






Bahasa
Halaman
Hukum


1
MASTER’S THESIS
Davide Ticchi
Normal Deformities Those Who Make Me Feel Like Many Others
Supervisor: Patrick Laviolette
Tallinn 2014
Department of Social and Cultural Anthropology
Estonian Humanities Institute – Tallinn University

2
For my parents,

3
Table of contents:
Summary 4 The Beginning of Our Stigmatic Journey 5
1. Chest Wall Deformities: Asymmetries of Lived Experience 11
2. Family Reactance and Individual Resilience 21
3. Those Who Make Me Feel Like Many Others 37
4. From Analogies To Meshwork Therapies: Narrative Deformities 55 The End of Our Stigmatic Journey 68 Acknowledgments 69 References 71
Notes 79
4
Summary:
This dissertation aims to make patients and therapists more aware of the psycho-social
and anthropological issues related to chest wall deformities (Pectus Excavatum, Pectus
Carinatum, Poland syndrome and so on). Stories of 'normal deformities' were recorded at two
children’s hospitals: Gaslini di Genova (in Italy) and Tallinna Lastehaigla (in Estonia). In
both settings, many deformed youngsters wanted to rid themselves of their uncomfortable
'stigma' through corrective surgery. Such a scenario allowed the collaboration between a
social scientist and two surgeons. It inspired a counselling psychology and medical
anthropology meshwork which encompasses the asymmetries of lived experience when being
conscious of chest wall deformities. Indeed, by listening, questioning and sharing with the
accounts of patient participants, owing to Interpretative Phenomenological Analysis, we enter
from this point forward into the kernel of a life-world for informants and the medical milieu
of body image disturbance (Smith, Flowers & Larkin, 2009).
The first-hand narratives recounted also inform an assessment model described in the
last chapter. This chronicles, perhaps even measures the degree of well-being for patients,
both in their social and private surrounding. Moreover, a discourse on family resilience and
resistance often appears throughout the dissertation. It assumes that how parents behave may
strongly encourage or hinder the success of teenagers in coping with their own ‘stigma’, thus
unfolding a lingering influence upon ‘normals’ who turn to those who do not feel like many
others. Taking into account the works of Gelya Frank, Erving Goffman and Linda Finlay,
ultimately this project aims to increase the attunement of therapists to patients – with their
physical stigma, either medically diagnosed or imagined.

5
The Beginning of Our Stigmatic Journey:
I started collecting fieldwork data within two unattractive hospital departments of
paediatric surgery. The first at Ospedale Gaslini di Genova and the other at Tallinna
Lastehaiga. Both consisted of rooms which run parallel to the corridor, plus one small
doctor’s office. In the beginning I tried to guess the different ‘home places’ from where my
informants originated. In Italy their accent and look helped me. My intention was to make
them feel comfortable, familiarising and finding a common ground based on widespread
imaginaries of wild but touristic islands in Sicily, or long and sandy beaches in Sardinia.
Apart from anthropologists ‘in search of respect’, indeed, I noticed that this strategy is shared
with other therapists too.1 It is no surprise the increasing relevance of psychological
anthropology along with the “evidence that understandings of illness and the consequent
social response may determine the prognosis of severe mental illness, independently of any
recourse to medical treatment” (Littlewood, Jadhav, Ryder, 2007: 172).
Thus, the credibility of psychological anthropology in hospitals is a serious matter of
bargaining, insofar as the discipline is not fully established. In this regard, Murphy reminds us
that:
The average general hospital must work according to a thoroughly “rationalized” system. There is
an elaborate division of labor, a meticulous allocation of responsibilities, and a careful scheduling
of activities. The hospital has all the features of a bureaucracy, and, like bureaucracies everywhere,
it both breeds and feeds on impersonality.2
1 Alluding to Bourgeois, Bourgeois, P. In Search of Respect: Selling Crack in El Barrio (Structural Analysis in the Social Sciences). 2 Murphy, pp. 20-21. << A key rule for being a successful sick person is: Don’t complain! The person who smiles and jokes while in obvious physical misery is honoured by all. Doctors and nurses are especially appreciative of this kind of patient, for he usually follows orders and seldom files malpractice suits. Hospital visitors also value cheeriness, and the sick person soon finds that he is expected to amuse them, and thus relieve their guilt at being well. These are front-area, or on-stage, performances – to use sociologist Erving Goffman’s celebrated theatrical metaphor for social interaction. The backstage behaviour may be totally different, however, and the public hero may become a whiner at home. >>

6
Luckily, both surgeons I assisted are enthusiast to work in a children’s hospital instead
of an ‘average general hospital’, and allowed me to try out a counselling model with their
patients – at Ospedale Gaslini during a monthly day hospital with a dozen of names on the
list, and at Lastehaigla when a few corrective procedures were completed. What differs is a
higher attention to others’ feelings in assessing the body. When naming anatomical parts, for
instance, their vocabulary shifts to childish words with early teenagers (e.g. Pectus
Excavatum → tiny hole), reverting to the official standard with older patients.
Owing to the run of time and a rather claustrophobic setting, I learned the importance of
having experienced already the same circumstance almost ten years before, when alone with
my parents I met the superior of Dr Torre – the Italian surgeon who operated me and allows
to make this project real. Since the moment when I experienced the impact of reality on the
realm of private worries, dreams and expectations, I have been wondering how other people
may feel, whether brave, afraid, or defiant. My fieldwork would answer that they are mostly
silent, letting someone or something else speak for them, conforming that what I experienced
in adolescence is true for many patients today. As though parents, clothes and eyes may say
more truths than opening their mouth, at least in public and before the operation. This is why
although medical examinations are usually private, alien to the either pleasant or unpleasant
routines of life, my descent into teenage lives has shown me that chest wall deformities
(CWDs) embrace both the private and social sphere of a person.
Thus, the intention of giving voice to them made me meet roughly forty teenagers and
young adults, everyone with his or her own story and peculiar impulse to leave the bedroom
and meet a surgeon. In addition, I met their families, also thrown into the hospital from far
and diverse places, with the hopeful need to find a sheet attesting officially the name of a
syndrome, a deformity, or just a don’t worry about it. I entered this world both with anxiety
and enthusiasm, aware of looking for answers to my old questions and new questions for my
informants. I met the uncertainty of researching what you can only guess is the right thing to
investigate, and above all the indefinability of being an anthropologist, a role that with
whatever prefix (medical, psychological, visual, etc.), is defined only in practice and
faithfulness. Relying on my instinct and the methodological skills I developed at university,
reading on buses, aircrafts and trains, but mostly living and experiencing the cultural jet-lag
moving from a ‘warm country’ like Italy to the small and reserved Estonia – as many of my
Nordic friends like to say.
As a matter of fact, comparing these two worlds I have not learnt that differences
prevail over similarities, but that life stories change according to one’s lived experience,

7
spoken language, and cultural imprinting. That is to say, when anthropologists look for an
exciting and exotic otherness, primarily they seek something that most people are resigned to
never find: truths. As such, finding myself inside all the people I encountered during this
fieldwork, I had gotten used to accept the obtrusiveness of being there without any formal
need, or as my professor Carlo A. Cubero reminded me, “giving them nothing” except for
counselling. All in all any fieldwork – especially at its earliest stage and in foreign countries –
helps us to find ourselves exactly where we are lost.
Further, I am happy that Dr Härma accepted to participate at the annual conference on
CWDs in Saint Etienne after Dr Torre invited him.3 By collaborating with them, now they can
join forces. Moreover, while I was becoming more competent on as a researcher-counsellor, I
never forgot patients and the importance of receiving their suggestions for my work. Overall,
I recorded almost thirty hours of chats, confessions, diagnoses, as well as proposed a multiple
answer questionnaire both in Italian and Estonian. As a result, the variety of the material
collected – digital recordings, statistics, scientific publications, field notes and footage, thanks
to MAXQDA and my photographer friend Anna Forgione – simplifies the process of cross-
validation and periodical update of information. Although my role has likely been unclear to
my informants, as a psycho-anthropologist who sits on a chair catching the feelings of
deformed teenagers, in the end I am able to illustrate how counselling worked with them.
Valorising ‘narrative’ as a way of coming back home with clear and available data, I hope to
raise the discussion around those psycho-social dynamics which influence boys and girls with
CWDs. This will show how anthropology can introduce new perspectives in certain medical
secrets that hide behind closed doors.
Moreover, the manner to elicit fragments of life from every patient in terms of familial
relationships, for example, has represented a phenomenological approach to anthropologists
who share similar topics and methods. It is reading Robert F. Murphy and Gelya Frank, in
particular, that I have been provided of a spotlight on a mosaic of individualities – or ‘cultural
biographies’, as the latter would rather call them.4 Here, the difference with these authors
consists in investing the time of my fieldwork with approximately thirty persons bearing
3 http://www.chirpediatric.fr/upload/documents/divers/Last_2de_Workshop_ENGLISH.pdf 4 Frank, p. 2. << It is an experiment I call cultural biography, which combines the genres of ethnography and life history. Ethnography is the cultural anthropologist’s stock-in-trade, a firsthand description of a people’s way of life. Unlike the early anthropologists, whose published works often consist of cultural inventories and static generalisations about the people they studied, contemporary anthropologists tend to write narrative ethnographies. These are stories based on events we have experienced – more as observing participants than as participant observers – through which we try to convey how people within a particular group or tradition create meaningful solutions to life’s challenges. >>

8
almost the same kind of problem, whereas Frank, for example, dedicated two decades of her
life to the key informant Diane DeVries, a lady born without limbs in Long Beach.
Conversely, I have been lacking a continuous update in my two field-sites – due to the
monthly time schedule of day-hospitals and operations – yet having the chance to keep in
touch with some informants, and to meet an eighteen years old Italian at his home place.
When I met David for the first time, his self-confidence surprised me. I sat from
lunchtime to dinnertime in Dr Torre’s studio. Meanwhile, patient after patient was called in
so that I had almost lost count of how many worries and diagnoses intertwined. I presented
myself as a researcher of medical anthropology – often forced to give a quick overview about
what that might be – then proposed my survey questionnaire for participants between thirteen
and twenty-three years old. In fact, I assumed that younger patients would not have enough
experience with topics of gender, sexuality and social influence to talk with me. It also
seemed, unlikely they would have answered my written questions without the obtrusive help
of parents. On the other hand, I had not the chance to meet any patient older than 23 years
old, as rarely but periodically both the Italian thoracic surgeon and the Estonian orthopaedist
do.
From this I discovered that I prefer a more circumscribed group of informants, not only
in terms of age but according to parameters of sex and diagnosis as well, since a detailed
spectrum of data avoids generalisations and makes comparisons easier. The reason why
quantitative data collected from patients of the two hospitals are differentiated by sex and age,
minimising the risk of vagueness. It also allows for these data to be made available to the
medical staff, as shown in the following example:
Survey conducted at Ospedale Gaslini during three days
of CWDs outpatient examinations
3
2
5 1
1
2
3
Age 13
14
15
16
18
19
23
14
3
Sex
Males Females

9
The typology of questions varies slightly whether the fifteen points of the questionnaire
are filled by pre or post-operative patients, covering those ‘blank spaces’ during the
conversation I could not discuss for their frequent embarrassment both in front of parents and
a stranger like me. Therefore, since it was not compulsory to answer every question because
of concern over reticence (an important finding in itself), one can find an example of how
much focus has been dedicated to patients’ own sense-making:
1) What made you decide to contact a surgeon who operates on deformed patients?
An evident deformity A physical imperfection
The wish to have a normal chest The wish to have a beautiful chest
Functional problems (breathe, heart) The discomfort of a different body’s look
My parents My relatives
Other ……………………………………………………………………………………….
The British film director Peter Greenaway says about cinema: “life is not a rectangle or
a parallelogram, so what are you doing sitting in the dark?”. Similarly, I consider the
questionnaire above as a compass and passkey, especially when an informal presentation
unsupported by papers is hard to identify or to trust, like in hospitals.5 Consequently, I have
been looking for an informant able to share with me what the others did not, carrying on a
relationship both friendly and fruitful according to this project’s goal: outlining the basics of
psycho-social care of deformed teenagers. For this purpose, after the initial stage of
‘hypothesis generation’, a ‘grounded theory’ approach provided this research with “the
progressive identification and integration of categories of meaning from the data obtained”
(Biggerstaff, 2012: 186). Developed from the collaboration of sociologists Glazer and Strauss
during the 1960s and 1970s, in fact, this methodology is designed to investigate social
processes from the bottom up, or the emergence of theory from data (Ibid.: 188, Willig, 2008:
44).
Thus, talking separately with David after the medical examination, we improvised a
counselling session where I could better understand his stubbornness to fix his physical
5 Peter Greenaway, “New Possibilities: Cinema is Dead, Long Live Cinema” , Avenali Chair in the Humanities, 13th September 2010.

10
imperfection. Though he ruled the way our conversation took place to make himself feel more
comfortable, (mostly by asking his mother to stay outside), he sought my personal viewpoint
on the severity of his aesthetic problem, which I would call instead an ‘imperfection’. From
this moment we started to communicate by email. I received his periodic updates about
summer challenges for people who are not proud of their body’s look. Most importantly,
however, I was getting closer to the social environment described in David’s own words.
Hence, invited to enter from the ‘back door’, I proposed to meet up with him again face to
face, both of us aiming to share something which may help those who feel bad for similar
reasons.
I travelled by train the same distance he covered with his mother to reach the hospital –
more than 700 kilometres from the province of Naples to Genoa – and during three days of
cohabitation, I could chronicle some of the dynamics which influence a teenager with
physical imperfections. My relatively young age facilitated me in bargaining access to his
home place. For David’s parents and sister, I seemed to represent a ‘mysterious object’, above
all strengthening his trust and my friendship with him. He still likes to hear “how am I
doing”.
On this sense of reciprocity and cooperation for a common and positive goal, I have
built up a mosaic of relationships and research outcomes, most of them belonging to the
category of ‘teenagers with CWDs’. Even though the narrative style of these chapters and
footage contributions will make sense of their struggles, either painful or exciting, the most
blurry and often mesmerising life experiences will hopefully find a place of inclusion as well.
In all likelihood, such experiential depictions will fall into one of the two following
categories: what for Augé is ‘oblivion’ and for Husserl a ‘phenomenological account’. Simply
put, patients may respectively reach a better understanding of their deformity using self-
reflection, or simply avoid to think about it, keeping everything inside.
It follows that Normal Deformities provides therapists with the perspective of patients,
and vice versa. Not only in order to give voice to them, but implementing a methodology of
counselling attuned to deformed patients. For this reason, next chapters spotlight both
existential and medical sides of dealing with an either stigmatised or fulfilling human chest.

11
1. Chest Wall Deformities: Asymmetries of Lived Experience
It takes courage to sit with
uncertainty and not-knowing, and
be open to what is emerging in the
“now” of the embodied dialogical
encounter.
Linda Finlay & Ken Evans –
To be, or not to be . . . registered:
A relational phenomenological
exploration of what State
Registration means to
psychotherapists
It is no surprise that Daniel’s father reported the case of his two cousins, respectively with a
Pectus Excavatum (PE) and a Pectus Carinatum (PC) – “one has a sunken chest, while the
other’s chest protrudes outward”. Summing up, Dr Torre thinks that “Daniel’s agenesis of the
pectoral muscle is aesthetically less harmful than a chest with a hole right in the middle”.
Similarly, scientific publications tend to classify CWDs according to their morphology, such
as a punch-shaped PE and a grand canyon shape PE among the most vivid examples. Thus,
let us have a look at the five CWDs classified by Acastello and conventionally accepted
among thoracic surgeons:

12
Cartilaginous
Pectus Excavatum,
Pectus Carinatum
PE: 90% of CWDs, (1:300-1000
live births), unknown aetiology,
40% familial
PC: Second most common CWD,
(1:1500 live births), unknown
aetiology, M:F (4-1), genetic
component
Costal
Simple or Complex,
Syndromics
Cartilaginous ribs are malformed
with unilateral or bilateral thoracic
wall depression, Simple (1-2 ribs)
Complex (>3 ribs)
Chondro-costal
Poland syndrome
Rare congenital anomaly,
(1:30.000 live births), unknown
aetiology, M:F (2-1), 4% familial
Sternal
Sternal Cleft
Rare CWD, midline fusion defect,
most common in females, 0.15%
incidence
Clavicle-scapular Scapular Combined
FIG. 1 - Acastello E. Patología de la pared torácica en pediatría.
Edit. El Ateneo, Bs.As. Argentina, 2006.
Despite this classification of CWDs, paediatric surgeons tend to customise their
vocabulary according to age, sex and behaviour of patients. Experienced doctors may also
diagnose the type of deformity without undressing the patient, since “PE patients have often a
typical aspect: they are slim and tall, with some degree of joint laxity, rounded shoulders with
a kyphotic habit and a ‘pot belly’ ” (Colombani, 2009: 119). Often, a troublesome lived
experience motivates patients to visit more than one doctor, travelling from Sicily to
Ospedale Pediatrico Gaslini di Genova and from Võru to Tallinna Lastehaigla. In these two
hospitals, for instance, I have met with more than twenty patients of thoracic surgeons
Michele Torre and Tiit Härma. Medical praxis for the diagnosis of CWDs consists in meeting

