







Bahasa
Halaman
Hukum

PUBLIC HEALTHDEVELOPING HEALTHY
COMMUNITIES
PART ONEHEALTH NEEDS ASSESSMENT PROFILE
PART TWOHEALTH PROMOTION PROPOSAL
Theresa Lowry-LehnenSpecialist Nurse Practitioner
Surrey University 2005
PUBLIC HEALTHPART ONE: HEALTH NEEDS ASSESSMENT PROFILE
CONTENTSPage
1. Introduction
1. Context and Theoretical Framework
4. Identification and Boundary of the Community
5. Practice Population Statistics
5. Wards and Deprivation Scores
6. Ethnicity
6. The Community’s Locality
7. The Community’s Social Structure
7. Lone Parent Households
8. Teenage Pregnancy Rates
8. Elderly Patients Living Alone
9. Children – Health Visitors Case Files 2004
11. Key Health Determinants
13. The Community’s Social Activity and Sentiment
14. What Is Being Done?15. Sutton and Merton PCT (Targets and Aims – 2003-
2006)
16. The Community’s Health
16. Chronic Illness Patients
17. Chronic Illness Patients and Smoking
18. Key facts –Smoking - DoH 2004
18. Governments Targets – Smoking – DoH 2004
19. Summary of Identified Community Health Needs
Main Health Need Identified ( Requiring
Intervention)
(Smoking Among The High Risk - Chronic Disease
Group Patients)
20. Conclusion
22. References
PUBLIC HEALTH
Theresa Lowry-LehnenGeneral Practice Nurse
PART ONE: HEALTH NEEDS ASSESSMENT PROFILE
INTRODUCTION
Since the first Public Health Act in 1875 there has been
a continuing development towards our current
understanding of public health, which is influenced by
legislation and policy, theory and practice-based
research. This paper focuses on current public health
policies and how they can be translated into practice.
Part One considers the wider determinants of health and
the concept of health needs and analyses and evaluates
collated data with regard to a community selected from my
practice area within the Sutton and Merton Primary Care
Trust. Part Two introduces a plan devised to address an
identified health need, i.e. smoking among high-risk
groups, and critically appraises an appropriate
intervention and evaluation strategy, based on the health
promotion model by Tannahill (1985). The proposed action
plan also incorporates the ‘stages of change’ model
developed by Prochaska and DiClemente (1984 cited by
Naidoo & Wills 2000).
Context and Theoretical FrameworkPublic health is not a new concept, but since the public
health movement of the 19th century the concept has
changed significantly. Evolving from a somewhat
paternalistic movement, public health now stresses the
participatory aspect of health promotion, with special
emphasis on the empowerment of patients.
The World Health Organisation has been pointed out as a
leading international influence on health care policy and
practice, with its development of worldwide health
initiatives aimed at addressing inequalities (Tinson:
1995). In Britain, the Black Report, published in 1982,
confirmed the extent of inequalities in health and health
care (Naidoo & Wills 2000). According to Ewles and
Simnett (2003), this report highlighted inappropriate
health care and a requirement to focus more on the health
needs of different groups.
The current view is expressed in the definition of public
health given by the Acheson Report (1988) “as the science
and art of preventing disease, prolonging life and
promoting health through the organised efforts of
society”.
The new public health aims to use regulations, fiscal
measures, policies and voluntary codes of practice to
provide the population with the opportunities to make the
healthier choice the easier choice (Naidoo & Wills 2000).
According to the World Health Organisation (1998), the
new public health is characterised by a comprehensive
understanding of the ways in which lifestyle and living
conditions determine health status and aims to protect
health by supporting lifestyles and creating supportive
environments for health.
“Making healthy choices easier” is the subtitle of the
current Labour government’s white paper “Choosing
Health”, which identifies an approach which respects the
freedom of individual choice and which addresses the fact
that too many people or groups have been left behind or
ignored in the past (DoH 2004a). Furthermore, the current
government stresses that health promotion, with a focus
on prevention and tackling inequalities, is one of the
key roles of primary care nurses (DoH 2002) and the
health service as a whole (DoH 2000, DoH 2004b).
A Health Assessment Profile can help to fulfil such a
role in a meaningful way. It has been acknowledged as the
most suitable assessment tool for community-based care,
marking a shift from the traditional assessment of health
needs by nurses on a one-to-one basis to a more
collective view which considers the wider and more
complex health needs of the community (Tinson 1995).
Such a profile has been defined as the systematic
collection of data to identify the health needs of a
defined population, and the analysis of that data to
assess and prioritise strategies in health promotion
(Twinn, Dauncey, Carnell 1990).
In determining health needs, the profiler must be aware
of the various ways in which they can be defined:
normative needs, felt needs, expressed needs, and
comparative needs (Bradshaw 1972 cited by Tinson 1995;
Blackie 1998).
A health needs assessment must also take into account
wider determinants of health, such as deprivation and
poverty, cultural and social influences, education,
housing, transport, and environmental factors (Naidoo &
Wills 2000, Ewles & Simnett 2003).
Both the various needs and the wider determinants will be
addressed in detail in the course of the Health Needs
Assessment Profile, which is based on the framework
suggested by Tinson (1995).
Tinson (1995) asserts that the first and most essential
task in compiling a profile is to identify the community
under examination and define its boundaries. It is also
important to consider the various dimensions within a
community, i.e. its locality (where it is), its social
structure (who lives there), its social activity (what
happens there) and its sentiment (what is it like to live
there) (Orr 1992 cited by Tinson 1995). Finally, the
dynamic nature of a chosen community should be taken into
account: Tinson (1995) suggests an approach using systems
theory as a framework, in which the community as a system
can be divided into subsystems, i.e. key health
determinants such as employment, education, housing,
crime, health care and transport. For this profile, data
was collected from a variety of sources, including a GP
practice profile I compiled at the surgery where I am
based, the Sutton and Merton PCT, local and national
government statistics, the latest Northern Wards
Participatory Needs Assessment and the national census.
Identification and Boundary of the Community The community chosen for this profile is the St Helier
(Merton) and St Helier North and South (Sutton) practice
population of Faccini House Surgery, Middleton Road,
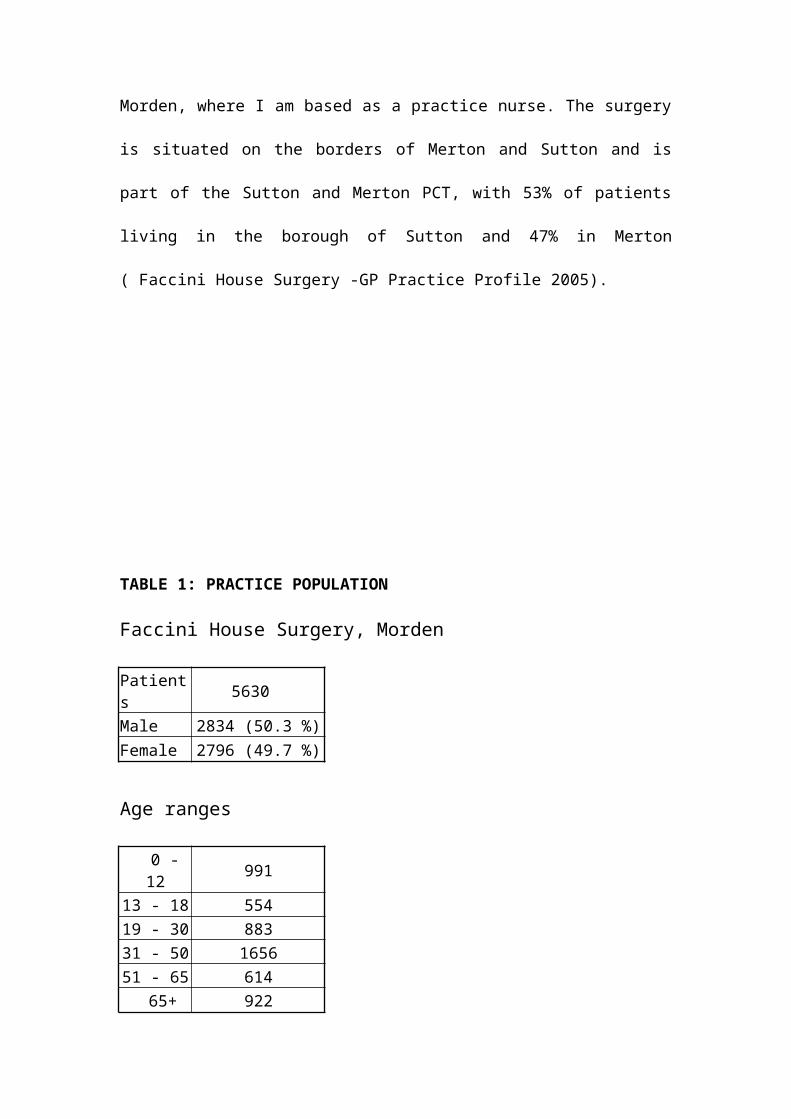
Morden, where I am based as a practice nurse. The surgery
is situated on the borders of Merton and Sutton and is
part of the Sutton and Merton PCT, with 53% of patients
living in the borough of Sutton and 47% in Merton
( Faccini House Surgery -GP Practice Profile 2005).
TABLE 1: PRACTICE POPULATION
Faccini House Surgery, Morden
Patients 5630
Male 2834 (50.3 %)Female 2796 (49.7 %)
Age ranges
0 -12 991
13 - 18 55419 - 30 88331 - 50 165651 - 65 614 65+ 922
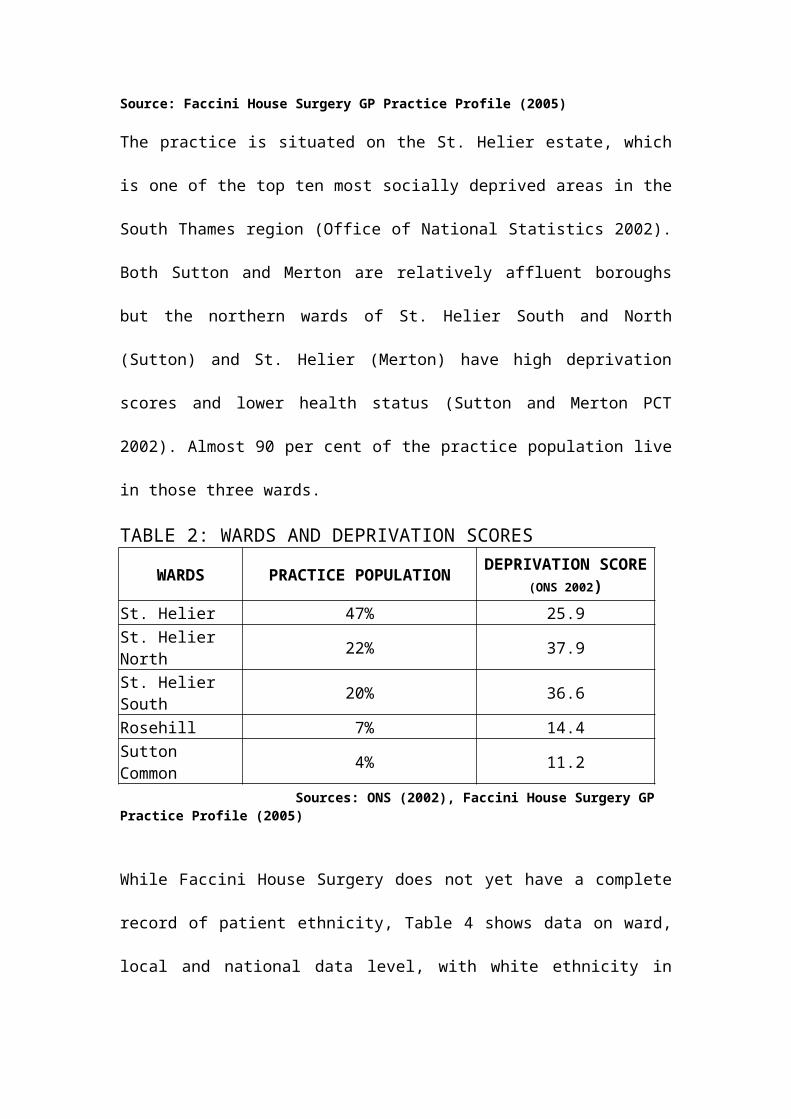
Source: Faccini House Surgery GP Practice Profile (2005)
The practice is situated on the St. Helier estate, which
is one of the top ten most socially deprived areas in the
South Thames region (Office of National Statistics 2002).
Both Sutton and Merton are relatively affluent boroughs
but the northern wards of St. Helier South and North
(Sutton) and St. Helier (Merton) have high deprivation
scores and lower health status (Sutton and Merton PCT
2002). Almost 90 per cent of the practice population live
in those three wards.
