







Bahasa
Halaman
Hukum


Ava i l ab l e on l i ne a t www.sc i enced i r ec t . com
Journal of Crohn's and Colitis (2012) 6, 913–923
Elevated levels of serum-soluble triggering receptorexpressed on myeloid cells-1 in patients with IBD donot correlate with intestinal TREM-1 mRNA expressionand endoscopic disease activityLeslie Saurer a,⁎,1, Silvia Rihs a,1, Michèle Birrer a, Nikolina Saxer-Seculic b,Markus Radsak c, Christoph Mueller a
The Swiss IBD Cohort Study d
a Division of Experimental Pathology, Institute of Pathology, University of Bern, Bern, Switzerlandb Division of Clinical Pathology, University Hospital of Geneva, Geneva, Switzerlandc Institute of Immunology, University of Mainz, 55131 Mainz, Germanyd See Appendix
Received 7 November 2011; received in revised form 9 February 2012; accepted 11 February 2012
Abbreviations: CD, Crohn's disease;Expressed on Myeloid Cells-1; UC, Ulce⁎ Corresponding author at: Institute o
fax: +41 31 381 87 64.E-mail address: leslie.saurer@path
1 The first two authors contributed e
1873-9946/$ - see front matter © 2012doi:10.1016/j.crohns.2012.02.010
KEYWORDS:Crohn's disease;Ulcerative colitis;TREM-1;TLR;Inflammatory bowel disease
Abstract
Background & aims: Triggering receptor expressed on myeloid cells-1 (TREM-1) is a potent am-plifier of pro-inflammatory responses. We have previously demonstrated a substantial increasein TREM-1-expressing macrophages in the inflamed intestinal mucosa of patients with inflamma-tory bowel diseases (IBD). TREM-1 is also produced as a soluble receptor (sTREM-1). Here, weaimed to determine whether serum sTREM-1 could be used as a surrogate marker of disease ac-
tivity in patients with IBD.Methods: Intestinal biopsies and concurrently collected sera from patients with Crohn's disease(CD) and Ulcerative colitis (UC) enrolled in the Swiss IBD cohort study were analyzed for intesti-nal TREM-1 mRNA and serum sTREM-1 expression. TREM-1 mRNA and sTREM-1 were correlatedwith the endoscopically determined disease activity. Serum sTREM-1 and TREM-1 mRNA expres-sion levels were further determined in sera and colonic tissues collected at various time-pointsIBD, inflammatory bowel diseases; TLR, Toll-like receptor (s); TREM-1, (soluble) Triggering Receptor-rative colitisf Pathology, University of Bern, Murtenstrasse 31, CH-3010 Bern, Switzerland. Tel.: +41 31 632 88 78;
ology.unibe.ch (L. Saurer).qually.
European Crohn's and Colitis Organisation. Published by Elsevier B.V. All rights reserved.

914 L. Saurer et al.
post disease induction in an experimental mouse model of colitis and correlated with diseaseactivity.Results: Expression of TREM-1 mRNA was upregulated in intestinal biopsies from patients withactive disease but not in patients with quiescent disease. Serum sTREM-1 was elevated in IBD pa-tients compared to normal controls. No substantial differences in sTREM-1 expression levelswere found in patients with active versus quiescent disease. In colitic mice, colonic TREM-1mRNA and serum sTREM-1 were also upregulated. While colonic TREM-1 mRNA expression levelscorrelated with disease activity, augmented serum sTREM-1 in fact associated with a mildercourse of disease.Conclusions: Analysis of sTREM-1 as a surrogate marker of disease activity in patients with IBDwarrants caution.© 2012 European Crohn's and Colitis Organisation. Published by Elsevier B.V. All rights reserved.
1. Introduction
Inflammatory bowel diseases (IBD) are a heterogeneousgroup of diseases comprising the two major disease entitiesCrohn's disease (CD) and ulcerative colitis (UC). While CDand UC differentially affect the gastrointestinal tract andlikely differ in their pathogenetic mechanisms, both CD andUC are believed to be driven by aberrant innate immune re-sponses to the commensal flora in genetically susceptible in-dividuals.1,2 A characteristic feature of both CD and UC isalso the fluctuating disease course with episodes of relapse(active disease) and remission (quiescent disease), whichcomplicate an adequate treatment of individual patients.Since endoscopy for accurate assessment of disease activityand treatment efficacy is time-consuming and expensive,considerable efforts have been undertaken to evaluatenon-invasive surrogate biomarkers and disease activity indi-ces based on clinical parameters. Among laboratory parame-ters, CRP, ESR and peripheral blood leukocyte counts areroutinely assessed, but representing acute phase reactants,exhibit low specificity for IBD. Clinical disease activity indi-ces such as the Crohn's disease activity index (CDAI) areprone to subjective judgements and have a low sensitivityin detecting subclinical inflammation or discriminating qui-escent from active disease.3
In contrast, and in keeping with the established role ofinnate immune cells in driving intestinal inflammation inIBD, presence of proteins derived from degranulating phago-cytes in the stool has been shown to closely correlate withendoscopic disease activity.3,4 Although these fecal bio-markers, such as calprotectin and lactoferrin, are now con-sidered the gold standard among the currently employedbiomarkers, analyses of fecal samples are not routinely per-formed and may not as well be accepted by patients andclinicians.
Triggering receptor expressed on myeloid cells-1 (TREM-1) is a member of the immunoglobulin superfamily predomi-nantly expressed on neutrophils and on subsets of monocytes/macrophages.5 Binding of the yet unidentified ligands toTREM-1 potently synergizes with distinct Toll-like receptor(TLR) ligands in amplifying oxidative burst and pro-inflammatory cytokine production.5–7 The TLR ligands LPSand lipoteichoic acid,6 but also the Nacht-LRR receptor(NLR) ligand muramyldipeptide8 and other stimuli such asthe pro-inflammatory cytokines TNFα and GM-CSF9 can
further upregulate surface TREM-1 expression. TREM-1 canalso be produced in a soluble form (sTREM-1)10,11 which isbelieved to originate from a protease-dependent shedding ofmembrane-bound TREM-1.12 Elevated serum levels of sTREM-1 are indicative of microbial infections,13,14 however, aug-mented sTREM-1 levels have also been reported for patientswith non-infectious inflammatory conditions such as rheuma-toid arthritis,15 acute pancreatitis,16 chronic obstructive pul-monary disease17 and cardiac arrest.18 Thus, sTREM-1 maynot only be considered a diagnosticmarker for microbial infec-tions, but may also have the potential to serve as a novelsurrogate marker to assess disease severity in other inflamma-tory diseases.
