







Bahasa
Halaman
Hukum

Kidney International, Vol. 61 (2002), pp. 1064–1078
Propionyl-l-carnitine prevents renal function deteriorationdue to ischemia/reperfusion
MARILENA MISTER, MARINA NORIS, JAROSLAW SZYMCZUK, NADIA AZZOLLINI, SISTIANA AIELLO,MAURO ABBATE, LECH TROCHIMOWICZ, ELENA GAGLIARDINI, ARDUINO ARDUINI,NORBERTO PERICO, and GIUSEPPE REMUZZI
Department of Immunology and Clinics of Organ Transplantation, Mario Negri Institute for Pharmalogical Research, Bergamo,Sigma-Tau, Pomezia, Roma, Italy
pletely prevented polymorphonuclear cell graft infiltration andPropionyl-L-carnitine prevents renal function deteriorationreduced tubular injury at 16 hours post-transplant.due to ischemia/reperfusion.
Conclusions. These data indicate that propionyl-l-carnitineBackground. Ischemia-reperfusion injury after organ trans-is of value in preventing decline of renal function that occursplantation is a major cause of delayed graft function. Preventionduring ischemia-reperfusion. The beneficial effect of propionyl-of post-transplant ischemia acute renal failure is still elusive.l-carnitine possibly relates to lowering lipid peroxidation andMethods. The present study was designed to examine whetherfree radical generation that eventually results in the preserva-propionyl-l-carnitine, an acyl derivative of carnitine involvedtion of tubular cell structure. The efficacy of propionyl-l-carni-in fatty acid oxidation pathway and adenosine 5!-triphosphatetine to modulate ischemia-reperfusion injury in these models(ATP) generation of mitochondria, prevented renal functionopens new perspectives for preventing post-transplant delayeddeterioration and structural injury induced by ischemia-reper-
fusion in an ex vivo rat model of isolated perfused kidney graft function.(IPK) preparation and in vivo in a model of syngeneic kidneytransplantation.
Results. In the model of ischemia (20 or 40 min)/reperfusion Transplantation of a solid organ from a donor has(90 or 70 min) in IPK, untreated kidneys showed a marked emerged as a treatment option for many diseases. Both thereduction of glomerular filtration rate (GFR) and renal perfu-
interruption and subsequent restoration of blood flow aresate flow (RPF) as compared to baseline, when perfusion wasoften the cause of tissue injury in any transplanted or-established by restoring effective perfusion pressure to 100
mm Hg. Exposure of kidneys to propionyl-l-carnitine before gan. Despite the progress in surgical techniques and pres-establishing the ischemia insult to tissue, largely prevented ervation conditions [1], every transplantation starts withrenal function impairment. Pre-exposure of ischemic kidneys an inevitable insult of the graft: the ischemia-reperfusionto propionyl-l-carnitine largely reduced the percent of lactate
syndrome. Ischemia-reperfusion injury may be consid-dehydrogenase (LDH), a cell injury marker, released into theperfusate after reperfusion as compared to untreated ischemic ered an inflammatory and vasomotor phenomenon. In re-kidneys. Histologic findings showed very mild post-ischemic nal transplant, delayed graft function is a relatively com-lesions in kidneys exposed to propionyl-l-carnitine as com- mon complication of this syndrome, occurring betweenpared to untreated ischemic kidneys. Immunohistochemical
20% and 60% of cadaveric kidney recipients [2]. It makesdetection of 4-hydroxynonenal protein adduct, a major productthe diagnosis of rejection more difficult, prolongs hospi-of lipid peroxidation, was very low in kidney infused with
propionyl-l-carnitine and exposed to ischemia/reperfusion as tal stay, renders allografts more immunogenic and pronecompared to untreated ischemic kidneys. ATP levels were not to rejection, and ultimately reduces short- and long-termaffected by propionyl-l-carnitine treatment. Renal function of graft survival rates [3–5]. Thus, the transplant communitykidneys exposed for four hours to cold Belzer UW solution
has focused increased attention on identifying drugs thatadded with propionyl-l-carnitine and transplanted to bineph-stabilize or reverse ischemia-reperfusion injury.rectomized recipients was largely preserved as compared to
untreated ischemic grafts. Propionyl-l-carnitine almost com- The primary events that can be considered responsiblefor the cascade of metabolic, functional and structuralalterations that develop after ischemia are energy imbal-Key words: acute renal failure, ischemia/reperfusion injury, isolatedance and alterations of cellular homeostasis [6]. More-perfused rat kidney, delayed graft function, kidney transplant, cold
organ storage. over, the reperfusion of previously ischemic tissue poten-tiates influx of calcium, release of intracellular enzymes,Received for publication December 18, 2000breakdown of phospholipids and disruption of cell mem-and in revised form October 18, 2001
Accepted for publication October 22, 2001 brane integrity, which either alone or in combination re-sults in ultimate cell death [6]. Current evidence leads 2002 by the International Society of Nephrology
1064

Mister et al: Propionyl-l-carnitine and ischemic injury 1065
to at least four major hypotheses concerning the media- if any, of propionyl-l-carnitine in this model; and (4)to explore whether addition of propionyl-l-carnitine totors of ischemia-reperfusion injury: calcium overloading,
generation of oxygen-derived free radicals, degradation Belzer UW solution during cold storage of donor kidneyprevents ischemia-reperfusion injury and facilitates im-of phospholipids, and accumulation of long-chain acyl-
carnitines [6–9]. mediate graft function in an experimental model of syn-geneic rat kidney transplantation.Interventions with calcium entry blockers [8, 10], free
radical scavengers [11–13], drugs that affect phospholipidmetabolism and activity [14, 15] or up-regulate "-oxida- METHODStion of long-chain fatty acids [16] have resulted in a
Animalssignificant but incomplete degree of protection in differ-ent experimental models of heart and renal ischemia- Adult male Sprague-Dawley rats of 300 to 350 g body
weight (Charles River Italia Spa, Calco, Italy) were usedreperfusion injury. Only very few studies have addressedthis issue in experimental renal transplantation. in IPK studies. Inbred adult male Lewis rats (RT1l,
Charles River) were used as donors and recipients inIn this regard, carnitine and propionyl-l-carnitinehave been reported to inhibit free radicals generation renal transplantation studies.
Animal care and treatment were conducted in accor-[17, 18], protect against impairment of fatty acid "-oxida-tion in mitochondria [19], inhibit platelet-activating fac- dance with institutional guidelines in compliance with
national (D.L. n.116, G.U. suppl. 40, February 18, 1992,tor [20] and preserves cell membrane integrity [21, 22]and induce vasodilation [23]. Thus, these agents could Circolare n.8, G.U. July 14, 1994) and international laws
and policies (European Economic Community Counciltarget simultaneously more than one pathogenetic factorof ischemia-reperfusion injury eventually providing bet- Directive 86/609, OJL 358, December 1987; “Guide for
the Care and Use of Laboratory Animals”, U.S. Nationalter therapeutic potential than that afforded by com-pounds so far explored in these experimental models. Research Council, 1996). All animals were allowed free
access to standard rat chow and tap water.Carnitine is an essential cofactor required for thetranslocation of activated long-chain fatty acids from
Isolated kidney perfusion procedures and apparatusextramitochondrial coenzyme A (CoA) into the innermitochondrial matrix and then to intramitochondrial The perfusion technique used in these experiments
has been previously described in detail [32]. The kidneyCoA, a process that requires carnitine and carnitine acyl-transferase [24]. This transport is essential to allow mito- was perfused in situ in a recirculating system with a
medium held at 37#C by a constant Haake D1 tempera-chondrial "-oxidation of long-chain fatty acid [24] andthus to provide energy supply to the cells. Therefore, ture circulator system (Haake, Berlin, Germany) and
gassed with a mixture of 95% O2-5%CO2 through a hal-carnitine is an important factor in regulating substrateflux and energy balance across cell membranes, which low-fiber membrane oxygenator. The perfusate was de-
livered to the renal artery cannula through a peristalticmight become critical in the context of ischemia-reperfu-sion, possibly preventing cell injury. Propionyl-l-carni- pump, an in-line 8-$m pore-size filter (Sartorius, Got-
tingen, Germany), and a glass bubble trap.tine, a short-chain acyl derivative of l-carnitine, has thepotential not only of restoring tissue carnitine stores, but The perfusate consisted of Krebs-Henseleit bicarbon-
ate buffer containing 3.5 g/dL of Ficoll 70 (Pharmaciaalso to replenish key mitochondrial tricarboxylic acidintermediates as documented by studies in skeletal mus- Fine Chemical, Uppsala, Sweden), 1 g/dL of bovine se-
rum albumin (BSA; Pentex BSA Fraction V; Bayer, Kan-cle mitochondria [25] and in ischemic heart tissues[26, 27] kakee, IL, USA), 200 mg/dL of glucose, 36 mg/dL of
urea, 50 mg/dL of creatinine, and a mixture of aminoThe beneficial effects of carnitine and propionyl-l-carnitine have been documented in animal models of acids as described [32]. The total volume of the perfusate
in the system was 250 mL.heart ischemia–reperfusion injury [26, 28–31]. Whetherthese compounds are also of value in preventing isch- Urine flow rate was determined gravimetrically. Perfu-
sate and urinary concentration of creatinine were mea-emia-reperfusion injury in the kidney has not been exam-ined so far. sured by Jaffe assay [33] and the glomerular filtration