TABLE 2: WARDS AND DEPRIVATION SCORES
WARDS PRACTICE POPULATION DEPRIVATION SCORE(ONS 2002)
St. Helier 47% 25.9St. Helier North 22% 37.9
St. Helier South 20% 36.6
Rosehill 7% 14.4Sutton Common 4% 11.2
Sources: ONS (2002), Faccini House Surgery GP Practice Profile (2005)
While Faccini House Surgery does not yet have a complete
record of patient ethnicity, Table 4 shows data on ward,
local and national data level, with white ethnicity in
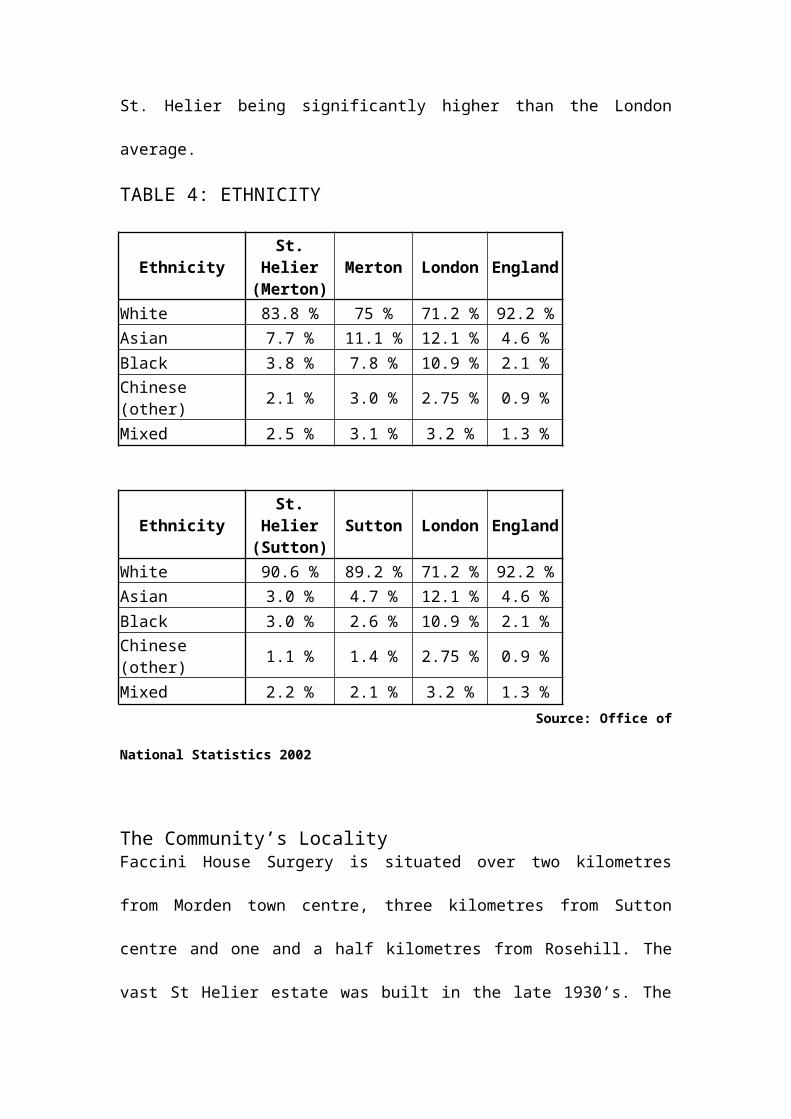
St. Helier being significantly higher than the London
average.
TABLE 4: ETHNICITY
EthnicitySt.
Helier(Merton)
Merton London England
White 83.8 % 75 % 71.2 % 92.2 %Asian 7.7 % 11.1 % 12.1 % 4.6 %Black 3.8 % 7.8 % 10.9 % 2.1 %Chinese (other) 2.1 % 3.0 % 2.75 % 0.9 %
Mixed 2.5 % 3.1 % 3.2 % 1.3 %
EthnicitySt.
Helier(Sutton)
Sutton London England
White 90.6 % 89.2 % 71.2 % 92.2 %Asian 3.0 % 4.7 % 12.1 % 4.6 %Black 3.0 % 2.6 % 10.9 % 2.1 %Chinese (other) 1.1 % 1.4 % 2.75 % 0.9 %
Mixed 2.2 % 2.1 % 3.2 % 1.3 % Source: Office of
National Statistics 2002
The Community’s LocalityFaccini House Surgery is situated over two kilometres
from Morden town centre, three kilometres from Sutton
centre and one and a half kilometres from Rosehill. The
vast St Helier estate was built in the late 1930’s. The
houses are small redbrick council style terraced houses,
each row backing on to another row of similar type
houses. The centralisation of facilities and services has
resulted in a lack of local services to meet the
population needs. To access most services in the locality
travel by bus or car is required. The closest
supermarkets are in Rosehill and Morden, and without
transport they are difficult for the elderly or those
with small children to access (Windshield Survey 2005).
There are four primary schools and one high school in the
immediate area, with lower educational achievements
compared to other schools in more affluent areas of
Merton and Sutton (Ofsted 2004). There is a significant
lack of green areas and playground facilities for
children and the nearest social centres and cafés are in
Rosehill and Morden centre (Windshield Survey 2005).
The Community’s Social Structure
The Census 2001 shows that the geographical area of the
Faccini House practice population has a high proportion
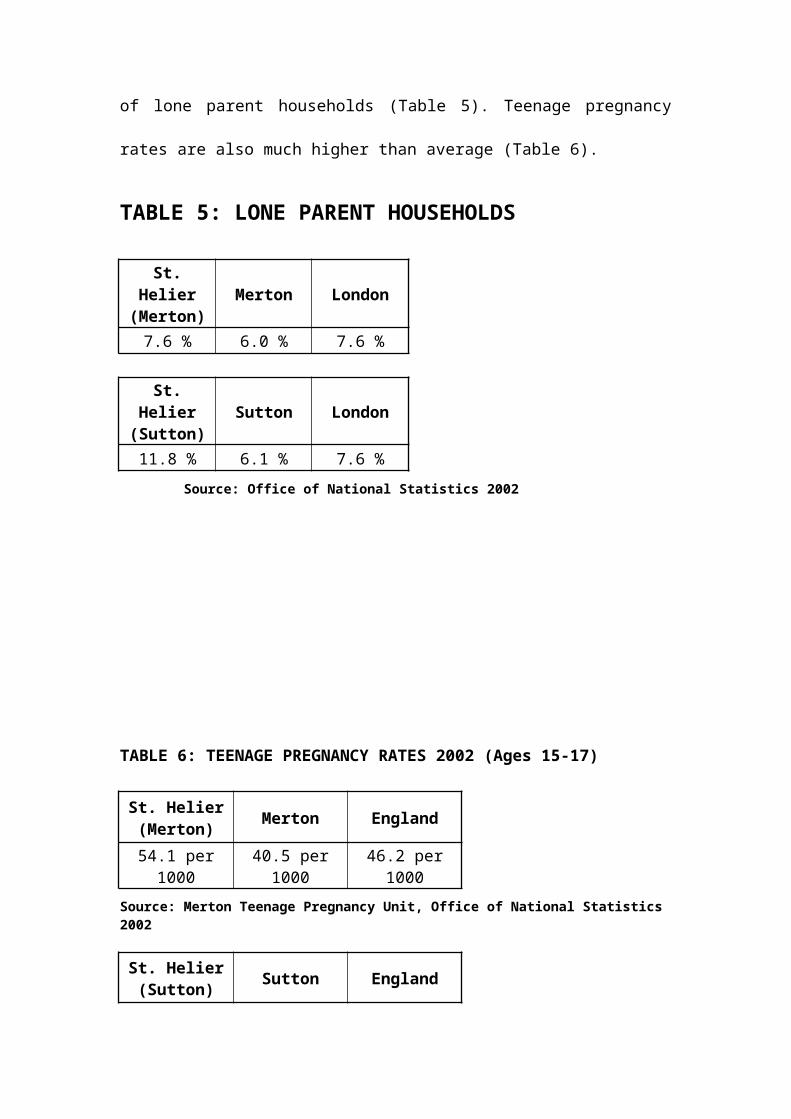
of lone parent households (Table 5). Teenage pregnancy
rates are also much higher than average (Table 6).
TABLE 5: LONE PARENT HOUSEHOLDS
St.Helier
(Merton)Merton London
7.6 % 6.0 % 7.6 %
St.Helier
(Sutton)Sutton London
11.8 % 6.1 % 7.6 % Source: Office of National Statistics 2002
TABLE 6: TEENAGE PREGNANCY RATES 2002 (Ages 15-17)
St. Helier(Merton) Merton England
54.1 per1000
40.5 per1000
46.2 per1000
Source: Merton Teenage Pregnancy Unit, Office of National Statistics 2002
St. Helier(Sutton) Sutton England
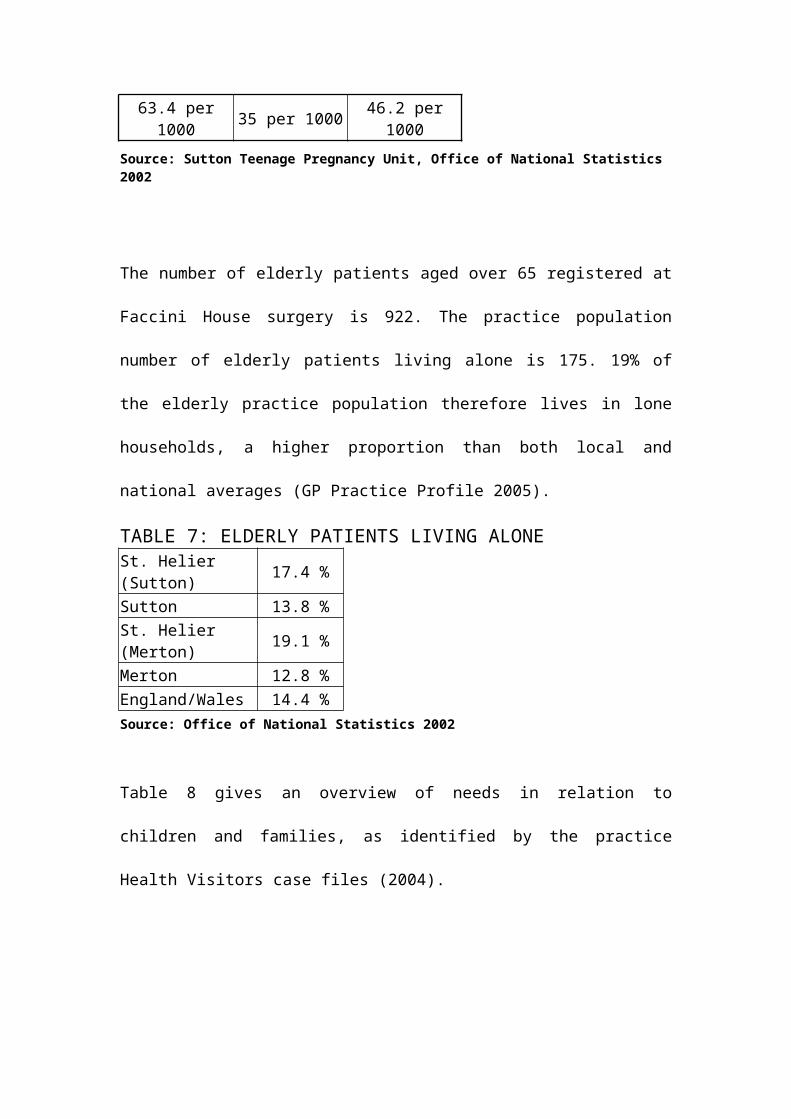
63.4 per1000 35 per 1000 46.2 per
1000Source: Sutton Teenage Pregnancy Unit, Office of National Statistics 2002
The number of elderly patients aged over 65 registered at
Faccini House surgery is 922. The practice population
number of elderly patients living alone is 175. 19% of
the elderly practice population therefore lives in lone
households, a higher proportion than both local and
national averages (GP Practice Profile 2005).
TABLE 7: ELDERLY PATIENTS LIVING ALONESt. Helier (Sutton) 17.4 %
Sutton 13.8 %St. Helier (Merton) 19.1 %
Merton 12.8 %England/Wales 14.4 %Source: Office of National Statistics 2002
Table 8 gives an overview of needs in relation to
children and families, as identified by the practice
Health Visitors case files (2004).
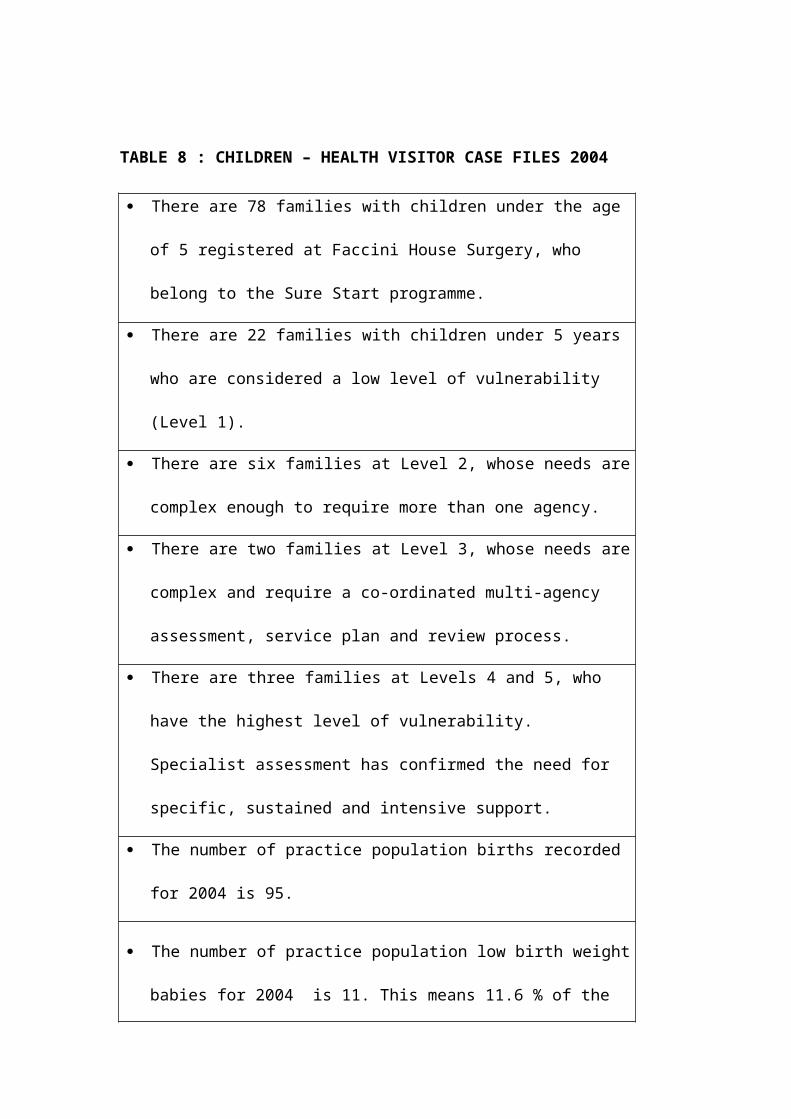
TABLE 8 : CHILDREN – HEALTH VISITOR CASE FILES 2004
There are 78 families with children under the age
of 5 registered at Faccini House Surgery, who
belong to the Sure Start programme.