We have recently demonstrated a significant increase inTREM-1 mRNA and protein, relating to an accumulation inTREM-1-expressing macrophages, in the inflamed intestinalmucosa of patients with IBD and mice with experimentalcolitis19,20 while TREM-1 expression was almost undetect-able in normal control samples and tissue specimens fromunaffected intestinal areas.19,21 Importantly, intestinal mac-rophages from patients with IBD but not from normal controlsproduced substantially increased levels of pro-inflammatorycytokines upon TREM-1-mediated activation in vitro,19 andblocking TREM-1 in two mouse models of experimental colitissignificantly attenuated disease.19 Based on the observedaccumulation of TREM-1-expressing cells in the inflamed intes-tinal tissue and the seemingly prominent role of TREM-1 inthe pathogenesis of IBD, we aimed to determine whetherincreased intestinal TREM-1 expression is reflected in elevatedlevels of serum sTREM-1 and whether sTREM-1 in the serumcould thus serve as a novel elegant tool to assess disease activ-ity in patients with IBD.
2. Materials and methods
2.1. Patients and samples
Criteria for inclusion of patients into the Swiss IBD cohortstudy (SIBDCS), the SIBDCS profile and ethical approvalhave been described previously.22 40 patients with Crohn'sdisease (CD) and 40 patients with Ulcerative colitis (UC)were selected from the cohort based on the availabilityof concurrently collected sera and intestinal biopsies. Serawere frozen at −80 °C within 24–48 h post collection.

915sTREM-1 as surrogate marker of disease activity in IBD
Intestinal biopsies were directly sampled into RNAlater RNAstabilization reagent (Ambion) and stored at −80 °C.
The 40 patients with CD or UC, respectively, included 20patients with quiescent disease and 20 additional patientswith active disease. Classification of disease activity intoquiescent and active was based on macroscopic findingsat the time-point of endoscopy. Mucosal healing or slighterythema were considered as quiescent disease whereasovert erythema and edema of the mucosa, aphthous diseaseor presence of ulcers were considered as active disease. Pa-tients with infectious colitis were excluded from the study.Mean age and gender distribution of patients with CD andUC were as follows: CD: 43±15 years, 42.5% females, andUC: 44.5±13 years, 45% females. The controls were healthypersons recruited from the laboratory staff who had provid-ed written consent for the collection of blood samples.
2.2. Mice
RAG2−/− mice were bred and maintained under SPF condi-tions in the central animal facility of the Medical School,University of Bern. All animal experiments were approvedby the state of Bern committee for animal experimentation(license number: 79/08).
2.3. Determination of sTREM-1 in sera and culturesupernatants
Human serum sTREM-1 levels were determined by an in-house optimized ELISA using the anti-human TREM-1 mAbclone 6B1.1 G12 (generous gift from M. Radsak, Universityof Mainz) at 10 μg/ml for coating and reagents from theHuman TREM-1 Duoset (R&D) for detection (according tomanufacturers' instructions). Mouse serum sTREM-1 wasmeasured by ELISA using the Mouse TREM-1 Duoset reagentsfrom R&D.
2.4. RNA isolation
RNA was isolated from one intestinal biopsy per patient usingthe Qiagen RNeasy Mini kit and following the manufacturers'instructions. RNA from mouse colonic tissue specimens wasisolated with the RNA isolation reagent Tri-reagent (Molecu-lar research center).
2.5. Quantitative RT-PCR for intestinal TREM-1 andS100A9 mRNA
RNA (≤2 μg) from human intestinal biopsies and mouse co-lonic tissue specimens was DNase treated using a RNAse-free DNase I (Ambion) and cDNA was generated with theHigh Capacity cDNA Reverse Transcription Kit (Applied Bio-systems). Expression of TREM-1 and S100A9 mRNA was ana-lyzed on a 7500 Real-time PCR System (Applied Biosystems)using Qiagen Quantitect Primer Assays. The house-keepinggene GAPDH was used for normalization of TREM-1 mRNAexpression.
2.6. Flow cytometry
TREM-1 surface expression was determined by staining withthe anti-human TREM-1 mAb clone 21C7 (hybridoma super-natant; generous gift from M. Colonna, Washington Univer-sity School of Medicine) followed by goat-anti-mouse Ig PE-labeled (Fab)2 (BD Biosciences). The mouse IgG1 cloneMOPC-21 of irrelevant specificity was used as isotype con-trol. Cells were acquired on a LSRII flow cytometer (BD Bio-sciences) and analyzed using Flowjo software (Tree Star).
2.7. Leukocyte isolations and in vitro cultures
Leukocytes from healthy controls were isolated from hepa-rinized blood by a 50′ sedimentation of erythrocytes over12% (w/v) Optiprep (Axis-Shiled, Oslo, Norway) and 16 g/lMethocel (Fluka, Buchs, Switzerland) in 130 mM NaCl. Theleukocyte-rich plasmawas subsequently collected andwashedwith IMDM 10% FCS (Sigma). Leukocytes were cultured at5×106 cells/well in 96-well flat bottom plates in the presenceof 100 ng/ml LPS (Sigma) for 24 h. Cell-free supernatantswere subsequently collected for analysis of sTREM-1.
2.8. CD4 CD45RBhi T cell adoptive transfer model ofcolitis
Colitis was induced in RAG2−/− mice by adoptive transfer of2×105 CD4+ CD25- CD45RBhi FACS-sorted T cells as describedpreviously.23 Mice were sacrificed at the indicated time-points or when they exhibited clinical signs of colitis (diarrhea,weight loss, signs of abdominal pain). Sera were obtainedby tail vein incision with a scalpel or by heart-puncture ofthe euthanized mice. Two pieces of the middle part of thecolon were removed for fixation in 4% paraformaldehyde inPBS (and subsequent paraffin embedding) or for storage inRNAlater (for subsequent isolation of RNA), respectively.
2.9. Clinical and histopathological assessments anddetermination of disease activity in colitic mice
Clinical scoring was based on the following parameters: % ofinitial weight loss (0–4%=0, 5–7%=1, 8–10%=2, 11–15%=3),extent of diarrhea (normal stool=0, soft stool=1, visiblediarrhea=2, absence of any stool=3) and macroscopic ap-pearance (i.e. thickening and shortening) of colons (normalappearance=0, mild-moderate-severe inflammation=1–3).Clinical scores for mice sacrificed at 10–12 days post diseaseinduction ranged from 0 to 8 (mean: 3.9±2.5). To assess the-presence of histopathological alterations, a scoring systemranging from 0 (no alterations) to 15 (most severe signs ofcolitis) was established, including the following parameters:cellular infiltration (0–3), loss of goblet cells (0–3), cryptabscesses (0–3), epithelial erosions (0–1), hyperemia (0–2),thickness of the colonic mucosa (0–3). Histological scoringwas performed by a pathologist (N.S.-S.) blinded to sampleidentity. Histopathological scores ranged from 1 to 8 (mean:3.9±2.6). For determination of disease activity in mice, clini-cal and histopathological scores were combined into a totalscore ranging from 1 to 15 (mean: 7.7±4).
