







Bahasa
Halaman
Hukum


www.elsevier.com/locate/schres
Schizophrenia Research
Risk factors for completed suicide in schizophrenia and other
chronic psychotic disorders: A case–control study
A. McGirr a, M. Tousignant a,b, D. Routhier b, L. Pouliot b, N. Chawky a,
H.C. Margolese c, G. Turecki a,*
a McGill Group for Suicide Studies, Douglas Hospital Research Centre, 6875 LaSalle blvd, Montreal QC, Canada H4H 1R3b University of Quebec, Montreal, Canada
c Department of Psychiatry, McGill University, Canada
Received 12 September 2005; received in revised form 20 February 2006; accepted 28 February 2006
Available online 19 April 2006
Abstract
Objective: Despite an increased risk for suicide among individuals diagnosed with psychotic disorders, risk factors for
completed suicide remain largely unexamined in this population. Using a case–control design, this study aimed to investigate
clinical and behavioural risk factors for suicide completion in schizophrenia and other chronic psychotic disorders.
Method: A total of 81 psychotic subjects were examined; of these, 45 died by suicide. Proxy-based interviews with, on average,
2 informants were conducted using the SCID I and II interviews and a series of personality trait assessments.
Results: Psychotic individuals at risk for suicide are most readily identified by the presence of depressive disorders NOS,
moderate to severe psychotic symptoms and a family history of suicidal behaviour. They also exhibited fewer negative
symptoms, had more comorbid diagnoses and, contrary to findings in other populations, we found that cluster A and C
personality trait symptoms seem to have protective effects against suicide in schizophrenics and other chronic psychotic
suicides.
Conclusions: Our study suggests that behavioural mediators of suicide risk, such as impulsive–aggressive behaviours, do not
play a role in schizophrenic and chronic psychotic suicide. This is contrary to findings in other diagnostic groups, thus implying
heterogeneity in predisposing mechanisms involved in suicide.
D 2006 Elsevier B.V. All rights reserved.
Keywords: Suicide; Schizophrenia; Alcohol abuse; Drug abuse; Personality disorders; Family history
0920-9964/$ - see front matter D 2006 Elsevier B.V. All rights reserved.
doi:10.1016/j.schres.2006.02.025
* Corresponding author. Tel.: +1 514 761 6131x2369; fax: +1 514
762 3023.
E-mail address: [email protected] (G. Turecki).
1. Introduction
The importance of suicide cannot be understated as
the United States alone sees more than 30000 suicide
victims annually (Centers for Disease Control and
84 (2006) 132–143
A. McGirr et al. / Schizophrenia Research 84 (2006) 132–143 133
Prevention: Advance report of final mortality statis-
tics, 1990, 1993). Among those particularly at risk for
committing suicide are individuals suffering from
schizophrenia and other chronic psychotic disorders
(Brown, 1997; Caldwell and Gottesman, 1990) with a
level of risk approaching that of individuals suffering
from affective disorders (Caldwell and Gottesman,
1990; Plutchik et al., 1989; Westermeyer et al., 1991).
Though recent estimates are becoming more conser-
vative (Palmer et al., 2005), suicide is still the leading
cause of premature death in this population (Fenton,
2000).
Although suicidal behaviour in psychotic patients
has received a great deal of attention, examinations
of individuals diagnosed with psychotic disorders
who die by suicide are few in number. Some
clinical characteristics, such as elevated levels of
depressive symptoms or the presence of depressive
disorders (Altamura et al., 2003; Fenton, 2000;
Hawton et al., 2005; Heila et al., 1997; Hu et al.,
1991; Kelly et al., 2004; Kreyenbuhl et al., 2002;
Kuo et al., 2005; Plutchik et al., 1989; Potkin et
al., 2003; Sinclair et al., 2004), have consistently
been associated with suicide and suicidal behaviour
among psychotic individuals, whereas others, such
as alcohol and substance abuse (Baca-Garcia et al.,
2005; Gut-Fayand et al., 2001; Kreyenbuhl et al.,
2002; Kuo et al., 2005; Sinclair et al., 2004) have
been associated with suicide attempts but not
completed suicide. Mixed findings have emerged
in studies of positive and negative symptoms
(Fenton, 2000; Hu et al., 1991; Kelly et al.,
2004; King et al., 2001; Sinclair et al., 2004).
Though an increased frequency of an active illness
phase among schizophrenic suicides has been
reported (Heila et al., 1997), and these individuals
are also more likely to have experienced psychotic
symptoms in the month preceding their suicides
(Hu et al., 1991), the association between the
severity of current psychotic symptoms and com-
pleted suicide has, to our knowledge, not been
examined in schizophrenia and other chronic
psychotic disorders. Recently, researchers have
begun to examine factors such as comorbidity
among this population (Kuo et al., 2005); additional
studies, however, are needed to confirm and better
characterize comorbidity patterns among psychotic
suicides. At the same time, structured information
on important clinical risk factors, such as person-
ality disorders, is, to our knowledge, absent from
the literature on suicide in schizophrenia and in
other chronic psychotic disorders.
Similarly, although there has been growing
evidence supporting the role of impulsive and
aggressive behaviours in suicide risk among unse-
lected suicides or in clinical subgroups, such as
those suicides whose primary psychiatric condition
was a major depressive disorder (Dumais et al.,
2005a), for the most part, data on impulsive and
aggressive behaviours in suicide completers are
limited and primarily based on indirect evidence
such as the prevalence of diagnostic categories
associated with aggressive and impulsive traits
(Brent, 1995; Cheng et al., 1997). Impulsive and
aggressive behaviours have, to our knowledge, not
been properly examined in psychotic completed
suicide and it remains unclear whether they mediate
suicide risk among psychotic individuals, as they
are believed to in other populations (Dumais et al.,
2005a).
The goal of the current study was to address the
lacunae and re-examine areas in which inconsistent
findings have emerged concerning the risk for
completed suicide in a sample of suicide victims
and matched living controls diagnosed with psy-
chotic disorders. More specifically, our primary
hypothesis was that concomitant psychopathology,
notably depression and psychopathology associated
with impulse discontrol (i.e. substance abuse dis-
orders and cluster B personality disorders), and
impulsive aggressive behaviours would be associ-
ated with completed suicide among psychotic
individuals. At the same time, we hypothesized
that the severity of psychotic symptoms would be
associated with completed suicide among this
population.
2. Methods
2.1. Subjects
Our sample consisted of 81 (62 male and 19
female) Caucasian subjects who were diagnosed with
schizophrenia or a chronic psychotic disorder. This
sample included 45 suicide completers and 36
A. McGirr et al. / Schizophrenia Research 84 (2006) 132–143134
matched controls. The mean age of the suicide group
was 34.45F11.61 years and 34.95F9.17 years for
the control group (t(79)= .197, p= .832). Diagnostic
distribution was similar (v2=4.284, df =4, p =.369)between groups: schizophrenia (86.0% vs. 83.8%),
schizoaffective disorder (7.0% vs. 13.5%), as well as
delusional disorder or psychotic disorder NOS (2.7%
vs. 12.5%). Moreover, no differences were observed
between groups in the proportion of schizophrenia
subtypes (v2=5.657, df =3, p =.130) nor in history
of hospitalization (3.18F3.68 vs. 5.31F8.27,
t(73)=1.457, p =.149). Suicide cases were recruited
during a period of approximately four years through an
ongoing collaboration with the Quebec Coroner’s
Office and the Montreal Central Morgue and cases
diagnosed with a psychotic disorder were identified
with help from the Quebec Statistics Institute and the
RAMQ, the Quebec Health Board. Methods of suicide
included hanging (51.2%), jumping (11.6%), stabbing
or laceration (11.6%), drowning (7.0%) and other
(19.4%).