There are 22 families with children under 5 years
who are considered a low level of vulnerability
(Level 1).
There are six families at Level 2, whose needs are
complex enough to require more than one agency.
There are two families at Level 3, whose needs are
complex and require a co-ordinated multi-agency
assessment, service plan and review process.
There are three families at Levels 4 and 5, who
have the highest level of vulnerability.
Specialist assessment has confirmed the need for
specific, sustained and intensive support.
The number of practice population births recorded
for 2004 is 95.
The number of practice population low birth weight
babies for 2004 is 11. This means 11.6 % of the
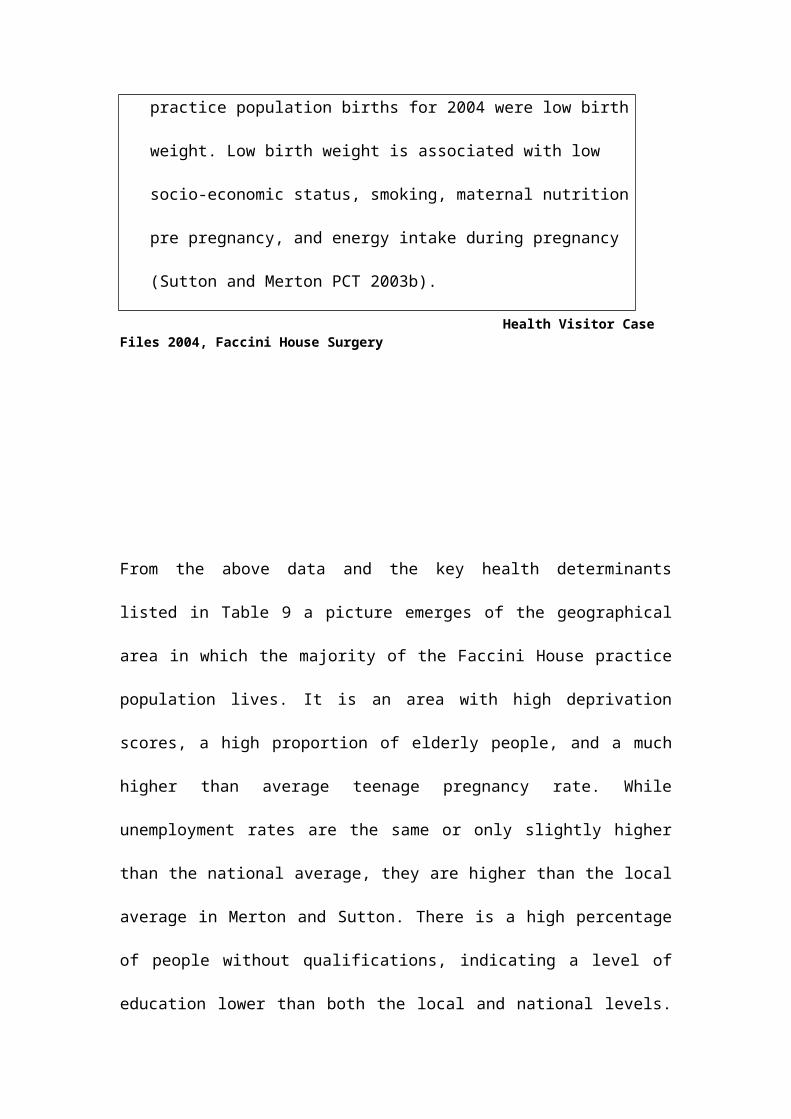
practice population births for 2004 were low birth
weight. Low birth weight is associated with low
socio-economic status, smoking, maternal nutrition
pre pregnancy, and energy intake during pregnancy
(Sutton and Merton PCT 2003b).
Health Visitor Case Files 2004, Faccini House Surgery
From the above data and the key health determinants
listed in Table 9 a picture emerges of the geographical
area in which the majority of the Faccini House practice
population lives. It is an area with high deprivation
scores, a high proportion of elderly people, and a much
higher than average teenage pregnancy rate. While
unemployment rates are the same or only slightly higher
than the national average, they are higher than the local
average in Merton and Sutton. There is a high percentage
of people without qualifications, indicating a level of
education lower than both the local and national levels.
There is also a higher than local and national average of
lone parent households. Rented council accommodation, as
opposed to owner occupied housing, is considerably higher
than both the local and national average, with a high
percentage of accommodation without central heating.
There is also a relatively high number of people without
private transport.
TABLE 9: KEY HEALTH DETERMINANTS
Limiting long term illness
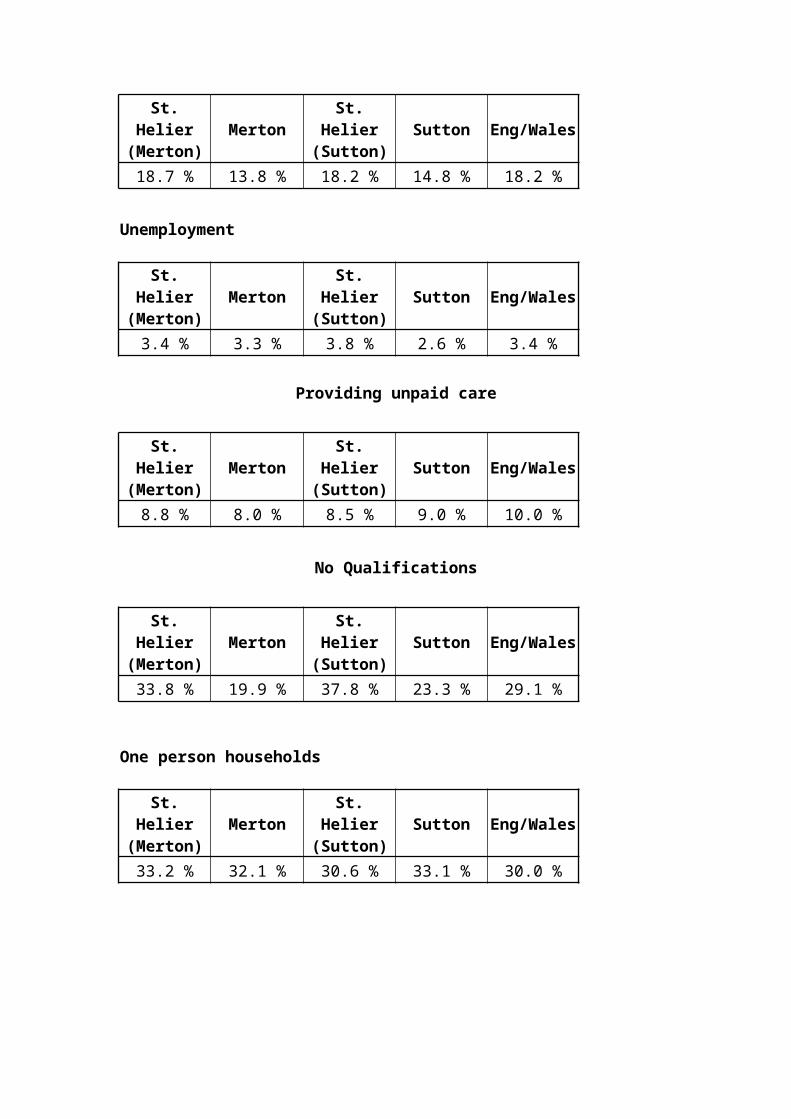
St.Helier
(Merton)Merton
St.Helier(Sutton)
Sutton Eng/Wales
18.7 % 13.8 % 18.2 % 14.8 % 18.2 %
Unemployment
St.Helier
(Merton)Merton
St.Helier(Sutton)
Sutton Eng/Wales
3.4 % 3.3 % 3.8 % 2.6 % 3.4 %
Providing unpaid care
St.Helier
(Merton)Merton
St.Helier(Sutton)
Sutton Eng/Wales
8.8 % 8.0 % 8.5 % 9.0 % 10.0 %
No Qualifications
St.Helier
(Merton)Merton
St.Helier(Sutton)
Sutton Eng/Wales
33.8 % 19.9 % 37.8 % 23.3 % 29.1 %
One person households
St.Helier
(Merton)Merton
St.Helier(Sutton)
Sutton Eng/Wales
33.2 % 32.1 % 30.6 % 33.1 % 30.0 %
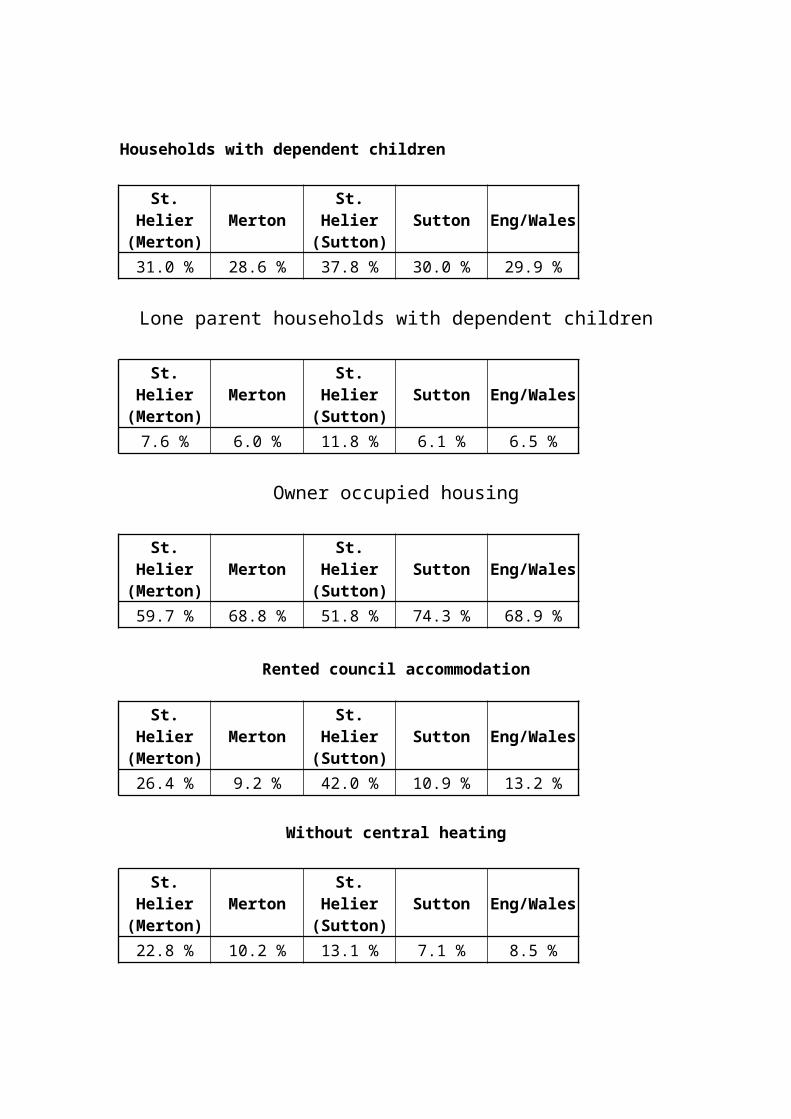
Households with dependent children
St.Helier
(Merton)Merton
St.Helier(Sutton)
Sutton Eng/Wales
31.0 % 28.6 % 37.8 % 30.0 % 29.9 %
Lone parent households with dependent children
St.Helier
(Merton)Merton
St.Helier(Sutton)
Sutton Eng/Wales
7.6 % 6.0 % 11.8 % 6.1 % 6.5 %
Owner occupied housing
St.Helier
(Merton)Merton
St.Helier(Sutton)
Sutton Eng/Wales
59.7 % 68.8 % 51.8 % 74.3 % 68.9 %
Rented council accommodation
St.Helier
(Merton)Merton
St.Helier(Sutton)
Sutton Eng/Wales
26.4 % 9.2 % 42.0 % 10.9 % 13.2 %
Without central heating
St.Helier
(Merton)Merton
St.Helier(Sutton)
Sutton Eng/Wales
22.8 % 10.2 % 13.1 % 7.1 % 8.5 %
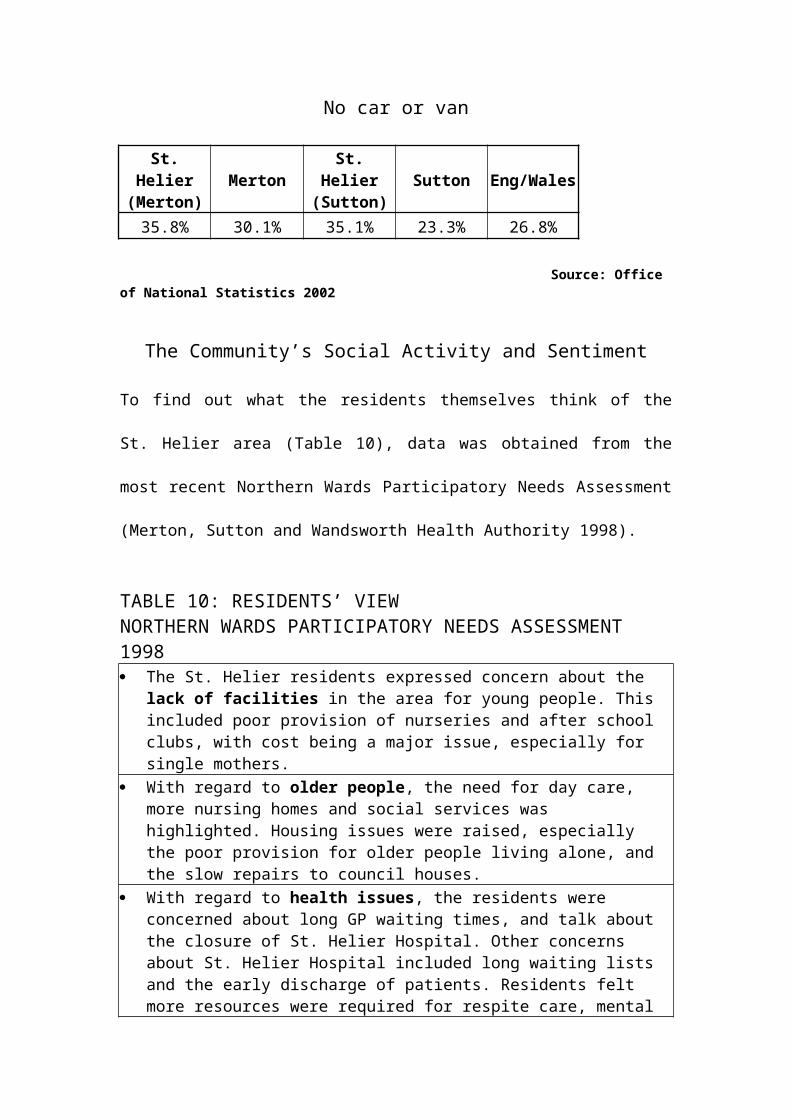
No car or van
St.Helier
(Merton)Merton
St.Helier(Sutton)
Sutton Eng/Wales
35.8% 30.1% 35.1% 23.3% 26.8%
Source: Office of National Statistics 2002
The Community’s Social Activity and Sentiment
To find out what the residents themselves think of the
St. Helier area (Table 10), data was obtained from the
most recent Northern Wards Participatory Needs Assessment
(Merton, Sutton and Wandsworth Health Authority 1998).
