theory is considered to be ‘true’ if it makes sense to those
being studied and if it allows others to understand the reality of those being studied (Neuman
2003, p. 79).
From an IS perspective, research is interpretive if knowledge of reality is gained through social
constructions such as language, shared meanings, documents, tools and other artefacts –
trying to understand situations through the meanings that people assign to these constructions
(Klein & Myers 1999). Orlikowski (1991) describes this as a ‘social action’ perspective on IT.
Walsham in Myers (2005) defines interpretive methods of research in IS as ‘aimed at
producing an understanding of the context of the information system; and the process whereby
Page 68

the information system influences and is influenced by the context’. Klein and Myers (1999)
suggest a set of interrelated principles to guide the interpretive approach in information
systems research:
• the hermeneutic circle
• contextualisation
• interaction between the researcher and the subject(s)
• abstraction and generalisation
• dialogical reasoning (acknowledging researcher preconceptions)
• multiple interpretations (influences of contradictions, social context, power etc. used in
revising understanding)
• suspicion.
The next approach, critical theory, is presented for completeness although it is not a stance
taken by this research. There is certainly a desire by the researcher to bring about change in
practice, but not in the social and political sense advocated by the critical approach.
3. 3.4.3 Critical theoryThis approach, which can be traced back to Karl Marx (1818-883) and Sigmund Freud (1856-
1939) is anti-positivist and anti-interpretive, using the argument that social research must be
reflective and is necessarily political (Neuman 2003, p. 81). It criticises Positivism for ignoring
social context and being anti-humanist (Neuman 2003, p. 81). In addition, it also disagrees with
Interpretivism in that Interpretivism defends the status quo (Crotty 1998, p. 113; Neuman 2003,
p. 81) and is seen to be too subjective and relativist – therefore amoral and passive (Neuman
2003, p. 81). Critical enquiry focuses on the reality of domination, distribution of power,
associated inequalities and ecological context and issues of sustainability (Miller & Crabtree
1999, p. 10). Fundamentally it adopts a realist position (that is, truth is out there) but sees
reality as constantly shaped by social, political, cultural and similar factors and evolving over
time (Neuman 2003, p. 82). Researchers taking this approach need to realise that their ability
to change circumstances is constrained by the various forms of social, cultural and political
domination (Myers 2005).
The empirical approach taken by this project must now include some discussion about data.
Although there is a clear separation is between data gathering and data analysis in quantitative
research, such a separation is problematic for many qualitative researchers (Myers 2005). This
is discussed next.
3. 3.5 Methods of analysis As the ‘analysis affects the data and the data affect the analysis’, Myers (2005) believes that
in qualitative research it is more accurate to speak of ’modes of analysis’ rather than ’data
Page 69

analysis’. These modes of analysis are the different approaches to gathering, analysing and
interpreting qualitative data. The common thread is that all qualitative modes of analysis are
concerned primarily with textual analysis (whether verbal or written) (Myers 2005). Three
approaches to data analysis are narrative metaphor, semiotics and hermeneutics; and these
are now considered.
In IS, narrative metaphor has mostly been used in understanding language, communication
and meaning among systems developers and organisational members (Myers 2005). This
approach sees people as organising their experience in the form of stories but, importantly,
there is a search for experiences which do not fit into the dominant (problem) narrative – the
potential meaningfulness to the alternative story is important (Zimmerman & Dickerson 1994).
By contrast, semiotics is primarily concerned with the meaning of signs and symbols in
language (Miller & Crabtree 1999, p. 29) where the objects function as the ‘vehicle of meaning’
but also communicate information that ‘overflows the object's use’ (Buckland 1998). The
essential idea is that words or signs can be assigned to primary conceptual categories; and
these categories represent important aspects of the theory to be tested. The importance of an
idea is revealed in the frequency with which it appears in the text. One form of semiotics
relevant to this project was content analysis – ’a technique for making replicable and valid
references from data to their contexts’ – based on patterns found in the text and used to make
inferences (Myers 2005). This approach underpinned the process of model development from
questionnaire, interview and work observation data. The implemented artefact, the digital
document, also represents a learning object as a ‘vehicle of meaning’.
The hermeneutic approach was particularly evident in this project as an underlying philosophy
and a specific mode of analysis (Myers 2005). It was true to the notion of the hermeneutic circle
regarding the connection between the understanding and interdependence of the whole and
the parts (Crotty 1998, p. 92; Klein & Myers 1999; Myers 2005). The iteration through the
different components uncovered shared meanings between the researcher and participants
(Klein & Myers 1999), developing what was already understood, and consequently clarifying
and broadening the starting point (Crotty 1998, p. 92). An affinity also existed between
participants and the researcher that helped with the emerging interpretation (Crotty 1998, p.
90). Importantly, in this research, determination of meaning was also about practical
judgement and common sense, not just abstract theorising (Crotty 1998, p. 91). Crotty (1998,
p. 91) suggests that skilled hermeneutic enquiry can gain an understanding that is deeper (in
the text) than an author's own understanding – interpreters may end up with a meaning and
assumptions that the authors themselves would have been unable to articulate.
Page 70
The discussion so far has considered research and methodological issues in the context of IS,
with the implicit assumption that these approaches would be suitable within the domain of
research – Health. The next section briefly examines the features of these two settings, and
argues that domain similarities support a similar approach for investigating a technology-
based intervention.
3. 3.6 Applicability of IS research approaches to the health environmentHealth professionals work in an increasingly complex area due to medical advances,
increasing specialisation, rising patient expectations, and the sheer size and diversity of health
service provision (Pope & Mays 1995) The interaction space within which clinicians carry out
their work is also complex as individuals communicate across rich social networks (Ash, Berg
& Coiera 2004). There are many similarities between the areas of Health and IS. Both are
multi-disciplinary fields and build on reference disciplines (Plummer 2001). Both also face
similar organisational issues when considering people and technology; and they share an
overall focus of successfully integrating people and technology to improve outcomes and
performance – they also share high failure rates of IS (Plummer 2001). Plummer (2001) also
considers health care issues to be more information intense, organisationally complex,
turbulent, paradoxical, subjective; and emotionally charged than other industries and
businesses.
The term socio-technical has equally been applied to the health system (Runciman & Moller
2001) and to IS research (Sutcliffe 2000) – the problems in both domains can also be
characterised as ‘wicked problems’ (Ritchey 2005). Much research in Health is applied
research (Pope & Mays 1995) involving human interaction; and this complexity and subjectivity
supports the need for appropriate qualitative methodologies (Plummer 2001).
As there are many parallels in IS research and HI in the nature of the organisational and
information issues (although they perhaps differ in the degree of intensity) it is reasonable to
assume that the same research methods would be useful to build theory and improve practice
in both. This topic is covered in detail in Chapter 4.
3.4 Methods in IS researchAs already mentioned, there is no single, correct approach to research and a decision must be
made about approach and consequently the methods to be used. This section gives a brief
taxonomy of research methods is IS (and appropriate in Health), overviews some research
methods that were candidates for this project; and justifies the selected method.
3. 4.1 A taxonomy of research methodsIn contrast to Computer Science (CS) which examines topics related to computer concepts at
Page 71

technical levels of analysis, IS examines topics related largely to organisational concepts
primarily at a behavioural level of analysis using evaluative research approaches (Glass,
Ramesh & Vessey 2004). IS has a number of referent disciplines (Glass, Ramesh & Vessey
2004), such as mathematics, logic, philosophy, psychology, sociology and management
(Gregor 2002), but is distinguished from these fields by the use of artefacts – and is thus at the
intersection of knowledge about properties of physical objects (machines) and knowledge
about human behaviour (Gregor 2002). One definition of IS is that it concerns ‘the effective
design, delivery, use and impact of information technology in organizations and society’
(Avison and Fitzgerald, 1995, p. xi) in Gregor (2002). Common methods in IS research are
presented in Table 3-2 (Choudrie & Dwivedi 2005).
This reliance on a range of reference disciplines (Barkhi & Sheetz 2001) can result in
significant theoretical diversity (Lee 2000; Barkhi & Sheetz 2001; Myers 2005). Also, added
confusion can arise through the use of different words for the same research methods in the
IS literature (Choudrie & Dwivedi 2005). Barkhi and Sheetz (2001) concluded that there was
not one dominant theory in use in IS research, and identified 111 separate theories from 273
articles. Despite concerns over the ‘babble effect’, a broad range of theories may in fact be
consistent with the diverse interests of the IS community, and probably not an issue as long as
the adopted theory is consistent with the situation for which it was described (Barkhi & Sheetz
2001).
Table 3-2: Common methods in IS research (Choudrie & Dwivedi 2005)
Research philosophy Minger's classification (2003) Gallier's classification (1992)
Positivist Observation (passive), measurements and analysis (statistical).
Laboratory experiments.
Experiments. Field experiments.
Survey, questionnaire or instrument. Survey.
Case study. Case study.
Theorem proof.
Forecasting.
Simulation. Simulation.
Interpretivist Interviews. Subjective/argumentative.
Ethnography. Action research.
Grounded theory. Descriptive/interpretive.
Participant observation. Futures research.
Role/game playing.
Methods involving interventions
Action research.
Critical theory.
Consultancy.
Page 72

3. 4.2 Comparison of candidate research methodsIn determining a suitable method for this thesis, the researcher considered five candidates.
The use of an artefact was central to the intervention and this intuitively suggested that Design
Research would be appropriate. Consequently, this section will not discuss the alternative
methods in detail but rather contrast their fundamental principles with Design Research to
justify selection by the researcher. A more detailed discussion of these methods can be found
in Appendix B. Design Research itself is briefly justified in this section, but is discussed in
detail in Chapter 4. The candidate methods were action research (AR), ethnography,
grounded theory, case study research and design research (DR).
3. 4.2.1 Action Research AR is applied research which treats knowledge as a form of power and abolishes the line
between research and social action; and is tied to political action where researchers try to
advance a cause or improve conditions by expanding public awareness (Neuman 1997). AR’s
strength lies in its focus on solving practical problems through intervention (Meyer 2000;
Davison, Martinsons & Kock 2004) and influencing practice positively, while simultaneously
gathering data to share more widely (Meyer 2000).
A number of principles underlie AR:
• a focus on the knowledge of action and outcomes from action (Chiasson & Dexter 2001)
• studying a phenomenon in its natural setting (Chiasson & Dexter 2001) seeking local
understandings (Stringer & Genat 2004, p. 15)
• interpreting and/or critiquing patterns of practice (Chiasson & Dexter 2001)
• playing an active role in the object of the study (Clarke 2000)
• valuing researcher and user experience in creating knowledge (Chiasson & Dexter 2001;
Davison, Martinsons & Kock 2004)
• requiring detailed data collection over a long period of time (Chiasson & Dexter 2001)
• a reflective, cyclical approach (Davison, Martinsons & Kock 2004; Stringer & Genat
2004, p.15)
• allowing findings to direct the research (Noffke 2004).
AR has been used in applied fields such as organisation development (Chiasson & Dexter
2001; Baskerville & Myers 2004), education (Baskerville & Myers 2004), system design,
training (Chiasson & Dexter 2001) and in health care settings (Meyer 2000). Scholars
researching socio-technical systems have been using forms of AR research for many years
(Baskerville & Myers 2004), e.g. for the design and study of electronic collaboration systems
(Schwabe & Krcmar 2000b).
Page 73

3. 4.2.2 EthnographyEthnography (field research or participant-observation research) (Neuman 2003, p. 363) aims
for ‘immersion’ in the lives of the people to be studied and placing the phenomena studied in
their social and cultural context (Neuman 2003, p. 363; Myers 2005). It is direct, face-to-face
social interaction with people in their natural setting (Neuman 2003, p. 364) using multiple
methods over extended periods (Miller & Crabtree 1999, p. 29). A critical part of ethnography
is ‘thick description’ – a rich detailed description of specifics rather than a summary,
standardisation, generalisation or variables (Neuman 2003, p. 367).
However, little generalisable knowledge, models or analytic methods emerge from
ethnography (Sutcliffe 2000). At the heart of ethnography is understanding beyond what is
explicitly seen or said to what is actually meant or implied in specific social contexts (Neuman
2003, p. 366). Ethnographic techniques have been applied to gather data for socio-technical
system requirements, as many problems in requirements engineering are known to have their
origins in complex social problems (Sutcliffe 2000). Ethnography has been widely used in the
study of IS in organisations, studying aspects of development and management, as a method
where multiple perspectives have been incorporated in systems design and as a general
approach in IS investigations (Myers 2005).
3. 4.2.3 Grounded theoryGrounded theory is a form of ethnographic enquiry which develops theory through a process
of systemically collecting and analysing data (Crotty 1998, p. 78; Myers 2005). More
specifically, it is inductive theory building based on empirical observations (Crotty 1998, p. 78;
Clarke 2000). The 'classic grounded theory‘ of Glaser and Strauss views induction as the key
process – ideas that are generated must be verified by the data (Douglas 2003; Heath &
Cowley 2004) – and is so called because theory is ‘grounded’ in the data from which it was
built (Power & Moynihan 2003). It shares goals with a positivist approach as it searches for
theory that is compatible with precise and rigorous evidence – and it is replicable and
generalisable (Neuman 2003, p. 52). Grounded theory is pragmatically oriented as it concerns
itself with social good and social usefulness (Seldén 2005).
As well as systematic data collection, central to Grounded Theory is data coding and writing
theoretical memos – these are used in parallel and iteratively to discover theory or revelations
in a given domain of study (Power & Moynihan 2003). Heath and Cowley (2004) note that the
aim is not to discover the theory, but a theory, to aid understanding and action. While having
its background in sociology, grounded theory has been used in tourism and hospitality
management, medical studies, psychology and, business and organisation studies (Douglas
2003), nursing and health care, and library and information science (Seldén 2005). Grounded
theory approaches are increasingly common in the IS research literature as the method is
Page 74

useful in developing context-based, process-oriented descriptions and explanations of
phenomenon (Myers 2005).
3. 4.2.4 Case study researchCase study research is the most common qualitative method used in IS (Plummer 2001; Myers
2005). The goal of case study research is to achieve exploration, description or explanation of
a particular situation, using extensive and purposeful sampling to obtain detailed information
from multiple sources (Neuman 1997; Kuzel 1999, p. 258; Clarke 2000; Yin 2003, p. 3). This
is also appropriate when researchers need to define their topics broadly or are faced with
contextual or complex multivariate conditions (Yin 2003, p. xi). This holistic approach is
particularly suited to IS research where interest has shifted to understanding complex
interactions among organisations, technologies and people (Dubé & Paré 2003); and
intangible concepts such as organisational performance and success (Plummer 2001). The
underlying principle is the in-depth examination of a few cases focusing on a few factors using
analytical logic (rather than induction) and considering the specific contexts in detail (Neuman
2003, p. 33). Often the process involves a pilot study to develop a conceptual framework and
operational measures for the ‘proper’ case study conducted later in a fresh environment (Yin
2003). While case studies can specify a causal process, generalisation is more difficult (Yin
1999; Neuman 2003, p. 33). Although this style of research is versatile as it can be positivist,
interpretive or critical (Plummer 2001; Dubé & Paré 2003; Myers 2005), it shares many
characteristics with other qualitative methodologies – the natural setting as a source of data,
the researcher as a key instrument of data collection, data collected as words and a focus on
participants' perspectives (Dubé & Paré 2003).
Case study research is considered ‘remarkably hard’ although traditionally considered to be
‘soft’ research – due to the challenges of designing a study in a systematic, manageable and
flexible manner while integrating the results into a coherent document (Dubé & Paré 2003). Yin
(1999) believes that the quality of case based studies can be improved by adopting a more
‘scientific’ approach. Case based studies are considered a suitable approach for studies in the
complex and changing domain of health, and have been used for studies in the areas of mental
health, methadone maintenance clinics, immunisation campaigns, single facility studies, policy
studies, for promising medical technologies (Yin 1999) patient illness experiences; and in
primary care in general (Kuzel 1999, p. 254). More generally, it has been used to study issues
of public policy and business administration (Yin 2003, p. xi), examine technology adoption
from organisational contexts (Choudrie & Dwivedi 2005),
3. 4.2.5 Design ResearchDesign research (science) is grounded in the ‘sciences of the artificial’ (Simon 1996), where
this is a body of knowledge about artificial (man made (sic)) objects and phenomena designed
Page 75

to meet certain desired goals (Vaishnavi & Kuechler 2005). From an IS perspective, design
science is fundamentally about addressing business needs or problem-solving (Hevner et al.
2004). The process for this is through constructing and applying innovative IT artefacts to
understand the problem addressed by the artefact and the likelihood of this approach providing
a solution (Hevner et al. 2004). As this research seeks to solve the ‘problem’ of decision-
making tools for medication management for pharmacists based on a digital artefact, this
appeared a natural fit with the design research method.
McKay and Marshall (2005) see parallels between design research and AR, in that
concomitant people, process and organisational structural changes are just as important and
relevant to improving the problem situation as the designed technical artefact. In addition (as
a socio-technical system), the essence of IS lies in the ‘contextualisation of the machine in the
social system’; and what makes design research resonate with a community that sensitivity to
social context (McKay & Marshall 2005).
The ontological and epistemological standpoints for design research suggested by Rossi and
Sein (2003) are realist (a real world exists but we are not seeking it) and that we can intervene
in the world to improve it. The research approach is qualitative and exploratory through the
development and design of systems and models (Rossi & Sein 2003).
Hevner et al. (2004) suggest that design research (in IS) addresses what are considered to be
‘wicked problems’ characterised by:
• unstable requirements and constraints based upon ill-defined environmental contexts
• complex interactions among subcomponents of the problem and its solution
• inherent flexibility to change design processes as well as design artefacts
• a critical dependence upon human cognitive abilities, i.e. creativity, to produce effective
solutions
• a critical dependence upon human social abilities (e.g., teamwork) to produce effective
solutions.
This approach is particularly usefully for new areas and where there are deficiencies in former
systems (Rossi & Sein 2003). Rigour is achieved by appropriately applying existing
methodologies, either using computational and mathematical methods, or empirical
techniques depending on the approach (Hevner et al. 2004) – and relevance is assured
through the investigation of existing problems and the contribution of new knowledge to a
community (Vaishnavi & Kuechler 2005). March and Smith (1995) in Hevner (2004) identify
two processes (build and evaluate) and four artefacts (constructs, models, methods and
instantiations) that are produced by design science (Hevner et al. 2004). The design research
Page 76

cycle consists of a number of steps: identify a need, build, evaluate, learn and theorise (Rossi
& Sein 2003). The important fundamental concepts of design research are that the process is
iterative and the philosophical perspective of the design researcher can change with progress
through the phases (Vaishnavi & Kuechler 2005). Thus, a reality created through a
constructive intervention can become the basis for new theorising and a further interventionist
cycle similar to AR methodology (Vaishnavi & Kuechler 2005).
3. 4.3 Selection and justification of the research methodThe preceding section has overviewed some candidate methods for this research project. The
intention of this research project was to investigate the application and utility of an electronic
document in the health environment for medication management. Although there is an overlap
between many of these methods from the perspectives of approach or analysis, the method
which best supported this research project was design research (DR), as central to this
research project were artefacts in the forms of the digital document and the information model
which underpinned it.
However, there were more similarities to DR than simply an artefact as a central concept. The
research was an iterative process travelling a development and refinement pathway through
hospital and community-based health scenarios. It addressed a problem of the lack of
support for informed decision-making for health professionals involved in medication
management. It was goal-oriented in attempting to understand the role of an electronic
document in supporting decision-making in health and to improve practice, in particular the
quality, safety and efficiency of the medication management process. It was contextual in that
it specifically addressed the needs of the pharmacist (and general practitioners to a different
degree) undertaking medication reviews. It involved engagement with health professionals
where the researcher was a participant-observer. In short, the project was characterised by an
ill-defined environmental context, complex interactions between problem and solution,
flexibility needed to change processes and artefact, a dependence on human cognitive abilities
to produce a solution; and a dependence on human social abilities (Hevner et al. 2004).
In addition, there were some fundamental aspects of the other methods which did not fit the
intent or nature of the project. There are obvious similarities with AR, in particular the reflective
cyclical approach to reveal a more detailed picture of the problem (and solution). However,
although the researcher had an influence on outcomes, this did not take the form of an ‘active’
participant to drive change or empower a group to change. Additionally, there was no socio-
political imperative of the sort which usually drives AR.
The main intention of ethnography is ’thick description’ – a rich description of a cultural context
Page 77

over time through immersion by the researcher. This thesis moved away from description of a
context to formulating models for practice improvement; and to a theme of iteration rather than
evolving description.
Some similarities do exist with the grounded theory approach, in particular the use of coding
to define and develop an information model. However, this was not considered a grounded
theory approach as the researcher went into the research project with prior domain experience
so the research was not ‘value-free’ (certainly not from the perspective of the original stance
of grounded theory methodology).
Case studies are common in the health environment, particularly in medicine. This research
project was not case study research as it did not seek to ‘raise questions and define
characteristics about a case’. It did rely on relatively few cases from which to empirically draw
conclusions, but, these were taken across three different scenarios, hospital, accredited
pharmacists (for benchtop testing) and in the general practitioner-pharmacist interaction
space. All data was not analysed in detail, but selected to address goals or the problems in
question. The iterative nature also differed, as with ethnography.
In summary, the strategy for this research project was empirical with an interpretivist, inductive
stance, adopting the design research method. Data collection and analysis were both
qualitative and quantitative; and data and participant triangulation were used to ensure validity.
The strategy of the research is now followed by the practical aspects of the project, the
research plan.
3.5 Research PlanAs mentioned by the researcher in the introduction to this chapter, the term 'research plan’, is
used here rather than 'research design' – so as to not confuse this with Design Research, the
research method. This section outlines the research plan, firstly in overview and then the
individual scenarios which formed the iterations through which the project proceeded.
The overall aim of this project was to improve medication management for health consumers,
through good medication management as observed by study participants. In a broader sense,
it also sought to investigate if and how digital documents could be used to support more
general requirements for a relevant health information and decision support structure. The
digital document was analysed by means of investigation of an information and work flow
model to support decision-making in the context of the evolving professional role of the
pharmacist. There was the potential to improve safety, quality and efficiency in the medication
review process with subsequent improvement in consumer outcomes.
Page 78

The information model and digital document were developed in parallel through the
investigation of three different use cases. Initially these were to be hospital clinical pharmacy
practice, home medication reviews (HMR) and the primary care community pharmacy in
Canada. The basis for the selection of these scenarios was their similar implications for
pharmacy decision support as similar requirements existed (to different degrees) in all three
scenarios. There was also a similar upstream reliance for information components (from the
medical professional writing medication orders or requests for HMR). The initial selection of
the Canadian health scenario was based on its strong parallels with the Australian scenario
and the similar patient-centred roles advocated by the Canadian Pharmacists Association. The
researcher considered that the use of a setting outside of Australia could provide additional
opportunities for providing greater richness to the model.
However, during the course of the research project it became evident that time and cost
constraints would not allow the researcher to investigate the Canadian scenario; and it was felt
that a greater focus on the community (HMR) environment would also add more depth to the
model and allow better evaluation of the artefact. The second scenario therefore became two
parts – a benchtop test of the document prototype and a field test. An advantage was that the
field test could be done with a more refined model than originally planned. In short, the use
cases became hospital clinical pharmacy practice and home medication reviews (comprising
bench top testing and field testing).
The project began with the hospital scenario (perceived to be more compact and information
dense), and this initial model was tested and refined through the other scenarios. The broad
plan was to iterate through an information collection, analysis, reflection, modelling and
prototyping loop to describe the information model and document metaphor in the context of
supporting pharmacy decision-making. Data triangulation and different approaches were used
in all scenarios to address validity.
3. 5.1 The hospital context (Part 1)Investigation of this scenario began with two questions, addressed consecutively.
A. Can medication management-related issues in the hospital environment be resolved by the use of technology?
Question A was addressed by data collection activities which for pharmacists, allowed an initial
understanding of medication-related information components, workflow and decision-process;
and for medical officers (MOs), the process for ordering medication and their perceptions to
requests for information. This allowed an understanding of important issues in medication
Page 79

management, suggested opportunities for decision support interventions, and provided a
repository of potentially helpful information flows.
This empirical, observational part of the project collected data through exploratory interviews,
observation of work practice, collection of demographic data and document analysis. Subjects
were hospital pharmacists and medical officers (MOs)1. Two to three of each group were to be
recruited from each of four major adult metropolitan hospitals in Adelaide, with the aim of
recruiting a total of at least 10 pharmacists and 10 doctors. Eligibility was based on the
participant having an appropriate role in their work scenario, i.e. a pharmacist designated as a
clinical pharmacist, and a MO who initiated medication therapy in the course of their clinical
practice. Selection was based on voluntary participation from potential subjects. There were
no specific exclusion criteria. The researcher recruited participants through Directors of
Pharmacy and Directors of Medical Administration. The former were known to the researcher
(as past colleagues). The Directors were initially approached informally by the researcher to
ascertain interest, and formal approaches for recruitment were instigated following approval
from each institutional Ethics Committee. Ethics approval was also obtained from the
University of South Australia (UniSA) Human Research Ethics Committee. The research
proposal for the hospital scenario (including data collection tools) is contained in Appendix E.
B. What technology approach might be appropriate to do this?
This question was addressed by the use of XForms technology. As the consideration of
technology was a major issue, this is discussed by the researcher in detail in Section 3.8.
3. 5.2 The community context: prototype bench testing (Part 2A)Part 1 provided the empirical basis for a model of information flow centred on the hospital
clinical pharmacist; and identified opportunities for improved support for that role. This next
scenario (Part 2A) addressed the next research question:
C. What are the differences in the community environment that affect the approach?
The data collection goals of this phase were to add to knowledge gained in the hospital
scenario, refine the information model for use in the community HMR scenario and develop the
digital document prototype. This used experiential information and opinion from pharmacists
carrying out HMRs; and who interacted with General Practitioners (GPs) in the community. In
addition, the process for GPs requesting HMRs needed to be understood; and goals needed
to be defined for the intervention planned in the field study.
1. Medical officer (MO) is a generic term commonly used in Australian hospitals to refer to doctors.
Page 80

Data were collected from interviews, prototype testing and a focus group. User reactions,
suggestions for improvement and innovation during testing of the digital document prototype
were used to progress the information and interface models. Participants in this scenario were
community pharmacists (a minimum of five pharmacists) undertaking HMR – prototype testing
aimed for pharmacists to enter a minimum of 25 HMR referrals (five each). Participant eligibility
was based on their being accredited to undertake HMRs; and inclusion into the project was
based on voluntary participation from potential subjects. The researcher recruited participants
through the HMR Pharmacist Facilitators of the Southern, Western and North-eastern
Divisions of General Practice in South Australia.
The research proposal for the benchtop testing scenario (also containing the data collection
tools) is shown in Appendix F.
3. 5.3 Medication review field study (Part 2B)This last part, 2B, concluded the project with a field study of the document prototype. In this
phase, the nature of research changed from exploration, understanding and development to
investigating effect, i.e. practice changes caused by the intervention. As for the previous
scenarios, initial research goals were transformed to research questions:
D. Can the intervention improve safety, quality and efficiency?
E. What is the contribution of the information model?
F. What is the contribution of the technology artefact (digital document)?
These questions were to be answered by perceptions from study participants and certain
qualitative markers shown in Table 3-3. These markers represented only a starting point as
the study sought opportunistic measures and opinions to measure the value or effect of the
intervention. Data were collected from analysis of prototype use, interviews, focus group and
document analysis. In addition, further document analysis for quality parameters was to be
undertaken by an independent review panel of three relevant domain experts consisting of at
least one doctor and one accredited pharmacist. Participants were pharmacists and general
practitioners (GPs).
A minimum of two practice groups were sought, where a group consisted of a community
medical practice undertaking medication reviews using accredited pharmacists. Participant
eligibility was based on informed, voluntary participation of individuals from identified
practices. The researcher recruited participants using direct approach to practices identified
Page 81

through the HMR pharmacist facilitators of the South Australian Divisions of General Practice,
participants from previous phases of this study or opportunistic communications with other
pharmacists. Patient consent is routinely required for patients undergoing HMRs, but the
researcher also determined whether the GPs and pharmacists had any additional consent
requirements for patients to be considered in the project.
Figure 3-1 graphically summarises the relationship of the research questions to the different
phases of research and the literature review. The research proposal for the field studies
(containing the data collection tools used) is shown in Appendix G
.
Table 3-3: Qualitative measures for the HMR field test
Can we improve? Measures/markers
Safety Reduced medication errors.Reduced adverse events.More timely consideration of HMR report.More current patient information.
Quality Improved clinical documentation.Increase time for direct patient care.Increased application of clinical guidelines/pathways.Health professional satisfaction.
Efficiency Increased speed of the MR process (report delivery, report acknowledgement).Reduced transcription.Reductions in tests.Changed patterns of drug prescribing.Improved pharmacist-GP communication.
Figure 3-1: Research questions in relation to research phases
Part 1 – The Hospital Scenario
Part 2 – The Community Scenario2A – Investigation of the
home medication review context: prototype bench testing
2B – Medication review field study
Literature review
Can we advance medication management for health consumers by supporting decision-making with a patient-
focused information model and technology-based intervention?
D. Can our intervention improve safety, quality and efficiency?E. What is the contribution of the information model?F. What is the contribution of the technology artefact (digital document)?
A. Can medication management-related issues in the hospital environment be addressed by the use of technology?
B. What is the best way of implementing this technology
approach?
C. What are the differences in the community environment that affect the approach?
What support is there for pharmacists for medication-related decision-making?
What technology might provide this support?
Page 82

3.6 Data collection techniquesThe research plan introduced the data collection techniques used in the project. These are
now described in more detail to demonstrate the nature of these techniques and the thought
required to use them. However, this is preceded by some discussion on the nature of the data
collected and the use of triangulation to ensure validity of the research.
3. 6.1 Quantitative and qualitative dataThe majority of data collected within the project (comparisons, documents, transcribed
recordings, observations and interviews) was descriptive and therefore qualitative (Coffey &
Atkinson 1996, p. 4; Neuman 1997, p. 30), although some quantitative data was collected for
descriptive statistics. In addition, as one of the research questions in the field study was
concerned with identifying improvement based on the intervention, appropriate data to allow
pre- and post-measurement was also planned.
The labels 'quantitative' and 'qualitative' are often used in the literature to describe schools of
research – this use is misleading, as these terms better describe the nature of the data
gathered in empirical research (Clarke 2000). Qualitative research does not constitute a
paradigm in its own right (Coffey & Atkinson 1996, p. 12) and the distinction between
qualitative and quantitative research occurs at the level of methods, not at the level of
epistemology or theoretical perspective (Coffey & Atkinson 1996, p. 13; Crotty 1998, p. 15). In
fact, the use of qualitative and quantitative techniques is seen to be complementary (Pope &
Mays 1995)
3. 6.2 Validity through triangulationThe important issue in qualitative research of how to ensure validity (Davison, Martinsons &
Kock 2004), reliability; and how to protect against bias (Mays & Pope 1995; Shaw 2001) is
addressed through triangulation. This is achieved by the use of more than one: source of data,
investigator, theory, methodological approach, environment; or setting (Malhotra & Grover
1998; Clarke 2000; Mays & Pope 2000; Guion 2001; Shaw 2001; Davison, Martinsons & Kock
2004). However, the type of triangulation used will depend on its feasibility and
appropriateness to the research question (Guion 2001).
Mays (2000) suggests that triangulation by data as a test of validity may be open to question
– it assumes that weaknesses in one data collection method will be compensated by strengths
in another and that it is always possible to judge between different narratives (e.g. from
interviews with clinicians and patients). However, data triangulation is commonly used; and
was used by the researcher in this project as being the easiest and most feasible. Data
collection techniques are described in section 3.6.3.
Page 83

3. 6.3 Data collection techniques
3. 6.3.1 Literature reviewThe literature review – the account of what has been published on a topic by accredited
scholars and researchers (Taylor & Procter 2005) – is considered an early step in the research
process irrespective of the approach adopted (Neuman 2003, p. 96). The principal literature
review undertaken for this project described in Chapter 2, sought to identify what support there
was for decision-making for pharmacists outside of traditional roles. This was in was in keeping
with the goal to ‘integrate and summarise what in is known in an area’ (Neuman 2003, p. 96);
and to provide the background and justification for the research questions (Bruce 1994).
Further literature was reviewed to gain familiarity with other bodies of knowledge – in
particular, to seek a possible technology solution – supported by literature on digital
documents and workflow, also discussed in Chapter 2. The researcher also sought
supplementary literature in the areas of research methodology, health (particularly relating to
medication safety, pharmacy practice and e-Health), standards (relating to the health-IT
environment) and technology such as XForms.
3. 6.3.2 Use of questionnairesThis project used semi-structured questionnaires as a primary exploration of medication
management issues. The mixture of closed and open-ended questions allowed some
quantification of responses as well as exploration of issues and attitudes (Kendall & Kendall
1988, p. 156; McColl et al. 2001, p. 45). Piloting a questionnaire on participants who are
representative of the target sample is seen to be a success factor for a good questionnaire
(Boynton 2004) – this was less of an issue for this project as the questionnaire was intended
as a preliminary step where (largely) open-ended questions allowed the participant time to
consider questions passively (Maciaszek 2001, p. 83). The follow-up interview (using a filled-
in questionnaire as the interview tool) solved any issues about clarifying questions (Maciaszek
2001, p. 83). Similarly, other factors such as the order of questions, format and choice of words
that can be important in self-administered questionnaires (to avoid issues such as bias)
(Kendall & Kendall 1988, p. 162-176) were not an issue because of the approach used.
However, the researcher acknowledges that because of the range of considerations that affect
questionnaire design (about which decisions have to be made) questionnaire research can
never be objective (Miller & Crabtree 1999).
3. 6.3.3 Use of interviewsIn keeping with an exploratory aim of the research, the interviews were face-to-face and in-
depth, building on the information collected through the initial questionnaire. The importance
of in-depth interviews using (the same) open-ended questions was to illicit rich, detailed
material (Mahoney 1997); and importantly for the researcher to capture opinion and not simply
uncover facts (Kendall & Kendall 1988, p. 125). The need for well-qualified interviewers was
Page 84

addressed by the fact that the researcher had significant domain experience – interviews with
domain experts are often a simple knowledge transfer process (Maciaszek 2001, p. 82). The
researcher’s domain knowledge also avoided problems of vocabulary, allowed participants to
be at ease and provided avenues of questioning in addition to those planned in the
questionnaire (Kendall & Kendall 1988, p. 130). Interviews were audio-taped as well as being
subject to further note-taking, as this was important to provide a complete record and an aid to
recall (Kendall & Kendall 1988, p. 140).
3. 6.3.4 Work practice observationObservations provided an opportunity for the researcher to collect data on behaviours,
interactions, and explore issues – important where this involves a sequence of, rather than
single events (Mahoney 1997). This was particularly valuable as it provided an opportunity to
view what was actually done (not simply documented or explained) and provided the
researcher with insight into participants’ communication with other individuals (Kendall &
Kendall 1988, p. 190). These observations also confirmed or contrasted findings from other
data collection methods (Kendall & Kendall 1988, p. 191). As noted by Miller and Crabtree
(1999, p. 15-16), this was a time-intensive and demanding method of data collection.
Observations in the hospital scenario were particularly important, as they revealed what
information was actually being used and how this was obtained, in contrast to information use
suggested by the participants at interview. This is in keeping with Mahoney’s (1997) opinion
that the ’observer is more than just an onlooker, but rather comes to the scene with a set of
target concepts, definitions, and criteria for describing events’. In this case it was to identify the
nature and sources of medication-related information that were used. For this exploratory
exercise the recording tool was essentially unstructured (Miller & Crabtree 1999, p. 15-16).
The researcher attempted passive rather than active observation to minimise observer
influence (Maciaszek 2001). However, it must be acknowledged that as a domain practitioner,
participants could have considered the researcher more as a ‘team’ member rather than
detached observer and therefore this could have brought about some behavioural changes in
participants.
3. 6.3.5 Use of focus groups Focus groups were important in this research project as natural interaction existed between
the two professional groups (GPs and accredited pharmacists) and it was valuable to obtain
their different perceptions of the information model and prototype. A focus group was also
thought to be useful in the evaluation of the document prototype by pharmacists with different
levels of experience in medication reviews. The usefulness of these focus groups in addition
to other techniques was that the group interaction would generate new data and understanding
unlikely to emerge without this interaction (Mahoney 1997) – particularly social contexts and
Page 85

important group dynamics (Mahoney 1997).
The approach used by the researcher to the focus group varied from that normally used.
Conducting a focus group would usually involve one or more moderator(s) who are there not
only to conduct the group, but also to help avoid biases that could be imposed on that group
by researchers (Kuzel 1999, p.119). However, with the notion that a ‘focus group is only as
good as its moderator’ (Kuzel 1999, p.120), the researcher decided to act as the moderator,
as his domain experience provided a particular level of understanding of hospital and
community pharmacy practice that could be used to stimulate discussion and improve the
quality of the data collection. However, understanding the problem of potential bias, the
researcher was clear in the intent to learn rather than to instruct (Sim 1998)
3. 6.3.6 DocumentsThis research project used purposive sampling (Kendall & Kendall 1988, p. 93) where one or
more examples of each type of medication-related document used by participants in decision
making were collected. This was useful in that documentation often provides insights into a
setting or group of people that cannot be observed or noted in any other way (Mahoney 1997).
Sampling included both public (e.g. reports, records) and personal (e.g. diaries, notes)
documents (Mahoney 1997). This required some documents to be de-identified to protect the
identity of patients and/or staff. Although there was a danger that these were incomplete,
documents provided an inexpensive and inconspicuous way of collecting data (Mahoney
1997).
3. 6.3.7 PrototypingPrototyping can be viewed from more than one perspective. It can be seen as a method used
to develop information systems (Middleton 1999) or a data-gathering technique (Kendall &
Kendall 1988, p. 219) – both occurred in this project.
Prototyping was used in Part 2A to test and refine the information and interface models through
user reactions and suggestions for improvement. The approach used to prototyping was not
the ‘traditional’ one of investigating options to determine the feasibility of a solution to a
problem (after elicitation of initial user requirements) (Pfleeger 1998, p. 169). Rather, it was
evolutionary (as opposed to exploratory and throw-away), intended to learn about a problem
and also used as part of the delivered (software) solution (Pfleeger 1998, p. 169). A rapid
prototyping approach is seen to be an advantage for developing expert systems where system
specifications are likely to change during the development (Bloom & Chung 2001), when there
is little previous design experience, the environment is uncertain or unstable, or decision-
making is unstructured or semi-structured (Kendall & Kendall 1988, p. 230). In addition, as the
HMR process is not a ‘highly-structured’ problem, it is a suitable problem for prototyping.
Page 86

Overall, prototyping matches the project domain well.
Prototyping can also serve as a basis for knowledge acquisition capturing smaller details that
are easily missed during requirements elicitation (Bloom & Chung 2001). This ability allowed
closer user participation and early feedback to the researcher that better reflected their real
world needs (Lenz & Kuhn 2004). This, in turn, was expected to lead to better acceptance
(Lenz & Kuhn 2004).
Prototyping in this project was also complementary to the chosen methodology, as DR is
underpinned by the construction of an artefact that can be used as an experimental proof of a
method or exploration of a method (or both) (Vaishnavi & Kuechler 2005).
Myers (2005) has suggested that in quantitative research, a clear separation between data
gathering and data analysis can be difficult (compared to quantitative research). The next
section therefore necessarily discusses data analysis as a follow-on from the data gathering
techniques in this section, to link but separate these activities.
3.7 Data analysisData analysis used a number of techniques, depending on the nature of the data and the
different aims within the project. This included modelling, prototyping, use of descriptive
statistics, content analysis and also a framework to evaluate the outcomes of the field study.
These are reported below.
3. 7.1 ModellingRevealing essential elements in relationship to one another (Friedman 2003) – in this case a
taxonomy of information components considered essential for medication management –
allowed the development of simple theory, rather than a dynamic model (describing process
or action) (Friedman 2003). As described in Chapter 2, the researcher was required to develop
an information model for medication as none were suitable for use within this project. However,
models in the health-care environment have been described for more complex tasks such as
clinical guidelines (Peleg et al. 2002), electronic health records (Beale & Heard 2003; Berg &
Toussaint 2003), clinical practice (Tange et al. 2003), business rules (Iyengar 2001) and drug
interactions (Solomon & Heathfield 1994). Many of these are commonly directed at building
blocks of medical knowledge or at the essence of medical decision-making (Berg & Toussaint
2003).
Modelling in the project proceeded through a number of iterations. Data from the hospital
scenario were analysed using QSR NUD*IST Vivo® (nVivo) version 2.0 software (Qualitative
Page 87
Solutions and Research Pty Ltd.) to form a preliminary qualitative model. The coding process
is described later under content analysis. This model was refined as a UML-based class
diagram to assist with hierarchical modelling, which also became the basis for the digital
document prototype. Subsequent refinements to the model after bench top testing and field
tests were incorporated into the UML model and document. A further intent was to ensure that
the information model was ‘aware’ of information flow – i.e. what information was relevant to
what user. However, this was not modelled explicitly but addressed by the context of
information use and implemented within the document.
3. 7.2 PrototypingAs alluded to earlier, evolutionary prototyping was used as method of data analysis to refine
the digital document prototype (and therefore the information model) from user interaction and
feedback. This was in line with the DR principles of ‘build... evaluate... learn’ (Rossi & Sein
2003). Prototype testing occurred in benchtop testing in Part 2A and in the subsequent field
trials in Part 2B. This iteration allowed the more specific information model relating to the
hospital scenario to evolve into one that incorporated features to support medication
management in the broader community setting.
3. 7.3 Descriptive statisticsThe statistics used in this project were largely descriptive and used to categorise data about
participants and findings in keeping with the qualitative data approach (Neely et al. 2002). This
relied on the use of nominal scales and on the researcher developing appropriate codes or
categories for behaviours, words, etc., to allow the use of some relative frequency distributions
(Morgan, Gliner & Harmon 1999). However, as statistical methods are fittingly chosen based
on what the question is and what the data ‘look like’ (Neely et al. 2002), the researcher used
comparative statistics opportunistically where the same variables were used across more than
one scenario, or pre- and post-data were available.
3. 7.4 Content analysisContent analysis is one form of semiotics where the fundamental idea is that words/signs are
assigned to conceptual categories and the frequency suggests their relative importance
(Myers 2005). This identification of key themes or categories depends on the process of coding
qualitative data (Coffey & Atkinson 1996, p. 27) through an interpretive process of describing,
organising, connecting, corroborating and representing the data (Miller & Crabtree 1999, p. 20-
24). How the data are organised also helps to answer the research question (Miller & Crabtree
1999, p. 20-24). Data were coded by the researcher using nVivo software after transcribed text
from questionnaires, interviews and work observations had been entered into the nVivo
software (again by the researcher). The approach to coding was consistent with the editing/
organising style of Miller and Crabtree (1999, p. 20-24) although the researcher’s domain
Page 88

knowledge assisted with the development of initial and emerging categories. This coding
served not only to ‘count’ (as in quantitative analysis) but as a ‘heuristic device’ for discovery
(Coffey & Atkinson 1996, p. 30).
The process of coding within nVivo involved the creating of links from selected (marked) text
in documents to nodes created in nVivo. An nVivo node is an object that can represent any
concept that users want to represent to (e.g. people, ideas, places, mental states). Nodes can
also be given attribute values and grouped in sets. The node trees created from the data
subsequently become the basis of qualitative models representing relationships between the
nodes – and used to form the preliminary information models.
3. 7.5 Evaluation of research goalsAs well as analysis of textual data, the evaluation of the project goals described for Part 2B
required the researcher to consider subjective concepts such as 'efficiency', 'quality' and
'safety'. While considering this, the Human-Organisation-Technology (HOT) Fit model
suggested itself as possible framework for the evaluation of the field studies (Yusof, Paul &
Stergioulas 2006). This framework was developed by Yusof, Paul and Stergioulas (2006) after
critical appraisal of existing Health Information System (HIS) evaluation studies. This model
contained dimensions of interest to this project (i.e. human and technology dimensions) and at
various levels described the goals for the field research – quality, efficiency and safety (clinical
outcomes). Further, this model also provided a mechanism for the evaluation of the interface
(the digital document artefact). The HOT Fit Model is shown as Figure 3-2 and elements of
evaluation suggested by Yusof, Paul and Stergioulas are shown in Appendix D.
One parameter of interest to the researcher was the ‘quality’ of home medication review
reports produced by the pharmacist for the GP. This could be assessed against a guideline
(the HMR Quality Assurance Form) developed as a quality assurance tool by the Southern
Divisions of General Practice (SDGP) and the Drug and Therapeutics Information Service
(DATIS) in South Australia. This guideline was used by accredited pharmacists as a ‘check list'
to determine the quality of HMR reports sent to the GP. This tool was an accepted and
pragmatic quality assurance tool that was highly relevant to pharmacists’ practice – and
therefore an appropriate tool for use in this research. This tool is shown in Appendix C.
This measure of quality was added to the list of Net Benefit evaluation items in the HOT Fit
Model.
The remaining question to be addressed in this chapter is (after question A, can medication
management-related issues in the hospital environment be resolved by the use of
technology?):
Page 89

B. What technology approach might be appropriate to do this?
This question has been left until the end of the chapter as it constitutes a significant topic of
discussion in its own right. Digital documents and the rationale for using this approach have
been discussed in Chapter 2; and the technology used to materialise the digital document is
described in the next section. As the health technology sector is also an area of significant
activity in regards to standards, standards with potential impact or applicability to the project
are also discussed.
3.8 Technology and Standards
3. 8.1 XForms The digital document artefact was implemented using a device-independent XML technology
called XForms. In contrast to HTML representations, XForms comprises separate sections
which describe what the form does and how the form looks, i.e. purpose and presentation,
allowing great flexibility (http://www.w3.org/MarkUp/Forms/, viewed 2006-01-05). Although a
recent standard, this offers considerable advantages because of platform independence, the
ability to develop forms to collect (XML) data, support for the structured interchange of data
and workflow, auto-filling and pre-filling of forms, and decoupled data, logic and presentation
(W3C 2004). Also, as a pivotal problem of medical data is the absence of machine-readable
structures, the document-oriented view of XML is seen to correspond well with the organisation
of health care data (Schweiger et al. 2005). Since this artefact is a ‘proof of concept’ rather than
Figure 3-2: The HOT fit model (Yusof, Paul & Stergioulas 2006)
HUMAN
Net Benefits
TECHNOLOGY
ORGANISATION
FitInfluence
InformationQuality
UserSatisfaction
Structure
Environment
System Use
System Quality
ServiceQuality
Page 90

a complete system; and there is a need to maximise flexibility and response in keeping with
the design research approach, XForms appeared to be a candidate approach. In addition, this
project will also serve to test the technology itself in a novel environment (the health care
domain) and suggest its suitability (or otherwise) to address these types of questions in this
domain.
3. 8.2 The impact of standardsThe advantages of standards and standardisation are well known and will not be discussed in
this thesis. However, it is important to restate that any technology-related research must be
aware of any standards which may affect its direction, or the ways in which the technology is
applied or implemented. This is particularly relevant for technology-related research in Health,
where there is significant interest in standardisation to improve communication, share data,
reduce cost, increase quality and improve outcomes. For example, in January 2005, 13 major
health and IT organisations in the United States (US) endorsed a ‘Common Framework’ to
support improved health information exchange (American Medical Informatics Association
2005).
The researcher undertook minor selective literature reviews to research emerging and/or
relevant technology standards for metadata, data representation and messaging. These
included XML Schema, the Resource Description Framework (RDF), Web Ontology Language
(OWL), HL7 messaging, openEHR, Clinical Document Architecture (CDA), archetypes, HL7
templates and Genre Taxonomy. Similar literature was also sought on discussions of
electronic guideline representations (e.g. GLIF, EON, Prodigy and GEM). The appropriate
standards initially seen to be relevant to the research project were XML schema, openEHR
and CDA. Genre and Pharmaceutical Care Network Europe (PCNE) (American
(Pharmaceutical Care Network Europe Foundation 2003) taxonomies were also investigated
for categorisation of concepts. CDA was seen to be particularly relevant in relation to the
intention of the digital document artefact; and this is discussed in the next sub-section.
3. 8.2.1 CDA/HL7The mission of the Health Level Seven (HL7) standards organisation is to create and promote
standards for the exchange, management and integration of electronic health care information
to increase the effectiveness and efficiency of health care delivery (http://www.hl7.org/about/,
viewed 2006-01-05). Enabling semantic interoperability across all platforms is a prime HL7
motivation (Dolin et al. 2001). The CDA was particularly relevant to this research project as it
is an XML-based document mark-up standard that specifies the hierarchical structure and
semantics of’ ‘clinical documents’ for information exchange (Liang, Bodorik & Shepherd 2003).
Page 91

A clinical document defined by HL7 has persistence, stewardship, potential for authentication,
wholeness, and human readability – and is defined as a complete information object that can
include text, images, sounds, and other multimedia content (Alschuler 2002). This approach
means that a XML document can at least be displayed at the recipient's site, using an
appropriate style sheet, and interpreted by a human, even if the contents of the document are
not ‘understood’ by the recipient's local system (Beyer et al. 2004). CDA document type
definitions describe data at three different levels of abstraction (Beyer et al. 2004) – CDA (at
Level 1) has been used to implement hospital discharge letters and summaries to
communicate information to the community setting (Paterson et al. 2002; Bludau, Wolff &
Hochlehnert 2003).
There are significant similarities between the CDA model and the intent of the digital document
in this research. In particular, this is the communication of clinical information, the use of XML
as an underlying representation and the importance of human readability. However, this
research emphasises an unrestricted approach to the information needs for medication
management, (i.e. without taking the HL7 Reference Information Model (RIM)1 as a starting
point). The focus of the project on human-to-human communication is also different from the
HL7 intent of supporting machine interchange. Therefore, the main differences are that CDA
intention is about communication (between systems) using XML schema and standardising
data representation with different granularities across its three levels. The approach with the
document metaphor is to communicate information to the human user, use the information
model to suggest the 'schema’ implicitly within the XForms model, and have different levels of
structure and granularity as suggested by the users to support appropriate decision-making.
The essential differences are initial intent rather than outcome (for the human user). However,
given the same underlying implementation technology, this does not preclude CDA
compliance in future work.
3. 8.3 User interface design‘Is it usable?’ – this is a question often asked about software (Weinshenk, Jamar & Yeo 1997,
p. xv). The research journey undertaken to formulate the information model and digital
document should in part answer this question, certainly from the perspective of the information
elements underpinning the medication-related decision process and their representation in the
digital document. However the user interface consists of a number of elements, such as
screens, windows, controls, menus and metaphors – the visual components that the user sees
and that affect how effective the user interaction will be (Weinshenk, Jamar & Yeo 1997, p. 7).
The goal here was to implement a well-designed interface that would reduce errors and make
people more productive as well as ensuring use (Weinshenk, Jamar & Yeo 1997, p. 7). The
1. The RIM is the source of information objects used in HL7 specifications
Page 92

principles for ‘intelligent interface design’ used in this project were taken from Weinschenk,
Jamar and Yeo (1997).
3.9 LimitationsThis research project has a number of limitations. The primary limitation results from it being
a sole researcher project. This potentially impacts on objectivity across a range of activities as
there is not a process to validate the reliability of interpretation or coding with other
researchers. This could have affected classification and/or coding within the literature review,
the qualitative coding used for model development; and direction chosen for development of
the digital document prototype. Similarly, as the sole recorder, moderator and interpreter of
questionnaire/interviews, work practices and focus groups, total objectivity was difficult
because of the researcher’s prior domain and personal experience. However, as the chosen
methodology (design research) is iterative and interactive through the artefact – it can react to,
and can change the direction of the research as knowledge of the problem increases
independently of the researcher – addressing some concerns about researcher bias. Further,
the project comprised only a small number of participants in both the hospital and community
scenarios – although data triangulation from a number of sources contributed to the validity of
the findings. However, the project is a proof of concept, intended to be further tested in
medication review field studies to validate the model and approach.
The chapter is summarised next in Section 3.10.
3.10 SummaryThis research project explored whether a digital document could be used to support decision-
making in health through a specific investigation of whether a digital document could be used
to support pharmacist decision-making in medication management. The need for the latter was
based on the researcher’s domain knowledge and was supported through examination of the
literature.
The digital document evolved in parallel with the development of an information model based
on data collection through an initial relatively information-rich hospital scenario to a more
general community environment. The methodological approach was empirical, with an
interpretivist, inductive stance using Design Research. The technology selected for
implementation of the digital document was XForms. The final aims were to investigate
whether this approach could improve the quality, efficiency and safety of the medication
management process in the community.
The next chapter discusses Design Research in more depth, in particular, its suitability for
Page 93

conducting research in complex and unstructured environments. From the foundations of its
use in education and IS, a case is made for its being an appropriate and novel method for
researching practice-based problems in the health care domain.
Page 94
Chapter 4
Design research in complex environments
4.1 IntroductionChapter 3 introduced methodology and candidate strategies to answer the research
questions; and concluded that Design Research was appropriate to use for a number of
reasons:
• the research environment was information-rich with ill-defined contexts
• there were complex interactions between problem and solution
• flexibility was required to allow changes to the processes and artefact
• there was a dependence on human cognitive abilities to produce a solution
• there was a dependence on human social abilities.
Similarly, the technology selected for implementation of the digital document was XForms,
based on the need to maximise flexibility and response in keeping with the Design Research
approach.
This chapter continues the discussion of Design Research (DR) and, in particular, its suitability
for research in complex and unstructured environments. This is approached from an
investigation of the use of DR in education and Information Systems (IS), with justification
made for it being an appropriate and novel method for researching practice-based problems
in the health care domain.
This chapter is structured as follows:
• it begins with Section 4.2 begins that considers the notion of design
• Section 4.3 discusses issues in dealing with complexity
• the use of Design Research in Education research is demonstrated in Section 4.4
• the use of Design Research in Information Systems research is demonstrated in Section
4.5
• the application of Design Research to the Health environment is justified in Section 4.6
• Section 4.7 discusses Design Research foundations
• the Design Research approach s aligned with the research plan in Section 4.8; and
• the chapter concludes with a summary in Section 4.9.
Page 95

4.2 Design – what’s in a name?Before DR can be discussed, it is useful to clarify terminology concepts identified in the (IS)
literature which may cause confusion. These are design, design theory, design science and
design research (DR) and, consequently, artefact.
Design is defined by the Merriam-Webster On-line Dictionary (http://www.m-w.com/cgi-bin/
dictionary, viewed 2006-06-26):
as a verb: ‘to create, fashion, execute, or construct according to plan’, or as a noun: ‘a plan or protocol for carrying out or accomplishing something (as a scientific experiment); also: the process of preparing this’
The design of artefacts has been carried out for centuries and distinguishes the sciences from
the professions (Simon 1996, p. 111; Vaishnavi & Kuechler 2005) such as engineering,
medicine, business and architecture (Simon 1996, p. xii). Most definitions of design share
three attributes: they refer to a process; the process is goal-oriented; and the goal is about
solving problems, meeting needs, improving situations, or creating something new or useful
(Friedman 2003).
‘Design ideal’ has also been described (at the most abstract level) where this describes the
values and standards which define the ultimate ‘good’ at which some design project aims – this
may be technical, economic or aesthetic standards, or a variety of other social ‘goods’ such as
equity, peace or conservation of natural resources (Klein & Hirschheim 2001).
Fallman (2003) presents three ‘accounts’ of design theory:
• the process-oriented conservative account (a linear process where every step is rational
and possible to describe)
• the product-oriented romantic account (guided by the designer’s values and tastes, such
as in poetry, drama, painting, sculpture and music); and
• the down-to-earth pragmatic account (a hermeneutic process of interpretation and
creation where designers interpret the effects of their designs in their settings).
Walls et al. (1992) consider Design Theory to be a package of three interrelated elements: a
set of user requirements; a set of system features (or principles for selecting system features);
and a set of principles deemed effective for guiding the development process. This can be
thought of as a complete package of guidance for designers (Markus, Majchrzak & Gasser
2002). Despite such formal guidance, however, there needs to be an unfolding ‘design
dialogue’ between the designer and customer that investigates the relationship between
details of the design and the problem to be solved (Fallman 2003).
Page 96
Design science has its origins in the ‘sciences of the artificial’ (Hevner et al. 2004), such as
architecture and engineering (McKay & Marshall 2005). This is a body of knowledge about
artificial (‘man made’ sic) objects and phenomena designed to meet certain desired goals
(Vaishnavi & Kuechler 2005). Design science is considered to be a systematic approach to
design, not just the use of scientific knowledge of artefacts.
Design itself, in some sense, can be seen as a scientific activity – although this is a
controversial concept challenged by many designers and design theorists (Cross 2002).
Nunamaker et al. (1990) classify design science as (applied) research which uses knowledge
to solve practical problems. It is technology-oriented and attempts to create things which serve
human purposes through the basic activities of building and evaluation (as opposed to natural
and social sciences, which try to understand reality) (Au 2001). Some comparisons made
between natural and design science enquiry (Lee 2000) are shown in Table 4-1.
Design science products are of four types – constructs, models, methods, and
implementations – but, absent from this list are theories, the ultimate products of natural
science research (March & Smith 1995). Fundamentally, from an IS perspective, design
science is about addressing business needs or problem-solving through constructing and
applying innovative IT artefacts to understand the problem addressed by the artefact and the
likelihood that this approach will provide a solution (Hevner et al. 2004).
There is some confusion in the literature, however, between the fields of practice and research
(Friedman 2003) on what constitutes design science and design science research (or DR) –
and the need to separate routine design (or system building) from DR (Hevner et al. 2004).
McKay and Marshall (2005) stress that the distinction between ‘designing’ (design science)
and ‘researching designing’ (DR) can be quite subtle; and more easily separated at a
conceptual level than at a practical level. Design researchers do not only design an artefact to
address a problem, but also conduct research into some aspect or dimension of the design
activity relevant to a particular problem. The process of design itself will add to knowledge, but
it is ‘the systematic and methodological enquiry into that practice’ that constitutes DR
Table 4-1: Comparisons of natural science and design science enquiry (Lee 2000)
The activity The purpose ExamplesNatural science enquiry Describing and explaining
nature and society.The description/explanation theory is true.
Physics.Biology.Economics.Psychology.
Design science enquiry Designing something new. The design is effective. Medicine.Architecture.Law.
Page 97

(Friedman 2003). In short, DR embodies the systematic acquisition of knowledge alongside
design and design activity (Bayazit 2004).
Thus, DR retains the goal of successful design but adds an additional goal of developing
useful, generalisable theories (Edelson 2002). However, Barab and Squire (2004) consider it
both critical and challenging to continually try to make two types of arguments for ‘experience-
near significance’ and ‘experience-distant relevance’, suggesting instead that the pragmatic
philosophical underpinning of DR is that the value of a theory lies in its ability to produce
changes in the world.
A further perspective on the ‘direction’ of design science is provided by McKay and Marshall
(2005) who identify a concern that DR is becoming narrowly framed with the pervasive view
that it is about ‘things’ of interest (e.g. decision support systems) or aspects of technical
systems (e.g. data models and CASE tools). This is in contrast to the view promulgated in the
Arts, where there is an attitudinal difference in definition:
design research regularly participates in the redefinition of the design process away from the stand-alone object and into the integrated system… By moving away from ‘mere styling’ of the product itself and into the interlocking systems that manifest, support, constrain and envelop products, designers can rightfully lay claim to a much farther-reaching contribution (McKay & Marshall 2005)
The central construct of DR – the artefact – is defined by the Merriam-Webster On-line
Dictionary (http://www.m-w.com/dictionary/artefact, viewed 2006-03-02) as: ’(1a) something
created by humans usually for a practical purpose’.
Simon (1996, p. 6) suggests that an artefact can be thought of as a meeting point ('interface')
between an 'inner' environment (the substance and organisation of the artefact itself) and an
'outer' environment (the surroundings in which it operates). If the inner environment is
appropriate to the outer environment, or vice versa, the artefact will serve its intended purpose.
There has been much discussion concerning what constitutes an ‘IT artefact’, seemingly
encompassing almost anything that is touched or affected by IT – suggesting a ‘boundary’
issue (Alter 2003b). Alter (2003b) suggests that this term – Benbasat and Zmud’s (2003)
definition – is too unclear to serve as a basic concept and better describes an ‘IT-reliant work
system’. The artefacts in this thesis are certainly IT artefacts, but the intended meaning here
is in line with the Dictionary definition above: ‘something created by humans usually for a
practical purpose’ – referring to the information model and its digital document implementation.
This section has discussed the various meanings associated with ‘design’ and introduced the
Page 98

artefact as being at a meeting point with the environment in which it will operate. A valuable
relationship in design is that understanding the design problem requires specific knowledge of
a domain; and designing a solution will lead to a further understanding of that domain
(Fitzpatrick 1998). DR can therefore be considered to be particularly appropriate for problem-
solving in complex environments; and this is introduced in the next section.
4.3 Dealing with complexityThe landmark article by Horst Rittel and Melvin Webber (1973) from UC Berkley, Dilemmas in
a General Theory of Planning, observed that there was a whole realm of social planning
problems which could not be successfully addressed by traditional linear, analytical
approaches (Ritchey 2005). These became known as ‘wicked problems’, as opposed to ‘tame
problems’.
Conklin (2001, p.11) in Ritchey (2005) defines a tame problem as one which:
• has a relatively well-defined and stable problem statement
• has a definite stopping point (we know when a solution is reached)
• has a solution which can be objectively evaluated as being right or wrong
• belongs to a class of similar problems which can be solved in a similar manner; and
• has solutions which can be tried and abandoned.
In contrast, wicked problems are ill-defined, ambiguous and can be associated with strong
moral, political and professional issues and, as they are strongly stakeholder dependent, there
is often little consensus about what the problem is, let alone how to resolve it (Ritchey 2005).
Further, wicked problems are sets of complex, interacting issues evolving in a dynamic social
context – and new forms of wicked problems can emerge as a result of trying to understand
and solve an existing problem (Ritchey 2005). Examples of important wicked problems include
complex, long-term social and organisational planning problems (Ritchey 2005), such as:
• what is a good national immigration policy?
• how should scientific and technological development be governed?
• how should we deal with crime and violence in our schools?
• how should an organisation develop in the face of an increasingly uncertain future?
Hevner et al. (2004) suggest that DR can address ‘wicked problems' through:
• the design of artefacts that embody complex interactions among subcomponents of the
problem and its solution
• allowing inherent flexibility to change design processes as well as artefacts
• acknowledging a critical dependence upon human cognitive abilities (i.e. use of
creativity) and human social abilities (e.g. teamwork) to produce effective solutions.
Page 99

