





Bahasa
Halaman
Hukum


Island Wide Pressure Ulcer
Prevention and Management Framework
July 2021
DOCUMENT PROFILE
Document Registration HSS-GD-CG-607-01
Document Type Framework
Short Title Island wide Pressure Ulcer Prevention Framework
Author Pressure Ulcer Taskforce Group under Chief Nurse Office
Publication Date July 2021
Target Audience Island wide health and social care sector
Circulation List All health and social care workers Island wide, HCS employees, external Partners, Safeguarding Partnership Board
Description Island wide Pressure Ulcer Prevention Policy including new safeguarding framework
Linked Policies HCS SI policy, HCS Conservative Sharp Debridement Policy
Approval Forum Organisations Policy and Procedure ratifying group
Review Date 2 years from approval
Contact Details Carole Brett [email protected] +44 (0) 1534 442055
HSS-GD-CG-607-01

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 2 of 35
CONTENTS LIST: 1. Introduction Page 3
2. Scope Page 3
3. Purpose Page 4
4. Definitions Page 4
5. Roles and Responsibilities Page 5
6. Prevention and Management of Pressure ulcers Page 5 6.1 Prevalence 6.2 Measurement of improvement 6.3 Causes of pressure injury’s 6.4 Prevention of pressure ulceration 6.5 Assessment of risk of developing a pressure injury 6.6 Re-assessment of risk 6.7 Implementation of prevention, treatment and care plans 6.8 Categorising and care planning for identified pressure ulcers 6.9 Dressing formulary 6.10 Debridement 6.11 Discharge 6.12 Access to specialist equipment 6.13 Statutory reporting 7. Safeguarding Page 13
8. Education, training and information Page 14
9. Consultation Page 15
10. Recommendations and approval process Page 16
11. Communication and dissemination Page 16
12. Implementation Page 17
13. Monitoring compliance and effectiveness of the document Page 17
14. Document review, frequency and version control Page 18
15. References Page 18
16. Appendices Page 20
Appendix 1: Healthcare Improvement Scotland (Standards) / JCC standards
Appendix 2: Categories of Pressure Ulcers
Appendix 3: SSKIN / aSSSKINg / Repositioning
Appendix 4: Notification of Incident Form (Jersey Care Commission)
Appendix 5: Root cause analysis templates.
Appendix 6: Pressure ulcers-when to raise a safeguarding concern
Appendix 7: Adult Decision Guide – Safeguarding
Appendix 8: Making Safeguarding Personal

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 3 of 35
1. INTRODUCTION This Framework has been developed to ensure an Island wide, standardised approach
for the provision of care to those people who have or may be at risk of developing pressure ulcers and to ensure consideration is given where there are potential safeguarding concerns.
1.1 Pressure ulcers are a global concern. In the NHS in England, 24,674 patients were reported to have developed a new pressure ulcer between April 2015 and March 2016, and treating pressure damage costs the NHS more than £3.8 million every day (NHS Improvement, 2018). In Jersey, our aim is to help prevent and reduce pressure ulcer development and associated complications, by working together to provide a framework that can be used across the Island by services that provide care to people who may be at risk of developing pressure ulcers.
1.2 This framework is designed to support a consistent and clear approach to prevention and management of pressure ulcers, across all settings and all age groups.
1.3 Each organisation, or service provider, will have specific policies and procedures in relation to personal care and risk assessment that reflect the principles of this framework. A holistic assessment or reassessment, that includes pressure ulcer risk assessment tools, will guide person-centred implementation of appropriate interventions to help reduce the incidence of, or deterioration in existing, pressure ulcers.
1.4 The framework supports delivery of person centred, optimal care standards by all health and social care providers, to prevent pressure ulcers and guide measurement for improvement.
(Aligns to Healthcare Improvement Scotland (HIS) Standards: 1,2,3,4,5,6 and Jersey Care Commission (JCC) Standards for Care Homes and Homecare:1,2,5) (Appendix 1)
2. SCOPE
2.1 The prevention and management of pressure ulcers is an Island wide priority. This Framework applies to employees and carers working for on-Island organisations, public, private and voluntary, responsible for the care of people who may at risk of developing pressure ulcers.
2.2 A collaborative approach, working within the principles of this framework and in conjunction with JCC and HIS standards, will ensure consistent delivery of best practice, ensuring inclusion of the person at risk in the decision making process.
(Aligns to HIS Standards: 1, 2, 5, 6 and JCC Standards for Care Homes and Homecare 1, 2, 5).

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 4 of 35
3. PURPOSE
3.1 The framework aims to promote a collaborative approach to prevention and management of pressure ulcers, in all health and social care settings, by adopting a standardised approach based on best practice and evidence to:
raise awareness of risks associated with pressure ulcers
reduce risk of developing pressure ulcers
increase knowledge and understanding of potential causes, preventative
interventions and identification of pressure ulcers
improve / drive delivery of high quality care by shared learning from incidents and
positive experiences
raise concerns where safeguarding issues are identified
3.2 This framework supports the individual’s right to prevent and manage pressure ulcers in alignment with recommendations for best practice
(HIS, 2020 and JCC Standards for Care Homes and Homecare 2019) (Appendix 1)
4. DEFINITIONS 4.1 For the purpose of this framework, the term “all age groups” includes:
adults
neonates
infants,
children
young people
4.2 A pressure ulcer is defined as localised damage to the skin and/or underlying tissue, usually over a bony prominence (or related to a medical or other device), resulting from sustained pressure (including pressure associated with shear and/or friction). The damage can present as intact skin or an open injury and may be painful. A pressure ulcer that has developed at the end of life due to skin failure is no longer referred to as a ‘Kennedy Ulcer’ and should be classified in the same way as all other pressure injuries. (NHSI, 2018)
4.3 Pressure ulcer categorisation is defined by NHSI (2019) (Appendix 2)
4.4 The definition of a pressure ulcer on admission (POA) should be that it is observed during the skin assessment undertaken within 6 hours of admission to an inpatient service or at first visit from Community Nursing Service.

