






Bahasa
Halaman
Hukum


http://qhr.sagepub.com/Qualitative Health Research
http://qhr.sagepub.com/content/early/2014/10/09/1049732314554096The online version of this article can be found at:
DOI: 10.1177/1049732314554096
published online 14 October 2014Qual Health ResElia Wyverkens, Hanna Van Parys and Ann Buysse
Experiences of Family Relationships Among Donor-Conceived Families: A Meta-Ethnography
Published by:
http://www.sagepublications.com
can be found at:Qualitative Health ResearchAdditional services and information for
http://qhr.sagepub.com/cgi/alertsEmail Alerts:
http://qhr.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Oct 14, 2014OnlineFirst Version of Record >>
by guest on October 14, 2014qhr.sagepub.comDownloaded from by guest on October 14, 2014qhr.sagepub.comDownloaded from
Qualitative Health Research 1 –18© The Author(s) 2014 Reprints and permissions: sagepub.com/journalsPermissions.navDOI: 10.1177/1049732314554096qhr.sagepub.com
Evidence for Practice
Worldwide, approximately 1 in 10 couples is affected by fertility problems (Boivin, Bunting, Collins, & Nygren, 2007; Covington & Burns, 2006). Research indicates that the inability to conceive alters one’s identity, strains rela-tionships, and diminishes self-esteem (Cousineau & Domar, 2007). New medical techniques, such as in vitro fertiliza-tion, enable couples to pursue parenthood. For some of these techniques, donor gametes are used: sperm or eggs of a person who will not be a future parent. This form of fam-ily building implies that the child has a genetic link to one parent (genetic parent) but not to the other parent (social parent). Within Euro-American cultures, building a family through donor conception is often challenging for parents given that (a) genetic connectedness is prevailing as the basis for family bonds and (b) the medical importance of genetic ties is often emphasized (for instance, genetic test-ing, bone marrow transplantation; Becker, Butler, & Nachtigall, 2005; Grace & Daniels, 2007; Hargreaves, 2006). Over the past several decades, empirical research on donor-conceived (DC) families has focused on the well-being of families and especially offspring (Golombok et al., 2002; Golombok, Cook, & Bish, 1995). This work has revealed that DC families are typically characterized by stable marital relationships, good parent–child relations, and good functioning, relative to naturally conceived fami-lies (see Bos & Van Balen, 2010; Brewaeys, 2001).
In recent years, researchers have shifted their focus from family well-being to how parents manage the
information about the donor origin in their family. This has resulted in a body of research on disclosure decisions about the nature of conception to the offspring (Daniels, Grace, & Gillett, 2011; Hahn & Rosenberg, 2002; Stevens, Perry, Burston, & Golombok, 2003). Much of this research has specifically focused on open-identity donation, in which DC offspring are given access to the donor’s identity once they reach maturity. Proponents of this trend argue that children have the right to know their genetic heritage (Daniels et al., 2011; Hahn & Rosenberg, 2002). Opponents stress the parents’ right for privacy and their freedom of choice with regard to their disclosure decision (Shehab et al., 2008). This ongoing debate has led many countries to abandon donor anonymity and to promote openness about the donor origin in families (e.g., Sweden, The Netherlands, Norway, Austria, Switzerland, United Kingdom, New Zealand, and Australia [Victoria and Western Australia]). Recently, Indekeu et al. (2013) synthesized the available qualitative, quantitative, and mixed-method evidence on disclosure decision-making process in heterosexual couples. Their article provides an intensive overview of intrapersonal, interpersonal, social,
554096QHRXXX10.1177/1049732314554096Qualitative Health ResearchWyverkens et al.research-article2014
1Ghent University, Ghent, Belgium
Corresponding Author:Elia Wyverkens, Faculty of Psychology and Educational Sciences, Ghent University, Henri Dunantlaan 2, 9000 Ghent, Belgium. Email: [email protected]
Experiences of Family Relationships Among Donor-Conceived Families: A Meta-Ethnography
Elia Wyverkens1, Hanna Van Parys1, and Ann Buysse1
AbstractIn this qualitative evidence synthesis, we explore how family relationships are experienced by parents who used gamete donation to conceive. We systematically searched four databases (PubMed, Web of Science, PsycINFO, and ProQuest) for literature related to this topic and retrieved 25 studies. Through the analysis of the qualitative studies, a comprehensive synthesis and framework was constructed. Following the meta-ethnography approach of Noblit and Hare, four main themes were identified: (a) balancing the importance of genetic and social ties, (b) normalizing and legitimizing the family, (c) building strong family ties, and (d) minimizing the role of the donor. Underlying these four main themes, a sense of being “different” and “similar” at the same time was apparent. Findings are discussed in terms of their implications for studying and counseling donor-conceived families.
Keywordsinfertility; meta-ethnography; reproduction; review
by guest on October 14, 2014qhr.sagepub.comDownloaded from

2 Qualitative Health Research
and family life cycle features that influence the disclosure decision in parents. With this review, the authors high-light the complexity of disclosure decisions as well as a lack of theoretical accounts that explain how the identi-fied factors influence disclosure.
Besides studies on disclosure outcomes, a number of qualitative studies have focused on different aspects of family relationships in this context: the meaning of resemblances (Becker et al., 2005), the construction of social and genetic ties (Hargreaves, 2006), and the role of the donor (Kirkman, 2004b). These studies offer insight into how parents build their families and how the mean-ing of social and genetic parenthood is constructed. Even though high-quality research has been published on this topic, it is difficult to obtain a comprehensive overview of these research findings. Moreover, studies have been conducted in different social–legal–cultural contexts and, as a consequence, have led to fragmented results.
In the current review, we synthesize the available qual-itative studies on family-building experiences and family relationships for DC families. In doing so, we aim to con-tribute to the field of family studies in particular and reproductive health care in general. Within the field of family psychology, a large body of quantitative research has been conducted to date, which has focused on the psy-chological well-being of parents and children as well as the quality of their relationships (e.g., Casey, Vasanti, Blake, & Golombok, 2013; Golombok et al., 2004). With our qualitative synthesis, we move beyond the study of family outcomes and investigate family processes in more detail. Applying the method of meta-ethnography (Noblit & Hare, 1988), we aimed to improve our understandings of family processes in DC families and the extent to which (the absence of) genetic connectedness plays a role in their experiences. Meta-ethnography is one of the most devel-oped and widely used methods for synthesizing qualita-tive data (Hannes & Lockwood, 2012; see, for instance, Varcoe, Rodney, & McCormick, 2003; Yick, 2008). This systematic and interpretative method goes beyond sum-marizing by classifying the identified concepts into a higher order theoretical structure (Dixon-Woods, Agarwal, Jones, Young, & Sutton, 2005).
Our decision to include only qualitative research find-ings was related to the assumption that qualitative research best fits experiential research questions and is able to provide a rich description of people’s meaning-making processes (Smith, Flowers, & Larkin, 2009). In addition, we focused on only one family type—hetero-sexual families—to be able to obtain consistency in our systematic review. Unlike lesbian- and gay-parented fam-ilies, heterosexual couples face fertility problems, and this can deny them the possibility to conceive genetic children of their own. This specific context, in which the traditional way of constituting a genetically related fam-
ily is unexpectedly impossible, was part of the family-building experiences we wanted to investigate.
Method
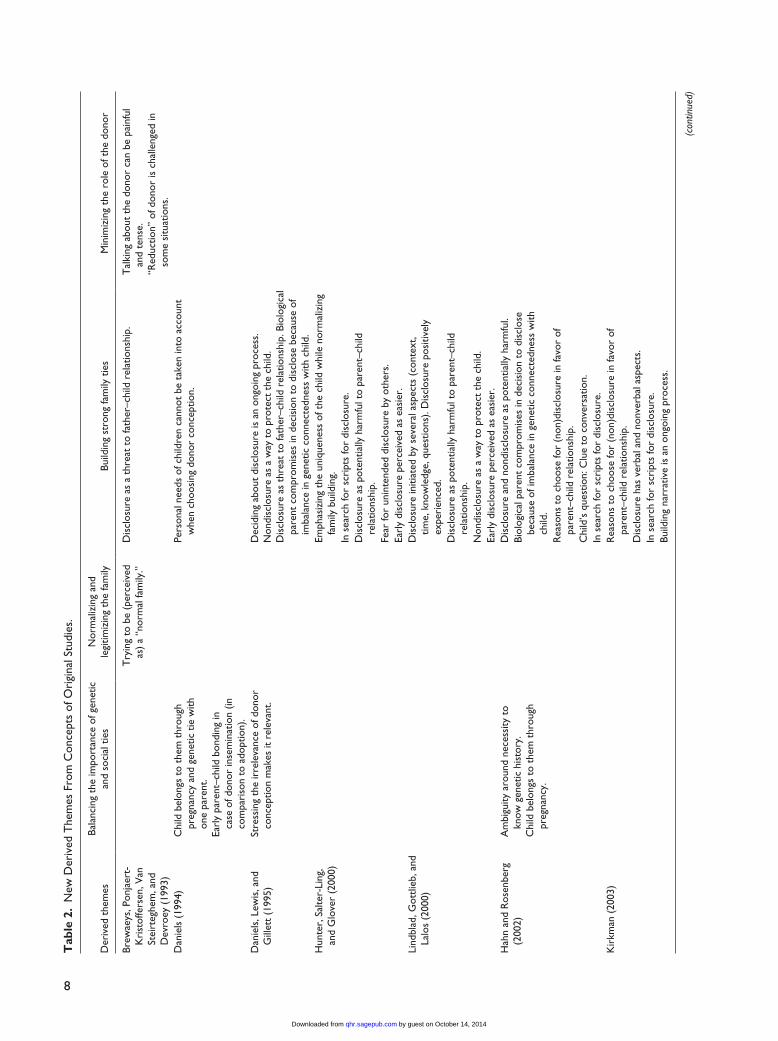
We conducted a systematic review of the qualitative research literature, following the meta-ethnography approach advocated by George Noblit and Dwight Hare (1988). Noblit and Hare developed this method in response to the practical problem of dealing with reports of different case studies on the same topic (Hannes & Lockwood, 2012). They both have a background in education research and were interested in the use of qualitative research meth-ods. In their conceptualization of this interpretative approach, Noblit and Hare sought to counter the prevailing positivist forms of knowledge synthesis which emphasized the aggregation of evidence through statistical meta-analy-sis (Hannes & Lockwood, 2012). Meta-ethnography was developed as a method of qualitative meta-synthesis that aimed to integrate and interpret findings from multiple qualitative studies (Kinn, Holgerson, Ekeland, & Davidson, 2013). The task of the synthesis is to translate studies into another, thereby providing new interpretations, rather than attempting to provide generalization (Hannes & Lockwood, 2012). This translative aspect distinguishes meta-ethnogra-phy from other methods for qualitative synthesis and proved useful in our review. The merits of meta-ethnogra-phy furthermore include its systematic approach and the high level of interpretation, which differentiates meta-eth-nography from traditional literature reviews (Dixon-Woods et al., 2005; Hannes & Lockwood, 2012). That said, one of the problems is the lack of guidelines on how to select and appraise studies, what to consider “data,” and how to synthesize the findings of the individual studies (Bondas & Hall, 2007; Kinn et al., 2013). Furthermore, the depth of the analysis and interpretations often differs from article to article (e.g., very descriptive or very theoretical), making it difficult to integrate findings. Zimmer (2006) argued that “metasynthesis is the synthesist’s interpretation of the interpretations of primary data by the original authors of the constituent studies” (p. 312). Therefore, the synthesis is always a result of constructed and intersubjec-tive meanings (Kinn et al., 2013). We tried to increase the transparency of the interpretative work by discussing every step in the research process within our research team and providing a detailed table with the identified concepts and themes (see Table 2). Below, we explain the seven phases of the meta-ethnography.
Identifying Topic of Interest and Search Strategy
In the first phase of the review, we identified our topic of interest: to discover how parents experience family
by guest on October 14, 2014qhr.sagepub.comDownloaded from

