







Bahasa
Halaman
Hukum

Chair of WEHAG: Dr Shyamal Mukherjee MBE Deputy Chair: Simon Barrigan
Administrator: Carol Davies (Email: [email protected])
Copyright protected WEHAG 2003 – 2009
WIRRAL ETHNIC HEALTH ADVISORY GROUP
(WEHAG)
INFORMATION & RESOURCE FILE
For use by all workers in health & social organisations in Wirral
(statutory, voluntary and community)
2nd Edition – January 2009
WEHAG website address: www.wehagwirral.nhs.uk
Page 2 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
CONTENTS Introduction & Foreword by Dr Shyamal Mukherjee...................................p.4
• Disclaimer .............................................................................................p.6 Mission Statement & Current Vision of WEHAG .........................................p.7 Guide to Using Resource File .......................................................................p.8 Advice for Health & Social Care Professionals .........................................p.10 1. Ethnic Minority Groups on Wirral
• History & Background..........................................................................p.11 • 2001 Census Data ..............................................................................p.12
2. Cross Cultural Communication & Consent Issues ...............................p.14
• How to contact trained interpreter or translation services....................p.16 3. Aspects of Culture – key points in the life cycle
• Black Caribbeans ................................................................................p.17 • Rastafarians ........................................................................................p.19 • Black Africans .....................................................................................p.21 • Somalis ...............................................................................................p.22 • Black British ........................................................................................p.24 • Chinese ...............................................................................................p.26 • Vietnamese-Chinese...........................................................................p.31 • South Asians
Indians......................................................................................p.34 Bangladeshis ............................................................................p.35 Pakistanis .................................................................................p.36 Muslims of South Asia ..............................................................p.37 Hindus ......................................................................................p.44 Sikhs.........................................................................................p.49
• Irish & Irish Travellers..........................................................................p.52 • Kosovan ..............................................................................................p.57 • Kurdish ................................................................................................p.58 • Polish ..................................................................................................p.60 • Somali .................................................................................................p.63 • Yemeni ................................................................................................p.65
4. Aspects of Faith .......................................................................................p.66
• Baha’I.............................................................................................p.67 • Buddhism.......................................................................................p.69 • Christianity .....................................................................................p.72 • Christian Scientists ........................................................................p.76 • Hari Krishna ...................................................................................p.78 • Hinduism........................................................................................p.79
Page 3 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
• Islam – Muslim...............................................................................p.82 • Jehovah’s Witnesses .....................................................................p.86 • Judaism .........................................................................................p.88 • Morman..........................................................................................p.91 • Quakers – Religious Society of Friends .........................................p.93 • Rastafarianism...............................................................................p.94 • Romany Origin ...............................................................................p.97 • Seventh Day Adventists...............................................................p.101 • Sikh..............................................................................................p.102
Calendar of Religious Festivals................................................................p.105 5. Asylum Seekers and Refugees
• Asylum Seeker Information & Support Group (Wirral).......................p.108 6. Gypsy Travellers ....................................................................................p.115 7. Practical Resources
• Interpretation and Translation Services.............................................p.117 • Websites ...........................................................................................p.118 • Other resources ................................................................................p.119 • Support Groups/Useful Contacts.......................................................p.120
8. The Race Relations (Amendment) Act 2000 & Wirral Ethnic Health Strategy 2003..............................................................................................p.125 9. Organisations’ Own Information
• Merseyside Police – Wirral Community Relations Unit .....................p.127 • Wirral Citizens Advice Bureau...........................................................p.130 • Forum Housing Association ..............................................................p.131 • Wirral Stop Smoking Service.............................................................p.132 • Wirral Drug & Alcohol Action Team (DAAT) ......................................p.133 • Wirral African Organisation ...............................................................p.134 • Wirral Black & Racial Minority Partnership (WBRMP).......................p.135 • Wirral African & Caribbean Community Voice...................................p.136 • Wirral Council BME Support Service.................................................p.137 • Wirral Refugee Action .......................................................................p.138
10. Examples of Good Practice
• Wirral Council ...................................................................................p.139 11. Acknowledgements .............................................................................p.151
Page 4 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
INTRODUCTION The Wirral Ethnic Health Advisory Group (WEHAG) has re-launched itself with a vision for this century. Building on the great work started by Lord Chan in 1995, the WEHAG will carry forward the legacy started by him. The WEHAG remains committed to work with all BME communities, agencies in the voluntary sector and corporate bodies to help develop an overarching strategy to identify and address health and social needs of the Wirral ethnic groups. The Information & Resource file is the culmination of a lot of hard work and will bring to us detailed information of different ethnic groups on the Wirral. It will become a great information source for professionals and others involved in patient care. I feel very privileged to be chairing this extraordinary group of dedicated people who remain committed to addressing health and inequality issues affecting the BME groups. I am extremely thankful to the BME groups, voluntary agencies and the corporate bodies without whose commitment this vision would remain unfulfilled. Dr Shyamal Mukherjee MBE Medical Director, NHS Wirral Chair of WEHAG
Original Foreword by Lord Chan of Oxton, Founder member and Chair Person of WEHAG
The Wirral Ethnic Health Advisory Group was formed when a needs survey of Asian communities, Chinese and Vietnamese in 1995 showed the need for trained interpreters in order for older people and new arrivals to access the NHS and statutory services. Two part-time trained interpreters with the appropriate language skills were employed in 1996 on a grant from the Wirral Health Authority to be link workers with the Bangladeshi and Chinese - Vietnamese communities. A new survey to locate ethnic minority groups who are new to Wirral is now being conducted by a project
Page 5 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
team at the Wirral Multicultural Centre. With the legislation of the Race Relations Amendment Act in 2000 requiring all public bodies including the NHS and other statutory bodies to promote have race equality schemes, the Wirral Ethnic Health Advisory Group decided to introduce an ethnic health strategy for Wirral. This was launched in March 2002 and all NHS bodies signed up to it. Since then, the Wirral Ethnic Health Advisory Group has extended its membership to these organisations and others such as St John's Hospice. Because the number of people from visible ethnic backgrounds in Wirral is around two per cent, there is a need for the staff of public bodies to have some basic information about their culture, language needs and religion. This Information and Resource File has been compiled with those requirements in mind. For example, cross-cultural communication has its problems particularly if you are unaware of the differences in body language such as eye contact and its significance in other cultures. Some information about the history of ethnic minority groups in Wirral will help you appreciate their limitation in the English language. So, when you use an interpreter, it is polite to look at the patient when asking questions rather than the interpreter. But just a word of caution - do not assume that all Bangladeshis, Chinese and Vietnamese residents in Wirral need interpreters. Those who are born and bred here or have been educated in Britain are fluent in English. Similarly, cultural preferences such as women wanting female doctors and health professionals occur among older White women as well as in ethnic minority women. I expect this information and resource file to be improved as we receive feedback from you. New information and updates will be introduced annually. We look forward to hearing from you Finally, all of us as professional people want to give the best service and care to our patients and clients. I trust this information and resource file will help you help people whose background you are not familiar.

Page 6 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Disclaimer
WEHAG have verified the information contained in this File and have consulted with local groups concerning the accuracy of the data. However, it is recognised that there may be some inaccuracies. Nevertheless, WEHAG have endeavoured to ensure that all the information is correct at the time of printing. If you wish to suggest amendments, please contact Carol Davies, Administrator, WEHAG: [email protected]
Page 7 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
WEHAG Mission Statement WEHAG is the Wirral’s advisory forum and information exchange, focusing on
ethnicity and health. It is a key driver for change, actively contributing towards
a reduction in health inequalities, accountable to local people and committed
to delivering actual results.
The Current Vision of WEHAG • To develop a common health strategy which addresses health issues
and unmet needs of all BME communities.
• To help promote a common corporate strategy to address the
requirements of different BME groups and feedback progress.
• To identify and develop specific health agendas (eg. Mental health,
diabetes, cardio-vascular disease, cancer, drugs and alcohol, social
isolation) relating to all BME groups.
Page 8 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Guide to using the Resource File
What is the purpose of the Ethnic Minorities Information & Resource File? To give all staff working in the NHS, health related organisations and Local Authority social care services basic background information of the visible ethnic minorities from South Asian, Black and Chinese people in Wirral, as well as Irish and Irish Travellers, Romany peoples, Asylum Seekers and Refugees. The Contents page: Indicates the layout with page numbers for the subsections:
• Introduction & Foreword is provided by Dr Shyamal Mukherjee MBE, Chair of WEHAG, Medical Director of NHS Wirral, and Chair of Wallasey Locality.
• Ethnic Minority Groups on Wirral – History & background, 2001 o Census Data: Britain is a multicultural and multi-ethnic country
with increasing numbers of non-European people living in the United Kingdom (UK), large numbers of Asylum seekers from Afghanistan, Iraq, Iran and parts of Southern Africa. Since the start of the 21st century, we can no longer ignore people whose first language is not English. On the other hand, the National Census of 2001 shows that more than 60% of black people, Indians, Pakistanis, Bangladeshis and Chinese living in the UK are born here. In fact, most young people from these countries are born and bred in the UK.
• Cross Cultural Communication: a practical perspective including
details on cultural differences
• Aspects of Culture contains general information on: Background & guide to naming systems Social customs & traditions.
• Aspects of Faith includes information under the following headings:
Key issues and special considerations, food & diet Care of the dying and what to do after death Festivals & holy days
• Calendar of Religious Festivals listed by month • Asylum Seekers & Refugees: details on definitions, documents &
support
Page 9 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
• Gypsy Travellers: general background information & contact details for support
• Practical Resources: contact details of Merseyside groups as well as
websites • Organisations’ Own Information
• Examples of Good Practice
• Acknowledgements
Braille, large print, audio & other formats also available on request:
Contact Carol Davies, Equality & Diversity Projects Officer, NHS Wirral, St
Catherine’s Hospital, Church Road, Tranmere, Birkenhead CH42 0LQ
Tel: 0151 651 0011 ext. 6039 or email [email protected]
Page 10 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Advice for Health and Social Care Professionals
Although we aim for all staff to have the opportunity to understand different
ethnic communities’ needs and requirements, there may be circumstances
where staff may not be familiar with, nor have the relevant information to
hand, in order to deliver the correct care relevant to the patient’s ethnicity.
If you are not familiar with the correct procedures, always ask a senior
member of staff.
When a Black or Minority Ethnic (BME) patient is known to be in their final
days of life, please be aware that, in most cases, there will be specific
religious needs which need to be met. Please refer to the relevant section of
this Information & Resource File, in the first instance. Additionally, it would be
wise to contact the patient’s family members/next of kin for further
advice/guidance on acceptable care.
For more information, please contact the Hospital Chaplain. For Arrowe Park
Hospital, please phone 0151 678 5111 ext. 2275. For Clatterbridge Hospital,
please phone 0151 334 4000 ext. 4008. Alternatively, please contact the
Hospital Switchboards (0151 678 5111/0151 334 4000).
Further information will be available on the WEHAG website
(www.wehagwirral.nhs.uk).
Page 11 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
1. Ethnic Minority Groups on Wirral – History & Background
Did you know ……Black soldiers of the Roman Empire served in Britain – a garrison of North African soldiers was stationed at Hadrian’s Wall in 253 AD!
• Black and ethnic minority people have been in and out of Britain through the ports of London, Bristol, Cardiff, Liverpool and Birkenhead for many centuries.
• Slaves from various parts of Africa were transported to the
Caribbean and North America via Liverpool from 1680 to 1800. There were some famous Black people in 19th Century, particularly Mary Seacole, a nurse who served in the Crimean War with Florence Nightingale. The Royal College of Nursing has a scholarship named after Seacole for nurses researching ethnic health issues. Mary Seacole is an honoured name in Toxteth.
• Jews from Eastern Europe came to Britain as refugees
• Many Irish people arrived here during the potato famine of
19thCentury
• The Chinese came to settle in Merseyside when the Holt family opened the first shipping line (Blue Funnel) from Liverpool to coastal cities of China in the 1860s.
After World War II, West Indians and South Asians from the Indian sub-continent were invited to Britain to take jobs in public transport, as nurses in the National Health Service and in industries such as the cotton mills of Lancashire and Yorkshire
• Displaced Europeans, especially the Italians, Poles and
Ukrainians came here to settle after the World War. Merseyside’s ethnic minority communities are unique in the UK because they have been settled here for a very long time. For example, there has been a ‘Chinatown’ in Liverpool around Pitt and Cleveland Streets since 1885, the oldest Chinese community in Europe.
• Black Liverpudlians have lived in Liverpool 8 for more than a century and many have one parent who is white.
Page 12 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
• Seamen from the Yemen settled in Granby and Toxteth to run corner-shops.
• Refugees have come here in the past 20 years from Vietnam, Somalia, Ethiopia and the Balkans (Bosnia and Kosovo)
• Immigrants from (the Republic of) Ireland have been coming
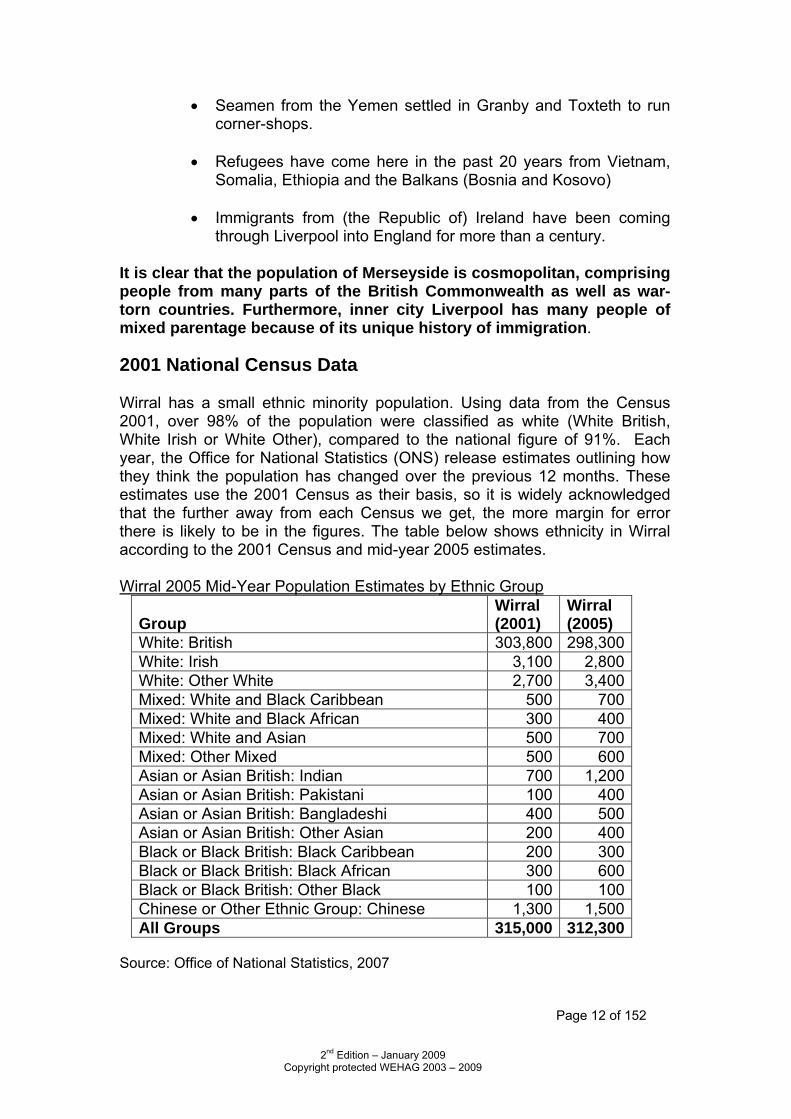
through Liverpool into England for more than a century. It is clear that the population of Merseyside is cosmopolitan, comprising people from many parts of the British Commonwealth as well as war-torn countries. Furthermore, inner city Liverpool has many people of mixed parentage because of its unique history of immigration. 2001 National Census Data Wirral has a small ethnic minority population. Using data from the Census 2001, over 98% of the population were classified as white (White British, White Irish or White Other), compared to the national figure of 91%. Each year, the Office for National Statistics (ONS) release estimates outlining how they think the population has changed over the previous 12 months. These estimates use the 2001 Census as their basis, so it is widely acknowledged that the further away from each Census we get, the more margin for error there is likely to be in the figures. The table below shows ethnicity in Wirral according to the 2001 Census and mid-year 2005 estimates. Wirral 2005 Mid-Year Population Estimates by Ethnic Group
Group
Wirral (2001)
Wirral (2005)
White: British 303,800 298,300 White: Irish 3,100 2,800 White: Other White 2,700 3,400 Mixed: White and Black Caribbean 500 700 Mixed: White and Black African 300 400 Mixed: White and Asian 500 700 Mixed: Other Mixed 500 600 Asian or Asian British: Indian 700 1,200 Asian or Asian British: Pakistani 100 400 Asian or Asian British: Bangladeshi 400 500 Asian or Asian British: Other Asian 200 400 Black or Black British: Black Caribbean 200 300 Black or Black British: Black African 300 600 Black or Black British: Other Black 100 100 Chinese or Other Ethnic Group: Chinese 1,300 1,500 All Groups 315,000 312,300
Source: Office of National Statistics, 2007
Page 13 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
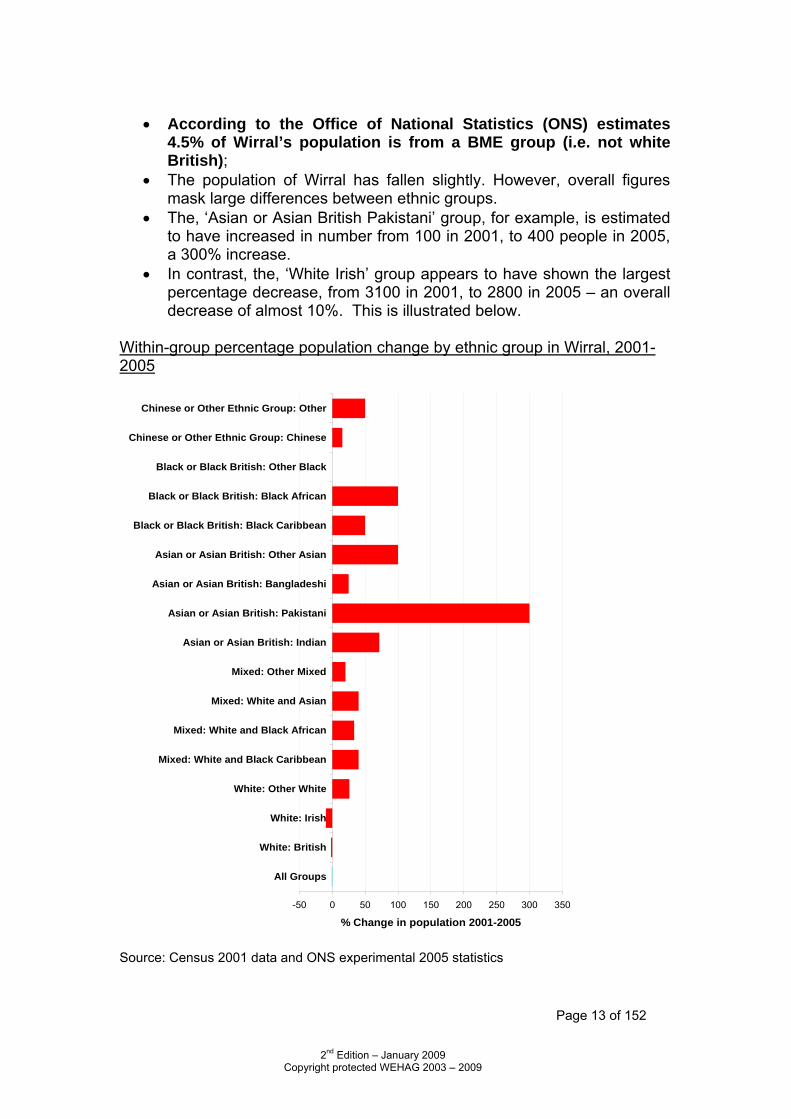
• According to the Office of National Statistics (ONS) estimates
4.5% of Wirral’s population is from a BME group (i.e. not white British);
• The population of Wirral has fallen slightly. However, overall figures mask large differences between ethnic groups.
• The, ‘Asian or Asian British Pakistani’ group, for example, is estimated to have increased in number from 100 in 2001, to 400 people in 2005, a 300% increase.
• In contrast, the, ‘White Irish’ group appears to have shown the largest percentage decrease, from 3100 in 2001, to 2800 in 2005 – an overall decrease of almost 10%. This is illustrated below.
Within-group percentage population change by ethnic group in Wirral, 2001-2005
-50 0 50 100 150 200 250 300 350
All Groups
White: British
White: Irish
White: Other White
Mixed: White and Black Caribbean
Mixed: White and Black African
Mixed: White and Asian
Mixed: Other Mixed
Asian or Asian British: Indian
Asian or Asian British: Pakistani
Asian or Asian British: Bangladeshi
Asian or Asian British: Other Asian
Black or Black British: Black Caribbean
Black or Black British: Black African
Black or Black British: Other Black
Chinese or Other Ethnic Group: Chinese
Chinese or Other Ethnic Group: Other
% Change in population 2001-2005
Source: Census 2001 data and ONS experimental 2005 statistics
Page 14 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
2. CROSS CULTURAL COMMUNICATION
• Communication is a tricky business. For example, just because someone sits silently does not mean that s/he necessarily understands what is being said, or that s/he feels that s/he has been adequately understood.
• Most people habitually ‘read’ behaviour in terms of their own familiar
cultural conventions. By doing this, they overlook the possibility that the other person’s behaviour may not be based on a similar culture.
• Ethnocentrism – the use of one’s “taken for granted” cultural
assumptions to (mis)interpret other people’s behaviour is a common human failing. Ethnocentric assumptions are a major source of the “unwitting processes” of social exclusion that the Macpherson Report (http://www.archive.official-documents.co.uk/document/cm42/4262/4262.htm)
• identified as institutional racism.
• Most of us initially look through the “taken for granted” spectacles of our own cultural tradition to make sense of the world around us. We also tend to be strongly attached to our own culture. Therefore, we should never underestimate the influence which our cultural background may have on our judgements and perceptions, no matter how open-minded we may consider ourselves to be.
• Cultural differences between Europeans and non-Europeans are
obvious in eye contact. In most European cultural traditions, a person who is willing to make eye contact with an interrogator is showing honesty and sincerity while one who does not make eye contact is showing shiftiness, uneasiness and possibly guilt.
• However other cultural traditions organise relationships differently.
• In South Asian and East Asian contexts, any woman who makes direct
eye contact with an unrelated man is regarded as brazen. Hence, modest and respectable women are expected to shield themselves from the direct gaze of men and, most especially, from senior male relatives. She may well keep her eyes lowered partly as a defensive measure.
• Similarly, Asian employees do not make direct eye contact with their
employers or superiors and people in authority. In any investigation, all Asian women should be approached and interviewed by a woman police officer using an appropriate female interpreter and not one of her male relatives such as her husband or brother.
Page 15 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
• Also, many of the African cultures do not make direct eye contact. It is, in fact, rude to look someone of social standing, significantly the elders, doctors, policemen, father figures etc in the eye. This is sometimes encouraged amongst the 1st and 2nd generation depending on the upbringing of the child and also the traditional practices of the parents.
When faced with a person who is not fluent in the English language, a trained interpreter should be called in order to improve the quality of communication. – see details below. For Wirral NHS employees, please refer to the relevant Trust’s Consent to Treatment policy. “Consent” is a patient’s agreement for a health professional to provide care. Patients may indicate consent non-verbally (for example by presenting their arm for their pulse to be taken), orally, or in writing. For the consent to be valid, the patient must
• be competent to take the particular decision • have received sufficient information • give consent voluntarily ie. not under any form of duress or undue influence from health professionals, family or friends.
Consent must be never be assumed, even for minor interventions.
Therefore, in order for the patient to receive sufficient information in a language which they understand, it may be necessary to arrange for an interpreter/translator.
• The interpreter must be fluent in English and in the language or dialect
of the person we wish to communicate with. Good quality communication begins with the correct pronunciation of a person’s name.
• We must avoid stereotypes because all individuals have rights
and feelings.
• Therefore, it would be inappropriate to ask a child to interpret for a parent because this puts unfair and disproportionate emotional and psychological stress and strain on the child. It may also cause embarrassment to the parent(s).
• Using a child or relative also breaches the patient’s right to
confidentiality.
Page 16 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
How to Contact a Trained Interpreter or Translation Service Language Line Language Line provides translation services over the telephone only. For Wirral NHS Trust employees, a department code will need to be quoted in order to access the services. This code number can be obtained from the department manager or the Equality & Diversity Team (ext. 6039). For urgent translations of documents i.e. same day or less, please ring Language Line who will then give you a number to fax the document to for them to be read back to you. Telephone Number: 0845 310 9900 Web address: www.languageline.co.uk Liverpool NOVAS They have an extensive list of interpreters. In the first instance, please telephone, followed by a fax. Telephone number: 0151 708 8640 Web address: www.novasscarman.org Wirral Multicultural Organisation The Wirral Multicultural Organisation provides interpreters for the Cantonese, Mandarin, Urdu, Punjabi, Hindi and Bengali speaking patients. To book an interpreter, please contact the Centre direct by telephone first. If necessary, this should be followed up by faxing or emailing the details of the work required. Emails should be directed to the individual at the WMO. Telephone Number: 0151 666 4547 Web address: www.wmo.org.uk Royal National Institute of the Deaf They provide Sign language interpreters, lip speakers and deaf-blind interpreters. Please contact them direct to book the interpreter. Telephone number: 0845 685 8000
Web address: www.rnid.org.uk
Page 17 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
3. ASPECTS OF CULTURE - Key points in the life cycle BLACK CARIBBEANS Black Caribbeans in Britain today came from the colonies of Jamaica, Guyana, Trinidad & Tobago, Barbados and the other islands stretching from the Bahamas to South America. They were invited by the British Government after World War II to work in public transport and as nurses. The first large group of Caribbeans arrived on the ship “Empire Windrush” in 1948. Language Although English is the main language spoken in the Caribbean, first generation migrants also speak Creole/Patois. Creole has a European root source of vocabularies such as Dutch, English, French and Portuguese. Naming Patterns Names of individuals are diverse and relate to their colonial histories. Many of the English names reflect those of British colonials and tend to be upper class names such as Winston, Allen and Shirley. Other names have origins in India (Patel, Singh and Kanhai), France (Pierre, Francois) and Holland (Maartens, Eickhof). History Britain, France, Holland and Spain and Portugal were the main countries involved in the slave trade. Most slaves were taken from West Africa (Ghana, Nigeria, Sierra Leone, and Cameroon) and, when put together, developed a language called Creole or Patois containing African and European language roots. Religion In Britain, the Caribbean communities are mostly Christians. They are more active in the black-led churches than in the mainline denominations. Caribbean Christians worship in numerous black-led churches such as the New Testament Church of God and Cherubim and Seraphim. Worship is taken seriously. It may consist of teachings from the Bible, praying, speaking “in tongues”, and audience participation, lively music and dancing.

Page 18 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
The Caribbean Family System The Caribbean family is matriarchal. The men migrated and the women were left in charge of the children. When the mothers or girlfriends migrated, grandmothers were left in charge. In Britain, long working hours, unemployment among black men and significant proportion of single parent mothers have aggravated family disruption. In the 2001 National Census, 9% of Black Caribbeans were aged over 65 or over compared with 16% of white people. Caribbean Diet Plantain looks like a large banana (yellow when ripe, green when unripe). Slices of ripe plantain are fried in oil and taste sweet. Ackee and saltfish is known as the national dish of Jamaica. Ackee grows on trees in the Caribbean. Yam forms a large part of the Caribbean diet. Patties (like Cornish pasties) are also popular.
Page 19 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
RASTAFARIANS Rastafarians have their origins in Jamaica and are said to have emerged as a direct result of the teachings of Marcus Garvey who died in England in 1940. Marcus Garvey believed that Africa was the beginning of civilization. He proclaimed that God would soon return in the 1930s, in living form, as stated in the biblical book of Revelation. Garvey said that this man, a direct descendant of Solomon and Sheba, would be crowned the King of Kings of one of Africa’s greatest nations; hence the significance of the crowning of Emperor Haile Selassie of Ethiopia. Rastafarianism had its origins in a ‘Back to Africa’ philosophy. The Rastas’ main aims are: One love, one aim and one destiny. Africa yesterday and today and forever more. In the Caribbean, Rastafarianism attracted working class Blacks. It became prominent with the black power movement of the 1960s and 1970s. In Britain, Rastafarianism is a conscious ideological and historical focal point. During the slave era, many Africans were forcibly removed from their homeland. They were taken mainly to the Caribbean Island and the Americas. Rastafarians feel that, although political slavery has ended both mentally and physically, slavery still exists and will end when the repatriation of all Africans to Africa is complete. Beliefs Rastafarians believe the Bible is the most important book for them. The Bible is read from Genesis through to Revelation at least one chapter a day. In the book of Revelation, God will return one day to the earth in his kingly glory. Rastafarians expect God to come as a man from an ancient lineage (“Jah Ras-tafari” means “God liveth always”). Emperor Haile Selassie, the former king of Ethiopia, is believed to be this man by Rastafarians. Today, Rastafarians try to live their lives as closely as possible to the teachings of the Bible. Rastafarians do not worship in a church building. Their regular weekly or monthly meetings take place in homes or community centres, they are spiritual where men and women (brethren and sisters) read and chant a chapter of the Bible, sing songs of praise and give thanks to the Most High, Jah Ras-tafari. The meetings are also used to give information of social issues and events. Festivals Festivals are celebrated in the Ethiopian calendar, the main two being Christmas and New Year. The birth of Emperor Haile Selassie is celebrated on 23 July. All festivals are celebrated by live shows, food and giving thanks to the Most High. New Year on the Rastafarian calendar is 1 April, the month of Reuben, the first born to Jacob.