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 5 of 35
4.5 The definition of a new pressure ulcer within a setting is that it is first observed after 6 hours of admission and within the current episode of care.
5. ROLES AND RESPONSIBILITIES
5.1 All health and social care providers across the Island will work together to ensure quality of care is maintained and improved through this framework.
5.2 All health and social care providers are responsible for seeking organisational support for the principles of this framework and the implementation of the recommendations.
6. PREVENTION AND MANGEMENT OF PRESSURE ULCERS
6.1 Prevalence 6.1.1 Despite raising public and professional awareness through national and local
initiatives, prevalence remains a concern. 6.1.2 NHS Improvement have recognised that systems used to monitor and report
pressure ulcers at local, regional and national levels are not standardised and as a result issued the revised definition and measurement document for pressure ulcers in 2018. This framework aligns itself to these recommendations.
(Aligns to HIS Standards: 1, 2 and JCC Standards for Care Homes 12 and
Homecare 9)
6.2 Measurement for Improvement
6.2.1 It is vital that processes as well as outcomes are measured to ensure an understanding of which part of the process needs strengthening in terms of reliability.
6.2.2 Examples of outcome measures:
number of new pressure ulcers;
location of the individual when the pressure injury was identified i.e. home,
hospital, other care setting
category of pressure ulcer;
rate of occurrence of new pressure ulcers per 1,000 bed days
rate of occurrence of new pressure ulcers per caseload
6.2.3 Organisations should decide what outcome measures are most appropriate and relevant to their care settings and all relevant information should be shared with all staff at team level in order to drive improvement.

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 6 of 35
6.2.4 Examples of process measures:
percent (%) compliance with risk assessment within an agreed period since
admission to service
level of compliance with SSKIN / aSSSKINg bundle (Appendix 3)
(Aligns to Healthcare Improvement Scotland Standards: 1, 2 &Jersey Care Commission Standards for Care Homes 12 and Homecare 9)
6.3 Causes of pressure ulcers
6.3.1 Pressure ulcers can affect anyone. Risk factors include age, medication, long lie, trauma, incontinence and pain (NHSI Core Curriculum, 2019)
6.3.2 The factors causing pressure injuries are divided into two groups:
1. Intrinsic – including disease, medication, malnourishment, age, dehydration/fluid status, lack of mobility, incontinence, skin condition and weight:
2. Extrinsic – external influences, which cause skin distortion including pressure and shearing forces.
6.3.3 Pressure ulceration to the foot of a service user has not always been recognised and reported. A number of these may be classified as device related pressure ulcers e.g. footwear or plaster casts.
6.3.4 NHS Improvement (2018) have recommended that the terms ‘avoidable’ and
‘unavoidable’ no longer be used. (Aligns to HIS Standards: 1,2,3,4 & JCC Standards for Care Homes and Homecare
1, 2, 3, 4)
6.4 Prevention of pressure ulceration
6.4.1 Each organisation has a responsibility to demonstrate leadership and commitment to the prevention and management of pressure ulcers.
6.4.2 For the prevention and management of pressure ulcers, the organisation can demonstrate:
implementation of policies, procedures, guidance and standards
a multi-professional approach
facilitation cross-organisational support

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 7 of 35
collection, monitoring, review and action on data
ongoing quality improvement
adherence to Duty of Candour
there is timely, effective, and person-centred communication, documentation and
transfer of information to ensure continuity of care between teams and settings.
(Aligns to HIS Standards: 3, 4, 5, 6 & JCC Standards for Care Homes and Homecare 1, 2, 3, 4, 5)
6.5 Assessment of risk of developing a pressure injury.
6.5.1 An initial risk assessment is undertaken as part of admission to a care setting and informs care planning.
6.5.2 Pressure ulcers can develop and deteriorate quickly, particularly in people considered to be at high risk, for example:
neonates
people with frailty
those with limited mobility
those with diabetes,
those who are nutritionally compromised
those at end of life
6.5.3 A risk assessment tool is used to support professional or clinical judgement.
6.5.4 Assessment and documentation of the risk of developing pressure ulcers or further
damage to existing pressure ulcers is:
within 6 hours of admission to hospital or care home
within 24 hours of admission to any other care setting
on the first visit from community services or teams, for example, community
nurse, hospital at home, social care or care at home
6.5.5 There are requirements for ‘valid consent’. For consent to be valid, it must be:
given by a person with capacity to consent or refuse consent to the intervention in question, or any other legal decision maker
given voluntarily and freely, without pressure or undue influence being exerted on the patient either to accept or refuse treatment

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 8 of 35
based on appropriate information and understood (informed). Acquiescence where the patient does not know what the intervention involves, is not consent
6.5.6 The Capacity and Self-Determination Law enshrines in legislation, a personal
autonomy and right to choose for themselves. There can be circumstances where a person may refuse part of, or all treatments. Where this occurs, it is important to spend time with the person, examining their views, whist given them appropriate information about the foreseeable consequences of deciding one way, or another or not deciding to take treatment at all.
(Aligns to HIS Standards: 3,4,5,6 & JCC Standards for Care Homes and
Homecare 1, 2, 3, 4, 5)
6.5.7 In the circumstances of a capacious refusal or care and treatment, the recording must include details of the information given to the patient, including the information regarding outcomes of refusing intervention. The recording must also contain details of the person’s understanding and retention of the given information about treatments(s), and how they used the information in making their decision to refuse treatment. A ‘Decision-Making Record’ can be extremely helpful in these circumstances.
6.5.8 Each formal assessment is undertaken by appropriately trained staff and includes:
with valid consent, inspection of the person’s skin, particularly areas over bony prominences and areas in contact with equipment and devices - careful attention is paid to those individuals with darkly pigmented skin in order to identify early skin damage
assessment of risk factors and other contributing factors, for example people with frailty, pain, limited mobility or diabetes, and those who are nutritionally compromised, or at end of life
assessment of the person’s needs within their home or care setting, including positioning and equipment
planned review of care plans and reassessment of risk
Where an assessment of risk or skin inspection has not been undertaken within the agreed time frames, staff record within the person’s care plan:
the reason, or reasons, assessment or inspection has not been undertaken or was delayed
the discussion with the person

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 9 of 35
6.6 Re-Assessment of Risk
6.6.1 Regular reassessment is used to evaluate an individual’s risk of developing a pressure ulcer, or experiencing further damage to an existing pressure ulcer(s).
6.6.2 Risk reassessment ensures that any changes in a person’s circumstances, for example if the person becomes acutely unwell, has a fall, undergoes an operation or their mobility is reduced, are recorded and used to inform care plans.
6.6.3 Regular review also ensures that an individual’s care plan is safe, effective and person-centred.
6.6.4 Reassessment, undertaken alongside the evaluation of existing care plans, also identifies whether existing interventions are managing the risk appropriately.
6.6.5 A reassessment of risk is undertaken and existing care plans are evaluated and
revised when:
an observed or reported change has occurred in the person’s condition or
changes noted on skin inspection
the person (and/or carer) report a change
the person is transferred to another care setting
the person is transferred between clinical areas e.g. transferring care between
wards
when the person is discharged from one care setting and receiving care setting
is provided with current assessment
according to organisational guidance
(Aligns to HIS Standards: 4, 5, 6 & JCC Standards for Care Homes and
Homecare 1, 2, 3, 4, 5)
6.7 Implementation of prevention, treatment and care plans
6.7.1 A Person-Centred Care Plan will be developed and implemented to reduce the risk of developing pressure ulcer(s) and to manage any existing pressure ulcer(s).
6.7.2 Preventative strategies such as the SSKIN / aSSSKINg care bundle (Appendix 3) should be initiated where a person is at risk of developing a pressure ulcer or to prevent further deterioration of an existing pressure ulcer(s).This should also include engagement with and support of the person and care providers, where indicated to self-manage their risk of developing pressure ulcers.

