







Bahasa
Halaman
Hukum


lable at ScienceDirect
Tuberculosis 94 (2014) 701e707
Contents lists avai
Tuberculosis
journal homepage: http : / / int l .e lsevierhealth.com/journals / tube
DRUG DISCOVERY AND RESISTANCE
Enhancement of in vitro activity of tuberculosis drugs by addition ofthioridazine is not reflected by improved in vivo therapeutic efficacy
Gerjo J. de Knegt a, *, Marian T. ten Kate a, Dick van Soolingen b, Rob Aarnoutse c,Martin J. Boeree d, Irma A.J.M. Bakker-Woudenberg a, Jurriaan E.M. de Steenwinkel a
a Erasmus MC, University Medical Centre Rotterdam, Department of Medical Microbiology & Infectious Diseases, Rotterdam, The Netherlandsb National Institute for Public Health and the Environment (RIVM), National Mycobacteria Reference Laboratory, Bilthoven, The Netherlandsc Radboud University Medical Centre, Department of Pharmacy, Nijmegen, The Netherlandsd Radboud University Nijmegen Medical Centre, University Centre for Chronic Diseases Dekkerswald, Nijmegen, The Netherlands
a r t i c l e i n f o
Article history:Received 20 June 2014Received in revised form21 August 2014Accepted 1 September 2014
Keywords:Murine modelTuberculosisThioridazineSynergyTime-kill kinetics
* Corresponding author. Department of Medical Meases, Erasmus MC, University Medical Centre RotterRotterdam, The Netherlands. Tel.: þ31 10 7037267.
E-mail address: [email protected] (G.J. de
http://dx.doi.org/10.1016/j.tube.2014.09.0021472-9792/© 2014 Elsevier Ltd. All rights reserved.
s u m m a r y
Objectives: Assessment of the activity of thioridazine towards Mycobacterium tuberculosis (Mtb), in vitroand in vivo as a single drug and in combination with tuberculosis (TB) drugs.Methods: The in vitro activity of thioridazine as single drug or in combination with TB drugs was assessedin terms of MIC and by use of the time-kill kinetics assay. Various Mtb strains among which the Beijinggenotype strain BE-1585 were included.In vivo, mice with TB induced by BE-1585 were treated with a TB drug regimen with thioridazine during13 weeks. Therapeutic efficacy was assessed by the change in mycobacterial load in the lung, spleen andliver during treatment and 13 weeks post-treatment.Results: In vitro, thioridazine showed a concentration-dependent and time-dependent bactericidal ac-tivity towards both actively-replicating and slowly-replicating Mtb. Thioridazine at high concentrationscould enhance the activity of isoniazid and rifampicin, and in case of isoniazid resulted in elimination ofmycobacteria and prevention of isoniazid-resistant mutants. Thioridazine had no added value in com-bination with moxifloxacin or amikacin.In mice with TB, thioridazine was poorly tolerated, limiting the maximum tolerated dose (MTD). Theaddition of thioridazine at the MTD to an isoniazid-rifampicin-pyrazinamide regimen for 13 weeks didnot result in enhanced therapeutic efficacy.Conclusions: Thioridazine is bactericidal towards Mtb in vitro, irrespective the mycobacterial growth rateand results in enhanced activity of the standard regimen. The in vitro activity of thioridazine in poten-tiating isoniazid and rifampicin is not reflected by improved therapeutic efficacy in a murine TB-model.
© 2014 Elsevier Ltd. All rights reserved.
1. Introduction
Resistance to tuberculosis (TB) drugs is rapidly emergingworldwide with nearly half a million cases of multi-drug resistantTB (MDR-TB) recorded annually [1]. MDR-TB is caused by Myco-bacterium tuberculosis (Mtb) strains that are resistant to the twomost prominent drugs in the treatment of TB; rifampicin (RIF) andisoniazid (INH). Extensively drug-resistant tuberculosis (XDR-TB) is
icrobiology & Infectious Dis-dam, P.O. Box 2040, 3000 CA
Knegt).
caused by Mtb strains that are resistant to RIF, INH to any of thefluoroquinolones and to any of the 3 second-line injectable drugssuch as amikacin (AMK), capreomycin or kanamycin [1]. Due to thevery poor treatment outcome of MDR-TB and XDR-TB [1], moreeffective treatment is urgently needed.
In Mtb, drug resistance is mainly caused by selection of bacteriawith spontaneous mutations in chromosomal genes, during sub-optimal treatment [2]. However, accumulative evidence suggestsan important role for mycobacterial efflux pumps in the extrusionof TB drugs and emergence of drug resistance [3,4]. Analysis of thegenome of Mtb reveals that it has one of the largest numbers ofputative efflux pumps among bacteria compared to its genome size[5]. These efflux pumps can extrude several compounds andchemicals out of the bacterial cell resulting in decreased intra-

G.J. de Knegt et al. / Tuberculosis 94 (2014) 701e707702
cellular drug concentrations [6]. It has also been demonstrated thatantibiotics can serve as inducers by regulating the expression ofefflux pumps at the level of gene transcription [7].
Phenothiazines are compounds that were previously used asanti-psychotic drugs. Additionally, phenothiazines also show asignificant inhibitory effect on the growth of various clinical Mtbisolates [8]. Although, the molecular mechanism of anti-mycobacterial activity of phenothiazines is still unclear, there areseveral hypotheses. Phenothiazines can interact with the DNAmetabolism [9], or can disturb the Ca2þ-calmodulin signalling [10]and can cause alterations in the bacterial cell membrane [11].Additionally, there is the alleged ability of phenothiazines to inhibitefflux pumps [4,12]. One of the phenothiazines is thioridazine(THZ), which is active against intra- and extracellular, drug-susceptible and drug-resistant Mtb and is concentrated by humanmacrophages [8,13,14].