Page 20 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Appearance Rastafarian men wear dreadlocks that denote power, freedom and defiance. Rastas object to the disfigurement of their God-given bodies and so do not shave, have no tattoos and do not cut their hair. Men often wear bright hats with Rastafarian colours: Red, symbolising blood of the martyrs, Black the colour of Africa, and Green the colour of vegetation and hope of the vision over oppression. Women tend to wear long skirts, socks with tights or trousers to keep their legs covered. Men and women wear badges or necklaces of the Star of David or the Ethiopian cross. Diet The Rastafarian diet is based mainly on natural foods of vegetables and cereals. Some Rastafarians may not be strictly vegetarians and they will eat fish or lamb (Halal or Kosher only). Pork is not eaten, as Rastafarians believe it is unclean meat. Alcohol, milk and coffee are not drunk or added to food. They do not use any prescribed medicines, preferring herbal remedies. No salt is used in cooking and the only oil used is dry coconut oil.
Page 21 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
BLACK AFRICANS Black Africans have been living in Britain for centuries. They originally came as slaves, seamen and for education. They have come from the former British colonial territories of West Africa (Ghana, Nigeria and Sierra Leone), East Africa (Kenya, Tanzania and Uganda) and Southern Africa (South Africa, Zambia and Zimbabwe). Many Black Africans held professional positions in their native countries eg. doctors, nurses, scientists before being recruited to come and work in this country. In the 1990s, Africans from French-speaking countries (e.g. Cameroon, Congo, and Rwanda) have found refuge in Britain.
• Most speak English and an African language. French is spoken by Africans from Francophone countries. However, the interpretation of English may differ. Mother tongue languages aid understanding. Other languages spoken include Arabic and Portuguese depending on which colonial power was in charge.
• Many came as students to British universities and colleges or as a
result of conflicts or persecution in their countries and were often professional people. In the case of Sierra Leone, some already had British citizenship. Many were also recruited to work in the UK and were issued with work permits.
• Since 1999, Black Zimbabweans have arrived in Britain as refugees
because of President Mugabe's intolerance of political opposition parties.
• Many have suffered racial discrimination. This discrimination has
included their experience of the police with frequent 'stop and search', or being followed by staff when shopping in departmental stores.
• Because of their daily experience of discrimination, Africans are
particularly sensitive when in contact with statutory services.
• Many Africans are practising Christians and are active in church. West African Diet
• Fried plantain is a common food
• Steamed mashed yam is a staple food of West Africa and looks like a large steamed dumpling. It is eaten with stew made of fish or meat (chicken or goat), using red palm oil.
• 'Jollof’ rice is a rice dish containing tomatoes, onions and meat or
vegetables
• Alcohol, in the form of beer and spirits, is drunk
Page 22 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
• Super malt is a popular non-alcoholic beverage Other lifestyle facts
• Young Black African men, Black Caribbeans, Pakistanis, and those belonging to mixed heritage have very high unemployment rates ranging between 25% and 31%. The comparable unemployment rate for young White men was 12% (2001 National Census).
Other African Communities SOMALI
• A 1993 study of the Somali community was done as part of a survey of Liverpool's ethnic minority groups by Eolas commissioned by Liverpool City Council. Many Somalis have come to Merseyside as refugees from the civil war in the Horn of Africa in the early 1980s.
• By 1993, there were 2500 Somali people living mainly in Granby and
Abercromby wards. More than half are young adults under the age of 25 years and only 8% pensioners over 65. Men outnumber women 6:4. Almost all Somalis are Muslim and adhere to social customs of gender separation.
• Over 70% of Somalis were unemployed in 1993. This proportion has
not altered and it includes professional people such as doctors whose medical qualifications are not recognised in the UK. In order to practice, they need to undergo clinical training for at least three years in a British medical school. However, the fees are prohibitive and most Somali doctors can only work as interpreters in the NHS in order to earn a living and to assist their peers to access GPs and hospital care. Somali health link workers, both men and women are based at Abercromby Health Centre.
• Somali women have problems with sexual intercourse and childbirth
because many have undergone female circumcision that distorts the female genitals. Special care is needed during labour and delivery because of this.
• Mental health problems are common among Somalis due to the trauma
of war and also associated, particularly among men, with the chewing of a plant quat (the leaves and stems having stimulant properties that keep users awake and hyperactive).
• Liverpool's Somali community is also divided by opposing political
parties carried over from their homeland. Suspicion of fellow Somalis exists as a result of political differences, competition for jobs and the aftermath of war. Because of these sensitivities, care should be taken to ascertain that a particular interpreter is acceptable to an individual Somali.
Page 23 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Wirral African Organisation c/o VCAW, 65 The Village, Bebington CH63 7PL The Wirral African Organisation has members from varied countries, such as Ghana, Zimbabwe, Egypt, Congo, Ethiopia, South Africa, Sierra Leone, Uganda, Zambia, Nigeria, Botswana, Gambia etc. The Wirral African Organisation meets on the first Friday of each month at Mayer Hall, Bebington from 7.00-9.00 p.m. The meetings are to promote positive African/BME culture, all topics relating to and affecting Africans/BME and issues concerning African/BME peoples’ health & well being. We support members of the organisation, and liaise/mediate on behalf of and/or between any service providers & stakeholders, including public, private and 3rd sector organisations. Please contact: Nurie Lamb, Chair person: 07773 35023 or Phillip Alliah, Vice Chair: 07988 236664
Page 24 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
BLACK BRITISH
• Most black children in our schools have been born in the UK. Some prefer to be known as Black British as they may not identify with their parents' cultural heritage. Some 4 in 10 black people born in Britain have a white parent. Among Liverpool-born black people, 9 in 10 have a white parent.
• School exclusions are high among black children and the Social
Exclusion Unit (of the Prime Minister's Office) is addressing this. The high level of exclusions is not because black children are more badly behaved than other children but that teachers often treat these children differently, being quicker to give sanctions for even trivial instances. Teachers also have lower expectations of black children, particularly boys.
• Recent research on black children and educational achievement found
that they do well in pre-school nursery and in the first years of primary education. But by 10 years, high levels of school exclusion take place among black children and they leave school with below average qualifications.
• Liverpool Blacks are particularly sensitive about their exclusion from
local authority discussions with ethnic minority groups.
• Increasing numbers of Liverpool-born black people with professional qualifications in law and management are active in community participation in health, social care and economic regeneration of the inner city.
• In Wirral, black people are usually working in the professions
associated with the NHS, in equal opportunity posts, the church and in the private sector. Others are students or postgraduates.
• Issues of racial discrimination in employment and in access to
entertainment services continue to upset black people born in Britain, particularly men. Although they are successful in sport such as athletics and football, the music industry and the media, black Britons feel vulnerable in their experience with the police including being stopped when driving and being stopped-and-searched when on the streets.
• Black people of mixed heritage are more likely to be victims of crime.
• Black people have expressed their desire not to be tolerated but
to be accepted and respected.
Page 25 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
WIRRAL AFRICAN AND CARIBBEAN COMMUNITY VOICE This association, formed in the year 2000, meets at the Charing Cross Methodist Church and the Wirral Multicultural Centre. The Group meets each Friday evening at 6.30 p.m.-8.30 p.m. at Charing Cross Methodist Centre, Birkenhead, Wirral. Health Issues Rates of compulsory admission to psychiatric hospitals are markedly higher for black and minority ethnic groups in comparison to whites. The significant differences in the use of the Mental Health Act between ethnic groups are present in all ages. There is greater involvement of the criminal justice system and, in particular, with the police in the referral pathway of minority groups. Less is known about suicide rates for Black African and African-Caribbean people living in the UK. Young black women may be vulnerable to suicide. Social risk factors may precipitate serious mental disorders and possibly suicidal behaviour in African and African-Caribbean people living in the UK.
Page 26 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
CHINESE
• The Chinese are the largest group of non-white minority ethnic residents in Wirral. They originate from Hong Kong (45%), China, Vietnam, Malaysia and Singapore and Britain. They speak Cantonese and Hakka, if from Hong Kong, and Mandarin, if from China. Many settled in Britain during the 1950s and 1960s. Most of our young Chinese aged less than 30 years are British-born and form 40% of the Chinese population.
• Although they run most of our fish-and-chips "takeaway" shops, a
significant number of Chinese work in the professions (doctors, pharmacists, dentists, nurses and engineers).
• When compared with Chinese living in Liverpool, Wirral's Chinese are
economically better off and more live in private housing.
• Half of Chinese over 45 years old are not fluent in English and need the help of interpreters to use statutory services including the police, health, social services and housing.
• They work in the catering trade and have limited formal education. In
their business, they experience racial harassment from customers (mostly young adults under the influence of alcohol) who refuse to pay for their food.
• The 4th National Survey of Ethnic Minorities in Britain published
in 1997 showed that the Chinese in England complained of racial harassment (16% compared with 15% of Caribbeans, 14% of African Asians and 13% of Pakistanis). A more recent survey of 1000 Chinese in England showed 2 in 5 had experienced racial abuse (Health Education Authority, 1999)
• Most families in the "takeaway" food business work Iong, unsociable
hours - 6 or 7 days every week. Children are expected to help at the sales counter. As a result, the family is isolated and women lack opportunities to learn English. Men tend to spend their leisure at a casino.
• Domestic violence can occur and depression affects women, in
particular.
• Older Chinese, who have been in catering for many years, suffer poor health and complain of arthritis, diabetes, high blood pressure and heart disease. These findings do not contradict the picture of good health and little long-term illness among the Chinese found in the 2001 National Census.
Page 27 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
History
• From 1885, the first Chinese communities appeared in Liverpool around Pitt Street and Cleveland Square. At the same time in London, Chinese seamen settled on Limehouse Causeway adjacent to the West India Docks.
• These early settlements were geared to servicing the needs of
Chinese crew arriving at British ports - Liverpool, London, Bristol and Cardiff. Laundries and lodging houses opened. The laundry business resulted in some dispersal from port areas but numbers remained small, with only 400 Chinese in Britain in 1900.
• From 15 settlers in 1881, the Chinese population of Liverpool grew to
502 in 1911. However, increase in the number of resident Chinese was restricted because of the implementation of the Aliens Act 1905 and the Aliens Restriction (Amendment) Act 1919.
• The first official reports on the Chinese in Britain appeared in the first
decade of the 20th century. They were about gambling and opium smoking among the men and their relations with white women which was a cause of official concern. Police reports from Liverpool, however, did not find evidence to substantiate these concerns.
• Opposition to the Chinese came from British seamen. Although there
were fewer of them than seamen from European countries, the Chinese were prepared to work for less and did not go on strike. Occasional assault or insult on the streets led the Chinese to set up organisations for self-protection such as mutual aid associations in Liverpool and London in 1907.
• These mutual aid associations also adjudicated in disputes between
members, provided financial support when members were ill or wanting to return to China, and attended to funeral rites and burial should they die in Britain.
• The associations organised celebrations of festivals such as the Lunar
New Year and All Souls Day. WIRRAL CHINESE ASSOCIATION (WCA) The WCA caters for the social and cultural needs of the 1,500 Chinese residents of Wirral. Based at the Wirral Multicultural Centre, it organises a weekly lunch club for Chinese pensioners and has an active Women’s Group that has an interest in health issues. The Chinese Health-Linkworker, also based at the Multicultural Centre, speaks Cantonese and Mandarin Chinese.
Page 28 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
The WCA celebrates the annual Chinese New Year festivities according to the Lunar Calendar. This includes a lavish lunch and karaoke. Chinese language classes are run by the WCA on Saturdays at the Multicultural Centre. Chinese Naming System
• The Chinese in Britain and other English-speaking countries have adopted western personal names. For many, this is a convenient way of helping their neighbours pronounce their name. However, for Chinese who are Christians, their Christian name is genuine and appears on baptismal and birth certificates. Some examples: Anthony Ping Kwan Wong (Christian name + Chinese name + Surname) or Mary Chan Wai Lin.
• Chinese names are usually split into three parts. In China, however,
the second and third names are combined and sometimes hyphenated e.g. Mao Tze-tung (Chairman Mao), Hu Jiantao (President).
• The surname is traditionally the first name, followed by the generation
name, with the personal name last. Brothers share the same surname and generation name but have a different personal name eg. Tan Eng Seng and Tan Eng Hock. Members of the same family but of another generation will have the same surname but the generation name will differ e.g. Tan Kong Meng and Tan Kong Teck.
• Chinese women may change their surname at marriage, but this is not
universal. An example would be: Wong Mei Ling becomes Chan Mei Ling. Occasionally, the new surname is a combination of both the husband's and the wife's names, as in: Chan-Wong Mei Ling.
• Vietnamese Chinese have names constructed on the same basis eg.
Tran Vhan Dong, Vong Hoa Lin. The important thing to remember is to ASK about the names of Chinese people.
Chinese Culture and Beliefs The culture of Chinese people in Britain tends to be westernised. Pop music and songs mainly from Hong Kong are sung in Cantonese but the tunes are familiar to western ears. Almost every home has TV and video-recorders to receive the two Chinese TV cable channels and play videos made in Hong Kong, China and Taiwan. Every regional radio station broadcasts an hour a week in Cantonese, but, in London, there is a Chinese radio station on FM seven days a week. Traditional Chinese culture of respect for elders, hard work and reliance on the family is practised here. The 4th National Survey of Ethnic Minorities in Britain found half the Chinese did not profess any religion, one quarter said they were Christians and one fifth (mainly over 50 years old) were Buddhists.
Page 29 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Chinese Buddhists put up a small altar/shrine on the wall of their kitchen or hall with an idol, flowers and burning incense sticks. Their system of beliefs is one of balance between Yin/Yang, light and darkness, male and female, hot and cold. The aim is to accept what is, to study the natural order of things (the Tao), and to work with it rather than against it. Worship is normally at either a temple or at a family altar/shrine. The five blessings of life are said to be-luck, food, long life, health and peace. Confucianism is not strictly a religion, rather a set of precepts governing relationships within the family and state. An ancient scholar, Kung Fu Tse, formulated these about 2000 years BC. Chinese Christians are evangelical Christians who believe the Bible is God's word that must be put into practise in daily life. They read the bible in Chinese and/or in English and worship in their own Chinese-language churches of which there are more than 100 in the UK.
• The Liverpool Chinese Gospel Church has 150 worshippers attending separate Cantonese and English language services for professionals and British-born Chinese.
• The church also conducts services in Cantonese thrice a month at Charing Cross Methodist Church, Birkenhead, on Sunday afternoons.
• The pastor of the Chinese Church conducts weddings and funerals. With the increasing number of Chinese from China coming to study in our universities, Mandarin is also being used for worship.
See also Christian Festivals & Holy days Diet
• Most Chinese eat seafood and their favoured meat is pork. • Stir-fried food cooked in a wok is typically Chinese. • Beef is the least favoured meat and cheese is not popular because of
its strong smell and taste. • Cow's milk causes diarrhoea among some Chinese because they have
no enzyme (lactase) to digest it. • Cantonese cuisine is renowned throughout the world, and it is eaten
with rice. • Northern Chinese food is based on bread and noodles. • Alcohol is consumed at banquets and festivals.
Dress Almost all Chinese wear western clothes. Women prefer trousers and blouse to dresses. Traditional clothes for women (e.g. "cheong-sum" or long close-fitting gown) are worn at Chinese New Year and celebrations.
Page 30 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Festivals – see calendar overleaf • The highlight of the calendar is the Chinese New Year or Yuan Tan.
This is a spring festival falling usually in late January or early February. • The Chinese New Year normally begins early February and continues
for 15 days. Chinese shops and businesses will normally take their only annual holiday at this time, closing for 2-3 days. Family meals are eaten and married couples give red envelopes containing money (Hung Pau) to children and single people. Guests and family are offered mandarin oranges or clementines.
• All debts are paid to start the New Year with a clean sheet.
• The Lantern Festival (Teng Chieh) marks the first full moon of the
year.
• Ching Ming (All Souls Day) usually takes place in April when family graves are visited. After cleaning and sweeping them, offerings of food and flowers are made to spirits followed by a 'picnic' when the family consumes the food.
• The Dragon Boat Festival is celebrated in summer with boat races on
the river. Rice dumplings containing either mung bean paste, meat or nuts and wrapped in bamboo leaves are eaten in remembrance of a saintly prime minister who sacrificed his life for the sake of his people.
• "The Mid-Autumn Festival in September is celebrated with the
sharing of "moon-cakes". Chinese Festivals listed by month: February Yuan Teh February Teng Chieh April Ch’ing Ming (Festival of Pure
Brightness) June Dragon Boat Festival October Chung Yuan
Page 31 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Current Issues for Chinese people Interpretation
• Interpreters are needed for new arrivals and people over 45 years of age. Most of them speak Cantonese and can read the Chinese script except for the poorly educated elderly.
• There is only one written language but pronunciation of the words varies a great deal from one Chinese dialect to another.
• The difference between Cantonese and Mandarin can be as much as the difference between spoken English and French.
Racial harassment
• This is a significant issue of concern for Chinese people in business, especially for those who are not fluent in English.
Care of the Older People
• Has increasingly led Chinese community groups such as the Wirral Chinese Association to seek grants from Local Authorities to organise Luncheon Clubs serving Chinese food for pensioners.
• The Chinese Luncheon Club in Birkenhead has 60-70 regulars attending once a week on Wednesday at the Wirral Multicultural Centre in Conway Street, Birkenhead.
Chinese health-seeking behaviour
• In the UK, Chinese people prefer to seek healthcare from the NHS particularly for acute infections and diagnosis of disease. Where a diagnosis of a chronic disease has been made such as diabetes, coronary heart disease, arthritis, some degree of disappointment may take place.
• It is important to stress the need to take medication regularly and to alter lifestyle and diet. Chinese are used to changing their diet when ill.
• A significant number of people would resort to traditional Chinese Medicine (TCM) in chronic disease, particularly as TCM is good for pain control.
• Continuing support is needed as much as it is in other communities among patients with chronic disease.
VIETNAMESE-CHINESE
• The Vietnamese Chinese came here between 1980 and 1982 when Local Councils on Merseyside accepted families of "boat people" rescued in the South China Sea by UK ships. They were equally drawn from North and South Vietnam, and from rural and urban backgrounds. Their plight was highlighted in the mass media with dramatic pictures of the ‘boat people’ and their precarious voyage on the South China Sea.
• Most of them suffered severe psychological trauma after they had survived the loss of houses and possessions in North Vietnam and of pirates who raped and pillaged them on the high seas. They had been
Page 32 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
expelled from Vietnam because they were ethnic Chinese. In fact, they suffered "ethnic cleansing" similar to that experienced in Bosnia and Kosovo in the 1990s.
• Many Vietnamese Chinese families who initially settled in Liverpool moved to South London when designated community workers to help them were withdrawn in the mid-1980s.
• Now, more Vietnamese (about 220) live in Wirral than in any other part of Merseyside. Most are members of the Wirral Vietnamese Association. Their children have been born here.
• A quarter of the current Vietnamese population speaks English as their first language and the majority of Vietnamese consider themselves to be permanent residents in the UK.
Religion Most Vietnamese are either Buddhists or Catholics. Some also follow Chinese and Vietnamese customs of ancestor worship. Language The predominant language of the Vietnamese is Vietnamese, although a few also speak Cantonese. Diet Vietnamese who are practicing Buddhists may not eat meat. Those who are practicing Catholics may not eat meat at Lent or on Fridays, when fish provides a suitable alternative. Naming System There are three parts to a Vietnamese name, with the family name coming first, followed by a complementary name and then a personal name. In the UK, many Vietnamese anglicise their names by giving their family name last. It is unusual for a married woman to adopt her husband’s family name. Often, it is not possible to determine gender from an individual’s personal name. However, complementary names can sometimes indicate sex: Van is often used by men and Thi by women as a complementary name. Death Traditionally, the body of a deceased family member is kept at the family home for between one and three days before the funeral. Upon death a person becomes an ancestor who must be respected. It is important to the Vietnamese that they bury the deceased as soon as possible because they believe that a body left above the ground allows its spirit to interfere with the living. Any shrines or objects in the home that are dedicated to the family’s ancestors should be treated with respect. To damage or remove them will cause great offence. Other information The tradition of guanxi (pronounced gwan-shi), which means ‘relationship’ or ‘connections’, underpins many relationships among the Chinese. This also

Page 33 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
applies to the ethnic Chinese originating from Vietnam. Refer to the section on guanxi within the Chinese section of this document. THE WIRRAL VIETNAMESE ASSOCIATION Participates with the Wirral Chinese Association and Wirral Asian Association on special occasions at the Wirral Multicultural Centre.
Page 34 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
SOUTH ASIANS INDIANS
• Indians form half of the South Asians in Merseyside. • Among them are Asian GPs and hospital doctors, but also some
market traders. • Most are English speakers with a limited number requiring an
interpreter. • The Overseas Doctors Association, whose members were trained in
South Asia, has many members resident in Wirral. • Indians speak Hindi, Punjabi and Gujarati. • Religion plays a significant part in the lives of Indian people, most of
whom are either Hindu or Muslim although some are Christians with family names identical to people in England eg. Mr John and Mrs George.
Gujarati
• Most Gujarati people came to the UK from East Africa. • Ugandan Gujaratis expelled by Idi Amin in 1972 fled to Britain. A
smaller proportion came from Gujarat, a state north of Bombay. • Most Gujaratis are self-employed in business.
Names
• Consist of a first name, a middle name and a family or sub-caste name (e.g. Chopra or Patel).
• The first and middle names are usually written as one name eg. Vijaykumar.
• It is the custom for Gujarati men and unmarried women to use their fathers' names as their middle names.
• Married women adopt their husband's name. • Traditional forms of address use first and second names only. Title
and family name, or title and full name, are acceptable in Britain eg. Mr Patel or Mrs Shushila Patel.
• The majority of Gujaratis are Hindus. • A small number belong to the Jain sect that bears some resemblance
to Buddhism with an emphasis on non-violence and respect for all living beings, as even the most insignificant insect is believed to have a soul.
• Jains also practice meditation and are strict vegetarians.
Page 35 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
BANGLADESHIS
• The first Bangladeshi people arrived in Britain in the early 1950s. They were mainly unaccompanied men intending to earn enough money to support their families back home.
• Most came from the Sylhet district, a rural region in North East
Bangladesh with British links from colonial times when the men worked on ships as cooks and manual labour. After World War II, many settled in port towns in Britain.
• Bangladeshis work mainly in catering as waiters and cooks. They, in
fact, run the majority of our 'Indian' restaurants.
• A significant number of Bangladeshi families live in Birkenhead. Their socio-economic status (and of Pakistanis) is the lowest of all ethnic groups in Britain. Their average wages are half that of white people. They tend to have about four children per family.
• Bangladeshi women usually do not go out to work, spending their time
caring for children and the home. Language and Culture
• Bangla (Bengali) is the state language of Bangladesh. • Most Bangladeshis in Britain speak a dialect of Bangla called Sylethi
that has no written script. • Some adults, especially women, cannot read or write Bengali as they
have had little formal education. Bengali literature is over a thousand years old.
• Modern Bengali literature, including poetry, is renowned. Rabindranath Tagore was awarded the Nobel Prize for literature before the First World War.
• Normal dress for women is a sari or shalwar kameez (a long blouse covering a pair of trousers). Men tend to wear Western clothes.
Beliefs
• Islam is the major religion with 87% being Muslims. • Others include Hindus (12%), Buddhists (0.6%) and Christians (0.3%).
Diet
• Bangladeshis eat rice and fish. In addition, they eat various lentils, vegetables and halal meat (goat, lamb and chicken).
• There is growing use of chapatis and naan bread. Health
• Bangladeshis in Britain have the worst health indicators for heart disease (affecting even young men) and diabetes in middle age.
Page 36 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
• Bangladeshi men have high rates of cigarette smoking and men and women chew “paan” - a leaf of a 'creeper' to which is added calcium carbonate and tobacco.
PAKISTANIS
• Pakistan is a large country, three times larger than the UK. Pakistan came into prominence after the tragedy of New York on 11 September 2001 as the neighbour of Afghanistan.
• Pakistanis have diverse backgrounds from the Pashtus or Pathans in the Northwest Frontier to Punjabis and Sindhis in the south.
• Urdu and English are the official languages in Pakistan. • Pakistanis in the UK do not speak Urdu (a language developed in
Delhi during the Mogul era and written in the Persian script) as a first language.
• Most will be more comfortable with Punjabi, Pashtun, Sindhi, Baluchi or even English
• Most Pakistanis are Muslim. Some are Christian and in the northern valleys of Pakistan, there are groups who are animistic including the "Black Infidels" in the Swat area.
Traditional Dress
• For Pakistani women, the shalwar kameez and dupatta equates to a long blouse, trousers and a scarf.
• It is customary to be covered from head to foot with only the hands and
face exposed to men. Only the father or husband would be exempted from this exclusion.
• For other cultural and religious customs, please see "Muslims
from South Asia"
• The social status of Pakistanis in Merseyside ranges from doctors to newsagents, waiters and cooks.
• Many Pakistanis are among the poorest people in Britain.
• Their health is also among the worst together with the Bangladeshis.
Page 37 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
MUSLIMS OF SOUTH ASIA
• Muslims on Merseyside come from Africa (Somalia, Sudan), Middle East (Yemen, Palestine) and South Asia (Bangladesh, Pakistan and India).
• They speak Arabic except for those from South Asia. • The majority of Muslims in the world are non-Arabs and they
outnumber Arabs six to one. • Indonesia is the world's largest Muslim nation with 152 million Muslims.
Naming systems and titles
• Muslim names are complex in Western terms. In the Muslim system, the last name is not usually a shared family name.
• In most Muslim families, each member has a completely different name, thus kinship cannot be identified or assumed.
Example: Father Mohammad Hafiz Mother Fatma Bibi Sons Saqib Bashir. Mohammad Sliarif Daughters Jameela Jan. Nahila Khatoon
• Members of a family should be identified by their own name followed
by their father’s or husband's name.
Example: Fatma Bibi w/o (wife of) Mohammad Hafiz Saqib Bashir s/o (son of) Mohammad Hafiz
• A typical pattern eg. the name is Mohammad Aftab Khan which consists of:
Religious name + Personal name + Clan name Religious Names
• These should not be used alone. • Any of the 99 names of Allah may be used as religious names, the
most common being Mohammad, Abdul, Shah, Syed, etc. • To address an Asian Muslim by any of these names alone may
cause offence because it is similar to addressing a devout Christian as Christ.
• In all of these names, as they are titles of the prophet Mohammad, the title name is always followed by a personal name eg. Abdul Quddus, Syed Akhtar, Shah Jehan.
Personal Names
• This is the equivalent of an English first name and is the one by which the person should be addressed.
Page 38 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
• It is not always clear which is the personal name, therefore you should ask.
• Often Muslims do not have a surname and use their personal name instead eg. Mohammad Yaqub could be Yaqub to his family and friends and Mr Yaqub on a formal basis.
• Many personal names used are of religious leaders or prophets eg. Ibrahim (Abraham); Fatma (daughter of Prophet Muhammad)
Female South Asian Muslim Naming System:
• This normally consists of two names, often three, none of which is a common family name eg. Nasreen Akthar.
• Recently, women have in Britain begun to choose their husband's last name as a shared family name eg. Fatma Begum married to Mohammad Akram would become Fatma Begum Akram in British records.
• As in the British system, the first name is always a personal name.
• Bibi, Begum, Khatoon are personal names which are often used as second names. They indicate that the person is female.
Male South Asian Muslim Naming System
• The full name usually consists of two or three parts eg. Mushtaq Mohammad, Mohammad Abdul Qureshi.
• The personal name can be the first or second part of a name. Some Muslims born in Britain have decided to have surnames such as Razaaq, Bhatti, and Shah etc.
REMEMBER: It is always best to ask a Muslim:
• what they use as their personal name • what they use as their surname in the United Kingdom, and • what they would like to be called
Please do not ask a Muslim for their 'Christian' name! Social Customs
• Muslims usually greet each other with a right handshake followed by their right hand touching their chest as a sign of friendship and sincerity.
• This is also the normal greeting between Muslims and non-Muslims. • However, cross-gender contact does not usually occur and may cause
offence among South Asian Muslims. • The traditional greeting is "Salaam aleikum" (“Peace of God be with
you”). You should be aware that, for cultural reasons, it might cause offence to have cross-gender contact eg a female member of staff speaking to a man and especially a male member of staff speaking to a woman. There
Page 39 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
will obviously be times when this is unavoidable and younger people will be less sensitive, but you should try to remember this, nonetheless.
• In your contact with South Asian Muslims, you may well need to find out how different people are related to one another.
• You should be aware that the traditional family is an extended one. In other words, you may find that, in addition to the parents and children who live in the house, there are grandparents and unmarried uncles and aunts.
• If a family member has recently moved into the area, it would be normal to stay with relatives until he or she is financially secure.
• This extended family also leads to differences in the terms that we use to refer to relatives.
• In South Asian languages, these terms can be very specific, indicating the relative's age and whether the relative is from the father's (paternal) of mother's (maternal) side of the family.
• In English, there are fewer terms and often you will encounter terms like "brother" or "uncle" being used in a very vague way.
• You will probably find it safer to try to ascertain the exact relationship if you do not want to end up quite confused!
• When having a meal with a Muslim, offer food and eat your food with your right hand only. The left hand is traditionally used for toilet purposes and should not be used for eating.
• Washing facilities for Muslims require bathing under a shower and washing with water after the toilet, with or without using toilet paper.
Diet
• Muslims may eat beef, lamb, mutton and chicken that have been ritually slaughtered. The meat is bled before slaughter in a manner similar to the Jewish practice of Kosher. This is called Halal (clean) meat.
• Although the practice may seem repugnant to you, hygiene benefits are significant, especially in relation to parasites in the blood. Halal meat is easily available in Britain. Pork is unclean and is not eaten
• These dietary considerations must be borne in mind if you have a Muslim patient of any nationality.
• Alcohol is forbidden to Muslims Beliefs – Some questions What is meant by 'Muslim' and who are Muslims?
• Islam (the religious faith of Muslims) has two meanings - Salaam means peace. It also means submission to the will of Allah (God).
• Both these meanings are linked since through submission to the will of Allah and obedience to his commands, believers should be able to achieve peace, both at a personal as well as at a community level.
• A Muslim is one who believes in Allah and in all the prophets, the last of whom was the Prophet Muhammad ("peace and blessings of Allah
Page 40 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
be upon him"), and bases his/her life on the revelation given to these prophets.