rate (GFR) calculated as creatinine clearance accordingThe present study was designed with the followingaims: (1) to investigate whether carnitine and propionyl- to standard formula [34]. Renal perfusion flow (RPF)
was determined volumetrically. The perfusion pressurel-carnitine prevented renal function deterioration andtubular injury induced by ischemia/reperfusion in a rat was kept constant at 100 mm Hg throughout the experi-
ments. Therefore, changes in RPF reflected changes inmodel of isolated perfused kidney (IPK); (2) to evaluatewhether the treatments may afford protection even when renal vascular resistance. For tissue collection a three-
way stop-cock was incorporated into the circuit near torenal injury is already established; (3) to examine thepossible mechanism(s) involved in the beneficial effect, the arterial cannula to allow perfusion with the fixative

Mister et al: Propionyl-l-carnitine and ischemic injury1066
solution at the same pressure applied during the func- fined as cell swelling, vacuolization, necrosis and loss ofbrush border) was assessed and graded according to ational study, for an additional 10 to 15 minutes. The
fixative solution contained 4% p-formaldehyde, (plus 5% semiquantitative scale (0 to 3) [36]. No or very mildischemic lesions were found in the glomeruli [36].sucrose), and butylated-hydroxy-toluene (50 $mol/L)
and 1 mmol/L ethylenediaminetetraacetic acid (EDTA). The degree of leukocyte infiltration in glomerular,perivascular and interstitial areas was determined by in-Kidney specimens were collected and processed for light
microscopy analysis. direct immunofluorescence. Mouse monoclonal antibod-ies were used for the detection of the following antigens:
Kidney transplantation (1) ED1 antigen, present in the rat monocytes and mac-rophages (Chemicon, Temecula, CA, USA); (2) a ratKidney transplantation was performed as described
previously [35]. The donor kidney was flushed with Bel- major histocompatibility complex (MHC) class II anti-gen monomorphic determinant (OX6; Serotec, Oxford,zer UW solution containing 1000 U/mL heparin and
added or not with propionyl-l-carnitine, according to UK); (3) rat CD8 cell surface glycoprotein expressed byT cytotoxic suppressor cells (OX8; Serotec). A mousethe experimental group and placed in an iced Belzer
UW solution for four hours with or without propionyl-l- anti-rat granulocyte monoclonal antibody (clone MOM/3F12/F2; Serotec) was used to stain infiltrating neutro-carnitine (cold ischemia) until transplant. After ischemia
time had elapsed, recipient rats underwent removal of phils. For these analyses tissue fragments were frozen inliquid nitrogen, sections (3 $m thick) cut using a Mikromthe native left kidney. Donor kidneys grafts were then
washed with saline solution and transplanted. An anasto- 500 O cryostat (Walldorf, Germany) and fixed in ace-tone. Tissue sections were blocked with phosphate-buf-mosis was created between the donor and recipient renal
artery as well as renal vein with end-to-end anastomosis. fered saline (PBS)/1% BSA, incubated overnight at 4#Cwith the primary antibody (ED1, 14 mg/mL; OX6, 5Vascular clamps were released after 30 minutes (warm
ischemia). Donor and recipient ureters were attached $g/mL; OX8, 1:100, MOM/3F12/F2, 1:10), washed withPBS, and then incubated with Cy3-conjugated donkeyend-to-end. The native right kidney was then removed.anti-mouse IgG antibodies (affinity-purified, absorbed
Histological examination with rat IgG, 5 $g/mL in PBS; Jackson ImmunoResearch,West Grove, PA, USA) for one hour at room tempera-Kidney specimens from IPK and syngeneic trans-
planted animals were fixed in Dubosq-Brazil and dehy- ture. For each marker, the number of cells was countedin at least ten randomly selected high-power microscopedrated in alcohol. After paraffin embedding, 3-$m sec-
tions of the blocks were cut and stained with periodic fields (%400) for each animal.acid-Schiff (PAS), Masson’s trichrome, and with hema-
Adenine nucleotides measurementtoxylin eosin (H&E). The histological evaluation wasperformed in a blinded fashion on representative sec- The freeze-clamped tissue was stored at &80#C until
analysis. Tissue was homogenized in HClO4 (14%, vol/tions of cortex and outer medullary regions. In controlIPK preparations only a mild and focal vacuolization vol) and subsequent adenine nucleotides analyses of the
neutralized perchloric extracts were carried out with aof proximal tubular epithelial cells was detected in thecortex. Histologic lesions in the medulla consisted of cell high-pressure liquid chromatography (HPLC) method,
as previously described [37].swelling and cytoplasmic disruption progressing to cellnecrosis in the thick ascending limbs, mainly in the inner
Immunocytochemistry of 4-hydroxynonenal proteinstripe region, and vacuolization, loss of brush border,adduct in IPKand luminal debris in proximal tubules. Structural changes
were assessed on H&E stained sections using a semi- Lipid peroxidation in IPK was localized by a specificanti-4-hydroxynonenal-lysine (4-HNE-lysine) antibodyquantitative scale with increasing severity of damage in
%20 randomly selected fields (at least 15 to 20 fields) (NA59, kindly provided by Dr. Witzum, The ScrippsResearch Institute, La Jolla, CA, USA) [38]. After perfu-for each section and the fields were assigned individual
scores. For thick ascending limbs, lesions were graded as sion fixation, biopsy slices (2 mm thick) were cut perpen-dicularly to the major axis of the kidney. Three-$m par-follows: 0 ' no abnormalities; 1 ' degenerative changes,
with only occasional necrotic cells; 2 ' lesions of moder- affin sections from renal tissue were processed forimmunohistochemistry using an avidin-biotin horserad-ate severity, with necrosis involving approximately (50%
profiles; 3 ' extensive necrosis. For proximal tubules, ish peroxidase complex technique (ABC method, ABC-Elite; Vector Laboratories, Burlingame, CA, USA) [39].lesions were graded as follows: 0 ' no abnormalities;
1 ' focal vacuolization and loss of brush borders; 2 ' Briefly, the sections were dewaxed, rehydrated and incu-bated for 30 minutes with 0.3% H2O2 in methanol tolesions of moderate severity with blebbing and loss of
individual cells; 3 ' severe lesions. quench endogenous peroxidase. Tissue was permeabil-ized in 0.1% Triton X-100 in PBS 0.01 mol/L, pH 7.2,In syngeneic kidney graft tissues, tubular damage (de-

Mister et al: Propionyl-l-carnitine and ischemic injury 1067
for 30 minutes and aspecificities were blocked by a 30- of urine output, glomerular filtration rate (GFR), andrenal perfusate flow (RPF).minute incubation with non-immune horse serum. All the
The same experimental protocol was repeated to as-above steps were carried out at room temperature. Slidessess the effect of propionyl-l-carnitine on renal functionwere then incubated overnight at 4#C in moist chamberin conditions of more severe ischemic insult to the kid-with the primary anti-4-HNE-lysine antibody (1:500) inneys, which more closely mimics the peritransplant statePBS/1% BSA, followed by the biotinylated horse-anti-that occurs when the ischemic period is prolonged upmouse IgG, ABC solution (Vector Laboratories) and de-to 40 minutes, again by reducing perfusion pressure toveloped with diaminobenzidine/nickel. The sections werethe IPK. Thus, kidneys undergoing ischemia/reperfusionthen counterstained with Harris hematoxylin (Biooptica,were exposed to vehicle (saline, group 5, N ' 3) orMilan, Italy). Negative controls were obtained by omit-propionyl-l-carnitine (3.6 mg/mL f.c.; infusion rate 0.4ting the primary antibody on a second section presentmL/min, group 6, N ' 3) with the infusion starting aton all the slides. The slides were examined under lightthe beginning of the experimental period (pre-ischemia/microscope by two pathologists blind to the nature ofreperfusion) and continued during the two-hour perfu-the experiment.sion period. Urine output, GFR, and RPF were moni-Multiple sections from each IPK were examined. Eachtored (Fig. 1A).section was scored for intensity of immunostaining (ab-
In additional experiments the therapeutic effect ofsent, faint, moderate, intense: 0 through 3). At least 8propionyl-l-carnitine was also investigated. Therefore,to 10 fields per section were examined. The mean valuesafter a ten-minute control clearance period and 20-for each section and for each IPK were determined.minute ischemia, kidneys were infused with propionyl-l-carnitine (3.6 mg/mL f.c., 0.4 mL/min, group 7, N 'Isolated perfused kidney study design6), starting immediately after reperfusion was restoredTo assess whether propionyl-l-carnitine may preserveand then continuing until the end of the perfusion period.renal function in conditions of ischemic insult to theRenal function was assessed as above.kidney, we first performed ex vivo experiments using a
To examine whether exposure to propionyl-l-carni-model of ischemia/reperfusion injury in isolated rat kid-tine affected tubular structure, some of the experimentsney perfused in a circulating system with an artificialanalyzed renal tissue specimens by light microscopy atcell-free medium (Fig. 1A). After surgery and a 20 tothe end of the perfusion period. Since minor differences25 minute equilibration period, a ten-minute baselinewere found in IPK exposed to 20 or 40 minutes of isch-urine collection and a perfusate sample were obtainedemia at histological examination, score values of the two(control clearance). Thereafter, kidneys were exposed sets of experiments were pooled for statistical analysis.