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 10 of 35
6.7.3 Where a care plan has not been implemented or followed, there should be documented explanation in their record and the reason care has not been delivered; e.g., it is their choice, where there is no access to specific services and evidence of the discussion with the person and any agreed actions.
6.7.4 Healthcare providers implement organisational policies and processes to deliver safe, effective and person-centred care. This includes criteria and timings for referral or liaison with specialist teams such as:
podiatry
dietetics
tissue viability service
vascular service
occupational therapy
physiotherapy
pain management services
6.7.5 The care plan is agreed with the person and includes:
the outcome from the risk assessment and skin inspection identification and
management of other risks or contributing factors, including, pain, skin tone,
incontinence, nutritional compromise (SSKIN / aSSSKINg bundle)
a treatment plan for any existing pressure ulcer(s)
frequency of repositioning
requirements for equipment
skin cleansing and maintenance regime
details of self-management strategies and information
planned reassessment of risk and care plan
6.7.6 The person-centred care plan is:
reviewed to ensure it meets the ongoing needs of the person
fully implemented and used to inform handovers, care transitions and discharge
planning
(Aligns to HIS Standards: 3,4,5,6 & JCC Standards for Care Homes and Homecare 1, 2, 3, 4, 5)

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 11 of 35
6.8 Categorising and care planning for identified pressure ulcers
6.8.1 People with an identified pressure ulcer(s) will receive a person-centred assessment, a categorisation of the pressure ulcer(s), comprehensive wound assessment and an individualised care plan.
6.8.2 Regular review is required to monitor the person’s condition, reduce the risk of deterioration in any identified pressure ulcer(s) and to help identify infection or sepsis.
6.8.3 Pressure ulcers categorised as 2 and above are reported using an organisational reporting system. (Please see statutory reporting section)
(Aligns to HIS Standards: 2, 5, 6 & JCC Standards for Care Homes and Homecare 1, 2, 3, 4, 5)
6.9 Dressing Formulary
6.9.1 The Dressing Formulary, intended to promote standardised selection of dressings across the Island is managed by the TVNs, and based on contemporary, evidence based, best practice guidance.
6.9.2 The type of dressing selected to promote healing of a pressure injury should be discussed with the individual and their family or carers, if appropriate.
(Aligns to HIS Standards: 5, 6 & JCC Standards for Care Homes and Homecare 6)
6.10 Debridement
6.10.1 If autolytic debridement is likely to take longer and prolong healing time, then the utilisation of conservative sharp debridement by a competent practitioner, such as a suitably trained and qualified TVNS, may be considered (NICE 2014). Each organisation will be responsible for policy development within their clinical area and ensure adherence to organisational guidelines for practice, including timely and appropriate referral to hospital from the community as and when required.
(Aligns to HIS Standards: 1, 2, 6 & JCC Standards for Care Homes and Homecare 6, HCS Conservative Sharp Debridement Policy 2021, FNHC Debridement Policy)
6.11 Discharge
6.11.1 All incidences of damage to skin integrity must be communicated to receiving providers of care on discharge or transfer and supported with documentation to ensure continuity between care settings and agencies. Communication should take place prior to discharge and include any need for specialist services, equipment or dressings.

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 12 of 35
(Aligns to HIS Standards: 1, 3, 5 & JCC Standards for Care Homes and Homecare 1, 2, 3, 4, 5)
6.12 Access to specialist equipment
6.12.1 People identified with an existing pressure ulcer or at significant risk of developing pressure ulceration, should be cared for on a pressure redistribution surface according to the holistic, risk assessment
6.12.2 Every care setting, should provide a basic level of equipment for the prevention of pressure ulcers for individuals, with the exception of custom made items. This includes; pressure redistributing cushions, heel and joint protectors and pressure redistributing mattresses. Maintenance of equipment is the responsibility of the care setting and should be carried out according to manufacturer’s guidelines.
6.12.3 For those individuals with capacity, fully informed of the risk, yet declining to purchase any recommended specialist equipment, when for use in their own homes, their decisions must be documented.
(Aligns to HIS Standards: 1,2,3,5 & JCC Standards for Care Homes and Homecare 1, 2, 3, 4, 5)
6.13 Reporting
6.13.1 All pressure ulcers, irrespective of category, should be recorded in the individual’s record. All pressure ulcers Category 2 and above, including suspected Deep Tissue Injury (sDTI) and unstageable pressure ulcers, should be reported into the organisation reporting system.
6.13.2 Pressure ulceration is considered as harm to people and therefore should be reported as an individual safety incident within the organisational risk management, reporting and learning system.
6.13.3 All POA (Pressure injury On Admission) category 2 or above should be reported in organisational reporting and learning systems.
6.13.4 All Medical Device Related Pressure Ulcers (MDRPU) should be reported and identified by using the appropriate category e.g. category 3 (MDRPU).
6.13.5 Moisture Associated Skin Damage (MASD) should be reported in local systems. Where skin damage is caused by a combination of moisture and pressure, the damage will be recorded as the category of pressure ulcer.
6.13.6 Care settings that are registered with the Jersey Care Commission have a statutory duty to notify the Commission of any pressure ulcers, Category 2 and above. The notification form is a requirement of compliance with registration in these settings (Appendix 4)