The control group was recruited among psychiatric
outpatients, from psychiatric community clinics affil-
iated with McGill University and the University of
Montreal. This study was approved by our local IRB
and suicide families, controls and informants signed
written informed consents.
2.2. Measures
A psychological autopsy method was used to
diagnose axis I and II DSM-IV psychiatric disorders,
personality, impulsivity, hostility and lifetime history
of aggression. This validated technique (Conner et al.,
2001a; Kelly and Mann, 1996; Zhang et al., 2003)
involves selecting the family member or friend best
acquainted with the subject to serve as an informant.
To ensure the comparability among cases and
controls, controls named an informant for the inter-
view process. Informants included mother (47.4% vs.
54.8%), father (13.2% vs. 6.5%), sibling (34.2% vs.
16.1%), child (2.6% vs. 6.5%) and significant other
(2.6% vs. 16.1%). We have previously reported that
the rate of specific disorders identified does not differ
between informants for a given subject (Dumais et al.,
2005a), nor does it vary as a function of the
informant’s relationship with the subject (Lesage et
al., 1994).
Psychiatric diagnoses were obtained using the
SCID-I (First et al., 2001) and SCID-II (First et al.,
1995) interviews. The severity of psychotic symp-
toms was determined using a section of the SCID-I
assessing functional impairment due to psychotic
symptoms. The assessment of axis II pathology
among psychotic individuals poses a unique chal-
lenge, for its presence must be established before the
onset of the disorder. Therefore, symptoms were
deemed present only if informants confirmed their
presence prior to the onset of psychotic symptoms;
this was further reviewed by a panel of psychiatrists
and psychologists (GT, NC and AM, who had
previous experience with the instrument). For a
subset of the current sample, agreement between
subject and informant was calculated: .77 depressive
disorder NOS; 1.0 substance abuse/dependence; 1.0,
schizophrenia and schizoaffective; 1.0, cluster A
personality disorders; 1.0 cluster B personality dis-
orders and .77, cluster C personality disorders. For a
different subset, two or more interviewers were asked
to separately rate the same subject; inter-rater
agreement was calculated: .72, depressive disorder
NOS; .77, substance abuse/dependence; .88, schizo-
phrenia and schizoaffective; 1.0, cluster A personality
disorders; 1.0 cluster B personality disorders and 1.0,
cluster C personality disorders.
Behavioural measures assessed in this study
focused on those commonly regarded as risk factors
for suicide, notably, personality traits and measures
of impulsive–aggressive behaviours. The Brown–
Goodwin History of Aggression (BGHA) (Brown
and Goodwin, 1986) is an 11-item assessment of
lifetime aggressive behaviours across childhood,
adolescence and adulthood. The Barratt Impulsive-
ness Scale (BIS-11) (Barratt, 1965) consists of 30
items and has been commonly used in the investi-
gation of impulsive behaviours. The Buss–Durkee
Hostility Inventory (BDHI) (Buss and Durkee, 1957)
is a 75-item assessment of impulsive aggression.
Last, the Trait and Character Inventory (TCI)
(Cloninger et al., 1994) was used to complete
information by assessing 4 basic temperament and
3 character dimensions. Consistent with our previous
studies in different clinical samples (Dumais et al.,
2005a,b) and with studies by other groups (Conner
et al., 2001a; Zhang et al., 2003), the internal
consistency estimates in this study were overall
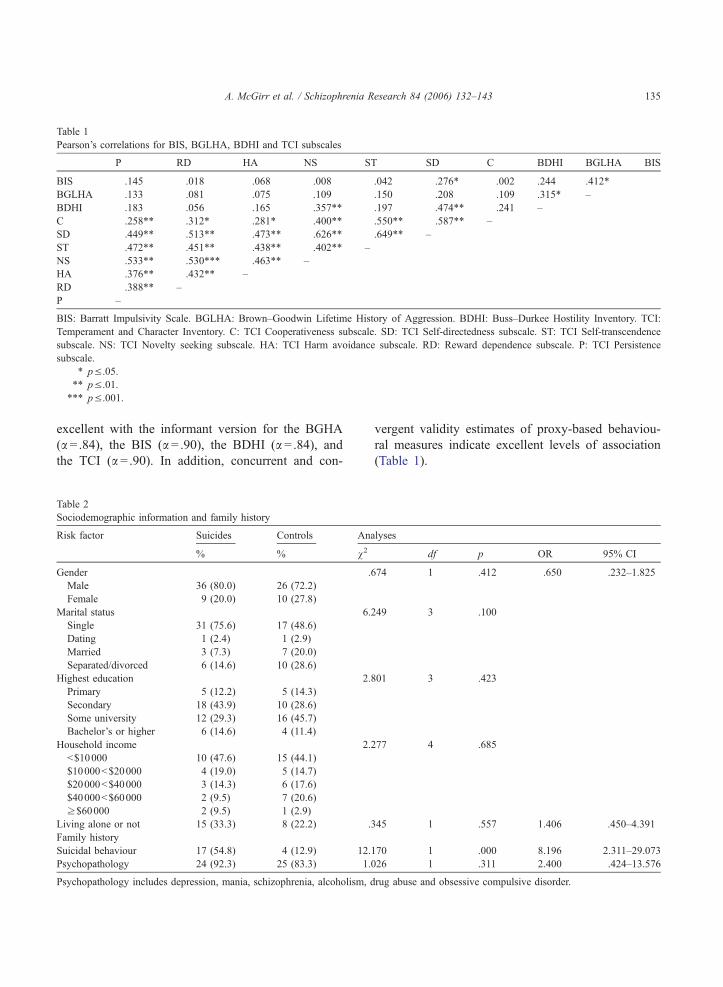
Table 1
Pearson’s correlations for BIS, BGLHA, BDHI and TCI subscales
P RD HA NS ST SD C BDHI BGLHA BIS
BIS .145 .018 � .068 � .008 � .042 � .276* � .002 .244 .412* �BGLHA � .133 .081 � .075 � .109 � .150 � .208 � .109 .315* –
BDHI � .183 � .056 � .165 � .357** � .197 � .474** � .241 –
C .258** .312* .281* .400** .550** .587** –
SD .449** .513** .473** .626** .649** –
ST .472** .451** .438** .402** –
NS .533** .530*** .463** –
HA .376** .432** –
RD .388** –
P –
BIS: Barratt Impulsivity Scale. BGLHA: Brown–Goodwin Lifetime History of Aggression. BDHI: Buss–Durkee Hostility Inventory. TCI:
Temperament and Character Inventory. C: TCI Cooperativeness subscale. SD: TCI Self-directedness subscale. ST: TCI Self-transcendence
subscale. NS: TCI Novelty seeking subscale. HA: TCI Harm avoidance subscale. RD: Reward dependence subscale. P: TCI Persistence
subscale.