to ischemia by markedly reducing perfusion pressure Control non-ischemic kidneys (N ' 3), ischemic kidneys(10 mm Hg) for 20 minutes. Perfusion pressure was then (N ' 5), ischemic kidneys exposed to propionyl-l-carni-restored to normal (100 mm Hg) and additional nine con- tine (N ' 6) were considered.secutive ten-minute clearance periods were performed. In additional experiments, to evaluate whether theThree experimental groups of IPKs were considered: potential protective effect of propionyl-l-carnitine oc-group 1 (N ' 10), was infused with vehicle (saline) di- curred by preserving renal cell viability, we measuredrectly into the renal artery; group 2 (N ' 10) was exposed the time course of lactate dehydrogenase (LDH) releaseto propionyl-l-carnitine (3.6 mg/mL, final concentration) (by an automatic analyzer) in the renal vein effluent ininfused at the rate of 0.4 mL/min. The concentration of control IPK preparations, in those exposed to 20 minutespropionyl-l-carnitine was chosen according to prelimi- of ischemia, and those in which propionyl-l-carnitinenary dose-response safety experiments in normal IPK had been infused before ischemia was established. Mea-preparations (data not shown). For comparison an addi- surements were performed in perfusate samples col-tional group (group 3, N ' 3), was infused with l-carnitine lected in subgroups of the above-mentioned set of exper-(3.6 mg/mL f.c.; Sigma Tau, Rome, Italy), at the same iments.rate of 0.4 mL/min. As a control group (group 4, N ' Moreover, whether the possible protective effect of pro-6), kidneys infused with vehicle but not undergoing isch- pionyl-l-carnitine on ischemia-reperfusion injury was re-emia/reperfusion injury were studied. All treatments lated to inhibition of lipid peroxidation process was inves-started at the beginning of the control clearance period tigated using two different methodological approaches:and continued for the two-hour perfusion period. Perfu- (1) by immunohistochemical detection of 4-hydroxyno-sion with vehicle, propionyl-l-carnitine, or l-carnitine nenal, a major aldehydic product of lipid peroxidationwas performed using an appropriate infusion pump con- [40], believed to be largely responsible for cytopathologi-nected with a catheter to the circuit very proximally to cal effects observed during oxidative stress [41], on thethe renal artery. For each collection period urine and renal tissue sections obtained for morphological analysis;
and (2) by evaluating the concentration of MDA, usingvenous effluent samples were collected for measurement
Mister et al: Propionyl-l-carnitine and ischemic injury1068
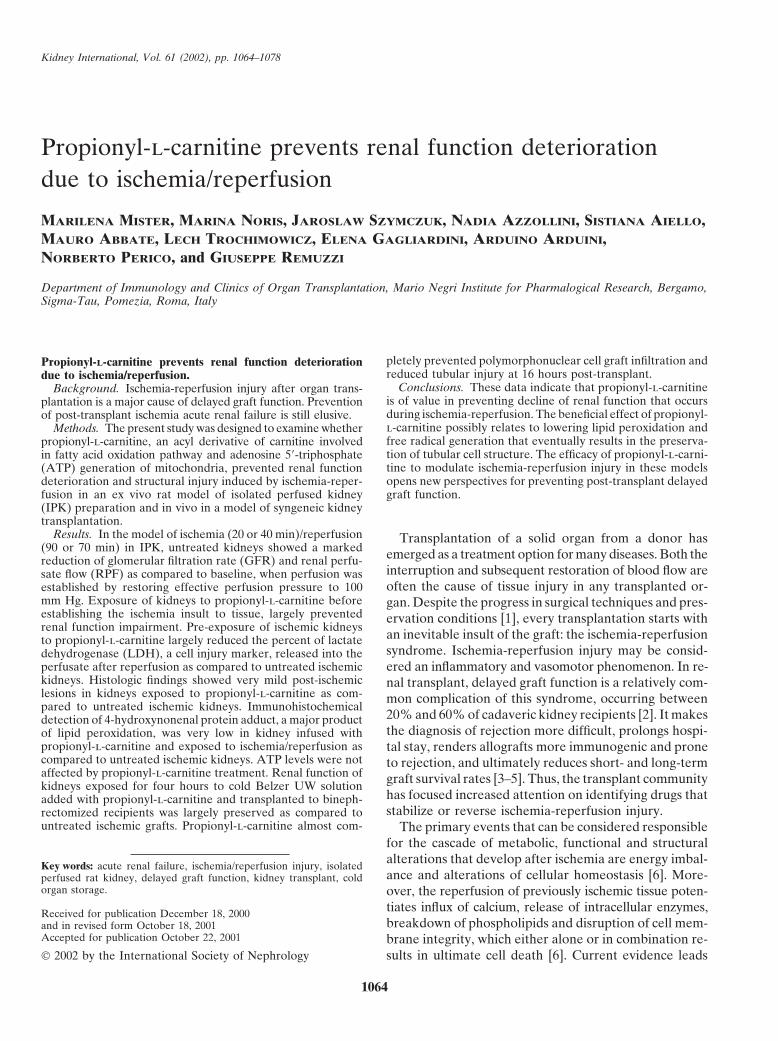
Fig. 1. Experimental protocol. (A) Isolated perfused rat kidney (IPK). After equilibration (time 0) and a 10 min. baseline period, kidneys wereexposed to ischemia by reducing perfusion pressure to 10 mm Hg. Perfusion pressure was then restored to normal (100 mm Hg) and additional9 consecutive 10-minute clearance periods were performed. Seven experimental groups were studied: group 1, IPK undergoing 20 minutes ofischemia and infused with vehicle; group 2, IPK undergoing 20 minutes of ischemia and infused with propionyl-l-carnitine from time 0; group 3,IPK undergoing 20 minutes ischemia and infused with l-carnitine from time 0; group 4, control IPK not undergoing ischemia; group 5, IPKundergoing 40 minutes of ischemia and infused with vehicle; group 6, IPK undergoing 40 minutes of ischemia and infused with propionyl-l-carnitine from time 0; group 7, IPK undergoing 20 minutes of ischemia and infused with propionyl-l-carnitine starting immediately after reperfusion(not shown in figure). (B) Syngeneic kidney transplant. Donor kidneys were transplanted in the syngeneic nephrectomized recipients after 4 hoursof cold ischemia time in Belzer UW solution. Five experimental groups were studied: group 8, donor kidney transplanted after a 4-hour coldischemia in Belzer plus vehicle; group 9, donor kidney transplanted after a 4-hour cold ischemia in Belzer plus propionyl-l-carnitine; group 10,donor kidney transplanted, no cold ischemia; group 11 (not shown), donor kidney transplanted after 4 hours of cold ischemia in Belzer plus vehicle,recipients sacrificed 16 hours post-transplantation; group 12, (not shown), donor kidney transplanted after 4 hours of cold ischemia in Belzer pluspropionyl-l-carnitine, recipients sacrificed 16 hours after transplantation.
the thiobarbituric acid method [42], in the venous efflu- end of the 120-minute perfusion period the kidneys werefreeze-clamped in liquid nitrogen for the evaluation ofent collected at various time points during the 120-mi-high energy phosphates.nute perfusion period.
To examine whether propionyl-l-carnitine improvedKidney transplant study designthe energy metabolism of the ischemic kidney, additional
experiments were performed with kidneys undergoing To evaluate whether propionyl-l-carnitine also mayexert a protective effect in vivo, experiments were per-20 minutes of ischemia/reperfusion exposed to vehicle
(saline, N ' 4) or propionyl-l-carnitine (N ' 4). At the formed in a model of syngeneic rat kidney transplanta-

Mister et al: Propionyl-l-carnitine and ischemic injury 1069
tion, and the impact of the treatment on renal function exposed to vehicle urine flow markedly declined at thebeginning of the ischemia period when perfusion pres-preservation during ischemia/reperfusion injury due to
cold kidney storage and revascularization was studied sure was intentionally lowered to allow a minimal perfu-sion flow. When reperfusion was established, diuresis(Fig. 1B). The absence of alloreactivity in this model
allowed us to isolate the effect of cold ischemia from progressively increased reaching pre-ischemia values 20minutes later (pre-ischemia, 107 ) 32 $L/min vs. 20 minimmunological factors. Donor kidneys were transplanted
in the syngeneic nephrectomized recipients after four post-ischemia, 113 ) 27 $L/min). This was maintainedfor the subsequent 30 minutes and then diuresis sponta-hours of cold ischemia time in Belzer UW solution (Via-
Span; DuPont Pharma, Firenze Italy; group 8, N ' 7) neously declined (end of perfusion, 104 ) 36 $L/min).In kidneys exposed to propionyl-l-carnitine before isch-or the same solution containing propionyl-l-carnitine
(1.2 mg/mL, group 9, N ' 7). This concentration of emia, urine output after reperfusion promptly recoveredand 20 minutes later was numerically higher than pre-propionyl-l-carnitine was chosen based on preliminary
experiments showing toxicity soon after transplantation ischemia values (pre-ischemia, 105 ) 11 $L/min vs. 20min post-ischemia, 128 ) 13 $L/min). Thereafter, urinewhen higher doses (3.6 and 1.8 mg/mL) of the compound
were used. Nephrectomized animals receiving a synge- output remained quite constant up to the end of the two-hour observation period (127 ) 26 $L/min). A similarneic graft not subjected to cold ischemia (non-ischemic
grafts) were used as controls (group 10, N ' 3). Warm profile of urine output was also found with l-carnitinepre-treatment (pre-ischemia, 90 ) 31 $L/min; end ofischemia time during surgical procedures was approxi-
mately 30 minutes. At 16 hours, 24 hours, and on days perfusion: 125 ) 16 $L/min). No significant differenceamong groups as far as urine output was documented at2, 5, 7 and 30 post-transplant, renal function was assayed
by measuring plasma creatinine concentration, by a Re- any time of the perfusion period.In control non-ischemic kidneys perfused with vehicleflotron creatinine test (Boehringer Mannheim, Mann-
heim, Germany), on whole blood collected from the tail renal function slightly declined during the two-hourstudy period, according to the characteristics of this prep-vein of anesthetized animals.
Two additional groups of rat recipients of a syngeneic aration [32] (baseline GFR, 1.09 ) 0.14; 60 min GFR,1.03 ) 0.15; 120 min GFR, 0.78 ) 0.14 mL/min). Askidney exposed to four hours of cold storage in Belzer
UW solution alone (group 11, N ' 4) or added with shown in Figure 2A, in ischemic kidneys treated withvehicle, the GFR that was not measurable during thepropionyl-l-carnitine (1.2 mg /ml, group 12, N ' 4) were
studied to specifically investigate the effect of propionyl- ischemia period was restored after establishing reperfu-sion, but the values were significantly lower than pre-l-carnitine on graft histology and inflammatory cell infil-
trate. The animals were sacrificed 16 hours after trans- ischemia GFR (0.47 ) 0.12 vs. 1.06 ) 0.19 mL/min,P * 0.01). After a mild tendency to increase during theplantation, the kidney grafts removed, and processed for
structural examination and immunohistochemical analy- subsequent 20 minutes of perfusion, a further progressivedecline of GFR was documented (end of perfusion, 0.48 )sis of polymorphonuclear cell, CD8 T lymphocyte, mac-
rophage, and MHC class II positive cell infiltrate. 0.16 mL/min). In kidneys exposed to propionyl-l-carni-tine before ischemia, GFR recovered more promptly
Statistical analysis than in vehicle-treated kidneys, as shown by a signifi-cantly higher mean value at the end of the first ten-Results are expressed as mean ) SD or SE as specified
in the Figure legends. Data were analyzed using two- minutes after reperfusion (0.74 ) 0.17 mL/min, P * 0.01vs. vehicle-treated kidneys). GFR progressively increasedway, one-way analysis of variance (ANOVA), or Krus-
kal-Wallis as appropriate. The significance level of differ- during the subsequent 30 minutes of perfusion, with aslight decrease thereafter, but the values were alwaysence between individual group means, subjected to the
two-way ANOVA, was established using the Tukey-Cic- significantly higher than in vehicle-treated kidneys forthe entire observation period (GFR at end of perfusion,chetti test for multiple comparisons [43]. Statistical sig-
nificance was defined as P * 0.05. 0.78 ) 0.17 mL/min, P * 0.01 vs. vehicle). Also, pre-treatment with l-carnitine largely prevented the declinein GFR after reperfusion, although a tendency for meanRESULTS values to decline with time was observed (pre-ischemia,
Effect of propionyl-L-carnitine on renal function 0.97 ) 0.12; 20 min of reperfusion, 0.72 ) 0.08; end ofdeterioration in a model of ischemia-reperfusion perfusion, 0.64 ) 0.07 mL/min).in the IPK As for RPF, a minor progressive decline of values with
time was found in control non-ischemic kidneys exposedIn control non-ischemic kidneys perfused with vehicle,urine output tended to increase progressively over the to vehicle (baseline RPF, 27.3 ) 1.5; 60 min RPF, 26.6 )
1.2; 120 min RPF, 25.5 ) 1.0 mL/min). In ischemic kid-two-hour perfusion period (baseline, 86 ) 21; 60 min,104 ) 15; 120 min, 118 ) 34 $L/min). In ischemic kidneys neys perfused with vehicle RPF declined from 26 ) 1
Mister et al: Propionyl-l-carnitine and ischemic injury1070
Table 1 shows the effect of vehicle or propionyl-l-carnitine on renal function parameters before and after amore severe (40 min) ischemia period. In vehicle-treatedkidneys, GFR increased after reperfusion but largelyremained below pre-ischemia values (P * 0.01 vs. base-line at all points considered). In kidneys exposed to pro-pionyl-l-carnitine GFR recovered more promptly thanin vehicle-treated kidneys (P * 0.05 at 60 min), butvalues were still significantly lower than pre-ischemia(P * 0.05). As for RPF, in vehicle-treated kidneys RPFtended to increase after reperfusion, but remained sig-nificantly lower than pre-ischemic values at all timepoints considered (Table 1). In kidneys exposed to propi-onyl-l-carnitine RPF recovered faster and at 90 minutesof perfusion was only numerically lower than pre-isch-emia values.