TABLE 10: RESIDENTS’ VIEW NORTHERN WARDS PARTICIPATORY NEEDS ASSESSMENT 1998 The St. Helier residents expressed concern about the
lack of facilities in the area for young people. This included poor provision of nurseries and after school clubs, with cost being a major issue, especially for single mothers.
With regard to older people, the need for day care, more nursing homes and social services was highlighted. Housing issues were raised, especially the poor provision for older people living alone, and the slow repairs to council houses.
With regard to health issues, the residents were concerned about long GP waiting times, and talk about the closure of St. Helier Hospital. Other concerns about St. Helier Hospital included long waiting lists and the early discharge of patients. Residents felt more resources were required for respite care, mental
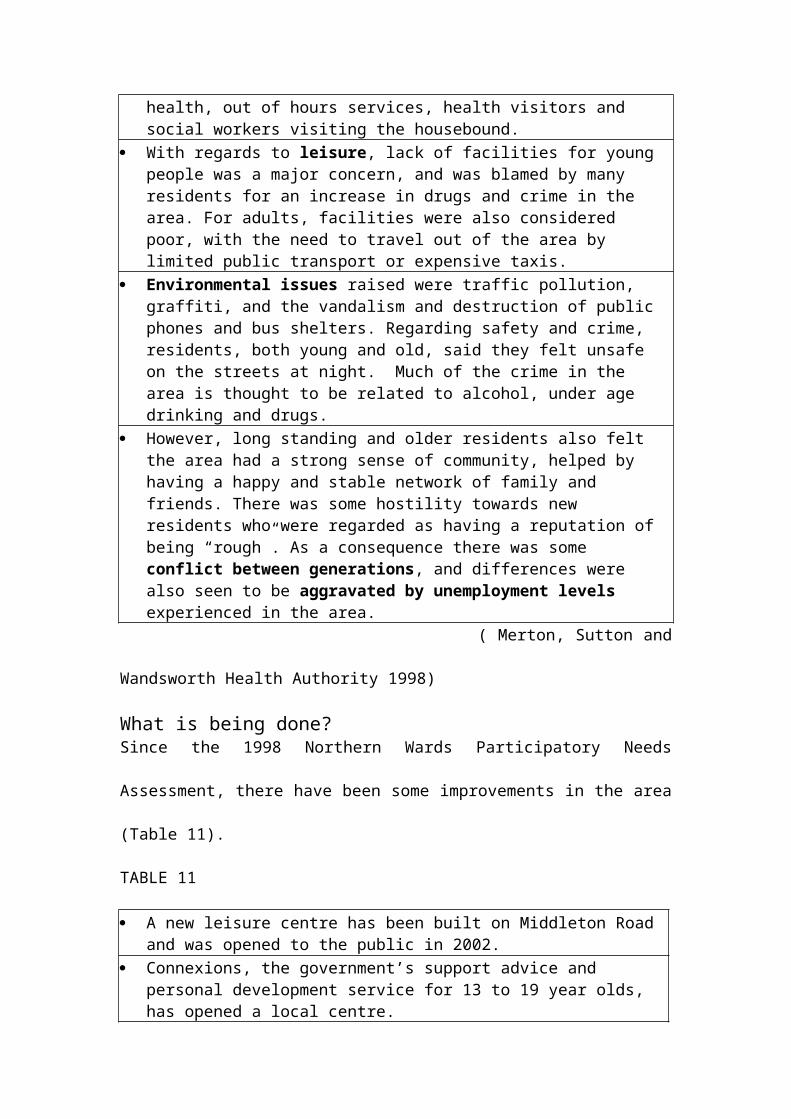
health, out of hours services, health visitors and social workers visiting the housebound.
With regards to leisure, lack of facilities for young people was a major concern, and was blamed by many residents for an increase in drugs and crime in the area. For adults, facilities were also considered poor, with the need to travel out of the area by limited public transport or expensive taxis.
Environmental issues raised were traffic pollution, graffiti, and the vandalism and destruction of public phones and bus shelters. Regarding safety and crime, residents, both young and old, said they felt unsafe on the streets at night. Much of the crime in the area is thought to be related to alcohol, under age drinking and drugs.
However, long standing and older residents also felt the area had a strong sense of community, helped by having a happy and stable network of family and friends. There was some hostility towards new residents who were regarded as having a reputation of being “rough”. As a consequence there was some conflict between generations, and differences were also seen to be aggravated by unemployment levels experienced in the area.
( Merton, Sutton and
Wandsworth Health Authority 1998)
What is being done?Since the 1998 Northern Wards Participatory Needs
Assessment, there have been some improvements in the area
(Table 11).
TABLE 11
A new leisure centre has been built on Middleton Road and was opened to the public in 2002.
Connexions, the government’s support advice and personal development service for 13 to 19 year olds, has opened a local centre.
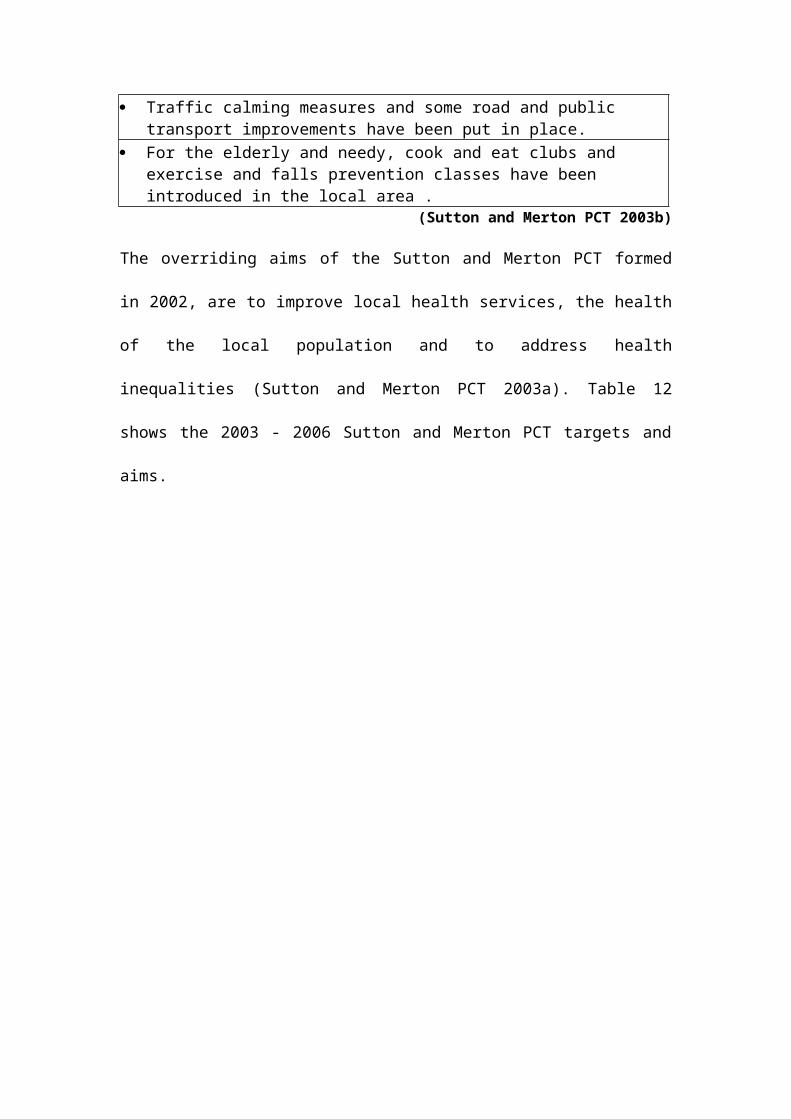
Traffic calming measures and some road and public transport improvements have been put in place.
For the elderly and needy, cook and eat clubs and exercise and falls prevention classes have been introduced in the local area .
(Sutton and Merton PCT 2003b)
The overriding aims of the Sutton and Merton PCT formed
in 2002, are to improve local health services, the health
of the local population and to address health
inequalities (Sutton and Merton PCT 2003a). Table 12
shows the 2003 - 2006 Sutton and Merton PCT targets and
aims.
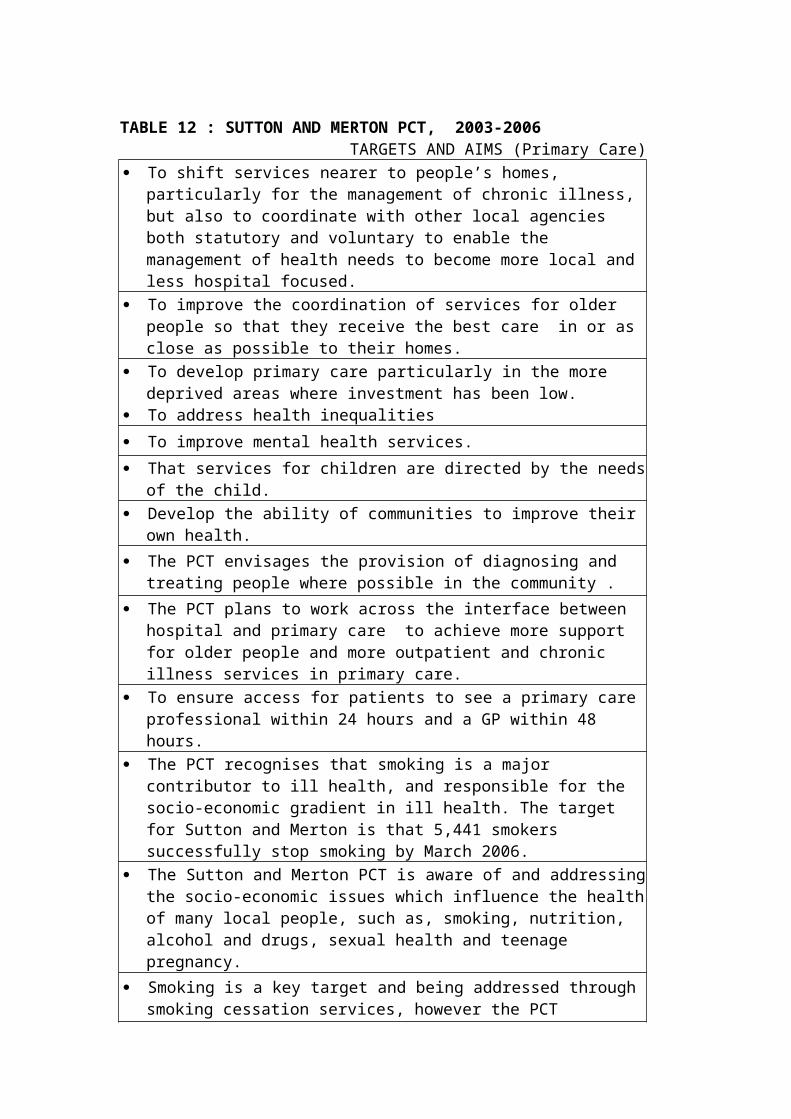
TABLE 12 : SUTTON AND MERTON PCT, 2003-2006 TARGETS AND AIMS (Primary Care) To shift services nearer to people’s homes,
particularly for the management of chronic illness, but also to coordinate with other local agencies both statutory and voluntary to enable the management of health needs to become more local and less hospital focused.