Wyverkens et al. 3
relationships when their traditional notion of a biologically related family is challenged. Subsequently, we consulted four search engines for our literature search: PubMed, Web of Science, PsycINFO, and ProQuest. Our threefold search string consisted of a combination of following keywords (and synonyms): (a) experiences, interview, qualitative; and (b) donor insemination, intracytoplasmic sperm injec-tion, in vitro fertilization, assisted reproductive technolo-gies, embryo donation, oocyte donation, sperm donation; and (c) kinship, family relationship, family building, fatherhood, motherhood. The systematic search yielded 1,321 references, which were reduced to 20 articles after evaluation of the title, the abstract, and the full text of the articles (see Figure 1). Through reference chaining, we included 5 additional studies, resulting in a total of 25 included studies.
Selection and Reading Process
In the second phase, we used the following inclusion criteria: Studies must (a) have reported empirical data on the experiences of family relationships after gamete donation, gathered from the perspective of heterosex-ual parents and (b) have made use of qualitative data collection methods and qualitative methods of analy-sis. No cutoff dates were set given that the field of family studies on donor gamete families is still in its infancy (our first included study dated from 1993). With regard to our first criterion, we systematically evaluated the “conceptual richness” of the articles and their relation to our review topic, and when the article
did not fit with the review question, it was excluded (e.g., it concerned a study about cell survival). Studies were also screened for their relevance using the fol-lowing screening questions: Does the article report on qualitative data? Does it mention a qualitative method of analysis? Does the analysis consist of an inductive phase in which codes result from a bottom-up analyti-cal process? and Are sufficient quotes given? In case one criterion was not met, inclusion decisions were made based on the relevance of the study and the rich-ness of the data. For instance, in Hargreaves (2006), no qualitative method of analysis was mentioned; how-ever, the findings proved to be a relevant contribution to our synthesis. Studies with a mixed sample (homo-sexual and heterosexual parents) or mixed methods (qualitative and quantitative data) were included in the review. However, in such cases, we only used qualita-tive data that were from the perspective of heterosex-ual couples. All phases of selection (on title, abstract, and full text) were carried out independently by the two main researchers (first and second author) and were followed by discussions to gain additional con-sensus on the final set of articles.
Identifying Key Concepts and Determining How Studies Are Related
In the third phase, each of the 25 articles was read, and characteristics of the studies were listed (see Table 1). Here, we sought to develop an in-depth understanding of the articles key concepts. Fourth, we extracted these key
Database search
Stage 1: evaluation of titlen = 1321 potentially relevant studies
Stage 2: evaluation of abstractn = 418 potentially relevant studies
Web of Science n =124
Stage 3: evaluation of full textn = 53 potentially relevant studies
Included in systematic reviewn = 25 relevant studies
PubMed n = 306
Studies excluded because of method, participants or topic n = 1296
Studies included after reference chainingn = 5
PsycInfon = 469
ProQuestn = 422
Figure 1. Process of study selection.
by guest on October 14, 2014qhr.sagepub.comDownloaded from

4
Tab
le 1
. C
hara
cter
istic
s of
Incl
uded
Stu
dies
in t
he R
evie
w.
Sour
ce a
rtic
leC
ount
ry s
ettin
gSe
ttin
gPa
rtic
ipan
t ch
arac
teri
stic
sD
ata
colle
ctio
nD
ata
anal
ysis
Beck
er, B
utle
r, a
nd
Nac
htig
all (
2005
)U
nite
d St
ates
Rec
ruitm
ent
thro
ugh
11 in
fert
ility
pr
actic
es +
1 s
perm
ban
k in
N
orth
ern
Cal
iforn
ia.
148
disc
losi
ng a
nd n
ondi
sclo
sing
he
tero
sexu
al c
oupl
es (
79 E
D/6
2 D
I/7 c
ombi
natio
n) C
hild
ren
from
in
fanc
y to
19
year
s ol
d.
Sem
istr
uctu
red
inte
rvie
ws:
C
oupl
e in
terv
iew
fo
llow
ed b
y so
lo
inte
rvie
w 3
mon
ths
late
r.
In-d
epth
pro
cess
of
code
dev
elop
men
t, co
mpa
ring
cod
es u
ntil
agre
emen
t of
95%
or
mor
e.Bl
ake,
Rea
ding
s, Ja
dva,
an
d G
olom
bok
(201
0)U
nite
d K
ingd
omR
ecru
itmen
t th
roug
h 9
fert
ility
cl
inic
s in
the
Uni
ted
Kin
gdom
. Pa
rt o
f a lo
ngitu
dina
l stu
dy.
23 d
iscl
osin
g m
othe
rs (
10 D
I, 13
ED
), 15
of t
heir
par
tner
s (7
DI,
8 ED
) an
d 12
chi
ldre
n (6
DI,
6 ED
). A
nony
mou
s do
natio
n an
d 1
know
n ED
. Chi
ldre
n ag
ed 7
yea
rs o
ld.
Sem
istr
uctu
red
stan
dard
ized
inte
rvie
ws
with
par
ents
sep
arat
ely
and
with
chi
ldre
n.
Con
tent
ana
lysi
s
Blyt
h, L
angr
idge
, and
H
arri
s (2
010)
Uni
ted
Kin
gdom
Rec
ruitm
ent
thro
ugh
2 U
nite
d K
ingd
om s
uppo
rt g
roup
s,
Don
or C
once
ptio
n N
etw
ork
and
the
Dai
sy N
etw
ork
(bot
h gr
oups
pro
mot
e di
sclo
sure
).
15 d
iscl
osin
g m
othe
rs a
nd 1
2 of
the
ir
part
ners
(13
DI,
2 ED
). C
hild
ren
aged
3-1
8 ye
ars
old.
Iden
tity-
rele
ase
dona
tion.
Sem
istr
uctu
red
inte
rvie
ws
with
par
ents
sep
arat
ely
Her
men
eutic
(in
terp
retiv
e)
phen
omen
olog
ical
ps
ycho
logy
Brew
aeys
, Pon
jaer
t-K
rist
offe
rsen
, Van
St
eirt
eghe
m, a
nd
Dev
roey
(19
93)
Belg
ium
Rec
ruitm
ent
thro
ugh
the
Cen
tre
for
Rep
rodu
ctiv
e M
edic
ine
of
the
Brus
sels
Uni
vers
ity H
ospi
tal.
25 h
omos
exua
l par
ents
(D
I) an
d 25
dis
clos
ing
and
nond
iscl
osin
g he
tero
sexu
al p
aren
ts (
DI)
thro
ugh
anon
ymou
s do
natio
n. C
hild
ren
aged
3
mon
ths
to 7
yea
rs.
Ope
n-en
ded
ques
tionn
aire
Qua
litat
ive
rese
arch
m
etho
d of
McC
rack
en
Burr
(20
09)
Uni
ted
Kin
gdom
Rec
ruitm
ent
thro
ugh
The
Fer
tility
C
entr
e (C
AR
E) a
nd t
he D
onor
C
once
ptio
n N
etw
ork.
10 w
omen
and
7 c
oupl
es (
DI),
di
sclo
sers
and
non
disc
lose
rs.
Ano
nym
ous
dona
tion.
Chi
ldre
n ag
ed 1
to
8 ye
ars
old.
Sem
istr
uctu
red
inte
rvie
ws,
10
alo
ne a
nd 7
con
join
t.Id
entif
icat
ion
of t
hem
es
follo
wed
by
mor
e de
taile
d in
terp
retiv
e co
ncep
tual
ana
lysi
s.D
anie
ls, G
race
, and
G
illet
t (2
011)
New
Zea
land
Rec
ruitm
ent
thro
ugh
a fe
rtili
ty
clin
ic in
Dun
edin
. Par
t of
a
long
itudi
nal s
tudy
.
12 h
eter
osex
ual n
ondi
sclo
sing
pa
rent
s (o
f sev
en fa
mili
es)
thro
ugh
DI.
Chi
ldre
n ag
ed 1
6-21
yea
rs.
Sem
istr
uctu
red
inte
rvie
ws,
co
njoi
nt a
nd s
epar
atel
yT
hem
atic
ana
lysi
s
Dan
iels
, Lew
is, a
nd
Gill
ett
(199
5)N
ew Z
eala
ndR
ecru
itmen
t th
roug
h th
e D
uned
in
Infe
rtili
ty C
linic
in N
ew Z
eala
nd.
48 d
iscl
osin
g an
d no
ndis
clos
ing
coup
les
who
had
a c
hild
/chi
ldre
n as
a
resu
lt of
DI.
Sem
istr
uctu
red
conj
oint
in
terv
iew
s an
d qu
antit
ativ
e da
ta.
Con
tent
ana
lysi
s
Dan
iels
(19
94)
New
Zea
land
Rec
ruitm
ent
thro
ugh
the
Dun
edin
In
fert
ility
Clin
ic in
New
Zea
land
.54
dis
clos
ing
and
nond
iscl
osin
g pa
rent
s th
roug
h D
I.Se
mis
truc
ture
d co
njoi
nt
inte
rvie
ws
and
quan
titat
ive
data
.
Con
tent
ana
lysi
s
Frie
se, B
ecke
r, a
nd
Nac
htig
all (
2008
)U
nite
d St
ates
Rec
ruitm
ent
thro
ugh
11 in
fert
ility
pr
actic
es +
1 s
perm
ban
k in
N
orth
ern
Cal
iforn
ia.
79 d
iscl
osin
g an
d no
ndis
clos
ing
hete
rose
xual
cou
ples
(ED
). C
hild
ren
from
infa
ncy
to 1
9 ye
ars
old.
Sem
istr
uctu
red
inte
rvie
ws:
C
oupl
e in
terv
iew
fo
llow
ed b
y so
lo
inte
rvie
w 3
mon
ths
late
r.
In-d
epth
pro
cess
of
code
dev
elop
men
t, co
mpa
ring
cod
es u
ntil
agre
emen
t of
95%
or
mor
e.G
race
and
Dan
iels
(2
007)
New
Zea
land
Part
of a
stu
dy c
ondu
cted
in
1990
with
het
eros
exua
l cou
ples
re
crui
ted
thro
ugh
an in
fert
ility
cl
inic
in N
ew Z
eala
nd.
41 d
iscl
osin
g an
d no
ndis
clos
ing
hete
rose
xual
cou
ples
(D
I) in
clud
ing
divo
rced
or
sepa
rate
d co
uple
s.
Ope
n-en
ded
inte
rvie
ws:
23
con
join
t in
terv
iew
s an
d 18
sep
arat
e in
terv
iew
s.
The
mat
ic a
naly
sis
(con
tinue
d)
by guest on October 14, 2014qhr.sagepub.comDownloaded from