What is the Qu’ran and what does it contain?
• The Quran is believed by Muslims to be the record of the exact words revealed by Allah through the Angel Gabriel to the prophet Mohammad.
• All of its 114 suras (chapters) have not been changed over the centuries, so that the Quran is in detail the text which was revealed to the Prophet Mohammad 14 centuries ago.
• Arabic, the language of the Quran is taught to all Muslims from childhood as they read the Quran.
• The main function of the Quran is guidance. The Quran is the prime source of every Muslim's faith and it contains principles, doctrines and direction for every sphere of human life and practice.
• It deals with all subjects that concern human beings: wisdom, religious doctrine, worship and law, but its basic theme is the relationship between Allah and his creations.
• At the same time, it provides guidelines for a just society, proper human conduct and an equitable economic system.
Belief in the Sunna as part of the Islamic faith
The Sunna, the practice and example of the Prophet, is the second authority for Muslims. A hadith is a reliably transmitted report of what the Prophet said, did or approved.
Ritual Worship consists of Prayer or Salah (five times a day)
• Alms giving or Zakah (2.5% of personal wealth each year) • Fasting or Saum (during the month of Ramadan) • Pilgrimage or Hajj (to Makkah/Mecca in Saudi Arabia once in a lifetime)
Prayer
• Shoes are removed for prayer and before entering a mosque. • Ritual cleansing of hands face and feet with water is necessary before
prayers, particularly at a mosque. • Prayers are said facing the direction of Makkah and using a
prayer mat. The worshipper bows and kneels and places his/her head on the mat.
Ramadan
• Islam teaches that Allah is close to all humanity and especially to those who earnestly seek His guidance and try to mould their lives according to His will in the blessed month of Ramadan.
• Fasting becomes compulsory for Muslim children when they reach puberty.
• During Ramadan, a Muslim fasts from dawn to sunset and does not eat any food, drink any water/fluids or indulge in sex. Fasting for one
Page 41 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
month of Ramadan develops, and helps to strengthen, the faith of Muslims.
• Exemption from Ramadan fasting includes the unwell, pregnant and menstruating women and those embarking on long journeys. But they are expected to fast the number of days missed afterwards.
• For people observing Ramadan, fasting should not have an adverse effect on their work, study and everyday life, especially their daily relations with other people. On the contrary, their behaviour should improve whilst fasting as the spiritual aspects of the month are kept in mind. However, it is almost inevitable that in mid to late afternoon, people who are fasting will start to feel tired and reluctant to do anything too strenuous.
Islamic Festivals
• Eid-ul-Fitr marks the end of the month of fasting. At this joyous festival, Muslims put on their new or best clothes and go to the mosques in the morning to pray in thanksgiving for the blessings they have received from Allah in the form of the Quran and in the keeping of the fast.
• In prayers, both at home and in the mosque, they also seek forgiveness of Allah and the ability to live by the Quran. After prayer, delicious meals are prepared and eaten by the family, friends and relatives.
Greetings for Eid-ul-Fitr are Eid-mubarak (Happy Eid) and Asalaam Alaikum (the peace of Allah be with you).
• Eid-ul-Adha is a major Muslim festival of the year to celebrate the life of the Prophet Ibrahim (Abraham) who lived 4000 years ago. Ibrahim's life serves as an inspiration and is a standard (along with the life of the Prophet Muhammad) for Muslims to aspire to. Eid-ul-Adha takes place at the time of the Pilgrimage to Makkah (over 2 months from Eld-ul-Fitr). After prayers, those who can afford to do so sacrifice an animal (as willingness to sacrifice his son at God's command), and share the meat with family, friends and the poor.
Pilgrimage to Makkah:
• The Hajj is an obligation for those who are physically and financially able to perform it. "Pilgrimage to the House is a duty that mankind owes to Allah for anyone who can find a way to do so" (Quran 3:97). To visit Makkah is to visit the Ka'bah, the house of God built by Ibrahim about 4000 years ago. Over 2 million Muslims make the pilgrimage each year.
• Everyone on pilgrimage wears the same simple garb of two unstitched sheets of white cloth, performs the same religious rites standing and bowing, and declaring "Labbaik, Allahumma Labbaik - Here I am, 0h Lord, here I am." On completing the Hajj, a Muslim gains the title Hajj and wears a white skullcap.
Page 42 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Women in Islam • Muslim women are held in high esteem. This has been made clear by
the Prophet Mohammad's saying "paradise lies under the feet of your mother" (An-Nasa'I). As is often the case, there is a mismatch between the Quran and the actual reality.
• Women may seem to have a second-class role but this may be a misrepresentation of the reality of the family or cultural group because, in Britain, Muslim women from South Asia may not speak English and want their husbands to accompany them.
• Islam lays down standards of dress and behaviour as part of a moral code.
• For girls, this means that the whole body, except face and hands, must be covered once they attain puberty. This applies only when the girls are in close proximity of people they are eligible to marry according to Islamic law ie. most males except close relatives.
• Most Muslim young women wear the hijab or headcover. Birth Rites
• Following the birth of a baby, a short prayer, the Azan, is recited into the baby's ear. It is equivalent to a christening in importance. If the child is male, it will be necessary for him to be circumcised as soon as possible.
Marriage Arranged marriages are still traditional in Muslim families. This can cause friction between parents and younger, westernised women who want to follow the example of their white friends.
• There are examples of parents forcing their daughters into marriages when they are visiting their home countries of India, Pakistan and Bangladesh.
• At the marriage ceremony, it is customary for the bridegroom to propose his intention to marry his bride.
• This proposal is conveyed to the bride who is asked if she agrees. • The groom is then told of the bride's acceptance, whereupon he is
asked to repeat the decision three times. • If both parties agree (ie. ceremony Nikah is carried out by the Imam (or
priest) who reads verses from the Quran. • Traditionally, a Muslim man may have up to four wives if he is able to
support them financially. • Having more than one wife is not common in the UK.
Divorce
• Traditional marriages can be ended by a man declaring three times that he divorces his wife.
• In the United Kingdom, all marriages, including Muslim marriages, are under British law and divorce has to take its usual course through the law courts. However, there have been requests made by some Muslim
Page 43 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
leaders that a Muslim (Shariah) court officiates over divorces and other legal matters affecting Muslims.
• Marriages between white women and Muslim men have come to the notice of the popular press when they fail and one party, usually the father, leaves the UK with his children and moves to a Muslim country.
Death rites
• When a Muslim person dies, it is important that he or she is buried as soon as possible after death and on the same day.
• This practice can only be delayed if the death is reported to the coroner and post-mortem examination is necessary.
• One person is buried per grave with the face of the deceased, when buried, facing Makkah. The grave itself should be raised by a minimum of six inches.
Islamic Traditions
• The majority of Muslims worldwide and in the UK is from the Sunni tradition.
• The other tradition of Shia Muslims is to be found in Iran and related areas.
• The Aga Khan, whose origin is in Pakistan, is the leader of Ismaili Muslims who belong to the Shiite (Shia) tradition.
Page 44 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
HINDUS • Hinduism is the dominant religion in India with about 80% of the
population being Hindu. • In Britain, Hindus comprise about 20% of the South Asian population.
They are predominantly from Gujarat and a limited number from Punjab.
Language
• Those from Gujarat speak Gujarati and Hindi. • People from Punjab speak Punjabi and Hindi.
Hindu Naming System
• Hindu names usually have three parts like the British system. Examples of typical names might include
Personal name + Middle name + Surname
Female Lalita Devi Sharma Male Raj Kumar Vasani
• Family and friends may use the first or personal name. The ending "Ji"
might be added to the personal name to denote respect as in Lalita-ji. • This form is used alone in informal conversation.
You should always address a Hindu using their title and full name as in:
Mrs Lalitadevi Sharma or Mr Rajkumar Vasani.
• Be aware that, although the wife and children usually take the same surname as the head of the family, the middle name may sometimes be used as a surname.
• Where this happens, don't be surprised if each member of the family
has a different surname eg. Mrs Devi might be the wife of Mr Lal. If in doubt, ask and clarify the relationship Beliefs
• Hinduism is a long established religion that has gone through many changes in Indian society. It is a complex religion.
• The basic belief is in one Supreme Being (the creator), but there are many gods or goddesses that are worshipped for different aspects of life and by different people according to their social class and economic status in Hindu society.
• Hindus believe in reincarnation and that any incorrect behaviour in this earthly life may lead to reincarnation as a lower order being eg. an animal, hence Hindus regard all life as related to them.
• Though there are many gods in Hinduism, the supreme god is Brahma, a god so great it is not possible to worship him directly. He is usually approached through one of the other gods and goddesses.
Page 45 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Hindu gods and goddesses
• Brahma The great creator has four heads, indicating that he thinks all
things.
• Shiva The destroyer has many sides to his character. Although frightening and appearing in graveyards and battlefields, he is also seen as the life force of the universe. People who follow Shiva see their god as loving, although there is animal sacrifice and some ascetics inflict pain on themselves.
• Vishnu
The preserver and god of love, sits in heaven with his wife but does come to earth usually disguised in one of 10 forms: Varana the boat, Buddha, Kalki; Krishna a popular god brave and fun loving; Matsya the fish; Narashima the lion; Kurma the tortoise, Vamana the dwarf; Parasurama the Rama with the axe; Rama the prince.
• Shakti
The Mother goddess. Many see her as the wife of God himself. She has two forms: one the fierce Durga or Kali, and the other the mild and gentle Parvati or Uma depicted as a beautiful young girl.
• Hanuman
The Monkey god is playful but wise.
• Surya The sun god
• Ganesh
The elephant god very wise and powerful Hereditary Caste system
• People tend to socialise and marry within the own caste. • Traditionally, caste defines not only social status but also a
limited range of acceptable jobs. The highest caste group is the Brahmin or priest.
• There are thousands of different caste groups according to the type of work which people do, or to their social status.
• Though Indian law forbids the caste system, it nevertheless continues as an 'accepted' tradition.
• The four caste groups are: Brahamins the priestly class or highest caste Kshatriyas the warriors and soldiers Vaishyas the traders
Page 46 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Sudras the peasants
• There are strict rules relating to caste. • One should only marry within one's own caste. • Eating with a lower caste is not allowed. • Some people have no caste and are casteless or "harijans" or
children of God, a name given to them by Mahatma Gandhi. • Harijans do all the menial tasks of society such as the dirty and
heavy work. Hindu beliefs In Hinduism, there is a fundamental belief that all living things have a soul (Atma) which passes from body to body in the cycle of birth and rebirth. Therefore, animals are regarded with great respect, particularly the following:
• The Cow has an honoured place because it provides the main necessities of life-milk, butter, and dung that is dried and used as fuel. It is used for pulling carts and ploughs. It is considered sacred and venerated as the embodiment of Mother Earth. White cows wander at will in cities and countryside in India. The cow should never be forced to do anything against its will and should not be injured. The bull, Nandi, is the god Shiva's attendant and his statue is seen in temples of Shiva.
• The Monkey is represented by the god Hanuman. It is worshipped
because of the part played by monkeys in the Ramayana, the epic of Rama and Sita where the monkey king, Hanuman, rescued Sita from captivity on the island of Sri Lanka. The events are remembered at the festival of Dussehra.
• The Elephant is represented by the elephant-headed god, Ganesh
(Shiva's son). He is thought of as the remover of obstacles and symbolises patience, strength and wisdom
• The Snake is considered holy and only killed in an emergency.
Anyone who kills a snake goes into mourning. People put out bowls of milk to feed snakes.
Page 47 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Religious Worship • There are many sacred books containing writings on Hinduism. They
include the Upanishads, the Bhagavad Gita and the Ramayana all written in Sanskrit. Many Hindus receive religious instruction from their family and local priests with the emphasis upon good Karma (internal spiritual well being) and avoidance of impurity and evil.
• In Britain, most Hindus carry out their daily individual worship in the
home combined with individual and communal worship in the Mandir (Hindu temple) on religious anniversaries and special occasions. The Mandir at Neasden, West London, is famous. Prior to worship, purification is necessary through ritual cleansing by fasting and removal of leather items including shoes.
• Women play an important role in worship at home and in the Mandir. In
the latter, they usually sit with younger children segregated from the men. Hindus place great importance to the reading of religious books such as the Bhagavad Gita and the Mahabharata in the same way as Christians do the Bible or Muslims the Quran.
Diet
• Generally, Hindus are vegetarians and do not eat eggs. Those who do eat meat do not eat beef as the cow is regarded a sacred animal
• Pig is regarded as unclean, so no pork products are eaten. • Devout and orthodox Hindus may be strict vegetarians and do not
smoke tobacco or drink alcohol. Many Hindus may be vegans who do not eat any meat, fish or dairy produce.
• Non-vegans eat chapatti (wheat pancakes), rice, peas, beans, lentils, vegetables, milk, curd (yoghurt), ghee (clarified butter) and fruit. Vegetables are often prepared as a 'curry'.
• Food has an important place in puja or religious worship. It is offered to the god in the temple or at the home shrine. Food, which is shared out after offering it to the god, is called prashada. The offerings can be choice fruits, nuts and sweetmeats.
Main Hindu Festivals Festivals closely follow the Indian lunar calendar and the seasons of the year. Actual timings vary according to different regions of India.
• Ram Navami in late March or April celebrates the birthday of Rama. In the home and temple, the priest tells the story of the Ramayana. Some foods are not eaten as it is a fast day but followed by celebration at night.
• Janam Ashtami is the birthday of Lord Krishna. Celebrations begin at midnight. Prayers are said at night with sharing of food after a fast the day before.
• Durga Ashtami is a celebration of the goddess of wealth and knowledge in late September or early October. It may last for 9-10 nights. Women and girls play a prominent role in this. Durga, the wife
Page 48 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
of Shiva, Lakshmi, wife of Vishnu and Sarasvati wife of Brahma are important characters in this celebration. In Bangladesh and West Bengal, it is called Durga Puja.
• Diwali is the festival of lights in late October or early November. The following day, the Hindu New Year's Day is associated with ceremonial lights and giving of presents. Diwali is the celebration of Rama and Sita's triumphal return to their kingdom and Ayodha and Rama's coronation.
• Holi in February or March takes place at the start of spring in India. It is devoted to the god of love, Kama, and to the great lover, Krishna. This is a time for playing practical jokes. In India, people throw coloured water at each other and the normal rules of everyday life are ignored for people sharing fun. In Western India, a large bonfire is lit and people share food.
• Ratha Yatra is held in May on the birthday of the lord of the universe, Jagannath. In India, especially Orissa, three huge carriages are drawn through the streets by thousands of pilgrims. The word "juggernaut" is derived from these events.
Life Cycle Birth
• The child is named after spending 10 days with his/her mother, the period considered to be of ritual impurity.
Marriage • The groom and his party travel to the bride's home with hospitality
provided by the bride's family. The couple sits in a temporary pavilion on either side of a curtain that is removed to the accompaniment of sacred verses in Sanskrit by a priest.
• The bride is given away by her father, the couple clasp hands and offer grain to the sacred fire and walk clockwise around the fire with ends of their garments knotted together, taking 7 steps together. They are then sprinkled with holy water and return after the festivities to the bridegroom's family home where they usually live.
Death • After death, the Hindu priest must be called to give his blessing to the
deceased. He may tie a thread around the neck or wrist and this should not be removed.
• The body must not be touched until the relatives arrive. • The body of the deceased is accompanied by relatives led by the
eldest son to the crematorium where he and the priest perform the last rites. Mourners may walk round the crematorium in an anti-clockwise direction. They return home led by the youngest son.
• Soon after the cremation, the ashes are taken with religious rites to flowing water where they are sprinkled on the outgoing sea tide or in a river. Many Hindus will take the ashes of their loved ones to be sprinkled in the Ganges River in India.
Page 49 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
SIKHS
• The Sikh community is both an ethnic and a religious group recognised under the Race Relations Act.
• In India, Sikhs form about 2% of the population compared to Hindus who constitute 80%.
• In Britain, however, both groups are approximately equal in numbers. More than 300,000 Sikhs now live in the UK, the largest Sikh community outside of India. Sikhs have also emigrated to East Africa, Australia, Canada, USA, Malaysia and most European countries.
• The Sikhs originate from the state of Punjab, a region divided between Pakistan and India in 1947. Since then, Sikhs have come to regard the smaller Indian State of Punjab as their spiritual homeland. Punjab means the land of 5 rivers (Beas, Chenab, Jhelum, Jumna and Satluj that flow into the Indus). The word Sikh derives from the Sanskrit word Shisya, which means "disciple" in Punjabi.
Language
• The spoken and written language is called Punjabi, written in its own Gurmukhi script, the mother tongue of the Sikhs.
• It is spoken by Hindu Punjabis and Muslim Punjabis. The difference is that the Hindu and Muslim people may use the Hindi and Urdu scripts respectively to write Punjabi.
Naming systems and titles
• Most Sikhs have three names: the first or personal name, a second or religious title (Singh meaning lion for men and Kaur meaning princess for all women). The third or family name is dropped in India but is used for administrative purposes in the UK.
Examples Personal name + Religious name + Family name Balbir Singh Bhogal - a Sikh man Harbans Kaur Gill - a Sikh woman
Points to remember
• Most Sikh first names do not indicate sex and can be both male and female.
• Calling out “Mr Singh” and “Mrs Kaur” causes confusion when there are many Sikhs waiting. One should, therefore, call out “Mr Gurdeep Singh” or “Mrs Surjit Kaur”.
• Most Sikh men are easy to recognise because of their turban and untrimmed beard.
• Sikhs are exempt from wearing crash helmets because of the protection afforded by 6 metres of tightly wound cloth in the turban. Sikh police officers wear black turbans with a chequered band and a badge at the front.
• There are some Sikhs who have given up the turban and beard to conform to western norms of appearance, but they will still be recognisable by the "Singh" in their names.
Page 50 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Sikhism - a religion
• Sikhs aim to unite their souls with God at death, achieving this by remembering God in daily life and truthful living.
• Their greeting, Sat sri akal, means truth is eternal. • Service to others is especially important. Sikhs follow the teachings of
a series of teachers and/or prophets called Gurus. Their scriptures are also given this status and are called the Guru Granth Sahib or Adi Granth.
• Devout Sikhs observe the " five Ks", These are: 1. Kesha - uncut hair 2. Kangha - a ceremonial comb 3. Kara - a steel bangle 4. Kirpan - a ceremonial sword or dagger 5. Kaccha - ceremonial cotton shorts
• Some Sikhs will have a prayer room in their homes and most will meet with others, often on a Sunday, at the Gurudwara (temple) for hymn singing, scripture reading and communal meals.
• In all Gurudwaras, people remove their footwear and ensure their heads are covered on entering, to show respect.
Festivals
• Festivals include the anniversary of the birth of Guru Nanak - often marked by a continuous reading of the scriptures.
• Baisakhi, on 13 April, commemorates the founding of Sikhism when the gurudwara flags are renewed and amrit (sugar-water) is taken.
• Diwali is an adaptation of the Hindu festival of light. Life Cycle Birth
• When a Sikh child is about a month old, it is taken to the Gurudwara. A prayer is offered in thanksgiving for a long and blessed life for the child. A name for the child is chosen at the same time by opening the Adi Granth at random and taking the first letter of the first word as the letter to start the name.
Marriage
• Sikhs are expected to marry. The couple are seated in the bride's home or the Gurudwara to the accompaniment of chanting of hymns from the Adi Granth, which is kept under a canopy beside them.
• The bride's father then gives his daughter to the groom; they are joined by a scarf or cloth and walk clockwise around the Adi Granth four times. They then sit down again to receive gifts and offerings from the guests.
• Sikhs do not expect non-Sikh partners to convert to Sikhism. However, they would expect the non-Sikh partner to accept the cultural aspects of the Sikh people.
Page 51 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
• Some people from the Sikh community do not marry non-Sikh partners but, on the whole, this is fairly limited.
Death
• When a Sikh is dying, friends and relatives gather at the bedside to recite parts of the Adi Granth.
• After death, the body is washed and dressed in new clothes by the family and taken for cremation.
• The cremation is started by the son or closest relative and the ashes are scattered over water. Sikhs wear white clothing during mourning.
Diet
• Although some Sikhs do eat meat, many that are religious are totally vegetarian.
• It is unusual to find a Sikh who smokes. • Most devout Sikhs are teetotal. • A typical evening Sikh meal would consist of rotis (chapatti), dahi
(yoghurt), dhaal (lentils) and sabzi (vegetables made into a curry, usually dry and fried with onions, garlic and ginger as a base.)
Sikh Culture
• Punjabi culture is a rich combination of folklore and popular traditions of art and craft. Folk songs and dances are shared by all Punjabis living in the Punjab and abroad.
• Music is an important part of the Sikh faith. • Traditional dance performed by women is known as Gidha. The origins
of Bhangra go back centuries and are embedded in the family traditions of the Punjab. Bhangra can be regarded as a harvest dance.
Page 52 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
IRISH & IRISH TRAVELLERS: A COMMUNITY PROFILE reproduced with kind permission of Irish Community Care, Merseyside The Irish community is the largest ethnic minority community in Britain. There are between two and eight million people born in Britain who identify as Irish ie. 10-13% of the population. Mid-year 2005 estimates indicate that there are 2800 Irish living in Wirral. This figure represents an overall decrease of almost 10% since 2001. The contribution of Irish people to the economy, to the political life and the culture of Britain has been a vital and powerful one. For many Irish people, Britain has been a place of welcome and opportunity. Yet, at the same time, there is evidence of INEQUALITY, DISADVANTAGE, DISCRIMINATION AND PREJUDICE. Because the majority of Irish people here are white and speak English as their first language, the Irish community has until recently been excluded from appropriate fora of debate around race, ethnicity and the ensuing barriers in accessing services and opportunities. There is a tendency to focus on the more visible and tangible elements of race/culture ie. colour, language, dress, diet, religion rather than the more invisible elements ie. values, traditions and beliefs. The Irish community is still fighting the cause of being recognised and included as a distinct ethnic minority community in Britain, even though it is officially recognised as such by the Commission for Racial Equality. The more recent recognition of Irish Travellers as a distinct minority ethnic group has been very much warmly welcomed; this community constitutes one of the most disadvantaged and excluded groups in its society. Facts about the Irish Community Health
• 18% of Irish-born people are affected by limiting long-term illness compared with 13% of white people and 8% of the other minority ethnic groups [Owen 1995].
• There are very high levels of cancers, coronary heart disease and
diabetes within the community.
• Irish people have the highest mortality rate of any ethnic minority community and this high mortality persists into second generation Irish people.
• Irish people have the highest rate of admission to psychiatric hospitals
and are over-represented in most diagnostic categories.
• Irish people have the highest rate of suicide and self-harm of any ethnic group and have undergone a worsening in their health status.
Page 53 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Housing Irish households are:
• More likely to be housed in private rented accommodation • More likely to share basic amenities • More likely to occupy non self-contained accommodation
There is evidence that only a small number of Irish people register on waiting lists for council housing which means that the community’s needs are going unrecorded [Cara 1995]
• A nationwide survey found that only 26 local authorities and only 51 of the largest 88 housing associations monitor Irish people as a separate ethnic group [CRE 1997]
Homelessness Homelessness is the most extreme form of housing needs and evidence shows that single Irish people are over-represented among the homeless population. ‘Single Irish people often go through the revolving door of being on the streets, then in temporary accommodation and then back on the streets again, with little or no prospect of a permanent solution to their housing problems’ [Cara 1994]
• Single Irish people represent about 9% of the residents in direct access hostels and 10% of winter shelters’ population [SHIL & LBGC 1996] London survey found that 22% of service users were Irish.
• In 1998, 24% of users of Irish service centres homeless [Kowarzik 2000]
• In 1997/1998, 24% of Irish households housed by housing associations were homeless [University of York, 1999]
Racism
• Anti-Irish racism is an everyday reality for Irish people and impacts on health, well-being and access to services [CRE 1997]
Barriers in accessing health services for the Irish Community Lack of awareness and understanding of the particular needs and experiences of the Irish community within existing services combined with the following cultural issues pose access barriers for Irish people:
• Low self esteem • Low expectations of their own health • Low expectations or lack of knowledge of existing health services • Culture of 'not troubling the doctor' leading to services being used
when illness is quite advanced • Culture of 'coping'
Page 54 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
• Culture of 'bottling up' stress and grief which may contribute to illness directly or result in coping through excessive use of tobacco, alcohol or illegal substances
• Tendency to absorb blame and to feel that illness or bad luck is their own fault even when the odds are clearly stacked against the person
• Reliance on prayer • High tolerance of pain and discomfort leaving medical help until much
later THE WAY FORWARD
• The recognition of the Irish community as a distinct ethnic minority community with particular needs and experiences.
• The introduction of a separate Irish category in all monitoring procedures [Irish by self-definition and not just an assumption based on place of birth].
• Irish issues to be a central feature in all equalities training. • Acknowledge the existence of anti-Irish racism as a reality for many
Irish people which needs to be challenged. • Irish community to be involved in all consultation processes. • Working in partnership with Irish community groups to develop health
promotion initiatives for our community which improve awareness of, and access to, the range of existing health services,
CONTACT Irish Community Care Merseyside, Liverpool Office 0151 707 4302 Irish Community Care Merseyside, Wirral Office 0151 650 5440 IRISH TRAVELLERS BACKGROUND Travellers have lived in this country for centuries. The Travelling community is not a homogenous one. There are many different groupings with different histories and work patterns ranging from Irish and Romani to English and East European. The rights of Travellers to lead a nomadic existence have always been challenged and they have faced hostile legislation and discrimination from the rest of society. The recent recognition of Irish Travellers as a distinct ethnic minority community has been very warmly welcomed, as this community constitutes one of the most excluded groups in our society. Irish Travellers have been settling and travelling through Merseyside for centuries. Irish Travellers traditionally earned a living by travelling from area to area helping with the harvest, trading horses or making pots and pans. The mechanisation of agriculture in post-war Britain and the introduction of plastic and enamel rendered much of the traditional work, carried out by Travellers, obsolete. Many Travellers have been forced to migrate to towns and cities
Page 55 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
where they face economic and social marginalisation. Irish Travellers are discriminated against both as Irish people and as Travellers. The ‘No Irish’ signs prevalent in the 1940s and 50s have disappeared, but the ‘No Traveller’ signs have not. For the Irish Travelling community, negative stereotyping, overt racism, social exclusion, lack of awareness of rights and services, coupled with very low literacy and numeracy skills and the transient nature of their lifestyle pose major barriers in accessing services and entitlements. The current health situation of Irish Travellers is equivalent to the health of the settled population in Britain in the 1940s. Families on official sites suffer due to poor design, location and management of sites and the forced movement of Travellers into temporary and permanent ‘tiled housing’ leads to increasing isolation and marginalisation as extended family support networks are weakened. The indicators are that this move does not enhance life chances of the Travelling community. BARRIERS IN ACCESSING HEALTH SERVICES FOR THE IRISH TRAVELLING COMMUNITY Lack of awareness and understanding of the particular needs and experiences of the Irish Travelling community combined with the following cultural issues pose access barriers for Irish Travellers:
• Transient nature of many Irish Traveller lifestyles leads to: difficulties in GP registration and follow up care, resulting in neglect of chronic illness and non-compliance with medication/treatments; and exclusion of the community from general health screening and health promotion programmes
• Poor literacy means that written appointments often are not understood and therefore missed. The importance of liaising through a third party community group, if possible, is crucial. For example, many Irish Travellers use Irish Community Care Merseyside as a safe mailing address and front-line workers make sure that appointments are read through and fully understood. They are written in the daybook and are contacted the day before the appointment to remind them.
• Poor literacy also means that following the instructions for medication is difficult and, unless it is explained very clearly, will mean that proper treatment cannot be accessed.
• Culture of coping leading to services being used when illness is quite advanced.
• High levels of stress and depression, following constant evictions from unauthorised encampments, which may contribute to illness directly or result in coping through excessive use of alcohol or tobacco.
• For male Irish Travellers, in particular, there is a tendency not to register at all with a GP practice. Health care is accessed through accident and emergency only when absolutely necessary.
Page 56 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
THE WAY FORWARD • The recognition of Irish Travellers as a distinct ethnic minority
community with particular needs and experiences • The introduction of a separate Irish Traveller category in all monitoring
procedures • Irish Traveller issues to be a central feature in all equalities training • Acknowledge the existence of very overt anti-Traveller racism as a
reality for the Travelling community that needs to be effectively challenged
• Irish Travelling community to be involved in all consultation processes • Working in partnership with Irish Traveller groups to develop health
promotion initiatives for the community which will work to improve access to the range of existing health services
Useful Contact Numbers Irish Community Care Merseyside, 60 Duke St. Liverpool L1 5AA Tel. 0151 707 4302 Merseyside Traveller and Gypsy Forum, c/o Irish Community Care Merseyside, 60 Duke Street. Liverpool L1 5AA National Gypsy Council, Green Acre Caravan Park, Hapsford, Helsby, Cheshire Tel: 01928 723 138. National Association for Health Workers with Travellers, 12 Lyndhurst Rd. Sheffield. Tel: 0114 271 6622. Irish Traveller Movement, The Old Library Building, Willesden Green Library Centre, 95 High Road, Willesden, London, NW10 2ST Tel: 020 8459 7638

Page 57 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
KOSOVAN Kosovo was once part of the Turkish Empire, but anti-Turkish resistance succeeded in expelling the Turks, and Kosovo became part of the newly founded state of Albania in 1912. However, in the following year the great European powers, including Britain, forced Albania to relinquish Kosovo to Serbia, which itself was incorporated into the new Kingdom of Yugoslavia in 1918. After the Second World War, Kosovo was granted autonomy within Serbia and this autonomy grew as a result of pressure and riots from the ethnic Albanian population. Riots in 1981 incited a Serbian backlash and increased Serbian resentment of Albanians. This led to the rise of power of the Serbian nationalist, Slobodan Milosevic. The Albanian media were suppressed, all Albanian language education was halted and the autonomous Kosovan parliament was abolished in 1990. In 1998/9, Serb militias, extremist groups from Belgrade and paramilitary police units drove Muslims from their homes in carefully planned operations, which were known as ‘ethnic cleansing’. The situation became so serious that in early 1999, NATO forces launched an air campaign to force the withdrawal of all Serbian military personnel from the province. Hundreds of thousands of Kosovar Albanians fled to neighbouring countries. Following Serbian withdrawal from the province in 1999, Kosovo is once again an autonomous region of Serbia under the present governance of an international peacekeeping force, KFOR (Kosovo Force). Although many of the Kosovar Albanian refugees have now returned home, Kosovo remains a dangerous place, with ethnic conflict still an everyday occurrence. Many Kosovar Albanian refugees remain in the UK, too frightened to return home. Religion The majority of Kosovar Albanians are Muslim, although they are not strict. The older generations tend to be more orthodox, although they are still less likely to be as orthodox as other Muslims. Many younger Kosovar Albanians are not strict about their diet and will eat meat that is not halal. This may differ among Kosovar Albanians who have originated from more rural areas. To the older, more orthodox generations of Kosovar Albanians the issue of whether or not meat is halal may be more important. Language Most Kosovans speak Albanian. Other information Many Kosovans had to leave their country in difficult circumstances. Some refugees may be wary of uniformed services because of their past experiences.