916 L. Saurer et al.
2.10. Statistical testing
Statistical analyses were carried out with a statistical pack-age program (GraphPad Prism software version 4.0). TheMann Whitney U test was employed for analysis of data pre-sented in Figs. 2, 4 and 5. Correlations were studied usingthe Spearman rank correlation test. The ability of sTREM-1and CRP to discriminate patients with either quiescent oractive IBD from healthy controls and to discriminate patientswith active IBD from patients with quiescent disease wasassessed by receiver operator characteristic analyses (ROC)and calculation of the area under the ROC (AUC) with a95% confidence interval.
3. Results
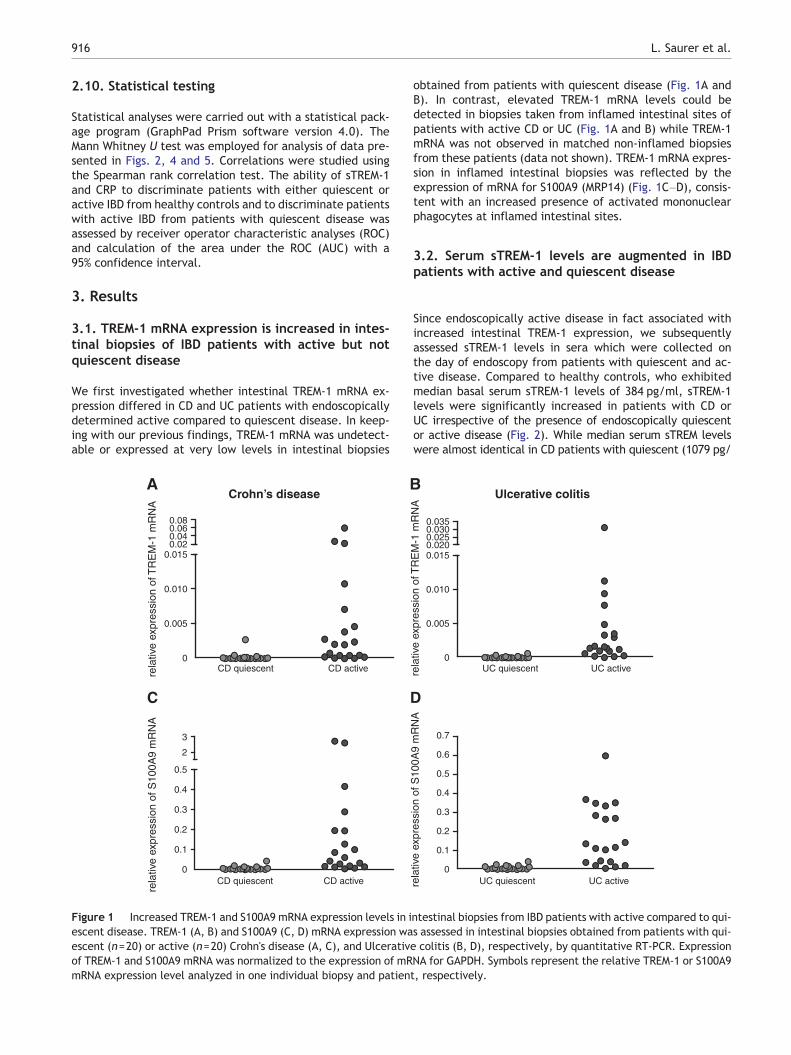
3.1. TREM-1 mRNA expression is increased in intes-tinal biopsies of IBD patients with active but notquiescent disease
We first investigated whether intestinal TREM-1 mRNA ex-pression differed in CD and UC patients with endoscopicallydetermined active compared to quiescent disease. In keep-ing with our previous findings, TREM-1 mRNA was undetect-able or expressed at very low levels in intestinal biopsies
CD quiescent CD activerela
tive
expr
essi
on o
f TR
EM
-1 m
RN
A
Crohn’s disease
0
0.1
0.2
0.3
0.4
0.5
2
3
CD quiescent CD active
rela
tive
expr
essi
on o
f S10
0A9
mR
NA
0
0.005
0.010
0.0150.020.040.060.08
A B
C
Figure 1 Increased TREM-1 and S100A9 mRNA expression levels in iescent disease. TREM-1 (A, B) and S100A9 (C, D) mRNA expression waescent (n=20) or active (n=20) Crohn's disease (A, C), and Ulcerativof TREM-1 and S100A9 mRNA was normalized to the expression of mRmRNA expression level analyzed in one individual biopsy and patien
obtained from patients with quiescent disease (Fig. 1A andB). In contrast, elevated TREM-1 mRNA levels could bedetected in biopsies taken from inflamed intestinal sites ofpatients with active CD or UC (Fig. 1A and B) while TREM-1mRNA was not observed in matched non-inflamed biopsiesfrom these patients (data not shown). TREM-1 mRNA expres-sion in inflamed intestinal biopsies was reflected by theexpression of mRNA for S100A9 (MRP14) (Fig. 1C–D), consis-tent with an increased presence of activated mononuclearphagocytes at inflamed intestinal sites.
3.2. Serum sTREM-1 levels are augmented in IBDpatients with active and quiescent disease
Since endoscopically active disease in fact associated withincreased intestinal TREM-1 expression, we subsequentlyassessed sTREM-1 levels in sera which were collected onthe day of endoscopy from patients with quiescent and ac-tive disease. Compared to healthy controls, who exhibitedmedian basal serum sTREM-1 levels of 384 pg/ml, sTREM-1levels were significantly increased in patients with CD orUC irrespective of the presence of endoscopically quiescentor active disease (Fig. 2). While median serum sTREM levelswere almost identical in CD patients with quiescent (1079 pg/
rela
tive
expr
essi
on o
f TR
EM
-1 m
RN
A
UC quiescent UC active
Ulcerative colitis
UC quiescent UC activerela
tive
expr
essi
on o
f S10
0A9
mR
NA
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0
0.005
0.010
0.0150.0200.0250.0300.035
D
ntestinal biopsies from IBD patients with active compared to qui-s assessed in intestinal biopsies obtained from patients with qui-e colitis (B, D), respectively, by quantitative RT-PCR. ExpressionNA for GAPDH. Symbols represent the relative TREM-1 or S100A9t, respectively.

917sTREM-1 as surrogate marker of disease activity in IBD
ml) compared to active (1124 pg/ml) disease (Fig. 2A), medianserum sTREM-1 was distinctly elevated in UC patients withactive (1441 pg/ml) compared to quiescent disease (950 pg/ml) (Fig. 2B). Patientswith IBD displayed a considerable degreeof heterogeneity with respect to serum sTREM-1 expressionlevels (Fig. 2A and B). A substantial overlap in expression levelsbetween patients with quiescent and active disease was alsoobserved for CRP, particularly in UC patients (Fig. 2C and D).No significant correlation was found for serum sTREM-1 andCRP levels, even in CD or UC patients with active disease (Sup-porting information Fig. 1).