We hypothesized that combining TB drugs with THZ results inenhancement of the efficacy of the TB drugs in vitro as well as in amurine TB model. The goal of this study is to show that adding THZto TB drugs will improve their efficacy.
In the current study, we conducted the in vitro concentration-dependent and time-dependent killing capacity (time-kill ki-netics) of THZ towards a Mtb strain of the Beijing genotype [15].Furthermore, we investigated whether the addition of THZ toseveral TB drugs leads to synergy between compounds and canenhance the time-kill kinetics of these TB drugs towards a Beijinggenotype strain.
Finally, we investigated the therapeutic potential of co-administration of THZ to a regimen of INH, RIF and pyrazinamide(PZA) in a murine TB-model, induced by a Beijing genotype strain[16]. Outcome parameters are mycobacterial elimination in infec-ted organs and the prevention of emergence of drug resistance andrelapse of TB.
2. Materials and methods
2.1. Mtb cultures
Mtb strains H37Rv (ATCC 27294), Beijing-1585 (BE-1585) andEast-African/Indian-1627 (EAI-1627) were used. Mtb suspensionswere cultured in Middlebrook 7H9 broth (Difco Laboratories,Detroit, MI, USA), supplemented with 10% oleic acid-albumin-dextrose-catalase enrichment (OADC, Baltimore Biological Labora-tories, Baltimore, MD, USA), 0.5% glycerol (Scharlau Chemie S.A,Sentmenat, Spain) and 0.05% Tween 20 (Sigma Chemical Co, St.Louis, MO, USA), under shaking conditions at 96 rpm at 37 �C.Cultures on solid media were grown on Middlebrook 7H10 agar(Difco), supplemented with 10% OADC and 0.5% glycerol for 28 daysat 37 �C with 5% CO2.
2.2. TB drugs
Isoniazid (INH, Hospital Pharmacy; Rotterdam, TheNetherlands), rifampicin (RIF, Rifadin®, Aventis Pharma B.V, Hoe-velaken, The Netherlands), amikacin (AMK, Hospira Benelux BVBA,Brussels, Belgium) moxifloxacin (MXF, Avelox®, Bayer ScheringPharma A.G, Berlin, Germany) and thioridazine (THZ, SigmaChemical Co, St. Louis, MO, USA) were prepared according to therecommendations of the manufacturers.
2.3. Minimal inhibitory concentration (MIC)
The solid media MIC of THZ for the Mtb strains was determinedin duplicate using the agar proportion method as described by theCLSI [17]. In short, colonies grown on solid media were suspended
in broth using glass beads and vortexed during 4 min. The sus-pension was allowed to settle down for 30 min, after which thesupernatant was taken and set to an optical density of McFarlandstandard 1. Using broth, a 1:10 dilution of this Mtb suspension wasplated onto solid media containing serial two-fold dilution con-centrations of TB drug. After incubation the degree of growth wasassessed. The MIC was defined as the lowest concentration of TBdrug that resulted in >99% growth inhibition.
2.4. In vitro time-kill kinetics
The concentration-dependent and time-dependent bactericidalactivity of THZ as a single drug were determined in liquid media asdescribed previously [18]. In short, low-density cultures of activelyreplicating (exponential-phase) BE-1585 or high-density culturesof slowly replicating (stationary-phase) BE-1585 were exposed totwo-fold increasing concentrations at 37 �C. On days 1, 3 and 6samples (200 ml) were taken, provided that the mycobacterialsuspension did not show visible aggregation, and were sub-cultured on drug-free solid media for CFU counts after 28 days ofincubation at 37 �C with 5% CO2.
The time-kill kinetics of the drug combinations in low-densitycultures of actively replicating BE-1585 were determined for THZin combination with INH, RIF, MXF and AMK. The concentrations ofTB-drugs selected for these experiments resulted in a maximum10-fold change of Mtb numbers after 6 days of single drug exposurecompared to day 0. THZ concentrations ranging from 1/4� MIC to4� the MIC were added to TB drugs at two-fold increasing con-centrations. On day 6 samples (200 ml) were taken, provided thatthemycobacterial suspension did not show visible aggregation, andwere sub-cultured on drug-free and drug-containing solid mediawith 4-fold the critical concentrations of the drug [17], i.e. 0.8 mg/LINH, 4 mg/L RIF, 8 mg/L MXF or 20 mg/L AMK to select drug-resistant mutants if present. After 28 days of incubation at 37 �Cwith 5% CO2 the number of CFU at the subculture plates wasdetermined.
Synergistic activity of drugs was determined after 6 days of drugexposure and was defined as a �100-fold (Dlog 2) decrease incolony count obtained using the drug combination compared to thecolony count obtained using the most active single agent, or whenthe drug combination resulted in complete mycobacterial elimi-nation while the most active single agent did not [19].
2.5. Animals
Specified pathogen-free female BALB/c mice were obtainedfrom Charles River (Les Oncins, France). At the day of infection,animals were 13e15 weeks old and weighed 20e25 g. Experi-mental protocols adhered to the rules specified in the Dutch AnimalExperimentation Act and are in concordance with the EU animaldirective 2010/63/EU. The Institutional Animal Care and Use Com-mittee of the Erasmus MC approved the present protocol (117-09-04).
2.6. Infection
Mice were infected as described previously [16]. In short, miceunder anaesthesia were infected by intratracheal instillation of asuspension containing 6.4 � 104 CFU of BE-1585, followed byproper inhalation.