* p V .05.** p V .01.*** p V .001.
A. McGirr et al. / Schizophrenia Research 84 (2006) 132–143 135
excellent with the informant version for the BGHA
(a =.84), the BIS (a= .90), the BDHI (a =.84), andthe TCI (a =.90). In addition, concurrent and con-
Table 2
Sociodemographic information and family history
Risk factor Suicides Controls Ana
% % v2
Gender .6
Male 36 (80.0) 26 (72.2)
Female 9 (20.0) 10 (27.8)
Marital status 6.2
Single 31 (75.6) 17 (48.6)
Dating 1 (2.4) 1 (2.9)
Married 3 (7.3) 7 (20.0)
Separated/divorced 6 (14.6) 10 (28.6)
Highest education 2.8
Primary 5 (12.2) 5 (14.3)
Secondary 18 (43.9) 10 (28.6)
Some university 12 (29.3) 16 (45.7)
Bachelor’s or higher 6 (14.6) 4 (11.4)
Household income 2.2
b$10000 10 (47.6) 15 (44.1)
$10000b$20000 4 (19.0) 5 (14.7)
$20000b$40000 3 (14.3) 6 (17.6)
$40000b$60000 2 (9.5) 7 (20.6)
z$60000 2 (9.5) 1 (2.9)
Living alone or not 15 (33.3) 8 (22.2) .3
Family history
Suicidal behaviour 17 (54.8) 4 (12.9) 12.1
Psychopathology 24 (92.3) 25 (83.3) 1.0
Psychopathology includes depression, mania, schizophrenia, alcoholism, d
vergent validity estimates of proxy-based behaviou-
ral measures indicate excellent levels of association
(Table 1).
lyses
df p OR 95% CI
74 1 .412 .650 .232–1.825
49 3 .100
01 3 .423
77 4 .685
45 1 .557 1.406 .450–4.391
70 1 .000 8.196 2.311–29.073
26 1 .311 2.400 .424–13.576
rug abuse and obsessive compulsive disorder.
A. McGirr et al. / Schizophrenia Research 84 (2006) 132–143136
2.3. Statistical analyses
Statistical analyses were performed using the SPSS
statistical package version 11.5 (SPSS Inc., Chicago,
IL). Chi-square analysis, and odds ratio (with exact
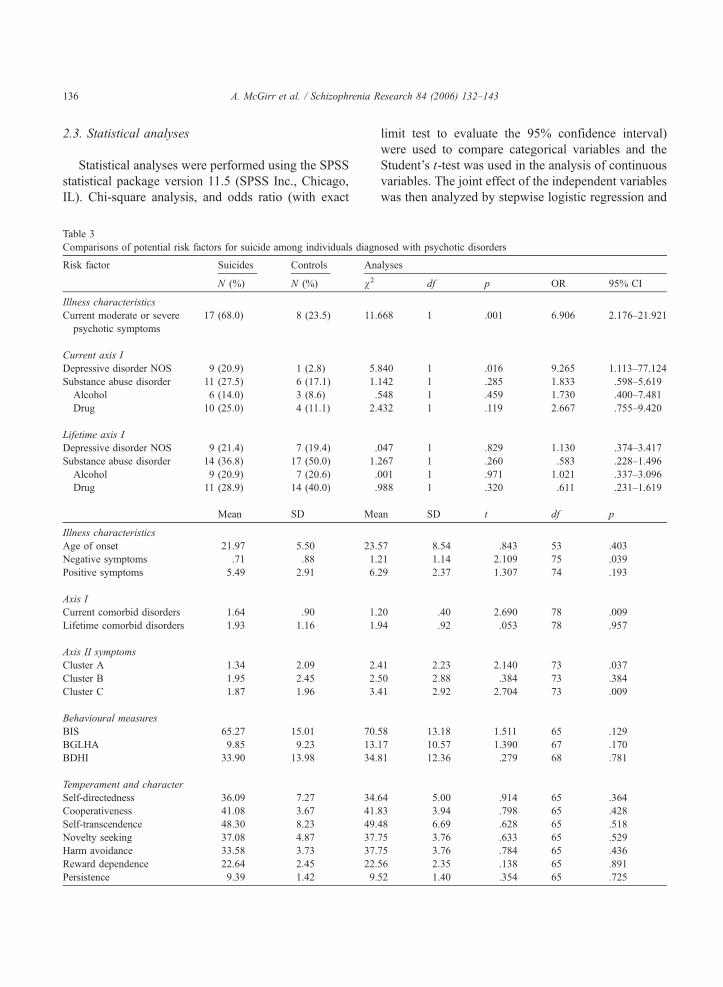
Table 3
Comparisons of potential risk factors for suicide among individuals diagn
Risk factor Suicides Controls An
N (%) N (%) v2
Illness characteristics
Current moderate or severe
psychotic symptoms
17 (68.0) 8 (23.5) 11.
Current axis I
Depressive disorder NOS 9 (20.9) 1 (2.8) 5.
Substance abuse disorder 11 (27.5) 6 (17.1) 1.
Alcohol 6 (14.0) 3 (8.6) .
Drug 10 (25.0) 4 (11.1) 2.
Lifetime axis I
Depressive disorder NOS 9 (21.4) 7 (19.4) .
Substance abuse disorder 14 (36.8) 17 (50.0) 1.
Alcohol 9 (20.9) 7 (20.6) .
Drug 11 (28.9) 14 (40.0) .
Mean SD Me
Illness characteristics
Age of onset 21.97 5.50 23.
Negative symptoms .71 .88 1.
Positive symptoms 5.49 2.91 6.
Axis I
Current comorbid disorders 1.64 .90 1.
Lifetime comorbid disorders 1.93 1.16 1.
Axis II symptoms
Cluster A 1.34 2.09 2.
Cluster B 1.95 2.45 2.
Cluster C 1.87 1.96 3.
Behavioural measures
BIS 65.27 15.01 70.
BGLHA 9.85 9.23 13.
BDHI 33.90 13.98 34.
Temperament and character
Self-directedness 36.09 7.27 34.
Cooperativeness 41.08 3.67 41.
Self-transcendence 48.30 8.23 49.
Novelty seeking 37.08 4.87 37.
Harm avoidance 33.58 3.73 37.
Reward dependence 22.64 2.45 22.