Page 58 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
KURDISH Kurds are, together with the Arabs, Persians, and Armenians, one of the most ancient peoples of the Near East. They originate from an area called Kurdistan, that encompasses eastern Turkey (approximately 15 million), north western Iran (6 million), northern Iraq (5 million), north eastern Syria (1 million) and parts of the Russian Federation (500,000), and there are believed to be about 35 million in total throughout the world. Many Kurds, including those who have emigrated to other countries, would like to see a separate country formed of those regions. As a result of the Gulf War in 1991, the Kurds in Iraq have enjoyed a relatively prolonged period of self-rule under the protection of the United States and Great Britain. In the 1920s and 1930s, the Turkish Kurds rebelled against the government who suppressed them with great ferocity deporting thousands from their homeland. The continued stringent suppression of over 9 million people has resulted in the rise of a Marxist guerrilla group. In Iran, the Kurds were similarly brought under control in the 1920s. In 1946, the Kurds of Mahabad succeeded in declaring an independent republic, but it only lasted a few months, and the authorities hanged the ringleaders. Tribal chiefs were allowed to register tribal lands as personal possessions and were welcomed into the Iranian ruling elite, in return for making sure their tribes obeyed the government. After the Shia revolution, the Kurdistan Democratic Party of Iran (KDPI) rebelled after demands for autonomy were refused by Tehran. In Iraq, there were numerous revolts against Baghdad, mainly by Mullah Mustafa Barzani, the famous leader of the Kurdistan Democratic Party of Iraq. From 1964 until 1975, Barzani was strong enough to maintain an intermittent state of war and peace negotiations. In 1974, the governing Ba’th party offered the Kurds autonomy but the Kurds believed it lacked substance and they reverted to war, strongly supported and encouraged by Iran. But in 1975 the Shah of Iran, who had supported Barzani, signed the Agreement of Algiers with the Iraqi government, abandoning the Iraqi Kurds to their fate and as a result the Kurdish resistance virtually collapsed and they were again repressed. The Kurdish language is actually a number of languages. The predominant languages within the Merseyside Kurdish Community are Sorani and Bahdini. Kurds may also speak a variety of languages, mainly Arabic and English, reflecting the society they are from. Kurdish communities are often male orientated, conservative and clan based. Religion The vast majority of Kurds are Sunni Muslims or Alevite Muslims, although there are some Shia Muslims, Jews and Christians.

Page 59 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Names, Conventions and Customs Kurds tend to follow the customs and conventions of the religion with which they are associated.
Page 60 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
POLISH Poland is situated in the centre of Europe. There is an interesting mixture of all European customs, religions and historical influences. Poland was dependant on the Soviet Union for 50 years and Polish borders were closed. Travelling anywhere abroad was made very difficult as visas were required. However, even with these issues, the Polish culture survived, and Polish faith and historical heritage is to be admired. Poland joined the European Union in 2004 and, as a result of EU regulations, there are now a significant number of new Polish settlers in Merseyside. The presence of the Polish settlers is apparent by the number of Polish food shops which now cater for the growing Polish communities in London, Manchester and Liverpool, and also on the Wirral. (4% of CAB’s clients are Polish). Wirral has a rapidly growing Polish population, although accurate figures are not available. Figures from MPA Cracow based in Birkenhead show that there are approximately 3000 Poles on the Wirral and that this number is growing systematically. There is a fast growing congregation at the Polish Mass held at Liverpool’s Catholic Cathedral. The congregation at Chester St. Francis’ is even larger. On 13 December 2008, the inauguration of Polish services was held in Birkenhead. Monthly services will be held at St Josef’s Parish Church, North Road, Tranmere. Further details can be obtained at www.mpacracow.org.uk In April 2007, the Polish government stated that the Polish population of the United Kingdom and Ireland is 1.2 million. Many Poles choose to migrate to the UK to seek better work opportunities as Poland has very high unemployment rates. A high proportion of Merseyside’s Polish community live in Liverpool Kensington, and Liverpool Walton. Many of these settlers work in the service industries around Ellesmere Port, Birkenhead and Flint, and in the agricultural industry in West Lancashire. Although only a small percentage of the Polish population live in Southport, this town is a popular leisure resort for the Poles. Religion The main religion in Poland is Roman Catholic. Other religions have settled in Poland and influenced its history - Tatar’s Muslim and Mongolian (settled in 15 century) and Protestants, Krishna’s, Units and Greek Catholic (all Eastern Catholics). A “Jewish clearance” was recorded before the 18th century (similar to Hitler in the 2nd World War). A small percentage followed Soviet ideology. Poland is not the most religiously devout country in Europe. However, even non-religious Poles were proud that Pope John Paul II was Polish. They wanted to show their respect and were very active in religion manifestations.
Page 61 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
To this day, Pope John Paul II is still considered a hero and a leading authority for most Poles. Language Polish. However, other languages are taught and these include German, Russian, English, French, Italian and Spanish. The level of education is similar to that in the UK. Poles can communicate with Slovakians and Czechs, the polish language being of the same language root. Most factory migrant workers do not speak English at all and therefore live alienated being unable to ask for any available services on the Wirral. Festivals Poles celebrate the following major Christian festivals: The Day of Remembering the Past is the1st November. It is a day to reflect on past ancestors, visit families, and to think and pray for them. Candles are lit in cemeteries. The same happens on Soul Day on 2nd November. Roads are extremely busy on these two days. Polish Christmas time starts by quiet time of meditation and fasting following the Roman Catholic announcement around St. Andrew’s Day. St. Andrew’s day is the last ball and dance fest opportunity before fasting. Kid’s festival of Swiety Mikolaj is celebrated on the Day of St Nicholas on December 6th. Gifts are exchanged within families and schools. Fasting and quiet time lasts until the 24th December. On this day, Poles are to abstain from food until the evening. The day is spent preparing the Christmas Tree, 12 traditional Christmas dishes and special types of cakes (poppy cake), soups and fishes. According to tradition and religion, only fish is eaten. Karp fish is preferred. 24th December – Wigilia - Christmas Eve The custom is to secure one empty place for any unexpected visitors who may arrive. The tradition is to end the evening in church singing carols. Holy Days are 24, 25, and 26 of December. New Year is celebrated in the same way as in the rest of Europe. Easter time consists of 3 days: Holy Saturday. Families are to prepare hard boiled home-decorated eggs and other bits of Easter food in decorated baskets. All eggs have to be blessed by a priest to start Easter time with dinner. The eggs are then to be shared between all. Again, no meat is to be provided before Sunday’s celebrated breakfast. Holy Sunday is celebrated by going to Mass and spending time with close relatives. Easter Monday is spent with friends going for walks.
Page 62 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Religious holidays are observed very strictly in Poland. Diet Diets are different dependant of individual life style. If catholic - no meat eating is allowed on Fridays. Naming System A Polish personal name, like names in most European cultures, consists of two main elements: imię, or the given name, followed by nazwisko, or the family name. Death As with other European countries, mourning after death is dependant upon religion.
Page 63 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
SOMALI Somalis originate from Somalia, located on the Horn of Africa. The Somalis or Samaal consist of six major clan-families. Four of the families represent about 70 per cent of Somalia’s population. These are the Dir, Daarood, Isaaq and Hawiye families who originally led a predominantly pastoral life style. The remaining two clan families, accounting for 30 per cent of the population, are the Digil and Rahanwayn clans who originally followed an agricultural way of life. The first refugees from Somalia came to the UK in the late 1980s at the outbreak of the civil war. They were mainly from the urban areas. Others followed later from the rural communities, their flights paid for by relatives already living in the UK, under a Home Office scheme that allowed residents to bring their families to the UK to join them. Despite sharing the same language, religion and customs, Somalis have developed a clear clan consciousness. This has led to conflict between different clans and sub-clans. Religion Somalis are generally Sunni Muslims. Dress Somali men in the UK will generally wear western clothes, although they may also wear a white cloth cap. Somali women wear a scarf to cover their heads and a long gown known as a jilbaab, which drapes from the neck to the ankles. This is because religious practice requires women to keep their bodies covered at all times. Language The predominant language of the Somali people is Somali. This had no written form until an official script was introduced in 1973. Because of this, many older people in the Somali community are unable to read and write, particularly those originating from the rural communities. Diet Somalis do not eat pork or pork products. Any meat consumed must be halal, which is produced by slaughtering the animal in accordance with religious practices. Alcohol is forbidden. Naming system The Somali naming system differs from most Muslims. A Somali name is made up of the first/personal name with either the father’s or grandfather’s name used as a last name/surname. This naming system is used by both men and women. A typical male name is: (Personal Father Family Name) Mohammed Jama Abdi

Page 64 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
A typical female name is: Sashra Omar Hassan Women have traditionally maintained their own name on marriage and a husband and wife will often have names that have no common element although a woman may take her husband’s name, if she wishes. Many Somalis had to leave their country in dangerous circumstances. To enable safe passage out of the country and avoid detection by rival clans, they had to use false names. These false names have subsequently appeared on their documentation in the host country and have by default become their legal names. However, members of their clan who are in their community in the host country are likely only to know them by the original name they had in Somalia. Other information Islam teaches high moral values, which require that men and women should remain separate in public places. Men may not be allowed to enter a house if a male family member is not present. A woman may refuse to be examined by a male doctor. Islam requires that Muslims keep their bodies covered at all times. Refugees who have limited contact with uniformed services may be afraid because of their past experiences of torture and brutality in Somalia. 14
Page 65 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
YEMENI The presence of Britain’s Yemeni communities can be traced back as far as 1885 in the NE of England. Many of the first settlers were sailors who had served on British merchant ships or soldiers in the army. Liverpool has one of the largest Yemeni communities in the UK. Aden, in Southern Yemen, was also a British Protectorate which allowed many Yemenis British Citizenship and ease of travel around Britain and her colonies. Many Yemenis came to Britain during the labour shortage in the steel industry trades across Yorkshire, but industrial decline led to unemployment and many left the UK between the 1970s and 1980s, yet many decided to stay. They diversified, improving educational qualifications and setting up a variety of businesses. Religion The majority of Yemenis in Merseyside are Muslims. As such, their religious festivals, death rites etc are laid out within the Muslim section of this File. Language The Yemeni is the largest Arabic speaking community in Liverpool. Death Due to the effects of high temperatures on the deceased in many Arabic countries, burial normally takes place as soon after death as possible, a practice which continues in this country. Death brings out the best of all grace which the occasion demands in Islam. It is treated as the start of real life – eternal life. It is paramount that the body is cleansed, bathed and buried immediately. 16
Page 66 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
4. Aspects of Faith The information in this section has been reproduced with kind permission of the Chaplaincy, Aintree University Hospitals NHS Foundation Trust. It is taken from their document entitled ‘Cultural and Religious Needs of Patients’. The preface to their document reads as follows: ‘These guidelines are intended to inform hospital staff and help them address the cultural and religious needs of patients in their care (particularly if no immediate family members are available). Wherever possible, the views of the individual patient or family should be sought. ‘….. The need for sensitivity when working with people who have different faith systems and values from those we might have is vitally important in facilitating the very best healthcare…..’ Their generosity in allowing us to present their material in this Information & Resource File is much appreciated. The Faith groups represented are as follows:
· Baha’i · Buddhism · Christianity · Christian Scientists · Hari Krishna · Hinduism · Islam – Muslim · Jehovah’s Witnesses · Judaism · Morman · Quakers – Religious Society of Friends · Rastafarianism · Romany Origin · Seventh Day Adventists · Sikh
Information has also been reproduced from the Home Office & Cabinet Office document entitled “The Needs of Faith Communities in Major Emergencies: Some Guidelines”, and also from the Merseyside Fire Service. Members of WEHAG have also contributed relevant and updated information. Thanks are extended to everyone concerned in producing this important information.
Page 67 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
BAHA’I FAITH The Baha’i Faith began in Persia in the middle of the last century since which time it has established itself throughout the world. Its founder, Baha’u’llah (a title meaning Glory of God), lived from 1817 – 1892 and is regarded by Bahais as a Messenger of God.
• His teachings centre on the unity of mankind and of religions and include:
o The harmony of religion and science o The equality of men and women o The abolition of prejudice
• The faith has no clergy and its affairs are in the hands of elected
administrative bodies known as “Spiritual Assemblies”.
• At present, there are some 200 of these in the UK. Although there are significant numbers of Bahai’s in this country of Persian origin, the majority of members here are of British background and their cultural approach and needs are basically the same as those of other patients.
• While they believe in the power of prayer, Bahai’s have no objection to
orthodox medical practice, seeing them as different aspects of the same God-given healing process. They are exhorted by their faith to trust and to follow the recommendations of the doctors treating them.
Key Issues and Special Considerations
• Members of the Faith observe a period of fasting each year. Those suffering chronic ill-health, children, elderly, expectant and nursing mothers are exempt.
• Under normal circumstances, Bahai’s abstain from alcohol and from
other harmful or habit-forming drugs. But it is permitted, where prescribed, as a bona fide part of treatment, as are Narcotics for control of pain.
• The bearing of children is regarded as one of the main reasons for the
institution of marriage but the details and extent of contraceptive practice are left to the conscience of the couple. Many will not use intra-uterine device as they regard it more as an abortifacient than a contraceptive.
Food and Diet
• There are no special requirements as far as food and diet are concerned except that the abstention from alcohol extends to cooking as well. Wine sauces, sherry trifle, etc are forbidden.
Page 68 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Care of the dying and what to do after death
• There is no objection to the giving or receiving of blood transfusions or of organ transplants.
• Donation of organs after death for transplanting to others is regarded
as praiseworthy.
• Bahais believe that, after death, the body should be treated with respect.
• Cremation is not permitted and burial should take place as near as
reasonably possible to the place of death, certainly within distance of an hour’s transport.
• There is no objection to necessary post mortem examination, provided
these stipulations can be met. Nursing Considerations Bahá'ís believe in the healing power of modern medicine for both physical and mental ills, while recognizing the role of the spirit, of prayer and of turning to God. There is no objection to being touched or treated by members of the opposite sex. The administration of prescription drugs and the like are all perfectly acceptable. There is no objection to mixed wards, but older Bahá'ís may prefer single-sex wards. Bahá'í patients will be ministered to by friends, by family and by those appointed as spiritual care givers by the community. Because the Bahá¹í faith has no sacraments, these spiritual care givers do not have a sacramental or priestly/ministerial role nor do they have any authority over the patient. BAHA’I faith Festivals and Holy Days listed by month: March Naw Ruz (new year) April Ridvan May Anniversary of the Declaration of the Bab May Anniversary of the Ascension of Baha’u’llah July Anniversary of the Martyrdom of the Bab October Anniversary of the Birth of the Bab November Anniversary of the Birth of Baha’u’llah
Page 69 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
BUDDHISM Buddhism means the teachings of Buddha. This is a way of life.
• It is the thought and practice associated with Buddha (The Enlightened) who lived in India in 5th/6th Century BC. He is revered, not as a God, but as the founder of a Way of Life.
• There are over 311 million Buddhists worldwide.
• There are many variations of Buddhism. Ethnic Buddhists are those
born into a Buddhist family or culture. Many Buddhists in the UK have consciously converted to Buddhism.
• Followers of Buddha seek to emulate his example of perfect morality,
wisdom and compassion culminating in a transformation of consciousness known as enlightenment.
• The Buddhist way of life involves:
o Keeping of special festivals o Pilgrimage to Buddhist sacred places o Social responsibility
Key Issues and Special Considerations Buddhism is divided into different schools. Since attitudes to a manner of things will vary considerably eg. dietary rules, disciplines and customs, it is important to find out from which school a Buddhist comes from. The individual or family will normally explain what is required.
• Normally there would be no physical contact across the genders. • Buddhists would appreciate a visit from a Buddhist Monk or Sister (this
can be arranged through the Chaplaincy team) • Peace and quiet for meditation and chanting would be appreciated. • Buddhists have no conflicts with modern medicine.
Food and Diet
• Because of their respect for all life, many are vegetarians.
Page 70 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Care of the dying and what to do after death
• A side room would be appreciated, where possible, as they require as much time as possible for meditation.
• Buddhists would like to have full information about their imminent
death to enable them to make their own preparation for death.
• Buddhists consider that dying is a very important part of life. It should be approached positively and in as clear and conscious state of mind as possible. This may mean a reduction of certain drugs which reduce consciousness.
• Post mortem and organ transplantation – there are unlikely to be any
objections as helping others is fundamental to the Buddhist belief.
• It is important that the body is wrapped in a sheet, without emblems.
• After death, cremation is generally preferred. Nursing Considerations There are no religious objections to blood transfusions, or transplants. In cases of hospital stays, the use of either a bath or a shower is a personal matter. Provision of a quiet space set aside in a hospital or rest centre is not a necessity but, if available, it can be used for silent reflection and meditation.
When caring for patients who are followers of the Buddhist religion, nurses need to understand that the patient's main goal is to bring back the body's yin/yang equilibrium that was disrupted because of illness. It is helpful to first discuss the patient's illness and care plan in relation to this concept before volunteering a medical or patho-physiological explanation. Because of the supreme importance of nature in Buddhists' lives, a culturally sensitive medical team will want to prescribe both herbal medicine and pharmaceutical medications, if appropriate. Remember, in these patients' eyes the goal is not curing but rather maintaining peace of body and mind that will ensure the rebirth process after death.
In terms of dietary assessments, the first step is obviously to find out whether the patient is a vegetarian, how strict or liberal he/she is in following the traditional vegetarian diet and whether there are any other dietary restrictions the patient must observe. The risk of vitamin B12 deficiency among pure vegetarians can be managed by increasing their daily intake of the different types of vegetable proteins.
Buddhist patients staying in a hospital that only serves western European food may appreciate being provided with a bottle of soy sauce that they can keep in their room to flavour their meals in the way they are accustomed to. The rule of thumb is: When in doubt, ask the patient what he or she would
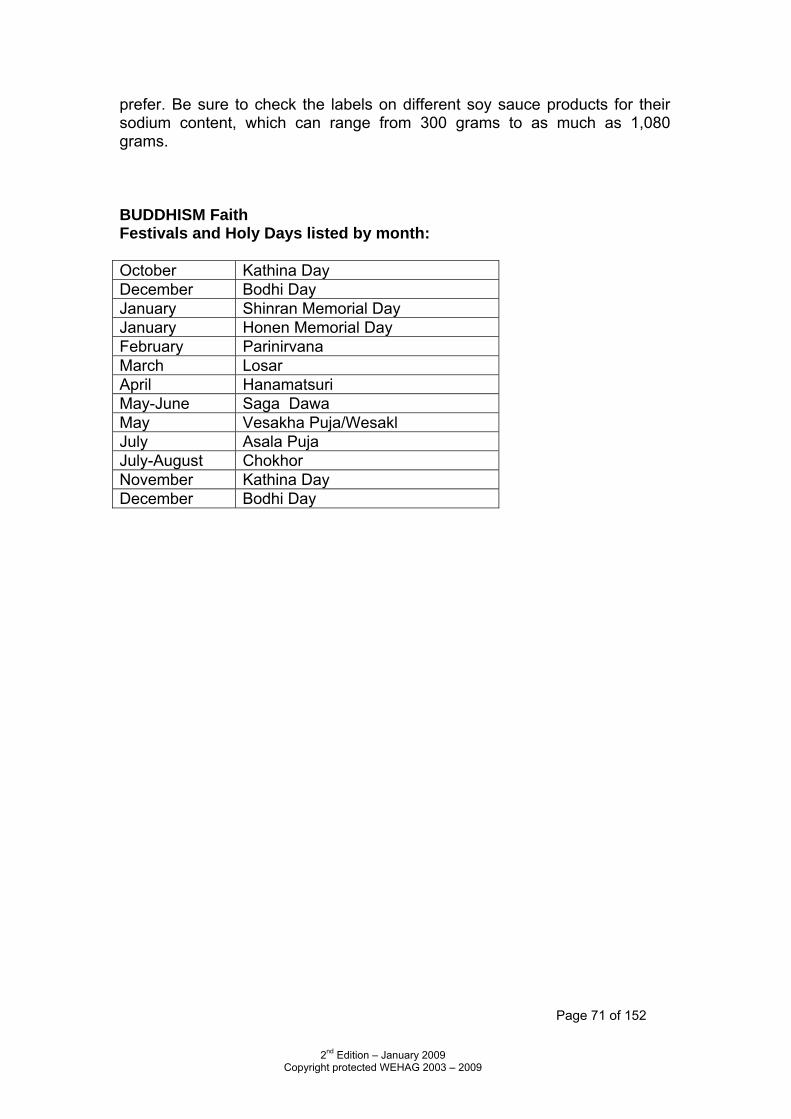
Page 71 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
prefer. Be sure to check the labels on different soy sauce products for their sodium content, which can range from 300 grams to as much as 1,080 grams.
BUDDHISM Faith Festivals and Holy Days listed by month: October Kathina Day December Bodhi Day January Shinran Memorial Day January Honen Memorial Day February Parinirvana March Losar April Hanamatsuri May-June Saga Dawa May Vesakha Puja/Wesakl July Asala Puja July-August Chokhor November Kathina Day December Bodhi Day
Page 72 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
CHRISTIANITY Christians believe that God became man in the person of Jesus Christ. He was crucified, rose from the dead, and ascended to heaven. Most Christians are baptised, either as babies or when they are old enough to profess their own faith in Jesus Christ. Approximately one third of the world’s population professes some form of Christianity. There are many different Christian churches with differing structures, beliefs and rituals but the concept of one God who reveals Himself as Father, Son and Holy Spirit (the Trinity) is central to all Christian teaching. Easter and Christmas are the most important Feast Days. Christian Churches include:
o Anglican/Church of England o Roman Catholicism o Free Churches (which do not conform to the Anglican or
Catholic traditions) Patients who belong to a particular denomination might be registered within one of the following:
o Methodist, Independent Methodist
o Unitarian
o Baptist o Plymouth or other Brethren o Free Church of England o Church of Nazarene o Church of Christ o 7th Day Adventists o Presbyterian Church o The Lutheran Church o Salvation Army o Pentecostal (Elim or Assembly of
God) o United Reformed Church o Independent Churches or
Missions (Bethesda, Ebenezer, Emmanuel etc)
o Church of Scotland o Quaker (Society of Friends) o The New Church
Key Issues and Special Considerations
• Patients may wish to see a Chaplain, especially before an operation so that they can be prayed for and receive Holy Communion. They may request a Bible and wish to attend services in the Chapel.
• Prayer cards and Bibles should be made available.
• There is no religious objection to the giving or receiving of blood or
organs, nor to the donation of the body for teaching or research.
• Roman Catholic patients will almost certainly wish to be visited by a Priest whilst in Hospital.
Page 73 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
• Roman Catholic Chaplains consider it their duty to visit all Catholic patients.
• Never hesitate to call the Roman Catholic Chaplain at any time in
appropriate situations.
• Church doctrine does forbid termination of pregnancy. Food and Diet There are no longer any general dietary requirements but some ‘high’ Anglicans (who may describe themselves as Anglo-Catholics) may wish to observe the traditional meatless Friday as a day of self-denial.
• Those awaiting Holy Communion may prefer to fast until after they receive the sacrament.
Afro-Caribbean Community
• The majority of Afro-Caribbeans in the UK are Christians and, as a result, their dietary patterns are free from religious influence but reflect the influence of the colonisers of the Caribbean islands.
• The diet is, therefore, based on cereals such as rice, maize and wheat;
roots and tubers such as yams, sweet potatoes and plantain. These are generally consumed with meats such as chicken and goat, both fresh and salted fish (eg salt fish and ackee (vegetables) is a traditional favourite). Dishes are well seasoned with herbs and spices and frequently eaten in the form of stew. Homemade soup is also very popular.
Chinese Christians: see page 26 Care of the dying and what to do after death Anglican/Church of England
• Prayers may be said at the bedside of the dying and sometimes it will be appropriate for the patient to be anointed. After death, some families may like to gather around the bed to give prayers of thanksgiving for the person’s life.
• Always ask the patient/significant others if they would like to see the
Chaplain or would like to make arrangements for their local priest to visit.
• Baptism for babies and young children should be offered.
Page 74 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Roman Catholic
• In addition to usual visits by the Chaplains, the Sacrament of the Sick is of particular important. The sacrament, however, is not the ‘Last Rites’ but a sacrament of healing administered at the beginning of illness or before a major operation.
• A Chaplain should be called to the dying patient or to the one who has
died, always respecting the wishes of both the patient and the relatives. He or she (it does not have to be a Priest) would be of assistance in consoling the relatives.
• Baptism of infants in danger of death is also important.
• Holy Communion is normally available through the Eucharistic
Ministers.
• There is no requirement for those who are ill, or those of retirement age to fast before receiving Holy Communion.
• The sacrament of reconciliation or Confession is also important.
Free Churches
• Free Church patients will welcome prayers but will not normally expect a sacramental ministry. As far as possible, ministry will be given by the Minister of their own church but visits by the Free Church Chaplain will be accepted.
• No religious objection to post mortem and transplants. • Last offices/rites are appropriate for all Christians.
Nursing Considerations Most would have no objections to being touched by members of the opposite sex for medical purposes. Treatment such as blood transfusions, surgery, organ transplants or the administration of drugs is permissible. Jehovah’s Witnesses (not regarded as Christians by most Christian organisations) are forbidden to receive blood transfusions and transplants. If a person is terminally ill, or dying, they may wish to keep a copy of the Bible close at hand. Survivors, their families and friends, should be allocated a quiet place at survivor and reception centres, which can be used for private prayer or to talk to a priest or minister.
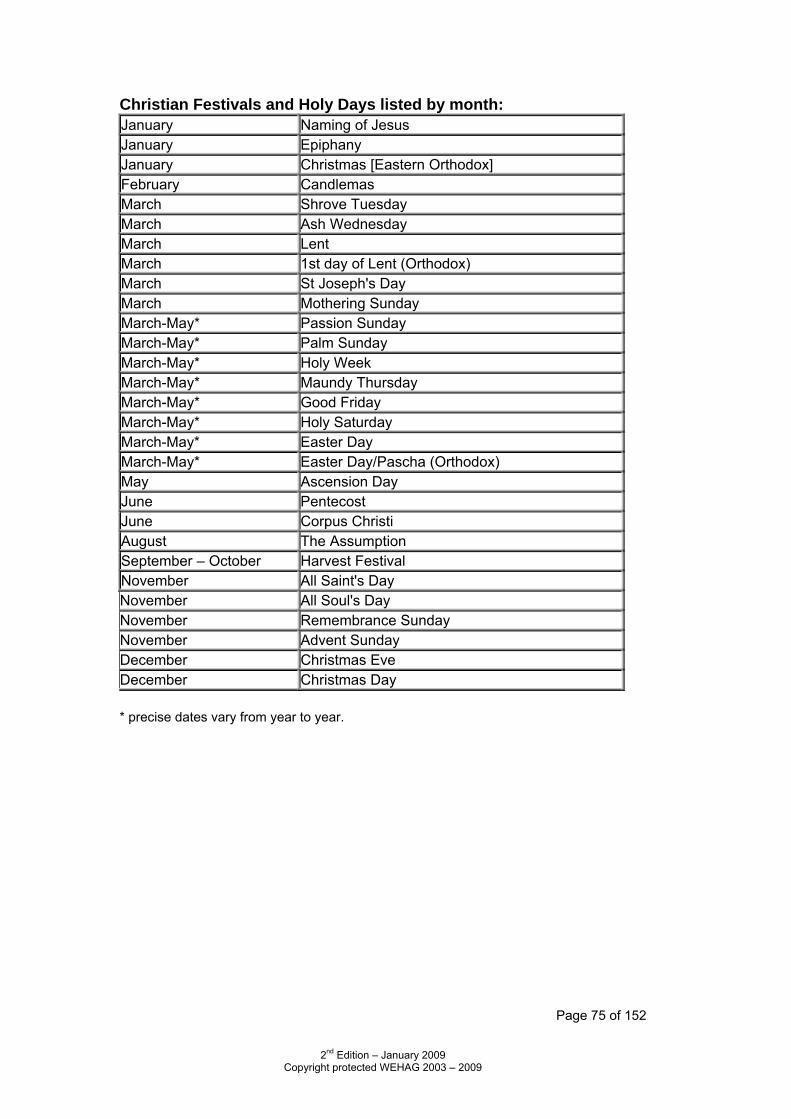
Page 75 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Christian Festivals and Holy Days listed by month: January Naming of Jesus January Epiphany January Christmas [Eastern Orthodox] February Candlemas March Shrove Tuesday March Ash Wednesday March Lent March 1st day of Lent (Orthodox) March St Joseph's Day March Mothering Sunday March-May* Passion Sunday March-May* Palm Sunday March-May* Holy Week March-May* Maundy Thursday March-May* Good Friday March-May* Holy Saturday March-May* Easter Day March-May* Easter Day/Pascha (Orthodox) May Ascension Day June Pentecost June Corpus Christi August The Assumption September – October Harvest Festival November All Saint's Day November All Soul's Day November Remembrance Sunday November Advent Sunday December Christmas Eve December Christmas Day * precise dates vary from year to year.
