clinical. studies on daul feel (filariasis) - ccrum
164
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of clinical. studies on daul feel (filariasis) - ccrum

CLINICAL. STUDIES ON DAUL FEEL (FILARIASIS)
A Technical Report
at The Regional Research Institute of Unani Medicine
1, West Mada Church Road, Madras 600 013
CENTRAL COUNCIL FOR RESEARCH IN UNANI MEDICINE MINISTRY OF HEALTH AND FAMILY WELFARE
GOVT. OF INDIA, NEW DELHI

Foreword
India is making a glorious entry into 21 st century holding high the banner of ancient heritage and vibrating new modern India. India's gallant march after independence with devastated economy, crippling health and hungry teeming millions is landmark in the history of human development. Our conquests over monstrous multifaceted crisis posing a dreadful threat to our stability at the dawn of independence are still fresh in our memory and sources of inspiration for younger generations. India with dedication and determination has found answers to many crushing problems and claims to have reached the pinnacles of glory. But yet we all have to run a marathon race to win laurels of success to carve out a dignified place in the world of medicines. The task ahead is stupendous.
India is a signatory to historic Alma Ata declaration of Health for All by 2000 AD. India's commitment is total. To attain the pious goal, the Ministry of Health and Family Welfare have focussed all attention to the problem areas, enlarged activities in health sector and geared up adminstative machineries to accelerate the pace of implementation of various programmes. Central Council for Research in Unani Medicine, an autonomous organisation of the Ministry of Health and Family Welfare is playing a very crucial role in Health Care Delivery. The Council with its capable manpower is engaged in various researcl"t activities with greater thrust on clinical research. Results in some areas are remarkable. Researches on scientific lines are in progress.
Prevalence of chronic and stubborn diseases has become a matter of grave concern for the Government and the nation. The Ministry of Health & Family Welfare have identified these dreadful · diseases as 'National Priorities' . 'Filariasis' is one of the major health problems of our country particulady in coastal areas. Agencies like NICD, ICMR, NFCP, CCRAS and CCRH are also doing work for finding a viable solution to this problem. CCRUM is up in arms to fight the menace and is poised for making significant contribution in National Health Care Programme.
The CCRUM took up the Clinical Research work on this gigantic problem at its Institutes located at Madras (T.N.), Bhadrak (Orissa) and Patna (Bihar). · The present study, however, is only related to Clinical Research work on 'Filariasis' carried out at Regional Research Institute of Unani Medicine, Madras. The time tested remedies reported in classical literature of Unani Medicine, have been clinically investigated on various scientific parameters to prove their work. We have had the collaborative support of Madras Medical College and other agencies. Some eminent experts of modem medicine have also been a.ssociated with these. The drug has proved efficacious without any side effects.
This work has possible only with the services and dedicated efforts of our researches at Madras Institute under the supervision of Prof. S. Khaleefathullah. The Council acknowl~ges their contribution and places on record deep appreciation:
Our studies are only a beginning and are open for evaluation. Suggestions are welcome.
(R.K. MUKHI) Director, CCRUM
& Director (ISM)
in the Ministry of Health & F.W.
Preface
Although important clinical advances continue to be made in the prevention and treatment of major diseases, there is an increasing consciousness of the responsibility in investigating effective and cheaper remedies.
The Regional Research Institute of Unani Medicine, Madras, which was established on 6th July 1979 and formally inaugurated on 28th October 1979, is engaged in extensive and exhaustive research on the following problems allotted by the Scientific Advisory Committee of the Central Council for Research in Unani -Medicihe, New Delhi.
1. DAUL FEEL (FILARIASIS)
2. ZIABITUS-e-SUKKARI (DIABETES MELLITUS)
3. WAJA-UL-MAFASIL (RHEUMATOID ARTHRITIS)
4. IL TEHAB-e-KAB/0-e-HAD (INFECTIVE HEPTITIS)
The Institute also has facilities for treating general out-patients. The building and land housing this ·Institute at No.1, West Mada Church Street, Royapuram, Madras-600 013, was placed at the disposal of the Central Council for Research in Unani Medicine, New Delhi, "by the Govenment of Tamil Nadu.
The Directors of Central Council for Research in Unani Medicine, both past and present have given full encouragement and support in not only establishing but also in equipping the Institute in a short span of time. The help Hakim M.A. Razzack has given during his tenure towards all the activities of the Institute is placed on record.
Daul Feel (Filariasis) is a major health problem especially prevalent in tropical Countries. In India it is endemic in Madras, Patna, Orissa and Coastal Antjhra Pradesh. This has prompted the Central Council for Research in Unani Medicine to undertake a clinical trial on Daul Feel (Filarisais) at Madras.
It is a pleasure to submit the Monograph on Clinical study of Daul Feel (Filariasis) comprising of 226 patients of Chronic . Filariasis. This Monograph will be of scientific importance not only to Unani Physicians, but also to colleagues of various other systems of medicine. It gives details about the linical aspects, pathological 1 bio-chemical I immunological aspects and botanical profile of the drugs used.
I am thankful to Dr. K.V. Thituvengadam and Dr. J.R. Shankaran and their team, Dept. of Clinical medicine of Govt. General Hospital, Madras for their collaboration in the double blind placebo cqntroiiP.d study.

I place on record our thanks to D.r. Sundarajan and his team of Department of Microbiology, Post-graduate Institute of Basic Medicine Sciences, Madras for their collaboration in the Immunological aspects of the study.
HAKIM SYED KHALEEFATHULLAH HONY. PROJECT. OFFICER
i

UNANI 1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11 .
SCIENTISTS ASSOCIATED WITH THE CLINICAL STUDIES ON DAUL FEEL (FIALRIASIS) AT REGIONAL RESEARCH INSTITUTE OF
UNANI MEDICINE, MADRAS
Hakim Giyasuddin Ahmed
Hakim (Mrs.) Rabia Begum
Hakim Darakshid Alam
Hakim ldris Ahmed )
Hakim (Mrs.) Gowher Sultana
Hakim Mushtaq Ahmed
Hakim L. 1 Samiullah
Hakim S.S. Hameed
Hakim K.B. Ansari
Hakim S. Kareemullah
Hakim Syed Jameeluddin
BIOCHEMISTRY
1. Dr. Najma Begum
2. Dr. Abdul Sattar
3. Dr. Abdul Kareem
PATHOLOGY
1. Dr. Shaik Dawood
2. Dr. (Mrs.) Rama Gopalan
3. Dr. (Mrs.) Doreen Gracias
STATISTICS
1. Mr. P. Ameer Basha
BOTA~Y
1. Mr. S.R. Nayar

CONTENTS
FOREWORD iii
PREFACE v
Scientists associated with the Clinical Studies on [')aul Feel (Filariasis) vii
1. Introduction
2.
3.
4.
5.
6.
7.
8.
9.
i. Concept of Daul Feel (Filariasis) in Unani Medicine ..
ii. Concept of Daul Feel (Filariasis) in Modern Medicine
Experimental protocol
Drugwise therapeutic trials
Discussion on the efficacy of different drugs used
Role of various factors in response to the treatment
Miscellaneous factors studied
Biochemical studies
Pathological studies
Herbal Drugs enterin·g in the composition of various recipes used for the treatment of Daul Feel (Filariasis)
APPENDICES
i) Abstract of papers presented on Daul Feel· (Filariasis) at different Seminars/Symposia
ii) Case Sheet for Daul Feel (Filariasis)
REFERENCES
1
2
9
12
79
79
80
80
81
105
131
138

CONCEPT OF DAUL FEEL (FILARIASIS) IN UNANI MEDICINE
Daul Feel has been defined by ancient Unani Physicians as a lymphatic disease characterized by unilateral or bilateral involvement of the lower limbs in the form of accumulation of fluid finally taking the shape of an elephant leg.
According to Unani Physicians Daul Feel occurs due to vesiation of humour, i.e. Balgham (Phlegm) and Sauda (Black bile) and this vesiated humour will accumulate in the body (or organ) due to weakness and obstruction of Urooq-e-Jauba (i.e. lymphatic vessels) thereby giving rise to the disease process.
The treatment regime employed for this chronic disease, according to the Unani Physicians,
comprises of two parts; one part being termed the "Munzij-Mushil ", and the other part, involves the administration of the appropriate herbal preparation.
The Munzij-Mushil therapy is a specialised mode of treatment, directed towards bringing
out coction in an already establ ished deranged humour and then causing expulsion . of this deranged humour through specific purgation thereby increasing the responsive potential of the patients to the other regime which is started after the completion of the MM Therapy. The change from Munzij to Mushil is indicated by the appearance of 'NUZJ' in the urine. During the treatment, patients are advised to refrain from phlegmatic diets such as bananas etc.
After completion of the Munzij-Mushil Therspy ,Musaffiyat (purification) and Muqaviat are administered orally, followed by external application termed 'ZIMAT' (Paste) to the affected part. They are also advised dressing of the affected part with bandage and also bed rest.
1

DIAGRAMATIC REPRESENTATION OF CLICNICAL SPECTRUM
A UNEXPOSED
B EXPOSED
UNINFECTED
AMICRQFILARAEMIC
UN INFECTED ASYMPTOMATIC
AMICROFILARAEMIC
- INNATE RESISTANCE
- TRANSFER OF IMMUNITY
FROM MOTHER
INFECTED
ASYMPTOMATIC ALLERGIC ASYMPTOMATIC SYMPTO ' MANIFESTATION MATIC
I I I AMICROFILARAEMIC AMICROFILARAEMIC MICROFILARAEMIC
Filarial Fever
Adenolymphangitis
eg. breast
(adult worms)
I Acute
(Adult worms)
3
I Granulomata
Chronic
(Adult worms)
TPE
Monoarthritis
(adult worms)

CONCEPT OF FILARIASIS IN MODERN MEDI·.·CINE
Filariasis is a complex of diseases caused by tissue dwelling nematodes which are responsible for some of the major helminth induced diseases of man. These worms invade the lymphatics,
1 •
subcutaneous and deep tissues c;>f human beings producing reactions ranging from acute in-flamation to chronic scarring. The viviparous females discharge microfilariae into the blood or subcutaneous tissues, where they live for weeks or months until taken up by hematophagus arthropods. Within these vectors they are then transformed into filariform larvae which then infect a new host when the arthropod takes another meal.
The larval forms of the parasite were first observed by Demarquay (1863) in the hydrocoe'lic fluid. Later Wucherer (1866) found them in the chylous urine and Lewis (1872) reported them in human blood. Bancroft (1876) identified the adult females hence the specific name was coined after the discoverer. The clicnical pictures produced by various species in this group are more
or less specific. The term lymphatic filariasis is commonly used to designate the disease produced by Wuchereria bancrofti and Brugia malayi, the organisms responsible for lymphatic blockade and elephantiasis. Loa loa causes loasis a disease charaterized by transient subcutaneous sewlling. Onchocerca volvulus produces blindness and pruritic s~in rash typical of onchocerciasis. Mansonella ozzardi, Dipetalonima perstans, and D. streptocerca cause infections of questionable clinical significance to humans. These parasites are identified by the location .• periodicity and morphologic characteristics of their microfilariae.
Clinical Spectrum
In the light of recent epidemiological and immunological studies it is being increasingly realised that in endemic areas some persons with the same exposure to infective larvae as others do not acquire infection or disease. These persons will be no different from those in non-endemic areas and will be asymptomatic.
On the other hand there are those who have been exposed to infective larvae and remain amicrofilariemic and asympytomatic because they have developed active immunity to infective larvae. These persons differ from the above categories in that they may show some serological or immunological reaction which ,demonstrates sensitisation to infective larvae. Other.individuals in whom the ineffective larvae reach L4 or young adult stage show allergic manifestations. These persons will be microfilaria negative but symptomatic. Others are asymptomatic microfilariemic.
Individuals with clicnical manifestations or filarial fever and adenolymphangitis are microfilaria positive or negative depending on the immunogenic response. At the extreme end of the spectrum are Tropical Pulmonary--Eosinophilia cases which are generally microfilaria negative
2

and represent an extreme hypersensitive state. Other forms of occult infections such as monoarthritis may also belong to this category.
Classical Filariasis
The cl inical manifestations vary with the geographic area, species of parasite and intensity of infection. Symptoms may occur within 3 months of infection but ordionarily the incubation period ranges from 8 to 12 months. Within 4 days of the infective larvae reaching the lymphatics there is a marked cell mediated response in the regional lymph gland folowed by an antibody mediated response in the afferent lymphatics by an antimacrofilarial antibody. This response is the cause of the local lymph gland enlargement in early filariasis. After the infective larvae migrate down the lymphatics considerable changes take place with a great increase in diameter and the formation of large tortuosities. These changes rapidly revert to normal following death of the worm from macrofilaricidal drugs. Distrubance of the lymph flow with lymphoedema results only when a strong resistancee to reinfection has developed with the appearance · of an antimocrofilaricidal antibody.
The Acute Stage
The acute eli nical manifestations of filariasis are characterised by recurrent. attacks of fever associated with lymphadenitis. Sometimes these are precipitated by hard physical exertion, while lymphadenitis in bancroftian filariasis (W.bancrofti) commonly 09curs in the inguinal region of the lymphatics of the male genitalia are also frequently affected, leading to funiculitis, epididmyitis or orchitis. In Brugian filariasis (B.m~layi or B.timori) the affected lymph nodes are mostly situated in the inguinal region and seldom It ever in the genitalia. Each attack of fever and lymphadenitis lasts for several days and usually subsides spontaneously following be_sj rest. It may be followed by retrograde lymphangitis, oedmatous infilteration of the surrounding subcutaneous tissue or even theJormation of abscesses which may ulcerate and lead to cicatrisation, lymphoedema is frequently present during these episodes but usually subside after the acute
stage. With time, resolution of the lymphoedema after each attack becomes less complete and the characteristic chronic changes develop. The whole acute clicnical course of an episode involving lymphadenitis and the complications leading to cicatrisation may last from .3 weeks to 3 months and can result in prolonged inability to work.
The Chronic Stage
The chronic signs of tila~iasis take many years to develop and only a small proportion of the infected community is attected. In bancroftian filariasis the major signs may differ from one area to another. These are hydrocoele, chyluria, lymphoedema and elephantiasis of the legs, scrotum, arms, vulva or breasts in order of decreasing frequency.
4

.. Occult Filariasis
mrs colit?"di'on /S cmmc/&.I?Z6!7' by &pl.>a?'es ol,ag/aKysmaJ nocJvmaJ covgh and wheezing,
and elevated erythrocyte sedimentation rate, pulmonary infilteration and an extremely high eosinophilia. It is commonly reported in South East Asia, Brazil and Africa. The syndrome is the result of an immune response in which the microfilariae are destroyed in the tissues without
reaching the peripheral blood.
Other clinical Manifestations include
Filarial granuloma of the breast : Lesions appear around the fpurth decade mostly in married
women and clinicaly resemble tumors (Chandrasoma & Mendis, 1978) MONOARTHRITIS :This
is commonly associated with fll~rlal lnf~etiM . W.bancrofti c~n ~lgo indUCQ POIV8nnriti~ wnicn stimulates rheumatism (Ismail and Nagaratnam 1 973)
Chyluria and Immune complex nephropathy : First descr ibed by Chugh e r a t 1978. I t Is
caused by the rupture of a varix in the wall of the bladder or elsewhere in the urinary tract. The contents of the lymphatics escape in the urine.
Worms in unusual sites : There have been several eariler records of lymphatic parasites in unusual sites. Two recent reports have been made of adult Brugia worms in the conjunctiva of patients in Malaysia (Dissanaike eta/, 1974, Mak eta/, 1974)
Aetiology
The genus Wuchereria contains only one species W.bancrofti a parasite which is found
only in man. There are two biologically different forms, one periodic with nocturnal periodicity of the microfilariae transmitted by night biting mosquitoes and the second subperiod ic with diurnal periodicity of the microfilariae transmitted by day biting mosquitoes. The adult worm can survive for 10 to 18 yrs.
The genus Brugia includes eight species :B. malayi, B.timori, B.pahangi, B.patei, B.beaveri, B.ceytonensis,B.granensis and B. tapiae. Only B.malayi and B.timor are known to occur as a natural infection in man.
The thread like adult worms live coiled together in human lymphatics. The male W.bancrofti . .
measures 35 mm and the female 80-1 00 mm. Gravid females release microfilariae in large numbers
into the lymphatics. The embryos are sheathed and measure 200-300 mm. They eventually reach the pheripheral blood where further development depends on their ingestion by a proper
mosquito vector. Species of Culex, Adis and Anopheles transmit bancroftian filariasis. Mansonia and Anopheles serve as vectors in Malyan disease. After development in the vector larvae migrate to the mouth parts. When the mosuqito feed~ on a human host they penetrate the punctured site and reach maturity in about a year. In the absense of reinfection man harbours microfilariae for 5-10 Yrs which is the reproductive life of the adult WO(ms.
5

The Homosepien is the only know~ vertebrate host for W.bancrofti, More than 250 Million people throughout the world are pr-esently infected and both the prevalence and distribution of the disease seems to be increasing in many parts of Africa and Asia.
PATHOLOGY
Invasion of man by the infective stage larva ( L 3 ) of W.bancrofti occurs without causing any symptoms. Only after moulting, the fourth stage larvae and young adults (1-3 months later) begin to induce local inflammatory reactions. While most of the pathology associated with infection occurs around adult worms in lymph nodes and afferent lymphatic vessels some pathology may develop elsewhere either around microfilariae cleared from blood or around adults located in ectopic sites. Such pathological changes have cell mediated humoral and foreign body components but. little is known about the factors that modulate the sequence and intensity of these reactions.
The most significant pathological changes are a consequence of adult worms living in the lymphatic vessels especially in lymph nodes, testes, epididymis and spermatic cord. These lymphatic vessels become dilated and the endothelial lining is thickened. In the adja.cent tissue a chronic inflammatory infilterate consisting of lymphocytes, histiocytes, plasma cells and eosinoptiils, surround the worms. A granulomatous reaction may develop and degenerating worms can provoke acute inflammation. The lumen of the lymphatic vessel eventually becomes obliterated. Microfilariae are seen within blood vessels and those that invade the walls of the blood vessels may provoke a focal vasculitis and lead to thrombosis. The pulmonary lesions in tropical eosinophilia contain microfilaria surrounded by inflammatioA. Much of the oedema in filariasis is caused by secondary infection llnd inflammation with subsequenty fibrosis and in
duration.
IMMUNOPATHOLOGY AND IMMUNOPATHOGENESIS
Patient with all forms of lymphatic filariasis except Tropical Pulmonary Eosinophilia are in general poorly responsive to filarial antigen. This hyporesponisveness appears limited almost exclusively to parasite antigens and is most prominent in patients with microfilaraemia. The lymphocytes show little or no response to filarial antigen in patients with microfilaraemia and only modest response in amicrofilaraemic individuals despite the fact that reactivity to non filarial
antigens and to mitogens is normal. The number of suppressor T cells and the ratio of these cells to helper T cells are abnormally high in most affected patients. Hyperglobulinemia with elevated levels of specific antibody occur in mocrofilaraemic patients having relatively deficient
antibody response, High levels ·of total and specific IGE antibodies are seen in all patients with filariasis along with · normal or increased numbers of basophils and mast cells. During the course of natural infection patients with lymphatic filariasis develop high levels of lgG or blocking antibodies that can supress or modulate lgE mediated allergic reactivity to parasite antigens. The modulation of allergic reactivity is filarial antigen specific. The antigens derived ·from W.bancrofti are s·urface or (E-S) excretory se~retory antigens.
6

Diagnosis
A parasitological diagnosis either by a positive blood examination or by a biopsy still remains the best means of identifying active or resident infection. No further advance have been
made in the methods of blood examination as given in the WHO expert committee on Filariasis, Third report (1974) and discussed by Denham and Me Gravy (1977) . Concentration techniques
and membrane filtration techniques are of importance in low l~vel of microfilaraemia and for conducting filarial surveys. Recent reviews have been made by Shibuya eta/ (1980) and Narisimhan et a/ (1981 ).
IMMUNOLOGICAL DIAGNOGIS : The numerous serological tests include skin test, complement fixation test, haemagglutination test and Immunofluorescence tests for antimicrofilarial and anti adult antibodies. The ideal immunological test is one that is sensitive, specific, qualitative and negative when infection is erad icated applicable in endemic area and economical (WHO!TDR
1979)
DIFFERENTIAL DIAGNOSIS :
The acute stages of filariasis must be distinguished from other causes of lymphangitis, lymphadinitis, funiculitis and orchitis. The obstructive stages and elephantiasis may be difficult
to differentiate except by the exclusion of other causes of obstruction of lymph flow such as metastatic carcinoma. Chyluria must be distinguished from the causes of lymphatic obstruction in the abdomen espe9ially tuberculosis. Mileoys' disease can be distinguished by lymphography by absent or atrophic lymph channel.
Treatment:
There are no recent advances in the treatment of chronic manifestations and chemotherapy contiues to be the only effective treatment for less chronic manifestation with diethylcarbamazine citrate DEC-C still remains the drug of choice (Duke, 1 980). However Levamizole and Mebendazole have recently been found to be effective (Temu and McMahan 1981) .
Macrofilaricidal Drugs:
Since filarial disease is due mostly to the reaction of the tissues against dead developing . . and adult filariae, macrofilaricidal drugs are not of much use in- the treatment, The death of the adult worms is shown by the disappearance of microfilariae from the blood after a period of up to 18 months. The drugs used are
1) Antimony (TWSb,Astiben)
2) Suremin (Antrypol)
3) Arsenic
7

Symptomatic treatment : This treatment Consists in removing any cause of irritation by rest, elevation of the affected part, applying cooling lotions, administering opium or morphine to
relieve pain and if tension is great, pricking or sacrifycing the swollen area under suitable aseptic
conditions, Subsequently the parts if their position permits should be elevated and firmly bandaged.
Surgical Treatment :
Abscesses caused by filariae must be opened and drained.
Parasite Related Aspects:
Control measures and many socio-economic developements have resulted in decline of infection by reduction of vector numbers and ineffective rates and reduced microfilarial rates. Raise in the general standards of living aid literacy with an increased awareness of the infection
and its possible treatment have also helped. Increased prevalence particularly of Wbancrofti
has occured in parts of Asia particularly India. Experimental studies have suggested that males are more susceptible than females and that the course of infection is probably related to sex hormones.
Prepatent period Life Span and Periodicity :
The earl iest recorded prepatent period is 12 months by Wijers and Kinyangi in Kenya. Microfi lariae tend to accumulate in the arterioles of the lungs where oxygen tension is lowest.
This has been referred to as the oxygen barrier. W.bancrofti microfilariae are very sensitive to change in the oxygen tension which is lower in the pulmonary capillaries at night so t~at the mocrofilariae moves through more read ily resulting in mocrofilarial counts raising up in the
peripheral blood.
Interrupted and continuous transmission : Wijers (1 977) stated that in areas with equal yearly
transmission, interrupted transmission tends to promote the development of amicrofilaraemia,
a continuous transmission permits the development of hydrocoele and other signs of the disease.
Zoonotic Aspects: As recently reviewed by Dissanaik 1979 animal fillariae that can affect man are the subperiodic strain of B.malayi and B.pahangi from sylvetic resources
Vector Aspects : Wijers {1977) has pointed out that vector density is not the main factor in determining prevalence but the relation between the human host an the vector density is equally important.
TRANSMISSION INTENSITY, MICROFILAREMIA AND DISEASE PATTERNS :
It has been reasonably assumed that the larger the nt,Jmber of infective larvae/infecrted mosquito that the population is exposed to the higher prevalance of infection and disease.
Dunn {1979) has studied the importance of human behavioural studies and indicated the relevance of behavioural research on multid isciplinary basis. Physical chemical and biological measure
8

must be integrated for control of vector and these must be continued with parasite control and community participation for the most effective control of lymphatic filariasis.
Prognosis: The progonosis lor life is exce#e!l/, pa!l!cularly If infected fnd(v(duafs have endemic areas or otherwise avoid reinfections. Disease control is accomplished by combining mass treatment with mosquito control measures.
EXPERIMENTAL PROTOCOL
Objective of the study :- The objective of the study was to assess the therapeutic efficacy of some Unani drugs in the treatment of DAUL FEEL (Filariasis). The study also aimed at maintaining the case history and the clicnical observations of the patients so as to get an idea about the aetiology of the disease. Pathological and Bio-Chemical changes occuring in Daul Feel (Filariasis) patients were also studied during the trials.
Criteria for selection of cases :- The patients belonging to either sex and different age group attending the out patient Department with the signs and symptoms of fever with rigor, lymphangitis and lymphadinitis followed by swelling of the lower limb and also the cases with swelling alone associated with previous history of frequent attacks of fever with rigor, lymphangitis and lymphadinitis were selected for study.
The criteria for selection was to include cases of Daul Feel free from other systemic diseases and having chronicity for upto 5 years. Pregnant women were excluded from the study.
The cases were classified into three groups according to the chronicity.
1. Group A Less than 2 Years
2. Group B 2 - 3 Years
3. Group C 3 - 5 Years
SELECTION OF DRUGS :- Numerous drugs have been prescribed for treatment of DAUL FEEL (Filariasis) in Unani literature. The drugs selected for trial were taken from the records of ancient
· Unani literature provided, and many authorities had agreed to on their efficacy. These drugs were used in the form of ,oral medicine and for external application (Zimad).
9
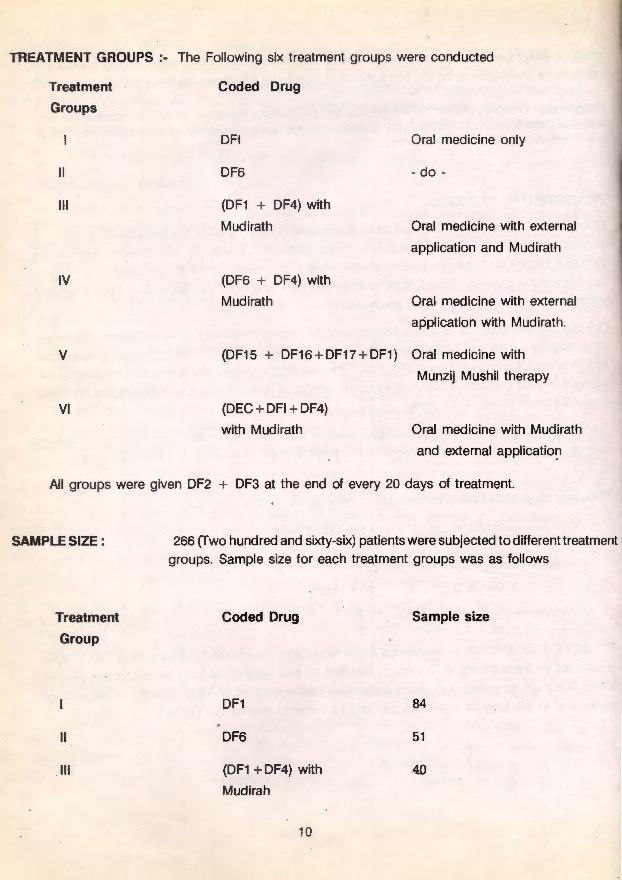
TREATMENT GROUPS :- The Following six treatment groups were conducted
Treatment
Groups
II
Ill
IV
v
VI
Coded Drug
OFI
DF6
(DF1 + DF4) with
Mudirath
(DF6 + DF4) with
Mudirath
Oral medicine only
- do -
Oral medicine with external
application and Mudirath
Oral medicine with external
application with Mudirath.
(DF15 + DF16 + DF17 + DF1) Oral medicine with
Munzij Mushil therapy
(DEC+ DFI + DF4)
with Mudirath Oral medicine with Mudirath
and external applicatio~
All groups were given DF2 + DF3 at the end of every 20 days of treatment.
SAMPLE SIZE :
Treatment
Group
II
Ill
266 (fwo hundred and sixty-six) patients were subjected to different treatment groups. Sample size for each treatment groups was as follows
Coded Drug
DF1
DF6
(DF1 + DF4) with
Mudirah
10
Sample size
84
51
-40

IV
v
VI
(DF6 + DF4) with
Mudiratr
(DF15 + DF16 + DF17 + DF1 )
(DEC + DF1 + DF4) with
Mudirah
34
30
27
DURATION OF TREATMENT :- Patients with Munzij Mushil therapy were treated for 104 days while
those without Munzij Mushil therapy were treated for 80 days.
METHOD ADOPTED :- Patients fulfilling the above mentioned diagnostic citeria were selected for
study in O.P.D. and I.P.D. of the Institute. On admission they were subjected to thorough clini<_;al examination and laboratory investigations including routine haemogram, microfilariaemia and Serum lgG, Urine analysis and stool examina ion. The base line data were recorded on a case sheet devised for the purpose of the study. Bio-chemical investigations including serum glutamate-oxaloacetate transaminase (SGOT) Serum Gl utamate Pyruvate transaminase (SGPT), Serum proteins, serum sodium, Serum Potassium, Serum cholesteral, blood sugar, and blood urea to rule out other associated diseases.
The measurement of the lower limbs were recorded and were also photographed. The clinical and pathological examinations and measurement of both the lower limbs were carried out on the base line and subsequently followed-up. Biochemical investigations were recorded on bas~ line and on
subsequent followups. Photographs of the limbs were taken on the base line, on 40th day and on the last day of the treatment. After the treatment all the cases were followed-up for one year in order to note any relapse.
DIETARY RESTRICTION AND RECOMMENDATION:- According to Unani System of Medicine as well as with support of available literature all "cold and phlegm producing" food and salt were restricted. ·
Food articles which are restricted and those recommended for "DAUL FEEL" (Fila,riasis) patients are given below.
RESTRICTED FOOD .- Food which is supposed to vasiated the blood (Fasad-addam) e.g. Fish (Specially salt-fish) , beef, pork and potatoes, arvi, natralu, pindalu and, birinjal 2. Food which is supposed to increase the Belgam (Phlegm) e.g. Banana and citrus fruits.
RECOMMENDED FOOD :-Rice, Wheat Indian Millet, Pulses, Pure ghee, broad beans, french beans, bittergourd, ridge gourd, onion, beet-root, carrot, red chillies, pepper, meat, bird's flesh, figs, almonds, walnut, dates, mango, apricot, papaya, fenugreek, drum sticks and turnip.
1 1

DRUGWISE THERAPEUTIC TRIALS
TRIAL N0.1
Coded Drug :- DF1 (oral medicine) along with
DF2 & DF3 (oral medicine)
Ingredients:- DF-1
1. Poost-e-Btskhopara sufaid - Two parts
2. Filfil Sufaid - Two parts
3. Bekh-e-Gule-Abbas - one part
4. Maghz-Tukhme-Karanjwa - One part
DF-2
1. Roghan Bed Anjir - 50ml
DF-3
1. Maghz Karanjwa - 4 Numbers.
Method of preparation : DF-1 : Each ingredient of the coded drug DF-1 was taken according to
the formula and pulverised separately into fine powder and then mixed throughly. DF-2 oil form; DF-3 : Powder form.
DOSAGE AND MODE OF ADMINISTRATION:
250mg of the powdered coded drug DF-1 was given in a capsule with the following dose schedule
Days of
tretment
2
3
4
5
No of
Capsules
2
3
2
Days of
treatment
6 -
7-
8-
9 -
10 -
10 -
days
Number of
capsules
2
3
2
3
20 Capsules
The capsules were administered in empty stomach early mornin·g for 80 days. During treatment the Mushil (Purgative) was given after every 20 days of treatment.
12