The design problem can be characterised as a ‘wicked problem’ where understanding and
designing are part of both the problem and the solution (Fitzpatrick 1998). This approach is
particularly usefully for new areas or where there are deficiencies in existing systems (Rossi &
Sein 2003).
Markus, Majchrzak and Gasser (2002) noted that emergent knowledge-intensive processes
(EKP) have challenging information requirements as they involve tacit and explicit knowledge;
and general and contextual knowledge – as well as requiring expertise to apply this
knowledge. Further, because knowledge is distributed across experts and non-experts, EKPs
also require knowledge to be shared. The researcher believes that these problems typify the
knowledge intensive areas of education and health. Furthermore, as all disciplines build
knowledge bases, how they do this is important, because it reveals processes which offer
cases for design (Owen 1997). Nonetheless, understanding what cooperative work means and
how to design systems to support this work are problems which defy simple definitions and
solutions (Fitzpatrick 1998). The use of design theory within these areas may allow the
development process to be more manageable by restricting the range of development
practices for developers to a more manageable set (Markus, Majchrzak & Gasser 2002).
The fields of education and IS are well characterised by problems of a wicked nature and are
supported by appropriate evidence of the usefulness of DR in those areas. The next two
sections examine this evidence, first in education and then in IS. For each domain, the
discussion begins with some background to DS, the suitability and advantages of DR; and also
some issues which require consideration.
4.4 Design research in educationThe origins of DR in education can be found almost a century ago with the recognition of the
difficulty of studying complex human functioning found in classrooms.
Thorndike (1910) in O'Donnell (2004) noted that:
(the) extreme complexity and intimate mixture with habits in the case of human instincts prevents studies of them, even when made with great care, from giving entirely unambiguous and elegant results
DR in education was introduced against a backdrop of criticism about the use of laboratory
studies (e.g. studying the memory process) that used artificial materials, when those contexts
and materials were so different from the ones which students would actually use in a real world
setting (O'Donnell 2004).
Page 100

The application of scientific methodology in education was seen to be problematic (Hoadley
2004) as:
• all the possible variables could not be controlled
• studies could not be double-blinded
• an intervention in an educational setting was a dependant rather than independent
variable
• there was a blurring of researcher-participant distinction
• generalisation was tentative (there was no expectation of universality of results)
• the researcher frequently followed discoveries where they led
• there was a need to record not only the intervention and rationale for design, but also the
changes over time and how a particular representation embodied (or did not) the
hypotheses being tested.
The term ‘design experiment’ was introduced by Brown and Collins in 1992, but was replaced
by design research (or design-based research) as being more appropriate in light of the nature
of the process (it was not really an ‘experiment’) (O'Donnell 2004). ’Developmental research’,
a form of DR, has been in use in Europe for some years (Kelly 2004). Educational interventions
are viewed as holistic, involving interactions between materials, teachers and learners; and
since the intervention is a product of the context in which it is implemented, the intervention
itself is the outcome (or at least an outcome) (The Design-Based Research Collective 2003).
These partnerships can also help distinguish between a ‘lethal mutation’ – a reinterpretation
that no longer captures the pedagogical essence of the innovation – and a productive
adaptation which preserves this essence and tailors the activity to the needs and
characteristics of particular classrooms (The Design-Based Research Collective 2003).
The primary goal of DR in education is to ’investigate how different learning environment
designs affect dependant variables in teaching and learning’ (O'Donnell 2004). Educational
research which is removed from practice may not account for the influence of contexts, the
complex nature of outcomes and the incompleteness of knowledge about which factors are
relevant for prediction (The Design-Based Research Collective 2003). In other words, learning,
cognition, knowing and context are inter-related and cannot be treated as isolated entities or
processes (Barab & Squire 2004).
DR in education is founded on the notion that important things can be learnt about the nature
of learning by attempting to engineer educational innovation amongst children in everyday
settings (Bell 2004). In addition, complex educational interventions can reveal phenomena of
interest to study that will subsequently promote specific educational outcomes and develop
Page 101
new theoretical insights about the nature of learning (Bell 2004). Importantly, DR also allows
research findings to be derived through adaptive evaluation (Collins, Joseph & Bielaczyc
2004). This provides the opportunity to advance the understanding of teaching, learning and
educational systems at the same time (Edelson 2002).
Shavelson et al. (2003) in Joseph (2004) describe DR in an educational context as:
such research, based strongly on prior research and theory and carried out in educational settings, seeks to trace the evolution of learning in complex, messy classrooms and schools, test and build theories of teaching and learning, and produce instructional tools that survive the challenges of everyday practice.
Three important intertwined goals for DR projects can be inferred from this definition –
research, design and pedagogical practice (Joseph 2004).
Edelson (2002) states that the objectives of DR (novelty and usefulness) are different from
traditional empirical research and thus this form of research should not be judged by the same
standards as ‘scientific method’ based research. The point of DR is to generate theories which
could not be generated either by isolated analysis or by traditional empirical approaches. The
blending of research and practice also fits well with the purposes of education, given its
fundamentally interventionist nature – without empirical research, it would be difficult to make
theoretical or practical progress in natural settings and refine use-centred theory (Bell 2004).
Further, because education is by nature an interventionist, designed endeavour, the scope of
DR may continue to expand and prove to as be productive as other established modes of
educational enquiry (e.g. experiment, historical, philosophical, anthropological or sociological
research) (Bell 2004). However, DR can still incorporate outcome-based evaluations which
characterise traditional theory testing (Edelson 2002), although traditional before-and-after
testing is less meaningful (Hoadley 2004).
The conventional role of design in educational research has been as a strategy for testing
theories – which assumed a fully developed theory that mapped directly into design (Edelson
2002). However, with an increasing concern for research to be educationally relevant and to
contribute to improvement (O'Donnell 2004), recent literature describes DR as a process
where design plays a critical role in the development of theories – not just evaluation (Edelson
2002). Kelly (2004) suggests that DR’s contribution is primarily its input into the thinking of
other researchers in similar contexts, who can take the foundations and use other
methodologies to allow generalisation. In fact, Kelly prefers the use of ‘working words’ such as
hypothesis, conjecture, model, framework, belief, rationale (amongst others) to ‘theory’, which
in science means a ‘well-substantiated explanation of some aspect of the natural world that
can incorporate facts, laws, inferences, and tested hypotheses’ (Kelly 2004).
Page 102

In DR, hypotheses about the learning phenomena are embodied in the designed artefacts
(Joseph 2004). Theory development often begins with an initial (incomplete) set of hypotheses
to guide the design process which progressively constructs a coherent theory – through a
parallel and retrospective process of reflection on design experiences and outcomes (Edelson
2002). However, a search guided only by the most general heuristics of 'interestingness' or
novelty can be an equally suitable mechanism for finding a suitable model for a social design
process (Simon 1996, p. 162).
As with many other research approaches, identification of gaps in the research literature can
originate questions (Joseph 2004). Consequently, design work is guided by the knowledge of
these gaps in current understanding to focus effort in areas which will make a useful
contribution (Edelson 2002) – empirical refinement can then identify results which can not only
lead to improvement of a particular learning design, but also to refinements in learning theory
itself (O'Donnell 2004).
O’Donnell states that the selection of questions in this domain should be those having a
meaningful relationship with student learning (O'Donnell 2004). Joseph (2004) agrees that
effective research requires a focus on specific questions – however, there are many design
considerations and there is a need to understand a large number of phenomena and variables
to improve a design. Thus, real-world practice and day-to-day needs do place constraints and
demands on design and research activities. Nevertheless, DR can use these design needs
and contextual demands as a way of determining the specific key questions of interest (Joseph
2004). Joseph (2004) asserts that there are some design questions which are critically
important – how are the artefacts used, how are they implicated in learning; and how might
they fail? A further issue is that, although design decisions (made within constraints) represent
opportunities for learning, they also provide a potential for researcher bias (Kelly 2004). Kelly
(2004) considers there is an association of ‘the contingent’ (parts that are more arbitrary) and
‘the necessary’ in these decisions; and that the real challenge is to connect the contingent to
the necessary.
A significant argument for DR is the usefulness of its results. If the ultimate goal of educational
research is the improvement of the education system, then results which directly address the
design of activities, materials and systems will be the most useful (Edelson 2002). The twin
goals of developing effective designs and contributing to basic understanding created through
the interactions of these goals is a ‘powerful engine for driving innovative work’ in education –
and because this takes place in a real-life context, design choices and research are closely
associated with that context (Joseph 2004). In fact, DR is something which: ‘might develop into
Page 103

a force sufficient to accelerate the ponderous educational system’ (Hake 2004).
There remain some key concerns and issues relating to DR in education:
• the relative certainty of its findings in comparison to traditional empirical research, as
explanatory power will be grounded in specific experiences rather than in statistical
methods (Edelson 2002)
• the ‘Bartlett effect’ – a tendency to select data that confirms the researcher's
expectations – particularly when portions of transcripts/interviews are selected to
illustrate a theoretical point, or when descriptions are selected from a large number of
potential examples. This risk is exacerbated by the amount of data collected (often too
much) (O'Donnell 2004)
• absence of standards for identifying when a design can be executed, should be
abandoned, or is promising enough to warrant exploration. The possibility of endless
revisions also has important resource implications for classrooms, curricula and
students' time (O'Donnell 2004)
• the question of when and how summative evaluation begins (Joseph 2004)
• problems with generalisation since relatively few participants are typically involved in
very in-depth analyses (Joseph 2004; O'Donnell, 2004)
• problems with generalisations across contexts (different schools, tools or circumstances)
(Joseph 2004) as complexity makes it difficult to identify contributors to success
(O'Donnell 2004)
• the context itself is not ’natural’ as it represents the joint efforts of researchers, teachers,
students and others who typically may not work so closely (O'Donnell 2004)
• the need to understand the role of the individual teacher, i.e. which aspect of activity
design and instruction belong to the model and which are due to the preferences of the
individual teacher (Joseph 2004)
• how to apply a useful model to new teachers and schools (Joseph 2004)
• the problem of managing large data sets produced by the DR process (Collins, Joseph &
Bielaczyc 2004).
DR in the educational setting has been employed in the fields of developmental psychology
(socio-cognitive development), cultural psychology, linguistic or cognitive anthropology; and
ethnography (Bell 2004). The focus of design efforts has varied with the interests of the
educational research community and has included design of curriculum, software, professional
development, school organisations, school-community collaborations (Edelson 2002); and
physics education (Hake 2004).
Page 104

The Design-Based Research Collective (2003) sees a number of prospects for Design
Research in education:
• exploring possibilities for creating novel learning and teaching environments
• developing theories of learning and instruction that are contextually based
• advancing and consolidating design knowledge; and
• increasing the capacity for educational innovation.
In summary, in education, design research activities are iterative, interventionist (innovative
and design-based) and theory-oriented enterprises whose theories do real work in practical
educational contexts (Cobb et al. 2003).
The use of DR as a research method in education ocurred in parallel with its use as a research
method in IS – this is discussed next in Section 4.5.
4.5 Design research in information systemsThe explorations of IS – unlike those of computer science (CS) and software engineering (SE)
which are often performed within the rules and practices of mathematics – usually occur in an
organisational (and therefore behavioural) context; and are based on relevant theories often
extracted from other disciplines (Glass, Ramesh & Vessey 2004). Although positivist science
shaped the field of IS in the 1980s, interpretive and critical science emerged as milestones in
the 1990s (Lee 2000). Lee (2000) considers that the IS research field has matured to the point
where substantive and methodological rigour make it the equal of any other business-school
discipline.
The prime focus of IS experts is on aligning IT artefacts within the organisational and social
contexts of use (i.e. the people who use them) – and on the implementation, evaluation and
consideration of related changes of these artefacts (Iivari, Hirschheim & Klein 2001).
However, some consider that the IS field has not deeply engaged its core subject matter – i.e.
the IT artefact (Orlikowski & Iacono 2001). One reason given is that IS researchers do not build
IT artefacts as most are not trained to do so (and so do not have the needed skills); and most
build their skills and experience around evaluating, theorising, and justifying existing artefacts
(Au 2001). There has been a call for more IT-reliant work in the IS field – with a greater
engagement with IT artefacts – as they are integral parts of work systems and therefore should
not be ignored when work systems are studied as systems (Alter 2003a).
The Conference on Design Methods held in London in 1962 (Jones and Thornley, 1963) is
generally regarded as the event that marked the launch of the design methods movement and
Page 105
design methodology as a field of enquiry in IS. A subsequent conference on the ‘design
method’ held in Birmingham in 1965 related 'the design method' to 'the scientific method' with
consequent reference to 'design science' (Cross 2002). Simon then further extended the
concept of design science in The Sciences of the Artificial published in 1969 (Lee 2000).
Lee (2000) considers that ‘design science is an old lesson just waiting for us to apply it’.
However, whereas natural science tries to understand reality, design science attempts to
create things which serve human purposes. It is technology-oriented, and its products are
assessed against criteria of utility or value – does it work, or is it an improvement? (March &
Smith 1995). This approach is particularly usefully for new areas where there are theories
which cannot be tested; and where there are identified deficiencies in existing systems (Rossi
& Sein 2003). Design is a key activity in fields such as architecture, engineering and urban
planning, which may not be thought of as ’sciences’ per se (March & Smith 1995).
Lee (2000) suggests that DR (or design science) contributes to resolving three dilemmas
facing IS:
• rigour vs. relevance
• reference vs. independent discipline in the development of the IS field; and
• technology vs. behaviour.
The first dilemma is addressed by DR’s application to real world problems, the discipline issue
is addressed by taking a system approach (therefore strengthening the notion of discipline
independence); and the latter through DR’s approach of treating the computer and behavioural
‘subsystems’ as being inseparable.
Purao (2002) does extend the concept of DR in IS to that of a paradigm. This is based on the
notion that DR creates new realities by ‘knowing through making’, something not anticipated
by the traditional philosophy of science. However, this discussion in this thesis will proceed
with the more conventional understanding of DR as a method.
From an IS perspective the main goal of DR is fundamentally about addressing business
needs or problem-solving (Hevner et al. 2004). Hevner et al. (2004) suggest that DR
addresses ‘wicked problems’ in IS characterised by:
• unstable requirements and constraints based upon ill-defined environmental contexts
• complex interactions among subcomponents of the problem and its solution
• inherent flexibility to change design processes as well as design artefacts
• a critical dependence upon human cognitive abilities, i.e. creativity, to produce effective
solutions
Page 106

• a critical dependence upon human social abilities (e.g., teamwork) to produce effective
solutions.
The challenge of designing decision support systems perhaps provides a good demonstration
of the wicked problems described by Hevner et al. – and it is not surprising that DR has been
used in the investigation of decision support systems (Arnott 2005).
DR begins with a perceived need which can originate in practice or be discipline-based (Purao
2002); and the IS field is particularly concerned with research and practice about problems and
solutions resulting from interactions between technology and (human) behaviour (Lee 2000).
In contrast to the natural science approach that aims at understanding phenomena, DR sets
out to develop ways to achieve human goals (March & Smith 1995) – DR researchers do not
believe that the 'truth' is 'out there', but help to create it through the generation of artefact
(Purao 2002). Lee (2000) believes that IS is about ‘technology-behaviour interactions’ rather
than ‘technology vs. behaviour’, i.e. they are inseparable. Similarly, as IS is viewed as a socio-
technical system (Sutcliffe 2000; McKay & Marshall 2005), the essence of IS lies in the
‘contextualisation of the machine in the social system’ and what makes DR resonate with
practice is its sensitivity to that social context (McKay & Marshall 2005).
The process of DR in IS involves the construction and application of innovative IT artefacts
which attempt to understand the problem addressed by the artefacts and the likelihood of this
approach providing a solution (Hevner et al. 2004). Artefacts can be expressed as constructs,
models, methods and instantiations or implementations (Au 2001; Vaishnavi & Kuechler
2005). As well as artefacts serving as models that represent situations as problems and
solution statements (March & Smith 1995), artefacts as ‘situated implementations’ can reveal
the knowledge to accomplish these solutions and then build theories about the problem and
solution (Purao 2002).This supports the beliefs of Morrison and George (1995) that the
dynamics of computer-based interventions cannot be understood unless we develop the
products that provide those interventions.
The interventionist, iterative cycle that underpins DR allows a prototype to serve as a system
specification or ‘evolutionary working system’ that can test an existing theory (Morrison &
George 1995); and become the basis for a new theory and new constructive intervention
(Vaishnavi & Kuechler 2005). However, although theorising about the IT artefact is intended to
uncover characteristics that are unique to IT, where IT artefacts significantly affect the task or
the environment, it can be beneficial to adapt theories from referent disciplines (March & Smith
1995).
Page 107

To return to the notion of truth, March and Smith (1995) suggest that the truth is essentially
what works in practice. As the implementation of an information system serves some human
interest, design choices will require value judgements and therefore necessarily select some
interests over others – this entails addressing what is ‘good’, ‘bad’, ‘right’ or ‘wrong’, as well as
technical issues about design (Klein & Hirschheim 2001). McKay and Marshall (2005) note that
concomitant people, processes and organisational structural changes are just as important
and relevant to improving a problem situation as a designed technical artefact. Consequently,
allowing the design process to capture the value judgements contained in organisational
decision-making and allowing them to be addressed rationally is important –- ignoring them
may not only be undesirable, but also may impose opportunity costs (Klein & Hirschheim
2001).
The DR approach also proposes a more realistic approach to the evaluation of systems. Simon
(1996, p. 28-29) talks about ‘satisficing’ where real world complexity means that the ‘best
answers’ to questions are unknowable; and since real world optimisation (with or without
computers) is impossible, a 'good enough' alternative is acceptable, not because this is
preferred but because there is no choice.
March and Smith (1995) however, identify a number of implications for IT research using
artefacts:
• there may not be an underlying deep structure to support a theory of IT per se so that
theories may need to be based on other theories of the natural phenomena (i.e. people)
that are impacted by the technology
• artefacts are perishable and consequently, so are the research results. As needs
change, therefore, the artefacts produced to meet those needs must also change
• as artefacts are being produced at an ever increasing rate, this results in innumerable
phenomena to study.
There is also a practical dilemma of competing design ideals – which design (ideal) should be
adopted, since development cannot be impartial and once the design ideal is made explicit,
development work is then bound by interest (Klein & Hirschheim 2001).
The suitability of DR for research in complex and unstructured environments is now discussed
in the context of the domain of interest for the research project – the health domain.
4.6 Designing a better health technology interventionDR has been discussed up to this point in relation to its suitability to address practical issues
and provide solutions in complex environments characterised by ‘wicked problems’ –
Page 108

education and IS. This research sought to apply DR in a new problem context in the health
domain – specifically, the problem of technology support for medication management. This
section describes the nature of the health care domain as a background for this decision; and
justifies the use of DR as appropriate and relevant for investigating a technology intervention
in this domain.
Health professionals work in an increasingly complex area characterised by advances in
medical science and technology, increasing specialisation, ever-greater patient expectations,
and, above all, the sheer size and diversity of health service provision (Pope & Mays 1995).
The interaction space within which clinicians carry out their work is also complex as individuals
must execute their tasks by communicating across rich social networks (Ash, Berg & Coiera
2004).
Information Systems in the health domain play an important role in improving health care
quality (Beyer et al. 2004). IT is seen as a valuable tool to provide productivity gains, cope with
demand, make health care delivery more consumer focused (European Commission 2004);
and address issues of quality and safety (Bates & Gawande 2003; Electronic Prescribing
Initiative 2004). IT plays a particularly significant role in information management (Sowerby
Centre for Health Informatics 2000), electronic prescribing (Electronic Prescribing Initiative
2004), clinical decision support and medication safety (Roughead & Semple 2002; Bates &
Gawande 2003). Safe care now requires a degree of individualisation that is becoming
unimaginable without computerised decision support (Bates & Gawande 2003) – information
systems are increasingly seen as an integral part of the health care process, rather than just
a tool (Beyer et al. 2004). However, health care processes are subject to change and health
information systems must be capable of adapting to this change where the driver for change
should be the need for the process improvement rather than the technology itself (Lenz et al.
2005).
Plummer (2001) describes Health Informatics (HI) has having ‘been concerned primarily with
the use of technology for the optimal use of health-related information for decision-making and
problem solving to improve health care outcomes’ – this term will be used in this thesis with
the same understanding. There are many similarities between the areas of HI and IS. Both are
multi-disciplinary fields. IS builds on reference disciplines including organisational theory,
decision science, information technology, and other management sciences – HI is also a blend
of referent disciplines including, but not limited to: psychology, sociology, anthropology,
organisational behaviour and management sciences (Plummer 2001).
HI and IS also face similar organisational issues when considering people and technology,
Page 109

including elements of power relationships, as well as politics and resistance – both share an
overall focus of successfully integrating people and technology to improve outcomes and
performance – both also share high failure rates in terms of information systems (Plummer
2001). Issues around health care, however, could be described as more information intense,
more organisationally complex, more turbulent, more paradoxical, more subjective; and more
emotionally charged than other industries and businesses (Plummer 2001).
Experiential knowledge is extremely significant in the practice of health professionals (e.g. in
medicine) – termed ‘knowledge work’ by Iivari, Hirschheim and Klein (2001). Such knowledge
work is differentiated from other work by: a body of knowledge; representations of the objects
of work; a deep theoretical understanding of the objects of work; and results which entail
knowledge as an essential ingredient (Iivari, Hirschheim & Klein 2001). Further, the complexity
of human behaviour within such environments is a reflection of the environment itself (Simon
1996, p. 80). The types of issues experienced in health clearly supports their classification as
‘wicked problems’ (Ritchey 2005) – similar to issues experienced in the fields of education and
IS. Subsequently, the researcher believed that a similar role existed for artefact-mediated
interventions – using design research – to produce effective problem solutions.
As with IS, socio-technical is a term also applied to the health system (Runciman & Moller
2001). The health system involves complex interactions between consumers, health
professionals and the health system framework itself (Runciman & Moller 2001). This
advocates for the use of IS research approaches that employ human-centric analyses of the
impact of computer systems on people; and consider how technology can be designed more
effectively for people (Sutcliffe 2000). However, the complexity of socio-technical evolution
should also never be underestimated (Lenz et al. 2005). Ash, Berg and Coiera (2004) caution
that when technologies become an integral part of health care work practices, behaviours
emerge out of the socio-technical coupling; and the behaviour of the overall system in any new
situation can never be fully predicted from the individual social or technical components.
Health information systems, as an integral part of these complex socio-technical systems,
must also cope with changing conditions and requirements (Beyer et al. 2004). The report of
the National Electronic Decision Support Taskforce referred to the need to investigate socio-
technical barriers which existed for health care providers and were preventing the uptake of
decision support systems (National Electronic Decision Support Taskforce 2002, p. 90).
Plummer (2001) identifies common organisational aspects that are critical to a system’s
success suggesting that these are critical in both IS and HI:
• organisational leadership and commitment
• the establishment of an appropriate coordinating body or mechanism
Page 110

• adoption of participatory approaches to IS development; and
• an iterative approach to development.
Some comparative dimensions of DR in education and IS have been synthesised from the
literature by the researcher; and summarised in Table 4-2. It is clear from this table that there
are many similarities in the approaches and problems encountered by researchers in both
domains. One of the curious elements of DR investigations is the parallel – but quite separate
– activities of these two groups of researchers over a comparatively long period of time. Table
4-2 also includes the equivalent DR dimensions for health, proposed by the researcher, based
on literature and domain knowledge – this summarises the reasons why DR methods are
appropriate for use in the HI environment.
Because of its applied nature, much research in the health environment is driven by specific
practical problems that are converted into research questions – rather than being derived from
the researcher’s theoretical perspectives (Pope & Mays 1995). Until recently, HI research has
tended to focus on the technical development of clinical systems and favoured the positivist
approach of medically trained researchers (Plummer 2001). But, as health care deals with
people, there is a whole set of questions about human interaction – and experimental and
quantitative methods are less suited to answer these questions (Pope & Mays 1995). It is this
complexity and subjectivity which supports the need for appropriate qualitative methodologies
for research and theory building in HI to improve success (Plummer 2001).
In summary, there are many parallels between the research in IS and HI in terms of the
organisational and information issues – although these two areas may differ in the degree of
intensity and ‘ways of knowing’ (how the discipline knowledge is evolved) (Owen 1997). It is
reasonable to assume, therefore, that the same research methods are appropriate to build
theory and improve practice in both. The issues of complexity and context addressed by DR
in educational research are also relevant to HI research – the DR approach in the present
research project clearly supports its interventionist nature as well as its desire to use scenarios
as test beds for innovation (Cobb et al. 2003). The DR approach – in particular, the DR cycle
and outputs – is outlined in the next section.
4.7 Design research foundationsIn keeping with the approach in Chapter 3 (Methodology), the discussion of DR will begin with
a philosophical perspective and then introduce the ontological and epistemological stances.
Sub-section 4.7.1 discusses the DR cycle in detail with outputs discussed subsequently in
Sub-section 4.7.2.
Page 111

Prior to this discussion, however, it is appropriate to provide an overview of DR – this is well
summarised by Vaishnavi and Kuechler (2005) in Figure 4-1, which shows the iterative nature
DR with process steps and associated outputs, as well as the knowledge flows which
contribute to understanding and theory development.
The DR approach uses qualitative and exploratory techniques through the development and
Table 4-2: Dimensions of DR in education, IS and health
Education Information Systems HealthBackground Teachers, students in complex,
'messy' classrooms and schools.
People, business, organisations and their existing or planned technologies, and work systems. Socio-technical systems.
Health professionals, support personnel, health consumers. Socio-technical systems. Substantial communication and distribution of general and local knowledge. Emergent knowledge processes.
Pre-emption Informed by prior research or incomplete theories.
Exploration of 'wicked problems'.
Exploration of 'wicked problems', related to quality, efficiency and safety.
Goal Test and build innovative theories / models of teaching and learning, and produce instructional tools that survive everyday practice.
Technology-based solutions to solve problems and improve performance of activities.
Solve problems of quality, efficiency and safety in the delivery of health care.
Artefact embodiment
Embody theory about learning phenomena in real-world context.
Define ideas, practices, technical capabilities and products and solutions.
Model or define practices, guidelines and processes.
Artefact expression
Activity structures, institutions, scaffolds, curricula, software, professional development, school organisations, school-community collaborations or conceptual frameworks.
Construct, model, method or instantiation. Software or hardware.
Construct, model, method or instantiation. Not necessarily technology-based.
Search process
Team needs to have collective expertise to accomplish the functions associated with developing design, conducting the experiment, and systematic retrospective analysis.
Requires domain knowledge. Explicitly represents only a subset or simplification of problem.
Requires domain knowledge. Explicitly represents only a subset or simplification of problem as much decision-making requires contextualisation and use of tacit knowledge.
Evaluation Improvement in value of a particular designed artefact or a process for carrying out design. Using methods able to document and connect learning processes with learning outcomes.
Typically 'satisficing' in light of practical constraints. Functionality, completeness, consistency, accuracy, reliability, fit with the organisation, and other relevant quality attributes.
Judged on perceived utility and impact on individuals and organisations. Notion of improvements in quality, safety and efficiency are important. Metrics from IS applied as appropriate.
Theory Theories of learning and instruction that are contextually based.
Predict or explain phenomena with respect the artefact's use. Knowledge represents operational principles.
Contribution to thinking of other researchers in similar contexts. Knowledge representing operational and decision-making principles / processes.
Relevance Theories of learning and instruction that are contextually based.
In respect to constituent community.
Contextually based.
Research outcomes
Novel learning and teaching environments and ultimately improvement of the education system.
Novelty, generality and significance of the artefact / solving an important previously unsolved problem.
Significance of artefact in solving problem / addressing issue, and ultimately improving delivery of health care.
Page 112

design of artefacts (systems and models) (Rossi & Sein 2003).
The ontological and epistemological standpoints for DR suggested by Rossi and Sein (2003)
are realist – the real world exists but we are not seeking it – but we can intervene in the world
to improve it. There are two general aspects of the realist view, existence and independence.
The realist claims that everyday life provides us with a familiar (and mundane) empirical
dependence on objects and their properties – but there is no further sense in which everyday
objects and their properties are dependent on anyone's linguistic practices or conceptual
schemes (Miller 2005).
Ontology for DR is evolutionary and complementary – an evolving artefact gradually takes
shape and becomes an object in the world – then, as the phenomenon of interest takes on
characteristics of the artefact, the changed version of the phenomenon assumes an emergent
ontological stance complementing the realist stance of the artefact (Purao 2002).
Epistemology in DR is ’knowing through making’, rather than truth through seeking; and the
stance can be described as reflective and hermeneutic (Purao 2002). It is reflective, since DR
moves between the phenomenon and artefact (generating data and theory), a cycle which
involves the gradual bridging of the gap between need and artefact (resonating with an action-
oriented view) (Purao 2002). As DR arrives at an understanding of the artefact and the
phenomenon at the same time, creation and understanding become part of the same
Figure 4-1: The Design Research cycle (Vaishnavi & Kuechler 2005)
Knowledge Flows Process Steps Outputs
Awareness of Problem
Suggestion
Development
Evaluation
Conclusion
Proposal
Tentative design
Operation and Goal Knowledge
Circumscription
Artefact
Performance measures
Results
Design Research Cycle
Page 113

epistemological process and cannot be separated (Purao 2002).
As DR researchers deepen their understanding of the phenomenon during their investigation,
it is important that they generate a comprehensive record of the ongoing design process and
the variety of data sources which may influence it (Cobb et al. 2003). For this reason, DR
typically triangulates multiple sources and kinds of data (connecting intended and unintended
outcomes to actions) in the pursuit of validity (The Design-Based Research Collective 2003).
However, the study of complex phenomena precludes complete specification of everything
that happens (Cobb et al. 2003), consequently it is important to distinguish between elements
which are the target of investigation and those which may be incidental, accidental or assumed
as background conditions (Cobb et al. 2003). This was an issue in the present research
project, as the artefacts under investigation could have been ‘muddied’ by participants’ desire
to include elements to ensure business needs were accommodated or only minimally
disrupted. The notion of maintaining a sense of central and incidental requirements was central
to the methodology (Cobb et al. 2003).
The Design-Based Research Collective (2003) proposes that good design-based research
exhibit the following five characteristics:
• the central goals (in an educational setting) of designing learning environments and
developing theories of learning are intertwined
• development and research take place through continuous cycles of design, enactment,
analysis, and redesign
• research on designs must lead to shareable theories which help communicate relevant
implications to practitioners and other designers
• research must account for how designs function in authentic settings; and must not only
document success or failure but also focus on interactions which refine understanding of
issues involved
• development of accounts relies on methods which can document and connect processes
of enactment to outcomes of interest.
This overall DR approach is now enlarged upon in the following two sub-sections, the design
research cycle and outputs of design research.
4. 7.1 The design research cycleThe DR cycle, the fundamental iterative approach of the DR method, describes the process
steps in the design science cycle as: awareness of problem, suggestion, development,
evaluation and conclusion (Vaishnavi & Kuechler 2005). These steps have also been
described as: identify a need, build, evaluate, learn and theorise (Rossi & Sein 2003). There
Page 114

is a fundamental concept there – the ability of the design researcher’s philosophical
perspective as progress is made through the phases. For example, if the design researcher
creates a reality through constructive intervention, s/he reflectively become a positivist
observer recording the behaviour of the system – the observations can then be interpreted to
become the basis for new theorising and a new, interventionist cycle begins – similar to action
research methodology (Vaishnavi & Kuechler 2005).
DR often begins with an early version of a design placed in a real-life context (Joseph 2004),
with that design typically evolving as the designers deepen their understanding of the design
context through analysis and formative evaluation (Edelson 2002). This process has been
described as akin to prototyping in software engineering (Joseph 2004). The design process
is thus a sequence of decisions made by the researcher to balance goals and constraints
regarding how the design process will proceed, what needs and opportunities are addressed;
and what form the resulting design will take (Edelson 2002).
There is also a stress on circumscription – an essential part of this methodology – which
assumes that each fragment of knowledge is valid only in certain situations, based on the
detection and analysis of contradictions, i.e. the researcher discovers when things don’t work
‘according to theory’ (Vaishnavi & Kuechler 2005). This does not happen because of a
misconstruction of the theory, but because of the inevitable incompleteness of any knowledge
– when the design process is forced to consider the problem in this way, valuable knowledge
is contributed to the understanding of the theories which motivated the original design
(Vaishnavi & Kuechler 2005). This iterative design process is thus seen as having two faces –
a prospective face (designs are implemented with a hypothesised learning process) and a
reflective face (design experiments are conjecture-driven tests) (Cobb et al. 2003).
The DR cycle raises an interesting issue of validity versus credibility. Hoadley (2004) states
that the concept of alignment is important to validity in DR – having the same individuals carry
ideas (theories) and intervention through explanation, prediction, falsification and application
ensures theories have practical application as a result of methodological alignment. In
contrast, when researchers are also the designers of the intervention, this can raise issues of
credibility (O'Donnell 2004; Barab & Squire 2004) because such interventions might be seen
to ‘taint’ the research context (Barab & Squire 2004). O’Donnell (2004) believes that the
iterative nature of DR can satisfy some of the issues of credibility (e.g. external comparisons,
replication, relationship between intervention and outcome; and ruling out alternative
explanations) – although this satisfaction is limited and objectivity is not really possible
(O'Donnell 2004). However, according to Cronbach (1982, p.108) in Bell (2004): ’validity is
subjective rather than objective: the plausibility of the conclusion is what counts. And
Page 115

plausibility, to twist a cliché, lies in the ear of the beholder’; and the: ‘truth essentially is what
works in practice’ (March & Smith 1995).
The main goal in DR is thus systemic validity (studies must inform theories which must inform
practice) rather than measurement validity (interpretation of the results accurately reflects the
truth of the theory being examined) (Hoadley 2004). Barab and Squire (2004) suggest that DR
offers a mode of enquiry which embraces consequential validity but while demonstrating this
local consequence and utility is necessary, it is not sufficient and theoretical assertions must
be made to go beyond the local context (Barab & Squire 2004). Cobb et al. (2003) also
consider that DR should investigate situations which can inform a broader class of
phenomena. This was in keeping with intention of the research project where the researcher
was investigating a specific medication-related case in health, but also had the intention of
informing just such a technology application to health in general.
The outputs of design research are discussed next, in Sub-section 4.7.2.
4. 7.2 Design research outputsDR outputs according to Vaishnavi and Kuechler (2005), include: proposal, tentative design,
artefact, performance measures; and results (assuming that some goal is achieved) – shown
in Figure 4-1. These outputs correspond to relevant and equivalent processes in the DR cycle.
March and Smith (1995) in Hevner et al. (2004) offer only two design processes but four design
artefacts. The two processes are ‘build’ and ‘evaluate’; and the artefacts are constructs
(vocabulary and symbols), models (abstractions and representations), methods (algorithms
and practices) and instantiations (implemented and prototype systems). Of interest, is that
Vaishnavi and Kuechler (2005) also make an analogy between the development of better
theories (as an output of DR based on artefact construction) to the outputs of experimental
natural science. Figure 4-2 shows an alternative view of DR outputs adapted by Purao (2002).
The main value of Purao’s model is that it shows how the artefact (as a situated
implementation) feeds back to knowledge (as operational principles) which in turn informs
emergent theory – the DR process as a mechanism for feedback. Purao demonstrates this by
means of a data retrieval example taken from Krishnan et al. (2001). The outputs of the
research project are also accommodated by this model – the situated implementation of the
digital document feeds back to knowledge articulated by the information model and the
XForms model; and these in turn fed back to the emergent theory of how medication
management could be supported by a digital document.
March and Smith (1995) state that theorising about instantiations may be also be viewed as a
Page 116

first step toward developing more general theories (e.g. explaining how electronic mail affects
communication may lead to more general theories of the effects of technology or more general
theories about human communication) or as the specialisation of an existing general theory
(March & Smith 1995). The research contribution lies in the novelty of the artefact and in the
persuasiveness of the claims that it is effective, e.g. a ’significant improvement’, or more
comprehensive or better performance (March & Smith 1995).
One notable limitation of this approach is that the technologies used to build artefacts are
perishable.The greater is the contribution of technology to the artefact, the weaker will be the
contribution of the artefact. Instead, the research it must be grounded in the problem which the
artefact was designed to solve – explaining why a particular approach to build the artefact
solved the problem more effectively than another approach. Ball (2001) cautions that
contributions which are based solely on the technology of the artefact are as perishable as the
technology itself. The artefact should outlast the study so it can be adopted, adapted and used
by others (Kelly 2004) – but ‘the theory must do real work’ (Cobb et al. 2003).
The Evaluation of DR centres around two sets of criteria, internal and external, shown in Table
4-3, as adapted from Rossi and Sein (2003). The description of the artefact – in terms of
organisation and function, as the interface between inner and outer environments – is a major
objective of design activity (Simon 1996, p. 9). The outer environment determines the
conditions for goal accomplishment; and if the inner system is properly designed, it will adapt
to the outer environment so that its behaviour will be determined in a large part by the
Figure 4-2: Design Research outputs (Purao 2002)
Artefact as Situated Implementation
Knowledge as Operational Principles
Emergent Theory about supporting a phenomenon
Information Retrieval Agent
How to generate access plans
to retrieve from heterogeneous databases
How to support retrieval from
multiple databases
Information model
Document technology (XForms)
The digital document
How to support medicationmanagement with a (digital) document
Example from Krishnan In current research
Page 117
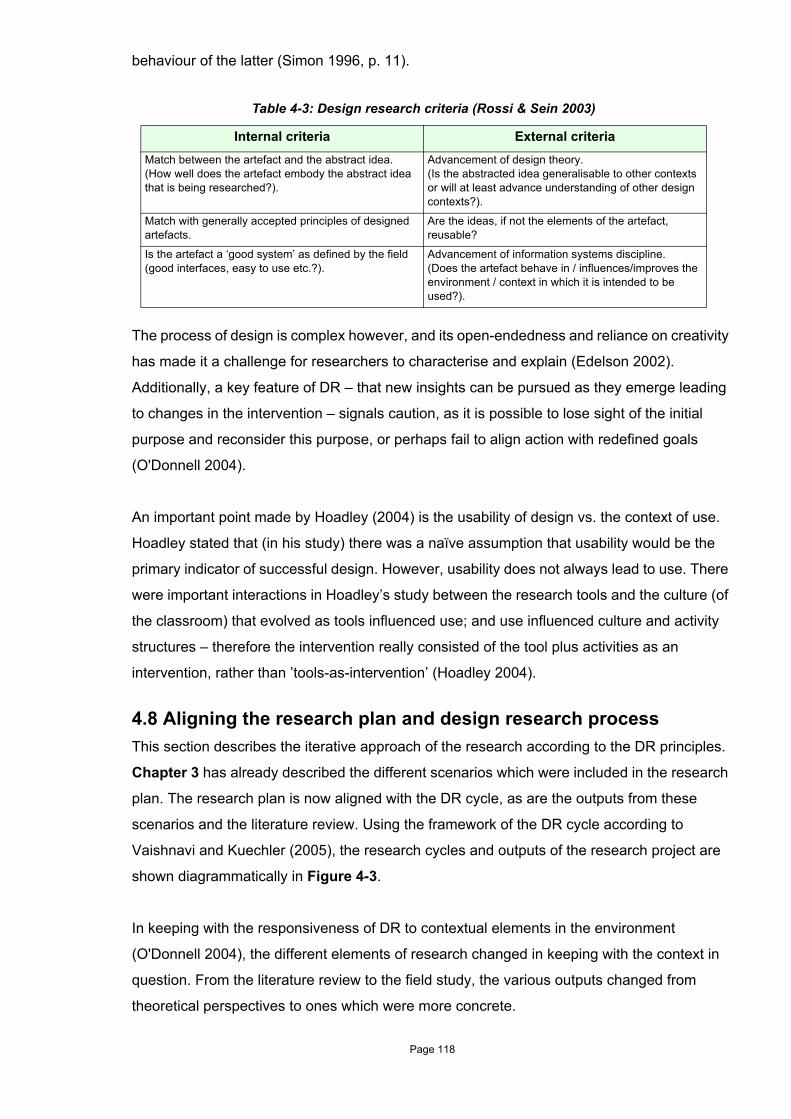
behaviour of the latter (Simon 1996, p. 11).
The process of design is complex however, and its open-endedness and reliance on creativity
has made it a challenge for researchers to characterise and explain (Edelson 2002).
Additionally, a key feature of DR – that new insights can be pursued as they emerge leading
to changes in the intervention – signals caution, as it is possible to lose sight of the initial
purpose and reconsider this purpose, or perhaps fail to align action with redefined goals
(O'Donnell 2004).
An important point made by Hoadley (2004) is the usability of design vs. the context of use.
Hoadley stated that (in his study) there was a naïve assumption that usability would be the
primary indicator of successful design. However, usability does not always lead to use. There
were important interactions in Hoadley’s study between the research tools and the culture (of
the classroom) that evolved as tools influenced use; and use influenced culture and activity
structures – therefore the intervention really consisted of the tool plus activities as an
intervention, rather than ’tools-as-intervention’ (Hoadley 2004).
4.8 Aligning the research plan and design research processThis section describes the iterative approach of the research according to the DR principles.
Chapter 3 has already described the different scenarios which were included in the research
plan. The research plan is now aligned with the DR cycle, as are the outputs from these
scenarios and the literature review. Using the framework of the DR cycle according to
Vaishnavi and Kuechler (2005), the research cycles and outputs of the research project are
shown diagrammatically in Figure 4-3.
In keeping with the responsiveness of DR to contextual elements in the environment
(O'Donnell 2004), the different elements of research changed in keeping with the context in
question. From the literature review to the field study, the various outputs changed from
theoretical perspectives to ones which were more concrete.
Table 4-3: Design research criteria (Rossi & Sein 2003)
Internal criteria External criteriaMatch between the artefact and the abstract idea.(How well does the artefact embody the abstract idea that is being researched?).
Advancement of design theory.(Is the abstracted idea generalisable to other contexts or will at least advance understanding of other design contexts?).
Match with generally accepted principles of designed artefacts.
Are the ideas, if not the elements of the artefact, reusable?
Is the artefact a ‘good system’ as defined by the field (good interfaces, easy to use etc.?).
Advancement of information systems discipline.(Does the artefact behave in / influences/improves the environment / context in which it is intended to be used?).
Page 118

For example, the proposal moved from developing decision support for pharmacists and the
consideration of digital documents in the literature review, through proposals to develop an
information model, to a generic tool to support decision-making and proposed intervention to
improve practice. Tentative design moved from consideration of data collection tools and
XForms technology to an ‘essential’ information model, hospital model and community model.
The instantiated artefact began with a hospital-derived information model, the next cycle
improved on that model by testing the hospital model and adding elements for community
context; and the field study tested the community-based model. Performance measures in
the bench-testing scenario tested the hospital model for completeness and refined it for the
community setting, while the field setting tested the community model for effectiveness in the
intervention. Finally, the results measured the intervention. Emergent features in the various
settings guided the direction of the research (The Design-Based Research Collective 2003).
To echo a previous concern, all features of all contexts could not receive attention; and so the
researcher was required to make decisions about what were considered important aspects for
investigation – with the consequent risk that other important aspects may have been
overlooked (O'Donnell 2004). However, the goal of this project was not to ‘sterilise’ the
Figure 4-3: Project iterative research cycle and outputs
ResultsDid the model & document contribute to quality, efficiency or safety of the medication management process
Performance measures (evaluation)Field testing in ‘real’ scenario
Performance measures (evaluation)Feed back from prototype testing
ArtefactCommunity-centric information modelEnhanced digital document prototype
ArtefactHospital-centric information modelDigital document prototype
ArtefactHospital-centric information modelDigital document prototype
Tentative designModel for community and hospital information
Tentative designHospital information model
Tentative design‘Essential information’ model
Tentative designXForms technologyTools for data collection
ProposalEvaluate intervention in medication review scenario
ProposalDevelop generic tool to support medication-related decision-making
ProposalDevelop knowledge of information use by pharmacists & doctors, decision-making, work flow
ProposalDevelop decision support (pharmacists)Use for digital documents
Literature review Part 1 – The Hospital Scenario2A – Investigation of the
home medication review context: prototype bench testing
2B – Medication review field study
Page 119
naturalistic contexts from all confounding variables, but to develop flexible and adaptive
theories which would remain useful even when applied to new local contexts – to strike a
balance between refinement and adaptability (Barab & Squire 2004).
A setting like this provides concerns about rigour and relevance, as interventions cannot be
entirely controlled and interactions cannot known in advance (thus the implications for other
contexts and ’successful intervention’ elsewhere) (Hoadley 2004). These concerns were
addressed by:
• the appropriate application of empirical techniques (rigour) (Hevner et al. 2004)
• the investigation of an existing problem (relevance, i.e. lack of medication management
support); and
• contribution of interesting new knowledge to a community (Vaishnavi & Kuechler 2005),
which was the community concerned with medication management.
Critical to this approach was the researcher’s need to monitor his own agenda and influence
over results; and not only document the perspective or starting point, but also any relevant
interventional strategies used by him or the participants (Hoadley 2004).
In search of answers, DR requires more than simply showing that a particular design works –
it demands that the researcher generate evidence-based claims to address theoretical issues
and further the theoretical knowledge of the field (Barab & Squire 2004). In real-world
complexity, however, ‘best answers’ are often unknowable and the ‘good enough answers’
must suffice (Simon 1996. p. 28-29). Simon (1996, p. 28-29) calls this ‘satisficing theory’,
where a person accepts a 'good enough' alternative, not because this is preferred, but because
there is no choice. Although human choices are not consistent and transitive, we need some
criteria of satisfaction (Simon 1996, p. 29). This was the approach taken by means of the
different contexts in which empirical data was gathered.
As discussed in Chapter 1, the ability to provide comprehensive decision support in a variety
of contexts is difficult, if not impossible. Thus, the approach to design of the artefacts taken by
the researcher had ‘satisfaction’ in mind where these artefacts would provide a pragmatic and
‘good enough’ basis of support (with the health professionals’ knowledge) to ensure good
medication management. This approach was also in keeping with the notion that complexity
(of a structure) depends on the way it is described; and as most of the complex structures
found in the world are enormously redundant, this can be used to simplify their description
(Simon 1996, p. 215) – this simplification involved finding the right representation – which was
the goal of this research project.
Page 120

4.9 Chapter summaryIn summary, the DR method appeared to be the most suitable approach to underpin this
research project. This was not only based on the fact that it was an artefact-based intervention,
but also that the health domain is characterised by a complex and dynamic environment where
solving problems requires careful consideration of the mutual interaction between the
technology and the human user.
The use of DR in similar (although possibly less information intense and emotional)
environments of education and IS also support this choice. Importantly, the pragmatic,
‘satisficing’ approach of DR was a realistic stance for the outcomes of this project.
This thesis now turns to the unfolding story of the DR journey iterating through the different
scenarios, beginning first with the hospital use case, presented in Chapter 5.
Page 121

Chapter 5
Formulating the information model: the hospitalscenario
5.1 IntroductionChapter 4 reviewed and discussed Design Research (DR) and concluded that this method
was the most suitable approach for the present research project, for several reasons:
• the health domain is characterised by a complex and dynamic environment, where
solving problems requires careful consideration of the mutual interaction between the
technology and the human user
• the project was an artefact-based intervention
• a number of iterations would be needed before the ideal medication management model
could be developed; and
• the project clearly required the development of a software solution – making this an
almost archetypal design research project.
This pragmatic, ‘satisficing’ approach of DR thus seemed ideal for this project.
The project iterates through three investigation scenarios: the hospital requirements analysis
setting, the benchtop testing of the prototype; and the field studies in which the developed
prototype was tested. This chapter describes the hospital scenario, in which the preliminary
data on which the initial model was based were collected. The empirical research undertaken
in this phase provided answers to the first two research questions:
A: Can medication management-related issues in the hospital environment be addressed by the use of technology?
Answering question A involved investigating the hospital context to provide an initial
understanding of both medication-related information components, including workflow and the
decision-process for pharmacists, as well as medical officer (MO)1 activities, including
1. Medical officer (MO) will be used as a generic term for hospital doctors, including resident medical offic-ers, registrars and consultants.
Page 122

processes for ordering medication and perceptions of requests for information. Data collection
was focused on revealing the medication management processes and activities within the
hospital context, but some questionnaire components were designed to identify broader
information, so as to obtain a richer background and help in identifying major themes and
issues. These became the basis for developing the initial medication management model. A
full analysis of this material can be found in Appendix J.
B: What technology approach might be appropriate to do this?
Question B was addressed by means of an XForms implementation of the information model.
The development process is too detailed to describe in full in this chapter, so the discussion
will concentrate on illustrating the major aspects of implementation; and will provide selected
examples of digital document views. The full implementation details, programming source files
and file structures are contained in a series of appendices, summarised in Table 5-1.
This chapter is structured as follows:
• the ways in which the data were gathered is reported in Section 5.2
• a structured analysis of the data is presented under the 'themes' which emerged from the
analysis process, together with an analysis of relevant documents in Section 5.3
• Section 5.4 describes the formulation of the resulting information model
• Section 5.5 reports the subsequent development of the digital document prototype; and
• the chapter is summarised in Section 5.6.
Authors not previously introduced in this thesis may be cited or quoted in this and subsequent
chapters. This new material appears only where it is necessary to support assertions or to
explain concepts.
5.2 The Data Gathering Process
5. 2.1 Questionnaires and interviewsThe recruitment process began with an approach to the Directors of Pharmacy Departments
of the candidate adult hospitals within the Adelaide metropolitan area, using a mixture of email
Table 5-1: Technical appendices
Appendix Content
K Full technical and development details.
L Visual Basic (VB) browser code.
M XForms document code.
N Patient XML file structure.
Page 123

and telephone. These people became the pathways to the pharmacists and Medical Directors
who, in turn, suggested a number of candidate Medical Officers (MOs) who were approached
directly by telephone.
Once individuals had agreed to participate, they were sent the questionnaire by email, allowing
them some time to consider the questions. They were contacted one to two weeks later to
make an appointment for an interview. A few participants completed the questionnaire quickly
and sent it back to the researcher within that time but for the majority, the follow-up call served
as a reminder to complete the questionnaire. The interview used the questionnaire as a
foundation and was conducted at a location which was convenient for the participant – usually
their workplace. For pharmacists, the researcher attempted to organise the interview for the
same day as a work practice observation, but this was unsuccessful as most pharmacists were
too busy to commit to both activities within a single day. The time required for the audio-taped
interviews ranged from 30 minutes to 1.5 hours, although most were about one hour in length.
Overall, 20 participants agreed to be involved (11 pharmacists and nine MOs); and data
collection ran from the end of October 2004 to late January 2005. The breakdown of
participants' locations is shown in Table 5-2.
The specialities of the MOs included: general medical; aged care and geriatrics; respiratory;
endocrinology; obstetrics; cardiology; emergency and psychiatry. Resident Medical Officers
(RMOs) had an average of 4 years' experience; registrars had, on average, 8 years of
experience; and the consultant had 39 years of experience. The practice areas of the
pharmacists who participated in the study were similar to those of the MOs and included:
general medicine and aged care; psychiatry; respiratory; cardiovascular; community liaison;
gastrointestinal; rehabilitation; orthopaedic; emergency and intensive care. Years of practice
for pharmacists were in the range of 2-30 (average 15.7, median 13); and clinical experience
ranged from 1-27 years (average 9.5, median 6.5). All pharmacists, except the most
inexperienced individual, were undertaking, or possessed, post-graduate qualifications.
Table 5-2: The distribution of hospital participants
Hospital PharmacistsResident
medical officers (RMOs)
Registrars Consultants
A 2 3 1 0
B 4 1 2 1
C 2 0 0 0
D 3 1 0 0
Page 124

5. 2.2 Work practice observationsThe questionnaires and interviews provided data relating to the medication-related information
individuals said they used, as well as identifying both what information was missing and the
material respondents would like to have. Those responses enabled the development of a set
of expectations concerning which components should be contained in the model. The data
obtained from questionnaires and interviews were then triangulated by observing actual
practice on the wards. Identifying the information which was actually used in practice helped
to confirm or refute the need for the components identified as a result of the interviews.
Work practice observation was designed to study the day-to-day activities of clinical
pharmacists and their related information and knowledge use. These were arranged at times
convenient for the pharmacists to observe an ‘average day’ (to the extent possible). No special
meetings or activities were arranged. There were 12 work practice observations of 11
pharmacists (as one pharmacist offered a second opportunity to be observed in a different
clinical setting). Pharmacists were observed for a total time of 23.8 hours (average 2.0 hours
per pharmacist, range 1.0 to 3.5 hours). During observations, there were a total of 95 'patient
information encounters’1 (average 8.6 per pharmacist, range 3 to 12).
As a background to these observations, it is useful to describe the expectations of the
pharmacists in this role and what the process generally entails – these explanations are
provided in the next two sub-sections.
5. 2.2.1 Clinical pharmacy practiceStandards for the practice of clinical pharmacy in Australian hospitals are compiled by the
Society of Hospital Pharmacists of Australia (SHPA) Committee of Specialty Practice in
Clinical Pharmacy (SHPA Committee of Specialty Practice in Clinical Pharmacy 2005). The
ideal is to develop a Medication Action Plan for each patient, where the six fundamental
components of this plan are: interpretation of patient-specific data; identification of clinical
problems; establishment of therapeutic goals; evaluation of therapeutic options;
individualisation of therapy; and monitoring of patient outcomes. Although formal medication
plans were not seen during work practice observations, these components were certainly
fulfilled by the pharmacists under observation.
5. 2.2.2 The medication review process in the wardThe medication review process involved pharmacists assessing relatively standard
components of information (drug chart, patient case notes, laboratory reports); and applying
their knowledge to ascertain if there was an issue and/or if there were missing information
1. A ‘patient information encounter’ was defined as an encounter where the pharmacist was involved in reviewing, evaluating or discussing a patient using documented information or information sought from another health professional. Each patient was only counted once even if there was more than one case of information use or exchange for that patient.
Page 125

components impeding an informed review. Some pharmacists carried reference information,
such as drug information texts and treatment guidelines, while some carried their own patient
summaries. A simplified process for medication reviews is shown in Figure 5-1, although this
can be much more complex and may involve many iterations.
The pharmacist’s clinical role was overwhelmingly seen as promoting the Quality Use of
Medicines (QUM), followed by the provision of information and education to patients and other
health professionals. Drug safety was also mentioned specifically, however, this is also
considered a goal of QUM. This role was described as being supportive and practical, offering
advice rather than only information. This often involved problem-solving, requiring professional
judgement to balance the positive and negative consequences of a course of action in the
absence of a definitive answer. Views were also expressed that often a pharmacist’s focus
may only be on drugs, but it was more important to think more broadly about the patient.
Page 126

5. 2.3 DocumentsCollecting working documents was important to uncover all the possible information
components that might be used in practice. The researcher did this opportunistically during
work practice observations; as well as during some pharmacist interviews. A total of 53 sample
documents were collected from pharmacists. Duplicates were collected only where they
illustrated different use or issues. There were many similar documents, as hospitals used local
variations of the same types of form (e.g. medication administration charts). Examples of
documents included one or more of: prescription forms (outpatient and discharge); inpatient
prescription and administration forms; medication charts (standard and intermittent drug
Figure 5-1: Hospital medication review process
Ward
Pharmacist checks patient information
Issue?
Urgent?Community Pharmacy, GP
Missing info.?
Nurse, MO, Allied Health
Patient, family member
yes
no
no
yes
no
yes
Entryinto
notes
Nurse, MO
MO
Drug chart
Lab. results
Own notes?
Case notes (med., nurse, & other)
no
Page 127

administration); observation charts; patient summary lists; pharmacists' own notes; nurse
hand-over sheet; and laboratory reports. A complete list is shown in Appendix J. Only 52
documents were analysed as one document was an audit tool for clinical pharmacists and thus
was not considered relevant for this purpose.
5.3 Analysis and discussionThis section analyses and discusses data from the different sources: questionnaires and
interviews, work practice observations; and document analysis. In order to keep this
discussion to a manageable size, the questionnaires themselves and the detailed analysis of
the raw data are contained in the appendices. Table 5.3 summarises the location of this
information.
Many of the same questions were used with both pharmacists and MOs, to allow comparisons
of fundamental issues, e.g. goals for medication management and patient outcomes, with the
result that a considerable amount of rich data emerged. It was not possible to examine all this
material in detail, e.g. the reflection of pharmacists and MOs on goals for medication
management or patient care. However, these data contributed to the researcher’s broader
understanding of the issues that affected pharmacists and MOs. The questions posed to
pharmacists and MOs are shown in Table 5-4.
Table 5-3: Data-related appendices
Appendix Content
H Pharmacist questionnaires.
I MO questionnaires.
J Full analysis of hospital data.
Page 128

Table 5-4: Questions posed to pharmacists and MOs
Pharmacists MOsWhat do you think are the main aims of a pharmacists' clinical role?
What do you think are the main goals in medication management?
What do think are the main goals in medication management?
What do you think are the main goals for patient care?
What do you think are the main goals for patient care?
Can you describe your relationships with other health professionals in achieving patient care goals?
What information components do you need to initiate a medication order?
What are the information sources you use in your work practice for patient medication management?
What information do you think pharmacists should have to allow them to contribute to effective medication management?
Have you ever needed to obtain information from sources other than in your practice environment?
Are you able to provide this type of information when you initiate the medication order? If not, what are the factors that prevent this?
Do you use any other (personal) knowledge in addition to information sources as part of your decision-making?
Are there any information components that are missing (if so, is this often?)
Are there ever any pieces of relevant information missing?
How do you manage with missing information components?
Do you think there are there any implications for medication management?
Do you think this has any implications for medication management?
Do you think there are there any implications for patient care or patient outcomes?
Do you think this has any implications for patient care or patient outcomes?
Are there any ways this information could be obtained / provided in your practice environment?
Are there any decision support tools in place to help with medication management?
Could a decision support tool help in supplying this information?
What is your understanding of the term 'decision support'?
How would you expect it to fit in to your work practice?
How would you expect this to fit into your work practice?
Is this realistic expectation in your current work scenario?
Is this a realistic expectation in your current work scenario?
What would expect from an 'ideal' decision support tool?
What features / support would you expect from an 'ideal' electronic decision support tool?
How generally acceptable do you think reminders / prompts are or would be from an electronic system (either decision support generally or from a prescribing system)
What factors would make alerts / prompts from an electronic system (more) acceptable?
Under what circumstances do you think it is acceptable to be asked to enter missing information required for a medication order, into an electronic system?
Would this be more acceptable if the request was accompanied by some justification?
Are there any occasions when you would accept such a system blocking the generation of a prescription or order?
Page 129

Grouping data and developing concepts was based on any relevant models from the literature
where possible, e.g. openEHR, CDA, Genres and PCNE – mentioned in Chapter 3. However,
as these models were not considered suitable for this project, concept development was based
on the researcher’s own domain experience and knowledge of the issues important for
medication management in the health sector. These were kept broad deliberately to allow
better awareness of the area rather than risk losing meaning through over-categorisation,
since the frequency and type of responses could potentially shed light on the relative
importance of particular concepts within and between groups.
A number of themes became apparent very early on during the data collection and analysis
process. Some of these themes were relevant to the project, directing the approach to the
information model, or suggesting factors which could impinge on the acceptability of using a
document approach for user-interaction. Other themes were of professional interest to the
researcher, such as the reporting of Complementary Medicines (CMs). Analysis and
discussion throughout this chapter (and, indeed, the next two chapters as well) is grouped
under these themes, so as to make the findings more readily comprehensible. This grouping
process combines data from questionnaires/interviews with findings from the work practice
observation, although the document analysis is discussed separately. The themes and their
respective sections are shown in Table 5.5.
5. 3.1 Missing information and surrogate valueThe many questions relating to this topic were based on the researcher's expectation that
missing information would be a significant problem for both pharmacists and MOs – this
expectation was quickly confirmed and, indeed, the issue of missing information also emerged
in the answers to other questions. This section brings together all the responses relating to
missing information, as well as techniques used by respondents to address or alleviate
information gaps.
Table 5-5: Research themes
Section Theme
5.3.1 Missing information and surrogate value.
5.3.2 Information granularity.
5.3.3 Conversation and communication.
5.3.4 Time constraints and summary information.
5.3.5 Decision support tools.
5.3.6 Systems for experts rather than expert systems.
5.3.7 Complementary and Over-the-Counter medication.
Page 130

