








Bahasa
Halaman
Hukum

NS Neurosurgery
Stewart Lo, Matt Stacey and Sara Temple, chapter editors Kathryn Howe and Kim Tsoi, associate editors Mark Pahuta, EBM editor Dr. Abhaya Kulkarni and Dr. Taufik Valiante, staff editors
Basic Anatomy Review 2
Differential Diagnoses of Common Presentions 4
INTRACRANIAL PATHOLOGY
Intracranial Pressure (ICP) Dynamics ...4 ICPNolume Relationship ICP Measurement Cerebral Blood Flow (CBF) Elevated ICP
Herniation Syndromes 6 Subfalcine Central Tentorial Lateral Tentorial Upward Tonsillar Treatment of Herniation Syndromes
Hydrocephalus 7
Benign Intracranial Hypertension 8 (Pseudotumour Cerebri)
Tumour 9 Metastatic Astrocytoma Meningioma Vestibular Schwannoma ("Acoustic Neuroma") Pituitary Adenoma
Pus 12 Cerebral Abscess
Blood 13 Extradural ("Epidural") Hematoma Subdural Hematoma
Cerebrovascular Disease 15 Subarachnoid Hemorrhage (SAH)� Intracerebral Hemorrhage (ICH)� Intracranial Aneurysms� Carotid Stenosis�
Vascular Malformations 20 Arteriovenous Malformations (AVMs) Cavernous Malformations
EXTRACRANIAL PATHOLOGY
Dermatomes/Myotomes 21
Approach to LimblBack Pain Extradural Lesion Intradural Intramedullary Lesion
22
Spinal Cord Syndromes Brown-Sequard Syndrome Anterior Cord Syndrome Central Cord Syndrome Posterior Cord Syndrome
24
Root Compression Cervical Disc Syndrome Lumbar Disc Syndrome Cauda Equina Syndrome Lumbar Spinal Stenosis Neurogenic Claudication
25
Peripheral Nerves Peripheral Nerve Injury Nerve Entrapment
27
SPECIALTY TOPICS
Neurotrauma Trauma Assessment Head Injury Brain Injury Late Complications of Head/Brain Injury Spine Injury Neurologically Determined Death
29
Pediatric Neurosurgery Spinal Dysraphism Intraventricular Hemorrhage Hydrocephalus in Pediatrics Dandy-Walker Malformation Chiari Malformations Craniosynostosis Pediatric BrainTumours
33
Functional Neurosurgery 36
Common Medications 36
Summary Key Questions 37
References 38
Toronto Notes 2008 Neurosurgery N51
Dr.JKR
NS2 Neurosurgery Basic Anatomy Review Toronto Notes 2008
See Functional Neuroanatomy software Basic Anatomy Review
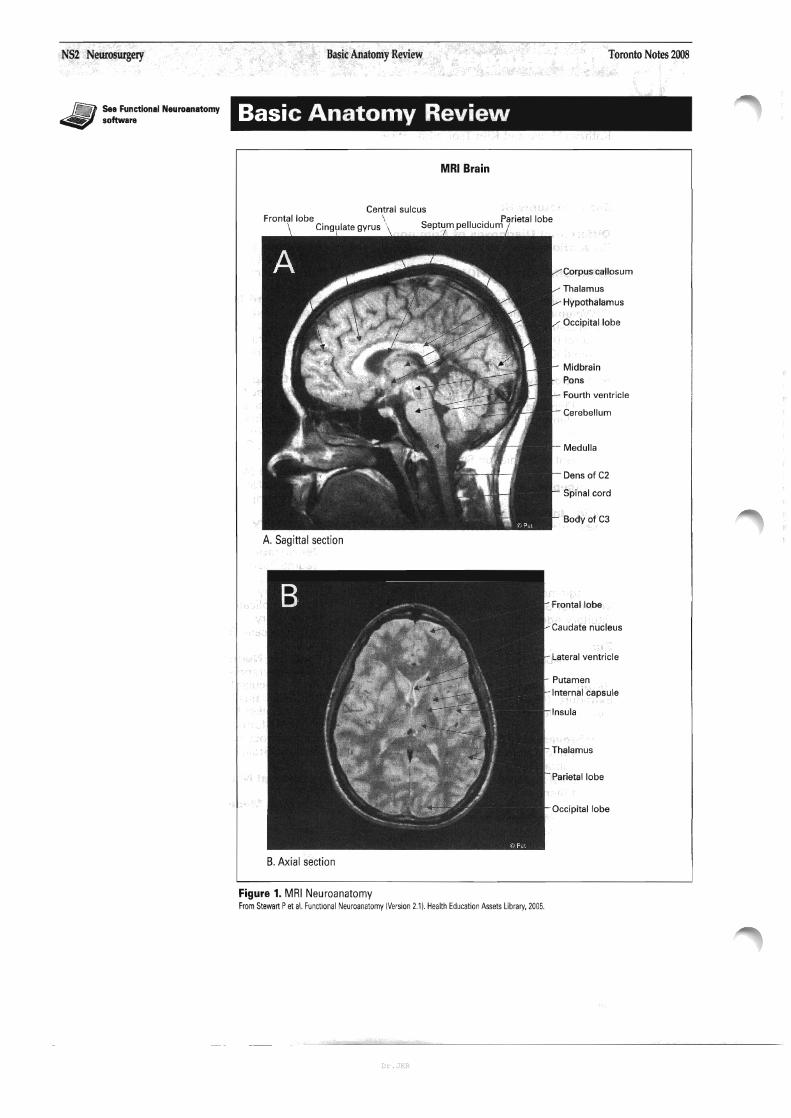
MRI Brain
Central sulcus� Frontal lobe \ . Parietal lobe�
Cingulate gyrus ' Septum pellucldum
Corpus callosum
Thalamus
Hypothalamus
Occipital lobe
Midbrain Pons
Fourth ventricle
Cerebellum
Medulla
Dens of C2
Spinal cord
Body of C3
A. Sagittal section
Frontal lobe
Caudate nucleus
Lateral ventricle
Putamen Internal capsule
Insula
Thalamus
Parietal lobe
Occipital lobe
B. Axial section
Figure 1. MRI Neuroanatomy� From Stewart Pet al. Functional Neuroanatomy (Version 2.1). Health Education Assets Library, 2005.�
Dr.JKR
Toronto Notes 2008� Basic Anatomy Review Neurosurgery NS3
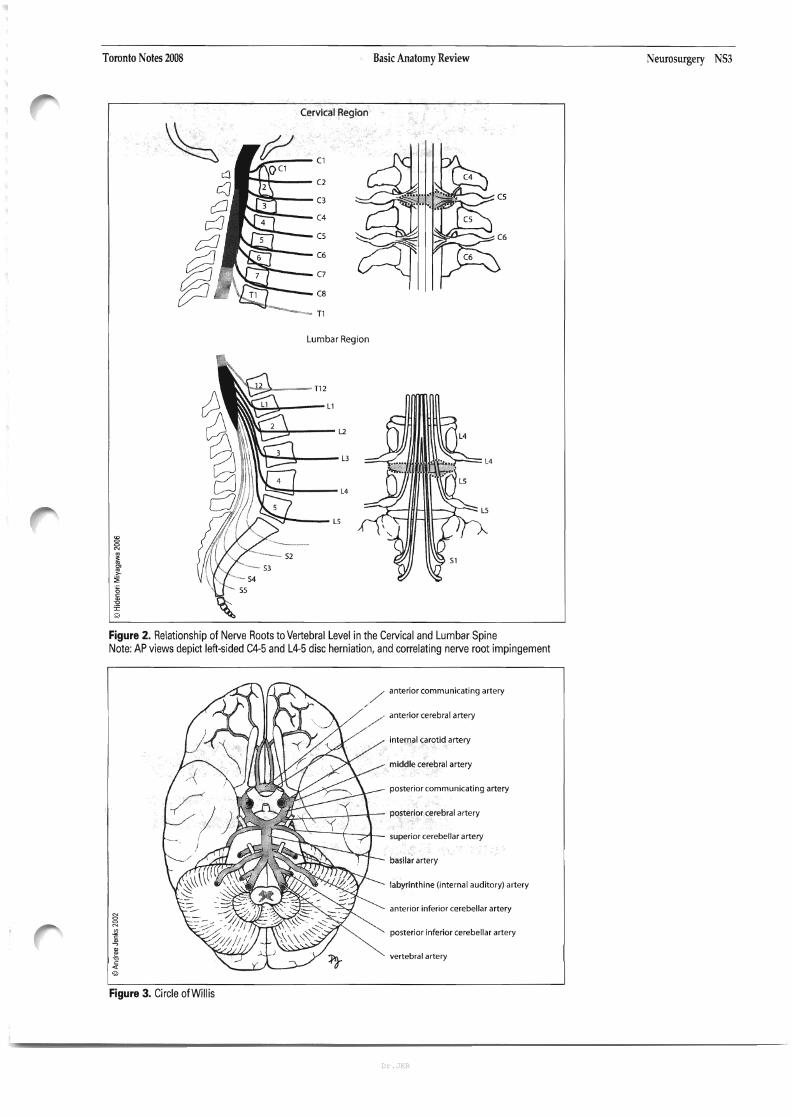
Cervical Region
~ (1
c:J c:]
(2
CJ C3
8 d (4�
(5�
(6�
C7�
(8�
T1�
fJB Lumbar Region
~~"""--L2
1\\\1~\"""':'~~-- L3
~",,==:=j----- L4
Figure 2. Relationship of Nerve Roots to Vertebral Level in the Cervical and Lumbar Spine Note: AP views depict left-sided C4-5 and L4-5 disc herniation, and correlating nerve root impingement
/ anterior communicating artery
/
.� anterior cerebral artery
internal carotid artery
middle cerebral artery
posterior communicating artery
L~~i-\~::/-l--;-- posterior cerebral artery
L~~-'.--...!....+-......l_ superior cerebellar artery
basilar artery
labyrinthine (internal auditory) artery
anterior inferior cerebellar artery
posterior inferior cerebellar artery
vertebral artery
Figure 3. Circle of Willis
Dr.JKR
NS4 Neurosurgery Differential Diagnoses of Common Presentionsflntracranial Pressure Dynamics Toronto Notes 2008
.....' ,.)-------------,
Primary eNS lymphoma reported ill 6-20% of IHIV-infectedl patients.
..... ' ,.\------------, Monro-Kellie hypothesis
Vbrain +Vblood +VCSF +Vles;on =� Vskull =constant�
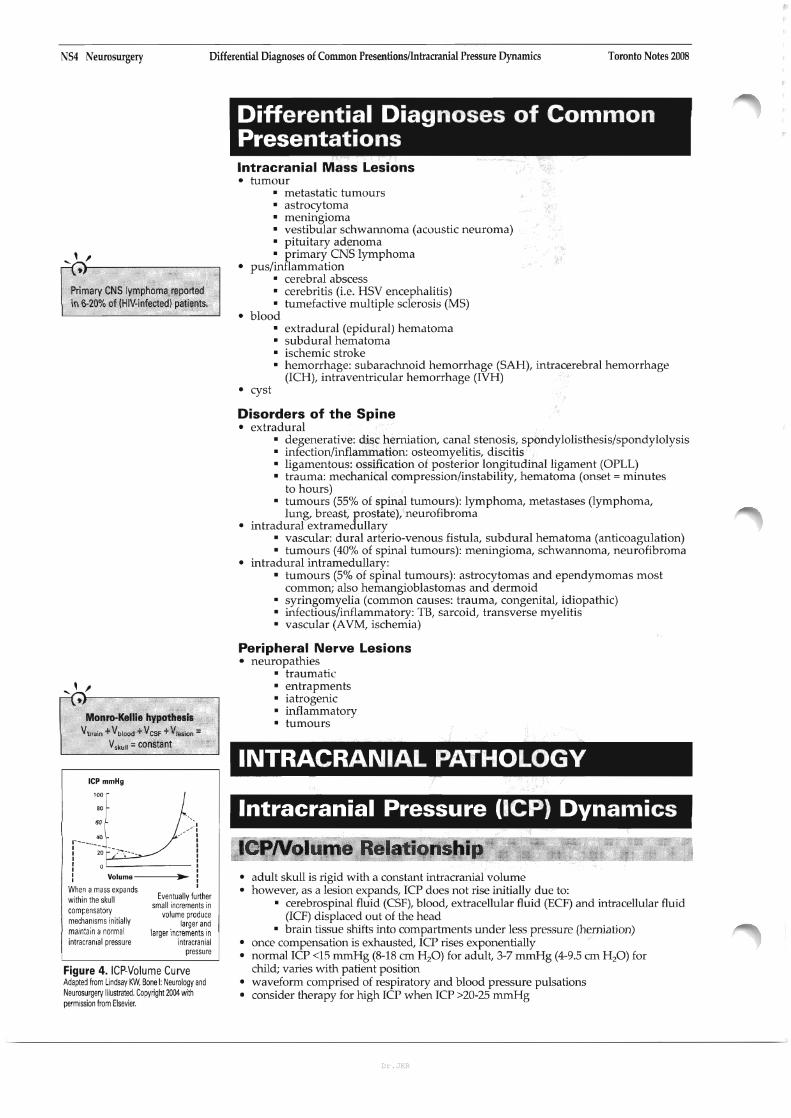
ICP mmHg
'~f~.):r-----J : : 20 '~-)...,---- : I� I
: 0 :
: Volume .. :
When amass expands I
within the skull Eventually further small increments in
com~ensatory volume produce mechanisms initially larger and mam:ain anormal larger increments in intracranial pressure intracranial
pressure
Figure 4. ICP·Volume Curve Adaptej from Lindsay 'fm, Bone I: Neurology and Neurosurgery Illustrated. Copyright 2004 with permission from Elsevier.
Differential Diagnoses of Common Presentations Intracranial Mass Lesions •� tumour
• metastatic tumours • astrocytoma • meningioma • vestibular schwannoma (acoustic neuroma) • pituitary adenoma •� primary CNS lymphoma
•� pus/inflammation • cerebral abscess • cerebritis (i.e. HSV encephalitis) • tumefactive multiple sclerosis (MS)
•� blood •� extradural (epidural) hematoma •� subdural hematoma • ischemic stroke • hemorrhage: subarachnoid hemorrhage (SAH), intracerebral hemorrhage
(rCH), intraventricular hemorrhage (rVH) •� cyst
Disorders of the Spine •� extradural
• degenerative: disc herniation, canal stenosis, spondylolisthesis/spondylolysis • infection/inflammation: osteomyelitis, discitis • ligamentous: ossification of posterior longitudinal ligament (OPLL) •� trauma: mechanical compression/instability, hematoma (onset = minutes
to hours) •� tumours (55% of spinal tumours): lymphoma, metastases (lymphoma,
lung, breast, prostate), neurofibroma •� intradural extramedullary
• vascular: dural arterio-venous fistula, subdural hematoma (anticoagulation) •� tumours (40% of spinal tumours): meningioma, schwannoma, neurofibroma
•� intradural intramedullary: •� tumours (5% of spinal tumours): astrocytomas and ependymomas most
common; also hemangioblastomas and dermoid • syringomyelia (common causes: trauma, congenital, idiopathic) • infectious/inflammatory: TB, sarcoid, transverse myelitis • vascular (AVM, ischemia)
Peripheral Nerve Lesions •� neuropathies
• traumatic •� entrapments • iatrogenic • inflammatory •� tumours
INTRACRANIAL PATHOLOGY
Intracranial Pressure (lCP) Dynamics
ICPNolume Relationshi •� adult skull is rigid with a constant intracranial volume •� however, as a lesion expands, rcp does not rise initially due to:
• cerebrospinal fluid (CSF), blood, extracellular fluid (ECF) and intracellular fluid (rCF) displacpd out of the head
• brain tissue shifts into compartments under less pressure (herniation) • once compensation is exhausted, rcp rises exponentially • normal rcp <15 mmHg (8-18 cm H20) for adult, 3-7 mmHg (4-9.5 em H 20) for
child; varies with patient position •� waveform comprised of respiratory and blood pressure pulsations • consider therapy for high rcp when rcp >20-25 rnmHg
Dr.JKR

Toronto Notes 2008� Intracranial Pressure Dynamics
ICP Measurement •� lumbar puncture (LP) (contraindicated with known/suspected intracranial mass lesion) •� intraventricular catheter/ventriculostomy/external ventricular drain ("gold standard",�
permits therapeutic drainage of CSF to decrease rcp; if mass and pressure gradient� present, drainage may increase gradient)�
•� other: fibreoptic monitor (intraventricular, intraparenchymal, subdural), subarachnoid bolt (Richmond screw), and epidural monitor
Cerebral Blood Flow (CBF) •� CBF depends on cerebral perfusion pressure (CPP) and cerebral vascular resistance •� normal CPP >50 mmHg in adults •� cerebral autoregulation maintains constant CBF by compensating for changes in CPP,�
unless:� • high rcp such that CPP <60 mmHg •� MAP>150 mmHg or MAP <50 mmHg • brain injury: Le. subarachnoid hemorrhage (SAH), severe trauma
Elevated ICP Etiology of Raised ICP •� increased intracranial blood volume
• hypoventilation --> increased pCO:Jdecreased paz .-+ vasodilatation •� venous outflow obstruction (venous sinus thrombosis, superior vena cava (SVC)
syndrome) • cranial dependency, Valsalva
•� cerebral edema: vasogenic (vessel damage), cytotoxic (cell death), osmotic (acute� hyponatremia, hepatic encephalopathy)�
•� hydrocephalus •� intracranial mass lesion (tumour, pus, blood, depressed skull fracture, foreign body) •� tension pneumocephalus •� status epilepticus • hypertensive encephalopathy (loss of autoregulation and cerebral edema)
CLINICAL FEATURES
Acute Raised ICP • headache (H/A) •� nausea and vomiting (N/V) •� decreased level of consciousness (LaC) if rcp =diastolic BP or midbrain compressed •� drop in Glasgow Coma Scale (GCS) --+ best index to monitor progress and predict�
outcome of acute intracranial process (see Neurotrauma, NS29)� •� papilledema ± retinal hemorrhages (may take 24-48 hours to develop) •� abnormal extra-ocular movements (EOM)
• CN VI palsy often falsely localizing (causative mass may be remote from nerve) •� upward gaze palsy (especially in children with obstructive hydrocephalus)
• herniation syndromes (see next page) • focal signs/symptoms due to lesion
Chronic Raised ICP • H/A
• postural: worsened by coughing, straining, bending over (Valsalva) • morning/evening H/A --+ vasodilatation due to increased CO2 with recumbency
•� visual changes • due to papilledema • enlarged blind spot, if advanced .-+ episodic constrictions of visual fields
("grey-outs")� • optic atrophy/blindness� • differentiate from papillitis (usually unilateral with decreased visual acuity)
Neurosurgery NS5
L CPP=MAP-ICP ~---------Autoregulation: CSF maintained despite�
change in CPP�
/~ ~j
<60 m~Hg i>150 mmHg
low BP or high ICP High BP
Cerebral perlusion pressure IMA~ICPI
Figure 5. Cerebral Autoregulation Curve Adapted from Lindsay et al: Neurology and Neurosurgery Illustrated. Copyright 2004 with permission from Elsevier.
..... ' ,..)-----------, Cushing'sTriad of Acute Raised ICP Full triad seen in 1/3 of cases 1. hypertension 2. bradycardia (late finding) 3. abnormal respiratory pattern
Dr.JKR