TABLE- 1
DF-1
SEX AND AGE-WISE DESTRIBUTION OF PATIENTS
AGE GROUP MALE FEMALE TOTAL PERCENTAGE
IN YEARS
1 - 10 Years - - - -
11 -20 Years 11 16 27 32
21 - 30 Years 12 16 28 33·
31 - 40 Years 3 10 13 15.5
41 - 50Years 9 4 13 15.5
51 - 60 Years 2 1 3 4
61 - 70 Years - - - -
Total 37 47 84 100
The coded drug DF-1 was tried in 84 cases (37 males and 47 females) .
Maximum number of patients were in the age group of 21-30 years followed by 11-20 years.
13

TABLE- 2
DF-1
DISTRIBUTION OF PATIENTS ACCORDING TO THE
CHRONICITY OF THE DISEASE
CHRONICITY NO. OF CASES PERCENTAGE
Less than 2 Years 55 65.5
2 - 3 Years 10 12
3 - 5 Years 19 22.5
Total 84 100 -- ·-----
Maximum number of cases were having chronicity of less than 2 years.
14

TABLE - 3
DF-1
RESPONSE IN RELATION TO THE CHRONICITY OF THE DISEASE
.-1
CHRONICITY RELIEVED PARTIALLY RELIEVED NOT RELIEVED
No. of percentage No.of percentage No.of Percentage
Patients Patients Patients
Less than 2 Years 12 21.8% 13 23.6% 30 54.55%
No. of pts .55
2 - 3 Years 1 10% 1 10% 8 80%
No. of pts.1 0 . 3 - 5 Years 4 21.1% 3 15.8% 12 63.2%
No of pts. 19
TOTAL 17 20.2% 17 20.2% 50 59.5%
No. of pts. 84 ---------
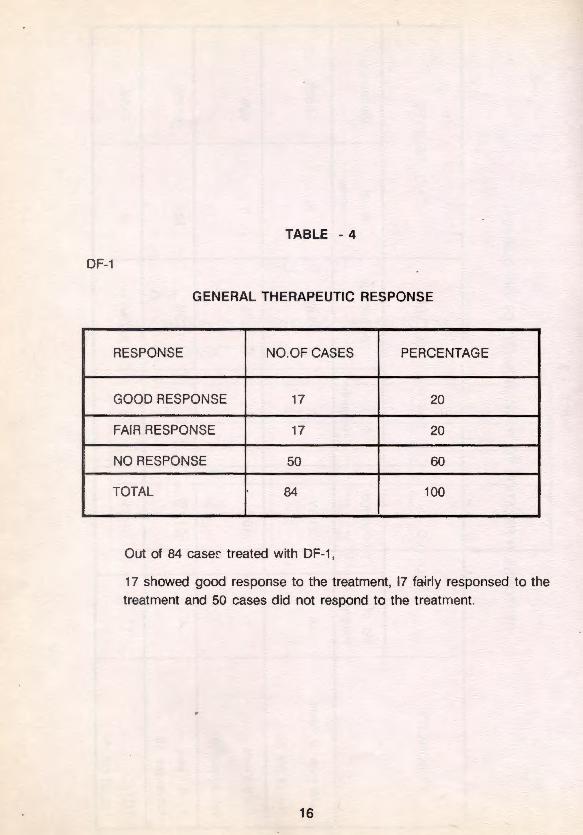
TABLE - 4
DF-1
GENERAL THERAPEUTIC RESPONSE
RESPONSE NO.OF CASES PERCENTAGE
GOOD RESPONSE 17 20
FAIR RESPONSE 17 20
NO RESPONSE 50 60
TOTAL 84 100
----- --- --------------- ----- ----- -- ----
Out of 84 caser treated with DF-1 ,
17 showed good response to the treatment, 17 fairly responsed to the treatment and 50 cases did not respond to the treatment.
16

...... --J
TABLE - 5
DRUGWISE DISTRIBUTION OF DIFFERENT SIGN AND SYMPTOMS AT THE TIME OF ADMISSION
AND DURING SUBSEQUENT FOLLOW-UPS
(CLINICAL FINDINGS)
Duration of No. of Fever Lymphangitis Lymphadinitis treatment cases
I
Base Line 84 12 3 12
' 40th Day 84 3 2 7
80th Day 84 6 1 6
~

())
TABLE • 6
DETAILS OF THE MEASUREMENTS OF OEDEMA IN CASES OF FILARIASIS WHO WERE TREATED WITH CODED DRUG "DF-1" FOR A PERIOD OF 80 DAYS
DAY OF EXAMINATION
Volume of Unit of Statistic measure Before Treatment After completion of
· (Oth day) 40 days treatment
Min. & Max 2510cc - 5030 cc 2430 cc - 4750 cc
' n 81 , 81
AFFECTED cc Mean + S.D 3560 + 550 3500 + 545 - -LEG t - value 2.636.
P: - <0.02
Min.&Max 2020 cc - 481 0 cc 2050 cc- 4720 cc
n 81 81
NORMAL cc Mean.zS.D 3160 + 560 3170 + 560 _,._ LEG t-value -1.01 2**
p: > 0.02
Min. & Max 25 cc - 1230 cc 0 cc - 1250 cc
- n 81 81
OEDEMA cc Mean + S.D 400 + 320 330 + 270 - .- -t.value 3.921*
p : - < 0.001
Note :- 1) The figures underlined represent the comparison between baseline and followup observations
2) The figures in rectangles represents the comparision between the follow-up observations
* The changes are significant at their respective probabil ity levels.
** The changes are not significant
After completion of 80 days treatment
2510 cc - 4950 cc 81
3520 + 550 - I -1.7405** I 1.6**
>0.02 > 0.02 .
2060 cc- 4710 cc
81
3195 + 550
-2.174* - 1 - 2.1629 • I < 0.05 < 0.05
10 cc - 1270 cc
81
325 + 260 ~-
I - 0.172 •• 1 3.532*
< 0.001 > 0.02
'

U)
Graphical repres-entation of the volume affected I Normal leg and oedema and the changes in them during treatment in cases of Filariasis who were treated with coded drug DF1 for 80 days.
A.C.40.DS.T
• P: <0.001
g + 600 400 t 320 325 ± 260
** 330 + 270 E • 3oo :J •• 0 P: <0.001 P: >0.02 >
B.L. A.C.40.DS.T A.C.80 .DS.T
The volume of oedema and the changes in it during treatment in terms of Mean~.D . and level of significance I Non-significance
NOTE :-
* The Changes are significant at their respective probability
' levels.
** The Changes are not significant
A.C40 DS.T = After completion of 40 days treatment
A.C.80 DS.T = After completion of 80
days trea!ment
B.L. -= Base line.

TABLE -7
BIO-CHEMICAL RESULTS OF DAUL FEEL (FILARIASIS) PATIENTS, TREATED WITH CODED DRUG DF-1 FOR 80 DAYS PATHOU
Investigation Unit of Statistics D A Y S 0 F EXAMINATION measure Base line After 40 days . After 80 days
R. Blood sugar Min & Max. 50 - 117 52 -125 56 -144 mg% n 42 42 42 Haem1
M .± S.D 80 ± 17 86 ± 18 80 ± 18
Blood Urea Min & Max. 10 - 38 10 - 39 10 - 34 mg% n 42 42 42 A.B. C.
M!. S.D. 19 ± 7 19 ± 7 18 ± 6
S .. Cholesterol Min& Max. 86 - 345 118 - 309 100 - 317 mg% n 42 42 42
W.B.C
M + S.D. F9 + 44 175 + 39 175 + 39 - ~ - -S .. .Total Proteins Min & Max. 5.9 - 8.0 6.1-8.0 6.0 - 8.0 I
gm% n 42 42 42 1-M + S.D 7.0 ±. 0.6 6.9 ! 0.6 7.1 ! 0:5 z
::> 0
S. Sodium Min & Max. 130 - 150 132 - 150 126 - 150 (.)
MEQ/1 n 42 42 42 M +S.D. 141 ± 6 140 ± 5 141 ± 7 -
...J
~ z w a:
S. Potasium Min & Max. 3.4 - 5.1 3.3 - 5.0 3.6 - 5.3 w u..
MEQ/1 n 42 42 42 u.. E 0 M .i S.D. 4.3 ± 0.5 4.2 ± 0.5 4.3 ± 0.4
S.G.O.T Min. & Max. · 7.6-36 8 - 40 8 - 33 f U/1 n 42 42 42
M + S.D . 22 ± 8 20 + 7 21 ± 6 .... - a: <ri
S.G.P.T Min & Max. 7.9 - 35 8 - 31 8 - 36 ui 1
U/1 n 42 42 42 M + S.D. 16 ± 7 17 ± 6 17 ± 7 ......
20
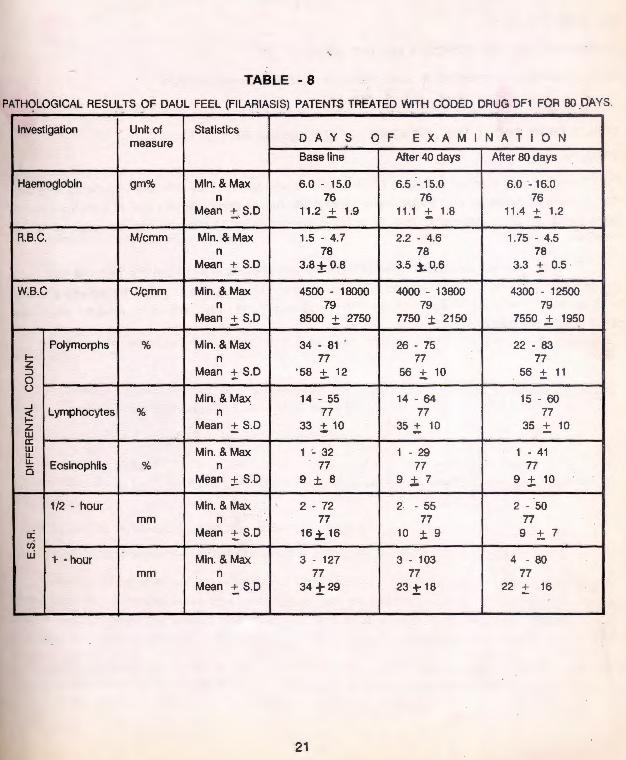
TABLE -8
30 DA PATHOLOGICAL RESULTS OF DAUL FEEL (FILARIASIS) PATENTS TREATED WITH CODED DRUG DF1 FOR 80 DAYS. - -
Investigation Unit of Statistics A Y S 0 0 measure D F E X A M I N A T I N
Base line After 40 days After 80 days
Haemoglobin gm% Min. & Max 6.0 - 15.0 6.5 - 15.0 6.0 - 16.0 n 76 76 76
Mean :!:.S.D 11 .2 + 1.9 11.1 + 1.8 11.4 + 1.2
R.B.C. M/cmm Min. & Max 1.5 - 4.7 2.2 - 4.6 1.75 - 4.5 n 78 78 78
Mean + S.D 3,8± 0.8 3.5 }.. 0_.6 3.3 .:!: 0.5
W.B.C C/cmm Min. & Max 4500 - 18000 4000 - 13800 4300 - 12500 n 79 79 79
Mean + S.D 8500 ± 2750 7750 ± 2150 7550 .± 1950
Polymorphs % Min. & Max 34 - 81 . 26- 75 22 - 83 1- n 77 77 77 z ::::> Mean + S.D ' 58 ±. 12 56 i 10 56 :!: 11 0 ()
Min. & Max 14 - 55 14 - 64 15 - 60 ...J
Lymphocytes % 77 77 77 <{ n 1- Mean + S.D 33 ±. 10 35 + 10 35 + 10 z w - -a: w Min. & Max 1 - 32 1 - 29 1 - 41 u. u. Eosinophils % n 77 77 77 0
Mean ± S.D 9 ± 8 9 ;!;. 7 9 + 10
1/2 - hour Min. & Max 2 - 72 2 - 55 2 - 50 mm n 77 77 77
a: Mean + S.D 16± 16 10 ± 9 9 ±. .,
uj uj
1- -hour Min. & Max 3 - 127 3 - 103 4 - 80 mm n 77 77 77
Mean + S.D 34 ±29 23 + 18 22 + 16 -
21

SIDE EFFECTS :- No side effets were noted during treatment and after treatment with the prescribed dossage of the coded drug D F-1
. RELAPSE :- 5 Cases
COMMENTS ON THE EFFICACY OF THE DRUG :
Good response was observed in cases having less than 2 years chronicity.
CONCLUSION ABOUT THE EFFICACY OF THE DRUGS DF-1
TRIAL N0.1
DF-1 The drug was tried on a sample of 84 cases. It was found to be effective in patients with less than 2 years chronicity of the disease. The general therapeutic response was that 17 patients showed good response to the treatment and 17 showed fair response 50 patinets did not re~pond to the treatment.
Patients having more than 2 years chronicity of the disease in whom the oedema was hard
and blackish in colour did not respond to the treatment. The drug was found to be equally effective In all patients irrespective of age and sex. The drug was found to be safe as no adverse effect was noted during the therapy.
22
·d
re IS
DOUBLE BLIND PLACEBO CONTROLLED COLLABORATIVE STUDY
DRUGS UNANIDRUG
DEC
PLACEBO
SAMPLE SIZE 116 (44, 36, 36)
CHRONICITY < 1Year in 83% cases
DURATION OF TREATMENT 80 days
Phase II Trial was ·double blind placebo controlled comprising of 116 cases and conducted in collaboration with the Department of Medical Chemistry, Government General Hospital, Madras under the guidance of Dr.K.V. Thiruvengadam.
Phase II Trial comprising of 116 ; patie~ were sub-divided into the following 3 groups :
1) Group A included 44 patients and received unani drug in the dose of 2 caps/day on empty stomach.
2) Group 8 consisted of 36 patients and received 300 mg of DEC 1n two capsules daily lin the morning
3) Group C also consisted of 36 patients and was treated with placebo (capsules containing sugar) . The elastocrepe bandage was used in all three groups.
The duration of treatment in phase II trial was 80days.
In phase II trial, chronicity of the disease was less than 1 year in 83% of cases, 1-2 years in 4.3% and 3 years in 1. 7%. Based on the chronicity,. homogeneity was maintained in group distribution of patients.
PATHOLOGICAL AN[) BIOCHEMICAL INVESTIGATIONS
Investigations were carried out at base line and at 40 and 80 days of treatment in trial II.
Samples of peripheral blood were drawn from patients and volunteers by venipuncture in acid citrate solution. A simultaneous 20)'tl bloOd smear was made for identifying microfilariae. The same amount was collected per person after 9.00 p.m. and thick smears were prepared. These sme~rs were then de-haemoglobinized, dried, fixed in acidified methyl alcohol and stained with JSB-1 stain.
Serum samples were stored at - 20 °C for the quantitative estimation of serum lgG, complement C3 and electrolytes. Other investigations included urine analysis for chyluria. Haemogram and other
23

biochemical investigations such as liver function tests, total proteins, urea, uric acid creatinine etc, were undertaken to rule out the toxicity of drugs. Motion examination was undertaken to rule out helminthic infestation.
lgG and Complement c3 were estimated by single radial immuno-diffusion technique using solugen SAID Plates and reference standards purchased from lmmuno-diagnostic P.Ltd., New Deihl
CONTROLS:
The control group consisted of 50 individuals from the laboratory staff and other volunteers of the Institute who did not have any evidence of filariasis.
RESULTS
Clicnical response in the double blind placebo controlled trial is also shown in tables and graphs/histograms. Relief was obtained in 72.72% patients receiving Unani drug, 37.5% patients receiving DEC and 19.5% patients treated with placebo. Drop out rate was highest (29.26%) in placebo treated group and lowest (18.18%) in patients receiving unani drug.
Relapse rate 1 year after treatment was lowest (12.5%) with unani drug, in comparision to DEC (37.5%) and placebo (42.8%).
56% reduction in oedema was observed with unani drug, 25% with DEC and 13% with placebo at the end of 80 days treatemnt.
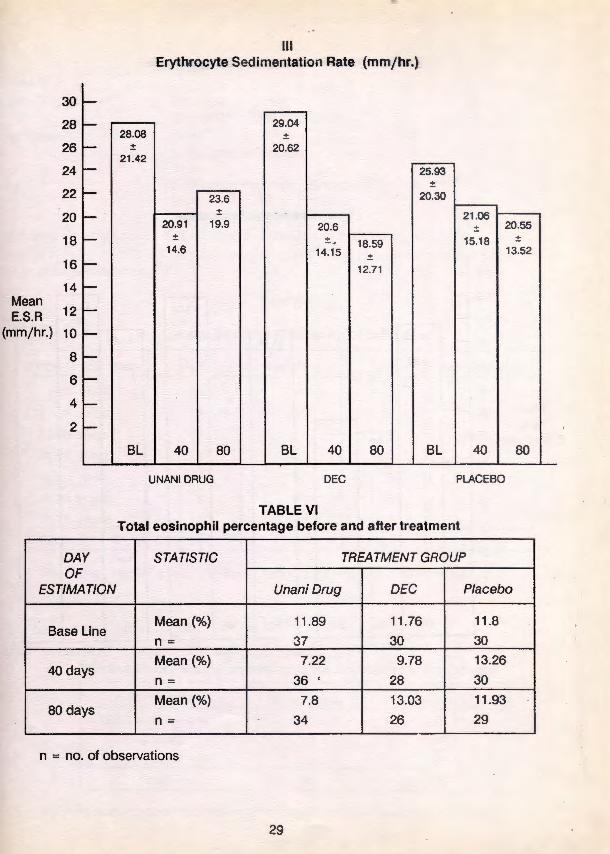
Erythrocyte sedimentation rate showed significant reduction only with DEC whereas total eosinophil count was significantly reduced by the unani drug as compared ot DEC and placebo. Biochemical parameters remained within normal limits.
24

~
. . - - - -~w-cn I» o -. ~~c;;
(") (") (1) ;::· (1) s (1) o e -· I» c:r_ c:r m a>:::::J:::::J 9~ 0 () 0.100.
TABLE I Clinical parameters before and after treatment
DRUG GROUP DAY
a -:::T (1)
Oc: (1) Cl)
:T :;· :-· 10
OF UNANIDRUG DEC I PLACEBO ESTIMATION
Total No. Lympha- Lymphan- Fever Total No. Lympha- Lymphan- Fever Total No. Lympha- Lymphan- Fever
ofpts. denitis gitis ofpts. denitis gitis ofpts. denitis gitis
' Base Line 44 36 17 23 44 34 23 14 41 37 15 18
40th day 36 3 4 3 34 29 16 9 29 8 2 7
80th day 36 2 2 1 34 8 5 4 29 3 4 9
TABLE II Filarial oedema in cubic centimeters before and after treatment •
TREATMENT GROUP No. of Days STATISTIC
Unani Drug DEC Placebo
Base Line Mean 286.79 35.11 212
I Follow-up MP;:~n 1f\Qm 234]3 11:in ?l:i
(40 days) % of reduction· 41.0% 33.2% 26.3%
II Follow-up Mean 127.0 263.68 186.66
(80 days) %of reduction 56.0% 25.0% 13.0% -- ---------- --- ----- - -- - ---

MEAN VOLUME
OF OEDEMA
(CC.)
360
330
100
90
80
MEAN 70
% 60 FBJ..CTrn
IN 50 SWELUNG
40
30
20
10
•
I FILARIAL OEDEMA (CC.)
(351 .11)
• • • •
~. ~ ~
~ . . ~ • DEC )
(286.79} • • • • (263.68
• •• • •• • . . I • • + UNAN • ) • • . + + DRUG • • (234.73 • • •
~1!4
.. . ..... (212) • • (186.66) .. ..,. .... ...... , . ....
' ' ' ••• (1 69.03) .... --
A.I(l:OO ' ' ~:: •• (156.25) •••••• (127)
0 40 80
NO. OF DAYS OF TREATMENT
II %REDUCTION IN FILARIAL OEDEMA AT 80 DAYS
r 56%
. 25%
n 13%
UNANI DRUG DEC PLACEBO
26
UNANIDRUG
DEC
PLACEBO

fiS .....,
100 90 80 70
(%) 60 50 40 30 20 10
-~--- - -- .~ --- .. - . ---~~.~
TABLE Ill Overall Clinical Response with different drugs
DRUG GROUP STATISTIC
Unani Drug n
%
DEC n
%
Placebo n
% - ---- --- --
n = No. of observations
(72.72%)
UNANI DRUG
RELIEVED
(37.5%)
(1 9.5%)
DEC PLACEBO
THERAPEUTIC RESPONSE
Relieved Not Relieved Droo Out
32 4 8 72.72 9.09 18.18
15 15 10 37.5 37.5 25
8 21 12 19.51 51 .21 29.26
v Overall Clinical Response
100 90
80 70
(%) 60 50 40 30 20 10 (9.09%)
UNANI DRUG
NOT RELIEVED
100 90 80 70
(51 .21 %) (%) 60
(37.5%)
DEC PLACEBO
50 40 30 20 10
TOTAL
44
40
41
(18.18%)
UNANI DRUG
DROPOUTS
(25%) (29.26%)
DEC PLACEBO
••

TABLE IV Relapse rate one year after treatment
TREATMENT GROUP STATISTIC
Unani Drug DEC
1 year followup n 24 16
Relapse n 3 6
% 12.5 37.5
n = no. of observations
Percentage of
Relapse
VI Relapse rate one year after treatment
100
90 80 70
60 50
40
30 20
10 (12.5%)
UNANI
DRUG
(37.5%)
DEC
TABLE V
(42.8%)
PLACEBO
Placebo
14 ~
6
42.86
Erythrocyte Sedimentation Rate in mmjhr. before and after treatment
DAY STATISTIC
TREATMENT GROUP
OF ESTIMATION Unani Drug DEC Placebo
Base Line Mean (mmj hr.) 28.08 29.04 25.93 n = 37 30 31
40 days Mean (mmjhr.) 20.3 20.6 21 .06
n= 36 29 31
80 days Mean (mmj hr) 23.6 18.59 20.55 n= 35 27 29
n = no. of observations
28
Ill Erythrocyte Sedimentation Rate (mmjhr.)
30 -28 - 29.04
28.08 ± 26 - ± 20.62
21 .42 24 - 25.93
± 22 - 23.6 20.30
20 ± 21 .06 - 20.91 19.9 20.6 ± 20.55
18
16
- ± ± . 18.59 15.18 ± 14.6 14.15 13.52
± ,__ 12.71
14 ,__ Mean E.S.R 12 I-
(mmjhr.) 10 ,__ 8 ,__ 6 I-
4 I-
2 I-
BL 40 80 BL 40 80 BL 40 80
UNANIDRUG DEC PLACEBO
TABLE VI Total eosinophil percentage before and after treatment
DAY STATISTIC TREA TMENT GROUP OF
ESTIMATION Unani Drug DEC Placebo
Mean(%) 11.89 11 .76 11.8 Base Line
n = 37 30 30
Mean(%) 7.22 9.78 13.26 40 days
36 ' 28 30 n =
Mean(%) 7.8 13.03 11.93 80 days
n = 34 26 29
n = no. of observations
29

IV Total Eosinophil Percentage
14 t-
13 t- 13.26 13.03
12
11
10
t- ± ±
10.56 8.33 11 .89 11 .88 11 .93
t- 11 .76 ± ± ± ±
~ 9.82 9.47 6.99 5.61
9 ~ 9.78
± Mean 8 r- 5.60
%of Eosinophils 7
7.8 ~ 7.22 ±
6 t- ± 6.7 6.31
5 ~
4 ~
3 t-
2 t-
1 !-
BL 40 80 BL 40 80 BL 40 80
UNANIDRUG DEC PLACEBO
30

Trial No.2
Coded Drug
Ingredients
DRUGWISE THERAPEUTIC TRIALS
DF 6 (oral medicine) DF 2 & DF 3 (Oral medicine)
DF6 1. Saboos-e-Gandom DF2 ' 1. Roghan Bed Anjir : 25 ml DF3 1. Magnz Karanjwa : 2 nos. ~
Method of Preparation
Dosage &
DF-6: Saboos-e-Gandom (Wheat Husk) Powdered
250 mg of coded drug DF-6 was given in capsule form as per the chart. mode of administration
TABLE-1 DF-6
Age and Sex Wise distribution of patients
Age Group in yrs. Male Female Total Percentage
1-10 years - - - -11-20 years 8 8 16 31
21-30 years 3 .5 8 16
31-40 years 3 13 16 31
41-50 · years - 5 5 10
51-60 years 3 2 5 10
61-70 years 1 - 1 2
Total 18 33 51 100
The coded drug DF-6 was tried on 51 patients (18 males and 33 females)
TABLE-2
DF-6 Distribution of Patients according to the Chronocity of the Disease
CHRONICITY No. ·of cases Percentaae
LESS than 2 years 34 66.7
2-3 years 8 15.7
3 - 5 years 9 17.6
Total 51 100
The maximum number of cases were having chronicity of less than 2 years.
31

TABLE-3 DF-6
Respdnse In Relation to the Chronicity of the Disease
Chronicity Relieved Partially Not Relieved Relieved
Less than 2 years 12(35.3%) . 9{26.5%) 13{38.2%) No. of pts.34
2-3years - 2(25%) 6(75%) No. of pts.a
3-5 years 3{33.3%) 1 (11 .1 %) 5(55.6%) ---No. of pts.9
Total 15{29.4%) 12(23.53%) 24(47.1%) No. of pts.51
---------- L....
Cases having less than 2 years chronicity showed maximum response. Response decreased with the increase in the chronocity of disease.
TABLE-4 DF-6
General Therapeutic Response
Response No. ofcases Percentage
Good response 15. 29
Fair response 12 24
No response 24 47
Total 51 100
General therapeutic response out of 51 cases treated with DF-6, 15 patients showed good response to the treatment, 12 faily responded to the treatment and 24 did not respond to the· tteatment.
DF-6 TABLE-5
Drugwise distribution of different sign and symptoms at the time of admission and during subsequent follow-ups
• (CLINICAL FINDINGS)
Duration of Treatment No. of cases Fever · Lymphangitis Lymphadintis
Base Line 51 1 8 11
40th Day 51 2 2 2
80th Day .51 1 1 2 ----- L_ _____ ---- - ---- -------
32
w w
I - ···I ceo _o 168.
TAB.LE-6
\U I» Cll
~
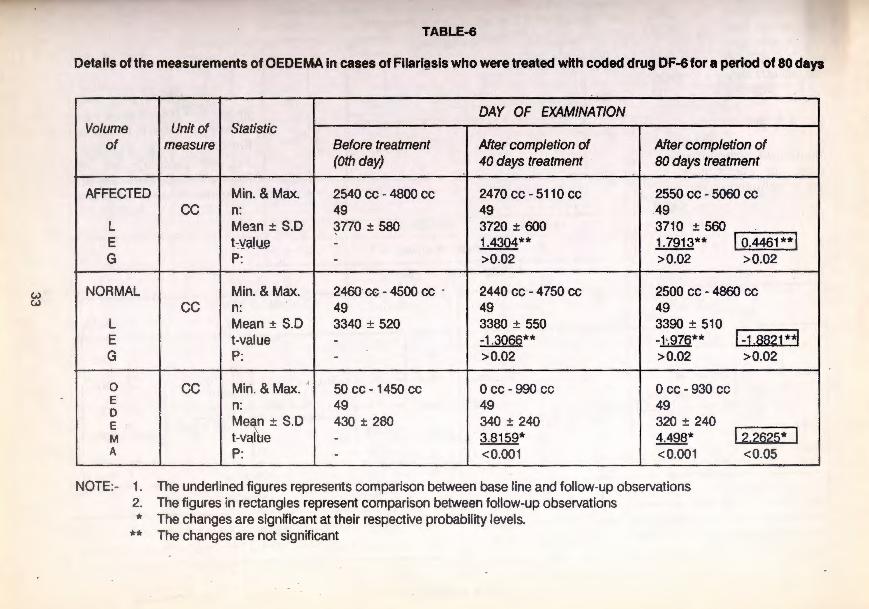
Details of the measurements of OEDEMA in cases of Filari@sis who were treated with coded drug DF-6 for a period of 80 days
-DAY OF EXAMINATION
Volume Unit of Statistic of measure Before treatment After completion of After completion of
(Oth day) 40 days treatment 80 days treatment
AFFECTED Min. & Max. 2540 cc - 4800 cc 2470 cc- 5110 cc 2550 cc - 5060 cc cc n: 49 49 49
l Me:m ± S.D 3770 ± 580 3720 ± 600 3710 ± 560 E t:va!u.e - 1.4304** 1.7913** I o.4461**1 G P: - >0.02 >0.02 >0.02
NORMAL Min. & Max. 2460 cc- 4500 cc . 2440 cc- 4750 cc 2500 cc - 4860 cc cc n: 49 49 49
l Mean± S.D 3340 ± 520 3380 ± 550 3390 ± 510 E t-value - -1.3066** -1•.976** 1-1,8821*3 G P: - >0.02 >0.02 >0.02
0 cc Miri. & Max. ' 50 cc- 1450 cc 0 cc- 990 cc Occ-930cc E n: 49 49 49 D
Mex ± S.D 430 ± 280 340 ± 240 320 ± 240 E M t-val e - 3.8159* 4.498* l2.222~* I A P: - <0.001 <0.001 <0.05
NOTE:- 1. The underlined figures represents comparison between base line and follow-up observations 2. The figures in rectangles represent comparison between follow-up observations * The changes are significant at their respective probability levels.
** The changes are not significant
!
' '
i

w -'>-
GRAPH N0.1
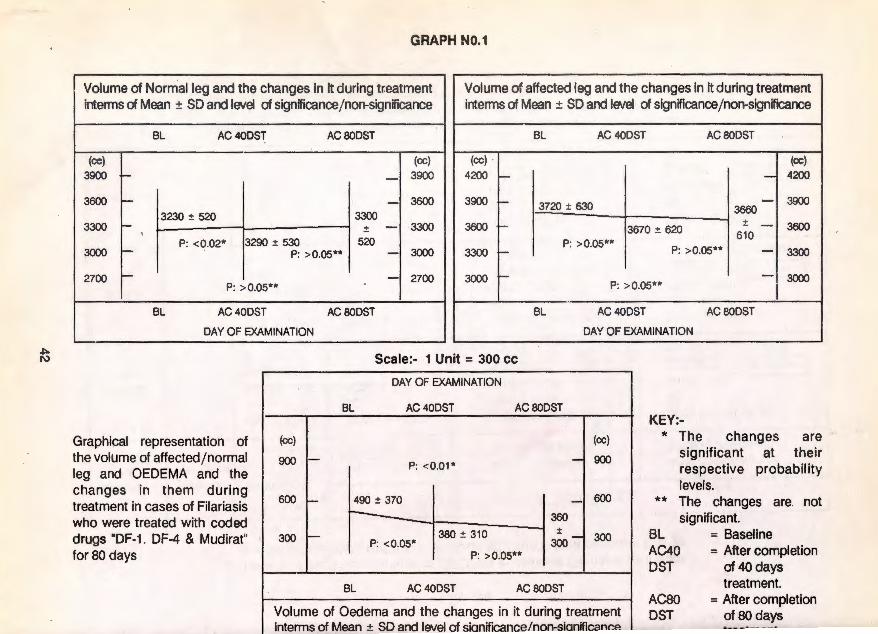
Volume of Normal leg and the changes in it during treatment Volume of affected leg and the changes in it during treatment interms of Mean ± SO and level of signifiCanGefnon-significance interms of Mean ± SO and level of signifiCancejnon-significance
BL AC40DST AC80DST BL AC40DST ACSODST
(cc) P: >0.02** (cc) (cc) (cc)
3900 r- I_ 3900 4200 - - 4200
3600 1-3340:!: 520 3390 - 3600 3900 - 3770:!: 580 3710 - 3900
:!: :!: 3300 1- 3380:!: 550 510 - 3300 3600 - - 3600 3720:!: 600 560
P: >El.02** 3000 - P: >0.02** - 3000
P: >0.02** P: > 0.02** 3300 - - 3300
2700 ~ . - 2700 3000 - - 3000 P: >0.02**
BL AC40DST ACSODST BL AC40DST ACSODST
DAY OF EXAMINATION DAY OF EXAMINATION
Graphical representation of the volume of affected/normal leg and OEDEMA and the changes in them during treatment in cases of Filariasis who were treated with coded drug "DF-6" for 80 days
Scale:- 1 Unit = 300 cc
DAY OF EXAMINATION
BL AC40DST AC80DST
900 1- - 900
600 r- P: <0.01* - 600
430 :!: 280
1340' 24<J
I 320 300 1- P: <0.01* 300 :!: -
240 P: < 0.05*
BL AC40DST ACSODST
Volume of Oedema and the changes in it during treatment interms of Mean ± SD and level of significance/non-significance
TABLE-7
KEY:-* The changes are
signif icant at their respect ive probability levels.
** The changes are not significant.
BL AC40 DST
ACBO DST
= Baseline = After completion
of40 days treatment.
= After completion ofBO days treatment