3.3. Intestinal TREM-1 mRNA expression and serumsTREM-1 levels do not correlate
In contrast to intestinal TREM-1 mRNA, which was barelydetectable in patients with quiescent CD or UC, IBD patientswith quiescent disease exhibited significantly elevatedserum sTREM-1 levels compared to normal controls (Figs. 1and 2). Hence, in IBD patients with endoscopically quiescentdisease, intestinal TREM-1 mRNA and serum sTREM-1 did notcorrelate (Fig. 3A and B). Since TREM-1 mRNA in inflamedbiopsies of patients with active disease and serum sTREM-1were expressed in a heterogeneous manner, ranging fromlow to high expression levels across the different patients,we considered the possibility that at least in IBD patientswith endoscopically active disease, increased intestinalTREM-1 mRNA expression could be reflected in higher
0
500
1000
1500
2000
2500
3000
3500
controls CD quiescent CD active
seru
m s
TR
EM
-1 (
pg/m
l)
0
10
20
305075
100
CR
P (
mg/
ml)
controls CD quiescent CD active
NS******
A B
DC ***NS ***
Crohn’s disease
Figure 2 Serum sTREM-1 levels are increased in patients with actidetermined in the sera of healthy controls (n=20) and in patients wrespectively. Each symbol represents a value obtained from an indivactive disease. Lines indicate median values. * pb0.05, *** pb0.001
serum sTREM-1 levels. However, also in IBD patients withactive disease, no significant correlation was found for intesti-nal TREM-1 mRNA and serum sTREM-1 expression (Fig. 3Cand D).
3.4. Differential expression of TREM-1 mRNA andserum sTREM-1 in patients with ileal versus colonic CD
Considering that in patients with endoscopically active dis-ease biopsies were analyzed from inflamed intestinal sitesonly, the heterogeneous expression pattern of mRNA forTREM-1 and S100A9 across the different patients' sampleswas striking. While these differences could be attributableto a distinct infiltration by myeloid cells, at least in patientswith CD they could also relate to the ileal versus colonic siteof disease, as reported previously for the release of calpro-tectin from intestinal tissue samples.24 Among the biopsiesanalyzed in the present study, half of the samples were de-rived from colonic versus ileal sites of inflammation in pa-tients with quiescent and active CD, respectively. Highestexpression levels of TREM-1 and S100A9 mRNA were indeeddetected in biopsies from inflamed colonic, but not ilealsites (Fig. 4A and B). Intriguingly, peak expression levels ofsTREM-1 were preferentially detected in patients with ilealcompared to colonic CD (Fig. 4C). These data further sug-gested that serum sTREM-1 may not be directly associatedwith TREM-1 expression in the inflamed intestine.
0
500
1000
1500
2000
2500
3000
3500
seru
m s
TR
EM
-1 (
pg/m
l)
controls UC quiescent UC active
Ulcerative colitis
0
10
20
305075
100
CR
P (
mg/
ml)
controls UC quiescent UC active
*******
** NS
ve and quiescent IBD. sTREM-1 (A, B) and CRP (C, D) levels wereith quiescent (n=20) and active (n=20) CD (A, C) and UC (B, D),idual healthy control or from a patient with either quiescent or.

NS
A B
DC
sTREM-1 (pg/ml)
quiescent quiescent
sTREM-1 (pg/ml)
active
NS
sTREM-1 (pg/ml)
NS
active
NS
sTREM-1 (pg/ml)
rela
tive
expr
essi
on o
f TR
EM
-1 m
RN
A
rela
tive
expr
essi
on o
f TR
EM
-1 m
RN
A
rela
tive
expr
essi
on o
f TR
EM
-1 m
RN
A
rela
tive
expr
essi
on o
f TR
EM
-1 m
RN
A
1000 2000 3000 4000 0
0.0005
0.0010
0.002
0.003
1000 2000 3000 4000 0
0.0002
0.00040.0006
0.0008
1000 2000 3000 40000
0.002
0.004
0.006
0.008
0.010
0.012
1000 2000 3000 40000
0.01
0.02
0.03
0.040.050.060.07
Ulcerative colitisCrohn’s disease
Figure 3 Intestinal TREM-1 mRNA and serum sTREM-1 levels do not correlate. TREM-1 mRNA and sTREM-1 expression levels deter-mined in intestinal biopsies and concurrently collected sera, respectively, from CD (A, C) or UC (B, D) patients with quiescent (A, B) oractive (C, D) disease were correlated using Spearman's rank correlation. NS=non significant.
918 L. Saurer et al.
3.5. Healthy control individuals differ with respectto serum sTREM-1 levels and surface TREM-1expression
Heterogeneity in serum sTREM-1 expression levels was notonly observed for patients with IBD but also for healthy con-trols, albeit to a lesser extent (Fig. 2). We thus speculatedthat serum sTREM-1 was not only subject to modulation byinflammatory responses but could also be influenced byinherent factors. Indeed, when six healthy controls weresystematically investigated with respect to their peripheralblood neutrophil counts, median surface expression ofTREM-1 and basal serum sTREM-1, those individuals withthe lowest serum sTREM-1 also exhibited reduced neutrophilcounts and, compared to healthy controls with intermediateserum sTREM-1, a distinctly lower TREM-1 surface expressionon their peripheral neutrophils (Table 1). Moreover, afterstimulation of leukocytes from these individuals with satu-rating concentrations of LPS in vitro, shedding of sTREM-1into the supernatant was still limited (Table 1). Notably, atleast in some of the healthy controls analyzed, low or highexpression of surface TREM-1 and serum sTREM-1 appearedto be a stable trait over time (data not shown). Hence, in-trinsic variations in surface TREM-1 and serum sTREM-1 maycontribute to the high degree of variability in serumsTREM-1 expression levels also in patients with IBD.
3.6. In mice with experimental colitis, intestinalTREM-1 mRNA expression is increased at later stagesof disease while a rise in sTREM-1 levels is observedearly post disease induction
In order to systematically follow the course and associationof intestinal TREM-1 mRNA and serum sTREM-1 expressionduring intestinal inflammation, we decided to employ an ex-perimental mouse model of colitis. Adoptive transfer of CD4CD45RBhi T cells into lymphopenic RAG2−/− recipients leadsto onset of weight loss, diarrhea and clinical signs of colitis,which depending on the microbial colonization of the recip-ients, may develop within 10–12 days post the colitogenicCD4 T cell transfer (Fig. 5A). In keeping with our previousresults and analogous to the situation in human individ-uals,19,20 TREM-1 mRNA expression was very low to unde-tectable in the colons of healthy control mice (Fig. 5B).In mice analyzed at 5 or 7 days post colitis induction, in-creased TREM-1 mRNA expression could still not be detected(Fig. 5B), consistent with the absence of macroscopic andhistopathological signs of colitis at these early time-points(Fig. 5A and data not shown). However, at 10–12 days postdisease induction, distinctly augmented TREM-1 mRNA ex-pression was observed in the colonic tissue samples fromthe majority of mice (Fig. 5B). TREM-1 expression correlatedwith the expression of mRNA for S100A9 (data not shown).