2.7. Treatment with TB drugs
For THZ a dose-finding study was performed in BE-1585 infec-ted mice with four different THZ dose-schedules added to a

G.J. de Knegt et al. / Tuberculosis 94 (2014) 701e707 703
combination of INH, RIF and PZA (HRZ) in human pharmacokinetic-equivalent doses, 25, 10 and 150 mg/kg respectively [20]. The basicexperimental scheme is shown in Table 1. A pilot experimentshowed that dose escalating of THZ was necessary because micebecame moribund when relative high doses (18e36 mg/kg/day) ofTHZ were used at the first administration due to toxic events (datanot shown). After slowly increasing the THZ dosage, mice showedinitially some discomfort but stayed alive and tolerate further in-crease of THZ dosage.
Briefly, treatment was started 2 weeks after infection and micewere randomly divided in five groups in which the THZ dosagesescalated every 3 weeks from 3 up to 12mg/kg/day in group 1, from6 up to 18 mg/kg/day in group 2, from 9 up to 27 mg/kg/day ingroup 3 and from 12 up to 36 mg/kg/day in group 4. Group 5 werecontrols receiving HRZ only. THZ in a total volume of 200 ml distilledwater was freshly prepared and daily administered intraperitone-ally, HRZ in human pharmacokinetic-equivalent doses in a totalvolume of 300 ml was daily administered subcutaneously [20].Treatment duration was 13 weeks. Subsequently, the treatmentschedule of THZ at the optimal dose obtained in the dose-findingstudy (6e18 mg/kg/day) in combination with HRZ was adminis-tered to determine therapeutic efficacy.
2.8. Determination of viable Mtb counts in infected organs
To provide more information about therapeutic efficacy andprevention of relapsemice (n¼ 4 per time point) were sacrificed byCO2 exposure at the start of therapy, after 3, 7 and 13weeks therapyand 13 weeks therapy followed by 13 weeks relapse assessment.The lung, spleen and liver were removed aseptically and processedas described previously [20]. To prevent carry-over of TB drugs,therapy was stopped 72 h before sacrificing the mice. In addition,tissue homogenate suspensions were centrifuged at 14,000 � g for10 min, and pellets were re-suspended in Phosphate Buffered Sa-line (PBS). From the tissue homogenates 10-fold serial dilutionswere performed and samples of 200 ml were cultured on drug-freeand drug-containing solid media with 4-fold the critical concen-trations of the drug [17], i.e. 0.8 mg/L INH or 4 mg/L RIF to selectdrug-resistant mutants if present.
2.9. Assessment of relapse of infection
The number of viable Mtb counts in lung, spleen and liver ofmice (n ¼ 4) was assessed 13 weeks after termination of TB treat-ment. Relapse was defined as Mtb-positive organ cultures, whileimmediately after termination of treatment organs were Mtb cul-ture-negative.
3. Results
3.1. In vitro MIC
The MICs of THZ for the three Mtb strains tested proved to besimilar, being 4e8 mg/L THZ.
Table 1Basic experimental scheme of the dose finding study.
Treatment groupY Time (weeks) /
0e2 3e5
1 Infection THZ 3 mg/kg þ HRZ2 Infection THZ 6 mg/kg þ HRZ3 Infection THZ 9 mg/kg þ HRZ4 Infection THZ 12 mg/kg þ HRZ5 Infection HRZ
3.2. In vitro time-kill kinetics
To assess synergy and the time and/or concentration dependentactivity, timeekill kinetic assays were performed for THZ as singledrug or in combination with INH, RIF, MXF and AMK for the BE-1585 strain. The activity of THZ against low-density cultures ofactively replicating BE-1585 is presented in Figure 1A. THZ showeda strong concentration- and time-dependent activity in the con-centration range tested (0.5 up to 128 mg/L). To achieve �99%mycobacterial killing, 16 mg/L THZ was needed. At a concentrationof 32 mg/L THZ, no Mtb were cultured anymore.
The activity of THZ in high-density cultures of slowly replicatingBE-1585 is presented in Figure 1B. Concentrations of 2e8 mg/L THZdid not show any activity, resulting in mycobacterial aggregation,whereas 16 mg/L THZ resulted in >99% mycobacterial killing. At aconcentration of 32 mg/L THZ, no Mtb were cultured anymore afterthree days of exposure.
The results of the time-kill kinetics in low-density cultures ofactively replicating BE-1585 after exposure to the drug combina-tions are presented in terms of Log 10 CFU/mL in Table 2. In thecontrol BE-1585 cultures CFU counts increased from 5.7 (5.6e5.8)to 7.3 (7.0e aggregation) within 6 days. Changes in CFU count of theBE-1585 cultures after 6 days of exposure to THZ as single agentwere (median þ range) 5.7 (5.6e5.8) to 5.8 (5.1e6.5), to 4.6(4.1e4.9) and to 1.9 (1.3e2.3) for 4, 8 and 16 mg/L THZ respectively.
Addition of THZ at 4, 8 or 16 mg/L to INH (0.063 mg/L) resultedin enhancedmycobacterial killing in vitro. A synergistic effect of thedrug combinationwas obtained, when THZ 8 or 16mg/L was added.No Mtb were cultured and emergence of INH resistance was pre-vented, while single drug exposure to INH resulted in selection ofINH-resistant mutants (Table 2). Addition of THZ to RIF (0.015mg/L)also showed enhancement of RIF activity, but only with the highestconcentration of THZ (16 mg/L) a synergistic activity was found. Incontrast, addition of THZ to MXF (0.031 mg/L) or AMK (0.25 mg/L)resulted in moderate improvement of the activity of MXF and AMK,but synergistic activity was not obtained.