Persistence 9.39 1.42 9.
limit test to evaluate the 95% confidence interval)
were used to compare categorical variables and the
Student’s t-test was used in the analysis of continuous
variables. The joint effect of the independent variables
was then analyzed by stepwise logistic regression and
osed with psychotic disorders
alyses
df p OR 95% CI
668 1 .001 6.906 2.176–21.921
840 1 .016 9.265 1.113–77.124
142 1 .285 1.833 .598–5.619
548 1 .459 1.730 .400–7.481
432 1 .119 2.667 .755–9.420
047 1 .829 1.130 .374–3.417
267 1 .260 .583 .228–1.496
001 1 .971 1.021 .337–3.096
988 1 .320 .611 .231–1.619
an SD t df p
57 8.54 � .843 53 .403
21 1.14 2.109 75 .039
29 2.37 1.307 74 .193
20 .40 �2.690 78 .009
94 .92 .053 78 .957
41 2.23 2.140 73 .037
50 2.88 .384 73 .384
41 2.92 2.704 73 .009
58 13.18 1.511 65 .129
17 10.57 1.390 67 .170
81 12.36 .279 68 .781
64 5.00 .914 65 .364
83 3.94 � .798 65 .428
48 6.69 � .628 65 .518
75 3.76 � .633 65 .529
75 3.76 � .784 65 .436
56 2.35 .138 65 .891
52 1.40 � .354 65 .725
A. McGirr et al. / Schizophrenia Research 84 (2006) 132–143 137
correlation matrix with suicide status as the dependent
variable.
3. Results
Sociodemographic characteristics of the sample
including family history are shown in Table 2. An
increased risk for suicide was associated with a family
history of suicidal behaviour (OR=8.19; 95% CI:
2.31–29.07); however, this was not conditional on an
increased family history of psychopathology, defined
as the presence of depression, mania, schizophrenia,
alcoholism, drug abuse, or obsessive compulsive
disorder (v2=1.02, df =1, p =.311). Further, those
with a family history of suicidal behaviour did not
differ from those without as relates to impulsivity
and aggression (BIS: 68.25F24.81 vs. 68.21F12.90,
t(43)=� .005, p = .996; BGLHA: 11.13F5.13 vs.
13.19F11.08, t(43)= .511, p =.430).
Table 3 addresses comparisons between psychotic
suicides and psychotic controls diagnosed with respect
to axis I and II characteristics, as well as behavioural,
character and temperament measures. Psychotic sui-
cide victims were more likely to have currently (last 6
months) met the criteria for a depressive disorder NOS
(OR=5.03; 95% CI: 1.08–26.02) and to have had two
Fig. 1. Predictors
or more comorbid axis I disorders (OR=3.39; 95 %CI:
1.22–9.40). Psychotic suicides were also more likely
to have been currently experiencing moderate to
severe psychotic symptoms (OR=6.90; 95% CI:
2.17–21.92) and to have exhibited lower levels of
negative symptoms (OR=.648; 95% CI: .26–1.60).
With respect to axis II diagnoses and symptoms,
psychotic suicides were characterized by lower levels
of cluster A symptoms (1.34F2.09 vs. 2.41F2.23,
t(73)=2.14, p b .05) and cluster C symptoms (1.87F1.96 vs. 3.41F2.92, t(73)=2.70, p b .01). No signif-
icant differences were found for any other axis I
disorders, cluster B symptoms, behavioural or temper-
ament and character measures.
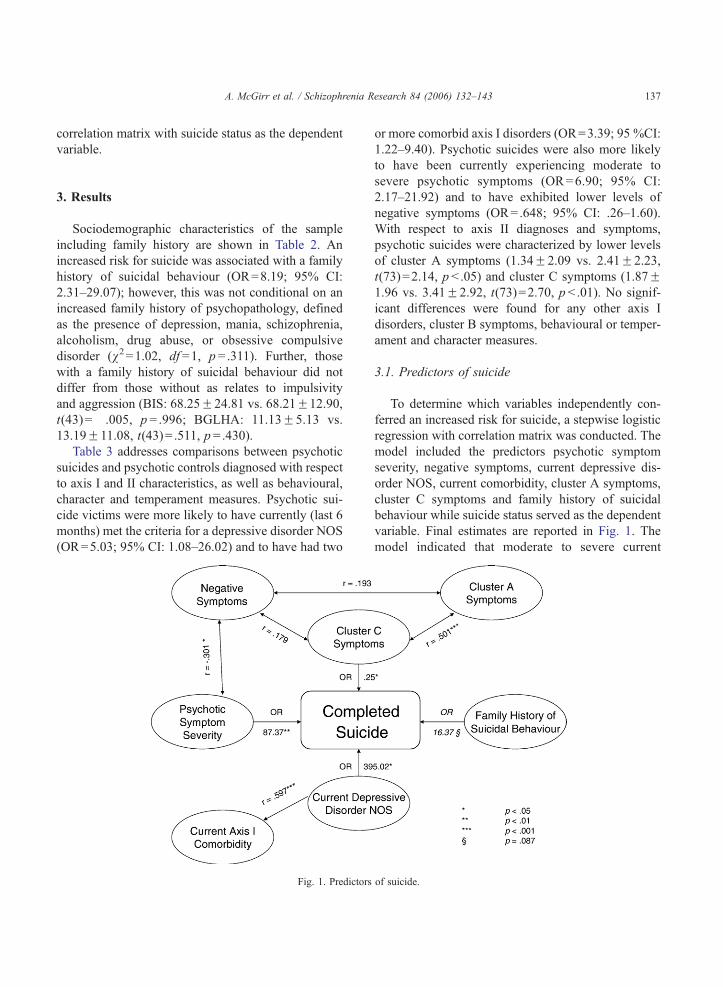
3.1. Predictors of suicide
To determine which variables independently con-
ferred an increased risk for suicide, a stepwise logistic
regression with correlation matrix was conducted. The
model included the predictors psychotic symptom
severity, negative symptoms, current depressive dis-
order NOS, current comorbidity, cluster A symptoms,
cluster C symptoms and family history of suicidal
behaviour while suicide status served as the dependent
variable. Final estimates are reported in Fig. 1. The
model indicated that moderate to severe current
of suicide.
A. McGirr et al. / Schizophrenia Research 84 (2006) 132–143138
psychotic symptoms (adjusted OR=87.37; 95% CI:
3.30–2309.72), current depressive disorder NOS
(adjusted OR=395.02; 95% CI: 1.47–106 140.5),
and cluster C symptoms (adjusted OR=.25; 95% CI:
.07–.91) were independent predictors of suicide, while
a trend towards significance was observed for a family
history of suicidal behaviour (adjusted OR=16.37;
95% CI: .66–403.06).
4. Discussion
In this study, 45 suicide victims diagnosed with
schizophrenia and other chronic psychotic disorders
were compared with 36 clinically similar controls. As
individuals diagnosed with psychotic disorders are at
an increased risk for suicide (Black et al., 1985;
Brown, 1997; Caldwell and Gottesman, 1990; Heila et
al., 1997; Henriksson et al., 1993), it is essential to
determine whether predictors of suicide among
psychotic individuals are similar to those recognized
to play a role in other clinical populations, such as
among patients with major depressive disorder. Few
studies on psychotic suicide completers have investi-
gated risk factors using a psychological autopsy with
a case–control design and standardized interviews to
retrieve information. Further, to our knowledge this is
the first study among this population to have
examined the relationship between completed suicide
and the potential risk factors a) impulsive aggressive
behaviours, b) personality disorders, and c) the current
severity of psychotic symptoms.