(...) 01
Volume of Oedema and the changes in it during treatment interms of Mean ± SD and level of signifiCance/non-significance
TABLE-7
DST ............ ..... _ ... ,.... .............. . . of80 days treatment
Bio-Chemical results of Daul Feel (Filariasis) patients treated with Coded Drug DF-6 for so days
v Unit DAY OF EXAMINATION
Investigation of Statistic ~easure Base line After 40 days After 80 days
-Min. &Max, 53 - 130 51 - 108 60 - 124
R.Biood Sugar mg% n 36 36 36 ' M ± S.O 83.3 ± 18.5 77.1 ± 12.9 81.2 ± 17.6
Min. & Max. 10 - 30 10-25 12 - 26 Blood Urea mg% n 36 36 36
M ± S.D . 17.9 ± 4.2 17.5 ± 5.1 16.9 ± 5.2
Min. & Max. 113-325 110-292 100-271 S. Cholesterol mg% n 36 36 36
M ± S.D 173 ± 43 . 172 ± 39 172 ± 41
Min. & Max. 6.0-8.0 5.5 - 8.0 6.0 - 8.0 S.Total Proteins gm% n 36 36 36
M ± S.D 7.1 ± 0.5 7.1 ± 0.6 ' 7.2 ± 0.4
Min. & Max. 133 - 150 130- 150 133- 150 S. Sodium meqjl n 36 36 36
M ± S.D 142 ± 5 142 ± 5 142 ± 5
Min. & Max. 3.6-5.0 3.4-5.0 3.2-4.7 S. Potassium meqjl n 36 36 36
M ± S.D 4.3 ± 0.4 4.1 ± 0.4 4.1 ± 0.4
Min. & Max. 6.7-44 7.0-35 6.9- 51/ S.G.O.T ujl n 36 36 36
M ± S.D 23 ± 8 20 ± 8 22 ± 10
Min. & Max. 8 -40 5.9-32 6-41 S.G.P.T ujl n 36 36 . 36
M ± S.D 17 ± 8 15 ± 7 17 ± 8

w 0>
T.ASLE-8
Pathological results of Daul Feel (Filariasis) patients, treated with Coded Drug DF-6 for 80 days
Unit DAY OF EXAMINATION Investigation cf Statistic
!measure Base line After 40 days After 80 days
Min. &Max. 6.0 - 16.5 6.0 -15.0 6.0 - 16.0 Haemoglobin , gm% 'l 49 . 49 49
Mean :!: S.D 11 .5 ..:!: 2.L 11 .1 :!: 2.0 11.4 :!: 2.0
Min. & Max. 1.75 - 4.8 1.5-4.5 2.0-4.75 .R.B.C Mfcmm n 4.9 49 49
Mean:!: S.D 3.6:!: 0.7 3.4 :!: 0.6 3.5:!: 0.7
Min. & Max. 4500 - 12200 4300 - 12000 4200-13500 W.B.C cj cmm n 49 49 49
Mean:!: S.D 8250:!: 1750 7650 :!: 2000 7650 :!: 1900
D Min. & Max. 35-77 32 - 72 38 - 77 I Polymorphs % n 48 48 48 F Mean:!: S.D 57 :!: 10 55 :!: 10 54 :!: 8 F C E 0 Min. &Max. 12-51 15 - 55 10 - 53 R U lymphocy1es % n 48 48 48 E N Mean:!: S.D 34 :!: 11 35 :!: 10 35 :!: 9 N T T Min. & Max. 0 - 33 0-33 1 - 37 I Eosinophils % n 48 48 48 A Mean:!: S.D 9 :!: 8 10:!: 6 11 :!: 9 l
Min. & Max. 2-60 1 - 50 2 - 40 E Yl hour mm n 48 48 48
s Mean:!: S.D 16 :!: 14 10 :!: 9 10:!: 7
Min. &Max. 4 - 97 2 - 110 4-84 R 1 hour mm n 48 48 48
Mean:!: S.D 36 :!: 26 25 :!: 20 25 :!: 17

Side Effects: No side effects were noted during treatment and after treatment with the prescribed dosage of the coded dn.)g DF-6.
Relapse: 5 cases Comments on the Efficacy of the Drug: On the above trial the coded drug DF-6 showed good response in less than 2 years Chronicity of the disease.
Conclusion about the Efficacy of the Drug DF-6
DF-6: The drug was tried on a sample of 51 cases. It was found to be effective in less than 2 years chronicity of disease. The general therapeutic response on the above trial was that 15 patients showed good response to the treatment and 12 exhibited .fair response to the treatment and 24 patients did not respond to the treatment.
It was observed that patients having more than 2 years chronicity of the disease and in whom the oedema was hard and blackish in colour did not respond to the treatment. The drug was found to be effective equally, irrespective of age and sex of the patients. The drug was found to be safe as no adverse effect was noted with the use of the drug.
37

Drugwise Therapeutic Trials Trial No.3 Coded Drug
Ingredients
DF-1, DF-4 with M (Oral medicine with external application) DF-2 & DF-3 (Oral medicine)
DF-1 1. Poost-e-Biskhopara sufaid - one part 2. Filfil sufaid - one part 3. Bekh-e-Gule-Abbas- 1h part 4. Maghz-Tukhme-Karanjwa - 1h part
Mudirat . 1. Khara-e-Khask
DF-4 1. Boora Armani, Basfaij (equal weight)
DF-2 2. Reghan Bed Anj ir
DF-3 1. Magnz Karanjwa
25ml
2 no.
Method of preparation : DF-1 was prepared as in Trial No.1 Mudirat: Prepared form of joshanda (Decoction) DF-4 : Each ingredient was powdered separately and mixed together thoroughly in glycerine.
Dosage and mode of administration: The dosage were administered as in trial no.1 250 mg Mudirat (Diuretics) given in the form of joshanda (decoction) daily. 10 gm DF-4 = was applied on the affected limb daily.
TABLE-1 DF-1 DF-4 with M
Sex and Agewise Distribution of Patients
Age Group in years Male Female Total Percentage
1-10 years - - - -11 -20 years 5 10 15 37.5 I
I
21 -30 years 5 9 14 35 I
31 -40 years 1 6 7 17.5
41 - 50 years 1 2 3 7.5
51 -60 years - 1 1 2.5
61 -70 years - - - -Total 12 28 40 100 '
The coded drug DF-1, DF-4 with M was tried in 40 cases (12 male and 28 female) . The :maximum number of patients were in the age group of 11 - 20 years followed by 21 - 30 years.
38

mg on
fhe
TABLE-2 DF-1, DF-4 with M
Distribution of Patients according to the Chronocity of the Disease
Chronicity No. of cases Percentage
LESS than 2 years 22 55
2 - 3 years 9 22.5
3-5 years 9 22.5
Total 40 . 100
The chronicity of disease is shown in table No.3.
The maximum number of cases were having chronicity of ~ess than 2 years.
TABLE-3
DF-1 + DF-4 with M
Response in Relation to the Chronicity of the Disease
Chronicity Relieved Partially Not Relieved Relieved
Less than 2 years 9(40.9%) 4(18.8%) 9(40.9%) No. of pts.22
2-3 years 2(22.2%) 2(22.2%) 5(55.6%) No. ofpts.9
3-5 years 1(11 .1%) 1(11.1 %) 7(77.8%) No. of pts.9
Total 12(30%) 7(17.5%) 21 (52.5%) ---t<ro. of pts.40
Cases having less than 2 years chronicity showed maximum response. Response decreased with the increase in the chronocity of disease.
39

TABLE-4 DF-1, DF-4 with M
General Therapeutic Response
Response No. of cases Percentage
Good response 12 30
Fair response 7 17.5
No response 21 52.5
Total 40 100 -----
Out of 40 cases treated with DF-1, DF-4 with M, 12 patients showed Good response to the treatment, 7 fairly responded to the treatment and 21 did not respond to the treatment.
. TABLE-5 DF-1, DF-4 with M
Drugwise distribution of different sign and symptoms at the time of admission and during subsequent follow-ups (CLINICAL FINDINGS)
Duration of Treatment No. of cases Fever Lymphangitis Lymphadintis
Base Line 40 3 12 9
40th Day 40 - - -·80th Day 40 1 - -
40

""" .....
iD
TABLE-6
Details of the measurements of OEDEMA in cases of Filariasis who were treated with coded drug "DF-1, DF-4and MUDIRAr' for a period of SOdays
DAY OF EXAMINATION Volume Unit of Statistic
of measure Before treatment After completion of After completion of (Oth day) 40 days treatment 80 days treatment
Min. & Max. 2770 cc- 5750 cc 2780 cc - 5850 cc 2680 cc - 60 20 cc n: 40 40 40
Affected cc Mean ± S.D 3720 ± 630 3670 ± 620 3660 ± 610 lo.1919**1 Leg t-value - 1.1958** 1.1839**
P: - >0.05 >0.05 >0.05
Min. & Max. 2430 cc - 4 720 ·cc 2500 cc - 4850 cc 2500 cc - 4850 cc n: 40 40 40
Normal cc Mean ± S.D 3230 ± 520 3290 ± 520 3300 ± 520 Leg t-value - -2.46* ' -1.916** l-a.18** I
P: - <0.02 >0.05 >0.05
Min. & Max. i 0 cc - 1140 cc 0 cc- 1100 cc 1 0 cc - 1170 cc n: 40 40 40
OEDEMA cc Mean± S.D 490 ± 370 380 ± 310 360 ± 300 t-value - 2.1319* 2.7836* lo.6723** 1 P: - <0.05 <0.01 >0.05
NOTE:- 1. The underlined figures represents comparison between base line and follow-up observations. 2. The figures in rectan~!es represents comparison between the follow-up observations. * The changes are significant at their respective probability levels.
** The c~anges are not significant.
!
I
I
I
!
~ 1\)
GRAPH N0.1
Volume of Nom\alleg and the changes in it during treatment Volume of affected leg and the changes in it during treatment interms of Mean ± SO and level of significancejnon-signif~eance interms of Mean ± SO and level of significancej non-significance
BL AC40DST AC SODST BL AC40DST AC SODST
(cc) (cc) (cc) (cc) 3900 - - 3900 4200 f- - 4200
3600 - - 3600 3230 :t 520 3300
3300 - :t - 3300 . P: < 0.02* 3290 :t 530 520
3900 f- 3720 :t 630 - 3900 3660
3600 f- 3670 :t 620 :t - 3600
61 0 P: >0.05**
3000 - P: > 0.05** - 3000 P: >0.05** 3300 :- - 3300 .
2700 -P: > 0.05**
BL AC 40DST
DAY OF EXAMINATION
Graphical representation of
I (cc) I
the volume of affected/normal 900 -leg and OEDEMA and the changes in them during treatment in cases of Filariasis ~~ who were treated with coded drugs "DF-1 . DF-4 & Mudirat" 300 -
for 80 days
- 2700 3000 1-
AC BOOST BL
Scale:- 1 Unit = 300 cc
DAY OF EXAMINATION
BL AC 40DST AC 80DST
I P: < 0.01 *
490 :t 370
360 +
- 3000 P: >0.05** I
AC 40DST AC80DST
DAY OF EXAMINATION
]: _I 600
KEY:-* The changes are
significant at their respective probability levels.
** The changes are not significant.
380 :t 310 300 -l 300 P: <0.05* BL AC40 DST
= Baseline = After completion
of 40 days treatment.
P: > 0.05**
BL AC 40DST AC SODST
Volume of Oedema and the changes in it during treatment interms of Mean ± SD and level of sianif~eance/non-sianificance
ACSO DST
= After completion of80 days

t;
TABLE- VII
r--· Investigation
A. Blood sugar
Blood urea
S. Cholesterol
S.Total Proteins
S. Sodium
S. Potasium
S.G.O.T.
S.G.P.T.
.;;,~~ - - - ---·--y -- --····-· ·-interms of Mean ± SO and level of signifteancejnon-significance
u.;,r u1 ov uay;,
treatment
BIOCHEMICAL RESULTS OF DUAL FEEL (FILARIASIS) PATIENTS, TREATED WITH CODED DF-1, DF-4 & M FOR 80 DAYS
Unit of DAY 0 F ESTIMATiON
Measure Statistic Base Line After 40 days After 80 days
Min. & Max. 59 - 114 58- 105 60- 115 mg% n 37 37 37
M±S.D. 84 .76± 11 .9 78.04± 14.2 80.97 ± 14.94
Min. & M;ix. 10-33 10 - 29 10 - 36 mg% n 37 37 37
M±S.D. 18.3±5.45 17.8±5.3 18.1 ±5.68
Min. & Max. 108-293 102 - 258 110-276 mg% n 37 37 37
M±S.D. 184±43 182±39 178±42
Min. & Max. 5.8±8.0 6. 1 ± 7.8 6.0±8.0 gm% n 3T 37 37
M±S.D. 6.9±0.6 6.4±0.8 6.7 ±0.5
Min. & Max. 132-152 133- 150 132 - 150 MEQ/L n 37 37 . 37
M±S.D. 142±6 140 ±4 142±4
Min. & Max. 3.3 - 5.1 3.5 - 5.2 3.3-5.1 MEQ/L n 37 37 37
M±S.D. 4.2±0.5 4.2±0.4 4.2±0.5
Min. & Max. 7.2-40 7.0- 46 11 -45 U/L n 37 37 37
M±S.D. 21 ± 7 21 ± 8 21 ±9
Min. & Max. 6.3 - 31 7.9 - 34 7 - 35 U/L n 37 37 37
M±S.D. 17 ± 7 16± 7 16 :± 7
~.QIE...;, Min. = Minimum value, Max. = Maximum value, n = no. of observations, M = Means

~ ~
TABLE- VIII
Investigation
Haemoglobin
' R.B.C.
W.B.C.
- Polymorphs c:: ::J 0
{.)
en Lymphocytes . ·.;::
c:: Cll ......
~ 'o Eosinophils
a: 1/2 - Hour (J) LU
1 - Hour
PATHOLOGICAL RESULTS OF DUAL FEEL (FILARIASIS) PATIENTS, TREATED WITH CODED DF-1, DF-4 & M FOR 80 DAYS
Unit of DAY 0 F ESTIMATION
Measure Statistic Base Line After 40 days After 80 days
Min. & Max. 6.0 - 17.0 6.0 - 15.0 6.5 - 14.5 gm% n 39 39 39
Mean ± S.D. 11.0 .± 2.1 10.7 .± 1.7 11 .0.± 1.7
Min. & Max. 2.5-4.5 2.0 - 4.75 2.0 - 4.25 c/mm n 38 38 38
Mean.± S.D. 3.6 .± 0.5 3.5 .± 0.55 3.5 .± 0.6
Min. & Max. 5500 - 16200 5500 - 11000 5500- 11500 c/mm n 38 38 38
Mean .± S.D. 9200 .± 2500 8000 ± 5000 8000 .± 2000
Min. & Max. 33 -84 28 - 78 26 - 70 % n 38 38 38
Mean.± S.D. 57.± 12 52.± 12 53± 11
Min. & Max. 14 - 60 17-59 15 -45 % Min 38 38 38
Mean.± S.D. 34 .± 10 36 .± 11 33 .± 7
Min. & Max. 0-30 0 - 31 2 - 50 % n 38 38 38
Mean± S.D. 9 .± 7 12 .± 10 14 .± 10
Min. & Max. 2 - 65 2 -40 2 - 34 mm n 38 38 38
Mean.± S.D. 16 .± 15 11 ± 8 10 .± 7
Min. & Max. \ 4 - 112 4- 80 4 - 70 mm n 38 38 38
Mean.± S.D. 36 .± 26 27 ± 18 27 .± 18
i
·'
SIDE EFFECTS :- No side effects were noted during treatment and after treatment with the prescribed dosage of the coded drugs DF-1, DF-4 with M.
RELAPSE:- 13 cases
COMMENTS ON THE EFFICACY OF THE DRUGS :- On the above trial the coded drugs DF-1, DF-4, with M was tried. Good response was seen in less than 2 years chronicity and 2-3 years chronicity. The cases having more than 3 years chronicity of the disease showed poor response to the treatment.
CONCLUSION ABOUT THE EFFICACY OF THE DRUG DF1 DF4 WITH M.
TRIAL N0.3
DF-1, DF-4 with M :- The drug was tried on a sample of 40 cases and it was found to be effective in less than 2 years chronicity of disease. The general therapeutic response was that 12 patients showed good response to the treatment and 7 fairly responded to the treatment, while 21 patients did not respond to the treatment.
It was observed that the patients having more than 2 years chronicity of the disease and in whom the oedema, was hard and blackish in colour, did not respond to the treatment. The drug was found to be equally effective irr~spective of age and sex of the patients. The drug was found to be safe as no adverse effect was noted with the use of DF1 DF4 with M.
DRUGWISE THERAPEUTIC TRIALS
TRIAL N0.4
Coded drug
Ingredients
METHOD CF PREPARATION
Dosage and mode of administration
DF-6, DF-4 with M (oral medicine with external application) DF2 & DF3 (Oral medicine)
DF-6: Saboos-e-Gandom (Wheat Husk) powdered
Mudirat: Khara-e-Khask
DF-4: Boora Armani, Basfaij (equal weight)
DF-2: Roghan Bed Anjir: 25 ml
DF-3: Magnz Karanjwa : 2 numbers
DF-6 was prepared as in trial No.2 Mudirat was prepared as in Trial No.3 DF-4 was prepared as in Trial No.3
The drug was administered as in Trial No.2 and 3.
45
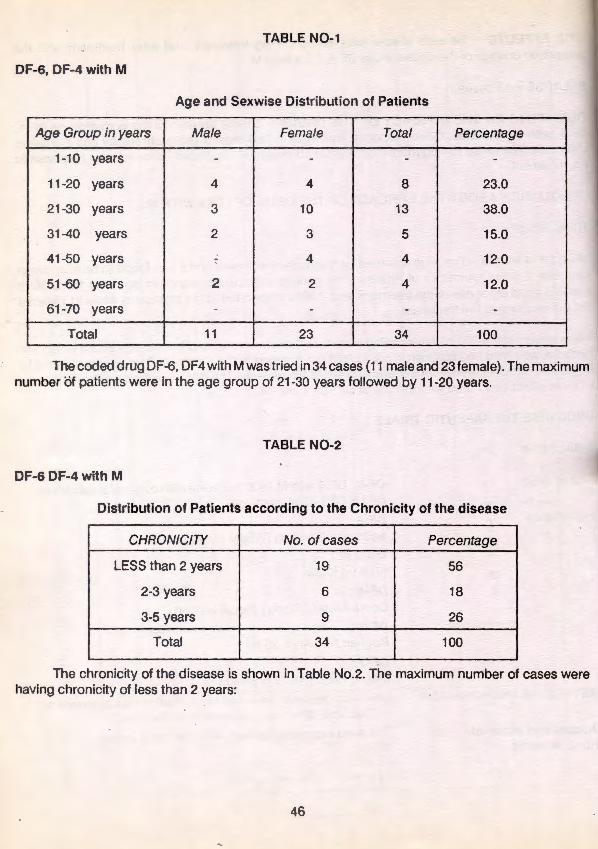
TABLE N0-1
DF-6, DF-4 with M
Age and Sexwise Distribution of Patients
Age Group in years Male Female Total Percentage
1-10 years - - - -
11-20 years 4 4 8 23.0
21-30 years 3 10 13 38.0
31-40 years 2 3 5 15.0
41 -50 years 7 4 4 12.0
51-60 years 2 2 4 12.0
61-70 years - - - -Total 11 23 34 100
The coded drug DF-6, DF4 with M was tried in 34 cases (11 male and 23 female) . The maximum number of patients were in the age group of 21-30 years followed by 11-20 years.
TABLE N0-2
DF-6 DF-4 with M
Distribution of Patients according to the Chronicity of the disease
CHRONICITY No. ofcases Percentage
LESS than 2 years 19 56
2-3 years 6 18
3-5 years 9 26
Total 34 100
The chronicity of the disease is shown in Table No.2. The maximum number of cases were having chronicity of less than 2 years~
46
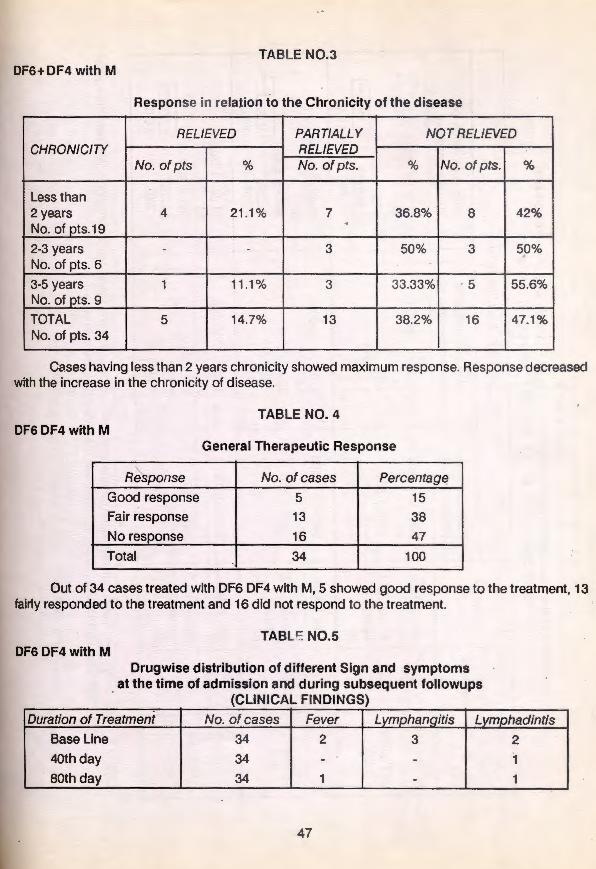
TABLE N0.3 DF6+ DF4 with M
Response in relation to the Chronicity of the disease
RELIEVED PARTIALLY NOT RELIEVED CHRONICITY RELIEVED
No. of pts % No. of pts. % No. ofpts. %
Less than 2 years 4 21 .1% 7 36.8% 8 42% No. of pts.19
. 2-3 years - - 3 50% 3 50% No. of pts. 6
3-5 years 1 11.1% 3 33.33% 5 55.6% No. of pts. 9
TOTAL 5 14.7% 13 38.2% 16 47.1% No. of pts. 34
CCI.ses having less than 2 years chronicity showed maximum response. Response decreased um with the increase in the chronicity of disease.
re
TABLE NO.4 DF6 DF4 with M
General Therapeutic Response
Response No.ofcases Percentag~
Good response 5 15
Fair response 13 38
No response 16 47
Total 34 100
Out of 34 cases treated with DF6 DF4 with M, 5 showed good response to the treatment, 13 fairly responded to the treatment and 16 did not respond to the treatment.
DF6 DF4 with M TABL~ N0.5
Drugwise distribution of different Sign and symptoms at the time of admission and during subsequent followups
(CLINICAL FINDINGS)
Duration of Treatment No. of cases Fever Lymphangitis Lymphadintis
Base Line 34 2 3 2
4oth day 34 - - 1
80th day 34 1 - 1
47

~
TABLE N0.6 Details of the measurements of Oedema in cases of Filariasis who were treated with
coded drugs "DF-6, DF-4 & MUDIRAT" for a period of 80 days r-.......
DAY OF EXAMINATION ltotume Unit ·of Statistic
of measure Before treatment After completion of After completion of
"'-.. (Oth day) 40 days treatment 80 days treatment
Min. & Max. 2800 cc .- 5870 cc 2690 cc- 5760 cc 2510 cc- 5510 cc n: 34 34 34
A.f:FECTED cc Mean± S.D 3860 ± 650 3780 ± 570 3780 ± 600 LEG
, t-value 1.8148** 1.5457** 11.4326**1 -P: - >0.05 >0.05 >0.05
..............
Min. & Max. 2400 cc - 4560 cc 2440 cc- 4560 cc 2390 cc - 4540 cc
~OR MAL n: 34 34 34
cc Mean± S.D 3370 ± 500 3390 ± 500 3420 ± 530 1-o 8081**1 LEG t-value - -1.2046** -1 .7584**
P: - >0.05 >0.05 >0.05 --........
Min. & Max. 30cc- 1310 cc 30 cc - 1200 cc 20 cc - 1170 cc
O~DEMA n: 34 34 34
cc Mean ± S.D 51 0 ± 470 390 ± 330 360 ± 320 t-value - 2.648* 2.7085* h .7783**1 P: - <0.02 <0.02 >0.05
- .........._ ------ - - -----------
NCJIE:- 1. The underlined ligures represents the comparison between base line and follow-up observations. Whereas the figures in rectangles represents comparison between the follow up observations.
2. * The changes are significant at their respective-probability levels. ** The changes are not significant.
GRAPH N0.1

""' <D
~- -** The changes are not significant.
GRAPH N0.1
Volume of Normal leg and the changes in it during treatment Volume of affected leg and the changes in it during treatment interms of Mean ± SD and level of significance/ non-significance interms of Mean ± SD and level of significance/non-significance
BL AC 40 DST AC 80DST BL AC 40 DST AC80DST
(cc) (cc) (cc) (cc) 3900 - - 3900 4500 f- P: >0.05** - 4500
3600 - 3370 + 500 ~420 - 3600
:!:
3300 - 3390:!: 500 530 - 3300
4200 1- - 4200
3880 :!: 650 3780 3900 r- - 3900 :!:
P: > 0.05** 3000 - P: >0.05** - 3000 P: >0.05** 3780 :!: 570 600
3600 r- - 3600 P: > 0.05**
2700 - - 2700 3300 1- - 3300 P: >0.05**
BL AC 40 DST AC 80DST BL AC 40 DST AC80DST
DAY OF EXAMINATION DAY OF EXAMINATION
Graphical representation of the volume of affected/normal leg and OEDEMA and the changes in them during treatment in cases of Filariasis who were treated with coded drugs "DF-6, DF-4 & Mudirat" for 80 days
Scale:- 1 Unit = 300 cc
DAY OF EXAMINATION
BL AC 40 DST AC 80DST
(cc) (cc)
900 - - 900 P: > 0.02*
600 - 510 :!: 470 - 600 ---- 360
300 - P: < 0.02* 390 :!: 330 :!: - 300
P: >0.05** 320
BL AC40 DST AC 80DST
· Volume of Oedema and the changes in it during treatment ~nterms of Mean ± SD and level of significance/non-significance
KEY:-* The changes are
sign ificant at their respective probability levels.
** The changes are not significant.
BL AC40 DST
AC80 DST
= Baseline = After completion
of 40 days treatment.
= After completion of 80 days treatment

(n 0
TABLE N0.7
Bio-Chemical results of "Daul Feel" (Filariasis) patients treated with coded drugs DF-6, DF-4 & M for so days
Unit DAY OF EXAMINATION Investigation of Statistic
measure Base line After 40 days After 80 days
Random Blood mg% Min. & Max. 51 - 114 60- 127 60-133 sugar n 33 33 33
Mean± S.D 82.1 ± 15.6 82.5 ± 14.7 83.1 ± 17.5
Min. & Max. 13-34 10-34 10-26 Blood urea mg% n 33 33 33
Mean± S.D 19 ± 5 19 ± 5 18 ± 4
Min. & Max. 86-262 100 ± 251 96 ± 245 S.Cholesterol mg% n 33 33 33
Mean± S.D 172 ±. 40 175 ± 40 182 ± 38
Min. & Max. 5.6-8.0 6.0 -8.0 6.4-8.0 S. Total Protein~ gm% n 33 33 33
Mean ± S.D 7.0 ± 0.6 7.0 ± 0.6 7.1 ±0.4
Min. & Max. 133- 150 130-150 130 -150 S.Sodium MEO/L n 33 33 33
Mean ± S.D 143 ± 5 144 ± 4 142 ± 5 .
Min. & Max. 3.7-5.5 3.4 - 5.0 3.5 -5.0 S.Potassium MEO/L n 33 33 33
Mean± S.D 4.4 ± 0.5 4.2 ± 0.4 4.3 ± 0.4
Min. & Max. 7.2 - 44 7.2 - 40 9 - 41 S.G.O.T. U/L n 33 33 33
Mean± S.D 18.3 ± 9.1 18.4 ± 8 22.2 ± 9.1
Min. & Max. 7.1 - 31 5.1 -27 8.0 - 42 S.G.P.T. U/L n 33 33 33
Mean± S.D 13.6 ± 5.6 13.7 ± 5.6 15.5 ± 6.8 --- - - --- · ---
NOTE :- Min. = Minimum value, Max : Maximum value, n = no. of observations