5
Sour
ce a
rtic
leC
ount
ry s
ettin
gSe
ttin
gPa
rtic
ipan
t ch
arac
teri
stic
sD
ata
colle
ctio
nD
ata
anal
ysis
Gra
ce, D
anie
ls, a
nd
Gill
ett
(200
8)N
ew Z
eala
ndPa
rt o
f a s
tudy
con
duct
ed in
19
90 w
ith h
eter
osex
ual c
oupl
es
recr
uite
d th
roug
h an
infe
rtili
ty
clin
ic in
New
Zea
land
.
41 d
iscl
osin
g an
d no
ndis
clos
ing
hete
rose
xual
cou
ples
(D
I) in
clud
ing
divo
rced
or
sepa
rate
d co
uple
s.
Ope
n-en
ded
inte
rvie
ws:
23
con
join
t in
terv
iew
s an
d 18
sep
arat
e in
terv
iew
s.
The
mat
ic a
naly
sis
Hah
n an
d R
osen
berg
(2
002)
Uni
ted
Stat
esR
ecru
itmen
t th
roug
h ce
nter
fo
r as
sist
ed r
epro
duct
ion
in
Mid
wes
tern
tea
chin
g ho
spita
l.
31 d
iscl
osin
g an
d no
ndis
clos
ing
pare
nts
thro
ugh
ED. A
nony
mou
s do
natio
n. C
hild
ren
aged
6 m
onth
s to
5 y
ears
.
Aud
iota
ped
tele
phon
e in
terv
iew
s an
d qu
antit
ativ
e da
ta.
Con
tent
ana
lysi
s
Har
grea
ves
(200
6)N
ew Z
eala
ndR
ecru
itmen
t th
roug
h N
ew
Zea
land
fert
ility
clin
ics
and
New
Zea
land
Infe
rtili
ty S
ocie
ty.
Exte
nded
fam
ily m
embe
rs w
ere
cont
acte
d by
the
par
ticip
atin
g pa
rent
s.
4 di
sclo
sing
and
non
disc
losi
ng
hete
rose
xual
cou
ples
(D
I) an
d th
e ex
tend
ed fa
mily
mem
bers
of t
wo
coup
les.
Chi
ldre
n fr
om in
fanc
y to
5
year
s ol
d.
Sem
istr
uctu
red
inte
rvie
ws
Des
crip
tion
of t
hem
atic
an
alys
is b
ut n
o ex
plic
it re
fere
nce
to t
hem
atic
an
alys
is
Har
grea
ves
and
Dan
iels
(2
007)
New
Zea
land
Rec
ruitm
ent
thro
ugh
New
Z
eala
nd fe
rtili
ty c
linic
s an
d N
ew Z
eala
nd In
fert
ility
Soc
iety
. Ex
tend
ed fa
mily
mem
bers
wer
e co
ntac
ted
by t
he p
artic
ipat
ing
pare
nts.
25 d
iscl
osin
g an
d no
ndis
clos
ing
hete
rose
xual
par
ents
(D
I) an
d 2
lesb
ian
coup
les
(DI).
Chi
ldre
n ag
ed
7 m
onth
s to
12
year
s.
Sem
istr
uctu
red
inte
rvie
ws
Des
crip
tion
of t
hem
atic
an
alys
is b
ut n
o ex
plic
it re
fere
nce
to t
hem
atic
an
alys
is
Hun
ter,
Sal
ter-
Ling
, and
G
love
r (2
000)
Uni
ted
Kin
gdom
Rec
ruitm
ent
thro
ugh
the
DI
Net
wor
k (s
uppo
rt g
roup
pr
omot
ing
disc
losu
re).
83 d
iscl
osin
g pa
rent
s (D
I; 39
cou
ples
an
d 5
wom
en).
Chi
ldre
n ag
ed 1
1 w
eeks
to
15 y
ears
.
Qua
ntita
tive
and
qual
itativ
e da
taC
onte
nt a
naly
sis
Kir
kman
(20
03)
Aus
tral
ia, C
anad
a,
Uni
ted
Stat
es,
Uni
ted
Kin
gdom
, and
A
rgen
tina
Cal
l for
par
ticip
atio
n vi
a se
vera
l ch
anne
ls: N
ewsl
ette
rs,
mag
azin
es, i
nfer
tility
clin
ics
in
Aus
tral
ia, s
now
ball
sam
plin
g.
55 d
iscl
osin
g an
d no
ndis
clos
ing
pare
nts
(thr
ough
DI,
ED, a
nd
embr
yo d
onat
ion)
and
12
child
ren.
A
nony
mou
s an
d kn
own
dona
tion.
32 in
terv
iew
s in
per
son,
18
audi
otap
ed in
terv
iew
s,
20 e
mai
l int
ervi
ews,
16
wri
tten
inte
rvie
ws,
and
1
tele
phon
e in
terv
iew
Nar
rativ
e an
alys
is
Kir
kman
(20
04b)
Aus
tral
ia, C
anad
a,
Uni
ted
Stat
es,
Uni
ted
Kin
gdom
, and
A
rgen
tina
Cal
l for
par
ticip
atio
n vi
a se
vera
l ch
anne
ls: N
ewsl
ette
rs,
mag
azin
es, i
nfer
tility
clin
ics
in
Aus
tral
ia, s
now
ball
sam
plin
g.
87 d
iscl
osin
g an
d no
ndis
clos
ing
part
icip
ants
(58
par
ents
, 22
dono
rs, a
nd 1
2 of
fspr
ing)
. Don
ors
and
reci
pien
ts o
f spe
rm, e
ggs,
or
embr
yos.
Ano
nym
ous
and
know
n do
natio
n.
32 in
terv
iew
s in
per
son,
18
audi
otap
ed in
terv
iew
s,
20 e
mai
l int
ervi
ews,
16
wri
tten
inte
rvie
ws,
and
1
tele
phon
e in
terv
iew
Nar
rativ
e an
alys
is
Kir
kman
(20
04a)
Aus
tral
ia, C
anad
a,
Uni
ted
Stat
es,
Uni
ted
Kin
gdom
, and
A
rgen
tina
Cal
l for
par
ticip
atio
n vi
a se
vera
l ch
anne
ls: N
ewsl
ette
rs,
mag
azin
es, i
nfer
tility
clin
ics
in
Aus
tral
ia, s
now
ball
sam
plin
g.
87 d
iscl
osin
g an
d no
ndis
clos
ing
part
icip
ants
(58
par
ents
, 22
dono
rs, a
nd 1
2 of
fspr
ing)
. Don
ors
and
reci
pien
ts o
f spe
rm, e
ggs,
or
embr
yos.
Ano
nym
ous
and
know
n do
natio
n.
32 in
terv
iew
s in
per
son,
18
audi
otap
ed in
terv
iew
s,
20 e
mai
l int
ervi
ews,
16
wri
tten
inte
rvie
ws,
and
1
tele
phon
e in
terv
iew
Nar
rativ
e an
alys
is
(con
tinue
d)
Tab
le 1
. (co
ntin
ued)
by guest on October 14, 2014qhr.sagepub.comDownloaded from

6
Sour
ce a
rtic
leC
ount
ry s
ettin
gSe
ttin
gPa
rtic
ipan
t ch
arac
teri
stic
sD
ata
colle
ctio
nD
ata
anal
ysis
Kir
kman
(20
08)
Aus
tral
ia, A
rgen
tina,
an
d C
anad
aC
all f
or p
artic
ipat
ion
via
seve
ral
chan
nels
: New
slet
ters
, m
agaz
ines
, inf
ertil
ity c
linic
s in
A
ustr
alia
, sno
wba
ll sa
mpl
ing.
21 d
iscl
osin
g an
d no
ndis
clos
ing
wom
en (
19 E
D a
nd 2
em
bryo
do
natio
n). (
Part
of p
roje
ct w
ith
87 p
artic
ipan
ts).
Ano
nym
ous
and
know
n do
natio
n.
10 in
terv
iew
s in
per
son,
4
by e
mai
l, 4
by le
tter
, 2
by a
udio
tap
e, a
nd 1
by
tele
phon
e
Nar
rativ
e an
alys
is
Lalo
s, G
ottli
eb, a
nd
Lalo
s (2
007)
Swed
enR
ecru
itmen
t th
roug
h 2
DI
cent
ers
in S
wed
en (
Kar
olin
ska
Uni
vers
ity H
ospi
tal,
Stoc
khol
m,
and
Uni
vers
ity H
ospi
tal,
Um
eå;
follo
w-u
p of
stu
dy in
200
0).
19 (
disc
losi
ng a
nd n
ondi
sclo
sing
) pa
rent
s th
roug
h D
I. Id
entit
y-re
leas
e do
natio
n. C
hild
ren
aged
1 t
o 15
ye
ars.
Sem
istr
uctu
red
tele
phon
e in
terv
iew
sT
ext
was
ana
lyze
d by
co
nten
t an
d cl
assi
fied
into
cat
egor
ies
and
them
es.
Lind
blad
, Got
tlieb
, and
La
los
(200
0)Sw
eden
Rec
ruitm
ent
thro
ugh
the
Um
eå U
nive
rsity
Hos
pita
l an
d K
arol
insk
a H
ospi
tal i
n St
ockh
olm
.
148
disc
losi
ng a
nd n
ondi
sclo
sing
pa
rent
s (D
I). Id
entit
y-re
leas
e do
natio
n. C
hild
ren
aged
1 t
o 11
ye
ars
and
olde
r.
Que
stio
nnai
re w
ith o
pen
and
clos
ed q
uest
ions
.O
pen
codi
ng
Lyce
tt, D
anie
ls, C
urso
n,
and
Gol
ombo
k (2
005)
Uni
ted
Kin
gdom
Rec
ruite
d fr
om K
ing’
s C
olle
ge
Hos
pita
l Ass
iste
d C
once
ptio
n U
nit
(pro
mot
ing
disc
losu
re).
46 d
iscl
osin
g an
d no
ndis
clos
ing
pare
nts
with
a 4
- to
8-y
ear-
old
DI-c
once
ived
chi
ld. I
dent
ity-r
elea
se
dona
tion.
Stan
dard
ized
and
se
mis
truc
ture
d in
terv
iew
s: 3
6 co
njoi
nt
inte
rvie
ws
and
10
inte
rvie
ws
with
mot
her
only
.
The
mat
ic a
naly
sis
Mac
Dou
gall,
Bec
ker,
Sh
eib,
and
Nac
htig
all
(200
7)
Nor
ther
n C
alifo
rnia
, U
nite
d St
ates
Rec
ruitm
ent
thro
ugh
11 m
edic
al
infe
rtili
ty p
ract
ices
and
1 s
perm
ba
nk.
112
disc
losi
ng c
oupl
es (
48 D
I and
64
ED).
Chi
ldre
n ag
ed 1
to
19 y
ears
.Et
hnog
raph
ic in
terv
iew
w
ith c
oupl
e, fo
llow
ed b
y in
divi
dual
inte
rvie
w w
ith
each
of t
he t
wo
part
ners
3
mon
ths
late
r
The
mat
ic a
naly
sis
Sheh
ab e
t al
. (20
08)
Nor
ther
n C
alifo
rnia
, U
nite
d St
ates
Rec
ruitm
ent
thro
ugh
11 m
edic
al
infe
rtili
ty p
ract
ices
and
1 s
perm
ba
nk.
141
disc
losi
ng a
nd n
ondi
sclo
sing
co
uple
s w
ho h
ad c
once
ived
a c
hild
us
ing
dono
r ga
met
es (
62 D
I and
79
ED).
Chi
ldre
n ag
ed 1
to
19 y
ears
.
Ethn
ogra
phic
inte
rvie
w
with
cou
ple,
follo
wed
by
indi
vidu
al in
terv
iew
with
ea
ch o
f the
tw
o pa
rtne
rs
3 m
onth
s la
ter
The
mat
ic a
naly
sis
Yee
, Bly
th, a
nd T
sang
(2
011)
Can
ada
Rec
ruitm
ent
thro
ugh
hosp
ital-
base
d IV
F cl
inic
in a
Can
adia
n ci
ty.
18 d
iscl
osin
g an
d no
ndis
clos
ing
mot
hers
and
15
know
n do
nors
(E
D).
Kno
wn
dona
tion.
Chi
ldre
n ag
ed 1
to
7.
Sem
istr
uctu
red
face
-to-
face
or
phon
e in
terv
iew
.T
hem
atic
ana
lysi
s
Not
e. IV
F =
in v
itro
fert
iliza
tion,
ED
= e
gg d
onat
ion,
DI =
don
or in
sem
inat
ion.
Tab
le 1
. (co
ntin
ued)
by guest on October 14, 2014qhr.sagepub.comDownloaded from