13
patients with their family, examining the chest shirtless, including CT scan, radiography or
spirometry test. Finally, consultants propose surgical correction if patients demonstrate two or
more of the following criteria (Kelly, 2008):
• symptoms;
• history of progression of the deformity;
• paradoxical movement of the chest wall with deep inspiration;
• a chest CT scan with Haller index greater than 3.25;
• cardiac compression;
• cava vein or pulmonary compression identified;
• abnormal pulmonary function studies showing significant restrictive disease;
• cardiac pathology secondary to the compression of the heart;
• history of failed previous repair;
• significant body image disturbance.
The assortment of criteria that may recommend corrective surgery induces Dr Torre and
Dr Härma to customise both diagnosis and therapy on a patient-centred basis. Indeed,
listening to patients before drawing conclusions is “now an accepted methodological
approach in psychological, health care and medical research, where our knowledge about
people is enhanced by our understanding of the individual case” (Biggerstaff, 2012: 175). For
instance, teenagers with a slight Poland syndrome like Daniel are recommended not to
undergo surgery. Psychological counselling is also important, since helps to make sense of
the lived experience of living with a deformity, and the many times you are concerned about
it. For example, Daniel’s mother is worried about next summer, knowing that he will not row
on the pedalo since his ‘thing’ is more visible when the arms rotate. Even though CWDs are
‘just’ physical abnormalities, often beget psychological discomfort and self-consciousness,
the reason why “a multidisciplinary approach is advisable in order to manage CWDs in all
their complexity” (Torre, M.; Rapuzzi, G.; Jasonni, V.; Varela, P., 2012: 131).
To sum up the result of a questionnaire filled out by twenty-two patients, 64 percent of
them consider a normal chest ‘a part of the body that looks like its anatomical representation’,
followed by ‘a part of the body with its own characteristics (nevus, anomalies, asymmetries
and so on)’, which more Estonians than Italians favour. Yet, the majority of them feels the
urge to narrate their own experience of a deformed chest. This is why Dr Torre considers also
14
the social and private surrounding of patients while keeping track of their life story, in order
to estimate the degree of motivation and domestic serenity before having the last word.
Overall, doctors prevent anyone from seeing corrective surgery as viaticum for ‘corrected’
relationships at home, which the operation alone hardly improves. In this regard, Goffman
pointed out the non- “acquisition of fully normal status, but a transformation of self from
someone with a particular blemish into someone with a record of having corrected a
particular blemish” (1963: 5). Yet the aesthetically enhancing minimally-invasive technique
called Nuss procedure (1987) – from the inventor Donald Nuss – catches the eye of many
viewers due to dozens of ‘pre and post’ videos on YouTube. The steep increase in sharing this
experience consists of video diaries often recorded in private, when the bedroom becomes the
stage of My Nuss Procedure before the eye of a webcam.
However, listening to these life stories bears the risk of taking for granted the outcome
of a still dangerous and painful operation, though the motivation of patients grows also thanks
to social media. Accordingly, the Foucauldian concept of ‘governmentality’ applied to CWDs
enlightens an individual urge of conformation to normals:
Governmentality can, therefore, be understood as the ‘art of government’ (2009: 79) or the
‘rationality immanent in the micro-powers’ (Senellart, 2009: 389) by which the state seeks to shape
the conduct of individuals. The exercise of power can take many forms and may involve coercion,
discipline, encouragement and the manipulation of desires and anxieties. Fundamentally, however,
it involves ‘acting upon an acting subject or acting subjects by virtue of their acting or being
capable of action’ (Foucault, 1982: 220). In other words, this art of governing depends on subjects
being free. (Pappa & Kennedy, 2012: 281)
Foucault explored also the dehumanising concept of ‘medical gaze’ in The Birth of the
Clinic: “that of a doctor supported and justified by an institution, that of a doctor endowed
with the power of decision and intervention” (1963: 109). Consequently, the hiding of CWDs
evokes shameful images of thieves who hold the loot under their coat, oversized like the t-
shirt of youngsters who make smoke and mirrors of their B-boy clothing style. Feeling unfree
to choose what to dress shows how ‘governmentality’ affects the decision of conforming to
normals by operating on a deformed chest. This is why parents expect surgeons to help their
son or daughter to overcome a low self-esteem. Yet, when the operation is not needed
surgeons suggest to contact a counsellor, a plastic surgeon or to try with sport. Roughly 77
percent of participants, indeed, answered that in alternative or in addition to surgery want to
improve the body’s look doing sport (only 5 percent do not feel this need, and 9 percent aim
15
for plastic surgery). Thus, physical activity applies to everyone without distinction of sex and
age, resulting in the most normalising, beautifying and ‘governmental therapy’ along with
corrective surgery.
Given the impact of malformations on lived experience, it is worth noting the
improvement of adolescent, adult and sexual life thanks to surgery, according to 53 percent of
informants. Suspects of ‘covering’ – “an effort to restrict the display of those failings most
centrally identified with the stigma”– applies to 47 percent of them (Goffman, 1963: 103).
Yet, without unfolding both their private and social surrounding we cannot understand the
strong hope for or aversion to corrective surgery. Since the typical wow! and 100% glad I did
it video diaries alone can motivate some patients, surgeons out to scout up the psychological
consequence of their diagnoses, recurring to multidisciplinary teamwork if necessary (e.g.
plastic surgeons, counselling psychologists).
Thanks to a ‘grounded theory’ approach that allows the emergence of categories from
the bottom up, we can also outline three typologies of video diaries: ‘institutional’, ‘corrected’
and ‘non-corrected’ (Biggerstaff, 2012: 188). Neat is the prevalence of clips that promote
corrective surgery in certain children’s hospitals, showing the young protagonists and their
family immensely grateful for what surgeons and medical staff do for them. Neither Dr Torre
nor Dr Härma recorded anything like this, though one corrective surgery per week makes of
Ospedale Gaslini one of the most active European hospital in the correction of CWDs. By
contrast, Tallinna Lastehaigla faces issues of limited funding for these procedures, yet
improving competence especially in the field of PC corrections. In fact, in the year 2012 these
two institutions report:
Ospedale Gaslini di Genova: 3 Pectus Carinatum (M) / 45 Pectus Excavatum (F 6 ; M 39)
Tallinna Lastehaigla: 3 Pectus Carinatum (F 1 ; M 2) / 13 Pectus Excavatum (M)
The number of operations shows a variance of 16 percent PC more in Tallinn than in
Genova, where the average of 12 year old patients is lower than in the former. Yet, leaving
behind the subtle influence of vloggers who look at the ‘miracle’, we find another side of
coping with CWDs in the encounter with a counsellor. Only a deep trust in him or her helps
youngsters to disclose their concerns, thanks to what Frank calls a ‘direct intuition’:

16
Empathy with another person's feelings is a direct intuition, an experience all its own, with no need
for symbols. In certain more complex states of empathy, however, Stein suggested that we assume
the place of the other person as the "I" at the center of her world, orienting toward the same objects
in the same way and using our imagination. (2000: 91)
Accordingly, an increasing number of boys and girls have been vlogging their story,
reporting what the doctor said and commenting each other’s posts, such as: “your deformity
look exactly like mine!”. Although these video diaries may look similar one another – eyes at
the camera and a stream of consciousness prepared beforehand – a kaleidoscope of facial
expressions and voices makes resonate each narration as unique. The most popular themes of
‘non-corrected’ videos are the years spent ignoring the name of your deformity, the concerns
about self-acceptance, and the difficulty of finding a partner that does not really care about it.
By taking off their t-shirt, they also prove the legitimacy to speak for those who have a
deformed body. Other than creating a ‘virtual community’ of deformed persons, this trend
separates those who hide their problem because too shy or ashamed of their body, from those
who deliberately film their physical beautification. However, thanks to this phenomenon:
People whose physical handicaps make it difficult to form new friendships find that virtual
communities treat them as they always wanted to be treated – as thinkers and transmitters of ideas
and feeling beings, not carnal vessels with a certain appearance and way of walking and talking (or
not walking and not talking). (Rheingold, 1993: 3)
As such, narrative accounts prevail on the visualisation of nude bodies, though often
displayed to show what the deformity looks like. Everyone seeks comments, good advices and
even diagnosis, when trying to understand if the depression of their chest is a PE or just
paranoia. The most common ‘non-corrected’ and ‘corrected’ YouTube headings are vivid,
such as My pectus excavatum life, Pectus excavatum and body transformation (Bodybuilding
motivation) and Pectus Carinatum Post-op. These examples give us the sentiment of an
intimately connected virtual community, more than the typical ‘institutional’ clip entitled
Pectus Excavatum Surgery and the Nuss Procedure plus the name of the hospital or the
doctor.i
Furthermore, video-sharing informs therapists about the way CWDs are experienced,
such as working out to develop disguising muscles or being alone with yourself. Some
vloggers also explain why avoid the beach, not far from what 50 percent of participants call
‘the desire to have a normal chest’. Another interesting aspect that emerges both from medical

17
examinations and video diaries is the concept of ‘imagined deformity’: an aesthetic
hypercriticism that lead to believe you are deformed, misinterpreting what CWDs actually are.
According to Goffman, this ‘awareness of inferiority’ is the reason why a person:
Is always insecure in his contact with other people; and this insecurity arises, not from mysterious
and somewhat disguised sources, as a great deal of our anxiety does, but from something which he
knows he cannot fix. Now that represents an almost fatal deficiency of the self-system, since the
self is unable to disguise or exclude a definite formulation that reads, ‘I am inferior. Therefore
people will dislike me and I cannot be secure with them’. (1963: 9)
Thus, surgeons must entrust their patients to a counsellor psychologist or a judicious
plastic surgeon before the growing ‘awareness of inferiority’ may frustrate those who cannot
undergo corrective surgery. Alternative therapies may avoid the risk of contemplating suicide,
which seems common among deformed patients who write on Pectus message boards. Beyond
the ‘governmentality’ of what Scheper-Hughes and Lock would call the ‘chest politic’ –
inspired by the “body politic, an artifact of social and political control”– we also find out that
a ‘beautiful chest’ is considered the best achievement of any corrective surgery (1987: 6). Yet,
59 percent of those who regard surgery as the necessary sacrifice to stop feeling ‘embarrassed
in public places (e.g. beach, swimming pool)’, must afford at least one general anaesthesia
plus an optional epidural anaesthesia, and other analgesics during rehabilitation. Arguably,
whatever the motivation to undergo corrective surgery is, doctors take it into account as a
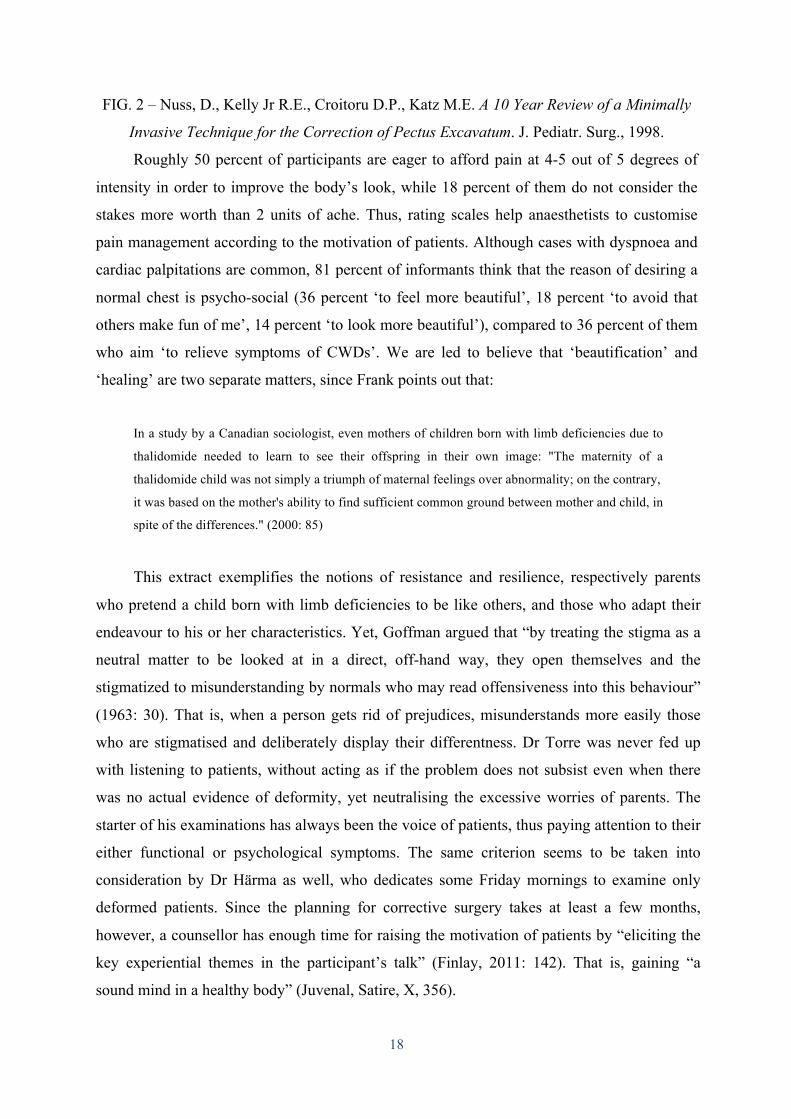
guarantee of collaboration with patients. The commitment between parties, indeed, lasts
roughly three years from the insertion to the removal of one or more titanium bars (FIG. 2).
18
FIG. 2 – Nuss, D., Kelly Jr R.E., Croitoru D.P., Katz M.E. A 10 Year Review of a Minimally
Invasive Technique for the Correction of Pectus Excavatum. J. Pediatr. Surg., 1998.
Roughly 50 percent of participants are eager to afford pain at 4-5 out of 5 degrees of
intensity in order to improve the body’s look, while 18 percent of them do not consider the
stakes more worth than 2 units of ache. Thus, rating scales help anaesthetists to customise
pain management according to the motivation of patients. Although cases with dyspnoea and
cardiac palpitations are common, 81 percent of informants think that the reason of desiring a
normal chest is psycho-social (36 percent ‘to feel more beautiful’, 18 percent ‘to avoid that
others make fun of me’, 14 percent ‘to look more beautiful’), compared to 36 percent of them
who aim ‘to relieve symptoms of CWDs’. We are led to believe that ‘beautification’ and
‘healing’ are two separate matters, since Frank points out that:
In a study by a Canadian sociologist, even mothers of children born with limb deficiencies due to
thalidomide needed to learn to see their offspring in their own image: "The maternity of a
thalidomide child was not simply a triumph of maternal feelings over abnormality; on the contrary,
it was based on the mother's ability to find sufficient common ground between mother and child, in
spite of the differences." (2000: 85)
This extract exemplifies the notions of resistance and resilience, respectively parents
who pretend a child born with limb deficiencies to be like others, and those who adapt their
endeavour to his or her characteristics. Yet, Goffman argued that “by treating the stigma as a
neutral matter to be looked at in a direct, off-hand way, they open themselves and the
stigmatized to misunderstanding by normals who may read offensiveness into this behaviour”
(1963: 30). That is, when a person gets rid of prejudices, misunderstands more easily those
who are stigmatised and deliberately display their differentness. Dr Torre was never fed up
with listening to patients, without acting as if the problem does not subsist even when there
was no actual evidence of deformity, yet neutralising the excessive worries of parents. The
starter of his examinations has always been the voice of patients, thus paying attention to their
either functional or psychological symptoms. The same criterion seems to be taken into
consideration by Dr Härma as well, who dedicates some Friday mornings to examine only
deformed patients. Since the planning for corrective surgery takes at least a few months,
however, a counsellor has enough time for raising the motivation of patients by “eliciting the
key experiential themes in the participant’s talk” (Finlay, 2011: 142). That is, gaining “a
sound mind in a healthy body” (Juvenal, Satire, X, 356).

19
This is what the new you stands for: a term used by Dr Barry LoSasso from Rady
Children’s Hospital in San Diego, and consisting in the new body’s look of patients once they
leave the operating theatre.ii Accordingly, if before the operation the posture was bowing, the
shoulders bent inward and the chest deformed, after roughly four hours under the knife each
this dented body is fixed, or even replaced with a new and dazzling model. As long as normal
bodies prove Juvenal’s equation: “mens sana in corpore sano”, those who correct their
deformity are expected to feel better, both physically and psychologically. Thus, thanks to the
‘corrected’ stories of Jimmy, Spencer and Sean, Dr LoSasso filmed the rush of emotions that
assaulted these guys when first saw their new you in the mirror. The ‘whoa!’ moment is when
you see the chest you dreamt when someone said: “something is wrong with you”. Now social
pressure pushes you in front of the same mirror with a different body, though:
O'Neill suggests that we have been "put on the machine" of biotechnology, some of us transformed
by radical surgery and genetic engineering into "spare parts" or prosthetic humans (1985: 153-
154). Lives are saved, or at least deaths are postponed, but it is possible that our humanity is being
compromised in the process. (Scheper-Hughes, Lock, 1987: 23)
Interested in the ‘compromising stage’ of the process that breaks the spell of bodies
grown deformed, O’Neill criticises the biotechnological authority of the ‘medical gaze’, as
though corrective surgery gives a better life to deformed persons but at a price. Yet, the
abilities of Dr Torre and Dr Härma make participants hope for ‘a happy adolescence’ (59
percent), ‘a happy adult life’ and ‘a happy sexual life’ (50 percent). Certain informants do not
even hide their wish to start living like their friends do, shining a light on the stronger peer
pressure and conformity behaviour among adolescents, expected to decrease in adulthood
(Sison, 2001; Brown, 2004). Although these aspirations concern the agenda of counselling
psychologists more than surgeons, Dr Torre and Dr Härma always take advantage from
motivated patients, especially when CWDs have latent symptoms. Once their chest will look
normal, 45 percent of participants plan to “change their life showing it shamelessly (e.g.
beach, swimming pool, sauna)”, thus highlighting a radical change in their habits and lifestyle.
Yet, as a study on Resilience in Competitive Athletes With Spinal Cord Injury demonstrates,
even their accidents “did not change who they were” (Machida, Iwrin, Feltz, 2013: 1060).
Finally, we must consider familial adaptation to physical stigmas, documenting how the
reactance and resilience of parents influence deformed teenagers. The next chapter thus dwells
on the analysis of phenomenological accounts coming from home straight to the hospital. It

20
shall verify if this really is “a custodial place within which the inmates live out all aspects of
their lives”, or rather a safe haven for some of their most asymmetric feelings (Murphy, 1990:
21).

21
2. Family Reactance and Individual Resilience
In every human voice there are echoes
of the mother’s tongue, echoes of
significant teachers, respected elders,
close friends; and there are accents, too,
which bind the voice to the history of a
region, a culture, and generations of
ancestors.
David Michael Levin –
The Body’s Recollection of Being:
Phenomenological Psychology and the
Deconstruction of Nihilism
Let us imagine that a CWD is an injury acquired throughout the childhood and
manifested in all its psychophysical complexity during the adolescence, and that nobody
excepting well-informed family doctors shed light on what to expect from a progressive
deformity right in the middle of my son’s or daughter’s chest. The first fear may assault
parents is the worsening of health conditions, as the sternum sinks into a deep hole or sticks
out every day a little further, all this while they are just passive audience. The sense of
impotence assaults them when deducing that their worries of parents may be even worse for
the youngster, who potentially keeps his bad feelings bottled up inside. What does a
deformed chest mean for him or her? As a researcher, “does my expertise involve
appropriation and suppression of her autonomous voice and self-determination?”, thus
jeopardising the chance of giving true voice to informants (Frank, 2000: 122). Or rather, I

22
“take control in a new humanistic sense by being clearly conscious of the choice of ensuring
co-researchers have both choice and voice themselves” (Krüger, 2007: 19).
Actually, making sure that their children feel free to book a surgical examination to
verbalise what they feel is the strategy that parents met in the hospital consider more fair.
Even when Dr Torre stated that there is no reason to worry about, usually parents admit they
could not avoid hearing the ‘call for help’ coming from a son or a daughter; as well as those
patients who really need further medical evaluations show that their family is ready to
undertake an often tiring journey in hospital. All in all CWDs require quick diagnoses in
order to guess the severity of each case. Given the evidence of a chest that likely
compromises the functionality of inner organs, the extent of time spent planning surgery is
usually shorter than the counselling session.
Going back to Daniel’s mother afraid of another troublesome summer for her teenage
son, here the parents’ fears prevail over the “very, very slight Poland syndrome” that Dr Torre
diagnosed. Indeed, though one pectoral muscle is missing, his ribs and sternum are fine and
the guy does not have any functional limitations in sports, that is an opening to any kind of
physical activity. Nonetheless, me and the surgeon know that, as Heidegger states:
When I am in a mood of sadness, then things address me quite differently or not at all. Here we do
not mean feeling in the subjective sense. Feeling [as existential mood] concerns my whole being-
in-the-world. Attunement belongs to being-in-the-world as being addressed by things. (Heidegger,
1987/2001: 202-203)
As a counsellor, thus, I must attune more to the ‘mood-as-atmosphere’ of my
interlocutors, and since Daniel is silent, at least his parents may feel free to express “their
vulnerabilities and feel that these are being heard appropriately” (Giorgi & Gallegos, 2005:
204).
Yet, Daniel is literally speechless. My focus is now his way of listening, as if a hundred
of times he heard the same words repeated, which are full of apprehension. His parents will
not hide their worries this time, rather adding some new preoccupation. Maybe it is because
Daniel experiences the Ken’s version of the ‘Barbie effect’ on women, his father argues. But
the fact of participating in this conversation does not make Daniel feel comfortable. Further,
it comes out that two older cousins of his father have both PE and PC, but he never mentioned
it to them. His high awareness of how a normal chest is supposed to look like seems partly
due to other CWDs in the family. Indeed, when taught about what are the most common

23
CWDs, punctually the two cousins come to his mind. Yet Dr Torre makes a clear distinction
between Poland syndrome and PE. When Daniel is getting dressed, I also play down saying
that nobody would ever feel ashamed of his body, excepting himself.
In the private, when Daniel is not forced to speak about it in front of a doctor, he may
think that when “symbols and cultural representations are not autonomous but, established
over long periods by complex patterns of practice, they become hugely influential” (King,
2012: 517). If so, his silence would manifest resignation to the script of family resistance.
Indeed, although his father says that “Daniel is able to weigh up the pros and cons, and at the
right time will take an independent decision”, his mother thinks that Daniel must do sport
from now, showing he has moved on from the problem.
When the surgeon writes that by his side no measures are to be taken, Daniel’s parents
ask what a severe Poland syndrome is:
1. Daniel’s minimal form (agenesis of one pectoral muscle)
2. Intermediate form (deficit of either one hand or some ribs associated to the agenesis of
one pectoral muscle, FIG. 4)
3. Serious form (deficit of both one hand and some ribs associated to the agenesis of one
pectoral muscle)
FIG. 4 - Digital mammogram (Mediolateral view) showing absence of the pectoralis major
muscle and architectural distortion on the left side and normal right breast – Salhab, M. et al.
International Seminars in Surgical Oncology, 2005.