U1 ......
NOTE :- Min. = Minimum value, Max : Maximum value, n = no. of observations
TABLE N0.8
Pathological results of Daul Feel (Filariasis) patients, treated with coded drug DF-6, DF-4 & M so days I
Unit DAY OF EXAMINATION i
Investigation of Statistic I
measure Base line After 40 days After 80 days I
Min. & Max. 7.0. 14.0 7.0. 14.5 5.0. 14.0 Haemoglobin gm% n 34 34 34
Mean :t S.D 11 .0:!: 1.8 11.3 :!: 1.7 11 .0 :!: 1.9
Min. & Max. 1.75. 4.45 2.0. 4.7 1.5. 4.65 A. B.C. Mjcmm n 34 34 34
Mean:!: S.D. 3.5:!: 0.8 3.6:!: 0.7 3.45:!: 0.9
Min. & Max. 5500-10600 4000-12700 5000-12400 W.B.C. cjcmm n 34 34 34
Mean :t S.D. 8050 £1350 8100:!: 1950 7750:!: 2000
Min. &Max. 35-72 27.81 39-80 D Polymorphs % n 34 34 34 I F Mean:!: S.D. 56:!: 10 56 :!: 12 . 55 :!: 11 F EC Min. & Max. 12 . 57 18.60 16.56 RO Lymphocytes % n 34 34 34 eu NN Mean :!: S.D 36:!: 10 35:!: 10 34:!: 10 T T I Min. & Max. 1. 24 1 -29 2. 26 A Eosinophils % n 34 34 34 L Mean:!: S.D 8:!:7 9:!:8 11 :!: 8
Min. & Max. 2 - 87 1. 38 2·22 E ~-hour mm n J4 34 34
Mean+ S.D. 15 + 16 11 + 9 10:!: 7 s
Min. & Max. 4. 122 2 - 80 4-58
R 1-hour mm n 34 34 34 Mean:!: S.D 34:!: 27 27 :!: 19 25:!: 17
- ---- -- -- -- -- ----- ---- --- - -

SIDE EFFECTS :- No .side effects were noted during treatment and after treatment with the prescribed dosage of the coded drug DF-6, DF-4 with M.
Relapse :- 6 cases
COMMENTS ON THE EFFICACY OF THE DRUGS:- The coded drugs DF-6, DF-4 with M tried . ·n the above trial showed good response In cases having less than 2 years chronicity, cases having more than 3 years chronicity of the disease did not respond.
CONCLUSION ABOUT THE EFFICACY OF THE DRUG DF6-DF4 WITH M
TRIAL N0.4
DF-6, DF-4 with M: The drug was tried on a sample of 34 cases, al)d was round to be effective in 11 patients with less than 2 years chronicity of disease. The general therapeutic response was as follows: - 5 patients showed good response to the treatment and 13 fairly responded to the treatment and 16 patients did not respond to the treatment.
It was observed that the patients having more than 2 years chronicity of the disease and In wnom the oedema was hard and blackish In colour did not respond to the treatment. The drug was found to be equally effective irrespective of age and sex of the patients. The drug was found to be safe as no side effects were noted with the use of DF6 DF4 with M.
DRUGWISE THERAPEUTIC TRIALS
TRIAL N0.5
Coded drug
Ingredients
DF 15, DF16 & DF17 (oral medicine) . DF2 & DF3 (oral medicine)
DF 15 1. Bekh-e-Karfas 2. Bekh-e-lzhkr 3. Bekh-e-Kasni 4. Bekh-e-Badiyan 5. Turbud
DF-16 (Mushil) 1. Jalapa 2. Habbul Neel 3. Magh-e-Fuloos
Khayar Shamber 4. Barg-e-Sana 5. Rogan Zaitoon
52
Apium graveolens Cymbopogon Jwarancusa Cichorium intvbus Foeniculum Vulgare Operculina turoethum
Ipomoea turoethum Ipomoea nil
Cassia fistula Cassia senna var senna Olea europea

OF 17 (Tabreed) 1. Khamlra Gujaban Sada 2. Behldana -3. Resha Klthmi 4. Barg-e-Gujaban-5. Unnab-
DF1
Borago Offlc lnalls Cydonia oblongs Althaea Officlnatfs Borago Qff!Cinalis ZiziQhys Jy!yba
1. Poost-e-Biskhapra Sufaid-2. Filfil Sufaid - Trianthema decandra 3. Bekh-e-Gule-Abbas - Mirabllis Jalapa 4. Maghz-Tukhme-Karanjwa-Caesalpinca bonduc
DF2 Roghan Beo Anjir : 25ml
DF3 Maghz Karanjwa 2 numbers
METfiOD OF PRt:PARATION : The ingredients of DF 15 {Munzij) were soaked in 350 ml of water over night boiled and reduced to half in the morning. Mushil & Tabreed : The Mushil and Tabreed were also prepared as for Munzij. DF-1 was prepared as mTrial No.1
DOSAGE AND MODE OF ADMINISTRATION: The prepared jo~nanda {decoction) was given In empty stomach early in the morning for a period of' 14 days. Mushil and Tabreed were administered alternately for 10 days {i.e. five Mushil and five Tabreed) . After completion of Munzij, Mushil therapy the coded dru·1 DF-1 was administered as in Trial No.1 .
TABLE N0.1 DF15 DF16 OF 17 & DF1
Age and Sexwise Distribution of Pat ients
Age Group in years Male Female Total Percentage
1-10 years - - - -11 -20 years 7 9 16 53
21 -30 years 3 5 8 27
31 -40 years 1 2 3 10
41 -50 years 2 - 2 7
51-60 years - - - -61 -70 years 1 - 1 3
Total 14 16 30 100
The coded drug DF15 DF16 DF17 & DF1 was tried in 30 cases {14 males and 16 females). The maximum number of patients were ~n the age of 11-20 years followed by 21-30 years.
53

TABLE N0.2 DF15 DF16 DF17 & DF1
Distribution of Patients according to the Chronicity of the Disease
CHRONICITY No. of cases Percentage
Less than 2 years 14 47
2-3 years g · 30
3 - 5 years 7 23
Total ao · 100
The chronicity of the disease is shown in Table No.2. The maximum number of cases having chronicity of less than 2 years.
TABLE N0.3 OF 15 + OF 16 + OF 17 + OF 1
Response in Relation to the Chronicity of the Disease
REUEVED PARTIALLY REUEVED NOTREUEVED CHRON/CfTY
No. ofpts % No. ofpts. "' No. ofpts. %
Less than 2 years 3 21 .4% 3 21 .4% 8 57.1% No. of pts. 14
2-3 years 2 22.2% 2 22.2'!1r 5 55.6% No. of pts.9
3-5years 1 14.3% - - 6 89.1% No. of pts.7
Total 6 20% 5 ! 16.7% 19 63.3" No. of pts.30
TABLE N0.4
GENERAL THERAPEUTIC RESPONSE
Response No. ofcases Percentage Good Response 6 20
Fair Response 5 17
No Response 19 63
Total 30 100
Out of 30 cases treated with OF 15 OF 16 OF 17 & OF 1 , 6 showed good response to the treatment, 5 fairly responded to the treatment and 19 did not respond to the treatment.
TABLE N0.5 OF 15 OF 16 DF17 &DF1
Drugwise Distribution of different sign and symptoms at the time of admission and during subsequent follow-ups (CLINICAL FINDINGS)
Duration of Treatment No. of cases Fever Lymphanaitis Lvmohadintis
Base line ' 30 2 6 6
L 40th day 30 1 - -80th day 30 1 2 2
---- -
54

c.n · 01
! -=r CD
TABLE N0.8
Details of measurements of OEDEMA in cases of Filariasis who were treated with coded drugs "DF-15, DF-16, DF-17 & DF-1 '
v u M
0 N E DAY- OF EXAMINATION
L 0 I A
U F T s Statistic Before treatment After completion After completion After completion After completion u M
0 R (Oth day) of Munzij Therapy of Mushil Therapy of40 days ofBOdays E
F E treatment treatment i
A Min. & Max. 3140cc - 5880cc 2950cc - 5580cc 2890cc - 5490cc 2890cc - 5450cc 3130cc - 5390cc !
F
F L n: 30 30 30 30 30 E E cc Mean:!: S.D 4230 :!: 750 4140:!: 710 4070:!: 680 4100:!: 660 4130:!: 650 C G T
12.8473* I 13.9653* 113 2854 * I &.6788* lio.8577** I 12.1803*1-2.441 * ~ 1.6887** 1 E t-value -D . P: - < 0.01 < 0.001 < 0.01 <0.01 <0.05 < 0.05 < 0.05 >0.05
••
Min. &Max. 2800cc - 531 Occ 2760cc - 5260cc 2750cc - 5060cc 2730cc - 5150cc 2810cc- 5120cc
N n: 30 30 30 30 30 0 L cc Mean:!: S.D 3740 :!: 630 3750:!: 630 3720:!: 600 3780:!: 610 3780:!: 610 A E M G t-value - 1-e.7oo2** 1 ~.6 1 o7** lh .8827** 1 -1.8886**1 1-2.5624* I l -2.1 524*j2.7623* fO.oao2** I A L
0 E D E M
cc A
'----·- . --- - ---
NOTE: 1.
2.
3.
4.
* **
Special Note:
P: - >0.05 >0.05 > 0.05 >0.05 >0.02 <0.05 < 0.02 >0.05 . Min. &Max. 80cc - 21 OOcc 130cc - 1900cc 50cc - 1510cc 30cc - 1650cc 20cc - 1720cc
n: 30 30 30 30 30
Mean:!: S.D 490:!: 410 390:!: 350 350:!: 310 320:!: 310 350:!: 330
t-value - 13.591* I 13.9032* lh .867** I ~b. 1448**1 13.6854*(9.2527**11 .5586**
P: - <0.01 <0.001 >0.05 <0.001 >0.05 <0.001 -- . - -- L____ _ ___
The figures in inverted rectangles represents the comparison between base line and follow-up observations;
The figures in rectangles opened upwards represents the comparison between Munzij and Mushil therapy observations.
The underlined figures represents the comparison between Mushil therapy and its consecutive follow-up observations.
The figures in rectangles represents the comparison between the follow-up observations during main course.
The changes are significant at their respective probability levels
The changes are not significant
The analysis are subjected to comparison between the changes_within the groups and not between the gro~< ;"lS .
>0.05 >0.05

01 Cl)
GRAPH N0.1
Volume of affected leg and the changes in it during treatment Volume of Normal leg and the changes in it during treatment interms of Mean ± SD and level of significance/non-significance interms of Mean ± SD and level of signif~cancejnon-significance
BL ACMZT ACMLT AC40DST A.CSOOST Bl ACMZT ACMLT AC40DST A.CSODST
(cc) (cc) (cc) (cc) 4800 1- P: >O.os•• - 4800 4500 r- P: >0.05•• - 4500
4500 - P: >0.05 .. P: <0.05• - 4500 4230:!: 750
4200 - P: <O.o:1• P: <0.02" - 4200
4200 r-, ____
4140 :!: 710 4070:!: 680 4130 - 4200 :!: 3900 r- 3750 :!: 630 3780:!: 610 3780 - 3900 4100:!: 660 650
3900 - P: <O.o1• P: <0.001• P: <0.02• - 3900 . :!:
3600 - 3740:!: 630 3720:!: 600 610 - 3600 P: >0.05 .. P: < O.o1• P: <o.os•
3600 - - 3600 P: >0.05** P: >0.05••
3300 - P: >0.05** P: <0.05• - 3300
BL ACMZT ACMLT AC40DST A.CSODST BL ACMZT ACMLT AC400ST A.CSODST
DAY OF EXAMINATION DAY OF EXAMINATION
Graphical interpretation of the volume of affected/normal leg and OEDEMA and the changes in them during treatment in cases of Filariasis who were treated with coded drugs "DF-15, DF-16, DF-17 & DF-1".
Scale:- 1 Unit = 300 cc
Volume of Oedema and the changes in it during treatment interms of Mean ± SD and level of signif~cancejnon-significance
BL ACMZT ACMLT AC400ST A.CSODST
(cc) - (cc)
900 i- P: >0.05** - 900 P: >0.05 ..
P: >0.05 ..
600 '-~ :!:41 0 390 :!: 350 - 600
350 :!: 310 350
300 - P: <0.01 • :m- 300 P: <0.001• P: >0.001• 320 :!: 310 P: >0.05 .. P: <O.oo1•
BL ACMZT ACMLT AC40DST A.CSODST
DAY OF EXAMINATION
KEY:-* The changes are
significant at their respective probability levels.
** The changes are not significant.
BL = Baseline ACMZT = After completion of
Munzij Therapy. ACMLT = After completion .of
Muzhnil Therapy. AC40DST = After completion of
40 days treatment. AC80DST = After completion of
80 days treatment
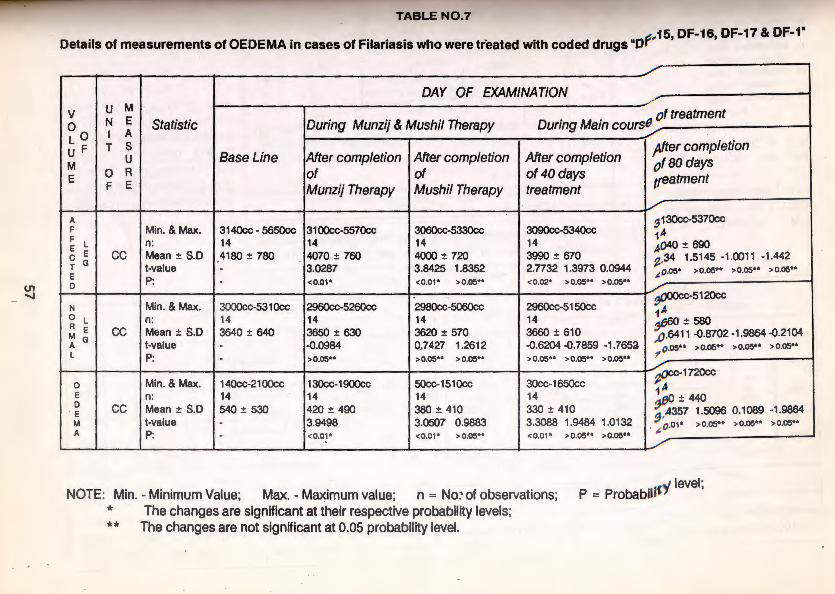
U'1 ......
I UA T Ut- t::XAMINATION I
TABLE N0.7
~ 15, DF-16, DF-17 & DF-1 " Details of measurements of OEDEMA In cases of Filariasis who were treated with coded drugs ·of
DAY OF EXAMINATION
v u M of treatment
0 N E Statistic During Munzij & Mushil Therapy During Main course Lo I A
U F T s /4fter completion
M u Base Line After completion After completion After completion
0taodays E 0 R of of of40days treatment F E Munzij Therapy Mushil Therapy treatment
A ~ 130ce-5370cc F Min. & Max. 3140cc • 5650cc 31 00cc-5570cc 3060cc-5330cc 3090cc-5340cc 14 F l n: 14 14 14 14 4040 ± 690 E E cc Mean± S.D 4180 ± 780 4070 ± 760 4000 ± 720 3990 ± 670 C G ~.34 1.5145 -1.0011 -1.442 T t-value . 3.0287 3.8425 1.8352 2.7732 1.3973 0.0944 ,1. 0.05* > 0.05** > 0.05.. > 0.05 .. E P: D
. <0.01* <0.01* >0.05*" < 0.02* > 0.05** > 0.05 ..
N Min. & Max. 3000cc-531 Occ 2960cc·5260cc 298Qcc-5060cc 2960cc·51 50cc ~-5120cc
14 0 L n: 14 14 14 14 ~660 ± 580 A E cc Mean± S.D 3640 ± 640 3650 ± 630 3620 ± 570 3660 ± 610 M G ,o.6411 -0.8702 -1.9864 -0.2104 A t-value . -0.0984 0_,7427 1.2612 -0.6204 -0.7859 -1 .7652 0.os.. > o.os** > o.o5"* > o.os•• L P: - >0.05** >0.05 .. >0.05** > 0.05... > 0.05** >0.05** 7
0 Min. & Max. 140cc-2100cc 130cc-1900cc 50cc-151 Occ 30cc-1650cc ~OCC-1720cc
A E n: 14 14 14 14 ~ ±440 D cc Mean± S.D 540 ± 530 420 ± 490 380 ± 410 330 ± 410 E 4357 1.5096 0.1089 -1 .9864 M t-value - 3.9498 3.0507 0.9883 3.3088 1.9484 1.0132 ~~ 01• >0.05.. >0.05** >0.05** A P: <0.01 * <0.01* >0.05** <0.0 1* > 0.05** > 0.05**
. ~ . ---- ---- - -- - -- - - --- - -· --
NOTE: Min. - Minimum Value; Max. - Maximum value; n = No:· of observations; P = Probabilro' level;
* The changes are significant at their respective probability levels; ** The changes are not significant at 0.05 probability level.
I
~

01 Q)
GRAPH N0.2
Volume of affected leg and the changes In It during treatment Volume of Normal leg and the changes in It during treatment interms of Mean ± SO and level of signifiC8ncejnon-significance interms of Mean ± SO and level of signifiCancejnon-significance
BL ACMZT ACMLT AC40DST AC80DS7 BL ACMZT ACMLT AC40DST AC80DS7
(cc) (cc) (cc) (cc)
4700 1- P: >0.05•• - 4700 P: >0.05 .. P: >0.05 ..
1-4180 :!: 780
4300 1--. 4000:!: 720 4040 - 4300
4200 - P: >0.05 .. P: >0.05 .. P: >0.05 .. - 4200 P: >0.05u
3880 3800 - 3620 + 570 _;_ - 3800
r-- - :!:
3900 1- P: <0.01 4070 :!: 780 690 - 3900
P: <0.02• 3990 :!: 670 , P: <O.o1• P: <0.05•
3500 f- - P: >0.05 .. - 3500 P: >0.05•• P: >0.05*•
3640:!: 640 3680:!: 610 580 3650 :!: 640 P: >0.05 ..
3400 - - 3400 P: >0.05 .. P: >0.05 ..
P: >0.05•• P: >0.05 .. 3000 - - 3000 P: >0.05 ..
BL ACMZT ACMLT •AC40DST AC80DS7 BL ACMZT ACMLT ~y.wosr AC800S7
DAY OF EXAMINATION DAY OF EXAMINATION
Graphical interpr~tion of the volume of affectedJRormal leg and OEDEMA ana the changes in them during treatment in cases of Filariasis who were treated with coded drugs "DF-15, DF-16, Df-17 & DF-1 " for 104 days.
..
Scale:- 1 Unit = 400 cc
Volume of Oedema and the changes in it during treatment interms of Mean ± SO and level of significancejnon-significance
(cc) .
800
400
0
BL ACMZT ACML T AC40DST AC800S7
P: <0.01· I P: <0.01 · I P: <0.01 · P: <0.01·
~ :!:530 P: >0.05 ..
380 :!: 410 380 :!:
420 = 490 I 440
P: > o.oe•• P: > o.oe .. 330 :!: 410
P: >0.05•• P: >O.oe ..
P: >O.oe ..
BL ACMZT ACMl T AC40DST M:.ltX)$7
DAY OF EXAMINATION
(cc)
800
400
0
KEY:-* The changes are
significant at their respective probability levels.
** The changes are not significant even at 0.05 probability level.
BL A9MZT
ACMLT
AC40DST
ACBOOST
Baseline ,. After completion of
Munzij Therapy. After completion of Muzhnil Therapy. After completion of 40 days treatment. After completion of 80 days treatment
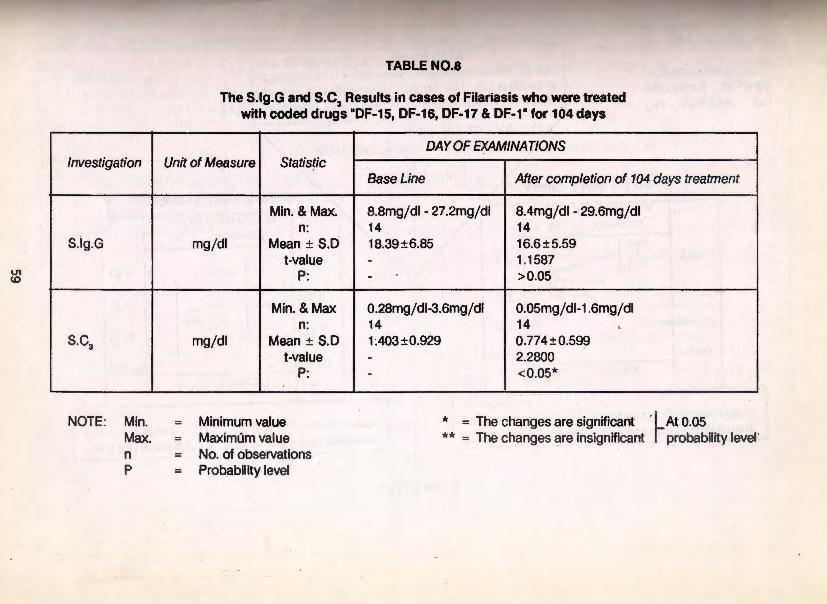
V1 co
Investigation
S.ig.G
S.C3
NOTE: Min. Max. n p
N:iftDfr1 80 days treatmMt
TABLE N0.8
The S.lg.G and S.C, Results in cases of Filariasis who were treated with coded drugs "DF-15, DF-16, DF-17 & DF-1" for 104 days
Unit of Measure Statistic
Min. &Max. n:
mgjdl Mean± S.D t-value
P:
Min. & Max n:
mgj dl Mean ± S.D t-value
P:
Minimum value Maximum value No. of observations
= Probability level
DAY OF EXAMINATIONS
Base Line After completion of 104 days treatment
8.8mgjdl - 27.2mgjdl 8.4mgjdl - 29.6mg/ dl 14 14 18.39±6.85 16.6±5.59 - 1.1587 - >0.05
0.28mgjdl-3.6mgjdl 0.05mgjdl-1.6mgjdl 14 14 ' 1.403±0.929 0.774±0.599 - 2.2800 - <0.05*
* = The changes are significant ·1 At 0.05 ** = The changes are insignificant r probability level'

0> 0
GRAPH NO.3
The S.lgG levels and the changes in it during treatment interms of Mean ± SO and level of significance/non- . significance
The S. C3 1evels and the changes in it during treatment interms of Mean ± SO and level of significance/nonsignificance
(mgj dl)
22.0
17.0 1-
112.0 ~
BL AC104DST
(mgjdl)
I I - 22.0 18.39 : 6.85
BL. AC104DST (mgj dl) (mgjdl)
8.0 I- - · 3.0
2.0 1- P: <o.os• ~ ·: · -117.0 5.59
-1 12.0
BL AC104DST
-l 2.0
1.0 t I~ I';'' -1 1.0 - l 0.599
v
Graphical interpretation of S.lg.G and S.C3 levels and the changes in them during treatment in cases of Filariasis who were treated with coded drugs OF-15, OF-16, OF-17 & OF-1" for 104 days.
*
**
= The changes are significant at 0.05 probability level.
= The changes are not significant.

Q) ......
- - ;:;~ ----- --· ·-·
GRAPH N0.4
The corr~lation and Regression analysis of the changes observed in SllgG. and Filarial Oedema during treatment in cases ot Filariasis who were treated with coded drugs DF-15, DF-16, DF-JJ &-~-1 for 104 days.
SCALE:-On Y -axis 1 unit
X-axis 1 unit
KEY:-
= 50 cc (Oedema) = 3 mgjdl (S.IgG)
1. The inclined lines are the Regression lines. 2. The Thick dots are the bivariate points in scatter
diagram. 3. .NS = Not Significant.
y The coefficient of correlation: r = 0.10785 P: >0.05 (NS)
NOTE:-No. of observation n = 14
S.lgG = 1.2195 + 0.00349(od) P: >0.025 (NS)
od = 158.491 + 3.333 (S.IgG) P: >0.025 (NS)
~S.IgG = 1.7929, Theaveragesof the respective
Oedema = 164.2857 observations
-X I I X -15 -12 -9 -6 -3 3 6 9 12 15 18
S.lgG
-Y

0) 1\)
GRAPH N0.5
The correlation and Regression analysis of the changes observed in SC3 and Filarial Oedema during treatment in cases of Filariasis who were treated with coded drugs DF-15, DF-16, DF-17 & DF-1 for 104 days.
SCALE:-On Y -axis 1 unit = 50 cc (Oedema)
X-axis 1 unit = 0.4 mgfdl (SC3)
KEY:-1. The inclined lines are the Regression lines. 350 2. The Thick dots are the bivariate points in scatter
diagram. 300 3. S = Significant.
The coefficient of correlation: r = 0.5844 p <0.025 (S)
SC3 = o:o75 + o.oo337(od) P: <0.025 (S)
NOTE:-No. of observation n = 14
od = 100.5827 + 101.341 (SC:J P: <0.025 (S)
~ SC3 = 0.6286 The averages of
the respective Oedema = 164.2857 observations
-X ,/"' ~I . X -1.6 -1.z:::?' -0.8 -0.4 0 0.4 0.8 1.2 1.6 2.0 2.4 2.8
sc3

I .. l_y_______ . , - J TABLE N0.9
Pathological Results Of Daul Feel (Filariasis) Patients, Treated With Coded Drugs DF-15, DF-16, DF-17 & DF-1
DAY OF EXAMINATION Unit
lnvetigation of Statistic During Munzij & Mushil Therapy During Main therapy measure Base Line
· After Munzij After Muzhil After 40 days After 80 days
Min.&Max. 7.0-13.5 6.0-14.0 6.0-14.5 5.4·13.5 6.0-14.0 Haemoglobin gm% n 26 . 26 26 26 26
Mean:tS.D 11.4±1.6 11.3±1.7 11 .3 :t 1.9 11.4±1.7 11.2 :t 1 7
Min.&Max. 2.75-4.0 2.75-3.9 2.5-4.0 2.0-4.0 2.5-4.0 I
R.B.C. Mjcmm n 26 26 26 26 26 I
Mean:tS.D 3.3±0.4 3.2±0.3 3.1 :t0.4 3.2±0.5 3.1 ±0.33 - --Min.&Max. 5600-15000 5000-16000 5000-13250 5000-11500 5000-10200
W.B.C. Cjcmm n 26 26 26 26 26 Mean:tS.D 8250±2400 83So:t2300 8100±2000 7850± 1750 7550± 1450
~ - -Min.&Max. 38-80 31-82 43-64 44-74 40-80
D Polymorphs % n 26 26 26 ' 26 26 I Mean:tS.D. 56±10 55±11 53:!:5 57±8 ' 53±9 F Fe
Min.&Max. 15-50 14-59 20-46 20-45 16-54 Eo Au Lymphocytes % n 26 26 26 26 26 EN Mean :t S.D. 35:t 10 33:t 12 37±7 36±8 38±8 NT T I Min.&Max. 2-30 3-32 4-24 0-15 1·27. A Eosinophils % n 26 26 26 26 26 L
Mean±S.D. 9:t7 12±8 10±7 7:t4 9:t6 ....
E Min.&Max. 1-70 1-54 1-43 0-23 0-75
~hour mm n 26 26 26 26 26
s Mean:tS.D. 19:t 18 17:!:16 14:t 11 10±6 11±14
Min.&Max. 2-1~6 2-95 2-105 2~2 2-105 R 1-hour mm n 26 26 26 · 26 26
Mean:tS.D. 41:t33 35±27 33±23 26:t 15 28.±24
Min.&Max. 22-45 23-45 22-45 20-40 20-45 ,P.C.V. % n . 25 25 25 25 25
Mean±S.D. 35:t5 36±5 36±5 35±6 36±5
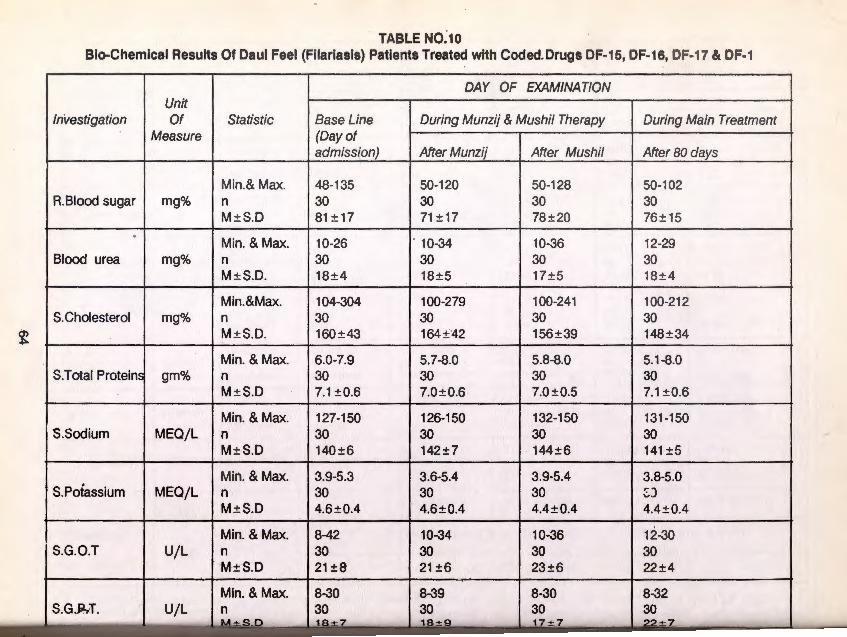
TABLE N0 .. 10 Bio-Chemical Results Of Daul Feel (Filariasis) Patients Treated with Coded. Drugs DF-15, DF-16, DF-17 & DF-1
DAY OF EXAMINATION Unit
Investigation I Of Statistic Base Line During Munzij & Mushil Therapy I During Main Treatment Measure (Day of
admissipn) After Munzij After Mushil After 80
Min.& Max. 48-135 50-120 50-128 50-102 R.Biood sugar I mg% In 30 30 30 30
M± S.D 81 ± 17 71 ±17 78±20 76±15
Min. & Max. 10-26 . 10-34 10-36 12-29 Blood urea I mg% In 30 30 30 30
M± S.D. 18 ±4 18±5 17±5 18±4
Min.&Max. 104-304 100-279 100-241 100-212 S. Cholesterol mg% n 30 30 30 30
~ M±S.D. 160±43 164±'42 156±39 148±34
Min. & Max. 6.0-7.9 5.7-8.0 5.8-8.0 5.1-8.0 S.Total Protein gm% n 30 30 30 30
M± S.D 7.1 ±0.6 7.0±0.6 7.0±0.5 7.1 ±0.6
Min. & Max. 127-150 126-150 132-150 131-150 S.Sodium I MEO/L In 30 30 30 30
M± S.D 140 ±6 142±7 144±6 141 ±5
Min. & Max. 3.9-5.3 3.6-5.4 3.9-5.4 3.8-5.0 S.Poiassium I MEO/L In 30 30 30 ::.J
M± S.D 4.6 ±0.4 4.6 ±0.4 4.4±0.4 4.4 ±0.4 -I Min. & Max. 8-42 10-34 10-36 12-30
S.G.O.T I U/L In 30 30 30 30 M±S.D 21±8 21 ±6 23 ±6 22 ±4
Min. & Max. 8-30 8-39 8-30 8-32 U/L In 30 30 30 30