Wyverkens et al. 7
concepts and explained and interpreted them in the con-text of the study as a whole (Hannes & Lockwood, 2012; Noblit & Hare, 1988). This process of identifying and interpreting concepts was conducted by the first two authors independently for 14 out of 25 articles. The remaining studies were analyzed by the first author and discussed with the second author to check for accuracy. In the fifth phase, we compared the identified concepts of each article with concepts of other articles to obtain broader themes across studies (on a meta-level). The syn-thesis focused on parents’ talk (first order constructs) and authors’ interpretations of their talk (second order con-structs; Noblit & Hare, 1988). In this phase, we mainly approached the analysis with a hermeneutics of faith, which means that we aimed to restore meaning to the text and to give “voice” to the participants (Josselson, 2004). The meta-analysis was performed in chronological order of publication, beginning with Brewaeys, Ponjaert-Kristoffersen, Van Steirteghem, and Devroey (1993) up to Yee, Blyth, and Tsang (2011) (see Table 2).
Translating Studies and Expressing the Synthesis
In the sixth phase, we attempted to create overarching themes while preserving the uniqueness of the individual studies. Both researchers participated in the development of the synthesis and the translation of the concepts. We com-bined studies by means of reciprocal translation analysis, meaning that concepts from individual studies were trans-lated into one another by constructing overarching concepts (Bondas & Hall, 2007; Kinn et al., 2013). We interpreted author’s interpretations (third-order constructs), mostly driven by a hermeneutics of suspicion, which means that we attempted to decode meanings that were more disguised (Josselson, 2004). Periodically, the synthesis was discussed with the third author until a coherent structure was achieved. The synthesis is expressed in the “Results” section, using quotes from the original studies. This is the seventh and final phase of the meta-ethnography.
Results
Study Characteristics
The set of included articles consisted of eight studies con-ducted in the United Kingdom, another eight in the United States, seven studies in New Zealand, five in Canada, four in Australia, four in Argentina, two in Sweden, and one in Belgium (see Table 1).1 The sample size ranged from 4 to 148 couples. Eight studies consisted of mixed samples with parents using egg donation, sperm dona-tion, and/or embryo donation. Thirteen studies solely focused on parents using sperm donation and four studies
solely on parents using egg donation. Policy and legisla-tive procedures varied from country to country. Sweden was in 1985 the first country to abandon donor anonym-ity. In Australia and New Zealand, only known donation is allowed, and openness about the donor conception is encouraged. More recently, the Human Fertilization Embryology Authority (HFEA) removed donor anonym-ity in the United Kingdom, allowing children to obtain identifying information on reaching age 18. In the United States, there are no regulations, only expert groups (e.g., American Society for Reproductive Medicine [ASRM]) that provide recommendations and guidelines. The remaining countries (Argentina, Canada, and Belgium) have an anonymous gamete donation policy and are char-acterized more by secrecy and taboo. Studies took place both before and after these legislative changes. Few stud-ies explicitly mentioned the type of donation (anony-mous, known, or identity-release), and information on the legal context and policy was often missing.
Description of Themes
Four major themes emerged when synthesizing the trans-lations: balancing the importance of genetic and social ties, normalizing and legitimizing the family, building strong family ties, and minimizing the role of the donor. Table 2 reflects the key concepts and themes we identi-fied. When we expressed the synthesis, we found the overarching notion that parents experienced “being dif-ferent” as well as “being similar,” compared with other families. We describe this dialectic tension after present-ing the four main themes.
Balancing the importance of genetic and social ties. Genes are regarded as significant connectors for the family, and parents are constantly reminded of the primacy of genes (Hargreaves, 2006). For DC families, the construction of family life based on genetic connection is challenged, and novel discourse needs to be built. Grace and Daniels (2007) show how couples tend to downgrade the impor-tance of genetics, except in medical contexts. One father using donor sperm states that providing information about the nature of conception can be important when confronted with a health crisis, but overall, genes are irrelevant for connectedness, relatedness, and the con-struction of the family:
Yeah, I don’t have a problem with that, I mean that’s important that that is the case. Um but ah, that’s just a, that’s just a genetic, ah, that’s just a medical thing. Ah, that isn’t, still to me, anything to do with who he is and who I am, and who [F] is, and who we are as a family. It’s not relevant. That’s just ah, that’s mechanics. It’s not the oil that makes the engine run. It’s just the bits of the engine, so yeah. (p. 703)
by guest on October 14, 2014qhr.sagepub.comDownloaded from
8
Tab
le 2
. N
ew D
eriv
ed T
hem
es F
rom
Con
cept
s of
Ori
gina
l Stu
dies
.
Der
ived
the
mes
Bala
ncin
g th
e im
port
ance
of g
enet
ic
and
soci
al t
ies
Nor
mal
izin
g an
d le
gitim
izin
g th
e fa
mily
Build
ing
stro
ng fa
mily
tie
sM
inim
izin
g th
e ro
le o
f the
don
or
Brew
aeys
, Pon
jaer
t-K
rist
offe
rsen
, Van
St
eirt
eghe
m, a
nd
Dev
roey
(19
93)
Try
ing
to b
e (p
erce
ived
as
) a
“nor
mal
fam
ily.”
Dis
clos
ure
as a
thr
eat
to fa
ther
–chi
ld r
elat
ions
hip.
Tal
king
abo
ut t
he d
onor
can
be
pain
ful
and
tens
e.“R
educ
tion”
of d
onor
is c
halle
nged
in
som
e si
tuat
ions
.D
anie
ls (
1994
) C
hild
bel
ongs
to
them
thr
ough
pr
egna
ncy
and
gene
tic t
ie w
ith
one
pare
nt.
Earl
y pa
rent
–chi
ld b
ondi
ng in
ca
se o
f don
or in
sem
inat
ion
(in
com
pari
son
to a
dopt
ion)
.
Pers
onal
nee
ds o
f chi
ldre
n ca
nnot
be
take
n in
to a
ccou
nt
whe
n ch
oosi
ng d
onor
con
cept
ion.
Dan
iels
, Lew
is, a
nd
Gill
ett
(199
5)
Stre
ssin
g th
e ir
rele
vanc
e of
don
or
conc
eptio
n m
akes
it r
elev
ant.
Dec
idin
g ab
out
disc
losu
re is
an
ongo
ing
proc
ess.
Non
disc
losu
re a
s a
way
to
prot
ect
the
child
.D
iscl
osur
e as
thr
eat
to fa
ther
–chi
ld r
elat
ions
hip.
Bio
logi
cal
pare
nt c
ompr
omis
es in
dec
isio
n to
dis
clos
e be
caus
e of
im
bala
nce
in g
enet
ic c
onne
cted
ness
with
chi
ld.
Hun
ter,
Sal
ter-
Ling
, an
d G
love
r (2
000)
Emph
asiz
ing
the
uniq
uene
ss o
f the
chi
ld w
hile
nor
mal
izin
g fa
mily
bui
ldin
g.
In s
earc
h fo
r sc
ript
s fo
r di
sclo
sure
.D
iscl
osur
e as
pot
entia
lly h
arm
ful t
o pa
rent
–chi
ld
rela
tions
hip.
Fear
for
unin
tend
ed d
iscl
osur
e by
oth
ers.
Earl
y di
sclo
sure
per
ceiv
ed a
s ea
sier
.Li
ndbl
ad, G
ottli
eb, a
nd
Lalo
s (2
000)
Dis
clos
ure
initi
ated
by
seve
ral a
spec
ts (
cont
ext,
time,
kno
wle
dge,
que
stio
ns).
Dis
clos
ure
posi
tivel
y ex
peri
ence
d.
D
iscl
osur
e as
pot
entia
lly h
arm
ful t
o pa
rent
–chi
ld
rela
tions
hip.
Non
disc
losu
re a
s a
way
to
prot
ect
the
child
.Ea
rly
disc
losu
re p
erce
ived
as
easi
er.
Hah
n an
d R
osen
berg
(2
002)
Am
bigu
ity a
roun
d ne
cess
ity t
o kn
ow g
enet
ic h
isto
ry.
Chi
ld b
elon
gs t
o th
em t
hrou
gh
preg
nanc
y.
Dis
clos
ure
and
nond
iscl
osur
e as
pot
entia
lly h
arm
ful.
Biol
ogic
al p
aren
t co
mpr
omis
es in
dec
isio
n to
dis
clos
e be
caus
e of
imba
lanc
e in
gen
etic
con
nect
edne
ss w
ith
child
.R
easo
ns t
o ch
oose
for
(non
)dis
clos
ure
in fa
vor
of
pare
nt–c
hild
rel
atio
nshi
p.C
hild
’s q
uest
ion:
Clu
e to
con
vers
atio
n.In
sea
rch
for
scri
pts
for
disc
losu
re.
Kir
kman
(20
03)
Rea
sons
to
choo
se fo
r (n
on)d
iscl
osur
e in
favo
r of
pa
rent
–chi
ld r
elat
ions
hip.
D
iscl
osur
e ha
s ve
rbal
and
non
verb
al a
spec
ts.
In s
earc
h fo
r sc
ript
s fo
r di
sclo
sure
.Bu
ildin
g na
rrat
ive
is a
n on
goin
g pr
oces
s.
(con
tinue
d)
by guest on October 14, 2014qhr.sagepub.comDownloaded from

