






Bahasa
Halaman
Hukum


doi: 10.1111/j.1472-8206.2010.00853.x
R E V I E W
A R T I C L E
Themed series on‘Sudden Cardiac Death –Cardiovascular Therapy’Meeting June 18–19, 2009Copenhagen, Denmark
Role of drugs and devices in patients at riskof sudden cardiac death
Giuseppe Boriania*, Igor Diembergera, Cinzia Valzaniaa, Mauro Biffia,Cristian Martignania, Emanuel Raschib, Valentina Mantovania,Matteo Ziacchia, Matteo Bertinia, Fabrizio De Pontib, Angelo Branzia
aInstitute of Cardiology, University of Bologna, Azienda Ospedaliera S. Orsola-Malpighi, Bologna, ItalybDepartment of Pharmacology, University of Bologna, Bologna, Italy
I N T R O D U C T I O N
Sudden cardiac death (SCD) is defined as an unexpected
death from cardiac causes following sudden cardiac
arrest occurring within 1 h of the onset of acute
symptoms [1]. Despite important progress, SCD contin-
ues to represent an important clinical challenge for
contemporary cardiology, and this is related to a series of
complex issues related to the extent of SCD epidemiology,
the variety of pathophysiological factors and mecha-
nisms that may lead to ventricular fibrillation as a
common final pathway, the incomplete knowledge of the
role of genetic factors in facilitating the occurrence of
malignant ventricular tachyarrhythmias, as well as the
difficulties in demonstrating the efficacy and effectiveness
of pharmacological or non-pharmacological interven-
tions (Figure 1).
A large number of studies have been dedicated to the
pathophysiology of SCD, and a specific experimental
model of SCD was developed to test the effect of various
classes of drugs [2]. In view of the complex interactions
among the mechanisms of arrhythmogenesis, the
anatomical and functional myocardial substrates, the
transient initiating events and genetic factors (Figure 1),
Keywords
anti-arrhythmic drugs,
cardioverter defibrillator,
sudden cardiac death,
ventricular fibrillation
Received 25 January 2010;
revised 19 March 2010;
accepted 4 May 2010
*Correspondence and reprints:
A B S T R A C T
The search for effective treatment for preventing sudden cardiac death (SCD) initially
started with anti-arrhythmic agents in high-risk patients, but the use of randomized
controlled trials clearly led to the conclusion that an approach based on anti-
arrhythmic agents is not useful, and sometimes potentially harmful (the risk of
arrhythmic death was increased up to 159% in CAST study). Today the approach to
SCD prevention includes considering both the setting of patients who have already
presented a cardiac arrest or a malignant ventricular tachyarrhythmias (secondary
preventions of SCD) and the much broader setting of primary prevention in patients
at variable degrees of identifiable risk. For secondary prevention of SCD, implantable
cardioverter defibrillation is now the standard of care (the risk of overall mortality
may be reduced by 20–31%), and anti-arrhythmic agents, specifically amiodarone,
have only a complementary role (for reducing device activations or for preventing
atrial fibrillation). For primary prevention of SCD in high-risk patients, cardioverter
defibrillators have nowadays specific indications in patients with left ventricular
dysfunction (often in combination with cardiac resynchronization therapy), where
the risk of overall mortality may be reduced by 23–54%. For the large number of
subjects who have some risk of SCD, but are not identified as at high risk of SCD, a
series of drugs could exert a favorable effect (beta-blockers, angiotensin-converting
enzyme inhibitors, angiotensin receptor blocker agents, statins, omega-3 fatty acids
and aldosterone antagonists), and for some of them evidence is emerging, from
subgroup analysis, of possible SCD prevention capabilities.
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594 575
Fund
amen
tal &
Cli
nica
l Pha
rmac
olog
y
randomized clinical trials are currently the crucial step to
validate any therapeutic intervention. Therefore, in this
review, we will focus on the clinical evaluation of the
therapeutic approaches for reducing SCD, with specific
reference to the result of randomized clinical trials.
The epidemiology of SCD as the basis for
therapeutic approaches
SCD is the most common cause of death in developed
Western countries where it is responsible every year for
more victims than AIDS (acquired immune deficiency
syndrome) or stroke [1,3,4], with around 460,000 SCDs
in the United States in 1998, accounting for nearly 60%
of all cardiac deaths.[5]. Worldwide, more than 3 million
people are estimated to die from SCD each year and only
<1–3% of SCD events are non-fatal [2]. It is estimated
that in Western countries, the overall incidence of SCD in
an unselected adult population is 1–2 per 1000 per year.
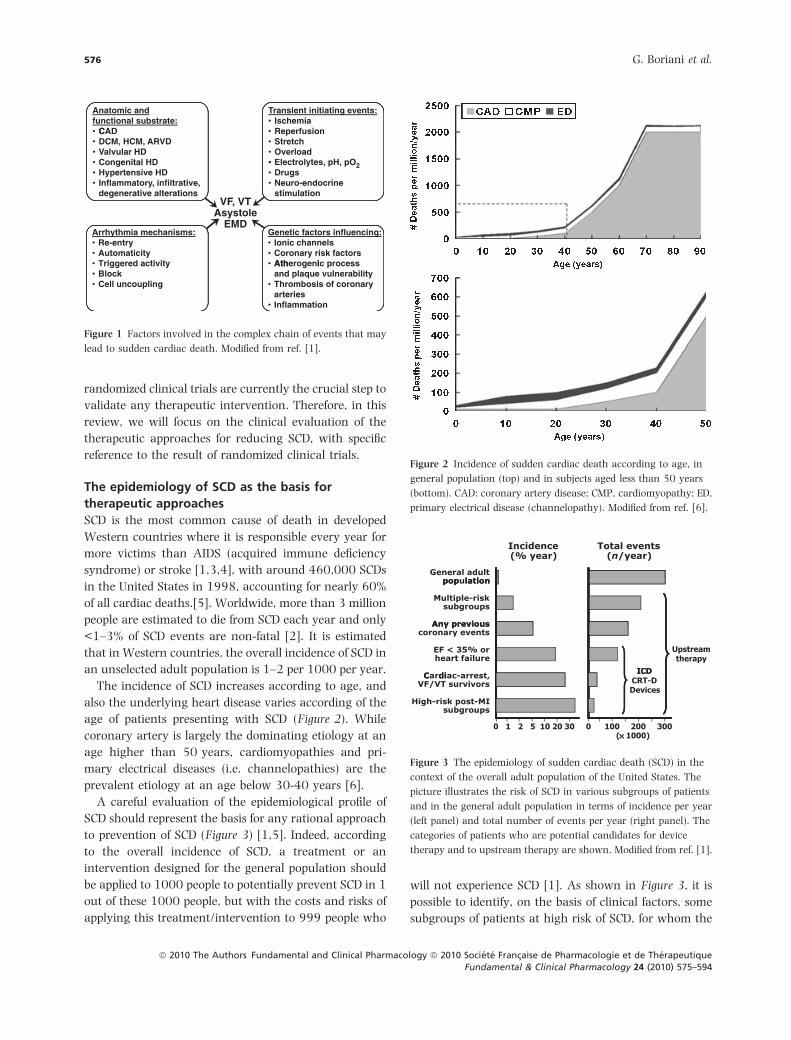
The incidence of SCD increases according to age, and
also the underlying heart disease varies according of the
age of patients presenting with SCD (Figure 2). While
coronary artery is largely the dominating etiology at an
age higher than 50 years, cardiomyopathies and pri-
mary electrical diseases (i.e. channelopathies) are the
prevalent etiology at an age below 30-40 years [6].
A careful evaluation of the epidemiological profile of
SCD should represent the basis for any rational approach
to prevention of SCD (Figure 3) [1,5]. Indeed, according
to the overall incidence of SCD, a treatment or an
intervention designed for the general population should
be applied to 1000 people to potentially prevent SCD in 1
out of these 1000 people, but with the costs and risks of
applying this treatment/intervention to 999 people who
will not experience SCD [1]. As shown in Figure 3, it is
possible to identify, on the basis of clinical factors, some
subgroups of patients at high risk of SCD, for whom the
Anatomic andfunctional substrate:
C
Transient initiating events:• Ischemia
• CAD• DCM, HCM, ARVD• Valvular HD
Congenital HD
• Reperfusion• Stretch• Overload••
• Hypertensive HD• Inflammatory, infiltrative,
•
• Drugs• Neuro-endocrine
stimulationdegenerative alterationsVF, VT
AsystoleEMD
Arrhythmia mechanisms:• Re-entry• Automaticity
Genetic factors influencing:• Ionic channels• Coronary risk factors
Ath i• Triggered activity• Block• Cell uncoupling
• Atherogenic processand plaque vulnerability
• Thrombosis of coronaryarteries
• Inflammation
Electrolytes, pH, pO2
Figure 1 Factors involved in the complex chain of events that may
lead to sudden cardiac death. Modified from ref. [1].
Figure 2 Incidence of sudden cardiac death according to age, in
general population (top) and in subjects aged less than 50 years
(bottom). CAD: coronary artery disease; CMP, cardiomyopathy; ED,
primary electrical disease (channelopathy). Modified from ref. [6].
Figure 3 The epidemiology of sudden cardiac death (SCD) in the
context of the overall adult population of the United States. The
picture illustrates the risk of SCD in various subgroups of patients
and in the general adult population in terms of incidence per year
(left panel) and total number of events per year (right panel). The
categories of patients who are potential candidates for device
therapy and to upstream therapy are shown. Modified from ref. [1].
576 G. Boriani et al.
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594

incidence of SCD events at 1 year may be at least 10-fold
greater than in the general population. These subgroups
of patients at high risk traditionally have been the
subject of investigations targeted to assess the risk and
cost-benefit ratio of a series of pharmacological and non-
pharmacological treatments (beta-blockers, amiodarone
and other anti-arrhythmic agents and, more recently,
implantable cardioverter defibrillators [ICDs]). These
subjects correspond to patients with coronary artery
disease, previous myocardial infarctions (MIs) associated
with left ventricular (LV) dysfunction and other high-risk
markers; patients with a recent ventricular tachyar-
rhythmia or recent cardiac arrest; and patients with LV
dysfunction or heart failure. However, approaches
directed to these high-risk patients will inevitably have
a limited effect on the overall number of SCD occurring
in the general population, as can be easily predicted by
data on the number of annual SCD events reported in
Figure 3 (right panel). The focus on high-risk patients
implies limiting the potential benefit of applied treat-
ments/interventions to a small fraction of the overall
number of subjects at risk. It is estimated that at least
two-thirds of all the events of SCD related to coronary
artery disease occur as the first clinical event in subjects
belonging to the general population or considered to be
at relatively low risk for SCD [(often relatively young
subjects with no more than one established cardiovas-
cular risk factor) [1,5]. For these reasons, although
present consensus guidelines [7] recommend highly
selective evidence-based SCD prevention strategies to
target the patients identified as at high risk for SCD, with
specific indications for ICDs, it should be highlighted that
this approach has the inherent limitation of targeting
only a relatively small proportion of all expected cases of
SCD. In this perspective, the ICD can be considered as
just one of the tools we have for fighting SCD: it is
obviously confined to high-risk subgroups and based on
prompt termination of ventricular tachyarrhythmias,
with an intervention which is ‘downstream’ of the chain
of events leading to life-threatening arrhythmias (i.e.
with effects acting directly on the electrophysiological
properties of cardiac fibers or specialized conducting
tissue). For patients at lower risk of SCD, or as a
complementary treatment in high-risk patients, there is
now increasing interest in the efficacy, effectiveness, and
cost-benefit ratio of a series of treatments that do not
have specific electrophysiological or anti-arrhythmic
effects, but may exert an ‘upstream’ effect on the
complex chain of events involved in SCD pathophysiol-
ogy, including interactions between substrate, triggers
and modulating factors [8]. As ‘upstream therapy’, we
can define all the pharmacological treatments without
electrophysiological actions on cardiac muscle or spe-
cialized conducting tissue [7]. In a rational approach to
SCD prevention, these upstream interventions (non-anti-
arrhythmic agents, such as b-blockers, aldosterone
antagonists, angiotensin-converting enzyme (ACE)
inhibitors, angiotensin II receptor blockers (ARB) agents,
statins and omega-3 fatty acids) should be considered as
attempts to prevent SCD in the much broader group of
patients at relatively low risk who have only coronary
risk factors, without specific markers of arrhythmic risk.
In this review, we will consider the evidence support-
ing the clinical use of anti-arrhythmic agents, ICDs and
non-anti-arrhythmic agents for upstream therapy, as a
rational and broad, full-spectrum approach to the
complex problem of SCD prevention. We will consider
both the selected setting of secondary prevention of SCD
[i.e. in patients with a previous aborted cardiac arrest or
a previous life-threatening ventricular tachycardia (VT)],
as well as the topical, larger setting of primary preven-
tion of SCD (i.e. in patients who had not previously
experienced life-threatening events but are identified as
patients at risk of SCD).
Anti-arrhythmic drugs: no evidence of benefit in
secondary and primary prevention of SCD
As ventricular fibrillation is the final common pathway
of a wide range of events leading to SCD (Figure 1), the
search for pharmacological agents to prevent SCD was
initially focused on agents that directly interact with the
ion channels of myocardial cells. Anti-arrhythmic agents
with characteristics typical of class I and class III
(including amiodarone) of the Vaughan Williams clas-
sification have been tested over time, also on the basis of
a series of considerations on the ‘vulnerable parameters’
that could be the most suitable targets for pharmaco-
logical interventions [9].