To improve the coordination of services for older people so that they receive the best care in or as close as possible to their homes.
To develop primary care particularly in the more deprived areas where investment has been low.
To address health inequalities To improve mental health services. That services for children are directed by the needs
of the child. Develop the ability of communities to improve their
own health. The PCT envisages the provision of diagnosing and
treating people where possible in the community . The PCT plans to work across the interface between
hospital and primary care to achieve more support for older people and more outpatient and chronic illness services in primary care.
To ensure access for patients to see a primary care professional within 24 hours and a GP within 48 hours.
The PCT recognises that smoking is a major contributor to ill health, and responsible for the socio-economic gradient in ill health. The target for Sutton and Merton is that 5,441 smokers successfully stop smoking by March 2006.
The Sutton and Merton PCT is aware of and addressingthe socio-economic issues which influence the healthof many local people, such as, smoking, nutrition, alcohol and drugs, sexual health and teenage pregnancy.
Smoking is a key target and being addressed through smoking cessation services, however the PCT
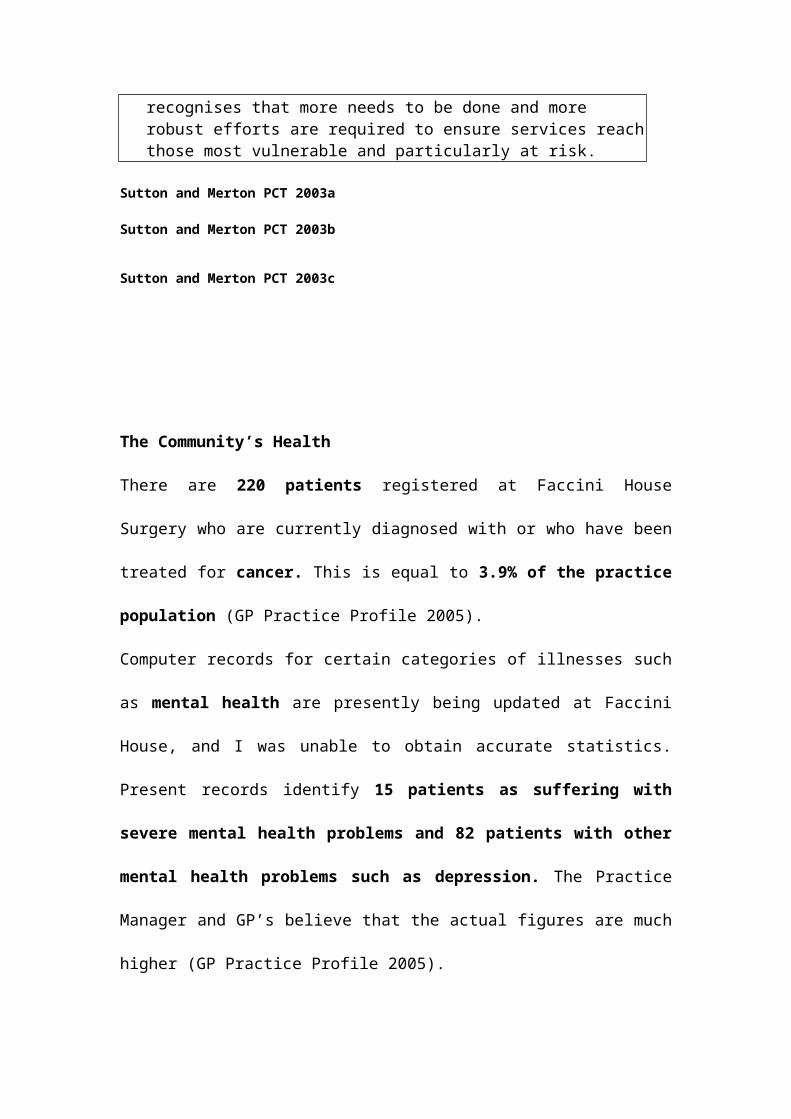
recognises that more needs to be done and more robust efforts are required to ensure services reachthose most vulnerable and particularly at risk.
Sutton and Merton PCT 2003a Sutton and Merton PCT 2003b Sutton and Merton PCT 2003c
The Community’s Health
There are 220 patients registered at Faccini House
Surgery who are currently diagnosed with or who have been
treated for cancer. This is equal to 3.9% of the practice
population (GP Practice Profile 2005).
Computer records for certain categories of illnesses such
as mental health are presently being updated at Faccini
House, and I was unable to obtain accurate statistics.
Present records identify 15 patients as suffering with
severe mental health problems and 82 patients with other
mental health problems such as depression. The Practice
Manager and GP’s believe that the actual figures are much
higher (GP Practice Profile 2005).
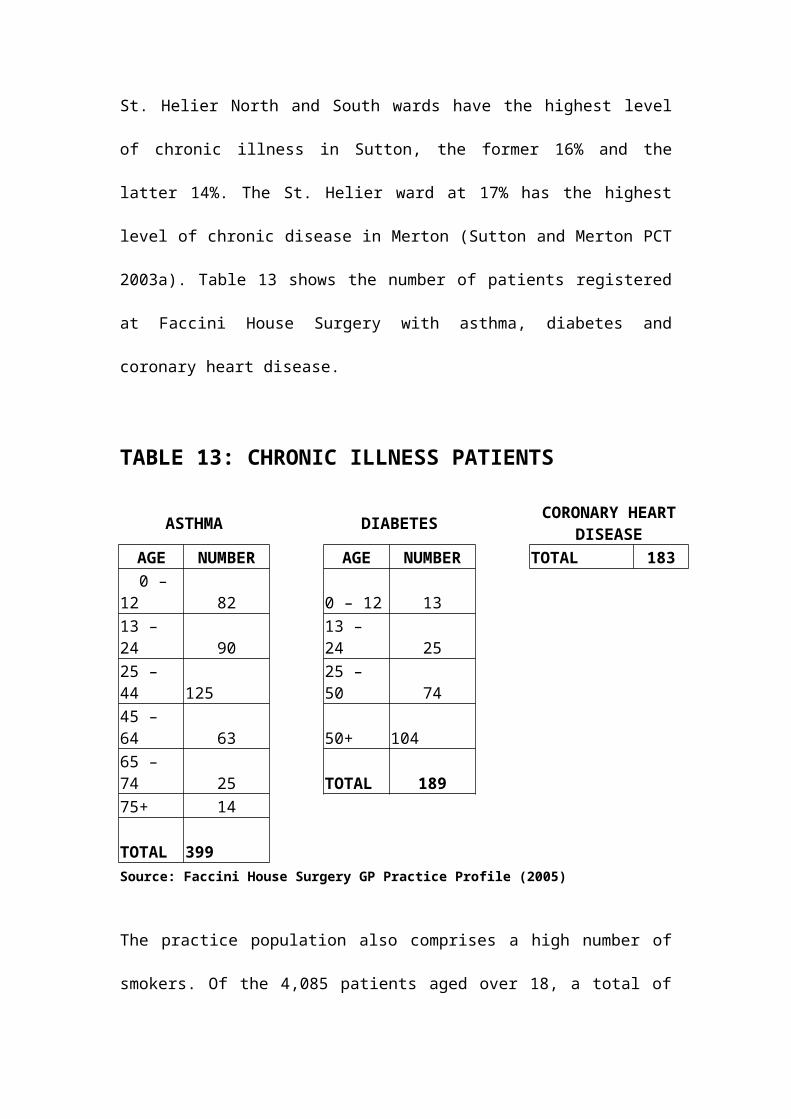
St. Helier North and South wards have the highest level
of chronic illness in Sutton, the former 16% and the
latter 14%. The St. Helier ward at 17% has the highest
level of chronic disease in Merton (Sutton and Merton PCT
2003a). Table 13 shows the number of patients registered
at Faccini House Surgery with asthma, diabetes and
coronary heart disease.
TABLE 13: CHRONIC ILLNESS PATIENTS
ASTHMA DIABETES CORONARY HEARTDISEASE
AGE NUMBER AGE NUMBER TOTAL 183 0 – 12 82 0 – 12 1313 – 24 90
13 – 24 25
25 – 44
125
25 – 50 74
45 – 64 63 50+
104
65 – 74 25 TOTAL 18975+ 14
TOTAL 399
Source: Faccini House Surgery GP Practice Profile (2005)
The practice population also comprises a high number of
smokers. Of the 4,085 patients aged over 18, a total of
1307, or 32%, are registered as smokers (GP Practice
Profile 2005). This is a higher proportion than the
national average of 26%, but close to the national
proportion of those in routine or manual employment who
smoke (31%) (DoH 2004a). Of 554 young people aged between
13 and 18 registered at the surgery, 55 smoke (GP
Practice Profile 2005), that is 10%, slightly higher than
the national average (9%) of 11 to 15 year-olds who smoke
(DoH 2004a).
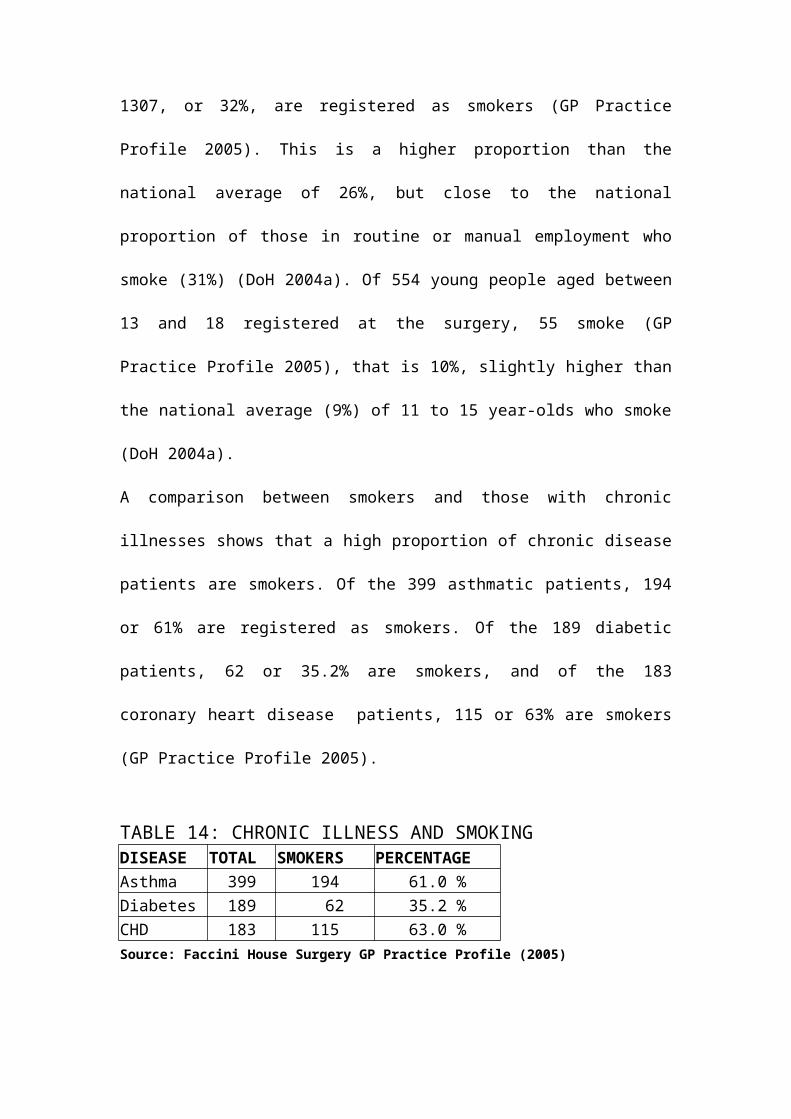
A comparison between smokers and those with chronic
illnesses shows that a high proportion of chronic disease
patients are smokers. Of the 399 asthmatic patients, 194
or 61% are registered as smokers. Of the 189 diabetic
patients, 62 or 35.2% are smokers, and of the 183
coronary heart disease patients, 115 or 63% are smokers
(GP Practice Profile 2005).