3.3. Assessment of the maximum tolerated dose
To assess the therapeutic efficacy of the combination of HRZ andTHZ, mice were inoculated with the BE-1585 strain. Two weeksafter inoculation, mice had developed a TB infection includingextra-pulmonary dissemination and treatment was initiated. Un-treated control animals became moribund by three weeks afterinfection and were euthanized. The highest dose schedule of THZ incombinationwith HRZ (group 4) resulted in severe toxic events andfinally all mice becamemoribund after 7 weeks of treatment. Of themice from group 3, one mouse died after 4 weeks of treatment andthe othermice became seriously ill andwere euthanized.Mice fromgroup 1 and 2 showed abnormal behaviour compared to the con-trols (group 5) but symptoms disappeared within 3 weeks. Basedupon these results the THZ schedule of group 2 (from 6 to 18 mg/kg/day) was set as the maximum tolerated dosage (MTD) in ourmouse model and used to assess the therapeutic efficacy (Figure 2).
6e8 9e15
THZ 6 mg/kg þ HRZ THZ 12 mg/kg þ HRZTHZ 12 mg/kg þ HRZ THZ 18 mg/kg þ HRZTHZ 18 mg/kg þ HRZ THZ 27 mg/kg þ HRZTHZ 24 mg/kg þ HRZ THZ 36 mg/kg þ HRZHRZ HRZ
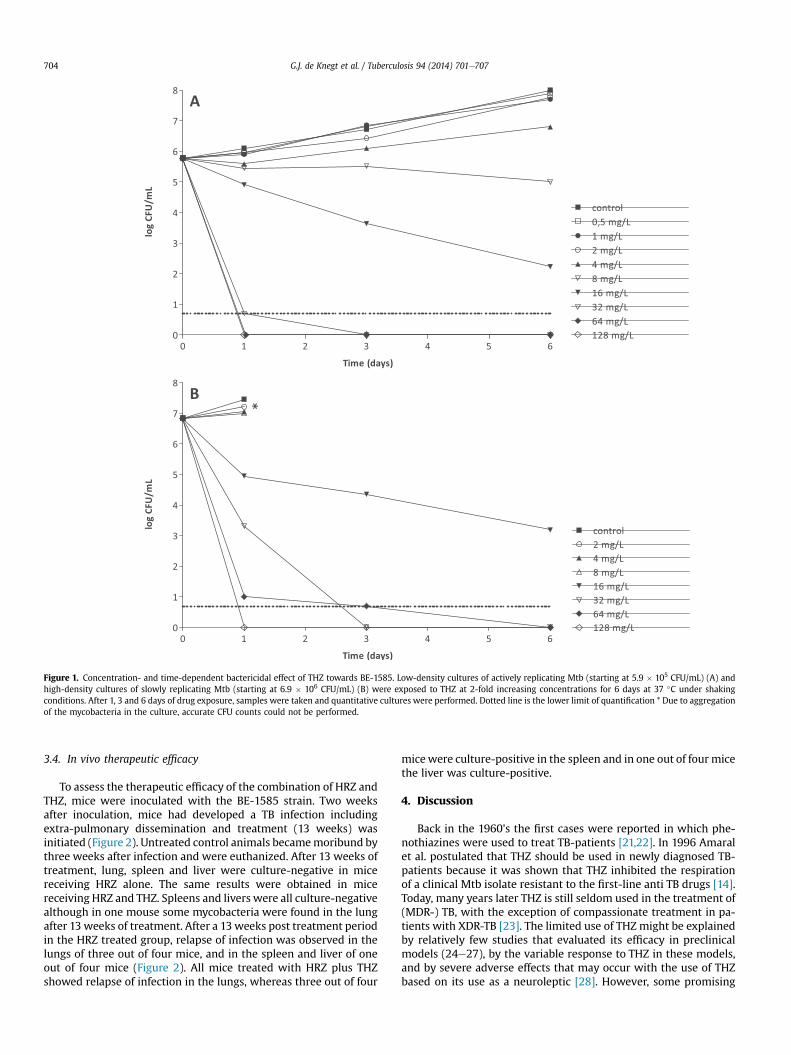
Figure 1. Concentration- and time-dependent bactericidal effect of THZ towards BE-1585. Low-density cultures of actively replicating Mtb (starting at 5.9 � 105 CFU/mL) (A) andhigh-density cultures of slowly replicating Mtb (starting at 6.9 � 106 CFU/mL) (B) were exposed to THZ at 2-fold increasing concentrations for 6 days at 37 �C under shakingconditions. After 1, 3 and 6 days of drug exposure, samples were taken and quantitative cultures were performed. Dotted line is the lower limit of quantification * Due to aggregationof the mycobacteria in the culture, accurate CFU counts could not be performed.
G.J. de Knegt et al. / Tuberculosis 94 (2014) 701e707704
3.4. In vivo therapeutic efficacy
To assess the therapeutic efficacy of the combination of HRZ andTHZ, mice were inoculated with the BE-1585 strain. Two weeksafter inoculation, mice had developed a TB infection includingextra-pulmonary dissemination and treatment (13 weeks) wasinitiated (Figure 2). Untreated control animals becamemoribund bythree weeks after infection and were euthanized. After 13 weeks oftreatment, lung, spleen and liver were culture-negative in micereceiving HRZ alone. The same results were obtained in micereceiving HRZ and THZ. Spleens and livers were all culture-negativealthough in one mouse some mycobacteria were found in the lungafter 13 weeks of treatment. After a 13weeks post treatment periodin the HRZ treated group, relapse of infection was observed in thelungs of three out of four mice, and in the spleen and liver of oneout of four mice (Figure 2). All mice treated with HRZ plus THZshowed relapse of infection in the lungs, whereas three out of four
micewere culture-positive in the spleen and in one out of four micethe liver was culture-positive.