9
Der
ived
the
mes
Bala
ncin
g th
e im
port
ance
of g
enet
ic
and
soci
al t
ies
Nor
mal
izin
g an
d le
gitim
izin
g th
e fa
mily
Build
ing
stro
ng fa
mily
tie
sM
inim
izin
g th
e ro
le o
f the
don
or
Kir
kman
(20
04b)
Irre
leva
nce
of g
enet
ics
to
conn
ecte
dnes
s vs
. abs
ence
of
gene
tic t
ie a
s lo
ss.
Sign
s of
diff
icul
t bo
ndin
g at
trib
uted
to
lack
of g
enet
ic c
onne
ctio
n.M
eani
ng o
f gen
etic
inhe
rita
nce
deco
ntex
tual
ized
from
con
text
of
fam
ily r
elat
ions
hips
.Fo
r so
cial
par
ent
bond
ing
with
ch
ildre
n in
crea
ses
over
tim
e.So
cial
fath
er fe
ars
to b
e re
ject
ed
duri
ng p
uber
ty.
Kir
kman
(20
04a)
V
alui
ng t
he s
perm
pro
vide
r im
plie
s de
valu
ing
the
soci
al fa
ther
.Sh
iftin
g id
eas
abou
t do
nor.
Lyce
tt, D
anie
ls,
Cur
son,
and
G
olom
bok
(200
5)
Mea
ning
of g
enet
ic in
heri
tanc
e de
cont
extu
aliz
ed fr
om c
onte
xt o
f fa
mily
rel
atio
nshi
ps.
Fear
for
unin
tend
ed d
iscl
osur
e by
oth
ers.
Dis
clos
ure
coul
d be
har
mfu
l to
pare
nt–c
hild
rel
atio
nshi
p.C
onfid
ence
in s
tren
gth
pare
nt–c
hild
rel
atio
nshi
p at
the
ba
se o
f dis
clos
ure.
Min
or r
eact
ions
of c
hild
ren
in c
ompa
riso
n to
ant
icip
ated
fe
ars.
Beck
er, B
utle
r, a
nd
Nac
htig
all (
2005
)
Irre
leva
nce
of g
enet
ics
to
conn
ecte
dnes
s vs
. abs
ence
of
gene
tic t
ie a
s lo
ss.
App
eari
ng a
s a
fam
ily in
th
e so
cial
con
text
.(N
on)r
esem
blan
ce t
alk
as d
iscu
rsiv
e ac
t.
Har
grea
ves
(200
6)
Irre
leva
nce
of g
enet
ics
to
conn
ecte
dnes
s vs
. abs
ence
of
gen
etic
tie
as
mea
ning
ful.
Mea
ning
of g
enet
ic in
heri
tanc
e de
cont
extu
aliz
ed fr
om c
onte
xt o
f fa
mily
rel
atio
nshi
ps.
Res
embl
ance
tal
k as
dis
curs
ive
act
(sup
port
ing
disc
ours
e of
rel
ated
ness
).
For
soci
al p
aren
t bo
ndin
g w
ith
child
ren
incr
ease
s ov
er t
ime.
Gra
ce a
nd D
anie
ls
(200
7)M
eani
ng o
f gen
etic
inhe
rita
nce
deco
ntex
tual
ized
from
con
text
of
fam
ily r
elat
ions
hips
.
Try
ing
to b
e (p
erce
ived
as
) a
“nor
mal
fam
ily.”
Con
trad
icto
ry a
ttitu
de t
owar
d di
sclo
sure
.
Ir
rele
vanc
e of
gen
etic
s to
co
nnec
tedn
ess
vs. a
bsen
ce o
f ge
netic
tie
as
loss
.
St
ress
ing
irre
leva
nce
of d
onor
co
ncep
tion
mak
es it
rel
evan
t.
(con
tinue
d)
Tab
le 2
. (co
ntin
ued)
by guest on October 14, 2014qhr.sagepub.comDownloaded from

10
Der
ived
the
mes
Bala
ncin
g th
e im
port
ance
of g
enet
ic
and
soci
al t
ies
Nor
mal
izin
g an
d le
gitim
izin
g th
e fa
mily
Build
ing
stro
ng fa
mily
tie
sM
inim
izin
g th
e ro
le o
f the
don
or
Har
grea
ves
and
Dan
iels
(2
007)
Dis
clos
ure
and
nond
iscl
osur
e as
pot
entia
lly h
arm
ful.
Rea
sons
to
choo
se fo
r (n
on)d
iscl
osur
e in
favo
r of
pa
rent
–chi
ld r
elat
ions
hip.
In s
earc
h fo
r sc
ript
s fo
r di
sclo
sure
.Bi
olog
ical
par
ent
com
prom
ises
in d
ecis
ion
to d
iscl
ose
beca
use
of im
bala
nce
in g
enet
ic c
onne
cted
ness
with
ch
ild.
Earl
y di
sclo
sure
per
ceiv
ed a
s ea
sier
.
Lalo
s, G
ottli
eb, a
nd
Lalo
s (2
007)
In s
earc
h fo
r sc
ript
s fo
r di
sclo
sure
.C
hild
’s q
uest
ion
as c
lue
for
conv
ersa
tion
or c
lue
for
prot
ectin
g th
e tr
uth
even
mor
e.C
onfid
ence
in s
tren
gth
pare
nt–c
hild
rel
atio
nshi
p at
the
ba
se o
f dis
clos
ure.
Belie
f “op
enne
ss le
ads
to g
ood
fam
ily r
elat
ions
hips
.”V
aria
bilit
y in
sto
ry t
ellin
g: F
rom
tec
hnic
al t
o fa
iry
tale
.
Mac
Dou
gall,
Bec
ker,
Sh
eib,
and
Nac
htig
all
(200
7)
Stru
gglin
g w
ith a
ssoc
iatio
n be
twee
n bi
olog
ical
link
and
rea
lnes
s of
pa
rent
hood
.
Try
ing
to b
e (p
erce
ived
as
) a
“nor
mal
” fa
mily
.St
reng
th p
aren
t–ch
ild r
elat
ions
hip
as b
uffe
r fo
r do
ubtin
g po
sitio
n so
cial
par
ent.
Dis
clos
ure
proc
ess
adju
sted
to
the
child
.C
reat
ing
cond
ition
s fo
r op
timal
acc
epta
nce
of d
onor
co
ncep
tion.
Dis
clos
ure
as a
n on
goin
g pr
oces
s.
Sheh
ab e
t al
. (20
08)
Res
embl
ance
tal
k as
cha
lleng
e an
d re
assu
ranc
e.
One
par
ent
com
prom
ises
in d
ecis
ion
to d
iscl
ose
in
vari
ous
way
s.
Frie
se, B
ecke
r, a
nd
Nac
htig
all (
2008
)C
once
rn a
bout
soc
ial
legi
timac
y of
fam
ily.
Fear
for
unin
tend
ed d
iscl
osur
e by
oth
ers.
Gra
ce, D
anie
ls, a
nd
Gill
ett
(200
8)T
ryin
g to
be
perc
eive
d as
a “
norm
al”
fam
ily.
Stre
ssin
g do
nor
is n
ot fa
ther
(in
co
mm
unic
atio
n w
ith c
hild
ren)
. Int
eres
t in
link
bet
wee
n do
nor
and
child
ren.
Er
asur
e of
don
or fa
cilit
ates
“se
nse
of
fam
ily.”
Red
uctio
n of
don
or c
halle
nged
in
som
e si
tuat
ions
.K
irkm
an (
2008
)M
eani
ng o
f gen
etic
inhe
rita
nce
deco
ntex
tual
ized
from
con
text
of
fam
ily r
elat
ions
hips
.
Stre
ngth
par
ent–
child
rel
atio
nshi
p as
buf
fer
for
doub
ting
posi
tion
soci
al m
othe
r.Ex
pres
sing
gra
titud
e an
d re
sent
men
t to
war
d un
know
n eg
g do
nor.
U
ncer
tain
ty a
bout
rea
lnes
s of
m
othe
rhoo
d.
(con
tinue
d)
Tab
le 2
. (co
ntin
ued)
by guest on October 14, 2014qhr.sagepub.comDownloaded from

11
Der
ived
the
mes
Bala
ncin
g th
e im
port
ance
of g
enet
ic
and
soci
al t
ies
Nor
mal
izin
g an
d le
gitim
izin
g th
e fa
mily
Build
ing
stro
ng fa
mily
tie
sM
inim
izin
g th
e ro
le o
f the
don
or
Burr
(20
09)
Soci
al a
nd p
hysi
cal b
ound
arie
s ar
ound
fam
ily m
ore
impo
rtan
t th
an la
ck o
f gen
etic
bon
d w
ith
child
.
Res
embl
ance
as
subs
titut
e fo
r m
issi
ng
gene
tic li
nk b
etw
een
fath
er a
nd c
hild
.
Am
bigu
ous
posi
tion
tow
ard
dono
r.
Blak
e, R
eadi
ngs,
Jadv
a,
and
Gol
ombo
k (2
010)
Preg
nanc
y an
d de
liver
y m
ore
impo
rtan
t th
an g
enet
ic t
ie (
for
fam
ily r
elat
edne
ss).
Mon
itori
ng p
aren
t–ch
ild r
elat
ions
hip
thro
ugho
ut
disc
losu
re p
roce
ss.
Chi
ld’s
neu
tral
/acc
eptin
g re
actio
n re
assu
ring
.C
once
rn a
bout
mea
ning
don
or c
once
ptio
n fo
r ch
ild’s
pe
rspe
ctiv
e on
par
ent–
child
rel
atio
nshi
p.
Blyt
h, L
angr
idge
, and
H
arri
s (2
010)
Coh
eren
t fa
mily
sto
ry a
s a
way
to
pres
erve
fam
ily b
onds
.Bo
okle
ts o
ffer
voca
bula
ry fo
r pa
rent
–chi
ld c
onve
rsat
ions
.Be
lief “
open
ness
lead
s to
goo
d fa
mily
rel
atio
nshi
ps.”
Dis
clos
ure
as im
pera
tive
(“go
od p
aren
t gi
ves
child
all
he
or s
he n
eeds
”).
Dis
clos
ure
open
s ne
w s
ocia
l com
plex
ity.
Dan
iels
, Gra
ce, a
nd
Gill
ett
(201
1)C
hild
’s q
uest
ion
as c
lue
for
conv
ersa
tion
and
to p
rote
ct
the
trut
h ev
en m
ore.
In
sea
rch
for
scri
pts
for
disc
losu
re.
Pa
rent
s en
tang
led
in v
icio
us s
ecre
cy c
ircl
e.
La
ck o
f con
fiden
ce in
str
engt
h pa
rent
–chi
ld r
elat
ions
hip
at
the
base
of n
ondi
sclo
sure
.
O
penn
ess
in p
aren
t–ch
ild r
elat
ion
enda
nger
ed b
y no
ndis
clos
ure.
Ea
rly
disc
losu
re p
erce
ived
as
easi
er.
Yee
, Bly
th, a
nd T
sang
(2
011)
Add
ed c
ompl
exity
in c
ase
of k
now
n do
natio
n.M
inor
rea
ctio
ns o
f chi
ldre
n in
com
pari
son
to a
ntic
ipat
ed
fear
s.Pa
rent
s (r
ecei
vers
) ar
e en
title
d to
dis
clos
e.V
aria
bilit
y in
sto
ry t
ellin
g: F
rom
tec
hnic
al t
o fa
iry
tale
.
Tab
le 2
. (co
ntin
ued)
by guest on October 14, 2014qhr.sagepub.comDownloaded from