quiescent activerela
tive
expr
essi
on o
f TR
EM
-1 m
RN
Are
lativ
e ex
pres
sion
of S
100A
9 m
RN
A
A
B
C
sTR
EM
-1 (
pg/m
l)
0
0.01
0.02
0.03
0.040.06
0.07
quiescent active
quiescent active quiescent active
colon colon
colon colon
ileum ileum
ileum ileum 0
0.25
0.50
0.75
12
3
controls CD ilealCD colon0
500
1000
1500
2000
2500
3000
3500 NS
Figure 4 Differential expression of TREM-1 mRNA and sTREM-1 in patients with ileal versus colonic CD. (A, B) TREM-1 andS100A9 mRNA expression levels in intestinal biopsies from pa-tients with quiescent (n=20) and active (n=20) CD accordingto the ileal or colonic biopsy sampling site. (C) serum sTREM-1levels in healthy controls and in patients with quiescent and ac-tive CD according to the ileal (n=20 patients) or colonic (n=20patients) site of disease. Each symbol represents values from ahealthy control or a patient with quiescent (grey circles) and ac-tive disease (black circles), respectively. Lines indicate medianvalues. NS=non significant.
Table 1 Healthy controls exhibit heterogeneous TREM-1surface expression and sTREM-1 levels.
Healthycontrols
SerumsTREM-1(pg/ml)
Neutrophilcount(×106/ml)
SurfaceTREM-1neutrophils(MFI)
LPS-inducedsTREM-1in vitro(pg/ml)
HC1 12 1.41 56 772HC2 330 3.53 277 1427HC3 254 1.67 78 1360HC4 75 1.21 57 452HC5 218 2.07 159 1198HC6 339 3.44 251 1191
TREM-1 surface expression on peripheral blood neutrophils fromsix healthy controls (HC1-6) was determined by flow cytometry.Mean fluorescence intensity (MFI) of TREM-1 expression wascalculated upon subtraction of the respective isotype controlvalues. For analysis of LPS-induced shedding of sTREM-1 in vitro,leukocytes were cultured o/n in vitro in the presence of 100 ng/mlLPS and sTREM-1 was determined in the cell-free culturesupernatants.
919sTREM-1 as surrogate marker of disease activity in IBD
Thus, in mice with experimental colitis, S100A9 and TREM-1expression in the intestinal mucosa represented a late ratherthan early event in the disease course. From control mice ormice sacrificed at the different time-points post colitis in-duction (Fig. 5C, filled circles) sera were also obtained andanalyzed for the presence of sTREM-1. Moreover, sTREM-1was assessed in sera from mice that were bled consecutivelyat days 5, 7 and 10–12 post CD4 T cell transfer (Fig. 5C, other
symbols). Serum sTREM-1 was expressed in a heterogeneousmanner in healthy control mice (mean: 102±42 pg/ml).Nonetheless, a distinct increase in serum sTREM-1 wasnoted as early as 5 days (mean: 141±42 pg/ml) and 7 days(mean: 169±80 pg/ml) post disease induction (Fig. 5C).Taken together, this kinetics indicated that activation ofTREM-1-expressing phagocytes in the inflamed intestinalmucosa and local shedding of TREM-1 did likely not repre-sent the predominant source of the increased serumsTREM-1 observed in experimental colitis.
Colonic TREM-1 mRNA expression and serum sTREM-1levels in control mice and mice sacrificed at 10–12 dayspost disease induction were subsequently correlated withdisease activity. To this end, mice were grouped into differ-ent categories of mild to moderate or severe diseasedepending on the overall scores for clinical and histopatho-logical signs of colitis (see Materials and methods). While aminority of mice (n=5) only developed a mild form of colitisand almost completely lacked colonic TREM-1 expressionsimilar to the healthy control group, the majority of mice(n=9) had moderate to severe disease, which associatedwith significantly increased TREM-1 mRNA expression(Fig. 5D). Intriguingly, an inverse relationship was observedfor serum sTREM-1 levels, and mice with a mild, but notsevere, form of colitis tended to exhibit increased serumsTREM-1 (Fig. 5E).
4. Discussion
With the present study we have aimed to assess the poten-tial of serum sTREM-1 to serve as a novel surrogate markerof disease activity in patients with IBD. Our findings demon-strate significantly upregulated levels of serum sTREM-1in patients with CD or UC compared to normal controls. How-ever, in contrast to intestinal TREM-1 mRNA, which was ex-clusively expressed in inflamed biopsies from patients withactive disease, elevated serum sTREM-1 was also detectedin patients with quiescent disease at similar levels as ob-served in patients with active disease. These results thus

rel.
expr
essi
on o
f TR
EM
-1 m
RN
A (
x 10
-3)
A
B C
0 2 4 6 8 10 1260
70
80
90
100
110
% in
itial
bod
y w
eigh
t
days post CD4 T cell transfer
0
0.1
0.21
3
5
7
9
11
13
day 0 day 5 day 7 days 10-12
400
300
200
100
0
sTR
EM
-1 (
pg/m
l)
day 0 day 5 day 7 days 10-12
D E
0
2
4
6
8
10
12
rel.
expr
essi
on o
f TR
EM
-1 m
RN
A (
x 10
-3)
controls mild moderate severe controls mild moderate severe
sTR
EM
-1 (
pg/m
l)
250
200
150
100
50
0
** ***
*
*NS
*
NS
Figure 5 Intestinal TREM-1 mRNA and serum sTREM-1 expression in mice with experimental colitis. (A) Adoptive transfer of 2×105
CD4 CD45RBhi T cells into lymphopenic RAG2−/− recipient mice leads to weight loss and onset of clinical colitis within 12 days postdisease induction. Mean values±SD for weight loss of n=14 mice are shown. (B) TREM-1 mRNA expression was assessed by qRT-PCRin colonic tissue specimens isolated from control RAG2−/− mice (n=11) and RAG2−/− mice at day 5 (n=6), day 7 (n=6) or days 10–12 (n=14) post disease induction. (C) sTREM-1 was determined by ELISA in the sera of control RAG2−/− mice (n=11) or of RAG2−/−
mice at various time-points post colitis induction. Filled circles indicate values for individual mice sacrificed at the indicated time-points while remaining symbols indicate values for individual mice which were bled consecutively (days 5, 7, and 10–12 post diseaseinduction) across the observation period. (D) Disease activity in mice sacrificed at 10–12 days post disease induction was determinedas described in Materials and methods. Mice with scores ranging from 1 to 5 were considered to exhibit mild disease while mice withscores from 6–10 and 11–15 were grouped into moderate and severe disease. Control mice, which had not received colitogenic CD4 Tcells had scores ≤1. TREM-1 mRNA expression in colonic tissue specimens of individual mice in relation to the disease activity isshown. (E) Serum sTREM-1 expression in control RAG2−/− mice and in RAG2−/− mice sacrificed at 10–12 days post disease inductionin relation to the disease activity is shown. (B–E) Lines indicate median values. * pb0.05, ** pb0.01.