Therapeutic effect of propionyl-L-carnitine onrenal function deterioration in a model ofischemia-reperfusion in IPK
Infusion of propionyl-l-carnitine starting at the begin-ning of reperfusion resulted in marked increase of GFR,despite the recovery of this parameter was less promptthan in kidneys pre-exposed to the compound (pre-isch-emia, 1.10 ) 0.06 mL/min; 10 min post-ischemia, 0.43 )0.05 mL/min). Thereafter, GFR values were comparableto those achieved in kidneys exposed to propionyl-l-carnitine from the beginning of the perfusion (end ofperfusion, 0.80 ) 0.07 mL/min vs. 0.78 ) 0.17 mL/min)and were significantly higher than in vehicle-treated kid-neys (P * 0.01). Similar results were obtained for RPF,
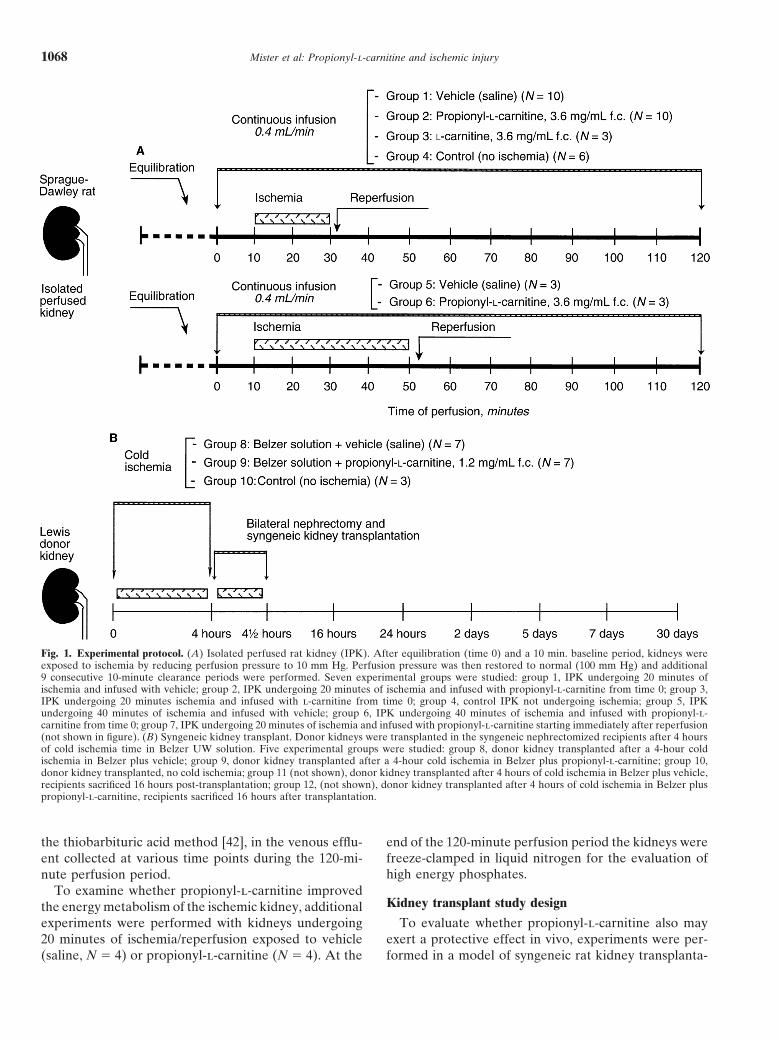
Fig. 2. Effect of propionyl-L-carnitine on changes in glomerular filtra- whose values increased with time to the same extenttion rate (GFR, A) and renal perfusate flow (RPF, B) induced by 20 independently of whether propionyl-l-carnitine infusionminutes of ischemia in an isolated perfused rat kidney preparation.
began before or after ischemia (end of perfusion, 25 )Vehicle (!; N ' 10), propionyl-l-carnitine ("; N ' 10) or l-carnitine(#; N ' 10) was infused into the renal artery starting before or immedi- 1 mL/min vs. 26 ) 2 mL/min).ately after the ischemic period. Values are mean ) SD. *P * 0.01 vs.propionyl-l-carnitine and baseline; P * 0.05 vs. baseline. Effect of propionyl-L-carnitine on biochemical and
histological markers of tissue damage in the modelof ischemia-reperfusion in IPK
In control kidneys a mild, progressive increase withmL/min at baseline to 5.7 ) 0.4 mL/min at the beginningof ischemia period (Fig. 2B). When normal perfusion time in the amount of LDH released in the perfusate
was found (Table 2). In those kidneys exposed to 20was re-established, RPF returned toward but did notreach pre-ischemia values (21 ) 2 mL/min, P * 0.01 minutes of ischemia, reperfusion was associated with a
marked percent increase of LDH release as compared tovs. pre-ischemia). Thereafter, RPF remained at valuessignificantly lower than baseline up to the end of the baseline pre-ischemia values, with a further progressive
increase through the end of the observation period. Per-two-hour perfusion (24 ) 1 mL/min). In kidneys exposedto propionyl-l-carnitine starting before ischemia, RPF cent LDH changes was significantly higher than that
reported in control kidneys. Pre-exposure of ischemicwas comparable to that in vehicle-treated kidneys before(27 ) 1 mL/min) and during the ischemia period (5.3 ) kidneys to propionyl-l-carnitine largely reduced, but not
normalized the percent of LDH released in the perfusate0.5 mL/min). After reperfusion, RPF recovered fasterand values were numerically but not significantly lower after reperfusion as compared to baseline.
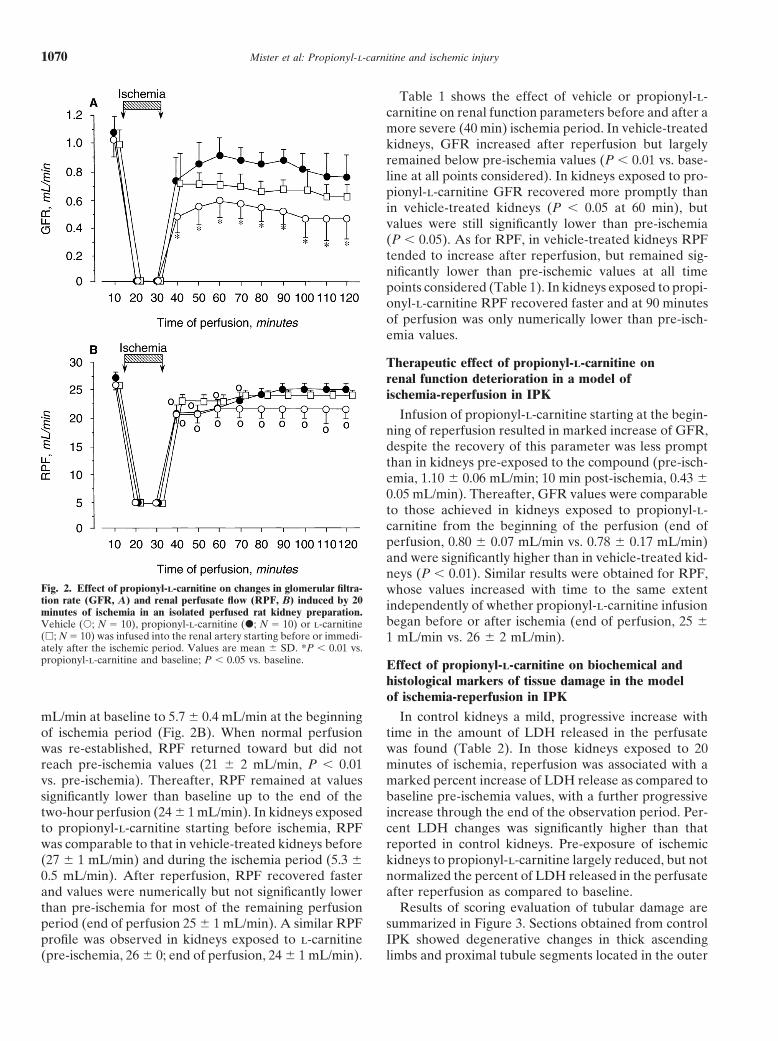
Results of scoring evaluation of tubular damage arethan pre-ischemia for most of the remaining perfusionperiod (end of perfusion 25 ) 1 mL/min). A similar RPF summarized in Figure 3. Sections obtained from control
IPK showed degenerative changes in thick ascendingprofile was observed in kidneys exposed to l-carnitine(pre-ischemia, 26 ) 0; end of perfusion, 24 ) 1 mL/min). limbs and proximal tubule segments located in the outer
Mister et al: Propionyl-l-carnitine and ischemic injury 1071
Table 1. Effect of propionyl-l-carnitine on renal function parameters in a model of ischemia(40 min)/reperfusion in isolated perfused kidneys
Vehicle (N ' 3) Propionyl-l-carnitine (N ' 3)
Baseline 60 min 120 min Baseline 60 min 120 min
Urine output lL/min 93)2 123)19 142) 11 109) 38 143) 14 120) 22GFR mL/min 1.21) 0.17 0.58) 0.04a 0.51 )0.08a 1.09 )0.20 0.80)0.06bc 0.74)0.05b
RPF mL/min 26)1 18)0 20) 0a 27)1a 19 )3a 24 )1
Values are mean ) SD.a P * 0.01, b P * 0.05 vs. baselinec P * 0.05 vs. vehicle
Table 2. Effect of propionyl-l-carnitine on lactate dehydrogenase (LDH) release into the perfusatevenous effluent in isolated perfused kidneys
Percent of LDH releasea
80 min 100 min 120 min
Controls (N ' 4) 28.3 (0–56.5) 10.0 (0–21.7) 89.0 (60.5–117.4)Ischemia/reperfusion + vehicle (N ' 6) 475.0 (246.0–703.3) 750.0 (422.4–1078) 835.0 (549–1121)Ischemia/reperfusion + propionyl-l-carnitine (N ' 6) 323.0 (219–427.2) 431.5 (322.2–540.7) 427.7 (364.3–491.0)b
Values are mean (range).a Over baseline (100%)b P * 0.05 vs. vehicle
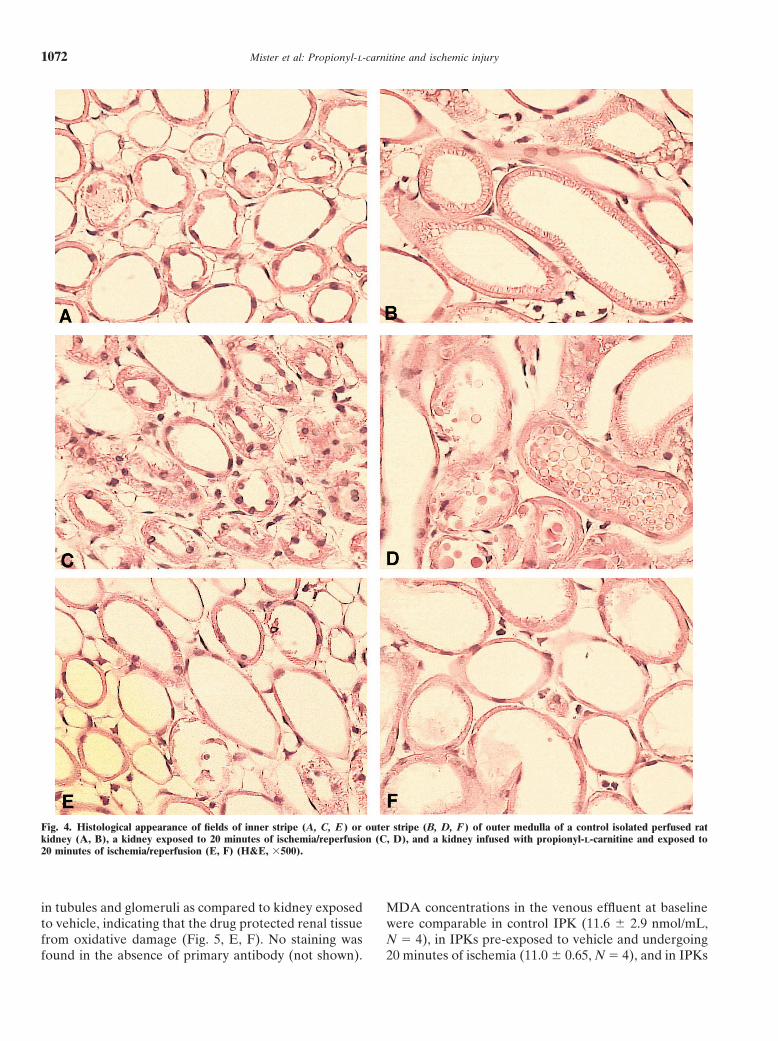
post-ischemic tubular lesions as compared to untreatedischemic kidneys. The protective effect of propionyl-l-carnitine was remarkable both in the thick ascendinglimbs and, to a lesser extent, in the proximal tubuli (Fig.4, E, F).