4. Discussion
Back in the 1960's the first cases were reported in which phe-nothiazines were used to treat TB-patients [21,22]. In 1996 Amaralet al. postulated that THZ should be used in newly diagnosed TB-patients because it was shown that THZ inhibited the respirationof a clinical Mtb isolate resistant to the first-line anti TB drugs [14].Today, many years later THZ is still seldom used in the treatment of(MDR-) TB, with the exception of compassionate treatment in pa-tients with XDR-TB [23]. The limited use of THZ might be explainedby relatively few studies that evaluated its efficacy in preclinicalmodels (24e27), by the variable response to THZ in these models,and by severe adverse effects that may occur with the use of THZbased on its use as a neuroleptic [28]. However, some promising

Table 2Effect of addition of THZ on the activity of INH, RIF, MXF or AMK towards BE-1585.
TB drugs tested (mg/L) Log 10 CFU/mL atday 0 LLQ ¼ 0.7
Log 10 CFU/mL atday 6 LLQ ¼ 0.7
TB-drug resistant mutants[1 per no. of bacteria]
Change in Log 10 CFU/mL of thedrug combination compared tothe most active single agent
Control 5.7 7.3 e
INH 0.063 5.6 5.4 [1:4.7 � 103]RIF 0.015 5.8 5.4 NFMXF 0.031 5.6 5.1 NFAMK 0.25 5.6 4.8 NFTHZ 4 5.7 (5.6e5.8) 5.8 (5.0e6.3) NDTHZ 8 5.7 (5.6e5.8) 4.6 (4.1e5.0) NDTHZ 16 5.7 (5.6e5.8) 1.9 (1.2e2.6) NDINH 0.063 þ THZ 4 5.6 2.8 NF �2.6*
INH 0.063 þ THZ 8 5.6 No bacteria cultured NF �4.0y
INH 0.063 þ THZ 16 5.6 No bacteria cultured NF �2.1y
RIF 0.015 þ THZ 4 5.8 3.7 NF �1.9RIF 0.015 þ THZ 8 5.8 3.4 NF �1.6RIF 0.015 þ THZ 16 5.8 No bacteria cultured NF �2.5y
MXF 0.031 þ THZ 4 5.6 4.7 NF �0.4MXF 0.031 þ THZ 8 5.6 4.1 NF �0.7MXF 0.031 þ THZ 16 5.6 2.1 NF þ0.4AMK 0.25 þ THZ 4 5.6 4.1 NF �0.7AMK 0.25 þ THZ 8 5.6 3.3 NF �1.3AMK 0.25 þ THZ 16 5.6 1.3 NF þ0.1
Low-density cultures of actively replicating BE-1585 were exposed to THZ for 6 days at 37 �C under shaking conditions. At day 6, samples were taken and quantitative cultureswere performed on drug free and drug containing solid media.LLQ ¼ lower limit of quantification.ND ¼ not determined.NF ¼ not found.
* Synergy.y Complete elimination of mycobacteria.
G.J. de Knegt et al. / Tuberculosis 94 (2014) 701e707 705
results were obtained with respect to the activity of THZ againstintracellular mycobacteria regardless the susceptibility status of themycobacteria [13], and this encouraged further investigation of theuse of THZ as a TB drug. Moreover, there is evidence that THZ is apotent inhibitor of efflux pumps, possibly causing accumulation ofdrugs inside phagocytic and bacterial cells and as such yielding asynergistic effect [4,12]. The present study evaluates the activity ofTHZ, as single drug or in combination with TB drugs, towardsactively replicating and slowly replicating mycobacteria of theBeijing genotype in vitro, and in murine TB caused by the sameBeijing strain in vivo.
In the present study the in vitro activity of THZ in terms of MICwas demonstrated towards H37Rv, BE-1585 and EAI-1627 strains.We found that THZ MIC values were similar and conclude that THZis active against extracellular Mtb, irrespective their genotype.
Among the in vitro susceptibility assays currently used, the solidmedia MIC assay provides endpoint data that are obtained after 4weeks of Mtb exposure to TB drugs. With such an assay only in-hibition of mycobacterial growth is detected. In the present studywe also performed the time-kill kinetic assay which is moreinformative with respect to the concentration-dependent andtime-dependent activity of the drug (Figure 1A and 1B), and alsodetermines mycobacterial killing. Using this assay, we concludethat THZ is effective in killing of extra-cellular BE-1585. As aremark, relatively high concentrations of THZ (�16 mg/L) areneeded to achieve mycobacterial killing in both the actively repli-cating Mtb (exponential-phase) (Figure 1A) as well as in the slowlyreplicating (stationary-phase) (Figure 1B). It is also shown that thebactericidal activity is irrespective of the replicating activity of themycobacteria. The relevance of this observation lies in the fact thatthe killing capacity of THZ towards slowly replicating mycobacteriais important from a therapeutic point of view, as it is thought thatdeep-seated Mtb in tissues during the dormant state probablyexhibit low metabolic activity. It is expected that these low-activeMtb are difficult to eliminate because most currently used TBdrugs are primarily active against actively replicating Mtb.
In the present study also combinations of several common TBdrugs and THZ were tested in low-density cultures of activelyreplicating BE-1585. In these studies the concentrations of TB drugswere selected that resulted in a maximum of 10-fold change in CFUcounts during 6 days of single drug exposure compared to day 0.The value of addition of THZ to the TB drugs was most pronouncedfor INH. With the three concentrations of THZ tested in combina-tion with INH, a substantial increased killing of Mtb was achievedand synergistic activity was obtained. With THZ 8 and 16 mg/L noMtb were cultured anymore. Furthermore, whereas INH-resistantmutants occurred after exposure of Mtb to INH as single drug, theaddition of THZ at all three concentrations prevented selection ofINH-resistant mutants. This result expands upon a prior study ofDutta et al. in which they presented in an acute murine model thattreatment with INH þ THZ reduced the frequency of INH-resistantmutants by 7-fold [24]. Machado et al. showed in vitro that INH-resistance can be reduced by inhibiting certain mycobacterialefflux pumps by exposure to THZ [29]. The potential of THZ in thisrespect is of high importance in view of the worldwide emergingINH resistance.