4.1. Illness characteristics
In this sample, suicide victims weremore likely than
controls to have experienced moderate to severe
psychotic symptoms at the time of suicide and suicide
completers exhibited fewer negative symptoms. A
logistic regression showed that greater psychotic
symptom severity was a good predictor of suicide with
an adjusted risk of 87.37, whereas negative symptoms
did not independently predict suicide. With respect to
current psychotic symptom severity, our findings are an
extension of previous findings that a large proportion of
schizophrenic suicides are in the active phase of the
illness (Heila et al., 1997) and that schizophrenic
suicides are more likely to experience psychotic
symptoms in the month preceding their suicides than
psychotic controls (Hu et al., 1991). A recent meta-
analysis has revealed an increased risk for suicide to be
associated with poor treatment compliance (Hawton et
al., 2005). Future studies should investigate the
independence with which current treatment compli-
ance and functional impairment due to psychotic
symptoms increase psychotic individuals’ risk for
suicide. The protective nature of negative symptoms
is in line with Fenton’s (Fenton, 2000; Fenton and
McGlashan, 1994; Fenton et al., 1997) deficit syn-
drome, a subtype of schizophrenia characterized by
insidious onset, the presence of negative symptoms at
onset, the progressing severity of negative symptoms
and a high probability of lifelong disability.
4.2. Axis I characteristics and behavioural measures
In line with previous findings of an increased risk
for suicide among schizophrenic and other psychotic
individuals associated with depressive disorders or
elevated levels of depressive symptoms (Altamura et
al., 2003; Cheng et al., 2000; Fenton, 2000; Foster et
al., 1997; Haw et al., 2002; Hawton et al., 2005;
Henriksson et al., 1993; Hu et al., 1991; Kelly et al.,
2004; Kreyenbuhl et al., 2002; Kuo et al., 2005;
Lesage et al., 1994; Mann et al., 2000; Plutchik et al.,
1989; Potkin et al., 2003; Roy, 1982; Rudd et al.,
1993; Shafii et al., 1988; Statham et al., 1998; Vieta et
al., 1992), we found an association between complet-
ed suicide and the presence of comorbid depressive
episodes. Further, a logistic regression revealed that
current depressive disorder NOS was the independent
predictor of suicide with the largest adjusted effect on
risk.
Consistent with previous reports (Kuo et al., 2005;
Sinclair et al., 2004), we did not find a significant
association between completed suicide and substance
abuse among schizophrenics and other chronic psy-
chotic individuals. Some studies, however, have
found such an association with suicide attempts in
this population (Altamura et al., 2003; Gut-Fayand et
al., 2001; Potkin et al., 2003) and consistent support
for the association between suicide risk and substance
abuse disorders has been reported in other clinical
populations (Brent et al., 2002; Castle et al., 2004;
Cheng et al., 2000; Hawton et al., 2003; King et al.,
2001; Lesage et al., 1994; Malone et al., 1995; Mann
A. McGirr et al. / Schizophrenia Research 84 (2006) 132–143 139
et al., 1999; Shafii et al., 1988; Statham et al., 1998).
Substance abuse appears to be a characteristic
frequently associated with psychotic illnesses and,
by nature of the design used, once we controlled for
the primary psychopathological condition, no effect of
substance-related disorders was observed on suicide
risk. A recent meta-analysis has reported that drug
abuse, but not alcohol abuse disorders, are associated
with an increased risk for suicide among schizo-
phrenics (Hawton et al., 2005). In line with these
findings, psychotic suicides and controls showed
different levels of current drug abuse (25.0% vs.
11.1%), yet this difference did not reach significance.
We did not find an association between impulsive
and aggressive behaviours and schizophrenia as well
as other chronic psychotic suicides. This is, to our
knowledge, the first study to have examined impul-
sive and aggressive behaviours using proxy-based
behavioural measures in this population. With respect
to aggression, our findings confirm previous studies
having used other means of assessing aggression
(Fenton, 2000; Sinclair et al., 2004). In the case of
impulsivity, other studies have found an association
between impulsivity and risk for suicide and suicidal
behaviour among schizophrenics, however they have
done so using indirect means by a) finding that
schizophrenic substance abusers are more impulsive
and assuming that, as in other populations, substance
abusers are more likely to attempt suicide (Gut-
Fayand et al., 2001), showing b) that a smaller
proportion of schizophrenic suicides appear to plan
their suicides (Kreyenbuhl et al., 2002), and c) that
such individuals had previously attempted suicide or
had been promiscuous (Fenton, 2000). This is, to our
knowledge, the first study to examine impulsivity
using a behavioural measure among psychotic suicide
completers, higher scores on which did not charac-
terize suicide completers. If confirmed in future
studies, these findings suggest that suicide risk may
be mediated differently across the major psychopath-
ological categories and provide further support for the
presence of heterogeneity in predisposing mecha-
nisms whereby suicide risk is increased in different
populations.
As it has been consistently reported among other
populations (Beautrais et al., 1996; Hawton et al.,
2003; Henriksson et al., 1993; Lesage et al., 1994;
Marttunen et al., 1991; Muller et al., 2005; Rudd et
al., 1993), and more recently, by Kuo et al. (Kuo et al.,
2005) among psychotic suicides, a significant rela-
tionship emerged between current comorbid axis I
disorders and psychotic completed suicide. In the
current sample, comorbidity appears to have been
driven by comorbid diagnoses of depressive disorder
NOS. Unlike reports in other diagnostic groups,
however, no excess lifetime comorbidity was ob-
served and the level of current comorbidity is of a
lesser magnitude than that reported among other
populations at risk for suicide (Kim et al., 2003).
This may be due to the lack of excess of levels of
impulsive–aggressive behaviours among the psychot-
ic suicides, as the comorbidity reported among
unselected suicides is primarily related to the con-
comitant presence of disorders that are related to
impulse discontrol, including substance abuse disor-
ders and cluster B personality disorders (Kim et al.,
2003).
4.3. Family history
We found an increased risk for suicide among
individuals with schizophrenia and chronic psychotic
disorders who had a family history of suicidal
behaviour. Moreover, our analyses indicated that this
increased risk operated independently from psycho-
pathology. Although these findings may be due to
possible artifacts such as a heightened awareness
about a family history of suicidal behaviour following
a suicide of a close family member, our findings are in
line with a large body of evidence coming from
studies using different methodologies supporting
familial aggregation of suicidal behaviour. For exam-
ple, in other diagnostic populations support for
familial clustering of suicide has been obtained (Roy
et al., 1991, 1995; Statham et al., 1998) and it has also
been reported that familial aggregation of suicidal
behaviour operates independently from psychopathol-
ogy (Brent et al., 1996; Cheng et al., 2000; Johnson et
al., 1998; Kim et al., 2005; Statham et al., 1998). In
previous studies it has been suggested that impulsive–
aggressive behaviours could mediate familial trans-
mission of suicidal behaviour (Brent et al., 1996,
2002, 2004; Brent and Mann, 2005; Kim et al., 2005),
however, in the current sample, measures of impulsive
aggression were not associated with family histories
of suicidal behaviour. Given that we were unable to
A. McGirr et al. / Schizophrenia Research 84 (2006) 132–143140
observe an association between suicide risk, impul-
sive–aggressive behaviours and their related psycho-
pathological conditions, it remains to be determined
what, if any, mechanisms at the behavioural level
could mediate familial transmission of suicide differ-
entiating those with chronic psychotic conditions and
other populations.