NS6 Neurosurgery Herniation Syndromes� Toronto Notes 2008
1. Subfalcine 2. Central 3. Uncal 4. Upward 5.Tonsillar
Figure 6. Herniation Types
Herniation Syndromes
Subfalcine (Cingulate) Herniation •� definition: cingulate gyrus herniates under falx •� etiology: lateral supratentorial lesion •� clinical features
•� usually asymptomatic, pathological/radiological observation warns of impending transtentorial herniation, risk of ACA compression
Central Tentorial (Axial) Herniation •� definition: displacement of diencephalon and midbrain through tentorial notch •� etiology: supratentorial midline lesion, diffuse cerebral swelling, late uncal herniation •� clinical features:
•� rostral to caudal deterioration (sequential failure of diencephalon --> medulla) • decreased LOC (midbrain compressed) •� EOM/upward gaze impairment ("sunset eyes") • brainstem hemorrhage ("Duret's" secondary to shearing of basilar artery
perforating vessels) • diabetes insipidus (traction on pituitary stalk and hypothalamus) --> end stage sign
Lateral Tentorial (Uncal) Herniation •� definition: uncus of temporal lobe herniates down through tentorial notch •� etiology: lateral supratentoriallesiun (often rapidly expanding trawnatic hematoma) •� clinical features:
•� ipsilateral non-reactive dilated pupil (earliest, most reliable sign), EOM paralysis (CN III compressed)
• decreased LOC (midbrain compressed) contralateral hemiplegia, ± extensor (upgoing) plantar response ± "Kernohan's notch": contralateral cerebral peduncle compressed due to shift of brain -> ipsilateral hemiplegia (a false localizing sign)
Upward Herniation •� definition: cerebellar vermis herniates through tentorial incisura, compressing
midbrain •� etiology: large posterior fussa mass causing herniation of cerebellum rostrally, common
after VP shunting •� clinical features:
•� superior cerebellar artery (SCA) compression * cerebellar infarct • compression of cerebral aqueduct --> hydrocephalus
Tonsillar Herniation (1IConing") •� definition: cerebellar tonsils herniate through foramen magnum •� etiology: infratentoriallesion or following central tentorial herniation •� clinical features:
• compression of cardiovascular and respiratory centers in medulla (rapidly fatal) may be precipitated by LP in presence of space occupying lesion (particularly in the posterior fossa)
Treatment of Herniation Syndromes---------' •� goals: keep Iep <20 mmHg, CPP >60-70 mmHg
General Measures •� elevate head of bed at 30-45° --> increases intracranial venous outflow •� prevent hypotension with fluid and pressors pm • ventilate to normocarbia (pC0235-40 mmHg) --> prevents vasodilatation • oxygen pm to maintain p02 >60 mmHg -> prevents hypoxic brain injury •� CT or Mill to identify etiology, assess for midline shift/herniation
Specific Measures (proceed stepwise prn) •� mannitol (20% IV solution 1-1.5 glkg, then 0.25 glkg q6h)
•� can give rapidly, acts in 30 minutes, must maintain sBP >90 mmHg •� hyperventiTate to pCO:? 30-35 mmHg
Dr.JKR

Toronto Notes 2008� Herniation Syndromes/Hydrocephalus Neurosurgery NS7
•� sedation ("light" e.g. codeine --> "heavy" e.g. fentanyl/MgS04 ± paralysis with vecuronium --> reduces sympathetic tone, HTN induced by muscle contraction)
•� corticosteroids • decreases edema over subsequent days around brain tumour, abscess, blood •� no proven value in head injury or stroke
•� surgeryd . 3 5 1CSF' . I h" . d d 1• ram - m VIa ventnc es, assess eac SItuation m epen ent y •� remove mass lesion, insert external ventricular drain (if acute) or shunt • decompressive craniectomy is a last resort
Hydrocephalus Definition •� increased CSF volume
Etiology •� decreased CSF absorption (majority) •� increased CSF production (rarely) - e.g. choroid plexus papilloma
(0.4-1% of intracranial tumours)
Epidemiology • estimated prevalence 1-1.5%; incidence of congenital hydrocephalus -] -2/1000 live births
Classification
1. Obstructive (Non-Communicating) Hydrocephalus •� absorption blocked within ventricular system proximal to the arachnoid granulations •� acquired causes:
• acquired aqueductal stenosis (adhesions following infection, hemorrhage) intraventricular lesions (tumours - e.g. 3rd ventricle colloid cyst, hematoma)
•� mass causing tentorial herniation, aqueduct/4th ventricle compression others: neurosarcoidosis, abscess/granulomas, arachnoid cysts
•� congenital causes: • aqueductal stenosis, Dandy-Walker malformation, Chiari malformation (see
Pediatric Neurosurgery, NS34) •� CT findings:
• ventricular enlargement proximal to block
2. Non-Obstructive (Communicating) Hydrocephalus •� CSF absorption blocked at extraventricular site = arachnoid granulations •� causes:
• post-infectious (#1 cause) -... meningitis, cysticercosis • post-hemorrhagic (#2 cause) --> SAH, NH, traumatic • Choroid plexus papilloma (rare, causes l' CSF production) • idiopathic normal pressure hydrocephalus
•� CT findings: • all ventricles dilated
3.� Normal Pressure Hydrocephalus (NPH) •� gradual onset of classic triad developing over weeks or months
• gait disturbance (ataxia and apraxia usually initial symptoms) • urinary incontinence • dementia
•� CSF pressure within clinically "normal" range, but symptoms abate with CSF shunting •� idiopathic etiology
4. Hydrocephalus Ex Vacuo •� enlargement of ventricles and sulci secondary to cerebral atrophy, not hydrocephalus •� usually a function of nonnal aging, also in Alzheimer's, Creutzfeldt-Jacob Disease
Clinical Features (see Pediatric Neurosurgery for infant/child, NS34) •� Acute Hydrocephalus
• signs and symptoms of acute raised ICP (see NS5) • impaired upward gaze ("sunset eyes") and/or CN VI palsy
•� Chronic Hy'droceEhalus• simIlar to NPH (see above)
Investigations •� CT'MRI
. • ventricular enlargement, may see prominent temporal horns • periventricular hypodensity (transependymal migration of CSF forced into
extracellular space) • narrow/absent sulci
•� ultrasound (through anterior fontanelle in infants) •� ICP monitoring (e.g. LP) may be used to investigate NPH, test response to shunting
(lumbar tap test) •� radionuclide cistemography can test CSF flow and absorption rate (unreliable)
~[ o
4� 5�
6� 1. Choroid plexus 2. Lateral ventricles 3. Third ventricle 4. Cerebral aqueduct (of Sylvius) ~
5. Fourth ventricle :-:: 6. Foramen Luschka and Magendie .~
7. Arachnoid granulations u:: 8. Subarachnoid space ~
9. Sagittal sinus @
Figure 7. The Flow of CSF
..... ' ,~}------------,
CSF produced by choroid plexuses, flows to: --t ventricles'" foramina of Luschka and Magendie ... subarachnoid space'" absorbed by arachnoid villi/granulations into venous sinuses.
Luschka =lateral, Magendie =medial
~,
NPH Progression "AID" =� Ataxia/Apraxia of gait ... Incontinence�
--t Dementia
..... ' ,~}------------,
CSF production =CSF reabsorption =� - 500mllday in normal adults�
Normal CSF volume -150 ml� (50% spinal, 50% intracranial'" 25 cc� intraventricular, 50 cc subarachnoid)�
Dr.JKR
NS8 Neurosurgery HydrocephaluslBenign Intracranial Hypertension� Toronto Notes 2008
Treatment •� surgical removal of obstruction (if possible) or excision of choroid plexus papilloma •� shunts:
• ventriculoperitoneal (VP) - most common ventriculo-atrial (VA) - not first choice because of l' infections, shunt emboli
• ventriculopleural • lumbopentoneal - for communicating hydrocephalus and pseudotumour cerebri
•� third ventriculostomy (for obstructive hydrocephalus) via ventricUloscopy •� LPs (for transient, IVH in premature infants, etc.)
Shunt Complications •� obstruction (most common cause of shunt malfunction)
• etiology: obstruction by choroid plexus, buildup of proteinaceous accretions, blood, cells (inflammatory or tumour), infection, disconnection or damage
• clinical features: acute hydrocephalus, increased ICP • investigations: "shunt series" (plain x-rays of entire shunt that only rule-out
disconnection, break, tip migration), CT, radionuclide "shuntogram" •� shunt tap and surgical exploration pm
•� infection (3-6%)• etiology: 5. epidermidis, 5. aureus, P. acnes, Gram-negative bacilli
clinical features: fever, N/V, anorexia, irritability, meningitis, peritonitis, signs and symptoms of shunt obstruction, shunt nephritis (VA shunt)
• investigations: CBC, blood culture, tap shunt for C&S (LP usually NOT recommended)
• overshunting (10% over 6.5 years) •� ± slit ventricle syndrome (collapse of ventricles leading to occlusion of shunt
ports by ependymal lining) •� ± subdural effusion, hematoma (collapsing brain tears bridging veins, especially
in NPH patients) •� ± secondary craniosynostosis (children) •� ± low pressure headache
•� seizures (5.5% risk in 1st year, 1.1% after 3rd year) •� inguinal hernia (17% incidence with VP shunt inserted in infancy), skin breakdown
over hardware
Benign Intracranial Hypertension (Pseudotumour Cerebri) Definition •� raised intracranial pressure and papilledema without evidence of any mass lesion,
hydrocephalus, infection or hypertensive encephalopathy (a diagnosis of exclusion)
Etiology •� unknown (majority), but associated with
• lateral venous sinus thrombosis • habitus/diet: obesity, hyper/hypovitaminosis A
endocrine: reproductive age, menstrual irregularities, Addison's/Cushing's disease, thyroid irregularities
• hematological: iron aeficiency anemia, polycythemia vera drugs: steroid administration or withdrawal, tetracycline, nalidixic acid, etc.
•� risk factors overlap with those of venous sinus thrombosis and similar to those for gallstones
Epidemiology •� incidence -0.5/100,000/year •� usually in 3rd and 4th decade (F>M)
Clinical Features •� symptoms and signs of raised ICP (H/A in >90%, pulsatile intracranial noise), but NO
decreased LaC or diplopia •� -J, visual acuity, papilledema, visual field defect, optic atrophy (key morbidity,�
preventable cause of often pennanent blindness)� •� usually self-limited, recurrence is common, chronic in some patients •� risk of blindness is not reliably correlated to symptoms or clmical course
Investigations •� CT: nonnal •� CSF studies: nonnal •� MRI: must look for venous sinus thrombosis
Treatment •� rio conditions that cause intracranial hypertension •� D/C offending medications, encourage weight loss, fluid/salt restriction •� phannacotherapy: acetazolamide (decreases CSF production), thiazide diuretic or�
furosemide� • if above fail ---> serial LPs, shunt� • optic nerve sheath decompression (if progressive impainnent of visual acuity)� •� 2-year follow-up with imaging to rule out occult tumour, ophthalmology follow-up
Dr.JKR

Toronto Notes 2008� Tumour Neurosurgery NS9
Tumour Definition •� primary vs. metastatic, intra-axial (parenchymal) vs. extra-axial, supratentorial vs.
infratentorial, adult vs. pediatric •� benign: non-invasive, but can be devastating due to expansion of mass in fixed
volume of skull •� malignant: implies rapid growth, invasiveness, but rarely extracranial metastasis
Table 1. TumourTypes: Age, Location Age Supratentorial� Infratentorial (posterior fossa)
<15 years . astrocytoma lall grades) 150%1 . medulloblastoma 115-20%)
• incidence: 2-51100.000Iyear - craniopharyngioma 15-10%) - cerebellar astrocytoma 115%1
• 60% infratentorial - others: pineal region tumours, choroid plexus - ependymoma 19%)
tumours, ganglioglioma, DNET - brainstem astrocytoma
>15 years • high grade astrocytoma (e.g. glioblastoma - metastasis
• 80% supratentorial multiforme (GBM) (12·15%) - acoustic neuroma Ischwannomal (5-10%)
• metastasis 115-30%, includes infratentorial) - hemangioblastoma 12%)
• meningioma 115-20%1 - meningioma
- low grade astrocytoma 18%)
- pituitary adenoma 15-8%)
- oligodendroglioma 15%)
- other: colloid cyst, eNS lymphoma,
dermoid/epidermoid cysts
Clinical Features •� progressive neurological deficit (70%) - usually motor weakness, ± CN deficits,
sensory, cognitive, personality, endocrine deficits may localize lesion •� HJA (50%) ± raised ICP (acute or chronic depending on growth rate), H/A
classically worse in am but non-specific (likely hypoventilation during sleep causing vasodilatation -->1' ICP), also may worsen with bending forwardNalsalva
•� NN (40%) •� seizures (25%) •� papilledema, obscured vision •� symptoms suggestive of TIA (ictal, post-ictal, or ischemic 2° to "steal phenomenon") •� rarely presents with hemorrhage •� familial syndromes associated with CNS tumours:
•� von Hippel-Lindau (hemangiomas) • tuberous sclerosis (astrocytomas) • neurofibromatosis type 1 and 2 (astrocytomas, acoustic neuromas respectively) • Li-Fraumeni (astrocytomas) • Turcot syndrome (GBMs) • multiple endocrine neoplasia type 1 (pituitary adenoma)
Investigations •� CT, MRI, stereotactic biopsy (tissue diagnosis), metastatic work-up pm
Treatment •� conservative - serial Hx, Px, imaging for slow growinglbenign lesions •� medical- corticosteroids to reduce cytotoxic cerebral edema, pharmacological (see
Pituitary Adenoma, NSll) •� surgical- total or partial excision (decompressive, palliative), shunt if hydrocephalus •� radiotherapy - conventional fractionated radiotherapy (XRT), stereotactic radiosurgery
(Gamma KnifeTM )
•� chemotherapy - e.g. alkylating agents (temozolomide)
MetastaticTumours •� most common brain tumour seen clinically •� 15-30% of cancer patients present with cerebral metastatic tumours • usually spread hematogenously
Location •� 80% are hemispheric, often at grey-white matter junction or junction of
temporal-parietal-occipital lobes (likely emboli spreading to terminal MCA branches)
OIl'
DDx for ring enhancing lesion on CT with contrast: "MAGICAL DR" 'Metastases� 'Abscess� 'Glioblastoma� (high grade astrocytomal� Infarct� Contusion� AIDS (toxoplasmosisl� Lymphoma� Demyelination� Resolving hematoma�
[' by far the 3 most common Ox's]
..... ' ,~)------------,
Primary Sources of Metastatic Brain Tumours Lung 44% Breast 10% Kidney (RCC) 7% GI 6% Melanoma 3%
Dr.JKR