The observation in intensive care units, that ventric-
ular fibrillation is preceded by frequent premature
ventricular beats (PVB) and initiated by PVBs with very
short coupling, coupled with the observations that the
occurrence of frequent PVBs in survivors of MI is
associated with increased risk of SCD led in the 1980s
to the concept of reducing SCD through PVB suppres-
sion. This concept was applied to the field of primary
prevention of SCD in patients with a previous MI, and
class I anti-arrhythmic agents of the Vaughan Williams
classification, which are potent suppressors of PVBs,
were tested in a series of studies, including randomized
Prevention of sudden cardiac death 577
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594
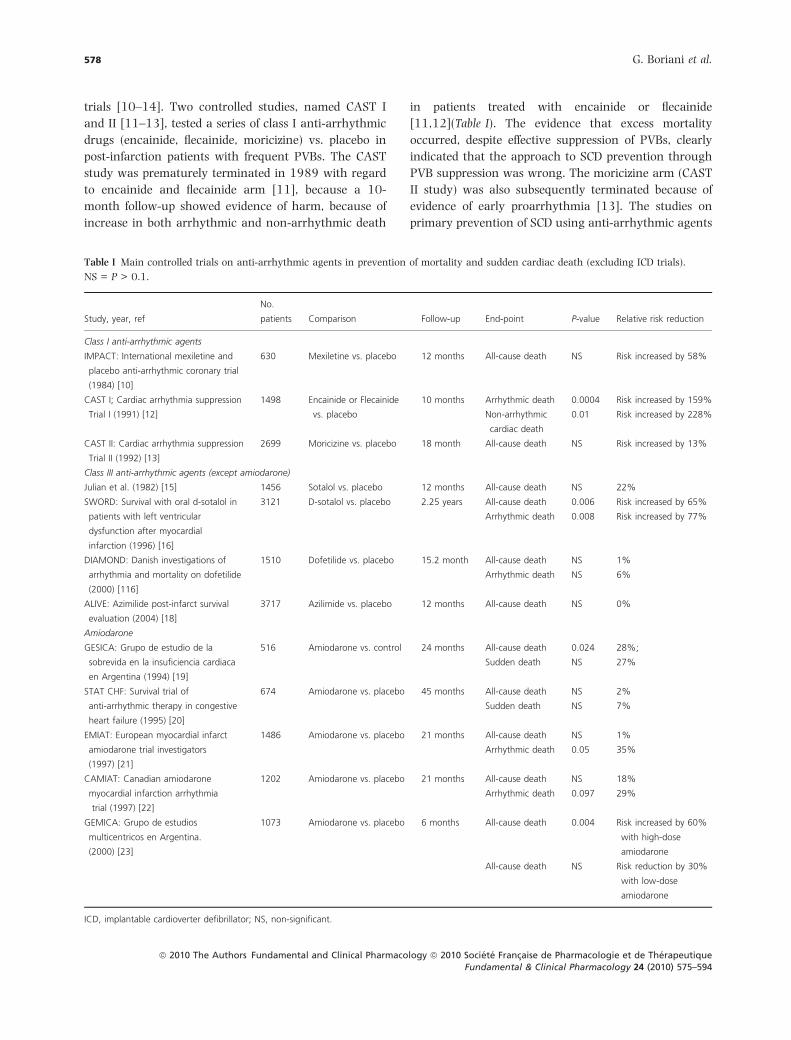
trials [10–14]. Two controlled studies, named CAST I
and II [11–13], tested a series of class I anti-arrhythmic
drugs (encainide, flecainide, moricizine) vs. placebo in
post-infarction patients with frequent PVBs. The CAST
study was prematurely terminated in 1989 with regard
to encainide and flecainide arm [11], because a 10-
month follow-up showed evidence of harm, because of
increase in both arrhythmic and non-arrhythmic death
in patients treated with encainide or flecainide
[11,12](Table I). The evidence that excess mortality
occurred, despite effective suppression of PVBs, clearly
indicated that the approach to SCD prevention through
PVB suppression was wrong. The moricizine arm (CAST
II study) was also subsequently terminated because of
evidence of early proarrhythmia [13]. The studies on
primary prevention of SCD using anti-arrhythmic agents
Table I Main controlled trials on anti-arrhythmic agents in prevention of mortality and sudden cardiac death (excluding ICD trials).
NS = P > 0.1.
Study, year, ref
No.
patients Comparison Follow-up End-point P-value Relative risk reduction
Class I anti-arrhythmic agents
IMPACT: International mexiletine and
placebo anti-arrhythmic coronary trial
(1984) [10]
630 Mexiletine vs. placebo 12 months All-cause death NS Risk increased by 58%
CAST I; Cardiac arrhythmia suppression
Trial I (1991) [12]
1498 Encainide or Flecainide
vs. placebo
10 months Arrhythmic death 0.0004 Risk increased by 159%
Non-arrhythmic
cardiac death
0.01 Risk increased by 228%
CAST II: Cardiac arrhythmia suppression
Trial II (1992) [13]
2699 Moricizine vs. placebo 18 month All-cause death NS Risk increased by 13%
Class III anti-arrhythmic agents (except amiodarone)
Julian et al. (1982) [15] 1456 Sotalol vs. placebo 12 months All-cause death NS 22%
SWORD: Survival with oral d-sotalol in
patients with left ventricular
dysfunction after myocardial
infarction (1996) [16]
3121 D-sotalol vs. placebo 2.25 years All-cause death 0.006 Risk increased by 65%
Arrhythmic death 0.008 Risk increased by 77%
DIAMOND: Danish investigations of
arrhythmia and mortality on dofetilide
(2000) [116]
1510 Dofetilide vs. placebo 15.2 month All-cause death NS 1%
Arrhythmic death NS 6%
ALIVE: Azimilide post-infarct survival
evaluation (2004) [18]
3717 Azilimide vs. placebo 12 months All-cause death NS 0%
Amiodarone
GESICA: Grupo de estudio de la
sobrevida en la insuficiencia cardiaca
en Argentina (1994) [19]
516 Amiodarone vs. control 24 months All-cause death 0.024 28%;
Sudden death NS 27%
STAT CHF: Survival trial of
anti-arrhythmic therapy in congestive
heart failure (1995) [20]
674 Amiodarone vs. placebo 45 months All-cause death NS 2%
Sudden death NS 7%
EMIAT: European myocardial infarct
amiodarone trial investigators
(1997) [21]
1486 Amiodarone vs. placebo 21 months All-cause death NS 1%
Arrhythmic death 0.05 35%
CAMIAT: Canadian amiodarone
myocardial infarction arrhythmia
trial (1997) [22]
1202 Amiodarone vs. placebo 21 months All-cause death NS 18%
Arrhythmic death 0.097 29%
GEMICA: Grupo de estudios
multicentricos en Argentina.
(2000) [23]
1073 Amiodarone vs. placebo 6 months All-cause death 0.004 Risk increased by 60%
with high-dose
amiodarone
All-cause death NS Risk reduction by 30%
with low-dose
amiodarone
ICD, implantable cardioverter defibrillator; NS, non-significant.
578 G. Boriani et al.
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594

were analyzed in a meta-analyses published by Teo el al.
[14], resulting in clear evidence that use of class I anti-
arrhythmic agents was associated with harm, expressed
by increased mortality in treated patients. The results of
these studies led to the conclusion of no role for class I,
and specifically for class Ic anti-arrhythmic agents in
SCD prevention in the setting of patient with previous
MI.
Agents with class III anti-arrhythmic properties have
been tested in a relatively small number of studies, while
much more data are available on amiodarone, a multi-
channel blocker that also exerts class III effects [15–26]
(Table I). Sotalol is a racemic mixture of a beta-blocker
and Ikr blocker, and in the study by Julian at al., its use
in post-infarction patients did not result in a significant
improvement in the outcome [15] (Table I). The SWORD
study tested d-sotalol, the isomer with pure class III
activity, in a population of patients with previous MI and
the result was negative, because of increased mortality
and only anti-arrhythmic death vs. placebo [16]
(Table I). Dofetilide is a class III anti-arrhythmic agent
developed to treat atrial fibrillation, which was tested in
a controlled study in post-infarction patients with LV
dysfunction, with evidence of no difference in overall
mortality and anti-arrhythmic mortality vs. placebo
[17]. More recently, azimilide, a complex class III anti-
arrhythmic agent, resulted in no improvement in the
outcome in a controlled study performed on post-
infarction patients with LV dysfunction [18].
Amiodarone has been the subject of several studies,
both in the field of primary and secondary prevention of
SCD. This agent has class III anti-arrhythmic properties,
but also exerts a broad spectrum of anti-arrhythmic
effects, through its multichannel activity, with a low rate
of proarrhythmic effects [9]. As shown in Table I, many
randomized, controlled trials were designed to assess the
efficacy of amiodarone either in patients with a previous
MI or in patients with heart failure [19–23]. As evident
from the results of the individual studies and from the
meta-analysis published in 1997 on more than 6500
patients [24], although amiodarone may reduce
arrhythmic death, there is no straight evidence that this
translated into a significant reduction in overall mortal-
ity. In the meta-analysis published in 1997, the reduc-
tion in overall mortality [13% relative risk (RR)
reduction] was significant or not significant depending
on the approach to meta-analysis (fixed effect or random
effect technique, respectively) [24]. A recent meta-
analysis on randomized studies on amiodarone was
published in 2009, based on 15 trials involving over
8500 patients [25]. This meta-analysis also confirms
that amiodarone treatment is associated with a signifi-
cant reduction in SCD and cardiovascular mortality (RR
reductions 28% and 18%, respectively), but without any
significant reduction in all-cause mortality [25].
Amiodarone was investigated also in SCD-HeFT trial, a
trial on the role of ICDs in primary prevention of SCD in
heart failure [26]. The lack of any significant improve-
ment in survival in the amiodarone arm vs. the placebo
arm of the SCD-HeFT trial (the trial with the largest
number of amiodarone-treated patients) strengthens the
notion that nowadays amiodarone has no role in
improving outcomes in patients at high risk [26]. For
this reason, and the evidence emerging from a series of
trials reported in Table II [27–35], amiodarone does not
currently represent a valid alternative to ICD therapy
which, unless not indicated for specific reasons [7], has
emerged as the landmark treatment for prevention of
SCD in high-risk patients, in the setting of either
secondary or primary prevention (the latter in patients
with LV dysfunction either of ischemic or of non-
ischemic etiology) [7,36–38].
Amiodarone has traditionally been the reference
treatment for patients with ventricular tachyarrhyth-
mias, i.e. in the setting of secondary prevention of SCD
(Table II). Its role in improving survival was initially
tested against anti-arrhythmic therapy guided by elec-
trophysiological testing in the CASCADE study, pub-
lished in 1993 [39]. In this study, 228 survivors of out-
of-hospital cardiac event were randomized to empiric
amiodarone or anti-arrhythmic therapy (predominantly
quinidine or procainamide) guided by the results of
programmed electrical stimulation. At 2 years, amioda-
rone treatment was associated with a significant lower
occurrence (8% vs. 31%, P = 0.007) of the combined
end-point of cardiac mortality, resuscitated cardiac event
or syncope because of ICD shock.
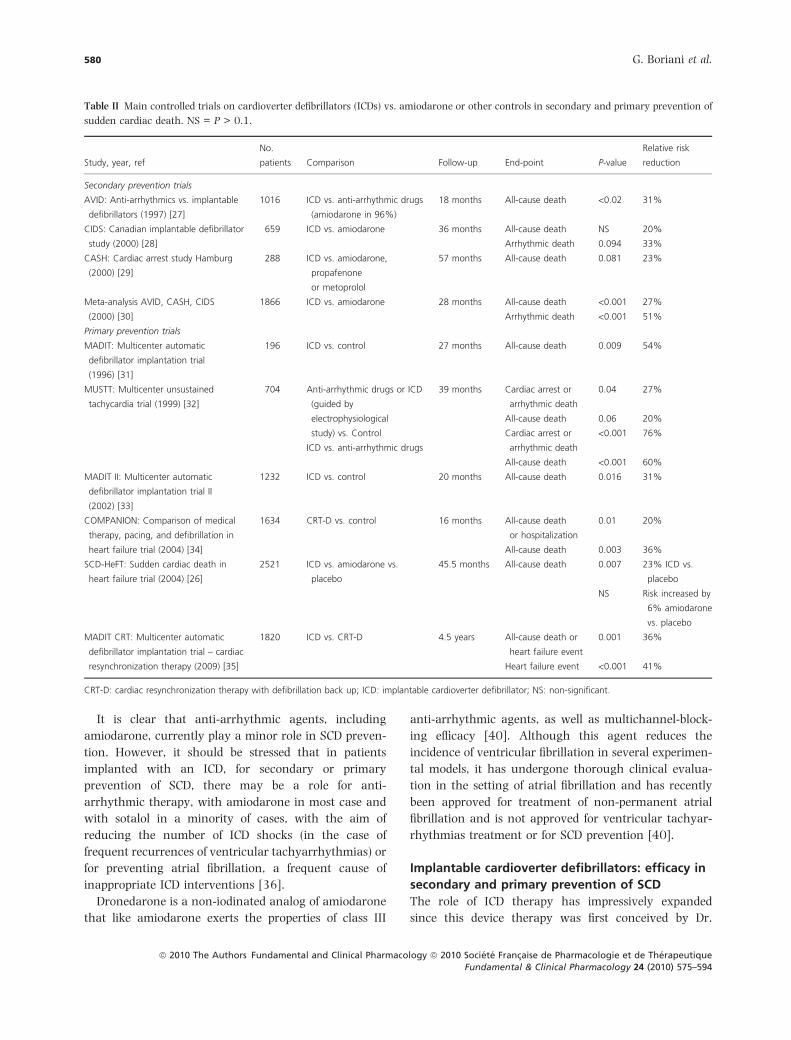
More recently, the development of ICDs has required
validation through randomized, clinical trials of ICD
therapy, and amiodarone has been the traditional
comparator in the field of either secondary or primary
prevention of SCD. The landmark trials comparing
amiodarone to ICD in the setting of secondary prevention
are shown in Table II, which also includes the results of a
meta-analysis [30]. Based on all the available trials, it
emerges that in the setting of secondary prevention, the
outcome of patients is improved by implanting an ICD,
which nowadays represents the standard of care for
secondary prevention of SCD, according to consensus
guidelines [7,38].
Prevention of sudden cardiac death 579
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594
It is clear that anti-arrhythmic agents, including
amiodarone, currently play a minor role in SCD preven-
tion. However, it should be stressed that in patients
implanted with an ICD, for secondary or primary
prevention of SCD, there may be a role for anti-
arrhythmic therapy, with amiodarone in most case and
with sotalol in a minority of cases, with the aim of
reducing the number of ICD shocks (in the case of
frequent recurrences of ventricular tachyarrhythmias) or
for preventing atrial fibrillation, a frequent cause of
inappropriate ICD interventions [36].
Dronedarone is a non-iodinated analog of amiodarone
that like amiodarone exerts the properties of class III
anti-arrhythmic agents, as well as multichannel-block-
ing efficacy [40]. Although this agent reduces the
incidence of ventricular fibrillation in several experimen-
tal models, it has undergone thorough clinical evalua-
tion in the setting of atrial fibrillation and has recently
been approved for treatment of non-permanent atrial
fibrillation and is not approved for ventricular tachyar-
rhythmias treatment or for SCD prevention [40].
Implantable cardioverter defibrillators: efficacy in
secondary and primary prevention of SCD
The role of ICD therapy has impressively expanded
since this device therapy was first conceived by Dr.