920 L. Saurer et al.
only partially consent with the findings from two previousstudies that have reported increased, but largely non-overlapping levels of serum sTREM-1 in IBD patients withmild compared to severe disease.25,26 Intriguingly, in these
studies median values measured for sTREM-1 were as lowas 0–50 pg/ml in healthy controls and in the case of Park'set al. investigation only reached 66.5 pg/ml even in pa-tients with IBD,26 illustrating potential differences in the

921sTREM-1 as surrogate marker of disease activity in IBD
methodological approach for detection of sTREM-1. Notably,when employing the commercialized specific ELISA kit thatwas likely utilized by the other two investigations, we consis-tently failed to detect serum sTREM-1 above backgroundlevels, and it was only with the use of an alternative (monoclo-nal) capture antibody and an in-house optimized ELISA that wewere able to successfully measure sTREM-1. While differencesin the ELISA protocols may account for some of the disparitiesin the results obtained with respect to the potential value ofsTREM-1 as surrogate marker of disease activity, other param-eters such as the size of the patient pool and determination ofactual disease activity are likely more relevant. In the presentstudy, we have analyzed equally sized groups of n=20 healthycontrols and CD or UC patients with either quiescent or activedisease, respectively. Importantly, since clinical activity indi-ces tend to correlate poorly with the actual endoscopic dis-ease activity, we have taken care to include only patientswith endoscopically determined disease activity and to ana-lyze sTREM-1 in serum samples that were actually obtainedon the day of endoscopy. This set-up, respectively, the con-current availability of intestinal biopsies and sera, has furtherallowed us to directly associate the presence of serum sTREM-1 with intestinal TREM-1mRNA expression. Based on our previ-ous observations that TREM-1-expressing mononuclear phago-cytes are substantially increased in the inflamed intestinalmucosa of patients with IBD and mice with experimental coli-tis,19,20 we have speculated that local activation-inducedshedding of surface TREM-1 may translate into increasedserum sTREM-1. Our latest results indeed show an associationof intestinal TREM-1 mRNA expression with endoscopically de-termined active versus quiescent IBD. It remains curious thatnot all of the inflamed biopsies from patients with active dis-ease exhibited substantially increased TREM-1 mRNA expres-sion. Since expression of TREM-1 mRNA significantlycorrelated with the expression of mRNA for S100A9 (data notshown), we assume that the heterogeneous expression levelsobserved for TREM-1 and S100A9may primarily be attributableto a distinct infiltration by myeloid cells. In addition, at leastin patients with active CD, the colonic versus ileal localizationof disease also appears to account for higher expression levelsof TREM-1 mRNA, similarly to what has previously beenreported for the release of S100 proteins from colonic tissuesamples.24 Unfortunately, due to the small size of the indi-vidual biopsies, a histological assessment of the extentand composition of the inflammatory infiltrate to further in-vestigate into the mechanism behind the heterogeneous ex-pression levels of TREM-1 and S100A9 mRNA was notattainable.
One of the most unanticipated and striking findings of thepresent study was the lack of correlation between intestinalTREM-1 mRNA expression and serum sTREM-1. Accordingly,while TREM-1 mRNA expression was undetectable in intestinalbiopsies from patients with quiescent disease, these patientsexhibited significantly increased levels of serum sTREM-1 com-pared to healthy controls. Moreover, even in patients with ac-tive disease, distinctly augmented expression of TREM-1mRNAdid not associate with peak levels of serum sTREM-1. Since inan experimental mouse model of colitis increased serumsTREM-1 levels clearly preceded an upregulated expressionof intestinal TREM-1 mRNA expression, we may concludethat, contrary to our initial assumptions, activation of TREM-1-expressing myeloid cells in the inflamed intestinal mucosa
and local shedding of TREM-1 can hardly represent the princi-pal source of the increased serum sTREM-1 observed in pa-tients with IBD.
Currently, we can at best speculate about the systemiccellular source of the elevated serum sTREM-1 observed inpatients with IBD, as well as the activating stimuli that trig-ger the release of surface TREM-1. Shedding of TREM-1 isinduced by TLR ligands such as LPS,10,11 but based on more re-cent evidence possibly also by non-microbial factors such asProstaglandin E2 (PGE2),27 hypoxic conditions28 or potentialligands of NOD family receptors such as monosodium uratecrystals.29 In contrast, pro-inflammatory cytokines such asTNFα, IL-1β or IFNγ appear insufficient in mediating substan-tial sTREM-1 release.11 Wewere not able to trigger the releaseof sTREM-1 by incubation of human PBMC with PGE2 or blockan LPS-induced shedding of sTREM-1 with synthetic Cox-inhibitors in vitro (data not shown), arguing against a simpleeffect of general pro-inflammatory mediators in stimulatingsTREM-1 release. We thus hypothesize that even in patientswith quiescent IBD and in mice with experimental colitis atthe early stages of disease induction, subclinical intestinal in-flammationmay be sufficient to causeminor intestinal epithe-lial barrier defects and translocation of bacterial productsinto the systemic circulation, which may subsequently triggerthe release of sTREM-1 distantly from the intestinal mucosa.The ability of serum sTREM-1 to detect subclinical inflamma-tion in IBD patients with quiescent disease is remarkable(AUC in CD patients compared to controls: 0.95±0.03 andin UC patients: 0.92±0.04) and in this respect appears superiorto CRP (AUC in CD patients: 0.60±0.09 and in UC patients:0.77±0.07). Nonetheless, like CRP, serum sTREM-1 cannot beconsidered a specific marker of IBD and thus has little valuefor an initial diagnosis of the disease. Furthermore, althoughmedian serum sTREM-1 levels were significantly elevated atleast in patients with active compared to quiescent UC, a sub-stantial overlap in expression levels was still observed be-tween the two patient groups. Hence, from the analysis ofthe confined number of patients included in this study, we de-duce that serum sTREM-1 only has limited potential to serve asa novel surrogate marker of disease activity in patients withIBD. This conclusion is corroborated by our findings from anexperimental mouse model of colitis, where serum sTREM-1levels tended to inversely associate, rather than directlycorrelate with disease activity. We have demonstrated previ-ously that administration of the synthetic peptide LP17, repre-senting the extracellular domain of TREM-1, to mice withestablished colitis was able to significantly attenuate the dis-ease process.19 Treatment with a recombinant TREM-1 fusionprotein or with LP17 peptide even protected mice from LPS-induced endotoxemic lethality,5,30 and in patients with sepsis,elevated serum sTREM-1 at the time-point of admission associ-ated with increased survival.31 Serum sTREM-1 thus not onlyhas to be looked at as a passive marker of infection or dis-ease, but also has to be considered as a decoy receptorwith protective functions that could actively modulate thedisease process.