NSIO Neurosurgery Tumour� Toronto Notes 2008
Investigations •� metastatic work-up (OCR, cr chest/abdo, abdominal D/S, bone scan, mammogram)• cr with contrast ~ round, well-circumscribed, often ring enhancing, ++ edema, often
multiple •� MRI more sensitive, especially for posterior fossa •� consider biopsy in unusual cases
Treatment •� medical
•� phenytoin for seizure prophylaxis if patient presents with seizure •� dexamethasone to reduce edema (often Significant cause of symptoms), given
with ranitidine •� chemotherapy (small cell lung cancer)
•� radiation Figure 8. Multiple Brain Metastases • whole brain radiation therapy (WERT) can help reduce symptoms in
inoperable cases (some tumours respond poorly e.g. melanoma), typically the sole treatment if multiple lesions
•� post-op WERT is commonly used • stereotactic radiosurgery •� multiple lesions:
1. metastatic work-up negative --+ brain biopsy 2.� metastatic work-up positive -. biOpsy affected sites other than the brain
•� surgical • single/solitary lesions ~ surgery + radiation
•� prognosis: median survival without treatment once symptomatic is -1 month, with optimal treatment 6-9 months but varies depending on primary
'jt ~ Astrocytom_a _ • most common primary intra-axial brain tumour
Table 2. Astrocytoma Grading System (one of many schemes)
World Health Organization (WHO) Typical CTIMRI Findings Survival
1- pilocytic astrocytoma No mass effect, no enhancement >10 years, cure if gross total resection .. 1
II-low grade/diffuse Mass effect, no enhancement 5years
--- 2 III - anaplastic� Complex enhancement 1.5-2 years
IV - glioblastoma multiforme Necrosis (ring enhancement) 9 months
Clinical Features •� middle aged, recent onset of new/worsening H/A, N/V, seizure ± focal
1. heterogenous contrast enhancement deficits or symptoms of increased ICP 2. ill-defined borders (infiltrativel 3. perilumour edema Investigations4. central necrosis
•� CT with contrast ~ variable appearance depending on grade (see Table 2) 5. compression of ventricles, midline shift • tissue biopsy ~ WHO grade correlates with prognosis, but 25% chance of sampling
Figure 9. High Grade Astrocytoma on error due to tumour heterogeneity CT
Treatment •� low grade astrocytoma:
•� close follow-up, radiation, chemotherapy, surgery all valid options •� surgery: not curative, trend towards better outcomes •� radiotherapy alone or post-op prolongs survival (retrospective evidence) •� chemotherapy - usually reserved for tumour progression
•� high grade astrocytomas (comprised of anaplastic astrocytoma and glioblastoma multiforme (GBM»
•� surgery: gross total removal with radiation to tumour bed ± WERT is the standard treatment unless: extensive dominant lobe GBM, Significant bilateral involvement, end of life near, extensive brainstern involvement
•� aim to prolong "quality" survival • chemotherapy: -20% response rate
•� multiple gliomas: WERT ± chemotherapy
Dr.JKR
Toronto Notes 2008� Tumour Neurosurgery NSll
Meningioma •� mostly benign (1% malignant), slow-growing, extra-axial, circumscribed
(non-infiltrative), arise from arachnoid membrane •� often cause hyperostosis of adjacent bone, often calcified, classically see Psammoma
bodies on histology
Common Locations •� parasagittal convexity or falx (70%), sphenoid wing, tuberculum sellae
Clinical Features •� middle aged, symptoms of increased rcp, focal deficits
Investigations •� CT with contrast: homogeneous, densely enhancing, along dural border ("dural tail"),
well circumscribed (see Figure 10) 1. homogenous contrast enhancement•� contrast enhanced MRI provides better detail 2. dural attachment•� angiography: most are supplied by external carotid feeders (meningeal vessels) 3. distinct margins• also assesses venous sinus involvement, "tumour blush" commonly seen�
(prolonged contrast image)� Figure 10. Meningioma on CT
Treatment •� conservative management for non-progressive, asymptomatic lesions •� surgery is treatment of choice if symptomatic or progression on sequential imaging
(curative if complete resection) •� stereotactic radiosurgery (SRS) may be an option for lesions <3 em •� endovascular embolization to facilitate surgery •� SRS or XRT for recurrent atypical/malignant meningiomas
Prognosis •� >90% 5-year survival, recurrence rate variable (often -10-20%) •� depends on extent of resection (Simpson's classification)
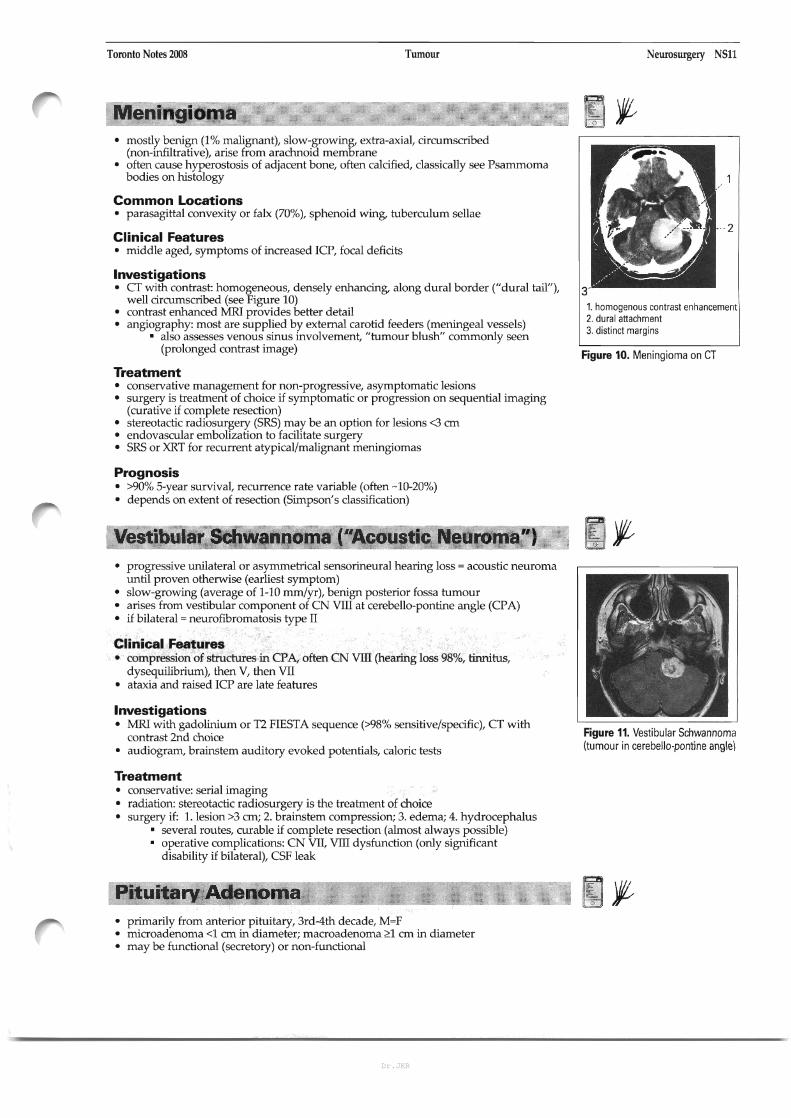
Vestibular Schwannoma e'Acoustic Neuroma") •� progressive unilateral or asymmetrical sensorineural hearing loss = acoustic neuroma
until proven otherwise (earliest symptom) •� slow-growing (average of 1-10 mm/yr), benign posterior fossa tumour •� arises from vestibular component of CN VITI at cerebello-pontine angle (CPA) •� if bilateral = neurofibromatosis type II
Clinical Features •� compression of structures in CPA, often CN VITI (hearing loss 98%, tinnitus,
dysequilibriurn), then V, then VII •� ataxia and raised rcp are late features
Investigations •� MRI with gadolinium or T2 FIESTA sequence (>98% sensitive/specific), CT with
Figure 11. Vestibular Schwannomacontrast 2nd choice (tumour in cerebella-pontine angle\•� audiogram, brainstem auditory evoked potentials, caloric tests
Treatment •� conservative: serial imaging •� radiation: stereotactic radiosurgery is the treatment of choice •� surgery if: 1. lesion >3 em; 2. brainstem compression; 3. edema; 4. hydrocephalus
• several routes, curable if complete resection (almost always possible) • operative complications: CN VII, VITI dysfunction (only significant�
disability if bilateral), CSF leak�
Pituitary Adenoma� o
•� primarily from anterior pituitary, 3rd-4th decade, M=F •� microadenoma <1 em in diameter; macroadenoma ~1 em in diameter •� may be functional (secretory) or non-functional
Dr.JKR

NSI2 Neurosurgery TumourlPus� Toronto Notes 2008
~,
Go Look For The Adenoma Please GH, LH, FSH,TSH, ACTH, Prolactin Acompressive adenoma in the pituitary will impair hormone production in this order (i.e. GH-secreting cells are most sensitive to compression)
Clinical Features •� mass effects
•� H/A • bitemporal hemianopsia (compression of optic chiasm) (see Neurology, N26
for details of visual field deficit) •� CN III, IV, Vv V'l' VI palsy (compression of cavernous sinus)
•� endocrine effects • hyperprolactinemia (prolactinoma) ---> infertility, amenorrhea,�
galactorrhea, decreased libido� •� ACTH production -. Cushing's disease, hyperpigmentation •� GH production ---> acromegaly/gigantism •� panhypopituitarism (hypothyroidism, hypoadrenalism, hypogonadism) •� associated MEN I syndrome •� diabetes insipidus •� pituitary apoplexy
•� apoplexy (sudden l:'xpansion of mass due to hemorrhage or necrosis) •� abrupt onset B/A, visual disturbances, ophthalmoplegia, and reduced
mental status, and panhypopituitarism •� CSF rhinorrhea and seizures (rare presenting signs of pituitary tumour) •� signs and symptoms of SAH (rare) (see NSI5)
Investigations •� formal visual fields, CN testing, endocrine tests (PRL level, TSH, 8 a.m. cortisol, fasting
glucose, FSH/LH, IGF-I), electrolytes, urine electrolytes and osmolarity, imaging (Mill with and without contrast)
Differential •� parasellar tumours (e.g. craniopharyngioma, tuberculum sellae meningioma), carotid
aneurysm
Treatment •� medical
•� rapid corticusteroid ..tdministration ± surgical decompression for apoplexy •� dopamine agonists (e.g. bromocriptine) for prolactinoma • serotonin antagonist (cyproheptadine), inhibition of cortisol production
(ketoconazole) for Cushing's •� somatostatin analogue (octreotide) ± bromocriptine for acromegaly • endocrine replacement therapy
•� surgical •� trans-sphenoidal. transethmoidal, transcranial approaches
Sources of Pus •� subdural empyema --> pus in pre-existing space with no capsule barrier thus rapid
expansion is commoll (from sinusitis, mastoiditis - rare, 20% mortality) • meningitis, encephalitis, toxoplasmosis (AIDS)� • osteomyelitis of skull (Pott's puffy tumour), usually seen with sinusitis� •� granuloma (TB, sarcoid)� •� cerebral abscess (see below)�
Cerebral Abscess Definition •� pus in brain substance, surrounded by tissue reaction (capsule formation)
Etiology •� modes of spread
• hematogenous spread (most common) •� adults: chest is #1 source --> lung abscess, bronchiectasis, empyema •� children: congenital cyanotic heart disease (CCHO) with R to L shunt •� immunosuppression (AIDS - toxoplasmosis)
•� contiguous spread (adjacent infection) • otitis media, mastoiditis, sinusitis, osteomyelitis, dental abscess
•� dural disruption •� surgery, trauma (especially with continued CSF leak) •� congenital defect (e.g. dermal sinus)
Dr.JKR

Toronto Notes 2008� PuslBlood Neurosurgery NS13
•� pathogens 3•� Streptococcus (most common), often anaerobic or microaerophilic
•� Staphylococcus (penetrating injury) •� Gram negatives, anaerobes •� immW1ocompromised: Toxoplasma, Nocardia, Candida albicans, Listeria�
monocytogmes, Mycobacterium and Aspergillus�
Risk Factors •� lW1g abnormalities (infection, AV fistulas (especially Osler-Weber-Rendu syndrome)) •� CCHD •� bacterial endocarditis •� penetrating head trauma •� AIDS
Clinical Features 1. surrounding edema •� focal neurological signs and symptoms 2. central low density (pus)•� mass effect, increased ICP and sequelae (cranial enlargement in children) 3. ring enhancement •� hemiparesis and seizures in 50% •� ± signs of systemic infection (mild fever, leukocytosis) Figure 12. Brain Abscess on CT
Investigations •� WBC/ESR may be normal, blood cultures rarely helpful and LP contraindicated •� CT scan often 1st test in emergency department •� ~fRl
• imaging of choice • diffusion/apparent diffusion coefficient (ADC) used to differentiate abscess�
(black) from tumour (white)�
Treatment •� multiple aspiration ± excision and send for Gram stain, acid fast bacillus (AFB), C&S,�
fungal culture� •� excision preferable if location suitable •� antibiotics
• empirically: vancomycin + ceftriaxone + metronidazole or chloramphenicol or� rifampin (6-8 weeks therapy)�
• revise antibiotics when C&S known •� anti-convulsants (1-2 years) •� follow up CT is critical (do weekly initially, more frequent if condition deteriorates)
Prognosis •� mortality with appropriate therapy -10%, permanent deficits in -50%
Blood
Extradural (6IEpidural") Hematoma Etiology •� temporal-parietal skull fracture ---+ ruptured middle meningeal artery
Epidemiology •� young adult, male> female
Clinical Features •� classically there is lucid interval between concussion and coma •� signs and symptoms depend on severity but can include H/A, N/V, amnesia, altered�
LaC�
Investigations •� CT without contrast ---+ high density biconvex mass against skull, "lenticular-shaped,"
1. compression of ventriclesusually with uniform density and sharp margins, usually limited by suture lines (midline shift)�
Treatment 2. blood� •� head elevation, mannitol pre-op, craniotomy to evacuate clot
Figure 13. Extradural Hematoma on Prognosis CT •� good with prompt management, as the brain is often not damaged
Dr.JKR
NS14 Neurosurgery Blood� Toronto Notes 2008
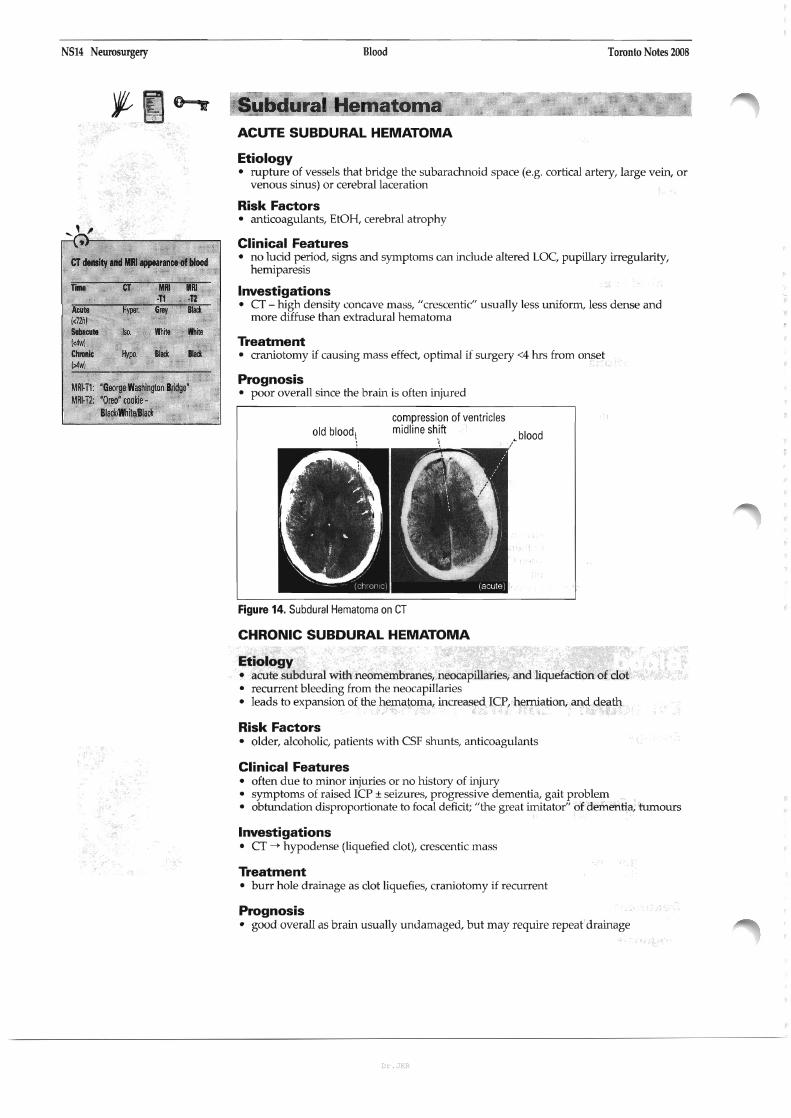
CT dInIity IIld III ..,.... of blood
tiiiit CT .. IIIIi ·n ·12
AMI Hyper. Grey BlICk «72hl SubIcuIe Iso. White White «4w) ClvIlIic Hypo. Blaci Blaci (>4wl
MR~ T1: 'George Washington Bridge' MRH2: 'Oreo' cookie -
BlackiWh~d1act
Subdural Hematoma ACUTE SUBDURAL HEMATOMA
Etiology •� rupture of vessels that bridge the subarachnoid space (e.g. cortical artery, large vein, or
venous sinus) or cerebral laceration
Risk Factors •� anticoagulants, EtOH, cerebral atrophy
Clinical Features •� no lucid period, signs and symptoms can include altered LOC, pupillary irregularity,
hemiparesis
Investigations •� CT - high density concave mass, "crescentic" usually less uniform, less dense and
more diffuse than extradural hematoma
Treatment •� craniotomy if causing mass effect, optimal if surgery <4 hrs from onset
Prognosis •� poor overall since the brain is often injured
compression of ventricles midline shiftold blood\ .blood
/
Figure 14. Subdural Hematoma on CT
CHRONIC SUBDURAL HEMATOMA
Etiology •� acute subdural with neomembranes, neocapillaries, and liquefaction of clot •� recurrent bleeding from the neocapillaries •� leads to expansion of the hematoma, increased rcp, herniation, and death
Risk Factors •� older, alcoholic, patients with CSF shunts, anticoagulants
Clinical Features •� often due to minor injuries or no history of injury • symptoms of raised rcp ± seizures, progressive dementia, gait problem • obtundation disproportionate to focal deficit; "the great imitator" of dementia, tumours
Investigations •� CT --+ hypodense (liquefied clol), crescentic mass
Treatment •� burr hole drainage as clot liquefies, craniotomy if recurrent
Prognosis •� good overall as brain usually undamaged, but may require repeat drainage
Dr.JKR
Toronto Notes 2008� Cerebrovascular Disease Neurosurgery NS15
Cerebrovascular Disease
Ischemic Cerebral Infarction (80%) •� embolic (heart, carotid artery, aorta) or thrombosis of intracerebral arteries (see Carotid
Stenosis section, NSI9, and Neurology. N59)
Intracranial Hemorrhage (20%) •� subarachnoid hemorrhage (SAH), spontaneous intracerebral hemorrhage (ICH),
intraventricular hemorrhage (IVH)
Subarachnoid Hemorrhage (SAH)-,:..----...---Definition •� bleeding into subarachnoid space (intracranial vessels between arachnoid and pia)
Etiology •� trauma (most common) •� spontaneous
•� aneurysms (75-80%) •� idiopathic (14-22%) • AVMs(5%)
•� coagulopathies (iatrogenic or primary), vasculitides, tumours (<5%)
Epidemiology •� -10-28/100,000 population/year •� peak age 55-60, 20% of cases occur under age 45
Risk Factors •� hypertension • pregnancy/parturition in patients with pre-existing AVMs, eclampsia • oral contraceptive pill •� substance abuse (cigarette smoking, cocaine, alcohol (debatable») •� conditions associated with high incidence of aneurysms (see Intracranial Aneurysms
section, NSI8)
Clinical Features of Spontaneous SAH •� sudden onset (seconds) severe headache: "worst headache of my life"
(up to 97% sensitive, 12-25% specific) •� history of exertion is common (straining, intercourse) •� nausea/vomiting, photophobia •� meningismus (neck pain/stiffness, positive Kernig's and Brudzinski's sign) •� decreased LOC (can include raised ICP, ischemia, seizure) •� focal deficits: cranial nerve palsy (e.g. III, IV), hemiparesis •� ocular hemorrhage in 20-40% (due to sudden raised ICP compressing
central retinal vein); subhyaloid/pre-retinal hemorrhages •� reactive hypertension •� sentineVwarningleaks
• SAH-like symptoms lasting <1 day ("thunderclap H/A") •� may have blood on CT or LP • -50% of patients with full blown SAH giw history suggestive of a warning leak
within past 3 weeks •� differential diagnosis of severe HIA, onset within seconds: SAH; thunderclap H/A;
dissection/thrombosis of aneurysm; venous sinus thrombosis; benign exertional H/A
Investigations •� non-contrast CT (see Figure 15) •� 98% sensitive within 12h, 93% within 24h; 100% specificity •� may be negative if small bleed or presentation delayed several days •� positive history for SAH with negative CT - MUST do LP (may be negative <12h) •� acute hydrocephalus, IVH, ICH, infarct or large aneurysm may be visible •� CT may also suggest site of aneurysm that has bled
o
..... ' ,~}-----------,
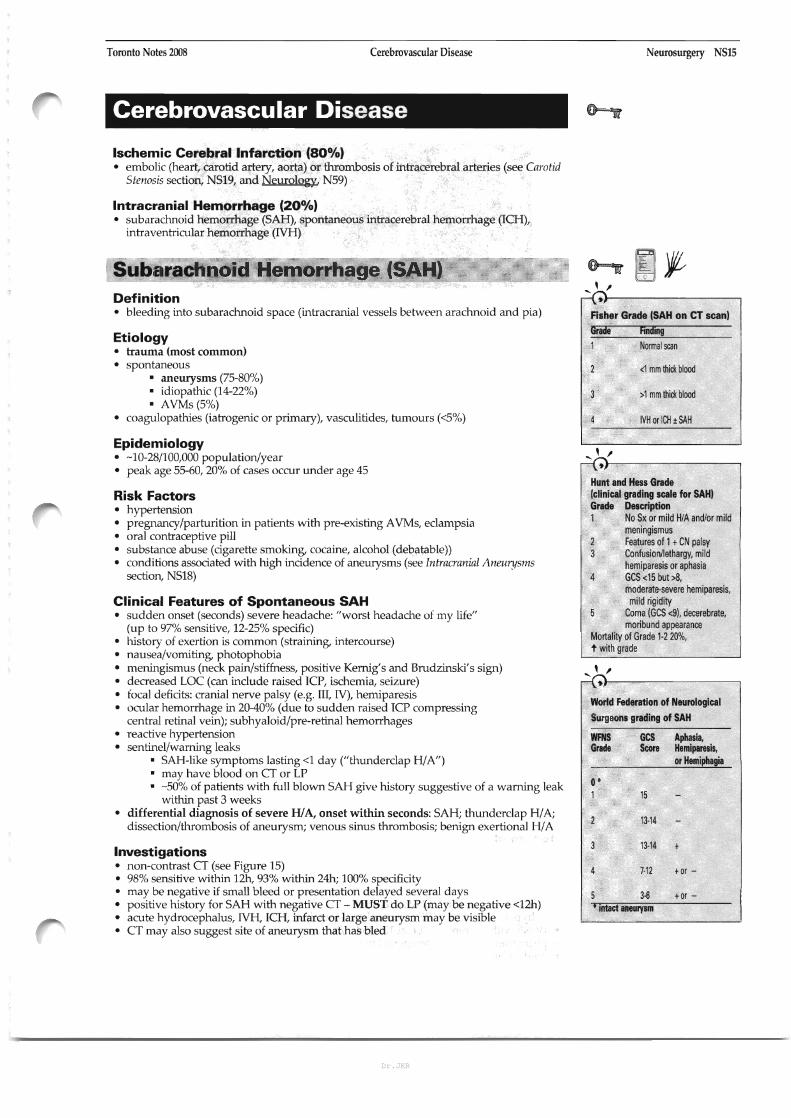
Fisher Grade (SAH on CT scan) Graae finding 1 Normal scan
<1 mm thick blood
>1 mm thick blood
IVH or ICH ±SAH
,� ~}-------------,
Hunt and Hess Grade (clinical grading scale for SAHI Grade Description 1 No Sx or mild H/A and/or mild
meningismus 2 Features of 1t CN palsy 3 Confusion/lethargy, mild
hemiparesis or aphasia 4 GCS <15 but>8,
moderate-severe hemiparesis, mild rigidity
Coma (GCS <9), decerebrate, moribund appearance
Mortality of Grade 1·2 20%, t with grade
.... ' ,~I------------,
World Federation of Neurological
Surgeons grading of SAH
WFNS Grade
GCS Score
Aphasia. Hemiparesis. or Hemiphagia
O' 1 15
13-14
13-14
7-'2 tor -
5 3-6 tor -, Intact aneurysm
Dr.JKR