TABLE N0.10 Bio-Chemical Results Of Daul Feel (Filariasis) Patients Treated with Coded. Drugs DF-15, DF-16, DF-1 7 & DF-1
DAY OF EXAMINATION Unit
Investigation I Of Statistic Base Line During Munzij & Mushil Therapy I During Main Treatment Measure (Day of
admiss(on) After Munzij After Mushil After 80
Min.& Max. 48-135 50-120 50-128 50-102 R.Biood sugar I mg% In 30 30 30 30
M ± S.D 81 ± 17 71 ±17 78±20 76±15
Min. & Max. 10-26 . 10-34 10-36 12-29 Blood urea I mg% In 30 30 30 30
M± S.D. 18±4 18±5 17±5 18±4
Min.&Max. 104-304 100-279 100-241 100-212 S. Cholesterol mg% n 30 30 30 30
~ M ± S.D. 160±43- 164±42 156±39 148 ±34
Min. & Max. 6.0-7.9 5.7-8.0 5.8-8.0 5.1-8.0 S.Total Protein gm% n 30 30 30 30
M ± S.D 7.1 ±0.6 7.0±0.6 7.0 ±0.5 7.1 ±0.6
Min. &Max. 127-150 126-150 132-150 131 -150 S.Sodium I MEQ/L I n 30 30 30 30
M ± S.D 140 ±6 142±7 144±6 141 ±5
Min. & Max. 3.9-5.3 3.6-5.4 3.9-5.4 3.8-5.0 S.Poiassium I MEO/L In 30 30 30 ~J
M±S.D 4.6±0.4 . 4.6±0.4 4.4±0.4 4.4 ±0.4
Min. &Max. 8-42 10-34 10-36 12-30 S.G.O.T I U/L In 30 30 30 30
M±S.D 21±8 21±6 23±6 22±4
Min. & Max. 8-30 8-39 ,8-30 18-32 S.G.M. ·I U/L In 30 30 30 30
M±S.D 18±7 -·- 18±9 17±7 22 ± 7

TABLE N0:1o Bio-Chemical Results Of Daul Feel (Filariasis) Patients Treated with Coded. Drugs DF-15, DF-16, DF-17 & DF-1
DAY OF EXAMINATION Unit
Investigation I Of Statistic Base Line During Munzij & Mushil Therapy I During Main Treatment Measure (Day of
admission) After Munzij After Mushil After 80
Min.& Max. 48-135 50-120 50-128 50-102 R.Biood sugar I mg% In 30 30 30 30
M±S.D 81 ±17 71 ±17 78±20 76±15
Min. & Max. 10-26 . 10-34 10-36 12-29 Blood urea I mg% I n 30 30 30 30
M± S.D. 18±4 18±5 17±5 18±4
Min.&Max. 104-304 100-279 100-241 100-212 S. Cholesterol mg% n 30 30 30 30
~ I M±S.D. 160±43 164±'42 156±39 148±34 I
Min. & Max. 6.0-7.9 5.7-8.0 5.8-8.0 5.1-8.0 S.Total Proteins gm% n 30 30 30 30
M±S.D 7.1 ±0.6 7.0±0.6 7.0 ±0.5 7.1 ±0.6
Min. & Max. 127-150 126-1 50 132-150 131-150 S.Sodium I MEO/L I n 30 30 30 30
M ±S.D 140±6 142±7 144±6 141 ±5
Min. & Max. 3.9-5.3 3.6-5.4 3.9-5.4 3.8-5.0 S.Poiassium I MEO/L I n 30 30 30 ::.J
M± S.D 4.6±0.4 4.6±0.4 4.4±0.4 4.4±0.4 I
Min. & Max. 8-42 10-34 10-36 12-30 S.G.O.T I U/ L In 30 30 30 30
M±S.D 21±8 21 ±6 23 ±6 22 ±4
Min. & Max. 8-30 8-39 18-30 18-32 S. G .Ji!.iT. ·I U/L In 30 30 30 30
±S.D 18± 7 18± 9 17 ± 7 22 ± 7

......
SIDE EFFECTS: No side effects were noted during treatment and after treatment with the prescribed dosage of the coded drug DF15 DF16 DF17 DF1
Relapse: 2 cases
Comments on the efficacy of the drug:- On the above trial the coded drug DF15 DF16 DF17 &DF1 were used. Good response was observed in less than 2 years and 2-3 years of the chronicity. Cases having more than 3 years chronicity of the disease did not respond to the treatment.
+I CONCLUSION ABOUT THE EFFICACY OF THE DRUG DF15 DF16 DF17 DF1 : C\1 C\1
m +I CX)
...... +I CX)
c CJ) +I ~
Trial No.5 DF15,DF16,DF17 AND DF-1 : The drug was tried on a sample of 30 cases and it was found to be effective in less than 2 years chronicity of disease. The general therapeutic response was - 6 patients showed good response to the treatment, 5 fairly responded to the treatment and 19 patients did not respond to the treatment.
It was observed that the patients having more than 2 years chronicity of the disease and in whom the oedema was hard and blackish in colour did not respond to the treatment. The drug was found to be effective equally irrespective of age and sex of the patients. The drug was found to be safe as no adverse effect was noted with the use of the drug DF15 DF16 DF17 DF1 .
DRUGWISE THERAPEUTIC TRIALS
TRIAL N0.6 Coded drug
Ingredients
DEC DF1 DF4 with M (oral medicine with external appl ication) DF2 & DF3 (oralmedicine)
DEC: Di-ethyl Carbomazine
DF1 : 1. Poost-e-Bishkapara sufaid • one part 2. Filfil Sufaid - one part 3. Bekh-e-Gule-Abbas - 1/2 part 4. Maghz-Tukhme-Karanjwa - 1 /2 part
Mudirat: Khara-e-Khask
DF-4: Boora Armani, Basfaij (equal weight)
DF2: Roghan Bed Anjir - 25ml
DF3: Maghz Karanjwa -2 Numbers.
65

"
METHOD OF PREPARATION DEC : , 150 mg Di-ethyl carbamazine citrate powder filled in the
capsule DF-1 : Each ingredient of the coded drug DF1 was taken according
to the formula and pulverised separately Into a fine powder and then mixed thoroughly
Mudirat: Prepared form of Joshanda (decoction)
DF-4: Each ingredient was powdered separately and mixed together thoroughly in glycerine
DOSAGE AND MODE OF ADMINISTRATION: DEC: 150 mg powder was filled in each capsule and administered daily once along with DF-1 for a period of 80 days.
DF1 : 250 mg of the powdered coded drug DF1 was given in capsule form as per the chart.
Days of Treatment No.of capsules Days of Treatment No. of Capsules 1 1 6 2 2 2 7 3 3 3 8 1 4 2 9 2 I
I
5 1 10 3 Total 1 0 days 20 Capsules
The capsules were administered in empty stomach early morning for 80 days. During treatment period the mushil (purgative) was given after every 20 days of treatment.
Mudirat & DF4: Mudirat (Diuretics) 250 ml was given in the form of joshanda (decoction) daily. DF-4 10gm wns applied on the affected limb daily.
TABLE N0.1 DEC DF1 DF4 with M
Sex and Agewise Distribution of Patients
Age Group in years Male Female Total Percentage
1-10 years - - - -11-20 years 4 7 11 41
21-30 years 1 2 3 11
31 -40 years •2 6 8 30
41-50 years 1 4 5 18
51-6U years - - - -61-70 years - - - -
Total 8 19 27 100
The coded c:Jrug DEC DF-1 DF-4 with Mwastried in 27 cases (8 males and 19females). The maximum number of patients were in the age group of 11-20 years followed by 31 -40 years.
66

I"+I
IC\J I C\J
I"+I
1 ~"-1 .,....
en +I
I CO .,....
0 u) +I ~
SIDE EFFECTS: No side effects were noted during treatment and after treatment with the prescribed dosage of the coded drug DF15 DF16 DF17 DF1
Relapse: 2 cases
Comments on the efficacy of the drug:- On the above trial the coded drug DF15 DF16 DF1 7 &DF1 were used. Good response was observed in less than 2 years and 2-3 years of the chronicity. Cases having more than 3 years chronicity of the disease did not respond to the treatment.
CONCLUSION ABOUT THE EFFICACY OF THE DRUG DF15 DF1 6 DF1 7 DF1:
Trial No.5 DF15,DF16,DF17 AND DF-1 : The drug was tried on a sample of 30 cases and it was found to be effective in less than 2 years chronicity of disease. The general therapeutic response was- 6 patients showed good response to the treatment, 5 fairly responded to the treatment and 19 patients did not respond to the treatment.
It was observed that the patients having more than 2 years chronicity of the disease and in whom the oedema was hard and blackish in colour d id not respond to the treatment. The drug was found to be effective equally irrespective of age and sex of the patients. The drug was found to be safe as no adverse effect was noted with the use of the drug DF15 DF16 DF17 DF1.
DRUGWISE THERAPEUTIC TRIALS
TRIAL N0.6 Coded drug
Ingredients
DEC DF1 DF4 with M (oral medicine with external application) DF2 & DF3 (oralmedicine)
DEC: Di-ethyl Carbomazine
DF1 : 1. Poost-e-Bishkapara sufaid • one part 2. Filfil Sufaid - one part 3. Bekh-e-Gule-Abbas - 1/2 part 4. Maghz-Tukhme-Karanjwa - 1/2 part
Mudirat: Khara-e-Khask
DF-4: Boora Armani, Basfaij (equal weight)
DF2: Roghan Bed Anjir - 25ml
DF3: Maghz Karanjwa -2 Numbers.
65

METHOD OF PREPARATION DEC : , 150 mg Di-ethyl carbamazine citrate powder filled in the
capsule DF-1 : Each ingredient of the coded drug DF1 was taken according
to the formula and pulverised separately Into a fine powder and then mixed thoroughly
Mudirat: Prepared form of Joshanda (decoction)
DF-4: Each ingre;dient was powdered separately and mixed together thoroughly in glycerine
DOSAGE AND MODE OF ADMINISTRATION: DEC: 150 mg powder was fill ed in each capsule and administered daily once along with DF-1 for a period of 80 days.
DF1: 250 mg of the powdered coded drug DF1 was given in capsule form as per the chart.
Days of Treatment No.of capsules Days of Treatment No. of Capsules 1 1 6 2
2 2 7 3 3 3 8 1
4 2 9 2 5 1 10 3
Total 1 0 days 20 Capsules
The capsules were administered in empty stomach early morning for 80 days. During treatment period the mushil (purgative) was given after every 20 days of treatment.
Mudirat & DF4: Mudirat (Diuretics) 250 ml was given in the form of joshanda (decoction) daily. DF-4 1 Ogm W<ls applied on the affected limb daily.
TAB.LE N0.1 DEC DF1 DF4 with M
Sex and Agewise Distribution of Patients
Age Group in years Male Female Total Percentage
1-10 years - - - - I
11-20 years 4 7 11 41
21-30 years 1 2 3 11
31-40 years 2 6 8 30
41-50 years 1 4 5 18
51-60 years - - - -61-70 years - - - -
Total 8 19 27 100 ----L__ _ _ ____________
The coded <:Jrug DEC DF-1 DF-4 with M was tried in 27 cases (8 males and 19 females) . The maximum number of patients were in the age group of 11-20 years followed by 31 -40 years.
66

DEC DF1 , DF4 with M TABLE N0.2.
D" ·b u 1stn u on o d" h Ch fP . at1ents accor mg to t e f h D" romc•tv o t e 1sease CHRONICITY No. of cases Percentage
Less than 2 years 12 44.5
2-3 years 3 11
3-5 years 12 44.5
Total 27 100
The chronicity of disease is shown in table no.2. The maximum number of cases were having chronicity of less than 2 years.
TABLE N0.3
DEC DF1 DF4 WITH M
Response in Relation to the Chronicity of the Disease RELIEVED PARTIALLY RELIEVED NOT RELIEVED
CHRONICITY
No. ofpts % No. ofpts. % No. ofpts. %
Less than 2 years 2 16.7% 5 41 .7% 5 41 .7% No. of pts.12
2-3 years 1 33.3% - - 2 66.7 No. of pts.3
3-5 years 3 25% 5 41 .7% 4 33.3% No. of pts.12
Total 6 22.2% 10 37% 11 40.7% No. of pts.27 -
TABLE N0.4
General Therapeutic Response
Response No.ofcases Percentage Good Response 6 22
Fair Response 10 37
No Resoonse 11 41
Total 27 100
Out of 27 cases treated w ith DEC, DF-1, DF-4 w ith M, 6 cases showed good response to the treatment, 10 fairly responded to the t reatment and 11 did not respond to the treatment.
TABLE N0.5
DEC, DF-1, DF-4 with M
Drugwise distribution of different sign and symptoms at the time of admission and during subsequent follow-ups (CLINICAL FINDINGS)
Duration of Treatment No. of cases Fever Lymphangitis /,..ymphadintis
Base line 27 2 4 9
40th day 27 - - -80th day 27 - - -
67
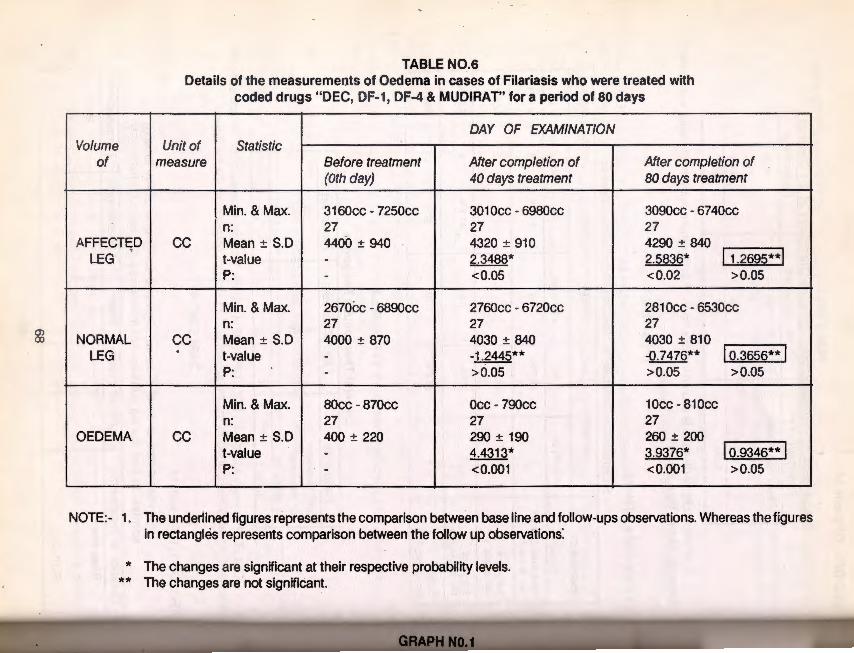
83
Volume of
AFFECTED ' LEG
NORMAL LEG
OEDEMA
TABLE N0.6 Details of the measurements of Oedema in cases of Filariasis who were treated with
coded drugs "DEC, DF-1, DF-4 & MUDIRAT" for a period of so days
DAY OF EXAMINATION Unit of Statistic
measure Before treatment After completion of After completion of (Oth day) 40 days treatment 80 days treatment
Min. & Max. 3160cc - 7250cc 301 Occ - 6980cc 3090cc - 67 40cc n: 27 27 27
cc Mean ± S.D 4400 ± 940 4320 ± 910 4290 ± 840 11.2695**1 t-value - 2.3488* 2.5836*
P: - <0.05 <0.02 >0.05
Min. & Max. 2670cc - 6890cc 2760cc - 6720cc 2810cc - 6530cc n: 27 27 27
cc Mean± S.D 4000 ± 870 4030 ± 840 4030 ± 810 . t-value -1.2445** -0.7476** I o.3656** I -P: - >0.05 >0.05 > 0.05
Min. & Max. 80cc - 870cc Occ -790cc 10cc- 810cc n: 27 27 27
cc Mean± S.D 400 ± 220 290 ± 190 260 ± 200 t-value - 4.4313* 3.9376* I o.9346** I P: - <0.001 <0.001 >0.05
-'
NOTE:- 1. The underlined figures represents the comparison between base line and follow-ups observations. Whereas the figures in rectangles represents comparison between the follow up observations:
* The changes are significant at their respective probability levels. ** The changes are not signifiCant.
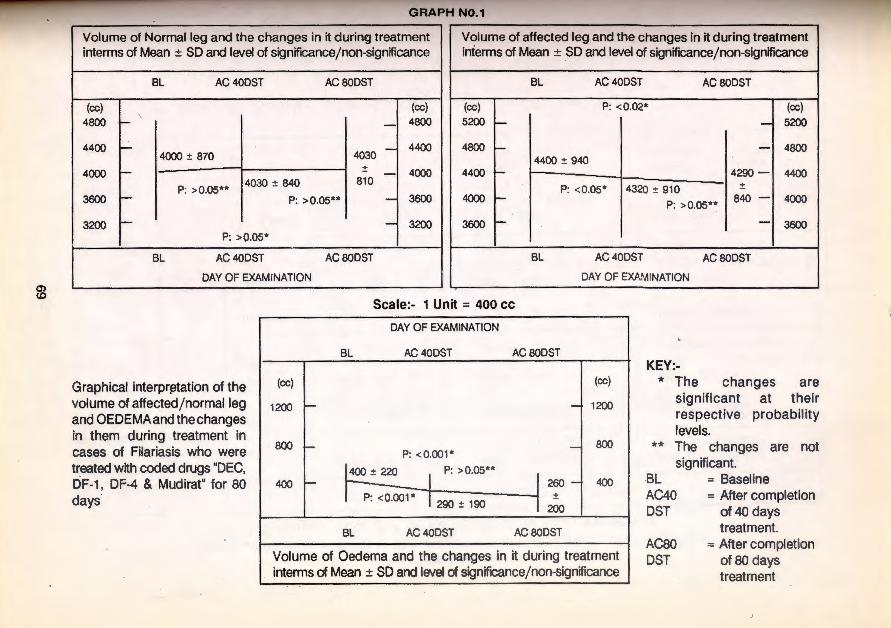
?6
GRAPH N0.1
Volume of Normal leg and the changes in it during treatment Volume of affected leg and the changes in it during treatment interms of Mean ± SD and level of significancejnon-significance interms of Mean ± SD and level of signif~cancejnon-significance
BL AC 40DST AC BOOST BL AC 40DST ACBODST
(cc) (cc) (cc) P: <0.02* (cc) 4BOO r- - 4800 I
5200 - - 5200
4400 f-4030 -
4400 4000:!: B70
4BOO - - 4BOO 4400 :!: 940
+ 4000 1- - - 4000 4400 r- 4290 - 4400
4030 :!: B40 B10 P: >0.05** P: < 0.05* 4320 :!: 910 :!:
3600 f- P: > 0.05** - 3600 4000 r-P: >0.05**
B40 - 4000
3200 1- - 3200 3600 1- - 3600 P: > 0.05*
BL AC40DST AC BOOST BL AC 40DST AC BOOST
I DAY OF EXAMINATION DAY OF EXAMINATION
Graphical interpr~tation of the volume of affected j normalleg and OEDEMA and the changes in them during treatment in cases of Filariasis who were treated with coded drugs "DEC, DF-1, DF-4 & Mudirat" for 80 days
Scale:- 1 Unit = 400 cc
DAY OF EXAMINATION
BL AC40DST AC BODST
(cc) (cc)
1200 - - 1200
BOO - - BOO P: <0.001*
400:!: 220 I P: >0.05** 1 260-400 - 400
P: <0.001 * 1290 :!: 190 l~ BL AC40DST ACBODST
Volume of Oedema and the changes in it during treatment interms of Mean ± SD and level of signif~cancejnon-significance
KEY:-* The changes are
significant at their respective probability levels.
** The changes are not significant.
BL AC40 DST
AC80 DST
= Baseline = After completion
of40 days treatment.
= After completion of80 days treatment

-....1 0
TABLE N0.7 Details of the measurements of Oedema in cases of Fil~riasis who were treated with
coded drugs "DEC, DF-1, DF-4 & MUDIRAT" fQr a period of so days
DAY 0~ EXAMINATION Volume Unit of Statistic
of measure Base Line After COfTJpletion of 40 days treatment
Min. & Max. 321 Occ - 6650cc 3320cc ~ 6540cc
' n: 14 14 AFFECTED cc Mean ± S.D 4420 ± 800 4370 ± ~70
LEG t-value - 1.4348 P: - >0.05**
Min. & Max. 2840cc - 5930cc 3190cc ~ 5940cc n: 14 14
NORMAL cc Mean ± S.D 4010 ± 670 4080 ± ~60 LEG t-value - -1 .9469
P: - >0.05** ,
Min. & Max. 1 OOcc - 720cc Occ - 79Ccc n: 14 14
OEDEMA cc Mean ± S.D 410 ± 210 290 ± 21 0 t-value - 3.7588 P: - <0.01*
NOTE:- Min./Max. = Minimum/Maximum value; n = No. of observations; p = Probability level
* The changes are significant at their respective probability levels. ** The changes are not significant.
After completion of 80 days treatment
3300cc - 5840cc 14 4300 ± 630 1.649 1.2362 >0.05 ** >0.05**
3250cc - 5830cc 14 4050 ± 640 -0.7339 0.9071 >0.05** >0.05**
10cc - 810cc 14 250 ± 220 2.8698 0.828 <0.02 * >0.05**

-...j _...
Volume of affected leg and the changes In it during treatment intenns of Mean ± SO and level of significance/non-significance
Volume of Normal leg and the changes In It during treatment intenns of Mean ± SO and level of significance/non-significance
BL AC 40DST ACBODST BL AC 40DST ACBODST
(cc) (cc) I
4900 1- - 4900 I
(cc) I (cc) 5200 - 5200
P: >0.05** 4500 f- - 4500
4010 :!: 670 4050
4100 - :!: - 4100 4080 :!: 660 640
P: > 0.05**
4800 P: > 0.05** __J 4800
4420 :!: 800 4300 4400 -1 4400
4370:!: 770 :!:
4000 t- I P: > 0.05** P: > 0.05** 630
j 4000 3700 - P: >0.05** - 3700
3600 r I I 3600 3300 r- - 3300
BL AC40DST ACBODST BL AC 40DST ACBODST
I DAY OF EXAMINATION DAY OF EXAMINATION
Graphical interpretation of the volume of affectedjnormalleg and OEDEMA and the changes in them during treatment in cases of Filariasis who were treated with coded drugs "DEC, DF-1, DF-4 & Mudirat" for 80 days
Scale:- 1 Unit = 400 cc
DAY OF EXAMINATION
BL AC 40DST AC 80DST
(cc) (cc)
800 - - 800
P: > 0.05**
400 1-410 :!: 210 ----J 250 -
400
P: <0.01* 1290:!: 210 :!:
0 - 220 - 0 P: <0.02*
BL AC 40DST AC 80DST
Volume of Oedema and the changes in it during treatment inferms of Mean ± SO and level of signif~eancejnon-significance
KEY:-* The changes are ' significant at their
respective probability levels.
** The changes are not significant.
BL AC40 DST
AC80 DST
= Baseline = After completion
of 40 days treatment.
= After completion of 80 days treatment

-....J 1\:)
Investigation .
S.lg.G
S.C3
NOTE· Min. Max. n p
TABLE N0.8
The S.lg.G and S.C3
Results in cases of Filariasis who were treated with coded drugs "DEC, DF-1, DF-4 & Mudirat" for 80 days
Unit of Measure Statistic
Min. & Max. n:
mgjdl Mean±S.D t-value
P:
Min.-Max n:
mgjdl Mean±S.D t-value
P:
Minimum value Maximum value No. of observations Probability level
DAY OF EXAMINATIONS
Base Line After completion of 80 days treatment
6.2 mgjdl - 29.6 mgjdl 11.8 mgjdl - 26.6 mgjdl 14 14 17.53 '± 6.96 20.01 ± 5.332 - -1 .7552 - >0.05**
0.1 mgjdl - 2.2 mgjdl 0.17 mgjdl - 3.4mgjdl 14 '14 1.21 ± 0.733 1.308 ± 0.8608 - -0.5282 - >0.05**
* = Th~ changes are significant ** = The changes are insignificant

" w
GRAPH N0.3
The correlation and Regression analysis of the changes observed in S.lgG and Filarial Oedema observed during treatment in cases of Filariasis who were treated with coded drugs DEC, DF-1, DF-4 & M for 80 days.
SCALE:-On Y-axis 1 unit
X-axis 1 unit
KEY:-
= 50 cc (Oedema) = 3 mgjdl (S.IgG)
1. The inclined lines are the Regression lines.
0 e d e m a
2. The Thick dots are the bivariate points in scatter diagram.
3. NS = Not Significant.
The coefficient of correlation: r = 0.4796 P: >0.025 (NS)
S.lgG = -4.479 + 0.01273 (od) P: > 0.025 (NS)
nd = 204.5869 + 19.1414 (S.IgG) P: > 0.025 (NS)
S.lgG
Oedema
-2.4786 IThe averages of the respective
157.143 I observations
NOTE:- No. of observation = 14
-X / I I X -1 8 -1 s -12 7 -9 -6 I -3 3 6 9 12 1s 18
S.lgG -100+--Y

- .,J ..,.
GRAPH NO.4
The SlgG levels and the changes in it during treatment interms of Mean ± SO and level of significance/nonsignificance
The SC3 levels and the changes in it during treatment interms of Mean ± SO and lev!')l of significance/nonsignificance
KEY:-
**
BL
AC800ST
Bl AC8oDST I (mgj dl) ~
22.0 ~I~" ~,,, " - 22.0 5.332
17.0 1- _, 17.0
12.0 1- P. >0.05 -1 12.0
BL AC80DST (mg j dl) ~ D (mg/ dQ 1.8
F-1·~ 1.8 1.3 f- 0~1.3 0.8 f- I -!0.8
P: > 0.05**
BL AC80DST DAY OF EXAMINATION BL ACSODST
DAY OF EXAMINATION Scale:- 1 Unit = 5 mgjdJ Scale:- 1 Unit = 0.5 mgjdl
= The changes are not significant at o.os probability level
~.· ......... .. · ... . ' · . ·• I > .· ·. ·. <01 ·Graphical inter~r~tatlon of SlgG an~ sc~ . } :·
. : . ;~y~·~::~m~·~m~ir••=~=h,~ ,n,~e,~;'!ir!;.tt,t#m!!,<i,Mt'r9.:•;;
Baseline
After completion of 80 days treatment
vl!~li~l~~~~lli~':~~@~W~illiiiiG

-...J 01
The correlation and Regression analyais of the changes observed in SC3 and Filarial Oedema during treatment in cases of Filariasis who were treated with coded drugs DEC, DF-1, DF-4 & M for 80 days.
The coefficient of correlation: r = 0.2398 P: >0.05 (NS)
NOTE:-No. of observation = 14
sc3
Oedema
350
-0.09643 The averages of~ tl:le respective
157.1 43 observations
y
On Y -axis 1 unit X-axis 1 unit
= 50 cc (Oedema) = 0.4 mg/dl (SC3)
SC3 = -a.2399 + o.ooo9131 (oo) P: >0.025 (NS)
od = 165.0636 + 82.1 381 (SC3)
P: >0.025 (NS)
1. The inclined lines are the Regression lines. 2. The Thick dots are the bivariate points in scatter
diagram. 3. NS = Not Significant.
-X X -1.6 -1.2 -0.8 0.4 0.8 1.2 1.6 2.0 2.4
-Y