24
Thus, Daniel’s father asks whether the problem is purely aesthetic or he could never
become a boxer, a tennis player or whatever he likes. The question is actually addressed to
the guy, who just intercepts the point but does not give an answer. By the way, comforted by
the negative diagnosis, now Daniel’s parents will to meet the plastic surgeon. The father
repeats he wants Daniel to do some sport. “Because he doesn’t?”, I ask. “He does”, he says,
“but developing only one pectoral muscle at the gym, he would highlight the agenesis of the
other half”. The surgeon nods, “many patients start working out thinking it will help them,
not realising that it’s actually worsening their body’s look”.
However, me and the family move to a separate studio, finding a more informal setting
where everyone is free to express further concerns, hoping that Daniel may also share some
of his thoughts. Once removed the ‘medical gaze’, in fact, Bremer et al. consider that:
Returning to everyday activities gives existence some stability, and clarity, and contributes to a
sense of coherence. There is a turn toward a changed life with new characteristics, where well-
being and meaning emerge through valuable human relationships. Well-being and suffering get
new meanings and coherence, which can be found when everyday existence incorporates the life
threat that, at least temporarily, has passed by. (Bremer et al., 2009: 328)
The above passage shows how interpersonal relationships train individuals in affording
their fears. As if anyone is able to reconsider one’s shame, frustration and silence, owing to
meeting the right persons and therapists. Those who make us feel like many others. Yet,
without pretending that valuable human relationships can be found only out of the family,
Daniel deals with both threats coming from his parents and the public surrounding. At the
same time, his mother and father are also afraid that either he will not accept his chest as it
looks like, or that someone, such as a girlfriend, will tell him: “I don’t like it”. Apparently,
both parents overthink Daniel’s struggles, persisting in their role of guides and tutors of their
body’s son. A topic that requires an additional research.
Maintaining a stubborn silence, Daniel aims to mark the separation from his parents’
worldview. For instance, when his mother provokes him saying that in case of breast cancer
she would recur to prosthesis, as not worth to live without one’s breast. The guy opposes that
for ladies is quite different, but she piles it on saying that actually anyone can see his physical
defect, even wearing a t-shirt. Daniel’s parents know that their son will to avoid any surgery.
He prefers to keep his chest for himself, incorporating what Bremer calls the ‘life threat’
temporarily passed by.

25
Yet, I assume that tired for the long series of medical examinations meeting doctors
who contradict each other, parents are more susceptible to misinterpret the aim of making
sure the well-being of their son or daughter. Consequently, the more his parents’ ideas are
blurry, the less Daniel will feel understood making his own choice. This is why the routine of
undertaking a sport activity is likely to play an important role in the resolution of his vow of
silence. As long as he is reserved and used to elaborate things in his own – ironic exception
among people from Tuscany – my advice is to evaluate his well-being by himself, “giving
feedback to mum and dad from time to time”. This seems to comfort them, Daniel first and
foremost.
With more enthusiasm his parents now list a series of workouts he can still do, such as
legs, abs, arms and back. Yet, his mother states that “Daniel has the problem of saying it out
loud”. Does this attitude necessarily have something to do with the stigmatising comments
and gazes at the beach? “I didn’t know what to answer them”, Daniel objects. But she insists:
“you should answer with a joke, though anyone would feel ashamed of it. Or next summer
you’ll behave spontaneously or we’ll take action”.
Vicariously, Daniel’s mother seems to experience the embarrassment of a woman
without breasts, though what is natural for her, the surgical operation, is not for her son.
Whether he wants to cope with his embarrassment because too afraid of surgery, it will just
take the time necessary to overcome his ‘blood phobia’. Although this example shows that
Daniel is better than the protagonist of My Private Pectus at coping with unease feelings, who
feels that:
The way Mike keeps looking at me doesn't help. It's not as if I don't like sex – or the idea of having
it – it's just that I might never get there. What with my chest and all. Mike goes on. ‘You've never
been laid?’ He's leaning towards me, eyebrows raised, pupils dilated. There's a million guys out
there who haven't got laid at seventeen – that’s what I tell myself. But I poke at the fire with a stick
feeling like I'm the only one. (Thamm, 2009: 29-30)
Analogies allow us to understand the battles between teenagers and the others,
emerging from the moment when an adolescent withdraws from beaches, swimming pools
and the spontaneity of being shirtless. Simple actions that recall the words of Daniel’s mother
when thinks that only a guy who behaves spontaneously is happy, a sort of ethical diktat –
“next summer Daniel will be confident with his chest or we will take action”. As every true
dilemma, however, ethics involve “the effort to constrain one’s freedom and spontaneity in
order to be open to the other person, or more precisely to allow oneself to be constrained by
26
the other” (Moran, 2000: 321). Put differently, the Foucauldian notion of ‘governmentality’
begets the ethical dilemma of what is considered right or wrong for deformed teenagers.
Shame, embarrassment, withdrawal and loneliness are definitely out of the running for a
successful adolescence. Yet, we risk to forget that untroubled stages of life do not exist and
deformities are just one aspect of a composite tableau vivant.
However, resilience to teenagers’ worries is highly demanding for parents, especially
when the social influence of peers acts not only at the beach but by means of social networks.
Moreover, a mother who is too concerned about the peer pressure coming from friends of her
son, risks to forget the bilateral nature of influence among peers. In this regard, Brown and
Larson consider that “we expect parents, teachers, coaches, or other adults to influence
children to a much greater extent than they are influenced by them” (2009: 78). Potentially,
we just believe in this theory because we know that young bodies in search of confidence are
more vulnerable to bullying than adults.
Daniel’s mother opens up the comparison between her son’s chest and “someone who
doesn’t have his problem”, sharply evoking a ‘governmental’ chest which outclasses the
deformed body. In this case Daniel must deal with those who make him feel like an alien,
commenting the agenesis of his right pectoral muscle. Of course his parents hope he will cope
with it, though by using the adverb spontaneously they seem to ignore the way teenagers
behave. Saint-Exupéry would say that “all grown-ups were once children... but only few of
them remember it” (1943). Accordingly, Daniel’s parents advocate their son by discouraging
him from living the difficulties of his age. Regardless of the Daniel’s attitude – “if it doesn’t
jeopardise my health, I will cope with it” – his parents feel allowed to seek medical advice
and offer him a host of surgical corrections.
Assuming that Daniel withdraws from friends, his mother makes a monster of the
private sphere where he spends most of his time. Yet, she seems to overlook the importance
of discovering one’s own body and senses at his age. Goodman and Baker, in this regard,
remind that “encountering the Other brings about a violent awakening to the self. Exposure to
the Other creates a denucleation and dethroning of the self ’s sovereignty and dismembers its
sense of security and comfort” (Finlay, 2011: 61). Hence, picking up the pieces of any
dethroning encounter with the other seems a positive way to grow up, and parents or
counsellors may help to make sense of such a destabilising experience.
Similarly, the capacity of being reflexive helps those who undertake psychotherapy to
find a balance in themselves. As therapists who deal with families and CWDs:

27
We need to reflect reflexively on meanings arising in our research and upon our role as (embodied)
researchers in constituting those meanings. At the same time, we also need to guard against
becoming too self-absorbed and caught up in self-indulgent introspection such that the focus of the
research shifts away from the phenomenon on to the researcher. Equally we want to avoid
situations where hyper-reflexivity results in objectifying ourselves and others. (Finlay, 2008: 79)
Finlay points out the carefulness required to therapists who enter the life-world of their
patients, when facing private issues that demand a non-interfering approach. However,
resilient families usually bargain a common and collaborative ground with deformed
adolescents and their social surrounding, normally constituted of trainers, teachers and
schoolmates. Yet, Blouin reminds us that being with others, as “in an erotic encounter it is not
just two bodies colliding but two resonating bodies evoking the surrounding world” (Finlay,
2011: 115). That is to say, in all likelihood Daniel and the other participants already know
what to expect from their social surrounding in relation to their deformity. It is no surprise
that Daniel got used to wear large t-shirts instead of tight-fitting clothes because of others.
And when his father says that “some of them behave like this because essentially they are
weaklings”, does it imply that Daniel is not?
A dichotomous thinking advantages conflicts and prejudices among teenagers,
discouraging them to place their trust in someone who may then phase you out. Educating to
consider deformities as important as a person’s character, however, would induce youngsters
“to focus even more on the cultural milieu as the source of discourses and practices in the
subject's life”, and not the body’s look alone (Frank, 2000: 153). For instance, Daniel’s father
makes up an ‘analogy of dogs’ in order to explain the attitude of his son’s friends, that is:
“our little mongrel dog growls at anyone and sometime bites too, whereas the other dog we
have is a quiet and peaceable Labrador if nobody annoys him”. Reading between the lines,
the man underlies a positive opinion of his son’s endeavour – as Daniel is quiet and peaceable
until nobody bothers him. Accordingly, favouring the implementation of physical activities
which discourage social isolation and release anger, bodily routines ensure a comfortable fit
between the lived body and surroundings (Finlay, 2011: 41).
Yet, Daniel’s mother recalls the limited freedom of swimming, as it may accentuate the
asymmetry of his pectoral muscles. Although understandably cautious, as a side effect, this
concern dissuades Daniel to relieve his stress of being commanded to do sport, dampening the
likelihood of making of physical activity an end in itself. Arguably, the fact that parents leave

28
their mark on these decisions also depends on a family-centred Italian education. Hypothesis
that Kraaykamp, Oldenkamp and Breedveld would endorse, as:
It seems likely that sport participation of children is related to the general (sport) climate in the
parental home. Parents, as initial and strongest agents of socialisation, will probably have a strong
influence on the sport activities of their children. (2012: 154)
Thus, assuming that the strongest agent who follows over a person’s life-course is a
wife or a husband, several studies confirm that “a partner may encourage and support doing
sport, but may also hinder sport, or make it less attractive. From all partner characteristics a
partner’s own sport participation is probably most influential” (Ibid.: 157).
As a matter of fact, the shift between Estonia and Italy shows that more youngsters
come to Dr Härma alone, than those who visit Dr Torre. Above all, these different trends
suggest that Estonian patients tend to undertake autonomously both decision-making and
corrective surgery. Unlikely their parents take an active part in this journey, with the result
that during the post-operative recovery more Estonians than Italians have nobody at their
bedside. Although we cannot generalise these tendencies, it seems rash to prefer one way or
another without considering both social context, made of different hospital norms and
therapeutic approaches. Hopefully, further researches on how differently patients with CWDs
experience the hospital will shed light on this comparison.
By the way, an ‘index of family manipulation’ may result by assessing how much
parents influence the sport activity of their children. Daniel’s mother already imagines how
long her son will ruminate on the many words we said today, hoping he will share some of his
thoughts with her, since what scares the most Italian parents seems to be teenagers’ silence.
Daniel’s parents are used to verbalise their fears in front of him, creating a mood-as-
atmosphere which does not allow him to answer back. Our encounter shows that what matters
to Daniel is not shared in front of his parents. Thus, how therapists may attune to both the son
and his parents? Do we have to choose one or the other?
In order to provide each party with the most fitting counselling, firstly we must resort to
‘attentive listening’, since “from the participant’s perspective, the experience of being truly
listened to – being witnessed and allowed to have a voice – can be profound” (Finlay, 2009:
210, bold is original). Further, counselling sessions already supply patients with the
therapist’s own sense-making, and a deeper understanding of how youngsters with CWDs
disguise their emotions may be achieved.

29
More precisely, Sinden points out that the a certain kind of emotions “describe a
process of struggle rather than an existing state of consensual domination that is continually
produced and reproduced” (2012: 615). Hence, only pointing out the feelings which
embarrass Daniel in front of others, a counsellor becomes able to negotiate a common ground
for the therapy. Arguably, the benefit from this practice is comparable to the gain of
professional athletes free “from the self-destructive consequences of repression, projection,
and identification” (Rose, 1998: 32). In short, allowing yourself to name the bad feelings
related to your chest, you stop living your fears alone and silent. Although competing in sport
is not the same of living with a CWD, their complementarity dwells on the need of concealing
social pressure.
******
On the other hand, Mark does not feel any pressure coming up from the sternum sunken
in his chest. Fearing an outbreak of health problems, he wants Dr Torre to reassure him. His
father is the only parent beside him, and confirms that the main reason for travelling from
Sicily to Genoa is to guarantee good health for his son. Indeed, sceptic of seeing CWDs
through the lens of psycho-social problems, Mark’s father says that his son “practices a sport
and goes to the beach regularly, as the deformity emerged a few years ago and perhaps is not
severe”. The time when deformities emerge seems to play an important role in the memory of
a family, especially when deformed teenagers change their habits as a way of adapting to a
stigmatic body. In all likelihood, straightforwardness is the attitude that allows Mark to take
up life challenges, preventing him from feeling the need of disguising himself. Indeed, both
father and son are well aware of the ‘hiding attitude’ of many deformed youngsters, yet
manifesting curiosity for the surgical techniques for the correction of CWDs.
Although Mark is defiantly self-confident, and does not take seriously the normal or
‘governmental’ body, his father asks if the gym may help him. This question gives Mark the
impression that there is always substantial room for improvement, as long as:
Normalisation works through structures of feelings, as individuals are “policed” and disciplined
through modes of internalised control. The creation of hierarchies, norms, and differentiations is
influenced by jealousy and feelings of inferiority, superiority, shame, and a desire for conformity.
(Boler, 1999: 21)

30
Mark’s father thinks that the internalised control of his son revolves around the PE, as
though physical stigmas were more accessible and intelligible than feelings. Probably, even
when Mark and his father referred to sunbathing at the beach and doing sport shamelessly, we
should keep well separated their understanding of the same activities. Brehm explains that “a
perceived diminution in freedom ignites an emotional state, called psychological reactance,
that elicits behaviors intended to restore this autonomy” (Brehm, 1966, 1972, Brehm &
Brehm, 1981). It follows that drawbacks of the body drive parents to react against CWD, seen
as a threat that may hinder their son’s or daughter’s fullness of life. This is why both Daniel’s
and Mark’s parents want to know the future prospects of living with PE.
Although the words of Mark’s father are rather optimistic, Dr Torre asks again to the
guy what drove him from Sicily to Ospedale Gaslini. Mark says he wants to know “whether it
may worsen, since at the moment does not bother me, but it is always better to know in
advance”. He is sixteen, a good age to disinter the sunken chest that systematically builds at
the gym, gaining enough muscles to feeling motivated in working out. Despite the high
resilience of the guy, thus, Dr Torre defines his PE of “a non-extremely severe kind”, yet
implying its severity. Indeed, Mark’s muscles may conceal important indicators of cardiac
compression, such as a Haller index greater than 3.25. A chest CT scan is needed before
having the last word, since both spirometry test and telecardiogram are negative. This is the
case when a surgeon misses patients’ shame when shirtless in front of people and their family
reactance, at least one necessary ally to even consider surgery. At the same time, as Daniel’s
story shown, family reactance alone may create more conflicts than solutions during decision-
making, which ultimately depends on teenagers’ will.
By making sense of wants and don’t wants of patients, Dr Torre seems eager to use
‘narrative analysis’ as “an interactive transaction with the potential for narrator and listener to
assign their own meanings to their experiences as the topic under discussion unfolds”
(Biggerstaff, 2012: 191). Thamm illustrates the case between Jack and his father in front of an
Australian doctor:
Dad starts, standing beside me as I sit in the seat by the desk. ‘Jack's got a condition. And he's
wanting to join up and I – we’, he looks at me, ‘want to know if they'll have him’ (in the army).
The doc peers at me. ‘So it's your appointment’ he asks.
I nod.
‘Do you want him here?’ the doc asks me while nodding in Dad's direction.
‘Course he does’ Dad says. ‘I mean, we both want to be here. We both want to know.’

31
The doc raises his eyebrows and lowers his glasses. ‘You sure about that?’ he says, looking
directly at me.
Immediately I like the guy. So I turn to Dad. ‘We won't be long, you can wait outside.’
Devastated, Dad mopes towards the door, but can’t help himself as he opens it. ‘You sure?
Sometimes it’s good to have some support.’
‘I’m fine.’
He leaves, but I can still make out his shadow behind the frosted glass. (2009: 192-193)
This extract shows that even a novel can inform therapists, and for positive
collaborations between therapists and parents, teenagers should feel free to speak, resorting to
their own sense- and decision-making. Even if no ‘sincerity threshold’ can be set, paediatric
surgeons know that the more young patients recount their problems by themselves, and the
less room is left for manipulated or misinterpreted accounts. Indeed, Jack’s father shows a
strong will of participating in the medical examination, as if he could take other advantage
than giving voice to his son. The reason why Dr Torre look at Mark and mentions future
discomforts that may derive from severe cases of PE: “body image disturbance, palpitation,
breathlessness, some bronchitis, limited resistance, pain and ailments”. Yet, as long as Mark
does not feel ashamed of his chest, though the deformity is severe, the surgeon prescribes a
chest CT scan whose result will be the Haller index (lateral diameter x antroposterior
diameter = > 3.25), a clarifying number (FIG. 5).
FIG. 5 – A CT scan of a 14 year old male with severe pectus excavatum showing a Haller
index of 3.58. A normal Haller index is about 2.5 – Wikimedia Commons, 2008.

32
In this case a counselling therapy seems unfitting, since would stress the guy more than
the deformity actually does. In fact, Mark is fully aware of the worsening of his PE, but does
not mention any discomfort because of this. He is pragmatic and likes to stop beating around
the bush, confirming that a chest CT scan is the only ‘counselling’ for confident patients.
Arguably, the attitude of Mark is rooted in “the contexts in which individuals have
lived, including the particular family milieu” (Frank, 2000: 149). Dr Torre is aware of both
the resilience of his patient, and the symptoms that threaten severely deformed persons. This
is why he schedules a new hospital appointment with Mark, both to analyse his CT scan and
keep track of his motivation for surgery. Somehow, the doctor expects him to change his
mind according to “(1) the importance of the freedom that is eliminated or threatened, and (2)
the proportion of free behaviours eliminated or threatened” in case of a positive diagnosis
(Brehm, 1966: 389). In other words, only meeting the criteria of a positive CT scan with the
necessary psychological motivation Mark should undergo surgery. His medical journey is to
be continued, and now he asks if Dr Torre has ever operated patients like him. Those who
make him feel like many others.
******
Isabelle was born with sternum bifidum – a deficiency in the midline embryonic fusion
of the sternal halves – the reason why has been operated as a child. She is a smart adoptive
girl in middle school age like her twin brother, and lives with a foster carer, who shows to Dr
Torre the chest CT scan he prescribed to Isabelle. He quickly notices that her sternum is too
close to the girl’s heart, and keeps rolling down with his eyes along the slices of body
displayed on the screen. The doctor is seeking the segment where the organ is more
compressed by the PE acquired as a post-surgical deformity. Then he stops and shows a
picture where the shape of Isabelle’s heart is similar to a shoe, saying that “the heart should
be right in the middle, but moved to the left because it did not have enough room”. Along
with the scroll wheel sound, the foster carer points at the heart shifting to the centre of the
screen. Isabelle does not say anything. Yet, Dr Torre is unsure of the most sunken part of
Isabelle’s chest, and keeps looking for it before assessing the Haller index, which in the end
results to be pathologic because 0.75 greater than 3.25. Isabelle is silent, and the foster carer
struggles to understand this parameter, also noticing that her sternum rotated and now is very
asymmetric. The girl asks if it is supposed to be symmetric, and the surgeon says: “flat,
sure… What do we plan to do? Did we talk about any operation before?”.