The enhanced activity of TB drugs following the addition of THZwas also observed in the combination of THZ-RIF. This is probablydue to an increase in intrabacterial concentrations of RIF [30]. Thisincrease is possibly caused by an increased cell wall permeability orinhibition of efflux pumps. The synergy found of THZ and RIF is inconcordance with a study of Viveiros et al. in which they alsodemonstrated an enhanced activity of RIF following addition of THZ[31]. However, they did not find enhanced activity of INH afteraddition of THZ [31], which might be explained by the use of poly-drug resistant Mtb strains or the much lower concentrations of INHapplied in their experiments.
The in vitro observations of the present study were realized withTHZ concentrations that are clinically not achievable. However, it isknown that accumulation of phenothiazines can occur withinalveolar macrophages [32], also Dutta et al. showed that THZ ac-cumulates at high concentration in lung tissue relative the serum
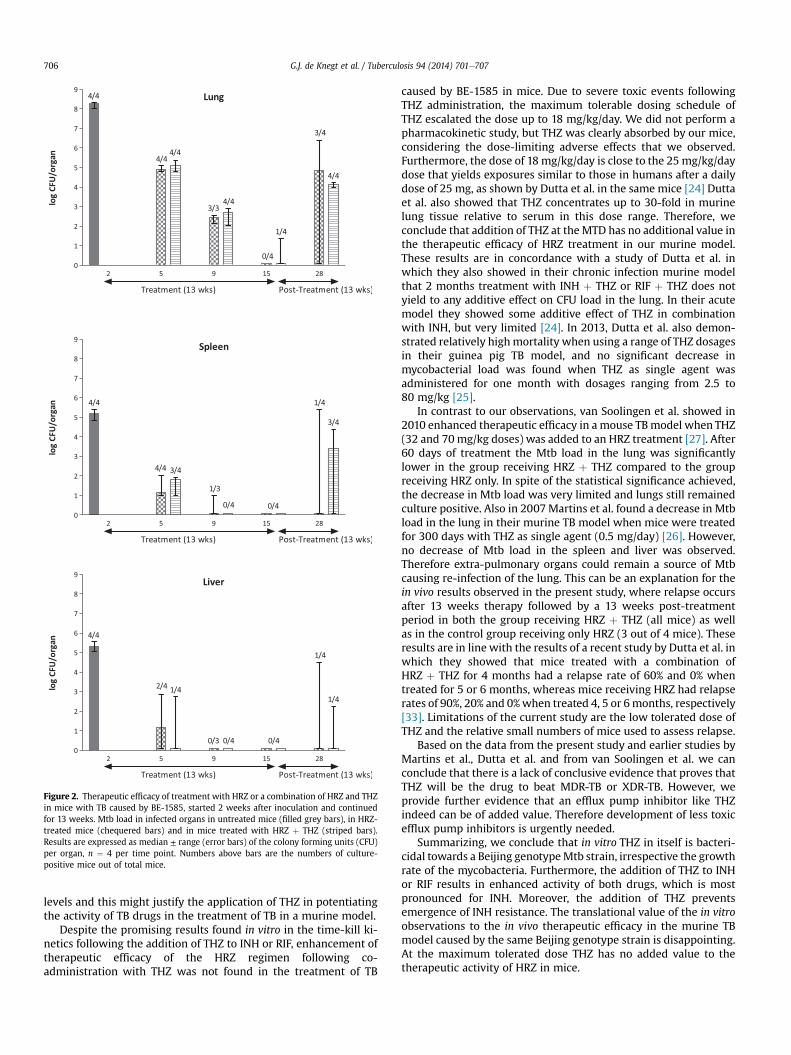
Figure 2. Therapeutic efficacy of treatment with HRZ or a combination of HRZ and THZin mice with TB caused by BE-1585, started 2 weeks after inoculation and continuedfor 13 weeks. Mtb load in infected organs in untreated mice (filled grey bars), in HRZ-treated mice (chequered bars) and in mice treated with HRZ þ THZ (striped bars).Results are expressed as median ± range (error bars) of the colony forming units (CFU)per organ, n ¼ 4 per time point. Numbers above bars are the numbers of culture-positive mice out of total mice.
G.J. de Knegt et al. / Tuberculosis 94 (2014) 701e707706
levels and this might justify the application of THZ in potentiatingthe activity of TB drugs in the treatment of TB in a murine model.
Despite the promising results found in vitro in the time-kill ki-netics following the addition of THZ to INH or RIF, enhancement oftherapeutic efficacy of the HRZ regimen following co-administration with THZ was not found in the treatment of TB
caused by BE-1585 in mice. Due to severe toxic events followingTHZ administration, the maximum tolerable dosing schedule ofTHZ escalated the dose up to 18 mg/kg/day. We did not perform apharmacokinetic study, but THZ was clearly absorbed by our mice,considering the dose-limiting adverse effects that we observed.Furthermore, the dose of 18 mg/kg/day is close to the 25 mg/kg/daydose that yields exposures similar to those in humans after a dailydose of 25 mg, as shown by Dutta et al. in the same mice [24] Duttaet al. also showed that THZ concentrates up to 30-fold in murinelung tissue relative to serum in this dose range. Therefore, weconclude that addition of THZ at theMTD has no additional value inthe therapeutic efficacy of HRZ treatment in our murine model.These results are in concordance with a study of Dutta et al. inwhich they also showed in their chronic infection murine modelthat 2 months treatment with INH þ THZ or RIF þ THZ does notyield to any additive effect on CFU load in the lung. In their acutemodel they showed some additive effect of THZ in combinationwith INH, but very limited [24]. In 2013, Dutta et al. also demon-strated relatively highmortality when using a range of THZ dosagesin their guinea pig TB model, and no significant decrease inmycobacterial load was found when THZ as single agent wasadministered for one month with dosages ranging from 2.5 to80 mg/kg [25].