NS16 Neurosurgery Cerebrovascular Disease� Toronto Notes 2008
blood inblood in� blood in interhemisphericbasal cisterns suprasellar cistern fissure
,, blood on blood 'in surface of sylvian tentorium fissures
Figure 15. Diagnosis of SAH
•� lumbar puncture (LP) - findings (highly sensitive): • elevated opening pressure (>18 em H20) • bloody initially, xanthochromic supernatant with centrifugation ("yellow") by
-12h, lasting 2 weeks • spectrophotometry is most sensitive for xanthochromia •� RBC count usually>100,000/mm3 without Significant drop from 1st to last tube
as in traumatic tap • protein elevated due to blood breakdown products
•� cerebral angiography ("gold standard for aneurysms") • demonstrates source of SAH in 80-85% of cases •� "angiogram negative SAH": repeat angiogram in 7-14 days, if negative-+
"perirnesencephalic SAH" •� magnetic resonance angiography (MRA) and CT angiography
• emerging technologies, sensitivity may be up to 95% for aneurysms
BP level of consciousness limb movements stiff neck fundi
conscious, alert, no neurological findings. I CT scanfundi normal
,-f
I�
[ i~bar puncture I~ negative I�
~i~-eJ
clear, colorless.� no microscopic blood�
T---�C.;o;;;;-J�
CTNMRNangiography
Figure 16. Approach to SAH
Treatment • admit to lCU or NICU • oxygen/ventilation pm •� NPO, bed rest, elevate head of bed 300, minimal external stimulation, neurological
vitals qlh •� aim to maintain sBP = 120-150 (balance of vasospasm prophylaxis, risk of re-bleed, risk
of hypotension since CBF autoregulation impaired by SAH) •� IV NS with 20 mmol KCl/L at 125-150 cclh •� phenytoin if seizure or temporal lobe clot •� mild sedation pm •� nimodipine for vasospasm neuroprotection --> 21 days; may d/c earlier if patient is
clinically well and ready for discharge
Dr.JKR
Toronto Notes 2008� Cerebrovascular Disease Neurosurgery NS17
•� cardiac rhythm monitor •� Foley pm, strict ins & outs •� 4 vessel angiography, early surgery or coiling to prevent rebleed
Complications •� vasospasm
• definition: constriction of blood vessels in response to arterial blood clot outside� vessels at the base of the brain�
• clinical features: confusion, -J., LOC, focal deficit (speech or motor)� • onset: 4-14 days post SAH (if deterioration within first 3 days, MUST look� "Triple H"Therapy for Vasospasm
for other cause) • Hypertension•� "radiographic" vasospasm in 30-70% of arteriograms performed 7 days • Hypervolemia
following SAH (peak incidence) • Hemodilution •� "symptomatic" vasospasm in 20-30% of SAH patients • detect clinically and/or with angiogram or transcranial Doppler (increased�
velocity of blood flow), CBC/electrolytes/CT urgently to rio other causes� •� risk factors: large amount of blood on CT (i.e. high Fisher grade), smoking, l'�
age, prior HTN� risk of cerebral infarct and death (biggest cause of morbidity and mortality in� patients who reach hospital)�
•� treatment •� "triple H" therapy (hypertension, hypervolemia, hemodilution) using�
fluids and pressors (examples: norepinenphrine, phenylephrine)� •� angioplasty for refractory cases
•� hydrocephalus (15-20%) - due to blood obstructing arachnoid granulations or subarachnoid space
•� can be acute or chronic - requiring intraventricular catheter or shunt� respectively�
•� neurogenic pulmonary edema •� hyponatremia - (SIADH, cerebral salt wasting) •� diabetes insipidus •� cardiac - arrhythmia (>50% have ECG changes), MI, CHF
Prognosis •� 10-15% mortality before reaching hospital, overall 50% mortality (majority within first
2-3 weeks) •� 30% of survivors have moderate - severe disability •� a major cause of mortality is rebleeding, for aneurysms:
•� risk of rebleed: 4% on first day, 15-20% within 2 weeks, 50% by 6 months •� if no rebleed by 6 months risk decreases to same incidence of unruptured
aneurysm (2%)� • only prevention is early clipping or coiling� • rebleed risk for "perimesencephalic SAH" is - same as for general population
Intracerebral Hemorrhage (lCH) --~-~----~---
Definition •� hemorrhage within brain parenchyma, accounts for -10% 01' strokes •� can dissect into ventricular system (NH) or through cortical surface (SAH)
Etiology •� hypertension (usually at putamen, thalamus, pons and cerebellum) •� hemorrhagic transformation (reperfusion post stroke, surgery, strenuous exercise, etc.) •� vascular anomalies
• aneurysm, AVMs and other vascular malformations (see Vascular Malformations,� NS20)�
•� venous sinus thrombosis • arteriopathies (cerebral amyloid angiopathy, lipohyalinosis, vasculitis)
•� tumours (1%) - often malignant (e.g. GBM, lymphoma, metastases) •� drugs (amphetamines, cocaine, EtOH, etc.) •� coagulopathy (iatrogenic (coumadin, tPA), leukemia, TTP, aplastic anemia) •� CNS infections (fungal, granulomas, herpes simplex encephalitis) •� post trauma (immediate or delayed, frontal and temporal lobes most commonly
injured via coup/contre-coup mechanism) •� eclampsia •� post-operative (carotid endarterectomy, craniotomy) •� idiopathic
Dr.JKR
NS18 Neurosurgery
Intemltionll Sublndmoid Aneurysm Trill (lSAn of IlIUIUIagicII clipping VI. IlldOVIICUIII coifing in 2143 petienlI with ruplUred intraCllllilllllturysms: IlindomiZld trill ILancet 2002; 360:1267-741 InllOduction: This randomized control trial aimed to compare endovascular detachable coil treatment against craniotomy and dipping for ruptured intracranial aneurysms in patients who were considered eligible for either modality of therapy. Mat!lods: 2143 patients were randomized to neurosurgical dipping In=10701 vs. treatment by endovascular coilln=10731.The primary clinical outcome was assessment using the modified Rankin scale for a score of 3-6 (dependellCf or death) at 1year. Results: Patients in this trial tended to be of good dillital grade prior to in!mention and amajority of aneurysms were in the anterior circulatory system. 190 out of 801123.7%1 patients who completed follow up in the endovascular treatment were dependent or dead at 1year compared with 243 of 793 130.6%1 in the neurosurgical treatment group (p:O,0019j.This showed arelative risk reduction of 22.6% {95% CI8.9-34.21 and an absolute risk reduction of 6.9 (95 CI2.5-11.3) when comparing endovascular to neurosurgical therapy, Conclusion: In patients with aruptured intracranial aneurysm who are suitable for either endovascular coiling or neurosurgical clipping, the outcome of dependellCf or death at one year favours the endovascular coiling therapy. Further neuropsychological assessment is being planned in subgroups to allow for subtle outcomes to be detected. Further follow up for dependency death is planned as well.
Cerebrovascular Disease
Epidemiology •� 12-15 cases/lOO,OOO population/year
Risk Factors •� increasing age (mainly >55 years) •� male gender •� hypertension •� Black/Asian> Caucasian •� previous CVA of any type (23x risk) •� both acute and chronic heavy EtOH use; cocaine, amphetamines •� liver disease
Clinical Features
Toronto Notes 2008
•� rIA-like symptoms often precede ICH, can localize to site of impending hemorrhage •� location: basal ganglia/internal capsule (50%), thalamus (15%), cerebral white matter
(15%), cerebellum/brainstem (15%) •� gradual onset of symptoms over minutes to hours, usually during activity •� H/A, vomiting, decreased LOC are common •� specific symptoms/deficits depend on location of ICH
Investigations •� high density blood on CT without contrast
Treatment •� medical:
•� decrease BP to pre-morbid level or by -20%; check PTT, INR, and correct coagulopathy (stop anticoagulation for 1-2 weeks)
•� control raised ICP •� phenytoin for seizure prophylaxis •� follow electrolytes (SIADH common) •� angiogram to rio vascular lesion UNLESS >45 yrs, known HTN, and
putamen/thalamic/posterior fossa ICH (yield - 0%) •� surgical:
•� craniotomy with evacuation of clot under direct vision, resection of source of ICH (Le. AVM, tumour, cavernoma), ventriculostomy to treat hydrocephalus
• indications: •� symptoms appear related to raised ICP or mass effect •� rapid deterioration (especially with signs of brainstem compression) •� favourable location, e.g. cerebellar, non-dominant hemisphere •� young patient (<50 y.o.) •� if tumour, AVM, aneurysm, or cavernoma suspected (resection or clip to
decrease risk of rebleed) •� contraindications:
•� small bleed: minimal symptoms, GCS >10 (not necessary) •� poor prognosis: massive hemorrhage (especially dominant lobe), low
GCS/coma, lost brainstem function •� medical reasons (e.g. very elderly, severe coagulopathy, difficult location
(e.g. basal ganglia, thalamus»
Prognosis •� 30-day mortality rate is 44%, mostly due to cerebral herniation •� rebleed rate is 2-6%, higher if HTN poorly controlled
Intracranial Aneurysms ___---....I~ l~
Epidemiology •� prevalence -5% (20% are multiple) •� female> male; age 35-65 years
Risk Factors •� autosomal dominant polycystic kidney disease (15%) •� fibromuscular dysplasia (7-21%) •� AVMs •� connective tissue diseases (Ehlers-Danlos, Marfan's) •� FHx •� bacterial endocarditis •� Osler-Weber-Rendu syndrome •� atherosclerosis and H1N •� trauma
Dr.JKR
Toronto Notes ZOOS� Cerebrovascular Disease Neurosurgery NS19
Types •� saccular (berry)
•� most common type • located at branch points of major cerebral arteries (Circle of Willis) •� 85-95% in carotid system, 5-15% in vertebrobasilar circulation
•� fusifonn • atherosclerotic •� more common in vertebrobasilar system, rarely rupture
•� mycotic • secondary to any infection of vessel wall, 20% multiple •� 60% Streptococcus and Staphylococcus •� 3-15% of patients with SBE
Clinical Presentation •� rupture (90%), most often SAH, but 30% ICH, 20% IVH, 3% subdural bleed •� sentinel hemorrhage ("thunderclap H/A") ---+ IMMINENT RISK •� mass effect (giant aneurysms)
• internal carotid or anterior communicating aneurysm may compress: • the pituitary stalk or hypothalamus causing hypopituitarism • the optic nerve or chiasm producing a visual field defect
• basilar artery aneurysm may compress midbrain, pons (limb weakness), or CN III
• posterior communicating artery aneurysm may produce CN III palsy •� intracavernous aneurysms (CN III, IV, Vv V~ VI)
•� small infarcts due to distal embolization (amaurosis fugax etc.) IMMINENT RISK •� seizures •� headache (without hemorrhage) •� incidental CT or angiography finding (asymptomatic)
Investigations •� CT, magnetic resonance angiography (MRA), angiogram
Treatment •� ruptured aneurysms:
• overall trend towards better outcome with early surgery or coiling (48-96 hours afterSAH)
•� choice of surgery vs. coiling not yet well defined, morphology/location can aid decision
•� treatment options: surgical placement of clip across aneurysm neck, trapping (clipping of proximal and distal vessels), thrombosing using Gugliemi detachable coils (endovascular technique), wrapping as last resort
•� unruptured aneurysms: •� 1% annual risk of rupture: risk dependent on size and location of aneurysm •� no clear evidence on when to operate: need to weigh life expectancy •� risk of morbidity/mortality of SAH (20%/50%) vs. surgical risk (2%/5%) • generally treat unruptured aneurysms>10 mm • consider treating when aneurysm 7-9 mm in middle-aged, yow1ger patients or
patients with a family history of aneurysms •� follow smaller aneurysms with serial angiography
Carotid Stenosis Definition •� narrowing of the internal carotid artery lumen due to atherosclerotic plaque
formation, usually near common carotid bifurcation into internal and external carotids
Risk Factors •� for plaque formation: HTN, smoking, OM, cva or CAD, dyslipidemia
Clinical Features •� may be asymptomatic •� symptomatic stenosis may present as transient ischemic attack (TlA), reversible
ischemic neurologic deficit (RIND), or stroke •� retinal insufficiency or infarct due to emboli occluding central retinal artery or
branches permanently or temporarily (amaurosis fugax) •� middle cerebral artery (MCA) occlusive symptoms
Prevention of dbabling and fatal strokas by� succeuful carotid endarterectomy in patiants� w~hout recent neurolGgical symptoms: ran·� domised controlled trial. - (lancet 2004;� 363:1491·1502.)�
Studr Asymptomatic Carotid Surgery TriaIIACST), a� randomized, controlled trial with follow·up at 5� years.� Patients: 3120 asymptomatic patienls with signifi·� cant carotid artery stenosis were randomized equally� between immediate carotid endarterectomy ICEAI� and indefinite deferral of CEA and were followed for� up to 5years Imean 3.4 yearsl.� Main Outeome: Any stroke lincluding fatal or dis�abling}.� Results: The risk of stroke or death within 30 days of� CEA was 3.1% (95% CI2.3-4.1). Comparing all� patients randomized to immediate CEA vs. deferral,� the 5-year stroke risks were 3.8% vs. 11% Igain 7.2%� [95% CI 5.0-9.41. p<tl.OOOll. This gain primarily� involved ischemic strokes in the carotid artery territo�ry 12.7% vs. 9.5%; gain 6.8% [4.8-8.81, p<O.OOOI}, of� which ha~ were disabling or fatal 11.6% vs. 5.3%;� gain 3.7% [2.1-5.21. p<O.OOOII. Combining the periop�erative and the non-perioperative strokes, the net 5�year risks were 6.4% vs. 11.8% for all strokes Igain� 5.4% 13.0-7.81. p<D.O001}, 3.5% vs. 6.1% for fatal or� disabling strokes Igain 2.5% [0.8-4.31, p=O.OO4I, and� 2.1% vs. 4.2% for fatal strokes Igain 2.1% [0.6-3.61.� p--o.0061.� Cone/u,ion,: In asymptomatic patients with signifi�taTll talo\\iI .1\ery menosis, immeiliate CEA reduced� the net 5-year stroke risk from about 12% to about� 6%. Half of this 5-year benefit involved disabling or� fatal strokes.�
Dr.JKR
NS20 Neurosurgery Cerebrovascular DiseaseNascular Malfonnations� Toronto Notes 2008
EndIrtmctomy for Asymptomatic Carotid AI1Iry SlInoIis - (JAMA 1995; 273:1421·1428.1
Sludy: Asymptomatic Carotid Atherosclerosis Study (flCASl, aprospective, randomized, multi· centretri.J1. Patients: 1662 patients with asymptOma1~ carotid artery stenosis of 60% or greater were randomized. Follow-up data are available on 1659. Recognized ri51: factors for stroke were similar be1ween Ilie two ~Iine.
• .Daily aspirin administration and medical ri51: factor management for all patients and carotid endarterectomy for patients randomized to rec~ve SlJrgery. IIIin 0IIfl:0mI: TlA or cerebral infarction occurring in the carotid artery territory and any TIA, stroke, or dealli occurring in the perioperative period. IIauIII:The risil for ipsilateral stroke and any peri· operative stroke or death based on a5-year follow· up lmedian of 2.7 yearsl was estimated to be 5.1% for surgical patients and 11.0% for patients treated medically (aggregate risk reduction of 53% (95% CI=22·72%1), CencIuaIotlI: Patients with asymptomatic carotid • artery steno~s of 60% or greater that are good can· didates for elective surgery will have a reduced 5year risl: of ipsilaterai stroke if carotid endarterectomy is perlormed in addition to aggressive management of modifiable risl: factors.
Investigations •� CBC, PIT, INR (hypercoagulable/hyperviscous states) •� fundoscopy > cholesterol emboli in retinal vessels (Hollenhorst plaques) •� auscultation over carotid bifurcation for bruits •� carotid duplex Doppler ultrasound: determines size of lumen and blood flow
velocity, safest but least accurate, unable to scan above mandible •� angiogram: "gold standard", 1/200 risk of stroke •� MRA: safer than angiogram, may overestimate stenosis •� CT angiogram (CTA)
Treatment •� control of HTN, lipids, diabetes (risk factor management) •� antiplatelet agents (ASA ± dipyridamole, clopidogrel) -25% relative risk reduction •� carotid endarterectomy (generally if symptomatic and >70% stenosis, see Prognosis) •� endovascular angioplasty ± stenting (utility being evaluated)
Prognosis
Table 3. Symptomatic Carotid Stenosis: North American Symptomatic Carotid EndarterectomyTrial (NASCET)
% Stenosis on Angiogram Risk of Major Stroke or Death
Medical Rx Medical +Surgical Rx 70-99 % 26% over 2years 9% over 2years 50-69% 22% over 5years 16% over 5years <50% Surgery has no benefit with 5% complication rate
Table 4. Asymptomatic Carotid Stenosis: Asymptomatic Carotic Atherosclerosis Study (ACAS) and Asymptomatic Carotid SurgeryTrial (ACsn
% Stenosis on Angiogram Risk of Major Stroke or Death
Medical Rx Medical + Surgical Rx 60-99% 11% over 5years 5.1% over 5years (ACASl 70-99% 11.8% over 5years 6.4% over 5years (ACSn
.... , ~
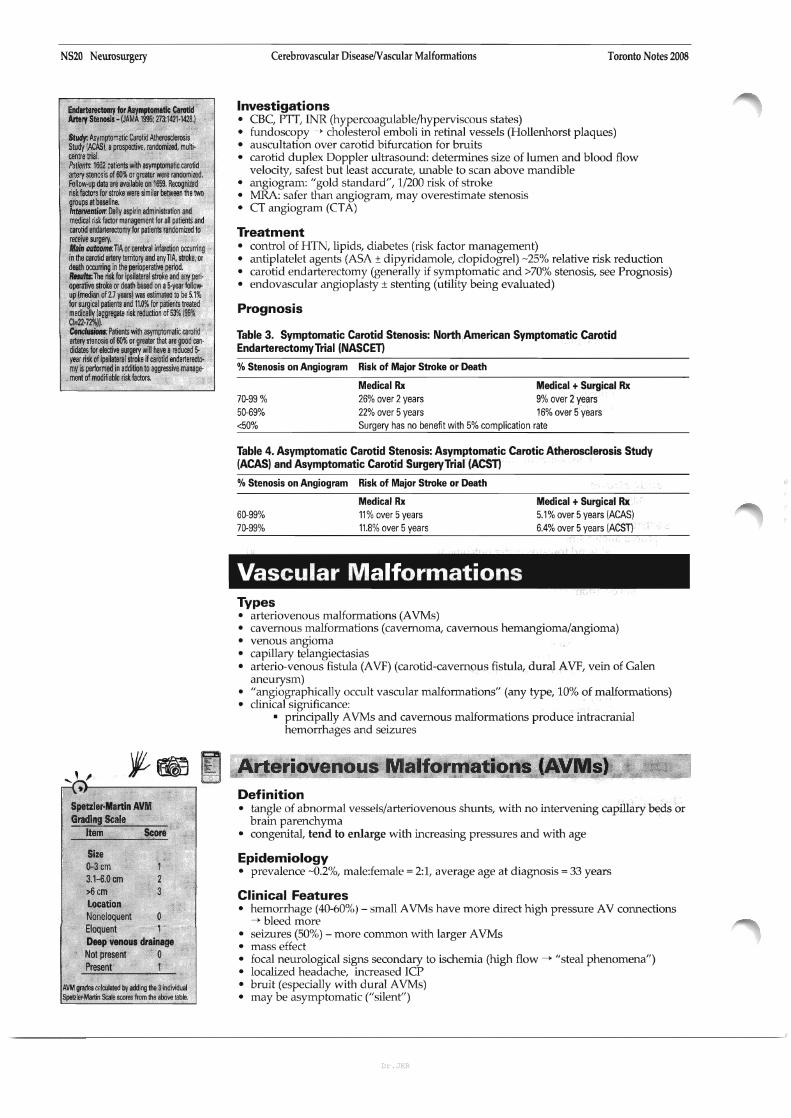
.)---------, Spetzler-Mertin AVM� Grading Scale�
Item Score�
Size D-3cm 3.1-6.0 cm >6cm Location Noneloquent Eloquent 1 Deep venous dreinage Not present 0 Present 1
AVM grades calcu/aled by adding 1Ile 3individual SpetzIer-Manin Scale scores from 1Ile above table.
Vascular Malformations Types •� arteriovenous malformations (AVMs) •� cavernous malformations (cavernoma, cavernous hemangioma/angioma) •� venous angioma •� capillary telangiectasias •� arterio-venous fistula (AVF) (carotid-cavernous fistula, dural AVF, vein of Galen
aneurysm) •� "angiographically occult vascular malformations" (any type, 10% of malformations) •� clinical Significance:
•� principally AVMs and cavernous malformations produce intracranial hemorrhages and seizures
Arteriovenous Malformations (AVMs) ----~-
Definition •� tangle of abnormal vessels/arteriovenous shunts, with no intervening capillary beds or
brain parenchyma •� congenital, tend to enlarge with increasing pressures and with age
Epidemiology •� prevalence -0.2%, male:female = 2:1, average age at diagnosis = 33 years
Clinical Features •� hemorrhage (40-60%) - small AVMs have more direct high pressure AV connections
-> bleed more •� seizures (50%) - more common with larger AVMs •� mass effect •� focal neurological signs secondary to ischemia (high flow -> "steal phenomena") •� localized headache, increased ICP •� bruit (especially with dural AVMs) •� may be asymptomatic ("silent")
Dr.JKR