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 13 of 35
6.13.7 Pressure ulcers, category 2 or above, that are thought to have been sustained in a care setting including hospital, hospice, prison, residential, nursing or other care setting, a Pressure Ulcer Specific Root Cause Analysis (RCA) tool should be completed by a Registered Nurse / Manager and reported within the organisations quality assurance process to support individual and organisational learning (Example hospital RCA given in Appendix 5)
6.13.8 For pressure ulcers, category 2 or above, that are thought to have been sustained in the person’s home where they are in receipt of nursing or social care at home. An RCA should be completed by a registered nurse / manager and reported in the organisations quality assurance process to support individual and organisational learning.
6.13.9 It is essential to identify incidents that indicate the most significant opportunities for learning and prevention of future harm.
6.13.10 If there are clusters of incidents, such as falls, pressure sores etc, investigating each individually using a full root cause analysis framework could lead to a debilitating process which does not support effective learning. (Aligns to HIS Standards: 1, 2, 3, 4 & 7 & JCC Standards for Care Homes 12 and Homecare 9)
7 SAFEGUARDING 7.1.1 Safeguarding is everyone’s business and in its broadest terms, abuse can happen
to anyone, anywhere. Responsibility for dealing with it lies with us all as members of the public, volunteers and professionals. It is, therefore, the responsibility of all staff to follow this framework and ensure referrals to Adult Safeguarding and Children and Families Hub are completed in a timely manner.
7.1.2 This policy should be read alongside the Jersey Safeguarding Partnership Board’s (SPB) procedures, additionally any relevant single agency policies.
7.1.3 Building relationships is key to achieving person-led, outcome-focused decisions that enhance the person’s involvement in decision making and optimises their choice and control. However this should not be a barrier to effective safeguarding when considering the wider risk to others. Please see Making Safeguarding Personal. (Appendix 7)
7.1.6 Pressure ulceration may be an indication that a person is being neglected; neglect
may involve deliberate withholding or unintentional failure of a carer to provide appropriate and adequate care and support. This may result in, significant preventable skin damage.
7.1.8 All health and social care providers are required to raise concerns around safeguarding. See Appendix 8 for the relevant pathway for specific areas to identify those pressure ulcers that need to be referred into the Safeguarding Alert

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 14 of 35
Process or those that can be managed within standard governance processes. Please include the adult decision guide once completed with the SPOR referral. If there are any concerns please discuss with the health Safeguarding Team.
7.1.9 A minority of cases may warrant raising a safeguarding concern. Adults should be referred to the Adult Safeguarding Team 01534 444440 or where a child is concerned, with the Children and Families Hub 01534 519000. The individual should be made aware they are being referred unless there is an identified reason not to share this with them such as lack of capacity in this area.
(Aligns to HIS Standards: 1, 2, 3 & 4, JCC Standards for Care Homes 4,6,7,9,10,11,12 and Homecare 3, 4, 5, 6, 7, 8, 9)
8 EDUCATION, TRAINING and INFORMATION
8.1 Ensuring staff are competent and confident to deliver safe and high quality care remains a key requirement for all health and social care providers. This framework supports the standards for education, training and information as described in Health Care Improvement Scotland (2019) (Appendix 1)
8.2 Each Organisation will demonstrate commitment to the education and training of staff involved in the prevention and management of pressure ulcers, appropriate to roles and workplace setting. The NHSI Core Curriculum (2018) should be used to guide content.
8.3 Information and support is available for anyone at risk of developing, or identified with, a pressure ulcer.
8.4 At community level, there are a number of individuals who may be at risk of pressure ulceration but only have contact with health professionals through their General Practitioner and Practice Nurses. Primary Care Services must have mechanisms in place to educate primary care staff in relation to this framework and to engage with individuals about the importance of skin checks and caring for their skin.
8.5 The framework supports a collaborative approach to on-going training across all health and social care provider organisations and encourages organisations to enable access to training sessions for staff regardless of their employing organisation.

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 15 of 35
9. CONSULTATION
9.1 This framework will be shared with all stakeholders in the Pressure Ulcer Taskforce Group for consensus.
9.2 Consultation Schedule
Name Job Title Organisation Date
Rose Naylor Chief Nurse Health & Community Services
27th March 2020
Aisling Adams Senior Nurse-Quality & Practice
Assurance
Health & Community Services
27th March 2020
Becky Sherrington Associate Chief Nurse
Health & Community Services
27th March 2020
Carole Brett Tissue Viability Nurse
Health Community Services
27th March 2020
Tia Hall Operational Lead for Adult Services
Family Nursing & Home Care
27th March 2020
Gilly Glendewar Tissue Viability Nurse
Family Nursing & Home Care
27th March 2020
Hilary Hopkins Head of Governance Jersey Hospice Care 27th March 2020
Cheryl Keneely Chair Person Care Federation 27th March 2020
Sam Lempriere Informatics Health & Community Services
27th March 2020
Paul Ahier Informatics Health & Community Services
27th March 2020
Emma O’Connor Patient Safety Officer Health & Community Services
27th March 2020
Tim Hill Practice Development
Health & Community Services
27th March 2020
Jessie Marshall Lead Nurse- Secondary
Scheduled care
Health & Community Services
27th March 2020
Claire Sambridge Lead Nurse-Primary, Preventative
Health & Community Services
27th March 2020
Paul McCabe Chief Pharmacist Health & Community Services
27th March 2020
Mary Munns Adult Safeguarding- Team Leader
Health & Community Services
27th March 2020
Patricia Marius Interim Designated Safeguarding Lead
Health & Community Services
27th March 2020
Claire Thompson Safeguarding Named Nurse for Adults
Health & Community Services
27th March 2020

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 16 of 35
Jenny Querns Safeguarding Lead Nurse for Adults and Children
Family Nursing & Home Care
27th March 2020
Geoff White Associate Chief Nurse
Health & Community Services
27th March 2020
Pam le Sueur Health & Community Services
24th August 2020
Wendy Baugh Lead nurse Health & Community Services
23rd October 2020
Valter Fernandes Lead nurse Health & Community Services
23rd October 2020
Alex Watts Lead Nurse Health & Community Services
23rd October 2020
Jan Auffret Lead Midwife Health & Community Services
23rd October 2020
Ward managers Grade 6 and 5 managers
Health & Community Services
23rd October 2020
Tarina Le Duc Head of Quality and Safety
Health & Community Services
29th October 2020
10 RECOMMENDATION AND APPROVAL PROCESS
10.1 This framework provides a standardised approach for provision of care to those people who may be at risk of developing pressure ulcers. The Chief Nurse Group in conjunction with Health and Community Services, Family Nursing and Home Care and Jersey Hospice Care will maintain oversight of this framework through the Pressure Ulcer Taskforce Group
10.2 This policy is ratified by the Organisations Policy and Procedure Ratifying Group.
11 COMMUNICATION / DISSEMINATION
11.1 Public Engagement 11.1.1 The risk of sustaining pressure ulceration is often seen to be the problem of the
health or social care professional; however, the individual at risk is central to successful prevention. Using the principles of adult safeguarding, ‘Empowerment, Prevention, Protection, Partnership, Proportionality and Accountability’ the desires and wishes of the individual should be considered.
11.1.2 This is particularly important when individuals suffer a life-changing event or illness
that significantly increases their risk of being susceptible to pressure ulceration. Consideration must be given to the application of the Capacity and Self-Determination (Jersey) Law 2016. If the individual has capacity, it is important to work with them to highlight the risk and identify actions that can reduce the risk.