33
The adoptive mother reminds Dr Torre that the last time Isabelle wanted to avoid
surgery if the reason was purely aesthetic. Consequently, the meeting of diagnostic and
psycho-social criteria seems to be missing again, forcing the surgeon to check the ECG as the
only other scientific index available, before diagnosing a severe CWD. However, Isabelle
plays football and everyone knows she has sufficient endurance. The ECG is negative,
indeed, forcing Dr Torre to take time and examine her chest once more, while saying that:
We are free to make the choice we prefer, there is no absolute right or wrong. Yet, the heart is a bit
displaced and compressed. Growing up it will not improve, but I see why you want to get away
with it, you have already some scars from the previous operations!
Certainly a tricky case, since both the personal and medical history of the girl cannot be
ignored, plus her lack of motivation rows against a pathologic Haller index. In this tension
lays the gap between the deontology of doctors – “objective outsiders looking in and
obtaining hard data to analyse” – and the ethic of a teenager – feeling that “objectivity is
constituted out of subjectivity” (Finlay, 2011: 46). Honouring Isabelle’s scars, which prove
her past medical journeys, here we move from family reactance to individual resilience, since
she plays football with passion and no deficits at all. Soon she will also compete in the track
and field Ligurian tournament, and the surgeon can only propose to wait one or two years
before drawing conclusions.
The foster carer asks whether the correction is aesthetic or functional, trying to advocate
Isabelle’s concerns, who just listens. Yet, Dr Torre considers the corrective procedure a win
for both sides. He is aware that Isabelle does not show to care of her body’s look, thus
stresses the importance of functional benefits owing to surgery. In this regard, Moi states that:
Problems do however arise if we are too sanguine about the actual possibility of making one's own
position clear. Hermeneutical theory, for instance, has pointed out that we cannot fully grasp our
own "horizon of understanding": there will always be unstated blind spots, fundamental
presuppositions and "pre-understandings" of which we are unaware. Psychoanalysis furthermore
informs us that the most powerful motivations of our psyche often turn out to be those we have
most deeply repressed. It is therefore difficult to believe that we can ever fully be aware of our
own perspective. The prejudices one is able to formulate consciously are precisely for that reason
likely to be the least important ones. (1985: 44)

34
Apart from distrusting definitive positions, Moi would invite the doctor to take time,
and Isabelle to gain experience before taking any decision. In fact, her chest may continue
worsening throughout the adolescence, as it might also stop earlier and bother the girl later.
Thus, Isabelle’s own ‘horizon of understanding’ must be open, aware that “to reach an
understanding in a dialogue is not merely a matter of putting oneself forward and successfully
asserting one’s own point of view, but being transformed into a communion in which we do
not remain what we were” (Gadamer, 1975/1996: 378–379). Only going through
transformative dialogues with significant others, Isabelle will reach a high degree of
consciousness that will beget all the answers she needs. As Gadamer highlights, indeed,
dialogue is a ‘transformative communion’ and cannot be truly experienced in the solitude of
‘pre-understandings’, such as believing that playing football will be always your first priority.
This is what Dr Torre seeks in Isabelle’s words when asks her: “do you feel pain when
playing football? Are you ashamed of your scars and hole in the chest at the beach?”.
Unperturbed, she plays down the importance of her physical defects, and fearing another
operation answers that “they are not visible”. The foster carer also explains that the swimming
costume hides properly both PE and scars.
In addition, the surgeon would prefer to correct a chest that has never been operated
before, since pushing outward a ‘non-virgin’ sternum may result less effective. The reason
why Dr Torre is doubtful and cautious before banging his head against a brick wall. He misses
the motivation of the patient that here becomes his own motivation, both necessary for taking
charge of any risky decision. At this point, Isabelle asks if another surgery means new scars
on her chest, though plastic surgery may easily fix them later. The surgeon foresees that the
development of an asymmetric breast may disturb her body-esteem in future, since among
adolescents and competitive athletes the female breast plays an important role. For instance,
Bissell and Duke undertook “a study of American television coverage of the US women’s
volleyball team games during the 2004 Olympics, and observed that a preponderance of
camera shots were focused on the breasts or buttocks of the athletes” (Keats, Keats-Osborn,
2012: 649).
Isabelle’s story shows that family reactance is more decisive than its resilience,
especially when surgical criteria are met but patient’s motivation is low. Perhaps she will
come to a decision after transformative dialogues with her foster carer, becoming aware that
well-being is both functional and aesthetic when it provides her with motivation for surgery.
Only answering to: “what will she gain by doing that?”, however, the twin brother sheds light
on the real change in Isabelle’s life after correcting her deformity. The surgeon answers that

35
“first she will gain a more beautiful body”, as long as at the moment she does not have any
symptom. Dr Torre focuses on the common sense of girls, who usually like to achieve a better
body’s look, and adds that “she could run into cardiorespiratory troubles that are harder to
treat at 40 years old when the sternum is calcified”. I argue that “after one or two years she
will be also more mature to take this decision”.
As a neither individual choice nor entirely influenced by social pressure, correcting
CWDs depends on lived experience and aspirations. For instance, “the young cyclists
suggested that the decision to dope did not happen immediately but could be affected by the
experience of losing a race and the pressure to win” (Pappa & Kennedy, 2012: 280). Hence,
self-esteem and social pressure may play a decisive role in Isabelle’s decision making, along
with the unfolding of her womanhood and personality. When asked if she has ever thought
about this operation, Isabelle answers: “yes, today it’s not the first time”. Yet, now she is
aware that undergoing surgery would imply:
Feeling pain, suspending sport activity for six month, doing a certain kind of post-operative
exercises you will hardly like. Therefore, more motivation inside of you will bring your journey to
a close. I will do my best, but you as a patient have to make an effort too, since if then you don’t
take rehabilitation seriously, why on earth should you do it? Whereas if you really want to do
something, then everything goes smoothly. (Dr Torre)
At this point, the curiosity of the foster carer spotlights what will happen if the girl
decides to undergo the Nuss procedure. Dr Torre explains that the praxis is: “five days of
post-operative recovery plus rehabilitation, but the correction is instant and should motivate
Isabelle to do it”. Nonetheless, Fitzpatrick and Finlay reminds us that:
The trauma of the original injury and surgery is followed by the dawning awareness of multiple
losses; despair and anxiety accompany the realization of dis-ability. The loss of function, of
confidence and motivation, of daily roles and activities, and of taken-for-granted physical safety,
all push the individual to retreat from the life they once lived. The result is a diminishment, a
shrinking of life. Without everyday roles and activities, life’s landscape feels barren and boring . . .
John retreats from socializing with his family and playing his sports. Jane abandons the final term
of her college, putting her life and her future on hold . . . At some point, the retreat must be halted
if rehabilitation is to be successful. So, the battle begins. The individual takes a stand to fight, to
get through, to subdue the enemy (the injury, the pain, the disability).The injured person moves
forward, determinedly and positively re-engaging with life. Helped by his wife ‘out of love’ to do
his exercises, John finds that this support fuels his determination to ‘beat the injury’. (2008: 149)
36
What may happen during the six months when I am removed from the field? Will I feel
as much energy and enthusiasm when playing football as I do now? These and other
questions haunt Isabelle, who now has to weigh pros and cons before taking her decision.
Here, both Isabelle and her family are supposed to take ‘a stand to fight’. Indeed, even if the
twin brother and the foster carer will subsume their help throughout Isabelle’s hospitalisation,
her adolescence will be necessarily diverted. For instance, the biggest threat to teenage habits
is the drop of what van Manen calls ‘existentials’, the four cardinal points in the life-world of
Isabelle in this case (1990: 101):
Lived space: the reassuring middle school classroom (stop for 1 month), the exciting football
pitch and locker room where to socialise and enjoy her favourite sport (stop for 6 months).
Lived body: her sunken chest and perhaps her scars are permanently corrected, physical
activity is suspended (swimming pool for 3 months, football for 6 months), breathing
exercises plus physiotherapy during the first month after the operation.
Lived time: the subjective perception of time passing endlessly or enjoyably before the
operation, dwelling in the hospital and after the recovery, when getting into her stride in daily
routine.
Lived relations: feeling protected or threatened by others throughout her medical journey,
reconsidering day-to-day relationships at home, on the football pitch and at school on the
basis of this exceptional circumstance.
Not only Isabelle must cope with all the physical precautions to succeed in corrective
surgery, but she will also deal with existential and social changes. In short, this decision
undermines both her private and social spheres. This is why Dr Torre asks to the girl whether
to schedule the next follow-up meeting after six or twelve months, implying the lot of
motivation she aims to gain by then. Isabelle favours the first option, thinking that six months
of stoppage time are quite enough.

37
3. Those Who Makes Me Feel Like Many Others
It’s not who I am underneath,
but what I do that defines me.
Bruce Wayne –
Batman Begins
David enters Dr Torre’s office with his mother, both look tired for the long trip from
Naples to Genoa. They sit calmly in front of me and the doctor, who gives way to the guy’s
own words to understand why they came there. “I would like to see if it is possible to solve
this problem…”, he seems to be concern about something implicit for him. Without using the
possessive adjective ‘my’, further, David shows embarrassment.
Dr Torre asks: “and then?”. “Then we will go back to Naples” is David’s laconic
answer. His mother points out that they booked a first clinical examination at Ospedale
Gaslini already two years ago, though they missed it because David had chicken pox. Now he
is eighteen years old, and admits that his problem is only aesthetic and “embarrasses me when
I go to the beach though physically doesn’t hurt me. I was twelve when it came out, and I
have been working out at the gym for three years”. After visiting him, Dr Torre describes his
deformity “of an ‘annoying’ kind, because it’s slight and limited to the right side of the
chest”. The reason why the cardiologist belied any anomaly of David’s heart.
His mother asks if genetic predisposition is conceivable in the field of CWDs, since
“after thorough observation I saw that in the middle of my chest there’s something, but well-
disguised”. Although the doctor agrees with most of the concerns of David and his mother, is
still sceptical about surgical solutions, since “the overall good condition of the chest makes
surgery worth only to reach perfection, and as a thoracic surgeon I cannot guarantee this
result without risks of failure and functional complications”.

38
This seems to confirm the hypothesis that correction of aesthetic problems by means of
traditional surgery is not advisable, and although his parents told David the same thing, he
does not accept the state of things. This is why both parents and the doctor are eager to
comply with his feelings, and Dr Torre explains him how plastic surgery can fill up with
tissues the excavated areas of his chest. In view of this chance David is still sceptic, knowing
that “when I am alone shirtless at home, I don’t know why but I feel bad watching myself,
and I am afraid that only filling up that hole might not help”. However, his mother opposes
that nobody would ever notice the imperfection again, “like a lady who makes up to disguise
her defects”. Yet, the thin line between making up and concealing yourself emerges
poignantly from Hathaway’s words:
Over and over I forgot what I had seen in the mirror. It could not penetrate into the interior of my
mind and become an integral part of me. I felt as if it had nothing to do with me; it was only a
disguise. But it was not the kind of disguise which is put on voluntarily by the person who wears
it, and which is intended to confuse other people as to one’s identity. My disguise had been put on
me without my consent or knowledge like the ones in fairy tales, and it was I myself who was
confuse by it, as to my own identity. (1943: 46-47)
Similarly, David knows that filling up his asymmetry would be just another disguise,
incapable of making him feel perfect as he wants. What his mother does not realise, indeed, is
the minor success of looking like many others, when you feel inside the burden of a mise-en-
scene. As Dr Torre argues, rather than the beautification of their body, “persons like David
seek the perfection here on earth, which is unfortunately hard to achieve, since if a severe PE
looks like your chest after the Nuss procedure, the patient is happy and I am too”. Although
respecting his discomfort, thus, the surgeon admits it is difficult to help out surgically: “we
could try, but is it sensible to operate without the guarantee of gaining a perfect result, that is
the only thing you would ever accept?”.
David aims to go the whole hog and find his answers, though he has none yet, and the
doctor suggests him to consider plastic surgery. By contrast, Diane DeVries strived to accept
“her body as ‘natural and fundamentally normal’ despite enormous social pressure to the
contrary” (Frank, 2000: 36). Similarly to David, Diane found much harder to cope with self-
acceptance, rather than bearing those who stigmatised her body since she was born. In fact,
Debra Kent reminds us that “our struggle is not unlike the striving for self-acceptance of the
millions of nonhandicapped who also fall short of the Beautiful People image. Our liberation
will be a victory for everyone” (Ibid.: 24).

39
The thin line between categories of normal and stigmatised persons, thus, brings into
question the attunement of surgery to the feelings of deformed patients. For instance,
teenagers who accept their deformity resiliently are still susceptible to meet two or more
criteria recommending surgery, such as Isabelle and probably Mark. Conversely, David feels
sad because traditional surgery does not give him hope. The question: who suffers most? is
less therapeutic than how differently do they suffer?. Attentive listening, for instance,
facilitates the elicitation of implicit meanings left aside because too painful or private, such as
David’s implicit question: “I don’t know why but I feel bad watching myself”. Assuming that
he knows from where his bad feeling takes its origin, I wonder what may hold him from
sharing ideas with the doctor, his mother and me?
Only moving to an empty office – where the surgeon and his mother did not enter –
partly answers to this question. According to Sartre, indeed, Finlay considers that:
The existential anxiety of consciousness in the face of its nothingness is allayed by what he calls
‘bad faith’. Bad faith is our refusal to take responsibility for our choices, instead we accept the
social attributions of others by conforming (self-)given roles. (Finlay, 2011: 60, bold is original)
This is why the informality of the relationship between me and David gives us enough
freedom from (self-)given roles, allowing us to start from scratch, negotiating the meaning of
words like deformity. He just asks me if the approach and methods I use are psychological, as
if he liked to undertake a psychotherapy. However, stressing the relevance of psycho-social
dynamics in the field of CWDs, we agree that “in seeking to empathise with an individual and
enter their life-world we embark on a psycho-social exploration” (Finlay, 2004: 15). David
thinks that much depends on “how one looks at the others”, and Frank wonders if:
Can anything be done by people without disabilities who want to subvert their own AB (able-
bodied) position? It takes time and effort to change one's consciousness and accord respect to
people with disabilities regarding their differences: Respect is a key concept in accepting
differentness. (2000: 80)
Reading between the lines, in this excerpt normals seem to keep ‘respect’ hostage of
prejudices before trying to subvert their able-bodied position. For example, David ignored
how his physical imperfection made him feel like until: “I was twelve years old, and at the
beach my grandmother and relatives pointed out that something was wrong with my chest”.
He never noticed it before, “only the others saw it, though problems began when I started to

40
go to the beach with my cousins and peers. The disgusted faces of some girls made me see it
as a problem, and I was ugly even in front of the mirror”. Thus, the parallel between the beach
and the mirror highlights the continuity of the public gaze into the private sphere. For
instance, “when I take a shower ‘that thing’ draws always my attention. I end up touching it,
though I will to rid myself of it wearing at least an undershirt in summer”.
This is the case of an extremely low body-esteem, and David persuaded that is the result
of social proof and authority (Cialdini, 2006). He does not consider any other conception of
his chest excepting the label of malformazione. Yet, aiming to unfold what deformities
actually are, he distinguishes deformed from normal persons to become more aware of his
own identity. His research laid the foundation of our ongoing relationship, and similarly to
Frank who wrote a cultural biography with Diane DeVries, we reconsidered the meaning of
deformities and unfolded David’s ‘identity beliefs’, since:iii
It seems possible for an individual to fail to live up to what we effectively demand of him, and yet
be relatively untouched by this failure; insulated by his alienation, protected by identity beliefs of
his own, he feels that he is a full-fledged normal human being, and that we are the ones who are
not quite human. He bears a stigma but does not seem to be impressed or repentant about doing so.
This possibility is celebrated in exemplary tales about Mennonites, Gypsies, shameless scoundrels,
and very orthodox Jews. (Goffman, 1963: 4)
Although David was far from feeling as ‘a full-fledged human being’, the variety of
bodies narrated in Daniel’s, Mark’s and Isabelle’s life stories gives him a chance to feel part
of a virtual community where he can feel like many others. In fact:
At the moment I cannot imagine to accept my chest, but maybe growing up... Since above all I
think it’s a state of mind. For example, I often participate in the Comicon Festival where people
disguise as superheroes, and I feel bad thinking that I can’t wear the Batman costume because
everybody would see everything, and it would be shocking. Even when nobody can see it, I feel as
they do, and this influences my posture, more curved than normal. I also feel shy to assert myself,
since once at the gym my friend’s eyes alighted on it, as if he was seeing an insect crawling on my
skin, though didn’t say anything. (David)
These memories constitute the ‘lived impairment’ of David, who barely name the
asymmetric chest in his narration. At the same time, sharing his emotions with a researcher-
counsellor contributes to legitimate David’s life history. Moreover, “similar background,
tastes, values, and interests propel individuals to select each other as friends, and as these
41
characteristics are affirmed within the relationship, the partners are likely to grow even more
similar to each other” (Brown, Larson, 2009: 76). Arguably, David finds himself unable to
share with friends what we address in our counselling session.
He admits to be extremely aware of his body’s look, and desires to pull up the problem
by the root. What also emerges from our encounter is the choice to verbalise these thoughts
without his mother, showing that David keeps a close eye on parental behaviour and will to
speak for himself. Moreover, the fact that we have just met each other allows him to say more
than he does with anyone else. Either choosing a surgical or conservative option, at the end of
his research David will know that he has not wasted time but gained self-awareness. After the
long walk, his resilience will be higher.
“At this stage, however, I want to consider more solutions and I would undergo surgery
even if the correction is partial, yet avoiding plastic surgery since I am sceptic about it”.
Telling me why he would prefer an incomplete correction with traditional surgery, David
shows a strong aversion to treatments which do not transform the chest wall anatomy. In other
words, “I fear the eventuality of a relapse and a weird body’s look after gaining mass”.
While David weighs up the different options, he can always update me by email until
will not feel good and healthy, depleting his:
Miserable thought that my problem isn’t severe enough, the reason why surgeons cannot correct it.
I am also eighteen years old, and if this problem bothers me is because at this age I am supposed to
feel bad. Even when a girl gets closer, I feel uneasy when touches me, and I withdraw from her
even if she likes me. Or when I play fighting with my classmates, I always cover my chest to avoid
the physical contact, though it doesn’t hurt me.
Like a cat that moves back from someone who twitches, David feels that something
limits his combat radius like Jack in Thamm’s novel, who would get rid of the crowd at the
beach instead of his embarrassment:
That night I stare into the fridge. I see nothing, but I'm thinking about the weekend, not my
stomach. I don't want the beach to be crowded. I don't want it to be too hot. I always surf with a
wettie to hide my chest. (Thamm, 2009: 16)
Thus, how shame may harm an able-bodied person? From a behavioural viewpoint,
shame makes David feel limited when experiences physical contact with peers or intimacy
with girls. “According to classic psychoanalytic theory, visible physical abnormalities