Toronto Notes 2008� Vascular Malformations/DermatomesIMyotomes Neurosurgery NS21
Investigations •� MRl (flow void), MRA •� angiography (7% will also have an aneurysm)
Treatment •� decreases risk of future hemorrhage and seizure
• surgical excision is treatment of choice for grade I and II lesions • endovascular embolization (glue, balloon) can facilitate surgery or stereotactic
radiosurgery (SRS) for suitable grade II to V lesiono:; •� SRS is treatment of choice for small (-S3 em in diameter) grade I and II lesions
surgery alone is unsuitable for grade IV and V lesions •� conservative (e.g. palliative embolization, seizure control if necessary)
Prognosis •� 10% mortality, 30-50% morbidity (serious neurological deficit) per bleed •� risk of major bleed: 2-4% per year (untreated AVMs)
Cavernous Malformations Definition •� benign vascular hamartoma consisting of irregular sinusoidal vascular channels
located within the brain
Epidemiology •� 0.1-0.2%, both sporadic and hereditary forms described
Clinical Features •� seizures (60%), progressive neurological deficit (50%), hemorrhage (20%), H/A •� hemorrhage risk less than AVM, usually minor bleeds
Investigations •� MRl (non-enhancing) •� usually not seen witb angiography
Treatment •� surgical excision - depending on presentation and location (supratentorial lesions
are less likely to bleed than infratentoriallesions)
EXTRACRANIAL PATHOLOGY
Dermatomes/Myotomes
~i===:Ll-1J;II; L2
L3 L4 L5
L1 L4 L2
'L3 L5 L4
/ L5
"'-, , ~}------------,
Important Dermatomes and� Myotomes� C2 - angle of jaw C4 - collar of shirt "C3,4.5 keeps the diaphragm alive" T4 - nipple line T6- xiphoid Tl0 - umbilical T12 - suprapubic "L3 above the knee" "$2,3,4 - keeps your stool off the floor"
Figure 17. Dermatomes
Dr.JKR

NS22 Neurosurgery
.... ' ,9)------------,
Myotom.. C5 - Shoulder abduction/elbow flexion C6 - Wrist extensors C7 - Elbow extension C8 - Squeeze hand T1 - Abduct fingers T2-9 -Intercostal (Abdominal reflexesl T9-10 - Upper abdominals T11·12 - Lower abdominals L2 - Flex hip L3 - Hip adduction l4 - Knee extension l5 - Dorsiflex ankle Sl - Plantarflex fool
~,
Reflexes� 1,2 tie my shoe. 51·2 Ankle jerit� 3, 4kid. the door >l3-4 Knee� 5, 6pick up sticks. C5·6 Biceps/Brachioradialis� 7. Slay them straight> C7·STrieeps
DermatomeslMyotomes/Approach to LimblBack Pain
Table 5. Myotomal Distribution of Nerve Roots
Roots
C14 C3, 4, 5
C5,6
C5,6
C6,7
C7,8
ca,Tl ca,Tl T2-9
T9.10 T11,12
Lt, 2. 3
L2,3,4
L4,5
L5, 51, 52
L5,51
51,52
52,3,4
Movement/action
Neck flexion, extension, rotation
Inspiration,lV, FEV, VC
Abduct arm (>90~
Flex and supinate forearm
Wrist extension
Forearm extension
Grasp
Abduct/adduct fingers
Hip flexion
Leg extension
Ankle dorsiflexion
Leg flexion
Great toe extension
Foot plantar flexion
Clamp down during rectal exam
Reflex
Biceps, brachioradialis
Supinator
Triceps
Finger jerk
Abdominal cutaneous reflex
Abdominal cutaneous reflex
Cremasteric
Knee jerk
Medial hamstring
Achilles tendon
(ankle jerkl
Anal cutaneous
Nerve
Cervical
Phrenic
Axillary
Musculocutaneous
Radial
Radial
Anterior interosseus
Ulnar
Intercostal Upper abdominals
Lower abdominaIs
Femoral
Femoral
Deep peroneal
Sciatic
Deep peroneal
Tibial
Pudendal
Toronto Notes 2008
Muscle
Deep neck
Diaphragm
Deltoid
Biceps brachii, brachioradialis
Extensor carpi radialis
Triceps brachii
Flexor digitorum profundus
Interossei
Intercostals
Iliopsoas
Quadriceps
Medial hamstring, tibialis anterior
Biceps femoris, semitendinosus,
semimembranosus
Extensor hallucis longus
Soleus, gastrocnemius
Bladder, lower bowel, anal sphincter
Approach to LimblBack Pain
I Pain I
Back pain (above gluteal fold) I Neuropathy r
(below gluteal foldl�
OR2t� --r L..'''i' Isee Orthopaedics (any limb)
With exertion or� sustained position� (/~ICo""'"'·""'"I/dependent
~+ / t -----.. Vascular claudicetion Perip/leral nerveNeurogenic Cord Root - sclerotomal pain and lperipherel neuropathy)claudication (myelopathy) (radiculopathy)sensory deficit - non-dermatomaV- dermatomal pain - LMN signs! -LMN signs!- reproduced by fixed myotomaland sensory deficit symptoms symptomsamount of exercise - sclerotomal- exercise or posture - UMN signs!- immediately relieved - autonomicinduced symptomswith dysfunction- prolonged reliefl below lesionrest or standing
posture dependent- signs of poor vascular
(need to sitlsupply to limb
Figure 18. Approach to Limb/Back Pain
Dr.JKR

Toronto Notes 2008� Approach to LimbfBack Pain
Clinical Features •� local pain at site of lesion •� radiculopathy (LMN)
•� fascieulations, atrophy •� motor: flaccid, weakness, decreased deep tendon reflex in root distribution • sensory: dermatomal .J,. pinprick sensation, numbness, paresthesia, pain • trophic changes: e.g. dry skin (if long-standing radieulopathy)
•� myelopathy •� LMN signs/symptoms at level of lesion •� UMN signs/symptoms below lesion
•� arms flexed, legs extended •� motor: proximal weakness and spasticity of lower extremities, increased
reflexes, clonus, Babinski sign (extensor plantar response), l-:loffman's sign (cervical), sphincter disturbance (decreased tone/sensation)
•� sensory: findings may be minimal (reduced vibration, proprioception), ± Lhermitte sign (shock sensation radiating down arms or legs with neck flexion)
Investigations •� plain x-ray of spine, CT, MRl, myelogram, electromyography (EMG),�
electrophysiology�
Extradural Lesion Cervical Stenosis (Cervical Spondylosis) •� etiology: combination of factors
• congenital spinal stenosis, degenerative disc process leading to osteophytes and central disc herniation
• hypertrophy of lamina/dura/facets/ligaments • subluxation, increased mobility, loss of normal spinal eurvature
•� epidemiology: increasing age (usually >50) •� clinical features:
• radieulopathy (at level of lesion) • AND/OR myelopathy (usually if >30% canal stenosis, below level of lesion) • AND/OR pain/paresthesia in neck/head/shoulders
•� investigations: x-ray of cervical spine ± flexion/extension views, MRl, CT/� myelogram�
•� treatment: • analgesics, collar • surgery -� indications: myelopathy, progressive neurologic impairment,
intractable pain, <1 year since presentation •� prognosis:
• myelopathy - 48% improve if treated within 1 year, 16% after 1 year • radieulopathy - variable, but better results than myelopathy
Intradural Intramedullary Lesion Syringomyelia •� definition: "syrinx", cavitation of spinal cord substance •� etiology: congenital, neoplastic, post-traumatic
• congenital craniovertebral anomalies (e.g. Chiari malformation, myelomeningocele, tethered cord)
• intramedullary tumours • arachnoiditis (traumatic)
•� clinical features: • suspended, dissociated sensory loss • pain and temperature loss in a cape-like distribution at level of cervical syrinx • preserved light touch and other modalities • LMN arm/hand weakness or wasting • may have spastic weakness of legs •� may have hydrocephalus, often asymptomatic • painless arthropathies (Charcot's joints)
•� investigations: MRI is best method, myelogram with delayed CT •� treahnent:
• conservative if NOT progressing •� treat underlying cause (e.g. posterior fossa decompression for Chiari 1, surgical
removal of tumour if causing a syrinx) •� prognosis: progressive deterioration in>1/3 despite therapy
Neurosurgery NS23
RED FLAGS for back pain "BACK PAIN": Bowel/bladder dysfunction Anesthesia (saddle) Constitutional symptoms (fever, night sweat, chills, weight loss) IKlhronic disease Paresthesia Age >50 IV drug use Neuromotor deficits
Figure 19.T, weighted� MRI of Syringomyelia�
Dr.JKR