Table II Main controlled trials on cardioverter defibrillators (ICDs) vs. amiodarone or other controls in secondary and primary prevention of
sudden cardiac death. NS = P > 0.1.
Study, year, ref
No.
patients Comparison Follow-up End-point P-value
Relative risk
reduction
Secondary prevention trials
AVID: Anti-arrhythmics vs. implantable
defibrillators (1997) [27]
1016 ICD vs. anti-arrhythmic drugs
(amiodarone in 96%)
18 months All-cause death <0.02 31%
CIDS: Canadian implantable defibrillator
study (2000) [28]
659 ICD vs. amiodarone 36 months All-cause death NS 20%
Arrhythmic death 0.094 33%
CASH: Cardiac arrest study Hamburg
(2000) [29]
288 ICD vs. amiodarone,
propafenone
or metoprolol
57 months All-cause death 0.081 23%
Meta-analysis AVID, CASH, CIDS
(2000) [30]
1866 ICD vs. amiodarone 28 months All-cause death <0.001 27%
Arrhythmic death <0.001 51%
Primary prevention trials
MADIT: Multicenter automatic
defibrillator implantation trial
(1996) [31]
196 ICD vs. control 27 months All-cause death 0.009 54%
MUSTT: Multicenter unsustained
tachycardia trial (1999) [32]
704 Anti-arrhythmic drugs or ICD
(guided by
electrophysiological
study) vs. Control
ICD vs. anti-arrhythmic drugs
39 months Cardiac arrest or
arrhythmic death
0.04 27%
All-cause death 0.06 20%
Cardiac arrest or
arrhythmic death
<0.001 76%
All-cause death <0.001 60%
MADIT II: Multicenter automatic
defibrillator implantation trial II
(2002) [33]
1232 ICD vs. control 20 months All-cause death 0.016 31%
COMPANION: Comparison of medical
therapy, pacing, and defibrillation in
heart failure trial (2004) [34]
1634 CRT-D vs. control 16 months All-cause death
or hospitalization
0.01 20%
All-cause death 0.003 36%
SCD-HeFT: Sudden cardiac death in
heart failure trial (2004) [26]
2521 ICD vs. amiodarone vs.
placebo
45.5 months All-cause death 0.007 23% ICD vs.
placebo
NS Risk increased by
6% amiodarone
vs. placebo
MADIT CRT: Multicenter automatic
defibrillator implantation trial – cardiac
resynchronization therapy (2009) [35]
1820 ICD vs. CRT-D 4.5 years All-cause death or
heart failure event
0.001 36%
Heart failure event <0.001 41%
CRT-D: cardiac resynchronization therapy with defibrillation back up; ICD: implantable cardioverter defibrillator; NS: non-significant.
580 G. Boriani et al.
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594
Michel Mirowski over 30 years ago for secondary SCD
prevention in selected patients with documented ven-
tricular tachyarrhythmias [41]. The first ICD was
implanted in a human in 1980, and in 1985, the
Food and drug administration approved use of this
device for patients who had survived two episodes of
cardiac arrest. Impressive technological advances have
made ICDs easier and safer to implant and better
accepted by patients, with the possibility of performing
the implant in a subcutaneous pectoral pocket, without
the need for thoracotomy [36,42]. In parallel, a series
of randomized, controlled trials tested the efficacy of
ICD in reducing SCD and improving overall survival,
not only in the selective field of secondary prevention
but also in high-risk patients without previous ventric-
ular tachyarrhythmias [26–35] (Table II). For all these
studies, the main criterion for selecting patients at high
risk of SCD was the presence of a depressed LV
function. Demonstrated efficacy of ICDs in primary
prevention was initially established in patients with
previous MI associated with LV dysfunction (MADIT I,
MUSTT, MADIT II trials) [31–33] and was then
extended to patients with LV dysfunction and heart
failure (NYHA class II and III) of either ischemic or
non-ischemic etiology (SCD-HeFT trial) [26]. These
findings were progressively translated into the recom-
mendations for ICD implantation provided by consen-
sus guidelines [7,38]. Considering the evidence from
the individual trials alongside the results of various
meta-analyses of efficacy [36,38], it seems clear that
ICDs are effective in improving overall survival at
2–5 years in appropriately selected patients with LV
dysfunction at high risk of SCD and that the number of
patients who need to be treated to prevent one death
ranges between 1 and 14 in a time perspective ranging
from 1 to 5 years [43].
Device therapy for SCD prevention has had a
substantial improvement since the development and
validation of cardiac resynchronization therapy, ini-
tially in patients with moderate to severe heart failure,
and more recently also in mild heart failure [35,44].
In patients with moderate to severe heart failure,
cardiac resynchronization therapy, through continuous
biventricular pacing, has been shown to improve
overall survival, as well as providing favorable effects
in terms of quality of life, exercise capacity and
reductions in hospitalization because of heart failure
[44]. In view of current guidelines [7,38] and the most
recent studies, definite indications are now available
for device therapy, i.e. ICDs or devices providing both
defibrillation and resynchronization therapy (CRTD
devices), both in the field of secondary and primary
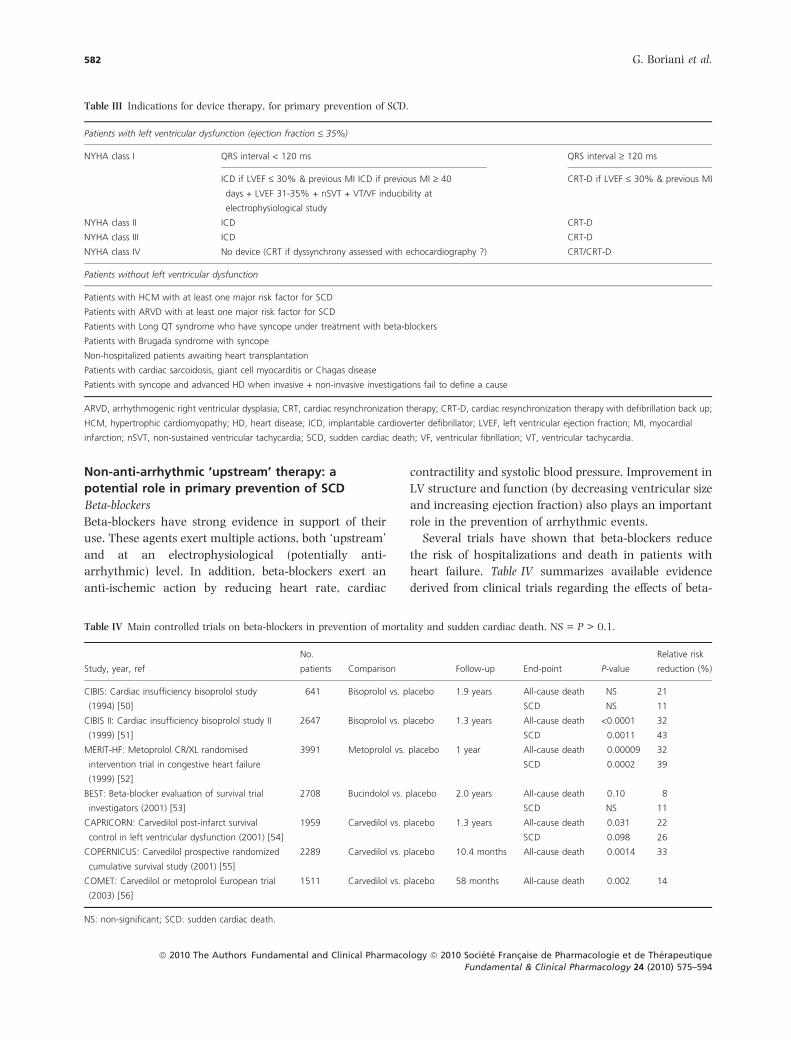
preventions of SCD. In Table III, indications to device
treatment for primary prevention of SCD and for heart
failure treatment are shown for a wide spectrum of
patients, including patients presenting with heart
failure and LV dysfunction. The presence of a wide
QRS complex (QRS duration ‡ 120 ms) is considered
an electrocardographic marker of ventricular dyssyn-
chrony and identifies those patients with heart failure
and LV dysfunction who can benefit from CRT [44].
As reported in Table III, patients with LV dysfunction
in the first 40 days following an acute MI are not
candidates to a prophylactic ICD, and this is in line
with the results of both DIAMOND and IRIS study
[45,46].
Some groups of patients are at risk of SCD even in the
absence of LV dysfunction, and specific indications for
ICD implant have been developed [7,38] for high-risk
subgroups of patients with hypertrophic cardiomyo-
pathy, arrhythmogenic right ventricular dysplasia, long
QT syndrome, Brugada syndrome or other clinical
entities, as indicated in Table III.
The challenging issue is now to what extent current
indications for device therapy for SCD prevention can be
applied in ‘real-world’ clinical practice, where health
care systems have to face the global financial and
economic crisis [36,43]. In this perspective, ICD is
commonly perceived as a rather expensive therapy, in
view of its high up-front costs at the time of device
implant, followed by maintenance costs for device
replacement and possible complications [43]. Despite
marked price reductions in the last decade, the cost issue
limits full acceptance and adoption of ICD therapy,
especially as regards widespread use for primary preven-
tion of SCD [36]. Even in economically developed
countries, the use of ICDs for primary prevention of
SCD represents an important public health consider-
ation, and implementation of consensus guidelines on
ICD use for primary prevention of SCD is fairly hetero-
geneous across Europe [36,43].
There is increasing interest on the role of VT
ablation, as a way for controlling ventricular tachyar-
rhythmias, either in patients who already have an
indication to ICD treatment [47,48] or in very selected
patients, as the unique intervention for preventing
recurrences of ventricular tachyarrhythmias [49]. The
latter application of VT ablation is still a matter of
clinical investigation, with regard to its impact on
patients’ outcomes at long term.
Prevention of sudden cardiac death 581
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594
Non-anti-arrhythmic ‘upstream’ therapy: a
potential role in primary prevention of SCD
Beta-blockers
Beta-blockers have strong evidence in support of their
use. These agents exert multiple actions, both ‘upstream’
and at an electrophysiological (potentially anti-
arrhythmic) level. In addition, beta-blockers exert an
anti-ischemic action by reducing heart rate, cardiac
contractility and systolic blood pressure. Improvement in
LV structure and function (by decreasing ventricular size
and increasing ejection fraction) also plays an important
role in the prevention of arrhythmic events.
Several trials have shown that beta-blockers reduce
the risk of hospitalizations and death in patients with
heart failure. Table IV summarizes available evidence
derived from clinical trials regarding the effects of beta-
Table IV Main controlled trials on beta-blockers in prevention of mortality and sudden cardiac death. NS = P > 0.1.
Study, year, ref
No.
patients Comparison Follow-up End-point P-value
Relative risk
reduction (%)
CIBIS: Cardiac insufficiency bisoprolol study
(1994) [50]
641 Bisoprolol vs. placebo 1.9 years All-cause death NS 21
SCD NS 11
CIBIS II: Cardiac insufficiency bisoprolol study II
(1999) [51]
2647 Bisoprolol vs. placebo 1.3 years All-cause death <0.0001 32
SCD 0.0011 43
MERIT-HF: Metoprolol CR/XL randomised
intervention trial in congestive heart failure
(1999) [52]
3991 Metoprolol vs. placebo 1 year All-cause death 0.00009 32
SCD 0.0002 39
BEST: Beta-blocker evaluation of survival trial
investigators (2001) [53]
2708 Bucindolol vs. placebo 2.0 years All-cause death 0.10 8
SCD NS 11
CAPRICORN: Carvedilol post-infarct survival
control in left ventricular dysfunction (2001) [54]
1959 Carvedilol vs. placebo 1.3 years All-cause death 0.031 22
SCD 0.098 26
COPERNICUS: Carvedilol prospective randomized
cumulative survival study (2001) [55]
2289 Carvedilol vs. placebo 10.4 months All-cause death 0.0014 33
COMET: Carvedilol or metoprolol European trial
(2003) [56]
1511 Carvedilol vs. placebo 58 months All-cause death 0.002 14
NS: non-significant; SCD: sudden cardiac death.
Table III Indications for device therapy, for primary prevention of SCD.
Patients with left ventricular dysfunction (ejection fraction £ 35%)
NYHA class I QRS interval < 120 ms QRS interval ‡ 120 ms
ICD if LVEF £ 30% & previous MI ICD if previous MI ‡ 40
days + LVEF 31-35% + nSVT + VT/VF inducibility at
electrophysiological study
CRT-D if LVEF £ 30% & previous MI
NYHA class II ICD CRT-D
NYHA class III ICD CRT-D
NYHA class IV No device (CRT if dyssynchrony assessed with echocardiography ?) CRT/CRT-D
Patients without left ventricular dysfunction
Patients with HCM with at least one major risk factor for SCD
Patients with ARVD with at least one major risk factor for SCD
Patients with Long QT syndrome who have syncope under treatment with beta-blockers
Patients with Brugada syndrome with syncope
Non-hospitalized patients awaiting heart transplantation
Patients with cardiac sarcoidosis, giant cell myocarditis or Chagas disease
Patients with syncope and advanced HD when invasive + non-invasive investigations fail to define a cause
ARVD, arrhythmogenic right ventricular dysplasia; CRT, cardiac resynchronization therapy; CRT-D, cardiac resynchronization therapy with defibrillation back up;
HCM, hypertrophic cardiomyopathy; HD, heart disease; ICD, implantable cardioverter defibrillator; LVEF, left ventricular ejection fraction; MI, myocardial
infarction; nSVT, non-sustained ventricular tachycardia; SCD, sudden cardiac death; VF, ventricular fibrillation; VT, ventricular tachycardia.
582 G. Boriani et al.
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594

blocker therapy on SCD and all-cause mortality [50–56].
The CIBIS II trial [51] demonstrated that treatment with
bisoprolol is associated with reduced all-cause mortality
in patients with heart failure symptoms and ejection
fraction of 35% or less (apparently irrespective of the
severity of heart failure etiology), and a reduction in SCD
was also recorded. In the MERIT-HF trial [52], addition
of metoprolol to standard therapy significantly reduced
both all-cause mortality in patients with NYHA func-
tional class II-IV symptoms and ejection fraction of
40% or less, and again seemed to lead to a reduction in
SCD.
Several meta-analyses [57–59] have reported that
beta-blocker therapy is associated with clinically mean-
ingful reductions in mortality in patients with congestive
heart failure. For example, in a meta-analysis [57] of 18
double-blind, placebo-controlled, parallel-group trials of
beta-blockers in heart failure, treatment with beta-
blockers provided a 32% reduction in the risk of death
and a 37% reduction in the combined risk of death or
hospitalization for heart failure.