TABLE 14: CHRONIC ILLNESS AND SMOKINGDISEASE TOTAL SMOKERS PERCENTAGEAsthma 399 194 61.0 %Diabetes 189 62 35.2 %CHD 183 115 63.0 %Source: Faccini House Surgery GP Practice Profile (2005)
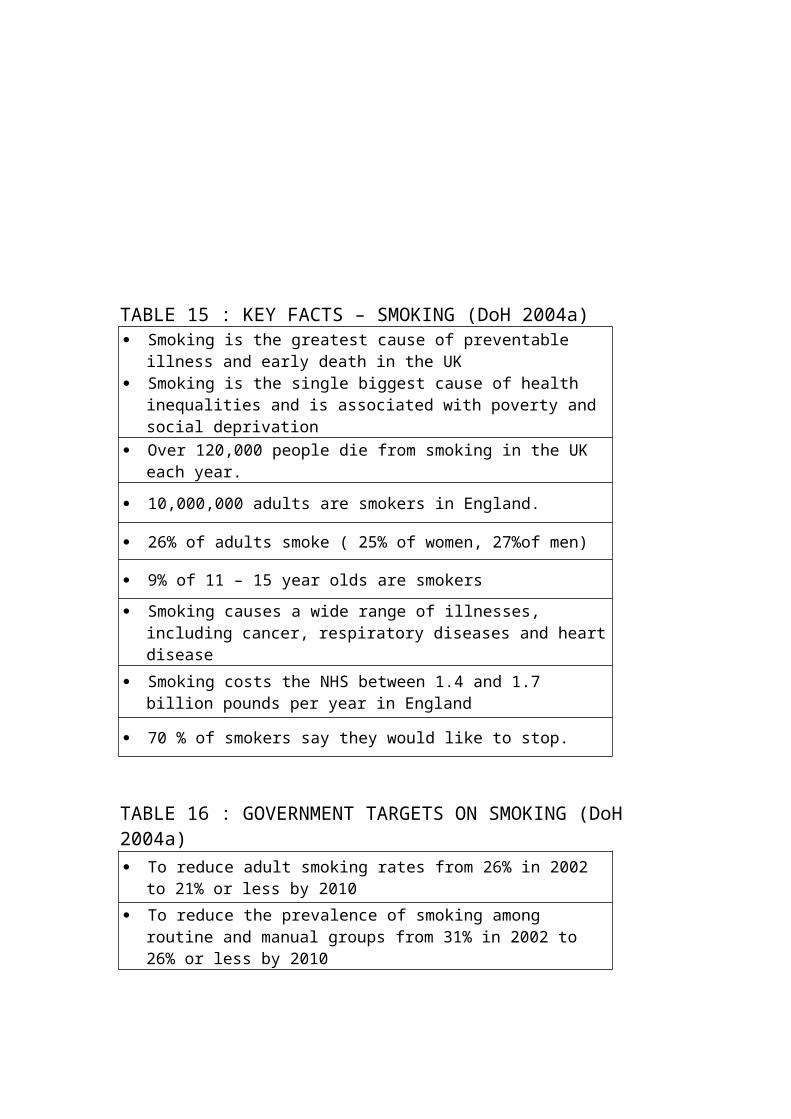
TABLE 15 : KEY FACTS – SMOKING (DoH 2004a) Smoking is the greatest cause of preventable
illness and early death in the UK Smoking is the single biggest cause of health
inequalities and is associated with poverty and social deprivation
Over 120,000 people die from smoking in the UK each year.
10,000,000 adults are smokers in England.
26% of adults smoke ( 25% of women, 27%of men)
9% of 11 – 15 year olds are smokers Smoking causes a wide range of illnesses,
including cancer, respiratory diseases and heartdisease
Smoking costs the NHS between 1.4 and 1.7 billion pounds per year in England
70 % of smokers say they would like to stop.
TABLE 16 : GOVERNMENT TARGETS ON SMOKING (DoH 2004a) To reduce adult smoking rates from 26% in 2002
to 21% or less by 2010 To reduce the prevalence of smoking among
routine and manual groups from 31% in 2002 to 26% or less by 2010
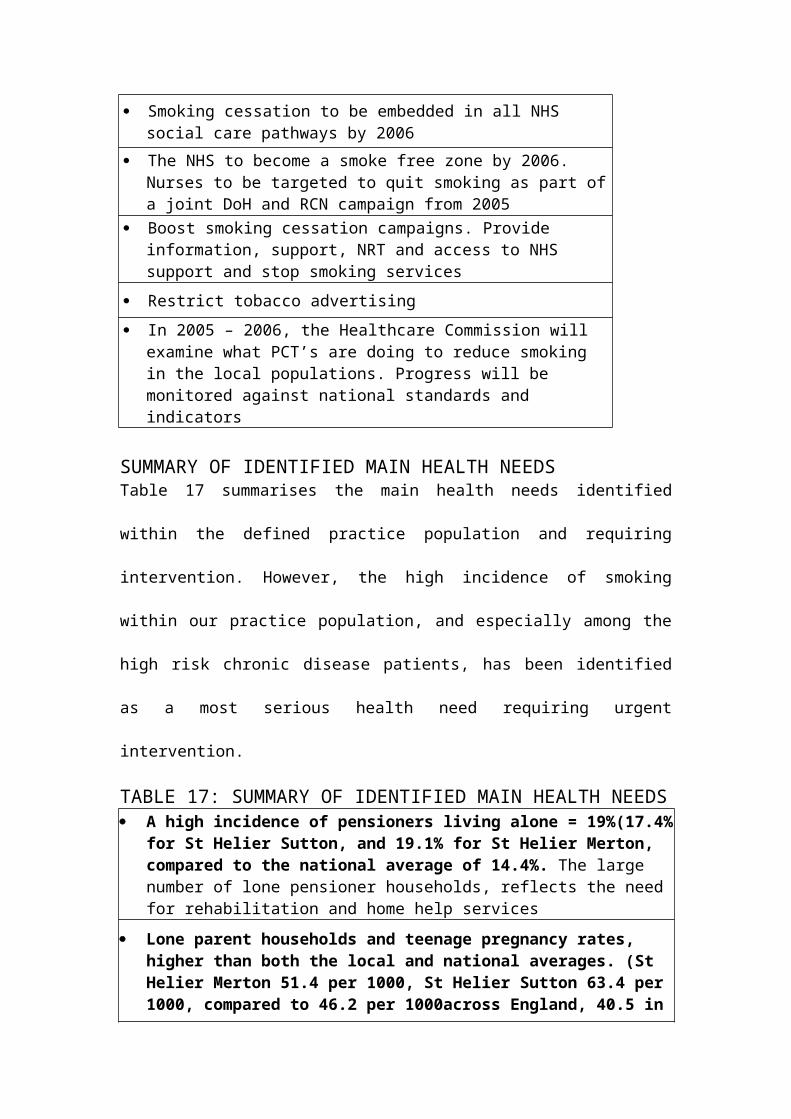
Smoking cessation to be embedded in all NHS social care pathways by 2006
The NHS to become a smoke free zone by 2006. Nurses to be targeted to quit smoking as part ofa joint DoH and RCN campaign from 2005
Boost smoking cessation campaigns. Provide information, support, NRT and access to NHS support and stop smoking services
Restrict tobacco advertising In 2005 – 2006, the Healthcare Commission will
examine what PCT’s are doing to reduce smoking in the local populations. Progress will be monitored against national standards and indicators
SUMMARY OF IDENTIFIED MAIN HEALTH NEEDSTable 17 summarises the main health needs identified
within the defined practice population and requiring
intervention. However, the high incidence of smoking
within our practice population, and especially among the
high risk chronic disease patients, has been identified
as a most serious health need requiring urgent
intervention.
TABLE 17: SUMMARY OF IDENTIFIED MAIN HEALTH NEEDS A high incidence of pensioners living alone = 19%(17.4%
for St Helier Sutton, and 19.1% for St Helier Merton, compared to the national average of 14.4%. The large number of lone pensioner households, reflects the need for rehabilitation and home help services
Lone parent households and teenage pregnancy rates, higher than both the local and national averages. (St Helier Merton 51.4 per 1000, St Helier Sutton 63.4 per 1000, compared to 46.2 per 1000across England, 40.5 in
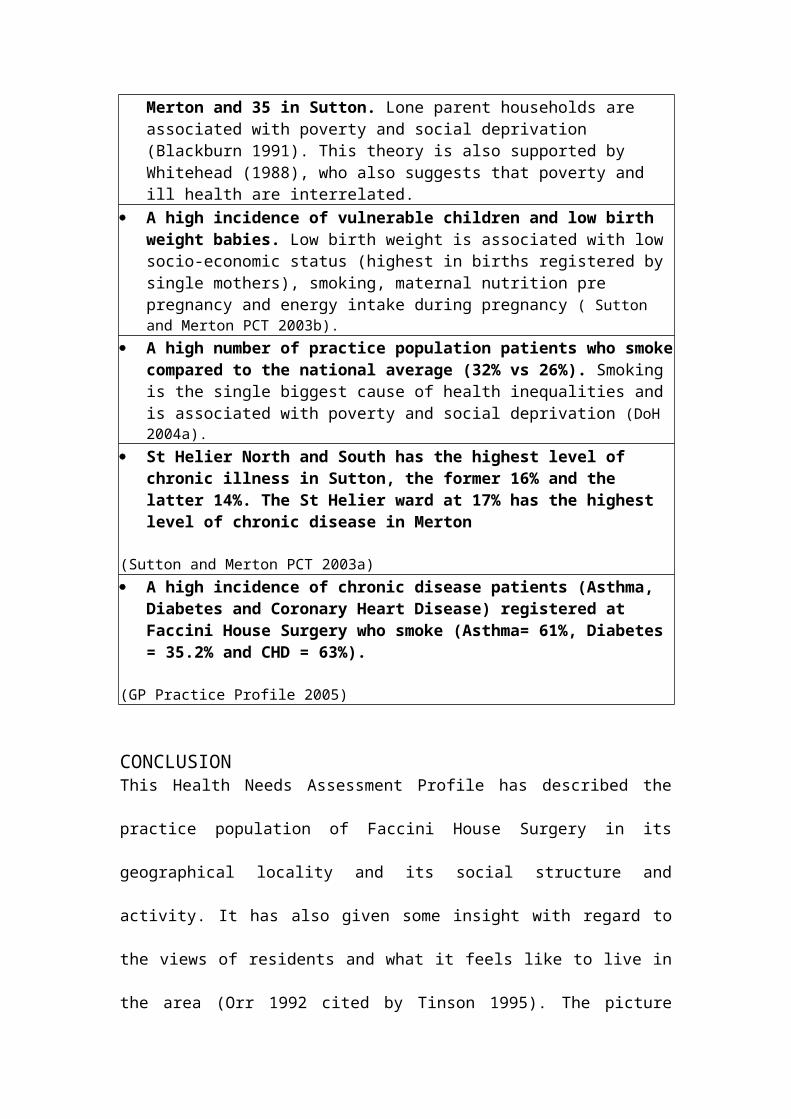
Merton and 35 in Sutton. Lone parent households are associated with poverty and social deprivation (Blackburn 1991). This theory is also supported by Whitehead (1988), who also suggests that poverty and ill health are interrelated.
A high incidence of vulnerable children and low birth weight babies. Low birth weight is associated with low socio-economic status (highest in births registered by single mothers), smoking, maternal nutrition pre pregnancy and energy intake during pregnancy ( Sutton and Merton PCT 2003b).
A high number of practice population patients who smokecompared to the national average (32% vs 26%). Smoking is the single biggest cause of health inequalities and is associated with poverty and social deprivation (DoH 2004a).
St Helier North and South has the highest level of chronic illness in Sutton, the former 16% and the latter 14%. The St Helier ward at 17% has the highest level of chronic disease in Merton
(Sutton and Merton PCT 2003a) A high incidence of chronic disease patients (Asthma,
Diabetes and Coronary Heart Disease) registered at Faccini House Surgery who smoke (Asthma= 61%, Diabetes = 35.2% and CHD = 63%).
(GP Practice Profile 2005)
CONCLUSIONThis Health Needs Assessment Profile has described the
practice population of Faccini House Surgery in its
geographical locality and its social structure and
activity. It has also given some insight with regard to
the views of residents and what it feels like to live in
the area (Orr 1992 cited by Tinson 1995). The picture
emerging from the collated data is one of an area of
relatively high social deprivation. From the locally
relevant data a number of comparative needs can be
identified, e.g. with regard to some key health
determinants such as education, transport, housing and
amenities, i.e. the subsystems mentioned above (Tinson
1995). A Participatory Needs Assessment by Merton, Sutton
and Wandsworth Health Authority (1998) has described both
felt and expressed needs.
This profile has also identified normative needs with
regard to the health of the practice population. One of
those needs is the high number of chronic disease
patients who are also smokers, thus exacerbating their
condition. While Tinson (1995) cautions that normative,
or professional, assessments can be problematic because
they do not always involve the client or community, the
identified health need is clearly one to be addressed
under the current government’s health targets, which
describe smoking as the UK’s single greatest cause of
preventable illness and early death and point out that 70
per cent of smokers say they want to give up (DoH 2004a).
“Smoking Kills – A White Paper on Tobacco” (1998)
describes smoking as the most identifiable factor
contributing to the gap in healthy life expectancy
between those most in need and those most advantaged (DoH
1998). Smoking is the single biggest cause of health
inequalities and is associated with poverty and social
deprivation (DoH 2004a).
“Liberating the Talents” (DoH 2002) highlights three main
core functions for nurses in primary care. As well as
being a point of first contact for patients and taking a
lead role in chronic disease and minor illness
management, they also have a responsibility to deliver
health protection and promotion programmes and the
various National Service Frameworks. The identified
community health need, i.e. smoking among the high-risk
chronic disease patients at Faccini House Surgery,
relates to the core functions of chronic disease
management, health protection and promotion and
delivering NSF’s (DoH 2001, DoH 2003) and will be
addressed by a health promotion intervention in the
second part of this paper.