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 17 of 35
Consideration for a referral to Adult Safeguarding should be undertaken if the individual is self-neglecting to the point where harm is occurring. If the individual lacks capacity, best interest decision making will be required.
11.1.3 It is recognised that a true partnership involves more than just giving information.
Individuals should be able to access information easily and be provided with the tools to help them assess their own risk of developing pressure ulcers, how to prevent them and who to contact should they be concerned.
11.1.4 If the individual lacks decision-specific capacity and continues to be non-concordant in the delivery of treatment; legal advice should be sought and consideration for an application to the court for protection may be required. All organisations should have clear processes in place to manage this.
11.1.5 All provider organisations should ensure that they can access a broad range of information and tools for individuals in order to encourage and support their participation in the prevention and management of pressure ulceration. All information should be culture and language specific.
(Aligns to: HIS Standards: 1, 2 & JCC Standards for Care Homes and Homecare 1, 2, 3, 4,
11.2 Communications 11.2.1 In order to engage with the wider audience of services caring for those at risk the
framework will be shared Island wide and to the general public via the GOV.JE website. There is an annual ‘Stop the Pressure Day’ which will include raising awareness of this framework.
(Aligns to HIS Standards: 1, 2 & JCC Standards for Care Homes and Homecare 7)
12 IMPLEMENTATION
12.1 This framework provides clear vision and standards that are understandable for both commissioners and providers of care. Successful implementation will require an Island Wide commitment with a common sense of purpose and a shared goal of harm free care. It is expected that all providers will adopt this framework.
(Aligns to HIS Standards: 1, 2, 3,4,5,6 & JCC Standards for Care Homes and Homecare 1, 2, 3, 4, 5)
13 MONITORING COMPLIANCE AND EFFECTIVENESS OF THE DOCUMENT
13.1 Each organisation will have audit in place for monitoring compliance with the pressure ulcer prevention strategies within this framework.
13.2 Any areas of concern identified, will result in the requirement for an improvement plan to be implemented and evaluated at next audit.

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 18 of 35
13.3 The Tissue Viability Nurses will continue to monitor and review the framework and report to their line managers
14 DOCUMENT REVIEW, FREQUENCY AND VERSION CONTROL 14.1 This document will be reviewed every two years, to take account of any changes in
national guidance. Necessary changes throughout the year will be issued as amendments to the framework. Such amendments will be clearly identifiable as to which section they refer and the date issued. These will be clearly communicated to all service providers.
15 REFERENCES
European Pressure Ulcer Advisory Panel Prevention and Treatment of Pressure Ulcer: Clinical Practice Guideline 2014
Health and Community Services Jersey (2017) Policy and Procedure for the Management of Serious Incidents within Health and Social Services link: https://soj/depts/HSS/Registered%20Documents/P%20Serious%20Incident%20Policy.pdf#search=SI
Healthcare Improvement Scotland (2020) http://www.healthcareimprovementscotland.org/our work/standards and guidelines/stnd s/pressure ulcer standards.aspx
Jersey Care Commission Home Care Standards (2019) link:
https://carecommission.je/wp-content/uploads/2019/02/JCC-Care-Standards-Home-Care-2019-v1..pdf
Jersey Care Commission Care Homes Standards (2019) link:
https://carecommission.je/wp-content/uploads/2019/08/JCC-Care-Standards-Care-Homes-Adults-2019v2.pdf
Jersey Safeguarding Board
(https://safeguarding.je/wp-content/uploads/2018/03/2018-MOU-amended-final.pdf)
NHS Improvement, pressure ulcers: revised definition and measurement, summary and recommendations. June 2018.
NHSI Core Curriculum, 2018. NHS Improvement (2018) Pressure Ulcer Core
Curriculum. Bit.ly/NHSIPUCoreCurriculum
National Pressure Ulcer Advisory Panel’s (NPUAP) 2015
Ousey K, Chadwick P and Cook L (2011) Diabetic foot or pressure ulcer on the foot? Wounds UK, Vol 7, No 3
Phister HR and Bohm G (2008). The Multiplicity of Emotions: A framework for emotional functions in decision making. Judgment and Decision making, 3, pp 5 – 17.
Vowden P, Vowden K (2015) Diabetic foot ulcer or pressure ulcer? That is the question. TheDiabetic Foot Journal 18: 62-

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 19 of 35
16. APPENDICIES Appendix 1: Summary of Healthcare Improvement Scotland Standards 2020 Summary of standards
Standard 1: leadership and governance The Organisation demonstrates leadership in the prevention and management of pressure ulcers.
Standard 2: staff education and training The Organisation demonstrates commitment to the education and training of all staff involved in the prevention and management of pressure ulcers, appropriate to roles and workplace setting.
Standard 3: person-centered information and support Information and support is available for people with, or at risk of developing, pressure ulcers, and/or their representatives where appropriate.
Standard 4: initial assessment of risk of developing a pressure ulcer An initial risk assessment is undertaken as part of admission to, or first contact with, a care service to inform care planning.
Standard 5: reassessment of risk Regular reassessment is used to re-evaluate an individual’s risk of developing pressure ulcers or experiencing further damage to existing pressure ulcers.
Standard 6: care planning for prevention of pressure ulcers A person-centered care plan is developed and implemented to reduce the risk of developing pressure ulcers.
Standard 7: assessment, grading and care planning for identified pressure ulcers. People with identified pressure ulcers will receive a holistic assessment and experience high quality and person-centered treatment and support
Hyperlink for full Standards:
https://www.healthcareimprovementscotland.org/our_work/standards_and_guidelines/stnds/pressure_ulcer_standards.aspx
The Jersey Care Commission Care Home Standards:
You will be given information that is shared in a way that you understand. This will tell you and others about the service and how you will be cared for.
You will be cared for and helped in a way which has been planned with you.
You will be cared for and helped by the right people with the right values, attitudes, understanding and training.
You will feel safe.