NS24 Neurosurgery Spinal Cord Syndromes� Toronto Notes 2008
... '•.l--------------,, Compartmentalize spinII cord ayncIromM anatomically by location.
o
o
~) . ~,
The pattern of impairment in Central Cord Syndrome is uMUO": Motor> sensory loss� Upper> lower extremity� Distal> proximal�
Spinal Cord Syndromes
•� see Neurology. N2 for Spinal Cord Anatomy
Complete Spinal Cord Lesion •� bilateral loss of motor/sensory and autonomic function at ;::4 segments below
lesion/injury, with UMN signs
Incomplete Spinal Cord Lesion •� any residual function at ;::4 segments below lesion •� signs include sensory/motor fimction in lower limbs and "sacral sparing" (perianal
sensation, voluntary rectal sphincter contraction) •� syndromes include Brown-Sequard's, central cord, anterior cord and posterior cord
Brown-Sequard Syndrome •� hemisection of spinal cord (lateral compression of one half of spinal cord) •� common causes:
•� trauma, tumour (extrinsic compression)
Signs and Symptoms •� motor
• ipsilateral loss of voluntary motor function below level of lesion with UMN signs • ipsilateral LMN signs at level of lesion
•� sensory• ipsilateral loss of vibration and proprioception; contralateral loss of pain
and temperature below level of lesion; "suspended" ipsilateral deficits (deficits are 1 to 2 levels below injury - Lissauer's tract)
• preserved light touch •� prognosis
• best prognosis of cord injuries (90% ambulate independently and have good sphincter control)
Anterior Cord Syndrome •� common causes
• anterior spinal artery territory compression or occlusion (anterior spinal artery supplies anterior 2/3 of cord)
Signs and Symptoms •� motor
• bilateral paraplegia (UMN below and LMN at level of lesion) • sphincter dysfunction (urinary retention)
•� sensory• bilateral loss of pain and temperature below level of lesion with preserved light
touch, vibration and proprioception (dissociated sensory loss)
Central Cord Syndrome •� most common incomplete spinal cord injury syndrome •� common causes:
• syringomyelia (progressive central cord cavitation), central tumours, spinal extension injuries
Signs and Symptoms •� motor
• bilateral motor paresis; upper (LMN lesion) > lower (UMN lesion) extremities; more pronounced in the hands
• sensory• variable bilateral suspended sensory loss (dissociated sensory loss -� pain and
temperature loss greater than vibration and proprioception loss) • intact sensation aoove and below affected dermatomes; sacral sparing
• other • bowel and/or bladder dysfunction is usually a late manifestation
•� prognosis•� 50% recover enough lower extremity function to ambulate, 90% ambulate
within 5 days, hand recovery variable
Dr.JKR

Toronto Notes 2008� Spinal Cord SyndromesfRoot Compression Neurosurgery S25
Posterior Cord S ndrome� [ o
•� common causes • posterior spinal artery infarction, trauma
Signs and Symptoms •� motor
• preserved motor function •� sensory
• bilateral loss of vibration and proprioception below level of lesion • preserved pain and temperature
•� prognosis •� more favourable than anterior cord syndrome
Root Compression
Differential Diagnosis •� herniated disk •� neoplasm (neurofibroma, schwannoma) •� synovial cyst, abscess •� hypertrophic bone/spur
Cervical Disc Syndrome Etiology • nucleus pulposus herniates through annulus fibrosis and impinges upon nerve root
Epidemiology •� most common levels C6-C7 (C7 root) > C5-C6 (C6 root)
Clinical Features •� pain down arm in nerve root distribution, worse with neck extension, ipsilateral�
rotation and lateral flexion (all compress the ipsilateral neural foramen)� •� LMN signs/symptoms
..... ' ,•� central cervical disc protrusion causes myelopathy as well as nerve root deficits .\-----------,
Investigations� Disc herniations impinge the nerve •� C-spine x-ray, CT, MRl (procedure of choice), EMG, nerve conduction studies root at the level below the inter
space in the cervical spine (i.e. C5Treatment 6 disc affects the C6 nerve root) •� conservative
•� no bedrest unless severe radicular symptoms • activity modification, patient education (reduce sitting, lifting) • physiotherapy (PT), exercise programs • analgesics; collar, traction may help
•� surgical indications • intractable pain despite adequate conservative treatment for >3 months • progressive neurological deficit • anterior cervical discectomy is usual surgical choice
Prognosis •� 95% improve spontaneously in 4 to 8 weeks
Table 6. lateral Cervical Disc Syndromes
C4-5 C5-6 C6-7 C7-T1
Root Involved C5 C6 C7 C8� Incidence 2% 19% 69% 10%� Sensory Shoulder Thumb Middle finger Ring finger, 5th finger� Motor Deltoid, biceps, Biceps Triceps Digital flexors,�
supraspinatus intrinsics� Reflex No change Biceps, Triceps Finger jerk�
Brachioradialis�
Dr.JKR

----------------
NS26 Neurosurgery Root Compression� Toronto Notes 2008
[uml)ar Disc Syn(lromeo
Figure 20. T2-weighted MRI of Lumbar Disc Herniation
Etiology •� same as cervical disease (laterally: compressing nerve root, centrally: cauda equina)
Epidemiology •� common (>95% of herniated lumbar disks) - L5 and S1 roots
Clinical Features •� leg pain> back pain •� limited back movement (especially forward flexion) due to pain •� symptoms and signs of radiculopathy (LMN) •� ± reflex paravertebral muscle spasm (functional scoliosis, loss of lordosis) •� nerve root tension signs:
• straight leg raise (SLR: Lasegue's test), crossed SLR ---+ LS, Sl roots • femoral stretch ---+ L4 root
Investigations •� x-ray spine (only to rule out other lesions), CT, MRl •� myelogram and post-myelogram CT (if surgery contemplated and plain CT not
conclusive)
Treatment •� conservative (same as cervical disc disease) •� surgical indications
•� same as cervical disc + cauda equina syndrome
Prognosis •� 95% improve spontaneously within 4 to 8 weeks
Table 7. Lateral Lumbar Disc Syndromes
1.34� L4-5 L5-S1
Root Involved L4� L5 S1
Incidence <10%� 45% 45%
Pain Femoral pattern� Sciatic pattern Sciatic pattern
Sensory Medial leg� Dorsal foot to hallux Lateral foot lateral leg
Motor Tibialis anterior (dorsiflexion)� Extensor hallucis longus Gastrocnemius, soleus (hallux extension) (plantar flexion)
Reflex Knee jerk� Medial hamstrings Ankle jerk
Cauda Equina Syndrome-----------------' Etiology •� compression of lumbosacral nerve roots below conus medullaris •� large central herniated disc (L4-5 or L5-S1) ± spinal stenosis, extrinsic mass
Clinical Features •� motor (LMN signs)
• weakness/paraparesis in multiple root distribution •� reduced deep tendon reflexes (knee and ankle) • sphincter disturbance (urinary retention and fecal incontinence due to loss of
anal sphincter tone) •� sensory
• pain in back radiating to legs� bilateral sensory loss or pain: involving multiple dermatomes�
• saddle anesthesia (most common sensory deficit) • sexual dysfunction (late finding)
Treatment •� requires urgent investigation and decompression «48 hrs) to preserve bowel and
bladder function
Dr.JKR

--------------
Toronto Notes 2008� Root Compression/Peripheral Nerves Neurosurgery NS27
___________~_~_--lLumbar SRinal StenosisEtiology •� congenital narrowing of spinal canal combined with degenerative changes
(herniated disk, hypertrophied facet joints and ligaments)
Clinical Features •� neurogenic claudication - 60% sensitive • neurologic exam may be normal, including straight leg raise test • often absent Achilles reflexes and diminished knee jerks •� symptoms relieved only by changing position (leaning forward, sitting down)
Investigations •� spine x-ray, CT, MRl, myelogram
Treatment •� conservative - NSAIDs, analgesia •� surgical -laminectomy with root decompression
enic ClaudicationEtiology •� ischemia of lumbosacral nerve roots secondary to vascular compromise and
increased demand from exertion, often associated with lumbar stenosis
Clinical Features •� dermatomal pain/paresthesia/weakness of buttock, hip, thigh, or leg initiated by
standing or walking •� slow relief with postural changes (sitting >30 min), NOT simply exertion cessation •� induced by variable degree of exercise or standing •� may be elicited with lumbar extension, but may not have any other neurological
findings, no signs of vascular compromise (e.g. ulcers, poor capillary refill, etc.)
Investigations •� bicycle test may help distinguish neurogenic claudication (NC) from vascular
claudication (with the waist flexed individuals with NC can last longer)
Treatment •� same as for lumbar spinal stenosis
Peripheral Nerves
Clinical Features •� peripheral polyneuropathy vs. peripheral nerve injury (entrapment/trauma) •� sclerotomal distribution (non-dermatomallmyotomal) •� loss of sensation, paraesthesia •� sensory deficits often symmetric, glove and stocking •� motor weakness •� trophic changes: cold extremities, cutaneous hair loss, brittle nails •� autonomic changes: local vasoconstriction (hypohidrosis) --> edema --> vasodilation�
(hyperhidrosis)�
Peripheral Nerve Inju Classification and Clinical Course •� neuropraxia: nerve intact but fails to function, recovery within hours to months •� axonotmesis: axon disrupted but nerve sheath intact --> Wallerian degeneration (of
axon segment distal to injury) --> recovery -1 mm/day •� neurotmesis: nerve completely severed, need surgical repair for recovery
Investigations •� radiologic (C-spine, chest/bone x-rays, myelogram, CT, MRl), bloodwork (CSF) •� electrophysiological studies (EMG, nerve conduction velocities (NCV)) may be helpful
in assessing nerve integrity
Treatment •� surgical repair of nerve sheath unless known to be intact (suture nerve sheaths or
nerve graft)
.... ' ,."l----------, Spinal cord ends at L1-2; dura� ends at 51-2�
.... ' ,.}--------------.., Key Features of Neurogenic vs.� V.scular Claudication� Neurogenic Claudication: der�matomal distribution with positional� relief occurring over minutes� Vascul.r Claudication: sclerotomal� distribution with relief occurring with� rest over seconds�
.,;.
Differential Diagnosis for Peripheral Neuropathy - "DANG THERAPIST" Diabetes or Drugs Alcohol or AIDS Nutritional (8'2 deficiency) Guillain-8arre Syndrome Traumatic Hereditary (Refsum's) Endocrine or Entrapment Renalluremia) Amyloid Porphyria Infectious� Sarcoid� Toxins�
Dr.JKR
NS28 Neurosurgery Peripheral Nerves� Toronto Notes 2008
L o
•� if sharp transection may consider primary repair •� most cases are dealt with in a delayed fashion •� conditions for ideal healing/regeneration
•� nerve transected sharply • clean wound� • optimal surgical facilities� • optimal cell metabolism� • possible spontaneous recovery/regeneration
•� delay surgical repair for a few weeks if first 3 conditions are not met
Nerve Entrapment •� definition: nerve compressed by nearby anatomic structures, often secondary to
localized, repetitive mechanical trauma with additional vascular injury to nerve •� clinical features: sensory loss in nerve distribution (often discriminative touch lost
first)
Carpal Tunnel Syndrome (CTS) •� see Plastic Surgery. PL17
Ulnar Nerve Entrapment at Elbow •� etiology: may be entrapped at several locations:
• behind medial epicondyle •� at medial intermuscular septum • distal to elbow at cubital tunnel
•� epidemiology: second most common entrapment neuropathy •� clinical features
• sensory: pain, numbness in ulnar 1.5 fingers • wasting of interossei (especially first dorsal interosseous) • weakness (especially abduction of index finger) - Wartenberg's sign • claw hand •� ± Tiner's sign from percussion of elbow (does not localize site of entrapment) • dislocation of ulnar nerve may be palpated at medial epicondyle with elbow
flexion/extension •� investigations: NCV ---> conduction delay across elbow •� treatment
• conservative: prevent repeated minor trauma (e.g. leaning on elbow or sleeping with hand under head), elbow pads, NSAIDs
• surgical: nerve decompression and transposition anterior to medial epicondyle
Less Common Entrapments •� Brachial plexus
• Erb's palsy ("Bellhop's tip position"): C5-6 injury; arm hangs at side, internally rotated, extension at elbow
• Klumpky's palsy: C8-Tl injury; clawed hand and wasting of small muscles of hand, ± flexed elbow
• Thoracic outlet syndrome • compression of the lower portion of the brachial plexus (which supplies the
ulnar nerve) as it emerges from the axilla, through a narrow passage beneath the clavicle and between the anterior and middle scalene muscles, while resting on the first rib
•� CXR to rule out Pancoast tumour (associated with Homer's syndrome) as this may mimic thoracic outlet syndrome, congenital cervical rib
•� Radial nerve ("Saturday Night Palsy") •� more often a pressure palsy (compression of axilla) • weakness of wrist and finger extensors (normal triceps)
•� Motor branch of ulnar nerve at wrist (Guyon's canal) • same as ulnar nerve entrapment but no sensory deficit on dorsum of hand
•� Common peroneal nerve • superficial and fixed behind fibular neck (sensitive to trauma, e.g. fracture) •� motor: decreased foot and toe extension ("foot drop"), decreased ankle eversion • sensory: decreased lateral foot and dorsum (less common)
•� Lateral cutaneous femoral nerve of the thigh ("meralgia paraesthetica") • pain over anterior/lateral aspect of thigh •� common in obese people, patients post-iliac bone grafts
•� Posterior tibial nerve ("tarsal tunnel") • pain/paresthesia in toes and sole of foot ± clawing of toes (Tiner's sign over
medial malleolus)
Dr.JKR

Toronto Notes 200S� Neurotrauma
SPECIALTV TOPICS
Neurotrauma Trauma Management (see also Emergenc;y Medicine. ER6)
Trauma Assessment
INITIAL MANAGEMENT
ABC's of trauma management take priority •� see Emergenc;y Medicine. ER2
NEUROLOGICAL ASSESSMENT
Mini-History •� period of LOC, post traumatic amnesia, loss of sensation/function, type of injury/�
accident�
Neurological Exam •� Glasgow Coma Scale (GCS) •� head and neck (lacerations, bruises, basal skull fracture signs, facial fractures, foreign
bodies) •� spine (palpable deformity, midline pain/tenderness) •� eyes (pupillary size and reactivity) •� brainstern (breathing pattern, CN palsies) •� cranial nerve exam •� motor exam, sensory exam (only if GCS is 15), reflexes •� sphincter tone •� record and repeat neurological exam at regular intervals
Investigations •� CT,L-spine x-rays
• AP, lateral, odontoid views for C-spine (must see from Cl to T1 (swimmer's view if necessary)) or CT
• oblique views looking for pars interarticularis fracture ("Scottie dog" sign) •� CT head and upper C-spine (whole C-spine if patient unconscious) look for fractures,
loss of mastoid or sinus air spaces, blood in cisterns, pneumocephalus •� Type and cross-match, ABG, CBC, drug screen (especially alcohol) •� chest and pelvic x-ray as indicated
TREATMENT
Treatment for Minor Head Injury • see also Canadian CT Head Rule sidebar, Emerenc;y Medicine. ER8)� • observation over 24-48 hours� •� wake every hour •� judicious use of sedatives or pain killers during this monitoring period
Treatment for Severe Head Injury (GCS :::;8) •� clear airway and ensure breathing (intubate if necessary) •� secure C-spine •� maintain adequate BP •� monitor to detect complications (GCS, CT, ICP) •� monitor and manage increased ICP if present (see Herniation, NS6) •� pharmacotherapy: anticonvulsants x 7 days, calcium channel blocker (CCB) for adult
cases only •� repair dural tears (>7 days)
Treatment of Spinal Injury • reduce dislocation if present by traction or surgery •� stabilize spine if unstable (halo vest, fusion, etc.) •� MRJ if neurological deficit is present to rule out cord compression
Neurosurgery NS29
"" ' ,.}-------------, Glasgow Coma Scale Eye IlIIponse VerbIIIItesponse Motor IlIIponse 4spontaneous 5oriented 6obeys commands 3opens eyes to 4confused 510calires to pain
voioe 3inappropliate words4 withdraws from 2opens eye to 2incomprehensible pain
pain soonds 3flexion to pain 1no eye opening 1no response (decorticate
posturingl 2exten~onto
pain (decerebrate posturingl
1no response
"'. Assessment of Spine CTlXray� (parasagittal view) - "ABCDS·� Alignment (Columns: anterior vertebral� line, posterior vertebral line, spinolami�nar line, posterior spinous line)� Bone (vertebral bodies, facets, spinous� processes)� Cartilage� Disc (disc space and interspinous space)� Soft tissues�
Dr.JKR
NS30 Neurosurgery
Vl/hich patients need CT head or transfer to aneurosurgical center? • remains unconscious after resuscitation • focal neurological signs • deteriorating
It'
Layer. of Scalp - "SCALP" Skin� Connective tissue (dense)� Aponeurosis (galea)� Loose connective tissue� Periosteum�
Neurotrauma� Toronto Notes 2008
•� emergent surgical decompression and/or fusion if necessary (i.e. patient with neurological deterioration)
•� more likely to be beneficial in incomplete cord injury • emergent surgery contraindicated for: complete spinal cord injury >8 hours,
medically unstable patient, and central cord syndrome •� urinary catheter, shifting in bed q2h, physiotherapy long-term •� ± high dose methylprednisolone (controversial)
Which patients should be admitted to hospital? •� skull fracture •� indirect signs of basal skull fracture •� confusion, impaired consciousness •� focal neurological signs •� extreme headache, vomiting •� seizures •� concussion with >5 minutes amnesia •� unstable spine •� use of alcohol •� poor social support (i.e. no friend/relative to monitor for next 24 hours) •� if there is any doubt, especially with children
KEY POINTS •� never do lumbar puncture in head injury •� all patients with head injury have C-spine injury until proven otherwise •� don't blame coma on alcohol- there may also be a hematoma •� low BP after head injury means injury elsewhere •� must clear spine both radiologically AND clinically (will require re-assessment
if/when patient improves clinically)
Head Injury-""--------------------_.....Scalp Injury •� rich blood supply •� considerable blood loss (vessels contract poorly when ruptured) •� minimal risk of infection due to rich vascularity
Skull Fractures� ~ •� depressed fractures ---> double density on skull x-ray (outer table of depressed segment
below inner table of skull), CT with bone windows is gold standard •� simple fractures (closed injury) ---> no need for antibiotics, no surgery •� compound fractures (open injury) ---> increased risk of infection, surgical debridement
within 24 hours is necessary • internal fractures into sinus ---> meningitis, pneumocephalus, risk of operative
bleed may limit treatment to antibiotics • basal skull fractures ---> not readily seen on x-ray, rely on clinical signs
• retroauricular ecchymoses (Battle's sign) • periorbital ecchymoses (raccoon eyes) • hemotympanum •� CSF rhinorrhea, otorrhea (suspect CSF if halo or target sign present)
suspect with Lefort II or ill midface fracture (seen on imaging)
Cranial Nerve Injury •� most traumatic causes of cranial nerve injury do not warrant intervention and have
at least minimal improvement •� surgical intervention:
• CN II -local eye/orbit injury •� CN ill, IV, VI - if herniation secondary to mass • CN VIII - repair of ossicles
•� CN injuries that improve: • CN I - recovery may occur in a few months; most do not improve • CN ill, IV, VI - majority recover •� CN VII - recovery with delayed lesions •� CN VITI - vestibular symptoms improve over weeks, deafness usually
permanent (except when resulting from hemotympanum)
Dr.JKR