Table 3 shows that the concentrations of energy com-pounds (ATP and ADP) and total energy charge [0.5(ADP+ 2ATP)/(ATP+ADP+AMP)] were low in IPKsundergoing ischemia/reperfusion, as a consequence ofischemia-induced loss [14, 22, 46]. Pre-exposure to propi-onyl-l-carnitine had no effect on ATP, energy charge,adenine nucleotides and adenine content in the IPKsundergoing ischemia/reperfusion (Table 3).
To evaluate the extent of generation of lipid peroxida-Fig. 3. Tubular histological change score in control isolated perfused tion products and their cell localization in the isolatedkidneys (IPKs; Control, N ' 3), in kidney exposed to 20 or 40 minutes kidneys after ischemia/reperfusion and the potential pro-of ischemia and treated with vehicle (Isch/reper + vehicle, N ' 5), or
tective effect of propionyl-l-carnitine, the amount andpropionyl-L-carnitine (Isch/reper + propionyl-L-carn nitine, N ' 6).Symbols are: (#) TAL, thick ascending limbs; ( ) PCT, proximal convo- the distribution of 4-HNE-modified proteins using a spe-luted tubules. Values are mean ) SD. *P * 0.05 vs. Isch/reper + vehicle, cific anti-4-HNE-lysine antibody were assessed [38, 47].§P * 0.05 vs. control and Isch/reper + propionyl-l-carn.
Indeed, it has been shown that the formation of adductsbetween 4-HNE, a major aldehydic product of lipid per-oxidation [40, 48–50], and the lysine residues of structural
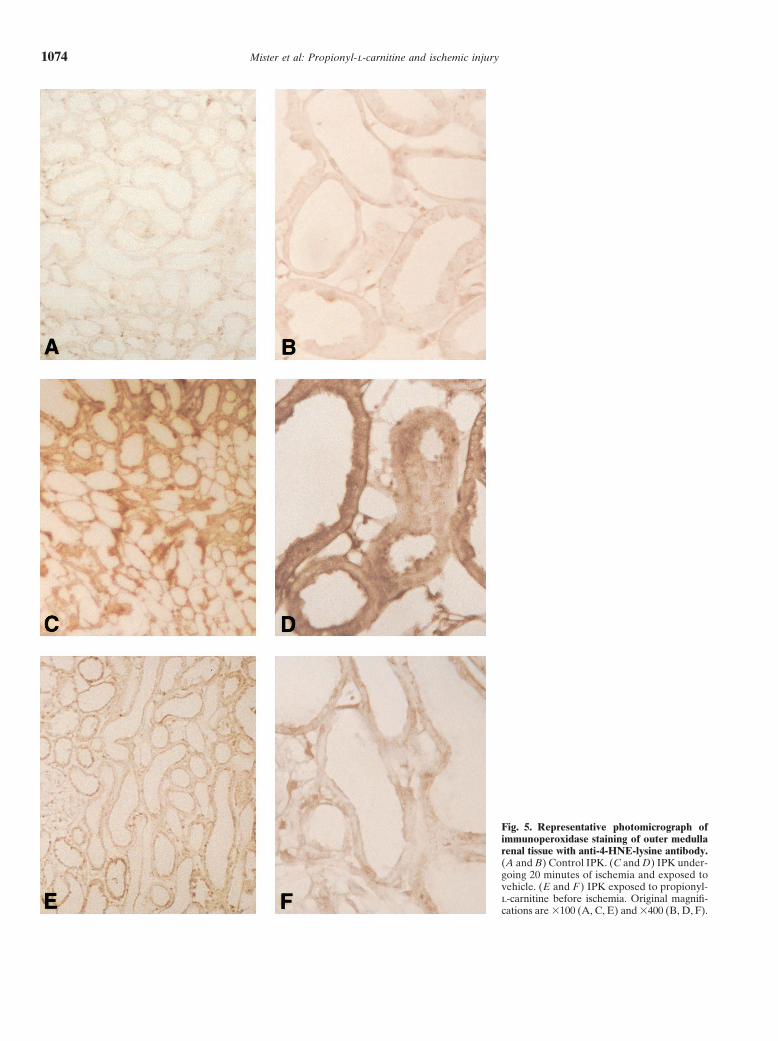
medulla (Fig. 4, A, B). Thick ascending limbs showed proteins, provides good evidence of local oxidative stresssevere changes, typical of this model [44, 45], with [51]. As shown in Figure 5 A and B, and Table 4, 4-HNE-marked swelling of the cytoplasm and cell detachment lysine staining was mostly faint in cortical and medullaryor necrosis. Lesions were more pronounced in kidneys tubules of control kidneys perfused with saline, whileexposed to 20 or 40 minutes ischemia, which in addition glomeruli were mostly negative. By contrast, IPKs un-to severe damage of thick ascending limbs showed much dergoing either 20 or 40 minutes of ischemia and exposedmore severe proximal tubular injury, including necrosis to vehicle showed moderate to intense 4-HNE-lysineand cell debris in tubular lumen (Fig. 4, C, D). IPKs pre- staining in medullary tubules (Fig. 5, C, D, and Tableexposed to propionyl-l-carnitine and undergoing isch- 4). In kidneys exposed to propionyl-l-carnitine before
ischemia, 4-HNE-lysine staining was impressively reducedemia/reperfusion had significantly (Fig. 3) less severe
Mister et al: Propionyl-l-carnitine and ischemic injury1072
Fig. 4. Histological appearance of fields of inner stripe (A, C, E ) or outer stripe (B, D, F ) of outer medulla of a control isolated perfused ratkidney (A, B), a kidney exposed to 20 minutes of ischemia/reperfusion (C, D), and a kidney infused with propionyl-L-carnitine and exposed to20 minutes of ischemia/reperfusion (E, F) (H&E, %500).
in tubules and glomeruli as compared to kidney exposed MDA concentrations in the venous effluent at baselinewere comparable in control IPK (11.6 ) 2.9 nmol/mL,to vehicle, indicating that the drug protected renal tissue
from oxidative damage (Fig. 5, E, F). No staining was N ' 4), in IPKs pre-exposed to vehicle and undergoing20 minutes of ischemia (11.0 ) 0.65, N ' 4), and in IPKsfound in the absence of primary antibody (not shown).

Mister et al: Propionyl-l-carnitine and ischemic injury 1073
Table 3. Adenine nucleotides, adenosine levels and energy charge in isolated perfused rat kidneys
ATP ADP AMP Adenosine Ec
Ischemia/reperfusion + vehicle 49.8)11.4 54.1)15.2 215.7)52.0 21.5) 1.9 0.3)0.01Ischemia/reperfusion + propionyl-l-carnitine 46.0)5.0 55.6) 4.0 193.9)21.0 20.1)4.8 0.3)0.01
Values (nmol/gr wet weight) are means ) SD, N ' 4 IPRK for each group; ischemia time is 20 minutes. Ec (energy charge) ' 1/2 ([ADP] + [2ATP]/[ATP] +[ADP] + [AMP]).