42
threaten the body image of the able-bodied”, a presumption that hold David back from those
activities where the body is assessed by others and not by himself (Frank, 2000: 85). Further,
seeing his chest worse than actually is allows him to comply with the surgical criteria of
corrective procedures. Attitude shared with Jack, protagonist of the previous extract, who
pretends to adapt the beach to his shame of surfing shirtless. Concerning his friends, David
explains that:
When some of my classmates discovered I was coming here, they called me ‘stupid’! It means that
they don’t see my dented chest as a problem, though being in my shoes they could go crazy for
much less, such as a protruding clavicle. Everyone has his own problems and goes through them in
the most unbearable way.
Here, David refers to his social surrounding and the teenage culture in Naples, a sort of
suffusing mood-as-atmosphere: “mood is like a pervasive atmosphere or cultural ambience
which surrounds us and is already ‘there’ before being experienced in the body” (Finlay,
2011: 27). As such, talking with friends about his chest, David sees how differently they
conceive the same body that is ashamed to show them, according to their own personality,
background and gender. Moreover, as Merlau-Ponty points out, “I perceive in a total way with
my whole being; I grasp a unique structure of the thing, a unique way of being, which speaks
to all my senses at once” (1964: 50). Hence, although David’s mother is not worried because
the asymmetry is slight, she respects the feelings of his son. The word ‘deformity’ means for
her an important need of David, the reason why she is at his side. Thus, the guy tries to
understand himself by following the rails of medicine, and although is not getting anywhere,
his goal of reflecting upon the body is accomplished by meeting therapists. This is why is
mother supports him, though as parents “we don’t see ‘that thing’, but he does. We don’t
perceive it strongly because I know that is slight, you have to deliberately look at it, observing
all details, but I respect his point of view”.
Yet, David’s parents would better understand the worries of their son if only grounded
in evidence-based medicine. That is to say, if the surgeon argues that there is one warning
symptom, the understanding of an even small defect would rapidly turns to pathology. No
matter whether the guy would continue hiding his chest to others, his deformity would
become a pathology only if symptomatic. This is why Eisenberg distinguishes “abnormalities
in the structure and/or function of organs and organ systems (disease), from the patient's

43
subjective experience of malaise (illness)” (1977). Accordingly, David goes only through the
subjective experience of deformity.
For instance, by describing his lived experience, our first meeting draws David’s social
surrounding. In this regard, Frank says that the “very inability to think, feel, and perceive like
a native can be a source of insight. It is often the failure of conventional empathy that forces
an anthropologist's effort to understand things "from within" ” (Frank, 2000: 100).
Anthropology addresses ‘from within’ issues of body image disturbance, taking into account
both one’s social and private surrounding. Thanks to attentive listening, moreover, therapists
assess the motivation that patients develop from these two contexts. Thus, counsellors should
participate in the medical examination of patients, preparing the most suitable counselling
session for each of them.
Yet, without considering the perspective of other parties involved in a patient’s life
story, therapists risk to turn into narrowed-minded advocates of deformed youngsters. In order
to maintain an ethical behaviour, thus, Giorgi suggests that phenomenological psychology
could just help to “make implicit ‘taken-for-granted’ elements of our lives explicit” (1995:
33). In other words, balancing emic and etic perspective of living with CWDs, patients taken
under therapists’ wing should reappraise their own body. The therapy should also fit with the
surgical needs of patients, without interfering with their clinical assessment, yet giving them
the chance to make sense of their deformity before having the last word. Consequently,
aiming to make implicit taken-for-granted elements of patients’ lives explicit, Biggerstaff
recommends four interchangeable approaches (2012: 189-193):
• Discursive psychology and Discourse Analysis: the discursive approach looks to verbal
behaviour as a more direct means of uncovering underlying cognitions rather than assigning a
numerical value ‘score’ or scale to a behaviour (Harré, 1995). This approach takes the view that
interpretation and empathy are involved in attempting to understand human behaviour. Self-report,
from people being studied, can then become a valuable resource in its own right.
• Narrative Analysis: a narrative approach entails examining people’s use of stories, accounts of
events etc. and also of listening to these stories (Sarbin, 1986). The related discipline of
‘narratology’ has developed from the disciplines of linguistics and literary criticism where
narratives are treated as a search for meaning in the lived experience of people (Bruner, 2002;
Holloway & Freshwater, 2007). Using psychology of narrative, for example, the researcher may
examine people’s life stories or their accounts of such experiences (Esin, 2011).
44
• Phenomenological psychology: phenomenology in psychology places the experience of the self at
the centre of the current psychological dialogue about people’s lived experiences and their
meanings (Cohen & Omery, 1994; Giorgi, 1995; Giorgi & Giorgi, 2008; Langdridge, 2007; Smith
et al., 1995; Spinelli, 2005). The qualitative psychologist is aiming to see and understand what
surrounds us (Cohen & Omery, 1994). When exploring the 'taken for granted' - the everyday lives
of participants, especially those aspects relating to the psychology of how people feel about an
issue, event, or experience for example - the use of a phenomenological approach highlights such
issues and brings them to the fore.
• Interpretative Phenomenological Analysis: acknowledges that the researcher’s engagement with
the participant’s ‘text’ has an interpretative element, in contrast to some other methods (e.g.,
discourse analysis, DA; see Potter, 1996). IPA assumes an epistemological stance whereby,
through its careful and explicit interpretative methodology, it becomes possible to access the
meanings an individual gives to their feelings and their cognitive inner world. DA aims to examine
the role of language in describing a person’s experience, whereas IPA intends to explore how
people may ascribe meaning to their experiences when interacting with their environment (Smith
et al., 1999). It is thus especially suited to behavioural and psychological studies that relate
findings to the bio-psycho-social theories informing discourse among healthcare professions
(Smith, 1996; Smith, 2004; Willig, 2008).
Since our first meeting David used ‘self-report’ to open up, alternating anecdotes about
his life in Naples with long pauses. Thanks to Discursive Psychology I could also analyse
nuances of conversation, such as the tone of voice and his facial expressions. Exploring “the
role of language in participants’ descriptions of events and conversations”, further, we elicit
some of David’s intimate feelings (Biggerstaff, 2012: 190). Thus, the fluctuation of the
dialogue between our different backgrounds invite us to make a new sense of CWDs.
Bracketing the idea of the ‘male chest’ as a banner of masculinity in Mediterranean countries,
David deconstructs the social side of his deformity saying: “I think it is a state of mind
deriving from the ideal of the perfect body, and what bothers me is that my problem is not
severe enough to be corrected”.
That said, the knowledge of the context from where patients come from narrows the gap
between them and therapists. By using a narrative approach, moreover, counsellors examine
how patients address their life story and for what purpose (e.g. to make sense of their shame,
loneliness, stigmatisation and so on). By mentioning Batman and his home place, for instance,
David follows the footprints of ‘narratology’ in a constant “search for meaning or significance

45
as we strive to make sense of our lives and our ‘being in the world’ ” (Biggerstaff, 2012: 190).
Therefore, the asymmetric look of his chest finds its narrative equivalent in the vivid picture
of his twelfth birthday:
Since when I discovered it I found that going to the beach was hard for me, as well as getting
undressed at the gym. It was also stressful to be on the sailing boat with my parents or with a
group of friends. Even when I was alone I tried to get undressed as less as I could after having a
shower, or when I was getting dressed, since I felt ashamed of myself.
Today, I think I have overcome the problem thanks to sociality, by meeting new persons and
realising that actually nobody judge you for a ‘characteristic’ like that. They all have their
problems and everyone faces them differently. For anyone problems are serious, but all in all do
not affect the idea we have of our friends or loved ones. (David)
Here, the centrality of lived experience informs therapists about the genesis of David’s
problem, which affected some of his attitudes, such as being extremely self-conscious in front
of others. This is why ‘narrative analysis’ is so helpful when we aim to interpret people’s
actions, since interpretation “is concerned with ‘reasons’ for things happening, rather than
strictly with their ‘causes’ ” (Bruner, 1991).
That said, explaining how sociality helped him to overcome his embarrassment, David
moves to the present life with the imaginary jump cut of his transformative experience. A
transition that rises meanings from the bottom up, making sense of David’s life-world through
the dialogue between therapist and patient. For this purpose, counsellors must be able to
assess patients’ traumatic memory riddled with negative emotions still pulsating in their heart.
For instance, David recalls the experience of sailing with his parents or a group of friends,
comparing the same experience today and in the past:
The sailing boat is for my father an end in itself. He likes sport, the sea, the sound of wind. I have
to admit I prefer the sailing boat as a chance to be with friends, at least now. Thus, I sail with him
only when I can invite someone I like to be with… Few years ago I sailed only if forced to do it,
since actually I wasn’t interested in sailing and bringing friends, or sailing just with my family.
Today, we go all together in summer on the sailing boat with the family and, if possible, I invite
someone else. Whether I have something better to do, then I’d rather quit to hang out with friends,
to spend time in group or, sometimes, to just read at home. Whatever. So it’s not really my
passion, as my father would desire. It’s his hobby and my enjoyment.

46
The time frame of narration is relevant as much as the words and images emerging from
the ‘retrospective description’ of David. In this regard, Finlay suggests that:
Participants might be guided to provide a description that starts prior to the event or experience
being described. Then the participant is asked to detail in a concrete way, their own thoughts,
feelings and behaviours as well as describing the environment and others involved. (2011: 97)
As a result, what addresses our therapeutic encounter is the very act of using words
suitable for the events that David lived through in the turmoil of adolescence. By using the
macro lens of Interpretative Phenomenological Analysis (IPA), we end up exploring David’s
social and private surrounding on the boat. He deliberately refers to thematic categories of
sport, sea, silence and wind, defining what makes incredible for his father the experience of
sailing, and implying that the same does not suits him. His description of natural phenomena
like sea and wind, therefore, offers a wide spectrum of possible interpretations, which shift
between David’s and his father’s life-world. As though, on the one hand, David understands
why the sensorial landscape of sailing seduces his father – “He likes sport, the sea, the sound
of wind”. On the other hand the guy draws a line between his own interpretation and his
father’s way of life. More than outlining two separate meanings of sailing, however, their
horizon depicts two different understandings of the same activity. When the father is
enthusiast of sailing on his boat, David feels anxious and uneasy with undressing in front of
him though he likes to sail around the Neapolitan gulf. This tension daunts David, unaware of
what Goffman argued about what may happen to those who get rid of their stigma:
For years the scar, harelip or misshapen nose has been looked on as a handicap, and its importance
in the social and emotional adjustment is unconsciously all embracing. When one removes this
factor by surgical repair, the patient is cast adrift from the more or less acceptable emotional
protection it has offered and soon he finds, to his surprise and discomfort, that life is not all
smooth sailing even for those with unblemished, “ordinary” faces. (1963: 6)
Changes in the interpretation of lived experience rely mostly on the appraisal of one’s
sense-making. No matter what sailing actually means, but David’s interpretation of this life
event. Indeed, the most influential forces of motivation, according to Dr Torre and Dr Härma,
consist in recollecting memories of the past relative to CWDs. Simply put, what they
intuitively figure out is a degree of alexithymia, an assessment model based on a low/high
number of negative experiences, such as going to the beach, feeling lonely and so on. As a
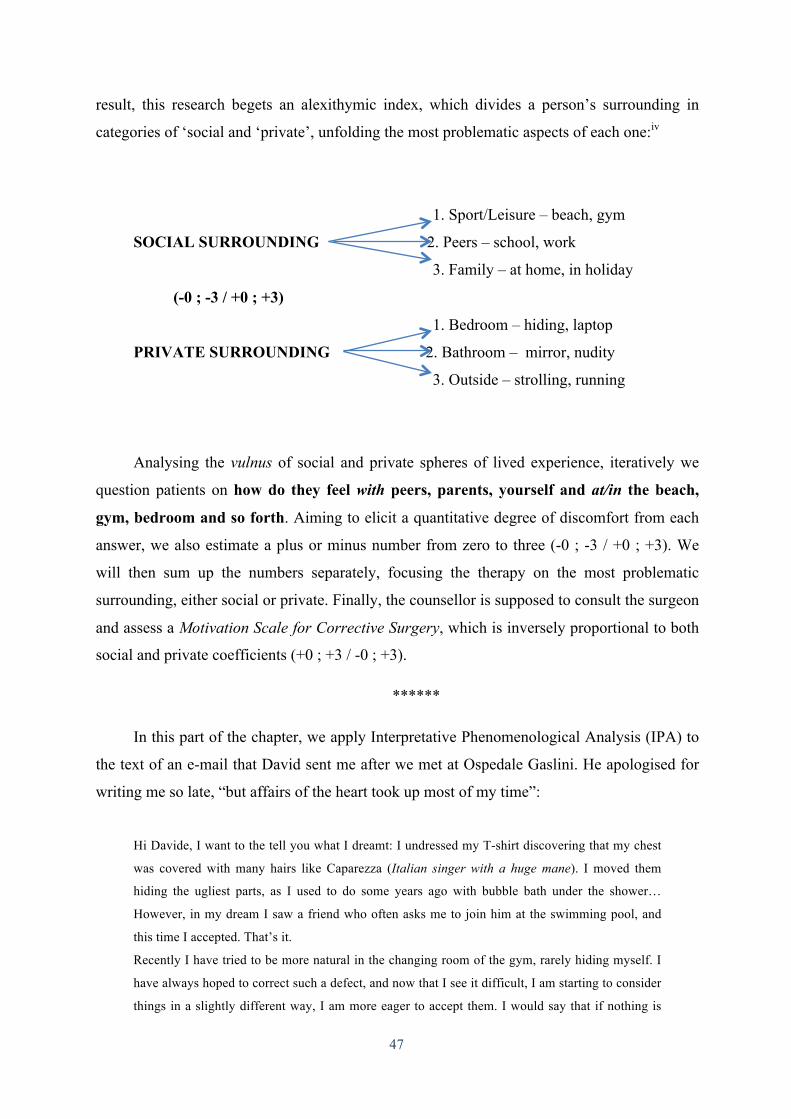
47
result, this research begets an alexithymic index, which divides a person’s surrounding in
categories of ‘social and ‘private’, unfolding the most problematic aspects of each one:iv
1. Sport/Leisure – beach, gym
SOCIAL SURROUNDING 2. Peers – school, work
3. Family – at home, in holiday
(-0 ; -3 / +0 ; +3)
1. Bedroom – hiding, laptop
PRIVATE SURROUNDING 2. Bathroom – mirror, nudity
3. Outside – strolling, running
Analysing the vulnus of social and private spheres of lived experience, iteratively we
question patients on how do they feel with peers, parents, yourself and at/in the beach,
gym, bedroom and so forth. Aiming to elicit a quantitative degree of discomfort from each
answer, we also estimate a plus or minus number from zero to three (-0 ; -3 / +0 ; +3). We
will then sum up the numbers separately, focusing the therapy on the most problematic
surrounding, either social or private. Finally, the counsellor is supposed to consult the surgeon
and assess a Motivation Scale for Corrective Surgery, which is inversely proportional to both
social and private coefficients (+0 ; +3 / -0 ; +3).
******
In this part of the chapter, we apply Interpretative Phenomenological Analysis (IPA) to
the text of an e-mail that David sent me after we met at Ospedale Gaslini. He apologised for
writing me so late, “but affairs of the heart took up most of my time”:
Hi Davide, I want to the tell you what I dreamt: I undressed my T-shirt discovering that my chest
was covered with many hairs like Caparezza (Italian singer with a huge mane). I moved them
hiding the ugliest parts, as I used to do some years ago with bubble bath under the shower…
However, in my dream I saw a friend who often asks me to join him at the swimming pool, and
this time I accepted. That’s it.
Recently I have tried to be more natural in the changing room of the gym, rarely hiding myself. I
have always hoped to correct such a defect, and now that I see it difficult, I am starting to consider
things in a slightly different way, I am more eager to accept them. I would say that if nothing is
48
possible to gain a perfect symmetry, I will not even undergo plastic surgery, but I still want to
sieve every solution.
Writing this letter, it is hard to find a name for my problem, since hole, dip or PE are all quite
annoying. Anyway, I hope these considerations could help you as much as it is useful for me to
write them. (21/04/2013)
“The habitus of a culture is a deeply emotional construct”, and no matter what the email
itself tells us about David (Jackson, 2004: 116). Our interpretation must be pertinent to his
life-world, informed by the social and private surrounding where he spends his life and writes
me his email. It follows that the data missing during the face-to-face encounter between
therapist and patient may also emerge at a later stage, either written by email or recounted in
the next counselling session.
Indeed, imagining David’s chest covered with a mass of hairs hiding his deformity is a
partial information, if I did not know that he used to do the same with bubble bath under the
shower. The need to make sense of perturbing life events convinced him to write me the email
– “I hope these considerations could help you as much as it is useful for me to write them”.
Further, his considerations are the result of self-reflection: “a shadow biography, a negative
image, for which the missing text could be found in the investigator's private thoughts,
interview questions, field notes, dreams, and letters home” (Frank, 2000: 84). An
interpretative approach helps therapists to bargain meanings elicited from the life-world of
informants. For instance, David shares with me information that went through a process of
reflexivity. Rarely the guy uses third person accounts, and shows courage in merging the
meaning of dreams with his intimacy, such as the shame of his naked body under the shower.
Yet, by talking with me he starts what Gadamer calls ‘fusion of horizons’, that is an
integration of broad-minded persons interpreting reflectively the same experience
(1975/1996). My attempt is to embody David’s dream, consequently, using embodiment as “a
methodological standpoint in which bodily experience is understood to be the existential
ground of culture and self, and therefore a valuable starting point for the analysis” (Csordas,
1994: 269).
First of all, accepting the invitation of a friend to go swimming with him, David dreams
the exposure of his naked body not only under the ‘medical gaze’. Although he avoids to
name a part of the body that looks repulsive to him, he knows that this is not mandatory
except for diagnoses. Further, his scepticism about plastic surgery match with the impossible
prediction of postoperative satisfaction. This is why doubts motivate him “to consider things

49
in a slightly different way”. David will to accept himself and behaves more naturally in the
changing room. However, the shower stall, the swimming pool and its changing room make
way for a holiday with friends in Barcelona, expanding the social surrounding of his physical
deformity as it follows:
Davide, at the moment I am in a very tricky situation because of my chest: the girl I like invited
me for one week in Barcelona with her friends, Barcelona is a seaside town. She is very cautious
in speaking and also very kind, she would never tell me anything bad and this does not make me
worry, but I care of what she thinks of me. You can’t imagine how strong, beautiful and buffed her
friends are, and how uninhibited she behaves with them. I know, I can’t compete with them and
that’s why I feel bad, thinking that she could even ignore me considering the kind of people she
hangs out with.
Concerning Batman, to tell you why I idolise him (it’s much more than a simple passion) I should
sum up all those experiences that disturbed me: exclusion from classmates, rejected by a girl, some
episodes of bullying. From the moral perspective, Batman represents the will to never give up. I
am not talking about the cinematic Batman but only its best comics. Batman is also the will of
redemption and much else. He incarnates the physical perfection as well, is a model to follow in all
his facets. At an irrational level, everything I do is a step toward Batman and to become like him.
This explains the ‘barrier’ of my chest. At the Comicon Festival there were some people disguised
and many others shirtless (a kind of rave party with literary, cinematic and musical themes), thus I
conceived my problem as a limitation of the freedom I want, and that these people have.
(13/05/2013)
This letter highlights the limited combat radius of planning summer holidays and
getting undressed where everyone else looks perfect. Essentially, the hamletian dilemma of
David emerges from the stigmatisation he would face accepting the invitation of his friend.
By making the chest responsible for this dilemma, however, he ignores the motives that
convinced the girl to invite him. That is, what Goffman called “a special discrepancy between
virtual and actual social identity” ends up in the terrifying vision of how friends would react
seeing something that David keeps out of their sight (1963: 2). His fear, thus, results to be
more powerful than any other benefit, holding him back from feeling the enthusiasm of
participation. Moreover, his comparison with the more ripped chests of the other male friends
suggests that low body-esteem is an alibi for marginalisation.
As a matter of fact, David prefers to continue hiding his chest, avoiding the risk that his
friends may ignore him after seeing how it looks like. Yet, this form of resilience discourages
sociality and favours withdrawal from the many life events that provide disclosure.