Based on the evidence of benefit, beta-blockers have to
be considered the mainstay of therapies for improving
patients’ outcome and for SCD prevention, both in
patients with and without heart failure [3–5,7].
Angiotensin-converting enzyme (ACE) inhibitors
The anti-arrhythmic effects of ACE inhibitors seem to be
mediated by several mechanisms [60]. A long series of
clinical trials have uniformly shown that ACE inhibitors
provide survival benefits in patients with congestive
heart failure or MI. Table V shows the trial results of the
main trials [61–74]. In a meta-analysis [75] of 15
randomized, controlled trials comparing ACE inhibitors
with placebo in patients following acute MI, ACE
inhibitor therapy resulted in a significant reduction in
risk of death (odds ratio: 0.83; 95%CI 0.71, 0.97),
cardiovascular death (odds ratio: 0.82; 95%CI 0.69,
0.97), and SCD (odds ratio: 0.80; 95%CI 0.70, 0.92).
The reduction in SCD risk seems therefore to be an
important component of the survival benefit observed
with ACE inhibitor therapy. A further systematic over-
view [76] of 5 long-term randomized trials comparing
ACE inhibitor treatment with placebo showed that ACE
inhibitors lower rates of mortality, MI, and hospital
admission for heart failure in patients with LV dysfunc-
tion with or without a recent MI, thus suggesting the use
of ACE inhibitors in patients with LV dysfunction
irrespective of the proximity to a MI. ACE inhibitors
now have an established role in improving the outcome
both of heart failure and post-infarction patients (with or
without LV dysfunction), but the preventive effect on
SCD does not appear to be a determinant of treatment
selection.
The impact of ACE inhibitors on the outcome of
larger groups of patients, such as patients with vascular
disease and preserved LV function has been evaluated
mainly in 3 large randomized, placebo-controlled trials:
HOPE [71,72], EUROPA [73], and PEACE [74], with
non-homogeneous results. A systematic review of these
three large trials [77] confirmed the benefits of ACE
inhibitors in patients with vascular disease without
heart failure or LV systolic dysfunction in terms of
reduced all-cause mortality (odds ratio: 0.86; 95%CI
0.79, 0.94) and cardiovascular mortality (odds ratio:
0.82; 95%CI 0.73, 0.91). Furthermore, two further
meta-analyses regarding randomized, controlled trials
of ACE inhibitors [78,79] showed beneficial effects on
total mortality and major cardiovascular end-points in
patients with coronary artery disease and preserved LV
function.
Based on the evidence of benefit, ACE inhibitors have a
crucial role for improving patients’ outcome and pre-
venting worsening of LV dysfunction in all the stages of
heart failure, including also the presence of LV dysfunc-
tion without overt heart failure; the overall benefit of
these agents may involve also favorable effects on the
risk of SCD [7].
Angiotensin receptor blocker agents
The potential benefit of angiotensin receptor blocker
agents (ARBs) is related to a series of neurohormonal
and haemodynamic mechanisms [60]. The main con-
trolled trials on ARBs in prevention of mortality and SCD
are shown in Table VI [80–88].
The ELITE trial [80] compared losartan with captopril
in elderly patients with heart failure: treatment with
losartan was associated with a significant decrease in
all-cause mortality (Table VI) [59–64]. The ELITE II
study [81] enrolled a larger number of patients with
heart failure but was unable to find any significant
difference between losartan and captopril in terms of all-
cause mortality or SCD. Similar results were obtained in
the OPTIMAAL trial [82]. The effects of adding an ARB
to the standard therapy for heart failure were investi-
gated in the Val–HeFT trial [83]. Overall mortality was
similar in the intervention and the placebo-controlled
arms. Subgroup analysis suggested significant survival
benefits from valsartan in patients not taking an ACE
inhibitor.
Prevention of sudden cardiac death 583
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594
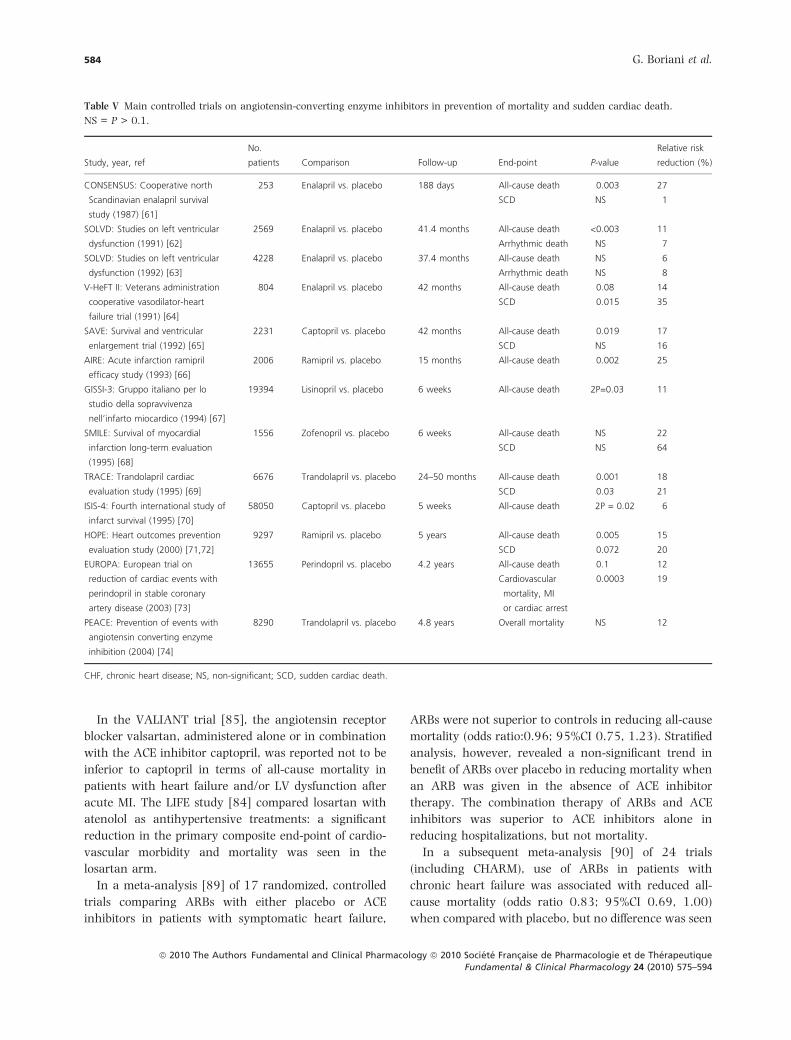
In the VALIANT trial [85], the angiotensin receptor
blocker valsartan, administered alone or in combination
with the ACE inhibitor captopril, was reported not to be
inferior to captopril in terms of all-cause mortality in
patients with heart failure and/or LV dysfunction after
acute MI. The LIFE study [84] compared losartan with
atenolol as antihypertensive treatments: a significant
reduction in the primary composite end-point of cardio-
vascular morbidity and mortality was seen in the
losartan arm.
In a meta-analysis [89] of 17 randomized, controlled
trials comparing ARBs with either placebo or ACE
inhibitors in patients with symptomatic heart failure,
ARBs were not superior to controls in reducing all-cause
mortality (odds ratio:0.96; 95%CI 0.75, 1.23). Stratified
analysis, however, revealed a non-significant trend in
benefit of ARBs over placebo in reducing mortality when
an ARB was given in the absence of ACE inhibitor
therapy. The combination therapy of ARBs and ACE
inhibitors was superior to ACE inhibitors alone in
reducing hospitalizations, but not mortality.
In a subsequent meta-analysis [90] of 24 trials
(including CHARM), use of ARBs in patients with
chronic heart failure was associated with reduced all-
cause mortality (odds ratio 0.83; 95%CI 0.69, 1.00)
when compared with placebo, but no difference was seen
Table V Main controlled trials on angiotensin-converting enzyme inhibitors in prevention of mortality and sudden cardiac death.
NS = P > 0.1.
Study, year, ref
No.
patients Comparison Follow-up End-point P-value
Relative risk
reduction (%)
CONSENSUS: Cooperative north
Scandinavian enalapril survival
study (1987) [61]
253 Enalapril vs. placebo 188 days All-cause death 0.003 27
SCD NS 1
SOLVD: Studies on left ventricular
dysfunction (1991) [62]
2569 Enalapril vs. placebo 41.4 months All-cause death <0.003 11
Arrhythmic death NS 7
SOLVD: Studies on left ventricular
dysfunction (1992) [63]
4228 Enalapril vs. placebo 37.4 months All-cause death NS 6
Arrhythmic death NS 8
V-HeFT II: Veterans administration
cooperative vasodilator-heart
failure trial (1991) [64]
804 Enalapril vs. placebo 42 months All-cause death 0.08 14
SCD 0.015 35
SAVE: Survival and ventricular
enlargement trial (1992) [65]
2231 Captopril vs. placebo 42 months All-cause death 0.019 17
SCD NS 16
AIRE: Acute infarction ramipril
efficacy study (1993) [66]
2006 Ramipril vs. placebo 15 months All-cause death 0.002 25
GISSI-3: Gruppo italiano per lo
studio della sopravvivenza
nell’infarto miocardico (1994) [67]
19394 Lisinopril vs. placebo 6 weeks All-cause death 2P=0.03 11
SMILE: Survival of myocardial
infarction long-term evaluation
(1995) [68]
1556 Zofenopril vs. placebo 6 weeks All-cause death NS 22
SCD NS 64
TRACE: Trandolapril cardiac
evaluation study (1995) [69]
6676 Trandolapril vs. placebo 24–50 months All-cause death 0.001 18
SCD 0.03 21
ISIS-4: Fourth international study of
infarct survival (1995) [70]
58050 Captopril vs. placebo 5 weeks All-cause death 2P = 0.02 6
HOPE: Heart outcomes prevention
evaluation study (2000) [71,72]
9297 Ramipril vs. placebo 5 years All-cause death 0.005 15
SCD 0.072 20
EUROPA: European trial on
reduction of cardiac events with
perindopril in stable coronary
artery disease (2003) [73]
13655 Perindopril vs. placebo 4.2 years All-cause death 0.1 12
Cardiovascular
mortality, MI
or cardiac arrest
0.0003 19
PEACE: Prevention of events with
angiotensin converting enzyme
inhibition (2004) [74]
8290 Trandolapril vs. placebo 4.8 years Overall mortality NS 12
CHF, chronic heart disease; NS, non-significant; SCD, sudden cardiac death.
584 G. Boriani et al.
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594
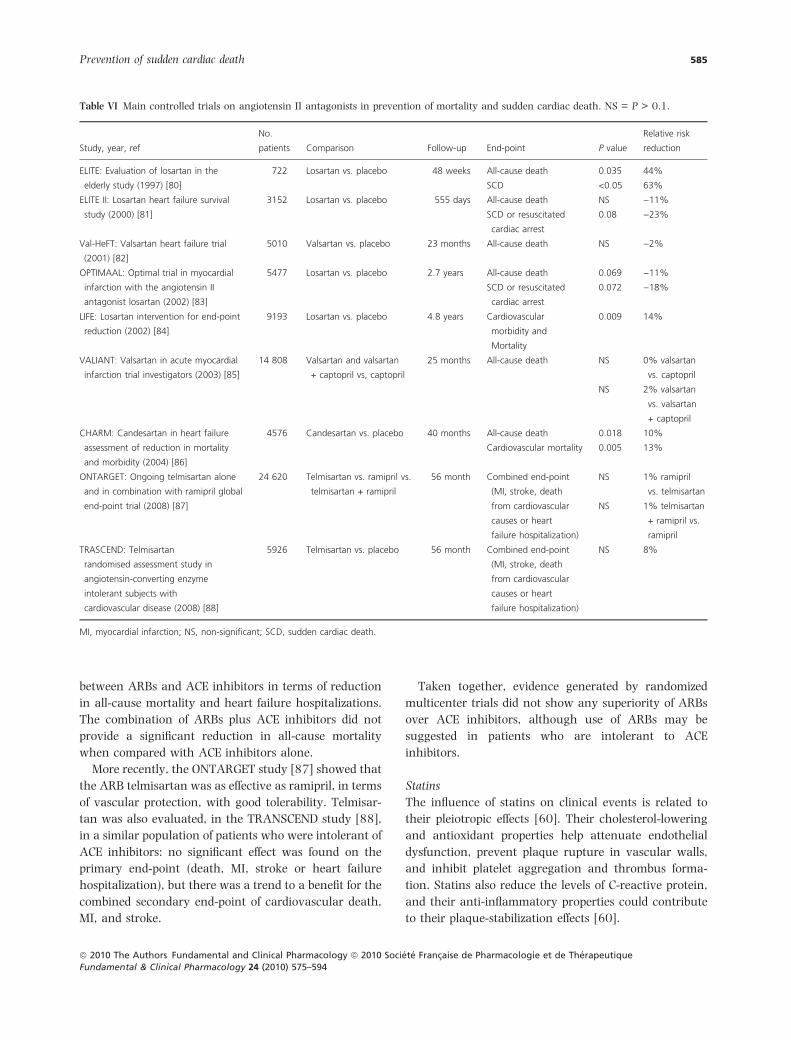
between ARBs and ACE inhibitors in terms of reduction
in all-cause mortality and heart failure hospitalizations.
The combination of ARBs plus ACE inhibitors did not
provide a significant reduction in all-cause mortality
when compared with ACE inhibitors alone.
More recently, the ONTARGET study [87] showed that
the ARB telmisartan was as effective as ramipril, in terms
of vascular protection, with good tolerability. Telmisar-
tan was also evaluated, in the TRANSCEND study [88],
in a similar population of patients who were intolerant of
ACE inhibitors: no significant effect was found on the
primary end-point (death, MI, stroke or heart failure
hospitalization), but there was a trend to a benefit for the
combined secondary end-point of cardiovascular death,
MI, and stroke.
Taken together, evidence generated by randomized
multicenter trials did not show any superiority of ARBs
over ACE inhibitors, although use of ARBs may be
suggested in patients who are intolerant to ACE
inhibitors.
Statins
The influence of statins on clinical events is related to
their pleiotropic effects [60]. Their cholesterol-lowering
and antioxidant properties help attenuate endothelial
dysfunction, prevent plaque rupture in vascular walls,
and inhibit platelet aggregation and thrombus forma-
tion. Statins also reduce the levels of C-reactive protein,
and their anti-inflammatory properties could contribute
to their plaque-stabilization effects [60].