4.4. Personality disorders
Our psychotic suicides were less likely to have
cluster A and C symptoms. While the role of
personality disorders in suicide risk has been exten-
sively investigated in unselected suicide completers
and suicide attempters (Apter et al., 1991; Beautrais et
al., 1996; Brent et al., 2002; Cheng et al., 2000, 1997;
Foster et al., 1997; Haw et al., 2001; Henriksson et al.,
1993; Lesage et al., 1994; Malone et al., 1995; Mann
et al., 1999; Shearer et al., 1988; Soloff et al., 1994),
the relationship between personality traits, personality
disorders and suicide risk has not yet been examined
in schizophrenic or psychotic suicides. Certainly, the
investigation of personality traits and disorders in
patients with schizophrenia and similar conditions is
potentially confounded by the natural course of
psychotic disorders and methodological difficulties
intrinsic to the retrospective investigation of premor-
bid personality traits in this diagnostic group. Never-
theless, our personality trait measures showed very
good reliability and good to excellent concurrent and
convergent validity, suggesting that personality meas-
ures in our sample are precise and accurate. Our
findings are in stark contrast with those from
examinations of personality variants in unselected
suicides, where personality disorders have emerged as
important risk factors for completed suicide (Apter et
al., 1991; Beautrais et al., 1996; Brent et al., 2002;
Cheng et al., 2000, 1997; Foster et al., 1997; Haw et
al., 2001; Henriksson et al., 1993; Lesage et al., 1994;
Malone et al., 1995; Mann et al., 1999; Shearer et al.,
1988; Soloff et al., 1994). Though further examina-
tions of personality disorders among individuals
diagnosed with psychotic disorders are needed, the
greater prevalence of cluster A and C symptoms
among controls has interesting implications. First,
higher cluster A symptoms are consistent with
negative symptom differences and hypothesized pre-
morbid psychotic features (Fenton, 2000; Fenton and
McGlashan, 1994; Fenton et al., 1997). Second,
cluster C symptoms may be associated with lower
social functioning, less exposure and thus lower levels
of interpersonal conflict or negative life event
occurrence. Last, lower levels of cluster A symptoms
may be associated with risk factors specific to suicide
among those suffering from psychotic disorders that
were not assessed, such as greater illness insight
(Schwartz and Smith, 2004) or fear of mental
disintegration (Hawton et al., 2005). These possibil-
ities require further investigation.
4.5. Limitations
In this study we opted for living controls of
comparable psychopathology and sociodemographic
characteristics and assessments using proxy-based
procedures. While controlling for the presence of
major psychopathology and using similar methods in
both groups helps avoid several methodological
shortcomings, our study has, nevertheless, limitations
that are inherent to post-mortem studies involving
proxy-based interviews. Informants may have imper-
fect and varying levels of information about the
subject from which the subject’s state of mind is
reconstructed. However, by using proxy-based inter-
views for both cases and controls, this possible bias
was controlled for. In addition, similar to studies
carried out by other groups (Conner et al., 2001a,b),
and in our studies of suicide in different diagnostic
subgroups (Dumais et al., 2005a,b), our instruments
had good concordance rates between proxy-based and
directly obtained information. Nonetheless, when
comparing suicides to living controls, it is important
to consider that family members in grief may
exaggerate or overemphasize symptoms and signs in
the deceased and that an asymmetry of information
may exist between the proxies of suicide completers
and living subjects. Other limitations of this study are
related to the relatively small sample, which is a
consequence of the low frequency of chronic psy-
chotic subjects (c7%) among unselected suicides.
Similarly, living controls may possess latent risk for
suicide, yet this is unlikely due to a lifetime risk of 5%
among psychotic individuals, decreasing risk with
time following illness onset and a window of risk
primarily limited to the first ten years following illness
onset. Should controls possess latent risk, this would

A. McGirr et al. / Schizophrenia Research 84 (2006) 132–143 141
result in reduced power and would not be likely to
influence our positive findings. Nevertheless, addi-
tional investigations among larger samples may be
required to identify differential risk for suicide
associated with risk factors such as drug abuse.
4.6. Conclusion
Our study suggests that behavioural mediators of
suicide risk, such as impulsive–aggressive behaviours
do not play a role in schizophrenic and chronic
psychotic suicide, contrary to findings in other clinical
populations. This implies heterogeneity in predispos-
ing mechanism involved in suicide, a possibility that
future studies should pursue both between and within
specific populations. We also found that cluster A and
C personality traits appear to have a protective effect
against suicide in schizophrenics and other chronic
psychoses, though further research is needed to
elucidate the interaction between personality, psychot-
ic disorders and suicide. The clinical implications of
our findings are important, as psychotic individuals at
risk for suicide are most readily identified by the
presence of depressive disorders NOS, moderate to
severe psychotic symptoms and a family history of
suicidal behaviour. Clinicians may also include an
illness profile including lower levels of negative
symptoms to further refine their identification of
individuals at risk for completed suicide.
References
Altamura, A.C., Bassetti, R., Bignotti, S., Pioli, R., Mundo, E.,
2003. Clinical variables related to suicide attempts in
schizophrenic patients: a retrospective study. Schizophr. Res.
60, 47–55.
Apter, A., Kotler, M., Sevy, S., Plutchik, R., Brown, S.L., Foster,
H., Hillbrand, M., Korn, M.L., van Praag, H.M., 1991.
Correlates of risk of suicide in violent and nonviolent
psychiatric patients. Am. J. Psychiatry 148, 883–887.
Baca-Garcia, E., Perez-Rodriguez, M.M., Diaz Sastre, C., Saiz-
Ruiz, J., de Leon, J., 2005. Suicidal behavior in schizophrenia
and depression: a comparison. Schizophr. Res. 75, 77–81.
Barratt, E.S., 1965. Factor analysis of some psychometric measures
of impulsiveness and anxiety. Psychol. Rep. 16, 547–554.
Beautrais, A.L., Joyce, P.R., Mulder, R.T., Fergusson, D.M.,
Deavoll, B.J., Nightingale, S.K., 1996. Prevalence and comor-
bidity of mental disorders in persons making serious
suicide attempts: a case–control study. Am. J. Psychiatry 153,
1009–1014.
Black, D.W., Warrack, G., Winokur, G., 1985. Excess mortality
among psychiatric patients. The Iowa Record–Linkage Study.
Jama 253, 58–61.
Brent, D.A., 1995. Risk factors for adolescent suicide and suicidal
behavior: mental and substance abuse disorders, family envi-
ronmental factors, and life stress. Suicide Life-Threat. Behav. 25
Suppl, 52–63.
Brent, D.A., Mann, J.J., 2005. Family genetic studies, suicide, and
suicidal behavior. Am. J. Med. Genet. C Semin. Med. Genet.
133, 13–24.
Brent, D.A., Bridge, J., Johnson, B.A., Connolly, J., 1996. Suicidal
behavior runs in families. A controlled family study
of adolescent suicide victims. Arch. Gen. Psychiatry 53,
1145–1152.