(2192 words excluding tables)
REFERENCES
Acheson (Chairman) 1998 Public Health in England HMSO, London
Blackburn C 1991 Poverty and Health: Working with families Open
University Press, Milton Keynes
Blackie C (ed.) 1998 Community Health Care Nursing Churchill
Livingstone, Edinburgh
Department of Health 1998 Smoking Kills - A White Paper on Tobacco
HMSO, London
Department of Health 2000 The NHS Plan: A Plan for Investment, a
Plan for Reform HMSO, London
Department of Health 2001 National Service Framework for Coronary
Heart Disease HMSO, London
Department of Health 2002 Liberating the Talents HMSO, London
Department of Health 2003 National Service Framework for Diabetes
HMSO, London
Department of Health 2004a Choosing health. Making healthy choices
easier. Executive summary HMSO, London
Department of Health 2004b Tackling Health Inequalities: A
Programme for Action HMSO, London
Ewles L, Simnett I 2003 Promoting Health: A Practical Guide 5th
ed. Bailliere Tindall, London
Faccini House Surgery 2004 Health Visitor Caseload 2004
Middleton Rd. Morden, SM4 6RS
Faccini House Surgery 2005 GP Practice Profile 2005 (compiled by
T Lowry-Lehnen) Middleton Road, Morden, SM4 6RS
Merton, Sutton and Wandsworth Health Authority 1998
Northern Wards Participatory Needs Assessment. Executive summary
Merton, Sutton and Wandsworth Health Authority,
London
Merton Teenage Pregnancy Unit 2004 Briefing paper on teenage
pregnancy in the London Borough of Merton Sutton and
Merton Primary Care Trust, London
Naidoo J, Wills J 2000 Health Promotion: Foundations for Practice 2nd
ed. Bailliere Tindall, London
Office of National Statistics 2002 Census 2001 HMSO, London
Ofsted 2004 Statistics (online) Available from: www.
ofsted.gov.uk (Accessed on 18 January 2005)
Sutton and Merton Primary Care Trust 2002 GLA Scrutiny of
Access to Primary Care in London Sutton and Merton Primary
Care Trust, London
Sutton and Merton Primary Care Trust 2003a Public Health
Annual Report 2002-2003 Sutton and Merton Primary Care
Trust, London
Sutton and Merton Primary Care Trust 2003b Local Delivery Plan
2003-2006 For Public Use Sutton and Merton Primary Care
Trust, London
Sutton and Merton Primary Care Trust 2003c Business Plan 2004
– 2005 Sutton and Merton Primary Care Trust, London
Sutton Teenage Pregnancy Unit 2002 Under 18 conception rates
1998-2002 Sutton and Merton Primary Care Trust,
London
Tannahill A 1985 What is Health Promotion? Health Education
Journal 44 (4): 167-168
Tinson S 1995 Assessing health need: a community
perspective In: Arnold Community Nursing: Dimensions
and Dilemmas Cain Hyde Hawkins: 144-165
Twinn S, Dauncey J, Carnell J 1990 The Process of Health Profiling
CPHVA, London
Whitehead M 1998 The Health Divide: Health Education Council,London
Windshield Survey 2005 St Helier Estate (compiled by T Lowry-
Lehnen) Sutton and Merton
World Health Organisation 1998 Health Promotion Glossary WHO, Geneva
PUBLIC HEALTHPART TWO: HEALTH PROMOTION PROPOSAL
CONTENTS Page
1. Introduction
1. Context and Theoretical Framework
2. Health Promotion Model – Tannahill (1985)
3. Intervention: Planning and Evaluation Framework
(Ewles & Simnett 2003)
4. The intervention
4. Needs and Priorities
4. Aims and Objectives
7. Best Way To Achieve Aims
8. Objectives and Methods
9. Ethical issues
9. Resources
10. Roles and Responsibilities
11. Evaluation Strategy
12. Action Plan
13. Conclusion
15. References
Appendix 1 TABLE 6: Action Plan (Intervention) Patient invitation letter Letter to PCT, requesting funding Proposed budget Poster Patient feedback / Evaluation questionnaire
Appendix 2 Determinants of health Jarman scores - Sutton Statistics St Helier Sutton and St Helier Merton Indices of Deprivation 2000 Sutton and Merton
PUBLIC HEALTH
Theresa Lowry-LehnenGeneral Practice Nurse
PART TWO: HEALTH PROMOTION PROPOSAL
INTRODUCTION
The Health Needs Assessment Profile in Part One has
identified smoking among the high risk groups (i.e.
patients with the chronic illnesses, asthma, coronary
heart disease and diabetes) within the GP practice
population of Faccini House Surgery as a major community
health need requiring intervention. Part Two of this
paper will devise and critically appraise a clinic-based
smoking cessation intervention, targeting chronic disease
patients within this GP practice population. It will use
the health promotion model suggested by Tannahill (1985)
and the planning and evaluation framework devised by
Ewles and Simnett (2003). The devised smoking cessation
action plan (Table 6, Appendix 1) also incorporates the
‘stages of change’ model developed by Prochaska and
DiClemente (1984 cited by Naidoo & Wills 2000).
CONTEXT AND THEORETICAL FRAMEWORK
Health Promotion – Definition
“Health Promotion” can mean a number of quite different
activities, and practitioners must be aware of the
available options (Naidoo & Wills 2000). The World Health
Organisation defines health promotion as the process of
enabling people to increase control over, and to improve,
their health (WHO 1984). The current government speaks of
delivering sustained improvement to the health of the
people by responding to people’s concerns about their
health with practical support on their own terms and by
providing the context and environment needed to make real
progress (DoH 2004a). Naidoo and Wills (2000) point out
that the phrase “making the healthier choice the easier
choice” has come to encapsulate the meaning of health
promotion. However, Tannahill (1985) claims that the term
“health promotion” has acquired so many meanings as to
become meaningless. A more detailed look at an
appropriate health promotion model will help to provide a
focus and a rationale for the proposed intervention.
Health Promotion Model – Tannahill (1985)
Tannahill (1985: 167) suggests reserving health promotion
“to define clearly a realm of health-enhancing activities”. He
proposes a model in which health promotion is seen as
comprising health education, prevention and protection as
three overlapping spheres of activity. Education is seen
as a communication activity aimed at enhancing well-being
and preventing or reducing ill health in individuals and
groups. Preventive action can take the form of prevention
of an illness or of avoidable complications of an already
established disease. Health protection is defined as
“legal or fiscal controls, other regulations or policies,
or voluntary codes of practice” (Tannahill 1985: 168).
While in an intervention such as the one proposed here
not all parts of Tannahill’s model may have equal weight,
it allows the practitioner to be aware of the possible
different activities and available options (Naidoo &
Wills 2000). It also enhances an awareness of current
policies and national service frameworks (DoH 2001, DoH
2003) and how the proposed intervention fits into
government policies and targets regarding smoking as the
“single greatest cause of preventable illness and early
death” (DoH 2004a).
Tannahill (1985) stresses that empowerment of individuals
and groups within the community is an important objective
for health promotion. He warns against a “top down”
approach and advocates a participatory process.
It should be pointed out that no health promotion model
can be seen in isolation. There is always a certain
overlap with other models, such as Caplan and Holland
(1990 cited by Naidoo & Wills 2000) and Beattie (1991
cited by Naidoo & Wills 2000). Similarly, the various
possible approaches to health promotion, such as medical,
behaviour change, educational, empowerment and social
change (Naidoo & Wills 2000), are not mutually exclusive
but should complement each other.
Intervention – Planning and Evaluation Framework

For the purpose of the proposed intervention the planning
and evaluation framework suggested by Ewles and Simnett
(2003) will be used. It sets out a seven-stage cycle. I
have adapted the planning process to include ethical
considerations, as shown in Table 1.
Table 1: Planning/Evaluation Cycle (adapted from Ewles &
Simnett 2003)
Identify needs and priorities Set aims and objectives Decide the best way of
achieving aims Consider ethical issues Identify resources Plan evaluation methods Set an action plan Implement plan, including
evaluation
THE INTERVENTION
Needs and priorities
The Health Needs Assessment Profile in Part One has
identified smoking cessation as a health need to be
addressed. In particular, the profile has identified a
high proportion of smokers among the chronic illness
patients at Faccini House Surgery. Smoking exacerbates
such illnesses as diabetes, respiratory and coronary
heart disease (DoH 2004a). The priority for this
intervention will therefore be smoking cessation targeted
at the chronic disease patients within the Faccini House
Surgery practice population.
While it may be pointed out that a cessation intervention
should be aimed at all smokers, not just those in high-
risk groups, the health belief model (Becker & Maiman
1975 cited by King 1984) may be used to support a more
targeted approach: As King (1984) states, most people do
not tend to think in terms of abstract statistics but
rather they think of concrete examples. It is hoped that
a cessation programme aimed at the identified high-risk
groups may allow a more targeted, and therefore, it is
hoped, more successful approach.
Aims and Objectives
According to Ewles and Simnett (2003) aims are broad
statements of the outcome one hopes to achieve while
objectives are much more specific, making the setting of
them a critical stage in the planning process.
The overall aim of this intervention is to address the
identified health need, i.e. to reduce the incidence of
smoking among chronic disease patients in line with
general government and local PCT targets (DoH 1998,
2004a, 2004b, Sutton and Merton PCT 2003a, 2003b, 2003c).
With regard to Tannahill’s (1985) model, this overall aim
should be approached in a comprehensive way. The aspect
of health protection can be seen in the context of
current government policies and targets with regard to
smoking cessation (DoH 2004a). Within this context, this
proposed intervention devises an educational approach in
the form of a communication activity aimed at enhancing
the well-being and preventing or reducing the ill health
in individuals and groups. The preventive aspect can be
seen in the attempt to avoid complications of an already
established disease.
It is possible to identify aspects of a number of health
promotion approaches (Naidoo & Wills 2002). There is a
medical component in that those at special risk have been
identified by the practitioner. Individuals may be
encouraged to take responsibility for their own health
and choose a healthier lifestyle in an approach aimed at
behaviour change. There is also the educational element
trying to increase knowledge and skills about healthier
lifestyles. The overall aim may be achieved by working
with clients within the community, thus strengthening
their empowerment (Naidoo & Wills 2002).
Objectives must be set in order to enable the
practitioner to work towards the overall aim. Ewles and
Simnett (2003) stress that objectives are the desired
outcome of an intervention and that, while challenging,
they should be attainable, relevant and as measurable as
possible. On the basis of Tannahill’s (1985) model, the
objectives should cover education, prevention and
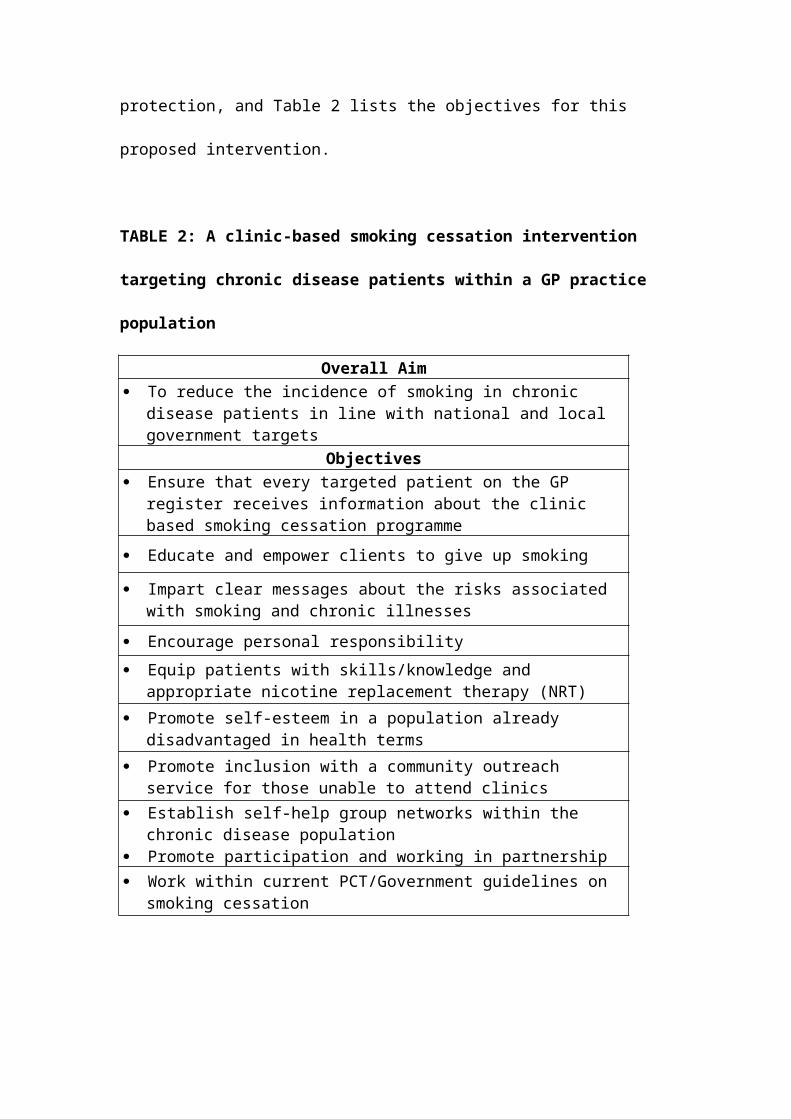
protection, and Table 2 lists the objectives for this
proposed intervention.
TABLE 2: A clinic-based smoking cessation intervention
targeting chronic disease patients within a GP practice
population
Overall Aim To reduce the incidence of smoking in chronic
disease patients in line with national and local government targets
Objectives Ensure that every targeted patient on the GP
register receives information about the clinic based smoking cessation programme
Educate and empower clients to give up smoking
Impart clear messages about the risks associated with smoking and chronic illnesses
Encourage personal responsibility Equip patients with skills/knowledge and
appropriate nicotine replacement therapy (NRT) Promote self-esteem in a population already
disadvantaged in health terms Promote inclusion with a community outreach
service for those unable to attend clinics Establish self-help group networks within the
chronic disease population Promote participation and working in partnership Work within current PCT/Government guidelines on
smoking cessation
Best Way to Achieve Aims
In choosing methods for an intervention, one must
consider whether they are appropriate and effective,
acceptable to clients and others involved and financially
viable (Ewles & Simnett 2003).