50
Interestingly, an attitude that overlaps with Batman’s life story, evoking a complicity between
the superhero and David, who wears the cloak of a “superhero with no superpowers” and
whose resilience to problems is a form of resistance (Langley, 2012). Batman is a universal
myth which crosses cultural confines before influencing David’s life-world with a sense of
justice and justification of withdrawing from peers. As such, the ‘shadow archetype’ of
Batman ends up representing the side of David “that is hidden, out of the light, the sum of
those characteristics you conceal from both the world and yourself” (Ibid.).
Although partly victimising, David’s batmanesque resilience to pain and bullies begets
a reactant sense-making of those vexations typical of adolescence. He feels that Batman’s
tragic biography supports him – Bruce Wayne became Batman after the brutal killing of his
parents under his eyes. Therefore, since the discovery of “not being perfect, that the human
body is not an infallible machine”, rather than passing over his physical stigma, David found
the way to interiorise his pain and rephrase it as a Batman’s story:
Batman arrived in the hardest time of my life, for many reasons. At the time I have only few
friends, my character was difficult, and things were getting worse at school with classmates. One
day I found the Batman videogame, and I liked it not much for his statuesque body or because he
fights villains, but as in the superheroic and fantasy imagery Batman is exceptional though
remaining an ordinary man. Often the circumstances make him feel subjected to someone and face
obstacles much stronger than his powers would allow him to take on, or at least this is how they
look like. Therefore, in the first half of the game there was a person defeated and rejected until he
was almost dying, and a sentence he said speaking to Joker is: “I will never let you take my life
obeying you”. Instead of the comic character fighting against bad people or the charming
superhero, in that moment Batman symbolized the idea I could overcome the adversities with my
own willpower. I can go forward, perhaps until I will win, like the lyric says: “sending a smile into
the arms of death”, so possibly winning against what is impossible to win.
FIG. 6 – David with a Batman poster in his bedroom.
51
Deconstructing Batman’s biography, David finds bits and pieces of his own life story.
Although seeing in an ordinary man like Bruce Wayne all the limits of human beings, he
admires his “very possession of a life-project” and knows that ‘in order to’ motives must
prevail over ‘because’ motives (Rapport, 2003: 6). Indeed, when David played Batman
videogame for the first time meeting a hero who fights bullies, he found dynamite for his
stigma. Whether this is not enough as a life-project, at least he finds an adolescence-project
that consists in reading life events through the lens of comics. Vicariously, thus, David faces
the enemy as Batman does in the second part of the videogame, after being “defeated and
rejected until he was almost dying”. This is a turning point in David’s adolescence, the time
when teenagers learn by heart quotations from Batman comics.
Indeed, as a cultural icon, Batman helps those who feel lonely for ‘in order to’ motives,
such as coping with significant body image disturbance. Asking ‘who is Batman?’, we should
rather wonder ‘who is the other’s Batman?’, as writers and artists “interpret him according to
the dictates of their own experience – the world outside their windows. It also allowed him to
be more than a mirror; he could be a receptacle, too” (Langley, 2012: 2). Imagining how the
world outside Wayne manor looks to Batman, we should also visualise the world from where
David wants to hide himself:
Actually I liked to hide myself above all to myself, since I was often alone. Sometimes a heavy
sweater was enough, a jacket or the blankets of a bed, when after falling asleep everything seemed
to disappear and nothing bothered me anymore. Mostly I stayed at home, or if I went on the sailing
boat I did not get undressed. I wore my t-shirt and while the others enjoyed, I did nothing except
dozing or sunbathing lying down on my belly.
The use of past tense shows that David is eager to overcome withdrawal from his social
surrounding. A puzzle of strategies and grey zones allowed him to disguise his chest,
especially just being alone with himself. As Dahlberg would argue, however, “Loneliness is
the figure against a background of commonality; being-alone is the other side of being-with;
loneliness is intertwined with togetherness” (2007: 206). It follows that David is never alone
but always with an ego built upon Batman storytelling, which adapts the script of his life story
to Bruce Wayne biography. Yet, Batman’s body is far from how David sees his own chest,
when we meet six months after our first encounter:
From a certain perspective, the discovery of not possessing a perfect body represented a process of
growth. I still remember that in my childhood, or early adolescence, I had a perception of my body

52
totally different than now, as if it was perfect, an abstract entity. For instance, I remember that
after having a shower I liked to lay on the bed feeling simply perfect. When I discovered that I
have physical defects, I realised that the most visible of them were not the only ones. Well, the
body is a machine and, as such, is not perfect. Suddenly this stroke me, somehow reminding me
the fallibility of the body-machine. That is, I could do nothing to solve this problem that actually
represented the missing solution of many other problems. For example, one day I may not manage
to fix my chest, and I may not do anything against life which will die out. Anyway, directly this
has never jeopardised any relationship with other people. Nobody has ever refused to talk with me,
and at the beach as well, friends don’t refuse me only because of that. Indirectly maybe yes, I had
prejudices, believing that someone could say something, that I could feel uncomfortable in
showing myself, going to the beach with friends or joining groups. Sure, above all we exist
because of what the others think about us. When the others started to think of me as a person like
many others, I felt like many others, and perhaps for this reason I overcame the problem.
Here, David spotlights a striking parallel between the impossibility of fixing his stigma,
and life that relentlessly dies out. As though both Batman and David agree that “meaning
making, finding value in tragedy or forging our own means to make it have positive
repercussions, helps many people cope and may be critical for posttraumatic growth”
(Langley, 2012: 47, italic is original). As such, David discovers that outside his window
bullying and injustice are all the rage, similarly to Batman. Moreover, in order to distance
himself from that underworld, the guy lives fully his private surrounding, making of the bed
sheets his Wayne manor.
Regardless of ‘because’ motives – the killing of parents or a low body-esteem –
resistance entails the struggles of a person in the environment where s/he lives. Accordingly,
David had only few friends, his character was difficult and only Batman toughened him. Yet,
compensating the lack of an active social life by reading Batman comics, David could find
people who share his same interest, those who make him feel like many others. In this regard,
poignantly Frank argues that:
Anthropologists highlight what it means to be a "person", a socially valued, fully participating
member of the group on the basis of the questions: is the individual included or excluded from
desirable life roles and daily occupations in their society? Which ones, and why? (2000: 45)
Although the community of comics’ fanatics welcomed David, fictional characters did
not make him feel a socially valued, fully participating member of a group. Thus, David is
more committed to his batmanesque role than his social status, though “as adolescents

53
consider or negotiate relationships with specific peers or peers groups, they must be sensitive
to status differentiations” (Brown & Larson, 2009: 76-77). Nowadays, David considers
solipsistic to lose oneself reading comics, yet mastering self-reflection when looking back at
the ‘because’ and ‘in order to’ motives of his past habits:
Sure, adolescence is a difficult period for everyone, I guess. Either big or small, everyone has his
own problems and goes through them in the most unbearable way. You overcome them simply
moving forward, growing up. For everyone this passage is marked by some particular episodes,
such as those who feel the burden of first responsibilities, who start working, who study for the
driving licence, the first girls. I’d say that responsibilities make us grow up. It’s not a real relief, a
truce perhaps, since between two bundles you can rest a bit, but I don’t think that in the end,
becoming an adult you can say that you are serene. Maybe you find a balance, maybe this is what
to grow up really means.
On one hand, he thinks that adulthood is a more balanced stage of life than adolescence,
less full of worries and mood swings about the body’s look. On the other hand, it is the time
of “the burden of first responsibilities”. For instance, David’s mother and father are in charge
of serious matters as respectively an architect and a policeman within a context of marked
illegality, such as the urban ring that surrounds Vesuvius. Thus, David seems to conceive an
even bigger gap between the adolescent and the adult script than other peers.
As a student of law who dreams to become a magistrate in the home of Camorra –
criminal organisation which takes origin in Campania – Batman represents his ideal of justice,
otherwise overwhelmed by the negative examples around him. In fact, along the roadsides
garbage and fires catch your eye, small towns swarm with suspicious gazes and the buzzing of
locals. The second time I visited David, first I found a bakery where to buy some pastries in a
small town of the Circumvesuviana, and the shady atmosphere pervaded me quickly. The
inhabitants were grumbling out of a few bars open, or driving their scooters slowly while
smoking and winking at somebody. For a moment I felt like Batman in a shrunk and sunny
Gotham City, an impression confirmed later by David’s parents when told me: “it’s not very
safe to walk there, be careful Davide”. I started to see why the mood-as-atmosphere of David
is largely shaped with contrasting feelings of justice and injustice.
Naturally, neither Batman alone could convince David to study law, nor just the social
context where he grew up, yet merging these factors with a low body-esteem, he might feel
motivated to afford a dangerous walk of life. Although in his early adolescence David was

54
more concerned with an ideal of the chest that should border on perfection, subsequently he
changed his mind:
When I arrived in Genoa and talked with you, I realised that even if you gave me a choice, it was a
little choice, really little. Yet I could think, reflect upon the problem trying to solve it
psychologically. Since I knew it was just a matter of conception. On the way back, thus, something
rather important happened to me. Instead of worrying for all these physical and material problems,
I started to think of a person who is very dear to me, who was waiting for me – she lives in
Campania – and how much I desired to see this person again. Hence, I focussed on other things.
Perhaps this helped me a lot, I mean, to consider other priorities.
At the time of our first meeting, David was finishing high school and expecting
university to change a good deal of unresolved problems. For example, the discovery of an
even little choice about his chest, and the feeling that loving someone does not entail the
imperfections of his body. Thus, David’s account seems to culminate in a sensual
daydreaming of the physical contact with the girl he loves:
I pull at her clothes. I want to hold her, feel her naked against me. I want to break through my
fears. She grabs at my shirt. She kisses my stomach, my chest. My skin tingles and finally I know I
can do it. I twist my hands in her thick hair in absolute excitement. (Thamm, 2009: 227)
David’s senses pass the psychological barrier of his dented body’s look to such a point
that he desires to meet the girl. Here, the role that senses play in the field of CWDs seems
comparable to those with severe disabilities, who can actually “have high self-esteem.
Asserting their abilities and desires, they can experience their own beauty, find lovers and life
partners, and enjoy the full spectrum of life's activities” (Frank, 2000: 35). Again, IPA helped
me to analyse David life story, useful for those with his same body’s look, age and gender, yet
bearing in mind that ‘deformed narratives’ differ both across cultures and individuals.

55
4. From Analogies To Meshwork Therapies: Narrative Deformities
As therapists, we know instinctively that some
things cannot be sensibly measured or quantified.
Linda Finlay –
Phenomenology for Therapists
Listening to persons with CWDs you bump into analogies and metaphors, meticulously
crafted to make explicit often unspoken concerns and fears. Thus, deformed patients who visit
doctors to diagnose their physical condition, also come to validate impressions and feelings
about their body:
The recognition that humans use narrative structure as a way to organize the events of their lives
and to provide a scheme for their own self-identity is of importance for the practice of
psychotherapy. The telling of the story in itself is held to have therapeutic value, and sharing one’s
own narrative with others helps bring cohesion to the support group. (Polkinghorne, 1988: 178)
As such, narrative is an important therapy for severe body image disturbance. Aware of
its healing outcome, indeed, surgeons and counsellors should listen attentively deformed
patients, measuring to what extent CWDs affect their lifestyle and alexithymia. Indeed, only
asking patients we can assess the helpfulness of both medical examination and counselling.
For instance, the majority of patients I met at Tallinna Lastehaigla and Ospedale Gaslini
were quite silent. Other than a manifestation of their embarrassment – and that some parents
were rather garrulous and bold – talking separately with them, I noticed that many of the
things we said about CWDs were too generic. That is, they know already what kind of
operation may or may not undergo, their disposition towards surgery, and some of them could
even predict the reaction of their parents. It is no surprise that Internet is a self-diagnosis tool
56
extremely popular nowadays. Yet, what is less clear in patients’ mind is the method of
therapists, who may also play dumb asking: “why you are here?”, or “tell me something about
yourself”. With this and other trickeries, Dr Torre and Dr Härma ask patients to metaphorise
their fears, proving that “when a text unfolds a new way of seeing a critique of how things are
becomes possible, along with a critique of the illusions of the interpreter” (Ricoeur,
1973/1990). Thanks to a therapy based on thorough interpretation of patients’ words,
consequently, we can unfold the vivid picture of their life-world. Yet, one’s lived experience
cannot be mechanically unravelled, since according to Frank “stories are not material to be
analysed; they are relationships to be entered” (1995).
Thus, collaborating with deformed teenagers, therapists become receptive to their
“volition, habituation, performance capacity, environments” and finally sense-making
(Kielhofner et al., 2002: 127). A whole spectrum of phenomena that crafts our understanding
of living with deformities of the upper body. For example, bracketing any taken-for-granted
conception of loneliness, the achievement of a better understanding of this phenomenon goes
hand in hand with the disclosure of patients who feel lonely or marginalised.
A good example of how metaphors can touch deformed persons profoundly is The Van
Analogy, a story written and read by unknown author and available on YouTube.v What
strikes here is the shift between a dented van and a deformed chest, as though putting “a great
big dent” in your van is the same of noticing a crevice in your chest. The voice-over states
that you are still angry after one week, and you wonder why. The second week you play
another song when driving, yet your anger is not chased away. Anger seems to be a common
symptom of body image disturbance among teenagers, since your body’s look makes you feel
as if you crafted the deformity with your own hands. Moreover, without enough money to
repair the dent in your van:
You find yourself with plenty of time to think differently about it. Does driving a dented van mean
I am a bad driver? Can I ever stop people from seeing the dent in my van and thinking what a bad
driver I am? Does the dent in my van stop me from getting where I want to go?
Although without the minimum criteria to undergo corrective surgery you, you struggle
every day with thoughts and worries about your body, feeling that you are responsible of such
an oddity and seeing yourself as worse than many others, unable to build the chest you desire.
In addition, pretending that people stop seeing this deformity as your failure, you are afraid of
their gaze. You start wondering if a CWD may hinder your chances of success in life, making

57
of your physical imperfection a social handicap, since “exclusionary conditions, not
impairments, are the root cause of disability” (Frank, 2000: 44). Yet, at the traffic lights,
when a van with a bigger dent pulls up alongside yours, you ask yourself:
Does it make you feel good about your own less dented van? Do you think about what it would be
like to be the driver of the van opposite you? What about the people walking on the street or the
car drivers waiting on the opposite side of the traffic lights?
Either positively or negatively, comparisons affect our self-esteem. Although someone
feels relieved seeing that people may have a worse body’s look than yours, you wonder what
would life be like putting yourself in their shoes. That said, Waldschmidt argues that “all of
us are always involved in the establishment of normal distribution curves: the normal mean,
the relevant transition zones, and the relevant periphery. Normalistic norms, in contrast to
normativity, are less static and less oriented to stability; they are based on change and
dynamics” (2005: 194). Thus, parking close to the workplace, someone you know comment:
‘Hey there is great big dent in your van. That's weird’. You reply ‘hey there is not a great big dent
in your van. That's weird’. You then decide whether to tell him the truth about why it looks that
way”. After three weeks you are driving along when you see a beautiful woman. You both smile at
each other. Do you worry about your van being dented? Do you think she notices the van has a
dent? Or is she just focused on your smile?
The way people react to what gets away from normality allows overthinking, a Pindaric
flight that deformed persons may experience when someone look at their body. Yet, not
necessarily other people’s eyes point at CWDs, but may uncover the beauty of a smile and
other peculiarities, thus breaking through your fears. Todres emphasises that:
In living a human life we come with the seasons, with dryness and wetness, with the rhythms of
darkness and light, of going away and coming back, of continuities and great discontinuities, with
its Janus-face of both potential anguish and renewal. Framing and permeating all this is finitude;
there, in the possibility of not being, and there, in the fragility of flowers, in the beauty of a sunset,
and in the passing of a smile. (Todres, 2007: 116)
As such, encounters fluctuate between fragility and power, presence and absence,
shame and pride. When someone stares at your body, you can still meet his or her eyes. The
ability to face what Bremer calls ‘life threats’ can be very high or very low in each of us. “We

58
come with the seasons”, Todres says, and we just conform to our mood-as-atmosphere.
Unlike the woman who winks at the driver of a dented van, many deformed persons think that
the body stands out more than a person’s aura. Thus, we end up reading our body through the
‘medical gaze’, forgetting that a dented chest is “an existential possibility where vulnerability
is embraced, enabling us to connect empathically with others (freedom for wound)” (Todres,
2007, italic is original). On the fourth week the mechanic proposes to beat the dent back into
shape, though it is not a total reconstruction and you cannot drive your van while it is being
fixed:
You consider it, but when you think about the dent in your van, you are no longer as angry when
the accident happened. You wonder why. On the fifth week you've got a hot date. You go to pick
her up in your dented van. Do you feel the need to tell her immediately about the dent in your van?
You are at the traffic lights and a Ferrari pulls up alongside your dented van. Your date Charlotte
sees it and you feel slightly uncomfortable, but it is not unbearable.
In other words, relationships with the opposite sex are avoided or frightening for some
people. The protagonist is not supposed to explain why there is a dent in his van, yet is afraid
that Charlotte may think that he hides something from her. As a matter of fact, he is ashamed
of his own shame, since he would rather show self-confidence when talking about himself.
Yet, as long as CWDs are a big part of a person, significant others may understand everything
without the need of explanations, like Jack’s girlfriend:
She kneels in front of me, lifts my shirt, runs her hands over my stomach, then upwards. My heart
bounds. I put my hand on hers as it inches to my chest but she says, ‘I don't care’, and rests her
palm in my depression. (Thamm, 2009: 227)
In conclusion, The Van Analogy draws an analogy between one’s deformity and the
lower status of a dented van driver:
On the sixth week, your dented van is not running as well as it used to. Could it be my dented van
that is slowing me down? By chance you are on vacation in the desert and buy fuel that you have
never heard of before from a very old cheap gas man. Upon driving from the desert, your van
seems to run a lot better compared to before. Eight years later your van’s engine life is coming to
an end. What do you think you will remember the most about your van? Two weeks later you are
at the local garage and the salesman is showing you a new van, which ironically has a dent in it.
Looking at the dent you ask yourself two questions – would it be my fault or make me angry if I