Page 76 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
CHRISTIAN SCIENTISTS
Founded by Mary Baker Eddy in 1879 (who suffered a great deal of ill-health, and experienced personal healing after reading of the healing power of Jesus Christ in the New Testament).
The Church of Christian Scientist aims to reinstate primitive Christianity and its lost element of healing. It is probably best known for its reliance on prayer for the healing of sickness and disease. This is believed to be in line with the healing practised by Jesus Christ and is seen as an integral part of the ministry of Christianity.
Christian Scientists are free moral agents and the Church does not control the actions of its members.
It is unusual for Christian Scientists to be patients in ordinary hospitals. Instead, they would seek help from a nursing home run by the Church, where the accent is on healing by prayer alone. However, the Church does not rebuke those who defer to the family or legal pressures to undergo conventional medical treatment.
Christian Scientists may be admitted to hospital for the following reasons: o Following accidents, a surgeon is allowed to set bones; o Childbirth, when a midwife is required by law to attend the woman; o Lack of finance; if they can no longer afford care in their own
hospital, even though the Church does give substantial financial support;
o Lack of faith; when faith is not strong enough to believe cure can be affected by spiritual means.
Key Issues and Special Considerations
The Christian Scientist, if in hospital voluntarily, is likely to accept minimal medical treatment.
They may also ask for drug therapy to be kept to a minimum. They may wish to contact a Christian Science practitioner to ask for
treatment through prayer. Food and Diet
The only dietary prohibitions are alcohol and tobacco.
Page 77 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Care of the dying and what to do after death Worship is kept free from ritual and there are no last rites. Post Mortem – Christian Scientists wish to be free from Post Mortems
unless required by law. Transfusions and organ transplantation – these are regarded as
material methods of treatment and neither donation nor reception would usually be acceptable for adults. Parents would consent to transfusion for their child if doctors were of the opinion that it was essential.
Routine last offices are appropriate. Female staff should handle a female body. Cremation is usually preferred, but this is a matter for family choice
Nursing Considerations If a Christian Scientist were taken to a hospital because of an accident, for example, and chose to decline conventional medical treatment, this would ordinarily mean that the individual was choosing instead, as a competent adult, to rely on prayer for healing (individually or with the help of a Christian Science practitioner). Such an individual would co-operate with authorities to take appropriate actions, such as quarantine, which may be considered necessary to protect others. Individuals relying on Christian Science may ask to be re-tested, or to have a pending procedure re-evaluated after having had time to pray for healing. If a Christian Scientist entered a hospital voluntarily, the individual would probably accept conventional medical treatment. He/she might ask that drugs/therapy be kept to a minimum. Individuals make their own decisions about blood transfusions and organ/tissue donation. Doctors, nurses, mental health professionals and chaplains will find that there are many meaningful ways in which they can show support for patients relying on Christian Science. Where possible, the best way to ascertain what would be most helpful in any circumstance is to ask the individual patient. Some of the following might be requested by a patient, or could be offered by the healthcare worker: ♦ providing the patient time and a quiet space to pray, during the various
stages of diagnosis and treatment. ♦ facilitating the patient’s contact with a Christian Science practitioner. ♦ making sure that the patient has access to the Bible and Science and
Health. ♦ Reading aloud to the patient requested passages from these books (or
other Christian Science literature).
Page 78 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
HARI KRISHNA
Hari Krishna is a religion with its basis in the sub-continent of India though now practised world-wide.
Its members are known as Devotees Although similar in some ways to Hinduism, it has a more ancient
base. Indian scriptures used by Krishna Devotees: Vheda, Baghavad and
Geta. Karma is a right or good spirit. Devotees need to achieve the right
Karma. Key Issues and Special Considerations
Chanting the Lord’s Holy names and prayers are a very important factor in the life of the Devotee.
A place of quiet should be provided for the Devotee to meditate. Often, they may wish to burn incense sticks.
Food and Diet
Devotees are Lacto Vegans. Eggs and certain vegetable products are not acceptable. Normally, patients will have food prepared with the right “Karma”
brought in by other Devotees, but will eat food prepared by non-Krishna people in an emergency.
Care of the dying and what to do after death
It is important that all the facts are disclosed to the patient. Krishna followers wish to prepare themselves for death.
It is paramount at the time of death to remember God. To this extent, other Devotees will be there to read Scripture and to chant the Hari Krishna mantra. This chanting may be done with musical instruments.
Nursing Considerations Devotees have no objection to blood products and will accept treatment offered.
Page 79 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
HINDUISM
Has no formal structure, but is the result of 5,000 years continuous cultural development.
It includes a number of extremely diverse, traditional and cultural beliefs and practices.
Hindus believe in the theory of re-birth and the principle of action ie. one has to face the consequences of actions in past lives.
It is extremely important to the Hindu patient that he is allowed to practice his religion in hospital.
Married women and children may wear red markings on their foreheads.
Married women may also wear a ‘nuptial thread necklace’ and male adults a ‘sacred thread’.
Key Issues and Special Considerations
Female patients prefer a female doctor, if possible, and consideration should be given to their modesty,
Hindus believe that the purification of the body is as essential as the purification of the soul. They try to bathe daily in running water and like to have a shower early in the day before saying their prayers.
Hindus are accustomed to having running water or a jug in the same room as the toilet and, if a bedpan is used, a bowl of water must be offered afterwards.
Hindus require time for meditation and this will certainly continue in cases of terminal illness. Often what may be required is somewhere to go to be alone.
The need for privacy is considerable amongst Hindus. It may be that the patient wants to keep small idols or pictures of gods beside his/her bed.
Food and Diet
The eating of beef is forbidden and pork is not usually acceptable. Many are vegetarians and do not eat eggs. They dislike plates that have been used for non-vegetarian food. Cow’s milk is acceptable to most Hindus. The cow is regarded as a sacred animal. Consequently, many are
vegetarian and, even among the non-vegetarian, beef is not generally eaten although they may eat mutton, poultry, fish and eggs.
Page 80 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Some vegetarians may include eggs and dairy products while others follow a completely vegan diet.
Fast days are common and may follow different patterns, from total elimination of food to a day where foods are restricted to those which are considered ‘pure’ eg. Rice and fruit.
The caste system also dictates who can prepare and share food. Care of the dying and what to do after death
Wherever possible, Hindu patients like to die at home. Before death, a Hindu desires to offer food and other articles of use to
the needy, religious persons or to the Temple. Coping with the unfamiliar organisational side of death in Britain can be
extremely distressing to bereaved relatives. Careful explanation and practical help may be needed to contact
undertakers and deal with the paperwork. Hindu priests can be very helpful.
Consult the family asking if they wish to perform the last rites, as distress may be caused if the body is touched by non-Hindus.
If no family is available, the following procedure should be
followed: o Wearing disposable gloves, close the eyes and straighten the
limbs; o Jewellery, sacred threads and other religious objects should not
be removed; o In most cases, the body should not be washed as this is part of
the funeral rites and will usually be carried out by relatives using Ganges water which is collected from the Temple;
o Wrap the body in a plain white sheet without religious emblems; o There are no religious objections to transplants; o Post Mortems are disliked but are accepted if required by law; o A Hindu is cremated.
Nursing Considerations A Hindu would prefer to be comforted by a person of the same sex. There is no stated preference in respect of medical examination and treatment. Blood transfusions, organ transplants, and all types of medicine for the purpose of saving life are permitted. Hindus traditionally live in extended families, so information or requests (e.g. for organ donation) should be made by the authorities to the head of the family to be passed on without delay to the rest of the family unit, where this
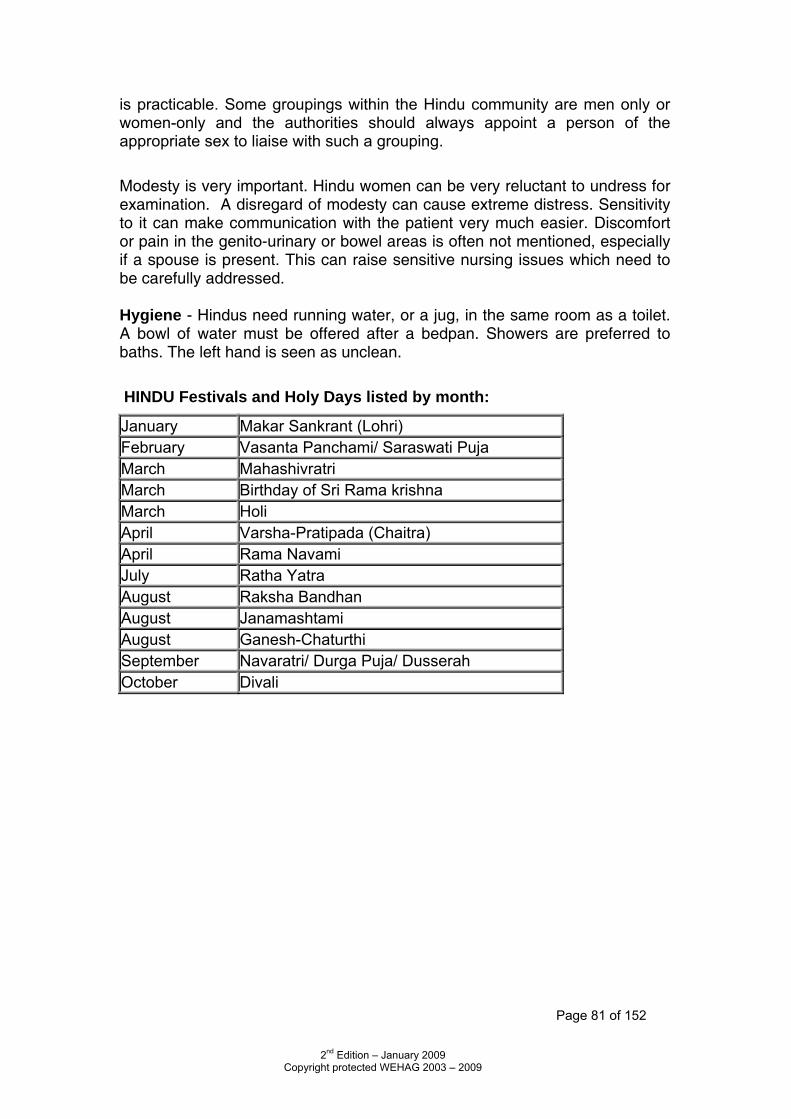
Page 81 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
is practicable. Some groupings within the Hindu community are men only or women-only and the authorities should always appoint a person of the appropriate sex to liaise with such a grouping. Modesty is very important. Hindu women can be very reluctant to undress for examination. A disregard of modesty can cause extreme distress. Sensitivity to it can make communication with the patient very much easier. Discomfort or pain in the genito-urinary or bowel areas is often not mentioned, especially if a spouse is present. This can raise sensitive nursing issues which need to be carefully addressed. Hygiene - Hindus need running water, or a jug, in the same room as a toilet. A bowl of water must be offered after a bedpan. Showers are preferred to baths. The left hand is seen as unclean. HINDU Festivals and Holy Days listed by month:
January Makar Sankrant (Lohri) February Vasanta Panchami/ Saraswati Puja March Mahashivratri March Birthday of Sri Rama krishna March Holi April Varsha-Pratipada (Chaitra) April Rama Navami July Ratha Yatra August Raksha Bandhan August Janamashtami August Ganesh-Chaturthi September Navaratri/ Durga Puja/ Dusserah October Divali
Page 82 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
ISLAM – MUSLIM
This is an Arabic word which means peace, purity, acceptance. The literal religious meaning of Islam is ‘surrender to the will of God’.
A Muslim is one who follows Islam. The Holy Book of Islam is the Quran which is the last revealed word of
God. Muslims are charged with the 5 Pillars of Islam:
o Declaration of Faith o The mandatory 5 daily prayers (facing Mecca) o The fast of Ramadan (in the 9th month of the Muslim calendar).
No Muslim must eat, drink or indulge in pleasure between the period of dawn to dusk.
o Give alms to the poor. o Pilgrimage to Mecca at least once in your lifetime (if you are
physically and financially able).
Key Issues and Special Considerations Muslims attach great importance to cleanliness
Hands, feet and mouth are always washed before prayers. After menstruation, the whole body is washed. A shower is preferred to a bath. After a bedpan is used, washing facilities should be offered. Women often react strongly to male Doctors and Nurses, and find
contact shameful. Muslims of both sexes are modest in their dress and outlook. Due
consideration should be given to this important factor during hospital procedures and routines. NB. Muslims may be reluctant to wear western style nightgowns.
Termination of pregnancy is not allowed. Following spontaneous abortion, tissue is treated as dead if before 130
days, after this period it is classed as a fully developed human being and must receive a funeral ceremony.
Food and Diet Halal food should be made available from the catering department (it is
food prepared in a special way. Pork, Bacon, Ham and alcohol are forbidden Islam provides directives regulating all aspects of life including food
preparation and eating. Food laws are derived from the Quran which forbids the consumption of alcohol, pork, carnivorous animals and
Page 83 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
some birds. Poultry and fish with scales are permitted. All meat consumed must be from animals killed by ritual slaughter (Halal).
Utensils which have come into contact with pork or pork products cannot be used for cooking.
During the lunar month of Ramadan, all Muslims should fast between Sunrise and Sunset. Those who are ill, pregnant or on a journey may be excused provided
that they make up the days of fasting on another occasion. Since it is more convenient to fast when the rest of the family is fasting, pregnant women may choose not to take up this dispensation and so may fast during their pregnancy.
Menstruating women are forbidden from fasting during Ramadan. The Quran advocates that children should be breast-fed up to the age
of two years. The staple food of Pakistani Muslims is the chapatti, made from wheat.
Meat, vegetables, and dhals are also eaten. Bangladeshi Muslims place a much greater emphasis on fish.
Care of the dying and what to do after death Patients may wish to sit or lie facing Mecca (South East) Family or friends may sit with the patient reading the Holy Quran and
make supplications. Post Mortem is only allowed if required by law. Organ donation may be refused but a special commission of 1982 did
declare organ donation permissible. Procedure at Death DO NOT WASH THE BODY
Where no relatives are available, staff should wear gloves. Avoid direct contact with the body. The body should face towards Mecca and the head should be turned
towards the right shoulder before rigor mortis begins. The body can be made respectable in the usual way ie. Combing hair
and straightening limbs BUT the family will ritually wash the body before burial.
Nursing Considerations The views of the family/Imam on whether organ donation, transplants and blood transfusions are acceptable should be sought in each case. In hospital, a shower is preferred to a bath. Muslims ritually wash after using the toilet, so a tap or container of water for washing should be provided
Page 84 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
whenever the toilet area is separate from the bathroom. In a rest centre, suitable facilities for pre-prayer washing, time to conduct prayer, and a clean prayer room with a prayer mat and a compass or sign pointing to Makkah (Mecca) - south-east in the United Kingdom are appreciated. Good communication and open dialogue is the key to providing culturally sensitive care. If possible, healthcare should be given by people of the same sex as the patient. This has become more possible with the advent of more males in nursing, and more females in medicine. For female patients, there is an overriding objective of modesty and privacy. In some cases, a close family member of the same sex may assist in the washing of the sick person. Muslims generally wear clothing that does not reveal the shape of their bodies. Hospital attire should be provided that meets these requirements, or if not, the patient can be advised to bring some of their own appropriate clothing. Unnecessary touching between non-related people of the opposite sex should be avoided. The left hand is considered unclean, so it is preferred that the right hand be used for feeding or administering medications. A beard is considered a very important religious symbol to the Muslim male patient. Like any other patient, permission must be obtained to shave any part of the beard, which should be done by a man. A sick Muslim patient who does not have freedom of movement may perform prayers while seated or even while lying down. Healthcare providers should be aware of this and not disturb the patient at prayer. Muslim patients may require special or additional assistance after toilet duties. It is of utmost importance that patients are given the necessary assistance to clean themselves after clearing their bowels (even in a pan). Having a jug in the bathroom/toilet is greatly appreciated, as Muslims prefer to wash with running water after using the toilet. The holy day for Muslims is Friday, when a patient may receive a number of hospital visitors above that normally expected
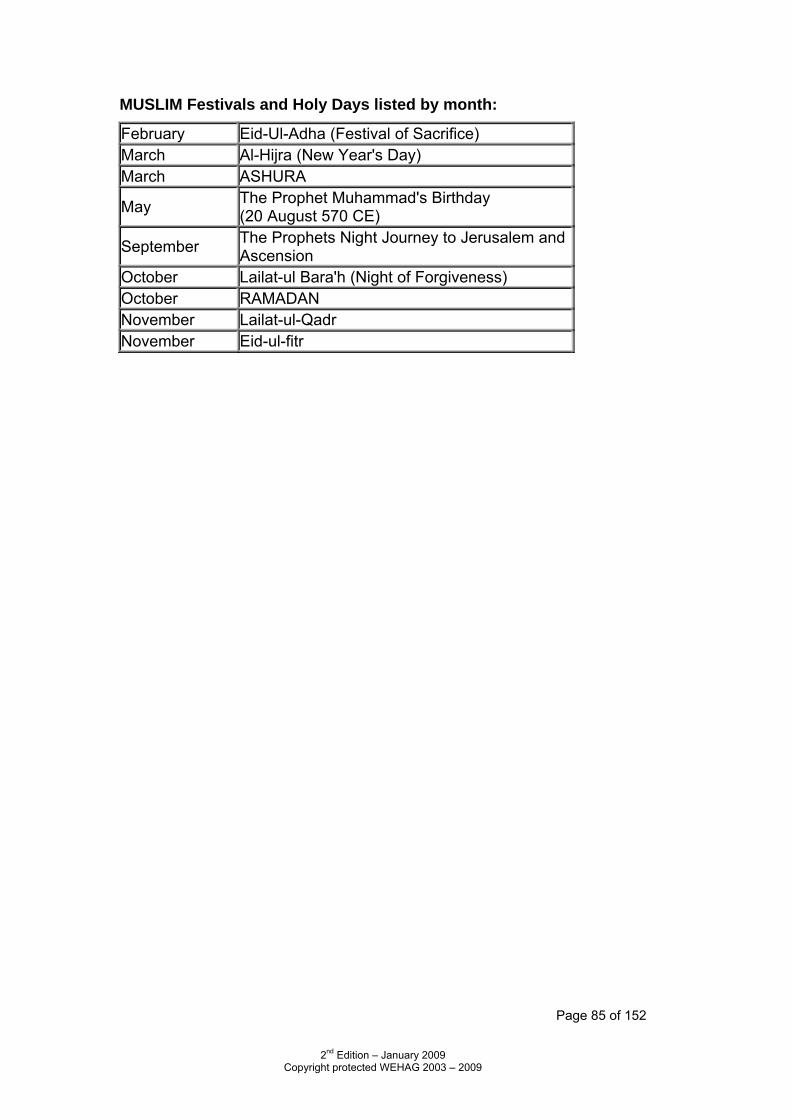
Page 85 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
MUSLIM Festivals and Holy Days listed by month:
February Eid-Ul-Adha (Festival of Sacrifice) March Al-Hijra (New Year's Day) March ASHURA
May The Prophet Muhammad's Birthday (20 August 570 CE)
September The Prophets Night Journey to Jerusalem and Ascension
October Lailat-ul Bara'h (Night of Forgiveness) October RAMADAN November Lailat-ul-Qadr November Eid-ul-fitr
Page 86 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
JEHOVAH’S WITNESSES Jehovah’s Witnesses believe in Almighty God, Jehovah, Creator of the Heavens and earth. They regard Jesus Christ as the Son of God and declare themselves to be Christian. They await the end of the present ‘world system’ which they believe will begin with the battle of Armageddon. Jehovah and His true witnesses will be the only survivors, His true witnesses being their sect. After Armageddon, there will be 1,000 years of peace and life under ‘favourable conditions’.
They are known for their door-to-door contact and believe in making a positive effort to reach the public, just as Jesus did when He went from city to city and town to town preaching and declaring the good news of the Kingdom of God.
Their worship centres are called Kingdom Halls where they conduct meetings on a weekly basis. They assemble in private homes to study the Bible each week.
The only festival celebrated is the annual memorial of the death of Christ, the date of which is calculated according to Biblical formula and so varies.
Key Issues and Special Considerations They believe medical treatment is a matter of informed consent of the
individual. They have strong views about the termination of pregnancy and are
totally against it (with the possible exception of ectopic pregnancy) Blood Transfusions
They are deeply religious people who have sincerely held Bible-based views that taking blood into one’s body is morally wrong.
They are pleased to co-operate with medical staff in alternative non-blood medical management, but will not accept treatment involving the use of blood or blood components.
They do not object to modern medicine. They believe that blood represents life itself and must be handled with respect.
Food and Diet Jehovah’s Witnesses reject food containing blood. They do not smoke or use tobacco products.
Page 87 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Care of the dying and what to do after death There are no special rituals or practices for those dying. The living body is dedicated to God, but the body has no particular
religious significance once the breath of life has passed from it. Patients who are very ill will appreciate a visit from one of their elders. They do not support euthanasia but if death is imminent/unavoidable,
then life should not be prolonged artificially. There are no religious objections to either Post Mortems or transplants
and the Witnesses view is that the use of cadaveric material for research or transplantation is a matter for personal conscientious decision.
There are no specific funeral rights, though a simple, personal service will likely be held at the deceased’s Kingdom Hall, or at the graveside or crematorium. Nursing Considerations For deeply-held reasons of religious faith there are basically only two medical interventions that Jehovah’s Witnesses object to: elective termination of pregnancy and allogeneic blood transfusion. Baptised Jehovah’s Witnesses usually carry on their person an Advance Medical Directive/Release document directing that no blood transfusions be given under any circumstances, and this document is renewed annually. A more detailed Health-Care Advance Directive form outlining their personal treatment choices may also be carried. Jehovah’s Witness are happy to sign hospital forms that state that no allogeneic blood transfusion or primary blood components be administered under any circumstances, while releasing doctors, medical personnel and hospitals from liability for any damages that might result from such refusal, despite otherwise competent care. They understand the challenge that their decisions can sometimes pose for doctors and nurses. In an effort to alleviate these situations, they have established a network of Hospital Liaison Committees throughout Britain. Members of these groups are trained to facilitate communication between medical staff and Jehovah’s Witness patients and are available at any time, night or day, to assist with difficulties either at the request of the treating team or the patient.
Page 88 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
JUDAISM The foundations of Judaism and the earliest stories of the Jewish people are found in the Hebrew Bible (ie. the Old Testament). The essential belief is that there is one Spiritual God who cannot be represented in any shape or form.
• The family has great importance to Jewish life.
• In Britain today, there is a wide spectrum of observance amongst Jews from ‘reform’ and ‘liberal’ to ‘ultra-orthodox’ communities, whose daily lives are guided by a code of laws contained in the five books of Moses (the Pentateuch).
Key Issues and Special Considerations
• The Feast of Yom Kippur – (Day of Atonement) – either September/October, when no food or water is taken for 24 hours.
• Most Jewish people who are hospitalised in Britain are not likely to
expect any particular considerations other than dietary ones. Ultra-Orthodox Jews
• Adhere very strictly to dietary requirements
• Women may not wish others to look at their hair and may wear a wig. In hospital, they may prefer a head scarf.
• It is considered immodest for men to touch women – other than their
wives. For such patients, thought needs to be given about what contact is necessary between nurse and patient.
Food and Diet
• Many Jews will ask for kosher food. Food is immensely important and, in essence, this means that specially prepared meat (only lamb, beef or chicken, no pig meat or rabbit) and only true fish (ie. with scales and fins) can be eaten.
• Some will require that strictly kosher meals are ordered. • Milk and meat products are not mixed. • The patient should be consulted about his/her level of dietary
observance.
Page 89 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Care of the dying and what to do after death
• The dying person should not be left alone. Many families will sit with their relative.
• A dying Jew may wish to hear or recite a special prayer or confession
(Vidui) or the Affirmation of Faith (The Shema). These prayers can be said on their behalf by a relative or Rabbi.
• Once death is established, the arms should be extended by the side
with the hands open.
• There are no Last Rites in Judaism.
• If a Rabbi should be called, first ascertain whether it is Orthodox, Reform or Liberal.
Traditionally, the body is left for about 8 minutes with a feather placed over the mouth and nose and watched for signs of breathing. If there are no signs, the eyes are closed by the son or nearest relative. The arms are then extended down the sides of the body and the lower jaw is bound up before rigor mortis sets in.
• Burial should take place within 24 hours of death and will be delayed only for the Sabbath.
• The family will set the ritual proceedings in motion.
• Where death must be notified to the Coroner, or where the attending
Doctor is unable to complete the death certificate, the family should contact their preferred undertaker who will be able to keep in contact with the Coroner’s Office.
• The Coroner’s Officers are very helpful in expediting arrangements for
Jewish bodies so that the funeral may not be unduly delayed.
• Orthodox Jews will resist Post Mortem unless required by law.
• The giving of organs, except corneas, is also frowned upon.
• Liberal or Reform Jews have different views, so check with the family, where possible.
Nursing Considerations Strictly Orthodox men and women actively avoid physical contact with people of the opposite sex and will not welcome being comforted by someone touching or putting an arm around them. All laws normally applying on the Sabbath or festival can be overruled for the purpose of saving life or
Page 90 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
safeguarding health. Blood transfusion is permitted and is a matter of personal choice. Transplants and organ donation are usually permissible, but may require advice from a Rabbi. A quiet area for prayer should be provided if possible. Orthodox Jews will not eat food that has been prepared in a hospital because of the need for the food to be kosher. JEWISH Festivals and Holy Days listed by month: January Tu B”Shevat March Purim April Passover (Pesach) April Yom Ha Shoah May Yom Ha’atzma’ut May Lag B’omer June Shavuot August Tisha B’ay September Rosh Hashana October Yom Kippur October Sukkot October Simchat Torah December Hanukhah
Page 91 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
MORMON – CHURCH OF LATTER-DAY SAINTS Properly known as the Church of the Latter-Day Saints. Began in America in the early 19th Century. Its headquarters are in Salt Lake City, Utah, USA. They believe that God, Christ and Holy Ghost are separate personages, although united in purpose.
• They believe in continuing revelation and that there is a living prophet, a man who received revelations from God and directs the churches here on earth.
• They believe that we are living in a time just before the Second
Coming of Christ and the Gospel should be taken through Missionary Work to the whole world.
• They believe in self-sufficiency in honouring, upholding and sustaining
the Law and in being of service in the community.
• Young people between the ages of 19 and 22 mainly do missionary work. They travel in pairs serving full-time without pay. They spread the word of the Mormon Church, visiting homes and the community.
Key Issues and Special Considerations Food and Diet
• Mormons drink neither tea nor coffee, as there is concern over the effects of stimulants including caffeine. Some will avoid all hot drinks.
• In hospital, water, milk or fruit juice will be acceptable.
• Alcohol and tobacco are forbidden.
• Mormons try to take care of their body, take proper rest and exercise
and eat a healthy diet.
• They are not usually vegetarians but will eat meat sparingly, avoiding products with much blood (eg. black pudding).
• Some Mormons who have undergone a special Temple ceremony
wear a sacred undergarment. This intensely private item will normally be worn at all times in life and in death. It may be removed for hygiene purposes and laundering and for surgical operations, but it must at all times be considered private and treated with respect.
Page 92 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Care of the dying and what to do after death
• Death, if inevitable, is regarded as a blessing and a purposeful part of external existence. There are no rituals for dying but spiritual contact is important and active members of the church will know how to contact their Bishop.
• Routine last offices are appropriate.
• The sacred garment, previously mentioned, must be replaced on the
body following last offices.
• There is no religious objection to post mortems or organ transplants or donation. Members are counselled that the decision is one for individuals and families to make.
• Blood transfusions – there is no religious objection, the Church
encourages blood donation and makes its meeting houses available for this purpose.
• Burial is preferred although cremation is not forbidden.
Nursing considerations Necessary medical treatment can be carried out without delay, and surgery and blood transfusions may be carried out as necessary. Transplants and organ donation are an individual and family matter; there are no religious objections 13
Page 93 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
RELIGIOUS SOCIETY OF FRIENDS (QUAKER) The Religious Society of Friends (Quaker) movement arose in mid 17th Century. Followers call themselves “Friends of Truth” or simply “Friends”. There are no ministers or pastors. Elders or Overseers are appointed to oversee the spiritual and pastoral wellbeing of Quaker meetings and its members.
• In their meetings for worship, Quakers do not sing hymns or use set prayers, but wait on God in silence, with a member occasionally speaking briefly, praying or reading from the Bible or other religious work.
• Quakers believe the whole of life to be sacred and the experience of
God is available to everyone.
• Quakerism is a group of insights, attitudes and practices which together form a way of life rather than a dogma or creed.
• It rests on a conviction that, by looking into their inmost hearts, people
can have direct communication with their creator. This experience cannot be described in words but Quakers base their whole lives on it.
Key Issues and Special Considerations
• A Quaker may like to be visited by another Quaker. Food and Diet
• No special considerations, some Quakers are vegetarian and a few are vegan.
Care of the dying and what to do after death
• There are no special rituals or practices for the dying. • Patients will appreciate a visit from an Elder or other Quakers who may
sit in silent worship. • A number of people are appointed to support and advise families after
death and to assist with practical arrangements. • No religious objections to post mortems or transplantation. • Burial or cremation, the wishes of the deceased are respected.
Page 94 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
RASTAFARIANISM This is a growing movement which began in the 1930s in the West Indies, mainly in Jamaica and Dominica among the descendants of slave families who had come from Africa. Identification with Africa is central to their doctrine. It is linked to the roots of resistance to slavery by the ‘Back to Africa’ movement led by Marcus Garvey which raised black consciousness and self respect and has inspired faith.
• Ras (Prince) Tafari, the Emperor of Ethiopia (Haile Selassie I in 1930) is central to their belief.
• He is considered to be a divine being, the Messiah of the human race,
who will ultimately lead all black people to freedom.
• Although many groups have contributed to the beliefs of the movement, it has rejected both Jamaican and European culture and the Christian Revivalist religion predominant in Jamaica - the result is a distinct entity.
• The Old and New Testament are still regarded as scriptures although
Rastafarians do not consider themselves to be Christians.