Brent, D.A., Oquendo, M., Birmaher, B., Greenhill, L., Kolko, D.,
Stanley, B., Zelazny, J., Brodsky, B., Bridge, J., Ellis, S.,
Salazar, J.O., Mann, J.J., 2002. Familial pathways to early-
onset suicide attempt: risk for suicidal behavior in offspring of
mood-disordered suicide attempters. Arch. Gen. Psychiatry 59,
801–807.
Brent, D.A., Oquendo, M., Birmaher, B., Greenhill, L., Kolko, D.,
Stanley, B., Zelazny, J., Brodsky, B., Melhem, N., Ellis, S.P.,
Mann, J.J., 2004. Familial transmission of mood disorders:
convergence and divergence with transmission of suicidal
behavior. J. Am. Acad. Child Adolesc. Psych. 43, 1259–1266.
Brown, S., 1997. Excess mortality of schizophrenia. A meta-
analysis. Br. J. Psychiatry 171, 502–508.
Brown, G.L., Goodwin, F.K., 1986. Human aggression and suicide.
Suicide Life-Threat. Behav. 16, 223–243.
Buss, A.H., Durkee, A., 1957. An inventory for assessing different
kinds of hostility. J. Consult. Psychol. 21, 343–349.
Caldwell, C.B., Gottesman, I.I., 1990. Schizophrenics kill them-
selves too: a review of risk factors for suicide. Schizophr. Bull.
16, 571–589.
Castle, K., Duberstein, P.R., Meldrum, S., Conner, K.R., Conwell,
Y., 2004. Risk factors for suicide in blacks and whites: an
analysis of data from the 1993 National Mortality Followback
Survey. Am. J. Psychiatry 161, 452–458.
Centers for Disease Control and Prevention: Advance report of final
mortality statistics, 1990, 1993, in Monthly Vital Statistics
Report, 41, pp. 1–52.
Cheng, A.T., Mann, A.H., Chan, K.A., 1997. Personality
disorder and suicide. A case–control study. Br. J. Psychiatry
170, 441–446.
Cheng, A.T., Chen, T.H., Chen, C.C., Jenkins, R., 2000.
Psychosocial and psychiatric risk factors for suicide. Case–
control psychological autopsy study. Br. J. Psychiatry 177,
360–365.
Cloninger, C.R., Przybeckm, T.R., Svrakic, D.M., Wetzel, R.D.,
1994. The Temperament and Character Inventory (TCI): A
Guide to Its Development and Use. Center for Psychobiology of
Personality, St-Louis, Missouri.
Conner, K.R., Conwell, Y., Duberstein, P.R., 2001. The validity of
proxy-based data in suicide research: a study of patients 50
years of age and older who attempted suicide. II. Life events,
social support and suicidal behavior. Acta Psychiatr. Scand. 104,
452–457.
A. McGirr et al. / Schizophrenia Research 84 (2006) 132–143142
Conner, K.R., Cox, C., Duberstein, P.R., Tian, L., Nisbet, P.A.,
Conwell, Y., 2001. Violence, alcohol, and completed suicide: a
case–control study. Am. J. Psychiatry 158, 1701–1705.
Dumais, A., Lesage, A.D., Alda, M., Rouleau, G., Dumont, M.,
Chawky, N., Roy, M., Mann, J.J., Benkelfat, C., Turecki, G.,
2005a. Risk factors for suicide completion in major depression:
a case–control study of impulsive and aggressive behaviors in
men. Am. J. Psychiatry 162, 2116–2124.
Dumais, A., Lesage, A.D., Lalovic, A., Seguin, M., Tousignant, M.,
Chawky, N., Turecki, G., 2005b. Is violent method of suicide a
behavioral marker of lifetime aggression? Am. J. Psychiatry
162, 1375–1378.
Fenton, W.S., 2000. Depression, suicide, and suicide prevention in
schizophrenia. Suicide Life-Threat. Behav. 30, 34–49.
Fenton, W.S., McGlashan, T.H., 1994. Antecedents, symptom
progression, and long-term outcome of the deficit syndrome in
schizophrenia. Am. J. Psychiatry 151, 351–356.
Fenton, W.S., McGlashan, T.H., Victor, B.J., Blyler, C.R., 1997.
Symptoms, subtype, and suicidality in patients with schizophre-
nia spectrum disorders. Am. J. Psychiatry 154, 199–204.
First, M.B., Spitzer, R.L., Gibbon, M., Williams, J.B.W., Lorna,
B., 1995. Structure Clinical Interview for DSM-IV Axis II
Personality Disorders (SCID-II). Biometrics Research Depart-
ment, New York State Psychiatric Institute, New York.
First, M.B., Gibbon, M., Spitzer, R.L., Williams, J.B.W., 2001.
Structured Clinical Interview for DSM-IV-TR Axis I Disorders,
Research Version, Patient Edition with Psychotic Screen.
Biometrics Research, New York State Psychiatric Institute,
New York.
Foster, T., Gillespie, K., McClelland, R., 1997. Mental disorders and
suicide in Northern Ireland. Br. J. Psychiatry 170, 447–452.
Gut-Fayand, A., Dervaux, A., Olie, J.P., Loo, H., Poirier, M.F.,
Krebs, M.O., 2001. Substance abuse and suicidality in
schizophrenia: a common risk factor linked to impulsivity.
Psychiatry Res. 102, 65–72.
Haw, C., Hawton, K., Houston, K., Townsend, E., 2001. Psychiatric
and personality disorders in deliberate self-harm patients. Br. J.
Psychiatry 178, 48–54.
Haw, C., Houston, K., Townsend, E., Hawton, K., 2002. Deliberate
self harm patients with depressive disorders: treatment and
outcome. J. Affect. Disord. 70, 57–65.
Hawton, K., Houston, K., Haw, C., Townsend, E., Harriss, L., 2003.
Comorbidity of axis I and axis II disorders in patients who
attempted suicide. Am. J. Psychiatry 160, 1494–1500.
Hawton, K., Sutton, L., Haw, C., Sinclair, J., Deeks, J.J., 2005.
Schizophrenia and suicide: systematic review of risk factors. Br.
J. Psychiatry 187, 9–20.
Heila, H., Isometsa, E.T., Henriksson, M.M., Heikkinen, M.E.,
Marttunen, M.J., Lonnqvist, J.K., 1997. Suicide and schizo-
phrenia: a nationwide psychological autopsy study on age- and
sex-specific clinical characteristics of 92 suicide victims with
schizophrenia. Am. J. Psychiatry 154, 1235–1242.
Henriksson, M.M., Aro, H.M., Marttunen, M.J., Heikkinen, M.E.,
Isometsa, E.T., Kuoppasalmi, K.I., Lonnqvist, J.K., 1993.
Mental disorders and comorbidity in suicide. Am. J. Psychiatry
150, 935–940.
Hu, W.H., Sun, C.M., Lee, C.T., Peng, S.L., Lin, S.K., Shen, W.W.,
1991. A clinical study of schizophrenic suicides. 42 cases in
Taiwan. Schizophr. Res. 5, 43–50.
Johnson, B.A., Brent, D.A., Bridge, J., Connolly, J., 1998. The
familial aggregation of adolescent suicide attempts. Acta
Psychiatr. Scand. 97, 18–24.