Table VI Main controlled trials on angiotensin II antagonists in prevention of mortality and sudden cardiac death. NS = P > 0.1.
Study, year, ref
No.
patients Comparison Follow-up End-point P value
Relative risk
reduction
ELITE: Evaluation of losartan in the
elderly study (1997) [80]
722 Losartan vs. placebo 48 weeks All-cause death 0.035 44%
SCD <0.05 63%
ELITE II: Losartan heart failure survival
study (2000) [81]
3152 Losartan vs. placebo 555 days All-cause death NS )11%
SCD or resuscitated
cardiac arrest
0.08 )23%
Val-HeFT: Valsartan heart failure trial
(2001) [82]
5010 Valsartan vs. placebo 23 months All-cause death NS )2%
OPTIMAAL: Optimal trial in myocardial
infarction with the angiotensin II
antagonist losartan (2002) [83]
5477 Losartan vs. placebo 2.7 years All-cause death 0.069 )11%
SCD or resuscitated
cardiac arrest
0.072 )18%
LIFE: Losartan intervention for end-point
reduction (2002) [84]
9193 Losartan vs. placebo 4.8 years Cardiovascular
morbidity and
Mortality
0.009 14%
VALIANT: Valsartan in acute myocardial
infarction trial investigators (2003) [85]
14 808 Valsartan and valsartan
+ captopril vs, captopril
25 months All-cause death NS 0% valsartan
vs. captopril
NS 2% valsartan
vs. valsartan
+ captopril
CHARM: Candesartan in heart failure
assessment of reduction in mortality
and morbidity (2004) [86]
4576 Candesartan vs. placebo 40 months All-cause death 0.018 10%
Cardiovascular mortality 0.005 13%
ONTARGET: Ongoing telmisartan alone
and in combination with ramipril global
end-point trial (2008) [87]
24 620 Telmisartan vs. ramipril vs.
telmisartan + ramipril
56 month Combined end-point
(MI, stroke, death
from cardiovascular
causes or heart
failure hospitalization)
NS 1% ramipril
vs. telmisartan
NS 1% telmisartan
+ ramipril vs.
ramipril
TRASCEND: Telmisartan
randomised assessment study in
angiotensin-converting enzyme
intolerant subjects with
cardiovascular disease (2008) [88]
5926 Telmisartan vs. placebo 56 month Combined end-point
(MI, stroke, death
from cardiovascular
causes or heart
failure hospitalization)
NS 8%
MI, myocardial infarction; NS, non-significant; SCD, sudden cardiac death.
Prevention of sudden cardiac death 585
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594
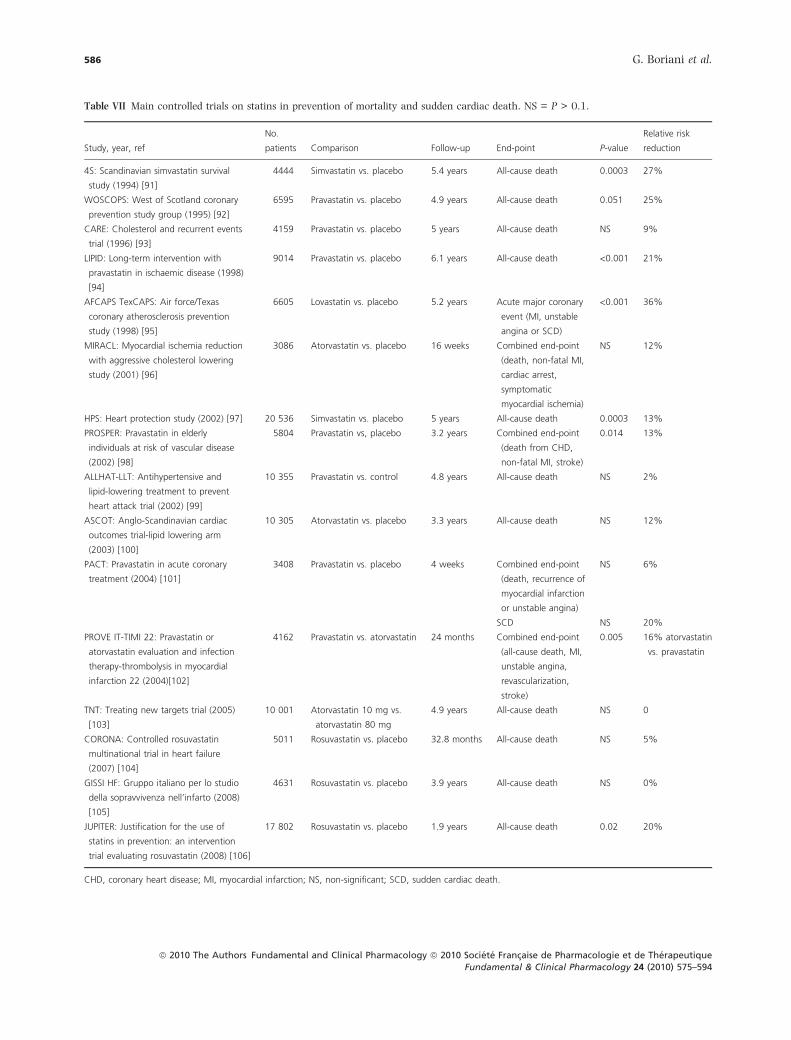
Table VII Main controlled trials on statins in prevention of mortality and sudden cardiac death. NS = P > 0.1.
Study, year, ref
No.
patients Comparison Follow-up End-point P-value
Relative risk
reduction
4S: Scandinavian simvastatin survival
study (1994) [91]
4444 Simvastatin vs. placebo 5.4 years All-cause death 0.0003 27%
WOSCOPS: West of Scotland coronary
prevention study group (1995) [92]
6595 Pravastatin vs. placebo 4.9 years All-cause death 0.051 25%
CARE: Cholesterol and recurrent events
trial (1996) [93]
4159 Pravastatin vs. placebo 5 years All-cause death NS 9%
LIPID: Long-term intervention with
pravastatin in ischaemic disease (1998)
[94]
9014 Pravastatin vs. placebo 6.1 years All-cause death <0.001 21%
AFCAPS TexCAPS: Air force/Texas
coronary atherosclerosis prevention
study (1998) [95]
6605 Lovastatin vs. placebo 5.2 years Acute major coronary
event (MI, unstable
angina or SCD)
<0.001 36%
MIRACL: Myocardial ischemia reduction
with aggressive cholesterol lowering
study (2001) [96]
3086 Atorvastatin vs. placebo 16 weeks Combined end-point
(death, non-fatal MI,
cardiac arrest,
symptomatic
myocardial ischemia)
NS 12%
HPS: Heart protection study (2002) [97] 20 536 Simvastatin vs. placebo 5 years All-cause death 0.0003 13%
PROSPER: Pravastatin in elderly
individuals at risk of vascular disease
(2002) [98]
5804 Pravastatin vs, placebo 3.2 years Combined end-point
(death from CHD,
non-fatal MI, stroke)
0.014 13%
ALLHAT-LLT: Antihypertensive and
lipid-lowering treatment to prevent
heart attack trial (2002) [99]
10 355 Pravastatin vs. control 4.8 years All-cause death NS 2%
ASCOT: Anglo-Scandinavian cardiac
outcomes trial-lipid lowering arm
(2003) [100]
10 305 Atorvastatin vs. placebo 3.3 years All-cause death NS 12%
PACT: Pravastatin in acute coronary
treatment (2004) [101]
3408 Pravastatin vs. placebo 4 weeks Combined end-point
(death, recurrence of
myocardial infarction
or unstable angina)
NS 6%
SCD NS 20%
PROVE IT-TIMI 22: Pravastatin or
atorvastatin evaluation and infection
therapy-thrombolysis in myocardial
infarction 22 (2004)[102]
4162 Pravastatin vs. atorvastatin 24 months Combined end-point
(all-cause death, MI,
unstable angina,
revascularization,
stroke)
0.005 16% atorvastatin
vs. pravastatin
TNT: Treating new targets trial (2005)
[103]
10 001 Atorvastatin 10 mg vs.
atorvastatin 80 mg
4.9 years All-cause death NS 0
CORONA: Controlled rosuvastatin
multinational trial in heart failure
(2007) [104]
5011 Rosuvastatin vs. placebo 32.8 months All-cause death NS 5%
GISSI HF: Gruppo italiano per lo studio
della sopravvivenza nell’infarto (2008)
[105]
4631 Rosuvastatin vs. placebo 3.9 years All-cause death NS 0%
JUPITER: Justification for the use of
statins in prevention: an intervention
trial evaluating rosuvastatin (2008) [106]
17 802 Rosuvastatin vs. placebo 1.9 years All-cause death 0.02 20%
CHD, coronary heart disease; MI, myocardial infarction; NS, non-significant; SCD, sudden cardiac death.
586 G. Boriani et al.
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594

Many trials have shown significant reductions in all-
cause mortality after statin therapy (Table VII) [91–106].
These benefits were mostly paralleled by reduced SCD,
although few specific data on this outcome measure were
separately reported.
In a meta-analysis of 15 lipid trials [107], statin
therapy significantly reduced the RR of coronary events
[RR 0.73; 95%CI 0.68, 0.77], cardiovascular disease
mortality (RR 0.78; 95%CI 0.73, 0.84), and all-cause
death (RR 0.85; 95%CI 0.81, 0,89). Another meta-
analysis of 10 outcome trials of statins [108] showed
that statin therapy reduces major coronary events by
27% (95%CI 23%, 30%), stroke by 18% (95%CI 10%,
25%), and all-cause mortality by 15% (95%CI 8%, 21%).
Coronary events were reduced by 23% (95%CI 18%,
29%) in pravastatin trials and 29% (95%CI 25%, 33%)
in five trials with other statins.
More recently, the ability of statins to improve
outcomes has been tested also independently of choles-
terol levels, i.e. in subjects with no conventional indica-
tion to statins. In patients with chronic heart failure,
GISSI-HF showed that rosuvastatin did not affect clinical
outcomes [105], while the CORONA trial [104] showed
that in older patients, rosuvastatin did not reduce
mortality, although the drug did reduce the number of
cardiovascular hospitalizations.
In JUPITER, rosuvastatin significantly reduced the
incidence of major cardiovascular events and death in
apparently healthy persons without hyperlipidemia but
with elevated high-sensitivity C-reactive protein levels
[106].
Based on the evidence from trials, statins have an
established therapeutic role in patients with coronary
artery disease, but the potential role in reducing SCD for
the broader population of patients at risk has still to be
assessed.
Omega-3 fatty acids
Omega-3 fatty acids may provide cardiovascular health
benefits derived from several effects, including decrease
in very low density lipoprotein and thereby in plasma
triglyceride levels; improvement in endothelial function;
cell membrane stabilization; platelet aggregation inhibi-
tion; suppression of smooth muscle cell proliferation; and
prevention of calcium overload [60].
Several clinical trials support the concept that omega-
3 fatty acids can reduce the risk of overall and
cardiovascular mortality in patients with coronary heart
disease [105,109–112] (Table VIII). In the GISSI-Preven-
tion study [112], the use of omega-3 fatty acids
significantly reduced the primary combined end-point
of death, non-fatal MI and non-fatal stroke, with a
benefit attributable to a decrease in the risk of overall
and cardiovascular death.
A systematic review has shown that the evidence for
the outcome benefits of n ) 3 fatty acids is stronger
in secondary- than in primary prevention trials [113].
Based on a literature review [114], Mozzafarian reported
that modest consumption of fish or fish oil substantially
reduces the risk of SCD and coronary deaths, with little
additional benefit with higher intakes.
Remarkably, no significant effect on all-cause death
was reported by a randomized, placebo-controlled trial
that evaluated the effects of n ) 3 fatty acids in patients
with ICDs [115].
A recent meta-analysis [116] of randomized trials on
omega-3 fatty acids in patients with coronary heart
disease, related to more than 20,000 patients, shows
that this treatment may reduce the incidence of SCD in
patients with previous MI (RR = 0.43; 95% CI:
0.20–0.91) but may have adverse effects in patients
with angina, where the risk of SCD may increase
(RR = 1.39; 95% CI: 1.01–1.92). Overall, the relative
risk for all-cause mortality was 0.77 (95% CI:
0.58–1.01), suggesting the need for further investiga-
tions in the setting of patients with angina. In patients
with chronic heart failure of New York Heart Associ-
ation class II–IV, GISSI-HF [105] reported that treat-
ment with n ) 3 PUFA (polyunsaturated fatty acid)
provided a significant beneficial advantage in terms of
mortality and admission to hospital for cardiovascular
reasons.
Based on the evidence derived from trials, omega-3
fatty acids result to be beneficial for patients with a
previous MI (with or without LV dysfunction). Their role
in other settings has still to be defined.