5. 3.1.1 Missing Information relevant to Medical Officers
All MOs confirmed the widespread problem that a great deal of information of all types was
missing – '90% of the time'. This situation could lead to 'diagnosis by treatment', because when
important information was missing, they frequently did not know what condition they were
treating for a few days, during which time the diagnosis was guided by a 'suspicion' or by
identifying what treatment did or didn't work. Another clear message was that MOs often did
not know what information was missing: i.e. 'you don't know what you don't know'.
Knowledge concerning the patient's medications was considered important, especially those
medications which had been tried in the past, as this could avoid repeating past medications
or overlooking a useful medication. One MO stated that, on patient admission, information
which would influence prescribing was missing in about 50% of cases - patients frequently
could not identify what they were currently taking (e.g. a 'little pink tablet'). A similar problem
applied to MOs in outpatient areas.
The disparate nature of information was also a problem – what laboratory tests patients had,
what the GP had done, social contexts, multiple patient presentations to GPs or pharmacies –
compounded by the MOs' inability to deal with this disparity because of time constraints.
5. 3.1.2 Missing Information relevant to Pharmacists Pharmacists actually described two types of missing information: one related to clinical
practice; and the other related to the medications themselves. Pharmacists often found that a
range of information was missing, but their particular focus was on medications, both past and
current; and on information which revealed the patient context (such as why drugs were
prescribed or background detail relating to an Adverse Drug Reaction (ADR)). A further
problem was information quality, since information was frequently ambiguous or poorly
documented – or, by contrast, well documented but inaccurate. Overall, participants believed
that the amount of information missing or requiring clarification was increasing.
Pharmacists, too, frequently mentioned the disparate nature of the information they needed.
They also added that it may not be 'missing' per se but was rather inappropriately located, e.g.
allergies and alerts might not have been filed in the correct location in the case notes. It was
seen as a major role of the pharmacist to ensure that information was transferred or clarified,
e.g. the nature or severity of allergies or ADRs. Where pharmacists kept their own patient
notes, a potential issue arose if they had important information about the patient and did not
Medical officers often found themselves guessing
Sometimes ‘you only get a partial glimpse of the patient’
Page 131

record this somewhere appropriate in the case notes, so that another decision-maker could
obtain this information when facing the same problem at a later date.
5. 3.1.3 Pharmacist techniques for obtaining missing informationPharmacists relied on multiple information sources (GPs, community pharmacists, patient or
family members, GPs' letters, compliance aids, patients’ lists and actual medications); and
routes (communication by paging MOs in hospital, or phone or fax).
Generally, missing components were first sought from available paper or on-line sources; if
this was not successful, pharmacists would turn to conversation with others. The importance
or urgency of the information to patient management dictated whether obtaining missing
information required immediate communication. The source(s) of this information depended
on both the type of information (e.g. community pharmacies to identify previously prescribed
medications, or patients themselves to confirm aspects of current medication); as well as on
the pharmacist's previous experience. In the latter case, knowledge of the 'system' meant a
pharmacist had the best chance of finding the relevant information. Multiple information
sources could reveal problems (e.g. therapeutic duplication) but, paradoxically, could
themselves cause additional problems, as it was difficult to determine the real scenario when
equally 'reliable' sources of information were in conflict - a resolution would still be required,
despite this uncertainty.
Professional colleagues were an important source of information, as participants felt that their
feedback would be based on clinical experience and would thus be more relevant. Often, there
was information pharmacists would not find unless they asked the right person the right
question.
Information could generally be found if sufficient effort was directed towards searching through
the numerous sources and the volumes of patient notes – and missing laboratory test results
could be re-ordered although, in some cases, this required the MO to reassess the clinical
situation and perhaps re-prescribe medications. Time lags in obtaining missing information
could be quite lengthy – occasionally, anomalies or missing information were found after the
patient had been discharged, requiring follow-up in the community.
An interesting issue was the transfer of information between the hospital and the community.
There was an expectation that both groups would provide information to one another, although
‘any scrap of information’
Information transfer between the hospital and the community was a 'minefield'
Page 132

participants believed that neither the hospital nor the community really did provide as much
information as was possible, leading to great frustration on both sides.
5. 3.1.4 Medical Officers as a source of information for pharmacistsThe aim of investigating this issue was to determine how far the roles of pharmacists and MOs
overlapped, that is whether information that was missing 'downstream' for pharmacists could
or would be provided upstream (into a system) by the MOs. An MO would not normally directly
supply a pharmacist with all the information required for a medication review – only with that
related to a medication order. The pharmacist would seek supplementary information from
other sources. However, it was important in a general sense to ascertain potential information
gaps for the pharmacist.
From a general perspective, it eventuated that MOs thought pharmacists should have access
to the same information they had themselves, believing that pharmacists were entitled to this
as members of the professional team. In addition, MOs believed that a further major
consideration was patient safety – the more people who were involved in managing the
patient's medication, the better the chance of obtaining the right information and reducing
medication errors. Pharmacists' different background and perspective were highly regarded by
MOs, especially in the case of long and complex medication history and in the case of chronic
patients, whose conditions might have evolved over decades.
This support by MOs for pharmacists to have access to all information meant that an
information model could consider any relevant information component without potential conflict
caused by issues of 'ownership' or professional barriers (real or imagined). The sole issue
raised was that of patient privacy and even this provided no hurdle since all participants
believed it was crucial for health professionals to understand one another in the course of
information sharing.
Many participants were willing to accept a system requesting information entry by MOs, but
this appeared to be relevant only in a small number of cases, such as: weight and creatinine
values for patients relating to renally-cleared drugs (e.g. gentamicin or enoxaparin), or INR
values in warfarin dosing. Other than for warfarin, there were probably only a minority of
patients who actually required 'fine tuning' based on laboratory values. A suggestion by one
MO that an estimated weight value could be used when accurate information was not available
was rejected by others, on the grounds that the estimated value might remain in the system
and not be corrected, leading to potential errors at a later date. Another MO believed that data
entry would not happen at all.
Page 133

Essentially, all MOs stated that it was not possible to provide all the required information. The
major problem was that the inpatient medication chart (the primary method of communication
between doctor and pharmacist) did not cater for conveying any information other than
allergies. A proposed Australian national standard inpatient medication chart (being
formulated at the time of the project) was suggested as going some way to resolve this lack
(e.g. allowing the communication of some laboratory values), but still would not provide all the
necessary information.
The researcher found it difficult to assess whether the information MOs were unable to provide
was the same information which pharmacists found difficult to obtain. This discussion proved
to be an introduction to the problems of the unavailability of, and disparate nature of,
information required for patient medication; and the lack of time to address this lacuna.
Although this question was originally designed to identify information gaps for the pharmacist,
its answer also revealed information gaps for MOs – clearly, information gaps are a
widespread problem right across the hospital system. Overall, a request for some specific
items of information was considered to be acceptable, as long as it was important information
and the need to enter the data could be bypassed. The researcher formed the impression that
a request for information from a computerised system would not be taken as seriously as if the
same request came from a person.
5. 3.1.5 Alternative information sources for MOsFurther information required by MOs was most often sought from General Practitioners (GPs),
although this was a time-intensive process. MOs did not often think of communicating with
community pharmacists and, where they did so, usually delegated this to more junior medical
staff or to hospital pharmacists. Communicating with GPs (i.e. other doctors) was part of the
medical culture and MOs were less aware of the role of community pharmacists.
The combination of much of medicine being 'guess work' with an abundance of information
sources was the source of much difficulty in obtaining accurate and timely information. Further,
not all information was useful, e.g. where a patient had numerous laboratory tests during a
single admission. However, there was a balance between too many tests (often requested by
younger and less experienced doctors) against the risk of errors of omission when doctors did
not order tests because they were confident of the likely results. This problem of the need to
obtain the 'right' information was further complicated by testing essentially for medico-legal
reasons (i.e. tests undertaken to protect the hospital against potential legal action at a later
date) which again could provide information unnecessary from the point of view of a patient's
medication management.
Page 134

5. 3.1.6 Work practice confirmation
The work practice observations confirmed the extent of missing information, which is
summarised in Table 5-6. As had been mentioned in interviews, missing information about
medication was the most significant problem, followed by information related to allergies.
Overall, almost three items of missing information were experienced each hour, or six per
pharmacist. On average, there were two items of information missing for every three patients.
These were all items of information deemed necessary for decision-making for that patient and
important enough to be pursued by the pharmacist. Conversely, where the missing information
was not sufficiently important, the pharmacist did not pursue it.
The need to pursue a piece of missing information could be seen as a surrogate for the value
of that component to the decision-making process and, consequently, became an interesting
hypothesis for the researcher and was a signal for the inclusion of that component into the
information model.
Missing information observed in work practice is also compared to that mentioned by
respondents during interviews in Table 5-7. It is clear from this table that pharmacists' and
MOs' views on what information was missing and how frequently they missed it did not relate
very accurately to the situation in practice. Missing patient information (notes) was not
specifically mentioned by either pharmacists or MOs, but was common in practice. However,
MOs did mention items such as treatment history, which are an information subset of patient
notes (the superset).
Table 5-6: Missing information experienced by pharmacists
Category pharmacist observation
percentage of total per hour per
pharmacist per patient
Current medication 26 42% 1.1 2.4 0.27
Allergies / sensitivities 10 16% 0.4 0.9 0.11
Specific patient information / social
7 11% 0.3 0.6 0.07
Patient notes 6 10% 0.3 0.5 0.06
Medication history 5 8% 0.2 0.5 0.05
Treatment history 5 8% 0.2 0.5 0.02
Laboratory tests 2 3% 0.1 0.2 0.02
Community pharmacy 1 2% 0.0 0.1 0.01
Total 62 100% 2.7 5.6 0.65
The value of information is based on its context of use
Page 135

An interesting observation was that allergies and sensitivities not mentioned by MOs as
missing information – although their importance was noted by this group of respondents – were
a real problem for pharmacists. This may be as simple as information being available to MOs
but not being transcribed to medication charts when prescribing occurs. Some items which
were described as missing during interviews were not recorded as missing during observation,
but this could be due to the length of the observation period – a longer period of observation
might provide a more accurate picture.
Additionally, for pharmacists, interpreting changing drug information was also an issue; and
constant revisions were needed to ensure up-to-date drug information – these were areas of
MOs' questions. Coping with missing drug information meant reassessing older information,
extrapolating from studies or, in some cases, using previous clinical experience. Where there
was limited evidence for uses of new drugs, no clinical trials or poor clinical trial design, it was
difficult to evaluate new therapy against existing therapy. Here the pharmacist would use
knowledge and experience to hypothesise answers.
5. 3.1.7 The implications of missing informationAlthough missing information was common, the more important question that arises is how
important is this. When asked, MOs and pharmacists both believed that missing information
had significant implications, particularly in terms of adverse effects and patient safety.
Table 5-7: Missing information – interviews and observed
Category MO interview pharmacist interview
pharmacist observation
Active problems 1
Adverse drugs events 3
All information 1 3
Allergies / sensitivities 1 4 10
Community pharmacy 1 1
Co-morbidities 1 1
Creatinine 1
Current medication 6 5 26
Drug supply 1
GP notes 1 1
Laboratory tests 3 2
Medication aids 1
Medication history 4 4 5
Patient notes 1 6
Specific patient information / social 1 7
Treatment history 4 5
Treatment indications 1 3
Weight 1 2
Page 136
In terms of medication management, MOs were primarily concerned about being unable to
carry out a proper patient assessment. They identified potential problems with retrying
previously unsuccessful medications, or overlooking medications that could be useful. These
were potentially important issues for 'sicker' patients who required immediate treatment. In
some cases, a patient could even be discharged with a condition that still required treatment;
and MOs were not confident that the GP would follow up on problems.
Similarly, pharmacists were concerned that an uninformed review of a patient might impair
good decision-making and appropriate drug use, risking duplication of existing medication; or
unnecessary, poor or unsafe use of drugs. They saw the 'best guess' approach, which
inevitably resulted from missing medication-related information, as being highly undesirable
because they were unable to offer sound advice under these circumstances.
As with medication management, all MOs stated that missing information had implications for
patient care. Their main concerns were poor patient outcomes – in particular, medication
errors leading to adverse effects, unplanned readmissions or, occasionally, poor or delayed
(disease) symptom control. Typical examples of potentially serious adverse events resulting
from missing information included: prescribing beta-blockers for cardiac patients having
underlying asthma or reversible broncho-spasm (a drug type contraindicated for this group);
prescribing drugs to patients allergic to them (e.g. penicillin, allopurinol); and drug class
duplications. The side effects of drugs it was not known a patient was taking could also be
misinterpreted as disease symptoms, leading to incorrect diagnoses or inappropriate
treatment.
Fortunately, even though missing information which could potentially lead to adverse
outcomes was common, ADRs were not – although the relationship between missing
information and poor outcomes was difficult to quantify. The issue was more likely to concern
quality of life than adverse outcomes per se. Despite the many factors that could contribute to
avoidable errors in hospital, MOs still felt that the chance of detecting medication-related
problems was greater in hospitals than in the community. The presence of trained
MOs were concerned about ‘being in the dark’ when beginning therapy
It was frustrating for pharmacists to be forced into making decisions which could inadvertently lead to errors
All MOs had seen adverse outcomes resulting from missing information
Page 137

professionals – doctors, pharmacists and nurses – within the hospital environment meant that
adverse reactions or events could be identified and treated quickly.
Pharmacists were primarily concerned about patients’ understanding of their medications and
compliance. Although ADRs were a concern of pharmacists, and were stated to be a common
occurrence, they were not often seen first-hand. This finding was in stark contrast to the
responses from the MOs, who believed ADRs were uncommon. Whether this contradiction
indicates a lack of awareness on the part of the MOs, or whether MOs were only concerned
with major adverse drug events, it is clear that there was a significant (and potentially very
important) difference in the views taken by MOs and pharmacists to the potentially adverse
outcomes of inadequate medication-related information in a hospital setting. Nursing staff
were of great value in terms of identifying the true state of affairs here: minor ADRs might well
not be documented, but nursing staff would be aware of them because of their more immediate
relationship with the patient.
Examples of serious ADRs volunteered by pharmacists included: patients receiving drugs to
which they were allergic; a patient with a bleeding ulcer given warfarin (and consequently
requiring intensive care); and a case of unintended bleeding when the dose of the
anticoagulant clexane was not reduced for a patient in renal failure. The impact could also be
secondary, e.g. an ADR might in itself be minor, such as increased ataxia, but this could result
in more frequent falls – potentially far more serious (as falls in the elderly are associated with
an increase in mortality (Donald & Bulpitt 1999)).
In summary, the widespread problem of missing information evident in the literature was
confirmed very early in this scenario. Any type of information could be missing, but the most
frequent – and of most relevance to this project – was medication, both current and historical.
Missing information clearly has a profound effect on the effectiveness of decision support
systems as they cannot function in the absence of relevant information e.g. calculation of dose
in the absence of patient weight, or prescribing recommendations in the absence of a coded
patient diagnosis.
A way forward may be to allow a decision support system to operate with missing information,
but to signal caution or limit recommendations; and to highlight the need for clinical judgement.
This approach would also minimise the impact on work process.
In terms of this project, a major outcome of the hospital scenario was that missing information
Not only could missing information lead to an ADR, but also lead to the inability to detect one
Page 138

became important as a basis for model development – its inclusion in the model was based on
the surrogate value of whether pharmacists pursued it for their decision-making.
5. 3.2 Information granularityOne important aspect of information (whether for use, requirements or because it was missing)
was granularity. This could range from patient case notes to specific data items such as a
laboratory value and was very much driven by the intent of the health professional.
5. 3.2.1 Information required by medical officers to initiate a medication orderMO’s information needs when initiating a medication order could be summarised as: what is
wrong (with the patients); what medications are they taking; and are they allergic to anything?
A particular aim was to streamline medications for the patient – polypharmacy, and its potential
to affect patients' ability to cope after hospital discharge was seen as very important. One MO
was concerned that once patients were discharged there was a danger GPs might simply (re-
)write repeat prescriptions for the medication(s) and that patients would then remain (possibly
wrongly) on those medications without further review.
5. 3.2.2 Information used by pharmacistsInitially, pharmacists were asked what types of medication-related and non medication-related
information they required. However, it became apparent to the researcher that all information
related either directly or indirectly to medication. For example, personal history might relate to
patients' ability to manage their medication at home.
The principal sources of patient-related information were the patient case notes and inpatient
medication chart. The sources could vary greatly in form and content; and information could
be obtained in person, by phone, formally or informally, internally or externally to the hospital,
from electronic or paper copy sources; or from other health professionals, laboratories,
patients or care givers. The availability of reference information was considered a lesser
problem than obtaining patient-related information.
The use of summaries proved very important. Some pharmacists kept their own patient
summaries of what was considered the most important information, although these were
difficult to maintain with large numbers of patients. Summary sources produced by other health
professionals were also considered useful, e.g. a nursing hand-over sheet was a simple and
efficient way to transfer basic information (e.g. diagnosis) between nursing shifts. On the other
hand, medication histories by MOs were not always trusted, as pharmacists considered
doctors were not sufficiently thorough in assessing sources. Notes from other pharmacists
Pharmacists sought information from ‘anywhere you can get it’ or from ‘anyone with anything to say’
Page 139
were more highly valued, as they had been developed by professionals with the same
perspective. Nonetheless, participants noted that such information could be out-of-date and
transcription errors were a common problem.
Patients themselves were considered a useful source of information, although not always
reliable, e.g. psychiatric patients or elderly patients with cognitive impairment such as
dementia were clearly unreliable sources. Sometimes patients were unsure of what they were
taking, or had not been fully informed by the doctor. Patients were thus most frequently used
for clarification of medication issues, rather than to compile an accurate history.
5. 3.2.3 Observed information use by pharmacistsThe information sources actually used by pharmacists during work practice observations are
summarised in Table 5-8. These were categorised by the researcher under the headings of:
conversation, on-line and paper sources, in line with Paepcke (1996), since Paepcke's intent
was to investigate the sharing of information by loosely coupled work groups needing to
structure information for flexible use – a use very similar to this project. The manner in which
information was obtained had implications for how it could be accommodated (or not) within
the information model.
The majority of information was obtained from paper or on-line media, with the bulk (not
surprisingly) coming from medication charts and patient case notes. Reference sources,
although mentioned by pharmacists as general requirements were seldom used in practice. A
vital amount of information gathering, however, took place during conversation, highlighting
information shortfalls in other sources. In some cases, conversation was the first route used –
especially where there was a need for a quick summary of 'where the patient was'. This could
save considerable time for the pharmacist in catching up with the patient's current situation,
especially where there had been a great deal of activity around the patient, or where the
pharmacist had not reviewed the patient for some time. This important issue is discussed
further in Subsection 5.3.3.
Page 140

In summary, the nature of information ranged from patient case notes to specific data items
such as a laboratory value, i.e. from aggregate to singular information sources. This was very
much driven by the health professional's particular need – did they know little about the current
situation, requiring more aggregate information such as the case notes, or did they just need
a data item on which to base a particular decision? In some cases, information was first sought
through conversation with others. This has significant implications for the representation of
information in clinical systems. Participants also mentioned they wanted 'everything', but a
more useful day-to-day source would take the form of a concise summary of important issues
for the patient. There is enormous difficulty in providing all patient data at an atomic level
suitable for patient-centric decision support – this is affirmed by the vast efforts in producing
taxonomies and terminologies on which to base decision support systems. In contrast, clinical
narrative (free text), although useful for communication, does not readily underpin decision
support (e.g. alerts and reminders).
The researcher believes that this contradiction represents a tension for the design of health
information systems – the need for atomic data to develop shared terminologies and
ontologies on which to base decision support systems and allow epidemiological research,
against the need to efficiently communicate and share contextual information for patient care.
Table 5-8: Information sources used by pharmacists
Sources Information encounters (%) Encounters
per hour
Encounters per
pharmacist
Encounters per patient
Conversation 91 28.4% 4.0 8.3 1.0Patients 20 6.3% 0.9 1.8 0.2
Nursing Staff 29 9.1% 1.3 2.6 0.3
Medical Officers 34 10.6% 1.5 3.1 0.4
Other 8 2.5% 0.4 0.7 0.1
On-line 20 6.3% 0.9 1.8 0.2Laboratory systems 14 4.4% 0.6 1.3 0.1
Other 6 1.9% 0.3 0.5 0.1
Paper 209 65.3% 9.2 19.0 2.2Medication 72 22.5% 3.2 6.5 0.8
Patient case notes 51 15.9% 2.2 4.6 0.5
Own documentation 40 12.5% 1.8 3.6 0.4
Patient medication or aids 9 2.8% 0.4 0.8 0.1
Other 37 11.6% 1.6 3.4 0.4
Total 320 100.0% 14.0 29.1 3.4
Page 141

From this researcher's perspective, as information needs were reported at different levels of
granularity, it became apparent that the information model, and subsequent decision support
tool, should also reflect this variety of levels of granularity.
5. 3.3 Conversation and communicationThe questions about seeking missing information made it clear that pharmacists
communicated with other health professionals frequently and often opportunistically e.g.
during ward rounds and at ward meetings. Communication tended to be of three main types:
seeking patient-related information; offering medication-related information (in patient
contexts); and providing more general drug information or education.
5. 3.3.1 Pharmacist communication with Medical OfficersCommunication with MOs' was routine and open. With the more junior MOs, this was more
informal; and tended to concern day-to-day management or clarification of drug therapy.
Communication with medical consultants was more infrequent and often more formal and
consultative, i.e. requiring more specialist knowledge, or further investigation of additional drug
information resources.
Importantly, some of the information gained from MOs was background patient information to
which pharmacists would not otherwise be privy. Scattered information meant that
communication with the MO was a much easier path for the pharmacist to obtain relevant and
important information about the patient. Moreover, as doctors often made the final decisions
about patient treatment, pharmacists believed it was important to communicate with them
directly.
5. 3.3.2 Communication with nursing professionalsCommunication with nurses also occurred frequently and opportunistically. Nurses usually
requested practical information about the administration of medications, dosages and safety,
while pharmacists sought day-to-day management and practical information from nurses
about patients.
Nurses were able to provide a quick picture of the patient and nursing notes were often
considered a better source of information than medical notes. Nurses could also be a better
source of patient-related information than the patients themselves could, as patients might be
Pharmacists believed they gained significant benefit in terms of communication by ‘being on the wards’
Nurses were the best source of observed patient information
Page 142

too subjective or unreliable. Nurses were also valuable in providing feedback about patient
response to changes in medication (e.g. the level of drowsiness); and could act as sentinels
for drug-related problems making the job a lot easier.
5. 3.3.3 Other pharmacistsCommunication between hospital pharmacists generally occurred where one was a specialist
in an area of practice, had greater experience, or possessed local knowledge. These were also
opportunities to obtain other pharmacists' opinions and obtain confirmation of initial thoughts.
Sometimes this allowed less experienced pharmacists to 'get a feel for ' a decision process
used by more experienced pharmacists. It could be difficult for younger pharmacists to deal
with questions where there was uncertainty and where no structure (other than experience)
existed to teach these skills. Not all communication, however, related to clinical issues, some
dealt with the practicalities of service delivery, e.g. service rosters. Communication with the
dispensary staff was also important, as this could lead to the detection of important or unusual
changes that had occurred in the ward. Pharmacists in the community were an important
source for information related to medications dispensed or supplied to patients in the
community, such as Over-the-Counter (OTC) medication.
5. 3.3.4 Other health professionalsInformation sought by other (Allied Health) professionals was invariably related to the
administration of medication, such as how and when to give medication. Information sought
from this group of professionals was largely concerned with patient issues affecting
compliance. For example, Speech Pathologists could advise on anatomical issues that
affected oral administration; and Social Workers could indicate whether social issues could
affect compliance.
5. 3.3.5 Pharmacist conversations observed during work practiceWork practice observations confirmed the importance of conversations as a method of
information transfer; and these were analysed on the basis of who was involved in the
conversation (Table 5-9). This table shows the number of conversations originated by the
pharmacist (From); and those originating from others.
A team approach and multi-disciplinary care was considered important by pharmacists
Page 143

.
The total number of conversations which took place between pharmacists and all other groups
during the 23.8 hours of observation was 152 (6.4 per hour), an average of almost 13 times for
the typical observation period. Eighty-nine conversations originated from pharmacists and 63
from other people. Pharmacists asked more questions of nurses, than nurses asked of
pharmacists, suggesting that pharmacists saw nurses as an important source of information.
During conversations, pharmacists often took the opportunity to provide more background
information or education, e.g. pharmacology, drug usage, formulations or availability; or drug
policy. This happened on 17 occasions with nurses and 21 occasions with MOs.
There were also a number of other interruptions not related to the specific role of pharmacists
that occurred on 16 occasions, including: answering the phone, or handling general ward
enquiries from patients, family or others etc.
A very important feature of conversation was that the information exchanged related
specifically to the patient and the immediate problem – there was no unnecessary information
to process and, consequently, this was very efficient. One weakness of exchanging
information in this way, however, is that it leaves no record of the information exchanged.
Other pharmacists or, indeed, MOs needing to take up the care of this particular patient at a
later time would therefore have no idea of the additional information sought or obtained.
The significant use of conversation by health professionals as means of information gathering
in the hospital environment suggests that it would be difficult for them to gather all the
information they require for decision-making without conversation. Further, there is some
information – the tacit knowledge of other health professionals – that is not available to
pharmacists other than by conversation. The implications for designing decision support
systems is that the information models that underpin them will be incomplete – missing will be
Table 5-9: Conversations between pharmacists and other professionals
Medical officers Nurses
Other pharmacist
sLaboratory Other Total
From pharmacist to..
35 42 8 1 3 89
From others (to pharmacist)
30 29 4 0 0 63
65 71 12 1 3 152
Conversation played an important role for pharmacists, for quick, contextual summary information about patients, relevant to their needs
Page 144

the information that health professionals exchange by conversation.
In addition, as health professionals have a strong desire to be able to communicate and share
information (including their peers in the wider community), the decision support solution needs
to be one which supports or, at least, does not hinder this desire.
5. 3.4 Time constraints and summary informationAnecdotally, lack of time is a considerable issue for health professionals when attending to
patients. This research project confirmed that the time to find, assimilate and interpret
information in the inpatient setting was a significant issue for pharmacists; and still more so for
MOs. This problem also affected MOs in outpatient areas, where lack of time to deal
adequately with patient problems was compounded by a lack of information on the part of
patients themselves concerning their medication.
Time also had an impact on where information was sought by pharmacists – depending on
how quickly the patient was moving through the system; and what or who was available as an
information source. This was also helps to explain why conversation played such an important
role for pharmacists. In addition, time was cited as a problem in using reference resources as
'one won't know the answer to a question simply because there is no time to look'.
Despite the need to have all information available for a particular clinical decision, the
possibility of presenting an artefact with summarised, relevant patient-related information was
seen as useful. A single page was suggested as a target length – if the summary was too long,
it would not be used. Bringing simplicity to actions was considered a worthwhile plan, e.g.
through a simple aggregation of 'one-line' problems and actions; and the use of flags.
One pharmacist engaged in medication reviews outside the hospital suggested a minimum
data set could provide a portable information representation suitable for a range of users.
However, as pharmacists in hospitals were used to accessing 'everything', this was seen as a
problem for a Decision Support System (DSS). Participants acknowledged that it would be
difficult to achieve a trade-off between displaying essential and all information. As further
evidence of the value of summary information, some pharmacists kept their own patient-
related summaries
The need to cope with many patients and press on with ward rounds is a major deterrent to interaction with decision support systems
The fact that medical staff did not have the time to focus on medications-related issues in sufficient detail, confirmed the important role of pharmacist interventions in preventing ADRs
Page 145

In summary, time was mentioned as being a significant issue to find and assess information;
and of relevance to this project, the ability to interact with a decision support tool. However, the
concept of a relevant information summary as the interface to a decision support tool was
considered a possible approach to address time constraints. The next section of this chapter
therefore discusses decision support tools – and the experience which participants have had
with such tools – in some detail.
5. 3.5 Decision support toolsAt the beginning of the interview, participants were asked about their experience with
electronic decision support tools, as prior experience could influence opinion and expectations
of such tools. Both groups had exposure to decision support tools, although many of these
were simple information retrieval or laboratory reporting systems existing at the hospitals –
reflecting the day-to-day activities. In addition to having more experience or exposure in this
area, pharmacists offered more opinions, particularly relating to the lack of success or
usefulness of the systems they had encountered – hampered by poor training or
understanding of how the systems functioned.
5. 3.5.1 Decision support tools used by pharmacistsPharmacists were asked explicitly about decision support tools which supported general or
clinical pharmacy practice, although there was generally no major distinction made between
these.
One hospital dispensing system in use did provide decision support features such as: drug-
drug interaction checking, checks for therapeutic duplication; and dose-checking. However,
drug information generally supporting the dispensing systems was rarely evidence-based and
not user-friendly - a 'best guess' was often still required. Other decision support tools were
unsophisticated, being largely passive information sources or on-line calculators. Pharmacists
also included paper-based information sources and guidelines, a drug information service; and
computer-based tools for personal use (spreadsheets). Much discussion concerning clinical
systems centred on OACIS (a South Australian repository of clinical information that includes
laboratory and radiological results). This had some ability to generate electronic discharge
summaries, although it was noted that the information in this system was not always correct.
The value of colleagues was again raised as an important resource, particularly in the
specialist area of drug information. One pharmacist highlighted texts as better, more portable
and more concise information compared to ward-based, on-line sources - a challenge for
developing useful tools.
Page 146

5. 3.5.2 Pharmacists' understanding of decision supportThere was a wide range of interpretations of decision support, with many views about
information integration, prompts and alerts; and mentions of evidence-based information. To
help with the analysis of decision support concepts mentioned by participants, the researcher
organised these into categories – supportive, prescriptive, explanatory, outcome; and ‘other’,
as this helped to explain the level of sophistication of the concepts. The concepts were also
graded according to the NEDST types previously described in Chapter 2 – this complete
analysis is shown in Appendix J.
One pharmacist saw decision support as: 'information used in conjunction with what you
already know (professional knowledge), and what you know about the patient, to make further
decisions about management' – undeniably, a tool to complement the use of personal
knowledge. However, most of the interpretations described the simplest NEDST types. Some
participants made no distinctions between computer, telephone or paper-based decision
support. The researcher believes that many pharmacists based their perception of what
decision support was on their personal experiences of simple hospital systems. It is hardly
surprising, then, that when clinicians (in the broadest meaning) are asked what they want in a
decision support system, they find it difficult to express their requirements succinctly and
clearly. Consequently, attempts to consolidate requirements are difficult and there is little
success in terms of workable systems. Further, there is a clear opportunity in these hospitals
to develop more sophisticated decision support for both pharmacists and MOs.
5. 3.5.3 Decision support and Medical OfficersAlthough MOs believed that a decision support tool could help in providing information, the
brevity of their replies suggested there was little familiarity with the notion of decision support
– one MO even required clarification of the term. This is not surprising, as the researcher’s
experience in hospitals reveals there is a lot of discussion and belief about the positive value
of ‘decision support’, without much understanding of what this actually entails.
5. 3.5.4 Fitting decision support into work practiceTo allow comparison between MOs and pharmacists, the researcher categorised responses
from participants as systems requirements based on Pleeger (1998). These categories
included: physical environment, interfaces, users and human factors, functionality, data,
resources, security and quality assurance.
One interesting difference was that pharmacists tended to concentrate on how decision
support might be delivered (the physical environment), whereas MOs were more focused on
what would be delivered (the nature of the information). There were no answers about the
resources that might be required for implementation, although this could be because the
Page 147

phrasing of the question was not designed to elicit answers of this type. Security and Quality
Assurance of systems were also not mentioned, but this may be because of the hospital
environment – hospital staff are inclined to assume that attention to such issues will be taken
care of by hospital IT departments.
Most pharmacists suggested that existing hospital computer networks could be used to deliver
decision support, as there were few issues about accessibility. Some did mention that PDAs
would be useful for increased portability, although there was a concern about the bulkiness
and speed of these devices. The level of information available on PDAs, however, was
expected to be the same as for PCs! Accessibility and speed were mentioned as the critical
factors to use – without these, other means would be used to find information.
There were some concerns expressed about how a DSS should fit in the workplace. One
pharmacist considered that overly simplified therapy guidelines were inappropriate – a better
solution would be to provide reference information, educate and allow interpretation.
Another view was that the DSS should function even in the absence of information. Of course,
with some information, e.g. weight, this would limit the ability to calculate or check doses.
Participants believed that although the system should be aware of the absence of some
information, it would be unable to judge the importance of that piece of information. In these
cases it would be better to have no information (and deal with that) than be given a wrong
answer.
Some discussion also touched on the use of default system values. It was felt to be critical that
users of such a system be able to distinguish between e.g. the absence of an allergy (i.e. no
allergy) and the absence of an answer to the question of whether the patient had a drug allergy
– since a missing answer to that question would leave open a potentially serious situation
should such an allergy exist.
Comments from MOs about decision support related to electronic prescribing – not
surprisingly, as this has been a (yet unrealised) goal for hospitals for many years. MOs
translated the 'fit' to mean nature or format of the information, including: treatment options;
flagging drugs with a narrow therapeutic index; and drug interactions. The nature of support
mentioned by MOs was of two types: reference information (e.g. to underpin the detection of
drug-drug interactions); and patient-related support (using patient data, e.g. weight and age;
An ‘idiot’s guide to therapy’ will only ‘lead to individuals acting like idiots’
Page 148

and laboratory data, e.g. creatinine clearance, so as to flag cautions, such as the need to
modify dose).
It was suggested that this support should be: available when required; flexible; easy to use and
understand; and time efficient – essentially integrated into existing IT systems and daily
practice. However, if such a system was not easy to use (an experience some respondents
had already had with an existing clinical system), individuals would turn to 'non-IT' solutions.
Increasing experience (and knowledge) of MOs could also decrease the need for such
support. Some MOs felt that this type of support would decrease the reliance on the doctor to
detect some of these issues; and this was not desirable as there were so many patient factors
to consider. Interestingly, PDAs were not mentioned by MOs despite two of them having past
experience of PDAs.
5. 3.5.5 Is decision support a realistic expectation?Pharmacists were more pragmatic about whether ward-based decision support was a realistic
expectation. This was seen to be possible for prescribing, but less likely for other more
sophisticated support. For several pharmacists, this view was based on previous experience
with attempts to integrate hospital data systems (laboratory and pharmacy) for use with a DSS.
These attempts were considered too ambitious for the technology available at the time; and
these relatively unsophisticated data systems required complex algorithms for interpretation.
Similarly, a trial of PDAs in ward rounds had failed as the required information could not be
retrieved quickly enough.
MO's generally thought that DSS within the hospital scenario was a realistic option and
equated this with access – using PCs in the wards or clinical areas, bedside access, or using
PDAs. The notion of using PDAs as a gateway to a computer-based system came with the
expectation that all information should be available through these interfaces – participants
believed it would not be desirable to use PDAs to find part of the information required – and
then have to obtain the remainder of the information via a PC. Such an approach, of course,
would be extremely challenging – the MOs responding to this question were naturally thinking
in terms of user requirements, rather than the demands this would place upon the hospital itself
and on the developers of such systems.
5. 3.5.6 An ideal decision support tool?The researcher once again grouped responses into requirements categories based on
Pfleeger (1998). There were many overlapping concepts which were difficult to classify, as
answers expressed different levels of granularity (e.g. 'list of patient information' as opposed
(it) ‘all got bigger than Ben Hur’
Page 149

to 'medication list'); or similar but different meanings could be attributed to the terms used (e.g.
'validated' vs. 'accurate').
Again, MOs were predominantly concerned with data (especially format and type), whereas
pharmacists were more interested in quality assurance. This may indicate MOs' concern with
obtaining necessary information quickly whereas, for pharmacists, the reliability of data is the
critical issue. This latter observation stems from the fact that pharmacists frequently need to
interpret (medication-related) information for others, so that being able to have confidence in
their information sources is very important.
Both groups considered an information summary desirable, although more MOs wanted this
summary to be a gateway to other information – possibly reflecting the dependence of MOs on
a wider range of information than is the case for pharmacists, not only for treatment but also
for diagnosis. Participants acknowledged that a satisfactory trade-off between displaying
essential and all information would be difficult to achieve. One page was again suggested as
a target length for information, but of course, available page information on a computer screen
is very different from what can be provided on a single screen of a PDA. The issue of how to
compress sufficient information to make a single PDA screen useful was not, however,
discussed.
In contrast to summaries, one pharmacist preferred to use all information available, on the
basis that it was better to discern the value of the information for oneself, than to allow a system
designer or programmer to make that decision. This is, of course, the classic problem of
requirements engineering – without adequate communication between end users and analysts
it is impossible to ensure that the subsequent system will truly reflect the needs of those users.
This problem becomes still more complex when there are a variety of users, with differing
needs, who must be able to use the system under conditions of extreme urgency. It is therefore
not surprising that responses to this question indicated a considerable level of concern about
the effectiveness of such decision support systems in an acute care setting.
Replacing professional function was a further issue to be raised by pharmacists who saw little
value in simply replicating what they did in daily practice. They believed there was no need to
flag every minor interaction, but rather sought to identify important, patient-specific information
such as co-morbidities and biochemistry; especially for groups such as renal or cardiac
patients.
A significant issue which emerged from this discussion was that the availability of wider
information depended on 'someone' to enter it; and that reliance on information entered by
Page 150

others could present problems of reliability or timeliness. Also, as it was possible for
information to be incorrect, e.g. a diagnosis could often be incomplete, being a 'work in
progress' for the first few days of admission – respondents were uncertain how decision-
making could be supported against a background of varied and changing information.
As different health professionals view the same information differently, there is an issue of how
information can be structured to accommodate a variety of purposes or intents; one solution
might be to maintain the status quo – continue to share the same information. This not only
allows simplicity of design but also perhaps contributes to patient safety through using
'different eyes'.
5. 3.5.7 The acceptability of alerts and remindersAlerts and reminders were seen as one of the most positive features of a DSS. Seven MOs
believed alerts and reminders would be acceptable and could, indeed, be an avenue to
promote good prescribing practice. Nevertheless, they were quick to add qualifications: the
overriding feeling was that the number of prompts and alerts had the potential to be a
significant problem – too many would be a serious nuisance, leading to users ignoring all
alerts, e.g. constant reminders that a particular medication causes drowsiness. They
suggested that useful alerts would be those relating to toxicity (e.g. previous ADRs for a
patient), interacting medications/biochemical values (e.g. stopping potassium supplements if
the serum potassium was high), areas unfamiliar to the MO (e.g. drug contraindications in
pregnancy), or issues which required immediate attention. However, even serious reminders
would be a nuisance if they occurred too often; and the threshold at which they became an
irritation could (and probably would) vary for each individual doctor. There was a common
belief that alerts had to have some patient context to be of value – but tailoring alerts for each
drug, interaction and health possibility was recognised as difficult.
Generally, it was felt that the acceptability of alerts would be better if they were supported by
references (as to why they were important). This was regarded as good for inexperienced staff
or in an intensive care scenario, although it would obviously introduce an extra level of reading
and inconvenience (and would clutter up the screen – a major problem for PDA users). Once
again, importance, relevance and presentation remained major issues. One possible solution
would be to personalise such a system, so that more experienced MOs could limit the number
and frequency of alerts, although this issue was not discussed by participants. One MO
declared that justification of alerts would probably make no difference at all to acceptability.
Clinical support from information systems was seen as the ‘holy grail’ but difficulties in the past only provide cynicism about the ability to realise the real needs of clinician in an acute care environment
Page 151

5. 3.5.8 The acceptance of blocking medication ordersThis issue was raised with MOs rather 'tongue in cheek', with little expectation of a positive
response. Five MOs were against this idea and four were in favour – although the 'yes'
answers were really 'yes but .. ' responses. The many problems identified with the concept of
blocking medication orders included: the difficulty of obtaining complete patient information
within the system; the need to avoid delay in patient treatment; the possibility that there might
be no alternatives to treatment choice (even where there was a contraindication to the drug
prescribed); the unavoidable fact that there would always be exceptions to every rule; and the
awareness that medicine was 'so grey'.
Although it was acceptable that having a DSS block a medication order might be a safety
mechanism, e.g. for checking interns, in cases of previous serious ADRs or allergies, or where
absolute contraindications occurred, respondents felt that this could be very frustrating and
could waste time. Participants noted that, in any case, such blocks would quickly be
circumvented and individuals would resort to the paper system or the telephone if they
believed the medication was really needed.
Reliance on anything other than a perfect system was seen as a source of other problems.
Much of the decision support discussion, particularly that relating to electronic prescribing,
really related to expert systems1. At one boundary, a high level of decision support can be
provided using captured knowledge. However, capturing and structuring knowledge to allow a
complete representation of the patient in an information system is exceedingly difficult because
of the issues mentioned – missing information, information granularity; and the need for health
professionals to communicate.
Another very important factor is the extensive use of personal (tacit) knowledge by health
professionals in their clinical practice. This thesis makes no attempt to quantify such use, but
statements from pharmacists to the researcher indicated extensive use of personal knowledge
– this was the first strategy in responding to a question.
1. Expert systems are rule-based systems that attempt to model the human thought processes, based on sets of hypotheses (Thornett 2001, 'Computer decision support systems in general practice', Interna-tional Journal of Information Management, vol. 21, no. 1, 2, pp. 39-47).
It was: ‘hard to think of absolute circumstances where we should be definitely and consistently prevented from prescribing something’
(I) ‘use my own knowledge 95% of the time’
Page 152

Gaining this knowledge took many years and was fed by a range of formal sources (e.g.
undergraduate and post-graduate training, ward rounds etc.) and informal sources (e.g.
clinical experience, personal research and communications with other health professionals).
Clinical practice and personal experience were particularly significant. For example, clinical
ward rounds were important to allow a pharmacist to 'marry up the medical side with
medications' – this was of significant value in placing medication use into context. Over time,
recall of previous situations became the knowledge base for approaching new problems.
Communication with other health professionals also tapped into others’ tacit knowledge.
Further, 'systems' knowledge of the environment outside the hospital allowed pharmacists to
consider patient care more broadly than simply in terms of the consideration of immediate
medication use.
One knowledge-based approach to information gathering was akin to 'reverse engineering',
where the patient diagnosis was used to infer which medications the patient should be taking,
e.g. a patient with hypercholesterolaemia would normally be taking a statin (based on standard
clinical guidelines) – the absence of that medication would indicate a possible omission in the
current medication list or a need to recommend therapy. This of course, could be the role
undertaken by a DSS – but again this presumes a large amount of accurate, contextual clinical
information.
Thus, the knowledge level of these pharmacists made them 'specialist' practitioners; and some
were also approached as consultants in their areas of practice, both from inside and outside
the pharmacy. This specialist knowledge co-existed with the general knowledge held by
pharmacists. This general knowledge was also valuable to MOs, e.g. cardiology pharmacists
might be asked about antibiotic therapy by cardiologists during ward rounds as cardiologists
would be familiar with 'their own' drugs but not antibiotics.
In summary, the enormous difficulty of capturing knowledge for a DSS ('expert system') and
the need for pharmacists and MOs to make use of their personal knowledge in dealing with
patients suggested a particular approach to the design of a decision support tool – providing
'essential' information and relying on a complement of human knowledge. The answer to
providing a practical technology tool for medication management seemed therefore to lie in
designing a system for experts, rather than an expert system.
5. 3.6 Complementary and Over-the-Counter medicationAlthough complementary medicines (CMs) and over-the-counter (OTC) preparations were not
specifically targeted by the researcher, it became clear that this area is a notable omission in
the information sought by pharmacists and MOs. Patients did not mention this group of
Page 153

medications often, nor bring them in to hospital – and neither MOs nor pharmacists asked
about them routinely. This was a surprising and disappointing lacuna, in light of the fact that
(certainly with CMs) there is increasing discussion in the medical literature about the potential
for interactions with prescribed medications against a background of growing use.
Discussions and observations revealed that CMs only came to mind in particular clinical
scenarios, e.g. with ‘hepatotoxicity of unknown origin’, or ‘funny neurologic (sic) symptoms and
seizures’, where this information might be vital for patient management.
However, this lack also presents an opportunity. As a goal of this project was to develop a
flexible approach for capturing medication information, the tool developed accommodates the
recording of CMs and OTCs, as well as prescription medications. Once recorded, instances in
the record would further serve to remind other health professionals to enquire about this group
of medications, thus providing a pathway for a complete medication record.
The recognition of themes from analysis of the questionnaire, interviews and work practice
observations provided the researcher with some fundamental concepts of medication-related
information use and approaches for dealing with this use. The final part of the data evaluation
process was document analysis, completing the picture of what information was essential to
medication-related decision-making. This is discussed in the next sub-section.
5. 3.7 Document analysisThe complete analysis of information components from document is shown in Appendix J.
These were modelled by the researcher using Unified Modelling Language (UML). The model,
shown in Figure 5-2, includes the frequency counts (in brackets) of the information
components.
Often a ‘blind eye’ was turned to complementary medicines
Page 154

The nature of the information components suggested initial categorisation under three main
information headings: patient, medication and laboratory. Not all components of all documents
were included in this analysis: some items were omitted because they were not components
per se, e.g. pharmacists use of a report from the hospital dispensing system, containing the
drugs and quantities dispensed for a patient – this report was a composite of information
elements that could be contained the model, rather that the report being an element itself.
Others, e.g. pharmacist names, doctor names and dates at the bottom of documents were not
considered important for the modelling exercise. Similarly, some inpatient drug chart details,
such as nurse administration codes, were too specific and were therefore omitted. Other
components (e.g. adverse drug reactions), despite having few occurrences, were represented
because they are so important.
Thus, the document analysis was not intended to be either an extensive or an exhaustive audit
which would capture every single information component that could be included in a hospital
patient case note – however, most components were represented. Some components
required a decision between alternatives. For example, medication components in inpatient
charts consisted of separate generic/brand name, dose, route and frequency elements. For
Figure 5-2: The information model from document analysis
Medication management document (occasions = 52)
Patient information Medication information Laboratory
Patient sticker (18)
Personal Reference
Name (38)
Address (7)
Patient record ID (34)
Date of Birth (27)
Age (11)
Sex (16)
Weight (4)
Height (2)
Internal
Allergies / sensitivities (13)
Adverse drug reactions (1)
External
GP details (4)
Community Pharmacy (3)
Reason for admission /Principal diagnosis (14)
Past medical history (7)
Lab. Comment (1)
Lab. test Date (3)
Lab. report Date (2)
Basic information Additional information
Medication managementIssues (3)
Ceased / changedDate (2)
Reasons summary fordose change (3)
Person responsiblefor change (2)
Start date (5)
Name (generic / brand)
Dose
Route
Frequency
AdditionalInstructions (7)
Supply source (3)
Duration ofTreatment (3)
Reconciliation of D/C or admit drugs (3)
Social History (4)
Others (9)
Discharge date (6)
Admit date (8)
Medical team (8)
Ward /cost centre (14)
Clinic (3)
Days in hospital (3)
Observations (1)
Observation dates (2)
Referral date (1)
Problem / action& outcome list (3)
Finish date (1)
Bed no. (1)
Progress summary (1)
Interview date (1)
Alcohol / drug history (1)
Administration date (2)
Warnings (1)
Person responsiblefor administration (2)
Administration aids (2)
Pharmacist contact (1)
Prescriber contact (1)
Information source(of medication history) (1)
Page 155

others (e.g. patient medication cards, medication lists in case notes) there was no separation,
i.e. all this information was usually combined in a single text phrase. It was also noted that
medication lists/cards for patient use were divided into 'regular' medications and 'when
required' medications; and could have separate columns for morning, midday, evening and
bedtime doses. The researcher chose to model the individual items separately, as this seemed
likely to provide a better basis for broad use within both hospitals and the community.
Formulation of the information model now began, and included the missing (and fundamentally
important) information components confirmed from interviews and work practice observation,
which were compared with high frequency information components identified from the
document analysis. This combination suggested the essential components which became the
basis of the initial information model, described in Section 5.4.
5.4 Formulation of the information modelThe first step towards development of the information model was construction of a qualitative
model, using nVivo, to provide a hierarchical view of the missing information components
observed in practice – shown in Figure 5-3. The main category nodes are shown in dark blue;
and instances within these categories are shown as pale blue nodes (without any quantitative
measures). Bracketed numbers under some of the nodes are not descriptive of node attributes
but merely indicate the node reference within nVivo. The main purpose of this exercise was to
group the information components which were important in themselves, or essential to
medication-related decision-making.
Page 156

Figu
re 5
-3: M
issi
ng in
form
atio
n m
odel
Miss
ing
info
rmat
ion
(ALL
10)
Alle
rgie
s (1
0 2)
Pote
ntia
l pro
blem
s (1
0 3)
Med
ical
not
es (1
0 4)
Patie
nt in
form
atio
n (1
0 5)
Inpa
tient
cha
rt (1
0 6)
Trea
tmen
t (10
7)
Labo
rato
ry (1
0 9)
Dru
g in
form
atio
n (1
0 10
)
Com
mun
ity p
harm
acist
(10
12)Med
icat
ion
(10
13)
Curre
nt m
edic
atio
n (1
0 13
1)
Med
icat
ion
hist
ory
(10
13 1
1)
Und
ocum
ente
d-no
alle
rgy
Unc
onfir
med
alle
rgy
Und
ocum
ente
d-kn
own
alle
rgy
Miss
ing
indi
cate
d m
edic
atio
n
Nur
ses
(10
8 1)
MO
(10
8 2)
Oth
er s
taff
(10
8)
Miss
ing
drug
stre
ngth
Inap
prop
riate
freq
uenc
y
Illegi
ble
med
icat
ion
Uni
dica
ted
med
icat
ion
Miss
ing
list (
e.g.
disc
harg
e lis
t)
Unk
now
n co
mpl
ianc
e
Unc
lear
adm
inist
ratio
n
Phar
mac
okin
etic
s
Dat
e
Miss
ing
dose
Miss
ing
stor
age
info
rmat
ion
Miss
ing
gene
ric /
bra
nd n
ame
Low
dos
e
Leng
th o
f the
rapy
Unc
onfir
med
sou
rce
Sam
ple
take
n?
Prod
uct i
dent
ificat
ion
Dos
ing
frequ
ency
Prod
uct a
vaila
bility
Dos
e
Taki
ng u
ndoc
umen
ted
med
icat
ion
Unk
now
n re
ason
for c
ease
d dr
ug
Ceas
ed m
edic
atio
n
Patie
nt id
entif
icat
ion
Ref
used
med
icat
ion
- alle
rgy
Patie
nt in
com
plet
e in
form
atio
n
Patie
nt u
nava
ilabl
e
Max
imum
dos
e
Caus
e of
adv
erse
effe
cts
Unc
lear
dia
gnos
is
Conf
lictin
g co
mpl
ianc
e
Shee
t miss
ing
Trea
tmen
t hist
ory-
OS
and
othe
r
Trea
tmen
t hist
ory-
GP
Miss
ing
wei
ght
Hist
ory
scat
tere
d
Miss
ing
lab
valu
es
Dru
g sa
fety
Chan
ging
dru
g in
foN
ew d
rug
info
rmat
ion
Uns
tudi
ed in
dica
tions
PBS
info
rmat
ion
Addi
tiona
l inst
ruct
ions
Alle
rgy
ambi
guou
s
Hist
ory
inco
rrect
Hist
ory
inco
mpl
ete

The refined model subsequently developed by the researcher is shown in Figure 5-4. This
contained four major categories of information: patient, treatment, medication and
investigations. Patient information contained review date, and personal and reference
information; treatment consisted of current treatment and history; medication information
contained current medications, medication history and medication management issues; and
investigations contained laboratory tests. The reason for the investigation level above
laboratory values was that although laboratory (e.g. drug or electrolyte) results were the most
commonly mentioned tests requested on patients, other investigations were also possible (e.g.
from AH professionals). This separation allowed for future flexibility in the model.
UML was selected as the representation method because it provided a means of mapping
components which needed to be implemented in the digital document. There was, however,
no code generation from the UML model, although of course this could be a basis for later
implementations of this model
So by the end of data analysis, an essential information model was formed that could support
a technology approach to help with the management of medication information in the hospital
Figure 5-4: The hospital information model
Medication management document
Patient information Treatment information Medication information Investigations
Date of review Personal Reference
Name
Address
Patient record ID
Date of Birth
Age
Sex
Weight
Height
Recent BP
Allergies / sensitivities
Adverse drug reactions
Recreational substance use
GP details
Community pharmacy
Current treatment
Reason for admission /Principal diagnosis
Active problem
Treatment History
Past medical history
Laboratory
Date
Item
Result
Currentmedications
Medicationhistory
Medicationmanagement
issues
Ceased / changed
date
Reasons fordose change
Person responsiblefor change
Medication
Date
Generic name
Brand name(s)
Dose
Route
Frequency
Additionalinstructions
Indication
Duration oftreatment
Patient indication
Maximumdose
Social history
Complianceissues
Page 158

setting – answering question A. The next section (Section 5.5) addresses this technology
approach to the digital document, which answers Question B.
5.5 The digital documentThe researcher chose XForms technology because it appeared to offer a number of technical
advantages for the development of a document-oriented view of (XML) data. For brevity's
sake, it is not possible to detail all the aspects of development and implementation – these can
be found in the various appendices mentioned at the beginning of this chapter (see Table 5-
1). The approach to this section will therefore be to 'walk through' development and
demonstrate the major steps and outcomes of the process. Similarly, not all screen shots will
be shown within this chapter, but rather those representative of the different faces of the digital
document.
5. 5.1 Some preliminary activitiesThere were two preliminary activities undertaken by the researcher prior to the development
of the digital document.
The first activity was an introduction to XForms technology. This involved using a server
implementation of XForms technology using an experimental medication-related information
model based on the researcher’s domain experience. This activity is reported in more detail in
Appendix K.
The second activity was concerned with what browser platform was going to be used in the
project to display the XForms document. This activity concluded that a suitable browser for the
display of the XForms document was Microsoft Internet Explorer® (IE) 6, together with a
required ‘plugin’ – formsPlayer® (x-port.net Ltd.). Formsplayer is responsible for the display of
the fP ( ) icons that will be subsequently seen in the screen shots of the digital document
in this thesis.
A further realisation was that there was a need to provide a user with file-related functions i.e.
for the digital document to be used with a variety of patient files. File-related functions were not
able to be implemented within the XForms document – this could only be done in a server
environment, creating a problem for ‘local’ use of the XForms document on e.g. a notebook
computer. This was solved by developing a very simple browser application using Microsoft
Visual Basic® (Version 5, Learning Edition), shown in Figure 5-5. This Visual Basic (VB)
browser provided functions to: view existing patient files, open patient files, add new patients
and close the browser. At this stage of the project, there was no need for a more sophisticated
environment as all that was required was a simple stand-alone application. The complete
Page 159

details about the VB browser are available in Appendix K.
5. 5.2 Developing the digital documentThe approach taken to implementing the digital document was that it should resemble a
conventional paper document as much as possible – avoiding (if possible) display elements
found in databases, such as grid elements and function buttons. The resultant ‘look’ of the
digital document was simple and ‘flat’ – similar to paper documents. Unfortunately, this ‘look’
was not able to be carried through to the sub-components of the digital document that were
used for data entry (i.e. data entry forms), however these forms were kept small to minimise
screen complexity for the user.
The translation of the information model to the digital document was based on each major
information category in the model being a separate ‘page’ in the digital document. Therefore,
e.g. the patient information node in the information model became the patient information
‘page’ in the digital document; and the elements within the patient information node (e.g. name,
address etc.) became information elements in the patient information page. This principle was
Figure 5-5: Visual Basic document viewer
Page 160

used for the other major information categories in the information model. This provided a good
alignment of the information model with document representation, which allowed changes in
the information model to be easily reflected in the digital document. The document could also
be described to participants as having tabbed pages – another paper metaphor familiar to
users e.g. an alphabetically indexed address book. There was a further advantage in using
tabbed pages as users would not need to scroll through an extra-ordinary long single page
document.
Minimising scrolling was also an aim within each document page – this led to the removal of
GP and pharmacy details from the front page of the document to a separate page. Although
not strictly in keeping with the information model, these components would not be used as
often as others would. (This pragmatic decision was later supported by pharmacist participants
during bench-top testing)
In keeping with the intent to not impede the work process, no fields were made mandatory as
the user should not be forced to enter anything as, of course, they might not possess this
information. A summary description of each page is provided in the subsections which follow.
5. 5.2.1 Patient details pageThe patient details page is shown in Figure 5-6. Information components for this page include:
patient name, address, Medicare number, date of birth and age (either could be entered), sex,
weight, height, blood pressure (systolic and diastolic values); and date of medication review.
When a value for weight, height or blood pressure was entered, XForms functions were used
to calculate the number of days since this took place (shown in blue). Flags could also be
displayed (the Omega symbol) if the difference was greater than 90 days. Using a similar
function, if the weight was missing, then the word ‘Missing’ would be displayed in lieu of the
weight value. These are examples of the dynamic functions available within XForms which can
be used to provide simple alerts and reminders.
Editing patient information required clicking on ‘edit personal details’. This opened a separate
form displayed in Figure 5-7. Hyperlinks were not underlined (as is the convention) to make
the document appear as much as possible like a paper document. Users were alerted to a link
when the cursor arrow changed to a hand-shaped cursor as the mouse pointer moved over
these links.
Allergies and adverse drug reactions were displayed as separate information groups, as
suggested by the model. The reason for this is that allergies are pharmacologically distinct (to
Page 161

ADRs) as they have an immunological basis, with a particular pattern of symptoms.
Recreational drug use (as defined by pharmacists) relates mainly to tobacco and alcohol
(although it is clearly not limited to those agents alone). The display of the editing options under
those groups uses the same style to maintain visual consistency and ease of use. This style
was maintained throughout the document as much as possible.
One feature that is common to all lists is colour highlighting of the line of information that has
current focus. For example, in Figure 5-6, the peanut allergy record has the current focus and
is shown in violet (as opposed to the amoxycillin record below coloured in black). This is also
Figure 5-6: Patient details page
Page 162

confirmed by the row number displayed next to the word ‘edit allergy’. The reason for both
these choices is that the coloured line is more immediately obvious. However, when display
on a monitor is less than optimal (e.g. one some notebook computers) or could influenced by
environmental lighting, the number proved to be more useful. The colour violet was selected
for use in the document simply because it complemented the violet colour of the fP logo.
The new allergy edit form is shown in Figure 5-8. The data entry fields are either text or, in the
case of Reaction date, xsd: these are formatted fields as defined by XForms 1.0. The
advantage of using date formatted fields was the availability of a drop-down calendar object
with the ability to do date arithmetic which this provided. Invalid values (e.g. the date in Figure
5-8) were flagged using violet bars to the right-hand side of the field.
Figure 5-7: Edit patient details form
Page 163

5. 5.2.2 Treatment information pageFigure 5-9 shows the simple treatment information page which displays principal diagnoses
(responsible for the patient’s hospital admission) and other active problems. This page
demonstrates the concept of a simple summary, suggested by participants being able
themselves to provide patient context – in this case, name of the condition and time frame. This
simplified representation was applied to other similar information components within other
pages.
Figure 5-8: New allergy form
Figure 5-9: Treatment information page
Page 164

5. 5.2.3 Medication information pageAlthough the medication page (Figure 5-10) is also displayed in a simple manner, there is
greater underlying complexity to this page.
The medication information components comprise: date (relating to supply or when first
recorded – the difference is not really important as the intention is to initially capture the use of
the medication at some point in time and establish a reference point); name (either generic or
brand); dose; route; frequency; instructions; indications (from the prescriber); duration; and
maximum dose (where appropriate). Although some of these components (e.g. indications or
duration) are not usually included on hospital prescriptions, this information which is normally
available from patient case notes, was considered important by pharmacists.
The medication editing forms are more complex as they contain more information components.
The edit medication form is shown in Figure 5-11; and the new medication form is shown in
Figure 5-12.
Figure 5-10: Medication page
Page 165

There is one significant difference between the edit and new medication forms – the edit form
also has fields for reason for change, by and date. When the edited information is saved, this
not only changes the current medication record, but also copies the information to a separate
section of the patient file containing the medication history. Capturing medication history (an
expressed information need) is thus supplemented by knowing why this was done, by whom
and when – providing a much better context for medication use.
Figure 5-11: Edit medication form
Figure 5-12: New medication form
Page 166

The medication history information display is displayed below the current medication
information after clicking on ‘view medication history’, shown in Figure 5-13. In the example,
the current medication is amoxycillin capsules 500mg. The previous dose was amoxycillin
capsules 250mg, shown as the bottom entry in medication history. The most recent medication
history item shows the current dose and the reason for change (‘dose increased’ by ‘jpc’ on
2006-08-28). Return to the previous display is by clicking ‘back to current medication’.
Medication-related issues, either Social or Compliance-related were implemented as two
simple text boxes, again on the basis that simple text would be the most flexible and expressive
(and thus most efficient) way of conveying information which could relate to a large number of
issues. These required only a simple editing box. The edit social issues form is shown in
Figure 5-14.
Figure 5-13: Medication history
Figure 5-14: Edit social issues form
Page 167

5. 5.2.4 Investigations pageThe investigations page (Figure 5-15) is as simple as the Treatment Information page;
including the information items: item, result and date of result. Item has been purposely left
generic and can represent a blood result value (e.g. serum potassium, blood sugar level, INR)
or radiological report text – again is to support a summary concept. The expectation was also
that not all values needed to be entered, only those considered important to a decision.
5. 5.2.5 Health Professional contacts pageAs already mentioned, health professional contacts were initially part of the patient information
components, but since they are not frequently used, were moved ‘to the side’. This page is
shown in Figure 5-16.
Figure 5-15: Investigations page
Page 168

5. 5.3 Experiences with XFormsAlthough XForms allowed quite rapid development (after the initial learning curve), the
researcher encountered a range of problems and issues quite early on.
These issues included:
• the lack of a dedicated XForms editor
• the lack of practical documentation (texts or examples) that could help with implementing
some of the required features in the digital document
• problems with different versions of the browser plugin (formsPlayer)
• the level of implementation of the XForms 1.0 standard in formsPlayer
• inconsistencies between how XForms and IE 6 interpreted Cascading Style Sheets,
causing problems with display of some elements in the digital document
• limitations with some of the functions supported by XForms.
In the last case of the issues presented, date functionality was a particular problem that
required some accommodation from users of the digital document. These issues are
presented in some detail in Appendix K.
Figure 5-16: Health professional contacts page
Page 169

5.6 Chapter summaryThis chapter reported the hospital scenario investigation that aimed to answer two research
questions – these are addressed consecutively below.
A: Can medication management-related issues in the hospital environment be addressed by the use of technology?
The strategy used to answer this first question was an investigation of information use by
pharmacists and MOs involved in medication management. Data triangulation of
questionnaires/interviews, work practice observations and document analysis allowed a
thorough examination of the type and nature of information components that were used.
Analysis of the data revealed a number of important themes that influenced the researcher’s
approach to developing the information model.
Missing information in the hospital scenario was common, particularly for medication-related
information; and was a potential problem for patient outcomes. This problem has major
implications for the successful implementation of decision support systems. However, in this
project, the researcher based whether pharmacists pursued missing information as a
surrogate for its value to the decision-making process; and subsequently inclusion in the
information model.
Information use by pharmacists MOs was also characterised by the need to use different types
of disparate sources of information, based on the decision-making context and the personal
knowledge of the individual. This ranged from patient case notes to specific data items such
as a laboratory value, i.e. from aggregate to singular, which has significant implications for the
representation of information in clinical systems. As information needs were reported at
different levels of granularity, this should be reflected in the consequent information model.
However, this represents a tension for the design of health information system – the need to
have atomic data to build decision support systems and support research, against the need to
efficiently communicate and share contextual information for patient care.
Conversation with other health professionals was a common method of obtaining information
that was missing from expected sources, but also when other multiple sources were available.
The importance of conversation was that it was a highly contextual and efficient means of
information transfer between health professionals, allowing access to tacit knowledge; and it
has other roles that cannot be mimicked by decision support tools. In light of this and the strong
desire for health professionals to communicate, the decision support solution needs to be one
that supports, or at least does not hinder this desire.
Page 170