In contrast to our observations, van Soolingen et al. showed in2010 enhanced therapeutic efficacy in a mouse TBmodel when THZ(32 and 70mg/kg doses) was added to an HRZ treatment [27]. After60 days of treatment the Mtb load in the lung was significantlylower in the group receiving HRZ þ THZ compared to the groupreceiving HRZ only. In spite of the statistical significance achieved,the decrease in Mtb load was very limited and lungs still remainedculture positive. Also in 2007Martins et al. found a decrease in Mtbload in the lung in their murine TB model when mice were treatedfor 300 days with THZ as single agent (0.5 mg/day) [26]. However,no decrease of Mtb load in the spleen and liver was observed.Therefore extra-pulmonary organs could remain a source of Mtbcausing re-infection of the lung. This can be an explanation for thein vivo results observed in the present study, where relapse occursafter 13 weeks therapy followed by a 13 weeks post-treatmentperiod in both the group receiving HRZ þ THZ (all mice) as wellas in the control group receiving only HRZ (3 out of 4 mice). Theseresults are in line with the results of a recent study by Dutta et al. inwhich they showed that mice treated with a combination ofHRZ þ THZ for 4 months had a relapse rate of 60% and 0% whentreated for 5 or 6 months, whereas mice receiving HRZ had relapserates of 90%, 20% and 0%when treated 4, 5 or 6months, respectively[33]. Limitations of the current study are the low tolerated dose ofTHZ and the relative small numbers of mice used to assess relapse.
Based on the data from the present study and earlier studies byMartins et al., Dutta et al. and from van Soolingen et al. we canconclude that there is a lack of conclusive evidence that proves thatTHZ will be the drug to beat MDR-TB or XDR-TB. However, weprovide further evidence that an efflux pump inhibitor like THZindeed can be of added value. Therefore development of less toxicefflux pump inhibitors is urgently needed.
Summarizing, we conclude that in vitro THZ in itself is bacteri-cidal towards a Beijing genotypeMtb strain, irrespective the growthrate of the mycobacteria. Furthermore, the addition of THZ to INHor RIF results in enhanced activity of both drugs, which is mostpronounced for INH. Moreover, the addition of THZ preventsemergence of INH resistance. The translational value of the in vitroobservations to the in vivo therapeutic efficacy in the murine TBmodel caused by the same Beijing genotype strain is disappointing.At the maximum tolerated dose THZ has no added value to thetherapeutic activity of HRZ in mice.
G.J. de Knegt et al. / Tuberculosis 94 (2014) 701e707 707
Transparency declarations: None to declare.
Funding: This work was financially supported by ZonMW(Priority Medicines Antimicrobi€ele Resistentie, project205200002).
Competing interests: None declared.
Ethical approval: Experimental protocols adhered to therules specified in the Dutch Animal Experimentation Act and arein concordance with the EU animal directive 2010/63/EU. TheInstitutional Animal Care and Use Committee of the Erasmus MCapproved the present protocol (117-09-04).
References
[1] WHO. Global tuberculosis control. 2011.[2] Ramaswamy S, Musser JM. Molecular genetic basis of antimicrobial agent
resistance in Mycobacterium tuberculosis: 1998 update. Tuber Lung Dis1998;79:3e29.
[3] Jarlier V, Nikaido H. Mycobacterial cell wall: structure and role in naturalresistance to antibiotics. FEMS Microbiol Lett 1994;123:11e8.
[4] Viveiros M, Leandro C, Amaral L. Mycobacterial efflux pumps and chemo-therapeutic implications. Int J Antimicrob Agents 2003;22:274e8.
[5] Paulsen IT, Chen J, Nelson KE, Saier Jr MH. Comparative genomics of microbialdrug efflux systems. J Mol Microbiol Biotechnol 2001;3:145e50.
[6] da Silva PE, Von Groll A, Martin A, Palomino JC. Efflux as a mechanism for drugresistance in Mycobacterium tuberculosis. FEMS Immunol Med Microbiol2011;63:1e9.
[7] Louw GE, Warren RM, Gey van Pittius NC, Leon R, Jimenez A, Pando RH,McEvoy CR, Grobbelaar M, Murray M, van Helden PD, Victor TC. Rifampicinreduces susceptibility to ofloxacin in rifampicin resistant Mycobacteriumtuberculosis through efflux. Am J Respir Crit Care Med 2011 Jul 15;184(2):269e76.
[8] Bettencourt MV, Bosne-David S, Amaral L. Comparative in vitro activity ofphenothiazines against multidrug-resistant Mycobacterium tuberculosis. Int JAntimicrob Agents 2000;16:69e71.
[9] Miskolci C, Labadi I, Kurihara T, Motohashi N, Molnar J. Guanine-cytosine richregions of plasmid DNA can be the target in anti-plasmid effect of pheno-thiazines. Int J Antimicrob Agents 2000;14:243e7.
[10] Martins M, Viveiros M, Amaral L. Inhibitors of Ca2þ and Kþ transport enhanceintracellular killing of M. tuberculosis by non-killing macrophages. In Vivo2008;22:69e75.
[11] Michalak K, Wesolowska O, Motohashi N, Molnar J, Hendrich AB. Interactionsof phenothiazines with lipid bilayer and their role in multidrug resistancereversal. Curr Drug Targets 2006;7:1095e105.