Aldosterone antagonists
On a pathophysiological basis, aldosterone antagonists
may have beneficial effects on cardiovascular mortality
and SCD through at least three mechanisms: a sympatho-
lytic effect, the reduction in both vascular and cardiac
fibrosis, and prevention of the negative effects of angio-
tensin II at vascular level, with reduction in vascular
endothelial dysfunction [60]. The effects of aldosterone
antagonists on SCD have been assessed in two random-
ized, placebo-controlled trials (Table IX). The RALES trial
evaluated the effects of spironolactone in patients with
congestive heart failure [117], while EPHESUS focused on
the use of eplerenone in MI survivors with LV dysfunction
Prevention of sudden cardiac death 587
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594
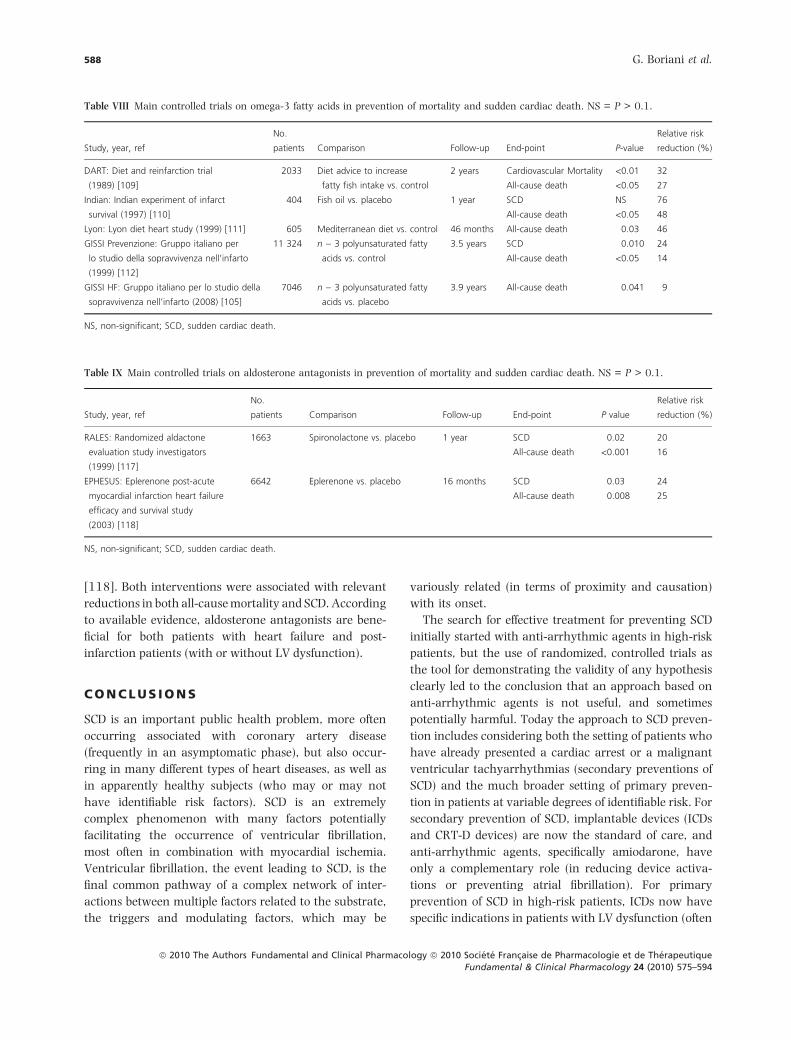
[118]. Both interventions were associated with relevant
reductions in both all-cause mortality and SCD. According
to available evidence, aldosterone antagonists are bene-
ficial for both patients with heart failure and post-
infarction patients (with or without LV dysfunction).
C O N C L U S I O N S
SCD is an important public health problem, more often
occurring associated with coronary artery disease
(frequently in an asymptomatic phase), but also occur-
ring in many different types of heart diseases, as well as
in apparently healthy subjects (who may or may not
have identifiable risk factors). SCD is an extremely
complex phenomenon with many factors potentially
facilitating the occurrence of ventricular fibrillation,
most often in combination with myocardial ischemia.
Ventricular fibrillation, the event leading to SCD, is the
final common pathway of a complex network of inter-
actions between multiple factors related to the substrate,
the triggers and modulating factors, which may be
variously related (in terms of proximity and causation)
with its onset.
The search for effective treatment for preventing SCD
initially started with anti-arrhythmic agents in high-risk
patients, but the use of randomized, controlled trials as
the tool for demonstrating the validity of any hypothesis
clearly led to the conclusion that an approach based on
anti-arrhythmic agents is not useful, and sometimes
potentially harmful. Today the approach to SCD preven-
tion includes considering both the setting of patients who
have already presented a cardiac arrest or a malignant
ventricular tachyarrhythmias (secondary preventions of
SCD) and the much broader setting of primary preven-
tion in patients at variable degrees of identifiable risk. For
secondary prevention of SCD, implantable devices (ICDs
and CRT-D devices) are now the standard of care, and
anti-arrhythmic agents, specifically amiodarone, have
only a complementary role (in reducing device activa-
tions or preventing atrial fibrillation). For primary
prevention of SCD in high-risk patients, ICDs now have
specific indications in patients with LV dysfunction (often
Table VIII Main controlled trials on omega-3 fatty acids in prevention of mortality and sudden cardiac death. NS = P > 0.1.
Study, year, ref
No.
patients Comparison Follow-up End-point P-value
Relative risk
reduction (%)
DART: Diet and reinfarction trial
(1989) [109]
2033 Diet advice to increase
fatty fish intake vs. control
2 years Cardiovascular Mortality <0.01 32
All-cause death <0.05 27
Indian: Indian experiment of infarct
survival (1997) [110]
404 Fish oil vs. placebo 1 year SCD NS 76
All-cause death <0.05 48
Lyon: Lyon diet heart study (1999) [111] 605 Mediterranean diet vs. control 46 months All-cause death 0.03 46
GISSI Prevenzione: Gruppo italiano per
lo studio della sopravvivenza nell’infarto
(1999) [112]
11 324 n ) 3 polyunsaturated fatty
acids vs. control
3.5 years SCD 0.010 24
All-cause death <0.05 14
GISSI HF: Gruppo italiano per lo studio della
sopravvivenza nell’infarto (2008) [105]
7046 n ) 3 polyunsaturated fatty
acids vs. placebo
3.9 years All-cause death 0.041 9
NS, non-significant; SCD, sudden cardiac death.
Table IX Main controlled trials on aldosterone antagonists in prevention of mortality and sudden cardiac death. NS = P > 0.1.
Study, year, ref
No.
patients Comparison Follow-up End-point P value
Relative risk
reduction (%)
RALES: Randomized aldactone
evaluation study investigators
(1999) [117]
1663 Spironolactone vs. placebo 1 year SCD 0.02 20
All-cause death <0.001 16
EPHESUS: Eplerenone post-acute
myocardial infarction heart failure
efficacy and survival study
(2003) [118]
6642 Eplerenone vs. placebo 16 months SCD 0.03 24
All-cause death 0.008 25
NS, non-significant; SCD, sudden cardiac death.
588 G. Boriani et al.
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594
in combination with CRT), although implementation in
clinical practice of this approach is still incomplete.
Moreover, both epidemiological and pathophysiologi-
cal considerations suggest that limiting the target of SCD
preventive strategies to the relatively limited number of
high-risk subjects (who are currently proposed for a
strictly ‘downstream’ intervention like the implantable
cardioverter defibrillator) will necessarily have a limited
impact on the overall number of SCD events occurring in
the general population. For the large number of subjects
who have some risk of SCD, but are not identified as at
high risk of SCD, a series of drugs that were initially
thought to be devoid of what is usually termed a true
‘anti-arrhythmic’ effect could conceivably help prevent
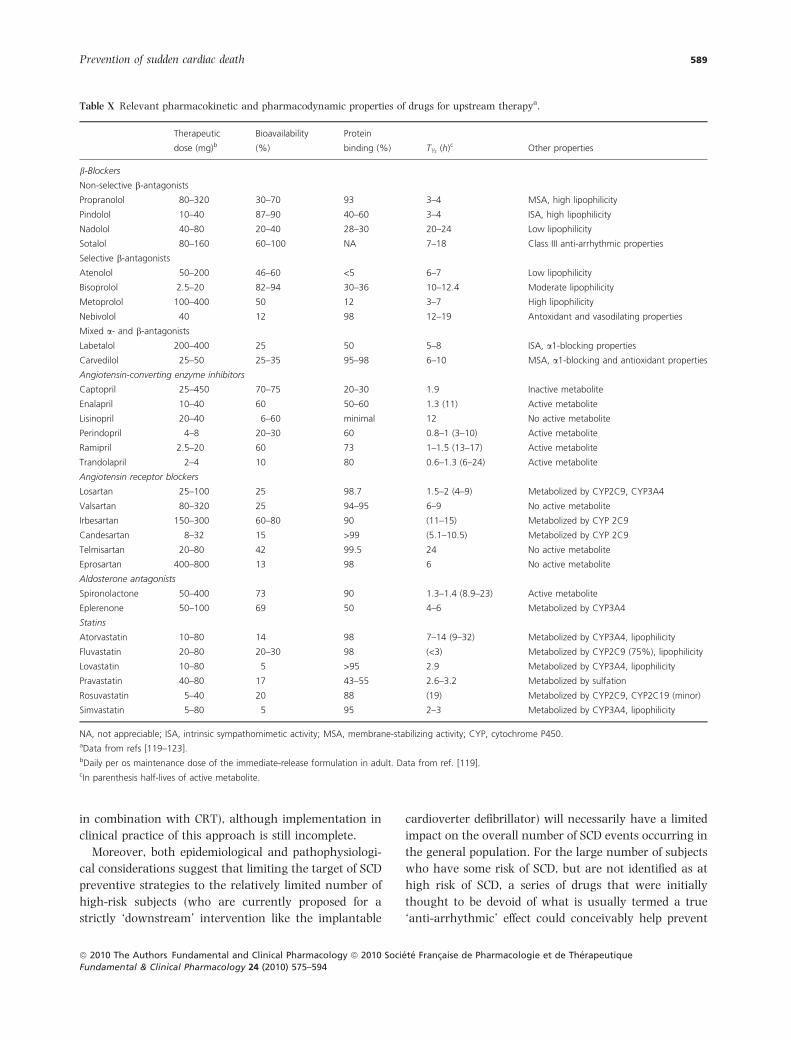
Table X Relevant pharmacokinetic and pharmacodynamic properties of drugs for upstream therapya.
Therapeutic
dose (mg)bBioavailability
(%)
Protein
binding (%) T½ (h)c Other properties
b-Blockers
Non-selective b-antagonists
Propranolol 80–320 30–70 93 3–4 MSA, high lipophilicity
Pindolol 10–40 87–90 40–60 3–4 ISA, high lipophilicity
Nadolol 40–80 20–40 28–30 20–24 Low lipophilicity
Sotalol 80–160 60–100 NA 7–18 Class III anti-arrhythmic properties
Selective b-antagonists
Atenolol 50–200 46–60 <5 6–7 Low lipophilicity
Bisoprolol 2.5–20 82–94 30–36 10–12.4 Moderate lipophilicity
Metoprolol 100–400 50 12 3–7 High lipophilicity
Nebivolol 40 12 98 12–19 Antoxidant and vasodilating properties
Mixed a- and b-antagonists
Labetalol 200–400 25 50 5–8 ISA, a1-blocking properties
Carvedilol 25–50 25–35 95–98 6–10 MSA, a1-blocking and antioxidant properties
Angiotensin-converting enzyme inhibitors
Captopril 25–450 70–75 20–30 1.9 Inactive metabolite
Enalapril 10–40 60 50–60 1.3 (11) Active metabolite
Lisinopril 20–40 6–60 minimal 12 No active metabolite
Perindopril 4–8 20–30 60 0.8–1 (3–10) Active metabolite
Ramipril 2.5–20 60 73 1–1.5 (13–17) Active metabolite
Trandolapril 2–4 10 80 0.6–1.3 (6–24) Active metabolite
Angiotensin receptor blockers
Losartan 25–100 25 98.7 1.5–2 (4–9) Metabolized by CYP2C9, CYP3A4
Valsartan 80–320 25 94–95 6–9 No active metabolite
Irbesartan 150–300 60–80 90 (11–15) Metabolized by CYP 2C9
Candesartan 8–32 15 >99 (5.1–10.5) Metabolized by CYP 2C9
Telmisartan 20–80 42 99.5 24 No active metabolite
Eprosartan 400–800 13 98 6 No active metabolite
Aldosterone antagonists
Spironolactone 50–400 73 90 1.3–1.4 (8.9–23) Active metabolite
Eplerenone 50–100 69 50 4–6 Metabolized by CYP3A4
Statins
Atorvastatin 10–80 14 98 7–14 (9–32) Metabolized by CYP3A4, lipophilicity
Fluvastatin 20–80 20–30 98 (<3) Metabolized by CYP2C9 (75%), lipophilicity
Lovastatin 10–80 5 >95 2.9 Metabolized by CYP3A4, lipophilicity
Pravastatin 40–80 17 43–55 2.6–3.2 Metabolized by sulfation
Rosuvastatin 5–40 20 88 (19) Metabolized by CYP2C9, CYP2C19 (minor)
Simvastatin 5–80 5 95 2–3 Metabolized by CYP3A4, lipophilicity
NA, not appreciable; ISA, intrinsic sympathomimetic activity; MSA, membrane-stabilizing activity; CYP, cytochrome P450.aData from refs [119–123].bDaily per os maintenance dose of the immediate-release formulation in adult. Data from ref. [119].cIn parenthesis half-lives of active metabolite.
Prevention of sudden cardiac death 589
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594

SCD in an attempt to reduce the overall SCD burden. As
a consequence of such an approach, for the large group
of patients at relatively low risk who have only coronary
risk factors, it could be possible to target the processes of
the complex cascade leading to SCD at an ‘upstream’
level. Such ‘upstream’ interventions could conceivably
include non-anti-arrhythmic agents, such as beta-block-
ers, angiotensin-converting enzyme inhibitors, angioten-
sin receptor blocker agents, statins, omega-3 fatty acids,
and aldosterone antagonists. The clinical use of these
agents should be based on an appropriate knowledge
of their pharmacokinetic/pharmacodynamic profile,
summarized in Table X [119–123]. Some of these agents
have already shown survival benefits in clinical trials,
largely focused on patients at relatively high risk of SCD,
and evidence is emerging from subgroup analysis of
possible SCD prevention capabilities. In patients at higher
risk of SCD, who are treated with an ICD or CRT-D
device, agents with ‘upstream’ effects can be associated
in an attempt to obtain additional, and synergetic, effects
on the outcome.
R E F E R E N C E S
1 Myerburg R.J., Kessler K.M., Castellanos A. Sudden cardiac
death. Structure, function, and time-dependence of risk.
Circulation (1992) 85(1 Suppl) I2–I10.
2 Billman G.E. A comprehensive review and analysis of 25 years
of data from an in vivo canine model of sudden cardiac death:
Implications for future anti-arrhythmic drug development.
Pharmacol. Ther. (2006) 111 808–835.
3 Zipes D., Wellens H.J. Sudden cardiac death. Circulation
(1998) 98 2334–2351.
4 Josephson M., Wellens H.J. Implantable defibrillators and
sudden cardiac death. Circulation (2004) 109 2685–2691.
5 Myerburg R.J. Sudden cardiac death exploring the limits of our
knowledge. J. Cardiovasc. Electrophysiol. (2001) 12 369–381.
6 Reducing the risk: a strategic approach. The report of the task
force on sudden cardiac death. Published by the Department of
Health and Children. Ireland (2006), 1–158.
7 Zipes D.P., Camm A.J., Borggrefe M. et al. ACC/AHA/ESC
2006 guidelines for management of patients with ventricular
arrhythmias and the prevention of sudden cardiac death: a
report of the American College of Cardiology/American Heart
Association Task Force and the European Society of Cardiol-
ogy Committee for Practice Guidelines (Writing Committee to
Develop Guidelines for Management of Patients With Ven-
tricular Arrhythmias and the Prevention of Sudden Cardiac
Death). Europace (2006) 8 746–837.