Time was raised as a significant issue affecting the ability to interact with a decision support
tool. However, using a relevant, concise information summary as the interface to a decision
support tool was seen as part of a possible solution to this issue.
The investigation of decision support tools used in the hospital found that those in use were
generally unsophisticated; and this also influenced perceptions of what an ‘ideal’ decision
support system should be. Despite agreement that these systems promised benefits, there
was widespread acknowledgement of the difficulty of implementing them and the barriers to
their use – supported by poor experiences in the past; and cynicism as to whether there would
be much success.
The researcher came to the conclusion that in light of the many issues uncovered above; and
the significant reliance of personal knowledge in clinical practice, this suggested that the
approach to design should consider systems for experts rather than expert systems – a
complement to human knowledge rather than attempt to model it completely. The final theme
was that of the inattention paid to complementary medicines and over-the-counter
preparations, possibly an opportunity for the digital document in practice.
The many difficulties experienced by pharmacists and doctors with medication management
suggested that technology could address these issues through a shareable model of essential
information components. This model would need to cope with missing information components
and acknowledge the use of knowledge.
B: What technology approach might be appropriate to do this?
This question was addressed by investigating the potential for XForms technology to realise
the digital document based on the information model identified for medication management.
XForms was selected as the underlying implementation technology based on the technical
advantages it offered, while using a document-oriented view. Development was made difficult
however, by a lack of practical supporting documentation, the level of standards
implementation in the formsPlayer browser plug-in; and the limited ability of some XForms
functions, particularly handing dates. However, the digital document prototype was developed
with XForms as intended; and this paved the way for the next phase – testing the information
model (through the document artefact) to measure its suitability for the community. This was
done through bench top testing with pharmacists accredited to carry out home medication
reviews in the community; and is described in Chapter 6.
Page 171

Chapter 6
Modelling for the community context: benchtoptesting
6.1 Introduction Chapter 5 described the first investigation scenario in the hospital setting; and the
development of the first information model and digital document prototype.
Although there was an expectation that many fundamental elements would be common to both
the hospital and wider community contexts, the information model required some modification
in order to fit the wider community. This modification took place during the second iteration; the
benchtop testing of the prototype. The empirical research undertaken in this phase sought to
answer the next research question:
C. What are the differences in the community environment that affect the approach?
This question was addressed as Part 2A of the project and involved: benchtop testing by
pharmacists accredited to perform home medication reviews (HMRs); further probing of the
questions explored in the hospital scenario; and some more focused questions about the
technology used to support HMRs.
This chapter reveals the differences in information requirements and use for accredited
pharmacists in the community. Themes which; emerged in the hospital context are also
examined here; and new themes identified. The full analysis of the data from this scenario is
contained in Appendix O. Full technical details for this chapter are contained in separate
appendices as shown in Table 6-1.
Page 172

This chapter is structured as follows:
• the ways in which the data were gathered is reported in Section 6.2
• analysis of the data is presented under the themes that are relevant to this scenario in
Section 6.3 – this provides consistency with the approach taken in chapter 5 and also
allows comparisons to be made with the hospital scenario
• changes that resulted in the revised, community-aligned information model are
discussed in Section 6.4
• the changes made to the digital document; and the development of the server service
are detailed in Section 6.5, and;
• the chapter is summarised in Section 6.6.
6.2 The data gathering processData gathering for the benchtop testing phase of the research included four separate
processes: firstly, a series of questionnaires and interviews with pharmacists accredited to
conduct HMRs; followed by testing of the prototype with this group of pharmacists; thirdly, a
focus group conducted with 3 members of this group, to enable a deeper and richer exploration
of issues arising out of the first two phases; and, finally, a detailed examination of relevant
documents – as was done in the initial, hospital-based, phase of exploration.
6. 2.1 Questionnaires and interviewsPotential participants for this scenario were identified by the researcher either as a result of
nominations made by Pharmacist Facilitators of the Divisions of General Practice, or during
discussions in the hospital scenario. The researcher approached the potential participants
directly and if they agreed to participate, the researcher sent them a questionnaire to them by
email or mail; and made an appointment made for an interview. The XForms document (and
formsPlayer plugin) was installed on participants’ computers – at the interview if possible or, if
not, during a subsequent meeting.
Table 6-1: Technical appendices
Appendix Content
P Full technical and development details.
Q Prototype development record (spreadsheet).
R Visual Basic (VB) browser code.
S Server (ASP) code.
T XForms document code.
U Patient XML file structure.
V XSL (report) code.
W Comparisons of information model elements (spreadsheet).
Page 173

This part of the study began in early 2005 and was completed in October 2005. Overall, six
pharmacists agreed to be involved. Pharmacists’ experience ranged from 5–32 years of
general practice (average 19.5 years), with 2–8 years of Home Medication Review (HMR)
experience (average 6.7 years).
6. 2.2 Prototype testingAs with the hospital scenario, the interviews provided an understanding of what information
was used, what was missing and what was desired to support medication management – or,
in this specific case, HMRs. Pharmacists testing the prototype with previous patient cases
would confirm the real information needs for those cases which offered parallels to the work
practice observations made in the hospital during the previous empirical research phase. Each
pharmacist was asked to enter five previous HMR patient cases into the digital document. The
researcher was able to observe two pharmacists, but time constraints made it impossible to
observe all five pharmacists during this phase of the research. Patient data was not viewed by
the researcher to maintain privacy.
As HMRs are a relatively new practice area for community pharmacists, the next two
subsections of this chapter provide some background about the skills of these pharmacists and
what the HMR process generally entails.
6. 2.2.1 Accredited pharmacistsPharmacists permitted to conduct medication reviews in the home or in Aged Care Facilities
(ACFs) are known in Australia as 'accredited pharmacists' (although the term 'consultant
pharmacist' is occasionally used). These pharmacists are accredited by the Australian
Association of Consultant Pharmacy (AACP) or the Society of Hospital Pharmacist of Australia
(SHPA). This accreditation not only ensures that these pharmacists have the additional skills
and knowledge required for undertaking medication reviews, but also allows them to claim
remuneration for their service from Medicare1.
Accreditation for pharmacists to undertake medication reviews in ACFs was first recognised in
1997; and this was extended to allow HMRs in 20002. HMRs were initially called Domiciliary
Medication Management Reviews (DMMRs) and although both terms are still in use, the more
recent term HMR will be used throughout this project. Similarly, the terms aged care facility
and residential care facility are used synonymously within the community, but the researcher
will use the term aged care facility (ACF). Without wishing to confuse the issue of acronyms
still further, medication reviews undertaken at an ACF are commonly referred to as Residential
Medication Management Reviews (RMMRs) – and this term will be used for this particular
1. Medicare is Australia’s universal public health system2. Personal communication, Sue Edwards, Pharmacy HMR Facilitator, 5/9/2006.
Page 174

category of medication reviews within this thesis.
6. 2.2.2 The HMR processThe goal of the HMR, according to the Australian Department of Health and Ageing, is to
maximise an individual patient's benefit from their medication regimen. Accordingly, the
Department has produced HMR guidelines for General Practitioners (GPs) undertaking HMRs
(http://www.health.gov.au/internet/wcms/publishing.nsf/content/health-epc-dmmr.htm/$FILE/
dmmrfactsheet.pdf; viewed 2006-09-12). This process is summarised in Figure 6-1, although
a more detailed description is contained in Appendix O.
By its very nature, the HMR process targets the elderly and/or individuals with chronic disease
who tend to have complex medication regimens – the disease groups of main concern in
medication management are cardiovascular disease, coronary heart failure and diabetes.
These individuals are at high risk of adverse events because of the complexity of their disease
processes or medications, or both. Medication management for patients at ACFs can still be
more difficult as these patients’ problems can be complicated by dementia and/or other self-
management issues (often the reason they are residents in an ACF).
As already noted in Section 6.2.2.1, the term ‘accredited pharmacist’ is the correct title for
pharmacists accredited to undertake medication reviews. The term ‘HMR pharmacist’ will
Figure 6-1: Home medication review process
HMR need identified(patient, carer, pharmacist,
other)Patient consent obtained
HMR referral form / relevant information sent to patient’s
preferred community pharmacy
Accredited Pharmacist conducts HMR
Pharmacist completes HMR report
GP develops draft medication management plan.Arranges follow-up
consultation with patient
GP & patient meet and agree on medication management plan
Copy of medication management plan to pharmacy,
Copy to GP & +/- copies to patient / other relevant health
professionals with patient agreement
Implementation of agreed actions with appropriate follow-
up and monitoring
HMR report sent to GP
Preferred pharmacy
Optional
Page 175

however, be used in this chapter – both because this term links the pharmacist to the process
undertaken, as well as to avoid confusion with a different medication review process which will
be described in Chapter 7.
HMR pharmacists consider their roles to be primarily focused upon patient education and the
optimisation of drug use (QUM) – a similar perception to that of their hospital colleagues. One
difference, however, is that the HMR pharmacist aims to identify any outstanding issues,
whereas for hospital patients, many issues already have been identified (or even have been
the reason for admission to hospital). A significant concern of HMR pharmacists was patients’
self-management, as this was important for patient independence, successful therapy and
safety. Respondents placed a significant emphasis on a holistic approach to patient care and,
with elderly patients in particular, believed that quality of life could often be more important than
specific management issues for medications or disease.
6. 2.3 The focus groupThe focus group enabled the participating pharmacists to come together after the benchtop
testing was complete, to share and describe their experiences of interacting with the digital
document. As already explained in Chapter 3 (Methodology), the group was moderated by the
researcher, as his domain experience provided allowed a level of understanding of hospital
and community pharmacy practice which could be used to stimulate discussion in a way which
would not have been possible for a less experienced moderator; as well as to improve the
quality of the data collection. In addition, as the focus group was small (3 pharmacists), data
collection could be achieved effectively through audio-taping, without requiring the researcher
to focus on note taking, at the expense of coordinating the group.
6. 2.4 Document analysisAs with the hospital scenario, document analysis was intended to uncover all the possible
information elements used by the participants. This task was simpler than was the case with
the hospital scenario, partly because there were fewer participants, but also because the range
of documents was smaller. Four of the five pharmacists supplied an example of their HMR
reports but, as this only provided a small number of samples, the researcher also sought
further representative HMR documents from other appropriate sources. This is detailed in
Sub-section 6.3.11.
6.3 Analysis and discussionThis section analyses and discusses the data from all sources: questionnaires and interviews,
prototype testing, the focus group; and document analysis. As with the previous chapter, in
order to keep the discussion to a manageable length, the detailed analysis and data collection
tools (pharmacist questionnaires, focus group tool etc.) are contained in appendices.
Page 176

Table 6-2 summarises the location of this information.
The questionnaires used for HMR pharmacists contained many of the same questions used
with hospital pharmacists to enable comparison of common issues. A further set of questions
was also applied to elucidate HMR workflow and the technology used by HMR pharmacists,
as this could impact on how the digital document might be implemented in the community
setting.
The set of questions used with HMR pharmacists is shown in Table 6-3.
Table 6-2: Data-related appendices
Appendix Content
Appendix F Data collection tools.
Appendix 0 Analysis of benchtop data.
Table 6-3: Questions posed to HMR pharmacists
Main questions
What do you think are the main aims of a HMR pharmacists' role?
What do you think are the main goals in medication management?
What do you think are the main goals for patient care?
Can you describe your relationships with other health professionals in achieving patient care goals?
What are the information sources you use in your work practice for patient medication management?
Have you ever needed to obtain information from sources other than in your practice environment? (what, when, how and for what?)
Do you use any other (personal) knowledge in addition to information sources as part of your decision-making? If so, please provide detail of the nature of the knowledge and how you acquired this knowledge.
Are there any information components that are missing (if so, is this often?)
How do you manage with missing information components?
Do you think there are there any implications for medication management?
Do you think there are there any implications for patient care or patient outcomes?
Are there any decision support tools in place to help with medication management?
What is your understanding of the term 'decision support'?
What would expect from an 'ideal' decision support tool?
How would you expect it to fit in to your work practice?
Is this a realistic expectation in your current work scenario? (please give reasons)
Workflow & Technology
How is the HMR request is received?
How is the HMR request processed (including any information transfer)?
What is the process for conducting HMR?
What is the process for report writing?
What is the process for the delivery of the report to the GP?
Page 177

Analysis of the data and discussion is, as in Chapter 5, grouped under the same themes
developed for the hospital scenario. The majority of the themes identified in the hospital
scenario were also relevant to the HMR pharmacists, although two new themes emerged
which were unique to this scenario. This result not only provided support for the findings from
the hospital scenario, but also identified the specific factors relevant to the community
scenario. This variation, anticipated by the researcher in light of his own clinical experience,
was crucial in terms of developing the digital document and ensuring its acceptability within the
community context – a medication management solution which only supported in-hospital use
would clearly be of only limited usefulness.
Prototype testing and document analysis are discussed separately. The themes and their
respective sections are shown in Table 6-4.
6. 3.1 Missing information
6. 3.1.1 Missing information for HMR pharmacists in GPs’ referralsThe problem of missing information was even more significant for HMR pharmacists than it had
been for hospital pharmacists. Whereas a hospital pharmacist had access to alternative
information sources, HMR pharmacists were able to rely on only two information sources: the
HMR referral from the GP and, optionally, a printout of the patient's medications dispensed by
their preferred pharmacy.
The amount of missing information within referrals used by HMR pharmacists was also
significant. Laboratory information was generally missing and, in some cases, this information
could be important e.g. information about renal function if the patient was taking metformin
(used in the treatment of Type II diabetes). Other potentially useful information which could be
missing included: the reasons for medication changes; patients' co-morbidities; whether a
Table 6-4: Research themes
Section Theme
6.3.1 Missing information
6.3.2 Information granularity
6.3.3 Conversation and communication
6.3.4 Time constraints and summary information
6.3.5 Decision support tools
6.3.6 Systems for experts rather than expert systems
6.3.7 A technology-poor practice paradigm
6.3.8 The ‘viewpoints’ of professional practice tools
6.3.9 Pharmacists’ perceptions of GPs in the HMR process
Page 178

medication had been tried and failed in a patient; and patients' drug sensitivities. Information
about the social situation or environment (e.g. was there a son with psychiatric problems, or a
potentially dangerous dog, at the patient's home?) could be important for pharmacist safety –
one pharmacist mentioned having been in an unsafe situation during an HMR interview with a
patient.
One potentially missing information component which generated a great deal of discussion
was the ‘real’ reason for referral. The reasons for referral usually given by the GP were one or
more of the risk factors for adverse outcomes for patients taking medications, shown in Table
6-5, provided as examples by the Health Insurance Commission (HIC)1.
These risk factors could, of course, be valid reasons for review. The HIC had originally
intended these risk factors merely as a guide for physicians, but they had instead become de
facto bases for GPs' HMR referrals. The pharmacists believed that these risk factors were
used by GPs as a 'pick list' to appease the HIC system and thus ensure payment for the HMR
referral. Pharmacists were concerned that sometimes these reasons did not indicate the real
reasons for the GP's concern (e.g. unstable INR levels for a patient). The lack of a more
targeted reason could mean that the real problem was not investigated and, consequently, not
appropriately reported back to the GP. The HIC guidelines are quite open (although this is
obviously not known by GPs), as a GP can initiate an HMR if it is clinically necessary to 'ensure
the quality use of medicines or to address a patient's needs' (http://
www.medicareaustralia.gov.au/providers/incentives_allowances/pharmacy_agreement/hmr/
patient_eligibility.htm; viewed 2006-09-10), i.e. if there is any concern about the patient's ability
to manage medication at home.
Overall, pharmacists felt they could place only precarious reliance on the GP to provide the
appropriate information for the HMR. One pharmacist stated that if, for example, pathology
1. The Health Insurance Commission is the Australian Federal government agency which pays GPs and pharmacists for HMRs.
Table 6-5: Risk factors for adverse outcomes for patients taking medications
Risk factor
Currently taking five or more regular medications, or more than 12 doses of medication per day.
Significant changes to the medication regimen in the last three months, including recent discharge from hospital.
Taking medication with a narrow therapeutic index or requiring therapeutic monitoring.
Symptoms suggestive of an adverse drug reaction.
Difficulty managing own medicines because of literacy or language difficulties, or impaired sight.
Attending a number of different doctors, both general practitioners and specialists.
Page 179

information was not provided in the referral, it was assumed the GP might not need feedback
in this area. This rationalisation is understandable, but does raise concern about the
effectiveness and consequent usefulness of an HMR.
6. 3.1.2 Pharmacists coping with missing information
Although the medication-related information from the GP could be ’scant’, pharmacists did not
usually contact the GP unless there was a ‘burning need’ to do so. Pharmacists could use the
local pharmacy to try and fill information gaps; and they routinely sought records of patients’
dispensed medications from the community pharmacy. Some pharmacists, indeed, expressed
rather pragmatic and pessimistic views about contacting GPs. In this rather precarious
situation, pharmacists often assumed that the GP might already possess the missing piece of
information (so pharmacists did not need to obtain it), or believed that the GP might have
already addressed the issue of concern. However, a contrasting view from one pharmacist was
that: ‘often things don't fall into place until you ask the GP later’.
This lack of information was taken into account by pharmacists when writing the HMR report;
and most pharmacists incorporated a disclaimer such as:
These comments are made without the full knowledge of (name)’s medical history. Any treatment decisions based on this information should be made in the context of the individual clinical circumstances of the patient.
The end result of missing information and the (possibly perceived) communication difficulties
between pharmacists and GPs was that the HMR report might well not be as useful to the GP
as it could be. This problem was addressed by pharmacists on the HMR report, by raising
issues which needed to be considered by the GP; and adding disclaimers to indicate that
recommendations were made without full knowledge of the patient.
Of course, the issue of missing information clearly depended on its type: some missing
information (e.g. date of birth) could be obtained by the pharmacist from the patient at the
interview, although (as in the hospital scenario), patients could be unreliable about their
medications. Obtaining some information could be especially difficult for the pharmacist, e.g.
patient weight (some pharmacists actually carried a set of bathroom scales with them to HMR
visits to weigh patients – not always an easy undertaking!). It became clear to the researcher
that pharmacists' skills were particularly important. Ensuring that they asked the right
questions and the ability to 'read' patients were important skills which improved over time – as
was the ability to gauge when there was no need to ask questions. A great deal of information
could also 'reveal itself in the home' e.g. if the blinds were pulled down or the carpet was torn,
(if the) ‘GP provided information is scant... then perhaps they are not interested in providing it’
Page 180

the pharmacist could infer a potential risk of patient falls.
6. 3.1.3 The implications of missing information
Pharmacists considered the main implication of missing information for medication
management was the quality and consequent usefulness of the HMR report to the GP. Missing
information meant that the review was not as comprehensive as it could have been, because
the right questions might not have been asked (of the patient) – and because a better
understanding of the reasons for the HMR referral might have avoided the need to ask
unnecessary questions.
Pharmacists expressed some pragmatic resignations about the effectiveness of highlighting
issues in an HMR report to the GP. In one example, where the metformin dose was high and
there was no indication of renal function, the pharmacist recommended (depending on the
patient's renal function) that a drop in the dose of metformin could be considered, or a newer
oral hypoglycaemic agent (more appropriate for renal problems) might be added. The patient's
dose of metformin was indeed dropped for a short while, but was then increased again without
(apparent) consideration of the newer agents, leaving the pharmacist with no idea at all of the
GP's decision process, nor the implications for the patient – and some considerable frustration!
The possible impact of missing information on patient outcomes was one significant difference
between the hospital and community settings. The community-based patient was often quite
well; and it was less likely there would be situations where missing information had an acute
effect on treatment – if there was a major problem the patient would be admitted to hospital.
Medication reviews in hospital were concerned with achieving control in acute situations,
whereas many of the community-based HMR issues (such as pain management, constipation
or incontinence) were ongoing. Nevertheless, although infrequent, community-based cases
did exist where acute issues (e.g. an adverse reaction to a medication) needed to be
addressed.
The main patient care goals for HMR pharmacists were: compliance with medications; patient
education; and optimising outcomes – the first two influencing the latter. However, as it was
often difficult to fully comprehend the situation – many pharmacists were unaware of patient
outcomes – it was generally assumed that the GP was managing the situation and that
Missing information meant that the HMR could be a ‘a bit of a pointless exercise’
However, there was ‘no point in chasing things up too much’; and patients were often considered to be ‘OK’ if nothing eventuated
Page 181

acceptable patient outcomes would eventuate.
In summary, as in hospital scenario, missing information was a significant problem for
accredited pharmacists in the HMR scenario. This problem was made more critical by the
pharmacist's dependence on the GP for patient-related information, although it was the
usefulness of the HMR report which was the main casualty – patient impact was less likely.
From the design perspective, the extent of missing information reinforced the researcher’s
belief that the digital document could not mandate the inclusion of information elements, only
suggest them and support their inclusion – aiming to collect missing information elements
where possible during the HMR loop.
6. 3.2 Information granularityThe issue of information granularity did not explicitly arise per se during this scenario,
although, as the researcher noted the information sources described by the HMR pharmacists,
the viewpoint formed during the hospital scenario was confirmed.
The main source of patient information, the HMR referral from the GP, was usually received in
the form of paper printouts from Medical Director® Version 2 (MD)1. These were accompanied
by a referral letter containing the patient’s consent and other administrative information
requirements for Medicare payment. An examination of relevant printouts available from MD
revealed a variety of levels of detail in the information provided, including:
• ‘full summary’ (containing patient details, family history, social history, current
medications, immunisations and past medical history)
• ‘full patient history’
• ‘limited patient history’ (containing patient details and past medical history); and
• ‘medication summary’ (containing patient details and current medications).
Other information sources used by HMR pharmacists primarily were drug information
resources, either textbooks or resources in electronic format on laptop computers. Drug
information centres and on-line resources were also mentioned by pharmacists.
Thus, although the issue of granularity did not explicitly arise, the nature of the information
elements used by HMR pharmacists was similar to those used by their hospital colleagues.
1. MD is the most common GP desktop system in Australia, where it is reportedly used by over 16,000 GPs (http://www.hcn.net.au/md3/stoppress.asp, viewed 2006-09-21).
Although patients could ‘miss out on something’, it was difficult for the pharmacists to know what this could be
Page 182
This confirmed to the researcher that the elements in the information model would have to be
provided at different levels of granularity to support the pharmacists’ natural work process.
6. 3.3 Conversation and communicationMost communication for pharmacists undertaking HMRs occurred with the GP through the
written report. Generally, there was little verbal communication and few pharmacists contacted
GPs before medication reviews – aided by the fact that most missing information was non-
urgent. However, good pharmacist-GP relationships were highly valued by pharmacists.
Where there was the possibility of multidisciplinary meetings (e.g. in the country or in hospital-
community interface programmes), communication with GPs was reported to be better. The
ACF environment provided much greater potential for communication for pharmacists, not only
with the nursing staff, but also with visiting GPs – ACFs essentially mimicked a hospital setting.
The researcher observed that relationships between pharmacists and GPs could be the basis
for some unease. There were some qualms about questioning the GP, as some were
considered ‘tricky’ – although this depended on the pharmacist’s acquaintance with the GP.
Part-time pharmacists also saw themselves as being at a disadvantage when it came to
communicating with GPs as they would have less familiarity.
Good communication always existed for pharmacists – verbally or by other means – with other
community pharmacists. Meetings for continuing education and peer review were also
mentioned by pharmacists within the context of relationships, as they were valued
opportunities for exchange with peers.
In summary, conversation with other health professionals was essentially limited to the GP but,
even when information was missing, this communication occurred only infrequently. This
behaviour was, in part, based on the pharmacists' beliefs about GPs' attitudes to HMRs; and
the fact that patient harm would be an unlikely result of missing information made the problem
less pressing.
Nonetheless, less than optimal levels of communication between GPs and pharmacists in the
community setting places a heavy reliance on the referral information to provide all the
necessary information for HMRs – which does not occur.
6. 3.4 Time constraints and summary informationAlthough the researcher did not observe time constraints as an issue for pharmacists
themselves (as this scenario was concerned with benchtop testing), respondents did raise time
Pharmacists could walk ‘a fine line between getting the message across and offending the doctor’.
Page 183

as an issue for GPs in dealing with HMR reports (and probably for initiating referrals, given the
poor quality many pharmacists noted). As pharmacists aimed for concise, summarised reports
to minimise the time impact (and maximise report impact) on GPs, the notion of summary
information as an efficient means of transfer seemed to be reaffirmed to the researcher.
In the hospital, an information summary was seen as a possible way to alleviate the need for
pharmacists and MOs to assimilate multiple information sources to gain a concise impression
of the patient. The information summary in the community context offers the same opportunity
– a concise and efficient impression of the patient after a medication review.
6. 3.5 Decision support tools
6. 3.5.1 Decision support tools used by pharmacistsThe use of decision support tools by HMR pharmacists was limited primarily to some on-line
and some computer-based drug information databases (i.e. of the simple NEDST Type 1
described in Chapter 2). Two pharmacists used Microsoft Access®-based databases which
had been developed to support RMMRs (but found useful for HMRs). Pharmacists found these
databases advantageous because they helped with report writing, although they could also
help the pharmacist undertake drug usage evaluations for ACFs. One database (Mediflags®)
incorporated a range of clinical information templates which could be used to formulate reports
for GPs. However, most pharmacists used Microsoft Word® (templates) for writing HMR
reports.
One pharmacist had substantially more information technology (IT) experience than the
others, having used MD (for reports), a ‘sticky notes’ application on a shared network and a
peer support network. This pharmacist also mentioned occasionally using a Palm application
for the 'easier ones' (i.e. HMRs) – although little detail was provided about this to the
researcher.
Drug information support for pharmacists came from a range of texts; and some on-line
resources. One pharmacist used the AACP website to access general treatment guidelines
and to pose on-line questions to other HMR pharmacists, especially about the use of CMs –
patients were frequent users of CMs at home and such information was often not available in
standard texts.
6. 3.5.2 Pharmacists’ understanding of decision support
As with their hospital colleagues, the understanding of decision support reflected the
pharmacists’ experience and no distinctions were made between the computer, telephone or
paper-based decision support. Pharmacists who were more IT-experienced offered views
such as: a ‘program that helps or guides to make better informed decisions, alongside use of
Page 184
knowledge’ – as with the hospital scenario, this suggested a tool to complement personal
knowledge.
Some of the paper-based decision support tools mentioned by pharmacists included
algorithms or clinical pathways (e.g. for cardiac failure or myocardial infarction) – these were
seen to encapsulate knowledge and eliminate the need for the pharmacist to seek further
information. The telephone-based support services mentioned by pharmacists included: the
Drugs and Therapeutics Information Service; and the Therapeutic Advice and Information
Service – ‘I ask a question and they give me an answer’.
6. 3.5.3 Fitting decision support into work practicePharmacists’ suggestions were about how decision support could be physically delivered, e.g.
notebook computer, PDA, telephones, on-line – or ‘electronic’ as a general term. However, the
researcher thought that an interesting aspect of these responses was the sense of where
decision support was expected to fit within the HMR process. A decision support tool was
unlikely to be used during an interview (other than perhaps if PDA-based, although again no
detail was offered as to how this could be done) as this was not convenient and pharmacists
wanted to concentrate on the patients themselves. The use of tools was more likely to occur
before an interview (e.g. to familiarise oneself with a disease), or after the interview (e.g. to
check about patient adverse effects). Pharmacists expressed a preference for use of a tool
after the interviews. This preference was based on the fact that, as information (about
medications and issues) on the referral was often incorrect, the referral information would not
reflect what was happening to the patient at home – this information would be more complete
after the pharmacist’s interview with the patient.
6. 3.5.4 Is decision support a realistic expectation?There was a general absence of opinion about this question. Pharmacists who were aware of,
or were using, tools (such as Mediflags®) thought decision support was realistic, but this was
based this on improvements in functionality of those tools. However, most pharmacists were
uncertain about how realistic decision support really was – although this uncertainty could also
stem from their general inexperience with technology.
6. 3.5.5 An ideal decision support tool
As with hospital participants, the expectations of HMR pharmacists about ideal decision
support tools reflected their personal experience. For example, the pharmacist who used
clinical pathways and guidelines mentioned these again at this point; and the pharmacist who
mentioned the use of drug information services also mentioned these once more. Expectations
Decision support was generally considered to be anything that helped professionals with decision-making
Page 185

tended to relate to content, rather than functionality – ideal decision support tools should be
based on up-to-date, evidence-based resources which consolidated information. Where types
of information were explicitly mentioned by pharmacists, these included: laboratory results;
diseases and, of course, medications (including drug interactions).
Of interest to the researcher was that pharmacists mainly mentioned drug-related or disease-
related information (i.e. reference information), but there was little reference to systems of
support for patient-related information – the area of greatest need. It is possible the reason for
this information 'bias' may be similar to that concerning pharmacists' perception of what a
decision support tool is – as pharmacists have not experienced a decision support system
which provides patient-related information, perhaps they cannot conceive of one.
‘Electronic sources’, however, were considered by pharmacists to be a more convenient way
to maintain information than paper-based sources; and electronic guidelines were considered
especially useful.
In summary, HMR pharmacists' day-to-day experience of decision support tools was far more
limited than that of their hospital colleagues. Because this HMR group was far less
sophisticated in technology use, there were also fewer clues available to the researcher about
technology needs. The main finding was an insight as to where a decision support tool might
fit within the HMR process – before or after the actual patient interview.
6. 3.6 Systems for experts rather than expert systemsPersonal knowledge emerged as a prominent issue for HMR pharmacists, just as it did for their
hospital colleagues.
HMR pharmacists' practical experience played a significant role in their knowledge acquisition
– e.g. acquired knowledge of common adverse effects in patients in particular situations
became the basis for caution in approaching new situations – to avoid repeating actions which
had previously led to errors or adverse events for the patient. In lieu of evidence, pharmacists
often used empirical judgement based on what had/had not worked in the past, to make
decisions about medication. However, one pharmacist issued a note of caution, stating that
that the more they knew, the more they realised they didn't know. This is a typical expert
judgement, and tends to confirm the expert status of the HMR pharmacists who participated in
a ‘quick screen’ to check for interactions or explain symptoms
(you are) ‘constantly thinking on your feet’
Page 186

the study.
In the same way that clinical pharmacists in hospitals evolve into 'specialists', so too do HMR
pharmacists evolve within the community setting. This is evidenced prima facie by the
requirement to undertake further training for accreditation. But in the presence of less
information (compared to the hospital), the reliance on use of personal knowledge was very
great. With even greater difficulty in capturing all the information for effective HMR reviews, it
seems highly appropriate to provide all the essential information needed to complement the
use of the pharmacist's personal knowledge. This finding helped to influence the design of the
prototype tool for the community environment.
6. 3.7 A technology-poor practice paradigmAlthough it was possible to for the researcher to establish the workflow process and technology
use by HMR pharmacists from the general questions in the interviews, the researcher felt an
additional, directed set of questions would provide richer data about these aspects which could
have implications for how the digital prototype might be used or should be implemented. A
summary of findings is shown in Table 6-6.
The paucity of technology use in the HMR environment throws up a paradox. Pharmacists
have used (computerised) dispensing systems for many years and many have experience of
Table 6-6: Workflow and technology use in the HMR process
Work flow item Information processing & transfer and technology used
How is the HMR request is received?
Notification to the pharmacist of the HMR was through the patient’s preferred pharmacy (unless they worked at the pharmacy and would therefore have the referral direct from the GP).The main delivery methods for referrals were by fax or mail. Where referral notification was by phone, the pharmacists would collect the referral from the GP practice in person. Two pharmacists mentioned the possibility of receipt by email (although this did not occur).
How HMR is the request processed (including any information transfer)?
There was generally little pre-processing of the referral before the medication review. Two pharmacists mentioned they pre-populated the HMR report with MS Word. Referrals were often 'screened' with the aim of browsing the medications, or for unfamiliar patient conditions.
What is the process for conducting HMR?
All pharmacists used hand-written notes on the paper copy referral (or partial report) at the time of patient interview. No pharmacist used a notebook computer during the interview.
What is the process for report writing?
Reports were prepared with a word processor (using Microsoft Word® templates), This often was in the form of a report that summarised patient issues and medication use. One pharmacist reported by exception using a ‘letter style’. Two pharmacists used a database for reporting.
What is the process for the delivery of report to the GP?
Fax, and then mail were the most common forms of HMR report delivery. One pharmacist faxed directly from a notebook computer. Delivery could also occur in person depending on proximity to the GP practice. Email was mentioned as an option for delivery of reports to pharmacies, but this seemed to be hampered by privacy concerns for a few pharmacists.
Page 187

computer-based information tools – they could be seen by others as quite ‘experienced’ in the
use of IT. However, the shortage of tools to support medication management (described in
Chapter 1), has been confirmed by the researcher in this scenario. All pharmacists were using
‘simple’ technology support, e.g. mainly word processing tools for HMR reporting. There was
very little (if any) use of technology-based communication tools, e.g. email or web-based tools
– the use of paper-based information sources prevailed. In light of these observations, perhaps
they should be considered ‘application-literate’ rather than ‘computer-literate’ (as would be
many health professionals).
Nevertheless, the pharmacists were certainly not adverse to trialling the digital document –
there was little effort required for the researcher to convince them to be involved in the project.
The researcher gained the impression that simple, useful tools to help with HMRs would be
welcomed.
There are two main implications of this ‘technology-poor practice paradigm’. Firstly, there is a
need for some technology to better support the communication of HMR information (this could
be as simple encrypted email); and secondly, a paradigm shift is required, from paper-based
to technology-based pharmacy practice in the community.
As mentioned earlier in this Chapter, two additional themes emerged from this phase of the
empirical research, which were specific to the community environment: the viewpoints of
professional practice tools; and pharmacists' perceptions of GPs in the HMR process. The next
two sub-sections of this chapter discuss these themes.
6. 3.8 The ‘viewpoints’ of professional practice toolsSome pharmacists held the view that the digital document should 'mesh' with a GP's desktop
system – and possibly even incorporate some features of (traditional) prescribing and
dispensing systems. This suggestion, however, would have led to a complete change in the
software solution being investigated and proposed in this thesis. There is no intention to
duplicate features of GPs' existing desktop systems, since they serve quite different purposes
to the medication management solution which forms the focus of this project. The researcher
considers these traditional systems have particular worldviews, or 'viewpoints'.
The function of a prescribing system is to allow selection of medication from a Pharmaceutical
Benefits Schedule (PBS)1 list – supported by features such as drug-drug interaction, some
drug-disease interaction checking etc. A dispensing system also allows selection of a
1. The Pharmaceutical Benefits Scheme subsidises payments for a high proportion of prescription medi-cations bought from pharmacies
Page 188

medication from a PBS list, with associated drug-drug interaction checking against the patients
prior supply record. Both these systems are built around supply of items to the patient from a
(common) list of medications: prescribing is concerned with the intention to supply (to the
patient); and dispensing with the actual supply of the medication. Neither, however, can lay
claim to actually representing what the patient is actually taking (although this can be the belief
of some GPs and pharmacists).
In relation to broader medication use, the prescribing system (MD) can record CM and OTC
medication taken by the patient (if this is volunteered by the patient) and if this medication is
included within MD. A dispensing system does not capture any such CM or OTC use.
The only way to reveal actual medication use is by means of a medication review; and the
purpose of the digital document investigated and prototyped in this research project is to
support that process. The digital document could truly represent the 'current medication record'
of an individual patient. It could only do so effectively, of course, if it is made available to both
patients and their relevant health care team on an ongoing basis – and, of course, no matter
how effective the solution proposed in this thesis, such an outcome can only be achieved if
both the GP and pharmacist are actively engaged with their patients in managing medication.
Nonetheless, a digital document living in its own ' electronic space' offers an opportunity to
provide a complete picture of a patient's medication use and compliance, whereas the
traditional systems are unable to do this. Prescribing a medication will not ensure it is
dispensed; and dispensing a medication will not ensure it is taken by the patient – neither can
represent actual use.
In this researcher's opinion, the desired ideal of integrating a current medication record
information (as advocated by the digital document) with existing prescribing and describing
systems is unlikely, because of the differing 'viewpoints' of the system types.
6. 3.9 Pharmacists’ perceptions of GPs in the HMR processAs reported earlier, communication between pharmacists and GPs was infrequent; and often
undertaken reluctantly. During this discussion, the researcher noted that pharmacists felt
some GPs were not convinced of the value of HMRs: a viewpoint reinforced by pharmacists'
experience of poor, or no, feedback from GPs. Not only is this situation unfortunate, it also has
implications for patient safety – pharmacists were often unaware of the outcomes of their
interventions. Pharmacists suggested that sharing the digital document on-line might not only
improve the information sharing process between these two groups – it might also contribute
to improving relationships between GPs and pharmacists.
Page 189

6. 3.10 Prototype testingPrototype testing is reported as a separate discussion as this was the true 'test' of the
information model and digital document. The discussion in this section combines data from
feedback about the prototype solution from the focus group, directly based upon participants'
reporting of their satisfaction with use, or by means of the researcher's owner observations. As
with much of the other data, this section will summarise findings. More substantial and detailed
reporting of the testing process can be found in Appendix O.
Where possible, the researcher attempted to observe prototype testing by pharmacists first-
hand, to reveal aspects of use which might not be reported by participants, e.g. which digital
document page they used first. Of course, as participants were being observed, use may not
have been 'normal' (the Heisenberg Uncertainty Principle1). Unfortunately, it proved possible
to observe only two of the five pharmacist participants, so only limited impressions could be
formed by the researcher on the basis of his observations. These pharmacists nevertheless
reported their use at the focus group or in other communication, so that observation was not
the only method of obtaining feedback from the usage of the prototype.
The researcher's impression, overall, was that pharmacists had little difficulty in using the
digital document and rapidly gained speed in using it once they had some initial familiarity with
the prototype. Speed of use only decreased when pharmacists were deciding how to word or
apportion text into fields (e.g. whether to describe a paracetamol dose as 1g or 2 tablets; or
whether to include an instruction of 'prn for pain' or place the word 'pain' in the indication field).
There were often questions about the intent of fields or what do in the case of a missing item
– the researcher made no specific suggestions about what to do in these cases, as the
intention was to observe actions, rather than to direct use. Observations also provided an
opportunity for the researcher to determine other needs (e.g. confirmation dialogue after some
actions, the need to resize or reformat screen components, etc.), or to note errors for
subsequent correction.
The following subsections summarise the results of the prototype testing, using the headings
which were used in the data gathering document.
1. The Heisenberg Uncertainty Principle has its foundations in quantum physics but its conservative inter-pretation is that uncertainty is a limitation imposed by our measuring techniques (http://plato.stan-ford.edu/entries/qt-uncertainty/#HeiRoaUncRel; viewed 2007-02-27).
Some pharmacists felt that the GP was ‘just following a (mechanical) process’
Page 190

6. 3.10.1 User reactions to the prototypePharmacists generally had positive reactions to the prototype and thought the concept was
good.
It was considered easy to use, although entering data was generally was found to be more time
consuming than pharmacists’ existing methods of entering data (using Word® templates), as
more information was requested by the digital document than was currently recorded for a
medication review (e.g. the start date for medication) – although one pharmacist declared that
‘it's about what you get used to’.
6. 3.10.2 User suggestions for the prototypeNot surprisingly, participants had many comments about the information elements or structure
of the document – this was expected, as not only was this the first test of functionally, but
testing was also intended to identify those elements required for the community context. A few
issues in particular were the basis of much discussion.
Opinion about the use of drop-down boxes was varied – some pharmacists considered these
useful (to save typing and time), while others preferred text boxes (to save searching through
long, e.g. medication lists, and time). This conflicting requirement is a good example of the
dilemma which can exist in satisfying user needs during development. In any case, the
researcher decided that (large) drop-down lists were not in keeping with the digital document’s
aim of being of a transportable and shareable medication-related record.
Pharmacists expressed some support for alerts and reminders during prototype testing, but the
consensus of the focus group was that these were not generally important. Using the examples
of weight and height, there would be only a small number of patients where such information
was considered important. Changes in weight were considered more important that an isolated
value of weight per se. The researcher considered this to be an interesting comment in light of
the poor information conveyed by GPs – they would probably be more likely to provide a weight
value than a more detailed comment about changes in weight.
Despite their overall advice that reminders were not critical for the system, pharmacists did
consider some alerts to be useful, including: a flag for any recent biochemistry; a more specific
flag for a recent INR; and a date indicating when the medication list had last been updated. In
the same thread of discussion, pharmacists considered that calculators for Body Mass Index
(BMI) and creatinine clearance (a measure of renal function) were useful, as many
pharmacists used these tools regularly. Some of the more important suggestions for changes
Generally (it) 'asked the right questions’; and was ‘logical with the right layout in the right order’
Page 191

to the digital document are shown in Table 6-7.
6. 3.10.3 User innovationsPharmacists also suggested many new features for the digital document. Many suggestions
were good ones, but a number would be difficult to implement or represented a direction
contrary to that of the digital document. Other suggestions were made by an individual
pharmacist, but were not representative of the group. The main issue for the researcher here
was not to succumb to the general trap of requirements elicitation, but rather to maintain the
goal of recognising essential information elements and appropriate digital document
functionality. Consequently, not all the ideas suggested were used to make changes to the
information model or (functional changes) to the document prototype. Suggestions which
were, and were not, implemented are summarised in Table 6-8.
Table 6-7: Pharmacists’ suggestions for changes to the digital document prototype
Changes
The date of birth should be recorded rather than age (as the next time the document was opened the age would be the same value and possibly incorrect); and the ability to record ‘unknown’ or other text value for date, as this may not be known.
Use of separate generic and brand names for medications.
Changing the cursor shape when this moved over a link. This changed from arrow to a ‘line cursor’ that was difficult to see – a hand-shaped cursor was suggested.
Highlighting the selected item on a list rather than having a box around it, as this was difficult to see.
Have the route of administration default to ‘oral’ (possibly with some other limited choices).
The ability to use headings on a report e.g. actions carried out, education undertaken and items for discussion.
Table 6-8: User innovations
Implemented Not implemented
Addition of patient risk factors (e.g. for cognition, eyesight).
Ability to print out a medication list for the patient.
Recording indications for medications from the patients’ perspectives.
Ability to record patient concerns.
A place to record social issues. Ability to use keyboard shortcuts as well as the mouse (Unable to do within project timeframe).
Capture medical / treatment history / inactive problems
Addition of yes/no confirmation when deleting entries (unable to do).
Tick box for common immunisations. An action plan (for the report).
Reason for referral field with an ability to add further comments (to be the basis of the report).
Ability to flag or highlight results and / or items indicating what was different in the report compared to the referral.
Separate lists for ‘regular’ and ‘when required’ (prn) medications.
Comments’ field after the medication information.
Add contact details for others (e.g. carers) Ability to print out a list of patients who underwent an HMR
Headings for information to share with the GP: issue (raised by GP), suggestion (by pharmacist after review), outcome (after the GP considers pharmacist recommendations).
‘Tick boxes' against issues to flag if they were resolved; and the same for the patient overall.
Ability to group drugs in the medication list.
Page 192

The term 'compliance' (as a text box label on the digital document) was considered
inappropriate – compliance was considered to be part of general management issues and it
was felt that a better approach would be to use the label 'medication management' with some
examples in brackets (e.g. compliance, handling, understanding). The recording of 'social
issues' was important to pharmacists, as many GPs were unaware of how these issues could
help the pharmacist undertake the HMR.
The ability to signal particular concerns about the patient, e.g. visual impairment, cognitive
problems etc. was deemed important, as these were patient aspects that could either affect
medication management or, in turn, be affected by the medication. One important addition was
the ability to indicate a recent fall – not featured on currently used referral documents.
One suggestion was to not include a feature: participants felt that a tick box listing the HIC
medication risk factors should not be provided within the document, believing that a text box
to enter the (real) reason for referral would provide more useful and actionable information.
6. 3.10.4 Functional prototype issues One area of significant discussion was dates, as all pharmacists experienced problems with
the way dates were handled within the prototype. The date field was displayed in an unfamiliar
format (yyyy-mm-dd) and entering an invalid date value prevented the document being saved.
Participants also discussed the more general issue of when dates should be used – believing
this to be important in certain cases e.g. when indicating a current course of medications, or
when weight or height were recorded. Such use would therefore depend on the particular
patient circumstances. The use of a default date value (of 'today') was seen as problematic, as
this could encourage users to take the easy option of leaving this value – which could give rise
to misinformation. This issue with unchallenged default date values often occurred with
referrals received from MD (i.e. they were wrong), but getting GPs to enter the correct dates
was considered 'a bit of a challenge'. It was felt that when there was no date to enter, values
such as 'unknown' or 'na' might be better options than a default date.
The medication and diagnosis lists were found to be cumbersome as a user needed to ‘flip’
back and forth between the display page of the document and the relevant data entry form
(these were the longest lists of items for any HMR document). A proposed solution was a
‘blank’ record for subsequent entries (similar to a database). The order of medication items
was also an issue as new items were inserted on the top of the medication list. A preference
emerged for the ability to group ‘important’ drugs (e.g. warfarin, anti-hypertensives, or drug
classes) at the top of the list; and to place the less important ones (e.g. laxatives) at the bottom.
Page 193

Further discussion arose over the labels of ‘diagnosis’ and ‘active problems’ as these reflected
hospital (discharge) and were confusing in an HMR context. As well, discussion revealed that
patient concerns and GP concerns might differ – a patient concern might not be a GP concern
and vice-versa – there was thus a need to record patient concerns (to feed back to the GP).
In summary, the main usability findings from prototype testing concerned issues associated
with date functionality, previously unnoticed errors in display; and changes required in the
underlying data structures based on the different context. Document analysis, which again
contributed to knowledge about information element frequency, is discussed next in Sub-
section 6.3.11.
6. 3.11 Document analysisDocument analysis was a simpler process for the researcher compared with the hospital
scenario, as the benchtop scenario had fewer participants, but also because there was a
smaller range of documents. Consequently, there was no need for the researcher to construct
a UML model (as with hospital-based documents). The documents used by this group
essentially were a referral from the GP, or report sent to the GP – these are discussed in the
next two sub-sections.
6. 3.11.1 Referral documentsThe referral documentation from the GP generally consisted of a referral letter accompanied
by one of a range of reports from MD. As the researcher was only able to obtain a small sample
of these documents from a comparatively few pharmacists, other representative sources of
HMR referral documents were sought. These included sample printouts from MD; and
documents published by the National Prescribing Service, Mediflags®, the Pharmacy Guild of
Australia and the Port Macquarie Division of GPs. As with the hospital scenario, the document
analysis was not intended to be either an extensive audit which would capture every single
information component that could be included in referral documents – rather, the components
that were most commonly represented. The researcher then analysed the information
elements contained in these documents and compared them with information elements of
models that he had formulated for the hospital scenario (for missing medication, patient
information and document analysis). These comparisons determined which information
components were common to both scenarios (confirming the importance of that information
component); and those which were needed to represent the community context – the latter
becoming candidates for inclusion into the information model. These comparisons confirmed
the need for the information elements identified for the hospital scenario, as well as suggesting
further community-related information elements. The spreadsheet contained in Appendix W
shows these comparisons in full.
Page 194
6. 3.11.2 ReportsThe HMR reports created by the pharmacists were invariably simple – some reports were
designed to be no longer than a single page. This brief report contained a concise summary of
the investigation of the issues raised by the GP (if any), any issues identified during the review;
and any subsequent recommendations for action. The reports from different pharmacists were
very similar as the Microsoft Word® templates used as the basis of the reports were often
shared through the HMR pharmacist 'network'. Some reports were based on Mediflags®
templates. The information components contained in a typical report included: patient details,
GP and pharmacist contact details, date of interview, patient diagnoses, social issues, (patient)
equipment used, concerns about the patient, allergies and Adverse Drug Reactions (ADRs),
current medication including indications, potential drug related problems/interactions, actions
taken by the pharmacist; and issues for consideration by the GP.
6. 3.12 Opportunities for the digital document to improve HMR practice
6. 3.12.1 The medication management review processPharmacists' opinions about ways in which the digital document could help the medication
management process, or improve patient outcomes, were of considerable importance to the
project – as well as to the researcher. In this, however, as with some of their suggestions for
new features for the prototype, pharmacists recommended features which were too broad to
be accommodated within this project. Nonetheless, these suggestions did serve to place the
digital document in a wider context than simply capturing HMR information.
Opportunities were seen to use the digital document to:
• complete the information loop between the pharmacist and GP. Participants suggested
that this would: enable the GP to acknowledging receipt of HMR information more
quickly and to send comments back to the pharmacist; increase GP accountability; and
potentially improve GP-pharmacist relationships. Such an approach might address the
problem of pharmacists not receiving medication action plans back from the GP, or
receiving feedback only after a further event occurs for that patient (e.g. going back to
hospital)
• streamline the HMR process for pharmacists, e.g. decrease the amount of typing
required after receiving the referral and, in particular, use the digital document as the
basis of an HMR report
(the current process was) ‘see the patient, write the report, send it to the doctor and eventually they get it, and think about it some time in the next few weeks’
Page 195

• enable the use of small, hand-held devices for data capture during patient visits, to avoid
having to later re-type information into a computer
• provide the basis for progressive plans as the patient moved through a number of HMRs,
hospital admissions, etc.
• standardise the format for HMR reporting
• form an audit tool for pharmacists (to review HMR practice)
• allow printing of material for patients (such as a medication list).
6. 3.12.2 Opportunities to improve the patient outcomesAlthough participants mentioned improving patient outcomes as a general benefit, they were
less specific on this topic than when discussing opportunities to improve the HMR process.
One improvement suggested in relation to improving patient outcomes was the idea of using
the digital document has an information tool – 'the more information the better' – although this
was disputed by other participants, because the act of recording more information does not, in
and of itself, improve patient outcomes. Improved outcomes were seen to be more associated
with the ability to improve communication (about the patient) between the health care team,
the patient and the family.
The timeliness of information, in particular, could affect patient outcomes. For example, during
a hospital ward round, a recommendation from a pharmacist could be enacted immediately,
so that the patient benefited immediately. With an HMR report, however, it was never known
if pharmacists' recommendations were put into action. If the information loop was completed,
therefore, important messages requiring immediate attention could be flagged to the GP, to the
benefit of the patient.
In summary, analysis of the data gathered from interviews, prototype testing, document
analysis; and the focus group provided the basis for amending the hospital-based information
model for HMR use in the community. Prototype testing also assessed visual and functional
components of the digital document in preparation for field testing. The community-aligned
model is discussed in Section 6.4; and changes to the digital document and other
implementation details in Section 6.5.
6.4 The community aligned information modelThe researcher's approach to refining the information model has been mentioned in some of
the previous sections of this thesis – not all elements or ideas suggested by HMR pharmacists
were adopted. Those which were adopted supported the project's goal of realising a portable
and flexible digital document to support medication management. This necessarily meant
avoiding complexity within the document which would not only divert the project from its
Page 196
intention, but also add issues of system size and performance. Some problems could not be
fully resolved satisfactorily, e.g. the date format problem, but had to be left for future work.
The major changes to the information model are shown in Table 6-9.
The revised information model is shown in Figure 6-2. This figure also shows the changes
made to the hospital model once the community material had been incorporated. Information
elements marked with a double asterisk (**) are new items added to the model; a single
asterisk (*) indicates that an item existing in the hospital model was amended in the community
model; and items marked with an ampersand (&) have been removed from the model. The
revised model included two calculators (##): one for Body Mass Index (BMI) and one for
creatinine clearance; as well as two alert functions (!!): one for the detection of warfarin in the
medication list and another which looks for warfarin and the presence of an INR in the
laboratory investigations list.
The implementation aspects of the model and other functional changes implemented in the
document are described in Section 6.5, with full details contained in Appendix P
Table 6-9: Information elements added to the model for the community context
Information group Information element Change from hospital to community context
Referral information All elements. This information was not required in the hospital.
Patient information Calculators for body mass index and creatinine clearance.
These would be available by in other ways in the hospital setting.
Recent BP (blood pressure). Available in other sources for hospital pharmacists.
Serum creatinine. Required by the calculator.
Other contacts. For family members, other health professionals in the community.
Physical information group. Factors that can affect adherence to medication for patients in the community (or can be affected by medication e.g. falls).
Medication information Immunisations group. An important consideration for the elderly in the community.
Generic and brand names. This existed as a single element in the hospital Mode, where the generic name is preferred.
Regular and when required medications.
This existed as a single group within the hospital model.
Alert for presence of warfarin. Added to test usefulness of alerts in the community setting.
Investigations group Alerts for presence of INR (and along with warfarin).
Added to test usefulness of alerts in the community setting.
Page 197

Figure 6-2: The community-aligned information model
Med
icat
ion
man
agem
ent d
ocum
ent
Pat
ient
info
rmat
ion
Trea
tmen
t inf
orm
atio
nM
edic
atio
n in
form
atio
nIn
vest
igat
ions
Ref
erra
l inf
orm
atio
n **
Ref
erra
l dat
e **
Dat
e of
revi
ew
Rep
ort d
ate
**
Com
plet
ed d
ate
**
Des
crip
tion
**
Rec
omm
enda
tion
**
Act
ion
**
Res
olve
d **
Res
olve
d da
te **
Per
sona
lR
efer
ence
Phys
ical
**
Nam
e
Add
ress
Med
icar
e nu
mbe
r(W
as P
atie
nt ID
)*
Dat
e of
Birt
h
Age Sex
Wei
ght
Hei
ght
Rec
ent B
P
Alle
rgie
s / s
ensi
tiviti
es
Adv
erse
dru
g re
actio
ns
Rec
reat
iona
l sub
stan
ce u
se
Syst
olic
Dia
stol
ic
Seru
m c
reat
inin
e **
GP
deta
ils *
Com
mun
ity
Phar
mac
y *
Oth
er c
onta
ct *
*
Cal
cula
tor #
#B
MI *
*
Prev
ious
falls
**
Cog
nitio
n **
Mem
ory
**
Lang
uage
**
Dex
terit
y **
Vis
ion
**
Hea
ring
**
Sw
allo
win
g **
Equi
pmen
t **
Oth
er *
*
Cur
rent
tre
atm
ent
& A
dmis
sion
reas
on /
Prin
cipa
l dia
gnos
is
Act
ive
prob
lem
Trea
tmen
t His
tory
Med
ical
his
tory
*(w
as p
ast
med
ical
his
tory
)
Labo
rato
ry
Dat
e
Item
Res
ult
Imm
unis
atio
ns **
Cur
rent
med
icat
ions
Med
icat
ion
hist
ory
Med
icat
ion
man
agem
ent
issu
es
Teta
nus
**
Influ
enza
**
Pneu
moc
occu
s **
Oth
er
Imm
unis
atio
ns *
*
Reg
ular
**m
edic
atio
ns
Whe
n re
quire
d **
med
icat
ions
(pm
)
Cea
sed
/ ch
ange
dda
te
Rea
sons
for
dose
cha
nge
Pers
on
resp
onsi
ble
for c
hang
e
Med
icat
ion
Dat
e
Gen
eric
nam
e *
Bra
nd n
ame(
s) *
Dos
e
Rou
te
Freq
uenc
y
Add
ition
alin
stru
ctio
ns
Indi
catio
n
Dur
atio
n of
treat
men
t
Pat
ient
indi
catio
n **
Freq
uenc
y
Max
imum
dose
Soc
ial
hist
ory
Med
icat
ion
man
agem
ent *
(was
co
mpl
ianc
eis
sues
)
Ale
rt !!
-war
farin
Aler
t !!
-war
farin
an
d IN
R
## C
alcu
lato
r!!
Aler
t C
hang
es to
mod
el fr
om h
ospi
tal v
ersi
on**
add
ed it
em* a
men
ded
item
& d
elet
ed it
em
Ref
erra
l rea
sons
**
Cal
cula
tor #
#C
reat
inin
e cl
eara
nce
**
Tele
phon
e **
Page 198

6.5 The digital document and the server serviceThis section describes the changes made to the Visual Basic (VB) viewer and the XForms
document, as a result of the bench top testing, together with the development of the server
service to support on-line access. Screen dumps in this chapter are only used to illustrate
major changes, rather than being used in all cases – sometimes only a small section of the
screen is shown (the area of interest), as a compromise between clarity and the use of space.
6. 5.1 The VB BrowserThere were minimal changes to the existing VB browser other than some minor formatting to
allow better sizing of the form for a lower resolution screen on a PC or notebook; and
maximising the display area for the digital document within the form.
However, the need to print a paper copy of the digital document required the researcher to
develop a new VB form. This ‘child’ form (VB Document Printer form) was launched from a new
[Print] button added at the top right of the VB form – shown in Figure 6-3.
The code contained within the VB Document Printer form used an XSL1stylesheet to transform
the patient’s XML file into an HTML format for display in the form’s window (for subsequent
printing). This child form option was faster and ‘cleaner’ than producing an HTML report in the
existing VB viewer, which would have required: saving the current document; producing the
HTML report; and then possibly re-opening the document again after printing. As opening the
document was a relatively slow process – the entire XForms document needed to be parsed
– avoiding this was clearly a better option. The source code for this second version of the VB
viewer is contained in Appendix R.
The VB Medication Management Document Printer form is shown in Figure 6-4 (on top of the
calling form).
1. eXtensible Stylesheet Language (XSL) stylesheets are designed to format output from XML docu-ments.
Figure 6-3: Visual Basic document viewer (version 2)
Page 199

The researcher designed the function of the buttons on the VB Document Printer form to be
similar to those on the calling form to the greatest extent possible. For example, the [View
patient documents] on the main form and [View existing patients] both opened a list of existing
patient documents. The button functions are explained in detail in Appendix P.
Figure 6-4: VB Medication Management Document Printer form
Page 200

A sample of a HTML report is shown in Figure 6-5. Clicking on [Send to printer] subsequently
opened a Microsoft Windows® printer dialogue box. The XSL code that causes the
transformation of the XML file to HTML output is contained in Appendix V.
The changes to the digital document pages required by the findings of the benchtop testing
phase of the project are now described, beginning in Section 6.5.2.
6. 5.2 The digital document Referral details page
The referral details page (shown in Figure 6-6) is new to the model; and is an obvious
consequence of the community context findings. The page contains the referral date, reasons
for referral (entered ideally by the GP) and the review date subsequently entered by the
pharmacist. The date values at this point are simply text values as there is no need for date
calculations on this page.
Figure 6-5: VB HTML output of the digital document
Page 201
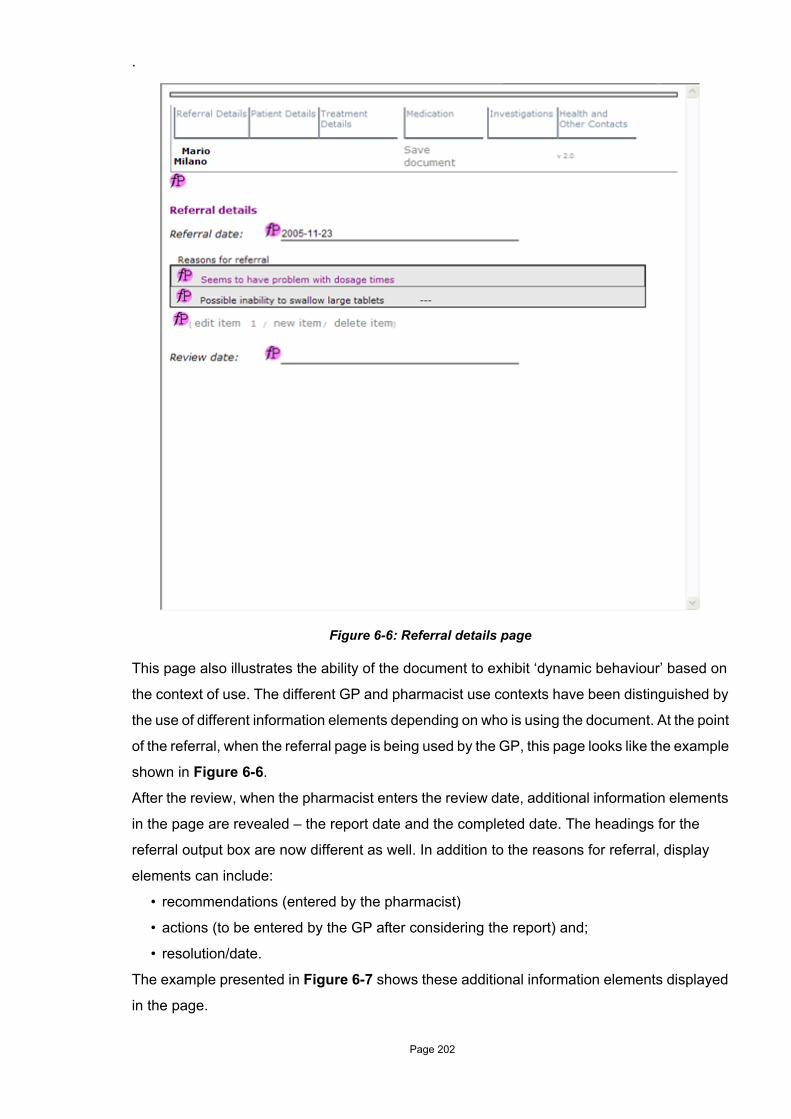
.
This page also illustrates the ability of the document to exhibit ‘dynamic behaviour’ based on
the context of use. The different GP and pharmacist use contexts have been distinguished by
the use of different information elements depending on who is using the document. At the point
of the referral, when the referral page is being used by the GP, this page looks like the example
shown in Figure 6-6.
After the review, when the pharmacist enters the review date, additional information elements
in the page are revealed – the report date and the completed date. The headings for the
referral output box are now different as well. In addition to the reasons for referral, display
elements can include:
• recommendations (entered by the pharmacist)
• actions (to be entered by the GP after considering the report) and;
• resolution/date.
The example presented in Figure 6-7 shows these additional information elements displayed
in the page.
Figure 6-6: Referral details page
Page 202

The same principle is used in editing reasons for referral where at the time of referral, reasons
for the referral can be added through use of a simple text entry form that appears once ‘new
item’ is clicked – shown in Figure 6-8.
The user's ability to add multiple referral entries using [Save and add another] was also added
to the documents functionality. This approach was also repeated for other potentially long lists
– such as medications and active problems.
In keeping with context awareness, once the HMR review date was entered, the form in Figure
6-8 changed to also reveal fields for the additional information elements, shown in Figure 6-9.
Figure 6-7: Referral details page – after the review
Figure 6-8: New reason for referral form
Page 203

These additional fields allow the pharmacist to add a recommendation alongside the referral
reason; and the GP to later add an action for the pharmacist’s recommendation. This
interchange between the pharmacist and the GP forms the basis of a potential action plan. The
resolved/date fields can be used by the pharmacist or GP if they consider the referral reason
is resolved.
6. 5.2.1 Patient details pageThe changes to the patient details page are shown in Figure 6-10. Differences from the
original page are: the display of calculated values of BMI and creatinine clearance, day values
(shown in blue) are now calculated as month values, the red Omega alert is now a * symbol;
and there are tick boxes to record patient concerns (cognition, memory etc.). Text areas were
also added for Other problems and Equipment used – both of these fields open to reveal
simple text editing forms. In the case of patient falls, ticking that option opens two fields to enter
additional information (fall details and date) – this is important as falls predispose the patient
to further falls (with a high mortality rate); and the circumstances of the falls can be particularly
important.
Figure 6-9: Extended reasons for referral form
Page 204