The use of serum sTREM-1 as surrogate marker of diseaseactivity may further be complicated by intrinsic parametersthat could influence its expression in the absence of overt in-flammation. Our preliminary analyses have indicated thathealthy control subjects can differ substantially with respectto their basal serum sTREM-1 levels. Moreover, low serum

922 L. Saurer et al.
sTREM-1 in some of these individuals associated with low sur-face expression of TREM-1 on neutrophils and appeared to bea stable trait over time. We are currently investigatingwhether these inherent differences in TREM-1 expressioncould be explained by polymorphisms in the TREM-1 gene,similar to what has been described for SNPs identified inthe CRP promoter region and CRP plasma levels.32
As intrinsic variations in TREM-1 expression in patientswith IBD may obscure any inflammation-induced changeson a population level, we have performed repeated analysesof serum sTREM-1 levels in eight patients with CD over atime-period of 38 months. Intriguingly, no consistent patternof upregulated or downmodulated serum sTREM-1 expressioncould be observed as these patients went through periods ofactive and quiescent disease, respectively (data not shown).Since in these analyses determination of disease activity wasnot strictly based on endoscopy but largely relied on clinicalassessments, more systematic time-course studies on indi-vidual patients will be required to conclusively investigatethe value of serum sTREM-1 in diagnosing or predicting re-lapses or even responses to treatments.
In summary, our current data argues against the use ofserum sTREM-1 as a straightforward novel marker of diseaseactivity in patients with IBD. However, considering the upre-gulated expression of TREM-1 mRNA in the inflamed intesti-nal mucosa of patients with active, but not quiescent IBD,and in mice with a severe, as opposed to a mild, form ofexperimental colitis, the potential role of TREM-1 in IBD can-not be overlooked. Thus, future evaluations on the possiblevalue of sTREM-1 as a fecal marker of disease activity orefforts to theurapeutically interfere with TREM-1 signallingmay still lead to a significant advances in the managementof IBD.
Supplementary materials related to this article can befound online at doi:10.1016/j.jcsr.2012.02.007.
Acknowledgements
The study was supported by research grants from theSwiss National Science Foundation (3200B0_122560 to CMand the Swiss IBD cohort 33CS30_134274). LS carried outexperiments, performed the analyses and wrote the manu-script. SR is responsible for the Swiss IBD Biobank and ac-quired the majority of the data. MB carried out some ofthe initial studies. N.S.-S. provided expert histopathologicalscoring of the mouse intestinal tissue specimens. M.R. pro-vided the anti-TREM-1 mAb 6B1.1G12 and technical assis-tance. CM designed and coordinated the study. The SIBDCSprovided access to tissue specimens from patients with IBDenrolled in the SIBDCS and ethical permission for use of thesamples.
Appendix
Members of the SIBDCS:Pierluigi Ballabeni, Peter Bauerfeind, Christoph Beglinger,
Stefan Begré, José Bengoa, Janek Binek, Daniel Boller, JanBorovicka, Christian Braegger, Bernard Burnand, RafaelCamara, Dominique Criblez, Philippe de Saussure, LukasDegen, Joakim Delarive, Tobias Ehmann, Matthias Engelmann,
Ali El Wafa, Christian Felley, Alain Frei, Remus Frei, MichaelFried, Michael Friedt, Florian Froehlich, Suzanne Gallot-Lavallé, Tilman Gerlach, Martin Geyer, Marc Girardin, OliverGoetze, Horst Haack, Serge Hediger, Peter Hengstler, KlaasHeyland, Patrick Janiak, Pascal Juillerat, Vera Kessler Bron-dolo, Christoph Knoblauch, Gerd A. Kullak-Ublick, MichaelManz, Rémy Meier, Christa Meyenberger, Pierre Michetti,Christian Mottet, Christoph Mueller, Beat Muellhaupt, ThierryNicolet, Andreas Nydegger, Isabelle Pache, Franziska Piccoli,Julia Pilz, Valérie Pittet, Ronald Rentsch, Jean-Pierre Rey,Silvia Rihs, Daniela Rogler, Gerhard Rogler, Markus Sagmeister,Bernhard Sauter, Niklaus Schaub, Susanne Schibli, Alain M.Schoepfer, Frank Seibold, Johannes Spalinger, PhilippeStadler, Michael Steuerwald, Alex Straumann, Michael Sulz,Michela Tempia-Caliera, Joel Thorens, John-Paul Vader,Stephan R. Vavricka, Jürg Voegtlin, Roland Von Kaenel,Gert Wachter, Juerg Wermuth, Paul Wiesel.
References
1. Strober W, Fuss I, Mannon P. The fundamental basis of inflam-matory bowel disease. J Clin Invest 2007;117:514–21.
2. Kaser A, Zeissig S, Blumberg RS. Inflammatory bowel disease.Annu Rev Immunol. 2010;28 573–1.
3. Schoepfer AM, Beglinger C, Straumann A, Trummler M, VavrickaSR, Bruegger LE, et al. Fecal calprotectin correlates more closelywith the Simple Endoscopic Score for Crohn's disease (SES-CD)than CRP, blood leukocytes, and the CDAI. Am J Gastroenterol.2010;105:162–9.
4. Foell D, Wittkowski H, Roth J. Monitoring disease activity bystool analyses: from occult blood to molecular markers of intes-tinal inflammation and damage. Gut 2009;58:859–68.
5. Bouchon A, Dietrich J, Colonna M. Cutting edge: inflammatoryresponses can be triggered by TREM-1, a novel receptor expressedon neutrophils and monocytes. J Immunol 2000;164:4991–5.
6. Bouchon A, Facchetti F, Weigand MA, Collonna M. TREM-1 am-plifies inflammation and is a crucial mediator of septic shock.Nature 2001;410:1103–7.
7. Radsak MP, Salih HR, Rammensee HG, Schild H. Triggering re-ceptor expressed on myeloid cells-1 in neutrophil inflammatoryresponses: differential regulation of activation and survival. JImmunol 2004;172:4956–63.
8. Netea MG, Azam T, Ferwerda G, Girardin SE, Kim SH, DinarelloCA. Triggering receptor expressed on myeloid cells-1 (TREM-1)amplifies the signals induced by the NACHT-LRR (NLR) patternrecognition receptors. J Leukoc Biol 2006;80:1454–61.