12 Qualitative Health Research
Participants engaged in a protective discourse favoring social relationships and stressed the importance of social bonds, commitment, love, time, and shared experiences. They seemed to decontextualize the meaning of genetic inheritance from the context of family relationships (Grace & Daniels, 2007; Hargreaves, 2006; Kirkman, 2004b, 2008; Lycett, Daniels, Curson, & Golombok, 2005). Although having genetically related children was always their first choice, they challenged the idea that bio-logical ties would bring them and their children intrinsi-cally closer (Hargreaves, 2006). However, throughout parents’ attempts to minimize the relevance of genetics to the family, genetics seem to become relevant anyway. Put another way, their efforts to create a new discourse (favor-ing social ties) show the importance that they attach to genetic relationships. Two seemingly contradictory stances became apparent: Sharing genes is unnecessary to form a family while the absence of genetic links is per-ceived as a loss and a difficulty. In five articles, this ambi-guity is evident (Becker et al., 2005; Grace & Daniels, 2007; Hargreaves, 2006; Kirkman, 2004b, 2008).
When it comes to family well-being, participants regard the intention to parent and the act of parenting as more essential than genetic links. Two notions are put forward with regard to the development of the parent–child bond in DC families. First, experiencing pregnancy (and the deliv-ery) seemed to be central in bonding with the child (Blake, Readings, Jadva, & Golombok, 2010; Hahn & Rosenberg, 2002). Parents refer to differences with adoption and sug-gest that through pregnancy and the genetic tie with one parent, they have the feeling that the child belongs to them from the start (Daniels, 1994). Second, the idea that bond-ing with the child does not occur immediately, but develops gradually, was also present in two studies (Hargreaves, 2006; Kirkman, 2004b). The social parent experiences increased bonding over time as well as increased confi-dence in the power of social family ties, which eventually becomes evident. However, as soon as bonding does not occur “naturally,” genetics become relevant again. Stated another way, in cases where “instant” attachment with the child is difficult, parents tend to emphasize the importance of genetics and attribute problems to the lack of genetic connection (Kirkman, 2004b). In several studies of Kirkman (2004b, 2008), concerns about the “realness” of social par-enthood are put forward. Parents fear being rejected by their children because they are not the “real” mother or father, suggesting that genetic parents are more genuine. However, it is also assumed that a good parent–child relation would form a “buffer” (Kirkman, 2008). Balancing the importance of genetic ties is strongly influenced by the outside world, which we address in the following theme.
Normalizing and legitimizing the family. Parents aim to be perceived and received as a “normal” family to join
society and facilitate integration (Becker et al., 2005; Brewaeys et al., 1993; Friese, Becker, & Nachtigall, 2008; Grace & Daniels, 2007; Grace, Daniels, & Gillett, 2008; Hunter, Salter-Ling, & Glover, 2000; Kirkman, 2008; Mac Dougall, Becker, Sheib, & Nachtigall, 2007). A key issue here is resemblance talk. In general, resem-blances within the family are experienced as a marker of kinship. When comments are made about (the presence or absence of) similarities, it has the potential to create dis-tance and feelings of loss as well as to embody connect-edness and feelings of happiness and pride. Parents relate to resemblance talk in a rather complex way; they use resemblance talk to support the sense of “being a family,” and they fear resemblance talk because it challenges the legitimacy of their family. Regarding the former, Becker et al. (2005) note how parents install resemblance talk to protect feelings of “familiarity” and “sameness.” Resem-blance talk is seen as a meaningful act, supporting a dis-course of relatedness (Hargreaves, 2006). Talking about likenesses forms a substitute for missing a genetic link between father and child (Burr, 2009), and parents tend to use physical resemblance to evoke relatedness with the social parent and to downgrade the connection to the donor (Hargreaves, 2006). However, when resemblance talk is initiated by others, it also threatens parents because it somehow questions their legitimacy as a family (Becker et al., 2005). Parents are sensitive to resemblance talk, as they want to normalize their family and to avoid the sense of “being different.” In addition, when comments are made about appearances, it triggers both disclosure and nondisclosure in parents (Becker et al., 2005; Shehab et al., 2008). Some parents clarify their situation by dis-closing the conception method, whereas nondisclosing parents use resemblance talk to reinforce and reassure their appearance as a seemingly genetically related fam-ily. This concept is made explicit by one woman:
We were open about it, and then as soon as we had the kids, our neighbours said, “Oh, your child looks just like you.” You don’t say, “That’s interesting because we used a donor.” I found myself not saying that and surprised I didn’t say it. I think as soon as you have children, you are so protective of them. You don’t want there to be a sense of they’re different. I’ve just found myself being totally private. (Becker et al., 2005, p. 1305)
Another way of normalizing the family is by maxi-mizing the resemblances between the child and the social parent. To do so, physical characteristics of the social parent are often matched with the donor (Becker et al., 2005; Grace & Daniels, 2007). Common to these strategies is the idea that families want to appear as a “normal” family by simulating genetic connectedness. One study about older motherhood touches on difficul-ties in this path to form a “normal” family and states that
by guest on October 14, 2014qhr.sagepub.comDownloaded from

Wyverkens et al. 13
appearing as an older mother can be socially interpreted as having used donor oocytes and cause unintended dis-closure (Friese et al., 2008). Mothers in this study fear being stigmatized, and as a result, they stress the legiti-macy of their motherhood. For instance, they “tried to link older motherhood with longstanding discourses regarding ‘good’ motherhood practices” (Friese et al., 2008, p. 70).
Finally, normalization is also present in communica-tion with the children, as parents try to present their way of family building as a “normal” and “natural” issue (Hunter et al., 2000; Mac Dougall et al., 2007)
It’s a difficult balance of bringing up the subject occasionally, or grabbing any opportunity as it suddenly arises, and not over emphasizing it to make him feel unusual. It has to seem the most natural thing in the world [mother of a 1-year-old]. (Hunter et al., 2000, p. 160)
Parents are careful not to picture the donor conception as something that “deviates” from the norm. This careful-ness that parents evince when communicating with their children is related to their more general focus on strong parent–child relationships and will be discussed in the next theme.
Building strong family ties. When we relate articles on the disclosure decisions and outcomes to our research ques-tion, what seems apparent are the concerns about family well-being and the strength of family relationships. In 13 studies, parents’ motivation to disclose—as well as their reasons to keep the donor origin secret—is presented as a choice that is made in the best interest of the child (Blake et al., 2010; Blyth, Langridge, & Harris, 2010; Brewaeys et al., 1993; Daniels et al., 2011; Daniels, Lewis, & Gillett, 1995; Hahn & Rosenberg, 2002; Hargreaves & Daniels, 2007; Hunter et al., 2000; Kirkman, 2003; Lalos, Gottlieb, & Lalos, 2007; Lindblad, Gottlieb, & Lalos, 2000; Lycett et al., 2005; Mac Dougall et al., 2007). Whether parents chose secrecy or (selective) disclosure, they express benign intentions: to protect their children from the pos-sible harm that secrecy or disclosure would cause. Specifi-cally, this means that some parents try to make the parent–child relationship stronger by being transparent and not keeping secrets, whereas others fear the prospect of endangering their relationship with their child by talk-ing about sensitive issues. Besides the effects that disclo-sure has on the strength of the relationships with their children, parents also regard the strength of the parent–child relationship as an important condition prior to telling (Daniels et al., 2011; Lalos et al., 2007; Lycett et al., 2005; Mac Dougall et al., 2007). High confidence in the strength of their relationship is foundational to disclosure, and a lack of confidence is one reason for nondisclosure.
Some parents chose to keep the DC a secret because they fear the psychological distance talking about this issue would create and the possible search for the donor: “[We] do not yet regard it as relevant whether we will tell . . . afraid that she will distance herself from her father. She is still so young” (Lindblad et al., 2000, p. 197). More arguments for nondisclosure are found across stud-ies. For instance, in four studies, participants claim that the donor origin is only a trivial matter. Through mini-mizing the importance of genetics, parents argue that knowing one’s genetic history is irrelevant, and therefore disclosing the conception method becomes superfluous (Daniels et al., 1995; Hahn & Rosenberg, 2002; Lindblad et al., 2000; Lycett et al., 2005):
We do not find it relevant to discuss this, when the legal father has always felt like the real dad. It is important to build a secure world for the child and not to talk about trifling matters. (Lindblad et al., 2000, p. 196)
At the same time, parents try to keep the DC silent, because it feels threatening to the family (Brewaeys et al., 1993; Grace & Daniels, 2007; Hargreaves & Daniels, 2007; Hunter et al., 2000). The “realness” of their parent-hood is questioned, and they are afraid that this might also become an issue for the child (Blyth et al., 2010). Thus, an apparent paradox is present as the donor concep-tion is not relevant or important to them, and at the same time, it feels threatening. The implicit primacy of genetic ties seems to prevail and causes parents to feel uncom-fortable with disclosing their family structure (Becker et al., 2005). On top of that, parents who keep the donor conception secret often feel bad about themselves and experience it as an instance of lying to their children (Daniels et al., 2011).
Other parents choose to be open because their great-est fear is that the child would devaluate the parent–child relationship, out of a sense of betrayal (in case of an accidental discovery). They believe that being trans-parent and valuing openness in their relationship will lead to strong and trusting family relationships (Blyth et al., 2010). In their narrative about the conception method, they emphasize how “special” and “unique” their child is (Hunter et al., 2000). In this way, they attempt to install an “acceptable” narrative to preserve the bond with the child (Blake et al., 2010). They also try to monitor the child’s meaning making by adapting the amount of information the child receives or the moments when donor conception is discussed. Blyth et al. (2010) also describe how disclosure opens new social complexity because, from that moment onward, children become storytellers themselves. Parents are no longer in control, and this is experienced as a threat to their privacy.
by guest on October 14, 2014qhr.sagepub.comDownloaded from

14 Qualitative Health Research
Many questions arise about the content, the manner, the timing, and the initiator of disclosure (Hunter et al., 2000; Lalos et al., 2007; Lindblad et al., 2000). Parents search for examples and advice to find out how, what, and when to tell. They navigate in a vacuum of scripts and construct their own strategies to do the best for their chil-dren. Hunter et al. (2000) highlight that the earlier parents informed the children, the easier it is. This was also found in three other studies where participants conveyed that late disclosure is more difficult (Daniels et al., 2011; Hargreaves & Daniels, 2007; Lindblad et al., 2000). Parents seem to be entangled in a vicious circle of delay-ing telling out of fear, which often makes disclosure even more difficult (Daniels et al., 2011).
In addition, disclosure decisions are embedded in mar-ital relationships, with biological parents mostly support-ing the social parent and giving more say to him or her in the decision to disclose or not. This is usually motivated by a perceived imbalance in connectedness with the child (Daniels et al., 1995; Hahn & Rosenberg, 2002; Hargreaves & Daniels, 2007). However, the study of Shehab et al. (2008) shows that one of the parents can compromise in the decision to disclose in various ways, for example, on the basis of experiential or emotional expertise in one of the partners. Hargreaves and Daniels (2007) point out that a loyalty conflict could occur in the biological parent between the needs of the children and the needs of the social parent. Besides taking care of the parent–child relationship, partners seemed to care for each other and to ensure that the position of the social parent is protected as well (Hargreaves & Daniels, 2007; Lindblad et al., 2000; Mac Dougall et al., 2007).
To summarize, the disclosure process seems a difficult and sometimes stressful task which challenges couples’ comfort and confidence in their parental role. In this pro-cess, building strong family ties is parents’ main concern.
Minimizing the role of the donor. To facilitate the experi-ence of “normative nuclear family bonds,” parents tend to “erase” the donor in their family constellation (Brewaeys et al., 1993; Burr, 2009; Grace et al., 2008). They stress the fact that in daily life, the donor’s existence is marginal and irrelevant (Grace et al., 2008). One female participant explains that “he just helped us get what we wanted at that time and then he was out of the picture, basically, for us. We’ve never thought about it in that respect again” (Grace et al., 2008, p. 306).
However, sometimes the donor issue arises once more in the family context (Brewaeys et al., 1993; Grace et al., 2008). For instance, when traits of the children cannot be recognized in the parents, this evokes thoughts about the donor. Also in medical contexts, parents are reminded of the donor’s existence. In three studies, the relation with the (sperm or oocyte) donor seems ambivalent (Burr,
2009; Kirkman, 2004a, 2008). Participants’ attitude toward the donor shifts from grateful to fear and resent-ment, and from curiosity to disinterest:
Helen: Yes, there was an amusing sort of situation as we walked back to the car parked round here [following their treatment] and we’re looking at people, going “Is that him? Or is that him? Nah surely not!” Mike: [Nodding in agreement] “It’s just a strange thing. There’s a sort of curiosity and a need to understand and know, but when you look you really don’t want to know.” (Burr, 2009, p. 711)
Parents are interested in the donor and the link he or she has with the children while they are trying to place him or her outside the family. Furthermore, they try to avoid talking about the donor because this is experienced as something painful, especially by the social parent who is reminded of his or her infertility (Brewaeys et al., 1993; Kirkman, 2004a). Families therefore struggle with the link society makes between a genetic parent and a “real” parent, whereas the social parent is the “real” parent for them (Hargreaves, 2006; Kirkman, 2004a; Mac Dougall et al., 2007). Grace et al. (2008) find that in family com-munication, the donor is systematically called “it” or “donor” instead of father, to minimize his role and to feel like they have a child of their own.
Dialectics of being different and being similar. All studies in our synthesis show how participants relate themselves to the nuclear family ideal and how they are occupied with acceptance by their social environment as they do not want to be considered as “abnormal” or “different” (e.g., Becker et al., 2005; Brewaeys et al., 1993). The concern parents feel with regard to the legitimacy of their family is not always directly described within the studied arti-cles. Rather, it seems to be present at a more implicit level. Most of the studies focus on ways to handle this concern, rather than providing experiential accounts of what parents exactly feel and fear. In this meta-ethnogra-phy, we sought to bring the experience of family relation-ships in this specific context to the fore. In doing so, we found that parents’ experiences are characterized by a dialectic tension of feeling “different” and “similar” at the same time. For instance, parents prove their “nor-malcy” by pointing out the irrelevance of genetic ties, and at the same time, they feel different because of the absence of genetic ties (first and second theme; e.g., Grace & Daniels, 2007; Hargreaves, 2006). Second, deci-sions about disclosure are found to be challenging for parents (e.g., Hunter et al., 2000; Lalos et al., 2007). Some thought it pointless to talk to the children about the method of conception because they feel like a normal family (Lindblad et al., 2000). Although they present the DC as something irrelevant, they put a lot of efforts into
by guest on October 14, 2014qhr.sagepub.comDownloaded from