Kelly, T.M., Mann, J.J., 1996. Validity of DSM-III-R diagnosis by
psychological autopsy: a comparison with clinician ante-mortem
diagnosis. Acta Psychiatr. Scand. 94, 337–343.
Kelly, D.L., Shim, J.C., Feldman, S.M., Yu, Y., Conley, R.R.,
2004. Lifetime psychiatric symptoms in persons with schizo-
phrenia who died by suicide compared to other means of
death. J. Psychiatr. Res. 38, 531–536.
Kim, C., Lesage, A., Seguin, M., Chawky, N., Vanier, C., Lipp, O.,
Turecki, G., 2003. Patterns of co-morbidity in male suicide
completers. Psychol. Med. 33, 1299–1309.
Kim, C.D., Seguin, M., Therrien, N., Riopel, G., Chawky, N.,
Lesage, A.D., Turecki, G., 2005. Familial aggregation of
suicidal behavior: a family study of male suicide com-
pleters from the general population. Am. J. Psychiatry 162,
1017–1019.
King, E.A., Baldwin, D.S., Sinclair, J.M., Baker, N.G., Campbell,
M.J., Thompson, C., 2001. The Wessex Recent In-Patient
Suicide Study, 1. Case–control study of 234 recently discharged
psychiatric patient suicides. Br. J. Psychiatry 178, 531–536.
Kreyenbuhl, J.A., Kelly, D.L., Conley, R.R., 2002. Circumstances
of suicide among individuals with schizophrenia. Schizophr.
Res. 58, 253–261.
Kuo, C.J., Tsai, S.Y., Lo, C.H., Wang, Y.P., Chen, C.C., 2005. Risk
factors for completed suicide in schizophrenia. J. Clin.
Psychiatry 66, 579–585.
Lesage, A.D., Boyer, R., Grunberg, F., Vanier, C., Morissette, R.,
Menard-Buteau, C., Loyer, M., 1994. Suicide and mental
disorders: a case–control study of young men. Am. J. Psychiatry
151, 1063–1068.
Malone, K.M., Haas, G.L., Sweeney, J.A., Mann, J.J., 1995. Major
depression and the risk of attempted suicide. J. Affect. Disord.
34, 173–185.
Mann, J.J., Waternaux, C., Haas, G.L., Malone, K.M., 1999.
Toward a clinical model of suicidal behavior in psychiatric
patients. Am. J. Psychiatry 156, 181–189.
Mann, J.J., Huang, Y.Y., Underwood, M.D., Kassir, S.A., Oppen-
heim, S., Kelly, T.M., Dwork, A.J., Arango, V., 2000. A
serotonin transporter gene promoter polymorphism (5-
HTTLPR) and prefrontal cortical binding in major depression
and suicide. Arch. Gen. Psychiatry 57, 729–738.
Marttunen, M.J., Aro, H.M., Henriksson, M.M., Lonnqvist, J.K.,
1991. Mental disorders in adolescent suicide. DSM-III-R axes
I and II diagnoses in suicides among 13- to 19-year-olds in
Finland. Arch. Gen. Psychiatry 48, 834–839.
Muller, D.J., Barkow, K., Kovalenko, S., Ohlraun, S., Fangerau, H.,
Kolsch, H., Lemke, M.R., Held, T., Nothen, M.M., Maier, W.,
Heun, R., Rietschel, M., 2005. Suicide attempts in schizophre-
nia and affective disorders with relation to some specific
demographical and clinical characteristics. Eur. Psychiatr. 20,
65–69.
A. McGirr et al. / Schizophrenia Research 84 (2006) 132–143 143
Palmer, B.A., Pankratz, V.S., Bostwick, J.M., 2005. The lifetime
risk of suicide in schizophrenia: a reexamination. Arch. Gen.
Psychiatry 62, 247–253.
Plutchik, R., van Praag, H.M., Conte, H.R., 1989. Correlates of
suicide and violence risk: III. A two-stage model of counter-
vailing forces. Psychiatry Res. 28, 215–225.
Potkin, S.G., Alphs, L., Hsu, C., Krishnan, K.R., Anand, R., Young,
F.K., Meltzer, H., Green, A., 2003. Predicting suicidal risk in
schizophrenic and schizoaffective patients in a prospective two-
year trial. Biol. Psychiatry 54, 444–452.
Roy, A., 1982. Suicide in chronic schizophrenia. Br. J. Psychiatry
141, 171–177.
Roy, A., Segal, N.L., Centerwall, B.S., Robinette, C.D., 1991.
Suicide in twins. Arch. Gen. Psychiatry 48, 29–32.
Roy, A., Segal, N.L., Sarchiapone, M., 1995. Attempted suicide
among living co-twins of twin suicide victims. Am. J.
Psychiatry 152, 1075–1076.
Rudd, M.D., Dahm, P.F., Rajab, M.H., 1993. Diagnostic comorbid-
ity in persons with suicidal ideation and behavior. Am. J.
Psychiatry 150, 928–934.
Schwartz, R.C., Smith, S.D., 2004. Suicidality and psychosis: the
predictive potential of symptomatology and insight into illness.
J. Psychiatr. Res. 38, 185–191.
Shafii, M., Steltz-Lenarsky, J., Derrick, A.M., Beckner, C.,
Whittinghill, J.R., 1988. Comorbidity of mental disorders in
the post-mortem diagnosis of completed suicide in children and
adolescents. J. Affect. Disord. 15, 227–233.
Shearer, S.L., Peters, C.P., Quaytman, M.S., Wadman, B.E., 1988.
Intent and lethality of suicide attempts among female borderline
inpatients. Am. J. Psychiatry 145, 1424–1427.
Sinclair, J.M., Mullee, M.A., King, E.A., Baldwin, D.S., 2004.
Suicide in schizophrenia: a retrospective case–control study of
51 suicides. Schizophr. Bull. 30, 803–811.
Soloff, P.H., Lis, J.A., Kelly, T., Cornelius, J., Ulrich, R., 1994. Risk
factors for suicidal behavior in borderline personality disorder.
Am. J. Psychiatry 151, 1316–1323.
Statham, D.J., Heath, A.C., Madden, P.A., Bucholz, K.K., Bierut,
L., Dinwiddie, S.H., Slutske, W.S., Dunne, M.P., Martin, N.G.,
1998. Suicidal behaviour: an epidemiological and genetic study.
Psychol. Med. 28, 839–855.
Vieta, E., Nieto, E., Gasto, C., Cirera, E., 1992. Serious suicide
attempts in affective patients. J. Affect. Disord. 24, 147–152.
Westermeyer, J.F., Harrow, M., Marengo, J.T., 1991. Risk for
suicide in schizophrenia and other psychotic and nonpsychotic
disorders. J. of Nerv. Ment. Dis. 179, 259–266.
Zhang, J., Conwell, Y., Wieczorek, W.F., Jiang, C., Jia, S., Zhou,
L., 2003. Studying Chinese suicide with proxy-based data:
reliability and validity of the methodology and instruments in
China. J. of Nerv. Ment. Dis. 191, 450–457.
Top Related
Copyright © 2022 FDOKUMEN