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 20 of 35
You will be supported to make your own decisions and you will receive care and support which respects your lifestyle, wishes and preferences.
Your care will be provided with consistency by competent care and support workers who have the necessary training and qualifications to meet your needs.
The environment will enhance your quality of life and the accommodation will be a pleasant place to live or stay.
Your meals will be varied, healthy and tasty and will be based around your preferences and requirements.
You won’t have to give up activities you enjoy when you live or stay in a care setting. There will be a range of things to do which will reflect your preferences and lifestyle.
Yours and other people’s thoughts, worries and complaints about how you are cared for will listened to and taken seriously.
The care service will be well managed.
The care service will be checked and reviewed regularly to sort out any issues and make things better for you and others
The Jersey Care Commission Homecare Standards:
1. You will be given information that is shared in a way that you understand. This will tell you and others about the service and how you will be cared for.
2. You will be cared for and helped in a way which has been planned with you.
3. You will be cared for and helped by the right people with the right values, attitudes, understanding and training.
4. You will feel safe.
5. You will be supported to make your own decisions and you will receive care and support which respects your lifestyle, wishes and preferences.
6. Your care will be provided with consistency and reliability by competent care and support workers who have the necessary training and qualifications to meet your needs.
7. Yours and other people’s thoughts, worries and complaints about how you are cared for will be listened to and taken seriously.
8. The home care service will be well managed.
9. The care service will be checked and reviewed regularly to sort out any issues and make things better for you and others.

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 21 of 35
Jersey Care Commission Home Care Standards (2019) link: https://carecommission.je/wp-content/uploads/2019/02/JCC-Care-Standards-Home-Care-2019-v1..pdf
Jersey Care Commission Care Homes Standards (2019) link: https://carecommission.je/wp-content/uploads/2019/08/JCC-Care-Standards-Care-Homes-Adults-2019v2.pdf

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 22 of 35
Appendix 2: Categories of pressure ulcer

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 23 of 35
Appendix 2

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 24 of 35

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 25 of 35
aSSSKINg tool: to be completed for
all patients with: - with any category
of PU or previous pressure ulcers
- with no pressure ulcer but at risk (as per pressure ulcer risk assess) Affix tit La
a
assessment
Complete risk assessment and holistic assessment to
determine level of risk and to guide plan of care, referrals,
equipment and interventions recommended/required.
Completed (date):
Documented level of risk: Yes/No
Care Plan: Yes/No
Referrals to:
Record in EMIS: Yes/No
S Safeguardin
g
Do you need to consider raising a Safeguarding alert?
Do you have any concerns, are you keeping the patient
safe? (consider capacity, risk assessment, MDT,
safeguarding policy, safeguarding trigger tool)
If Yes discuss with team leader and Safeguarding lead
Yes No
S Surface
Select an appropriate support surface based on
patients level of risk:
Mattress Type (state):
Cushion type (state):
Heel Protector (state):
Other (state):
Ensure equipment is in good working order and on correct settings
Yes or No
Is patient comfortable? Yes or No
Individual is bedbound/wheelchair bound? Yes or No
Does the person sleep in their chair? Yes or No
S Skin
Perform “Skin tolerance test” regularly and identify any
evidence of pressure damage to:
Determine frequency of checks:
Buttocks
Elbow
Sacrum
Trochanter (hips)
Spine
Heels
Occiput
Toes
Pressure Ulcer Prevention
aSSSKINg Tool Name:
URN:
ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
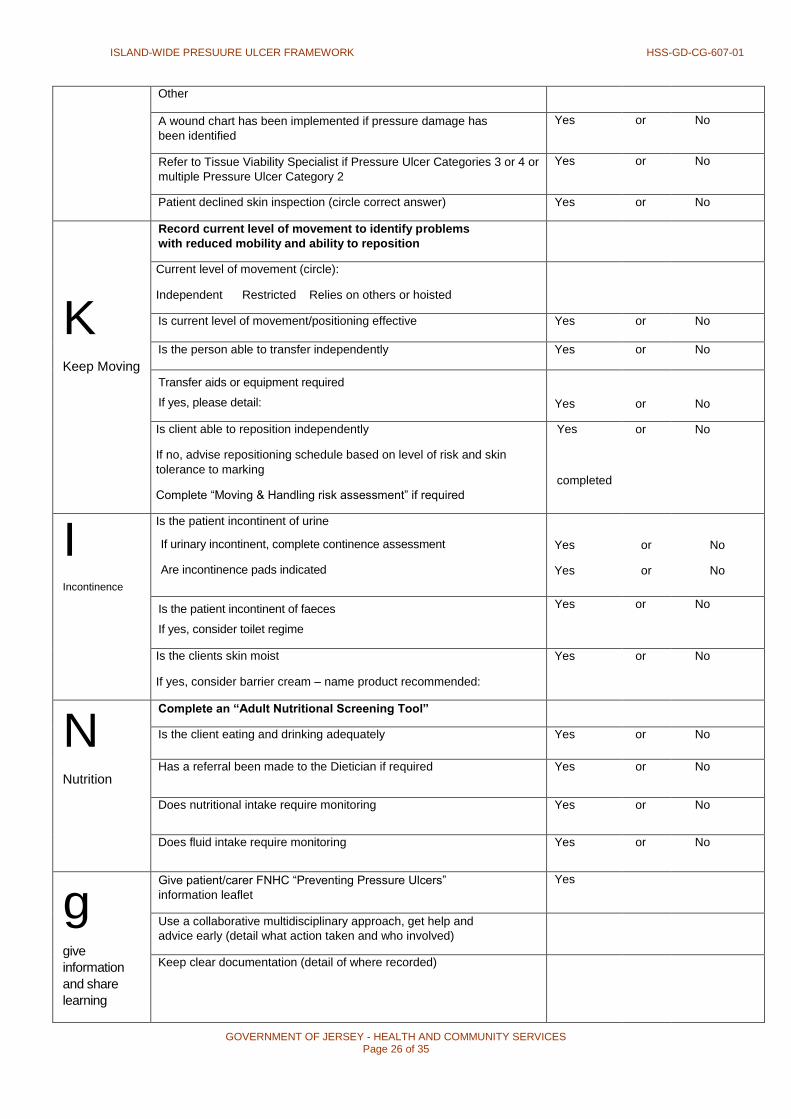
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 26 of 35
Other
A wound chart has been implemented if pressure damage has
been identified
Yes or No
Refer to Tissue Viability Specialist if Pressure Ulcer Categories 3 or 4 or
multiple Pressure Ulcer Category 2
Yes or No
Patient declined skin inspection (circle correct answer) Yes or No
K Keep Moving
Record current level of movement to identify problems
with reduced mobility and ability to reposition
Current level of movement (circle):
Independent Restricted Relies on others or hoisted
Is current level of movement/positioning effective Yes or No
Is the person able to transfer independently Yes or No
Transfer aids or equipment required
If yes, please detail: Yes or No
Is client able to reposition independently
If no, advise repositioning schedule based on level of risk and skin
tolerance to marking
Complete “Moving & Handling risk assessment” if required
Yes
completed
or No
I Incontinence
Is the patient incontinent of urine
If urinary incontinent, complete continence assessment
Are incontinence pads indicated
Yes
Yes
or
or
No
No
Is the patient incontinent of faeces
If yes, consider toilet regime
Yes or No
Is the clients skin moist
If yes, consider barrier cream – name product recommended:
Yes or No
N Nutrition
Complete an “Adult Nutritional Screening Tool”
Is the client eating and drinking adequately Yes or No
Has a referral been made to the Dietician if required Yes or No
Does nutritional intake require monitoring Yes or No
Does fluid intake require monitoring Yes or No
g give
information
and share
learning
Give patient/carer FNHC “Preventing Pressure Ulcers”
information leaflet
Yes
Use a collaborative multidisciplinary approach, get help and
advice early (detail what action taken and who involved)
Keep clear documentation (detail of where recorded)