9. Bleharski JR, Kiessler V, Buonsanti C, Sieling PA, Stenger S,Colonna M, et al. A role for triggering receptor expressed on my-eloid cells-1 in host defense during the early-induced and adap-tive phases of the immune response. J Immunol 2003;170:3812–8.
10. Knapp S, Gibot S, de Vos A, Veersteg HH, Colonna M, van derPoll T. Cutting edge: expression patterns of surface and solubletriggering receptor expressed on myeloid cells-1 in humanendotoxemia. J Immunol 2004;173:7131–4.
11. Gibot S, Kolopp-Sarda MN, Bene MC, Bollaert PE, Lozniewski A,Mory F, et al. A soluble form of the triggering receptorexpressed on myeloid cells-1 modulates the inflammatory re-sponse in murine sepsis. J Exp Med 2004;200:1419–26.
12. Gomez-Pina V, Soares-Schanoski A, Rodriguez-Rojas A, DelFresno C, Garcia F, Vallejo-Cremades MT, et al. Metalloprotei-nases shed TREM-1 ectodomain from lipopolysaccharide-stimulated human monocytes. J Immunol 2007;179:4065–73.
13. Gibot S, Kolopp-Sarda MN, Bene MC, Cravoisy A, Levy B, FaureGC, et al. Plasma level of a triggering receptor expressed on

923sTREM-1 as surrogate marker of disease activity in IBD
myeloid cells-1: its diagnostic accuracy in patients with sus-pected sepsis. Ann Intern Med 2004;141:9–15.
14. Gibot S, Cravoisy A, Levy B, Bene MC, Faure G, Bollaert PE. Sol-uble triggering receptor expressed on myeloid cells and the di-agnosis of pneumonia. N Engl J Med 2004;350:451–8.
15. Collins CE, La DT, Yang HT, Massin F, Gibot S, Faure G, et al. El-evated synovial expression of triggering receptor expressed onmyeloid cells 1 in patients with septic arthritis or rheumatoidarthritis. Ann Rheum Dis 2009;68:1768–74.
16. Yasuda T, Takeyama Y, Ueda T, Shinzeki M, Sawa H, Takahiro N,et al. Increased levels of soluble triggering receptor expressedon myeloid cells-1 in patients with acute pancreatitis. Crit CareMed 2008;36:2048–53.
17. Radsak MP, Taube C, Haselmayer P, Tenzer S, Salih HR,Wiewrodt R, et al. Soluble triggering receptor expressed on my-eloid cells 1 is released in patients with stable chronic obstruc-tive pulmonary disease. Clin Dev Immunol 2007;2007:52040.
18. Adib-Conquy M, Monchi M, Goulenok C, Laurent I, Thuong M,Cavaillon JM, et al. Increased plasma levels of soluble triggeringreceptor expressed onmyeloid cells 1 and procalcitonin after car-diac surgery and cardiac arrest without infection. Shock 2007;28:406–10.
19. Schenk M, Bouchon A, Seibold F, Mueller C. TREM-1–expressingintestinal macrophages crucially amplify chronic inflammationin experimental colitis and inflammatory bowel diseases. JClin Invest 2007;117:3097–106.
20. Weber B, Saurer L, Schenk M, Dickgreber N, Mueller C. CX3CR1defines functionally distinct intestinal mononuclear phagocytesubsets which maintain their respective functions during ho-meostatic and inflammatory conditions. Eur J Immunol.2011;41:773–9.
21. Schenk M, Bouchon A, Birrer S, Colonna M, Mueller C. Macro-phages expressing triggering receptor expressed on myeloidcells-1 are underrepresented in the human intestine. J Immu-nol 2005;174:517–24.
22. Pittet V, Juillerat P, Mottet C, Felley C, Ballabeni P, Burnand B,et al. Cohort profile: the Swiss Inflammatory Bowel Disease Co-hort Study (SIBDCS). Int J Epidemiol 2009;38:922–31.
23. Dayer Schneider J, Seibold I, Saxer-Sekulic N, Paredes BE,Saurer L, Mueller C. Lack of TNFR2 expression by CD4(+) T
cells exacerbates experimental colitis. Eur J Immunol2009;39:1743–53.
24. Foell D, Wittkowski H, Ren Z, Turton J, Pang G, Daebritz J, et al.Phagocyte-specific S100 proteins are released from affectedmucosa and promote immune responses during inflammatorybowel disease. J Pathol 2008;216:183–92.
25. Tzivras M, Koussoulas V, Giamarellos-Bourboulis EJ, Tzivras D,Tsaganos T, Koutoukas P, et al. Role of soluble triggering receptorexpressed on myeloid cells in inflammatory bowel disease.WorldJ Gastroenterol 2006;12:3416–9.
26. Park JJ, Cheon JH, Kim BY, Kim DH, Kim ES, Kim TI, et al. Cor-relation of serum-soluble triggering receptor expressed on mye-loid cells-1 with clinical disease activity in inflammatory boweldisease. Dig Dis Sci 2009;54:1525–31.
27. Murakami Y, Kohsaka H, Kitasato H, Akahoshi T. Lipopolysac-charide-induced up-regulation of triggering receptor expressedon myeloid cells-1 expression on macrophages is regulated byendogenous prostaglandin E2. J Immunol 2007;178:1144–50.
28. Bosco MC, Pierobon D, Blengio F, Raggi F, Vanni C, Gattorno M,et al. Hypoxia modulates the gene expression profile of immu-noregulatory receptors in human mature dendritic cells: identi-fication of TREM-1 as a novel hypoxic marker in vitro and in vivo.Blood. 2011;117:2625–9.
29. Murakami Y, Akahoshi T, Hayashi I, Endo I, Kawai S, Inoue M,et al. Induction of triggering receptor expressed on myeloidcells 1 in murine resident peritoneal macrophages by monoso-dium urate monohydrate crystals. Arthritis Rheum 2006;54:455–62.
30. Gibot S, Cravoisy A. Soluble form of the triggering receptorexpressed on myeloid cells-1 as a marker of microbial infection.Clin Med Res 2004;2:181–7.
31. Gibot S, Cravoisy A, Kolopp-Sarda MN, Bene MC, Faure G,Bollaert PE, et al. Time-course of sTREM (soluble triggering recep-tor expressed on myeloid cells)-1, procalcitonin, and C-reactiveprotein plasma concentrations during sepsis. Crit Care Med2005;33:792–6.
32. Carlson CS, Aldred SF, Lee PK, Tracy RP, Schwartz SM, Rieder M,et al. Polymorphisms within the C-reactive protein (CRP) pro-moter region are associated with plasma CRP levels. Am JHum Genet 2005;77:64–77.
Top Related
Copyright © 2022 FDOKUMEN