Toronto Notes 2008� Neurolraurna
Arterial Injury •� e.g. carotid-cavernous (C-C) fistula, carotid/vertebral artery dissection
Intracranial Bleeding (see Blood, NS13 and Cerebrovascular Disease, NSI5)
Brain Injury Primary Impact Injury •� mechanism of injury determines pathology: penetrating injuries, gunshot wounds
• low velocity~ local damage • high velocity -. distant damage possible (due to wave of compression),
concussion •� American Academy of Neurology (AAN) definition of concussion: "a trauma-induced
alteration in mental status that mayor may not involve loss of consciousness" •� AAN Classification:
•� Grade 1: altered mental status <15 min •� Grade 2: altered mental status>15 min •� Grade 3: any loss of consciousness
•� no parenchymal abnormalities on CT •� coup (damage at site of blow) •� contre-coup (damage at opposite site of blow)
•� acute decompression causes cavitation followed by a wave of acute compression •� contusion (hemorrhagic)
• high density areas on CT ± mass effect • commonly occurs with brain impact on bony prominences (inferior frontal lobe,
pole of temporal lobe) •� diffuse axonal injury/shearing
• may tear blood vessels ---> hemorrhagic foci • wide variety of damage results • all brain injury causes shear • often the cause of decreased LOC if no space occupying lesion on CT
Secondary Pathologic Processes •� 1/3 of in-hospital mortalities following head injury were able to talk after the injury •� delayed and progressive injury to the brain due to:
• edema • intracranial hemorrhages • ischemia/infarction • raised rcp
Extracranial Conditions •� hypoxemia
•� trauma: chest, upper airway, brainstem • exceptionally damaging to traumatized brain cells • leads to ischemia, raised rcp
•� hypercarbia • leads to raised rcp (secondary to vasodilation)
•� systemic hypotension • caused by blood loss, not by head injury (e.g. ruptured spleen) • cerebral autoregulation lost in trauma • leads to decreased CPP, ischemia
•� hyperpyrexia • leads to increased brain metabolic demands ---> ischemia
•� fluid and electrolyte imbalance • iatrogenic (most common) • syndrome of inappropriate antidiuretic hormone (SlADH) secretion (from head
injury) • diabetes insipidus (Dr) from head injury • may lead to cerebral edema and raised rcp
•� coagulopathy
Intracranial Conditions •� raised rcp due to traumatic cerebral edema OR traumatic intracranial hemorrhage
Neurosurgery NS31
... ' ,9}-----------,
AAN Classification� Grade 1: altered mental status <15 min� Grade 2: altered mental status> 15 min� Grade 3: any loss of consciousness�
Management Associated w~h AAN Concussion Grades AANGrede Management Options 1 Examine 15min for amnesia and other
symptoms Return to normal activity it symptoms clear within 15mins
Remove from activity for 1day, then reexamine CT or MRI if HlA or other symptoms worsen or last>1week Return to normal activity after 1week without symptoms
Emergent neuro exam t imaging If initial exam is normal, may go home with close follow up Admit if any signs of pathology or persistent abnormal mental status CT or MRI if H/A or other symptoms If brief concussion 1(1 mini, return to normal activity after 1week without symptoms If prolonged concussion 1>1 min), return to normal activity only after 2 weeks wnhout symptoms
Coup
ContF"CCO~
Figure 21. CT Showing Coup-Contre-Coup Injury
... , , 9}-----------,
SIAOH -> hyponatremia,� 01-> hypernatremia�
Dr.JKR

NS32 Neurosurgery
.....� Type 2 I \
, I0�
© Hidenori Miyagawa 2006
Figure 22. Odontoid Fracture Classification D-,r
Neurotrauma� Toronto Notes 200S
Late Com~lications of HeadIBrain Inju~
•� seizures •� 5% of head injury patients develop seizures • incidence related to severity and location of injury -> increased with local brain
damage or intracranial hemorrhage • post-traumatic seizure may be immediate, early, or late •� presence of early (within first week) post-traumatic seizure raises incidence of
late seizures to 25% •� meningitis: associated with CSF leak from nose or ear •� hydrocephalus: acute hydrocephalus or delayed normal pressure hydrocephalus (NPH)
•� see Orthopaedics. ORlO and Emergency Medicine. ER9
Vertebral Column (See Assessment of Spine sidebar, NS29) •� stable fracture •� compression fracturf' •� unstable fracture
•� burst fracture (note: not all burst fractures are unstable) • dislocation, locked facets
•� "special" fractures • odontoid (Type I, II, III): Type 11/111 unstable; II requires fixation • Jefferson (fractures in ring of CI): due to axial loading • hangman's (fractured C2 pedicles at pars interarticularis, spondylolisthesis of
the axis): due to hyperextension • clay shoveler's fracture (avulsion of spinous process, usually C7)
•� assess ligamentous instability using flexion/extension x-ray views of C-spine ± MRI •� thoracolumbar spine unstable if 4/6 segments disrupted (3 columns divided into left
and right) • anterior column: anterior half of vertebral body, disc and anterior longitudinal
ligament • middle column: posterior half of vertebral body, disc and posterior longitudinal
ligament • posterior column: posterior arch, facet joints, and ligaments
Spinal Cord •� cord injury with initial bony or ligamentous trauma or after moving an unstable
vertebral column •� complete: no preservation of sensory/motor function below lesion, no recovery • incomplete lesions (see Spinal Cord Syndromes, NS24)
Nerve Roots •� avulsion (e.g. bracrual plexus in motorcycle accident)
Neurologically Determined Deatli________--11
Definition •� irreversible and diffuse brain injury resulting in absence of clinical brain function •� cardiovascular activity may persist for up to two weeks
Criteria of Diagnosis •� prerequisites: no CNS depressant drugs/neuromuscular blocking agents, no drug
intoxication/poisoning, temperature >32"C, no electrolyte/acid-base/endocrine disturbance
•� absent brainstem reflexes: • absent pupillary light reflex • absentcornealreflpxes • absent oculocephalic response • absent caloric responses (i.e. no deviation of eyes to irrigation of each ear
with 50cc of ice water - allow 1 min after injection, 5 min between sides) • absent pharyngeal and tracheal reflexes • absent cough with tracheal suctioning • absent respiratory drive at PaC02 >60mmHg or >20mmHg above baseline
(apnea test) • 2 evaluations separated by time, usually performed by two specialists
(e.g. neurologist, anesthetist, neurosurgeon) •� confirmatory testing: flat EEG, absent perfusion assessed with cerebral angiogram
Dr.JKR
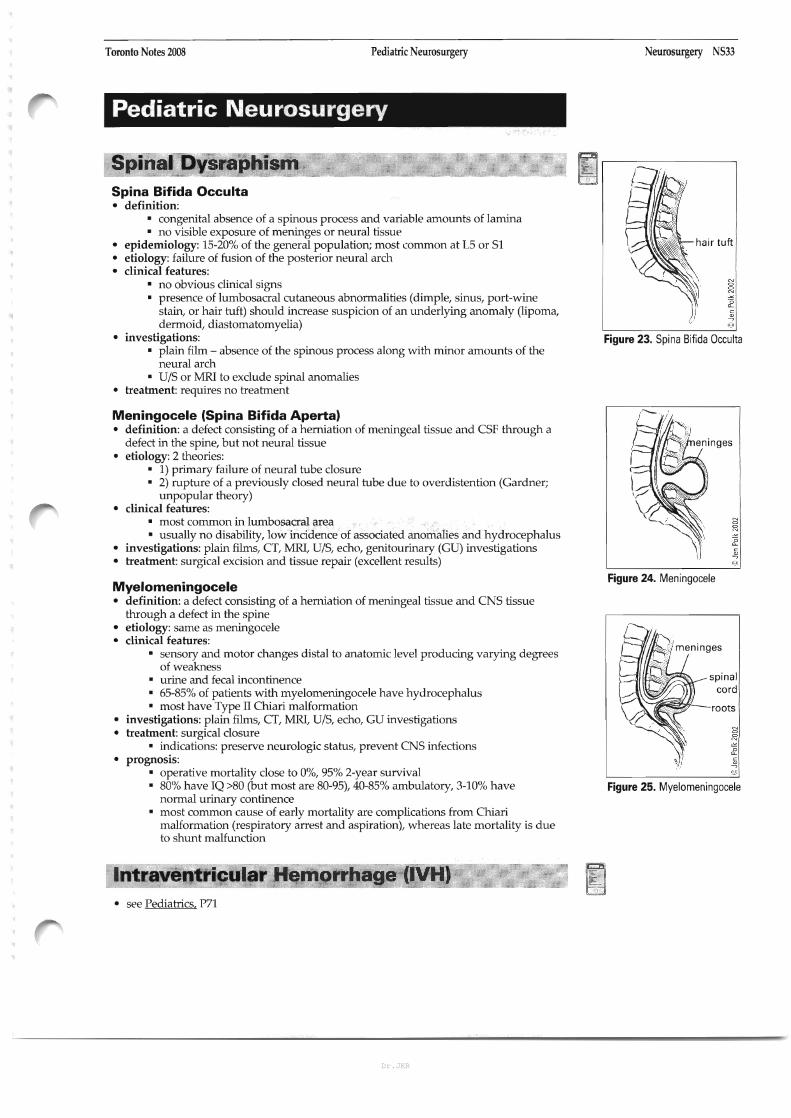
Toronto Notes 2008� Pediatric Neurosurgery Neurosurgery NS33
Pediatric Neurosurgery
Spinal Dysraphism Spina Bifida Occulta •� definition:
• congenital absence of a spinous process and variable amounts of lamina •� no visible exposure of meninges or neural tissue
•� epidemiology: 15-20% of the general population; most common at L5 or Sl •� etiology: failure of fusion of the posterior neural arch •� clinical features:
•� no obvious clinical signs • presence of lumbosacral cutaneous abnormalities (dimple, sinus, port-wine�
stain, or hair tuft) should increase suspicion of an underlying anomaly (lipoma,� dermoid, diastomatomyelia)�
•� investigations: Figure 23. Spina Bifida Occulta • plain film -� absence of the spinous process along with minor amounts of the�
neural arch� •� DIS or MRI to exclude spinal anomalies
•� treatment: requires no treatment
Meningocele (Spina Bifida Aperta) •� definition: a defect consisting of a herniation of meningeal tissue and CSF through a�
defect in the spine, but not neural tissue� •� etiology: 2 theories:
•� 1) primary failure of neural tube closure •� 2) rupture of a previously closed neural tube due to overdistention (Gardner;�
unpopular theory)� •� clinical features:
•� most common in lumbosacral area • usually no disability, low incidence of associated anomalies and hydrocephalus
•� investigations: plain films, CT, MRI, DIS, echo, genitourinary (GD) investigations •� treatment: surgical excision and tissue repair (excellent results)
Figure 24. MeningoceleMyelomeningocele •� definition: a defect consisting of a herniation of meningeal tissue and CNS tissue�
through a defect in the spine� •� etiology: same as meningocele •� clinical features:
• sensory and motor changes distal to anatomic level producing varying degrees� of weakness�
spinal• urine and fecal incontinence •� 65-85% of patients with myelomeningocele have hydrocephalus :::~~~~IJ-- cord• most have Type II Chiari malformation� roots
•� investigations: plain films, CT, MRI, DIS, echo, GD investigations •� treatment: surgical closure g:
• indications: preserve neurologic status, prevent CNS infections� ~
£ •� prognosis: :/ ~
• operative mortality close to 0%, 95% 2-year survival @
•� 80% have IQ >80 (but most are 80-95), 40-85% ambulatory, 3-10% have Figure 25. Myelomeningocele normal urinary continence
• most common cause of early mortality are complications from Chiari� malformation (respiratory arrest and aspiration), whereas late mortality is due� to shunt malfunction�
Intraventricular Hemorrhage (lVH) •� see Pediatrics. P71
Dr.JKR