Figure 6-10: Patient details page
Page 205
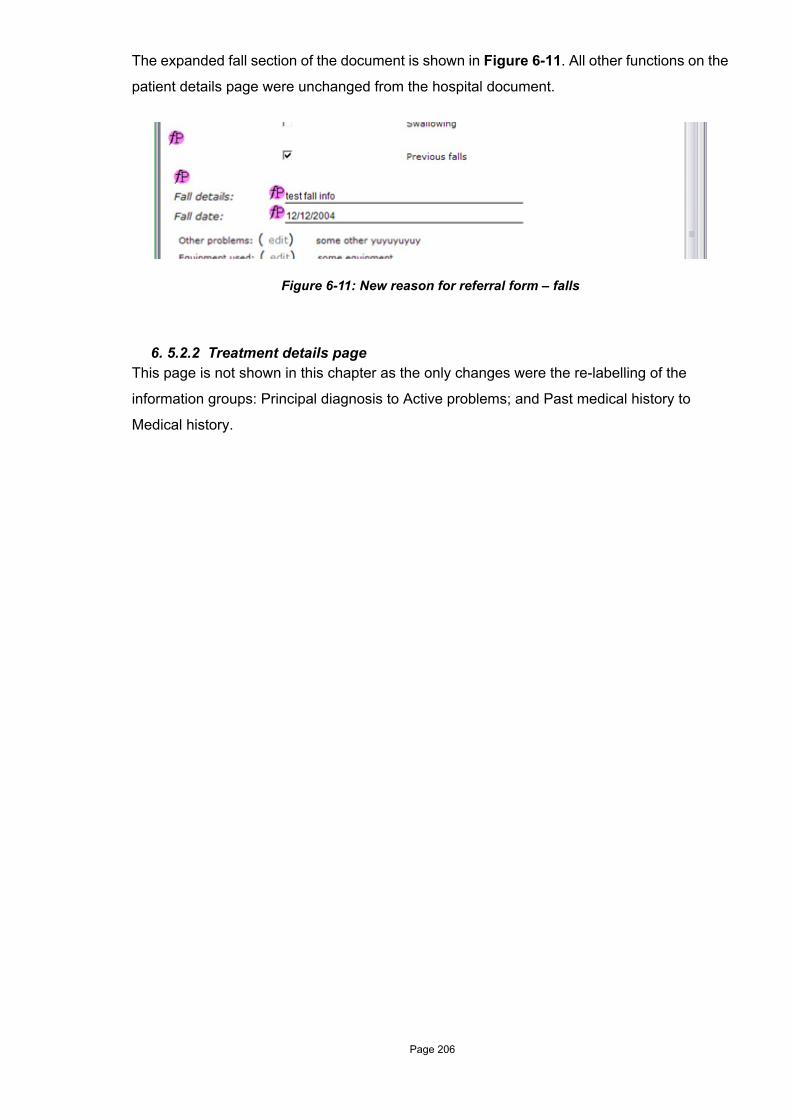
The expanded fall section of the document is shown in Figure 6-11. All other functions on the
patient details page were unchanged from the hospital document.
6. 5.2.2 Treatment details pageThis page is not shown in this chapter as the only changes were the re-labelling of the
information groups: Principal diagnosis to Active problems; and Past medical history to
Medical history.
Figure 6-11: New reason for referral form – falls
Page 206

6. 5.2.3 Medication pageThe medication page (Figure 6-12) underwent the most significant changes of any previously
existing page.
The first change was the addition of a section for immunisations which are commonly used for
elderly patients: including tetanus, influenza vaccine and pneumococcus vaccine; and an area
to record others. The edit form for these is shown in Figure 6-13.
Figure 6-12: Medication page
Page 207

The other significant change is the division of medication into two groups: regular medications;
and when-required medications. These have similar edit, new and delete functions and, as
before, there is the option to display medication history. This display of medication history also
needed amendment to accommodate the two different types of medication.
Current medication was shown as a combined block of the current regular and when-required
medications; and history was shown as two separate groups of regular and when-required
medication. An issue not initially considered on the hospital document was that the edit, new
and delete function options (triggers) were still visible when the medication history was
displayed. These were removed from the display, leaving only a 'hide medication history'
option. The medication history report is shown in Figure 6-14.
Figure 6-13: Edit immunisations form
Page 208

Figure 6-14: Medication history
Page 209
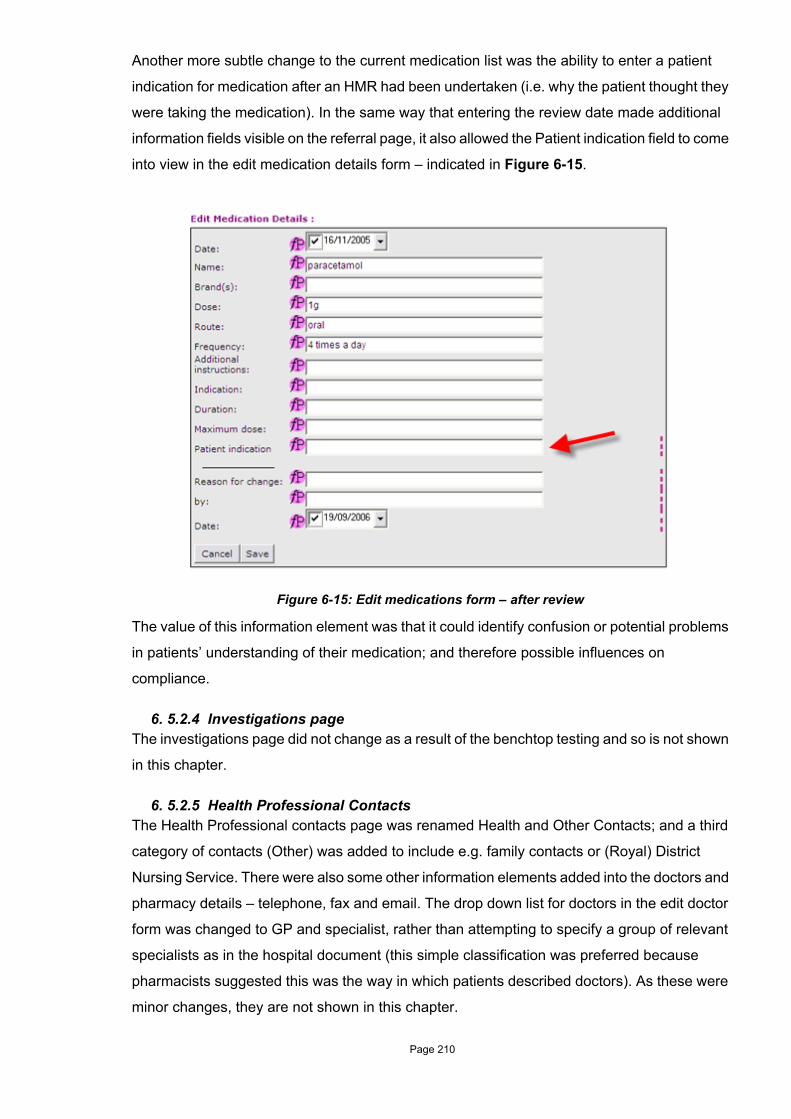
Another more subtle change to the current medication list was the ability to enter a patient
indication for medication after an HMR had been undertaken (i.e. why the patient thought they
were taking the medication). In the same way that entering the review date made additional
information fields visible on the referral page, it also allowed the Patient indication field to come
into view in the edit medication details form – indicated in Figure 6-15.
The value of this information element was that it could identify confusion or potential problems
in patients’ understanding of their medication; and therefore possible influences on
compliance.
6. 5.2.4 Investigations pageThe investigations page did not change as a result of the benchtop testing and so is not shown
in this chapter.
6. 5.2.5 Health Professional ContactsThe Health Professional contacts page was renamed Health and Other Contacts; and a third
category of contacts (Other) was added to include e.g. family contacts or (Royal) District
Nursing Service. There were also some other information elements added into the doctors and
pharmacy details – telephone, fax and email. The drop down list for doctors in the edit doctor
form was changed to GP and specialist, rather than attempting to specify a group of relevant
specialists as in the hospital document (this simple classification was preferred because
pharmacists suggested this was the way in which patients described doctors). As these were
minor changes, they are not shown in this chapter.
Figure 6-15: Edit medications form – after review
Page 210

6. 5.3 The server serviceAn important outcome of this scenario was the development of a server service to allow on-
line access. This was important, in keeping with the participants’ desires to able to
communicate medication-related information (i.e. the digital document). In this on-line
environment, the researcher aimed to duplicate, as closely as possible, the functions provided
by the VB viewer – the display of the digital document and the same patient file functions. In
addition, there was also a need to be able to upload and download patient files between the
server and a PC (or notebook computer). The ability to use the digital document on-line,
‘locally’ or as a combination of both, by transferring patient files between the server and local
computer, provided a great deal of flexibility so that the participants could accommodate their
work preferences (or try new methods).
The options available to users included:
• Using the document in isolation, i.e. for the pharmacist to use the patient documents on a
notebook or desktop using the VB browser-based approach (this would mean that the
pharmacist received a paper copy referral (mail or fax); and returned a paper copy report
to the GP).
• Using the document completely via the server. This offered the best option for efficient
sharing of the document. In this case, the GP referral would ‘change’ into the report after
the review information was entered by the pharmacist. (It was still likely that the
pharmacist would take a paper copy of the referral to the interview – no pharmacists
indicated that they used a notebook computer during interviews).
• Use a combination of both options, e.g. the patient referral could be created by the GP
on the server and later downloaded by the pharmacist, or the pharmacist could perform
the first part of the review process using paper and then load a completed referral report
onto the server for the GP to view. Other variations of this were possible.
The patient XML file could also be exchanged using encrypted email of course (as the average
patient XML file size was only in the order of 8–17Kb), although this option was not specifically
considered at this stage of the project. The different pathways for use of the document are
graphically summarised in Figure 6-16.
Although the server service supported exchange of the medication document, however, the
researcher did not attempt to accommodate the business aspects of the HMR process, i.e. the
referral letter required for HMR payment by HIC. This issue falls into the Future Work category
and is discussed in Chapter 8.
The researcher began developing the server environment using Apache Tomcat®, as this was
Page 211

a common approach within the University. But despite some initial success, this approach did
not allow the digital document to be delivered to users in its own browser ‘shell’ (like the VB
viewer). The researcher considered a number of approaches, including Java Server Pages,
Java Servlets and Java Swing. However, the learning curve for these was too steep for the
time frame remaining for the project and eventually the service was implemented using
Microsoft Internet Information Server® (IIS) version 5.1. A major advantage of this approach
was that Microsoft Active Server Pages® (ASP) used procedural code very similar to that used
for the VB viewer. An unfortunate disadvantage was that there was little (no) support for this
strategy within the University environment. Some of the development steps for the server
service appear in the development record are shown in Appendix Q.
A visual representation of the server service (detailing the relevant ASP files) is presented in
Figure 6-17. The code for all server pages is shown in Appendix S
Figure 6-16: Pathways for the HMR digital document
HMR documentDesktop PC
PC/notebook
Server
GP
Home Medicines Review
View HMR report
Enter HMR info
HMR report
EnterHMR
report info.
HMR info
Enter HMRinfo.
Enter review
info.HMR document
Pharmacist
Page 212
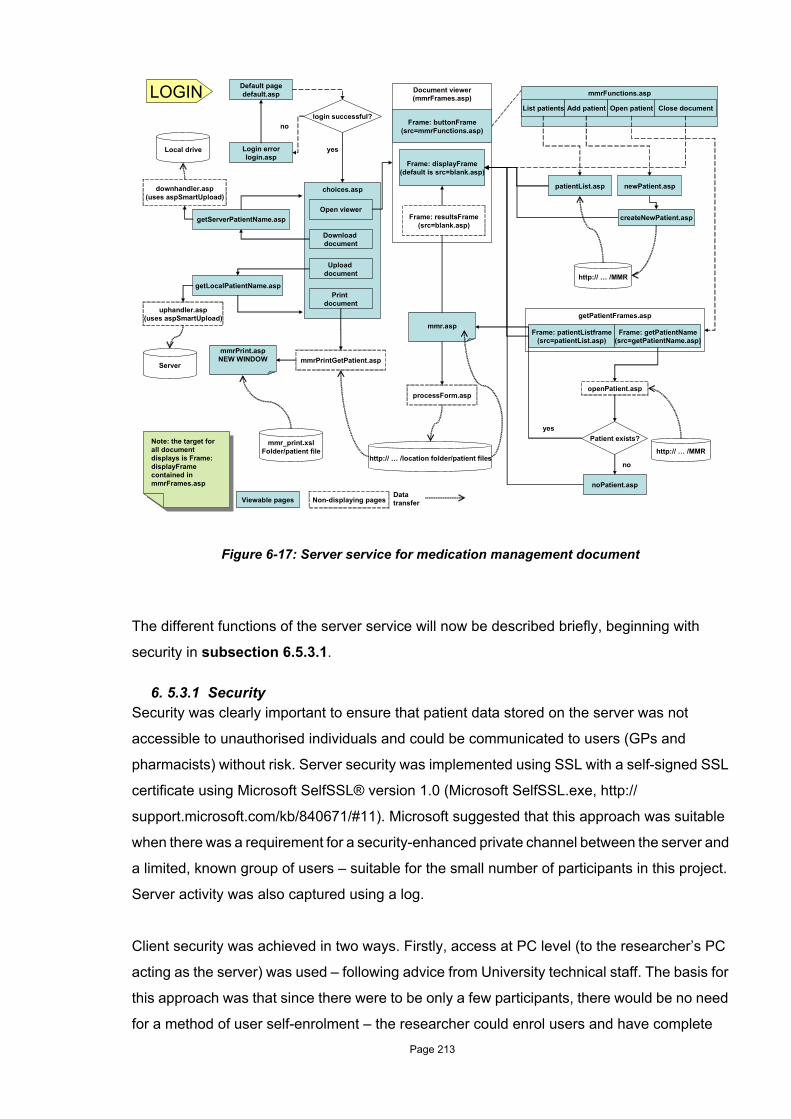
The different functions of the server service will now be described briefly, beginning with
security in subsection 6.5.3.1.
6. 5.3.1 SecuritySecurity was clearly important to ensure that patient data stored on the server was not
accessible to unauthorised individuals and could be communicated to users (GPs and
pharmacists) without risk. Server security was implemented using SSL with a self-signed SSL
certificate using Microsoft SelfSSL® version 1.0 (Microsoft SelfSSL.exe, http://
support.microsoft.com/kb/840671/#11). Microsoft suggested that this approach was suitable
when there was a requirement for a security-enhanced private channel between the server and
a limited, known group of users – suitable for the small number of participants in this project.
Server activity was also captured using a log.
Client security was achieved in two ways. Firstly, access at PC level (to the researcher’s PC
acting as the server) was used – following advice from University technical staff. The basis for
this approach was that since there were to be only a few participants, there would be no need
for a method of user self-enrolment – the researcher could enrol users and have complete
Figure 6-17: Server service for medication management document
login successful?
Patient exists?
mmrFunctions.asp
List patients Add patient Open patient Close document
patientList.asp
createNewPatient.asp
newPatient.asp
http:// … /MMR
getPatientFrames.asp
Frame: patientListframe(src=patientList.asp)
Frame: getPatientName(src=getPatientName.asp)
Non-displaying pages
mmrPrintGetPatient.asp
processForm.aspopenPatient.asp
Viewable pages
http:// … /MMR
noPatient.asp
mmr.asp
http:// … /location folder/patient files
choices.asp
Open viewer
Download document
Upload document
Print document
mmr_print.xslFolder/patient file
Default pagedefault.asp
getServerPatientName.asp
getLocalPatientName.asp
yes
no
Document viewer(mmrFrames.asp)
Frame: buttonFrame(src=mmrFunctions.asp)
Frame: displayFrame(default is src=blank.asp)
Frame: resultsFrame(src=blank.asp)
Local drive
Server
uphandler.asp(uses aspSmartUpload)
downhandler.asp(uses aspSmartUpload)
no
yes
Data transfer
Note: the target for all document displays is Frame: displayFrame contained in mmrFrames.asp
Note: the target for all document displays is Frame: displayFrame contained in mmrFrames.asp
mmrPrint.aspNEW WINDOW
LOGIN
Login errorlogin.asp
Page 213

control.
Secondly, a server service log-in further validated users; and pointed them to specific folders
where they had appropriate rights to create and manage their patient documents. The user
name and password were set by the researcher; and all security and privacy details were
discussed with participants. Further detail about security; and the log-in screens seen by the
users are contained in Appendix P.
Once users had successfully logged-in, they were presented with the browser view shown in
Figure 6-18, showing the options available to them.
The different ASP pages of the service are now described in the following subsections and, in
keeping with the intention of brevity used throughout this thesis, the fine detail, including
source code, is confined to appendices.
6. 5.3.2 Server pagesSelecting the [Open Document Viewer] option resulted in the display of the page shown in
Figure 6-19. This page was essentially the same as the VB browser form, showing function
buttons at the top to: list patients, add new patients; open patient files; and close the document.
The only difference between this and the VB browser was the document printing button
available on the VB viewer, which was located differently on the server service, i.e. on the very
Figure 6-18: Server options after log-in
Page 214
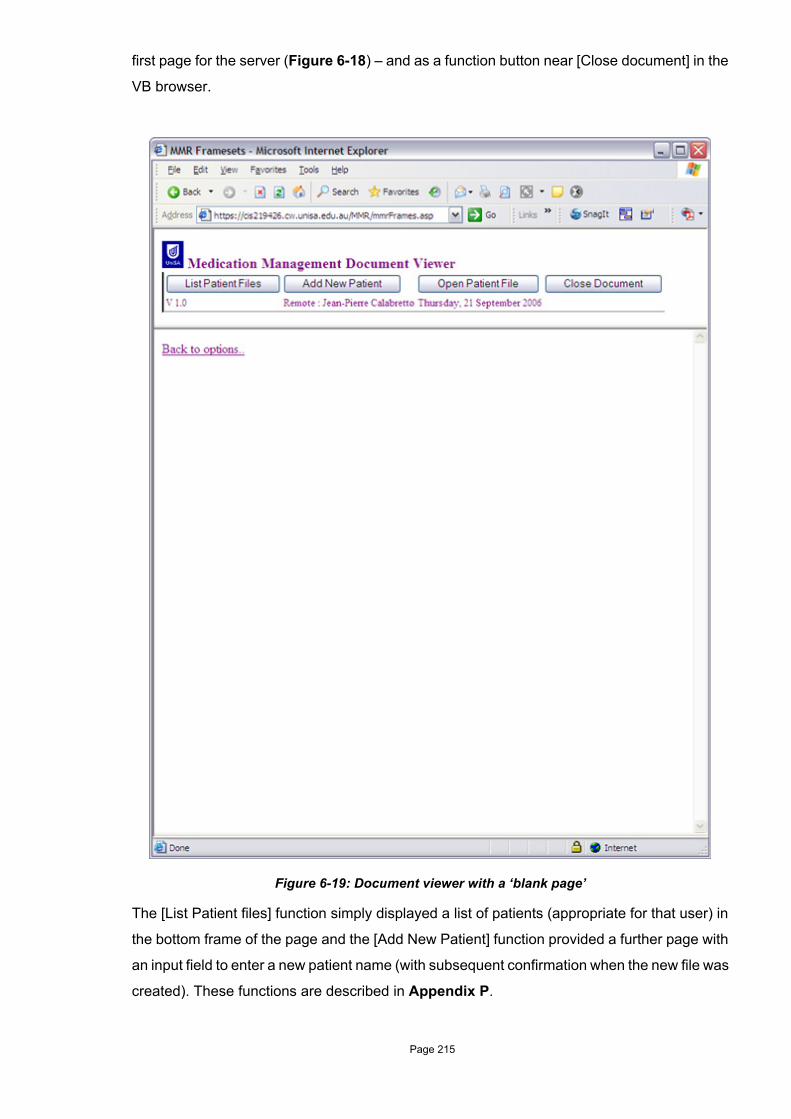
first page for the server (Figure 6-18) – and as a function button near [Close document] in the
VB browser.
The [List Patient files] function simply displayed a list of patients (appropriate for that user) in
the bottom frame of the page and the [Add New Patient] function provided a further page with
an input field to enter a new patient name (with subsequent confirmation when the new file was
created). These functions are described in Appendix P.
Figure 6-19: Document viewer with a ‘blank page’
Page 215

The [Open Patient File] function displayed the page shown in Figure 6-20.
The list of patients available to the user was shown in the left-hand frame so that users would
not need to remember what the patients they had in their list. Typing the name of the patient
in the input field and clicking on [Open document] would consequently display the appropriate
patient document in the bottom frame – shown in Figure-21.
Figure 6-20: Open patient document
Page 216

The [Close Document] function caused the document in the bottom frame to be replaced with
a ‘blank page’ to bring the user back to the view displayed in Figure 6-19. As with the VB
browser implementation, the document could be closed on the server without saving changes
that had been made to the information contained within it. Therefore the [Close Document]
option also displayed a confirmation message (using a simple VB Script message form) to
remind the user to save any changes to the document before proceeding.
Figure 6-21: The patient document displayed on the server
Page 217

By using the approach of ‘duplicating’ the features of the VB browser in the server
implementation, the researcher was able to provide a similar ‘look and feel’ in both
environments (as much as possible). Therefore, although some of the ‘surroundings’ of the
document would have to be different, the digital document itself would always be displayed in
the same familiar way for users.
The process of printing a paper copy of the digital document began with selecting the [Prepare
document for printing] choice on the Options page (Figure 6-18); and this displayed the page
shown in Figure 6-22.
Entering the patient name and clicking on [Get document] would call the ASP procedure to
cause the XSL transformation of the appropriate patient XML file and send the HTML output
to a new (IE) browser window instance. This window is shown, tiled over the calling window in
Figure 6-23.
Figure 6-22: Print patient document from the server
Page 218

The HTML report output could then be checked for accuracy by pharmacist and then printed
using the local Microsoft Windows® printing options available on the computer. The XSL
transformation process was a very quick and efficient way of generating a report and, since the
same XSL stylesheet was used for both the VB viewer and the server, the 'same' report would
be seen by users – ensuring further consistency.
To exchange patient files between the server and local PC/notebook, users could use the
[Retrieve document from the server] and [Send document to the server] functions on the
Options page. For these functions, the researcher used some public domain VBScript code –
Figure 6-23: HMR report output in new browser window
Page 219

smartASPUpload (http://aspzone.com/blogs/john/archive/2003/07/03/160.aspx) – which had
the advantage that, in addition to using a procedure which had already been tested, this also
saved considerable development and testing time. An example of [Retrieve document from the
server] is shown in Figure 6-24.
6. 5.3.3 Summary of the technical changesIn summary, the researcher did not implement all changes to the document suggested during
prototype testing, as some conflicted with the intention of providing a simple model containing
essential information elements. Other changes were outside the scope of the project and a
further group were too difficult to implement. To reiterate, as this project was a proof of concept
seeking indicative data about usefulness, implementation complexity was kept to a minimum,
rather than seeking to implement a fully featured system.
Figure 6-24: Save patient file locally
Page 220

A major undertaking for the researcher was to provide the ability to use the digital document
on-line, allowing an effective means of communicating the medication management document
between GPs and pharmacists. The combination of the server service and the ability to work
locally provided flexibility and allowed adaptation to GPs' or pharmacists' working styles – this
allowed the medication management document to be truly portable.
Only one potentially serious problem was experienced by the researcher during the
development of the server service – a sudden and debilitating failure in which the XForms
document could not display dynamic components (such as date objects). This was caused by
security patch updates for IE, provided by Microsoft. This problem is not detailed in this
chapter, but is mentioned by the researcher as a note of caution for those relying on widely
used applications (i.e. IE) to behave consistently.
6.6 Chapter summaryThis chapter reported the benchtop testing phase of this project, where the researcher took the
information model developed for the hospital context and assessed it for community use by
prototype testing by HMR pharmacists. The intent was to answer the research question:
C. What are the differences in the community environment that affect the approach?
The strategy used to answer this question was to investigate how medication-related
information was used by HMR pharmacists through the data triangulation of a combination of
questionnaires/interviews, work practice observations, document analysis, prototype testing
and a focus group.
Although the goals of HMR pharmacists for medication management and patient care were
similar to those of their hospital colleagues – medication optimisation and safety – this group
had a more holistic approach to patient care. Efforts were concentrated on ensuring patient
self-management, education; and improvement in the quality of life. In fact, the quality of life
for patients was often considered to be a more important issue than the management of
patients' medications or disease.
Some of the themes that arose in the hospital context were also relevant in this context.
Information use by pharmacists was characterised by a critical reliance on the GP – the result
was a great deal of missing information. The flexibility of the information model to cope with
this information lack was thus even more important. Notwithstanding the addition of the
necessary information elements for the community context, the good fit of existing information
Page 221
components to HMR pharmacists confirmed to the researcher that the information needed to
exist at different levels of granularity.
In contrast to the hospital situation, information seeking by conversation was rare in the
community context, increasing the importance of, and reliance upon information provided by
the referral document – a difficult dilemma. This also raised the issue of relationships with GPs
and how this affected the attitude towards information seeking behaviour.
Although time constraints did not emerge here for pharmacists, they perceived lack of time to
be important for GPs' ability to deal with the HMR report – and for any subsequent feedback
the pharmacist might receive. This issue supported the notion that an artefact with
summarised, relevant patient-related information which was appropriate for hospital use could
also be relevant here for use by the GP.
Against the background of the scarcity of appropriate information, the significant reliance on
personal knowledge by pharmacists during HMRs (and specific training for this role) suggested
that they were experts within their own context. This suggests that the hospital-based
approach of an essential information model to complement the use of personal knowledge is
also appropriate in this context.
As well as the lack of availability of decision support tools in this scenario, another important
theme that emerged was the general lack of technology use by pharmacists in the HMR
process. Although pharmacists were willing to consider the use of technology, the researcher
considers that the 'technology-poor practice' in the community signals the need for a paradigm
shift, but also has implications for what technology approach would be useful.
The last theme to emerge, but one which was of significant importance to design and
implementation strategies, was that of the 'viewpoints' of professional practice tools. The digital
document and its intentions were fundamentally different to those of the GP desktop systems
and the current pharmacy dispensing systems – the quest for a shareable, current medication
record does not fit well with the design approaches of these existing systems. This mismatch
of intentions poses a significant issue for integration of the digital document and these
systems.
From the perspective of the information model, the hospital medication elements were a
relatively good fit, with a few changes. The major changes to the model were additions of
patient-related information elements, in particular, the reasons for referral and supporting
patient physical information (e.g. falls etc.). These are information elements that are generally
Page 222

available to hospital pharmacists from patient case notes or other health professionals. So in
a way, these extensions to the model reflects a need for the same type information by
community and hospital pharmacists, although the acuity of the patients has an effect on what
this information might be – for a hospital patient this may be about a stroke suffered by the
patient, but for a community patient it may be about the management of chronic pain. An
important change to the digital document was that the researcher made ‘context-aware’ –
based on whether it was being used by the GP for referral, or pharmacist for the HMR – an
important step towards supporting individual use.
This chapter has discussed and analysed the changes to the hospital-based information model
after testing by HMR pharmacists. What the artefacts of this project – the information model
and the digital document – now required were testing in actual use.
The field studies which assessed the suitability of the community-aware model, the ability of
the digital document to support information sharing; and any impact on the HMR process are
described in Chapter 7.
Page 223

Chapter 7
Evaluating the digital document: field studies
7.1 IntroductionChapter 6 discussed the benchtop testing by Home Medication Review (HMR) pharmacists
which laid the foundations for modifying the hospital-based information model and XForms
prototype to suit a community-based context. The benchtop testing phase also further explored
the questions raised in the hospital scenario and sought answers to some more focused
questions about the use of technology for HMRs.
This chapter describes Part 2B of the project, the third and final iteration of the investigation
which evaluated the digital document prototype. The empirical research undertaken in this
phase provided the answers to the last three research questions.
D. Can our intervention improve safety, quality and efficiency?
E. What is the contribution of the information model?
F. What is the contribution of the technology artefact (digital document)?
These questions were answered by field testing the digital document as an intervention into
HMRs carried out in the community. This chapter reveals how the digital document was used
by pharmacists and General Practitioners (GPs); their impressions of the digital document; the
impact of the intervention; and the roles played by the information model and digital document
in the intervention.
The full analysis of these field studies is reported in Appendix X. Additional forms the
researcher needed to develop during the field study – a GP practice-specific patient consent
forms; user log-in guide; and a patient data collection form – are shown in Appendix Y.
As with the previous data chapters, the full technical aspects are described separately in a
number of appendices summarised in Table 7-1.
Page 224

This chapter is structured as follows:
• how the data were gathered is reported in Section 7.2
• a structured analysis of the data is presented under themes, consistent with the previous
two chapters, together with a report of field use and an evaluation of the intervention in
Section 7.3
• Section 7.4 discusses the changes that occurred to the information model as a result of
the field studies
• the impacts of the field studies on the digital document and server service are discussed
in Sections 7.5; and
• the chapter is summarised in Section 7.6.
7.2 The data gathering processThe data gathering process was considerably more varied during this phase of the research
than was the case for either of the two previous scenarios. For this scenario, the enrolment
process was considerably longer and more complex; and the data sources were more diverse.
Further, there were issues which affected both the success of enrolment and the collection of
data. Consequently, enrolment, data sources; and the issues which had an impact on the
conduct of this phase of the project are discussed separately in the following subsections.
7. 2.1 Enrolling the participantsPrior to the recruitment process, potential pharmacist participants for the field studies were
identified through the group of pharmacists involved in the previous benchtop scenario and
through personal communication with Pharmacy HMR Facilitators for the Divisions of General
Practice.
The recruitment process began with the researcher contacting the potential pharmacist
participant. As pharmacists agreed to participate, they were asked by the researcher to
nominate relevant GPs who might also be interested in participating in the field study (the GP,
in turn, was able to suggest still further pharmacists). This process resulted in an informal
'network' of participants.
Table 7-1: Technical appendices
Appendix Content
Z Full technical and development details.
AA XForms document code.
AB Patient XML file structure.
AC XSL (report) code.
Page 225

The researcher organised formal, face-to-face meetings with GPs to assess their interest in
participating in the field study, as well as to agree on how patient confidentiality (and server
security) would be addressed. This meeting also served to obtain agreement on the process
for their involvement and on how continuing communication between GPs and the researcher
would be handled.
The field test also involved two Hospital Outreach Medication Review (HOMR) pharmacists,
once again initially recommended by a pharmacist previously enrolled in the benchtop testing
phase; and then these pharmacists were also approached directly by the researcher. The
involvement of HOMR pharmacists was a serendipitous, but valuable, event, because the
HOMRs provided a unique opportunity to test the digital document’s effectiveness with
medication-related information concerning hospital patients about to be discharged into the
community.
It is pertinent to briefly describe the HOMR process at this point in the chapter, before any
analysis of the digital document use in that setting. The HOMR project was a component of a
larger Chronic and Aged Care project, funded by the Australian Federal Government. The aim
of the HOMR project was to facilitate an HMR for individuals who were elderly, or who had
chronic illness, soon after hospital discharge (the HMR process was discussed in Chapter 6).
These hospital patients were targeted because they were believed to be at special risk of
adverse events after hospital discharge. The HOMR project aimed to incorporate additional
HMR referral information into an existing Medication Transfer Summary form (MTS) already
developed by the hospital pharmacy; and send it to the GP, who could use the document as
the basis for an HMR referral. Part of the HOMR pharmacists' role was to liaise with the
patient's GP and ensure there was an accredited pharmacist who could provide an HMR in an
appropriate time frame (1-2 weeks after discharge).
In summary, then, from a total of 10 pharmacists and 8 GPs contacted as potential participants
in the field studies, 6 pharmacists and 5 GPs were finally enrolled. Four of the 6 pharmacists
were involved in the HMR process; and 2 were part of the HOMR project. The recruitment
history (for both GPs and pharmacists) is summarised in Appendix X.
Patient enrolment was usually handled by GPs – but some patients were also enrolled by
pharmacists (with the approval of the patient's GP). A total of 47 patients were enrolled in the
field studies.
Page 226

7. 2.2 Data sourcesData for this phase of the research came from five primary sources:
• field use of the digital document by pharmacists and GPs;
• digital document testing by HOMR pharmacists in the hospital discharge setting;
• interviews with GPs;
• a detailed examination of relevant, de-identified patient data, medication review referrals
and reports – complementing the document analysis which was done in the hospital-
based and bench-top testing phases of exploration; and, finally,
• a focus group conducted with pharmacists at the end of the field studies, to enable a
deeper exploration of the issues arising from prototype use.
Although the field studies were the principal test of the digital document intervention, further
sources of data emerged during the field activities (in addition to the sources of data mentioned
above), including: attendance by the researcher at accredited pharmacists' meetings;
conversations and meetings with various individuals involved with, or interested in medication
reviews; and logs of telephone calls and email communication.
In keeping with the Design Research method, the researcher retained data from all interactions
with participants (the complete data set for this scenario is shown in Table 7-2). The tools used
for data collection during this research phase are contained in Appendix G.
Not all these data, of course, contributed directly to the evaluation of the model or digital
document. They did, however, add to the researcher's general understanding of the
medication management environment; and the likely role of this technology intervention.
These data sources are described in the following subsections.
7. 2.2.1 Field use of the digital documentData resulting from field use of the digital document by pharmacists and GPs was collected
from the individuals concerned by the researcher, each time the digital document was used for
Table 7-2: Summary of data sources from the field studies
Data source
Field use of the digital document by pharmacists and GPs.
Hospital Outreach Medication Review (HOMR) testing.
General practitioner interviews.
Patient-related data (HMR referrals and reports).
Accredited pharmacists’ meetings.
Other incidental conversations and meetings.
Logs of telephone calls and email communication.
Pharmacist focus group.
Page 227

an HMR case: in some cases pharmacists notified the researcher the digital document had
been used; while in those cases where the researcher acted as the 'interface' between the GP
and the pharmacist, the researcher followed-up the pharmacist to check on usage. Data were
collected for a total of 28 HMRs. One pharmacist also suggested trialling the digital document
in an Aged Care Facility for Residential Medication Management Reviews (RMMRs), resulting
in additional data collection for 3 RMMRs. There was a great deal of variability in the way data
were collected from pharmacists and GPs – this is discussed in Sub-section 7.2.3.
7. 2.2.2 HOMR testingData collection for the HOMR scenario was very straightforward compared with the HMR
setting and consisted of a meeting with the HOMR pharmacists where the researcher sought
feedback about their experiences with the digital document. The value of testing the digital
document within the HOMR process was that the document had already been modelled for an
HMR referral – i.e. it was ‘ready’ to be used in the community. This scenario resulted in the
testing of 16 HOMRs.
7. 2.2.3 General Practitioner discussions and interviewsThe meetings with GPs provided the researcher with a range of data including data which was
important to the conduct of the project, such as how patient confidentiality and data security
needed to be addressed; and how the researcher would communicate with the GP during the
project. However, the data that emerged from these meetings also pertained to: GPs’ overall
impressions of the project; views on current HMR practices (including problems and potential
solutions); feedback on the digital document prototype (demonstrated either on a notebook
computer or as a paper example based on the opportunities afforded to the researcher); and
business and other issues that impacted on HMR practices.
7. 2.2.4 Patient-related data used for the trialPatient-related data collected by the researcher included paper copies of HMR referrals and
reports and, where possible, copies of the corresponding XML files from participants'
computers. These patient XML files were generated by the digital document when participants
used the digital document to enter referral information, or information for a report. Patients
were de-identified by the pharmacist or the researcher, as previously agreed with the GP and/
or pharmacist.
The paper HMR referral document identified the principal information provided by the GP. In
addition, the difference between the information contained in the GP's paper referral and the
pharmacist's XML referral file provided insight into what information was, or could be, entered
into the digital document. The GP's referral document also revealed what information was
missing and provided a basis for identifying which decisions the pharmacist might have made
in deciding which information from the document would be used.
Page 228

The researcher used the same strategy of collecting all possible paper documents in the case
of reports as well (i.e. both paper documents and XML files) to ensure that the information
entered into the digital document following the HMR reflected what had actually been sent to
the GP. This ensured there were no additional hand-written entries on the paper copy reports
sent to the GP, or to observe if additional information had accompanied the paper report (e.g.
information pamphlets). The researcher also anticipated that using XML files would allow
easier comparison of information elements used between patients – and this was the case.
7. 2.2.5 Accredited pharmacists’ meetingsAttendance at these meetings provided the researcher with valuable insights into both the
HMR process as well as identifying issues common to HMR pharmacists. The researcher was
first invited to attend a meeting on HMR software availability in June 2004, well before the
commencement of the field studies themselves. This led to subsequent attendances at (6)
other meetings relevant to the project which were presentations on HMR-related topics
(Quality Assurance featured highly) and contained case studies of HMRs as practical
exercises for the HMR pharmacists. One meeting was attended by a GP and another by a
clinical pharmacologist – and these two meetings provided further valuable data on doctors’
perceptions of the HMR process.
7. 2.2.6 Other conversations and meetingsOne serendipitous outcome of the project was the networking with other pharmacists and
individuals interested in the project. In addition to providing material which confirmed the
project's approach, these encounters were also excellent sources of ideas for further research
– particularly important for verifying the value of the project – for example:
• interest in the project's modelling approach by a Division of General Practice HMR
project group
• meetings and conversations with Pharmacist Facilitators (endorsing the direction of the
project)
• interest from the Head of a Clinical Pharmacology Department at a metropolitan adult
hospital which is leading a discharge project involving cardiac patients; and
• meetings with lecturers at the University of South Australia's School of Pharmacy and
Medical Sciences, who were interested in potential applications of the digital document.
7. 2.2.7 Logs of telephone calls and email communicationTelephone calls were normally used by the researcher to arrange meetings, follow-up on
previous meetings or to discuss practical aspects of the project with participants. The log of
project-related telephone calls contained primarily administrative data and is therefore not
discussed explicitly in this chapter – although any information obtained from telephone calls
which was useful to the project has been incorporated into other discussions
Page 229

Email communication with participants was used by the researcher wherever possible, not only
because this provided a written record of communications, but also because, as an
asynchronous negotiations medium, it was far less intrusive into the participants' busy
schedules than, for example, telephone calls or face-to-face meetings. As with telephone calls,
the record of emails is not reported here because of its size and nature but, as with the
telephone log, any information useful in the context of the project is included in other
discussion.
7. 2.2.8 HMR pharmacists’ focus groupThe focus group, which ran for approximately 1.5 hours, was held at the end of the field study
and was attended by 3 of the 4 HMR pharmacists. A summary of the focus group findings was
circulated to all participants for verification and to ensure the major issues had been
adequately captured. The one pharmacist who was unable to attend the focus group was
subsequently interviewed by the researcher, enabling him to comment on issues from the
focus group, as well as providing his feedback on the prototype testing more generally.
Although these field studies began with a simple plan for the data gathering process, the many
practice differences of pharmacists and GPs made this process more complex than
anticipated. Some of the issues contributing to this complexity are discussed in the next sub-
section.
7. 2.3 Issues encountered during data gathering
7. 2.3.1 Field studiesBecause of the different HMR practices of GPs and pharmacists, their level of involvement in
the field study needed to be flexible, being based on their level of comfort with the use of the
digital document (and technology in general); and on how they believed this might fit into (or
change) their work practice.
This resulted in a range of different 'paths' for the digital document during the field studies,
depending on whether the server service was used and how the digital document was used –
and, consequently, affecting the quantity and quality of the data available to the researcher
(e.g. where the referral was sent by the pharmacist directly to the researcher, there was no
ability to evaluate the GP's experience of entering data into the digital document).These digital
document paths are summarised in Table 7-3.
Page 230

7. 2.3.2 HOMR testingAlthough hospital environment provided an ideal opportunity to test the server service
(because of the networking and Internet access in place), the HOMR project pharmacists did
not use the server service – stating this was because of time commitments. The researcher
did detect a level of discomfort from one pharmacist about server use, although the reason for
this discomfort was unclear. Perhaps one explanation was that patient information entered into
the server would be stored 'elsewhere' (leading to unvoiced concerns about patient privacy).
Consequently, the VB viewer was installed on two PCs within the pharmacy department; and
testing by the pharmacists occurred quickly after this.
7. 2.3.3 Meetings with GPsIt has already been mentioned that differing requirements between one general practice and
another prevented complete data collection, but a number of other issues which arose during
meetings with GPs affected the conduct of the project.
One minor issue (easily resolved) was that most GPs required a patient consent form for use
in their practice – these forms are shown in Appendix Y.
Table 7-3: The digital document paths in the field studies
GP and Pharmacist IDs
GP1 and P1 GP1 and P2GP faxed referral to pharmacist who entered detail into
notebook computer. Report done on notebook and paper copy faxed back to GP.
(GP1 did not want patient data entered onto server)
GP faxed referral to pharmacist who entered detail into notebook computer. Report done on notebook and paper
copy faxed back to GP.(GP1 did not want patient data entered onto server)
GP2 and P4GP mailed the referrals to the researcher who added them to the server. The researcher added the patient files to the pharmacist’s computer – the pharmacist did not want to use the server directly. The amended patient files were taken from this computer and loaded back onto the server, but a paper report was delivered to the GP by the pharmacists.
The GP did not use any on-line access
GP3 and P1 GP3 and P3
For one HMR patient, GP faxed referral to pharmacist. Pharmacist used local browser to enter referral information and report. Paper copy of report sent to GP by pharmacist. For three ACF patients, the pharmacist entered information for the HMR reports using local browser, and sent paper
copies to GP
GP faxed referral to pharmacist. Pharmacist used local browser to enter referral information and report. Paper copy
of report sent to GP by pharmacist.
GP4 and P4GP emailed the referrals to the researcher who added them to the server. The researcher added the patient files to the pharmacist’s computer – the pharmacist did not want to use the server directly. The amended patient files were taken
from this computer and loaded back onto the server to allow GP on-line access.
Page 231

One theme which has clearly been significant throughout this project is that of time and its
impact on the HMR process. A rather different impact of time was on the conduct of the project
itself. Lack of time was the reason given by 3 of the 8 GPs (contacted as potential participants)
for not participating in the field studies. Using the same justification, only one of the remaining
five GPs used the digital document personally. All five GPs were happy to have their patients
considered for inclusion in the studies although, here again, one GP claimed he was too busy
even to obtain consent from patients (this was to be done by the researcher or the HMR
pharmacist). The main reason for GP involvement at all was their common desire to be able to
help improve the HMR process in any way – for some GPs, the whole issue was about patient
care but, for others, the major focus appeared to be on improving their business processes.
This focus on lack of time also affected the researcher's meetings with GPs. During the field
studies the researcher was acutely aware that GPs expected him to waste as little as possible
of their time, which meant that interviews with GPs were not as valuable to the project as they
could have been. And, although a demonstration of the digital document (on a laptop
computer) had been planned for all GP participants, only two of the GPs ultimately participated
in such a demonstration. In fact, GP-researcher communication always occurred with the
practice nurse who acted as an intermediary, except in the case of one GP with whom there
was direct communication and with whom meetings were of sufficient length to enable
appropriate data collection.
Finally, although a final (exit) interview had been planned for all GPs, this took place only with
one GP in person – though a second GP's practice provided a telephone interview (with the
practice nurse!).
A summary of the researcher’s interactions with GPs and their involvement is shown in Table
7-4.
Page 232

7. 2.3.4 Patient-related dataThe wide variability in HMR practices amongst GPs and pharmacists described earlier meant
that collection of documents (or patient XML files) could not be achieved in a consistent
manner.
For HMRs, a copy of the paper referral was obtained for all (28) patients. There were several
possible avenues for the paper HMR referral documents, each with different implications for
data analysis. The paper referral could be sent:
• to the researcher (this occurred when the researcher was acting as the 'interface'
between the GP desktop system and the digital document – entering the referral
information into the digital document on the server so it could be accessed on-line by the
pharmacist). Where the information was entered into a digital document by the
researcher, it was the same information that was contained on the paper referral;
Table 7-4: Summary of interaction with GPs
GP Practice details / background Summary of interaction Level of
involvement
GP1 Shared practice with Practice Nurse. Site had been compulsory acquired and was in the process of negotiation. Practice was to go ‘paperless’.
GP was very interested in use of technology. No initial interest due to lack of time and no interface to GP desktop system. After first meeting was happy to involve patients and nominated other pharmacists. Did not want patient data stored on project server. Despite much communication with the Practice Nurse (email), no further meetings eventuated due to time commitments.
First meeting.Seven patients.
GP2 Shared practice with Practice Nurse.
Agreed to participate based on no changes to his existing process. Referrals to be sent to researcher by mail to enter into the server service. Nominated local pharmacist. Some communication by email with Practice Nurse. Had final interview.
First meeting and final interview.Five patients.
GP3 Single practice with Practice Nurse.
Meeting with both where they agreed to participate based on current process. Subsequently demonstrated digital document on notebook to Practice Nurse. Communication occurred through Practice Nurse (email and phone). There was confusion about the HMR process at this practice. Final interview unable to be organised.
First meeting with subsequent demonstration of prototype on notebook.Two patients; and additional three patients for RMMR.
GP4 Single practitioner. First meeting with demonstration of digital document; and agreed to participate. This GP had not previously done HMRs. The GP’s notebook was set up for local and server use of the digital document. There were five meetings including the final interviews, and communication occurred with the GP throughout. The GP provided a written evaluation.
Total of five meetings. GP use of the digital document locally and via server. Fourteen patients.
GP5 Shared practice with Practice Nurse. Same practice as GP2.
First meeting with demonstration of the prototype. Agreed to participate based on no changes to existing process; and researcher / pharmacist to obtain patient consent.
First meeting. No patients.
Page 233

• to the pharmacist, in which case data could only be collected by the researcher after the
HMR was completed – so that the (XML) file represented the situation after the HMR, i.e.
it was the report, not the referral. In these cases, there was no opportunity to see what
information the pharmacist had entered into the digital document compared with that
contained in the paper referral. In the case of the (3) RMMRs, there was no paper copy
of a referral, as the GP arranged these by telephone; or,
• not at all, as was the case for the HOMR scenario. For the (16) HOMR patients, there
were only pharmacist-generated (XML) referral files, as the pharmacist was responsible
for generating the referrals.
For HMR reports, both a paper copy and a matching XML file were available for all HMR
patients (in the sole exception, a pharmacist sent additional (paper) drug information material
to the GP).
A summary of all medication review documents collected during field studies is shown in Table
7-5. The numbers in the table represent the number of documents (or files) collected by the
researcher out of the total possible, i.e. the number of patients.
.
These inconsistencies made it impossible to compare 'before' and 'after' information from the
referral and the report. It was possible, however, to analyse which information elements were
missing from the referrals, how often they were missing; and how this might be influenced by
the information sources available to the pharmacist – missing information is discussed in
Section 7.3.1.
Further, the reporting 'style' of the pharmacists did not really change before or after the
intervention – pharmacists used the digital document to prepare a paper-based HMR report
very similar to that they were using prior to the intervention – which prevented the researcher
from evaluating the HMR reports (using the HMR QA form – see Appendix C) with an
independent panel to assess HMR report quality.
Table 7-5: Patient data sources
HMR HOMR RMMR
Paper referral 28/28 NA NA
XML referral file 20/28 16/16 NA
Paper report 3/28 NA 3/3
XML report files 28/28 NA No
Page 234

7. 2.3.5 EmailAlthough email appeared to be the ‘ideal’ communication medium with which to capture
researcher-participant (remote) interactions, email use varied between participant groups and
was not as useful as anticipated.
All pharmacists had access to email, either at work or at home. Email use was not a regular
practice for all pharmacists, however, but was used effectively by four pharmacists.
All GPs had email addresses for their practices, but messaging was usually done by the
Practice Nurse, rather than by the GP. In these cases, it was often not clear whether the
message had actually been received by the GP – for some, therefore, there was still a need
for follow-up telephone calls from the researcher. For three GPs, email was used to deliver
draft patient consent forms. One notable exception – the most technology-aware GP – used
email directly and effectively, both to communicate with, and to deliver patient referrals to, the
researcher.
7. 2.3.6 The focus groupThe focus group had been planned to include both pharmacists and GPs involved in the
project. In the event, however, no GPs were invited to attend the focus group, because time
constraints made it unlikely they would be able (or willing) to do so.
In summary, the data gathering process did not proceed for the project as expected and
compromised the researcher's ability to collect and evaluate (some) data. The final number of
patients cases used to test the digital document was 47, comprising: 28 HMRs; 3 Residential
Medication Management Reviews (RMMRs); and 16 HOMRs. Attention turns next to the
analysis and discussion of this data in Section 7.3. Participants are referred to in this chapter
using abbreviations, e.g. P1 and GP1 for pharmacist one and GP one respectively, to maintain
anonymity.
7.3 Analysis and discussion of findingsAs with the previous two chapters, time and space constraints prohibit the fully detailed
analysis of the material gathered for this chapter. A full analysis is, however, contained in
Appendix X.
The approach to analysis in this scenario was different to that taken in the previous two
scenarios in several ways. Firstly, there were no formal questionnaires to analyse. Secondly,
this phase was designed to observe the effect of the digital document intervention on
medication management as it occurred. Thirdly, the overall goal of this phase of the research
was to determine the contributions of the information model and the digital document.
Page 235

Impressions of these effects were determined as a combination of the more specific feedback
about use of the digital document (and, naturally, the underlying information model); and the
researcher's analysis of the many and varied sources of data.
This chapter once again makes use of thematic headings within which to discuss the results,
as was the case for the previous two chapters. Some themes which emerged in this scenario
were (not surprisingly) the same as those identified in the benchtop scenario. However, the
ability of the researcher to directly investigate the 'other side' of the HMR equation – the GP –
allowed some of these themes to be further developed and revealed others. The themes which
frame the discussion are shown in Table 7-6, where it is clear that both 6.3.10 and 6.3.11 are
new themes.
7. 3.1 Missing informationIt appeared possible the researcher might be able to measure the extent of missing information
in the field studies since, although overall document collection was incomplete, HMR referral
documents were obtained for all (28) patients
A detailed tabular comparison of missing information is contained in Appendix X. The
discussion in this chapter will, of necessity, only summarise this comparison, but some
sections of some tables in the appendix have been reproduced here where they contained
especially important observations.
One particular difficulty for the researcher was attempting to measure whether missing
information was important, i.e. whether its absence was an issue for patient care. For example,
if a laboratory result such as an INR was missing for a patient taking warfarin, it was impossible
to know whether this omission was acceptable because the patient had been stabilised on
Table 7-6: Research themes
Section Theme
6.3.1 Missing information
6.3.2 Information granularity and the language of health professionals
6.3.3 Conversation and communication
6.3.4 Time constraints and summary information
6.3.5 Alerts & reminders
6.3.6 Systems for experts rather than expert systems
6.3.7 A technology-poor practice paradigm
6.3.8 The ‘viewpoints’ of professional practice tools
6.3.9 Pharmacists’ perceptions of GPs in the HMR process
6.3.10 The Practice nurse
6.3.11 Complementary medicines & Over-the-counter medication
Page 236

warfarin for some time (if the patient had only recently commenced taking warfarin and there
was no recent INR, it was clearly both relevant (and important) that this laboratory value be
provided). To resolve this problem, the researcher introduced a number of categories to
describe the presence of information elements, including:
• yes – information was entered
• not entered (ne) – there was a heading in the referral source for this information, but no
information was provided. This information may not be relevant for the patient.
• no – no heading for this information in the referral source, so that no information could be
provided
• to follow – this was information which could be conveyed via other sources (e.g. the
referral letter from the GP)
• NA – not applicable (e.g. a referral reason in the RMMR report).
Some information on the referral could be implied – sex, by 'Mr.' or 'Mrs.' (although not where
the patient's title was 'Dr.' or 'Prof.'); and medication route from the type of medication product
(e.g. a tablet would generally suggest the oral route of administration). One GP also included
additional information elements which were not part of the information model (e.g. pulse rate).
The discussion of some aspects of information availability follows in the next sub-sections,
based on the major information categories of the information model, i.e. referral, personal,
treatment, medication; and laboratory information.
As described during the discussion of bench-top testing in Chapter 6, specific reasons for
referral (Table 7-7) were infrequent and, even when provided, were still framed in Health
Insurance Commission (HIC) terms (i.e. medication risk factors). Of course, there may not
have been any specific issues of concern for these patients. For HOMRs, the hospital
admission was reason in itself for an HMR follow-up in the community, although pharmacists
did list other specific patient issues as well. For the RMMRs, a review was a routine event, so
that a specific referral reason was not required.
Table 7-7: Comparison of missing information in referral documents – referral information
Information type (document page)
Information element
HMR (28) HOMR (16) RMMR Reports (3)
Referral information
referral description
yes (standard reasons) - 5/28yes, free text - 7/28to follow - 5/28no - 11/28 (10 from same GP, but perhaps later via referral letter).
yes - 15/16ne - 1/16Individual reasons (for admission) as well as the summary above.
NA
Page 237

A substantial amount of personal patient information could be missing (see Table 7-8); and the
use of certain terminology could create uncertainty about the information which had been
provided. In the case of allergies, for example, the term 'none known' was often used – which
is not at all the same as 'none': 'none' means that this patient has no allergies; but 'none known'
does not make it clear whether allergies have been ruled out or not. Weight was another item
which was also frequently missing. This was problematic because weight is the basis for
checking doses and performing a number of important calculations (e.g. BMI). The tables also
show that for some missing HMR information (e.g. weight, height), there appeared to be a
pattern based on the source of the referral information – this is discussed in detail in Section
7.3.8 (the 'viewpoints' of professional practice tools).
HOMR pharmacists, in theory, had access to any hospital-based information they required. In
reality, however, these pharmacists could experience the same missing information issues as
their colleagues described in the hospital scenario (see Chapter 5) but because they did not
need to make prompt decisions about therapy, they had more time to find the missing
information (in fact, these pharmacists made no mention of missing information). Nonetheless,
certain information was only entered if the pharmacist felt it relevant for the patient, e.g. a
serum creatinine level would only be entered if there was an issue about renal function. So,
although some information appeared to be missing, it was possible these lacunae were
deliberate omissions by the pharmacist.
Page 238

.
Table 7-9 provides a summary of missing treatment-related information within the different
types of medication management review. The reporting of treatment information for HMRs is
actually misrepresented in this table, however, because treatment information could be
contained under either 'active problems' or 'history', depending on where GPs had initially
entered this information within their desktop system (over which the trial had no influence).
Only 4 HMR referrals listed information under both the active problems and history heading –
giving a true indication of the patient’s disease status. One referral contained no treatment
information at all – providing the pharmacist with no basis against which to judge the
appropriateness of the medication prescribed for the patient.
Table 7-8: Comparison of missing information in referral documents – personal information
Information type (document page)
Information element
HMR (28) HOMR (16) RMMR Reports (3)
Personaldob(date of birth)
yes - 21/28no - 7/28 (these were not supplied with an alternative age below).
yes - 8/16: ne - 8/16 yes.
age NA - 21/28 (as dob was entered)no - 7/28
age - 5/16 (de-identified) ne - 11/16
NA.
sex no - 28/28, on lab. reports if they were provided
yes - 12/16: ne - 4/16 yes.
weight yes - 7/28: no - 21/28 yes - 6/10: ne - 10/16 yes
height yes - 7/28: no - 21/28 yes - 4/16: ne - 12/16 ne. As above.
BP yes - 7/28: no - 21/28 yes - 12/16: ne - 4/16 ne. As above.
Se creat yes - 8/28no - 20/28
yes - 8/16ne - 8/16
ne.As above.
allergies yes - 28/28(many were ‘none known’).
yes - 10/16ne - 6/16
ne.As above.
ADR (warnings)
yes - 5/28: no - 19/28ne - 4/28
yes - 4/16: ne - 12/16 yes. Stated ‘nil known’ in all cases.
recreational subs
yes - 12/28no - 16/28
ne - 16/16 ne.
Physicalfalls no - 28/28 yes - 1/16: ne - 15/16 ne.
cognition yes - 7/28: no - 21/28 ne - 16/16 ne.
memory no - 28/28 ne - 16/16 ne.
language, dexterity, vision, hearing, swallowing
yes - 7/28no - 21/28
ne - 16/16 ne.
Page 239

A medication list (Table 7-10) was the information provided most consistently on the paper
referrals – although even this was missing on two occasions!
The source of medication information was a 'dump' from the GP desktop system output under
four headings in the report:
• drug name (actually a product name from the medication list available within the GP
desktop system)
• Ltd.Elapse (the purpose of this is unknown, as nothing ever appeared under this
heading)
• Strength (this could duplicate information contained in the drug name); and
• Dose/Freq./Special (this heading concatenated all dosing frequency and additional
information – an example of the information that could be listed under this heading is: '2
inh q.4.h. p.r.n.'). These information components reflected the abbreviated pick lists of
instructions available within the GP desktop system.
Although pharmacists tended to separate 'regular' from 'when required' medications in HMR
reports, these divisions were never used in the referrals they received; and very little social,
family, or compliance information was provided to pharmacists.
The HOMR entries were more detailed because information was tailored by pharmacists and
this information often included additional instructions – both with Latin abbreviations, as well
as with additional English phrases e.g. '2 puffs inh bd rinse mouth after dose and inhale via
spacer'.
Table 7-9: Comparison of missing information in referral documents – treatment information
Information type (document page)
Information element
HMR (28) HOMR (16) RMMR Reports (3)
Treatmentactive problems
yes - 13/28: no - 14/28ne - 1/28
yes - 15/16: ne - 1/16 ne.
history yes - 18/28: no - 10/28Some used history for all problems.
yes - 15/16: ne - 1/16 ne.
Page 240

Laboratory information (Table 7-11) was not provided regularly by the GP and, where it was
provided, was included in a separate paper document printed from the laboratory reports
stored in the GP desktop system. HMR pharmacists tended not to add any laboratory values
(from the paper sources) into the digital document for reporting back to the GP, so that
laboratory values seldom ended up in the digital documents. By contrast, the HOMR
pharmacists did enter laboratory values when they were considered important for
communicating to others (which was precisely the reason for including this section in the digital
Table 7-10: Comparison of missing information in referral documents – medication information
Information type (document page)
Information element
HMR (28) HOMR (16) RMMR Reports (3)
Immunisationstetanus yes - 9/28: no - 11/28
ne - 8/28yes- 2/16: ne - 14/16 ne.
flu yes - 17/28 (some were extensive records).no - 11/28
yes - 2/16ne - 14/16
yes - 1/3ne - 2/3
pneumococcus
yes - 17/28: no - 11/28 yes 2/16: ne - 14/16 yes - 1/3: ne - 2/3
immun. Dates
yes - 16/28: no - 12/28 ne 16/16 yes - 1/3: ne - 2/3
Medications-regular
date no - 28/28 two had no medication list at all.
yes - 6/116ne - 10/16
no.
generic yes - 22/28: no - 6/28 yes - 15/16: no - 1/16 yes.
brand yes - 22/28: no - 2/28 yes - 14/16: no - 2/16 yes.
dose yes - 26/28: no - 2/28 yes 16/16 yes.
route yes - 6/28: no - 3/28no (but implied from medication form) - 19/28
yes - 16/16 yes.
frequency yes - 25/28: no - 2/28no (but implied) - 1/28
yes 16/16 yes.
instructions yes - 6/28: ‘mdu’ - 11/28no - 11/28
yes - 14/16: no - 1/16ne - 1/16
no.
indication yes - 2/28: no - 26/28 yes - 14/16: ne - 2/16 no.
duration yes - 1/28: no - 27/28 yes - 13/16: ne - 3/16 no.
Medications-prn.
no specific prn list. yes - 7/16: ne - 9/16 ne. One patient did have prn medication.
HistoriesSocial yes - 3/28: no - 19/28
ne - 6/28ne - 16/16 ne.
Family yes - 2/28: no - 19/28ne - 7/28
no - 16/16 ne.
Compliance no. yes - 9/16: ne - 7/16 ne.
Page 241

document).
In summary, missing information was as serious a problem as originally anticipated, with a
clear reliance on the GP (often with an unsuccessful outcome). Pharmacists, however,
appeared to be resigned to the fact that this would occur and would carry out the review despite
any missing information – there was little evidence of pharmacists contacting GPs to fill in
information gaps in their referral documents. A printout of the dispensing history from the local
pharmacy was, however, used to supplement medication information if required.
The focus on chronic disease management also seemed to alter the importance of missing
information because, as these patients were not acutely unwell, pharmacists assumed that the
missing information would be unlikely to have much immediate impact on the patient's
management. Since, although this was a small study, no cases of patient misadventure were
reported, missing information in a community setting may indeed be less important than in the
hospital environment.
An interesting missing information pattern in relation to the report used from GP desktop
system is discussed in detail in Section 7.3.8.
As the HMR system exists now, there is no incentive for GPs to have complete information in
their desktop system – pharmacists will simply cope with this lack and come back to the GP if
there are any major problems. GPs' demand for a summary of issues (despite their
consistently vocalised desire for a complete, current medication record) suggests that this
situation is unlikely to change.
Nevertheless, pharmacists saw an opportunity to collect a complete set of information by
sharing the digital document with GPs (and other pharmacists involved in the patient’s care),
believing that this would allow better decision-making about the patient. Overall, this problem
of missing information further reinforced the notion that the document could only suggest and
support inclusion of information elements, not mandate that health professionals use them.
Table 7-11: Comparison of missing information in referral documents – laboratory information
Information type (document page)
Information element
HMR (28) HOMR (16) RMMR Reports (3)
Laboratorydate yes - 8/28: no - 20/28 yes - 10/16: ne - 6/16 ne.
item yes - 9/28: no - 19/28 yes - 16/16 ‘no results’ - 3/3/
result yes - 8/28: no - 19/28ne - 1/28
yes - 10/16ne - 6/16
ne.
Page 242