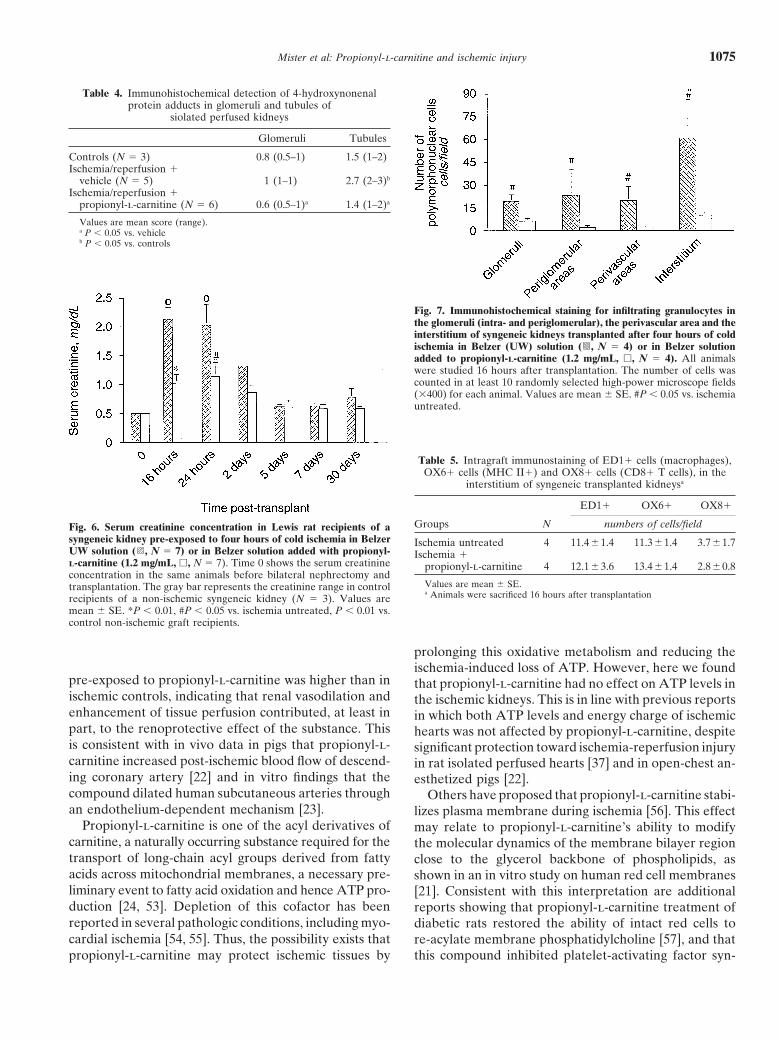
pre-exposed to propionyl-l-carnitine and undergoing 20 hours after transplantation showed moderate tubular ne-minutes of ischemia (11.8 ) 2.6, N ' 4). In control IPKs crosis manifested by swollen, vacuolated proximal tubu-MDA concentration in the venous effluent remained lar cells with pyknotic nuclei and cell detachment (semi-quite stable during the perfusion time. By contrast, in quantitative mean score, 1.1 ) 0.3). Additional changesthose kidneys exposed to 20 minutes of ischemia, reper- included tubular dilation, flattening of tubular epithe-fusion was associated with a marked increase of MDA lium and cell debris in tubular lumens [36, 52]. Propionyl-release in the venous effluent as compared to baseline l-carnitine partially reduced tubular damage (meanpre-ischemia values, with a maximal increase during the score, 0.8 ) 0.2).first 10 minutes of reperfusion (40 min, 41 ) 10% in- A detailed immunohistologic evaluation of intragraftcrease over baseline, P * 0.05, vs. 40 min control IPK, leukocyte infiltration at 16 hours post-transplantation5 ) 3% increase over baseline). Pre-exposure of ischemic was also undertaken. Figure 7 summarizes the resultskidneys to propionyl-l-carnitine completely abolished of quantitative evaluation of neutrophils infiltration bythe increase of MDA in the venous effluent after reperfu- immunohistochemical staining. In untreated ischemicsion, as compared to baseline (40 min, &2.4 ) 6% in- kidneys a large number of granulocytes was found in thecrease over baseline, P * 0.05, vs. IPKs pre-exposed to interstitium, and to a lesser extent in intra- and periglom-vehicle and undergoing 20 min ischemia). erular areas as well as in perivascular areas. Addition of
propionyl-l-carnitine to the cold storage solution sig-Effect of propionyl-L-carnitine on ischemia- nificantly decreased graft granulocyte infiltration at 16reperfusion-induced graft dysfunction hours post-transplant (P * 0.05 vs. untreated ischemicin syngeneic kidney transplants grafts). In contrast to granulocytes, a low number of
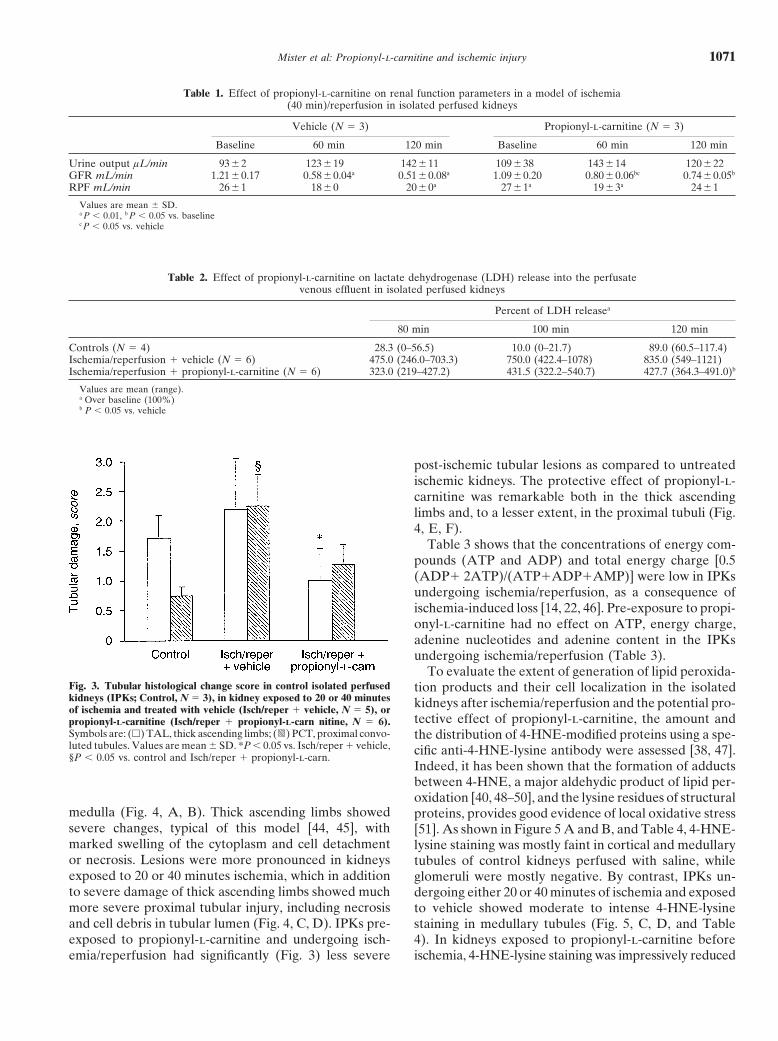
Figure 6 shows the time course of serum creatinine ED1+ monocytes/macrophages, MHC class II+ cells, andconcentration in Lewis rats recipients of syngeneic kid- CD8+ cells was found in kidneys transplanted followingney transplants pre-exposed to a four-hour cold ischemia four hours of ischemia, mainly in the interstitium (Tableperiod. In animals receiving untreated donor ischemic 5). No difference was found in monocyte and T-cell infil-kidneys (group 8) renal dysfunction occurred early post- tration between untreated and propionyl-l-carnitinetransplant, as documented by serum creatinine values treated grafts (Table 5).significantly higher than in control rats transplanted withnon-ischemic kidneys and studied at 16, 24 hours and at
DISCUSSIONday 2 post-surgery. Thereafter renal function progres-In an ex vivo model of ischemia-reperfusion injury insively improved with serum creatinine reaching normal
an isolated perfused rat kidney preparation, exposurevalues in most animals at day 5 of follow-up. Three outof kidneys to propionyl-l-carnitine before the ischemicof seven rats, however, did not completely recover graftinsult largely prevented renal function impairment thatfunction, and one of them died at day 19 post-transplant.instead occurred after restoring normal perfusion in con-By contrast, in animals receiving kidneys treated withtrol untreated ischemic kidneys. This study also con-propionyl-l-carnitine during the pre-transplant four-hourfirmed in vivo the efficacy of propionyl-l-carnitine ofischemia period, serum creatinine at 16 and 24 hoursmodulating ischemia-reperfusion injury in a syngeneicpost-surgery was significantly lower than values in ani-rat kidney transplant model to the extent that post-trans-mals transplanted with untreated ischemic kidneys (16plant delayed graft function was mostly prevented.hr, P * 0.01; 24 hr, P * 0.05). Renal function completely
Several mechanisms by which propionyl-l-carnitinerecovered in these animals by day 5 post-transplant.protected ischemic kidney improving functional recovery
Effect of propionyl-L-carnitine on ischemia- during reperfusion have been explored.reperfusion-induced graft injury and cell In the IPK preparation, perfusion pressure is main-infiltration in syngeneic kidney transplants tained constant at 100 mm Hg by a flow pump; thus,
the change in RPF is an indirect measurement of renalHistologic examination of sections from kidneys trans-planted after four-hour cold ischemia and studied 16 vascular resistance. During reperfusion RPF in kidneys
Mister et al: Propionyl-l-carnitine and ischemic injury1074
Fig. 5. Representative photomicrograph ofimmunoperoxidase staining of outer medullarenal tissue with anti-4-HNE-lysine antibody.(A and B) Control IPK. (C and D) IPK under-going 20 minutes of ischemia and exposed tovehicle. (E and F ) IPK exposed to propionyl-l-carnitine before ischemia. Original magnifi-cations are %100 (A, C, E) and %400 (B, D, F).
Mister et al: Propionyl-l-carnitine and ischemic injury 1075
Table 4. Immunohistochemical detection of 4-hydroxynonenalprotein adducts in glomeruli and tubules of
siolated perfused kidneys
Glomeruli Tubules
Controls (N ' 3) 0.8 (0.5–1) 1.5 (1–2)Ischemia/reperfusion +
vehicle (N ' 5) 1 (1–1) 2.7 (2–3)b
Ischemia/reperfusion +propionyl-l-carnitine (N ' 6) 0.6 (0.5–1)a 1.4 (1–2)a
Values are mean score (range).a P * 0.05 vs. vehicleb P * 0.05 vs. controls
Fig. 7. Immunohistochemical staining for infiltrating granulocytes inthe glomeruli (intra- and periglomerular), the perivascular area and theinterstitium of syngeneic kidneys transplanted after four hours of coldischemia in Belzer (UW) solution ( , N ' 4) or in Belzer solutionadded to propionyl-L-carnitine (1.2 mg/mL, #, N ' 4). All animalswere studied 16 hours after transplantation. The number of cells wascounted in at least 10 randomly selected high-power microscope fields(%400) for each animal. Values are mean ) SE. #P * 0.05 vs. ischemiauntreated.