NS34 Neurosurgery Pediatric Neurosurgery� Toronto Notes 2008
I.� o
o
Hydrocephalus in Pediatrics Etiology •� congenital
• aqueductal anomalies, primary aqueductal stenosis in infancy • secondary gliosis due to intrauterine viral infections (mumps, varicella,
TORCH) • Dandy-Walker malformation (2-4%) • Chiari malformation, especially Type II • myelomeningocele
•� acquired • post meningitis • post hemorrhage (SAH, IVH) •� masses (vascular malformation, neoplastic)
Clinical Features •� symptoms and signs of hydrocephalus are age related in pediatrics •� increased head circumference (HC), bulging anterior fontanelle, widened cranial
sutures •� irritability, lethargy, poor feeding and vomiting •� "cracked pot" sound on cranial percussion •� scalp vein dilation (increased collateral venous drainage) •� sunset sign - forced downward deviation of eyes •� episodic bradycardia and apnea
Investigations •� skull x-ray, DIS, CT, }"IRI, ICP monitoring
Treatment •� similar to adults (see Hydrocephalus, NS7)
Definition •� atresia of foramina of Magendie and Luschka, resulting in:
• complete or incomplete agenesis of the cerebellar vermis with widely separated, hypoplastic cerebellar hemisphere
• posterior fossa cyst, enlarged posterior fossa • dilatation of 4th ventricle (also 3rd and lateral ventricles)
•� associated anomalies • hydrocephalus (90%) • agenesis of corpus callosum (17%)� • occipital encephalocele (7%)�
Epidemiology •� 2-4% of pediatric hydrocephalus
Clinical Features •� 20% are asymptomatic, seizures occur in 15% •� symptoms and signs of hydrocephalus combined with a prominent occiput in infancy •� ataxia, spasticity, poor fine motor control common in childhood
Investigations •� skull x-ray, CT
Treatment •� asymptomatic patients require no treatment •� associated hydrocephalus requires surgical treatment •� supratentorial lateral ventricular or cystoperitoneal shunt
•� Prognosis: 75-100% survival, 50% have normal IQ
Dr.JKR
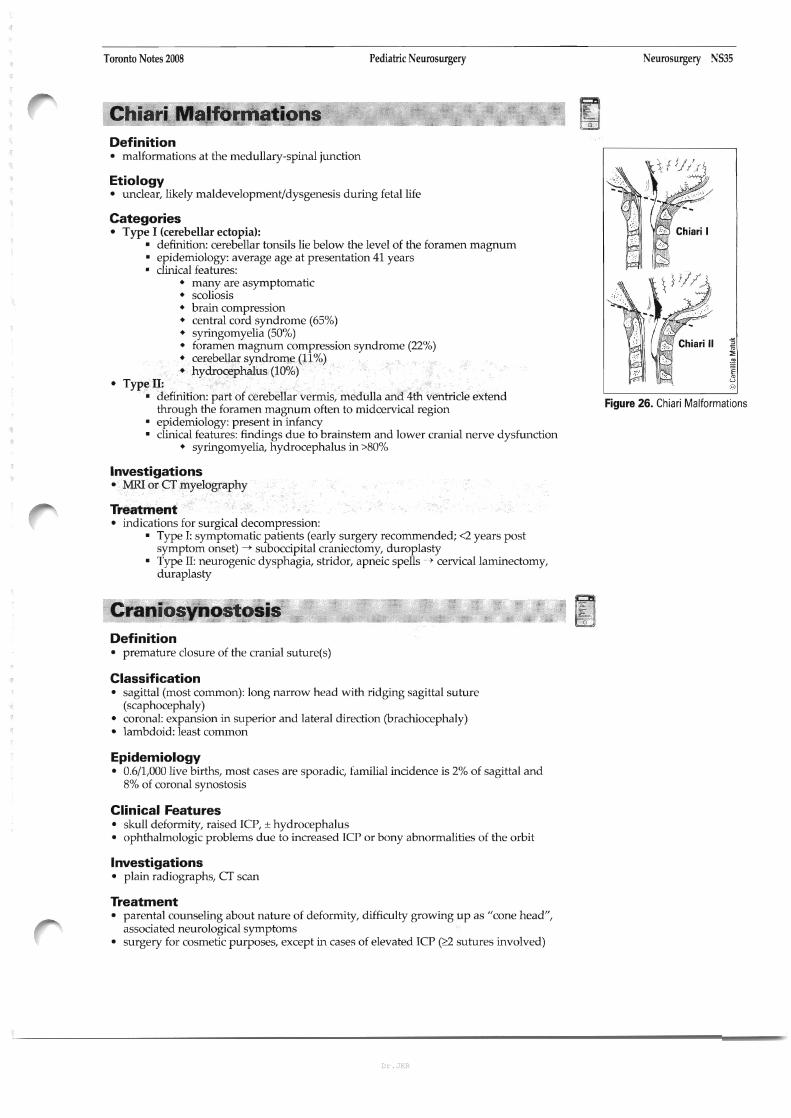
Toronto Notes 2008� Pediatric Neurosurgery Neurosurgery !lJS35
Chiari Malformations o
Definition •� malformations at the medullary-spinal junction
Etiology •� unclear, likely maldevelopment/dysgenesis during fetal life
Categories •� Type I (cerebellar ectopia):
• definition: cerebellar tonsils lie below the level of the foramen magnum • epidemiology: average age at presentation 41 years • clinical features:
•� many are asymptomatic •� scoliosis •� brain compression •� central cord syndrome (65%) •� syringomyelia (50%) •� foramen magnum compression syndrome (22%) •� cerebellar syndrome (11%) •� hydrocephalus (10%)
• Type II: • definition: part of cerebellar vermis, medulla and 4th ventricle extend
Figure 26. Chiari Malformationsthrough the foramen magnum often to midcervical region • epidemiology: present in infancy • clinical features: findings due to brainstem and lower cranial nerve dysfunction
•� syringomyelia, hydrocephalus in >80%
Investigations • MRI or CT myelography
Treatment •� indications for surgical decompression:
• Type I: symptomatic patients (early surgery recommended; <2 years post� symptom onset) -> suboccipital craniectomy, duroplasty�
• Type II: neurogenic dysphagia, stridor, apneic spells ---> cervical laminectomy,� duraplasty�
Craniosynostosis o
Definition •� premature closure of the cranial suture(s)
Classification •� sagittal (most common): long narrow head with ridging sagittal suture�
(scaphocephaly)� •� coronal: expansion in superior and lateral direction (brachiocephaly) •� lambdoid: least common
Epidemiology •� 0.6/1,000 live births, most cases are sporadic, familial incidence is 2% of sagittal and�
8% of coronal synostosis�
Clinical Features • skull deformity, raised ICP, ± hydrocephalus� • ophthalmologic problems due to increased ICP or bony abnormalities of the orbit�
Investigations •� plain radiographs, CT scan
Treatment •� parental counseling about nature of deformity, difficulty growing up as "cone head",�
associated neurological symptoms� •� surgery for cosmetic purposes, except in cases of elevated ICP (~ sutures involved)
Dr.JKR

NS36 Neurosurgery Pediatric NeurosurgerylFunctional Neurosurgery/Common Medications Toronto Notes 2008
Pediatric Brain Tumours Relative frequency of pediatric • see also Tumour, NS9 brain tumours
Tumour type Percent Epidemiology • 20% of all pediatric cancers (second only to leukemia)
Astrocytoma, low-grade 40 • 60% of pediatric tumours are infratentorial Supratentorial (23) • pediatric brain tumours arise from various cellular lineages: Infratentorial (17)�
Medulloblastoma 20� • glia: low-grade astrocytoma (supra- or infratentorial), anaplastic astrocytoma, Brainstem glioma 8 glioblastoma multiforme (largely supratentorial) (see NSlO for details) Ependymoma 8 • primitive nerve cells: supratentorial (primitive neuroectodermal tumour, Malignant glioma 6 PNET), infratentorial (medulloblastoma), pineal gland (pineoblastoma) Craniopharyngioma 6 • non-neuronal cells: germ cell tumour, craniopharyngioma, dermoid, PNET 4 meningioma, neurinoma, pituitary adenoma, others Pineal, germ cell tumour 3 Other 5 Clinical Features
• vomiting, seizure, macrocrania, hydrocephalus Reprinted from Pediatric Clinics of North America, Vol, 44(41, Kun LE, Brain Tumors: chal • developmental delay, poor feeding, failure to thrive� lenges and directions, pp. 907-17. Copyright� 1997, with permission from Elsevier.�
Functional Neurosurgery
Surgical Treatment of the following disorders (see Neurology for details) • Parkinson's disease and tremor, N32 and N34 • spasticity (including dystonias), N36 • surgical management of pain, N51
Common Medications The following are guidelines ONLY: follow clinical jUdgment and up-to-date prescription recommendations in practice: dosages refer to adults unless otherwise specified
Table 8. Common Medications Drug Name� Dosing Schedule Indications Side Effects Contnlincications Comments
lorazepam IAtivan"l� 4mg IV over 2minutes, Statusepilepticus •drowsiness, sedation •other CNS depressants, •start phenytoin loading ql()'15 minutes digoxin lincreases simuhaneously ldo not exceed 8mg/12hr) digoxin levelsl
ClIIbamazep'me lTegtelol")� rIC douloureux (Trigeminal neuralgial: Tic douloureux •worsening of seizures, • lithium lincreases lithium •hypersensnivity toTCAs, •monnor CSC (potential 100 mg PO bid, increase by 200 mg/day ITrigeminal neuralgial heart failure, arrhythmias, toxicity!. MAOI previous bone marrow hematological toxidtyl up 10 amaximum of 1,200 mg/day Se~ures AV blad, aplastic anemia, other meds may increase suppression, MAOI in 200 mg tidl agranulocytosis, carbamazepine levels or past 14 days Seizures: 200 mg PO bid, increase by thrombocytopenia, have decreased effects 200 mg (inpatient q3 days: hepatnis, erythema outpatient q7 daysj until therapeutic muhrrorme, Stevens-Johnson level achieved lusual optimum syndrome dosage: 8O()'1,200 mg/day: range: 600-2,000 mg/dayl
phenytoin (Dilantin")� Seizures: Loading dose: 18m!Jl<g Seizures •thrombocytopenia, •other meds may increase •bradyarrhythmias, heart blod< •important to give over time to slow IV or 3O().600 mg PO/day Statusepilepticus leukopenia, phenytoin levels and prevent causing acardiac arrest divided bitl'tid, agranulocytosis, toxicity or have decreased Maintenance: 2O().500 mg IV/day pancytopenia, toxic effects [max. rate: (4().50 mg/min or hepatitis,Stevens300 mg PO q4hl: Johnson syndrome, average maintenance dose: toxic epidermal 300 mg/day PO necrolysis Status epilepticus: 200 mg IV over 30 minutes 1- 20 m!Jl<g: ifnotta~ng regularly),or 500 mg IV over 10 minutes (if already on phenytoinl
dexameltlasone loading dose: 1()'20 mg IV: Cerebral edema le.g. •pseudotumour cerebri, 'aminoglutethimide, •systemic fungal infections, •no longer used in acute spinal C()rd IDecadron"\ Maintenance: 4-£ mg IV/day secondary to tumour, seizures, heart failure, antidiabetics, /!.SA, immunosuppressive dose injury
divided qid (may be POI� head injury, arrhythmias, NSAlDs, barbiluates, with live virus vaccines pseudotumour cerebri) thromboembolism, phenytoin, rifampin, Preoperative preparation pancrealitis, acute adrenal cardiac glycosides, for patients with insufficiency; avoid cyclosporine, ephedrine, increased ICP abrupt withdrawal oral anticoagulants, secondary to brain potassium-depleting neoplasms drugs, salicylates,
skin-testing antigens, toxoids, vacdnes
Dr.JKR

Toronto Notes 2008� Common Medications/Summary Key Questions
Table 8. Common Medications (continued) DNg Name� Dosing Schedule Indications Side Effeots Corrvnon Interactions
mannitol� 1-1.5 g/lg IV rapid infusion Raised ICP •seizures, heart failure • lithium (increases� (350 mL of 10% solutionl excretion of lithium)� followed by 0.15 glkg IV q6h�
mimodipine INimotop'"l� 60 mg PO/NG q4h x11 days Vasospasm in SAH •decreased blood •antihypertensives (may ~arted within 96 hours of SAH pressure, tachycardia, increase hypotensive effects),
dyspnea� CCB (may increase effects!. cimetidine (increases nimodipine bioavailabilityl
Summary Key Questions Questions� Answers
1.� What are the contraindications to lumbar puncture? Uncorrected coagulopathy� Known or suspected intracranial mass lesion� Non-communicating hydrocephalus� Skin infections near site of puncture�
2. What is the most common CNS neoplasm in adults?� Metastasis
3. What is the most common CNS neoplasm in children?� Astrocytoma
4.� What is the clinical features of acute raised ICP? Headache, nausea, vomiting, decreased LOC, papilledema ± retinal hemorrhage, abnormal extra-ocular movements, herniation syndromes, focal deficits due to lesion
5.� What is the likely source of bleeding causing an Middle meningeal artery tear� epidural hematoma?�
6. What are the risk factors for subdural hematoma?� Alcohol, anticoagulants, cerebral atrophy
7. What is the most common site for an intracranial aneurysm?� Anterior communica~ng artery
8.� What are the symptoms of subarachnoid hemorrhage? "Worst headache of my life", nausea/vomiting, photophobia, meningismus, sleepiness, focal deficits
9.� What are the top three etiologies for a Metasta~c neoplasm, GBM, abscess� rim-enhancing intraparenchymal lesion?�
lO.ln asevere, unstable stroke patient, what do Intubate� you do before sending them to CT?�
11. If apatient had increased ICP, what position do you not Trendelenberg� want them in?�
12.60 year-old man has aseizure for the first time. Space-occupying lesion !tumour)� What's the most likely cause?�
13. Ahockey player gets hit in the head and becomes Epidural hematoma� unconscious for afew minutes. He wakes up after afew� minutes. Next day: drowsy and headache.� What could be the cause of these symptoms?�
14. What is the GCS of apatient who can open their 3+4+6=13� eyes to voice, obeys commands, and has confused speech?�
15. L4/L5 herniated disc, what motor effects may be observed?� Foot Drop
16. Best test to investigate subarachnoid hemorrhage?� CT Scan
17. Would rupture of an intracranial artery cause an No, it would cause asubarachnoid hemorrhage� epidural hematoma?�
18. Loss of plantar re1\ex, what level would you expect the lesion? L5-S1
19. If C5-6 disk herniation, which root affected?� C6
20. What are the early signs and symptoms of increased ICP?� Headache, nausea, vomi~ng, papilledema
Contraindications
•anuria, severe pulmonary oonge~ion, frank pulmonary edema, severe heart failure, severe dehydration, metabolic edema, progressive renal disease or dysfunction, active intracranial bleeding except during craniotomy
•none known
Neurosurgery NS37
Comments
•effect OCC\lrs in 1-5mins, maximal at 1D-OO mins
•often altemated with furosemide 10-10 mg IV q6h
• indwelling urinary catheter to measure ins and outs
•causes vasodilation •only calcium channel blader ICCBI
to cross BBB (blood brain bamerl •use half the normal dose for liver
failure; monitor BP always
Dr.JKR
NS38 Neurosurgery Summary Key PointslReferences Toronto Notes 2008
Questions Answers
21. What are the 3divisions of the brain stem? Midbrain, pons, medulla
22. What region olthe bram governs comprehension of speech? Wernicke's area, dominanttemporallobe Which lobe is it located?
23. What is the normal cerebral perfusion pressure? >50 mm Hg
24. Which sensory level corresponds to the shoulders? C4
25. What name is given to cn C2? Cl =Atlas, C2 =Axis
26. How many cervical vertebrae are there? Cervical nerve roots? 7 cervical vertebrae, 8cervical nerve roots
27. What is the most common cervical disc herniation? C6fl
28. What physical findings would you expect from a C7 radiculopathy? Triceps muscle weakness, decreased triceps reflex
29. What is the usual treatment of acervical disc herniation? Watchful waiting, over 95% heal spontaneously
30. What is the most likely position of a lesion leading to Left frontal lobe expressive dysphasia and mild arm weakness?
31. What nerve root exits between L4 &L5? L4 nerve root
32. What root is usually affected with an L415 disc herniation? L5
33. Can an L4 disc ever impinge on an L4 nerve root? Yes. With afar lateral disc herniation
34. What is sciatica? Pain traveling down the leg associated with nerve root impingement
35. What are 3main signs of an Sl radiculopathy? Weak plantar flexion of foot Decreased sensation over lateral foot Decreased ankle jerk
36. What are the most common presentations of brain tumours? Progressive neurologic deficit, headache, seizure
37. Pituitary tumours are most commonly associated MENI with what endocrine syndrome?
38. What are the most common metastases to the brain? Lung>Breast>RenaI>GI>Melanoma
39. What nerve is trapped in carpal tunnel syndrome Median nerve
References Ahn NU, Ahn UM, Nallamshetty L, et al. Cauda equina syndrome in ankylosing spondylitis (the CES-AS syndrome): meta-analysis of� outcomes after medical and surgical treatments. Journal of Spinal Disorders 2001;14:427-33.� Aids to the examination of the peripheral nervous system. London, UK: BalliereTindall, 1986.� AI-Shahi R, Warlow CP Interventions for treating brain arteriovenous malformations in aduhs. The Cochrane Library 2004;Volume 2.� Barker FG 20d
, Ogilvy CS. Efficacy of prophylactic nimodipine for delayed ischemic deficit after subarachnoid hemorrhage: ametaanaly�sis. Journal of Neurosurgery 1996;84:405-14.� Barnett H, Taylor W, Eliasziw M, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis.� NEJM 1998;339:1415-25.� Bracken MB, Shepard MJ, HolfordTR, et al. Methylprednisolone or tirilazad mesylate administration after acute spinal cord injury: 1�year follow up. Results of the third National Acute Spinal Cord Injury randomized controlled trial. Journal of Neurosurgery 1998;89:699�706.� Crossman AR, Neary D. Neuroanatomy: an illustrated colour text. Toronto, ON: Churchill Livingston, 1998.� Edlow J, Caplan L. Avoiding pitfalls in the diagnosis of subarachnoid hemorrhage. NEJM. 2000;342(11:29-36.� Executive Committee for the Asymptomatic Carotid Atherosclerosis Study IACAS). Endarterectomy for asymptomatic carotid artery� stenosis. JAMA 1995;273:1421-28.� Fitzgerald MJ1 Neuranatomy: basic and clinica/13rd edition). Philadelphia: WB Saunders, 1997.� Goetz CG, Pappert EJ. Textbook ofclinical neurology 11 st edition). Toronto, ON: WB Saunders, 1999.� Greenberg MS. Handbook of neurosurgery 15th edition). NewYork:Thieme, 2001.� Kun, LE. Brain Tumours: Challenges and Directions. Pediatric Clinics of North America. 1997; Vol 44141:907-17.� Lindsay KW, Bone I. Neurology and neurosurgery illustrated. NewYork: Churchill Livingstone, 2004.� MRC Asymptomatic Carotid SurgeryTrial (ACSTI Collaborative Group. Prevention of disabling and fatal strokes by successful carotid� endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet 2004;363:1491-502.� Nieuwenhuys R, Voagd J, van Huijzen C. The human central nervous system 13rd edition). NewYork: Springer-Verlag, 1988.� Nursing 2004 Drug Handbookl24th editianl. New York, NY: Springhouse LippincottWiliiams &Wilkins, 2004.� Ogilvy CS, Stieg PE, Awad I., et al. Recommendations for the management of intracranial arteriovenous malformations. Circulation� 2001 ;103:2644-57.� Porter PJ, Willinsky RA, HarperW, et al. Cerebral cavernous malformations: natural history and prognosis after clinical deterioration� with or without hemorrhage. Journal of Neurosurgery 1997;87:190-7.� Saal JS, Saal JA,Yurth EF. Nonoperative management of herniated cervical intervertebral disc with radiculopathy, Spine. 21(161:1877-83,� 1996.� Shapiro S. Medical realities of cauda equina syndrome secondary to lumbar disc herniation. Spine. 25(3):348-51; discussion 352, 2000.� Shemie S, Doig C, Dickens B, et al. Severe brain injury to neurological determination of Death: Canadian forum recommendations.� CMAJ 2006; 174(6): SI-30.� Short OJ, EI Masry WS, Jones PW. High dose methylprednisolone in the management of acute spinal cord injury - asystematic review� from aclinical perspective. Spinal Cord 2000;38:273-86.� Spetzler RF. Martin NA. A proposed grading system for arteriovenous malformations. Journal of Neurosurgery 1986;65:476-83.� The North American Symptomatic Carotid EndarterectomyTrial INASCET). Beneficial effects of carotid endarterectomy in symptomatic� patients with high-grade carotid stenosis. NEJM 1991;325:445-53.�
Dr.JKR
Top Related
Copyright © 2022 FDOKUMEN