7. 3.2 Information granularity and the language of health professionalsThe issue of information granularity – the need for the provide information elements at different
levels of detail to support the pharmacists' natural work processes – was raised in the hospital
phase (Chapter 5) and confirmed in the benchtop testing phase (Chapter 6). The researcher
believes the need for information elements at different levels of granularity was further
confirmed by the field studies, although this confirmation was more implicit than explicit. The
GPs accepted the content of the digital document without further suggestions for changing the
nature of the information elements – and both the pharmacists and the single GP who made
use of the digital document directly commented on the appropriateness of the information
elements which the digital document provided.
A further factor emerged during the field observations. Pharmacists and GPs commonly used
abbreviations, acronyms and personal 'shorthand' when entering diseases and symptoms, or
as part of the clinical narratives entered into referral or report documents (as well as the
common use of Latin abbreviations for directions for medication use). This, of course, also
happens in the hospital setting but, as the clinical narrative text itself was not the subject of
investigation, this issue was not as apparent as it was in the field studies setting.
Examples of clinical narratives and expressions used during field studies included:
• In HMR referrals from GPs
‘Breast cancer (left), radiotherapy/axillary lymph node clearance/tamoxifen – 2000’
‘Necrosis – infection, post radiotherapy’
‘Scaphoid Fracture (left), got lateral epicondylitis from POP’
• In HOMR referrals (from a pharmacist)
‘Lipid studies were suboptimal – consider introducing a statin, if an appropriate trial of lifestyle
and diet modification does not produce improvements’
• In HMR reports
‘CCF, IHD, PCI to LAD’
‘It was also noted that Ostelin is on the medication list. Mrs W's free Calcium is at the lower
end of normal i.e. 1.11 (1.10-1.25). On this basis, it may be worth considering the addition of
Calcium.’
There is clearly the possibility of supporting the use of acronyms for diseases (e.g. CCF)
through dictionaries, or using terminologies (such as SNOMED CT1). This possibility is unlikely
to be successful, however, if GPs (or pharmacists) need to navigate through enormous
terminology lists to locate the clinical terms that they require (and if this processing power
1. SNOMED CT® is a clinical, computerised language designed to enable unambiguous communication between health care institutions and professionals.
Page 243

existed in GP’s desktop systems).
Another issue was the use of free text fields: both HMR and HOMR pharmacists commented
positively on this feature, as it allowed flexibility in terms of what – and how much – information
could be entered into the document. Free text fields were considered more desirable than
drop-down template text for reporting, because drop-down fields can: make reports appear too
similar, do not easily allow pharmacists to express their clinical judgement; and could direct the
nature of the report in a manner which was not intended.
The use of passages of text thus presents some particular problems for the design of decision
support tools. Firstly, how could structured lists be used to compose meaningful (and readable)
clinical narrative. Secondly, the information exchanged between these health professionals
requires a knowledge of other patient details – the patient context – if it is to be meaningful to
health professionals. Meaning occurs now through health professionals using their commonly
shared and understood ‘language’.
The researcher also gained the impression from pharmacists' meetings that the amount and
nature of the information to be provided back to the GP should include whatever is important
– this leaves the notion of any data structure quite open. It is very difficult to imagine how more
granular information elements would support pharmacists' requirements. Moreover, it is
foreseeable that any structure imposed by decision support tools on these ‘conversations’ will
be met with resistance from health professionals.
In summary, while providing support to the findings from the first two phases of the research
that there is a need to support the information granularity which best fits with the information
use of the health professionals involved in medication management, the field studies made it
clear that the information communicated by the digital document should be couched in the
everyday 'language of practice' of health professionals. The researcher therefore considers
that the dilemma facing technology which attempts to support health professionals is an
impasse resulting from the need for data categorisation to underpin decision support (e.g.
alerts) and allow information to be communicated 'seamlessly' between technology systems
(enabling inter-connectivity) – while simultaneously providing humans with simple and flexible
support to complement their work processes, without losing the high-level richness they
require in their information.
Information provided back to the GP should be ‘whatever is important’
Page 244
7. 3.3 Conversation and communicationThe opinion of the HMR pharmacists in this phase echoed the views of the pharmacists
involved in the benchtop testing phase – that issues such as GP-pharmacist relationships and
the attitudes of GPs to HMRs affected whether the pharmacist would actively seek information
from the GP.
During the field studies there were only a few occasions when pharmacists reported talking to
GPs – e.g. for one pharmacist, this involved establishing the initial HMR process details with
a GP new to ordering HMRs; and for other pharmacists, conversation occurred during
combined GP-pharmacist educational meetings. For the field study pharmacists, however,
there was little reluctance to contact GPs, compared with the reluctance expressed by other
pharmacists at accredited pharmacists' meetings and during the benchtop testing phase. Yet,
although the researcher observed that field study pharmacist-GP relationships were quite
good, communication between these two groups was still infrequent – and much of the 'front-
line' communication between pharmacists and medical practices which did occur involved a
Practice Nurse.
Pharmacists did not appear to hold conversations with other (allied) health professionals,
although it was difficult for the researcher to be entirely sure of this.
The lack of communication might have meant that the patients encountered in this field study
were straight-forward and did not require additional follow-up by pharmacists. Clearly, our
wider field study is required before any definitive comments can be made about the overall
breadth and quality of pharmacist conversations with GPs and other health professionals.
Most communication between pharmacists and GPs, therefore, occurred by means of the
paper documentation which flowed between them. This resulted in some significant delays in
the reporting of HMRs to GPs – and in GPs being unaware of whether HMR reports had been
received from pharmacists. As the researcher has already suggested during the reports of the
benchtop scenario, this presents a quandary – having the referral document function as the
sole effective source of information from the GP to the pharmacist means that this document
absolutely must be comprehensive – but this does not occur! One of the main benefits of the
digital document as perceived by pharmacists was communication – whether because of or
despite the uncertainty of the information they received – the potential to communicate (and
thus share) information more quickly between themselves and GPs was seen as an important
and useful feature.
The researcher believes there are two points to be made here. Firstly, when the digital
Page 245

document is seen as an intervention in the relationship between GPs and pharmacists, this
intervention may be realised more successful where good relationships (and communication)
already exist, as it would be easier to 'intervene' in a relationship which already has a co-
operative basis (as seen in this field study). Secondly, and perhaps paradoxically, where
pharmacist-GP relationships are uncertain, using the digital document may enable the
development of some common ground to help communication – and perhaps even improve
relationships (as suggested by field study pharmacists).
7. 3.4 Time constraints and summary informationPharmacists in the benchtop phase remarked that time was a critical issue for GPs in the HMR
process, affecting the GP's ability to order HMRs initially, as well as to deal with HMR reports
received back from the pharmacist. This issue was confirmed by these field studies: not only
by observing the impact on the HMR process, but also in terms of the (lack of) project
involvement by GPs described earlier in this section.
As GPs attempted to minimise their time demands, they expected that HMR reports would
always contain concise summaries of important information, rather than including detailed
accounts. GPs could actually be quite disparaging about detailed reports.
The unnecessary information in the HMR reports to which GPs referred also included the
addition of pharmacological or pharmaceutical detail by pharmacists (e.g. commonly-known
drug side effects).
Time was also the reason why some GPs wanted a 'one-button' approach from desktop
systems designed to initiate HMRs (although one GP considered this approach to be
undesirable, as it did not allow the patient to be properly assessed prior to the review). Lack of
time also prevented GPs from gaining a clear understanding of a patient's medication use (one
reason why GPs were reluctant to stop medications prescribed by specialists), or from
communicating changes in medications to patients (who quickly forgot these details in any
case). These two issues highlight the value of an HMR to the GP, not only to clarify medication
use, but also to uncover issues which might not be identified during the necessarily brief
Where good communication exists, so might better outcomes for patients
..it was important to keep the information succinct and report on the main points, rather than the 'small stuff’
GPs did not want to be told ‘what they knew’
Page 246

meetings between GPs and their patients.
GPs' lack of time was well understood by pharmacists, who noted that this was the reason for
poor HMR referral rates from GPs (only about 10% of all GPs ordered HMRs). Consequently,
pharmacists aimed to provide simple, practical HMR reports which would place minimal time
demands on the GP.
One topic which arose during the field studies was the amount of information 'returned' to the
GP by the (paper version of the) digital document report, compared with the amount of
information in the summary-style HMR report normally prepared by the pharmacist. Although
GPs felt that this provided too much information, in (electronic) use the structure of the digital
document would address this perception, as the 'front page' of the digital document carried
only the summary information required by the GP – the remaining information could be viewed
by the GPs if they wanted to do so.
Further, HMRs take place in a small business environment (of GP and community pharmacy
practices) with financial gains being the main incentive for some GPs and pharmacists to
engage in the practice of HMRs. The challenge for technology is to support information sharing
and communication as a balance between the quality required for safe patient care; and the
expediency required for business efficiency. Unless there is an increase in the amount of time
available for GPs to deal with HMRs, or a change in the HMR process to make it easier, GPs'
enthusiasm for HMRs is likely to remain low.
7. 3.5 The use of alerts and remindersThe benchtop focus group suggested that alerts and reminders would be of limited use (other
than perhaps for weight and height) – this suggestion was substantiated during field studies.
Missing data (again) was a central problem. For example, weight and height values were only
conveyed in the referral information on 7 of 28 occasions (25%); and creatinine on 8 of 28
occasions (29%) – and these 7 occasions for weight were all from one GP. But even when
weight was flagged as missing on the digital document when used by the pharmacist, the
pharmacist did not enter that information. Of course, there is no way of knowing if that
information would have been entered by GPs had they used the digital document directly.
Warfarin alerts were a good example of this problem, from several perspectives. 2 HMR
patients, 3 HOMR patients and one RMMR patient within the field tests were taking warfarin.
Neither of the HMR patients had an INR value in their laboratory information, causing the alert
(requesting the availability of an INR) to be displayed in the document – but no INR value was
Page 247

added to report by the pharmacist. Two of the 3 HOMR patients had INR values entered in the
laboratory information, but the text value of 'warfarin' which had been entered into the
medication list was capitalised (i.e. Warfarin), which is not the convention for generic names –
which are invariably lower case – so the warfarin-INR alert was not triggered. The ACF patient
had recently been prescribed warfarin, but there was no INR value in the laboratory information
of the report sent to the GP by the pharmacist. As with the HOMR cases, the text value of
'warfarin' was capitalised so the alert did not appear.
These findings not only showed that HMRs can fail to include crucial information, but also
highlighted a problem with the input validation of the test system (which had failed to effectively
and accurately verify text). Although the researcher had discussed these alerts with the
participating pharmacists previously, they did not even consider the alerts even when they
'malfunctioned' (as was the case with the HOMR and RMMR) – this may suggest that alerts
are not as important to the pharmacist as anticipated; and poses some important questions
about the effectiveness of these to a HMR system.
Further, as laboratory values for HMRs were provided on separate (paper) documents, values
were never entered into the digital document by HMR pharmacists. For HOMRs, values were
only entered if they were considered important. These practices served to circumvent the
alerts provided in the digital document – once again suggesting that alerts might not prove
particularly useful in the HMR environment.
In contrast, however, one pharmacist did actively use calculators – she was the recipient of the
more detailed HMR referral reports from the GP; and thus had better information available.
One can surmise that if more information is provided, there may be better use of such features.
Despite this one helpful example, this small field study suggests that alerts may not be as
useful as hoped for because of missing information and current information management
practices. However, this would need to be confirmed by larger and better controlled studies.
7. 3.6 Systems for experts rather than expert systemsThe conclusions from the hospital phase (Chapter 5) were that clinical pharmacists evolved
into specialists, characterised by high levels of use of personal knowledge during their
medication-related decision-making. The benchtop testing phase (Chapter 6) also supported
this view of accredited pharmacists. Field studies confirmed that the substantial levels of
missing information forced HMR pharmacists to use personal knowledge to a significant level
– the HMR environment is not an area for novices.
Page 248

Thus, across the continuum of medication management, the fact that we are dealing with
specialists suggests a particular approach to the design of decision support tools. As
mentioned in previous chapters, this approach has less to do with providing a wide range of
structured information, or attempting to adapt this information across a range of patient
contexts and a wide range of health professionals’ abilities and knowledge. A more suitable
approach might involve providing essential information to support decision-making, where the
human can more appropriately understand and deal with different contexts. Thus, the design
of systems for experts rather than expert systems, seems to be the most appropriate approach
to designing tools for medication management, both in the hospital and in the community.
7. 3.7 A technology-poor practice paradigmFrom an accredited pharmacist’s meeting about HMR software availability, the researcher
gained the strong impression that, of the six available software products, many were too
expensive, too complex or required a level of technological understanding which was beyond
the comfort level of the audience. The products included databases, Palm® applications, a
Microsoft Word ® macro tool; and a application that allowed encrypted emailing of HMR
referrals and reports. The vast majority of pharmacists were using the tools previously
described to the researcher – word processing templates in Microsoft Word® and, for a few,
Microsoft Access®-based applications.
Nevertheless, against a background of poor availability of, or inexperience with decision
support tools, field study pharmacists (and benchtop test pharmacists) were happy to ‘try
something new’ – although they appeared to be more comfortable with a process which
reflected their usual one. Therefore, when they had a choice of using the server service or a
‘local’ tool, they chose the local tool (e.g. using the digital document on a notebook computer).
This provided the best evidence of pharmacists’ discomfort with technology – the many
different ‘paths’ that resulted for the digital document during the field studies (described in Sub-
section 7.2.3.1).
Pharmacists universally agreed, however, that sharing the digital document on-line would
realise the greatest benefits. A technology environment of low IT availability and low IT
utilisation such as the one within which community pharmacists exist has been described as
having a state of ‘limited assimilation’ of IT (Bajwa et al. 2007).
GPs’ bondage to their GP desktop system had major implications for their ability to envisage
or accept anything different from their usual practice. Just as researcher considers
pharmacists to be ‘application literate’ (see Chapter 6), the GPs could be described as
Page 249

‘application bound’.
The need to better support the communication of information remains evident from these field
studies, but this requires a paradigm shift from a paper-based to a digital-based approach. A
suitable technology approach might be one which can be implemented incrementally, is
flexible in use; and complements the work flow of individuals. The document-oriented user
interaction approach used in this project is one possible way to achieve this paradigm shift.
Addressing the community health technology predicament is a matter of the right, rather than
the most sophisticated, technology.
7. 3.8 The ‘viewpoints’ of professional practice toolsThe functions and ‘viewpoints’ of prescribing and dispensing systems were initially described
in Chapter 6. To recap, the viewpoint of the GP desktop system has major implications for the
use of the digital document, as the information in the GP desktop system can only be a
snapshot of the patient when last seen by the GP, representing a prescription audit trail rather
than actual current medication use.
The desire expressed by GPs to have ‘everything’ in their system presents a challenge to the
notion of information sharing – the underlying structure of the information in the GP system
does not allow the representation a current medication record. For example, only medications
contained within the lists included in GP desktop systems can be recorded – this hampers the
ability to enter CMs and OTCs (reportedly widely used by the elderly).
Interestingly, although CMs were mentioned by pharmacists in their reports (in the
commentary field), no pharmacist entered a CM into the digital document medication lists. It
could be surmised that, as the original medication lists from the GP desktop system contained
only prescribed medications, this could be an influence on how the pharmacist reports back,
i.e. not including the CMs in with the prescribed medications.
Another influence of the GP desktop system in the referral information given to pharmacists
was the ‘pattern’ of information that was determined by the GP’s report, shown in Figure 7-12.
In this case, the GP desktop system is Medical Director®.
The digital document approach was considered the 'next step', as many GPs and pharmacists were ‘not ready for this yet’
Page 250

These reports, other than for the Home medicines review referral report, were ‘one-button’
reports which assembled patient information contained in the GP desktop system. In contrast,
the HMR review referral is based on a template containing information personalised for the GP.
This required more effort from the GP, but the pharmacist received information that was clearly
superior and more relevant to the HMR.
Of course, just because there was a heading for information in these reports did not mean that
information was conveyed under those headings. But headings did dictate what possible
information could be provided – further affected by the amount of information entered into the
GP desktop system by the GP. If information did not appear under a heading, however, the
researcher was unable to ascertain why this was so – the information might not have been
available to the GP, or the GP might simply have chosen not enter it. Referral documents could
thus vary from one extreme of a simple medication summary, to an extensive array of
information at the other extreme.
Table 7-12: GP desktop reports used to provide HMR referral information
Information type
Health summary
Sheet
Medication summary
Full summary
Limited patient history
Full patient history
Home medicines
review referral
Patient-related
Personal details, smoking and alcohol use, allergies and warnings.Social and family history.
Personal details, allergies.
Personal details, allergies and warnings.Social and family history.
Personal details, allergies.Social and family history.
Personal details, allergies.
Personal details, smoking and alcohol use, allergies. Blood pressure, weight & height (with dates)Other issues (list of vision, language, cognition etc.).Patient consent.
Medication Current &Immunisations.
Headed as ‘Medications’
Current &Immunisations.
Current Headed as ‘Medication’.
Medications and vaccinations.
Treatment Current active problems & past medical history.
nil. Past medical history.
Past medical history.
Past medical history.
Conditions / diagnosis.
Laboratory nil. nil. nil. nil. nil. nil.
Other nil. nil. nil. nil. nil. Doctor, Pharmacy & pharmacist details. Medication administrator. Reason for referral. Aids used.
Page 251

This was an interesting observation in light of the Royal Australian College of General
Practitioners' Standards for General Practice, which stipulate that patients' health summaries
are required to contain current problems, past history, allergies, medications, risk factors (e.g.
smoking); and relevant family and social history (Mara 2006). The digital document trialled in
the field studies would seem to offer both GPs and pharmacists an effective means of
complying with the RACGP standards.
GPs did not appear to place much importance on information categories – one GP put all the
illness-related information into 'medical history'. Unfortunately, as no observation of how
information was entered into the GP desktop system was possible in this field trial, the effect
of GP data entry habits remains unknown for this project.
The final issue relating to professional tools which arose during field study was the influence
of the 'business' aspects of HMRs and GP practices in general. The Medicare requirement for
an audit trail, i.e. evidence of a HMR referral, action plan etc., necessitated a 'paper trail' to be
located in one place – GP's wanted this to be within the GP desktop system. The medical
billing system was also currently incorporated into the (clinical) GP desktop system.
Consequently, GPs considered that any change in 'systems' necessitated having all this
information together in the new system. Thus, GPs' desires to have a 'single record' for both
clinical and business information created a perception that it would be too difficult for them to
change anything about their current practice.
The influence of the GP desktop viewpoint is therefore very significant for the likely success of
the system trialled in this research project, but it should not be allowed to impede progress.
While the functional role of a prescribing system will never be in question, this needs to be
acknowledged as only one role. The GP desktop system does not (in its current guise) allow
information sharing, nor does it represent a current medication record. Whether the providers
of the GP desktop systems can be involved in subsequent research is unclear, but such a
solution would obviously be ideal.
Although the digital document is seen as an additional entity, it will have to exist in its own
communication space to realise its intent of being a shareable, communicable and ultimately
current, medication record.
Pharmacists mentioned that having something ‘more universal that sat outside of Medical Director’ was ‘sensible and useful’, but also a problem.
Page 252

7. 3.9 Pharmacists’ perceptions of GPs in the HMR processThis theme first emerged in the benchtop testing phase where pharmacists perceived GPs to
be unconvinced of the value of HMRs.
The consensus of pharmacists' meetings (attended by the researcher) was also that GPs'
acceptance of and attention to HMRs was poor. This lack of conviction of the value of HMRs,
by GPs, together with their lack of time, meant that many pharmacists felt uneasy in
approaching GPs. Consequently, pharmacists were frequently unable to obtain the information
they wanted from GPs – pharmacists were especially uncomfortable in raising particular issues
e.g. had the patient been investigated for a particular condition.
During field studies, there was a great deal of variation in how individual pharmacists and GPs
approached HMRs. For some GPs, HMRs did appear to a mechanical business process –
some GPs were concerned about remuneration and the 'red tape' that came with the HMR
process. This attitude of GPs may be part of the reason, re-iterated by pharmacists, that many
GPs provided minimal information (and, for some GPs, information could still be hand-written).
All these reasons contributed to the view held by pharmacists that, while the digital document
tool had the potential to allow GPs to provide better information, it was not clear that GPs would
use it, especially in small practices.
As mentioned previously, the participating pharmacists and GPs were considered to be more
motivated than most however (possibly the reason why they chose to take part in the project
in the first place). There seems no doubt to the researcher that the better the GP-pharmacist
relationship, the better the HMR process generally. Perhaps, if the digital document can
provide an environment to improve GP-pharmacist communication and relationships more
generally, GPs' perceptions of HMRs might also improve, increasing their uptake by GPs and
potentially providing better outcomes for patients.
7. 3.10 The Practice nurseThe Practice Nurse was introduced in Section 7.3.3. Not all GP practices had a Practice Nurse
(particularly small practices) but where they existed, it became apparent that part of their role
was to be a channel for ‘direct’ communication to the GP. This was true for the researcher and
appeared to be true for many of the HMR pharmacists. Of course, where there were important
clinical issues about the patient for the pharmacist to discuss with the GP, communication
would take place directly with the GP.
Some GPs saw HMRs as 'extras'.
Page 253
However, the direct patient involvement of Practice Nurses could be substantial. In one case
the Practice Nurse carried out patient health assessments and flagged those patients requiring
medication reviews to the GP. Interestingly, one GP mentioned using receptionists to fill out
part of the medication action plan – this would require caution, as receptionists are unlikely to
have the skill or background for this role – but Practice Nurses do have these skills. Therefore,
there may be an opportunity to extend the role of the Practice Nurse to include greater
involvement in the generation of HMR referrals.
Since Practice Nurses already serve as intermediates between the GP and pharmacist; and
because of their knowledge of the patient and ability to access to patient information, Practice
Nurses are in an ideal position to generate a more complete referral document – using the
digital document. This may be one solution to GPs’ inability to use the digital document
because of time constraints (and possibly because of technology issues). This suggestion is
made by the researcher, of course, without any knowledge of the work loads which exist for
these individuals. However, as many Practice Nurses already perform health assessments,
the next step to generating a medication referral document seems logical, given the
overlapping nature of information contained in a health assessment and a HMR referral –
providing a possible way to increase the number and quality of HMRs.
7. 3.11 Complementary medicines and over-the-counter medicationCMs and OTCs were a notable omission in the information sought by pharmacists and Medical
Officers (MOs) in the hospital. During the field studies, GPs also failed to include this
information in the medication lists included in their referral documents. However, pharmacists
did note these (e.g. vitamins, topical analgesic and anti-inflammatory creams; and antacids) in
the HMR report for the GP – but still did not include them in the actual medication list.
The researcher believes that CMs and OTCs should be captured within the list used for other
(prescription) medications. This can not only contribute to the development of a complete
medication list, but existing entries can act as reminders for later visits to the GP or in other
reviews. It is arguable whether this information is always important (e.g. vitamins – although
even in this case some fat-soluble vitamins, such as Vitamin A or D, can have significant side-
effects used in high doses in long-term use), but a number of CMs (e.g. St. John's Wort), have
potentially serious interactions with prescribed medications. One reason for this omission may
be that the HMR is, at least in part, driven by the information is contained in the GP desktop
systems and how this information is expressed, i.e. only reflecting medications identified within
that system. Although the pharmacist updates the GP on the accuracy of that information, CMs
and OTCs remain a separate consideration, rather than being components of a complete
medication list. The current systems actually hinder the assimilation of this information
Page 254

Yet, as the digital document would exist 'outside' GP desktop systems – and therefore outside
their influence – it provides an ability to record this information to the advantage of the GP and
the pharmacist; and ultimately the patient, as more informed decisions can be made about
their therapy. Once again, of course, this raises the issue of how to persuade at least some
GPs of the benefit of using two quite separate patient-related desktop systems.
Attention next turns to the digital document use experiences of the pharmacists and GP,
discussed in Section 7.3.12.
7. 3.12 Field study experiences
7. 3.12.1 HMRsThe general impressions of pharmacists about the digital document were the same here as in
benchtop testing – the digital document was logical and easy to use; and became easier with
repeated use. Overall, however, time to complete a HMR report using the digital document was
longer compared to the usual practice of this group of only returning a one page (paper)
summary to the GP (because for the digital document, the HMR pharmacists were entering all
the information forwarded to them by the GP – previously, pharmacists only entered
summarised information into the word-processed reports).
Field use of the digital document led to only one change in the information model – the addition
of a ‘commentary’ field to enable an overall summary of the HMR to be conveyed to the GP.
This reflected the practice of all HMR pharmacists to produce a succinct summary – whether
they provided other information or not.
Prior to the field studies, pharmacists had suggested a need to record the (‘real’) reason for
referral. However, this could not be tested as no GPs used the digital document directly to
produce the referral. One GP did write his own referral reasons on the paper referral, but these
were still in general terms (e.g. ‘education – on multiple medication’ or ‘review of medications
and husband’s understanding’). There were no instances of a GP indicating a more specific
issue which needed to be addressed (e.g. an assessment for a dosing aid). The inclusion of
the commentary field can also be seen as a result of the absence of targeted referral reasons
– this allowed pharmacists to report back to the GP more generally (and more flexibly) in the
absence of specific reasons.
As the paper report copy of the digital document had been the main avenue for pharmacists to
report back to the GP, there was a deal of comment about this report – although comment was
largely to do with formatting (display and grouping of information) rather than with information
content. Two changes were made to the paper report during field studies:
Page 255

• The first change in the report output reflected the change made to the digital document,
i.e. the addition of the commentary element. The researcher also made this a dynamic
field, as its appearance depended on the presence of the review date – prior to the
review, this field was not displayed on the report and, consequently, was less cluttered;
but after entering the review date, the commentary text was displayed on the report. One
pharmacist did use the paper printout as a working document during the review – the
document could thus be considered to be a practical working document, being used in
different roles at different times.
• The second change was enabling the display of the calculated values for the creatinine
clearance (CCl) and body mass index (BMI) calculators – initially absent because no way
had been found to achieve this during the XSL transformation that produced the report.
Although the paper report was not a prime focus of the project, it became clear that it could
very well be used to support the current (manual) process as an interim step to realising an
more technologically sophisticated HMR setting.
7. 3.12.2 HOMRsThe general reactions of the HOMR pharmacists were very similar to those of the HMR
pharmacists – information flow within the document was logical, it was easy to use and
became easier with repeated use. The date field (not surprisingly) provided some problems.
Pharmacists commented positively about some information elements, e.g. being able to
identify who changed medication information and when – important in a hospital setting with
many health professionals. No essential information items were considered to be missing
(although existing ones were not necessarily going to be used). The 'empty slots' were seen
as a good way of eventually collecting all appropriate (and perhaps complete) information.
A major finding in this setting was that some additional hospital-related information elements
would allow the model to fit with hospital use (as well as community use).
Some suggested information elements included:
• administrative data (e.g. admission date, ward, treating team)
• details of the patient’s progress during admission
• details of correspondence during admission (between health professionals)
• a ‘comments’ element alongside medication (e.g. for monitoring requirements); and
• a separate section for ‘short-term’ medications (e.g. tapering prednisolone or antibiotic
courses).
HOMR pharmacists considered that these elements would make the digital document a
‘working document’ which could capture the flow of information within the hospital. Some of
Page 256

these additions may not be a natural fit with the intention of the information model, e.g.
correspondence details, as this is more in the direction of a complete electronic health record.
Other information elements, e.g. reasons for referral, were probably unnecessary (although
these pharmacists had used this element to record patient summaries (that could be later used
by the GP). Fundamentally, the model was a good fit and some suggested ‘variations’ in the
display of information elements in the digital document could be accommodated by different
contextual views enabled by XForms.
In summary, this opportunistic test suggested an extended use of the digital document as a
‘working document’ within the hospital environment – requiring relatively minor changes to the
information model. This working document would not only be of value within the hospital, but
could also be the vehicle for information flow into the community for HMRs (supporting the
similar paper-based process already begun in this hospital). The ability to have a digital
document that could be used within the hospital and community settings suggests a real
opportunity to improve the continuity of care for patients, at least from the perspective of
medication management.
However, as this direction differed from that of the original project aim, changes were not made
to the information model – these suggestions would more appropriately form the basis of a
future investigation.
7. 3.12.3 RMMRsMedication reviews in ACFs (i.e. RMMRs) can be seen as a hybrid of HMRs and HOMRs.
RMMRs are similar to HOMRs as information can be sought from patient records at the ACF
(although no investigation was made during this project of the degree to which problems exist
with missing or uninterpretable information in that setting). RMMRs are also similar to HMRs
in intention, i.e. this is a medication review of the patient for the GP.
The experience of using the digital document with RMMRs did not add significantly to the
findings of the field study. If anything, this simply re-enforced the notion that conciseness was
a goal for reports. Very little information contained in the RMMR reports was sent to the GP
and the pharmacist again re-iterated that the GP only needed a summary of patient issues –
rather than duplicate information which could be located at the ACF or by the GP
7. 3.12.4 The technically aware GPAs one GP (GP4) did use the digital document and was the only participant who used the on-
line service, the researcher considers this to be a significant event; and thus worthy of separate
discussion. This GP was also able to download patient files from the server to his PC on one
occasion when there was a temporary problem with digital document display on the server –
Page 257

proof of the value of providing alternative work processes.
The data provided by the GP (based on the HOT Fit model) are reported in full in Appendix
X, but are summarised here.
The GP considered the digital document to be easy to learn and data entry methods simple to
use. The information categories were considered relevant and the ability to add as much
information as required was valued.
He stated that the usefulness of the digital document for medication management was 'good',
although he would have preferred to have drugs and related issues on the same page of the
document. Although this GP regarded the digital document as easy to use, he thought 'non
computer literate people' might have some initial reservations about using it. The only
problems which required resolution, however, were some minor formatting issues.
The GP phrased the perceived gains of the digital document in terms of safety, quality,
efficiency and patient outcomes. However, some of the gains mentioned by the GP could
actually describe the gains of the HMR process itself, not just the intervention (this is a not-
infrequent result of automating any complex process – and is a phenomenon encountered by
almost all researchers investigating technology transfer and innovation diffusion). This GP was
motivated to do HMRs for the first time as a result of involvement in this project. He stated that
there were safety gains because of the pharmacist's 'excellent review' (this external audit could
detect drug interactions). He also felt that the peer review process would improve quality
assurance, but quality was also improved as the GP was 'forced' to keep records up-to-date.
Increased efficiency, though, was perceived by the GP as something that would occur once
the system was operational (rather than within this limited project – an opinion also echoed by
pharmacists).
The GP also mentioned that there had been (positive) clinical outcomes for several of his
patients (through changes to medication therapy). However, as mentioned, this could be as a
result of the overall process; and the effect of the intervention cannot be removed from the
HMR process itself. Nevertheless, the fit of the information model was substantiated for its
purpose by this especially technically literate (and technophilic) GP. The net benefits of the
intervention reported by the GP are reproduced verbatim in Table 7-13.
Information was: ‘not too much, not too little’
The digital document had ‘great potential’
Page 258

.
This concludes the discussion of data analysis. The next important considerations for this
project are: what impact did the intervention have on the medication management process?
and what, if any, were the outcomes? The evaluation of the intervention is discussed next in
Sub-section 7.3.13.
7. 3.13 Evaluation of the interventionAs planned, the tool used to evaluate the intervention was the Human-Organisation-
Technology Fit (HOT Fit) Model advocated by Yusof, Paul and Stergioulas (2006).
As there was poor use of the server service, with only one GP providing feedback, assessment
of this service can essentially only be made on the perceptions of possible use by users.
However, as the digital document was used (locally) by all pharmacists and one GP, the
information model and digital document can be assessed with reasonable confidence against
the evaluation model.
Not all the components represented in the HOT Fit model were relevant to this project. The
researcher therefore selected those which were relevant and included one further element –
quality, in the net benefits – because quality (as a broad concept) was often at the centre of
accredited pharmacists' discussions of the HMR process. The adapted HOT Fit Model is
shown in Figure 7-2 and the original model in Appendix D.
To allow easier evaluation, the researcher has separated the HOT Fit model components into
tables (Tables 7-14 to Table 7-20) which deal independently with the human, organisation,
technology and net benefit aspects of the model. The HOT Fit model and tables have also
been numbered to show the links between them. Within these tables, there is a further sub-
Table 7-13: Net benefit comments from GP4
Net benefits1. Provide seamless communication between pharmacist / doctor /patient if adequate computer skills and computer access.2. Effectively alters clinical outcomes, provides opportunity for audit & peer reviews3. Could be a source of information for ADRAC (‘adverse reactions’ body) by pharmacist alerta4. Cost effective from my viewpoint5. Link in with government payments6. Viable for me to put into practice7. A potential for other uses, e.g. doctor -> hospital, hospital -> allied health, intrahospital communication pharmacy -> medical staff, check for discharge summaries, ‘smart card - credit card for patients transferring information’8. Download laptop facility means data cold be collected at remote point and transferred at base
a. The Adverse Drug Reactions Advisory Committee (ADRAC) is the central Australian body responsible for collecting and reporting adverse drug reactions.
Page 259
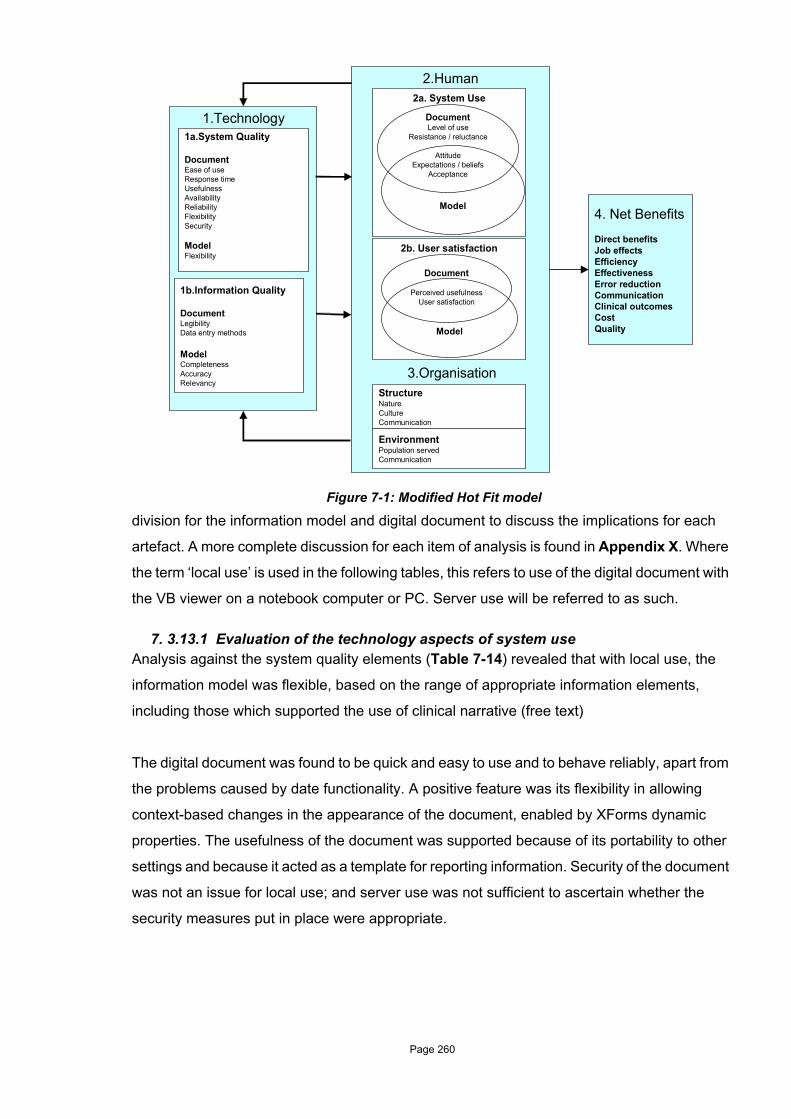
division for the information model and digital document to discuss the implications for each
artefact. A more complete discussion for each item of analysis is found in Appendix X. Where
the term ‘local use’ is used in the following tables, this refers to use of the digital document with
the VB viewer on a notebook computer or PC. Server use will be referred to as such.
7. 3.13.1 Evaluation of the technology aspects of system useAnalysis against the system quality elements (Table 7-14) revealed that with local use, the
information model was flexible, based on the range of appropriate information elements,
including those which supported the use of clinical narrative (free text)
The digital document was found to be quick and easy to use and to behave reliably, apart from
the problems caused by date functionality. A positive feature was its flexibility in allowing
context-based changes in the appearance of the document, enabled by XForms dynamic
properties. The usefulness of the document was supported because of its portability to other
settings and because it acted as a template for reporting information. Security of the document
was not an issue for local use; and server use was not sufficient to ascertain whether the
security measures put in place were appropriate.
Figure 7-1: Modified Hot Fit model
2.Human
1.Technology
1b.Information Quality
DocumentLegibilityData entry methods
ModelCompletenessAccuracyRelevancy
1a.System Quality
DocumentEase of useResponse timeUsefulnessAvailabilityReliabilityFlexibilitySecurity
ModelFlexibility
2b. User satisfaction
2a. System Use
DocumentLevel of use
Resistance / reluctance
AttitudeExpectations / beliefs
Acceptance
Model
Document
Perceived usefulnessUser satisfaction
Model
StructureNatureCultureCommunication
EnvironmentPopulation servedCommunication
3.Organisation
4. Net Benefits
Direct benefitsJob effectsEfficiencyEffectivenessError reductionCommunicationClinical outcomesCostQuality
Page 260

Although system quality is clearly important for user acceptability, the researcher considers
that information quality is particularly relevant to this project, as information quality may have
an impact on the outcomes for the ultimate focus of this project – the patient.
Evaluation of the information quality (Table 7-15) supports the view that the information model
is complete and relevant for the purposes of HMR reviews. There was no opportunity to test
whether the intervention bettered the accuracy of medication-related information but this was
perceived by participants as this model (or at least its implementation) could be shared.
However, accuracy was discerned to be at least as good as for existing systems.
Improvements in legibility ascribed to the digital document resulted from the move from hand-
written reports. Data entry methods were considered simple and useable, with information flow
being logical although, once again, the date entry method was a problem.
Table 7-14: Technology aspects of the intervention – 1a. System quality
1. Technology
HOT Fit Model element Information model Digital document
1a. System qualityEase of use Easy to use, improving over time. Date
functionality caused some difficulties.
Response time Good for local use. Server response was acceptable over a broadband.
Usefulness Useful as a template for gathering, sharing and reporting information for HMRs; and as a ‘working’ document within a hospital. Usefulness also suggested in other settings. Portability suggested document use on PDA and USB devices.
Availability No problems with document operation at local use. No problems with server availability during development, testing and field access (although had limited use)
Reliability Behaved reliably throughout field use. One issue with a Microsoft security patch.
Flexibility Based on the range and nature of the information elements – free text elements allowed expression of clinical narratives too difficulty to capture otherwise. Flexibility was suggested by use in scenarios other than HMR.
XForms allowed dynamic behaviour to hide or reveal information based on context of use. Pharmacists considered the document very flexible. GP user commented that layout was not flexible (but this was not intended). Document was a useable artefact in a number of scenarios.
Security Not an issue as most use of the document use was at local level. This would be a more significant issue with a bigger group of self-enrolling users and on-line use.
Page 261

7. 3.13.2 Evaluation of the human aspects of system useOverall, the evaluation of the human aspects of system was positive (Table 7-16).
There was a positive attitude towards the use of a simplified model, although GPs’ attitudes on
what information should be contained within GP prescribing systems (compared to the
information model) affected attitudes about possible use of this tool in the future. Despite the
expectation (of GPs) that succinct information should be located in their desktop system, all
participants believed there was value in using this modelling approach to support the
communication of relevant, summarised information. However, pharmacists also believed this
‘next step’ would be difficult for GPs to take. Acceptance of this ‘essential’ information model
was good.
The digital document was viewed positively and had good use locally (for participants that
elected to use it), although there was variation on how it was used because of pharmacists’
current work practices or GPs’ wishes about patient confidentiality. The level of use of the
server-based alternative was poor. The main expectation of the digital document was that it
have some interfacing ability to the GP desktop system.
Table 7-15: Technology aspects of the intervention – 1b. Information quality
1. Technology – Information quality
HOT Fit Model element Information model Digital document
1b. Information qualityCompleteness Confirmed, as only one element added to the
model during HMR field use. Pharmacists and GPs considered no essential elements were missing. Sharing the document would improve the completeness of information over time.
Accuracy No opportunity to determine information accuracy, but was considered to be as good as for use of existing systems. Sharing would improve accuracy over time.
Legibility This was considered largely in comparison to hand-written reports.
Relevancy The elements were considered logical and relevant. Relevancy of information elements was also patient-context dependant. The relevancy of alerts and reminders remains unclear.
Data entry methods Found to be simple, generally acceptable and flow was logical. A free text field for some elements was valued. Drop-down boxes were considered of limited use. Date fields could be a problem leading to inadvertent errors. Overall, data entry took longer, but not considered a major problem (by pharmacists).
Page 262

Overall acceptability of the digital document was good, with an additional benefit being that the
report, which was not a focus of the investigation, was valued in its own right. Although
pharmacists did not use the server service, they saw no acceptance issues for on-line of the
digital document.
The only reluctance encountered with the system was for on-line use (other than for one GP),
because of concern about patient privacy in some cases, or because this was too different to
the current work process. Importantly, time featured highly as an overall deterrent for any use
by GPs.
Table 7-16: Human aspects of the intervention – 2a System use
2. Human – System use
HOT Fit Model element Information model Digital document
2a. System UseLevel of use Good use at local level by all pharmacists. None
used the server service. The level of use was dictated by pharmacists’ current work practices or the GPs’ wishes about patient confidentiality.Use at local and server level by one GP (time constraints prevented other GPs from use).
Attitude Positive attitude towards the use of a simplified model. How this model related to the information contained within GP prescribing systems affected attitudes about possible use in the future.
There was a positive attitude to using the digital document for those that used it.
Expectations / beliefs
GPs expected succinct information to be located in their desktop system, wanting a ‘one-button’ approach to HMRs. Despite this, they felt there was value in this approach to communicate relevant, summarised information between pharmacists and themselves.Pharmacists considered this a ‘next step’ and although desirable, questioned whether GPs would take it up.
The main expectation was for the digital document to have some interfacing ability to the GP desktop system. GPs particularly wanted the ability to produce a referral document with minimal effort.
Acceptance The model of ‘essential’ information was acceptable, having a good balance of information items. The field trial did not have any major impact on the design of the model. GPs would find it difficult to move away from current work patterns.
The digital document was acceptable in use overall. Minor changes were suggested to the layout of the document; and the paper report (although not a focus of investigation). The paper report was valued in its own right. Pharmacists saw no acceptance issues for digital document use on-line.
Resistance / reluctance
There was no reluctance to local use of the document, but some reluctance to use the server. This was concern about patient privacy in some cases, or was too different to the current work process. Time featured highly as an overall deterrent for any use by GPs.
Page 263

User satisfaction with the system in the intervention was good, as summarised in Table 7-17.
The information model was found to be useful as a basis for the communication of essential
information. Further, users felt that this approach could be useful in other settings. Pharmacists
particularly, considered that an approach which enabled information sharing ‘outside’ of the
GP desktop systems was very useful. The researcher’s general observation was that users
were satisfied with the information model.
The digital document was considered useful as a template for information gathering and
reporting, although the usefulness of alerts and reminders and calculators is unclear and
requires further investigation. There was also good user satisfaction with the document
interface (again, other than the problem with date functionality).
Evaluation of the structural components of the HMR ‘organisation’ within which the intervention
took place is summarised in Table 7-18.
The nature of the environment is one of independent, communicating professional practices
where there is no natural coordination of activities, but these rather occur on a push basis as
the patients are ‘pushed’ between health providers or services. The culture is similarly
concerned with independence – in decision-making and professional practice – with the added
complexity of being a small business environment. There is no structure in place which allows
good communication between the members of this HMR ‘organisation’; and communication
and information-sharing uses mainly a range of conventional methods (e.g. telephone and
facsimile).
Table 7-17: Human aspects of the intervention – 2b. User satisfaction
2. Human – User satisfaction
HOT Fit Model element Information model Digital document
2b. User satisfactionPerceived usefulness
The usefulness of the model to support communication of essential information was upheld by users. This was reinforced by suggestions for use in other settings and applications. Pharmacists considered something ‘outside’ of the GP desktop system allowing information to be shared as desirable.
Usefulness was considered to be high, as a standard template for information gathering and reporting. The usefulness of alerts and reminders and calculators is unclear and requires further investigation. The GP that used the document considered that it had ‘great potential’.
User satisfaction The general observation was that users were satisfied with the information model – supported by the fact that users’ experiences were straightforward with few problems.
Users were satisfied with the document interface (other than the problem with date functionality). The additional time required (by pharmacists) to add data was not considered a major problem. User satisfaction of the GP was also positive.
Page 264

The implication of this structural evaluation is that this environment requires a structure to be
put into place. This structure will need to accommodate a ‘push-based’ style of communication
of information; information-sharing that allows multi-disciplinary input, but independent
decision-making; and can operate in a low technology environment. The digital document
approach advocated by this project may be an appropriate structural approach.
The environmental aspects of the HMR ‘organisation’ are evaluated in Table 7-19. The
population served in this intervention project was composed of those pharmacists and GPs
involved in HMRs in the community. However, the population which could be served by the
artefacts in this project is wider, including other health professionals involved in the patient’s
care and, of course, the patients themselves – this is the basis of some of the Future Work
described in the next chapter.
Communication emerged as the major issue in this intervention. The ability to improve
communication foresees many benefits, such as improved: information sharing between
health professionals (and across health care settings); information collection, accuracy and
use; medication-related decision-making; pharmacist-GP relationships; and ultimately better
outcomes for patients.
Table 7-18: Organisational aspects of the intervention – Structure
3. Organisation – Structure
HOT Fit Model element
StructureNature The structure of the ‘organisation’ involved can be considered a set of independent,
communicating professional practices. This is the case in the community, whether the entities are GPs, pharmacies, pharmacists, other health professionals or hospitals. There is no easy way to coordinate patient processes across these practices. It largely occurs through a ‘push’ mechanism, i.e. a health care process occurs around a patient and follows them as they are ‘pushed’ from one health care setting or provider to another, based on the outcome of the previous service. The ability to communicate medication-related information across this ‘organisation’ promises to address some of the problems of information sharing and communication inherent in its nature.
Culture The culture of health professionals in the community is one of independent decision-making, with or without input from other health professionals. As the importance and benefit of a multi-disciplinary approach gains acceptance, the value of shared information and others’ opinion is increasing. However, this is more difficult in the community (compared to the hospital), because of the poor physical proximity of health professionals; and communication issues in part resulting from perceptions about other professionals. This environment is also a small business environment that draws payment for carrying out HMRs. A communication framework suggested by the intervention may alleviate some of these issues, although a significant challenge will be alignment with, or accommodation of, business issues.
Communication There is no structure in place which facilitates good communication. Communication of HMR information occurs by mail or fax; and direct pharmacist-GP communication if it occurs, is by telephone. There is essentially no communication by email or by other on-line means. Communication of information could be easily achieved using current technology, as the digital document approach purposefully used existing standards and pursued a ‘low tech’ approach. The portability of the digital document is a major enabler of this.
Page 265

The net benefits of the intervention are listed in Table 7-20. These are a compilation of benefits
mentioned by user; and those observed by the researcher. Some of these are not easily
discerned between the information model and its instantiation as the digital document. Some
benefits mentioned by GPs would be an expected outcome of a HMR in any case, e.g.
providing an opportunity for audit and peer review. Also, some others are less specifically
concerned with the model or document, than with the nature of the (technology-based)
intervention, e.g. source of information for ADRAC or links to government payment. However,
these are all described as they were all benefits perceived by participants. Many participants
mentioned future applications or potential applications for the digital document approach –
these are discussed under future work in Chapter 8.
Table 7-19: Organisational aspects of the intervention – Environment
3. Organisation – Environment
HOT Fit Model element
EnvironmentPopulation served Although the population served in this project was GPs and community pharmacists, users saw
the potential for information sharing between other health professionals, including across the hospital-community interface. This could also include patients. The population which could be served by the digital document could be anyone that was involved in patient care that had an interest in medication management.
Communication Communication in this ‘organisation’ is a significant issue. Frequent pharmacist-GP communication is not the norm, even in the presence of missing information; and this is often compounded by professional perceptions. Good relationships with GPs were highly valued by pharmacists; and communication was much easier in these cases. The potential to improve the communication of information was the most important aspect of the intervention. This was a positive feature seen by both GPs and pharmacists. Communication could be extended to include other health professionals; and also between different communities of practice, e.g. hospital-community, intra-hospital; and with patients themselves.
Page 266

Table 7-20: Net benefits of the intervention
4. Net benefits
HOT Fit Model element Information model Digital Document
Direct benefits The information model provides a template of essential medication-related information which is to the point, relevant; and can be understood and shared by health professionals. This is the basis of many of the other benefits.
The digital document approach allows a flexible way of communicating and sharing medication-related information through a simple, easy-to-use artefact.
Job effects Simplifies the need to determine what information needs to be collected as this is suggested by the ‘template’. This can standardise expectations of what information is transferred between health professionals.
Provides opportunities for audit and peer review (although this is done by the HMR process anyway).Could be a source of information for ADRAC (through pharmacist alerting)
Efficiency The model acts as a suitable communication template to streamline the medication management process since the information structure is known to participants in the medication management process.
Timeliness and availability were seen as the main contributors to efficiency; and other benefits (e.g. safety) also flow from these.
Effectiveness Aids completeness of information collection. The digital document appeared to be an effective (and flexible) way to represent and communicate information.
Error reduction The model act as a prompt for collection of relevant information, increasing the chances of errors being detected and rectified.
Accuracy of information improves as the document is shared and updated by a number of health professionals. Encouraging the move from hand-written documents also adds to safety.
Communication Provides an expected set of information which will be communicated (although not necessarily a complete set).
Seen as a way to provide ‘seamless’ communication between pharmacist, doctor and patient (given adequate computer skills).Provides flexibility for the work process (e.g. directly on server, or patient files can be downloaded / uploaded from laptop computers).
Clinical outcomes Model will be the basis for greater clarity of information presentation (to GP) possibly increasing the uptake of recommendations.
Patient outcomes are likely to be improved if there is greater communication between health professionals. As information can be communicated more quickly, recommendations may be effected more quickly leading to better patient outcomes.
Cost No cost benefits were attributed to the information model.
It is not anticipated that direct costs of the HMR process would be decreased as a result of the intervention. However, one can surmise that a more efficient process and better outcomes could lead to cost benefits more broadly over time.
Quality Standard elements guide the depth and quality of information for reporting; and this assists Quality Assurance.
Mainly as a move from hand-written documents. But overall, this was seen as a step to generally improving the quality of reporting.
Page 267

In summary, because the intervention in the field trial was influenced by some practice issues
(as noted in Section 7.2.3), the researcher's ability to measure the effect of the intervention on
HMRs was less than perfect. Nonetheless, all pharmacists and one GP made direct use of the
digital document (locally) on a notebook computer or PC. An unexpected – but valuable –
outcome of the field study was the potential to use the digital document in a hospital discharge
setting which confirmed the flexibility of the document (and model).
The only major change to the information model which occurred as a result of the field studies
was the addition of a single information element – a free text field. These were highly valued
as they could be used to express clinical judgements, but presented a dilemma when
attempting to use categorised information as the basis for alerts. Although some data entry
issues interfered with the testing of the alert functions, they were not used by pharmacists
(although this, in itself, is a cause for some concern – as alerts in relation to drugs such as
warfarin should certainly be taken seriously). Similarly, there is no suggestion that reminders
made any difference to whether pharmacists added missing information. Whether alerts and
reminders would have made any difference to GPs' behaviour remains untested.
The digital document was generally found simple and easy-to-use; and information flow
through the document was considered logical. The requirement of the digital document for
pharmacists to add more information compared to the current word processed reports added
a little more time to the current HMR process – but was not considered a problem.
Evaluation against the modified HOT Fit model revealed benefits to the intervention: some real
and some perceived.
The fundamental benefits of the information model arise from its being a template of essential
medication-related information which is focused and relevant; and which can be understood
and shared by health professionals. This formed the basis of other perceived benefits, such as
a shared understanding of what information elements should be provided, helping with the
completeness this information, improving information quality; and improving the uptake of
recommendations (by GPs).
The fundamental benefits of the digital document are due to its flexible approach to
communicating and sharing medication-related information through a simple, easy-to-use
artefact. The document paradigm was a comfortable fit for these health professionals. Sharing
this document on-line was seen to be of particular potential value in improving the timeliness
and availability of information and communication between health professionals – contributing
to better patient outcomes.
Page 268

There were also two incidental benefits from this intervention. One GP who had not previously
undertaken HMRs was motivated to do so by this project; and a pharmacist who had previously
produced hand-written reports subsequently produced more legible reports for GPs. In the
latter case, it will be interesting to see if this improvement continues after the completion of the
project.
Issues which limited the researcher’s ability to evaluate the intervention were mainly the time
available for GPs to participate and the poor use of the server service. GPs also had the
expectation that the digital document should be interfaced with, or be part of, their GP desktop
system. This was not possible during the project – and is perhaps not appropriate, given the
different intents of the GP systems and the digital document. It was evident, however, that
there is no clear way that information communication between a number of health
professionals can be supported by the GP systems.
Nevertheless, as a proof of concept for this approach to support medication management, the
results are encouraging. Clearly, there is now a need for larger field trials to realise the full
potential of such an intervention.
The final information model which resulted from the field studies is now discussed in Section
7.4.
7.4 The information modelThe final information model which emerged after the field studies is shown in Figure 7-2. This
simply includes the additional commentary information element – the other minor re-
arrangements suggested for some of the elements have not been included as these do not
affect the model overall. Further, the dynamic components of the model – alerts and
calculators – have been retained as these should remain for future field tests. As mentioned
by the researcher, any changes suggested by the HOMR experience are issues for a future
project in a hospital environment.
The implementation aspects of the model and other functional changes resulting from the field
studies are now described in Section 7.5, with full technical details contained in Appendix Z.
Page 269

Figure 7-2: The final information model
Med
icat
ion
man
agem
ent d
ocum
ent
Patie
nt in
form
atio
nTr
eatm
ent i
nfor
mat
ion
Med
icat
ion
info
rmat
ion
Inve
stig
atio
nsR
efer
ral i
nfor
mat
ion
Ref
erra
l dat
e
Dat
e of
revi
ew
Rep
ort d
ate
Com
plet
ed d
ate
Des
crip
tion
Rec
omm
enda
tion
Actio
n
Res
olve
d
Res
olve
d da
te
Pers
onal
Ref
eren
cePh
ysic
al
Nam
e
Addr
ess
Med
icar
e nu
mbe
r
Dat
e of
Birt
h
Age
Sex
Wei
ght
Hei
ght
Rec
ent B
P
Alle
rgie
s / s
ensi
tiviti
es
Adve
rse
drug
reac
tions
Rec
reat
iona
l sub
stan
ce u
se
Sys
tolic
Dia
stol
ic
Seru
m c
reat
inin
e
GP
deta
ils
Com
mun
ity
phar
mac
y
Oth
er c
onta
cts
Cal
cula
tor:
BM
I
Prev
ious
falls
Cog
nitio
n
Mem
ory
Lang
uage
Dex
terit
y
Visi
on
Hea
ring
Swal
low
ing
Equi
pmen
t
Oth
er
Cur
rent
tre
atm
ent
Activ
e pr
oble
m
Trea
tmen
t His
tory
Med
ical
his
tory
Labo
rato
ry
Dat
e
Item
Res
ult
Imm
unis
atio
nsC
urre
ntm
edic
atio
nsM
edic
atio
nhi
stor
yM
edic
atio
nm
anag
emen
tis
sues
Teta
nus
Influ
enza
Pneu
moc
occu
s
Oth
er
Reg
ular
med
icat
ions
Whe
n re
quire
dm
edic
atio
ns
Cea
sed
/ ch
ange
dda
te
Rea
sons
for
chan
ge
Pers
on
resp
onsi
ble
Med
icat
ion
Dat
e
Gen
eric
nam
e
Bran
d na
me(
s)
Dos
e
Rou
te
Freq
uenc
y
Addi
tiona
l ins
truct
ions
Indi
catio
n
Dur
atio
n of
trea
tmen
t
Patie
nt in
dica
tion
Max
imum
dose
Soci
al
hist
ory
Med
icat
ion
man
agem
ent
Aler
t: -w
arfa
rin
Aler
t:
-war
farin
an
d IN
R
Cal
cula
tor
Aler
t
Ref
erra
l rea
sons
Cal
cula
tor:
Cre
atin
ine
clea
ranc
e
Com
men
tary
Page 270

7.5 The digital document and the server serviceThe nature of possible changes were those which:
• were required for the document (and model) to function in the field
• were minor format changes to the document or re-arrangements to model elements
suggested near the end of the field study and were thus not implemented, or
• would take the model to different environments in future work (e.g. the hospital working
document).
Changes made are now discussed in the following sub-sections.
7. 5.1 The VB BrowserThere was no need for any changes to the existing VB browser or the (‘child’) VB Medication
Management Document Printer form during the field study.
7. 5.2 The digital documentAs mentioned earlier, the one change made to the digital document was the addition of the
additional commentary field, reflecting the addition of this element in the information model –
this change was consequently reflected in the patient XML file and the XSL report.
In keeping with having the document view reflect the context of use, the researcher made the
commentary field visible contingent on the presence of the review date. Prior to the review, the
referral page in the digital document displayed the referral date, reason for referral and
(‘empty’) review date (see Figure 7-3).
Page 271

The addition of the review date by the pharmacist (after the review) allows the commentary
field to become visible (as well as the previous information elements which became visible –
recommendations etc. – described in Chapter 6). The pharmacist could then add summary
information about the review. An example is shown in Figure 7-4.
Figure 7-3: Digital document referral page prior to review
Page 272

There were no changes to any other pages of the digital document. Changes to the XSL report
are detailed next.
7. 5.3 The XSL reportThe researcher has mentioned the two changes to the XSL report earlier in the chapter. The
first change reflected the addition of the commentary field to the referral page on the digital
document. The second change was the ability to perform Body Mass Index (BMI) and
Creatinine Clearance (CCl) calculations during the XSL transformation of the patient XML file
into HTML output.
As a paper copy of the XSL report could be taken to the review as a working document, it was
important for it to carry only the referral information and not be cluttered by other detail e.g. an
‘empty’ commentary field. Prior to the review, the XSL report was that shown in Figure 7-5.
Figure 7-4: Digital document referral page after review
Page 273

Once the pharmacist entered the review date into the digital document, this act triggered the
ability to display the commentary information on the report; and output ‘signature’ alongside
which the pharmacist could sign their name (once printed on paper) (Figure 7-6). As this
commentary was the main summary of the HMR produced by the pharmacist for the GP, it was
important that it captured the attention of the GP. The researcher thus chose to output this
information at the top of the report, immediately under the dates – this ensured that the GP
saw the summary of the HMR before other information. With the ability to display (or not) the
commentary information the paper document could function as both a working review
document for the pharmacist and a report for the GP.
Figure 7-5: HTML output of document before the HMR review
Page 274

The second change was the ability to display calculated values of the BMI and CCl in the
report. Initially, the researcher had not found a way of calculating values during an XSL
transformation of the patient XML file. BMI and CCl were calculated in the digital document and
could be manually transferred onto the paper report by the pharmacist – this was not ideal. The
solution to the calculation problem was through the use of embedded VBScript functions in the
XSL file.
An example of these calculated values on a section of a report is highlighted in Figure 7-7.
Figure 7-6: HTML output of document after review
Page 275

Figure 7-7: HTML report output – calculated values
Page 276

7. 5.4 The server serviceThe server service was not changed other then the need to update the XSL file (for consistency
with the VB browser).
Two errors were encountered by the GP who used the server service: the first of these was
that a complete list of his patients did not appear on the server. On investigation, the patients
were there and viewable by the researcher, so it was not clear why this information had not
appeared on the GP's first log-in.
The second error was an inability to open some patient files. Investigation by the researcher
revealed that this problem was resulted from a parsing error with the naming convention used
for the patient XML file – due to the presence of a comma (,), e.g. lastname,firstname.xml. This
problem had not occurred when using the VB browser, as the VB code was able to deal with
the presence of commas when parsing the filename (text). The server problem was resolved
by changing the file name format to lastname-firstname.xml format.
Page 277

7.6 Chapter Summary This chapter has reported the field study interventions which sought to evaluate the information
model and digital document prototype in operation in the medication management community,
prepared for this context by prior benchtop testing by accredited pharmacists. The chapter now
concludes by addressing the three research questions posed at the beginning of the field
study. This is done consecutively under each question heading below.
D. Can our intervention improve safety, quality and efficiency?
As a proof of concept, the intervention was sufficient to perceive benefits for the medication
management process, health professionals and patients.
Contribution to safety was likely to arise through prompting pharmacists and GPs for
medication-related information which is relevant to decision-making. Relevant information
increases the chance that pharmacists and GPs will be able to detect and correct errors. As
the document would be used and updated by health professionals over a period of time, this
revision of the document would also improve the accuracy of the information contained within
the document. The ability to share information in a more timely manner, together with better
information availability (particularly for the GP) means that recommendations about patients'
medication could be effected more quickly; and thus lead to better patient outcomes. Where
use of the digital document encouraged moving from hand-written reports, gains in legibility
were also likely to contribute to patient safety. Nevertheless, although safety gains were
perceived, this would need to be confirmed through more extensive field studies.
Quality was examined under system and information headings using modified HOT Fit model.
Although system quality is important for usability and acceptance, the researcher considers
that it is information quality, or rather the impact of information quality which is of most
relevance to this project. Quality was a persistent issue in accredited pharmacists’ meetings –
for the HMR process itself and the HMR report. The ideal suggested by pharmacists was: to
have adequate, relevant information to review the patient; to be able to communicate a
succinct summary of the essential issues to the GP in a timely manner; and to receive GP
feedback though a medication action plan. The digital document approach provides a possible
solution for this ideal. In addition, promoting the use of standard (and essential) information
elements can guide the depth and quality of information required for reporting. The move away
from hand-written reports certainly adds to quality overall.
Efficiency gains in the HMR process were envisaged by participants through the ability to
convey the information electronically – again improving the timeliness and availability of
Page 278
information. Not only could this allow patient-related decisions to be made more quickly, but
also could facilitate feedback to the pharmacist – currently an uncommon event.
E. What is the contribution of the information model?
The contribution of the model is to provide a template of essential medication-related
information which is succinct, relevant and can be understood and shared by health
professionals. This contribution is reinforced by the digital document’s ability to be used in
different medication management scenarios. Thus, the principle contribution is a relevant
framework for medication management-related information.
F. What is the contribution of the technology artefact (digital document)?
The contribution of the digital document is to allow a flexible means of communicating and
sharing medication-related information through a simple, easy-to-use artefact. Although the
information model could be implemented with other approaches, the document-centric
approach was a comfortable fit with health professionals’ practice. The advantage of being
able to use the document in a number of ways in the project (on-line or ‘locally’) demonstrated
its flexibility in different work flows. The ability to provide some dynamic functionality in the
digital document, still offers potentially useful (although probably limited) application. In brief,
the principle contribution of the digital document is its natural fit with the work environment; and
it’s flexibility in use and communication.
This chapter concludes the analysis and discussion of the field studies, the last of the three
iterations which developed, tested and evaluated the artefacts of interest in this project – the
information model and digital document.
The next and final chapter, Chapter 8, collects and addresses all the research questions
posed in this project. It also considers themes and coincidental findings which emerged during
the project; and reflects on the contributions of the project. Finally, it will discuss future work
realised by the researcher or suggested by project participants.
Page 279