Working with individuals and small groups has been
identified as effective for changing attitudes, feelings
and behaviour (Ewles & Simnett 2003).
The objectives identified in the previous section can be
listed under such headings as health awareness,
improvement of knowledge, empowerment, changing attitudes
and behaviour, and societal change, which also correspond
to the three spheres of activity identified in
Tannahill’s (1985) model. Adapting the aims and methods
identified by Ewles and Simnett (2003), the chosen
methods for the objectives in this intervention are group
work, group teaching and talks with the opportunity of
one-to-one counselling and the appropriate use of NRT,
audio visual and written materials. Table 3 groups the
objectives under overall goals as well as activities

corresponding to Tannahill’s (1985) model and shows the
chosen methods.
TABLE 3: Objectives and Methods (Adapted from Ewles & Simnett 2003 and Tannahill 1985)
GOALS / ACTIVITY Health Awareness/ Promotion Education Knowledge Empowerment Changing attitudes and behaviour Health protection and illness prevention Reducing inequalities Participation and partnership working Societal change/protection
METHODS

Specialist nurses: Talks, education, specialist knowledge
Expert patients: Motivate, support, encourage, role models
Counselling: Change behaviour/attitudes, support, motivate
Outreach nurse: Visit patients unable to attend in the community
Group-work : Patient networking and forming self help groups
Literature: Education, information
Nicotine replacement therapyOBJECTIVES
Ensure every targeted patient receives information about local smoking cessation programme, impart clear messages about the risks associated with smoking and chronic conditions
Equip and empower patients with skills/knowledge and appropriate nicotine replacement therapy (NRT)
Promote inclusion with a community outreach service forthose unable to attend clinics
Educate and empower clients to give up smoking Encourage personal responsibility Promote self-esteem Establish self-help group networks within the chronic
disease population Work within current PCT/Government guidelines on
smoking cessation
Ethical Issues
Having set aims and objectives and having decided on the
best way of achieving them, it is appropriate at this
point to adapt Ewles and Simnett’s (2003) planning and
evaluation framework by including a consideration of
ethical issues. As Jenkins and Emmett (1997) point out,
nurses may assume that their perceptions and assessments
of a patient’s health is accurate and corresponds with
those of the patient, but there is a danger of
manipulating a patient under the guise of health
promotion. Not only is it important to establish what
health promotion itself is but also what impact nurses’
own perceptions may have on the implementation of a
health intervention (Gott & O’Brien 1990). If the concept
of empowerment is to be taken seriously, then the
patient’s autonomy must be respected. Group work and
group teaching are appropriate methods to allow patients
a say in matters which concern them. Those methods also
allow the practitioner to take into account the fact that
health education cannot be effective without
consideration of patients’ beliefs and attitudes. The
“health belief model” can help to illustrate how a
patient’s beliefs can influence his health-related
behaviour (King 1984). In the context of this
intervention it means that it must be taken into account
how patients may perceive risks and benefits.
Resources
As has already been demonstrated, the proposed
intervention fits in with the priorities and targets set
by current government policy (DoH 2004a). In terms of
material resources, use will be made of nicotine
replacement therapy, written material /literature, audio
and visual aids and display materials. It is also
important to identify existing local self-help groups for
the targeted chronic illnesses as well as voluntary
organisations such as the British Heart Foundation,
Diabetes UK and Asthma UK. The people involved in the
intervention (clients and staff) and their commitment,
time, skills, knowledge and expertise are the most
important resources. Table 4 proposes roles and
responsibilities.
TABLE 4: Roles and Responsibilities
Practice Nurses Co-ordinate the cessation programme
Point of contact/support
Overall responsibility Budgets/ Timetable
Evaluate programme
Specialist Nurses Respiratory nurse specialist Education CHD nurse specialist Specialist
information Diabetes nurse specialist Empowerment
GP Prescriptions for NRT Point of contact and support
Expert patients(CHD, Asthma, Diabetes) Empowerment
Motivation/encouragementRole models
Smoking cessation counsellor NRT adviceOne-to-one and group
counsellingEducation /Support/
Encouragement
Outreach nurse Communityoutreach visits Support /Education/ Counselling
Patients Participation Share experiences
Provide ongoing supportForm own support networksPart of decision and evaluation
process
Practice manager HousekeepingHealth and safety
Administrative staff Letters/posters/information Phone calls Point of contact
Evaluation Strategy
In setting out an evaluation strategy, it is worthwhile
assessing both the outcome and the process of the health
intervention (Ewles & Simnett 2003). While it may be
difficult to measure the outcome for some of the stated
objectives, such as encouraging personal responsibility
and promoting self-esteem, there are ways in which the
overall objective can be measured to some degree. Given
the nature of the proposed intervention, two methods of
measuring the outcome are most appropriate. Firstly,
feedback will be sought from the participants, patients
as well as practitioners, both in a more informal way
such as a group feedback session and through a more
formal questionnaire (Appendix 1). Secondly, and most
importantly given the overall aim of the intervention,
participating patients will be monitored on a voluntary
basis in order to record whether they have given up
smoking. It is suggested that the patients will be
approached after one month, three months, six months and
twelve months to update the record of their progress. For
those patients who have given up smoking their health
indicators and their own perceptions about their health
may be recorded at future appointments.
With regard to evaluating the process, it is suggested
that all input in terms of time, money and materials will
be recorded, enabling the course facilitator to set the
costs against the benefits of the intervention. In
addition, the facilitator should keep a diary to allow
self-evaluation. Finally, feedback from clients and other
practitioners will be sought, both at the end of group
sessions and through a suggestion box (Ewles & Simnett
2003).
TABLE 5: Evaluation Strategy
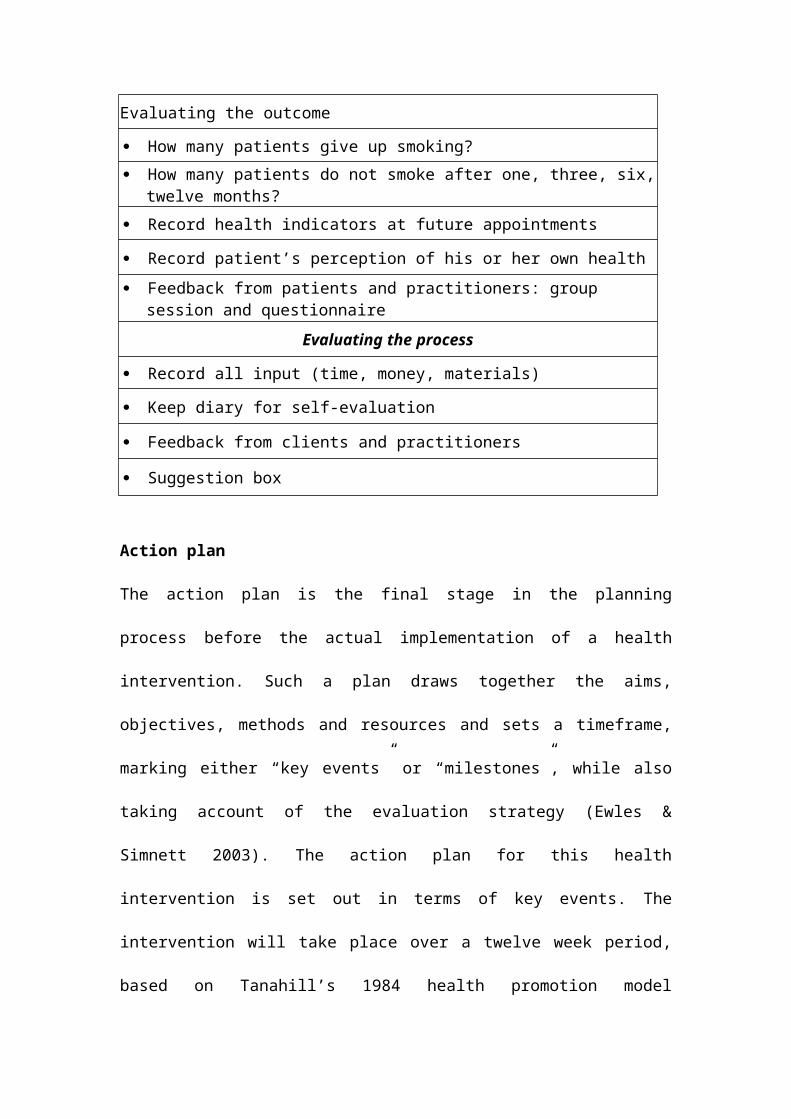
Evaluating the outcome
How many patients give up smoking? How many patients do not smoke after one, three, six,
twelve months? Record health indicators at future appointments
Record patient’s perception of his or her own health Feedback from patients and practitioners: group
session and questionnaireEvaluating the process
Record all input (time, money, materials)
Keep diary for self-evaluation
Feedback from clients and practitioners
Suggestion box
Action plan
The action plan is the final stage in the planning
process before the actual implementation of a health
intervention. Such a plan draws together the aims,
objectives, methods and resources and sets a timeframe,
marking either “key events” or “milestones”, while also
taking account of the evaluation strategy (Ewles &
Simnett 2003). The action plan for this health
intervention is set out in terms of key events. The
intervention will take place over a twelve week period,
based on Tanahill’s 1984 health promotion model
(education, prevention and protection) and incorporating
the “Stages of Change” model developed by Prochaska and
DiClemente (1984, cited by Naidoo & Wills 2000). This
model describes how clients change their behaviour
through various stages ranging from pre-contemplation and
contemplating change to then making the change (action
stage) before a final stage of maintenance, at which the
new behaviour is sustained and the client moves into a
healthier lifestyle. Table 6 (Appendix 1) sets out the
action plan and key events within a set timeframe.
CONCLUSION
This paper has devised and critically appraised a clinic-
based smoking cessation intervention, targeting chronic
disease patients within a GP practice population. The
intervention concerns one of the main needs identified in
the Health Needs Assessment Profile undertaken in Part
One. Using Tannahill’s (1985) health promotion model, the
planning and evaluation framework suggested by Ewles and
Simnett (2003), and the ‘stages of change’ model
developed by Prochaska and DiClemente (1984 cited by
Naidoo & Wills 2000), the intervention has been designed
to enable people to increase control over, and to
improve, their health, thus reflecting the World Health
Organisation’s definitions of health promotion (WHO 1984)
and the “new public health” (WHO 1998). The intervention
also takes into account current government policies by
responding to people’s concerns about their health with
practical support on their own terms and by providing the
context and environment needed to make real progress (DoH
2004a). In a wider socio-political context, the current
government describes health promotion as one of the key
roles of primary care nurses (DoH 2002) and the health
service as a whole (DoH 2000, DoH 2004b). In that
respect, the Health Needs Assessment Profile and the
health promotion intervention can also be seen as a
contribution to delivering relevant National Service
Frameworks (DoH 2001, DoH 2003).
Above all, the intervention aims not only to improve the
health of patients but also to empower them to make the
right choices about their own health, providing them with
the appropriate knowledge and guidance. This is made
possible by taking into account the three overlapping
spheres of activity – education, prevention and
protection - identified by Tannahill (1985) with regard
to health promotion. That health promotion should be a
comprehensive concept is reflected in the fact that the
intervention in this paper includes elements of various
approaches, medical, behaviour change, educational and
empowerment, as described by Naidoo and Wills (2000).
Using theoretical models and frameworks to explore and
address practice-based health needs and interventions
allows practitioners to gain a deeper understanding of
the concepts of public health. These models and
frameworks are useful tools for translating the aims of
health promotion, protection and illness prevention into
practice. This in turn makes it possible to enhance
practice with the ultimate aims of reducing inequalities,
improving health and providing better outcomes for
individuals and society as a whole.
REFERENCES
Department of Health 1998 Smoking Kills - A White Paper on Tobacco
HMSO, London
Department of Health 2000 The NHS Plan: A Plan for Investment, a
Plan for Reform HMSO, London
Department of Health 2001 National Service Framework for Coronary
Heart Disease HMSO, London
Department of Health 2002 Liberating the Talents HMSO, London
Department of Health 2003 National Service Framework for Diabetes
HMSO, London
Department of Health 2004a Choosing health. Making healthy choices
easier. Executive summary HMSO, London
Department of Health 2004b Tackling Health Inequalities: A
Programme for Action HMSO, London
Ewles L, Simnett I 2003 Promoting Health: A Practical Guide 5th
ed. Bailliere Tindall, London
Gott M, O’Brien M 1990 Attitudes and beliefs in health
promotion Nursing Standard 5 (2): 30-32
Jenkins D, Emmett S 1997 The ethical dilemma of health
education Professional Nurse 12 (6): 426-428
King J 1984 The health belief model Nursing Times 24
October: 53-55
Naidoo J, Wills J 2000 Health Promotion: Foundations for Practice 2nd
ed. Bailliere Tindall, London
Sutton and Merton Primary Care Trust 2003a Public Health
Annual Report 2002-2003 Sutton and Merton Primary Care
Trust, London
Sutton and Merton Primary Care Trust 2003b Local Delivery Plan
2003-2006 For Public Use Sutton and Merton Primary Care
Trust, London
Sutton and Merton Primary Care Trust 2003c Business Plan 2004
– 2005 Sutton and Merton Primary Care Trust, London
Tannahill A 1985 What is Health Promotion? Health Education
Journal 44 (4): 167-168
World Health Organisation 1984 Health Promotion: A Discussion
Document on the Concept and Principles WHO Regional Office
for Europe, Copenhagen

World Health Organisation 1998 Health Promotion Glossary WHO,
Geneva
Top Related
Copyright © 2022 FDOKUMEN