8 Boriani G., Valzania C., Diemberger I. et al. Potential of non-
antiarrhythmic drugs to provide an innovative upstream
approach to the pharmacological prevention of sudden cardiac
death. Expert Opin. Investig. Drugs (2007) 16 605–623.
9 Members of the Sicilian Gambit: The ‘‘Sicilian Gambit.’’ A new
approach to the classification of antiarrhythmic drugs based
on their actions on arrhythmogenic mechanisms. The Task
Force of the Working Group on Arrhythmias of the European
Society of Cardiology. Eur. Heart J. (1991) 12 1112–1131.
10 Impact Research Group. International mexiletine and placebo
antiarrhythmic coronary trial: I. Report on arrhythmia and
other findings. J. Am. Coll. Cardiol. (1984) 4 1148–1163.
11 The Cardiac Arrhythmia Suppression Trial (CAST) Investiga-
tors. Preliminary report: effect of encainide and flecainide on
mortality in a randomized trial of arrhythmia suppression
after myocardial infarction. N. Engl. J. Med. (1989) 321, 406–
412.
12 Echt D., Liebson P., Mitchell B. et al. Mortality and morbidity
in patients receiving encainide, flecainide, or placebo: the
Cardiac Arrhythmia Suppression Trial (CAST I). N. Engl. J.
Med. (1991) 324 781–788.
13 The Cardiac Arrhythmia Suppression Trial II Investigators.
Effect of the antiarrhythmic agent moricizine on survival after
myocardial infarction. N. Engl. J. Med. (1992) 327 227–233.
14 Teo K.K., Yusuf S., Furberg C.D. Effects of prophylactic
antiarrhythmic drug therapy in acute myocardial infarction:
an overview of results from randomized controlled trials.
JAMA (1993) 270 1589–1595.
15 Julian D.G., Prescott R.J., Jackson F.S., Szekely P. Controlled
trial of sotalol for one year after myocardial infarction. Lancet
(1982) 1 1142–1147.
16 Waldo A., Camm J., deRuyter H. et al. Survival with oral
d-sotalol in patients with left ventricular dysfunction after
myocardial infarction (SWORD: Survival With Oral D-sotalol).
Lancet (1996) 348 7–12.
17 Kober L., Bloch Thomsen P., Moller M. et al. Effect of dofetilide
in patients with recent myocardial infarction and left-ven-
tricular dysfunction: a randomised trial. Lancet (2000) 356
2052–2058.
18 Camm A.J., Pratt C.M., Schwartz P.J. et al. on behalf of the
AzimiLide post Infarct surVival Evaluation (ALIVE) Investi-
gators. Mortality in patients after a recent myocardial
infarction: a randomized, placebo-controlled trial of azimilide
using heart rate variability for risk stratification. Circulation
(2004) 109 990–996.
19 Doval H.C., Nul D.R., Grancelli H.O., Perrone S.V., Bortman
G.R., Curiel R. Randomised trial of low-dose amiodarone in
severe congestive heart failure. Grupo de Estudio de la
Sobrevida en la Insuficiencia Cardiaca en Argentina (GESICA).
Lancet (1994) 344 493–498.
20 Singh S.N., Fletcher R.D., Fisher S.G. et al. Amiodarone in
patients with congestive heart failure and asymptomatic
ventricular arrhythmia. Survival Trial of Antiarrhythmic
Therapy in Congestive Heart Failure. N. Engl. J. Med. (1995)
333 77–82.
21 Julian D.G., Camm A.J., Frangin G. et al. Randomised trial of
effect of amiodarone on mortality in patients with left-
ventricular dysfunction after recent myocardial infarction:
EMIAT. European Myocardial Infarct Amiodarone Trial
Investigators. Lancet (1997) 349 667–674.
590 G. Boriani et al.
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594

22 Cairns J.A., Connolly S.J., Roberts R., Gent M. Randomised
trial of outcome after myocardial infarction in patients with
frequent or repetitive ventricular premature depolarisations:
CAMIAT. Canadian Amiodarone Myocardial Infarction
Arrhythmia Trial Investigators. Lancet (1997) 349 675–
682.
23 Elizari M.V., Martinez J.M., Belziti C. et al. Morbidity and
mortality following early administration of amiodarone in
acute myocardial infarction. GEMICA study investigators.
Eur. Heart J. (2000) 21 198–205.
24 Amiodarone Trials Meta-Analysis Investigators. Effect of
prophylactic amiodarone on mortality after acute myocardial
infarction and in congestive heart failure: meta-analysis of
individual data from 6500 patients in randomised trials.
Lancet (1997) 350 1417–1424.
25 Piccini J.P., Berger J.S., O’Connor C.M. Amiodarone for the
prevention of sudden cardiac death: a meta-analysis of
randomized controlled trials. Eur. Heart J. (2009) 30 1245–
1253.
26 Bardy G.H., Lee K.L., Mark D.B. et al. Amiodarone or an
implantable cardioverter-defibrillator for congestive heart
failure. N. Engl. J. Med. (2005) 352 225–237.
27 The Antiarrhythmics versus Implantable Defibrillators (AVID)
Investigators. A comparison of antiarrhythmic-drug therapy
with implantable defibrillators in patients resuscitated from
near-fatal ventricular arrhythmias. N. Engl. J. Med. (1997)
337, 1576–1583.
28 Connolly S.J., Gent M., Roberts R.S. et al. Canadian implant-
able defibrillator study (CIDS): a randomized trial of the
implantable cardioverter defibrillator against amiodarone.
Circulation (2000) 101 1297–1302.
29 Kuck K.H., Cappato R., Siebels J., Ruppel R. Randomized
comparison of antiarrhythmic drug therapy with implantable
defibrillators in patients resuscitated from cardiac arrest : the
Cardiac Arrest Study Hamburg (CASH). Circulation (2000)
102 748–754.
30 Connolly S.J., Hallstrom A.P., Cappato R. et al. Meta-analysis
of the implantable cardioverter defibrillator secondary pre-
vention trials. AVID, CASH and CIDS studies. Eur. Heart J.
(2000) 21 2071–2078.
31 Moss A.J., Hall W.J., Cannom D.S. et al. Improved survival
with an implanted defibrillator in patients with coronary
disease at high risk for ventricular arrhythmia. N. Engl. J.
Med. (1996) 335 1933–1940.
32 Buxton A.E., Lee K.L., Fisher J.D., Josephson M.E., Prystowsky
E.N., Hafley G. A randomized study of the prevention of
sudden death in patients with coronary artery disease.
N. Engl. J. Med. (1999) 341 1882–1890.
33 Moss A.J., Zareba W., Hall W.J. et al. Prophylactic implanta-
tion of a defibrillator in patients with myocardial infarction
and reduced ejection fraction. N. Engl. J. Med. (2002) 346
877–883.
34 Bristow M.R., Saxon L.A., Boehmer J. et al. Cardiac resyn-
chronization therapy with or without an implantable defi-
brillator in advanced chronic heart failure. N. Engl. J. Med.
(2004) 350 2140–2150.
35 Moss A.J., Hall W.J., Cannom D.S. et al. Cardiac-resynchro-
nization therapy for the prevention of heart-failure events. N.
Engl. J. Med. (2009) 361 1329–1338.
36 Boriani G., Ricci R., Toselli T., Ferrari R., Branzi A., Santini M.
Implantable cardioverter defibrillators: from evidence of trials to
clinical practice. Eur. Heart J. Suppl (2007) 9(Suppl I) I66–I73.
37 Ezekowitz J.A., Rowe B.H., Dryden D.M. et al. Systematic
review: implantable cardioverter defibrillators for adults with
left ventricular systolic dysfunction. Ann. Intern. Med. (2007)
147 251–262.
38 Epstein A.E., Dimarco J.P., Ellenbogen K.A. et al. ACC/AHA/
HRS 2008 Guidelines for device-based therapy of cardiac
rhythm abnormalities. Heart Rhythm (2008) 5 e1–e6.
39 Cardiac arrest in Seattle: conventional versus amiodarone
drug evaluation (CASCADE Study). Am. J. Cardiol. (1993) 72
280–287.
40 Hoy S.M., Keam S.J. Dronedarone. Drugs (2009) 69 1647–
1663.
41 Mirowski M., Reid P.R., Mower M.M. et al. Termination of
malignant ventricular arrhythmias with an implanted auto-
matic defibrillator in human beings. N. Engl. J. Med. (1980)
303 322–324.
42 Sutton R., Fisher J.D., Linde C., Benditt D.G. History of
electrical therapy for the heart. Eur. Heart J. Suppl. (2007) 9
I3–I10.
43 Boriani G., Biffi M., Martignani C. et al. Expenditure and value
for money: the challenge of implantable cardioverter defibril-
lators. QJM (2009) 102 349–356.
44 Leclercq C., Bleeker G.B., Linde C. et al. Cardiac resynchroni-
zation therapy: clinical results and evolution of candidate
selection. Eur. Heart J. Suppl. (2007) 9 I94–I106.
45 Hohnloser S.H., Kuck K.H., Dorian P. et al. Prophylactic use
of an implantable cardioverter-defibrillator after acute
myocardial infarction. N. Engl. J. Med. (2004) 351
2481–2488.
46 Steinbeck G., Andresen D., Seidl K. et al. Defibrillator
implantation early after myocardial infarction. N. Engl. J. Med.
(2009) 361 1427–1436.
47 Reddy V.Y., Reynolds M.R., Neuzil P. et al. Prophylactic
catheter ablation for the prevention of defibrillator therapy. N.
Engl. J. Med. (2007) 357 2657–2665.
48 Kuck K.H., Schaumann A., Eckardt L. et al. Catheter ablation of
stable ventricular tachycardia before defibrillator implantation
in patients with coronary heart disease (VTACH): a multicentre
randomised controlled trial. Lancet (2010) 375 31–40.
49 Viana-Tejedor A., Merino J.L., Perez-Silva A. et al. Effective-
ness of catheter ablation of ventricular tachycardia in elderly
patients with structural heart disease. Rev. Esp. Cardiol.
(2010) 63 156–160.
50 CIBIS Investigators. A randomized trial of beta-blockade in
heart failure. The Cardiac Insufficiency Bisoprolol Study
(CIBIS). CIBIS Investigators and Committees. Circulation
(1994) 90 1765–1773.
51 CIBIS II Investigators. The Cardiac Insufficiency Bisoprolol
Study II (CIBIS-II): a randomised trial. Lancet (1999) 353 9–
13.
Prevention of sudden cardiac death 591
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594
52 MERIT-HF Study group. Effect of metoprolol CR/XL in chronic
heart failure: Metoprolol CR/XL Randomised Intervention
Trial in Congestive Heart Failure (MERIT-HF). Lancet (1999)
353 2001–2007.
53 The beta-blocker evaluation of survival trial investigators. A
trial of the beta-blocker bucindolol in patients with advanced
chronic heart failure. N. Engl. J. Med. (2001) 344 1659–1667.
54 Dargie H.J. Effect of carvedilol on outcome after myocardial
infarction in patients with left-ventricular dysfunction: the
CAPRICORN randomised trial. Lancet (2001) 357 1385–
1390.
55 Paker M., Coast A.J., Flower M.B. et al. Effect of carvedilol on
survival in severe chronic heart failure. N. Engl. J. Med.
(2001) 344 1651–1658.
56 Poole-Wilson P.A., Swedberg K., Cleland J.G. et al. Compar-
ison of carvedilol and metoprolol on clinical outcomes in
patients with chronic heart failure in the Carvedilol Or
Metoprolol European Trial (COMET): randomised controlled
trial. Lancet (2003) 362 7–13.
57 Lechat P., Packer M., Chalon S., Cucherat M., Arab T., Boissel
J.P. Clinical effects of beta-adrenergic blockade in chronic
heart failure: a meta-analysis of double-blind, placebo-con-
trolled, randomized trials. Circulation (1998) 98 1184–1191.
58 Freemantle N., Cleland J., Young P., Manson J., Harrison J.
Beta blockade after myocardial infarction: systematic review
and meta regression analysis. BMJ (1999) 318 1730–1737.
59 Brophy J.M., Joseph L., Roleau J.L. Beta-blockers in congestive
heart failure. A Bayesian meta-analysis. Ann. Intern. Med.
(2001) 134 550–560.
60 Alberte C., Zipes D.P. Use of nonantiarrhythmic drugs for
prevention of sudden cardiac death. J. Cardiovasc. Electro-
physiol. (2003) 9(Suppl) S87–S95.
61 The CONSENSUS trial study group. Effects of enalapril on
mortality in severe congestive heart failure. Results of the
Cooperative North Scandinavian Enalapril Survival Study
(CONSENSUS). The CONSENSUS Trial Study Group. N. Engl. J.
Med. (1987) 316 1429–1435.
62 The SOLVD investigators. Effect of enalapril on survival in
patients with reduced left ventricular ejection fractions and
congestive heart failure. The SOLVD Investigators. N. Engl. J.
Med. (1991) 325 293–302.
63 The SOLVD investigators. Effect of enalapril on mortality and
the development of heart failure in asymptomatic patients
with reduced left ventricular ejection fractions. The SOLVD
Investigators. N. Engl. J. Med. (1992) 327 685–691.
64 Cohn J.N., Johnson G., Ziesche S. et al. A comparison of
enalapril with hydralazine-isosorbide dinitrate in the treat-
ment of chronic congestive heart failure. N. Engl. J. Med.
(1991) 325 303–310.
65 Pfeffer M.A., Braunwald E., Moye L.A. et al. Effect of captopril
on mortality and morbidity in patients with left ventricular
dysfunction after myocardial infarction. Results of the survival
and ventricular enlargement trial. The SAVE Investigators.
N. Engl. J. Med. (1992) 327 669–677.
66 The AIRE investigators. Effect of ramipril on mortality and
morbidity of survivors of acute myocardial infarction with
clinical evidence of heart failure. The Acute Infarction
Ramipril Efficacy (AIRE) Study Investigators. Lancet (1993)
342 821–828.
67 The GISSI-3 investigators. GISSI-3: effects of lisinopril and
transdermal glyceryl trinitrate singly and together on
6-week mortality and ventricular function after acute
myocardial infarction. Gruppo Italiano per lo Studio della
Sopravvivenza nell’infarto Miocardico. Lancet (1994) 343
1115–1122.
68 Ambrosioni E., Borghi C., Magnani B. The effect of the
angiotensin-converting-enzyme inhibitor zofenopril on mor-
tality and morbidity after anterior myocardial infarction. The
Survival of Myocardial Infarction Long-Term Evaluation
(SMILE) Study Investigators. N. Engl. J. Med. (1995) 332
80–85.