Wyverkens et al. 15
trying to keep it a secret, thus making it relevant. Other parents struggle with integrating the narrative of DC in family life while seeking normalcy and recognition by the society (e.g., Blyth et al., 2010). Both disclosing and nondisclosing parents want to be good parents and are afraid of being judged for their decisions. Therefore, it could be that they rationalize and justify their choices as being made in the best interest of the child. Finally, the donor seems to be both absent and present in the family narrative (fourth theme). Parents erase the donor and yet are sometimes curious or concerned about genetic inheri-tance (e.g., Burr, 2009). Overall, they both refuse and embrace differences in their family narrative.
Discussion
With our meta-ethnography, we attempted to integrate the qualitative literature and to gain additional insight into the experiences of family relationships in DC families. We found that parents’ attempts to minimize the impor-tance of genetics, to normalize their family, to build strong families, and to minimize the role of the donor were characterized by a dialectic tension between feeling “different” and “similar” at the same time.
The participants of the studies in our review all lived in Western cultures where genetic connectedness is taken for granted and considered as inherently attached to the parent–child relationship (Hargreaves, 2006). However, for these couples, the most logical way (societal and bio-logical) to build a family seemed impossible. This might lead parents to revise their attitudes toward the relevance of genetics. Whereas the meaning of social and genetic ties is intertwined in the general population, these parents can consider the meaning of these bonds separately. As a consequence, an artificial division of family relationships is created (genetic and nongenetic). In this respect, the meaning that would be attributed to the “hybrid” of social and genetic bonds is sometimes attributed to social ties alone, because genetic ties are partly missing. In our review, we found that parents focused on the importance of love, time, and shared experiences and built a protec-tive discourse favoring social bonds as the basis for fam-ily ties (Grace & Daniels, 2007; Hargreaves, 2006; Kirkman, 2004b, 2008; Lycett et al., 2005). However, parents’ efforts to underplay the genetic connection intrinsically point at the fact that genes seemed signifi-cant to them. The heterosexual nuclear family (based on blood ties) remains the reference point and dominant definition of “the family.” In this respect, the contempo-rary focus on genetic explanations for health, illness, and personality and the increasing medicalization puts pres-sure on parents. They become responsible for the genetic makeup of the family (or the absence of genetic connec-tion in the family). Also, on a legal and ethical level, the
focus is on children’s right to know their genetic origin (Ravelingien, Provoost, & Pennings, 2013), again high-lighting the dominance of the genetic discourse.
Central to our synthesis was the parents’ underlying wish to be recognized as a “normal” family and their attempts to preserve strong familial bonds. In doing so, parents simultaneously minimized genetics and found it relevant, talked about their way of building a family and wanted to keep it secret, erased the donor and brought him to the fore, and so forth. While these attitudes might seem contradictory, we interpreted them as dialectic ten-sions that coexist as opponent forces. In general, dialec-tics refer to the assumption that in social life, people experience tensions between opposites and contradic-tions they cannot resolve. The theory of dialectics goes back to philosophical writings of Hegel (1807/1977) in his work, The Phenomenology of Mind, and the Russian philosopher Bakhtin (1981). Within family psychology, some researchers have studied dialectical processes in marital relationships (Baxter, 2011; Baxter & Montgomery, 1996), parent–child relationships (De Mol, Lemmens, Verhofstadt, & Kuczynski, 2013), and thera-peutic relationships (Rober & Seltzer, 2010). The way we interpreted the dialectic tension in our synthesis is differ-ent from these dialectical approaches in the sense that we did not identify dialectics within family relationships but rather in relation to the ideas about families in society. Parents see their families as “normal” families, which might lead them to keep the DC secret or to normalize their family situation to others. At the same time, they are confronted with medical narratives, resemblance talk, and societal ideas privileging blood ties, which make them feel “different.” The dialectic tension thus takes place between (interpersonal and intrapersonal) experi-ences of difference and normalcy, experiences that are influenced by ideas about families in society.
The tensions we identified are not entirely new to the existing literature on nontraditional families. Empirical studies with lesbian families show similar processes as identified here. For example, Nordqvist (2010) found that talking about family resemblances can create distance as well as connectedness in the context of lesbian families. Nordqvist and Smart (2014) also described how connec-tions to the donor introduce unanticipated questions and how parents manage ideas about genetic connectedness, which has become central in contemporary society. Hequembourg and Farrell (1999) and Ben-Ari and Livni (2006) also identified a dialectic tension between the mar-ginal and mainstream identity in lesbian mothers. By becoming mothers, they join the mainstream identity as a mother, whereas lesbianism is still considered as marginal in society. Also for adoptive single mothers, tensions occur as they feel autonomous and empowered by becoming a single mother on a personal level, whereas from an
by guest on October 14, 2014qhr.sagepub.comDownloaded from

16 Qualitative Health Research
interpersonal viewpoint they are considered as deviant (Ben-Ari & Weinberg-Kurnik, 2007). Although we found similar tensions in the broader literature on nontraditional families, the struggle to become a “normal” family seemed more difficult for lesbian-parented families or single moth-ers because they are more “visible” as a DC family, and they are confronted with social stigma related to the lack of a (male) parent. Besides becoming a nongenetic parent, they also face difficulties in building a nonheterosexual family. Nordqvist and Smart (2014) argue,
Donor-conceived families are the most recent of the new families and they are facing sensitive issues about whether they can fit in and look just like other families or whether they should embrace their difference while still insisting that they are perfectly proper families. (p. 7)
With our review, we have shown that this tension char-acterizes current research findings on DC families and points at a core issue that should be taken into account in counseling practice.
Some limitations need to be addressed. In line with Indekeu et al. (2013), we found it difficult to translate results from one country to other countries with different legislative contexts. At the same time, we identified very similar debates and concerns in all countries where donor-assisted conception was practiced. These debates generally focused on whether or not donor anonymity should be abandoned and whether or not openness about DC should be promoted. In the primary data, all parents expressed their concerns and doubts about disclosure and information about the donor. However, the way these debates and con-cerns are presented is very context specific. For example, Lindblad et al. (2000) presented the disclosure process as a positive experience, with parents feeling relieved and chil-dren reacting with curiosity. However, this study was con-ducted in Sweden, where disclosure is very much promoted, and this message was implicitly (even explicitly) reflected by the authors. Also, Hunter et al. (2000) recruited parents via the Donor Insemination Network in the United Kingdom and found that the earlier parents told their chil-dren about DC the better, but this is also recommended by those support groups. Thus, the social climate and the advices in counseling practice might have influenced find-ings. A more detailed study on the impact of policies and social climates is needed to make statements about its influence on family life. Second, in our attempt to analyze the family experiences in detail, we found our themes to be closely intertwined. We are aware that the presented struc-ture is only one way of interpreting the studies. However, our methodological rigor (by analyzing independently and systematically) helped to support our findings.
Our review demonstrates that—instead of studying the needs of isolated family members, motivated by societal
debates (for instance, “the need of the child to know his genetic origin”)—we need to take into account the family context. Therefore, we argue that it is necessary to hold on to a more systemic approach and to pay attention to the long-term goals in family relationships (De Mol & Buysse, 2008), as they might explain how parents relate to disclo-sure decisions and the importance they attach to genetics. In general, parents looked for ways to preserve strong family bonds and good parent–child relations (i.e., long-term goals), and their alternative way of conceiving played a marginal role in their family building. Our findings also indicate that posttreatment counseling could be beneficial to provide support and space for parents to talk about their concerns (for instance, regarding disclosure decisions). However, the identified tension of feeling “similar but dif-ferent” could prevent parents from going to counseling. Counseling usually takes place in the context of the fertil-ity centers, which possibly symbolizes parents’ experi-ences of feeling “different” (in comparison to naturally conceiving couples) because they are reminded of the fact that their children are DC. By contrast, the medicalization and narrow focus on the goal of procreating, together with the clinics’ efforts to create “normal” families and to mini-mize the differences from a genetically related two-parent family (for instance, through matching the social parent with the donor), ignore and create little space for parents’ sense of “otherness.” For counseling practice, we suggest that these dialectic tensions in trying to be seen as a nor-mal family while feeling different, as well as parents’ needs to talk and not to talk about the donor origin, should be acknowledged.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Special Research Fund of Ghent University.
Note
1. Four studies included participants from different countries: Australia, Canada, United States, United Kingdom, and Argentina.
References
Bakhtin, M. (1981). The dialogic imagination. Austin: University of Texas Press.
Baxter, L. A. (2011). Voicing relationships: A dialogical per-spective. London: SAGE.
Baxter, L. A., & Montgomery, B. M. (1996). Relating: Dialogues & dialectics. New York: Guilford Press.
by guest on October 14, 2014qhr.sagepub.comDownloaded from
Wyverkens et al. 17
Becker, G., Butler, A., & Nachtigall, R. D. (2005). Resemblance talk: A challenge for parents whose children were conceived with donor gametes in the US. Social Science & Medicine, 61, 1300–1309. doi:10.1016/j.socsci-med.2005.01.018
Ben-Ari, A., & Livni, T. (2006). Motherhood is not a given thing: Experiences and constructed meanings of biological and nonbiological lesbian mothers. Sex Roles, 54, 521–531. doi:10.1007/s11199-006-9016-0
Ben-Ari, A., & Weinberg-Kurnik, G. (2007). The dialectics between the personal and the interpersonal in the experi-ences of adoptive single mothers by choice. Sex Roles, 56, 823–833. doi:10.1007/s11199-007-9241-1
Blake, L., Readings, C. J., Jadva, V., & Golombok, S. (2010). “Daddy ran out of tadpoles”: How parents tell their chil-dren that they are donor conceived, and what their 7-year-olds understand. Human Reproduction, 25, 2527–2534. doi:10.1093/humrep/deq208
Blyth, E., Langridge, D., & Harris, R. (2010). Family building in donor conception: Parents’ experiences of sharing infor-mation. Journal of Reproductive and Infant Psychology, 28, 116–127. doi:10.1080/02646830903295018
Boivin, J., Bunting, L., Collins, J. A., & Nygren, K. G. (2007). International estimates of infertility prevalence and treat-ment-seeking: Potential need and demand for infertil-ity medical care. Human Reproduction, 22, 1506–1512. doi:10.1093/humrep/dem046
Bondas, T., & Hall, E. O. C. (2007). Challenges in approaching metasynthesis research. Qualitative Health Research, 17, 113–121. doi:10.1177/1049732306295879
Bos, H. M. W., & Van Balen, F. (2010). Children of the new reproductive technologies: Social and genetic parent-hood. Patient Education and Counseling, 81, 429–435. doi:10.1016/j.pec.2010.09.012
Brewaeys, A. (2001). Review: Parent-child relationships and child development in donor insemination families. Human Reproduction Update, 7, 38–46. doi:10.1093/humupd/7.1.38
Brewaeys, A., Ponjaert-Kristoffersen, I., Van Steirteghem, A. C., & Devroey, P. (1993). Children from anonymous donors: An inquiry into homosexual and heterosexual par-ents’ attitudes. Journal of Psychosomatic Obstetrics & Gynecology, 14, 23–35.
Burr, J. (2009). Fear, fascination and the sperm donor as “abjec-tion” in interviews with heterosexual recipients of donor insemination. Sociology of Health & Illness, 31, 705–718. doi:10.1111/j.1467-9566.2009.01171.x
Casey, P., Vasanti, J., Blake, L., & Golombok, S. (2013). Families created by donor insemination: Father–child relationships at age 7. Journal of Marriage and Family, 7, 858–870. doi:10.1111/jomf.12043
Cousineau, T. M., & Domar, A. D. (2007). Psychological impact of infertility. Best Practice & Research Clinical Obstetrics & Gynaecology, 21, 293–308. doi:10.1016/j.bpobgyn.2006.12.003
Covington, S. N., & Burns, L. H. (2006). Infertility counseling: A comprehensive handbook for clinicians. Cambridge, UK: Cambridge University Press.
Daniels, K. R. (1994). Adoption and donor insemination: Factors influencing couples’ choices. Child Welfare, 73(1), 5–14.
Daniels, K. R., Grace, V. M., & Gillett, W. R. (2011). Factors associated with parents’ decisions to tell their adult off-spring about the offspring’s donor conception. Human Reproduction, 26, 2783–2790. doi:10.1093/humrep/der247
Daniels, K. R., Lewis, G. M., & Gillett, W. (1995). Telling donor insemination offspring about their conception: The nature of couples’ decision-making. Social Science & Medicine, 40, 1213–1220. doi:10.1016/0277-9536(94)00251-N
De Mol, J., & Buysse, A. (2008). The phenomenology of chil-dren’s influence on parents. Journal of Family Therapy, 30, 163–193. doi:10.1111/j.1467-6427.2008.00424.x
De Mol, J., Lemmens, G., Verhofstadt, L., & Kuczynski, L. (2013). Intergenerational transmission in a bidirectional context. Psychologica Belgica, 53(3), 7–23. doi:10.5334/pb-53-3-7
Dixon-Woods, M., Agarwal, S., Jones, D., Young, B., & Sutton, A. (2005). Synthesising qualitative and quanti-tative evidence: A review of possible methods. Journal of Health Services Research & Policy, 10, 45–53. doi:10.1258/1355819052801804
Friese, C., Becker, G., & Nachtigall, R. D. (2008). Older moth-erhood and the changing life course in the era of assisted reproductive technologies. Journal of Aging Studies, 22, 65–73. doi:10.1016/j.jaging.2007.05.009
Golombok, S., Brewaeys, A., Giavazzi, M. T., Guerra, D., MacCallum, F., & Rust, J. (2002). The European study of assisted reproduction families: The transition to adoles-cence. Human Reproduction, 17, 830–840. doi:10.1093/humrep/17.3.830
Golombok, S., Cook, R., & Bish, A. (1995). Families created by the new reproductive technologies: Quality of parent-ing and social and emotional development of the children. Child Development, 66, 285–298. doi:10.2307/1131578
Golombok, S., Lycett, E., MacCallum, F., Vasanti, J., Murray, C., Rust, J., . . . Margara, R. (2004). Parenting infants con-ceived by gamete donation. Journal of Family Psychology, 18, 443–452. doi:10.1037/0893-3200.18.3.443
Grace, V. M., & Daniels, K. R. (2007). The (ir)relevance of genetics: Engendering parallel worlds of procreation and reproduction. Sociology of Health & Illness, 29, 692–710. doi:10.1111/j.1467-9566.2007.01010.x
Grace, V. M., Daniels, K. R., & Gillett, W. (2008). The donor, the father, and the imaginary constitution of the family: Parents’ constructions in the case of donor insemination. Social Science & Medicine, 66, 301–314. doi:10.1016/j.socscimed.2007.08.029
Hahn, S. J., & Rosenberg, M. C. (2002). The disclosure deci-sions of parents who conceive children using donor eggs. Journal of Obstetric Gynecologic & Neonatal Nursing, 31, 283–293. doi:10.1111/j.1552-6909.2002.tb00050.x
Hannes, K., & Lockwood, C. (2012). Synthesizing qualitative research: Choosing the right approach. West Sussex, UK: Wiley-Blackwell.
Hargreaves, K. (2006). Constructing families and kinship through donor insemination. Sociology of Health & Illness, 28, 261–283. doi:10.1111/j.1467-9566.2006.00492.x
Hargreaves, K., & Daniels, K. (2007). Parents dilemmas in sharing donor insemination conception stories with their children. Children & Society, 21, 420–431. doi:10.1111/j.1099-0860.2006.00079.x
by guest on October 14, 2014qhr.sagepub.comDownloaded from