59
bought a van that already had a dent? Is it possible to always be a good driver and avoid putting a
dent in my next van?
Overall, what The Van Analogy claims in the end is a great deal of faith for living all
your life with a CWD, but also when correcting your physical stigma. Since King et al. point
out that “losing myself, also felt slightly scary. Who would I be and who would I become if I
was to disappear to be replaced by a paler-shade of me? I became aware that I felt somehow
sad at the loss of my customary embodied way of being” (2008: 95-96). Thus, by answering
the latter question we unfold the impact of body transformation on one’s existence,
comparable with new driving habits when you change your car.
For instance, Dimitri comes from the north-east of Estonia, where during his early
adolescence discovered that CWDs might be corrected. Since then, he thinks that the
operation could ameliorate both his chest and life, in addition to the gym where he works out
regularly. At first Dr Härma diagnosed him a “not so deep PE, but he insisted. He wanted the
operation. I asked him whether he was absolutely sure, and he looks nice now!”. Indeed, the
Nuss technique was a success, and the result of training plus the operation now make him
look like many others. The decision to undergo surgery was taken autonomously, and he also
deals with the recovery alone, since nobody is beside him when pain management shifts from
anaesthetics to his endurance. Arguably, living with his previous body was more unbearable
than the physical pain he feels now. Despite David – the protagonist of Chapter 3 – Dimitri
does not say much about his past, manifesting a lesser need for counselling than his Italian
peer. Overall, operated patients seem less eager to talk with counsellors during the recovery,
whereas David chose to reflect upon his body instead of any surgical procedure. He needed to
express the role of his body in life, and this is why he opened his heart to me. Since as a
counsellor, “I can sustain an approach to the Other that is open, respectful, non-instrumental
and relationally oriented. I can dwell with them as they seek to describe their journey in all its
richness and complexity” (Finlay, 2011: 13). Further, the encounter with David showed that
an open approach is therapeutic, and the in-depth analysis of one’s life-world leads to a
customised counselling therapy. As any new method, however, the counselling of patients
with a CWD is in search of support from today’s medical establishment, and above all from
thoracic surgeons. In fact, other than assisting patients throughout the recovery, its
motivational function before and after the operation is at hand.
Yet, Dimitri finds the doctor who can give his torso a new shape. As if looking for the
tattoo designer who better interprets his draft, unlikely he would change his mind talking with
60
someone who argues that tattooing is not the only choice. Indeed, correcting his deformity
Dimitri will restart working out in order to get ripped, rather than just disguising the hole in
his chest. By contrast, Daniel’s mother claimed in the second chapter that “developing only
one pectoral muscle at the gym, he would highlight the agenesis of the other half”. In view of
this drawback Dimitri is more lucky, since he afforded the Nuss technique to play his ripped
chest up.
That said, CWDs are intermingled with the ambiguities of psycho-social influence, and
nowhere is written that the ‘acquired normality’ after corrective surgery is necessarily
curative. Some patients found pain and post-operative scars hard to bear, and maintained
antisocial habits with a low joie de vivre. Yet, many of those who made it now look the
doctor in the eyes, thanking him for the important role played in their life. In this context,
counselling therapy becomes a chance to unfold one’s complex self, as David explains six
months after our first encounter:
Yes Davide, our relationship has been very important for me, and putting me in front of a choice
has been also important. That is, mine is obviously a small problem, unlikely treatable surgically,
but you and the doctor spoke to me as if the choice was up to me, showing me both pro and cons.
In this way, I made my choice without feeling forced to. The emails and the opportunity to share
my thoughts with someone helped me, albeit I have to say that I met you at a particular moment of
my life, a moment when I started to build up deeper friendships. It was a very important
relationship, but not the only one and not the most decisive. Yours and the doctor’s method,
indeed, consisted in putting me in front of a choice to the extent that I could make it mine.
I must admit that what I told you was not a news for me, I had everything in my mind already.
Your function was above all to clarify my thoughts with a great empathy, because probably we
experienced often the same, and you found my story in the story of other persons, or in your story
too. I wanted to be understood, and I wanted to clarify my ideas by sharing them with you.
Something I neither said out easily, nor with many people. For me it was a relief and this is
another important aspect. I mean, the very fact of saying those things to a person who wanted to
listen me and understand me played an important role.
Firstly, from the relationship between me and David we both needed something – my
research and his counselling. Yet, our collaboration has also been supported by Dr Torre and
David’s family. Overall, we managed to keep in touch by email, and we met two other times
after our first meeting. We understood the importance of sharing and updating his life story
with continuity, always analysing the content of his lived experience, fears and even dreams –
as reported in Chapter 3. Further, my anthropological background allowed me to consider

61
both his private and social surrounding for a better attunement. Above all, the aim of making
David feel responsible of his own decisions allowed him to start our ‘collaborative therapy’
“without feeling forced to”. As he said, both me and the doctor put him “in front of a choice”:
either counselling therapy or an appointment with a plastic surgeon. Thus, David was given a
chance to stop passing his blameworthy past and present, as Goffman outlined:
He who passes finds unanticipated needs to disclose discrediting information about himself, as
when a wife of a mental patient tries to collect her husband’s unemployment insurance or a
‘married’ homosexual tries to insure his house and finds he must try to explain his peculiar choice
of beneficiary. He also suffers from “in-deeperism”, that is, pressure to elaborate a lie further and
further to prevent a given disclosure. His adaptive techniques can themselves give rise to hurt
feelings and misunderstandings on the part of others. His effort to conceal incapacities may cause
him to display other ones or give the appearance of doing so: slovenliness, as when a near-blind
person, affecting to see, trips over a stool, or spills drink down his shirt; inattentiveness,
stubbornness, woodenness, or distance, as when a hard of hearing person fails to respond to a
remark proffered him by someone ignorant of his shortcoming; sleepiness as when a teacher
perceives a student’s petit mal epilepsy seizure as momentary daydreaming; drunkenness, as when
a man with cerebral palsy finds that his gait is always being misinterpreted. (1963: 83)
What the ‘passing’ of a deformity cannot hide is when your eye fells upon your chest.
This is why we cannot be indifferent about patients’ self-esteem during the assessments of
CWDs, and diagnostic procedures must consider the alexithymic index of patients, focusing
on the discomforts that follow them at home and to the beach. Neither pointing up analogies
between deformed and near-blind persons nor omitting them, thus, we may find out in what
category deformed people place themselves. Thanks to the Motivation Scale for Corrective
Surgery, we could even take advantage of disclosing one’s discrediting information about him
or herself for therapeutic purposes.
Eager to give patients a choice between surgical and conservative therapy, nowadays
surgeons and psychotherapists should pursue the well-being of deformed persons working on
a team. When corrective surgery is the best way to help unmotivated patients, then
counselling therapy could help to reconsider this first option for their physical well-being.
Nevertheless, the last word in the framework of CWDs rests with the uniqueness of each case.
Regardless of patients’ decision, everyone should accept it, including parents. Indeed,
Dr Torre recounts that “amongst those to persuade of the benefits deriving from corrective
surgery, parents are usually the most afraid of complications and the least motivated”. It takes
time to convince adults that a teenager may be so brave to afford pain after surgery, and

62
psychological support may help a lot, since the counsellor’s as well as “the researcher’s
approach is one of openness where we pay close attention to the other with curiosity,
empathy and compassion” (Finlay, 2011: 166, bold is original). Also parents are led to
reconsider the others’ life-world through the lens of a therapist, hearing that the words of
adolescents may resonate in a new and vibrant way.
Here, what Finlay calls ‘transferences/counter-transferences’ is the capacity of
attunement to the person who lives beside you, such as a son or a daughter. Being receptive to
his or her words brackets preconceptions and makes room for the unknown and unheard side
of our beloved ones. For this reason, we should start from the tough experience of
encountering deformed persons who live close at our hand, without stigmatising them and
being indifferent to their concern. Asking ‘how deformities make one feel about his or her
body?’, we are “faced with the challenge of meeting the other in all his/her complexity”
(Evans & Gilbert, 2005: 74-75). We avoid the risk of what Goffman called ‘in-deeperism’:
the attitude of hiding your chest believing and making others believe that you are fine with it,
though you are only acting this way.
This partly explain the surprise of David’s friends when decides “to visit a thoracic
surgeon in the north”, as they cannot see the problem but only its disguise. Somehow, the
same duality is echoed in Michael’s story, whose mother introduces by saying that her:
Fear is whether heart and lungs may grow well, more than an aesthetic problem. Actually, growing
up he developed a quite ironic character, having a laugh about it with his friends, without creating
a problem for himself. Although he actually lives it as a problem, as long as he speaks with me
about it and since others’ eye fells upon there. Hence, as a mum, I thought that if the doctor says
that there is no critical condition, a tiny tattoo there… making of this small imperfection a strong
point, would make sense.
Again, the positions of parents and son are verbalised independently – with a
dominance of the adults’ account. Trying to empathise her son, Michael’s mother admires his
coping strategies saying he is ironic about his deformity. Yet, she never mentions this word,
replaced with the more generic term ‘imperfection’ and the symbolic strength of a tattoo.
During the clinical examination the woman admits to feel “upset when his sternum moves up
and down for the heartbeat. It scares me”. Kindly, Dr Torre opposes that the same may
happen to people without PE as well, and only the CT scan will reveal if these worries are
grounded or not. The doctor holds the balance of power between two different attitudes: the
maternal preference of correcting the deformity, and Michael’s fear of the operation.
63
Naturally, without knowing the motives that led them to their position, doctors are not
supposed to take a stand but to check if at least two surgical criteria meet or not.
Of course, patients have parents who need also to break their fears and to deal with their
empathetic deformity, usually making sure that this anomaly does not jeopardise their son’s or
daughter’s well-being. Less frequently, however, parents may have to accept the choice of
teenagers in one way or another, that is what surgeons are responsible for: the respect of
patients’ decision. According to the General Medical Council:
You must respect a patient’s decision to refuse an investigation or treatment, even if you think
their decision is wrong or irrational. You should explain your concerns clearly to the patient and
outline the possible consequences of their decision. You must not, however, put pressure on a
patient to accept your advice. (2008: 19)
At the same time, parents must be considered and aware of medical issues, since other
than signing the surgery agreement on minor’s place, they affect patients’ well-being either
prior and after the operation, or without it. Carl’s mother, for instance, understands that we
would rather talk just the two of us, and leaves the room with a smile. He does not want to
hear a thing about correcting with two titanium bars the canyon valley which grooves his
chest. Rather, he looks at the bright side of his adolescence:
I have many friends, and although they trot out my problem, I don’t get angry. I have parents and
relatives who love me, and therefore I don’t feel out of my element. Of course, when someone
comes to tell you “but do you drink from it?”, obviously this gets a bit under your skin.
Here, we find that Carl switches the first with the second person only when someone
makes a fool of you and gets on your nerves. His firsthand narrative becomes a ‘universal
you’, upon which listeners reflect their solidarity with the guy. Yet, IPA methodology takes
empathy into account more as a prerequisite of interpretation, than an end in itself. Instead of
“straightforward, unreflected absorption in the objects of experience, the phenomenological
approach involves reflection upon experience. The task is to elucidate and render explicit the
taken-for-granted assumptions of everyday life and, particularly, to bring to the fore one’s
consciousness of the world” (Toombs, 1993: xii). No matter if Carl recounts a compelling life
story, since therapist do not probe high moral values of patients but the meaningfulness of
their accounts to raise new questions about problems and solutions. This is why future

64
treatments of CWDs should aim to weave lived-experience into ‘meshwork therapies’, as
Ingold’s SPIDER suggests in the analogy When ANT Meets SPIDER:
My point is that the web is not an entity. That is to say, it is not a closed in, self-contained object
that is set over against other objects with which it may then be juxtaposed or conjoined. It is rather
a bundle or tissue of strands, tightly drawn together here but trailing loose ends there, which tangle
with other strands from other bundles. For the twigs or stems to which I attach these trailing ends
are themselves but the visible tips of complex underground root systems. Every plant, too, is a
living tissue of lines. And so, indeed, am I. It is as though my body were formed through knotting
together threads of life that run out through my many legs into the web and thence to the wider
environment. The world, for me, is not an assemblage of bits and pieces but a tangle of threads and
pathways. Let us call it a meshwork, so as to distinguish it from your network. My claim, then, is
that action is not the result of an agency that is distributed around the network, but rather emerges
from the interplay of forces that are conducted along the lines of the meshwork. (2011: 91-92,
italic is original)
Accordingly, the therapy is not an entity that separates the chest of deformed persons
from the complexity of their social and private surrounding, which Ingold’s ANT reduces to
an “assemblage of bits and pieces” (2011: 92). The ‘medical gaze’ on Daniel’s, Mark’s and
especially David’s body boosts their self-reflection, bringing issues of sexual identity to the
fore. However, Mol opposes that masculinity and femininity are performed only when
“staging oneself as a woman or a man” (2002: 39). That is, whenever you get undressed, your
chest’s look reduces yourself to a manifestation of these two gender roles, and what is not
typical of a man or a woman calls your identity into question.
“By conceiving every hybrid as a mixture of two pure forms”, Latour claims that a
modern thinking split therapies in separated entities, and the new challenge is to meswhork
them (1993: 78, italic is original). Therefore, Carl’s excavated chest should not be taken as an
entity separated from himself, since he could never undergo surgery without considering the
many beloved ones, hideous and happy memories put at risk. As an embodied though
stigmatic thread of life, his deformity constitutes a necessary strand in the tangle of pathways
among which he chooses the best for himself. Carl’s meshwork, above all, is made of people
who support his decision-making without interfering. Carl is not a sportsman, he plays
ocarina, an instrument:

65
As particular as the sports and the music I like. I’d love to play fencing but in Sardinia it’s hard to
find a place for this sport, so I gave in. I really like to listen Irish folk music, its ballads and
storytelling, as well as blues, but also rock and metal sometimes.
By recounting his hobbies, Carl conveys what makes him feel good. Yet, this
description of himself stands in opposition to the idea that “participant validation is flawed,
since the ‘atmosphere of safety’ that would allow the individual to lower his or her defences
and act in open candour is hardly likely to be achieved in the research encounter” (Ashworth,
1993: 15). Yet, Carl wants to make sure if his deformity may threat his health, since he would
rather avoid the implantation of two titanium bars, “though I am also afraid that after few
years I could regret my decision, especially if it will worsen”. His fourteen years do not let
him foresee how he will feel and what he will think about his body.
As a folk music fan, he dreams to make dance people forever with a certain ballad. Carl
describes his way of being as eternal, though fearing a backlash of his future self for the
decision he must take in a few weeks. For this purpose, therapists must help patients to be
aware but not threatened, informed but not obsessed, hopeful yet staying grounded, avoiding
the risk that:
Everything that goes on without us paying explicit attention to it when we are healthy – walking,
thinking, talking – now offers resistance. The body, our thinking, the world, everything is now ‘out
of tune’, colored by feelings of pain, weakness and helplessness. This way of being in the world in
illness is best understood as a form of homelessness. (Svenaeus, 2001: 89–90)
Since Svenaeus analogy of ‘homelessness’ speaks to youngsters who first see their
CWD, therapists must be ready to give a home to those who have lost it. Associations of
young patients and parents supported by medical professionals (e.g. Associazione Italiana
Sindrome di Poland, www.sindromedipoland.org), also organise events and conferences
providing deformed persons an agora for mutual aid. In contrast to what Ashowrth defines an
‘atmosphere of safety’ made up by participant and researcher together, here people who share
the same way of being experience a ‘fusion of horizons’ (Gadamer, 1960/1996: 302). By
socialising with others, indeed, we see “from a particular advantage point. We speak of
narrowness of horizon, of the possible expansion of horizon, of the opening up of new
horizons and so forth” (Ibid.). However, Carl makes explicit that “what challenges me the
most is to take a decision. Although my ideas are clear, this is the first time I have to choose

66
something so delicate”. Before taking a decision that may drive him to surgery, he also points
out that:
Other than the fear of the two bars, I think that I’ve never been recovered in hospital before, and
what bothers me is that after the operation I must say to friends who jostle me: ‘please don’t touch
me because there’s a metal bar in my chest’.
Carl seems more concerned about his freedom of behaving as many others, than the
anguish of looking weird compared to them. There is a tension between way of being and way
of looking in this account, if we take the freedom of jostling friends as a good reason to avoid
corrective surgery. Similarly, in the culture of track and field Pappa and Kennedy outline that:
“deviations from the norm, including the assertion of personal freedom, are strongly
discouraged if sporting victory is to be achieved” (2012: 282). Yet, disliking alcohol, parties
and smoking, Carl is against habits and stereotypes typical of the Italian teenage culture. As
such, according to Sartre ‘shame’ is a way to objectify oneself, as “I see myself because
somebody sees me. Shame reveals to me that I am this being” (Sartre, 1943/1969: 259–262,
italic is original). Carl does not like to feel like many others, he copes with a severe deformity
thanks to his family, though builds an egocentric fence that makes him wander away from
friends and peers. Since the cultural surrounding influences the well-being of deformed
persons, it is important that therapists situate their listening in both anthropological and
psycho-social terms. For instance, Carl lives in a touristic area of Sardinia:
Where it’s hard to find young people with the same interests as me. Further, everyone plays soccer
there, and I can’t even remember the name of a single football player or team, while one of my
classmates knows all of them by heart. I also tried volleyball and then quitted since I wasn’t good
enough, though I could easily smash the ball as I am tall 190 cm!
Frank would argue that anthropological investigations do not bring any scientific truth,
but give an insight about researcher and informant:
My fascination with Diane prompted me at once to explore the sources in myself that made the
image of a woman without limbs so intriguing. Through systematic self-reflection I probed my
identification and empathy with her situation, uncovering my own invisible disabilities and then
disentangling them from the way Diane sees herself. (2000: 4)

67
Making sense of patients’ life-world lays the foundations of collaborative therapies,
where specialists must be aware of their influential power and the ‘chain of authority’ that
may lead deformed persons to make a choice or another (Murphy, 1990: 21). Thus, their
priority in the treatment of CWDs should shift from assessing to monitoring, and from
advising to listening. Yet, this does not prevent doctors from finding the best therapy
according to both the Motivation Scale for Corrective Surgery and functional problems that
vary on a case-by-case basis. In this scenario, counselling is still the favoured option for the
many patients unconvinced by the operation.
Thus, we should equip ‘Pectus teams’ with a counselling psychologist and an
established methodology that would offer patients a new home. By using the Operation-
Expectation-Questionnaire, Frankfurter Body Concept Scales and the Motivation Scale for
Corrective Surgery, further, we are able to apply standardised evaluation criteria (Hadolt et
al., 2011: 666-667). Parameters acknowledge by both surgeons and counsellors would also
provide patients with a cross-validated diagnosis. Moreover, since many teenagers without a
severe CWD schedule more than one appointment with surgeons, counselling may help them
to understand why corrective surgery is not a good idea and what alternatives they have.
As Hadolt et al. point out: “the wish for a standardised psychological support
(supporting the development of coping strategies with the goal of psycho-social health)
during the period of treatment was expressed by one patient” (2011: 669). Although the
sample of their research is quite small – seventeen adolescents who has undergone the Nuss
procedure – the issue at hand consists in establishing routine CWD counselling for both
corrected and non-corrected patients (Ibid.: 665-666). As such, the number of surgeons who
deal with unmotivated or asymptomatic patients will likely decrease.