Table 5. Intragraft immunostaining of ED1+ cells (macrophages),OX6+ cells (MHC II+) and OX8+ cells (CD8+ T cells), in the
interstitium of syngeneic transplanted kidneysa
ED1+ OX6+ OX8+
Groups N numbers of cells/fieldFig. 6. Serum creatinine concentration in Lewis rat recipients of asyngeneic kidney pre-exposed to four hours of cold ischemia in Belzer Ischemia untreated 4 11.4) 1.4 11.3) 1.4 3.7)1.7UW solution ( , N ' 7) or in Belzer solution added with propionyl- Ischemia +L-carnitine (1.2 mg/mL, #, N ' 7). Time 0 shows the serum creatinine propionyl-l-carnitine 4 12.1)3.6 13.4)1.4 2.8)0.8concentration in the same animals before bilateral nephrectomy and
Values are mean ) SE.transplantation. The gray bar represents the creatinine range in controla Animals were sacrificed 16 hours after transplantationrecipients of a non-ischemic syngeneic kidney (N ' 3). Values are
mean ) SE. *P * 0.01, #P * 0.05 vs. ischemia untreated, P * 0.01 vs.control non-ischemic graft recipients.
prolonging this oxidative metabolism and reducing theischemia-induced loss of ATP. However, here we found
pre-exposed to propionyl-l-carnitine was higher than in that propionyl-l-carnitine had no effect on ATP levels inischemic controls, indicating that renal vasodilation and the ischemic kidneys. This is in line with previous reportsenhancement of tissue perfusion contributed, at least in in which both ATP levels and energy charge of ischemicpart, to the renoprotective effect of the substance. This hearts was not affected by propionyl-l-carnitine, despiteis consistent with in vivo data in pigs that propionyl-l- significant protection toward ischemia-reperfusion injurycarnitine increased post-ischemic blood flow of descend- in rat isolated perfused hearts [37] and in open-chest an-ing coronary artery [22] and in vitro findings that the esthetized pigs [22].compound dilated human subcutaneous arteries through Others have proposed that propionyl-l-carnitine stabi-an endothelium-dependent mechanism [23]. lizes plasma membrane during ischemia [56]. This effect
Propionyl-l-carnitine is one of the acyl derivatives of may relate to propionyl-l-carnitine’s ability to modifycarnitine, a naturally occurring substance required for the the molecular dynamics of the membrane bilayer regiontransport of long-chain acyl groups derived from fatty close to the glycerol backbone of phospholipids, asacids across mitochondrial membranes, a necessary pre- shown in an in vitro study on human red cell membranesliminary event to fatty acid oxidation and hence ATP pro- [21]. Consistent with this interpretation are additionalduction [24, 53]. Depletion of this cofactor has been reports showing that propionyl-l-carnitine treatment ofreported in several pathologic conditions, including myo- diabetic rats restored the ability of intact red cells tocardial ischemia [54, 55]. Thus, the possibility exists that re-acylate membrane phosphatidylcholine [57], and that
this compound inhibited platelet-activating factor syn-propionyl-l-carnitine may protect ischemic tissues by

Mister et al: Propionyl-l-carnitine and ischemic injury1076
thesis in human neutrophils and platelets [20]. That in- duced early intragraft granulocyte infiltration. This find-deed propionyl-l-carnitine preserved cell membrane in- ing indicates that, in addition to directly limiting freetegrity is supported by our findings of consistent reduction radical formation by renal parenchymal cells, propionyl-l-of LDH release, a cell injury marker [51, 58], into the per- carnitine may have contributed to restore graft functionfusate of IPKs exposed to ischemia/reperfusion. More- by largely avoiding the additional tissue damage thatover, the possibility that the protective action of propio- would have been triggered by granulocytes recruited intonyl-l-carnitine involved a cellular effect other than the the graft after ischemia-reperfusion.energy-linked one after experimental ischemia rests also It also should be taken into account that propionyl-l-on the histological findings of very mild post-ischemic le- carnitine has been shown to be beneficial by amelioratingsions both in the thick ascending limbs and in the proximal ischemic damage to the mitochondria through inhibitiontubules in kidneys exposed to the drug, a pattern even bet- of the toxic effect of amphiphilic compounds like lyso-ter than that of non-ischemic control IPKs. This is sup- phospholipids or long chain acylcarnitines [9, 19, 67, 68].ported also by in vivo data that propionyl-l-carnitine par- This could be an additional mechanism by which propio-tially reduced tubular damage in syngeneic transplanted nyl-l-carnitine afforded protection in our models of renalkidneys pre-exposed to four hours of cold ischemia. ischemia-reperfusion injury.
The effects of propionyl-l-carnitine on membrane in- In summary, propionyl-l-carnitine is of value in pre-tegrity and phospholipids also may account for attenua- venting the renal function deterioration that occurs aftertion of oxidant stress. Indeed, evidence is available that tissue ischemia-reperfusion injury in ex vivo isolated per-the compound protects from lipid peroxidation and free fused rat kidney preparation as well as in a model ofradical formation [59, 60]. This suggests that infusion of syngeneic kidney transplantation. The beneficial effectcarnitine derivatives into the renal artery may have pre- of propionyl-l-carnitine possibly relates to its ability ofvented deterioration in renal function by limiting oxygen reducing lipid peroxidation and free radical generation,radical generation during ischemia-reperfusion. Indeed, which contributes to the preservation of tubular cell struc-immunohistochemical detection of 4-hydroxynonenal pro- ture and function as well as prevention of tissue inflamma-tein adducts, a major product of lipid peroxidation [40, tory cell infiltration. Further studies, however, are re-48, 49], was very low in kidneys infused with propionyl- quired to get more insights on the relevant mechanismsl-carnitine and exposed to ischemia/reperfusion as com- through which propionyl-l-carnitine exerts its beneficialpared with untreated ischemic kidneys. Interestingly, re- effect on renal ischemia-reperfusion injury. Nevertheless,duction of 4-hydroxynonenal protein adduct generation these findings open perspectives for treatment to preventmainly occurred at cortical and medullary tubules, the post-transplant delayed graft function, which may improvestructures more susceptible to the ischemic-reperfusion patient outcome after renal transplantation.injury. In line with these findings also are data that inIPKs, propionyl-l-carnitine completely prevented the in- ACKNOWLEDGMENTScrease of MDA concentration in the venous effluent after
This work was partially supported by a grant from Sigma-Tau.reperfusion.We thank Dr. Nerina Corsico (Sigma-Tau, Industrie FarmaceuticheBy limiting free radical formation and preserving tubu- Riunite S.p.a., Rome, Italy) for kindly providing propionyl-l-carnitine
lar cell integrity propionyl-l-carnitine also is expected to and l-carnitine, and Mr. Alessandro Peschechera for performing theATP measurements. The authors also thank Dr. Agnieszka Czauz forprevent the active inflammatory responses associated withtechnical assistance, Mr. Gianfranco Marchetti for the work on tissueparenchymal injury after ischemia-reperfusion through histology, and Ms. Daniela Rottoli for technical assistance. Ms. Feder-
the release of cytokines and chemokines [61]. Available ica Casiraghi helped to prepare the manuscript.evidence shows that sublethally or even lethally injured
Reprint requests to Marina Noris, Chem. Pharm. D., Mario Negriproximal tubular and endothelial cells as a consequenceInstitute for Pharmacological Research, Via Gavazzeni 11, 24125 Ber-
of tissue hypoxia/reperfusion injury may act as a trigger gamo, Italy.E-mail: [email protected] this inflammatory reaction [61–63]. In particular, poly-
morphonuclear cells (PMNs) recruited during reperfu-sion have long been implicated as critical mediators of REFERENCESthe early renal parenchymal injury in ischemic acute 1. Belzer FO: Evaluation of preservation of the intra-abdominalrenal failure [64, 65]. PMNs, by amplifying an inflamma- organ. Transplant Proc 25:2527–2530, 1993
2. Cecka JM, Cho YW, Terasaki PI: Analyses of the UNOS scientifictory response that leads to the generation of vasocon-renal transplant registry at three years: Early events affecting trans-strictor agents [52], cytokines, and toxic mediators such plant success. Transplantation 53:59–63, 1992
as reactive oxygen species and proteases [66], may ulti- 3. Gaston RS, Schlessinger SD: Delayed graft function after re-nal transplantation: Causes, implications, and clinical management.mately induce additional damage in post-ischemic renalJ Nephrol 7:313–321, 1994injury. Our results found that propionyl-l-carnitine added
4. Shoskes DA, Halloran PF: Delayed graft function in renalto the cold storage solution of kidneys undergoing four transplantation: Etiology, management and long-term significance.