TABLE N0.9
Pathological results of Daul Feel (Filariasis) patients, treated with coded drug DEC, DF-1, DF-4 & M for 80 days
Unit DAY OF EXAMINATION Investigation of Statistic
measure Base line After 40 days After 80 days
Min. & Max. 8.0 - 14.0 7.5- 14.0 8.0 - 14.5 Haemoglobin gm% n 27 27 27
Mean :!: S.D 11.6 :!: 1.4 11 .6 :!: 1.4 11.4 :!: 1.6
Min. &Max. 2.0 -4.0 2.0:!: 4.25 2.5:!: 4.2 A.B. C. Mfcmm n 27 27 27
Mean:!: S.D. 3.2:!: 0.5 3.17:!: 0.4 3.3 :!: 0.27
Min. & Max. 6000 - 12300 6000-12000 5700 -1 3000 I
W.B.C. cjcmm n 27 27 27 · Mean :!: S.D. 7500 :!: 1500 7600:!: 1600 7850 :!: 1800
~ Min. & Max. 37 - 67 41-69 32 - 68 D Polymorphs % n 27 27 27 I F Mean :!: S.D. 57 :!: 7 55:!: 6 57 :!: 8 F E C Min. & Max. 27-50 20 - 57 20 - 63 RO Lymphocyt.es % n 27 27 27 EU
Mean:!: S.D 38 :!: 7 39 :!: 7 36:!: 9 NN T T I Min. & Max. 0- 15 1 - 13 0-22 A Eosinophils % n 27 27 27 L Mean:!: S.D 5:!:4 6:!:4 7:!:6
Min. & Max. 1-90 1-39 2-40 E 'h-hour mm n 27 27 27
Mean+ S.D. 23 + 25 11 :!: 10 12:!: 10 s
Min. &Max. 2 - 106 2-80 5-88
R 1-hour mm n 27 27 27 Mean :!: S.D 45:!: 34 29:!: 21 29 :!: 21
Min. & Max. 24-42 25-45 23-48 P.C.V % n 15 15 15
Mean:!: S.D 35:!: 5 35:!: 6 35:!: 6
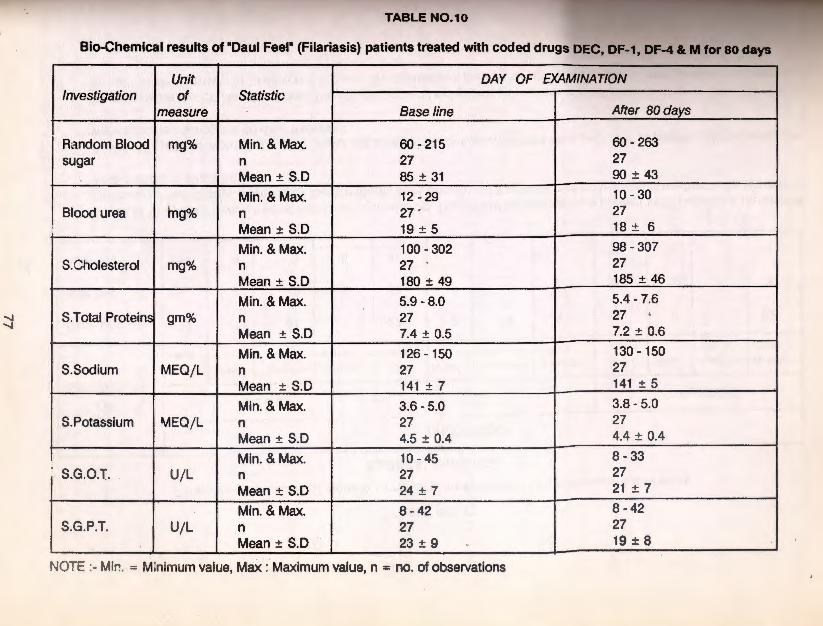
.......,
.......,
1 - ~r 1 Mean :!: s.o I 35 ± 5 35 ± s 35
± 6
__ I ow - ~ 115 I
TABLE N0.10
Bio-Chemical results of "Caul Feel" (Filariasis) patients tteated with coded drugs DEC, DF-1, DF-4 & M for ao days
Unit DAY OF EXAMINATION Investigation of Statistic
measure Base line After 80 days
Random Blood mg% Min. & Max. 60-215 60-263
sugar n 27 27
Mean± S.D 85 + 31 90 ± 43
Min. & Max. 12-29 10-30
Blood urea lng% n 27 . 27
Mean ± S.D 19 + 5 18 ± 6
Min. &Max. 100 - 302 98 - 307
S. Cholesterol mg% n 27 . 27
Mean+ S.D 180 + 49 185 + 46
Min. & Max. 5.9 - 8.0 5.4-7.6
S.Total Proteins gm% n 27 27 ' Mean ± S.D 7.4 ± 0.5 7.2 ± 0.6
Min. & Max. 126 - 150 130- 150
S.Sodium MEQjL n 27 27
Mean + S.D 141 + 7 141 + 5
Min. & Max. 3.6 -5.0 3.8 - 5.0
S.Potassium MEQ/L n 27 27
Mean± S.D 4.5 ± 0.4 4.4 ± 0.4
Min. & Max. 10-45 8-33 . S.G.O.T. U/L n 27 27
Mean ± S.D 24 ± 7 21 ± 7
Min. & Max. 8-42 8-42
S.G.P.T. U/L n 27 27 Mean ± S.D · 23 ± 9 19 ± 8
NOTE :- Min. = Minimum value, MaX :· Maximum value, n = no. of observations
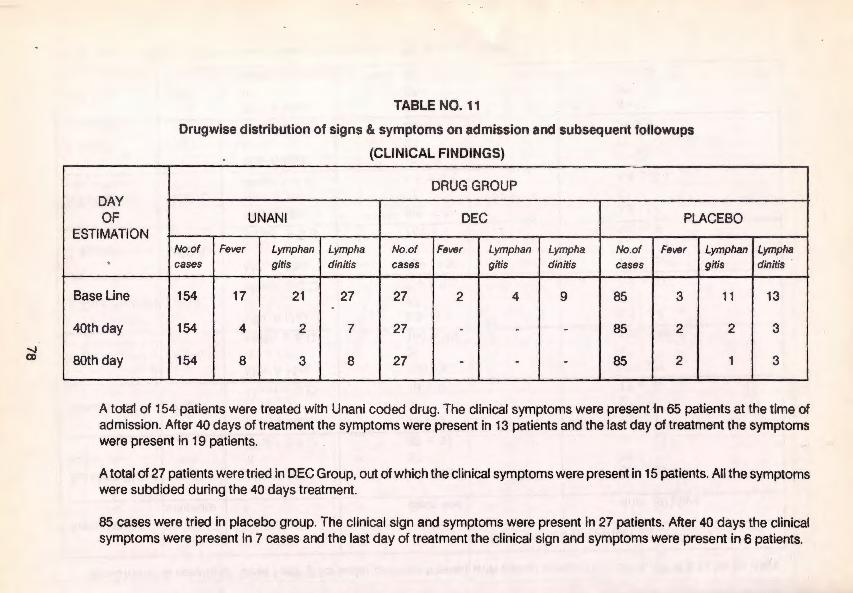
....... CJ)
DAY OF
ESTIMATION
'
Base Line
40th day
80th day
TABLE NO. 11
Drugwise distribution of signs & symptoms on admission and subsequent followups
(CLINICAL FINDINGS)
DRUG GROUP
UN ANI DEC PLACEBO
No.of Fever Lymphan Lympha No.of Fever Lymphan Lymph a No.of Fever Lymphan cases gitis dinitis cases gitis dinitis cases gitis
154 17 21 27 27 2 4 9 85 3 11
154 4 2 7 27 - - - 85 2 2
154 8 3 8 27 - - - 85 2 1 -------
Lympha dinitis ·
13
3
3
A total of 154 patients were treated with Unani coded drug. The clinical symptoms were present ·In 65 patients at the time of admission. After 40 days of treatment the symptoms were present in 13 patients and the last day of treatment the symptoms were present in 19 patients.
A total of 27 patients were tried in DEC Group, out of which the clinical symptoms were present in 15 patients. All the symptoms were subdided during the 40 days treatment.
85 cases were tried in placebo group. The clinical sign and symptoms were present in 27 patients. After 40 days the clinical symptoms were present in 7 cases and the last day of treatment the clinical sign and symptoms were present in 6 patients.
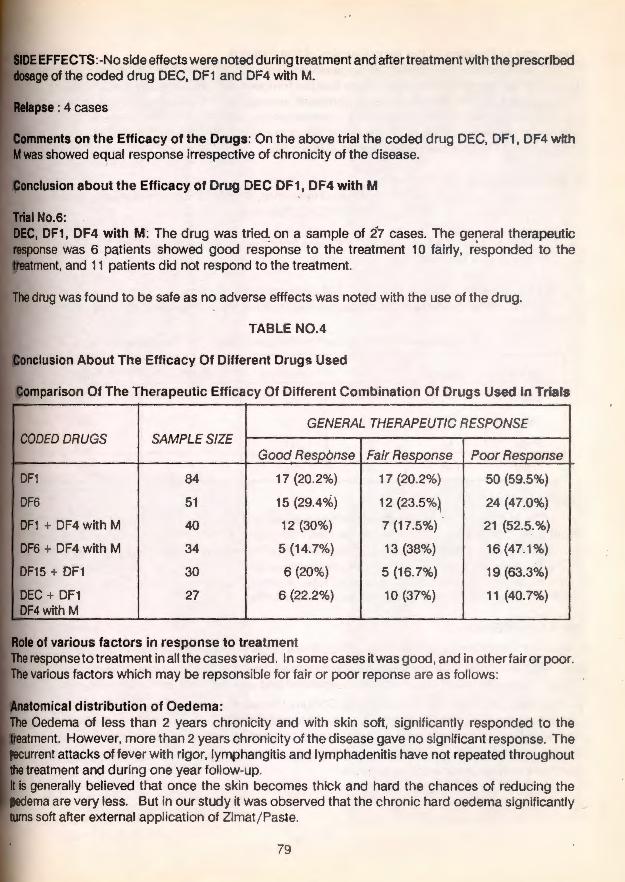
EFFECTS: -No side effects were noted during treatment and after treatment with the prescribed of the coded drug DEC, DF1 and DF4 with M.
r.ftll~m,!nt !ll on the Efficacy of the Drugs: On the above trial the coded drug DEC, DF1, DF4 with was showed equal response irrespective of chronicity of the disease.
Conclusion about the Efficacy of Drug DEC DF1, DF4 with M
Trial No.6: DEC, DF1 , DF4 with M: The drug was tried on a sample of 27 cases. The general therapeutic response was 6 patients showed good response to the treatment 10 fairly, responded to the treatment, and 11 patients did not respond to the treatment.
The drug was found to be safe as no adverse efffects was noted with the use of the drug.
TABLE N0.4
usion About The Efficacy Of Different Drugs Used
Comparison Of The Therapeutic Efficacy Of Different Combination Of Drugs Used in Trials
GENERAL THERAPEUTIC RESPONSE CODED DRUGS SAMPLE SIZE
Good
84 17 (20.2%) 17 (20.2%) 50 (59.5%)
51 15 {29.4°k) 12 (23.5%~ 24 (47.0%)
40 12 {30%) 7 (17.5%) 21 (52.5.%)
34 5 (14.7%) 13 {38%) 16(47.1%)
30 6 (20%) 5 (16.7%) 19 (63.3%)
27 6 (22.2%) 10 (37%) 11 (40.7%)
of various factors in response to treatment response to treatment in all the cases varied. In some cases it was good, and in other fair or poor. various factors which may be repsonsible for fair or poor reponse are as follows:
,anllrnmical distribution of Oedema: Oedema of less than 2 years chronicity and with skin soft, significantly responded to the
However, more than 2 years chronicity of the disease gave no significant response. The attacks of fever with rigor, lymphangitis and lymphadenitis have not repeated throughout
treatment and during one year follow-up. Is generally believed that once the skin becomes thick and hard the chances of reducing the
are very less. But in our study it was observed that the chronic hard oedema significantly turns soft after external application of Zimat j Pas.te.
79

Response in Rel,tion to the temperament of the patients Out of the 266 cases, 144 cases had Balgaml temperament, 51 cases had Damavi temperament, 64 cases Safravi temperament, and 7 cases Saudavi temperament. In our study, it is observed that the temperament of the disease is more dominant among Balgami(Phlegm) temperament that the patients also showed good response on comparison to patients with other temperaments. According to Unani literature, the disease will occur due to the Balgam-e-Gairtabaee(Abnormal Phlegm) and Sauda-e-Gairtabee(Abnormal Black Bile)
Miscellaneous factors studied · Various factors such as Social status, place of residence, dietary habits were studied in order to study th~ significance of these factors in 'DAUL FEEL' (Filariasis).
Social Status:- OUt of the 266 cases 206 were from the low income group, 41 were from middle income group and 19 from high income group.
Place of Residence:- Out of the 266, 204 cases were, loca! resident 53 cases were from other districts of Tamil Nadu and rest of the 9 cases were from neighbouring States of Andhra Pradesh and Pondicherry.
Response In Relation To The Temperament Of The Patients
Reponse Balgami Damavi Safrawi Saudavi Total
Good 43 7 13 1 64
Fair 42 16 10 2 70
Poor 59 28 41 4 132
Total 144 51 64 7 266 - - - - - - -----
Dietary .Habits:
Out of the 266 cases the incidence of the d isease was prevalent more common (263) among nonvegetarian compared to vegetarian: It has also been noted that its prevalence is more common in coastal areas e.g. coastal Tamil Nadu, Coastal Andhra Pradesh and Pondicherry etc. where fish and
, salt fish Is generally a part of the daily diet and hence eaten in plenty. This observation correlates with a similar con~ept In Unanl medicine as this type of_ dietary habits may cause 'Daul Feel (Filariasis). However, this contradi~ts with several modern researches.
Biochemical Studies:
A total number of 266 patients were studied. These patients were treated with various coded Unanl
drug regimes. Blood samples were collected from all the patients at the time of admission i.e. base line a.nd at regular follow-ups. Serum was separated and used for biochemical investigations, sugar,
urea, cholesterol, Total protein, Electrolytes, Sodium, Potassium and enzymes, Glutamate oxaloacetate transaminase (GOT) and Glutamate Pyruvate transaminase (GPT) were the biochemical parameters studied. Standard laboratory procedures were employed for these investigations.
Results showed that there is no changes in the bioch~mical parameters studied, during and after treatment with coded unani drug regimes.
80
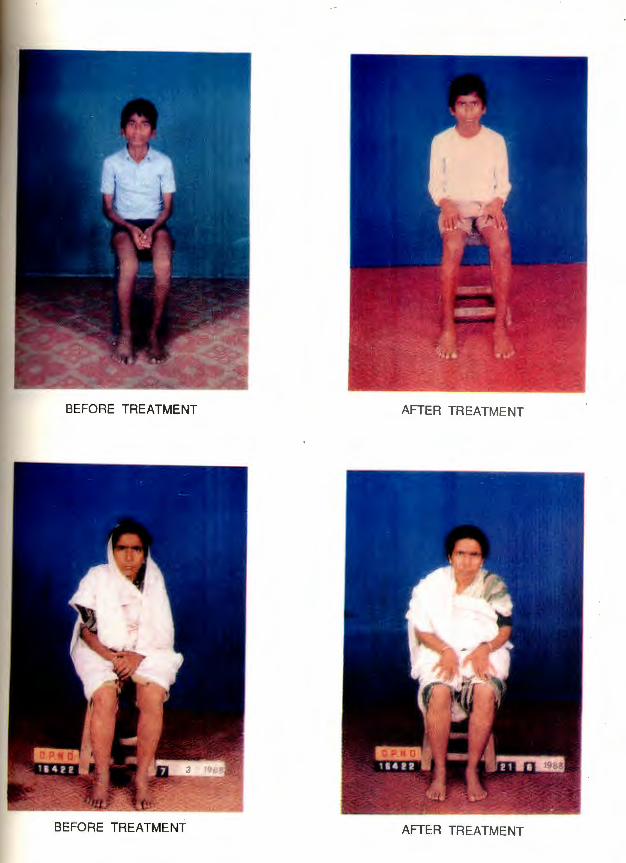
,64 the the
11al
ldy
:Jie
ter
BEFORE TREATMENT AFTER TREATMENT
BEFORE TREATMENT AFTER TREATMENT

BEFORE TREATMENT AFTER TREATMENT
BEFORE TREATMENT

BEFORE TREATMENT AFTER TREATMENT
BEFORE TREATMENT ArTER TREATMENT

The maintenance of normal levels of serum cholesterol and protein, transaminases GOT & GPT suggests that the liver function is not impaired, also there is no hepatocellular damage. In other . words the coded unani drug therapy did not have hepatotoxic side effects.
The maintenance of normal levels of urea, etectrocytes sod ium, potassium revealed that the unani drug therapy did not have any nephrotoxic side effects.
The biochemical studies carried out in these patients treated with various coded unani drug regimes suggested that the drug therapy did not have toxic side effects.
f'atl,olc,qical investigations were undertaken for 266 patients.. being treated with the various Unani regimes. The investigations included complete haemograms (haemoglobin, TC,differential count,
and ESR) urine analysis and motion examination. The samples of peripheral blood were drawn patients and volunteers by venipuncture in EDT A solution. A simultaneous 20 blood smear
made for identifying microfilariae. The same amount was collected per person after 9 p.m. and smears were prepared. These smears were then dehaemoglobinized, dried fixed in acidified
methyl alcohol and stained in JSB 1. Serum samples were stored at -20°C for the quantitative estimation of lgG and C3.
control group consisted of ind ividuals from the laboratory staff and other volunteers of the i.~•lll·mult: who did not have any evidence of filariasis. These served for establishing laboratory
Concentration and filteration techniques were employed for detection of microfilariae especially in cases with low density.
eveluation of the pathological parameters showed that there was mild reduction in E.S.R. in all groups with the exception of the group treated with DEC DF1 DF4 c M in which no change in was observed throughout the treatment. The reduction in E.S.R. observed in other groups was
statistically significant. No significant changes were observed in the Total Leukocyte count and total eosinophil count.
rftA.r~rn•3•haematological parameters such as haemoglobin and P.C. V. were within the normal range all the trials.
Immunological Responses
of the patients showed elevated lgG levels, of these, 60% showed reduction towards the normal and 20% showed maintenance.
was observed in 49% of the patients of these 80% showed reduction, and 16% showed ~aln1ton::>nr•o. The reduction in elevated complement C3 levels was statistically significant.
lnm~tatil'ln & Regression Analysis correlation between complement C3 and filarial oedema was statistically significant, whereas between serum lgG and filarial oedema was not statistically significant.
DF1 DF4 with M lgG and Complement C3, did not show any significant change throughout the treatment.
81
munological Evaluati on of tients of Filariasis
83

Materials and Methods 51 patients of either sex within the age range of 1 0-55 years with unilateral lower
1mb involvement were selected for the study after a careful clinical history and physical examination. The two Unani temperaments observed in these patients were Safravi lnd Balgami. 26 patients were diagnosed as acute and 25 as chronic cases of lariasis. The patients were randomly subdivided into four groups. Three groups comprised of 14 patients e~ch and the fourth group of 9 patients. Each of the four groups of patients received the following coded Unani regimes over a period of 1 05 days.
Group I : DF15, DF16, DF17 DF1, DF4 & M
Group II : DF15, DF16, DF17 , DF1
Group Ill : DEC DF1, DF4 and M
Group IV : Formed part of a double blind study
conducted at the Govt.General Hospital: Madras in which a comparative study was done between Unani drug DEC and Placebo in a dose of 2 B.D for 80 days.
The treatment regime employed consists of .two parts, one part being termed the. -MUNZIJ MUSHIL" and the other part the coded Unani Drug. The Munzij Mushil therapy is a specialized mode of treatment in the Unani System of Medicine directed towards bringing oot coction in an already established deranged humour and then causing · expulsion of this deranged humour through specific purgation thereby increasing the IISPOnsive pc;>tential of the patient to the other coded regime which is started after ~he completiq_n of the M.M.therapy. The change ·from Munzij to Mushil is indicated by the appearance of turbidity called Nuzj in the urine. During this therapy patients are • .:Misea to refrain from phlegmatic diets such as banana, etc.
The control group consisted of 14 individuals from the laboratory staff and other - .. "......... of the Institute who did not have any evidence of filariasis.
Samples of peripheral blood were drawn from patients and volunteers by venipuncture acid citrate solution. A Simultaneous 2QJ.q blood smear was made for identifying
The same amount was collected per. person after 9 p.m. and thick were prepared. These smears ·were then dehaemoglobinized, dried, fixed . in methyl alcohol and stained in JSB-1.
1
Serum samples were stored at - 200C for the quantitative estimation of lgG, C3 and Other investigations included urine analysis for chyluri.a. Haemogram and
biochemical investigations such as liver function tests, total proteins, urea, uric creatinine etc. were undertaken to rule <>Ot the toxicity of the drugs. Motion
were undertaken to rule out helmenthic infestation.
and C 3 were estimated by single radial immuno ~~~~~~~;;;;~t;~ Pvt':'L~d~ ~~\Q ?\a\es and re\erence standards purchased from

Materials and Methods 51 patients of either sex within the age range of 10-55 years with unilateral lower
limb involvement were selected for the study after a careful clinical history and physical examination. The two Unani temperaments observed in these patients were Safravi and Balgami. 26 patients were diagnosed as acute and 25 as chronic cases of filariasis. The patients were randomly subdivided into four groups. Three groups comprised of 14 patients each and the fourth group of 9 patients. Each of the four groups of patients received· the following coded Unani regimes over a period of 1 05 days.
Group I : DF15, DF16, DF17 DF1, DF4 & M . Group II : DF15, DF16, DF17 , DF1
Group Ill : DEC DF1, DF4 and M
Group IV : Formed part of a double blind study
conducted at the Govt.General Hospital·, Madras in which a comparative study was done between Unani drug DEC and Placebo in a dose of 2 B.D for 80 days.
The treatment regime employed consists of two parts, one part being termed the. "MUNZIJ MUSHIL" and the other part the coded Unani Drug. The Munzij Mushil therapy is a specialized mode of treatment in the Unani System of Medicine directed towards bringing oot coction in an already established deranged humour and then causing expulsion of this deranged humour through specific purgation thereby increasing· the responsive P<?tential of the patient to the other coded regime which is started after the completiq_n of the M.M.therapy. The ch~nge from Munzij to Mushil is indicated by the appearance of turbidity called Nuzj in the urine. During this therapy patients are advised to refrain from phlegmatic diets such as banana, etc.
The control group consisted of 14 individuals from the laboratory staff and other of the Institute who did not have any evidence of filariasis.
Samples of peripheral bk>od were drawn from patients and volunteers by venipuncture citrate solution. A simultaneous 20J.J ~ blood smear was made for identifying
!llnfimri!ll:l The same amount was colrected per. person after 9 p.m. and thick were prepared. These smears ·were then dehaemoglobinized, dried, fixed . in methyl alcohol and stained in JSB-1 . 1
samples were stored at - 20"C for the quantitative estimation of lgG, C3 and . Other investigations included urine analysis for chyluri.a. Haemogram and
biochemical investigations such as liver function tests; total proteins, urea, uric creatinine etc. were undertaken to rule -out the toxicity of the drugs. Motion
were undertaken to rule out helmenthic infestation.
and C 3 were estimated by single radial immuno diffusion techniques using SRID plates and reference standards purchased from lmmunodiagnostic Pvt.Ltd.
Delhi. •
85
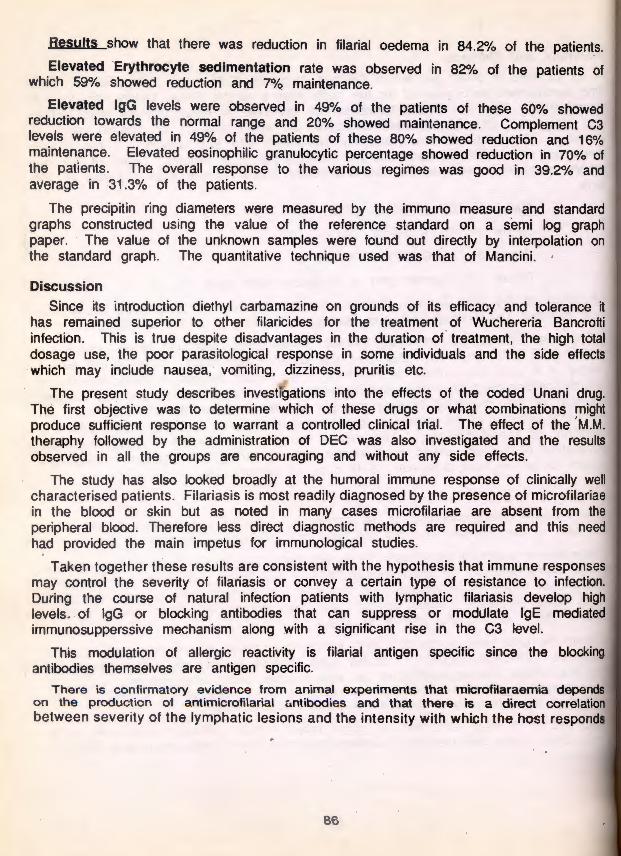
Results show that there was reduction in filarial oedema in 84.2% of the patients.
Elevated ·Erythrocyte sedimentation rate was observed in 82% of the patients of which 59% showed reduction and 7% maintenance.
Elevated lgG levels were observed in 49% of the patients of these 60% showed reduction towards the normal range and 20% showed maintenance. Complement C3 levels were elevated in 49% of the patients of these 80% showed reduction and 16% maintenance. Elevated eosinophilic granulocytic percentage showed reduction in 70% of the patients. The overall response to the various regimes was good in 39.2% and average in 31.3% of the patients.
The precipitin ring diameters were measured by the immuno measure and standard graphs constructed using the value of the reference standard on a semi log graph paper. The value of the unknown samples were found out directly by interpolation on the standard graph. The quantitative technique used was that of Mancini. ·
Discussion
Since its introduction diethyl carbamazine on grounds of its efficacy and tolerance it has remained superior to other filaricides for the treatment of Wuchereria Bancrofti infection. This is true despite disadvantages in the duration o( treatment, the high total dosage use, the poor parasitological response in some individuals and the side effects which may include nausea, vomiting, dizziness, pruritis etc.
The present study describes investigations into the effects of the coded Unani drug. The first objective was to determine which of these drugs or what combinations might produce sufficient response to warrant a controlled clinical trial. The effect of the · ~.tM. theraphy followed by the administration of DEC was also investigated and the results observed in all the groups are encouraging and without any side effects.
The study has also looked broadly at the humoral immune response of clinically well characterised patients. Filariasis is most readily diagnosed by the presence of microfilariae in the blood or skin but as noted in many cases microfilariae are absent from the peripheral blood. Therefore less direct diagnostic methods are required and this need had provided the main impetus for immunological studies.
Taken together these results are consistent with the hypothesis that immune responses may control the severity of filariasis or convey a certain type of resistance to infection. During the course of natural infection patients with lymphatic filariasis develop high levels . . of lgG or blocking antibodies that can suppress or modulate lgE mediated immunosupperssive mechanism along with a significant rise in the C3 level.
This modulation of allergic reactivity is filarial antigen specific since the , antibodies themselves are antigen specific.
There is confirmatory evidence from animal experiments that microfilaraemia depends on the production of antimicrofilarial c:.ntibodies and that there is a direct correlation between severity of the lymphatic lesions and the intensity with which the host responds
86
to tl
T in th depE resp their

to the parasitic antigens.
The Broad spectrum of clinico pathological aberrations observed may reflect variations in the immune response to a large numbers of antigens . The clinical spectrum therefore depends upon the indirect mechanism evolved by the parasite that evade the host response or suppress immunological responsiveness during the course of infection for their survival in long association with the host.
TABLE IV Results of
Day of Ex ami- CJ)
nation - () ;= CJ)
i= <( f-CJ)
Base Line Mean + -
S.D.
After Mean treatment + -
S.D.
lgG and complement C3 Befor~ and after treatment
Statistics Serum lgG (mglml)
Drug Groups
M.M.T + M.M.T+ unani Unani drug drug
with EA
18.4 18.25 + + - -
6.54 9.14
16.6 15.13 + + - -
5.4 6.06
87 I I
M.M.T+ DEC
17:5 + -
6.7
20.01 + -
5.1
Serum c3 (mg/ml)
Drug Groups
M.M.T+ M.M.T M.M.T+ Unani Unani DEC drug drug with
EA
1.4 1.37 1.2 + + + - - -
0.89 0.74 0.7
0.70 1.17 1.31 + + .+ - - -
0.56 0.53 0.83

20
18 -
16
E 14 0, E
CJ 12 ..2>
-~ 10 ;::)
a: w Cl)
8 z <: w ::E 6
4
2
)
Immunoglobulin levels ln-mghnl.
18.54 +
6.54 16.6 +
5.4
BL AT
MM Therapy +.
Unani Drug
18.25 +
9.14 15.13
+
6.06
BL AT ...
PY +
Unani Drug+ Ex. App.,
88
20.01 +
~ 17.5 I
+
6.7
-
BL AT
+ Placebo
py
I
!
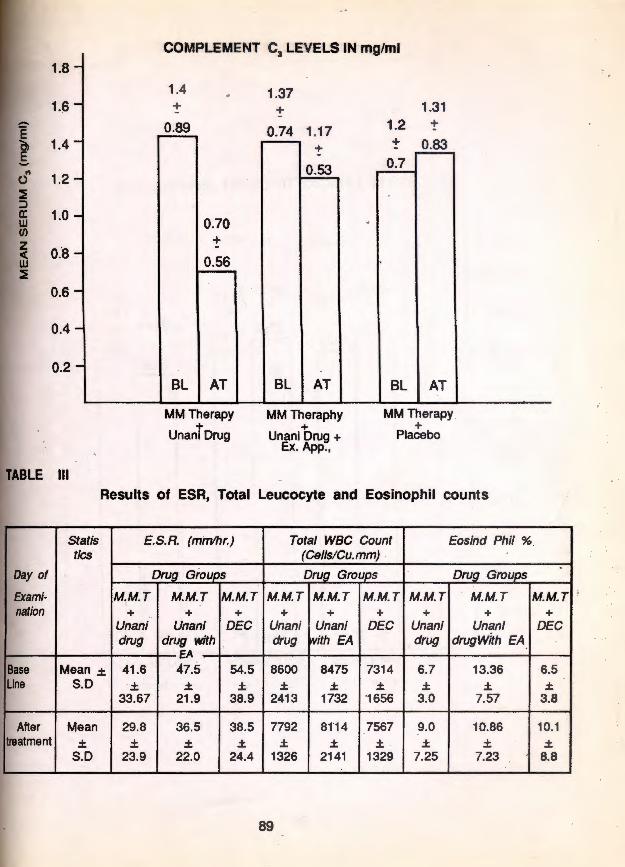
COMPLEMENT C3 LEVELS IN mg/ml
1.8 -. '
1.4 . 1.37 1.~ - + + 1.31
0.89 0.74 1.17 1.2 +
1.4 - + 0.83 +
.. 1.2 0
0.53 0.7 -
~ ::> a: 1.0 w (/)
z 0.8 < w
- 0.70 . +
- 0.56 ~
0.6 -
0.4 -
0.2 -BL AT BL AT BL AT
MM Therapy MM Theraphy MM Therapy . + + +
Unanl Drug Unani Drug+ Placebo Ex. App.,
Ill Results of ESR, Total Leucocyte and Eosinophil counts
Stat is E.S.R. (minlhr.) Total WBC Count Eosind Phil % tics (Cells/Cu.mm) .
Day of
Ex ami- M.M.T M.M.T M.M.T M.M.T M.M.T M.M.T M.M.T M.M.T M.M_T . nation + + + + + + + + +
Unani Unani DEC Unani Unani DEC Unani Unani DEC drug dmg With drug ith EA drug drugWith EA
EA Base Mean .± 41 .6 47.5 54.5 8600 8475 7314 6.7 13.36 6.5 Line S.D .± .± .± .± .± .± .± .± .±
33.67 21.9 38.9 2413 1732 '1656 3.0 7.57 3.8
After Mean 29.8 36.5 38.5 7792 81'14 7567 9.0 10.86 10.1 treatment .± .± .± .± .± .± .± .± .± .±
S.D 23.9 22.0 24.4 1326 2141 1329 7.25 7.23 8.8
89
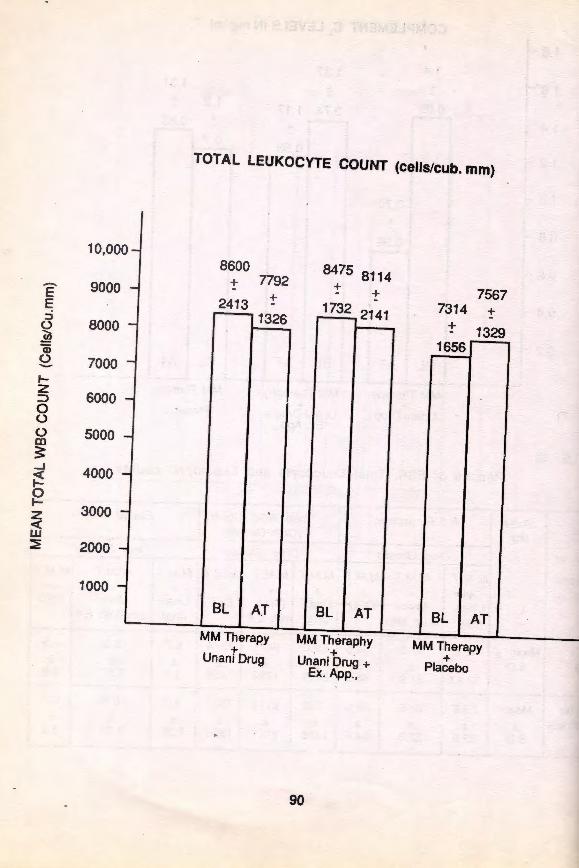
10,000 -
E 9000 -E
-::J 8000 0 ...._
.!!l a; £ 7000 -1-z
6000 ::::> 0 0
-0 5000 m 3:
--J 4000 < b
-1-3000 z
< w ~ 2000 -
1000 -
TOTAL LEUKOCYTE COUNT (cells/cub. mm)
8600 + 7792
2413 +
1326
BL AT
MM Therapy +
Unani Drug
8475 8114 + + -
1732 2141
BL AT
MM Theraphy '+
Unani Drug + Ex. App.,
90
7567 7314 +
+ 1329 1656
BL AT
MM Therapy +
Placebo