• For them, Christ’s spirit has been reborn in Ras Tafari, the New Messiah.
• They believe they are the true Jews who will eventually be redeemed
by repatriation to Africa, their true home and heaven on earth.
• It is a personal religion with no church buildings, set services or official clergy.
• All members share in the religious aspects and have a deep love of
God.
• Many Rastafarians are converts to the religion and members of the faith are readily identified by their distinctive hairstyle. Dreadlocks or ‘locks’ are the symbol of faith and a sign of black pride.
Key Issues and Special Considerations
• Rastafarian women dress modestly at all times and this must be respected in hospital.
• There is a taboo on the wearing of second-hand clothing. Therefore,
they may be unwilling to wear hospital garments which have been worn by others. Disposable theatre gowns may be preferred.
Page 95 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Food and Diet
• All forms of pig meat are forbidden • Some feel that all meat is unnecessary and follow a vegetarian diet. • Certain fish are regarded as unwholesome: herring and sardines, in
particular, are not acceptable. • Orthodox Rastafarians do not take stimulants ie. alcohol, caffeine or
tobacco. • Rastafarians follow the dietary regulations with varying degrees of
strictness. The most orthodox eat ‘I-tal’ or ‘natural’ foods. • Processed and preserved foods are excluded since food additives are
believed to pollute the body and soul. • Canned food is also avoided. • Meat, poultry, eggs and diary products are unacceptable, while alcohol
and salt are prohibited. • A second group of Rastafarians accept the central tenets of the ‘I-tal’
code, but consume dairy products, small quantities of scaled fish, sea-salt and other seasonings.
Care of the dying and what to do after death
• Family members may pray at the bedside but there are no rites or rituals before or after death.
• At death, routine last offices are appropriate. • Few Rastafarians would agree with a post mortem unless it is ordered
by the Coroner. • Organ donation/transplantation is considered extremely distasteful,
although reception to and from family members may be considered. • Fear of contamination of the body will influence the attitude of
transfusion and transplantation. • There is also a belief that to do so is to interfere with God’s plan for
mankind. • Burial is preferred but cremation is not forbidden.
Nursing Considerations
• They will be unwilling to receive any treatment which might contaminate the body and some may reject western style treatments eg. Blood transfusions, blood donors, organ transplants. There is a belief that to do so is to interfere with God’s plan for mankind.
• Some will prefer to try alternative therapies such as herbalism,
homeopathy or acupuncture.
• Visiting the sick is important and visits are often made in groups. As the visiting allocation is usually two visitors to a bed, Rastafarian visitors often feel they are made unwelcome in the hospital environment.
Page 96 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
RASTAFARIAN Festivals and Holy Days listed by month: July Birthday of Haile Selassie I September Ethiopian New Year’s Day November Anniversary of the Crowning of Haile Selassie I December Christmas
Page 97 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
ROMANY ORIGIN Includes English, Irish, Scottish and Welsh Travellers and those who live on a permanent site. Those in transit and travellers who are settled in houses, although relinquishing their nomadic lifestyle, do not lose their ethnic identity.
• Many people of Romany origin are Christians. • Travellers often experience difficulties in seeing a GP. When this
happens, they will present themselves at A&E (their only means of gaining health care needed)
• Romanes (Romany language) is still spoken today. However, the majority of travellers speak English.
• They may need assistance with the filling in of forms. Key Issues and Special Considerations
• Romanies do not believe in washing clothes in the same bowl in which vegetables or food are prepared. A separate bowl is kept for washing face and hands etc. Many feel it is mochardi (unclean) to do otherwise.
• From the age of eleven and throughout adulthood, people of Romany
origin do not like undressing in front of others (out of modesty). In addition to this, they prefer to keep legs and feet covered – it is considered to be rude to do otherwise.
• Older Romany people will not wash their hair – it is clean from its own
natural process and cleanliness is aided by the use of hedgehog oil.
• Older people often use bacon fat as a moisturiser, particularly on their arms.
• Patients may wish to see a Chaplain and/or request a Bible.
• Catholicism does forbid the termination of pregnancy and, indeed,
many Travellers (irrespective of religion) do not agree with abortion other than on medical grounds.
Food and Diet
• There are no general dietary requirements
Page 98 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Nursing Considerations
To increase a sense of trust when working with Romani patients and families, remain consistent, reliable, and clear. Ensure that the plan of care addresses issues that are important to the patient and family. Review the plan of care in shift report and stress to all staff the importance of closely following the plan as written. Be a reliable nurse: Let the patient and family know when you will be in the room and how to reach you on the floor. Either inform them of when you will do specific nursing interventions or negotiate a time with them. Consider using an interpreter if the patient’s first language is not English. Since illiteracy is common in the Romani population, provide a variety of educational materials, including videos, photos, pictures, and diagrams, as well as written information. Respect cultural traditions and taboos when caring for Romani patients and their families and consider addressing Romani cultural traditions and taboos in the plan of care as applicable.
Loyalty to the family and community (also referred to as the tribe and clan) is the most important universal value in Romani culture. During hospitalization, many members of the extended family will want to be with the patient at all times. Up to 100 family members may be present when a patient is hospitalized. The number increases with the seriousness of the health problem. Understanding Romani family structure and the importance of family presence during hospitalization will help nurses provide more effective interventions for the patient.
Being present with sick family members is a sign of respect and a duty. Try to provide a private room for patients and a visiting room for family members, who will want to remain with the patient — or at least on the hospital premises — while he or she is hospitalized. Often family members will want to participate in the care of the patient. Negotiate this with family members, allowing them to participate as appropriate. Provide education and equipment as indicated. For example, allowing the family to give the patient a bed bath and help with meals will increase the satisfaction of both patient and family. The patient feels cared for, and family members know that they are helping the patient.
When a Romani patient is hospitalized, ask the patient and the nuclear family to identify one to two contact people. The family will typically choose family decision makers. This supports the concept that family input is important in developing the plan of care. These contacts will be the people to whom you provide daily updates. Ask the family to inform the rest of the community of this arrangement, explaining that you cannot communicate with more than two members of the family without it interfering with your care of the family member and other patients.
Several authors note that Romani family members have the reputation of being “demanding” and “aggressive” in the hospital. Family members may insist that their loved one be cared for by older, well-known physicians. They
Page 99 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
may also demand a specific treatment or medication. Clearly explain how clinical decisions are made in your organization and how to interact with staff. Ask the contact people to keep a list of questions to give you once or twice per shift. If the family exhibits unacceptable behaviours, talk directly with those who are acting inappropriately and follow up with the contact people.
Romani rules about hygiene and cleanliness are based upon the concept of impurity. This concept includes ideas of physical impurity or uncleanliness as well as moral impurity. For the body to be clean, the top and bottom halves of the body must be kept separate. The bottom of the body, from the navel down, is considered unclean. Secretions from the bottom of the body are thought to be dirty and shameful. The top of the body is clean, and secretions from the top of the body are not considered unclean or shameful. For example, sputum is considered to have curative properties, and Roma use it to clean cuts and scratches. Serious illness can occur when a Romani person fails to keep sections of the body separate.
To respect a Romani patient’s beliefs about cleanliness, be diligent about caring for the top and bottom of the patient’s body separately. When bathing a Romani patient, bring two sets of soap and towels to the room. Wash the patient below the navel with one bar of soap and one set of towels and use a fresh set when you wash the top of the body. If you are using a basin, use two separate basins or thoroughly wash the basin before moving to the other part of the body. Make sure to wash your hands before you touch a patient or family member. If you are examining a patient, wash your hands after you have touched the lower part of the patient’s body. Since the lower part of the body is considered unclean and shameful, be sure to provide privacy during examinations and use draping for modesty.
Ask female patients whether they would like a chaperone during exams; many women will want a family member to chaperone rather than a healthcare worker they do not know. Allow Romani patients to wear their own bedclothes when possible. It is humiliating for a Romani patient to wear a hospital gown and expose his or her legs.
Care of the dying and what to do after death
• Travellers family and friends, from around the country will want, need to see, and be with the person before they die. This often means there will be large numbers of people visiting.
• After death, the family will request that the person be laid out in
clothing of their choice.
• Family and friends will often place items in the coffin; these will be things that the deceased person was fond of eg. jewellery, photographs, children’s toys etc.
Page 100 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
• The family will also want to take the person back with them in order to sit up all night with them, allowing family and friends to pay their last respects before the funeral the next day.
• Burial is preferred but cremation is not forbidden. However, the
majority of Romanies do not believe in cremation.
• There are no religious/cultural objections to the giving or receiving of blood or organs.
Festivals and Holy Days – see Christian Faith
Page 101 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
SEVENTH DAY ADVENTISTS The Seventh Day Adventists grew out of the world-wide religious revival in the mid 19th Century, believing biblical prophecies that the Second Coming of Christ is imminent. When this did not happen by 1840, a group of disappointed Adventists continued their study and concluded that the second coming of Christ was still in the future. The Church began formally in 1863 and based its faith and practice on 27 fundamental beliefs. Key Issues and Special Considerations
• They do not smoke or drink alcohol. • They will only take prescribed drugs.
Food and Diet
• Some choose not to take caffeinated drinks. • Pork and shellfish will not normally be eaten. • Some choose to be vegetarians or vegan.
Care of the dying and what to do after death
• There is no objection to the giving or receiving of blood transfusions or organ transplant or donation.
• A service by an Adventist Minister may be requested just prior to death, when the patient will be anointed.
• The family will want to be present for this service • Burial or cremation is a personal choice.
Page 102 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
SIKH Sikhs believe in one God, and many cycles of rebirth. They request equality of all people, regardless of caste, colour, creed or sex. The birth place of Sikhism was in Punjab, India. They believe that God is the only reality and that spiritual release can be obtained by taming the ego through devotional singing, recitation of the divine mane, meditation and service.
• Prayers are read five times daily. • Sikhs do not smoke and adultery is forbidden. • To indicate equality, all men are given the name Singh (which means
Lion). All women receive the name Kaur (princess).
Sikhs, as an act of faith, wear: o Kesh (long hair which is kept under a turban) o Kangha (a small comb which is worn in the hair at all times) o Kara (a steel bracelet or ring which is worn on the right wrist) o Kachhla (a special type of underwear) o Kirpaan (a sword symbolically worn by baptised Sikhs)
These are known as the “5 K’s”. Key Issues and Special Considerations
• Female doctors for female patients, whenever possible.
• The five K’s worn by Sikh men should not be disturbed. If it becomes necessary for the removal of one of these, the reasons should be explained very carefully to patient and family.
• The Kara should only be removed if surgery or x-ray is to be performed
on the right arm. For other operative procedures, this should be concealed with tape.
• Most Sikhs are accustomed to having water in the same room as the
toilet. Therefore, a bowl of water should always be provided when a bedpan has been used.
Food and Diet
• Sikhs are basically Lacto-vegetarian. • Beef and pork are not normally eaten. • Many will not accept fish, eggs and meat. • The Sikh community primarily originates from the Indian Punjab. Their
religion, Sikhism, draws upon both Hindu and Muslim traditions. Consequently, vegetarianism is not uncommon and Sikhs who do eat meat will not eat beef or pork.
Page 103 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
• However, non-vegetarian Sikhs will usually consume mutton, poultry, fish, eggs and dairy products such as yoghurt, buttermilk and panir (home-made cheese).
• The staple cereal for Punjabs is wheat. Although rice is eaten, it is less important in the diet.
Care of the dying and what to do after death
• The family will normally be present and say prayers. • At death, routine procedure may be performed. Do not remove the
Five K’s. • There is no religious objection to post mortem or transplantation. • The body should be released as soon as possible to enable the funeral
to take place. • Sikhs are always cremated.
Nursing Considerations - Respect modesty and privacy (knock on the door; announce your
arrival, etc.).
- Do not interrupt a praying patient for routine care.
- Respect the patient's personal space by limiting unnecessary touching.
- Be sensitive to the significance of the Sikh's five K's, (religious symbols or articles of faith) which they may choose to wear on their person at all times. Again, they are uncut hair (Kesh), a wooden comb (Kangha), a steel bracelet (Kara), underwear (Kachhehra), and a ceremonial sword (Kirpaan)· After removing their headdress, Sikh patients may want to keep their head covered with an alternative covering such as a small turban or a scarf. (A surgical bouffant cap is acceptable.) The headdress should be respected and, if removed, should be given to the family or placed with the patient's personal belongings. Do not place the headdress with the shoes.· Infants may be required to wear religious symbols e.g. "Kara" (a steel bracelet).
- Consult patient, family (or the parents in case of a child) prior to shaving or removing hair from any part of the patient's body. This applies to both male and female patients.
- Sikh women may insist on covering their bodies with more than a hospital gown. They may request that when possible, examinations be done while a female patient wears a gown.
- Although Sikhism does not ban treatment from being provided by a practitioner of the opposite sex, providing the patient with of the same sex practitioner when possible is preferable, especially if the patient requests it.·
Page 104 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
- Many Sikhs are new immigrants from Punjab, or other countries and may have language comprehension problems. Therefore, take time to explain tests, procedures, side effects and treatments to the patient and appropriate family members. It may be necessary to arrange for a Punjabi language interpreter.
- Cleanliness is part of the Sikh way of life. Daily bathing and personal hygiene care should be provided unless advised otherwise by the attending physician due to a medical reason. Washing and conditioning of hair, including male facial hair, with shampoo or soap should be done as frequently as needed. Hair can be dried naturally or with an electric hair dryer. Hair should be combed daily at a minimum.· It is a Sikh cultural and religious practice to visit the sick. Be open and understanding of visits by family members, children and well wishers, when practical.
SIKH Festivals and Holy Days listed by month: January Birthday of Guru Gobind Singh April Vaisakhi (Baisakhi) June Martyrdom of Guru Arjan October Divali November Birthday of Guru Nanak November Martyrdom of Guru Tegh Bahadur
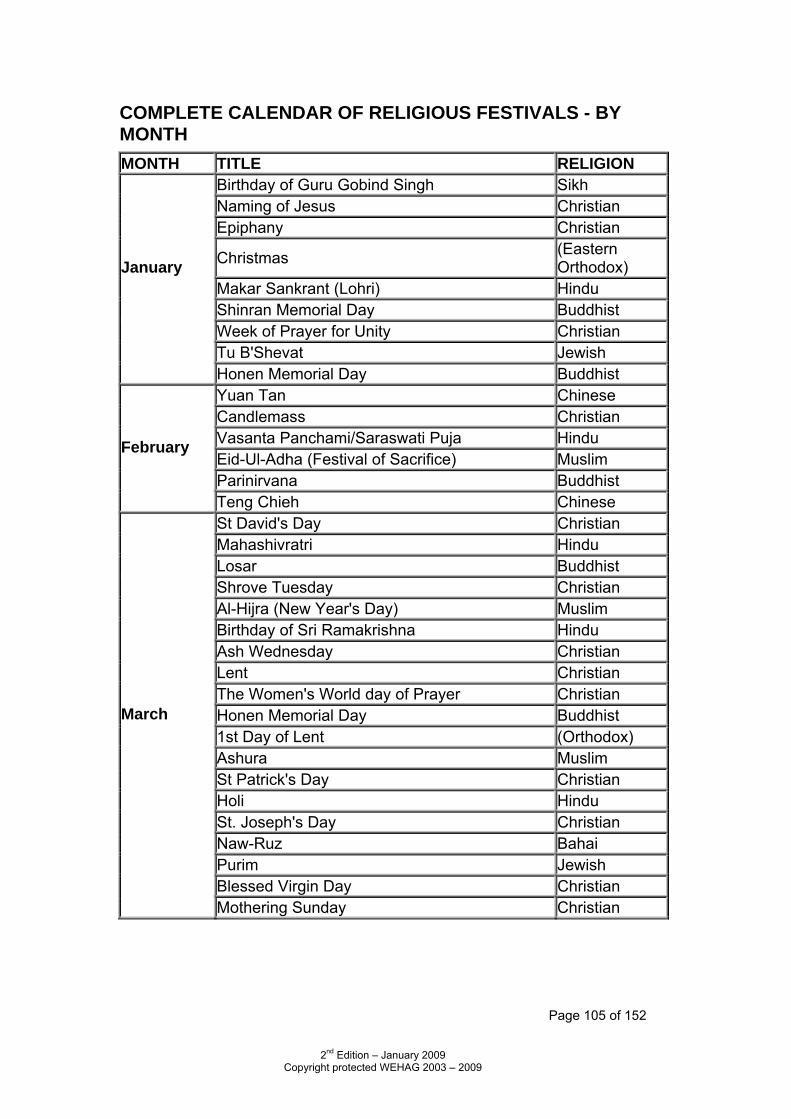
Page 105 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
COMPLETE CALENDAR OF RELIGIOUS FESTIVALS - BY MONTH MONTH TITLE RELIGION
Birthday of Guru Gobind Singh Sikh Naming of Jesus Christian Epiphany Christian
Christmas (Eastern Orthodox)
Makar Sankrant (Lohri) Hindu Shinran Memorial Day Buddhist Week of Prayer for Unity Christian
January
Tu B'Shevat Jewish Honen Memorial Day Buddhist
Yuan Tan Chinese Candlemass Christian Vasanta Panchami/Saraswati Puja Hindu Eid-Ul-Adha (Festival of Sacrifice) Muslim Parinirvana Buddhist
February
Teng Chieh Chinese St David's Day Christian Mahashivratri Hindu Losar Buddhist Shrove Tuesday Christian Al-Hijra (New Year's Day) Muslim Birthday of Sri Ramakrishna Hindu Ash Wednesday Christian Lent Christian The Women's World day of Prayer Christian Honen Memorial Day Buddhist 1st Day of Lent (Orthodox) Ashura Muslim St Patrick's Day Christian Holi Hindu St. Joseph's Day Christian Naw-Ruz Bahai Purim Jewish Blessed Virgin Day Christian
March
Mothering Sunday Christian
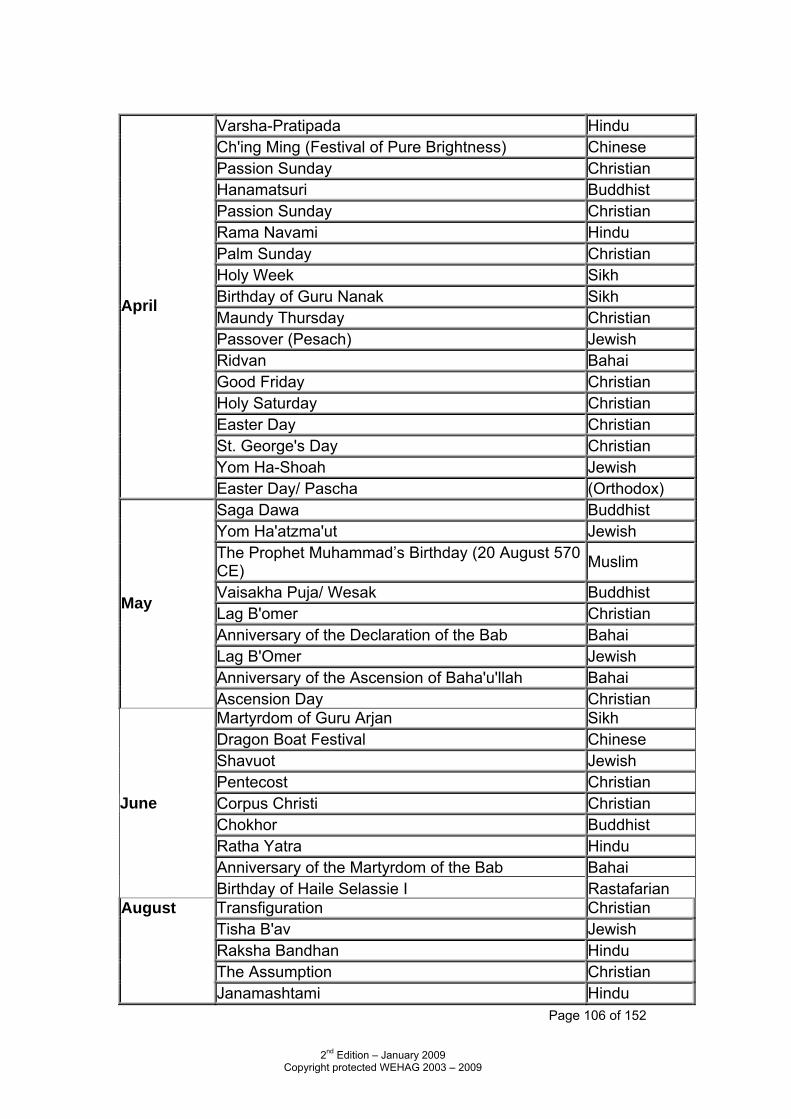
Page 106 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Varsha-Pratipada Hindu Ch'ing Ming (Festival of Pure Brightness) Chinese Passion Sunday Christian Hanamatsuri Buddhist Passion Sunday Christian Rama Navami Hindu Palm Sunday Christian Holy Week Sikh Birthday of Guru Nanak Sikh Maundy Thursday Christian Passover (Pesach) Jewish Ridvan Bahai Good Friday Christian Holy Saturday Christian Easter Day Christian St. George's Day Christian Yom Ha-Shoah Jewish
April
Easter Day/ Pascha (Orthodox) Saga Dawa Buddhist Yom Ha'atzma'ut Jewish The Prophet Muhammad’s Birthday (20 August 570 CE) Muslim
Vaisakha Puja/ Wesak Buddhist Lag B'omer Christian Anniversary of the Declaration of the Bab Bahai Lag B'Omer Jewish Anniversary of the Ascension of Baha'u'llah Bahai
May
Ascension Day Christian Martyrdom of Guru Arjan Sikh Dragon Boat Festival Chinese Shavuot Jewish Pentecost Christian Corpus Christi Christian Chokhor Buddhist Ratha Yatra Hindu Anniversary of the Martyrdom of the Bab Bahai
June
Birthday of Haile Selassie I Rastafarian Transfiguration Christian Tisha B'av Jewish Raksha Bandhan Hindu The Assumption Christian
August
Janamashtami Hindu
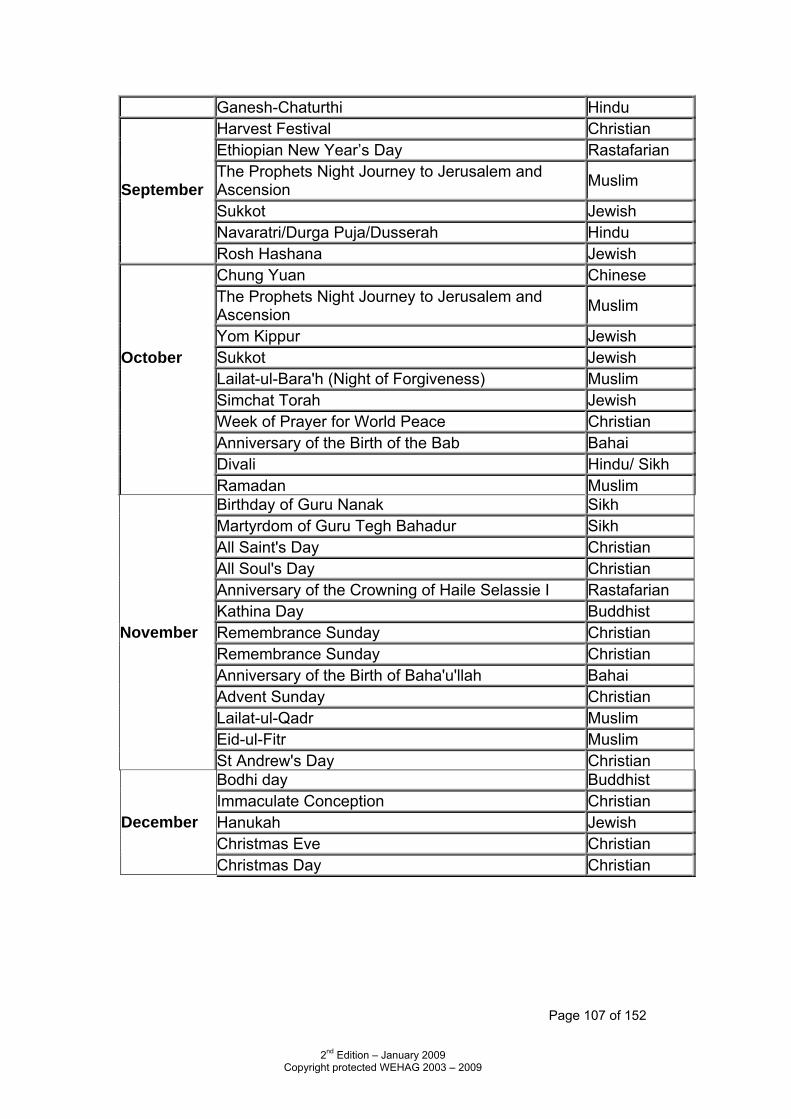
Page 107 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Ganesh-Chaturthi Hindu Harvest Festival Christian Ethiopian New Year’s Day Rastafarian The Prophets Night Journey to Jerusalem and Ascension Muslim
Sukkot Jewish Navaratri/Durga Puja/Dusserah Hindu
September
Rosh Hashana Jewish Chung Yuan Chinese The Prophets Night Journey to Jerusalem and Ascension Muslim
Yom Kippur Jewish Sukkot Jewish Lailat-ul-Bara'h (Night of Forgiveness) Muslim Simchat Torah Jewish Week of Prayer for World Peace Christian
October
Anniversary of the Birth of the Bab Bahai Divali Hindu/ Sikh Ramadan Muslim
Birthday of Guru Nanak Sikh Martyrdom of Guru Tegh Bahadur Sikh All Saint's Day Christian All Soul's Day Christian Anniversary of the Crowning of Haile Selassie I Rastafarian Kathina Day Buddhist Remembrance Sunday Christian Remembrance Sunday Christian Anniversary of the Birth of Baha'u'llah Bahai Advent Sunday Christian Lailat-ul-Qadr Muslim Eid-ul-Fitr Muslim
November
St Andrew's Day Christian Bodhi day Buddhist Immaculate Conception Christian Hanukah Jewish Christmas Eve Christian
December
Christmas Day Christian
Page 108 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
5. ASYLUM SEEKERS AND REFUGEES The following information is accurate at the time of print. Home Office policies and procedures can and do change making it advisable to check details with an Office of the Immigration Services Commissioner (OISC) registered advice agency eg. Refugee Action Liverpool. (Extract from DOH Resource Information Pack: Providing Health & Personal Social Services for Asylum Seekers dispersed through the National Asylum Support Service) Although asylum seeker/refugees are not a homogenous group, but people who come from diverse backgrounds and cultures, some of the components of refugee experience will be common to all.
The refugee experience is made up of three parts: 1 Pre-flight Experience
This may include oppression, persecution, harassment, conflict, witnessing combat, imprisonment, violence, torture, rape, fear, famine, death of family and friends.
2 Flight
This may involve escape, paying traffickers to cross borders, hazardous conditions, the fear of being discovered and imprisoned, uncertainty, physical and sexual abuse, deprivation, separation and loss of family members.
3 Exile
The most common are anxiety about the outcome of asylum claim, fear of deportation, detention, poverty, homelessness, cultural shock, language barrier, racism, isolation, unemployment, boredom, homesickness, separation and loss of family, friends, community, status, occupation, income and home, and guilt and anxiety about those left behind. Feelings of insecurity, powerlessness and inability to settle.
Asylum seekers/refugees are often very resourceful people who have survived extremes of stress. Mental health problems that they may suffer from are no different to those of indigenous people but their problems may be expressed in ways that reflect their cultural backgrounds which may be very different to those of many indigenous people, and also reflect stresses and strains that may not be familiar to mental health staff.
Page 109 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Key Definitions & Documentation This section contains both definitions commonly used in reference to refugees and information on the most common documents issued to asylum seekers, refugees and those with leave to remain by the Home Office and the Immigration Service. 1951 United Nations Convention relating to the status of Refugees The convention was drafted in the context of an estimated 30 million refugees inside post war Europe, and only applied to European nationals. In 1967, a UN protocol extended the convention to cover anybody, anywhere in the world. Currently, 136 countries have signed up to the UN convention on refugees and are committed to certain duties, including: • Non-refoulement (not returning someone to a country where s/he would
be in danger) • Protection (having a system in place to protect refugees) • Equal rights (to award recognised refugees the same rights as other
members of society) The interpretation of these duties varies from country to country. Asylum seeker - a person who has made an application for refugee status in line with Immigration Rules and the guidance set out in the Refugee Convention (the Refugee Convention is a general phrase used to cover the 1951 Convention and its 1967 Protocol). Once a person’s asylum application has been assessed by the Home Office, they are given a decision. This could be: 1. Person granted asylum - a person will be granted asylum if they meet the requirements of paragraph 334 of the Immigration Rules. In general terms, where a person is able to demonstrate a fear of persecution, if returned to their country, for reasons of race, religion, nationality, membership of a particular social group or political opinion and the person doesn't fall to be excluded from the provisions of the Refugee Convention, they will be granted asylum. A grant of asylum means that a person has been recognised as a refugee. Since August 2005, people are now only granted 5 years refugee status, during which time the Home Office can review their claim in some situations eg. If something changes in the country of origin so UKBA considers it now safe for them to return. If the 5 years goes by and UKBA have not reviewed their claim, refugees can then apply for indefinite leave to remain. 2. Refusal - the person’s application is rejected. When a person is refused refugee status, they will either have a suspensive or a non-suspensive right of appeal (some may choose not to appeal). If someone has a non-suspensive appeal, they will be required to return to their own country in order to exercise that right of appeal. This applies to 17 countries at the moment.