Chapter 8
Summary and conclusions
8.1 IntroductionChapter 7 described the third and last investigation scenario of this project, the field studies
that evaluated the artefacts of interest – the information model and digital document. In
particular, these artefacts were evaluated for their ability to support medication reviews
undertaken by community pharmacists and General Practitioners (GPs), the impact on the
medication review process; and any implications for patient outcomes.
In this, the final chapter of the thesis, the researcher summarises the project, brings together
the main conclusions drawn from the research findings, provides answers to the research
questions; and suggests avenues for further research.
This chapter is structured as follows:
• a summary of the project is given in Section 8.2
• the themes that emerged during the project and directed the development of the
information model and digital document are summarised and discussed in Section 8.3
• a summary of the changes to the information model which occurred through the different
research scenarios is presented in Section 8.4
• the research questions are brought together and answered in Section 8.5
• Section 8.6 summarises contribution of the research to theory and practice; and
• the chapter concludes by suggesting future work in Section 8.7.
8.2 Project summaryThis project explored whether a technology tool could be used to improve medication
management from a patient-focused perspective. Pharmacists were the main target of this
project as they have an important and evolving role in medication management, specifically in
medication reviews. The project had the potential to improve safety, quality and efficiency in
the medication review process for patients and more generally, to consider influences which
might have an impact on the development and uptake of technology tools in the medication
management environment. Some of the project findings also have broader implications for how
Page 280

technology tools are taken up within the Health sector; and for the consequent effect on
outcomes for health consumers.
In the absence of existing and relevant information models for medication management, the
researcher developed such a model himself by means of an investigation of information needs
and work flow. A document-based approach was chosen as the implementing solution for this
model, because documents are the prevailing information-sharing paradigm in Health. This
was a natural way to communicate and support clinical documentation for health professionals;
and the solution could readily be implemented as a digital document, using XForms – an XML-
based, next-generation markup language with promise for modelling human-computer
interactions and decision support, based on a document metaphor.
The information model and digital document evolved in parallel during the investigation of three
different use cases. In the first iteration, the information model and, subsequently, the digital
document prototype, were developed in the information-rich hospital scenario with clinical
pharmacists and medical officers. The second iteration prepared the information model and
digital document for the community context by testing by pharmacists accredited to undertake
Home Medication Reviews (HMRs). The third and final iteration tested these artefacts by
means of an intervention in the community medication review environment, where pharmacists
and GPs jointly undertook the medication reviews. The researcher then evaluated the
community intervention to assess its contribution to quality, safety; and efficiency, on the
medication review process.
The Design Research loops consisted of: data collection and analysis, reflection, modelling;
and prototyping – enabling the information model and document to evolve within the context
of supporting pharmacy decision-making and, as is normal with Design Research, feeding the
each iteration's findings into the planning for the next. Data triangulation was also used in these
scenarios to address the validity of both the data gathering, as well as the approach taken.
Before addressing the research questions specifically, it is appropriate to reflect on the themes
which emerged during the project. These were not only important as a framework within which
the researcher analysed and discussed findings, but also because they had direct implications
for the approach taken to developing the artefacts; and because they also have possible
implications for the adoption of technology tools by health professionals more generally. These
themes are discussed next in Section 8.3.
Page 281

8.3 ThemesAll the themes identified had implications for the design of the digital prototype – but one theme
was of particular professional interest to the researcher (himself a pharmacist).
Complementary and over-the-counter medications were not a specific target of investigation,
but were shown to be important for patient care. It became clear that these additions to patient
medication were not covered by existing methods of undertaking community medication
reviews, although these medications have significant potential implications for patients' health.
The electronic document recommended by this research project does, by contrast, enable the
inclusion of this group of self-recommended medications – and thus provides community
health care professionals with the ability to ensure a more thorough (and consequently safer)
understanding of patients' existing medication.
Other themes identified during the empirical research, such as the role of the practice nurse,
provide the potential for future work. The themes have been grouped under two headings: the
hospital and the community (as benchtop testing and field studies were both community
settings). The full set of themes is shown in Figure 8-1; and discussed in the subsequent sub-
sections, beginning with Sub-section 8.3.1. The implications of these themes are summarised
in Table 8-1.
Figure 8-1: Project themes
Hospital
CommunityMissing information
Conversation & communication
Information granularity & the language of health professionals
Time constraints & summary information
Decision support tools
Alerts and reminders
Systems for experts
Complementary &
over-the-counter medications
Perceptions about GPs
Technology-poor practice paradigm
Viewpoints of professional practice tools
The role of the Practice Nurse
Page 282

8. 3.1 Missing informationThe widespread problem of missing information evident in the literature was confirmed
immediately in the hospital scenario. The most common – and of most consequence to this
project – was that of medication-related information (and its lack). Missing information was also
a significant problem identified by community pharmacists during benchtop testing; and this
fact was confirmed during field tests.
The problem of missing information was more critical for HMR pharmacists than for hospital
pharmacists, as they had fewer information sources on which they could rely. Field studies
observed that a broad range of information could be missing; although an immediate impact
on the patient was less likely in the community than in a hospital, because the focus of care in
the community was on chronic disease management, rather than on acute situations as in
hospital. In other words, patients in hospital are generally much sicker than those being treated
in the community, so that missing or inaccurate information relating to their medication is likely
to have a much more serious effect.
Pharmacists could obtain information during patient interviews, but this ability was limited in
both hospital and community scenarios, because patients were not always reliable sources of
information. Although hospital pharmacists were able to elicit some missing information from
other health professionals, HMR pharmacists had only themselves to rely on and would often
press on with a medication review despite a lack of information; merely suggesting to the GP
that the HMR could be of limited value.
Other aspects of missing information were seen in the community: predominantly 'pattern'-
based missing information, founded on the patient reports from GP desktop systems provided
to the HMR pharmacist as the basis for the referral.
The most significant importance of missing information is its profound effect on the
effectiveness of decision support systems, which cannot function in the absence of relevant
information, e.g. the inability to calculate a dose in the absence of a patient weight value or
making prescribing recommendations in the absence of a coded patient diagnosis. Until this
problem can be resolved, one way forward may be to allow a decision support system to
operate with missing information, but to signal caution or limit recommendations; and to
highlight the need for clinical judgement. This approach would also have less impact on the
work process of health professionals.
From the point of view of this project, missing information became important as a basis for
formulating the initial information model. Whether hospital pharmacists pursued missing
Page 283

information for their decision-making was dependent on the importance of that information to
their decision. The researcher therefore concluded that a decision to pursue an information
element actively could be used as a surrogate for the value of that information element to the
decision-making process – and, consequently, as a surrogate for inclusion into the information
model. Further, because the digital document (the implementation of the model) is
communicated and shared among health professionals, the decision to identify sought
information elements consequently provides an opportunity to collect these missing elements
and thus provide a more complete, possibly current, record of medication use.
8. 3.2 Information granularityOne important aspect of information for both doctors and pharmacists was the varying levels
of granularity of information elements, which became evident both during the formulation of
requirements for information modelling, as well as during the analysis of missing information.
In the hospital environment, the nature of information ranged from patient case-notes to
specific data items such as a laboratory value, i.e. from aggregate to atomic levels of
information. The level of the information sought was driven by the need of the health
professional, for example, whether they knew little about the current situation and required
aggregated information such as a patient's case notes; or whether a pharmacist simply needed
a specific data item on which to base a decision. Participants mentioned during interviews that
they wanted 'everything' but conceded that a more useful day-to-day form of information would
be a concise summary, representative of important issues for the patient.
The changes to the hospital-based information model for the community context also
confirmed the need for elements at different levels of granularity – additions included
aggregated items (e.g. a field for patient indications) as well as atomic elements (e.g. a serum
creatinine value). It appeared that community pharmacists and GPs had a greater need for
aggregate data items than was the case in hospital scenario. The researcher considers the
granularity of information has two implications for information in clinical systems:
representation and communication.
Representation: there is enormous difficulty in providing all patient data at an atomic level
suitable for patient-centric decision support (attested by the vast efforts in producing
taxonomies and terminologies on which to build decision support systems). By contrast, the
clinical narratives (which include acronyms and 'shorthand'), used and valued by pharmacists
and GPs, do not readily underpin decision support. This represents a tension for the design of
health information systems – the need for atomic data to develop shared terminologies and
ontologies on which to build decision support systems and allow epidemiological research, vs.
Page 284

the need to share contextual information for patient care. The reporting of information needs
at different levels of granularity suggested that the information model and, consequently, the
decision support tool, should also reflect this granularity. Passages of text present particular
problems. How can structured lists (in decision support tools) be used to compose meaningful
(and readable) clinical narrative?
The information exchanged between these health professionals requires additional knowledge
– the patient context – to make it meaningful. Meaning occurs now because health
professionals make use of their shared and understood 'language'. It is expected that any
structure imposed by decision support tools on these 'conversations' will be met with
resistance from health professionals. Thus, the information communicated by the digital
document should be in the everyday language of practice of health professionals.
Communication: the information communicated between health care professionals should
occur in a way which complements their work processes and information flows. This project
identified simplicity and flexibility as important aspects of information communication between
pharmacists and doctors. The issue is, once again, how aggregate information can be
communicated between systems to allow humans to retain and share the rich narrative that is
meaningful to them – while simultaneously supporting the categorisation of the information
needed for 'seamless' inter-connectivity?
8. 3.3 Conversation and communicationConversation was revealed as a very important information pathway for hospital pharmacists:
primarily to chase missing information, but also as an efficient way of obtaining contextual
information about the patient, even when other sources were available. There are also many
occasions when tacit knowledge held by other health professionals would not otherwise be
available to the pharmacist. Conversation has other important roles, e.g. social roles, or
opportunistic interventions for education of other health professionals; and these cannot be
usurped by decision support tools.
HMR pharmacists' conversation opportunities were essentially limited to the GP, although field
studies observed the Practice Nurse as a 'front-line' to GPs. Although conversations with GPs
occurred infrequently – even when information was missing – pharmacists valued good
relationships with GPs. The importance of good communication was also supported by the fact
that pharmacists believed the digital document could provide common ground between
pharmacists and GPs to assist communication – and perhaps even improve relationships.
The use of conversation as a significant means of communicating information has a number
Page 285

of implications for decision support tools. Firstly, it is unlikely that all the information required
for decision-making will be captured for any decision support system – much of the
communicated information is the tacit knowledge of other health professionals. Secondly,
information about a patient will be summarised and can be highly contextual to the decision-
making process – this is a very efficient way of transferring information; and is the reason why
pharmacists often used conversation as their first information-gathering option. Thirdly,
conversation plays other social roles which can not be directly supported by decision support
tools.
It is clear that decision support tools can only in part support the information needs of health
professionals. The 'conversations' between health professionals must be supported, alongside
other means of communication, by decision support tools.
8. 3.4 Time constraints and summary informationTime, or the lack of time, was a constant influence on the health care process
In hospitals, the time to find, assimilate and interpret information was a significant issue for
pharmacists; and even more so for MOs. The need to cope with many patients and press on
with ward rounds was a major deterrent to MOs' interaction with decision support systems.
Despite pharmacists' and MOs' desire to have all patient-related information available to aid in
their decision-making, the concept of an artefact with summarised, relevant, patient-related
information was seen as a practical solution. Participants acknowledged that a trade-off
between displaying essential and all information would be difficult to achieve.
In the community, time was mainly an issue for GPs, affecting the quality of the HMR referral
sent to the pharmacist; as well as their ability to deal with HMR reports sent back to them by
pharmacists. Time also adversely affected GPs' level of involvement in the project. Many GPs
wanted a 'one-button' approach to generating HMR referrals; and expected reports from
pharmacists to be short and to the point. Pharmacists' awareness of these issues meant that
they strived to produce summarised reports which would minimise the time impact and
maximise report impact on GPs.
The impact of time, therefore, was on 'shaping' the information required or produced by health
professionals. This information shape always took the form of high-level information
summaries which could be considered quickly.
In the community setting, therefore, unless there is a significant change to the time available
to GPs, or the nature of the HMR process, GPs' enthusiasm for HMRs is likely to remain low.
Page 286

Thus, even with the possibility of providing information in the correct shape, any technology
must realise a balance between the information quality required for safe patient care and the
expediency required for business efficiency.
8. 3.5 Alerts and remindersAlerts and reminders are generally held to be practical and useful components of decision
support tools. Certainly, within the hospital setting, alerts and reminders were seen as the most
positive features of a decision support system – an avenue to promote good prescribing
practice. However, the value of alerts and reminders to decision-making was qualified by their
ability to perform within an appropriate patient context – but tailoring alerts for each drug,
disease and patient possibility is difficult. Alerts were considered to be of value in areas relating
to toxicity (e.g. previous ADRs for a patient); in unfamiliar areas (e.g. drug contraindications in
pregnancy); or in the case of issues requiring immediate attention. However, even these
serious reminders would become a nuisance if they occurred too often; and the threshold at
which they became an irritation could (and probably would) vary for each individual doctor.
Even if alerts were supported by reference information (as to why they were important), it was
their relevance which was the most important issue for acceptance by health professionals.
The introduction of reference information, however, would obviously introduce an extra level
of reading and inconvenience, limiting its usefulness. The possibility of personalising such a
system, so that more experienced MOs could control the number and frequency of alerts, was
not discussed by participants and should form the subject of future research.
Although the concept of alerts and reminders was supported in the hospital setting, this was
not the case in the community. HMR pharmacists suggested that alerts and reminders
provided in the digital document would be of limited use; and this view was confirmed during
the field studies, where it became apparent that the information required to trigger alerts was
often missing in the digital document – either because it had not been included in the original
HMR referral from the GP, or because the pharmacist did not act to the alert (by entering the
missing information).
In summary, the researcher believes that alerts and reminders pose a quandary for decision
support tools. With the ever-increasing amount of information available, the inclusion of alerts
and reminders in the 'background' of such a system to assist health professionals in recalling
crucial issues is intuitively desirable. For alerts and reminders to be truly useful, however, they
must also capture and structure information so that it is relevant to decision-making in both
hospitals and the community.
Page 287

A further issue in the community setting is that current information management practices by
pharmacists did not permit the evaluation of alerts and reminders in this project – so that the
usefulness of even the simple alerts and reminders implemented in the digital document
remains unclear. Clearly, this issue needs to be confirmed by larger and better controlled
studies.
8. 3.6 Decision support toolsAll hospital participants had exposure to decision support tools, although many of these were
simple information retrieval or laboratory reporting systems, reflecting day-to-day activities. In
addition to having more experience or exposure in this area, pharmacists offered more
opinions, particularly relating to the lack of success or usefulness of the systems they had
encountered – hampered by poor training or understanding of how the systems functioned.
HMR pharmacists' experience with decision support tools also reflected their work
environment: the availability of technology-based tools in the community was significantly less
than in the hospital setting, with HMR pharmacists being exposed only to a small range of
paper-based and electronic drug information resources. The only support for the HMR role was
a word processor! Interestingly, pharmacists in both settings failed to distinguish between
technology-based and other sources of decision support – whether paper-based, telephone-
based, or interaction with other health professionals.
What information a decision support system should provide – and whether this would be
possible – were areas of much discussion. In the hospital, many MOs and pharmacists saw
patient summaries as useful output from a decision support system, with the added ability of
the decision support system to allow links to more detailed patient information; although they
also believed that all information should be presented, on the basis that it was better to discern
the value of the information for oneself, than to allow a system designer or programmer to
make that decision. This difficulty of requirements engineering – ensuring that a subsequent
system will truly reflect the needs of its users – becomes still more complex when there are a
variety of users, with differing needs. It was not surprising to find a considerable level of
concern about the effectiveness of decision support systems in an acute care setting.
Participants also noted that the availability of wider information depended on 'someone' to
enter it; that reliance on such systems could present other problems; and that it was possible
for information to be incorrect, e.g. a diagnosis could often be incomplete, being a 'work in
progress' for the first few days of admission. How can decision-making be supported against
a background of varied and changing information?
Page 288

While expressing opinions about 'ideal' decision support, participants offered a wide range of
interpretations of decision support, with many views about information integration, mentions of
prompts and alerts and discussions of evidence-based information. The researcher believes
that, because participants' perceptions of the nature of a decision are generally based on their
(less than ideal) experiences, it is hardly surprising that clinicians, when asked what they want
from a decision support system, find it difficult to express their requirements succinctly and
clearly.
Hospital pharmacists' ability to access the same information as MOs was viewed positively
because this was seen as important for patient safety – viewing the same information through
'different eyes'.
It seems logical that the approach to designing decision support systems should take note of
the requirements of different user groups, e.g. pharmacists and MOs. However, there are a
number of problems to be solved:
• the conflicting requirements, not only between user groups, but within those groups
• the difficulty of incorporating all the required information to represent patient contexts
• the problem of structuring information to accommodate a variety of purposes.
Even when these problems are solved, there is still no assurance that data in the system will
be correct. Perhaps one solution would be to maintain the status quo – allow health
professionals to continue to share the same information, but assist them to do so by means of
technology. This not only allows simplicity of design for decision support systems, but also
continues to enable the 'different eyes' to contribute to patient safety. What does remain clear,
however, is the opportunity in these hospitals to develop more sophisticated decision support
for both pharmacists and MOs.
The situation in the community was different, in that HMR pharmacists' day-to-day experience
of decision support tools was far less than that of their hospital colleagues. In part, as this HMR
group was far less sophisticated in their technology use in general, there were fewer clues
available to the researcher about decision support needs. The main finding was an insight
about where a decision support tool might fit within the HMR process – before or after the
HMR. However, the more significant effort in the community is likely to be about enabling
information sharing through decision support, rather than prospective discussions about how
it should be shared.
Page 289

8. 3.7 Systems for experts rather than expert systemsMuch of the decision support discussion which arose in hospitals (particularly that relating to
electronic prescribing) was very much in the spirit of expert systems. The researcher has
already described the problems of capturing and structuring knowledge to allow a complete
representation of a patient in an information system.
A further factor to consider is the extensive use of personal (tacit) knowledge by health
professionals in their clinical practice. This thesis made no attempt to quantify such use, but
statements from pharmacists indicated the extensive use of personal knowledge – this was the
first strategy in responding to a question. Within the hospital environment, gaining this
knowledge took many years, fed by a range of formal sources and informal sources. Clinical
practice and personal experience were particularly significant. Over time, pharmacists' recall
of previous situations became the knowledge base for approaching new problems.
Pharmacists' understanding of the 'systems' outside the hospital environment also allowed
them to consider patient care more broadly than simply in terms of immediate medication use
within the hospital admission.
One knowledge-based approach to information gathering by pharmacists was to infer which
medications a patient should be taking on the basis of that patient's diagnosis – the absence
of a particular medication in the patient's list could indicate a possible omission in the current
medication list, or a need for the pharmacist to recommend a therapy option to the patient's
doctor. This, of course, is a role which could be undertaken by a decision support system –
but, once again, this presumes a large amount of accurate, contextual clinical information and
is an outcome which might well be unacceptable to both MOs and pharmacists.
Within the hospital, the knowledge level and experience of the pharmacists made them
'specialist' practitioners – some approached as consultants in their areas of practice, both from
inside and outside the pharmacy.
Just as clinical pharmacists in hospitals evolved into 'specialists' so, too, did HMR pharmacists
evolve within the community setting. This is evidenced prima facie by the requirement to
undertake further training for accreditation. But, in the presence of even less information
available for medication reviews (compared to the hospital), the reliance on use of personal
knowledge was very high.
The researcher believes that the enormous difficulty of capturing knowledge for a decision
support system and the extensive use of personal knowledge across the continuum of
medication management suggests a particular approach to the design of a decision support
Page 290

tool: the idea of designing 'systems for experts', rather than expert systems. This approach has
less to do with providing a wide range of information and attempting to adapt this information
across a range of patient and user contexts, than with providing essential information to
support decision-making, where a human can more appropriately understand and deal with
differing contexts.
8. 3.8 A technology-poor practice paradigmThe paucity of technology use in the HMR environment throws up a paradox.
Pharmacists have used (computerised) dispensing systems for many years and many have
experience of computer-based information tools – they could be seen both by health
professionals and others as quite 'experienced' in the use of IT, i.e. 'IT-literate'. Yet the
shortage of tools to support medication management has been confirmed by the researcher in
this scenario. All pharmacists were using 'simple' technology support, e.g. mainly word
processing tools for HMR reporting. There was very little (if any) use of technology-based
communication tools, e.g. email or web-based tools – paper-based information sources
prevailed. In light of these observations, the researcher considers that pharmacists should be
considered 'application-literate' rather than 'computer-literate' (as, indeed, would many health
professionals). Nevertheless, pharmacists were not adverse to trialling the digital document.
In fact, they were happy to 'try something new', but were more comfortable with a process
which reflected their usual one. When they had a choice of using the server service or a local
tool, therefore, they chose the latter. Although they were 'not ready for this yet', the researcher
gained the impression that simple, useful tools to help with HMRs would be welcomed.
Bondage to the GP desktop system had major implications for GPs' ability to envisage or
accept anything outside this desktop system. As the pharmacists have been described as
'application literate', the researcher considers the GPs to be 'application bound'.
There are two main issues arising from this technology-poor practice paradigm. Firstly, there
is a need for some technology to better support communication. Secondly, the ability to use
any technology-based tools will require a paradigm shift in community pharmacy practice.
From the perspective of this project, the shift required is that from communicating paper-based
information to communicating digital information. A possible way forward would be to use an
approach which can be implemented incrementally; is flexible in use; and complements the
work flow of individuals. The document-oriented user interaction approach trialled in this
project may be a way to achieve this goal. Addressing this predicament is a matter of the right
technology, not of more sophisticated technology.
8. 3.9 The ‘viewpoints’ of professional practice toolsGPs expressed the view that an interface to, or interaction with, the GP desktop system was
Page 291

needed for the digital document. This desire was to some extent mirrored by pharmacists, who
believed GPs would not use two separate systems. Further, there were some early
suggestions by pharmacists that the digital document could incorporate some features of
existing prescribing and dispensing systems: primarily drop-down lists.
The project, however, has no intention of duplicating features of these systems, as they serve
entirely specific and different purposes. The researcher takes the view that prescribing
systems and dispensing systems are built around the supply of medications. Prescribing is
concerned with the intention to supply a medication to a patient; and dispensing with the actual
supply of medication to a patient. However, neither can lay claim to representing what the
patient is actually taking – although this can be the belief of some GPs and pharmacists.
In relation to representing broader medication use, the prescribing system encountered in the
project had some limited ability to record Complementary Medicines (CMs) and Over-the-
Counter (OTC) medications taken by the patient, if this medication was included by the GP. A
CM or OTC, however, cannot be recorded in a dispensing system by the pharmacist. The only
way to reveal what actual medication the patient is taking is though a medication review.
The digital document used in this project has the potential to record all medication used by a
patient – it can become the 'current medication record', based on its ability be shared by the
relevant health professionals (and, ultimately, the patient). GPs' desire to have 'everything'
included in the GP desktop system presents a major impasse. Not only are the viewpoints of
the digital document and the GP desktop system different, the underlying data structures of
these proprietary systems are unlikely to exist in a form which allows the representation of a
current medication record. The researcher's own experience suggests that the proprietary
nature of many GP desktop systems makes even simple data interchange difficult.
The influence of the GP desktop viewpoint is therefore significant. But it should not impair
progress. While the functional role of a prescribing system will never be in question, it needs
to be acknowledged that it has one role only. The GP desktop system does not (in its current
guise) allow information sharing, nor does it represent a current medication record. Although
the digital document may be seen as an additional entity, it will need to exist in its own
communication space to be a shareable, communicable and, ultimately, current medication
record.
A further influence of the GP desktop system on the referral information given to pharmacists
was the 'pattern' of information determined by the report used by the GP. This pattern was the
result of the different information headings in the reports. These headings dictated what
Page 292

possible information could be provided to the pharmacist – although there was no certainty that
this information was provided. The variability of the information under these headings was
likely to be due to the data entry habits of GPs into the GP desktop systems, although the effect
of GP data entry habits was not studied during this project – this is another area of future
research.
8. 3.10 Complementary and Over-the-Counter medicationAlthough the researcher has mentioned that CMs and OTCs were not specifically targeted by
the project, they were notable omissions from the information sought by pharmacists and
medical officers in hospitals. Patients seldom considered or brought in CMs and OTCs when
they came in to hospital – but, in any case, CMs and OTCs were not included in the routine
questioning of patients about their medications by MOs or pharmacists. Against a background
of increasing consumer self-medication with CMs and OTCs, this appears surprising, as well
as being disappointing, considering that there is increasing discussion in the medical literature
about potential interactions of CMs with prescribed medications. It appears a 'blind eye' was
turned to CMs, except perhaps where they came to mind in particular clinical scenarios.
There was a greater awareness of CMs and OTCs by community pharmacists carrying out
medication reviews, who often reported their use back to the GP in HMR summaries (although
they were not included in the digital document medication list).
It is, of course, debatable whether recording information about CMs and OTCs is always
important (e.g. for vitamins), but it will be important for some medications where there are
potential interactions with prescribed medications (e.g. St. John's Wort). However, for CMs
and OTCs to be part of an ongoing medication record, they should be captured in the list of
other (prescription) medications. Their inclusion not only aids in obtaining a complete
medication list, but also serves as a reminder to ask the patient about CM and OTC use in later
visits to the GP, or for other medication reviews. This ability could also extend to the hospital
setting, if the digital document became more broadly shared.
Because the collection of information for HMR referrals is driven by the type of information
contained in the GP desktop systems, CM and OTC information is rarely collected. That is, as
the GP desktop system only contains information about prescription medication, the 'prompt'
for the pharmacist is only for prescription medication to be updated within the GP system. So
when the pharmacist updates the accuracy of the 'GP's list', CMs and OTCs will be reported
separately; and the GP's medication list will remain a separate, incomplete medication list.
The researcher's belief that the digital document should exist 'outside' GP systems (and,
therefore, outside their influence), is based on the observation that these systems have
Page 293

different viewpoints; and that independence is required to allow the communication of
information between health professionals. This independence also now provides an
opportunity to record information about CMs and OTCs to the advantage of the GP and the
pharmacist and, ultimately, the patient to enable informed decisions about therapy.
8. 3.11 Pharmacists’ perceptions of GPs in the HMR processFollowing the hospital scenario, the researcher concluded that pharmacists had no hesitation
in communicating with medical officers (or any other health professionals) to seek information,
or for any other purpose. However, for community pharmacists, communication with GPs was
infrequent and often undertaken reluctantly. This reluctance by pharmacists was expressed in
accredited pharmacists' meetings, benchtop testing and field studies. There was a uniform
understanding by pharmacists that GPs were busy; and that they should not be bothered
inappropriately. However, there was also a perception that many GPs were not convinced of
the value of the HMR process – suggested by pharmacists as a reason for the poor uptake of
HMRs by GPs. Other GPs appeared to approach HMRs as a mechanical business process –
reinforced by pharmacists' experience of poor, or no, feedback from GPs after HMRs. Not only
is this situation unfortunate, but it has potential implications for patient safety, evidenced by
pharmacists being unaware of the outcomes of HMRs for patients.
Where good GP-pharmacist communication existed, this was highly valued by pharmacists.
For the field study group, relationships between GPs and pharmacists were good, but this
study group was atypical, being unusually motivated about HMRs compared with the norm.
The researcher feels no doubt, however, that the better the GP-pharmacist relationship, the
better the HMR process generally.
This has two possible implications for the digital document. Firstly, as an intervention tool, the
digital document may initially be more successful where good relationships (and
communication) already exist – the intervention will be seen as an avenue to improve the HMR
process. Secondly, using the digital document may itself provide an environment which not
only helps communication, but also could improve relationships – by providing a focus for HMR
improvement and 'forcing' communication. This latter point was implied by pharmacists in the
benchtop and field study groups. And where good communication exits so, too, might there be
better outcomes for patients.
8. 3.12 The role of the Practice NurseNot all GP practices have a Practice Nurse, especially small GP practices. During the project,
it was evident to the researcher that the Practice Nurse was often the channel for 'direct'
communication with the GP. This was true for the researcher; and appeared true for many of
the pharmacists undertaking HMRs. The pharmacist, of course, would still discuss important
Page 294

clinical issues with the GP. The direct patient involvement of a Practice Nurse is often
substantial, e.g. carrying out patient health assessments and flagging patients who require
medication reviews to the GP.
There is an opportunity here to extend the role of the Practice Nurse to include more direct
involvement in the generation of the HMR referral, as time was a major deterrent to digital
document use for GPs. Interestingly, one GP mentioned using receptionists to enter data into
a Medication Action plan – an area of some concern, as receptionists are unlikely to have the
skill or background for this role. Practice Nurses, however, do have both the school and the
background for this task. As Practice Nurses are an intermediary between the GP and
pharmacist, have knowledge of the patient; and have access to patient information, they are
in an ideal position to generate a referral document i.e. using the digital document. The
researcher makes this statement without knowledge of work loads for these individuals – but,
as many Practice Nurses perform health assessments, the creation of a medication referral
document seems a logical next step, given the overlapping natures of these documents. In
light of the issues of time and GP desktop system interfaces, extending the role of the Practice
Nurse provides a possible way of increasing the number and quality of HMRs.
Reflection on the themes which emerged during the project now concludes with a summary of
the themes presented in Table 8-1, in which the themes are considered within and across the
hospital and community settings. The table identifies implications for design or implementation
which arose during this project; and also highlights implications the researcher considers may
have a broader impact on the uptake of decision support tools within the health care sector
more generally.
Table 8-1: The implications of project themes
Theme Hospital scenario Community scenarioMissing information The value of an information element can be
determined by whether a health professional needs to pursue that information element for their decision-making – this suggests the inclusion of that information element into a model of essential information.
The implementation of an information model should suggest but not mandate the entry of essential information elements.
Information granularity and the language of health professionals
Information-based models and support tools for health professionals should reflect the information granularity evident in everyday practice and the ‘language’ used by health professionals. This poses a significant dilemma for the notion using categorisation for the exchange of information between systems and for the use of information for research.
Page 295

Conversation and communication
Conversation is a significant and very efficient way for health professionals to access contextual information and knowledge not available through other means.
Conversation also serves social and other roles and is highly valued by pharmacists. The information available through conversation is unlikely to be captured and structured for use within decision support systems and some roles cannot be duplicated within decision support systems.
Time constraints and summary information
Time was perceived to be a major influence in the ability to use decision support tools.
Time was a major influence for GPs to initiate referrals and cope with HMR reports received from pharmacists.
A concise, contextually-relevant summary of medication-related information is an approach to providing information for time-poor health professionals.
Decision support tools
The perception of what decision support tools are is influenced by the personal experiences of health professionals. It is difficult for health professionals to express requirements for decision support tools and to not be influenced by these experiences.
Alerts & reminders Alerts and reminders are perceived to be the most useful features of decision support tools. However, the acceptance of these features will be impacted upon severely by their usefulness (based on patient context), ability to access the appropriate information, repetition and impact on the work process.
The role for alerts and reminders in the context of a community-based decision support tool is still unclear but likely to be of limited application.
Systems for experts rather than expert systems
Pharmacists exhibit expert behaviours across the medication management continuum. Supporting the work practice of these individuals is better achieved by providing essential information to complement their professional knowledge, rather than attempt the onerous task of collecting and shaping the range of necessary information to support a range of patient and user contexts.
A technology-poor practice paradigm
The paucity of technology use in the community suggests the best technology will be the ‘right’ technology, implemented incrementally; and which is flexible and complements work flow. A document-oriented user interaction approach may be suitable.
The ‘viewpoints’ of professional practice tools
The viewpoints of GP desktop systems (and dispensing systems) do not support information sharing and preclude interfacing to concepts such as the digital document. GP desktop systems also ‘shape’ the information use of pharmacists.
Pharmacists’ perceptions of GPs in the HMR process
Many GPs are not convinced of the value of HMRs. Better communication between pharmacists and GPs, by a means such as the digital document, may improve communication and help with the uptake of; and value of HMRs to GPs.
The Practice nurse There may be a role for Practice Nurses to generate HMRs using the digital document to alleviate the problem of the number and quality of HMRs from GPs.
Complementary medicines (CMs) & Over-the-counter (OTC) medication
Information about CMs and OTCS is not routinely sought.
Information about CMs and OTCs is not routinely recorded in GP desktop systems. Pharmacists report the use of CMs and OTCs ‘alongside’ prescription medications/
Against the increasing use of CMs and OTCs in the community and potential for drug interactions with prescribed medications, there is a need capture use of these agents alongside prescription medications. There is an opportunity to do so with a shared record of medication-related information such as the digital document.
Table 8-1: The implications of project themes
Theme Hospital scenario Community scenario
Page 296

The evolution of the information model through the three iterations of the project is now
discussed in Section 8.4.
8.4 The evolution of the information modelThe information model and, consequently, its expression as a digital document underwent
three changes as a result of the iterations through the three research scenarios. Within each
scenario, analysis of the data suggested which information elements should be included in the
model and which additional functional requirements were needed in the digital document
prototype. A summary of these changes is shown in Figure 8-2. The figure shows the
transition of information elements in the model, represented as a series of documents.
Page 297

Figure 8-2: The evolution of the information model
PATI
ENT
INFO
RM
ATIO
Npe
rson
al nam
e, a
ddre
ssM
edic
are
num
ber
date
of b
irth,
age
, sex
wei
ght,
heig
ht, b
lood
pre
ssur
ese
rum
cre
atin
ine
alle
rgie
sad
vers
e dr
ug re
actio
nsre
crea
tiona
l sub
stan
ces
refe
renc
eG
P de
tails
, Com
mun
ity P
harm
acy
Oth
er c
onta
cts
phys
ical fa
lls, c
ogni
tion,
mem
ory,
lang
uage
, de
xter
ity, v
isio
n, h
earin
g, s
wal
low
ing,
eq
uipm
ent,
othe
r--
----
----
-----
----
----
-----
----
-----
----
TREA
TMEN
T IN
FOR
MAT
ION
curr
ent t
reat
men
tac
tive
prob
lem
str
eatm
ent h
isto
rym
edic
al h
isto
ry--
----
----
-----
----
----
-----
----
-----
-M
EDIC
ATIO
N IN
FOR
MAT
ION
imm
unis
atio
nste
tanu
s, fl
u, p
neum
ococ
cus,
oth
er
imm
unis
atio
ns
curr
ent m
edic
atio
nsre
gula
rw
hen
requ
ired
date
date
gene
ric n
ame
gene
ric n
ame
bran
d na
me
bran
d na
me
dose
, rou
tedo
se, r
oute
frequ
ency
frequ
ency
inst
ruct
ions
inst
ruct
ions
indi
catio
nin
dica
tion
dura
tion
dura
tion
patie
nt in
dica
tion
patie
nt in
dica
tion
med
icat
ion
hist
ory
chan
ge d
ate
chan
ge d
ate
chan
ge re
ason
chan
ge re
ason
chan
ge b
ych
ange
by
med
icat
ion
man
agem
ent i
ssue
sso
cial
med
icat
ion
man
agem
ent
----
----
----
----
----
----
-----
----
INVE
STIG
ATIO
NS
la
bora
tory
date
, ite
m, r
esul
tw
arfa
rin a
nd IN
R a
lert
s
PATI
ENT
INFO
RM
ATIO
Npe
rson
al nam
e, a
ddre
ssM
edic
are
num
ber
date
of b
irth,
age
, sex
wei
ght,
heig
ht, b
lood
pre
ssur
ese
rum
cre
atin
ine
alle
rgie
sad
vers
e dr
ug re
actio
nsre
crea
tiona
l sub
stan
ces
refe
renc
eG
P de
tails
, Com
mun
ity P
harm
acy
Oth
er c
onta
cts
phys
ical fa
lls, c
ogni
tion,
mem
ory,
lang
uage
, de
xter
ity, v
isio
n, h
earin
g, s
wal
low
ing,
eq
uipm
ent,
othe
r--
----
----
-----
----
----
-----
----
-----
----
TREA
TMEN
T IN
FOR
MAT
ION
curr
ent t
reat
men
tac
tive
prob
lem
str
eatm
ent h
isto
rym
edic
al h
isto
ry--
----
----
-----
----
----
-----
----
-----
-M
EDIC
ATIO
N IN
FOR
MAT
ION
imm
unis
atio
nste
tanu
s, fl
u, p
neum
ococ
cus,
oth
er
imm
unis
atio
ns
curr
ent m
edic
atio
nsre
gula
rw
hen
requ
ired
date
date
gene
ric n
ame
gene
ric n
ame
bran
d na
me
bran
d na
me
dose
, rou
tedo
se, r
oute
frequ
ency
frequ
ency
inst
ruct
ions
inst
ruct
ions
indi
catio
nin
dica
tion
dura
tion
dura
tion
patie
nt in
dica
tion
patie
nt in
dica
tion
med
icat
ion
hist
ory
chan
ge d
ate
chan
ge d
ate
chan
ge re
ason
chan
ge re
ason
chan
ge b
ych
ange
by
med
icat
ion
man
agem
ent i
ssue
sso
cial
med
icat
ion
man
agem
ent
----
----
----
----
----
----
-----
----
INVE
STIG
ATIO
NS
la
bora
tory
date
, ite
m, r
esul
tw
arfa
rin a
nd IN
R a
lert
s
REF
ERR
AL IN
FOR
MAT
ION
refe
rral
dat
ere
view
dat
ere
port
date
com
plet
ed d
ate
refe
rral
des
crip
tion
refe
rral
reco
mm
end.
refe
rral
act
ion
refe
rral
reso
lved
reso
lved
dat
e
REF
ERR
AL IN
FOR
MAT
ION
refe
rral
dat
ere
view
dat
ere
port
date
com
plet
ed d
ate
refe
rral
des
crip
tion
refe
rral
reco
mm
end.
refe
rral
act
ion
refe
rral
reso
lved
reso
lved
dat
e
med
icat
ion
revi
ew d
ate
PATI
ENT
INFO
RM
ATIO
Npe
rson
al nam
e, a
ddre
ssun
it re
cord
num
ber
date
of b
irth,
age
, sex
wei
ght,
heig
ht, b
lood
pre
ssur
e
alle
rgie
sad
vers
e dr
ug re
actio
nsre
crea
tiona
l sub
stan
ces
refe
renc
eG
P de
tails
, Com
mun
ity P
harm
acy
----
----
----
-----
----
-----
----
-----
----
--TR
EATM
ENT
INFO
RM
ATIO
Ncu
rren
t tre
atm
ent
adm
issi
on re
ason
& d
iagn
oses
trea
tmen
t his
tory
past
med
ical
his
tory
----
----
----
-----
----
-----
----
-----
---
MED
ICAT
ION
INFO
RM
ATIO
Ncu
rren
t med
icat
ions
date
gene
ric n
ame
dose
, rou
tefre
quen
cy, i
nstru
ctio
nsin
dica
tion
dura
tion
med
icat
ion
hist
ory
chan
ge d
ate
chan
ge re
ason
chan
ge b
ym
edic
atio
n m
anag
emen
t iss
ues
soci
alco
mpl
ianc
e--
----
----
-----
----
----
-----
----
-----
---
INVE
STIG
ATIO
NS
labo
rato
ryda
te, i
tem
, res
ult
war
farin
and
INR
ale
rts
med
icat
ion
revi
ew d
ate
PATI
ENT
INFO
RM
ATIO
Npe
rson
al nam
e, a
ddre
ssun
it re
cord
num
ber
date
of b
irth,
age
, sex
wei
ght,
heig
ht, b
lood
pre
ssur
e
alle
rgie
sad
vers
e dr
ug re
actio
nsre
crea
tiona
l sub
stan
ces
refe
renc
eG
P de
tails
, Com
mun
ity P
harm
acy
----
----
----
-----
----
-----
----
-----
----
--TR
EATM
ENT
INFO
RM
ATIO
Ncu
rren
t tre
atm
ent
adm
issi
on re
ason
& d
iagn
oses
trea
tmen
t his
tory
past
med
ical
his
tory
----
----
----
-----
----
-----
----
-----
---
MED
ICAT
ION
INFO
RM
ATIO
Ncu
rren
t med
icat
ions
date
gene
ric n
ame
dose
, rou
tefre
quen
cy, i
nstru
ctio
nsin
dica
tion
dura
tion
med
icat
ion
hist
ory
chan
ge d
ate
chan
ge re
ason
chan
ge b
ym
edic
atio
n m
anag
emen
t iss
ues
soci
alco
mpl
ianc
e--
----
----
-----
----
----
-----
----
-----
---
INVE
STIG
ATIO
NS
labo
rato
ryda
te, i
tem
, res
ult
war
farin
and
INR
ale
rts
REF
ERR
AL IN
FOR
MAT
ION
refe
rral
dat
ere
view
dat
ere
port
date
com
plet
ed d
ate
com
men
tary
refe
rral
des
crip
tion
refe
rral
reco
mm
end.
refe
rral
act
ion
refe
rral
reso
lved
reso
lved
dat
e--
----
----
-----
----
----
-----
----
-----
--PA
TIEN
T IN
FOR
MAT
ION
pers
onal
refe
renc
eph
ysic
al--
----
----
-----
----
----
-----
----
-----
---
TREA
TMEN
T IN
FOR
MAT
ION
curr
ent t
reat
men
ttr
eatm
ent h
isto
ry--
----
----
-----
----
----
-----
----
-----
-M
EDIC
ATIO
N IN
FOR
MAT
ION
imm
unis
atio
ns
curr
ent m
edic
atio
nsre
gula
rw
hen
requ
ired
med
icat
ion
hist
ory
med
icat
ion
man
agem
ent i
ssue
s--
----
----
-----
----
----
-----
----
-IN
VEST
IGAT
ION
Sla
bora
tory
war
farin
and
INR
ale
rts
REF
ERR
AL IN
FOR
MAT
ION
refe
rral
dat
ere
view
dat
ere
port
date
com
plet
ed d
ate
com
men
tary
refe
rral
des
crip
tion
refe
rral
reco
mm
end.
refe
rral
act
ion
refe
rral
reso
lved
reso
lved
dat
e--
----
----
-----
----
----
-----
----
-----
--PA
TIEN
T IN
FOR
MAT
ION
pers
onal
refe
renc
eph
ysic
al--
----
----
-----
----
----
-----
----
-----
---
TREA
TMEN
T IN
FOR
MAT
ION
curr
ent t
reat
men
ttr
eatm
ent h
isto
ry--
----
----
-----
----
----
-----
----
-----
-M
EDIC
ATIO
N IN
FOR
MAT
ION
imm
unis
atio
ns
curr
ent m
edic
atio
nsre
gula
rw
hen
requ
ired
med
icat
ion
hist
ory
med
icat
ion
man
agem
ent i
ssue
s--
----
----
-----
----
----
-----
----
-IN
VEST
IGAT
ION
Sla
bora
tory
war
farin
and
INR
ale
rts
Hos
pita
l inf
orm
atio
n m
odel
Com
mun
ity-a
ligne
d in
form
atio
n m
odel
Fina
l inf
orm
atio
n m
odel
Med
icat
ions
spl
it in
to
regu
lar &
whe
n re
quire
d
Adde
d se
rum
cr
eatin
ine
Adde
d ot
her c
onta
cts
Adde
d ph
ysic
al
com
pone
nts
Cha
nged
labe
l
Cha
nged
labe
l
Mov
ed re
view
dat
e
Adde
d ne
w
Ref
erra
l In
form
atio
n pa
ge
Adde
d co
mm
enta
ry
Adde
d br
and
nam
e
Adde
d pa
tient
indi
catio
n
Cha
nged
labe
l
Adde
d BM
I &
crea
tinin
e cl
eara
nce
calc
ulat
or
Cal
cula
tor
Cal
cula
tor
Page 298

Attention now turns to answering the questions which guided the project. The research in this
project was encapsulated in one main research question and a number of sub-questions.
These are brought together next in section 8.5.
8.5 research questionsThe main research question for this project was:
Can we advance medication management for health consumers by supporting decision-making with a patient-focused information model and technology-based intervention?
This complex was answered through a number of sub-questions used in the different phases
of the project, summarised in Figure 8-3. Each sub-question will be addressed on the way to
answering the main research question.
At the beginning of the project, prior to the investigation, two preliminary questions were
addressed by means of investigation of the relevant literature.
What support is there for pharmacists for medication-related decision-making?
The researcher found there was very little evidence of suitable technology to support the
pharmacy profession with its medication-related decision-making other than for a few
Figure 8-3 Research questions in relation to research phases
Part 1 – The Hospital Scenario
Part 2 – The Community Scenario2A – Investigation of the
home medication review context: prototype bench testing
2B – Medication review field study
Literature review
Can we advance medication management for health consumers by supporting decision-making with a patient-
focused information model and technology-based intervention?
D. Can our intervention improve safety, quality and efficiency?E. What is the contribution of the information model?F. What is the contribution of the technology artefact (digital document)?
A. Can medication management-related issues in the hospital environment be addressed by the use of technology?
B. What is the best way of implementing this technology
approach?
C. What are the differences in the community environment that affect the approach?
What support is there for pharmacists for medication-related decision-making?
What technology might provide this support?
Page 299

examples of relatively simple support tools and the traditional practice tools for dispensing and
information retrieval. This finding suggested a clear need to develop an appropriate tool to
support pharmacists with decision-making or additional information needs to support their
expanding, patient-centred medication management roles. The need for this project was
consequently justified.
What technology might provide this support?
The concept of a document metaphor, implemented as a digital document, was identified as a
suitable approach, promising to support information sharing and communication by means of
a metaphor familiar to health professionals. A document approach was also a good way to
satisfy the requirements for flexible information representation required for the dynamic and
complex health environment. Documents, by their nature, also offered other potential
advantages, such as support for some of the social aspects of the work.
As the need for the research was justified; and a technology approach for the project identified,
more specific research sub-questions could be addressed. These follow below.
A: Can medication management-related issues in the hospital environment be addressed by the use of technology?
The strategy for answering this first question was to understand information use by
pharmacists and medical officers involved in medication management within hospitals. The
hospital scenario was investigated first, as the researcher considered it to be a more
'information rich' environment, which would allow a fuller investigation of the issues
surrounding information use by health professionals. The medication management related
issues which emerged in this environment included:
• the inefficiency and uncertainty of decision-making due to the need to use disparate and
quite distinct sources of information
• the fact that information, particularly that related to medication, was often missing, which
led to concerns by medical officers and pharmacists about the effect on safety and
quality of life for patients
• the fact that conversation was an important method for pharmacists to seek missing
information – conversation was also a very important and efficient way of pharmacists
obtaining highly contextual patient-related information from other health professionals,
even when other sources of information were available
Page 300

• the prominent use of individual knowledge in medication-related decision-making of
pharmacists; and
• the differences between the information which health professionals: stated they would
like use; stated they did use; and were actually observed to use by the researcher.
The many difficulties experienced by pharmacists and doctors in accessing need information
suggested that technology could help address these issues through a shareable model of
essential information elements. This information model would need to cope with missing
information elements, recognise the use of personal knowledge; and represent and
communicate information in the same way that health professionals used information.
B: What technology approach might be appropriate to do this?
This question was addressed by investigating the potential for XForms technology to
implement the digital document which was based on the information model.
The researcher selected XForms as the underlying implementation technology based on
XForms' technical advantages such as: ease of authoring, flexibility; and the ability it provided
for the researcher to investigate alerts and reminders – while using a document-oriented view.
Despite some issues due to XForms being an evolving standard, the digital document
prototype was implemented as intended and the researcher's experience confirmed the
potential of XForms to realise a portable and dynamic document, suitable for supporting
information sharing and communication by health professionals.
C. What are the differences in the community environment that affect the approach?
This question was answered through benchtop testing of the digital document prototype by
accredited pharmacists. The major changes to the model were related to the inclusion of
patient information elements required in the community environment (e.g. reasons for referral),
or supporting physical information (e.g. falls etc.) which were not available to the community
pharmacists (compared with their hospital colleagues). The inclusion of these information
elements actually reflected the similar information needs of community and hospital
pharmacists. But, in the case of community pharmacists, the model required extensions to
make up for the unavailability of information sources (including conversation) available to their
hospital colleagues – although the depth of information required by community pharmacists
Page 301

was less, as patient management is concerned with (more stable) chronic disease compared
to the acute disease episodes experienced in hospitals. The main intention of community
pharmacists was supporting patients in managing at home and, consequently, in keeping
patients out of hospital. Further, in the community, the document needed to be 'context-aware'
of its use, depending on whether it was used by the GP for referral, or by the pharmacist for
the HMR.
D. Can our intervention improve safety, quality and efficiency?
This question was answered by field study interventions into the HMR setting in the
community. This intervention, though limited in terms of the number of subjects, was sufficient
for GPs and pharmacists to perceive benefits for the medication management process, health
professionals; and patients. There were a number of contributions to safety:
• encouraging the collection of information relevant to medication management-related
decision-making, thus increasing the chances of errors being detected and corrected by
pharmacists
• increased accuracy of medication-related information as the result of document sharing
by health professionals
• more timely sharing and better availability of information for the GP, so that patient
recommendations from pharmacists could be effected more quickly by GPs
• encouraging pharmacists to move from hand-written reports
Although these safety gains were perceived, they would need to be confirmed through more
extensive field studies.
Quality was examined under system and information headings, but the researcher believes
information quality was the most important issue for pharmacists carrying out home medication
reviews, both from the perspective of the review process and that of the report. Quality
improvements were perceived by the:
• use of standardised essential information elements to guide pharmacists with the depth
and quality of information required for HMR reporting – this was also seen to assist
pharmacists with quality assurance evaluations
• move away from hand-written reports
• ability to communicate a succinct summary of essential information to the GP in a timely
manner; and
• potential for pharmacists to receive GP feedback though an action plan
Efficiency was illustrated in two ways, through improvements in:
Page 302

• the timeliness of information; and
• availability of information.
This would allow patient-related decisions to be made more quickly by the GP and facilitate
feedback to the pharmacist.
E. What is the contribution of the information model?
The model provides a template of essential medication-related information which is succinct,
relevant and can be understood and shared by health professionals. This was reinforced by
the model’s ability to be used in different medication management scenarios. Thus, the
principal contribution of the information model is a relevant framework for medication
management-related information.
F. What is the contribution of the technology artefact (digital document)?
The digital document allows a flexible way of communicating and sharing medication-related
information through a simple, easy-to-use artefact. The document-centric approach is a
comfortable fit with health professionals’ practice. The ability to provide some dynamic
functionality has limited, although potentially useful application. In brief, the principle
contribution of the digital document is its natural fit with the work environment and its flexibility
in use and communication.
The researcher now returns to the main question for this research project.
Can we advance medication management for health consumers by supporting decision-making with a patient-focused information model and technology-based intervention?
The answer to this question is 'yes'. However, this answer is contingent on the approach used
to develop the technology used in the intervention. This project has identified a number of
important, information-related issues which can affect decision-making in the practice area of
medication management, including: missing information, the context of information use; and
the relationship of information use by health professionals alongside use of their personal
knowledge. These factors all affect the approach to designing and implementing technology
tools. An affirmative answer, based on this project, is therefore contingent on the use of the
correct technology, as a complement to, rather than an intruder into, human decision-making.
Page 303

The suggested contributions of this research to theory and practice are now discussed in
Section 8.6.
8.6 Research contributions
8. 6.1 Contributions to theoryThis project has contributed to the development of theory in the area of medical information
models, especially those relating to the support of medication management, as well as to the
understanding of the support role offered by a digital document as the potential means of
implementation of such a model.
• Decision support theory has tended to concentrate on: the identification and
development of taxonomies or guidelines suitable for inclusion into a DSS software
implementation; knowledge translation into active rules; and development of software
which appropriately combines the knowledge and rules (and local data) to provide
appropriate decision support functionality on a user’s desktop. This research project, by
contrast, has focused on identifying the issues which underpin the development of the
information model. A particularly important finding is that decision-making can be most
effectively supported by a collection of essential information elements as a complement
to human knowledge, rather than attempting to represent all information and knowledge
within a model. This stance acknowledges the difficulty of categorising complex, health-
related information; the need for humans to apply information in a wide variety of
differing and variable contexts; and the manner in which health care professionals use
and communicate language which is meaningful for their purposes. These findings cast
a different light on the analysis of both decision support and expert systems – and make
a significant contribution to theory in the area of medical support systems.
• The role of the document, in either paper or electronic form, to represent and
communicate information is well understood. The role of paper-based documents in
Health is also well known. This project has added to this knowledge by confirming the fit
of a digital document for the process of the medication management for doctors and
pharmacists; and that the digital document can serve as a suitable boundary object
between these practice groups in Health. An important finding was that the application of
dynamic properties of digital documents may be limited, as these documents exist in an
environment of information uncertainty. These results suggest both that there is great
promise for the use of digital documents in Health; but that at the same time the
complexity of the health care environment demands particular attention.
Page 304

• Finally, the project adds to the empirical evidence for the need for decision support tools
for pharmacists involved in medication management, particularly the emerging
community role of medication reviews. It does this while identifying issues which affect
the approach to development and implementation, or the success of these tools.
8. 6.2 Contributions to practiceThis project has contributed to medication management practice by suggesting a framework
which can be used to improve the conduct of medication reviews. Further, the project has
identified problems and possible solutions which can contribute to the better uptake of
technology in the area of medication management and, in general.
• The digital document approach in this project provides a framework which can be used
to improve the sharing and communication of relevant medication-related information
between doctors and pharmacists. This promises gains in safety, quality and efficiency
of the medication management process; and ultimately improvements in outcomes for
patients.
• The project has identified that sophisticated technology is not required to implement
changes in the medication management environment. The approach is one of providing
the ‘right’ technology which accommodates the work processes of individuals – a
‘lightweight’ approach advocated the project, using the digital document, is adequate for
supporting a paradigm change in the community.
• The project has diagnosed issues that impact on the conduct of medication reviews in
the community. The inability of existing medical and pharmacy systems to represent
actual current medication taken by patients suggests that practice of medication
management may not be served adequately by a single decision support tool.
• Opportunities for practice improvement have also been suggested: an approach to
enable the recording of complementary and over-the-counter medications, addressing a
current practice problem; and an opportunity to improve the number and quality of home
medication review referrals through the involvement of other health professionals (the
medical practice nurse).
• Future work suggested by the project (and one project already begun) suggests other
opportunities to contribute to improved patient outcomes in the area of medication
management and, more broadly in Health.
This chapter now concludes with suggestions for future work in Section 8.7.
Page 305

8.7 Future workThe future work suggested here is based on opportunities envisaged during the project; and is
expressed as high level concepts. Clearly, issues such as technology infrastructure and
privacy/security would need to be considered more fully in these future projects than they have
in the present project. In addition, redevelopment of the proof of concept digital document
might well require redevelopment in other languages or on other platforms.
8. 7.1 More extensive field trialsThe project began with the understanding that results would be indicative and that, as a proof
of concept, wider extrapolation of results would be inappropriate. Participants in field studies
did perceive benefits, particularly with communication and how information could be better
shared. They also considered there would be benefits to medication management for safety,
quality and efficiency. But as the researcher was not able to directly measure benefits, more
extensive field trials are now required. As GPs and pharmacists fall into informal geographical
groups around patients requiring HMRs, opportunities for trials within these community
'networks' would be both possible and appropriate.
8. 7.2 A ‘working document’ for medication management in a hospitalThis suggestion arose during testing of the digital document by the Hospital Outreach
Medication Review pharmacists. These pharmacists used a paper medication and allergy
history tracking form within the hospital and a further medication transfer summary form to
convey patients’ medication information to GPs. The close fit of the digital document to the
purposes of both these forms suggested the digital document’s use as a shared ‘working
document’ to achieve both functions, with interest shown by this group as a possible future
project. This project has already begun within the University of South Australia.
8. 7.3 HMR referral generation by Practice Nurses The Practice Nurse played a significant role in medical practices, this role emerging as a
‘theme’ in the project. As discussed earlier, Practice Nurses are ideally placed in the
communication pathway to GPs, have access to patient data and are already involved in
patient-related activities such as performing health assessments. In light of the time constraint
on GPs which causes problems in the number and quality of HMRs being generated, there
may be a role for Practice Nurses to generate HMRs using the digital document.
8. 7.4 A digital document approach in an Aged Care FacilityThe intent of a review in an Aged Care Facility (ACF) is the same as that of an HMR and the
digital document in its present state would come close to supporting this. The digital document
was tested only on a few ACR reviews but did not identify any issues that would obviate or
even limit its use for such a purpose. In the ACF scenario, in the absence of any other systems,
the digital document could become a current medication record, useful to facility staff, the
Page 306

reviewing pharmacist and the visiting GP. With the possibility of on-line sharing, remote access
by the GP would also be possible.
8. 7.5 A digital document approach for information exchange for discharged hospital cardiac patientsInterest was expressed by an adult hospital to use the digital document for cardiac patients
discharged into the community. As a high-risk group, these cardiac patients required an HMR
to be undertaken within a short period once in the community to ensure that they were
managing their medication appropriately. Part of this hospital’s needs was to communicate the
relevant information to the HMR pharmacists; and then the HMR pharmacists’ review
information back to hospital. The leader of the hospital project (who was also head of the
cardiac unit) suggested signalled his interest in discussing the results of the project with the
researcher.
8. 7.6 A portable medication recordThe portability of the digital document suggested its use as a mobile medication record for
patients. This was suggested by a GP who saw an opportunity for using the digital document
on a USB drive, so the patient could take their medication records with them to the GP, or for
emergency visits etc. This could be achieved using a similar approach to the local use of the
document, e.g. using a Visual Basic form and browser (such as Firefox Portable®) stored on
a USB drive. There would be issues to consider such as loss and size of the device, privacy
and security etc. However, this approach may be promising as USB drives are more likely to
be able to connect easily to relatively recent computers (compared to e.g. Smartcards that
would require dedicated device readers and software). The advantages here would be that the
GP, community pharmacist and hospital pharmacist could all contribute to maintaining the
currency of the information on the USB record when they were with the patient.
8. 7.7 A digital document approach for patient groups with extensive medica-tion use As well as the elderly patient population targeted in this project, there are other groups of
individuals that have extensive medication use because of chronic illness. From the
researcher’s experience in a Women’s and Children’s hospital, two pertinent groups are
patients with Cystic Fibrosis and Oncology patients. Both of these groups can be diagnosed at
a very early age, have treatment and support that heavily involves the use of medication and
nutrition and are users of complementary medicines. There is a great deal of effort required of
these patients and their parents or guardians to manage medications. The digital document
approach, either on-line or as local record may help by providing a shareable, maintainable
current record. The approach of a portable record perhaps may be particularly useful in an
adolescent context. There is also a more general question of how useful the approach of a
portable record might be in a general paediatric context, for use by parents.
Page 307

8. 7.8 A shared record with health consumersIt is ironic that the term ‘patient-focused’ usually fails to include the direct involvement of the
patient. As suggested during the field study, there may be an opportunity for the digital
document, or at least the information contained in it, to be shared amongst a number of users
(the patient, the pharmacist and the GP). However, in light of the evidence suggesting that
involving patients more directly in decision-making about their own health can lead to better
medication adherence and better outcomes, the logical step would be to involve consumers
directly. The potential is there with the digital document approach – it would be a very
interesting project looking at which consumers wanted to share their medication information
with health professionals; and also the attitude of health professionals who would no longer
‘control’ the record.
8. 7.9 A shared record with other health professionalsAs the idea of much future work is about sharing information, other useful projects may involve
medication-related information-sharing by health professionals other than GPs and
pharmacists e.g. district nurses and community pharmacists. The (district) nursing profession
increasingly provides care to patients in the home that includes the administration of
medications. A current medication record may be of use to this group, although it is difficult to
suggest what value this would be without greater knowledge of what current district nursing
processes entail.
8. 7.10 GP information behaviour with GP desktop systemsThis project brought to light the reliance of pharmacists on the information contained in the GP
desktop systems. A study of GP data entry habits with their GP desktop systems may shed
some light what issues affect the amount and quality of information that GPs enter into these
systems. This could provide suggestions to improve the information contained in those
systems to the mutual benefit for the GP and the pharmacist dependant on that information for
medication reviews.
Page 308

References
Ahearn, MD & Kerr, SJ 2003, 'General practitioners' perceptions of the pharmaceutical decision-support tools in their prescribing software', Medical Journal of Australia, vol. 179, pp. 34-37
Alschuler, L 2002, 'CDA Introductory Tutorial', paper presented at the 1st International Conference on the Clinical Document Architecture, Berlin, Germany, October 7-9.
Alter, S 2003a, '18 Reasons Why IT-Reliant Work Systems Should Replace ìThe IT Artifactî as the Core Subject Matter of the IS Field', Communications of the Association for Information Systems, vol. 12, pp. 365-394.
Alter, S 2003b, 'Sidestepping the IT Artifact, Scrapping the IS Silo, and Laying Claim to ‘Systems in Organizations’, Communications of the Association for Information Systems, vol. 12, pp. 494-526.
American Medical Informatics Association 2005, Leading Health Care and Information Technology Groups Endorse Common Framework for Health Information Exchange to Support Improvements in Health and Healthcare, American Medical Informatics Association.
Ammenwerth, E 2006, 'Health technology assessment - Findings from the section on assessing information technologies for health ', Methods of Information in Medicine, vol. 45, no. S1, pp. 16-19.
Amsden, D 2003, 'Push technology in the pharmacy. Clinical decision support helps the pharmacy department of a South Carolina medical center automate monitoring of medication effectiveness', Health Management Technology, vol. 24, no. 1, pp. 28-31.
Armstrong, EP & Denemark, CR 1998, 'How Pharmacists Respond to On-line, Real-Time DUR Alerts', Journal of the American Pharmaceutical Association, vol. 38, no. 2, pp. 149-154.
Arnott, D 2005, Cognitive biases and decision support systems development: A design science approach Working paper), updated 2005, Melbourne, Australia, viewed 2006-05-01, <http://www.business.uq.edu.au/events/speakers/arnott-paper.pdf >.
Arshad, U, Mascolo, C & Mellor, M 2003, 'Exploiting Mobile Computing in Health-care', paper presented at the 23rd International Conference on Distributed Computing Systems (ICDCS’03), Providence, Rhode Island USA, May.
Ash, JS, Berg, M & Coiera, E 2004, 'Some Unintended Consequences of Information Technology in Health Care: The Nature of Patient Care Information System-related Errors', Journal of the American Medical Informatics Association, vol. 11, no. 2, pp. 104-112.
Au, YA 2001, 'Design Science I: The Role of Design Science Electric Commerce Research', Communications of the Association for Information Systems, vol. 7, no. Article 1.
Australian Institute of Health and Welfare 2006, Australia’s health 2006, Canberra, Australia.
Bajramovic, J, Emmerton, L & Tett, SE 2004, 'Perceptions around concordance - focus groups and semi-structured interviews conducted with consumers, pharmacists and general practitioners', Health Expectations, vol. 7, no. 3, pp. 221-234.
Page 309