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 27 of 35
Repositioning chart
Sig
natu
re /
Oth
er c
om
men
ts- i
ncl
ude
Pai
n
Iden
tifie
d rep
osi
tion in
g
Ski
n In
spec
tion
Reposi
tionin
g (u
sin
g le
gend)
sched
ule
(hrs
) Com
men
ts Des
igna
tion
e.g
. M
outh
care
, eye c
are
, tra
ctio
n o
bs e
tc
To Fro
m
Time
Date
Leg
en
d - L
eft (L), R
ight (
R), B
ack
(B
), P
rone (P
), S
ittin
g U
p (S
U), C
hair (C
), M
obilisi
ng (M
)
Ple
ase
Com
ple
te o
r Affi
x A
ddre
ssogra
ph
Surna
me:
Forena
me:
War
d / A
rea:
She
et N
o:
Dat
e of
Birth
:
Nam
e / D
esig
natio
n URN N
o:
Sign
ature
She
et N
o:
Rep
ositio
nin
g C
hart
fo
r all th
ose id
en
tified
at ri
sk o
f p
ressu
re d
am
ag
e, w
ith
exis
tin
g p
ressu
re d
am
ag
e o
r re
cen
tly h
ad
pre
ssu
re d
am
ag
e
* E
ncoura
ge a
ll th
ose id
entif
ied a
s b
ein
g a
t ri
sk o
f pre
ssure
dam
age to c
hange their p
ositi
on fre
quently
and a
t le
ast six
hourly.
* E
ncoura
ge a
ll th
ose id
entif
ied a
s b
ein
g a
t h
igh
ris
k o
f pre
ssure
dam
age to c
hange their p
ositi
on fre
quently
and a
t le
ast fo
ur
hourly.
* In
div
idual t
issue tole
rance tim
e s
hould
be taken in
to c
onsi
dera
tion w
hen d
ete
rmin
ing r
eposi
tionin
g s
chedule
s.T
he a
bove a
re a
vaila
ble
as
a g
uid
e o
nly
.
Insp
ect th
e p
atients
skin
reg
ula
rly. P
atien
ts o
n p
ressu
re r
edis
trib
ution
eq
uip
ment still
req
uir
e s
kin
insp
ectio
n a
nd
regu
lar
rep
ositio
nin
g

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 28 of 35
Appendix 4: Notification of injury

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 29 of 35
Appendix 5: Root cause analysis templates

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 30 of 35

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 31 of 35
Appendix 6
Pressure Ulcers: When to raise a Safeguarding Concern This flow chart is to be used for inpatient services (HCS) and all community
providers
An individual who develops Pressure ulceration is considered at risk and therefore consideration must be given to the safeguarding process. This process is inclusive of all ages:
children through to adult. All agencies must be aware of indicators in determining when safeguarding issues may arise.
An individual develops pressure ulcer(s)
Pressure ulcer(s) verified as Category 1 or 2 by registered professional: complete Datix, Assure or appropriate incident reporting mechanism
Pressure ulcer(s) verified as multiple category 2, Category 3, 4, unstageable, deep tissue injury by Tissue viability nurse or trained professional: complete Datix, Assure or appropriate incident reporting mechanism
Ensure reasonable steps are taken to
prevent / manage pressure ulceration.
Follow up so that these measures are seen
to be effective. Seek advice from Tissue
Viability Nurse if additional support/advice
is required
Complete Adult Safeguarding Decision Guide. Record conclusion in incident reporting and records. If threshold for adult safeguarding alert is met (Score of 15 or more) or clinical judgement concern, refer to Safeguarding following Safeguarding Adult’s procedure.
Health and Community Services
All Community including: FNHC, Hospice, GP, Care Homes & agencies, Children’s services, charities
Complete Root Cause Analysis
Complete Root Cause Analysis Key points for all situations:
Involve individual in decisions where possible.
Take action and put preventative management measures in place.
Ensure that the person, family and all carers communicate effectively
Call a Multi-Disciplinary team meeting
Refer to Tissue Viability Specialist Nurses where appropriate
Ensure that follow up is robust and that if there is further deterioration consideration must be given to raising a Safeguarding Alert
Organisational investigations to be carried out
Consider level of harm and reporting to relevant organisations
Identify lessons to be learned: consider Practice Learning Events for staff and carers
Link for Adult Safeguarding Referral: https://soj/depts/HSS/Documents/Read%20only%20forms/F%20Adult%20Safeguarding%20Alert
%20Form.doc
Decision by Safeguarding team as to whether a Safeguarding concern is to be pursued in conjunction with the Health Safeguarding team or the Tissue Viability Nurse Specialists.
Complete Adult Safeguarding Decision Guide. Record conclusion in incident reporting and records. If threshold for adult safeguarding alert is met (Score of 15 or more) or clinical judgement concern, refer to Safeguarding following Safeguarding Adult’s procedure.