Page 110 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
However, most will have a suspensive right of appeal, meaning their removal is suspended until they have exhausted all appeal rights. Some people, on appealing, may be given granted asylum or otherwise. A person who no longer has any appeal rights in the United Kingdom will be removed or expected to leave the United Kingdom. If they do not leave, they will be an over-stayer. Sometimes, although a person has exhausted their appeal routes, it is not possible for them to return to their country – for example, if there is no safe route in existence or if the person is in the late stages of pregnancy. Such people can apply for section 4 or ‘hard case’ support, which comprises basic accommodation and £35 in vouchers per week. Support does not continue until the person can safely return. It is regularly reviewed, has very strict criteria, and is withdrawn unless the person can prove that they are unable to leave the UK (eg. because they would not survive the journey back/because they have outstanding legal rights to be in the UK/because there is no route of return to their country). Support continues until the person can safely return to their country of origin. The majority of refused asylum seekers are not eligible for any form of support and a large number become destitute in the UK. 3. Person given humanitarian protection status - will be granted to a person who has failed to demonstrate a claim for asylum but is able to demonstrate that, if returned, they would face a serious threat to life or person (subject to certain exclusions) arising from:
• the death penalty • unlawful killing • torture, inhumane or degrading treatment or punishment.
Since August 2005, humanitarian status is given for up to five years and is similar to refugee status (UKBA can review this during the 5 years if the situation changes in the country of origin) but humanitarian protection in practice is rarely granted. After 5 years, people can apply for ILR. 4. Person given discretionary leave to remain - will be granted to an applicant who:
• has an Article 8 claim (a claim to stay based on keeping a family united);
• has an Article 3 claim only on medical grounds or severe humanitarian cases;
• is an Unaccompanied Asylum Seeking Child (UASC) for whom adequate reception arrangements are not available in their own country;
• would have qualified for asylum or Humanitarian Protection but has been ‘excluded’ (eg. if the person is a known terrorist or serious criminal);
• is able to demonstrate particularly compelling reasons why removal would not be appropriate.
Page 111 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Discretionary leave to remain is given for up to three years and is normally only given to unaccompanied children seeking asylum. People can apply for the leave to be extended for up to 3 more years. If so, the claim is reviewed. After 6 years, people can apply for ILR but the claim is first reviewed again.
5. Person given exceptional leave to remain (pre-April 2003 only) - exceptional leave would have been granted where a person was able to demonstrate compelling compassionate or humanitarian reasons why they should not be removed from the United Kingdom. Exceptional leave to remain was replaced by humanitarian protection status and discretionary leave to remain on April 1st 2003, though persons given a decision before April 1st 2003 could be in the UK under this status. Exceptional leave to remain was given for up to 4 years.
Documentation SAL1: The Standard Acknowledgement Letter or 'SAL' is given to a person who has claimed asylum at a port of entry. It confirms that a claim for asylum has been made and that the person is currently awaiting an initial decision. It is issued if an immigration officer is satisfied with an asylum seeker’s identity documents and that the person should be given Temporary Admission. The SAL can be used as an identity document in establishing entitlement to a range of services. SAL2: The SAL2 Standard Acknowledgement Letter is given to a person who has claimed asylum after entry into the UK. It confirms that a claim for asylum has been made and that the person is currently awaiting an initial decision. The SAL can be used as an identity document. In some instances, a SAL1 can be replaced with a SAL2 if, for example, a child subsequently joins the main applicant. However, this person is still considered an “on arrival” applicant. ARC: this Application Registration Card will replace SAL1/SAL2 and will store asylum seeker data on the micro-chip
IS96: a document notifying a person that they have been granted 'Temporary Admission'. It is given at the port of entry. If the person was not able to satisfy the immigration officer of their identity they may only be issued with an IS96. Since April 1998, an asylum seeker should have been given a SAL even if they did not have documentary proof of their identity. Thus, if someone has a SAL1 they should also have an IS96. If they have a SAL2, they would not normally be expected to have an IS96.

Page 112 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
GEN19: a document indicating that an individual has been granted ELR in the UK. Since July 1998, a grant of ELR has consisted of four years’ leave to remain, after which time, an application for 'indefinite leave to remain' can be made. All asylum seekers are entitled to free healthcare, as are all refugees, those with humanitarian protection and discretionary leave. As a result of a recent court case, refused asylum seekers are also entitled to free healthcare (though this may change if UKBA appeals the decision). All emergency healthcare is free of charge irrelevant of immigration status. If a hospital believes that someone is required to pay, they should first treat the patient, then consider payment. In terms of primary care, GPs always have the discretion to register refused asylum seekers and it would be discriminatory to refuse to register a patient on the grounds of their race or ethnicity. All asylum seekers and refugees (and those with humanitarian protection and discretionary leave) are entitled to free primary healthcare and can apply for an HC2 for help with prescription charges etc dependent on their income (just as for a British resident).
Page 113 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Asylum Seeker Resources HARP - www.harpweb.org.uk The Health of Asylum Seekers and Refugee Portal is a key source of information for health professionals working with asylum seekers. Information currently available includes: • Vital Resources - introduces health workers to key policies & issues
along with funding opportunities. • Social Information - includes information on unaccompanied minors &
refugee health professionals. • Cultural Information - includes reference to cross-cultural issues, country
profiles & a guide to languages. • Practical Resources - includes a model asylum seeker “welcome pack”,
translated instructions for taking medicines, multi-cultural leaflets on identifying child abuse and more.
• Multi-lingual Appointment Card - a downloadable resource allowing you
to print a patient’s appointment card in over 30 different languages. • General Care - general health information with some information specific
to women, children and men. • Health Events/Training Opportunities Other guidance Health staff who are working with asylum seekers and refugees are also recommended to read ‘Meeting the Health Needs of Refugee and Asylum Seekers in the UK’ by Angela Burnett and Yohannes Fassil. This is a resource pack aimed at both clinicians and service planners, particularly those with less experience of working with asylum seekers and refugees. The pack contains a wealth of information on detailed aspects of healthcare not provided here – from dermatology to dental problems, along with background information on the asylum process and discussion of related issues such as legal support, schooling/education and tracing missing family members. Many practical suggestions and models of good practice are given throughout. The pack is available at: http://www.london.nhs.uk/newsmedia/publications/AsylumRefugee.pdf
Page 114 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Asylum Seeker Information Support Group (Wirral)
This group was formed in 2002 by health, local authority and police as a means of providing support for both asylum seekers and staff needing to provide health, social, housing and educational services.
Although Wirral is not a designated Dispersal area, there have been,
and still are, a number of Asylum Seekers who have resided on Wirral for certain periods of time and who require appropriate services to meet their needs as either individuals or families.
A Protocol is currently being developed (awaiting approval by the
Caldicott Guardians) in order that information can be shared across agencies on a ‘need to know‘ basis for the benefit and in the best interests of the individual requiring care and or support from the various agencies.
A hand held record will be introduced for Asylum Seekers and New
Immigrants and use will be made of the DOH Resource Information Pack: Providing Health & Personal Social Services for Asylum Seekers dispersed through the National Asylum Support Service due for publication mid-June 2003.
The group has already circulated information to various agencies re.
the Harp website and the multilingual appointment card and also receives the monthly Asylum Seeker Newsletter from the DOH Asylum Seeker Co-ordination Team.
The Education & Cultural Services Department of Wirral Borough Council has produced GUIDELINES FOR TEACHERS WORKING WITH REFUGEE CHILDREN issued in May 2002 by the Team for English as an Additional language (TEAL). This most useful booklet advises on use of interpreters, preparation before entry to school, language development and the linguistic background of refugee children in Britain, as well as practical information on making information guides and classroom posters. The information contained would be useful for any agencies dealing with refugee children and young families. The Team is based at Professional Excellence Centre, Acre Lane, Bromborough, Wirral and the contact is Yvonne Gibson Tel: 0151 346 6518.
Page 115 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
6. Gypsy Travellers (an extract from The Educator, the
online magazine for the professionals in Education) Who are gypsy travellers?
Gypsies, or travellers, have been one of Great Britain’s ethnic minorities for about 5000 years.
Research shows that they are descended from nomadic tribal groups who left Northern India about 1000 years ago, and moved Westwards across Europe, some groups remaining and settling in each country which they passed through.
The Romani language, of which an Anglicised form is still used by travellers in England, has its roots in Sanskrit. Throughout their history, they have followed a distinctive way of life as a nomadic people.
They have, to a large extent, remained separated from the house dwelling society, while maintaining links with it as a resourceful and versatile mobile workforce.
Although usually marrying within their own group, the Gypsies have, over the centuries, linked in with other travelling groups, who were on the road due to a variety of different circumstances – traders, craftsmen, journeymen, entertainers, the Irish travellers and the Scottish Tinkers.
They travelled and continue to travel in England, Scotland, Ireland and Wales and the families who today refer to themselves as Gypsies or Travellers, are members of ethnic groups whose claim is primarily on descent, with shared values, habits and customs.
Their transport, living accommodation and means of earning a living have changed with the times, as the house-dwellers have also changed. Some have settled in houses, on private family sites or on council sites and travel much less than before.
There are indeed many individual differences and standards of living between extended family groups of travellers, as in any community. However, all have a strong cultural bond in the common heritage of the Traveller.
Contacts listed:
GYSPY COUNCIL FOR EDUCATION, CULTURE, WELFARE & CIVIL RIGHTS
European & UK Office, Aveley Clinic, 8 Hall Road, Aveley, Essex, RM15 4HD
Tel. 01708 868986
NATIONAL GYPSY COUNCIL
Greenacres Caravan Park, Hapsford, Helsby, Warrington, WA6 0JS
Tel. 01937 842782
Page 116 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
GYSPY & TRAVELLER EVANGELICAL MOVEMENT
Tel. 01922 478965 (Midlands) 01372 376912 (South)
ADVISORY COUNCIL FOR THE EDUCATION OF ROMANIES AND OTHER TRAVELLERS (ACERT)
Moot House, The Stow, Harlow, Essex, CM20 3A
Page 117 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
7. PRACTICAL RESOURCES Interpretation and Translation Services
• NHS Communication strategies are being subject to review in order to comply with the Race Relations (Amendment) 2000 Act and the NHS Plan so that information will be available to non-English speakers as well as English speakers who, for whatever reason, are unable to read written I Information. Use will be made of audio tapes as well as translated material. Contact has already been made with the Institute of Public Service Linguists.
• Each NHS Trust now employs a Communications Manager who deals with all aspects of strategic and operational communications.
• For initial assessment and consent purposes with a non-English speaking patient, various NHS Trusts have contracted Language Line a telephone interpretation and translation service to be used by their staff. Training has been given to the healthcare workers who are involved in this contract.
• NHS Direct has also recently introduced a telephone helpline service for non-English speaking patients and have produced a series of leaflets in 27 languages to enable access to this service. These leaflets are being made available across the NHS organisations and GP surgeries in Wirral so that a similar language line service will be available for a direct caller.
THE NHS DIRECT HELPLINE NUMBER IS: 0845 4647
• The North West Ambulance Service NHS Trust has issued to all its paramedics a copy of the Multilingual Emergency Phrase Book (developed by the Ambulance Service Association of which NWAS is an affiliated body) with information on a Question and Answer format in 31 languages. A page of the various language scripts plus an illustration of British Sign Language is also incorporated into this handy booklet.
• Liverpool NOVAS (Liverpool Council) have an extensive list of
interpreters. Tel: 0151 708 8640
• Wirral Multicultural Centre provides interpreters for Cantonese, Mandarin, Urdu, Punjabi, Hindi and Bengali speaking patients. Tel: 0151 666 4547
Page 118 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Websites
• Centre for Research in Ethnic Relations www.warwick.ac.uk/go/crer • Positively Diverse http://www.nhsemployers.org/excellence/excellence-449.cfm • The Equality & Human Rights Commission www.cre.gov.uk • Tackling Racial Harassment in the NHS http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4009459 • Zero Tolerance http://www.dh.gov.uk/en/Publicationsandstatistics/Lettersandcirculars/Dearcolleagueletters/DH_4002920 • North West Ethnic Health www.ethnichealth-northwest.net • Tackling Health Inequalities: Consultation on a Plan for delivery http://www.dh.gov.uk/en/Publichealth/Healthinequalities/index.htm • Harpweb www.harpweb.org.uk
Page 119 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Other Resources The NHS Plan 2000, DOH, London http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/AnnualReports/Browsable/DH_5277178 Valuing Diversity – Black & Ethnic Health Liverpool NHS Action Plan 2001-2002, LHA http://www.nwph.net/nwpho/Publications/ethnicminority.pdf Race Equality in the Department of Health http://www.dh.gov.uk/en/Managingyourorganisation/Equalityandhumanrights/Raceequality/index.htm The Vital Connection – NHS Equalities Framework http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4007652 Study of Black, Asian & Ethnic Minority Issues, Ziggi Alexander 1999, DOH London http://www.library.nhs.uk/ethnicity/ViewResource.aspx?resID=251365 The Health Survey for England - The Health of Minority Ethnic Groups ’99. Erens B et al, 2001, The Stationery Office, London http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsStatistics/DH_4006420 Health Visitor & School Nurse Development Programme – Resource Packs, 2001, DOH, London http://www.dh.gov.uk/en/Publicationsandstatistics/Lettersandcirculars/Professionalletters/Chiefnursingofficerletters/DH_4004240
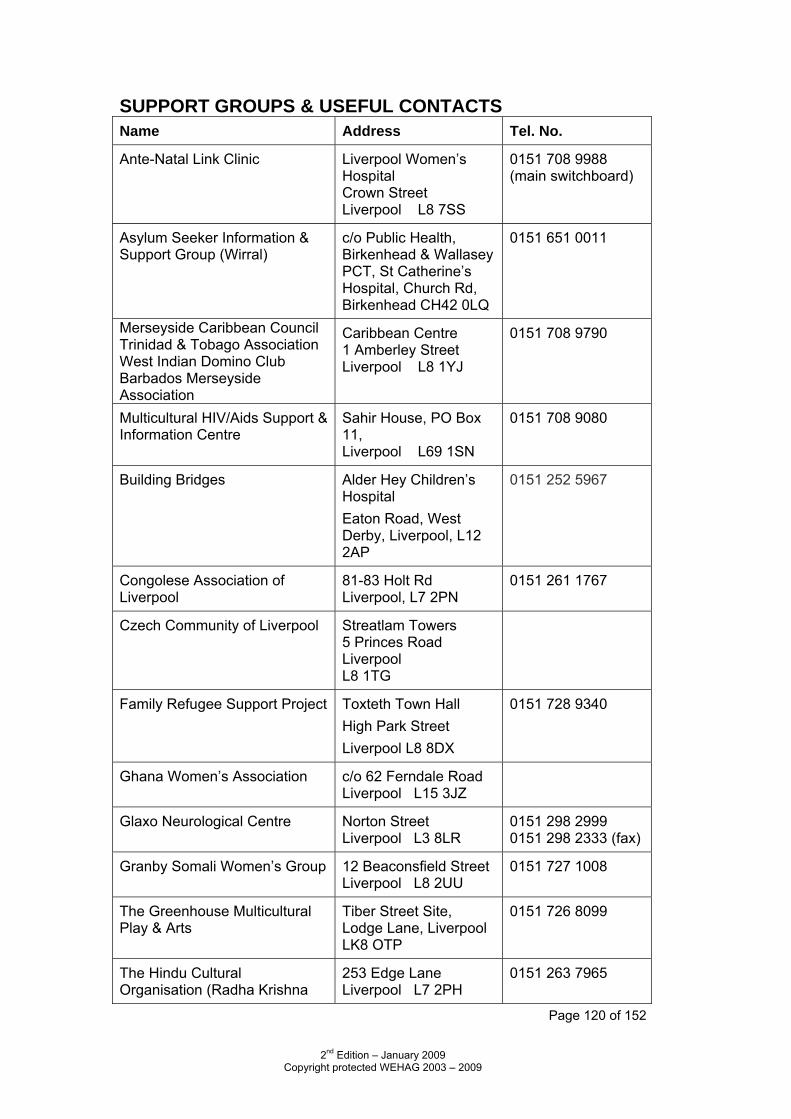
Page 120 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
SUPPORT GROUPS & USEFUL CONTACTS Name Address Tel. No.
Ante-Natal Link Clinic Liverpool Women’s Hospital Crown Street Liverpool L8 7SS
0151 708 9988 (main switchboard)
Asylum Seeker Information & Support Group (Wirral)
c/o Public Health, Birkenhead & Wallasey PCT, St Catherine’s Hospital, Church Rd, Birkenhead CH42 0LQ
0151 651 0011
Merseyside Caribbean Council Trinidad & Tobago Association West Indian Domino Club Barbados Merseyside Association
Caribbean Centre 1 Amberley Street Liverpool L8 1YJ
0151 708 9790
Multicultural HIV/Aids Support & Information Centre
Sahir House, PO Box 11, Liverpool L69 1SN
0151 708 9080
Building Bridges Alder Hey Children’s Hospital Eaton Road, West Derby, Liverpool, L12 2AP
0151 252 5967
Congolese Association of Liverpool
81-83 Holt Rd Liverpool, L7 2PN
0151 261 1767
Czech Community of Liverpool Streatlam Towers 5 Princes Road Liverpool L8 1TG
Family Refugee Support Project Toxteth Town Hall High Park Street Liverpool L8 8DX
0151 728 9340
Ghana Women’s Association c/o 62 Ferndale Road Liverpool L15 3JZ
Glaxo Neurological Centre Norton Street Liverpool L3 8LR
0151 298 2999 0151 298 2333 (fax)
Granby Somali Women’s Group 12 Beaconsfield Street Liverpool L8 2UU
0151 727 1008
The Greenhouse Multicultural Play & Arts
Tiber Street Site, Lodge Lane, Liverpool LK8 OTP
0151 726 8099
The Hindu Cultural Organisation (Radha Krishna
253 Edge Lane Liverpool L7 2PH
0151 263 7965
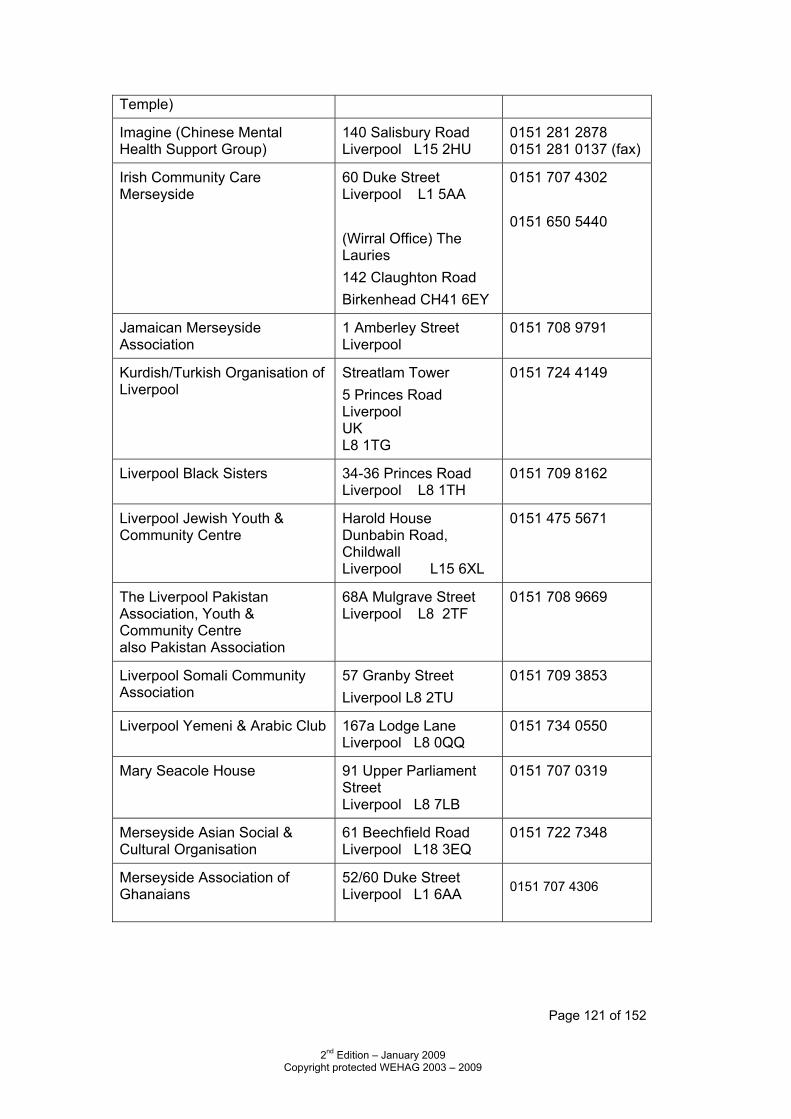
Page 121 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Temple)
Imagine (Chinese Mental Health Support Group)
140 Salisbury Road Liverpool L15 2HU
0151 281 2878 0151 281 0137 (fax)
Irish Community Care Merseyside
60 Duke Street Liverpool L1 5AA (Wirral Office) The Lauries 142 Claughton Road Birkenhead CH41 6EY
0151 707 4302 0151 650 5440
Jamaican Merseyside Association
1 Amberley Street Liverpool
0151 708 9791
Kurdish/Turkish Organisation of Liverpool
Streatlam Tower 5 Princes Road Liverpool UK L8 1TG
0151 724 4149
Liverpool Black Sisters 34-36 Princes Road Liverpool L8 1TH
0151 709 8162
Liverpool Jewish Youth & Community Centre
Harold House Dunbabin Road, Childwall Liverpool L15 6XL
0151 475 5671
The Liverpool Pakistan Association, Youth & Community Centre also Pakistan Association
68A Mulgrave Street Liverpool L8 2TF
0151 708 9669
Liverpool Somali Community Association
57 Granby Street Liverpool L8 2TU
0151 709 3853
Liverpool Yemeni & Arabic Club 167a Lodge Lane Liverpool L8 0QQ
0151 734 0550
Mary Seacole House 91 Upper Parliament Street Liverpool L8 7LB
0151 707 0319
Merseyside Asian Social & Cultural Organisation
61 Beechfield Road Liverpool L18 3EQ
0151 722 7348
Merseyside Association of Ghanaians
52/60 Duke Street Liverpool L1 6AA
0151 707 4306
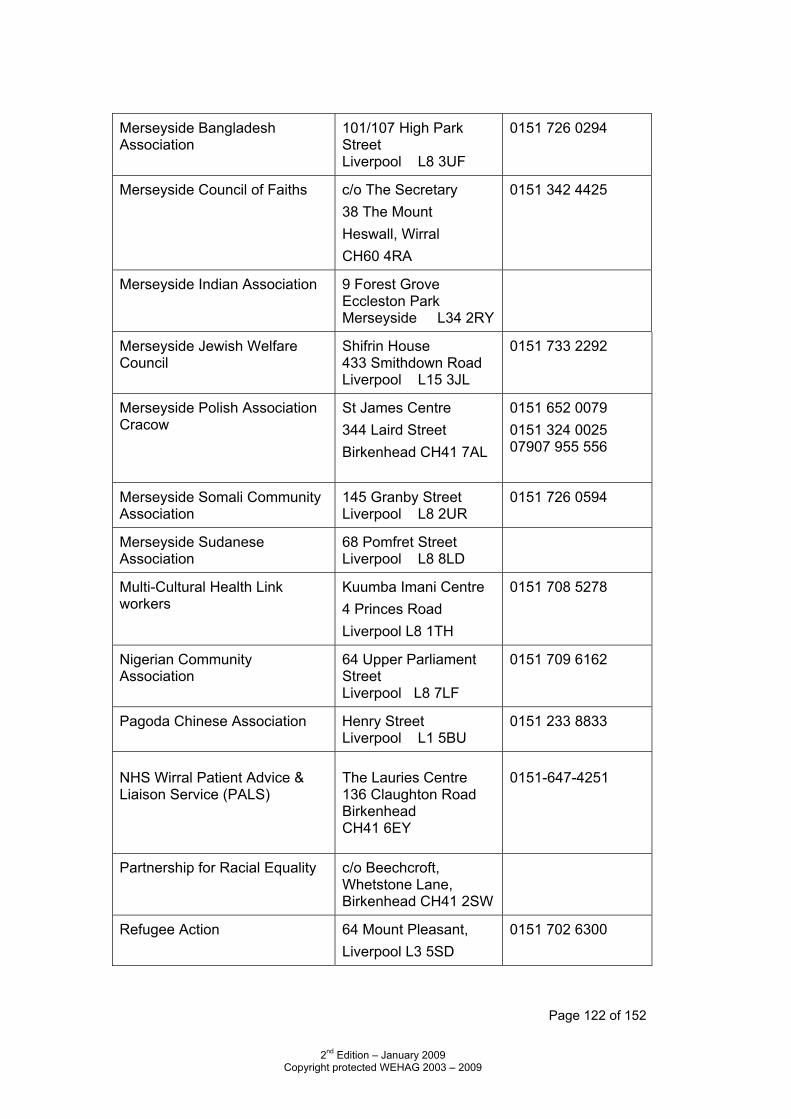
Page 122 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Merseyside Bangladesh Association
101/107 High Park Street Liverpool L8 3UF
0151 726 0294
Merseyside Council of Faiths c/o The Secretary 38 The Mount Heswall, Wirral CH60 4RA
0151 342 4425
Merseyside Indian Association 9 Forest Grove Eccleston Park Merseyside L34 2RY
Merseyside Jewish Welfare Council
Shifrin House 433 Smithdown Road Liverpool L15 3JL
0151 733 2292
Merseyside Polish Association Cracow
St James Centre 344 Laird Street Birkenhead CH41 7AL
0151 652 0079 0151 324 0025 07907 955 556
Merseyside Somali Community Association
145 Granby Street Liverpool L8 2UR
0151 726 0594
Merseyside Sudanese Association
68 Pomfret Street Liverpool L8 8LD
Multi-Cultural Health Link workers
Kuumba Imani Centre 4 Princes Road Liverpool L8 1TH
0151 708 5278
Nigerian Community Association
64 Upper Parliament Street Liverpool L8 7LF
0151 709 6162
Pagoda Chinese Association Henry Street Liverpool L1 5BU
0151 233 8833
NHS Wirral Patient Advice & Liaison Service (PALS)
The Lauries Centre 136 Claughton Road Birkenhead CH41 6EY
0151-647-4251
Partnership for Racial Equality c/o Beechcroft, Whetstone Lane, Birkenhead CH41 2SW
Refugee Action 64 Mount Pleasant, Liverpool L3 5SD
0151 702 6300
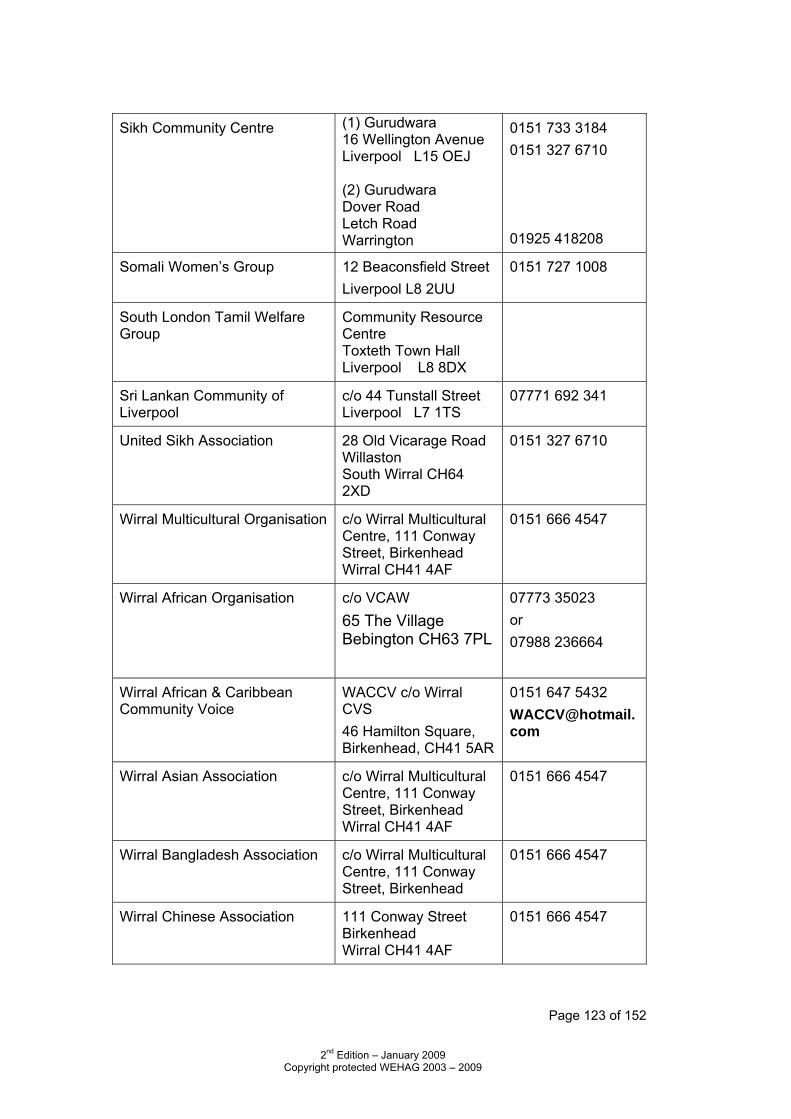
Page 123 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Sikh Community Centre (1) Gurudwara
16 Wellington Avenue Liverpool L15 OEJ (2) Gurudwara Dover Road Letch Road Warrington
0151 733 3184 0151 327 6710 01925 418208
Somali Women’s Group 12 Beaconsfield Street Liverpool L8 2UU
0151 727 1008
South London Tamil Welfare Group
Community Resource Centre Toxteth Town Hall Liverpool L8 8DX
Sri Lankan Community of Liverpool
c/o 44 Tunstall Street Liverpool L7 1TS
07771 692 341
United Sikh Association 28 Old Vicarage Road Willaston South Wirral CH64 2XD
0151 327 6710
Wirral Multicultural Organisation c/o Wirral Multicultural Centre, 111 Conway Street, Birkenhead Wirral CH41 4AF
0151 666 4547
Wirral African Organisation c/o VCAW 65 The Village Bebington CH63 7PL
07773 35023 or 07988 236664
Wirral African & Caribbean Community Voice
WACCV c/o Wirral CVS 46 Hamilton Square, Birkenhead, CH41 5AR
0151 647 5432 [email protected]
Wirral Asian Association c/o Wirral Multicultural Centre, 111 Conway Street, Birkenhead Wirral CH41 4AF
0151 666 4547
Wirral Bangladesh Association c/o Wirral Multicultural Centre, 111 Conway Street, Birkenhead
0151 666 4547
Wirral Chinese Association 111 Conway Street Birkenhead Wirral CH41 4AF
0151 666 4547
Page 124 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Wirral Ethnic Health Advisory Group
Administrator: Carol Davies
0151 651 0011
Wirral Islamic Centre & Shahjalal Mosque
309 Borough Road, Birkenhead, Wirral
0151 666 2089
NHS Wirral St Catherine’s Hospital Church Road, Birkenhead CH42 0LQ
0151 651 0011
Wirral Vietnamese Association 111 Conway Street Birkenhead Wirral CH41 4AF
0151 666 4547
Yemeni Community Association 167 Lodge Lane Liverpool L8 OQQ
0151 734 4965
Page 125 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
The Race Relations (Amendment) Act 2000 & Wirral Ethnic
Health Strategy Facts about the Race Relations (Amendment) Act 2000 This Act places a new statutory duty on all public bodies to promote race equality and to ensure that unlawful discrimination on the grounds of race does not occur. Its aim is to encourage the development of a change in culture, including policy making, service delivery and employment practice. In order to comply, the organisations must aim to:
Eliminate unlawful racial discrimination Promote equality of opportunity Promote good relations between people of different ethnic groups.