16 -
14 -~ 0 _I 12 -i c.. 0 10 z -Ci5 0
8 w -z <( w
6 ::E -
4 -2 -
TOTAL EOSINOPHIL PERCENTAGE
9.0 +
6.7 7.25 +
3.0
BL AT
MM Therapy +
Unani Drug
13.36 +
7.~7 10.86 +
7.23
BL AT
MM Theraphy +
Unani Drug+ Ex. App.,
91
10.1 +
8.8
6.5 +
3.8
BL AT
MM Therapy +
Placebo
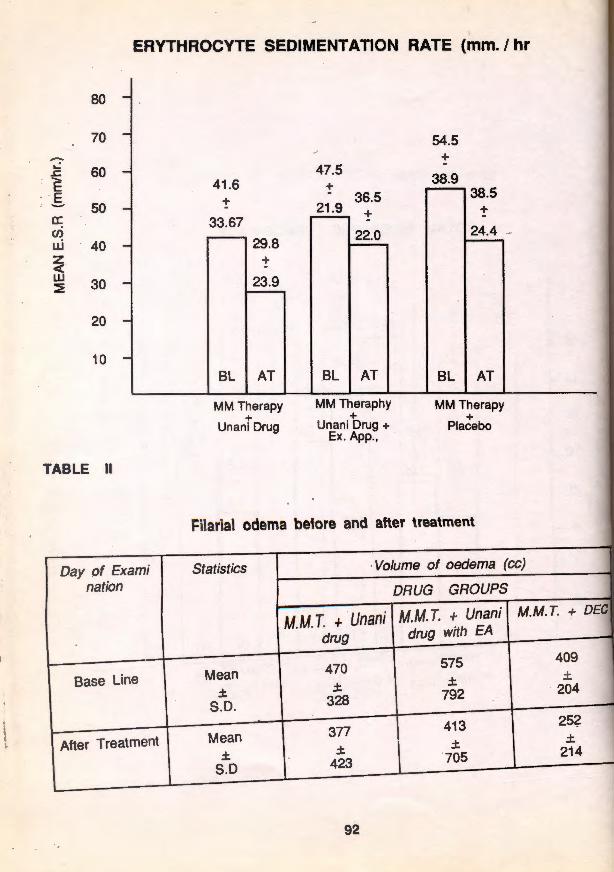
ERYTHROCYTE SEDIMENTATION RATE (mm. I hr
80
70
-...: 60 .s:::. e .s 50 a: (/)
u.i 40 z < w 30 ::E -
20
10
TABLE II
Day of Exami I nation
Base Line I
After Treatment 1
41 .6 + -
33.67 29.8
+
23.9
BL AT
MM Therapy +
Unani Drug
47.5 +
36.5 21 .9 +
22.0
BL AT
MM Theraphy +
Unani Drug+ Ex. App.,
54.5 +
38.9 38.5
+
24.4 -
BL AT
MM Therapy +
Placebo
Filarial odema betore and after treatment
Statistics I ·Volume of oedema (cc)
DRUG GROUPS
M.M. T. + Unani M.M. T. + Unani I M.M. T.
drug drug with EA
470 575
\ 409
Mean I ± ± ± ± 204
S.D. 328 792
377 413 I 252 Mean
\. ± ± ± ± 705 214
S.D 423
92
lf -~ Q w 0
& w ::& ::;)
~ ~ ::&

600 -
550 -
500 -
450 -
4QO -
350 --
300 -
250 -
200 -
150 -
100 -
50 -
FILARIAL OEDEMA (cc.)
470 +
328
377 +
423
BL AT
MM Therapy +
Unani Drug
575 +
792
413 +
705
BL AT
MM Theraphy +
Unani Drug + Ex. App.,
93
.
409 +
204
252 +
214
B.L AT
MM Therapy +
Placebo

Use of homologous/heterologous antigens I antibodies in the
diagnosis of patients of filariasis along with the study of clinical status (Cell-Mediated Immunity).
95 .·

A collaborative study with department of Microbiology, Dr. A.L. Mudaliar Post Graduate Institute of Basic Medical Sciences
Taramani, Madras.
Introduction Bancroftian Filariasis is a major public health problem in India. Around 24 million
people harbour microfilariae in the blood while · 18 million suffer with filarial disease manifestation such as hydrocoele, elephantiasis, etc. lmmunodiagnosis of filariasis is one of the major challenges of to-day. Extensive studies have been made to explore the use of heterologous as well as homologous somatic antigen in immounodiagnosis.
Parasitological diagnosis either by positive blood examination or by biopsy still remains the best means of identifying active or resident infection . Since this is not always possible in asymptomatic non-patent infection, early prepatent infection with or without acute inflammatory signs and in late obstruct ive cases , the present study was undertaken to study the sensit ivity and specificity of heterologous with homologous antigen/antibodies in the serodiagnosis of Bancroftian Filariasis along with the cross reactivity of bancroftian filariasis sera with heterologous antigen/antibodies.
Since studies on the characterization of cell mediated immuneresponse have suggested that patients with patent infection respond poorly or no( at all to both heterologous and homologous filarial antigens, observation on cell mediated immune response (T-cells and Leukocyte Migration Inhibition) were made during this study.
The Study group consisted of 40 filarial cases and 16 controls. The filarial cases were further divided into asymptomatic microfilariae carriers (22) and clinically diagnosed cases of chronic filariasis (MF-ve) (18). The patients of chronic filariasis were treated by the coded Unani drug formulae. The controls comprised of 16 healthy endemic · individuals (MF-ve) ·
Parasitological Investigation: Nocturnal blood smears were examined for the presence of microfilariae. Whenever
the parasite was present the count per 20 mm3 of blood was estimated. The stools of all cases were examined by wet preparation and the formal ether concentration technique for any evidence of intestinal nematode infestation.
Serological Investigations : 5 ml of venous blood were aseptically collected in Heparin and 5 ml in plain tubes
sera were preserved at -20°C in . O.Sml . aliquotes with addition of 0.1% NaNi
: Homologous antigen collection : Concentration of microfilariae from blood of mF + carriers by nucleop re fi lateration
Known mF + ive carrier density 30mF/20c.mm. Blood was
97

¢entrifuged at 2000 rpm for 20 mts. at 37°C. To 1ml of the sediment 10ml of physiological saline was added then incubated at 37°C for 10 mts. The RBCs were lysed completely. It was taken into 20ml syringe and filtered through nucleopore filter of 5A.I porosity. The filter papers were washed with 2ml physiological saline. The washing was collected and centrifuged at 2,500 rpm for 1 Omts. at -4 to 1 ooc. The supernatant was discarded. The sediment was re-suspended in saline stored at -20°C (0.5ml aliquots with addition of 0.1% NaN2).
Heterologous Antigen Collection : Adult worms .of Setaria digjtata were cotlected . from the pentonial fluid of cows. These were washed with the normal saline follwed with 0.05M PB pH 7.2 and stored at -20°C. These were ground and then homogenised for 1 0 min. They were then sonicated for 1 0 minutes/ 9K cyls. They were then centrifuged at 10,000 rpm - 10 min 4°C. The superintend is used as a whole worm antigen. It is used to immunise rabits and in the production of antibodies.
Antibody Production : Rabit Anti MF Antiserum : Purified . mF preparation (3000 mF/ml) was homogenised in a glass homogenizer and
sonicated (10 times for 1.5 mts) at 4°C. It was then centrifuged at 10,000 rpm/10mts. Rabbits were immunized with sonicated mF antigens emulsified in an equal vol.of Freunds complete adjuvant. Three injections were given at 15 days interval initially two doses of 1 ml mF/animal were . given intramuscularly and the final injection (0.1 ml) without adjuvant was given intravenously. Antiserum was treated exclusively first with glutaraldehyde insolubilized normal human AB Serum and subsequently with buffy coat cells from normal 0 group blood to absorb out any contaminating antibodies against these blood components.
Double Diffusion : Double diffusion was carried out in 1% Agarose gel prepared in PBS pH 7.2 - 7.4
to find out the cross reactivity.
Counter lmmuno Electrophoresis was performed using heterologous/homologus antigens/antibodies.
, Leukocyte Migration Inhibition : Peripheral blood leukocyte, migration inhibition test was used for the study of cell
mediatecHmmunity. The CMI test was done according to the procedure of Soborg and as described by Sundaraj .e1 at.. The cone. of the antigen was 50 ·J.l g/ml of the final medium. Migration inhibition of more than 20% was considered to oe positive.
Absolute and % T cell counts was done by rosetting with sheep RBC following the procedure described. by Jondal .e1 at.. At each assessment the absolute number of peripheral blood lymphocytes was determined from the total blood cell count and the differential count.
98

investigations :
Complete Haemograms, urine analysis and Biochemical Investigation· (LFT, Serum ~'""""'g"') etc. These investigations were undertaken to rule out toxicity of the
unani formulae.
and Dosage : Coded Unani regimes (DFI & DF6 and DF4 an external application) were adminstered the patients of chronic filariasis over a period · of 80 days. The patients_ were
to refrain from phlegmatic diets such as bananas etc.
positive) : Using homologous antibodies antigen could be detected Using heterologous antibodies antigen could be detected in 60% of
In chronic cases : (mF negative) : Both heterologous and homologous systems detect antigen equally.
In endemic normal : 6% could be detected by homologous system.
Celt Mediated Immune Response : Reduction of absolute T cell number was observed in patients of chronic filariasis .
subsequent improvement during the treatment. Leukocyte Migration Inhibition was , than 20% and kept increasing throughout the treatment indicating an good immune
Total lymphocyte count : No significant elevations ~f the total lymphocyte count was during the therapy.
Discussion and conclusion An expected homologous system of ag/ab had a higher sensitivity but in the absence
of non-availability of sufficient quantity of antigen heterologous antigen can be used as I gave 60% of antigen detection. It did not give any cross reactivity and specificity was good.
For diagnosis these serological tests clearly show their advantage over the conventional parasitological examination. ·The concentration technique which can detect even low levels of parasitemia can hardly be applied for diagnosis and epidemiological studies ooe to its technical . difficulties.
Host response to parasitic infection is often reflected in . the peripheral blood picture. this has been studied in some non nelminthic infection, there is paucity of data
case of filarial infection,_ After an initial phase of normal vigorous responsiveness to parasite antigen there is lowering of the cell mediated immunity ·. during the chronic
of filariasis.
One of the hypothesis to explain the immuno-pathology of the infected fi larial patient -is that the filarial parasite actively suppresses the host immune system so that the
ite can thrive without interference. Active rosette test detects a population of T involved in active aspects of cellular immunity. It has been observed· that all s with known defects in cellular immunity have decreased active rosetters. Hence ~ -
99

the reduction of T cell number observed in the study possibly reflects a decreased cellular immunity. Further work is indicated to confirm this observation. The production of migration inhibition factor by T cells on incubation with antigen is widely accepted as an in vivocorrelation of cell mediated hyper sensitivity. Migration inhibition assessed in the ·presence of an antigen correlates with the intensity of delayed hypers~nsitivity.
TABLE 1
Detection of Ag/Antibody in sera using homologous Ag* and Ab** by CIE
Sera No. Examined Serum antigen Serum antibody Positivity Positivity
% %
Microfilaraemia 22 19/22(86.36) 17/22 (77.27) (mf + ve)
Chronic 18 8/1 8(44.44) 11/18(61 .11) filariasis (mf-ve)
Endemic Normals 16 1/16(6.25) 3/16 (18.75) (mf-ve)
* Antigen - W bancroftj mf Ag. ** Antibody - Anti W.bancroftj mf.
TABLE 2. Detection of Ag/Antibody In sera of patients using heterologous antigen
* and ant.lbody •• by CIE
Sera No Examined
Microfilaraemia 22 (mf + ve)
Chronic 20 Filariasis (mf-ve)
Endemic Normals 16 (mf-ve)
* Antigen - S.digitata W.W Ag. ** Antibody - Anti .s...d.lgjtata w.w Ab
Berum antigen Positivity
(%)
13/22 (59.09)
10/20(50)
0/16(0)
100
Serum anti-body Positivity
(%)
12122 (54.54)
7/20 (35)
4/16(25)

sed TABLE 3. lion 1ted Comparison of (%) reactivity of sonicated mf Ag/Ab and Setaria ;ed digitata whole worm Ag/Antibodies with different filarial Sera •ity. (using positive predictive value theory)
Sera No. No showing Antigen tve in CIE with : Examined
W.bancrofti % S. digitata W.W.Ag 0/o
. Microfilaraemia 22 19 86.56 13 60 (mf + ve)
Chronic 18 8 44.44 10 55 Filariasis (mf + ve)
Endemic Normals 16 1 6.25 0 0
Sera No. examined No. Showing A ntigen +VEin CIE with
w.bancroffi 0/o S. Digitata %
mf antibodies antibodies
Microfilaraemia 22 17 77.27 12 54.5 (mf + ve)
Chronic 18 11 61.11 7 35 Filariasis (mf-ve)
Endemic Normals 16 . 3 18.75 4 25
101

1800
, 1600
1400 ..... 0 E 1\)
; 1200 (.) .......
~ 1000 -J w (.)
BOO r 600
CMI IN CHRONIC FILARIAL PATIENTS TREATED WITH CODED UNANI DRUGS
ABSOLUTE 'T' CELL COUNT
LEUCOCYTE MIGRATION INHIBITION
\
70 1615.5
60
50
~ 40 -J
'*-889.1 30
30.6 30.6 28.5 27.07
0 20 40 DAYS
80
0
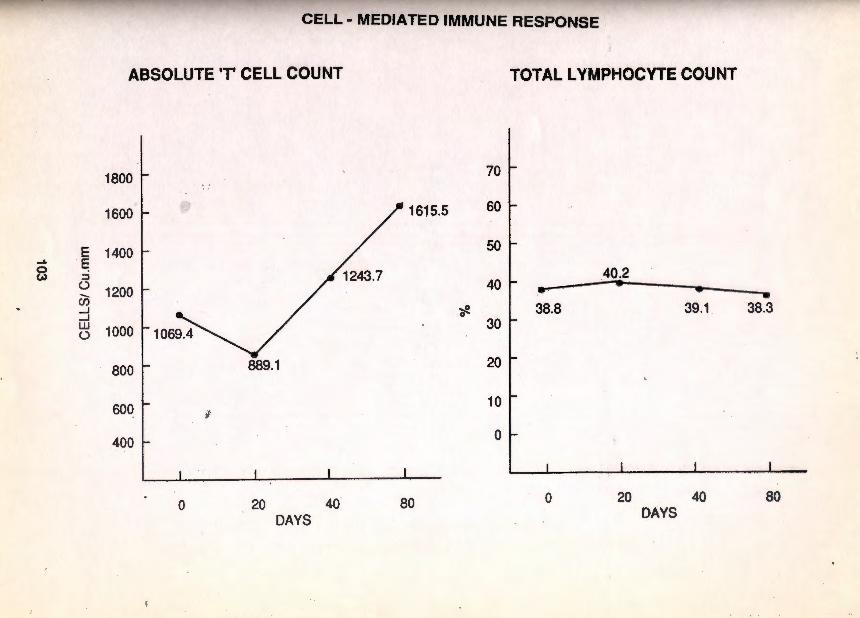
CELL- MEDIATED IMMUNE RESPONSE
ABSOLUTE ·r CELL COUNT TOTAL LYMPHOCYTE COUNT
1800 [ 70
1600 0 /1615.5 60
E 1400 - 50 .... · ~ 0 c.> ::J 1243.7
40 I 40.2 (..) ..._ 1200 .... ... en • _.J
• _.J
~ 38.8 39.1 38.3 LU
0
(..) 1000 30
800 889.1 20
600 l 10
400 I 0
0 20 40 DAYS
80 0 20 40 DAYS
80

Herbal Drugs

1. Unani name
Botanical name
Family
Tamil name
Distribution
Description
Part used
Actions
Uses
107
BISKHOPRA SAFAID
Trianthema decandra Linn.
Aizoaceae •
Chattaranai, Vellai Charuvelai
South Maharashtra, Decqnn, Camatic, on dry soil . lands : a common weed on roadsides.
Prostrate herbs with woody roots, leaves ellegtic-oblong, flowers pink indense umbel like clusters in the axils of leaves, capsule 4-seeded
Root · bark
Root aperient
Roots aperient ; useful in hepatitis, asthma and suppression of menses; ground with milk and given internally, considered specific for orchitis.
Decoction of the root-bark aperient
2. Unani name
Botanical name
Family
Tamil name
Distribution
.Description
Part used
Chemical constituents
Temperament
Actions
Correctives
Uses
108
FULFIL SAFAID
Piper nigrum Linn.
Piperaceae
Milagu
Cultivated in hot and damp parts of common
A stout glabrous climbing shrub; at nodes; leaves small, cordate, g getting larger; flowers greenish-yellow; red, round, on axially spiks.
Fruits, dehusked seeds
Fruits contain piperetine; alkaloids like line, chavicine, piperidine and essential
Hot 3°, Dry 3°
Removes belgham; carminative, aphrodisiac stomachic stimulant
·For hot temperament - Vinegar, fruits and ·for cold temperament -honey
As an aromatic; stimulant in cholera, in weakness following fevers; in dyspepsia, as antiperiodic in malarial fevers, alternative in paraplegia and arthritic diseases; externally as a rubefacient
~

2. Unani name
Botanical name
Family
Tamil name
Distribution
.Description
Part used
Chemical constituents
Temperament
Actions
Correctives
Uses
FULFIL SAFAID
Piper nigrum Linn.
Piperaceae
Milagu
Cult ivated in hot and damp parts of India, commOn
A stout glabrous climbing shrub; .rooting at nodes ; leaves small, cordate, graduafiy getting larger; flowers greenish-yellow; fruits red, round, on axially spiks.
Fruits, dehusked seeds
Fruits contain piperetine; alkaloids like piper line, chavicine, piperidine and essential oils
Hot 3°, Dry 3°
Removes belgham; carminative, aphrodisiac stomachic stimulant
·For hot temperament- Vinegar, fruits and ·for cold temperament -honey
As an aromatic; stimulant in cholera, in weakness following fevers; in dyspepsia, as antiperiodic in malarial fevers, alternative in paraplegia and arthritic diseases; externally as a rubefacient
•
108

nd
in
FILFIL- E- SIYAH (Piper nigrum L.)
BISKHOPRA SAFAID (Triantnema decandra L.)
FILFIL- E- SAFAID (Piper nigrum L.)
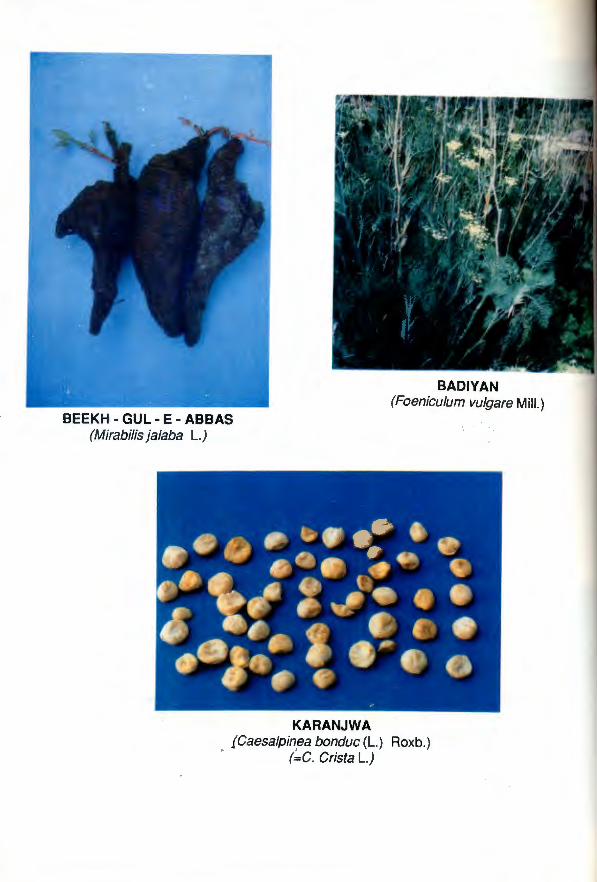
BEEKH- GUL-E- ABBAS (Mirabilis jalaba L.)
BADlY AN (Foeniculum vulgare Mill.)
KARANJWA fCaesalpinea bonduc (L. ) Roxb.)
(~C. Crista L.)
3. Unani name
Botanical name
Family
Tamil name
Distribution
Description
Part used
Chemical constituents
Actions
Uses
109
GUL-E-ABBAS
Mirabilis jalapa Linn.
Nyetaginaceae
Anthi Malligai
Cultivated or spontaneous over the greater part of India; also common in the hotter valleys of N.W.Himalayas
Tuberous herbs with jointed stems; leave ovate, acuminate; flowers red, yellow white or variegated, with a long tube and spreading limb opening in the evening; fruits black
Tuberous roots
Roots contain a small quantity of trigonellin
Roots : purgative; properties similar to Jalap
Roots: aphrodisiac, purgative Leaves: maturant ; lessen inflammation; applied to boils phlegmons, and whitlow
Unani name
Botanical name
Family
Tamil name
Distribution
Description
Part used.
Chemical constituents
Temperament
Actions
Substitutes
Uses
KARANJWA
Caesalpina bonduc (L) Roxb
(== C. Crista L.)
Caesalpinaiceae
Kazhanchikay, Gasakkay
Through the hotter parts of India upto BOOm, in hills; common in Bengal and South India
A large straggling thorny shrub; leaves with 6-8 pinnae; leaflets oblong-elleptic, stipules large pinnately divided; flowers yellow in larg.e racemes; fruit an oblong prickly pod; with one or two round grey seeds
Kernel
Seeds contain bitter sub-stance phytosterinin; bonducin; Saponin, fatty oil 20-40%, starch , sucrose, two phytosterols; bitter amorphous glycoside bonducin in oil
Hot 3° Dry 3°
Anti-inflammatory, Antipyretic, styptic
Barg-e-Karanjwa
Seeds as an external application in skin ~ses. Oil from seeds; useful in cutneous affections, herpes, scabies; used in rheumatism.
110

5. Unani name
Botanical Name
Family
Tamil name
Distribution
Description
Part used
Chemical constituents
Temperament
Actions
Harmful effects
Correctives
Uses
111
BEIKH KARAFS
Apium graveolens Linn.
Apiaceae
Om am
Foot of N.W.Himalayas and outlying hills in the Punjab and U.P.
Biennial herbs with branching stems; radical leaves pinnate; with largely lobed segments, cauline, 3-partite; flowers greenish-yellow, with characteristic smell; mericarps . 2, jointed, small with narrow ridges
Root
Fruits yield 2-3% of a pale yellow volatile oil which consists of d- limonene 60, dsefmene 1 a, seaanonic ac1a an hydride 0-5, and sedanolide 2.5 to 3%
Hot 2<' Dry 2<'
De-obstruant and resolvant, diuretic, emmenagogue alexipharmic
Qn those having hot temperament
Kishneez
Fruits : preventive of rheumatism and gout. Internally as pectoral and as tonic, carmir~ative adjunct to purgatives

6. Unani name
Botanical name
Family
Tamil name
Distribution
Description
Part used
Chemical constituents
Temperament
Actions
Substjtutes
Uses
Wild form
112
BEEKH KANSI
Cichorium· lntybus Linn Asteraceae
Chikkari, Kasini chedi
Wild in Punjab, N.W.Frontier Provinces Hyderabad. Cultivated in Nadiad, and Amabad in Bombay
An erect perennial herb; radical pinnatified leaves toothed; heads terminal or axially spikes, solitary clusters; flowers bright blue, smooth, angled, crowned with a ring pappus scales.
Root; seeds
Roots contain glucosides, cichorin ; substances lactucin, intybin
Seeds cold 2'> Dry 2"
Diuretic; Antipyretic Stomachic, increases bile secretion and p digestion, alternative, bitter
Tukhm-e-Kasoos, Tukhm-e-Kurta
Cultivated plant: used as tonic, in fevers, vomiting diarrhoea; and enlargement of spleen
considered to be tonic, emmenagogue alex it eric

6. Unani name
Botanical name
Family
Tamil name
Distribution
Description
Part used
Chemical constituents
Temperament
Actions
Subs~itutes
Uses
Wild form
112
BEEKH KANSJ
Cichorium· lntybus Linn Asteraceae
Chikkari, Kasif.li chedi
Wild in Punjab, N.W.Frontier Provinces Hyderabad. Cultivated in Nadiad, and Amabad in Bombay
An erect perennial herb; radical pinnatified leaves toothed; heads ligu terminal or axially spikes, solitary or clusters; flowers bright blue, smooth, angled, crowned with a ring pappus scales.
Root; seeds
Roots contain glucosides, cichorin ; substances lactucin, intybin
Seeds cold ~ Dry ~
Diuretic; Antipyretic Stomachic, tonic, increases bile secretion and promotes digestion, alternative, bitter
Tukhm-e-Kasoos, Tukhm-e-Kurfa
Cultivated plant: used as vomiting diarrhoea; and spleen
considered to be tonic, emmenagogue alex it eric

6. Unani name
Botanical name
Family
Tamil name
Distribution
Description
Part used
Chemical constituents
Temperament
Actions
Substjtutes
Uses
Wild form
112
BEEKH KANSI
Cichorium· lntybus Linn
Asteraceae
Chikkari, Kasini chedi
Wild in Punjab, N.W.Frontier Provinces and Hyderabad. Cultivated in Nadiad, Broach and Amabad in Bombay
An erect perennial herb; radical leaves pinnatified leaves toothed; heads ligulate, terminal or axially spikes, solitary or in clusters ; flowers bright blue, achenes smooth, angled, crowned with a ring of pappus scales.
Root; seeds
Roots contain glucosides, cichorin; bitter substances lactucin, intybin
Seeds cold 2" Dry 2"
Diuretic; Antipyretic Stomachic, tonic, increases bile secretion and promotes digestion, alternative, bitter
Tukhm-e-Kasoos, Tukhm-e-Kurfa
Cultivated plant: used as tonic, in fevers, vomiting diarrhoea; and enlargement of spleen
considered to be tonic, emmenagogue alex it eric
Unani name
Botanical name
Family
Tamil name
Distribution
Description
Part used
Chemical constituents
Temperament
Actions
Uses
113
BED ANJEER (ARAND)
Ricinus communis Linn.
Euphorbiaceae
Aamanakku
Cultivated throughout India and naturalised near hill stations
A small tree, leaves palmately lobed ; lobes serrate, acuminate; flowers on long terminal racemes ; · fruits echinate; seeds oblong smooth~ mott led with white spongy portion
Oil
Seeds contain alkaloid ricinine, toxalbumin, ricin. Seeds yield 45-50% of a fixed oil
Hot 2", Dry 2"
Purgative of all akhlats, carminative, emmenagogue
Seeds counter irritant in scorpion sting; fish poison Oil: applied to the head to relieve head ache and poultice for boils
8. Unani Name
Botanical name
Family
Distribution
Description
Part used
Chemical constituents
Actions
Uses
;)
114
AZKHAR
Cymbopogon jwarancusa Schult
Poaceae
Himalayas from Kashmir to Assam, ascending upto 3000m; and in the northwestern plains reaching down to Bombay
A tall grass with aromatic roots; leaves flat upto 60 em long Smm awide, linear, narrow; ending , in a long capillary tip; panicles long, narrow spikelets ; 3-4 pairs pedicelled spikelets rather equal or longer than sessile , narrowly, lanceolate; purplish;lower involucra! glume 7-9 nerved
Roots
Essential 9H, about 1% which contains 90% of d-piperitione, oil from grass grown ·in Sind contains 44% Ketone
Aromatic, tonic, stimulant
Grass used to purify:blood; and in coughs, chro.nic rheumatism, and cholera; aromatic, tonic in dyspepsia ; stimulant and sudorific in gout, fever and rheumatism .
../7"

am, rthbay
ves ~ar,
tip;
9. Unani Name
Botanical name
Family
Tamil name
Distribution
Description
Part used
Chemical constituents
Temperament
Actions
Fruits
Correctives
Uses
115
BADlY AN
Foeniculam vulgare Mill. Apiaceae
Sompu
Extensively cultivated in India
Glabrous herbs; leave~ 3-.4 times compound, having lineatr ultimate segments with strong smell when crushed; flowers small, yellow; . tru.i!s . ct>mpos1ng of 2 meric.arps, straw· yellow
Root
Essential oil
Hot 2" Dry 2"
, Root ·: Purgative
Stimulant, stomachic, carminative
Sandal and Sikanjabean
Carminative, stomachic
' ·

1 o. Unani name Botanical name
Family
Tamil name
Distribution
Description
Part used
Chemical constituents
Temperament
Actions Correctives
Uses
Resin
TURBUD SAFAID Operculinal turpethum Silvamanso
Convolvulaceae
Sivadai, Sivedai
'Throughout India upto 1 OOOm, also occasionally grown in gardens
Perennial herbs with long roots; stems twining; leaves ovate or oblong; cymes few flowered, white; capsules 1.3 mm across, globose, enclosed in enlaroed brittle sepals Stem
Resin similar to Jalap resin, glycoside turpethin
Hot and Dry 3°
Root purgative, phlegmagogue
Frying the hollow pieces of stem in Badam oil
Root: purgative; prescribed in scorpion sting and snake~bite
similar to Jalap resin used in phlegmatary diseases
1 f.s
Ur
Be
Fa
Ta
Dii
De~
Pa: c~ Tel A
Sul
us1

Unani name
Botanical name
Family
Tamil name
Distribution
Description
Part used
Chemical constituents
Temperament
Actions
117
HABBUL NEEL
· Ipomoea nil . {L.) Roth
(=1. hederacea (L) Jacq)
Convolvulaceae
Kakkattan
Throughout India, both cultivated and apparently wild upto 2000m in the Himalayas
A slender climber ; stem covered with black pointing hairs; leaves palmately 3-lobed, ovate, · cordate at base; flowers 1-3 on a peduncle, pink; seeds glabrous, black
Seeds
Seeds contain glycoside and resin
Hot 3°, Dry 3°
Purgative, attenuant; relieving the system of 'Safra' and Balgam
Cathartic
Tukhm-e-Sadab, Beikh~e-Hanzal
Seeds purgative; substitute for Jalap

'•
12. Unani name
Botanical name
Family
Tamil name
Distribution
_ Description
Parts used
Cherl)ical constituents
Temperament
Actions
Harmful effects
Correctives
Substitutes
Uses
KHAYAR SHAMBER
Cassia fistula Linn.
Caesalpiniaceae
Chara Konrai, Konrai
Throughout India; as an ornamental plant in avenues
A medium sized tree; leaflets 8-16, ovate, glabrous; . flowers in long hanging racemes, axiallary. yellow; fruit a cylindrical pod, · 30-60 em long; black; seeds arrangea transversely
Pulp on tne seeds
Pulp contains rhein, the major anthraquinone derivative; small amount of volatile oil , three waxy substances and a resinous substance
Hot 1°, moist 1°
Pulp purgative, tonic, febrifuge
Sometimes causes gripping and diarrhoea
Mastagi, Anisoon and oils
Turbud, Turanjbeen
In liver diseases; intestinal ulceration; externally as a paste to resolve, as gargle, useful in chest diseases of children
118
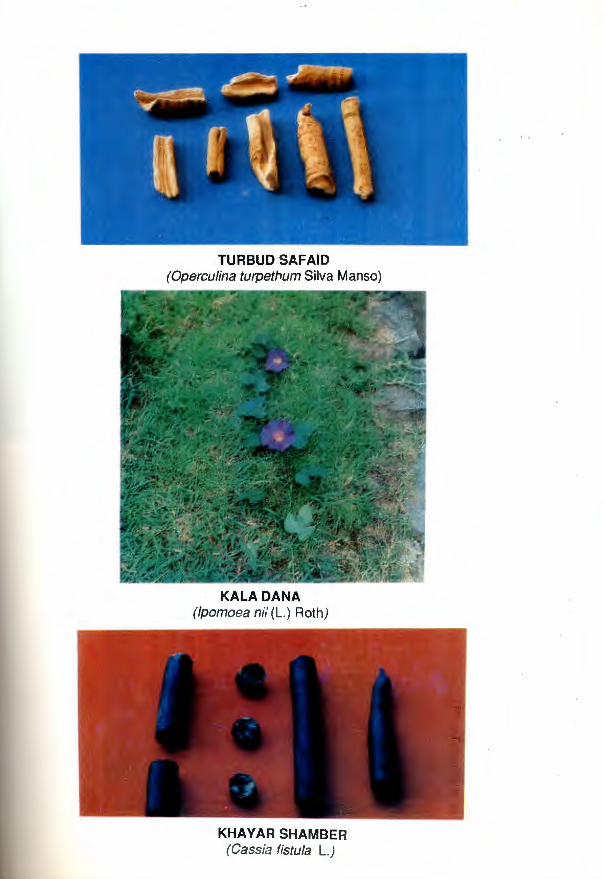
.e, [lg :a I
r of a
TURBUD SAFAID (Operculina turpethum Silva Manso)
KALA DANA (Ipomoea nii (L.) Roth)
KHA Y AR SHAMBER (Cassia fistula L.)