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 32 of 35
ADULT DECISION GUIDE-Safeguarding
Risk Category Level of Concern Evidence 1 Has the patient’s skin deteriorated to either grade 3/4/
unstageable or multiple grade 2 from healthy
unbroken skin since the last opportunity to assess/
visit
Yes. e.g. record of blanching /
non- blanching erythema
5 E.g. evidence of redness or skin
breaks with no evidence of provision of
repositioning or pressure relieving
devices provided
No e.g. no previous skin integrity
issues or no previous contact health
or social care services
0
2 Has there been a recent change, i.e. within days or
hours, in their / clinical condition that could have
contributed to skin damage? e.g. infection, pyrexia,
anaemia, end of life care, critical illness
Change in condition contributing
to skin damage
0
No change in condition that could
contribute to skin damage
5
3 Was there a pressure ulcer risk assessment or
reassessment with appropriate pressure ulcer care plan
in place and documented? In line with each
organisations policy and guidance
Current risk assessment and care
plan carried out by a health care
professional and documented
appropriate to patients needs
0 State date of assessment Risk tool used
Score / Risk level
Risk assessment carried out and
care plan in place documented but
not reviewed as person’s needs
have changed
5 What elements of care plan are in place
No or incomplete risk
assessment and/or care plan
carried out
15 What elements would have been
expected to be in place but were not
4 Is there a concern that the Pressure Ulcer developed as
a result of the informal carer wilfully ignoring or
preventing access to care or services
No/Not Applicable 0
Yes 15 5 Is the level of damage to skin inconsistent with the
patient’s risk status for pressure ulcer development?
e.g. low risk–Category/ grade 3 or 4 pressure ulcer
Skin damage less severe than
patient’s risk assessment suggests
is proportional
0
Skin damage more severe than patient’s risk assessment suggests is proportional
10
6 Answer (a) if your patient has capacity to consent to
every element of the care plan.
Answer (b) if your patient has been assessed as not
having capacity to consent to any of the care plan or
some capacity to consent to some but not the entire care
plan.
a Was the patient compliant with the care plan
having received information regarding the risks of
non- compliance?
Patient has not followed care plan
and local non Concordance policies
have been followed.
0
Patient followed some aspects of
care plan but not all
3
Patient followed care plan or not given
information to enable them to make
an informed choice.
5
b Was appropriate care undertaken in the patient’s best
interests, following the best interests’ checklist in the
Mental Capacity Act Code of Practice? (supported by
documentation, e.g. capacity and best interest
statements and record of care delivered)
Documentation of care being
undertaken in patient’s best
interests
0
No documentation of care being
undertaken in patient’s best interests
10
If the score is 15 or over, discuss with the HCS (safeguarding) as determined by local procedures and reflecting the urgency of the situation. Please send
this decision guide along with the referral through to Adult Safeguarding team. When the decision guide has been completed, even when there is no
indication that a safeguarding alert needs to be raised the tool should be stored in the Datix record. The individual should be made aware they are being
referred unless there is an identified reason not to share this with them such as lack of mental capacity in this area.

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 33 of 35
Appendix 8: Making Safeguarding Personal "Safeguarding may be everyone's business but making safeguarding personal means
it is my business"
Our multi-agency safeguarding policy and procedures provide a firm foundation
for Making Safeguarding Personal in Jersey.
Making Safeguarding Personal (MSP) is a philosophical approach to promote
responses to safeguarding situations in a way that enhances a person's involvement,
choice and control as well as improving quality of life, alongside their well-being and
safety.
The key focus is on developing a real understanding of what people wish to achieve. This
includes agreeing, negotiating and recording their desired outcomes, working out with
them (and their representatives or advocates if they lack capacity) how best those
outcomes might be reached, and the extent to which desired outcomes have been
realised at the end of the intervention
The full participation of people in all decisions affecting their lives should be encouraged.
In the past, people involved in adult safeguarding related incidents have said they can
sometimes feel they have little control in respect of what is happening to them; are not
involved in discussions; are rushed to make decisions or have little say over outcomes.
'Making Safeguarding Personal' therefore promotes a shift in culture and practice,
which ensures that any intervention is more effective from the perspective of the person
involved in the matter.
Whilst pressure ulceration may indeed be a matter for clinicians the principles of making
safeguarding personal must remain at the forefront of our thinking. It is an expectation
that the fullest involvement of the person will be explored.
Fundamentally, effective safeguarding is about people and organisations working
together to prevent and reduce both the risk and experience of abuse or neglect.
Safeguarding means protecting the health, wellbeing and human rights of people at risk,
enabling them to live safely, free from abuse and neglect. Safeguarding also means
making sure that the adult's wellbeing is supported and their views, wishes, feelings and
beliefs are respected when agreeing on any action. In Jersey we endorse the ethos of
making no decision about me, without me. Effective safeguarding is keeping people in
control and aware of their rights.
In Jersey, we pride ourselves on the strength of partnership arrangements we have in place, and we recognise the skills, strengths and knowledge of all our partners in delivering quality safeguarding interventions to our citizens. Safeguarding is more effective when we work together cooperatively.
Remember: patients, community based clients, their carers, and their representatives are partners too.
1. Concerns raised with the Safeguarding Adults Team about Pressure Care

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 34 of 35
In respect of concerns relating pressure care – the Safeguarding Adults Team (SAT) will become involved where neglect is indicated.
Neglect can be caused through omissions of care or treatment – or less in less likely circumstances through deliberate acts of failures to care appropriately. For pressure related matters, that are not adjudged to be caused through neglect, the SAT do not have a role.
In light of our new multi-agency policy driver around making safeguarding personal – the SAT expect that a discussion with the patient (or their representative if they lack capacity) will have been held prior to a concern being submitted.
Health and Community Services (SAT) will:
Ensure that any Safeguarding Adults concern is acted on in line with the Safeguarding Adults Procedures;
Coordinate the actions that relevant organisations take in accordance with their own duties and responsibilities;
Ensure a continued focus on the adult at risk and consideration of other adults or children;
Ensure that key decisions are made to an agreed timescale; Ensure that any Safeguarding Plans (when required) are put in place
with adequate arrangements for review and monitoring; Ensure that any actions and interventions are proportionate to the level of risk and
enable the adult at risk to be in control, unless there are clear recorded reasons why this should not be the case;
The Safeguarding Adults Team will make enquiries, or request partner agencies to do so, if they reasonably suspect a person who meets the criteria is, or is at risk of, being abused or neglected.
It is highly likely that partner agencies with the relevant clinical skills and knowledge will be called upon to carry out enquiries into pressure care related matters.
The SAT Safeguarding Coordinator is the Officer who has overall responsibility for ensuring there is an appropriate response to the concerns raised.
The Safeguarding Coordinator must ensure arrangements are made for the continued involvement of the person (patient) in all decisions made about them in accordance with their wishes and desired outcomes.
In relation to care settings, the consideration of risks to other people/patients’ needs to be duly considered and factored. In such circumstances where there is believed to be a culture of neglect or poor care, then discussions with the individual need to be mindful of the likelihood, that any enquiries made are likely to go beyond their individually expressed outcome.

ISLAND-WIDE PRESUURE ULCER FRAMEWORK HSS-GD-CG-607-01
GOVERNMENT OF JERSEY - HEALTH AND COMMUNITY SERVICES Page 35 of 35
Top Related
Copyright © 2022 FDOKUMEN