Alongside these duties, the Trusts must fulfill other specific duties laid down by the amended Act which include preparation and delivery of a Race Equality Scheme. A Race Equality Scheme involves a wide ranging review of the functioning of the organisation, including: assessing how the activities of the Trust affect ethnic minority patients and staff, monitoring service impact on ethnic groups, monitoring of employment issues by ethnic group and publishing the Scheme, together with the results of monitoring. “The NHS Plan sets out a vision that places equality, fair treatment and social inclusion at the heart of plans to modernise the service” Background to Wirral Ethnic Health Strategy In February 2001, Wirral Ethnic Health Advisory Group (WEHAG) agreed to go ahead with developing a Strategy. The first meeting was held in June with nominated representatives from all healthcare organisations on Wirral. The late Lord Chan presented an overview of Ethnic Health, and group work took place around a vision and strategic objectives. A further six meetings took place which involved the group in preparation and agreement upon standards of care and monitoring arrangements which underpin the strategy. Following the January 2002 meeting, the Strategy was duly signed by all the partners prior to the launch, in the presence of Lord Chan and Lord Hunt, the then Minister of Health on 22 March 2002. The 2003 Strategy was launched in the presence of Lord Chan and the mayor of Wirral on June 3rd 2003.

Page 126 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
• WEHAG meets bi-monthly to monitor progress of the Strategy, share best practice and disseminate information. Implementing the Strategy is part of NHS Wirrals commitment to the NHS vision of equality, fair treatment and social inclusion and, as such, is incorporated into the NHS Wirrals Race Equality Scheme, a requirement to the Race Relations (Amendment) Act 2000.
Page 127 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
9. ORGANISATIONS’ OWN INFORMATION
Merseyside Police - Wirral Community Relations Unit
The role of Wirral’s Community Relations Unit is to ensure links with individual groups and sections of the community are established, maintained and developed. What we learn from these relationships is passed on to departments across Wirral allowing us to deliver our services more effectively.
The dialogue that exists provides the community with an opportunity to share their concerns, issues and fears with us and allows us to work together with them to ensure they are addressed.
Areas of Responsibility
The Community Relations Unit works with a variety of minority communities to establish whether the service that Merseyside Police provides meets their needs.
Our areas of responsibility are listed below.
• Race, Disability & Gender Equality Schemes • Stop Search • Black & Racial Minorities • Young People • Gypsies/Travellers • Social Exclusion (Sex workers, homeless) • Asylum Seekers • Lesbian, Gay, Bisexual & Transgender Persons • Older Persons • Disability • Community Engagement
Contact Details for Wirral Community Relations Unit
Sergeant Simon Barrigan Community Relations Co-ordinator
Phone 0845 408 0508 Fax 0151 606 5464 Email [email protected] Address The Old Courthouse
Manor Road Wallasey Merseyside CH44 1BU
Page 128 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
SIGMA Units
Merseyside Police has a specialist team, Sigma, to investigate Hate Crime across the county. Hate Crime incidents will be dealt with by dedicated investigators whose sole job will be to investigate hate crime incidents in their area.
A Hate Incident is defined as: Any incident, which may or may not constitute a criminal offence, which is perceived by the victim or any other person, as being motivated by prejudice or hate.
A Hate Crime is defined as: Any Hate Incident which constitutes a criminal offence, perceived by the victim or any other person, as being motivated by prejudice or hate.
The prejudice or hate perceived can be based on any identifying factor, including the six strands of diversity, age, disability, gender, race, religion/belief or sexual orientation.
Reporting Hate Crime
You have the right to live free from harassment, as does any other person in this country. Laws exist to protect all people regardless of immigration status, race, religion, disability, transgender or sexual orientation.
Many hate crimes go unreported because people do not always report it. Victims may feel embarrassed. They may be scared that they will be attacked again or they are worried at how they will be treated by the Police. If you are witness to or a victim of crime, please contact the Police.
If you are the victim of crime or hate crime, do not suffer in silence, report it to the Police.
What number should I ring?
In an Emergency call 999.
An emergency is when:
• A crime is happening now • People are injured • People are being threatened or are in danger • The offender is still there or is nearby
You can call 999 for free from any phone. You can also use your mobile number even if you have no credit left on it.
Page 129 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Say which language you speak and, if you can, where you are. There is an interpreter service for those whose first language is not English. This means that you are able to have access to an interpreter from Language Line and there is a three-way conferencing facility between the caller, the interpreter and the operator. It may take a couple of minutes to connect to the translation service so the call handler will ask for you to remain on the line. Police officers in police cars will then come to assist you, if required.
Non-emergency
Go to a police station:
• If you are worried about being seen, you can go to a police station away from your area. We can get an interpreter for you. We can also provide you with a male or female officer, as appropriate.
Or,
Call a police station on 0151 709 6010:
• Say which language you speak and they can get an interpreter for you. Plain clothes police officers can visit you at home in a private car, so your neighbours will not know who they are. You will have to make arrangements for this first.
Report it online
Use the online reporting form at www.merseyside.police.uk. Your completed form will be transmitted to our Contact Centre and you will receive an acknowledgement email, following which our Contact Centre staff will be in touch with you within 2 hours of receipt.
If you do not receive an acknowledgement or contact from us within 2 hours, please ring 0151 709 6010.
Please tell us if you fear you will be in danger by reporting it to us.
You can also report it at specific organisations in Merseyside or designated phone lines if you do not want to tell the police. Some agencies can also help you fill in a reporting form.
• Crimestoppers is an independent charity working to stop crime. You can call anonymously on 0800 555 111
• Hate Crime can also be reported to the independent charity Stop Hate UK 24 hours a day on 0800 138 1625. Trained operators will give you advice and take the report.
Page 130 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Wirral Citizens Advice Bureau Wirral Citizens Advice Bureau (CAB), in conjunction with Wirral Advocacy, have been commissioned by the PCT since September 2006 to provide advice, information, and advocacy to people with mild to moderate mental health problems in 19 GP surgeries within NRF areas in the Wirral. The Primary Care Advice team (PCAL) consists of 3 advisers who work alongside the GPs and 2 further advisers who provide ongoing support. Each surgery has 3 appointments per session. Referrals are made through GPs and other health professionals within the surgery. We work closely with other health professionals such as the Harm Reduction Team, Primary Care Mental Health Team, Alcohol and Drugs Misuse team and Clinical Psychology. We have also built working relationships with Wirral Change, BME support service, Chairman of the Mosque, Black and Racial Minority Women’s Network and Merseyside Polish Association. We have recently been successful with our application to the Third Party Health Innovation Fund for funding to extend our project so that we can employ 2 trained advisers, one from the Eastern European Community who speaks Polish and Russian and one from the Southern Asian Community who speaks Urdu, Hindi and Bengali. By increasing the team, we will be able to engage more fully with those communities and assist in improving mental health services for these people.

Page 131 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Forum Housing Association Mission Statement - “It’s all about you” Forum Housing Association is a Registered Social Landlord and is a provider of supported housing and services for young people aged between 16 – 25. The Association has properties throughout Merseyside including Wirral, Bootle, Southport and Ellesmere Port. Each of the Association’s properties (projects) vary, some with 24 hour support, others with a limited amount. This is dependent upon specific need and the range of services required to those housed. The Association’s aim is to provide accommodation and support to young people to enable them to realise their full potential. Young people have a big voice in the Association which impacts upon service delivery. Partnership working is crucial to the Association’s success and we work with over 80 partners to deliver services to our residents and, in addition, residents and staff are involved in local community initiatives. Forum Housing Association is fully committed to the Equality and Diversity Agenda and has been recognised for being so, especially with regard to the Association’s passion to see young people grow. The Association is opposed to discrimination on any grounds and is committed to creating a culture of inclusiveness by developing a work place which reflects the local population with which we work and to help heighten staff and resident awareness to help people understand and deal with difference. The Association’s commitment to Equality and Diversity can be further highlighted by the partnership working it does with the Wirral Ethnic Health Advisory Group and the Strategic Housing Partnership Diversity subgroup. More information on Forum Housing Association, including information on our accommodation and services, can be found by visiting: www.forumhousing.co.uk Or, by contacting 0151 649 9718
Page 132 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Wirral Stop Smoking Service
Wirral Stop Smoking Service Health and Wellbeing Team Gibraltar House Kelvin Road Wallasey CH44 7JW Tel 0151 630 8383 Fax 0151 630 8390
• We are a free and confidential NHS service to help people stop using tobacco
• We offer community based support to people from BME groups, to stop smoking and chewing tobacco.
• We want to raise awareness of the health issues surrounding tobacco use in the various communities
• We aim to offer culturally appropriate support in familiar community venues, for example Wirral Multicultural Centre, Wirral Change, St James’ Centre, some GP surgeries, and can organise translation services if required.
Page 133 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Wirral Drug And Alcohol Action Team (DAAT)
DAAT brings together a wide range of local public bodies, community and voluntary organisations that are all concerned with the effects of drug and alcohol use in Wirral. We are responsible for meeting local targets, set by the Government, to reduce the harmful and health risks caused by substance misuse.
Our Vision: A Wirral society free of all the problems caused by drug and alcohol misuse.
Our Key aims are to: • Prevent harm to children, young people and families affected by
substance misuse • Protect communities through tackling drug supply, drug-related crime
and anti-social behaviour. • Deliver new approaches to drug treatment and social reintegration • Public information campaigns, communications and community
engagement DAAT is not in itself a treatment service. People seeking advice, support or treatment can access these services through our Website www.wirraldaat.org and clicking on contacts or ring free phone: ACT 0800 028 1300 – a 24/7 helpline for drug users Damage Limitation 0800 988 1421 – a local free phone for alcohol advice Frank 0800 77 66 00 – National helpline for drug and alcohol advice PADA (Parents against Drug Abuse) Local 24 hour helpline 08457 023867 www.Kooth.com – A confidential online advice and information service for young people.
Page 134 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Wirral African Organisation Address: c/o VCAW, 65 The Village, Bebington CH63 7PL The Wirral African Organisation has members from varied countries, such as Ghana, Zimbabwe, Egypt, Congo, Ethiopia, South Africa, Sierra Leone, Uganda, Zambia, Nigeria, Botswana, Gambia etc. The Wirral African Organisation meets on the first Friday of each month at Mayer Hall, Bebington from 7.00-9.00 p.m. The meetings are to promote positive African/BME culture, all topics relating to and affecting Africans/BME and issues concerning African/BME peoples’ health & well being. We support members of the organisation, and liaise/mediate on behalf of and/or between any service providers & stakeholders, including public, private and 3rd sector organisations. Please contact: Nurie Lamb, Chair person: 07773 35023 or Phillip Alliah, Vice Chair: 07988 236664
Page 135 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Wirral Black and Racial Minority Partnership (WBRMP)
Wirral Black and Racial Minority Partnership (WBRMP) is a voluntary umbrella organisation, made up of several smaller black and racial minority groups. Currently, there are 17 groups who are members, including Sudanese, Bangladeshi, African, Arab, Caribbean, Polish, Irish, and female representation.
The Partnership allows Wirral’s BRM communities to speak with one united voice.
It is one of the main engagement tools for BRM consultation within
Wirral for all its sectors.
The Partnership provides representation in the public and private arena in all matters relating to Wirral’s BRM communities.
The Partnership promotes diversity, equality and cultural awareness.
Training and information is provided to ensure that all members are
empowered and confident of their representation within local government and the services arena.
The Partnership is a Multi-Faith organisation.
The Partnership monitors, lobbies and challenges how services are
delivered in Wirral for its BRM community members.
The Partnership provides the BRM communities in Wirral with a platform to discuss and develop issues specifically relating to BRM communities.
The Partnership deals with all BRM issues, whether it relates to an
individual, a specific community, service providers or local government. The Partnership can be contacted at [email protected] or by telephoning: 07894-162612.

Page 136 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Wirral African and Caribbean Community Voice This association, formed in the year 2000, meets at the Charing Cross Methodist Church and the Wirral Multicultural Centre. The Group meets each Friday evening at 6.30 p.m.-8.30 p.m. at Charing Cross Methodist Centre, Birkenhead, Wirral.
Page 137 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Wirral Council Black Minority Ethnic (BME) Support Service Aims of the Service “To ensure effective housing support, and greater choice for the BME community across Wirral. The long term aim is to enable individuals to access services for themselves, as and when needed. Better support for better lives”. BME Support Service help The BME Support Service focuses on support services that ensure people can live safely and securely in their own homes. The support includes:
Help with managing budget and accessing welfare benefits Help to maintain their own safety in the home Helping people gain access to other services relating to housing
needs, including health and social activities Advice and support on repair works Directing people to community resources Identifying community concerns and gaps in services Addressing language barriers to access services Highlighting the importance of culture in providing services
Who is eligible for support? Anyone from the BME community including Asian, Eastern Europeans, Irish, Gypsy and Travellers, Black, South East Asian, Middle Eastern (or other ethnicity) and people of dual heritage who are employed or unemployed:
Young people (aged 18 and above) at risk People with drug or alcohol problems People with learning disabilities People with physical and sensory disabilities Older people with support needs Women at risk of domestic violence People with mental health problems People at risk of offending Homeless people/families with support needs People with HIV/AIDS Refugees Teenage parents
Contact: To find out more about the service and to check if you are eligible please contact the support officers below: Angela Sumner 0151 691 8689 Mizanur Rahman 0151 691 8685

Page 138 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Refugee Action
Refugee Action is an independent, national charity working to enable refugees to build new lives in the UK. We provide practical advice and assistance for newly arrived asylum seekers and long-term commitment to their settlement through community development work, and received 43,000 visits from asylum seekers last year. As one of the country’s leading agencies in the field, Refugee Action has 25 years’ experience in pioneering innovative work in partnership with refugees. 64 Mount Pleasant Liverpool L3 5SD Tel: 0151 702 6300
Page 139 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
10. EXAMPLES OF GOOD PRACTICE
Wirral One Stop Shops The Council is committed to improving access to services for Wirral residents. As part of that commitment, we have established a network of 13 One Stop Shops to make sure that everyone can access our services. The service has been running for over ten years and continues to improve and expand. In every One Stop Shop there are free phone links to council departments and a range of general advice leaflets. To make life easier we provide:
• comfortable seating areas • private interview rooms, if needed • disabled car parking spaces • wheelchair access • toilets with adapted access • baby changing facilities
One Stop Shop staff link services together and anticipate your needs, for example: If you are moving house then in one visit you could:
• sort out your Council Tax bill, • find out what you need to do if you are claiming Housing or Council
Tax Benefit, • find out about new childcare provision, • what days your bins are collected, • what catchment area for schools your new home is in, • where your nearest doctor or dentist is, • registering on the electoral roll
Page 140 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Below are some of the things that One Stop Shops can help you with: Housing Benefit/Council Tax Access to rented accommodation Blue Badge Scheme Electoral Register It's Your Call ( ASBO) Parking Appeals Council Job Applications Waste / Environmental Services Licensing Wirral Children’s Information Service Student Support Services Registrar Services School Admissions and Home to School Transport
Council Meetings / Agendas / Councillor & MP queries
Home Improvement Grants Leisure Services / Schemes Tourism Social Services areas Consumer Advice Pest Control / Environmental Health Education & Welfare Benefits Homeless Service Planning and Building Control Community Legal Service
One Stop Shops work with other organisations to provide help and assistance on non-council services. (Please note that some surgeries are only provided at selected sites). We work with:
Department for Work and Pensions Age Concern Merseyside Police Wirral Alcohol Services Fire Service - making referrals to Merseyside Fire and Rescue Service
for Home Fire Safety Checks Mersey travel Job Centre Plus – electronic Job points at some sites allow searches
for job vacancies. At other sites we display a small selection of available positions.
Accessibility All One Stop Shops are accessible and meet the requirements of the Disability Discrimination Act. We offer a telephone interpreting service and for customers whose first or preferred language is not English, language identification cards and dual handsets are available to make it easier to communicate with us. This service covers over 150 languages and on average it takes 30 seconds to be connected to an interpreter.
Page 141 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
ONE STOP SHOPS
Birkenhead One Stop Shop Conway Centre Conway Street Birkenhead Wirral CH41 6JD Mon – Fri 9.00 a.m. – 5.00 p.m. Open Saturday 9.00 a.m. – 12.30 p.m.
Bebington One Stop Shop Pennant House Municipal Buildings Bebington Wirral CH63 7PL Mon – Fri 9.00 a.m. – 5.00 p.m. except Wednesdays 9.00 a.m. – 4.00 p.m.
Moreton One Stop Shop Moreton Municipal Buildings Knutsford Road Moreton Wirral CH46 8TN Mon – Fri 9.00 a.m. – 5.00 p.m. except Wednesdays 10.00 a.m. – 5.00 p.m.
Heswall One Stop Shop Heswall Library Telegraph Road Heswall Wirral CH60 0AF Closed Wednesdays Open Saturday 9.00 a.m. – 1.00 pm
Seacombe One Stop Shop Dave Jackson Suite Town Hall Brighton Street Wallasey Wirral CH44 8ED Mon – Fri 9.00 a.m. – 5.00 p.m. except Wednesdays 10.00 a.m. – 5.00 p.m.
Rock Ferry One Stop Shop 257 Old Chester Road Rock Ferry Wirral CH42 3TD Mon – Fri 9.00 a.m. – 5.00 p.m. except Wednesdays 10.00 a.m. – 5.00 p.m.
West Kirby One Stop Shop The Concourse Grange Road, West Kirby Wirral CH48 4HX Mon – Fri 9.00 a.m. – 5.00 p.m. except Wednesdays 10.00 a.m. – 5.00 p.m.
Eastham One Stop Shop Mill Park Drive Eastham Wirral CH62 9AL Mon – Fri 9.00 a.m. – 5.00 p.m. except Wednesdays 9.00 a.m. – 4.00 p.m.
Page 142 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
New Brighton One Stop Shop New Brighton Community Centre 1A Hope Street New Brighton Wirral Merseyside CH45 2LN Open 11a.m. – 3 p.m. Mon - Fri
Bromborough One Stop Shop (Within Job Centre Plus) Port Causeway House, Bromborough Wirral CH62 4TG Mon & Fri 9.00a.m–1.00 pm & 2– 5.00 p.m. Wed 10.00 a.m. – 1.00p.m. & 2.00 - 4.00 pm
Hoylake One Stop (Within Job Centre Plus) Town Hall Chambers 1 The Quadrant Hoylake CH47 2HR Mon & Tues 9.00 a.m. – 1.00 p.m. Wed 1.00 p.m. – 5.00 p.m.
Liscard One Stop Shop (Within Job Centre Plus) Dominick House St Albans Road Liscard CH44 5XS Mon - Fri 9.00 a.m. – 1.00 pm & 2-5.00 p.m. Wednesdays 10.00 a.m. 1.00 pm & 2– 5.00 p.m.
Upton One Stop Shop (Within Job Centre Plus) 52 Arrowe Park Road Upton CH49 0UE Mon, Tues & Thursday 9.00 a.m. – 1.00 p.m.
Page 143 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Page 144 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
One Stop Shops: An A-Z of help that you can receive Staff within the One Stop Shops are able to provide help and advice on a wide range of issues, some of which you might not traditionally think of as being Council Services. The One Stop Shops are spread throughout Wirral and are placed in well known and easily accessible buildings. Access to rented Housing (Wirral Homes Scheme) Registering customers onto the Wirral Homes database, establishing if there are any particular circumstances in relation to their application eg. Homelessness, urgent need status being applied, help customers when making expressions of interest on properties advertised, amending details on the database. Adult Social Services Providing information about aids and adaptations, luncheon clubs, linking to the CSCI website and giving details of residential homes, inspection reports on care homes, giving information about the different types of care available, providing information to carers about their rights and what help is available to them. Blue Badge Scheme This scheme is to help people with mobility issues. Staff will explain the criteria, help customers complete the form, issue the badge to the customer if it's an automatic issue, write to the doctor if it's a discretionary award, deal with follow up queries, prepare and issue the badge for collection for the customer in discretionary cases, advise customers about how to appeal against a decision made. Council Tax Explaining how a bill has been worked out, seeing if the customer is eligible for any discounts to help reduce the bill, advice on what to do if a reminder or summons for non payment is received, advice on eligibility for the fair debt scheme, taking debit / credit card payments for your Council Tax. Consumer Advice First stage Consumer Advice given to customers, providing them with the consumer support pack, helping them complete letters to traders rejecting goods etc, giving advice on subsequent remedies, providing details of businesses who have joined the Wirral Fair Traders scheme
Page 145 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Council Meetings / Agendas / Councillor & MP queries Dealing with customer queries about minutes of meetings, dates / times / agendas of meetings, advising of when the and where Councillors & MPs hold their surgeries, provide contact details of Councillors & MPs Education & Welfare Benefits Advising customers who qualify that their children would be eligible to receive free school meals / milk. Electoral Register Link in with customers advising of change of address for Council Tax / Housing Benefit by downloading the form whilst in the OSS for them to complete or advising that a household member has turned 18, dealing with queries for confirmation of entry on the register, produce confirmation letter. Fire Service Making referrals to Merseyside Fire and Rescue Service for Home Fire Safety Checks Homeless Service Acting as the initial contact point for customers presenting themselves as homeless, giving first stage advice on what constitutes homelessness, liaising with the homeless section to arrange an appointment and, liaising with the homeless families unit, liaising with the tenancy support team to try and prevent customers becoming homeless Home Improvements Giving advice / raising service requests for disabled adaptations, promote energy efficiency grants e.g. warm front, cosy loans, contacting the handyman service for residents living who are eligible, give advice on what help they can get from the home improvement agency, make referrals to the POPIN (Promoting Older People's Independence Network) service where appropriate. Housing & Council Tax Benefit Advice on eligibility to benefit, help in filling out forms, explaining how benefit has been worked out, taking, receipting and scanning proofs when information is required.
Page 146 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
It's Your Call Offering support to customers who are suffering from neighbour nuisance / anti social behaviour, providing self help guidance / leaflets, recording the details, completing an initial complaint record for any Wirral Partnership Home tenants.
Job Applications Printing off Council job application details, receiving returned job applications, issuing system generated receipts. Leisure Services / Schemes Provide information on the Wirral passport and the Invigor8 scheme including eligibility criteria and fees, receipt the passport scheme documents Licensing Providing help with new and renewal applications for hackney and private hire cabs, new / renewal vehicle applications, temporary events notices, street / house collection licenses, Premises licences. Parking Appeals Taking payments for parking fines issued, explaining the process and helping customers appeal against the fine Pest Control / Environmental Health Providing information about the charges for dealing with the different types of pest ( rats / mice / wasps nests / bugs etc ), making service requests via the CRM, acting as a reception point at Seacombe for members of the public dropping off specimens of pests / suspect items of food. Planning and Building Control Providing copies of plans for customers to view, liaising with planning / building control officers to provide basic advice. Registrar Services Explaining who can and what you need to do to register a birth or a death, what information needs to be taken when attending the appointment, helping the customer contact the registrar if there is any coroner involvement, advising of any costs involved with the registrar service, helping to obtain copy birth and death certificates.
Page 147 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Student Support Services Providing information to students and helping with the application process for a loan with living costs, dealing with subsequent changes in circumstances. Tourism Information on tourist attractions in Wirral - beaches/country parks/theatres/museums etc providing information from the "Visit Wirral" website, providing information about any ongoing initiatives. Waste Environmental Services Information provided on waste and recycling issues and raising service requests for street cleansing issues, help with any missed bin collection Wirral Children’s Information Service Access to the Wirral children’s Information system to provide information on how to become a childcare provider, information on early years education for 3 & 4 year olds, carrying out a childcare search for the area / postcode requested by the customer, providing Ofsted inspection reports. Wirral Partnership Homes Check rent accounts, liaising with Wirral Partnership Homes income teams, making arrangements, dealing with estate management queries, tenancy terminations, garage queries, first stage neighbour nuisance issues (as above), advice on support cost queries, home insurance queries, providing right to buy information, generating duplicate payment cards, taking payments of rent on payment portal, dealing with first stage complaints, information on paint and repair programmes. Working in Partnership with other organizations Different surgeries are run across the One Stop Shops, including
• Age Concern • Merseyside Police • Pension Service • Wirral Alcohol Services
Page 148 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Wirral Council’s Call Centre
The Council is committed to improving access to services and launched its Call Centre in 2004 having listened to the views of Wirral residents. Since it was launched, the Call Centre has expanded the range of services that it delivers and has extended its opening hours for certain areas. The Call Centre numbers and opening hours are detailed below: General Enquiries / Switchboard
If you are unsure who you should be contacted the switchboard operators will direct you to the appropriate Department or person as quickly as possible. Tel: 0151 606 2000. Available: 8.45am to 5pm Monday to Friday Revenues and Benefits
The team provides a generic telephone point of contact for customers making enquiries relating to both Council Tax accounts and Housing/Council Tax Benefit claims. Tel: 0151 606 2002 Minicom: 0151 606 2575 Available: 8am to 6.30 pm Monday to Thursday 8am to 5pm Friday 9am to 12.30pm Saturday Streetscene
The team responds to calls and emails with regard to all street related services and ensure the enquiry is referred to the appropriate department for resolution Tel: 0151 606 2004 Minicom: 0151 606 2575 Available: 8am to 5pm Monday to Friday For emergencies outside of normal hours call 0151 647 7810
Page 149 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Central Advice & Duty Team
The Central Advice and Duty Team (CADT) provide a single point of contact by telephone, letter and fax for anyone wishing to contact Social Services for support or advice 24 hours a day, seven days a week Tel: 0151 606 2006 Minicom: 0151 606 2573 Available: 9am to 5pm Monday to Friday Contact Address – CADT, PO Box 32, Birkenhead, Wirral, CH41 5WE
For emergencies outside of normal hours: The emergency duty team provides out of hours cover from 5.00 pm to 9.00 am and covers weekends and bank holidays (including Christmas, New Year's Day and Easter). Tel: 0151 652 4991.
Information and Advice
The Information and Advice team offer a more generic service. Advisors are able to offer general advice and book appointments for a range of council services. Tel: 0151 606 2020 Available: 9am to 5pm Monday to Friday An answer phone facility operates outside of normal hours for reports of Anti Social Behaviour Automated Telephone Payments
Payments can be made in respect of many council services using this 24 hour facility Tel: 0151 606 2345
Page 150 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Library Information Points You might already be familiar with how Wirral Council’s One Stop Shops can help with council-related enquiries, but did you know that you can also receive initial advice and information through the Information Point network? The network is based in seven libraries and complements the One Stop Shops by providing further access to council services. How can Information Points help me? Here are just some of the first stage advice and information areas they deal with:
• Issuing forms, leaflets and other literature e.g. Housing Benefit forms and leaflets
• Taking payments via credit / debit cards for things like Council Tax • Provide details of traders registered on the Council’s Fair Trade
scheme if you are looking to get work done on your home • Information on energy efficiency schemes • Advising you on refuse and recycling collections
Where’s my nearest Information Point? You’ll find the information Points at libraries in:
Beechwood Bromborough Greasby Irby Prenton Ridgeway St James
What about the other libraries? Videolinks have been installed in a further 6 libraries:
Birkenhead Central Higher Bebington Leasowe Upton Wallasey Central Wallasey Village
This enables customers to speak directly with specialist advice staff in the Council’s Call Centre. Wirral Council is committed to improving the quality of life for its residents and making its services more accessible. The Information Point network is part of that commitment.
Page 151 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
11. ACKNOWLEDGEMENTS Special thanks go to Dr Shyamal Mukherjee for his overall guidance and future vision for WEHAG. Thanks are also extended to:
Simon Barrigan for his advice and guidance and also for providing information on Merseyside Police (Wirral Community Relations Unit); Raza Moula (Wirral Multicultural Organisation) for designing the WEHAG logo; Dave Bolton (Wirral Health Informatics Service - WHIS) for producing the WEHAG logo; and Bill Douglas, Head of Intranet/Internet Services - WHIS for assisting in the formatting of the File. Craig Lewis (The Little Design Shop) for arranging the printing of the Information & Resource File; Nurie Lamb, Susie Goligher and Helen Renner for contributing information on the African communities; Helen Renner for providing information on the Caribbean section. Brendan Collins, Public Health Department, NHS Wirral for providing statistical data; Renata Ziolkowska for contributing to the section on the Polish community; Natasha Smith for producing information on Wirral Drug and Alcohol Action Team; Nazma Khatun for information on Wirral Black & Racial Minority Partnership; Patricia Smye for producing information on Wirral’s Stop Smoking Service; Anne Jou for contributing to the section on the Chinese community; Sarah Patterson, Merseyside Fire Association, for access to information contained in their Communities Handbook. Mal Reston for contributing information on the Wirral Multicultural Organisation.

Page 152 of 152
2nd Edition – January 2009 Copyright protected WEHAG 2003 – 2009
Siafullah Syed for providing contact details for the Wirral Bangladesh Association. Sagal Jama for information on the Somali community. Paul McAvoy and Kat Lorenz for providing information on asylum seekers. Carol Davies Administrator for WEHAG January 2009
Top Related
Copyright © 2022 FDOKUMEN