[12] Kaatz GW, Moudgal VV, Seo SM, Kristiansen JE. Phenothiazines and thio-xanthenes inhibit multidrug efflux pump activity in Staphylococcus aureus.Antimicrob Agents Chemother 2003;47:719e26.
[13] Ordway D, Viveiros M, Leandro C, Bettencourt R, Almeida J, Martins M,Kristiansen JE, Molnar J, Amaral L. Clinical concentrations of thioridazine killintracellular multidrug-resistant Mycobacterium tuberculosis. AntimicrobAgents Chemother 2003;47:917e22.
[14] Amaral L, Kristiansen JE, Abebe LS, Millett W. Inhibition of the respiration ofmulti-drug resistant clinical isolates of Mycobacterium tuberculosis by thio-ridazine: potential use for initial therapy of freshly diagnosed tuberculosis.J Antimicrob Chemother 1996;38:1049e53.
[15] de Steenwinkel JE, ten Kate MT, de Knegt GJ, Kremer K, Aarnoutse RE,Boeree MJ, Verbrugh HA, van Soolingen D, Bakker-Woudenberg IA. Drugsusceptibility of Mycobacterium tuberculosis Beijing genotype and associationwith MDR TB. Emerg Infect Dis 2012;18:660e3.
[16] de Steenwinkel JE, Ten Kate MT, de Knegt GJ, Verbrugh HA, Aarnoutse RE,Boeree MJ, den Bakker MA, van Soolingen D, Bakker-Woudenberg IA. Con-sequences of noncompliance for therapy efficacy and emergence of resistancein murine tuberculosis caused by the Beijing genotype of Mycobacteriumtuberculosis. Antimicrob Agents Chemother 2012;56:4937e44.
[17] NCCLS. Susceptibility testing of mycobacteria, nocardia, and other aerobicactinomycetes; approved standarddsecond edition. 31. 2012.
[18] de Steenwinkel JE, de Knegt GJ, ten Kate MT, van Belkum A, Verbrugh HA,Kremer K, van Soolingen D, Bakker-Woudenberg IA. Time-kill kinetics of anti-tuberculosis drugs, and emergence of resistance, in relation to metabolic ac-tivity of Mycobacterium tuberculosis. J Antimicrob Chemother 2010;65:2582e9.
[19] Doern CD. When does 2 þ 2 ¼ 5?: a review of antimicrobial synergy testing.J Clin Microbiol 2014 Jun 11. pii: JCM.01121-14.
[20] De Steenwinkel JE, De Knegt GJ, Ten Kate MT, Van Belkum A, Verbrugh HA,Hernandez-Pando R, Van Soolingen D, Bakker-Woudenberg IA. Immunolog-ical parameters to define infection progression and therapy response in awell-defined tuberculosis model in mice. Int J Immunopathol Pharmacol2009;22:723e34.
[21] Gover DM. Thioridazine and chlorprothixene in the management of anxiety intuberculous patients. Am Rev Respir Dis 1962;85:587e90.
[22] Hollister LE, Eikenberry DT, Raffel S. Chlorpromazine in nonpsychotic patientswith pulmonary tuberculosis. Am Rev Respir Dis 1960;81:562e6.
[23] Abbate E, Vescovo M, Natiello M, Cufre M, Garcia A, Gonzalez Montaner P,Ambroggi M, Ritacco V, van Soolingen D. Successful alternative treatment ofextensively drug-resistant tuberculosis in Argentina with a combination oflinezolid, moxifloxacin and thioridazine. J Antimicrob Chemother 2012;67:473e7.
[24] Dutta NK, Pinn ML, Karakousis PC. Reduced emergence of isoniazid resistancewith concurrent use of thioridazine against acute murine tuberculosis. Anti-microb Agents Chemother 2014 Jul;58(7):4048e53.
[25] Dutta NK, Pinn ML, Zhao M, Rudek MA, Karakousis PC. Thioridazine lacksbactericidal activity in an animal model of extracellular tuberculosis.J Antimicrob Chemother 2013;68:1327e30.
[26] Martins M, Viveiros M, Kristiansen JE, Molnar J, Amaral L. The curative activityof thioridazine on mice infected with Mycobacterium tuberculosis. In Vivo2007;21:771e5.
[27] van Soolingen D, Hernandez-Pando R, Orozco H, Aguilar D, Magis-Escurra C,Amaral L, van Ingen J, Boeree MJ. The antipsychotic thioridazine showspromising therapeutic activity in a mouse model of multidrug-resistanttuberculosis. PLoS One 2010;5.
[28] Alvarez PA, Pahissa J. QT alterations in psychopharmacology: proven candi-dates and suspects. Curr Drug Saf 2010;5:97e104.
[29] Machado D, Couto I, Perdigao J, Rodrigues L, Portugal I, Baptista P, Veigas B,Amaral L, Viveiros M. Contribution of efflux to the emergence of isoniazid andmultidrug resistance in Mycobacterium tuberculosis. PLoS One 2012;7:e34538.
[30] Sharma S, Singh A. Phenothiazines as anti-tubercular agents: mechanisticinsights and clinical implications. Expert Opin Investig Drugs 2011;20:1665e76.
[31] Viveiros M, Amaral L. Enhancement of antibiotic activity against poly-drugresistant Mycobacterium tuberculosis by phenothiazines. Int J AntimicrobAgents 2001;17:225e8.
[32] Crowle AJ, Douvas GS, May MH. Chlorpromazine: a drug potentially useful fortreating mycobacterial infections. Chemotherapy 1992;38:410e9.
[33] Dutta NK, Pinn ML, Karakousis PC. Sterilizing activity of thioridazine incombination with the first-line regimen against acute murine TB. AntimicrobAgents Chemother 2014 Sep;58(9):5567e9.
Top Related
Copyright © 2022 FDOKUMEN