(l spe6tnll ·a =) (II!V\1 &6UO(qO &fUOpA:J)
VNVOIH38
(l S!fEWfO!JJO &8&4l/V) IIIII!IH>t-3-HS31:1
(&uuas · JBA ·1 &uuas &fSS&:J) VNvS
13. Unani name
Botanical name
Family
Tamil name
Dist.ribution
Description
Part used
Chemical constituents
Temperament
Actions
Harmful effects
Correctives
Substitutes
Uses
119
SANA
Cassia senna L. Var senna
(=C. angustifolia Vahl
Caesalpiniaceae
Nila Avakkay
Cultivated in South India in Tirunelveli, Madura and Tiruchi. Recently introduced in Mysore
WOOJJy herbs; leaves with 8-16 leaflets; leaflets eliptic-ovate; flowers yellow on axiallary and terminal racemes; fruits flat, broad curved with 4-6 seeds.
Leaves, pods
Leaves contain, anthraquinone, essential oil, Chrysophanic acid
1 Sorbamnetin and calcium oxalate 12% in leaves.
Two glycosides, sennasoide - A and seenosoid-B, and oxymethyl anthraquinone in fru its
Hot ~. Dry 1°
Purgative, laxative
Produces nausea and uneasiness
Namak-e-Taam, Roghan Badam & Ward
Turbud
Used as purgatives

14. Unani name
Botanical name
Family
Tamil name
Distribution
Description
Part used
Chemical consthuents
Actions
Uses
1.20
ZAITOON
Olea europea Linn.
Oleaceae
Saidun
Baluchistan
A medium sized evergree tree; leaves oblong-lanceolate, cuspidate, dark green, shipping above; flowers white, in axially trichotomous panicles; drupes 5-7mm long ovoid, supported by the . persistent calyx, black when ripe; pulp scanty, endocarp bony
Oil
Fruits contain glycoside oleuropein and fatty oil
Oil demulcent, emollient
As demulcent and emollient
1

15. Unani Name
Botanical name
Family
Tamil name
Distribution
Description
Part used
Chemical constituents
Actions
Uses
121
BEHIDANA
Cydonia oblonga Mill.
(=C.vulgaris Pers)
Rosaceae
Simai madalai
Cultivated in north west Frontier Provinces; Punjab, Kashmir and in the Nilgiris
Large deciduous shrubs ; leaves ovate elleptic,· dark gr~en ; flowers. : Y(hite or pink, solitary axillarv fruits a p6me, pyriform, ribbed, fleshy, aromatip; seeds many mucilaginous
Seeds
Seed kernel contains glycoside amygdalin
Seeds demulcent
Seeds : used in diarrhoea, dysentery sore throat and fever, mucilage as an external application for scalds and ulcers.

16. Unani nam~
Botanical name
Family
Tamil name
Distribution
Description
Part used
Chemical constituents
Temperament
Actions
Harmful effects
Correctives
Substitutes
Uses
122
KHITMJ
Althaea officina/is Linn.
Malvaceae
Simaithuthi
Kashmir and Punjab
A perennial uniformly downy herb upto 90cm; leaves ovate ovoid, simple, slightly lobed, cordate, flowers peduncled in axillary clusters, rosy; ovary many celled; seed solitary in each carpel
Root
Root col')tains mulage 35 and starch 37%
Hot 1°, Dry 1°
Emollient, suppurant. .Laxative
On stomach
Zarishk, Asal and Saunf
Tukjm-e-Khubhazi
Used in cough and asthma; infusion of flowers in bronchial catarrh and bronchitis
Di
D
P.
4 u

upto
of it is
17. Una{li name
Botanical
Family
Distribution
Description
Part used
Actions
Uses
--
123
GAUZABAN
Onosma echioides Linn.
Boraginacease
Kashmir 1600 to 2700 m; also in kumaon and Baluchistan
A biennial patently hispid herb with cauline leaves; leaves oblong; racemes elongate, often forked; corolla yellow; nutlets 5-6mm long, stony, white shining, smooth, often speckled
Leaves
Alterative Leaves alterative in power form given to children as purgative
..
18. Unani name
Botanical name
Family
Tamil name
Distribution
. Description
Parts used
Chemical constituents
Actions
Uses
124
UN NAB Ziziphus jujuba (L) Lam
Rhamnaceae
Elandai
Indigenous and naturalised throughout India and in outer Himalayas upto 1600m
A small thorny tree; leaves ovate elliptic, softly hairy beneath, flowers in small axilliary clusters, yelow; fruits yellow to orange, globose upto 2cm across
Fruits
Fruits contain tannin 1.22%; total phenolics 3.48%; alkaloids 0.25%; gum, mucilage and sugar (free reducing sugar (12.18% total 22.8%) and minerals 2.89%
Fruits : Stomachic, styptic;
Fruits mucilaginous ; styptic; considered to purify blood, and aid digestion

.,
II )
GAUZABAN (Onosma echioides L.)
UN NAB (Ziziphusjujuba (L.) Lam)
KHA RE KHASAK (Tribulus terrestris L.)

19. Unani name
Botanical name
Family
Tamil name
Distribution
Description
Part used
Chemical constituents
Actions
Uses
125
GANDUM
Triticum aestivum Linn.
Poaceae
Gothumai
Widely cultivated in many parts of North India and the Deccan Peninsula, especially in the North West ; and upto 4000m in the Himalayas and Tibet
Tufted annual grasses ; leaves glabrous, or having one or both surfaces hairy; spikes glabrous, hairy aconed; spikelet 3, ovate oblong, swollen, more or less according to the quality with a groove on one face, blunt at both ends or pointed, surrounded by a hairy tuft.
Fruit rind (Husk)
1 Kg grains contains As2 0 2
Seeds cooling, tonic
0.03 mg
Seeds colling, tonic, fattening, increase appetite and relish for food; useful in medicine in general disorders of health

20. Unani name
Temperament
Substitutes
Usses
r
126
BORA ARMANI
Silicate of Alumina, Magnesia and of Iron
A calcerous mineral often made into cakes and stamped with ce impressions. It is usually prepared mixing pipe clay or common chalk oxide of iron and red ochre. It in powder or regular pieces of brown or variegated colours. It is and somewhat heavy. On section ~ granular and sprinkled with white particles, and the cut portion resembles a piece rhubarb.
Hot & Dry 4-4°
Salt - Natroon
Refrigerant, antiseptic. paste~
astringent, It is used

Unani name
Botanical name
Family
Tamil name
Distribution
Description
Part used
Chemical constituents
Temperament
Actions
Correctives
Substitutes
Uses
127 ....
KKARE-KHASAK
Tribulus terrestris Linn.
Zygophyllaceae
Nerinji
Throughout India and upto 3200m in Kashmir
Branching prostrate herbs; leaves compound, leaflets small, oblong, 3-7 pairs; flowers yellow, star shaped; fruits roundish, woody, with. few hard stout spines.
Fruits
Fruit contains traces of an alkaloid a fixed oil, a small quantity of essential oil, resins and nitrates
Hot 1°, Dry 1°
Diuretic, aphrodisiac
Badam, Shireen (Prunusi amygdalus Batsch.
Khar-e-khasak Kalan (Pedelium murex L)
Cooling; used in painful micturition calculus affections; in the form of infusion usefut as a diuretic in gout, kidney diseases and gravel.
~ .

Appendices

Clinical Evaluation of coded Unani Drug in comparl.on with Diethyl C8rbamazine and Placebo in DAUL-FEEL (Filariasis)
C.Sultana, M.Ahmad, D.Gracias and S.Khaleefathullah
Regional Research Institute of Unani Medicine, Madras-600 013.
Abstract
Although Diethyl Carbamazine (DEC) continues . to be drug of choice in filariasis in modern system of medicine, the efficacy is not uniform in all patients and acceptance is limited by severe side reactions, warranting search for new and safe therapies for effective management of this disease.
A large variety of herbal drugs are claimed to be useful in the treatment of filariasis by ancient Unani Physicians but . no clinical data is available to support such claims.
The present trial was, therefore, carried out to cl inically evaluate a coded Unani formulation on patients of either sex, different age groups and chronically varying between 1 yr to 5 yrs . with unilateral lower limb involvement.
A preliminary trial with Unani drug on 111 patients was followed by a double blind trial on 116 cases using Unani drug, DEC and placebo over a period of 80 days. Results suggest that Unani drug is superior to DEC as it relieved more than 70% patients in comparison to 37% by DEC. Similarly 56% and 25% reduction in filarial oedema was caused by Unani drug and DEC respectively . Drop out and relapse rate was also less in patients treated with Unani drug.
Significant reduction in elevated ESR and total eosinophil count was observed with both the drugs and chronicity had negative effect on response to treatment Results will be discussed in detail.
• Research Officer (Unani) •• Research Officer (Unani) - Presenting Author
••• Research Officer (Pathology)
**** Hony. Project Officer
131
A study of the Antigen/Antibodies of Bancroftian Filarisis by the use of Heterologous Antigen/Antibodies (Setaria digitata) with Reference to the clinical
status
D.Gracias *N.Mallikarjun ** T.Sundarajan *** and S.Khaleefathullah****
A collaborative STUDY with Dept. of Mi~robiology Dr.ALM. P.G.I.B.M.S. Taramani Madras
Abstract Non"availability of sufficient antigens from Wuchereria Bancrofti Microfilarias has led
to the present study in which an attempt has been made to diagnose patients of chronic filariasis by the use of heterologous antigen/antibody in the detection of antigen/ antibody of Wuchereria Bancrofti. The specificity and sensitivity of results were compared with the same prepared from homologous W. Bancrofti filarial antigen.
Counter-lmmuno Electrophoresis was performed. Filarial antibodies were detected in 12 of 22 mF positive carriers, 7 of 20 chronic filarial patients and 4 of 16 endemic normal sera by the use of hetrologous ag/ab.
Counter lmmuno Electrophoresis with homologous ag/ab detected filarial antibodies in 17 of 21 mF positive carriers, 11 of 18 chronic filarial patients and 3 of 16 endemic sera. The heterolocous antigen appears to be ~ensitive and specific and has practical diagnostic value for Wuchereria Bancrofti. Observation on the immune status (cell mediated immunity) of patients being treated with coded unani formulae was made during the study.
* Research Officer (Path.) RRIUM, Madras
** Research Scholar, Dept. of Microbilogy, Dr.A.L.M. PGIBMS
••• Reader in Microbiology, Dept. of Microbiology, Dr. A.L.M., PGIBMS
Hony.Project Officer, RRIUM, Madras ****
132

Evaluation · of the Immunopathological Response in patients of Filarisis being Treated with various coded Unani Regimes
Doreen Gracious, Abdul Kareem, Giyasuudin Ahmed, Gowher Sultana and Syed Khaleefathullah
Regional Research Institute of Unanl Medicine, Madras-13.
Abstract
The present study was conducted over a period of 2 years (1985-1987) on 51 filarial patients with unilateral lower limb involvement. Th~ chronicity of the disease varied from 3 months - 3 years. All patients were clinically assessed at the time of admission and subsequently at regular intervals over a period of 80-150 days. Measurement of filarial oedema was done by water displacement' method. Complement C3 and lmmunoalobulin lgG were quantitatively estimated by single radical immunodiffusion technique of ~ Mancini
Results show that there was reduction in filarial oedema in 84.~/o of the patients. Elevated erythrocyte sedi,entation rate was observed in 8~/o of the patients of which 59% showed reduction and 7% marntenance. Elevated lgG levels were observed in 49% of patients of these 60% showed reduction towards the normal range and20% showed maintenance. Similarly complement C3 levels were elevated in 49% of .. the patients, of these 80% showed reduction and 16% maintenance. Elevated eosinophilic granulocytic percentage showed reduction in 70% of the patients. The overall response to the various regimes was good in 39..2% and average in 31 .3% of the patients.
* Research Officer (Pathology)
** Research Officer (Bio-chemistry)
*** Research Officer (Unani)
**** Hony. Project Officer
133

Clinical Evaluation of coded Unani Drugs DF1 DF4 c M In co"'parison with DF6 DF4 CM along with MM therapy in cases of' J;;aul Feel (Filaliasisl
Giyasuddin Ahmed Syed,, Jameeluddin Ahmed, Abdul Kareem•••
Doreeh Gracias, P.Ameer Basha and Syed Khaleefathullah
Abstract DrrriTfg the period of four y.ears patients with clinical diagnosis of "Daul Feel" (Filariasis)
was conducted on 81 cases with unilateral lower 4imb .involvement. The chronicity of the disease varies from 3 months to 5 years. All cases were cfinicaHy assessed at the time of admission and at regular followups, over a period of 108 days. Measurement of filarial oedema was done by water displacement method.
The present study show that there was definite clinical relief and reduction in filarial · oedema. The detail study will be discussed in the full paper.
* Research Officer (Unani)
**
***
****
*****
Research Assistant (Unani)
Research Officer (Bio-Chemistry)
Research Officer (Pathology)
Investigator
****** Hony.Project Officer, RRIUM, Madras
134

A co:laborative study on Daul Feel (Filariasis) A clinical Study
Hakim Gowher Sultana* Hakim ·syed Khaleefathullah.
Abstract
Collaborative studies with Government General Hospital, Madras in the tre~tment of Daul Feel (Filariasis) cases with Unani drug, Allopathic drug ·and placebo were under taken.
In this paper results of treatment of 30 cases in all, ten cases in each group, the course of treatment lasting for 80 days and fo llow-up for one year are presented . .
Especially as there is no treatment for Daul Feel in Modern medicine, results of treatment with Unani Medicine, without side effects as compared to allopathic drug DEC and Placebo are encouraging.
It is a matter of interest, to note that the resuhs of placebo group also compare little favourably.
This study reveals that the patients having Balgami Mizaj (Barid Ratab) are more susceptible for disease.
* Research Officer (Unani) R.R .I.U.M, Madras
** Hony.Project Officer, R.R .I.U.M. , Madras
135
Biochemical Evaluation of Daul Feel {Filari.asis) patients treated with various coded Unani Regimes.
M. Abdul kareem• Dordeen Gracias•• Gtyasuddin Ahmed*** and Syed Khaleefathullah****
Abstract
The present study was conducted to observe the changes in Biochemical parameten in Daul Feel (Filariasis) patients treated with various coded Unani Drugs. The studl was carried out on 94 filarial patients of either sex, with chronicity varying between ~ months - 4 years with unilateral lower limb involvement. Biochemical investigation! were carried out at the time of admission and ·at subsequent follow-ups.
Results showed that there was no changes in the Biochemical parameters durinQi after drug therapy. Elevated Erthrocyte sedimentation rate was observed in 81.9% 01
the patients of which 62.3% showed reduction. Significant reduction in Filarial OedemE was also observed.
* Research Officer (Bio-chemistry)
•• Research Officer (Pathology)
*** Research Officer (Unani)
**** Hony.Project Officer
136

Biochemical Evaluation of Daul Feel . {Filariasis) patie.nts treated with various coded Unani Regimes.
M. Abdul kareem• Dordeen Gracias•• Giyasuddln Ahmed*** and Syed Khaleefathullah****
Abstract
The present study was conducted to observe the changes in Biochemical parameters in Daul Feel (Filariasis) patients treated with various coded Unani Drugs. The study was carried out on 94 filarial patients of either sex, with chronicity varying between 3 months - 4 years with unilateral lower limb involvement. Biochemical investigations were carried out at the time of admission and ·at subsequent follow-ups.
Results showed that there was no changes in the Biochemical parameters during/ after drug therapy. Elevated Erthrocyte sedimentation rate was observed in 81.9% of the patients of which 62.3% showed reduction. Significant reduction in Filarial Oedema was also observed.
• Research Officer (Bio-chemistry)
•• Research Officer (Pathology)
*** Re.search Officer (Unani)
**** Hony. Project Officer
136

Plants vsed in Daul Feel (Filariasis) and its distribution in South India
S R.Nayar" and Syed Khaleefathullah**
Abstract
In· Unani system of Medicine, plants and their products are used to prepare a number of pharmaceutical preparations. Research findings of the council in Daul Feel (Filariasis) proves that, this disease can be treated withqut much side effects using plant drugs singly or in combination. Preparation of standard pharmaceutical products mainly depends in unadulterated crude drugs the present communication envisages the distributional pattern of some Unani Medicinal plants of Sounth India used in Daul Feel (Filariasis). Efforts are also made to analyse these drugs Uantitatively.
* Assistant Research Officer, (Botany)
** Hony. Project Offic~r. RRIUM, Madras
137
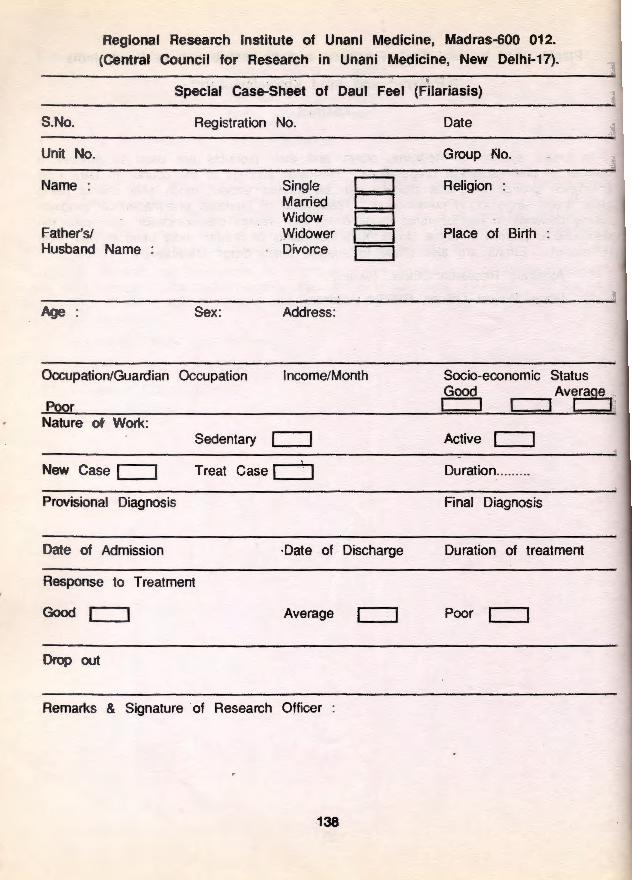
Regional Research Institute of Unani Medicine, Madras-600 012. (Central Council for Research in Unani Medicine, New Delhi-17).
Special Case-Sheet of Daul Feel (Filariasis)
S.No.
Unit No.
Name
Father's! Husband Name
Age
Registration No.
Single c:J Married c:J Widow c:J Widower CJ Divorce c:J
Sex: Address:
Occupation/Guardian Occupation Income/Month
Poor Nature of Work:
Sedentary c:::::J
New Case c:J Treat Case c:::::J Provisional Diagnosis
Date of Admission ·Date of Discharge
Response to Treatment
Good c=J Average c=J
Drop out
Remarks & Signature of Research Officer
138
Date
Group f\Jo.
Religion
Place of Birth
Socio-economic Status Good Avrage
1 c:::J c:::J
Active c:J
Duration ..... ... .
Final Diagnosis
Duration of treatment
Poor c=J

Khas Shikayat (Presenting Complaints)
Rudad-e-Merz Mojuda (History of Present Illness)
History of fever attacks :
History of lymphadenopathy
History of ~yrnphangitis :
Mojuda Shikayat (presenting complaints)
Fever : Present CJ With Rigor c:J
lymphadenopathy Present If Present, Give details
lymphangitis : Present If present, give details
Oedema : Present
Other · ·complaints
Headache CJ Nausea CJ Vomiting
Rashes CJ Funiculitis CJ Epididymitis
Orchitis CJ Hydrocele CJ Vulvae
Chylurea CJ Varicose Veins CJ Ascites
Skin Conditions: Soft skin [:=J · Thick skin
Hyperkeratosis [:=J Warts
Affect~ Body Parts
Upper Extremities
lower Extremities
Other Parts :
Coarsening
Nodules
Right Arm c:J Right Leg c:J
139
Absent CJ Without Rigor CJ
Absent
Absent
Absent
CJ c:J CJ CJ
Urticarial c:J
Corrugation
Fissure
Left Arm c::J Left Leg c::J

Date of Onset :
Age_ at onset : Youngc:J _Adult CJ Mode of Onset :
Stage of disease at time of Registration :
Acute c=J Sub-acute c=J History _ of Past Illness
Malaria c:::J Gonorrhoea c=J Others
Tuberclosis c=J
History of Previous
Unani c:::J Siddha c:::J
treatment of Present complaint :
Ayurveda c=J Allopathy c:::J Homoeopathy c=J Others :' c=J
Response
Habits:
Diet : Vegetarian c=J Non-Vegetarian c::::J
Alcohol : Occasional [:::J Moderate CJ Tobacco Chewwing : Occasional c=J Moderate c:J Smoking : . Occasional c:J Moderate c=J Others
Patient Mizaj (Temperament)
According to Qualitative State (Kaifiyat)
According to Quantitative . State (Kumiyat)
General Physical Examination
Physique : Good c=J Average c::::J Poorc::::J
Poorc::::J Nutrition : Good c:J Aver~ge c::=J Tongue
Gums
Teeth
140
Oldc:J
Chronic [::J
Syphilis c:::J
Heavy c:::J Heavy C==:J Heavy C==:J

Systematic Examination :·
Eyes
E.N .T.
Dermatology
Cardiovascular system :
Central Nervous System
Respiratory System
Digestive System
Urino-genital System
Lymph Nodes
Condition of Peripheral arteries
Features
Good CJ Regular c:::::J Sound c:::::J
141
Average CJ
Irregular c:::J
Disturbed c::J
Poor c:::::J
Insomnia

Systematic Examination :·
Eyes
E.N.T.
Dermatology
Cardiovascular system :
Central Nervous System
Respiratory System
Digestive System
Urino-genital System
Lymph Nodes
Condition of Peripheral arteries
Other Features
Appetite
Bowels:
Sleep:
Good c::J Regular c:::J Sound c:J
141
Average c::J Irregular c:J Disturbed c:::J
Poor c:::J
Insomnia

Micturition
If Abnormal, clarify
Menstruation
Height
Date
Pulse
Temperature
Blood Pressure
Weight
Treatment
Principal Medicine
Dose
Timings
Supportive Medicine
Other Medicines
Diet
Normal [:=::J Abnormal [:=::J
Regular c=J With pain [:=::J
Weight ·:
142
Irregular c=J Without pain c=J
Ideal Weight c=J
Under Weightc=J
Over Weight c=J
Complete Blood Picture
Haemoglobin
Total W.B.C.
· Differential Count
Polyrnorphs
Eosinophils
Basophils
Smear for microfilaria
Peripheral Smear
E.S.R. 1/2 Hr.
Urine Examination
Laboratory Test ~ppearance
Reaction
Sugar
Deposits Epithelial Cells ·
Bacteria
A.B. C.
Stool Examination
Laboratory Test :
Ova
Laboratory Investigations
: ..... ..... ... .... ..... .......... gmo/o R.B.C. ................ ... ......... .. .......... /em
. ...... ............... ... .. ......... /em.
.... ... .. ... ............. ..... .. .. ... ... o/o Lymphocytes ..... .. ........................... %
••• . ••• •.• • . ••. • • • • •• • .. •. ......• • . . . ••• 0/o Monocytes .............. ........................ 0k
•• • • •• ••• •• ••• •••• •• ••• •• • • ••••••••• • • • • 0/o
Day Night :
1 Hr.
(Nazari Muaina (naked eye Examination)
Quantity
Albumin ........................ ................... .
Phosphates .................. ................... .
Pus cells ............................ .. .. ........ .
Casts .... ................................... .. .... .
Crystals ........................................... .
(Nazari Muaina)
Cyst
143
I

References
1. Sengupta G, T.M.Mohapatra and P.C. Sen, 1986 lmmunodiagnosis of Filariasis Jr. Trop.Med. and Hygiene 89, 313-317
2. Kaliraj P. and B.C.Harinath. 1982 Fractionation and Evaluation of W.Bancrofti microfilarial antigens in immunodiagnosis of Bancroftian Filariasis /.J. of Expt. Biology 20: 440-444
3. Dhanvantari Y. Naidu M.V.V.L Narasimhan, Ch.Krishna Rao Hemanth Kumar and C.K.Rao Relative efficacy of W.Bancrofti microfilarial and infective larval antigens in the detection. of filarial antiboides.
4. Reddy M.V. et al 1986 Isolation and evaluatipn of antigens from microfilaraemia plasma and immunocomplexes for diagnosis of Bancroftian Filarriasis I.J.P.M. 29: 179 -183
5. Robert, S. Desowitz and Steven, R . . Uma .1970, Detection of antibodies in human and ·animal Filariasis by counter immunoelectrophoresis with DiroJilarae immities antigens. J.of Helminthology 50: 53-57
6. Otlesen, A. et a/ 1987, Immunological aspects - Immunoglobulin complement and specific antifilarial lgg, lgM, lgE antibodies Am. J. Trop.Med. and Hyg. 34: 953-961
7. Ambrose-Thomas, P, 1974 Immunological diagnosis of human filariasis, prese~ possibilities and limitations (A Review) Acta Tropica, 31, 108
8. S.Dissanayake and M.M.Ismail 1980, Antigens of Setaria Digitata: Cross reaction with surface antigens of Wuchereria Bancrofti microfilariae and serum antibodies of W.bancrofti infected subjects Bulletin of World Health Organization 58(4) : 649
9. Ogilvie B.M. and Worm M.J. 1976, Immunity to nematode parasites of man with .special reference to Ascaris, hook worm and filariae. Immunology of parasitic disease S.Cohen and E.M.Sandun Eds (Blackwell London) p.397
10. Kagan I.G.: 1963, A review of immunologic methods for the diagnosis of filariasis. J.Parasitol 49, 773
11 . Chugh K.S, Singhol P.C, Tewari S.C et a/ 1978 Am.Jr.of Trop. Med. and Hyg. 27 : 630 - 631
12. Denham D.A, MC Gruvy PB 1977 Advances in Parasitology 15: 243 - 309
13. Denham D.A, Roger R 1975 Trans. of the Roy. Soc. Trop Med. & Hyg. 69 173 - 176
14. Dissanik As , Quah CH, Thien SM 1974 Am. Jr. of Trop. Med. and Hyg. 23 1023-1206
149

15. Dunn FL 1979 Bulletin of the World Health Organisation 57: 499 - 512
16. Narashimhan MVVL, Roychowdhury SP, et al 1979, Jr. of Comm. Dis. 13: 204-206
17. Shibuya T, Cabrera BD, Tanaka H et a/ 1980 Jap. Jr. of Exp.Med. 59: 463-468
18. WHOffDR 1979 A Report of the fourth meeting of the scientific Working Group on Filariasis: Progress in the immunology of filariasis TDR/Fii-SWG (4) 79.3.
19. Wijen D JB 1977 Annals of Trop. Med. and Parasitol. 71: 451-463
20. Manson Bahr and Apted 1982, Mansons' tropical disease 18th Ed. London, ELBS 148-180
21. Ottensen E.A. 1977, Specific Cellular irresponsiveness in human filariasis. Immunology 33 & 13
22. Jondal M.Holm G. and Wigzell H 1972, Surface marker of human T and B lymphocytes. A large population of lymphocytes forming non-immune rosetters with sheep red blood cells J.Exp.Med 136 (1972) 207
23. Urbantak S.J . White A.G.Barclay, G.R. Wood S.M. and Kay A.B. 1978, Test of immune function . In : Handbook of experimental immunology Vol.3 D.M. Weir Ed (Blackwell London) p.47
24. Malviya A.N.Kumar, R.Bhuyan, L.N. and Mohapatra, L.N .Rosette 1974, forming lymphocytes. A modified technique for better stability and reproductivity . Di-stribution in lymphoid tissue of rhesus monkey. lnd.J.Med.Res. 72 640.
150

AL Qanoon Fl TIB volume Ill page 487
Locknao 1906
Ghanni Manni - Abul Hasan Maasur
AL Oatari
Lackhno Page 287-288
Zakhira Khauazam Shahi
Volume Vlth Page 553-652
Chopra, R.N. Nayar, S.L. and Chopra I.C., 1956 Glossary of Indian Medicinal Plants CSIR, New Delhi pp.330
Mathew, K.M. 1983 The Flora of Tamil Nadu Carnatic, vol 1-11, Rapinet Herbarium, Tiruchi, pp 2154
Anonymous 1983
National Formulary of Unani Medicine (ed 1 ), Min. Health & Family Welfare, New Delhi.
151