68
The End of Our Stigmatic Journey
Despite symptoms and physical limitations typical of CWDs, what leaves its mark at
the end of our journey is likely the eagerness to empathise with those who cope with
disturbance of body image. For different reasons, indeed, the accounts of our children, friends
and partners with anomalous bodies beget a deeper understanding of one’s own adolescence.
Meeting Daniel, Mark, Carl, David, Isabelle and their family, anyone has the chance to think
retrospectively how harassing it must have been to live through the lens of so young a
‘troubled’ body. While the world outside opened up new horizons and infatuations with
persons and hobbies, many of us were unsure of playing a winning role, even on our own.
‘Chameleonic’ enough, however, we ended up seeking advice from others, believing in
getting better, becoming more sociable and sharing little things that became big things.
Finally, we got off on the right foot. With courage we afforded a painful and delicate growth,
still looking ahead with stomach in and chest out!
Nowadays, an increasing number of researchers highlight the relevance of CWDs’ care
in the field of paediatric surgery and psychology (Hadolt, Steinmann, Kelly Jr, Lawson and so
on). Less attention is paid to the phenomenological and therapeutic aspects, as perspectives
for attuning to the complex lived experience of patients. As such, counsellors may hopefully
draw inspiration from this research and its tailored meshwork of patients, families and
therapists – aiming to shed light on the grey areas of deformed life-worlds.

69
Acknowledgements
Firstly, I cannot get out of thanking all the patients who dedicated me their time giving
life to this project. Although concerned about themselves, indeed, they contributed to
encourage those who still seek their disclosure. In particular, Davide Politi and his beautiful
family kindly welcomed me in their home, allowing us to grow a relationship of reciprocal
trust and understanding. What his life story taught me cannot be reduced to any dissertation.
Further, I will not forget parents, siblings and foster carers of patients, always beside
them with love and fears, willing to help their son or daughter as best as they can. In fact,
only few of them pretended to know the truth about their children or have the last word,
whereas the majority took our meeting as a chance to learn from each other.
Dr Michele Torre, moreover, believed in this project since the beginning, opening the
heavy doors of his Surgical Dept. at Ospedale Pediatrico Gaslini di Genova, which I warmly
thank for accepting me (FIG. 7). I hope this dissertation may reflect the passion and
uprightness he devotes to his profession. At the same time, I must thank Dr Tiit Härma for the
precious time he spent with me, aiming to increase the expertise about CWDs at the Surgical
Dept. of Tallinna Lastehaigla. His humanity and competence are important for Estonian guys
and girls. Further, without the introduction to the health care system in Estonia of Dr Marika
Tammaru, this project would have been less consistent.
Yet, the audiovisual support of Anna Forgione is the cherry on top, owing to Davide
Politi’s interview recorded in Naples and the photos taken in Tallinn. Her work finds way into
deformed persons’ heart, as much as in the eyes of professional photografers. The careful
listening and advices of Anna-Kristina, my parents’ love, the closeness of both friends and
relatives are also worthy of note.
Last but not least, I cannot forget to thank Patrick Laviolette and Carlo A. Cubero,
anthropologists who always encouraged me to find myself in the other’s voice. Thus, I am
also greatful to my colleagues and the Estonian Humanities Institute at Tallinn University,
whose open discussions still resonate in my mind.

70
FIG. 7 – Dr Torre explains the Nuss procedure to a patient.

71
References:
Andres, F., Castanier, C., Le Scanff, C. 2014. ‘Attachment and alcohol use amongst athletes:
The mediating role of conscientiousness and alexithymia’, Addictive Behaviors. Vol. 39, 2,
pp. 487-490.
Ashworth, P.D. 1993. Participant agreement in the justification of qualitative findings,
Journal of Phenomenological Psychology. Vol. 24, pp. 3–16.
Augé, M. 2004. Oblivion. University of Minnesota Press, Minneapolis, MN, USA.
Biggerstaff, D. 2012. Qualitative Research Methods in Psychology, Psychology - Selected
Papers, Dr. Gina Rossi (Ed.). ISBN: 978-953-51-0587-9, InTech, Rijeka, Croatia, Available
from:
http://www.intechopen.com/books/psychology-selected-papers/qualitative-research-methods-
in-psychology
Boler, M. 1999. Feeling Power: Emotions and Education. Routledge, New York, USA.
Bourgeois, P. 2002. In Search of Respect: Selling Crack in El Barrio (Structural Analysis in
the Social Sciences). Cambridge University Press, Cambridge, U.K.
Brehm, J. W. 1966. A theory of psychological reactance. Academic Press, New York, USA.
Brehm, J. W. 1972. Responses to loss of freedom: A theory of psychological reactance.
General Learning Press Morristown, NJ, USA.
Brehm, J. W., Brehm, S. S. 1981. Psychological reactance: A theory of freedom and control.
Academic Press, San Diego, CA, USA.

72
Bremer, A., Dahlberg, K. and Sandman, L. 2009. To survive out-of-hospital cardiac arrest: a
search for meaning and coherence, Qualitative Health Research. Vol. 19, pp. 323–338.
Brown, B. B., Larson J. 2009. ‘Peer Relationships in Adolescence’, Handbook of Adolescent
Psychology. Chapter 3 (Oct., 2009), pp. 74-103.
Bruner, J. 1990. Acts of Meaning. Harvard University Press, Cambridge, MA, USA.
Bruner, J. 1991. The narrative construction of reality, Critical Inquiry. Vol. 18, pp. 1-21.
Cialdini, R. B. 2006. Influence: The Psychology of Persuasion. William Morrow and
Company, Inc., New York, USA.
Colombani, P. 2009. Preoperative assessment of chest wall deformities. Semin Thorac
Cardiovasc Surg. Vol. 21, No.1, pp. 58-63.
Csordas, J. T. 1994. Embodiment and Experience: The Existential Ground of Culture and Self.
Cambridge University Press, Cambridge, U.K.
Dahlberg, K. 2007. The enigmatic phenomenonof loneliness, International Journal of
Qualitative Studies on Health and Well-being. Vol. 2, pp. 195-207.
Douglas, M. 1966. Purity And Danger: An Analysis of The Concept of Pollution And Taboo.
Routledge, New York, USA.
Eisenberg, L. 1977. Disease and Illness: Distinctions Between Professional and Popular Ideas
of Sickness, Culture, Medicine and Psychiatry. Vol. 1, pp. 9-23.
Evans, K.R., Gilbert, M. 2005. An Introduction to Integrative Psychotherapy. Palgrave
Macmillan, Basingstoke, Hampshire, U.K.
Evans, Ken, Finlay, L. 2009. To be, or not to be . . . registered: A relational
phenomenological exploration of what State Registration means to psychotherapists,
European Journal for Qualitative Research in Psychotherapy. Vol. 4, pp. 4-12.

73
Finlay, L. 2004. The Practice of Psychosocial Occupation Therapy. Nelson Thornes,
Celtenham, U.K.
Finlay, L. 2011. Phenomenology for Therapists: Researching the Lived World. Wiley-
Blackwell, Oxford, U.K.
Fitzpatrick, N., Finlay, L. 2008. ‘Frustrating disability’: The lived experience of coping with
the rehabilitation phase following flexor tendon surgery, International Journal of Qualitative
Studies on Health and Well-being. Vol. 3, pp. 143-154.
Frank, A. W. 1995. The Wounded Story Teller: Body, Illness, and Ethics. University of
Chicago Press, Chicago, IL, USA.
Frank, G. 2000. Venus on Wheels: Two Decades of Dialogue on Disability, Biography, and
Being Female in America. University of California Press, Berkley and Los Angeles, CA,
USA.
Foucault, M. 1963. The Birth of the Clinic. Routledge, Oxon, U.K.
Gadamer, H.-G. 1975/1996. Truth and Method. Second revised edition, originally published
in German in 1965. Sheed and Ward, London, U.K.
General Medical Council. 2008. Consent: patients and doctors making decisions together.
GMC, London, U.K.
Giorgi, A. 1995. Phenomenological Psychology. In J. A. Smith, R. Harré, K. Van
Langenhove (Eds.) Rethinking Psychology. Sage Publications, London, U.K.
Giorgi, A., Gallegos, N. 2005. Living through some positive experiences of psychotherapy,
Journal of Phenomenological Psychology. Vol. 36, pp. 195-218.
Glaser, B. G., Strauss, A. L. 1967. The discovery of grounded theory. Aldine, Chicago, USA.
74
Goffman, E. 1963. Stigma: Notes on the Management of Spoiled Identity. Simon & Shuster
Inc., New York, USA.
Hadolt, B., Wallisch, A., Egger, J. W., Höllwarth, M. E. 2011. Body-image, self-concept and
mental exposure in patients with pectus excavatum, Paediatric Surgery International. Vol.
27, pp. 665–670.
Hathaway, K. B. 1943. The Little Lockersmith. Coward-McCann, New York, USA.
Heidegger, M. 1987/2001. Zollikon Seminars: Protocols-Conversations-Letters. M. Boss
(Ed), Evanston, IL: Northwestern University Press (Originally published in German in 1987).
Ingold, T. 2011. Being Alive: Essays on Movement, Knowledge and Description. Routledge,
Abingdon, U.K.
Jackson, P. 2004. Inside clubbing: Sensual Experiments in the Art of Being Human. Berg,
Oxford, U.K.
Keats, P.A., Keats-Osborn, W.R. 2012. Overexposed: Capturing a secret side of sports
photography. International Review for the Sociology of Sport. Vol. 48, 6, pp. 643-657.
Kelly Jr, RE. 2008 Pectus Excavatum: Historical background, clinical picture, preoperative
evaluation and criteria for operation, Semin Pediatr Surg. Vol. 17, 3, pp. 181-193.
Kelly Jr, RE et al. 2008. Surgical repair of Pectus Excavatum markedly improves body image
and perceived ability for physical activity: Multicenter study, Pediatrics. Vol. 122, pp. 1218-
1222.
Kent, D. 1987. In Search of Liberation, Women: Images and Realities: A Multicultural
Anthology. McGraw-Hill Humanities/Social Sciences/Languages, 5 edition, Columbus, OH,
USA.
Kielhofner, G., Borell, L., Freidheim, L., Goldstein, K., Helfrich, C., Jonsson, H., Josephsson,
S., Mallinson, T. and Nygård, L. 2002. Crafting occupational life. In G. Kielhofner (Ed),

75
Model of Human Occupation: Theory and Application. 3rd edn.: Lippincott Williams and
Wilkins, Baltimore, MA, USA.
King, N., Finlay, L., Ashworth, P., Smith, J.A., Langdridge, D. and Butt, T. 2008. ‘Can’t
really trust that, so what can I trust?’: A polyvocal, qualitative analysis of the psychology of
mistrust, Qualitative Research in Psychology. Vol. 5, pp. 80-102.
King, A. 2012. The naked female athlete: The case of Rebecca Romero. International Review
for the Sociology of Sport. Vol. 48, 5, pp. 515-534.
Kraaykamp, G., Oldenkamp, M., Breedveld, K. 2012. Starting a sport in the Netherlands: A
life-course analysis of the effects of individual, parental and partner characteristics,
International Review for the Sociology of Sport. Vol. 48, 2, pp. 153-170.
Krüger, A. 2007. An introduction to the ethics of gestalt research with informants, European
Journal for Qualitative Research in Psychotherapy. Vol. 2, pp. 17-22.
Langley, T. 2012. Batman and Psychology: A Dark and Stormy Knight. John Wiley & Sons,
Inc., Hoboken, NJ, USA.
Latour, B. 1993. We Have Never Been Modern. Harvard University Press, Cambridge, MA,
USA.
Lawson, ML. et al. 2003. A pilot study of the impact of surgical repair on disease-specific
quality of life among patients with pectus excavatum, Journal of Paediatric Surgery. Vol. 38,
pp. 916-918.
Levin, D.M. 1985. The Body’s Recollection of Being: Phenomenological Psychology and the
Deconstruction of Nihilism. Routledge & Kegan Paul, London, U.K.
Littlewood, R., Jadhav, S., Ryder, A. G. 2007. A Cross National Study of The Stigmatisation
of Severe Psychiatric Illness: Historical Review, Methdological Considerations, and
Development of the Questionnaire, Transcultural Psychiatry. Vol. 44, 2, pp. 171-202.
76
Machida, M., Irwin, B., Feltz, D. 2013. Resilience in Competitive Athletes With Spinal Cord
Injury: The Role of Sport Participation, Qualitative Health Research. Vol. 23, pp. 1054-1065.
Merleau-Ponty, M. 1964. The film and the new psychology, In M. Merleau-Ponty (Ed), Sense
and Non-Sense. Northwestern University Press Evanston, IL, USA.
Moi, T. 1985. Sexual/Textual Politics: Feminist Literary Theory. Routledge, New York, USA.
Mol, A. 2002. The Body Multiple: Ontology in Medical Practice. Duke University Press,
Durham, NC, USA.
Moran, D. 2000. Introduction to Phenomenology. Routledge, London, U.K.
Murphy, F. R. 1990. The Body Silent. W. W. Norton, New York, USA.
Pappa, E., Kennedy, E. 2012. ‘It was my thought… he made it a reality’: Normalization and
responsibility in athletes’ accounts of performance-enhancing drug use, International Review
for the Sociology of Sport. Vol. 48, 3, pp. 277-294.
Polkinghorne, D. E. 1988. Narrative Knowing and the Human Sciences. State University of
New York Press, Albany, New York, USA.
Rapport, N. 2003. I am Dynamite: An Alternative Anthropology of Power. Routledge, London,
U.K.
Ricoeur, P. 1973/1990. Hermeneutics and the critique of ideology. In G.L. Ormiston and A.D.
Schrift (Eds), The Hermeneutic Tradition: From Ast to Ricoeur. pp. 298–334, State of
University of New York Press, Albany, NY, USA.
Rose, N. S. 1998. Inventing Our Selves: Psychology, Power, and Personhood. Cambridge
University Press, Boston, MA, USA.
Rheingold, H. 1993. The Virtual Community: Homesteading on the Electronic Frontier.
Addison Wesley, Boston, USA.

77
Saint-Exupéry, A. 1943. The Little Prince. Reynal & Hitchcock, New York, USA.
Sartre, J.-P. 1943/1969. Being and Nothingness. Trans. H. Barnes, 1958, Routledge, London,
U.K.
Scheper-Hughes, N., Lock, M. M. 1987. The Mindful Body: A Prolegomenon to Future Work
in Medical Anthropology, Medical Anthropology Quarterly New Series. Vol. 1, 1, pp. 6-41.
Sifneos, P. E. 1973. The prevalence of alexithymic characteristics in psychosomatic patients,
Psychotherapy and Psychosomatics. 26, pp. 270-285.
Sinden, J. L. 2012. The sociology of emotion in elite sport: Examining the role of
normalization and technologies, International Review for the Sociology of Sport. Vol. 48, 5,
pp. 613-28.
Smith, J. A., Flowers, P., Larkin, M. 2009. Interpretative phenomenological analysis: Theory,
method and research. Sage, London, U.K.
Steinmann, C., Krille, S., Mueller, A., Weber, P., Reingruber, B., Marin, A. 2011. Pectus
excavatum and pectus carinatum patients suffer from lower quality of life and impaired body
image: a control group comparison of psychological characteristics prior to surgical
correction, European Journal of Cardio-Thoracic Surgery. Vol. 40, 5, pp. 1138-1145.
Svenaeus, F. 2001. The phenomenology of health and illness. In S.K. Toombs (Ed),
Handbook of Phenomenology and Medicine. pp. 87–108, Kluwer Academic, Dordrecht,
Netherlands.
Thamm, S. 2009. My Private Pectus. Ford Street Publishing, Clifton Hill, Australia.
Todres, L. 2007. Embodied Enquiry: Phenomenological Touchstones for Research,
Psychotherapy and Spirituality. Palgrave Macmillan, Basingstoke, Hampshire, U.K.
Toombs, S.K. 1993. The Meaning of Illness: A Phenomenological Account of the Different
Perspectives of Physician and Patient. Kluwer Academic: Dordrecht, Netherlands.

78
Torre M., Rapuzzi G., Jasonni V. and Varela P., 2012. Chest Wall Deformities: An Overview
on Classification and Surgical Options, Topics in Thoracic Surgery, Prof. Paulo Cardoso
(Ed.). ISBN: 978-953-51-0010-2, InTech, Rijeka, Croatia, Available from:
http://www.intechopen.com/books/topics-in-thoracicsurgery/chest-wall-deformities-an-
overview-on-classification-and-surgical-options
van Manen, M. 1990. Researching Lived Experience: Human Science for an Action Sensitive
Pedagogy. State University of New York Press, New York, USA.
Waldschmidt, A. 2005. Who Is Normal? Who Is Deviant? “Normality” and “Risk” in Genetic
Diagnostics and Counseling. In S. Tremain (Ed.) Foucault And The Governmentality Of
Disability. University of Michigan, MI, USA.
Willig, C. (2008) Introducing qualitative research methods in psychology: Adventures in
theory and method. 2nd ed. McGrawHill / Open University Press, Maidenhead, U.K.
Picture on the cover: © Anna Forgione

79
Notes: i YouTube accessed on 16/01/2014 searching: ‘pectus excavatum Nuss diary’, ‘pectus excavatum how to
accept it’, ‘pectus excavatum’, ‘pectus excavatum workout’.
ii Barry Lo Sasso. 2012. The New You and Beyond
https://www.youtube.com/watch?v=UOHB9GBZMRU
iii It is an experiment I call cultural biography, which combines the genres of ethnography and life history.
Ethnography is the cultural anthropologist’s stock-in-trade, a firsthand description of a people’s way of life.
Unlike the early anthropologists, whose published works often consists of cultural inventories and static
generalisations about the people they studied, contemporary anthropologists tend to write narrative
ethnographies. These are stories based on events we have experienced – more as observing participants than as
participant observers – through which we try to convey how people within a particular group or tradition create
meaningful solutions to life’s challenges. (…) The life history is a related anthropological genre that traces how
a culture influences the experiences of a specific individual. Most life histories consist of autobiographies or life
stories in the oral tradition. (Frank, 2000)
iv Alexithymia refers to difficulties identifying and describing emotions, constricted imagined processes
and an externally oriented cognitive style (Sifneos, 1973). Some authors stress that alexithymia is a personality
trait that places individuals at a greater risk of alcohol-related disorders due to maladaptive emotional regulation
strategies (Coriale et al., 2012). Recent studies suggest that alexithymia is related to dysfunctional parenting
(Thorberg et al., 2011) and therefore to insecure attachment (Montebarocci, Codispoti, Baldaro, & Rossi, 2004).
(Andres, Castanier, LeScanff, 2014)
v Unknown author. 2012. Pectus Excavatum The Van Analogy
http://www.youtube.com/watch?v=03IgQwePjCM
80
Lihtlitsents lõputöö reprodutseerimiseks ja lõputöö üldsusele kättesaadavaks tegemiseks Mina ___________________________________________ (sünnikuupäev: _____________)
(autori nimi) 1. annan Tallinna Ülikoolile tasuta loa (lihtlitsentsi) enda loodud teose
________________________________________________________________________________________________________________________________________________________________________________________________________________________
(lõputöö pealkiri) mille juhendaja on ________________________________________________________,
(juhendaja nimi) säilitamiseks ja üldsusele kättesaadavaks tegemiseks Tallinna Ülikooli Akadeemilise Raamatukogu repositooriumis.
2. olen teadlik, et punktis 1 nimetatud õigused jäävad alles ka autorile. 3. kinnitan, et lihtlitsentsi andmisega ei rikuta teiste isikute intellektuaalomandi ega
isikuandmete kaitse seadusest tulenevaid õigusi. Tallinnas/Haapsalus/Rakveres/Helsingis, ______________________________
(digitaalne) allkiri ja kuupäev
Top Related
Copyright © 2022 FDOKUMEN