Bajwa, DS, Lewis, LF, Pervan, G, Munkvold, BE, Lai, V & Schwabe, G 2007, 'Organizational Assimilation of Collaborative Information Technologies: Global Comparisons', paper presented at the 40th Hawaii International Conference on System Sciences (HICSS-40), Hawaii, USA, January.
Ball, NL 2001, 'Design Science II: The Impact of Design Science on e-Commerce Research and Practice', Communications of the Association for Information Systems, vol. 7, no. Article 2.
Barab, S & Squire, K 2004, 'Design-Based Research: Putting a Stake in the Ground', The Journal of the Learning Sciences, vol. 13, no. 1, pp. 1-14.
Barkhi, R & Sheetz, SD 2001, 'The State of Theoretrical Diversity in Information Sysems', Communications of the Association for Information Systems, vol. 7, no. Article 6.
Baron, RJ, Fabens, EL, Schiffman, M & Wolf, E 2005, 'Electronic Health Records: Just around the Corner? Or over the Cliff?' Annals of Internal Medicine, vol. 143, no. 3, pp. 222-226.
Barrett, G, Cassell, JA, Peacock, JL & Coleman, MP 2006, 'National survey of British public's views on use of identifiable medical data by the National Cancer Registry', British Medical Journal, vol. 332, no. 7549, pp. 1068-1072.
Barretta, JR, Strayera, SM & Schubarta, JR 2004, 'Assessing medical residents’ usage and perceived needs for personal digital assistants', International Journal of Medical Informatics, vol. 73, pp. 25-34.
Barretto, SA, Warren, J, Goodchild, A, Bird, L, Heard, S & Stumptner, M 2003, 'Linking Guidelines to Electronic Health Record Design for Improved Chronic Disease Management', paper presented at the American Medical Informatics Association Symposium (AMIA 2003), Washington DC, USA, 8-12 November.
Baskerville, R & Myers, MD 2004, 'Special issue on action research in information systems: making is research relevant to practice- foreword', Management Information Systems Quarterly, vol. 28, no. 3, pp. 329-355.
Bates, DW & Gawande, AA 2003, 'Improving Safety with Information Technology', New England Journal of Medicine, vol. 348, no. 25, pp. 2526-2534.
Bates, DW, Kuperman, GJ, Wang, S, Gandhi, T, Kittler, A, Volk, L, Spurr, C, Khorasani, R, Tanasijevic, M & Middleton, B 2003, 'Ten Commandments for Effective Clinical Decision Support: Making the Practice of Evidence-based Medicine a Reality', Journal of the American Medical Informatics Association, vol. 10, no. 6, pp. 523-530.
Bayazit, N 2004, Investigating Design: A Review of Forty Years of Design Research, 16-29, SpringerLink, viewed 2006-06-26, <http://www.mitpressjournals.org/doi/abs/10.1162/074793604772933739 >.
Beale, T & Heard, S 2003, Archetype Definition Language (ADL), Revision 1.1 edn, updated 24 Jan 2004, The openEHR Foundation, Ocean Informatics Australia, viewed 2004-03-09, <http://www.oceaninformatics.biz/adl/adl_1_1.pdf>.
Beers, MH 1997, 'Explicit criteria for determining potentially inappropriate medication use by the elderly. An update', Archives of Internal Medicine, vol. 157, no. 14, pp. 1531-1536.
Bell, P 2004, 'On the Theoretical Breadth of Design-Based Research in Education', Educational Psychologist, vol. 39, no. 4, pp. 243-253.
Benbasat, I & Zmud, RW 2003, 'The Identity Crisis within the IS Discipline: Defining and Communicating the Discipline's Core Properties', Management Information Systems Quarterly, vol. 27, no. 2, pp. 183-194.
Page 310

Berg, M & Goorman, E 1999, 'The contextual nature of medical information', International Journal of Medical Informatics, vol. 56, no. 1-3, pp. 51-60.
Berg, M & Toussaint, P 2003, 'The mantra of modeling and the forgotten powers of paper: a sociotechnical view on the development of process-oriented ICT in health care', International Journal of Medical Informatics, vol. 69, no. 2-3, pp. 223-234.
Bernauer, M, Kappel, G & Michlmayr, E 2003, 'Traceable Document Flows.' paper presented at the International Workshop on Web Semantics (WebS), in conjunction with the 15th International Conference on Database and Expert Systems Applications (DEXA). Zaragoza, Spain, 1-5 September.
Berner, ES 2002, 'Ethical and Legal Issues in the Use of Clinical Decision Support Systems', Journal of Healthcare Information Management, vol. 16, no. 4, pp. 34-37.
Beyer, M, Kuhn, KA, Meiler, C, Jablonski, S & Lenz, R 2004, 'Towards a flexible, process-oriented IT architecture for an integrated healthcare network', paper presented at the 2004 ACM symposium on Applied computing, Nicosia, Cyprus, 14--17 March.
Bindoff, IK, Tenni, PC, Peterson, GM, Kang, BH & Jackson, SL 2007, 'Development of an intelligent decision support system for medication review', Journal of Clinical Pharmacy and Therapeutics, vol. 32, no. 1, pp. 81-88.
Bloom, PC & Chung, QB 2001, 'Lessons learned from developing a mission-critical expert system with multiple experts through rapid prototyping', Expert Systems with Applications, vol. 20, no. 2, pp. 217-227.
Bludau, HB, Wolff, A & Hochlehnert, AJ 2003, 'Presenting XML-based medical discharge letters according to CDA', Methods of Information in Medicine, vol. 42, no. 5, pp. 552-556.
Bobb, A, Gleason, K, Husch, M, Feinglass, J, Yarnold, PR & Noskin, GA 2004, 'The Epidemiology of Prescribing Errors: The Potential Impact of Computerized Prescriber Order Entry', Archives of Internal Medicine, vol. 164, no. 7, pp. 785-792.
Boynton, PM 2004, 'Administering, analysing, and reporting your questionnaire', British Medical Journal, vol. 328, no. 7452, pp. 1372-1375.
Bradley, C & Blenkinsopp, A 1996, 'Over the Counter Drugs: The future for self medication', British Medical Journal, vol. 312, no. 7034, pp. 835-837.
Brown, JS & Duguid, P 1995, The Social Life of Documents, viewed 2005-06-23, <http://www2.parc.com/ops/members/brown/papers/sociallife.html>.
Browne, E 2001, Workflow in Healthcare - Musing on State, Healthbase Australia, viewed 2004-09-15, <http://workflow.healthbase.info/monographs/mon_state.html>.
Bruce, CS 1994, 'Research students' early experiences of the dissertation literature review', Studies in Higher Education, vol. 19, no. 2, pp. 217-229.
Buckland, M 1998, 'What is a digital document?' Document NumÈrique (Paris), vol. 2, no. 2, p. 221.
Calabretto, J-P, Warren, J & Bird, L 2005, 'Pharmacy decision support: where is it? A systematic literature review', The International Journal of Pharmacy Practice, vol. 13, no. 3, pp. 157-163.
Cameron, K 2005, 'Comment on medication management models and other pharmacist interventions: implications for policy and practice.' Home Health Care Services Quarterly, vol. 24, no. 1-2, pp. 73-85.
Page 311

Campbell, EM, Sittig, DF, Ash, JS, Guappone, KP & Dykstra, RH 2006, 'Types of Unintended Consequences Related to Computerized Provider Order Entry', Journal of the American Medical Association, vol. 13, no. 5, pp. 547-556.
Canadian Pharmacists Association 2004a, e-Therapeutics — Drug Therapy Management Tools to Improve Safety and Outcomes, updated January 2004, viewed 2004-07-05, <http://www.pharmacists.ca/content/about_cpha/whats_happening/cpha_in_action/pdf/CPhAPHCTF_e-TherapeuticsExecSummary.pdf>.
Canadian Pharmacists Association 2004b, Pharmacists and Primary Health Care, updated May 2004, viewed 2004-07-05, <http://www.pharmacists.ca/content/about_cpha/whats_happening/cpha_in_action/pdf/primaryhealth2a.pdf>.
Carmichael, J, Alvarez, A, Chaput, R, DiMaggio, J, Magallon, H & Mambourg, S 2004, 'Establishment and outcomes of a model primary care pharmacy service system.' American journal of health-system pharmacy, vol. 61, no. 5, pp. 472-482.
Carroll, AE & Christakis, DA 2004, 'Pediatricians’ Use of and Attitudes About Personal Digital Assistants', Pediatrics, vol. 113, pp. 238-242.
Chen, H, Zeng, D, Atabakhsh, H, Wyzga, W & Schroeder, J 2003, 'COPLINK: managing law enforcement data and knowledge ', Communications of the ACM, vol. 46, no. 1, pp. 28-34.
Chiasson, M & Dexter, AS 2001, 'System development conflict during the use of an information systems prototyping method of action research:Implications for practice and research', Information Technology & People, vol. 14, no. 1, 91-108.
Choudrie, J & Dwivedi, YK 2005, 'Research Design: Investigating the Research Approaches for Examining Technology Adoption Issues', Journal of Research Practice, vol. 1, no. 1, p. Article D1.
Clarke, R 2000, Appropriate Research Methods for Electronic Commerce, updated 19/4/2000, Xamax Consultancy Pty Ltd, Canberra, Australia, viewed 2005-10-24 2005, < http://www.anu.edu.au/people/Roger.Clarke/EC/ResMeth.html>.
Cobb, P, Confrey, J, diSessa, A, Lehrer, R & Schauble, L 2003, 'Design Experiments in Educational Research', Educational Researcher, vol. 32, no. 1, pp. 9-13.
Coffey, A & Atkinson, P 1996, Making Sense of Qualitative Data: Complementary Research Strategies, SAGE Publications Inc., Thousand Oaks, California, USA.
Cohen, JP, Paquette, C & Cairns, CP 2005, 'Switching prescription drugs to over the counter', British Medical Journal, vol. 330, no. 7481, pp. 39-41.
Coiera, E 2003a, 'Chapter 25 - Clinical Decision Support Systems', in Guide to Health Informatics 2nd Edition, Second edn, Hodder & Stoughton Educational, London, UK.
Coiera, E 2003b, 'Interaction design theory', International Journal of Medical Informatics, vol. 69, no. 2-3, pp. 205-222.
Coiera, E, Westbrook, J & Wyatt, J 2006, 'The safety and quality of decision support systems ', Methods of Information in Medicine, vol. 45, no. S1, pp. 20-25.
Coiera, EW & Westbrook, JI 2006, 'Should clinical software be regulated?' Medical Journal of Australia, vol. 184, no. 12, pp. 600-601.
Collins, A, Joseph, D & Bielaczyc, K 2004, 'Design research: Theoretical and methodological issues', Journal of the Learning Sciences, vol. 13, no. 1, pp. 15-42.
Page 312

Commonwealth of Australia 2002, The National Strategy for Quality Use of Medicines: PLAIN ENGLISH EDITION, Commonwealth of Australia, Canberra, Australia.
Cooper, J, Alcock, C & Burgess, L 2003, 'The adoption of PDAs within health the care sector: improving work practices and service delivery in ambulatory care', paper presented at the CollECTeR (Europe) Conference, National University of Ireland, Galway, Ireland, 24 June.
Cross, N 2002, 'Design as a Discipline', paper presented at the 'The Inter-disciplinary Design Quandary’ Conference, De Montfort University, Leicester, UK., 13 February.
Crotty, M 1998, The foundations of social research: meaning and perspective in the research process, Allen & Unwin Pty Ltd, St Leonards NSW, Australia.
Currie, LM, Graham, M, Allen, M, Bakken, S, Patel, V & Cimino, JJ 2003, 'Clinical Information Needs in Context: An Observational Study of Clinicians While Using a Clinical Information System', paper presented at the American Medical Informatics Association Symposium, Washington DC, USA, 8-12 November.
Davis, K, Schoenbaum, SC, Scott Collins, K, Tenney, K, Hughes, DL & Audet, A-MJ 2002, Room for Improvement: Patients Report on The Quality of their Health Care, The Commonwealth Fund, New York, NY, USA.
Davison, RM, Martinsons, MG & Kock, N 2004, 'Principles of canonical action research', Information Systems Journal, vol. 14, pp. 65-86.
Delaney, BC, Fitzmaurice, DA, Riaz, A & Hobbs, FDR 1999, 'Can computerised decision support systems deliver improved quality in primary care?' British Medical Journal, vol. 319, no. 7220, 1999, pp. 1281-.
Delbridge, A (ed.) 1982, The Macquarie Dictionary, Macquarie Library Pty Ltd, McMahons Point NSW, Australia.
Department of Health 2002, Delivering 21st Century IT Support for the NHS, updated 2002, Department of Health, UK, viewed 2004-05-28, <http://www.worcestershirehealth.nhs.uk/EXTRANET_Library/GreeningC/whip_strategy/nat_strat/ict/d21cit.pdf>.
Department of Health Social Services and Public Safety 2004, Pharmacy in Practice, Belfast, Northern Ireland, viewed 2004-05-28, <http://www.dhsspsni.gov.uk/pgroups/pharmaceutical/pharmacy.asp#comm_role>.
Dolin, RH, Alschuler, L, Beebe, C, Biron, PV, Boyer, SL, Essin, D, Kimber, E, Lincoln, T & Mattison, JE 2001, 'The HL7 Clinical Document Architecture', Journal of the American Medical Informatics Association, vol. 8, no. 6, pp. 552-561.
Donald, IP & Bulpitt, CJ 1999, 'The prognosis of falls in elderly people living at home', Age Ageing, vol. 28, no. 2, pp. 121-125.
Dooley, MJ, Allen, KM, Doecke, CJ, Galbraith, KJ, Taylor, GR, Bright, J & Carey, DL 2003, 'A prospective multicentre study of pharmacist initiated changes to drug therapy and patient management in acute care government funded hospitals', British Journal of Clinical Pharmacology, vol. 57, no. 4, pp. 513-521.
Douglas, D 2003, 'Inductive theory generation: A grounded approach to business inquiry', Electronic Journal of Business Research Methods, vol. 2, no. 1, pp. 47-54.
Dubé, L & Paré, G 2003, 'Rigor in Information Systems Positivist Case Research: Current Practices, Trends, and Recommendations', Management Information Systems Quarterly, vol. 27, no. 4, pp. 597-563.
Page 313

Eccles, M, McColl, E, Steen, N, Rousseau, N, Grimshaw, J, Parkin, D & Purves, I 2002, 'Effect of computerised evidence based guidelines on management of asthma and angina in adults in primary care: cluster randomised controlled trial', British Medical Journal, vol. 325, no. 7370, pp. 941-.
Edelson, DC 2002, 'Design Research: What We Learn When We Engage in Design', The Journal Of The Learning Sciences, vol. 11, no. 1, pp. 105-121.
Elder, NC & Hickner, J 2005, 'Missing Clinical Information: The System Is Down', Journal of the American Medical Association, vol. 293, no. 5, pp. 617-619.
Electronic Prescribing Initiative 2004, Electronic Prescribing: Toward Maximum Value and Rapid Adoption. Recommendations for Optimal Design and Implementation to Improve Care, Increase Efficiency and Reduce Costs in Ambulatory Care, updated April 14, 2004, eHealth Initiative, Washington, D.C., viewed 2004-05-28, <http://ehr.medigent.com/assets/collaborate/2004/04/14/eHealth%20Initiative%20Electronic%20Prescribing%20Report%2004.14.04%20Executive%20Summary.pdf>.
Elkin, PL, Peleg, M, Lacson, R, Bernstam, E, Tu, S, Boxwala, A, Greenes, R & Shortliffe, EH 2001, Toward Standardization of Electronic Guideline Representation, updated 2004-03-25, viewed 2004-04-06, <http://www-smi.stanford.edu/pubs/SMI_Reports/SMI-2001-0865.pdf>.
Ely, JW, Osheroff, JA, Gorman, PN, Ebell, MH, Chambliss, ML, Pifer, EA & Stavri, PZ 2000, 'A taxonomy of generic clinical questions: classification study', British Medical Journal, vol. 321, no. 7258, pp. 429-432.
England, I 2001, 'The Status of Health IT Expenditure: A Qualitative Study of Senior Executives in Regard to IT Investment', paper presented at the Ninth National Health Informatics Conference (HIC 2001), Canberra, Australia, 29 - 31 July.
Erwig, M 2003, 'Xing: a visual XML query language', Journal of Visual Languages & Computing, vol. 14, no. 1, 2003/2, pp. 5-45.
European Commission 2004, e-Health - making healthcare better for European citizens: An action plan for a European e-Health Area, COMMISSION OF THE EUROPEAN COMMUNITIES, Brussels.
Fallman, D 2003, 'Design-oriented human-computer interaction', paper presented at the Conference on Human Factors in Computing Systems, Ft. Lauderdale, Florida, USA, 5-10 April.
Fällman, D & Grönlund, Å 2002, 'Rigor and Relevance Remodeled', paper presented at the Information Systems Research in Scandinavia Conference (IRIS25), Bautahoj, Denmark, 10-13 August.
Fick, DM, Cooper, JW, Wade, WE, Waller, JL, Maclean, JR & Beers, MH 2003, 'Updating the Beers Criteria for Potentially Inappropriate Medication Use in Older Adults: Results of a US Consensus Panel of Experts', Archives of Internal Medicine, vol. 163, no. 22, pp. 2716-2724.
Fitzpatrick, G 1998, 'The Locales Framework: Understanding and Designing for Cooperative Work', Department of Computer Science and Electrical Engineering, PhD thesis, The University of Queensland.
Fitzpatrick, G 2000a, ' Understanding the Paper Health Record in Practice: Implications for EHR', paper presented at the Health Informatics Conference (HIC2000), Adelaide, South Australia, 3-5 September.
Fitzpatrick, G 2000b, 'Centres, Peripheries and Electronic Communication: Changing Work Practice Boundaries', Scandinavian Journal of Information Systems, vol. 12, pp. 115-148.
Page 314

Forum 2000, '2000 and counting - the application of IT to modern pharmacy practice', The Pharmaceutical Journal, vol. 264, no. 7089, pp. 487-490.
Frey, D 2003, 'The Medication Management Model: An Effective Tool for Home Health Providers', Home Health Care Management Practice, vol. 15, no. 3, pp. 222-230.
Frey, D & Rahman, A 2003, 'Medication Management: An evidence based model that decreases adverse events', Home Healthcare Nurse, vol. 21, no. 6, pp. 404-412.
Friedman, K 2003, 'Theory construction in design research: criteria: approaches, and methods', Design Studies, vol. 24, no. 6, pp. 507-522.
Furuta, R 1995, 'Documents in the Digital Library', paper presented at the International Symposium on Digital Libraries (ISDL'95), University of Library and Information Science, Tsukuba Science City, Japan, 22-25 August.
Garg, AX, Adhikari, NKJ, McDonald, H, Rosas-Arellano, MP, Devereaux, PJ, Beyene, J, Sam, J & Haynes, RB 2005, 'Effects of Computerized Clinical Decision Support Systems on Practitioner Performance and Patient Outcomes: A Systematic Review', Journal of the American Medical Association, vol. 293, no. 10, pp. 1223-1238.
General Practice Computing Group 1999, 'Strategic Future Directions', paper presented at the General Practice Electronic Decision Support Workshop, Canberra, 23-24 September.
Gilbert, AL, Roughead, EE, Beilby, JJ, Mott, K & Barratt, JD 2002, 'Collaborative medication management services: improving patient care', Medical Journal of Australia, vol. 177, no. 4, pp. 189-192.
Giles-Burness, DA & Roberts, RI 2002, 'Modernising pharmacy the Stockport experience of producing a pharmacy development strategy in the new National Health Service', The Pharmaceutical Journal, vol. 268, no. 7185, pp. 218-20.
Ginsburg, M 2000, 'Intranet Document Management Systems as Knowledge Ecologies', paper presented at the 33rd Hawaii International Conference on System Sciences (HICSS-33), Hawaii, USA, January.
Glass, RL, Ramesh, V & Vessey, I 2004, 'An analysis of research in computing disciplines', Communications of the Association for Computing Machinery, vol. 47, no. 6, pp. 89-94.
Glassman, P, Simon, B, Belperio, P & Lanto, A 2002, 'Improving recognition of drug interactions: benefits and barriers to using automated drug alerts', Med Care, vol. 40, no. 12, pp. 1161-1171.
Gowan, J & Roller, L 2004, 'The pharmacist and patient-focused care', Australian Journal of Pharmacy, vol. 85, no. 1009, pp. 275-279.
Greenes, RA 2001, 'Realizing Quality with Effective Decision Support: The Premise, the Present, and the Promise', paper presented at the Ninth National Health Informatics Conference (HIC 2001), Canberra, Australia, 29 - 31 July.
Gregor, S 2002, 'A theory of theories in information systems', in Information Systems Foundations: Building the Theoretical Base, eds. S Gregor & D Hart, Australian National University, Canberra, Australia, pp. 1-20.
Guion, LA 2001, Triangulation: Establishing the Validity of Qualitative Studies1, Institute of Food and Agriculure Sciences, Florida, USA.
Hake, RR 2004, 'Design-Based Research: Old PER Wine in a New Bottle', paper presented at the Physics Education Research Conference (PERC 2004), Sacramento, California, USA, 4-5 August.
Page 315

Hameed, K 2003, Telematics and Informatics vol. 20, no. 2, pp. 99-106.
Heath, H & Cowley, S 2004, 'Developing a grounded theory approach: a comparison of Glaser and Strauss', International Journal of Nursing Studies, vol. 41, pp. 141-150.
Heeks, R 2006, 'Health information systems: Failure, success and improvisation', International Journal of Medical Informatics, vol. 75, no. 2, pp. 125-137.
Hevner, AR, March, ST, Park, J & Ram, S 2004, 'Design Science in Information Systems Research', Management Information Systems Quarterly, vol. 20, no. 1, pp. 75-105.
Hoadley, CM 2004, 'Methodological Alignment in Design-Based Research', Educational Psychologist, vol. 39, no. 4, pp. 203-212.
Holleran, K, Pappas, J, Lou, H, Rubalcaba, P, Lee, R, Clay, S, Cutone, J, Flammini, S, Kuperman, G & Middleton, B 2003, 'Mobile Technology in a Clinical Setting', paper presented at the American Medical Informatics Association Symposium (AMIA 2003), Washington DC, USA, 8-12 November.
Honkaranta, A 2001, 'Developing Document and Content Management in Enterprises using a ‘GENRE LENS’, paper presented at the 5th International Conference on Enterprise Information Systems (ICEIS2003), Angers, France, 23-26April.'
Ihara, E, Summer, L & Shirey, L 2002, 'Prescription drugs: a vital component of health care', in Challenges for the 21st Century: Chronic and Disabling Conditions, Center on an Aging Society, Georgetown University, Washington DC.
Iivari, J, Hirschheim, R & Klein, HK 2001, 'Towards more professional Information Systems Development: ISD as Knowledge Work', paper presented at the The 9th European Conference on Information Systems, Bled, Slovenia, 27-29 June.
Institute of Medicine 2001, Crossing the Quality Chasm : A New Health System for the 21st Century, Washington, DC.
Iyengar, S 2001, Model Driven Architecture(MDA) meets (trying to!) Business Modeling and Rules, November 6, 2001 edn, Unisys, New Orleans, viewed 2004-03-29 2001, <http://www.businessrulesforum.com/2001_Presentations/Iyengar.pdf>.
Jadad, AR & Enkin, MW 2007, 'Computers: transcending our limits?' British Medical Journal, vol. 334, no. suppl_1, pp. s8-.
Jørgensen, HD 2002, 'Interactive Process Models for Knowledge Intensive Process Work', PhD thesis, Norwegian University of Science and Technology & SINTEF Telecom and Informatics.
Joseph, D 2004, 'The Practice of Design-Based Research: Uncovering the Interplay Between Design, Research, and the Real-Work Context', Educational Psychologist, vol. 39, no. 4, pp. 235-242.
Kaplan, B 2001, 'Evaluating informatics applications--some alternative approaches: theory, social interactionism, and call for methodological pluralism', International Journal of Medical Informatics, vol. 64, no. 1, pp. 39-56.
Karjalainen, A, Päivärinta, T, Tyrväinen, P & Rajala, J 2000, 'Genre-Based Metadata for Enterprise Document Management', paper presented at the 33rd Hawaii International Conference on System Sciences (HICSS-33), Hawaii, USA, January.
Kelly, AE 2004, 'Design Research in Education: Yes, but is it Methodological?' Journal of the Learning Sciences, vol. 13, no. 1, pp. 115-128.
Page 316

Kendall, KE & Kendall, JE 1988, Systems analysis and design, Prentice-Hall International Inc., Englewood Cliffs NJ, USA.
Klein, HK & Hirschheim, R 2001, 'Choosing Between Competing Design Ideals in Information Systems Development', Information Systems Frontiers, vol. 3, no. 1, pp. 75-90.
Klein, HK & Myers, MD 1999, 'A set of principles for conducting and evaluating interpretive field studies in information systems', Management Information Systems Quarterly, vol. 23, no. 1, pp. 67-94.
Klischewski, R & Wetzel, I 2003, 'Serviceflow management for health provider networks', Logistics Information Management, vol. 16, no. 3/4, pp. 259-269.
Kohn, LT, Corrigan, JM & Donaldson, MS (eds) 1999, To Err Is Human: Building a Safer Health System, National Academy Press, Washington DC.
Koppel, R, Metlay, JP, Cohen, A, Abaluck, B, Localio, AR, Kimmel, SE & Strom, BL 2005, 'Role of Computerized Physician Order Entry Systems in Facilitating Medication Errors', Journal of the American Medical Association, vol. 293, no. 10, pp. 1197-1203.
Kuilboer, MM, van der Lei, J, Bohnen, AM & van Bemmel, JH 1997, 'The availability of unavailable information', paper presented at the American Medical Informatics Association Symposium, Nashville TE, USA, October 25-29.
Kuperman, GJ & Gibson, RF 2003, 'Computer Physician Order Entry: Benefits, Costs, and Issues', Annals of Internal Medicine, vol. 139, no. 1, pp. 31-39.
Kuzel, AJ 1999, 'Sampling in Qualitative Inquiry', in Doing Qualitative Research, Second edn, eds. BF Crabtree & WL Miller, Sage Publications Inc., Thousand Oaks, California, USA.
LaMarca, A, Edwards, WK, Dourish, P, Lamping, J, Smith, I & Thornton, J 1999, 'Taking the Work out of Workflow: Mechanisms for Document-Centered Collaboration', paper presented at the European Conference on Computer Supported Cooperative Work (ECSCW), Copenhagen, Denmark, September
Lee, A 2000, 'Keynote address: Systems Thinking, Design Science and Paradigms: Heeding Three Lessons from the Past to Resolve Three Dilemmas in the Present to Direct a Trajectory for Future Research in the Informations Systems Field', paper presented at the 11th National Conference on Information Management, Kaohsiung, Taiwan, 20 May.
Lee, JK, Grace, KA & Taylor, AJ 2006, 'Effect of a Pharmacy Care Program on Medication Adherence and Persistence, Blood Pressure, and Low-Density Lipoprotein Cholesterol: A Randomized Controlled Trial', Journal of the American Medical Association, p. 296.21.joc60162.
Lenz, R, Buessecker, F, Herlofsen, H, Hinrichs, F, Zeiler, T & Kuhn, K 2005, 'Demand-driven evolution of IT systems in healthcare - A case study for improving interdisciplinary processes', Methods of Information in Medicine, vol. 44, no. 1, pp. 4-10.
Lenz, R, Elstner, T, Siegele, H & Kuhn, KA 2002, 'A Practical Approach to Process Support in Health Information Systems', Journal of the American Medical Informatics Association, vol. 9, no. 6, pp. 571-585.
Lenz, R & Kuhn, KA 2004, 'Towards a continuous evolution and adaptation of information systems in healthcare', International Journal of Medical Informatics, vol. 73, no. 1, pp. 75-89.
Liang, Z, Bodorik, P & Shepherd, M 2003, 'Storage Model for CDA Document', paper presented at the 36th Annual Hawaii International Conference on System Sciences (HICSS-36), Hawaii, USA, January.
Page 317

Little, P, Everitt, H, Williamson, I, Warner, G, Moore, M, Gould, C, Ferrier, K & Payne, S 2001, 'Observational study of effect of patient centredness and positive approach on outcomes of general practice consultations', British Medical Journal, vol. 323, no. 7318, pp. 908-911.
Maciaszek, L 2001, 'Chapter 3: Requirements Determination', in Requirements analysis and system design : developing information systems with UML, Addison-Wesley, Harlow, England, pp. 80-105.
Mack, TA 1998, 'Decision support considerations in the development and implementation of an electronic medical record', Pharmacy Practice Management Quarterly, vol. 18, no. 1, pp. 21-34.
Mahoney, C 1997, Part II. Overview of Qualitative Methods and Analytic Techniques. Chapter 3. Common Qualitative Methods, Directorate for Education and Human Resources, Division of Research, Evaluation and Communication, National Science Foundation, Arlington, Virginia, USA, viewed 2004-07-26, <http://www.ehr.nsf.gov/EHR/REC/pubs/NSF97-153/CHAP_3.HTM>.
Malhotra, MK & Grover, V 1998, 'An assessment of survey research in POM: from constructs to theory', Journal of Operations Management, vol. 16, no. 4, pp. 407-425.
Mara, P 2006, 'Accreditation and electronic medical records', Pulse+IT, vol. 1, no. 1, pp. 36-37.
March, ST & Smith, GF 1995, 'Design and natural science research on information technology', Decision Support Systems, vol. 15, no. 4, pp. 251-266.
Markus, ML, Majchrzak, A & Gasser, L 2002, 'A Design Theory For Systems That Support Emergent Knowledge Processes', Management Information Systems Quarterly, vol. 26, no. 3, pp. 179-212.
Mathiassen, L 2002, 'Collaborative practice research', Information Technology & People, vol. 15, no. 4, pp. 321-345.
Mays, N & Pope, C 2000, 'Qualitative research in health care: Assessing quality in qualitative research', British Medical Journal, vol. 320, no. 7226, pp. 50-52.
Mays, N & Pope, C 1995, 'Qualitative Research: Rigour and qualitative research', British Medical Journal, vol. 311, no. 6997, pp. 109-112.
McColl, E, Jacoby, A, Thomas, L, Soutter, J, Bamford, C, Steen, N, Thomas, R, Harvey, E, Garratt, A & Bond, J 2001, Design and use of questionnaires: a review of best practice applicable to surveys of health service staff and patients, updated December 2001, viewed 2006-01-03, <http://www.ncchta.org/fullmono/mon531.pdf>
McGregor, JC, Weekes, E, Forrest, GN, Standiford, HC, Perencevich, EN, Furuno, JP & Harris, AD 2006, 'Impact of a Computerized Clinical Decision Support System on Reducing Inappropriate Antimicrobial Use: A Randomized Controlled Trial', Journal of the American Medical Informatics Association, vol. 13, no. 4, pp. 378-384.
McKay, J & Marshall, P 2005, 'A Review of Design Science in Information Systems', paper presented at the Australasian Conference on Information Systems (ACIS 2005), Sydney, Australia, 29 Nov – 2 Dec.
McNurlin, BC & Sprague, RH 2005, Information systems management in practice, 7th edn, Pearson-Prentice Hall, Upper Saddle River, NJ, USA.
Mendonca, EA, Chen, ES, Stetson, PD, McKnight, LK, Lei, J & Cimino, JJ 2004, 'Approach to mobile information and communication for health care', International Journal of Medical Informatics, vol. 73, no. 7-8, pp. 631-638.
Page 318

Meyer, J 2000, 'Qualitative research in health care: Using qualitative methods in health related action research', British Medical Journal, vol. 320, no. 7228, pp. 178-181.
Michalsky, G 1991, 'The World of Documents', Byte, vol. 16, no. 4, pp. 159-170.
Middleton, P 1999, 'Managing information system development in bureaucracies', Information and Software Technology, vol. 41, no. 8, pp. 473-482.
Miller, A 2005, 'Realism', in The Stanford Encyclopedia of Philosophy (Fall 2005 Edition), ed. EN Zalta.
Miller, WL & Crabtree, BF 1999, 'Clinical Research: A Multimethod Typology and Qualitative Roadmap', in Doing qualitative research, Second edn, eds. BF Crabtree & WL Miller, Sage Publications Inc., Thousand Oaks, California, USA.
Millonig, MK, Jackson, TL & Ellis, WM 2002, 'Improving Medication Use Through Pharmacists' Access to Patient-Specific Health Care Information', Journal of the American Pharmaceutical Association, vol. 42, no. 4, pp. 638-645.
Monane, M, Matthias, DM, Nagle, BA & Kelly, MA 1998, 'Improving Prescribing Patterns for the Elderly Through an Online Drug Utilization Review Intervention: A System Linking the Physician, Pharmacist, and Computer', Journal of the American Medical Association, vol. 280, no. 14, pp. 1249-1252.
Moody, DL 2000, 'Building links between IS research and professional practice: improving the relevance and impact of IS research', paper presented at the International Conference on Information Systems (ICIS), Brisbane, Queensland, Australia, 10-13 December.
Morgan, GA, Gliner, JA & Harmon, RJ 1999, 'Measurement and Descriptive Statistics', Journal of the American Academy of Child & Adolescent Psychiatry, vol. 38, no. 10, pp. 1313-1315.
Morrison, J & George, JF 1995, 'Exploring the software engineering component in MIS research', Communications of the ACM, vol. 38, no. 7, pp. 80-91.
Mueser, K, Drake, R & Wallach, M 1998, 'Dual diagnosis: a review of etiological theories.' Addictive behaviour, vol. 23, no. 6, pp. 717-734.
Müller, A, Dörre, J, Gerstl, P & Seiffert, R 1999, 'The TaxGen Framework: Automating the Generation of a Taxonomy for a Large Document Collection', paper presented at the 32nd Hawaii International Conference on System Sciences (HICSS-32), Hawaii, USA, January.
Mumford, E 2001, 'Advice for an action researcher', Information Technology & People, vol. 14, no. 1, pp. 12-27.
Murphy, LD 1998, 'Digital Document Metadata in Organizations: Roles, Analytical Approaches, and Future Research Directions', paper presented at the 31st Hawaii International Conference on System Sciences (HICSS-31), Hawaii, USA, January.
Murphy, LD 2001, 'Digital Documents in Organizational Communities of Practice: A First Look', paper presented at the 34th Annual Hawaii International Conference on System Sciences (HICSS-34), Hawaii, USA, January.
Murray, MD, Loos, B, Tu, W, Eckert, GJ, Zhou, X-H & Tierney, WM 1998, 'Effects of Computer-based Prescribing on Pharmacist Work Patterns', Journal of the American Medical Informatics Association, vol. 5, no. 6, pp. 546-553.
Myers, MD 2005, Qualitative Research in Information Systems, Management Information Systems Quarterly (21:2), June 1997, pp. 241-242. , MISQ Discovery, archival version, June 1997, http://www.misq.org/discovery/MISQD_isworld/. MISQ Discovery, updated version, updated July 26, 2005, viewed 2005-10-25 2005, <http://www.qual.auckland.ac.nz/>.
Page 319

National Electronic Decision Support Taskforce 2002, Electronic decision support for Australia’s health sector, Department of Health and Aged Care, Commonwealth of Australia, Canberra, Australia.
National Electronic Health Records Taskforce 2000, A health information network for Australia, Department of Health and Aged Care, Commonwealth of Australia, Canberra, Australia.
National Health Information Management Advisory Council 2001, HEALTH ONLINE: A health information action plan for Australia - second edition, Commonwealth Government of Australia, Canberra, Australia.
Neely, JG, Stewart, MG, Hartman, JM, Forsen Jr, JW & Wallace, MS 2002, 'Tutorials in Clinical Research, Part VI: Descriptive Statistics', Laryngoscope, vol. 112, no. 7, pp. 1249-1255.
Neuman, WL 2003, Social research methods : qualitative and quantitative approaches, Fifth edn, Pearson Education Inc., Boston, Massachusetts, USA.
Neuman, WL 1997, Social research methods: qualitative and quantitative approaches, Third edn, Allyn and Bacon, Boston, MA, USA.
Noffke, SE 2004, 'Theorising and practicing social justice issues through action research', paper presented at the Action Research Seminar, Underdale Campus, University of South Australia, Adelaide, 22 June.
O'Donnell, AM 2004, 'A Commentary on Design Research', Educational Psychologist, vol. 39, no. 4, pp. 255-261.
OpenClinical 2004, Decision Support Systems, updated Mon, 17 May 2004, OpenClinical, viewed 2004-05-27 2004, <http://www.openclinical.org/dss.html#definition>.
Orlikowski, WJ & Iacono, CS 2001, 'Research Commentary: Desperately Seeking the "IT" in IT Research-A Call to Theorizing the IT Artifact', Information Systems Research, vol. 12, no. 2, pp. 121-134.
Orlikowski, WJ & Robey, D 1991, 'Information Technology and the Structuring of Organizations', Information Systems Research, vol. 2, no. 2, pp. 143-169.
Ortiz, E, Meyer, G & Burstin, H 2002, 'Clinical Informatics and Patient Safety at the Agency for Healthcare Research and Quality', Journal of the American Medical Informatics Association, vol. 9, pp. S2-7.
Osterberg, L & Blaschke, T 2005, 'Adherence to Medication', New England Journal of Medicine, vol. 353, no. 5, pp. 487-497.
Owen, CL 1997, 'Understanding Design Research. Toward an Achievement of Balance', Japanese Society for the Science of Design, vol. 5, no. 2, pp. 36-45.
Panzarasa, S, Bellazzib, R, Larizzab, C & Stefanelli, M 2004, 'A careflow management system for chronic patients', paper presented at the Medinfo 2004, San Francisco, USA, Sept 7-11, 2004.
Paterson, GI, Shepherd, M, Wang, X, Watters, C & Zitnera, D 2002, 'Using XML-based Clinical Document Architecture for Exchange of Structured Discharge Summaries', paper presented at the 35th Hawaii International Conference on System Sciences ( HICSS-35), Hawaii, USA, January.
Peabody, JW, Luck, J, Jain, S, Bertenthal, D & Glassman, P 2004, 'Assessing the accuracy of administrative data in health information systems', Medical Care, vol. 42, no. 11, pp. 1066-72.
Page 320

Peleg, M, Tu, S, Bury, J, Ciccarese, P, Fox, J, Greenes, RA, Hall, R, Johnson, PD, Jones, N, Kumar, A, Miksch, S, Quaglini, S, Seyfang, A, Shortliffe, EH & Stefanelli, M 2002, Comparing Models of Decision and Action for Guideline-Based Decision Support: a Case-Study Approach (Part 1 of 2), SMI-2002-0922, viewed 2004-03-17, <http://www.smi.stanford.edu/pubs/SMI_Reports/SMI-2002-0922.pdf>.
Peters, DH, Kohli, M, Mascarenhas, M & Rao, K 2006, 'Can computers improve patient care by primary health care workers in India?' International Journal of Quality in Health Care, vol. 18, no. 6, pp. 437-445.
Pfleeger, SL 1998, '4: Capturing the Requirements', in Software Engineering: theory and practice, Prentice Hall, Upper Saddle River, NJ,, pp. 135-177.
Pharmaceutical Care Network Europe Foundation 2003, The PCNE Classification V 5.00, updated 2006-08-03, 2003 Pharmaceutical Care Network Europe Foundation, viewed 2004-12-03, <www.pcne.org>.
Phillips, EM & Pugh, DS 2000, How to get a PhD : a handbook for students and their supervisors, 3rd. edn, Open University Press, Buckingham, England.
Plummer, A 2001, 'Information Systems Methodology for Building Theory in Health Informatics: The Argument for a Structured Approach to Case Study Research', paper presented at the 34th Hawaii International Conference on System Sciences (HICCS-34), Hawaii, USA, January.
Poon, EG, Blumenfeld, B, Hamann, C, Turchin, A, Graydon-Baker, E, McCarthy, PC, Poikonen, J, Mar, P, Schnipper, JL, Hallisey, RK, Smith, S, McCormack, C, Paterno, M, Coley, CM, Karson, A, Chueh, HC, Van Putten, C, Millar, SG, Clapp, M, Bhan, I, Meyer, GS, Gandhi, TK & Broverman, CA 2006, 'Design and Implementation of an Application and Associated Services to Support Interdisciplinary Medication Reconciliation Efforts at an Integrated Healthcare Delivery Network', Journal of the American Medical Informatics Association, vol. 13, no. 6, pp. 581-592.
Poon, IO, Lal, L, Brown, EN & Braun, UK 2007, 'The impact of pharmacist-managed oral anticoagulation therapy in older veterans', Journal of Clinical Pharmacy and Therapeutics, vol. 32, no. 1, pp. 21-29.
Pope, C & Mays, N 1995, 'Qualitative Research: Reaching the parts other methods cannot reach: an introduction to qualitative methods in health and health services research', British Medical Journal, vol. 311, no. 6996, pp. 42-45.
Porter, SC, Forbes, P, Feldman, HA & Goldmann, DA 2006, 'Impact of Patient-Centered Decision Support on Quality of Asthma Care in the Emergency Department', Pediatrics, vol. 117, no. 1, pp. e33-42.
Power, N & Moynihan, T 2003, 'A Theory of Requirements Documentation Situated in Practice', paper presented at the SIGDOC, San Francisco, California, USA., 12-15 October.
Purao, S 2002, Design Research in the Technology Information Systems: Truth or Dare (Working paper), viewed 2005-11-01, <http://purao.ist.psu.edu/working-papers/dare-purao.pdf>.
Purcell, GP 2005, 'What makes a good clinical decision support system', British Medical Journal, vol. 330, no. 7494, pp. 740-741.
Quaglini, S, Stefanelli, M, Lanzola, G, Caporusso, V & Panzarasa, S 2001, 'Flexible guideline-based patient careflow systems', Artificial Intelligence in Medicine, vol. 22, no. 1, pp. 65-80.
Remmlinger, E 2002, 'Next generation clinical systems: is it time to jump?' paper presented at the HIMSS 2002 Conference, Atlanta GA, USA, January.
Page 321

Rich, DS 2004, 'New JCAHO Medication Management Standards for 2004', American journal of health-system pharmacy, vol. 61, no. 13, pp. 1349-1358.
Ritchey, T 2005, Wicked Problems: Structuring Social Messes with Morphological Analysis, Swedish Morphological Society, viewed 2006-04-17, <http://www.swemorph.com/pdf/wp.pdf>.
Rittel, HWJ & Webber, MM 1973, 'Dilemmas in a General Theory of Planning', Policy Sciences, vol. 4, no. 2, pp. 155-169.
Rossi, M & Sein, M 2003, 'Design Research Workshop: A Proactive Research Approach', paper presented at the Information Systems Research in Scandinavia Conference (IRIS26), Finland, 9-12 August.
Rothschild, JM, Fang, E, Liu, V, Litvak, I, Yoon, C & Bates, DW 2006, 'Use and Perceived Benefits of Handheld Computer-based Clinical References', Journal of the American Medical Informatics Association, vol. 13, no. 6, pp. 619-626.
Roughead, EE & Lexchin, J 2006, 'Adverse drug events: counting is not enough, action is needed', Medical Journal of Australia, vol. 184, no. 7, pp. 315-316.
Roughead, EE, Semple, SJ & Vitry, AI 2005, 'Pharmaceutical care services: a systematic review of published studies, 1990 to 2003, examining effectiveness in improving patient outcomes', International Journal of Pharmacy Practice, vol. 13, no. 1, pp. 53–70.
Roughead, L & Semple, S 2002, Second National Report on Patient Safety: Improving Medication Safety, Australian Council for Safety and Quality in Health Care, Canberra, Australia.
Roukema, J, Los, RK, Bleeker, SE, van Ginneken, AM, van der Lei, J & Moll, HA 2006, 'Paper Versus Computer: Feasibility of an Electronic Medical Record in General Pediatrics', Pediatrics, vol. 117, no. 1, pp. 15-21.
Runciman, W & Moller, J 2001, Iatrogenic Injury in Australia, Australian Patient Safety Foundation, Adelaide, Australia.
Runciman, WB, Roughead, EE, Semple, SJ & Adams, RJ 2003, 'Adverse drug events and medication errors in Australia', International Journal of Quality in Health Care, vol. 15, no. 90001, pp. 49-59.
Saini, B, Krass, I & Armour, C 2004, 'Development, implementation, and evaluation of a community pharmacy-based asthma care model.' Annals of Pharmacotherapy, vol. 38, no. 11, pp. 1954-1960.
Sargent, J, Burgess, L, Cooper, J, Alcock, C & Ryan, D 2005, 'Enhancing User Acceptance of Mandated Technology Implementation in a Mobile Healthcare Setting: A Case Study ', paper presented at the 16th Australasian Conference on Information Systems, Sydney, Australia, 29 Nov – 2 Dec.
Schauder, D, Stillman, L & Johanson, G 2005, 'Sustaining a community network: the information continuum, e-democracy and the case of VICNET', The Journal of Community Informatics, vol. 1, no. 2, pp. 79-102,.
Schloeffel, P 2004a, Current EHR Developments: an Australian and International Perspective - Part 1. Health Care and Informatics Review OnlineTM, updated September 2004, ProCare Health Limited, viewed 2004-12-08 2004, <http://www.enigma.co.nz/hcro/website/index.cfm?fuseaction=articledisplay&featureid=010904>.
Page 322

Schloeffel, P 2004b, Current EHR Developments: an Australian and International Perspective - Part 2. Health Care and Informatics Review OnlineTM, updated September 2004, ProCare Health Limited, viewed 2004-12-08 2004, <http://www.enigma.co.nz/hcro/website/index.cfm?fuseaction=articledisplay&featureid=010904>.
Schwabe, G 1999, 'Understanding and Supporting Knowledge Management and Organizational Memory in a City Council', paper presented at the 32nd Hawaii International Conference on System Sciences (HICSS-32), Hawaii, USA, January.
Schwabe, G & Frohberg, D 2006, 'Facilitating mobile groups - experiences and requirements', paper presented at the Group Decision and Negotiation 2006 Conference, Karlsruhe, Germany, 25-28 June.
Schwabe, G & Krcmar, H 2000a, 'Electronic Meeting Support for Councils', AI & Society, vol. 14, no. 1, pp. 48-70.
Schwabe, G & Krcmar, H 2000b, 'Piloting Socio-technical Innovation', paper presented at the Eighth European Conference on Information Systems (ECIS), Vienna, Austria, 3-5 July.
Schweiger, R, Brumhard, M, Hoelzer, S & Dudeck, J 2005, 'Implementing health care systems using XML standards', International Journal of Medical Informatics, vol. 74, no. 2-4, pp. 267-277.
Seldén, L 2005, 'On Grounded Theory – with some malice', Journal of Documentation, vol. 61, no. 1, pp. 114-129.
Shaw, RL 2001, 'Why use interpretative phenomenological analysis in Health Psychology?' Health Psychology Update, vol. 10, no. 4, pp. 48-52.
Shepherd, M, Abidi, SSR, Gao, Q, Chen, Z & Qi, Q 2006, 'Information systems and health care ix: accessing tacit knowledge and linking it to the peer-reviewed literature', Communications of the Association for Information Systems, vol. 17, pp. 873-894.
Shepherd, M & Watters, C 1998, 'The Evolution of Cybergenres', paper presented at the 31st Hawaii International Conference on System Sciences (HICSS-31), Hawaii, USA, January.
Shepherd, M, Watters, C & Kennedy, A 2004, 'Cybergenre: automatic identification of home pages on the Web', Journal of Web Engineering, vol. 3, no. 3 & 4, pp. 236-251.
SHPA Committee of Specialty Practice in Clinical Pharmacy 2005, 'SHPA Standards of Practice for Clinical Pharmacy', Journal of Pharmacy Practice and Research, vol. 35, no. 2, pp. 122-146.
Sim, I & Berlin, A 2003, 'A Framework for Classifying Decision Support Systems', paper presented at the American Medical Informatics Association Symposium (AMIA 2003), Washington DC, USA, 8-12 November.
Sim, J 1998, 'Collecting and analysing qualitative data: issues raised by the focus group', Journal of Advanced Nursing, vol. 28, no. 2, pp. 345-352.
Simon, HA 1996, Sciences of the artificial, Third edn, MIT Press, Cambridge, Massachusetts, USA.
Simpson, SH, Eurich, DT, Majumdar, SR, Padwal, RS, Tsuyuki, RT, Varney, J & Johnson, JA 2006, 'A meta-analysis of the association between adherence to drug therapy and mortality', British Medical Journal, vol. 333, no. 7557, pp. 15-20.
Simpson, SH, Johnson, JA, Biggs, C, Biggs, RS, Kuntz, A, Semchuk, W, Taylor, JG, Farris, KB & Tsuyuki, RT 2001, 'Practice-based research: lessons from community pharmacist participants', Pharmacotherapy, vol. 21, no. 6, pp. 731-9.
Page 323

Sintchenko, V & Coiera, EW 2003, 'Which clinical decisions benefit from automation? A task complexity approach*', International Journal of Medical Informatics, vol. 70, no. 2-3, 309-316.
Smith, DH, Perrin, N, Feldstein, A, Yang, X, Kuang, D, Simon, SR, Sittig, DF, Platt, R & Soumerai, SB 2006, 'The Impact of Prescribing Safety Alerts for Elderly Persons in an Electronic Medical Record: An Interrupted Time Series Evaluation', Archives of Internal Medicine, vol. 166, no. 10, pp. 1098-1104.
Smith, PC, Araya-Guerra, R, Bublitz, C, Parnes, B, Dickinson, LM, Van Vorst, R, Westfall, JM & Pace, WD 2005, 'Missing clinical information during primary care visits', Journal of the American Medical Association, vol. 293, no. 5, pp. 565-71.
Solomon, WD & Heathfield, HA 1994, 'Conceptual Modelling Used to Represent Drug Interactions', paper presented at the International Conference of the European Federation for Medical Informatics, Lisbon, Portugal, May.
Southon, G 2003, ' Advancing Knowledge in Health: A Knowledge-based Health System', paper presented at the Eleventh National Health Informatics Conference (HIC2003) and Twelfth National RACGP Computer Conference ; HINZ 2003: Second National Health Informatics and Management Conference, Sydney, Australia, 10-12 August.
Southon, G & Cook, R 2001, 'Knowledge and Informatics: The Critical Role of Knowledge', paper presented at the Ninth National Health Informatics Conference (HIC 2001) Canberra, Australia, 29-31 July.
Sowerby Centre for Health Informatics 2000, eHealth Horizons, University of Newcastle, Newcastle, UK.
Stowasser, DA, Allinson, YM & O'Leary, KM 2004, 'Understanding the Medicines Management Pathway', Journal of Pharmacy Practice and Research, vol. 34, no. 4, pp. 293-296.
Straub, D, Gefen, D & Boudreau, M-C 2004, The ISWorld Quantitative, Positivist Research Methods Website, (Ed) Dennis Galletta,, updated January 7, 2005., Association for Information Systems, Atlanta, Georgia, USA, viewed 2005-10-24 2005, <http://dstraub.cis.gsu.edu/quant/>.
Stringer, E & Genat, WJ 2004, Action research in health, Pearson - Merrill Prentice Hall, Upper Saddle River, NJ, USA.
Sutcliffe, AG 2000, 'Requirements Analysis for Socio-technical System Design', Information Systems, vol. 25, no. 3, pp. 213-233.
Swatman, PM, Bytheway, A, Cavill, M, Cooper, J & Wilde, WD 1996, 'Virtual Communities: Linking people and markets electronically', paper presented at the 7th Australasian Conference on Information Systems (ACIS96), Hobart, Tasmania, Australia, 11-13 December.
Tange, H, Dietz, JLG, Hasman, A & de Vries Robbe, PF 2003, 'A generic model of clinical practice - A common view of individual and collaborative care.' Methods of Information in Medicine, vol. 42, pp. 203-211.
Taylor, D & Procter, M 2005, The Literature Review: A Few Tips On Conducting It, updated Last modified July 9, 2005, University of Toronto, Toronto, Canada, viewed 2006-01-04 2006, <http://www.utoronto.ca/writing/litrev.html>.
The Design-Based Research Collective 2003, 'Design-Based Research: An Emerging Paradigm for Educational Inquiry', Educational Researcher, vol. 32, no. 1, pp. 5-8.
The National Institute of Clinical Studies 2002, Report of the Electronic Decision Support Governance Workshop, Melbourne, Australia.
Page 324
Thornett, A 2001, 'Computer decision support systems in general practice', International Journal of Information Management, vol. 21, no. 1, pp. 39-47.
Toms, EG & Campbell, DG 1999, 'Genre as Interface Metaphor: Exploiting Form and Function in Digital Environments', paper presented at the 32nd Hawaii International Conference on System Sciences (HICSS-32), Hawaii, USA, January.
Toomey, L, Adams, L & Churchill, EF 1998, 'Meetings in a Virtual Space: Creating a Digital Document', paper presented at the 31st Hawaii International Conference on System Sciences (HICSS-31), Hawaii, USA, January.
Truex III, DP 2001, 'Three Issues Concerning Relevance in IS Research: Epistemology, Audience and Method', Communications of the Association for Information Systems, vol. 6, no. Article 24.
Tyrväinen, P & Päivärinta, T 1999, 'On Rethinking Organizational Document Genres for Electronic Document Management', paper presented at the 32nd Hawaii International Conference on System Sciences (HICSS-32), Hawaii, USA, January.
Uijlenbroek, JJM 1997, 'Designing electronic document infrastructures', School of Systems Engineering, Policy Analysis and Management, PhD thesis, Delft University of Technology, Netherlands.
UK Audit Commission 2001, A spoonful of sugar: medicines management in NHS hospitals, Audit Commission, London, UK.
Vaishnavi, V & Kuechler, B 2005, Design Research in Information Systems, Association for Information Systems, Atlanta, Georgia, USA, viewed 2005-10-11 2005, <http://www.isworld.org/Researchdesign/drisISworld.htm>.
van der Aalst, WMP & Kumar, A 2001, 'A reference model for team-enabled workflow management systems', Data & Knowledge Engineering, vol. 38, no. 3, pp. 335-363.
Varian, HR 1995, 'The information economy', Scientific American, September, pp. 200-201.
W3C 2004, XForms - The Next Generation of Web Forms, updated 2004/06/22, viewed 2004-06-23 2004, <http://www.w3.org/MarkUp/Forms/>.
Wagner, MM & Hogan, WR 1996, 'The accuracy of medication data in an outpatient electronic medical record', Journal of the American Medical Informatics Association, vol. 3, no. 3, pp. 234-44.
Walther, M, Nguyen, K, Garsden, H, Coiera, E & Lovell, NH 2002, Architecture for querying heterogeneous data sources for online decision-support in primary care, For special issue on Mining and Searching the Web (IEEE Transactions on Knowledge and Data Engineering), updated 1 Sep 2002, viewed 2004-03-31, <http://ranger.uta.edu/~alp/ix/readings/queryingHealthSources.pdf>.
Wang, JK, Herzog, NS, Kaushal, R, Park, C, Mochizuki, C & Weingarten, SR 2007, 'Prevention of Pediatric Medication Errors by Hospital Pharmacists and the Potential Benefit of Computerized Physician Order Entry', Pediatrics, vol. 119, no. 1, pp. e77-85.
Watt, N, Cooper, J, Lois Burgess & Alcock, C 2002, 'Are Business Websites Complying with Government Privacy Legislation?' paper presented at the 15th Bled Electronic Commerce Conference, eReality: Constructing the eEconomy, Bled, Slovenia, June 17 - 19.
Weigand, H & van den Heuvel, W-J 2002, 'Cross-organizational workflow integration using contracts', Decision Support Systems, vol. 33, no. 3, pp. 247-265.
Page 325

Weingart, SN, Toth, M, Sands, DZ, Aronson, MD, Davis, RB & Phillips, RS 2003, 'Physicians' Decisions to Override Computerized Drug Alerts in Primary Care', Archives of Internal Medicine, vol. 163, no. 21, pp. 2625-2631.
Weinshenk, S, Jamar, P & Yeo, SC 1997, GUI design essentials for Windows 95, Windows 3.1 World Wide Web, John Wiley & Sons Inc, New York; Chichester, USA.
Wenger, EC & Snyder, WM 2000, 'Communities of Practice: The Organizational Frontier.' Harvard Business Review, vol. 78, no. 1, pp. 139-145.
Westfall, RD 1999, 'An IS Research Relevance Manifesto', Communications of the Association for Information Systems, vol. 2, no. Paper 14.
Whitehead, PA, Sunderland, V & Benrimoj, S 2003, 'The 'general practice' pharmacist', The Australian Journal of Pharmacy, vol. 84, no. pp. 24-27.
Win, KT & Cooper, J 2004, 'Information Age, Electronic Health Record and Australia Healthcare', International Journal of The Computer, the Internet and Management, vol. 12, no. 3, pp. 14-21.
Winthereik, BR & Vikkelsø, S 2005, 'ICT and Integrated Care: Some Dilemmas of Standardising Inter-Organisational Communication', Computer Supported Cooperative Work (CSCW), vol. 14, pp. 43-67.
Workflow Management Coalition 1999, The Workflow Management Coalition Specification: Terminology & Glossary, Workflow Management Coalition, Winchester, United Kingdom.
World Health Organisation 2003a, Adherence to long-term therapies: evidence for action., World Health Organisation, Geneva, Switzerland.
World Health Organisation 2003b, Diet, Nutrition and the Prevention of Chronic Diseases, World Health Organization, Geneva, Switzerland.
World Health Organisation 2002, The World Health Report 2002, Reducing Risks, Promoting Healthy Life, Geneva, Switzerland
Worley-Louis, MM, Schommer, JC & Finnegan, JR 2003, 'Construct identification and measure development for investigating pharmacist-patient relationships', Patient Education and Counselling, vol. 51, no. 3, pp. 229-238.
Wu, JYF, Leung, WYS, Chang, S, Lee, B, Zee, B, Tong, PCY & Chan, JCN 2006, 'Effectiveness of telephone counselling by a pharmacist in reducing mortality in patients receiving polypharmacy: randomised controlled trial', British Medical Journal, vol. 333, no. 7567, pp. 522-.
Wyatt, J & Spiegelhalter, D 1991, 'Field trials of medical decision-aids: potential problems and solutions', paper presented at the Symposium on Computer Applications in Medical Care, Washington DC, USA, 1991.
Wyatt, JC 2000, 'Decision support systems', Journal of the Royal Society of Medicine, vol. 93, December, pp. 629-633.
Wyatt, JC & Sullivan, F 2005, 'Keeping up: learning in the workplace', British Medical Journal, vol. 331, no. 7525, pp. 1129-1132.
Yach, D, Hawkes, C, Gould, C & Hofman, K 2004, 'The global burden of chronic diseases - Overcoming impediments to prevention and control', Journal of the American Medical Association, vol. 291, no. 21, pp. 2616-2622.
Yin, R 1999, 'Enhancing the quality of case studies in health services research', Health Services Research, vol. 34, no. 5 (Part 2), pp. 1209-1224.
Page 326

Yin, RK 2003, Applications of case study research, Second edn, Sage Publications, Thousand Oaks, California, USA.
Yoshioka, T, Herman, G, Yates, J & Orlikowski, W 2001, 'Genre Taxonomy: A Knowledge Repository of Communicative Actions', ACM Transactions on Information Systems, vol. 19, no. 4, pp. 431-456.
Yusof, MM, Paul, RJ & Stergioulas, LK 2006, 'Towards a Framework for Health Information Systems Evaluation', paper presented at the 39th Annual Hawaii International Conference on System Sciences (HICSS-39), Hawaii, USA, January.
Zimmerman, JL & Dickerson, VC 1994, 'Using a Narrative Metaphor: Implications for Theory and Clinical Practice', Family Process, vol. 33, no. 3, pp. 233-245.
Page 327

Page 328
Appendices
As described at the beginning of this thesis, all appendices are contained on CD-ROM as PDF-formatted files. The file names are prefixed by the Appendix number as shown in the list below:
Appendix AA-Field Studies XForms Code.pdf
Appendix A-Analysis of Pharmacy DS Literature.pdf
Appendix AB-Field Studies Patient XML File.pdf
Appendix AC-Field Studies XSL Code.pdf
Appendix AD-Bibliography.pdf
Appendix B-An investigation of Methodology.pdf
Appendix C-HMR Quality Assurance Form.pdf
Appendix D-HOT Fit Model items.pdf
Appendix E-Hospital Ethics Approval & Correspondence.pdf
Appendix F-Benchtop Testing Ethics Approval.pdf
Appendix G-Field Studies Ethics Approval.pdf
Appendix H-Pharmacist Questionnaire.pdf
Appendix I-Medical Officer Questionnaire.pdf
Appendix J-Hospital Full Analysis.pdf
Appendix K-Hospital Technical & Development.pdf
Appendix L-Hospital VB Viewer Code.pdf
Appendix M-Hospital XForms Code.pdf
Appendix N-Hospital Patient XML File.pdf
Appendix O-Benchtop Full Analysis.pdf
Appendix P-Benchtop Technical & Development.pdf
Appendix Q-Development Record (Excel).pdf
Appendix R-Benchtop VB Viewer Code.pdf
Appendix S-Benchtop ASP Code.pdf
Appendix T-Benchtop XForms Code.pdf
Appendix U-Benchtop Patient XML File.pdf
Appendix V-Benchtop XSL Code.pdf
Appendix W-Benchtop Comparison of Model Elements.pdf
Appendix X-Field Studies Full Analysis.pdf
Appendix Y-Field Studies Additional Forms.pdf
Appendix Z-Field Studies Technical & Development.pdf
Top Related
Copyright © 2022 FDOKUMEN