J Urol 155:1831–1840, 1996hours of cold ischemia before transplantation largely re-
Mister et al: Propionyl-l-carnitine and ischemic injury 1077
5. Lu CY: Ischemia, injury and renal allograft rejection. Curr Opin 28. Suzuki Y, Kamikawa T, Kobayashi A: Effects of L-carnitine ontissue levels of acyl carnitine, acyl coenzyme A and high energyNephrol Hyper 5:107–110, 1996
6. Paller MS, Greene EL: Role of calcium in reperfusion injury of phosphate in ischemic dog hearts. Jpn Circ J 45:687–694, 198129. Folts JD, Shug AL, Koke JR: Protection of the ischemic dogthe kidney, in Cellular, Biochemical, and Molecolar Aspects of
Reperfusion Injury, edited by Dipak KD, New York, Annals of myocardium with carnitine. Am J Cardiol 41:209–214, 197830. Ferrari R, Ceconi C, Curello S, et al: Protective effect of propio-the New York Academy of Sciences, 1994, p 59
7. Burke TJ, Schrier RW: Pathophysiology of cell ischemia, in Dis- nyl-L-carnitine against ischemia and reperfusion damage. Mol CellBiochem 88:161–168, 1989eases of the Kidney, edited by Schrier RW, Gottschalk CW,
Boston, Little Brown & Co., 1997, p 1013 31. Liedtke AJ, Demaison L, Nellis SH: Effect of L-propionyl-carni-tine on mechanical recovery during reflow in intact hearts. Am J8. Schrier RW, Arnold PE, Van Putten VJ, Burke TJ: Cellular
calcium in acute renal failure. Role of calcium entry blockers. Physiol 255:169–176, 198832. Perico N, Delaini F, Tagliaferri M, et al: Effect of platelet-Kidney Int 32:313–321, 1987
9. Yamada KA, Kanter EM, Newatia A: Long-chain acylcarnitine activating factor and its specific receptor antagonist on glomerularpermeability to proteins in isolated perfused rat kidney. Lab Investinduces Ca2+ efflux from the sarcoplasmic reticulum. J Cardiovasc
Pharmacol 36:14–21, 2000 58:163–171, 198833. Bonsnes RW, Taussky HA: The colorimetric determination of10. Weir MR: Calcium channel blockers in organ transplantation:
Important new therapeutic modalities. J Am Soc Nephrol 1(Suppl creatinine by the Jaffe reaction. J Biol Chem 158:581–586, 194534. Boyce NW, Holdsworth SR: Direct anti-GBM antibody induced1):S28–S38, 1990
11. Chambers DJ, Braimbridge MV, Hearse DJ: Free radicals and alteration in glomerular permselectivity. Kidney Int 30:666–672, 198635. Noris M, Azzollini N, Mister M, et al: Peripheral donor leuko-cardioplegia: Allopurinol and oxypurinol reduce myocardial injury
following ischemic arrest. Ann Thorac Surg 44:291–297, 1987 cytes prolong survival of rat renal allografts. Kidney Int 56:1101–1112, 199912. Myers ML, Bolli R, Lekich CJ, et al: Enhancement of recovery
of myocardial function by oxygen free radical scavengers after 36. Dragun D, Tullius SG, Park JK, et al: ICAM-1 antisense oligode-soxynucleotides prevent reperfusion injury and enhance immediatereversible regional ischemia. Circulation 72:915–921, 1985
13. Przyklenk K, Kloner RA: Superoxide dismutase plus catalase graft function in renal transplantation. Kidney Int 54:590–602, 199837. Di Lisa F, Menabo R, Barbato R, Siliprandi N: Contrastingimprove contractile function in the canine model of the stunned
myocardium. Circ Res 58:148–156, 1986 effects of propionate and propionyl-L-carnitine on energy-linkedprocesses in ischemic hearts. Am J Physiol 267:H455–H461, 199414. Hauet T, Bauza G, Goujon JM, et al: Effects of trimetazidine on
lipid peroxidation and ph metabolites during cold storage and 38. Uchida K, Szweda LI, Chae H-Z, Stadtman ER: Immunochemi-cal detection of 4-hydroxynoneal protein adducts in oxidized hepa-reperfusion of is perfused rat kidneys. J Pharmacol Exp Ther 285:
1061–1067, 1998 tocytes. Proc Natl Acad Sci USA 90:8742–8746, 199339. Aiello S, Noris M, Todeschini M, et al: Renal and systemic nitric15. Riera M, Torras J, Herrero I, et al: Neutrophils accentuate renal
cold ischemia-reperfusion injury, role of PAF and beneficial effect oxide synthesis in rats with renal mass reduction. Kidney Int 52:171–181, 1997of a PAF antagonist. J Pharmacol Exp Ther 280:786–794, 1997
16. Portilla D, Dai G, Peters JM, et al: Etomoxir-induces PPAR- 40. Esterbauer H, Cheeseman KH, Dianzani MU, et al: Separationand characterization of the aldehydic products of lipid peroxidationalpha-modulated enzymes protect during acute renal failure. Am
J Physiol 278:F667–F675, 2000 stimulated by ADP-Fe2+ in rat liver microsomes. Biochem J 208:129–140, 198217. Lango R, Smolenski RT, Narkiewicz M, et al: Influence of
L-carnitine and its derivatives on myocardial metabolism and func- 41. Esterbauer H, Schaur RJ, Zollner H: Chemistry and biochemis-try of 4-hydroxynoneal, malonaldehyde and related aldehydes.tion in ischemic heart disease and during cardiopulmonary bypass.
Cardiovasc Res 51:21–29, 2001 Free Radic Biol Med 11:81–128, 199142. Noris M, Ruggenenti P, Todeschini M, et al: Increased nitric ox-18. Sayed-Ahmed MM, Salman TM, Gaballah HE, et al: Propionyl-
L-carnitine as protector against adriamycin-induced cardiomyopa- ide formation in recurrent thrombotic microangiopathies: A pos-sible mediator of microvascular injury. Am J Kidney Dis 27:790–thy. Pharmacol Res 43:513–520, 2001
19. Sayed-Ahmed MM, Shouman SA, Rezk BM, et al: Propionyl- 796, 199643. Wallenstein S, Zucker CL, Fleiss JL: Some statistical methodsL-carnitine as potential protective agent against adriamycin-in-
duced impairment of fatty acid beta-oxidation in isolated heart useful in circulation research. Circ Res 47:1–9, 198044. Brezis M, Rosen S, Silva P, Epstein FH: Transport activity mod-mitochondria. Pharmacol Res 41:143–150, 2000
20. Triggiani M, Oriente A, Golino P, et al: Inhibition of platelet- ifies thick ascending limb damage in the isolated perfused kidney.Kidney Int 25:65–72, 1984activating factor synthesis in human neutrophils and platelets by
propionyl-L-carnitine. J Biochem Pharmacol 58:1341–1348, 1999 45. Shanley PF, Shapiro JI, Chan L, et al: Acidosis and hypoxicmedullary injury in the isolated perfused kidney. Kidney Int 34:791–21. Arduini A, Gorbunov N, Arrigoni-Martelli E, et al: Effects of
L-carnitine and its acetate and propionate esters on the molecular 796, 199846. Hauet T, Mothes D, Goujon JM, et al: Protective effect of polyeth-dynamics of human erythrocyte membrane. Biochim Biophys Acta
1146:229–235, 1993 ylene glycol against prolonged cold ischemia and reperfusion in-jury: Study in the isolated perfused rat kidney. J Pharmacol Exp22. Sassen LMA, Bezstarosti K, Van Der Giessen WJ, et al: L-pro-
pionylcarnitine increases postischemic blood flow but does not ef- Ther 297:946–952, 200147. Neale TJ, Ojha PP, Exner M, et al: Proteinuria in passive Hey-fect recovery of energy charge. Am J Physiol 261:H172–H180, 1991
23. Cipolla MJ, Nicoloff A, Rebello T, et al: Propionyl-L-carnitine mann nephritis is associated with lipid peroxidation and formationof adducts on type IV collagen. J Clin Invest 94:1577–1584, 1994dilates human subcutaneous arteries through an endothelium-
dependent mechanism. J Vasc Surg 29:1097–1103, 1999 48. Benedetti A, Comporti M, Esterbauer H: Identification of4-hydroxynonenal as a cytotoxic product originating from the per-24. Bremer J: Carnitine—metabolism and functions. Physiol Rev 63:
1420–1480, 1983 oxidation of liver microsomal lipids. Biochem Biophys Acta 620:281–296, 198025. Davies EJ, Spyderold O, Bremer J: Pyruvate carboxylase and
propionyl-Co-A carboxylase as anaplerotic enzymes in skeletal 49. Benedetti A, Pompella A, Fulceri R, Comporti M: Detection of4-hydroxynonenal and other lipid peroxidation products in themuscle mitochondria. Eur J Biochem 110:255–262, 1980
26. Paulson DJ, Traxler J, Schmidt M: Protection of the ischaemic liver of bromobenzene-poisoned mice. Biochem Biophys Acta 876:658–666, 1986myocardium by propionyl-L-carnitine. Effect on the recovery of
cardiac output after ischaemia and reperfusion, carnitine transport 50. Rosenfeld ME, Palinski W, Yla-Herttuala S, et al: Distributionof oxidation specific lipid-protein adducts and apolipoprotein B inand fatty acid oxidation. Cardiovasc Res 20:536–541, 1986
27. Tassani V, Cattapan F, Magnanimi L, Pescherchera A: Anapler- atherosclerotic lesions of varying severity from WHHL rabbits.Arteriosclerosis 10:336–349, 1990otic effect of propionyl carnitine in rat heart mitochondria. Bio-
chem Biophys Res Commun 199:949–953, 1994 51. Hauet T, Mothes D, Goujon J-M, et al: Trimetazidine reverses

Mister et al: Propionyl-l-carnitine and ischemic injury1078
deleterious effects of ischemia-reperfusion in the isolated perfused tives on heart mitochondrial damage induced by lipid peroxidation.Pharmacol Res Comm 20:125–132, 1988pig kidney model. Nephron 80:296–304, 1998
60. Kotaka K, Miyazaki Y, Ogawa K, et al: Reversal of ischemia-52. Herrero I, Torras J, Riera M, et al: Prevention of cold ischae-induced mitochondrial dysfunction after coronary reperfusion.mia-reperfusion injury by an endothelin receptor antagonist inJ Mol Cell Cardiol 14:223–231, 1982experimental renal transplantation. Nephrol Dial Transplant 14:
61. Bonventre JV: Mechanisms of ischemic acute renal failure. Kidney872–880, 1999Int 43:1160–1178, 199353. Siliprandi N, Ciman M, Sartorelli L: Myocardial carnitine trans- 62. Bonventre JV, Colvin RB: Adhesion molecules in renal disease.
port. Basic Res Cardiol 82:53–62, 1987 Curr Opin Nephrol Hyper 5:254–261, 199654. Schwartz A, Wood JM, Allen JC: Biochemical and morphologic 63. Bevilacqua MP, Nelson RM, Mannori G: Endothelial-leukocyte
correlates of cardiac ischemia. I. Membrane systems. Am J Cardiol adhesion molecules in human disease. Ann Rev Med 45:361–378,32:46–61, 1973 1994
55. Shug AJ, Thomsen JH, Folts JD: Changes in tissue levels of car- 64. Thornton M, Winn R, Alpers CE, Zager RA: An evaluation ofthe neutrophil as a mediator of in vivo ischemic-reperfusion injury.nitine and other metabolites during myocardial ischemia and an-Am J Pathol 135:509–515, 1989oxia. Arch Biochem Biophys 187:25–33, 1978
65. Brady HR: Leukocyte adhesion molecules and kidney disease.56. Hulsmann WC: Biochemical profile of propionylcarnitine. Cardio-Kidney Int 45:1285–1300, 1994vasc Drugs Ther 5(Suppl 1):7–9, 1991
66. Heinzelmann M, Mercer-Jones MA, Passmore IS: Neutrophils57. Arduini A, Dottori S, Sciarroni AF, et al: Effect of propionyl-and renal failure. Am J Kidney Dis 34:384–399, 1999L-carnitine treatment on membrane phospholipid fatty acid turn- 67. Mutomba MC, Yuan H, Konyavko M, et al: Regulation of the
over in diabetic rat erythrocytes. Mol Cell Biochem 152:31–37, 1995 activity of caspases by L-carnitine and palmitoylcarnitine. FEBS58. Heyman SN, Rosen S, Epstein FH, et al: Loop diuretics reduce Lett 478:19–25, 2000
hypoxic damage to proximal tubules of the isolated perfused rat 68. Xiao CY, Chen M, Hara A, et al: Palmitoyl-L-carnitine modifieskidney. Kidney Int 45:981–985, 1994 the myocardial levels of high-energy phosphate and free fatty acids.
Basic Res Cardiol 92:320–330, 199759. Ferrari R, Ceconi C, Curello S, et al: Effect of L-carnitine deriva-
Top Related
Copyright © 2022 FDOKUMEN