69 Kober L., Torp-Pedersen C., Carlsen J.E. et al. A clinical trial of
the angiotensin-converting-enzyme inhibitor trandolapril in
patients with left ventricular dysfunction after myocardial
infarction. Trandolapril Cardiac Evaluation (TRACE) Study
Group. N. Engl. J. Med. (1995) 333 1670–1676.
70 The ISIS-4 investigators. ISIS-4: a randomised factorial trial
assessing early oral captopril, oral mononitrate, and intra-
venous magnesium sulphate in 58,050 patients with sus-
pected acute myocardial infarction. ISIS-4 (Fourth
International Study of Infarct Survival) Collaborative Group.
Lancet (1995) 345 669–685.
71 Tusuf S., Sleight P., Pogue J., Bosch J., Davies R., Dagenais G.
Effects of an angiotensin-converting-enzyme inhibitor, ram-
ipril, on cardiovascular events in high-risk patients. The Heart
Outcomes Prevention Evaluation Study Investigators. N. Engl.
J. Med. (2000) 342 145–153.
72 Teo K.K., Mitchell L.B., Pogue J. et al. Effect of ramipril in
reducing sudden deaths and nonfatal cardiac arrests in high-
risk individuals without heart failure or left ventricular
dysfunction. Circulation (2004) 110 1413–1417.
73 Fox K.M. Efficacy of perindopril in reduction of cardiovascular
events among patients with stable coronary artery disease:
randomised, double-blind, placebo-controlled, multicentre
trial (the EUROPA study). Lancet (2003) 362 782–788.
74 Braunwald E., Domanski M.I., Fowler S.E. et al. Angiotensin-
converting-enzyme inhibition in stable coronary artery dis-
ease. N. Engl. J. Med. (2004) 351 2058–2068.
75 Domanski M.I., Exner D.V., Borkowf C.B., Gellar N.L., Rosen-
berg Y., Pfeffer M.A. Effect of angiotensin converting
enzyme inhibition on sudden cardiac death in patients
following acute myocardial infarction. A meta-analysis of
randomized clinical trials. J. Am. Coll. Cardiol. (1999) 33
598–604.
76 Flather M.D., Yusuf S., Kober L. et al. Long-term ACE-
inhibitor therapy in patients with heart failure or left-
ventricular dysfunction: a systematic overview of data from
individual patients. ACE-Inhibitor Myocardial Infarction Col-
laborative Group. Lancet (2000) 355 1575–1581.
77 Dagenais G.R., Pogue J., Fox K., Simoons Ml., Yusuf S.
Angiotensin-converting-enzyme inhibitors in stable vascular
disease without left ventricular systolic dysfunction or heart
592 G. Boriani et al.
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594
failure: a combined analysis of three trials. Lancet (2006) 368
581–588.
78 Al-Mallah M.H., Tleyjeh I.M., Abdel-Latif A.A., Weaver W.D.
Angiotensin-converting enzyme inhibitors in coronary artery
disease and preserved left ventricular systolic function: a
systematic review and meta-analysis of randomized controlled
trials. J. Am. Coll. Cardiol. (2006) 47 1576–1583.
79 Danchin N., Cucherat M., Thuillez C., Durand E., Kadri Z., Steg
P.G. Angiotensin-converting enzyme inhibitors in patients
with coronary artery disease and absence of heart failure or
left ventricular systolic dysfunction: an overview of long-term
randomized controlled trials. Arch. Intern. Med. (2006) 166
787–796.
80 Pitt B., Segal R., Martinez F.A. et al. Randomised trial of
losartan versus captopril in patients over 65 with heart failure
(Evaluation of Losartan in the Elderly Study, ELITE). Lancet
(1997) 349 747–752.
81 Pitt B., Poole-Wilson P.A., Segal R. et al. Effect of losartan
compared with captopril on mortality in patients with
symptomatic heart failure: randomised trial–the Losartan
Heart Failure Survival Study ELITE II. Lancet (2000) 355
1582–1587.
82 Cohn J.N., Tognoni G. A randomized trial of the angiotensin-
receptor blocker valsartan in chronic heart failure. N. Engl. J.
Med. (2001) 345 1667–1675.
83 Dickstein K., Kjekshus J. Effects of losartan and captopril on
mortality and morbidity in high-risk patients after acute
myocardial infarction: the OPTIMAAL randomised trial.
Optimal Trial in Myocardial Infarction with Angiotensin II
Antagonist Losartan. Lancet (2002) 360 752–760.
84 Dahlof B., Devereux R.B., Kjeldsen S.E. et al. Cardiovascular
morbidity and mortality in the Losartan Intervention For
Endpoint reduction in hypertension study (LIFE): a rando-
mised trial against atenolol. Lancet (2002) 359 995–1003.
85 Pfeffer M.A., Mcmurray J.I., Velazquez E.J. et al. Valsartan,
captopril, or both in myocardial infarction complicated by
heart failure, left ventricular dysfunction, or both. N. Engl. J.
Med. (2003) 349 1893–1906.
86 Young J.B., Dunlap M.E., Pfeffer M.A. et al. Mortality and
morbidity reduction with Candesartan in patients with
chronic heart failure and left ventricular systolic dysfunction:
results of the CHARM low-left ventricular ejection fraction
trials. Circulation (2004) 110 2618–2626.
87 Yusuf S., Teo K.K., Pogue J. et al. Telmisartan, ramipril, or
both in patients at high risk for vascular events. N. Engl. J.
Med. (2008) 358 1547–1559.
88 TRANSCEND Investigators. Effects of the angiotensin-receptor
blocker telmisartan on cardiovascular events in high-risk
patients intolerant to angiotensin converting enzyme inhibi-
tors: a randomised controlled trial. Lancet (2008) 372 1174–
1183.
89 Jong P., Demers C., Mckelvie R.S., Liu P.P. Angiotensin
receptor blockers in heart failure: meta-analysis of randomized
controlled trials. J. Am. Coll. Cardiol. (2002) 39 463–470.
90 Lee V.C., Rhew D.C., Dylan M., Badamgarav E., Braunstein
G.D., Weingarten S.R. Meta-analysis: angiotensin-receptor
blockers in chronic heart failure and high-risk acute myo-
cardial infarction. Ann. Intern. Med. (2004) 141 693–704.
91 Scandinavian simvastatin survival study group Randomised
trial of cholesterol lowering in 4444 patients with coronary
heart disease: the Scandinavian Simvastatin Survival Study
(4S). Lancet (1994) 344 1383–1389.
92 Shepherd J., Cobbe S.M., Ford I. et al. Prevention of coronary
heart disease with pravastatin in men with hypercholesterol-
emia. West of Scotland Coronary Prevention Study Group. N.
Engl. J. Med. (1995) 333 1301–1307.
93 Sacks F.M., Pfeffer M.A., Moye L.A. et al. The effect of
pravastatin on coronary events after myocardial infarction in
patients with average cholesterol levels. Cholesterol and
Recurrent Events Trial investigators. N. Engl. J. Med. (1996)
335 1001–1009.
94 The LIPID study group. Prevention of cardiovascular events and
death with pravastatin in patients with coronary heart disease
and a broad range of initial cholesterol levels. The Long-Term
Intervention with Pravastatin in Ischaemic Disease (LIPID)
Study Group. N. Engl. J. Med. (1998) 339 1349–1357.
95 Downs J.R., Clearfield M., Weis S. et al. Primary prevention of
acute coronary events with lovastatin in men and women
with average cholesterol levels: results of AFCAPS/TexCAPS.
Air Force/Texas Coronary Atherosclerosis Prevention Study.
JAMA (1998) 279 1615–1622.
96 Schwartz G.G., Olsson A.G., Ezekowitz M.D. et al. Effects of
atorvastatin on early recurrent ischemic events in acute
coronary syndromes: the MIRACL study: a randomized
controlled trial. JAMA (2001) 285 1711–1718.
97 Heart protection study collaborative group. MRC/BHF Heart
Protection Study of cholesterol lowering with simvastatin in
20,536 high-risk individuals: a randomised placebo-controlled
trial. Lancet (2002) 360 7–22.
98 Shepherd J., Blauw G.J., Murphy M.B. et al. Pravastatin in
elderly individuals at risk of vascular disease (PROSPER): a
randomised controlled trial. Lancet (2002) 360 1623–1630.
99 ALLHAT collaborative research group. Major outcomes in
moderately hypercholesterolemic, hypertensive patients ran-
domized to pravastatin vs usual care: The Antihypertensive
and Lipid-Lowering Treatment to Prevent Heart Attack Trial
(ALLHAT-LLT). JAMA (2002) 288 2998–3007.
100 Sever P.S., Dahlof B., Poulter N.R. et al. Prevention of
coronary and stroke events with atorvastatin in hypertensive
patients who have average or lower-than-average cholesterol
concentrations, in the Anglo-Scandinavian Cardiac Outcomes
Trial – Lipid Lowering Arm (ASCOT-LLA): a multicentre
randomised controlled trial. Lancet (2003) 361 1149–1158.
101 Thompson P.L., Meredith I., Amerena J. et al. Effect of
pravastatin compared with placebo initiated within 24 hours
of onset of acute myocardial infarction or unstable angina: the
Pravastatin in Acute Coronary Treatment (PACT) trial. Am.
Heart J. (2004) 148 e2.
102 Cannon C.P., Braunwald E., Mccabe C.H. et al. Intensive
versus moderate lipid lowering with statins after acute
coronary syndromes. N. Engl. J. Med. (2004) 350 1495–
1504.
Prevention of sudden cardiac death 593
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594
103 Larosa J.C., Grundy S.M., Waters D.D. et al. Intensive lipid
lowering with atorvastatin in patients with stable coronary
disease. N. Engl. J. Med. (2005) 352 1425–1435.
104 CORONA Group Rosuvastatin in older patients with systolic
heart failure. N. Engl. J. Med. (2007) 357 2248–2261.
105 Gissi-HF Investigators. Effect of rosuvastatin in patients with
chronic heart failure (the GISSI-HF trial): a randomised,
double-blind, placebo-controlled trial. Lancet (2008) 372
1231–1239.
106 JUPITER Study Group. Rosuvastatin to prevent vascular
events in men and women with elevated C-reactive protein. N.
Engl. J. Med. (2008) 359 2195–2207.
107 Vrecer M., Turk S., Drinovec J., Mrhar A. Use of statins in
primary and secondary prevention of coronary heart disease
and ischemic stroke. Meta-analysis of randomized trials. Int. J.
Clin. Pharmacol. Ther. (2003) 41 567–577.
108 Cheung B.M., Lauder I.J., Lau C.P., Kumana C.R. Meta-
analysis of large randomized controlled trials to evaluate the
impact of statins on cardiovascular outcomes. Br. J. Clin.
Pharmacol. (2004) 57 640–651.
109 Burr M.L., Fehily A.M., Gilbert J.F. et al. Effects of changes in
fat, fish, and fibre intakes on death and myocardial reinfarc-
tion: diet and reinfarction trial (DART). Lancet (1989) 2 757–
761.
110 Singh R.B., Niaz M.A., Sharma J.P., Kumar R., Rastogi V.,
Moshiri M. Randomized, double-blind, placebo-controlled
trial of fish oil and mustard oil in patients with suspected
acute myocardial infarction: the Indian experiment of
infarct survival – 4. Cardiovasc. Drugs Ther. (1997) 11
485–491.
111 De Lorgeril M., Salen P., Martin J.L., Monjaud I., Delaye J.,
Mamelle N. Mediterranean diet, traditional risk factors, and
the rate of cardiovascular complications after myocardial
infarction: final report of the Lyon Diet Heart Study. Circu-
lation (1999) 99 779–785.
112 GISSI-prevenzione investigators. Dietary supplementation
with n-3 polyunsaturated fatty acids and vitamin E after
myocardial infarction: results of the GISSI-Prevenzione trial.
Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto
miocardico. Lancet (1999) 354 447–455.
113 Wang C., Harris W.S., Chung M. et al. n-3 Fatty acids from
fish or fish-oil supplements, but not alpha-linolenic acid,
benefit cardiovascular disease outcomes in primary- and
secondary-prevention studies: a systematic review. Am. J.
Clin. Nutr. (2006) 84 5–17.
114 Mozaffarian D. Fish and n-3 fatty acids for the prevention of
fatal coronary heart disease and sudden cardiac death. Am. J.
Clin. Nutr. (2008) 87 1991S–1996S.
115 Brouwer I.A., Zock P.L., Camm A.J. et al. Effect of fish oil on
ventricular tachyarrhythmia and death in patients with
implantable cardioverter defibrillators: the Study on Omega-3
Fatty Acids and Ventricular Arrhythmia (SOFA) randomized
trial. JAMA (2006) 295 2613–2619.
116 Zhao Y.T., Chen Q., Sun Y.X. et al. Prevention of sudden
cardiac death with omega-3 fatty acids in patients with
coronary heart disease: a meta-analysis of randomized con-
trolled trials. Ann. Med. (2009) 41 301–310.
117 Pitt B., Zannad F., Remme W.J. et al. The effect of spirono-
lactone on morbidity and mortality in patients with severe
heart failure. Randomized Aldactone Evaluation Study Inves-
tigators. N. Engl. J. Med. (1999) 341 709–717.
118 Pitt B., Remme W., Zannad F. et al. Eplerenone, a selective
aldosterone blocker, in patients with left ventricular dysfunc-
tion after myocardial infarction. N. Engl. J. Med. (2003) 348
1309–1321.
119 Micromedex Thomson� Healthcare system; DRUGDEX�evaluations, available at http://www.thomsonhc.com (last
access 15/03/2010).
120 Mason R.P., Giles T.D., Sowers J.R. Evolving mechanisms of
action of beta blockers: focus on nebivolol. J. Cardiovasc.
Pharmacol. (2009) 54 123–128.
121 Burnier M. Angiotensin II type 1 receptor blockers. Circulation
(2001) 103 904–912.
122 Corsini A., Bellosta S., Baetta R., Fumagalli R., Paoletti R.,
Bernini F. New insights into the pharmacodynamic and
pharmacokinetic properties of statins. Pharmacol. Ther.
(1999) 84 413–428.
123 Bellosta S., Paoletti R., Corsini A. Safety of statins: focus on
clinical pharmacokinetics and drug interactions. Circulation
(2004) 23(Suppl 1) III50–III57.
594 G. Boriani et al.
ª 2010 The Authors Fundamental and Clinical Pharmacology ª 2010 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 24 (2010) 575–594
Top Related
Copyright © 2022 FDOKUMEN