18 Qualitative Health Research
Hegel, G. W. F. (1977). The phenomenology of mind (translated by A. V. Miller). Oxford, UK: Clarendon Press. (Original work published 1807)
Hequembourg, A. L., & Farrell, M. P. (1999). Lesbian mother-hood: Negotiating marginal-mainstream identities. Gender & Society, 13, 540–557. doi:10.1177/0891243990-13004007
Hunter, M., Salter-Ling, N., & Glover, L. (2000). Donor insemination: Telling children about their origins. Child Psychology & Psychiatry Review, 5, 157–163. doi:10.1017/S1360641700002355
Indekeu, A., Dierickx, K., Schotsmans, P., Daniels, K. R., Rober, P., & D’Hooghe, T. (2013). Factors contributing to parental decision-making in disclosing donor conception: A systematic review. Human Reproduction Update, 19, 714–733. doi:10.1093/humupd/dmt018
Josselson, R. (2004). The hermeneutics of faith and the hermeneutics of suspicion. Narrative Inquiry, 14, 1–28. doi:10.1075/ni.14.1.01jos
Kinn, L. G., Holgerson, H., Ekeland, T.-J., & Davidson, L. (2013). Metasynthesis and bricolage: An artistic exercise of creating a collage of meaning. Qualitative Health Research, 23, 1285–1292. doi:10.1177/1049732313502127
Kirkman, M. (2003). Parents’ contributions to the narrative identity of offspring of donor-assisted conception. Social Science & Medicine, 57, 2229–2242. doi:10.1016/S0277-9536(03)00099-6
Kirkman, M. (2004a). Genetic connection and relationships in narratives of donor-assisted conception. Australian Journal of Emerging Technologies and Society, 2(1), 1–20.
Kirkman, M. (2004b). Saviours and satyrs: Ambivalence in nar-rative meanings of sperm provision. Culture, Health & Sexuality, 6, 319–335. doi:10.1080/136910503 10001645041
Kirkman, M. (2008). Being a “real” mum: Motherhood through donated eggs and embryos. Women’s Studies International Forum, 31, 241–248. doi:10.1016/j.wsif.2008.05.006
Lalos, A., Gottlieb, C., & Lalos, O. (2007). Legislated right for donor-insemination children to know their genetic origin: A study of parental thinking. Human Reproduction, 22, 1759–1768. doi:10.1093/humrep/dem063
Lindblad, F., Gottlieb, C., & Lalos, O. (2000). To tell or not to tell—What parents think about telling their children that they were born following donor insemination. Journal of Psychosomatic Obstetrics & Gynecology, 21, 193–203. doi:10.3109/01674820009085588
Lycett, E., Daniels, K., Curson, R., & Golombok, S. (2005). School-aged children of donor insemination: A study of parents’ disclosure patterns. Human Reproduction, 20, 810–819. doi:10.1093/humrep/deh703
Mac Dougall, K., Becker, G., Sheib, J. E., & Nachtigall, R. D. (2007). Strategies for disclosure: How parents approach telling their children that they were conceived with donor gametes. Fertility and Sterility, 87, 524–533. doi:10.1016/j.fertnstert.2006.07.1514
Noblit, G. W., & Hare, R. D. (1988). Meta-ethnography: Synthesizing qualitative studies. Newbury Park, CA: SAGE.
Nordqvist, P. (2010). Out of sight, out of mind: Family resem-blances in lesbian donor conception. Sociology, 44, 1128–1144. doi:10.1177/0038038510381616
Nordqvist, P., & Smart, C. (2014). Relative strangers: Family life, genes and donor conception. Hampshire, UK: Palgrave Macmillan.
Ravelingien, A., Provoost, V., & Pennings, G. (2013). Donor-conceived children looking for their sperm donor: What do they want to know? Facts, Views & Vision in Obstetrics and Gynaecology, 5, 257–264.
Rober, P., & Seltzer, M. (2010). Avoiding colonizer positions in the therapy room: Some ideas about the challenges of dealing with the dialectic of misery and resources in fami-lies. Family Process, 49, 123–137. doi:10.1111/j.1545-5300.2010.01312.x
Shehab, D., Duff, J., Pasch, L. A., Mac Dougall, K., Sheib, J. E., & Nachtigall, R. D. (2008). How parents whose children have been conceived with donor gametes make their disclo-sure decision: Contexts, influences and couple dynamics. Fertility and Sterility, 89, 179–187. doi:10.1016/j.fertn-stert.2007.02.046
Smith, J. A., Flowers, P., & Larkin, M. (2009). Interpretative phenomenological analysis: Theory method and research. London: SAGE.
Stevens, M., Perry, B., Burston, A., & Golombok, S. (2003). Openness in lesbian-mother families regarding mother’s sexual orientation and child’s conception by donor insemi-nation. Journal of Reproductive and Infant Psychology, 21, 347–362. doi:10.1080/0264683031000-1622141
Varcoe, C., Rodney, P., & McCormick, J. (2003). Health care relationships in context: An analysis of three eth-nographies. Qualitative Health Research, 13, 957–973. doi:10.1177/1049732303253483
Yee, S., Blyth, E., & Tsang, A. K. T. (2011). Views of donors and recipients regarding disclosure to children following altru-istic known oocyte donation. Reproductive BioMedicine Online, 23, 851–859. doi:10.1016/j.rbmo.2011.06.003
Yick, A. G. (2008). A metasynthesis of qualitative findings on the role of spirituality and religiosity among culturally diverse domestic violence survivors. Qualitative Health Research, 18, 1289–1306. doi:10.1177/1049732308321772
Zimmer, L. (2006). Qualitative meta-synthesis: A question of dialoguing with texts. Journal of Advanced Nursing, 53, 311–318. doi:10.1111/j.1365-2648.2006.03721.x
Author Biographies
Elia Wyverkens, MaPsy, is a doctoral student at the Department of Experimental Clinical and Health Psychology, Faculty of Psychology and Educational Sciences, University of Ghent, Belgium.
Hanna Van Parys, PhD, is a postdoctoral researcher at the Department of Experimental Clinical and Health Psychology, Faculty of Psychology and Educational Sciences, University of Ghent, Belgium. She is also a family therapist at the Psychiatric Unit of the University Hospital Ghent, Belgium.
Ann Buysse, PhD, is a full professor in family psychology at the Department of Experimental Clinical and Health Psychology, Faculty of Psychology and Educational Sciences, University of Ghent, Belgium.
by guest on October 14, 2014qhr.sagepub.comDownloaded from
Top Related
Copyright © 2022 FDOKUMEN

